Aug 24, 2023 | Volume 13 - Issue 2
Chloe Lancaster, Michelle W. Brasfield
The COVID-19 pandemic led to an unparalleled disruption of student learning, disengaged students from school and peers, increased exposure to trauma, and had a negative impact on students’ mental health and well-being. School counselors are the most accessible mental health care professionals in a school, providing support for all students’ social and emotional needs and academic success. This study used an exploratory survey design to investigate the perspectives of 207 school counselors in Tennessee regarding students’ COVID-19–related mental health, academic functioning, and interpersonal skills; interventions school counselors have deployed to support students; and barriers they have encountered. Results indicate that students’ mental health has significantly declined across all grade levels and is interconnected with academic, social, and behavioral problems; school counselors have provided support consistent with crisis counseling; and caseload and non-counseling duties have created significant barriers in the provision of care.
Keywords: COVID-19, school counselors, student mental health, interventions, barriers
The psychological cost of the COVID-19 pandemic has been profound and wide-reaching. Although the K–12 population has been less susceptible to the adverse physical effects of COVID-19, for many, the pandemic has left an indelible mark on their mental health (Karaman et al., 2021). Before the outbreak of COVID-19 in 2020, youth mental health had become an issue of national concern, with one in six minors struggling with mental illness (Whitney & Peterson, 2019). Research has emerged to indicate that COVID-19 has further elevated the mental health problems of K–12 students across the nation (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). The end of COVID-19 lockdown restrictions may have alleviated immediate issues associated with social isolation and online learning; however, for those students experiencing COVID-19–related trauma and crisis, symptomatology has persisted beyond school reentry (Centers for Disease Control and Prevention [CDC], 2022; Patterson, 2022). As frontline helping professionals with training in mental health and school systems, school counselors are often the first responders to students in crisis (Karaman et al., 2021; Lambie et al., 2019), yet researchers have not explored reentry problems from the school counselor’s perspective. We conducted this study to understand school counselors’ experience of COVID-19–related student issues, their strategies to assist students, and their encountered barriers. We theorized that persistent problems related to the organizational structures within which counselors work, such as large caseloads, assignment of non-counseling duties, and under-resourced schools and communities (Lambie et al., 2019), may have greatly impacted their ability to meaningfully help students in high need of mental health support.
Literature Review
Students and COVID-19–Related Distress
From the outset of the COVID-19 pandemic, scholars predicted that disruptions to schooling, COVID-19–related stress, family conflict, and frequent media exposure to the pandemic would amplify mental health problems in children and youth (Imran et al., 2020). Empirical studies published in 2020 and 2021 have substantiated this concern, with findings indicating that COVID-19 restrictions adversely affected youth in multiple ways, including the development of unhealthy eating habits, increased screen time, reduced physical activity, sleep disturbances, academic delays, social problems, and an overall escalation in mental health concerns (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). The preponderance of research focused on adolescents, particularly as extended time in social isolation disrupted their developmental reliance on peer interactions for social and emotional support (Imran et al., 2020). Multiple studies found that not feeling connected to friends, high social media usage, and general COVID-19–related fears were associated with higher levels of depression and anxiety (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021).
Although less is known about the impact of COVID-19 on younger children, evidence is emerging to indicate that the COVID-19 pandemic has elevated adverse childhood experiences (ACEs; Bryant et al., 2020). From a developmental perspective, children are less able to communicate and process their thoughts and feelings and are greatly affected by the emotional state of their caregivers (Zimmer-Gembeck & Skinner, 2011). Thus, exposure to parental anxieties related to housing, food, and economic insecurity likely exerted a destabilizing effect on children during the stay-at-home mandate and beyond (Imran et al., 2020). Further, children in poverty may be particularly vulnerable to an amplification of ACEs due to their families being disproportionately impacted by economic hardships and family mortality during the pandemic (Bryant et al., 2020).
Students’ Mental Health Pre-Pandemic
The COVID-19 pandemic increased intra-family adversity, which has long-term implications for the well-being of children and adolescents (CDC, 2022). However, in pre–COVID-19 times, with the rise in school shootings and teen suicide, the mental health of K–12 populations had already become a public health concern. According to the National Alliance on Mental Illness, one in six children aged 6–17 experienced a mental health disorder (Whitney & Peterson, 2019). Since reentry following COVID-19 shutdowns, indicators suggest the COVID-19 pandemic has worsened children’s mental health (CDC, 2022; Karaman et al., 2021), with widespread reports of student learning gaps, chronic absenteeism, declines in social skills, and increased behavior problems (CDC, 2022; Patterson, 2022). Further, previous research on children’s responses to a variety of traumatic events has found that children and adolescents can develop long-term mental illness following a traumatic experience, which is unlikely to abate without intervention (Udwin et al., 2000). For youth, the experience of mental health problems increases their risk factors in other areas, such as a decline in academic performance, poor decision-making, drug use, and high-risk sexual behaviors (CDC, 2022). In this regard, the responsiveness of schools to flex their organizational resources to address the psychological changes in their student body seems instrumental in assuaging the long-term effects of COVID-related trauma and the mitigation of adverse educational outcomes (Savitz-Romer et al., 2021).
School Counselors’ Role in Provision of Mental Health Services
Schools have long been discussed as a primary access point for mental health services, given that children spend much of their day in school, and children and adolescents in need of mental health care are more likely to receive assistance in a school as opposed to a clinical setting (Lambie et al., 2019). Conversations about students’ access to mental health care in school settings segue to the role of school counselors and students’ access to school counseling services. School counselors are the most accessible mental health care professionals in schools, with 80.7% of schools employing full-time or part-time school counselors (Lambie et al., 2019). By contrast, only 66.5% employ a school psychologist, and 41.5% employ a school social worker (National Center for Educational Statistics, 2016). Further, school counselors are trained in crisis prevention and responsive services, including individual and group counseling; consultation with administrators, teachers, parents, and professionals; and coordination of services within a multi-tiered system of supports (MTSS; Pincus et al., 2020).
Evidence to support school counselors’ work in times of crisis comes from multiple sources. Salloum and Overstreet (2008) found that a school counselor–led small group implemented after Hurricane Katrina improved PTSD symptoms among elementary school students. Similarly, Udwin and colleagues (2000) found that students who received psychological support at school following a national crisis experienced a reduction in PTSD symptomology. Additionally, scholars have proposed that school counselors utilize their skill set in assessment to administer universal mental health screenings to identify students at greater risk of having or developing mental health concerns (Lambie et al., 2019; Pincus et al., 2020).
Barriers School Counselors Face in the Provision of Services
Although school counselors have the training and skills necessary to assist students transitioning back to school from a disruption like COVID-19, they face multiple barriers to their work. Most notably, they struggle with unmanageable caseloads. The American School Counselor Association (ASCA) recommends that counselor-to-student ratios not exceed 1:250 (ASCA, 2019). Yet, the average ratio in the United States is 1:455, with Tennessee experiencing an average ratio of 1:450 (Patel & Clinedinst, 2021). Research indicates that large school counselor caseloads adversely affect student outcomes, insofar as attendance, graduation, and disciplinary problems are more prevalent in schools with high school counselor caseloads (Parzych et al., 2019). Unfortunately, minority students in under-resourced schools are disproportionately impacted by high counselor ratios (Whitney & Peterson, 2019) and are more likely to experience adverse educational outcomes, as well as unmet mental health needs (Kaffenberger & O’Rorke-Trigiani, 2013). These findings raise concern for students whose mental health and academics have declined since the emergence of COVID-19 who attend schools with overstretched counselors struggling to meet the needs of their student body. This study was conducted in part to explore if caseload correlates to school counselors’ perceived ability to attend to students’ COVID-related problems and if differences were more pronounced in schools with lower socioeconomic status (SES).
In addition to ratios, ASCA recommends that school counselors spend 80% of their time providing direct and indirect services to students. Program elements within direct service include curriculum delivery, individual student planning, and responsive services. Indirect services include referrals to other agencies and programs within and outside the school system and consultation and collaboration with stakeholders, particularly for crisis response (ASCA, 2019). Researchers have documented the favorable effects on student academics and behaviors when school counselors follow these national guidelines for time and role allocations (Cholewa et al., 2015). Nonetheless, school counselors are often assigned non-counseling duties by their campus and district administrators (Gysbers & Henderson, 2012), preventing them from fulfilling their appropriate roles. These duties include test coordination, record keeping, attendance monitoring, substitute teaching, and student discipline (ASCA, 2019). Data indicate that non-counseling duties may be more problematic at the secondary level, with high school counselors over-reporting non-counseling duties, when compared to elementary school counselors (Chandler et al., 2018). Geographic differences have also been documented, with rural school counselors reporting higher levels of non-counseling duties in comparison to urban school counselors (Chandler et al., 2018). In the current study, we were curious to understand the impact of non-counseling duties on school counselors’ response to students’ COVID-19 concerns and to explore the intersection of counselor responsiveness to COVID-19 by non-counseling duties, grade level, and geographic region (e.g., urban, suburban, rural), respectively.
School Responses to COVID-19 in Tennessee
In response to the COVID-19 pandemic, Tennessee’s governor ordered all Tennessee public schools closed from March 20 until March 31, 2020, and extended this closure through the end of the 2019–2020 school year. To complete the school year outside of the physical educational space, districts created their own plans to address student learning, often dependent on available technology and resources (Tennessee Office of the Governor, 2020). Districts made decisions for returning in the fall 2020 semester based on guidelines from the Tennessee Department of Education (DOE), which included social distancing, smaller class size, assigned seats, and alternating in-person days with distance learning (Tennessee DOE, 2020). To provide further context to our survey responses, in 2019, the state DOE (Tennessee State Board of Education, 2017) updated its school counseling policy and standards to require school counselors to spend 80% of their time in direct service to students, a specification consistent with the ASCA National Model for allocation of school counselor time. Although the policy stated counselor ratios should not exceed 1:500 in elementary and 1:350 in secondary schools, this specification falls short of the ASCA 1:250 recommendation. Further, because of the state funding formula that permits school districts to hire administrators in lieu of school counselors, depending on school needs, we expected many of the school counselors would have caseloads that exceeded DOE policy.
Purpose of Study
School counselors are uniquely positioned to assist students with their mental health, including COVID-19–related concerns, in a school context (Pincus et al., 2020). Yet, even before the COVID-19 pandemic, school counseling programs were frequently under-equipped to meet the magnitude of students’ mental health needs (DeKruyf et al., 2013). This study was conducted to understand, from the perspective of school counselors in Tennessee, the ongoing impact of COVID-19 upon students’ mental health, examine strategies they have deployed to assist students, and discover barriers encountered in providing care to meet their students’ needs. Because poor mental health manifests in a plethora of academic, behavior, and social skill adjustment issues for children and adolescents (CDC, 2022), we also examined school counselors’ perceptions of changes in those domains from pre-pandemic to current times. Given documented patterns of variability in school counselor programs, we also investigated school counselors’ perceived barriers to assisting students by location, SES, and assigned non-counseling duties. To address the aim of the study, we posited three related research questions (RQs):
| RQ1: |
How has COVID-19 affected students’ mental health, academics, and social skills in Tennessee? What issues presented the greatest concern, and how did interventions differ by grade level (elementary, middle, or high school)? |
| RQ2: |
What interventions do school counselors in Tennessee use to assist students with their COVID-19–related concerns, and how do interventions differ by grade level (elementary, middle, or high school)? |
| RQ3: |
What barriers do school counselors in Tennessee report as interfering with their ability to address students’ COVID-19 concerns? Do reported barriers differ by grade level (elementary, middle, or high), location (urban, suburban, or rural), socioeconomic status, non-counseling duties, size of caseload (small, medium, or large), or following the state guideline for spending 80% of the time in student services? |
Method
Study Design and Instrumentation
Given the absence of research examining school counselors’ perspectives of how the pandemic has affected student mental health, their response to students’ COVID-19 issues, and barriers encountered in their efforts, we employed an exploratory research design. Exploratory designs are used when there is limited prior research to warrant the examination of a directional hypothesis (Swedberg, 2020). Within the framework of an exploratory design, we developed a non-standardized instrument to answer the three research questions. Although this constitutes a limitation of the study, we endeavored to address validity concerns by following the principles of the tailored design method of survey research (Dillman, 2007). Prior to constructing the survey, we reviewed the extant literature on students’ COVID-19–related issues, school counselors’ roles, and professional issues, in addition to conducting a focus group (N = 7) with school counselors and school counseling supervisors from across the state in which the study was conducted to explore their perceptions in changes to student functioning, strategies they have deployed to assist students, and obstacles they have encountered. Focus group data were used to inform the development of survey items and ensure the instrument covered relevant content. For example, the focus group provided expert insight into the non-counseling duties that are frequently assigned to counselors in the state, as well as the nature of students’ psychological, academic, and behavioral problems witnessed since the onset of COVID-19. Before launching the survey, we piloted the survey with 19 school counselors in Tennessee to elicit feedback about the flow and coverage of the survey. Based on their responses, we added an item addressing universal intervention and edited language on multiple items to align with state-specific terminology (e.g., “MTSS coordination” was expanded to “RTI2B/MTSS/PBIS coordinator” to reflect more state-recognized school counselor titles when operating in these capacities).
The final survey consisted of 64 items in predominantly binary, checkbox, and Likert scale formats. Demographic items were informed by categories outlined by the U.S. Census, the Tennessee DOE, and inclusive practices for data collection (Fernandez et al., 2016). Twenty-one items gathered demographic data related to school counselor characteristics (e.g., age, race, gender), counseling program variables (e.g., caseload, division of time, non-counseling duties, fair-share responsibilities), and school variables (e.g., school level, Title I status, location, staffing patterns). SES was measured using a school’s designated Title I status, with response categories of “yes,” “no,” and “unsure.” Likewise, to determine if school counselors dedicated 80% of their time to direct service, we created a multiple-choice item with the options of “yes,” “no,” and “unsure.” A concise description of the state guidelines was embedded into the survey to promote accurate responses to this item. We gathered data on counselors’ perspectives of their students’ current functioning in areas of mental health, academics, social skills, and behaviors through multiple-choice items with a 5-point range of “much better” to “much worse.” For each area of functioning, school counselors were required to indicate the areas of concern via a checkbox item. Additionally, checkbox items were used to identify school counselors’ strategies to assist students, barriers encountered, and needed resources. As noted, these response categories were based on extant literature and expert input.
Cronbach’s alphas were computed to determine the reliability of the survey items in indicating overall post–COVID-19 functioning of students according to school counselors. These values indicate that these four areas were moderately related with acceptable consistency (α = .653). When making additional comparisons among the four constructs, two areas—behavior and social skills—were found to be more consistent (α = .705; Sheperis et al., 2020). Further, reliability scores likely reflect the exploratory design, which requested participants respond to conceptually related but not converging constructs (e.g., academics, mental health, social skills, and behavior). For example, a change in student academics would not necessarily signify a change in student mental health and vice versa. Thus, participant responses would not necessarily be uniform across items measuring students’ mental health, academics, and social skills, and overall instrument consistency would not be affected in turn.
Participants
We recruited a state-level sample of professional school counselors employed in K–12 public schools in Tennessee. Following the pilot study, in December 2021, we recruited participants through an anonymous Qualtrics link utilizing multiple platforms: the state school counselor association’s listserv, social media, respondent referrals, and dissemination via school counseling supervisors. Participants were eligible to complete the survey if they were currently employed in a K–12 public school in Tennessee. Upon examination of our survey data, we found 276 total responses with 220 complete for a completion rate of 79.7%. Because the survey was distributed through the above-mentioned methods, we were unable to calculate the response rate without knowing how many of the approximately 2,000 public school counselors in Tennessee received the survey. Upon further examination of the survey respondents, we removed one school counseling supervisor; four school counselors whose students were remote/hybrid; and eight school counselors in private, charter, or alternative schools to maintain focus on the experiences of traditional public school counselors working with students in person during the ongoing COVID-19 pandemic for a final sample of 207 participants. An examination of the respondents’ demographics revealed a sample that was predominantly female and White/Caucasian and worked in Title I, suburban, or rural elementary schools. The sample’s mean years serving as a school counselor was 11.7 (SD = 7.5), with mean years at current school of 6.8 (SD = 6.4). See Table 1 for more demographic information. For analysis purposes, we divided the school counselors into three groups by the size of their reported caseload. These categories were informed by a national study of school counselor ratios (National Association of College Admission Counselors, 2019) and consisted of ratios in the range of small (1:100–1:300; 14.0%, n = 29), medium (1:301–1:550; 69.6%, n = 144), and large (1:551 and higher; 15.0%, n = 31).
Table 1
Demographic Characteristics of the Sample
| Characteristic |
n |
% |
| Age |
|
|
| 18–24 years |
3 |
1.4 |
| 25–44 years |
99 |
47.8 |
| 45–64 years |
102 |
49.3 |
| 65 years plus |
3 |
1.4 |
| Race/Ethnicity |
|
|
| Black/African American |
17 |
8.2 |
| Latinx/Hispanic |
1 |
0.5 |
| White/Caucasian |
183 |
88.4 |
| American Indian/Alaskan Native |
1 |
0.5 |
| Other |
5 |
2.4 |
| Gender |
|
|
| Female |
192 |
92.8 |
| Male |
15 |
7.2 |
Note. N = 207.
Data Analysis
We ran a post hoc power analysis using the G*Power 3.1.9.7 statistical software to determine if our sample size was sufficient at the .80 power level with α = .05 and found that a minimum sample size of 100 was required for our analyses. Given our sample size of 207 participants, the power analysis indicated that our sample size was sufficient (Faul et al., 2007). We utilized SPSS version 26 to calculate the following analyses for this study: (a) descriptive statistics; (b) Fisher’s exact test for two dichotomous nominal variables; (c) an extension of Fisher’s exact test, the Freeman-Halton exact test, for one dichotomous nominal variable and one nominal variable with three levels; and (d) point-biserial correlation analysis for one nominal variable and one interval variable (Frey, 2018). We also examined effect size to determine practical importance using the following levels for examining nominal data (Rea & Parker, 1992), precedence for which has been established by complementary studies in educational research (K. Erickson & Quick, 2017; Kotrlik et al., 2011): negligible [0, .1), weak [.1, .2), moderate [.2, .4), relatively strong [.4, .6), strong [.6, .8), and very strong [.8, 1.0). Phi (ϕ) indicates the effect size for the exact tests, and the correlation is the effect size for the point-biserial correlation. We only included statistical analyses that resulted in moderate associations or higher. Three school counselors (1.4%) who reported caseloads that were unusually small (< 100) and outside our specified caseload parameters were removed from the analysis. Additionally, we excluded school counselors who indicated “unsure” in the categories of location (rural, suburban, urban), Title I status, and adherence to state policy for direct service to students. See Table 2 for school characteristics.
Results
Research Question 1
RQ1 examined school counselors’ perspectives of the impact of COVID-19 on students’ mental health, academics, and social skills as well as variation by grade level (elementary, middle, or high school). When asked about the mental health changes they have witnessed in their students post–COVID-19 pandemic, 93.7% (n = 194) of school counselors reported negative changes with 42.5% (n = 88) reporting “much worse” and 51.2% (n = 106) reporting “somewhat worse” changes. Specifically, school counselors reported issues regarding anxiety (92.8%, n = 192), depression (77.3%, n = 160), family dysfunction (71.0%, n = 147), COVID-19–related grief and loss (63.8%, n = 132), technology addiction (52.7%, n = 109), suicidality (50.7%, n = 105), fear of COVID-19 (49.8%, n = 103), substance use issues (21.7%, n = 45), and other issues (12.6%, n = 26) such as separation anxiety, self-harm, and anger. The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and depression (p < .001, ϕ = .301) with a moderate positive association, suicidality (p < .001, ϕ = .499) with a relatively strong positive association, and substance use (p < .001, ϕ = .583) with a relatively strong positive association. For depression, 90.0% (n = 54) of high school counselors and 85.7% (n = 36) of middle school counselors reported this issue as compared to 63.0% (n = 51) of elementary school counselors. For suicidality, 76.2% (n = 32) of middle school counselors and 71.7% (n = 43) of high school counselors reported this concern as compared to 23.5% (n = 19) of elementary school counselors. For substance use, 58.3% (n = 35) of high school counselors and 20.0% (n = 8) of middle school counselors reported this concern as compared to 1.2% (n = 1) of elementary school counselors. All other mental health concerns were not significant with grade level.
When queried regarding academic changes post–COVID-19, 90.3% (n = 187) of school counselors reported negative changes to students’ academics with 35.3% (n = 73) reporting “much worse” and 55.1% (n = 114) reporting “somewhat worse” changes. School counselors reported an overall decline across all subjects (80.7%, n = 167). Additionally, school counselors reported non-cognitive factors regarding lack of motivation (84.1%, n = 174), lack of parental support during the school day (75.4%, n = 156), attention issues (71.0%, n = 147), poor mental health (64.7%, n = 134), sleep deprivation (41.1%, n = 85), limited technology during virtual learning (33.3%, n = 69), lack of space to work at home during virtual learning (30.4%, n = 63), poor physical health (17.9%, n = 37), and other (3.9%, n = 8). The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and lack of motivation (p = .001, ϕ = .265), poor mental health (p = .001, ϕ = .269), and attention issues (p = .009, ϕ = .232), all with positive moderate associations. For lack of motivation, 96.7% (n = 58) of high school counselors and 88.1% (n = 37) of middle school counselors reported this issue as compared to 75.3% (n = 61) of elementary school counselors. For poor mental health, 78.3% (n = 47) of high school counselors and 69.0% (n = 29) of middle school counselors reported this outcome as compared with 49.4% (n = 40) of elementary school counselors. For attention issues, 79.0% (n = 64) of elementary school counselors and 73.8% (n = 31) of middle school counselors reported concerns as compared to 55.0% (n =33) of high school counselors.
Table 2
School/Program Characteristics
| Characteristic |
n |
% |
| Location |
|
|
| Urban |
31 |
15.0 |
| Suburban |
95 |
45.9 |
| Rural |
72 |
34.8 |
| Unsure |
9 |
4.3 |
| Title I Status |
|
|
| Yes |
121 |
58.5 |
| No |
57 |
27.5 |
| Unsure |
29 |
14.0 |
| Grade Level |
|
|
| Elementary |
81 |
39.1 |
| Middle |
42 |
20.3 |
| High |
60 |
29.0 |
| Other |
24 |
11.6 |
| Follows 80% Direct Service Guideline |
|
|
| Yes |
112 |
54.1 |
| No |
65 |
31.4 |
| Unsure |
30 |
14.5 |
| School Counselor-to-Student Ratio (caseload) |
|
|
| 1:1–1:300 |
29 |
14.0 |
| 1:301–1:550 |
144 |
69.6 |
| 1:551 and higher |
31 |
15.0 |
| Other |
3 |
1.4 |
Note. N = 207
When asked about behavioral changes, 87.4% (n = 181) of school counselors reported negative changes to behaviors with 30.4% (n = 63) reporting “much worse” and 57.0% (n = 118) reporting “moderately worse” changes. Comparably, when asked about social skills changes, 87.0% (n = 180) of school counselors reported negative changes to students’ social skills with 36.2% (n = 75) reporting “much worse” and 50.7% (n = 105) reporting “moderately worse” changes. Specifically, school counselors reported trouble socializing with peers (84.1%, n = 174), absence of social flexibility (58.0 %, n = 120), increase of physical aggression (55.1%, n = 114), increase in relational aggression (50.7%, n = 105), increase in cyberbullying (23.7%, n = 49), increase in bullying (19.3%, n = 40), and other (8.2%, n = 17) such as issues with conflict resolution and preference for technology. The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and cyberbullying (p = .003, ϕ = .255), with a moderate positive association with 42.9% (n = 18) of middle school counselors, 23.3% (n = 14) of high school counselors, and 14.8% (n = 12) of elementary school counselors reporting an increase in this area. All other social skills changes were not significant with grade level.
Research Question 2
RQ2 examined the interventions that school counselors used in assisting students with their COVID-19–related concerns and if this differed by grade level. School counselors reported the various supports that they provided to their students who struggled with COVID-19–related issues, including individual counseling (95.7%, n = 198), consultation with parents/teachers (85.5%, n = 177), referrals (80.7%, n = 167), collaboration with other school-based helpers (77.3%, n = 160), coping skills instruction (71.5%, n = 148), group counseling (44.0%, n = 91), universal health screenings (17.9%, n = 37), and other interventions (4.3%, n = 9) such as food programs, holiday donation programs, peer support, and academic support meetings. We used the Freeman-Halton exact test to examine the relationship between grade level (n = 183) and these supports and found that small group counseling (p < .001, ϕ = .405) and coping skills instruction (p = .028, ϕ = .200) were significant, both with moderate positive association. For small group counseling, 63.0% (n = 51) of elementary school counselors and 45.2% (n = 19) of middle school counselors provided this support as compared to 16.7% (n = 10) of high school counselors. For coping skills instruction, 77.8% (n = 63) of elementary school counselors and 71.4% (n = 30) of middle school counselors reported this intervention as compared to 56.7% (n = 34) of high school counselors.
Research Question 3
RQ3 examined the barriers school counselors encountered in their ability to provide services and if this differed by grade level, SES, location, number of non-counseling duties, caseload size, and following the state guideline to spend 80% of time providing student services. When asked if they had encountered barriers to assisting their students with their COVID-19–related needs, 54.6% (n = 113) of school counselors reported that they had experienced barriers, and 45.4% (n = 94) reported that they had not. For those counselors who answered “yes,” barriers included: high caseload (44.4%, n = 92), number of non-counseling duties (20.3%, n = 42), lack of administrator support (12.1%, n = 25), being included on master schedule for guidance classes (10.1%, n = 21), lack of training to address COVID-19 needs (8.2%, n = 17), too much time coordinating the MTSS program (7.7%, n = 16), and other reasons (9.7%, n = 20). Examples of other reasons include students’ attendance, lack of resources (both space and personnel), and focus on academics over mental health. Of note, 47.3% (n = 98) of school counselors reported an increase in non-counseling duties since COVID-19, ranging from a substantial to a slight increase.
We used the Freeman-Halton exact test to examine the aforementioned barriers by grade level (n = 183) and found that being on the master schedule (p < .001, ϕ = .297) was significant with moderate positive association with 19.8% (n = 16) of elementary school counselors reporting this task as compared to 2.4 % (n = 1) of middle school counselors and 1.7% (n = 1) of high school counselors. We used point-biserial correlation analysis to examine how the number of new post–COVID-19 non-counseling duties related to the perceived barriers to providing services to students and found this to be significant (rpb = .211, p = .002) with a positive moderate association. School counselors who reported barriers to providing services had been allocated more non-counseling duties since the pandemic (n = 113, M = 1.22, SD = 1.49) than those who did not report barriers (n = 94, M = .66, SD = 1.04). We used a Freeman-Halton exact test to examine the specific barriers by caseload (n = 204) and found school counselors with a high caseload reported significantly more difficulty in addressing students’ COVID-19–related needs (p < .001, ϕ = .284), with a moderate positive association for large (58.1%, n =18) and medium (47.2%, n = 68) caseloads, as compared to those with a small (10.4%, n = 3) caseload. Investigating the state DOE guideline for 80% of time in service to students (n = 177), excluding those who were unsure, revealed that 63.3% (n = 112) followed the guideline and 36.7% did not (n = 65). We used a Fisher’s exact test to examine the relationship between following the 80% guideline and specific barriers and found that reporting too many non-counseling duties (p < .001, ϕ = -.358) was significant, with a moderate negative association for those who did not follow the guideline (41.5%, n = 27) in comparison to those who did follow the 80% guideline (10.7%, n = 12). All other barriers were not significant with grade level, SES, location, number of non-counseling duties, caseload size, and following the 80% state guideline. We used a Fisher’s exact test to examine SES by Title I (n = 178) classification and found that it was not significant with any of the barriers.
Discussion
Our results render a disturbing picture of students’ post–COVID-19 mental health functioning and school counselors’ perceived ability to effectively meet their students’ needs since a return to in-person learning, as reported by this sample of 207 school counselors in Tennessee. For RQ1, over 93% of our respondents indicated that their students’ mental health had worsened, with anxiety and depression identified as the most pronounced psychological concern, followed by family dysfunction, grief, technology addiction, and suicidality. These results confirm our predictions that the COVID-19 pandemic would exert a harmful impact on the mental health of children and adolescents (Bryant et al., 2020; Cénat & Dalexis, 2020). Depression and suicidality were significant concerns for middle and high school counselors, and substance abuse was significant at the high school level. The reported spike in diagnosable mental health problems by secondary school counselors aligns with research indicating that half of all mental health and substance use disorders begin at 14 (Quinn et al., 2016). The CDC recently reported that depression, substance abuse, and suicide have increased among adult populations since COVID-19, with young adults presenting the most significant risk (Czeisler et al., 2020). Our results provide preliminary evidence indicating that COVID-19–related trends have similarly impacted adolescents. Further, given the relationship between ACEs and substance misuse (CDC, 2022; Quinn et al., 2016), it may be reasonable to conjecture that an increase in family dysfunction, grief, fear of COVID-19, and severance of social relationships underscored a rise in substance use problems, particularly among high school students.
In addition to mental health, student academics notably declined according to school counselors in Tennessee, with 90.3% of participants reporting negative changes to students’ academics. Previous research attributed students’ COVID-19 pandemic–related academic issues to the vagaries of online instruction, a lack of parental supervision, inadequate technology, and limited workspace, among other factors (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). Our results aligned with these findings by explicitly connecting delays in students’ academic progress to psychological factors. Of note, we found a significant relationship between grade level, lack of motivation, poor mental health, and attention issues, with middle and high school counselors reporting greater concerns in the areas of motivation and mental health, and elementary and middle school counselors identifying attention problems as the greatest concern. The developmental onset of mental health disorders (Lambie et al., 2019) likely accounts for increased student mental health problems reported by middle and high school counselors. However, motivation and attentional issues across the grades were problematic, and because both are symptomatic of depression and anxiety, they raise a red flag for the mental health of all K–12 students in Tennessee.
Alongside academics, 87.0% of school counselors reported negative changes in students’ social skills and 87.4% reported worsened behaviors among students, with trouble socializing with peers, absence of social flexibility, and an increase in physical and relational aggression being the most pronounced problems. Declines in students’ ability to get along with peers may be uniquely linked to social isolation during lockdown (Ellis et al., 2020; Karaman et al., 2021); however, of great concern is the increase in all forms of bullying, with cyberbullying being particularly problematic in middle school. Youth aggression is a long-term consequence of ACEs and has implications for overall school safety, with victimization and perpetration both positively associated with school violence (Forster et al., 2020).
RQ2 investigated what interventions school counselors used to assist students with their COVID-19–related concerns and examined interventions by grade level. The preponderance of school counselors relied on individual counseling (95.7%), consultation (85.5%), referrals (80.7%), collaboration with other school-based helpers (77.3%), and coping skills instruction (71.5%), all of which are consistent with crisis-level supports. Nonetheless, only 44% of the sample, primarily elementary school counselors, had used small group counseling, despite its proven efficacy with children exposed to trauma (Salloum & Overstreet, 2008). The underutilization of group work at the high school level presents a concern, given that group work provides context for peer support and social learning, both considered critical therapeutic factors for adolescents (Gysbers & Henderson, 2012). Nonetheless, this finding resonates with previous results that high school counselors are more apt to assume administrative roles in place of the provision of direct student services (Chandler et al., 2018). Universal assessment has been proffered as an efficient and empirically grounded method for the early identification of at-risk students in need of COVID-19–related interventions (A. Erickson & Abel, 2013; Karaman et al., 2021; Pincus et al., 2020). Unfortunately, only 17.9% of the sample reported administering universal mental health screeners, a finding aligned with other studies that indicate schools have resisted adopting mental health screeners because of inadequate resources and related concerns about following up with students identified as being at risk (Burns & Rapee, 2022).
