Dec 5, 2024 | Volume 14 - Issue 3
Fei Shen, Ying Zhang, Xiafei Wang
Intimate partner violence (IPV) has consistently been shown to have deleterious effects on survivors’ interpersonal and intrapersonal relationships. Despite the negative outcomes of IPV, distress after IPV varies widely, and not all IPV survivors show a significant degree of distress. The present study examined the impact of IPV on adult attachment and self-esteem, as well as the moderating role of childhood attachment on the relationships between IPV, adult attachment, and self-esteem using path analysis. A total of 1,708 adult participants were included in this study. As hypothesized, we found that IPV survivors had significantly higher levels of anxious and avoidant adult attachment than participants without a history of IPV. Additionally, childhood attachment buffered the relationship between IPV and self-esteem. We did not find that childhood attachment moderated the relationship between IPV and adult attachment. These results provide insight on attachment-based interventions that can mitigate the negative effects of IPV on people’s perceptions of self.
Keywords: intimate partner violence, childhood attachment, adult attachment, self-esteem, moderation
More than 10 million adults experience intimate partner violence (IPV) victimization annually in the United States (Black et al., 2011); therefore, it undoubtedly remains a prominent public health concern. IPV victimization has been consistently associated with deleterious effects on survivors’ physical and mental health. It is well established that IPV survivors demonstrated increased risks for chronic pain, injury, insomnia, disabilities, post-traumatic stress disorder, depression, and suicidality (Burke et al., 2005; Gilbert et al., 2023; Matheson et al., 2015; McLaughlin et al., 2012). Historically, empirical studies on trauma and violence have focused on psychopathology and symptoms (McLaughlin et al., 2012; Sayed et al., 2015). However, there is limited research on exploring the link between IPV victimization and intrapersonal and interpersonal relationship outcomes. Attachment theory (Bowlby, 1969) not only provides a rich theoretical framework for conceptualizing an individual’s psychopathology, but also establishes a foundation for understanding the intrapersonal and relational sequelae of IPV (Levendosky et al., 2012; Sutton, 2019). IPV survivors often experience a violation of trust and a sense of betrayal in the aftermath and develop ineffective coping mechanisms (e.g., distancing themselves emotionally), which could potentially impact their new intimate relationships (St. Vil et al., 2021).
Despite the negative outcomes of IPV victimization, the levels of distress following such incidents can vary (Scott & Babcock, 2010). Although evidence has implicated numerous risk factors related to IPV victimization (e.g., childhood trauma, gender inequity; Jewkes et al., 2017; Meeker et al., 2020), limited effort has been put forth to recognize protective factors that contribute to IPV survivors’ coping and healing processes. Childhood attachment has been proposed as a potential protective factor for IPV survivors’ coping with traumatic experiences and a moderator for buffering the negative psychological outcomes of IPV (Pang & Thomas, 2020), which provides a meaningful foundation for us to further investigate childhood attachment as a moderator buffering relational outcomes. To our knowledge, no study to date has investigated the potential moderating role of childhood attachment security on the association between IPV, interpersonal outcomes (e.g., adult attachment), and intrapersonal outcomes (e.g., self-esteem) in a non-clinical sample. Understanding the moderating role of childhood attachment can potentially provide further directions toward protecting survivors from negative outcomes and creating interventions that foster healthier interpersonal relationships. In tackling the gaps in the literature, we aim to: (a) investigate the impact of IPV on adult attachment and self-esteem; and (b) examine the moderating role of childhood attachment on the relationships between IPV, adult attachment, and self-esteem.
Theoretical Framework—Attachment Theory
Attachment theory (Bowlby, 1969) offers an explanation of how the relationship between children and their primary caregiver(s) develops and how it impacts children’s subsequent developmental process. According to Bowlby (1973), children develop mental representations of themselves and others, known as internal working models, through their interactions with their primary caregiver(s). Children with secure attachment are more likely to form positive self-perceptions and relationships with others (Bowlby, 1969). In contrast, children who develop insecure attachment are more likely to struggle with coping with distress and form poor relationships with others, resulting from caregivers responding to their needs insensitively.
Although evidence suggests the continuity of attachment from childhood to adulthood (Bowlby, 1969), there are distinctions between these two variables based on individuals’ attachment needs, developmental stages, and characteristics of different relationships. As children grow into adolescents and emerging adults, they often continue to maintain connections with their primary caregivers while exploring new social roles outside of the family and forming close relationships with peers and romantic partners to develop adult attachment (Moretti & Peled, 2004). Secure adult attachment is generally characterized by flexibility, the ability to work independently and cooperatively with others, the ability to seek support from intimate partners, and the capacity to manage loss in a healthy manner (Brennan et al., 1998). Adult romantic relationships are thought to be underlined by two fundamental attachment-related dimensions: anxiety and avoidance. Adults with anxious attachment tend to experience worry and fear regarding abandonment or rejection by their partner, leading them to seek constant reassurance and validation from their partner. On the other hand, avoidant-attached individuals often feel uncomfortable with being close to their partner, which can lead them to withdraw from intimacy and emotional closeness in the relationship (Brennan et al., 1998). Thus, understanding the similarities and differences of attachment categories as well as dynamics of the attachment system is warranted (Lopez & Brennan, 2000).
Childhood Attachment, IPV Victimization, and Adult Attachment
Various researchers have extensively investigated the significant association between attachment developed with romantic partners and its involvement in IPV dynamics (Bradshaw & Garbarino, 2004; Duru et al., 2019; Levendosky et al., 2012). However, most studies explored the relationship between adult attachment and IPV perpetration (Gormley & Lopez, 2010; McClure & Parmenter, 2020). Specifically, individuals with insecure attachment present intense fear of abandonment or rejection and activate their aggressive behaviors to control their partners (Gormley & Lopez, 2010). Regarding IPV victimization circumstances, few studies have examined attachment security among IPV survivors. Specifically, simultaneously exploring attachment with primary caregivers in childhood and attachment with romantic partners in adulthood could capture the complexity of the impact of IPV victimization experiences on relational and emotional outcomes. Ponti and Tani (2019) investigated both childhood attachment and adult attachment among 60 women who experienced IPV and indicated that the attachment to the mother could influence IPV victimization both directly and indirectly through the mediation effect of adult attachment with romantic partners. In other words, attachment with the mother could serve as a protector for not entering a violent romantic relationship or healthily managing the aftermath of traumatic experiences.
Childhood attachment has been identified as a potential moderator that may contribute to the variations of the healing process among IPV survivors in a small but growing number of studies (e.g., Scott & Babcock, 2010). Pang and Thomas (2020) examined the moderating role of childhood attachment on the relationship between exposure to domestic violence in adolescence and psychological outcomes and adult life satisfaction with a sample of 351 adult college students. They found that childhood attachment moderated the relationship between IPV exposure and adult life satisfaction but not psychological outcomes. This study provides empirical support for the moderating role of childhood attachment on early IPV exposure and later adult psychological and relationship outcomes. Given the context in which IPV occurs in the intimate relationships, not addressing the association between childhood attachment and adult attachment together would not fully capture the complexity of the attachment process in the adult population. It is possible that the relationship between IPV victimization and adult attachment security would be attenuated in conditions of childhood attachment. Therefore, the moderation effect of childhood attachment in the context of IPV needs to be empirically substantiated.
Childhood Attachment, IPV Victimization, and Self-Esteem
Self-esteem generally refers to a person’s overall evaluation and attitude toward themself (Rosenberg, 1965). Experiencing IPV was found to have detrimental effects on an individual’s self-esteem; IPV survivors often have lower levels of self-esteem than non-abused individuals (Childress, 2013; Karakurt et al., 2014; Tariq, 2013). Experiencing IPV (e.g., emotional and psychological abuse) can lead to feelings of worthlessness and hopelessness, making it difficult for survivors to maintain autonomy and make decisions that are in their best interest (Tariq, 2013). IPV survivors consistently reported feeling burdened with a sense of guilt, shame, and self-blame for being victimized (Lindgren & Renck, 2008). Unfortunately, this can contribute to a vicious cycle, as survivors who have low self-esteem are less likely to take steps to leave abusive relationships (Karakurt et al., 2014), which leads to further victimization (Eddleston et al., 1998). Understanding the link between IPV victimization and self-esteem is crucial, as rebuilding self-esteem can also help survivors develop stronger relationships with others, gain strength toward ending abusive relationships, reduce risks of mental health problems, and feel more empowered to seek help and support (Karakurt et al., 2022).
The development of the self can be seen to unfold in the context of attachment and the internalization of important others’ perceptions and expectations. Numerous studies have shed some light on the association between childhood attachment and self-esteem, suggesting that secure attachment with primary caregivers can serve as a key protective factor for developing higher levels of self-esteem (Shen et al., 2021; Wilkinson, 2004). In contrast, individuals who reported insecure attachment with their primary caregivers tended to demonstrate lower levels of self-esteem (Gamble & Roberts, 2005). However, interpersonal trauma such as IPV can produce long-term dysfunctions of self (Childress, 2013). Although no study has directly explored the moderating role of childhood attachment buffering the relationship between IPV and self-esteem, several studies have indicated that parental support serves as a moderator role in the relationship between interpersonal violence and self-esteem (Duru et al., 2019). Indeed, if a person had secure attachment experiences in childhood, they may have developed a positive sense of self-worth and the belief that they deserve love and respect, which could buffer the negative effects of IPV on their self-esteem. Considering the existing literature and theoretical explanations as a whole, it seems reasonable to postulate that childhood attachment might serve as a potential moderator of the association between IPV and self-esteem.
Taken together, the literature consistently supports the significance of exploring protective factors contributing to IPV survivors’ healing process, yet no study to date has investigated the potential moderating role of childhood attachment on the association between IPV, adult attachment, and self-esteem in a non-clinical diverse sample. In tackling these gaps, we pose two research questions (RQs):
RQ1: How is IPV associated with adult attachment and self-esteem?
RQ2: How does childhood attachment moderate the relationships between IPV, adult
attachment, and self-esteem?
We hypothesized that: 1) IPV victimization is significantly positively associated with adult attachment (i.e., anxious attachment, avoidant attachment) and negatively associated with self-esteem; 2) Childhood attachment moderates the relationship between IPV victimization and adult attachment (i.e., anxious attachment, avoidant attachment); and 3) Childhood attachment moderates the relationship between IPV victimization and self-esteem.
Method
Sampling Procedures
With approval from the university IRB, research recruitment information was posted on various social media platforms (e.g., Facebook, Craigslist, university announcement boards). Individuals who were 18 years of age or older and able to fill out the questionnaire in English were eligible for the study. Participants were directed to an online Qualtrics survey to voluntarily complete the informed consent and the measures listed in the following section. At the end of the survey, participants were prompted to enter their email addresses to win one of 10 $15 e-gift cards. Their email addresses were not included for data analysis.
Participants
Of the 2,373 voluntary adult participants who took the survey, 1,708 (71.76%) individuals were retained for the final analysis, including 507 (29.68%) participants who experienced IPV in adulthood and 1,191 (69.73%) participants without a history of IPV in adulthood. We eliminated participants who either did not consent to the study (n = 36, 1.51%), were younger than 18 years old (n = 33, 1.39%), or did not complete 95% of the survey questions (n = 596, 25.11%). We examined whether those who were excluded from the sample because of missing or invalid data differed from those who were retained. There was a significant difference in age between the included sample (M = 28.89, SD = 12.38) and excluded sample (M = 32.10, SD = 13.51); t (2,255) = −3.48, p = 0.001. Therefore, excluding participants with missing data was less likely to significantly impact our results. Table 1 shows that 76.23% of the participants were female. The age range of the sample was broad, from 18 to 89 years old, with an average age of 30.
Table 1
Demographic and Key Variables Information (N = 1,708)
| Variables |
N |
Percent |
Range |
M(SD) |
| Childhood attachment |
1,708 |
100% |
1–5 |
3.34(0.92) |
| IPV status
IPV
Non-IPV |
1,698
507
1,191 |
99.41%
29.68%
69.73% |
0–1 |
|
| Self-Esteem |
1,704 |
99.77% |
3–40 |
26.98(7.46) |
| Anxious Attachment |
1,708 |
100% |
1–7 |
4.11(1.26) |
| Avoidant Attachment |
1,708 |
100% |
1–7 |
3.71(1.16) |
| Control Variables |
|
|
|
|
| Gender
Male
Female |
1,683
381
1,302 |
98.54%
22.31%
76.23% |
|
|
| Household Income
Less than $5,000
$5,000–$9,999
$10,000–$14,999
$15,000–$19,999
$20,000–$24,999
$25,000–$29,999
$30,000–$39,999
$40,000–$49,999
$50,000–$74,999
$75,000–$99,999
$100,000–$149,999
$150,000 or more |
1,514
183
96
119
83
98
78
128
141
239
143
139
67 |
88.64%
10.70%
5.60%
7.00%
4.90%
5.70%
4.60%
7.50%
8.30%
14.00%
8.40%
8.10%
3.90% |
|
|
Measures
Childhood Attachment
The parental attachment subscale of the Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987) was used to measure childhood attachment. Participants rated their attachment to their parent(s) or caregiver(s) who had the most influence on them during their childhood. The subscale consists of 25 items divided into three dimensions, including 10 items on Trust (e.g., “My mother/father trusts my judgment”), nine items on Communication (e.g., “I can count on my mother/father when I need to get something off my chest”), and six items on Alienation (e.g., “I don’t get much attention from my mother/father”). Participants rated the items using a 5-point Likert scale ranging from 1 (almost never or never true) to 5 (almost always or always true). Responses were averaged, with a higher score reflecting more secure childhood attachment. This subscale has demonstrated relatively high internal consistency, with a Cronbach’s alpha of .93 (Armsden & Greenberg, 1987), and construct validity (Cherrier et al., 2023; Gomez & McLaren, 2007). In the present study, the Cronbach’s alpha coefficient for this subscale was .96.
Intimate Partner Violence
Participants’ experiences of IPV were assessed through the question “Have you ever experienced intimate partner violence (physical, sexual, or psychological harm) by a current or former partner or spouse since the age of 18?” Responses were coded as 1 = Yes, 0 = No.
Adult Attachment
Adult attachment was measured using the Experience in Close Relationships Scale (ECR; Brennan et al., 1998). The ECR consists of 36 items with 18 items assessing each of the two dimensions: anxious attachment (e.g., “I worry about being abandoned”) and avoidant attachment (e.g., “I try to avoid getting too close to my partner/friends”). To reduce confounding factors with childhood attachment with their parent(s) or primary caregiver(s), we only assessed adult attachment with close friends and/or romantic partners. Responses were rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Two scores were computed by averaging items on each subscale, with a higher score reflecting a higher level of anxious or avoidant attachment. Two subscales demonstrated high construct validity in various studies (Gormley & Lopez, 2010; Ponti & Tani, 2019) and a relatively high consistency for anxiety (α = .91) and avoidance (α = .94; Brennan et al., 1998). Cronbach’s alpha coefficients for the present study were .93 for anxiety and .92 for avoidance.
Self-Esteem
The Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1965) is a 10-item self-report measure of overall feelings of self-worth or self-acceptance (e.g., “I am satisfied with myself”). All items were coded using a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Items were summed, with a higher score indicating a higher level of self-esteem. RSES has been frequently used in various studies, demonstrating high reliability and validity (Brennan & Morris, 1997; Rosenberg, 1979). The Cronbach’s alpha for the present study was .89.
Control Variables
To make more accurate estimates, we included control variables that are potentially associated with IPV exposures, such as gender and household income. Gender was dummy coded as 1 = Male, 2 = Female.
Data Analysis
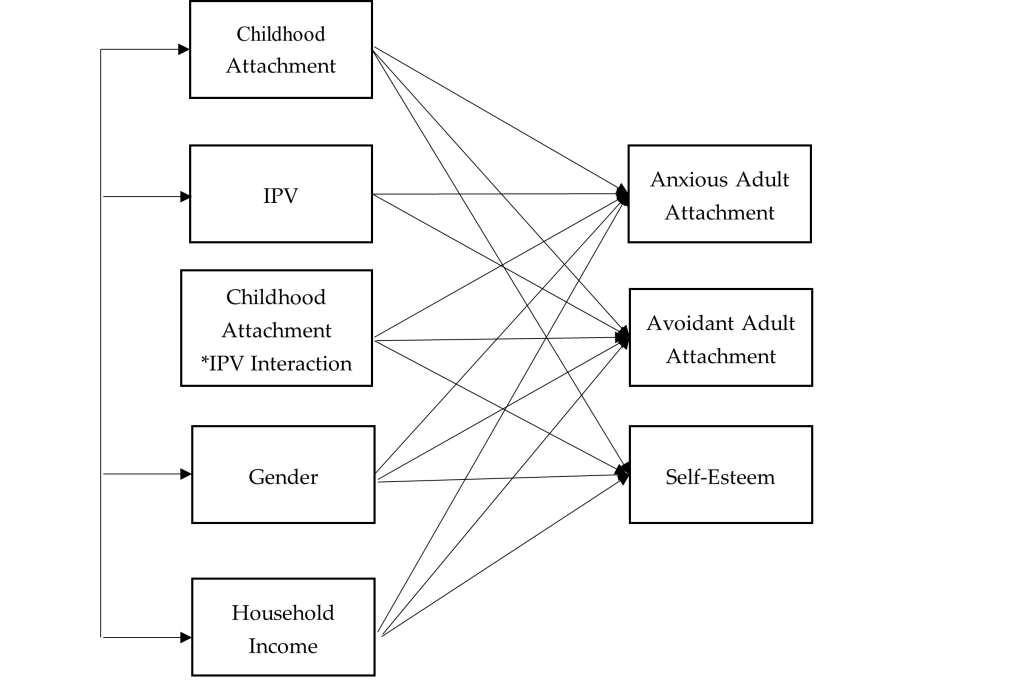
We used SPSS 27 for data preparation and Mplus 8 for data analysis. Missing data were treated with the full information maximum likelihood in Mplus as recommended (Acock, 2005). We examined all the bivariate relationships between all the variables within our study including IPV, childhood attachment, adult attachment (anxious and avoidant attachment), self-esteem, and control variables (i.e., gender and household income). We conducted path analysis to examine the moderating role of childhood attachment between IPV, self-esteem, and adult attachment (see Figure 1). We computed an interaction term by multiplying the predictor (IPV) and the moderator (childhood attachment). A moderation relationship is identified if the interaction item significantly predicts the dependent variables (Baron & Kenny, 1986). The goodness of model fit was evaluated by recommended indices with a non-significant chi-square value, RMSEA < .08, CFI > .90, TLI > .90, and SRMR < .05 (Hooper et al., 2008).
