Oct 31, 2023 | Volume 13 - Issue 3
Byeolbee Um, Lindsay Woodbridge, Susannah M. Wood
This content analysis examined articles on international counseling students published in selected counseling journals between 2006 and 2021. Results of this study provide an overview of 18 articles, including publication trends, methodological designs, and content areas. We identified three major themes from multiple categories, including professional practices and development, diverse challenges, and personal and social resources. Implications for counseling researchers and counselor education programs to increase understanding and support for international counseling students are provided.
Keywords: international counseling students, counseling journals, content analysis, publication trends, counseling researchers
International counseling students (ICSs) can be defined as individuals from outside the United States who seek professional training by enrolling in counselor education programs in the United States. After graduation, they often keep contributing to the counseling field as professional counselors or counselor educators, either in the United States or their home countries (Behl et al., 2017). In 2021, non-resident international students accounted for 1.02% of master’s students and 3.81% of doctoral students in counseling programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2022). However, because these percentages do not include international students who have resident alien status in the United States (Karaman et al., 2018), the actual numbers of international students in counseling programs may be higher. Despite the underestimated number of ICSs in CACREP-accredited programs, Ng (2006) found that at least one international student was enrolled in 41% of CACREP-accredited programs, which suggested that many counselor education programs already had some degree of global cultural diversity. Considering that the number of ICSs in the United States has risen within a few decades (CACREP, 2022; Ng, 2006), additional research is needed on this population and how best to prepare them for professional practice.
Research on International Students in Counseling Programs
While in training, ICSs, like domestic students, experience pressure to perform across academic, practical, and personal contexts (Thompson et al., 2011). However, ICSs face the additional challenges of adapting to a new culture and practicing counseling in that culture (Ju et al., 2020; Kuo et al., 2021; Ng & Smith, 2009). These challenges stem from having varying levels of experience using English in an academic context, adapting to new sociocultural and interpersonal patterns, and navigating key clinical factors of counselor education such as supervision and therapeutic relationships (Jang et al., 2014; C. Li et al., 2018; Y. Mori et al., 2009). Researchers have found that ICSs perceive more barriers and concerns regarding their training, such as academic problems and role ambiguity in supervision (Akkurt et al., 2018; Ng & Smith, 2009).
Regarding the experiences of ICSs, researchers have paid scholarly attention to the concept of acculturation, which is the assimilation process an individual experiences in response to the psychological, social, and cultural forces they are exposed to in a new dominant culture (C. Li et al., 2018; Ng & Smith, 2012). According to counseling studies, ICSs’ levels of acculturation and acculturative stress were associated with several variables related to their professional development, including counseling self-efficacy, language anxiety, and diverse academic and life needs (Behl et al., 2017; Interiano-Shiverdecker et al., 2019; C. Li et al., 2018). For example, Interiano-Shiverdecker et al. (2019) found that two domains of acculturation—ethnic identity and individualistic values—were positively associated with counseling self-efficacy for international counseling master’s students. Researchers have also uncovered the potential issues ICSs can experience related to a lack of acculturation: Behl et al. (2017) found that students’ acculturative stress was positively associated with their academic, social, cultural, and language needs.
With goals of uncovering effective coping strategies and identifying characteristics of high-quality training environments, researchers have investigated the personal and academic experiences of ICSs (Lau & Ng, 2012; Nilsson & Wang, 2008; Park et al., 2017; Woo et al., 2015). Woo and colleagues (2015) identified several coping tools of ICSs. These tools included self-directed strategies such as engaging in reflection and keeping up with the latest literature, support from mentors, and networking among international students and graduates (Woo et al., 2015). Researchers have attended to strategies that support ICSs’ development of cultural competence and commitment to social justice (Delgado-Romero & Wu, 2010; Karaman et al., 2018; Ng & Smith, 2012). For example, Delgado-Romero and Wu (2010) piloted a social justice group intervention with six Asian ICS participants and found the intervention to be a useful way to empower students and enhance their critical consciousness about inequity.
Supervision has been another area of focus in ICS research. Through interviews and surveys of ICSs, researchers have identified supervision strategies that support ICSs’ developing cultural competence, professional development, and self-efficacy (Mori et al., 2009; Ng & Smith, 2012; Park et al., 2017). A shared theme across these studies is the importance of clear communication. Findings of two studies (Mori et al., 2009; Ng & Smith, 2012) support supervisors engaging ICS supervisees in communication about critical topics such as cultural differences and the purpose and expectations of supervision. Based on a consensual qualitative analysis of interviews with 10 ICS participants, Park et al. (2017) recommended that programs and supervisors make sure to share basic information about systems of counseling, health care, and social welfare in the United States.
Necessity of ICS Research
Across academic units, there has been a growing attention to international graduate students (Anandavalli et al., 2021; Vakkai et al., 2020). Given the increasing representation of international students in counseling programs, researchers have called for academic and practical strategies to support ICSs’ success in training (Lertora & Croffie, 2020; Woo et al., 2015). These calls are aligned with the values of professional counseling organizations. Specifically, the American Counseling Association (ACA; 2014) endorsed respect for diversity and multiculturalism as elements of counselor competence. This value is reflected in the ACA Code of Ethics, including Standard F.11.b, which urges counselor educators to value a diverse student body in counseling programs. Similarly, the CACREP standards have identified counseling programs as responsible for working to include “a diverse group of students and to create and support an inclusive learning community” (CACREP, 2015, p. 6). Because counselors must have a profound comprehension of and commitment to diversity, experiences with multiculturalism during professional training programs are essential (O’Hara et al., 2021; Ratts et al., 2016). In this vein, the presence of international students in counseling programs can be beneficial for both domestic and international students by enhancing trainees’ understanding of diversity and multicultural counseling competencies (Behl et al., 2017; Luo & Jamieson-Drake, 2013). Given that there is a substantially increasing need for addressing multiculturalism, diversity, and social justice in the counseling profession, counseling programs’ efforts to recruit various minority student groups, including ICSs, will contribute to not only counselor training but also client outcomes in the long term.
However, despite the importance of the topic, researchers have consistently indicated that research on ICSs has been quite limited (Behl et al., 2017; Lau et al., 2019). In counseling research, there is a history of researchers using content analysis to provide a comprehensive overview of topics that are underrepresented but have growing importance. For example, Singh and Shelton (2011) published a content analysis of qualitative research related to counseling lesbian, gay, bisexual, transgender, and queer clients. Involving the summarization of findings from a body of literature into a few key categories or content areas (Stemler, 2001), content analysis is a useful methodology for expanding the field’s knowledge and understanding of the topic. Considering ICSs’ unique challenges and their potential contributions to enriching diversity in counseling programs and in the profession (Park et al., 2017), a comprehensive understanding of the current ICS literature is needed. This content analysis can identify how the research on ICSs has progressed and what remains unexplored or underexplored, which can provide meaningful implications for researchers interested in conducting ICS research in the future.
Purpose of the Study
The purpose of this study is to identify major findings in literature recently published on ICSs in the United States and to draw useful implications for counseling researchers and counseling programs seeking to better understand and support international students in counseling programs. Our content analysis, which focused on ICS research published between 2006 and 2021 in selected counseling journals, was driven by the following research questions: 1) What are the publication trends in ICS research, such as prevalence, publication outlets, authorship, methodological design, and sample size and characteristics?; and 2) What is the content of the ICS research published in counseling journals? Based on the findings, this study aimed to suggest recommendations for counseling researchers to fill the scholarly gap in ICS research and for counselor education programs to provide more effective training experiences to their international trainees.
Method
Content analysis is a useful methodology to expand our knowledge and understanding of the field through an overview of the current literature (Stemler, 2001). This approach makes it possible to effectively summarize a large amount of data using a few categories or content areas. In counseling research, content analysis has been used to provide an overview of a profession that is underrepresented but with growing importance (e.g., LGBTQ; Singh & Shelton, 2011), which is aligned with the aim of this study. This study employed both quantitative and qualitative content analysis to provide an overview of ICS research. Quantitative content analysis refers to analyzing the data in mathematical ways and applying predetermined categories that do not derive from the data (Forman & Damschroder, 2007). After reviewing existing content analysis articles in the counseling field, Byeolbee Um and Susannah M. Wood determined the scope of our quantitative analysis as: (a) journal and authorship, (b) research design, (c) participant characteristics, and (d) data collection methods.
Research Team
The research team consisted of two doctoral candidates and one full professor, all of whom were affiliated with the same CACREP-accredited counselor education and supervision program at a Midwestern university. Um and Lindsay Woodbridge were doctoral candidates in counselor education and supervision when conducting this research project and are currently counselor educators. Um is an international scholar from an East Asian country. She has drawn on her experiences in quantitative and qualitative courses and research projects to engage in research of marginalized counseling students, including ICSs. Woodbridge is a domestic scholar who has taken classes and collaborated with international student peers and worked with international students in instructional and clinical capacities. She has taken quantitative and qualitative research courses and completed several research projects. The first and second authors met regularly to establish the scope of the investigation, collect data, and form a consensus on coding emerging categories and sorting them into themes. Wood, an experienced researcher and instructor, has worked as a counselor educator for more than 15 years. She has worked with international students in teaching, supervision, advising, and mentoring capacities. She audited the research process, reviewed emergent categories and themes, and provided constructive feedback at each phase of the study.
Data Collection
To identify a full list of ICS studies that satisfy the scope of this study, Um and Woodbridge independently performed electronic searches using research databases including EBSCO, PsycINFO, and ERIC. Because ICSs have attracted scholarly attention relatively recently and because Ng’s (2006) study that estimated the number of ICSs in CACREP-accredited programs was the first published research on ICSs in counselor education programs, we set 2006 as the initial year of our search. We used the following search criteria to identify candidate articles: (a) published between 2006 and 2021 in ACA division, branch, and state journals and major journals under the auspices of professional counseling organizations; (b) containing one or more of the following keywords: international students, international counseling students, international counseling trainees, international counseling programs, counselor education; and (c) involving original empirical findings from ICSs in the United States.
We conducted an extensive search of ICS research across various journals in the counselor education field and identified ICS articles from several ACA-related journals, including Counselor Education and Supervision (CES), Journal of Multicultural Counseling and Development (JMCD), The Journal of Counselor Preparation and Supervision (JCPS), The Journal for Specialists in Group Work (JSGW), and the Journal of Professional Counseling: Practice, Theory & Research (JPC). Additionally, we found ICS articles from the International Journal for the Advancement of Counselling (IJAC) and the Journal of Counselor Leadership and Advocacy (JCLA), which are associated with the International Association for Counselling and Chi Sigma Iota, respectively. Although they are not under the broader umbrella of ACA, these journals have contributed to enriching scholarship in the counseling field.
After the initial searches, Um and Woodbridge made a preliminary list of the articles identified based on the search results. Subsequently, they re-screened the articles independently. Among the 27 identified articles, we excluded five conceptual papers, three articles that examined counselors’ or counselor educators’ experiences after graduation, and one article about ICSs in Turkey. Consequently, the final data consisted of 18 articles published by seven selected counseling journals.
Data Analysis
The research team analyzed content areas of the ICS research as an extension of qualitative content analysis, which requires performing the systematical coding and identifying categories/themes (Cho & Lee, 2014). We followed a series of steps suggested by Downe-Wamboldt (1992), which included selecting the unit of analysis, developing and modifying categories, and coding data. Several methods were used to ensure the trustworthiness of this content analysis study (Kyngäs et al., 2020). For credibility, Um and Woodbridge conducted multiple rounds of review on determining an adequate unit of analysis and tracked all discussions and modifications in great detail. For dependability, we calculated interrater reliability coefficients and Wood provided feedback about the results. Um also secured confirmability by utilizing audit trails, which described the specific steps and reflections of the project. Finally, to support transferability, we carefully examined other content analysis articles, reflected core aspects in the current study, and depicted the research process transparently.
Coding Protocol
After completing the quantitative content analysis, we conducted the qualitative content analysis as Downe-Wamboldt (1992) suggested. In so doing, we applied the inductive category development process suggested by Mayring (2000), which features a systematic categorization process of identifying tentative categories, coding units, and extracting themes from established categories. Specifically, after discussing the research question and levels of abstraction for categories, Um and Woodbridge determined the preliminary categories based on the text of the 18 ICS articles. We practiced coding the data using two articles and then performed independent coding of the remaining articles. Using a constructivist approach, we agreed to add additional categories as needed. Subsequently, the categories were revised until we reached a consensus. In the final step, established categories were sorted into three themes to identify the latent meaning of qualitative materials (Cho & Lee, 2014; Forman & Damschroder, 2007). Regarding validity, the congruence between existing conceptual themes and results of data coding secures external validity, which is regarded as the purpose of content analysis (Downe-Wamboldt, 1992).
Interrater Reliability
We used various indices of interrater reliability to assess the overall congruence between the researchers who performed the qualitative analysis and ensure trustworthiness. In this study, we used the kappa statistic (κ) suggested by Cohen (1960), which shows the extent of consensus among raters for selecting an article or coding texts (Stemler, 2001). Cohen’s kappa has been used extensively across various academic fields to measure the degree of agreement between raters. More specifically, the kappa statistic was calculated in two phases: 1) after screening articles and 2) after coding the texts according to the categories. The kappa results between Um and Woodbridge were .68 for screening articles and .71 for coding the text, both of which are considered substantial (.61–.80; Stemler, 2004).
Results
Results of Quantitative Content Analysis
Based on our electronic search, we identified a total of 18 ICS articles published between 2006 and 2021 in seven selected counseling journals, including three ACA division journals, one ACA state-branch journal, one ACES regional journal, and two journals from professional counseling associations (see Table 1). Specifically, two articles were published in CES, three in JMCD, one in JCPS, one in JSGW, three in JPC, seven in IJAC, and one in JCLA. Across the 18 ICS articles, a total of 35 researchers were identified as authors or co-authors with six authoring more than one article. According to researchers’ positionality statements in qualitative articles, eight researchers reported that they were previous or current ICSs in the United States. The institutional affiliations of researchers include 22 U.S. universities and two international universities, with three institutional affiliations appearing more than once across the studies.
Table 1
Summary of International Counseling Student Research in Selected Counseling Journals Between 2006 and 2021
| Journal and Author |
Research Design |
Participants |
Data Collection |
Topic |
| Counselor Education and Supervision (CES) |
Behl et al.
(2017) |
Quantitative
(Pearson product-moment correlations) |
38 counseling master’s and doctoral students |
Online survey |
Stress related to acculturation and students’ language, academic, social, and cultural needs |
D. Li & Liu
(2020) |
Qualitative (Phenomenology) |
11 doctoral students |
Semi-structured interview |
ICSs’ experiences with teaching preparation |
| Journal of Multicultural Counseling and Development (JMCD) |
Kuo et al.
(2021) |
Qualitative (Consensual
qualitative research) |
13 doctoral students |
Semi-structured interview |
ICSs’ professional identity development influenced by their multicultural identity and experience |
Nilsson &
Dodds (2006) |
Quantitative (Exploratory factor analysis, ANOVA, and hierarchical multiple regression analysis) |
115 master’s and doctoral students in counseling and psychology |
Online survey |
Development of a scale to measure issues in supervision |
Woo et al.
(2015) |
Qualitative (Consensual qualitative research) |
8 counselor education doctoral students |
Semi-structured interview |
Coping strategies used during training in supervision |
| The Journal of Counselor Preparation and Supervision (JCPS) |
Park et al.
(2017) |
Qualitative (Consensual qualitative research) |
10 counseling master’s and doctoral students |
Semi-structured interview |
Practicum and internship experiences of ICSs |
| The Journal for Specialists in Group Work (JSGW) |
Delgado-Romero
& Wu (2010) |
Qualitative
(Not identified) |
6 Asian counseling graduate students |
Counseling
practice |
Social justice–focused group intervention |
| Journal of Professional Counseling: Practice, Theory & Research (JPC) |
Interiano-
Shiverdecker
et al. (2019) |
Quantitative (Hierarchical multiple regression analysis) |
94 counseling master’s and doctoral students |
Online survey |
Relationship between acculturation and self-efficacy |
| Ng (2006) |
Quantitative (Descriptive analysis) |
96 CACREP-accredited
counseling programs |
Responses via email/telephone |
Enrollment in CACREP-accredited programs |
Sangganjanavanich
& Black (2009) |
Qualitative (Phenomenology) |
4 master’s students
and 1 doctoral student
in counseling |
Semi-structured interview |
Perceptions of supervision |
|
|
|
|
|
| International Journal for the Advancement of Counselling (IJAC) |
|
|
Akkurt et al.
(2018) |
Quantitative (Moderation analysis) |
71 counseling master’s and doctoral students |
Online survey |
Relationships between acculturation, counselor self-efficacy, supervisory working alliance, and role ambiguity moderated by frequency of multicultural discussion |
Interiano & Lim
(2018) |
Qualitative (Interpretive phenomenology) |
8 foreign-born doctoral students |
Semi-structured interview |
Influence of acculturation on ICSs’ professional development |
Lertora & Croffie
(2020) |
Qualitative (Phenomenology) |
6 counseling master’s students |
Demographics survey, focus
group, and semi-structured
interview |
Lived experiences of master’s-level ICSs in counseling program, including challenges and support, cultural differences, and future career paths |
C. Li et al.
(2018) |
Quantitative
(Linear regression analysis) |
72 counseling master’s and doctoral students |
Online survey |
Influence of acculturation and foreign language anxiety on ICSs’ counseling self-efficacy |
Ng & Smith
(2009) |
Quantitative
(F-tests) |
56 international counseling students
82 domestic
counseling students |
Survey |
Perceived barriers and concerns of ICSs in their training compared to domestic counseling students |
Ng & Smith
(2012) |
Quantitative (Hierarchical regression analysis) |
71 counseling master’s and doctoral students |
Online survey |
Relationships among ICSs’ training level, acculturation, counselor self-efficacy, supervisory working alliance, role ambiguity, and multicultural discussion |
Smith & Ng
(2009) |
Mixed methods (Descriptive analysis, constant comparative method of analysis, and phenomenology) |
11 master’s students and 10 doctoral students (including 7 recent graduates) |
Online survey |
ICSs’ experiences, resources, hindrances, and recommendations regarding multicultural counseling training |
| Journal of Counselor Leadership and Advocacy (JCLA) |
Kuo et al.
(2018) |
Qualitative (Consensual qualitative research) |
13 doctoral students |
Semi-structured interview |
ICSs’ professional identity development influenced by their multicultural identity and experience |
Note. ICS = international counseling student.
In terms of research design, eight articles employed quantitative research designs with diverse statistical methods including hierarchical multiple regression analysis, ANOVA, exploratory factor analysis, descriptive analysis, linear regression analysis, and moderation analysis. Another nine articles used qualitative approaches including phenomenology and consensual qualitative research, while one article (Smith & Ng, 2009) applied mixed methods design including both quantitative and qualitative analyses. Regarding participants, eight quantitative studies reported having between 38 to 115 ICS participants, including Ng’s (2006) study in which the author collected information on ICSs from 96 CACREP-accredited counseling programs. The numbers of participants in the eight qualitative ICS articles were relatively smaller, ranging from 5 to 13, which is natural given the characteristics of quantitative and qualitative research designs. Finally, the mixed methods study included 21 ICS participants. Quantitative researchers most frequently used online surveys to collect data, although one researcher (Ng, 2006) gathered information via email or telephone. Researchers using qualitative methodologies primarily used semi-structured interviews to collect data, while Delgado-Romero and Wu (2010) performed a group counseling intervention and interpreted the results, including the feedback of group members.
Results of Qualitative Content Analysis
The content areas of the ICS research included personal and professional aspects of ICSs’ adjustment and development. These aspects were influenced by ICSs’ unique circumstances along with their needs, potential stressors, and accessible resources and strategies. During qualitative content analysis, we generated and established preliminary categories. We then developed the preliminary categories into three main themes encompassing ICS research: (a) professional practices and professional development, (b) academic, social, and cultural challenges, and (c) personal and social resources. Each theme consisted of several identified categories.
Professional Practices and Professional Development
Many studies examined ICSs’ perceptions, concerns, needs, and suggestions of professional training experiences, including practicum and internship (e.g., Lertora & Croffie, 2020; Park et al., 2017), supervision (e.g., Ng & Smith, 2012; Nilsson & Dodds, 2006), multicultural training (e.g., Akkurt et al., 2018; Smith & Ng, 2009), social justice group intervention (Delgado-Romero & Wu, 2010), and teaching preparation (D. Li & Liu, 2020) from the unique perspective of ICSs. Furthermore, in relation to the professional practices, several categories of ICSs’ professional development were identified, such as counseling self-efficacy (e.g., Interiano-Shiverdecker et al., 2019; C. Li et al., 2018), professional identity development (e.g., Kuo et al., 2018, 2021), role ambiguity (Akkurt et al., 2018; Ng & Smith, 2012), and multicultural competencies (Smith & Ng, 2009).
Academic, Social, and Cultural Challenges
The second theme included unique challenges that ICSs encountered across academic, social, and cultural domains. The most commonly identified category from 12 studies was acculturation (e.g., Behl et al., 2017; Interiano & Lim, 2018; Lertora & Croffie, 2020). In addition, ICSs faced other cultural barriers involving cultural differences (e.g., Behl et al., 2017; Woo et al., 2015), difficulties in performing teaching and supervision practices (e.g., Li & Liu, 2020; Woo et al., 2015), and struggles in understanding cultural values and U.S. culture (e.g., Kuo et al., 2021; Sangganjanavanich & Black, 2009). ICSs reported that their academic and social concerns included English proficiency (e.g., Kuo et al., 2021; Nilsson & Dodds, 2006) and experiences of language anxiety (C. Li et al., 2018); stigma, biases, and discrimination (e.g., Ng & Smith, 2009; Sangganjanavanich & Black, 2009); and interpersonal isolation (e.g., Behl et al., 2017).
Personal and Social Resources
The third theme emerged from multiple categories of personal and social resources that supported ICSs. In terms of personal resources, researchers identified several characteristics such as self-reflection, self-regulation, and self-efficacy, which contributed to ICSs’ professional development (e.g., Delgado-Romero & Wu, 2010; Interiano-Shiverdecker et al., 2019; Woo et al., 2015). Additionally, the sources of social support for ICSs included their peers and other ICSs (e.g., D. Li & Liu, 2020; Woo et al., 2015), faculty and mentors (e.g., Smith & Ng, 2009; Woo et al., 2015), department and college (e.g., Delgado-Romero & Wu, 2010; D. Li & Liu, 2020), and family (Kuo et al., 2018).
Discussion
The purpose of this content analysis was to provide an organized overview of counseling studies conducted for ICSs over the past 16 years both from quantitative and qualitative perspectives. The aggregated findings, including publication trends and content areas of ICS research, are expected to present the missing pieces in research to better understand and support ICSs and provide meaningful recommendations to better support their professional development. Specifically, we identified 18 articles published in selected counseling journals during the 16-year period from 2006 to 2021. Our findings included the journals, authorship and affiliation, research orientation, participant characteristics, data collection method, and content areas. In general, researchers from many educational institutions have conducted collaborative research focusing on ICSs, with a balance of quantitative and qualitative methodologies. Research participants were ICSs at master’s and doctoral levels, with larger participant groups for quantitative studies and smaller groups for qualitative studies. The most frequently employed methods for data collection were online surveys and semi-structured interviews. Among the 18 identified ICS articles, three main content themes emerged, with each theme consisting of several categories.
In terms of the content, counseling researchers have consistently examined the professional practices of ICSs in their programs. Our findings indicate that many researchers were interested in supervision as an essential aspect of counselor education. Supervision involves intricate dynamics between the supervisor, supervisee, and client, and it can have a substantial influence on counselor competency development (Falender & Shafranske, 2007; Nilsson & Dodds, 2006). For this reason, ICS research has focused not only on investigating the supervisory concerns, needs, and satisfaction of ICSs, but on providing an integrative supervision model for this population (Nilsson & Dodds, 2006; Park et al., 2017; Sangganjanavanich & Black, 2009). Beyond supervision, researchers have also explored other topics, including teaching preparation and social justice counseling (Delgado-Romero & Wu, 2010;
D. Li & Liu, 2020). We found that researchers have attended to ICSs’ professional competencies as well as their training processes, including counseling self-efficacy, professional identity, and multicultural and social justice competencies (Kuo et al., 2021; C. Li et al., 2018; Smith & Ng, 2009). These professional competencies and training processes are regarded as important indices of successful and effective counselor training (Center for Substance Abuse Treatment, 2014; Woo et al., 2015). As a whole, ICS research has addressed diverse student training experiences and resultant developmental outcomes, although the absolute number of studies remains limited.
Our results highlight cultural and language differences as a primary barrier for many ICSs when they initiated their study in a foreign country. This finding is consistent with previous studies, including Mori’s (2000) seminal work. Most studies we examined identified acculturation as a key construct of ICSs’ adjustment and growth in a foreign country (Interiano & Lim, 2018; Ng & Smith, 2012). Many ICS participants sought to maintain a balance between engaging in U.S. language and culture and sustaining their own cultural identity (Interiano-Shiverdecker et al., 2019; D. Li & Liu, 2020; Sangganjanavanich & Black, 2009). Specifically, ICSs reported cultural challenges in several areas, including the educational system, teaching styles, personal interactions, social justice issues, and cultural values and practices (Behl et al., 2017; Delgado-Romero & Wu, 2010; D. Li & Liu, 2020). One study found that doctoral-level ICSs experienced greater cultural adjustment problems and conflicts compared to master’s-level ICSs (Ng & Smith, 2009), which implies that differentiated understanding and approaches may be required according to ICSs’ developmental stages. Also, our findings echoed the existing literature that one of the main obstacles for international students is language proficiency (Kuo et al., 2021; C. Li et al., 2018), as ICSs who had difficulty using English reported greater academic needs and concerns than their peers (Behl et al., 2017).
A notable finding is that the cultural barriers ICSs experienced were intertwined with their social concerns. ICSs are exposed to social dangers involving stigma, discrimination, and interpersonal isolation (Behl et al., 2017; Delgado-Romero & Wu, 2010). Although several researchers explored the potential relationship between ICSs’ length of time in the United States and their stress and cultural development (Behl et al., 2017; Nilsson & Dodds, 2006), their findings did not indicate any significant relationship. This lack of an effect may imply that other risks and protective factors have more influence on the successful adjustment and achievement of ICSs regardless of the amount of time they have spent in the United States. As such, our findings have shown that ICSs face unique challenges across their professional and personal lives in acculturating to two or more cultures and satisfying counseling training requirements.
Corresponding to these challenges, various personal and social resources have been regarded as protective factors of ICS development. Specifically, in terms of social support, researchers identified the importance of support from mentors, supervisors, peers, and other international graduate students (e.g., Woo et al., 2015). Given that ICSs often experience a lack of social support, it is noteworthy that the current ICS literature highlights the need for counselor training programs to promote students’ personal strengths and social connections.
