Broaching the Social Determinants of Mental Health in Counseling Practice
Danielle Pester Boyd, Laura K. Jones, Courtney Maier, Danica G. Hays
The intentional exploration or broaching of topics related to the social determinants of mental health (SDoMH) throughout the counseling process helps align clinical practice with the profession’s focus on multicultural and social justice counseling competency. This article identifies six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences, (e) addressing emergent needs, and (f) termination practices. These SDoMH broaching behaviors span counselor preparation, assessment, intervention, and termination, empowering counselors to address SDoMH in their work. We conclude with implications for fostering SDoMH broaching behaviors within counselor education.
Keywords: broaching, social determinants of mental health, multicultural, counseling competency, counselor education
Counselors are increasingly called upon to integrate multicultural competence and social justice advocacy into their practice, particularly when addressing systemic and environmental factors that shape client well-being. The Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) and relevant constructs, such as the social determinants–based counseling model (SDCM; Pester Boyd et al., 2025) and the multidimensional model of broaching behavior (MMBB; Day-Vines et al., 2020), provide guiding frameworks for ensuring culturally responsive care. Taken together, these models inform concrete methods for integrating discussions of systemic, environmental, and structural influences into counselor–client interactions, which create a foundation for a set of broaching behaviors focused specifically on the social determinants of mental health (SDoMH).
Social determinants of health (SDOH) refer to “the conditions in which people are born, grow, live, work, and age that shape health outcomes” (World Health Organization [WHO], 2025, para. 1). These determinants include economic stability (e.g., employment, income), health care access, education, neighborhood safety, and social relationships, all of which impact physical and mental health. The SDoMH focus specifically on the social and structural factors influencing mental health outcomes, such as exposure to discrimination, adverse childhood experiences, community violence, economic disparities, and barriers to mental health care (Compton & Shim, 2020), influences that are reflected in the MSJCC.
The SDCM is an empirically based systemic framework for addressing SDoMH across various practice settings (Pester Boyd et al., 2025). It guides counselors in identifying barriers, such as economic hardship, discrimination, and limited access to resources, and then provides a structured process for broaching these concerns in session. Beyond simple recognition, the SDCM emphasizes implementing culturally responsive interventions, including connecting clients with community supports, advocating for policy changes, or adapting treatment plans to account for systemic stressors. This systemic responsiveness communicates to clients that their external challenges are legitimate and central to their mental health care, which reinforces the therapeutic alliance by integrating advocacy with clinical practice. Given the links among the MSJCC, SDoMH, and therapeutic outcomes, it is imperative that counselors are familiar with SDoMH, understand their impact, and are prepared to broach topics related to SDoMH with clients. Therefore, integrating the SDCM with known broaching models like the MMBB can serve to operationalize these action strategies as concrete methods to demonstrate the MSJCC.
The MMBB provides a framework to explicitly explore or broach racial, ethnic, and cultural (REC) factors with clients throughout the therapeutic process (Day-Vines et al., 2020, 2021). These broaching behaviors focus on four distinct contexts: intracounseling, intraindividual, intra-REC, and inter-REC domains. Specifically, counselors acknowledge REC concerns that impact the counselor–client relationship (intracounseling), the intersections of the client’s identity (intraindividual), the client’s cultural group membership (intra-REC), and their experiences with structural inequality (inter-REC). By intentionally attending to these layers, counselors demonstrate cultural humility and multicultural competency that affirms the realities of clients’ REC concerns. Effective broaching has been linked to enhanced client trust, increased depth of client self-disclosure, higher levels of client satisfaction, and improved therapeutic outcomes, which make it a critical component of effective multicultural counseling (Depauw et al., 2025; Gantt-Howrey et al., 2024; King & Borders, 2019; Zhang & Burkard, 2008).
By integrating the SDCM with the MMBB, we developed a set of SDoMH-specific broaching behaviors. The MMBB strengthens the relational dimension of counseling through cultural engagement while the SDCM equips counselors to act on systemic barriers that influence client well-being. Together, these models ultimately foster trust, collaboration, and empowerment and establish counseling as a space where both individual experiences and broader structural inequities are acknowledged and addressed.
SDoMH Broaching Behaviors
This article describes six SDoMH broaching behaviors for counselors grounded in the MMBB and the SDCM: counselor development, client psychoeducation, contextualization, attending to differences of lived experience, addressing emergent needs, and SDoMH-informed termination practices. These SDoMH broaching behaviors represent an interactive approach in which counselors shift among the behaviors throughout their own development as well as during assessment, intervention, and termination within the counseling relationship.
Counselor Development
The first SDoMH broaching behavior is initiated during a counselor’s preparation to work with clients. In alignment with the MSJCC (Ratts et al., 2016), counselors are expected to continually foster both knowledge and self-awareness related to the multicultural and social justice issues facing their clients, including client experiences with SDoMH. In order to develop their knowledge of SDoMH scholarship, counselors can familiarize themselves with the seminal SDOH/SDoMH frameworks (e.g., Compton & Shim, 2020; Lund et al., 2018; WHO, 2025); guiding practice models related to broaching behaviors and best practices for addressing the SDoMH (e.g., MMBB, SDCM; Day-Vines et al., 2020; Pester Boyd et al., 2025); general scholarship on SDoMH application in training, practice, and research (e.g., Johnson et al., 2023; Lenz & Lemberger-Truelove, 2023; Lenz & Litam, 2023; Mason et al., 2023; Neal Keith et al., 2023; Pester et al., 2023); and, when applicable, setting-specific SDoMH resources for school counselors (e.g., Brookover, 2024; Johnson & Brookover, 2021), career counselors (Johnson et al., 2024), and family counselors (Robins et al., 2022).
Next, to facilitate self-awareness, counselors are encouraged to engage in reflective practices that identify areas of strength in addressing SDoMH with clients and areas that require skill and dispositional development. First, counselors should reflect on any personal experiences with SDoMH and how those experiences may both inform and potentially bias their work with clients. For example, counselors who have dealt with their own experiences of economic instability may need to watch for emerging countertransference with clients having similar experiences. We recommend that counselors review existing SDoMH frameworks and identify which determinants have affected them personally and interpersonally with peers, family members, and colleagues. In addition, they can consider what strategies were helpful or harmful as they personally navigated SDoMH.
