Eric M. Brown, Kristy L. Carlisle, Melanie Burgess, Jacob Clark, Ariel Hutcheon
Despite an emphasis on self-care to avoid burnout and increase compassion satisfaction within the counseling profession, there is a dearth of research on the developmental experiences of counselors that may increase the likelihood of burnout. We examined the impact of mental health counselors’ (N = 140) experiences of adverse childhood experiences and positive childhood experiences on their present rates of compassion satisfaction, burnout, and secondary traumatic stress. We used a cross-sectional, non-experimental correlational design and reported descriptive statistics as well as results of multiple regression models. Results indicated significant relationships among counselors’ rates of adverse childhood experiences, positive childhood experiences, and compassion satisfaction and burnout. We include implications for the use of both the adverse and positive childhood experiences assessments in the training of counseling students and supervisees.
Keywords: counselors, burnout, childhood experiences, compassion satisfaction, secondary traumatic stress
Over the past 20 years, public health research on adverse childhood experiences (ACEs) and their deleterious effects on physical and mental health has proliferated and branched out to various disciplines (Campbell et al., 2016; Frampton et al., 2018). More recently, the importance of understanding the implications of ACEs for the mental health of clients has entered the counseling literature (Wheeler et al., 2021; Zyromski et al., 2020), yet the ways in which a counselor’s own experience of ACEs may affect their work have not been examined. The absence of such research is significant given the report that mental health workers have the highest rates of ACEs among those in the helping professions (Redford, 2016).
A thorough literature search of PsycINFO, ProQuest, and Google Scholar using terms including, but not limited to, adverse childhood experiences, positive childhood experiences (PCEs), compassion satisfaction (CS), burnout, secondary traumatic stress (STS), and mental health counselors (MHCs), found no peer-reviewed articles that examined the relationship between ACEs or PCEs and counselors’ rates of CS and burnout. Therefore, we chose to examine the effects of early developmental adversity, as well as early protective factors, on the professional quality of life of counselors, as measured by assessing the counselor’s levels of CS, burnout, and STS.
Adverse Childhood Experiences (ACEs)
In the mid-nineties, Felitti et al. (1998), with the support of the Centers for Disease Control, created the ACE Study Questionnaire to study early childhood trauma and deprivation experiences. The ACE Study Questionnaire consists of 10 questions related to whether a person before the age of 18 experienced emotional or physical abuse, substance addiction in the home, parental divorce or separation, a caretaker with mental illness, or emotional deprivation. Each question that is answered in the affirmative results in one “ACE,” with respondents’ scores ranging from 1 to 10. Studies have found that ACEs have a dose-response effect; therefore, every point increase can significantly raise the chance of experiencing negative mental and physical health effects into adulthood (Boullier & Blair, 2018; Campbell et al., 2016; Merrick et al., 2017). Additionally, individuals with four or more ACEs are significantly more likely to suffer from mental illness or substance addiction, be further traumatized as adults, and succumb to an early death (Anda et al., 2007; Metzler et al., 2017).
More recently, researchers have found that Black and Latinx individuals have significantly higher rates of ACEs compared to White individuals (R. D. Lee & Chen, 2017; Merrick et al., 2017; Strompolis et al., 2019). In a study involving 60,598 participants, R. D. Lee and Chen (2017) discovered not only that Black and Hispanic participants had higher rates of ACEs, but also that there was a correlation between ACEs and drinking alcohol heavily. In a sample of 214,517 participants across 23 states in the United States, Merrick et al. (2017) found that racially minoritized individuals, sexual minorities, the unemployed, those with less than a high school education, and those making less than $15,000 a year had significantly higher rates of ACEs than White individuals, heterosexuals, the employed, and those with higher education and income, respectively. Zyromski et al. (2020) noted that the preponderance of ACEs within marginalized communities, such as ethnic minority populations, make ACEs “a social justice issue” (p. 352).
There is scarce research related to the potential impact of ACEs on practitioners and graduate students in helping professions. Thomas (2016) evaluated the rates of ACEs with Master of Social Work (MSW) students, discovering that MSW students were 3.3 times more likely to have four or more ACEs compared to a general sample of university students. Similarly, counselors-in-training are not immune to the effects of childhood adversity; in fact, researchers noted that counselors-in-training may pursue a counseling degree because of personal trauma that drives their aspirations to help others (Conteh et al., 2017). Evans (1997) found that 93% of counselors-in-training reported at least one traumatic experience in their lives, while Conteh et al. (2017) discovered that 95% of counselors-in-training reported between one and eight traumas throughout their lifetime. Considering these results, researchers have suggested that practitioners with a history of trauma may be vulnerable to re-experiencing trauma with clients, which could negatively impact client care and increase the rate of counselor burnout (Conteh et al., 2017; Thomas, 2016). Because the rates of ACEs in practicing MHCs are unknown, it is difficult to determine how ACEs may play a role in impacting CS, burnout, and STS. Furthermore, we lack research on early developmental factors that may contribute to CS, burnout, and STS.
Positive Childhood Experiences (PCEs)
In recent years, childhood development researchers have explored protective factors that may reduce the harmful effects of ACEs. In 2018, Crouch et al. (2019) examined the relationship between two protective factors and their mitigating effects on individuals reporting at least four ACEs. In a sample of 7,079 respondents, the researchers discovered that individuals who reported growing up “with an adult who made them feel safe and protected were less likely to report frequent mental distress or poor health” (Crouch et al., 2019, p. 165). Bethell et al. (2019) found significant correlations between seven positive interpersonal experiences with family and friends and decreased negative effects of ACEs. They also discovered that these factors have a dose-response effect in relation to ACEs so that with each additional PCEs, the harmful effects of ACEs are lessened. The discovery of PCEs has become important in understanding developmentally protective factors that guard from the damaging effects of childhood adversity. Specifically, higher rates of PCEs decrease the chances of mental health disorders of adults, even in those with higher numbers of ACEs (Bethell et al., 2019). An examination of the rates of PCEs in MHCs may provide insight into the well-being of counselors.
