Brian J. Clarke, Michael T. Hartley, Austin M. Guida
Impostor phenomenon (IP), characterized by persistent self-doubt despite objective success, is prevalent during the early stages of counselor development, often emerging as individuals transition from training into professional practice. This study examined whether self-compassion mediates relationships between IP, resilience, and mental health among 281 counselors-in-training enrolled in departments accredited by the Council for the Accreditation of Counseling and Related Educational Programs. Mediation analyses showed that self-compassion fully mediated the effects of IP on resilience and depression and partially mediated the effect on anxiety. MANOVA results indicated that higher self-compassion corresponded with lower IP, anxiety, and depression, and greater resilience, with robust effects. Findings identify self-compassion as a developmental competency that supports balanced self-evaluation, emotional regulation, and sustainable counselor well-being. Integrating self-compassion training into counselor education and supervision may help developing counselors manage impostor-related distress, strengthen resilience, and promote ethical, sustainable professional practice.
Keywords: impostor phenomenon, counselor development, self-compassion, resilience, mental health
Building resilience and prioritizing mental health are vital during the formative stages of counselor development. During the early stages of training and supervised practice, developing counselors experience the inherent emotional demands and elevated anxiety common while learning to integrate theoretical knowledge into clinical practice (Skovholt & Trotter-Mathison, 2024; Stoltenberg & McNeill, 2010). Although these feelings may diminish with increased experience, enduring self-doubt and inadequacy may signal impostor phenomenon (Clance & Lawry, 2024). Imposter phenomenon (IP), characterized by persistent feelings of fraudulence and incompetence despite evidence of success, impacts nearly all developing counselors (Clarke et al., 2025; Tigranyan et al., 2021). Those experiencing IP may struggle to internalize mastery experiences and fail to consolidate moments of success into genuine confidence (Gadsby & Hohwy, 2024; Roskowski, 2010). Individual differences in coping with IP may be partially explained by self-compassion, which may buffer IP’s negative effects on counseling self-efficacy and well-being (Clarke et al., 2025).
The persistent fear of being exposed as a fraud becomes a harmful cycle whereby individuals ruminate on perceived shortcomings, discount positive feedback, and misattribute positive outcomes to external factors (Clance & Lawry, 2024). Behaviors associated with IP include extreme perfectionism, procrastination, and/or exhausting overpreparation, which can inhibit counselor development (Clarke et al., 2025; Nguyen, 2023). Because IP is rooted in shame and feelings of inadequacy, it contributes to isolation, burnout, and compassion fatigue (Garba et al., 2024; Ojeda, 2024).
IP undermines the reflective, relational, and self-evaluative capacities that are central to counselor development. Counselors who experience chronic self-doubt may hesitate to disclose errors in supervision, question their competence, and struggle to sustain resilience, patterns that can jeopardize client care and professional longevity (Delaney, 2018; Housenecht & Swank, 2022). Given the demands of counselor training and practice, protective factors such as resilience and self-compassion may be critical for developing counselor well-being and persistence.
Resilience is a protective factor to cope with mental distress and burnout (Gerber & Anaki, 2021; Webb & Rosenbaum, 2019). Emerging from the positive psychology movement, resilience explains why some individuals behave adaptively under great stress while others do not. Beyond recovery from adversity, resilience is a process of successful adaptation and coping during challenging or threatening circumstances (Webb & Rosenbaum, 2019). Cultivating new coping mechanisms and fostering personal growth, resilience can sustain well-being and performance during difficult experiences. The limited research on resilience among developing counselors has identified self-awareness and self-compassion as critical protective factors to cope with the emotional demands of becoming a counselor (Hou & Skovholt, 2020).
As a protective factor, self-compassion can play an important role in the resilience and mental health of developing counselors, especially in the presence of IP (Clarke et al., 2025; Neff et al., 2005). Self-compassion is comprised of three interrelated dimensions: mindfulness, common humanity, and self-kindness (Neff, 2023). Mindfulness, the core of self-compassion, involves maintaining awareness of present experiences with reduced reactivity and self-judgment. The common humanity dimension refers to the acceptance that suffering is inherent to our shared human experience. By normalizing challenging experiences, this perspective helps prevent the isolation that may arise from perceiving failures as uniquely personal. Finally, self-kindness encompasses behaviors and ways of relating intrapersonally that offer support and comfort during times of suffering or setbacks. Rather than defaulting to self-criticism, overidentification with failures, or isolation, self-compassion enables understanding and resilience, reducing the impact of IP and the fear of failure during counselor development (Clarke et al., 2025; Warren et al., 2016).
The theoretical alignment between self-compassion and resilience is rooted in their shared emphasis on adaptive emotional regulation, growth through adversity, and the development of a stable and supportive inner identity (Warren et al., 2016). Self-compassion supports sustainable resilience by reducing self-criticism and perfectionism and fostering a growth mindset (Neff, 2023; Warren et al., 2016). Indeed, a recent meta-analysis indicated that self-compassion is consistently linked to positive outcomes among mental health professionals, including enhanced competence, improved therapeutic presence, and a greater willingness to seek guidance and supervision (Crego et al., 2022).
Because of its regulating effects, self-compassion may help developing counselors to tolerate the stress of IP through improved emotional self-regulation (Crego et al., 2022; Neff, 2023). In this way, self-compassion can function as an emotion-focused coping mechanism that reduces the mental distress associated with IP (Clarke, 2024; Crego et al., 2022; Gerber & Anaki, 2021). Ultimately, when individuals experience IP-related distress, self-compassionate responses (mindfulness, common humanity, self-kindness) may interrupt the IP cycle, preserving resilience and mental health (Neff et al., 2005).
