Oct 31, 2023 | Volume 13 - Issue 3
Wesley B. Webber, W. Leigh Atherton, Kelli S. Russell, Hilary J. Flint, Stephen J. Leierer
The COVID-19 pandemic and efforts to manage it have affected mental health around the world. Although early research on the COVID-19 pandemic showed a general decline in mental health after the pandemic began, mental health in later stages of the pandemic might be improving alongside other changes (e.g., availability of vaccines, return to in-person activities). The present study utilized data from a mental health service intervention for individuals at a southeastern university who were exposed to COVID-19 following the university’s return to in-person operations. This study tested whether time period (August–September 2021 vs. January–February 2022) predicted individuals’ likelihood of being mild or above in depression and anxiety ratings. Results showed that individuals were more likely to be mild or above in both depression and anxiety ratings during August–September of 2021 than January–February of 2022. Suggestions for future research and implications for professional counselors are discussed.
Keywords: COVID-19, mental health, depression, anxiety, university
The novel coronavirus (COVID-19), first detected in 2019, spread globally at a rapid pace, with the first confirmed case in the United States occurring on January 20, 2020, in the state of Washington (Centers for Disease Control and Prevention [CDC], 2023). By April 2020, the United States had the most reported deaths in the world due to COVID-19. It was not until December of 2020 that the first round of vaccines, authorized under emergency use authorization, was made available (Food and Drug Administration [FDA], 2021). As of October 2022 in the United States, a total of 97,063,357 cases of COVID-19 had been reported, from which there were 1,065,152 COVID-19–related deaths (CDC, 2023). A reported 111,367,843 individuals aged 5 and above in the United States had received their first booster dose of a COVID-19 vaccine as of October 2022 (CDC, 2023). Previous research has shown that the COVID-19 pandemic and efforts to manage it (e.g., lockdowns, quarantine, isolation) had negative effects on mental health in the United States and internationally (Huckins et al., 2020; Pierce et al., 2020; Son et al., 2020). Based on the extended duration of the pandemic and changes that have occurred during it (e.g., vaccine availability, lessening of initial social restrictions), more recent research has investigated possible changes in mental health in later stages of the COVID-19 pandemic (Fioravanti et al., 2022; McLeish et al., 2022; Tang et al., 2022). The present study adds to this literature by exploring whether psychosocial symptomatology (i.e., depression and anxiety) at a university in the Southeastern United States differed in individuals exposed to COVID-19 during August–September 2021 as compared to individuals exposed to COVID-19 during January–February 2022 (following the university’s return to on-campus operations in August 2021).
Challenges to Mental Health During the COVID-19 Pandemic
Since the beginning of the COVID-19 pandemic, conceptual and empirical research has focused on ways in which the pandemic and associated stressors might impact mental health (Bzdok & Dunbar, 2020; Marroquín et al., 2020; Şimşir et al., 2022). Implementation of lockdowns to deter spread of the virus led to concerns that social isolation might have severe impacts on mental health (Bzdok & Dunbar, 2020). This hypothesis was empirically supported, as stay-at-home orders and individuals’ reported levels of social distancing were positively associated with depression and anxiety (Marroquín et al., 2020). Individuals’ views on the COVID-19 pandemic evolved quickly at the outset of the pandemic, and perceptions of risk were shown to increase during the pandemic’s first week in the United States (Wise et al., 2020). Growing awareness of the dangers of the virus likely had deleterious effects on mental health; Şimşir et al. (2022) found through a meta-analysis that fear of COVID-19 was associated with a variety of mental health problems. Mental health was also negatively affected by stigmatization associated with the COVID-19 pandemic, as was the case for those exposed to COVID-19 while at their place of work (Schubert et al., 2021). Such stigmatization associated with COVID-19 exposure was found to increase risk for depression and anxiety (Schubert et al., 2021).
The lockdowns and social distancing measures that accompanied early stages of the COVID-19 pandemic also resulted in changes to routines that likely impacted mental health. For some individuals facing lockdowns or other disruptions to typical routines, reductions in physical activity occurred. Individuals who reported greater impact of COVID-19 on their level of physical activity showed greater symptoms of depression and anxiety (Silva et al., 2022). Early in the COVID-19 pandemic, based on people’s increased time spent at home and their concerns about COVID-19 developments, some people increased their media usage (e.g., news outlets, social media). Such increases in media usage were associated with decreases in mental health (Meyer et al., 2020; Riehm et al., 2020). The COVID-19 pandemic had less significant impact on mental health for those with greater tolerance of uncertainty (Rettie & Daniels, 2021) and psychological flexibility (Dawson & Golijani-Moghaddam, 2020). Thus, some individuals were uniquely suited to face the many changes and stressors brought about by the COVID-19 pandemic.
One population that previous research has identified as being especially at risk for negative mental health outcomes during the COVID-19 pandemic is college students (Xiong et al., 2020). For college students, the COVID-19 pandemic occurred alongside other stressors known to be typical for this population such as adjusting to leaving home, navigating new peer groups, and making career decisions (Beiter et al., 2015; Liu et al., 2019). Thus, for many college students, the COVID-19 pandemic disrupted a period of life already filled with many transitions. For example, shortly after the COVID-19 pandemic began, many college students were forced to leave their dormitories and peers as universities transitioned to online delivery of classes (Copeland et al., 2021). Xiong et al. (2020) found through a systematic review that college students were especially vulnerable to negative mental health outcomes at the outset of the COVID-19 pandemic as compared to others in the general population. In the United States, college students’ reported degree of life disruption due to the COVID-19 pandemic was positively associated with depression at the conclusion of the spring 2020 semester (Stamatis et al., 2022). During fall 2020, COVID-19 concerns and previous COVID-19 infection were each found to be associated with higher levels of depression and anxiety among U.S. college students (Oh et al., 2021). Overall, previous research has supported the notion that changes associated with the COVID-19 pandemic had general negative effects on mental health in the general population and in college students specifically.
Changes in Psychosocial Symptomatology Across the COVID-19 Pandemic
Although research has shown that the COVID-19 pandemic introduced unprecedented challenges and stressors that were associated with mental health problems, another important direction for research has been to characterize overall changes in psychosocial symptomatology as the COVID-19 pandemic progressed. Such research is important given that individuals might psychologically adapt to constant COVID-19 stressors or might benefit from changes that have occurred as the COVID-19 pandemic has progressed (e.g., vaccine availability, lessening of societal restrictions). Initial longitudinal studies comparing individuals’ symptomatology before the COVID-19 pandemic and after its beginning showed that mental health deteriorated after the COVID-19 pandemic began (Elmer et al., 2020; Huckins et al., 2020; Pierce et al., 2020). Prati and Mancini (2021) conducted a meta-analysis of 28 studies that used longitudinal or natural experimental designs and found that depression and anxiety showed small but statistically significant increases after implementation of the initial lockdowns in response to COVID-19. The various changes to ways of life associated with the COVID-19 pandemic appeared to result in a general deterioration in mental health.
Previous research has also explored possible changes in mental health beyond those that were observed in the initial phase of the COVID-19 pandemic. In support of the notion that individuals adapted to changes associated with the COVID-19 pandemic, Fancourt et al. (2021) found that anxiety and depression decreased across the initial lockdown period in the United Kingdom. In contrast, Ozamiz-Etxebarria et al. (2020) found that levels of depression and anxiety were higher 3 weeks into the initial lockdown period in Spain as compared to the beginning of the lockdown. Fioravanti et al. (2022) assessed psychological symptoms longitudinally in an Italian sample at three time points—the beginning of the COVID-19 pandemic and first lockdown (March 2020), the end of the first lockdown phase (May 2020), and during a second wave of COVID-19 with increased societal restrictions (November 2020). Their findings pointed to possible influences of COVID-19 waves and societal restrictions on specific psychosocial symptoms. Specifically, depression, anxiety, obsessive-compulsive disorder, and post-traumatic stress disorder all decreased at the end of the first lockdown phase (Fioravanti et al., 2022). However, all symptoms besides obsessive-compulsive disorder significantly increased from the end of the first lockdown phase to the second wave of COVID-19 (Fioravanti et al., 2022).
Recent research on mental health among college students in later stages of the COVID-19 pandemic has also focused on possible mental health changes over time (McLeish et al., 2022; Tang et al., 2022). Tang et al. (2022) reported reductions in anxiety and depression in a longitudinal study of university students in the United Kingdom between a first time point (July–September 2020, after the end of lockdown) and a second time point (January–March 2021, when vaccinations were becoming available). In contrast, McLeish et al. (2022) found through a repeated cross-sectional study that depression and anxiety among students at a specific university increased from spring 2020 to fall 2020, with the increases being maintained in spring 2021. The authors noted that vaccines were not widely available at the university until the end of spring 2021 (McLeish et al., 2022). Thus, recent studies have found mixed results as to whether psychosocial symptomatology improved over time during the COVID-19 pandemic. These discrepancies may be due to contextual differences between studies (e.g., differences in data collection time periods, availability of vaccines, or levels of COVID-19 restrictions being implemented during data collection).
The Present Study
The present study was conducted based on the need for continued research on mental health across the evolving COVID-19 pandemic and based on previous conflicting findings on possible mental health changes in later stages of the COVID-19 pandemic. Given previous research showing detrimental effects of the COVID-19 pandemic on mental health in the general population and in college students, the present study utilized data from a university population. Specifically, an archival dataset was used in the present study to examine data collected during 2021–2022 at a university in the Southeastern United States and to test whether time period would predict severity of depression and anxiety symptoms. Individuals in the study had been exposed to COVID-19 between August–September 2021 or between January–February 2022 and had requested a mental health contact during university-conducted contact tracing. These two time periods corresponded to surges in COVID-19 cases at the university due to the delta and omicron COVID-19 variants, respectively. August–September 2021 also coincided with a return to on-campus operations at the university and therefore captured psychosocial symptomatology at the beginning of a significant transition in the COVID-19 pandemic (i.e., a return to organized in-person activities on a college campus during the evolving pandemic). This study was designed to answer the following research questions:
- Among those requesting mental health contact after COVID-19 exposure, was the likelihood of having at least mild depression symptoms different for those whose contact occurred between August–September 2021 as compared to those whose contact occurred between January–February 2022?
- Among those requesting mental health contact after COVID-19 exposure, was the likelihood of having at least mild anxiety symptoms different for those whose contact occurred between August–September 2021 as compared to those whose contact occurred between January–February 2022?
Method
Design
A retrospective research design was used to analyze the possible effect of time period on severity of depression and anxiety symptoms among members of a university population who had been exposed to COVID-19 and requested a mental health check-in. The study used a de-identified dataset obtained from the service providers who completed the mental health check-in. We confirmed through consultation with the IRB that the use of archival, de-identified data does not necessitate IRB review.
COVID-19 Mental Health Check-In Dataset
The archival, de-identified dataset used in the present study was compiled as part of a mental health service occurring between February 2021 and February 2022. Participants in the dataset had tested positive for COVID-19 or been exposed to COVID-19 without a positive test. During university-conducted contact tracing, they were offered and elected to receive a subsequent mental health check-in. Individuals who were contact traced and thereby offered a mental health check-in had become known to contact tracers through one of two routes: (a) they reported their own COVID-19 diagnosis or exposure through a self-reporting mechanism as instructed by the university, or (b) they were reported by another individual as having been diagnosed with or exposed to COVID-19. The dataset used in this study included data collected during the mental health check-ins for those who elected to receive them. This data was collected over the phone and documented in RedCap (a secure web browser–based survey protocol designed for clinical research) at the time of the phone call or within 24 hours. The dataset consisted of data for 211 individuals’ check-ins. For each check-in, the dataset included participants’ demographic information, screening data (for depression, anxiety, and trauma), identified needs of the participant, resources shared with the participant, and the date of data entry.
The present study focused on check-in data for all individuals from the COVID-19 Mental Health Check-in Dataset whose check-in had occurred during one of the two time periods of focus—August–September 2021 or January–February 2022. These two time periods corresponded to surges in COVID-19 cases at the university associated with the delta and omicron COVID-19 variants, respectively. The 149 individuals who checked in during these 4 months represented 70.62% of the total number of check-ins over the 12-month dataset (N = 211), reflecting the surges in COVID-19 cases during these two periods. Of the 149 individuals in the present study, 96 (64.43%) received their check-in during August–September 2021, and 53 (35.57%) received their check-in during January–February 2022. The selection of these two time periods from the larger dataset allowed for comparison of psychosocial symptomatology during comparable levels of COVID-19 infection (i.e., surges associated with two subsequent COVID-19 variants) at comparable points in subsequent academic semesters (i.e., the first 2 months of the fall 2021 and spring 2022 semesters). The present study used only the screening data for depression and anxiety, as the scales for each of these constructs showed good internal consistency (Cronbach’s alpha > .80).
Participants
The sample in the present study consisted of 149 individuals. The selected individuals’ ages ranged from 17 to 52 (M = 22.21, SD = 7.43). With regard to gender, 67.11% identified as female, 32.21% as male, and 0.67% as non-binary. The reported races of individuals in the study were as follows: 60.4% White, 20.13% African American, 6.71% Hispanic, 3.36% Other, 2.68% Two or more races, 1.34% Middle Eastern, 1.34% Native American, and 0.67% Asian. Some participants preferred not to indicate their race (3.36%). In responding to a question about their ethnicity, 87.25% of individuals identified as not Latinx, 9.40% identified as Latinx, and 3.36% preferred not to answer. With regard to academic level/job title, 32.89% were freshmen, 20.13% were sophomores, 14.09% were juniors, 15.44% were seniors, 7.38% were graduate students, 8.05% were faculty/staff, and 2.01% preferred not to answer. Regarding employment, 53.69% were not employed (including students), 30.20% were employed part-time, 12.75% were employed full-time, and 3.36% preferred not to answer. The relationship statuses of individuals were reported as the following: 87.92% single (never married), 4.7% married, 2.01% single but cohabitating with a significant other, 1.34% in a domestic partnership or civil union, 1.34% separated, 0.67% divorced, and 2.01% preferred not to answer. Table 1 summarizes demographic responses within each of the two time periods and for the full sample.
Measures
Demographic Questionnaire
Participants responded to seven demographic questions (age, gender, race, ethnicity, academic year/job title, current employment status, and relationship status). They were informed that this information was optional and that they could choose not to answer particular questions.
Table 1
Demographic Characteristics of the Sample
|
Demographic
Characteristic |
|
| August–September 2021 |
January–February 2022 |
Full Sample |
|
n |
% |
n |
% |
n |
% |
| Gender |
|
|
|
|
|
|
| Female |
69 |
71.88 |
31 |
58.49 |
100 |
67.11 |
| Male |
27 |
28.13 |
21 |
39.62 |
48 |
32.21 |
| Non-binary |
0 |
0 |
1 |
1.89 |
1 |
0.67 |
| Race |
|
|
|
|
|
|
| White |
56 |
58.33 |
34 |
64.15 |
90 |
60.40 |
| African American |
23 |
23.96 |
7 |
13.21 |
30 |
20.13 |
| Hispanic |
8 |
8.33 |
2 |
3.77 |
10 |
6.71 |
| Other race |
1 |
1.04 |
4 |
7.55 |
5 |
3.36 |
| Two or more races |
4 |
4.17 |
0 |
0 |
4 |
2.68 |
| Middle Eastern |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Native American |
1 |
1.04 |
1 |
1.89 |
2 |
1.34 |
| Asian |
1 |
1.04 |
0 |
0 |
1 |
0.67 |
| Prefer not to answer |
0 |
0 |
5 |
9.43 |
5 |
3.36 |
| Ethnicity |
|
|
|
|
|
|
| Not Latinx |
82 |
85.42 |
48 |
90.57 |
130 |
87.25 |
| Latinx |
12 |
12.50 |
2 |
3.77 |
14 |
9.40 |
| Prefer not to answer |
2 |
2.08 |
3 |
5.66 |
5 |
3.36 |
| Academic Year / Job Title |
|
|
|
|
|
|
| Freshman |
38 |
39.58 |
11 |
20.75 |
49 |
32.89 |
| Sophomore |
18 |
18.75 |
12 |
22.64 |
30 |
20.13 |
| Junior |
15 |
15.63 |
6 |
11.32 |
21 |
14.09 |
| Senior |
15 |
15.63 |
8 |
15.09 |
23 |
15.44 |
| Graduate Student |
6 |
6.25 |
5 |
9.43 |
11 |
7.38 |
| Faculty/Staff |
4 |
4.17 |
8 |
15.09 |
12 |
8.05 |
| Prefer not to answer |
0 |
0 |
3 |
5.66 |
3 |
2.01 |
| Employment |
|
|
|
|
|
|
| Not Employed (including student) |
62 |
64.58 |
18 |
33.96 |
80 |
53.69 |
| Employed Part-Time |
26 |
27.08 |
19 |
35.85 |
45 |
30.20 |
| Employed Full-Time |
8 |
8.33 |
11 |
20.75 |
19 |
12.75 |
| Prefer not to answer |
0 |
0 |
5 |
9.43 |
5 |
3.36 |
| Relationship Status |
|
|
|
|
|
|
| Single, never married |
87 |
90.63 |
44 |
83.02 |
131 |
87.92 |
| Married |
3 |
3.13 |
4 |
7.55 |
7 |
4.70 |
| Single, but cohabitating with a
significant other |
2 |
2.08 |
1 |
1.89 |
3 |
2.01 |
| In a domestic partnership or civil union |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Separated |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Divorced |
0 |
0 |
1 |
1.89 |
1 |
0.67 |
| Prefer not to answer |
0 |
0 |
3 |
5.66 |
3 |
2.01 |
| Note. Average age was 21.51 (SD = 6.98) in August–September 2021 group, 23.49 (SD = 8.11) in January–February 2022 group, and 22.21 (SD = 7.43) in the full sample. |
Patient Health Questionnaire-9 (PHQ-9)
The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) is a 9-item self-report questionnaire that measures the frequency and severity of depression symptoms over the past 2 weeks. The PHQ-9 has been validated for screening for depression in the general population (Kroenke et al., 2001; Martin et al., 2006). The questionnaire measures frequency of symptoms such as “feeling down, depressed, or hopeless,” and “little interest or pleasure in doing things.” The PHQ-9 uses a 4-point Likert scale to measure frequency of symptoms over the past 2 weeks with the response options of not at all, several days, more than half the days, and nearly every day. Scores of 0, 1, 2, and 3 are assigned to each of the four response categories, and a PHQ-9 total score is derived by adding the scores for each of the nine PHQ-9 items. Minimal depression is indicated by PHQ-9 total scores of 0–4, mild depression by scores of 5–9, moderate depression by scores of 10–14, moderately severe depression by scores of 15–19, and severe depression by scores of 20–27. Question 9 on the PHQ-9 is a single screening question assessing suicide risk. Interviewers were trained in appropriate protocol in the event of a positive screen for this question. Cronbach’s alpha for the PHQ-9 in the present study was .86.