Counselor Well-Being
As defined by the American Counseling Association (ACA; 2014), professional counselors work to empower diverse clients to achieve their personal goals. Specifically, MHCs provide client-driven services in agencies, hospitals, and private practices (American Mental Health Counselors Association [AMHCA], 2020). Counselors are trained to cultivate and monitor their own sense of well-being while providing their expertise and leadership to clients and students who have experienced difficulties related to trauma, injustice, abuse, loss, violence, and distress (Council for Accreditation of Counseling and Related Educational Programs [CACREP], 2015; S. M. Lee et al., 2010). Self-care, or the act of cultivating a subjectively defined state of health, is now ubiquitous in counselor education programs and promoted among practitioners (ACA, 2014; CACREP, 2015); however, scholars note that many counselors do not routinely prioritize their own sense of well-being and monitor CS, burnout, and STS (Coaston, 2017). While working closely with clients, practitioners may benefit from reflecting on how their own experiences of personal adversity may influence their work and possibly create a predisposition toward burnout.
Burnout of Counselors
Burnout is defined as the emotional and physical response to chronic stressors in the workplace that lead to substantial negative consequences (Maslach et al., 2001). Scholars have evaluated the external facets of professional counselors’ work that lead to increased burnout, such as time spent on non-counseling duties, lack of on-the-job support, and negative working environments (Thompson et al., 2014); however, internal factors that lead to burnout, such as counselors’ experiences of adversity, remain unstudied. The ubiquitous nature of trauma and its lifelong impact on clients has gained more attention over the past 20 years (Bemak & Chung, 2017; Debellis, 2001; Webber et al., 2017), yet researchers are only beginning to explore the impact of trauma on the lives and professional experiences of counselors (Conteh et al., 2017; McKim & Smith-Adcock, 2014).
Recently, scholars have sought to understand contributing factors that diminish CS and increase burnout (S. M. Lee et al., 2010). In a study of 86 counselors-in-training, Can and Watson (2019) found that a trainee’s degree of resilience and wellness predicted burnout, whereas empathy and supervisory working alliance did not. They did not assess for internal or experiential factors that may have contributed to burnout.
Cook et al. (2021) conducted a qualitative inquiry with 246 novice counselors to explore symptoms of burnout that may not be captured in commonly used assessments. The researchers found several predominant themes, including negative emotional experiences such as anxiety, depression and crying spells; fatigue and tiredness; and unfulfillment in work. Participants also reported physical illness and weight gain or loss, self-perceived ineffectiveness as a counselor, and cognitive impairment. Close to 10% of participants stated that an unhealthy environment contributed to their experience of burnout. Cook et al. did not inquire about any personal history that may have also contributed to symptoms of burnout.
Counselors and STS
Distinct from but related to burnout, STS has been discussed in the literature relating to the well-being of helping professions across numerous disciplines (Branson, 2019; Butler et al., 2017; Molnar et al., 2017). Secondary traumatic stress, also called vicarious trauma, is distinguished from burnout by its symptoms overlapping with post-traumatic stress disorder (PTSD), such as intrusive thoughts, hypervigilance, and avoidance of distressing memories (Ivicic & Motta, 2017; Molnar et al., 2017). In a study of 220 counselors, Lanier and Carney (2019) discovered that 49.5% of counselors experienced symptoms of vicarious trauma, with 85.5% reporting “I thought about my work with clients when I didn’t intend to” and 80.5% confirming that “I felt emotionally numb” (p. 339). Lakioti et al. (2020) found in a study of 163 Greek mental health practitioners that there was a significant positive correlation between burnout and STS (r = .48) and that practitioners who scored high in empathy also scored high in STS (r = .34). In their meta-analysis of 38 studies examining risk factors for STS in therapeutic work, Hensel et al. (2015) found small yet significant effect sizes for “trauma caseload volume (r = .16), caseload frequency (r = .12), caseload ratio (r = .19), and having a personal trauma history (r = .19)” in relation to STS (p. 83).
Research regarding counselors’ own personal trauma is still emerging and a consensus is not yet formed. In a recent study of 90 psychotherapy trainees, Klasen et al. (2019) indicated that secure attachments play a modifying role in limiting the severity of trauma’s expression. McKim and Smith-Adcock (2014) evaluated characteristics of trauma counselors to understand how frequent exposure to indirect trauma might influence burnout and CS, as assessed by the Professional Quality of Life Scale (ProQOL; Stamm, 2010). Their results indicated that higher levels of exposure to client trauma, in combination with less perceived control over the workplace, led to increased burnout (McKim & Smith-Adcock, 2014). Consistent with the ACA Code of Ethics (2014), counselors are expected to self-monitor for impairment issues that could impact clients such as burnout, STS, and the decrease of CS.
Compassion Satisfaction
CS has been studied nominally and may serve as a protective factor against burnout (Coaston, 2017). Compassion satisfaction is defined as a psychological benefit derived from working effectively with clients to produce meaningful and positive change in their lives (McKim & Smith-Adcock, 2014; Stamm, 2010). McKim and Smith-Adcock (2014) discovered that trauma counselors who experienced higher levels of personal trauma also exhibited higher levels of CS or fulfillment derived from their role in the helping alliance. Although these emergent results contradict older literature that demonstrates how counselors with more personal trauma have higher levels of burnout (Baird & Kracen, 2006; Nelson-Gardell & Harris, 2003), presently, the relationship between CS, burnout, and STS in counselors in relation to ACEs is still unclear.