The purpose of this study is to examine how self-compassion functions as a protective factor in the relationship between IP, resilience, and mental health during counselor development. Research has found self-compassion to support resilience among health care providers (Delaney, 2018), yet much less is known about the relationship between self-compassion and resilience among developing counselors who experience IP. Addressing the negative impact of IP on counselor development, this article explores how self-compassion might mitigate IP’s negative relationships with resilience and mental health (Clarke et al, 2025; Roskowski, 2010; Tigranyan et al., 2021). The guiding research questions were:
- To what extent does self-compassion mediate the relationships between IP and the outcomes of resilience and mental health?
- How do levels of self-compassion relate to variations in IP, resilience, and mental health among the sample?
We hypothesized that IP would have a significant negative relationship with resilience and mental health, and that self-compassion will significantly mediate these negative associations. Specifically, higher levels of self-compassion will relate to lower IP and improved mental health and resilience. Our findings offer valuable insights into how self-compassion can enhance resilience and promote mental health during counselor development.
Methods
Procedure
The study received IRB approval prior to the recruitment of master’s-level counseling students from across the United States. Data were collected between April and October 2023, using an online survey disseminated via email to Council for the Accreditation of Counseling and Related Educational Programs (CACREP)–accredited program liaisons. These emails described the study and outlined informed consent procedures and inclusion criteria. Eligible participants were individuals enrolled in CACREP-accredited counseling programs aged 18 or older. After consenting, participants were presented with the measures and a demographic questionnaire developed by the authors. Engagement with the study concluded once participants either completed or exited the survey.
Participants
The sample consisted of 281 counseling students attending CACREP-accredited counseling programs from 37 U.S. states and the District of Columbia. Although the present sample consisted of counselors-in-training (CITs), the term developing counselors is used throughout this paper to reflect the broader developmental continuum that spans counselor training and early professional practice (Stoltenberg & McNeill, 2010).
Consistent with the population of CITs, most participants identified as White (n = 190, 67.29%) with lower percentages identifying as Hispanic or Latinx (n = 43, 15.2 %), Asian (n = 17, 6.0%), African American or Black (n = 13, 4.6%), multiracial (n = 13, 4.6%), American Indian or Alaskan Native (n = 3, 1.1%) and Middle Eastern (n = 2, 0.7%). The majority (n = 237, 83.7%) identified as female, with 32 (11.3%) identifying as male, 6 (2.1%) as non-binary, 4 (1.4%) as genderqueer, and 2 (0.7%) choosing not to disclose their gender identity. Participants were from clinical mental health (n = 170, 60.1%), school counseling (n = 49, 17.3%), rehabilitation counseling (n = 49, 17.3%), and marriage and family counseling (n = 13, 4.6%) programs. The average participant age was 32 years (SD = 10.35), with an age range from 21 to 67 years.
Measures
Self-Compassion Scale-Short Form (SCS-SF)
The SCS-SF is a short form of the Self-Compassion Scale (Neff, 2003), consisting of 12 self-report items selected from the original scale (Raes et al., 2011). Items are rated on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Examples include “I try to see my failings as part of the human condition” and “I’m disapproving and judgmental about my own flaws and inadequacies” (Neff, 2003, p. 2). SCS-SF scores have shown good internal consistency (α = .86), with its total scores strongly correlating with those of the full version (r = .98; Raes et al., 2011). Factor analysis has confirmed that the SCS-SF shares the same factor structure as the original scale (Neff et al., 2019; Raes et al., 2011). Scores are interpreted as levels of self-compassion: low (1–2.4), moderate (2.5–3.5), and high (3.51–5). In the present study, SCS-SF scores demonstrated good internal consistency reflected in an alpha of .85, and omega of .85.
Academic Resilience Scale-6 (ARS-6)
The ARS-6 is a concise self-report scale designed to measure academic resilience, defined as the ability to manage challenges, stress, and setbacks within a learning environment (Martin & Marsh, 2006). Items include statements such as “I’m good at bouncing back from a poor grade or difficult feedback” and “I don’t let a bad grade or feedback affect my confidence.” Responses are rated on a 7-point Likert-type response scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater academic resilience. Item and factor level construct validity was supported through factor score estimates, correlation, path analysis, and cluster analysis, showing the ARS scores were closely aligned with related constructs including self-efficacy, control, planning, low anxiety, and persistence (Martin & Marsh, 2006). ARS-6 scores have demonstrated good internal consistency, with an alpha coefficient of .89 (Martin & Marsh, 2006). In the current study, the ARS-6 scores showed acceptable reliability supported by alpha and omega scores of .83.
Clance Impostor Phenomenon Scale (CIPS-10)
The CIPS-10 (Wang et al., 2022) is a condensed, 10-item version of the original 20-item Clance Impostor Phenomenon Scale (CIPS) designed to assess impostor feelings (Clance, 1985). A systematic review by Mak et al. (2019) supported the CIPS-20 as a valid (construct, criterion, and content) measure of IP. The CIPS-10 utilizes a Likert-type response scale ranging from 1 (not at all true) to 5 (very true) and includes items from the CIPS-20, such as “I’m afraid people important to me may find out that I’m not as capable as they think I am” and “I feel my success was due to some kind of luck rather than competence.” Wang et al. (2022) reported strong internal reliability for the CIPS-10 (α = .93), with total scores closely aligning with those of the CIPS-20. Construct validity was supported through factor score estimates, revealing a single-factor structure similar to the 20-item version. In this study, CIPS-10 scores were interpreted using adjusted categories from Clance (1985): few IP (less than 20), moderate IP (20–29), frequent IP (30–39), and intense IP (40–50). Within the current sample, CIPS-10 scores demonstrated good internal consistency with an alpha of .88 and omega of .90.
