May 17, 2021 | Article



Melissa Sitton, Tina Du Rocher Schudlich, Christina Byrne, Chase M. Ochrach, and Seneca E. A. Erwin received the 2020 Outstanding Scholar Award for Quantitative or Qualitative Research for their article, “Family Functioning and Self-Injury in Treatment-Seeking Adolescents: Implications for Counselors.”
Melissa Sitton, MS, is currently a doctoral student studying clinical psychology at Southern Methodist University in Dallas, Texas. She earned her BA in psychology and individual and family development from Seattle Pacific University, and her MS in experimental psychology from Western Washington University. Her research interests include experiences of stress and interpersonal violence in adolescence and young adulthood, and factors that might exacerbate or ameliorate outcomes following those stressful events.
Tina Du Rocher Schudlich, PhD, MHP, is a professor of psychology at Western Washington University. She serves as the director for the Psychology Department’s Counseling Training Clinic, where she oversees graduate counseling students providing free counseling services to community members. Her research interests examine the role of parent and family processes in the development, maintenance, and treatment of psychopathology in children. Areas of specific focus include understanding reciprocal relations between mood disorders and families’ well-being and the role of parent participation in treatment for youth self-harm and autism spectrum disorder. Another emerging area of her research explores barriers and ways to increase access to mental health treatment for culturally and linguistically diverse youth and their family. She incorporates multi-method approaches to her research and is especially fond of qualitative methods, such as behavioral observations, interviews, and diary methods.
Christina A. Byrne, PhD, is an associate professor in the psychology department at Western Washington University, in Bellingham, Washington, where she serves as Director of the Clinical Mental Health Counseling Program. Dr. Byrne’s research interests include psychological trauma and interpersonal violence. (Dr. Byrne is not pictured above.)
Chase M. Ochrach, MS, is finishing her third year in the counseling psychology doctoral program at the University of Wisconsin–Madison. She earned her bachelor’s degree in psychology from the University of California, Santa Cruz, and her master’s in clinical mental health counseling from Western Washington University. Ochrach currently works with adjudicated youth at Mendota Juvenile Treatment Center in Madison, Wisconsin, and with veterans at the Zablocki VA Medical Center in Milwaukee. She recently proposed her dissertation study, titled Boy’s Search for Meaning: Meaning Making as a Predictor of Trajectories of Adaptation in Formerly Incarcerated Youth. She hopes to continue with research and clinical work with forensic juvenile populations and will be applying to clinical internships this year.
Seneca E. A. Erwin, MA, recently received her master’s in educational psychology from the University of Northern Colorado. She works in the recruiting sphere at a Fortune 500 technology company. Her research interests focus on social justice, domestic violence, mindfulness, and play therapy.
Read more about the TPC scholarship awards here.
Apr 9, 2021 | Book Reviews
by Kathy M. Evans and Aubrey L. Sejuit
Coursework and trainings in cultural competencies are often approached as an afterthought, a perspective used to enhance and improve existing practice. Counseling programs often include a course in multiculturalism and diversity focused on teaching theories of cultural and identity development, but this has a drawback: Students become responsible for integrating the course content into their intended area of practice. For career professionals, that can be a huge task—integrating counseling skills, career development theory, practical knowledge of vocations and employment law, cultural competencies, and social justice initiatives. Kathy Evans and Aubrey Sejuit’s second edition of Gaining Cultural Competence in Career Counseling is a valuable tool in this process; it seamlessly weaves together these categories to provide a thorough guide for the culturally competent career counselor.
The text is structured similarly to a typical multicultural counseling course. Chapters 1 through 4 discuss the importance of culturally competent career counseling, highlighting issues including the history of discrimination against marginalized groups in the workplace. Readers are introduced to concepts, such as worldview, locus of control and responsibility, and bias, and encouraged to explore their own biases and values. Each concept is framed from the perspective of career development, with examples and reflective activities emphasizing stereotypes or microaggressions related specifically to work- and workplace-related issues.
Chapters 5 through 7 delve into the application of cultural competencies in widely used career development theories and assessments. Evans and Sejuit examine classical career development theories (Parsons, Super, Holland) as well as newer theories to provide career professionals with guidance on how to reconcile those theories’ cultural shortcomings with ethical practice. Dimensions that are often measured in career assessments—interest, personality, and cognitive ability—are discussed, including the monochromatic landscape in which these assessments were developed. Evans and Sejuit then take the topic one step further, providing a framework for career professionals to administer and interpret assessments in a culturally informed manner.
Chapters 8 and 9 explore specific applications of cultural competencies, including in work with children and adolescents and social justice and advocacy. This is the text’s strongest section. Evans and Sejuit provide a multitude of evidence demonstrating how career information received in childhood and adolescence shapes adult career decisions, disproportionately affecting minority and low–socioeconomic status communities. Evans and Sejuit demonstrate that by simply engaging children and adolescents in an ethical and informed manner, practitioners are affecting outcomes. This is especially crucial information, as children and adolescents are often overlooked in the field of career counseling and development.
My only complaint is that Evans and Sejuit do not dive into more material in working with specific populations. The text is energizing and leaves the reader wanting to know more. However, this simplicity is also the text’s strength. At the core, the text is not only about working with and advocating for marginalized populations, but also about learning to effectively work with clients who differ from yourself as a practitioner. Activities and reflections are incorporated into each chapter of the text to provide a starting point for this process.
Gaining Cultural Competence in Career Counseling contains introductory information that will serve any professional looking to begin their journey toward cultural competency in career counseling. However, it is also an excellent tool for experienced practitioners who want to develop their knowledge of incorporating cultural competencies and social justice in their work. Again, Gaining Cultural Competence in Career Counseling takes practitioners beyond the material covered in social justice and multicultural and diversity trainings and provides a comprehensive guide for professionals of all levels.
Evans, K. M. & Sejuit, A. L. (2021). Gaining Cultural Competence in Career Counseling (2nd ed.). National Career Development Association.
Reviewed by: Erin Connelly, MS, EdS, University of North Georgia
The Professional Counselor
https://tpcwordpress.azurewebsites.net
Apr 1, 2021 | Volume 11 - Issue 2
Fei Shen, Yanhong Liu, Mansi Brat
The present study examined the relationships between childhood attachment, adult attachment, self-esteem, and psychological distress; specifically, it investigated the multiple mediating roles of self-esteem and adult attachment on the association between childhood attachment and psychological distress. Using 1,708 adult participants, a multiple-mediator model analysis following bootstrapping procedures was conducted in order to investigate the mechanisms among childhood and adult attachment, self-esteem, and psychological distress. As hypothesized, childhood attachment was significantly associated with self-esteem, adult attachment, and psychological distress. Self-esteem was found to be a significant mediator for the relationship between childhood attachment and adult attachment. In addition, adult attachment significantly mediated the relationship between self-esteem and psychological distress. The results provide insight on counseling interventions to increase adults’ self-esteem and attachment security, with efforts to decrease the negative impact of insecure childhood attachment on later psychological distress.
Keywords: childhood attachment, adult attachment, self-esteem, psychological distress, mediator
Attachment has been widely documented across disciplines, following Bowlby’s (1973) foundational work known as attachment theory. Attachment, in the context of child–parent interactions, is defined as a child’s behavioral tendency to use the primary caregiver as the secure base when exploring their surroundings (Bowlby, 1969; Sroufe & Waters, 1977). Research has shed light on the significance of childhood attachment in predicting individuals’ intrapersonal qualities such as self-esteem and emotion regulation during adulthood (Brennan & Morris, 1997), interpersonal orientations examined through attachment variation and adaptation across different developmental stages (Sroufe, 2005), and overall psychological well-being (Cassidy & Shaver, 2010; Wright et al., 2014).
Given its clinical significance, attachment has gained increased interest across disciplines. For example, childhood attachment was found to significantly predict coping and life satisfaction in young adulthood (Wright et al., 2017). Relatedly, a 30-year longitudinal study reinforces the vital role of childhood attachment in predicting individuals’ development of “the self and personality” (Sroufe, 2005, p. 352). Sroufe’s (2005) study reinforced the vital role of attachment across the life span. As an outcome variable, attachment is asserted to be associated with empathy (Ruckstaetter et al., 2017) and parenting practice in the adoptive population (Liu & Hazler, 2017). Considering the interplay between individuals’ relationship evolvement and their living contexts (Bowlby, 1973; Sroufe, 2005), attachment is examined at different stages generally labelled as childhood attachment and adult attachment, with the former focusing on the infant/child–parent relationship and the latter on adults’ generalized relationships with intimate others (e.g., romantic partners, close friends). Because of the abstract nature of attachment, it is commonly measured in the form of childhood attachment styles (Ainsworth et al., 1978) or adult attachment orientations (Turan et al., 2016).
Conceptual Framework
The present study is grounded in attachment theory, which is centered around a child’s ability to utilize their primary caregiver as the secure base when exploring surroundings, involving an appropriate balance between physical proximity, curiosity, and wariness (Bowlby, 1973; Sroufe & Waters, 1977). A core theoretical underpinning of attachment theory is the internal working model capturing a child’s self-concept and expectations of others (Bretherton, 1996). Internal working models of self and other are complementary. Namely, a child with strong internal working models is characterized with a perception of self as being worthy and deserving of love and a perception of others as being responsive, reliable, and nurturing (Bowlby, 1973; Sroufe, 2005).
In the context of attachment theory, childhood attachment is considered an outcome of consistent child–caregiver interactions and serves as the foundation for individuals’ later personality development (Bowbly, 1973; Sroufe, 2005). In line with child–caregiver interactions, Ainsworth et al. (1978) came up with three attachment styles based upon Bowlby’s seminal work, including secure, anxious-ambivalent, and anxious-avoidant attachment, following sequential phases of laboratory observations. Attachment theory was subsequently extended beyond the child–parent relationship to include later relationships in adulthood, given the parallels between these relationships (Cassidy & Shaver, 2010). Likewise, four distinct adult attachment styles (i.e., secure, dismissing, preoccupied, and fearful) are referred to based on the two-dimensional models of self and other (Konrath et al., 2014). Adult attachment styles are commonly examined under two orientations: attachment avoidance and attachment anxiety (Turan et al., 2016). Individuals showing low avoidance and low anxiety are considered securely attached, whereas those with high levels of anxiety and avoidance tend to be insecurely attached. Although childhood attachment and adult attachment are broadly considered distinct concepts in the literature, they share a spectrum of behaviors spanning from secure to insecure attachment. The levels of avoidance and anxiety involved in these behaviors are used as parameters to differentiate securely attached individuals from those who are insecurely attached.
Childhood Attachment, Self-Esteem, and Adult Attachment
Despite the conceptual overlaps, childhood attachment to caregivers and adult attachment to intimate others are commonly investigated as two distinct variables associated with individuals’ needs and features of different relationships. Childhood attachment captures a child’s distinct relationship with the primary caregiver (e.g., the mother figure) as well as their ability to differentiate the primary caregiver from other adults (Bowlby, 1969, 1973), whereas adult attachment may involve an individual’s multiple relationships (with parents, a romantic partner, or close friends). Noting the general stability of attachment from childhood to adulthood (Fraley, 2002), previous conceptual work stresses the importance of contexts in individuals’ attachment evolvement, highlighting that “patterns of adaptation” and “new experiences” reinforce each other in a reciprocal way (Sroufe, 2005, p. 349). For instance, an individual may develop secure attachment in adulthood because of healthy interpersonal experiences likely facilitated by trust, support, and nurturing received from significant others or their relationships, despite showing insecure attachment patterns in early childhood. A dynamic view of attachment development is thus warranted.
From a dynamic lens, researchers have generated evidence for the association between childhood attachment and adult attachment (Pascuzzo et al., 2013; Styron & Janoff-Bulman, 1997). For example, in a study of 879 college students (Styron & Janoff-Bulman, 1997), participants’ perception of their childhood attachment to both mother and father significantly predicted 7.9% of the variance in their adult attachment scores. Similarly, Pascuzzo et al. (2013) followed 56 adolescents at age 14 through age 22 and found that attachment insecurity to both parents and peers during adolescence was significantly associated with anxious romantic attachment in adulthood as measured by the Experience in Close Relationships Scale (ECR; Brennan et al., 1998). Studies that rely on retrospective data to assess childhood attachment (e.g., Styron & Janoff-Bulman, 1997) may be limited in validity because of time elapsed and potential compounding variables.
Childhood attachment is well recognized as the foundation for the growth of self-reliance and emotional regulation (Bowlby, 1973). Aligning with self-reliance, self-esteem appears to be frequently studied primarily through self-liking and self-competence (Brennan & Morris, 1997). Brennan and Morris (1997) defined self-liking as general self-evaluation based on perceived positive regard from others, and self-competence as concrete self-evaluation based on personal abilities and attributes. Previous research has suggested that secure attachment (to parents and peers) is significantly associated with higher levels of self-esteem (e.g., Wilkinson, 2004). In contrast, individuals who reported insecure attachment tended to endorse low self-esteem (Gamble & Roberts, 2005).
These results provide theoretical and empirical evidence for links between childhood attachment and adult attachment, but these links are likely to be indirect and mediated by other relevant variables from developmental perspectives. To our knowledge, no study has investigated the effect of self-esteem on the relationship between childhood attachment and adult attachment. The theoretical framework of attachment theory indicates that childhood attachment can have not only direct effects on adult attachment, but also indirect effects on adult attachment via self-esteem. In order to develop effective interventions tackling issues with adult attachment, it is important to examine potential mediators (e.g., self-esteem) between childhood attachment and adult attachment. To address this gap, the present study tests this hypothesized mediation function of self-esteem with a nonclinical sample of adults.
Self-Esteem, Attachment, and Psychological Distress
The extant literature comprises prolific information on the relationship between attachment and psychological well-being (Gnilka et al., 2013; Karreman & Vingerhoets, 2012; M. E. Kenny & Sirin, 2006; Turan et al., 2016; Wright et al., 2014). Existing evidence focuses on the relationship between adult attachment orientations and individuals’ psychological well-being (e.g., Karreman & Vingerhoets, 2012; Lynch, 2013; Roberts et al., 1996; Sowislo & Orth, 2013). Nevertheless, previous research has shed some light on the role of early childhood attachment in predicting psychological distresses in adulthood, including depression and anxiety (Bureau et al., 2009; Lecompte et al., 2014; Styron & Janoff-Bulman, 1997). Lecompte and colleagues (2014) conducted a longitudinal study of a sample of preschoolers (N = 68) with data collected at 4 years and again at 11–12 years; results of the study suggested that children with disorganized attachment at the baseline scored higher in both anxiety and depressive symptoms compared to those classified as securely attached.
Likewise, the effect of self-esteem on psychological distress is well established. A meta-analysis on 80 longitudinal studies published between 1994 and 2010 yielded consistent evidence supporting the relationship between low self-esteem and depressive symptoms (Sowislo & Orth, 2013). More recently, Masselink et al. (2018) examined data collected at four different points of participants’ development from early adolescence to young adulthood, which demonstrated that low self-esteem constitutes a persistent risk factor for participants’ depressive symptoms across developmental stages. Moreover, self-esteem scores in early adolescence significantly predicted the participants’ depressive symptoms at later stages, specifically during late adolescence and young adulthood.
Research has also supported the association between self-esteem, adult attachment, and psychological distress. Lopez and Gormley (2002) followed 207 college students from the beginning to the end of their freshman year and identified adjustment outcomes in association with the participants’ attachment styles and changes of their attachment styles measured by the ECR (e.g., secure-to-insecure attachment, insecure-to-secure attachment). The authors found that participants who remained securely attached scored higher in self-confidence and lower in both psychological distress and reactive coping compared to those who reported consistent insecure attachment. Moreover, participants who maintained secure attachment presented better outcomes in self-confidence and psychological well-being than the comparative group with secure-to-insecure or insecure-to-secure attachment changes (Lopez & Gormley, 2002). Adult attachment (measured by the ECR) was also found to be a mediator for the effects of traumatic events on post-traumatic symptomatology among a sample of female college students (Sandberg et al., 2010). In addition, Roberts et al. (1996) suggested attachment insecurity contributed to negative beliefs about oneself, which in turn activated cognitive structures of psychological distress, such as depression and anxiety, with a sample of 152 undergraduate students.
Taken together, the literature provides consistent support for the significant relationships between childhood attachment and various outcome variables in later adulthood, including adult attachment, self-esteem, and psychological distress. It further reveals a two-fold gap: (a) the variables tended to be investigated separately in previous studies, yet the mechanisms among these variables remained underexplored; and (b) little is known about the role of self-esteem and adult attachment in the association between childhood attachment and psychological distress. Disentangling the mechanisms, including potential mediating roles, involved in the variables will enrich the current knowledge based on attachment and can facilitate counseling interventions surrounding the effects of childhood attachment. In tackling the gap, three hypotheses were posed:
1. Childhood attachment is significantly associated with adult attachment, self-esteem, and psychological distress.
2. Self-esteem mediates the relationship between perceived childhood attachment and adult attachment.
3. Adult attachment mediates the relationship between self-esteem and
psychological distress.