Overall, we identified patterns and trends in research on international students in counseling programs based on studies published in selected counseling journals. Despite our efforts to reflect on diverse ICS experiences, the paucity of ICS research across selected counseling journals, particularly ACA journals, is notable. Given the increasing representation of ICSs in the wider counseling student body (Ng, 2006), further studies addressing the resources and barriers of this student population are needed. Furthermore, international students were exposed to unprecedented difficulties and mental health threats during the COVID-19 pandemic (Chen et al., 2020). These challenges necessitate more scholarly attention toward supporting and advocating for ICSs, including their adjustment, professional development, and transition from training to practice.
Implications
Because members of the counseling profession have expressly emphasized the importance of enriching multiculturalism and diversity (D. Li & Liu, 2020), we expect our findings to provide meaningful implications for counselor education programs. First, counseling researchers are encouraged to conduct more ICS research given the limited available studies and the increasing representation of international students in counseling programs. Even though they attempted to examine diverse training experiences and competency development of ICSs, many areas are understudied, such as their teaching and social justice practices. The existing ICS research mostly concentrated on identifying factors that influence ICSs’ academic and social lives. However, given the continuous increase of ICSs in the counseling field, research about strengths and support strategies of counselor education programs having many ICSs is worth studying. Also, in future studies, researchers can try to reflect the actual voices of ICSs about what they want from their training programs, whether they feel their program is affordable, and whether their program is effective in supporting their professional development. In addition, counseling researchers can develop projects considering cultural differences of ICSs in order to better understand them not as a single group but as multiple individuals having unique cultural backgrounds. Overall, this content analysis study underscores the need for more research on this student population.
Regarding counselor education programs, programs can provide specific resources to support the professional development of ICSs. To help ICSs overcome language barriers, for instance, institutions can provide professional assistance in the use of English, such as writing centers and speaking centers. Departments can provide language support specifically relevant to counseling, including workshops and seminars about practical language tips for counseling practice and research writing. For example, Jang and colleagues (2014) recommended instituting mock supervision sessions before practicum and/or internship to further prepare international counseling trainees for their duties. Counselor education programs are expected to address the unique language and academic needs of ICSs.
Counselor education programs should also facilitate ICSs’ cultural understanding and adjustment. Counselor education programs can design and provide opportunities for ICSs to socially interact with colleagues and faculty members in the program. Existing studies that highlight the importance of mentoring (e.g., Delgado-Romero & Wu, 2010; Ng, 2006; Woo et al., 2015) are further proof that faculty members in counselor education programs can play a significant role in the personal and professional development of ICSs. Because ICSs share unique challenges and learning experiences (D. Li & Liu, 2020; Sangganjanavanich & Black, 2009), faculty members who were ICSs or have experience advising or collaborating with ICSs can serve as essential mentors for this population.
Counselor education programs might benefit from developing and employing curriculum and courses that apply the empirical findings of ICS research, including the results of this study. These studies serve as a reference for designing more effective counselor training. Programs that design their training to support the needs of ICSs may also find that they are more effective in recruiting and retaining international students. For example, faculty members can respond to ICSs’ anxiety and concerns before they enter clinical practice (Ellis et al., 2015; Nilsson & Wang, 2008). Also, ICSs are expected to benefit from synthesized results about ICS research, promoting a deeper understanding of themselves and enabling them to develop their own coping strategies and access potential resources. Furthermore, counselor education programs need to prepare different training trajectories for master’s students and doctoral students. Compared to ICSs in doctoral programs, ICSs are relatively rare at the master’s level, comprising only 1% of master’s-level counseling trainees (CACREP, 2015). Because master’s-level ICSs may feel like they belong to the minority, helping them feel connected is an essential task for counselor education programs. Therefore, programs are required to prioritize the effective delivery of knowledge and adequate practical opportunities for supervisees at the master’s level.
Finally, counselor education programs should work toward a program culture that supports diversity. Although fostering multiculturalism has emerged as a priority for counselor education programs, more work is needed to support internationally diverse perspectives. For example, Taephant and colleagues (2015) examined the experiences of U.S.-educated international counselors practicing in non-Western counseling environments. Drawing upon these findings and other relevant references, counselor educators may design a class discussing the limitations of Western-style training. As is evidenced by existing literature, open discussions about cultural differences can be effective for the psychosocial adjustment and professional development of ICSs.
Limitations and Future Research
This study includes some limitations to note. The first and most important limitation is the concerning lack of research focusing on international students in the counseling profession (D. Li & Liu, 2020; Nilsson & Dodds, 2006; Woo et al., 2015). Even though ICSs have recently begun to attract scholarly attention (Lau et al., 2019), the number of articles published recently may not be sufficient to discuss the diverse purposes and areas of focus for ICS research. Although our study specifically highlighted the need for more research on ICSs, an extensive range of discussion was not possible due to the limited number of articles. Thus, we encourage more professional counseling organizations and counseling researchers to consider ICSs’ professional development as a research topic. Also, because this study was limited to articles published in journals related to ACA and selected other professional organizations, future research with a more comprehensive search may elicit rich and diverse discussion. Finally, content analysis has a few methodological limitations, such as no existence of unified rules and a precise analytical process, and potential biases in coding, which necessitates further research on ICSs using other methodologies for more in-depth investigations.
Conclusion
ICSs can contribute to increasing program diversity and cultivating students’ multicultural counseling competency but have been understudied despite their growing representation. This study provided a comprehensive overview of ICS research across 18 articles within a 16-year period, using both quantitative and qualitative content analysis. Counseling researchers can pay more scholarly attention to the academic and social lives of ICSs from a strength-based approach. Counseling programs and counselor educators can support ICSs by providing resources for adjustment, developing curricular and extracurricular activities involving ICSs, and working toward a more multicultural and inclusive program environment.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Akkurt, M. N., Ng, K.-M., & Kolbert, J. (2018). Multicultural discussion as a moderator of counseling supervision-related constructs. International Journal for the Advancement of Counselling, 40(4), 455–468.
https://doi.org/10.1007/s10447-018-9337-z
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Anandavalli, S., Borders, L. D., & Kniffin, L. E. (2021). “I am strong. Mentally strong!”: Psychosocial strengths of international graduate students of color. The Professional Counselor, 11(2), 173–187.
https://doi.org/10.15241/sa.11.2.173
Behl, M., Laux, J. M., Roseman, C. P., Tiamiyu, M., & Spann, S. (2017). Needs and acculturative stress of international students in CACREP programs. Counselor Education and Supervision, 56(4), 305–318.
https://doi.org/10.1002/ceas.12087
Center for Substance Abuse Treatment. (2014). A treatment improvement protocol: Improving cultural competence. Substance Abuse and Mental Health Services Administration.
Chen, J. H., Li, Y., Wu, A. M. S., & Tong, K. K. (2020). The overlooked minority: Mental health of international students worldwide under the COVID-19 pandemic and beyond. Asian Journal of Psychiatry, 54, 102333. https://doi.org/10.1016/j.ajp.2020.102333
Cho, J. Y., & Lee, E.-H. (2014). Reducing confusion about grounded theory and qualitative content analysis: Similarities and differences. The Qualitative Report, 19(32), 1–20. https://doi.org/10.46743/2160-3715/2014.1028
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20(1), 37–46. https://doi.org/10.1177/001316446002000104
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2022). CACREP vital statistics 2021. https://www.cacrep.org/wp-content/uploads/2023/01/vital-statistics-report-2021.pdf
Delgado-Romero, E. A., & Wu, Y.-C. (2010). Asian international students in counseling programs: A group intervention to promote social justice. The Journal for Specialists in Group Work, 35(3), 290–298.
https://doi.org/10.1080/01933922.2010.492896
Downe-Wamboldt, B. (1992). Content analysis: Method, applications, and issues. Health Care for Women International, 13(3), 313–321. https://doi.org/10.1080/07399339209516006
Ellis, M. V., Hutman, H., & Chapin, J. (2015). Reducing supervisee anxiety: Effects of a role induction intervention for clinical supervision. Journal of Counseling Psychology, 62(4), 608–620. https://doi.org/10.1037/cou0000099
Falender, C. A., & Shafranske, E. P. (2007). Competence in competency-based supervision practice: Construct and application. Professional Psychology: Research and Practice, 38(3), 232–240.
https://doi.org/10.1037/0735-7028.38.3.232
Forman, J., & Damschroder, L. (2007). Qualitative content analysis. In L. Jacoby & L. A. Siminoff (Eds.), Empirical methods for bioethics: A primer (pp. 39–62). Elsevier.
Interiano, C. G., & Lim, J. H. (2018). A “chameleonic” identity: Foreign-born doctoral students in U.S. counselor education. International Journal for the Advancement of Counselling, 40(3), 310–325.
https://doi.org/10.1007/s10447-018-9328-0
Interiano-Shiverdecker, C. G., Foxx, S. P., & Flowers, C. (2019). Acculturation domains and counselor self-efficacy. Journal of Professional Counseling: Practice, Theory & Research, 46(1–2), 48–63.
https://doi.org/10.1080/15566382.2019.1669373
Jang, Y. J., Woo, H., & Henfield, M. S. (2014). A qualitative study of challenges faced by international doctoral students in counselor education supervision courses. Asia Pacific Education Review, 15(4), 561–572.
https://doi.org/10.1007/s12564-014-9342-9
Ju, J., Merrell-James, R., Coker, J. K., Ghoston, M., Pérez, J. F. C., & Field, T. A. (2020). Recruiting, retaining, and supporting students from underrepresented racial minority backgrounds in doctoral counselor education. The Professional Counselor, 10(4), 581–602. https://doi.org/10.15241/jj.10.4.581
Karaman, M. A., Schmit, M. K., Ulus, I. C., & Oliver, M. (2018). International counseling students’ perception of ethics. Journal of International Students, 8(2), 677–695. https://doi.org/10.5281/zenodo.1250370
Kuo, P., Washington, A., & Woo, H. (2021). Professional identity development and multicultural identity among international counselor education doctoral students. Journal of Multicultural Counseling and Development, 49(2), 116–128. https://doi.org/10.1002/jmcd.12210
Kuo, P., Woo, H., & Washington, A. (2018). Professional identity development of international counselor education doctoral students. Journal of Counselor Leadership and Advocacy, 5(2), 153–169.
https://doi.org/10.1080/2326716X.2018.1452079
Kyngäs, H., Kääriäinen, M., & Elo, S. (2020). The trustworthiness of content analysis. In H. Kyngäs, K. Mikkonen, & M. Kääriäinen (Eds), The application of content analysis in nursing science research (pp. 41–48). Springer. https://doi.org/10.1007/978-3-030-30199-6_5
Lau, J., & Ng, K.-M. (2012). Effectiveness and relevance of training for international counseling graduates: A qualitative inquiry. International Journal for the Advancement of Counselling, 34(1), 87–105.
https://doi.org/10.1007/s10447-011-9128-2
Lau, J., Su, Y.-W., Chen, C.-C., & Dai, C.-L. (2019). Using a collaborative model in supervision with international counseling students. The Journal of Humanistic Counseling, 58(2), 150–164. https://doi.org/10.1002/johc.12103
Lertora, I. M., & Croffie, A. L. (2020). The lived experiences of international students in a CACREP counseling program. International Journal for the Advancement of Counselling, 42(2), 174–190.
https://doi.org/10.1007/s10447-019-09394-6
Li, C., Lu, J., Bernstein, B., & Bang, N. M. (2018). Counseling self-efficacy of international counseling students in the U.S.: The impact of foreign language anxiety and acculturation. International Journal for the Advancement of Counselling, 40(3), 267–278. https://doi.org/10.1007/s10447-018-9325-3
Li, D., & Liu, Y. (2020). International counseling doctoral students’ teaching preparation: A phenomenological study. Counselor Education and Supervision, 59(3), 200–215. https://doi.org/10.1002/ceas.12184
Luo, J., & Jamieson-Drake, D. (2013). Examining the educational benefits of interacting with international students. Journal of International Students, 3(2), 85–101. https://files.eric.ed.gov/fulltext/EJ1056457.pdf
Mayring, P. (2000). Qualitative content analysis. Forum: Qualitative Social Research, 1(2).
Mori, S. C. (2000). Addressing the mental health concerns of international students. Journal of Counseling & Development, 78(2), 137–144. https://doi.org/10.1002/j.1556-6676.2000.tb02571.x
Mori, Y., Inman, A. G., & Caskie, G. I. L. (2009). Supervising international students: Relationship between acculturation, supervisor multicultural competence, cultural discussions, and supervision satisfaction. Training and Education in Professional Psychology, 3(1), 10–18. https://doi.org/10.1037/a0013072
Nilsson, J. E., & Dodds, A. K. (2006). A pilot phase in the development of the International Student Supervision Scale. Journal of Multicultural Counseling and Development, 34(1), 50–62.
https://doi.org/10.1002/j.2161-1912.2006.tb00026.x
Nilsson, J. E., & Wang, C. (2008). Supervising international students in counseling and psychology training. In A. K. Hess, K. D. Hess, & T. H. Hess (Eds.), Psychotherapy supervision: Theory, research, and practice
(2nd ed.; pp. 70–81). Wiley.
Ng, K.-M. (2006). International students in CACREP-accredited counseling programs. Journal of Professional Counseling: Practice, Theory & Research, 34(1–2), 20–32. https://doi.org/10.1080/15566382.2006.12033821
Ng, K.-M., & Smith, S. D. (2009). Perceptions and experiences of international trainees in counseling and related programs. International Journal for the Advancement of Counselling, 31(1), 57–70.
https://doi.org/10.1007/s10447-008-9068-7
Ng, K.-M., & Smith, S. D. (2012). Training level, acculturation, role ambiguity, and multicultural discussions in training and supervising international counseling students in the United States. International Journal for the Advancement of Counselling, 34(1), 72–86. https://doi.org/10.1007/s10447-011-9130-8
O’Hara, C., Chang, C. Y., & Giordano, A. L. (2021). Multicultural competence in counseling research: The cornerstone of scholarship. Journal of Counseling & Development, 99(2), 200–209.
https://doi.org/10.1002/jcad.12367
Park, S., Lee, J. H., & Wood, S. M. (2017). Experiences of international students in practicum and internship courses: A consensus qualitative research. The Journal of Counselor Preparation and Supervision, 9(2).
https://digitalcommons.sacredheart.edu/cgi/viewcontent.cgi?article=1137&context=jcps
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Sangganjanavanich, V. F., & Black, L. L. (2009). Clinical supervision for international counselors-in-training: Implications for supervisors. Journal of Professional Counseling: Practice, Theory & Research, 37(2), 52–65. https://doi.org/10.1080/15566382.2009.12033860
Singh, A. A., & Shelton, K. (2011). A content analysis of LGBTQ qualitative research in counseling: A ten-year review. Journal of Counseling & Development, 89(2), 217–226.
https://doi.org/10.1002/j.1556-6678.2011.tb00080.x
Smith, S. D., & Ng, K.-M. (2009). International counseling trainees’ experiences and perceptions of their multicultural counseling training in the United States: A mixed method inquiry. International Journal for the Advancement of Counselling, 31(4), 271–285. https://doi.org/10.1007/s10447-009-9083-3
Stemler, S. (2001). An overview of content analysis. Practical Assessment, Research, and Evaluation, 7(17). https://doi.org/10.7275/z6fm-2e34
Stemler, S. E. (2004). A comparison of consensus, consistency, and measurement approaches to estimating interrater reliability. Practical Assessment, Research, and Evaluation, 9(1).
https://doi.org/10.7275/96jp-xz07
Taephant, N., Rubel, D., & Champe, J. (2015). A grounded theory of Western-trained Asian group leaders leading groups in Asia. The Journal for Specialists in Group Work, 40(1), 74–101.
https://doi.org/10.1080/01933922.2014.993054
Thompson, E. H., Frick, M. H., & Trice-Black, S. (2011). Counselor-in-training perceptions of supervision practices related to self-care and burnout. The Professional Counselor, 1(3), 152–162. https://doi.org/10.15241/eht.1.3.152
Vakkai, R. J. Y., Harris, K., Chaplin, K. S., Crabbe, J. J., & Reynolds, M. (2020). Sociocultural factors that impact the health status, quality of life, and academic achievement of international graduate students: A literature review. Journal of International Students, 10(3), 758–775. https://files.eric.ed.gov/fulltext/EJ1265821.pdf
Woo, H., Jang, Y. J., & Henfield, M. S. (2015). International doctoral students in counselor education: Coping strategies in supervision training. Journal of Multicultural Counseling and Development, 43(4), 288–304. https://doi.org/10.1002/jmcd.12022
Byeolbee Um, PhD, is an assistant professor at the University of Oklahoma. Lindsay Woodbridge, PhD, LMHC, LPC, is an assistant professor at the University of Wisconsin-Stout. Susannah M. Wood, PhD, NCC, is a professor at the University of Iowa. Correspondence may be addressed to Byeolbee Um, 820 Van Vleet Oval, Rm 303, Norman, OK 73019, byeolbee.um-1@ou.edu.
May 10, 2023 | Volume 13 - Issue 1
Erin E. Woods, Alexandra Gantt-Howrey, Amber L. Pope
To better understand how women portray obsessive-compulsive disorder (OCD) on social media, we conducted a critical content analysis of TikTok videos. We examined a sample of 50 TikTok videos tagged with “#OCD” that were created by women, yielding two themes and multiple subthemes: 1) minimizes OCD symptoms and 1a) uses OCD as a synonym for cleanliness and organization; 2) accurately depicts OCD symptoms, 2a) corrects misunderstanding, and 2b) shares obsessive fears. Results revealed that TikToks perpetuating stigma about OCD were prevalent, though women also posted TikToks presenting OCD in more accurate and comprehensive ways. Implications for mental health counselors are explained.
Keywords: obsessive-compulsive disorder, TikTok, women, content analysis, stigma
Obsessive-compulsive disorder (OCD) is often used in the popular vernacular to describe someone who likes things tidy or who is particular about a certain issue. Individuals commonly use phrases like “I’m so OCD” as captions of social media posts (Pavelko & Myrick, 2016), which may perpetuate stigma and misunderstanding about this complicated condition. According to the American Psychiatric Association (APA), OCD is a serious mental health condition that often results in significant impairment and distress due to the presence of time-consuming obsessions and compulsion (APA, 2022; Fennell & Liberato, 2007). Obsessions are urges, images, or thoughts that are unwanted, distressing, intrusive, and repetitive (APA, 2022) and may adhere to certain themes, such as doubt, contamination, harm, religious ideas, unwanted sexual thoughts, perfectionism, or fear of losing control (Clark & Radomsky, 2014; International Obsessive Compulsive Disorder Foundation [IOCDF], n.d.b.). Moreover, due to the distressing nature of obsessions, individuals with OCD often try to ignore, neutralize, or suppress these thoughts through compulsive acts—repeated mental or behavioral actions that individuals feel they must do to reduce the distress associated with obsessions or to prevent an undesirable event from occurring. Compulsions usually adhere to strict rules, are excessive, and are not realistically related to the concern they attempt to prevent or eliminate. Compulsions often are classified into common groupings, such as checking, cleaning, ordering or repeating, and/or mental actions (APA, 2022; Starcevic et al., 2011). According to prevalence data, women are slightly more likely than men to be diagnosed with OCD in adulthood and often experience later symptom onset than men (APA, 2022).
Appropriate diagnosis and effective treatment of OCD often takes an average of 17 years (IOCDF, n.d.a). Individuals with OCD often delay seeking treatment because of concerns of being viewed in a negative manner and the fear of stigma related to being diagnosed with a mental health disorder (Belloch et al., 2009; Steinberg & Wetterneck, 2017). Conceptualization of OCD ranges from viewing OCD as a less serious concern compared to other mental health disorders, to deeming OCD a chronic illness, to considering OCD as a positive trait. The medicalization of OCD may help individuals feel less stigmatized by identifying OCD as an illness (Fennell & Liberato, 2007). As Fennell and Liberato noted, “Societal conceptions [of OCD] are constantly relevant to respondents, affecting their self-conception and anticipated stigma” (p. 327). To this effect, accurate portrayal of OCD and factually based education for the public have been noted as important action steps to reduce stigma (Webb et al., 2016).
The stigma associated with OCD impacts the disclosure of symptoms to others, including social supports as well as mental health providers. Some may hide their OCD symptoms or make excuses for their behavior out of shame or embarrassment. Further, some individuals report negative perceptions or reactions after disclosing their OCD diagnosis to friends, family, or employers (Fennell & Liberato, 2007). However, some individuals benefit from disclosing symptoms of OCD to their support systems, and others find it helpful to engage and interact with people who also have an OCD diagnosis. Hence, societal conceptions of OCD can impact how individuals cope with their symptoms, including help-seeking behaviors (Fennell & Boyd, 2014; Ma, 2017; Steinberg & Wetterneck, 2017).
OCD Representations on Social Media
Researchers have called for continued examination of the representation of OCD in the media, particularly on social media platforms (Pavelko & Myrick, 2016; Robinson et al., 2019). Although increased social media discussions about OCD may decrease stigma, the often trivial nature of such depictions downplays the seriousness of this disorder (Fennell & Liberato, 2007). For instance, Robinson and colleagues (2019) explored attitudes toward five mental health and five physical health diagnoses on Twitter and found OCD to have the highest rate of trivialization of the 10 disorders, concluding that minimization of OCD symptoms and related suffering is a form of stigma.
How individuals describe OCD in the common vernacular on social media impacts societal conceptualizations of OCD (Fennell & Boyd, 2014; Pavelko & Myrick, 2016). In a quantitative study examining the use of “#OCD” on Twitter, Pavelko and Myrick (2016) identified post after post in which Twitter users employed “#OCD” when referring to non-disordered actions, such as organizing pencils. Tweets labeled “#OCD” were presented to participants, assessing their emotional reactions, stereotypes about OCD, and behavioral intentions to support individuals with OCD after reviewing the hashtagged tweets. Participants indicated increased irritation and decreased sympathy when OCD was framed in trivial language (i.e., language downplaying the seriousness of OCD) versus objective clinical language in the tweets. Further, these correlations varied by gender of the tweeter, with participants reporting increased negative emotional reactivity to women who utilized trivial language rather than to men. Pavelko and Myrick concluded that “Messages regarding trifling, detail-oriented behaviors frequently belittle or downplay the severity of OCD in 140 characters or less” (p. 42).
In a qualitative study, Fennell and Boyd (2014) examined how media portrayals of OCD were interpreted by individuals who have been diagnosed with or believe they have OCD. Similar to Pavelko and Myrick’s (2016) findings, participants reported feeling frustrated by the seemingly casual use of “OCD” in the vernacular and by depictions of OCD that were presented in stereotypical and comedic manners, at times making light of the symptoms (Fennell & Boyd, 2014). Participants noted users exhibited certain symptoms of OCD more frequently than others, namely contamination obsessions, washing and cleaning compulsions, and hoarding behaviors, all of which may portray OCD as a habit rather than a disorder. However, participants expressed appreciation for depictions of OCD in the media, acknowledging that media portrayals helped them identify what they were experiencing as OCD. Hence, media representations of OCD are varied and complex, eliciting mixed emotional reactions and divergent understandings of OCD from individuals who are consuming those messages (Fennell & Boyd, 2014; Pavelko & Myrick, 2016).
Moreover, OCD and associated symptoms are frequently misunderstood, even among mental health professionals who are trained to diagnose the disorder. In a quantitative study of mental health counselors and graduate students, participants exhibited stigma toward OCD symptoms related to sexual thoughts, violent thoughts, and contamination (Steinberg & Wetterneck, 2017). Further, Glazier et al. (2013) found issues pertaining to the accurate and timely diagnosis of OCD among APA members due to misidentification of OCD symptoms. In this quantitative study, participants were asked to provide a diagnosis for five case vignettes, each depicting various OCD obsessive symptoms. There was a 38.9% misidentification rate of OCD across the vignettes, with variation in rates based on the symptoms presented in each vignette. The vignette describing symptoms related to contamination was misidentified at the lowest rate of 15.8%, although the vignette describing symptoms of obsessions related to “homosexuality” was misdiagnosed at a rate of 77.0% (Glazier et al., 2013). In sum, OCD is an often stigmatized and misunderstood disorder, resulting in challenges for individuals living with OCD and for mental health counselors attempting to accurately diagnose OCD in their clients (Fennell & Boyd, 2014; Fennell & Liberato, 2007; Glazier et al., 2013; Steinberg & Wetterneck, 2017).
TikTok: Social Media Phenomenon and Social Change Agent
Although researchers have explored the use of the term OCD in the vernacular and on social media, along with associated impacts on people living with OCD (Fennell & Boyd, 2014), researchers have yet to explore how particular mental health diagnoses such as OCD are portrayed and discussed on TikTok, a popular social media application, or “app,” released globally in 2017 (Iqbal, 2022). TikTok’s content consists of brief videos created by users, which can be viewed and interacted with by other users (Anderson, 2020). TikTok uses an algorithm to show users videos that appeal to their interests. Users interact on the platform through likes, comments, reactions, and direct messages. Hashtags are added to videos to help individuals search for specific types of content. To have full access to TikTok, a user must have an active account; individuals with accounts can create a profile page, which can be used with various privacy settings (Anderson, 2020). The scope of TikTok is vast, reaching an average of 689 million users worldwide every month, with 100 million users in the United States (Iqbal, 2022). According to Iqbal (2022), TikTok reached over 1.4 billion users in 2022. The app is frequented by individuals of various ages, nationalities, genders, and socioeconomic statuses and in 2022, TikTok was downloaded over 3.3 billion times (Iqbal, 2022).
Based on TikTok’s wide reach, it is reasonable to assume that content shared on the app has implications for how society views certain topics, including mental health disorders, as meaning is constructed through interactions with others on the application. Vitikainen et al. (2020) described TikTok as a social change agent, noting that despite the app’s ban on political campaign–related content, users have utilized TikTok for political movements, such as joining together to sabotage a Donald Trump rally in 2020 (Lorenz et al., 2020). Further, TikTok videos and hashtags were used to spread information about wearing masks during the COVID-19 pandemic (Basch, Fera, et al., 2021). The World Health Organization TikTok videos related to wearing a mask were viewed over 57 million times, and just 100 TikToks with the hashtag “#WearaMask” were viewed over 500 million times (Basch, Fera, et al., 2021).
As the app has such an extensive user base, “TikTok has great potential in conveying important public health messages to various segments of the population” (Basch, Fera, et al., 2021, para. 18). It stands to reason that if TikTok videos can influence social action and aid in the spread of public health information, they also could be a powerful tool in either upholding or dismantling misunderstanding and stigma around mental health disorders such as OCD. However, researchers have highlighted the existence of misinformation on popular social media platforms, including TikTok (Sharevski et al., 2023). For example, in various studies on COVID-19 information conveyed via TikTok, researchers found that much of the information is misinformation (Basch, Meleo-Erwin, et al., 2021; McCashin & Murphy, 2022). Sharevski et al. (2023) found that in viewing TikToks that included debunked abortion misinformation, approximately 30% of participants believed the information to be true. These findings highlight the prevalence of health-related misinformation on TikTok and related implications for professionals and the general public alike. Therefore, to better understand current social discourse around OCD, we conducted a content analysis to answer the following research question: How are women portraying OCD on TikTok?