For RQ3, we explored the school counselors’ perspectives of the barriers they have encountered in assisting their students with their COVID-19 concerns. The proliferation of barriers reported by school counselors (high caseload, non-counseling duties, lack of administrator support, being on the master schedule for guidance classes, and a lack of training) verifies our concern that school counselors in Tennessee did not receive the support instrumental to their ability to provide effective student services at this critical time. Our state-level findings resonate with studies conducted in other states that indicate school counselors’ non-counseling duties increased during the pandemic while administrator support declined (Savitz-Romer et al., 2021). Other studies have also drawn attention to widespread staffing shortages associated with COVID-related absences and a reduced pool of substitute teachers (Patterson, 2022). Although we did not examine staff resources explicitly, with almost 50% of our Tennessee sample witnessing an increase in their non-counseling duties, it would be reasonable to infer that campus administrators are deploying school counselors to triage critical gaps in staffing patterns. Interestingly, despite a widespread increase in non-counseling duties post–COVID-19, only 20.3% of counselors reported non-counseling duties as a barrier to providing care. The discrepancy between these two results may be indicative of the phenomenon of role diffusion in school counseling, a problem that emerges when school counselors begin to integrate non-counseling duties as part of their accepted role and thus do not perceive them as antithetical to their professional identity (Astramovich et al., 2013). Furthermore, neither SES (Title I) nor location (rural, suburban, urban) were significant with barriers, and although this could reflect our relatively small sample, it could also be indicative of staff shortages adversely affecting the role of school counselors across all settings, regardless of the school’s demographic status.
The most notable barrier reported by respondents was a large caseload. School counselors with large and medium-sized caseloads reported more barriers and were less likely to follow the 80% guideline. Thus, those students who were negatively impacted by large counselor caseloads before COVID-19 faced further obstacles in accessing their school counseling services despite an overall increase in their mental health and academic needs. Further, elementary school counselors listed on the master schedule for guidance classes faced additional barriers to addressing their students’ needs outside of their prevention-focused (Tier 1) activities. Classroom guidance is considered helpful in elementary school for building social skills and study habits; however, when counselors are placed on the master schedule, it can impact their ability to provide responsive student services (Gysbers & Henderson, 2012) which seemed to be the case with our respondents.
Implications for Professional Advocacy
The results of this study illustrate a decline in student functioning, pronounced in the area of mental health, and have implications for school counselor advocacy in the areas of policy and practice. Advocating for policy change takes time and is beyond the individual efforts of school counselors, who are often beholden to their principal’s limited understanding of school counselors’ appropriate role and function (Lancaster & Reiner, 2022) and subsumed by untenable caseloads in under-resourced schools (Lambie et al., 2019). We, therefore, assert that advocacy is the professional imperative for all vested school counseling professionals (state counseling associations, school counselor educators, school counseling supervisors, and school counselors), all of whom could be working in tandem to advance the profession.
At the policy level, state and national counseling associations should reconsider the important role school counselors play in supporting students’ mental well-being and re-examine policies that delineate the appropriate use of school counselors’ time. Currently, the state school counseling model (Tennessee Policy 5.103) mirrors the national model (ASCA, 2019), perennially focusing on school counselors’ role in supporting student academics and delimiting their counseling role to prevention services, crisis counseling, and referrals to other mental health professionals. For state and national counseling associations, positioning school counselors as primarily focused on student academics demonstrated their value during the No Child Left Behind Act (NCLB; 2001) era, which prioritized unidimensional outcome measures of student success, particularly in math and reading (Savitz-Romer, 2019). However, the Every Student Succeeds Act (ESSA) replaced NCLB in 2015 and emphasizes more holistic aspects of student development and school climate. Many scholars argue that the ESSA (2015) combined with the rise in mental health issues has created a policy window for school counselors, led by their state and national professional associations (Savitz-Romer, 2019), to focus on the non-cognitive aspects that undergird healthy student development and to reclaim mental health as a domain central to school counselor practice (Lambie et al., 2019).
Redefining school counselors’ role in terms of mental health would require them to receive more clinical supervision (Lambie et al., 2019). In comparison to counselors in clinical settings, school counselors receive little to no supervision for their clinical efforts, which affects their clinical identity and weakens their counseling skills over time (Lancaster & Reiner, 2022). To address this gap, symbiotic partnerships could be formed with counselor education programs, particularly those that offer doctoral degrees in counselor education and supervision, to provide clinical supervision to local school counselors. Progress in this area may be forthcoming in the state, as institutions of higher education that operate school counseling, school psychology, and school social work programs have been invited to apply for grants funded through COVID-19 relief funding to support student internships in high-need schools. In addition, funds are available to support clinical supervision experiences that extend beyond students’ graduate training programs (Tennessee DOE, 2023).
MTSS programs also offer a promising prevention and intervention framework for meeting students’ comprehensive needs, including mental health, and align to both state and national school counseling models (Goodman-Scott et al., 2019). Further, the Tennessee DOE (2018) has developed a resource guide based on a tiered model for supporting students’ differential mental health needs, which school counselors could efficiently implement within their existing MTSS programs. Of note, within the Tennessee model, Tier 1 mental health practices build a foundation for mental wellness for all students. Advanced supports at Tiers 2 and 3 provide students who are at risk because of behavioral and/or mental health concerns with access to small groups and mental health interventions. One dimension of the state’s tiered mental health model is universal screening to identify students with internalizing behavioral disorders. Although few counselors in this study utilized universal screening, we recommend school counselors and their supervisors leverage the preexisting Tennessee DOE guidelines to petition their districts to adopt universal mental health screening.
Although the state mandated reduced counselor ratios in 2017 (Policy 5.103.), the funding formula allowed for uneven adoption of this policy (Tennessee Comptroller of the Treasury, n.d.), and target ratios fell short of national recommendations (ASCA, 2019). Thus, a function of this research was to utilize results in policy contexts to advocate for ratio realignments. In partnership with the state school counselor association, we produced a one-page results summary, written in simple language, to disseminate to state politicians to illuminate the acuity of mental health issues faced by K–12 students and proposed a solution through increased school counselor access. An advocacy effort led by the state association resulted in proposed legislation TN HB0364/SB0348, which would require one licensed full-time professional school counselor position for every 250 students and is currently advancing through the state Senate and House committees. A significant takeaway from this study is the importance and potency of coordinated partnerships between researchers, state counseling associations, and school counselors—an alliance that could be replicated in other states by school counselor stakeholders to advocate for the profession.
Limitations
The generalizability of these findings is limited because of the use of a state-level sample and a non-standardized, self-report survey. First, self-report surveys are sensitive to respondents’ tendency to rate themselves more favorably. Thus, it would be reasonable to conjecture that school counselors overestimated their adherence to the state guideline to spend 80% of their time in service to students and underreported their non-counseling duties. Second, although the items were informed by previous research on the psychological issues faced by children and adolescents during COVID-19 (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021) and those factors that affect school counselors’ ability to provide direct services (Kaffenberger & O’Rorke-Trigiani, 2013; Parzych et al., 2019; Whitney & Peterson, 2019), the use of an ad hoc survey precluded us from performing more robust analyses (e.g., regression analysis). Third, because we only gathered data on students’ mental health issues and academic functioning post–COVID-19 pandemic, we have no benchmark data of students’ pre–COVID-19 functioning with which to make objective comparisons.
Fourth, although the sample was large enough to find some significant results, it was a small percentage of the state’s total population of public school counselors, which is estimated to be over 2,000. A larger sample would have increased the generalizability of findings and impacted the significance levels and practical importance of the results. Fifth, our sample lacks racial and gender diversity; however, it does align with the state’s overall population of educators (Tennessee DOE, 2021). Finally, regarding data analysis, interpreting correlations on a small population sample needs to be performed cautiously because of the possibility of sampling error. Additionally, point-biserial correlation can be impacted by the dichotomous nature of one of the variables, which constrains the variability of the results (Hinkle et al., 2002). Nonetheless, correlational analyses of ordinal and nominal variables in small-scale research are consistent with our exploratory design, and the results provide evidence that the variables examined share some type of relationship and provide direction for future research.
Future Research
Given that we conducted this study in the aftermath of the COVID-19 pandemic and have utilized data and policy to advocate for expanded student access to school counseling services in Tennessee, this study design could be replicated by future researchers in the event that another pandemic or crisis of similar scale affects K–12 populations. Nonetheless, our exploratory design is an inherent limitation with the preponderance of our findings based on correlational analysis of largely non-parametric data. Future studies could explore dimensions of students’ mental health utilizing student data from empirical inventories. Rather than relying on school counselor perception data, researchers could use results from universal screenings, such as the Behavior Assessment System for Children-3rd edition (BASC-3), to better understand the nature of student issues and examine differential risk by demographic factors (e.g., age, gender, ethnicity), which could be used to inform evidence-based interventions with at-risk and high-risk populations. Further, researchers could employ quasi-experimental designs to assess outcomes of school counselor-led interventions, such as small groups, with students who have scored as being at risk based on universal screening. Studies of this nature can help build a case for the efficacy of school counselors and, in turn, protect them from role misallocation. Qualitative research could also be conducted in those schools in which school counselors implement a universal screening, intervention, and referral system to glean an implementation blueprint practical to other school counselors within and outside the state.
Conclusion
With elevated rates of depression, anxiety, substance use, and bullying, it is reasonable to conjecture that students in Tennessee have experienced COVID-19–related trauma, which according to research is unlikely to abate without intervention (CDC, 2022; Savitz-Romer et al., 2021). Although our state-level respondents indicated that they provided services consistent with crisis counseling (e.g., individual counseling, group counseling, consultation, and referrals), almost 50% of the counselors had been burdened with additional non-counseling duties, which could reduce their capacity to work with students at different levels of risk. Large caseload was a significant barrier, leaving counselors struggling to provide an appropriate level of care. This finding raises considerable concern about the risk faced by students who have experienced deterioration in their mental health and academics since the onset of COVID-19, yet attend schools in Tennessee with elevated school counselor-to-student caseloads. Nationally and at the state level, school counselors are the most prevalent mental health professionals in schools and are trained in crisis response (National Center for Education Statistics, 2016). Unfortunately, Tennessee school counselors appear to be facing barriers in the provision of student services related to high caseload and non-counseling duties, which presents cause for professional advocacy within the state and beyond.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2019). ASCA national model: A framework for school counseling programs (4th ed.).
Astramovich, R. L., Hoskins, W. J., Gutierrez, A. P., & Bartlett, K. A. (2013). Identifying role diffusion in school counseling. The Professional Counselor, 3(3), 175–184. https://doi.org/10.15241/rla.3.3.175
Bryant, D. J., Oo, M., & Damian, A. J. (2020). The rise of adverse childhood experiences during the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S193–S194.
https://doi.org/10.1037/tra0000711
Burns, J. R., & Rapee, R. M. (2022). Barriers to universal mental health screening in schools: The perspective of school psychologists. Journal of Applied School Psychology, 38(3), 1–18.
https://doi.org/10.1080/15377903.2021.1941470
Cénat, J. M., & Dalexis, R. D. (2020). The complex trauma spectrum during the COVID-19 pandemic: A threat for children and adolescents’ physical and mental health. Psychiatry Research, 293, 113473.
https://doi.org/10.1016/j.psychres.2020.113473
Centers for Disease Control and Prevention. (2022, March 31). New CDC data illuminate youth mental health threats during the COVID-19 pandemic [Press release]. https://tinyurl.com/yckv6v9d
Chandler, J. W., Burnham, J. J., Riechel, M. E. K., Dahir, C. A., Stone, C. B., Oliver, D. F., Davis, A. P., & Bledsoe, K. G. (2018). Assessing the counseling and non-counseling roles of school counselors. Journal of School Counseling, 16(7), 1–33. https://files.eric.ed.gov/fulltext/EJ1182095.pdf
Cholewa, B., Burkhardt, C. K., & Hull, M. F. (2015). Are school counselors impacting underrepresented students’ thinking about postsecondary education? A nationally representative study. Professional School Counseling, 19(1), 144–154. https://doi.org/10.5330/1096-2409-19.1.144
Czeisler, M. É., Lane, R. I., Petrosky, E., Wiley, J. F., Christensen, A., Njai, R., Weaver, M. D., Robbins, R., Facer-Childs, E. R., Barger, L. K., Czeisler, C. A., Howard, M. E., & Rajaratnam, S. M. W. (2020). Mental health, substance use, and suicidal ideation during the COVID-19 pandemic. Morbidity & Mortality Weekly Report, 69(32), 1049–1057. https://www.cdc.gov/mmwr/volumes/69/wr/mm6932a1.htm
DeKruyf, L., Auger, R. W., & Trice-Black, S. (2013). The role of school counselors in meeting students’ mental health needs: Examining issues of professional identity. Professional School Counseling, 16(5), 271–282. https://doi.org/10.1177/2156759X0001600502
Dillman, D. A. (2007). Mail and internet surveys: The tailored design method (2nd ed.). Wiley.
Ellis, W. E., Dumas, T. M., & Forbes, L. M. (2020). Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement, 52(3), 177–187.
https://doi.org/10.1037/cbs0000215
Erickson, A., & Abel, N. R. (2013). A high school counselor’s leadership in providing school-wide screenings for depression and enhancing suicide awareness. Professional School Counseling, 16(5), 283–289.
https://doi.org/10.1177/2156759X1201600501
Erickson, K., & Quick, N. (2017). The profiles of students with significant cognitive disabilities and known hearing loss. The Journal of Deaf Studies & Deaf Education, 22(1), 35–48.
https://doi.org/10.1093/deafed/enw052
Every Student Succeeds Act, Pub. L. No. 114–95 § 114 Stat. 1177 (2015, Dec. 10). https://www.congress.gov/114/plaws/publ95/PLAW-114publ95.pdf
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
https://doi.org/10.3758/bf03193146
Fernandez, T., Godwin, A., Doyle, J., Verdin, D., Boone, H., Kirn, A., Benson, L., & Potvin, G. (2016). More comprehensive and inclusive approaches to demographic data collection. School of Engineering Education Graduate Student Series. Paper 60. https://tinyurl.com/2p9p2ct7
Forster, M., Gower, A. L., McMorris, B. J., & Borowsky, I. W. (2020). Adverse childhood experiences and school-based victimization and perpetration. Journal of Interpersonal Violence, 35(3–4), 662–681.
https://doi.org/10.1177/0886260517689885
Frey, B. B. (2018). The SAGE encyclopedia of educational research, measurement, and evaluation. SAGE.
Goodman-Scott, E., Betters-Bubon, J., & Donohue, P. (Eds.). (2019). The school counselor’s guide to multi-tiered systems of support. Routledge.
Gysbers, N. C., & Henderson, P. (2012). Developing and managing your school guidance and counseling program (5th ed.). American Counseling Association.
Hinkle, D. E., Wiersma, W., & Jurs, S. G. (2002). Applied statistics for the behavioral sciences (5th ed.). Houghton Mifflin Company.
Imran, N., Zeshan, M., & Pervaiz, Z. (2020). Mental health considerations for children & adolescents in COVID-19 pandemic. Pakistan Journal of Medical Sciences, 36(COVID19-S4), S67–S72.
https://doi.org/10.12669/pjms.36.COVID19-S4.2759
Kaffenberger, C. J., & O’Rorke-Trigiani, J. (2013). Addressing student mental health needs by providing direct and indirect services and building alliances in the community. Professional School Counseling, 16(5), 323–332. https://doi.org/10.1177/2156759X1201600505
Karaman, M. A., Eşici, H., Tomar, İ. H., & Aliyev, R. (2021). COVID-19: Are school counseling services ready? Students’ psychological symptoms, school counselors’ views, and solutions. Frontiers in Psychology, 12. https://doi.org/10.3389/fpsyg.2021.647740
Kotrlik, J. W., Williams, H. A., & Jabor, M. K. (2011). Reporting and interpreting effect size in quantitative agricultural education research. Journal of Agricultural Education, 52(1), 132–142.
https://doi.org/10.5032/jae.2011.01132
Lambie, G. W., Stickl Haugen, J., Borland, J. R., & Campbell, L. O. (2019). Who took “counseling” out of the role of professional school counselors in the United States? Journal of School-Based Counseling Policy and Evaluation, 1(3), 51–61. https://doi.org/10.25774/7kjb-bt85
Lancaster, C., & Reiner, S. (2022). Supervision in K–12 school settings. In A. S. Lenz & B. Flamez (Eds.), Practical approaches to clinical supervision across settings: Theory, practice, and research (pp. 223–241). Pearson.
Magson, N. R., Freeman, J. Y. A., Rapee, R. M., Richardson, C. E., Oar, E. L., & Fardouly, J. (2021). Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. Journal of Youth and Adolescence, 50(1), 44–57. https://doi.org/10.1007/s10964-020-01332-9
National Association for College Admission Counseling. (2019). State-by-state student-to-counselor ratio maps by school district: Data visualizations. https://public.tableau.com/profile/nacac.research#!
National Center for Education Statistics. (2016). National teacher and principal survey. https://nces.ed.gov/surveys/ntps
No Child Left Behind Act of 2001, Pub. L. No. 107–110, 115 Stat. 1425 (2002). https://www.congress.gov/107/plaws/publ110/PLAW-107publ110.htm
Parzych, J. L., Donohue, P., Gaesser, A., & Chiu, M. M. (2019). Measuring the impact of school counselor ratios on student outcomes. ASCA Research Report. https://tinyurl.com/3sbuk5dd
Patel, P., & Clinedinst, M. (2021). State-by-state student-to-counselor ratio maps by school district. National Association for College Admission Counseling. https://files.eric.ed.gov/fulltext/ED615227.pdf
Patterson, J. (2022, March 4). School counselors and social workers struggle to meet student needs. National Education Association Today. https://tinyurl.com/yckwhhc4
Pincus, R., Hannor-Walker, T., Wright, L., & Justice, J. (2020). COVID-19’s effect on students: How school counselors rise to the rescue. NASSP Bulletin, 104(4), 241–256. https://doi.org/10.1177/0192636520975866
Quinn, K., Boone, L., Scheidell, J. D., Mateu-Gelabert, P., McGorray, S. P., Beharie, N., Cottler, L. B., & Khan, M. R. (2016). The relationships of childhood trauma and adulthood prescription pain reliever misuse and injection drug use. Drug and Alcohol Dependence, 169, 190–198. https://doi.org/10.1016/j.drugalcdep.2016.09.021
Rea, L. M., & Parker, R. A. (1992). Designing and conducting survey research: A comprehensive guide. Jossey-Bass.
Salloum, A., & Overstreet, S. (2008). Evaluation of individual and group grief and trauma interventions for children post disaster. Journal of Clinical Child & Adolescent Psychology, 37(3), 495–507.
https://doi.org/10.1080/15374410802148194
Savitz-Romer, M. (2019). Fulfilling the promise: Reimagining school counseling to advance student success. Harvard Education Press.
Savitz-Romer, M., Rowan-Kenyon, H. T., Nicola, T. P., Alexander, E., & Carroll, S. (2021). When the kids are not alright: School counseling in the time of COVID-19. AERA Open, 7. https://doi.org/10.1177/23328584211033600
Sheperis, C., Drummond, R. J., & Jones, K. D. (2020). Assessment procedures for counselors and helping professionals (9th ed.). Pearson.
Swedberg, R. (2020). Exploratory research. In C. Elman, J. Gerring, & J. Mahoney (Eds.), The production of knowledge: Enhancing progress in social science (pp. 17–37). Cambridge University Press.
Tennessee Comptroller of the Treasury. (n.d.). Tennessee basic education program: Handbook for computation. https://tinyurl.com/twazjrut
Tennessee Department of Education. (2018). Tennessee comprehensive school-based mental health resource guide. https://tinyurl.com/2bfetw3t
Tennessee Department of Education. (2020). Reopening schools: Overview guide for LEAs. https://tinyurl.com/2hry8hs6
Tennessee Department of Education. (2021). TDOE, TERA releases 2021 Tennessee Educator Survey results. https://tinyurl.com/523b5hmn
Tennessee Department of Education. (2023). Project RAISE internship opportunities. https://web.cvent.com/event/c34c10c7-31e5-48ec-aaa2-7d343e00af77/websitePage:fa84d4fc-c565-4872-98eb-86552d79a670
Tennessee Office of the Governor. (n.d.). COVID-19 timeline. https://www.tn.gov/governor/covid-19/covid19timeline.html
Tennessee State Board of Education. (2017). School counseling model & standards policy 5.103. https://tinyurl.com/39a7jhyx
Udwin, O., Boyle, S., Yule, W., Bolton, D., & O’Ryan, D. (2000). Risk factors for long-term psychological effects of a disaster experienced in adolescence: Predictors of post traumatic stress disorder. Journal of Child Psychology & Psychiatry, 41(8), 969–979. https://doi.org/10.1111/1469-7610.00685
Whitney, D. G., & Peterson, M. D. (2019, February 11). US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatrics, 173(4), 389–391.
https://doi.org/10.1001/jamapediatrics.2018.5399
Zimmer-Gembeck, M. J., & Skinner, E. A. (2011). Review: The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development, 35(1), 1–17. https://doi.org/10.1177/0165025410384923
Chloe Lancaster, PhD, is an associate professor at the University of South Florida. Michelle W. Brasfield, EdD, LPSC, is an assistant professor at the University of Memphis. Correspondence may be addressed to Chloe Lancaster, 422 E. Fowler Ave, EDU 105, Tampa, FL 33620, clancaster2@usf.edu.
Nov 9, 2022 | Volume 12 - Issue 3
Derron Hilts, Yanhong Liu, Melissa Luke
The authors examined whether school counselors’ emotional intelligence predicted their comprehensive school counseling program (CSCP) implementation and whether engagement in transformational leadership practices mediated the relationship between emotional intelligence and CSCP implementation. The sample for the study consisted of 792 school counselors nationwide. The findings demonstrated the significant mediating role of transformational leadership on the relationship between emotional intelligence and CSCP implementation. Implications for the counseling profession are discussed.
Keywords: emotional intelligence, school counselors, transformational leadership, comprehensive school counseling program, implementation
School counselors have been called upon to design and implement culturally responsive comprehensive school counseling programs (CSCPs) that have a deliberate and systemic focus on facilitating optimal student outcomes and development (American School Counselor Association [ASCA], 2017, 2019b). To this end, school counselors are expected to align their activities with the ASCA National Model (ASCA, 2019b) with an aim toward facilitating students’ knowledge, attitudes, skills, and behaviors to be academically and socially/emotionally successful and preparing students for college and career (ASCA, 2021). Relatedly, ASCA (2019a) urges school counselors to apply and enact a model of leadership in the process of program implementation. Several studies (e.g., Mason, 2010; Mullen et al., 2019; Shillingford & Lambie, 2010) have provided empirical evidence that supports the predictive role of school counselors’ leadership on their program implementation outcomes. Still, little is known about the relationship between school counselors’ program implementation and their leadership practices grounded in a specific model such as transformational leadership (Bolman & Deal, 1997; Kouzes & Posner, 1995). Understanding this relationship may allow school counselors to better align their practices within a specific leadership framework consistent with best practice (ASCA, 2019a).
Although leadership has been broadly established as a macro-level capability, emotional intelligence has started to gain interest in recent literature, as intra- and interpersonal competencies are central to school counselors’ practice (Hilts et al., 2019; Hilts, Liu, et al., 2022; Mullen et al., 2018). For instance, school counselors must be emotionally attuned to themselves and others to more effectively navigate the complexities of systems in which they operate (Mullen et al., 2018). One way to achieve such emotional attunement may be by respecting and validating others’ perspectives and providing emotional support to enact interpersonal influence aimed at facilitating educational partners’ keenness toward programmatic efforts (Hilts et al., 2019; Hilts, Liu, et al., 2022; Jordan & Lawrence, 2009). The purpose of the current study is to examine the mechanisms between school counselors’ emotional intelligence, transformational leadership, and CSCP implementation.
Comprehensive School Counseling Programs
Although school counseling programs will vary in structure based on the unique needs of school and community partners (Mason, 2010), programs should be comprehensive in scope, preventative by design, and developmental in nature (ASCA, 2017). CSCP implementation, which comprises a core component of school counseling practice, involves multilevel services (e.g., instruction, consultation, collaboration) and assessments (e.g., program assessments, annual results reports). The functioning of these services and assessments is further defined and managed within the broader school community by the CSCP (Duquette, 2021). Moreover, CSCPs are generally aligned with the ASCA National Model (ASCA, 2019b) to create a shared vision among school counselors to have a more deliberate and systemic focus on facilitating optimal student outcomes and development.
Over the past 20 years, researchers have consistently found positive relationships between CSCP implementation and student achievement reflected through course grades and graduation/retention rates (Sink et al., 2008) and achievement-related outcomes such as behavioral issues and attendance (Akos et al., 2019). Students who attend schools with more well established and fully implemented CSCPs are more likely to perform well academically and behaviorally (Akos et al., 2019). Additionally, researchers have found that school counselors who engage in multilevel services associated with a CSCP are more likely to have higher levels of wellness functioning compared to those who are less engaged in delivering these services (Randick et al., 2018). As such, CSCP implementation seems to not only be positively related to student development and achievement but also the overall well-being of school counselors.
Designing and implementing a culturally responsive CSCP demands a collaborative effort between both school counselors and educational partners to create and sustain an environment that is responsive to students’ diverse needs (ASCA, 2017). This ongoing and iterative process requires school counselors to be emotionally attuned with school, family, and community partners to co-construct, facilitate, and lead initiatives to more efficaciously implement equitable services within their programs (ASCA, 2019b; Bryan et al., 2017). School counselors must engage in leadership and be attentive toward their self- and other-awareness and management to traverse diverse contexts involving differences in personalities, values and goals, and ideologies (Mullen et al., 2018). Although researchers have reported that school counselors’ CSCP implementation is positively related to their leadership (e.g., Mason, 2010), no studies have investigated the relationship between emotional intelligence and CSCP implementation.
Emotional Intelligence
Emotional intelligence generally refers to the ability to recognize, comprehend, and manage the emotions of oneself and others to accomplish individual and shared goals (Kim & Kim, 2017). Scholars have purported that emotional intelligence can be subsumed into two overarching forms: trait emotional intelligence and ability emotional intelligence (Petrides & Furnham, 2000a, 2000b, 2001). Trait emotional intelligence, also known as trait emotional self-efficacy, involves “a constellation of behavioral dispositions and self-perceptions concerning one’s ability to recognize, process, and utilize emotional-laden information” (Petrides et al., 2004, p. 278). Ability emotional intelligence, also referred to as cognitive-emotional ability, concerns an individual’s emotion-related cognitive abilities (Petrides & Furnham, 2000b). Said differently, trait emotional intelligence is in the realm of an individual’s personality (e.g., social awareness), whereas ability emotional intelligence denotes an individual’s actual capabilities to perceive, understand, and respond to emotionally charged situations.
Over the past two decades, scholars have expanded the scope of emotional intelligence to have a deliberate focus on how emotional intelligence occurs within teams or groups in the workforce context (Jordan et al., 2002; Jordan & Lawrence, 2009). Given the salience of emotions in various professional and work contexts (e.g., Jordan & Troth, 2004), Jordan and colleagues’ (2002) Workgroup Emotional Intelligence Profile (WEIP) facilitates a better understanding of how emotional intelligence manifests in teams. The WEIP centralizes emotional intelligence around the “understanding of emotional processes” (Jordan et al., 2002, p. 197). Using the WEIP, researchers revealed that higher emotional intelligence scores are positively related to job satisfaction, organizational citizenship (e.g., performing competently under pressure), organizational commitment, and school and work performance (Miao et al., 2017a, 2017b; Van Rooy & Viswesvaran, 2004). Conversely, higher scores of emotional intelligence were negatively associated with turnover intentions and counterproductive behavior (Miao et al., 2017a, 2017b).
Emotional intelligence has also gained increased attention in the counseling literature. For example, Easton et al. (2008) found emotional intelligence as a significant predictor of counseling self-efficacy in the areas of attending to the counseling process and dealing with difficult client behavior. Following a two-phase investigation, Easton and colleagues demonstrated the stability of emotional intelligence during a 9-month timeframe in both groups of professional counselors and counselors-in-training; thus, the researchers argued that emotional intelligence may be an inherent characteristic associated with the career choice of counseling. In an earlier study with a sample with 108 school counselors, emotional intelligence was found to be significantly and uniquely related to school counselors’ multicultural counseling competence (Constantine & Gainor, 2001). More recently, school counselors’ emotional intelligence was found to be positively related to leadership self-efficacy and experience (Mullen et al., 2018).
School Counseling Leadership Practice
Leadership practice is a dynamic, interpersonal phenomenon within which school counselors engage in behaviors that mobilize support from educational partners to achieve programmatic and organizational objectives aimed at promoting student achievement and development (Hilts, Peters, et al., 2022). The focus on leadership practice entails an emphasis on the actual behavior of the individual, which scholars have contended is a byproduct of both individual and contextual factors in which these behaviors occur (Hilts, Liu, et al., 2022; Mischel & Shoda, 1998; Scarborough & Luke, 2008). For instance, school counselors’ support from other school partners (Dollarhide et al., 2008; Robinson et al., 2019) and previous leadership experience (Hilts, Liu, et al., 2022; Lowe et al., 2017) have been found to influence school counselors’ engagement in leadership. Hilts, Liu, and colleagues (2022) found that intra- and interpersonal factors significantly predicted school counselors’ engagement in leadership such as multicultural competence, leadership self-efficacy, and psychological empowerment. Across several models of leadership (e.g., Bolman & Deal, 1997; Kouzes & Posner, 1995), transformational leadership has been situated in the context of school counseling (Gibson et al., 2018).
Transformational School Counseling Leadership
Transformational leadership is described as behaviors aimed at encouraging others to enact leadership, challenge the status quo, and actively pursue learning and development to achieve higher performance (Bolman & Deal, 1997; Kouzes & Posner, 1995). Individuals employing transformational leadership foster a climate of trust and respect and inspire motivation among others by facilitating emotional attachments and commitment to others and the organization’s mission. More recently, Gibson et al. (2018) constructed and validated the School Counseling Transformational Leadership Inventory (SCTLI) in an effort to support school counselors in conceptualizing and informing their approach to leadership. The SCTLI (Gibson et al., 2018)—grounded in the ASCA National Model (ASCA, 2012) and the general transformational leadership literature (e.g., Avolio et al., 1991)—offers a framework to support engagement in leadership within a school context. For example, school counselors build partnerships with important decision-makers in the school and community and empower educational partners to act to improve the program and the school. School counselors engaging in transformational leadership ascribe to an egalitarian structure in which they engage in shared decision-making, promote a united vision, and inspire others to work toward positive change among students and the broader school community (Lowe et al., 2017). Beyond being studied as an outcome variable itself (Hilts, Liu, et al., 2022), school counselors’ enactment of leadership has also been found to be positively associated with their outcomes of CSCP implementation (Mason, 2010; Mullen et al., 2019).