Method
Participants
Of the 2,373 voluntary adult participants who took the survey, 1,708 (72%) completed 95% of all the questions and were retained for final analysis. Among the participants, 76.2% (n = 1,302) were female, 22.3% (n = 381) were male, and 1.3% (n = 25) chose not to specify their gender. The mean age of the participants was 29.89, ranging from 18 to 89 years old (SD = 12.44). A total of 66.3% (n = 1,133) of participants described themselves as White/European American, 8.7% (n = 148) as African American, 10.2% (n = 175) as Asian/Pacific Islander, 2.6% (n = 44) as American Indian/Native American, 7.3% (n = 124) as biracial or multiracial, 3.6% (n = 61) as other race, and 1.3% (n = 23) did not specify.
Sampling Procedures
The study was approved by the university’s IRB. We posted the recruitment information on various websites (e.g., Facebook, discussion board, university announcement board, Craigslist) in order to recruit a diverse pool of participants. Individuals who were 18 years old or above and were able to fill out the questionnaire in English were eligible for participating in this project. Participants were directed to an online Qualtrics survey consisting of the measures discussed in the following section. An informed consent form was included at the beginning of the survey outlining the confidentiality, voluntary participation, and anonymity of the study. Participants were prompted to enter their email addresses to win one of ten $15 e-gift cards. Participants’ email addresses were not included in the survey questions and data analysis.
Measures
Psychological Distress
Psychological distress was measured using the 10-item Kessler Psychological Distress Scale (K10; Kessler et al., 2003). Participants were asked about their emotional states in the past four weeks (e.g., “How often did you feel nervous?”). Responses were rated on a 5-point scale ranging from 0 (None of the time) to 4 (All of the time). Scores were averaged, with a higher score indicating a higher level of psychological distress. Previous studies using K10 have provided evidence of validity (Andrews & Slade, 2001). The internal consistency for K10 has been well established with a Cronbach’s alpha coefficient ranging from .88 (Easton et al., 2017) to .94 (Donker et al., 2010). In this study, the Cronbach’s alpha coefficient was .94.
Childhood Attachment
Childhood attachment was measured using the Parental Attachment subscale of the Inventory of Parent and Peer Attachment (IPPA; Armsden & Greenberg, 1987). Previous research has demonstrated evidence that this measure has great convergent and concurrent validity (M. E. Kenny & Sirin, 2006). The IPPA has been used to recall childhood attachment in adult populations (Aspelmeier et al., 2007; Cummings-Robeau et al., 2009). This 25-item subscale directs participants to recall their attachment to the parent(s) or caregiver(s) who had the most influence on them during childhood. The subscale consists of three dimensions, including 10 items on trust, nine items on communication, and six items on alienation. Some sample items are: “My parent(s)/primary caregiver(s) accepts me as I am” for trust, “I tell my parent(s)/primary caregiver(s) about my problems and troubles)” for communication, and “I do not get much attention from my parent(s)/primary caregiver(s)” for alienation. Participants rated the items using a 5-point Likert scale ranging from 1 (Almost never or never true) to 5 (Almost always or always true). Items were averaged to form the subscale, with a higher score reflecting more secure childhood attachment. The subscale has demonstrated high internal consistency with a Cronbach’s alpha of .93 (Armsden & Greenberg, 1987). In the present study, Cronbach’s alpha for the subscale was .96.
Adult Attachment
Adult attachment was measured using the ECR (Brennan et al., 1998). The ECR consists of 36 items with 18 items assessing each of the two orientations: attachment anxiety and attachment avoidance. In order to avoid confounding factors, we only assessed adult attachment with close friends or romantic partners, as relationships with parents can confound the childhood attachment outcomes. Responses were rated on a 7-point Likert scale ranging from 1 (Strongly disagree) to 7 (Strongly agree). Two scores were averaged, with a higher score reflecting a higher level of attachment anxiety or avoidance. In terms of validity, the ECR subscales have been found to be positively associated with psychological distress and intention to seek counseling, and negatively associated with social support (Vogel & Wei, 2005). The ECR has a high internal consistency for both the anxiety (α = .91) and avoidance (α = .94) dimensions (Brennan et al., 1998). For this study, Cronbach’s alphas for attachment anxiety and attachment avoidance were .93 and .92, respectively.
Self-Esteem
Rosenberg’s Self-Esteem Scale (RSES; Rosenberg, 1965) is a 10-item scale designed to assess an adult’s self-esteem. The scale assesses both self-competency (e.g., “I feel that I have a number of good qualities”) and self-liking (e.g., “I certainly feel useless at times”). Responses were coded using a 4-point Likert scale ranging from 1 (Strongly disagree) to 4 (Strongly agree). Negatively worded statements were reverse-coded. Scores were averaged, with a higher score reflecting a higher level of self-esteem. RSES has been frequently used in various studies with high reliability and validity (Brennan & Morris, 1997; Chen et al., 2017). In this study, the Cronbach’s alpha coefficient was .89.
Data Analysis
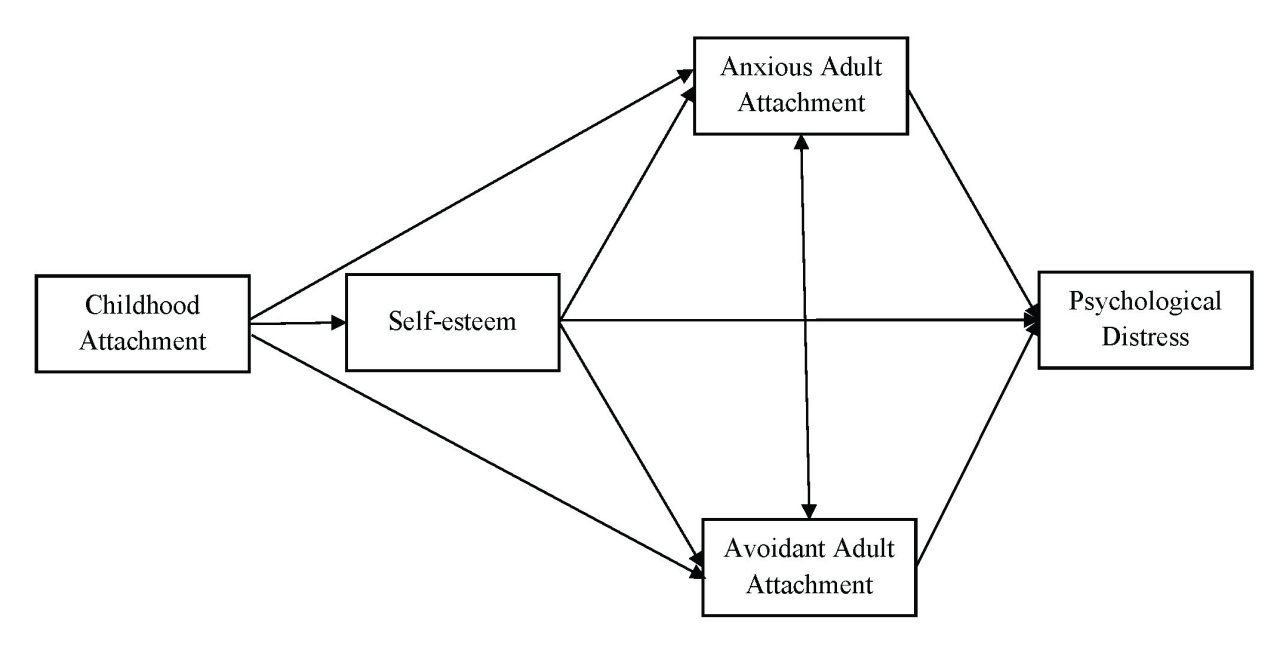
Descriptive statistics were computed using SPSS version 23 followed by a multiple-mediator model analysis using Mplus version 7.4 (Muthén & Muthén, 2012). Missing data were treated with the full information maximum likelihood estimation in Mplus, which was one of the most pragmatic approaches in producing unbiased parameter estimates (Acock, 2005). The multiple-mediator model includes childhood attachment as the predictor, self-esteem and adult attachment anxiety and avoidance as mediators, and psychological distress as the outcome variable (see Figure 1). The mediation analysis was conducted using bootstrapping procedures (J = 2,000), which was a resampling method to construct a confidence interval for the indirect effect (Preacher & Hayes, 2008). Several model fit indices based on Kline’s (2010) guidelines were employed, including the ratio of chi-square to degree of freedom (χ2/df), root-mean-square error of approximation (RMSEA), Tucker-Lewis index (TLI), comparative fit index (CFI), and standardized root-mean-square residual (SRMR). Indicators of good model fit are a nonsignificant chi-square value, a CFI and TLI of .90 or greater, RMSEA of .08 or less, and an SRMR of .05 or less (Hooper et al., 2008).
Figure 1
Multiple-Mediator Model: Self-Esteem, Anxious Adult Attachment, and Avoidant Adult Attachment as Multiple Mediators Between Childhood Attachment and Psychological Distress
Results
Descriptive Statistics and Correlations
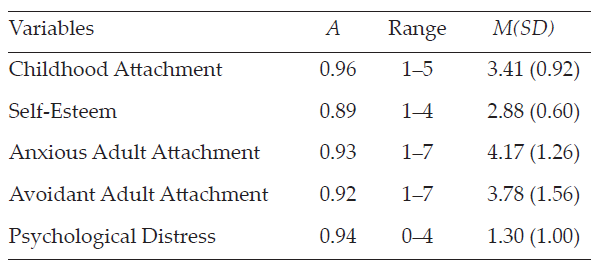
The descriptive statistics of each variable are reported in Table 1.
Table 1
Descriptive Statistics for Variables (N = 1,708)
Pearson’s correlations between variables were computed. All bivariate statistics are presented in Table 2 and provided full support for our Hypothesis 1. For instance, childhood attachment was positively associated with self-esteem (r = .38, p < .001) and negatively correlated with adult attachment anxiety (r = -.26, p < .001) and avoidance (r = -.45, p < .001), as well as with psychological distress (r = -.35, p < .001). Significant negative correlations were found between self-esteem and adult attachment anxiety (r = -.49, p < .001) and avoidance (r = -.46, p < .001), and between self-esteem and psychological distress (r = -.63, p < .001). Both adult attachment anxiety (r = .57, p < .001) and avoidance (r = .42, p < .001) were positively associated with psychological distress. Significant correlation was found between adult attachment anxiety and avoidance (r = .31, p < .001).
Table 2
Correlation Matrix of Variables (N = 1,708)
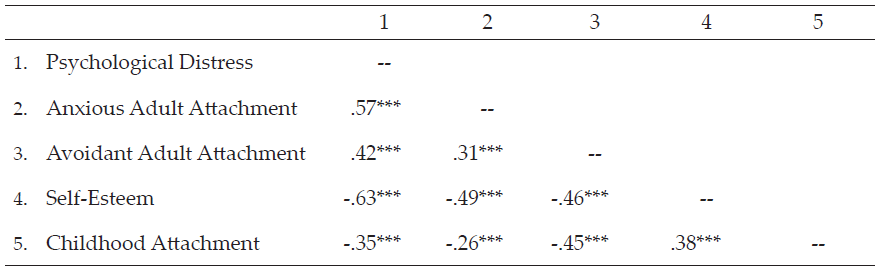
*p < .05. **p < .01. ***p < .001 (two-tailed).
The Multiple-Mediator Model
The multiple-mediator model involving self-esteem and adult attachment as mediators, with bootstrapping procedures, yielded satisfactory fit indices: χ2(1) = 12.24, p < .001, CFI = 1.00, TLI = 0.96, SRMR = .01. However, the index of RMSEA = .08, 90% CI [0.05, 0.12] indicated a mediocre fit, with the upper value of 90% CI larger than the suggested cutoff score of 0.08. D. A. Kenny et al. (2015) suggested that the models with small degrees of freedom had the average width of the 90% CI above 0.10, unless the sample size was extremely large. The nonsignificant χ2 value was interpreted as a good fit index.
The present study further revealed that secure childhood attachment was associated with high self-esteem (β = .25, p < .001) and low levels of anxiety (β = -.12, p < .001) and avoidance (β = -.41, p < .001) of adult attachment. Meanwhile, high self-esteem was associated with low anxiety (β = -.95, p < .001) and low avoidance (β = -.64, p < .001) of adult attachment. In addition, high self-esteem (β = -.68, p < .001) and low adult attachment anxiety (β = .26, p < .001) and avoidance (β = .11, p < .001) were significantly associated with low psychological distress. The results supported both Hypotheses 2 and 3 in that self-esteem mediated the relationship between childhood attachment and adult attachment, and adult attachment mediated the relationship between self-esteem and psychological distress.
The mediating role of self-esteem was examined using bootstrapping procedures. Results demonstrated that self-esteem significantly mediated the association between childhood attachment and adult attachment anxiety (b = -.24, 95% CI [-0.27, -0.21]) and avoidance (b = -.16, 95% CI [-0.19, -0.14]).
The present study further supported the mediating role of adult attachment (i.e., anxiety and avoidance). The association between self-esteem and psychological distress was significantly mediated by both adult attachment anxiety (b = -.24, 95% CI [-0.29, -0.21]) and avoidance (b = -.07, 95% CI [-0.10, -0.05]). Mediation effects are denoted in Table 3.
Table 3
Mediation Analysis With Bootstrapping: Unstandardized and Standardized Estimates and Confidence Intervals for Mediation Effects
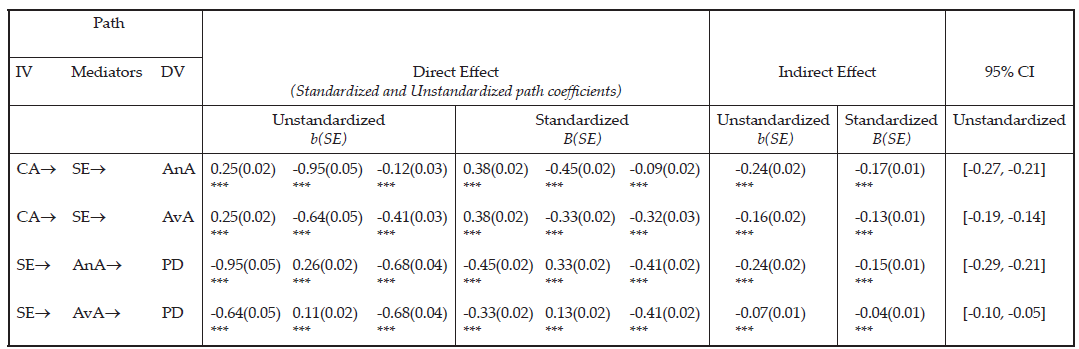
Note. Bootstrap J = 2,000, CI = confidence interval; IV = independent variable; DV = dependent variable; CA = Childhood Attachment; SE = Self-Esteem; AnA = Anxious Adult Attachment; AvA = Avoidant Adult Attachment; PD = Psychological Distress. Direct effect of path direction, IV® Mediator, Mediator ® DV, IV ® DV. Statistical significance was evaluated based on whether 95% bias corrected bootstrap CIs include zero or not. If zero was included in the CI, then it was not a significant indirect effect. Model fit: χ2(1) = 12.24, p < .001, CFI = 1.00, TLI = 0.96, SRMR = .01, RMSEA = .08 (90% CI [0.05, 0.12]).
Discussion
The present study highlights the significance of childhood attachment and its associations with self-esteem and psychological distress in adulthood. Participants who reported secure childhood attachment scored higher on self-esteem and lower on psychological distress. Secure childhood attachment was also found to be associated with low adult attachment anxiety and avoidance. Our study builds upon previous research (e.g., Sroufe, 2005) to capture the complexity of key variables related to attachment and its evolvement from childhood to adulthood. The results shed further light on the mechanisms among childhood attachment, self-esteem, adult attachment, and psychological distress. Self-esteem was found to be a significant mediator between childhood attachment and adult attachment; meanwhile, adult attachment was found to be a mediator between self-esteem and psychological distress.
The findings support Hypothesis 1 in that individuals with more secure childhood attachment reported higher levels of self-esteem, lower levels of adult attachment anxiety and avoidance, and less psychological distress. The results echo attachment theory (Bowlby, 1973), positing childhood attachment as a predictor of later adjustment as well as self-esteem, indicating that the quality of attachment appears to be intimately related to how to cope with stress and how to perceive oneself (Wilkinson, 2004). The results are also consistent with previous research that highlighted secure childhood attachment as a protective factor against anxiety, depression, and later emotional and relational distress (e.g., Karreman & Vingerhoets, 2012).
Results also lend support to Hypothesis 2 in that self-esteem mediated the relationship between childhood attachment and adult attachment. Self-esteem as a mediator echoed previous research that indicated the influence of childhood attachment on one’s self-esteem may be mitigated by expanded social networks in adulthood (Steiger et al., 2014). For instance, it is likely that improving self-esteem through peer connections (e.g., friendship; romantic relationships) may contribute to individuals’ adaptation to close relationships and enhance attachment security in adulthood, despite their insecure attachment with primary caregivers in childhood (Fraley, 2002; Sroufe, 2005).
Congruent with Hypothesis 3, adult attachment was a mediator for the relationship between self-esteem and psychological distress. Previous research provided evidence that low self-esteem increases the risk of developing psychological distress such as depressive and anxious symptoms (Li et al., 2014); nevertheless, individuals may experience less psychological impact with secure attachment manifested through their close relationships. Little is known about the relationship between insecure adult attachment (i.e., anxious and avoidant attachment) and psychological distress, and the mediating role of adult attachment has rarely been addressed. In a sample of 154 women in a community context, Bifulco et al. (2006) found that fearful and angry-dismissive attachment partially mediated the relationship between childhood adversity and depression or anxiety. The present study extends the Bifulco et al. study to include a larger, gender-inclusive, and racially diverse population that captures a wider age range. Further, using continuous measurements, the present study counteracts the limitations of dichotomous measures used in Bifulco et al.’s study, thus reflecting the spectrum and complexity of attachment.