Counselors should also reflect on any prior experiences working with clients who were dealing with SDoMH and how those prior professional experiences might inform and potentially bias their ability to help new clients with SDoMH. For example, counselors might view clients as resistant if they do not consistently attend counseling sessions, although those clients may be dealing with circumstances impacted by SDoMH (e.g., unstable transportation, lack of childcare, unreliable internet access). Mechanisms such as supervision or consultation can be helpful for facilitating counselor awareness and development related to being nonjudgmental, showing unconditional positive regard, and embodying congruence, which are all vital components of creating and maintaining a strong therapeutic alliance.
Additionally, counselors or counseling supervisors can administer the Addressing Client Needs with Social Determinants of Health Scale (ACN:SDH, Johnson, 2023) to more formally assess readiness for addressing SDoMH. This tool measures a provider’s SDOH competency related to knowledge, awareness, biases, skills, and preparedness. The ACN:SDH findings can be reviewed within supervision or consultation. For areas where data reflect a lack of readiness, counselors can process feelings associated with their limited readiness and brainstorm resources that may be useful for building readiness. Ultimately, as counselors focus inward to broach and support their professional development related to the SDoMH framework, they will be more prepared to implement the remaining SDoMH broaching behaviors in client interactions.
Client Psychoeducation
Client psychoeducation is the next SDoMH broaching behavior that begins during the intake and assessment process. Psychoeducation is an evidence-based intervention that integrates client education into the counseling process by connecting clinical outcomes to increased client self-awareness and skill development across many mental health presenting concerns (e.g., anxiety, depression, schizophrenia; Dolan et al., 2021; Luo et al., 2025). We suggest that counselors mindfully introduce SDoMH psychoeducation into the intake and assessment process to increase client knowledge and awareness about the potential impact of SDoMH on well-being.
Furthermore, there is growing support for universal SDoMH screening (Gantt-Howrey et al., 2024; Johnson & Brookover, 2021; Johnson et al., 2023), with many available screeners for counselors to use, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE; 2022); the Accountable Health Communities Health-Related Social Needs Screening Tool (Center for Medicare and Medicaid Innovation, n.d.); and the WE CARE Survey (Garg et al., 2007). These screeners can be incorporated into intake processes to establish a baseline of SDoMH data for clients. For example, the PRAPARE assessment identifies both individual areas of risk related to social determinants and an overall risk tally score. Counselors can use this data to inform both the focus of the psychoeducation intervention and the client’s treatment plan.
Many clients may not fully understand why they are being asked about these areas of their lives or be aware of how these determinants may influence well-being. Therefore, counselors should first define SDoMH and explain the overall framework using jargon-free language. For example:
Social determinants of mental health are different social and environmental factors that can positively or negatively influence our physical and mental health. These can be factors like having your basic needs of food, housing, and employment met; having access to quality education and health care; living in a safe environment free of violence and risk; and having strong social and community support. The more people are surrounded by supportive social and environmental conditions, the easier it is to improve overall health and mental health. When people do not have adequate access to these conditions, it can lead to a higher risk of health and mental health concerns. It is important for the work that we are going to do together to have a clear picture of how your environment is influencing your physical and mental health so that we can work to increase conditions that will support the positive mental health changes you are wanting to make.
Counselors can also consider using visual tools in session, such as handouts that depict SDoMH in an easily understandable format (see Figure 1 for a sample).
Counselors should then use the SDoMH data collected through the assessment process to provide data-driven psychoeducation about the specific social determinant risk areas identified in a client’s assessment, outlining the research and known physical and mental health risks and outcomes of those determinants. For example, one item on the PRAPARE assessment asks, “How often do you see or talk to people that you care about and feel close to?” If a client answers less than three times per week, they are flagged for a risk tally on this item; the counselor could provide psychoeducation on the impact of social connection and community support alongside the risks of social isolation (U.S. Department of Health and Human Services, 2023). A counselor might broach the topic by saying:
I noticed when you were asked how many times you see or talk to people you care about that you answered less than three times per week. I ask this question on the screener because at times the number and quality of our social connections can have an influence on our physical and mental health. For example, social isolation has been linked to increased risk of anxiety and depression, lower academic and job performance, greater susceptibility to viruses and respiratory illnesses, and even long-term risk of diseases such as heart disease and stroke. Healthy social connection can protect us from disease and increase our sense of safety, meaning, and resilience. Tell me more about what social connection looks like in your life.
By broaching the subject in this way, the counselor can intentionally assess the impact of a specific social determinant on the client’s overall well-being and health. In the example, the counselor would seek to understand the quantity, quality, and impact of the client’s relationships while also screening for any potential physical symptoms that might require an external referral. This practice of broaching SDoMH through client psychoeducation and assessment allows the counselor to implement data-driven practices that provide a multitiered therapeutic framework to conceptualize client concerns across various socioecological levels (e.g., individual, interpersonal, community, public policy). This in turn supports the development of a more holistic treatment plan that incorporates both individual and community interventions.
