Apr 1, 2021 | Volume 11 - Issue 2
Melissa J. Sitton, Tina Du Rocher Schudlich, Christina Byrne
A psychosocial approach to predicting self-injurious behavior (SIB) may allow for more accurate predictions and enhance intervention for individuals who engage in SIB. We examined psychosocial predictors of SIB within and between two populations: individuals with traits of borderline personality disorder (BPD; N = 60) and college students (N = 116). All participants met the inclusion criteria of engaging in SIB at least once in the past year. All participants completed measures of psychological distress, social functioning, and SIB. Methods of SIB did not vary across samples, but SIB rates did. Psychological distress and population type (BPD or student) predicted SIB, whereas social factors did not. Additionally, we found a significant interaction wherein psychological distress was more related to SIB in individuals with traits of BPD. Accordingly, we recommend that counselors consider population and psychological distress when assessing SIB risk in clients.
Keywords: self-injurious behavior, borderline personality disorder, college students, psychological distress, social functioning
Self-injurious behavior (SIB), the deliberate act of self-inflicted bodily harm, is of growing concern to counselors and clinicians. According to Nock (2010), SIB is a broad concept encompassing self-injury completed with suicidal intent (i.e., suicide attempts), without suicidal intent (i.e., nonsuicidal self-injury), or with ambivalence toward life (i.e., ambivalent, meaning neither strictly suicidal nor nonsuicidal). In other words, an individual can engage in SIB with differing goals that vary in intent from harming themselves to dying. The American Psychiatric Association (2013) considers suicide behavior disorder and nonsuicidal self-injury to be “conditions for further study” (p. 801). Individuals who engage in SIB over time are likely to do so with greater frequency, more methods, and increasing lethality (Andrews et al., 2013). Therefore, there is a great need for counselors and clinicians to assess their clients for SIB.
Although there are differing theories of the development and maintenance of SIB based on intent, particularly regarding the development of suicidal and nonsuicidal SIB, there are similar intrapersonal and interpersonal themes across theories. For instance, in their four-function model of nonsuicidal SIB, Nock and Prinstein (2004, 2005) proposed that intrapersonal (e.g., affective) and interpersonal (e.g., help-seeking) factors act as positive and negative reinforcers of nonsuicidal SIB. Similarly, in their renowned interpersonal–psychological theory of suicide, Joiner and colleagues (Joiner, 2005; Van Orden et al., 2010) proposed that individuals who attempt suicide are characterized both by a desire to die (i.e., interpersonal factors of perceived burdensomeness and thwarted belongingness) and the acquired capability to attempt (i.e., intrapersonal factors such as past SIB).
Notably, there is no specific theory to date regarding ambivalent SIB. Researchers and clinicians often differentiate SIB into two categories (Nock, 2010). In the first category, there is no explicit intent to die, and therefore it is considered nonsuicidal SIB. In the second category, there is no clear lack of suicidal intent, and therefore it is considered suicidal SIB. Thus, ambivalent SIB is often categorized as suicidal SIB, rather than as a unique experience. Regardless of how ambivalent SIB is classified, it is likely that both intrapersonal and interpersonal factors relate to ambivalent SIB given that both are relevant to suicidal and nonsuicidal SIB. Furthermore, individuals who engage in SIB often report multiple intents behind their past SIB (Andover et al., 2012; Klonsky & Olino, 2008). Because of these similarities and the clinical significance of each, we examined intrapersonal (i.e., psychological distress) and interpersonal (i.e., social functioning) predictors of SIB in the current study.
Predicting SIB With Psychosocial Functioning
The relations between psychological distress and SIB are well established in the literature. Researchers have found positive associations between SIB and depression (Andover et al., 2005; Kirkcaldy et al., 2007), anxiety (Andover et al., 2005; Klonsky & Olino, 2008), obsessive-compulsion (Kirkcaldy et al., 2007), and interpersonal sensitivity (Kim et al., 2015; Kirkcaldy et al., 2007). These studies and others examined specific experiences of psychological distress as it relates to SIB in adults and adolescents and in community and inpatient samples.
Previous studies have also demonstrated relations between social functioning and SIB. For instance, SIB is associated with less social support from family and friends (Rotolone & Martin, 2012; Tuisku et al., 2014). Similarly, SIB is related to more negative interactions or negative relational dynamics with family (Halstead et al., 2014; Van Orden et al., 2010) and friends (Adrian et al., 2011).
Predicting SIB in Different Populations
Some individuals may be at greater risk for developing SIB. In particular, SIB is especially prevalent in individuals with borderline personality disorder (BPD). According to the American Psychiatric Association (2013), BPD is characterized by “marked impulsivity” along with “a pervasive pattern of instability of interpersonal relationships, self-image, and affects” (p. 663). Notably, one diagnostic criterion of BPD is “recurrent suicidal behavior, gestures, threats, or self-mutilating behavior” (p. 663). Additionally, some risk factors for developing BPD (e.g., high emotion dysregulation, trauma exposure, etc.; Crowell et al., 2009) are also risk factors for engaging in SIB (Nock, 2009, 2010). Although lifetime rates of SIB in individuals with BPD vary, one study found that 92.2% of individuals who sought outpatient treatment for symptoms of BPD had engaged in nonsuicidal SIB within the past 2 months (Andión et al., 2012). Additionally, up to 75% of individuals with BPD reported at least one instance of suicidal SIB (Black et al., 2004). Furthermore, there appear to be differences in SIB engagement when comparing individuals with BPD to a community sample. For example, adults with BPD reported engaging in nonsuicidal SIB more recently and frequently, using more varied methods, and causing more physically severe injuries that require medical attention, compared to individuals without BPD who engaged in nonsuicidal SIB (Turner et al., 2015).
Although the rates and severity of SIB are higher in individuals with BPD than in the general population (Bentley et al., 2015), SIB is considered relatively common in other populations, including nonsuicidal SIB among college students (e.g., Whitlock et al., 2006, 2013). College students are thought to engage in SIB more than the general population (as suggested by Wilcox et al., 2012) with approximately 17%–41% of college students participating in nonsuicidal SIB (Whitlock et al., 2006) compared to 5.9% of adults in the general population (Klonsky, 2011). Most college students are also in the highest risk age group for nonsuicidal SIB (Rodham & Hawton, 2009), and suicide is the second leading cause of death during this period (18–25 years old; Centers for Disease Control and Prevention, 2017). Notably, college students and non–college students of the same age (i.e., 16–24 years old) do not appear to differ in rates of SIB (McManus & Gunnell, 2020).
Current Study
A wealth of research has identified important psychological and social factors that may be associated with the occurrence of SIB. However, it remains unclear how these factors intersect to predict SIB. Additionally, as Turner et al. (2015) suggested, most research on SIB has considered either individuals with BPD or nonclinical samples (e.g., college students) without considering potential differences in predictors between these populations.
The current study used a comprehensive psychosocial approach to examine psychological distress and social functioning in two samples: a high-risk, treatment-seeking sample of individuals with traits of BPD and a sample of college students. This allowed us to characterize how key factors may intersect in predicting SIB. Our objectives were to (a) examine SIB within and between the two populations, (b) evaluate which psychosocial factors predicted total lifetime SIB for both populations, and (c) determine whether the predictors of total lifetime SIB varied by population (i.e., test for an interaction between psychosocial predictors and sample).
Method
Participants and Procedure
This study included a sample of individuals with BPD traits and a college student sample. For both samples, our inclusion criteria required that participants have a history of SIB with at least one self-reported episode of SIB (i.e., SIB of any intent) in the past year. We required recent SIB so that the measures of current psychological and social functioning would be appropriate predictors, rather than examining current functioning with a retrospective report of SIB after several years.
Sample 1: Individuals With Traits of BPD
The first sample consisted of data from a larger study on dialectical behavior therapy (DBT) in teens and adults (Sitton et al., 2020). Participants sought treatment for BPD symptoms from community-based counselors, although not all participants had formal diagnoses of BPD. The counselors obtained informed consent from participants and collaborated with a local university for this larger IRB-approved study. Of the 62 participants in this larger study, 96.8% (n = 60) reported engaging in SIB in the past year and constituted the BPD-Tx sample.
BPD-Tx participants (n = 60) were mostly young adults (M = 23.53 years, SD = 6.85 years, range = 18–48 years old). Based on self-reports, there were 49 females (81.7%), eight males (13.3%), and three participants who identified as non-binary or androgynous (5%). This sample was mostly White/European American (83.1%), followed by multiracial (10.2%), Asian American (1.7%), and Hispanic/Latinx (1.7%), with an additional 3.4% identifying as “other” or not reporting. Most (80%) reported no counseling experience prior to receiving DBT from the community counselors (i.e., at the time of recruitment). Data on sexual orientation was not available for this sample.
Sample 2: Undergraduate College Students
The second sample consisted of undergraduate students in introductory psychology courses at a university in the Pacific Northwest. We recruited students to participate in a study called “Emotional and Behavioral Responses to Stress” and informed all participants that they might experience distress as part of the study. After giving their informed consent, participants completed the measures online in a campus computer lab so any questions or concerns could be immediately addressed by a research assistant trained in suicide prevention. Debriefing included an extensive form that included on- and off-campus mental health resources.
Of the 536 students who completed the survey, 43.8% reported engaging in SIB during their lifetime, and 116 students (21.6%) met the inclusion criteria of engaging in SIB in the past year. This proportion of students is high compared to some student samples (e.g., Whitlock et al., 2006; Wilcox et al., 2012), but it is comparable to the lifetime rate from at least one other university sample (Gratz et al., 2002).
Student participants included in this study (n = 116) were mostly young adults (M = 19.62 years, SD = 1.58 years, range = 18–27 years old). Based on self-reports, there were 89 females (78.4%), 23 males (19.8%), and four participants who identified as non-binary or androgynous (4%). This sample was mostly White/European American (69%), followed by multiracial (19.8%), Asian American (6%), and Hispanic/Latinx (4.3%). Participants’ sexual orientations were as follows: 60.3% heterosexual, 18.1% bisexual, 7.8% pansexual, 6.9% homosexual, 1.7% asexual, and 1.8% who identified as “other.” Most (77.6%) reported previous counseling experiences, with about one-fifth currently seeing a counselor (22.4%). Other studies have found rates of prior experience with counseling services to be closer to 55% in college students (e.g., Niegocki & Ægisdóttir, 2019). Most student participants reported seeking counseling services for stress- and mood-related symptoms, and none reported seeking treatment specifically for BPD.
Measures
Self-Injurious Behavior (SIB)
We used the Lifetime Suicide Attempt Self-Injury Interview (LSASI; Linehan & Comtois, 1996) to assess participants’ history of SIB, including frequency, method, and intent. This 20-item measure asks about the dates of the most recent and most severe SIB act (e.g., “When was the most recent time that you intentionally injured yourself?”) and assesses the total lifetime frequency for 11 methods of SIB, as well as the separate intent(s) of each SIB act (suicidal, nonsuicidal, or ambivalent). Higher scores indicate more SIB acts.
Internal consistency was adequate for both samples (BPD-Tx sample, Cronbach’s α = .75; student sample, Cronbach’s α = .73). Notably, the LSASI was created for clinical use rather than research use; therefore, there are no known studies of its reliability or validity. However, the LSASI was already in use by the counselors in the larger study of DBT described, and they chose to use it to assess SIB in the BPD-Tx sample. We used it for the student sample to be consistent with the existing sample data. Following Linehan and Comtois’s (1996) scoring instructions, we calculated a total lifetime frequency for each participant by summing all SIB of any intent.
Psychological Distress
The Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1975) is a broad-spectrum psychiatric symptom checklist. Participants rate their distress level in the past week on a Likert-type scale from 0 (not at all) to 4 (extremely) for each of 90 items (e.g., “How much were you distressed by feeling critical of others?”). This measure assesses nine factors of psychological distress. For this study, we were interested in the factors of Depression, Anxiety, Obsessive-Compulsion, and Interpersonal Sensitivity. The internal consistency of this measure was very high in the BPD-Tx sample (α = .97).
To reduce participant burden, we used the Brief Symptom Inventory (BSI; Derogatis & Spencer, 1982), a 53-item version of the SCL-90-R, for student participants. The internal consistency was very high in the student sample (α = .96).
To assess the comparability of the SCL-90-R and the BSI for subsequent analysis, we separately averaged all items for the factors of Anxiety, Depression, Obsessive-Compulsion, and Interpersonal Sensitivity to determine BPD-Tx participants’ scores of psychological distress using these two measures. We found strong correlations between the SCL-90-R factors and the BSI factors (Depression: r = .92, p < .001; Anxiety: r = .97, p < .001; Obsessive-Compulsion: r = .95, p < .001; Interpersonal Sensitivity: r = .90, p < .001; and Average Psychological Distress: r = .98, p < .001). Following Derogatis (1993), who found no significant difference in validity between the SCL-90-R and the BSI, we used only the BSI items to create symptom factors for both samples. The internal consistency of the BSI items for the
BPD-Tx sample was very high (α = .95).
Social Functioning
The Network of Relationships Inventory-Behavioral Systems Version (NRI; Furman & Buhrmester, 2009) is a 33-item self-report measure of social support and negative interactions in various relationships (i.e., one’s mother, father, friends, and romantic partner). Participants rate the frequency of positive support or negative interactions on a Likert-scale from 1 (little or none) to 5 (the most). The Positive Support scale includes five subscales: Seeks Secure Base, Provides Secure Base, Seeks Safe Haven, Provides Safe Haven, and Companionship. The Negative Interactions scale includes three subscales: Conflict, Antagonism, and Criticism. Higher scores indicate more of each factor. The internal consistency was high for both samples (BPD-Tx, α = .93; student sample, α = .94).
We calculated the mean score of the Positive Support subscales, including Seeks Secure Base, Seeks Safe Haven, and Companionship. We did not include Provides Secure Base or Provides Safe Haven because Furman and Buhrmester (2009) described these as “caretaking” factors rather than “attachment” or “affiliation” factors. We also calculated the mean score of all three Negative Interactions subscales.
Data Analysis Plan
To begin, we tested for the assumptions of analysis, following guidelines proposed by Tabachnick and Fidell (2019). We defined outliers as data points beyond three standard deviations from the mean. We evaluated outliers within each group and replaced them with the value that was three standard deviations above the group mean. We chose this more liberal approach to outliers to maximize variability in the data. It was especially important to maintain variability in the outcome variable of total SIB given that higher levels of SIB have great clinical significance. For skewness and kurtosis of the composite variables, we used ±2 as our acceptable range of values. We transformed variables that did not meet our criteria for normality. We also utilized the missing completely at random test and found no systematic patterns to missing data, and thus used the group means to replace missing values for analysis.
To assess SIB in the two samples, we examined the intent of SIB acts separately for each sample and analyzed if SIB rates differed based on demographic information. To examine psychosocial predictors of SIB, we conducted a multiple linear regression. We used total SIB (including suicidal, nonsuicidal, and ambivalent SIB) as the outcome variable. We also examined differences in predictors of total SIB between the BPD-Tx and student samples by including interaction terms (e.g., psychological distress x sample). Statistically significant interactions were graphed to aid interpretation (Howell, 2013).