Generalized Anxiety Disorder 7-Item Scale (GAD-7)
The Generalized Anxiety Disorder 7-Item Scale (GAD-7; Spitzer et al., 2006) is a 7-item self-report anxiety questionnaire that measures the frequency and severity of anxiety symptoms over the past 2 weeks. The GAD-7 has demonstrated reliability and validity as a measure of anxiety in the general population (Löwe et al., 2008). The questionnaire measures symptoms such as “feeling nervous, anxious, or on edge,” and “not being able to stop or control worrying.” The format of the GAD-7 is similar to the PHQ-9, using a 4-point Likert scale to measure frequency of symptoms over the past 2 weeks with response options of not at all, several days, more than half the days, and nearly every day. GAD-7 scores are calculated by assigning scores of 0, 1, 2, and 3 for response categories and then adding the scores from the 7 items to derive a total score ranging from 0 to 21. Minimal anxiety is indicated by total scores of 0–4, mild anxiety by scores of 5–9, moderate anxiety by scores of 10–14, and severe anxiety by scores of 15– 21. Cronbach’s alpha for the GAD-7 in the present study was .86.
Analytic Strategy
Total scores for the PHQ-9 and GAD-7 were found to be positively skewed for both groups of participants. Binary logistic regression was therefore an appropriate method of analysis for this dataset, as binary logistic regression does not require normality of dependent variables (Tabachnick & Fidell, 2019). For two separate binary logistic regression models, individuals were classified as being either minimal or mild or above in depression (PHQ-9) and anxiety (GAD-7) to create binary outcome variables. This choice of cutoff allowed each model (with time period as predictor) to satisfy the recommendation of Peduzzi et al. (1996) that there be at least 10 cases per outcome per predictor in binary logistic regression.
Prior to performing these intended primary analyses to answer the research questions, preliminary analyses were conducted to determine whether adding control variables to the logistic regression models was warranted. Chi-square tests of independence, Fisher-Freeman-Halton Exact tests, Fisher’s Exact tests, and an independent samples t-test were used to test for possible differences between the two time periods in individuals’ responses to demographic questions. In cases in which responses to demographic questions were shown to be significantly different across the two groups, appropriate tests were used to determine whether the demographic responses in question were associated with either of the two intended dependent variables.
Following the preliminary analyses, the intended two binary logistic regressions were conducted to answer the research questions. In the first binary logistic regression, time period was the predictor
(1 = August–September 2021, 0 = January–February 2022) and PHQ-9 depression category was the outcome (1 = mild or above, 0 = minimal). In the second logistic regression, time period was the predictor (1 = August–September 2021, 0 = January–February 2022) and GAD-7 anxiety category was the outcome (1 = mild or above, 0 = minimal). All analyses were conducted using SPSS Version 28.
Results
Preliminary Demographic Analyses
Prior to the primary analyses, preliminary analyses were conducted to determine whether the two groups differed in their responses to demographic questions. Fisher-Freeman-Halton Exact tests and an independent samples t-test were used to test for differences between groups in their responses to the seven demographic questions. Two of the seven tests were statistically significant at Bonferroni-corrected alpha level. Specifically, Fisher-Freeman-Halton Exact tests found significant differences between time periods on the race (p = .004) and employment (p < .001) demographic variables.
Based on the above significant results for the race and employment variables across the time periods, 2 x 2 tests were conducted to test for differences between specific race responses and specific employment responses across the two time periods. For these 2 x 2 tests, a chi-square test of independence was used when all expected cell counts were 5 or greater and Fisher’s Exact test was used when any expected cell counts were less than 5. To follow up the significant result for race, 2 x 2 tests were conducted for all pairs of race responses in which 2 x 2 tests were possible (i.e., in which there was at least one observation for each of the two race responses at both time periods). These follow-up 2 x 2 tests of responses to the race question across time periods found no statistically significant differences between pairs of race responses across time periods using Bonferroni-corrected alpha level. Follow-up 2 x 2 tests comparing all pairs of responses to the employment question across time periods found two statistically significant differences using Bonferroni-corrected alpha level. A chi-square test of independence showed that individuals were more likely to be employed full-time during January–February 2022 than August–September 2021 as compared to those not employed (including students), X2 (1, N = 99) = 9.29, p = .002. Fisher’s Exact test showed that individuals were more likely to indicate “prefer not to answer” during January–February 2022 than during August–September 2021 as compared to those indicating “not employed (including students),” p = .001.
The statistically significant tests for race and employment across time periods were followed up with additional tests to determine if depression or anxiety category (minimal vs. mild or above for each) was associated with individuals’ responses to the relevant race and employment questions. A Fisher-Freeman-Halton Exact test showed that depression category was not associated with individuals’ responses to the race question, p = .099. A Fisher-Freeman-Halton Exact test also showed that individuals’ anxiety category was not associated with individuals’ responses to the race question,
p = .386. With regard to employment, tests of association were conducted between the intended dependent variables and the specific employment responses that were found to differ between the two groups. A chi-square test of independence showed that individuals’ status as “not employed” vs. “employed full-time” was not associated with depression category, X2 (1, N = 99) = .63, p = .429. A chi-square test of independence also showed that these employment statuses were not associated with anxiety category, X2 (1, N = 99) = .27, p = .601. Similarly, Fisher’s Exact tests showed that individuals’ employment responses of “prefer not to answer” vs. “not employed (including students)” were not associated with depression category (p = .156) or anxiety category (p = .317). These results were interpreted as indicating that the ways in which individuals in the two time periods differed demographically did not have significant impact on the study’s dependent variables of interest. Therefore, binary logistic regressions were conducted with only time period as a predictor of each dependent variable.
Relationship Between Time Period and Severity of Depression Symptoms
Most individuals in the study were in the minimal depression range on the PHQ-9 as compared to the other four categories. Figure 1 shows the percentage of individuals falling into each of the five PHQ-9 categories during each of the two time periods.
Figure 1
Percentages of Individuals Falling Into Each of the PHQ-9 Categories for Each of the Two Time Periods
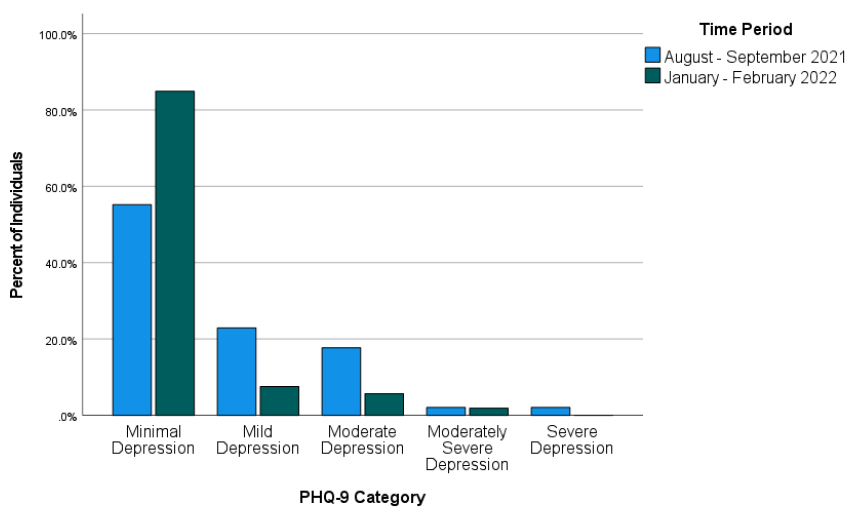
Across both time periods combined (August–September 2021 and January–February 2022), 51 individuals (34.23%) were mild or above in depression while 98 (65.77%) were in the minimal range. Binary logistic regression was used to test whether time period predicted severity of depression symptoms. Time period was entered as a predictor (1 = August–September 2021, 0 = January–February 2022) of depression (1 = mild or above, 0 = minimal depression). The overall binary logistic regression model was found to be statistically significant, χ2(1) = 14.46, p < .001, Cox & Snell R2 = .092, Nagelkerke R2 = .128. In the model, time period was found to be a significant predictor of depression, Wald χ2(1) = 12.17, B = 1.52, SE = .44, p < .001. The model estimated that the odds of being mild or above in depression were 4.56 times higher during August–September 2021 than during January–February 2022 for individuals requesting a mental health check-in following COVID-19 exposure. Specifically, the predicted odds of being mild or above in depression were .81 during August–September 2021 and .18 during January–February 2022.
Relationship Between Time Period and Severity of Anxiety Symptoms
Most individuals in the study were in the minimal anxiety range on the GAD-7 as compared to the other three categories. Figure 2 shows the percentage of individuals falling into each of the four GAD-7 categories during each of the two time periods.
Figure 2
Percentages of Individuals Falling Into Each of the GAD-7 Categories for Each of the Two Time Periods
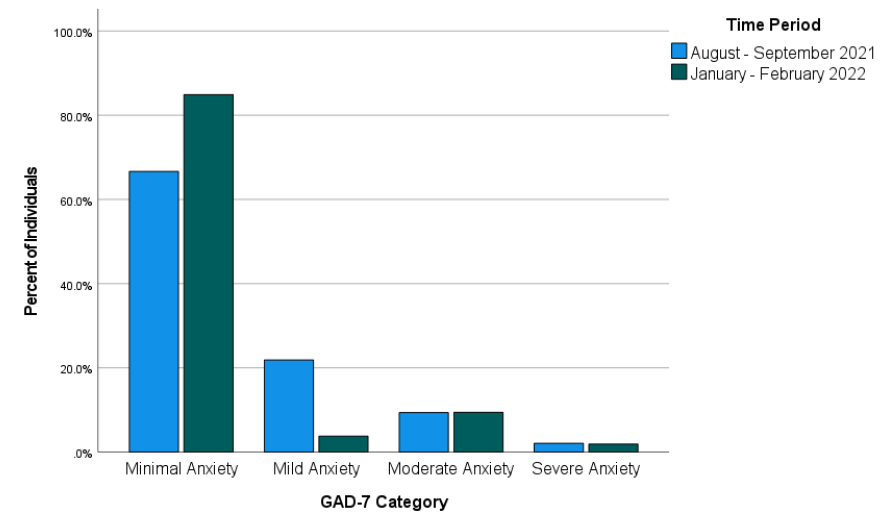
Across both time periods combined, 40 individuals (26.85%) reported anxiety at levels of mild or above and 109 individuals (73.15%) reported minimal anxiety. Binary logistic regression was used to test whether time period predicted severity of anxiety symptoms. Time period was entered as a predictor (1 = August–September 2021, 0 = January–February 2022) of anxiety (1 = mild or above, 0 = minimal anxiety). The overall binary logistic regression model was statistically significant, χ2(1) = 6.16, p = .013, Cox & Snell R2 = .041, Nagelkerke R2 = .059. In the model, time period was a significant predictor of anxiety, Wald χ2(1) = 5.51, B = 1.03, SE = .44, p = .019. Odds of being mild or above in anxiety were estimated by the model to be 2.81 times higher during August–September 2021 than during January–February 2022 for individuals requesting a mental health check-in after exposure to COVID-19. Specifically, the predicted odds of being mild or above in anxiety were .50 during August–September 2021 and .18 during January–February 2022.
Discussion
This study examined whether time period would predict severity of depression and anxiety symptoms in a sample of individuals exposed to COVID-19 at a university in the Southeastern United States. More specifically, the study addressed the possibility that the likelihood of being mild or above in depression and anxiety would differ between two time periods following the university’s return to in-person operations in August 2021. The results of the study showed that the likelihood of being mild or above in depression and the likelihood of being mild or above in anxiety after exposure to COVID-19 were both higher during August–September 2021 than during January–February 2022. This finding is in line with previous research that found improvements in psychosocial symptomatology in later stages of the COVID-19 pandemic (Tang et al., 2022) and in contrast to research that did not find such improvements (McLeish et al., 2022). Based on the results of the present study, it appears likely that factors that differed between the two assessed time periods (first two months of fall 2021 vs. first two months of spring 2022) contributed to the observed difference in likelihood of depression and anxiety symptoms. McLeish et al. (2022) noted that vaccines were not widely available in their study that did not find such differences, while Tang et al. (2022), who did find significant differences, noted that vaccines were available at their second data collection point (January–March 2021). For individuals in the present study, COVID-19 vaccinations were available. Vaccination was strongly encouraged by university administrators following the return to campus, and more individuals on campus were vaccinated in spring 2022 than in fall 2021. Vaccinations might have lessened individuals’ COVID-19 concerns and contributed to more positive psychosocial outcomes during spring 2022 than fall 2021.
Besides vaccinations possibly lessening depression and anxiety symptoms, other environmental circumstances might also have played a role. The two time periods on which this study focused also differed in their proximity to a significant environmental event—a return to in-person operations on the campus where the individuals studied and/or worked. Early research on the mental health impact of COVID-19 highlighted the negative mental health effects of factors such as reduced physical activity (Silva et al., 2022), life disruptions due to the COVID-19 pandemic (Stamatis et al., 2022), and social distancing (Marroquín et al., 2020). Therefore, it is possible that symptoms of depression and anxiety in spring 2022 were affected by changes in specific circumstances known to have negatively impacted mental health earlier in the COVID-19 pandemic. For example, individuals’ physical activity likely increased because of a return to campus, and they might have perceived less disruption to their lives through being able to resume in-person activities. Although individuals in the present study who were exposed to COVID-19 during the first 2 months after the return to campus might have reaped some benefits from the return to more normal environmental circumstances, they might also have faced a period of adjustment. In contrast, individuals exposed to COVID-19 between January and February 2022 might have been more readjusted and reaped greater benefits from the return to campus, thereby reducing depression and anxiety symptoms.
Implications
This study’s findings on psychosocial symptomatology across time during the COVID-19 pandemic have important implications for the work of counselors. Based on the results of the present study, counselors planning outreach efforts to individuals exposed to COVID-19 should consider that as time passes, these individuals might be more stable with regard to symptoms of depression and anxiety. However, some individuals directly affected by COVID-19 might still be interested in receiving mental health information despite low levels of depression and anxiety. Many individuals in the present study scored as minimal in depression and anxiety but were still interested in receiving a mental health check-in. Thus, counselors should advocate for mental health information and resources to be made available to individuals who are known to be facing stressors related to COVID-19. Counselors should be prepared to have conversations to determine the contextual needs of individuals exposed to COVID-19 rather than relying only on standardized measures of psychosocial symptomatology. For example, counselors working with employees (such as university employees in the present study) should be attentive to the possibility that employees exposed to COVID-19 may be concerned about facing stigma in their workplace due to their exposure (Schubert et al., 2021).
Given that the present study focused on individuals from a university population, the study’s results also have specific implications for college counselors. College counselors should develop approaches to reach students during circumstances that might make traditional outreach challenging. For example, the present study used data from a mental health intervention in which service providers collaborated with university contact tracers to safely provide mental health resources by telephone to individuals exposed to COVID-19. College counselors should be prepared to connect clients with services at a distance. Previous research during the COVID-19 pandemic found that college students were interested in using teletherapy and online self-help resources, particularly if such services were made available for free (Ahuvia et al., 2022).
Besides preparing for flexible modes of service delivery, college counselors should be prepared to deliver interventions most likely to be useful to college students during the COVID-19 pandemic or similar pandemics. Those recently exposed to COVID-19 might benefit from discussing possible fears associated with COVID-19, experiences of stigmatization they might have experienced due to their exposure, and ways to maintain mental health during any period of quarantine or isolation that might be required. Those not recently exposed to COVID-19 might instead benefit from interventions that address other issues that might have resulted from the COVID-19 pandemic or societal responses to it. For example, if circumstances associated with the COVID-19 pandemic led to reductions in a client’s amount of exercise, a counselor can help the client identify ways they might increase their physical activity. Interventions promoting physical activity were found to reduce anxiety and depression in college students during the COVID-19 pandemic (Luo et al., 2022).
Limitations
This study had limitations that should be considered. First, with the study being retrospective and using secondary data from a clinical intervention, it was not possible to include measures that might have better clarified mechanisms of the changes that were observed in psychosocial symptoms. Thus, the possible explanations above of what might have driven these changes are tentative and future research should test them more directly. Second, individuals in the present study were likely to have been in greater distress than the general university population based on their exposure to COVID-19, which might limit the generalizability of the study’s findings. Third, individuals in the present study were from a single university in the Southeastern United States. Thus, our findings might not generalize to other regions where university-related COVID-19 policies might have differed. Fourth, the decision to create a binary independent variable to reflect time periods (August–September 2021 and January–February 2022) in the present study also entails a limitation. This decision was justifiable on the basis that it allowed for comparisons of individuals at similar points in academic semesters and during comparable periods of COVID-19 infection. However, this analysis decision means that inferences from the study’s results are limited to the two specific time periods that were analyzed. Fifth, individuals in the present study responded to items on the GAD-7 and PHQ-9 through a phone conversation with interviewers. Interviewer-administered surveys have been previously associated with greater tendencies toward socially desirable responses than self-administered surveys (Bowling, 2005). This might limit the present study’s generalizability in contexts where self-administrations of the GAD-7 and PHQ-9 are used.