Figure 1
Visual Depiction of the Social Determinants of Mental Health for Clinical Use
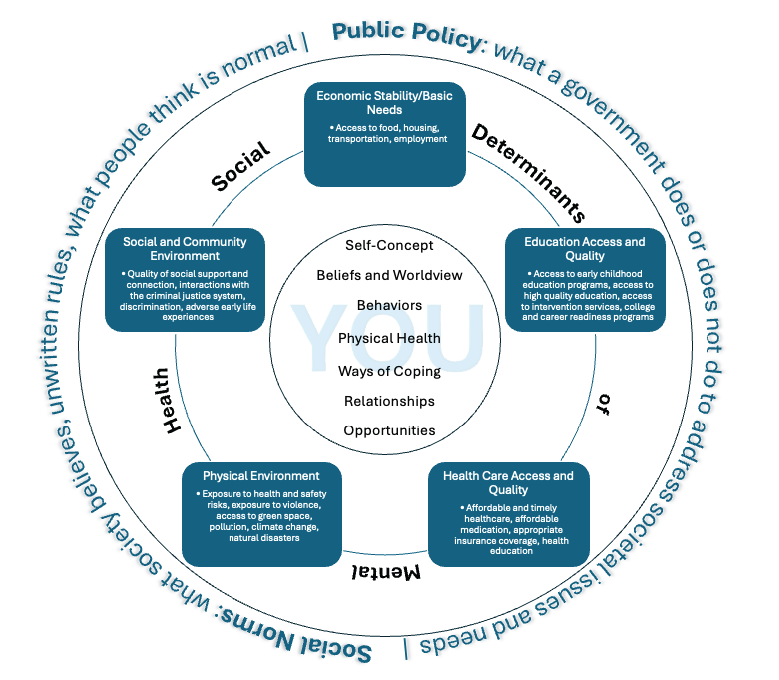
Note. Adapted from Social Determinants of Health, by Office of Disease Prevention and Health Promotion, 2025 (https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health) and “Social Determinants of Mental Health” by Compton, M. T., & Shim, R. S., 2015, Focus, 13(4), p. 420 (https://doi.org/10.1176/appi.focus.20150017).
Contextualizing SDoMH for Each Client
As a client develops understanding and awareness of the social determinants impacting their well-being, the counselor should also use broaching to contextualize that knowledge on an individual level. In this way, counselors go beyond educating clients about SDoMH in general and instead seek to collaborate with the client to understand how they are uniquely impacted by those factors. This practice of contextualizing SDoMH allows the client to make connections between their lived experiences, intrapsychic concerns, and the larger social and environmental context.
This broaching behavior aligns well with the MMBB and its intraindividual, intra-REC, and inter-REC broaching dimensions. Counselors can apply these broaching dimensions to the contextualization process. For example, intraindividual broaching can be used to acknowledge how SDoMH impact a client’s identity dimensions (e.g., race, gender, socioeconomic status, sexual orientation, immigration status). A counselor could say, “It sounds like financial strain has limited your transportation options to get to your appointments. Let’s find some free or low-cost alternatives that might better fit within your budget.” Intra-REC broaching, or the exploration of within–cultural group concerns, can help the counselor discuss any client issues impacted by SDoMH that are culture-specific. A counselor might say to the client, “I imagine it could be difficult to ask family and friends for a ride to your appointments if mental health is stigmatized in those relationships.” Finally, a counselor may apply inter-REC broaching by exploring a client’s experiences with discrimination:
Relying on public transportation resources in this city has caused you to miss important appointments and events. It sounds like these public resources don’t meet the needs of residents. I plan to write a letter to the city council explaining some of the issues. Is there anything specific that you would like me to communicate or any way that you would like to advocate for changes?
By integrating these specific broaching dimensions, counselors can help clients gain both self and situational awareness by better understanding the possible role of social determinants in their own lives. In turn, this allows the counselor and client to better address challenges by understanding the client’s unique needs in context. From the previous example, the counselor might consider the following: Does the client need help identifying additional transportation resources? Would virtual counseling sessions be a more accessible option? Can I advocate for improved public transportation in the local community by providing key context to local leaders about how unreliable transportation affects the health of their constituents? Are there self-advocacy skills that I could help the client develop? Through targeted discussions on SDoMH like these, counselors can ensure that they are providing culturally responsive care that meets their clients’ unique needs.
Broaching Differences in the Counselor–Client Relationship
As SDoMH factors are integrated into the therapeutic process, counselors must also attend to the interpersonal process of the therapeutic alliance by intentionally broaching any differences that may exist between the counselor and client. Clients from historically marginalized backgrounds may experience factors that may differ significantly from their counselor’s lived experiences, such as heightened economic instability, community violence, and health care barriers (Compton & Shim, 2015). The MMBB, through its intracounseling domain, emphasizes that a counselor must actively acknowledge and explore REC differences between the counselor and client to attend to any disruptive interpersonal processes that might impact the therapeutic relationship (Day-Vines et al., 2020). We suggest that differences in lived experience related to SDoMH be treated comparably to ensure culturally responsive and effective care.
Research suggests that counselors who fail to broach REC concerns and SDoMH-related disparities risk reinforcing dominant cultural narratives that dismiss or minimize the structural challenges clients face, potentially leading to client disengagement, cultural miscommunication, and premature termination of counseling services (Day-Vines et al., 2021; Drinane et al., 2018; Owen et al., 2014). Thus, it is incumbent upon counselors to broach these differences with cultural humility, openness, and a willingness to engage in difficult but necessary conversations (Newton & Steele, 2025). To effectively broach these conversations, a counselor should adopt a collaborative, client-centered approach by acknowledging potential differences in lived experiences while affirming the client’s perspective.
One strategy is for the counselor to invite open discussions by saying:
I recognize that my experiences may be different from yours, and I don’t want to make assumptions about the challenges that you face. I’d like to understand more about how factors like financial stress, health care access, or discrimination may be affecting your mental health. Would you be open to sharing what that has been like for you?
This type of broaching explicitly acknowledges differences in identity, privilege, and lived experience between the counselor and client while creating a nonjudgmental and validating therapeutic space for the client to share their reality (Day-Vines et al., 2021).
Another example of effective intracounseling broaching can be seen in a case where a White counselor works with a Black client who describes frequent racial discrimination in the workplace. To avoid deflecting or minimizing the client’s experience, the counselor might say, “I want to acknowledge that my lived experience may not reflect what you’re describing, but I want to understand how these challenges impact your well-being.” This affirming, non-defensive approach allows for deeper exploration of SDoMH factors such as racial stress, economic opportunity, and access to mental health care (Newton & Steele, 2025). Such intentional broaching behaviors can also help mitigate client mistrust, validate sociocultural realities, and strengthen the therapeutic alliance (Day-Vines et al., 2021).