Implications for Counseling Practice
The present study sheds light on interventions for clients’ psychological distress. The results corroborated positive associations between psychological distress and insecure childhood attachment and attachment anxiety and avoidance during adulthood. Although adults can no longer change their childhood experiences, including their attachment-related adversities, interventions that target improving adult attachment may still mitigate the negative effect of childhood attachment on psychological distress later during adulthood. Considering the reciprocal influence noted between self-esteem and adult attachment (Foster et al., 2007), counseling strategies encompassing both self-esteem and adult attachment are thus desirable.
Specifically, counselors could conceptualize self-esteem in a relational context in which they may incorporate clients’ support systems (e.g., partner, close friends, parents) into the treatment. A key treatment goal may be utilizing close relationships to boost self-esteem. On the contrary, counselors may engage clients with low self-esteem in communicating their attachment needs while involving significant others (e.g., partners) to enact positive responses, such as attentive listening and validation of mutual needs. Counselors are encouraged to assess how childhood attachment experiences may have influenced the client’s adult attachment, as insecure attachment may lead to challenges with perceived trustworthiness of self and others, which could hinder growth in the interpersonal relationships. Clients may further benefit from reflecting over specific attachment behaviors and interactional patterns within close relationships (e.g., how they manage proximity to an attachment figure when they experience distress) in order to restructure and enhance their attachment security internally and externally (Cassidy et al., 2013).
The finding of self-esteem as a significant mediator supports the proposition that self-esteem is responsive to life events and that these can influence one’s perception and evaluation of self. Previous research indicated that individuals with low self-esteem may be easily triggered by stressful life events and consequently respond irrationally and negatively (Taylor & Montgomery, 2007). Counselors may consider adapting Fennell’s (1997) Cognitive Behavioral Therapy model comprising early experience, bottom line, and rules for living to help clients enhance self-esteem. Fennell’s model suggests that clients’ early experiences (e.g., childhood attachment, traumatic experience, cultural context) may have an influence on the development of a fundamental bottom line about themselves (e.g., “I am not good enough,” “I am worthless”). Counselors may further assist clients with mapping out the rules for living (e.g., dysfunctional assumptions) related to distorted thoughts on what they should do in order to cultivate their core beliefs (as being loved or accepted or vice versa). For example, if clients have formed insecure attachment during childhood (early experience), they may develop a bottom line that “I am not good enough.” In making efforts to feel accepted in the family, they may have the rules for living that “I have to receive all As in all my classes.” If clients fail to achieve the rules for living, they likely would develop anxious and depressive symptoms, which may activate the confirmation of the bottom line. To counteract the negative patterns, counselors may work with clients to process the impact of early experience (e.g., early insecure attachment) on their bottom line and revise the rules of living to develop healthier coping strategies. When clients develop alternative rules of living, counselors may further help them to re-evaluate the bottom line and enhance self-acceptance.
Limitations and Future Research Directions
Although the results supported all three hypotheses, the present study was subject to a few limitations. First, the self-report measures may have been subject to biases, especially for the memory of childhood attachment. Another limitation pertains to a retrospective assessment of perceptions of childhood attachment that may be changed over time because of life experiences (e.g., death, parental divorce). Relatedly, the cross-sectional study could not capture the changes over a period of time. Not knowing the types of childhood attachment (i.e., anxious attachment, avoidant attachment) presented as another limitation for researchers’ understanding of the variations of attachment and how each type might impact long-term outcomes. In the future, researchers may consider longitudinal studies to explore the variations and changes in attachment over the life span and examine what other mechanisms contribute to the changes to protect against the negative impact. Future research may also incorporate other-report data filled out by significant others (e.g., parents, romantic partners) to minimize social desirability and provide multiple perspectives.
Conclusion
Attachment theory provides a strong theoretical framework in understanding individuals’ psychological well-being over the life span (DeKlyen & Greenberg, 2008). Informed by attachment theory, the present study investigated the mediating roles of self-esteem and adult attachment (measured through the levels of anxiety and avoidance) on the relations between childhood attachment and psychological distress, and between self-esteem and psychological distress, respectively. The multiple-mediator analysis with bootstrapping supports both self-esteem and adult attachment as significant mediators. Our results also support the associations between childhood attachment with self-esteem, adult attachment, and psychological distress. The study contributes to the gap pertaining to adult attachment and provides practical implications for counselors working in various settings in their work with clients surrounding attachment security, self-esteem, and psychological well-being.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Acock, A. C. (2005). Working with missing values. Journal of Marriage and Family Therapy, 67(4), 1012–1028.
https://doi.org/10.1111/j.1741-3737.2005.00191.x
Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of attachment: A psychological study of the strange situation. Lawrence Erlbaum.
Andrews, G., & Slade, T. (2001). Interpreting scores on the Kessler Psychological Distress Scale (K10). Australian and New Zealand Journal of Public Health, 25(6), 494–497. https://doi.org/10.1111/j.1467-842x.2001.tb00310.x
Armsden, G. C., & Greenberg, M. T. (1987). The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. https://doi.org/10.1007/BF02202939
Aspelmeier, J. E., Elliott, A. N., & Smith, C. H. (2007). Childhood sexual abuse, attachment, and trauma symptoms in college females: The moderating role of attachment. Child Abuse & Neglect, 31(5), 549–566.
https://doi.org/10.1016/j.chiabu.2006.12.002
Bifulco, A., Kwon, J., Jacobs, C., Moran, P. M., Bunn, A., & Beer, N. (2006). Adult attachment style as mediator between childhood neglect/abuse and adult depression and anxiety. Social Psychiatry and Psychiatric Epidemiology, 41, 796–805. https://doi.org/10.1007/s00127-006-0101-z
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. Basic Books.
Bowlby, J. (1973). Attachment and loss. Vol. 2: Separation: Anxiety and anger. Basic Books.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). Guilford.
Brennan, K. A., & Morris, K. A. (1997). Attachment styles, self-esteem, and patterns of seeking feedback from romantic partners. Personality and Social Psychology Bulletin, 23(1), 23–31.
https://doi.org/10.1177/0146167297231003
Bretherton, I. (1996). Internal working models of attachment relationships as related to resilient coping. In G. G. Noam & K. W. Fischer (Eds.), Development and vulnerability in close relationships (pp. 3–27). Lawrence Erlbaum.
Bureau, J. F., Easlerbrooks, M. A., & Lyons-Ruth, K. (2009). Attachment disorganization and controlling behavior in middle childhood: Maternal and child precursors and correlates. Attachment & Human Development, 11(3), 265–284. https://doi.org/10.1080/14616730902814788
Cassidy, J., Jones, J. D., & Shaver, P. R. (2013). Contributions of attachment theory and research: A framework for future research, translation, and policy. Development and Psychopathology, 25(4), 1415–1434.
https://doi.org/10.1017/S0954579413000692
Cassidy, J., & Shaver, P. R. (Eds.). (2010). Handbook of attachment: Theory, research, and clinical applications (2nd ed.). Guilford.
Chen, W., Zhang, D., Pan, Y., Hu, T., Liu, G., & Luo, S. (2017). Perceived social support and self-esteem as mediators of the relationship between parental attachment and life satisfaction among Chinese adolescents. Personality and Individual Differences, 108, 98–102. https://doi.org/10.1016/j.paid.2016.12.009
Cummings-Robeau, T. L., Lopez, F. G., & Rice, K. G. (2009). Attachment-related predictors of college students’ problems with interpersonal sensitivity and aggression. Journal of Social and Clinical Psychology, 28(3),
364–391. https://doi.org/10.1521/jscp.2009.28.3.364
DeKlyen, M., & Greenberg, M. T. (2008). Attachment and psychopathology in childhood. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (2nd ed., pp. 637–665). Guilford.
Donker, T., Comijs, H., Cuijpers, P., Terluin, B., Nolen, W., Zitman, F., & Penninx, B. (2010). The validity of the Dutch K10 and extended K10 screening scales for depressive and anxiety disorders. Psychiatry Research, 176(1), 45–50. https://doi.org/10.1016/j.psychres.2009.01.012
Easton, S. D., Safadi, N, S., Wang, Y., & Hasson, R. G., III. (2017). The Kessler Psychological Distress Scale: Translation and validation of an Arabic version. Health and Quality of Life Outcomes, 15(1), 215.
https://doi.org/10.1186/s12955-017-0783-9
Fennell, M. J. V. (1997). Low self-esteem: A cognitive perspective. Behavioural and Cognitive Psychotherapy, 25(1), 1–26. https://doi.org/10.1017/S1352465800015368
Foster, J. D., Kernis, M. H., & Goldman, B. M. (2007). Linking adult attachment to self-esteem stability. Self and Identity, 6(1), 64–73. https://doi.org/10.1080/15298860600832139
Fraley, R. C. (2002). Attachment stability from infancy to adulthood: Meta-analysis and dynamic modeling of developmental mechanisms. Personality and Social Psychology Review, 6(2), 123–151.
https://doi.org/10.1207/S15327957PSPR0602_03
Gamble, S. A., & Roberts, J. E. (2005). Adolescents’ perceptions of primary caregivers and cognitive style: The roles of attachment security and gender. Cognitive Therapy and Research, 29, 123–141.
https://doi.org/10.1007/s10608-005-3160-7
Gnilka, P. B., Ashby, J. S., & Noble, C. M. (2013). Adaptive and maladaptive perfectionism as mediators of adult attachment styles and depression, hopelessness, and life satisfaction. Journal of Counseling & Development, 91(1), 78–86. https://doi.org/10.1002/j.1556-6676.2013.00074.x
Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modeling: Guidelines for determining model fit. Electronic Journal on Business Research Methods, 6(1), 53–60.
Karreman, A., & Vingerhoets, A. J. J. M. (2012). Attachment and well-being: The mediating role of emotion regulation and resilience. Personality and Individual Differences, 53(7), 821–826.
https://doi.org/10.1016/j.paid.2012.06.014
Kenny, D. A., Kaniskan, B., & McCoach, D. B. (2015). The performance of RMSEA in models with small degrees of freedom. Sociological Methods & Research, 44(3), 486–507. https://doi.org/10.1177/0049124114543236
Kenny, M. E., & Sirin, S. R. (2006). Parental attachment, self-worth, and depressive symptoms among emerging adults. Journal of Counseling & Development, 84(1), 61–71. https://doi.org/10.1002/j.1556-6678.2006.tb00380.x
Kessler, R. C., Barker, P. R., Colpe, L. J., Epstein, J. F., Gfroerer, J. C., Hiripi, E., Howes, M. J., Normand, S.-L. T., Manderscheid, R. W., Walters, E. E., & Zaslavsky, A. M. (2003). Screening for serious mental illness in the general population. Archives of General Psychiatry, 60(2), 184–189. https://doi.org/10.1001/archpsyc.60.2.184
Kline, R. B. (2010). Principles and practice of structural equation modeling (3rd ed.). Guilford.
Konrath, S. H., Chiopik, W. J., Hsing, C. K., & O’Brien, E. (2014). Changes in adult attachment styles in American college students over time: A meta-analysis. Personality and Social Psychology Review, 18(4), 326–348.
https://doi.org/10.1177/1088868314530516
Lecompte, V., Moss, E., Cyr, C., & Pascuzzo, K. (2014). Preschool attachment, self-esteem and the development of preadolescent anxiety and depressive symptoms. Attachment & Human Development, 16(3), 242–260. https://doi.org/10.1080/14616734.2013.873816
Li, S. T., Albert, A. B., & Dwelle, D. G. (2014). Parental and peer support as predictors of depression and self-esteem among college students. Journal of College Student Development, 55(2), 120–138.
https://doi.org/10.1353/csd.2014.0015
Liu, Y., & Hazler, R. J. (2017). Predictors of attachment security in children adopted from China by US families: Implication for professional counsellors. Asia Pacific Journal of Counselling and Psychotherapy, 8(2), 115–130. https://doi.org/10.1080/21507686.2017.1342675
Lopez, F. G., & Gormley, B. (2002). Stability and change in adult attachment style over the first-year college transition: Relations to self-confidence, coping, and distress patterns. Journal of Counseling Psychology, 49(3), 355–364. https://doi.org/10.1037/0022-0167.49.3.355
Lynch, M. F. (2013). Attachment, autonomy, and emotional reliance: A multilevel model. Journal of Counseling & Development, 91(3), 301–312. https://doi.org/10.1002/j.1556-6676.2013.00098.x
Masselink, M., Van Roekel, E., & Oldehinkel, A. J. (2018). Self-esteem in early adolescence as predictor of depressive symptoms in late adolescence and early adulthood: The mediating role of motivational and social factors. Journal of Youth and Adolescence, 47, 932–946. https://doi.org/10.1007/s10964-017-0727-z
Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide (7th ed.). http://www.statmodel.com/download/users
guide/Mplus%20user%20guide%20Ver_7_r3_web.pdf
Pascuzzo, K., Cyr, C., & Moss, E. (2013). Longitudinal association between adolescent attachment, adult romantic attachment, and emotion regulation strategies. Attachment & Human Development, 15(1), 83–103.
https://doi.org/10.1080/14616734.2013.745713
Preacher, K. J., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40(3), 879–891.
https://doi.org/10.3758/BRM.40.3.879
Roberts, J. E., Gotlib, I. H., & Kassel, J. D. (1996). Adult attachment security and symptoms of depression: The mediating roles of dysfunctional attitudes and low self-esteem. Journal of Personality and Social Psychology, 70(2), 310–320. https://doi.org/10.1037/0022-3514.70.2.310
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press.
Ruckstaetter, J., Sells, J., Newmeyer, M. D., & Zink, D. (2017). Parental apologies, empathy, shame, guilt, and attachment: A path analysis. Journal of Counseling & Development, 95(4), 389–400.
https://doi.org/10.1002/jcad.12154
Sandberg, D. A., Suess, E. A., & Heaton, J. L. (2010). Attachment anxiety as a mediator of the relationship between interpersonal trauma and posttraumatic symptomatology among college women. Journal of Interpersonal Violence, 25(1), 33–49. https://doi.org/10.1177/0886260508329126
Sowislo, J. F., & Orth, U. (2013). Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychological Bulletin, 139(1), 213–240. https://doi.org/10.1037/a0028931
Sroufe, L. A. (2005). Attachment and development: A prospective, longitudinal study from birth to adulthood. Attachment & Human Development, 7(4), 349–367. https://doi.org/10.1080/14616730500365928
Sroufe, L. A., & Waters, E. (1977). Attachment as an organizational construct. Child Development, 48(4), 1184–1199. https://doi.org/10.2307/1128475
Steiger, A. E., Allemand, M., Robins, R. W., & Fend, H. A. (2014). Low and decreasing self-esteem in adolescence predict adult depression two decades later. Journal of Personality and Social Psychology, 106(2), 325–338. https://doi.org/10.1037/a0035133
Styron, T., & Janoff-Bulman, R. (1997). Childhood attachment and abuse: Long-term effects on adult attachment, depression, and conflict resolution. Child Abuse & Neglect, 21(10), 1015–1023.
https://doi.org/10.1016/S0145-2134(97)00062-8
Taylor, T. L., & Montgomery, P. (2007). Can cognitive-behavioral therapy increase self-esteem among depressed adolescents? A systematic review. Children and Youth Services Review, 29(7), 823–839.
https://doi.org/10.1016/j.childyouth.2007.01.010
Turan, N., Kocalevent, R.-D., Quintana, S. M., Erdur-Baker, Ö., & Diestelmann, J. (2016). Attachment orientations: Predicting psychological distress in German and Turkish samples. Journal of Counseling & Development, 94(1), 91–102. https://doi.org/10.1002/jcad.12065
Vogel, D. L., & Wei, M. (2005). Adult attachment and help-seeking intent: The mediating roles of psychological distress and perceived social support. Journal of Counseling Psychology, 52(3), 347–357.
https://doi.org/10.1037/0022-0167.52.3.347
Wilkinson, R. B. (2004). The role of parental and peer attachment in the psychological health and self-esteem of adolescents. Journal of Youth and Adolescence, 33, 479–493.
https://doi.org/10.1023/B:JOYO.0000048063.59425.20
Wright, S. L., Firsick, D. M., Kacmarski, J. A., & Jenkins-Guarnieri, M. A. (2017). Effects of attachment on coping efficacy, career decision self-efficacy, and life satisfaction. Journal of Counseling & Development, 95(4), 445–456. https://doi.org/10.1002/jcad.12159
Wright, S. L., Perrone-McGovern, K. M., Boo, J. N., & White, A.V. (2014). Influential factors in academic and career self-efficacy: Attachment, supports, and career barriers. Journal of Counseling & Development, 92(1), 36–46. https://doi.org/10.1002/j.1556-6676.2014.00128.x
Fei Shen, PhD, is a staff therapist at Syracuse University. Yanhong Liu, PhD, NCC, is an assistant professor at Syracuse University. Mansi Brat, PhD, LPC, is a staff therapist at Syracuse University. Correspondence may be addressed to Fei Shen, 150 Sims Drive, Syracuse, NY 13210, fshen02@syr.edu.