For the multiple linear regression analysis, we used effect coding for sample type (Daly et al., 2016), which allows comparison of a sample mean to the overall mean instead of using one sample as a reference group. Additionally, we centered the predictor variables around the grand mean for the whole sample to reduce the risk of multicollinearity. We inspected the tolerance and variance inflation factors, and used multiple sources (e.g., correlations between variables, p-values, and the standard error of the regression coefficients) to determine if multicollinearity was an issue.
Results
We used SPSS 24.0 to analyze the data. Using one-way analysis of variance (ANOVA), we found no differences between the samples based on gender or ethnicity (all p values > .05). However, using an independent samples t-test, we found that the BPD-Tx sample (M = 23.53, SD = 6.85) was older on average than the student sample: M = 19.62, SD = 1.58, t(173) = 5.85, p < .001. Additionally, the BPD-Tx sample (13.3%) reported prior experience with counseling (dichotomous variable) less often than the student sample (77.6%) on average: χ2(1) = 59.39, p < .001.
Sample Differences in SIB
We conducted descriptive analyses for all SIB variables. See Table 1 for descriptive statistics of the different intents of SIB (nonsuicidal, ambivalent, and suicidal), total SIB (including the untransformed total score), and the reported number of SIB methods. Table 1 also includes difference scores of SIB acts based on independent sample t-tests in consideration of the two samples. Individuals in the BPD-Tx sample engaged in more nonsuicidal, ambivalent, and total SIB in their lifetime compared to the student sample. Although there appeared to be no difference between samples in suicidal SIB, it is worth noting that this variable did not meet our criteria for normality in either sample even after transformation.
Table 1
Means (With Standard Deviations) and Difference Scores for Self-Injurious Behavior (SIB) by Sample
| Variable |
BPD-Tx
(N = 60) |
Student
(N = 116) |
t(df) |
p |
| Nonsuicidal SIB |
3.13 (1.81) |
2.34 (1.55) |
t(174) = 3.01 |
.003 |
| Ambivalent SIB |
1.92 (2.02) |
1.07 (1.33) |
t(86.25) = 2.94 |
.004 |
| Suicidal SIB |
0.66 (0.90) |
0.45 (0.81) |
t(174) = 1.61 |
.110 |
| Total SIB |
3.87 (1.84) |
2.86 (1.43) |
t(96.56) = 3.73 |
< .001 |
| Total SIB (untransformed) |
166.31 (268.69) |
44.10 (75.60) |
t(63.88) = 3.45 |
.001 |
| Number of SIB methods |
3.28 (1.53) |
3.28 (2.11) |
t(174) = -0.004 |
.997 |
Note. BPD-Tx = participants with traits of borderline personality disorder; Total SIB (untransformed) =
untransformed values after adjusting the outliers in the raw reported values. Significant p values are in bold.
Although the normality of suicidal SIB was improved using a transformation, we were unable to meet our
acceptable range of ±2 for kurtosis (BPD-Tx kurtosis = 4.22; student kurtosis = 2.71).
In the BPD-Tx sample, we found no differences in SIB frequency based on gender, age, ethnicity, or counseling experience using one-way ANOVA. In the student sample, we found no differences in SIB frequency based on age, ethnicity, living situation, or counseling experience using one-way ANOVA. However, SIB frequency differed by gender such that those who identified as non-binary (M = 4.64, SD = 1.35) reported significantly higher rates of SIB than both males (M = 2.80, SD = 1.31) and females (M = 2.95, SD = 1.20). There were no differences in SIB frequency or severity based on sexual orientation in the student sample.
Psychosocial Predictors of SIB
We compared the two samples on the predictor variables first by using independent sample t-tests. We found that BPD-Tx participants reported less psychological distress (M = 2.21, SD = 0.78) than student participants: M = 2.78, SD = 0.89, t(174) = −4.16, p < .001. The BPD-Tx participants (M = 3.25, SD = 0.49) also reported less positive social support than student participants: M = 3.44, SD = 0.54, t(174) = −2.26, p = .025. Lastly, BPD-Tx participants (M = 1.22, SD = 0.43) reported more negative interactions than student participants: M = 1.07, SD = 0.43, t(174) = 2.15, p = .033.
We conducted bivariate correlations between all predictor variables and the outcome variable for each sample. In the BPD-Tx sample, total SIB was positively correlated with average psychological distress (r = .37, p = .004). In the student sample, total SIB was negatively correlated with positive social support (r = −.18, p = .049). In both samples, average psychological distress was positively associated with negative interactions (BPD-Tx: r = .36, p = .005; student: r = .24, p = .008). No other variables were significantly correlated in either sample.
Next, we conducted a multiple linear regression using total SIB as the outcome variable for both samples together. We entered seven predictors simultaneously: psychological distress, positive social support, negative interactions, sample type, and the interactions between sample type and the three other predictors. Together, these seven variables significantly predicted total SIB: F(7,168) = 5.01, p < .001, MSE = 2.33, r2 = .17. As shown in Table 2, psychological distress (sr2 = .06), sample type (sr2 = .12), and the interaction between psychological distress and sample type (sr2 = .03) were each significant unique predictors of total SIB. Specifically, based on the positive β weights, more psychological distress and being in the BPD-Tx sample were both associated with higher lifetime rates of SIB. Notably, multicollinearity did not appear to be an issue in this regression given the moderate to low correlations between factors, sufficiently high tolerance values, acceptable variance inflation factor values (ranging from 1.25–1.55), and the low standard error of regression coefficients relative to their scale.
Table 2
Multiple Regression Analysis Predicting Total Self-Injurious Behavior for the Whole Sample (N = 176)
|
|
CI |
| Variable |
B |
SE B |
β |
t |
p |
sr2 |
Lower |
Upper |
| Psych. distress |
0.57 |
0.16 |
.31 |
3.55 |
.001 |
.06 |
0.25 |
0.89 |
| Pos. social support |
−0.48 |
0.25 |
−.16 |
−1.96 |
.052 |
.02 |
−0.97 |
0.00 |
| Neg. interactions |
−0.26 |
0.30 |
−.07 |
−0.85 |
.399 |
.003 |
−0.85 |
0.34 |
| Sample type |
0.68 |
0.14 |
.39 |
4.87 |
< .001 |
.12 |
0.40 |
0.95 |
| Psych. distress x sample |
0.40 |
0.16 |
.21 |
2.46 |
.015 |
.03 |
0.08 |
0.71 |
| Pos. social support x sample |
0.00 |
0.25 |
.00 |
0.00 |
.997 |
.001 |
−0.49 |
0.49 |
| Neg. interactions x sample |
−0.08 |
0.30 |
−.02 |
−0.25 |
.801 |
.001 |
−0.67 |
0.52 |
|
|
|
|
|
|
|
|
|
|
Note. Psych. = psychological; Pos. = positive; Neg. = negative; sr2 = squared semipartial correlation. Sample type was
coded so that BPD-Tx sample = 1, student sample = -1. Significant p values are in bold.
Sample Differences in SIB Predictors
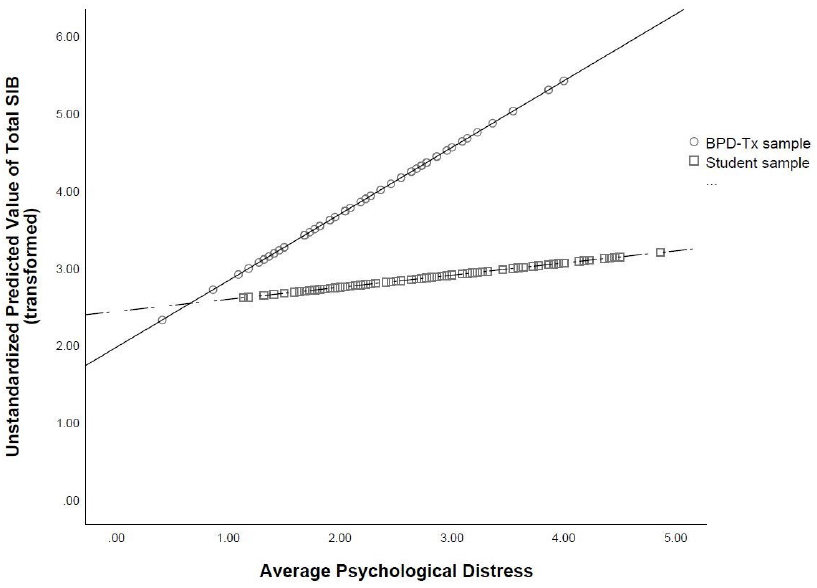
To further probe the statistically significant interaction, we plotted the regression paths for psychological distress predicting total SIB by sample type. As shown in Figure 1, more psychological distress was related to higher lifetime rates of total SIB in both samples, which supports the main effect of psychological distress found in the multiple regression analysis. However, the relation between psychological distress and total SIB was stronger in the BPD-Tx sample than in the student sample (as evidenced by the steeper slope of the regression line representing the BPD-Tx sample compared to that of the student sample).
Figure 1
Regression Lines of Average Psychological Distress Predicting Total Self-Injurious Behavior (SIB) by Sample Type
Discussion
The primary goals of the current study were to establish a more comprehensive set of predictors of SIB and to better understand how the experience of SIB varied by population (BPD-Tx vs. college students). This study was unique in its psychosocial approach to predictors. Additionally, we tested for interactions between sample type and the psychosocial predictors of SIB. This singular examination of interacting predictors has seldom been conducted in the literature, and thus is an important strength of this study.
SIB Engagement and Psychosocial Functioning
The results demonstrate a very high lifetime frequency of SIB in both samples. Although most studies do not report the lifetime frequency rates of SIB of their participants, the frequency of SIB in our student sample was comparable to that found in another study of students using the same SIB methods with nonsuicidal intent (Croyle & Waltz, 2007). The frequency rate of SIB in the BPD-Tx sample appeared to be lower than found in some other studies with individuals with BPD (e.g., Turner et al., 2015).
Additionally, we found that the lifetime frequency rates of SIB were higher in the BPD-Tx sample than in the student sample, which aligns with previous studies (e.g., Klonsky & Olino, 2008; Turner et al., 2015). This makes sense given the maladaptive behaviors often seen in individuals with BPD. Additionally, given that the BPD-Tx sample was older than student participants on average, it is also possible that their increased lifetime rates of SIB reflected a greater number of years to engage in it. Alternatively, the higher SIB frequency reported by the BPD-Tx participants may serve an interpersonal function. According to Linehan (1993), nonsuicidal SIB is commonly used by individuals with BPD to communicate with and gain attention from others.
Interestingly, despite higher rates of total SIB, BPD-Tx participants reported less psychological distress than did student participants. This was contrary to many other studies showing a strong association between psychological distress and engagement in nonsuicidal SIB for individuals with BPD (e.g., Sadeh et al., 2014; Turner et al., 2015). One possible explanation for the lower rates of psychological distress reported by BPD-Tx participants is that their baseline level of psychological distress was higher, leading these negative emotions to be considered normal and therefore not “distressing.” Additionally, given that fewer BPD-Tx participants reported prior experience with counseling than student participants, it could be that BPD-Tx participants reported less psychological distress because of a lack of emotional self-awareness. This aligns with Turner et al.’s (2015) finding that participants with BPD who engage in nonsuicidal SIB reported less awareness of their emotional states. Another explanation is that the BPD-Tx participants were recruited from a community-based clinic wherein they were preparing to start DBT. Although the data used in the current study represents pretest data gathered prior to treatment, it is possible that the BPD-Tx participants were experiencing lowered distress at the time of data collection because of the hope and positive expectations that are often associated with starting a new treatment (Dew & Bickman, 2005).
Socially, the BPD-Tx participants reported less positive support than student participants. This finding aligns with the biosocial theory of BPD (Linehan, 1993), which suggests that individuals with BPD may experience or perceive an invalidating environment. Alternatively, BPD-Tx participants may be more likely to interpret interactions with others as negative, which aligns with Peters et al.’s (2015) finding that individuals with traits of BPD often demonstrated maladaptive responses to emotional experiences, leading them to interact negatively with others.
Psychosocial Predictors of SIB
An important finding of the current study is that psychological distress predicted total SIB with a small to moderate effect size. This suggests that psychological distress (including experiences of anxiety, depression, obsessive-compulsion, and interpersonal sensitivity) is an important component of SIB of various intents. Specifically, psychological distress may act as a catalyst for SIB, wherein individuals engage in SIB to decrease their psychological distress. This explanation aligns with Nock and Prinstein’s (2004, 2005) theory of the intrapersonal negative reinforcement function of nonsuicidal SIB. Namely, that one might engage in SIB in order to reduce tension or psychological distress, particularly anxiety.
Contrary to the majority of extant literature (e.g., Wilcox et al., 2012), neither positive social support nor negative interactions predicted total SIB in the current study. We also did not find an interaction between either social variable and sample type, suggesting that social functioning might not be a direct, distinct predictor of total SIB for either population. However, it is possible that social functioning is indirectly related to total SIB. For example, we found a significant positive correlation between negative interactions and psychological distress in both samples. Given these correlations, negative interactions may contribute to experiences of psychological distress, which then predict total SIB. This proposed indirect relation is supported by Adrian et al.’s (2011) study, which found that emotion dysregulation partially mediated the relation between interpersonal problems (i.e., problems with one’s family and peers) and nonsuicidal SIB.
Another possible explanation for the lack of significant social predictors of SIB in the current study is the variability in the data that stems from inconsistent timing of social support. Specifically, it is unclear if positive support preceded SIB engagement, followed the SIB act, or both. Turner et al. (2016) found that perceived social support increased after participants disclosed their nonsuicidal SIB acts to others. However, they also found that this increased support was associated with increased nonsuicidal SIB urges and acts the following day, presumably because the SIB had achieved the desired interpersonal function. Thus, similar to Turner et al.’s (2016) study, the lack of a clear, linear relation between SIB and social support may have contributed to nonsignificant findings of social predictors in the current study.
Notably, the strongest single predictor of total SIB was sample type, with BPD-Tx participants showing greater frequency of total lifetime SIB than student participants. This aligns with Turner et al. (2015), who found that individuals with BPD traits engage in nonsuicidal SIB more often than do those without BPD traits.
Sample Differences in SIB Predictors
The relation between psychological distress and total SIB was stronger for the BPD-Tx sample than for the student sample. This finding is somewhat supported by previous literature; for example, Klonsky and Olino’s (2008) latent class analysis revealed that the group with the most nonsuicidal SIB also reported more symptoms of BPD and psychological distress and reported regularly engaging in nonsuicidal SIB to help regulate their emotions. In comparison, individuals with BPD traits in the current study reported engaging in more total SIB (as well as nonsuicidal SIB) but did not report greater levels of psychological distress than did the student participants. However, if our BPD-Tx participants used SIB for emotion regulation, too, then perhaps this strategy allowed them to experience lower levels of psychological distress day-to-day than student participants. This aligns with Sadeh et al.’s (2014) finding that BPD symptoms related to the affect-regulating function of SIB, especially nonsuicidal SIB.