Building rapport and trust is central to the broaching process, particularly when addressing systemic disparities. Trust building requires empathy, active listening, and a willingness to acknowledge one’s own biases (Day-Vines et al., 2021). Integrating clients’ interests, cultural values, and lived experiences into sessions makes counseling more relevant, while creating a safe space grounded in unconditional acceptance encourages openness and authenticity. Together, these broaching practices foster trust, empower clients to take an active role in the process, and strengthen the foundation for growth and change.
Broaching Emergent Needs in Session
Counselors should also be mindful to broach emergent client needs throughout the therapeutic process. Though counselors may assess clients for SDoMH at the beginning of the counseling process, that information must be viewed within a dynamic client context that requires an ongoing response rather than a one-time assessment. Therefore, counselors must remain attuned to emerging SDoMH needs throughout the therapeutic process and utilize immediacy skills to broach and address concerns as they arise.
Many clients face barriers related to income, health care access, transportation, and social support networks, all of which can create stressors that directly influence mental health outcomes because they add layers of stress that can overshadow therapeutic work (Compton & Shim, 2015). When basic needs are not met, clients may experience heightened anxiety, hopelessness, or distraction, which can limit their ability to fully engage in treatment.
Ongoing systemic barriers can also reinforce feelings of disempowerment and make it harder for clients to trust the counseling process or believe change is possible. As a result, unresolved SDoMH challenges often lead to inconsistent attendance, premature termination, or reduced treatment effectiveness. By addressing these barriers within the counseling process, counselors not only improve client retention and engagement but also enhance overall wellness by affirming that external stressors are legitimate and integral to mental health care.
For example, a client who discloses heightened anxiety over an overdue utility bill may struggle to engage in therapy until the pressing financial stressor is addressed. A counselor might broach this concern by saying, “I can see how this situation is overwhelming and I want to support you in finding a solution. Would it be helpful to take a few minutes to explore assistance programs or a payment plan?” This response validates the client’s distress while offering immediate, actionable support to address a pressing external challenge. Similarly, a client struggling with transportation barriers may benefit from a session in which the counselor helps them identify local transit options, employer benefits, or community-based ride services to ensure consistent access to mental health care. Meeting such immediate, concrete needs within the session fosters greater trust, retention, and engagement in the counseling process (Day-Vines et al., 2021; Newton & Steele, 2025). Additionally, addressing pressing SDoMH concerns in real time reinforces the message that both psychological distress and external stressors are valid therapeutic concerns. This approach ensures that counseling remains responsive and supportive of the client’s holistic well-being.
Beyond directly helping clients address pressing needs in session, the counselor can support self-advocacy and empowerment by equipping clients with the knowledge and skills to independently resolve their emergent needs. Developing self-advocacy skills enables clients to engage more effectively with health care providers, employers, and social service agencies providing skills that bridge the counseling office into everyday life (Compton & Shim, 2020). Self-advocacy intervention empowers clients to actively pursue resources, assert their rights, and confront systemic barriers with confidence. Moreover, self-advocacy skills foster resilience and equip clients to not only overcome immediate obstacles but to also sustain progress in the face of future challenges. In this way, developing self-advocacy skills is not just a counseling technique but a vital outcome that supports long-term growth and empowerment.
The counselor can facilitate the development of self-advocacy skills by helping clients identify resources, role-play difficult conversations, and anticipate potential barriers they may encounter when seeking support. For example, a client experiencing housing insecurity may feel intimidated about reaching out to a local housing agency because of past negative experiences or uncertainty about eligibility requirements. A counselor might role-play the conversation by saying, “Let’s practice how you might explain your situation when calling the housing agency. You could start by saying, ‘I’m looking for assistance with securing stable housing. Can you help me understand the eligibility requirements and next steps?’” This approach allows the client to rehearse the interaction in a supportive setting, boosting their confidence before making the actual call. Additionally, the counselor can help the client identify potential challenges, such as long wait times or required documentation, and develop strategies to navigate them, ensuring that they feel prepared and empowered when seeking resources.
Through active collaboration, counselors can help clients recognize their strengths; build resilience to adapt, recover, and grow when faced with adversity; and gain confidence in advocating for themselves in settings that may otherwise feel disempowering. This approach fosters an environment where clients feel seen, supported, and empowered to navigate both personal and systemic challenges as they arise.
Termination Considerations
Finally, SDoMH need to be broached in the context of termination because of their impact on client dropout rates and early termination of treatment (Roberts et al., 2022). Although counselors are traditionally taught that termination should be gradual and that clients should share readiness, that is not always the reality because of the influence of social determinants. For example, electricity or phone service may be terminated because of an inability to pay bills, thereby limiting the client’s access to virtual sessions; limited transportation or childcare may prevent continued session attendance. Although counselors hope that they will be able to have a final session, that is not always realistic.
Nevertheless, the termination period represents a critical phase of the clinical process and must be attended to as part of the counseling process (Baum, 2005; Goode et al., 2017; Knox et al., 2011; Lee et al., 2023; Vasquez et al., 2008). Therefore, incorporating SDoMH broaching behaviors throughout the counseling relationship lays the foundation for effective clinical termination, even if termination occurs prematurely. For example, enhancing skills such as self-advocacy and incorporating discussions of resource identification and utilization can help empower clients in the event of unexpected termination.
When a formal termination is possible, continuing to broach SDoMH throughout that process can strengthen therapeutic gains and enhance overall therapeutic outcomes. As such, a counselor may engage clients in discussions around how SDoMH have impacted their therapeutic experience and goal attainment during counseling. This conversation can extend to how SDoMH may influence goal attainment after counseling, including brainstorming potential challenges that may arise. Discussions around how to apply skills gained during counseling to navigate those challenges and address relevant social determinants can also be impactful.
Additionally, a counselor should recognize that clients who discontinue care because of SDoMH-related barriers may choose to reengage in counseling once those barriers have been resolved. Thus, using a screen door approach (Pester Boyd et al., 2025) to termination can be helpful. This may include broaching the process of how clients can return to counseling (e.g., whether a new intake is required, potential waitlist considerations), available options for returning (e.g., in person, telehealth, in-home), and factors that might warrant reengagement in counseling.
