Regina Gavin Williams, Stanley B. Baker, ClarLynda R. Williams-DeVane
Three female foster care youth, aged 15, 17, and 17, volunteered to participate in customized counseling interventions. A theory-based presentation framework was used to conduct an A-B-A single-case research design. A female licensed professional counselor collaborated with the participants in customizing interventions, delivering the intervention, and collecting the outcome data, with the three participants engaging in self-monitoring to provide outcome data. Four career and college readiness self-efficacy factor scores were used to determine the components of the customized interventions and to assess the participants’ progress. The factors were: (a) college knowledge, (b) positive personal characteristics, (c) academic competence, and (d) potential to set and achieve future goals. Positive trends occurred for each participant, although different factor-specific outcome data patterns occurred for each participant. Effect sizes ranged from small to large across the participants and factors, and the participants found value in their respective customized interventions.
Keywords: foster care youth, customized counseling interventions, single-case research design, career readiness self-efficacy, college readiness self-efficacy
Appropriate assistance is important for effective navigation of the demanding postsecondary education preparation process and is vital for attaining admittance into higher education (Pecora, Williams, et al., 2006). Youth who are academic low achievers from middle-to-low income families, underrepresented minorities, the disabled, and youth from families in which no one has previously attended college find it especially difficult to navigate access to higher education (College Board, 2006). Moreover, youth in the foster care system potentially face all of the listed access challenges.
Foster care youth have been removed from their family units through decisions determined in the courts. Judges may decide to place youth in foster homes, in group homes, or with their relatives (i.e., kinship foster care; C. M. Kirk, Lewis, Nilsen, & Colvin, 2013). More long-term placement outcomes include adoption or aging out of foster care. According to statistics from the Adoption and Foster Care Analysis and Reporting System (AFCARS; 2013), there were approximately 402,378 youth in foster care, and 47% of these youth resided in non-relative foster care homes. Additionally, foster placements spent 20 months on average in multiple placement settings (AFCARS, 2013). These circumstances create various multiple educational attainment barriers for foster care youth.
According to C. M. Kirk et al. (2013), about 10% of former foster care youth were enrolled in college, and only 4% of these youth obtained a bachelor’s degree. Youth in foster care are more likely to drop out of high school, repeat a grade, or be suspended or expelled (Unrau, Font, & Rawls, 2012). Only one third of foster care youth who age out of the foster care system after their 18th birthday possess a driver’s license, own basic necessities for living, or have money upon leaving the foster system (Pecora, Kessler, et al., 2006). Furthermore, very little is known about the readiness of foster care youth to undertake a postsecondary education, the developmental necessities of these youth during their transition to postsecondary education, and ways professionals in the child welfare system and in higher education can be of assistance (Unrau et al., 2012).
- Kirk et al. (2013) found indications that many youth in foster care have aspirations to pursue a postsecondary education. There is a dearth of information about foster care youth who have become successful in adulthood (Hudson, 2013), or their readiness to make a successful transition to adulthood (Lemon, Hines, & Merdinger, 2005). R. Kirk and Day (2011) found that an experiential learning program for youth aging out of foster care located in a college setting increased their knowledge about college admissions and campus life. Pecora, Williams, et al. (2006) found from a survey of 1,609 foster care alumni that foster care youth who received tutoring and independent living training and had employment experiences had high postsecondary education graduation rates.
Lemon et al. (2005) compared former foster care youth who experienced independent living programs (ILPs) and were attending 11 different colleges with former foster care youth not attending colleges and individuals with low-income backgrounds who were attending colleges. The findings indicated that the ILP participants were more likely to have acquired concrete skills such as finding employment; managing budgets; attaining housing; developing psycho-emotional skills, such as goal setting; and discovering opportunities for training and education (Lemon et al., 2005). Related recommendations for improving the career and college readiness of foster care youth include individual and group counseling focused on adjustment challenges and negative educational attitudes (Geroski & Knauss, 2000). Kaplan, Skolnik, and Turnbull (2009) also recommended career and college readiness counseling interventions.
Conley (2010) defined career ready as possessing the content knowledge and key learning skills and techniques to begin studies in a career pathway. Achieve, Inc. (n.d.) defined college ready as being prepared for postsecondary education training experiences that lead to obtaining credentials such as a bachelor’s or associate degree, a license, or a certificate. The reviewed literature cited above presented foster care youth as being at risk because they lacked the career and college readiness preparation needed for successful transitions from foster care to the postsecondary education opportunities essential for successful futures in the 21st century. Fortunately, there is evidence that group and individual counseling interventions can be helpful (Geroski & Knauss, 2000; Kaplan et al., 2009). The literature cited above also indicated that interventions based on an understanding of the unique circumstances foster care youth experience and focused on enhancing their career and college readiness may improve their potential to have access to postsecondary education opportunities.
A critical component of the challenge to achieve career and college readiness seems to be whether or not foster care youth believe they can successfully attain postsecondary education and develop meaningful careers. The general dependent variable in the present study was self-efficacy—that is, an individual’s personal beliefs about his or her ability to perform a specific behavior or achieve a specific personal goal (Bandura, 1997). The specific self-efficacy variable in the present study was career and college readiness self-efficacy (Baker & Parikh Foxx, 2012). The readiness construct was derived from Savickas’ (2011) career construction theory, built on the classic career readiness construct by Super (1990). The goal for the treatment approach in the study was to help foster care youth connect insights with future work and career opportunities and take possession of their lives.
The authors’ purpose in conducting the present study was to examine the effects of customized individual counseling interventions on the career and college readiness self-efficacy of a small sample of foster care youth. The research hypotheses for all three participants were focused on the effects of the respective customized interventions across baseline, intervention, and withdrawal phases in a single-case research design.