Emotional Intelligence and the Mediating Role of Transformational Leadership
Over the past several decades, emotional intelligence has been increasingly attributed as a critical trait and ability of individuals employing effective leadership (Kim & Kim, 2017). For instance, Gray (2009) asserted that effective school leaders are able to perceive, understand, and monitor their own and others’ internal states and use this information to guide the thinking and actions of themselves and others. Mullen and colleagues (2018) found that, among a sample of 389 school counselors, domains of emotional intelligence (Jordan & Lawrence, 2009) were significant predictors of leadership self-efficacy and leadership experience. Specifically, Mullen et al.’s (2018) results showed that (a) awareness of own emotions and management of own and others’ emotions were positively related to leadership self-efficacy; (b) management of own and others’ emotions significantly predicted leadership experience; and (c) awareness and management of others’ emotions was positively associated with self-leadership.
Moreover, initial research has revealed that not only is emotional intelligence an antecedent of leadership (Barbuto et al., 2014; Harms & Credé, 2010; Mullen et al., 2018), but that leadership, particularly transformational leadership, mediates the relationship between emotional intelligence and job-related behavior such as job performance (Hur et al., 2011; Hussein & Yesiltas, 2020; Rahman & Ferdausy, 2014). For example, Hussein and Yesiltas’s (2020) results indicated that not only were higher scores of emotional intelligence positively associated with organizational commitment, but that transformational leadership partially mediated the relationship between emotional intelligence and organizational commitment. In another study, Hur and colleagues (2011) sought to examine whether transformational leadership mediated the link between emotional intelligence and multiple outcomes among 859 public employees across 55 teams. The researchers’ results showed that transformational leadership mediated the relationship between emotional intelligence and service climate, as well as between emotional intelligence and leadership effectiveness. Scholars have explained this relationship as the ability of individuals employing transformational leadership to inspire and motivate others to accomplish beyond self- and organizational expectations and redirect feelings of frustration from setbacks to constructive solutions (Hur et al., 2011; Hussein & Yesiltas, 2020).
Purpose of the Study
Taken together, emotional intelligence has been identified in the counseling literature as a significant predictor of counseling self-efficacy and competence (Constantine & Gainor, 2001; Easton et al., 2008). It has also been well established in the workforce literature as being positively related to job performance and leadership outcomes (Hussein & Yesiltas, 2020; Kim & Kim, 2017). The broader leadership literature also comprises evidence in support of the mediating role of transformational leadership between emotional intelligence and performance outcomes (Hur et al., 2011; Hussein & Yesiltas, 2020; Rahman & Ferdausy, 2014). Emotional intelligence has not been examined in relation to school counselors’ CSCP implementation and service outcomes, although CSCP implementation has been widely embraced as a core of the ASCA National Model. Likewise, although emotional intelligence has been studied with counseling practice and leadership separately, we identified no empirical research that has examined the mechanisms between school counselors’ emotional intelligence, transformational leadership practice, and outcomes of program implementation. The present study seeks to address these gaps. Thus, the two research questions that guided our study were: (a) Does school counselors’ emotional intelligence predict their CSCP implementation? and (b) Does engagement in transformational leadership practice mediate the relationship between emotional intelligence and CSCP implementation? Given the synergistic focus on collaboration (or teamwork) shared by the school and workforce contexts coupled with previous empirical evidence, we hypothesized that (a) school counselors’ emotional intelligence predicts their CSCP implementation, and (b) transformational leadership practice mediates the relationship between emotional intelligence and CSCP implementation.
Method
Research Design
In the present study, we utilized a correlational, cross-sectional survey design. We used the Statistical Package for Social Sciences (SPSS, version 27). To test our hypotheses, we performed a mediation analysis using Hayes’s PROCESS in order to establish the extent of influence of an independent variable on an outcome variable (through a mediator; Hayes, 2012). Mediation analysis answered how an effect occurred between variables and is based on the prerequisite that the independent variable/predictor is often considered the “causal antecedent” to the outcome variable of interest (Hayes, 2012, p. 3). Furthermore, we expected that the effects of school counselors’ emotional intelligence on their CSCP implementation would be partly explained by the effects of their engagement in transformational leadership.
Participants
Participants included for final analysis were 792 practicing school counselors in the United States, 94.6% (n = 749) of which reported to be certified/licensed as school counselors and 5.4% (n = 43) indicated to be either not certified/licensed or “unsure.” The sample’s geographic location was mostly suburban (n = 399, 50.4%), followed by rural (n = 195, 24.6%) and urban (n = 184, 23.2%); and 1.8% of participants (n = 14) did not disclose their setting. Public schools accounted for 86.2% (n = 683) of participants’ work settings, followed by charter (n = 42, 5.3%) and private (n = 40, 5.1%), while 3.4% (n = 27) of participants indicated “other” or did not disclose. For grade levels served by participants, 13% (n = 103) worked at the PK–4 level, 20.8% (n = 165) at the 5–8 level, 28.4% (n = 225) at the 9–12 level, and 37.8% (n = 299) worked at the combined K–12 level. Participants’ race/ethnicity included Asian/Native Hawaiian/Pacific Islander (n = 26, 3.3%), Multiracial (n = 47, 5.9%), Black/African American (n = 56, 7.1%), Hispanic/Latino (n = 70, 8.8%), and White (n = 593, 74.9%). Lastly, participants’ mean age was 43, ranging from 23 to 77 years of age. Of the 792 participants, 82.4% (n = 653) identified as cisgender female, 11.0% (n = 88) as cisgender male, 0.3% (n = 2) as transgender female, 0.3% (n = 2) as transgender male, 3.8% (n = 30) chose “prefer to self-identify,” and 2.2% (n = 17) chose “not to answer.” Our sample was representative of the larger population based on the results of a recent nationwide study by ASCA (2021), in which approximately 7,000 school counselors were surveyed; demographic statistics from that study similar to ours included 88% of participants working in public, non-charter schools; 19% working at the middle school level; and 24% working in urban schools..
Procedures and Data Collection
Prior to engaging in data collection, we received approval from our university’s IRB. According to our a priori power analysis conducted using G*Power 3.1 Software (Faul et al., 2007), a sample size of 558 participants would be considered sufficient for the current study, assuming a small effect size ( f 2 = 0.1); therefore, we attempted to achieve a nationally representative sample through a variety of recruitment methods. In efforts to represent the target population, non-probability sampling methods (Balkin & Kleist, 2016) were used and included either sending, posting, or requesting dissemination of a research recruitment message and survey link to (a) school counselors of current or former Recognized ASCA Model Program (RAMP)-designated school counseling programs, (b) state school counseling associations, (c) several closed groups on Facebook for school counselors, (d) the ASCA Scene online discussion forum, and (e) the university’s school counselor listserv. In addition, similar to recruitment methods used by Hilts and colleagues (2019) in previous school counseling research, we emailed ASCA members directly with an invitation to participate. We shared one to two follow-up announcements through these same methods between 2 to 4 weeks after the initial recruitment message.
The link within the research recruitment announcement directed participants to an informed consent page. After indicating their willingness to participate in the study, participants were then directed to the online survey managed by the Qualtrics platform. On average, the survey took approximately 15 minutes to complete.
Instrumentation
Demographic Questionnaire
The demographic questionnaire consisted of 18 questions asked of all eligible participants. The demographic form included questions about participants’ school level, geographic location, school type, and student caseload. We also asked participants about other demographic information including race/ethnicity, gender, age, and years of experience.
Workgroup Emotional Intelligence Profile
The Workgroup Emotional Intelligence Profile-Short Version (WEIP-S; Jordan & Lawrence, 2009), a shortened version of the WEIP (Jordan et al., 2002) and the WEIP-6 (Jordan & Troth, 2004), is a 16-item, self-report scale that measures participants’ emotional intelligence within a team context. Jordan and Lawrence (2009) selected just 25 behaviorally based items from the 30-item WEIP-6 (Jordan & Troth, 2004). Through confirmatory factor analyses (CFA) to achieve the best fit model, the final WEIP-S measure consisted of 16 items with four factors, each of which had good internal consistency reliability in the sample: awareness of own emotions (4 items, ⍺ = .85), management of own emotions (4 items, ⍺ = .77), awareness of others’ emotions (4 items, ⍺ = .88), and management of others’ emotions (4 items, ⍺ = .77). To enhance construct validity of the WEIP-S, Jordan and Lawrence employed model replication analyses and test-retest stability across three time periods. Examples of items from each dimension are (a) “I can explain the emotions I feel to team members” (awareness of own emotions); (b) “When I am frustrated with fellow team members, I can overcome my frustration” (management of own emotions); (c) “I can read fellow team members ‘true’ feelings, even if they try to hide them” (awareness of others’ emotions); and (d) “I can provide the ‘spark’ to get fellow team members enthusiastic” (management of others’ emotions). The items are measured on a Likert-type scale ranging from 1 (strongly disagree) to 7 (strongly agree). For analyses, we summed scores of all dimensions, with higher scores indicating a greater amount of emotional intelligence. Cronbach’s ⍺ and McDonald’s omega (ω) for the WEIP-S were both .93, which indicated good internal consistency.
School Counseling Transformational Leadership Inventory
The SCTLI (Gibson et al., 2018) is a 15-item, self-report inventory that measures the leadership practices of school counselors. The items are measured on a Likert-type scale ranging from 1 (never) to 5 (always or almost always) and a total score indicates the self-reported level of engagement in overall leadership practices. Sample items on the SCTLI include “I have empowered parents and colleagues to act to improve the program and the school” and “I have used persuasion with decision-makers to accomplish school counseling goals.” Findings from Gibson et al.’s (2018) exploratory factor analyses (EFAs) and CFAs revealed a one-factor model of transformational leadership practices based on transformational leadership theory and responsibilities as described within the ASCA National Model (ASCA, 2019b; CFI = .94, TLI = .93, RMSEA = .08). Through Pearson’s correlation, the researchers revealed that concurrent validity was significant (r = .68, p < .01). Additionally, in their sample, Gibson et al. reported strong internal consistency reliability with a Cronbach’s α = .94. In the current study, Cronbach’s α and McDonald’s (ω) for the SCTLI were .93 and .94, respectively.
School Counseling Program Implementation
The School Counseling Program Implementation Survey-Revised (SCPIS-R; Clemens et al., 2010; Fye et al., 2020) is a self-report survey that measures school counselors’ level of CSCP implementation. The SCPIS-R (Fye et al., 2020), used in the current study, is a 14-item Likert-type scale ranging from 1 (not present) to 4 (fully implemented). The factor structure was established through two studies that utilized EFA (Clemens et al., 2010) and CFA (Fye et al., 2020) to test the factor structure. The data from the original study (Clemens et al., 2010) yielded a three-factor model structure of the SCPIS, which includes programmatic orientation (7 items, α = .79), school counselors’ use of computer software (3 items, α = .83), and school counseling services (7 items, α =. 81), and a total SCPIS of α = .87. That said, Fye et al.’s (2020) CFA findings suggested a modified two-factor model was a more appropriate fit; thus, the modified two-factor model structure of the SCPIS includes only programmatic orientation (7 items, α = .86) and school counseling services (7 items, α = .83) and a total SCPIS of α = .90. Examples from each factor are (a) needs assessments are completed regularly and guide program planning (programmatic orientation) and (b) services are organized so that all students are well served and have access to them (school counseling services). We calculated participants’ total SCPIS scores with higher scores indicating greater CSCP implementation (Mason, 2010; Mullen et al., 2019). In the present study, the SCPIS-R demonstrated good reliability (Cronbach’s α = .90; McDonald’s ω = .90) in our sample.
Data Analysis
Missing Data Analysis and Assumptions Test
We received a total of 1,128 responses. Of all these responses, 336 respondents missed a significant portion (over 70%) of one or more of the main scales (i.e., WEIP-S, SCTLI, and SCPIS-R). We assessed this portion of values as not missing completely at random (NMCAR), and we proceeded with employing listwise deletion to 336 cases. The data NMCAR may be because of the survey length and time commitment, which is discussed more in the Limitations section. With the remaining 792 cases, the missing values counted for 0.1%–0.7% of missing values across respective scales. We performed a Little’s Missing Completely at Random test using SPSS Statistics Version 26.0 with a nonsignificant chi-square value (p > .05), which suggested that the missing values (across cases) were missed completely at random. Therefore, we retained all 792 cases and followed multiple imputation (Scheffer, 2002) to replace the missing values, using SPSS. Our data met assumptions for mediation analysis, normality based on histograms, and linearity and homoscedasticity as demonstrated through the scatterplots generated from univariate analysis.
Mediation Analysis
In our mediation model (see Figure 1), given its combined trait-ability nature and stability over time, school counselors’ emotional intelligence was hypothesized as the causal antecedent to program implementation; we then hypothesized transformational leadership practice to be a mediator for the effect of school counselors’ emotional intelligence on program implementation. We tested our mediation model based on Baron and Kenny’s (1986) approach. Specifically, our mediation analysis entailed four steps involving (a) the role of school counselors’ emotional intelligence (X) in predicting CSCP implementation (Y), with the coefficient denoted as c to reflect the total effect that X has on Y; (b) the predictive role of school counselors’ emotional intelligence (X) on transformational leadership practice (M), with the coefficient denoted as a; (c) the effect of transformational leadership practice (M) on CSCP implementation (Y), controlling for the effect of emotional intelligence (X), with the coefficient denoted as b; and (d) the association between school counselors’ emotional intelligence (X) and CSCP implementation (Y), using transformational leadership practice (M) as a mediator with coefficient denoted as c’ (MacKinnon et al., 2012). The difference between the coefficients c and c’,
(c – c’), is the mediation effect of transformational leadership practice.
Figure 1
The Hypothesized Mediation Model
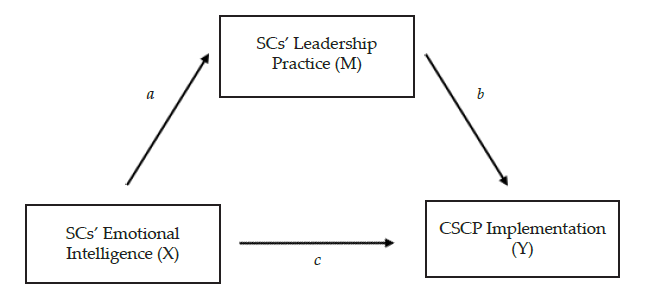
Note. SC = school counselors; CSCP = Comprehensive School Counseling Program.
Hayes’s PROCESS v3.5 (with 5,000 regenerated bootstrap samples) was used to perform the mediation analysis. Hayes’s PROCESS is an analytical function in SPSS used to specify and estimate coefficients of specified paths using ordinary least squares (OLS) regression (Hayes, 2012). We consulted Fritz and MacKinnon (2007) regarding sample adequacy for detecting a mediation effect. Specifically, in order to allow .80 power and a medium mediation effect size, a sample of 397 is recommended for Baron and Kenny’s test, and a sample of 558 is considered adequate to detect small effects via percentile bootstrap (Fritz & MacKinnon, 2007). As such, our sample size of 792 met both criteria. According to MacKinnon et al. (2012), the mediation effect is significant, if zero (0) is excluded from the designated confidence interval (95% in our study).
Results
Correlations
We performed a bivariate analysis on the main study variables of school counselors’ emotional intelligence (measured using the WEIP-S), transformational leadership practice (measured using the SCTLI), and school counselors’ CSCP implementation (measured using the SCPIS-R). School counselors’ emotional intelligence scores were positively correlated with their transformational leadership practice (r = .42, p < .001) and were positively correlated with their CSCP implementation (r = .34, p < .001). Similarly, school counselors’ transformational leadership practice was found to be positively correlated with CSCP implementation (r = .56, p < .001). Table 1 denotes the correlations among variables.
Table 1
Correlation Matrix of Study Variables
| Variable |
EI |
TL |
CSCP |
| EI |
– |
.42** |
.34** |
| TL |
.42** |
– |
.56** |
| CSCP |
.34** |
.56** |
– |
Note. EI = school counselors’ emotional intelligence scores; TL = school counselors’ transformational
leadership; CSCP = school counselors’ comprehensive school counseling program implementation.
**p < .001
Mediation Analysis Results
With the total effect model (Step 1), we found a positive relation between school counselors’ emotional intelligence (X) and their CSCP implementation (Y; coefficient c = 0.24; p < .001; CI [0.20, 0.29]). Namely, school counselors’ emotional intelligence scores significantly predicted their CSCP implementation. In Step 2, we found a positive association between school counselors’ emotional intelligence scores (X) and their transformational leadership practice (M; coefficient a = 0.38; p < .001; CI [0.32, 0.43]). In Step 3, school counseling transformational leadership practice (M) was found to significantly predict their CSCP implementation (Y; coefficient b = 0.40; p < .001, CI [0.35, 0.45]) while controlling for the effect of emotional intelligence (X). Lastly, after adding transformational leadership practice as a mediator, we noted a significant direct effect of emotional intelligence on school counselors’ CSCP implementation (coefficient c’ = 0.09; p = .0001; CI [0.05, 0.14]). We also detected a mediation effect (coefficient ab = 0.15 which equaled c – c’; p < .001; CI [0.12, 0.18]) of emotional intelligence on CSCP implementation through transformational leadership practice. The 95% confidence intervals did not include zero (0), so the path coefficients were significant.
We performed a Sobel test to further evaluate the significance of the mediation effect by school counseling transformational leadership practice, which yielded a Sobel test statistic of 9.97 with a p value of < .001. The Sobel outcome corroborated the significance of our mediated effect. To calculate the effect size of our mediation analysis, we generated kappa-squared value (k2; Preacher & Kelley, 2011). Our kappa-squared (k2) value of .17 suggested a medium effect size (Cohen, 1988). Table 2 demonstrates regression results for the effect of school counselors’ emotional intelligence on their CSCP implementation outcomes mediated by transformational leadership practice.
Table 2
Regression Results for Mediated Effect by Leadership Practice
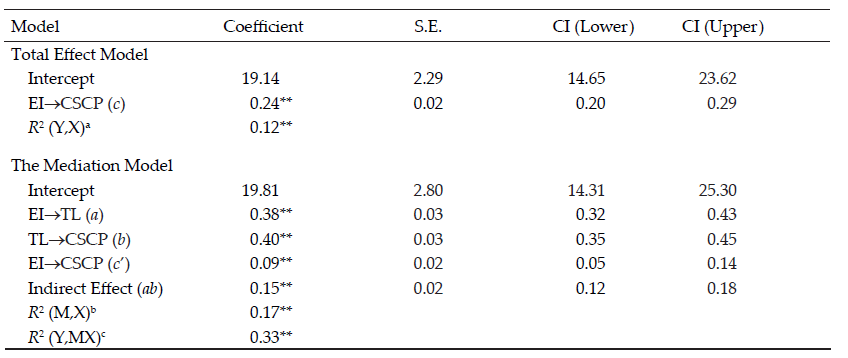
Note. N = 792. EI = emotional intelligence; TL = transformational leadership; CSCP = comprehensive school counseling program; CI = 95% Confidence Interval. The 95% CI for ab is obtained by the bias-corrected bootstrap with 5,000 resamples.
aR2 (Y,X) is the proportion of variance in CSCP implementation explained by EI.
bR2 (M,X) is the proportion of variance in TL explained by EI.
cR2 (Y,MX) is the proportion of variance in CSCP implementation explained by EI and TL.
**p < .001.
Discussion
In this national sample of 792 practicing school counselors, we examined whether school counselors’ emotional intelligence predicts their CSCP implementation. We also investigated whether engagement in transformational leadership practice mediated the relationship between school counselors’ emotional intelligence and CSCP implementation. First, we found that school counselors who reported higher scores of emotional intelligence were also more likely to score higher in CSCP implementation. Given that designing and implementing a CSCP requires school counselors to engage in a culturally responsive and collaborative effort (ASCA, 2017), our result that suggested emotional intelligence is positively correlated with CSCP implementation is not entirely unpredicted. This result was consistent with previous evidence supporting the positive correlation between emotional intelligence and work performance (Miao et al., 2017a, 2017b; Van Rooy & Viswesvaran, 2004). The result also illustrated the predictive role of school counselors’ emotional intelligence on their CSCP implementation, beyond its significant association with counseling competencies (Constantine & Gainor, 2001; Easton et al., 2008).
Secondly, school counselors’ emotional intelligence was found to be positively associated with their engagement in transformational leadership. This result aligned with previous evidence that school counselors’ emotional intelligence is linked to leadership outcomes demonstrated through the workforce literature (Barbuto et al., 2014; Harms & Credé, 2010; Kim & Kim, 2017). Similarly, the result echoed Mullen et al.’s (2018) finding on the positive relationship between school counselors’ emotional intelligence and leadership scores measured by the Leadership Self-Efficacy Scale (LSES; Bobbio & Manganelli, 2009). Noteworthily, the LSES was normed and validated with college students. Our results advanced the school counseling literature and corroborated the relationship between emotional intelligence and school counseling transformational leadership measured by the SCTLI, a scale developed specifically for school counselors. Our results suggest that school counselors may actively attend to emotional processes in order to effectively enact transformational leadership practice.
Thirdly, we found that school counselors’ engagement in transformational leadership significantly mediated the relationship between their emotional intelligence and CSCP implementation. Because leadership is woven into the ASCA National Model and is considered an integral component of a CSCP (ASCA, 2019b), and school counselors are required to develop collaborative partnerships with a range of educational partners (ASCA, 2019a; Bryan et al., 2017), we were not surprised to find these two concepts were related to CSCP implementation. This result also aligns with empirical evidence in the broader leadership literature that transformational leadership mediated the relationship between emotional intelligence and work performance (Hur et al., 2011; Hussein & Yesiltas, 2020). This result is particularly meaningful in that it demonstrates school counseling leadership as either a significant predictor (Mason, 2010; Mullen et al., 2019) or an outcome variable itself (Hilts, Liu, et al., 2022; Mullen et al., 2018). It enables a more nuanced understanding of mechanisms involved in emotional intelligence, leadership, and program implementation in a school counseling context. To our best knowledge, the current study was the first study that found that through leadership practice, school counselors’ emotional intelligence may offer an indirect effect on their CSCP implementation.
Implications
Results of this study have implications for school counselor practice and school counselor training and supervision. Given the significant relationships between emotional intelligence, transformational leadership, and CSCP implementation, we suggest that practicing school counselors begin by assessing their emotional intelligence, transformational leadership, and CSCP implementation and then set goals to enhance their performance. This may be especially important considering that other research has suggested that school counselors’ engagement in leadership, as well as their other roles and responsibilities (e.g., multicultural competence; challenging co-workers about discriminatory practices) have changed since the onset of the COVID-19 pandemic (Hilts & Liu, 2022). For instance, Hilts and Liu’s (2022) results indicated that school counselors’ leadership practice scores were higher during the pandemic compared to prior to the COVID-19 outbreak.
Next, school counselors can seek resources and professional development opportunities to support their goals. For example, school counselors may benefit from professional development focused on social-emotional learning (SEL), given SEL’s competency approach to building collaborative relationships (Collaborative for Academic, Social, and Emotional Learning, n.d.). That said, school counselors should also seek supports to experientially integrate their intrapersonal, interpersonal, and systemic skills associated with emotional intelligence, transformational leadership, and CSCP implementation. Intentional application of the Model for Supervision of School Counseling Leadership (Hilts, Peters, et al., 2022) may provide one such example for both school counseling practitioners and those in training.
School counselor training programs can also identify meaningful opportunities to infuse emotional intelligence and transformational leadership into school counselor coursework and supervision. Scarborough and Luke (2008) identified the important role of exposure in training to models of successful CSCP implementation and related resources on subsequent self-efficacy. As such, not only can school counseling coursework infuse the ASCA National Model Implementation Guide: Manage & Assess (ASCA, 2019b) and the Making DATA Work: An ASCA National Model publication (ASCA, 2018) along with additional emotional intelligence and transformational leadership resources, school counseling faculty and supervisors should intentionally incorporate school counseling students’ ongoing exposure to practicing school counselors and supervisors with high scores of emotional intelligence and transformational leadership.
Limitations
As with all research, the results of this study need to be understood in consideration of the methodological strengths and limitations. Despite obtaining a large national sample, the data collection procedures used in this study prevented our ability to determine the survey response rate. As such, we are unable to make any claim about non-response bias and it is possible that school counselors who declined to participate significantly differed from those who completed the study. Relatedly, the sample included a proportionately large number of participants who started the survey but did not finish. It is possible that the attrition of these school counselors reflected an as of yet unidentified confounding construct that is also related to the variables under study (Balkin & Kleist, 2016). Our sample is nonetheless generally representative of the national school counselor demographic data reported in the recent state of the profession survey of approximately 7,000 school counselors (ASCA, 2021), strengthening the validity and subsequent generalizability of our results.
Another limitation of our study is that all data were cross-sectional and non-experimental. The correlation and mediation analyses used in the study demonstrate the strength of associations between the examined constructs, and do not reflect temporal or causal relationships. The cross-sectional design does not allow statistical control for the predictor and outcome variables; thus, it may not accurately specify the effect of the predictor on the mediator (Maxwell & Cole, 2007). Therefore, any inclination to impose intuitive logic or imbue directionality that emotional intelligence is an antecedent to either transformational leadership or CSCP implementation should be interpreted with caution. Further, all data from this study were collected at the same time and relied upon self-report. As such, common-method variance could have inflated the identified relationships between the constructs.
An important consideration is that this study was delineated to focus on illustrating individual path coefficients between emotional intelligence, leadership, and CSCP implementation and provides limited insight into understanding of complex relationships among latent variables. Likewise, we used Hayes’s PROCESS to examine our mediation model which features procedure rather than overall model fit created through more sophisticated statistical analyses such as structural equation modeling (SEM). Given that PROCESS is a modeling tool that relies on OLS regression, it may be biased in estimating effects without taking into consideration measurement error (Darlington & Hayes, 2017).
Suggestions for Future Research
The results of this study have numerous implications for future research. Future studies may explore the relationship between emotional intelligence and other forms of leadership prevalent in the counseling literature, such as charismatic democratic or servant leadership (Hilts, Peters, et al., 2022). In addition, because self-report emotional intelligence measures have been described as better to assess intrapersonal processes and ability emotional intelligence measures have been shown to be related to emotion-focused coping and work performance (Miao et al., 2017a, 2017b), future research may consider incorporating ability and mixed emotional intelligence measurements to examine a causal model of emotional intelligence and transformational leadership (or other forms of leadership).
Future research could extend the unit of analysis in this study (e.g., individual school counselor) and adopt a similar perspective to Lee and Wong (2019) to examine emotional intelligence in teams. Studies could similarly expand the use of self-report emotional intelligence measures and include ability or mixed emotional intelligence measurement. Relatedly, as Miao et al. (2017b) described significant moderator effects of emotional labor demands of jobs on the relationship between self-report emotional intelligence and job satisfaction, future research could assess this in the school counseling context, wherein the emotional labor demands of the work may vary. Given the robust workforce literature grounding associations between emotional intelligence and job performance, job satisfaction, organizational commitment, and resilience in the face of counterproductive behavior in the workplace (Hussein & Yesiltas, 2020), future school counseling research can examine emotional intelligence and other constructs, including ethical decision-making, belonging, attachment, burnout, and systemic factors.
Lastly, as most constructs involved in school counseling practice are latent variables in nature, we recommend future scholars consider SEM when it comes to investigating overall model fit between the variables of interest. SEM offers more specification to the model including goodness of fit of the model to the data (Hayes et al., 2018). It minimizes bias involved in mediation effect estimation with consideration of individual indicators for each latent variable (Kline, 2016).
Conclusion
As an initial examination of the relationship between emotional intelligence and CSCP implementation, as well as the role of school counselors’ transformational leadership in mediating the relationship between emotional intelligence and CSCP implementation, this study was grounded in the empirical scholarship on leadership in both school counseling and allied fields. We found support for our hypothesized model of school counselors’ emotional intelligence and their CSCP implementation, mediated by their engagement in transformational leadership. Our examination yielded evidence in support of the significant mediating role of school counselors’ transformational leadership engagement on the relationship between emotional intelligence and CSCP implementation. In the meantime, our results supported the robust reliability of three instruments in our sample: the WEIP-S (Jordan & Lawrence, 2009), the SCTLI (Gibson et al., 2018), and the SCPIS-R (Clemens et al., 2010; Fye et al., 2020), which can be useful for future school counseling researchers and practitioners. This study serves as an important necessary step in establishing these relationships, and we anticipate that our results will ground further investigation related to school counselors’ emotional intelligence, leadership practices, and CSCP implementation, including the development of additional measurements.
Conflict of Interest and Funding Disclosure
This study was partially funded by Chi Sigma
Iota International’s Excellence in Counseling
Research Grants Program.
References
Akos, P., Bastian, K. C., Domina, T., & de Luna, L. M. M. (2019). Recognized ASCA Model Program (RAMP) and student outcomes in elementary and middle schools. Professional School Counseling, 22(1), 1–9. https://doi.org/10.1177/2156759X19869933
American School Counselor Association. (2012). The ASCA national model: A framework for school counseling programs (3rd ed.).
American School Counselor Association. (2017). The school counselor and school counseling programs.
https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-School-Counseling-Program
American School Counselor Association. (2018). Making data work: An ASCA National Model publication (4th ed.).
American School Counselor Association. (2019a). ASCA school counselor professional standards & competencies. https://www.schoolcounselor.org/getmedia/a8d59c2c-51de-4ec3-a565-a3235f3b93c3/SC-Competencies.pdf
American School Counselor Association. (2019b). The ASCA national model: A framework for school counseling programs (4th ed.).
American School Counselor Association. (2021). ASCA research report: State of the profession 2020. https://www.sch
oolcounselor.org/getmedia/bb23299b-678d-4bce-8863-cfcb55f7df87/2020-State-of-the-Profession.pdf
Avolio, B. J., Waldman, D. A., & Yammarino, F. J. (1991). Leading in the 1990s: The four I’s of transformational leadership. Journal of European Industrial Training, 15(4), 9–16. https://doi.org/10.1108/03090599110143366
Balkin, R. S., & Kleist, D. M. (2016). Counseling research: A practitioner-scholar approach. American Counseling Association.
Barbuto, J. E., Gottfredson, R. K., & Searle, T. P. (2014). An examination of emotional intelligence as an antecedent of servant leadership. Journal of Leadership & Organizational Studies, 21(3), 315–323.
https://doi.org/10.1177/1548051814531826
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
Bobbio, A., & Manganelli, A. M. (2009). Leadership Self-Efficacy Scale. A new multidimensional instrument. TPM–Testing, Psychometrics, Methodology in Applied Psychology, 16(1), 3–24. https://www.tpmap.org/wp-content/
uploads/2014/11/16.1.1.pdf
Bolman, L. G., & Deal, T. E. (1997). Reframing organizations: Artistry, choice, and leadership (2nd ed.). Jossey-Bass.
Bryan, J. A., Young, A., Griffin, D., & Holcomb-McCoy, C. (2017). Leadership practices linked to involvement in school–family–community partnerships: A national study. Professional School Counseling, 21(1), 1–13. https://doi.org/10.1177/2156759X18761897
Clemens, E. V., Carey, J. C., & Harrington, K. M. (2010). The school counseling program implementation survey: Initial instrument development and exploratory factor analysis. Professional School Counseling, 14(2), 125–134. https://doi.org/10.1177/2156759X1001400201
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum. https://www.ut
stat.toronto.edu/~brunner/oldclass/378f16/readings/CohenPower.pdf
Collaborative for Academic, Social, and Emotional Learning. (n.d.). SEL in school districts. https://casel.org/systemic-implementation/sel-in-school-districts
Constantine, M. G., & Gainor, K. A. (2001). Emotional intelligence and empathy: Their relation to multicultural counseling knowledge and awareness. Professional School Counseling, 5(2), 131–137.