Broaching SDoMH during termination should also include providing and discussing a list of referrals and resources to support clients beyond counseling. These resources should address both immediate mental health needs and the social determinants that impact overall well-being. Clients may wish to discuss these referrals and resources further to better understand the process of accessing them. This may include empowering clients with language they can use in various settings, such as navigating legal, social services, or medical resources, or even role-playing those conversations.
Given the potential role of SDoMH in early termination, such discussions should begin early in the clinical process. For example, a counselor might say, “You mentioned concerns that you may lose your health insurance. Can we talk through what that may look like if that were to happen?” This helps the counselor address factors related to counseling and mental health while also helping the client brainstorm challenges, solutions, and resources. Using the other SDoMH broaching behaviors to sustain these conversations throughout the counseling process can lead to effective client termination, even if termination occurs unexpectedly.
SDoMH Broaching Behaviors and Counselor Education
There is a growing call within counseling and related mental health fields to enhance SDoMH training and increase counselor readiness to broach these topics in practice (Gantt-Howrey et al., 2024; Johnson & Robins, 2021; Newton & Steele, 2025; Pester Boyd et al., 2025). As such, counselor education programs at the master’s and doctoral levels should incorporate discussion and clinical practice opportunities to help counselors-in-training (CITs) build awareness of SDoMH and develop best practices for broaching and addressing their impact on client well-being. Counselor education programs can embed SDoMH broaching across coursework, supervision, and experiential learning to prepare CITs for ethical and effective practice.
Integrating SDoMH in Coursework and Supervision
SDoMH training may be integrated in a number of counselor education courses and aligns with Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2023) standards (Gantt-Howrey et al., 2024; Pester Boyd et al., 2025). For example, suggested activities per course/CACREP core area include: (a) examining ethical considerations of broaching SDoMH, including advocacy responsibilities and potential boundary issues when addressing systemic barriers (i.e., professional orientation and ethics); (b) helping CITs connect the MSJCC to SDoMH through case study analysis (i.e., social and cultural diversity); (c) highlighting how developmental outcomes are shaped by SDoMH (i.e., human growth and development); (d) addressing how economic stability, employment, and educational inequities intersect with career counseling (i.e., career development); (e) having CITs practice broaching SDoMH through role-plays to become aware of how SDoMH affects rapport, trust, and client disclosure (i.e., counseling and helping relationships); (f) integrating experiential activities in which students design psychoeducational groups focused on wellness promotion, social support, or navigating systemic barriers (i.e., group counseling and group work); (g) teaching CITs to administer and interpret SDoMH screening tools and to incorporate results into case conceptualizations (i.e., assessment and evaluation); and (h) requiring that CITs design projects to investigate the impact of SDoMH on client outcomes or evaluate community-based interventions (i.e., research and program evaluation).
In addition, practicum and internship supervision provides an important space for modeling SDoMH broaching and supporting CITs in developing cultural humility and ethical decision-making through structured activities. Supervisors might, for example, guide CITs in identifying protective factors through a strengths mapping exercise that charts client supports across individual, relational, community, and cultural identities. They can also facilitate role-plays in which CITs practice acknowledging the protective role of extended family, religious communities, cultural traditions, or neighborhood engagement. Site supervisors may also connect practicum activities to systemic issues, such as collaborating with schools or agencies on wellness or resource initiatives. Finally, reflective supervision discussions can help CITs analyze their own responses to client strengths and SDoMH barriers and notice whether they default to problem-solving or strength-building.
SDoMH Broaching in Experiential Learning
Experiential activities provide CITs with opportunities across coursework, practicum, and internship to connect theory to practice. Experiential activities may include case analysis, role-plays, assessment practice, community engagement, and classroom discussions focused on ethical dilemmas. First, CITs can analyze case vignettes to examine how SDoMH affect individuals and families. For example, dyads might review a case through the lens of a specific determinant such as housing insecurity or underemployment, discuss the client’s presenting concerns in context, and brainstorm broaching strategies. Second, structured role-plays further allow students to develop confidence in directly addressing SDoMH with clients. For example, in triadic supervision, CITs can rotate roles as counselor, client, and observer, while peers and supervisors provide feedback on the clarity and effectiveness of broaching behaviors.
Third, assignments that incorporate SDoMH assessment tools (e.g., PRAPARE, WE CARE Survey) also prepare CITs to integrate systemic factors into case conceptualization. CITs may practice administering and interpreting screeners with hypothetical clients and then learn to translate results into simple, jargon-free explanations for use in sessions. Fourth, community engagement projects deepen this preparation by connecting CITs to the systemic realities clients face. Examples include researching local issues such as food insecurity and mapping neighborhood resources.
Ethical reflection is also a part of experiential learning. Classroom discussions may explore balancing advocacy efforts with professional boundaries or managing countertransference when counselors share similar systemic challenges with their clients. In addition, classroom dialogue can highlight positive determinants of mental health by fostering empathy and compassion. Storytelling circles or guided conversations can invite CITs to share their own lived experiences of belonging or exclusion and consider how these experiences influence their empathy and ethical decision-making.
Cultural humility is the foundation for effective SDoMH broaching. To strengthen cultural humility and responsiveness, counselor education programs can embed the abovementioned experiential learning strategies across coursework and supervision. Self-reflection exercises may include journaling prompts such as: “What identities give me privilege and how might that shape my assumptions with clients?”; “How have I responded when a client’s worldview or values conflicted with my own? What could I do differently to remain open and nonjudgmental?”; and “Recall a time you felt excluded, misunderstood, or powerless. How does that experience shape your empathy for clients navigating systemic inequities?” These reflections can be revisited across the program to track growth in self-awareness and cultural responsiveness.
Guided discussions can be facilitated through fishbowl discussions in which CITs share and listen to experiences of privilege, discrimination, or cultural differences, followed by role-plays that practice broaching these issues in counseling. Counselor educators can model effective broaching and provide feedback on student language and presence during these exercises.