Purpose of Study
The purpose of this study was to examine the effects of early developmental adversity as well as early protective factors on the CS, burnout, and STS of MHCs. Despite the ongoing concern for factors that contribute to the CS, burnout, and STS of counselors, there is a dearth of research on personal experiences that may predispose counselors to burnout (Conteh et al., 2017; McKim & Smith-Adcock, 2014). Considering the detrimental effects of burnout on counselors’ health and well-being, as well as the decrease in empathy that often accompanies burnout, it is imperative that we understand the various causes of burnout (Can & Watson, 2019; Cook et al., 2021; Maslach et al., 2001). This knowledge will assist clinical MHCs, supervisors, and counselor educators in knowing which professional counselors or counselors-in-training may be more susceptible to burnout, STS, and decreased CS.
Research on ACEs within the counseling profession, as proposed by the original Felitti et al. (1998) study, is scant. Zyromski et al. (2020) discovered in their content analysis of ACA and American School Counselor Association journals that only three articles contained any focus on ACEs as defined in the original study. They suggested that by incorporating such a well-defined and researched concept as ACEs, counselors will be better equipped to address the deleterious effects of early adverse experiences. In order to address the gap within the literature, we chose to focus on the rates of ACEs and PCEs of counselors and how they potentially impact CS, burnout, and STS. After conducting an exhaustive search of the literature, we found no other study that examined the potential relationship between counselors’ developmental history using the ACEs and PCEs assessments and their levels of burnout, CS, and STS.
Method
This study entailed a cross-sectional, non-experimental correlational design and reported descriptive statistics, as well as results of multiple regression models. Relationships among MHCs’ ACEs, PCEs, CS, burnout, and STS were examined. Research questions (RQs) guiding the study were: RQ1 (descriptive): What are the mean scores of MHCs for ACEs, PCEs, CS, burnout, and STS constructs? and RQ2 (regression): To what extent do MHCs’ ACEs, PCEs, gender, race, socioeconomic status, and educational level predict CS, burnout, and STS?
Power Analysis
The target number of participants for the study was at least N = 138, based on a power analysis. Researchers used G*Power 3.1.9.6 (Faul et al., 2009) to calculate an a priori power analysis with a .05 alpha level (Cohen, 1988, 1992), a medium effect size for multiple R2 of .09 (Cohen, 1988), and a power of .80 (Cohen, 1992).
Participants
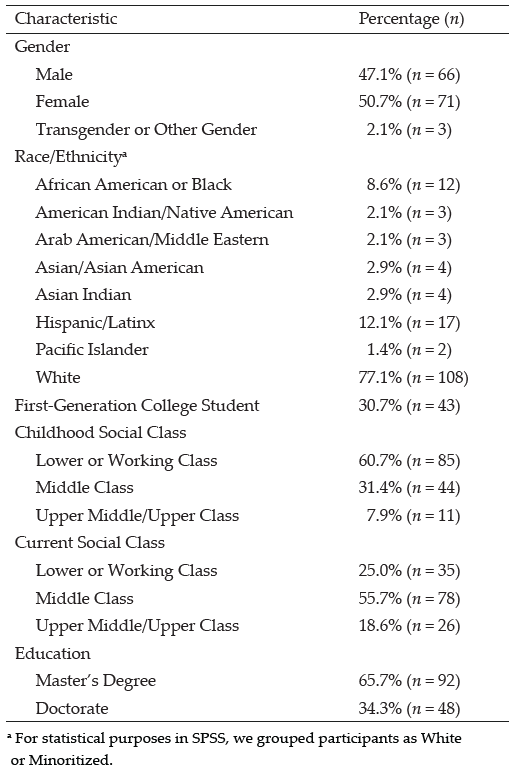
The eligibility criteria for this study were to be a clinical MHC, 18 years or older, who worked 30 hours or more per week in the field of mental health counseling. After soliciting participants nationally through emails, we collected data from 140 participants who met the criteria. MHCs ranged in age from 22 to 72 years old with an average age of 38 (SD = 11.01). Table 1 shows the diverse sample. Slightly more than half (n = 71) identified as female and a little less than half (n = 66) as male. More than three-quarters (n = 108) identified as White. The majority of participants (n = 85) reported their childhood SES as lower or working class, while more than half (n = 78) reported their current social class as middle class. Our sample with predominantly female and predominantly White participants is similar both to known counselor demographics (Norton & Tan, 2019) and to the Felitti et al. (1998) ACEs study.
Instrumentation
Three instruments with good validity and reliability were used to measure ACEs, PCEs, CS, burnout, and STS. We created a demographic questionnaire to collect information on participants’ identities (e.g., race, gender) and childhood backgrounds (e.g., ACEs, PCEs, SES).
Adverse Childhood Experiences (ACE) Study Questionnaire
The ACE Study Questionnaire (Felitti et al., 1998) is a 10-item survey of the most common examples of childhood abuse and neglect. It was developed out of research that connected childhood trauma to subsequent mental and physical ailments. Subsequent research found good test-retest reliability of the measure in an adult population (Dube et al., 2004; Frampton et al., 2018) and a Cronbach’s alpha score of .78 (Ford et al., 2014). The survey produces self-report scores between 0 and 10. The higher the score, the greater the risk for mental and physical health issues as well as decreased quality of life. Consistent research (e.g., Anda et al., 2006; Dube et al., 2004; Hughes et al., 2017) shows that a score of 4 or more indicates serious risk.
Table 1
Participant Demographics
Positive Childhood Experiences (PCE) Questionnaire
The PCE Questionnaire (Bethell et al., 2019) is a 7-item survey of PCEs (i.e., connection with family, friends, and community) that are statistically predictive of good mental health in adulthood. After accounting for ACEs, higher PCE scores reduce mental health and interpersonal problems later in life. Specifically, scores in the 6 to 7 range are most protective from harmful effects of ACEs, and scores in the 3 to 5 range are moderately protective. A Cronbach’s alpha score of .77 reported in the original 2019 study indicates good reliability.