Method
Research Design
An A-B-A single-case experimental research design (SCRD) was employed in the present study. Components of the design were A1 = baseline phase, B = treatment phase, and A2 = withdrawal of treatment phase. The study participants’ responses during the clinical withdrawal phase provided evidence of the effect of the intervention after it had been withdrawn (Engel & Schutt, 2013; Hinkle, 1992; Martin-Causey & Hinkle, 1995).
Participants
The three participants were attending a voluntary, state-funded, county-administered life-skills development program in a Southeastern metropolitan county. The intervention focus of the program was on helping foster care youth transition to adulthood. The program served foster care youth from age 13 to 18 years old, those who aged out of foster care on their 18th birthday, and those voluntarily remaining in foster care after their 18th birthday. Approximately 50 foster care youth were enrolled in the program, although only six to 12 attended monthly meetings at any given time.
The first author had served as a volunteer for the program prior to providing the customized interventions in the present study. Following approval by the university institutional review board, the first author recruited participants for the intervention while attending one of the monthly skills development programs. Initially, four participants volunteered, and one withdrew after the second individual counseling session; being 18 and eligible to leave the system, this participant moved elsewhere. The three continuing participants professed an interest in pursuing postsecondary education. They were interested in exploring career and academic options and in becoming more confident that they could achieve future success in spite of their familial circumstances. Individual information about the participants is given below (pseudonyms are used in place of their real names).
Rose. Rose was a 17-year-old African American female high school senior enrolled in a non-traditional high school in a Southeastern city that served as a gateway to a community college. She decided to attend the community college because of the advantages of the gateway arrangement. Her current grade point average (GPA) was 2.6. She lived in a stable home, although she often had disagreements with her foster parents. Several other foster care youth lived in the same apartment, making privacy difficult to achieve.
Janelle. Janelle was a 15-year-old biracial (Caucasian/African American) female 10th grade student enrolled in a traditional public high school in a Southeastern city. She was an honor roll student with a 3.9 GPA. Her sexual orientation was lesbian, and she believed her foster parents would not accept her if they knew her orientation. She wanted to attend a four-year college and was uncertain about fields of study and potential career goals.
Kara. Kara was a 17-year-old African American female high school senior enrolled in a large comprehensive Southeastern urban high school. She had a 3.4 GPA and planned to attend college following graduation. Deciding on a major was her primary goal. She lived in a kinship foster care setting with two aunts and appeared to have considerable support at home.
The Counselor
The intervention was designed by the first author, who also served as the counselor presenting the customized interventions to the three participants. She was a 30-year-old African American female with a bachelor’s degree in psychology and a master’s degree in school counseling. She was a licensed professional counselor, a National Certified Counselor, and a recipient of a National Board for Certified Counselors minority fellowship. Her professional experience has included college access interventions, outpatient therapy employment, student services in higher education, and transitional living intervention programming. She previously served children and adolescents from underserved backgrounds, a significant number of whom were in foster care. She has had previous research experience; however, the present study was her first SCRD experience.
Instrumentation
Career and college readiness self-efficacy. The Career and College Readiness Self-Efficacy Inventory (CCRSI; Baker & Parikh Foxx, 2012) was completed by participants across all three phases of the study. The CCRSI readiness construct is based on Savickas’ (2011) career constructivist theory, and the self-efficacy concept was derived from Bandura’s (1997) social cognitive theory. Item content represents broad contextual goals (e.g., “I have confidence in being able to achieve a good life 10 years from now”) and specific content (e.g., “I know about various ways to pay for post-high school education”). Responses to each item range from strongly agree (5 points) to strongly disagree (1 point). There are 14 items in the total scale with scores ranging from 14 to 70. Higher scores indicate higher levels of self-efficacy.
In the present study, the customized interventions were based on the four CCRSI factors, and the factor scores were used in the data analyses. The CCRSI factors are: (a) college knowledge (5 items; scores ranging from 5 to 25); (b) positive personal characteristics (4 items; scores ranging from 4 to 20); (c) academic competence (3 items; scores ranging from 3 to 15); and (d) potential to set and achieve future goals (2 items; scores ranging from 2 to 10). An exploratory factor analysis of the CCRSI identified the four factors as accounting for 51% of the variance (Baker et al., 2017), and a confirmatory factor analysis supported the four-factor model (Martinez, Baker, & Young, 2017). Alpha reliability estimates for the total scale from two previous studies were .86 and .87. For the factor scales, they were: (a) college knowledge (.76 and .80), (b) positive personal characteristics (.69 and .70), (c) academic competence (.75 and .75), and (d) potential to set and achieve future goals (.46 and .51; Baker et al., 2017).
Social validity measure. Social validity refers to the social significance of the intervention (Wolf, 1978). According to Hott, Limberg, Ohrt, and Schmit (2015), evidence of social validity serves as a quality indicator in SCRDs and should be presented clearly in the results sections of said studies. Client satisfaction is one of the indicators of social validity recommended by Hott et al. (2015). An extant self-report measure designed to assess participants’ attitudes about research interventions upon their completion was used in the present study.
The Attitude Toward Treatment (ATT; Baker, 1983) scale was used to assess satisfaction with the intervention in the present study. The ATT was used previously as a post-treatment measure of satisfaction with psychoeducational group intervention. Content validity for using the ATT to assess client attitudes toward the interventions they received in clinical settings, as was the case in the present research, had been established in previous studies. The ATT consists of 14 seven-point Likert items with the wording presented in the past tense (e.g., How beneficial do you think this program was for you?). Scores range from a low of 14 to a high of 98.
