Apr 1, 2026 | Volume 16 - Issue 1
Danielle Pester Boyd, Laura K. Jones, Courtney Maier, Danica G. Hays
The intentional exploration or broaching of topics related to the social determinants of mental health (SDoMH) throughout the counseling process helps align clinical practice with the profession’s focus on multicultural and social justice counseling competency. This article identifies six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences, (e) addressing emergent needs, and (f) termination practices. These SDoMH broaching behaviors span counselor preparation, assessment, intervention, and termination, empowering counselors to address SDoMH in their work. We conclude with implications for fostering SDoMH broaching behaviors within counselor education.
Keywords: broaching, social determinants of mental health, multicultural, counseling competency, counselor education
Counselors are increasingly called upon to integrate multicultural competence and social justice advocacy into their practice, particularly when addressing systemic and environmental factors that shape client well-being. The Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) and relevant constructs, such as the social determinants–based counseling model (SDCM; Pester Boyd et al., 2025) and the multidimensional model of broaching behavior (MMBB; Day-Vines et al., 2020), provide guiding frameworks for ensuring culturally responsive care. Taken together, these models inform concrete methods for integrating discussions of systemic, environmental, and structural influences into counselor–client interactions, which create a foundation for a set of broaching behaviors focused specifically on the social determinants of mental health (SDoMH).
Social determinants of health (SDOH) refer to “the conditions in which people are born, grow, live, work, and age that shape health outcomes” (World Health Organization [WHO], 2025, para. 1). These determinants include economic stability (e.g., employment, income), health care access, education, neighborhood safety, and social relationships, all of which impact physical and mental health. The SDoMH focus specifically on the social and structural factors influencing mental health outcomes, such as exposure to discrimination, adverse childhood experiences, community violence, economic disparities, and barriers to mental health care (Compton & Shim, 2020), influences that are reflected in the MSJCC.
The SDCM is an empirically based systemic framework for addressing SDoMH across various practice settings (Pester Boyd et al., 2025). It guides counselors in identifying barriers, such as economic hardship, discrimination, and limited access to resources, and then provides a structured process for broaching these concerns in session. Beyond simple recognition, the SDCM emphasizes implementing culturally responsive interventions, including connecting clients with community supports, advocating for policy changes, or adapting treatment plans to account for systemic stressors. This systemic responsiveness communicates to clients that their external challenges are legitimate and central to their mental health care, which reinforces the therapeutic alliance by integrating advocacy with clinical practice. Given the links among the MSJCC, SDoMH, and therapeutic outcomes, it is imperative that counselors are familiar with SDoMH, understand their impact, and are prepared to broach topics related to SDoMH with clients. Therefore, integrating the SDCM with known broaching models like the MMBB can serve to operationalize these action strategies as concrete methods to demonstrate the MSJCC.
The MMBB provides a framework to explicitly explore or broach racial, ethnic, and cultural (REC) factors with clients throughout the therapeutic process (Day-Vines et al., 2020, 2021). These broaching behaviors focus on four distinct contexts: intracounseling, intraindividual, intra-REC, and inter-REC domains. Specifically, counselors acknowledge REC concerns that impact the counselor–client relationship (intracounseling), the intersections of the client’s identity (intraindividual), the client’s cultural group membership (intra-REC), and their experiences with structural inequality (inter-REC). By intentionally attending to these layers, counselors demonstrate cultural humility and multicultural competency that affirms the realities of clients’ REC concerns. Effective broaching has been linked to enhanced client trust, increased depth of client self-disclosure, higher levels of client satisfaction, and improved therapeutic outcomes, which make it a critical component of effective multicultural counseling (Depauw et al., 2025; Gantt-Howrey et al., 2024; King & Borders, 2019; Zhang & Burkard, 2008).
By integrating the SDCM with the MMBB, we developed a set of SDoMH-specific broaching behaviors. The MMBB strengthens the relational dimension of counseling through cultural engagement while the SDCM equips counselors to act on systemic barriers that influence client well-being. Together, these models ultimately foster trust, collaboration, and empowerment and establish counseling as a space where both individual experiences and broader structural inequities are acknowledged and addressed.
SDoMH Broaching Behaviors
This article describes six SDoMH broaching behaviors for counselors grounded in the MMBB and the SDCM: counselor development, client psychoeducation, contextualization, attending to differences of lived experience, addressing emergent needs, and SDoMH-informed termination practices. These SDoMH broaching behaviors represent an interactive approach in which counselors shift among the behaviors throughout their own development as well as during assessment, intervention, and termination within the counseling relationship.
Counselor Development
The first SDoMH broaching behavior is initiated during a counselor’s preparation to work with clients. In alignment with the MSJCC (Ratts et al., 2016), counselors are expected to continually foster both knowledge and self-awareness related to the multicultural and social justice issues facing their clients, including client experiences with SDoMH. In order to develop their knowledge of SDoMH scholarship, counselors can familiarize themselves with the seminal SDOH/SDoMH frameworks (e.g., Compton & Shim, 2020; Lund et al., 2018; WHO, 2025); guiding practice models related to broaching behaviors and best practices for addressing the SDoMH (e.g., MMBB, SDCM; Day-Vines et al., 2020; Pester Boyd et al., 2025); general scholarship on SDoMH application in training, practice, and research (e.g., Johnson et al., 2023; Lenz & Lemberger-Truelove, 2023; Lenz & Litam, 2023; Mason et al., 2023; Neal Keith et al., 2023; Pester et al., 2023); and, when applicable, setting-specific SDoMH resources for school counselors (e.g., Brookover, 2024; Johnson & Brookover, 2021), career counselors (Johnson et al., 2024), and family counselors (Robins et al., 2022).
Next, to facilitate self-awareness, counselors are encouraged to engage in reflective practices that identify areas of strength in addressing SDoMH with clients and areas that require skill and dispositional development. First, counselors should reflect on any personal experiences with SDoMH and how those experiences may both inform and potentially bias their work with clients. For example, counselors who have dealt with their own experiences of economic instability may need to watch for emerging countertransference with clients having similar experiences. We recommend that counselors review existing SDoMH frameworks and identify which determinants have affected them personally and interpersonally with peers, family members, and colleagues. In addition, they can consider what strategies were helpful or harmful as they personally navigated SDoMH.
Counselors should also reflect on any prior experiences working with clients who were dealing with SDoMH and how those prior professional experiences might inform and potentially bias their ability to help new clients with SDoMH. For example, counselors might view clients as resistant if they do not consistently attend counseling sessions, although those clients may be dealing with circumstances impacted by SDoMH (e.g., unstable transportation, lack of childcare, unreliable internet access). Mechanisms such as supervision or consultation can be helpful for facilitating counselor awareness and development related to being nonjudgmental, showing unconditional positive regard, and embodying congruence, which are all vital components of creating and maintaining a strong therapeutic alliance.
Additionally, counselors or counseling supervisors can administer the Addressing Client Needs with Social Determinants of Health Scale (ACN:SDH, Johnson, 2023) to more formally assess readiness for addressing SDoMH. This tool measures a provider’s SDOH competency related to knowledge, awareness, biases, skills, and preparedness. The ACN:SDH findings can be reviewed within supervision or consultation. For areas where data reflect a lack of readiness, counselors can process feelings associated with their limited readiness and brainstorm resources that may be useful for building readiness. Ultimately, as counselors focus inward to broach and support their professional development related to the SDoMH framework, they will be more prepared to implement the remaining SDoMH broaching behaviors in client interactions.
Client Psychoeducation
Client psychoeducation is the next SDoMH broaching behavior that begins during the intake and assessment process. Psychoeducation is an evidence-based intervention that integrates client education into the counseling process by connecting clinical outcomes to increased client self-awareness and skill development across many mental health presenting concerns (e.g., anxiety, depression, schizophrenia; Dolan et al., 2021; Luo et al., 2025). We suggest that counselors mindfully introduce SDoMH psychoeducation into the intake and assessment process to increase client knowledge and awareness about the potential impact of SDoMH on well-being.
Furthermore, there is growing support for universal SDoMH screening (Gantt-Howrey et al., 2024; Johnson & Brookover, 2021; Johnson et al., 2023), with many available screeners for counselors to use, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE; 2022); the Accountable Health Communities Health-Related Social Needs Screening Tool (Center for Medicare and Medicaid Innovation, n.d.); and the WE CARE Survey (Garg et al., 2007). These screeners can be incorporated into intake processes to establish a baseline of SDoMH data for clients. For example, the PRAPARE assessment identifies both individual areas of risk related to social determinants and an overall risk tally score. Counselors can use this data to inform both the focus of the psychoeducation intervention and the client’s treatment plan.
Many clients may not fully understand why they are being asked about these areas of their lives or be aware of how these determinants may influence well-being. Therefore, counselors should first define SDoMH and explain the overall framework using jargon-free language. For example:
Social determinants of mental health are different social and environmental factors that can positively or negatively influence our physical and mental health. These can be factors like having your basic needs of food, housing, and employment met; having access to quality education and health care; living in a safe environment free of violence and risk; and having strong social and community support. The more people are surrounded by supportive social and environmental conditions, the easier it is to improve overall health and mental health. When people do not have adequate access to these conditions, it can lead to a higher risk of health and mental health concerns. It is important for the work that we are going to do together to have a clear picture of how your environment is influencing your physical and mental health so that we can work to increase conditions that will support the positive mental health changes you are wanting to make.
Counselors can also consider using visual tools in session, such as handouts that depict SDoMH in an easily understandable format (see Figure 1 for a sample).
Counselors should then use the SDoMH data collected through the assessment process to provide data-driven psychoeducation about the specific social determinant risk areas identified in a client’s assessment, outlining the research and known physical and mental health risks and outcomes of those determinants. For example, one item on the PRAPARE assessment asks, “How often do you see or talk to people that you care about and feel close to?” If a client answers less than three times per week, they are flagged for a risk tally on this item; the counselor could provide psychoeducation on the impact of social connection and community support alongside the risks of social isolation (U.S. Department of Health and Human Services, 2023). A counselor might broach the topic by saying:
I noticed when you were asked how many times you see or talk to people you care about that you answered less than three times per week. I ask this question on the screener because at times the number and quality of our social connections can have an influence on our physical and mental health. For example, social isolation has been linked to increased risk of anxiety and depression, lower academic and job performance, greater susceptibility to viruses and respiratory illnesses, and even long-term risk of diseases such as heart disease and stroke. Healthy social connection can protect us from disease and increase our sense of safety, meaning, and resilience. Tell me more about what social connection looks like in your life.
By broaching the subject in this way, the counselor can intentionally assess the impact of a specific social determinant on the client’s overall well-being and health. In the example, the counselor would seek to understand the quantity, quality, and impact of the client’s relationships while also screening for any potential physical symptoms that might require an external referral. This practice of broaching SDoMH through client psychoeducation and assessment allows the counselor to implement data-driven practices that provide a multitiered therapeutic framework to conceptualize client concerns across various socioecological levels (e.g., individual, interpersonal, community, public policy). This in turn supports the development of a more holistic treatment plan that incorporates both individual and community interventions.