Additionally, the significant interaction we found between psychological distress and sample type resembles Andover et al.’s (2005) finding that BPD symptoms accounted for the relation between anxiety and nonsuicidal SIB. However, in our study, psychological distress was a significant unique predictor of total SIB (in addition to the significant interaction between psychological distress and sample type). In other words, sample type seems to be a moderator between psychological distress and SIB in our study, as opposed to a mediator.
Counseling Implications
Our findings have several treatment implications. Many counselors will not be surprised by the high rates of SIB found in our BPD-Tx sample. However, we also found a clinically important high rate of SIB in college students. Given that past engagement in SIB is one of the strongest predictors of future SIB (including nonsuicidal and suicidal SIB; Tuisku et al., 2014), the high lifetime rates of SIB found in both samples in the current study are noteworthy for service providers. Specifically, our results suggest that universities and other institutions concerned with mental health in college students should consider utilizing SIB screening tools. Additionally, the high prevalence of students with a lifetime history of any SIB suggests the need for widespread intervention programs for student populations. For example, some research (e.g., Kannan et al., 2021) has examined the implementation of DBT skills groups in college counseling centers for students with a variety of presenting issues, including SIB. Such intervention programs could benefit a wider range of students and help improve quality of life for many, especially those struggling with SIB.
Given that psychological distress predicted total SIB, it may be beneficial for counselors to regularly assess the level of psychological distress in all clients, including those with BPD and college students. Clients with high psychological distress, including anxiety, depression, obsessive-compulsion, and interpersonal sensitivity, will likely engage in more SIB than those with low psychological distress, and thus the counselor may be able to intervene before the client escalates to a high frequency of SIB. Assessing and tracking affective distress levels may be common with suicide assessment and safety planning, but there may be less awareness about the need for this with SIB. Treatment protocols could also focus on lowering psychological distress to see if that will decrease SIB. For example, DBT, which emphasizes psychological distress tolerance, has been increasingly implemented in college campus counseling centers (see Chugani, 2015). However, given that the current study’s findings are not causal, we cannot definitively conclude that lowering psychological distress will affect SIB.
Importantly, the interaction between psychological distress and sample type is noteworthy given that it contributes to the small extant evidence of divergence between populations of individuals with symptoms of BPD and other, more community-based populations like college students. Specifically, we found differences in SIB prevalence, in lifetime frequency, and in one predictor (i.e., psychological distress) in our two samples. This aligns with Turner et al.’s (2015) findings that individuals who engaged in SIB with and without BPD differed in SIB frequency, severity, and comorbid affective symptomology.
It is also worth noting that the correlational analysis revealed a difference between these two samples in social functioning. In particular, there was a statistically significant negative correlation between total SIB and positive social support in the student sample, but not in the BPD-Tx sample. Because of this, although we only found one statistically significant interaction between psychosocial predictors and sample type, it is plausible that there are other notable differences in SIB risk factors between these two populations. Thus, when treating SIB, it may be worth assessing for other symptoms of BPD to form a more accurate representation of a client’s experience and to help form a specific treatment plan.
Limitations and Future Studies
One potential limitation of the current study is that we included only individuals who reported engaging in SIB in the past year because we wanted to examine current predictors of current SIB. However, it is possible that psychological distress and social support are more effective predictors of future SIB acts. In other words, the current study examined predictors of the frequency of SIB using current psychosocial functioning, yet the psychosocial variables might have been better at predicting whether or not an individual will engage in SIB in the future. This theory aligns with Heath et al.’s (2009) interpretation of their lack of results linking social support to lifetime rates of nonsuicidal SIB. Specifically, that social support may better relate to differences between those who will engage in SIB compared to those who will not, as opposed to the degree (i.e., frequency) of SIB. It is unclear how the results may have differed if we included a comparison group of individuals who do not engage in SIB or have never engaged in SIB.
A second limitation was the need to use specific measures to compare the student sample to the existing BPD-Tx sample data. Although the LSASI measure has the advantage of thoroughly examining SIB methods and intent, it was intended for clinical use rather than research. Additionally, the LSASI is a lifetime measure of SIB as opposed to assessing recent SIB; although our inclusion criteria required participants to have engaged in SIB at least once in the past year, it is unknown how recent or severe the SIB was in the past year relative to one’s lifetime. Because of this, a dichotomous measure of past-year engagement in SIB may have better suited our need for recent SIB assessment. Nonetheless, the LSASI provided a great depth and variability in the data that was not only valuable in the current research study, but also clinically important to the counselors with whom we collaborated in the larger DBT study.
A third limitation is that there may be other variables involved in predicting SIB that were not assessed, such as emotion regulation skills or trauma exposure. For example, SIB frequency might be more strongly related to one’s ability to regulate distress rather than the presence of distress itself. Given that emotional reactivity and trauma exposure are both risk factors for SIB (Nock, 2009, 2010) and for the development of BPD (Crowell et al., 2009), future studies may want to further explicate these relations.
It is also worth noting that the samples in the current study may include theoretically overlapping populations. Specifically, we did not screen the BPD-Tx group for current academic status, and therefore it is possible that some participants in the BPD-Tx group were also college students. We decided not to exclude BPD-Tx participants based on academic status in order to reduce barriers to study participation and so that the BPD-Tx sample would represent people who seek treatment for BPD in the community, not just those who are not college students. Additionally, although we screened the student sample for the explicit endorsement of BPD diagnosis, it is possible that some participants in the student sample had subthreshold symptoms of BPD (especially considering that SIB itself is a symptom of BPD) or simply had not received a diagnosis of BPD at the time of this study.
Future studies should continue to examine psychosocial predictors of SIB with larger and more diverse samples in order to explore the relations between psychological and social predictors. Additionally, future studies should explore other relevant factors with the psychosocial predictors (e.g., emotion regulation, trauma exposure) to determine if other factors may better explain (or mediate the relations with) SIB. Moreover, longitudinal and experience-sampling designs would allow researchers to gain better understanding of how changes in psychosocial functioning relate to decisions to engage in SIB as well as the exact sequence of events for SIB acts. Although some studies have recently begun using these techniques, a more psychosocial approach to predictors and consequences of SIB (also considering various intents) may provide more prudent information for intervention and treatment of individuals who engage in SIB.
Conclusion
The current study sought to identify psychosocial predictors of SIB in two clinically different populations and to compare predictors between these populations. We found high lifetime frequency rates of SIB in both samples, suggesting a need for more widespread assessment of SIB in young adults from different populations. We also found that population type itself was the strongest predictor of SIB—individuals with traits of BPD engaged in more SIB in their lifetimes than did college students. Additionally, psychological distress predicted SIB; however, we also found a significant interaction between population and psychological distress, which suggests that psychological distress may be more related to SIB in individuals with traits of BPD than in more community-based populations like college students. Consequently, counselors should consider population and psychological distress when assessing SIB risk in clients.
Conflict of Interest and Funding Disclosure
Data from the existing BPD sample was partially
funded by an internal grant awarded to coauthor
Christina Byrne. The authors reported no conflict
of interest or other funding for the development
of this manuscript.
References
Adrian, M., Zeman, J., Erdley, C., Lisa, L., & Sim, L. (2011). Emotional dysregulation and interpersonal difficulties as risk factors for nonsuicidal self-injury in adolescent girls. Journal of Abnormal Child Psychology, 39(3), 389–400. https://doi.org/10.1007/s10802-010-9465-3
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Andión, Ó., Ferrer, M., Matali, J., Gancedo, B., Calvo, N., Barral, C., Valero, S., Di Genova, A., Diener, M. J., Torrubia, R., & Casas, M. (2012). Effectiveness of combined individual and group dialectical behavior therapy compared to only individual dialectical behavior therapy: A preliminary study. Psychotherapy, 49(2), 241–250. https://doi.org/10.1037/a0027401
Andover, M. S., Morris, B. W., Wren, A., & Bruzzese, M. E. (2012). The co-occurrence of non-suicidal self-injury and attempted suicide among adolescents: Distinguishing risk factors and psychosocial correlates. Child and Adolescent Psychiatry and Mental Health, 6. https://doi.org/10.1186/1753-2000-6-11
Andover, M. S., Pepper, C. M., Ryabchenko, K. A., Orrico, E. G., & Gibb, B. E. (2005). Self-mutilation and symptoms of depression, anxiety, and borderline personality disorder. Suicide and Life-Threatening Behavior, 35(5), 581–591. https://doi.org/10.1521/suli.2005.35.5.581
Andrews, T., Martin, G., Hasking, P., & Page, A. (2013). Predictors of continuation and cessation of nonsuicidal self-injury. Journal of Adolescent Health, 53(1), 40–46. https://doi.org/10.1016/j.jadohealth.2013.01.009
Bentley, K. H., Cassiello-Robbins, C. F., Vittorio, L., Sauer-Zavala, S., & Barlow, D. H. (2015). The association between nonsuicidal self-injury and the emotional disorders: A meta-analytic review. Clinical Psychology Review, 37, 72–88. https://doi.org/10.1016/j.cpr.2015.02.006
Black, D. W., Blum, N., Pfohl, B., & Hale, N. (2004). Suicidal behavior in borderline personality disorder: Prevalence, risk factors, prediction, and prevention. Journal of Personality Disorders, 18(3), 226–239. https://doi.org/10.1521/pedi.18.3.226.35445
Centers for Disease Control and Prevention. (2017). Leading causes of death reports. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html
Chugani, C. D. (2015). Dialectical behavior therapy in college counseling centers: Current literature and implications for practice. Journal of College Student Psychotherapy, 29(2), 120–131.
https://doi.org/10.1080/87568225.2015.1008368
Crowell, S. E., Beauchaine, T. P., & Linehan, M. M. (2009). A biosocial developmental model of borderline personality: Elaborating and extending Linehan’s theory. Psychological Bulletin, 135(3), 495–510. https://doi.org/10.1037/a0015616
Croyle, K. L., & Waltz, J. (2007). Subclinical self-harm: Range of behaviors, extent, and associated characteristics. American Journal of Orthopsychiatry, 77(2), 332–342. https://doi.org/10.1037/0002-9432.77.2.332
Daly, A., Dekker, T., & Hess, S. (2016). Dummy coding vs effects coding for categorical variables: Clarifications and extensions. Journal of Choice Modelling, 21, 36–41. https://doi.org/10.1016/j.jocm.2016.09.005
Derogatis, L. R. (1975). The SCL-90-R. Clinical Psychometric Research.
Derogatis, L. R. (1993). BSI Brief Symptom Inventory: Administration, Scoring, and Procedure Manual (4th ed.). National Computer Systems.
Derogatis, L. R., & Spencer, P. (1982). The Brief Symptom Inventory: Administration, scoring and procedures manual—1. Clinical Psychometric Research.
Dew, S. E., & Bickman, L. (2005). Client expectancies about therapy. Mental Health Services Research, 7(1), 21–33. https://doi.org/10.1007/s11020-005-1963-5
Furman, W., & Buhrmester, D. (2009). Methods and measures: The Network of Relationships Inventory: Behavioral Systems Version. International Journal of Behavioral Development, 33(5), 470–478. https://doi.org/10.1177/0165025409342634
Gratz, K. L., Conrad, S. D., & Roemer, L. (2002). Risk factors for deliberate self-harm among college students. American Journal of Orthopsychiatry, 72(1), 128–140. https://doi.org/10.1037/0002-9432.72.1.128
Halstead, R. O., Pavkov, T. W., Hecker, L. L., & Seliner, M. M. (2014). Family dynamics and self-injury behaviors: A correlation analysis. Journal of Marital and Family Therapy, 40(2), 246–259.
https://doi.org/10.1111/j.1752-0606.2012.00336.x
Heath, N. L., Ross, S., Toste, J. R., Charlebois, A., & Nedecheva, T. (2009). Retrospective analysis of social factors and nonsuicidal self-injury among young adults. Canadian Journal of Behavioural Science/Revue Canadienne des sciences du comportement, 41(3), 180–186. https://doi.org/10.1037/a0015732
Howell, D. C. (2013). Statistical methods for psychology (8th ed.). Cengage.
Joiner, T. (2005). Why people die by suicide. Harvard University Press.
Kannan, D., Chugani, C. D., Muhomba, M., & Koon, K. (2021). A qualitative analysis of college counseling center staff experiences of the utility of dialectical behavior therapy programs on campus. Journal of College Student Pychotherapy, 35(1), 1–17. https://doi.org/10.1080/87568225.2019.1620662
Kim, K. L., Cushman, G. K., Weissman, A. B., Puzia, M. E., Wegbreit, E., Tone, E. B., Spirito, A., & Dickstein, D. P. (2015). Behavioral and emotional responses to interpersonal stress: A comparison of adolescents engaged in non-suicidal self-injury to adolescent suicide attempters. Psychiatry Research, 228(3), 899–906.
https://doi.org/10.1016/j.psychres.2015.05.001
Kirkcaldy, B. D., Brown, J. M., & Siefen, G. R. (2007). Profiling adolescents attempting suicide and self-injurious behavior. International Journal on Disability and Human Development, 6(1), 75–86. https://doi.org/10.1515/IJDHD.2007.6.1.75
Klonsky, E. D. (2011). Non-suicidal self-injury in United States adults: Prevalence, sociodemographics, topography and functions. Psychological Medicine, 41(9), 1981–1986. https://doi.org/10.1017/S0033291710002497
Klonsky, E. D., & Olino, T. M. (2008). Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. Journal of Consulting and Clinical Psychology, 76(1), 22–27. https://doi.org/10.1037/0022-006X.76.1.22
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford.
Linehan, M. M., & Comtois, K. A. (1996). Lifetime parasuicide count. Unpublished manuscript, Department of Psychology, University of Washington, Seattle.