Assessing unforeseen participant and setting changes. To control for threats to internal validity caused by unforeseen changes in the participants, the counselor-investigator kept field notes for each participant throughout the study (Hott et al., 2015).
Procedure
Customized interventions framework. The independent variables were the customized interventions for each participant. The customized intervention framework was entitled Students That Are Achieving Success (S.T.A.R.S). Explicating the foundations of the customized intervention process is necessary for establishing the fidelity of the treatment (Hott et al., 2015). All three customized interventions were embedded in a single conceptual framework. The conceptual framework was based on an integration of tenets of social cognitive career theory (SCCT; Lent, Brown, & Hackett, 1994), cognitive information processing (CIP; Peterson, Sampson, Lenz & Reardon, 2002), and the American School Counselor Association’s National Model (ASCA; 2012). The SCCT (Lent et al., 1994) is a useful instrument for researchers wishing to stress the importance of addressing external factors that influence career self-efficacy beliefs and outcome expectations. Therefore, the interventions were designed to identify external barriers for each participant and attempt to introduce ways to overcome them. The CIP (Peterson et al., 2002) was designed to help individuals understand the content and process of career decision-making and problem solving. The ILP component of the CIP framework was used during the initial meeting with each participant to identify at least three goals and establish mutually agreed-upon action steps. A focus on helping participants establish personal academic, career, and social goals; develop future plans; and monitor their learning aligned with the individual student planning component of the ASCA National Model.
Specific customizing strategies for each participant. Activities listed on the ILPs reflected the participants’ postsecondary education and career-related needs based on CCRSI (Baker & Parikh Foxx, 2012) scores acquired a week prior to the initial meetings. The counselor and each participant identified the desired activities and related outcomes, estimated time needed to complete activities, matched activities and goals, and prioritized the activities. CCRSI (Baker & Parikh Foxx, 2012) pre-treatment factor scores for each participant were used in the customizing process.
Rose’s customized goals. The pre-treatment CCRSI scores for Rose indicated that she needed assistance in believing in her academic competence and potential to achieve future goals. She already knew she would attend a community college; however, she had difficulty meeting academic expectations while in high school. Consequently, she wanted to explore strategies to help her improve academically and be eligible for admission to the community college. Not knowing what her major would be or how she would pay for college seemed to be interfering with her future goals. Her customized goals were exploring: (a) ways to improve her academic performance, (b) potential academic majors, and (c) ways to pay for college.
Janelle’s customized goals. The pre-treatment CCRSI scores for Janelle indicated that she needed assistance with believing in her academic competence and potential to achieve future goals. As a high school sophomore with no family focus on higher education, Janelle was uninformed about postsecondary education. She indicated that her time-management skills related to academic work were deficient. Consequently, her customized goals were: (a) understanding the college application and admission process, ways to receive financial aid, requirements for academic success in college, and cultural differences between high school and college; (b) exploring college majors and career choices; (c) learning to set short- and long-term goals; and (d) improving her time-management skills.
Kara’s customized goals. The pre-treatment CCRSI scores for Kara indicated that she needed assistance with believing in her academic competence and potential to achieve future goals. Although planning to attend college after graduation, Kara was struggling to maintain academic motivation while balancing academic and extracurricular activities. She also experienced doubts about future goals and achieving them. These circumstances led to the following customized goals: (a) enhancing her time-management skills, (b) engaging in short- and long-term goal setting, (c) exploring potential academic majors, (d) learning more about how to pay for college, and (e) understanding how college education influences one’s future income and lifestyle.
Data collection. The CCRSI (Baker & Parikh Foxx, 2012) was distributed electronically via Qualtrics survey software to the participants upon their submission of the informed consent forms. The pre-treatment CCRSI data served as the baseline (Phase A1) for the study. A common self-monitoring schedule was distributed with instructions for each participant to complete the CCRSI four times during the 2 weeks prior to the beginning of the intervention. The intervention (Phase B) lasted 8 weeks for each participant. Participants completed the CCRSI at the end of each weekly session. During the 2-week withdrawal phase (A2) following the last intervention session, participants were again instructed to follow a common self-monitoring schedule for completing the CCRSI four times. The three participants received a dinner, a gift card, and a certificate of completion from the counselor-investigator at the end of the study.
Data analysis. Visual and non-parametric analyses were used to assess the outcomes for each experiment, and non-parametric analyses provided information about the effects of the treatments (Hott et al., 2015).
Temporal analysis. The time series data were plotted graphically on x (temporal independent variable) and y (dependent variable) axes for each participant and CCRSI factor. Autocorrelation and regression analyses were used to determine the appropriate statistical analysis procedure. Autocorrelation analysis was used to determine whether each observation within each phase and factor of the study was truly independent. Observations that were not correlated to each other could not be predicted (Bloom, Fischer, & Orme, 2006). Regression analysis was used to determine whether significant trends were present for each phase of each CCRSI factor for each participant (alpha <.05). In cases where there was significant trend and autocorrelation, as well as outliers within each phase, the Robust Conservative Dual-Criteria (RCDC; Borckardt, 2008) method was used as the primary statistical analysis tool. RCDC was used to compare differences between phases for each participant as opposed to traditional parametric methods like the student’s t-test and analysis of variance (ANOVA).
Intervention effects. Providing effect sizes in addition to visual analyses enhances the credibility, reliability, and defensibility of single-case research findings (Vannest & Ninci, 2015). Vannest and Ninci (2015) reported that there are several strategies available to estimate effect sizes for SCRD studies. In cases where there is a significant trend and autocorrelation, the G-index (Cohen, 1988) is used to estimate effect sizes. The G-index results were determined by using the regression line and the mean or median from the baseline. The effect size was calculated by using the proportion of participants’ scores in the desired zone above the regression line, which was an expected increase in scores from the baseline to treatment phases. The baseline average was then subtracted from the intervention average, with a positive value indicating improved effects and a negative value indicating decreased effects. Metrics for interpreting G-index effect sizes are: small (< 0.3), medium (0.31 to 0.50), and large (> 0.51).