Methods
We conducted a deductive, qualitative content analysis of 50 TikTok videos to examine how OCD is being discussed and portrayed by women on the large-scale social media platform of TikTok, which encompasses the power to disrupt stigma and influence the narratives attributed to OCD. Our decision to utilize content analysis was influenced by the use of this methodology in existing literature exploring OCD and media (Fennell & Boyd, 2014; Robinson et al., 2019), and a content analysis aligned with our intent to interpret women’s portrayal of OCD through social discourse on TikTok. A content analysis is a systematic yet flexible process utilized to derive meaning from a set of data (Schreier, 2014). Qualitative content analysis is aligned with social constructivism and is concerned with exploring the “meaning and interpretation . . . of symbolic material, [and] the importance of context in determining meaning” (Schreier, 2014, p. 173). To describe meaning from our sample of TikTok videos, we followed the steps of a qualitative content analysis (Schreier, 2014): define the research question; select the content to analyze; develop a coding frame; segment and trial code the data; evaluate the coding frame; conduct the main analysis; and interpret and present the findings.
After determining our research question, we selected TikTok videos that met the following criteria: a) the TikTok video included the hashtag OCD (#OCD), and b) the primary person in the video presented as a woman and/or included she/her pronouns in their profile bio. We chose to focus on individuals presenting as women in this study because OCD symptomology varies based on gender in studies comparing cisgender women to cisgender men, with women having slightly higher rates of OCD diagnoses than men. Further, women exhibit cleaning-related symptoms more often than men (APA, 2022), and excessive cleanliness is commonly displayed in media depictions of OCD (Fennell & Boyd, 2014). Women also have unique experiences related to the intersectionality of gender, social discourse, and mental health diagnosis and treatment, or lack thereof (Bondi & Burman, 2001; Robinson et al., 2019). Further, women’s trivialization of OCD on social media may elicit stronger negative emotional reactions from consumers, such as annoyance and decreased sympathy toward individuals with OCD (Pavelko & Myrick, 2016).
We chose the 50 TikTok videos with the most views for our sample (Dworkin, 2012). We were able to determine these videos by searching for “#OCD” within the TikTok app in February 2021. The sample was analyzed in March 2021. Similarly, in another content analysis, Fowler et al. (2021) selected the first 50 TikTok videos using a particular hashtag for their sample. They noted the influence of the TikTok algorithm, as the algorithm determines which videos are shown and in which order. Moreover, we determined the sample size based on other studies that engaged qualitative methods to analyze videos on various social media platforms, some of which utilized a sample size of fewer than 50 (Fowler et al., 2021; Johnson et al., 2019, 2021; Wallis, 2011). Next, we deductively determined codes in a concept-driven way (Schreier, 2014) based on the extant literature surrounding OCD, stigma, and popular understanding of the diagnosis. These initial codes were stigma perpetuated and accurate information about OCD shared. It is important to note that at the time of data analysis, the current edition of the Diagnostic and Statistical Manual of Mental Disorders was the DSM-5 (APA, 2013). The DSM-5-TR (APA, 2022) was released in 2022; however, there were no updates to the OCD diagnostic criteria in the text revision.
The research team identified more codes during the review of the data, and we altered codes to be more specific to the data, including daily routine, checking OCD, and feeling misunderstood. During the segmentation phase of the coding process, the research team divided the data into individual units, or segments, based on a thematic criterion. More specifically, we divided the larger chunks of data (i.e., the entirety of what was said in a TikTok) into individual units (i.e., sentences) based on the aforementioned codes. Next, we went through a pilot round of coding using the predetermined codes on approximately 50% of the data. We evaluated and made changes to the coding frame as necessary, developing more specific codes to best represent the data. From there, we proceeded to the main analysis phase, in which the research team coded all data according to our final coding framework and determined themes and subthemes based on the coded data. Each team member individually determined themes, and then the team members met to compare, discuss, and alter the themes until we reached consensus on the themes and subthemes that best represented the data. Of the total sample, 48 videos comprise the two final categories.
Increasing Trustworthiness
The research team for the content analysis consisted of the first two authors of this article, Erin E. Woods and Alexandra Gantt-Howrey, who are cisgender heterosexual (cishet) White women and are mental health counselors familiar with OCD. To increase trustworthiness, Woods and Gantt-Howrey practiced weekly reflexive journaling to become more aware of and bracket our biases throughout the data analysis, with the recognition that bias cannot be completely bracketed (Creswell, 2003). As part of the reflexive journaling process, we recognized and considered various sociocultural factors at play in our own lives, including our existence as cishet White women in the United States. Moreover, we identified various biases and expectations we held, including expectations of seeing OCD used as a non-clinical descriptor, previous knowledge related to OCD misdiagnosis and misunderstanding, and the belief that OCD should be used only in reference to the actual disorder. In an attempt to bracket these biases throughout the data analysis process, we engaged in frequent dialogue with one another to consider and evaluate assumptions that arose during the data analysis. Finally, to increase trustworthiness, the third author, Amber L. Pope, a licensed mental health counselor and counselor educator who identifies as a cishet White woman, acted as an auditor and reviewed the final themes and subthemes according to the data (Creswell, 2003). More specifically, Pope reviewed the data as well as the themes and subthemes developed by Woods and Gantt-Howrey. Pope then offered feedback on the results (e.g., use of theme names to accurately represent the data), and Woods and Gantt-Howrey integrated Pope’s feedback into the final results presented below.
Results
This investigation explored how women communicate about OCD on TikTok. Two themes and three subthemes emerged from the data: 1) minimizes OCD symptoms and 1a) uses OCD as a synonym for cleanliness and organization; 2) accurately depicts OCD symptoms, 2a) corrects misunderstanding, and 2b) shares obsessive fears. A clear dichotomy was found: Many TikTok videos depicted women using OCD as an inaccurate descriptor, perpetuating stigma surrounding the diagnosis, while others shared factually based information in alignment with the DSM-5 description of OCD, often representing their own experiences with OCD. Below, our findings are illustrated with rich descriptions from the data.
Minimizes OCD Symptoms
The first category, minimizes OCD symptoms, describes participants’ portrayals of OCD in a way that either minimized or negated symptom severity, and/or described the disorder in a manner that does not align with the DSM-5 definition of OCD. Twenty-eight videos (56%) from the sample are included in this category. Many TikToks in this category used the term “OCD” as a synonym for being very clean or organized, or to portray an unrelated phenomenon, such as collecting items or creating a spreadsheet. One TikTok of a woman describing her father exemplifies this misuse of the term “OCD”: “This is my dad and he has a problem . . . because he has the OCD. And you might have it too if your 800-count DVD collection is in alphabetical order from ‘8 Mile’ to ‘Young Frankenstein.’” This quote is representative of the trivialization of the OCD diagnosis. Moreover, a TikTok about a mother’s feelings of frustration over her daughter’s messy painting further demonstrates the stigma perpetuated by many TikTok videos, as the mother stated:
Do any other moms relate to the extreme anxiety this gives me? I can sit here and watch but I’m dying on the inside. This is very hard for me. But I will sit here . . . and not let my anxiety and OCD get the best of me.
Uses OCD as a Synonym for Cleanliness and Organization
The subcategory uses OCD as a synonym for cleanliness and organization represents TikTok videos in which women used OCD as a descriptor for a clean person, and includes 10 of the 28 videos in this category. Building upon the first category, minimizes OCD symptoms, this subcategory further demonstrates explanations, examples, and use of the term OCD in ways that do not accurately describe the disorder. A popular audio clip was utilized frequently in our sample and was often paired with visual content of individuals organizing or cleaning various objects and spaces. The woman in the audio stated:
When they come into my house and they also think that I am a sociopath, that I take the time to do this once a month. Like, you know what? You say OCD is a disease, I say it’s a blessing.
Through equating OCD to “a blessing” and also trivializing the term “sociopath” to simply describe someone who is well-organized, such TikTok videos minimize the OCD diagnosis and the experiences of individuals with OCD, equating the disorder to something it is not—a proclivity for cleanliness and organization. Furthermore, other TikToks with #OCD were solely about cleaning or organizing. A woman in one TikTok described a “bathroom hack for a deep clean” as she displayed bleach and a bowl of hot water. In another TikTok, these words crossed the screen for the viewer to read: “*My bff being messy*” and, subsequently, “*My OCD kicking in*,” while the video displays an unmade bed.
Accurately Depicts OCD Symptoms
The second category, accurately depicts OCD symptoms, is defined as women portraying information that aligns with the DSM-5 description of OCD symptom constellations and current research on OCD. Twenty videos (40%) comprise this category. Women in the TikToks in this category typically indicated they had an OCD diagnosis, describing their unique experiences with OCD and explaining how their symptoms align with the DSM-5 definition. For example, TikToks in our sample represented the following aspects of the DSM-5 symptoms of OCD (APA, 2013): recurrent intrusive thoughts, performance of a compulsion, and “clinically significant distress or impairment in social, occupational, or other important areas of functioning” (p. 237). For example, one TikTok begins with the words “Live with ______ for a day” across the screen. A woman is then pictured “selecting” OCD from a variety of mental health diagnoses. In other TikToks, users describe their compulsions, such as a woman narrating her need to perform various rituals like choosing a certain color shirt, or another in which a woman flips a light switch repeatedly.
Corrects Misunderstanding
The first subcategory, corrects misunderstanding, encompasses videos in which women with OCD sought to correct misinformation or inaccurate portrayals about OCD. Eight of the 20 videos from the second category are included in this subcategory. The following quote demonstrates a woman debunking popular misconceptions of OCD symptoms: “What people think OCD is *picture of an organized desk.* What it’s like for me: *woman spraying perfume.* My brain: ‘spray it 3 times or your mum will die.’” In another TikTok, a woman lamented the prevalent, stigmatized view of OCD:
OCD is not cute. She doesn’t wear big glasses and chunky sweaters while she neatly lines up her stationary in color order. She’s probably the most misunderstood disorder, to the point where people nonchalantly use her name to describe a neat person.
Importantly, the speaker describes OCD as “misunderstood,” directly contradicting the previously described “version” of OCD as simply a proclivity for neatness or organization.
Shares Obsessive Fears
In this subcategory, shares obsessive fears, women provided more specific information and details in their TikToks to depict OCD in a more holistic, accurate manner. Eleven videos are included in this subcategory. The fears women shared included the deaths of loved ones, losing one’s job, accidentally setting one’s house on fire, losing a relationship, and not locking one’s front door. One woman’s TikTok portrayed the intrusive thoughts and subsequent fears she experienced frequently:
Documenting a side of OCD that people don’t usually see: Did I tell my mom I love her before she went to bed? What if she dies on the way to work tomorrow? Should I wake her up and tell her just in case? No, that will make her mad. Wait, but did I lock the doors? Did my sister make it home safe? She didn’t text me; her location is off. Oh, she’s fine; she just responded. Should I check the locks?
This quote demonstrates the intrusive thoughts that individuals with OCD often experience. More specifically, the intrusive thoughts in this example include fears such as death of a loved one, uncertainty, and potential lack of safety for self and others.
Discussion
The purpose of this study was to increase understanding of how women are portraying OCD on TikTok to inform counselors on the current social discourse around OCD. Our findings substantiate the extant literature and provide new insight, possibilities, and practice implications given this novel exploration of how women discuss OCD on TikTok. The categories that emerged from our content analysis reveal the variety in the types of TikToks women created and hashtagged with the term “OCD,” with the two main themes being minimizes OCD symptoms, demonstrating the trivialization of OCD by women on TikTok, and accurately depicts OCD symptoms, in which women attempted to correct inaccurate perceptions about OCD by sharing their own experiences and factual information about the diagnosis. Our results also suggested that women with an OCD diagnosis shared more factually based depictions of the disorder than the women who did not indicate a diagnosis in their TikTok videos. Our findings of two dichotomous themes are unsurprising given other findings on health-related misinformation on TikTok (e.g., Basch, Meleo-Erwin, et al., 2021; McCashin & Murphy, 2022), yielding opportunities for professionals to provide accurate information on the platform.
The majority of women whose content fell in the accurately depicts OCD symptoms theme indicated they had an OCD diagnosis. These women corrected misinformation about OCD and also shared their own experiences of living with OCD, depicting the seriousness and pervasiveness of their obsessive thoughts. Our results indicate that women with OCD may desire to see OCD portrayed correctly in the media, in ways that are different from the stereotypical or comedic depictions often prevalent in mainstream media (Fennell & Boyd, 2014). These negative stereotypes may contribute to women’s oppression through the perpetuation of misinformation. Women with OCD also may be motivated by the fear of stigma (Steinberg & Wetterneck, 2017) and the desire to have their mental health diagnosis taken seriously. Fennell and Liberato (2007) noted the importance of societal conceptions of OCD to those with the diagnosis; therefore, the creators in our sample may be motivated to alter the popular understanding and trivialization of OCD (Pavelko & Myrick, 2016; Robinson et al., 2019) through their TikTok content as a result of living with the disorder themselves and the impact of their OCD symptoms on their functioning. Moreover, motivation to post publicly about one’s experience with OCD may help women connect with others (Fennell & Liberato, 2007) through a large social media platform.
Yet our other main theme of minimizes OCD symptoms supports findings from previous research (e.g., Pavelko & Myrick, 2016; Robinson et al., 2019) that OCD is frequently depicted in the media and popular culture in a manner that minimizes the symptomatology or severity of OCD symptoms. Our results illustrate that the content created by women on TikTok often portrays OCD as synonymous with cleanliness and organization, hence trivializing OCD symptoms. Multiple TikToks (n = 4) utilized a popular audio: “You say OCD is a disease; I say it’s a blessing,” over a video of someone organizing, often some sort of household item, which aligns with previous findings that OCD is typically portrayed in the media by characters with washing and cleaning compulsions (Fennell & Boyd, 2014). Additionally, multiple videos in the uses OCD as a synonym for cleanliness or organization subtheme included language and descriptions that stigmatized cleaning symptoms, such as “*My bff being messy*,” *My OCD kicking in*,” and “I literally saved my toothbrush to like get the corners and clean cuz I’m OCD.” Despite cleanliness being the most visible depiction of OCD (Steinberg & Wetterneck, 2017) and more often seen in women with OCD than in men (APA, 2022), the way these symptoms are portrayed do not holistically represent OCD or encompass the potential effects of this disorder and instead contribute to the continued trivialization of this disorder.
Implications
Our findings yield various implications for counselors and future research. Because of the popularity and breadth of TikTok content, both clients and counselors are likely to use the app and subsequently view TikToks that contain minimizing, trivializing, or stigmatizing information about OCD. Counselors are not immune to holding stigmatizing views about OCD (Steinberg & Wetterneck, 2017). Exposure to trivializing content may influence how counselors view OCD symptoms and the severity of OCD with their clients, potentially contributing to misdiagnosing OCD. Our results indicate cleanliness and organization were the common depictions of OCD on TikTok, which could result in counselors having a limited understanding of OCD symptomatology and misidentifying other types of OCD symptoms that fall into groupings such as unwanted sexual thoughts or religious obsessions (Glazier et al., 2013). Mental health counselors responded with social rejection and general concerns to case vignettes of clients with contamination obsessions and cleaning compulsions (Steinberg & Wetterneck, 2017); consumption of social media that equates OCD to cleanliness and organization could perpetuate similar stigmas toward OCD among counselors.
For clients, exposure to content that trivializes and/or stigmatizes OCD may lead to hesitancy to seek treatment (Steinberg & Wetterneck, 2017) or even a failure to recognize one’s symptoms as indicative of a mental health issue (Fennell & Liberato, 2007). Hence, our results stress the importance of counselors increasing their knowledge of OCD in its various presentations and examining their own beliefs and biases toward OCD symptoms, recognizing that our reactions as counselors may impact how clients choose to present or hide their symptoms of OCD out of fear of stigmatization. During the mental health assessment process, counselors may want to ask clients displaying OCD symptoms questions related to their perceptions of the disorder such as, “How have you seen OCD depicted by characters on TV or in the movies?” or “What do you believe about OCD according to what you have seen/read on social media?” For clients who indicate inaccurate or negative conceptualization of OCD, psychoeducation may be useful to correct misinformation or misconceptions about OCD that clients obtained from the media. Counselors also may want to help clients develop media literacy skills, particularly for clients who consume a lot of social media, so clients can effectively analyze and reflect on the messages they encounter regarding OCD.
To enhance counselors’ knowledge of OCD, counselor educators can use the portrayals of OCD on social media to inform classroom discussion and activities when teaching about mental health diagnosis. For example, counselor educators can ask students to describe what they have seen about OCD in the media and explore how these examples do or do not align with the DSM-5 description of OCD. Counselor educators also can encourage students to explore their own biases and perceptions about OCD, which may help reduce the stigma held by mental health counselors related to OCD symptoms (Steinberg & Wetterneck, 2017) and increase accurate diagnosis of OCD (Glazier et al., 2013).
Further, our results demonstrate the importance of public education to decrease stigma related to mental health disorders (Webb et al., 2016), particularly targeted to individuals who do not have an OCD diagnosis, as they may be more likely to share or create trivializing content. As Fennell and Liberato (2007) stated, “the need for more public information on the lived experience of OCD and mental ‘disorders’ cannot be stressed enough” (p. 328). TikTok shows great potential to spread health information (Basch, Fera, et al., 2021), and this social media platform could be utilized to help share more accurate depictions of OCD. For example, counselors, individuals with OCD, and other advocates may consider utilizing the power of a targeted “hashtag” campaign, with the goal of reducing stigma toward OCD through countering the impact of stigmatizing content (Robinson et al., 2019). This type of positive and factual representation of OCD also may help to combat societal inequalities that can be perpetuated through the stigmatization and trivialization of OCD, and hashtag campaigns may be enacted by individuals and larger counseling organizations alike.
TikTok has a unique feature called “stitch” that allows users to combine another user’s video with the one they are creating. Some counselors are already using the “stitch” function as a means of psychoeducation and advocacy to correct misconceptions of mental health in TikTok videos, where counselors can directly connect their educated responses to the original video that contained inaccurate information. To effectively challenge the stigma surrounding mental health diagnoses, counselors need to be aware of the current public discourse occurring on social media platforms and use this information to develop advocacy-based interventions. In line with the American Counseling Association’s Code of Ethics (2014), counselors should consider other means of engaging in advocacy to benefit those diagnosed with OCD, such as providing public education in their local contexts and supporting public policies that could help provide affordable treatment of the disorder. The IOCDF’s Advocate Program (IOCDF, 2022) may prove to be a beneficial resource for such work.
Concerning future research, we suggest utilizing a larger sample of TikTok videos, analyzing social media content on other platforms, and including gender-expansive individuals and cisgender men as part of the sample to gather more perspectives. Additionally, researchers can compare who is creating the social media content and where accurate or inaccurate portrayals of OCD are occurring on social media. Quantitative research may provide more insight into how individuals with an OCD diagnosis create media content compared to those who do not have a diagnosis. Understanding the nuances in how OCD is portrayed across platforms or creators can enhance counselors’ knowledge of how to use social media as appropriate resources or social connections for their clients with OCD. Finally, more information on how OCD is depicted on social media can help counselors better recognize the messages their clients receive about OCD when using social media and improve their ability to correct the unreliable information their clients consume on these platforms.
Limitations
Various limitations should be taken into consideration. Given the nature of qualitative research, the findings of this study cannot be generalized to larger groups. We did not obtain IRB approval for this study, given that we used publicly available information for our data, and we did not directly contact the video creators to clarify gender identity, OCD diagnosis, or other demographic information that would have enhanced the description of our sample or allowed us to explore how intersectionality impacts depictions of OCD. Because we did not gather demographic information, we determined inclusion based on the individuals’ presentation as a woman and/or use of she/her pronouns in their profile, and our results are based solely on the content the women disclosed in their videos. For example, we cannot conclusively determine that women with a diagnosis share more accurate information about OCD on TikTok as compared to those without a diagnosis. Additionally, we did not contact the creators to gain a more thorough understanding of their intended message when creating the video. Finally, it should be noted that by utilizing the 50 most viewed TikToks with #OCD, videos that were less widely viewed and shared were not included in our sample, perhaps limiting our understanding of more nuanced portrayals of OCD on TikTok. Utilizing the most viewed TikToks as our sample may have contributed to the resulting dichotomous themes, capturing only the predominant trends of minimizing or accurately depicting OCD symptoms.
Conclusion
OCD is a serious and often debilitating mental health disorder (APA, 2022) that is frequently misunderstood and misrepresented in mainstream culture (Pavelko & Myrick, 2016; Steinberg & Wetterneck, 2017). Through a content analysis of TikTok videos created by women with the hashtag “OCD,” our resulting themes and subthemes revealed a mix of perpetuating stereotypes and minimizing OCD symptoms and of sharing accurate information and personal experiences concerning OCD. These findings can assist counselors and counselor educators to better understand the types of social media content clients are viewing and potential harmful messages clients may internalize about OCD through exposure to media. Further, counselors should consider their own consumption of social media and examine their perceptions of and biases toward OCD throughout the treatment process. Likewise, counselor educators should adjust their pedagogy to encourage student exploration of misconceptions and enhance training in how to accurately diagnose and treat OCD in their future work as mental health counselors. Although social media can perpetuate stigma, it can also be used as a tool for powerful positive change, and we encourage all readers to consider the accuracy of the content they post on social media when it comes to depicting mental health disorders.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Anderson, K. E. (2020). Getting acquainted with social networks and apps: It is time to talk about TikTok. Library Hi Tech News, 37(4), 7–12. https://doi.org/10.1108/LHTN-01-2020-0001
Basch, C. H., Fera, J., Pierce, I., & Basch, C. E. (2021). Promoting mask use on TikTok: Descriptive, cross-sectional study. JMIR Public Health and Surveillance, 7(2), e26392. https://doi.org/10.2196/26392
Basch, C. H., Meleo-Erwin, Z., Fera, J., Jaime, C., & Basch, C. E. (2021). A global pandemic in the time of viral memes: COVID-19 vaccine misinformation and disinformation on TikTok. Human Vaccines & Immunotherapeutics, 17(8), 2373–2377. https://doi.org/10.1080/21645515.2021.1894896
Belloch, A., del Valle, G., Morillo, C., Carrió, C., & Cabedo, E. (2009). To seek advice or not to seek advice about the problem: The help-seeking dilemma for obsessive-compulsive disorder. Social Psychiatry and Psychiatric Epidemiology, 44(4), 257–264. https://doi.org/10.1007/s00127-008-0423-0
Bondi, L., & Burman, E. (2001). Women and mental health A feminist review. Feminist Review, 68(1), 6–33. https://doi.org/10.1080/01417780122133
Clark, D. A., & Radomsky, A. S. (2014). Introduction: A global perspective on unwanted intrusive thoughts. Journal of Obsessive-Compulsive and Related Disorders, 3(3), 265–268. https://doi.org/10.1016/j.jocrd.2014.02.001
Creswell, J. W. (2003). Research design: Qualitative, quantitative, and mixed methods approaches (2nd ed.). SAGE.
Dworkin, S. L. (2012). Sample size policy for qualitative studies using in-depth interviews. Archives of Sexual Behavior, 41, 1319–1320. https://doi.org/10.1007/s10508-012-0016-6
Fennell, D., & Boyd, M. (2014). Obsessive-compulsive disorder in the media. Deviant Behavior, 35(9), 669–686. https://doi.org/10.1080/01639625.2013.872526
Fennell, D., & Liberato, A. S. Q. (2007). Learning to live with OCD: Labeling, the self, and stigma. Deviant Behavior, 28(4), 305–331. https://doi.org/10.1080/01639620701233274
Fowler, L. R., Schoen, L., Stevens Smith, H., & Morain, S. R. (2021). Sex education on TikTok: A content analysis of themes. Health Promotion Practice, 23(5). https://doi.org/10.1177/15248399211031536
Glazier, K., Calixte, R. M., Rothschild, R.2013). High rates of OCD symptom misidentification by mental health professionals. Annals of Clinical Psychiatry, 25(3), 201–209. https://www.ingentaconnect.com/contentone/fmc/acp/2013/00000025/00000003/art00006
International Obsessive Compulsive Disorder Foundation. (2022). IOCDF Advocate Program. https://iocdf.org/advocate-program/#:~:text=The%20IOCDF%20Advocate%20Program%20i
s%20about%20OCD%20and%20related%20disorders
International Obsessive Compulsive Disorder Foundation. (n.d.a). IOCDF Training Institute. https://iocdf.org/professionals/training-institute/
International Obsessive Compulsive Disorder Foundation. (n.d.b.) What is OCD? https://iocdf.org/about-ocd/
Iqbal, M. (2022). TikTok revenue and usage statistics. Business of Apps. https://www.businessofapps.com/data/tik-tok-statistics/
Johnson, K. F., Brookover, D. L., Borden, N. J., Worth, A. K., Temple, P., & Mahan, L. B. (2021). What YouTube narratives reveal about online support, counseling entrance, and how Black Americans manage depression symptomology. Informatics for Health and Social Care, 46(1), 84–99. https://doi.org/10.1080/17538157.2020.1865967
Johnson, K. F., Worth, A., & Brookover, D. (2019). Families facing the opioid crisis: Content and frame analysis of YouTube videos. The Family Journal, 27(2), 1–12. https://doi.org/10.1177/1066480719832507
Lorenz, T., Browning, K., & Frenkel, S. (June, 2020). TikTok teens and K-pop stans say they sank Trump rally. The New York Times. https://www.nytimes.com/2020/06/21/style/tiktok-trump-rally-tulsa.html
Ma, Z. (2017). How the media cover mental illnesses: A review. Health Education, 117(1), 90–109. https://doi.org/10.1108/HE-01-2016-0004
McCashin, D., & Murphy, C. M. (2022). Using TikTok for public and youth mental health—A systematic review and content analysis. Clinical Child Psychology and Psychiatry, 28(1). https://doi.org/10.1177/13591045221106608
Pavelko, R., & Myrick, J. G. (2016). Tweeting and trivializing: How the trivialization of obsessive–compulsive disorder via social media impacts user perceptions, emotions, and behaviors. Imagination, Cognition and Personality, 36(1), 41–63. https://doi.org/10.1177/0276236615598957
Robinson, P., Turk, D., Jilka. S., & Cella, M. (2019). Measuring attitudes towards mental health using social media: Investigating stigma and trivialisation. Social Psychiatry and Psychiatric Epidemiology, 54(1), 51–58. https://doi.org/10.1007/s00127-018-1571-5
Schreier, M. (2014). Qualitative content analysis. In U. Flicke (Ed.), The SAGE handbook of qualitative data analysis (pp. 170–183). SAGE. https://doi.org/10.4135/9781446282243
Sharevski, F., Loop, J. V., Jachim, P., Devine, A., & Pieroni, E. (2023). Abortion misinformation on TikTok: Rampant content, lax moderation, and vivid user experiences. arXiv preprint. https://doi.org/10.48550/arXiv.2301.05128
Starcevic, V., Berle, D., Brakoulias, V., Sammut, P., Moses, K., Milicevic, D., & Hannan, A. (2011). Functions of compulsions in obsessive–compulsive disorder. Australian & New Zealand Journal of Psychiatry, 45(6), 449–457. https://doi.org/10.3109/00048674.2011.567243
Steinberg, D. S., & Wetterneck, C. T. (2017). OCD taboo thoughts and stigmatizing attitudes in clinicians. Community Mental Health Journal, 53, 275–280. https://doi.org/10.1007/s10597-016-0055-x
Vitikainen, S., Buzzell, M., de Regt, L., & Timmermans, L. (2020). “Stop licking the boots and start marching them”—An exploratory research proposal into peer-to-peer political discussion on TikTok. Masters of Media. http://mastersofmedia.hum.uva.nl/blog/2020/10/21/stop-licking-the-boots-and-start-marching-them/
Wallis, C. (2011). Performing gender: A content analysis of gender display in music videos. Sex Roles, 64(3–4), 160–172. https://doi.org/10.1007/s11199-010-9814-2
Webb, M., Peterson, J., Willis, S. C., Rodney, H., Siebert, E., Carlile, J. A., & Stinar, L. (2016). The role of empathy and adult attachment in predicting stigma toward severe and persistent mental illness and other psychosocial or health conditions. Journal of Mental Health Counseling, 38(1), 62–78. https://doi.org/10.17744/mehc.38.1.05
Erin E. Woods, PhD, LPC, serves as Clinic Director at the College of William & Mary. Alexandra Gantt-Howrey, PhD, NCC, is an assistant professor at New Mexico State University. Amber L. Pope, PhD, LPC, LMHC, CCTP, is an assistant professor at the College of William & Mary. Correspondence may be addressed to Alexandra Gantt-Howrey, P.O. Box 30001, MSC 3AC, Las Cruces, New Mexico 88003, aghowrey@nmsu.edu.