Apr 1, 2021 | Volume 11 - Issue 2
Autumn L. Cabell, Dana Brookover, Amber Livingston, Ila Cartwright
The purpose of this study was to contribute to the literature surrounding school counselors and their support of underrepresented high school students who are interested in science, technology, engineering, and math (STEM). The influence of context on school counseling was also explored, in particular practicing during the COVID-19 pandemic. Through this phenomenological study, nine high school counselors were individually interviewed, and four themes emerged. These themes were: (a) professional knowledge surrounding issues of diversity in STEM, (b) training related to the needs of underrepresented students in STEM, (c) active engagement in supporting underrepresented students’ STEM career interests, and (d) barriers related to supporting underrepresented students’ STEM interests. This article includes implications for (a) how school counselors can support underrepresented students’ STEM interests, particularly during the COVID-19 pandemic; (b) how counselor educators can contribute to STEM-related research and training; and (c) how school administrators can support school counselors’ STEM initiatives.
Keywords: STEM, school counseling, underrepresented students, high school, COVID-19
The science, technology, engineering, and math (STEM) fields in the United States comprise a large and growing sector of the economy (National Science and Technology Council [NSTC], 2018). Currently, there are more than 9 million people employed in STEM careers (U.S. Bureau of Labor Statistics [BLS], 2020). This is approximately 6% of the United States workforce (BLS, 2020). According to the BLS (2020), computer science, engineering, and physical science occupations; managerial and postsecondary teaching occupations related to those areas; and sales occupations requiring scientific knowledge at the postsecondary level are considered STEM occupations. STEM occupations require the knowledge and skills to solve problems, make sense of information, and gather and evaluate evidence to make decisions (U.S. Department of Education [U.S. ED], n.d.). In order to meet the demands of the evolving workforce and society, the United States needs students who are fluent in STEM fields and are pursuing careers in STEM (U.S. ED, n.d.).
The demand for professionals and employees with STEM skill sets is a national priority (NSTC, 2018). Estimates indicate that there will be a shortage of over 1 million STEM workers (Xue & Larson, 2015), and the need for workers will grow by 8% before 2030 (BLS, 2020). In contrast, non-STEM occupations are only projected to grow by 3% before 2030 (BLS, 2020). Because of the need for professionals with STEM skill sets, choosing to pursue a career in the STEM sector leads to the potential for positive job marketability. In addition, students who major in STEM programs during college may earn a higher salary upon graduation than other students (Cataldi et al., 2014; Vilorio, 2014). However, not all students have equitable opportunities to pursue careers in STEM.
The Need for Diversity in STEM
Diversity in STEM continues to be a concern in the United States (National Science Foundation, 2019). Beginning in high school, fewer women and minorities expect to have a career in STEM at age 30 (Mau & Li, 2018). Then, in college, significantly more men than women declare STEM majors and significantly more Asian and White students declare STEM majors (Mau, 2016). Although women now make up over half of the overall workforce, they are underrepresented in certain STEM sectors, such as computer jobs and engineering (Funk & Parker, 2018). Relatedly, in 2015–2016, more bachelor’s degrees were awarded to females (58%) than males (42%), yet females only made up 36% of bachelor’s degrees in STEM fields (National Center for Education Statistics [NCES], 2019). Additionally, the gender wage gap is wider in the STEM fields than in non-STEM jobs (Funk & Parker, 2018).
Further, Black, Latinx, and Native American workers are underrepresented in STEM occupations when compared to White and Asian workers (Funk & Parker, 2018; Mau, 2016). Though racial minorities are gradually becoming more represented in STEM fields, there is still more work to be done. For example, in 2015–2016, White students were awarded approximately 90% of the bachelor’s degrees in STEM fields (NCES, 2019). The percentages of Latinx (15%), Black (12%), and Native American (14%) students who received degrees in STEM was disproportionately lower than that of White students.
These gender and racial disparities in STEM begin even before students enter college. High school is a critical timepoint to address gender and racial disparities in STEM. High school provides students with an opportunity to engage in higher-level STEM coursework and gain self-efficacy in their STEM skills and abilities. Chen (2013) suggested that when students do not have the opportunity to engage with higher-level coursework in STEM, they are less likely to complete college degrees in STEM. Further, Grossman and Porche (2014) explained that during the high school years, encouragement to pursue STEM coursework is critical to developing students’ STEM self-efficacy. Mau and Li (2018) found that ninth grade students with higher math and science self-efficacy were more likely to have STEM career expectations and aspirations.
However, girls and underrepresented minorities in K–12 are more likely to experience stereotype threat (i.e., anxiety about their performance or ability based on negative stereotypes) and less likely to be enrolled in advanced STEM coursework during high school (Curry & Shillingford, 2015; Hamilton et al., 2015). This results in gaps in advanced STEM skills and a lack of further interest in STEM careers. Thus, professional school counselors must address the inequities in opportunity for their students through targeted STEM career interventions. Often, high school is a student’s last opportunity to develop their interest in STEM careers (Falco & Summers, 2019; Schmidt et al., 2012; Shillingford et al., 2017).
School Counselors and STEM
Under their role as defined by the American School Counselor Association (ASCA) National Model (2012), professional school counselors play an integral part in utilizing career counseling to support and encourage students to pursue STEM education and careers (Schmidt et al., 2012). Falco (2017) provided a conceptual model for school counselors to guide their STEM academic and career support with their students, including: (a) encouraging students to take advanced math and science courses, (b) providing classroom instruction on the benefits of pursuing STEM education, and (c) improving self-efficacy through providing mentoring and small group counseling opportunities. Other suggested roles for professional school counselors in STEM counseling involve ensuring equitable gender and racial ethnic ratios in STEM classes, integrating STEM knowledge into goal setting, and involving parents and guardians in academic and career planning (Schmidt et al., 2012). Although the topic of STEM counseling within the school counseling profession is still emerging, school counselors and researchers have highlighted the importance of working with girls and underrepresented racial minorities regarding STEM pursuits (Falco & Summers, 2019; Shillingford et al., 2017).
School Counselors and STEM for Girls and Underrepresented Racial Minorities
In order to provide equitable and anti-racist school counseling services, professional school counselors must be knowledgeable and aware of the factors perpetuating the opportunity gaps in STEM for girls and underrepresented minorities. Potential reasons for the opportunity gaps in STEM higher education include: (a) young people not being engaged in higher-level STEM coursework in high school, (b) inability to meet the financial or time commitment required by STEM programs, and (c) motivation and confidence concerns (Chen, 2013). Additionally, starting in adolescence, underrepresented students in the STEM fields also face a lack of support and encouragement and, oftentimes, direct discouragement from educators regarding enrollment in rigorous STEM coursework (Grossman & Porche, 2014).
Unfortunately, underrepresented students are less likely to expect their school counselors to share postsecondary information with them, and school counselors often miss opportunities to improve underrepresented students’ STEM outcomes (Dockery & McKelvey, 2013; Shillingford et al., 2017). Yet, emerging evidence shows that school counselors can impact STEM aspirations in students. For instance, one school counseling intervention that showed promising results in promoting STEM self-efficacy was a career group intervention with adolescent girls, half of whom identified as Latina (Falco & Summers, 2019). The school counseling intervention focused on targeting STEM self-efficacy and career decision self-efficacy. The results indicated that participants in the treatment group improved significantly on both outcomes and even increased those gains 3 months post-intervention when compared to the control group (Falco & Summers, 2019).
In another study, researchers aimed to investigate the influence that school counselors’ leadership had on STEM engagement, their collaboration between parents and students of color, and barriers that inhibited them from giving students more tools and resources to contribute to their success (Shillingford et al., 2017). The school counselors in the study aligned with a leadership style that integrated collaborative and motivational techniques and suggested other school counselors can utilize their leadership style to communicate more effectively with parents and support racially underrepresented students’ STEM aspirations (Shillingford et al., 2017). However, there are barriers surrounding these efforts, including inadequacy of education around STEM for school counselors; challenges with supporting parents, especially parents from marginalized racial identities; and having insufficient resources to benefit students (Shillingford et al., 2017). These studies show that school counselors can target STEM self-efficacy and emphasize school counselors’ roles in promoting STEM career aspirations with racially underrepresented students. However, the current context of the COVID-19 pandemic should be taken into consideration when surveying the current climate of STEM counseling with students.
COVID-19 and School Counselors
The COVID-19 pandemic has highlighted the inequities within our education system (Aguilar, 2020). For example, there is a digital equity gap, which includes a lack of access to adequate technology or internet, which must be taken into consideration and addressed in the virtual and hybrid learning settings many school divisions have adopted (Aguilar, 2020). During the pandemic, students often come to their virtual learning environments disengaged and having experienced various traumas (Savitz-Romer et al., 2020). These considerations call for flexibility, empathy, and perseverance from educators, including school counselors.
School counselors are trained in promoting students’ social-emotional, academic, and postsecondary development and hence are key to supporting students’ readjustment, learning, and continued college and career readiness progress during this time (Savitz-Romer et al., 2020). The work of the school counselor has not halted, especially with the challenges inherent in transitioning to a new way of school counseling. These challenges during the pandemic have led to less time spent in their usual counseling about social-emotional issues, career development, or postsecondary plans; notably, 50% of school counselors reported they spent less time than usual on career planning, and 25% reported less time spent on college planning (Savitz-Romer et al., 2020). Still, school counselors are pushing forward and adapting their practices to continue their work, including STEM counseling (ASCA, 2021).
Purpose of the Current Study
As reviewed, professional school counselors play a vital role in the development and motivation of students interested in STEM. Shillingford and colleagues (2017) called attention to the necessity of educating school counselors on how to support students of color interested in the STEM fields, as well as the influence of having a collaborative relationship between parents, students, and school counselors to assist with students’ STEM career development and exploration. Although Shillingford et al. emphasized the leadership role school counselors take in impacting the pipeline of students of color in STEM, their work (a) does not address the intersectionality of the race and gender disparities in STEM and (b) does not specifically address the critical, and perhaps last, opportunity for counseling intervention that can take place at the high school level.
Given the need for gender and racial diversity in STEM and the limited literature that emphasizes the role of school counselors in STEM counseling and education, the purpose of this transcendental phenomenological study was to increase understanding of the lived experiences of high school counselors who support girls’ and underrepresented minority students’ interests in STEM. As students begin to prepare for their next step in life, high school is the last chance school counselors have to intervene and influence students who have shown interest in STEM-related careers and minimize potential barriers that may come their way. Thus, the following research questions guided this inquiry: 1) What are the experiences of high school counselors who support girls’ and underrepresented minority students’ STEM interests and career aspirations? and 2) What contexts (including the COVID-19 pandemic) influence high school counselors’ support of girls’ and underrepresented minority students’ STEM interests and career aspirations?
Method
A transcendental phenomenological approach was used to develop understanding of the experiences of high school counselors who support underrepresented students’ STEM career interests and the contexts that influence their support. Transcendental phenomenology is a suitable design when the aim is to discover the essence, or the nature, of a phenomenon, experience, or concept (Moustakas, 1994). Our research team included four members. Our first author, Cabell, is a Black, cisgender female counselor educator. As the primary researcher, her role was to recruit and interview participants and to assist with coding. The research team also included two Black, cisgender female counselor education and supervision doctoral students, Livingston and Cartwright, and one White, cisgender female counselor education doctoral candidate, Brookover. Cabell, Brookover, and Cartwright hold master’s degrees in school counseling. Cabell and Brookover previously worked as high school counselors and Cartwright worked as an elementary school counselor at the time of the study. In addition, Cabell has professional experience providing career counseling to undergraduate engineering students. Livingston earned a master’s degree in college counseling and has professional experience working with diverse populations of college students.
Sample
The recommended sample size for phenomenological qualitative research is 5–25; thus, participants were recruited with this range in mind (Creswell & Poth, 2017), using purposeful sampling. Criteria for inclusion were school counselors or school counselor interns who worked in a high school within the past 2 years. A total of nine school counselors participated in this study.
Participants were seven school counselors who worked in a high school at the time of the study, one school counselor who worked in a high school within the past 2 years, and one college counselor who worked in a high school at the time of the study. Participants were racially diverse with six identifying as Black, two identifying as White, and one identifying as Mexican American/Chicano. Regarding gender, seven identified as cisgender women and two identified as cisgender men. Participants’ ages ranged from 26 to 46. In addition, the sample included participants who worked in various states, including two each in California and Virginia; one each in Indiana, Maryland, Michigan, and Washington, D.C.; and one who worked in both Kansas and Missouri. Three participants stated that they worked at a Catholic private high school. As part of their role, all participants stated that they provided career counseling services to students on a weekly basis. Most participants (n = 5) explained that the high school where they worked was diverse with regard to students’ race and gender. Lastly, participants had 4–18 years of experience working as high school counselors. See Table 1 for participant pseudonyms and demographics.
Table 1
Participant Pseudonyms and Demographics
| Pseudonym |
Gender |
Age |
Race |
State |
Years of Experience |
Role and Work Experience |
| Jane |
Female |
38 |
Black |
MD |
7 |
Counselor at a Catholic high school |
| Kate |
Female |
40 |
Black |
CA |
5 |
College counselor at a Catholic high school |
| Christy |
Female |
26 |
Black |
D.C. |
4 |
Counselor at a Catholic high school |
| Lauren |
Female |
37 |
White |
KS/MO |
7 |
Counselor who just switched from
high school to elementary school |
| Dawn |
Female |
30 |
Black |
VA |
4 |
Counselor at a public high school |
| Kelly |
Female |
37 |
Black |
MI |
13 |
Counselor at a public high school |
| Jo |
Male |
46 |
Mexican American/Chicano |
CA |
18 |
Counselor at a public high school |
| Tina |
Female |
35 |
Black |
IN |
4 |
Counselor at a public high school |
| Mark |
Male |
38 |
White |
VA |
6 |
Counselor at a public high school |
Data Collection
First, the study was approved by the university’s IRB. After approval, our first author, Cabell, sent recruitment flyers and emails to high school counselors using social media platforms (e.g., Twitter, Facebook, and LinkedIn) and state and national school counseling listservs (e.g., ASCA SCENE). Volunteers who met the eligibility criteria were encouraged to email Cabell in order to schedule a virtual interview through Zoom. Volunteers confirmed via email that they were a school counselor or school counseling intern at a high school within the past 2 years. Then, volunteers were sent the informed consent form and information on how to schedule their interview. Once scheduled, participants were emailed a Zoom link and directions on how to start their interview. Each interview lasted approximately 30–45 minutes and was audio-recorded.
At the beginning of each semi-structured interview, participants were asked demographic questions. Cabell developed interview questions based on the literature regarding (a) school counselors’ involvement in STEM education, (b) the underrepresentation of girls and racial minorities (e.g., Black, Latinx, and Native American) in STEM, and (c) the impact of COVID-19 on school counseling and K–12 education. The interview included 11 questions (see Appendix for the full list). Example interview questions included: What is your understanding of the issues of diversity in STEM? What has been your experience in promoting STEM careers to underrepresented students? What barriers do you face in promoting STEM careers to underrepresented students? and How has the COVID-19 pandemic impacted your role in supporting underrepresented students’ STEM career aspirations and interests? Following each interview, the audio recordings were transcribed using a website (Rev.com) and checked for accuracy by both Cabell and the participants. Cabell reviewed the transcripts for accuracy and made any changes due to typographical errors. She then emailed the transcripts to participants to review and make any changes. Two participants identified typographical errors in their transcript and emailed Cabell with edits.
Data Analysis
Data from the interview transcripts were analyzed. First, the raw data from the transcripts were examined to note significant quotes (i.e., horizontalization). Each transcript was reviewed individually by Cabell and Cartwright for exemplary quotes related to the research questions. Then, clusters of meaning were developed from these quotes and compiled into themes. These themes were used to develop descriptions of the participants’ experiences and explain how contextual factors influenced their support of underrepresented students’ STEM career interests and aspirations.
Trustworthiness
Trustworthiness is critical to establishing the validity of qualitative research; thus, several measures were implemented (Maxwell, 2005). First, in order to set aside personal biases, experiences, and feelings regarding the purpose of the research, all members of our research team engaged in bracketing our own experiences (i.e., epoché) before beginning this research (Creswell & Poth, 2017; Moustakas, 1994). Bracketing was completed in the form of concept maps and journaling. We individually bracketed our potential biases and then discussed our process with the team. Potential biases that were discussed included: (a) the impact of our first author’s experience providing career counseling to engineering undergraduate students, (b) our race and gender, and (c) our prior school counseling experience with underrepresented minorities.
In addition, throughout each semi-structured interview, Cabell completed check-ins to ensure understanding of the participant’s experience and perspective. Also, after each interview was transcribed, participants were sent their transcripts for member checking. Any inaccuracies in the transcript were changed based on the participant’s responses. Only transcripts that were reviewed by the participant were analyzed. Next, Cabell and Cartwright independently coded each transcript. Then, we established group consensus for all themes and exemplary quotes. Lastly, after the codebook was developed with themes and participant quotes, we sent the codebook to two counseling graduate students, who served as external auditors after being trained by Cabell on qualitative research and auditing. They reviewed the codebook to identify any discrepancies and ensure the significant quotes, themes, and codes aligned.
Results
We sought to (a) highlight the experiences of high school counselors who support the STEM interests of girls and underrepresented minority students and (b) identify the contexts that impact their ability to support these students, particularly taking into account the COVID-19 pandemic. Specifically, participants reflected on supporting girls; Black, Latinx, and Native American students; and those students at the intersections of both identities (e.g., Black girls, Latinx girls). We identified four themes in the analysis of the high school counselors’ experiences: 1) professional knowledge of issues of diversity in STEM; 2) training related to the needs of underrepresented students in STEM; 3) active engagement or taking an active role in supporting underrepresented students’ STEM career interests; and 4) barriers related to supporting underrepresented students’ STEM interests, including COVID-19, school, administration, students’ self-efficacy, and language.