Assessing social validity and unforeseen changes in participants. Each participant completed the ATT measure following the final session of their respective interventions. The counselor-investigator kept field notes for each participant throughout the study.
Results
Statistical Analyses
Descriptive statistics. Descriptive statistics were computed for each of the participants across each of the factors which are presented in Table 1. Rose’s responses were very stable as indicated by the consistent means and medians across all phases of the study. Further, the standard deviation values were close to zero, indicating a lack of variation in stability. Janelle’s responses were less stable. The large range in the treatment phase is indicative of the presence of outliers in the treatment phase for Janelle. Kara exhibited more variability than Rose, but there were no outliers.
Table 1
Descriptive Statistics
| Participant | n | Mean | Median | SD | Range (min, max) | |||||||||||
| A1 | B | A2 | A1 | B | A2 | A1 | B | A2 | A1 | B | A2 | A1 | B | A2 | ||
| Rose | College Knowledge | 4 | 12 | 4 | 24.75 | 25.00 | 25.00 | 25 | 25 | 25 | 0.5 | 0.0 | 0.0 | (24,25) | (25,25) | (25,25) |
| Positive Personal Characteristics | 4 | 12 | 4 | 20.00 | 19.91 | 20.00 | 20 | 20 | 20 | 0.00 | 0.29 | 0.000 | (20,20) | (19,20) | (20,20) | |
| Academic Competence | 4 | 12 | 4 | 13.0 | 14.5 | 15.0 | 13 | 15 | 15 | 0.00 | 0.67 | 0.000 | (13,13) | (13,15) | (15,15) | |
| Potential to Achieve Future Goals | 4 | 12 | 4 | 10 | 9.91 | 10 | 10 | 10 | 10 | 0.00 | 0.29 | 0.000 | (10,10) | (9,10) | (10,10) | |
| All Factors | 4 | 12 | 4 | 67.75 | 69.33 | 70.00 | 68.0 | 69.5 | 70.0 | 0.50 | 0.78 | 0.000 | (67,68) | (68,70) | (70,70) | |
| Janelle | College Knowledge | 4 | 12 | 4 | 13.00 | 17.17 | 25.00 | 12 | 19 | 25 | 2.71 | 7.38 | 0.00 | (11,17) | (5,25) | (25,25) |
| Positive Personal Characteristics | 4 | 12 | 4 | 16.25 | 15.42 | 20.00 | 16 | 19 | 20 | 0.50 | 0.68 | 0.00 | (16,17) | (4,20) | (20,20) | |
| Academic Competence | 4 | 12 | 4 | 14.25 | 12.00 | 15.00 | 14 | 15 | 15 | 0.50 | 5.43 | 0.00 | (14,15) | (3,15) | (15,15) | |
| Potential to Achieve Future Goals | 4 | 12 | 4 | 9.75 | 8.00 | 10.00 | 10 | 10 | 10 | 0.50 | 3.62 | 0.00 | (9,10) | (2,10) | (10,10) | |
| All Factors | 4 | 12 | 4 | 53.25 | 52.58 | 70.00 | 52.0 | 63.5 | 70.0 | 3.20 | 22.67 | 0.00 | (51,58) | (14,69) | (70,70) | |
| Kara | College Knowledge | 4 | 12 | 4 | 17.00 | 21.33 | 23.75 | 17.5 | 21.0 | 24.0 | 2.45 | 2.39 | 0.50 | (14,19) | (23,24) | (19,25) |
| Positive Personal Characteristics | 4 | 12 | 4 | 14.50 | 17.83 | 18.25 | 14.5 | 17.5 | 18.0 | 0.58 | 1.03 | 0.50 | (14,15) | (17,20) | (18,19) | |
| Academic Competence | 4 | 12 | 4 | 10.25 | 13.08 | 13.50 | 1.5 | 13.0 | 13.5 | 0.96 | 1.08 | 0.58 | (9,11) | (12,15) | (13,14) | |
| Potential to Achieve Future Goals | 4 | 12 | 4 | 9.25 | 9.58 | 10.00 | 9.5 | 10.0 | 10.0 | .96 | 0.67 | 0.00 | (8.10) | (8,10) | (10,10) | |
| All Factors | 4 | 12 | 4 | 51.00 | 61.83 | 65.50 | 50.0 | 60.5 | 65.5 | 2.71 | 4.67 | 1.29 | (49,55) | (57,70) | (64,67) | |
Note. The descriptive statistics show stability for both Rose and Kara. More variability was present for Janelle, indicative of outliers leading to the use of non-parametric analysis methods.
Autocorrelation. Autocorrelation was measured and evaluated at the .05 significance level. There was significant autocorrelation for Rose for the Academic Competence factor (p = 0) in the treatment phase. There was no significant correlation for Janelle. There was significant autocorrelation in several areas for Kara: college knowledge (p = 0.003), positive personal characteristics (p = 0.001), and academic competence (p = 0) in the treatment phase. No transformations were applied to correct for autocorrelation because of lack of independence between data points, the small sample size, and the significant trends in some of the phases; therefore, non-parametric data analyses were used.