Figure 1
Path Analysis: Moderating Effect of Childhood Attachment on the Relationship Between IPV, Self-Esteem, and Adult Attachment
Results
Descriptive statistics and bivariate correlations of the study variables are demonstrated in Tables 1 and 2. Our model demonstrated good fit to the data, with χ2(4) = 41.90, p = .001, RMSEA = .07, 90% CI [.05, .08], CFI = .99, TLI = .99, SRMR = .02.
The standardized coefficients of the path model revealed that IPV survivors tended to have higher levels of anxious adult attachment (b = .67, p < .001) and avoidant adult attachment (b = .62, p < .001), and lower levels of self-esteem (b = −.29, p < .001) compared with participants without a history of IPV (see Table 3). Individuals with more secure childhood attachment tended to have lower levels of anxious adult attachment (b = −.38, p < .001) and avoidant adult attachment (b = −.31, p < .001), and higher levels of self-esteem (b = .22, p < .001). We found that childhood attachment buffered the relationship between IPV and self-esteem (b = .12, p < .001). Specifically, IPV survivors with more secure childhood attachment demonstrated higher levels of self-esteem. Although the moderation effect was statistically significant, the magnitude of the effect was small. Moreover, IPV survivors with more secure childhood attachment did not demonstrate significant differences on anxious or avoidant adult attachment compared to participants without a history of IPV.
Table 2
Bivariate Correlation Matrix of Variables
| |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
| 1. Anxious Adult Attachment |
– |
|
|
|
|
|
|
| 2. Avoidant Adult Attachment |
.40*** |
– |
|
|
|
|
|
| 3. Self-Esteem |
−.18*** |
−.15*** |
– |
|
|
|
|
| 4. Childhood Attachment |
−.45*** |
−.47*** |
.18*** |
– |
|
|
|
| 5. IPV |
.26*** |
.54*** |
−.17*** |
−.31*** |
– |
|
|
| 6. Gender |
−.10*** |
−.06** |
.14*** |
−.01 |
−.08*** |
– |
|
| 7. Household Income |
.03 |
.08*** |
−.05* |
−.08** |
−.06* |
−.01 |
– |
*p < .05 (two-tailed). **p < .01. ***p < .001.
Table 3
Unstandardized and Standardized Path Coefficients (Standard Errors) for Path Analysis
| Parameter Estimates |
|
Anxious Adult
Attachment |
Avoidant Adult
Attachment |
Self-esteem |
| Childhood Attachment |
Unstandardized |
−.37(.01)*** |
−.33(.02)*** |
.26(.04)*** |
| |
Standardized |
−.38(.01)*** |
−.31(.02)*** |
.22(.03)*** |
| IPV |
Unstandardized |
.61(.01)*** |
.62(.02)*** |
−.33(.04)*** |
| |
Standardized |
.67(.01)*** |
.62(.02)*** |
−.29(.03)*** |
| IPV*Childhood Attachment
Interaction |
Unstandardized |
.00(.00) |
.01(.01) |
.10(.02)*** |
| Standardized |
.01(.01) |
.01(.01) |
.12(.02)*** |
| Control Variables |
| Gender |
Unstandardized |
−.03(.01)** |
−.08(.03)** |
.18(.06)** |
| |
Standardized |
−.02(.01)** |
−.04(.01)** |
.07(.02)** |
| Household Income |
Unstandardized |
.01(.00)*** |
.01(.00)*** |
−.02(.01)** |
| |
Standardized |
.02(.01)*** |
.04(.01)*** |
−.06(.02)** |
*p < .05 (two-tailed). **p < .01. ***p < .001.
Female participants tended to have lower levels of anxious (b = −.02, p < .01) or avoidant adult attachment (b = −.04, p < .01), and higher levels of self-esteem (b = .07, p < .01). Individuals with higher household income reported higher levels of anxious adult attachment (b = .02, p < .001), avoidant adult attachment (b = .04, p < .001), and lower levels of self-esteem (b = −.06, p < .01).
Discussion
Although most existing literature predominantly focuses on revealing how the attachment style of the IPV perpetrators may influence their behavior (Velotti et al., 2018), our study contributes to the field by exploring the potential association between IPV victimization and adult attachment. Using a non-clinical sample, this study identified a positive association between IPV victimization and adult insecure attachment, including both anxious and avoidant dimensions. Meanwhile, a negative association was observed between IPV victimization and self-esteem. These findings concur with the tenets of attachment theory, which posits that individuals who experienced IPV would have a sense of betrayal of trust within intimate relationships. Rather than serving a secure attachment base in intimate adult relationships, IPV experience altered internal models of self as a victim and the other as perpetrator if the individuals stay in the abusive relationships for long enough (Levendosky et al., 2012). IPV survivors may adopt maladaptive coping strategies to mitigate the distress stemming from such intimate relationships. Consequently, these individuals might manifest anxious or avoidant attachment (Levendosky et al., 2012). At the same time, our results indicating reduced self-esteem among IPV victims resonates with previous studies, underscoring the detrimental effects of IPV on self-esteem (Childress, 2013; Karakurt et al., 2014). Enduring undeserved maltreatment from partners can persistently undermine an individual’s sense of self-efficacy and competency (Tariq, 2013).
Our findings do not identify childhood attachment as a significant moderating factor between IPV victimization and insecure attachment in adulthood. There is currently no study to compare with this finding, as the present study is the first to investigate the moderating role of childhood attachment on the relationship between adult IPV victimization and adult attachment.
Although previous research implied that childhood attachment can mitigate the adverse effects of IPV on psychological health and adult life satisfaction (Pang & Thomas, 2020), those studies assessed IPV experiences during an individual’s childhood. Nevertheless, we speculate that IPV targets an individual’s sense of security, which is predominantly influenced by adult romantic relationships (Dutton & White, 2012). This IPV-related sense of security distinguishes itself from childhood attachment, which primarily arises from interactions between parents and children. For instance, the fear associated with intimate relationships and feelings of betrayal, as a result of sustained physical and emotional abuse from an intimate partner, may not be readily alleviated by the sense of security instilled by one’s primary caregivers during childhood. Survivors who were abused by their partner may attempt to manage their distress by deactivating their attachment system, which would reflect more insecure working models of self and others, less self-confidence, and lack of trust in others (Kobayashi et al., 2021).
Conversely, our research determined that childhood attachment acts as a moderator between IPV victimization and self-esteem, aligning with previous studies showing parental support as a vital protective mechanism for the self-esteem of individuals subjected to interpersonal violence (Duru et al., 2019). As posited by attachment theory, secure childhood attachment fosters a robust self-concept, equipping individuals with the belief that they are valuable and deserving of love (Bowlby, 1969). This foundational belief may serve as an effective counterbalance, attenuating the damage to self-esteem precipitated by IPV. We acknowledge that although the moderating effect of childhood attachment on the relationship between IPV victimization and self-esteem was statistically significant, the magnitude standardized coefficients were fairly low. One possible explanation could be that when transitioning to adulthood, individuals expand their social relationships with their peers, romantic partners, and offspring, which may increasingly take on their attachment organizations (Allen et al., 2018; Guarnieri et al., 2015). Future studies could further explore the level of effectiveness of childhood attachment mitigating the negative impact of IPV experience on interpersonal and intrapersonal outcomes in adulthood.
Limitations and Future Directions
Although the present study adds important contributions to the literature on IPV victimization and attachment, several limitations must be acknowledged. First, the dichotomous question of IPV could not fully capture all of the complexity of IPV victimization experiences. Future research should consider other factors related to IPV, including severity of the violence, types of IPV, age of onset, frequency, and duration. Second, retrospective reporting of childhood attachment with the primary caregiver(s) may lead to bias, or distortion in the recall of traumatic events from family of origin. However, previous studies have shown that retrospective reports only have a small amount of bias and that it is not strong enough to invalidate the results for adverse childhood experiences (Hardt & Rutter, 2004).
A growing body of literature has identified adult attachment as a risk factor of IPV (Doumas et al., 2008); here, we were not able to determine the causal relationship between adult attachment and IPV. We did conduct a path analysis using childhood attachment and adult attachment to predict IPV and self-esteem, but the model did not demonstrate a good fit. It is possible that attachment and IPV do not have a simple causal relationship; other childhood trauma experiences may contribute to the complexity of the IPV (Li et al., 2019).
Finally, not knowing the types of attachment in childhood limited our exploration regarding the changes of attachment styles from childhood to adulthood. The cross-sectional design of assessing childhood attachment and adult attachment concurrently did not provide sufficient evidence to determine the cause and effect. Bowlby (1969) believed that there is a continuity between childhood attachment and adult attachment over the life course. An individual’s security in adult relationships may be a partial reflection of their experiences with primary caregivers in early childhood (Ammaniti et al., 2000). However, one of the common misconceptions about attachment theory is that attachment is always stable from infancy to adulthood (Hazan & Shaver, 1994). It is possible that adults’ attachment patterns would change if their relational experiences were disturbed by relational trauma such as IPV (West & George, 1999) or childhood trauma (Shen & Soloski, 2024), which partially explains that childhood attachment is not a significant moderator between IPV and adult attachment from our findings. Future research could conduct longitudinal studies to examine the changes of attachment and how childhood trauma and IPV influences attachment over time.
Implications
The findings of the present study provide insights that may inform clinical interventions for adult survivors who have experienced IPV to rebuild trusting interpersonal relationships and relationships with self. First, IPV experiences were significantly associated with anxious and avoidant adult attachment. During a traumatic experience, such as IPV, the attachment security system is activated, and survivors are in a surviving mode and tend to seek protection. Unfortunately, IPV involves power, control, and betrayal within an intimate relationship, which may damage internal working models of self and others if they stay for long enough (Levendosky et al., 2012). Thus, clinical interventions could focus on altering survivors’ negative internal working models to increase security within non-abusive close relationships. Close friends and family members could remain as a secure base for IPV survivors while they rebuild their personal and social lives that IPV have damaged. Additionally, therapeutic relationships could potentially serve as a secure base for survivors to explore their attachment behaviors. Survivors with avoidant attachment demonstrate deactivation attachment behaviors (Brenner et al., 2021), such as minimizing the impact of their trauma experiences, having a tendency to perceive and present themselves as strong, or avoiding discussing their trauma experiences to avoid the possible pain (Muller, 2009). Therefore, clinicians need to hold a safe space to challenge survivors with avoidant attachment to reactivate their attachment systems, such as by validating their avoidance and ambivalence or facilitating conversations to turn toward trauma-related experiences and emotions instead of turning away. Survivors with anxious attachment, on the other hand, demonstrate hyperactivation attachment behaviors, including fear of rejection and abandonment, hypersensitivity to and preoccupation with relationships and intimacy, utilization of negative emotional regulation strategies, as well as difficulties with leaving abusive relationships (Kural & Kovacs, 2022; Velotti et al., 2018). Clinicians could teach anxious-attached survivors some effective coping strategies, including self-regulation skills, creating boundaries, establishing safety plans, maintaining relationships with others, and increasing self-compassion (Rizo et al., 2017), which may help them to perceive themselves as worthy, lovable, and less dependent on others.
Furthermore, group counseling is a powerful way to learn about trusting oneself and others and to improve interpersonal relationship skills. Clients’ attachment patterns will be activated through interactions with the group members and the facilitators. Clients with anxious attachment tend to react to group members’ rejections, while clients with avoidant attachment tend to demonstrate withdrawal behaviors (e.g., disengagement; Zorzella et al., 2014). Therefore, when working with these clients, clinicians should stimulate the change of internal working models by using the group as a secure base to foster corrective emotional exchanges that challenge group members’ maladaptive beliefs about themselves and others (Marmarosh et al., 2013).
One of the important findings of the current study is that childhood attachment with the primary caregiver(s) buffered the relationship between IPV and self-esteem. From a clinical point of view, the result may bring hope for adult survivors of interpersonal violence regarding their healing process; primary caregivers could still serve as a secure base to offer a crucial opportunity to strengthen the internal working models that would positively affect later adjustment. Counselors could assess survivors’ attachment with their primary caregivers and give them autonomy to determine if it is beneficial to get their non-abusive primary caregivers involved in the treatment to provide support. Although the moderation result from the present study was statistically significant, the magnitude of moderating effect was small. During adulthood, individuals expand their relationship networks with their peers (e.g., friends) and romantic partners, as these relationships become more central in their daily life (Guarnieri et al., 2015). Therefore, the effectiveness of childhood attachment mitigating the adverse effect of IPV in adulthood clinically needs to be further investigated.
Conclusion
The present study empirically examines the moderation role of childhood attachment on the association between IPV, adult attachment, and self-esteem. Specifically, we found that childhood attachment was a significant moderator buffering the relationship between the experience of IPV and self-esteem. A theoretical and empirical understanding of the role of attachment in the context of IPV has implications for researchers and clinicians working with survivors and their families.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Acock, A. C. (2005). Working with missing values. Journal of Marriage and Family, 67(4), 1012–1028.
https://doi.org/10.1111/j.1741-3737.2005.00191.x
Allen, J. P., Grande, L., Tan, J., & Leob, E. (2018). Parent and peer predictors of change in attachment security from adolescence to adulthood. Child Development, 89(4), 1120–1132. https://doi.org/10.1111/cdev.12840
Ammaniti, M., Van Ijzendoorn, M. H., Speranza, A. M., & Tambelli, R. (2000). Internal working models of attachment during late childhood and early adolescence: An exploration of stability and change. Attachment & Human Development, 2(3), 328–346. https://doi.org/10.1080/14616730010001587
Armsden, G. C., & Greenberg, M. T. (1987). The inventory of parent and peer attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. https://doi.org/10.1007/BF02202939
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
Black, M. C., Basile, K. C., Breiding, M. J., Smith, S. G., Walters, M. L., Merrick, M. T., Chen, J., & Stevens, M. R. (2011). The National Intimate Partner and Sexual Violence Survey: 2010 summary report. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. Basic Books.
Bowlby, J. (1973). Attachment and loss, Vol. 2: Separation: Anxiety and anger. Basic Books.
Bradshaw, C. P., & Garbarino, J. (2004). Social cognition as a mediator of the influence of family and community violence on adolescent development: Implications for intervention. In J. Devine, J. Gilligan, K. A. Miczek, R. Shaikh, & D. Pfaff (Eds.), Youth violence: Scientific approaches to prevention (pp. 85–105). New York Academy of Sciences.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). Guilford.