Darlington, R. B., & Hayes, A. F. (2017). Regression analysis and linear models: Concepts, applications, and implementation. Guilford.
Dollarhide, C. T., Gibson, D. M., & Saginak, K. A. (2008). New counselors’ leadership efforts in school counseling: Themes from a year-long qualitative study. Professional School Counseling, 11(4), 262–271. https://doi.org/10.1177/2156759X0801100407
Duquette, K. (2021). “We’re powerful too, you know?” A narrative inquiry into elementary school counselors’ experiences of the RAMP process. Professional School Counseling, 25(1), 1–15.
https://doi.org/10.1177/2156759X20985831
Easton, C., Martin, W. E., Jr., & Wilson, S. (2008). Emotional intelligence and implications for counseling
self-efficacy: Phase II. Counselor Education and Supervision, 47(4), 218–232.
https://doi.org/10.1002/j.1556-6978.2008.tb00053.x
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Fye, H. J., Memis, R., Soyturk, I., Myer, R., Karpinski, A. C., & Rainey, J. S. (2020). A confirmatory factor analysis of the school counseling program implementation survey. Journal of School Counseling, 18(24). http://www.jsc.montana.edu/articles/v18n24.pdf
Gibson, D. M., Dollarhide, C. T., Conley, A. H., & Lowe, C. (2018). The construction and validation of the school counseling transformational leadership inventory. Journal of Counselor Leadership and Advocacy, 5(1), 1–12. https://doi.org/10.1080/2326716X.2017.1399246
Gray, D. (2009). Emotional intelligence and school leadership. International Journal of Educational Leadership Preparation, 4(4), n4.
Harms, P. D., & Credé, M. (2010). Emotional intelligence and transformational and transactional leadership: A meta-analysis. Journal of Leadership & Organizational Studies, 17(1), 5–17. https://doi.org/10.1177/1548051809350894
Hayes, A. F. (2012). PROCESS: A versatile computational tool for observed variable mediation, moderation, and conditional process modeling [White paper].
Hayes, A. F., Montoya, A. K., & Rockwood, N. J. (2017). The analysis of mechanisms and their contingencies: PROCESS versus structural equation modeling. Australasian Marketing Journal, 25(1), 76–81.
https://doi.org/10.1016/j.ausmj.2017.02.001
Hilts, D., Kratsa, K., Joseph, M., Kolbert, J. B., Crothers, L. M., & Nice, M. L. (2019). School counselors’ perceptions of barriers to implementing a RAMP-designated school counseling program. Professional School Counseling, 23(1), 1–11. https://doi.org/10.1177/2156759X19882646
Hilts, D., & Liu, Y. (2022). School counselors’ perceived school climate, leadership practice, psychological empowerment, and multicultural competence before and during COVID-19. Niagara University [Unpublished manuscript].
Hilts, D., Liu, Y., Li, D., & Luke, M. (2022). Examining ecological factors that predict school counselors’ engagement in leadership practices. Professional School Counseling, 26(1), 1–14. https://doi.org/10.1177/2156759X221118042
Hilts, D., Peters, H. C., Liu, Y., & Luke, M. (2022). The model for supervision of school counseling leadership. Journal of Counselor Leadership and Advocacy, 1–16. https://doi.org/10.1080/2326716X.2022.2032871
Hur, Y., van den Berg, P. T., & Wilderom, C. P. M. (2011). Transformational leadership as a mediator between emotional intelligence and team outcomes. The Leadership Quarterly, 22(4), 591–603.
https://doi.org/10.1016/j.leaqua.2011.05.002
Hussein, B., & Yesiltas, M. (2020). The influence of emotional intelligence on employee’s counterwork behavior and organizational commitment: Mediating role of transformational leadership. Revista de Cercetare si Interventie Sociala, 71, 377–402. https://doi.org/10.33788/rcis.71.23
Jordan, P. J., Ashkanasy, N. M., Härtel, C. E., & Hooper, G. S. (2002). Workgroup emotional intelligence: Scale development and relationship to team process effectiveness and goal focus. Human Resource Management Review, 12(2), 195–214. https://doi.org/10.1016/S1053-4822(02)00046-3
Jordan, P. J., & Lawrence, S. A. (2009). Emotional intelligence in teams: Development and initial validation of the short version of the Workgroup Emotional Intelligence Profile (WEIP-S). Journal of Management and Organization, 15(4), 452–469. https://doi.org/10.1017/S1833367200002546
Jordan, P. J., & Troth, A. C. (2004). Managing emotions during team problem solving: Emotional intelligence and conflict resolution. Human Performance, 17(2), 195–218. https://doi.org/10.1207/s15327043hup1702_4
Kim, H., & Kim, T. (2017). Emotional intelligence and transformational leadership: A review of empirical studies. Human Resource Development Review, 16(4), 377–393. https://doi.org/10.1177/1534484317729262
Kline, R. B. (2016). Principles and practice of structural equation modeling (4th ed.). Guilford.
Kouzes, J. M., & Posner, B. Z. (1995). The leadership challenge: How to keep getting extraordinary things done in organizations (1st ed.). Jossey-Bass.
Lee, C., & Wong, C.-S. (2019). The effect of team emotional intelligence on team process and effectiveness. Journal of Management & Organization, 25(6), 844–859. https://doi.org/10.1017/jmo.2017.43
Lowe, C., Gibson, D. M., & Carlson, R. G. (2017). Examining the relationship between school counselors’ age, years of experience, school setting, and self-perceived transformational leadership skills. Professional School Counseling, 21(1b), 1–7. https://doi.org/10.1177/2156759X18773580
MacKinnon, D. P., Cheong, J., & Pirlott, A. G. (2012). Statistical mediation analysis. In H. Cooper, P. M. Camic, D. L. Long, A. T. Panter, D. Rindskopf, & K. J. Sher (Eds.), APA handbook of research methods in psychology, Vol. 2. Research designs: Quantitative, qualitative, neuropsychological, and biological (pp. 313–331). American Psychological Association.
Mason, E. C. M. (2010). Leadership practices of school counselors and counseling program implementation. National Association of Secondary School Principals Bulletin, 94(4), 274–285. https://doi.org/10.1177/0192636510395012
Maxwell, S. E., & Cole, D. A. (2007). Bias in cross-sectional analyses of longitudinal mediation. Psychological Methods, 12(1), 23–44. https://doi.org/10.1037/1082-989X.12.1.23
Miao, C., Humphrey, R. H., & Qian, S. (2017a). A meta-analysis of emotional intelligence and work attitudes. Journal of Occupational and Organizational Psychology, 90(2), 177–202. https://doi.org/10.1111/joop.12167
Miao, C., Humphrey, R. H., & Qian, S. (2017b). Are the emotionally intelligent good citizens or counterproductive? A meta-analysis of emotional intelligence and its relationships with organizational citizenship behavior and counterproductive work behavior. Personality and Individual Differences, 116, 144–156. https://doi.org/10.1016/j.paid.2017.04.015
Mischel, W., & Shoda, Y. (1998). Reconciling processing dynamics and personality dispositions. Annual Review of Psychology, 49, 229–258. https://doi.org/10.1146/annurev.psych.49.1.229
Mullen, P. R., Gutierrez, D., & Newhart, S. (2018). School counselors’ emotional intelligence and its relationship to leadership. Professional School Counseling, 21(1b), 1–12. https://doi.org/10.1177/2156759X18772989
Mullen, P. R., Newhart, S., Haskins, N. H., Shapiro, K., & Cassel, K. (2019). An examination of school counselors’ leadership self-efficacy, programmatic services, and social issue advocacy. Journal of Counselor Leadership and Advocacy, 6(2), 160–173. https://doi.org/10.1080/2326716X.2019.1590253
Petrides, K. V., Frederickson, N., & Furnham, A. (2004). The role of trait emotional intelligence in academic performance and deviant behavior at school. Personality and Individual Differences, 36(2), 277–293.
https://doi.org/10.1016/S0191-8869(03)00084-9
Petrides, K. V., & Furnham, A. (2000a). Gender differences in measured and self-estimated trait emotional intelligence. Sex Roles, 42, 449–461. https://doi.org/10.1023/A:1007006523133
Petrides, K. V., & Furnham, A. (2000b). On the dimensional structure of emotional intelligence. Personality and Individual Differences, 29(2), 313–320. https://doi.org/10.1016/S0191-8869(99)00195-6
Petrides, K. V., & Furnham, A. (2001). Trait emotional intelligence: Psychometric investigation with reference to established trait taxonomies. European Journal of Personality, 15(6), 425–448. https://doi.org/10.1002/per.416
Preacher, K. J., & Kelley, K. (2011). Effect size measures for mediation models: Quantitative strategies for communicating indirect effects. Psychological Methods, 16(2), 93–115. https://doi.org/10.1037/a0022658
Rahman, S., & Ferdausy, S. (2014). Relationship between emotional intelligence and job performance mediated by transformational leadership. NIDA Development Journal, 54(4), 122–153. https://doi.org/10.14456/ndj.2014.1
Randick, N. M., Dermer, S., & Michel, R. E. (2018). Exploring the job duties that impact school counselor wellness: The role of RAMP, supervision, and support. Professional School Counseling, 22(1).
https://doi.org/10.1177/2156759X18820331
Robinson, D. M., Mason, E. C. M., McMahon, H. G., Flowers, L. R., & Harrison, A. (2019). New school counselors’ perceptions of factors influencing their roles as leaders. Professional School Counseling, 22(1), 1–15. https://doi.org/10.1177/2156759X19852617
Scheffer, J. (2002). Dealing with missing data. Research Letters in the Information and Mathematical Sciences, 3, 153–160. http://hdl.handle.net/10179/4355
Shillingford, M. A., & Lambie, G. W. (2010). Contribution of professional school counselors’ values and leadership practices to their programmatic service delivery. Professional School Counseling, 13(4), 208–217. https://doi.org/10.1177/2156759X1001300401
Sink, C. A., Akos, P., Turnbull, R. J., & Mvududu, N. (2008). An investigation of comprehensive school counseling programs and academic achievement in Washington state middle schools. Professional School Counseling, 12(1). https://doi.org/10.1177/2156759X0801200105
Van Rooy, D. L., & Viswesvaran, C. (2004). Emotional intelligence: A meta-analytic investigation of predictive
validity and nomological net. Journal of Vocational Behavior, 65(1), 71–95.
https://doi.org/10.1016/S0001-8791(03)00076-9
Derron Hilts, PhD, NCC, is an assistant professor at Niagara University. Yanhong Liu, PhD, NCC, is an associate professor at Syracuse University. Melissa Luke, PhD, NCC, is a dean’s professor at Syracuse University. Correspondence may be addressed to Derron Hilts, 5795 Lewiston Rd, Niagara University, NY 14109, dhilts@niagara.edu.
Feb 7, 2022 | Volume 12 - Issue 1
Clark D. Ausloos, Madeline Clark, Hansori Jang, Tahani Dari, Stacey Diane Arañez Litam
Trans youth experience discrimination and marginalization in their homes, communities, and schools. Professional school counselors (PSCs) are positioned to support and advocate for trans youth as dictated by professional standards. However, an extensive review of literature revealed a lack of confidence and competence in counselors working with trans youth and their families. Further, there is a dearth of literature that addresses factors leading to increased school counselor competence with trans students. The current study uses a cross-sectional survey design to contribute to the extant literature and explore how PSCs in the United States work with students in the K–12 public school system. Results from multiple regression analyses indicate that PSCs who have had postgraduate training and report personal and professional experiences with trans students are more competent in working with trans students. Implications for PSCs and school counselor education programs are discussed.
Keywords: trans youth, school counselors, competence, counselor education, multiple regression analysis
Trans people experience an incongruence between their sex assigned at birth and their gender identity (GI; Ginicola et al., 2017; McBee, 2013). The term trans encompasses a wide range of gender-expansive identities, including trans (transgender), nonbinary (one who identifies outside the gender binary of male or female), genderqueer or gender-fluid (one who identifies with gender in a fluid, dynamic way) and agender (one who does not identify as having a gender). Trans people face pervasive discrimination and marginalization (Whitman & Han, 2017), leading to severe physical and mental health disparities, like depression, anxiety, and suicidality (James et al., 2016). In schools, trans students face 4 times higher rates of discrimination when compared with cisgender peers (Kosciw et al., 2020; Williams et al., 2021). Trans students are more vulnerable to mental health disorders, a lack of social support, and an increase in self-harm, suicidal ideations, and suicide attempts (Kosciw et al., 2020; Reisner et al., 2014), especially among transmale and nonbinary students (Toomey et al., 2018). These rates are increasing in national trends and are even higher among Black and Latinx trans students (Vance et al., 2021). The COVID-19 pandemic further exacerbated barriers and inequities for trans students, with increasing health concerns, isolation, economic hardships, issues with housing, and limited access to essential clinical care (Burgess et al., 2021).
Increasingly, trans students face systemic legal barriers to their health and well-being (Wang et al., 2016). States including Arkansas, Idaho, Montana, South Dakota, and Tennessee have introduced bills that ban trans students from participating in sports that are congruent with their GI (Transgender Law Center, 2021). In April of 2021, Arkansas banned medical gender-affirming services to students under 18 years of age (American Civil Liberties Union [ACLU], 2021). New Hampshire’s House Bill 68 proposed adding gender-affirming treatments to the definition of child abuse (ACLU, 2021). Beyond political oppression, trans youth experience overt discrimination, verbal abuse, physical and sexual assault, and marginalization within their homes, schools, and places of employment (Human Rights Campaign [HRC], 2018; James et al., 2016). Trans youth additionally face disaffirming and incompetent teachers and medical professionals (Grant et al., 2011; James et al., 2016; Whitman & Han, 2017) and embedded systemic transmisia (the hatred of trans persons; Simmons University Library, 2019). Despite the pervasive mental health concerns faced by trans students (i.e., depression, anxiety, disordered eating, self-harm, suicide), professional school counselors (PSCs) continue to be ill equipped in supporting and advocating for this marginalized population within schools (Simons, 2021). Based upon an analysis of the extant body of research, we found that counselor education training programs lack rigor in working with trans students (O’Hara et al., 2013; Salpietro et al., 2019), counselor educators may hold biased views about trans students (Frank & Cannon, 2010), and there is an absence of quality professional development opportunities on trans issues (Salpietro et al., 2019; Shi & Doud, 2017). It is therefore of paramount importance for PSCs and counselor education programs to obtain a deeper understanding of how to better prepare for and support trans students in schools.
Professional School Counselors and Trans Students
PSCs focus on academic, career, and social-emotional growth and work as leaders alongside teachers, administration, families, and other stakeholders. PSCs are therefore well positioned to provide safety and support for trans students, promote change, and act as social justice advocates within schools (Bemak & Chung, 2008). The American School Counselor Association (ASCA) mandates that PSCs “promote affirmation, respect, and equal opportunity for all individuals regardless of . . . gender identity, or gender expression . . . and promote awareness of and education on issues related to LGBT students” (2016a, p. 37). PSCs who work with trans students may provide services through the Multitiered Systems of Support lens (MTSS; ASCA, 2019), through collaboration, by supporting school administration and staff (e.g., trainings, meetings, workshops), and through provision of direct student services (e.g., individual and group counseling, working with families). More specifically, PSCs advocate for and with students for name and pronoun changes within schools, trans-inclusive school policies, and increased visibility and normalization of trans people and issues.
ASCA (2016b) adopted a position that PSCs recognize that “the responsibility for determining a student’s gender identity rests with the student rather than outside confirmation from medical practitioners . . . or documentation of legal changes” (p. 64). It is clear that PSCs should possess knowledge and skills in working with and advocating for trans youth through a range of services at various levels and in coordination with other stakeholders in schools, all while respecting students’ autonomy and authenticity (ASCA, 2016a, 2016b, 2019; Bemak & Chung, 2008).
Counselor Education Programs
Although professional standards provide best practices (ALGBTIC LGBQQIA Competencies Taskforce, 2013; ASCA, 2016a), many PSCs never receive the training necessary to effectively serve trans students (Bidell, 2012; O’Hara et al., 2013; Salpietro et al., 2019). Salpietro and colleagues (2019) reported that counselor incompetence was related to a lack of rigorous training that attends to family systems, intersectionality, and medical issues through gender-affirming therapies (i.e., blockers, hormones, or surgeries). These researchers indicated a need for comprehensive, standardized, and thorough formal training (i.e., graduate school) and informal professional development opportunities. These findings are consistent with Shi and Doud (2017), who recommended PSCs specifically take advantage of conferences and workshops to supplement formal educational curricula. The Gay, Lesbian, and Straight Education Network (GLSEN) conducted a survey that reported about 81% of school mental health professionals received “little to no competency training in their graduate programs related to working with [trans] populations,” and about 74% of participants rated their graduate training programs as “fair or poor” in preparing them for work with trans students (GLSEN et al., 2019, p. xviii). GLSEN and other professional organizations additionally reported about two-thirds of school professionals do not feel prepared to work with trans students (GLSEN et al., 2019). Although there are some professional development opportunities, such as those offered through the World Professional Association for Transgender Health (WPATH), the HRC, and the Society for Sexual, Affectional, Intersex, and Gender-Expansive Identities (SAIGE), there is still a lack of concrete training within graduate programs and through fieldwork experiences and an overall lack of accessible, professional trainings. There is a clear need for increased attention to trans issues in formal educational programs and professional development offerings.
Purpose of the Study and Research Questions
This study examines factors that contribute to PSC competence in working with trans students in K–12 public schools. We highlight the need for PSCs and counselor education training programs to better focus on and support trans students. More specifically, we examine the following PSC factors: (a) the PSC’s GI, (b) whether the PSC has received postgraduate training on trans issues or populations, (c) whether the PSC has worked with self-identified trans students, and (d) whether the PSC knows someone who identifies as trans outside of the school setting.
PSC Gender Identity
Researchers recommend that special attention is given within a category of interest (i.e., gender identity) to historically marginalized groups, encouraging counselor-researchers to view all samples “in terms of their particularity and to attend to diversity within samples” (Cole, 2009, p. 176). We were intentional in using PSC GI demographic factors in data analysis, attending to diversity among PSC gender identities, as research indicates there may be relationships between counselor GI, privilege and oppression, and multicultural counselor competence (Cole, 2009). Culturally competent counselors engage in self-reflection, examine their own biases and stereotypes, consider how their positions of privilege or oppression impact the therapeutic alliance, and deliver culturally responsive counseling interventions.
Postgraduate Training Addressing Trans Issues
Researchers note that graduate programs in counselor education are not adequately preparing school counseling students to work with trans students (Bidell, 2012; Farmer et al., 2013; Frank & Cannon, 2010; GLSEN et al., 2019; O’Hara et al., 2013) and that much of the awareness, knowledge, and skills gained in working with this population are result of counselors’ self-seeking professional trainings, education, and workshops that are focused on trans issues and students (Salpietro et al., 2019; Shi & Doud, 2017).
Professional Experiences With Trans Students
O’Hara and colleagues (2013) reported no significance on scores of competence in working with trans clients between counseling students who completed practicum or internship and those who did not. In the present study, our variable relates to PSCs who have already graduated, reflecting on their professional tenure as PSCs, and if these experiences provided opportunities to work with trans students.
Personal Relationships With Trans People
O’Hara and colleagues (2013) reported that participants in their study identified informal sources as necessary for gaining trans-affirming knowledge and skills, such as “exposure to or personally knowing someone who [is trans]” (p. 246). Research supports the concept that increasing affirming attitudes and mitigating negative attitudes and beliefs toward trans individuals can be accomplished by exposure and intentional engagement in fostering personal and professional relationships with trans people (Salpietro et al., 2019; Simons, 2021). In forming relationships with trans people, we can listen to and learn from the lived experiences of this community, examine our own biases, and position ourselves as supportive allies, personally and professionally.
Research Questions
With these factors in mind, the following research questions were identified:
- What is the relationship between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personally knowing someone who is trans) and levels of PSC self-perceived competence in working with trans students in schools?
- What is the relationship between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personally knowing someone who is trans) and PSC awareness in working with trans students in schools?
- What is the relationship between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personally knowing someone who is trans) and PSC knowledge in working with trans students in schools?
- What is the relationship between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personally knowing someone who is trans) and PSC skills in working with trans students in schools?
We hypothesized there would be a statistically significance difference (p > .05) between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personally knowing someone who is trans) and levels of PSC self-perceived competence in working with trans students in schools. More specifically, we hypothesized that cisfemale PSCs who have had postgraduate training on trans issues, who have worked with trans students, and who personally know someone who is trans, would report higher scores in measures of awareness, knowledge, skills, and overall competence. Cisgender (cis) refers to someone who experiences congruence between their sex assigned at birth and their GI. Research demonstrates that cismales may express more negative attitudes and hold restrictive views toward queer and trans people when compared with cisfemales (Landén & Innala, 2000; Norton & Herek, 2012).
Method
Participants
With an anticipated medium effect size of 0.15, a desired statistical power level of 0.95, and desired probability level of 0.05 (Israel, 2013), we determined an appropriate minimum sample size for the proposed study was 120 PSCs. Initially, 499 responses were recorded. Of those, 110 were incomplete or had missing data, yielding a total of 389 fully completed surveys. Participants in this study (N = 389) were PSCs with a valid school counseling license working in a public school setting, from kindergarten through 12th grade, in the United States. Participant demographic information can be found in Table 1.
Table 1
Demographic Characteristics of Professional School Counselors (PSCs)
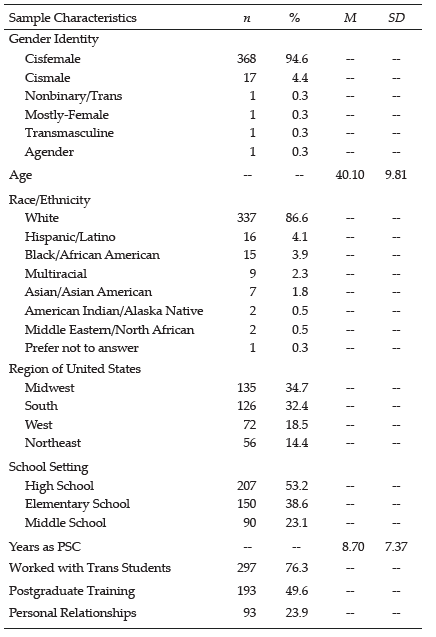
Procedures
For ease of use and accuracy of representation, we used probability sampling, more specifically, a simple random sample selection process (Creswell, 2013). Upon approval by the IRB, we posted a series of three recruitment letters (with 2 weeks between each posting) to PSCs through an online professional forum, ASCA Scene. We also posted our recruitment letter on ASCA Aspects, a monthly e-newsletter. Data were collected over a period of 6 weeks. PSCs who elected to participate were directed to the electronic informed consent document and the survey.
Instrumentation
Demographic Questionnaire
Participants completed a questionnaire with write-in options for both age and gender and forced-choice responses to gather racial-ethnic identity, years working as a licensed school counselor, the region in which they practiced, and grade levels in which the participants worked. Our four independent variables were collected through the demographic questionnaire. Participants indicated their experiences, if any, with trans students, experiences with postgraduate training on trans issues, and personal relationships with trans people.
Gender Identity Counselor Competency Scale
The Gender Identity Counselor Competency Scale (GICCS), a revised version of the Sexual Orientation Counselor Competency Scale (Bidell, 2005), was used to assess PSC competence, the dependent variable in the study. This is the instrument best suited for intended measurement of self-perceived competence (Bidell, 2012; O’Hara et al., 2013). Bidell (2005) developed the instrument based on Sue and colleagues’ (1992) research of multicultural counseling competencies, with the domains of attitudinal awareness, knowledge, and skills. Bidell (2005) reported the Cronbach’s alpha of .90, with subscale scores for internal consistency of .88 for the Awareness subscale, .71 for the Knowledge subscale, and .91 for the Skills subscale (Bidell, 2005, 2012). Test-retest reliability for the overall instrument was found to be .84, with .85 for the Awareness subscale, .84 for the Knowledge subscale, and .83 for the Skills subscale (Bidell, 2005). The GICCS is a 29-item self-report assessment on a 7-point Likert scale (where 1 is not at all true and 7 is totally true). Examples of questions include: “I have received adequate clinical training and supervision to counsel transgender clients” and “The lifestyle of a transgender client is unnatural or immoral” (O’Hara et al., 2013, p. 242). Cronbach’s alpha in the present study was .70, adequate for our analysis.
Awareness Subscale. The Awareness subscale consists of 10 items focused on counselors’ attitudinal awareness and prejudice about trans clients, including statements like “It would be best if my clients viewed a [cisgender] lifestyle as ideal” and “I think that my clients should accept some degree of conformity to traditional [gender] values” (Bidell, 2005, p. 273). Cronbach’s alpha for the Awareness subscale has been reported as .88 (Bidell, 2005) and was .89 in the present sample. Self-awareness and reflection are critical skills for counselors in examining deeply held biases and beliefs and in asking culturally responsive questions to strengthen the therapeutic alliance.
Knowledge Subscale. This subscale of the GICCS consists of eight items focused on counselors’ experiences and skills with trans clients, including statements like “I am aware that counselors frequently impose their values concerning [gender] upon [trans] clients” and “I am aware of institutional barriers that may inhibit [trans] clients from using mental health services” (Bidell, 2005, p. 273). Cronbach’s alpha for the Knowledge subscale was reported as .76 (Bidell, 2005), and was .73 in the present sample. Counselors who impose their own values on a client may cause rifts in the therapeutic alliance and could potentially even harm clients.
Skills Subscale. This subscale of the GICCS consists of 11 items focused on counselors’ experiences and skills with trans clients, including statements like “I have experience counseling [trans male] clients” and “I have received adequate clinical training and supervision to counsel [trans] clients” (Bidell, 2005, p. 273). Cronbach’s alpha for the Skills subscale was reported as .91 (Bidell, 2005) but was .75 in the present sample. Counselors working with trans students need to understand the importance of evolving language and terminologies; utilize affirmative, celebratory, and liberating counseling; and have knowledge of and connection to medical providers who support gender-affirming interventions.
Data Analysis Procedures
Data Cleaning
We first screened the data to ensure it was usable, reliable, and valid to proceed with statistical analyses. We continued data cleaning by coding the demographic variable of GI 1 through 4: cisfemale (1); cismale (2); nonbinary, trans, and/or genderqueer (3); and agender (4). Racial-ethnic identities were coded 1 through 10: American Indian or Alaska Native (1); Asian or Asian American (2); Black or African American (3); Hispanic, Latino, or Spanish Origin (4); Middle Eastern or North African (5); Native Hawaiian or Other Pacific Islander (6); White (7); Some Other Race, Ethnicity, or Origin (8); Prefer Not to Answer (9); and Multiracial Identity (10). PSC location was also coded 1 through 6: Midwest (1), Northeast (2), South (3), West (4), Puerto Rico or other U.S. Territories (5), and Other (6). Last of the demographic variables, we coded PSC School Level 1 through 4: Elementary (1), Middle School (2), High School (3), and Other (4). In addition, we cleaned variables highlighting PSC professional and personal training and experiences with trans persons. The first variable was dummy coded to reflect participants who had worked with trans students (1; n = 297, 76.3%) and participants who indicated not working with trans students (0; n = 92, 23.7%). The next variable, PSC postgraduate training, was dummy coded for use in data analyses, reflecting those who indicated they engaged in postgraduate training (1; n = 193, 49.6%) and participants who indicated they did not engage in postgraduate training (0; n = 196, 50.4%). The final variable was dummy coded to reflect participants who know someone who is trans outside of the school setting (1; n = 93, 23.9%) and those participants who do not know someone who is trans outside of the school setting (0; n = 296, 76.1%). Per Bidell (2005), we started by reverse scoring coded GICCS items and created new variables for the GICCS total mean score, attitudinal Awareness, Skills, and Knowledge subscales.
Data Analysis
Post–data cleaning, we entered all the data from the demographic questionnaire and the GICCS into SPSS 26. To best answer the research questions, we used a series of standard multiple regression analyses to determine “the existence of a relationship and the extent to which variables are related, including statistical significance” (Sheperis et al., 2017, p. 131). Although multiple regression analysis can be used in prediction studies, it can also be used to determine how much of the variation in a dependent variable is explained by the independent variables, which is what we intended to measure (Johnson, 2001). Our independent variables were four categorical variables measured by our demographic questionnaire: PSC GI, postgraduate training, PSC work with trans students, and PSC personal relationships with someone who is trans. Our dependent variable was school counselor competence in working with trans students, as measured by the GICCS (Bidell, 2005).
There are many assumptions to consider when conducting a multiple regression analysis, including (a) two or more continuous or categorical independent variables, (b) a continuous dependent variable, (c) independence of residuals (or observations), (d) linearity (both between dependent variable and each of the independent variables, and between the dependent variable and the independent variables as a whole), (e) homoscedasticity, (f) absence of multicollinearity, (g) no significant outliers, and (h) normally distributed residuals (Flatt & Jacobs, 2019). The research variables met assumptions (a) and (b) in conducting multiple regressions. In analyzing data in SPSS, independence of residuals was determined by using the Durbin-Watson statistic, which ranges in value from 0 to 4, with a value near 2 indicating no correlation between residuals. Assumption (c) was met, as the Durbin-Watson value found was 1.46 (Savin & White, 1977). Additionally, we plotted a scatterplot using variables, as well as a partial regression with each of the independent variables and the dependent variable, and observed linear relationships, attending to the assumptions of linearity (d; i.e., a linear relationship between dependent and independent variables) and homoscedasticity (e; i.e., residuals are equal for all values of the predicted dependent variable). Homoscedasticity was also assessed by visual inspection of a plot of studentized residuals versus unstandardized predicted values. To assess the absence of multicollinearity (f), we considered the variance inflation factors (VIF) indicated in the coefficients table (Flatt & Jacobs, 2019). We found VIF values ranging from 1.01 to 1.05, indicating an absence of multicollinearity (f). VIF is a measure of the amount of multicollinearity in a set of multiple regression variables (Flatt & Jacobs, 2019). We checked for unusual points (g): outliers, high leverage points, and highly influential points. We did identify a significant outlier (−3.10) in case number 133 by examining the range of standardized residuals ([−3.10 to 2.34]), which is outside the common cut-off range of three standard deviations (SD). We then inspected the studentized deleted residual values and found a value in case number 133 (−3.15), which falls outside the common cut-off range of 3 SD.
Additionally, we determined two cases of problematic leverage values that were greater than the safe value of 0.2 (0.36 and 0.23). The cases that violated assumptions were filtered out and the standard multiple regression analysis was run again. This time, the data did not violate assumptions (a) through (g). Last, we observed normally distributed standardized residuals (h). To determine if any cases were influential in the data, we examined the Cook’s Distance values, which ranged from .000 to .090. As there were no values above 1, there were no highly influential points. To answer the first research question (the relationship between PSC factors and levels of PSC self-perceived competence in working with trans students in schools as measured by total scores on the GICCS), we used a standard multiple regression analysis (Sheperis et al., 2017). To answer research questions 2 through 4, we conducted standard multiple regression analyses using the Awareness, Knowledge, and Skills subscales as the dependent variables, respectively.