Figure 1
Visual Depiction of the Social Determinants of Mental Health for Clinical Use
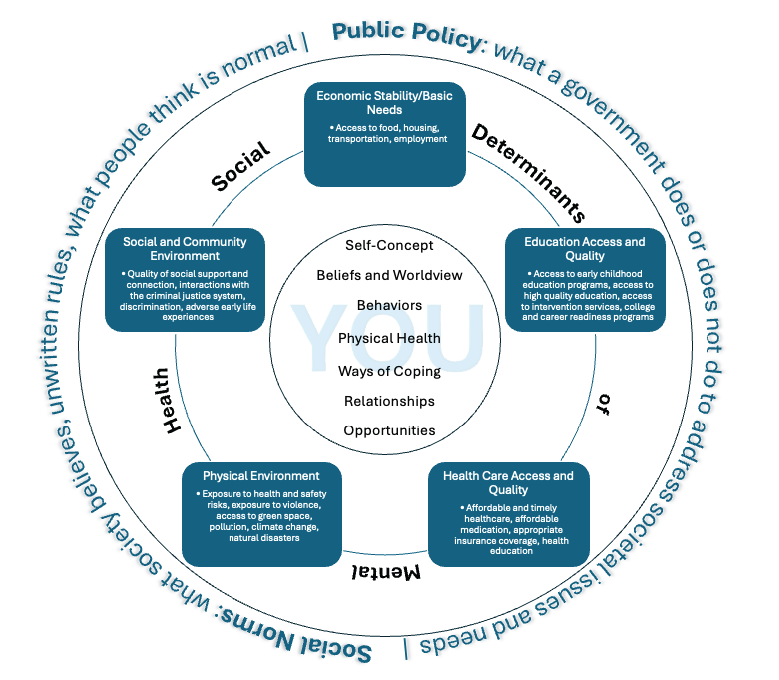
Note. Adapted from Social Determinants of Health, by Office of Disease Prevention and Health Promotion, 2025 (https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health) and “Social Determinants of Mental Health” by Compton, M. T., & Shim, R. S., 2015, Focus, 13(4), p. 420 (https://doi.org/10.1176/appi.focus.20150017).
Contextualizing SDoMH for Each Client
As a client develops understanding and awareness of the social determinants impacting their well-being, the counselor should also use broaching to contextualize that knowledge on an individual level. In this way, counselors go beyond educating clients about SDoMH in general and instead seek to collaborate with the client to understand how they are uniquely impacted by those factors. This practice of contextualizing SDoMH allows the client to make connections between their lived experiences, intrapsychic concerns, and the larger social and environmental context.
This broaching behavior aligns well with the MMBB and its intraindividual, intra-REC, and inter-REC broaching dimensions. Counselors can apply these broaching dimensions to the contextualization process. For example, intraindividual broaching can be used to acknowledge how SDoMH impact a client’s identity dimensions (e.g., race, gender, socioeconomic status, sexual orientation, immigration status). A counselor could say, “It sounds like financial strain has limited your transportation options to get to your appointments. Let’s find some free or low-cost alternatives that might better fit within your budget.” Intra-REC broaching, or the exploration of within–cultural group concerns, can help the counselor discuss any client issues impacted by SDoMH that are culture-specific. A counselor might say to the client, “I imagine it could be difficult to ask family and friends for a ride to your appointments if mental health is stigmatized in those relationships.” Finally, a counselor may apply inter-REC broaching by exploring a client’s experiences with discrimination:
Relying on public transportation resources in this city has caused you to miss important appointments and events. It sounds like these public resources don’t meet the needs of residents. I plan to write a letter to the city council explaining some of the issues. Is there anything specific that you would like me to communicate or any way that you would like to advocate for changes?
By integrating these specific broaching dimensions, counselors can help clients gain both self and situational awareness by better understanding the possible role of social determinants in their own lives. In turn, this allows the counselor and client to better address challenges by understanding the client’s unique needs in context. From the previous example, the counselor might consider the following: Does the client need help identifying additional transportation resources? Would virtual counseling sessions be a more accessible option? Can I advocate for improved public transportation in the local community by providing key context to local leaders about how unreliable transportation affects the health of their constituents? Are there self-advocacy skills that I could help the client develop? Through targeted discussions on SDoMH like these, counselors can ensure that they are providing culturally responsive care that meets their clients’ unique needs.
Broaching Differences in the Counselor–Client Relationship
As SDoMH factors are integrated into the therapeutic process, counselors must also attend to the interpersonal process of the therapeutic alliance by intentionally broaching any differences that may exist between the counselor and client. Clients from historically marginalized backgrounds may experience factors that may differ significantly from their counselor’s lived experiences, such as heightened economic instability, community violence, and health care barriers (Compton & Shim, 2015). The MMBB, through its intracounseling domain, emphasizes that a counselor must actively acknowledge and explore REC differences between the counselor and client to attend to any disruptive interpersonal processes that might impact the therapeutic relationship (Day-Vines et al., 2020). We suggest that differences in lived experience related to SDoMH be treated comparably to ensure culturally responsive and effective care.
Research suggests that counselors who fail to broach REC concerns and SDoMH-related disparities risk reinforcing dominant cultural narratives that dismiss or minimize the structural challenges clients face, potentially leading to client disengagement, cultural miscommunication, and premature termination of counseling services (Day-Vines et al., 2021; Drinane et al., 2018; Owen et al., 2014). Thus, it is incumbent upon counselors to broach these differences with cultural humility, openness, and a willingness to engage in difficult but necessary conversations (Newton & Steele, 2025). To effectively broach these conversations, a counselor should adopt a collaborative, client-centered approach by acknowledging potential differences in lived experiences while affirming the client’s perspective.
One strategy is for the counselor to invite open discussions by saying:
I recognize that my experiences may be different from yours, and I don’t want to make assumptions about the challenges that you face. I’d like to understand more about how factors like financial stress, health care access, or discrimination may be affecting your mental health. Would you be open to sharing what that has been like for you?
This type of broaching explicitly acknowledges differences in identity, privilege, and lived experience between the counselor and client while creating a nonjudgmental and validating therapeutic space for the client to share their reality (Day-Vines et al., 2021).
Another example of effective intracounseling broaching can be seen in a case where a White counselor works with a Black client who describes frequent racial discrimination in the workplace. To avoid deflecting or minimizing the client’s experience, the counselor might say, “I want to acknowledge that my lived experience may not reflect what you’re describing, but I want to understand how these challenges impact your well-being.” This affirming, non-defensive approach allows for deeper exploration of SDoMH factors such as racial stress, economic opportunity, and access to mental health care (Newton & Steele, 2025). Such intentional broaching behaviors can also help mitigate client mistrust, validate sociocultural realities, and strengthen the therapeutic alliance (Day-Vines et al., 2021).
Building rapport and trust is central to the broaching process, particularly when addressing systemic disparities. Trust building requires empathy, active listening, and a willingness to acknowledge one’s own biases (Day-Vines et al., 2021). Integrating clients’ interests, cultural values, and lived experiences into sessions makes counseling more relevant, while creating a safe space grounded in unconditional acceptance encourages openness and authenticity. Together, these broaching practices foster trust, empower clients to take an active role in the process, and strengthen the foundation for growth and change.
Broaching Emergent Needs in Session
Counselors should also be mindful to broach emergent client needs throughout the therapeutic process. Though counselors may assess clients for SDoMH at the beginning of the counseling process, that information must be viewed within a dynamic client context that requires an ongoing response rather than a one-time assessment. Therefore, counselors must remain attuned to emerging SDoMH needs throughout the therapeutic process and utilize immediacy skills to broach and address concerns as they arise.
Many clients face barriers related to income, health care access, transportation, and social support networks, all of which can create stressors that directly influence mental health outcomes because they add layers of stress that can overshadow therapeutic work (Compton & Shim, 2015). When basic needs are not met, clients may experience heightened anxiety, hopelessness, or distraction, which can limit their ability to fully engage in treatment.
Ongoing systemic barriers can also reinforce feelings of disempowerment and make it harder for clients to trust the counseling process or believe change is possible. As a result, unresolved SDoMH challenges often lead to inconsistent attendance, premature termination, or reduced treatment effectiveness. By addressing these barriers within the counseling process, counselors not only improve client retention and engagement but also enhance overall wellness by affirming that external stressors are legitimate and integral to mental health care.
For example, a client who discloses heightened anxiety over an overdue utility bill may struggle to engage in therapy until the pressing financial stressor is addressed. A counselor might broach this concern by saying, “I can see how this situation is overwhelming and I want to support you in finding a solution. Would it be helpful to take a few minutes to explore assistance programs or a payment plan?” This response validates the client’s distress while offering immediate, actionable support to address a pressing external challenge. Similarly, a client struggling with transportation barriers may benefit from a session in which the counselor helps them identify local transit options, employer benefits, or community-based ride services to ensure consistent access to mental health care. Meeting such immediate, concrete needs within the session fosters greater trust, retention, and engagement in the counseling process (Day-Vines et al., 2021; Newton & Steele, 2025). Additionally, addressing pressing SDoMH concerns in real time reinforces the message that both psychological distress and external stressors are valid therapeutic concerns. This approach ensures that counseling remains responsive and supportive of the client’s holistic well-being.
Beyond directly helping clients address pressing needs in session, the counselor can support self-advocacy and empowerment by equipping clients with the knowledge and skills to independently resolve their emergent needs. Developing self-advocacy skills enables clients to engage more effectively with health care providers, employers, and social service agencies providing skills that bridge the counseling office into everyday life (Compton & Shim, 2020). Self-advocacy intervention empowers clients to actively pursue resources, assert their rights, and confront systemic barriers with confidence. Moreover, self-advocacy skills foster resilience and equip clients to not only overcome immediate obstacles but to also sustain progress in the face of future challenges. In this way, developing self-advocacy skills is not just a counseling technique but a vital outcome that supports long-term growth and empowerment.
The counselor can facilitate the development of self-advocacy skills by helping clients identify resources, role-play difficult conversations, and anticipate potential barriers they may encounter when seeking support. For example, a client experiencing housing insecurity may feel intimidated about reaching out to a local housing agency because of past negative experiences or uncertainty about eligibility requirements. A counselor might role-play the conversation by saying, “Let’s practice how you might explain your situation when calling the housing agency. You could start by saying, ‘I’m looking for assistance with securing stable housing. Can you help me understand the eligibility requirements and next steps?’” This approach allows the client to rehearse the interaction in a supportive setting, boosting their confidence before making the actual call. Additionally, the counselor can help the client identify potential challenges, such as long wait times or required documentation, and develop strategies to navigate them, ensuring that they feel prepared and empowered when seeking resources.