Patient Health Questionnaire-4 (PHQ-4)
The PHQ-4 is a 4-item, self-report assessment screening tool for depression and anxiety (Kroenke et al., 2009). The Likert-type responses are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). A total score of 3 or more, across both items, indicates the presence of moderate-to-severe symptoms (Kroenke et al., 2009). In meta-analyses, PHQ-4 scores have shown good internal consistency (α = .89) and have yielded valid and diagnostically accurate depression and anxiety scores (Khubchandani et al., 2016; Kroenke et al, 2009). Construct validity was supported using a varimax-rotated principal components analysis conducted on the four screening items (PHQ-2 and GAD-2), yielding two components that together explained 83% of the overall variance. Likewise, criterion validity was indicated by individuals diagnosed with depression or anxiety by a health care professional scoring significantly higher on the PHQ-2, GAD-2, and PHQ-4 compared to participants without a clinical diagnosis (Khubchandani et al., 2016). In the present sample, the PHQ-4 scores showed good internal consistency with an alpha score of .87 and omega of .84.
Data Analysis
Portions of this data set informed a previously published manuscript that focused on how self-compassion can mitigate IP’s negative relationship with counselor self-efficacy (Clarke et al., 2025). Although the two manuscripts share IP and self-compassion data, the current manuscript is distinct and extends this line of inquiry by its unique focus on the benefits of self-compassion for counselor resilience and mental health, despite the presence of IP.
All analyses were performed using SPSS (v29) with a p ≤ .01 benchmark to reduce the likelihood of Type I error and ensure that the most reliable effects are interpreted as statistically meaningful. Preliminary analyses were conducted to examine statistical assumptions for the mediation and MANOVA models. Normality was confirmed for all variables via Shapiro-Wilk (all p > .05). Box’s M test supported homogeneity of variance–covariance matrices (p = .021), and observations were independent. In addition to all VIF scores being < 2, no bivariate correlations exceeded r = .80, suggesting that multicollinearity was not a concern. Collectively, these results suggest that the data met all assumptions necessary for the planned analyses (Tabachnick & Fidell, 2019).
We selected a regression-based mediation analysis because of the study’s focus on specific indirect effects of self-compassion and the moderate sample size, both of which made alternative analyses less ideal (Hayes, 2022). Because the variables tested were represented by composite scores rather than latent constructs, a mediation was statistically appropriate and provided a parsimonious method to examine self-compassion as a buffer for IP. Although cross-sectional mediation cannot establish temporal precedence or causation, it can identify statistical pathways that warrant future longitudinal investigation (Fairchild & McDaniel, 2017; Hayes, 2022). The 99% confidence intervals (CI) of the effects were derived from 10,000 bootstrap samples. If the upper and lower bounds of the CI did not include zero, they were considered statistically significant.
Finally, MANOVA was used to determine how the severity of IP affected its relationships with resilience, anxiety, depression, and self-compassion. The four levels of IP used in this analysis were defined as few, moderate, frequent, and intense IP according to the CIPS author (Clance, 1985). MANOVA effect size was described using partial eta squared values of 0.01 (small), 0.059 (medium), and 0.14 (large; Richardson, 2011). Cohen’s d was used to interpret effect sizes for follow up Tukey analyses, small effect (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8; Gignac & Szodorai, 2016).
A priori power analysis for mediation effects (Fritz & MacKinnon, 2007) indicated a minimum sample of 148 participants would provide .80 power to detect medium-sized indirect effects using bias-corrected bootstrapping. For MANOVA with three groups and four dependent variables, G*Power indicated 158 participants would yield .80 power for detecting medium effects (f² = .25). Our sample of 281 exceeded both requirements.
Results
Descriptives
Pearson correlations indicated significant (< .01) bivariate relationships among self-compassion, impostor phenomenon, depression, anxiety, and academic resilience (Table 1). There were no significant differences in self-compassion, IP, resilience, anxiety, or depression across demographics or counseling program emphasis.
Table 1
Descriptive Statistics and Bivariate Correlations
| Mean | SD | 1 | 2 | 3 | 4 | ||
| 1. Self-Compassion | 3.06 | 0.74 | – | ||||
| 2. Impostor Phenomenon | 32.81 | 8.22 | −.54* | – | |||
| 3. Depression | 1.27 | 1.60 | −.42* | .35* | – | ||
| 4. Anxiety | 2.54 | 1.78 | −.55* | .46* | .59* | – | |
| 5. Academic Resilience | 27.66 | 6.51 | .53* | −.36* | −.23* | −.40* | |
*p ≤ .01.
The sample included high levels of impostor phenomenon (M = 32.81, SD = 8.22), with over 65% falling in the frequent-to-intense range. IP showed strong negative correlations with self-compassion (r = −.54) and resilience (r = −.36), and strong positive correlations with anxiety (r = .46) and depression (r = .35).
Mediation Analysis
Mediation analyses were used to explore the statistical associations among IP, self-compassion, and the outcome variables of resilience, anxiety, and depression. Results indicated that self-compassion functioned as a statistical mediator in the relationships between IP and each outcome.
Figure 1
Mediation Analysis: Impostor and Resilience
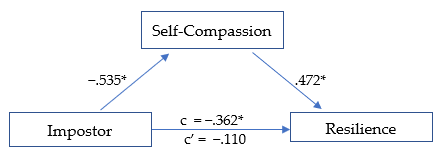
*p ≤ .01
The first model (Figure 1) was significant, R² = .290, F(1, 278) = 59.78, p < .01. The total effect (c) of IP on academic resilience was negative and significant, β = −.362, SE = .126, t = −2.868, p < .01, suggesting that higher IP scores were associated with lower resilience. When self-compassion was included in the model, the direct effect (c′) of IP on resilience was no longer significant, β = −.110, SE = .060, t = −1.838, p = .07, consistent with full statistical mediation (Hayes, 2022). The indirect pathway through self-compassion represented 69.6% of the total standardized association. IP was negatively associated with self-compassion (β = −.535, p < .01; large effect), and self-compassion was positively associated with resilience (β = .472, p < .01; large effect). The overall indirect effect was significant (β = −.252, p < .01).