Regression. Regression was measured for each participant, factor, and phase to determine if there is a trend in each phase of the study. All three participants exhibited unique trend patterns for each of the factors. Rose exhibited a significant trend for academic competence in the treatment phase. The strong positive slope (R2 = 0.7399, Slope = 0.16084, p = .000332) suggested a steady increase during the treatment phase. Janelle exhibited negative treatment phase trends for positive personal characteristics (R2 = 0.3392, Slope = -1.094, p = 0.049), academic competence (R2 = 0.411, Slope = -0.9650, p = 0.0247), and potential to achieve future goals (R2 = 0.411, Slope = -0.6434, p = 0.0247). The negative slopes suggest a decrease in self-efficacy across all factors except college knowledge. Lastly, Kara exhibited significant positive trends for college knowledge (R2 = 0.7142, Slope = 0.5594, p = 0.000538), positive personal characteristics (R2 = 0.6138, Slope = 0.22378, p = 0.00257), and academic competence (R2 = 0.6823, Slope = 0.24825, p = 0.00093) in the treatment phase, suggesting a steady increase in these factors. The overall findings indicated that further parametric data analyses (e.g., ANOVAs) would not be appropriate because of the significant trends in various factors.
RCDC. The autocorrelation indications, regression trends, and additional complexity of outlier scores indicated that the RCDC (Borckardt, 2008), a robust non-parametric method, should be used rather than the Conservative Dual-Criteria method (Fisher, Kelley, & Lomas, 2003; Swoboda, Kratochwill, & Levin, 2010) and parametric methods such as student’s t-test and ANOVA. The RCDC significance threshold is based on the mean and regression lines and the number of comparisons in the comparison phase. Datum that fall above or below the desired zone, as determined by the mean and regression lines, are considered significant. The sign of the slope determines the direction of the difference. For Rose, there were significant increases in the academic competence scores in the treatment phase. Enhancing her academic competence was one of the customized goals set at the beginning of the treatment phase. For Janelle, college knowledge and academic competence scores improved significantly in the treatment phase. These were the two customized goal categories for Janelle. For Kara, positive personal characteristics and academic competence scores improved significantly. Enhancing academic competence was one of the customizing goals set for Kara.
Visual Analyses
The graphic data are presented in Figure 1. The baseline, treatment, and withdrawal phase CCRSI factor scores for each participant are presented visually. The visual analysis confirmed the findings of the RCDC analyses.
Effect Sizes
Cohen’s (1988) G-index effect size findings varied across the three participants, indicating that the interventions had differential treatment effects. For Rose, there was a large effect size (1.00) for academic competence from baseline to end of treatment, with a medium negative effect size from end of treatment to end of withdrawal (-0.5). In her case, the treatment effect appears to have decreased somewhat after the intervention was withdrawn.
Janelle experienced large treatment effect sizes on college knowledge (0.75), positive personal characteristics (0.75), and academic competence (0.75) from the baseline to end of withdrawal, with a negative medium effect size for potential to achieve future goals (-0.5). All four effect sizes were medium (0.5) from end of treatment to end of withdrawal phases. The treatment effect appeared to have declined somewhat during withdrawal for the first three factors, while the effect for potential to achieve future goals appeared to have improved during withdrawal.
Kara’s data indicated effects on three CCRSI factors from baseline to end of treatment: college knowledge (0.25; small), positive personal characteristics (0.5; medium), and academic competence (0.5; medium). All of the effect sizes were negative (-0.5) at the end of the withdrawal phase. Her findings indicated treatment effects across all four CCRSI factors during the intervention with a clear drop off after withdrawal of the intervention.
Social Validity
As stated above, client satisfaction was assessed as an indicator of social validity (Hott et al. 2015). The ATT (Baker, 1983) scores for all three participants were quite high, with Rose scoring 97, Janelle 89, and Kara 89 on a scale ranging from 14 to 98. These findings were assumed to represent evidence of social validity for the study.
Unforeseen Changes in Participants
The counselor-investigator’s field notes provided important information that helped to explain unclear or puzzling visual findings, especially for Janelle. Her scores across all four self-efficacy factors were either quite high or increasing from the beginning of the intervention to the fifth session, and then the scores dropped dramatically over the next three sessions only to dramatically rise to very high levels at the end of the treatment phase. Observing the graphic visual representation of her data was indeed puzzling and would have remained puzzling without the field notes data. Fortunately, the counselor-investigator had recorded Janelle’s sharing of a significant current personal problem that caused concern about the impact of the issue on her future beyond high school. The circumstances led to Janelle’s being in a negative mood that the counselor-investigator was eventually able to help her address in addition to continuing the customized treatment protocol.
Rose informed the counselor-investigator that she lacked privacy in her foster home, and arrangements were made to meet with her for the treatment sessions in a community setting. She eventually decided to join an independent living program and was excited about being on her own with limited assistance.
Summary of the Results
The data indicated that positive trends occurred for each participant. Although the trends were positive, different CCRSI factor-specific outcome data patterns occurred for each participant. The effect sizes ranged from small to large across the participants and factors. There was evidence of statistical effects for each participant; however, the effect-size patterns differed across the three participants.