Brennan, K. A., & Morris, K. A. (1997). Attachment styles, self-esteem, and patterns of seeking feedback from romantic partners. Personality and Social Psychology Bulletin, 23(1), 23–31. https://doi.org/10.1177/0146167297231003
Brenner, I., Bachner-Melman, R., Lev-Ari, L., Levi-Ogolnic, M., Tolmacz, R., & Ben-Amitay, G. (2021). Attachment, sense of entitlement in romantic relationships, and sexual revictimization among adult CSA survivors. Journal of Interpersonal Violence, 36(19–20), NP10720–NP10743. https://doi.org/10.1177/0886260519875558
Burke, J. G., Thieman, L. K., Gielen, A. C., O’Campo, P., & McDonnell, K. A. (2005). Intimate partner violence, substance use, and HIV among low-income women: Taking a closer look. Violence Against Women, 11(9), 1140–1161. https://doi.org/10.1177/1077801205276943
Cherrier, C., Courtois, R., Rusch, E., & Potard, C. (2023). Parental attachment, self-esteem, social problem-solving, intimate partner violence victimization in emerging adulthood. The Journal of Psychology, 157(7), 451–471. https://doi.org/10.1080/00223980.2023.2242561
Childress, S. (2013). A meta-summary of qualitative findings on the lived experience among culturally diverse domestic violence survivors. Issues in Mental Health Nursing, 34(9), 693–705. https://doi.org/10.3109/01612840.2013.791735
Doumas, D. M., Pearson, C. L., Elgin, J. E., & McKinley, L. L. (2008). Adult attachment as a risk factor for intimate partner violence: The “mispairing” of partners’ attachment styles. Journal of Interpersonal Violence, 23(5), 616–634. https://doi.org/10.1177/0886260507313526
Duru, E., Balkis, M., & Turkdoğan, T. (2019). Relational violence, social support, self-esteem, depression and anxiety: A moderated mediation model. Journal of Child and Family Studies, 28, 2404–2414.
https://doi.org/10.1007/s10826-019-01509-2
Dutton, D. G., & White, K. R. (2012). Attachment insecurity and intimate partner violence. Aggression and Violent Behavior, 17(5), 475–481. https://doi.org/10.1016/j.avb.2012.07.003
Gamble, S. A., & Roberts, J. E. (2005). Adolescents’ perceptions of primary caregivers and cognitive style: The roles of attachment security and gender. Cognitive Therapy and Research, 29, 123–141. https://doi.org/10.1007/s10608-005-3160-7
Gilbert, L. K., Zhang, X., Basile, K. C., Breiding, M., & Kresnow, M. (2023). Intimate partner violence and health conditions among U. S. adults—National Intimate Partner Violence Survey, 2010–2012. Journal of Interpersonal Violence, 38(1–2), 237–261. https://doi.org/10.1177/08862605221080147
Gomez, R., & McLaren, S. (2007). The inter-relations of mother and father attachment, self-esteem and aggression during late adolescence. Aggressive Behavior, 33(2), 160–169. https://doi.org/10.1002/ab.20181
Gormley, B., & Lopez, F. G. (2010). Psychological abuse perpetration in college dating relationships: Contributions of gender, stress, and adult attachment orientations. Journal of Interpersonal Violence, 25(2), 204–218. https://doi.org/10.1177/0886260509334404
Guarnieri, S., Smorti, M., & Tani, F. (2015). Attachment relationships and life satisfaction during emerging adulthood. Social Indicators Research, 121(3), 833–847. https://doi.org/10.1007/s11205-014-0655-1
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. https://doi.org/10.1111/j.1469-7610.2004.00218.x
Hazan, C., & Shaver, P. R. (1994). Deeper into attachment theory. Psychological Inquiry, 5(1), 68–79. https://doi.org/10.1207/s15327965pli0501_15
Hooper, D., Coughlan, J., & Mullen, M. (2008). Structural equation modeling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6(1), 53–60. https://doi.org/10.21427/D7CF7R
Jewkes, R., Fulu, E., Tabassam Naved, R., Chirwa, E., Dunkle, K., Haardörfer, R., Garcia-Moreno, C., & the UN Multi-country Study on Men and Violence Study Team. (2017). Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the Pacific. PloS Medicine, 14(9), e1002381. https://doi.org/10.1371/journal.pmed.1002381
Karakurt, G., Koç, E., Katta, P., Jones, N., & Bolen, S. D. (2022). Treatments for female victims of intimate partner violence: Systematic review and meta-analysis. Frontiers in Psychology, 13, 793021. https://doi.org/10.3389/fpsyg.2022.793021
Karakurt, G., Smith, D., & Whiting, J. (2014). Impact of intimate partner violence on women’s mental health. Journal of Family Violence, 29(7), 693–702. https://doi.org/10.1007/s10896-014-9633-2
Kobayashi, J. E., Levendosky, A. A., Bogat, G. A., & Weatherill, R. P. (2021). Romantic attachment as a mediator of the relationships between interpersonal trauma and prenatal representations. Psychology of Violence, 11(2), 133–143. https://doi.org/10.1037/vio0000361
Kural, A. I., & Kovacs, M. (2022). The role of anxious attachment in the continuation of abusive relationships: The potential for strengthening a secure attachment schema as a tool of empowerment. Acta Psychologica, 225, 103537. https://doi.org/10.1016/j.actpsy.2022.103537
Levendosky, A. A., Lannert, B., & Yalch, M. (2012). The effects of intimate partner violence on women and child survivors: An attachment perspective. Psychodynamic Psychiatry, 40(3), 397–433.
https://doi.org/10.1521/pdps.2012.40.3.397
Li, S., Zhao, F., & Yu, G. (2019). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. Child Abuse & Neglect, 88, 212–224. https://doi.org/10.1016/j.chiabu.2018.11.012
Lindgren, M. S., & Renck, B. (2008). “It is still so deep-seated, the fear”: Psychological stress reactions as consequences of intimate partner violence. Journal of Psychiatric and Mental Health Nursing, 15(3), 219–228. https://doi.org/10.1111/j.1365-2850.2007.01215.x
Lopez, F. G., & Brennan, K. A. (2000). Dynamic processes underlying adult attachment organization: Toward an attachment theoretical perspective on the healthy and effective self. Journal of Counseling Psychology, 47(3), 283–300. https://doi.org/10.1037/0022-0167.47.3.283
Marmarosh, C. L., Markin, R. D., & Spiegel, E. B. (2013). Attachment in group psychotherapy. American Psychological Association. https://doi.org/10.1037/14186-000
Matheson, F. I., Daoud, N., Hamilton-Wright, S., Borenstein, H., Pedersen, C., & O’Campo, P. (2015). Where did she go? The transformation of self-esteem, self-identity, and mental well-being among women who have experienced intimate partner violence. Women’s Health Issues, 25(5), 561–569. https://doi.org/10.1016/j.whi.2015.04.006
McClure, M. M., & Parmenter, M. (2020). Childhood trauma, trait anxiety, and anxious attachment as predictors of intimate partner violence in college students. Journal of Interpersonal Violence, 35(23–24), 6067–6082. https://doi.org/10.1177/0886260517721894
McLaughlin, J., O’Carroll, R. E., & O’Connor, R. C. (2012). Intimate partner abuse and suicidality: A systemic review. Clinical Psychology Review, 32(8), 677–689. https://doi.org/10.1016/j.cpr.2012.08.002
Meeker, K. A., Hayes, B. E., Randa, R., & Saunders, J. (2020). Examining risk factors of intimate partner violence victimization in Central America: A snapshot of Guatemala and Honduras. International Journal of Offender Therapy and Comparative Criminology, 68(5), 468–487. https://doi.org/10.1177/0306624X20981049
Moretti, M. M., & Peled, M. (2004). Adolescent-parent attachment: Bonds that support healthy development. Paediatrics & Child Health, 9(8), 551–555. https://doi.org/10.1093/pch/9.8.551
Muller, R. T. (2009). Trauma and dismissing (avoidant) attachment: Intervention strategies in individual psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 46(1), 68–81. https://doi.org/10.1037/a0015135
Pang, L. H. G., & Thomas, S. J. (2020). Exposure to domestic violence during adolescence: Coping strategies and attachment styles as early moderators and their relationship to functioning during adulthood. Journal of Child & Adolescent Trauma, 13(2), 185–198. https://doi.org/10.1007/s40653-019-00279-9
Ponti, L., & Tani, F. (2019). Attachment bonds as risk factors of intimate partner violence. Journal of Child and Family Studies, 28, 1425–1432. https://doi.org/10.1007/s10826-019-01361-4
Rizo, C. F., Givens, A., & Lombardi, B. (2017). A systematic review of coping among heterosexual female IPV survivors in the United States with a focus on the conceptualization and measurement of coping. Aggression and Violent Behavior, 34, 35–50. https://doi.org/10.1016/j.avb.2017.03.006
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press.
Rosenberg, M. (1979). Conceiving the self. Basic Books.
Sayed, S., Iacoviello, B. M., & Charney, D. S. (2015). Risk factors for the development of psychopathology following trauma. Current Psychiatry Reports, 17, 70. https://doi.org/10.1007/s11920-015-0612-y
Scott, S., & Babcock, J. C. (2010). Attachment as a moderator between intimate partner violence and PTSD symptoms. Journal of Family Violence, 25(1), 1–9. https://doi.org/10.1007/s10896-009-9264-1
Shen, F., Liu, Y, & Brat, M. (2021). Attachment, self-esteem, and psychological distress: A multiple-mediator model. The Professional Counselor, 11(2), 129–142. https://doi.org/10.15241/fs.11.2.129
Shen, F., & Soloski, K. L. (2024). Examining the moderating role of childhood attachment for the relationship between child sexual abuse and adult attachment. Journal of Family Violence, 39, 347–357.
https://doi.org/10.1007/s10896-022-00456-9
St. Vil, N. M., Carter, T., & Johnson, S. (2021). Betrayal trauma and barriers to forming new intimate relationships among survivors of intimate partner violence. Journal of Interpersonal Violence, 36(7–8), NP3495–NP3509. https://doi.org/10.1177/0886260518779596
Sutton, T. E. (2019). Review of attachment theory: Familial predictors, continuity and change, and intrapersonal and relational outcomes. Marriage & Family Review, 55(1), 1–22. https://doi.org/10.1080/01494929.2018.1458001
Tariq, Q. (2013). Impact of intimate partner violence on self esteem of women in Pakistan. American Journal of Humanities and Social Sciences, 1(1), 25–30. https://doi.org/10.11634/232907811604271
Velotti, P., Beomonte Zobel, S., Rogier, G., & Tambelli, R. (2018). Exploring relationships: A systematic review on intimate partner violence and attachment. Frontiers in Psychology, 9, 1166. https://doi.org/10.3389/fpsyg.2018.01166
West, M., & George, C. (1999). Abuse and violence in intimate adult relationships: New perspectives from attachment theory. Attachment & Human Development, 1(2), 137–156. https://doi.org/10.1080/14616739900134201
Wilkinson, R. B. (2004). The role of parental and peer attachment in the psychological health and self-esteem of adolescents. Journal of Youth and Adolescence, 33, 479–493. https://doi.org/10.1023/B:JOYO.0000048063.59425.20
Zorzella, K. P. M., Muller, R. T., & Classen, C. C. (2014). Trauma group therapy: The role of attachment and therapeutic alliance. International Journal of Group Psychotherapy, 64(1), 24–47. https://doi.org/10.1521/ijgp.2014.64.1.24
Fei Shen, PhD, LMFT, is an assistant professor at Kean University. Ying Zhang, PhD, is an assistant professor at Clarkson University. Xiafei Wang, PhD, is an assistant professor at Syracuse University. Correspondence may be addressed to Fei Shen, 1000 Morris Ave., Union, NJ 07083, fshen@kean.edu.
May 22, 2024 | Volume 14 - Issue 1
Emily Horton
Body neutrality is a concept wherein individuals embody a neutral attitude toward the body that is realistic and flexible, appreciate and care for the function of the body, and acknowledge that self-worth is not defined by one’s outward appearance. Family behavior regarding body image has been related to higher levels of body dissatisfaction and unhealthy eating behavior among children and adolescents. Caregivers need knowledge and support on how to cultivate healthy body image for their children and adolescents. Limited studies explore how to parent in a way that promotes healthy relationships with one’s body, food, and exercise. I conducted a grounded theory study to explore the experiences of caregivers who integrate tenets of body neutrality. Semi-structured interviews were conducted with 10 caregivers of children and adolescents who self-identified as approaching parenting from a place of body neutrality. Through constructivist grounded theory, I discerned insights regarding how caregivers can support their children and adolescents in developing healthy relationships with their bodies and how this corresponds with self-esteem. Considerations for counselors using body neutrality to support children, adolescents, and caregivers are provided.
Keywords: body neutrality, body image, parenting, children and adolescents, self-esteem
Body image and related low self-esteem are frequently under-addressed or unaddressed in counseling children, adolescents, and their caregivers (Damiano et al., 2020). Too often, counselors may take a reactive approach to addressing unhealthy relationships with food, bodies, and exercise in the family system, such as counseling after an adolescent is diagnosed with an eating disorder (Liechty et al., 2016). Thus, counselors may benefit from considering how to take a preventative, proactive approach to supporting children’s mental health specific to their relationship with food, bodies, and movement (Siegel et al., 2021). Because the family system has tremendous impact on children’s body image and relationship with food, counselors need to consider how to provide appropriate psychoeducation and support to caregivers on how to manage food and body talk (Gutin, 2021). Positive caregiver influence on body image can prevent disordered eating, negative body image, and low self-worth, and many families need a licensed mental health professional to cultivate said positive influence (Veldhuis et al., 2020).
Researchers have found that children as young as 3 to 5 years old experience body image issues (Damiano et al., 2015; Dittmar et al., 2006). Caregivers often communicate body dissatisfaction, engage in dieting, and demonstrate a drive for thinness, messages that children can internalize (National Eating Disorders Association, 2022). Families can inadvertently pass down unhealthy ideals regarding body image to their children (Kluck, 2010). Kluck (2010) emphasized that a family’s focus on appearance was related to their child’s body image dissatisfaction, and the dissatisfaction predicted increased disordered eating. Counselors with appropriate training can play an important role in mitigating the harmful cycle before disordered thinking turns into disordered eating (Klassen, 2017). Counselors have the unique opportunity to support families in encouraging a healthy relationship with their bodies (Horton, 2023; Horton & Powers, 2024).
In this study, I sought to explore the experiences of caregivers who integrate tenets of body neutrality. Body neutrality is a concept wherein individuals embody a neutral attitude toward the body that is realistic and flexible, appreciate and care for the function of the body, and acknowledge that self-worth is not defined by one’s outward appearance (Pellizzer & Wade, 2023). Examples of body neutrality can include not describing food as healthy or unhealthy, talking about what our bodies do for us rather than what they look like, and moving for enjoyment rather than to burn calories. Because the tripartite model emphasizes that parental influence, in addition to peer and media influence, is significant for children’s body image development, I explored existing research on parental influence on body image and self-esteem (Thompson et al., 1999).
Parental Influence on Body Image and Self-Esteem
Some family members negatively impact children’s and adolescents’ body image (Pursey et al., 2021). Neumark-Sztainer et al. (2010) found that over half of the adolescents in their study experienced weight-based and appearance-based teasing from family, and these experiences correlated to higher levels of body dissatisfaction, disordered eating, and related mental health difficulties, such as depression. Parental influence on body image includes both direct (e.g., criticism about their child’s weight) and indirect (e.g., parents’ attitudes about their own bodies, food, and exercise) behaviors (Rodgers & Chabrol, 2009). Abraczinskas and colleagues (2012) conducted a study exploring parent direct influence, including weight- and eating-related comments, and modeling, including parental modeling of dieting and related behavior. In the study of over 360 participants, Abraczinskas and colleagues found that parental influence is a risk factor in the development of a drive for thinness, body shape dissatisfaction, and eating disorder symptomology.
Moreover, Wymer and colleagues (2022) emphasized the importance of parent engagement in body image and self-esteem development. Often, families recognize the importance of discussing body image with their children but do not feel confident or competent in doing so (Siegel et al., 2021). The lack of confidence and competence leads to messages about health being conflated with messages about thinness (Siegel et al., 2021). In addition, researchers highlighted that although parental influence has a significant impact on body image and self-esteem, siblings, friends, and the media are also perceived to have influence over youth’s feelings about their bodies (Ricciardelli et al., 2000). The exiguous literature on parental influence on body image repeatedly emphasizes the negative impact of parents on body image yet seldom explores preventative and therapeutic ways of promoting healthy body image (Phares et al., 2004). Thus, I sought to explore how counselors might integrate body neutrality when supporting families and provide early intervention and prevention for adverse relationships with food, body, and movement.
Body Neutrality
Body neutrality is a concept wherein individuals accept their bodies as a vessel that carries them through life, and as such, do not attach positive or negative feelings to their physicality. For example, body neutrality can entail nurturing and respecting the body, being mindful of body talk, engaging in body gratitude and functionality appreciation, and recognizing self-worth that is not focused on appearance (Pellizzer & Wade, 2023). Body neutrality is an approach taken to help with the healing of body image, particularly in the field of eating disorders (Perry et al., 2019). Body neutrality tenets appear to be integral in the prevention of body image dissatisfaction and disordered eating (Herle et al., 2020). Practicing body neutrality positively impacts body satisfaction, self-esteem, and negative affect with adults, though continued empirical research is needed on its impact with youth (Walker et al., 2021). Although counselors and other allied professionals integrate body neutrality into their clinical practice, there is minimal research on its efficacy outside of eating disorder treatment. Existing research has emphasized the need for counseling approaches with youth that highlight body neutrality tenets, such as mindful eating and awareness-building conversations about societal messaging (Klassen, 2017). However, researchers have yet to explore how body neutrality could be integrated into a parenting approach. The bulk of the limited understanding of body neutrality is treatment based, rather than prevention oriented.
Thus, the purpose of this study was to cultivate a grounded theory or an abstract theoretical understanding of body neutral parenting (Charmaz, 2014). Further insight into the experiences, challenges, and potential barriers in parenting with body neutrality can enable a deeper understanding of how parents seek to promote healthy body image and self-esteem for children and adolescents. In this study, I aimed to offer a newfound understanding to mental health professionals supporting children, adolescents, and caregivers in the areas of body, food, movement, and related mental health implications.
Method
Methodology
To address the paucity of literature, a grounded theory study was conducted to examine the following research question: How do caregivers conceptualize and actualize body neutral parenting with their children? The study derived from constructivist grounded theory (CGT; Charmaz, 2014). CGT is an interpretative, qualitative methodology that acknowledges that researchers and participants co-create the theory (Charmaz, 2014). Given a desire to understand how caregivers conceptualize and utilize body neutral parenting, CGT was deemed appropriate. The purpose of the study was to generate a new theory through inductive analysis of data gleaned from caregivers who self-identify as using body neutral parenting.
Role of the Researcher
Congruent with CGT, I maintained a position of distant expert (Charmaz, 2014). The theoretical meaning was constructed by turning participants’ experiences into digestible theoretical interpretations. While staying as true to the experiences of the participants as possible, I reconstructed the participants’ stories in the development of the grounded theory via balancing conceptual analysis of participants’ stories and creating a sense of their presence in the narrative (Mills et al., 2006). I sought to examine the impact of my privilege and preconceptions as a White, cisgender woman and professional in the field of mental health counseling, with experience supporting families navigating eating disorders and disordered eating (Charmaz, 2014). Also, as a parent who integrates body neutrality into my approach with my child, I practiced reflexive journaling and other trustworthiness strategies to bracket my biases throughout the study.