Future Research
The results of this study provide important directions for future research. Future researchers who can conduct prospective studies or who have access to larger retrospective datasets should aim to determine specific factors that might lead to improvement in mental health outcomes over time during the COVID-19 pandemic. Knowledge produced by such studies could contribute to clinical applications in the future regarding COVID-19 or other pandemics that might occur. Relatedly, future research with larger samples of demographically diverse participants should explore possible demographic differences in specific mental health trajectories in later stages of the COVID-19 pandemic.
Future research should continue to focus specifically on those who are interested in mental health information and interventions during the COVID-19 pandemic. To follow up this study’s findings, future quantitative and qualitative studies should aim to identify which individuals are interested in receiving mental health services and determine the best ways to deliver services to them. As a globally experienced stressor, the COVID-19 pandemic might have changed some individuals’ views of mental health and/or their receptiveness to mental health outreach. More specifically, some might be more receptive to available mental health information even at lower thresholds of anxiety, depression, or other psychosocial symptoms. Such clients might be interested in preventive services or their interest in mental health information might be driven by other factors. Future studies should address these possibilities more directly than was possible in the present retrospective study.
Conclusion
Overall, the present study provided a positive picture regarding psychosocial symptomatology in later stages of the COVID-19 pandemic. Results from this study of students and employees at a university in the Southeastern Unites States following their return to campus found that many individuals requesting mental health information after exposure to COVID-19 showed minimal levels of depression and anxiety. Individuals in the study were more likely to be in these minimal ranges during January–February 2022 than August–September 2021. COVID-19 will continue to have effects in individuals’ lives through future infections and potentially through lasting effects of previous stages of the COVID-19 pandemic. As organized in-person activities resume and COVID-19 infections continue, counseling researchers and practitioners should continue efforts to best characterize and address individuals’ mental health needs associated with the COVID-19 pandemic.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ahuvia, I. L., Sung, J. Y., Dobias, M. L., Nelson, B. D., Richmond, L. L., London, B., & Schleider, J. L. (2022). College student interest in teletherapy and self-guided mental health supports during the COVID-19 pandemic. Journal of American College Health. Advance online publication.
https://doi.org/10.1080/07448481.2022.2062245
Beiter, R., Nash, R., McCrady, M., Rhoades, D., Linscomb, M., Clarahan, M., & Sammut, S. (2015). The prevalence and correlates of depression, anxiety, and stress in a sample of college students. Journal of Affective Disorders, 173, 90–96. https://doi.org/10.1016/j.jad.2014.10.054
Bowling, A. (2005). Mode of questionnaire administration can have serious effects on data quality. Journal of Public Health, 27(3), 281–291. https://doi.org/10.1093/pubmed/fdi031
Bzdok, D., & Dunbar, R. I. M. (2020). The neurobiology of social distance. Trends in Cognitive Sciences, 24(9), 717–733. https://doi.org/10.1016/j.tics.2020.05.016
Centers for Disease Control and Prevention. (2023, March 15). COVID-19 timeline. https://www.cdc.gov/museum/timeline/covid19.html
Copeland, W. E., McGinnis, E., Bai, Y., Adams, Z., Nardone, H., Devadanam, V., Rettew, J., & Hudziak, J. J. (2021). Impact of COVID-19 pandemic on college student mental health and wellness. Journal of the American Academy of Child & Adolescent Psychiatry, 60(1), 134–141.e2. https://doi.org/10.1016/j.jaac.2020.08.466
Dawson, D. L., & Golijani-Moghaddam, N. (2020). COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. Journal of Contextual Behavioral Science, 17, 126–134.
https://doi.org/10.1016/j.jcbs.2020.07.010
Elmer, T., Mepham, K., & Stadtfeld, C. (2020). Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE, 15(7), Article e0236337. https://doi.org/10.1371/journal.pone.0236337
Fancourt, D., Steptoe, A., & Bu, F. (2021). Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. The Lancet Psychiatry, 8(2), 141–149. https://doi.org/10.1016/S2215-0366(20)30482-X
Fioravanti, G., Benucci, S. B., Prostamo, A., Banchi, V., & Casale, S. (2022). Effects of the COVID-19 pandemic on psychological health in a sample of Italian adults: A three-wave longitudinal study. Psychiatry Research, 315, Article 114705. https://doi.org/10.1016/j.psychres.2022.114705
Food and Drug Administration. (2021, August 23). FDA approves first COVID-19 vaccine. https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine
Huckins, J. F., daSilva, A. W., Wang, W., Hedlund, E., Rogers, C., Nepal, S. K., Wu, J., Obuchi, M., Murphy, E. I., Meyer, M. L., Wagner, D. D., Holtzheimer, P. E., & Campbell, A. T. (2020). Mental health and behavior of college students during the early phases of the COVID-19 pandemic: Longitudinal smartphone and ecological momentary assessment study. Journal of Medical Internet Research, 22(6), Article e20185.
https://doi.org/10.2196/20185
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Liu, C. H., Stevens, C., Wong, S. H. M., Yasui, M., & Chen, J. A. (2019). The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depression and Anxiety, 36(1), 8–17. https://doi.org/10.1002/da.22830
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., & Herzberg, P. Y. (2008). Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Medical Care, 46(3), 266–274. https://doi.org/10.1097/MLR.0b013e318160d093
Luo, Q., Zhang, P., Liu, Y., Ma, X., & Jennings, G. (2022). Intervention of physical activity for university students with anxiety and depression during the COVID-19 pandemic prevention and control period: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 19(22), 15338. https://doi.org/10.3390/ijerph192215338
Marroquín, B., Vine, V., & Morgan, R. (2020). Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Research, 293, Article 113419. https://doi.org/10.1016/j.psychres.2020.113419
Martin, A., Rief, W., Klaiberg, A., & Braehler, E. (2006). Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. General Hospital Psychiatry, 28(1), 71–77.
https://doi.org/10.1016/j.genhosppsych.2005.07.003
McLeish, A. C., Walker, K. L., & Hart, J. L. (2022). Changes in internalizing symptoms and anxiety sensitivity among college students during the COVID-19 pandemic. Journal of Psychopathology and Behavioral Assessment, 44, 1021–1028. https://doi.org/10.1007/s10862-022-09990-8
Meyer, J., McDowell, C., Lansing, J., Brower, C., Smith, L., Tully, M., & Herring, M. (2020). Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. International Journal of Environmental Research and Public Health, 17(18), Article 6469.
https://doi.org/10.3390/ijerph17186469
Oh, H., Marinovich, C., Rajkumar, R., Besecker, M., Zhou, S., Jacob, L., Koyanagi, A., & Smith, L. (2021). COVID-19 dimensions are related to depression and anxiety among US college students: Findings from the Healthy Minds Survey 2020. Journal of Affective Disorders, 292, 270–275. https://doi.org/10.1016/j.jad.2021.05.121
Ozamiz-Etxebarria, N., Idoiaga Mondragon, N., Dosil Santamaría, M., & Picaza Gorrotxategi, M. (2020). Psychological symptoms during the two stages of lockdown in response to the COVID-19 outbreak: An investigation in a sample of citizens in Northern Spain. Frontiers in Psychology, 11, Article 1491.
https://doi.org/10.3389/fpsyg.2020.01491
Peduzzi, P., Concato, J., Kemper, E., Holford, T. R., & Feinstein, A. R. (1996). A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology, 49(12), 1373–1379. https://doi.org/10.1016/S0895-4356(96)00236-3
Pierce, M., Hope, H., Ford, T., Hatch, S., Hotopf, M., John, A., Kontopantelis, E., Webb, R., Wessely, S., McManus, S., & Abel, K. M. (2020). Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. The Lancet Psychiatry, 7(10), 883–892.
https://doi.org/10.1016/S2215-0366(20)30308-4
Prati, G., & Mancini, A. D. (2021). The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychological Medicine, 51(2), 201–211. https://doi.org/10.1017/S0033291721000015
Rettie, H., & Daniels, J. (2021). Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. American Psychologist, 76(3), 427–437. https://doi.org/10.1037/amp0000710
Riehm, K. E., Holingue, C., Kalb, L. G., Bennett, D., Kapteyn, A., Jiang, Q., Veldhuis, C. B., Johnson, R. M., Fallin, M. D., Kreuter, F., Stuart, E. A., & Thrul, J. (2020). Associations between media exposure and mental distress among U.S. adults at the beginning of the COVID-19 pandemic. American Journal of Preventive Medicine, 59(5), 630–638. https://doi.org/10.1016/j.amepre.2020.06.008
Schubert, M., Ludwig, J., Freiberg, A., Hahne, T. M., Romero Starke, K., Girbig, M., Faller, G., Apfelbacher, C., von dem Knesebeck, O., & Seidler, A. (2021). Stigmatization from work-related COVID-19 exposure: A systematic review with meta-analysis. International Journal of Environmental Research and Public Health, 18(12), 6183. https://doi.org/10.3390/ijerph18126183
Silva, D. T. C., Prado, W. L., Cucato, G. G., Correia, M. A., Ritti-Dias, R. M., Lofrano-Prado, M. C., Tebar, W. R., & Christofaro, D. G. D. (2022). Impact of COVID-19 pandemic on physical activity level and screen time is associated with decreased mental health in Brazillian adults: A cross-sectional epidemiological study. Psychiatry Research, 314, Article 114657. https://doi.org/10.1016/j.psychres.2022.114657
Şimşir, Z., Koç, H., Seki, T., & Griffiths, M. D. (2022). The relationship between fear of COVID-19 and mental health problems: A meta-analysis. Death Studies, 46(3), 515–523. https://doi.org/10.1080/07481187.2021.1889097
Son, C., Hegde, S., Smith, A., Wang, X., & Sasangohar, F. (2020). Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. Journal of Medical Internet Research, 22(9), Article e21279. https://doi.org/10.2196/21279
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097.
https://doi.org/10.1001/archinte.166.10.1092
Stamatis, C. A., Broos, H. C., Hudiburgh, S. E., Dale, S. K., & Timpano, K. R. (2022). A longitudinal investigation of COVID-19 pandemic experiences and mental health among university students. British Journal of Clinical Psychology, 61(2), 385–404. https://doi.org/10.1111/bjc.12351
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Tang, N. K. Y., McEnery, K. A. M., Chandler, L., Toro, C., Walasek, L., Friend, H., Gu, S., Singh, S. P., & Meyer, C. (2022). Pandemic and student mental health: Mental health symptoms amongst university students and young adults after the first cycle of lockdown in the UK. BJPsych Open, 8(4), Article e138.
https://doi.org/10.1192/bjo.2022.523
Wise, T., Zbozinek, T. D., Michelini, G., Hagan, C. C., & Mobbs, D. (2020). Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States.
Royal Society Open Science, 7(9), Article 200742. https://doi.org/10.1098/rsos.200742
Xiong, J., Lipsitz, O., Nasri, F., Lui, L. M. W., Gill, H., Phan, L., Chen-Li, D., Iacobucci, M., Ho, R., Majeed, A., & McIntyre, R. S. (2020). Impact of COVID-19 pandemic on mental health in the general population: A systematic review. Journal of Affective Disorders, 277, 55–64. https://doi.org/10.1016/j.jad.2020.08.001
Wesley B. Webber, PhD, NCC, is a postdoctoral scholar at East Carolina University. W. Leigh Atherton, PhD, LCMHCS, LCAS, CCS, CRC, is an associate professor and program director at East Carolina University. Kelli S. Russell, MPH, RHEd, is a teaching assistant professor at East Carolina University. Hilary J. Flint, NCC, LCMHCA, is a clinical counselor at C&C Betterworks. Stephen J. Leierer, PhD, is a research associate at the Florida State University Career Center. Correspondence may be addressed to Wesley B. Webber, Department of Addictions and Rehabilitation Studies, Mail Stop 677, East Carolina University, 1000 East 5th Street, Greenville, NC 27858-4353, webberw21@ecu.edu.
Nov 9, 2021 | Volume 11 - Issue 4
Jennifer Scaturo Watkinson, Gayle Cicero, Elizabeth Burton
It is widely documented that practicum students experience anxiety as a natural part of their counselor development. Within constructivist supervision, mindfulness exercises are used to help counselors-in-training (CITs) work with their anxiety by having them focus on their internal experiences. To inform and strengthen our practice, we engaged in a practitioner inquiry study to understand how practicum students experienced mindfulness as a central part of supervision. We analyzed 25 sandtray reflections and compared them to transcripts from two focus groups to uncover three major themes related to the student experience: (a) openness to the process, (b) reflection and self-care, and (c) attention to the doing. One key lesson learned was the importance of balancing mindfulness exercises to highlight the internal experiences related to anxiety while providing adequate opportunities for CITs to share stories and hear from peers during group supervision.
Keywords: supervision, mindfulness, counselors-in-training, anxiety, practitioner inquiry
It is widely documented that counselors-in-training (CITs) experience anxiety as part of the developmental process (Auxier et al., 2003; Kuo et al., 2016; Moss et al., 2014). Reasons for anxiety include CITs’ doubts about their ability to perform competently within their professional role (Moss et al., 2014) coupled with perfectionism (Kuo et al., 2016). Additionally, Auxier et al. (2003) noted that CITs’ anxiety also stems from the pressure associated with external evaluation provided by supervisors. Wagner and Hill (2015) added that CITs’ need for external validation from their supervisors, coupled with the belief that there is only one right way to counsel clients, also generates anxiety. This need for external validation creates an overreliance on a supervisor’s judgment that could render a CIT helpless (Wagner & Hill, 2015). Although a moderate amount of anxiety may increase a person’s focus and positively impact productivity, too much anxiety impedes learning and growth (Kuo et al., 2016). Hence, there is a need for supervisors to address anxiety early in a CIT’s development to foster self-reliance and professional growth (Ellis et al., 2015; Mehr et al., 2015).
The two lead authors of this article, Jennifer Scaturo Watkinson and Gayle Cicero, are counselor educators who supervised school counseling practicum students and ascribed to a constructivist approach to supervision. While discussing supervision pedagogy, we shared our observations on how anxious our practicum students were to be evaluated and our belief that their anxiety often limited their professional growth and development as counselors. Within constructivist supervision, mindfulness exercises are used to help CITs work with their anxiety by having them focus on their internal experiences of discomfort (Guiffrida, 2015). Thus, we utilized mindfulness as a central approach to helping our students work with their anxiety associated with the counselor developmental process.
To assist in our planning, we reviewed the supervision literature and found that discussions on mindfulness were largely conceptual (Guiffrida, 2015; Johnson et al., 2020; Schauss et al., 2017; Sturm et al., 2012) or outcome-based (Bohecker et al., 2016; Campbell & Christopher, 2012; Carson & Langer, 2006; Daniel et al., 2015; Dong et al., 2017), with limited focus on supervision pedagogy to guide supervisors on how to integrate mindfulness into their practicum seminars, particularly from the perspective of the practitioner. Further, Barrio Minton et al. (2014) and Brackette (2014) confirmed that there was a scarcity of counselor education literature that focused on teaching pedagogy and argued that more research in this area was needed to improve counselor preparation. To add to the current literature on supervision pedagogy and inform our practice, we engaged in a practitioner inquiry study (Cochran-Smith & Lytle, 2009) and formed a professional learning community to investigate how utilizing mindfulness within our supervision could help school counseling practicum students work with their anxiety.
Literature Review
Constructive Supervision
Supervisors who utilize constructivist principles help CITs make meaning of their experience by examining how their approach benefits their clients (Guiffrida, 2015). Constructivism is built upon the belief that knowledge is not derived from absolute realities but rather localized to specific contexts and personal experiences. McAuliffe (2011) argued that knowledge is “continually being created through conversations” and is not given to the learner through a one-sided expert account. Constructivists believe that learning is “reflexive and includes a tolerance for ambiguity” (McAuliffe, 2011, p. 4). Constructivist supervisors prioritize CITs’ experiences, encouraging them to examine the intent behind their approach and reach their own conclusions. Hence, constructive supervisors help supervisees deconstruct experiences that have multiple “right” approaches to client care while normalizing the anxiety associated with professional growth. Within a constructivist supervision framework, moderate amounts of anxiety are not viewed as problematic but rather are seen as a catalyst for change (Guiffrida, 2015) and part of the learning process (McAuliffe, 2011). Guiffrida (2015) asserted that the aim of supervision in the early stages of counselor development is not to remove feelings of anxiety but rather to help the CIT acknowledge and live with the anxiety. Utilizing mindfulness, supervisors acknowledge CITs’ internal experiences and guide them through intentional mindfulness practices to generate personal and professional reflection and meaning making.
Within constructivist supervision, mindfulness is a central approach to helping CITs work with their anxiety (Guiffrida, 2015). Kabat-Zinn (2016) defined mindfulness as “paying attention in a sustained and particular way: on purpose, in the present moment and nonjudgmentally” (p. 1). Constructive supervisors facilitate learning experiences that promote introspection and intentionally direct CITs to examine their internal experience, without judgment, during times of disequilibrium. Rather than helping a CIT rid themselves of anxiety, the constructivist supervisor acknowledges that anxiety is a normal response to the uncertainty of doing something for the first time (Guiffrida, 2015). Mindfulness provides a platform for a supervisor to normalize anxiety within the supervisory relationship (Sturm et al., 2012). Hence, supervisors can utilize mindfulness to prioritize the CITs’ internal experiences (e.g., doubt, uncertainty, fear) and foster self-reliance.
Mindfulness as an Approach
Mindfulness practices are linked to the personal and professional growth of CITs (Bohecker et al., 2016; Campbell & Christopher, 2012). Campbell and Christopher (2012) compared counseling students who participated in a mindfulness-based stress reduction (MBSR) program to a control group and found that those who participated in MBSR reported significant decreases in stress, negative affect, rumination, and state and trait anxiety while noting a significant increase in positive affect and self-compassion when compared to participants in the control group. Additionally, Christopher and Maris (2010) reported that supervisees who were exposed to mindfulness were “more open, aware, self-accepting, and less defensive in supervision” (p. 123). Similarly, Bohecker et al. (2016) discovered that CITs who participated in a mindfulness experiential small group saw the benefits of attending to their emotions (e.g., internal experiences) and acknowledged that mindfulness increased self-awareness and promoted objectivity when attending to their thoughts. Having objectivity allowed them to be in the present, which positively affected their behavioral responses (Bohecker et al., 2016).