Promoting Positive Social Determinants
In addition to addressing negative SDoMH (e.g., discrimination, housing insecurity, poverty, community violence), counselor educators can help CITs recognize and promote positive SDoMH that build resilience. These determinants include self-care practices, strong social support, inclusive environments, cultural affirmation, and opportunities for growth and connection. In addition, counselor educators can model and encourage strengths-based approaches that affirm client identities, such as validating cultural, gender, or spiritual expressions, during intake and treatment planning.
Wellness models and self-care planning can be integrated into coursework to benefit both CITs and future clients. For example, assignments might include creating a personal self-care plan; evaluating wellness models and interventions across cultures; or designing a client-friendly handout that translates wellness strategies (e.g., mindfulness, exercise, nutrition, social connection) into accessible, culturally responsive language.
Counselor education programs can embed advocacy projects across coursework to promote systemic conditions that support mental health equity. Examples include partnering with schools to develop anti-bullying campaigns; creating culturally inclusive mental health awareness workshops for parents and teachers; and collaborating with community agencies to expand access in areas such as housing assistance, after-school programs, health care access, or transportation services. CITs might also design stigma-reduction campaigns with public health organizations.
Service-learning projects can further immerse students in community contexts by mapping resources, conducting needs assessments, or partnering with organizations addressing issues such as refugee resettlement, food insecurity, or housing justice. As service-learning projects conclude, CITs can be asked, “What systemic barriers did you observe and how might they affect mental health?”; “How did this experience shape your understanding of your role as advocate?”; and “How might insights from this project influence how you broach SDoMH with clients in practice?”
Preparing for SDoMH Broaching Challenges
Although broaching SDoMH is a critical counseling skill, CITs may face obstacles when attempting to apply it in future practice. Agency settings may limit the time available to explore systemic issues, and some trainees may feel anxious about making missteps when discussing topics such as poverty, discrimination, or community violence. Clients themselves may hesitate to disclose experiences of marginalization out of fear of judgment or because such issues have been dismissed in past encounters with helping professionals.
Counselor educators can support student development by intentionally acknowledging these challenges within the classroom and supervision spaces. For example, they might facilitate a structured dialogue in which CITs share their concerns about broaching while the counselor educator normalizes discomfort and models language for difficult conversations. In these dialogues, they might ask CITs, “What feelings come up for you when you think about broaching SDoMH with a client?”; “What makes these conversations challenging in practice?”; or “How might you respond if a client resists or shuts down when SDoMH are introduced?” Such discussions can help trainees recognize that hesitation is common and that growth comes from practice and feedback rather than perfection.
Another way to strengthen readiness is through guided debriefing of role-plays or client simulations. After a broaching exercise, counselor educators can ask CITs to reflect on moments in which they felt stuck, explore how power dynamics may have shaped the exchange, and brainstorm alternative approaches. For instance, a CIT might role-play broaching transportation barriers with a hypothetical client who frequently misses sessions. After the role-play, other CITs within the classroom or supervision session could examine the CIT’s wording and the client’s reaction and then suggest alternative ways to frame the issue that both validate the client’s struggle and highlight systemic factors.
Counselor educators can also discuss the limitations of broaching within supervision. When reviewing case presentations, supervisors might ask CITs not only how they addressed SDoMH but also what structural limitations they encountered and how those shaped the counseling process. For example, a CIT might describe working with a client who lacked consistent childcare and therefore missed several sessions. The supervisor could guide the student to consider how systemic gaps in affordable childcare both constrained the counseling process and required exploration of advocacy or referral options. These conversations emphasize that although broaching can validate client experiences, it cannot by itself dismantle inequities, thus highlighting the importance of community collaboration and ongoing advocacy. As counselor educators intentionally and thoroughly analyze the process together, CITs can learn to approach barriers not as failures but as opportunities to deepen cultural humility.
Evaluating SDoMH Broaching Behaviors
Currently, there are no existing measures to evaluate SDoMH broaching behaviors, and future research should prioritize the development of validated tools to assess both counselor competency in SDoMH broaching and client perceptions of these efforts. Quantitative studies could focus on designing and testing new measures that assess the clarity, timing, cultural responsiveness, and impact of SDoMH broaching within the counseling relationship. Counseling researchers could utilize these instruments to conduct longitudinal studies and controlled intervention studies exploring the influence that SDoMH broaching has on client trust, client engagement in counseling, and therapeutic outcomes.
Until instruments specific to SDoMH broaching have been developed, researchers can use existing scales that independently measure broaching behaviors (e.g., Day-Vines et al., 2013; Day-Vines et al., 2024), SDoMH readiness (e.g., Johnson, 2023) and SDoMH assessment (e.g., Gantt-Howrey et al., 2024) to understand effective counseling behavior related to these constructs.
In addition to quantitative approaches, qualitative studies can help inform the impact of broaching behaviors on clients, CITs, and counselors. Studies that explore client experiences with counselors who broach SDoMH can provide contextual nuance and enhance multiculturally competent practice. For instance, interviews or focus groups with clients might uncover how broaching influences their feelings of safety, empowerment, or stigma reduction. Furthermore, researchers could conduct case studies of counselors in varied settings to examine how SDoMH broaching unfolds in practice. Data from session transcripts and client and counselor interviews could reveal additional best practices for addressing SDoMH, promoting positive social determinants, and counteracting challenges that counselors may have while broaching SDoMH.
Conclusion
Learning to effectively broach SDoMH provides an opportunity for counselors to further operationalize Ratts et al.’s (2016) MSJCC. As the cross-disciplinary call for universal SDoMH screening practices continues to grow across health professions, to remain leaders among the mental health professions, counselors must begin intentionally broaching SDoMH with clients. However, as a profession, broaching SDoMH may require reexamining the professional counselor identity, expanding advocacy roles, and reviewing ethical standards that may inadvertently create barriers to effectively addressing the impact of social determinants on clients’ lives.