Participant Recruitment
I obtained IRB approval prior to data collection. Per the IRB, all participants verbally consented before partaking in the research study. I used purposive sampling (Patton, 2014) for participant selection. Selection criteria included: (a) being a caregiver to at least one child under the age of 18, (b) identifying as integrating body neutrality into their parenting approach, and (c) willingness to participate in an interview lasting roughly 1 hour. I circulated electronic flyers detailing the focus of the study to social media pages for caregivers and professional networks. The recruitment flyers provided examples of body neutral parenting, including not describing food as healthy or unhealthy, talking about what our bodies do for us rather than what they look like, and moving for enjoyment rather than to burn calories.
Ten participants were interviewed. Of the 10 participants, nine identified as cisgender women and one identified as nonbinary. All 10 participants described themselves as being middle class. Nine participants were married and one was single. All of the participants had graduate-level or doctorate-level educations; four had master’s degrees and six had doctoral degrees. Participants lived in seven different states and two different countries. Participants had at least one child, with the number of children ranging from 1 to 5. Table 1 provides detailed demographic data.
Table 1
Participants’ Demographic Data
| Pseudonym |
Age |
Race |
Number
of Children |
Age of Children |
Race of Children |
| Logan |
27 |
White |
1 |
20 months |
White |
| Esmeralda |
38 |
Hispanic |
2 |
8 and 5 years |
White |
| Imani |
29 |
Black, White |
2 |
6 and 3 years |
White |
| Kimberly |
33 |
White |
2 |
5 and 2 years |
White |
| Heather |
42 |
White |
2 |
3 years, 8 months |
White |
| Cassie |
45 |
White |
5 |
16, 13, 11, 9, and 7 years |
White |
| Shanice |
36 |
African American |
4 |
15, 9, and 2 years; 4 months |
African American |
| Scarlett |
36 |
White |
3 |
17, 5, and 4 years |
White |
| Leilani |
43 |
White |
1 |
9 years |
Polynesian, White |
| Jennifer |
36 |
White |
1 |
2 years |
Middle Eastern, White |
Data Collection and Analysis
As guided by Charmaz’s (2014) CGT protocol, data collection and data analysis proceeded simultaneously, and the inclusion criteria evolved to include caregivers with children of all ages. The semi-structured interviews occurred via confidential videoconferencing software and lasted between 60 and 75 minutes. Interviews were an open-ended, detailed exploration of an aspect of life in which the participants had substantial experience and considerable insight: parenting with body neutrality principles (Charmaz & Liska Belgrave, 2012). During the interviews, I inquired about caregivers’ experiences, challenges, and insights of body neutral parenting. With the emergent categories, the guide evolved to emphasize the nuances of the parenting approach in alignment with three-cycle coding or focused coding (Charmaz, 2014).
Grounded theorists try to elicit their participants’ stories and attend to whether the participants’ interpretations are theoretically plausible (Charmaz & Liska Belgrave, 2012). As such, the interview protocol began with an initial open-ended question: “Tell me about a time in which you used body neutral parenting.” Then, I asked intermediate questions, such as “How, if at all, have your thoughts and feelings about body neutral parenting changed since your child was born?” I also asked ending questions, including: “How has taking the approach with your children impacted you as a parent? As a person?” The interview questions were informed by the literature and were reviewed by another content matter expert.
In addition to the in-depth interview, I used information from other data sources to support the depth of the data and theory construction. Other triangulated data sources included field notes of observations during the interviews, a reflexive journal, literature and previous research on body neutrality, and a demographic survey. In this way, the constant comparative analysis unique to CGT increases rigor through complex coding procedures more so than other methods of qualitative data analysis (Hays & McKibben, 2021). The constant comparative analysis examines nuanced relationships between participants through negative case analysis to strengthen findings (Hays & McKibben, 2021).
Three-cycle coding and constant comparative analysis drove the data analysis process (Charmaz, 2014). Through the data analysis process, I constantly compared data (Mills et al., 2006). Inductive in nature, the constant comparison through the data analysis grounded my theories from the participants’ experiences (Mills et al., 2006). In alignment with CGT, I coded the interviews through a fluid process of initial coding, focused coding, and theoretical coding. During initial coding, I focused on “fragments of data,” such as words, lines, segments, and incidents (Charmaz, 2014, p. 109). The initial coding process not only included the transcripts, but also continued the interaction and data collection to facilitate the continuous analytical process. I also engaged with focus coding, wherein I used the most significant and frequent codes that made the most analytic sense (Charmaz, 2014). The focused codes were more theoretical than line-by-line coding practices. I engaged in theoretical coding of the data; theoretical coding is a way of “weaving the fractured story back together” (Charmaz, 2014, p. 63). In accordance with Charmaz (2014), theoretical coding involved clarifying the “general context and specific conditions” and discovering “participants’ strategies for dealing with them” (p. 63). As I moved throughout the three-cycle coding process, the number of codes, categories, and emerging core categories decreased and refined, leaving me with the final core categories described below (Khanal, 2018).
Rigor and Trustworthiness
Throughout the totality of the research process, I engaged with five strategies to ensure trustworthiness. In the data analysis process, significant care was taken to ground analytic claims in the data obtained and remain true to the raw material provided by participants (Charmaz, 2014). I fostered trustworthiness through member checking and memo-writing (Creswell & Poth, 2017). I sent the transcript and the themes to participants and had six of 10 participants verify the themes as being congruent with their experiences. The other participants did not respond to the email with the transcript. Memo-writing was critical in constructing theoretical categories (Charmaz, 2014). I stopped and analyzed my ideas about the codes and emerging categories via memo-writing. Successive memos kept me immersed in the analysis and increased the abstraction of my ideas (Charmaz, 2014). In the theory construction, I also triangulated data sources, including semi-structured interviews, field notes of observations during the interviews, memo-writing, literature and previous research on body neutrality, and a demographic survey. Charmaz (2014) emphasized the importance of “thick descriptions” (p. 14), which I captured via writing extensive field notes of observations during the interviews and compiling detailed narratives from transcribed tapes of interviews.
I also shared my memos and data analysis process with an external auditor (Hays & McKibben, 2021). The external auditor was a researcher with experience in qualitative research and content familiarity. After the external auditor reviewed the data analysis trail, including the three stages of coding, I reviewed her written feedback and we met to process the feedback. The external auditor offered several pieces of feedback regarding the analytic process, including leaning more into the theory rather than the stories and removing quotes that captured pieces outside of the theory (i.e., removing content rooted in diet culture and body positivity). Feedback was integrated to strengthen the study’s development and explication of the theory based on data.
Results
This study involved the caregivers and researcher co-constructing the parenting theory while integrating body neutrality concepts. The theory stemmed from the perspectives shared by caregivers who parent in such a way as to promote body acceptance, such as focusing on what our bodies can do for us, avoiding body talk, eating the foods we want to eat, listening to our bodies, not focusing compliments on appearance, etc. As such, the grounded theory below explains caregivers interacting and experiencing body neutral parenting (Charmaz, 2014).
The emergent core category was the balancing of internal experiences with external parenting, moving toward body neutral parenting. The emergent core category captured the essence of the theory—parents integrating body neutrality balance internal experiences (e.g., their own relationship with their bodies and food) with external parenting (e.g., their parenting skills of how to handle food in the household). Figure 1 depicts a conceptual diagram of the body neutral parenting grounded theory. The “mobile” emphasizes the movement and interconnectedness within the body neutral parenting process. At the top of the diagram, there is a seesaw balance between the external parenting skills and internal experiences, processing, and regulating. The internal and external experiences teeter and totter and inform one another as a parent integrates body neutrality. The mobile diagram showcases that if one piece moves, the other pieces move as well. To illustrate, if a parent’s external parenting skills move (e.g., a parent no longer says negative things about their body in front of their children), their internal experiences are impacted (e.g., their own unmet childhood mental health needs related to body image are addressed). The core category of balancing internal experiences with external parenting moving toward body neutral parenting included two categories: (a) De-moralizing Food, Bodies, and Movement, and (b) Reprogramming and Re-Parenting. Each of the two emergent categories has associated subcategories.
De-moralizing Food, Bodies, and Movement
The first category is De-moralizing Food, Bodies, and Movement (n = 10). Within this category, there were three subcategories: De-moralizing Food, De-moralizing Bodies, and De-moralizing Movement. The category embodied acknowledging and countering the large cultural narrative of “good” foods and “bad” foods as well as “good” bodies and “bad” bodies. Participants emphasized the impact of removing the reward and punishment that accompanies the moralization of food, bodies, and movement. As captured by Kimberly, body neutral parenting is about “giving children more of a voice”and trusting them: “When they say that they’re hurt, believing them; when they say that they’re hungry, believing them. Letting them speak for themselves and not speaking for them or for their body. Trusting that they know their body the best.”
Figure 1
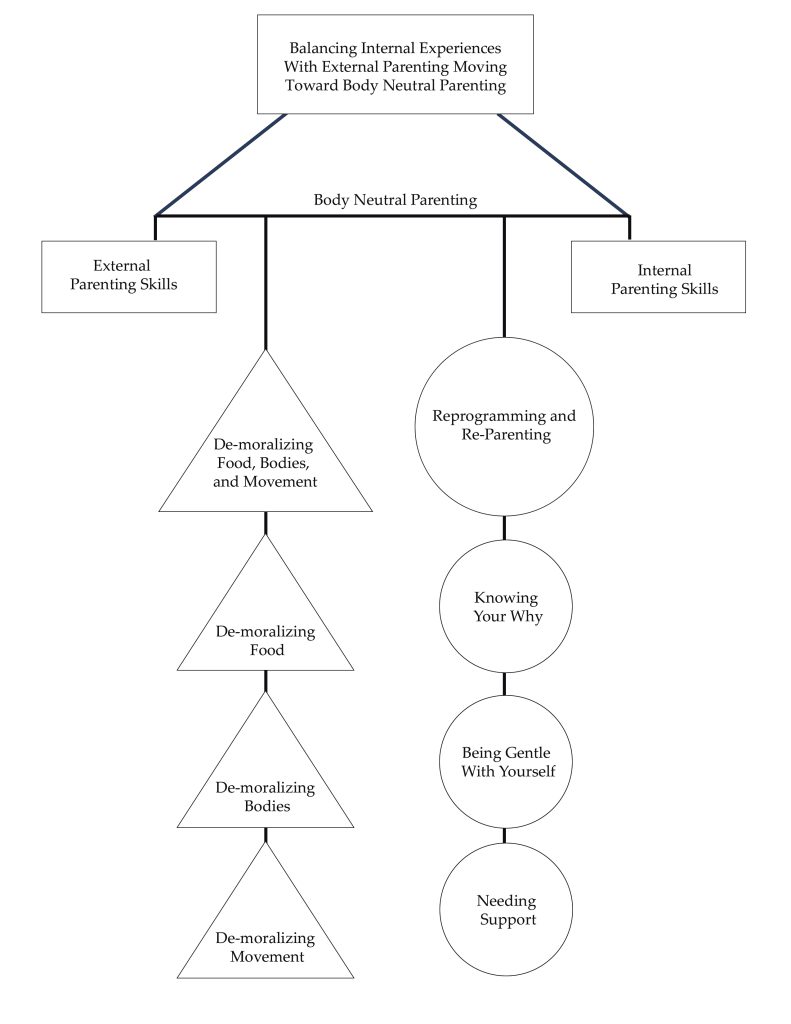
Note. This figure showcases the diagram of the body neutral parenting theory. The diagram shows a visual representation of the emergent core category, two categories, and six subcategories and their relationships (Charmaz, 2014).
De-moralizing Food
The first subcategory (n = 10) was De-moralizing Food. Participants consistently noted that food was “one of the biggest” parts of body neutral parenting—specifically, approaching food not as “good” or “bad,” not as “healthy” or “unhealthy,” but simply, neutrally, as “fuel” for the body. Cassie articulated that “A big piece is trying to take the moral piece out of it too. That it’s somehow good to have a certain body or foods are good or bad. Just trying to get away from that.”
The demoralization of food, moving toward neutrality with food, presented in numerous ways across participants’ approaches to caregiving. A primary way in which participants showcased their beliefs about food with regard to body neutrality was to present different foods in a neutral way. For example, the neutral presentation of different foods could look like desserts on the child’s plate from the beginning of the meal, rather than something to be “earned” after eating the “good” foods first. Esmeralda articulated a way in which she demoralized foods and presented them neutrally through what she coined as “Tasting Tuesdays.” She shared:
Instead of making a meal that you serve up in bowls or on plates, you basically charcuterie board the whole meal. . . . I noticed the effect it had on my kids to present a bunch of options, including desserts or traditional treats—it was all presented together. I was laying out all the foods on equal ground, lots of options. And many traditionally unhealthy foods and many traditionally healthy foods just all on the table together. There was no instruction. They just got an empty plate, and they could fill it with whatever they wanted, and I think for them there was some autonomy built into that. They could decide exactly what and how much they wanted to eat off the table. But it also, I think, inspired some adventurousness in them.
Presenting foods neutrally mitigated food judgment, created variety and exposures to food, and met the developmental needs of her children by making mealtime fun.
Another pivotal element of de-moralizing food and moving toward neutrality with food was to create space for children to practice noticing their hunger and fullness cues. Jennifer shared about her experience helping her child learn to trust their body and its cues. She explained:
Trying to trust him and listening to his body, even though he’s 2, and knowing where to intervene and where I shouldn’t intervene. If I make dinner and I put it in front of him and he touches nothing and wants to get down, the way that I was raised was you finish your plate no matter what. Reading everything that I’m reading and trying to move to this neutral space. What I want to say is “At least taste it. At least take a bite. Take one bite. Take three bites.” And what I’m choosing to do is, “Okay, you don’t have to eat right now. We’ll have a bedtime snack later.” I was conditioned to think that first thought.
While not explicitly using the language, participants spoke to helping their children with their hunger, fullness, and satiety cues. Practicing satiety looked like the children being able to say, as Scarlett’s son said, “My body is hungry for ice cream.” Also, Kimberly shared trying to instill autonomy within her children as they learn their hunger, fullness, and satiety cues:
We do defer to them a lot in terms of what they eat or when they’re eating. My daughter wanted canned cooked carrots for breakfast. It was like, well, okay, that’s not maybe socially typical, eating cooked carrots for breakfast. But if that’s what your body wants, go for it. . . . They asked her a question at school when she was graduating from preschool. What would you spend $1,000,000 on? A doughnut. So, it’s like, okay, we’re not going to demonize your doughnuts. You can have your doughnuts when you want your doughnuts.
Here, Kimberly also captured body neutral parenting’s emphasis on avoiding “healthy” vs. “unhealthy” food and other dichotomous language, stemming from diet culture.
Neutral beliefs and behaviors regarding food also manifest via portion sizes for children. Scarlett highlighted differences she noticed in how her family members wanted to portion food for her two sons: one in a larger body and one in a smaller body. She explained that her family members will “offer to my one son and not to the other” while also saying “Oh, do you need that?” to the son in a larger body. Thus, integrating body neutral parenting entails presenting food neutrally, rather than being driven by internalized societal messages about food and thin privilege (e.g., suggesting to a child in a larger body that they may not need the amount of food they are being served perhaps because of anti-fat bias). Body neutral parenting applies for children of all body types.
Moreover, caregivers practicing body neutrality with their children talked about food in a way that emphasizes how it “fuels the body” rather than being about “reward or punishment.” Esmeralda explained:
It’s like you have to basically find a whole new system of rewards. Sweet things are good motivators. They’re reward systems. And they’re also seen as the desirable food after you choke down the “healthy” food . . . these are the “good” foods you have to eat in order to get the “bad” foods that you get rewarded with after dinner. That just is such an insidious concept.
Counter to food being a “reward” or “punishment,” children get to choose rather than falling into the power struggle with food. Cassie described
taking the power out of the food situation. With little kids, everyone thinks like, “Oh, you have to control it and you have to make sure they get vegetables in and all that stuff.” Then it becomes about this power dynamic and just trying to take power out of it and then it is about letting them listen to their body and learn about their body.
Avoiding using food as a reward or as a punishment was integral to the body neutral parenting approach.
De-moralizing Bodies
The second subcategory (n = 9) was De-moralizing Bodies, wherein there are not “good” bodies and “bad” bodies. Leilani described, “In relation to size, shape, behavior, disposition, bad habits . . . everybody’s different.” Body neutral parenting conceptualizes bodies in neutral ways, emphasizing what they help people do. As Cassie explained, “You need food to do the things you want to do, and so we take care of our bodies . . . not to look pretty, but to be able to do—focus more on the doing.” Similarly, Leilani shared,
My go-to approach is to say things like “Everyone’s body is growing at its own pace” and “We have to let our bodies grow at their own pace.” I’m freaked out by stats on how many U.S. girls are dieting around age 10-ish. I’m hoping that my emphasis on letting our bodies do what they need to do will have some impact against pre-teen dieting fads taking hold in our home.
Many participants spoke about their goal for their children of “listening to their bodies.” Kimberly explained, “We tell our children a lot, ‘Listen to your body.’ So, what your body is feeling, what your body is saying, if your body is not hungry anymore, that’s fine. Or if it is hungry.” Further, participants named the impact of modeling, and not modeling, ideals about bodies. To illustrate, Imani explained,
Not talking about other people, that is a huge thing in our family, is just to not talk negatively about people that we don’t know or about people we do know. We don’t talk negatively about our own bodies in front of our kids or anybody else’s body in front of our kids. That’s honestly probably one of the more impactful things that we do.