CITs also experienced benefits to having mindfulness incorporated into their practicum and internship seminar classes. Dong et al. (2017) examined CITs’ response to mindfulness-based activities and discussions during internship seminar. Results suggested that CITs who engaged in mindfulness practices were more focused on the moment and responded to stressors with acceptance and nonjudgment. As a result, CITs were more likely to be “okay with not being okay” when faced with challenging situations (Dong et al., 2017, p. 311). Additionally, Dong and his colleagues noted that participants were able to validate themselves when they made mistakes and were more accepting of their rough edges. Carson and Langer (2006) agreed and added that CITs who received mindfulness as part of their supervision were better able to examine the thoughts that contributed to their anxiety and were more open to accepting their mistakes as learning opportunities. As a result, CITs minimized the focus they put on self-criticism and were less vulnerable when they made mistakes (Carson & Langer, 2006). These studies highlight how CITs benefited from integrating mindfulness into group supervision, yet there is limited research on how counselor educators might structure their practicum seminars to include mindfulness as an integrated approach to supervision.
Purpose of the Present Study
The purpose of this practitioner inquiry was to inform Watkinson and Cicero’s practice as supervisors of practicum school counseling students within a CACREP-accredited program. We utilized mindfulness as a central approach to group supervision during practicum seminar and wanted to understand how intentional mindfulness exercises that prioritized the CITs’ internal experiences (e.g., uncertainty, doubt, fear) were perceived by our students. By understanding the student experience, we could make informed decisions about how we might improve upon the way we integrate mindfulness into future seminar meetings. Specifically, we were guided by this research question: How are CITs experiencing mindfulness as part of group supervision provided during practicum seminar?
Method
We engaged in a practitioner inquiry study (Cochran-Smith & Lytle, 2009) to examine the application of mindfulness within the context of our practice. Cochran-Smith and Lytle (2009) argued that the examination of one’s practice privileges practitioner knowledge and adds to the overall discourse on teaching pedagogy, as “deep and significant changes in practice can only be brought about by those closest to the day-to-day work of teaching and learning” (p. 6). Although not intended to generalize knowledge, practitioner inquiry positions the researcher as a participant to uncover tensions and challenges that come from applying theory to practice while enhancing the knowledge of the practitioner doing the investigation (Cochran-Smith & Lytle, 2009). Thus, we intended to reflect upon how we integrated mindfulness into supervision by understanding the experiences of our practicum students.
Participants
We gained approval from our university’s IRB to conduct the study and invited all 33 CITs enrolled in our practicum sections to participate. Twenty-five (76%) CITs agreed to participate. Of the 25 participants, 24 identified as female (96%) and one identified as male (4%). Sixteen students (64%) self-identified as White/Caucasian, five (20%) as African American, three (12%) as Hispanic, and one (4%) as other. Eighty-four percent of participants were full-time students and 16% identified as part-time. Students were told they could withdraw their participation at any time. All practicum students completed their field experience in public schools.
To safeguard participants from believing they were required to join the study, Watkinson and Cicero were not aware of which students agreed to participate until the end of the semester, when grades were submitted. To protect participant identity until after the semester, we took the following steps: 1) the third author, Elizabeth Burton, was the only one who knew the identity of the participants; 2) Burton recruited participants, stored data (erasing identifying information), and communicated with the participants; 3) the data source labeled sandtray reflections included activities that all CITs completed as part of a required seminar experience; 4) a focus group was held after the semester concluded and grades were submitted; and 5) during data collection, Watkinson and Cicero never discussed the study with any of the CITs enrolled in practicum.
Seminar Context
The practicum course is the first field experience for CITs enrolled in the school counseling master’s program. As per the CACREP 2016 Standards, the practicum experience is a 100-hour experience in which 40% of those hours are in direct service. In addition to meeting those direct hours by working with several individual clients, practicum students are also required to design and run a small counseling group and deliver several classroom lessons within schools. Further, CACREP-accredited programs must provide practicum students with 1.5 hours on average of group supervision per week throughout the duration of the semester. Thus, our practicum seminars were designed to provide CITs with the required group supervision.
All practicum seminar sessions met in person except for one, which was held synchronously through Zoom, a web conferencing platform. There were three sections of practicum, two taught by Cicero and one taught by Watkinson. Watkinson and Cicero drew upon constructive supervision principles and mindfulness core concepts (e.g., self-compassion, present moment, and nonjudgment) to guide the planning of the practicum seminars. We maintained similar course structures, objectives, and learning outcomes utilizing similar room arrangements, mindfulness exercises, and structured learning experiences. Mindfulness exercises were central to the practicum seminar and were focused on the practicum students’ internal experiences. The 15 weekly practicum seminars were 90 minutes in length, and student-to-faculty ratios were 9:1 for two of the practicum sections and 6:1 for the third. The room arrangement consisted of a circle of chairs for students to use during the opening and closing of the seminar, along with a designated workspace for students to sit at tables to take notes or complete reflective class experiences. Soft meditation music played as students entered the room and was turned off to signal the beginning of class.
Watkinson and Cicero engaged in weekly collaborative planning meetings throughout the 15-week semester to plan their seminar meetings and share insights related to student learning. The instructional design was experiential and incorporated mindfulness exercises during the opening of the seminar to bring attention to the “here and now,” breath, nonjudgment, and self-compassion. Cicero was previously trained in mindfulness and exercises were selected based upon her training; Cicero taught Watkinson how to implement those mindfulness exercises during their weekly meetings. Many of the opening mindfulness exercises can be found through internet searches.
Structure of Seminar Meetings
The structure and room arrangement for each practicum seminar were consistent across the three sections. Fourteen of the 15 seminar meetings began with the CITs participating in a 5-minute mindfulness opening that transitioned into structured learning experiences and ended with a sharing circle. Seminar Meeting 11 was entirely dedicated to mindfulness, engaging practicum students in several mindfulness activities for the purpose of drawing their attention to breath and reflection.
Mindfulness Openings
The 5-minute mindfulness openings were scripted and consisted of either a guided meditation (e.g., Calm Still Lake, A River Runs Through It), intentional breathing exercises (e.g., Balloon Breath, Meditative Chimes) or chair yoga (e.g., Mountain Pose, Warrior 2). Each mindfulness opening concluded with reflective questions to increase awareness of the present moment (e.g., What was this experience like for you?). The meditation exercises were varied to introduce CITs to different approaches they might want to try outside of seminar for personal use or in their own practice with K–12 students.
Structured Learning Experiences
After the mindfulness opening, CITs participated in structured learning experiences that focused on either counselor development, case conceptualization, group counseling leadership, evidence-based planning, or classroom curriculum development and instruction. Guided by constructivist supervision principles, two of the structured learning experiences implemented were metaphorical case drawing (Guiffrida, 2015) and sandtray (Guiffrida, 2015; Saltis et al., 2019).
Metaphorical Case Drawing. Guiffrida’s (2015) metaphorical case drawing was used to assist CITs in the development of their case conceptualization skills. In Guiffrida’s work, a metaphorical case drawing has three steps. First, CITs reflect upon six items that highlight their internal experiences and perspectives specific to an individual counseling session with one of their clients: 1) identification of the client’s primary concern, 2) description of the client and CIT interaction, 3) CIT’s intention for the session, 4) CIT’s description of how they viewed their performance as a counselor during the session, 5) general assessment of how the session went, and 6) statement on what the CIT thought the client gained from the session. Second, CITs use images and/or metaphors to respond to three of the six items above to create a case drawing. Lastly, utilizing their case drawings, CITs share their cases with the supervisor and other supervisees. Through the presentation of their case, the CITs interpreted their work while the supervisor and other supervisees listened and asked questions to facilitate deeper insight by offering alternative perspectives.
Sandtray. Although sandtray is typically used in supervision to help CITs develop their case conceptualization skills (Anekstein et al., 2014; Guiffrida, 2015; Guiffrida et al., 2007), we modified our use of sandtray to focus the CITs on their developmental journey as counselors. Like the metaphorical case drawing, the sandtray facilitates an internal examination where CITs get to interpret their own experience (Guiffrida et al., 2007). The sandtray was used in Seminar Meetings 6 and 13 to document how CITs were encountering practicum at two different times in the semester. The written reflections that followed the sandtray were used as a data source for this study and are therefore described in further detail.
Prior to creating an image in the sandtray, CITs were asked to journal about their experience as a practicum student. The prompt was left open so that CITs would have the freedom to focus on the most salient part of their experience. Next, CITs were partnered to create a sandtray image and each pair were given a large box that contained sand and a small baggie filled with a variety of miniature objects. CITs had 5 minutes to create an image in response to this prompt: Create an image that represents your practicum experience thus far. At the conclusion of the 5 minutes, CITs shared their stories with their partners. After everyone created a sandtray image and shared, CITs wrote a reflection in response to this prompt: Drawing from the sandtray exercise and sharing, describe your experience in practicum thus far. Identify and describe the thoughts and feelings you have as you begin your work with students. These written reflections were submitted to the professor at the conclusion of the seminar meeting.
At Seminar Meeting 13, CITs created and shared their sandtray images. Following the same procedure as identified in Seminar Meeting 6, CITs engaged in the sandtray activity again to create a new image in response to a new prompt: Create an image that described your overall experience in practicum. After creating and sharing of their image with a partner, students reflected and responded in writing to a final prompt: Drawing from the sandtray exercise, describe your experience in practicum. Identify and describe your thoughts and feelings now that practicum has come to an end. What have you learned about yourself? Written reflections were completed during the seminar meeting and submitted to the professor when class ended.
Sharing Circle
After the structured learning experience, each seminar concluded with a 5–10 minute sharing circle where students summarized new insights and identified actions to implement at their practicum site. The sharing circle was guided by two questions: What are some key takeaways from today’s seminar? and How might we use what we have learned today within our own practice?
Structure of Mindfulness Seminar Meeting
Seminar Meeting 11 was fully dedicated to the practice of mindfulness and did not follow the above seminar format and structure. During this one 90-minute class, CITs identified an intention, created a mindfulness jar, journaled, and walked a labyrinth. Johnson et al. (2020) argued that CITs who receive mindfulness as part of their supervision should start or maintain a mindfulness practice of their own. Yet there is nothing in the research that identifies specific mindfulness exercises as being essential to that practice, only that CITs should be exposed to mindfulness as part of the classroom experience (Johnson et al., 2020). Thus, our intent for this seminar meeting was to engage CITs in mindfulness exercises that would encourage meditation and reflection. For this class we requested a large room to accommodate a small circle arrangement of 10 chairs and three stations: a labyrinth, creating a mindfulness jar, and journaling. During this seminar meeting, the CITs were instructed to visit the three stations at their own pace and to self-select the order in which they participated in those stations. Class opened with a mindfulness exercise that focused on breath and ended with a sharing circle to debrief. An example of a closing question posed by the professors during the sharing circle is: What insights would you like to share about your experience in seminar today?
Labyrinth. CITs were given a brief description of a labyrinth along with written instructions on how to set an intention and walk the labyrinth. We created a floor labyrinth for use during the seminar. CITs set their intention prior to walking the labyrinth. Some examples of intentions were to be open to the process or to demonstrate self-compassion. Once inside the labyrinth, CITs would follow the path and could walk the labyrinth as many times as they desired.
Creating Mindfulness Jars. CITs created a mindfulness jar from an empty 8-ounce bottle, fine glitter, clear hand soap, confetti, and water. Directions on how to create a mindfulness jar were provided at the station. CITs were encouraged to use the mindfulness jar during the 90-minute seminar as a focal point to guide their breath during reflection time.
Journaling. CITs were provided paper, pens, markers, and crayons for journaling at the beginning of the seminar. CITs were provided minimal directions on what they were to journal, outside of selecting a quiet place in the room to write and reflect upon their experience during the session. Journals were private and CITs were not asked to share what they wrote with the professors or other CITs.
Data Sources and Collection
We used three data sources to understand CITs’ experience with mindfulness as part of supervision: supervisor observations, sandtray reflections from weeks 6 and 13, and focus group transcripts. Watkinson and Cicero captured supervisor observations in their meeting minutes, which also included specific plans for each seminar session along with assumptions and observations about CIT learning. The written sandtray reflections captured CITs’ overall experience in practicum at two different points in the semester. Using a multi-step process, the sandtray served as a structured learning experience completed and collected during the seminar meetings. Data from sandtray reflections taken at the end of the semester (week 13) were analyzed to examine how CITs reflected on their overall practicum experience at the completion of the semester.
All 25 participating CITs were invited to participate in a focus group. Of the 25, nine (36%) attended and two different focus groups were held to accommodate their schedules. Each focus group was held virtually on Zoom, recorded, and transcribed, and took place at the end of the academic semester after grades were issued. Focus groups lasted 60 minutes, were co-led by Watkinson and Cicero, and served as a type of member checking. Guiding questions/prompts were: Describe your experience in practicum this semester, Describe your feelings throughout the semester, and What was it like for you to engage in mindfulness as part of your development as a counselor?
Trustworthiness
Watkinson and Cicero are both counselor educators at a university located within the Mid-Atlantic region of the United States. Watkinson is a Caucasian middle-aged female with 14 years of experience as a school counselor and over 10 years of experience as a counselor educator. Cicero is a Caucasian middle-aged female with 30 years of experience in a large public school district as a teacher, school counselor, and a district-level administrator of school counseling and student service programs, as well as 3 years of experience as a counselor educator. Watkinson and Cicero are licensed professional counselors, board approved certified supervisors, and certified school counselors. Burton was a first-semester school counseling student and served as Watkinson’s graduate assistant. She is a Caucasian female with no prior experience in schools or as a counselor. At the time of data analysis, she had finished her first year of coursework and offered an additional perspective on how the data could be interpreted.
Watkinson and Cicero held certain biases and assumptions about how mindfulness might be experienced by CITs in their practicum sections. We assumed that mindfulness was beneficial to CIT counselor development yet had no preconceived ideas as to the type of benefit it would have on their professional growth outside of our assumption that mindfulness could help CITs work with their anxiety. Additionally, we found that CITs, particularly at the practicum level, were anxious and worried about their performance and believed that supervision was needed to attend to that anxiety. Lastly, we shared a strong desire to better understand our own practice and were therefore open and expected feedback to strengthen that practice.
Trustworthiness was addressed in a variety of ways. In practitioner research, validation is obtained through a form of peer review, where practitioner researchers collaborate to discuss and reflect upon their experiences through peer feedback (Anderson & Herr, 1999; Cochran-Smith & Lytle, 2009). Thus, Watkinson and Cicero met weekly during the 15-week semester to share observations and obtain feedback related to their own practice. Further, during these meetings we engaged in critical dialogue to disrupt previously held assumptions and biases. For example, we challenged each other to share evidence to support the interpretations we made about how students were experiencing the course, asking the question, How do you know? Observations that included peer feedback were recorded in our meeting minutes.
Second, we engaged in prolonged observation of participants as we worked alongside CITs, acting in the role of both inside and outside observers during the 15-week semester. As Creswell (2013) asserted, validation of findings comes from prolonged engagement and persistent observation of participants. Third, we triangulated data, comparing Seminar Meeting 13 sandtray reflection data across the three practicum sections to the focus group transcripts (Merriam, 2009). Fourth, the focus groups served as a type of member checking (Merriam, 2009) to validate and refine our analysis of the final sandtray reflections to the perceptions that were shared by students in the focus groups.
Data Analysis
We formed a research team and regularly met to debate and discuss the data during the analysis process. Data from the sandtray reflections taken during Seminar Meeting 13 were organized into a table for analysis so that we could track individual responses and practicum sections. Drawing from Creswell’s (2013) process for analyzing data, we each familiarized ourselves with the data by independently engaging in multiple readings of the final sandtray reflections and focus group transcripts, including memoing to capture initial impressions and key concepts. After familiarizing ourselves with the data, we met as a research team to share initial insights and bracket assumptions. Next, we reviewed each line of the final sandtray reflection data independently to identify initial codes. As a research team, we shared our codes, discussed discrepancies, and reviewed units of data until consensus was reached and a codebook was created. Next, codes from the final sandtray reflections were compared to the focus group transcripts and refined. Lastly, we looked for patterns in the data and organized them into themes.
Findings
To examine our supervision practice, we sought to understand how CITs experienced mindfulness as a supervision approach. Prioritizing mindfulness within our practicum seminar meetings focused our students on the examination and understanding of their internal experiences and meeting uncertainty with nonjudgment and self-compassion. After analyzing the data, three major themes emerged: openness to the process of becoming, reflection and self-care, and attention to the doing.
Openness to the Process of Becoming
Although CITs acknowledged the challenges associated with their experience, they also expressed an openness to becoming a counselor who generated personal insight, self-compassion, and wisdom. As one participant stated, “It’s natural to feel uncertain when learning new concepts. However, uncertainty should not consume you and cause your thoughts to become negative. Give yourself permission to grow.” Another wrote, “The biggest growth I’ve seen in myself is self-awareness. Regardless of my weaknesses and shortcomings, I am good enough!! The greatest gift I can give to students is to be myself.”
CITs felt hopeful and purposeful in their development as counselors and expressed excitement about their professional growth. As one participant remarked, “In the beginning everything seemed new and scary, but when I look at the end, I see so much growth. I will continue to grow and expand. I look forward to my career.” Another wrote:
At the beginning of practicum, I felt awkward and unsure of myself. I felt self-conscious. At the end of practicum, I can feel the growth I’ve made. I no longer feel awkward or self-conscious. I know who I am and what kind of counselor I am.