Theme 1: Professional Knowledge
The first theme of professional knowledge of issues of diversity in STEM encompassed participants’ knowledge of the issues of gender and racial disparities in STEM fields nationally (i.e., representation in STEM occupations) and issues of diversity in STEM at their school (i.e., STEM courses). All participants were aware of the lack of racial and gender diversity in STEM nationally. Jane explained:
People of color, especially Black students, people who identify as female or women are vastly underrepresented in many of the STEM fields. . . . I know that there are many initiatives in K–12 [and] higher education to bring in or recruit or encourage students of color in particular and female students of color to explore STEM.
Similarly, Kate discussed that the STEM fields overall are “moving in a more diverse direction” yet are still dominated by men. She noticed that the majority of the students at her high school who are interested in STEM “are not Black or Brown students, they’re usually everything else.” According to Christy, “there’s a huge gap with our minorities. They don’t have the access to the education of the different jobs in STEM, and how to even reach those positions. . . . It ends up being a cyclical effect.”
Further, Dawn reflected on the lack of representation in STEM fields and the initiatives that she knows aim to diversify the images of STEM professionals. For example, Dawn discussed a social media campaign and stated:
There’s been a cool campaign, like what a scientist looks like. And it’s all of these cool Black women in lab coats. . . . So I’m pretty sure it’s just fighting against stereotypes of who should be in STEM, and what kind of person.
Kelly also spoke to the lack of diversity in STEM, not only as a national issue but also in her high school. Kelly mentioned the STEM opportunity gap: “If students are in STEM programs and they are of color, they don’t really see a lot of support, and they definitely don’t see teachers and staff that look like them.” Likewise, Jo explained that girls in particular “sometimes doubt their ability even though they’re within our top 5% of our school.” Tina acknowledged that there is a need for more girls in STEM and girls of color in STEM nationally, so she explained, “I’ve definitely been pushing my girls, especially my girls of color, my Latinx and my Black girls to definitely go out” and “I often tell them ‘paint engineering with your red lipstick,’ because I think that’s what we need to see is more women out there.”
Theme 2: Training
The second theme of training related to the needs of underrepresented students in STEM was identified through participants’ reflections on formal and informal training opportunities they completed to effectively meet their students’ needs. Some of the participants received informal training with regard to STEM counseling and education. For example, Jane explained that when she first became a school counselor, she “became friends with a few school counselors who were also women of color. And they were . . . fierce advocates for girls of color in the computer science field specifically.” The informal professional development that this group of school counseling peers provided her then led to more formal training on “some of the various tools that are out there, programs that are available, ways in which you can target girls of color and just some of the roadblocks that we as school counselors might run into.” Though Jane received both formal and informal training, she explained, “I’m still learning . . . ways in which we can do better in terms of exposing students, building it into our program, collecting data around it.” Similar to Jane, Mark also had the opportunity to attend both formal and informal training. Mark stated, “I’ve attended the occasional webinar here and there that focuses specifically on that particular demographic.” He also added that he had conversations with “some of the professors and the advisors [at neighboring colleges] within those STEM programs that really helped develop a broader understanding.”
In contrast, many participants (n = 7) could not discuss informal or formal training opportunities with regard to STEM and supporting underrepresented students. Kate explained that she received “nothing in the formal sense” with regard to STEM counseling or education training. Similarly, Christy stated, “I would say formally none, nothing professional regarding development, or seminars, workshops, or anything like that.” However, she did have some informal training because supporting underrepresented students’ STEM interests has been “a conversation that we have had with our counseling department of how to bring different types of professionals into the school and bringing them into the career days.” Dawn expressed that “STEM is such a big field. I still need help learning and understanding everything that STEM offers.” Sharing a similar sentiment in needing to know more, Tina explained, “I wish I knew more. . . . It’s just, I want to know more. I want to be able to support them. My goodness.”
Theme 3: Active Engagement
The third theme of active engagement in supporting underrepresented students’ STEM career interests emphasized the roles the high school counselors took to support students with STEM career interests. Many participants recognized their role as high school counselors in providing students with exposure to STEM career fields and supporting students’ prior knowledge of STEM. Embedded into the interviews with participants was the role of the school counselor and STEM. Christy stated, “It’s really our role to bridge that gap and make the connections that may not have been made previously, or the students might not have had access to before.” Mark shared his role in optimizing students’ strengths:
“Every student is going to present his or her own set of talents and abilities. . . . it’s my job to make sure that I can help them recognize what those talents and abilities are and help them cultivate a passion.”
Participants also took pride in building relationships with students early in their high school experience to assist them in discovering STEM careers. Kelly stated, “We definitely talk about it when students come to our offices. When we meet with our eighth graders coming into high school, we definitely let them know, here are your options.”
A method of bridging the gap for underrepresented students is by providing access to academic and postsecondary STEM opportunities. Christy spoke to her experience of supporting underrepresented students by providing that access:
We introduced that summer bridge class for the students. So, this will be the first year that we will potentially see the benefit of that. And hopefully seeing stronger grades in those students, especially students coming from public schools, minority students who are just now having access to the private school resources.
Similarly, Jane found value in encouraging her underrepresented students with passions in STEM to take advantage of all opportunities. Jane spoke of an encounter with a previous student. She recalled, “Last year I had a Black female student who said that she had started coding classes in middle school. . . . She really liked it, so I was like, ‘Great. We’re going to do all of them.’” In increasing access for students, the participants were intentional to ensure underrepresented students have opportunities. Kate stated, “I keep a lookout for virtual fly-in opportunities, especially when I know I have a student that’s interested in STEM and they are of a minority group, I always nominate them for those fly-ins.”
Jane summarized her role in supporting underrepresented students’ interests in STEM by saying:
“The school counselor has a huge role in not only exposing students to the possibilities of STEM careers but really targeting and explicitly encouraging Black students, Latino students to participate in and learn more about the STEM field.”
Further, regarding taking an active role in encouraging underrepresented students to pursue STEM, one participant, Kate, reflected on how her own racial identity motivates her to encourage students of color:
Me being a woman of color, I can’t help but feel like I’m rooting for everybody Black. . . . That’s not to say that I don’t encourage my non-students of color to also pursue STEM. . . . I feel like I have to really look out for my students of color, in my counseling department, I’m the only Black counselor. So, I do feel more pressure to really look out for them because I know, prior to me getting there, they weren’t inviting Historical Black Colleges and Universities [HBCUs] to come out. There was no HBCU session at our college fairs and so forth. No one was sending out information about the multicultural fly-ins. . . . Now I’m doing it and I forward it to my coworkers.
Lauren discussed how she actively identifies underrepresented students for STEM-related opportunities. Communication is key, she said: “Good communication with my teachers, so of course, math and science teachers, if they’re in tune with their students, that’s really helpful, identify the students and let me know.” In addition to communication with teachers, Lauren found value in using college and career cluster surveys with students. Lauren said the most impact her role has with students with regard to STEM is during career assessments “when they’re identifying that their talents or their personality matches up with any of the STEM fields.” She noted, “I think that’s brought in the most numbers of kids.” Other participants also used more formal career development tools. Christy stated, “We use Naviance at our school for college planning,” and Jo stated, “Our school uses Xello. It does a lot of interest surveys and gets students to see where they’re at, their personality, their interests and then matches it to careers.”
Theme 4: Barriers
Barriers related to supporting underrepresented students’ STEM interests emerged as the fourth theme, with participants reflecting on hindrances to their ability to support underrepresented students’ STEM careers and opportunities. These barriers included: COVID-19, school, administration, students’ self-efficacy, and language.
COVID-19
COVID-19 is a barrier that was presented in most of the participants’ interviews (n = 8). It was primarily identified as a context impacting students negatively and also one that resulted in changes to school counselors’ roles and day-to-day practice. When reflecting on the beginning of the pandemic, Lauren expressed, “All I did from March through May was call, email, and bother parents and seniors about graduation and making sure they were alive. That completely impacted my role for minority students pursuing STEM. . . . We were down to basic needs.” Christy also reflected on COVID-19 and said, “It’s really been bad. I would say that minorities in general, that’s probably the hardest group to get to virtually” with regard to communicating with students as a result of virtual schooling. Jo echoed Christy’s sentiments and stated, “I think the biggest challenge has been the distance, like not being able to meet them one-on-one.” Jo further explained, “Some of our students do not have all the technology they need, so they can’t jump on a Zoom, or maybe they do and the Wi-Fi is really bad.”
School
Participants also highlighted requirements at the school level that hinder students from accessing STEM careers and opportunities. Jo stated, “A student could do everything they need to graduate high school but not necessarily be ready for the university.” Jo was referring to the lack of college readiness and opportunity his school provides. Moreover, Kelly stated, “So they’re interested in that…the medical or the engineering. But when they find out, ‘I can get more credit in an AP,’ it kind of turns them off a little bit.” AP courses can help students with a weighted GPA, bring students closer to meeting graduation requirements, and give them college credits. In Kelly’s experience, her students are interested in STEM fields; however, it is hard to combat the course credit hours linked to an AP course versus a STEM course. Furthermore, in relation to school barriers, Kate mentioned the importance of anti-racist school practices:
I would probably even go as far as to say, knowing that all of our STEM teachers and faculty are anti-racist and I don’t know that all of them are. And the reason why I think that that’s important is because it’s possible that they receive opportunities for students, and are they aggressively sending or communicating those opportunities out to students of color?
Administration
In addition to COVID-19 and school barriers, participants also highlighted the lack of time and some administrative issues as barriers to supporting underrepresented students who are interested in STEM. For example, Jane discussed that high school is late in a student’s educational experience to only just begin discussing STEM:
I think the primary barrier is getting them so late. I mean, high school is late. It’s not too late, of course. It’s never too late. Students can always find their interest and their passion. But it’s not like the super early stages.
Jane further emphasized that by the time students of color are in high school, they may already lack the necessary exposure to STEM coursework:
I don’t know if any of my Black students are coming into ninth grade with that previous exposure. . . . I know that some of them are not. And so, I think that is a huge barrier. Not having them already exposed to a lot of what the STEM fields can offer.
Another challenge that participants highlighted was not having enough time to meet with students individually because of their caseload or administrative tasks. For example, Christy mentioned, “Another barrier is just time. Even with my caseload this year, I have 350 students.” Similarly, Lauren discussed “the lack of time, and the bulk of so many other responsibilities being given to counselors by administrators” as an impediment.
She further explained that the wide list of administrative duties at the high school level not only impeded her ability to meet students’ needs but also prompted her to leave high school and work at the elementary school level. Likewise, Kelly also explained how administrative tasks hinder her ability to have “meaningful conversations in a smaller school setting” because instead of meeting with students individually, she highlighted that she has “19 other things to do . . . because of the makeup of my job.”
Students’ Self-Efficacy
Participants also identified barriers regarding underrepresented students’ beliefs about STEM and their STEM abilities. Mark explained that one of the biggest issues he faces in supporting students from diverse backgrounds who are interested in STEM “is that they struggle with some of the challenging courses.” Similarly, Jane expressed that students may have struggled in STEM coursework during elementary and middle school, resulting in negative self-efficacy beliefs like “I’m not a math person or I’m not good at math.” In a similar vein, Jo explained that some of his underrepresented students do have the academic foundation; however, they “sometimes don’t feel as confident” about their STEM abilities. He stated, “I think a lot of my students, when they’re looking at these careers, sometimes they don’t see themselves in those careers and so that steers them away. . . . They just don’t feel it’s a possibility.”
Language
Lastly, some participants recognized the prevalence of barriers specific to the Latinx community. Tina mentioned the role of a counselor when helping students make the connections to various career options:
Working with Latinx and some undocumented or DACA students, the students of color, and even first-generation students . . . our role is very influential. In certain situations, especially for my kiddos whose parents don’t speak English, we are the adult, we are the person that’s helping them make those important decisions.
Some families Jo worked with did not always understand the materials about a STEM opportunity because of language barriers. He emphasized the importance of having materials in languages all families can understand:
We can sometimes talk about opportunities, but if it’s not getting into the hands of the families and if they’re not understanding what the opportunity is, they may not be as willing to allow their kid to attend maybe a 6-week program or a college program.
Discussion
STEM fields are growing in demand and are in need of talented and diverse individuals from varying gender identities and racial backgrounds (BLS, 2020; NCES, 2019). High school is the last opportunity in the K–12 system to promote and increase the pipeline of underrepresented students pursuing STEM careers. This study sought to support and extend the literature on the role of school counselors in supporting underrepresented students’ STEM career interests while also exploring the impact of context, including the COVID-19 pandemic, on STEM counseling. The findings emphasize the importance of high school counselors in promoting, encouraging, and supporting girls, racial minorities, and students at the intersections of both identities who are interested in STEM careers.
The results of this study aligned with the findings of Shillingford and colleagues (2017) that knowledge and training related to STEM professions was lacking for school counselors. Similarly, in the present study, some participants were able to identify concrete formal and informal training that they received in regard to STEM careers and diversity issues, but many of the participants in this study stated that they either received no training or were in need of more information and training related to STEM careers and diversity concerns. Further, time was similarly identified as a barrier. In both studies, school counselors explained that there is not enough time in the day to dedicate to discussing STEM career pathways with students individually.
Our findings have added a more nuanced understanding of time as a barrier for students and school counselors given its emphasis on high school. School counselors (n = 3) discussed how lack of prior STEM academic experiences can have negative consequences for high school students’ interest in STEM. For example, if a student is missing the foundational academic understanding of STEM before they get to high school, then they can fall further behind in the academic work even though they may express an interest in STEM careers. In addition, although high school is not too late to intervene and support students’ STEM interests, it is late in the academic journey to both (a) supplement academic understanding and (b) combat the internalized beliefs that students may have because of their prior educational experiences with STEM.
Similar to the work of Falco and Summers (2019), the importance of self-efficacy was explained by the participants in this study. For example, both Jo and Jane explained how Black and Latinx girls may lack confidence in themselves and not see themselves as being capable of pursuing and excelling in STEM careers. In interviews, they both observed how students either struggling in STEM coursework previously or not seeing themselves represented in STEM careers experienced diminished self-confidence regarding STEM. Although none of the participants explicitly discussed the term self-efficacy, they explained that Black and Brown students and girls may have low STEM-related self-efficacy and school counselors can play a role in increasing students’ exposure to STEM. The role high school counselors play in exposing students to diversity in STEM and diverse STEM careers is integral to challenging students’ distorted STEM self-efficacy beliefs. Moreover, Christy discussed her role in supporting students with STEM bridge courses—school counselors’ participation in these programs can help students develop STEM skills and self-efficacy.
Furthermore, in alignment with ASCA’s (2021) emphasis on school counselors’ role in supporting the social-emotional learning and career development of students, the findings in this study also revealed the importance of career development assessments in high school counselors’ ability to support students. Career assessment tools and platforms such as Naviance, Xello, CollegeBoard, etc., provided participants in this study with the tools to 1) identify students who may be interested in STEM careers and 2) help students connect their interests and abilities to STEM careers. Though school counselors might be pressed for time, utilizing career assessments can help structure individual meetings with students and open the door to follow-up conversations and programming surrounding careers in STEM.
In addition, the findings also revealed the importance of making community connections and utilizing social media to further support underrepresented students as they pursue STEM careers. Participants mentioned the importance of connecting students with HBCUs or other colleges in the area in order to help underrepresented students explore postsecondary options in STEM. Moreover, to increase students’ access to representation, as Dawn mentioned, high school counselors can expose students to social media campaigns that emphasize the representation of Black women in STEM, Latinx women in STEM, Native American men in STEM, and more. Increasing students’ access to more diverse images and professionals in STEM can help students to think about what being in STEM can look like after high school and, therefore, begin to see themselves in those STEM positions.
With the current emphasis on anti-racist educational processes in mind, the findings revealed the importance of communication. Participants explained that specifically, communication with math and science teachers is critical to identifying and supporting underrepresented students who are exhibiting strong potential in STEM. Additionally, Kate pointed out the importance of knowing that everyone in the school, including teachers and school counselors, are engaging in anti-racist practices in order to communicate with underrepresented students surrounding opportunities that increase access to STEM. Schmidt and colleagues (2012) also emphasized the importance of school counselors encouraging teachers to remove systemic barriers to students’ educational success. Moreover, Jo and Tina highlighted the importance of having materials for students and parents in various languages in order to communicate STEM possibilities. In engaging in anti-racist practices, it is important for school counselors to collaborate with school administrators to reduce barriers in communication, particularly surrounding the languages used to share STEM opportunities targeted to underrepresented students.
Overall, the findings of this study revealed that COVID-19 has resulted in additional barriers to supporting underrepresented high school students’ STEM career interests. In alignment with the emerging literature surrounding COVID-19 and its impact on the educational system, participants explained the technology gap is even wider for their Black and Brown students (Aguilar, 2020). Students’ inadequate access to technology has made it difficult for school counselors even to check in with students, much less discuss students’ STEM career aspirations. As Lauren mentioned, many school counselors have been addressing students’ basic needs during the pandemic. Although many STEM companies are still hiring during the pandemic and STEM careers are still projected to grow even after the pandemic, school counselors’ conversations with underrepresented students regarding STEM may be stalled at this time.