McManus, S., & Gunnell, D. (2020). Trends in mental health, non-suicidal self-harm and suicide attempts in 16–24-year-old students and non-students in England, 2000–2014. Social Psychiatry and Psychiatric Epidemiology, 55(1), 125–128. https://doi.org/10.1007/s00127-019-01797-5
Niegocki, K. L., & Ægisdóttir, S. (2019). College students’ coping and psychological help-seeking attitudes and intentions. Journal of Mental Health Counseling, 41(2), 144–157. https://doi.org/10.17744/mehc.41.2.04
Nock, M. K. (2009). Why do people hurt themselves? New insights into the nature and functions of self-injury. Current Directions in Psychological Science, 18(2), 78–83. https://doi.org/10.1111/j.1467-8721.2009.01613.x
Nock, M. K. (2010). Self-injury. Annual Review of Clinical Psychology, 6, 339–363.
https://doi.org/10.1146/annurev.clinpsy.121208.131258
Nock, M. K., & Prinstein, M. J. (2004). A functional approach to the assessment of self-mutilative behavior. Journal of Consulting and Clinical Psychology, 72(5), 885–890. https://doi.org/10.1037/0022-006X.72.5.885
Nock, M. K., & Prinstein, M. J. (2005). Contextual features and behavioral functions of self-mutilation among adolescents. Journal of Abnormal Psychology, 114(1), 140–146. https://doi.org/10.1037/0021-843X.114.1.140
Peters, J. R., Smart, L. M., & Baer, R. A. (2015). Dysfunctional responses to emotion mediate the cross-sectional relationship between rejection sensitivity and borderline personality features. Journal of Personality Disorders, 29(2), 231–240. https://doi.org/10.1521/pedi_2014_28_151
Rodham, K., & Hawton, K. (2009). Epidemiology and phenomenology of nonsuicidal self-injury. In M. K. Nock (Ed.), Understanding nonsuicidal self-injury: Origins, assessment, and treatment (pp. 37–62). American Psychological Association. https://doi.org/10.1037/11875-003
Rotolone, C., & Martin, G. (2012). Giving up self-injury: A comparison of everyday social and personal resources in past versus current self-injurers. Archives of Suicide Research, 16(2), 147–158.
https://doi.org/10.1080/13811118.2012.667333
Sadeh, N., Londahl-Shaller, E. A., Piatigorsky, A., Fordwood, S., Stuart, B. K., McNiel, D. E., Klonsky, E. D., Ozer, E. M., & Yaeger, A. M. (2014). Functions of non-suicidal self-injury in adolescents and young adults with borderline personality disorder symptoms. Psychiatry Research, 216(2), 217–222.
https://doi.org/10.1016/j.psychres.2014.02.018
Sitton, M., Du Rocher Schudlich, T., Byrne, C., Ochrach, C. M., & Erwin, S. E. A. (2020). Family functioning and self-injury in treatment-seeking adolescents: Implications for counselors. The Professional Counselor, 10(3), 351–364. https://doi.org/10.15241/ms.10.3.351
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Tuisku, V., Kiviruusu, O., Pelkonen, M., Karlsson, L., Strandholm, T., & Marttunen, M. (2014). Depressed adolescents as young adults: Predictors of suicide attempt and non-suicidal self-injury during an 8-year follow-up. Journal of Affective Disorders, 152, 313–319. https://doi.org/10.1016/j.jad.2013.09.031
Turner, B. J., Cobb, R. J., Gratz, K. L., & Chapman, A. L. (2016). The role of interpersonal conflict and perceived social support in nonsuicidal self-injury in daily life. Journal of Abnormal Psychology, 125(4), 588–598. https://doi.org/10.1037/abn0000141
Turner, B. J., Dixon-Gordon, K. L., Austin, S. B., Rodriguez, M. A., Rosenthal, M. Z., & Chapman, A. L. (2015). Non-suicidal self-injury with and without borderline personality disorder: Differences in self-injury and diagnostic comorbidity. Psychiatry Research, 230(1), 28–35. https://doi.org/10.1016/j.psychres.2015.07.058
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & Joiner, T. E., Jr. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575–600. https://doi.org/10.1037/a0018697
Whitlock, J., Eckenrode, J., & Silverman, D. (2006). Self-injurious behaviors in a college population. Pediatrics, 117(6), 1939–1948. https://doi.org/10.1542/peds.2005-2543
Whitlock, J., Muehlenkamp, J., Eckenrode, J., Purington, A., Baral Abrams, G., Barreira, P., & Kress, V. (2013). Nonsuicidal self-injury as a gateway to suicide in young adults. Journal of Adolescent Health, 52(4), 486–492. https://doi.org/10.1016/j.jadohealth.2012.09.010
Wilcox, H. C., Arria, A. M., Caldeira, K. M., Vincent, K. B., Pinchevsky, G. M., & O’Grady, K. E. (2012). Longitudinal predictors of past-year non-suicidal self-injury and motives among college students. Psychological Medicine, 42(4), 717–726. https://doi.org/10.1017/S0033291711001814
Melissa J. Sitton, MS, is a doctoral student at Southern Methodist University. Tina Du Rocher Schudlich, PhD, MHP, is a professor at Western Washington University. Christina Byrne, PhD, is an associate professor at Western Washington University. Correspondence may be addressed to Melissa J. Sitton, Department of Psychology, Southern Methodist University, P.O. Box 750442, Dallas, TX 75275-0442, msitton@smu.edu.
Jun 26, 2015 | Article, Volume 5 - Issue 3
Kathleen Brown-Rice, Susan Furr
College Greek life students self-report high rates of binge drinking and experience more alcohol-related problems than students who are not members of the Greek system. But little research has been conducted to measure differences in alcohol-free housing (dry) and alcohol-allowed housing (wet). The purpose of this quantitative study was to investigate the alcohol consumption of Greek houses (dry sorority, wet fraternity, dry fraternity). It was found that in the Greek community, university students’ scores on the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) were significantly lower for dry sorority housing members than both the wet fraternity and dry fraternity housing members, with no significant difference found between the wet and dry fraternity participants. Regardless of type, Greek-affiliated students’ drinking levels appear to be high and exceed what is considered safe on the AUDIT-C for both female and male Greek students.
Keywords: binge drinking, college students, AUDIT-C, Greek system, wet/dry housing
Throughout the literature, research findings indicate that university students affiliated with the Greek system consume more alcohol and experience more alcohol-related problems than students who are not members of the Greek system (Barry, 2007; Borsari, Hustad, & Capone, 2009; Ragsdale et al., 2012). In particular, self-reported binge drinking is significantly higher among members of this community (Barry, 2007; Chauvin, 2012; Page & O’Hegarty, 2006). Research also indicates that students who come to college with a prior drinking history may seek out venues for continuing this behavior in college, as indicated by the variable of high school binge drinking being the best predictor of Greek student binge drinking (Chauvin, 2012). Borsari et al. (2009) concluded that students who use alcohol heavily in high school may self-select into the Greek system in order to find an environment supportive of their behavior. However, it also has been found that students who join a fraternity in their first year significantly increase their drinking and alcohol-related consequences compared to those who do not join (Park, Sher, & Krull, 2008).
Consequences of Binge Drinking
There are numerous costs associated with college students engaging in binge drinking behaviors, both to the students themselves and others. It is estimated that per university, the total yearly cost of alcohol-related emergency department visits is around $500,000 (Mundt & Zakletsaia, 2012). Negative consequences of binge drinking can range in severity from a hangover to alcohol-related problems with law enforcement to suicide attempts (Gillespie, Holt, & Blackwell, 2007). Alcohol consumption among undergraduate college students contributes annually to an estimated 600,000 alcohol-related unintentional injuries, 700,000 assaults by another student who was drinking, 1,500 alcohol-related student deaths, 97,000 sexual assaults, 400,000 acts of alcohol-related unprotected sex and 100,000 incidences of being too intoxicated to know if sex was consensual (Hingson, Zha, & Weitzman, 2009). Further, it has been found that 50% of men who commit rape on college campuses were drinking at the time of the offense (Cole, 2006), and women who drink on college campuses are more likely to be the victim of a sexual assault (McCauley, Calhoun, & Gidycz, 2010).
The literature provides that college students who are members of the Greek community are at greater risk for experiencing negative consequences from heavy drinking (LaBrie, Kenney, Mirza, & Lac, 2011; Nguyen, Walters, Rinker, Wyatt, & DeJong, 2011; Soule, Barnett, & Moorhouse, 2015). Fraternity and sorority membership has been positively associated with driving after drinking (LaBrie et al., 2011) and owning a fake ID (Nguyen et al., 2011). Fraternity and sorority members reported that they were twice as likely as non-Greek college students to engage in sex with someone without getting consent and were one and a half times more likely to forget what they did or where they were after drinking (Soule et al., 2015). In fact, sorority members who binge drink are significantly more likely to be injured, drive under the influence of alcohol, be sexually victimized and engage in unwanted sex than non-Greek female binge drinkers (Ragsdale et al., 2012). Given that Greek membership and binge drinking are correlated with more severe negative consequences and that fraternity and sorority members report more peer pressure to drink (Knee & Neighbors, 2002; Young, Morales, McCabe, Boyd, & D’Arcy, 2005), it is important to consider the effect of the type of housing on college student drinking behaviors.
Alcohol-Free University Housing
Because of the influence of the Greek housing environment on drinking norms, interventions at the residential level have been cited as a strategy for reducing risky drinking levels (Borsari et al., 2009). But what happens when alcohol-free policies are implemented? Do levels of risky drinking decrease? Examining alcohol-free Greek housing in general provides a mixed picture of results. First, at colleges that only allow dry housing, students are significantly less likely to drink alcohol than students at wet schools (29.1% abstainers at dry schools versus 16.1% abstainers at wet schools). But when examining only those students who report drinking while attending colleges that ban alcohol, their drinking patterns do not differ from drinkers at non-ban schools (Wechsler, Lee, Gledhill-Hoyt, & Nelson, 2001). Overall, there are lower rates of secondhand effects of alcohol use (e.g., insults, serious arguments, property damage, interrupted sleep) at schools where alcohol is banned. In residences where both alcohol and smoking are banned, there are lower levels of drinking, but not in residences where only alcohol is banned. Wechsler, Lee, Nelson, and Lee (2001) concluded that this type of substance-free residence may help protect those students who were not heavy drinkers in high school from becoming engaged in episodic drinking in college, but it does not lower drinking levels among those who did drink heavily in high school. It appears that students who are not heavy drinkers in high school are more likely to choose substance-free housing in college.
Colleges also have attempted to establish alcohol-free events as a means of decreasing alcohol use on campus. Wei, Barnett, and Clark (2010) found that during the semester that was surveyed, less than half of the students (43.9%) attended an alcohol-free party. However, for students who attended both alcohol and alcohol-free parties, their level of alcohol consumption and intoxication was lower on the nights of the alcohol-free events versus their typical drinking nights. In another study, it was found that students drank less on days they attended alcohol-free programming than when they went to other events where alcohol was present, drinking 41% fewer drinks on the evenings of late-night planned activities (Patrick, Maggs, & Osgood, 2010).
Greek Life Housing
The question remains as to how these results apply to the Greek system. Greek housing has been found to create an enabling environment for drinking (Ashmore, Del Boca, & Beebe, 2002; Borsani et al., 2009; Glindemann & Geller, 2003; Harford, Wechsler, & Seibring, 2002; Paschall & Saltz, 2007). There has been some movement toward fraternities establishing alcohol-free housing as a means of reducing risky drinking. Sororities have a history of providing alcohol-free houses, yet members still display higher levels of drinking than students who are not members of sororities (Ragsdale et al., 2012). In general, implementation of alcohol-free housing has not been found to reduce high levels of drinking (Crosse, Ginexi, & Caudill, 2006). In a study of one national college fraternity, Caudill et al. (2006) found that chapters that implement an alcohol-free policy have almost identical drinking levels compared to chapters that do not have an alcohol-free policy. However, fraternities continue to grapple with reducing the impact of alcohol use on their chapters in terms of issues such as the deterioration of living facilities and stabilizing rising liability insurance costs through the development of guidelines for alcohol-free fraternity housing (Whipple, 2005). Thus, there is limited research on whether there are any differences in drinking behaviors based upon type of Greek housing and whether decreases in drinking occur over time.
Based on a quantitative study of an alcohol-free fraternity, Robison (2007) found that members joined for environmental factors such as cleaner living conditions, better academic conditions, the ability to separate home and party life, and friendships built on a common bond. Most of the members did drink but drank at different locations. The fraternity was able to maintain its membership through focusing on recruitment, promoting the benefits of environmental factors, providing social alternatives, focusing on brotherhood and friendship, and enforcing alcohol-related rules. Information was not provided for drinking levels, but through examining grade point average, Robinson stated that this fraternity consistently ranked in the top tier academically. However, by-products of alcohol consumption still occurred, such as disturbing the peace, vandalism and threatening behavior. In some cases, students created other opportunities for drinking, such as car bars, where members would park a car in a nearby location and drink from the car. Therefore, it would appear that dry houses have a different set of risk factors. As with some of the other descriptions of alcohol-free fraternities, information on level of drinking was not reported.
Given that Greek membership is correlated with more negative consequences when members drink (LaBrie et al., 2011; Nguyen et al., 2011; Soule et al., 2015) and that there is a lack of research determining the differences in binge drinking based upon type of Greek housing and across an academic year, the purpose of the current study was to investigate the alcohol consumption of Greek houses (dry sorority, wet fraternity, dry fraternity) for two independent samples (fall and spring semesters). It is the policy of the National Panhellenic Council that College Panhellenic planned or sponsored events be alcohol free (National Panhellenic Conference, 2015). At this university, there were no sorority houses that allowed alcohol, but the inclusion of data on the drinking patterns of female members provides another aspect of drinking patterns of those involved in the Greek community. We hypothesized that members of dry sorority houses would report lower alcohol consumption than members of wet and dry fraternity houses for both fall and spring semesters, and that members of dry fraternity houses would report lower alcohol consumption than members of wet fraternity houses for both fall and spring semesters.
Methodology
Participants and Procedures
The population for this study was students residing in Greek housing at a Midwestern university during the 2012–2013 academic year (N = 735). Recruitment of participants was conducted to obtain two independent samples in the fall semester of 2012 and the spring semester of 2013 via announcements at fraternity and sorority chapter meetings. A total of 385 Greek members living in Greek housing took part in the fall recruitment, resulting in a response rate of 50.3%. Respondents with missing or invalid data (n = 22, less than 6%) were eliminated via listwise deletion, leaving a total number of 363 participants who were classified in the fall semester group. For spring, 379 Greek members participated, resulting in a response rate of 49.5%. Respondents with missing or invalid data (n = 7, less than 2%) were eliminated via listwise deletion, leaving a total number of 372 participants classified in the spring semester group.
During regular scheduled house meetings, the first author asked participants to complete a researcher-designed survey consisting of five demographic questions (i.e., Greek house, gender, age, cultural/racial background, academic year). The Alcohol Use Disorders Identification Test-Consumption (AUDIT-C) was utilized to obtain information about participants’ alcohol use (Babor, Higgins-Biddle, Saunders, & Monteiro, 2001; Bush, Kivlahan, McDonell, Fihn, & Bradley, 1998). Prior to administration, the participants were provided with narrative and visual aids that defined one drink as one 12-ounce beer, one 8.5-ounce malt beverage, one 5-ounce glass of wine, one mixed drink containing one (1.5-ounce) shot of alcohol, or one single (1.5-ounce) shot of liquor. On the Audit-C, the following three questions assess frequency of drinking: (a) How often do you have a drink containing alcohol? (Never = 0 points, Monthly or less = 1 point, 2–4 times a month = 2 points, 2–3 times a week = 3 points, 4 or more times a week = 4 points); (b) How many drinks containing alcohol do you have on a typical day when you are drinking? (1 or 2 = 0 points, 3 or 4 = 1 point, 5 or 6 = 2 points, 7–9 = 3 points, 10 or more = 4 points); and (c) How often do you have six or more drinks on one occasion? (Never = 0 points, Less than monthly = 1 point, Monthly = 2 points, Weekly = 3 points, Daily or almost daily = 4 points). Responses to each item are scored from 0–4, generating a maximum possible score on the AUDIT-C of 12. Higher scores reflect higher intensity of drinking. For men a score of 4 or above and for women a score of 3 or above indicates hazardous drinking or an active alcohol use disorder (Bush et al., 1998). The AUDIT-C has been found to be a valid screening tool for alcohol misuse for men and women, with optimal screening thresholds for alcohol misuse among men being a score of 4 and for women a score of 3 (Bradley et al., 2007; Frank et al., 2008), and valid and reliable for assessing alcohol consumption in college students (Barry, Chaney, Stellefson, & Dodd, 2015). Prior to each administration of the survey, the purposes and procedures of the study, confidentiality of data, and participants’ rights were explained to respondents. All participants gave informed consent prior to completing the survey. All procedures were approved by the first author’s Institutional Review Board, and participants were not offered any incentive for completing the survey. Demographic information regarding participants for fall and spring semesters is provided
in Table 1.