Results
Correlations Between Variables of Interest
Prior to the regression analysis, we examined correlations between the variables: PSC GI (cisfemale, cismale, trans, agender), having worked with trans students, postgraduate training experiences, personally knowing someone who is trans, the GICCS Awareness subscale, the GICCS Skills subscale, the GICCS Knowledge subscale, and the GICCS total score. Correlations of variables of interest are found in Table 2. There were multiple significant correlations as determined by Pearson product moment correlations (r). The GICCS total score was significantly correlated with the Awareness subscale (r = −.65, p < .001), the Skills subscale (r = .83, p < .001), and the Knowledge subscale (r = .66, p < .001). The Awareness subscale was significantly correlated with the Skills subscale (r = −.26, p < .001) and the Knowledge subscale (r = .30, p < .001). The Knowledge subscale was also significantly correlated with the Skills subscale (r = .30, p < .001). In examining demographic factors, cisfemale GI was significantly correlated with cismale GI (r = −.90, p < .001), trans GI (r = −.37, p < .001), and agender GI (r = −.21, p < .001). Additionally, cisfemale GI was significantly correlated with having worked with trans students (r = −.12, p = .036), as well as the GICCS total score (r = −.14, p = .005), the Skills subscale (r = −.14, p = .005), and the Knowledge subscale (r = −.15, p = .003). Cismale GI was significantly correlated with the GICCS total score (r = .11, p = .038), the Skills subscale (r = .12, p = .017), and the Knowledge subscale (r = .11, p = .003). Trans GI was significantly correlated with personally knowing someone who is trans (r = .12, p = .002), as well as with the GICCS total score (r = .12, p = .034). Having worked with trans students was significantly correlated with the GICCS total score (r = .41, p <.001), the Skills subscale (r = .55, p < .001), and the Awareness subscale (r = −.11,
p = .032). Postgraduate training was significantly correlated with many variables, including personally knowing someone who is trans (r = .14, p = .005), and with the GICCS total scores (r = .36, p < .001), the Skills subscale (r = .41, p < .001), the Knowledge subscale (r = .19, p < .001), and the Awareness subscale (r = −.10, p = .040). Last, personally knowing someone who is trans was significantly correlated with the GICCS total score (r = .35, p < .001), the Skills subscale (r = .29, p < .001), the Knowledge subscale
(r = .25, p < .001), and the Awareness subscale (r = −.22, p < .001).
Table 2
Correlation Table for Variables of Interest
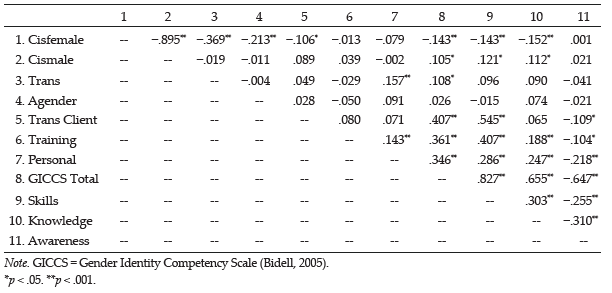
Model 1: PSC Competency
R² for the overall model was 35.2%, with an adjusted R² of 34.1%, a small to moderate size according to Cohen (1988). PSC factors significantly predicted levels of PSC self-perceived competence in working with trans students in schools, F(6, 381) = 34.430, p < .001. In examining beta weights (β), having worked with trans students received the strongest weight in the model (β = .35), followed by postgraduate training (β = .29) and personally knowing someone who is trans (β = .27). The variable with the most weight, having worked with trans students, had a structure coefficient (rs) of .67, and rs2 was 45.2%, meaning that of the 35.2% effect (R2), this variable accounts for 45.2% of the explained variance by itself. This shows that PSCs’ competence is increased by experiences with trans students, engaging in postgraduate trainings, and personally knowing someone who is trans. A summary of regression coefficients and standard errors can be found in Table 3.
Table 3
Multiple Linear Regression Analyses Exploring Professional School Counselor Competence
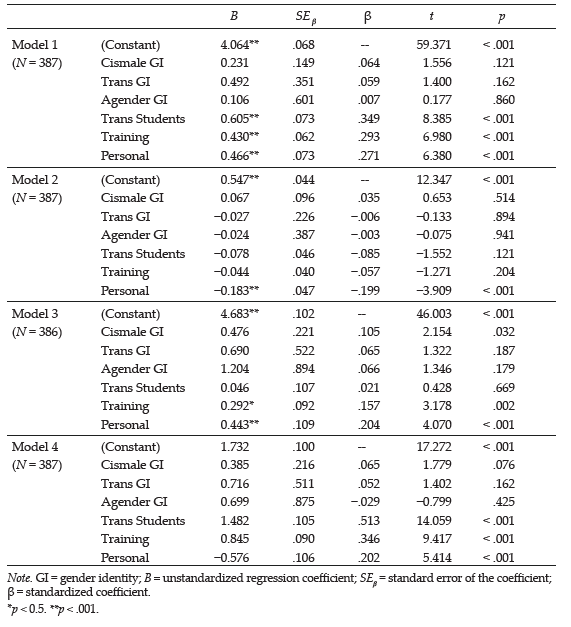
Model 2: PSC Awareness
R² for the overall model was 5.8%, with an adjusted R² of 6.2%, a very small effect size (Cohen, 1988). PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personal relationship with someone who is trans) significantly predicted awareness of PSC self-perceived competence in working with trans students in schools, F(6, 380) = 3.873, p = .001. Personally knowing someone who is trans was the only significant predictor in this model. We examined the regression coefficients and corresponding data (β = −.20, rs = −0.90, rs2 = 80%). Of the 5.8% effect (R²), personally knowing someone who is trans accounted for 80% of the explained variance by itself.
Model 3: PSC Knowledge
R² for the overall model was 10.3%, with an adjusted R² of 8.9%, a small effect size (Cohen, 1988). PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personal relationship with someone who is trans) significantly predicted knowledge of PSC self-perceived competence in working with trans students in schools, F(6, 379) = 7.257, p < .001. Personally knowing someone who is trans, postgraduate training, and cismale GI were all significant in this model. Personally knowing someone who is trans received the strongest weight in the model (β = .20, rs = .76), followed by postgraduate training (β = .16, rs = .58) and cismale GI (β = .12, rs = .35). After examining regression coefficients and corresponding data, we determined that of the 10.3% effect (R2), personally knowing someone who is trans accounted for 58.3% of the explained variance by itself. These findings demonstrate that PSC knowledge is strongly supported through fostering personal relationships with trans people.
Model 4: PSC Skills
R² for the overall model was 50.2%, with an adjusted R² of 49.5%, a medium effect size according to Cohen (1988). PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personal relationship with someone who is trans) significantly predicted self-perceived PSC skills in working with trans students in schools, F(6, 380) = 63.945, p < .001. Having worked with trans students, postgraduate training, and personally knowing someone who is trans were all significant in this model. Having worked with trans students received the strongest weight in the model (β = .51), followed by postgraduate training (β = .35) and personally knowing someone who is trans (β = .20). After examining regression coefficients and corresponding data, we determined that of the 50.2% effect (R2), having worked with trans students accounted for 79% of the explained variance by itself. Counselors can augment their skills by staying updated on appropriate language and terminologies and by fostering relationships with affirming providers and medical professionals in the community.
Discussion
The most salient finding in this model is that PSCs who worked with trans students were strongly positively correlated with GICCS total scores (r = .61, p < .001). This finding may indicate that increased exposure to trans students may subsequently increase competency in working with trans populations. Our research findings supplement existing studies that reported a relationship between affirming attitudes toward trans students and professional exposure to trans people (Salpietro et al., 2019; Simons, 2021). Avoidance of counseling trans students because of discomfort is not only unethical (ASCA, 2016b) but inhibits a PSC’s ability to develop their GI competence (Henry & Grubbs, 2017). Thus, it is imperative that PSCs receive opportunities to work with trans students (through practicum or internship experiences); consult with experienced, gender-affirming PSCs who have worked with trans students; and “expose themselves to published texts . . . films . . . [and] service-learning activities . . . to gain a better understanding of the experiences of [trans] persons” (O’Hara et al., 2013, p. 251). Additionally, PSCs must engage in constant self-reflection, introspection, and processing of biases and worldviews to provide culturally competent care to trans students.
Counseling Competence
Postgraduate training was moderately positively correlated with GICCS total score (r = .43, p < .001), indicating that additional postgraduate training in trans issues increased competence in the present sample (Model 1). This is consistent with extant literature, which demonstrated that PSCs who received postgraduate training were more competent in providing affirming services to trans students compared to PSCs who had not received the training (Salpietro et al., 2019; Shi & Doud, 2017). Finally, the presence of personal relationships with trans people was moderately positively correlated with GICCS total scores (r = .47, p < .001). These results support current literature in that PSCs who currently have or have had personal relationships with trans people were more competent in providing affirming services to trans students (GLSEN et al., 2019; O’Hara et al., 2013; Salpietro et al., 2019; Simons, 2021).
Awareness
We explored the relationship between PSC factors on the Awareness subscale of the GICCS in the second research question (Model 2). In examining coefficients for the model, having personal relationships with trans people is associated with a decrease in GICCS Awareness subscale scores, a weak, negative correlation (r = −.19, p = .001). This finding may indicate that people who did not know someone personally who is trans would score slightly higher on the Awareness subscale. These unexpected findings are contrary to existing research, which reported that engaging in personal relationships with trans people increased affirming attitudes and mitigated negative attitudes (Henry & Grubbs, 2017; Salpietro et al., 2019). Because of the lack of practical significance of PSC factors (i.e., GI, postgraduate training, PSC work with trans students, and PSC personal relationship with someone who is trans) on the Awareness subscale, these results should be considered with caution.
Knowledge
In the third research question, we explored the relationship between PSC factors on the Knowledge subscale of the GICCS (Model 3). In examining coefficients for the model, PSC cisgender male GI was moderately positively correlated with the Knowledge subscale scores (r = .476, p = .032), indicating that cismale PSCs scored moderately higher on the Knowledge subscale when compared with other PSC gender identities in the present sample. One possible explanation is the present study’s sample of cisfemales (N = 368, 94.6%) and cismales (N = 17, 4.4%). Within this sample, the ages of the cismale PSCs could reflect a time in which counselor education programs increased attention to diversity, whereas this was not always a main tenet in training among older PSCs (who may be more represented by cisfemale PSCs in this sample [Bemak & Chung, 2008]). Presently, the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015) requires accredited counselor education programs to deliver a counseling curriculum that includes specific attention to social and cultural diversity, an essential foundation of competent counselors. Additionally, PSC postgraduate training was weakly positively correlated with Knowledge subscale scores (r = .292, p = .002), which supports the literature that PSCs who engage in professional training opportunities outside of graduate school increase their knowledge of trans students and trans issues (Salpietro et al., 2019; Shi & Doud, 2017). Having personal experiences with trans people was moderately positively correlated with Knowledge subscale scores (r = .434, p < .001), indicating that those PSCs who personally knew a trans person felt more confident and competent in their knowledge about trans students and issues. This supports current literature (GLSEN et al., 2019; Henry & Grubbs, 2017; O’Hara et al., 2013; Salpietro et al., 2019) showing that PSCs who intentionally engaged in and fostered personal relationships with trans people reported greater competence.
Skills
Finally, we explored the relationship between PSC factors (GI, postgraduate training, PSC work with trans students, and PSC personal relationship with someone who is trans) on the Skills subscale of the GICCS in research question 4 (Model 4). In examining coefficients for the model, having worked with trans students was moderately positively correlated with Skills subscale scores (r = .545, p < .001), which may indicate that PSCs who work with trans students will be more likely to employ the necessary supports to ensure growth in “academic, career and social/emotional development” (ASCA, 2016a, para. 1). This is supported by literature in which researchers reported number of students worked with and “interpersonal contact” (personal exposure) as positive predictors of affirmative counselor competence (Bidell, 2012; Farmer et al., 2013). PSCs play an essential role in advocating for and removing barriers for trans students, which improves trans students’ well-being, academic success, and interpersonal growth. PSC postgraduate training was strongly positively correlated with Skills subscale scores (r = .845, p < .001), which may indicate that PSCs who engage in professional development opportunities and trainings gain essential skills for working with trans students. This finding is consistent with extant research that reported the importance of postgraduate training and professional development opportunities on trans topics (Bidell, 2012; Frank & Cannon, 2010; GLSEN et al., 2019; O’Hara et al., 2013). Finally, knowing someone personally who is trans was moderately positively correlated with Skills subscale scores (r = .576, p < .000), which may mean that having familiarity and exposure to trans folks increases PSC’s self-perceived skills.
Implications
Professional School Counselors
Based on the results of our study, PSCs who worked with trans students reported significantly higher scores of overall self-perceived competence compared to PSCs who had not worked with trans students. Specifically, our results indicate a link between PSCs having worked with trans students and higher scores on the Knowledge subscale. The GICCS Knowledge subscale addresses PSC knowledge of trans psychosocial issues (Bidell, 2005). This supports the idea that PSCs who work with self-identified trans students have a deeper understanding of the social and psychological challenges faced by trans people, and these experiences increase their comfort in working with trans students. All PSCs are required to protect and support the well-being of queer and trans youth and must have foundational knowledge and familiarity with trans students and issues (ASCA, 2016b). PSCs must attend professional development offerings on trans issues, and counselor education programs must provide increased time and attention to discussing trans issues, clients, and students.
PSC postgraduate training experiences are significantly linked to an overall increase in scores on the GICCS, indicating that PSC postgraduate experiences contribute to PSCs feeling more confident and competent in working with trans students. We conceptualized postgraduate training experiences as any training or education focused on trans persons or issues that a PSC received after their graduate program education. These results indicate that to increase competence and provide affirming, ethical care to trans students, PSCs should engage in some type of postgraduate training on trans issues and students, especially if they are unfamiliar with trans issues. These results are congruent with other studies, which found no significance in the relationship between groups on the Awareness subscale, but significant relationships on both the Knowledge and Skills subscales, with professional training experiences (Bidell, 2005; Rutter et al., 2008). PSCs are therefore encouraged to join professional organizations that promote best practices in working with trans students, like WPATH, the HRC, and SAIGE, as these organizations often offer professional development opportunities. It is essential that PSCs seek out trainings that are specific to trans students and issues, attend to unique psychosocial barriers, outline best practices, describe social/medical affirming care, and provide an overview of ethical and legal issues.
Of all the variables in the present study, PSCs knowing someone who identifies as trans was significantly linked to an increase in overall confidence and competence, as well as a significant increase in both Knowledge and Skills. Surprisingly, PSCs who indicated they did not know someone who identified as trans scored slightly higher on the Awareness subscale scores when compared with PSCs who did. The Awareness subscale of the GICCS examines a PSC’s self-awareness of anti-trans biases and stigmatization (Bidell, 2005). This result is contrary to existing research, which reported that engaging in personal relationships with trans folks increased affirming attitudes and mitigated negative attitudes (Henry & Grubbs, 2017; Salpietro et al., 2019). The link between a PSC personally knowing someone who is trans and a counselor’s competence in knowledge and skills supports extant literature that speaks to the importance of non–work-related experiences with trans people (e.g., personal, familial, social) and an increase in counselors’ competence in working with trans students (Whitman & Han, 2017). It is important that PSCs continue to monitor and increase their personal engagement with trans communities, as this significantly links to PSCs feeling more comfortable and more competent in working with trans students. Personal experiences may include fostering connections to trans family members, friends, and trans people through community organizations (GLSEN et al., 2019; Henry & Grubbs, 2017; Salpietro et al., 2019). Given the findings of our study, it is important for PSCs to connect to affirming resources in their communities. PSCs may consider exploring the multitude of resources offered by GLAAD (glaad.org), the National Center for Transgender Equality (NCTE; transequality.org), and PFLAG (pflag.org).
Counselor Education Programs
Our results indicate that those PSCs who engage in professional development are more competent than those who do not. Professional counseling organizations (i.e., ASCA) and accrediting bodies (i.e., CACREP) mandate that school counselors-in-training receive formal training in social and cultural diversity (F.2; CACREP, 2015), including multicultural counseling competencies (F.2.c.; CACREP, 2015), and deliver a comprehensive “counseling program that advocates for and affirms all students . . . including . . . gender, gender identity and expression” (ASCA, 2016a, para. 3). Although current standards call for the inclusion of LGBTQIA+ issues within counselor education curricula, the reality is that counselors-in-training receive minimal training in working with trans and gender-expansive students (Frank & Cannon, 2010; O’Hara et al., 2013). It is imperative that CE programs and counselor educators broaden the scope of learning about trans issues, going beyond the minimal requirements (CACREP, 2015) and providing depth and rigor in gender-related coursework in diversity courses. This research supports other emergent literature which recommends that counselor education programs offer additional, specific courses related to affectional and sexual identities (LGBQ+), and gender-expansive identities (trans, nonbinary), as covering specific issues and populations increases counselor competency (Bidell, 2012; Henry & Grubbs, 2017; O’Hara et al., 2013, Salpietro et al., 2019).
Limitations and Directions for Future Research
Limitations of the study include potential social desirability factors and inattentive responding, which may influence the quality of the data, as the study relied on self-report. Particularly, we note that the findings of higher self-awareness for PSCs who did not know someone who identified as trans could be a potential result of social desirability factors. Although the present study confirms that certain professional and personal factors contribute to PSCs increased competence in working with trans students in the present sample, additional research should be conducted. Also, much of our sample consisted of White ciswomen and, therefore, we caution readers about generalizing these findings to school counselors outside of those identities. The revised GICCS has not been used in many studies focusing on trans populations and additional research is needed to assess its validity with PSCs and trans youth (Bidell, 2005, 2012). Future researchers should consider additive studies that more deeply examine the types of professional development opportunities that promote PSC competency, including length, location, modality, themes, and expertise of presenter(s). Knowing these factors is important for crafting and delivering meaningful and competence-fostering professional development opportunities for PSCs. Also, future studies should examine unique nuances within trans groups, such as nonbinary and gender-fluid students (Toomey et al., 2018), and highlight the voices of trans students of color (Vance et al., 2021). Finally, future studies should also include demographic factors like religiosity and spirituality and their correlation to PSC GI competence, building on the work of Farmer and colleagues (2013).
Conclusion
This study highlights the need for increased attention to trans issues in many domains: among PSCs, within school counseling training programs, and in existing professional development offerings. ASCA mandates that PSCs be advocates for trans students, but there is a lack of attention to trans issues in school counseling training programs, leading PSCs to feel unprepared and to seek outside professional development offerings. The study also highlights the importance of building community and connections with trans people in and outside of professional settings, leading to increased PSC competence in professional settings. PSCs should continue to learn about the evolving language, trends, and needs of the trans community, ideally from those who are part of that community. Additionally, PSCs should engage with and use resources from professional trans-affirming organizations, such as WPATH, HRC, SAIGE, GLAAD, NCTE, and PFLAG.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
ALGBTIC LGBQQIA Competencies Taskforce. (2013). Association for Lesbian, Gay, Bisexual, and Transgender Issues in counseling competencies for counseling with Lesbian, Gay, Bisexual, Queer, Questioning, Intersex, and Ally individuals. Journal of LGBT Issues in Counseling, 7(1), 2–43. https://doi.org/10.1080/15538605.2013.755444
American Civil Liberties Union. (2021). Legislation affecting LGBTQ rights across the country 2021.
https://www.aclu.org/legislation-affecting-lgbt-rights-across-country
American School Counselor Association. (2016a). ASCA ethical standards for school counselors. https://www.schoolcounselor.org/getmedia/f041cbd0-7004-47a5-ba01-3a5d657c6743/Ethical-Standards.pdf
American School Counselor Association. (2016b). The school counselor and transgender/gender-nonconforming youth. https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Transgender-Gender-noncon
American School Counselor Association. (2019). ASCA school counselor professional standards & competencies.
https://www.schoolcounselor.org/getmedia/a8d59c2c-51de-4ec3-a565-a3235f3b93c3/SC-Competencies.pdf
Bemak, F., & Chung, R. C.-Y. (2008). New professional roles and advocacy strategies for school counselors: A multicultural/social justice perspective to move beyond the nice counselor syndrome. Journal of Counseling & Development, 86(3), 372–381. https://doi.org/10.1002/j.1556-6678.2008.tb00522.x
Bidell, M. P. (2005). The Sexual Orientation Counselor Competency Scale: Assessing attitudes, skills, and knowledge of counselors working with lesbian, gay, and bisexual clients. Journal of Counselor Education and Supervision, 44(4), 267–279. https://doi.org/10.1002/j.1556-6978.2005.tb01755.x
Bidell, M. P. (2012). Examining school counseling students’ multicultural and sexual orientation competencies through a cross-specialization comparison. Journal of Counseling & Development, 90(2), 200–207.
https://doi.org/10.1111/j.1556-6676.2012.00025.x
Burgess, C. M., Batchelder, A. W., Sloan, C. A., Ieong, M., & Streed, C. G., Jr. (2021). Impact of the COVID-19 pandemic on transgender and gender diverse health care. The Lancet, 9(11), 729–731.
https://doi.org/10.1016/S2213-8587(21)00266-7
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed). Routledge.
Cole, E. R. (2009). Intersectionality and research in psychology. American Psychologist, 64(3), 170–180. https://doi.org/10.1037/a0014564
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards
Creswell, J. W. (2013). Research design: Qualitative, quantitative, and mixed methods approaches (4th ed.). SAGE.
Farmer, L. B., Welfare, L. E., & Burge, P. L. (2013). Counselor competence with lesbian, gay, and bisexual clients: Differences among practice settings. Journal of Multicultural Counseling and Development, 41(4), 194–209. https://doi.org/10.1002/j.2161-1912.2013.00036.x
Flatt, C., & Jacobs, R. L. (2019). Principle assumptions of regression analysis: Testing, techniques, and statistical reporting of imperfect data sets. Advances in Developing Human Resources, 21(4), 484–502.
https://doi.org/10.1177/1523422319869915
Frank, D. A., II, & Cannon, E. P. (2010). Queer theory as pedagogy in counselor education: A framework for diversity training. Journal of LGBT Issues in Counseling, 4(1), 18–31. https://doi.org/10.1080/15538600903552731
Ginicola, M. M., Smith, C., & Filmore, J. M. (2017). Affirmative counseling with LGBTQI+ people. American Counseling Association.
Gay, Lesbian, & Straight Education Network, American School Counselor Association, American Council for School Social Work, & School Social Work Association of America. (2019). Supporting safe and healthy schools for lesbian, gay, bisexual, transgender, and queer students: A national survey of school counselors, social workers, and psychologists. GLSEN. https://www.glsen.org/sites/default/files/2019-11/Supporting_Saf
e_and_Healthy_Schools_%20Mental_Health_Professionals_2019.pdf
Grant, J. M., Mottet, L. A., Tanis, J., Harrison, J., Herman, J. L., & Keisling, M. (2011). Injustice at every turn: A report of the National Transgender Discrimination Survey. National Center for Transgender Equality and National Gay and Lesbian Task Force. https://transequality.org/sites/default/files/docs/resources/NTDS_Report.pdf
Henry, H. L., & Grubbs, L. (2017). Best practices for school counselors working with transgender students. In G. R. Walz & J. C. Bleuer (Eds), Ideas and research you can use: VISTAS 2016. https://bit.ly/HenryTrans2017
Human Rights Campaign. (2018). 2018 LGBTQ Youth Report. https://bit.ly/HRCLGBTQReport
Israel, G. D. (2013). Determining sample size. Agricultural Education and Communication Department, UF/IFAS Extension. https://bit.ly/Israel2013SampleSize
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. https://transequality.org/sites/default/file
s/docs/usts/USTS-Full-Report-Dec17.pdf
Johnson, B. (2001). Toward a new classification of nonexperimental quantitative research. Educational Researcher, 30(2), 3–13. https://doi.org/10.3102/0013189X030002003
Kosciw, J. G., Clark, C. M., Truong, N. L., & Zongrone, A. D. (2020). The 2019 National School Climate Survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation’s schools. GLSEN. https://www.glsen.org/sites/default/files/2020-10/NSCS-2019-Full-Report_0.pdf
Landén, M., & Innala, S. (2000). Attitudes toward transsexualism in a Swedish national survey. Archives of Sexual Behavior, 29(4), 375–388. https://doi.org/10.1023/A:1001970521182
McBee, C. (2013). Towards a more affirming perspective: Contemporary psychodynamic practice with trans* and gender non-conforming individuals. The University of Chicago School of Social Service Administration (Org.) Advocates’ Forum: The University of Chicago, 37–52. The University of Chicago. https://crownschool.uchicago.edu/contemporary-psychodynamic-trans-and-gender-non-conforming-individuals
Norton, A. T., & Herek, G. M. (2012). Heterosexuals’ attitudes toward transgender people: Findings from a national probability sample of U.S. adults. Sex Roles, 68, 738–753. https://doi.org/10.1007/s11199-011-0110-6
O’Hara, C., Dispenza, F., Brack, G., & Blood, R. A. C. (2013). The preparedness of counselors in training to work with transgender clients: A mixed methods investigation. Journal of LGBT Issues in Counseling, 7(3), 236–256. https://doi.org/10.1080/15538605.2013.812929
Reisner, S. L., White, J. M., Dunham, E. E., Heflin, K., Begenyi, J., Cahill, S., & Project VOICE Team. (2014). Discrimination and health in Massachusetts: A statewide survey of transgender and gender nonconforming adults. The Fenway Institute. http://fenwayfocus.org/wp-content/uploads/2014/07/The-Fenway-Institut
e-MTPC-Project-VOICE-Report-July-2014.pdf
Rutter, P. A., Estrada, D., Ferguson, L. K., & Diggs, G. A. (2008). Sexual orientation and counselor competency: The impact of training on enhancing awareness, knowledge and skills. Journal of LGBT Issues in Counseling, 2(2), 109–125. https://doi.org/10.1080/15538600802125472
Salpietro, L., Ausloos, C., & Clark, M. (2019). Cisgender professional counselors’ experiences with trans* clients. Journal of LGBT Issues in Counseling, 13(3), 198–215. https://doi.org/10.1080/15538605.2019.1627975
Savin, N. E., & White, K. J. (1977). The Durbin-Watson Test for serial correlation with extreme sample sizes or many regressors. Econometrica, 45(8), 1989–1996. https://doi.org/10.2307/1914122
Sheperis, C. J., Young, J. S., & Daniels, M. H. (2017). Counseling research: Quantitative, qualitative, and mixed methods (2nd ed.). Pearson.
Shi, Q., & Doud, S. (2017). An examination of school counselors’ competency working with lesbian, gay and bisexual and transgender (LGBT) Students. Journal of LGBT Issues in Counseling, 11(1), 2–17.
https://doi.org/10.1080/15538605.2017.1273165
Simmons University Library. (2019). Anti-Oppression: Anti-Transmisia. https://simmons.libguides.com/anti-opp
ression/anti-transmisia
Simons, J. D. (2021). School counselor advocacy for gender minority students. PLoS ONE, 16(3), e0248022. https://doi.org/10.1371/journal.pone.0248022
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Counseling & Development, 70(4), 477–486. https://doi.org/10.1002/j.1556-6676.1992.tb01642.x
Toomey, R. B., Syvertsen, A. K., & Shramko, M. (2018). Transgender adolescent suicide behavior. Pediatrics, 142(4), e20174218. https://doi.org/10.1542/peds.2017-4218
Transgender Law Center. (2021). National equality map. https://transgenderlawcenter.org/equalitymap
Vance, S. R., Jr., Boyer, C. B., Glidden, D. V., & Sevelius, J. (2021). Mental health and psychosocial risk and protective factors among Black and Latinx transgender youth compared with peers. JAMA Network Open, 4(3), e213256. https://doi.org/10.1001/jamanetworkopen.2021.3256
Wang, T., Solomon, D., Durso, L. E., McBride, S., & Cahill, S. (2016). State anti-transgender bathroom bills threaten transgender people’s health and participation in public life: Policy brief. The Fenway Institute and Center for American Progress. https://fenwayhealth.org/wp-content/uploads/2015/12/COM-2485-Transgender-Bathroom-Bill-Brief_v8-pages.pdf
Whitman, C. N., & Han, H. (2017). Clinician competencies: Strengths and limitations for work with transgender and gender non-conforming (TGNC) clients. International Journal of Transgenderism, 18(2), 154–171. https://doi.org/10.1080/15532739.2016.1249818
Williams, A. J., Jones, C., Arcelus, J., Townsend, E., Lazaridou, A., & Michail, M. (2021). A systematic review and meta-analysis of victimisation and mental health prevalence among LGBTQ+ young people with experiences of self-harm and suicide. PLoS ONE, 16(1), e0245268.
https://doi.org/10.1371/journal.pone.0245268
Clark D. Ausloos, PhD, NCC, LPC, LPSC, is a clinical assistant professor at the University of Denver. Madeline Clark, PhD, NCC, ACS, LPC (VA), LPCC (OH), is an associate professor at the University of Toledo. Hansori Jang, PhD, NCC, is an assistant professor at Hankuk University of Foreign Studies. Tahani Dari, PhD, NCC, LPC (MI), LPSC, is an assistant professor at the University of Toledo. Stacey Diane Arañez Litam, PhD, NCC, CCMHC, LPCC-S, is an assistant professor at Cleveland State University. Correspondence may be addressed to Clark D. Ausloos, 15578 John F. McCarthy Way, Perrysburg, OH 43551, clark.ausloos@du.edu.
Aug 20, 2021 | Volume 11 - Issue 3
Alexander T. Becnel, Lillian Range, Theodore P. Remley, Jr.
In a national sample of current school counselors with membership in the American School Counselor Association (N = 226), we examined the prevalence of suicide training among school counselors as well as differences in suicide assessment self-efficacy and workplace anxiety between school counselors who were exposed to student suicide and those who were not. The results indicate that 38% of school counselors were not prepared for suicide prevention during graduate training. Although school counselors’ exposure to suicide was not related to their workplace anxiety, those who were exposed to a student suicide attempt had higher suicide assessment self-efficacy scores than those who were not. This study demonstrates the impact of suicide exposure on school counselors and the need for additional suicide assessment training.
Keywords: school counselors, suicide, suicide assessment, self-efficacy, workplace anxiety
Suicide continues to be a growing concern for young people in the United States. Suicide is the second leading cause of death among children between the ages of 11 and 18, claiming the lives of 2,127 middle school– and high school–aged children in 2019 alone (Centers for Disease Control and Prevention [CDC], 2021). In 2019, a nationwide survey found that 18.8% of high school students reported seriously considering attempting suicide, 15.7% reported making a plan to attempt suicide, and 8.9% reported attempting suicide (Ivey-Stephenson et al., 2019). As youth suicide rates continue to rise (National Institute of Mental Health [NIMH], 2019), it is becoming increasingly important to understand how school counselors are prepared to work with suicidal youth, as well as the impact of suicidality on them.
Children and adolescents spend significant amounts of time at school, making school counselors the primary suicide and risk assessors for this population (American School Counselor Association [ASCA], 2020b). School counselors are more likely to assess youth for suicide risk than any other mental health professional (Schmidt, 2016). In 2002, a national study of ASCA members found that 30% of professional school counselors experienced a suicide-related crisis event while they were graduate student interns (Allen et al., 2002). In a more recent study, about two thirds of school counselors reported that they were conducting multiple suicide assessments each month (Gallo, 2018). Stickl Haugen et al. (2021) found that 79.8% of school counselors worked with a student who had previously attempted suicide and 36.7% experienced a student’s death by suicide. As school counselors become more frequently exposed to student suicide, it is important to understand their preparation for this role and the impact of these events on the school counselors themselves.