Implications
The present study has implications for school counseling practice, counselor education, and school administration. As expressed in the participants’ interviews, high school counselors care deeply about supporting underrepresented students’ STEM interests, despite the barriers. At the same time, high school counselors may be limited in their own training and their knowledge of STEM opportunities. Furthermore, COVID-19 has resulted in additional barriers for school counselors who may already be confronted with limited time and resources.
School Counseling
Students may benefit from school counselors sharing more STEM postsecondary options. For example, when discussing postsecondary options related to STEM, none of the participants discussed students participating in apprenticeships. Most participants reflected on connecting students to universities, including HBCUs. However, apprenticeships are paid industry-driven experiences in which students can receive specialized training with a company (U.S. Department of Labor, n.d.). Many apprenticeship programs are related to STEM. For example, there are apprenticeships for information technology specialists, medical laboratory specialists, and pharmacy technicians. In addition, a main benefit of completing an apprenticeship program in a STEM industry after high school is that after the completion of their apprenticeship, over 90% of employers retain their apprentices for full-time employment.
Moreover, although COVID-19 has shifted many schools to virtual formats, there are still opportunities for school counselors to help underrepresented students. For example, many STEM companies, such as Boeing, AT&T, Abbott, and more, are offering students virtual internship experiences. Websites such as Vault.com have offered virtual internship job search tools during the pandemic. In addition, online tools such as LinkedIn Learning can provide students ages 16 and above with access to training opportunities related to coding, math, and science concepts. School counselors increasing their knowledge about practical virtual STEM resources can help increase underrepresented students’ access to STEM careers during the pandemic. Through connecting with local university and community college career services departments, school counselors can learn more about STEM resources to share with students. In addition, there are several STEM-focused social media groups that school counselors can join in order to learn more about STEM. School counselors with an interest in STEM can develop more state or regional interest networks within their school counseling organizations in order to share resources and information with each other.
Counselor Education
This study also has several implications for counselor educators who will train the next generation of school counselors. Several participants highlighted that they had limited or no training on STEM career opportunities. In order to help increase school counselors’ knowledge regarding the need for STEM professionals and the ways that they can support underrepresented students, counselor educators can incorporate this learning into career counseling coursework. For instance, as an assignment, counselor educators can help school counseling graduate students utilize career counseling theory to develop a program aimed at promoting STEM to underrepresented high school students. Utilizing career counseling coursework to encourage students to find creative solutions to career-related issues can help make this course more meaningful and practically significant for future school counselors.
In addition, counselor educators can engage in research endeavors to build the literature connecting school counseling and STEM education. In doing so, counselor educators can host webinars, present at conferences, and disseminate information in both school counseling newsletters and professional journals in order to help increase school counselors’ knowledge on the needs of underrepresented students who may be interested in STEM. Additionally, counselor educators can collaborate with ASCA to conduct professional development opportunities for school counselors that explain relevant literature on STEM and how school counselors help develop students’ STEM career aspirations.
School Administration
Similarly, school administrators can support and encourage school counselors to attend professional development opportunities regarding STEM. This support can entail sharing STEM-related professional development opportunities with school counselors and giving school counselors the time to attend these professional development opportunities. Additionally, school administrators could benefit from listening to school counselors’ recommendations for how schools can better support underrepresented students and ensure equitable access to STEM coursework. Further, school administrators can review policies to incorporate anti-racist practices that promote STEM to diverse populations of students. These practices can include: (a) reviewing the racial and gender makeup of STEM courses to ensure equitable representation of students in STEM courses; (b) building connections with community organizations and stakeholders that provide resources to underrepresented students who are interested in STEM; and (c) ensuring that school counselors have access to documents regarding STEM opportunities to share with students and their parents in multiple languages, including both English and Spanish. Moreover, school administrators can work to ensure that the duties assigned to school counselors align with the ASCA National Model (2012) and allow school counselors to focus on STEM-related career development interventions for students.
Limitations and Future Research
There are several limitations to this study that warrant discussion. First, many of the participants in this study were counselors of color. Thus, there may be an element of self-selection bias wherein participants (school counselors of color) were more inclined to value the purpose of the study and be more connected to the experiences of underrepresented students. Hence, future research can emphasize the importance of all school counselors, regardless of race, addressing the needs of underrepresented students in STEM. Similarly, all the counselors in this study were several years removed from their graduate school experience. School counselors who have graduated recently may have more training and awareness of the disparities in STEM; thus, future studies can explore beginning counselors’ knowledge of STEM issues and support of underrepresented students.
In addition, all interviews were conducted virtually, which can increase the likelihood of response inhibition, wherein participants were uncomfortable with confidentiality and privacy when speaking across the internet (Janghorban et al., 2014). Future studies that are not limited by a pandemic or geography may benefit from doing in-person interviews in participants’ schools or an environment where the participants feel more comfortable. Although validity practices such as journaling, external auditing, and check-ins were utilized by our lead researcher, her closeness to the topic as both a professional and a Black woman may have impacted the objectivity of the study. The sample size was in accordance with phenomenological research; however, an increased sample size that is even more representative of school counselors from high schools across the nation could help increase this study’s generalizability.
Future research studies can explore the educational experiences of underrepresented professionals (e.g., Black women) in STEM in order to better understand what makes students pursue and stay in STEM fields as well as the role of the school counselor in their future success in STEM. In addition, future studies can explore how school counselors can collaborate with career advisors at local colleges in order to increase diversity in the STEM pipeline. In a similar vein, future studies can explore the experiences of underrepresented high school students who received STEM-related support from their school counselors and transitioned to college to pursue a major in STEM. Also, very few of the participants in this study explicitly spoke to their experience supporting Native American and Indigenous students. Given the lack of Indigenous and Native American professionals in STEM, future studies can specifically focus on their needs with regard to STEM education.
Conclusion
In sum, school counselors play a vital role in supporting the academic and career success of all students. For students who may find themselves underrepresented in STEM, high school counselors can make the difference by exposing them to possibilities and opportunities in STEM. High school might be some students’ last opportunity to (a) explore and discover varying career paths, (b) complete the preparation needed for a smooth transition to college, and/or (c) access resources to support diversity in STEM. In spite of barriers and limitations, school counselors ensure that students, regardless of gender or race, do not fall through the cracks and are encouraged to pursue any profession they desire, including a career in STEM.
Conflict of Interest and Funding Disclosure
This study was made possible by a grant from
the Virginia Counseling Association Foundation.
The authors reported no conflict of interest
for the development of this manuscript.
References
Aguilar, S. J. (2020). Guidelines and tools for promoting digital equity. Information and Learning Sciences, 121(5/6), 285–299. https://doi.org/10.1108/ILS-04-2020-0084
American School Counselor Association. (2012). ASCA national model: A framework for school counseling programs (3rd ed.).
American School Counselor Association. (2021). School counseling and school reentry during COVID-19. https://schoolcounselor.org/Publications-Research/Publications/Free-ASCA-Resources/COVID-19-Resources
Cataldi, E. F., Siegel, P., Shepherd, B., & Cooney, J. (2014). Baccalaureate and beyond: A first look at the employment experiences and lives of college graduates, 4 Years On (B&B:08/12) (NCES 2014-141). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. https://nces.ed.gov/pubs2014/2014141.pdf
Chen, X. (2013). STEM attrition: College students’ paths into and out of STEM fields (NCES 2014-001). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. https://nces.ed.gov/pubs2014/2014001rev.pdf
Creswell, J. W., & Poth, C. N. (2017). Qualitative inquiry & research design: Choosing among five approaches (4th ed.). SAGE.
Curry, J. R., & Shillingford, M. A. (2015). African American students’ career college readiness: The journey unraveled. Lexington Books.
Dockery, D. J., & McKelvey, S. (2013). Underrepresented college students’ experiences with school counselors. Journal of School Counseling, 11(3), n3. https://files.eric.ed.gov/fulltext/EJ1012298.pdf
Falco, L. D. (2017). The school counselor and STEM career development. Journal of Career Development, 44(4), 359–374. https://doi.org/10.1177/0894845316656445
Falco, L. D., & Summers, J. J. (2019). Improving career decision self-efficacy and STEM self-efficacy in high school girls: Evaluation of an intervention. Journal of Career Development, 46(1), 62–76.
https://doi.org/10.1177/0894845317721651
Funk, C., & Parker, K. (2018). Diversity in the STEM workforce varies widely across jobs. Pew Research Center.
https://www.pewsocialtrends.org/2018/01/09/diversity-in-the-stem-workforce-varies-widely-across-jobs
Grossman, J. M., & Porche, M. V. (2014). Perceived gender and racial/ethnic barriers to STEM success. Urban Education, 49(6), 698–727. https://doi.org/10.1177%2F0042085913481364
Hamilton, A. F., Malin, J., & Hackmann, D. (2015). Racial/ethnic and gender equity patterns in Illinois high school career and technical education coursework. Journal of Career and Technical Education, 30(1), 29–52.
https://doi.org/10.21061/jcte.v30i1.712
Janghorban, R., Latifnejad Roudsari, R., & Taghipour, A. (2014). Skype interviewing: The new generation of online synchronous interview in qualitative research. International Journal of Qualitative Studies on Health and Well-Being, 9(1), 24152. https://doi.org/10.3402/qhw.v9.24152
Mau, W.-C. J. (2016). Characteristics of US students that pursued a STEM major and factors that predicted their persistence in degree completion. Universal Journal of Educational Research, 4(6), 1495–1500.
https://doi.org/10.13189/ujer.2016.040630
Mau, W.-C. J., & Li, J. (2018). Factors influencing STEM career aspirations of underrepresented high school students. The Career Development Quarterly, 66(3), 246–258. https://doi.org/10.1002/cdq.12146
Maxwell, J. A. (2005). Qualitative research design: An interactive approach (2nd ed.). SAGE.
Moustakas, C. (1994). Phenomenological research methods. SAGE.
National Center for Education Statistics. (2019). Status and trends in the education of racial and ethnic groups.
https://nces.ed.gov/programs/raceindicators/indicator_reg.asp
National Center for Education Statistics. (2020). High School Longitudinal Study of 2009 (HSLS:09). https://nces.ed.gov/surveys/hsls09/hsls09_data.asp
National Science Foundation. (2019). Women, minorities, and persons with disabilities in science and engineering: 2019. National Center for Science and Engineering Statistics Special Report NSF 19–304. https://www.nsf.gov/statistics/wmpd
National Science and Technology Council. (2018). Charting a course for success: America’s strategy for STEM education. Office of Science and Technology Policy. https://www.energy.gov/sites/prod/files/2019/05/f62/STEM-Education-Strategic-Plan-2018.pdf
Savitz-Romer, M., Rowan-Kenyon, H. T., Nicola, T. P., Carroll, S., & Hecht, L. (2020). Expanding support beyond the virtual classroom: Lessons and recommendations from school counselors during the COVID-19 crisis. Harvard Graduate School of Education & Boston College Lynch School of Education and Human Development. https://www.gse.harvard.edu/sites/default/files/documents/School-Counseling-Covid-19-Report.pdf
Schmidt, C. D., Hardinge, G. B., & Rokutani, L. (2012). Expanding the school counselor repertoire through STEM-focused career development. The Career Development Quarterly, 60(1), 25–35.
https://doi.org/10.1002/j.2161-0045.2012.00003.x
Shillingford, M. A., Oh, S., & Finnell, L. R. (2017). Promoting STEM career development among students and parents of color. Professional School Counseling, 21(1b), 1–11. https://doi.org/10.1177/2156759X18773599
U.S. Bureau of Labor Statistics. (2020). Employment projections: Employment in STEM occupations. https://www.bls.gov/emp/tables/stem-employment.htm
U.S. Department of Education. (n.d.). Science, technology, engineering, and math, including computer science.
https://www.ed.gov/stem
U.S. Department of Labor. (n.d.). Discover apprenticeship: Earn while you learn today. https://www.apprenticeship.gov/sites/default/files/Career_Seeker_Fact_Sheet.pdf
Vilorio, D. (2014). STEM 101: Intro to tomorrow’s jobs. https://www.bls.gov/careeroutlook/2014/spring/art01.pdf
Xue, Y., & Larson, R. C. (2015). STEM crisis or STEM surplus? Yes and yes. https://www.bls.gov/opub/mlr/2015/article/stem-crisis-or-stem-surplus-yes-and-yes.htm
Appendix
Interview Questions
What is your understanding of the issues of diversity in STEM?
What training did you receive regarding the needs of underrepresented students who are interested in STEM?
What do you believe is the role of a school counselor in supporting underrepresented students’ interest in STEM careers?
What is your role in supporting STEM academic and career opportunities for underrepresented students?
What has been your experience in promoting STEM careers to underrepresented students?
How do you identify underrepresented students who may have potential or interest in STEM careers?
What barriers do you face in promoting STEM careers to underrepresented students?
What school and community factors influence your ability to support underrepresented students’ STEM career aspirations and interests?
How do you prepare underrepresented students for postsecondary opportunities in STEM?
What do you wish was different about how you support underrepresented students’ STEM career interests and aspirations?
How has the COVID-19 pandemic impacted your role in supporting underrepresented students’ STEM career aspirations and interests?
The authors would like to thank and acknowledge the Virginia Counseling Association Foundation; and Lexi Caliendo and Kirsten Nozime for their feedback, which improved the quality of this study. Autumn L. Cabell, PhD, NCC, LPC, CCC, CCTP, is an assistant professor at DePaul University. Dana Brookover, PhD, NCC, is an assistant professor at the University of Scranton. Amber Livingston, MEd, is a doctoral student at Virginia Commonwealth University. Ila Cartwright, MEd, is a doctoral student at Virginia Commonwealth University. Correspondence may be addressed to Autumn L. Cabell, DePaul University, 2247 N Halsted St., Rm. 246, Chicago, IL 60614, acabell@depaul.edu.
Apr 1, 2021 | Volume 11 - Issue 2
Samara G. Richmond, Amber M. Samuels, A. Elizabeth Crunk
The COVID-19 pandemic has brought about collective experiences of grief; thus, counselors-in-training (CITs) and their doctoral student supervisors may encounter increases in grief-oriented clinical work. In considering how to support CITs’ work with grieving clients, doctoral supervisors should be prepared to help CITs manage experiences of vicarious grief (VG). Given the ubiquity of loss and the limited amount of grief-specific coursework in counselor training, CITs could benefit from exploring their experiences of VG with their doctoral supervisors in clinical supervision—a core area of training for doctoral students enrolled in counselor education programs accredited by the Council for Accreditation of Counseling and Related Educational Programs. In this manuscript, we (a) provide an overview of the literature on VG, (b) discuss the potential impact of VG on CITs, (c) present a case study illustrating attention to VG in supervision, and (d) provide practical strategies doctoral supervisors can employ when addressing VG in supervision, drawing on Bernard and Goodyear’s discrimination model.
Keywords: vicarious grief, counselors-in-training, doctoral supervisors, clinical supervision, discrimination model
Loss, and the resulting grief response, is a universal human experience that individuals are likely to encounter at multiple points across the life span (Chan & Tin, 2012). As such, grief presents in counseling as a common client concern (Hill et al., 2018) and can stem from the loss of a loved one through death, non-death loss (e.g., relationship loss, loss of lifestyle), or normal life transitions (e.g., retirement, relocating; Sullender, 2010). Given the ubiquity of these experiences, counselors should anticipate working with clients who are facing loss and grief throughout their years of practice (Doughty Horn et al., 2013).
Current events may also elicit collective and global grief responses as we have seen with the COVID-19 pandemic and the unexpected death of professional basketball player Kobe Bryant early in 2020 (Milstein, 2017; Weir, 2020). These bring the pervasiveness of grief to the forefront of our awareness. Counselors, not immune to these events at the macro or micro level, must cope with their own grief responses and be prepared to experience grief through exposure to their clients’ presenting concerns, recognized as a vicarious grief (VG) response (Chan & Tin, 2012; Kirchberg et al., 1998; Rando, 1997). This reality, highlighted by the growing awareness and impact of collective grief in 2020, supports the need for increased loss and grief competencies within the profession of counseling.
Although calls have been made to more purposefully integrate loss and grief competencies into counselor education (Doughty Horn et al., 2013), we aim to highlight the importance of supporting doctoral students in growing loss and grief competencies related to their roles as future counselor educators and supervisors. As the most recent Council for Accreditation of Counseling and Related Educational Programs (CACREP) standards identify supervision as one of the five core areas of doctoral-level student training (CACREP, 2015), we propose that doctoral students should be trained to identify VG observed within counselors-in-training (CITs) and themselves. Further, they should be prepared to facilitate supervisory discussion to explore VG and help CITs learn strategies for effectively managing VG they might experience in response to their clinical work. Drawing on the existing literature on vicarious trauma, loss, and grief in counseling and supervision, as well as Bernard and Goodyear’s (1992, 2019) discrimination model, with this article we (a) provide an overview of the literature on VG, (b) discuss the potential impact of VG on CITs, (c) present a case study illustrating VG in supervision, and (d) provide practical strategies doctoral supervisors can employ when addressing VG in supervision.