Aug 20, 2021 | Volume 11 - Issue 3
Hannah B. Bayne, Danica G. Hays, Luke Harness, Brianna Kane
We conducted a content analysis of counseling scholarship related to Whiteness for articles published in national peer-reviewed counseling journals within the 35-year time frame (1984–2019) following the publication of Janet Helms’s seminal work on White racial identity. We identified articles within eight counseling journals for a final sample of 63 articles—eight qualitative (12.7%), 38 quantitative (60.3%), and 17 theoretical (27.0%). Our findings outline publication characteristics and trends and present themes for key findings in this area of scholarship. They reveal patterns such as type of research methodology, sampling, correlations between White racial identity and other constructs, and limitations of White racial identity assessment. Based on this overview of extant research on Whiteness, our recommendations include future research that focuses on behavioral and clinical manifestations, anti-racism training within counselor education, and developing a better overall understanding of how White attitudes and behaviors function for self-protection.
Keywords: Whiteness, White racial identity, counseling scholarship, counseling journals, content analysis
Counselors are ethically guided to understand and address the roles that race, privilege, and oppression play in impacting both themselves and their clients (American Counseling Association [ACA], 2014). Most practitioners identify as White despite the population diversity in the United States (U.S. Census Bureau, 2020), which holds implications for understanding how Whiteness impacts culturally competent counselor training and practice (Helms, 1984, 1995, 2017). It is important, then, to understand the role of racial identity within counseling, particularly in terms of how Whiteness can be deconstructed and examined as a constant force impacting power dynamics and client progress (Helms, 1990, 2017; Malott et al., 2015). Whiteness models (i.e., Helms, 1984) describe how White people make meaning of their own and others’ racial identity as a result of personal and social experiences with race (Helms, 1984, 2017). The Helms model, along with other constructs, such as color-blindness (Frankenberg, 1993), White racial consciousness (Claney & Parker, 1989), and White fragility (DiAngelo, 2018), implicates the harmful impacts of Whiteness and invites critical reflection of how these constructs impact the counseling process.
Though much has been theorized regarding Whiteness and its impact within the helping professions, the contributions of Whiteness scholarship within professional counseling journals are unclear. An understanding of the specific professional applications and explorations of Whiteness within counseling can help identify best practices in counselor education, research, and practice to counter the harmful impacts of Whiteness and encourage growth toward anti-racist attitudes and behaviors.
White Racial Identity and Related Constructs
The Helms (1984) model of White racial identity (WRI) presents Whiteness as a developmental process centering on racial consciousness (i.e., the awareness of one’s own race), as well as awareness of attitudes and behaviors toward other racial groups (Helms, 1984, 1990, 1995, 2017). According to Helms, White people have the privilege to restrict themselves to environments and relationships that are homogenous and White-normative, thus limiting their progression through the stages (DiAngelo, 2018; Helms, 1984). The initial model (Helms, 1984) contained five stages (i.e., Contact, Disintegration, Reintegration, Pseudo-Independence, and Autonomy), each with a positive or negative response that could facilitate progression toward a more advanced stage, regression to earlier stages of the model, or stagnation at the current stage of development. Helms (1990) later added a sixth status, Immersion/Emersion, to the model as an intermediary between Pseudo-Independence and Autonomy. These final three stages of the model (i.e., Pseudo-Independence, Immersion/Emersion, Autonomy) involve increasing levels of racial acceptance and intellectual and emotional comfort with racial issues, which in turn leads to the development of a positive and anti-racist WRI (Helms, 1990, 1995).WRI requires intentional and sustained attention toward how Whiteness impacts the self and others, with progression through the stages leading to beneficial intra and interpersonal outcomes (Helms, 1990, 1995, 2017).
Since Helms (1984), several additional components of Whiteness have been introduced, primarily within psychology, counseling psychology, and sociology scholarship. White racial consciousness is distinct from the WRI model in its focus on attitudes toward racial out-groups, rather than using the White in-group as a reference point (Choney & Behrens, 1996; Claney & Parker, 1989). Race essentialism refers to the degree to which a person believes that race reflects biological differences that influence personal characteristics (Tawa, 2017). Symbolic/modern racism refers to overt attitudes of White people related to their perceived superiority (Henry & Sears, 2002; McConahay, 1986). A fourth Whiteness component, color-blind racial ideology, enables color-evasion (i.e., “I don’t see color”) and power-evasion roles (i.e., “everyone has an equal chance to succeed”), which allow White people to deny the impact of race and therefore evade a sense of responsibility for oppression (Frankenberg, 1993; Neville et al., 2013). White privilege refers to the systemic and unearned advantages provided to White people over people of color (McIntosh, 1988). There are also psychosocial costs accrued to White people as a result of racism that include (a) affective (e.g., anxiety and fear, anger, sadness, guilt and shame); (b) cognitive (i.e., distorted views of self, others, and reality in general related to race); and (c) behavioral (i.e., avoidance of cross-racial situations or loss of relationships with White people) impacts (Spanierman & Heppner, 2004). White fragility (DiAngelo, 2018) reflects defensive strategies White people use to re-establish cognitive and affective equilibrium regarding their own Whiteness and impact on others.
Whiteness concepts are thus varied, with different vantage points of how White people might engage in the consideration of power, privilege, and racism, and what potential implications these constructs might have on their development. These constructs also seem largely rooted in psychology research, and it is therefore unclear the extent to which counselor educators and researchers have examined and applied these constructs to training and practice. Such an analysis can assist in situating Whiteness within the specific contexts and professional roles of counseling and can identify areas in need of further study.
The Present Study
Because of the varied components of Whiteness, as well as its potential impact on counselor development and counseling process and outcome (Helms, 1995, 2017), there is a need to examine how these constructs have been examined and applied within counseling research. We sought to identify how and to what degree Whiteness constructs have been explored or developed within the counseling profession since the publication of the Helms (1984) model. We hope to summarize empirical and theoretical constructs related to Whiteness in national peer-reviewed counseling journals to more clearly consider implications for training and practice. Such analysis can highlight the saliency of WRI, demonstrating the need for continued focus on the influences and impacts of Whiteness within counseling. The following research questions were addressed: 1) What types of articles, topics, and major findings are published on Whiteness?; 2) What are the methodological features of articles published on Whiteness?; and 3) What are themes from key findings across these publications?
Method
We employed content analysis to identify publication patterns of national peer-reviewed counseling journals regarding counseling research on Whiteness in order to understand the scope and depth of this scholarship as it applies to fostering counselor training and practice. Content analysis is the systematic review of text in order to produce and summarize numerical data and identify patterns across data sources regarding phenomena (Neuendorf, 2017). In addition, content analysis has been used to summarize and identify patterns for specific topics, including multicultural counseling (e.g., Singh & Shelton, 2011).
Data Sources and Procedure
The sampling units for this study were journal articles on Whiteness topics published in national peer-reviewed journals (N = 24) of the ACA and its divisions, the American School Counselor Association, the American Mental Health Counselors Association, the National Board for Certified Counselors, and Chi Sigma Iota International. We used the following search terms: White supremacy, White racial identity, White privilege, White fragility, White guilt, White shame, White savior, White victimhood, color-blindness, race essentialism, anti-racism, White racism, reverse racism, White resistance, and Whiteness. We selected a 35-year review period (i.e., 1984–2019) to correspond with Helms’s (1984) foundational work on WRI.
We reviewed article abstracts to identify an initial sampling unit pool (N = 185 articles; 29 qualitative [15.6%], 56 quantitative [30.3%], and 100 theoretical [54.1%]). In pairs, we reviewed the initial pool to more closely examine each sampling unit for inclusion in analysis. We excluded 122 articles upon closer inspection (e.g., special issue introductions, personal narratives or profiles, broader focus on social justice issues, ethnic identity, multiculturalism, or primary focus on another racial group). This resulted in a final sample of 63 articles—eight qualitative (12.7%), 38 quantitative (60.3%), and 17 theoretical (27.0%; see Table 1).
Research Team
Our team consisted of four researchers: two counselor education faculty members and two counselor education doctoral students. We all identify as White. Hannah B. Bayne and Danica G. Hays hold doctorates in counselor education, and Luke Harness and Brianna Kane hold master’s degrees in school counseling and mental health counseling, respectively. We were all trained in qualitative research methods, and Bayne and Hays have conducted numerous qualitative research projects, including previous content analyses. Bayne and Hays trained Harness and Kane on content analysis through establishing coding protocols and coding together until an acceptable inter-rater threshold was met.
Table 1
Exclusion and Inclusion of Articles by Journal and Article Type
| Journal |
Excludeda |
Included |
Total
Sample |
% of
Final
Sample |
| Quant |
Qual |
Theory |
Quant |
Qual |
Theory |
| Journal of Counseling & Development |
5 |
0 |
11 |
16 |
4 |
5 |
24 |
38.1% |
Journal of Multicultural Counseling and
Development |
3 |
3 |
14 |
14 |
3 |
8 |
24 |
38.1% |
| Counselor Education and Supervision |
1 |
0 |
1 |
4 |
1 |
2 |
7 |
11.1% |
| The Journal of Humanistic Counseling |
1 |
2 |
14 |
1 |
1 |
1 |
3 |
4.8% |
| Journal of Mental Health Counseling |
0 |
0 |
2 |
1 |
0 |
3 |
2 |
3.2% |
| Counseling and Values |
0 |
0 |
0 |
1 |
0 |
0 |
1 |
1.6% |
| The Family Journal |
1 |
1 |
5 |
0 |
0 |
2 |
1 |
1.6% |
| Journal of Creativity in Mental Health |
0 |
2 |
4 |
0 |
0 |
1 |
1 |
1.6% |
| Adultspan Journal |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| The Career Development Quarterly |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Counseling Outcome Research
and Evaluation |
0 |
2 |
0 |
0 |
0 |
0 |
0 |
0% |
Journal for Social Action in Counseling
and Psychology |
0 |
0 |
3 |
0 |
0 |
0 |
0 |
0% |
| The Journal for Specialists in Group Work |
0 |
1 |
6 |
0 |
0 |
0 |
0 |
0% |
Journal of Addictions & Offender
Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| Journal of Child and Adolescent Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| Journal of College Counseling |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Journal of Counselor Leadership
and Advocacy |
1 |
5 |
6 |
0 |
0 |
0 |
0 |
0% |
| Journal of Employment Counseling |
2 |
0 |
4 |
0 |
0 |
0 |
0 |
0% |
| Journal of LGBTQ Issues in Counseling |
0 |
1 |
2 |
0 |
0 |
0 |
0 |
0% |
Journal of Military and Government
Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Measurement and Evaluation in
Counseling and Development |
1 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
| Professional School Counseling |
0 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
| Rehabilitation Counseling Bulletin |
3 |
1 |
2 |
0 |
0 |
0 |
0 |
0% |
| The Professional Counselor |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0% |
| Professional School Counseling |
0 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
Note. Quant = quantitative research articles; Qual = qualitative research articles; Theory = theoretical articles.
aArticles were excluded from analysis if they did not directly address Whiteness or White racial identity (e.g., special issue introductions, personal narratives or profiles, broader focus on social justice issues, ethnic identity, multiculturalism, or primary focus on another racial group).
Coding Frame Development
Dimensions and categories for our coding frame included: journal outlet, publication year, author characteristics (i.e., name, institutional affiliation, ACES region), article type, sample characteristics (e.g., composition, size, gender, race/ethnicity), research components (e.g., research design, data sources or instrumentation, statistical methods, research traditions, trustworthiness strategies), topics discussed (e.g., WRI attitudes, counselor preparation models, intervention use, client outcomes, counseling process), article implications and limitations, and a brief statement of key findings. Over the course of research team meetings, we reviewed and operationalized the coding frame dimensions and categories. We then selected one empirical and one conceptual article to code together in order to refine the coding frame, which resulted in further clarification of some categories.
Data Analysis
To establish evidence of replicability (Neuendorf, 2017), we coded eight (12.7%) randomly selected cases proportionate to the sample composition (i.e., two conceptual, four quantitative, two qualitative). We analyzed the accuracy rate of coding using R data analysis software for statistical analysis (LoMartire, 2020). Across 376 possible observations for eight cases, there was an acceptable rate of coding accuracy (0.89). In addition, pairwise Pearson-product correlations among raters indicated that coding misses did not follow a systematic pattern for any variable (r = −.10 to .65), and thus there were no significant variations in coding among research team members. After pilot coding, we met to discuss areas of coding misses to ensure understanding of the final coding frame.
For the main coding phase, we worked in pairs and divided the sample equally for independent and consensus coding. Upon completion of consensus coding of the entire sample, we extracted 29 keywords describing the Whiteness topics discussed in the articles. Bayne and Hays reviewed the 29 independent topics and collapsed the topics into eight larger themes. To identify themes across the key findings, Bayne and Harness reviewed 125 independent statements based on coder summaries of article findings, and through independent and consensus coding collapsed statements to yield three main themes.
Results
Article Characteristics
We focused on several article characteristics (Research Question 1): article type (conceptual, quantitative, qualitative); number of relevant articles per journal outlet; the relationship between journal outlet and article type; and frequency of Whiteness topics within and across journal outlets. Of the 24 national peer-reviewed counseling journals, eight journals (33.3%) contained publications that met inclusion criteria (i.e., contained keywords for Whiteness from our search criteria and focused specifically on WRI). The number of publications in those journals ranged from 1 to 24 (M = 2.5; Mdn = 7.88; SD = 10.15) and are listed in order of frequency in Table 2). There was not a significant relationship between the journal outlet and article type (i.e., quantitative, qualitative, conceptual) for this topic (r = 0.04, p = .39).
Table 2
Articles Addressing Whiteness and Associated Keywords in National Peer-Reviewed Counseling Journals
| Journal |
Articles Addressing Whiteness |
Percent of Total Sample |
| Journal of Counseling & Development |
24 |
38.1% |
| Journal of Multicultural Counseling and Development |
24 |
38.1% |
| Counselor Education and Supervision |
7 |
11.1% |
| The Journal of Humanistic Counseling |
3 |
4.8% |
| Journal of Mental Health Counseling |
2 |
3.2% |
| Counseling and Values |
1 |
1.6% |
| The Family Journal |
1 |
1.6% |
| Journal of Creativity in Mental Health |
1 |
1.6% |
| Adultspan Journal |
0 |
0% |
| The Career Development Quarterly |
0 |
0% |
| Counseling Outcome Research and Evaluation |
0 |
0% |
| Journal for Social Action in Counseling and Psychology |
0 |
0% |
| The Journal for Specialists in Group Work |
0 |
0% |
| Journal of Addictions & Offender Counseling |
0 |
0% |
| Journal of Child and Adolescent Counseling |
0 |
0% |
| Journal of College Counseling |
0 |
0% |
| Journal of Counselor Leadership and Advocacy |
0 |
0% |
| Journal of Employment Counseling |
0 |
0% |
| Journal of LGBTQ Issues in Counseling |
0 |
0% |
| Journal of Military and Government Counseling |
0 |
0% |
Measurement and Evaluation in Counseling and
Development |
0 |
0% |
| Professional School Counseling |
0 |
0% |
| Rehabilitation Counseling Bulletin |
0 |
0% |
| The Professional Counselor |
0 |
0% |
| Professional School Counseling |
0 |
0% |
Additionally, we identified eight themes of topics discussed within counseling research on Whiteness (see Table 3). For qualitative research, the three most frequently addressed topics were theory development, intrapsychic variables, and multicultural counseling competency (MCC). The most frequent topics discussed in theoretical articles were theory development, counselor preparation, Whiteness and WRI expression, cultural identity development, and counseling process.
Table 3
Themes in Topics Discussed Within Whiteness and WRI Articles
| Theme |
Description |
N
% |
Quant
n / % |
Qual
n / % |
Theory
n / % |
Examples |
| Whiteness and WRI Expression |
Attitudes and knowledge related to WRI and Whiteness constructs, with some (n = 5) examining pre–posttest changes
|
43
68.3% |
32 74.4% |
3
7.0% |
8
18.6% |
WRI attitudes, color-blind racial attitudes, racism and responses, White privilege and responses, and developmental considerations
|
| Cultural Identity Development |
Cultural identities and developmental processes outside of race
|
27
42.9% |
21
77.8% |
1
3.7% |
5
18.5% |
Ethnic identity, womanist identity, cultural demographics such as gender and age
|
| Counselor Preparation |
Training implications, with some presenting training intervention findings (n = 6)
|
23
36.5% |
17
73.9% |
1
4.3% |
5
21.8% |
Pedagogy, training interventions, and supervision process and outcome
|
| Theory Development |
Development or expansion of theoretical concepts |
18
28.6% |
5
27.8% |
5
27.8% |
8
44.4% |
White racial consciousness versus WRI, prominent responses to White privilege, psychological dispositions of White racism
|
| Multicultural Counseling Competency |
Measurements of perceived multicultural counseling competency
|
12
19.0% |
10
83.3% |
2
16.7% |
0
0.0% |
Perceived competency,
link with WRI |
| Counseling Process |
Counseling process and outcome variables
|
11
17.5% |
8
72.7% |
1
9.1% |
2
18.2% |
Client perceptions, working alliance, and clinical applications
|
| Intrapsychic Variables |
Affective and cognitive components that influence Whiteness and WRI
|
11
17.5% |
8
72.7% |
2
18.2% |
1
9.1% |
Personality variables, cognitive development, ego development
|
| Assessment Characteristics |
Development and/or critique of Whiteness and WRI measurements
|
9
14.3% |
8
88.9% |
0
0.0% |
1
11.1% |
Limitations of WRI scales, development of White privilege awareness scales |
| Totala |
|
154
|
111
72.1% |
15
9.7% |
30
19.5% |
|
Note. Quant = quantitative research articles; Qual = qualitative research articles; Theory = theoretical articles.
aPercentage total exceeds 100% because of rounding and/or topic overlap between articles.
Methodological Features
To address Research Question 2, we explored the methodological features of articles. These features included sample composition, research design, data sources, and limitations as reported within each empirical article (n = 46).
Sample Composition
For the 45 studies providing information about the racial/ethnic composition of their samples, White individuals accounted for a mean of 91% of total participants (range = 55%–100%; SD = 14). An average of 14% Black (SD = 6.7), 7.1% Latinx (SD = 4.7), 5.4% Asian (SD = 2.3), and less than 5% each of multiracial, Arab, and Native American respondents were included across the samples. Of studies reporting gender (n = 44), women accounted for an average of 68% of total participants (range = 33–100; SD = 14.7), and men accounted for 31% of total samples (range = 12–67; SD = 14). The age of participants, reported in 71.7% of the empirical studies, ranged from 16 to 81 (M = 29, SD = 8.2).
Of the 61 independent samples across the articles, a majority focused on student populations, with master’s trainees (n = 20, 32.8%), undergraduate students (n = 14, 21.9%), and doctoral trainees (n = 10, 16.4%) representing over 70% of the sample. The remainder of the samples included practitioners (n = 8, 13.1%), unspecified samples (n = 3, 4.9%), university educators (n = 2, 3.3%), educational specialist trainees (n = 2, 3.3%), site supervisors (n = 1, 1.6%), and general population adult samples (n = 1, 1.6%). The target audience of the articles (N = 63) focused primarily on counselor trainees (n = 34, 49.3%) or clients in agency/practice settings (n = 12, 17.4%). Other audiences included practitioners (n = 9, 13%), researchers (n = 3, 4.3%), general population (n = 6, 8.7%), counselor educators (n = 1, 1.4%), and general university personnel (n = 1, 1.4%).
Research Design and Data Sources
Of the 38 quantitative articles, 10 (26.3%) included an intervention as part of the research design. The majority employed a correlational design (n = 27, 71.1%), with the remainder consisting of four (10.5%) descriptive, four (10.5%) quasi-experimental, one (2.6%) ex post facto/causal comparative, one (2.6%) pre-experimental, and one (2.6%) true experimental design. In recruiting and selecting samples, most researchers used convenience sampling (n = 27, 57.4%), while the rest used purposive (n = 12, 31.6%), simple random (n = 5, 10.6%), stratified (n = 2, 4.3%), and homogenous (n = 1, 2.1%) sampling methods.
Regarding study instrumentation, 37 quantitative studies utilized self-report forced-choice surveys, with one study employing a combination of forced-choice and open-ended question surveys. Across the 38 quantitative studies, 13 of 50 (26%) assessments were used more than once. The most frequently used assessment was the White Racial Identity Attitudes Scale (n = 24; Helms & Carter, 1990). The 50 assessments purported to measure the following targeted variables: race/racial identity/racism (n = 17, 34%); MCC (n = 9, 18%); cultural identity (n = 6, 12%); counseling process and outcome (n = 5, 10%); social desirability (n = 2, 4%); and other variables such as personality, anxiety, and ego development (n = 11, 22%). Finally, data analysis procedures included ANOVA/MANOVA (n = 25, 30.9%), correlation (n = 23, 28.4%), regression (n = 17, 21%), t-tests (n = 7, 8.6%), descriptive (n = 5, 6.2%), exploratory factor analysis (n = 1, 1.2%), confirmatory factor analysis (n = 1, 1.2%), SEM/path analysis (n = 1, 1.2%), and cluster analysis (n = 1, 1.2%).
We identified the research traditions of the eight qualitative studies as follows: phenomenology (n = 3, 37.5%), grounded theory (n = 2, 25%), and naturalistic inquiry (n = 1, 12.5%); two were unspecified (25%). The most common qualitative recruitment method was criterion sampling (n = 5, 62.5%), followed by convenience (n = 3, 37.5%), homogenous (n = 2, 25%), snowball/chain (n = 2, 25%), intensity (n = 2, 25%), and stratified purposeful (n = 1, 12.5%) sampling procedures. (Several studies used multiple recruitment methods, resulting in totals greater than 100%.) There were 12 data sources reported across the eight qualitative studies, falling into the following categories: individual interviews (n = 7, 58.3%), focus group interviews (n = 2, 16.7%), artifacts/documents (n = 2, 16.7%), and observations (n = 1, 8.3%). Trustworthiness strategies included prolonged engagement (n = 7, 13.7%); use of a research team (n = 6, 11.8%); researcher reflexivity, triangulation of data sources, thick description, and simultaneous data collection and analysis (n = 5 each, 9.8%); peer debriefing, audit trail, and member checking (n = 4 each, 7.8%); theory development (n = 3, 5.9%); and one each (2%) of external auditor, memos and/or field notes, and persistent observation.
Limitations Within Sampled Studies
Of the 46 empirical studies, 44 (95.7%) reported limitations. Limitations included design issues related to sampling/generalizability (n = 38, 82.6%); self-report/social desirability (n = 23, 50.0%); instrumentation (n = 20, 43.5%); research design concerns related to the ability to directly measure a variable of interest (e.g., clinical work, training activities; n = 7, 15.2%); experimenter/researcher effects (n = 3, 6.5%); use of less sophisticated statistical methods (n = 3, 6.5%); and use of an analogue design (n = 2, 4.3%). Within identified limitations, researchers most often cited limited generalizability with regard to sample composition (i.e., lack of diversity, small sample sizes, homogenous samples). Social desirability was noted as a potential limitation given the nature of the topics (i.e., racism, prejudice, privilege). Instrumentation issues pertained to weak reliability for samples, limited validity evidence, and disadvantages of self-administration. Researchers also acknowledged the difficulty of conceptualizing WRI constructs as distinct, noting the multidimensional nature of WRI and the challenge in discriminating between complex constructs.
Key Findings
There were three main categories of key findings. The largest category (i.e., 51 codes) consisted of identification of correlates and predictors of Whiteness/White racial identity. Findings related to gender and WRI were mixed, with several articles (n = 7) noting differences in WRI stages among men and women (i.e., women more frequently endorsing Contact and Pseudo-Independent stages, men more frequently endorsing Disintegration and Reintegration), and others determining gender differences were not significant in predicting WRI (n = 2). Additional findings included significant positive correlations and predictive effects between WRI, racism, MCC, personality variables (i.e., Openness linked with higher WRI and Neuroticism linked with lower WRI), and working alliance. Other constructs, such as ego defenses, emotional states, social–cognitive maturity, fear, and religious orientation, also demonstrated significant alignment with WRI stages. White guilt, the impact of personal relationships with communities of color, and lower levels of race salience (i.e., race essentialism) were also linked to Whiteness.
The next largest category (i.e., 32 codes) related to critiques of White racial identity models and measures. Most of the conceptual articles focused in some way on this category, often criticizing WRI models as subjective and lacking in complexity, or critiquing WRI measurement and previous research because of issues of reliability and validity. Several stressed caution for interpreting WRI according to existing models, suggesting a more nuanced approach of contextualizing individuals and accounting for within-group variation. Empirical articles also suggested that achieving and maintaining higher levels of WRI, particularly anti-racist identities and attitudes, may be more difficult than originally conceptualized and may require levels of engagement that are difficult to maintain in a racist society.
Training implications and impact (i.e., 24 codes), noted within empirical and conceptual studies, included tips for addressing Whiteness in counselor education (e.g., offering courses focused on Whiteness and anti-racism) and in supervision (e.g., openly discussing race, privilege, and oppression; matching supervisors and supervisees by racial identity when possible). Empirical studies noted mixed improvement in WRI stages and MCC as a result of both general progression through a counselor training program as well as specific multicultural training: Training was linked to increased White guilt and privilege awareness (n = 15), though others did not find significant effects of training (n = 2). Conceptual articles emphasized focusing training on anti-racist development. Collectively, these findings and subsequent implications encourage further research and reflection on the correlates of WRI and MCC, factors facilitating growth, and ways to improve research and measurement to enhance critical engagement with these topics.