Figure 2
Mediation Analysis: Impostor and Anxiety
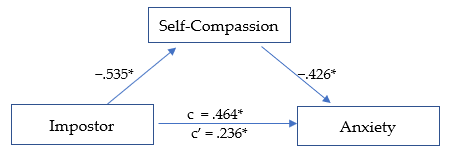
*p ≤ .01.
The second model (Figure 2) was significant, R² = .345, F(1, 278) = 73.159, p < .01. The total effect (c) of IP on anxiety was positive and significant, β = .464, SE = .053, t = 8.747, p < .01, indicating that higher IP scores were related to higher anxiety levels. After including self-compassion, the direct effect (c′) was reduced but remained significant, β = .236, SE = .057, t = 4.110, p < .01, suggesting partial statistical mediation. The indirect pathway through self-compassion accounted for 49.2% of the total standardized association. IP was negatively associated with self-compassion (β = −.535,p < .01; large effect), and self-compassion was negatively associated with anxiety (β = −.426, p < .01; medium effect). The overall indirect effect was significant, β = −.228, p < .01.
Figure 3
Mediation Analysis: Impostor and Depression
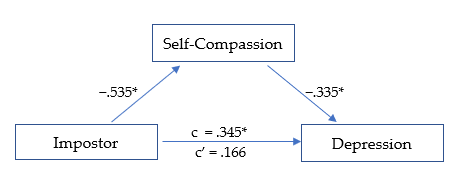
*p ≤ .01.
The third model (Figure 3) was significant, R² = .199, F(1, 278) = 34.484, p < .01. The total effect (c) of IP on depression was positive and significant, β = .345, SE = .056, t = 6.135, p < .01, indicating that higher IP scores were associated with higher depression levels. After accounting for self-compassion, the direct effect (c′) was reduced and no longer significant, β = .166, SE = .064, t = 2.611, p = .02, suggesting full statistical mediation. The indirect pathway through self-compassion represented 51.9% of the total standardized association. IP was negatively related to self-compassion (β = −.535, p < .01; large effect), and self-compassion was negatively related to depression (β = −.335, p < .01; medium effect). The overall indirect effect was significant, β = −.179, p < .01.
MANOVA
Self-compassion scores were divided into three levels (low, moderate, and high) as suggested by Neff (2003) to determine if the effect of self-compassion was consistent across each level. MANOVA analyses revealed that IP, resilience, depression, and anxiety each varied significantly based on level of self-compassion, F(8, 550) = 20.790, p < .01, Wilk’s Λ = 0.590, ηp2 = .232, indicating a large effect size.
The MANOVA results revealed that IP scores varied according to level of self-compassion, F(2, 281) = 48.807, p < .01, ηp2 = .260, with a large effect size. IP decreased significantly at each rising level of self-compassion, from low to moderate (d = 0.666, p < .01) and moderate to high (d = 0.987, p < .01), with medium and large effect sizes, respectively. The greatest decrease in IP was seen as self-compassion rose from moderate to high.
Resilience was significantly higher at each increasing level of self-compassion F(2, 281) = 39.323, p < .01, ηp2 = .221, with a large overall effect size. Resilience rose linearly across each level of self-compassion, from low to moderate (d = −0.756, p < .01), and from moderate to high (d = −0.790, p < .01), each with a medium-high effect size.
Depression scores lowered significantly as self-compassion level increased, F(2, 281) = 20.232, p < .01, ηp2 = .127, with an overall medium effect size. The decrease in depression was noted across levels of self-compassion, from low to moderate (d = 0.446, p < .01), and from moderate to high (d = 0.625, p < .01), each with a medium effect size. The largest decrease in depression was observed as self-compassion rose from moderate to high.
Anxiety scores decreased significantly as the level of self-compassion increased, F(2, 281) = 45.898, p < .01, ηp2 = .248, with a large overall effect size. Anxiety scores were lower as self-compassion rose from low to moderate (d = 0.895, p < .01), and from moderate to high (d = 0.711, p < .01), with large and medium effect sizes, respectively. The largest decrease in anxiety was noted as self-compassion increased from low to moderate.
Discussion
Our findings indicate that self-compassion is a strong protective factor and may enhance resilience and promote mental health among developing counselors, despite impostor feelings. Specifically, self-compassion fully mediated the negative relationship between IP, resilience, and depression, while partially mediating the relationship between IP and anxiety. This suggests that even when experiencing IP, higher self-compassion may help to maintain greater resilience and significantly reduced anxiety and depression. The results are promising and suggest that cultivating self-compassion may facilitate professional growth by interrupting the IP cycle. Our results offer further insights into how self-compassion can support resilience and mental health (Housenecht & Swank, 2022).
Descriptive Statistics
Descriptive analyses revealed a notably high prevalence of IP in the sample, with 96.1% (n = 270) reporting moderate to intense symptoms. Scores were skewed toward the higher end of the scale, with 65.1% of participants in the frequent-to-intense range and 21% in the highest category. Compared with earlier samples, these findings suggest that the severity of IP has increased substantially over the past 15 years (Roskowski, 2010; Tigranyan et al., 2021). For example, only 27.6% of a 2010 sample fell into the frequent-to-intense categories, compared with nearly two-thirds in the present study. Likewise, the proportion of students in the highest IP range has risen fivefold, from 4.1% in 2010 to 21% here. Although this increase may be influenced by broader cultural or educational factors, the trend underscores the importance of implementing effective coping strategies to support counselor well-being and persistence.