Grief in Counseling
In order to more thoroughly understand counselors’ and supervisors’ experiences of VG, it is necessary to first explore how loss and grief may present within the therapeutic context. Contrary to traditional stage models of bereavement, contemporary research indicates that grief is a more nuanced, nonlinear psychological response to loss that can vary significantly between individuals with respect to duration of grief and the presentation and intensity of symptoms (Crunk et al., 2017; Doughty Horn et al., 2013). For example, although the majority of individuals experience more normative grief responses, about 10% of bereaved individuals experience a protracted, debilitating, and sometimes life-threatening grief response known as complicated grief (Shear, 2012), also referred to as prolonged grief disorder (Prigerson et al., 1995) or persistent complex bereavement disorder (American Psychiatric Association, 2013). As doctoral student supervisors and CITs inevitably encounter clinical presentations of loss and grief, the ability to identify and discuss both common and complicated grief reactions not only serves to support determination of treatment interventions, but also promotes the introspection necessary to identify, explore, and cope with their own VG responses (Ober et al., 2012), which is the focus of this present article.
Vicarious Grief
Prior literature within the counseling profession has largely focused on vicarious trauma—the negative emotional or psychological changes and altered view of self, others, or the world experienced by counselors resulting from repeated engagement with clients’ trauma-related stories, memories, pain, and fear (American Counseling Association [ACA], n.d.; Trippany et al., 2004). It is widely recognized by practitioners and counselor educators that vicarious trauma can be personally and professionally disruptive, with counselors experiencing behavior changes, interpersonal issues, shifts in personal values and beliefs, and diminished job performance as a result (ACA, n.d.). However, less attention has been directed toward VG (i.e., bereavement), a phenomenon originally documented by Kastenbaum (1987) that describes “the experience of loss and consequent grief and mourning that occurs following the deaths of others not personally known by the mourner” (Rando, 1997, p. 259). The two types of VG include (a) Type 1, exclusively VG (i.e., the griever feels what it is like to be in the initial griever’s position) and (b) Type 2, the experience of VG for a griever along with feeling reminded of one’s own losses and unfinished grieving (Rando, 1997; Sullender, 2010). Although there is overlap between grief and trauma, there are also important differences for counselors to be aware of and attend to in counselor training, practice, and supervision, particularly given the pervasiveness of loss and grief.
In light of prior literature suggesting that counselors can experience negative outcomes following vicarious traumatization, we propose that issues of loss and grief, too, can elicit unexpected and unwanted grief responses that might impact counselors’ well-being or even their ability to provide client care. CITs and doctoral supervisors would benefit from greater awareness of the potential impacts of VG on themselves and their ability to deliver ethical and effective services to clients. Research has indicated training and experience in grief counseling are among the strongest predictors of grief counseling competence (Ober et al., 2012); thus, counselors who have little or no training in grief and loss may be at risk for being unable to manage clients’ grief presentations. With counselor wellness essential to providing adequate clinical services, and counselors holding an ethical obligation to be prepared to work with a variety of client presentations, including loss and grief, it is suggested that increased attention to VG serves to promote counselor wellness, clinical preparedness, and positive client outcomes (Hill et al., 2018).
Although the long-term effects of our current experiences of collective, widespread grief have yet to be fully identified and understood, the immediate impact brings to the forefront the professional necessity of recognizing reactions to grief within clinical work and supervision. Sufficient evidence exists that counselors who work with clients facing issues of loss and grief are vulnerable to compassion fatigue, burnout, and secondary traumatization. Best practices reflect the necessity for practitioners to attend to their emotional responses to clients presenting with these issues (Chan & Tin, 2012; Gentry, 2002; Kirchberg et al., 1998), but little empirical evidence has been established surrounding how counselors respond to discussion of loss and grief in supervision. Therefore, to promote recognition and understanding of VG, it is beneficial for counselors and counselor educators to consider the separate and distinct impacts of VG on a counselor’s work. This includes how VG can permeate into supervisory relationships—space that has traditionally been used for counselors to process and attend to their emotional reaction to clients’ presenting concerns (Bernard & Goodyear, 2019).
Vicarious Grief in Supervision
Although supervision is evaluative and hierarchical by nature, it can serve a “simultaneous purpose of enhancing the professional functioning” (Bernard & Goodyear, 2019, p. 9) of the CIT. When applied to loss- and grief-oriented clinical work, it may be understood to include assisting CITs in exploring how their own reactions contribute to their ability to deliver clinical services. For doctoral students in the role of supervisor, this task requires that they not only support the connection of classroom learning to clinical practice, but also promote personal reflection and growth in the service of clients. As such, in cases of clients presenting with issues of loss and grief, doctoral students can utilize supervision and the supervisory working alliance to facilitate identification and understanding of a VG response, ultimately supporting more effective clinical work.
The supervision literature suggests that VG may affect counselors differently depending on their level of clinical experience. For example, more advanced clinicians have been found to experience less distress when faced with death-related client concerns (Terry et al., 1996), whereas beginning counselors, particularly those in a practicum course, rate death and loss as highly uncomfortable clinical topics to handle (Kirchberg & Neimeyer, 1991). In addition, the interplay of personal and contextual factors may exacerbate the distress that students experience when faced with these clinical topics, emphasizing the necessity of not only acquiring appropriate knowledge and skills related to grief work, but also personal awareness and competencies to manage their emotional responses (Chan & Tin, 2012; Kirchberg et al., 1998). Doctoral students must be prepared through their own education and introspective abilities to support this process for their CITs.
As it presents for CITs, sufficient evidence can be derived from the loss and grief and vicarious trauma literature to suggest that client outcomes may be affected when CITs cannot adequately identify or cope with vicarious responses (ACA, n.d.; Hill et al., 2018). When experiencing VG, it may be more difficult for CITs to attend to client presentations during session and engage in pre-session planning or post-session reflection (Lonn & Haiyasoso, 2016). Without standards for grief training or practice in the professional counseling field (Doughty Horn et al., 2013; Ober et al., 2012), much of the responsibility to promote CIT wellness and attention to VG responses falls on doctoral student supervisors engaging with CITs in their practicum experiences. As such, doctoral student supervisors, also ethically charged with promoting client welfare and proficiency of practitioners across presenting concerns, should be prepared to attend to VG and its likelihood to impact CIT ability to lead client sessions effectively.
Given that the vicarious trauma literature suggests that supervisors monitor their own responses to trauma-focused clinical information presented by their CITs, doctoral student supervisors and their supervisors (i.e., counselor educators and supervisors) supporting grief work must also be aware of their own risk for VG (Lonn & Haiyasoso, 2016). Supervisors may also experience emotional reactions to CITs’ disclosures of their own VG reactions in supervision (Bernard & Goodyear, 2019). Through utilizing introspective practices, doctoral student supervisors and their supervising counselor educators and supervisors can attend to this heightened possibility of VG by examining their physical, emotional, and cognitive reactions to their CITs, their workload, and any personal issues pertaining to unresolved grief that may be shaping how they in turn conduct supervision around topics of loss and grief (Ladany et al., 2000; Walker & Gray, 2002, as cited in Bernard & Goodyear, 2019). The following sections outline recommendations for addressing VG in supervision with doctoral-level supervisors and CITs.
Supervision and Vicarious Grief: Leveraging Roles and Relationships
Clinical supervision is essential to basic counselor training and has become a major emphasis of counseling doctoral training programs (Bernard & Goodyear, 2019; CACREP, 2015). Supervision as a practice has been found to increase counselor objectivity, empathy, and compassion (Trippany et al., 2004), providing an ideal environment for doctoral student supervisors to intervene and address the ripple effects of client grief presentations. Although grief is a common client concern, literature addressing VG in supervision is scarce. Generally recognized standards for addressing VG in supervision do not yet exist. Thus, in the absence of best practices, in this article, we extrapolate from existing supervision literature strategies for effectively fostering CIT growth and adapting our understanding of how these factors may also serve to support CITs and their supervisors as they navigate grief-related content and possible VG experiences in supervision.
Just as it has been studied in psychotherapy research, common factors of supervision can be examined to better conceptualize the supervisor’s role and ability to shift a CIT’s experience of VG. In considering common and specific factors of supervisory models, it has been suggested that the supervisory relationship is paramount to positive clinical outcomes (Crunk & Barden, 2017). Doctoral student supervisors, in being asked to address the intense emotional reactions of VG with their CITs, may benefit from focusing on the quality of the supervisory relationship to encourage openness, honesty, and increased willingness to process feelings of grief that arise in relation to work with their clients.
Per Bernard and Goodyear’s (1992, 2019) discrimination model, it can also be helpful to consider how the supervisory roles of counselor, consultant, and teacher may inform a doctoral student supervisor’s approach to VG with trainees. Often as a new supervisor, it can be difficult to navigate these roles and best determine which to utilize within supervision (Bernard & Goodyear, 2019; Nelson et al., 2006). The counselor role may be most familiar, given previous clinical experience, but the consultant and teacher role hold value in striking an “optimal balance between support and challenge” (Bernard & Goodyear, 2019, p. 106) for the CIT. Purposefully integrating the roles of counselor, consultant, and teacher can support doctoral student supervisors in addressing CIT factors, such as resistance, anxiety, and transference, which inherently contribute to a trainee’s experience of VG (Bernard & Goodyear, 2019; Chan & Tin, 2012; Gentry, 2002; Kirchberg et al., 1998).
To facilitate this integration of roles within the context of supervision, it is also crucial to recognize that doctoral student supervisors, early in their own training as clinical supervisors, may struggle with this task (Bernard & Goodyear, 2019; Nelson et al., 2006). In response to COVID-19 impacts to clinical services, doctoral student supervisors may be asked to provide consultation to CITs regarding navigating a client crisis via teletherapy. Overlapping with the role of consultant is also the necessity for doctoral student supervisors to teach CITs about ethical usage of teletherapy platforms for the delivery of clinical services. Further, doctoral student supervisors may recognize the need to provide counseling support to CITs around anxiety that manifests from the plethora of changes in a short period of time. These examples highlight the complex tasks facing doctoral student supervisors in the context of the current COVID-19 pandemic and draw attention to the support doctoral student supervisors may benefit from in order to remain best equipped to meet their CITs’ needs. Group or individual supervision with faculty members or senior clinic staff members may prove useful to provide an opportunity for doctoral student supervisors to examine their perspectives, emotional reactions, and the challenges of their new professional identity, coupled with the potential parallel process of experiencing their own VG through their work with CITs (Trippany et al., 2004).
As supervision provides opportunities for professional and personal growth critical to the learning experience of CITs, doctoral student supervisors must consider how best to support CITs in both of these domains. The bereavement literature suggests that a larger focus is often placed on the development of professional competencies, knowledge, and skills, as compared to an emphasis on the personal nature, or the role of self, in loss and grief (Balk et al., 2007; Stroebe et al., 2008). Thus, it is common for CITs and supervisors alike, particularly those who have not received formal academic instruction on topics of loss and grief, to be less open to topics of death and loss with clients, have less insight into their own beliefs regarding death, and have a greater fear of death (Doughty Horn et al., 2013).
This suggests that for supervisors to effectively address VG within supervision, they should engage in their own self-study of loss and grief to support their acquisition of knowledge and increased personal understanding of responses to death and loss. Because coursework that focuses specifically on loss and grief is not required by CACREP standards (Doughty Horn et al., 2013), it is unlikely that doctoral students coming from master’s programs in counseling or marriage and family therapy have had substantive training specific to loss and grief (Ober et al., 2012). Seeking out learning opportunities will further prepare doctoral student supervisors to embody the roles of counselor, consultant, and teacher to both educate and process their CITs’ reactions related to loss, grief, and death. Much like vicarious trauma has been approached within supervision, doctoral student supervisors who have engaged in the study and self-reflection of loss and grief can serve in the important role of helping CITs “stay in their own chairs” (Rothschild, 2006, p. 201). They can more effectively support identification of CITs’ gaps in knowledge or reactions to the material presented by the client and utilize supervision as a space for both education and emotional processing.
Doctoral student supervisors working with CITs must recognize the inherent challenges CITs may have in sharing clinical and personal information within supervision (Lonn & Haiyasoso, 2016). New counselors may be less aware of their emotional reactions in session (Dowden et al., 2014), further necessitating attention to VG by supervisors. Doctoral student supervisors, in guiding CITs to gain insight into their own reactions, may find benefit in incorporating discussion of countertransference and VG in an effort to differentiate the experiences for CITs. Countertransference—a counselor’s emotional, cognitive, or behavioral reactions that occur in response to the client or clinical content and are rooted in the counselor’s own life and relational experiences (Bernard & Goodyear, 2019; Hayes et al., 2011)—can be understood as distinct from VG, which, adapted from the vicarious trauma literature, is the response to the loss-oriented client material unrelated to personal experiences (Trippany et al., 2004). Although countertransference may also occur for a CIT as it relates to loss and grief, the literature supports the likelihood that as clients experience existential crises of meaning around loss, professional helpers are likely to share in the existential challenges, including the experience of VG (Chan & Tin, 2012). It is beneficial for doctoral student supervisors to support CITs in making this distinction, as each may require different attention within the supervision process.
The COVID-19 pandemic has elicited a surge of global loss, grief, and trauma, increasing the likelihood of supervisors and CITs encountering VG in supervision. Generally speaking, it is important and necessary for doctoral students to attend to the previously mentioned tasks of supporting CITs who may encounter VG, while recognizing the likelihood of a parallel process between supervision and the trainee’s clinical work (Bernard & Goodyear, 2019). Just as it can be hard for a CIT to manage responses to grief, so too may it be challenging for a new supervisor to cope without thorough discussion of loss and grief topics in supervision. Given the current widespread and collective grief specific to COVID-19, and the ubiquity of loss and grief in general, we recommend that counselor education programs help doctoral student supervisors to become more aware of the potential for VG to emerge in supervision. Strategies may include introducing case studies of VG in supervision to support doctoral students in applying strategies and exploring the impacts for themselves and their CITs.
Implications for Training: Doctoral Student Curricular Preparation
A review of the existing literature revealed that there is both minimal research and limited curricular focus on loss and grief education in the profession of counseling (Doughty Horn et al., 2013). Although this conversation has largely focused on master’s-level curricula, it is important to consider the impact of this lack of focus within doctoral education as well. Counselor education doctoral students, lacking education on clinical competencies in loss and grief from within their master’s programs, are preparing themselves to become educators of the next generation of counselors. Therefore, it is imperative that we rectify this lack of competency around loss and grief in order to best meet the moral and ethical obligation of counselors and counselor educators to promote and facilitate client growth both in their own clinical work and through the instruction and supervision of students’ work (Cicchetti et al., 2016).
Doctoral programs, although held by CACREP (2015) standards to include training in counseling, supervision, teaching, research, and advocacy, currently have no requirement to address topics of loss and grief, including VG within these domains. In order to most effectively implement the strategies discussed above, doctoral student supervisors would benefit from more focused training, both to enhance their supervisory competencies and fill gaps within introductory counselor education. Despite the existence of master’s CACREP standards that address life span development issues, there exist no CACREP standards to date that address topics of loss and grief, including VG. Hence, in this article, we examine how VG can perhaps be incorporated into doctoral supervisory curriculum.
Within counselor education doctoral programs, supervision is a core area of counselor educator education and training (CACREP, 2015). Given the ubiquity and salience of grief (Doughty Horn et al., 2013), VG is an arguably crucial phenomenon to be acknowledged and addressed by both CITs and doctoral supervisors. Hence, it is worthwhile to examine the content of courses that meet this standard. Whether a didactic course prior to direct supervisory experience or an experiential course, CACREP (2015) calls for course material to include a variety of components (e.g., purposes of clinical supervision, skills and modalities, ethical responsibilities, culturally relevant strategies). Despite the likelihood of issues of loss and grief to be present in clinical scenarios, CACREP supervision standards remain broad, meaning important topics, like loss and grief, may be neglected in course development and discussion. Just as students build on their prior knowledge of theory, interventions, cultural competence, and trauma-informed practice, so too can loss and grief be discussed as it relates to growing supervision knowledge, skills, and competencies.
The incorporation of these topics into doctoral courses may need to include foundational instruction related to loss and grief to facilitate basic competencies in addition to more complex applications of loss and grief clinical content to supervision frameworks, ethical issues, and modalities of supervision. Counselor educators and doctoral program coordinators may consider integrating VG both to draw attention to the possibility of one’s own encounter with VG as a counselor and counselor educator, and to provide opportunities for processing and self-reflection. Through purposeful instruction and modeling of strategies for supervision, doctoral student supervisors are better equipped not only to manage their own reactions, but also to recognize and facilitate understanding of their CITs’ reactions, ultimately supporting client well-being (Cicchetti et al., 2016). As such, we suggest that faculty of doctoral programs critically examine clinical topics discussed within courses meeting the CACREP supervision standards and purposefully integrate loss, grief, and VG into course content. Further, the use of case studies as a means of illustrating practical strategies that counselors and supervisors can use is a well-documented practice within the counseling scholarship (Kelly, 2016). Hence, in order to support doctoral students in their preparedness to apply the practical strategies discussed in this article, we present a case study as an example that can be used with doctoral students to support their training around VG in supervision.
Case Study
The following fictional case study illustrates features of VG (i.e., Type 1 and Type 2; Kastenbaum, 1987; Rando, 1997; Sullender, 2010) evident with Cynthia, a CIT, during clinical supervision with a doctoral supervisor. Doctoral supervisors working with CITs experiencing VG are advised to use the information previously outlined to pay attention to the grief reactions presented in the case. Drawing on Bernard and Goodyear’s (1992, 2019) discrimination model, we discuss interventions that supervisors can use to attend to VG in supervision. Supervisor collaboration with practicum instructors to facilitate the management and potential amelioration of VG is also discussed. The case study highlights the important role supervision plays in facilitating the CIT’s awareness about the process of both leaving and returning to one’s “chair” (Rothschild, 2006, p. 201).