Through active collaboration, counselors can help clients recognize their strengths; build resilience to adapt, recover, and grow when faced with adversity; and gain confidence in advocating for themselves in settings that may otherwise feel disempowering. This approach fosters an environment where clients feel seen, supported, and empowered to navigate both personal and systemic challenges as they arise.
Termination Considerations
Finally, SDoMH need to be broached in the context of termination because of their impact on client dropout rates and early termination of treatment (Roberts et al., 2022). Although counselors are traditionally taught that termination should be gradual and that clients should share readiness, that is not always the reality because of the influence of social determinants. For example, electricity or phone service may be terminated because of an inability to pay bills, thereby limiting the client’s access to virtual sessions; limited transportation or childcare may prevent continued session attendance. Although counselors hope that they will be able to have a final session, that is not always realistic.
Nevertheless, the termination period represents a critical phase of the clinical process and must be attended to as part of the counseling process (Baum, 2005; Goode et al., 2017; Knox et al., 2011; Lee et al., 2023; Vasquez et al., 2008). Therefore, incorporating SDoMH broaching behaviors throughout the counseling relationship lays the foundation for effective clinical termination, even if termination occurs prematurely. For example, enhancing skills such as self-advocacy and incorporating discussions of resource identification and utilization can help empower clients in the event of unexpected termination.
When a formal termination is possible, continuing to broach SDoMH throughout that process can strengthen therapeutic gains and enhance overall therapeutic outcomes. As such, a counselor may engage clients in discussions around how SDoMH have impacted their therapeutic experience and goal attainment during counseling. This conversation can extend to how SDoMH may influence goal attainment after counseling, including brainstorming potential challenges that may arise. Discussions around how to apply skills gained during counseling to navigate those challenges and address relevant social determinants can also be impactful.
Additionally, a counselor should recognize that clients who discontinue care because of SDoMH-related barriers may choose to reengage in counseling once those barriers have been resolved. Thus, using a screen door approach (Pester Boyd et al., 2025) to termination can be helpful. This may include broaching the process of how clients can return to counseling (e.g., whether a new intake is required, potential waitlist considerations), available options for returning (e.g., in person, telehealth, in-home), and factors that might warrant reengagement in counseling.
Broaching SDoMH during termination should also include providing and discussing a list of referrals and resources to support clients beyond counseling. These resources should address both immediate mental health needs and the social determinants that impact overall well-being. Clients may wish to discuss these referrals and resources further to better understand the process of accessing them. This may include empowering clients with language they can use in various settings, such as navigating legal, social services, or medical resources, or even role-playing those conversations.
Given the potential role of SDoMH in early termination, such discussions should begin early in the clinical process. For example, a counselor might say, “You mentioned concerns that you may lose your health insurance. Can we talk through what that may look like if that were to happen?” This helps the counselor address factors related to counseling and mental health while also helping the client brainstorm challenges, solutions, and resources. Using the other SDoMH broaching behaviors to sustain these conversations throughout the counseling process can lead to effective client termination, even if termination occurs unexpectedly.
SDoMH Broaching Behaviors and Counselor Education
There is a growing call within counseling and related mental health fields to enhance SDoMH training and increase counselor readiness to broach these topics in practice (Gantt-Howrey et al., 2024; Johnson & Robins, 2021; Newton & Steele, 2025; Pester Boyd et al., 2025). As such, counselor education programs at the master’s and doctoral levels should incorporate discussion and clinical practice opportunities to help counselors-in-training (CITs) build awareness of SDoMH and develop best practices for broaching and addressing their impact on client well-being. Counselor education programs can embed SDoMH broaching across coursework, supervision, and experiential learning to prepare CITs for ethical and effective practice.
Integrating SDoMH in Coursework and Supervision
SDoMH training may be integrated in a number of counselor education courses and aligns with Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2023) standards (Gantt-Howrey et al., 2024; Pester Boyd et al., 2025). For example, suggested activities per course/CACREP core area include: (a) examining ethical considerations of broaching SDoMH, including advocacy responsibilities and potential boundary issues when addressing systemic barriers (i.e., professional orientation and ethics); (b) helping CITs connect the MSJCC to SDoMH through case study analysis (i.e., social and cultural diversity); (c) highlighting how developmental outcomes are shaped by SDoMH (i.e., human growth and development); (d) addressing how economic stability, employment, and educational inequities intersect with career counseling (i.e., career development); (e) having CITs practice broaching SDoMH through role-plays to become aware of how SDoMH affects rapport, trust, and client disclosure (i.e., counseling and helping relationships); (f) integrating experiential activities in which students design psychoeducational groups focused on wellness promotion, social support, or navigating systemic barriers (i.e., group counseling and group work); (g) teaching CITs to administer and interpret SDoMH screening tools and to incorporate results into case conceptualizations (i.e., assessment and evaluation); and (h) requiring that CITs design projects to investigate the impact of SDoMH on client outcomes or evaluate community-based interventions (i.e., research and program evaluation).
In addition, practicum and internship supervision provides an important space for modeling SDoMH broaching and supporting CITs in developing cultural humility and ethical decision-making through structured activities. Supervisors might, for example, guide CITs in identifying protective factors through a strengths mapping exercise that charts client supports across individual, relational, community, and cultural identities. They can also facilitate role-plays in which CITs practice acknowledging the protective role of extended family, religious communities, cultural traditions, or neighborhood engagement. Site supervisors may also connect practicum activities to systemic issues, such as collaborating with schools or agencies on wellness or resource initiatives. Finally, reflective supervision discussions can help CITs analyze their own responses to client strengths and SDoMH barriers and notice whether they default to problem-solving or strength-building.
SDoMH Broaching in Experiential Learning
Experiential activities provide CITs with opportunities across coursework, practicum, and internship to connect theory to practice. Experiential activities may include case analysis, role-plays, assessment practice, community engagement, and classroom discussions focused on ethical dilemmas. First, CITs can analyze case vignettes to examine how SDoMH affect individuals and families. For example, dyads might review a case through the lens of a specific determinant such as housing insecurity or underemployment, discuss the client’s presenting concerns in context, and brainstorm broaching strategies. Second, structured role-plays further allow students to develop confidence in directly addressing SDoMH with clients. For example, in triadic supervision, CITs can rotate roles as counselor, client, and observer, while peers and supervisors provide feedback on the clarity and effectiveness of broaching behaviors.
Third, assignments that incorporate SDoMH assessment tools (e.g., PRAPARE, WE CARE Survey) also prepare CITs to integrate systemic factors into case conceptualization. CITs may practice administering and interpreting screeners with hypothetical clients and then learn to translate results into simple, jargon-free explanations for use in sessions. Fourth, community engagement projects deepen this preparation by connecting CITs to the systemic realities clients face. Examples include researching local issues such as food insecurity and mapping neighborhood resources.
Ethical reflection is also a part of experiential learning. Classroom discussions may explore balancing advocacy efforts with professional boundaries or managing countertransference when counselors share similar systemic challenges with their clients. In addition, classroom dialogue can highlight positive determinants of mental health by fostering empathy and compassion. Storytelling circles or guided conversations can invite CITs to share their own lived experiences of belonging or exclusion and consider how these experiences influence their empathy and ethical decision-making.
Cultural humility is the foundation for effective SDoMH broaching. To strengthen cultural humility and responsiveness, counselor education programs can embed the abovementioned experiential learning strategies across coursework and supervision. Self-reflection exercises may include journaling prompts such as: “What identities give me privilege and how might that shape my assumptions with clients?”; “How have I responded when a client’s worldview or values conflicted with my own? What could I do differently to remain open and nonjudgmental?”; and “Recall a time you felt excluded, misunderstood, or powerless. How does that experience shape your empathy for clients navigating systemic inequities?” These reflections can be revisited across the program to track growth in self-awareness and cultural responsiveness.
Guided discussions can be facilitated through fishbowl discussions in which CITs share and listen to experiences of privilege, discrimination, or cultural differences, followed by role-plays that practice broaching these issues in counseling. Counselor educators can model effective broaching and provide feedback on student language and presence during these exercises.
Promoting Positive Social Determinants
In addition to addressing negative SDoMH (e.g., discrimination, housing insecurity, poverty, community violence), counselor educators can help CITs recognize and promote positive SDoMH that build resilience. These determinants include self-care practices, strong social support, inclusive environments, cultural affirmation, and opportunities for growth and connection. In addition, counselor educators can model and encourage strengths-based approaches that affirm client identities, such as validating cultural, gender, or spiritual expressions, during intake and treatment planning.
Wellness models and self-care planning can be integrated into coursework to benefit both CITs and future clients. For example, assignments might include creating a personal self-care plan; evaluating wellness models and interventions across cultures; or designing a client-friendly handout that translates wellness strategies (e.g., mindfulness, exercise, nutrition, social connection) into accessible, culturally responsive language.
Counselor education programs can embed advocacy projects across coursework to promote systemic conditions that support mental health equity. Examples include partnering with schools to develop anti-bullying campaigns; creating culturally inclusive mental health awareness workshops for parents and teachers; and collaborating with community agencies to expand access in areas such as housing assistance, after-school programs, health care access, or transportation services. CITs might also design stigma-reduction campaigns with public health organizations.
Service-learning projects can further immerse students in community contexts by mapping resources, conducting needs assessments, or partnering with organizations addressing issues such as refugee resettlement, food insecurity, or housing justice. As service-learning projects conclude, CITs can be asked, “What systemic barriers did you observe and how might they affect mental health?”; “How did this experience shape your understanding of your role as advocate?”; and “How might insights from this project influence how you broach SDoMH with clients in practice?”
Preparing for SDoMH Broaching Challenges
Although broaching SDoMH is a critical counseling skill, CITs may face obstacles when attempting to apply it in future practice. Agency settings may limit the time available to explore systemic issues, and some trainees may feel anxious about making missteps when discussing topics such as poverty, discrimination, or community violence. Clients themselves may hesitate to disclose experiences of marginalization out of fear of judgment or because such issues have been dismissed in past encounters with helping professionals.
Counselor educators can support student development by intentionally acknowledging these challenges within the classroom and supervision spaces. For example, they might facilitate a structured dialogue in which CITs share their concerns about broaching while the counselor educator normalizes discomfort and models language for difficult conversations. In these dialogues, they might ask CITs, “What feelings come up for you when you think about broaching SDoMH with a client?”; “What makes these conversations challenging in practice?”; or “How might you respond if a client resists or shuts down when SDoMH are introduced?” Such discussions can help trainees recognize that hesitation is common and that growth comes from practice and feedback rather than perfection.
Another way to strengthen readiness is through guided debriefing of role-plays or client simulations. After a broaching exercise, counselor educators can ask CITs to reflect on moments in which they felt stuck, explore how power dynamics may have shaped the exchange, and brainstorm alternative approaches. For instance, a CIT might role-play broaching transportation barriers with a hypothetical client who frequently misses sessions. After the role-play, other CITs within the classroom or supervision session could examine the CIT’s wording and the client’s reaction and then suggest alternative ways to frame the issue that both validate the client’s struggle and highlight systemic factors.