Kimberly, too, emphasized being mindful of modeling how to think and talk about bodies:
Making sure that we model kindness to our bodies in front of them as well. So not saying things that are self-deprecating about the way that we look. Making sure that our children don’t hear us saying, “Oh my gosh, I’m just so fat,” those kinds of messages.
Also, participants emphasized integrating body neutrality into clothing approaches with their children. Scarlett described being mindful of the language she uses regarding clothes and bodies: “You’re too big for that versus those clothes don’t fit your body, or you’re too small for that versus that doesn’t really look like it’s comfortable on your body. Let’s find something that works best for you.”
De-moralizing Movement
The last subcategory (n = 7) was De-moralizing Movement, which included engaging in movement for fun and being mindful of how we speak about exercise. Imani explained:
And so I think that for us, we really try to keep those things [exercise, body image, and food] disconnected. If you’re doing gymnastics, it’s because you’re interested in it and you think it’s a fun thing, not because it’s going to impact your body, not because you know it’s going to make you thin. It’s because you think it’s fun.
Cassie conceptualized movement as being fun, not for compensation, as well: “Being excited about things our bodies are doing and not just kind of the emphasis on like, well, if it’s fun, let’s do it. But if it’s not fun, then we’re not going to push ourselves or torture ourselves.” Moreover, Scarlett emphasized the importance of being conscientious of language used to describe her children’s bodies:
How big they are. We use that term especially with male children. But you are such a big boy is always the thing. You’re such a big boy . . . instead trying to just say things like, “Oh, hey, that’s really awesome that you can do X, Y, and Z.” Trying to make it very concrete, it’s very cool that your body allows you to run around and play.
When it came to De-moralizing Food, Bodies, and Movement, a theme of removing the “shoulds” prevailed across participants. Kimberly described trying to “stay neutral with foods so that we don’t end up so much down the should line of what they should be eating or what they should be doing in terms of physical activity or those kinds of things.” Taking out the “should” entailed avoiding dictating what children “should be eating, “should look like,” or how they “should be exercising.” In summary, as poignantly articulated by Logan, “just focusing on the objectivity of what’s there without having the positive or negative associations.”
Reprogramming and Re-Parenting
The second category (n = 10) was Reprogramming and Re-Parenting. Beyond the skills of body neutral parenting, a key tenet of the approach was ample self-reflection. Caregivers engaged in deep reflection of their own relationship with food, their body, and movement while supporting their children in their body image development. The self-reflection process entailed identifying, rewiring, and, often, re-parenting oneself through the sociocultural messages that have permeated one’s life span. Scarlett shared that body neutral parenting “makes me reflect on myself and why I’m saying the things I’m saying and why I feel the way I’m feeling.” Subcategories of Reprogramming and Re-Parenting included: Knowing Your Why, Being Gentle With Yourself, and Needing Support.
To illustrate, Leilani increased her awareness of her history with disordered eating and exercising for compensation and shared the impact her daughter has had on rewiring her way of thinking:
If I had a child who was very thin, it would have reinforced that dysfunction for me, because then I’m someone who produced a very thin child, and that makes me even better. . . . And then when you have a kid who’s really big and she’s pretty chubby, that you have to make such a hard shift to undo. Being the skinniest person in the room isn’t your greatest value in life and really reestablishing that personal value system. That’s been a massive kind of change for me.
This is a tangible example of the rewiring that happened for Leilani, though all of the parents spoke to their rewiring process and need to re-parent themselves alongside their children.
Knowing Your Why
The first subcategory (n = 10) of Reprogramming and Re-Parenting was Knowing Your Why. Participants acknowledged the value they put into the parenting approach. Jennifer captured common collective values of body neutral parenting when she shared:
Number one, reducing shame. Number two, increasing quality of life and self-confidence . . . that would probably eventually help with any mental health issues or any relationship issues because he’ll have the self-confidence to say where his boundaries are and trust his body. And at the same time listen to other people and be empathetic.
Similarly, Kimberly emphasized how much it means to be parenting without shame: “I love that we know we’re not parenting with shame . . . as the hidden motivator. That’s why you don’t eat that extra food you might be hungry for.”
A significant challenge for many participants was the “internalized messaging” they experienced regarding their body image, food, and movement. Almost all of the participants (n = 8) directly spoke to their experiences with an eating disorder or disordered eating driving their desire to parent from a body neutral stance. Cassie, for example, cited her eating disorder recovery as sparking her passion for body neutral parenting:
Right when my husband and I got married, I went into treatment for an eating disorder, and so that shaped me a lot. . . . I was using all of the things that I had learned and trying to really instill it in them. How we talk about food, how we talk about bodies. It was such an integral part of my parenting.
Being Gentle With Yourself
The second subcategory was Being Gentle With Yourself. Each participant (n = 10) criticized themselves in some fashion about not perfectly integrating body neutrality into their parenting approach. They were quick to highlight their failures and slow to honor their successes. Body neutral parenting, given its emphasis on countering long-standing sociocultural messaging, requires offering oneself a great deal of grace. Body neutral parenting entails tremendous learning, and that learning starts with reminding caregivers that they are doing the best that they can with the knowledge, support, and resources that they have. Imani spoke to how she navigated thoughts from these internalized messages and filtered them:
I think about things like, “She’s thinning out.” . . . It’s so ingrained, it’s hard not to think those things. And so then even if that’s something that goes across my mind or I think about the things that they’re eating and how that might impact their body or their physical health, just stopping that conversation with me and not actually talking about that with them, it’s not something that they need to hear. So, I think that it’s just as much what we don’t say as much as what we do say to them.
Having thoughts stemming from diet culture and stumbling and saying the “wrong” thing is inevitable when rewiring these deeply embedded messages. Not only are those moments of “messing up” normal, but they also create space for beautiful moments to repair. Scarlett explained her process of repairing the inevitable ruptures:
Which all sounds well and good and wonderful until you are running around with a 4-year-old and a 5-year-old on your day to day. I will also balance that, it’s also trying to catch myself when I say things that I’ve just internalized from society in my own childhood and being like, “Hey, isn’t that interesting.” Just talking out loud to them. Saying, “Isn’t it interesting that I said X, Y, and Z? Is that really maybe the best way to talk about our bodies?” Trying to just be reflective and knowing that I’m not always going to be body neutral but trying to be intentional about noticing when I’m not.
The participants reflected that parenting is an imperfect, human process.
Needing Support
The third subcategory was Needing Support. All of the caregivers in the study (n = 10) spoke to the importance of feeling support in their parenting approach. Support looked different for each family; some received support through social media, and others described finding support from their partner or other like-minded caregivers. Every participant described the role that social media had in their body neutral parenting approach. Many described learning about the approach via social media and experiencing continued support through certain social media pages. For example, common social media pages referenced by participants included Feeding Littles, Our Mama Village, Dr. Becky, and Kids Eat in Color. Most participants recommended that caregivers interested in starting body neutral parenting seek out social media for knowledge and support.
Additionally, participants emphasized the importance of being on the same page with other primary caregivers. Consistently, participants accentuated the need to talk through how to navigate situations in advance, to be on the same page for how to handle them. To illustrate, Scarlett described how to navigate their child “wanting ice cream after not eating all of their dinner” and how she and her partner talked through how to approach that situation. Esmeralda emphasized a need for support that she felt she was not getting:
I don’t think I’ve really found a group of parents or moms where we can talk through these things or troubleshoot together. I feel like I’m a consumer of some social media on the topic, and then I’m just sort of alone.
Feeling supported appeared to be integral to body neutral parenting.
Discussion
This co-created grounded theory on body neutral parenting is a valuable addition to the literature, given the gaps in understanding how counselors can help guardians support healthy body image amongst children (Klassen, 2017). Given the significant familial influence on body image development, counselors can consider this study’s findings through a preventative lens (Liechty et al., 2016). The findings align with the scant literature on body neutrality, suggesting the need for continued exploration of how to support children, adolescents, and their families in their conceptualizations of body, food, and movement (Gutin, 2021). Mental health counselors can consider body neutral parenting as an avenue to foster positive familial influence in body image development. Positive familial influence on body image and related self-worth can prevent disordered eating, negative body image, and low self-worth (Veldhuis et al., 2020). Thus, body neutral parenting appears to have the potential to have significant impact on the mental health and self-efficacy of children, as well as their caregivers.
Based on the findings of this study, critical tenets of body neutral parenting include de-moralizing food, bodies, and movement, and reprogramming and re-parenting. The co-created parenting theory constructed in this study can be utilized as a way of conceptualizing a parenting practice that facilitates healthy body image development for families. Specifically, counselors can help families learn that food is not “healthy” or “unhealthy” and there are not “good” or “bad” bodies. In addition, the co-created theory emphasizes the need for counselors to help family members heal from internalized messages and misconceptions about health that can perpetuate body image dissatisfaction and disordered eating across generations.
Implications for Counselors and Caregivers
Counselors and caregivers are uniquely positioned to use the findings of this study to inform how they support children and their body image development. In this study, parents offered their approach to integrating body neutral parenting with their children. The co-created theory of body neutral parenting offers a baseline for counselors and parents to consider, and future research on the theory is needed. Thus, counselors and parents can consider learning about body neutrality and integrating the principles in supporting the mental health of families.
Counselors
Body neutral parenting gives families and counselors alike a framework of how to navigate conversations of body, food, and movement to promote a healthy relationship with body image. Families need the language, including specific scripts of what to say and do, and what to avoid saying and doing, to support their children in their body image development. It appears that many families would be interested in shifting the larger sociocultural narrative, including diet culture, with their approach to raising their children, if they had the appropriate psychoeducation and support (Siegel et al., 2021). Clinical mental health counselors can meet that need. The co-created grounded theory in this study and further research can provide a launching pad for counselors who want to take a more preventative approach to body image and related mental health support for youth. Counselors can teach families about de-moralizing food, bodies, and movement in their household, for example, as part of the counseling process for children and adolescents who are at risk for disordered eating and body image concerns.
Counselors can consider how to be of support to families with an interest in integrating body neutrality into their childrearing approach. Mental health professionals can consider how to be of support through the arduous, though meaningful, process of simultaneously parenting one’s children and re-parenting oneself. Some ways in which mental health counselors can support families include normalizing and validating how difficult body neutrality can be and offering specific scripts of what to avoid saying and what to say instead. To illustrate, a counselor might provide psychoeducation to a parent on how to talk to their child about food. Rather than saying “Apples are good for you,” the caregiver could say, “Red food gives you a strong heart” (Kids Eat in Color, 2022). Moreover, families will need support as they navigate the tremendous amount of rewiring involved for body neutral parenting. Counselors can keep in mind the larger overarching goal to drive their clinical decisions in supporting families through body neutral parenting and avoid the negative experience of shame (Ruckstaetter et al., 2017). Counselors can support families in realizing that parenting is an imperfect, human process. Reminding caregivers that imperfect moments will happen, and how to be gentle with themselves, is critical for caregivers continuing the body neutral lifestyle.
As practicing counselors, we must engage in deep reflective practice ourselves to support families and children with body neutrality. In order to be culturally responsive and meet the needs of diverse families, we must “gain knowledge, personal awareness, sensitivity, dispositions, and skills” specific to body neutrality (ACA, 2014, C.2.a). All people have internalized messages and “shoulds” about food, bodies, and exercise, and those internalized biases can hinder the counselor’s ability to support the intricate needs of diverse families healing their relationships with food, bodies, and exercise. Thus, it is an ethical imperative for counselors to engage in self-reflective work about their internalized messages and how those biases might impact the body image needs of children. To illustrate, a counselor might have thin privilege and internalized messages of fat phobia and unknowingly perpetuate the social justice issue of sizeism. Similarly, a parent might make negative comments about the larger body individuals on a TV show. When working with a client in a larger body, a counselor might congratulate the client on their weight loss, when the client might actually be struggling with restricting food and exercising for compensation. It remains an ethical and social justice requirement to engage in both self-reflective work and learning new skills, such as de-moralizing food, to be a culturally responsive, ethical counselor.
Parents and Caregivers
Relatedly, parents and caregivers can consider body neutrality when supporting their children with their body image development. For example, parents might consider the findings of this study and consider what de-moralizing food, bodies, and movement might look like in their home as well as reflect on their own healing process related to reprogramming and re-parenting. Parents might first identify how they engage in power struggles with food; use food as a reward; or use moralized language around food, bodies, and movement. Then, they might work toward identified areas for growth that can help move toward a more neutral relationship with food, bodies, and movement in their home.
Parents might be intentional about their use of language related to food, bodies, and movement with their children. For example, parents might avoid using the terms “healthy” and “unhealthy” related to food, but rather, emphasize the nutrients in the food, how the body feels after food, and other concepts congruent with intuitive and mindful eating. Further, in this study, many parents prefer the term “movement” over “exercise,” as it more accurately captures the relationship with moving the body. “Exercise” has a connotation for many clients as being punitive, exhausting, or for compensation, as opposed to “movement” embodying the mindful moving of the body for fun concepts aligned with body neutrality. In addition to language considerations, parents might consider how they maneuver mealtimes and integrate suggestions from the findings of this study, such as offering sweet foods at the same time as the meal, rather than having the dessert afterward as something to be earned.
Parents might also engage in their own healing and reflective practices, such as identifying their own food rules and reprogramming their internalized messages about food. Parents can model body neutrality with their own body by avoiding negative body talk, such as “I am so fat” or “I am bad for eating that, now I need to walk off those calories,” and replacing those comments with more body neutral statements. Similarly, caregivers can be mindful of how they talk about others’ bodies, such as avoiding negative comments about the larger body individuals on a TV show. Examples of body neutral statements might be: “My body is hungry for” and “I love that my body allows me to give you big hugs.”
Limitations
The sampling procedure is a limitation of this study. Onwuegbuzie and Collins (2007) suggested an ideal sample size between 12 and 15 for a grounded theory investigation using interviews. Although the study met theoretical saturation, the sample size was slightly under some recommended sources for a grounded theory investigation with 10 interviews. Moreover, although attempts were made to have a diverse sample and a geographically diverse sample was acquired, the study primarily captured the experiences of highly educated, middle-class mothers.
In addition, another primary limitation is the self-report from parents. Although parents self-reported as enacting body neutral parenting practices, I did not confirm if their self-report aligned with their actual parenting practices. As such, this study was not able to confirm how or in what way the participants’ parenting was effective. Moreover, research has not yet confirmed that body neutral parenting practices are helpful for children, necessitating further outcome research.
Future Research
Future studies could cast a more comprehensive, representative net and capture the experiences of other caregivers of more diverse gender, socioeconomic, and educational backgrounds. Researchers could explore the nuances of caregivers integrating body neutrality into their approach caring for their children, such as specific developmental considerations. Research exploring current counseling practices, including how counselors support families through body neutral parenting, would also be a helpful addition to a scant literature base.
Conclusion
This study uncovered body neutral practices that caregivers and mental health professionals alike can use to support the body image development of children and adolescents. In particular, findings emphasized the importance of the caregiver’s reflective work and de-moralizing food, bodies, and movement. Body neutrality as an approach to parenting appears to underpin the healthy development of body image and related self-esteem in children and adolescents.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Abraczinskas, M., Fisak, B., Jr., & Barnes, R. D. (2012). The relation between parental influence, body image, and eating behaviors in a nonclinical female sample. Body Image, 9(1), 93–100.
https://doi.org/10.1016/j.bodyim.2011.10.005
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/Resources/aca-code-of-ethics.pdf
Charmaz, K. (2014). Constructing grounded theory: A practical guide through qualitative analysis (2nd ed.). SAGE.
Charmaz, K., & Liska Belgrave, L. (2012). Qualitative interviewing and grounded theory analysis. In J. F. Gubrium, J. A. Holstein, A. B. Marvasti, & K. D. McKinney (Eds.), The SAGE handbook of interview research: The complexity of the craft (2nd ed., pp. 347–365). SAGE.
Creswell, J. W., & Poth, C. N. (2017). Qualitative inquiry and research design: Choosing among five approaches (5th ed.). SAGE.