Acknowledging the emotional challenges of their professional journey, CITs highlighted the emotional discomfort they felt at the start of practicum. One student stated: “Anxiety from the beginning—feeling of anxiety and not knowing what to expect.” Another mentioned in her reflection, “I definitely had feelings of inadequacy. I just didn’t think that I was doing what I needed to do.” Some students expressed this discomfort as cyclical:
Understanding everything that was going to be happening and everything that was expected and what it all entails, I definitely started to get more anxious and got comfortable and then getting [anxious] again. So, kind of like back and forth a lot.
Students compared this back and forth feeling to that of a rollercoaster: “I feel like some weeks I’d be on fire, like, yeah, I did really good . . . there would be other days where it’s like my timing is off and I’m uncomfortable in the classrooms . . . it was definitely a rollercoaster feeling.”
Another student agreed, sharing that they “would definitely second the rollercoaster. The beginning was very overwhelming for sure . . . that rollercoaster of like the expectation of learning . . . feeling like you’re doing really bad and then learning what is good.”
There was also a sense of wisdom in how the participants described what they gained from this experience of becoming. One participant mentioned “feeling depressed and anxious. . . . Fast forward 2 months and I had grown so much. I can’t believe in only 60 days my attitude toward practicum changed so dramatically. . . . change and growth take time, but it does happen.” Another CIT stated:
In my first reflection, there seemed to be a lot of low points, but I was hopeful things would get better. In my second reflection, I realized that the things I have done have made an impact and the highs and lows both got me to this point.
CITs expressed recognition of the highs and lows experienced and within that recognition focused on a greater purpose. As one wrote,
I started out being very unaware and doubtful of myself. I was overwhelmed and wasn’t seeing the beauty in the process of learning who I am as a counselor. I began to see the small and big impacts that I had with my students in 15 weeks. I saw the power that comes with being a counselor and am more mindful of the impact I have and will make.
Another reflected:
The biggest growth I’ve seen in myself is self-awareness. Awareness of my strengths and weaknesses so that I can be mindful of how to be the best I can be for all students. So that I can strive to have a positive impact on others.
Another mentioned:
At this point in the journey, I finally met my passion. I always wanted to have an impact not because I taught a great lesson, but because I helped a student and showed I cared. I grew by knowing how to use my tools to make a difference while finding my style of counseling in the process. The growth hasn’t stopped and needs refinement, but I want each day to be better for myself and the students.
Additionally, CITs perceived feedback to be essential to their growth process. One CIT reflected that they “learned to be open to change . . . accepting feedback and letting it help me make positive changes throughout this journey. There is always a need for continued growth and development.” Another remarked:
I’ve realized that in order for me to learn and grow I have to be more open [to feedback]. Being closed off means that I am only working with what I know, which is not helpful to me personally, but also what we tell students not to do. Being open has forced me to become a more active participant in my learning and take more risks . . . it will all be worth it in the end.
Another practicum student focused on gratitude:
Feedback and supervision helped to change my perspective and boost my confidence. Things about myself that I thought had nothing to do with being a counselor were highlighted and the areas for improvement were spoken of and tended to with genuine care. I’m grateful to have had the experience of becoming so reflective. I’m grateful for the lows and the moments where I felt as though I was at a standstill. I’m grateful for falling so hard that my only option was to reach out and ask for help. I’m grateful for the hurdles . . . and I’m grateful for the ever-flowing river. I’m grateful for the art and the science of counseling. I’m grateful for who I’m becoming in the process of becoming. I’m grateful for grace and for the realization of how necessary it is. I’m grateful for family and adopted big sisters in the program. I’m grateful to have had the chance to say “I don’t know” and keep learning.
The theme of openness to the journey was also highlighted in the acknowledgement of not being in control. There was an openness to embracing the unknown and the chaos associated with not having everything figured out, as one CIT concluded:
In the beginning, I was working really hard to try to figure everything out. I saw obstacles everywhere. As I moved on, I started to focus on counseling in a way that didn’t put pressure on me to do all of the right things. I started to grasp the essence of counseling and what makes the profession unique.
Another noted:
One major insight is that it was a chaotic journey. It’s not straightforward, and I don’t always know the path I’ll take, but I am continuously growing and learning about myself as a person and as a school counselor. . . . I am enjoying the unknown. I like what I am doing, and I like moving forward, even if I am unsure at times.
Reflection and Self-Care
CITs reported that the seminar was very reflective, which gave them a sense of calm and a new appreciation for self-care. As one student commented, “I did, like everyone else, find [the seminar class] to be calming, enjoyable, and reflective.” Reflection generated by the mindfulness exercises gave CITs an opportunity to get to know themselves:
It was definitely a positive experience for sure. I would agree it was very calming and super reflective. I felt like I understood myself as a counselor and also just like as a person on my own personal journey. Even aside from that I felt like I learned a lot.
Further, CITs expressed the importance of reflection and giving themselves the space to be in the present moment as a means of self-care:
I am so wrapped up in everything that is going on in my life and getting everything done. And school takes a lot of everything I’ve got . . . to be reminded and practice [mindfulness] on a regular basis . . . but doing it each week in class, helped me to do it at home. So that was giving me that practice and repetition and it really made a huge difference.
Another mentioned, “There’s just so many things going on in your life . . . to be reflective and just calm my inner self and learn how to breathe . . . this was a life skill class for me,” and a different student elaborated, “I was so grateful for it because I realized how much self-reflection I have to do . . . that I need to keep doing it and making it a priority.”
Attention to the Doing
Although students valued the priority that we placed upon mindfulness to better understand their internal experiences, some wished that we had provided more time for them to share stories about their practicum sites. As one CIT stated, “I would have liked to have had time each week for all of us to share what was going on and to learn from each other’s situations and to support each other in those situations.” Additionally, CITs desired to know more about what was happening at different practicum sites because of the belief that they were missing an experience. As one CIT explained, “I didn’t have a role model so it was nice to hear everyone else’s role models . . . so I could just learn from pieces I wasn’t getting [at my site].” Another CIT agreed: “I think it definitely would have helped to hear more about other people’s sites just because I wasn’t really getting a ton out of my site. Or I did get things, but differently.” Another mentioned, “I wanted to hear other people’s experiences because I felt like everyone was at such different schools and different levels . . . we’re all experiencing different things.”
Discussion
We sought to understand how practicum students experienced mindfulness exercises within supervision to improve our own practice. To help practicum students work with their anxiety, mindfulness exercises were heavily integrated into the course structure to engage all CITs in weekly reflective exercises that directed their attention toward their internal experiences. Practicum students were invited to acknowledge their anxiety and respond to it with nonjudgment and self-compassion. Mindfulness core concepts (e.g., being present, nonjudgment, self-compassion) served as a framework for how practicum students made meaning of their internal experiences. Although our focus was not to determine the impact mindfulness had on our practicum students, to inform our practice we did seek to gain a descriptive understanding of how our students experienced mindfulness as part of their group supervision.
Open to the Process of Becoming
Our CITs reported being open to the process of becoming a counselor that included acceptance of where they were in the developmental process. Through acceptance, CITs reported being aware of the uncertainty associated with learning a new skill and leaned into that anxiety with self-compassion and nonjudgment. Further, they were able to acknowledge the ambiguity (e.g., “rollercoaster”) associated with learning something new and the tension that comes with being uncomfortable. Bohecker et al. (2016) found similar results in their qualitative study, acknowledging that CITs who integrated mindfulness practices into their daily lives were better able to handle the ambiguity associated with counselor development. As part of her correlational study, Fulton (2016) found that self-compassion, a core principle of mindfulness, was predictive of a CIT’s tolerance to handle ambiguity. Thus, our findings support and add to the current literature by describing qualitatively how practicum students made meaning of that uncertainty to normalize the tension that was associated with it.
Self-Care
Participants saw reflection as a form of self-care, finding meditation to be relaxing, and they acknowledged that meditating each week during seminar allowed them to stay in the present moment. Similarly, Duffy and colleagues (2017) found that CITs in their qualitative study who participated in weekly mindfulness exercises as part of a core class described mindfulness as reflective, providing them with a sense of calm and ability to stay within the present. Banker and Goldenson (2021) noted that CITs within their qualitative study also reported personal benefits to utilizing mindfulness within their practicum seminar, including being able to better transition to the present moment. Thus, the experiences our practicum students had connecting reflection as a form of self-care are similar to the experiences of other CITs who practiced regular meditation.
Attention to the Doing
Although CITs saw value in participating in group supervision that integrated mindfulness as a central approach within their practicum seminars, some CITs wanted more focus on learning about the experiences other practicum students had at their school sites. Specifically, CITs desired to know more about school counselor practice by sharing stories of what their peers were doing, as well as the work being done by the practicing school counselor. Participants sought more understanding on school counselor practice either because of a lack of modeling at their own schools or professional curiosity. Similarly, Watkinson et al. (2018) noted that counselor educators reported discrepancies between how school counseling CITs were being prepared versus what they experienced in the field. For example, counselor educators shared that they often taught content (e.g., implementing a comprehensive school counseling program) that their school counseling CITs did not see modeled at their schools. Thus, it would seem logical that CITs at the practicum level would want to have more exposure to activities that school counselors were doing at other sites, especially if what they were observing was not aligned with their training.
Reflecting on Our Own Practice: Lessons Learned
Through this practitioner inquiry, we gained some valuable insight into how CITs experienced mindfulness that has informed our practice. First, by analyzing our CITs’ experiences in practicum, we believed that they benefited from the mindfulness exercises as a way to work with their anxiety. Specifically, we were encouraged that practicum students expressed an openness to the process of becoming a counselor, which included self-acceptance. CITs stated they were more open to feedback and less critical of themselves, recognizing they still had much to learn. Second, we learned that although the integration of mindfulness as a central approach to our supervision could be helpful to practicum students, CITs also expressed a desire to have more time dedicated to hearing about the work their peers and other practicing school counselors were doing within schools. This was particularly important if the CIT believed their site was lacking. Hence, as supervisors we needed to create a balance between engaging our CITs in mindfulness practices and the need that our CITs had to share work stories and gain some practical insight into the work of school counselors.
Cochran-Smith and Lytle (2009) highlighted that a benefit to practitioner inquiry was the uncovering of professional dilemmas that naturally occur when you apply a concept to practice. For us, seeking balance challenged us to consider what specific mindfulness exercises were critical to maintain. Watkinson et al. (2018) also found that counselor educators struggled with balancing the amount of content that needs to be covered in a course versus the depth of understanding that is needed for CITs to apply the content learned. Thus, we too needed to decide on depth versus breadth, which boiled down to identifying the frequency with which we had our practicum students participate in mindfulness exercises in each seminar meeting to gain benefit.
Because the recent literature suggested that exposure to weekly mindfulness exercises within core courses and clinical seminars benefited CITs (Campbell & Christopher, 2012; Dong et al., 2017; Fulton, 2016), we decided to keep the opening mindfulness meditative exercises and remove the one seminar session we had dedicated to mindfulness. Further, we increased the time CITs spent in sharing circles to include space for CITs to talk about the work being done by school counselors (or themselves) at practicum sites. Lastly, we looked for opportunities to highlight mindfulness principles in case conceptualization.
To integrate mindfulness principles into case conceptualization, Sturm and colleagues (2012) proposed using metaphors (i.e., Earth, Air, Water, Space and Fire) that represent ancient Buddhist principles when conceptualizing cases. For instance, the Earth metaphor symbolizes grounding, and when applied to case conceptualization enables CITs to consider what grounds them personally and theoretically when treating a client (Sturm et al., 2012). Another example of integrating core mindfulness principles into supervision is through free association (Schauss et al., 2017). Schauss et al. (2017) used free association to help CITs attend to the present by asking questions that focused CITs on the here and now (Schauss et al., 2017). Sample questions include: What are you feeling in this moment? When and in what ways has this feeling surfaced during your counseling experiences at your school site? How does your body respond to this type of feeling and what is the impact on your counseling experiences? By integrating mindfulness principles into skill development (e.g., case conceptualization), our practicum students would be further exposed to core mindfulness principles.
Limitations and Future Research
Our intention of sharing the findings from this study was to offer a practitioner’s perspective on how CITs experienced mindfulness within supervision to contribute to the broader discussions on counselor education pedagogy. Generalization was not the objective, and findings need to be interpreted within the context of practice. Further, this study did not examine the impact that mindfulness had on CIT anxiety, and we are not able to infer such causal relationships. To strengthen our understanding of counselor education pedagogy, future studies could build upon our findings to identify which mindfulness exercises had the greatest impact on helping CITs work with their anxiety. Understanding which mindfulness exercises impact anxiety, counselor educators could be more intentional with the exercises they include, thus making room for other supervision priorities (e.g., CITs hearing about the work of practicing school counselors).
Future research could also investigate how supervisors’ modeling of core mindfulness principles could impact counselor development and the supervisory alliance. Daniel et al. (2015) have called upon researchers to increase understanding of how supervisors’ mindfulness behaviors impact the supervisory relationship. Future research could attend to this deficiency within the literature by looking at the relationship between a supervisor’s mindfulness behaviors and the supervisory relationship through a practitioner lens.
Conclusion
By incorporating a mindfulness approach into supervision, we learned that CITs were open to working with the anxiety associated with becoming a counselor. This openness or self-acceptance gave them the perspective to appreciate the impact this experience had on them and others while also valuing the benefits of reflection through meditation. The intent of this study was not to generalize the experience of these CITs to others; rather, it was to generate conversation and an understanding of how CITs experienced mindfulness to better our practice as supervisors. Although CITs saw benefits of mindfulness within supervision, they also desired more conversations on counselor practice to better their understanding of the role school counselors have in schools. As supervisors, we understand mindfulness should be balanced with the need for CITs to learn about the work of the school counselor through the sharing of experiences at their practicum sites. Beginning each session with a mindfulness exercise and infusing mindfulness core principles into case conceptualization could be a means to achieve such balance.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Anderson, G. L., & Herr, K. (1999). The new paradigm wars: Is there room for rigorous practitioner knowledge in schools and universities? Educational Researcher, 28(5), 12–21. https://www.jstor.org/stable/1176368
Anekstein, A. M., Hoskins, W. J., Astramovich, R. L., Garner, D., & Terry, J. (2014). Sandtray supervision: Integrating models and sandtray therapy. Journal of Creativity in Mental Health, 9(1), 122–134. https://doi.org/10.1080/15401383.2014.876885
Auxier, C. R., Hughes, F. R., & Kline, W. B. (2003). Identity development in counselors-in-training. Counselor Education and Supervision, 43(1), 25–38.
https://doi.org/10.1002/j.1556-6978.2003.tb01827.x
Banker, J. E., & Goldenson, D. (2021). Mindfulness practices in supervision: Training counselors’ experiences. The Family Journal, 29(1), 17–23. https://doi.org/10.1177/1066480720954204
Barrio Minton, C. A., Wachter Morris, C. A., & Yaites, L. D. (2014). Pedagogy in counselor education: A 10-year content analysis of journals. Counselor Education and Supervision, 53(3), 162–177.
https://doi.org/10.1002/j.1556-6978.2014.00055.x
Bohecker, L., Vereen, L. G., Wells, P. C., & Wathen, C. C. (2016). A mindfulness experiential small group to help students tolerate ambiguity. Counselor Education and Supervision, 55(1), 16–30.
https://doi.org/10.1002/ceas.12030
Brackette, C. M. (2014). The scholarship of teaching and learning in clinical mental health counseling. New Directions for Teaching and Learning, 2014(139), 37–48. https://doi.org/10.1002/tl.20103
Campbell, J., & Christopher, J. (2012). Teaching mindfulness to create effective counselors. Journal of Mental Health Counseling, 34(3), 213–226. ttps://doi.org/10.17744/mehc.34.3.j75658520157258l
Carson, S. H., & Langer, E. J. (2006). Mindfulness and self-acceptance. Journal of Rational-Emotive and Cognitive-Behavior Therapy, 24(1), 29–43. https://doi.org/10.1007/s10942-006-0022-5
Christopher, J. C., & Maris, J. A. (2010). Integrating mindfulness as self-care into counselling and psychotherapy training. Counselling and Psychotherapy Research, 10(2), 114–125. https://doi.org/10.1080/14733141003750285
Cochran-Smith, M., & Lytle, S. L. (2009). Inquiry as stance: Practitioner research for the next generation. Teachers College Press.
Creswell, J. W. (2013). Qualitative inquiry & research design: Choosing among five approaches. (3rd ed.). SAGE.
Daniel, L., Borders, L. D., & Willse, J. (2015). The role of supervisors’ and supervisees’ mindfulness in clinical supervision. Counselor Education and Supervision, 54(3), 221–232. https://doi.org/10.1002/ceas.12015
Dong, S., Campbell, A., & Vance, S. (2017). Examining the facilitating role of mindfulness on professional identity development among counselors-in-training: A qualitative approach. The Professional Counselor, 7(4), 305–317. https://doi.org/10.15241/sd.7.4.305
Duffy, J. T., Guiffrida, D. A, Araneda, M. E., Tetenov, S. M. R., & Fitzgibbons, S. C. (2017). A qualitative study of the experiences of counseling students who participate in mindfulness-based activities in a counseling theory and practice course. International Journal for the Advancement of Counselling, 39(1), 28–42. https://doi.org/10.1007/s10447-016-9280-9
Ellis, M. V., Hutman, H., & Chapin, J. (2015). Reducing supervisee anxiety: Effects of a role induction intervention for clinical supervision. Journal of Counseling Psychology, 62(4), 608–620.
https://doi.org/10.1037/cou0000099
Fulton, C. L. (2016). Mindfulness, self-compassion, and counselor characteristics and session variables. Journal of Mental Health Counseling, 38(4), 360–374. https://doi.org/10.17744/mehc.38.4.06
Guiffrida, D. A. (2015). Constructive clinical supervision in counseling and psychotherapy. Routledge.