Counselor educators can also discuss the limitations of broaching within supervision. When reviewing case presentations, supervisors might ask CITs not only how they addressed SDoMH but also what structural limitations they encountered and how those shaped the counseling process. For example, a CIT might describe working with a client who lacked consistent childcare and therefore missed several sessions. The supervisor could guide the student to consider how systemic gaps in affordable childcare both constrained the counseling process and required exploration of advocacy or referral options. These conversations emphasize that although broaching can validate client experiences, it cannot by itself dismantle inequities, thus highlighting the importance of community collaboration and ongoing advocacy. As counselor educators intentionally and thoroughly analyze the process together, CITs can learn to approach barriers not as failures but as opportunities to deepen cultural humility.
Evaluating SDoMH Broaching Behaviors
Currently, there are no existing measures to evaluate SDoMH broaching behaviors, and future research should prioritize the development of validated tools to assess both counselor competency in SDoMH broaching and client perceptions of these efforts. Quantitative studies could focus on designing and testing new measures that assess the clarity, timing, cultural responsiveness, and impact of SDoMH broaching within the counseling relationship. Counseling researchers could utilize these instruments to conduct longitudinal studies and controlled intervention studies exploring the influence that SDoMH broaching has on client trust, client engagement in counseling, and therapeutic outcomes.
Until instruments specific to SDoMH broaching have been developed, researchers can use existing scales that independently measure broaching behaviors (e.g., Day-Vines et al., 2013; Day-Vines et al., 2024), SDoMH readiness (e.g., Johnson, 2023) and SDoMH assessment (e.g., Gantt-Howrey et al., 2024) to understand effective counseling behavior related to these constructs.
In addition to quantitative approaches, qualitative studies can help inform the impact of broaching behaviors on clients, CITs, and counselors. Studies that explore client experiences with counselors who broach SDoMH can provide contextual nuance and enhance multiculturally competent practice. For instance, interviews or focus groups with clients might uncover how broaching influences their feelings of safety, empowerment, or stigma reduction. Furthermore, researchers could conduct case studies of counselors in varied settings to examine how SDoMH broaching unfolds in practice. Data from session transcripts and client and counselor interviews could reveal additional best practices for addressing SDoMH, promoting positive social determinants, and counteracting challenges that counselors may have while broaching SDoMH.
Conclusion
Learning to effectively broach SDoMH provides an opportunity for counselors to further operationalize Ratts et al.’s (2016) MSJCC. As the cross-disciplinary call for universal SDoMH screening practices continues to grow across health professions, to remain leaders among the mental health professions, counselors must begin intentionally broaching SDoMH with clients. However, as a profession, broaching SDoMH may require reexamining the professional counselor identity, expanding advocacy roles, and reviewing ethical standards that may inadvertently create barriers to effectively addressing the impact of social determinants on clients’ lives.
Preliminary research suggests that effectively broaching SDoMH throughout the counseling process supports a number of short- and long-term benefits to clinical practice, which warrants its further integration and evaluation in the counseling profession. Counselors perceive that in the short term, broaching SDoMH strengthens the therapeutic relationship while fostering MSJCC (Pester Boyd et al., 2025). These early benefits can give way to enhanced client empowerment and improved access to interprofessional resources and services, both of which can lead to better treatment outcomes. Long-term, effectively broaching SDoMH can result in improved overall health of the client, improved community health, and decreased marginalization.
The MMBB (Day-Vines et al., 2020) and SDCM (Pester Boyd et al., 2025) provide needed frameworks to enhance these client outcomes. Using the integration of these frameworks as a foundation, we identified six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences of lived experience, (e) addressing emergent needs, and (f) SDoMH-informed termination practices. These broaching behaviors provide specific guidance for how to integrate SDoMH into counseling practice, which operationalizes the mandate of the MSJCC to address systemic and environmental factors impacting client mental health. We suggest that counselors integrate the identified SDoMH broaching behaviors throughout all stages of the therapeutic process to support a strong counselor–client relationship, enhanced client self-disclosure, increased client satisfaction, and improved therapeutic outcomes.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Baum, N. (2005). Correlates of clients’ emotional and behavioral responses to treatment termination. Clinical Social Work Journal, 33(3), 309–326. https://doi.org/10.1007/s10615-005-4946-5
Brookover, D. L. (2024). The career development and social determinants framework: An integrative approach. Professional School Counseling, 28(1), 1–12. https://doi.org/10.1177/2156759X241290494
Center for Medicare & Medicaid Innovation. (n.d.). The accountable health communities health-related social needs screening tool. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
Compton, M. T., & Shim, R. S. (2015). The social determinants of mental health. Focus, 13(4), 419–425. https://doi.org/10.1176/appi.focus.20150017
Compton, M. T., & Shim, R. S. (2020). Why employers must focus on the social determinants of mental health. American Journal of Health Promotion, 34(2), 215–219. https://doi.org/10.1177/0890117119896122c
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2024/04/2024-Standards-Combined-Version-4.11.2024.pdf
Day-Vines, N. L., Bryan, J., and Griffin, D. (2013). The Broaching Attitudes and Behavior Survey (BABS): An exploratory assessment of its dimensionality. Journal of Multicultural Counseling and Development, 41(4), 210–223. https://doi.org/10.1002/j.2161-1912.2013.00037.x
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., & Gubara, S. (2021). Strategies for broaching the subjects of race, ethnicity, and culture. Journal of Counseling & Development, 99(3), 348–357. https://doi.org/10.1002/jcad.12380
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., Gubara, S., & Otabil, N. A. A. (2020). The multidimensional model of broaching behavior. Journal of Counseling & Development, 98(1), 107–118. https://doi.org/10.1002/jcad.12304
Day-Vines, N. L., Zhang, J., Cluxton-Keller, F., Hicks, D., Jones, C., Spann, R. T., Daga, D., & Agorsor, C. (2024). The development and validation of an instrument to examine clients’ perspectives about their counselors’ ability to broach racial, ethnic, and cultural concerns. Journal of Multicultural Counseling and Development, 52(3), 173–188. https://doi.org/10.1002/jmcd.12300
Depauw, H., Van Hiel, A., Talal, H., Dierckx, K., Geenen, F., Valcke, B., & De Clercq, B. (2025). The development of the Broaching Assessment Scale: A client-rated measure of therapists’ broaching behaviour in clinical counselling. Psychotherapy Research, 35(3), 424–440. https://doi.org/10.1080/10503307.2024.2301948
Dolan, N., Simmonds-Buckley, M., Kellett, S., Siddell, E., & Delgadillo, J. (2021). Effectiveness of stress control large group psychoeducation for anxiety and depression: Systematic review and meta-analysis. British Journal of Clinical Psychology, 60(3), 375–399. https://doi.org/10.1111/bjc.12288
Drinane, J. M., Owen, J., & Tao, K. W. (2018). Cultural concealment and therapy outcomes. Journal of Counseling Psychology, 65(2), 239–246. https://doi.org/10.1037/cou0000246
Gantt-Howrey, A., Lin, M., Shaikh, A., Johnson, K. F., Preston, J. W., & Wilson, L. (2024). Assessing social determinants of mental health: Client experiences and counselor practices. Journal of Counseling & Development, 102(4), 394–405. https://doi.org/10.1002/jcad.12519
Garg, A., Butz, A. M., Dworkin, P. H., Lewis, R. A., Thompson, R. E., & Serwint, J. R. (2007). Improving the management of family psychosocial problems at low-income children’s well-child care visits: The WE CARE Project. Pediatrics, 120(3), 547–558. https://doi.org/10.1542/peds.2007-0398
Goode, J., Park, J., Parkin, S., Tompkins, K. A., & Swift, J. K. (2017). A collaborative approach to psychotherapy termination. Psychotherapy, 54(1), 10–14. https://doi.org/10.1037/pst0000085
Johnson, K. F. (2023). Development and initial validation of the Addressing Client Needs with Social Determinants of Health Scale (ACN: SDH). BMC Health Services Research, 23(1), 374. https://doi.org/10.1186/s12913-023-09292-z
Johnson, K. F., & Brookover, D. L. (2021). School counselors’ knowledge, actions, and recommendations for addressing social determinants of health with students, families, and in communities. Professional School Counseling, 25(1). https://doi.org/10.1177/2156759X20985847
Johnson, K. F., Cunningham, P. D., Tirado, C., Moreno, O., Gillespie, N. N., Duyile, B., Hughes, D. C., Scott, E. G., & Brookover, D. (2023). Social determinants of mental health considerations for counseling children and adolescents. Journal of Child and Adolescent Counseling, 9(1), 21–33. https://doi.org/10.1080/23727810.2023.2169223
Johnson, K. F., Gantt-Howrey, A., Duyile, B. E., Robins, L. B., & Dockery, N. (2024). Career counselors addressing social determinants of mental health in rural communities. The Professional Counselor, 14(1), 1–14. https://doi.org/10.15241/kfj.14.1.1
Johnson, K., & Robins, L. B. (2021). Counselor educators experiences and techniques teaching about social-health inequities. Journal of Counselor Preparation and Supervision, 14(4). https://research.library.kutztown.edu/jcps/vol14/iss4/ 7
King, K. M., & Borders, L. D. (2019). An experimental investigation of White counselors broaching race and racism. Journal of Counseling & Development, 97(4), 341–351. https://doi.org/10.1002/jcad.12283
Knox, S., Adrians, N., Everson, E., Hess, S., Hill, C., & Crook-Lyon, R. (2011). Clients’ perspectives on therapy termination. Psychotherapy Research, 21(2), 154–167. https://doi.org/10.1080/10503307.2010.534509
Lee, P.-S., Wang, L.-F., & Swift, J. K. (2023). Clients’ and counselors’ termination decisions and experiences in counseling. Current Psychology, 42, 3734–3744. https://doi.org/10.1007/s12144-021-01725-4
Lenz, A. S., & Lemberger-Truelove, M. E. (2023). The social determinants of mental health and professional counseling: A call to action. Journal of Counseling & Development, 101(4), 375–380. https://doi.org/10.1002/jcad.12489
Lenz, A. S., & Litam, S. D. A. (2023). Integrating the social determinants of mental health into case conceptualization and treatment planning. Journal of Counseling & Development, 101(4), 416–428. https://doi.org/10.1002/jcad.12487
Lund, C., Brooke-Sumner, C., Baingana, F., Baron, E. C., Breuer, E., Chandra, P., Haushofer, J., Herrman, H., Jordans, M., Kieling, C., Medina-Mora, M. E., Morgan, E., Omigbodun, O., Tol, W., Patel, V., & Saxena, S. (2018). Social determinants of mental disorders and the sustainable development goals: A systematic review of reviews. The Lancet Psychiatry, 5(4), 357–369. https://doi.org/10.1016/S2215-0366(18)30060-9
Luo, H., Li, Y. L., Luo, X. J., Xia, L., Xiao, J., Xiao, H., & Chen, J. (2025). The efficacy of psychoeducation-based programs on internalized stigma in patients with schizophrenia: A systematic review and meta-analysis. Psychiatry Research, 350, 116540. https://doi.org/10.1016/j.psychres.2025.116540