Discussion and Implications
In this content analysis of 63 articles covering a 35-year period across eight national counseling journals, we found that a third of counseling journals featured scholarship specifically related to Whiteness, with the Journal of Counseling & Development and the Journal of Multicultural Counseling and Development accounting for more than 76% of the total sampling units. The majority of the articles were quantitative, followed by theoretical and qualitative articles. Topical focus was centered on correlates of Whiteness with variables such as racism and color-blindness, other non-racial components of cultural identity, training implications, and theory development (see Table 3). Interestingly, many Whiteness constructs discussed in the general literature (e.g., White fragility, modern racism, psychosocial costs) were not addressed in counseling scholarship; the primary constructs discussed were WRI and White privilege.
The sample composition across empirical studies was primarily White and female with a mean age in the late 20s and with undergraduate students comprising on average 22% of the article samples. In addition, practitioners, site supervisors, the general population, and EdS trainees only comprised between 1.6% and 13.1% of the samples. Schooley et al. (2019) cautioned against the overuse of undergraduate students when measuring Whiteness constructs because of the complexities and situational influences of WRI development, and this warning seems to hold relevance for counseling scholarship. Methodological selection mirrored previously found patterns in counseling research (Wester et al., 2013), with most quantitative studies relying upon convenience sampling and correlational design with ANOVA/MANOVA as the selected statistical analyses. In addition, 26.3% of the articles included an intervention. For the qualitative studies, the most frequently used tradition and method was phenomenology and individual interviews.
Overall, findings from the sample support theoretically consistent relationships with Whiteness and/or WRI, including their predictive nature of MCC, social desirability, working alliance, and lower race salience. However, findings were mixed on the role of gender and MCC in connection to a training intervention. Additionally, some studies in our sample critiqued WRI models, cautioning against oversimplification of a complex model and highlighting issues in measurement due to subjectivity and social desirability. This critique aligns with previous researchers who have suggested that WRI is more complex than previously indicated (see Helms, 1984, 1990, 2017). WRI may be highly situational and affected by within-group differences and internal and external factors that complicate accuracy in assessment and clinical application. Of particular concern in previous research is the ability to properly conceptualize and measure the Contact and Autonomy stages (Carter et al., 2004). Both stages have demonstrated difficulty in assessment due to an individual’s lack of awareness of personal racism at each stage (Carter et al., 2004; Rowe, 2006). The Autonomy status, in particular, could be impacted by what DiAngelo (2018) referred to as “progressive” or “liberal” Whiteness, in which efforts are more focused on maintaining a positive self-image than engaging with people of color in meaningful ways (Helms, 2017). Therefore, although there are some consistencies and corroborations within counseling literature and other scholarship on Whiteness, the critiques and complexities of the topic suggest further inquiry is needed.
Implications for Counseling Research
Based on our findings, we note several directions for future research. First, future studies could include greater demographic diversity as well as more participation from counselor educators, site supervisors, practitioners, and clients across the ACES regions. Including counselor educators in empirical studies can highlight aspects of Whiteness that influence their approach to training and scholarship. With regard to increasing scholarship involving site supervisors, practitioners, and clients, Hays et al. (2019) highlighted several strategies for recruiting sites to participate as co-researchers as well as obtaining clinical samples through strengthening research–practice partnerships. Additionally, recruiting more heterogenous samples—in terms of sample composition and demographics—could provide much-needed psychometrics for available measures as well as refined operationalization of Whiteness. Additional research can further explore individual correlates and predictors to enhance counselor training, supervision, and practice by identifying opportunities for assessment and development at each level of WRI.
Second, most reports of empirical studies in our sample noted concerns with sampling and generalizability, social desirability, and instrumentation. Given these concerns, researchers are to be cautious about the interpretation and application of previous study findings using the White Racial Identity Attitudes Scale (WRIAS). In particular, scholarship within counseling and related disciplines reveals substantial psychometric concerns with the WRIAS’s Contact and Autonomy stages (Behrens, 1997; Carter et al., 2004; Hays et al., 2008; Malott et al., 2015). The complex nature of assessing WRI-related behaviors that may run counter to a person’s intentions (Carter et al., 2004; DiAngelo, 2018) needs further study. Additionally, given the concerns with self-report measures due to socially desirable responses, it seems problematic that none of the current quantitative articles used performance measures, which could help to compare self-report with behaviors and client outcomes. Future research can therefore emphasize behavioral assessments and clinical outcomes to correlate findings with WRI models.
Third, the use of intervention-based research could explore core components of instruction, awareness, and experience to identify facilitative strategies for enhancing WRI in both counselor trainees and within client populations. Because White people are negatively impacted by racism and restricted racial identity, encouraging growth in WRI in both clinical and educational settings can be a means of promoting wellness for counselors and clients. Thus, research is needed that can carefully examine the complexities of WRI development and address difficulties in assessment due to defensive strategies such as White fragility and lack of insight into the various intra- and interpersonal manifestations of racism.
Finally, though the research examined within this analysis advances the application of WRI theory and practices within the counseling profession, opportunities exist for further exploration of WRI development and the intersection with multiple constructs of Whiteness discussed across the helping professions (e.g., White fragility, color-blindness, race essentialism). The articles analyzed for the present study reflect an assumption that more advanced WRI attitudes, lower color-blind attitudes, greater anti-racism attitudes, and greater awareness of White privilege can yield more positive clinical outcomes. However, given some of the aforementioned limitations, this assumption has not been empirically tested in counseling. Because clients’ and counselors’ affective, cognitive, and behavioral responses to Whiteness can affect the counseling relationship, process, and treatment selection and outcomes (Helms, 1984, 2017), it is imperative that this assumption is properly tested. Empirical and conceptual work should therefore further explore Whiteness constructs to elucidate how White attitudes and behaviors at each stage function for self-protection and move toward aspirational goals of anti-racism and ethical and competent clinical application.
Implications for Counseling Practice, Training, and Supervision
In addition to future research directions related to Whiteness and WRI, findings allow for recommendations for counseling practice, training, and supervision. For example, extant literature emphasizes the importance of racial self-awareness, including an understanding of White privilege and racism. The practice of centering discussions on the harmful impacts of Whiteness, as well as the various ways Whiteness can manifest in therapeutic spaces, allows counselors to examine racial development within and around themselves. White counselors who are able to reflect on their own racial privileges and begin the conversation (i.e., broaching) about racial differences can increase the working alliance quality with clients of color (Burkard et al., 1999; Day-Vines et al., 2007; Helms, 1990).
Furthermore, counselors should heed the themes within the key findings of our sample, following recommendations for taking a broad, contextual, and critical view when understanding and applying WRI models. Counselors can be encouraged to view WRI as Helms (2019) intended—as a broad and complex interplay of relational dynamics, connected with other Whiteness constructs, and following an intentional progression toward anti-racism and social justice. Counselors should take particular caution with viewing the Autonomy stage as a point of arrival, given conflicting findings and the possibility that White people in higher stages may engage in behaviors to assuage guilt rather than to be true allies for people of color. The Helms model associates such attitudes and actions with the Pseudo-Independence stage (Helms, 2019), yet findings cast some doubt as to whether White people who score within the Autonomy stage have actually reached that level of WRI development. Counselors should thus interpret assessment scores with caution and ensure they are also assessing their own level of development and subsequent impact on others through continued and honest reflection and positive engagement in cross-racial relationships.
Regarding training, course content focusing on exploring Whiteness, WRI, and other racial identities through use of an anti-racism training model integrated throughout the curriculum can help students become comfortable with potential cross-racial conflicts and broaching Whiteness (Malott et al., 2015). The Council for Accreditation of Counseling and Related Educational Programs (CACREP) can similarly stress these desired student outcomes when updating standards for counselor training, specifically mentioning the importance of WRI as part of multicultural preparation. It is imperative to begin conversations about race and identity development to create opportunities for growth for any student who may be challenged with their racial identity and how it might impact their clients. Furthermore, counselor educators and supervisors can ask counselors in training to brainstorm how counseling and other services might be developed or adapted in order to contribute toward anti-racist goals and outcomes.
Limitations
The current findings are to be interpreted with caution, as the scope of our study presents some limitations. First, we chose to limit inclusion criteria to national peer-reviewed counseling journals in order to focus on scholarship within professional counseling journals, and therefore our results cannot be generalized to similar disciplines, dissertation research, book chapters, or more localized outlets such as state journals. Our coding sheet was also limited in the information it collected, including sample demographics. Though not all studies included the same demographic variables, we did not capture specifics related to a sample’s political affiliation, religious orientation, ability status, socioeconomic status, diversity exposure, or other details that could have better conceptualized the samples and findings. Additionally, we limited our search to the keywords related to Whiteness that we had identified in related literature but may have missed studies employing constructs outside of our search criteria. Our own identities as White academics may also have influenced the coding process as well as the subsequent interpretation of findings.
Conclusion
This content analysis provides a snapshot of Whiteness scholarship conducted in the counseling profession during a 35-year period. Patterns of study design and analysis were noted, and key findings were summarized to provide context and comparison within the broader literature. Identified themes and relationships highlight theoretically consistent findings for some Whiteness constructs, as well as showcase research gaps that need to be addressed before counselors can apply findings to practice and training. Finally, this content analysis demonstrates the need for a greater understanding of Whiteness and related constructs in counselor education, training, and practice.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
Behrens, J. T. (1997). Does the White Racial Identity Attitude Scale measure racial identity? Journal of Counseling Psychology, 44(1), 3–12. https://doi.org/10.1037/0022-0167.44.1.3
Burkard, A. W., Ponterotto, J. G., Reynolds, A. L., & Alfonso, V. C. (1999). White counselor trainees’ racial identity and working alliance perceptions. Journal of Counseling & Development, 77(3), 324–329. https://doi.org/10.1002/j.1556-6676.1999.tb02455.x
Carter, R. T., Helms, J. E., & Juby, H. L. (2004). The relationship between racism and racial identity for White Americans: A profile analysis. Journal of Multicultural Counseling and Development, 32(1), 2–17. https://doi.org/10.1002/j.2161-1912.2004.tb00357.x
Choney, S. K., & Behrens, J. T. (1996). Development of the Oklahoma Racial Attitudes Scale Preliminary Form (ORAS-P). Multicultural Assessment in Counseling and Clinical Psychology. https://digitalcommons.unl.edu/burosbookmulticultural/10
Claney, D., & Parker, W. M. (1989). Assessing White racial consciousness and perceived comfort with Black individuals: A preliminary study. Journal of Counseling & Development, 67(8), 449–451. https://doi.org/10.1002/j.1556-6676.1989.tb02114.x
Day-Vines, N. L., Wood, S. M., Grothaus, T., Craigen, L., Holman, A., Dotson-Blake, K., & Douglass, M. J. (2007). Broaching the subjects of race, ethnicity, and culture during the counseling process. Journal of Counseling & Development, 85(4), 401–409. https://doi.org/10.1002/j.1556-6678.2007.tb00608.x
DiAngelo, R. (2018). White fragility: Why it’s so hard for White people to talk about racism. Beacon Press.
Frankenberg, R. (1993). White women, race matters: The social construction of Whiteness. University of Minnesota Press.
Hays, D. G., Bolin, T., & Chen, C.-C. (2019). Closing the gap: Fostering successful research-practice partnerships in counselor education. Counselor Education and Supervision, 58(4), 278–292. https://doi.org/10.1002/ceas.12157
Hays, D. G., Chang, C. Y., & Havice, P. (2008). White racial identity statuses as predictors of White privilege awareness. The Journal of Humanistic Counseling, Education and Development, 47(2), 234–246. https://doi.org/10.1002/j.2161-1939.2008.tb00060.x
Helms, J. E. (1984). Toward a theoretical explanation of the effects of race on counseling: A Black and White model. The Counseling Psychologist, 12(4), 153–165. https://doi.org/10.1177/0011000084124013
Helms, J. E. (Ed.) (1990). Black and White racial identity: Theory, research, and practice. Praeger.
Helms, J. E. (1995). An update of Helms’ White and people of color racial identity models. In J. G. Ponterotto, J. M. Casas, L. A. Suzuki, & C. M. Alexander (Eds.), Handbook of multicultural counseling (1st ed.; pp. 181–196). SAGE.
Helms, J. E. (2017). The challenge of making Whiteness visible: Reactions to four Whiteness articles. The Counseling Psychologist, 45(5), 717–726. https://doi.org/10.1177/0011000017718943
Helms, J. E. (2019). A race is a nice thing to have: A guide to being a White person or understanding the White persons in your life (3rd ed.). Cognella.
Helms, J. E., & Carter, R. T. (1990). Development of the White Racial Identity Inventory. In J. E. Helms (Ed.), Black and White racial identity: Theory, research, and practice (pp. 67–80). Greenwood Press.
Henry, P. J., & Sears, D. O. (2002). The Symbolic Racism 2000 Scale. Political Psychology, 23(2), 253–283. https://doi.org/10.1111/0162-895X.00281
LoMartire, R. (2020). Rel: Reliability coefficients. R package version. 1.4.1. https://cran.r-project.org
Malott, K. M., Paone, T. R., Schaefle, S., Cates, J., & Haizlip, B. (2015). Expanding White racial identity theory: A qualitative investigation of Whites engaged in antiracist action. Journal of Counseling & Development, 93(3), 333–343. https://doi.org/10.1002/jcad.12031
McConahay, J. B. (1986). Modern racism, ambivalence, and the Modern Racism Scale. In J. F. Dovidio & S. L. Gaertner (Eds.), Prejudice, discrimination, and racism (pp. 91–125). Academic Press.
McIntosh, P. (1988). White privilege and male privilege: A personal account of coming to see correspondences through work in women’s studies (Wellesley College, Center for Research on Women Working Paper, No. 189). Wellesley College. https://www.wcwonline.org/images/pdf/White_Privilege_and_Male_Privilege_Personal_Account-Peggy_McIntosh.pdf
Neuendorf, K. A. (2017). The content analysis guidebook (2nd ed.). SAGE.
Neville, H. A., Awad, G. H., Brooks, J. E., Flores, M. P., & Bleumel, J. (2013). Color-blind racial ideology: Theory, training, and measurement implications in psychology. American Psychologist, 68(6), 455–466. https://doi.org/10.1037/a0033282
Rowe, W. (2006). White racial identity: Science, faith, and pseudoscience. Journal of Multicultural Counseling & Development, 34(4), 235–243. https://doi.org/10.1002/j.2161-1912.2006.tb00042.x
Schooley, R. C., Debbiesiu, L. L., & Spanierman, L. B. (2019). Measuring Whiteness: A systematic review of instruments and call to action. The Counseling Psychologist, 47(4), 530–565. https://doi.org/10.1177/0011000019883261
Singh, A. A., & Shelton, K. (2011). A content analysis of LGBTQ qualitative research in counseling: A ten-year review. Journal of Counseling & Development, 89(2), 217–226. https://doi.org/10.1002/j.1556-6678.2011.tb00080.x
Spanierman, L. B., & Heppner, M. J. (2004). Psychosocial Costs of Racism to Whites Scale (PCRW): Construction and initial validation. Journal of Counseling Psychology, 51(2), 249–262. https://doi.org/10.1037/0022-0167.51.2.249
Tawa, J. (2017). The Beliefs About Race Scale (BARS): Dimensions of racial essentialism and their psychometric properties. Cultural Diversity and Ethnic Minority Psychology, 23(4), 516–526. https://doi.org/10.1037/cdp0000151
U.S. Census Bureau. (2020). Public Use Microdata Sample data. https://www.census.gov/programs-surveys/acs/data/pums.html
Wester, K. L., Borders, L. D., Boul, S., & Horton, E. (2013). Research quality: Critique of quantitative articles in the Journal of Counseling & Development. Journal of Counseling & Development, 91(3), 280–290. https://doi.org/10.1002/j.1556-6676.2013.00096.x
The authors would like to thank Cheolwoo Park for his invaluable assistance in this study. Hannah B. Bayne, PhD, LMHC (FL), LPC (VA), is an assistant professor at the University of Florida. Danica G. Hays, PhD, is a dean and professor at the University of Nevada Las Vegas. Luke Harness is a doctoral student at the University of Florida. Brianna Kane is a doctoral student at the University of Florida. Harness and Kane contributed equally to the project and share third authorship. Correspondence may be addressed to Hannah B. Bayne, 140 Norman Hall, Gainesville, FL 32611, hbayne@coe.ufl.edu.
Feb 26, 2021 | Volume 11 - Issue 1
Ryan M. Cook, Heather J. Fye, Janelle L. Jones, Eric R. Baltrinic
This study explored the self-reported symptoms of burnout in a sample of 246 novice professional counselors. The authors inductively analyzed 1,205 discrete units using content analysis, yielding 12 categories and related subcategories. Many emergent categories aligned with existing conceptualizations of burnout, while other categories offered new insights into how burnout manifested for novice professional counselors. Informed by these findings, the authors implore counseling scholars to consider, in their conceptualization of counselor burnout, a wide range of burnout symptoms, including those that were frequently endorsed symptoms (e.g., negative emotional experience, fatigue and tiredness, unfulfilled in counseling work) as well as less commonly endorsed symptoms (e.g., negative coping strategies, questions of one’s career choice, psychological distress). Implications for novice professional counselors and supervisors are offered, including a discussion about counselors’ experiences of burnout to ensure they are providing ethical services to their clients.
Keywords: novice professional counselors, burnout, content analysis, conceptualization, symptoms
The term high-touch professions refers to the fields that require professionals to provide ongoing and intense emotional services to clients (Maslach & Leiter, 2016). Although such work can be highly rewarding, these professionals are also at risk for burnout (Bardhoshi et al., 2019). In counseling, professionals are called to provide ongoing and intensive mental health services to clients with trauma histories (Foreman, 2018) and complicated needs (Freadling & Foss-Kelly, 2014). The risk of burnout is exacerbated by the fact that counselors often work in professional environments that are highly demanding and lack resources to serve their clients (Freadling & Foss-Kelly, 2014; Maslach & Leiter, 2016).
The consequences of burnout for counselors and clients can be considerable (Bardhoshi et al., 2019). Potential impacts include a decline in counselors’ self-care, strain of personal relationships, and damage to their overall emotional health (Bardhoshi et al., 2019; Cook et al., 2020; Maslach & Leiter, 2016). Unaddressed burnout might also lead to more serious professional issues like impairment (e.g., substance use, mental illness, personal crisis, or illness; Lawson et al., 2007). Thus, self-monitoring symptoms of burnout is of the utmost importance for counselors to ensure they are providing ethical services to their clients (American Counseling Association [ACA], 2014).
Although burnout is an occupational risk to all counselors (e.g., Bardhoshi et al., 2019; J. Lee et al., 2011; S. M. Lee et al., 2007), novice professional counselors may be especially vulnerable to burnout (Thompson et al., 2014; Westwood et al., 2017; Yang & Hayes, 2020). In the current study, we define novice professional counselors as those who are currently engaged in supervision for licensure in their respective states. Novice professional counselors face a multitude of challenges, such as managing large caseloads, working long hours for low wages, and receiving limited financial support for client care (Freadling & Foss-Kelly, 2014). Even though their professional competencies are still developing (Freadling & Foss-Kelly, 2014; Rønnestad & Skovholt, 2013), these counselors receive minimal direct oversight from a supervisor (Cook & Sackett, 2018). However, to date, no study has exclusively examined novice professional counselors’ descriptions of their experiences of burnout. Input from these counselors is important to understand their specific issues of counselor burnout. Other helping professionals have studied a rich context of practitioners’ burnout experiences. For example, Warren et al. (2012) examined open-ended text responses of people who treated clients with eating disorders and found nuanced contributors to burnout among these providers, including patient descriptors (e.g., personality, engagement in treatment), work-related descriptors (e.g., excessive work hours, inadequate resources), and therapist descriptors (e.g., negative emotional response, self-care). Accordingly, we employed a similar approach to examine the open-ended qualitative responses of 246 novice professional counselors’ self-reported symptoms of burnout.
Conceptual Framework of Burnout
Burnout is defined as “a psychological syndrome emerging as a prolonged response to chronic interpersonal stressors on the job” (Maslach & Leiter, 2016, p. 103). Although there are multiple conceptual frameworks of burnout (e.g., Kristensen et al., 2005; S. M. Lee et al., 2007; Maslach & Jackson, 1981; Shirom & Melamed, 2006; Stamm, 2010), the predominant model used to study burnout is the one developed by Maslach and Jackson (1981), which is measured by the Maslach Burnout Inventory (MBI). Informed by qualitative research, Maslach and Jackson (1981) developed the MBI and conceptualized burnout for all human service professionals as a three-dimensional model consisting of Exhaustion, Depersonalization, and Decreased Personal Accomplishment. Exhaustion is signaled by emotional fatigue, loss of energy, or feeling drained. Depersonalization is characterized by cynicism or negative attitudes toward clients, while Decreased Personal Accomplishment is indicated by a lack of fulfillment in one’s work or feeling ineffective. This conceptualization of burnout has been used to develop several versions of the MBI that are targeted for different professions (e.g., human services, education) and for professionals in general.
Despite the prominence of the MBI model in the burnout literature (Koutsimani et al., 2019), other scholars (e.g., Kristensen et al., 2005; Shirom & Melamed, 2006) have argued for a different conceptualization of burnout, noting several shortcomings of Maslach and Jackson’s (1981) three-dimensional model. Shirom and Melamed (2006) criticized the lack of theoretical framework of the MBI and noted that the factors were derived via factor analysis. They developed the Shirom-Melamed Burnout Measure (Shirom & Melamed, 2006), a measure informed by the Conservation of Resources theory (Hobfoll, 1989), which measures burnout as a depletion of physical, emotional, and cognitive resources using two subscales: Physical Fatigue and Cognitive Weariness.
Kristensen et al. (2005) also criticized the utility of the MBI for numerous reasons, including the lack of theoretical underpinnings of the instrument. Therefore, they developed the Copenhagen Burnout Inventory to capture burnout in professionals across disciplines, most notably human service professionals. From Kristensen et al.’s perspective, the underlying cause of burnout is physical and psychological exhaustion, which occurs across three domains: Personal Burnout (i.e., burnout that is attributable to the person themselves), Work-Related Burnout (i.e., burnout that is attributable to the workplace), and Client-Related Burnout (i.e., burnout that is attributable to their work with clients; Kristensen et al., 2005).
Stamm (2010) conceptualized the construct of professional quality of life for helping professionals, which included three dimensions: Compassion Satisfaction, Burnout, and Secondary Traumatic Stress. Burnout, as theorized by Stamm, is marked by feelings of hopelessness, frustration, and anger, as well as a belief that one’s own work is unhelpful to others, which results in a decline in professional performance. The experience of burnout may also be caused by an overburdening workload or working in an unsupportive environment (Stamm, 2010). Stamm’s model is reflected in the Professional Quality of Life Scale (ProQOL), and this instrument has been used by counseling scholars (e.g., Lambert & Lawson, 2013; Thompson et al., 2014).
A reason for variations in the conceptualization of burnout is that it manifests differently across professions (Maslach & Leiter, 2016). The only counseling-specific model of burnout is conceptualized by S. M. Lee et al. (2007), who developed the Counselor Burnout Inventory (CBI). The CBI was informed by the three dimensions of the MBI and additionally captured the unique work environment of professional counselors and its impact on their personal lives. As such, the CBI poses a five-dimensional model consisting of Exhaustion, Incompetence, Negative Work Environment, Devaluing Client, and Deterioration in Personal Life. In recent years, the CBI has been the instrument predominantly used by researchers to study counselor burnout (e.g., Bardhoshi et al., 2019; Fye et al., 2020; J. Lee et al., 2011).
The Current Study
J. Lee et al. (2011) noted the challenges of studying counselor burnout across diverse samples. They encouraged scholars to examine burnout within homogenous samples of counselors in order to offer more nuanced implications for each group. Prior scholarship (e.g., Freadling & Foss-Kelly, 2014; Thompson et al., 2014) suggested that novice professional counselors may be at risk of burnout, and despite the aforesaid vulnerabilities (e.g., low wages, work with high need clients, professional competency limitations), their self-reported manifestation of burnout symptoms have yet to be studied.
We acknowledge the critical importance of studying burnout in the profession of counseling. However, repeatedly relying on data from similar instruments to measure burnout may fail to capture new or relevant information about the phenomenon (Kristensen et al., 2005) for human service professionals (e.g., Maslach & Jackson, 1981) or professional counselors (e.g., S. M. Lee et al., 2007). Alternatively, content analysis, which focuses on the analysis of open-ended qualitative text (Krippendorff, 2013), may better capture the intricacies of burnout that could not be measured using quantitative instruments (e.g., Warren et al., 2012). Thus, we aimed to address the following research question: What are novice professional counselors’ self-reported symptoms of burnout?
Methodology
Participants
Participants in the current study were 246 postgraduate counselors who were currently receiving supervision for licensure. The age of participants ranged from 23 to 69, averaging 36.91 (SD = 10.15) years. The majority of participants identified as female (n = 195, 79.3%), while 22 participants identified as male (8.9%), four identified as non-binary (1.6%), nine indicated that they did not want to disclose their gender (3.7%), and 16 participants did not respond to the item (6.5%). The participants’ race/ethnicity was reported as follows: White (n = 186; 75.6%), Multiracial (n = 15, 6.1%), Latino/Hispanic (n = 7, 3.3%), Black (n = 6, 2.4%), Asian (n = 6, 2.4%), American Indian or Alaska Native (n = 3, 0.8%), Native Hawaiian or Pacific Islander (n = 1, 0.4%), and Other (n = 7, 3.3%), while 15 participants declined to respond to the item (6.1%). The self-reported race/ethnicity demographic information is comparable to all counselors in the profession, based on DataUSA (2018). The participants’ client caseload ranged from 1 to 650 (M = 41.88; Mdn = 30.0; SD = 53.74). On average, participants had worked as counselors for 5 years (Mdn = 3.3; SD = 4.87). The provided percentages may not total to 100 percent because of rounding and because participants were afforded the option to select more than one response.
Procedure
To answer our research question, we used data from a larger study of novice professional counselor burnout, which included both quantitative and qualitative data. After receiving IRB approval, we obtained lists of names and email addresses of counselors engaged in supervision for licensure from the licensing boards in seven states: Florida, Nebraska, New Mexico, Oregon, Utah, Washington, and Wisconsin. We aimed to recruit a nationally representative sample by purposefully choosing at least one state from each of the ACA regions. In addition, states were selected based upon our ability to obtain a list of counselors who were engaged in supervision for licensure from the respective licensure boards. We were able to survey at least one state from each ACA region except the North Atlantic Region. After removing invalid email addresses, we invited 6,874 potential participants by email to complete an online survey in Qualtrics. This survey was completed by 560 counselors, yielding a response rate of 8.15%. This response rate is consistent with other studies that employed a similar design (Gonzalez et al., 2020). All participants were asked, Do you believe you are currently experiencing symptoms of burnout?, to which participants responded (a) yes or (b) no. Participants who responded yes were then prompted with the direction, Describe your symptoms of burnout, using an open-ended text box, which did not have a character limit. A total of 246 participants (43.9%) responded yes and qualitatively described their symptoms of burnout. On average, participants provided 30.31 words (SD = 36.30). We answered our research question for the current study using only the qualitative data, which aligns with the American Psychological Association’s Journal Article Reporting Standards for Qualitative Research (JARS-Qual; Levitt et al., 2018).