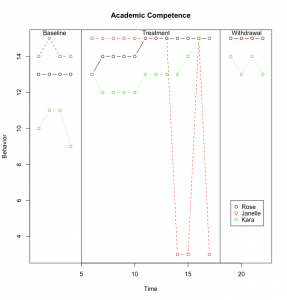
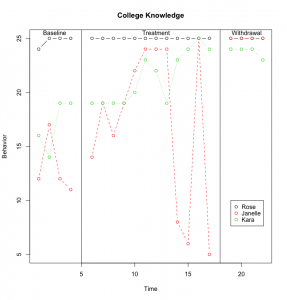
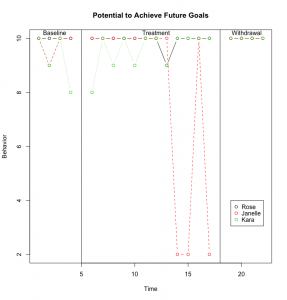
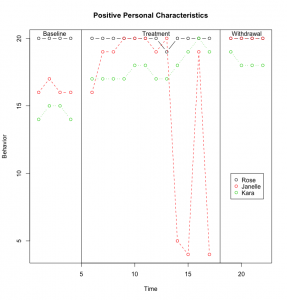
Figure 1. Baseline, Treatment, and Withdrawal Phase CCRSI Data for Each Participant
Discussion
The social validity data was analytically useful in determining that the participants believed they received something of value from their respective customized interventions. The CCRSI data were supportive of each participant, providing some evidence of enhanced career and college readiness self-efficacy during the intervention. The baseline data over 2 weeks for the three foster care participants indicated neither a decline nor an improvement during that phase, leading to an inference that, where there were significant positive changes during the treatment phase, the intervention likely caused them (Ray, 2015). The theory-based framework for the interventions provided an important structure for the counselor when attempting to design customized interventions for each participant. Given the differences in pre-treatment demographic characteristics across the three participants and the differences in CCRSI data for each of them, customizing the interventions seemed to be an appropriate strategy, and the two research strategies seemed to complement each other. Customized treatment interventions allow counselors to focus on specific goals for individual clients. Likewise, a theory-based framework provides a common client treatment process for a broad range of customized interventions. Additional important ingredients are independent and dependent variables that can be clearly defined, translated into intervention strategies, and measured objectively over time.
Although sharing a status—being in foster care—the three participants were not mirror images of each other. Rose was a high school senior with a relatively low GPA who had identified a postsecondary gateway to a community college. Her baseline scores were high on all four CCRSI factors. They remained high throughout the intervention with a statistically significant enhancement on the academic competence self-efficacy factor. The effect size for that factor was large, and her ATT score was categorized as very high.
Janelle was younger than the other participants, had a relatively high GPA, and wanted to attend a four-year college. She had negative treatment trends on all of the factors except college knowledge during the treatment phase, yet an upward trend became statistically significant at the end of the withdrawal phase for the positive personal characteristics and academic competence factors as well. A dramatic drop in her scores near the end of the treatment phase accounted for the negative trend. Significant personal challenges, documented by the counselor’s notes, were problematic for Janelle during treatment. The counselor was able to successfully address Janelle’s concerns and her CCRSI data improved. Her ATT score was high as well. Her lower scores on the college knowledge factor seemed indicative of being a 15-year-old high school student. The less effective impact on the potential to achieve future goals factor may have reflected the ongoing sexual orientation challenge she was experiencing.
Kara was a senior in a comprehensive high school with a strong GPA who wanted to attend college. Her baseline data across the four CCRSI factors was low enough to provide room for a positive trend during the treatment phase, and statistically significant trends occurred on the positive personal characteristics and academic competence factors during the treatment phase. Those effect sizes were medium. There also was a small effect size for the college knowledge factor. The findings indicated that the effects of the treatment dropped off somewhat during the withdrawal phase for Kara. Her ATT score was high.
Having at least three participants in an SCRD study is a recommended criterion (Lenz, 2015; Ray, 2015). This criterion is viewed as a safeguard against attrition and allows for inclusion of diverse participant characteristics. Having multiple participants enhances the opportunity to better understand the phenomenon being studied and supports attempted generalizations. Common findings across the three participants were as follows: (a) all three foster care participants experienced significant positive trends on at least one CCRSI factor in spite of relatively high baseline scores; (b) all participants rated the value of their respective customized interventions highly; (c) field notes were important for counselors when engaged in SCRD interventions; (d) the participants’ demographic differences demonstrated at the beginning of the present study supported the customized intervention idea; and
(e) combining inferential statistical and visual analyses of the data provided important information when the visual data alone were unclear.
Limitations
Although the treatments were customized, the duration of the baseline, treatment, and withdrawal phases were similar for all participants. Consequently, because the three treatment interventions had to be the same length of time within the A-B-A single-case design, the counselor was unable to customize the duration of the interventions. Each foster care participant may have benefitted from being able to engage in the treatment phase as long as needed. Unfortunately, the scheduling circumstances did not allow for this option. Scheduling challenges also forced restricted time frames for the baseline and withdrawal phases. The data collection process required participants to follow a prescribed self-monitoring schedule. They did not consistently conform to it, especially during the baseline and withdrawal phases. This inconsistency caused the counselor to issue reminders more often than desired and led to some inconsistencies in data collection protocols. The varied settings in which the interventions occurred may have caused a reactive effect. Regarding the generally high baseline scores, the participants may have been influenced by a halo effect at the outset. The gender and ethnicity of the participants, two African American females and one Caucasian/African American female, caused the sample to be somewhat homogeneous. During the repeated collections of the CCRSI data, the items were presented in the same order. Consequently, the internal validity of the study may have been enhanced if the items were presented randomly each time.
The study was conducted in the field setting rather than in a laboratory. Although field settings are more realistic than laboratory research, it is more difficult to control events that may reduce the internal validity of a study (Heppner, Wampold, Owen, Thompson, & Wang, 2016). Therefore, the limitations cited above are not unusual for experimental field studies.
Recommendations for Future Research
The recommendations focus on further research using the SCRD model. Two SCRD experimental research thrusts are presented herein. One focuses on serving foster care youth, and the other focuses on understanding and enhancing career and college readiness self-efficacy for diverse populations.
Assuming that the usefulness of a customized approach with a common framework similar to the S.T.A.R.S. model has been established in this study, additional independent variables that have potential for enhancing the postsecondary education readiness of foster care youth can be developed. Self-efficacy represents an attitude or belief variable, and other interventions can be developed to address either additional attitudinal variables (e.g., aspirations) or knowledge and behavior variables that are important for successful access to postsecondary education.