Mason, S., Ragan, M., Gilbert, S. H., & Lenz, A. S. (2023). Social determinants of mental health: Implications for measurement, research, and evaluation. Journal of Counseling & Development, 101(4), 440–448. https://doi.org/10.1002/jcad.12490
Neal Keith, S., Coleman, M. L., Hicks Becton, L. Y., & Springfield, J. (2023). Assessing the social determinants of mental health in counseling practice. Journal of Counseling & Development, 101(4), 381–391. https://doi.org/10.1002/jcad.12470
Newton, C., & Steele, J. M. (2025). The broaching readiness framework: A path for psychologists to embrace cultural opportunities. Counselling Psychology Quarterly, 38(4), 1135–1152. https://doi.org/10.1080/09515070.2025.2458034
Office of Disease Prevention and Health Promotion. (2025). Social determinants of health. https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health
Owen, J., Tao, K. W., Imel, Z. E., Wampold, B. E., & Rodolfa, E. (2014). Addressing racial and ethnic microaggressions in therapy. Professional Psychology: Research and Practice, 45(4), 283–290. https://doi.org/10.1037/a0037420
Pester, D. A., Jones, L. K., & Talib, Z. (2023). Social determinants of mental health: Informing counseling practice and professional identity. Journal of Counseling & Development, 101(4), 392–401. https://doi.org/10.1002/jcad.12473
Pester Boyd, D. A., Hays, D. G., & Jones, L. K. (2025). Assessing and addressing social determinants of mental health in counseling: A grounded theory investigation. Journal of Counseling & Development, 103(4), 469–483. https://doi.org/10.1002/jcad.70003
PRAPARE. (2022). Protocol for responding to and assessing patient assets, risks, and experiences: Implementation and action toolkit. https://prapare.org/wp-content/uploads/2022/09/Full-Toolkit_June-2022_Final.pdf
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Roberts, T., Esponda, G. M., Torre, C., Pillai, P., Cohen, A., & Burgess, R. A. (2022). Reconceptualising the treatment gap for common mental disorders: A fork in the road for global mental health? The British Journal of Psychiatry, 221(3), 553–557. https://doi.org/10.1192/bjp.2021.221
Robins, L. B., Johnson, K. F., Duyile, B., Gantt-Howrey, A., Dockery, N., Robins, S. D., & Wheeler, N. (2022). Family counselors addressing social determinants of mental health in underserved communities. The Family Journal, 31(2), 213–221. https://doi.org/10.1177/10664807221132799
U.S. Department of Health and Human Services. (2023). Our epidemic of loneliness and isolation: The U.S. Surgeon General’s advisory on the healing effects of social connection and community. https://www.hhs.gov/sites/default/files/surgeon-general-social-connection-advisory.pdf
Vasquez, M. J. T., Bingham, R. P., & Barnett, J. E. (2008). Psychotherapy termination: Clinical and ethical responsibilities. Journal of Clinical Psychology, 64(5), 653–665. https://doi.org/10.1002/jclp.20478
World Health Organization. (2025). Social determinants of health. https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1
Zhang, N., & Burkard, A. W. (2008). Client and counselor discussions of racial and ethnic differences in counseling: An exploratory investigation. Journal of Multicultural Counseling and Development, 36(2), 77–87. https://doi.org/10.1002/j.2161-1912.2008.tb00072.x
Danielle Pester Boyd, PhD, NCC, LPC (TX), RPT, is an assistant professor at Auburn University. Laura K. Jones, PhD, is an associate professor at the University of North Carolina at Asheville. Courtney Maier, MEd, NCC, APC, is a doctoral student at Auburn University. Danica G. Hays, PhD, is a dean and professor at the University of Nevada Las Vegas. Correspondence may be addressed to Danielle Pester Boyd, 345 West Samford Avenue, Suite 3188, Auburn, AL 36849, danielle.boyd@auburn.edu.
Apr 1, 2026 | Volume 16 - Issue 1
Brian J. Clarke, Michael T. Hartley, Austin M. Guida
Impostor phenomenon (IP), characterized by persistent self-doubt despite objective success, is prevalent during the early stages of counselor development, often emerging as individuals transition from training into professional practice. This study examined whether self-compassion mediates relationships between IP, resilience, and mental health among 281 counselors-in-training enrolled in departments accredited by the Council for the Accreditation of Counseling and Related Educational Programs. Mediation analyses showed that self-compassion fully mediated the effects of IP on resilience and depression and partially mediated the effect on anxiety. MANOVA results indicated that higher self-compassion corresponded with lower IP, anxiety, and depression, and greater resilience, with robust effects. Findings identify self-compassion as a developmental competency that supports balanced self-evaluation, emotional regulation, and sustainable counselor well-being. Integrating self-compassion training into counselor education and supervision may help developing counselors manage impostor-related distress, strengthen resilience, and promote ethical, sustainable professional practice.
Keywords: impostor phenomenon, counselor development, self-compassion, resilience, mental health
Building resilience and prioritizing mental health are vital during the formative stages of counselor development. During the early stages of training and supervised practice, developing counselors experience the inherent emotional demands and elevated anxiety common while learning to integrate theoretical knowledge into clinical practice (Skovholt & Trotter-Mathison, 2024; Stoltenberg & McNeill, 2010). Although these feelings may diminish with increased experience, enduring self-doubt and inadequacy may signal impostor phenomenon (Clance & Lawry, 2024). Imposter phenomenon (IP), characterized by persistent feelings of fraudulence and incompetence despite evidence of success, impacts nearly all developing counselors (Clarke et al., 2025; Tigranyan et al., 2021). Those experiencing IP may struggle to internalize mastery experiences and fail to consolidate moments of success into genuine confidence (Gadsby & Hohwy, 2024; Roskowski, 2010). Individual differences in coping with IP may be partially explained by self-compassion, which may buffer IP’s negative effects on counseling self-efficacy and well-being (Clarke et al., 2025).
The persistent fear of being exposed as a fraud becomes a harmful cycle whereby individuals ruminate on perceived shortcomings, discount positive feedback, and misattribute positive outcomes to external factors (Clance & Lawry, 2024). Behaviors associated with IP include extreme perfectionism, procrastination, and/or exhausting overpreparation, which can inhibit counselor development (Clarke et al., 2025; Nguyen, 2023). Because IP is rooted in shame and feelings of inadequacy, it contributes to isolation, burnout, and compassion fatigue (Garba et al., 2024; Ojeda, 2024).
IP undermines the reflective, relational, and self-evaluative capacities that are central to counselor development. Counselors who experience chronic self-doubt may hesitate to disclose errors in supervision, question their competence, and struggle to sustain resilience, patterns that can jeopardize client care and professional longevity (Delaney, 2018; Housenecht & Swank, 2022). Given the demands of counselor training and practice, protective factors such as resilience and self-compassion may be critical for developing counselor well-being and persistence.
Resilience is a protective factor to cope with mental distress and burnout (Gerber & Anaki, 2021; Webb & Rosenbaum, 2019). Emerging from the positive psychology movement, resilience explains why some individuals behave adaptively under great stress while others do not. Beyond recovery from adversity, resilience is a process of successful adaptation and coping during challenging or threatening circumstances (Webb & Rosenbaum, 2019). Cultivating new coping mechanisms and fostering personal growth, resilience can sustain well-being and performance during difficult experiences. The limited research on resilience among developing counselors has identified self-awareness and self-compassion as critical protective factors to cope with the emotional demands of becoming a counselor (Hou & Skovholt, 2020).
As a protective factor, self-compassion can play an important role in the resilience and mental health of developing counselors, especially in the presence of IP (Clarke et al., 2025; Neff et al., 2005). Self-compassion is comprised of three interrelated dimensions: mindfulness, common humanity, and self-kindness (Neff, 2023). Mindfulness, the core of self-compassion, involves maintaining awareness of present experiences with reduced reactivity and self-judgment. The common humanity dimension refers to the acceptance that suffering is inherent to our shared human experience. By normalizing challenging experiences, this perspective helps prevent the isolation that may arise from perceiving failures as uniquely personal. Finally, self-kindness encompasses behaviors and ways of relating intrapersonally that offer support and comfort during times of suffering or setbacks. Rather than defaulting to self-criticism, overidentification with failures, or isolation, self-compassion enables understanding and resilience, reducing the impact of IP and the fear of failure during counselor development (Clarke et al., 2025; Warren et al., 2016).
The theoretical alignment between self-compassion and resilience is rooted in their shared emphasis on adaptive emotional regulation, growth through adversity, and the development of a stable and supportive inner identity (Warren et al., 2016). Self-compassion supports sustainable resilience by reducing self-criticism and perfectionism and fostering a growth mindset (Neff, 2023; Warren et al., 2016). Indeed, a recent meta-analysis indicated that self-compassion is consistently linked to positive outcomes among mental health professionals, including enhanced competence, improved therapeutic presence, and a greater willingness to seek guidance and supervision (Crego et al., 2022).
Because of its regulating effects, self-compassion may help developing counselors to tolerate the stress of IP through improved emotional self-regulation (Crego et al., 2022; Neff, 2023). In this way, self-compassion can function as an emotion-focused coping mechanism that reduces the mental distress associated with IP (Clarke, 2024; Crego et al., 2022; Gerber & Anaki, 2021). Ultimately, when individuals experience IP-related distress, self-compassionate responses (mindfulness, common humanity, self-kindness) may interrupt the IP cycle, preserving resilience and mental health (Neff et al., 2005).
The purpose of this study is to examine how self-compassion functions as a protective factor in the relationship between IP, resilience, and mental health during counselor development. Research has found self-compassion to support resilience among health care providers (Delaney, 2018), yet much less is known about the relationship between self-compassion and resilience among developing counselors who experience IP. Addressing the negative impact of IP on counselor development, this article explores how self-compassion might mitigate IP’s negative relationships with resilience and mental health (Clarke et al, 2025; Roskowski, 2010; Tigranyan et al., 2021). The guiding research questions were:
- To what extent does self-compassion mediate the relationships between IP and the outcomes of resilience and mental health?
- How do levels of self-compassion relate to variations in IP, resilience, and mental health among the sample?
We hypothesized that IP would have a significant negative relationship with resilience and mental health, and that self-compassion will significantly mediate these negative associations. Specifically, higher levels of self-compassion will relate to lower IP and improved mental health and resilience. Our findings offer valuable insights into how self-compassion can enhance resilience and promote mental health during counselor development.