Data Analysis
To answer our research question, we analyzed participants’ open-ended responses using content analysis, which allows for systematic and contextualized review of text data (Krippendorff, 2013). As recommended by Krippendorff (2013), we followed the steps of conducting content analysis: unitizing, sampling, recording, and reducing. We first separated the responses of the 246 participants into discrete units. For example, “feeling exhausted and back pain” was coded as two units: (a) feeling exhausted and (b) back pain. This process resulted in a total of 1,205 discrete units. We reduced our data into categories using an inductive approach, which allowed for new categories to emerge from the data without an a priori theory (Krippendorff, 2013). Although there are multiple conceptualizations of burnout (Maslach & Jackson, 1981; S. M. Lee et al., 2007) that could have informed our analysis (i.e., deductive approach; Krippendorff, 2013), we chose an inductive approach to capture the conceptualization of burnout for novice professional counselors—generating categories based on participants’ explanations of their own symptoms of burnout (Kondracki et al., 2002).
To that end, we developed a codebook by randomly selecting roughly 10% of the discrete units to code as a pretest. Our first and third authors, Ryan M. Cook and Janelle L. Jones, independently reviewed the discrete units, met to discuss and develop categories and corresponding definitions, and coded the pretest data together to enhance reliability. This process yielded a codebook that consisted of 12 categories. Cook and Jones then used the codebook (categories and definitions) to independently code the remaining 90% of the data across three rounds (i.e., 30% increments). After each round, Cook and Jones met to discuss discrepancies and to reach consensus on the final codes. The overall agreement between Cook and Jones was 97% and the interrater reliability was acceptable (Krippendorff α = .80; Krippendorff, 2013), which was calculated using ReCal2 (Freelon, 2013). At the end of the coding process, Cook and Jones reviewed their notes for each code and further organized them into subcategories based on commonalities. The second author, Heather J. Fye, served as the auditor (see Researcher Trustworthiness section) and reviewed the entire coding process.
Researcher Trustworthiness
The research team consisted of four members, three counselor educators and one counselor education and supervision doctoral student. The first and third authors, Cook and Jones, served as coders, while the second author, Fye, served as the auditor and the fourth author, Eric R. Baltrinic, served as a qualitative consultant. The counseling experience of the four authors ranged from 4 to 18 years, and the supervision experience of the authors ranged from 3 to 9 years. Cook, Fye, and Baltrinic are licensed professional counselors and three of the authors are credentialed as either a National Certified Counselor or Approved Clinical Supervisor.
We all acknowledged our personal experiences of burnout to some degree as practicing counselors as well as observing the consequences of burnout to our students and supervisees. All members of the research team had prior experience studying counselor burnout. Although these collective experiences enriched our understanding of the subject matter, we also attempted to bracket our assumptions and biases throughout the research process. To increase the trustworthiness of the coding process, the auditor, Fye, reviewed the codebook, categories and subcategories, discreteness, and two coders’ notes coding process after the pretest and rounds of coding. Fye provided feedback on the category definitions, coding process, and coding decisions during the analysis process.
Results
Using an inductive approach, 12 categories and related subcategories emerged from the 1,205 discrete self-reported symptoms of burnout. Full results, including the 12 categories and subcategories, as well as the frequencies of the categories and subcategories, are presented in the Appendix. We discuss each category in detail and provide illustrative examples of each category using direct participant quotes (Levitt et al., 2018).
Negative Emotional Experience
Of the 1,205 coded units, 218 units (18.1%) were coded into the category negative emotional experience. This category reflected participants’ descriptions of experiencing negative feelings related to their work as counselors (e.g., anxiety, depression, irritability) or unwanted negative emotions (e.g., crying spells). This category included 15 subcategories, and the units coded into these subcategories reflected the participants’ descriptions of a wide range of negative feelings. For example, one participant reported she was “struggling to feel happy,” while another participant shared that she “is carrying a heavy burden [that] no one understands or is aware of.” Some participants also reported crying spells. One participant shared she “has fits of crying,” while another reported she “[cries] in the bathroom at work.”
Fatigue and Tiredness
The category fatigue and tiredness was coded 195 times (16.2%) and included four subcategories. This category captured participants’ descriptions of feeling exhausted, fatigued, or tired. Units coded into this category included the participants’ indications that they feel exhausted, despite sleeping well. For example, one participant described feeling perpetually exhausted—“nothing recharges my batteries”— while another participant stated that her fatigue worsened as the week progressed: “[I feel] more and more exhausted throughout the week.”
Unfulfilled in Counseling Work
The category unfulfilled in counseling work captured the participants’ descriptions of no longer deriving joy at work, dread in going to work or completing work-related responsibilities, or lacking motivation to do work. This category was coded 140 times (11.6%) and subcategories included five subcategories. Avoidance of burdensome administrative responsibilities (e.g., paperwork) were commonly reported units that were captured in this category. For example, a participant noted “putting off doing notes.” Units also captured in this category reflected participants’ self-report of no longer feeling motivated or deriving joy from their work, which ultimately led some participants to stop seeking training. For instance, a participant described herself as “going through the motions at work,” and another added that she was no longer “motivated to improve [her] skills.”
Unhealthy Work Environment
Across all coded units, 128 units (10.6%) were coded in the category unhealthy work environment, which included 15 subcategories. This category captured participants’ descriptions of their work environment that contribute to a counselor experiencing burnout. For example, units captured in this category commonly described participants’ reports of working long hours with few or no breaks throughout the day, and participants feeling pressured to take on additional clients. Some participants described managing large client caseloads or caseloads with “high risk or high needs” clients. The units reflecting participants’ perceived lack of supervisor support were also coded into this category. For example, a participant noted that she was “scared to make a mistake or ask questions about doing my job,” while another participant described a supervisor as not “supportive or trustworthy.” Finally, units that signaled participants’ feelings of being inadequately compensated were coded into this category, such as this participant’s response: “I do not get paid enough for the work that I do.”
Physical Symptoms
The category physical symptoms reflected participants’ descriptions of physical ailments, physical manifestations of burnout (e.g., soreness, pain), physical illnesses, or physical descriptors (e.g., weight gain, weight loss). There were 107 coded units (8.9%) that referenced physical symptoms. The seven subcategories captured in this category reflected a wide range of physical ailments. The most commonly coded units were participants’ descriptions of headaches, illnesses, and weight changes, although some less commonly coded units reflected more serious physical and medical issues. For example, a participant noted, “I have TMJ [temporomandibular joint dysfunction] pain most days from clenching my jaw,” while another participant stated that she “recently began to have debilitating stomach symptoms, which were identified as small ulcerations.”
Negative Impact on Personal Interest or Self-Care
Across all coded units, 101 units (8.4%) were coded in the category negative impact on personal interest or self-care, which included eight subcategories. This category reflected the participants’ descriptions of reduced self-care or inability to engage in self-perceived healthy behaviors (e.g., cannot fall asleep), or lacking personal interest. Units coded in this category most commonly reflected participants’ experience of sleep issues—difficulty either falling asleep or staying asleep. Other units reflected participants’ lessening desire to engage in once-enjoyable activities. For example, one participant noted, “I find myself knowing that I need more time for play, rest, recovery, socializing, and personal interests, but [I am] feeling confused about how to fit that in.” Another participant described her self-care as unconstructive: “It often feels like no amount of self-care is helpful, which makes it more difficult to engage in any self-care.”
Self-Perceived Ineffectiveness as a Counselor
We coded 127 units (10.5%) into the category self-perceived ineffectiveness as a counselor, which included six subcategories. This category reflected the participants’ descriptions of their self-perceived decrease in self-efficacy as a counselor, difficulty in developing or maintaining therapeutic relationships with clients, decreased empathy toward clients, or questioning of their own abilities as counselors (e.g., ability to facilitate change). For example, one participant noted that she did not “have as much empathy for clients as before,” while another participant expressed, “I often feel like clients are being demanding and trying to waste my time.” Units coded into this category also reflected participants’ feelings of inadequacy or struggles to develop a meaningful professional relationship with clients. One participant stated that she must “reach very deep every morning for the presence of mind and spirit to pay close attention and to care deeply for each of these people.” Although less frequently coded, some units described participants’ feelings of compassion satisfaction or self-reported secondary traumatic stress. For example, one participant shared that she was “personally disturbed” by her work.
Cognitive Impairment
Across all coded units, 75 units (6.2%) were coded in the category cognitive impairment, and this category included seven subcategories. The units coded into this category reflected the participants’ descriptions of their cognitive abilities being negatively impacted in different ways. For example, one participant described “feeling like I am in a fog at work,” while another participant shared that she found it “hard to concentrate at work.” Some units captured in this category reflected participants’ rumination of clients or work; for example, one participant noted “shifting my attention to ruminating about dropouts at times, when I need to be present with a [current] client.”
Negative Impact on Personal Relationships
The category negative impact on personal relationships captured 63 coded units (5.2%). Participants’ descriptions of strained relationships as a result of their self-reported burnout were coded into this category, which included three subcategories. For example, one participant described “not [feeling] available for emotional connects with others in my personal life,” while another participant said that they “lashed out sometimes at family members after a stressful day of work.” Another example of the negative impact on personal relationships was a participant’s description of “struggling to find joy at home with my wife and two kids.”
Negative Coping Strategies
We coded 22 units (1.8%) into the category negative coping strategies. This category included five subcategories that captured participants’ descriptions of using unhealthy or negative coping strategies to cope with burnout. Units coded into this category described participants’ use of a variety of negative coping strategies. For example, participants noted an increase in “alcohol consumption” or “smoking.” Relatedly, a participant expressed one of her coping strategies was “the excessive use of Netflix,” while another participant stated that she was “not eating or eating way too much.”
Questioning of One’s Career Choice
Units that reflected participants’ descriptions of the questioning of one’s career choice and potential or planned desire to leave the profession were coded into the category questioning of one’s career choice. There were 21 coded units (1.7%) for this category, which included two subcategories. An example of units coded into this category is a participant who stated that she has “thoughts that I have made a mistake in pursuing this line of work.” Another participant shared feelings of “wanting to quit [my] job.” Some units coded into this category captured participants who were already making plans to leave their jobs or the field. For example, one participant shared that she “recently put in [my] notice at agency,” while another participant stated plans to leave the profession “within one year.”
Psychological Distress
The least number of units were coded into the category psychological distress, which was coded eight times (0.7%) and included two subcategories. This category captured the participants’ discussions of a mental health diagnosis, which they attributed as a symptom of burnout, or suicidal ideations. For example, one participant shared, “I have been diagnosed with major depressive disorder and my job is a factor,” while another participant stated, “I sought therapy for myself and I had to increase my anti-depressant medication.” Finally, two participants endorsed experiencing suicidal ideations at some previous point related to their burnout.
Discussion
The content analysis yielded insights of self-reported burnout symptoms by capturing the phenomenon in novice professional counselors’ own words. Many of the 12 categories that emerged from the data generally aligned with prior conceptualizations of burnout for human service professionals (e.g., Maslach & Jackson, 1981) and counselors (S. M. Lee et al., 2007), while some categories provided novel insights into how burnout manifested in this sample. Further, we observed trends in common self-reported descriptors of burnout for novice professional counselors (negative emotional experiences) to the least commonly endorsed descriptors (psychological distress). We assert that these findings enrich the scholarly understanding of the burnout phenomenon in novice professional counselors.
Discussion of the Conceptual Framework of Burnout
Maslach and Jackson (1981) emphasized in their earlier work that exhaustion and fatigue are core features of burnout, and the category of fatigue and tiredness was the second most commonly coded category (16.2% of all coded units) in our study. Our findings reaffirm exhaustion (or fatigue or tiredness) as a central feature of burnout, and specifically self-reported symptoms of burnout in novice professional counselors. Scholars (e.g., Kristensen et al., 2005; Maslach & Jackson, 1981; Shirom & Melamed, 2006) have conceptualized that the interconnectedness between the emotional, physical, and psychological fatigue of burnout is different. Shirom and Melamed (2006) distinguished emotional, physical, and cognitive resources, while Kristensen et al. (2005) made no distinction between physical and psychological exhaustion. Stamm (2010) also viewed exhaustion as a feature of burnout but did not specify how this exhaustion manifested in human service professionals. In the current study, we chose to distinguish emotional, physical, and cognitive symptoms to best capture the participants’ experiences in their own words (Kondracki et al., 2002). However, we found supportive evidence that novice professional counselors’ burnout included emotional, physical, and cognitive symptoms. Our findings suggest that all three components should be examined to adequately capture this phenomenon.
The category negative emotional experience, which reflected participants’ reports of experiencing negative feelings associated with their work as counselors, was the most commonly endorsed symptom of burnout (18.1% of all coded units). In other models of burnout (e.g., Kristensen et al., 2005; Shirom & Melamed, 2006), feelings or emotions are most often conceptualized as emotional exhaustion, emotional fatigue, or emotional distress. However, the participants in the current study richly described their negative emotional experiences, as captured in the subcategories, with irritability, anxiety, depression, and stress being the most commonly endorsed negative emotions. These findings most closely align with Stamm’s (2010) conceptualization of burnout, which suggested that feelings of hopelessness, anger, frustration, and depression are evidence of burnout. Relatedly, a similar content analysis performed with eating disorder treatment professionals also found that their participants most frequently described emotional distress (61% of their sample, n = 94) as a way in which their worry for clients impacts their personal and professional lives (Warren et al., 2012). Scholars (e.g., Maslach & Leiter, 2016) have postulated about the relationship between workplace burnout and affectional distress (e.g., depression, anxiety, stress); however, such an investigation has yet to be conducted in the profession of counseling. Our findings suggest that novice professional counselors commonly describe their manifestation of burnout as an emotional experience, and as such, this represents a gap in the current conceptualization of counselor burnout.
Two other categories captured in the current study were physical symptoms and cognitive impairment symptoms. Physical symptoms were coded for 8.9% of the 1,205 units coded, while cognitive symptoms were coded for 6.1% of all coded units. In the existing burnout literature (e.g., Maslach & Jackson, 1981; Shirom & Melamed, 2006), physical symptoms of burnout often paralleled or referenced fatigue or exhaustion. For example, in Shirom and Melamed’s (2006) model, physical symptoms were reflective of feeling physically tired. However, in the current study, participants most commonly described their physical symptoms as back pain, illnesses, and headaches. This finding aligns with Kaeding et al. (2017), who found that counseling and clinical psychology trainees attributed their back and neck pain to sitting for long periods of time. We assert that specific physical symptoms may have been inadequately captured by the existing models of burnout.
Relatedly, Shirom and Melamed (2006) suggested that psychological fatigue or psychological manifestations of burnout should be distinguished from those of emotional and physical symptoms, while Kristensen et al. (2005) made no such distinctions. The participants in the current study described numerous cognitive manifestations of burnout, and the most commonly coded subcategories included concentration or focus, rumination, and forgetfulness. These self-reported symptoms closely align with the model of Shirom and Melamed, which describes psychological fatigue as an inability to think clearly and difficulty processing one’s own thoughts. Further, Kristensen et al. described one symptom of personal burnout as being at risk of becoming ill. However, no items of cognitive impairment or worsening cognitive abilities are included in the CBI. Informed by our findings, descriptors of cognitive impairment should be considered to understand burnout in novice professional counselors.
Two of the three dimensions of burnout as conceptualized by Maslach and Jackson (1981) were Depersonalization (i.e., cynicism or negative attitudes toward clients) and Decreased Personal Accomplishment (i.e., diminished fulfillment in one’s work or feeling ineffective in their work). These two dimensions are similar to Stamm’s (2010) conceptualization of burnout for human service professionals, which included the features of perceiving that one’s own work is unhelpful and no longer enjoying the work. In the current study, two of the categories that emerged closely aligned with these conceptualizations of burnout: unfulfilled in counseling work (11.6% of all coded units) and self-perceived ineffectiveness as a counselor (10.5% of all coded units). Collectively, these two categories and related subcategories provide rich descriptors of how novice professional counselors experience their own depersonalization and diminished personal accomplishment (Maslach & Jackson, 1981).
Our findings align with qualitative studies of novice professional counselors’ experiences (e.g., Freadling & Foss-Kelly, 2014; Rønnestad & Skovholt, 2013). For example, Freadling and Foss-Kelly (2014) found that novice professional counselors sometimes question if their graduate training adequately prepared them for their current positions. As such, questioning of one’s clinical abilities by counselors at this developmental level was also a common experience by participants in our study (Freadling & Foss-Kelly, 2014).
Our findings were consistent with the counselor-specific burnout model in which S. M. Lee et al. (2007) noted the importance of including the unique work environment of counselors and related impact on their personal life. Our findings support the burnout conceptualization with novice professional counselors. For example, participants in the current study described an unhealthy work environment (10.6% of all coded units). The most commonly coded subcategories included unsupportive employer or supervisor, frustrated with system, burdened by documentation, and overburdened by amount of work or multiple roles.
In terms of the impact of counseling work on their personal lives (S. M. Lee et al., 2007), evidence of this dimension was captured in the current study in two categories: negative impact on personal interest or self-care and negative impact on personal relationships. There is a high degree of interconnectedness between burnout and self-care (Maslach & Leiter, 2016; Warren et al., 2012). Thus, it is unsurprising that participants reported a decrease in their self-care; however, some of the specific self-care behaviors that are affected as a result of novice professional counselors experiencing burnout are less understood. In the current study, the most commonly coded subcategory was difficulty falling asleep or staying asleep, followed by lack of interest in hobbies, poor work/life balance, and general decrease in self-care. As defined in the CBI, lack of time for personal interest and poor work/life balance are both indicators of Deterioration in Personal Life. While sleep onset and maintenance issues are associated with burnout (Yang & Hayes, 2020), counselors’ experiences with sleep issues appears to be a novel finding. Another indicator of deterioration in counselors’ personal lives as theorized by S. M. Lee et al. was a lack of time to spend with friends, which was also observed in our study. Relatedly, some participants indicated that they isolated from their social support system. Other participants described strained personal relationships (i.e., conflict in personal relationships, poor emotional connection with others), which are unique findings.
Counselor Burnout Versus Counselor Impairment
Although uncommonly reported, some participants in the current study described using negative coping strategies (1.8% of all coded units) and psychological distress (0.7% of all coded units) as evidence of their self-reported burnout. Examples of negative coping strategies reported by participants included increased substance use (e.g., alcohol, caffeine, nicotine) and overeating or skipping meals, while examples of psychological distress included having received a psychological diagnosis and experiencing increased suicidal ideations, which participants attributed to burnout. These self-reported symptoms of burnout align more closely with the definition of counselor impairment (Lawson et al., 2007) as opposed to the definition of counselor burnout. Our findings are significant for two reasons. First, any study of counselor burnout that utilized one of the commonly used instruments of burnout (e.g., CBI, MBI) would have failed to capture these participants’ experiences. Second, these findings suggest that a small number of counselors may be experiencing significant impairment in their personal and professional lives, despite being early in their professional careers. Finally, another infrequently coded category was questioning of one’s career choice (1.7% of all coded units). Coded units in this category indicated that some counselors were wondering if counseling was a good professional fit for them, while others expressed their intention to seek employment in another profession. It is possible that prolonged disengagement from one’s professional work (i.e., cynicism; Maslach & Jackson, 1981) could result in counselors wanting to explore other career options.
Limitations
There are limitations of this study which we must address. The purpose of content analysis is not to generalize findings, so our findings may only reflect the experiences of burnout for the participants in the current study. Their experiences may be influenced by developmental levels, experiences in their specific state, or other reasons that we did not capture.
Another limitation is our response rate of 8.15%. A possible reason for our low response rate is self-selection bias—counselors who were currently experiencing burnout responded to the open-ended items as opposed to those who were not feeling burnout. Future research is needed to see how burnout presents in larger or different populations of counselors. It might also be important to study the career-sustaining behaviors and work environments of those counselors who did not endorse burnout. The final limitation is that this study was descriptive in nature. Future researchers are encouraged to explore the factors that may predict burnout while also considering the novel findings generated from this study.
Implications
Our findings offer implications for counseling researchers, counselors, and supervisors. Although many of the findings from the current study align with prior research, there appears to be some degree of discrepancy between how burnout is conceptualized by scholars and how novice professional counselors describe symptoms of burnout. We implore scholars to further examine the specific descriptors of burnout as reported by participants in this study and to see if the frequency of these self-reported symptoms can be duplicated. Specifically, scholars should focus on the emotional experience of novice professional counselors, fatigue and tiredness, and feeling unfulfilled in their work, which were the most commonly reported symptoms. It also seems critically important to explore the less commonly reported descriptors of burnout, like negative coping strategies, questioning of one’s career choice, and psychological distress. Each of these categories could signal counselor impairment and would have been otherwise missed by scholars who relied exclusively on existing Likert-type burnout inventories.
Novice professional counselors sometimes experience self-doubt about their counseling skills or even the profession (Rønnestad & Skovholt, 2013), given the difficult work conditions in which these counselors practice (e.g., low wages, long hours; Freadling & Foss-Kelly, 2014). Novice professional counselors should understand that experiences of burnout appear to be commonly occurring. The illumination of these descriptors may encourage other novice professional counselors to seek guidance from their supervisors on how best to manage these feelings. For those novice professional counselors who are experiencing more serious personal and professional issues associated with burnout (e.g., using negative coping strategies and psychological distress), they should consider whether they are presently able to provide counseling services to clients and seek consultation from a supervisor (ACA, 2014).
Our findings have implications for supervisors. For example, supervisors should be willing to openly discuss burnout with their supervisees. Our results can provide supervisors with descriptors that capture novice professional counselors’ experiences of burnout. Supervisors might find it helpful to disclose some of their own experiences of burnout (or mitigating burnout) with their supervisees, which can normalize the supervisees’ experiences (Knox et al., 2011). Finally, to the extent that supervisors are able, they should protect novice professional counselors from experiencing an unhealthy work environment or potentially harmful behaviors. For example, in response to supervisees’ self-reported symptoms of burnout, supervisors could limit caseloads, allow counselors time to complete documentation, or mandate regular breaks throughout the day (including lunchtime).
Conclusion
There are many novice professional counselors experiencing a wide range of symptoms of burnout. A career in counseling can be rewarding, but prolonged burnout can lead to both personal and professional consequences, as evidenced by the findings from this study. Counselors must attend to their own symptoms of burnout in order to provide quality care to their clients and lead a fulfilling personal life. Supervisors and educators can support these counselors by discussing the experiences of burnout, and future scholars can better understand the experiences of counselor burnout by studying the phenomenon using definitions and symptoms in the words of counselors as opposed to generic definitions.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
Bardhoshi, G., Erford, B. T., & Jang, H. (2019). Psychometric synthesis of the Counselor Burnout Inventory. Journal of Counseling & Development, 97(2), 195–208. https://doi.org/10.1002/jcad.12250
Cook, R. M., Fye, H. J., & Wind, S. A. (2020). An examination of the Counselor Burnout Inventory using item response theory in early career post-master’s counselors. Measurement and Evaluation in Counseling and Development. Advance online publication. https://doi.org/10.1080/07481756.2020.1827439
Cook, R. M., & Sackett, C. R. (2018). Exploration of prelicensed counselors’ experiences prioritizing information for clinical supervision. Journal of Counseling & Development, 96(4), 449–460. https://doi.org/10.1002/jcad.12226
DataUSA. (2018). Counselors. https://datausa.io/profile/soc/counselors#demographics
Foreman, T. (2018). Wellness, exposure to trauma, and vicarious traumatization: A pilot study. Journal of Mental Health Counseling, 40(2), 142–155. https://doi.org/10.17744/mehc.40.2.04
Freadling, A. H., & Foss-Kelly, L. L. (2014). New counselors’ experiences of community health centers. Counselor Education and Supervision, 53(3), 219–232. https://doi.org/10.1002/j.1556-6978.2014.00059.x
Freelon, D. (2013). ReCal OIR: Ordinal, interval, and ratio intercoder reliability as a web service. International Journal of Internet Science, 8(1), 10–16.
Fye, H. J., Cook, R. M., Baltrinic, E. R., & Baylin, A. (2020). Examining individual and organizational factors of school counselor burnout. The Professional Counselor, 10(2), 235–250. https://doi.org/10.15241/hjf.10.2.235
Gonzalez, E., Sperandio, K. R., Mullen, P. R., & Tuazon, V. E. (2020). Development and initial testing of the Multidimensional Cultural Humility Scale. Measurement and Evaluation in Counseling and Development, 54(1), 56–70. https://doi.org/10.1080/07481756.2020.1745648
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44(3), 513–524. https://doi.org/10.1037/0003-066X.44.3.513
Kaeding, A., Sougleris, C., Reid, C., van Vreeswijk, M. F., Hayes, C., Dorrian, J., & Simpson, S. (2017). Professional burnout, early maladaptive schemas, and physical health in clinical and counselling psychology trainees. Journal of Clinical Psychology, 73(12), 1782–1796. https://doi.org/10.1002/jclp.22485
Knox, S., Edwards, L. M., Hess, S. A., & Hill, C. E. (2011). Supervisor self-disclosure: Supervisees’ experiences and perspectives. Psychotherapy, 48(4), 336–341. https://doi.org/10.1037/a0022067
Kondracki, N. L., Wellman, N. S., & Amundson, D. R. (2002). Content analysis: Review of methods and their applications in nutrition education. Journal of Nutrition Education and Behavior, 34(4), 224–230.
https://doi.org/10.1016/S1499-4046(06)60097-3
Koutsimani, P., Montgomery, A., & Georganta, K. (2019). The relationship between burnout, depression, and anxiety: A systemic review and meta-analysis. Frontiers in Psychology, 10(284), 1–19.
https://doi.org/10.3389/fpsyg.2019.00284
Krippendorff, K. (2013). Content analysis: An introduction to its methodology (3rd ed.). SAGE.
Kristensen, T. S., Hannerz, H., Høgh, A., & Borg, V. (2005). The Copenhagen Psychosocial Questionnaire: A tool for the assessment and improvement of the psychosocial work environment. Scandinavian Journal of Work, Environment & Health, 31(6), 438–449. https://doi.org/10.5271/sjweh.948
Lambert, S. F., & Lawson, G. (2013). Resilience of professional counselors following Hurricanes Katrina and Rita. Journal of Counseling & Development, 91(3), 261–268. https://doi.org/10.1002/j.1556-6676.2013.00094.x
Lawson, G., Venart, E., Hazler, R. J., & Kottler, J. A. (2007). Toward a culture of counselor wellness. Journal of Humanistic Counseling, 46(1), 5–19. https://doi.org/10.1002/j.2161-1939.2007.tb00022.x
Lee, J., Lim, N., Yang, E., & Lee, S. M. (2011). Antecedents and consequences of three dimensions of burnout in psychotherapists: A meta-analysis. Professional Psychology: Research and Practice, 42(3), 252–258.
https://doi.org/10.1037/a0023319
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., Ogle, N. T., Powell, M. L., Quinn, J. J., Wallace, S. L., & Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40(3), 142–154.
https://doi.org/10.1080/07481756.2007.11909811
Levitt, H. M., Bamberg, M., Creswell, J. W., Frost, D. M., Josselson, R., & Suárez-Orozco, C. (2018). Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publication and Communications Board task force report. American Psychologist, 73(1), 26–46. https://doi.org/10.1037/amp0000151
Maslach, C., & Jackson, S. E. (1981). The measurement of experienced burnout. Journal of Organizational Behavior, 2(2), 99–113. https://doi.org/10.1002/job.4030020205
Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. https://doi.org/10.1002/wps.20311
Rønnestad, M. H., & Skovholt, T. M. (2013). The developing practitioner: Growth and stagnation of therapists and counselors. Routledge.