Damiano, S. R., Gregg, K. J., Spiel, E. C., McLean, S. A., Wertheim, E. H., & Paxton, S. J. (2015). Relationships between body size attitudes and body image of 4-year-old boys and girls, and attitudes of their fathers and mothers. Journal of Eating Disorders, 3(1), 1–10. https://doi.org/10.1186/s40337-015-0048-0
Damiano, S. R., McLean, S. A., Nguyen, L., Yager, Z., & Paxton, S. J. (2020). Do we cause harm? Understanding the impact of research with young children about their body image. Body Image, 34, 59–66.
https://doi.org/10.1016/j.bodyim.2020.05.008
Dittmar, H., Halliwell, E., & Ive, S. (2006). Does Barbie make girls want to be thin? The effect of experimental exposure to images of dolls on the body image of 5- to 8-year-old girls. Developmental Psychology, 42(2), 283–292. https://doi.org/10.1037/0012-1649.42.2.283
Gutin, I. (2021). Body mass index is just a number: Conflating riskiness and unhealthiness in discourse on body size. Sociology of Health & Illness, 43(6), 1437–1453. https://doi.org/10.1111/1467-9566.13309
Hays, D. G., & McKibben, W. B. (2021). Promoting rigorous research: Generalizability and qualitative research. Journal of Counseling & Development, 99(2), 178–188. https://doi.org/10.1002/jcad.12365
Herle, M., De Stavola, B., Hübel, C., Abdulkadir, M., Ferreira, D. S., Loos, R. J. F., Bryant-Waugh, R., Bulik, C. M., & Micali, N. (2020). A longitudinal study of eating behaviours in childhood and later eating disorder behaviours and diagnoses. The British Journal of Psychiatry, 216(2), 113–119. https://doi.org/10.1192/bjp.2019.174
Horton, E. (2023). “I want different for my child”: An interpretative phenomenological analysis of mothers’ histories of disordered eating and the impact on their parenting approach. The Family Journal, 31(2), 314–321. https://doi.org/10.1177/10664807221151171
Horton, E., & Powers, M. (2024). Demoralizing food, bodies, and movement: A phenomenological exploration of caregivers’ experience in a body neutral parenting support group. The Family Journal.
https://doi.org/10.1177/10664807231226232
Khanal, K. P. (2018). Constructivist grounded theory practice in accountability research. Journal of Education and Research, 8(1), 61–88. https://doi.org/10.3126/jer.v8i1.25480
Kids Eat in Color [@kids.eat.in.color]. (2022, April 21). How to talk: May not help, may help a lot [Photograph]. Instagram. https://www.instagram.com/p/Ccnn7CMr2D5/?utm_source=ig_web_copy_link
Klassen, S. (2017). Free to be: Developing a mindfulness-based eating disorder prevention program for preteens. Journal of Child and Adolescent Counseling, 3(2), 75–87. https://doi.org/10.1080/23727810.2017.1294918
Kluck, A. S. (2010). Family influence on disordered eating: The role of body image dissatisfaction. Body Image, 7(1), 8–14. https://doi.org/10.1016/j.bodyim.2009.09.009
Liechty, J. M., Clarke, S., Birky, J. P., & Harrison, K. (2016). Perceptions of early body image socialization in families: Exploring knowledge, beliefs, and strategies among mothers of preschoolers. Body Image, 19, 68–78. https://doi.org/10.1016/j.bodyim.2016.08.010
Mills, J., Bonner, A., & Francis, K. (2006). The development of constructivist grounded theory. International Journal of Qualitative Methods, 5(1), 25–35. https://doi.org/10.1177/160940690600500103
National Eating Disorders Association. (2022). Body image. https://www.nationaleatingdisorders.org/body-image
Neumark-Sztainer, D., Bauer, K. W., Friend, S., Hannan, P. J., Story, M., & Berge, J. M. (2010). Family weight talk and dieting: How much do they matter for body dissatisfaction and disordered eating behaviors in adolescent girls? Journal of Adolescent Health, 47(3), 270–276. https://doi.org/10.1016/j.jadohealth.2010.02.001
Onwuegbuzie, A. J., & Collins, K. M. T. (2007). A typology of mixed methods sampling designs in social science research. The Qualitative Report, 12(2), 281–316. https://doi.org/10.46743/2160-3715/2007.1638
Patton, M. Q. (2014). Qualitative research and evaluation methods: Integrating theory and practice. SAGE.
Pellizzer, M. L., & Wade, T. D. (2023). Developing a definition of body neutrality and strategies for an intervention. Body Image, 46, 434–442. https://doi.org/10.1016/j.bodyim.2023.07.006
Perry, M., Watson, L., Hayden, L., & Inwards-Breland, D. (2019). Using body neutrality to inform eating disorder management in a gender diverse world. Child and Adolescent Health, 3(9), 597–598.
https://doi.org/10.1016/s2352-4642(19)30237-8
Phares, V., Steinberg, A. R., & Thompson, J. K. (2004). Gender differences in peer and parental influences: Body image disturbance, self-worth, and psychological functioning in preadolescent children. Journal of Youth and Adolescence, 33(5), 421–429. https://doi.org/10.1023/B:JOYO.0000037634.18749.20
Pursey, K. M., Burrows, T. L., Barker, D., Hart, M., & Paxton, S. J. (2021). Disordered eating, body image concerns, and weight control behaviors in primary school aged children: A systematic review and meta-analysis of universal–selective prevention interventions. International Journal of Eating Disorders, 54(10), 1730–1765. https://doi.org/10.1002/eat.23571
Ricciardelli, L. A., McCabe, M. P., & Banfield, S. (2000). Body image and body change methods in adolescent boys: Role of parents, friends and the media. Journal of Psychosomatic Research, 49(3), 189–197.
https://doi.org/10.1016/S0022-3999(00)00159-8
Rodgers, R., & Chabrol, H. (2009). Parental attitudes, body image disturbance and disordered eating amongst adolescents and young adults: A review. European Eating Disorders Review, 17(2), 137–151. https://doi.org/10.1002/erv.907
Ruckstaetter, J., Sells, J., Newmeyer, M. D., & Zink, D. (2017). Parental apologies, empathy, shame, guilt, and attachment: A path analysis. Journal of Counseling & Development, 95(4), 389–400.
https://doi.org/10.1002/jcad.12154
Sharpe, H., Patalay, P., Choo, T.-H., Wall, M., Mason, S. M., Goldschmidt, A. B., & Neumark-Sztainer, D. (2018). Bidirectional associations between body dissatisfaction and depressive symptoms from adolescence through early adulthood. Development and Psychopathology, 30(4), 1447–1458. https://doi.org/10.1017/S0954579417001663
Siegel, J. A., Ramseyer Winter, V., & Cook, M. (2021). “It really presents a struggle for females, especially my little girl”: Exploring fathers’ experiences discussing body image with their young daughters. Body Image, 36, 84–94. https://doi.org/10.1016/j.bodyim.2020.11.001
Thompson, J. K., Heinberg, L. J., Altabe, M., & Tantleff-Dunn, S. (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance (1st ed.). American Psychological Association.
https://doi.org/10.1037/10312-000
Veldhuis, J., Alleva, J. M., Bij de Vaate, A. J. D., Keijer, M., & Konijn, E. A. (2020). Me, my selfie, and I: The relations between selfie behaviors, body image, self-objectification, and self-esteem in young women. Psychology of Popular Media, 9(1), 3–13. https://doi.org/10.1037/ppm0000206
Walker, D. C., Gorrell, S., Hildebrandt, T., & Anderson, D. A. (2021). Consequences of repeated critical versus neutral body checking in women with high shape or weight concern. Behavior Therapy, 52(4), 830–846. https://doi.org/10.1016/j.beth.2020.10.005
Wymer, B., Swartz, M. R., Boyd, L., Zankman, M., & Swisher, S. (2022). A content analysis of empirical parent engagement literature. Journal of Child and Adolescent Counseling, 8(1), 16–30. https://doi.org/10.1080/23727810.2022.2037987
Emily Horton, PhD, LPC, RPT, is an assistant professor at the University of Houston–Clear Lake. Correspondence may be addressed to Emily Horton, 2700 Bay Area Boulevard, Houston, TX 77058, horton@uhcl.edu.
Apr 1, 2021 | Volume 11 - Issue 2
Fei Shen, Yanhong Liu, Mansi Brat
The present study examined the relationships between childhood attachment, adult attachment, self-esteem, and psychological distress; specifically, it investigated the multiple mediating roles of self-esteem and adult attachment on the association between childhood attachment and psychological distress. Using 1,708 adult participants, a multiple-mediator model analysis following bootstrapping procedures was conducted in order to investigate the mechanisms among childhood and adult attachment, self-esteem, and psychological distress. As hypothesized, childhood attachment was significantly associated with self-esteem, adult attachment, and psychological distress. Self-esteem was found to be a significant mediator for the relationship between childhood attachment and adult attachment. In addition, adult attachment significantly mediated the relationship between self-esteem and psychological distress. The results provide insight on counseling interventions to increase adults’ self-esteem and attachment security, with efforts to decrease the negative impact of insecure childhood attachment on later psychological distress.
Keywords: childhood attachment, adult attachment, self-esteem, psychological distress, mediator
Attachment has been widely documented across disciplines, following Bowlby’s (1973) foundational work known as attachment theory. Attachment, in the context of child–parent interactions, is defined as a child’s behavioral tendency to use the primary caregiver as the secure base when exploring their surroundings (Bowlby, 1969; Sroufe & Waters, 1977). Research has shed light on the significance of childhood attachment in predicting individuals’ intrapersonal qualities such as self-esteem and emotion regulation during adulthood (Brennan & Morris, 1997), interpersonal orientations examined through attachment variation and adaptation across different developmental stages (Sroufe, 2005), and overall psychological well-being (Cassidy & Shaver, 2010; Wright et al., 2014).
Given its clinical significance, attachment has gained increased interest across disciplines. For example, childhood attachment was found to significantly predict coping and life satisfaction in young adulthood (Wright et al., 2017). Relatedly, a 30-year longitudinal study reinforces the vital role of childhood attachment in predicting individuals’ development of “the self and personality” (Sroufe, 2005, p. 352). Sroufe’s (2005) study reinforced the vital role of attachment across the life span. As an outcome variable, attachment is asserted to be associated with empathy (Ruckstaetter et al., 2017) and parenting practice in the adoptive population (Liu & Hazler, 2017). Considering the interplay between individuals’ relationship evolvement and their living contexts (Bowlby, 1973; Sroufe, 2005), attachment is examined at different stages generally labelled as childhood attachment and adult attachment, with the former focusing on the infant/child–parent relationship and the latter on adults’ generalized relationships with intimate others (e.g., romantic partners, close friends). Because of the abstract nature of attachment, it is commonly measured in the form of childhood attachment styles (Ainsworth et al., 1978) or adult attachment orientations (Turan et al., 2016).
Conceptual Framework
The present study is grounded in attachment theory, which is centered around a child’s ability to utilize their primary caregiver as the secure base when exploring surroundings, involving an appropriate balance between physical proximity, curiosity, and wariness (Bowlby, 1973; Sroufe & Waters, 1977). A core theoretical underpinning of attachment theory is the internal working model capturing a child’s self-concept and expectations of others (Bretherton, 1996). Internal working models of self and other are complementary. Namely, a child with strong internal working models is characterized with a perception of self as being worthy and deserving of love and a perception of others as being responsive, reliable, and nurturing (Bowlby, 1973; Sroufe, 2005).
In the context of attachment theory, childhood attachment is considered an outcome of consistent child–caregiver interactions and serves as the foundation for individuals’ later personality development (Bowbly, 1973; Sroufe, 2005). In line with child–caregiver interactions, Ainsworth et al. (1978) came up with three attachment styles based upon Bowlby’s seminal work, including secure, anxious-ambivalent, and anxious-avoidant attachment, following sequential phases of laboratory observations. Attachment theory was subsequently extended beyond the child–parent relationship to include later relationships in adulthood, given the parallels between these relationships (Cassidy & Shaver, 2010). Likewise, four distinct adult attachment styles (i.e., secure, dismissing, preoccupied, and fearful) are referred to based on the two-dimensional models of self and other (Konrath et al., 2014). Adult attachment styles are commonly examined under two orientations: attachment avoidance and attachment anxiety (Turan et al., 2016). Individuals showing low avoidance and low anxiety are considered securely attached, whereas those with high levels of anxiety and avoidance tend to be insecurely attached. Although childhood attachment and adult attachment are broadly considered distinct concepts in the literature, they share a spectrum of behaviors spanning from secure to insecure attachment. The levels of avoidance and anxiety involved in these behaviors are used as parameters to differentiate securely attached individuals from those who are insecurely attached.
Childhood Attachment, Self-Esteem, and Adult Attachment
Despite the conceptual overlaps, childhood attachment to caregivers and adult attachment to intimate others are commonly investigated as two distinct variables associated with individuals’ needs and features of different relationships. Childhood attachment captures a child’s distinct relationship with the primary caregiver (e.g., the mother figure) as well as their ability to differentiate the primary caregiver from other adults (Bowlby, 1969, 1973), whereas adult attachment may involve an individual’s multiple relationships (with parents, a romantic partner, or close friends). Noting the general stability of attachment from childhood to adulthood (Fraley, 2002), previous conceptual work stresses the importance of contexts in individuals’ attachment evolvement, highlighting that “patterns of adaptation” and “new experiences” reinforce each other in a reciprocal way (Sroufe, 2005, p. 349). For instance, an individual may develop secure attachment in adulthood because of healthy interpersonal experiences likely facilitated by trust, support, and nurturing received from significant others or their relationships, despite showing insecure attachment patterns in early childhood. A dynamic view of attachment development is thus warranted.
From a dynamic lens, researchers have generated evidence for the association between childhood attachment and adult attachment (Pascuzzo et al., 2013; Styron & Janoff-Bulman, 1997). For example, in a study of 879 college students (Styron & Janoff-Bulman, 1997), participants’ perception of their childhood attachment to both mother and father significantly predicted 7.9% of the variance in their adult attachment scores. Similarly, Pascuzzo et al. (2013) followed 56 adolescents at age 14 through age 22 and found that attachment insecurity to both parents and peers during adolescence was significantly associated with anxious romantic attachment in adulthood as measured by the Experience in Close Relationships Scale (ECR; Brennan et al., 1998). Studies that rely on retrospective data to assess childhood attachment (e.g., Styron & Janoff-Bulman, 1997) may be limited in validity because of time elapsed and potential compounding variables.
Childhood attachment is well recognized as the foundation for the growth of self-reliance and emotional regulation (Bowlby, 1973). Aligning with self-reliance, self-esteem appears to be frequently studied primarily through self-liking and self-competence (Brennan & Morris, 1997). Brennan and Morris (1997) defined self-liking as general self-evaluation based on perceived positive regard from others, and self-competence as concrete self-evaluation based on personal abilities and attributes. Previous research has suggested that secure attachment (to parents and peers) is significantly associated with higher levels of self-esteem (e.g., Wilkinson, 2004). In contrast, individuals who reported insecure attachment tended to endorse low self-esteem (Gamble & Roberts, 2005).
These results provide theoretical and empirical evidence for links between childhood attachment and adult attachment, but these links are likely to be indirect and mediated by other relevant variables from developmental perspectives. To our knowledge, no study has investigated the effect of self-esteem on the relationship between childhood attachment and adult attachment. The theoretical framework of attachment theory indicates that childhood attachment can have not only direct effects on adult attachment, but also indirect effects on adult attachment via self-esteem. In order to develop effective interventions tackling issues with adult attachment, it is important to examine potential mediators (e.g., self-esteem) between childhood attachment and adult attachment. To address this gap, the present study tests this hypothesized mediation function of self-esteem with a nonclinical sample of adults.
Self-Esteem, Attachment, and Psychological Distress
The extant literature comprises prolific information on the relationship between attachment and psychological well-being (Gnilka et al., 2013; Karreman & Vingerhoets, 2012; M. E. Kenny & Sirin, 2006; Turan et al., 2016; Wright et al., 2014). Existing evidence focuses on the relationship between adult attachment orientations and individuals’ psychological well-being (e.g., Karreman & Vingerhoets, 2012; Lynch, 2013; Roberts et al., 1996; Sowislo & Orth, 2013). Nevertheless, previous research has shed some light on the role of early childhood attachment in predicting psychological distresses in adulthood, including depression and anxiety (Bureau et al., 2009; Lecompte et al., 2014; Styron & Janoff-Bulman, 1997). Lecompte and colleagues (2014) conducted a longitudinal study of a sample of preschoolers (N = 68) with data collected at 4 years and again at 11–12 years; results of the study suggested that children with disorganized attachment at the baseline scored higher in both anxiety and depressive symptoms compared to those classified as securely attached.
Likewise, the effect of self-esteem on psychological distress is well established. A meta-analysis on 80 longitudinal studies published between 1994 and 2010 yielded consistent evidence supporting the relationship between low self-esteem and depressive symptoms (Sowislo & Orth, 2013). More recently, Masselink et al. (2018) examined data collected at four different points of participants’ development from early adolescence to young adulthood, which demonstrated that low self-esteem constitutes a persistent risk factor for participants’ depressive symptoms across developmental stages. Moreover, self-esteem scores in early adolescence significantly predicted the participants’ depressive symptoms at later stages, specifically during late adolescence and young adulthood.
Research has also supported the association between self-esteem, adult attachment, and psychological distress. Lopez and Gormley (2002) followed 207 college students from the beginning to the end of their freshman year and identified adjustment outcomes in association with the participants’ attachment styles and changes of their attachment styles measured by the ECR (e.g., secure-to-insecure attachment, insecure-to-secure attachment). The authors found that participants who remained securely attached scored higher in self-confidence and lower in both psychological distress and reactive coping compared to those who reported consistent insecure attachment. Moreover, participants who maintained secure attachment presented better outcomes in self-confidence and psychological well-being than the comparative group with secure-to-insecure or insecure-to-secure attachment changes (Lopez & Gormley, 2002). Adult attachment (measured by the ECR) was also found to be a mediator for the effects of traumatic events on post-traumatic symptomatology among a sample of female college students (Sandberg et al., 2010). In addition, Roberts et al. (1996) suggested attachment insecurity contributed to negative beliefs about oneself, which in turn activated cognitive structures of psychological distress, such as depression and anxiety, with a sample of 152 undergraduate students.