Consistently elevated IP scores across studies suggest that impostor feelings may be a common element of counselor development. Such feelings are often fueled by both internal and environmental pressures, particularly graduate students’ unreasonably high expectations of their performance and rapid development (Clance & Lawry, 2024). These unrealistic standards can generate unnecessary self-doubt, distorted self-assessments, and persistent self-criticism (Gadsby & Hohwy, 2024). Importantly, the current results indicate that self-compassion is a powerful counterbalance to IP. Higher self-compassion was associated with lower IP, anxiety, and depression, and with greater resilience, findings that align with previous research (Liu et al., 2023).
Mediation Models
Self-Compassion, IP, and Resilience
The first mediation analysis revealed that self-compassion fully mediated the negative relationship between IP and resilience. When accounting for self-compassion, the negative relationship between IP and resilience was rendered statistically non-significant. This outcome suggests that developing counselors with higher self-compassion may more easily adapt and recover when experiencing impostor-related distress. Self-compassion may assist key aspects of resilience, including stress management, coping with adversity, and maintaining a stable and supportive inner identity (Webb & Rosenbaum, 2019).
Although IP encourages harsh self-criticism and rumination on perceived failures, it is possible that through increased self-acceptance and soothing kindness, counselors can embody greater resilience when confronting areas of growth with less fear of failure. Additionally, a common humanity perspective can encourage acceptance of struggles as a normal part of counselor development and one shared by their peers. These soothing and normalizing aspects of self-compassion can encourage community rather than isolation when struggling, helping counselors to maintain resilience amidst adversity (Hou & Skovholt, 2020; Neff, 2023). Without effective coping practices, the challenges of counselor development can wear down resilience, creating vulnerability to mental distress, burnout, and counselor impairment (Cook et al., 2021; Gerber & Anaki, 2021).
Self-Compassion, IP, and Mental Health
Our results indicate that self-compassion is associated with less anxiety among those experiencing IP. Because anxiety is prevalent in this population and a primary emotional response to IP, efforts to increase self-compassion can have widely beneficial outcomes (Crego et al., 2022; Garba et al., 2024). The common humanity and mindfulness components of self-compassion may be critical to this outcome, as they can help limit emotional reactivity, normalize the IP experience, and reduce the isolation and fear of being exposed as an impostor (Clarke & Guida, 2025). This process involves mindfully recognizing that others share similar experiences and feelings, empowering developing counselors to seek support and reduce fear of failure (Neff, 2023). Likewise, practicing self-kindness may counter the harsh self-criticism associated with IP and encourage them to embrace the developmental process, including their imperfections (Patzak et al., 2017; Warren et al., 2016).
Anxiety and depression are closely linked and often co-occur (Beck & Alford, 2009). Though depression may not correlate as strongly with IP as anxiety does, it remains a common outcome (Garba et al., 2024). IP is persistent and sustained by cognitive distortions and misattributions, which also contribute to depressive thought patterns (Beck & Alford, 2009). However, our analysis revealed that self-compassion fully mediated the relationship between IP and depression. This suggests that a combination of mindful awareness and active self-kindness may facilitate more balanced self-assessment, countering perfectionism and harsh self-criticism commonly associated with IP (Clarke & Hartley, 2025; Pákozdy et al., 2023).
Although IP significantly predicted anxiety and depression, the buffering effect of self-compassion suggests that those with more compassionate self-perceptions may better tolerate the uncertainty and challenges common to counselor training. For example, those with a self-compassionate mindset may reinterpret failures as growth opportunities, a shift that may protect against anxious and depressive symptoms (Crego et al., 2022; Warren et al., 2016). These findings highlight the regulatory potential of self-compassion in reducing emotional reactivity to impostor-related distress.
Level of Self-Compassion in Relation to IP, Resilience, and Mental Health
MANOVA was utilized to determine whether the level of self-compassion (categorized as low, moderate, or high) was related to the level of IP, resilience, anxiety, and depression (Neff, 2003). Self-compassion had a significant positive relationship with mental health and resilience; however, the relationships varied significantly based on level of self-compassion (Figure 4). The results demonstrate that even lower levels of self-compassion were related to significantly lower IP, anxiety, and depression, as well as increased resilience. This pattern suggests that even modest improvements in self-compassion can correspond to improved well-being among developing counselors (Luo et al., 2023). For example, IP severity decreased significantly as self-compassion levels increased, revealing a linear reduction in IP from low to high self-compassion levels, with the most pronounced decrease occurring between the moderate and high categories.
Similarly, resilience scores also increased consistently across each level of self-compassion. The increase was linear, with the most substantial increase occurring when self-compassion rose from low to moderate. The steady increase in resilience across all self-compassion levels points to a possible dose-response relationship. Initial gains in self-compassion may bolster developing counselors’ ability to persevere through challenges (Neff et al., 2005), and interventions resulting in modest enhancements in self-compassion could yield significant improvements in resilience.
Figure 4
IP, Resilience, Depression, and Anxiety Across Levels of Self-Compassion
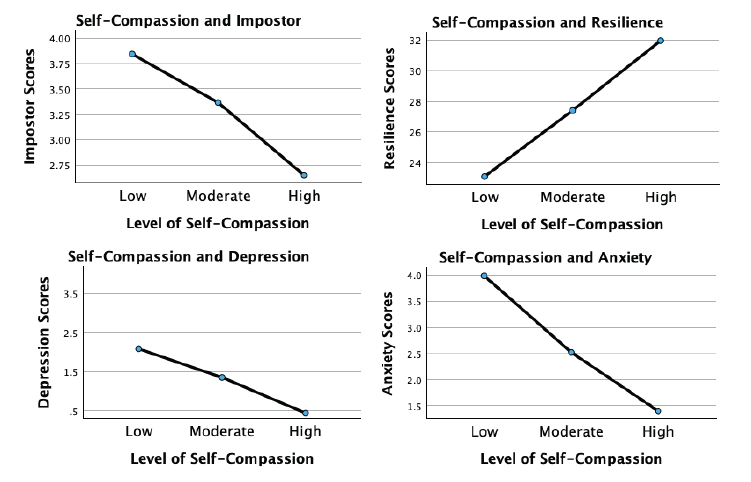
Although more variable, the association of self-compassion with anxiety and depression was similarly beneficial. Anxiety levels decreased significantly with each incremental increase in self-compassion, with the largest reduction occurring from low to moderate levels. This underscores the potential that even lower levels of self-compassion may still meaningfully alleviate anxiety. For depression, a significant decrease occurred across self-compassion levels, with the most substantial reduction noted as self-compassion increased from moderate to high. This suggests that self-compassion may interrupt the internal feedback loop of shame, self-criticism, and hopelessness that sustains depressive thinking in the context of IP.