Guiffrida, D. A., Jordan, R., Saiz, S., & Barnes, K. L. (2007). The use of metaphor in clinical supervision. Journal of Counseling & Development, 85(4), 393–400.
https://doi.org/10.1002/j.1556-6678.2007.tb00607.x
Johnson, D. A., Ivers, N. N., Avera, J. A., & Frazee, M. (2020). Supervision guidelines for fostering state-mindfulness among supervisees. The Clinical Supervisor, 39(1), 128–145.
https://doi.org/10.1080/07325223.2019.1674761
Kabat-Zinn, J. (2016). Mindfulness for beginners: Reclaiming the present moment—and your life. Sounds True, Inc.
Kuo, H.-J., Landon, T. J., Connor, A., & Chen, R. K. (2016). Managing anxiety in clinical supervision. Journal of Rehabilitation, 82(3), 18–27.
McAuliffe, G. (2011). Constructing counselor education. In G. McAuliffe & K. Eriksen (Eds.), Handbook of counselor preparation: Constructivist, developmental, and experiential approaches (pp. 3–12). SAGE.
Mehr, K. E., Ladany, N., & Caskie, G. I. L. (2015). Factors influencing trainee willingness to disclose in supervision. Training and Education in Professional Psychology, 9(1), 44–51.
https://doi.org/10.1037/tep0000028
Merriam, S. B. (2009). Qualitative research: A guide to design and implementation (3rd ed.). Jossey-Bass.
Moss, J. M., Gibson, D. M., & Dollarhide, C. T. (2014). Professional identity development: A grounded theory of transformational tasks of counselors. Journal of Counseling & Development, 92(1), 3–12. https://doi.org/10.1002/j.1556-6676.2014.00124.x
Saltis, M. N., Critchlow, C., & Smith, J. A. (2019). Teaching through sand: Creative applications of sandtray within constructivist pedagogy. Journal of Creativity in Mental Health, 14(3), 381–390.
https://doi.org/10.1080/15401383.2019.1624995
Schauss, E., Steinruck, R. E., & Brown, M. H. (2017). Mindfulness and free association for multicultural competence: A model for clinical group supervision. Journal of Counselor Practice, 8(2), 102–119. https://doi.org/10.22229/xpw610283
Sturm, D. C., Presbury, J., & Echterling, L. G. (2012). The elements: A model of mindful supervision. Journal of Creativity in Mental Health, 7(3), 222–232. https://doi.org/10.1080/15401383.2012.711718
Wagner, H. H., & Hill, N. R. (2015). Becoming counselors through growth and learning: The entry transition process. Counselor Education and Supervision, 54(3), 189–202. https://doi.org/10.1002/ceas.12013
Watkinson, J. S., Goodman-Scott, E. C., Martin, I., & Biles, K. (2018). Counselor educators’ experiences preparing preservice school counselors: A phenomenological study. Counselor Education and Supervision, 57(3), 178–193. https://doi.org/10.1002/ceas.12109
Jennifer Scaturo Watkinson, PhD, LCPC, is a certified school counselor and serves as an associate professor and the School Counseling Program Director at Loyola University Maryland. Gayle Cicero, EdD, LCPC, is a certified school counselor and serves as an assistant clinical professor at Loyola University Maryland. Elizabeth Burton is a certified professional school counselor for Baltimore County Public Schools. Correspondence may be addressed to Jennifer Watkinson, Timonium Graduate Center, 2034 Greenspring Dr., Lutherville-Timonium, MD 21093, jswatkinson@loyola.edu.
Mar 23, 2016 | Article, Volume 6 - Issue 1
Ellen W. Armbruster, David C. Witherington
The attachment work of John Bowlby (1988) affords clinicians and researchers the opportunity to view psychopathology as relationally based, rather than as unique to the individual to whom a specific label has been given. Anxiety is a particularly fitting place to focus this type of investigation since understanding the meaning and function of anxiety within the context of human development lies at the center of attachment theory. Bowlby integrated the time-honored notion that the early child-caregiver bond is critical to the child’s survival and well-being into his knowledge of scientific facts and meaning and provided an interpersonal understanding of healthy as well as pathological development. Bowlby’s thoughts, flowing as they did from psychoanalysis and object relations, revolutionized the analytic world by removing dysfunction from the center of the individual and placing it in the space between interacting humans. Through the use of instruments designed to measure attachment style, early bonding memories and five different types of anxiety, this study utilizes Bowlby’s viewpoint as a springboard from which to examine the correlations between adults’ perception of their past and present relational experiences and their current levels of anxiety.
Relationship of Attachment and Bonding to Anxiety Disorders
There is a sizeable body of research suggesting a relationship between anxiety and attachment or bonding experiences (e.g., Cassidy, Lichtenstein-Phelps, Sibrava, Thomas, & Borkovec, 2009; Cavedo & Parker, 1994; Chorpita & Barlow, 1998; Eng & Heimberg, 2006; Eng, Heimberg, Hart, Schneier, & Liebowitz, 2001; Manicavasagar, Silove, Wagner, & Hadzi-Pavlovic, 1999; Marazziti et al., 2007; Meites, Ingram, & Siegle, 2012; O’Connor & Elklit, 2008; Pacchierotti et al., 2002; Parker, 1979; Renaud, 2008; Seganfredo et al., 2009; Turgeon, O’Connor, Marchand, & Freeston, 2002). We will first review the literature explicating the anxiety–attachment paradigm and then consider research that has looked at anxiety and bonding, before turning to the studies that have incorporated measures of both attachment and bonding in an examination of individuals with specific anxiety states.
Anxiety and Attachment
Substantial investigation has considered anxiety-attachment associations. Potential links have been found between generalized anxiety disorder (GAD) and attachment, with indications that increasing perceptions of difficult early attachment experiences are tied to a risk for GAD (Cassidy et al., 2009). Furthermore, investigation has shown individuals with GAD to report less secure parental attachment, less trust, increased difficulty with communication, and more alienation than individuals without the disorder (Eng & Heimberg, 2006). In other work, participants with panic disorder (PD), obsessive-compulsive disorder (OCD), major depressive disorder or bipolar disorder were found to have higher levels of preoccupied attachment style, and participants without these conditions had higher levels of secure attachment (Marazziti et al., 2007). Social anxiety also has been considered in light of adult attachment, and individuals with an anxious-preoccupied attachment style have reported higher levels of social fear and avoidance than participants with a secure attachment style (Eng et al., 2001).
Attachment anxiety and avoidance have been connected to increased symptoms of post-traumatic stress disorder (PTSD) in veterans (Renaud, 2008). However, the vast majority of participants in Renaud’s (2008) study reported a preference for attachment avoidance (either fearful or dismissing), and PTSD symptoms were higher among these individuals. In young adults, secure attachment has been associated with fewer PTSD symptoms; however, dismissing and fearful attachment preferences have been tied to a higher number of PTSD symptoms (O’Connor & Elklit, 2008). Associations of this nature may indicate that secure attachment offers potential protection against the development of PTSD, whereas dismissing and fearful attachment may increase risk (O’Connor & Elklit, 2008).
Anxiety and Bonding
A noteworthy number of studies have looked at the relationship between anxiety and bonding. For instance, associations have been demonstrated between both PD and GAD and the condition of affectionless control (lack of attunement and overprotection) by parents (Chorpita & Barlow, 1998). In other research (Chambless, Gillis, Tran, & Stekettee, 1996), people with PD or OCD also most commonly perceived their parents’ style of caregiving to fall within the affectionless control category. In addition, individuals who rated their mothers most highly on the overprotection scale experienced the earliest onset of anxiety disorders.
Associations have been found between mother overprotection and PD in men and between father overprotection and PD in women (Seganfredo et al., 2009), and a relationship has been noted between perception of parental overprotection and adult symptoms of separation anxiety (Manicavasagar et al., 1999). Furthermore, in a study matching participants diagnosed with PD and healthy controls, individuals with PD reported lower parental care than those without the disorder (Pacchierotti et al., 2002). A relationship also has been demonstrated between low parental care and generalized fear among a large sample of undergraduates (Meites et al., 2012). Other researchers have conceded that the development of GAD may be related to unfavorable parental behavior (Silove, Parker, Hadzi-Pavlovic, Manicavasagar, & Blaszczynski, 1991). However, they also suggested the alternative possibility that maternal overprotection could be a response to early signs of anxiety in people with PD.
Early bonding memories and obsessionality have been shown to be related as well. Positive correlations were noted between obsessionality and parental overprotection for both males and females, and between obsessionality and maternal care in females; however, negative correlations were found between obsessionality and parental care in males (Cavedo & Parker 1994). In other work, outpatients with OCD or PD remembered their parents as being more overprotective than did a control group of non-anxious participants, leading researchers to the conclusion that parental overprotection may increase the risk that children will develop anxiety disorders (Turgeon et al., 2002). However, in another study investigating the link between early bonding memories and obsessive-compulsive behaviors in a non-clinical population, researchers concluded that low parental care may represent a risk for emotional suffering in adulthood, but does not predict a specific psychiatric disorder (Mancini, D’Olimpio, Prunetti, Didonna, & Del Genio, 2000).
The relationship between early bonding memories and agoraphobia or social phobia also has been assessed (Parker, 1979). Parker (1979) found that people with agoraphobia reported their mothers to be less caring than did participants in the control group, but differed in no other way. Individuals with social phobia reported both their mothers and fathers to be less caring and more overprotective than did the control group individuals.
Anxiety, Attachment and Bonding
Despite substantial evidence of correlation between adult attachment and anxiety and between early bonding memories and anxiety, fewer empirical studies explicitly differentiate between adult attachment and parental bonding constructs, or consider both in relation to specific anxiety types. Here, we will review studies that have investigated the association between anxiety and both adult attachment and parental bonding.
Myhr, Sookman, and Pinard (2004) examined adult attachment and early parental bonding memories in a sample of individuals with OCD or depression. More relationship anxiety was evident among participants with OCD or depression and more dependency discomfort (avoidance) was seen in participants with depression and in unmarried participants with OCD. With regard to early bonding memories, individuals with OCD did not differ from controls, and there was no clear correlation between adult attachment and early bonding memories. The researchers suggested two potential reasons for this finding: (a) the bonding instrument they were using may not have measured relational elements necessary for adult attachment security; or (b) the responses may have reflected a bias based on attachment security or specific diagnosis.
Ghafoori, Hierholzer, Howsepian, and Boardman (2008) investigated the protective value of adult attachment, parental bonding and divine love in adjustment to trauma experienced in the military. They found that current PTSD symptoms in veterans who participated in the study negatively correlated with secure attachment and positively correlated with insecure attachment. However, no significant relationship emerged between current PTSD symptoms and early childhood bonding memories. Findings did indicate that adult attachment style contributes to the severity of PTSD and that perceived parental care moderates that relationship (i.e., since parental care negatively correlated with insecure attachment).
Yarbro, Mahaffey, Abramowitz, and Kashdan (2013) used online self-report measures to explore the relationship between memories of low care in early child–caregiver relationships and reports of obsessive beliefs in a sample of undergraduate college students. Their findings indicated significant associations between the two variables, lending support to the idea that there is a relationship between obsessive beliefs and affectionless and neglectful parenting (Yarbro et al., 2013). The researchers also considered whether attachment anxiety or avoidance may mediate this relationship. Through the use of hierarchical regression models, they demonstrated that attachment anxiety may serve as a partial mediator of the relationship between memories of low care and self-reported obsessive beliefs, but that attachment avoidance did not function in this way (Yarbro et al., 2013).
As well as providing additional support in favor of the relationship between attachment, bonding and anxiety, the Myhr et al. (2004), Ghafoori et al. (2008) and Yarbro et al. (2013) studies lead us to consider a further possibility. We offer the idea that adult attachment and parental bonding may address qualitatively distinct aspects of human interaction, especially when considered in light of different types of anxiety. The work of the aforementioned authors highlights the need to investigate adult attachment and parental bonding as distinct yet potentially interdependent constructs that illuminate, from different viewpoints, the intricacies of interpersonal connection.
Constructs of Adult Attachment and Parental Bonding
The construct of adult attachment may be understood as resolving to two primary dimensions: model of self and model of others (Bartholomew & Horowitz, 1991). In Bartholomew and Horowitz’s (1991) work, the degree of positivity an individual experiences with regard to his or her representation of self meets the degree of positivity that person experiences with regard to his or her representation of others to yield four potential patterns of preference in relationships. Those who have a positive view of themselves and of others are at ease in intimate and in autonomous situations and have a secure style of attachment. Individuals with a preoccupied style of attachment have a negative view of self, but see others in a positive light; they look to their intimate relationships for fulfillment and validation. The fearful style of attachment involves a wish for closeness that remains unfulfilled due to fears of rejection, whereas the dismissing style is typified by denial that intimacy with others is needed or desired. According to Bartholomew and Horowitz’s (1991) model, the fearful style reflects a negative view of self (undeserving of the love and support of others), as well as a negative view of others, whereas the dismissing style reflects a positive view of self (minimizing the awareness of needs or distress) and a negative view of others.
The construct of parental bonding and its classificatory scheme also can be understood as resolving to two primary dimensions: (perceived) parental care and (perceived) parental overprotection (Parker, Tupling, & Brown, 1979). The dimensions are presumed to contribute to the bond that develops between a parent and a child early in life and, when considered together, result in four potential bonding experiences. Optimal bonding is said to occur when parental care (emotional warmth and acceptance) is high and overprotection (psychological control and intrusion) is low; whereas affectionate constraint refers to bonding in which parents are highly overprotective of their children while exhibiting some caring behaviors toward them (Gladstone & Parker, 2005). When parental care and overprotection are both low, the parent–child bond that develops may be weak or absent, and when care is low (emotional coldness and rejection) and overprotection is high, affectionless control typifies the bonding relationship.
Although the constructs of adult attachment and parental bonding tap into the nature of relationship quality, each construct views human connection from a different vantage point. Whereas Bartholomew and Horowitz’s (1991) four-category adult attachment model considers individuals’ perceptions of their current close relationships with peers, Parker et al.’s (1979) conceptualization of parental bonding involves recollections of early relationships with caregivers. That is, the attachment construct targets the manner in which people perceive their own worth and that of others in the context of current relationships; the bonding construct, however, targets a present-day characterization of past caregiver style. Rather than addressing the perception of one’s upbringing, adult attachment focuses on a current sense of worth and the expectation of how others will respond in relationship. Parental bonding, in contrast, focuses upon memories of early child–caregiver interactions and the sense of how one was treated by one’s caregivers.
In consideration of the distinctions between the adult attachment and parental bonding constructs, we may view the assessment of adult attachment as eliciting a general sense of how one fits into current relationships and the assessment of parental bonding as specific to the memory of past child–caregiver interactions. In other words, adult attachment and parental bonding, while certainly interrelated in that both tap into the quality of relationships individuals form with others, nonetheless do not actually target the same general conceptualization of relationship quality, but are instead distinct constructs that capture slightly different aspects of human interaction from divergent points of view.
Purpose of the Study and Predictions
This study, in light of the relative paucity of research involving single-sample assessments of our constructs of interest, was designed to address more systematically the interconnections that may exist between adult attachment, memories of early parental bonding experiences and various forms of anxiety. To accomplish this, we specifically targeted adults’ reports of early interactions with caregivers, as well as their present interpersonal approach in relation to five different types of self-reported anxiety: obsessive-compulsive behavior, panic symptomatology, experience of worry and generalized anxiety, post-trauma symptomatology, and experience of social anxiety.
Predictions for the study flowed from our premise that adult attachment and parental bonding are interconnected but separate aspects of relational experience. Although Myhr et al. (2004) found no significant correlation between attachment and early bonding memories, the authors suggested potential reasons for this finding, including instrument limitations and attachment or diagnosis biases of the participants. Taking into account this explanation and our premise that the attachment and bonding constructs, while interrelated, capture relationship quality from different vantage points, we first conjectured that we would find a low to moderate relationship between these two variables.
With respect to relationships among adult attachment and anxiety, since the preponderance of the literature (Cassidy et al., 2009; Eng & Heimberg, 2006; Eng et al., 2001; Ghafoori et al., 2008; Marazziti et al., 2007; Myhr et al., 2004; O’Connor & Elklit, 2008; Renaud, 2008) indicates associations between self-reports of adult attachment style and self-reports of anxiety, we predicted that the tendency toward each of several different anxiety types would negatively correlate with secure attachment style and positively correlate with the insecure styles of attachment, and that these associations would be strong.
With respect to relationships between parental bonding and anxiety, some of the literature indicates a clear association (Chambless et al., 1996; Chorpita & Barlow, 1998; Pacchierotti et al., 2002; Parker, 1979; Turgeon et al., 2002; Yarbro et al., 2013), whereas other investigations have yielded mixed results (Cavedo & Parker, 1994; Ghafoori et al., 2008; Mancini et al., 2000; Manicavasagar et al., 1999; Myhr et al., 2004; Parker, 1979; Silove et al., 1991). Given these inconsistencies and our assumption of adult attachment and parental bonding as measuring distinct aspects of relational quality, we anticipated fewer significant correlations between parental bonding and different forms of anxiety. Nevertheless, where significant correlations arose, we predicted positive correlations between anxiety and the overprotection dimension of parental bonding and negative correlations between anxiety and the care dimension.
Method
Participants
Participants for the study were 201 undergraduate psychology students (152 female, 48 male, with one person not reporting gender) at a university located in the Southwestern United States. Latino/Hispanic participants comprised 36.8% of the sample and Caucasian participants comprised 49.8%. The remaining participants reported race or ethnicity as African American (3%), Asian (2%), Native American (2%), Pacific Islander (.5%), or Other (6%). Participants’ ages ranged from 17 to 50 years, with a mean of 19.86 (SD = 3.78).
Procedures
Approval for the study was granted by the Institutional Review Board at our university. Participants were recruited through a Web-based recruitment system and their participation was an optional part of their psychology course requirement. A description of the study and the dates and times during which data collection would take place were posted on the Web site and participants signed up for the test period that was convenient for them. As participants arrived at the testing location, they were greeted by the test administrator and seated around a table. After informed consent was explained and a questionnaire packet provided, participants were allowed up to 1.5 hours to complete the surveys. A maximum of 25 participants were permitted to sign up for each test period.