Data Analysis
The Statistical Package for Social Sciences software (version 21) was utilized to screen and analyze the data. All statistical analyses are reported with alpha set at 0.05. Preliminary analyses were conducted to check the data for any outliers or errors, and no violations of linearity, normality and homoscedasticity were found. The frequencies of each variable were checked for minimums and maximums. Again, no errors or outliers were found.
Table 1
Demographic Variables by Group
|
Fall Semester 2012
|
Spring Semester 2013
|
|
n
|
%
|
n
|
%
|
| Greek House: |
|
|
|
|
| Sorority – Dry |
148
|
40.8
|
234
|
62.9
|
| Fraternity – Dry |
50
|
13.8
|
58
|
15.6
|
| Fraternity – Wet |
165
|
45.5
|
80
|
21.5
|
| Gender: |
|
|
|
|
| Female |
148
|
40.8
|
234
|
62.9
|
| Male |
215
|
59.2
|
138
|
37.1
|
| Age: |
|
|
|
|
| 18–20 |
268
|
73.8
|
287
|
77.2
|
| 21 and older |
95
|
26.2
|
85
|
22.8
|
| Ethnicity: |
|
|
|
|
| African American |
2
|
.6
|
5
|
1.3
|
| Asian/Pacific Islander |
3
|
.8
|
4
|
1.1
|
| Caucasian |
344
|
94.8
|
351
|
94.4
|
| Hispanic/Latino |
1
|
.3
|
2
|
.5
|
| Native American |
5
|
1.4
|
4
|
1.1
|
| Multi-Racial |
8
|
2.2
|
6
|
1.6
|
| Academic Year: |
|
|
|
|
| Freshman |
84
|
23.1
|
107
|
28.8
|
| Sophomore |
128
|
35.3
|
138
|
37.1
|
| Junior |
82
|
22.6
|
74
|
19.9
|
| Senior |
69
|
19.0
|
51
|
13.7
|
| Graduate |
0
|
0
|
2
|
.5
|
Results
For the fall semester sample, a one-way analysis of variance (ANOVA) was used to test for AUDIT-C score differences among the Greek house variable. AUDIT-C scores differed significantly across the three house categories, F(2, 360) = 39.958, p = .000. Scheffe post-hoc comparisons of the three groups indicated that the sorority dry house group (M = 5.02, 95% CI [4.60, 5.44]) had significantly lower scores than the fraternity dry house group (M = 7.94, 95% CI [7.40, 8.48]), p = .000 and the fraternity wet house group (M = 7.42, 95% CI [6.97, 7.88]), p = .000. AUDIT-C scores were not significantly different between the fraternity dry house group and the fraternity wet house group at p = .489. When looking specifically at how often participants consume six or more drinks on one occasion, significant differences were found among the Greek house variable. AUDIT-C scores differed significantly across the three house categories, F(2, 360) = 40.858, p = .000. Scheffe post-hoc comparisons of the three groups indicated that the sorority dry house group (M = 1.22, 95% CI [1.07, 1.38]) had significantly lower scores than the fraternity dry house group (M = 2. 40, 95% CI [2.17, 2.63]), p = .000 and the fraternity wet house group (M = 2.10, 95% CI [1.93, 2.26]), p = .000. Scores were not significantly different between the fraternity dry house group and the fraternity wet house group at p = .175.
When looking at the spring respondents, a one-way ANOVA showed that AUDIT-C scores differed significantly across the three Greek house categories, F(2, 369) = 9.526, p = .000. Scheffe post-hoc comparisons of the three groups indicated that the sorority dry group (M = 4.76, 95% CI [4.41, 5.11]) had significantly lower scores than the fraternity dry house group (M = 5.97, 95% CI [5.15, 6.79]), p = .011 and the fraternity wet house group (M = 6.09, 95% CI [5.48, 6.70]), p = .001. AUDIT-C scores were not significantly different between the fraternity dry house group and the fraternity wet house group at p = .967. When looking specifically at how often participants consume six or more drinks on one occasion, significant differences among the Greek house variable were found. AUDIT-C scores differed significantly across the three house categories, F(2, 369) = 10.450, p = .000. Scheffe post-hoc comparisons of the three groups indicated that the sorority dry house group (M = 1.07, 95% CI [.95, 1.19]) had significantly lower scores than the fraternity dry house group (M = 1.57, 95% CI [1.29, 1.85]), p = .002 and the fraternity wet house group (M = 1.53, 95% CI [1.30, 1.75]), p = .002. Scores were not significantly different between the fraternity dry house group and the fraternity wet house group at p = .966.
These findings supported our hypothesis that members of dry sorority houses would report lower alcohol consumption than members of wet and dry fraternity houses for both fall and spring semesters. However, the second hypothesis, that members of dry fraternity houses would report lower alcohol consumption than members of wet fraternity houses for both fall and spring, was not supported. Table 2 details Greek house scores for the three AUDIT-C questions.
Table 2
Mean Scores and Standard Deviations by Semester and Greek House Responses to AUDIT-C Questions
| Question by House |
Fall Semester 2012
|
Spring Semester 2013
|
|
|
n
|
M
|
SD
|
n
|
M
|
SD
|
| Question 1: |
|
|
|
|
|
|
| Sorority – Dry |
148 |
1.96 |
.95 |
234 |
1.76 |
.92 |
| Fraternity – Dry |
50 |
2.50 |
.71 |
58 |
2.03 |
.99 |
| Fraternity – Wet |
165 |
2.45 |
.97 |
80 |
2.21 |
.94 |
| Question 2: |
|
|
|
|
|
|
| Sorority – Dry |
148 |
1.89 |
.98 |
234 |
1.91 |
1.11 |
| Fraternity – Dry |
50 |
3.10 |
.86 |
58 |
2.36 |
1.19 |
| Fraternity – Wet |
165 |
2.87 |
1.18 |
80 |
2.35 |
1.19 |
| Question 3: |
|
|
|
|
|
|
| Sorority – Dry |
148 |
1.22 |
.97 |
234 |
1.07 |
.93 |
| Fraternity – Dry |
50 |
2.40 |
.81 |
58 |
1.57 |
1.06 |
| Fraternity – Wet |
165 |
2.10 |
1.08 |
80 |
1.53 |
1.01 |
| Total AUDIT-C: |
|
|
|
|
|
|
| Sorority – Dry |
148 |
5.02 |
.42 |
234 |
4.76 |
.35 |
| Fraternity – Dry |
50 |
7.94 |
.54 |
58 |
5.97 |
.82 |
| Fraternity – Wet |
165 |
7.42 |
.45 |
80 |
6.09 |
.61 |
Limitations
This study has four main limitations. First, this study used a convenience sample of Greek members from one university that is not likely to represent the population of all Greek members. The second limitation is that volunteers may have answered the survey questions differently than members of the population who did not agree to participate would have. Another limitation is that the samples might not be truly independent; some participants could have filled out the survey in both the fall and spring. The final limitation is related to the survey being a self-report measure; participants may have provided answers that did not represent their true behaviors. However, previous researchers have found a statistically significant relationship between college respondents’ self-reported alcohol use when compared to the report from a collateral informant (Hagman, Cohn, Noel, & Clifford, 2010; Laforge, Borsari, & Baer, 2005).
Discussion and Implications
Regardless of whether Greek houses have a dry or wet status, drinking levels appear to be high and exceed what is considered safe on the AUDIT-C for both men and women living in Greek housing. Sororities have generally had policies that prohibit alcohol use in sorority houses, yet report levels of drinking that are considered hazardous. The lack of differences in drinking levels between men who live in dry fraternity houses versus wet fraternity houses is disappointing, but not totally unexpected given previous studies (Caudill et al., 2006; Crosse et al., 2006). It appears that residents in the Greek system accept the norms of heavy drinking that are associated with Greek membership. Although members may have some benefits from living in dry houses, such as a cleaner environment and less disruption to academic performance, the risks of alcohol abuse continue.
The cross-sectional research provides the most interesting results, with a significant difference between drinking levels in the fall semester compared to the spring semester. In particular, a general linear univariate analysis revealed that the scores of the fall groups and the spring groups were significantly different, F(1,729) = 26.179, p = .000, with a significant interaction effect, F(2, 729) = 38.901, p = .005, where fraternity members, whether living in a dry or wet house, reported higher AUDIT-C scores than sorority members living in Greek housing. Because this study is not a repeated measures design, the results do not evaluate changes in individuals. It is not possible to determine whether some of the same students took the survey both semesters, but there is probably some overlap in the two populations. The one environmental change that occurred between the two assessment periods was the implementation of alcohol education programs that a majority of Greek students (75.8%) attended in the fall. We cannot determine that this educational program facilitated the decrease in risky drinking and need to further examine the possibility that continued programming about how to drink alcohol safely and the effects of acute alcohol intoxication may expand students’ knowledge and thus impact their choices. Another consideration may be football tailgating. Glassman, Dodd, Sheu, Rienzo, and Wagenaar (2010) assessed college students at one university to examine their extreme ritualistic alcohol consumption, which is defined as consuming 10 or more drinks on game day for a male, and eight or more drinks for a female. Glassman et al. found that participants who were male, White, a Greek community member and of legal drinking age reported disproportionately higher rates of alcohol consumption on game day. Although tailgating is not observed as a major event on this campus, there may be other variables that contributed to higher drinking levels in the fall semester versus the spring semester.
Directions for Future Research
This research study offers contributions and implications for professional counselors. As a result of these findings, some important considerations for future research have emerged. First, if Greek members in dry houses are engaging in risky drinking behaviors at the same degree as members in wet houses, it is important to ascertain where they are drinking since they are not allowed to drink in their residence. Consequently, examining where the drinking occurs and how the alcohol is obtained would be beneficial. If these students are selecting other avenues for drinking that may encourage risky behaviors, such as driving, then dry houses may present some additional risks that need to be addressed. Also, little is known about members of Greek organizations who live in non-Greek housing. Do these students engage in drinking patterns similar to those who live in Greek housing when they attend Greek activities? How might their drinking patterns change when involved in activities in their non-Greek setting? In addition, drinking patterns among females in the Greek system generally reflect risky drinking patterns. Even though alcohol is not permitted in the living environments of the sororities in this sample, females still drink at high levels. More investigation into the role that the interaction of fraternities and sororities plays in levels of drinking needs to conducted. The question of whether females drink more when engaged in fraternity activities needs to be addressed.
The second research consideration is related to other communities of which the Greek members may be a part. College athletes have been found to drink more alcohol and engage more often in binge drinking than non-athletes (Hildebrand, Johnson, & Bogle, 2001; Nelson & Wechsler, 2001). In fact, Huchting, Lac, Hummer, and LaBrie (2011) compared independent samples of Greek members’ and athletes’ drinking patterns and found that athletes experienced significantly greater conformity reasons for drinking (i.e., social pressures that push an individual to conform and engage in alcohol use) than Greek members. Greek members experienced significantly more social problems from drinking. However, it is unknown whether there are differences between drinking behaviors of Greek members who are athletes and those who are not. This could be important information to assist clinicians in determining where to target prevention strategies. The final research consideration relates to gaining a better understanding of how individual Greek member’s drinking patterns change over an academic year. Therefore, future studies should include identifiers for participants to determine whether individual changes occur.
Conclusion
Consistent with other research, banning alcohol in Greek housing does not appear to reduce levels of drinking. Students may benefit from alcohol-free environments for reasons other than reducing drinking, but alcohol-free environments seem to have little impact on student drinking behaviors. There may even be some concerns about the risks involved in drinking away from one’s residence such as driving while intoxicated. The larger issue around alcohol use in the Greek system is how to challenge the established drinking norms in ways that encourage students to drink safely. Helping students focus on the deeper meaning of Greek membership that promotes a sense of community and enhances the values of the fraternity or sorority may be a direction for future interventions.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ashmore, R. D., Del Boca, F. K., & Beebe, M. (2002). “Alkie,” “frat brother,” and “jock”: Perceived types of college students and stereotypes about drinking. Journal of Applied Social Psychology, 32, 885–907. doi:10.1111/j.1559-1816.2002.tb00247.x
Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., & Monteiro, M. G. (2001). AUDIT: The Alcohol Use Disorders Identification Test—Guidelines for use in primary care (2nd ed.) World Health Organization: Geneva, Switzerland.
Barry, A. E. (2007). Using theory-based constructs to explore the impact of Greek membership on alcohol-related beliefs and behaviors: A systematic literature review. Journal of American College Health, 56, 307–315. doi:10.3200/JACH.56.3.307-316
Barry, A. E., Chaney, B. H., Stellefson, M. L., & Dodd, V. (2015). Evaluating the psychometric properties of the AUDIT-C among college students. Journal of Substance Use, 20, 1–5. doi:10.3109/14659891.2013.856479
Borsari, B., Hustad, J. T. P., & Capone, C. (2009). Alcohol use in the Greek system, 1999–2009: A decade of progress. Current Drug Abuse Reviews, 2, 216–255.
Bradley, K. A., DeBenedetti, A. F., Volk, R. J., Williams, E. C., Frank, D., & Kivlahan, D. R. (2007). AUDIT-C as a brief screen for alcohol misuse in primary care. Alcoholism: Clinical & Experimental Research, 31, 1208–1217. doi:10.1111/j.1530-0277.2007.00403
Bush, K., Kivlahan, D. A., McDonell, M. B., Fihn, S. D., & Bradley, K. A. (1998). The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Archives of Internal Medicine, 158, 1789–1795.
Caudill, B. D., Crosse, S. B., Campbell, B., Howard, J., Luckey, B., & Blane, H. T. (2006). High-risk drinking among college fraternity members: A national perspective. Journal of American College Health, 55, 141–155. doi:10.3200/JACH.55.3.141-155
Chauvin, C. D. (2012). Social norms and motivations associated with college binge drinking. Sociological Inquiry, 82, 257–281. doi:10.1111/j.1475-682X.2011.00400.x
Cole, T. B. (2006). Rape at US colleges often fueled by alcohol. Journal of the American Medical Association, 296, 504–505. doi:10.1001/jama.296.5.504
Crosse, S. B., Ginexi, E. M., & Caudill, B. D. (2006). Examining the effects of a national alcohol-free fraternity housing policy. The Journal of Primary Prevention, 27, 477–495. doi:10.1007/s10935-006-0049-5
Frank, D., DeBenedetti, A. F., Volk, R. J., Williams, E. C., Kivlahan, D. R., & Bradley, K. A. (2008). Effectiveness of the AUDIT-C as a screening test for alcohol misuse in three race/ethnic groups. Journal of General Internal Medicine, 23, 781–787. doi:10.1007/s11606-008-0594-0
Gillespie, W., Holt, J. L., & Blackwell, R. L. (2007). Measuring outcomes of alcohol, marijuana, and cocaine use among college students: A preliminary test of the shortened inventory of problems– alcohol and drugs (SIP-AD). Journal of Drug Issues, 37, 549–567.