Methods
Procedure
The study received IRB approval prior to the recruitment of master’s-level counseling students from across the United States. Data were collected between April and October 2023, using an online survey disseminated via email to Council for the Accreditation of Counseling and Related Educational Programs (CACREP)–accredited program liaisons. These emails described the study and outlined informed consent procedures and inclusion criteria. Eligible participants were individuals enrolled in CACREP-accredited counseling programs aged 18 or older. After consenting, participants were presented with the measures and a demographic questionnaire developed by the authors. Engagement with the study concluded once participants either completed or exited the survey.
Participants
The sample consisted of 281 counseling students attending CACREP-accredited counseling programs from 37 U.S. states and the District of Columbia. Although the present sample consisted of counselors-in-training (CITs), the term developing counselors is used throughout this paper to reflect the broader developmental continuum that spans counselor training and early professional practice (Stoltenberg & McNeill, 2010).
Consistent with the population of CITs, most participants identified as White (n = 190, 67.29%) with lower percentages identifying as Hispanic or Latinx (n = 43, 15.2 %), Asian (n = 17, 6.0%), African American or Black (n = 13, 4.6%), multiracial (n = 13, 4.6%), American Indian or Alaskan Native (n = 3, 1.1%) and Middle Eastern (n = 2, 0.7%). The majority (n = 237, 83.7%) identified as female, with 32 (11.3%) identifying as male, 6 (2.1%) as non-binary, 4 (1.4%) as genderqueer, and 2 (0.7%) choosing not to disclose their gender identity. Participants were from clinical mental health (n = 170, 60.1%), school counseling (n = 49, 17.3%), rehabilitation counseling (n = 49, 17.3%), and marriage and family counseling (n = 13, 4.6%) programs. The average participant age was 32 years (SD = 10.35), with an age range from 21 to 67 years.
Measures
Self-Compassion Scale-Short Form (SCS-SF)
The SCS-SF is a short form of the Self-Compassion Scale (Neff, 2003), consisting of 12 self-report items selected from the original scale (Raes et al., 2011). Items are rated on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Examples include “I try to see my failings as part of the human condition” and “I’m disapproving and judgmental about my own flaws and inadequacies” (Neff, 2003, p. 2). SCS-SF scores have shown good internal consistency (α = .86), with its total scores strongly correlating with those of the full version (r = .98; Raes et al., 2011). Factor analysis has confirmed that the SCS-SF shares the same factor structure as the original scale (Neff et al., 2019; Raes et al., 2011). Scores are interpreted as levels of self-compassion: low (1–2.4), moderate (2.5–3.5), and high (3.51–5). In the present study, SCS-SF scores demonstrated good internal consistency reflected in an alpha of .85, and omega of .85.
Academic Resilience Scale-6 (ARS-6)
The ARS-6 is a concise self-report scale designed to measure academic resilience, defined as the ability to manage challenges, stress, and setbacks within a learning environment (Martin & Marsh, 2006). Items include statements such as “I’m good at bouncing back from a poor grade or difficult feedback” and “I don’t let a bad grade or feedback affect my confidence.” Responses are rated on a 7-point Likert-type response scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater academic resilience. Item and factor level construct validity was supported through factor score estimates, correlation, path analysis, and cluster analysis, showing the ARS scores were closely aligned with related constructs including self-efficacy, control, planning, low anxiety, and persistence (Martin & Marsh, 2006). ARS-6 scores have demonstrated good internal consistency, with an alpha coefficient of .89 (Martin & Marsh, 2006). In the current study, the ARS-6 scores showed acceptable reliability supported by alpha and omega scores of .83.
Clance Impostor Phenomenon Scale (CIPS-10)
The CIPS-10 (Wang et al., 2022) is a condensed, 10-item version of the original 20-item Clance Impostor Phenomenon Scale (CIPS) designed to assess impostor feelings (Clance, 1985). A systematic review by Mak et al. (2019) supported the CIPS-20 as a valid (construct, criterion, and content) measure of IP. The CIPS-10 utilizes a Likert-type response scale ranging from 1 (not at all true) to 5 (very true) and includes items from the CIPS-20, such as “I’m afraid people important to me may find out that I’m not as capable as they think I am” and “I feel my success was due to some kind of luck rather than competence.” Wang et al. (2022) reported strong internal reliability for the CIPS-10 (α = .93), with total scores closely aligning with those of the CIPS-20. Construct validity was supported through factor score estimates, revealing a single-factor structure similar to the 20-item version. In this study, CIPS-10 scores were interpreted using adjusted categories from Clance (1985): few IP (less than 20), moderate IP (20–29), frequent IP (30–39), and intense IP (40–50). Within the current sample, CIPS-10 scores demonstrated good internal consistency with an alpha of .88 and omega of .90.
Patient Health Questionnaire-4 (PHQ-4)
The PHQ-4 is a 4-item, self-report assessment screening tool for depression and anxiety (Kroenke et al., 2009). The Likert-type responses are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). A total score of 3 or more, across both items, indicates the presence of moderate-to-severe symptoms (Kroenke et al., 2009). In meta-analyses, PHQ-4 scores have shown good internal consistency (α = .89) and have yielded valid and diagnostically accurate depression and anxiety scores (Khubchandani et al., 2016; Kroenke et al, 2009). Construct validity was supported using a varimax-rotated principal components analysis conducted on the four screening items (PHQ-2 and GAD-2), yielding two components that together explained 83% of the overall variance. Likewise, criterion validity was indicated by individuals diagnosed with depression or anxiety by a health care professional scoring significantly higher on the PHQ-2, GAD-2, and PHQ-4 compared to participants without a clinical diagnosis (Khubchandani et al., 2016). In the present sample, the PHQ-4 scores showed good internal consistency with an alpha score of .87 and omega of .84.
Data Analysis
Portions of this data set informed a previously published manuscript that focused on how self-compassion can mitigate IP’s negative relationship with counselor self-efficacy (Clarke et al., 2025). Although the two manuscripts share IP and self-compassion data, the current manuscript is distinct and extends this line of inquiry by its unique focus on the benefits of self-compassion for counselor resilience and mental health, despite the presence of IP.
All analyses were performed using SPSS (v29) with a p ≤ .01 benchmark to reduce the likelihood of Type I error and ensure that the most reliable effects are interpreted as statistically meaningful. Preliminary analyses were conducted to examine statistical assumptions for the mediation and MANOVA models. Normality was confirmed for all variables via Shapiro-Wilk (all p > .05). Box’s M test supported homogeneity of variance–covariance matrices (p = .021), and observations were independent. In addition to all VIF scores being < 2, no bivariate correlations exceeded r = .80, suggesting that multicollinearity was not a concern. Collectively, these results suggest that the data met all assumptions necessary for the planned analyses (Tabachnick & Fidell, 2019).
We selected a regression-based mediation analysis because of the study’s focus on specific indirect effects of self-compassion and the moderate sample size, both of which made alternative analyses less ideal (Hayes, 2022). Because the variables tested were represented by composite scores rather than latent constructs, a mediation was statistically appropriate and provided a parsimonious method to examine self-compassion as a buffer for IP. Although cross-sectional mediation cannot establish temporal precedence or causation, it can identify statistical pathways that warrant future longitudinal investigation (Fairchild & McDaniel, 2017; Hayes, 2022). The 99% confidence intervals (CI) of the effects were derived from 10,000 bootstrap samples. If the upper and lower bounds of the CI did not include zero, they were considered statistically significant.
Finally, MANOVA was used to determine how the severity of IP affected its relationships with resilience, anxiety, depression, and self-compassion. The four levels of IP used in this analysis were defined as few, moderate, frequent, and intense IP according to the CIPS author (Clance, 1985). MANOVA effect size was described using partial eta squared values of 0.01 (small), 0.059 (medium), and 0.14 (large; Richardson, 2011). Cohen’s d was used to interpret effect sizes for follow up Tukey analyses, small effect (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8; Gignac & Szodorai, 2016).
A priori power analysis for mediation effects (Fritz & MacKinnon, 2007) indicated a minimum sample of 148 participants would provide .80 power to detect medium-sized indirect effects using bias-corrected bootstrapping. For MANOVA with three groups and four dependent variables, G*Power indicated 158 participants would yield .80 power for detecting medium effects (f² = .25). Our sample of 281 exceeded both requirements.
Results
Descriptives
Pearson correlations indicated significant (< .01) bivariate relationships among self-compassion, impostor phenomenon, depression, anxiety, and academic resilience (Table 1). There were no significant differences in self-compassion, IP, resilience, anxiety, or depression across demographics or counseling program emphasis.
Table 1
Descriptive Statistics and Bivariate Correlations
|
Mean |
SD |
1 |
2 |
3 |
4 |
|
| 1. Self-Compassion |
3.06 |
0.74 |
– |
|
|
|
| 2. Impostor Phenomenon |
32.81 |
8.22 |
−.54* |
– |
|
|
| 3. Depression |
1.27 |
1.60 |
−.42* |
.35* |
– |
|
| 4. Anxiety |
2.54 |
1.78 |
−.55* |
.46* |
.59* |
– |
| 5. Academic Resilience |
27.66 |
6.51 |
.53* |
−.36* |
−.23* |
−.40* |
*p ≤ .01.
The sample included high levels of impostor phenomenon (M = 32.81, SD = 8.22), with over 65% falling in the frequent-to-intense range. IP showed strong negative correlations with self-compassion (r = −.54) and resilience (r = −.36), and strong positive correlations with anxiety (r = .46) and depression (r = .35).
Mediation Analysis
Mediation analyses were used to explore the statistical associations among IP, self-compassion, and the outcome variables of resilience, anxiety, and depression. Results indicated that self-compassion functioned as a statistical mediator in the relationships between IP and each outcome.
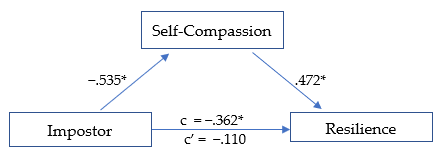
Figure 1
Mediation Analysis: Impostor and Resilience
*p ≤ .01
The first model (Figure 1) was significant, R² = .290, F(1, 278) = 59.78, p < .01. The total effect (c) of IP on academic resilience was negative and significant, β = −.362, SE = .126, t = −2.868, p < .01, suggesting that higher IP scores were associated with lower resilience. When self-compassion was included in the model, the direct effect (c′) of IP on resilience was no longer significant, β = −.110, SE = .060, t = −1.838, p = .07, consistent with full statistical mediation (Hayes, 2022). The indirect pathway through self-compassion represented 69.6% of the total standardized association. IP was negatively associated with self-compassion (β = −.535, p < .01; large effect), and self-compassion was positively associated with resilience (β = .472, p < .01; large effect). The overall indirect effect was significant (β = −.252, p < .01).
Figure 2
Mediation Analysis: Impostor and Anxiety
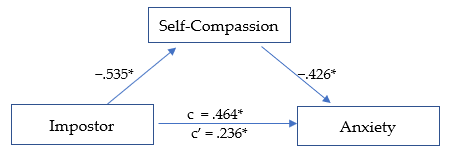
*p ≤ .01.