Professional Quality of Life Scale (ProQOL)
The ProQOL (Stamm, 2010) is a 30-item survey with good construct validity measuring both positive and negative responses to the work of helping professionals. It measures three constructs: CS, which has a Cronbach’s alpha score of .88; burnout, which has a Cronbach’s alpha score of .75; and STS, which has a Cronbach’s alpha score of .81. For CS, or positive feelings about one’s ability to help, a score below 23 indicates problems at work. For burnout, or feelings of exhaustion, frustration, anger, or depression, scores below 23 indicate feeling good about work, while scores above 41 indicate feeling ineffective. For STS, or feelings of fear related to trauma in the workplace, scores above 43 indicate something frightening at work.
Procedure
After IRB approval, we used purposeful sampling methods to recruit participants. We emailed over 6,000 MHCs from a data set purchased from a national data bank. Furthermore, we posted invitations to participate on Facebook groups for MHCs. Invitations included informed consent, as well as a link to a Qualtrics survey containing all instruments and demographic questions. Researchers cleaned all collected data leading to 140 usable cases, computed instruments and transformed variables into usable form, and checked for assumptions for multiple regression. For each instrument, we assessed for reliability with Cronbach’s alpha tests. The ACEs instrument produced a Cronbach’s alpha of .89, the PCEs instrument produced .81, and the ProQOL produced .79, all within the good to excellent range. We used SPSS 28 for all analyses.
Data Analysis and Results
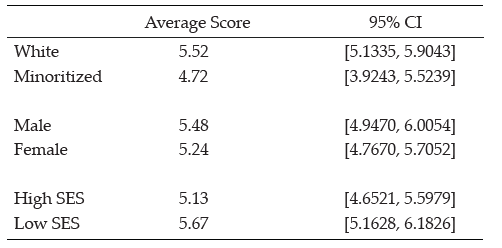
To answer our first research question, we evaluated the mean scores for ACEs, PCEs, CS, burnout, and STS. Respondents in the study had a mean ACE score of 3.42, 95% CI [2.8577, 3.9852], beneath the threshold of 4 and just below the range for significant risk. Their mean PCE score of 5.34, 95% CI [5.0006, 5.6957], was at the upper end of moderately protective. White MHCs had a lower average ACE score and higher average PCE score than minoritized MHCs. Male MHCs had higher average ACE and PCE scores than females, and MHCs with lower childhood SES had lower average ACE scores and higher average PCE scores than those with higher SES (see Tables 2 and 3).
Table 2
Average Adverse Childhood Experience Scores by Demographics
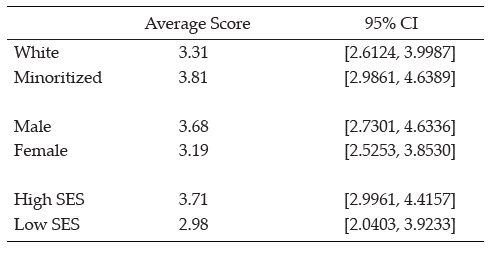
Table 3
Average Positive Childhood Experience Scores by Demographics
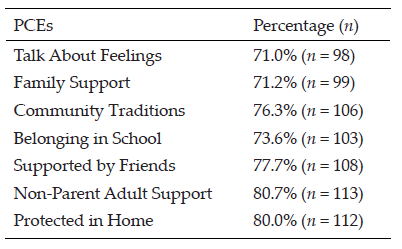
Type of scores are shown in percentages for each type of ACE and PCE to show what percentage of MHCs reported an adverse or protective childhood experience (see Tables 4 and 5).
Table 4
Type of Adverse Childhood Experience Score
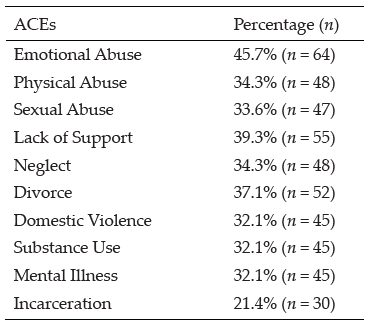
Table 5
Type of Positive Childhood Experience Score
Next, we analyzed MHCs’ scores related to CS, burnout, and STS. Participants’ mean CS score of 31.81, 95% CI [30.6005, 33.0138], was well above the threshold of 23, which indicates a positive level of CS. Their overall mean burnout score of 24.59, 95% CI [23.5793, 25.5921], was well below the threshold of 41, which indicates that the average MHC was not suffering from burnout. Their overall mean STS score of 26.37, 95% CI [25.0346, 27.7083], was also well below the threshold of 43, which indicates the average MHC was not experiencing STS.
For RQ 2, we also tested whether and to what extent MHCs’ ACEs, PCEs, and demographic variables predict CS, burnout, and STS. We ran three linear regression models to assess significant predictors of CS, burnout, and STS. In the first model, a regression of CS on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 40.5% of the variance in CS, F (5, 134) = 17.558, p < .001. Specifically, significant predictors of CS were ACEs (β = −.550), gender (β = −.218), race/ethnicity (β = −.160), and childhood SES (β = −.171). PCEs were nonsignificant in relation to CS. Items negatively related to CS were ACEs (i.e., higher ACE scores predicted lower CS), gender (i.e., being female predicted higher CS), race/ethnicity (i.e., being minoritized predicted higher CS), and childhood SES (i.e., lower levels of SES predicted higher CS; see Table 6).
In the second model, a regression of burnout on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 18.9% of the variance in burnout, F (5, 134) = 6.032, p < .001. Specifically, both ACEs and PCEs were significant predictors of burnout (β = .309 and β= −.197, respectively). Gender, race/ethnicity, and SES were nonsignificant predictors of burnout. ACEs were positively related to burnout (i.e., higher ACE scores indicated higher burnout), and PCEs were negatively related to burnout (i.e., higher PCEs indicated lower burnout; see Table 7).