Preliminary research suggests that effectively broaching SDoMH throughout the counseling process supports a number of short- and long-term benefits to clinical practice, which warrants its further integration and evaluation in the counseling profession. Counselors perceive that in the short term, broaching SDoMH strengthens the therapeutic relationship while fostering MSJCC (Pester Boyd et al., 2025). These early benefits can give way to enhanced client empowerment and improved access to interprofessional resources and services, both of which can lead to better treatment outcomes. Long-term, effectively broaching SDoMH can result in improved overall health of the client, improved community health, and decreased marginalization.
The MMBB (Day-Vines et al., 2020) and SDCM (Pester Boyd et al., 2025) provide needed frameworks to enhance these client outcomes. Using the integration of these frameworks as a foundation, we identified six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences of lived experience, (e) addressing emergent needs, and (f) SDoMH-informed termination practices. These broaching behaviors provide specific guidance for how to integrate SDoMH into counseling practice, which operationalizes the mandate of the MSJCC to address systemic and environmental factors impacting client mental health. We suggest that counselors integrate the identified SDoMH broaching behaviors throughout all stages of the therapeutic process to support a strong counselor–client relationship, enhanced client self-disclosure, increased client satisfaction, and improved therapeutic outcomes.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Baum, N. (2005). Correlates of clients’ emotional and behavioral responses to treatment termination. Clinical Social Work Journal, 33(3), 309–326. https://doi.org/10.1007/s10615-005-4946-5
Brookover, D. L. (2024). The career development and social determinants framework: An integrative approach. Professional School Counseling, 28(1), 1–12. https://doi.org/10.1177/2156759X241290494
Center for Medicare & Medicaid Innovation. (n.d.). The accountable health communities health-related social needs screening tool. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
Compton, M. T., & Shim, R. S. (2015). The social determinants of mental health. Focus, 13(4), 419–425. https://doi.org/10.1176/appi.focus.20150017
Compton, M. T., & Shim, R. S. (2020). Why employers must focus on the social determinants of mental health. American Journal of Health Promotion, 34(2), 215–219. https://doi.org/10.1177/0890117119896122c
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2024/04/2024-Standards-Combined-Version-4.11.2024.pdf
Day-Vines, N. L., Bryan, J., and Griffin, D. (2013). The Broaching Attitudes and Behavior Survey (BABS): An exploratory assessment of its dimensionality. Journal of Multicultural Counseling and Development, 41(4), 210–223. https://doi.org/10.1002/j.2161-1912.2013.00037.x
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., & Gubara, S. (2021). Strategies for broaching the subjects of race, ethnicity, and culture. Journal of Counseling & Development, 99(3), 348–357. https://doi.org/10.1002/jcad.12380
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., Gubara, S., & Otabil, N. A. A. (2020). The multidimensional model of broaching behavior. Journal of Counseling & Development, 98(1), 107–118. https://doi.org/10.1002/jcad.12304
Day-Vines, N. L., Zhang, J., Cluxton-Keller, F., Hicks, D., Jones, C., Spann, R. T., Daga, D., & Agorsor, C. (2024). The development and validation of an instrument to examine clients’ perspectives about their counselors’ ability to broach racial, ethnic, and cultural concerns. Journal of Multicultural Counseling and Development, 52(3), 173–188. https://doi.org/10.1002/jmcd.12300
Depauw, H., Van Hiel, A., Talal, H., Dierckx, K., Geenen, F., Valcke, B., & De Clercq, B. (2025). The development of the Broaching Assessment Scale: A client-rated measure of therapists’ broaching behaviour in clinical counselling. Psychotherapy Research, 35(3), 424–440. https://doi.org/10.1080/10503307.2024.2301948
Dolan, N., Simmonds-Buckley, M., Kellett, S., Siddell, E., & Delgadillo, J. (2021). Effectiveness of stress control large group psychoeducation for anxiety and depression: Systematic review and meta-analysis. British Journal of Clinical Psychology, 60(3), 375–399. https://doi.org/10.1111/bjc.12288
Drinane, J. M., Owen, J., & Tao, K. W. (2018). Cultural concealment and therapy outcomes. Journal of Counseling Psychology, 65(2), 239–246. https://doi.org/10.1037/cou0000246
Gantt-Howrey, A., Lin, M., Shaikh, A., Johnson, K. F., Preston, J. W., & Wilson, L. (2024). Assessing social determinants of mental health: Client experiences and counselor practices. Journal of Counseling & Development, 102(4), 394–405. https://doi.org/10.1002/jcad.12519
Garg, A., Butz, A. M., Dworkin, P. H., Lewis, R. A., Thompson, R. E., & Serwint, J. R. (2007). Improving the management of family psychosocial problems at low-income children’s well-child care visits: The WE CARE Project. Pediatrics, 120(3), 547–558. https://doi.org/10.1542/peds.2007-0398
Goode, J., Park, J., Parkin, S., Tompkins, K. A., & Swift, J. K. (2017). A collaborative approach to psychotherapy termination. Psychotherapy, 54(1), 10–14. https://doi.org/10.1037/pst0000085
Johnson, K. F. (2023). Development and initial validation of the Addressing Client Needs with Social Determinants of Health Scale (ACN: SDH). BMC Health Services Research, 23(1), 374. https://doi.org/10.1186/s12913-023-09292-z
Johnson, K. F., & Brookover, D. L. (2021). School counselors’ knowledge, actions, and recommendations for addressing social determinants of health with students, families, and in communities. Professional School Counseling, 25(1). https://doi.org/10.1177/2156759X20985847
Johnson, K. F., Cunningham, P. D., Tirado, C., Moreno, O., Gillespie, N. N., Duyile, B., Hughes, D. C., Scott, E. G., & Brookover, D. (2023). Social determinants of mental health considerations for counseling children and adolescents. Journal of Child and Adolescent Counseling, 9(1), 21–33. https://doi.org/10.1080/23727810.2023.2169223