The second model (Figure 2) was significant, R² = .345, F(1, 278) = 73.159, p < .01. The total effect (c) of IP on anxiety was positive and significant, β = .464, SE = .053, t = 8.747, p < .01, indicating that higher IP scores were related to higher anxiety levels. After including self-compassion, the direct effect (c′) was reduced but remained significant, β = .236, SE = .057, t = 4.110, p < .01, suggesting partial statistical mediation. The indirect pathway through self-compassion accounted for 49.2% of the total standardized association. IP was negatively associated with self-compassion (β = −.535,p < .01; large effect), and self-compassion was negatively associated with anxiety (β = −.426, p < .01; medium effect). The overall indirect effect was significant, β = −.228, p < .01.
Figure 3
Mediation Analysis: Impostor and Depression
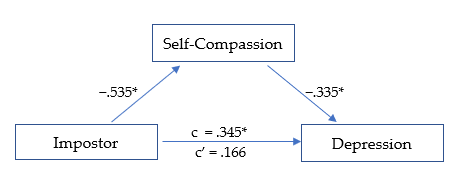
*p ≤ .01.
The third model (Figure 3) was significant, R² = .199, F(1, 278) = 34.484, p < .01. The total effect (c) of IP on depression was positive and significant, β = .345, SE = .056, t = 6.135, p < .01, indicating that higher IP scores were associated with higher depression levels. After accounting for self-compassion, the direct effect (c′) was reduced and no longer significant, β = .166, SE = .064, t = 2.611, p = .02, suggesting full statistical mediation. The indirect pathway through self-compassion represented 51.9% of the total standardized association. IP was negatively related to self-compassion (β = −.535, p < .01; large effect), and self-compassion was negatively related to depression (β = −.335, p < .01; medium effect). The overall indirect effect was significant, β = −.179, p < .01.
MANOVA
Self-compassion scores were divided into three levels (low, moderate, and high) as suggested by Neff (2003) to determine if the effect of self-compassion was consistent across each level. MANOVA analyses revealed that IP, resilience, depression, and anxiety each varied significantly based on level of self-compassion, F(8, 550) = 20.790, p < .01, Wilk’s Λ = 0.590, ηp2 = .232, indicating a large effect size.
The MANOVA results revealed that IP scores varied according to level of self-compassion, F(2, 281) = 48.807, p < .01, ηp2 = .260, with a large effect size. IP decreased significantly at each rising level of self-compassion, from low to moderate (d = 0.666, p < .01) and moderate to high (d = 0.987, p < .01), with medium and large effect sizes, respectively. The greatest decrease in IP was seen as self-compassion rose from moderate to high.
Resilience was significantly higher at each increasing level of self-compassion F(2, 281) = 39.323, p < .01, ηp2 = .221, with a large overall effect size. Resilience rose linearly across each level of self-compassion, from low to moderate (d = −0.756, p < .01), and from moderate to high (d = −0.790, p < .01), each with a medium-high effect size.
Depression scores lowered significantly as self-compassion level increased, F(2, 281) = 20.232, p < .01, ηp2 = .127, with an overall medium effect size. The decrease in depression was noted across levels of self-compassion, from low to moderate (d = 0.446, p < .01), and from moderate to high (d = 0.625, p < .01), each with a medium effect size. The largest decrease in depression was observed as self-compassion rose from moderate to high.
Anxiety scores decreased significantly as the level of self-compassion increased, F(2, 281) = 45.898, p < .01, ηp2 = .248, with a large overall effect size. Anxiety scores were lower as self-compassion rose from low to moderate (d = 0.895, p < .01), and from moderate to high (d = 0.711, p < .01), with large and medium effect sizes, respectively. The largest decrease in anxiety was noted as self-compassion increased from low to moderate.
Discussion
Our findings indicate that self-compassion is a strong protective factor and may enhance resilience and promote mental health among developing counselors, despite impostor feelings. Specifically, self-compassion fully mediated the negative relationship between IP, resilience, and depression, while partially mediating the relationship between IP and anxiety. This suggests that even when experiencing IP, higher self-compassion may help to maintain greater resilience and significantly reduced anxiety and depression. The results are promising and suggest that cultivating self-compassion may facilitate professional growth by interrupting the IP cycle. Our results offer further insights into how self-compassion can support resilience and mental health (Housenecht & Swank, 2022).
Descriptive Statistics
Descriptive analyses revealed a notably high prevalence of IP in the sample, with 96.1% (n = 270) reporting moderate to intense symptoms. Scores were skewed toward the higher end of the scale, with 65.1% of participants in the frequent-to-intense range and 21% in the highest category. Compared with earlier samples, these findings suggest that the severity of IP has increased substantially over the past 15 years (Roskowski, 2010; Tigranyan et al., 2021). For example, only 27.6% of a 2010 sample fell into the frequent-to-intense categories, compared with nearly two-thirds in the present study. Likewise, the proportion of students in the highest IP range has risen fivefold, from 4.1% in 2010 to 21% here. Although this increase may be influenced by broader cultural or educational factors, the trend underscores the importance of implementing effective coping strategies to support counselor well-being and persistence.
Consistently elevated IP scores across studies suggest that impostor feelings may be a common element of counselor development. Such feelings are often fueled by both internal and environmental pressures, particularly graduate students’ unreasonably high expectations of their performance and rapid development (Clance & Lawry, 2024). These unrealistic standards can generate unnecessary self-doubt, distorted self-assessments, and persistent self-criticism (Gadsby & Hohwy, 2024). Importantly, the current results indicate that self-compassion is a powerful counterbalance to IP. Higher self-compassion was associated with lower IP, anxiety, and depression, and with greater resilience, findings that align with previous research (Liu et al., 2023).
Mediation Models
Self-Compassion, IP, and Resilience
The first mediation analysis revealed that self-compassion fully mediated the negative relationship between IP and resilience. When accounting for self-compassion, the negative relationship between IP and resilience was rendered statistically non-significant. This outcome suggests that developing counselors with higher self-compassion may more easily adapt and recover when experiencing impostor-related distress. Self-compassion may assist key aspects of resilience, including stress management, coping with adversity, and maintaining a stable and supportive inner identity (Webb & Rosenbaum, 2019).
Although IP encourages harsh self-criticism and rumination on perceived failures, it is possible that through increased self-acceptance and soothing kindness, counselors can embody greater resilience when confronting areas of growth with less fear of failure. Additionally, a common humanity perspective can encourage acceptance of struggles as a normal part of counselor development and one shared by their peers. These soothing and normalizing aspects of self-compassion can encourage community rather than isolation when struggling, helping counselors to maintain resilience amidst adversity (Hou & Skovholt, 2020; Neff, 2023). Without effective coping practices, the challenges of counselor development can wear down resilience, creating vulnerability to mental distress, burnout, and counselor impairment (Cook et al., 2021; Gerber & Anaki, 2021).
Self-Compassion, IP, and Mental Health
Our results indicate that self-compassion is associated with less anxiety among those experiencing IP. Because anxiety is prevalent in this population and a primary emotional response to IP, efforts to increase self-compassion can have widely beneficial outcomes (Crego et al., 2022; Garba et al., 2024). The common humanity and mindfulness components of self-compassion may be critical to this outcome, as they can help limit emotional reactivity, normalize the IP experience, and reduce the isolation and fear of being exposed as an impostor (Clarke & Guida, 2025). This process involves mindfully recognizing that others share similar experiences and feelings, empowering developing counselors to seek support and reduce fear of failure (Neff, 2023). Likewise, practicing self-kindness may counter the harsh self-criticism associated with IP and encourage them to embrace the developmental process, including their imperfections (Patzak et al., 2017; Warren et al., 2016).
Anxiety and depression are closely linked and often co-occur (Beck & Alford, 2009). Though depression may not correlate as strongly with IP as anxiety does, it remains a common outcome (Garba et al., 2024). IP is persistent and sustained by cognitive distortions and misattributions, which also contribute to depressive thought patterns (Beck & Alford, 2009). However, our analysis revealed that self-compassion fully mediated the relationship between IP and depression. This suggests that a combination of mindful awareness and active self-kindness may facilitate more balanced self-assessment, countering perfectionism and harsh self-criticism commonly associated with IP (Clarke & Hartley, 2025; Pákozdy et al., 2023).
Although IP significantly predicted anxiety and depression, the buffering effect of self-compassion suggests that those with more compassionate self-perceptions may better tolerate the uncertainty and challenges common to counselor training. For example, those with a self-compassionate mindset may reinterpret failures as growth opportunities, a shift that may protect against anxious and depressive symptoms (Crego et al., 2022; Warren et al., 2016). These findings highlight the regulatory potential of self-compassion in reducing emotional reactivity to impostor-related distress.
Level of Self-Compassion in Relation to IP, Resilience, and Mental Health
MANOVA was utilized to determine whether the level of self-compassion (categorized as low, moderate, or high) was related to the level of IP, resilience, anxiety, and depression (Neff, 2003). Self-compassion had a significant positive relationship with mental health and resilience; however, the relationships varied significantly based on level of self-compassion (Figure 4). The results demonstrate that even lower levels of self-compassion were related to significantly lower IP, anxiety, and depression, as well as increased resilience. This pattern suggests that even modest improvements in self-compassion can correspond to improved well-being among developing counselors (Luo et al., 2023). For example, IP severity decreased significantly as self-compassion levels increased, revealing a linear reduction in IP from low to high self-compassion levels, with the most pronounced decrease occurring between the moderate and high categories.
Similarly, resilience scores also increased consistently across each level of self-compassion. The increase was linear, with the most substantial increase occurring when self-compassion rose from low to moderate. The steady increase in resilience across all self-compassion levels points to a possible dose-response relationship. Initial gains in self-compassion may bolster developing counselors’ ability to persevere through challenges (Neff et al., 2005), and interventions resulting in modest enhancements in self-compassion could yield significant improvements in resilience.
Figure 4
IP, Resilience, Depression, and Anxiety Across Levels of Self-Compassion
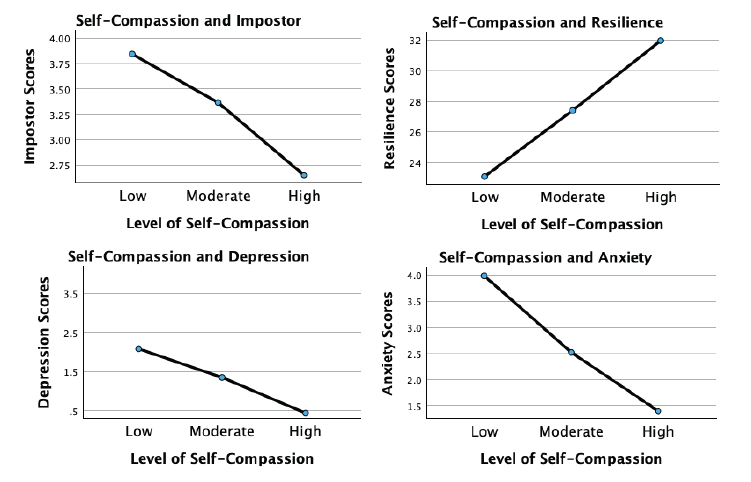
Although more variable, the association of self-compassion with anxiety and depression was similarly beneficial. Anxiety levels decreased significantly with each incremental increase in self-compassion, with the largest reduction occurring from low to moderate levels. This underscores the potential that even lower levels of self-compassion may still meaningfully alleviate anxiety. For depression, a significant decrease occurred across self-compassion levels, with the most substantial reduction noted as self-compassion increased from moderate to high. This suggests that self-compassion may interrupt the internal feedback loop of shame, self-criticism, and hopelessness that sustains depressive thinking in the context of IP.