The Case of Cynthia
Cynthia is a master’s-level CIT who is approaching the end of her practicum experience in the midst of COVID-19. During supervision, Cynthia discusses her clients’ experiences with multiple forms of loss and associated grief resulting from the pandemic, ranging from the deaths of loved ones to COVID-19, to job loss, loss of financial security, loss of special plans, loss of social connection, and an overall loss of “normal life” as they knew it. When Cynthia’s supervisor asks her how it has felt for her to help clients process their feelings of grief, Cynthia shares that when her clients share their grief with her, she becomes simultaneously reminded of her own losses (e.g., loss of social connection, daily routine, and normalcy) resulting from the pandemic, as well as her own associated grief response that she finds becomes activated in and outside of session. Cynthia shares that her own grief has been triggered by hearing her clients’ experiences and that her satisfaction with and sense of personal accomplishment surrounding her clinical work is starting to diminish.
Cynthia shares that she has also begun avoiding talking or thinking about their grief-related experiences in session. In supervision, she shares that since the pandemic, she worries that she is not doing enough for her clients and reports feeling a general sense of hopelessness associated with her work with them. Although she feels as though she is hearing her clients share stories about their loss and grief “constantly,” she also indicates that she is trying to stay motivated to continue to work with her clients and believes in her ability to help them. She also reports, however, that bearing continuous witness to their grief, fear, and overall uncertainty associated with the losses they are enduring because of the pandemic is becoming emotionally difficult to manage.
A Brief Analysis: Type 1 and Type 2 VG. As illustrated above, the case of Cynthia depicts manifestations of Type 1 and Type 2 VG during supervision. First, Type 2 VG is evidenced by Cynthia’s report of being reminded of her own losses following those of her clients and her resulting grief response. Within this instance of Type 2 VG, in response to the reported grief of her clients, Cynthia is reminded of her own losses as well as her own unfinished grieving. Second, Type 1 VG is evidenced by Cynthia’s report that her own grief response has been triggered after hearing her clients’ experiences of grief. Unlike Cynthia’s experience of Type 2 VG, in which her own unfinished grief was elicited, in this instance, Cynthia exclusively feels what it is like to be in the griever’s (i.e., client’s) position. When using a case study such as this with doctoral students, it may be beneficial to have them identify and discuss the types of VG present and begin to process how they might attend to both within supervision.
Attending to VG in Supervision. According to Bernard and Goodyear (1992, 2019), the three primary roles that are associated with clinical supervision are: counselor, teacher, and consultant. Given that these roles all fall within the domain of supervision, CITs can be afforded a broad variety of developmentally appropriate interventions throughout supervision. In considering common and specific factors of supervisory models, it has been suggested that the supervisory relationship is paramount to positive clinical outcomes (Crunk & Barden, 2017). Doctoral student supervisors, when addressing the intense emotional reactions of VG with their CITs, may benefit from focusing on the quality of the supervisory relationship to encourage openness, honesty, and increased willingness to process feelings of grief related to client work. When using a case study for experiential purposes, doctoral students can be asked to consider how, along with the use of common factors, the trifecta of roles presented by the discrimination model can be called on by supervisors to offer CITs guidance surrounding the challenging terrain of VG, regardless of the supervisor’s theoretical supervisory orientation.
Counselor. Although the intent is not to provide therapy, doctoral students can consider how the role of counselor remains constant throughout the supervisory relationship and can facilitate CITs’ understanding of and ability to manage their personal feelings and reactions as they emerge throughout their work with clients (Bernard & Goodyear, 2019). Initially, after the origination of the COVID-19 pandemic and its loss-related effects on Cynthia’s clients, Cynthia exhibited VG as well as hopelessness surrounding her clinical work during supervision. By facilitating Cynthia’s processing through reflecting her feelings of hopelessness and asking her to reflect on how her feelings may be affecting her work with clients, the doctoral student supervisor might guide Cynthia in expressing her underlying emotions that are associated with her VG response and impacting her clinical work. Given the potential for CITs to feel challenged in sharing clinical and personal information within supervision (Lonn & Haiyasoso, 2016), doctoral students examining this case study can consider how as a supervisor they might also use a check-in with Cynthia at the beginning of supervision (Doyle, 2017), in order to normalize her personal grief reactions and encourage her to be proactive about self-care surrounding her VG. Furthermore, in the case of COVID-19, this case study can highlight for doctoral students how a supervisor might attend to their own feelings of grief and demonstrate their willingness to model transparency and vulnerability to Cynthia in order to assist her in acknowledging and managing countertransference and VG. Ultimately, in more closely examining the role of counselor, doctoral students can more clearly imagine how they might be able to help Cynthia examine her feelings and emotions associated with her VG to her clients and her clinical work to reduce the potential for disturbance in her therapeutic relationship.
Teacher. In the role of teacher, the supervisor assumes the primary responsibility for the CIT’s learning (Bernard & Goodyear, 2019). In the case of Cynthia, as teacher, doctoral students can contemplate and discuss how as a supervisor they might work to help her understand her reactions to her clinical work as VG. In addition to providing education about how counselors are called to attend to their clients’ needs during a crisis, the supervisor might also provide Cynthia with psychoeducation about VG, as well as examples of symptoms and information pertaining to distinguishing it from countertransference, compassion fatigue, or burnout. This knowledge would be provided to Cynthia to help normalize and validate manifestations of indirect grief which makes these reactions easier to manage, with the case study providing opportunity for doctoral students to evaluate their own knowledge of these areas and seek support from peers or faculty to grow their knowledge.
Furthermore, doctoral students examining this case study may also be prompted to examine how they could bolster Cynthia’s learning and enhance her preparedness to work with her grieving clients by bringing Cynthia’s experiences to the attention of her practicum instructor. This provides opportunity for doctoral students to consider how to collaborate with faculty so that instructors might provide additional educational support surrounding the concept of VG during group supervision. Through discussion around how to effectively integrate didactic components into the supervisory process and attend to Cynthia’s learning, doctoral students are able to practice how a supervisor can work toward ameliorating a CIT’s VG.
Consultant. In the role of consultant, the supervisor might work with Cynthia to identify strategies that minimize the impact of VG and allow her to engage in self-care practices. By examining this case study, doctoral students can consider how to balance the teaching role, in which they adopt the role of the expert, with the consultant role, in which the supervisor works to foster Cynthia’s independence, autonomy, and empowerment (Bernard & Goodyear, 2019). Given that Cynthia demonstrated motivation to engage in supervision and learn more about her VG, as consultant, the supervisor might provide her with structured guidance surrounding how to approach her work with clients. Doctoral students may benefit from discussion around how to promote amelioration of Cynthia’s VG through providing her with resources regarding self-regulation and offering to help her brainstorm ways to be more present with her clients in session during discussions of grief. By examining a case study, doctoral students are provided the opportunity to further consider how, as consultant, they might communicate to Cynthia that she handled this situation ethically and professionally by sharing her feelings of VG with the supervisor.
Limitations
Given the dearth of research on grief literacy in counselor education and without sufficient standards around loss and grief training for counselors (Doughty Horn et al., 2013; Ober et al., 2012),
our conceptualizations, discussion, and recommendations for doctoral student supervisors and CITs encountering VG in supervision are inherently limited. Thus, we cannot be certain these recommendations would significantly influence the supervisory experience and its effect on client and counselor well-being. We believe there is sufficient evidence within the current literature suggesting that attention to VG within supervision is warranted, but further research is necessary to more completely understand the role of supervision in identifying and managing VG responses.
Further, our exploration of VG is limited to an academic setting as we believe specific attention to these competencies lies in the inclusion of loss and grief training within counselor education (Doughty Horn et al., 2013). However, given the ubiquity of grief in life and within counseling (Chan & Tin, 2012; Doughty Horn et al., 2013; Hill et al., 2018), it would be remiss for us to not acknowledge that this discussion about doctoral student supervisors is just one of many situations in which a counselor or clinical supervisor may find themselves faced with experiences of VG. Our conceptualization of VG and many of our suggestions may even ring true for clinical supervisors at various stages of their career within that role. Further research must consider how supervision occurs in contexts outside of academia and the impact of VG for counselors and supervisors at more advanced stages of their career.
Future Directions
Given the continued pervasiveness of the COVID-19 pandemic, it is impossible to understand its long-term effects, but the immediate impacts to the profession of counseling speak to the necessity of recognizing reactions to grief within clinical work and supervision. Although the supervision literature abounds with approaches for supervising counselors, as highlighted by this article, the counseling literature lacks empirical studies on VG in supervision, despite its occurrence and impact on clinicians and supervisors alike. In the absence of such research, we call for VG in supervision to be an emerging area of focus for the profession of counseling, particularly within doctoral counselor education.
However, although the scope of this article is aimed at recognizing and managing VG by doctoral student supervisors, it is our hope that drawing attention to the complexities of this experience brings further conversation to experiences of VG in all types of clinical supervision. It is of benefit to all supervisors, doctoral students, and clinicians both new to the role and with seasoned experience that increased attention is directed toward validating specific supervisory techniques developed to attend to counselors’ experience of VG in supervision. It is our goal that this discussion acknowledges the impact of VG on clinicians and promotes further research and development of best practices for managing VG in supervision, both within counselor education and beyond.
Conclusion
CITs and counselor educators face the possibility of experiencing VG in their respective work with clients and CITs who have experienced loss. Counselor educators in supervisory roles can help CITs mitigate VG through facilitating awareness of the impacts of grief-related clinical content into the supervision process and attending to CITs’ unique needs in the roles of teacher, counselor, and consultant. In light of the COVID-19 pandemic and its resulting landscape of increased loss and related mental health needs, it is especially critical for counselor educators and supervisors to be equipped to attend to the needs of CITs who are experiencing VG. In this article, we aimed to address this need by defining VG, discussing its potential impact on CITs and doctoral supervisors, and presenting a case study illustrating interventions that counselor educators can use when addressing VG in supervision.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (n.d.). Fact sheet #9: Vicarious trauma. https://www.counseling.org/docs/trauma-disaster/fact-sheet-9—vicarious-trauma.pdf?sfvrsn=f0f03a27_2
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Balk, D., Wogrin, C., Thornton, G., & Meagher, D. (Eds.). (2007). Handbook of thanatology: The essential body of knowledge for the study of death, dying, and bereavement (1st ed.). Routledge/Taylor & Francis Group.
Bernard, J. M., & Goodyear, R. K. (1992). Fundamentals of clinical supervision (1st ed.). Allyn & Bacon.
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Chan, W. C. H., & Tin, A. F. (2012). Beyond knowledge and skills: Self-competence in working with death, dying, and bereavement. Death Studies, 36(10), 899–913. https://doi.org/10.1080/07481187.2011.604465
Cicchetti, R. J., McArthur, L., Szirony, G. M., & Blum, C. R. (2016). Perceived competency in grief counseling: Implications for counselor education. Journal of Social, Behavioral, and Health Sciences, 10(1), 3–17.
https://doi.org/10.5590/JSBHS.2016.10.1.02
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Crunk, A. E., & Barden, S. M. (2017). The Common Factors Discrimination Model: An integrated approach to counselor supervision. The Professional Counselor, 7(1), 62–75. https://doi.org/10.15241/aec.7.1.62
Crunk, A. E., Burke, L. A., & Robinson, E. H. M., III. (2017). Complicated grief: An evolving theoretical landscape. Journal of Counseling & Development, 95(2), 226–233. https://doi.org/10.1002/jcad.12134
Doughty Horn, E. A., Crews, J. A., & Harrawood, L. K. (2013). Grief and loss education: Recommendations for curricular inclusion. Counselor Education and Supervision, 52(1), 70–80.
https://doi.org/10.1002/j.1556-6978.2013.00029.x
Dowden, A. R., Warren, J. M., Kambui, H. A. (2014). Three tiered model toward improved self-awareness and self-care. In G. R. Walz & J. C. Bleuer (Eds.), Ideas and research you can use: VISTAS 2014. http://www.counseling.org/docs/default-source/vistas/article_30.pdf
Doyle, K. A. (2017). Modeled wellness: Using perceived supervisor wellness and the supervisory relationship to predict supervisee personal wellness [Doctoral dissertation, Virginia Tech].
Gentry, J. E. (2002). Compassion fatigue: A crucible of transformation. Journal of Trauma Practice, 1(3–4), 37–61. https://doi.org/10.1300/J189v01n03_03
Hayes, J. A., Gelso, C. J., & Hummel, A. M. (2011). Managing countertransference. Psychotherapy, 48(1), 88–97. https://doi.org/10.1037/a0022182
Hill, J. E., Cicchetti, R. J., Jackson, S. A., & Szirony, G. M. (2018). Perceptions of grief education in accredited counseling programs: Recommendations for counselor education. Journal of Social, Behavioral, and Health Sciences, 12(1), 74–83. https://doi.org/10.5590/JSBHS.2018.12.1.05
Kastenbaum, R. (1987). Vicarious grief: An intergenerational phenomenon? Death Studies, 11(6), 447–453.
https://doi.org/10.1080/07481188708252209
Kelly, V. A. (2016). Addiction in the family: What every counselor needs to know. American Counseling Association.
Kirchberg, T. M., & Neimeyer, R. A. (1991). Reactions of beginning counselors to situations involving death and dying. Death Studies, 15(6), 603–610. https://doi.org/10.1080/07481189108252548
Kirchberg, T. M., Neimeyer, R. A., & James, R. K. (1998). Beginning counselors’ death concerns and empathic responses to client situations involving death and grief. Death Studies, 22(2), 99–120.
https://doi.org/10.1080/074811898201623
Ladany, N., Constantine, M. G., Miller, K., Erickson, C. D., & Muse-Burke, J. L. (2000). Supervisor countertransference: A qualitative investigation into its identification and description. Journal of Counseling Psychology, 47(1), 102–115. https://doi.org/10.1037/0022-0167.47.1.102
Lonn, M. R., & Haiyasoso, M. (2016). Helping counselors “stay in their chair”: Addressing vicarious trauma in supervision. In G. R. Walz & J. C. Bleuer (Eds.), Ideas and research you can use: VISTAS 2016. https://www.counseling.org/docs/default-source/vistas/article_90_2016.pdf?sfvrsn=cbe2482c_4
Milstein, C. (Ed.). (2017). Rebellious mourning: The collective work of grief. AK Press.
Nelson, K. W., Oliver, M., & Capps, F. (2006). Becoming a supervisor: Doctoral student perceptions of the training experience. Counselor Education and Supervision, 46(1), 17–31.
https://doi.org/10.1002/j.1556-6978.2006.tb00009.x
Ober, A. M., Granello, D. H., & Wheaton, J. E. (2012). Grief counseling: An investigation of counselors’ training, experience, and competencies. Journal of Counseling & Development, 90(2), 150–159.
https://doi.org/10.1111/j.1556-6676.2012.00020.x
Prigerson, H. G., Maciejewski, P. K., Reynolds, C. F., III, Bierhals, A. J., Newsom, J. T., Fasiczka, A., Frank, E., Doman, J., & Miller, M. (1995). Inventory of Complicated Grief: A scale to measure maladaptive symptoms of loss. Psychiatry Research, 59(1–2), 65–79. https://doi.org/10.1016/0165-1781(95)02757-2
Rando, T. A. (1997). Vicarious bereavement. In S. Strack (Ed.), Death and the quest for meaning: Essays in honor of Herman Feifel (pp. 257–274). Jason Aronson.
Rothschild, B. (2006). Help for the helpers: Self-care strategies for managing burnout and stress. W. W. Norton.
Shear, M. K. (2012). Getting straight about grief. Depression and Anxiety, 29(6), 461–464.
https://doi.org/10.1002/da.21963
Stroebe, M. S., Hansson, R. O., Schut, H., & Stroebe, W. (Eds.). (2008). Handbook of bereavement research and practice: Advances in theory and intervention. American Psychological Association.
Sullender, R. S. (2010). Vicarious grieving and the media. Pastoral Psychology, 59, 191–200.
https://doi.org/10.1007/s11089-009-0227-5
Terry, M. L., Bivens, A. J., & Neimeyer, R. A. (1996). Comfort and empathy of experienced counselors in client situations involving death and loss. Omega – Journal of Death and Dying, 32(4), 269–285.
https://doi.org/10.2190/WJ89-KCTY-DBWG-8QTX
Trippany, R. L., White Kress, V. E., & Wilcoxon, S. A. (2004). Preventing vicarious trauma: What counselors should know when working with trauma survivors. Journal of Counseling & Development, 82(1), 31–37. https://doi.org/10.1002/j.1556-6678.2004.tb00283.x
Weir, K. (2020). Grief and COVID-19: Mourning our bygone lives. American Psychological Association News.
https://www.apa.org/news/apa/2020/04/grief-covid-19
Samara G. Richmond, MA, MS, NCC, LGPC, is a doctoral candidate at The George Washington University. Amber M. Samuels, MS, NCC, LGPC, is a doctoral candidate at The George Washington University. A. Elizabeth Crunk, PhD, NCC, LGPC, is an assistant professor at The George Washington University. Correspondence may be addressed to Samara G. Richmond, 2136 G St NW, Washington, D.C. 20052, sgelb@gwmail.gwu.edu.