These findings indicate that self-compassion is an important protective factor for developing counselor mental health. Contrary to expectations, even lower levels of self-compassion significantly relate to reduced IP, anxiety, and depression while increasing resilience (Luo et al., 2023). Integrating strategies to enhance self-compassion into counselor training programs could incrementally increase self-compassion, build emotional tolerance, and create a more stable internal environment from which resilience and well-being can emerge.
Implications and Future Directions for Counselor Development
Despite IP’s prevalence and association with diminished resilience and psychological distress, it remains underexamined in the counseling literature. Beyond a self-care strategy, self-compassion may build resilience and maintain mental health during and after counselor training. Integrating self-compassion into counselor education and early career development may cultivate a more supportive environment and provide counselors with evidence-based ways to manage IP and enhance resilience. Whereas, if left unaddressed, IP can lead to unnecessary distress, burnout, and professional attrition (Coaston & Lawrence, 2019; Ojeda, 2024).
Growing evidence suggests that self-compassion is vital for counselor development and ethical practice (Clarke et al., 2025; Coaston & Lawrence, 2019). The American Counseling Association (ACA) Code of Ethics (2014) emphasizes that professional counselors must engage in ongoing self-assessment and maintain their effectiveness through self-care practices. Similarly, CACREP (2023) standards require counselor education programs to integrate “self-care, self-awareness, and self-evaluation strategies for ethical and effective practice” (3.A.11.). Without meaningful coping strategies, IP can directly undermine these ethical mandates by diminishing well-being and distorting self-evaluation necessary for competent practice (Gadsby & Hohwy, 2024).
Regular engagement in reflective activities promoting balanced self-evaluation is essential to counselor development. If such exercises lack a compassionate focus, they may inadvertently reinforce impostor-related distortions by encouraging rumination and inaccurate self-critique. Matching reflective self-assessment with self-compassion practice may allow developing counselors to internalize feedback and move attention away from self-criticism and toward a growth mindset, transforming internal narratives dominated by IP (Warren et al., 2016).
Counselor educators and professional agencies can integrate self-compassion training through multiple pathways. Brief interventions, such as abbreviated versions of the Mindful Self-Compassion program (Germer & Neff, 2019), offer evidence-based approaches for enhancing counselor resilience. If limited by time and resources, supervisors and mentors can model self-compassionate practices by normalizing struggles, demonstrating constructive self-talk, and providing balanced growth-oriented feedback. The disclosure of faculty or supervisor IP experiences may be particularly powerful, reframing vulnerability and self-care as professional strengths rather than weaknesses.
Because IP is a contextual and environmentally fueled experience, counseling agencies and community mental health settings can foster organizational climates that prioritize compassion and collaboration and normalize challenges during the growth process (Coaston, 2019). When institutions reward openness, reflection, and learning from error, rather than perfection and productivity, developing counselors are more likely to engage in authentic self-assessment and seek help when struggling.
Early career peer support groups and compassion-focused initiatives can also counter the competitive, perfectionistic culture that sustains IP in professional practice (Clark et al., 2022). These approaches challenge the isolating belief that self-doubt is uniquely shameful, and foster community and belonging (Clarke & Guida, 2025; Hou & Skovholt, 2020). Future research should employ longitudinal and experimental designs to test targeted self-compassion interventions, clarifying causal relationships between self-compassion, resilience, and mental health outcomes in counselor education and professional contexts.
Clinical Supervision
Developmentally, the transition from classroom learning to applying theory and skills in clinical practice naturally provokes stress and anxiety (Skovholt & Trotter-Mathison, 2024). Although clinical supervision provides an ideal context for fostering openness and resilience (Coaston, 2019), experiencing IP may be a barrier to disclosing challenges because of emotional distress and fear of exposing perceived inadequacies (DeCandia Vitoria, 2021). Maintaining a façade of competence can compromise development and hinder the supervisory relationship (Thériault et al., 2009). These perfectionistic tendencies and IP are often motivated by context, suggesting that supervisors’ approaches may significantly alleviate these patterns.
Coaston (2019) provides a practical framework for applying self-compassion principles and philosophy in clinical supervision. Rooted in humanistic and developmental theory, this approach emphasizes that supervisors can accompany supervisees through the inevitable discomfort and vulnerability of professional growth by responding with compassion rather than judgment. By adopting a compassionate approach, the supervisory relationship can deepen, normalizing challenges and facilitating an authentic dialogue about IP-related uncertainties. In this way, clinical supervisors can address common cognitive and affective challenges.
A compassionate supervisory environment promotes balanced self-reflection and can reduce the shame-based fear of exposure that drives impostor defenses. This may allow supervisees to explore their conceptual skills openly, reframe unrealistic expectations, and persist despite challenges (Hou & Skovholt, 2020; Stoltenberg & McNeill, 2010). Future research can investigate how self-compassion contributes to the supervisory relationship, comfort with disclosure, and the integration of constructive feedback during supervised practice.