School Counselor Suicide and Crisis Training
Although school counselors are often exposed to student suicide, many school counselors lack appropriate crisis intervention and suicide assessment training (Allen et al., 2002; Springer et al., 2020; Wachter Morris & Barrio Minton, 2012) and lack confidence in their ability to assess students for suicide risk (Gallo, 2018; Schmidt, 2016). About 20 years ago, one third of school counselors entered the field without any formal crisis intervention coursework and nearly 60% did not feel adequately prepared to handle a school crisis event (Allen et al., 2002). Ten years later, school counselors did not fare any better, with less than a quarter of school counselors reporting that they completed a course in crisis intervention and nearly two thirds reporting that a crisis intervention course was not even offered during their master’s program (Wachter Morris & Barrio Minton, 2012). Not surprisingly, therefore, school counselors feel unprepared. In a national survey, 44% of school counselors reported being unprepared for a student suicide attempt, and 57% reported being unprepared for a student’s death by suicide (Solomonson & Killam, 2013). In another national survey, Gallo (2018) found that only 50% of school counselors thought that their training adequately prepared them to assess suicidal students, and only 59% felt prepared to recognize a student who was at risk. These results are especially troubling considering that the Council for Accreditation of Counseling and Related Educational Programs (CACREP) requires school counselor education programs to provide both suicide prevention and suicide assessment training (CACREP, 2015).
Exposure to Suicide and Self-Efficacy
Mental health professionals often question their professional judgment following an exposure to suicide (Sherba et al., 2019; Thomyangkoon & Leenars, 2008). Consequently, it is imperative to explore school counselor self-efficacy in the aftermath of a student suicide. Self-efficacy is the degree to which individuals believe that that they can achieve self-determined goals, and individuals are more likely to be successful in achieving those goals simply by belief in their success (Bandura, 1986). Counselor self-efficacy is defined as counselors’ judgment of their ability to provide counseling to their clients (Larson et al., 1992). As counselors spend more years in practice, their self-efficacy increases (Goreczny et al., 2015; Kozina et al., 2010; Lent et al., 2003). Further, counselor education faculty have significantly higher levels of suicide assessment self-efficacy than their students (Douglas & Wachter Morris, 2015). The relationship between counselor self-efficacy and work experience is well documented, so it is imperative to control for years of counseling experience as a potential covariate when studying other factors that can affect counselor self-efficacy.
Although the literature regarding school counselors’ exposure to suicide is sparse, more studies have focused on the experiences of related professions, such as clinical counselors, social workers, psychiatrists, and psychologists. In a national survey, 23% of clinical counselors experienced a client’s death by suicide at some point in their career (McAdams & Foster, 2002). In the aftermath of their clients’ deaths by suicide, those counselors reported a loss of self-esteem and an increase of intrusive thoughts. They increased referrals for hospitalization for clients at risk, gave increased attention to signs for suicide, and increased their awareness of legal liabilities in their practices. In a study of community-based mental health professionals who experienced a client death by suicide, one third considered changing careers and about 15% considered early retirement in the aftermath of the suicide (Sherba et al., 2019). Psychologists who felt responsible for the death were more likely to experience a sense of professional incompetence (Finlayson & Graetz Simmonds, 2018). Among psychiatrists, those who experienced a patient’s suicidal death were more likely in the future to suggest hospitalization for patients who showed risk signs for suicide (Greenberg & Shefler, 2014). Additionally, 20% of the psychiatrists in Thomyangkoon and Leenars’s (2008) study considered changing professions after experiencing a patient death by suicide. Given the similarities in these professions, it is reasonable to suggest that school counselors may feel more anxious about their jobs following a suicide exposure.
To date, there are only three published studies that explore suicide exposures among school counselors (Christianson & Everall, 2008; Gallo et al., 2021; Stickl Haugen et al., 2021). In a qualitative study, high school counselors felt a lack of personal support from their fellow staff members and noted the importance of self-care in the aftermath of a student death by suicide. Additionally, those who lost students to suicide thought that a lack of practice standards made it difficult to navigate these difficult situations (Christianson & Everall, 2008). In another qualitative study, elementary school counselors who worked with suicidal students recognized their important work in preventing suicide but also reported a lack of suicide prevention training opportunities tailored toward working with young children (Gallo et al., 2021). In a quantitative study, most school counselors thought that a student’s death by suicide left both personal and professional impacts on their lives. These school counselors most often reported low mood, a sense of guilt or responsibility, and preoccupation with the incident as personal impacts. They also identified heightened awareness of suicide risk, more professional caution around suicide, and seeking additional training as professional impacts. The researchers suggested that future studies should determine if the number of student deaths by suicide influences the impact of the suicide exposure (Stickl Haugen et al., 2021). However, this study did not examine anxiety, an important personal impact, nor did it examine self-efficacy in dealing with suicide attempts, a more likely occurrence than suicide deaths.
Research Questions
The following research questions guided this study:
- What is the prevalence of graduate and postgraduate training in suicide prevention, crisis intervention, and suicide postvention among current school counselors?
- Are there differences in suicide assessment self-efficacy between school counselors exposed and not exposed to student deaths by suicide and suicide attempts, controlling for years of school counseling experience as a covariate?
- Does the number of suicide exposures relate to school counselors’ level of suicide assessment self-efficacy when controlling for years of school counseling experience as a covariate?
- Are there differences in workplace anxiety between school counselors exposed and not exposed to student deaths by suicide and suicide attempts, controlling for years of school counseling experience as a covariate?
Method
Procedure
We obtained approval from our university’s Human Subjects Protection Review Committee prior to conducting this study. Using a random number generator, we randomly selected 5,000 members from the ASCA member directory to receive a link to the survey. When potential participants clicked the link, they viewed and agreed to an informed consent statement before they were permitted to view the survey. This statement also informed participants that they could stop participation or withdraw their participation at any time. Upon agreement to the informed consent statement, participants were directed to the survey. This online survey was administered via Qualtrics, which allowed them to respond anonymously.
Participants
From the 5,000 potential participants, 422 began the survey. From these participants, 101 opened the survey and did not answer any questions, 5 did not agree to the informed consent statement, 29 reported that they were not current school counselors, and 60 did not complete the survey. Thus, 226 of the 5,000 ASCA members completed the survey (4.52%). An a priori power analysis (Cohen, 1992) with a power of .8, a medium effect size, and α = .05 determined that the required sample size for our most robust test was 175.
Participants were 226 current school counselors (201 women, 88.9%; 25 men, 11.1%). The racial categories included 192 White (85%), nine Black or African American (4%), eight “other” races (3.5%), six Asian (2.7%), five biracial or multiracial (2.2%), three American Indian or Alaska Native (1.3%), and three not reporting race (1.3%). The ethnicity categories included 210 participants (92.9%) who were not of Hispanic or Latino or Spanish origin and 16 (7.1%) who were of Hispanic or Latino or Spanish origin. The mean age was 39 years (SD = 10.68), and the mean years of experience working as a school counselor was 7 (SD = 6.98). With regard to school setting, 52 school counselors worked in an elementary or primary school (23%), 58 worked in a middle or junior high school (25.7%), 81 worked in a high school (35.8%), 19 worked in a K–12 school (8.4%), and 16 worked in another type of school not listed (7.1%). Although ASCA does not provide demographic information about their members, this sample is similar in its demographic makeup to the sample in Gilbride et al.’s (2016) study, which sought to describe the demographic identity of ASCA’s membership.
Instrumentation
The survey packet consisted of three instruments: the demographic questionnaire, the Counselor Suicide Assessment Efficacy Survey (CSAES; Douglas & Wachter Morris, 2015), and the Workplace Anxiety Scale (WAS; McCarthy et al., 2016).
Demographic Questionnaire
Using a demographic questionnaire, we asked participants to identify the following information: sex, race, ethnicity, age, years of school counseling experience, and school type (e.g., high school, middle school). Additionally, we asked participants to identify the types of suicide exposures that they have encountered in their school counseling careers. If they reported exposure to either deaths by suicide or suicide attempts, the survey followed up with additional questions about the number of exposures, the amount of time since the first suicide exposure, and the amount of time since the most recent suicide exposure. We asked participants if their schools had crisis plans or crisis teams. We also asked participants if they had training in suicide prevention, crisis intervention, and suicide postvention during graduate school and the number of postgraduate training hours in each of these areas.
CSAES
The CSAES evaluates counselors’ confidence in their ability to assess clients for suicide risk and intervene with a client at risk of suicide. It includes 25 items in four subscales: General Suicide Assessment, Assessment of Personal Characteristics, Assessment of Suicide History, and Suicide Intervention. Each item is rated on a 5-point Likert scale from 1 (not confident) to 5 (highly confident). High scores indicate high self-efficacy. Among school counselors in the original study, each subscale had good internal consistency (α = .88–.81) and acceptable goodness of fit. As suggested by Douglas and Wachter Morris (2015), we scored each subscale separately and averaged each score. This process created four comparable subscale scores.
WAS
The WAS measures participants’ job-related anxiety. This scale asks participants to rate eight items such as “I worry that my work performance will be lower than that of others at work” on a 5-point scale from 1 (strongly disagree) to 5 (strongly agree). High scores on the WAS indicate higher levels of job-related anxiety. The WAS demonstrated good internal consistency (α = .94) and acceptable goodness of fit (McCarthy et al., 2016).
Data Analysis
To address our first research question, we used descriptive statistics to examine the prevalence of training among the participants. We used analysis of covariance (ANCOVA) to detect differences in both suicide assessment self-efficacy (CSAES scores) and workplace anxiety (WAS scores) while controlling for years of school counseling experience between school counselors who were exposed to student suicide and those who were not. We considered exposure to deaths by suicide and exposure to suicide attempts as different types of exposure. Therefore, we performed a total of four ANCOVAs: (a) differences in CSAES scores between school counselors exposed to deaths by suicide and those not exposed, (b) differences in CSAES scores between school counselors exposed to suicide attempts and those not exposed, (c) differences in WAS scores between school counselors exposed to deaths by suicide and those not exposed, and (d) differences in WAS scores between school counselors exposed to suicide attempts and those not exposed. We also used analysis of variance (ANOVA) to determine the difference in years of school counseling experience between those exposed to suicide and those not exposed. To determine the relationship between the number of suicide exposures and counselor suicide assessment self-efficacy, we also completed two partial correlations between the number of exposures to student death by suicide and CSAES scores, and the number of exposures to student suicide attempts and CSAES scores.
Results
A total of 64 school counselors reported that they experienced a student death by suicide during their school counseling experience (28.3%), with a mean of 2.11 deaths (SD = 2.21). On average, their first suicide death was 6.72 years ago (SD = 5.87), and the most recent suicide death was 3.84 years ago (SD = 3.88). A total of 124 participants experienced a student suicide attempt during their school counseling experience (54.9%), with a mean of 5.36 attempts (SD = 10.54). On average, the first suicide attempt was 5.91 years ago (SD = 6.07), and the most recent attempt was 1.82 years ago (SD = 2.10). Of all 226 school counselors, 195 worked in schools that have crisis plans (86.3%), and 170 worked in schools that have crisis teams (75.2%).
Suicide Training
Regarding suicide prevention training during their graduate program, 140 (62%) received some training, but 86 (38%) received no training. Regarding crisis intervention training during their graduate program, 142 (63%) received some, but 84 (37%) received none. Regarding suicide postvention, only 87 (38.5%) received some, but 139 (61.5%) received none. The number of postgraduate training hours varied widely for each preparation type. For suicide prevention, training hours averaged 12.20 (SD = 28.61); for crisis intervention, training hours averaged 9.04 (SD = 15.51); and for suicide postvention, training hours averaged 6.45 (SD = 18.14). We removed one participant’s postgraduate training data that was more than 3 standard deviations higher than the mean. In order to better illustrate the distribution of postgraduate training hours, we grouped the number of training hours into four categories: 0 hours, 1–10 hours, 11–50 hours, and more than 50 hours of postgraduate training. Nearly a quarter of the participants (24.3%) received no postgraduate training in suicide prevention, about a third of the participants (30.5%) received no postgraduate training in crisis intervention, and half (50.4%) received no postgraduate training in suicide postvention.
To further demonstrate the disparity of suicide training, cross-tabulation was performed between graduate training and the number of postgraduate training hours. We reported this data in Table 1. Most surprisingly, 25 school counselors (11.1%) received no graduate training in suicide prevention, nor any postgraduate hours of training in suicide prevention; another 45 (19.9%) received no graduate training and only 10 or fewer hours of postgraduate training in suicide prevention, making nearly 1 in 3 school counselors unprepared to provide suicide prevention services. Crisis intervention fared similarly with 26 school counselors (11.5%) reporting no graduate training and no postgraduate training hours and 41 school counselors (18.1%) reporting no graduate training and 10 or fewer postgraduate training hours. Again, nearly 1 in 3 school counselors were not adequately prepared to provide this important service. Crisis postvention fared the worst, with 80 school counselors (35.4%) reporting that they received no graduate training and no postgraduate training hours, and 46 school counselors (20.4%) reporting no graduate training and fewer than 10 hours of postgraduate training. More than half of the school counselors surveyed are unprepared to face the aftermath of a suicide.
Table 1
Graduate Training and Postgraduate Training Hours
| Number of postgraduate training hours |
Received graduate training |
Did not receive graduate training |
|
Frequency |
Percentage |
Frequency |
Percentage |
| Suicide Prevention |
|
|
|
|
| 0 hours |
30 |
13.3 |
25 |
11.1 |
| 1–10 hours |
73 |
32.3 |
45 |
19.9 |
| 11–50 hours |
29 |
12.8 |
15 |
6.6 |
| 50 or more hours |
8 |
3.6 |
1 |
0.4 |
| Total |
140 |
62.0 |
86 |
38.0 |
|
|
|
|
|
| Crisis Intervention |
|
|
|
|
| 0 hours |
43 |
19.0 |
26 |
11.5 |
| 1–10 hours |
69 |
30.5 |
41 |
18.1 |
| 11–50 hours |
26 |
11.5 |
16 |
7.0 |
| 50 or more hours |
4 |
1.8 |
1 |
0.4 |
| Total |
142 |
63.0 |
84 |
37.0 |
|
|
|
|
|
| Suicide Postvention |
|
|
|
|
| 0 hours |
34 |
15.0 |
80 |
35.4 |
| 1–10 hours |
37 |
16.4 |
46 |
20.4 |
| 11–50 hours |
12 |
5.3 |
11 |
4.8 |
| 50 or more hours |
4 |
1.8 |
2 |
0.9 |
| Total |
87 |
38.5 |
139 |
61.5 |
Suicide Exposure and Suicide Assessment Self-Efficacy
An ANOVA indicated that school counselors exposed to a student death by suicide had significantly more years of school counseling experience (M = 11.9, SD = 7.87) than school counselors not exposed to a student death by suicide (M = 5.1, SD = 5.56): F(1, 224) = 21.512, p < .001. Controlling for years of school counseling experience as a covariate, an ANCOVA indicated that there was no significant difference between these two groups in General Suicide Assessment, F(1, 223) = .316, p = .574; Assessment of Personal Characteristics, F(1, 223) = .156, p = .694; Suicide Intervention, F(1, 223) = .028, p = .867; or Assessment of Suicide History, F(1, 223) = 1.095, p = .133.
Similarly, results of an ANOVA indicated that school counselors exposed to student suicide attempts had significantly more years of school counseling experience (M = 8.8, SD = 7.31) than counselors not exposed (M = 4.9, SD = 5.94): F(1, 224) = 8.055, p = .005. Controlling for years of school counseling experience, an ANCOVA indicated significant differences between the two groups in General Suicide Assessment, F(1, 223) = 6.014, p = .015; Assessment of Personal Characteristics, F(1, 223) = 7.140, p = .008; and Suicide Intervention, F(1, 223) = 6.671, p = .010; but not Assessment of Suicide History, F(1, 223) = .763, p = .383. Overall, effect sizes were small.
Number of Exposures and Self-Efficacy
A partial correlation between the number of suicide exposures and CSAES scores while controlling for years of school counseling experience was not statistically significant. There was no significant relationship between the number of death by suicide exposures and General Suicide Assessment, r(61) = .137, p = .285; Assessment of Suicide History, r(61) = .207, p = .104; Assessment of Personal Characteristics, r(61) = .170, p = .184; or Suicide Intervention, r(61) = .077, p = .551. Likewise, there was also no significant relationships between the number of suicide attempt exposures and General Suicide Assessment, r(121) = −.028, p = .762; Assessment of Suicide History, r(121) = .087, p = .336; Assessment of Personal Characteristics, r(121) = .131, p = .150; or Suicide Intervention, r(121) = .076, p = .401. We reported data regarding the frequency of suicide exposure in Table 2.
Suicide Exposure and Workplace Anxiety
In WAS scores, an ANCOVA revealed that there were no significant differences between school counselors exposed and not exposed to a student death by suicide when controlling for years of school counseling experience: F(1, 223) = .412, p = .522. Likewise, an ANCOVA revealed that there was no significant difference in WAS scores between school counselors exposed and not exposed to student suicide attempts when controlling for years of school counseling experience: F(1, 223) = .238, p = .626. To further illustrate the relationship between years of school counseling experience and workplace anxiety, a correlation coefficient indicated that these measures were significantly related, r(224) = −.260, p < .001.
Discussion
Among these school counselors, more than a quarter experienced a student’s death by suicide and over half experienced a student’s suicide attempt. These results are consistent with previous studies indicating that many school counselors will eventually be exposed to a student suicide during their careers (Allen et al., 2002; Gallo, 2018; Schmidt, 2016; Stickl Haugen et al., 2021). Given how common suicide experiences are, school counselors need to be trained to manage suicide-related crises.
Training
A surprising result in our study was the overall lack of suicide and crisis training reported. As seen in Table 1, nearly 2 in 5 school counselors (38%) reported that they received no suicide prevention training during their graduate education. Additionally, a quarter of the school counselors in this study reported that they received no postgraduate training in suicide prevention, and half reported between 1 and 10 hours. Thus, a sizeable portion of these school counselors were not adequately trained to incorporate suicide prevention programs into their school counseling practice. This finding echoes Gallo (2018), who reported that only 60% of school counselors felt prepared to identify students at risk for suicide. These rates are poor considering that CACREP requires suicide assessment and suicide prevention training as a standard of all counselor education programs (CACREP, 2015). Further, ASCA states that school counselors are responsible for identifying students at risk for suicide and ensuring that suicide prevention programs are in place in schools (ASCA, 2020a). The lack of training reported in this study is particularly troubling given that all of the participants in this study were members of ASCA.
Table 2
Frequency of Student Suicide Exposure
| Variable |
Frequency |
Percentage |
| Number of student deaths by suicide (n = 64) |
|
|
| 1 |
37 |
57.8 |
| 2 |
15 |
23.4 |
| 3–5 |
8 |
12.5 |
| > 5 |
4 |
6.3 |
| Years since first death by suicide (n = 64) |
|
|
| Within 1 year |
12 |
18.8 |
| 1 and 5 years |
25 |
39.0 |
| 6 and 10 years |
12 |
18.8 |
| More than 10 years |
15 |
23.4 |
| Years since most recent death by suicide (n = 64) |
|
|
| Within 1 year |
23 |
35.9 |
| Between 1 and 5 years |
26 |
40.6 |
| Between 6 and 10 years |
11 |
17.2 |
| More than 10 years |
4 |
6.3 |
| Number of student suicide attempts (n = 124) |
|
|
| 1 |
29 |
23.4 |
| 2 |
29 |
23.4 |
| 3–5 |
44 |
35.5 |
| > 5 |
22 |
17.7 |
| Years since first student attempt (n = 124) |
|
|
| Within 1 year |
30 |
24.2 |
| Between 1 and 5 years |
51 |
41.1 |
| Between 6 and 10 years |
21 |
17.0 |
| More than 10 years |
22 |
17.7 |
| Years since most recent attempt (n = 124) |
|
|
| Within 1 year |
84 |
67.7 |
| Between 1 and 5 years |
33 |
26.6 |
| Between 6 and 10 years |
6 |
4.8 |
| More than 10 years |
1 |
0.8 |
Crisis intervention training among school counselors also was poor. Comparable to the finding on suicide prevention training, a third of these school counselors reported no graduate training in crisis intervention. Further, more than a third reported that they did not receive postgraduate training hours in crisis intervention, and nearly half received between 1 and 10 hours of postgraduate training. A significant portion of these school counselors were not adequately prepared to respond to crises in their schools. These findings are slightly worse than the findings from 20 years ago when one third of a sample of school counselors reported that they entered the field with no formal crisis intervention coursework (Allen et al., 2002). However, these findings are much better than Wachter Morris and Barrio Minton’s (2012) study in which only 20% of school counselors completed a course in crisis intervention during their master’s degree program. Although preparation has increased, crisis preparation for school counseling students must continue to improve given that school counselors regularly experience crises (Wachter, 2006) and school counseling students often experience crises while still in graduate school completing their practicum or internship (Wachter Morris & Barrio Minton, 2012). The number of school counselors who experienced a student suicide event in the current study also supports the notion that school counselors regularly experience crises.
Most of these school counselors (61.5%) were not trained in their graduate programs for suicide postvention. Half of the surveyed school counselors reported that they received no postgraduate training hours in suicide postvention, with an additional 38% reported having received between 1 and 10 hours of postgraduate training. These results demonstrate that the vast majority of school counselors are not prepared to respond to a student’s suicidal death. This finding is distressing because school counselors play a vital role in the aftermath of a student suicide (Maples et al., 2005; Substance Abuse and Mental Health Services Administration [SAMHSA], 2016).
Suicide Assessment Self-Efficacy
Among these counselors, exposure to suicide alone did not make a difference with their suicide assessment self-efficacy or workplace anxiety. Years of school counseling experience appears to have a much more important role in suicide assessment self-efficacy and reduced anxiety than experiencing a student’s death by suicide. This result supports previous studies that found that years of experience has a positive relationship with self-efficacy (Douglas & Wachter Morris, 2015; Kozina et al., 2010; Lent et al., 2003). It also parallels the previous finding that the impact of a client’s suicidal death on a mental health practitioner decreases as the practitioner gains years of experience (McAdams & Foster, 2002). This result is different from Stickl Haugen et al.’s (2021) finding that school counselors who were exposed to a student death had higher levels of suicide assessment self-efficacy than those not exposed. However, Stickl Haugen et al. did not control for years of school counseling experience.
In contrast, exposure to suicide attempts did make a difference in suicide assessment self-efficacy. Even after controlling for years of experience, counselors with suicide attempt experience reported more efficacy in three of four subscales: General Suicide Assessment, Assessment of Personal Characteristics, and Suicide Intervention. One explanation for this outcome is that a student suicide attempt experience might motivate school counselors to learn about suicide and the risk factors associated. This explanation echoes Wagner et al.’s (2020) finding that counselors found additional training in the aftermath of a suicide very helpful. Many of the school counselors in the current study received no formal training, so it is possible that these experiences helped them fill in knowledge gaps, which in turn increased their self-efficacy. Training increases self-efficacy (Al-Darmaki, 2004; Mirick et al., 2016; Wachter Morris & Barrio Minton, 2012), so it is also possible that this experience worked as an in vivo training for these school counselors, increasing their self-efficacy.
Workplace Anxiety
Although mental health clinicians often experience symptoms of anxiety in the wake of a student suicide (McAdams & Foster, 2002; Sherba et al., 2019), present results suggest that a student’s death or suicide attempt does not have an impact on school counselors’ workplace anxiety. One explanation for this finding is the relationship between self-efficacy and anxiety. Overall, these school counselors had high self-efficacy scores in each of the four subscales. Previous research indicated that as self-efficacy increases, anxiety decreases (Bodenhorn & Skaggs, 2005; Gorecnzy et al., 2015; Larson et al., 1992). The death by suicide experience might not have impacted the counselors’ anxiety in this study because of their overall high self-efficacy. Another explanation is that the school counselors in this study had on average several years of experience (M = 7.05). Workplace anxiety levels decrease as school counselors spend more time on the job.
Implications
These results have several implications for school counselors and school counselor educators. First, school counselor educators and school counseling graduate programs should be aware of both the overall disparity of graduate-level suicide and crisis training as well as the benefits that training can provide to future school counselors. Regarding suicide prevention, crisis intervention, and suicide postvention, there are far too many untrained school counselors among the current body of school counselors. School counseling students are a vulnerable group when it comes to suicide assessment self-efficacy (Douglas & Wachter Morris, 2015), so it is imperative to support their professional development. School counseling graduate programs must increase their efforts to adequately train and prepare school counselors for suicide prevention, assessment, and intervention.
Second, school counselors should prepare to face the probability of having to deal with student suicide attempts and student deaths by suicide. If school counselors do not receive this training during their graduate programs, then they must seek continuing education opportunities that address suicide prevention, crisis intervention, and suicide postvention. Suicide and crisis training increases counselor self-efficacy (Mirick et al., 2016; Wachter Morris & Barrio Minton, 2012), making appropriate preparation vital. Additionally, school counselors could consider clinical supervision as a supplemental layer of support. School counselors receive supervision at much lower rates than their clinical counterparts (Perera-Diltz & Mason, 2012) even though many school counselors desire more supervision (Cook et al., 2012). Given that school counseling–focused supervision can increase self-efficacy (Tang, 2019) and school counselors feel a lack of personal support in the aftermath of a suicide (Christianson & Everall, 2008), school counselors must seek clinical supervision.
Finally, school counselor educators should consider training efforts that focus specifically on student suicide attempts. In the current study, school counselors exposed to a suicide attempt were more efficacious than school counselors not exposed to a student suicide attempt. Modeling these experiences through the use of specific role plays could help school counseling students feel more confident about their suicide assessment capabilities. Although CACREP does not require counselor education programs to provide suicide postvention training (CACREP, 2015), perhaps standards should adapt to include this important training area. Regardless, programs should also emphasize this training to best prepare school counselors.
Limitations and Suggestions for Future Research
Some factors limited this study. Although we had a national sample, we surveyed only current members of ASCA. It is possible that school counselors who are not members of ASCA might have responded differently. The study also had a low response rate (4.64%). Those school counselors who responded may be uniquely interested in this area, so the results may not reflect all school counselors. This study also did not limit the types of school counselors who could participate. It is possible that school counselors who work with younger children, such as elementary and primary school counselors, have less familiarity with suicide assessment and intervention than those school counselors who work with older children. The inclusion of these counselors could have affected the results of this study. Finally, this study did not ask participants if they graduated from a CACREP-accredited program. Because suicide prevention and assessment training are required components of CACREP-accredited programs, it is possible that school counselors who graduated from these programs may have different levels of training and self-efficacy than those trained in unaccredited programs.
For future studies, researchers should consider limiting their samples to specific levels of schooling such as elementary, middle, or high school. This change would help illustrate the nuanced differences among school counselors in different academic environments as well as increase focus on the school counselors who most often work with suicidal students. Future studies should also consider surveying a sample that includes all school counselors, not just ASCA members. Researchers should also differentiate between school counselors who graduated from CACREP-accredited programs and those who did not. Collecting this data would allow researchers to detect if there are any differences in suicide assessment training and self-efficacy between these two groups. Finally, future researchers should consider designing a study that seeks to identify the factors that most impact suicide assessment self-efficacy. Although this study showed that a suicide attempt experience could impact suicide assessment self-efficacy, other factors, such as self-confidence, could have a larger influence.
Suicide continues to be understudied in school counseling. Even though this study demonstrates the high likelihood that a school counselor will experience a student suicide, school counselors continue to report a lack of preparation in suicide prevention, crisis intervention, and suicide postvention. Although school counselors who experienced a student suicide attempt appeared to gain self-efficacy from their experiences, additional training in counseling suicidal students might help school counselors feel prepared before they face such serious situations. If additional training can help school counselors save students from suicide, then efforts must be made to adequately prepare them.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Al-Darmaki, F. R. (2004). Counselor training, anxiety, and counseling self-efficacy: Implications for training psychology students from the United Arab Emirates University. Social Behavior and Personality: An International Journal, 32(5), 429–439. https://doi.org/10.2224/sbp.2004.32.5.429
Allen, M., Burt, K., Bryan, E., Carter, D., Orsi, R., & Durkan, L. (2002). School counselors’ preparation for and participation in crisis intervention. Professional School Counseling, 6(2), 96–102.
American School Counselor Association. (2020a). The school counselor and suicide risk assessment. https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Suicide-Risk-Assessment
American School Counselor Association. (2020b). The school counselor and student mental health. https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Student-Mental-Health
Bandura, A. (Ed.). (1986). Social foundations of thought and action: A social cognitive theory. Prentice Hall.
Bodenhorn, N., & Skaggs, G. (2005). Development of the School Counselor Self-Efficacy Scale. Measurement and Evaluation in Counseling and Development, 38(1), 14–28. https://doi.org/10.1080/07481756.2005.11909766
Centers for Disease Control and Prevention. (2021). Injury center: Violence prevention: Suicide prevention. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html
Christianson, C. L., & Everall, R. D. (2008). Constructing bridges of support: School counsellors’ experiences of student suicide. Canadian Journal of Counselling, 42(3), 209–221.
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037//0033-2909.112.1.155
Cook, K., Trepal, H., & Somody, C. (2012). Supervision of school counselors: The SAAFT model. Journal of School Counseling, 10(21). https://files.eric.ed.gov/fulltext/EJ981202.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Douglas, K. A., & Wachter Morris, C. A. (2015). Assessing counselors’ self-efficacy in suicide assessment and intervention. Counseling Outcome Research and Evaluation, 6(1), 58–69. https://doi.org/10.1177/2150137814567471
Finlayson, M., & Graetz Simmonds, J. (2018). Impact of client suicide on psychologists in Australia. Australian Psychologist, 53(1), 23–32. https://doi.org/10.1111/ap.12240
Gallo, L. L. (2018). The relationship between high school counselors’ self-efficacy and conducting suicide risk assessments. Journal of Child and Adolescent Counseling, 4(3), 209–225. https://doi.org/10.1080/23727810.2017.1422646
Gallo, L. L., Rausch, M. A., Beck, M. J., & Porchia, S. (2021). Elementary school counselors’ experiences with suicidal students, Journal of Child and Adolescent Counseling, 7(1), 26–41. https://doi.org/10.1080/23727810.2020.1835419
Gilbride, D. D., Goodrich, K. M., & Luke, M. (2016). The professional peer membership of school counselors and the resources used within their decision-making. The Journal of Counselor Preparation and Supervision, 8(2). https://repository.wcsu.edu/jcps/vol8/iss2/4
Goreczny, A. J., Hamilton, D., Lubinski, L., & Pasquinelli, M. (2015). Exploration of counselor self-efficacy across academic training. The Clinical Supervisor, 34(1), 78–97. https://doi.org/10.1080/07325223.2015.1012916
Greenberg, D., & Shefler, G. (2014). Patient suicide. Israel Journal of Psychiatry & Related Sciences, 51(3), 193–198.