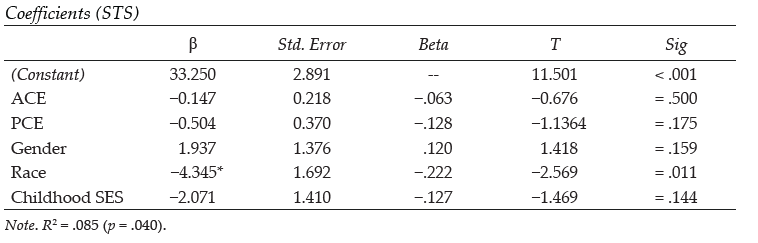
In the third model, a regression of STS on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 8.5% of variance in STS, F (5, 134) = 2.402, p < .001. Only race/ethnicity was a significant predictor of STS (β= −.222; i.e., being White indicated lower STS). ACEs, PCEs, gender, and SES produced nonsignificant results related to STS (see Table 8).
Table 6
Regression Results Using Compassion Satisfaction as the Criterion
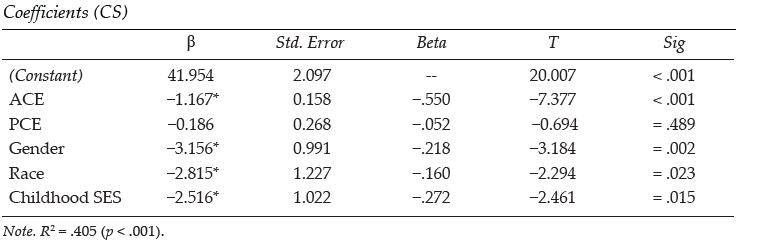
Table 7
Regression Results Using Burnout as the Criterion
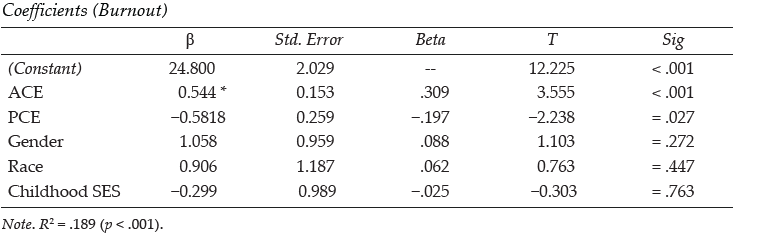
Table 8
Regression Results Using Secondary Traumatic Stress as the Criterion
Discussion
After conducting an exhaustive literature review, we found no other study that examined the relationship between a counselor’s personal history of childhood adversity and protective factors (i.e., ACEs and PCEs) and their professional experience with burnout, STS, and CS. As the counseling profession is placing a greater emphasis on counselors becoming trauma-informed (e.g., Bemak & Chung, 2017; Debellis, 2001; Webber et al., 2017), recent research has examined counselor wellness, burnout, PTSD symptoms, and possible contributing factors (Can & Watson, 2019; Cook et al., 2021; Lanier & Carney, 2019). In line with other studies, we found that some individuals drawn to the profession of counseling are more likely to have had adversity and hardship events in their personal histories (Conteh et al., 2017; McKim & Smith-Adcock, 2014). What is unique in this study is the examination of how both adverse and positive childhood experiences may impact the CS, burnout, and STS of MHCs.
Similar to Thomas (2016), who found that social work students had higher rates of ACEs than the general population, the results of this study indicated that counselor participants had higher rates of ACEs for all 10 experiences than the original Felitti et al. (1998) ACEs study. This was also aligned with Conteh and colleagues (2017), who found that counselors-in-training may have higher rates of trauma than the average population. The results also indicated that almost 43% (n = 60) of MHCs scored four or more ACEs, which placed them at high risk for mental and physical health problems (Boullier & Blair, 2018; Campbell et al., 2016; Merrick et al., 2017). As may be surmised from other studies on the deleterious effects of ACEs on emotional well-being, having higher numbers of ACEs was a significant predictor of burnout. Lower ACEs scores also significantly predicted CS with a high effect size (.55). Similarly, higher PCEs were linked to lower burnout. However, PCEs were not found to significantly predict CS.
We examined the average rates of and relationships between ACEs, PCEs, CS, burnout, and STS in a sample of MHCs. McKim and Smith-Adcock (2014) examined the burnout rates of trauma counselors, finding that counselors with more personal trauma had an increase in CS, perhaps due to personal growth. In contrast, this study found that counselors with more ACEs were more likely to experience less CS. This difference may be a result of this study utilizing the ACE Study Questionnaire (Felitti et al., 1998) whereas McKim and Smith-Adcock (2014) used Stamm’s (2008) Stressful Life Experiences – Short Form to assess for experiences that may have happened in adulthood or to someone outside of the family. Developmentally, painful childhood experiences may be harder to process, which may in turn produce further-reaching negative outcomes. McKim and Smith-Adcock also found that having a sense of control in the workplace and the number of years of experience as a counselor also positively correlated with CS. The results from our analysis indicated that greater attention needs to be given to the traumatic experiences of counselors and how these events may impact professional resilience.
This study may also be the first to examine the demographic factors of counselors, including gender, racial identity, and childhood SES, as potential predictive factors of burnout, STS, and CS. All three demographic variables were found to be predictive of CS, but none were predictive of burnout. The results from our analysis indicated that greater attention needs to be given to the traumatic experiences of counselors and how these events may impact CS, burnout, and STS.
It should be noted that ethnically minoritized counselors had higher rates of CS than their White peers. Given that higher ACEs scores had a negative relationship with CS with a high effect size, and that minoritized counselors had higher average rates of ACEs and lower average rates of PCEs when compared to White counselors, we expected minoritized counselors to experience lower CS. However, the current study found that being a minoritized counselor actually predicted higher CS and lower burnout. It may encourage all counselors to know that greater CS among minoritized counselors indicates that ACEs and PCEs are not determinative of whether a person experiences burnout or satisfaction.