Clinical supervisors can also create a culture of shared vulnerability by modeling self-compassion and transparency about their own developmental struggles and self-doubt. This enables supervisees to internalize feedback and approach self-evaluation with less emotional reactivity. Enhancing collaboration within the alliance empowers supervisees to feel more competent in navigating their development independently (Skovholt & Trotter-Mathison, 2024). Given the potential benefits of this approach, we recommend that future research examine how embodiment and facilitation of self-compassion affect counselor development and well-being.
Limitations
Although the results of this study are encouraging, there are limitations. The cross-sectional design limits the data to a single point in time rather than showing fluctuations in self-compassion, IP, resilience, and mental health over time. Likewise, the present results do not establish causality. Replicating this study using a longitudinal approach can provide greater insight into these fluctuations. Furthermore, self-report measures introduce limitations such as social desirability bias and reliance on participant self-awareness. Likewise, individuals with a personal connection to IP may have been more likely to participate, potentially skewing results.
Participants were not asked about their matriculation status as counseling students, leaving their stage of development unknown. Future research should include clinical experience (i.e., none, practicum, internship) and matriculation status. This information would provide greater insight into how experience and counselor development interact with IP. The current study used a general IP assessment, while future research should use the Counselor Impostor Scale (CIS; Nguyen, 2023), which was published after data collection for this study was complete. The CIS is designed specifically for the counseling domain and could provide more nuanced insights. Additionally, because maladaptive coping strategies such as procrastination and perfectionism sustain IP, subsequent studies should explore these constructs, which could inform more targeted interventions.
Conclusion
The growth process during counselor training is inherently challenging and often gives rise to IP, which increases anxiety and depression while diminishing resilience. Self-compassion is a promising method for enhancing resilience and well-being, despite the presence of IP. Once learned, self-compassion is an accessible practice and relies on applying skills with which counselors are familiar, such as kindness and compassion toward themselves. The results of this study are encouraging and robust, suggesting that self-compassion can enhance resilience by supporting adaptive emotional regulation and fostering a growth-oriented mindset. Self-compassionate counselors can maintain their well-being despite experiencing IP. Importantly, the positive impact of self-compassion was consistent and significant even at lower levels, which is especially important given the prevalence and severity of IP among CITs. The findings support integrating self-compassion into counselor training and clinical supervision through modeling, training, and practice. This approach can provide effective coping for IP and improve resilience, mental health, and persistence.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default- document-library/ethics/2014-aca-code-of-ethics.pdf
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). University of Pennsylvania Press.
Council for the Accreditation of Counseling and Related Educational Programs (2023). 2024 standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Clance, P. R. (1985). Clance Impostor Phenomenon Scale (CIPS). [Database record]. APA PsycTests. https://doi.org/10.1037/t11274-000
Clance, P., & Lawry, S. (2024). Impostor phenomenon: Origins and treatment. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 17–43). American Psychological Association.
Clark, P., Holden, C., Russell, M., & Downs, H. (2022). The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy, 44(2), 185–197. https://doi.org/10.1007/s10591-021-09580-y
Clarke, B. J. (2024). Emerging adult life satisfaction and mental health: The mediating role of self-compassion and social support. Emerging Adulthood, 12(6), 1137–1147. https://doi.org/10.1177/21676968241279490
Clarke, B. J., & Guida, A. M. (2025). Self-compassion to community: The mediating effect of belonging on college student mental health and life satisfaction. Journal of College Student Mental Health. Advance online publication. https://doi.org/10.1080/28367138.2025.2552484
Clarke, B. J., & Hartley, M. T. (2025). Contemplative dispositions and mental health: The supportive role of self-compassion and mindfulness on college students’ resilience. Journal of College Student Mental Health, 39(1), 142–164. https://doi.org/10.1080/28367138.2024.2331931
Clarke, B. J., Hartley, M. T., & Button, C. (2025). Impostor phenomenon and counselor development: The critical role of self-compassion. Journal of Counseling & Development, 103(2), 149–160. https://doi.org/10.1002/jcad.12544
Coaston, S. C. (2019). Cultivating self-compassion within the supervision relationship. The Clinical Supervisor, 38(1), 79–96. https://doi.org/10.1080/07325223.2018.1525596
Coaston, S. C., & Lawrence, C. (2019). Integrating self-compassion across the counselor education curriculum. Journal of Creativity in Mental Health, 14(3), 292–305. https://doi.org/10.1080/15401383.2019.1610536
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in developing professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Crego, A., Yela, J. R., Riesco-Matías, P., Gómez-Martínez, M. Á., & Vicente-Arruebarrena, A. (2022). The benefits of self-compassion in mental health professionals: A systematic review of empirical research. Psychology Research and Behavior Management, 15, 2599–2620. https://doi.org/10.2147/PRBM.S359382
DeCandia Vitoria, A. (2021). Experiential supervision: Healing impostor phenomenon from the inside out. The Clinical Supervisor, 40(2), 200–217. https://doi.org/10.1080/07325223.2020.1830215
Delaney, M. C. (2018). Caring for the caregivers: Evaluation of the effect of an eight-week pilot Mindful Self-Compassion (MSC) training program on nurses’ compassion fatigue and resilience. PLoS ONE, 13(11), e0207261. https://doi.org/10.1371/journal.pone.0207261
Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gadsby, S., & Hohwy, J. (2024). Negative performance evaluation in the impostor phenomenon. Current Psychology, 43, 9300–9308. https://doi.org/10.1007/s12144-023-05030-0
Garba, R., Coleman, C., & Kelley, T. (2024). The impostor phenomenon and mental health. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 61–79). American Psychological Association.
Gerber, Z., & Anaki, D. (2021). The role of self-compassion, concern for others, and basic psychological needs in the reduction of caregiving burnout. Mindfulness, 12, 741–750. https://doi.org/10.1007/s12671-020-01540-1
Germer, C., & Neff, K. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. Guilford.
Gignac, G. E., & Szodorai, E. T. (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. https://doi.org/10.1016/j.paid.2016.06.069
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford.