Ivey-Stephenson, A. Z., Demissie, Z., Crosby, A. E., Stone, D. M., Gaylor, E., Wilkins, N., Lowry, R., & Brown, M. (2019). Suicidal ideation and behaviors among high school students — Youth Risk Behavior Survey, United States, 2019. Morbidity and Mortality Weekly Report, Supplement 69(1), 47–55. https://doi.org/10.15585/mmwr.su6901a6
Kozina, K., Grabovari, N., De Stefano, J., & Drapeau, M. (2010). Measuring changes in counselor self-efficacy: Further validation and implications for training and supervision. The Clinical Supervisor, 29(2), 117–127. https://doi.org/10.1080/07325223.2010.517483
Larson, L. M., Suzuki, L. A., Gillespie, K. N., Potenza, M. T., Bechtel, M. A., & Toulouse, A. L. (1992). Development and validation of the Counseling Self-Estimate Inventory. Journal of Counseling Psychology, 39(1), 105–120. https://doi.org/10.1037/0022-0167.39.1.105
Lent, R. W., Hill, C. E., & Hoffman, M. A. (2003). Development and validation of the Counselor Activity Self-Efficacy Scales. Journal of Counseling Psychology, 50(1), 97–108. https://doi.org/10.1037/0022-0167.50.1.97
Maples, M. F., Packman, J., Abney, P., Daugherty, R. F., Casey, J. A., & Pirtle, L. (2005). Suicide by teenagers in middle school: A postvention team approach. Journal of Counseling & Development, 83(4), 397–405. https://doi.org/10.1002/j.1556-6678.2005.tb00361.x
McAdams, C. R., III., & Foster, V. A. (2002). An assessment of resources for counselor coping and recovery in the aftermath of client suicide. Journal of Humanistic Counseling, Education and Development, 41(2), 232–242.
McCarthy, J. M., Trougakos, J. P., & Cheng, B. H. (2016). Are anxious workers less productive workers? It depends on the quality of social exchange. Journal of Applied Psychology, 101(2), 279–291. https://doi.org/10.1037/apl0000044
Mirick, R. G., Bridger, J., McCauley, J., & Berkowitz, L. (2016). Continuing education on suicide assessment and crisis intervention for social workers and other mental health professionals: A follow-up study. Journal of Teaching in Social Work, 36(4), 363–379. https://doi.org/10.1080/08841233.2016.1200171
National Institute of Mental Health. (2019). Mental health information: Statistics: Suicide. https://www.nimh.nih.gov/health/statistics/suicide.shtml
Perera-Diltz, D. M., & Mason, K. L. (2012). A national survey of school counselor supervision practices: Administrative, clinical, peer, and technology mediated supervision. Journal of School Counseling, 10, 1–34. https://files.eric.ed.gov/fulltext/EJ978860.pdf
Substance Abuse and Mental Health Services Administration. (2016). Preventing suicide: A toolkit for high school. Center for Mental Health Services, Substance Abuse and Mental Health Services Administration. https://store.samhsa.gov/product/Preventing-Suicide-A-Toolkit-for-High-Schools/SMA12-4669
Schmidt, R. C. (2016). Mental health practitioners’ perceived levels of preparedness, levels of confidence and methods used in the assessment of youth suicide risk. The Professional Counselor, 6(1), 76–88. https://doi.org/10.15241/rs.6.1.76
Sherba, R. T., Linley, J. V., Coxe, K. A., & Gersper, B. E. (2019). Impact of client suicide on social workers and counselors. Social Work in Mental Health, 17(3), 279–301. https://doi.org/10.1080/15332985.2018.1550028
Solomonson, L. L., & Killam, W. (2013). A national study on crisis intervention: Are school counselors prepared to respond? Ideas and Research You Can Use: VISTAS 2013. https://www.counseling.org/docs/default-source/vistas/a-national-study-on-crisis-intervention.pdf?sfvrsn=b3b9af05_11
Springer, S., Paone, C. H., Colucci, J., & Moss, L. J. (2020). Addressing suicidality: Examining preservice school counselors’ perceptions of their training experiences. Journal of Child and Adolescent Counseling, 6(1), 18–36. https://doi.org/10.1080/23727810.2018.1556990
Stickl Haugen, J., Waalkes, P. L., & Lambie, G. W. (2021). A national survey of school counselors’ experiences with student death by suicide. Professional School Counseling, 25(1), 1–11. https://doi.org/10.1177/2156759X21993804
Tang, A. (2019). The impact of school counseling supervision on practicing school counselors’ self-efficacy in building a comprehensive school counseling program. Professional School Counseling, 23(1), 1–11. https://doi.org/10.1177/2156759X20947723
Thomyangkoon, P., & Leenars, A., (2008). Impact of death by suicide of patients on Thai psychiatrists. Suicide & Life-Threatening Behavior, 38(6), 728–740. https://doi.org/3994/10.1521/suli.2008.38.6.728
Wachter, C. A. (2006). Crisis in the schools: Crisis, crisis intervention training, and school counselor burnout (Publication No. 3221458). [Doctoral dissertation, University of North Carolina at Greensboro]. ProQuest Dissertations Publishing.
Wachter Morris, C. A., & Barrio Minton, C. A. (2012). Crisis in the curriculum? New counselors’ crisis preparation, experiences, and self-efficacy. Counselor Education and Supervision, 51(4), 256–269. https://doi.org/10.1002/j.1556-6978.2012.00019.x
Wagner, N. J., Grunhaus, C. M. L., & Tuazon, V. E. (2020). Agency responses to counselor survivors of client suicide. The Professional Counselor, 10(2), 251–265. https://doi.org/10.15241/njw.10.2.251
Alexander T. Becnel, PhD, NCC, LPC, is a doctoral candidate at the University of Holy Cross. Lillian Range, PhD, is a professor at the University of Holy Cross. Theodore P. Remley, Jr., JD, PhD, NCC, is a professor at the University of Holy Cross. Correspondence may be addressed to Alexander T. Becnel, 4123 Woodland Drive, New Orleans, LA 70131, abecnel2@uhcno.edu.
Aug 20, 2021 | Volume 11 - Issue 3
Louisa L. Foss-Kelly, Margaret M. Generali, Michael J. Crowley
The consequences of adolescent drug and alcohol use may be serious and far-reaching, forecasting problematic use or addictive behaviors into adulthood. School counselors are particularly well suited to understand the needs of the school community and to seamlessly deliver sustainable substance use prevention. This pilot study with 46 ninth-grade students investigates the impact of the Making Choices and Reducing Risk (MCARR) program, a drug and alcohol use prevention program for the school setting. The MCARR curriculum addresses general knowledge of substances and their related risks, methods for evaluating risk, and skills for avoiding or coping with drug and alcohol use. Using a motivational interviewing framework, MCARR empowers students to choose freely how they wish to behave in relation to drugs and alcohol and to contribute to the health of others in the school community. The authors hypothesized that the implementation of the MCARR curriculum would influence student attitudes, knowledge, and use of substances. Results suggest that the MCARR had a beneficial impact on student attitudes and knowledge. Further, no appreciable increases in substance use during the program were observed. Initial results point to the promise of program feasibility and further research with larger samples including assessment of longitudinal impact.
Keywords: MCARR, school counselors, drug and alcohol use, substance use prevention, motivational interviewing
Adolescent substance use continues to wreak havoc in the United States, resulting in tragic consequences for adolescents, their families, and communities. Although some substances of abuse and modes of delivery have faded in prominence, others have taken their place. For instance, data from the National Institute on Drug Abuse’s Monitoring the Future Survey reflect an alarming rise in e-cigarette use, which may predict an easier transition to combustible cigarettes and cause serious lung injuries (Johnston et al., 2020; Singh et al., 2020). Use of illicit drugs among adolescents is down, yet cannabis use has increased among younger adolescents to levels that the Food and Drug Administration has described as epidemic (Johnston et al., 2020; Yu et al., 2020). Reports have shown a rise in 30-day marijuana vaping, a common metric for assessing recent use, which has doubled or tripled among eighth, 10th, and 12th graders (Johnston et al., 2020). Concerns remain that early initiation of drug use may further fuel the United States’ ongoing opioid epidemic (D. A. Clark et al., 2020; D. J. Clark & Schumacher, 2017). Historically, alcohol has been the most prominent substance of abuse among adolescents (Substance Abuse and Mental Health Services Administration [SAMHSA], 2018); however, binge alcohol use, defined as more than five drinks on a single occasion, has been declining since the 1970s (Johnston et al., 2020). Regardless, alcohol use and its related risks, such as homicide, suicide, and motor vehicle crashes, continue to be a significant problem for youth (Hadland, 2019; Lee et al., 2018).
Among adolescent risk-taking behaviors, substance use is particularly concerning because of potential impacts on the developing brain (Jordan & Andersen, 2017; Renard et al., 2016). Adolescence offers a “window of opportunity” for the establishment of neural pathways that may protect against the development of drug and alcohol use problems (Whyte et al., 2018). Brain structure may impact function in the areas of working memory, attention, and cognitive and social skill development in adolescence (Fuhrmann et al., 2015; Randolph et al., 2013). The developmental tasks of adolescence, such as identity formation, social connectedness, and patterns of interpersonal relatedness, may also be negatively impacted by substance use (Finkeldey et al., 2020; Lee et al., 2018). Incidents of adolescent intoxication may lead to early sexual debut, high-risk sexual activity, physical altercations, or other regrettable behavior (Clark et al., 2020). Moreover, drug use has consistently been linked to depression, anxiety, and poor school performance (e.g., D’Amico et al., 2016; M. S. Dunbar et al., 2017; Ohannessian, 2014). Suicidality and non-suicidal self-injury have also been associated with substance use (e.g., Carretta et al., 2018; Gobbi et al., 2019). In a study of 4,800 adolescents, illicit drug use was more strongly associated with suicidal behavior than other high-risk behaviors (Ammerman et al., 2018). The risks of adolescent drug and other substance use are sweeping, significant, and important for informing prevention efforts.
Early identification and intervention for adolescents is critical for preventing later substance use disorders and staving off this public health problem (Levy et al., 2016). In 2011, of young adults aged 18–30 admitted for substance use disorder treatment, 74% initiated use at age 17 or younger (SAMHSA, 2014). Research suggests that the increase of lifetime problem alcohol use increases by a factor of four when adolescents drink prior to age 15, compared to those who drink prior to age 20 (Kuperman et al., 2013). The current literature identifies a clear relationship between early alcohol and marijuana use and future patterns of prescription opioid abuse (B. R. Harris, 2016). A recent study of over 1,300 adolescents found that those who screened positive for highest risk in a simple 2-question assessment were shown to have a higher number of drinking days and to be at higher risk for alcohol use disorder 3 years later (Linakis, 2019).
School Personnel as Frontline Responders to Adolescent Substance Use Risk
School personnel and the school community have important roles to play in promoting mental health and preventing substance use among students (E. T. Dunbar et al., 2019; Eschenbeck et al., 2019; Lintz et al., 2019). School-based services may range from prevention to treatment, with efficacious results demonstrated using motivational interviewing and other evidence-based approaches (Winters et al., 2012). A number of prevention programs implemented by school leaders or trained youth facilitators have demonstrated efficacy, including Youth to Youth (Wade-Mdivanian et al., 2016), an empowerment-focused, positive youth development approach for ages 13–17 in a 4-day summer conference format. Another is Refuse, Remove, Reasons (RRR; Mogro-Wilson et al., 2017), a 5-session curriculum for ages 13–17 delivered in health classrooms by clinical service providers from the community. The RRR involves caregivers and uniquely focuses on mutual aid between students.
The keepin’ it R.E.A.L. program (Hecht et al., 2003), designed for younger adolescents, Grades 6–9, involves urban or rural culturally grounded curricula focused on social norms and networking to make behavior change and has been adopted by the national Drug Abuse Resistance Education (D.A.R.E.) program. The Life Skills Training program (Botvin & Griffin, 2004), designed for middle school students, relies on cognitive behavioral principles to help students develop self-management and social skills. Also designed for middle school students, the All Stars curriculum (McNeal et al., 2004), emphasizes social skills, social norms, and debunking inaccurate beliefs about adolescent substance use, violence, and early sexual debut. All Stars uses 22 sessions, with some groups outside of class and in a one-on-one meeting format. Each of the programs described here has contributed to the efforts to prevent drug and alcohol abuse among young people; however, none of these offer a school counselor–implemented classroom guidance curriculum specifically designed for middle adolescence, including students aged 14–17 years.
The Role of School Counselors
As stable members of the school community, school counselors hold knowledge of their students and the culture of the school and surrounding community, allowing for a seamless response to student needs. The schoolwide multi-tiered system of supports (MTSS) model used to prevent and respond to academic and behavioral difficulties in children provides a structure for delivering prevention in comprehensive school counseling services (Pullen et al., 2019). MTSS utilizes student assessment for the development of tiers of intervention or support to address identified student needs in comprehensive school counseling services (Ziomek-Daigle, 2016). MTSS defines a Tier 1 intervention as primary prevention and includes evidence-based programming for all students. These interventions are used to support student knowledge, skill acquisition, and healthy decision-making and are appropriate for addressing conflict resolution, nutrition and health, and substance use.
The comprehensive school counseling model provides a sound means for delivering substance use prevention interventions. Classroom guidance education, a key responsibility of school counselors, provides an ideal opportunity to implement primary prevention of substance use for all students. However, to date no comprehensive substance use prevention program has focused specifically on delivery by school counselors.
The MCARR Program
Making Choices and Reducing Risk (MCARR) is a school counseling–based program for addressing substance use among adolescents. MCARR utilizes a structured classroom educational program. The program is implemented throughout the academic year as a Tier 1 schoolwide approach with ninth graders in a classroom setting (Ziomek-Daigle, 2016). The program involves meeting once per month to deliver psychoeducation and to engage in reflective and team-oriented learning experiences as part of a health education or related class. MCARR is a naturally sustainable intervention based on school community concepts and highly effective adolescent counseling interventions, described below.
Motivational Interviewing
The MCARR is based on motivational interviewing (MI) and risk reduction principles, both of which are well-established approaches in clinical settings (e.g., Cushing et al., 2014; DiClemente et al., 2017) and in schools (Rollnick et al., 2016). MI focuses primarily on the decision-making process, including resolving ambivalence about change and respecting the client’s autonomy to make their own choices (Miller & Rollnick, 2013). MI has been described as more of a philosophy or method of communication rather than a set of specific techniques. Alongside the Rogerian value of respect, MI offers a form of freedom by providing a validating, encouraging, and safe space to explore one’s identity and learn to make adaptive life choices. Other MI concepts include developing and amplifying discrepancies between one’s current behavior and desired behavior. MI also calls counselors to “roll with resistance” when clients verbalize a lack of desire to change or refusal to change or make healthy choices (Miller & Rollnick, 2013). Rolling with resistance is particularly helpful for adults working with adolescents familiar with authority figure conflict. These adults may quickly slide into an authoritarian tug-of-war to win the adolescent over to behaving in a certain way, inadvertently causing even more resistance. MI may be ideal for supporting adolescents who yearn for personal freedom and the right to make their own choices (Naar-King & Suarez, 2011).
Risk Reduction
Risk reduction is a widely used public health concept in drug and alcohol treatment, especially in terms of relapse prevention (Hendershot et al., 2011). Risk reduction is not directed at abstinence—rather it aims to help those who use alcohol or drugs to engage in use at a lower risk level. The concept of risk reduction is a response to data suggesting that abstinence-only approaches may not be effective for adolescents (Blackman et al., 2018). There is arguably no acceptably low risk level for adolescents. However, when used as a complement to MI, risk reduction ideas can be used to demonstrate that the ultimate decision to use can only be made by the adolescent. Instead of fighting against the developmental task of individuation, this approach could allow adolescents to freely choose whether or not to use and begin to consider future levels of substance use as an adult.
Evaluating Consequences: The CRAFFT
The CRAFFT (Car, Relax, Alone, Forget, Friends, and Trouble) is a simple screening instrument incorporated into MCARR to assess substance use consequences and identify problem substance use (Knight, 2016; Knight et al., 1999). The CRAFFT 2.0 instrument is composed of six questions related to use of drugs and alcohol in the prior year, in various situations such as use in motor vehicles, use to relax or when alone, problems with memory related to intoxication, problems with friends, and violations resulting in trouble with school or legal entities. The MCARR curriculum encourages students to consider substance use situations presented on the CRAFFT not to screen peers, but rather as “red flags” to inform healthier decision-making and action.
Neurobiological Education for Risk Literacy
In the MCARR program, students learn about the neurological and physiological impacts of substance abuse in adolescence, including neural plasticity and the functional and structural changes that may permanently affect working memory, attention, and other processes in the developing brain (Fuhrmann et al., 2015). A meta-analytic study by Day and colleagues (2015) suggested that alcohol use can lead to problems with executive functioning, including attention and mental flexibility, as well as mechanisms of self-control. Some drinking and drug use behaviors may be associated with the development of mood and anxiety-related problems (Pedrelli et al., 2016). In addition to this information, MCARR also presents the physiological impact of alcohol and specific drugs, including fatigue, muscle weakness, and damage to organs. MCARR applies these concepts to the daily routine of an adolescent, including specific examples of how these changes may impact athletic performance, academic performance, or social interactions. This information may inform decision-making and contribute to risk literacy, or the ability to consider, interpret, and act on accurate information to make decisions about whether one will engage in substance use (Nagy et al., 2017).
Refusal Skills
Adolescent expectations about the positive or negative effects of substance use may be an important factor in prevention and refusal skills (Lee et al., 2020). For instance, cannabis use is less likely when adolescents perceive it as riskier (Miech et al., 2017). Knowledge about the various impacts of drugs and alcohol have been correlated with the development of beliefs about use, including social aspects, physiological aspects, and general expectancies of use (Zucker et al., 2008). Attitudes about drugs and alcohol and their risks appear to be an important part of effective prevention efforts (Miech et al., 2017; Stephens et al., 2009). For these reasons, the development of healthy attitudes about drug and alcohol use becomes an important life task (Schulenberg & Maggs, 2002).
Peer Influence
Understanding the power of peer influence in adolescent substance use (Henneberger et al., 2019), the MCARR approach also employs the social context of the caring school community to support primary prevention efforts and promote overall student wellness. It is well documented that social pressures are particularly heightened during adolescence, when the desire to affiliate with peers and find acceptance within a peer group is highly valued (Trucco et al., 2011). During the adolescent developmental period, decision-making reference points are more likely to shift away from family and important adults and toward peer groups. According to normative social behavior theory, perceptions that most of one’s peers use drugs and alcohol may increase the likelihood of one’s own substance use (Rimal & Real, 2005). Students often overestimate the frequency and level of use of alcohol and other substances by their peers, resulting in increased likelihood of earlier experimentation (Prestwich et al., 2016). Community-building efforts have the potential to promote a climate wherein students are aware of the risks related to substance use and support positive decision-making among their peers. In this way, students can learn to advocate for others as well as themselves.
Coping and Self-Regulation
The MCARR program also emphasizes coping and emotion regulation skills, both of which are associated with decreased risk-taking behaviors among adolescents (Wills et al., 2016). Skills for coping with stress have been shown to impact future substance use (Zucker et al., 2008). The development of coping skills and substance use knowledge is combined to support informed choices and reduced risk throughout adolescence. Additionally, the MCARR curriculum includes skill-building instruction and practice on drug refusal skills, as these skills have been shown to increase self-efficacy for resisting use (Karatay & Baş, 2017). To support decision-making, students are taught how to analyze and cope with the increasing prevalence of marketing messages in video and social media. These media messages have been shown to significantly impact adolescent perceptions of substance use, resulting in calls for educational interventions to help students cope with messages that encourage substance use (Romer & Moreno, 2017). Ideally, group norms that encourage emotional well-being and self-care may facilitate a student’s receptivity to healthy messages about the risks of drug and alcohol use and may help students make choices accordingly.
Purpose of the Present Study
The purpose of this pilot study was to examine the feasibility of a primary prevention intervention delivered by school counselors targeting decision-making and attitudes around substance use in a Northeastern urban high school with ninth-grade students. We posed the following questions: First, does the MCARR program impact student attitudes and knowledge related to substance use, including perceived risk and readiness to change? Second, does the MCARR program impact substance use behaviors? Using research and literature cited above, we hypothesized that the implementation of the MCARR curriculum would influence student attitudes, knowledge, and use of substances as measured by paired-samples t-tests of data gathered prior to and following implementation of the curriculum.
Method
Participants and Sampling Procedures
This study was approved by both the school district and researchers’ university IRB. Participants of this study were 46 ninth-grade students at an urban high school (54.2% female, 45.8% male), ages 13–15 years (M = 14.13, SD = .57), who provided responses before and after participating in the MCARR program. The ethnic background of participants was as follows: 37% Hispanic or Latino, 30.4% African American, 21.7% Caucasian, 6.5% Mixed ethnic background, 2.2% Asian, and 2.2% preferred not to say.
The families of all ninth graders were notified of the MCARR lessons being delivered within their child’s dramatic arts classroom. The MCARR program and study procedures were described in the informed consent letter to parents. Students gave assent to participate by signing an assent form that was both read aloud and provided to each student. Data collection via a survey was explained along with the risks and benefits of study participation. Although this curriculum was approved for all ninth graders at the school, parents were given the option to opt their child out of the survey portion of this lesson. The study survey was given prior to their first lesson, then repeated following their ninth lesson. None of the students or families opted out of the survey portion of the MCARR program.
Measure
The survey we constructed included non-identifying demographic items, 20 Likert-type scale items, and two open-ended questions. The 20 Likert-type scale items included items from the following subscales: Substance Use Days, CRAFFT Items, Readiness to Change, and Attitudes Regarding Riskiness of Substance Use. The following sources of material informed the development of our MCARR survey: the Youth Risk Behavior Surveillance System (Kann et al., 2018); the CRAFFT 2.0 survey (Knight, 2016); Screening, Brief Intervention, and Referral to Treatment (SBIRT) screening and interviewing (S. K. Harris et al., 2014); and the National Institute on Alcohol Abuse and Alcoholism guidelines (NIAAA; 2011).
Substance use was measured by asking participants to retrospectively estimate their drug or alcohol use in the prior 30 days, a time period consistent with national surveys of youth substance use (Zapolski et al., 2017). Then participants completed six items from the CRAFFT 2.0 survey (Knight, 2016). These questions used a yes/no format, each question relating to a letter in the CRAFFT acronym describing situations or circumstances involving drug or alcohol use. Using the 30-day interval, our survey asked participants the following CRAFFT questions: “Have you ever ridden in a CAR driven by someone (including yourself) who was ‘high’ or had been using alcohol or drugs?,” “Do you ever use alcohol or drugs to RELAX, feel better about yourself or fit in?,” “Do you ever use alcohol or drugs while you are by yourself, or ALONE?,” “Do you ever FORGET things you did while using alcohol or drugs?,” “Do your FAMILY or FRIENDS ever tell you that you should cut down on your drinking or drug use?,” and “Have you ever gotten into TROUBLE while you were using alcohol or drugs?” In general, higher scores indicate higher risk for a substance use disorder (Knight, 2016; Knight et al., 2002). The CRAFFT can be used as a self-report screening tool and has been shown to have strong psychometric properties (e.g., Dhalla et al., 2011; Levy et al., 2004). In an early study of 538 participants, the CRAFFT demonstrated sensitivity, specificity, and predictive value in identifying adolescents with substance use problems (Knight et al., 2002). Further, in a study of 4,753 participants, the CRAFFT 2.0 demonstrated strong concurrent and predictive validity (Shenoi et al., 2019).
Readiness to Change items were informed by components of the brief negotiation interview in SBIRT (D’Onofrio et al., 2005; Whittle et al., 2015) and substance use attitudes items were adapted from the Youth Risk Behavior Surveillance System (Kann et al., 2018). Knowledge items were developed based on NIAAA guidelines and norms, such as alcohol volume in various types of beverages and adult low-risk use levels (Alcohol Research Editorial Staff, 2018). Item composition of the four subscales is presented in the supplementary materials (Appendix A).
Procedure
The MCARR is intended to be a universal intervention for students in at least one grade, with ninth graders as the primary target population. MCARR consists of nine learning modules each lasting 1.5 hours, offered once per month in a classroom with 15–20 students in each meeting. The nine modules are: 1) Orientation to the MCARR Program and Community Building, 2) Personal Coping, 3) Attitudes and Messages About Use, 4) Alcohol, 5) Community Partners, 6) Assumptions and Low-Risk Limits, 7) Cannabis, Nicotine, and E-Cigarettes, 8) Opioids and Cocaine, and 9) Review: Decisions. Each module, including the learning objectives and a summary of activities, is provided in Appendix B.
The education curriculum (MCARR) was delivered each month within the dramatic arts classroom at the school. School counselors delivered the curriculum via overhead slides and brief videos, with related reflection and application activities throughout. Each lesson closed with an exit slip used to support and monitor lessons learned that day. The exit slip helped remind students of key concepts in the lesson and gave counselors a sense of the relevance of the lesson and the content retained. In this way, the school counselor could address confusing concepts in the following lesson as needed and continuously improve the program. The survey was administered via computer immediately preceding the presentation of the first module and at the conclusion of the last module.
Results
Descriptive statistics for major study variables are provided in Table 1. Data reported by participants on each of the four scales used in the study were evaluated by way of paired-samples t-tests. The first research question explored the impact of the MCARR curriculum on substance use attitudes and knowledge. We observed significant increase in readiness to change, t(45) = −3.70, p < .001, and a significant increase in knowledge and perception about the riskiness of substance use, t(45) = −4.91, p < .001. The second research question compared student self-reported substance use pre- and post-intervention. Notably, we observed no significant change in substance use days. The absence of significant increases in use may be important during an adolescent period when experimentation with substance use typically increases. However, CRAFFT scores did increase from pre- to post-intervention: t(45) = −2.41, p = .020. We further explored significant increases in the CRAFFT at both the participant level and the item level (see Table 2). Individual CRAFFT items data revealed clear differences in relative impact of each item, with the motor vehicle item “Have you ever ridden in a CAR driven by someone (including yourself) who was ‘high’ or had been using alcohol or drugs?” presenting prominently with the greatest increase in student endorsement (3 at pre- to 12 at post-intervention). The Relax item remained the same (2 at both pre- and post). There was an increase in reported use of substances while Alone (1 to 4), and a slight increase in scores related to Family/Friends (0 to 1), Forgetting (0 to 3), and Trouble (0 to 1). During the course of the study, students with a total CRAFFT items score of 2 or higher, the established CRAFFT 2.0 threshold for suggesting higher risk (Shenoi et al., 2019), rose from 1 participant to 7 participants (N = 46). These results appear to be linked to the motor vehicle item in the CRAFFT, which could point to a potential refinement of MCARR, discussed below. The design of this study does not permit these patterns to be conclusively linked with participation in the MCARR program; however, our data provide promising preliminary evidence for the effectiveness of the MCARR curriculum for targeting attitudes around substance use and readiness for behavior change.
Discussion
In this pilot study, we show the feasibility of the MCARR program delivered by school counselors to ninth-grade students in an urban setting. This primary prevention curriculum was particularly well-suited for universal implementation in the classroom setting. Promising results included significant increases in healthy attitudes about substances, which are important in helping prevent future substance use problems (Nagy et al., 2017). Pre- and post-CRAFFT data showed a slight increase in risky use, with a clear increase in students riding in a car with a person who had been using substances. It should be noted that participants spending more time with others who use while in motor vehicles, not the student’s own use per se, appears to have contributed substantially to the rise in overall CRAFFT scores in this particular study. In fact, because we did not see an appreciable change in self-reported substance use from pre- to post-intervention, which remained low, we believe the uptick in the CRAFFT motor vehicle item does not reflect the adolescent reporting on their own use in a car, but rather an increase in riding with others who are under the influence of substances. This finding has significance for future curriculum development, which may increase content related to managing situations involving substance use and motor vehicles.
Table 1
Means and Standard Deviations of Major Study Variables
| |
Pre-Assessment |
Post-Assessment |
|
| |
Mean |
SD |
Mean |
SD |
t |
p |
| Substance Use Days |
0.58 |
3.04 |
0.59 |
2.21 |
0.09 |
.930 |
| CRAFFT Items |
0.15 |
0.52 |
0.52 |
1.03 |
−2.41 |
.020 |
| Readiness to Change |
12.10 |
7.84 |
16.50 |
7.85 |
−3.70 |
< .001 |
| Attitudes Regarding Riskiness of Substance Use |
14.33 |
2.87 |
16.65 |
2.80 |
−4.91 |
< .001 |
|
|
|
|
|
|
|
|
|
|
Note. Maximum score for Substance Use Days: 30, CRAFFT Items: 6, Readiness to Change: 24, and Attitudes
Regarding Riskiness of Substance Use: 18. No significant changes were found in substance use days.
Significance was also found in increased readiness for change among those reporting current substance use, perhaps reflecting the utility of offering decisional freedom during a time associated with increasing ambivalence about the choice to initiate drug and alcohol use (Hohman et al., 2014). We did not observe appreciable increases in substance use or abuse across the length of the program, which is noteworthy, as the adolescent years may commonly be a time of increasing substance experimentation and use (Johnston et al., 2020).
Adolescent drug and alcohol use continues to cause ongoing, intractable public health problems (Whyte et al., 2018). As established members of the school community network, school counselors are ideally positioned to play an important role in preventing and reducing drug and alcohol use and other mental health problems among adolescents (Fisher & Harrison, 2018; Haskins, 2012). Their unique integrated role in the school and in the students’ school life offers background knowledge of student experience, positive relational influence, and access to school and community resources when support is needed. Moreover, a program such as MCARR, which aligns with the roles of school personnel such as the school counselor, could lead to a sustainable approach for mitigating teen substance use. The spirit of MI, allowing individuals to make life choices freely, is a sound approach to counseling adolescents and lends itself well to school counseling interventions and changes in attitudes (Naar-King & Suarez, 2011). Further, the MCARR curriculum may increase general knowledge of drugs and alcohol and related risk literacy, which likely contributes to delaying drug and alcohol use until adulthood (Kuperman et al., 2013). Consistent with prior research, the MCARR may effectively use student connections and interaction to teach skills for coping with challenges related to drug and alcohol use (Henneberger et al., 2019).
Table 2
Pre- and Post-MCARR CRAFFT Endorsement by Item and Total Score
| CRAFFT Individual Items Endorsed |
|
Pre |
Post |
1. Have you ever ridden in a car driven by someone (including yourself) who
was “high” or had been using alcohol or drugs? |
no |
43 |
34 |
| yes |
3 |
12 |
| 2. Do you ever use alcohol or drugs to relax, feel better about yourself, or fit in? |
no |
44 |
44 |
| yes |
2 |
2 |
| 3. Do you ever use alcohol or drugs while you are by yourself, or alone? |
no |
45 |
42 |
| yes |
1 |
4 |
| 4. Do you ever forget things you did while using alcohol or drugs?
|
no |
46 |
43 |
| yes |
0 |
3 |
5. Do your family or friends ever tell you that you should cut down on your
drinking or drug use? |
no |
46 |
45 |
| yes |
0 |
1 |
| 6. Have you ever gotten into trouble while using alcohol or drugs? |
no |
46 |
45 |
| |
yes |
0 |
1 |
| Student CRAFFT Total Scoresa |
Score |
Pre |
Post |
| |
0 |
41 |
33 |
| |
1 |
4 |
6 |
| |
2 |
0 |
5 |
| Number of items endorsed “yes” |
3 |
1 |
1 |
| |
4 |
0 |
0 |
| |
5 |
0 |
1 |
| |
6 |
0 |
0 |
a This portion of the table shows the number of students endorsing 0–6 items on the CRAFFT survey. Students with higher-risk scores (total score ≥ 2) changed from 1 student at pre to 7 students at post.