Shirom, A., & Melamed, S. (2006). A comparison of the construct validity of two burnout measures in two groups of professionals. International Journal of Stress Management, 13(2), 176–200.
https://doi.org/10.1037/1072-5245.13.2.176
Stamm, B. H. (2010). Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL).
http://www.proqol.org.
Thompson, I., Amatea, E., & Thompson, E. (2014). Personal and contextual predictors of mental health counselors’ compassion fatigue and burnout. Journal of Mental Health Counseling, 36(1), 58–77.
https://doi.org/10.17744/mehc.36.1.p61m73373m4617r3
Warren, C. S., Schafer, K. J., Crowley, M. E., & Olivardia, R. (2012). A qualitative analysis of job burnout in eating disorder treatment providers. Eating Disorders, 20(3), 175–195.
https://doi.org/10.1080/10640266.2012.668476
Westwood, S., Morison, L., Allt, J., & Holmes, N. (2017). Predictors of emotional exhaustion, disengagement and burnout among improving access to psychological therapies (IAPT) practitioners. Journal of Mental Health, 26(2), 172–179. https://doi.org/10.1080/09638237.2016.1276540
Yang, Y., & Hayes, J. A. (2020). Causes and consequences of burnout among mental health professionals: A practice-oriented review of recent empirical literature. Psychotherapy, 57(3), 426–463.
https://doi.org/10.1037/pst0000317
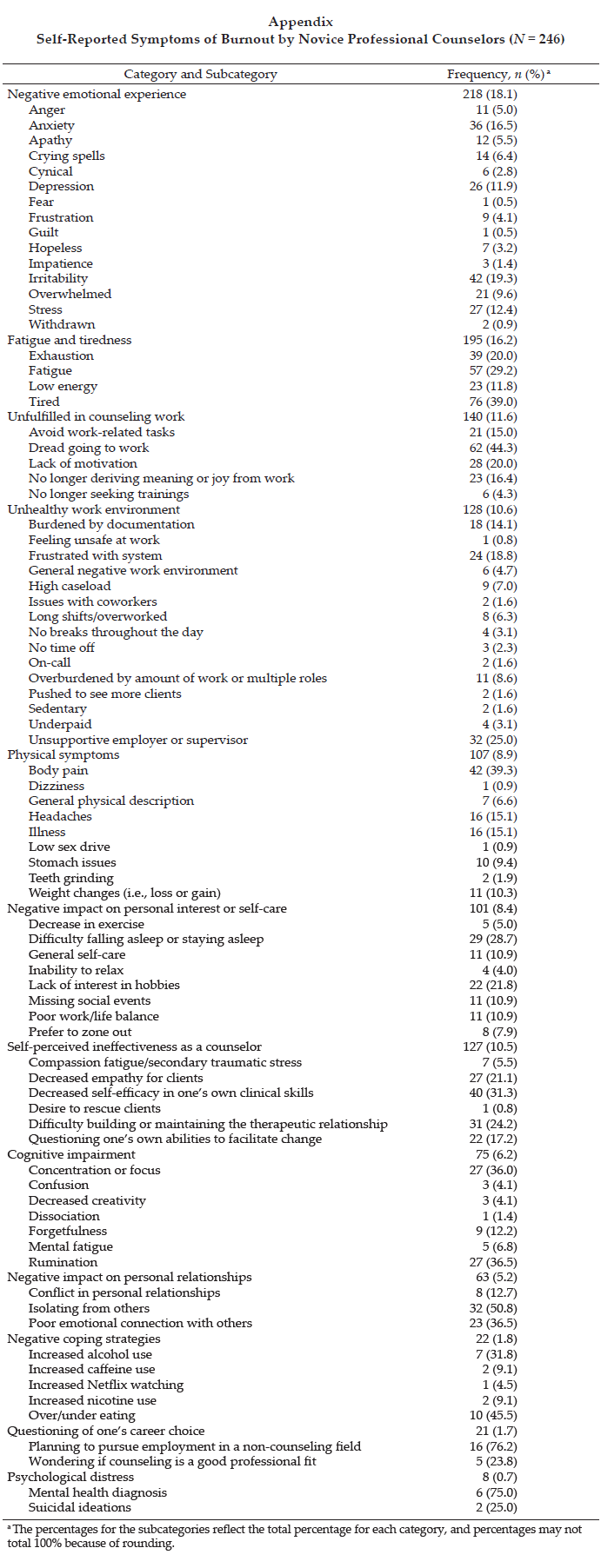
Ryan M. Cook, PhD, ACS, LPC, is an assistant professor at the University of Alabama. Heather J. Fye, PhD, NCC, LPC, is an assistant professor at the University of Alabama. Janelle L. Jones, MS, NCC, is a doctoral student at the University of Alabama. Eric R. Baltrinic, PhD, LPCC-S (OH), is an assistant professor at the University of Alabama. Correspondence may be addressed to Ryan M. Cook, 310A Graves Hall, Box 870231, Tuscaloosa, AL 35475, rmcook@ua.edu.
Jun 28, 2018 | Volume 8 - Issue 2
Ryan M. Cook, Laura E. Welfare, Devon E. Romero
Studies from allied professions suggest that intentional nondisclosure in clinical supervision is common; however, the types of intentional nondisclosure and reasons for nondisclosure have yet to be examined in an adequate sample of counselors-in-training (CITs). The current study examined intentional nondisclosure by CITs during their onsite supervision experience. We utilized content analysis to examine examples of intentional nondisclosure. Sixty-six participants provided examples of intentionally withholding information from their supervisors they perceived as significant. The most common types of information withheld were negative reactions to supervisors, general client observations, and clinical mistakes. The most common reasons cited were impression management, perceived unimportance, negative feelings, and supervisor incompetence. We offer implications for both supervisees and supervisors on how they might mitigate intentional nondisclosure; for example, we present strategies to address ineffective or harmful supervision, discuss techniques to openly address intentional nondisclosure, and explore ways to integrate training on best practices in clinical supervision.
Keywords: intentional nondisclosure, counselors-in-training, supervision, content analysis, best practices in clinical supervision
Counselors-in-training (CITs) in programs accredited by the Council for Accreditation of Counseling & Related Educational Programs (CACREP) are required to complete two supervised onsite field experiences (i.e., practicum and internship) in their area of interest (e.g., clinical mental health, school, rehabilitation; CACREP, 2015). The purpose of this onsite field experience is for CITs to learn the roles and responsibilities of being a professional counselor by applying what they learn in their training programs to their work in a counseling setting (CACREP, 2015). Given CITs’ limited clinical experience, onsite supervisors provide weekly supervision to aid CITs in their professional development (Borders et al., 2011; Borders et al., 2014). Although supervision is a unique opportunity, CITs receive problematic mixed messages about the expectations of the supervisory process (Borders, 2009). CITs are encouraged to discuss the topics and concerns that are the most important to their professional growth (Bordin, 1983), but the information shared is then used by their supervisors to evaluate their clinical performance (Bernard & Goodyear, 2014). These evaluations have a definitive impact on CITs’ ability to pass a practicum or internship course or graduate (CACREP, 2015) and subsequently secure employment in the counseling field. Thus, it is not surprising that studies in allied professions (e.g., clinical psychology, counseling psychology, social work) have shown that trainees commonly withhold potentially unflattering information from their supervisors (Hess et al., 2008; Ladany, Hill, Corbett, & Nutt, 1996; Mehr, Ladany, & Caskie, 2010, 2015; Pisani, 2005). While CITs’ concern to maintain a favorable image in the eyes of their supervisor is understandable, withholding information can result in missed learning opportunities for CITs and negatively impact their clients (Hess et al., 2008).
To date, only two studies have examined supervisee intentional nondisclosure in a sample of counselor education students (Cook & Welfare, 2018; Lonn & Juhnke, 2017). However, neither study examined specific examples of the types and reasons of CIT nondisclosure during onsite supervision. Counselors submit to a unique training model, with specific requirements and goals for master’s-level counselors (e.g., CACREP, 2015). CITs enrolled in CACREP-accredited programs can specialize in one of seven tracks: (a) addictions counseling; (b) career counseling; (c) clinical mental health counseling; (d) clinical rehabilitation counseling; (e) college counseling and student affairs; (f) marriage, couple, and family counseling; (g) school counseling; and (h) rehabilitation counseling. As a result, CITs work in diverse settings with a wide variety of responsibilities that are unique to the counseling profession (CACREP, 2015; Lawson, 2016). Without a study focused on CITs’ experiences in onsite supervision, CITs and supervisors must rely on findings from allied professions that may or may not reflect the counseling training model. Thus, in the current study we aimed to examine the types of intentional nondisclosure and the reasons for the nondisclosure during CITs’ supervised onsite field experience.
Supervised Onsite Field Experience in CACREP-Accredited Programs
Given the growing importance of attending a CACREP-accredited program as an educational requirement for professional counselors (Lawson, 2016), we chose to specifically target intentional nondisclosure by CITs enrolled in CACREP-accredited training programs. State licensure boards are encouraging or mandating that those pursuing professional licensure as counselors must have a degree from a CACREP-accredited program (Lawson, 2016). Additionally, as of January 1, 2022, those applying to be National Certified Counselors (NCCs) will need to graduate from a CACREP-accredited program (National Board for Certified Counselors, 2014). Thus, the standards for onsite field experiences outlined in the 2016 CACREP Standards provide clear guidelines for counselor training. Furthermore, the activities during the onsite field experience are designed to mimic those of a professional counselor in the field (CACREP, 2015). Exploring CIT intentional nondisclosure within the CACREP educational structure can help to inform best practices in counselor training.
Intentional Nondisclosure in Clinical Supervision
The supervision process is reliant on CITs to self-identify important information to share with their supervisors (Ladany et al., 1996); however, identifying this important information is not always clear to CITs given the intricacies of the client–counselor relationship (Farber, 2006; Knox, 2015). Farber (2006) suggested that some nondisclosure “is normative and unavoidable in supervision” (p. 181). Yet, there are instances in which CITs purposefully withhold information they know is relevant because of concerns for what could happen if they shared the information with their supervisor (Hess et al., 2008; Yourman & Farber, 1996).
So why would CITs, who are held to the same ethical standards as practicing counselors (American Counseling Association [ACA], 2014), knowingly choose to withhold information that could be harmful to their professional development or their clients’ treatment? During an onsite field experience, CITs learn the day-to-day tasks of being a professional counselor (e.g., establishing rapport, planning treatment, managing paperwork), but they also must meet the demands of their graduate training programs. Most CITs want to perform counselor functions at a high level, if not perfectly (Rønnestad & Skovholt, 2003). Avoiding clinical mistakes is a dubious belief that CITs hold for themselves (Knox, 2015). These high expectations create a reasonable desire to present oneself favorably to their supervisors, even though supervisors know that perfection is impossible (Farber, 2006). Moreover, CITs are told to share information that is most salient to their personal and professional development with their supervisors, but disclosing information that may be potentially unflattering or embarrassing can then be used by supervisors to evaluate performance (Borders, 2009).
Types and Reasons for Intentional Nondisclosure
In a seminal study on intentional nondisclosure, Ladany et al. (1996) investigated the types and reasons for nondisclosure in a sample of clinical and counseling psychology trainees. Participants were asked to identify instances in which they withheld information from their supervisors and then provide a rationale for why they failed to share that information. The authors found that 97.2% of the participants withheld information from their supervisors.
Through categorizing the content of the nondisclosures, Ladany et al. identified 13 types of nondisclosure, providing definitions and examples of each type: (a) negative reactions to supervisor (e.g., unfavorable thoughts or feelings about supervisors or their actions); (b) personal issues (e.g., information about an individual’s personal life that may not be relevant); (c) clinical mistakes (e.g., an error made by a counselor); (d) evaluation concerns (e.g., worry about the supervisor’s evaluation);
(e) general client observations (e.g., reactions about the client or client treatment); (f) negative reactions to client (e.g., unfavorable thoughts or feelings about clients or clients’ actions); (g) countertransference (e.g., seeing oneself as similar to the client); (h) client–counselor attraction issues (e.g., sexual attraction between client and counselor); (i) positive reactions to supervisor (e.g., favorable thoughts or feelings about supervisors or their actions); (j) supervision setting concerns (e.g., concerns about the placement or tasks required at placement); (k) supervisor appearance (e.g., reactions to supervisor’s outward appearance); (l) supervisee–supervisor attraction issues (e.g., sexual attraction between supervisee and supervisor); and (m) positive reactions to client (e.g., favorable thoughts or feelings about clients or their actions).
They also identified 11 reasons for intentional nondisclosure: (a) perceived unimportance (e.g., information not worth discussing with supervisor); (b) too personal (e.g., information about one’s personal life that is private); (c) negative feelings (e.g., embarrassment, shame, anxiety); (d) poor alliance with supervisor (e.g., poor working relationship with supervisor); (e) deference (e.g., inappropriate for a counselor to bring up because of their role as intern or supervisee); (f) impression management (e.g., desire to be perceived favorably by supervisor); (g) supervisor agenda (e.g., supervisor’s views, roles, and beliefs that guide supervisor’s actions or reactions to supervisee); (h) political suicide (e.g., fear that the disclosure will be disruptive in the workplace and lead to the supervisee being unwelcome or unsupported); (i) pointlessness (e.g., addressing the issue would not influence change); (j) supervisor not competent (e.g., supervisor is inaccessible or unfit for supervisory role); and (k) unclear (e.g., researchers unable to read participants’ statements). The most common types of intentional nondisclosure in the study by Ladany et al. (1996) were negative reactions to supervisor, CITs’ personal issues, clinical mistakes, and evaluation concerns, while the most common reasons for the nondisclosures were perceived unimportance, too personal, negative feelings, and a poor alliance with the supervisor.
Subsequent studies, also from allied professions (e.g., social work, clinical psychology), have found similar results in regard to the types and reasons for intentional nondisclosure (Hess et al., 2008; Mehr et al., 2010; Pisani, 2005). Mehr and colleagues (2010) found 84.2% of psychology trainees reported withholding information from their supervisors, and the most common types of nondisclosures were negative perception of supervision, personal life concerns, and negative perception of the supervisor, while the most common reasons for nondisclosure were impression management, deference, and fear of negative consequences. Additionally, Pisani (2005) found the most commonly withheld information for social work trainees included supervisor–supervisee attraction issues, negative reactions to supervisor, and supervision setting concerns. Finally, in a qualitative study, Hess et al. (2008) explored the differences in a single example of intentional nondisclosure based on psychology trainees’ perceptions of the quality of the supervisory relationship—for example, good (i.e., only one instance of a problem in the supervisory relationship) versus problematic supervisory relationships (i.e., ongoing issues in the supervisory relationship). They found that supervisees in both good and problematic supervisory relationships withheld information about client-related issues. However, supervisees in problematic relationships more commonly withheld supervision-related concerns (e.g., negative reactions to supervisor) compared to supervisees in good relationships. The findings described above provide empirical evidence that nondisclosure in allied professions is common.
The Current Study
Although there is evidence that supervisees from allied professions withhold information, there is currently a dearth of literature regarding intentional nondisclosure by CITs in the field of counseling. Cook and Welfare (2018) found that the quality of the supervisory working alliance and supervisee avoidant attachment style predicted supervisee nondisclosure. In a qualitative study, Lonn and Juhnke (2017) examined supervisee nondisclosure in triadic supervision. They found that the supervisee’s perception of their relationships, the presence of a peer, and opportunity to share were important to whether supervisees withheld information. However, these studies failed to examine the types of information being withheld by CITs as well as their reason for withholding information. Considering that professional counselors have a unique training model (CACREP, 2015), professional identity (Lawson, 2016), and code of ethics (ACA, 2014), the purpose of the current study was to examine the types and reasons of intentional nondisclosure by CITs during their supervised onsite internship experience.
Method
We utilized content analysis (Hsieh & Shannon, 2005) to examine the examples of intentional nondisclosures provided by CITs that occurred in supervision with their onsite internship supervisors. Hsieh and Shannon (2005) defined qualitative content analysis as “a research method for the subjective interpretation of the content of text data through the systematic classification process of coding and identifying themes or patterns” (p. 1278). Our analysis was guided by the findings from Ladany et al. (1996), which allowed us to compare the findings from the current study with those from allied professions while also examining how the phenomenon of intentional nondisclosure might present uniquely in the counseling profession (Hsieh & Shannon, 2005). The current study was designed to answer two research questions: (a) What are the types of information that CITs intentionally withhold from their supervisors during their internship’s onsite supervision? and (b) What are the reasons for their nondisclosure?
Research Team
Our research team included three members. The first and third authors served as coders while the second author served as a peer reviewer. The first and second authors are counselor educators at different universities in the Southeast United States, and the third author was a doctoral student at the same institution as the first author. We all have experience as professional counselors, supervisees, supervisors, and researchers; consequently, we have experienced all parts of the nondisclosure cycle. Prior to the analysis process, we discussed how our previous experiences might impact the analysis. Likewise, we intentionally discussed and bracketed potential influences of bias throughout the project. We also employed triangulation (e.g., multiple coders), utilized frequent peer debriefs, and employed a peer reviewer (Creswell, 2013). Our items also were reviewed by four consultants with counseling, supervision, and research experience to minimize bias and maximize clarity.
Recruitment Procedure and Participants
After securing IRB approval, we recruited participants currently enrolled in internship for the current study through the assistance of counselor education faculty at CACREP-accredited institutions. Fifteen counselor educators at 14 institutions offered paper-and-pencil instrument packets to CITs during one of their class periods. As indicated by the key informants, 152 of the 173 CITs present in class on the day the packets were offered agreed to participate in the study. This resulted in an in-class response rate of 87.86%.
Participants were CITs currently enrolled in internship in a CACREP-accredited program and receiving supervision at their internship sites. The age of the participants ranged from 22 to 60 years old (M = 28.13, SD = 7.43, n = 107). Eighty-eight participants identified as female (80%), 17 participants identified as male (15.5%), three participants identified as nonbinary (gender identity not male and not female, 2.7%), and two participants indicated that they did not want to disclose their gender (1.8%). Regarding race, the majority of participants identified as White (non-Hispanic; n = 71, 64.5%), while 23 participants identified as African American (20.9%), four participants identified as Asian/Pacific Islander (3.6%), three participants identified as Hispanic/Latinx (2.7%), three participants identified as multiracial (2.7%), one participant identified as Native American (0.9%), one participant responded “none of the above categories” (0.9%), and four participants responded that they preferred not to disclose (3.6%). Regarding CACREP track, 64 participants were enrolled in a clinical mental health counseling track (58.2%), 32 participants were enrolled in a school counseling track (29.1%), nine were enrolled in a college counseling and students affairs track (8.2%), and five were enrolled in a marriage, couples, and family track (4.5%).
Instrument
The instrument was designed to gather information about participants’ experiences with their current onsite internship supervisors. Two items were the focus of this study: (a) “Describe a time when you decided not to share something you thought was significant with your current onsite internship supervisor” and (b) “What brought you to that decision to not share it with your current onsite internship supervisor?” In addition, the questionnaire included 15 items to collect demographic information about the participants and their current onsite internship supervisors. Of the 152 participants who began participation, 42 participants (27.6%) were removed from the analysis as they did not complete the open-ended questions, resulting in a final sample of 110 participants. We utilized the demographic variables to check for evidence of nonresponse bias using Chi-square tests of independence and independent t-tests. We did not find evidence of response bias when comparing those who answered the open-ended questions and those who did not.
Data Analysis
We analyzed participants’ responses to the open-ended questions utilizing content analysis. We categorized the types of intentional nondisclosure and the reasons for nondisclosure into categories as recommended by Hsieh and Shannon (2005). For our analysis, we utilized the types of nondisclosure and the reasons for nondisclosure originally identified by Ladany et al. (1996). To reiterate, Ladany et al. identified 13 types of intentional nondisclosure and 11 reasons for nondisclosure (1996). Also, as recommended by Hsieh and Shannon (2005), we allowed for new categories to emerge that did not fit within the categories from Ladany et al. The rationale for this approach was two-fold. First, we could best understand the phenomenon of intentional nondisclosure by comparing our findings to that of previous research from allied professions, while also generating new knowledge of how nondisclosure might uniquely manifest in the counseling profession (Lawson, 2016). Second, utilizing previous research provided structure to our coding procedures and informed the researchers’ interpretation of participant responses (Hsieh & Shannon, 2005).
Coding process. The first and third authors coded the responses of 110 participants for (a) whether or not the participant identified an incident of intentional nondisclosure and (b) to categorize the participant responses that indicated intentional nondisclosure by the type and reasons for the nondisclosure. Each response was coded into one category of type of nondisclosure and one category of reason for the nondisclosure. First, the two coders selected 10 participant responses and coded them as a team. Next, the two coders selected an additional 10 participant responses and coded them independently of each other. They then came together to reach a consensus on the categorization of participant responses. The remaining 90 participant responses were coded independently, and the two coders regularly engaged in peer debriefings throughout the process to ensure consistency (Creswell, 2013). After all 110 participant responses were analyzed, the first and third authors met to finalize the categorization of participant responses and to generate names for the new categories that emerged during the analysis (Hsieh & Shannon, 2005). Regarding the categorization of participant responses in terms of the participant-identified incident of intentional nondisclosure, the coders’ agreement was 100%. Regarding the types and reasons for the nondisclosure, the coders initially disagreed on 15 types of intentional nondisclosure and 23 reasons for the nondisclosure. The two coders established consensus through discussion, resulting in an agreement of 100% (Creswell, 2013). Finally, the second author, serving as a peer reviewer, evaluated the entire coding process. She was chosen based on her expertise with supervision delivery (e.g., protocol, practice) and the topic of intentional nondisclosure. She did not recommend any changes to the categorization of participant responses; however, she recommended renaming two of the new categories for the types of nondisclosures that emerged from the data to better reflect the content of participant responses. Eleven types of intentional nondisclosure and 13 reasons emerged from our analysis.
Results
Forty-four (40%) participants reported that they had never withheld something significant from their current onsite internship supervisors, while 66 (60%) reported that they had. Examples of responses coded as never having withheld something significant from their onsite supervisors include “N/A,” “At this time, I have not withheld any information that I felt was significant with my supervisor,” and “I don’t think there has been one.” For the responses that included an example of intentional nondisclosure (n = 66), 11 types of intentional nondisclosure and 13 reasons for withholding information emerged from the data. The types of intentional nondisclosure included eight types of nondisclosure that were from Ladany et al.’s (1996) research on nondisclosure and three new types of intentional nondisclosure that emerged in this data set: (a) CIT professional developmental needs, (b) a peer’s significant issue, and
(c) experiencing sexual harassment. Regarding the reasons for the intentional nondisclosures, 10 reasons mirrored the findings from Ladany et al. and three reasons were unique to the current study: (a) did not want to harm client or confidentiality concerns, (b) consulted with another supervisor, and (c) issue with other professional in supervision setting.
The Types and Reasons for Intentional Nondisclosures
The most common type of intentional nondisclosures identified by the researchers in the current study were negative reactions to supervisor (n = 18, 27.3%), general client observations (n = 16, 24.2%), and clinical mistakes (n = 15, 22.7%). The most common reasons for intentional nondisclosures were impression management (n = 12, 18.2%), perceived unimportant (n = 8, 12.1%), negative feelings, (n = 8, 12.1%), and supervisor not competent (n = 8, 12.1%). Complete results of the coding and category frequencies of the types of nondisclosures are presented in Table 1, and the final coding and category frequencies of the reasons for nondisclosure are presented in Table 2.
| Table 1
Types of Intentional Nondisclosure |
| Type of Intentional Nondisclosure |
n (%) |
Examples |
| Negative Reactions to Supervisor |
18 (27.3%) |
When my supervisor asked if there is anything that is hindering our relationship, I lied and said that there wasn’t anything and the relationship is fine.
I feel that I am not getting feedback about my counseling from my supervisor in the supervision meetings. Instead I am only getting suggestions of how the supervisor would have handled the client.
Made a comment behind my back. My onsite supervisor is new and so I don’t share too much because he’s easily overwhelmed. |
General Client
Observations |
16 (24.2%) |
I gave [clients] more chances to skip/miss an appointment than [my supervisor] would allow so sometimes don’t let her know when people cancel or no show.
When a client disclosed personal family issues; client’s past trauma. |
| Clinical Mistakes |
15 (22.7%) |
I put a client in danger by a lack of knowledge and being new in a position.
Too much self-disclosure in a session; getting behind on case notes/paperwork.
Having a chronically suicidal client and . . . not assessing for SI in a session and feeling as if when assessed it was not done so well. |
Client–Counselor
Attraction Issues |
4 (6.1%) |
I felt attracted to an assessment client.
During a session, a client told me that he liked how I looked in my pants. He then told me that he got excited at the sound of my voice. |
| Countertransference |
3 (4.5%) |
A client reminded me of my late mother.
Early in internship, I had strong countertransference with a client. |
| Supervision Setting Concerns |
3 (4.5%) |
I was concerned if I was going to have to find another site to finish hours.
Frustration with internship duties. |
| Personal Issues |
2 (3.0%) |
I did not tell my supervisor that I chose to cut it off with a potential romantic partner. |
| CIT Developmental Need |
2 (3.0%) |
When I was first starting out I had a hard time letting my supervisor know when I needed something extra from them whether it be time or information. |
| Negative Reactions to Client |
1 (1.5%) |
Anger toward a student. |
| A Peer’s Significant Issue |
1 (1.5%) |
A client wrote a letter to my co-intern about his sexual desires and love for her. |
| Experiencing Sexual Harassment |
1 (1.5%) |
When I felt sexually harassed by a colleague. |
| Note. Not all types of intentional nondisclosure from Ladany et al. (1996) were present in this sample, and three new types emerged: (a) CIT developmental need, (b) a peer’s significant issue, and (c) experiencing sexual harassment.
|
| Table 2
Reasons for Intentional Nondisclosure |
| Reasons |
n (%) |
Examples |
Impression
Management |
13 (19.7%) |
Concerned about evaluations by those who supervise my supervisors.
Fear of looking bad or being perceived as not being a good counselor.
[Supervisor] might pass judgment because I can’t possibly know what I’m talking about being only an intern.
I worried she will think I’m unprofessional or not trust me with future clients. |
| Negative Feelings |
8 (12.1%) |
Poor self-confidence.
Fear of rejection.