Hou, J.-M., & Skovholt, T. M. (2020). Characteristics of highly resilient therapists. Journal of Counseling Psychology, 67(3), 386–400. https://doi.org/10.1037/cou0000401
Housenecht, A., & Swank, J. (2022). Motivation, belonging, and support: Examining persistence in counseling programs. Teaching and Supervision in Counseling, 4(2), Article 3. https://doi.org/10.7290/tsc04g4iv
Khubchandani, J., Brey, R., Kotecki, J., Kleinfelder, J., & Anderson, J. (2016). The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Archives of Psychiatric Nursing, 30(4), 457–462. https://doi.org/10.1016/j.apnu.2016.01.014
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Liu, S., Wei, M., & Russell, D. (2023). Effects of a brief self-compassion intervention for college students with impostor phenomenon. Journal of Counseling Psychology, 70(6), 711–724. https://doi.org/10.1037/cou0000703
Luo, X., Che, X., & Lei, Y. (2023). Characterizing the effects of self-compassion interventions on anxiety: Meta-analytic evidence from randomized controlled studies. Journal of Contextual Behavioral Science, 30, 132–141. https://doi.org/10.1016/j.jcbs.2023.10.004
Mak, K. K. L., Kleitman, S., & Abbott, M. J. (2019). Impostor phenomenon measurement scales: A systematic review. Frontiers in Psychology, 10, 671. https://doi.org/10.3389/fpsyg.2019.00671
Martin, A. J., & Marsh, H. W. (2006). Academic resilience and its psychological and educational correlates: A construct validity approach. Psychology in the Schools, 43(3), 267–281. https://doi.org/10.1002/pits.20149
Neff, K. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2023). Self-compassion: Theory, method, research, and intervention. Annual Review of Psychology, 74, 193–218. https://doi.org/10.1146/annurev-psych-032420-031047
Neff, K. D., Hsieh, Y. P., & Dejitterat, K. (2005). Self-compassion, achievement goals, and coping with academic failure. Self and Identity, 4(3), 263–287. https://doi.org/10.1080/13576500444000317
Neff, K. D., Tóth-Király, I., Yarnell, L. M., Arimitsu, K., Castilho, P., Ghorbani, N., Guo, H. X., Hirsch, J. K., Hupfeld, J., Hutz, C. S., Kotsou, I., Lee, W. K., Montero-Marin, J., Sirois, F. M., de Souza, L. K., Svendsen, J. L., Wilkinson, R. B., & Mantzios, M. (2019). Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: Support for use of a total score and six subscale scores. Psychological Assessment, 31(1), 27–45. https://doi.org/10.1037/pas0000629
Nguyen, L. T. (2023). Development and validation of the Counseling Impostor Scale (Doctoral dissertation). Texas A&M University–Corpus Christi.
Ojeda, L. (2024). Impostor phenomenon and burnout. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 81–110). American Psychological Association.
Pákozdy, C., Askew, J., Dyer, J., Gately, P., Martin, L., Mavor, K. I., & Brown, G. R. (2023). The impostor phenomenon and its relationship with self-efficacy, perfectionism, and happiness in university students. Current Psychology, 43, 1–10. https://doi.org/10.1007/s12144-023-04672-4
Patzak, A., Kollmayer, M., & Schober, B. (2017). Buffering impostor feelings with kindness: The mediating role of self-compassion between gender-role orientation and the impostor phenomenon. Frontiers in Psychology, 8, Article 1289. https://doi.org/10.3389/fpsyg.2017.01289
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Roskowski, J. C. R. (2010). Impostor phenomenon and counseling self-efficacy: The impact of impostor feelings (Doctoral dissertation). Ball State University.
Skovholt, T. M., & Trotter-Mathison, M. (2024). The elevated stressors of the novice practitioner. In T. M. Skovholt & M. Trotter-Mathison (Eds.), The resilient practitioner: Burnout and compassion fatigue prevention and self-care strategies for the helping professions (4th ed., pp. 42–68). Taylor & Francis.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Thériault, A., Gazzola, N., & Richardson, B. (2009). Feelings of incompetence in developing therapists: Consequences, coping, and correctives. Canadian Journal of Counselling, 43(2), 105–119.
Tigranyan, S., Byington, D. R., Liupakorn, D., Hicks, A., Mathis, M., & Rodolfa, E. (2021). Factors related to the impostor phenomenon in psychology doctoral students. Training and Education in Professional Psychology, 15(4), 298–305. https://doi.org/10.1037/tep0000321
Wang, B., Andrews, W., Bechtoldt, M. N., Rohrmann, S., & de Vries, R. E. (2022). Validation of the short Clance Impostor Phenomenon Scale (CIPS-10). European Journal of Psychological Assessment, 40(2), 158–168. https://doi.org/10.1027/1015-5759/a000747
Warren, R., Smeets, E., & Neff, K. (2016). Self-criticism and self-compassion: Risk and resilience. Current Psychiatry, 15(12), 18–33. https://self-compassion.org/wp-content/uploads/2016/12/Self-Criticism.pdf
Webb, R. E., & Rosenbaum, P. (2019). Resilience and thinking perpendicularly: A meditation or morning jog. Journal of College Student Psychotherapy, 33(1), 75–88. https://doi.org/10.1080/87568225.2018.1449687
Brian J. Clarke, PhD, NCC, LAC, is an assistant professor at the University of Arizona. Michael T. Hartley, PhD, CRC, is a professor at the University of Arizona. Austin M. Guida, PhD, NCC, LAC, is an assistant professor at Northern Arizona University. Correspondence may be addressed to Brian J. Clarke, Department of Disability and Psychoeducational Studies, College of Education, 1430 E. 2nd Street, Room 422, Tucson, AZ, 85721-0069, bclarke14@arizona.edu.