Given that the customized intervention approach with the independent and dependent variables derived from the career and college readiness self-efficacy construct proved useful for a sample of foster care adolescents, applying the same approach to more diverse populations is recommended. All K–12 students can benefit from interventions designed to enhance their career and college readiness self-efficacy. Can this be accomplished across other populations?
Efforts to pursue research related to both foci presented above can benefit from more sophisticated SCRDs and more temporally flexible experimental interventions. More sophisticated designs can enhance the internal validity of SCRD studies. For example, multiple baseline designs (e.g., A-B-A-B) provide for multiple relevant outcomes and increased data points (e.g., A-B-A-B-A-B), and allow researchers to replicate the intervention effects within one study (Lenz, 2015). Also, a combination of statistical and visual data analyses will enhance the probability of finding trends when they are difficult to see visually.
Recommendations for Practice
Recommendations for serving foster care youth herein might be generalizable to some extent for serving all youth. The individual student planning component of the ASCA National Model (2012) will be a useful framework for customizing interventions, providing ongoing activities that will help students with goal setting and planning for the future, and developing learning and graduation plans. Furthermore, school counselors can use appraisal and advisement strategies to enhance career and college readiness by helping students to evaluate their own interests, skills, and abilities in order to make informed decisions about their future (ASCA, 2012).
School counselors are encouraged to create support and educational programming for students in foster care. Because multiple foster care placement switches may serve as an impediment to high school completion and, overall, cause a disruption to educational progression, school counselors are challenged to organize career and college readiness programming that will permit foster care youth to receive a satisfactory amount of information regardless of when they arrive at their schools. School counselors may also engage in and coordinate legislative or policy-level advocacy efforts by organizing social and political advocacy endeavors, such as a legislative day, that tackle the educational needs of foster care youth and assemble individuals to get involved in these efforts. Counselors in the schools can accomplish this goal through participation in either state- or national-level counseling-specific organizations.
Community and school counselors can collaborate with stakeholders to familiarize foster care youth with programs that will aid them with their transition into institutions of postsecondary education. They can acquaint themselves with programs geared toward providing postsecondary education services to both current and former foster care youth who are in college. College counselors can create support groups for adolescents aging out of foster care that address and normalize the transition challenges they face, provide academic and personal support services and resources, and help incoming students build community in their new environment.
Furthermore, counselor educators can inform their students about the career and college readiness self-efficacy construct and how multiple barriers impact the postsecondary education aspirations of all students. In so doing, they also can include career and college readiness enhancement strategies for working with underserved student populations within their course curriculums. Counselors in school, community, and college settings can contribute to enhancing the postsecondary education access of foster care youth specifically, and all youth generally. In so doing, counselors often find themselves providing individualized student planning or counseling services. Within the broad context of career and college readiness, individual student clients, including foster care youth, present varied access circumstances that challenge counselors to customize their responsive services in order to address situation-specific needs.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
Achieve, Inc. (n.d.). College and career readiness. Washington, DC: Author. Retrieved from https://www.achieve.org/college-and-career-readiness
Administration for Children and Families. (2013). The AFCARS report. Retrieved from https://www.acf.hhs.gov/sites/default/files/cb/afcarsreport21.pdf
American School Counselor Association. (2012). ASCA national model: A framework for school counseling programs (3rd ed.). Alexandria, VA: Author.
Baker, S. B. (1983). Attitude Toward Treatment. Unpublished scale. Raleigh, NC: Counselor Education Program, North Carolina State University.
Baker, S. B., & Parikh Foxx, S. (2012). Career College Readiness Self-Efficacy Inventory. Raleigh, NC: North Carolina State University.
Baker, S. B., Parikh Foxx, S., Akcan-Aydin, P., Gavin Williams, R., Ashraf, A., & Martinez, R. R. (2017). Psychometric properties of the Career and College Readiness Self-Efficacy Inventory. In Ideas and research you can use: VISTAS 2017. Retrieved from https://www.counseling.org/docs/default-source/vistas/article_3166ce2bf16116603abcacff0000bee5e7.pdf?sfvrsn=f8d84b2c_4
Bandura, A. (1997). Self-efficacy: The exercise of control. New York, NY: Freeman.
Bloom, M., Fischer, J., & Orme, J. G. (2006). Evaluating practice: Guidelines for the accountable professional (5th ed.). Needham Heights, MA: Allyn & Bacon.
Borckardt, J. J. (2008). User’s guide: Simulation modeling analysis: Time series analysis program for short time series data streams: Version 8.3.3. Retrieved from http://www.clinicalresearcher.org/SMA_Guide.pdf
Bragg, D. D., Kim, E., & Barnett, E. A. (2006). Creating access and success: Academic pathways reaching underserved students. New Directions for Community Colleges, 135, 5–19.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillside, NJ: Lawrence Erlbaum Associates, Inc.
College Board. (2006). College Ed: Creating a college-going culture guide. Retrieved from http://www.collegeboard.com/prod_downloads/collegeed/collegeEd-create-college-going-culture.pdf
Conley, D. T. (2010). College and career ready: Helping all students succeed beyond high school. San Francisco, CA: Jossey-Bass.
Engel, R. J., & Schutt, R. K. (2013). The practice of research in social work (3rd ed). Thousand Oaks, CA: Sage.
Fisher, W. W., Kelley, M. E., & Lomas, J. E. (2003). Visual aids and structured criteria for improving visual inspection ad interpretation of single-case design. Journal of Applied Behavior Analysis, 36, 387–406. doi:10.1901/jaba.2003.36-387
Geroski, A. M., & Knauss, L. (2000). Addressing the needs of foster children within a school counseling program. Professional School Counseling, 3(3), 152–161.