Our findings that female counselors were more likely to have higher CS than their male peers, and that counselors from low-income or working-class SES had higher CS than those from middle and upper classes, are also noteworthy. It is possible that the more collectivist tendencies of minoritized individuals in general, and of female counselors regardless of race, may help foster greater professional resilience or quality of life (Graham et al., 2020; Jordan, 2017). Counselors from lower- or working-class childhood SES may also maintain the collectivist orientation of their upbringing. This proposition is supported by previous research, which indicates that social support is a significant factor that promotes CS in therapists (Ducharme et al., 2008). This may also relate to Crouch et al.’s (2019) finding that the most significant PCE that mitigates the effects of ACEs is having a safe relationship with an adult. These results are further supported by research indicating that secure attachments in adulthood moderate the effect of childhood adversity (Klasen et al., 2019). Despite a limited sample size, Conteh et al. (2017) found that 95% of their sample of 86 counselors-in-training reported having experienced at least one trauma. Although male participants in Conteh’s study were significantly more likely to report more traumas than women—4.93 to 3.46 respectively—women reported more post-traumatic growth than men. Similar to our findings, this may indicate why female counselors were more likely to experience greater CS than male counselors.
Although close to half of our participants (42.9%) met the critical threshold of four ACEs, it is encouraging that the average participant indicated that they were not experiencing burnout. This may be the result of more than half of our participants having five or more PCEs, with PCEs predicting lower burnout. It should also be noted that in this study, ACEs were not significantly correlated with STS, which may be counterintuitive as one may assume that childhood adversity may leave one more susceptible to STS. The strongest findings in the current study, as demonstrated by high effect sizes, are that lower ACE scores predict higher CS and lower burnout. However, the potentially mitigating influence of PCEs only predicted burnout, not CS, with a lower effect size.
Limitations
Threats to internal and external validity are unavoidable in descriptive studies. As such, one limitation of this study is that it focused on descriptive and predictive relationships and therefore does not describe causation. Furthermore, this study used self-report data which may threaten internal validity. Finally, selection bias may be a risk to generalizability. However, the sample in this study is demographically similar to other studies examining the counseling population, so this risk may be minimal.
Implications
Both professional organizations (e.g., ACA, AMHCA) and CACREP can promote counselor wellness by putting policies in place recognizing that individuals going into the counseling profession are likely to have personal histories shaped by adverse experiences. These policies may include a more systemic understanding of wellness strategies for counselors. Self-care is often conceptualized as a personal endeavor achieved outside of work hours, yet policies may be put in place to promote organizational wellness by providing space and emotional support for counselor wellness. For example, far too often grants require caseloads that are too heavy to foster and maintain the well-being of counselors.
The results of this study may also have implications for counselor education. Given that 42% of our participants had four or more ACEs, it may be likely that close to half of students within counseling programs have also suffered from a significant amount of childhood adversity. This may have implications for how we educate counselors to work with trauma. Trauma-informed training generally focuses on the effects of trauma on the life of clients and supports evidence-based practices that aid in recovery, resilience, and improved quality of life. Training that is trauma-attuned may focus more on the counselor’s awareness of how their own history of adversity may shape their professional stamina. This may also lead to more research on trauma-attuned supervision.
Considering the substantial percentage of MHCs who may have four or more ACEs, it is possible that many clinical supervisors have also been greatly affected by their personal histories. Trauma-attuned supervisors will continually reflect on how their past adversity may be influencing the supervisory relationship while also monitoring both their own as well as their supervisee’s levels of burnout and emotional reactivity toward clients.
As Zyromski et al. (2020) posited, the use of ACEs as a construct can provide clarity and focus to the harmful experiences that may impede the healthy development of a client. Likewise, knowledge about ACEs and PCEs can help supervisors and counselor educators train counselors who are at greater risk for burnout. It is important that the privacy of the counselor’s childhood experiences be protected, but trainees can be given the ACE and PCE assessments and told of the risk factors that high ACE and low PCE scores have with regard to burnout and CS. Furthermore, clinical and faculty supervisors can provide assessments for CS and burnout at key points during a trainee’s internship or first few years of postgraduate experience. Counselor educators and supervisors may then help trainees develop a self-care plan that will help to foster CS.
Directions for Future Research
Future studies may further examine the difference between demographic groups based on gender, race, and education in relation to potential protective factors that female and minoritized MHCs have that may decrease the likelihood they will experience burnout. Further research may also examine which ACEs, if any, may have higher correlations with burnout and which PCEs are more likely to serve as protective factors. Furthermore, our results indicate a need to study the CS and burnout of minoritized counselors, female counselors, and those coming from lower childhood SES. Examination of potential cultural and protective factors of these groups may contribute significantly to the literature on burnout prevention.
Given the percentage of counselors who have ACE scores that fall within the range of concern, future research may examine potential differences of counselors who are trauma-attuned and not simply trauma-informed. As stated above, ACEs were not significantly correlated with STS. It may be helpful for future researchers to use different measurements of secondary stress to further assess whether there is any correlation between ACEs and STS.