Glassman, T. J., Dodd, V. J., Sheu, J.-J., Rienzo, B. A., & Wagenaar, A. C. (2010). Extreme ritualistic alcohol consumption among college students on game day. Journal of American College Health, 58, 413–423.
Glindemann, K. E., & Geller, E. S. (2003). A systematic assessment of intoxication at university parties: Effects of the environmental context. Environment and Behavior, 35, 655–664. doi:10.1177/0013916503254751
Hagman, B. T., Cohn, A. M., Noel, N. E., & Clifford, P. R. (2010). Collateral informant assessment in alcohol use research involving college students. Journal of American College Health, 59, 82–90. doi:10.1080/07448481.2010.483707
Harford, T. C., Wechsler, H., & Seibring, M. (2002). Attendance and alcohol use at parties and bars in college: A national survey of current drinkers. Journal of Studies on Alcohol, 63, 726–733.
Hildebrand, K. M., Johnson, D. J., & Bogle, K. (2001). Comparison of patterns of alcohol use between high school and college athletes and non-athletes. College Student Journal, 35, 358–365.
Hingson, R. W., Zha, W., & Weitzman, E. R. (2009). Magnitude of and trends in alcohol-related mortality and morbidity among U.S. college students aged 18–24, 1998–2005. Journal of Studies on Alcohol and Drugs Supplement, 16, 12–20.
Huchting, K. K., Lac, A., Hummer, J. F., & LaBrie, J. W. (2011). Comparing Greek-affiliated students and student athletes: An examination of the behavior-intention link, reasons for drinking, and alcohol-related consequences. Journal of Alcohol & Drug Education, 55, 61–81.
Knee, C. R., & Neighbors, C. (2002). Self-determination, perception of peer pressure, and drinking among college students. Journal of Applied Social Psychology, 32, 522–543. doi:10.1111/j.1559-1816.2002.tb00228.x
LaBrie, J. W., Kenney, S. R., Mirza, T., & Lac, A. (2011). Identifying factors that increase the likelihood of driving after drinking among college students. Accident Analysis & Prevention, 43, 1371–1377. doi:10.1016/j.aap.2011.02.011
Laforge, R. G., Borsari, B., U., & Baer, J. S. (2005). The utility of collateral informant assessment in college alcohol research: Results from a longitudinal prevention trial. Journal of Studies on Alcohol, 66, 479–487.
McCauley, J. L., Calhoun, K. S., & Gidycz, C. A. (2010). Binge drinking and rape: A prospective examination of college women with a history of previous sexual victimization. Journal of Interpersonal Violence, 25, 1655–1668. doi:10.1177/0886260509354580
Mundt, M. P., & Zakletsaia, L. I. (2012). Prevention for college students who suffer alcohol-induced blackouts could deter high-cost emergency department visits. Health Affairs, 31, 863–870. doi:10.1377/hlthaff.2010.1140
National Panhellenic Conference. (2015). NPC policies and best practices. Retrieved from https://www.npcwomen.org/resources/pdf/College%20Panhellenic%20Policies%20and%20Best%20Practices.pdf
Nelson, T. R, & Wechsler, H. (2001). Alcohol and college athletes. Medicine & Science in Sports & Exercise, 33, 43–47.
Nguyen, N., Walters, S. T., Rinker, D. V., Wyatt, T. M., & DeJong, W. (2011). Fake ID ownership in a US sample of incoming first-year college students. Addictive Behaviors, 36, 759–761. doi:10.1016/j.addbeh.2011.01.035
Page, R. M., & O’Hegarty, M. (2006). Type of student residence as a factor in college students’ alcohol consumption and social normative perceptions regarding alcohol use. Journal of Child & Adolescent Substance Abuse, 15, 15–31. doi:10.1300/J029v15n03_02
Park, A., Sher, K. J., & Krull, J. L. (2008). Risky drinking in college changes as fraternity/sorority affiliation changes: A person-environment perspective. Psychology of Addictive Behaviors, 22, 219–229. doi:10.1037/0893-164X.22.2.219
Paschall, M. J., & Saltz, R. F. (2007). Relationships between college settings and student alcohol use before, during and after events: A multi-level study. Drug and Alcohol Review, 26, 635–644. doi:10.1080/09595230701613601
Patrick, M. E., Maggs, J. L., & Osgood, D. W. (2010). LateNight [sic] Penn State alcohol-free programming: Students drink less on days they participate. Prevention Science, 11, 155–162. doi:10.1007/s11121-009-0160-y
Ragsdale, K., Porter, J. R., Mathews, R., White, A., Gore-Felton, C., & McGarvey, E. L. (2012). ‘Liquor before beer, you’re in the clear’: Binge drinking and other risk behaviours among fraternity/sorority members and their non-Greek peers. Journal of Substance Use, 17, 323–339. doi:10.3109/14659891.2011.583312
Robison, A. (2007). Case study analysis of a college fraternity utilizing alcohol-free housing. Dissertation Abstracts International: Section A. Humanities and Social Sciences, 68(10), 4227.
Soule, E. K., Barnett, T. E., & Moorhouse, M. D. (2015). Protective behavioral strategies and negative alcohol-related consequences among US college fraternity and sorority members. Journal of Substance Use, 20, 16–21. doi:10.3109/14659891.2013.858783
Wechsler, H., Lee, J. E., Gledhill-Hoyt, J., & Nelson, T. F. (2001). Alcohol use and problems at colleges banning alcohol: Results of a national survey. Journal of Studies on Alcohol, 62, 133–141.
Wechsler, H., Lee, J. E., Nelson, T. F., & Lee, H. (2001). Drinking levels, alcohol problems and secondhand effects in substance-free college residences: Results of a national study. Journal of Studies on Alcohol, 62, 23–31.
Wei, J., Barnett, N. P., & Clark, M. (2010). Attendance at alcohol-free and alcohol-service parties and alcohol consumption among college students. Addictive Behaviors, 35, 572–579. doi:10.1016/j.addbeh.2010.01.008
Whipple, E. G. (2005). Brotherhood: Our substance of choice. Retrieved from http://www.phideltatheta.org/resources/10_year_anniversary_whitepaper.pdf
Young, A. M., Morales, M., McCabe, S. E., Boyd, C. J., & D’Arcy, H. (2005). Drinking like a guy: Frequent binge drinking among undergraduate women. Substance Use & Misuse, 40, 241–267. doi:10.1081/JA-200048464
Kathleen Brown-Rice, NCC, is an Assistant Professor at the University of South Dakota. Susan Furr is a Professor at the University of North Carolina-Charlotte. Correspondence may be addressed to Kathleen Brown-Rice, 414 E. Clark Street, Vermillion, SD 57069, kathleen.rice@usd.edu.
Sep 10, 2014 | Article, Volume 2 - Issue 1
Kylie P. Dotson-Blake, David Knox, Marty E. Zusman
Despite growing attention to the subject, a dearth of information exists regarding college students’ perceptions and process of meaning-making related to the act of oral sex. Such perspectives and allied social sexual scripts can have considerable consequences on the sexuality and sexual health of older teens and college-aged populations. The present research serves to elucidate such perspectives and presents a profile of college students’ degree of agreeing that oral sex is not sex. Over half (62.1%) of a sample of college students (N = 781) at a large southeastern university agreed that oral sex is not sex. Response rates across demographic groups are presented and factors that influence such perspectives are examined. Sexual script theory serves as the theoretical framework. Implications and limitations are explored.
Keywords: oral sex, social sexual scripts, college students, script theory, sexuality, sex counseling
Television talk show hosts, The Washington Post (Stepp, 2005) and Science Daily (University of California, San Francisco, 2005) have all had recent headlines related to oral sex in the older teen and college-aged populations. Because of these and other popular media sources, sex educators, parents and others have become more aware of oral sex engagement among college students and more concerned about the impacts of this engagement. Although society members are becoming concerned about this topic, limited information regarding college students’ perceptions and process of meaning-making related to the act of oral sex is available in the literature. To develop sexuality education curriculum and resources targeted at young people engaging in oral sex, professionals must first identify those most likely to engage in oral sex, their process of meaning-making around this engagement and risks young people are exposed to as a function of their engagement in oral sex.
In an effort to provide insight into this population’s process of meaning-making related to engagement in oral sex and initial information about characteristics of college students likely to engage in oral sex, this article presents the findings of a survey conducted at a large southeastern university. An initial profile of undergraduates who agreed with the statement “Oral Sex is Not Sex” is offered and findings are analyzed through the lens of social sexual script theory to explore the process of meaning-making related to the perceptions of participants regarding oral sex. We hope this information will assist sex educators, counselors, health professionals and parents in efforts to target individuals likely to engage in oral sex to minimize risks related to oral sex in the college student population. Thus, the purpose of this study was to provide a profile of undergraduates who agreed with the assertion that oral sex is not sex and to explore the links between participant responses and sexual scripts to illuminate fully how these participants perceived oral sex engagement. This profile is important because recent research suggests that young people perceive oral sex as safe, with few potential health risks (Halpern-Felsher, Cornell, Kropp, & Tschann, 2005). However, engaging in oral sex may expose individuals to the risk of viral and bacterial infections, including chlamydia, gonorrhea and herpes (Edwards & Carne, 1998a, 1998b). Consequently, it is critical that counselors fully understand the context and perceptions of college students in order to provide information to assist with healthy decision-making in developmentally-appropriate ways for these clients.
Theoretical Foundation
Sexual script theory situates perceptions of sexual interactions within the social context to explain how sexual identity and sexuality are shaped by social cultural messages (Frith & Kitzinger, 2001). Consequently, what is perceived to be “real” sex is defined by the society within which one exists, individual identity and socio-cultural normative sexual scripts. Sexual scripts vary across individuals, but often common elements exist within sexual scripts associated with particular cultural groups (Wiederman, 2005). As a social constructionist approach to exploring the development of sexuality, sexual script theory has been primarily used as a qualitative method of research (Simon & Gagnon, 2003). However, recent research has applied sexual script theory in quantitative research exploring the impact of exposure to sexually explicit material on young people (Stulhofer, Busko, & Landripet, 2010). For the study presented in this article, results were found using quantitative methods and then a qualitative exploration of themes that emerged from the quantitative data yielded links to sexual scripts postulated by sexual script theory.
Sexual Scripts and Heterocentric Standards
One sexual script prevalent in Western cultures, the traditional sexual script (Rostosky & Travis, 2000), serves to situate sexual intercourse between heterosexuals as real sex. This sexual script serves to disenfranchise sexual minorities by failing to recognize the full spectrum of sexual acts occurring between persons of any gender and the meanings attributed to these acts. Furthermore, not only is sex limited to heterosexual intercourse, but the concept fundamentally depends on male ejaculation since it is the male orgasm that denotes both the number of times a couple has sex and is the culmination (the climax) of sex (Frye, 1990). This phallocentric approach with regard to the concept of sex limits the power of women to be equal partners in a heterosexual relationship (Bhattacharyya, 2002). Consequently, these heterocentric standards for what qualifies as sex means that lesbians do not have real sex since lesbian sex does not involve penile penetration.
Within this sexual value system, vaginal-penile penetration/intercourse is at the apex of what constitutes sex, such that all other non-coital sexual practices/behaviors—such as oral sex—are considered foreplay and as a result have not been researched as fully and comprehensively as vaginal-penile penetration/intercourse. Much of sexual research has been situated within Western culture, resulting in the firm entrenchment of the traditional sexual script (Rostosky & Travis, 2000) within research methods and processes. This social entrenchment of heteronormative standards impacts the social sexual scripts college-aged individuals hold and apply in their sexual engagement (Bhattacharyya, 2002).
Peer groups have a strong influence on sexual behaviors, particularly among young adults. Peer group shifts in perceptions and values, when it comes to sex and sexual activity, will in turn impact sexual trends and patterns within peer groups. For college students, peer group perceptions powerfully impact individual perceptions and behaviors (Carter & McGoldrick, 1999). Prinstein, Meade, and Cohen (2003) discerned a positive relationship between young people’s reports of oral sex engagement and peer popularity. This suggests that peer culture for college students supports oral sex practice.
Peer group perceptions are formed within the context of the larger society and events, media and social issues within the society. One such societal event relevant to this discussion is the Clinton-Lewinsky scandal. At the heart of the scandal is Clinton’s famous utterance, “I did not have sexual relations with that woman, Miss Lewinsky” (Clinton, 1998). Whether his perception of oral sex as not real sex is due more to his personal perception based upon the traditional sexual script (Rostosky & Travis, 2000) or Clinton’s cunning sense of self-preservation will never be known. What is known, however, is that his statement and the subsequent maelstrom of controversy that ensued solidly asserted the question: “Is oral sex really sex?” into the public domain for debate.
Prevalence of Oral Sex Engagement in Young Adult and College-Age Population
In 2002, as part of the National Survey of Family Growth, 10,208 people ages 15–19 were included in the overall sample, and, of these respondents, more than half of males (55%) and females (54%) reported engaging in oral sex (Mosher, Chandra, & Jones, 2005). Richters, de Visser, Rissel, & Smith (2006) analyzed data from the Australian Study of Health and Relationships from a representative sample of 19,307 Australians aged 16 to 59 and found that almost a third (32%) of the respondents reported that oral sex was included in their last sexual encounter. Similarly, in a study of 212 participants ranging in age from 15 to 17, Prinstein, Meade, and Cohen (2003) reported that a third of the males and half of the females had engaged in oral sex in the past year. These studies reveal that many of the college-aged population are engaging in oral sex.
Oral Sex Scripts and Pop Culture
As dialogue about oral sex entered contemporary popular culture, it also became mainstreamed into the young adult vernacular and embedded into the tapestry of social mores and norms. Sexual script theory (Gagnon & Simon, 1973) emphasizes that social norms play a significant role in governing college students’ processes of meaning-making regarding health information and subsequent health and sexual behaviors. This theory holds at its foundation the understanding that sexuality is borne from cultural norms and messages that define what is deemed sex and socially-appropriate responses in sexual situations and encounters (Frith & Kitzinger, 2001).
In considering the impact of culturally-laden sexual norms and social sexual messages, one may infer that as oral sex has entered contemporary discourse, the social norms emerging from this discourse have impacted college students’ perceptions of and participation in oral sex. Understanding this process of social norm-belief-behavior interaction and possible consequences, including sexually transmitted infections (STIs), is critically important for sex educators, counselors and therapists working with the college-aged population, as these clients have intense levels of interactions with peers attuned to contemporary popular culture.