Study Limitations
Although an important first step in developing and evaluating a primary prevention curriculum for school personnel, this pilot study has limitations worth noting. First, this is an open trial. Thus, without a matched control group or an active control group in the context of an experiment, we cannot make strong causal inferences about the impact of our intervention on youth attitudes and readiness for change around substance use. Second, this was a small sample study. A larger sample would more strongly speak to the robustness of the results we report here. Third, the incorporation of more comprehensive substance use instruments into the survey would improve the strength of inferences about the impact of MCARR on substance use behavior. Fourth, the assessment of readiness to change was only applicable to students self-reporting substance use. Future studies may focus on readiness to change among all participants, regardless of substance use self-assessment. In addition, in spite of the specificity of the curriculum, it is possible that the methods of content delivery and program facilitation were impacted by the personal style or characteristics unique to the instructor. These factors could be measured in future work. Lastly, we did not include a follow-up assessment that could speak to the robustness of our observed effects and longer term impact on substance use as students move through their high school years and beyond.
Future Directions
Research is needed to establish evidence to support school interventions such as the MCARR. Future research may support the efficacy of the MCARR through measures of substance use knowledge, risk assessment evaluation competencies, and attitudes about substance use. Longitudinal studies may explore how the MCARR impacts students’ future drug and alcohol use, and research should also explore the relevance of the MCARR for students of different ages, in a variety of school settings, across a diverse range of communities. Future research should focus on the feasibility of this curriculum in online learning environments, including possible delivery adaptations and content considerations. Collaboration with school staff, health educators, and other members of the school community could improve any impact offered by the MCARR. Using school counselors, the MCARR curriculum offers promise in mitigating drug and alcohol use, heading off problematic use, and encouraging students to intentionally reflect on their choices. For the longer term, we hope that a program such as the MCARR could be sustainable, drawing on the roles that counselors already fill within schools and with bridges to counselor education programs, where new school counselors enter the workforce with the MCARR program on board. Problematic substance use continues to plague our youth. We hope that the MCARR, realized through school counselors and other school professionals, can address an important gap via a systemic approach to mitigating youth substance use risk. For the future, we are planning a larger, multi-school study that addresses the limitations just noted and a deeper phenotyping of student characteristics and assessment of processes that may affect the potency of our program (e.g., student relationship with school, peer and parental attitudes about substance use).
In conclusion, with MCARR we provide the profession with a promising primary preventive school-based approach for reducing adolescent substance use behaviors. MCARR is the first program designed specifically to harness the professional strengths of school counselors, with findings in an open trial suggesting impacts on student attitudes and knowledge related to substance use including perceived risk and readiness to change, but without appreciable increases in substance use during a high-risk period. Future work in a randomized trial and follow-up across the high school years will further evaluate MCARR impacts and sustainability in the school milieu.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alcohol Research Editorial Staff. (2018). Drinking patterns and their definitions. Alcohol Research, 39(1), 17–18.
Ammerman, B. A., Steinberg, L., & McCloskey, M. S. (2018). Risk-taking behavior and suicidality: The unique role of adolescent drug use. Journal of Clinical Child & Adolescent Psychology, 47(1), 131–141. https://doi.org/10.1080/15374416.2016.1220313
Blackman, S., Bradley, R., Fagg, M., & Hickmott, N. (2018). Towards ‘sensible’ drug information: Critically exploring drug intersectionalities, ‘Just Say No,’ normalisation and harm reduction. Drugs: Education, Prevention and Policy, 25(4), 320–328. https://doi.org/10.1080/09687637.2017.1397100
Botvin, G. J., & Griffin, K. W. (2004). Life skills training: Empirical findings and future directions. The Journal of Primary Prevention, 25, 211–232. https://doi.org/10.1023/B:JOPP.0000042391.58573.5b
Carretta, C. M., Burgess, A. W., Dowdell, E. B., & Caldwell, B. A. (2018). Adolescent suicide cases: Toxicology reports and prescription drugs. The Journal for Nurse Practitioners, 14(7), 552–558.
https://doi.org/10.1016/j.nurpra.2018.05.010
Clark, D. A., Donnellan, M. B., Durbin, C. E., Nuttall, A. K., Hicks, B. M, & Robins, R. W. (2020). Sex, drugs, and early emerging risk: Examining the association between sexual debut and substance use across adolescence. PLoS ONE, 15(2). https://doi.org/10.1371/journal.pone.0228432
Clark, D. J., & Schumacher, M. A. (2017). America’s opioid epidemic: Supply and demand considerations. Anesthesia & Analgesia, 125(5), 1667–1674. https://doi.org/10.1213/ANE.0000000000002388
Cushing, C. C., Jensen, C. D., Miller, M. B., & Leffingwell, T. R. (2014). Meta-analysis of motivational interviewing for adolescent health behavior: Efficacy beyond substance use. Journal of Consulting and Clinical Psychology, 82(6), 1212–1218. https://doi.org/10.1037/a0036912
D’Amico, E. J., Tucker, J. S., Miles, J. N. V., Ewing, B. A., Shih, R. A., & Pedersen, E. R. (2016). Alcohol and marijuana use trajectories in a diverse longitudinal sample of adolescents: Examining use patterns from age 11 to 17 years. Addiction, 111(10), 1825–1835. https://doi.org/10.1111/add.13442
Day, A. M., Kahler, C. W., Ahern, D. C., & Clark, U. S. (2015). Executive functioning in alcohol use studies: A brief review of findings and challenges in assessment. Current Drug Abuse Reviews, 8(1), 26–40. https://doi.org/10.2174/1874473708666150416110515
Dhalla, S., Zumbo, B. D., & Poole, G. (2011). A review of the psychometric properties of the CRAFFT instrument: 1999–2010. Current Drug Abuse Reviews, 4(1), 57–64. https://doi.org/10.2174/1874473711104010057
DiClemente, C. C., Corno, C. M., Graydon, M. M., Wiprovnick, A. E., & Knoblach, D. J. (2017). Motivational interviewing, enhancement, and brief interventions over the last decade: A review of reviews of efficacy and effectiveness. Psychology of Addictive Behaviors, 31(8), 862–887. https://doi.org/10.1037/adb0000318
D’Onofrio, G., Pantalon, M. V., Degutis, L. C., Fiellin, D. A., & O’Connor, P. G. (2005). Development and implementation of an emergency practitioner-performed brief intervention for hazardous and harmful drinkers in the emergency department. Academic Emergency Medicine, 12(3), 249–256.
https://doi.org/10.1197/j.aem.2004.10.021
Dunbar, E. T., Jr., Nelson, M. D., & Tarabochia, D. S. (2019). Substance use disorders: What school counselors should know. Journal of School Counseling, 17(21), 1–29.
Dunbar, M. S., Tucker, J. S., Ewing, B. A., Pedersen, E. R., Miles, J. N. V., Shih, R. A., & D’Amico, E. J. (2017). Frequency of e-cigarette use, health status, and risk and protective health behaviors in adolescents. Journal of Addiction Medicine, 11(1), 55–62. https://doi.org/10.1097/ADM.0000000000000272
Eschenbeck, H., Lehner, L., Hofmann, H., Bauer, S., Becker, K., Diestelkamp, S., Kaess, M., Moessner, M., Rummel-Kluge, C., & Salize, H.-J. (2019). School-based mental health promotion in children and adolescents with StresSOS using online or face-to-face interventions: A study protocol for a randomized controlled trial within the ProHEAD Consortium. Trials, 20. https://doi.org/10.1186/s13063-018-3159-5
Finkeldey, J. G., Longmore, M. A., Giordano, P. C., & Manning, W. D. (2020). Identifying as a troublemaker/partier: The influence of parental incarceration and emotional independence. Journal of Child and Family Studies, 29, 802–816. https://doi.org/10.1007/s10826-019-01561-y
Fisher, G. L., & Harrison, T. C. (2018). Substance abuse: Information for school counselors, social workers, therapists, and counselors (6th ed.). Pearson.
Fuhrmann, D., Knoll, L. J., & Blakemore, S.-J. (2015). Adolescence as a sensitive period of brain development. Trends in Cognitive Sciences, 19(10), 558–566. https://doi.org/10.1016/j.tics.2015.07.008
Gobbi, G., Atkin, T., Zytynski, T., Wang, S., Askari, S., Boruff, J., Ware, M., Marmorstein, N., Cipriani, A., Dendukuri, N., & Mayo, N. (2019). Association of cannabis use in adolescence and risk of depression, anxiety, and suicidality in young adulthood: A systematic review and meta-analysis. JAMA Psychiatry, 76(4), 426–434. https://doi.org/10.1001/jamapsychiatry.2018.4500
Hadland, S. E. (2019). Epidemiology and historical drug use patterns. In J. W. Welsh & S. E. Hadland (Eds.), Treating adolescent substance use: A clinician’s guide (pp. 3–14). Springer.
Harris, B. R. (2016). Talking about screening, brief intervention, and referral to treatment for adolescents: An upstream intervention to address the heroin and prescription opioid epidemic. Preventive Medicine, 91, 397–399. https://doi.org/10.1016/j.ypmed.2016.08.022
Harris, S. K., Louis-Jacques, J., & Knight, J. R. (2014). Screening and brief intervention for alcohol and other abuse. Adolescent Medicine State of the Art Review, 25(1), 126–156.
Haskins, N. H. (2012). The school counselor’s role with students at-risk for substance abuse. VISTAS 2012, Vol. 1, 1–8. American Counseling Association.
Hecht, M. L., Marsiglia, F. F., Elek, E., Wagstaff, D. A., Kulis, S., Dustman, P., & Miller-Day, M. (2003). Culturally-grounded substance use prevention: An evaluation of the keepin’ it R.E.A.L. curriculum. Prevention Science, 4, 233–248. https://doi.org/10.1023/A:1026016131401
Hendershot, C. S., Witkiewitz, K., George, W. H., & Marlatt, G. A. (2011). Relapse prevention for addictive behaviors. Substance Abuse Treatment, Prevention, and Policy, 6(17). https://doi.org/10.1186/1747-597X-6-17
Henneberger, A. K., Gest, S. D., & Zadzora, K. M. (2019). Preventing adolescent substance use: A content analysis of peer processes targeted within universal school-based programs. The Journal of Primary Prevention, 40, 213–230. https://doi.org/10.1007/s10935-019-00544-5
Hohman, Z. P., Crano, W. D, Siegel, J. T., & Alvaro, E. M. (2014). Attitude ambivalence, friend norms, and adolescent drug use. Prevention Science, 15(1), 65–74.
https://doi.org/10.1007/s11121-013-0368-8
Johnston, L. D., Miech, R. A., O’Malley, P. M., Bachman, J. G., Schulenberg, J. E., & Patrick, M. E. (2020). Monitoring the future national survey results on drug use: 1975–2019: Overview, key findings on adolescent drug use. Institute for Social Research, The University of Michigan.
Jordan, C. J., & Andersen, S. L. (2017). Sensitive periods of substance abuse: Early risk for the transition to dependence. Developmental Cognitive Neuroscience, 25, 29–44.
https://doi.org/10.1016/j.dcn.2016.10.004
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B., Lowry, R., Chyen, D., Whittle, L., Thornton, J., Lim, C., Bradford, D., Yamakawa, Y., Leon, M., Brener, N., & Etheir, K. A. (2018). Morbidity and mortality weekly report: Youth risk behavior surveillance—United States, 2017. Surveillance Summaries, 67(8), 1–114. https://doi.org/10.15585/mmwr.ss6708a1
Karatay, G., & Baş, N. G. (2017). Effects of role-playing scenarios on the self-efficacy of students in resisting against substance addiction: A pilot study. The Journal of Health Care Organization, Provision, and Financing, 54, 1–6. https://doi.org/10.1177/0046958017720624
Knight, J. R. (2016). The CRAFFT interview (version 2.0). Boston Children’s Hospital. https://crafft.org/wp-content/uploads/2019/02/CRAFFT-2.0_Clinician-Interview.pdf
Knight, J. R., Sherritt, L., Shriter, L. A., Harris, S. K., & Chang, G. (2002). Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of Pediatric Adolescent Medicine, 156(6), 607–614. https://doi.org/10.1001/archpedi.156.6.607
Knight, J. R., Shrier, L. A., Bravender, T. D., Farrell, M., Vander Bilt, J., & Shaffer, H. J. (1999). A new brief screen for adolescent substance abuse. Archives of Pediatric Adolescent Medicine, 153(6), 591–596. https://doi.org/10.1001/archpedi.153.6.591
Kuperman, S., Chan, G., Kramer, J. R., Wetherill, L., Bucholz, K. K., Dick, D., Hesselbrock, V., Porjesz, B., Rangaswamy, M., & Schuckit, M. (2013). A model to determine the likely age of an adolescent’s first drink of alcohol. Pediatrics, 131(2), 242–248. https://doi.org/10.1542/peds.2012-0880
Lee, C.-K., Corte, C., & Stein, K. F. (2018). Drinker identity: Key risk factor for adolescent alcohol use. Journal of School Health, 88(3), 253–260. https://doi.org/10.1111/josh.12603
Lee, C.-K., Corte, C., Stein, K. F., Feng, J.-Y., & Liao, L.-L. (2020). Alcohol-related cognitive mechanisms underlying adolescent alcohol use and alcohol problems: Outcome expectancy, self-schema, and self-efficacy. Addictive Behaviors, 105, 106349. http://doi.org/10.1016/j.addbeh.2020.106349
Levy, S., Sherritt, L., Harris, S. K., Gates, E. C., Holder, D. W., Kulig, J. W., & Knight, J. R. (2004). Test-retest reliability of adolescents’ self-report of substance use. Alcoholism: Clinical and Experimental Research, 28(8), 1236–1241. https://doi.org/10.1097/01.alc.0000134216.22162.a5
Levy, S. J. L., Williams, J. F., & Committee on Substance Abuse Use and Prevention. (2016). Substance use screening, brief intervention, and referral to treatment. Pediatrics, 138(1), 143.
http://doi.org/10.1542/peds.2016-1211
Linakis, J. G., Bromberg, J. R., Casper, T. C., Chun, T. H., Mello, M. J., Richards, R., Mull, C. C., Shenoi, R. P., Vance, C., Ahmad, F., Bajaj, L., Brown, K. M., Chernick, L. S., Cohen, D. M., Fein, J., Horeczko, T., Levas, M. N., McAninch, B., Monuteaux, M. C., . . . Dean, J. M. (2019). Predictive validity of a 2-question alcohol screen at 1-, 2-, and 3-year follow-up. Pediatrics, 143(3). https://doi.org/10.1542/peds.2018-2001
Lintz, M. J., Thurstone, C., Hull, M., & Ladegard, K. (2019). Development of a school-based substance treatment model. Journal of Child & Adolescent Substance Abuse, 28(2), 127–131.
https://doi.org/10.1080/1067828X.2019.1623145
McNeal, R. B., Jr., Hansen, W. B., Harrington, N. G., & Giles, S. M. (2004). How All Stars works: An examination of program effects on mediating variables. Health Education & Behavior, 31(2), 165–178. https://doi.org/10.1177/1090198103259852
Miech, R., Patrick, M. E., O’Malley, P. M., & Johnston, L. D. (2017). E-cigarette use as a predictor of cigarette smoking: Results from a 1-year follow up of a national sample of 12th grade students. Tobacco Control, 26(E2), e106–e111. https://doi.org/10.1136/tobaccocontrol-2016-053291
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). Guilford.
Mogro-Wilson, C., Allen, E., & Cavallucci, C. (2017). A brief high school prevention program to decrease alcohol usage and change social norms. Social Work Research, 41(1), 53–62.
https://doi.org/10.1093/swr/svw023
Naar-King, S., & Suarez, M. (2011). Motivational interviewing with adolescents and young adults. Guilford.
Nagy, E., Verres, R., & Grevenstein, D. (2017). Risk competence in dealing with alcohol and other drugs in adolescence. Substance Use & Misuse, 52(14), 1892–1909. https://doi.org/10.1080/10826084.2017.1318149
National Institute on Alcohol Abuse and Alcoholism. (2011). Alcohol screening and brief intervention for youth: A practitioner’s guide. www.niaaa.nih.gov/YouthGuide
Ohannessian, C. M. (2014). Anxiety and substance use during adolescence. Substance Abuse, 35(4), 418–425. https://doi.org/10.1080/08897077.2014.953663
Pedrelli, P., Shapero, B., Archibald, A., & Dale, C. (2016). Alcohol use and depression during adolescence and young adulthood: A summary and interpretation of mixed findings. Current Addiction Reports, 3(1), 91–97. https://doi.org/10.1007/s40429-016-0084-0
Prestwich, A., Kellar, I., Conner, M., Lawton, R., Gardner, P., & Turgut, L. (2016). Does changing social influence engender changes in alcohol intake? A meta-analysis. Journal of Consulting and Clinical Psychology, 84(10), 845–860. https://doi.org/10.1037/ccp0000112
Pullen, P. C., van Dijk, W., Gonsalves, V. E., Lane, H. B., & Ashworth, K. E. (2019). Response to intervention and multi-tiered systems of support: How do they differ and how are they the same, if at all? In P. C. Pullen & M. J. Kennedy (Eds.), Handbook of response to intervention and multi-tiered systems of support (pp. 5–10). Routledge.
Randolph, K., Turull, P., Margolis, A., & Tau, G. (2013). Cannabis and cognitive systems in adolescents. Adolescent Psychiatry, 3(2), 135–147. https://doi.org/10.2174/2210676611303020004
Renard, J., Vitalis, T., Rame, M., Krebs, M.-O., Lenkei, Z., Le Pen, G., & Jay, T. M. (2016). Chronic cannabinoid exposure during adolescence leads to long-term structural and functional changes in the prefrontal cortex. European Neuropsychopharmacology, 26(1), 55–64. https://doi.org/10.1016/j.euroneuro.2015.11.005
Rimal, R. N., & Real, K. (2005). How behaviors are influenced by perceived norms: A test of the theory of normative social behavior. Communication Research, 32(3), 389–414. https://doi.org/10.1177/0093650205275385
Rollnick, S., Kaplan, S. G., & Rutschman, R. (2016). Motivational interviewing in schools: Conversations to improve behavior and learning. Guilford.
Romer, D., & Moreno, M. (2017). Digital media and risks for adolescent substance abuse and problematic gambling. Pediatrics, 140(S2), S102–S106. https://doi.org/10.1542/peds.2016-1758L
Schulenberg, J. E., & Maggs, J. L. (2002). A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. Journal of Studies on Alcohol, 14, 54–70. http://doi.org/10.15288/jsas.2002.s14.54
Shenoi, R. P., Linakis, J. G., Bromberg, J. R., Casper, T. C., Richards, R., Mello, M. J., Chun, T. H., & Spirito, A. (2019). Predictive validity of the CRAFFT for substance use disorder, 144(2).
https://doi.org/10.1542/peds.2018-3415
Singh, S., Windle, S. B., Filion, K. B., Thombs, B. D., O’Loughlin, J. L., Grad, R., & Eisenberg, M. J. (2020). E-cigarettes and youth: Patterns of use, potential harms, and recommendations. Preventive Medicine, 133, 106009. http://doi.org/10.1016/j.ypmed.2020.106009
Stephens, P. C., Sloboda, Z., Stephens, R. C., Teasdale, B., Grey, S. F., Hawthorne, R. D., & Williams, J. (2009). Universal school-based substance abuse prevention programs: Modeling targeted mediators and outcomes for adolescent cigarette, alcohol and marijuana use. Drug and Alcohol Dependence, 102(1–3), 19–29. https://doi.org/10.1016/j.drugalcdep.2008.12.016
Substance Abuse and Mental Health Services Administration. (2014). The Center for Behavioral Health Statistics and Quality (CBHSQ) Report. https://pubmed.ncbi.nlm.nih.gov/26913315
Substance Abuse and Mental Health Services Administration. (2018). Key substance use and mental health indicators in the United States: Results from the 2017 National Survey on Drug Use and Health (HHS Publication No. SMA 18-5068, NSDUH Series H-53). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHFFR2017/NSDUHFFR2017.pdf
Trucco, E. M., Colder, C. R., & Wieczorek, W. F. (2011). Vulnerability to peer influence: A moderated mediation study of early adolescent alcohol use initiation. Addictive Behaviors, 36(7), 729–736. https://doi.org/10.1016/j.addbeh.2011.02.008
Wade-Mdivanian, R., Anderson-Butcher, D., Newman, T. J., Ruderman, D. E., Smock, J., & Christie, S. (2016). Exploring the long-term impact of a positive youth development-based alcohol, tobacco and other drug prevention program. Journal of Alcohol and Drug Education, 60(3), 67–89.
Whittle, A. E., Buckelew, S. M., Satterfield, J. M., Lum, P. J., & O’Sullivan, P. (2015). Addressing adolescent substance use: Teaching Screening, Brief Intervention, and Referral to Treatment (SBIRT) and Motivational Interviewing (MI) to residents. Substance Abuse, 36(3), 325–331.
https://doi.org/10.1080/08897077.2014.965292
Whyte, A. J., Torregrossa, M. M., Barker, J. M., & Gourley, S. L. (2018). Editorial: Long-term consequences of adolescent drug use: Evidence from pre-clinical and clinical models. Frontiers in Behavioral Neuroscience, 12(83), 6–8. https://doi.org/10.3389/fnbeh.2018.00083
Wills, T. A., Simons, J. S., Sussman, S., & Knight, R. (2016). Emotional self-control and dysregulation: A dual-process analysis of pathways to externalizing/internalizing symptomatology and positive well-being in younger adolescents. Drug and Alcohol Dependence, 163(S1), S37–S45.
http://doi.org/10.1016/j.drugalcdep.2015.08.039
Winters, K. C., Fahnhorst, T., Botzet, A., Lee, S., & Lalone, B. (2012). Brief intervention for drug-abusing adolescents in a school setting: Outcomes and mediating factors. Journal of Substance Abuse Treatment, 42(3), 279–288. https://doi.org/10.1016/j.jsat.2011.08.005
Yu, B., Chen, X., Chen, X., & Yan, H. (2020). Marijuana legalization and historical trends in marijuana use among US residents aged 12–25: Results from the 1979–2016 National Survey on Drug Use and Health. BMC Public Health, 20, 156. https://doi.org/10.1186/s12889-020-8253-4
Zapolski, T. C. B., Fisher, S., Banks, D. E., Hensel, D. J., & Barnes-Najor, J. (2017). Examining the protective effect of ethnic identity on drug attitudes and use among a diverse youth population. Journal of Youth and Adolescence, 46, 1702–1715. https://doi.org/10.1007/s10964-016-0605-0
Ziomek-Daigle, J. (Ed.). (2016). School counseling classroom guidance: Prevention, accountability, and outcomes. SAGE.
Zucker, R. A., Donovan, J. E., Masten, A. S., Mattson, M. E., & Moss, H. B. (2008). Early developmental processes and the continuity of risk for underage drinking and problem drinking. Pediatrics, 121(S4), S252–S272. http://doi.org/10.1542/peds.2007-2243B
Appendix A
Study Subscales
| |
Substance Use
0 days; 1–2 days; 3–5 days; 6–9 days; 10–19 days; 20–29 days; everyday |
| 1 |
In the past 30 days, how many days did you have at least one drink of alcohol? |
| 2 |
In the past 30 days, how many days have you used marijuana? |
| 3 |
In the past 30 days, how many days have you vaped? |
| 4 |
In the past 30 days, how many days have you used tobacco? |
| 5 |
In the past 30 days, how many days have you used prescription drugs in a way other than prescribed? |
| 6 |
In the past 30 days, how many days have you used illegal drugs? |
| 7 |
In the past 30 days, how many days have you used other means to get high? |
| |
Self-Assessment of Use
Yes or No |
| 1 |
Have you ever ridden in a car driven by someone (including yourself) who was “high” or using alcohol or drugs? |
| 2 |
Do you ever use alcohol or drugs to relax, feel better about yourself, or fit in? |
| 3 |
Do you ever use alcohol or drugs while you are by yourself, or alone? |
| 4 |
Do you ever forget things you did while using alcohol or drugs? |
| 5 |
Do your family or friends ever tell you that you should cut down on your drinking or your drug use? |
| 6 |
Have you ever gotten in trouble while you were using alcohol or drugs? |
| 7 |
Are you worried about alcohol or drug abuse among your friends? |
| 8 |
Are you worried about alcohol or drug abuse in your family? |
| |
Attitudes About Use
1 – not very bad for you; 2 – somewhat bad for you; 3 – very bad for you |
| 1 |
How harmful is it to occasionally use alcohol? |
| 2 |
How harmful is it to occasionally use marijuana? |
| 3 |
How harmful is it to occasionally use e-cigs or vaporizers (vaping)? |
| 4 |
How harmful is it to occasionally use tobacco? |
| 5 |
How harmful is it to occasionally use prescription drugs in a way other than prescribed? |
| 6 |
How harmful is it to occasionally use illegal drugs or other ways to get high? |
| |
Readiness to Change |
| |
1 – very likely; 2 – somewhat likely; 3 – somewhat unlikely; 4 – not at all likely |
| |
If you currently use any of the substances below, on a scale of 1–4, how likely is it you would reduce or stop your use? |
| 1 |
Alcohol |
| 2 |
Marijuana |
| 3 |
Vaping |
| 4 |
Tobacco |
| 5 |
Prescription drugs outside of their intended purpose |
| 6 |
Illegal drugs or other ways to get high |
Appendix B
MCARR Curriculum
| MCARR Curriculum |
| Module 1
Orientation to the MCARR Program and Community Building |
| Learning Objectives
At the end of this lesson, students will:
Establish the foundation for the development of community within the classroom group.
Recognize community and civic responsibility within the students’ own school.
Identify the benefits of being a part of a classroom community, including the value in being socially and emotionally supported by others in social environments.
Activities
Psychoeducational lecture.
Team-building activity.
Scenarios: Students consider scenarios of school- and community-related challenges that require social connectedness and help students develop solutions that promote stronger social bonds and support. |
| Module 2
Personal Coping |
| Learning Objectives
At the end of this lesson, students will:
Recall the potential impact of stress and how it may correlate with less healthy choices, such as drug and alcohol use, including warning signals within self and others.
Identify coping skills that can mediate the negative impact of stress on student well-being.
Recognize healthy stress-reducing behaviors already used by students and introduce new coping strategies for managing stress.
Activities
Psychoeducational lecture.
Students practice several basic methods for managing life stress, including diaphragmatic breathing and abbreviated progressive muscle relaxation.
Students identify life stress and coping strategies, with special emphasis on the potential for strategies to reduce the risk of drug and alcohol use. |
| Module 3
Attitudes and Messages About Use |
| Learning Objectives
At the end of this lesson, students will:
1. Recognize the impact of societal attitudes and messages on adolescent substance use.
2. Identify the messages received through the media about substances and the impact on student
decision-making.
3. Define the impact of stress and normalization of common responses to stress.
Activities
Psychoeducational lecture.
Group discussion on a series of photos and statements made by popular musicians. Students assume the perspective of the popular figure, theorize about attitudes they may have had, and evaluate the impact of those attitudes on the lives of those figures.
Students are then challenged to understand other popular culture influences on drug and alcohol use. |
| Module 4
Alcohol |
| Learning Objectives
At the end of this lesson, students will:
1. Identify the physiological and neurological mechanisms of alcohol use and potential harm and
consequences of use.
2. Recognize the impact of alcohol on the body.
3. Define the long-term and short-term physiological and psychosocial effects of alcohol on adolescents.
Activities
Psychoeducational lecture.
Students complete and share a body map worksheet to draw arrows and make linkages of the impact of alcohol use on the adolescent body.
Small groups are given scenarios to consider a day in the life of an alcoholic beverage, from the perspective of the beverage as a character in the scenario.
Students consider elements of the CRAFFT as applied to hypothetical characters involved in their story. |
| Module 5
Community Partners |
| Learning Objectives
At the end of this lesson, students will:
1. Discuss the influence of the community on adolescent drug and alcohol use and methods by which
the community can be used to support those at risk of drug and alcohol problems.
2. Describe the potential benefit or harm of specific peer attitudes and behaviors related to drug and
alcohol use.
3. Recognize signs of possible alcohol or drug use problems among members of the community.
Activities
Psychoeducational lecture
In small groups, students describe a caring school community, followed by a group discussion of harmful and helpful aspects of peer influence.
Exposure to assessment methods such as yellow and red flags that may indicate a substance use problem and the CRAFFT screening tool.
Using role play, students practice methods for communicating with a peer that may minimize defensiveness and identify points of intervention. |
| Module 6
Assumptions and Low-Risk Limits |
| Learning Objectives
At the end of this lesson, students will:
Recognize assumptions made about substance use in school and society.
Classify facts and myths about drug and alcohol use.
Understand risk levels of use for both adolescents and adults and how these may present in various situations.
Activities
Psychoeducational lecture.
Team-building activity, with processing focused on the dynamics of group decision-making.
Myths are presented in a series of group discussion true/false questions about descriptive norms to help students understand that drug or alcohol use is not an inevitable part of the adolescent experience.
Established guidelines for adult limits and moderate use of alcohol are presented, while simultaneously emphasizing that no amount of alcohol represents low or moderate risk for minors.
Case studies are used to apply yellow and red flag warning signs discussed in prior lesson. |
| Module 7
Cannabis, Nicotine, and E-Cigarettes |
| Learning Objectives
At the end of this lesson, students will:
1. Identify a variety of hazards associated with cannabis and nicotine, with special focus on e-cigarettes.
2. Comprehend the physiological and neurological impacts of cannabis and nicotine on adolescents.
3. Describe and practice refusal skills related to cannabis and nicotine.
Activities
Students are provided with an overview of the mechanisms involved in cannabis use and learn about the impact of cannabis on the developing brain, such as learning and memory deficits, loss of motivation, and mood swings.
In the “Whose truth is it, anyway?” discussion, students are given a series of statements and asked to measure the likelihood of the statement’s veracity, depending on the source of the statement and other influencing factors.
After this content, students move around the classroom to find classmates who can answer various questions correctly. |
| Module 8
Opioids and Cocaine |
| Learning Objectives
At the end of this lesson, students will:
Recognize the classes of drugs related to opioids and cocaine and trends in use and abuse of these drugs, including risk of serious injury or death.
Recall facts about physiological and neurological impacts of various forms of opioids and cocaine.
Summarize the dangers of opioid use.
Activities
Psychoeducational lecture.
Video to demonstrate neurological dynamics and physiological mechanisms, including the potential for overdose.
Students brainstorm resources in their school community and receive information on community resources for helping those with addiction, including professional networks, such as counselors and other mental health providers, and informal networks, such as neighborhood and faith leaders.
In dyads, students are asked to role-play skills for persuading a peer or loved one to seek professional help and weigh the pros and cons of these decisions. |
| Module 9
Review: Decisions |
| Learning Objectives
At the end of this lesson, students will:
1. Identify the experiences and information presented throughout the curriculum, with an overarching
theme of decisional balance.
2. Recall key information related to each module.
3. Describe what the curriculum has meant to each student and how they envision the experience
impacting future decisions.
Activities
Students participate in a learning game in which teams compete to give correct answers about key concepts, including facts about the dynamics of problem alcohol and drug use and its consequences and risks.
Students report on identifying and coping with stress, connecting with a caring community, and advocating for their and others’ needs.
Students are reminded of the influence of myths, attitudes, and assumptions on the use of alcohol and drugs and recollect components of the CRAFFT. |
Louisa L. Foss-Kelly, PhD, NCC, ACS, LPC, is a professor at Southern Connecticut State University. Margaret M. Generali, PhD, is a certified school counselor and a professor and department chair at Southern Connecticut State University. Michael J. Crowley, PhD, is a licensed psychologist and an associate professor at Yale University. Correspondence may be addressed to Louisa L. Foss-Kelly, Counseling and School Psychology, Southern Connecticut State University, 501 Crescent St., New Haven, CT 06515, fossl1@southernct.edu.