Taken together, the literature provides consistent support for the significant relationships between childhood attachment and various outcome variables in later adulthood, including adult attachment, self-esteem, and psychological distress. It further reveals a two-fold gap: (a) the variables tended to be investigated separately in previous studies, yet the mechanisms among these variables remained underexplored; and (b) little is known about the role of self-esteem and adult attachment in the association between childhood attachment and psychological distress. Disentangling the mechanisms, including potential mediating roles, involved in the variables will enrich the current knowledge based on attachment and can facilitate counseling interventions surrounding the effects of childhood attachment. In tackling the gap, three hypotheses were posed:
1. Childhood attachment is significantly associated with adult attachment, self-esteem, and psychological distress.
2. Self-esteem mediates the relationship between perceived childhood attachment and adult attachment.
3. Adult attachment mediates the relationship between self-esteem and
psychological distress.
Method
Participants
Of the 2,373 voluntary adult participants who took the survey, 1,708 (72%) completed 95% of all the questions and were retained for final analysis. Among the participants, 76.2% (n = 1,302) were female, 22.3% (n = 381) were male, and 1.3% (n = 25) chose not to specify their gender. The mean age of the participants was 29.89, ranging from 18 to 89 years old (SD = 12.44). A total of 66.3% (n = 1,133) of participants described themselves as White/European American, 8.7% (n = 148) as African American, 10.2% (n = 175) as Asian/Pacific Islander, 2.6% (n = 44) as American Indian/Native American, 7.3% (n = 124) as biracial or multiracial, 3.6% (n = 61) as other race, and 1.3% (n = 23) did not specify.
Sampling Procedures
The study was approved by the university’s IRB. We posted the recruitment information on various websites (e.g., Facebook, discussion board, university announcement board, Craigslist) in order to recruit a diverse pool of participants. Individuals who were 18 years old or above and were able to fill out the questionnaire in English were eligible for participating in this project. Participants were directed to an online Qualtrics survey consisting of the measures discussed in the following section. An informed consent form was included at the beginning of the survey outlining the confidentiality, voluntary participation, and anonymity of the study. Participants were prompted to enter their email addresses to win one of ten $15 e-gift cards. Participants’ email addresses were not included in the survey questions and data analysis.
Measures
Psychological Distress
Psychological distress was measured using the 10-item Kessler Psychological Distress Scale (K10; Kessler et al., 2003). Participants were asked about their emotional states in the past four weeks (e.g., “How often did you feel nervous?”). Responses were rated on a 5-point scale ranging from 0 (None of the time) to 4 (All of the time). Scores were averaged, with a higher score indicating a higher level of psychological distress. Previous studies using K10 have provided evidence of validity (Andrews & Slade, 2001). The internal consistency for K10 has been well established with a Cronbach’s alpha coefficient ranging from .88 (Easton et al., 2017) to .94 (Donker et al., 2010). In this study, the Cronbach’s alpha coefficient was .94.
Childhood Attachment
Childhood attachment was measured using the Parental Attachment subscale of the Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1987). Previous research has demonstrated evidence that this measure has great convergent and concurrent validity (M. E. Kenny & Sirin, 2006). The IPPA has been used to recall childhood attachment in adult populations (Aspelmeier et al., 2007; Cummings-Robeau et al., 2009). This 25-item subscale directs participants to recall their attachment to the parent(s) or caregiver(s) who had the most influence on them during childhood. The subscale consists of three dimensions, including 10 items on trust, nine items on communication, and six items on alienation. Some sample items are: “My parent(s)/primary caregiver(s) accepts me as I am” for trust, “I tell my parent(s)/primary caregiver(s) about my problems and troubles)” for communication, and “I do not get much attention from my parent(s)/primary caregiver(s)” for alienation. Participants rated the items using a 5-point Likert scale ranging from 1 (Almost never or never true) to 5 (Almost always or always true). Items were averaged to form the subscale, with a higher score reflecting more secure childhood attachment. The subscale has demonstrated high internal consistency with a Cronbach’s alpha of .93 (Armsden & Greenberg, 1987). In the present study, Cronbach’s alpha for the subscale was .96.
Adult Attachment
Adult attachment was measured using the ECR (Brennan et al., 1998). The ECR consists of 36 items with 18 items assessing each of the two orientations: attachment anxiety and attachment avoidance. In order to avoid confounding factors, we only assessed adult attachment with close friends or romantic partners, as relationships with parents can confound the childhood attachment outcomes. Responses were rated on a 7-point Likert scale ranging from 1 (Strongly disagree) to 7 (Strongly agree). Two scores were averaged, with a higher score reflecting a higher level of attachment anxiety or avoidance. In terms of validity, the ECR subscales have been found to be positively associated with psychological distress and intention to seek counseling, and negatively associated with social support (Vogel & Wei, 2005). The ECR has a high internal consistency for both the anxiety (α = .91) and avoidance (α = .94) dimensions (Brennan et al., 1998). For this study, Cronbach’s alphas for attachment anxiety and attachment avoidance were .93 and .92, respectively.
Self-Esteem
Rosenberg’s Self-Esteem Scale (RSES; Rosenberg, 1965) is a 10-item scale designed to assess an adult’s self-esteem. The scale assesses both self-competency (e.g., “I feel that I have a number of good qualities”) and self-liking (e.g., “I certainly feel useless at times”). Responses were coded using a 4-point Likert scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). Negatively worded statements were reverse-coded. Scores were averaged, with a higher score reflecting a higher level of self-esteem. RSES has been frequently used in various studies with high reliability and validity (Brennan & Morris, 1997; Chen et al., 2017). In this study, the Cronbach’s alpha coefficient was .89.
Data Analysis
Descriptive statistics were computed using SPSS version 23 followed by a multiple-mediator model analysis using Mplus version 7.4 (Muthén & Muthén, 2012). Missing data were treated with the full information maximum likelihood estimation in Mplus, which was one of the most pragmatic approaches in producing unbiased parameter estimates (Acock, 2005). The multiple-mediator model includes childhood attachment as the predictor, self-esteem and adult attachment anxiety and avoidance as mediators, and psychological distress as the outcome variable (see Figure 1). The mediation analysis was conducted using bootstrapping procedures (J = 2,000), which was a resampling method to construct a confidence interval for the indirect effect (Preacher & Hayes, 2008). Several model fit indices based on Kline’s (2010) guidelines were employed, including the ratio of chi-square to degree of freedom (χ2/df), root-mean-square error of approximation (RMSEA), Tucker-Lewis index (TLI), comparative fit index (CFI), and standardized root-mean-square residual (SRMR). Indicators of good model fit are a nonsignificant chi-square value, a CFI and TLI of .90 or greater, RMSEA of .08 or less, and an SRMR of .05 or less (Hooper et al., 2008).
Figure 1
Multiple-Mediator Model: Self-Esteem, Anxious Adult Attachment, and Avoidant Adult Attachment as Multiple Mediators Between Childhood Attachment and Psychological Distress
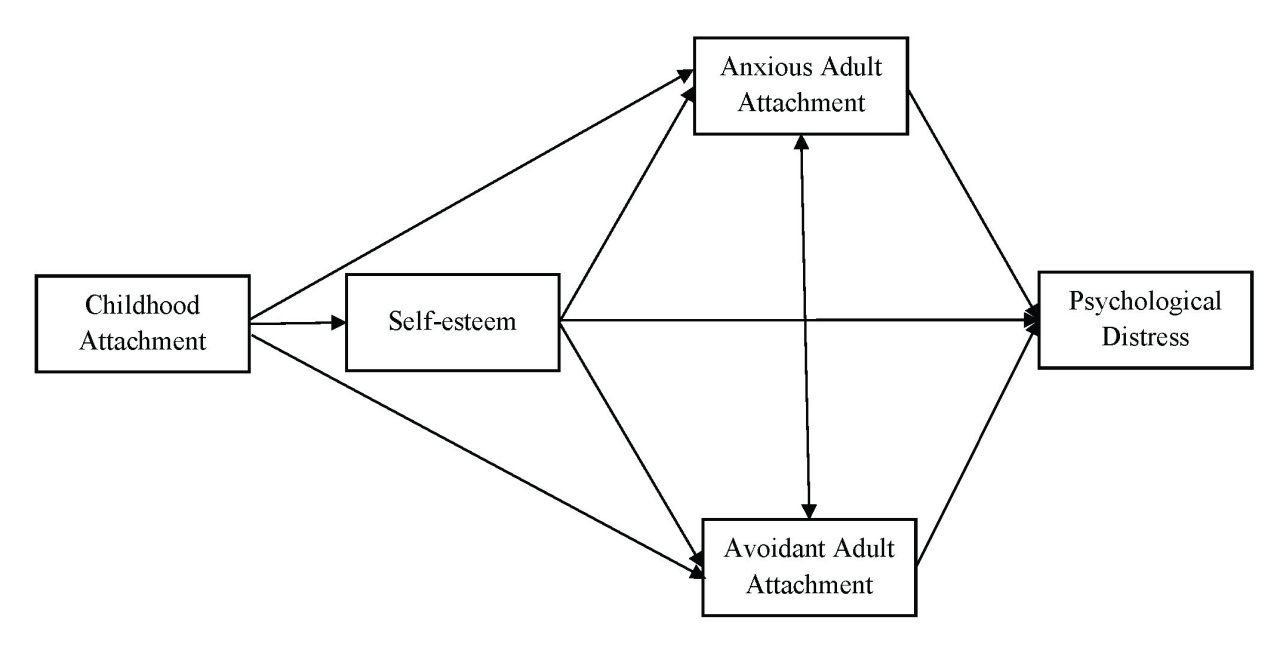
Results
Descriptive Statistics and Correlations
The descriptive statistics of each variable are reported in Table 1.
Table 1
Descriptive Statistics for Variables (N = 1,708)
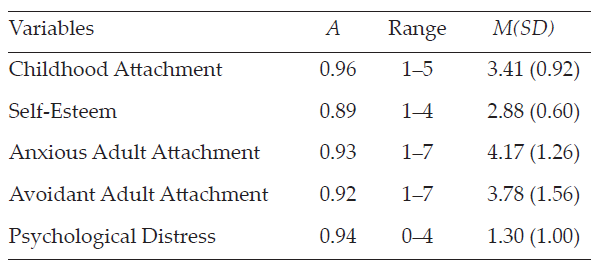
Pearson’s correlations between variables were computed. All bivariate statistics are presented in Table 2 and provided full support for our Hypothesis 1. For instance, childhood attachment was positively associated with self-esteem (r = .38, p < .001) and negatively correlated with adult attachment anxiety (r = -.26, p < .001) and avoidance (r = -.45, p < .001), as well as with psychological distress (r = -.35, p < .001). Significant negative correlations were found between self-esteem and adult attachment anxiety (r = -.49, p < .001) and avoidance (r = -.46, p < .001), and between self-esteem and psychological distress (r = -.63, p < .001). Both adult attachment anxiety (r = .57, p < .001) and avoidance (r = .42, p < .001) were positively associated with psychological distress. Significant correlation was found between adult attachment anxiety and avoidance (r = .31, p < .001).
Table 2
Correlation Matrix of Variables (N = 1,708)
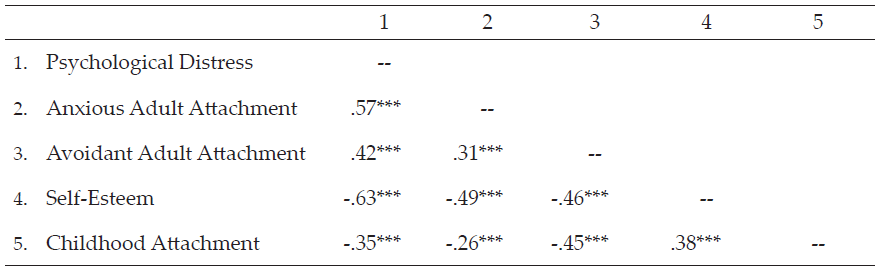
*p < .05. **p < .01. ***p < .001 (two-tailed).
The Multiple-Mediator Model
The multiple-mediator model involving self-esteem and adult attachment as mediators, with bootstrapping procedures, yielded satisfactory fit indices: χ2(1) = 12.24, p < .001, CFI = 1.00, TLI = 0.96, SRMR = .01. However, the index of RMSEA = .08, 90% CI [0.05, 0.12] indicated a mediocre fit, with the upper value of 90% CI larger than the suggested cutoff score of 0.08. D. A. Kenny et al. (2015) suggested that the models with small degrees of freedom had the average width of the 90% CI above 0.10, unless the sample size was extremely large. The nonsignificant χ2 value was interpreted as a good fit index.
The present study further revealed that secure childhood attachment was associated with high self-esteem (β = .25, p < .001) and low levels of anxiety (β = -.12, p < .001) and avoidance (β = -.41, p < .001) of adult attachment. Meanwhile, high self-esteem was associated with low anxiety (β = -.95, p < .001) and low avoidance (β = -.64, p < .001) of adult attachment. In addition, high self-esteem (β = -.68, p < .001) and low adult attachment anxiety (β = .26, p < .001) and avoidance (β = .11, p < .001) were significantly associated with low psychological distress. The results supported both Hypotheses 2 and 3 in that self-esteem mediated the relationship between childhood attachment and adult attachment, and adult attachment mediated the relationship between self-esteem and psychological distress.
The mediating role of self-esteem was examined using bootstrapping procedures. Results demonstrated that self-esteem significantly mediated the association between childhood attachment and adult attachment anxiety (b = -.24, 95% CI [-0.27, -0.21]) and avoidance (b = -.16, 95% CI [-0.19, -0.14]).
The present study further supported the mediating role of adult attachment (i.e., anxiety and avoidance). The association between self-esteem and psychological distress was significantly mediated by both adult attachment anxiety (b = -.24, 95% CI [-0.29, -0.21]) and avoidance (b = -.07, 95% CI [-0.10, -0.05]). Mediation effects are denoted in Table 3.
Table 3
Mediation Analysis With Bootstrapping: Unstandardized and Standardized Estimates and Confidence Intervals for Mediation Effects
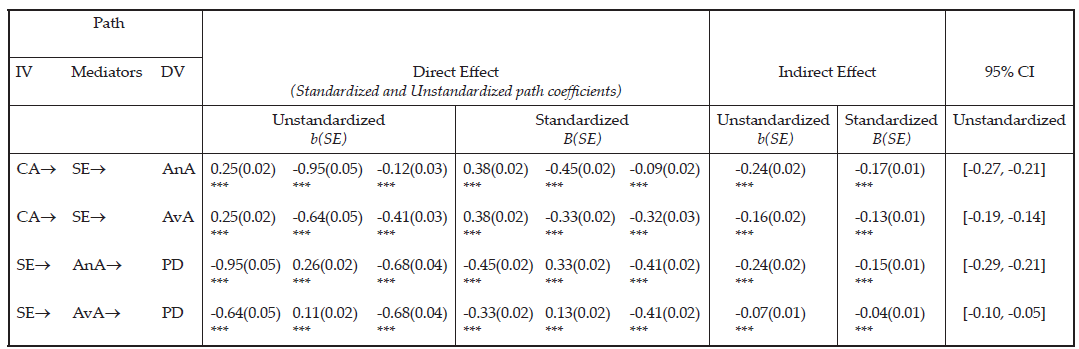
Note. Bootstrap J = 2,000, CI = confidence interval; IV = independent variable; DV = dependent variable; CA = Childhood Attachment; SE = Self-Esteem; AnA = Anxious Adult Attachment; AvA = Avoidant Adult Attachment; PD = Psychological Distress. Direct effect of path direction, IV® Mediator, Mediator ® DV, IV ® DV. Statistical significance was evaluated based on whether 95% bias corrected bootstrap CIs include zero or not. If zero was included in the CI, then it was not a significant indirect effect. Model fit: χ2(1) = 12.24, p < .001, CFI = 1.00, TLI = 0.96, SRMR = .01, RMSEA = .08 (90% CI [0.05, 0.12]).
Discussion
The present study highlights the significance of childhood attachment and its associations with self-esteem and psychological distress in adulthood. Participants who reported secure childhood attachment scored higher on self-esteem and lower on psychological distress. Secure childhood attachment was also found to be associated with low adult attachment anxiety and avoidance. Our study builds upon previous research (e.g., Sroufe, 2005) to capture the complexity of key variables related to attachment and its evolvement from childhood to adulthood. The results shed further light on the mechanisms among childhood attachment, self-esteem, adult attachment, and psychological distress. Self-esteem was found to be a significant mediator between childhood attachment and adult attachment; meanwhile, adult attachment was found to be a mediator between self-esteem and psychological distress.
The findings support Hypothesis 1 in that individuals with more secure childhood attachment reported higher levels of self-esteem, lower levels of adult attachment anxiety and avoidance, and less psychological distress. The results echo attachment theory (Bowlby, 1973), positing childhood attachment as a predictor of later adjustment as well as self-esteem, indicating that the quality of attachment appears to be intimately related to how to cope with stress and how to perceive oneself (Wilkinson, 2004). The results are also consistent with previous research that highlighted secure childhood attachment as a protective factor against anxiety, depression, and later emotional and relational distress (e.g., Karreman & Vingerhoets, 2012).
Results also lend support to Hypothesis 2 in that self-esteem mediated the relationship between childhood attachment and adult attachment. Self-esteem as a mediator echoed previous research that indicated the influence of childhood attachment on one’s self-esteem may be mitigated by expanded social networks in adulthood (Steiger et al., 2014). For instance, it is likely that improving self-esteem through peer connections (e.g., friendship; romantic relationships) may contribute to individuals’ adaptation to close relationships and enhance attachment security in adulthood, despite their insecure attachment with primary caregivers in childhood (Fraley, 2002; Sroufe, 2005).