Young Adults and Sexually Transmitted Infections
Researchers also have found that young people are increasingly experiencing high rates of sexually transmitted infections (STIs) (Prinstein, Meade, & Cohen, 2003). According to the Centers for Disease Control and Prevention (2006), females who are 15–19 years of age reported the highest rates of all other demographic groups for chlamydia and gonorrhea. Of the 19 million STIs reported each year in the U.S., Weinstock, Berman, and Cates (2004) estimated that almost 50% occur in individuals who are 15–24 years of age. From these high rates of STIs in the young adult population, it can be inferred that more education around protection and safe sex engagement is necessary. Recent research has shown that young people also are concerned about the need for safety in sexual engagement and as such have turned to oral sex because they feel it presents fewer health risks (Halpern-Felsher, Cornell, Kropp, & Tschann, 2005). However, oral sex also presents risks of STIs. In a summary of research over more than 35 years regarding oral sex as a possible means of transmitting STIs, Edwards and Carne (1998a, 1998b) noted that oral sex may transmit viral and bacterial infections, including gonorrhea, chlamydia and herpes. Consequently, college students need to be educated about the risks of STI transmission through oral sex to minimize the harmful consequences.
The Need to Explore Perceptions of Oral Sex
In view of the various studies reporting the frequency and consequences of oral sex among young adults and college students, we emphasize the importance of educating this population about safe practices related to oral sex. A first step in this process is to assess the perceptions of this population in regard to oral sex. In short, though the research suggests that this population is engaging in oral sex (Prinstein, Meade, & Cohen, 2003), little is known about how they perceive the act and what meaning they attribute to the behavior in terms of their sense of self and sexual identity development. How do college students perceive oral sex? Do they perceive it to be real (i.e., intercourse) sex? How does it shape a young adult’s sense of self? Do college students feel that by engaging in oral sex and other non-coital behaviors that they are practicing a form of abstinence, that they are maintaining their virginity? Finding the answers to these questions may assist sex educators, counselors and therapists in developing comprehensive sexuality education programs incorporating resource awareness, prevention and health-focused knowledge for this population (Bay-Cheng, 2003).
In an effort to begin to address these questions and process, this article presents the findings of a study exploring the perceptions and behaviors of college students regarding oral sex. The purpose of the research was to identify a profile of undergraduates who agree with the assertion oral sex is not sex. This profile can be used to identify college students who may be more likely to engage in oral sex, allowing clinicians and educators to plan and implement developmentally-appropriate measures in contexts most likely to reach this population. An exploration of the intersection of social norms, utilizing sexual script theory, with characteristics prevalent in the profile that emerged will be discussed, as well as the implications and limitations of the study.
Sexual Script Theory and Perceptions of Oral Sex
By exploring research focused on oral sex engagement, the college-aged population and prevalent social sexual scripts, one may make significant inferences regarding this population’s perceptions of oral sex and process of meaning-making related to this sexual act. Again, it is important that the authors note that sexual scripts are based upon individual experience and social engagement and as such are impacted by the intersecting identity characteristics of individuals. Sexual scripts are reflective of culture and thus some elements will be common to members of the identified cultural group to which the script refers (Geer & Broussard, 1990). However, personal identity is multi-faceted and individuals belong to many different cultural groups by the nature of their race, ethnicity, religion, social class, sexual identity, education status, etc. Consequently, there may be wide variation in sexual scripts across individuals, even within a specific cultural group or sub-group (Wiederman, 2005).
Remaining cognizant of the diversity of sexual scripts across cultural groups, the authors will lead an exploration of selected dominant sexual scripts that may impact college-aged individual’s perceptions of and engagement in oral sex in the U.S. This exploration is not intended to be exhaustive; it is simply meant to serve as a foundation for understanding the potential of sexual scripts to impact these individuals’ processes of meaning-making related to oral sex. Finally, the authors recognize that sex extends far beyond penile penetration of a vagina. Unfortunately, the majority of research findings gleaned from a comprehensive review of the professional literature promote heteronormative standards by focusing solely on sex as the act of sexual intercourse between individuals of different genders. Consequently, the discussion of current professional research is limited in scope, indicating the need for additional research exploring the full range of sexual activities and sexual scripts impacting young adults and the college student population of any gender and sexuality.
Perception One: Oral Sex is Safe
The current professional literature suggests that young adults and college students articulate diverse reasons for engagement in oral sex. A reason that emerges dominantly from multiple studies is the perception that oral sex is safe with minimal risk and consequence (Halpern-Felsher et al., 2005; Remez, 2000). In a study of ninth-graders in California, participants were unlikely to use barrier protection when engaging in oral sex (Halpern-Felsher et al., 2005), indicating that they felt the practice of oral sex carried minimal risk for STIs. Possibly contributing to adolescent and teen perceptions of oral sex as safe are the sex education programs to which this population is exposed. Data suggest that abstinence-only and faith-based sex education programs do little to educate young adults on the very real and possible dangers associated with oral sex—i.e., the spread of STIs (Lindau, Tetteh, Kasza, & Gilliam, 2008). This lack of information may lead to the perception that because risks related to oral sex are not talked about, it must be safe. Surveys find that most young adults are misinformed, in that they are taught that STI risks are only associated with vaginal-penile intercourse. In sum, we surmise that these sex education programs, shifts in societal perceptions of and sexual scripts related to oral sex, and the use of oral sex as a substitute for intercourse may have a strong effect on the perceptions of the college age population reflecting that oral sex is safe sex.
Perception Two: Oral Sex Mitigates Religiosity and Sex Guilt Tension
Studies have shown strong correlations between degree of religiosity and patterns of sexual behavior. Kinsey, Pomeroy and Martin (1948, 1953) were some of the first to show empirically that religious identification limits sexual behaviors among the unmarried. Schulz, Bohrnstedt, Borgatta, and Evans (1977) also found that religiosity had a significant inhibiting effect on sexual behavior for both men and women. A study conducted by Wulf, Prentice, Hansum, Ferrar, and Spilka (1984) examined the sexual attitudes and behaviors among evangelical Christian singles, and found overall a more conservative outlook in sexual beliefs compared to the cultural norms. Of this group, those that were intrinsically faithful—that is, the more intensely religious who had a strong identification with traditional Christian values—and were not involved in a relationship, displayed the most conservative sexual attitudes. Among the more devout and single, the strongest correlations were found with respect to premarital intercourse and oral sex, in that these individuals were least likely to have engaged in these two activities.
Numerous studies have shown strong relationships between religiosity and sex guilt (Langston, 1973; Mosher & Cross, 1971). Those with conventional religious beliefs are more likely to have sex guilt, which in turn inhibits sexual behavior (Sack, Keller & Hinkle, 1984). Individuals with sex guilt are more absolutist in their orientations to sex and are less sexually active, since transgressing these strict sexual parameters might elicit intense displeasure and an antagonistic relationship with their religious community. By perceiving oral sex as not real sex, young adults and college students may be able to mitigate the tension between religious beliefs and sex guilt. For instance, a meta-analysis of studies looking at sexual attitudes and practices among young adults found that a majority believe oral sex to be less intimate compared to intercourse and that oral sex does not spoil virgin status (Remez, 2000). Many abstinence-only and faith based sex education programs now include a new push for virginity pledges, reinforcing the notion that vaginal intercourse is what is most at stake when it comes to preserving one’s virgin status.
Perception Three: Oral Sex Requires Less Commitment
Studies examining sexual attitudes and practices have found that sexual experience seems to be associated with a more liberal orientation to sex. This more liberal orientation to sex has been linked with “hooking up,” defined as having sex with someone one has just met (Richey, Knox, & Zusman, 2009). Paul, McManus, and Hayes (2000) examined the hookup culture within a college setting. They found that students high on impulsivity had a more noncommittal orientation with regard to relationships, displayed a high level of autonomy, and were much more likely to engage in both coital and non-coital hookups.
Social scripts are shared interpretations and have three functions: to define situations, name actors, and plot behaviors. For example, the social sexual script operative between two college students who are hooking up is to define the situation (a hookup, not a relationship where they will see each other tomorrow), name the actors (male and female college students out to meet someone for an evening of fun), and plot behaviors (go back to one’s dorm room or apartment, fool around, and not see each other again.). This hookup process leads to lessened intimacy and expectations for commitment in sexual encounters. Related to oral sex, findings (Halpern-Felsher et al., 2005) show that among teens and the college-aged population, oral sex is used as a substitute for vaginal-penile intercourse and as such may take the place of vaginal-penile intercourse in heterosexual hookup events. This perception of oral sex as less intimate by the college-aged population stands in contrast to perceptions of older adults, particularly older women, who view oral sex as equally intimate (or more so) to vaginal sex (Remez, 2000).
Perception Four: Oral Sex is Not Sex
The authors posit that each of the preceding sexual scripts is subsumed by an over-arching sexual script prevalent within the college-aged population: oral sex is not sex. By positioning oral sex as a less risky, less intimate sex practice that allows one to maintain his/her virginity with minimal religion-based sex guilt, the college-aged population may not identify oral sex as real sex. According to Remez (2000), peer culture socializes young adults to perceive oral sex as abstinence, allowing one to maintain and protect one’s virginity. Many factors related to contemporary social sexual scripts for oral sex support the assertion that the college-aged population does not identify oral sex as sex, including beliefs that oral sex does not impact their virgin status, is thought to be less dangerous, is less likely to lead to deterioration in the student’s reputation, and leads to less guilt than vaginal-penile penetration (Hollander, 2005).
All of the aforementioned sexual scripts contribute to the perceptions of college-aged individuals regarding oral sex. By raising awareness of the social sexual scripts, we hope to illuminate the process of meaning-making college-aged individuals attach to the act of oral sex. Further illumination of specific characteristics aligned with the over-arching social sexual script of oral sex is not sex will allow sex educators, counselors and others to target initiatives aimed at reducing risks related to oral sex in a more intentional, focused effort on individuals within the college-aged population who are most vulnerable to those risks.
Method
Sample
The data for this study were taken from a larger nonrandom sample of 781 undergraduates at a large southeastern university who answered a 100-item questionnaire (approved by the Institutional Review Board of the university) on “Sexual Attitudes and Behaviors of College Students.” Respondents completed the questionnaire anonymously (the researcher was not in the room when the questionnaire was completed and no identifying information or codes allowed the researcher to know the identity of the respondents). Listwise deletion was used to address issues of missing data and two participants were excluded from statistical calculations due to missing data.
Measures
The measure used to collect data was a 100-item survey developed by Knox and Zussman (2007): Sexual Attitudes and Behaviors of College Students. The survey was developed based on a review of the professional literature related to sexuality among undergraduates. For the purpose of this research, demographic characteristics including gender, race, age and class level and the survey domains of sexual practices, religious identification and sexual values were included in the analysis. Within the domain of sexual practices were items asking participants to respond to whether they have given or received oral sex. Items surveying participants’ perceptions of themselves as religious and their beliefs about the importance of marrying someone of their same religion were included in the domain of religious identification. The domain of sexual values included items asking participants to choose the sexual value of absolutism, relativism, or hedonism, that best described their sexual values, and items asking participants to indicate their willingness to have sex without love.
Data Analysis
Data analysis was conducted using SPSS 17.0. Pearson product moment correlations and non-parametric statistics including cross-classification and Chi Squares were calculated to assess relationships among demographic characteristics and the selected domains. Following the quantitative analysis, themes within the results were explored through the lens of sexual script theory.
Results
Analysis of the data revealed several relationships that may be related to the dominant social sexual scripts affecting teen and college-aged individual’s engagement in oral sex. The majority of participants (62%) indicated their agreement with the statement that oral sex is not sex. In comparing the characteristics of those who agreed and disagreed, five statistically significant relationships emerged. Through statistical analysis of the responses, a profile of participants who asserted that oral sex is not sex emerged. Of the respondents, 76.4% were females and 25.4% were males. Racial background included 79.5% European American, 15.7% Blacks (respondent self-identified as African-American Black, African Black, or Caribbean Black), 1.9% Biracial, 1.7% Asian, and 1.3% Hispanic. The majority, (95%) of the sample identified as heterosexual, 2.9% identified as bisexual and 2% identified as homosexual. The mean age of the sample was 19 years-old.
Underclassmen-Freshmen & Sophomores
Freshmen and sophomores were the most likely to agree that oral sex does not take away one’s virginity, with the majority of freshmen and sophomores indicating their agreement that engaging in oral sex does not constitute having sex (see Table 1). Juniors and seniors were less likely than underclassmen to agree that oral sex is not having sex. Hence, there was a general pattern that the lower the class rank of the student, the more likely the student to hold the belief that he or she could have oral sex and remain a virgin.

European American
Race was significantly related to perceptions of oral sex as not being sex (see Table 2). European American undergraduates were more likely than Blacks (respondent self-identified as African-American Black, African Black, or Caribbean Black) to agree that oral sex is not sex. In this study, the limited number of Asian and Latino participants renders the data of minimal use, however 61.5% of Asian participants (N=13) and 70% of Hispanic participants (N=10) indicated that they agreed that oral sex is not sex.

Self-Identified as Religious
Students who noted that they considered themselves to be religious by indicating that they agreed or strongly agreed with the statement, “I am a religious person,” were more likely to agree that oral sex is not sex than students who reported that they were not religious at all (61.3% vs. 14.3%). Participant responses revealed an inverse relationship between self-identification as “a religious person” and having never “given oral sex to a partner,” r(4) = -.121, p = .001, and having “never received oral sex,” r(4) = -.099, p = .006. An inverse relationship between perceptions of the importance of marrying someone with the same religious identification as oneself and giving and receiving oral sex respectively also was noted, r(4) = -.114, p = .001 and r(4) = -.129, p = .000. Participants who identified as religious were thus more likely to agree that oral sex is not sex and also indicated that they have engaged in oral sex.
Sexual Value
Given the alternative sexual values of relativism (“the appropriateness of intercourse depends on the nature of the relationship”), absolutism (“no intercourse before marriage”) and hedonism (“if it feels good, do it”), students who self-identified as hedonistic were more likely than those who viewed themselves as relativists and absolutists to agree that oral sex is not sex (65.8% vs. 62.9%, and 48.0%) (p < .05). Expressed another way, over 50% of absolutists compared to 34% of hedonists say the idea that one is still a virgin after having oral sex is not true. This 16% difference is striking. Participants who reported having engaged in sex without love also indicated they had engaged in both giving and receiving oral sex r(2) = -.229, p = .000, and r(2) = -.206, p =.000. These findings reflect that students who express more hedonistic perspectives are more likely to agree that oral sex is not sex and does not impact one’s status as a virgin.
Safe Sex Practices
A significant inverse relationship existed between participants who reported requiring the use of a condom before intercourse and never having given oral sex (r(4) = -.120, p = .001), and never having received oral sex (r(4) = -.092, p = .010). These findings indicate that the participants from this study who engaged in oral sex also used protective methods when engaging in intercourse outside of oral sex.
Gender
Gender was not significantly related to participant perceptions of oral sex as not being real sex and sex only referring to sexual intercourse. Gender was, however, significantly related to having never given oral sex χ2 (1, N = 781) = 3.843, ρ = .05) and having never received oral sex χ2 (1, N = 781) = 4.016, =.045), with males indicating in greater levels than females that they have received oral sex, and also that they have never given oral sex. These findings indicate that the gendered experiences of giving and/or receiving oral sex are important to explore, because it appears from the participant responses in this study that there may be gender differences in the likelihood of an individual giving or receiving oral sex.
Discussion
This research sought to gain information about college-aged individuals most likely to agree that oral sex is not sex and to share information about individuals within this population’s perceptions about engagement in oral sex. The results allowed for the development of a demographic profile of participants who agreed that oral sex is not sex. In considering the results and demographic profile of participants who agreed that oral sex is not sex, relationships between sexual scripts and participant responses emerged.