Embarrassment, inferiority felt with supervisor. |
Supervisor Not
Competent |
8 (12.1%) |
I see the way she counsels clients and I know she thinks taking time to establish rapport and positive therapeutic relationships is not always necessary.
Everyone in the office says she is burnt-out and I want to be more compassionate. |
Perceived
Unimportant |
8 (12.1%) |
I did not feel it was necessary.
I was running late to class and I didn’t consult with her because she was in a session with a client so I figured I’d tell her the next day. |
| Deference |
6 (9.1%) |
I did not feel like it would be taken well, and that I am only an intern and should not correct her.
Didn’t want to hurt/upset her or burn a professional relationship. |
| Poor Alliance with Supervisor |
5 (7.6%) |
The power differential.
She berated me in supervision to the point of tears. I feel unsafe with her and our clinical styles contrast.
I knew she would make me feel inferior. |
| Supervisor Agenda |
4 (6.1%) |
I thought he would immediately notify people in charge.
Knowing my supervisor would want to tell [client’s] mother. |
| Political Suicide |
4 (6.1%) |
I want to get hired where I’m working and I don’t feel . . . safe during supervision.
It’s a small practice and I have to share a wall with this offender every day. |
Did Not Want to Harm Client or
Confidentiality
Concerns |
4 (6.1%) |
I didn’t want to put client in a bad situation.
That student was not positive of her status and was not in any danger. Revealing her secret at that point would have damaged the relationship.
Confidentiality issues. |
| Too Personal |
3 (4.5%) |
It was too personal.
I didn’t want to talk about my grief. |
| Pointlessness |
1 (1.5%) |
Thought that was between student and personal physician. |
Consulted with
Another
Supervisor |
1 (1.5%) |
Other supervisor suggestions. |
Issues with Other Professionals in
Supervision Setting |
1 (1.5%) |
The teacher expressed frustration. Hopes to prevent future conflict. |
| Note. Not all categories and reasons from Ladany et al. (1996) were present in this sample, and three new reasons emerged: (a) did not want to harm client or confidentiality concerns, (b) consulted with another supervisor, and (c) issues with other professionals in supervision setting. |
Specific Examples of the Types and Reasons for Intentional Nondisclosure
To provide a more complete picture of the phenomenon of intentional nondisclosure (Hsieh & Shannon, 2005), this section is presented to highlight specific examples provided by participants for each type of nondisclosure and the reasons they withheld the information. Our coded reason for the type of intentional nondisclosure is included in parentheses below (e.g., deference, impression management, political suicide).
Negative reactions to supervisor. One participant stated that she did not disclose that her supervisor “was not helpful during a time that I needed her to be” because the participant “did not want to . . . upset her or burn a professional relationship” (deference). Another participant did not tell her supervisor at her school internship that she disapproved of the way the supervisor addressed a student: “I felt she was being too harsh on a student and not considering other factors.” This participant did not want her supervisor to perceive her as “being wrong” (impression management). A participant stated that even though her supervisor sits in on all of her sessions at her internship site, she still withheld that she is not satisfied with the quality of their relationship and did not share how she felt “in the relationship with her.” She added that she did not disclose this information because “I am afraid she’ll be angry and it will damage the relationship we do have” (negative feelings). Finally, for a clinical mental health CIT, even her supervisor directly asking if she had concerns about the supervisory relationship was not enough to encourage her disclosure: “When my supervisor asked if there is anything that is hindering our relationships I lied and said that there wasn’t anything and the relationship is fine.” The CIT stated she lied because “the power differential, being videotaped, and concerns with confidentiality . . . stopped me from being completely honest about my comfort with our relationship” (poor alliance with supervisor).
General client observations. General client observations differed from clinical mistakes because participants did not self-identify that they perceived the specific examples they provided to be mistakes. Rather, participants indicated that the examples they provided were relevant; however, they failed to disclose this significant information to their supervisors. One school counseling CIT stated that she did not share with her supervisor that she was having trouble “breaking the ice with a client” because she “knew my [supervisor] would make me feel inferior” (poor alliance with supervisor). Another school counseling CIT shared that she failed to disclose that one of her clients was “drinking alcohol on campus” because she thought her supervisor would “immediately notify people in charge of discipline rather than talking to the student first” (supervisor agenda). Finally, another school counseling CIT stated that a client told her she was pregnant, but she failed to notify her supervisor because “that student was not positive of her status and was not in any danger. Revealing her secret at that point would have damaged the relationship” (did not want to harm client; confidentiality concerns).
Clinical mistakes. Participants reported a range of clinical mistakes, from minor clerical errors to potentially more problematic mistakes such as failure to assess for client risk. One clinical mental health CIT did not share that she was “behind on my case notes” because she “did not feel it was necessary” and she “caught up quickly” (perceived unimportant). A student affairs CIT stated that he did not let his supervisor know that he “lacked confidence in theories” because he felt “inadequate” and “embarrassed” (negative feelings). A clinical mental health CIT shared that she failed to disclose something in supervision that her supervisor had previously told her not to do: “My supervisor had previously verbalized that she would be upset.” She withheld this information because “I didn’t want to seem . . . incompetent and I respected her and want her to think I’m doing my best” (impression management). Multiple participants provided specific examples of intentional nondisclosures related to failing to adequately assess for client risk or failing to notify their supervisors that a client was engaging in risk-related behavior. A school counseling CIT shared that she did not discuss with her supervisor that “a client (minor on a school campus) was engaging in [non-suicidal self-injury] again” because “we discussed before how she is obligated to pass that info to school principal who tells parents” (supervisor agenda). This participant added that she decided not to share this information with her supervisor because she perceived the self-injury to be non–life threatening and she wanted to “save rapport” with the client (did not want to harm client; confidentiality concerns). Finally, a school counseling CIT stated that she withheld from her supervisor that she “put a client in danger by my lack of knowledge and being new in my position.” This CIT did not discuss this with her supervisor because “my supervisor wasn’t available” (supervisor not competent).
Client–counselor attraction issues. One clinical mental health counseling CIT stated that her client “told me that he liked how I looked in my pants. He then told me that he got excited at the sound of my voice.” She stated that she did not disclose this information to her supervisor because “I told myself that I did not understand how he meant the comment and I thought he would stop the flirting if I ignored him” (perceived unimportant). Two participants indicated that they experienced sexual attraction to a client but failed to share it with their supervisor. One student affairs CIT stated that she felt “embarrassed” (negative feelings), while a clinical mental health counseling CIT shared that he “did not want anyone to find out and I felt like I handled it fine” (impression management).
Countertransference. One marriage, couples, and family CIT stated that she did not disclose to her supervisor that a client “reminded me of [my] late mother” because she “did not want to talk about [my] grief” (too personal). A clinical mental health counseling CIT echoed the previous participant’s thinking process. She stated she did not tell her supervisor she was experiencing “countertransference” with a client because “it was too personal” (too personal). Finally, another marriage, couples, and family CIT stated that early in her internship she had “strong countertransference with a client” as a result of a personal grieving process. She shared that she did not tell her supervisor because she wasn’t sure “how much I trusted her with this information as it was only several weeks into internship” (poor alliance with supervisor).
Supervision setting concerns. A clinical mental health counseling CIT stated that she did not express her “frustration with internship duties” to her supervisor because “he was unavailable” (supervisor not competent). Another clinical mental health counseling CIT was concerned that she “would need to find another site to finish [internship] hours,” but did not tell her supervisor because “I did not choose to add to stress [of my] site supervisor by posing my concern” (deference).
Personal issues. One participant enrolled in a clinical mental health counseling program withheld from the supervisor that “sad and depressed” feelings because of a “fear of rejection” (negative feelings) arose during supervision. A school counseling CIT did not disclose to her supervisor that she had recently ended a relationship “with a potential romantic partner” even though it was causing her to “feel drained and emotional during the day at her internship” because “I felt that it would be silly to and I thought I did a good enough job ignoring the feelings while with students” (too personal).
CIT developmental need. One clinical mental health counseling CIT shared that she had a difficult time “letting my supervisor know when I needed something extra from them whether it be time or information” because she “felt nervous about [her] position as ‘just an intern’” (negative feelings). Another clinical mental health counseling CIT stated that she failed to let her supervisor know that she is “concerned about being in an individual session with a male client” because she is fearful that her supervisor would think she is “unprofessional or not trust me with future clients” (impression management).
Negative reactions to client. Only one participant indicated that she failed to disclose a negative reaction to a client with her supervisor. This student affairs CIT stated that she did not disclose her “anger towards a client” because she “did not think it was important enough to share” (perceived unimportant).
A peer’s significant issue. One clinical mental health counseling CIT noted that there was a failure to disclose to the supervisor that “a client wrote a letter to my co-intern about his sexual desires and love for her.” This CIT stated that the co-intern did not want this information shared and that the participant “did not think it was my place” (deference).
Experiencing sexual harassment. A clinical mental health counseling CIT stated that she was “sexually harassed by a colleague,” but failed to disclose to her supervisor because “it’s a small practice and I have to share space with this offender every day” (political suicide).
Discussion
The current investigation was designed to examine the types of and reasons for intentional nondisclosure by CITs during their onsite supervision. Sixty percent of the participants provided an example of withholding something significant from their onsite internship supervisors, suggesting that, similar to allied professions, intentional nondisclosure by counseling CITs is common (Ladany et al., 1996; Pisani, 2005; Yourman & Farber, 1996). Participants also provided detailed examples of the types of intentional nondisclosures as well as the reasons they withheld the information. These findings provide insight into the experiences of CITs at their internship placement. In this section, we will connect our findings to those from previous research as well as offer implications for counselors, supervisors, and counselor training programs.
The Types of Intentional Nondisclosure and Reasons for Nondisclosure
Overall, the types of intentional nondisclosure and the reasons for these nondisclosures are comparable to the findings of previous studies in allied professions. There were four categories of the types of intentional nondisclosure that emerged in the study by Ladany et al. (1996) that were not present in the current study: (a) positive reactions to supervisor, (b) supervisor appearance, (c) supervisee–supervisor attraction issues, and (d) positive reactions to client. The category of “unclear” in regard to the reasons for nondisclosure also was not found in the current study, as all participant responses in the current study were legible. Participants of differing CACREP tracks all provided examples of intentional nondisclosure to their supervisors in regard to their field placement. These findings suggest that despite the differences in training models (CACREP, 2015) and professional identities (Lawson, 2016), CITs experience many of the same situations that result in intentional nondisclosure as those from allied professions. The most commonly withheld information in the current study was negative reactions to supervisor, which also was true for psychology trainees in the study by Ladany et al. Supervisees appear most hesitant to discuss their concerns about their supervisor or supervision experience (Hess et al., 2008; Mehr et al., 2010; Pisani, 2005). In addition, CITs also commonly withheld general observations about clients and clinical mistakes similar to allied professions (Hess et al., 2008; Ladany et al., 1996; Mehr et al., 2010; Pisani, 2005).
The CITs in the current study provided many reasons for their intentional nondisclosure, but some reasons were more commonly reported than others. Like the findings from Mehr et al. (2010), participants in the current study most commonly withheld information in order to make a favorable impression on their supervisors. Others reported they withheld because of negative feelings such as “shame” or “embarrassment.” Farber (2006) suggested that internalized negative feelings are often a reason for nondisclosure. Consistent with findings from allied professions (Hess et al., 2008; Ladany et al., 1996), CITs also withheld because (a) they believed a supervisor was not competent, (b) they believed information was not quite important enough to disclose, and (c) they wanted to perform perfectly in their new roles.
Novel Findings Regarding Types and Reasons for Intentional Nondisclosure
An important aspect of content analysis is discussing findings that may extend existing knowledge of a given phenomenon (Hsieh & Shannon, 2005). The current study is the first to examine the types of intentional nondisclosure and reasons for nondisclosure in a sample of CITs. As such, there are several novel findings that warrant discussion. For example, two participants indicated that they did not discuss their professional development needs with their onsite supervisor. This is particularly interesting, given a central function of clinical supervision is to facilitate CIT professional development (Bernard & Goodyear, 2014). CITs who internalize their professional developmental needs as a flaw or who desire to hide these needs for fear of their supervisors’ reactions also may desire to perform perfectly (Rønnestad & Skovholt, 2003). Discussing opportunities for growth as a CIT can be difficult (Mehr et al., 2010); thus, supervisors may need to prompt their supervisees to discuss their needs more directly.
Another novel finding is that one participant indicated that she withheld from her supervisor about her peer’s ethical dilemma (the client letter revealing romantic interest). This participant explained that she did not feel it was her place to share her peer’s information, but all counselors and CITs share some responsibility to address ethical concerns. Ladany et al. (1996) found that 53% of those who withheld information from their supervisors told a peer in the field about their concern. Therefore, it seems likely that other CITs may be placed in a similar position as the participant in the current study. Knowing one’s ethical responsibility to disclose unethical behavior, as in the situation germane to this study, could be prudent (ACA, 2014). Finally, one participant indicated that she was being sexually harassed by a colleague. This report of intentional nondisclosure is particularly concerning given the increased attention to Title IX and attempts to mitigate sexual harassment and sexual assault in university and workplace settings (Welfare, Wagstaff, & Haynes, 2017). This participant’s willingness to share her trauma through the data collection process in this study presents an opportunity for counselor educators and supervisors to explore strategies to prevent these experiences for future CITs.
Regarding the reasons for intentional nondisclosure, there also were novel findings because three new reasons emerged in the current study. First, five participants did not disclose information to their supervisor because they did not want to harm their clients or violate a client’s confidentiality. However, the sharing of information with a supervisor would never violate client confidentiality (ACA, 2014). Perhaps the supervisees’ confusion about the parameters of confidentiality or misdirected efforts to protect clients from the actions of a supervisor they perceived as incompetent led to this decision. A second novel reason for intentional nondisclosure was evidenced by one participant who reported consulting with a supervisor who was not her site supervisor. Ladany et al. (1996) found that 15% of psychology trainees consulted with “another supervisor” outside their primary supervisor (p. 16). Ladany et al. did not ask their participants to clarify the role of another supervisor; however, this finding is relevant to the current study and the training of CITs. Throughout a CIT’s internship experience, they have two supervisors: one onsite supervisor and one university supervisor (CACREP, 2015). It is unclear if the supervisor with whom the participant discussed their concern was another supervisor at the site or the university supervisor. However, this could be an inherent challenge for CITs to identify who to share information with, particularly if there are issues in one of the two relationships. Finally, one school counseling CIT indicated that she had an issue with a teacher and addressed this issue with the teacher directly. Counselors work in diverse settings (ACA, 2014; CACREP, 2015) and may often work with persons outside the counseling profession. Counseling programs and supervisors may need to better prepare students to work with other professionals in their specific setting.
Implications for CITs
The findings from the current study provide empirical evidence that, when faced with the decision to share in clinical supervision, CITs sometimes chose to withhold information from their supervisors despite knowing its relevance. CITs of all CACREP tracks will likely be faced with this difficult decision. We hope that these findings, which offer insights into the experience of intentional nondisclosure, help to normalize the challenges that CITs face and identify strategies to prevent nondisclosure.
Some of the participants described harmful supervision experiences in which they were berated by their supervisors, feared fallout if they were to disclose illegal sexual harassment by another site employee, were concerned about a supervisor’s clinical competence, or did not feel safe to share even blatantly inappropriate client behaviors. Harmful supervision such as this has also been described by Ellis et al. (2014) and is a major concern for counseling and related professions. CITs who find themselves in harmful supervision situations can consider seeking support from another professional, a peer, or a professional association ethics consultant who might help rectify these issues.
Even for those CITs who are not enduring harmful supervision, there are costs to nondisclosure such as stalled development, safety concerns, and ethical or legal violations. Ultimately, the decision to withhold information from one’s clinical supervisor rests with the CIT (Murphy & Wright, 2005). Advocating for a safe and productive supervisory experience may result in a change that serves as a catalyst for supervisee growth or prevents client harm. No supervisee needs to be concerned about burdening a supervisor with disclosures about training issues or ethics; it is the supervisor’s responsibility to address supervisee needs, no matter how burdensome. Relatedly, supervisees who are reluctant to discuss their observations of clients or clinical mistakes for fear of being evaluated poorly or perceived as unqualified should consider ways to demonstrate quality work in order to balance the areas for growth. Making mistakes is expected for all CITs, but it is important to use supervision to learn from these mistakes (Pearson, 2001). In fact, reflecting on previous experiences—and learning from those experiences—is key to becoming a skilled and seasoned counselor (Rønnestad & Skovholt, 2003). CITs also might find it helpful to pursue their own personal counseling as another strategy to facilitate personal and professional growth (Oden, Miner-Holden, & Balkin, 2009).
Several CITs shared their hesitancy in disclosing information to their supervisor for fear of violating their clients’ confidentiality or harming the therapeutic alliance. Although client confidentially is critical, disclosing information to one’s supervisor would not violate a client’s confidentiality (ACA, 2014). In fact, some of the concerns expressed seemed to be more about the limits of confidentiality in the setting more broadly (e.g., high school rules), rather than with the supervisor specifically. Counselors are encouraged to not tell a client that the information shared during the counseling process will remain absolutely confidential. Rather, counselors are encouraged to include a passage in their informed consent about the boundaries of client confidentiality and discuss this information with their clients (ACA, 2014). Finally, predicting when ethical or legal issues will occur may be impossible. Counselors should regularly consult with supervisors to discuss treatment options and legal and ethical issues (ACA, 2014).
Implications for Supervisors and Counselor Education Training Programs
Supervisors and counselor educators play a central role in reducing CIT intentional nondisclosures. The findings from the current study suggest there is a wide range of topics that CITs are reluctant to discuss with their supervisors and a wide range of reasons for withholding. The varying nature of intentional nondisclosures highlights the necessity of individualized interventions. Broadly speaking, supervisors are encouraged to facilitate an open and safe environment that invites disclosure (Bordin, 1983). This might also mean supervisors must be willing to purposefully solicit feedback from their supervisees (Murphy & Wright, 2005). Additionally, supervisors must be proactive in utilizing the knowledge gained from studies like this one to normalize the experiences of their supervisees. Perhaps by discussing each of the types of nondisclosure described above with CITs, supervisors can reduce the pressures associated with performing perfectly (Rønnestad & Skovholt, 2003) or diminish the negative emotions (e.g., shame, embarrassment) associated with making mistakes (Farber, 2006; Knox, 2015).
Finally, some of the experiences described by the participants in the current study are deeply troubling, as they shared specific examples of ineffective and harmful supervision. The burden of providing evidence and reporting instances of harmful supervision is often placed on the CIT (Ellis, Taylor, Corp, Hutman, & Kangos, 2017). We outlined some strategies for CITs in case they were to experience harmful supervision; however, the findings from the current study suggest that CITs are withholding this information for any number of reasons. The participants in this study are not unlike those from other allied professions who have similar supervision experiences (for specific examples of harmful supervision, see Ellis, 2017). Thus, supervisors and counselor education programs must work to prevent CITs from experiencing the damaging effects of ineffective or harmful supervision. We encourage counselor education programs to be proactive by reviewing the signs of ineffective and harmful supervision practices with students before they begin their internships and to regularly check in with students about the supervision experience. Counselor education programs may find it beneficial to solicit student feedback about their practicum/internship site at the end of each term—specifically targeting concerns related to ineffective and harmful supervision.
Encouraging students to disclose their experiences with ineffective or harmful supervision while they are in the process of graded program work might not be possible because of the reasons described above; however, preventing similar experiences for future students may be. Finally, CACREP (2015) requires that all site supervisors receive supervision training prior to serving in this capacity. Accidental instances of ineffective or harmful supervision may be prevented by adding training for site supervisors in this content area (Ellis et al., 2017).
Limitations and Future Research
The current study has limitations that create opportunities for future research. First, we utilized the categories originally identified in the study conducted by Ladany et al. (1996). Although we allowed for the creation of new categories, it is possible that selecting a different study to guide our investigation would have yielded different findings (Hsieh & Shannon, 2005). Also, prompting for a single example of significant intentional nondisclosure may have influenced the findings. Future studies should include the opportunity to provide multiple examples, which could result in different findings. Finally, participants were asked to provide examples of intentional nondisclosure with their onsite supervisors during their internship. These participants were receiving supervision from a university supervisor (CACREP, 2015), meaning the information withheld from the onsite supervisor may have been discussed with the university supervisor. It is also plausible that supervisees withheld the information from both the onsite and university supervisors. Site supervisors and university supervisors might have conflicting agendas, presenting a burden on supervisees to decide what to disclose to whom. Future studies should examine how supervisees decide what to disclose when they have multiple supervisors at one time. Finally, participants in the current study reported they were most hesitant to disclose their negative reactions about their supervisors. Future research should explore how supervisors can better monitor their supervisees’ reactions to them.
Conclusion
Although previous research from allied professions provides evidence of how nondisclosure manifests within those professions, the findings from this study provide empirical evidence of how CIT intentional nondisclosure presents during onsite supervision. These findings provide valuable insights into the types of information that CITs withhold as well as the reasons for their nondisclosure during their onsite supervision. Given that the counseling profession has a unique training model (CACREP, 2015) and professional identity (Lawson, 2016), these findings can be used by CITs, onsite supervisors, and counselor educators to generate targeted solutions to address this critical issue.
Conflict of Interest and Funding Disclosure
This research was supported by a grant from the Association for Counselor Education and Supervision.
References
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author.
Bernard, J. M., & Goodyear, R. K. (2014). Fundamentals of clinical supervision (5th ed.). Boston, MA: Pearson.
Borders, L. D. (2009). Subtle messages in clinical supervision. The Clinical Supervisor, 28, 200–209. doi:10.1080/07325220903324694
Borders, L. D., DeKruyf, L., Fernando, D. M., Glosoff, H. L., Hays, D. G., Page, B., & Welfare, L. E. (2011). Best practices in clinical supervision. Retrieved from https://www.acesonline.net/sites/default/files/ACES-Best-Practices-in-clinical-supervision-document-FINAL_0_0.pdf
Borders, L. D., Glosoff, H. L., Welfare, L. E., Hays, D. G., DeKruyf, L., Fernando, D. M., & Page, B. (2014). Best practices in clinical supervision: Evolution of a counseling specialty. The Clinical Supervisor, 33, 26–44.
Bordin, E. S. (1983). A working alliance based model of supervision. The Counseling Psychologist, 11, 35–42. doi:10.1177/0011000083111007
Cook, R. M., & Welfare, L. E. (2018). Examining predictors of counselor-in-training intentional nondisclosure. Counselor Education and Supervision, 57, 211–226.
Council for Accreditation of Counseling & Related Educational Programs. (2015). 2016 CACREP standards.
Retrieved from https://www.cacrep.org/for-programs/2016-cacrep-standards
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). Thousand Oaks, CA: Sage.
Ellis, M. V. (2017). Narratives of harmful clinical supervision. The Clinical Supervisor, 36, 20–87.
doi:10.1080/07325223.2017.1297752
Ellis, M. V., Berger, L., Hanus, A. E., Ayala, E. E., Swords, B. A., & Siembor, M. (2014). Inadequate and harmful clinical supervision: Testing a revised framework and assessing occurrence. The Counseling Psychologist, 42, 434–472. doi:10.1177/0011000013508656
Ellis, M. V., Taylor, E. J., Corp, D. A., Hutman, H., & Kangos, K. A. (2017). Narratives of harmful clinical supervision: Introduction to the special issue. The Clinical Supervisor, 36, 4–19.
doi:10.1080/07325223.2017.1297753
Farber, B. A. (2006). Self-disclosure in psychotherapy (1st ed.).New York, NY: Guilford Press.
Hess, S. A., Knox, S., Schultz, J. M., Hill, C. E., Sloan, L., Brandt, S., . . . Hoffman, M. A. (2008). Predoctoral interns’ nondisclosure in supervision. Psychotherapy Research, 18, 400–411. doi:10.1080/10503300701697505
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15, 1277–1288. doi:10.1177/1049732305276687
Knox, S. (2015). Disclosure—and lack thereof—in individual supervision. The Clinical Supervisor, 34, 151–163. doi:10.1080/07325223.2015.1086462
Ladany, N., Hill, C. E., Corbett, M. M., & Nutt, E. A. (1996). Nature, extent, and importance of what psychotherapy trainees do not disclose to their supervisors. Journal of Counseling Psychology, 43, 10–24. doi:10.1037/0022-0167.43.1.10
Lawson, G. (2016). On being a profession: A historical perspective on counselor licensure and accreditation. Journal of Counselor Leadership and Advocacy, 3, 71–84. doi:10.1080/2326716X.2016.1169955
Lonn, M. R., & Juhnke, G. (2017). Nondisclosure in triadic supervision: A phenomenological study of counseling students. Counselor Education and Supervision, 56, 82–97. doi:10.1002/ceas.12064
Mehr, K. E., Ladany, N., & Caskie, G. I. L. (2010). Trainee nondisclosure in supervision: What are they not telling you? Counselling & Psychotherapy Research, 10, 103–113. doi:10.1080/14733141003712301
Mehr, K. E., Ladany, N., & Caskie, G. I. L. (2015). Factors influencing trainee willingness to disclose in supervision. Training and Education in Professional Psychology, 9, 44–51. doi:10.1037/tep0000028
Murphy, M. J., & Wright, D. W. (2005). Supervisees’ perspectives of power use in supervision. Journal of Marital and Family Therapy, 31, 283–295. doi:10.1111/j.1752-0606.2005.tb01569.x
National Board for Certified Counselors. (2014). NBCC educational requirements to change in 2022. The National Certified Counselor, 30(3), 1–2.
Oden, K. A., Miner-Holden, J., & Balkin, R. S. (2009). Required counseling for mental health professional trainees: Its perceived effect on self-awareness and other potential benefits. Journal of Mental Health, 18, 441–448. doi:10.3109/09638230902968217
Pearson, Q. M. (2001). A case in clinical supervision: A framework for putting theory into practice. Journal of Mental Health Counseling, 23, 174–183. doi:10.1111/ppc.12003
Pisani, A. (2005). Talk to me: Supervisee disclosure in supervision. Smith College Studies in Social Work, 75, 29–47. doi:10.1300/J497v75n01_03
Rønnestad, M. H., & Skovholt, T. M. (2003). The journey of the counselor and therapist: Research findings and perspectives on professional development. Journal of Career Development, 30, 5–44. doi:10.1177/089484530303000102
Welfare, L. E., Wagstaff, J., & Haynes, J. R. (2017). Counselor education and Title IX: Current perceptions and questions. Counselor Education and Supervision, 56(3), 193–207. doi:10.1002/ceas.12072
Yourman, D. B., & Farber, B. A. (1996). Nondisclosure and distortion in psychotherapy supervision. Psychotherapy: Theory, Research, Practice, Training, 33, 567–575. doi:10.1037/0033-3204.33.4.567
Ryan M. Cook is an assistant professor at The University of Alabama. Laura E. Welfare, NCC, is an associate professor at Virginia Tech. Devon E. Romero, NCC, is an assistant professor at The University of Texas at San Antonio. Correspondence can be addressed to Ryan Cook, 310A Graves Hall, The University of Alabama, Tuscaloosa, AL 35487, rmcook@ua.edu.