Heppner, P. P., Wampold, B. E., Owen, J., Thompson, M. N., & Wang, K. T. (2016). Research design in counseling (4th ed.). Boston, MA: Cengage Learning.
Hinkle, J. S. (1992). Computer-assisted career guidance and single-subject research: A scientist-practitioner approach to accountability. Journal of Counseling & Development, 70, 391–395. doi:10.1002/j.1556-6676.1992.tb01622.x
Hott, B. L., Limberg, D., Ohrt, J. H., & Schmit, M. K. (2015). Reporting results of single-case studies. Journal of Counseling & Development, 93, 412–417. doi:10.1002/jcad.12039
Hudson, A. L. (2013). Career mentoring needs of youths in foster care: Voices for change. Journal of Child and Adolescent Psychiatric Nursing, 26, 131–137. doi:10.1111/jcap.12032
Kaplan, S. J., Skolnik, L., & Turnbull, A. (2009). Enhancing the empowerment of youth in foster care: Supportive services. Child Welfare, 88, 133–161.
Kirk, C. M., Lewis, R. K., Nilsen, C., & Colvin, D. Q. (2013). Foster care and college: The educational aspirations and expectations of youth in the foster care system. Youth & Society, 45, 307–323. doi:10.1177/0044118X11417734
Kirk, R., & Day, A. (2011). Increasing college access for youth aging out of foster care: Evaluation of a summer camp program for foster youth transitioning from high school to college. Children and Youth Services Review, 33, 1173–1180. doi:10.1016/j.childyouth.2011.02.018
Lemon, K., Hines, A. M., & Merdinger, J. (2005). From foster care to young adulthood: The role of independent living programs in supporting successful transitions. Children and Youth Services Review, 27, 251–270. doi:10.1016/j.childyouth.2004.09.005
Lent, R. W., Brown, S. D., & Hackett, G. (1994). Toward a unifying social cognitive theory of career and academic interest, choice, and performance [Monograph]. Journal of Vocational Behavior, 45, 79–122. doi:10.1006/jvbe.1994.1027
Lenz, A. S. (2015). Using single-case research designs to demonstrate evidence for counseling practices. Journal of Counseling & Development, 93, 387–393. doi:10.1002/jcad.12036
Martin-Causey, T., & Hinkle, J. S. (1995). Multimodal therapy with an aggressive preadolescent: A demonstration of effectiveness and accountability. Journal of Counseling & Development, 73, 306–310. doi:10.1002/j.1556-6676.1995.tb01753.x
Martinez, R. R., Baker, S. B., & Young, T. (2017). Promoting career and college readiness, aspirations, and self-efficacy: Curriculum field test. The Career Development Quarterly, 65(2), 173–188. doi:10.1002/cdq.12090
Pecora, P. J., Kessler, R. C., O’Brien, K., White, C. R., Williams, J., Hiripi, E., . . . Herrick, M. A. (2006). Educational and employment outcomes of adults formerly placed in foster care: Results from the Northwest Foster Care Alumni Study. Children and Youth Services Review, 28, 1459–1481.
doi:10.1016/j.childyouth.2006.04.003
Pecora, P. J., Williams, J., Kessler, R. C., Hiripi, E., O’Brien, K., Emerson, J., . . . Torres, D. (2006). Assessing the educational achievements of adults who were formerly placed in family foster care. Child & Family Social Work, 11, 220–231. doi:10.1111/j.1365-2206.2006.00429.x
Peterson, G. W., Sampson, J. P., Jr., Lenz, J. G., & Reardon, R. C. (2002). A cognitive information processing approach to career problem solving and decision making. In D. Brown and Associates (Eds.), Career choice and development (pp. 312–369). San Francisco, CA: Jossey-Bass.
Ray, D. C. (2015). Single-case research design and analysis: Counseling applications. Journal of Counseling & Development, 93, 394–402. doi:10.1002/jcad.12037
Savickas, M. L. (2011). Career counseling. Washington, DC: American Psychological Association.
Super, D. E. (1990). A life-span, life space approach to career development. In D. Brown & L. Brooks (Eds.), Career choice and development: Applying contemporary theories to practice (2nd ed., pp. 197–261). San Francisco, CA: Jossey-Bass.
Swoboda, C. M., Kratochwill, T. R., & Levin, J. R. (2010). Conservative dual-criterion method for single-case research: A guide for visual analysis of AB, ABAB, and multiple-baseline designs. Wisconsin Center for Education Research Working Paper No.13, 495–512.
Unrau, Y. A., Font, S. A., & Rawls, G. (2012). Readiness for college engagement among students who have aged out of foster care. Children and Youth Services Review, 34, 76–83. doi:10.1016/j.childyouth.2011.09.002
Vannest, K. J., & Ninci, J. (2015). Evaluating intervention effects in single-case research designs. Journal of Counseling & Development, 93, 403–411. doi:10.1002/jcad.12038
Wolf, M. M. (1978). Social validity: The case for subjective measurement or how applied behavioral analysis is finding its heart. Journal of Applied Behavioral Analysis, 11, 203–214. doi:10.1901/jaba.1978.11-203
Regina Gavin Williams, NCC, is the Director of Student Engagement and Diversity Coordinator at North Carolina State University. Stanley B. Baker, NCC, is a professor at North Carolina State University. ClarLynda R. Williams-DeVane is an associate professor at North Carolina Central University. Correspondence can be addressed to Regina Gavin Williams, 2310 Stinson Dr., CB 7801, North Carolina State University, Raleigh, NC 27695-7801, rjgavin@ncsu.edu.