Variables and Instrumentation
Relationship Scales Questionnaire. To index adult attachment, we used the Relationship Scales Questionnaire (RSQ; Griffin & Bartholomew, 1994). The RSQ consists of 30 items and asks participants to rate, on a 5-point scale, how well each of the items fits their perception of the style they use in their close relationships. Individuals are scored on each of four attachment patterns: secure, fearful, preoccupied, and dismissing. Internal consistencies for the RSQ range from .41 for secure attachment to .71 for dismissing attachment. Although these alpha values may appear low, it is a natural result of combining two orthogonal dimensions, including model of self and model of others. It also is important to note that test–retest reliability may be inferred from the data on internal consistency, since the RSQ indexes attachment using a dimensional approach (Griffin & Bartholomew, 1994). A psychometric examination of the RSQ in a French population demonstrated good construct validity, test–retest reliability and internal consistency (Guédeney, Fermanian, & Bifulco, 2010). We chose the RSQ for its widespread application in counseling and other mental health venues to study attachment as it relates to topics such as parental bonding and anxiety (Ghafoori et al., 2008; Yarbro et al., 2013), perfectionism (Chen, Hewitt, & Flett, 2015), interpersonal sensitivity (Otani et al., 2014), and problematic substance use (Massey, Compton, & Kaslow, 2014).
Parental Bonding Instrument. To index parental bonding, we used the Parental Bonding Instrument (PBI) developed by Parker et al. (1979). The instrument consists of 25 items, including 12 parental care items and 13 parental overprotection items, and asks participants to rate on a 4-point scale how they remember their primary caregiver. A test–retest reliability study yielded a Pearson correlation coefficient for the care scale of .761 and a Pearson correlation coefficient for the overprotection scale of .628 (Parker et al., 1979). A comparison of the psychometric properties of the PBI and another measure of parenting behavior demonstrated that the PBI may be more stable over time (Safford, Alloy, & Pieracci, 2007), and a Persian version showed high internal consistency and test–retest reliability (Behzadi & Parker, 2015). We chose the PBI for its long history of utilization in the study of familial relationships. It continues to be a frequently employed instrument in the investigation of caregiver–offspring interactions in the context of problems such as anxiety (Meites et al., 2012; Seganfredo et al., 2009), pathological gambling (Villalta, Arévalo, Valdepérez, Pascual, & Pérez de los Cobos, 2015), intermittent explosive disorder (Lee, Meyerhoff, & Coccaro, 2014) and suicidality (Goschin, Briggs, Blanco-Lutzen, Cohen, & Galynker, 2013).
Obsessive-Compulsive Inventory-Revised. To assess tendency toward obsessive-compulsive behavior, we used the Obsessive-Compulsive Inventory-Revised (OCI-R; Foa et al., 2002). This questionnaire consists of 18 items and asks participants to rate, on a 5-point scale, how much each item has bothered them in the last month. In their examination of the psychometric properties of the OCI-R, Foa et al. (2002) demonstrated that test–retest reliability ranged from .74 to .91 for individuals with OCD, and from .57 to .87 for non-anxious controls. In a recent psychometric examination, the OCI-R was shown to be valid, reliable and diagnostically sensitive (Wootton et al., 2015). The OCI-R also demonstrated good validity and reliability in an older adult population (Calamari et al., 2014).
Panic Disorder Severity Scale-Self Report. To assess tendency toward panic symptoms, we used the Panic Disorder Severity Scale-Self Report (PDSS-SR; Houck, Speigel, Shear, & Rucci, 2002). The PDSS-SR consists of seven questions rated on a 5-point scale. The questions explore the presence and degree of panic in the lives of participants. Test–retest reliability was shown by Shear et al. (2001) to be satisfactory, with a Pearson correlation coefficient of .71. More recently, a psychometric evaluation of the self-report and clinician-administered versions of the PDSS indicated adequate or promising reliability and validity for each form (Wuyek, Antony, & McCabe, 2011). An examination of the Spanish version of the PDSS-SR demonstrated that the psychometric properties were comparable to those of other versions of this instrument (Santacana et al., 2014).
Penn State Worry Questionnaire. To assess tendency toward worry and generalized anxiety, we used the Penn State Worry Questionnaire (PSWQ; Meyer, Miller, Metzger, & Borkovec, 1990). This measure consists of 16 items and asks participants to rate, on a 5-point scale, how characteristic each item is of them. Meyer et al. (1990) found the PSWQ to possess high internal consistency and good test–retest reliability (r[45] = .92, p < .001) in clinical as well as in non-clinical samples, with alpha coefficients ranging from .88 to .95 for both groups. More recent examinations of the PSWQ have indicated that the instrument is psychometrically sound in African American populations (DeLapp, Chapman, & Williams, 2015), in online administrations of the Hungarian version (Pajkossy, Simor, Szendi, & Racsmány, 2015) and among older adults (Wuthrich, Johnco, & Knight, 2014). The PSWQ continues to be used to index worry in the study of therapeutic concerns such as psychological inflexibility (Ruiz, 2014), negative mood (Dash & Davey, 2012), and distress tolerance (Macatee, Capron, Guthrie, Schmidt, & Cougle, 2015).
PTSD Checklist-Civilian Version. To assess tendency toward post-trauma symptoms, we used the PTSD Checklist-Civilian Version (PCL-C; Weathers, Litz, Herman, Huska, & Kean, 1993). The PCL-C consists of 17 items asking participants to rate, on a 5-point scale, how often each item has bothered them in the last month. Weathers et al. (1993) studied veterans in their original research on the psychometric properties of the PCL and found that test–retest reliability was .96 over a period of 2 to 3 days. Recent investigation of the psychometric properties of the PCL-C indicated continued high internal consistency and high test–retest reliability in a non-clinical population; in addition, convergent and discriminant validity were satisfactory when compared to other assessments of PTSD (Conybeare, Behar, Solomon, Newman, & Borkovec, 2012).
Social Interaction Anxiety Scale. To assess tendency toward social anxiety, we used the Social Interaction Anxiety Scale (SIAS; Mattick & Clarke, 1998). The SIAS consists of 20 items. This questionnaire asks participants to rate, on a 5-point scale, how characteristic each item is of them. In their examination of the psychometric properties of the SIAS, Mattick and Clark (1998) found the alpha coefficient for test–retest reliability to be .92 at both 4 weeks (range 3–5 weeks) and 12 weeks (range 11–13 weeks). More recently, the SIAS has been evaluated in several settings and formats, including the Internet (Hedman et al., 2010; Hirai, Vernon, Clum, & Skidmore, 2011) and in a shortened version (Fergus, Valentiner, Kim, & McGrath, 2014) with consistently adequate results. The SIAS continues to be used to index social anxiety in the study of mental health related topics such as participation in Alcoholics Anonymous (Moser, Turk, & Glover, 2015) and efficacy of cognitive-behavioral group therapy versus group psychotherapy (Bjornsson et al., 2011).
Data Analyses
Scoring. Scores and, when relevant, sub-scores were calculated for each instrument. Although the PBI can yield specific categories of parental bonding (i.e., optimal bonding or affectionless control), for the purposes of our study each dimension of this instrument (care and overprotection) was scored continuously. Like the PBI, the RSQ may be employed categorically; we elected, instead, to utilize the multi-item nature of the RSQ to permit participants to express their attachment preferences on a continuous scale so that overall attachment preferences would incorporate aspects of each of the four attachment patterns (Griffin & Bartholomew, 1994). This approach allowed us to develop a correlation matrix that included continuous scores not only for the PBI and RSQ, but also for each of the anxiety indices utilized. Data analysis also involved the calculation of Pearson’s r for the relationships between RSQ and PBI scores, between RSQ scores and scores on each of the five anxiety indices we used, and between PBI scores and scores on each of the five anxiety indices.
Reliability of scores. Reliability coefficients were calculated for each of the instruments utilized, including the subscales of the PBI, the RSQ, and the OCI-R. Cronbach’s alpha for the instruments ranged from .420 for the secure subscale of the RSQ to .938 for the PSWQ (see Tables 1 and 2). Due to the low reliability for several of the scales, all observed correlations were disattenuated (corrected to account for measurement error) using the following equation (Osborne, 2003):
The reliability coefficients are represented by r11 and r22, while r12 is the observed correlation and r*12 is the disattenuated correlation. Disattenuated correlations are listed in parentheses below the observed correlations in Tables 1 and 2.
Significance level and magnitude of correlations. In order to reduce the risk of a Type I Error in this study, a more stringent alpha level was adopted: only correlations that were significant at p < .01 were considered, while correlations significant at p < .05 were disregarded.
Correlation coefficients of 0 to .3 were considered to be of small magnitude, whereas correlation coefficients of .4 to .7 were considered to be of moderate magnitude, and correlation coefficients of .8 or greater were considered to be of high magnitude.
With respect to correlations between RSQ scores and ratings on each of the five self-report measures of anxiety (OCI-R, PDSS-SR, PSWQ, PCL-C, and SIAS), higher scores for the RSQ’s secure attachment preference negatively correlated with higher scores on all five self-report measures of anxiety (p < .01). The disattenuated correlation between scores for the RSQ’s secure attachment preference and ratings on the SIAS was of high magnitude (r = -.805), while the magnitudes of the disattenuated correlations for scores for the RSQ’s secure attachment preference and scores on the other anxiety indices were all moderate (secure attachment–obsessive-compulsive, r = -.642; secure attachment–panic, r = -.467; secure attachment–worry, r = -.567; secure attachment–post-trauma, r = -.622). Higher scores for the RSQ’s preoccupied and fearful attachment preferences positively correlated with higher scores on every type of anxiety indexed (p < .01), with all disattenuated correlations nearing or reaching moderate magnitude. Dismissing attachment style was not correlated with scores for any type of anxiety assessed in this study.
With respect to correlations between PBI scores and ratings on each of the five self-report measures of anxiety (OCI-R, PDSS-SR, PSWQ, PCL-C, and SIAS), neither PBI’s care nor overprotection dimension correlated with obsessive-compulsive symptoms, panic, or worry. However, higher scores on the PBI care dimension negatively correlated with higher scores for post-trauma and social anxiety symptoms (p < .01), and higher scores on PBI’s overprotection dimension positively correlated with higher scores for post-trauma and social anxiety (p < .01). All correlations were of small magnitude (care–post-trauma, r = -.276; care–social anxiety, r = -.317; overprotection–post-trauma, r = .220; overprotection–social anxiety, r = .220).
Discussion
This study examined the relationship between participant reports of adult attachment style, early bonding interactions with caregivers, and five different anxiety types. Results of the study supported our predictions of (a) a low to moderate relationship between adult attachment and parental bonding, (b) strong negative correlations between a secure attachment preference and all types of anxiety, (c) strong positive correlations between preoccupied and fearful attachment preferences and all types of anxiety, and (d) fewer significant correlations between early bonding memories and different anxiety types. With regard to this last prediction, only two types of anxiety (post-traumatic and social) were negatively associated with the care dimension of bonding and positively associated with the overprotection dimension; the other anxiety types were not correlated with either bonding dimension. Contrary to prediction, dismissing attachment did not correlate with any anxiety type or with either the care or overprotection dimension of parental bonding.
The positive correlation we found between secure attachment and early memories of high care and low overprotection contrasts with the absence of significant correlation in Myhr et al.’s (2004)
results, but is in keeping with our assumption that adult attachment and parental bonding constructs are distinct, as well as interrelated (hence our prediction of a low to moderate relationship). Also noteworthy was the absence of significant correlation between dismissing attachment style and both the care and overprotection scales of the PBI. Since insecure attachment is considered to result from relationship experiences that do not support the optimal development of a child (Bowlby, 1988), it is interesting that only fearful and preoccupied attachment preferences were correlated with less-than-optimal caregiving (lower care scores and higher overprotection scores).
Further explanation for this result may lie in the inherent qualities of the dismissing attachment pattern. Bartholomew (1993) suggested that dismissing attachment is characterized by a denial of the need for close relationships and George, Kaplan, and Main (1996) posited that individuals with a dismissing attachment state of mind often idealize their caregivers. Participants with a dismissing attachment style may have failed to report less-than-optimal caregiving, because they did not feel close to their caregivers and were thus unaware of their caregivers’ deficiencies or even dismissed unpleasant early bonding memories. In addition, the absence of significant correlation between dismissing attachment and total scores for all types of anxiety indexed in our sample suggests that individuals with a dismissing attachment style may experience a lower level of the subjectively disagreeable physiological reactivity that is often present alongside anxiety. If so, this may help explain the decreased reporting of anxiety and unpleasant early bonding memories among individuals who reported a preference for the dismissing attachment pattern.
As expected, lower correlations emerged between memories of early parental bonding (both care and overprotection) and different types of anxiety than those observed between anxiety and the secure, preoccupied, and fearful styles of adult attachment. Neither the care nor the overprotection dimension of bonding significantly correlated with total obsessive-compulsive symptoms, panic symptoms or generalized anxiety symptoms, which is partly consistent with Manicavasagar et al. (1999), who determined that PD may not be correlated with parental overprotection. Congruent with Parker’s (1979) investigation, which found that people with social phobia reported decreased care and increased overprotection in their caregivers, our results revealed significant correlations between parental bonding and anxiety only with respect to post-trauma and social anxiety symptomatology, and these correlations were of low magnitude.
Given that our study revealed associations between early bonding memories and experiences of both post-trauma and social anxiety, but not the other types of anxiety indexed, it is necessary to consider a possible etiology for this finding. Since our sample consisted of undergraduate psychology students, we thought it likely that many of our participants might be young people who were away from their homes and families for the first time and could be experiencing fear about their new social environment and possibly even feel traumatized by the separation from their caregivers. Indeed, our thinking is supported by the work of Manicavasagar et al. (1999), which indicated a potential association between the perception of parental overprotection and adult symptoms of separation anxiety.
Although results were consistent with predictions of lower correlations between parental bonding and anxiety than between attachment and anxiety, our findings diverged from the work of several other researchers. For example, Silove et al. (1991), Cavedo and Parker (1994), and Turgeon et al. (2002) found significant correlations between various types of anxiety and early bonding memories. It is possible that the lack of significant correlation in our sample between early bonding memories
and obsessive-compulsive, panic or generalized anxiety symptoms may indicate that people with these types of anxiety remembered fewer adverse early bonding experiences as a means of self-soothing during a difficult time (i.e., first experience living away from home). Even though these individuals did not report enough positive or negative experiences with caregivers to result in care
or overprotection correlations, they may have been unconsciously attempting to calm (or neutralize) their anxiety by remembering their early experiences in a more favorable light.
Treatment Implications of Attachment Style and Early Bonding Memories
Given the findings of our study, we believe that awareness of client attachment style may enhance therapeutic outcome in the treatment of anxiety conditions. For example, anxiety in individuals with secure attachment may be due to recent trauma rather than to long-term pathology, and the counselor’s role will be to help these individuals traverse their current obstacles and regain previous effectual functioning (Pistole, 1989). On the other hand, fearful clients may need extra time to form an attachment to their counselors and to use them as a “secure base” from which to explore the world in
a less anxious way. Anxious individuals with a preoccupied style of attachment may have difficulty managing their emotional responses and counselors may find it helpful to respond with empathic listening, rather than becoming frustrated by emotional behavior (Pistole, 1989). Individuals with a dismissing attachment style may deny anxiety, as well as any desire or need for closeness, and the counselor may find it necessary to confront the dismissal of important relationships (including the therapeutic bond) and the denial of emotions like anxiety (Pistole, 1989).
Awareness of clients’ early bonding memories may also inform therapeutic intervention when working with anxious individuals. In this study, post-trauma and social anxiety symptoms correlated with memories of early bonding, and understanding these connections may be meaningful in the treatment of anxiety. Young adults, who are potentially living away from their families of origin for the first time, may be particularly susceptible to post-trauma and social anxiety and may seek counseling for their concerns. A therapeutic understanding that these anxiety symptoms may be related to a less-than-optimal early environment, triggered by the uncertainties of being away from home, could result in treatment that is more relevant and individualized to the situation. Although medication may be appropriate for some clients contending with these circumstances, in other instances it could be especially beneficial to approach the treatment from the perspective of understanding the early family environment.
In contrast to post-trauma and social anxiety symptoms, obsessive-compulsive, panic and generalized anxiety symptoms were not correlated with early bonding memories. This may indicate that these conditions have fewer roots originating within the family, and the use of medications to control these particular anxiety symptoms may be appropriate. Despite the apparent lack of association between these three types of anxiety and early bonding memories, however, we suggest that involvement in counseling simultaneous to the use of any medication may increase the efficacy of treatment by providing a safe place for clients to discuss their concerns and consider solutions to the difficulties they encounter as a result of their anxiety conditions.
Considering the findings of this study, it is fair to assume that those counselors who bear in mind client attachment style and early bonding memories will provide a potentially more successful treatment for clients with anxiety conditions. The idea that attachment and bonding are related but distinct and separate constructs has the potential to broaden counselors’ conceptualization of the manner in which relational involvement may impact anxiety and therefore contribute to enhanced treatment efficacy. Ideally, treatment of anxious clients will include an individualized approach that takes into account the manner and style in which each person forms attachments to others and with regard for the relationship between the type of anxiety being treated and memories of the early child–caregiver bond.
Limitations and Future Directions
The choice to focus our investigation on a non-clinical population is consistent with the method of several studies concerning this literature (e.g., Eng et al., 2001; Mancini et al., 2000; Meites et al., 2012; O’Connor & Elklit, 2008; Yarbro et al., 2013). Nevertheless, the use of a non-clinical undergraduate sample may have resulted in more limited variation within anxiety states, creating a potential restriction of scores. Clearly, a clinical sample of individuals with previously diagnosed anxiety disorders is necessary to substantiate the non-clinical findings of this study. In addition, our sample’s overrepresentation of women relative to men may be considered a limitation in that the associations between attachment, bonding, and anxiety could vary according to gender.