Johnson, K. F., Gantt-Howrey, A., Duyile, B. E., Robins, L. B., & Dockery, N. (2024). Career counselors addressing social determinants of mental health in rural communities. The Professional Counselor, 14(1), 1–14. https://doi.org/10.15241/kfj.14.1.1
Johnson, K., & Robins, L. B. (2021). Counselor educators experiences and techniques teaching about social-health inequities. Journal of Counselor Preparation and Supervision, 14(4). https://research.library.kutztown.edu/jcps/vol14/iss4/ 7
King, K. M., & Borders, L. D. (2019). An experimental investigation of White counselors broaching race and racism. Journal of Counseling & Development, 97(4), 341–351. https://doi.org/10.1002/jcad.12283
Knox, S., Adrians, N., Everson, E., Hess, S., Hill, C., & Crook-Lyon, R. (2011). Clients’ perspectives on therapy termination. Psychotherapy Research, 21(2), 154–167. https://doi.org/10.1080/10503307.2010.534509
Lee, P.-S., Wang, L.-F., & Swift, J. K. (2023). Clients’ and counselors’ termination decisions and experiences in counseling. Current Psychology, 42, 3734–3744. https://doi.org/10.1007/s12144-021-01725-4
Lenz, A. S., & Lemberger-Truelove, M. E. (2023). The social determinants of mental health and professional counseling: A call to action. Journal of Counseling & Development, 101(4), 375–380. https://doi.org/10.1002/jcad.12489
Lenz, A. S., & Litam, S. D. A. (2023). Integrating the social determinants of mental health into case conceptualization and treatment planning. Journal of Counseling & Development, 101(4), 416–428. https://doi.org/10.1002/jcad.12487
Lund, C., Brooke-Sumner, C., Baingana, F., Baron, E. C., Breuer, E., Chandra, P., Haushofer, J., Herrman, H., Jordans, M., Kieling, C., Medina-Mora, M. E., Morgan, E., Omigbodun, O., Tol, W., Patel, V., & Saxena, S. (2018). Social determinants of mental disorders and the sustainable development goals: A systematic review of reviews. The Lancet Psychiatry, 5(4), 357–369. https://doi.org/10.1016/S2215-0366(18)30060-9
Luo, H., Li, Y. L., Luo, X. J., Xia, L., Xiao, J., Xiao, H., & Chen, J. (2025). The efficacy of psychoeducation-based programs on internalized stigma in patients with schizophrenia: A systematic review and meta-analysis. Psychiatry Research, 350, 116540. https://doi.org/10.1016/j.psychres.2025.116540
Mason, S., Ragan, M., Gilbert, S. H., & Lenz, A. S. (2023). Social determinants of mental health: Implications for measurement, research, and evaluation. Journal of Counseling & Development, 101(4), 440–448. https://doi.org/10.1002/jcad.12490
Neal Keith, S., Coleman, M. L., Hicks Becton, L. Y., & Springfield, J. (2023). Assessing the social determinants of mental health in counseling practice. Journal of Counseling & Development, 101(4), 381–391. https://doi.org/10.1002/jcad.12470
Newton, C., & Steele, J. M. (2025). The broaching readiness framework: A path for psychologists to embrace cultural opportunities. Counselling Psychology Quarterly, 38(4), 1135–1152. https://doi.org/10.1080/09515070.2025.2458034
Office of Disease Prevention and Health Promotion. (2025). Social determinants of health. https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health
Owen, J., Tao, K. W., Imel, Z. E., Wampold, B. E., & Rodolfa, E. (2014). Addressing racial and ethnic microaggressions in therapy. Professional Psychology: Research and Practice, 45(4), 283–290. https://doi.org/10.1037/a0037420
Pester, D. A., Jones, L. K., & Talib, Z. (2023). Social determinants of mental health: Informing counseling practice and professional identity. Journal of Counseling & Development, 101(4), 392–401. https://doi.org/10.1002/jcad.12473
Pester Boyd, D. A., Hays, D. G., & Jones, L. K. (2025). Assessing and addressing social determinants of mental health in counseling: A grounded theory investigation. Journal of Counseling & Development, 103(4), 469–483. https://doi.org/10.1002/jcad.70003
PRAPARE. (2022). Protocol for responding to and assessing patient assets, risks, and experiences: Implementation and action toolkit. https://prapare.org/wp-content/uploads/2022/09/Full-Toolkit_June-2022_Final.pdf
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Roberts, T., Esponda, G. M., Torre, C., Pillai, P., Cohen, A., & Burgess, R. A. (2022). Reconceptualising the treatment gap for common mental disorders: A fork in the road for global mental health? The British Journal of Psychiatry, 221(3), 553–557. https://doi.org/10.1192/bjp.2021.221
Robins, L. B., Johnson, K. F., Duyile, B., Gantt-Howrey, A., Dockery, N., Robins, S. D., & Wheeler, N. (2022). Family counselors addressing social determinants of mental health in underserved communities. The Family Journal, 31(2), 213–221. https://doi.org/10.1177/10664807221132799
U.S. Department of Health and Human Services. (2023). Our epidemic of loneliness and isolation: The U.S. Surgeon General’s advisory on the healing effects of social connection and community. https://www.hhs.gov/sites/default/files/surgeon-general-social-connection-advisory.pdf
Vasquez, M. J. T., Bingham, R. P., & Barnett, J. E. (2008). Psychotherapy termination: Clinical and ethical responsibilities. Journal of Clinical Psychology, 64(5), 653–665. https://doi.org/10.1002/jclp.20478
World Health Organization. (2025). Social determinants of health. https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1
Zhang, N., & Burkard, A. W. (2008). Client and counselor discussions of racial and ethnic differences in counseling: An exploratory investigation. Journal of Multicultural Counseling and Development, 36(2), 77–87. https://doi.org/10.1002/j.2161-1912.2008.tb00072.x
Danielle Pester Boyd, PhD, NCC, LPC (TX), RPT, is an assistant professor at Auburn University. Laura K. Jones, PhD, is an associate professor at the University of North Carolina at Asheville. Courtney Maier, MEd, NCC, APC, is a doctoral student at Auburn University. Danica G. Hays, PhD, is a dean and professor at the University of Nevada Las Vegas. Correspondence may be addressed to Danielle Pester Boyd, 345 West Samford Avenue, Suite 3188, Auburn, AL 36849, danielle.boyd@auburn.edu.