Conclusion
The purpose of this study was to examine personal factors in the developmental history of clinical MHCs that may influence their likelihood of experiencing professional burnout. This is the first known study we can identify using the ACE Study Questionnaire as a measure to inquire about a potential relationship between the counselors’ developmental adversity and their rates of burnout, CS, and STS. Results indicated that higher ACE scores correlate positively with burnout, and yet PCEs may serve as protective factors. Finally, we found that women and minoritized counselors were more likely to experience compassion satisfaction than males and White counselors. This was true for minoritized counselors despite their having slightly higher rates of ACEs and lower rates of PCEs. We recommend that counselors become aware of how their own experiences of ACEs and PCEs may be impacting their current practice.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
American Mental Health Counselors Association. (2020). AMHCA code of ethics. https://bit.ly/AMHCAcodeofethics
Anda, R. F., Brown, D. W., Felitti, V. J., Bremner, J. D., Dube, S. R., & Giles, W. H. (2007). Adverse childhood experiences and prescribed psychotropic medications in adults. American Journal of Preventive Medicine, 32(5), 389–394. https://doi.org/10.1016/j.amepre.2007.01.005
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., Dube, S. R., & Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256, 174–186. https://doi.org/10.1007/s00406-005-0624-4
Baird, K., & Kracen, A. C. (2006). Vicarious traumatization and secondary traumatic stress: A research synthesis. Counselling Psychology Quarterly, 19(2), 181–188. https://doi.org/10.1080/09515070600811899
Bemak, F., & Chung, R. C.-Y. (2017). Refugee trauma: Culturally responsive counseling interventions. Journal of Counseling & Development, 95(3), 299–308. https://doi.org/10.1002/jcad.12144
Bethell, C., Jones, J., Gombojav, N., Linkenbach, J., & Sege, R. (2019). Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatrics, 173(11), e193007. https://doi.org/10.1001/jamapediatrics.2019.3007
Boullier, M., & Blair, M. (2018). Adverse childhood experiences. Pediatrics and Child Health, 28(3), 132–137. https://doi.org/10.1016/j.paed.2017.12.008
Branson, D. C. (2019). Vicarious trauma, themes in research, and terminology: A review of literature. Traumatology, 25(1), 2–10. https://doi.org/10.1037/trm0000161
Butler, L. D., Carello, J., & Maguin, E. (2017). Trauma, stress, and self-care in clinical training: Predictors of burnout, decline in health status, secondary traumatic stress symptoms, and compassion satisfaction. Psychological Trauma: Theory, Research, Practice, and Policy, 9(4), 416–424. https://doi.org/10.1037/tra0000187
Campbell, J. A., Walker, R. J., & Egede, L. E. (2016). Associations between adverse childhood experiences, high- risk behaviors, and morbidity in adulthood. American Journal of Preventive Medicine, 50(3), 344–352. https://doi.org/10.1016/j.amepre.2015.07.022
Can, N., & Watson, J. C. (2019). Individual and relational predictors of compassion fatigue among counselors-in-training. The Professional Counselor, 9(4), 285–297. https://doi.org/10.15241/nc.9.4.285
Coaston, S. C. (2017). Self-care through self-compassion: A balm for burnout. The Professional Counselor, 7(3), 285–297. https://doi.org/10.15241/scc.7.3.285
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. (2nd ed.) Routledge.
Cohen, J. (1992). Statistical power analysis. Current Directions in Psychological Science, 1(3), 98–101. https://doi.org/10.1111/1467-8721.ep10768783
Conteh, J. A., Huber, M. J., & Bashir, H. A. (2017). Examining the relationship between traumatic experiences and posttraumatic growth among counselors-in-training. The Practitioner Scholar: Journal of Counseling and Professional Psychology, 6, 32–36.
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in novice professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Crouch, E., Radcliff, E., Strompolis, M., & Srivastav, A. (2019). Safe, stable, and nurtured: Protective factors against poor physical and mental health outcomes following exposure to adverse childhood experiences (ACEs). Journal of Child & Adolescent Trauma, 12, 165–173. https://doi.org/10.1007/s40653-018-0217-9
Debellis, M. D. (2001). Developmental traumatology: the psychobiological development of maltreated children and its implications for research, treatment, and policy. Development and Psychopathology, 13(3), 539–564. https://doi.org/10.1017/s0954579401003078
Dube, S. R., Williamson, D. F., Thompson, T., Felitti, V. J., & Anda, R. F. (2004). Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse & Neglect, 28(7), 729–737. https://doi.org/10.1016/j.chiabu.2003.08.009
Ducharme, L. J., Knudsen, H. K., & Roman, P. M. (2008). Emotional exhaustion and turnover intention in human service occupations: The protective role of coworker support. Sociological Spectrum, 28(1), 81–104. https://doi.org/10.1080/02732170701675268
Evans, J. H. (1997). Trauma and post-traumatic growth among graduate level counselor education students: What is their relative incidence and what relationships do they share? (Order No. 9732654) [Doctoral dissertation, Ohio University]. ProQuest Dissertations & Theses Global.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/brm.41.4.1149
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Ford, D. C., Merrick, M. T., Parks, S. E., Breiding, M. J., Gilbert, L. K., Edwards, V. J., Dhingra, S. S., Barile, J. P., & Thompson, W. W. (2014). Examination of the factorial structure of adverse childhood experiences and recommendations for three subscale scores. Psychology of Violence, 4(4), 432–444. https://doi.org/10.1037/a0037723
Frampton, N. M. A., Poole, J. C., Dobson, K. S., & Pusch, D. (2018). The effects of adult depression on the recollection of adverse childhood experiences. Child Abuse & Neglect, 86, 45–54. https://doi.org/10.1016/j.chiabu.2018.09.006