The demographic profile which emerged indicated that participants most likely to agree that oral sex is not sex were underclassmen (freshmen and sophomores), European American and self-identified as religious. Inferences from the results were made through a parallel exploration of sexual scripts and the quantitative data from the studied domains and the demographic profile.
Oral Sex is Safe
The negative relationship that emerged between requiring the use of contraception before intercourse and engagement in oral sex may have many meanings. From the limited information provided through this analysis concerning safe sex practices and perceptions of oral sex, few inferences regarding the relationship between these issues can be made. Although the literature would suggest that college-aged students believe oral sex to be safe, this study did not provide enough information to definitively make this inference. However, the negative relationship between participants who required the use of contraception and previous experience with oral sex indicated that participants with previous experience giving and receiving oral sex were more likely to require the use of a condom before intercourse than were participants with no prior experience giving and receiving oral sex. From this finding, it could be inferred that participants who engage in oral sex are more likely to engage in safe sex practices, aligning congruently with the social sexual script posited in the professional literature of the perceptions that oral sex is safe. However, there could be many contributing factors to this relationship and further study is necessary to make clear inferences.
Oral Sex Potentially Mitigates Religiosity and Sex Guilt Tension
Supporting the sexual script that oral sex mitigates sex guilt because it is not real sex, the findings of this study discerned a strong relationship between religious identification and engagement in oral sex. Participants who reported strong self-identification as religious also reported having engaged in giving and receiving oral sex. Additionally, a significant relationship existed between participant responses to “I am a religious person” and “oral sex is not sex” χ2 (4, N = 781) = 10.310, p = .036). Other studies have shown that teens and young adults engage in oral sex because they view it as something that they do before they are ready to have sex (Remez, 2000). This of course implies that the only thing that counts as sex is vaginal-penile intercourse, and that this type of sexual activity breaks the threshold of virgin status.
These findings are not enough to conclude fully that oral sex is used to mitigate sex guilt-religiosity tension. However, the findings do suggest that college students who view themselves as religious also engage in oral sex, indicating that oral sex may be viewed as less likely to violate religious mores related to sexual engagement, since it is not viewed as real sex.
Oral Sex Requires Less Commitment
Perceptions of oral sex as less intimate and requiring less commitment may be better understood by exploring the class level, racial and sexual value components of the profile that emerged. Students at the beginning of their college careers, freshman and sophomores, were more likely to agree that oral sex is not sex. Developmentally, individuals at more advanced stages of one’s college career, such as juniors and seniors, may be more likely to be searching for a life-partner for a more committed, intimate relationship than students at the beginning of the college experience. By engaging in sexual acts perceived by this population as not real sex, these participants are able to avoid more deeply committed relationships.
In terms of racial background and the perception of oral sex as requiring less commitment, previous researchers have revealed that European Americans are more likely to engage in oral sex. In a national sample, 81% of European American men, 66% of African American men, and 65% of Latino men reported ever having received fellatio (Mahay, Laumann, & Michaels, 2001). Of European American, Latino and African Americans receiving fellatio, 82%, 68%, and 55%, respectively, reported the experience as “appealing” (Mahay et al., 2001). In the same study, 75% of European American women, 56% of Latina women, and 34% of African American women reported ever having provided fellatio for a male partner. Of European American, Latina and African American women providing fellatio, 55%, 46% and 25%, respectively, regarded the experience as “appealing” (Mahay et al., 2001). Mahay’s findings suggest that European Americans are more willing to engage in oral sex because they view it as less intimate, involved, or serious (Mahay et al., 2001). Like deep kissing or manual stimulation, they may perceive it as not sex. In contrast, African Americans may view oral sex as more “intimate, involved, and serious” and hence would be more likely to agree that oral sex is sex. The findings of this study support Mahay’s findings with European Americans being statistically more likely than African Americans to agree that oral sex is not sex.
Indicated sexual values also were related to the sexual script of oral sex as requiring less commitment. Participants who self-identified as hedonists (65.8%), with an if it feels good do it approach to sex, also agreed with the assertion that oral sex is not sex and will allow one to maintain virgin status. Since persons who “hookup” and had sex without love are more likely to be hedonists, it also is not surprising that students who reported that they had experienced having sex without love were more likely to report having engaged in giving and receiving oral sex. These findings support Young’s (1980) analysis of college students’ behaviors and attitudes relative to oral-genital sexuality, which revealed that college students who engaged in oral sex, had experienced sexual intercourse and were sexually active, possessed more favorable attitudes toward oral-genital sexual engagement.
In conclusion, Chambers (2007) studied college students and found agreement with oral sex is not sex, that oral sex is less intimate than sexual intercourse, and that the interpersonal context for being most comfortable about engaging in oral sex is a committed relationship, not a married relationship. Similarly, in the current study, we found that more than 60 percent of the respondents (62.1%) agreed that oral sex is not sex. Specifically, 62.1% responded “yes” to the statement “Having sex is having sexual intercourse, not having oral sex.” In contrast, 37.9% responded “no” to the statement.
Implications
Recognizing undergraduates who are more likely to agree with the assertion that oral sex is not sex will enable counselors and sex educators to provide targeted, specific education experiences to this population. This study revealed that undergraduates who were European American, religious, and underclassmen were more likely to agree that oral sex is not sex. However, although certain statistical differences existed among participants who believed that oral sex is not sex, over 60% of the total participant group in this study agreed that oral sex allows one to maintain one’s virgin status because it is not sex. This indicates that we do need specific targeted sex education opportunities for those most likely to agree that oral sex is not sex, but we also need broad, far-reaching education opportunities for the rest of the college-age population. Furthermore, this study explored the impact of dominant social sexual scripts on college-aged students’ perceptions of oral sex. By understanding the potential of social sexual scripts to ascribe meaning to an act of sexual engagement, sex educators and counselors will be better prepared to engage in discourse with young adults and college-aged individuals in a timely, developmentally-appropriate manner.
Limitations
The data for this study should be interpreted with caution. The data used in this study were pulled from a convenience sample of 781 undergraduates at one southeastern university. This sample cannot be considered representative of the total college-aged population in the U.S. However, it may provide some information from which larger, more representative studies can be developed.
A major limitation of this study is the lack of diversity within the sample. With small numbers of gay, lesbian and bisexual participants, it was impossible to discern the perceptions and likelihood for engagement in oral sex by this demographic segment of the college-aged population. The literature would suggest that college students identifying as gay, lesbian or bisexual may have unique perceptions of oral sex and processes for making meaning of this experience (Feldmann & Middleman, 2002). Unfortunately, this study had limited participants identifying as gay, lesbian or bisexual and did not fully explore this population’s experiences and perceptions. This is a major limitation of this research and should be addressed by additional research specifically exploring the perceptions and engagement of college-aged individuals who identify as gay, lesbian or bisexual in giving and receiving oral sex. Additionally, there were few individuals of Latino or Asian descent included in the sample, limiting the utility of the findings with these individuals.
Another significant limitation of the study was the lack of in-depth exploration about the gendered experience of giving and receiving oral sex. From the initial results, it was determined that a significant relationship existed between gender and giving and/or receiving oral sex. This is an important consideration to explore, particularly when considering the impact of social sexual scripts on the sexual engagement of young people. It is quite possible that males and females in the young adult and college-aged population have very different experiences with and perceptions of the process of engaging in oral sex. This is an area that needs further research and not including a thorough investigation of the impact of gender on the responses of participants was a limitation of this study.
References
Bay-Cheng, L. Y. (2003). The trouble of teen sex: The construction of adolescent sexuality through school-based sexuality education. Sex Education, 3, 61–74. doi:10.1080/1468181032000052162
Bhattacharyya, G. (2002). Sexuality and society. New York, NY: Routledge.
Carter, B., & McGoldrick, M. (Eds.). (1999). The expanded family life cycle: Individual, family, and social perspectives (3rd ed). Boston, MA: Allyn & Bacon.
Centers for Disease Control and Prevention, Division of Sexually Transmitted Diseases. (2006). Trends in reportable sexually transmitted diseases in the United States, 2005. Retrieved from http://www.cdc.gov/STD/STATS/trends2006.htm.
Chambers, W. C. (2007). Oral sex: Varied behaviors and perceptions in a college population. Journal of Sex Research, 44, 28–42. doi:10.1207/s15598519jsr4401_4
Clinton, W. J. (1998). Response to the Lewinsky allegations. Miller Center of Public Affairs, University of Virginia. Retrieved March 9, 2009 from http://millercenter.org/scripps/archive/speeches/detail/3930.
Edwards, S., & Carne, C. (1998a). Oral sex and the transmission of non-viral STIs. Sexually Transmitted Infections, 74, 95–100. doi:10.1136/sti.74.2.95
Edwards, S., & Carne, C. (1998b). Oral sex and the transmission of viral STIs. Sexually Transmitted Infections, 74, 6–10. doi:10.1136/sti.74.1.6
Feldmann, J., & Middleman, A. B. (2002, October). Adolescent sexuality and sexual behavior. Current Opinion in Obstetrics & Gynecology, 14(5), 489–493.
Frith, H., & Kitzinger, C. (2001). Reformulating sexual script theory: Developing a discursive psychology of sexual negotiation. Theory and Psychology, 11, 209–232. doi:10.1177/0959354301112004
Frye, M. (1990). Lesbian sex. In J. Allen (Ed.), Lesbian philosophies and cultures (pp. 305–315). New York, NY: State University of New York Press.
Gagnon, J. H., & Simon, W. (1973). Sexual conduct: The social sources of human sexuality. Chicago, IL: Aldine.
Geer, J. H., & Broussard, D. B. (1990). Scaling heterosexual behavior and arousal: Consistency and sex differences. Journal of Personality and Social Psychology, 58, 664–671. doi:10.1037/0022-3514.58.4.664
Halpern-Felsher, B. L., Cornell, J. L, Kropp, R. Y., & Tschann, J. M. (2005). Oral versus vaginal sex among adolescents: Perceptions, attitudes and behavior. Pediatrics, 115, 845–851. doi:10.1542/peds.2004-2108
Hollander, D. (2005). Many young teenagers consider oral sex more acceptable and less risky than vaginal intercourse. Perspectives on Sexual and Reproductive Health, 37(3), 155–157. doi:10.1111/j.1931-2393.2005.tb00051.x
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1953). Sexual behavior in the human female. Philadelphia, PA: Saunders.
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1948). Sexual behavior in the human male. Philadelphia, PA: Saunders.
Langston, R. D. (1973). Sex guilt and sex behavior in college students. Journal of Personality Assessment, 37, 467–472.
Lindau, S. T., Tetteh, A. S., Kasza, K., & Gilliam, M. (2008). What schools teach our patients about sex: Content, quality and influences on sex education. Obstetrics & Gynecology, 111(2) Part 1, 256–266.
Mahay, J., Laumann, E. O., & Michaels, S. (2001). Race, gender, and class in sexual scripts. In E. O. Laumann & R. T. Michael (Eds.), Sex, love, and health in America: Private choices and public policies (pp. 197–238). Chicago, IL: University of Chicago Press.
Mosher W. D., Chandra A., & Jones J. (2005). Sexual behavior and selected health measures: Men and women 15–44 years of age, United States, 2002. Advance data from vital and health statistics; no 362. Hyattsville, MD: National Center for Health Statistics.
Mosher, D. L., & Cross, H. J. (1971). Sex guilt and premarital sexual experiences of college students. Journal of Consulting and Clinical Psychology, 36, 22–32. doi:10.1037/h0030454
Paul, E., McManus, B., & Hayes, A. (2000). “Hookups”: Characteristics and correlates of college students’ spontaneous and anonymous sexual experiences. The Journal of Sex Research, 37, 76–88. doi:10.1080/00224490009552023
Prinstein, M. J., Meade, C. S., & Cohen, G. L. (2003). Adolescent oral sex, peer popularity, and perceptions of best friends’ sexual behavior. Journal of Pediatric Psychology, 28, 243–249. doi:10.1093/jpepsy/jsg012
Remez, L. (2000). Oral sex among adolescents: Is it sex or is it abstinence? Family Planning Perspectives, 32, 298–304. doi:10.2307/2648199
Richey, E., Knox, D., & Zusman, M. (2009). Sexual values of 783 undergraduates. College Student Journal, 43, 175–180.
Richters, J., de Visser, R., Rissel, C., & Smith, A. (2006). Sexual practices at last heterosexual encounter and occurrence of orgasm in a national survey. Journal of Sex Research, 43, 217–226. doi:10.1080/00224490609552320
Rostosky, S. S., & Travis, C. B. (2000). Menopause and sexuality: Ageism and sexism unite. In C. B. Travis & J. W. White (Eds.), Sexuality, society, and feminism (pp. 181–209). Washington, DC: American Psychological Association. doi:10.1037/10345-008
Sack, A., Keller, J., & Hinkle, D. E. (1984). Premarital sexual intercourse: A test of the effects of peer group, religiosity, and sexual guilt. The Journal of Sex Research, 20, 168–185. doi:10.1080/00224498409551215
Schulz, B., Bohrnstedt, G. W., Borgatta, E. R., & Evans, R. R. (1977). Explaining premarital sexual intercourse among college students: A causal model. Social Forces, 56, 148–165. doi:10.2307/2577418
Simon, W., & Gagnon, J. H. (2003). Sexual scripts: Origins, influences and changes. Qualitative Sociology, 26, 491–497. doi:10.1023/B:QUAS.0000005053.99846.e5
Stepp, L. S. (2005, September 16). Study: Half of all teens have had oral sex. The Washington Post, p. A07.
Stulhofer, A., Busko, V., & Landripet, I. (2010). Pornography, sexual socialization, and satisfaction among young men. Archives of Sexual Behavior, 39, 168–178. doi:10.1007/s10508-008-9387-0
University Of California, San Francisco (2005, April). Teens believe oral sex is safer, more acceptable to peers. ScienceDaily. Retrieved May 10, 2009, from http://www.sciencedaily.com/releases/2005/04/050411135016.htm.
Weinstock H., Berman S., & Cates W. (2004). Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspectives on Sexual and Reproductive Health, 36, 6–10. doi:10.1363/3600604
Wiederman, M. W. (2005). The gendered nature of sexual scripts. The Family Journal, 13, 496–502. doi: 10.1177/1066480705278729
Wulf, J., D., Prentice, D., Hansum, D., Ferrar, A., & Spilka. B. (1984). Religiosity and sexual attitudes and behaviors among evangelical Christian singles. Review of Religious Research, 26(2), 119–131. doi:10.2307/3511697
Young, M. (1980). Attitudes and behavior of college students relative to oral-genital sexuality. Archives of Sexual Behavior, 9, 61–67. doi:10.1007/BF01541401
Kylie P. Dotson-Blake, NCC, is an Assistant Professor and David Knox is a Professor at East Carolina University. Marty E. Zusman is Professor Emeritus at Indiana University Northwest. Correspondence can be addressed to Kylie P. Dotson-Blake, East Carolina University, 706 River Hill Drive, Greenville, NC 27858, blakek@ecu.edu.