Congruent with Hypothesis 3, adult attachment was a mediator for the relationship between self-esteem and psychological distress. Previous research provided evidence that low self-esteem increases the risk of developing psychological distress such as depressive and anxious symptoms (Li et al., 2014); nevertheless, individuals may experience less psychological impact with secure attachment manifested through their close relationships. Little is known about the relationship between insecure adult attachment (i.e., anxious and avoidant attachment) and psychological distress, and the mediating role of adult attachment has rarely been addressed. In a sample of 154 women in a community context, Bifulco et al. (2006) found that fearful and angry-dismissive attachment partially mediated the relationship between childhood adversity and depression or anxiety. The present study extends the Bifulco et al. study to include a larger, gender-inclusive, and racially diverse population that captures a wider age range. Further, using continuous measurements, the present study counteracts the limitations of dichotomous measures used in Bifulco et al.’s study, thus reflecting the spectrum and complexity of attachment.
Implications for Counseling Practice
The present study sheds light on interventions for clients’ psychological distress. The results corroborated positive associations between psychological distress and insecure childhood attachment and attachment anxiety and avoidance during adulthood. Although adults can no longer change their childhood experiences, including their attachment-related adversities, interventions that target improving adult attachment may still mitigate the negative effect of childhood attachment on psychological distress later during adulthood. Considering the reciprocal influence noted between self-esteem and adult attachment (Foster et al., 2007), counseling strategies encompassing both self-esteem and adult attachment are thus desirable.
Specifically, counselors could conceptualize self-esteem in a relational context in which they may incorporate clients’ support systems (e.g., partner, close friends, parents) into the treatment. A key treatment goal may be utilizing close relationships to boost self-esteem. On the contrary, counselors may engage clients with low self-esteem in communicating their attachment needs while involving significant others (e.g., partners) to enact positive responses, such as attentive listening and validation of mutual needs. Counselors are encouraged to assess how childhood attachment experiences may have influenced the client’s adult attachment, as insecure attachment may lead to challenges with perceived trustworthiness of self and others, which could hinder growth in the interpersonal relationships. Clients may further benefit from reflecting over specific attachment behaviors and interactional patterns within close relationships (e.g., how they manage proximity to an attachment figure when they experience distress) in order to restructure and enhance their attachment security internally and externally (Cassidy et al., 2013).
The finding of self-esteem as a significant mediator supports the proposition that self-esteem is responsive to life events and that these can influence one’s perception and evaluation of self. Previous research indicated that individuals with low self-esteem may be easily triggered by stressful life events and consequently respond irrationally and negatively (Taylor & Montgomery, 2007). Counselors may consider adapting Fennell’s (1997) Cognitive Behavioral Therapy model comprising early experience, bottom line, and rules for living to help clients enhance self-esteem. Fennell’s model suggests that clients’ early experiences (e.g., childhood attachment, traumatic experience, cultural context) may have an influence on the development of a fundamental bottom line about themselves (e.g., “I am not good enough,” “I am worthless”). Counselors may further assist clients with mapping out the rules for living (e.g., dysfunctional assumptions) related to distorted thoughts on what they should do in order to cultivate their core beliefs (as being loved or accepted or vice versa). For example, if clients have formed insecure attachment during childhood (early experience), they may develop a bottom line that “I am not good enough.” In making efforts to feel accepted in the family, they may have the rules for living that “I have to receive all As in all my classes.” If clients fail to achieve the rules for living, they likely would develop anxious and depressive symptoms, which may activate the confirmation of the bottom line. To counteract the negative patterns, counselors may work with clients to process the impact of early experience (e.g., early insecure attachment) on their bottom line and revise the rules of living to develop healthier coping strategies. When clients develop alternative rules of living, counselors may further help them to re-evaluate the bottom line and enhance self-acceptance.
Limitations and Future Research Directions
Although the results supported all three hypotheses, the present study was subject to a few limitations. First, the self-report measures may have been subject to biases, especially for the memory of childhood attachment. Another limitation pertains to a retrospective assessment of perceptions of childhood attachment that may be changed over time because of life experiences (e.g., death, parental divorce). Relatedly, the cross-sectional study could not capture the changes over a period of time. Not knowing the types of childhood attachment (i.e., anxious attachment, avoidant attachment) presented as another limitation for researchers’ understanding of the variations of attachment and how each type might impact long-term outcomes. In the future, researchers may consider longitudinal studies to explore the variations and changes in attachment over the life span and examine what other mechanisms contribute to the changes to protect against the negative impact. Future research may also incorporate other-report data filled out by significant others (e.g., parents, romantic partners) to minimize social desirability and provide multiple perspectives.
Conclusion
Attachment theory provides a strong theoretical framework in understanding individuals’ psychological well-being over the life span (DeKlyen & Greenberg, 2008). Informed by attachment theory, the present study investigated the mediating roles of self-esteem and adult attachment (measured through the levels of anxiety and avoidance) on the relations between childhood attachment and psychological distress, and between self-esteem and psychological distress, respectively. The multiple-mediator analysis with bootstrapping supports both self-esteem and adult attachment as significant mediators. Our results also support the associations between childhood attachment with self-esteem, adult attachment, and psychological distress. The study contributes to the gap pertaining to adult attachment and provides practical implications for counselors working in various settings in their work with clients surrounding attachment security, self-esteem, and psychological well-being.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Acock, A. C. (2005). Working with missing values. Journal of Marriage and Family Therapy, 67(4), 1012–1028.
https://doi.org/10.1111/j.1741-3737.2005.00191.x
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Lawrence Erlbaum.
Andrews, G., & Slade, T. (2001). Interpreting scores on the Kessler Psychological Distress Scale (K10). Australian and New Zealand Journal of Public Health, 25(6), 494–497. https://doi.org/10.1111/j.1467-842x.2001.tb00310.x
Armsden, G. C., & Greenberg, M. T. (1987). The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. https://doi.org/10.1007/BF02202939
Aspelmeier, J. E., Elliott, A. N., & Smith, C. H. (2007). Childhood sexual abuse, attachment, and trauma symptoms in college females: The moderating role of attachment. Child Abuse & Neglect, 31(5), 549–566.
https://doi.org/10.1016/j.chiabu.2006.12.002
Bifulco, A., Kwon, J., Jacobs, C., Moran, P. M., Bunn, A., & Beer, N. (2006). Adult attachment style as mediator between childhood neglect/abuse and adult depression and anxiety. Social Psychiatry and Psychiatric Epidemiology, 41, 796–805. https://doi.org/10.1007/s00127-006-0101-z
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. Basic Books.
Bowlby, J. (1973). Attachment and loss. Vol. 2: Separation: Anxiety and anger. Basic Books.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). Guilford.
Brennan, K. A., & Morris, K. A. (1997). Attachment styles, self-esteem, and patterns of seeking feedback from romantic partners. Personality and Social Psychology Bulletin, 23(1), 23–31.
https://doi.org/10.1177/0146167297231003
Bretherton, I. (1996). Internal working models of attachment relationships as related to resilient coping. In G. G. Noam & K. W. Fischer (Eds.), Development and vulnerability in close relationships (pp. 3–27). Lawrence Erlbaum.
Bureau, J. F., Easlerbrooks, M. A., & Lyons-Ruth, K. (2009). Attachment disorganization and controlling behavior in middle childhood: Maternal and child precursors and correlates. Attachment & Human Development, 11(3), 265–284. https://doi.org/10.1080/14616730902814788
Cassidy, J., Jones, J. D., & Shaver, P. R. (2013). Contributions of attachment theory and research: A framework for future research, translation, and policy. Development and Psychopathology, 25(4), 1415–1434.
https://doi.org/10.1017/S0954579413000692
Cassidy, J., & Shaver, P. R. (Eds.). (2010). Handbook of attachment: Theory, research, and clinical applications (2nd ed.). Guilford.
Chen, W., Zhang, D., Pan, Y., Hu, T., Liu, G., & Luo, S. (2017). Perceived social support and self-esteem as mediators of the relationship between parental attachment and life satisfaction among Chinese adolescents. Personality and Individual Differences, 108, 98–102. https://doi.org/10.1016/j.paid.2016.12.009
Cummings-Robeau, T. L., Lopez, F. G., & Rice, K. G. (2009). Attachment-related predictors of college students’ problems with interpersonal sensitivity and aggression. Journal of Social and Clinical Psychology, 28(3),
364–391. https://doi.org/10.1521/jscp.2009.28.3.364
DeKlyen, M., & Greenberg, M. T. (2008). Attachment and psychopathology in childhood. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (2nd ed., pp. 637–665). Guilford.
Donker, T., Comijs, H., Cuijpers, P., Terluin, B., Nolen, W., Zitman, F., & Penninx, B. (2010). The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research, 176(1), 45–50. https://doi.org/10.1016/j.psychres.2009.01.012
Easton, S. D., Safadi, N, S., Wang, Y., & Hasson, R. G., III. (2017). The Kessler Psychological Distress Scale: Translation and validation of an Arabic version. Health and Quality of Life Outcomes, 15(1), 215.
https://doi.org/10.1186/s12955-017-0783-9
Fennell, M. J. V. (1997). Low self-esteem: A cognitive perspective. Behavioural and Cognitive Psychotherapy, 25(1), 1–26. https://doi.org/10.1017/S1352465800015368
Foster, J. D., Kernis, M. H., & Goldman, B. M. (2007). Linking adult attachment to self-esteem stability. Self and Identity, 6(1), 64–73. https://doi.org/10.1080/15298860600832139
Fraley, R. C. (2002). Attachment stability from infancy to adulthood: Meta-analysis and dynamic modeling of developmental mechanisms. Personality and Social Psychology Review, 6(2), 123–151.
https://doi.org/10.1207/S15327957PSPR0602_03
Gamble, S. A., & Roberts, J. E. (2005). Adolescents’ perceptions of primary caregivers and cognitive style: The roles of attachment security and gender. Cognitive Therapy and Research, 29, 123–141.
https://doi.org/10.1007/s10608-005-3160-7
Gnilka, P. B., Ashby, J. S., & Noble, C. M. (2013). Adaptive and maladaptive perfectionism as mediators of adult attachment styles and depression, hopelessness, and life satisfaction. Journal of Counseling & Development, 91(1), 78–86. https://doi.org/10.1002/j.1556-6676.2013.00074.x
Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modeling: Guidelines for determining model fit. Electronic Journal on Business Research Methods, 6(1), 53–60.
Karreman, A., & Vingerhoets, A. J. J. M. (2012). Attachment and well-being: The mediating role of emotion regulation and resilience. Personality and Individual Differences, 53(7), 821–826.
https://doi.org/10.1016/j.paid.2012.06.014
Kenny, D. A., Kaniskan, B., & McCoach, D. B. (2015). The performance of RMSEA in models with small degrees of freedom. Sociological Methods & Research, 44(3), 486–507. https://doi.org/10.1177/0049124114543236
Kenny, M. E., & Sirin, S. R. (2006). Parental attachment, self-worth, and depressive symptoms among emerging adults. Journal of Counseling & Development, 84(1), 61–71. https://doi.org/10.1002/j.1556-6678.2006.tb00380.x
Kessler, R. C., Barker, P. R., Colpe, L. J., Epstein, J. F., Gfroerer, J. C., Hiripi, E., Howes, M. J., Normand, S.-L. T., Manderscheid, R. W., Walters, E. E., & Zaslavsky, A. M. (2003). Screening for serious mental illness in the general population. Archives of General Psychiatry, 60(2), 184–189. https://doi.org/10.1001/archpsyc.60.2.184
Kline, R. B. (2010). Principles and practice of structural equation modeling (3rd ed.). Guilford.
Konrath, S. H., Chiopik, W. J., Hsing, C. K., & O’Brien, E. (2014). Changes in adult attachment styles in American college students over time: A meta-analysis. Personality and Social Psychology Review, 18(4), 326–348.
https://doi.org/10.1177/1088868314530516
Lecompte, V., Moss, E., Cyr, C., & Pascuzzo, K. (2014). Preschool attachment, self-esteem and the development of preadolescent anxiety and depressive symptoms. Attachment & Human Development, 16(3), 242–260. https://doi.org/10.1080/14616734.2013.873816
Li, S. T., Albert, A. B., & Dwelle, D. G. (2014). Parental and peer support as predictors of depression and self-esteem among college students. Journal of College Student Development, 55(2), 120–138.
https://doi.org/10.1353/csd.2014.0015
Liu, Y., & Hazler, R. J. (2017). Predictors of attachment security in children adopted from China by US families: Implication for professional counsellors. Asia Pacific Journal of Counselling and Psychotherapy, 8(2), 115–130. https://doi.org/10.1080/21507686.2017.1342675
Lopez, F. G., & Gormley, B. (2002). Stability and change in adult attachment style over the first-year college transition: Relations to self-confidence, coping, and distress patterns. Journal of Counseling Psychology, 49(3), 355–364. https://doi.org/10.1037/0022-0167.49.3.355
Lynch, M. F. (2013). Attachment, autonomy, and emotional reliance: A multilevel model. Journal of Counseling & Development, 91(3), 301–312. https://doi.org/10.1002/j.1556-6676.2013.00098.x
Masselink, M., Van Roekel, E., & Oldehinkel, A. J. (2018). Self-esteem in early adolescence as predictor of depressive symptoms in late adolescence and early adulthood: The mediating role of motivational and social factors. Journal of Youth and Adolescence, 47, 932–946. https://doi.org/10.1007/s10964-017-0727-z
Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide (7th ed.). http://www.statmodel.com/download/users
guide/Mplus%20user%20guide%20Ver_7_r3_web.pdf
Pascuzzo, K., Cyr, C., & Moss, E. (2013). Longitudinal association between adolescent attachment, adult romantic attachment, and emotion regulation strategies. Attachment & Human Development, 15(1), 83–103.
https://doi.org/10.1080/14616734.2013.745713
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891.
https://doi.org/10.3758/BRM.40.3.879
Roberts, J. E., Gotlib, I. H., & Kassel, J. D. (1996). Adult attachment security and symptoms of depression: The mediating roles of dysfunctional attitudes and low self-esteem. Journal of Personality and Social Psychology, 70(2), 310–320. https://doi.org/10.1037/0022-3514.70.2.310
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press.
Ruckstaetter, J., Sells, J., Newmeyer, M. D., & Zink, D. (2017). Parental apologies, empathy, shame, guilt, and attachment: A path analysis. Journal of Counseling & Development, 95(4), 389–400.
https://doi.org/10.1002/jcad.12154
Sandberg, D. A., Suess, E. A., & Heaton, J. L. (2010). Attachment anxiety as a mediator of the relationship between interpersonal trauma and posttraumatic symptomatology among college women. Journal of Interpersonal Violence, 25(1), 33–49. https://doi.org/10.1177/0886260508329126
Sowislo, J. F., & Orth, U. (2013). Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychological Bulletin, 139(1), 213–240. https://doi.org/10.1037/a0028931
Sroufe, L. A. (2005). Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development, 7(4), 349–367. https://doi.org/10.1080/14616730500365928
Sroufe, L. A., & Waters, E. (1977). Attachment as an organizational construct. Child Development, 48(4), 1184–1199. https://doi.org/10.2307/1128475
Steiger, A. E., Allemand, M., Robins, R. W., & Fend, H. A. (2014). Low and decreasing self-esteem in adolescence predict adult depression two decades later. Journal of Personality and Social Psychology, 106(2), 325–338. https://doi.org/10.1037/a0035133
Styron, T., & Janoff-Bulman, R. (1997). Childhood attachment and abuse: Long-term effects on adult attachment, depression, and conflict resolution. Child Abuse & Neglect, 21(10), 1015–1023.
https://doi.org/10.1016/S0145-2134(97)00062-8
Taylor, T. L., & Montgomery, P. (2007). Can cognitive-behavioral therapy increase self-esteem among depressed adolescents? A systematic review. Children and Youth Services Review, 29(7), 823–839.
https://doi.org/10.1016/j.childyouth.2007.01.010
Turan, N., Kocalevent, R.-D., Quintana, S. M., Erdur-Baker, Ö., & Diestelmann, J. (2016). Attachment orientations: Predicting psychological distress in German and Turkish samples. Journal of Counseling & Development, 94(1), 91–102. https://doi.org/10.1002/jcad.12065
Vogel, D. L., & Wei, M. (2005). Adult attachment and help-seeking intent: The mediating roles of psychological distress and perceived social support. Journal of Counseling Psychology, 52(3), 347–357.
https://doi.org/10.1037/0022-0167.52.3.347
Wilkinson, R. B. (2004). The role of parental and peer attachment in the psychological health and self-esteem of adolescents. Journal of Youth and Adolescence, 33, 479–493.
https://doi.org/10.1023/B:JOYO.0000048063.59425.20
Wright, S. L., Firsick, D. M., Kacmarski, J. A., & Jenkins-Guarnieri, M. A. (2017). Effects of attachment on coping efficacy, career decision self-efficacy, and life satisfaction. Journal of Counseling & Development, 95(4), 445–456. https://doi.org/10.1002/jcad.12159
Wright, S. L., Perrone-McGovern, K. M., Boo, J. N., & White, A.V. (2014). Influential factors in academic and career self-efficacy: Attachment, supports, and career barriers. Journal of Counseling & Development, 92(1), 36–46. https://doi.org/10.1002/j.1556-6676.2014.00128.x
Fei Shen, PhD, is a staff therapist at Syracuse University. Yanhong Liu, PhD, NCC, is an assistant professor at Syracuse University. Mansi Brat, PhD, LPC, is a staff therapist at Syracuse University. Correspondence may be addressed to Fei Shen, 150 Sims Drive, Syracuse, NY 13210, fshen02@syr.edu.