Graham, C., Chun, Y., Grinstein-Weiss, M., & Roll, S. (2020, June 24). Well-being and mental health amid COVID-19: Differences in resilience across minorities and whites. Brookings. https://www.brookings.edu/research/well-being-and-mental-health-amid-covid-19-differences-in-resilience-across-minorities-and-whites
Hensel, J. M., Ruiz, C., Finney, C., & Dewa, C. S. (2015). Meta-analysis of risk factors for secondary traumatic stress in therapeutic work with trauma victims. Journal of Traumatic Stress, 28(2), 83–91. https://doi.org/10.1002/jts.21998
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., Jones, L., & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), 356–366. https://doi.org/10.1016/S2468-2667(17)30118-4
Ivicic, R., & Motta, R. (2017). Variables associated with secondary traumatic stress among mental health professionals. Traumatology, 23(2), 196–204. https://doi.org/10.1037/trm0000065
Jordan, J. V. (2017). Relational–cultural theory: The power of connection to transform our lives. The Journal of Humanistic Counseling, 56(3), 228–243. https://doi.org/10.1002/johc.12055
Klasen, J., Nolte, T., Möller, H., & Taubner, S. (2019). Aversive kindheitserfahrungen, bindungsrepräsentationen und mentalisierungsfähigkeit von psychotherapeuten in ausbildung [Adverse childhood experiences, attachment representations and mentalizing capacity of psychotherapists in training]. Zeitschrift für Psychosomatische Medizin und Psychotherapie, 65(4), 353–371. https://doi.org/10.13109/zptm.2019.65.4.353
Lakioti, A., Stalikas, A., & Pezirkianidis, C. (2020). The role of personal, professional, and psychological factors in therapists’ resilience. Professional Psychology: Research and Practice, 51(6), 560–570. https://doi.org/10.1037/pro0000306
Lanier, B. A., & Carney, J. S. (2019). Practicing counselors, vicarious trauma, and subthreshold PTSD: Implications for counselor educators. The Professional Counselor, 9(4), 334–346. https://doi.org/10.15241/bal.9.4.334
Lee, R. D., & Chen, J. (2017). Adverse childhood experiences, mental health, and excessive alcohol use: Examination of race/ethnicity and sex differences. Child Abuse & Neglect, 69, 40–48. https://doi.org/10.1016/j.chiabu.2017.04.004
Lee, S. M., Cho, S. H., Kissinger, D., & Ogle, N. T. (2010). A typology of burnout in professional counselors. Journal of Counseling & Development, 88(2), 131–138. https://doi.org/10.1002/j.1556-6678.2010.tb00001.x
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. https://doi.org/10.1146/annurev.psych.52.1.397
McKim, L. L., & Smith-Adcock, S. (2014). Trauma counsellors’ quality of life. International Journal for the Advancement of Counselling, 36, 58–69. https://doi.org/10.1007/s10447-013-9190-z
Merrick, M. T., Ports, K. A., Ford, D. C., Afifi, T. O., Gershoff, E. T., & Grogan-Kaylor, A. (2017). Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse & Neglect, 69, 10–19. https://doi.org/10.1016/j.chiabu.2017.03.016
Metzler, M., Merrick, M. T., Klevens, J., Ports, K. A., & Ford, D. C. (2017). Adverse childhood experiences and life opportunities: Shifting the narrative. Children and Youth Services Review, 72, 141–149.
Molnar, B. E., Sprang, G., Killian, K. D., Gottfried, R., Emery, V., & Bride, B. E. (2017). Advancing science and practice for vicarious traumatization/secondary traumatic stress: A research agenda. Traumatology, 23(2), 129–142. https://doi.org/10.1037/trm0000122
Nelson-Gardell, D., & Harris, D. (2003). Childhood abuse history, secondary traumatic stress, and child welfare workers. Child Welfare, 82(1), 5–26.
Norton, A. L., & Tan, T. X. (2019). The relationship between licensed mental health counselors’ political ideology and counseling theory preference. American Journal of Orthopsychiatry, 89(1), 86–94. https://doi.org/10.1037/ort0000339
Redford, J. (Director). (2016). Resilience: The biology of stress and the science of hope [Film]. KPJR Films. https://kpjrfilms.co/resilience/
Stamm, B. H. (2008). Design theory and psychometrics of the stressful life experiences screening (SLES). https://bit.ly/StammSLES
Stamm, B. H. (2010). The concise manual for the professional quality of life scale (ProQOL). https://proqol.org/proqol-manual
Strompolis, M., Tucker, W., Crouch, E., & Radcliff, E. (2019). The intersectionality of adverse childhood experiences, race/ethnicity, and income: Implications for policy. Journal of Prevention & Intervention in the Community, 47(4), 310–324. https://doi.org/10.1080/10852352.2019.1617387
Thomas, J. T. (2016). Adverse childhood experiences among MSW students. Journal of Teaching in Social Work, 36(3), 235–255. https://doi.org/10.1080/08841233.2016.1182609
Thompson, I., Amatea, E., & Thompson, E. (2014). Personal and contextual predictors of mental health counselors’ compassion fatigue and burnout. Journal of Mental Health Counseling, 36(1), 58–77. https://doi.org/10.17744/mehc.36.1.p61m73373m4617r3
Webber, J. M., Kitzinger, R., Runte, J. K., Smith, C. M., & Mascari, J. B. (2017). Traumatology trends: A content analysis of three counseling journals from 1994 to 2014. Journal of Counseling & Development, 95(3), 249–259. https://doi.org/10.1002/jcad.12139
Wheeler, N. J., Regal, R. A., Griffith, S.-A. M., & Barden, S. M. (2021). Dyadic influence of adverse childhood experiences: Counseling implications for mental and relational health. Journal of Counseling & Development, 99(1), 24–36. https://doi.org/10.1002/jcad.12351
Zyromski, B., Baker, E., Betters-Bubon, J., Dollarhide, C. T., & Antonides, J. (2020). Adverse childhood experiences: A 20-year content analysis of American Counseling Association and American School Counselor Association journals. Journal of Counseling & Development, 98(4), 351–362. https://doi.org/10.1002/jcad.12338
Eric M. Brown, PhD, LPC, is an assistant professor at DePaul University. Kristy L. Carlisle, PhD, is an assistant professor at Old Dominion University. Melanie Burgess, PhD, is an assistant professor at the University of Memphis. Jacob Clark, BS, is a graduate student at Old Dominion University. Ariel Hutcheon, MA, is a doctoral student at Old Dominion University. Correspondence may be addressed to Eric M. Brown, 2247 N. Halsted St., Chicago, IL 60614, ebrow107@depaul.edu.