We also suggest that ongoing investigation of anxiety and attachment incorporate the use of instruments that do not require participants to discern their own degree of relational capacity. For example, the Adult Attachment Interview (George et al., 1996) provides a method for assessing attachment state of mind through unconscious processes. The dismissing attachment style, which itself merits further study, could be illuminated through the use of an instrument such as this. In addition to this concern, several of the instruments we elected to use were older measures. Although they continue to be utilized for investigatory purposes in the mental health field, their age may have bearing upon the data they yield, particularly since several of the instruments have not been re-normed or validated with current populations.
Finally, although Latino participants comprised nearly 37% of our sample, we advocate that future study of attachment, bonding and anxiety include a specific focus on multicultural populations. There may well be differences in the ways individuals from varied backgrounds experience anxiety and this should be investigated. People who have recently immigrated, for example, may experience change of this magnitude as stressful and anxiety provoking. Understanding the role of attachment and early bonding relationships in this population ultimately may provide information to support individuals, families and children who transition from their original culture into a new one.
Conflict of Interest and Funding Disclosure
The authors reported that the research was supported
in part by UNM’s Regent’s Fellowship Award and
Research Project and Travel Grant.
References
Bartholomew, K. (1993). From childhood to adult relationships: Attachment theory and research. In S. W. Duck (Ed.), Understanding relationship processes 2: Learning about relationships (pp. 30–62). Thousand Oaks, CA: Sage.
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four-category model. Journal of Personality and Social Psychology, 61, 226–244. doi:10.1037/0022-3514.61.2.226
Behzadi, B., & Parker, G. (2015). A Persian version of the Parental Bonding Instrument: Factor structure and psychometric properties. Psychiatry Research, 225, 580–587. doi:10.1016/j.psychres.2014.11.042
Bjornsson, A. S., Bidwell, L. C., Brosse, A. L., Carey, G., Hauser, M., Mackiewicz Seghete, K. L., . . . & Craighead, W. E. (2011). Cognitive–behavioral group therapy versus group psychotherapy for social anxiety disorder among college students: A randomized controlled trial. Depression and Anxiety, 28, 1034–1042.
doi:10.1002/da.20877
Bowlby, J. (1988). A secure base: Parent-child attachment and healthy human development. New York, NY: Basic Books.
Calamari, J. E., Woodard, J. L., Armstrong, K. M., Molino, A., Pontarelli, N. K., Socha, J., & Longley, S. L. (2014).
Assessing older adults’ obsessive-compulsive disorder symptoms: Psychometric characteristics of
the Obsessive Compulsive Inventory-Revised. Journal of Obsessive-Compulsive and Related Disorders, 3,
124–131. doi:10.1016/j.jocrd.2014.03.002
Cassidy, J., Lichtenstein-Phelps, J., Sibrava, N. J., Thomas, C. L., Jr., & Borkovec, T. D. (2009). Generalized anxiety disorder: Connections with self-reported attachment. Behavior Therapy, 40, 23–38.
doi:10.1016/j.beth.2007.12.004
Cavedo, L. C., & Parker, G. (1994). Parental Bonding Instrument: Exploring for links between scores and obsessionality. Social Psychiatry and Psychiatric Epidemiology, 29, 78–82.
Chambless, D. L., Gillis, M. M., Tran, G. Q., & Steketee, G. S. (1996). Parental bonding reports of clients with obsessive-compulsive disorder and agoraphobia. Clinical Psychology & Psychotherapy, 3(2), 77–85.
Chen, C., Hewitt, P. L., & Flett, G. L. (2015). Preoccupied attachment, need to belong, shame, and interpersonal perfectionism: An investigation of the perfectionism social disconnection model. Personality and Individual Differences, 76, 177–182. doi:10.1016/j.paid.2014.12.001
Chorpita, B. F., & Barlow, D. H. (1998). The development of anxiety: The role of control in the early environment. Psychological Bulletin, 124, 3–21. doi:10.1037/0033-2909.124.1.3
Conybeare, D., Behar, E., Solomon, A., Newman, M. G., & Borkovec, T. D. (2012). The PTSD Checklist—Civilian Version: Reliability, validity, and factor structure in a nonclinical sample. Journal of Clinical Psychology, 68, 699–713. doi:10.1002/jclp.21845
Dash, S. R., & Davey, G. C. L. (2012). An experimental investigation of the role of negative mood in worry: The role of appraisals that facilitate systematic information processing. Journal of Behavior Therapy and Experimental Psychiatry, 43, 823–831. doi:10.1016/j.jbtep.2011.12.002
DeLapp, R. C. T., Chapman, L. K., & Williams, M. T. (2015). Psychometric properties of a brief version of the Penn State Worry Questionnaire in African Americans and European Americans. Psychological Assessment. doi:10.1037/pas0000208
Eng, W., & Heimberg, R. G. (2006). Interpersonal correlates of generalized anxiety disorder: Self versus other perception. Journal of Anxiety Disorders, 20, 380–387. doi:10.1016/j.janxdis.2005.02.005
Eng, W., Heimberg, R. G., Hart, T. A., Schneier, F. R., & Liebowitz, M. R. (2001). Attachment in individuals with social anxiety disorder: The relationship among adult attachment styles, social anxiety, and depression. Emotion, 1, 365–380. doi:10.1037/1528-3542.1.4.365
Fergus, T. A., Valentiner, D. P., Kim, H.-S., & McGrath, P. B. (2014). The Social Interaction Anxiety Scale (SIAS) and the Social Phobia Scale (SPS): A comparison of two short-form versions. Psychological Assessment, 26, 1281–1291. doi:10.1037/a0037313
Foa, E. B., Huppert, J. D., Leiberg, S., Langner, R., Kichic, R., Hajcak, G., & Salkovskis, P. M. (2002). The Obsessive-Compulsive Inventory: Development and validation of a short version. Psychological Assessment, 14, 485–496. doi:10.1037/1040-3590.14.4.485
George, C., Kaplan, N., & Main, M. (1996). Adult Attachment Interview. Unpublished manuscript, Department of Psychology, University of California, Berkeley (3rd ed.).
Ghafoori, B., Hierholzer, R. W., Howsepian, B., & Boardman, A. (2008). The role of adult attachment, parental bonding, and spiritual love in the adjustment to military trauma. Journal of Trauma & Dissociation, 9, 85–106. doi:10.1080/15299730802073726
Gladstone, G. L., & Parker, G. B. (2005). The role of parenting in the development of psychopathology: An overview of research using the Parental Bonding Instrument. In J. L. Hudson & R. M. Rapee (Eds.), Psychopathology and the family (pp. 21–33). New York, NY: Elsevier Science.
doi:10.1016/B978-008044449-9/50003-4
Goschin, S., Briggs, J., Blanco-Lutzen, S., Cohen, L. J., & Galynker, I. (2013). Parental affectionless control and suicidality. Journal of Affective Disorders, 151, 1–6. doi:10.1016/j.jad.2013.05.096
Griffin, D. W., & Bartholomew, K. (1994). The metaphysics of measurement: The case of adult attachment. In K. Bartholomew & D. Perlman (Eds.), Advances in personal relationships, Vol. 5: Attachment processes in adulthood (pp. 17–52). London: Jessica Kingsley Publishers.
Guédeney, N., Fermanian, J., & Bifulco, A. (2010). La version française du relationship scales questionnaire de
Bartholomew (RSQ, questionnaire des échelles de relation): Étude de validation du construit. L’Encéphale:
Revue de Psychiatrie Clinique Biologique et Thérapeutique, 36, 69–76. doi:10.1016/j.encep.2008.12.006
Hedman, E., Ljótsson, B., Rück, C., Furmark, T., Carlbring, P., Lindefors, N., & Andersson, G. (2010). Internet administration of self-report measures commonly used in research on social anxiety disorder: A psychometric evaluation. Computers in Human Behavior, 26, 736–740. doi:10.1016/j.chb.2010.01.010
Hirai, M., Vernon, L. L., Clum, G. A., & Skidmore, S. T. (2011). Psychometric properties and administration measurement invariance of social phobia symptom measures: Paper-pencil vs. internet administrations. Journal of Psychopathology and Behavioral Assessment, 33, 470–479. doi:10.1007/s10862-011-9257-2
Houck, P. R., Speigel, D. A., Shear, M. K., & Rucci, P. (2002). Reliability of the self-report version of the Panic Disorder Severity Scale. Depression and Anxiety, 15, 183–185. doi:10.1002/da.10049
Lee, R., Meyerhoff, J., & Coccaro, E. F. (2014). Intermittent explosive disorder and aversive parental care. Psychiatry Research, 220, 477–482. doi:10.1016/j.psychres.2014.05.059
Macatee, R. J., Capron, D. W., Guthrie, W., Schmidt, N. B., & Cougle, J. R. (2015). Distress tolerance and pathological worry: Tests of incremental and prospective relationships. Behavior Therapy, 46, 449–462. doi:10.1016/j.beth.2015.03.003
Mancini, F., D’Olimpio, F., Prunetti, E., Didonna, F., & Del Genio, M. (2000). Parental bonding: Can obsessive symptoms and general distress be predicted by perceived rearing practices? Clinical Psychology & Psychotherapy, 7, 201–208. doi:10.1002/1099-0879(200007)7:3
Manicavasagar, V., Silove, D., Wagner, R., & Hadzi-Pavlovic, D. (1999). Parental representations associated with adult separation anxiety and panic disorder-agoraphobia. Australian and New Zealand Journal of Psychiatry, 33, 422–428. doi:10.1046/j.1440-1614.1999.00566.x
Marazziti, D., Dell’Osso, B., Dell’Osso, M. C., Consoli, G., Del Debbio, A., Mungai, F., . . . & Dell’Osso, L. (2007). Romantic attachment in patients with mood and anxiety disorders. CNS Spectrums, 12, 751–756.
Massey, S. H., Compton, M. T., & Kaslow, N. J. (2014). Attachment security and problematic substance use in low-income, suicidal, African American women. The American Journal on Addictions, 23, 294–299. doi:10.1111/j.1521-0391.2014.12104.x
Mattick, R. P., & Clarke, J. C. (1998). Development and validation of measures of social phobia scrutiny fear and social interaction anxiety. Behaviour Research and Therapy, 36, 455–470. doi:10.1016/S0005-7967(97)10031-6
Meites, T., Ingram, R. E., & Siegle, G. J. (2012). Unique and shared aspects of affective symptomatology: The role of parental bonding in depression and anxiety symptom profiles. Cognitive Therapy and Research, 36, 173–181. doi:10.1007/s10608-011-9426-3
Meyer, T. J., Miller, M. L., Metzger, R. L., & Borkovec, T. D. (1990). Development and validation of the Penn State Worry Questionnaire. Behaviour Research and Therapy, 28, 487–495. doi:10.1016/0005-7967(90)90135-6
Moser, J. C., Turk, C. L., & Glover, J. G. (2015). The relationship between participation in Alcoholics Anonymous and social anxiety. Psi Chi Journal of Psychological Research, 20, 97–101. Retrieved from http://search.proquest.com/docview/1710260749?accountid=10181.
Myhr, G., Sookman, D., & Pinard, G. (2004). Attachment security and parental bonding in adults with obsessive-compulsive disorder: A comparison with depressed out-patients and healthy controls. Acta Psychiatrica Scandinavica, 109, 447–456. doi:10.1111/j.1600-0047.2004.00271.x
O’Connor, M., & Elklit, A. (2008). Attachment styles, traumatic events, and PTSD: A cross-sectional investigation of adult attachment and trauma. Attachment and Human Development, 10, 59–71. doi:10.1080/14616730701868597
Osborne, J. W. (2003). Effect sizes and the disattenuation of correlation and regression coefficients: Lessons from educational psychology. Practical Assessment, Research and Evaluation, 8. Retrieved from http://pareonline.net/getvn.asp?v=8&n=11
Otani, K., Suzuki, A., Matsumoto, Y., Shibuya, N., Sadahiro, R., & Enokido, M. (2014). Correlations of interpersonal sensitivity with negative working models of the self and other: Evidence for link with attachment insecurity. Annals of General Psychiatry, 13. Retrieved from http://www.annals-general-psychiatry.com/content/13/1/5.
Pacchierotti, C., Bossini, L., Castrogiovanni, A., Pieraccini, F., Soreca, I., & Castrogiovanni, P. (2002). Attachment and panic disorder. Psychopathology, 35, 347–354.
Pajkossy, P., Simor, P., Szendi, I., & Racsmány, M. (2015). Hungarian validation of the Penn State Worry Questionnaire (PSWQ): Method effects and comparison of paper-pencil versus online administration. European Journal of Psychological Assessment, 31, 159–165. doi:10.1027/1015-5759/a000221
Parker, G. (1979). Reported parental characteristics of agoraphobics and social phobics. The British Journal of Psychiatry, 135, 555–560. doi:10.1192/bjp.135.6.555
Parker, G., Tupling, H., & Brown, L. B. (1979). A Parental Bonding Instrument. British Journal of Medical Psychology, 52, 1–10. doi:10.1111/j.2044-8341.1979.tb02487.x
Pistole, C. (1989). Attachment: Implications for counselors. Journal of Counseling & Development, 68, 190–193. doi:10.1002/j.1556-6676.1989.tb01355.x
Renaud, E. F. (2008). The attachment characteristics of combat veterans with PTSD. Traumatology, 14(3), 1–12. doi:10.1177/1534765608319085
Ruiz, F. J. (2014). The relationship between low levels of mindfulness skills and pathological worry: The mediating role of psychological inflexibility. Anales De Psicología, 30, 887–897. doi:10.6018/analesps.30.3.150651
Safford, S. M., Alloy, L. B., & Pieracci, A. (2007). A comparison of two measures of parental behavior. Journal of Child and Family Studies, 16, 375–384. doi:10.1007/s10826-006-9092-3
Santacana, M., Fullana, M. A., Bonillo, A., Morales, M., Montoro, M., Rosado, S., . . . & Bulbena, A. (2014). Psychometric properties of the Spanish self-report version of the Panic Disorder Severity Scale. Comprehensive Psychiatry, 55. doi:10.1016/j.comppsych.2014.04.007
Seganfredo, A. C. G., Torres, M., Salum, G. A., Blaya, C., Acosta, J., Eizirik, C., & Manfro, G. G. (2009). Gender differences in the associations between childhood trauma and parental bonding in panic disorder. Revista Brasileira de Psiquiatria, 31, 314–321. doi:10.1590/S1516-44462009005000005
Shear, M. K. (1996). Factors in the etiology and pathogenesis of panic disorder: Revisiting the attachment-separation paradigm. The American Journal of Psychiatry, 153(Suppl.), 125–136.
Shear, M. K., Rucci, P., Williams, J., Frank, E., Grochocinski, V., Vander Bilt, J., . . . & Wang, T. (2001). Reliability and validity of the Panic Disorder Severity Scale: Replication and extension. Journal of Psychiatric Research, 35, 293–296. doi:10.1016/S0022-3956(01)00028-0
Silove, D., Parker, G., Hadzi-Pavlovic, D., Manicavasagar, V., & Blaszczynski, A. (1991). Parental representations of patients with panic disorder and generalised anxiety disorder. The British Journal of Psychiatry, 159, 835–841. doi:10.1192/bjp.159.6.835
Turgeon, L., O’Connor, K. P., Marchand, A., & Freeston, M. H. (2002). Recollections of parent-child relationships in patients with obsessive-compulsive disorder and panic disorder with agoraphobia. Acta Psychiatrica Scandinavica, 105, 310–316. doi:10.1034/j.1600-0447.2002.1188.x
Villalta, L., Arévalo, R., Valdepérez, A., Pascual, J. C., & Pérez de los Cobos, J. (2015). Parental bonding in subjects with pathological gambling disorder compared with healthy controls. Psychiatric Quarterly, 86, 61–67. doi:10.1007/s11126-014-9336-0
Weathers, F. W., Litz, B. T., Herman, D. S., Huska, J. A., & Kean, T. M. (1993). The PTSD Checklist: Reliability, validity, and diagnostic utility. Paper presented at the Annual Meeting of the International Society for Traumatic Stress Studies, San Antonio, TX, October.
Wootton, B. M., Diefenbach, G. J., Bragdon, L. B., Steketee, G., Frost, R. O., & Tolin, D. F. (2015). A contemporary psychometric evaluation of the Obsessive Compulsive Inventory—Revised (OCI-R). Psychological Assessment, 27, 874–882. doi:10.1037/pas0000075
Wuthrich, V. M., Johnco, C., & Knight, A. (2014). Comparison of the Penn State Worry Questionnaire (PSWQ) and abbreviated version (PSWQ-A) in a clinical and non-clinical population of older adults. Journal of Anxiety Disorders, 28, 657–663. doi:10.1016/j.janxdis.2014.07.005
Wuyek, L. A., Antony, M. M., & McCabe, R. E. (2011). Psychometric properties of the Panic Disorder Severity
Scale: Clinician-administered and self-report versions. Clinical Psychology & Psychotherapy, 18, 234–243.
doi:10.1002/cpp.703
Yarbro, J., Mahaffey, B., Abramowitz, J., & Kashdan, T. B. (2013). Recollections of parent-child relationships, attachment insecurity, and obsessive-compulsive beliefs. Personality and Individual Differences, 54, 355–360. doi:10.1016/j.paid.2012.10.003
Ellen W. Armbruster, NCC, is an Assistant Professor at Central Michigan University. David C. Witherington is an Associate Professor at the University of New Mexico. The authors also wish to acknowledge the contributions of David Olguin, Jay Parkes, Gene Coffield, and Jeffrey Katzman. Correspondence can be addressed to Ellen Armbruster, Education and Human Services Bldg. #353, Central Michigan University, Mt. Pleasant, MI 48859, armbr1ew@cmich.edu.