These findings indicate that self-compassion is an important protective factor for developing counselor mental health. Contrary to expectations, even lower levels of self-compassion significantly relate to reduced IP, anxiety, and depression while increasing resilience (Luo et al., 2023). Integrating strategies to enhance self-compassion into counselor training programs could incrementally increase self-compassion, build emotional tolerance, and create a more stable internal environment from which resilience and well-being can emerge.
Implications and Future Directions for Counselor Development
Despite IP’s prevalence and association with diminished resilience and psychological distress, it remains underexamined in the counseling literature. Beyond a self-care strategy, self-compassion may build resilience and maintain mental health during and after counselor training. Integrating self-compassion into counselor education and early career development may cultivate a more supportive environment and provide counselors with evidence-based ways to manage IP and enhance resilience. Whereas, if left unaddressed, IP can lead to unnecessary distress, burnout, and professional attrition (Coaston & Lawrence, 2019; Ojeda, 2024).
Growing evidence suggests that self-compassion is vital for counselor development and ethical practice (Clarke et al., 2025; Coaston & Lawrence, 2019). The American Counseling Association (ACA) Code of Ethics (2014) emphasizes that professional counselors must engage in ongoing self-assessment and maintain their effectiveness through self-care practices. Similarly, CACREP (2023) standards require counselor education programs to integrate “self-care, self-awareness, and self-evaluation strategies for ethical and effective practice” (3.A.11.). Without meaningful coping strategies, IP can directly undermine these ethical mandates by diminishing well-being and distorting self-evaluation necessary for competent practice (Gadsby & Hohwy, 2024).
Regular engagement in reflective activities promoting balanced self-evaluation is essential to counselor development. If such exercises lack a compassionate focus, they may inadvertently reinforce impostor-related distortions by encouraging rumination and inaccurate self-critique. Matching reflective self-assessment with self-compassion practice may allow developing counselors to internalize feedback and move attention away from self-criticism and toward a growth mindset, transforming internal narratives dominated by IP (Warren et al., 2016).
Counselor educators and professional agencies can integrate self-compassion training through multiple pathways. Brief interventions, such as abbreviated versions of the Mindful Self-Compassion program (Germer & Neff, 2019), offer evidence-based approaches for enhancing counselor resilience. If limited by time and resources, supervisors and mentors can model self-compassionate practices by normalizing struggles, demonstrating constructive self-talk, and providing balanced growth-oriented feedback. The disclosure of faculty or supervisor IP experiences may be particularly powerful, reframing vulnerability and self-care as professional strengths rather than weaknesses.
Because IP is a contextual and environmentally fueled experience, counseling agencies and community mental health settings can foster organizational climates that prioritize compassion and collaboration and normalize challenges during the growth process (Coaston, 2019). When institutions reward openness, reflection, and learning from error, rather than perfection and productivity, developing counselors are more likely to engage in authentic self-assessment and seek help when struggling.
Early career peer support groups and compassion-focused initiatives can also counter the competitive, perfectionistic culture that sustains IP in professional practice (Clark et al., 2022). These approaches challenge the isolating belief that self-doubt is uniquely shameful, and foster community and belonging (Clarke & Guida, 2025; Hou & Skovholt, 2020). Future research should employ longitudinal and experimental designs to test targeted self-compassion interventions, clarifying causal relationships between self-compassion, resilience, and mental health outcomes in counselor education and professional contexts.
Clinical Supervision
Developmentally, the transition from classroom learning to applying theory and skills in clinical practice naturally provokes stress and anxiety (Skovholt & Trotter-Mathison, 2024). Although clinical supervision provides an ideal context for fostering openness and resilience (Coaston, 2019), experiencing IP may be a barrier to disclosing challenges because of emotional distress and fear of exposing perceived inadequacies (DeCandia Vitoria, 2021). Maintaining a façade of competence can compromise development and hinder the supervisory relationship (Thériault et al., 2009). These perfectionistic tendencies and IP are often motivated by context, suggesting that supervisors’ approaches may significantly alleviate these patterns.
Coaston (2019) provides a practical framework for applying self-compassion principles and philosophy in clinical supervision. Rooted in humanistic and developmental theory, this approach emphasizes that supervisors can accompany supervisees through the inevitable discomfort and vulnerability of professional growth by responding with compassion rather than judgment. By adopting a compassionate approach, the supervisory relationship can deepen, normalizing challenges and facilitating an authentic dialogue about IP-related uncertainties. In this way, clinical supervisors can address common cognitive and affective challenges.
A compassionate supervisory environment promotes balanced self-reflection and can reduce the shame-based fear of exposure that drives impostor defenses. This may allow supervisees to explore their conceptual skills openly, reframe unrealistic expectations, and persist despite challenges (Hou & Skovholt, 2020; Stoltenberg & McNeill, 2010). Future research can investigate how self-compassion contributes to the supervisory relationship, comfort with disclosure, and the integration of constructive feedback during supervised practice.
Clinical supervisors can also create a culture of shared vulnerability by modeling self-compassion and transparency about their own developmental struggles and self-doubt. This enables supervisees to internalize feedback and approach self-evaluation with less emotional reactivity. Enhancing collaboration within the alliance empowers supervisees to feel more competent in navigating their development independently (Skovholt & Trotter-Mathison, 2024). Given the potential benefits of this approach, we recommend that future research examine how embodiment and facilitation of self-compassion affect counselor development and well-being.
Limitations
Although the results of this study are encouraging, there are limitations. The cross-sectional design limits the data to a single point in time rather than showing fluctuations in self-compassion, IP, resilience, and mental health over time. Likewise, the present results do not establish causality. Replicating this study using a longitudinal approach can provide greater insight into these fluctuations. Furthermore, self-report measures introduce limitations such as social desirability bias and reliance on participant self-awareness. Likewise, individuals with a personal connection to IP may have been more likely to participate, potentially skewing results.
Participants were not asked about their matriculation status as counseling students, leaving their stage of development unknown. Future research should include clinical experience (i.e., none, practicum, internship) and matriculation status. This information would provide greater insight into how experience and counselor development interact with IP. The current study used a general IP assessment, while future research should use the Counselor Impostor Scale (CIS; Nguyen, 2023), which was published after data collection for this study was complete. The CIS is designed specifically for the counseling domain and could provide more nuanced insights. Additionally, because maladaptive coping strategies such as procrastination and perfectionism sustain IP, subsequent studies should explore these constructs, which could inform more targeted interventions.
Conclusion
The growth process during counselor training is inherently challenging and often gives rise to IP, which increases anxiety and depression while diminishing resilience. Self-compassion is a promising method for enhancing resilience and well-being, despite the presence of IP. Once learned, self-compassion is an accessible practice and relies on applying skills with which counselors are familiar, such as kindness and compassion toward themselves. The results of this study are encouraging and robust, suggesting that self-compassion can enhance resilience by supporting adaptive emotional regulation and fostering a growth-oriented mindset. Self-compassionate counselors can maintain their well-being despite experiencing IP. Importantly, the positive impact of self-compassion was consistent and significant even at lower levels, which is especially important given the prevalence and severity of IP among CITs. The findings support integrating self-compassion into counselor training and clinical supervision through modeling, training, and practice. This approach can provide effective coping for IP and improve resilience, mental health, and persistence.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default- document-library/ethics/2014-aca-code-of-ethics.pdf
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). University of Pennsylvania Press.
Council for the Accreditation of Counseling and Related Educational Programs (2023). 2024 standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Clance, P. R. (1985). Clance Impostor Phenomenon Scale (CIPS). [Database record]. APA PsycTests. https://doi.org/10.1037/t11274-000
Clance, P., & Lawry, S. (2024). Impostor phenomenon: Origins and treatment. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 17–43). American Psychological Association.
Clark, P., Holden, C., Russell, M., & Downs, H. (2022). The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy, 44(2), 185–197. https://doi.org/10.1007/s10591-021-09580-y
Clarke, B. J. (2024). Emerging adult life satisfaction and mental health: The mediating role of self-compassion and social support. Emerging Adulthood, 12(6), 1137–1147. https://doi.org/10.1177/21676968241279490
Clarke, B. J., & Guida, A. M. (2025). Self-compassion to community: The mediating effect of belonging on college student mental health and life satisfaction. Journal of College Student Mental Health. Advance online publication. https://doi.org/10.1080/28367138.2025.2552484
Clarke, B. J., & Hartley, M. T. (2025). Contemplative dispositions and mental health: The supportive role of self-compassion and mindfulness on college students’ resilience. Journal of College Student Mental Health, 39(1), 142–164. https://doi.org/10.1080/28367138.2024.2331931
Clarke, B. J., Hartley, M. T., & Button, C. (2025). Impostor phenomenon and counselor development: The critical role of self-compassion. Journal of Counseling & Development, 103(2), 149–160. https://doi.org/10.1002/jcad.12544
Coaston, S. C. (2019). Cultivating self-compassion within the supervision relationship. The Clinical Supervisor, 38(1), 79–96. https://doi.org/10.1080/07325223.2018.1525596
Coaston, S. C., & Lawrence, C. (2019). Integrating self-compassion across the counselor education curriculum. Journal of Creativity in Mental Health, 14(3), 292–305. https://doi.org/10.1080/15401383.2019.1610536
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in developing professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Crego, A., Yela, J. R., Riesco-Matías, P., Gómez-Martínez, M. Á., & Vicente-Arruebarrena, A. (2022). The benefits of self-compassion in mental health professionals: A systematic review of empirical research. Psychology Research and Behavior Management, 15, 2599–2620. https://doi.org/10.2147/PRBM.S359382
DeCandia Vitoria, A. (2021). Experiential supervision: Healing impostor phenomenon from the inside out. The Clinical Supervisor, 40(2), 200–217. https://doi.org/10.1080/07325223.2020.1830215
Delaney, M. C. (2018). Caring for the caregivers: Evaluation of the effect of an eight-week pilot Mindful Self-Compassion (MSC) training program on nurses’ compassion fatigue and resilience. PLoS ONE, 13(11), e0207261. https://doi.org/10.1371/journal.pone.0207261
Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gadsby, S., & Hohwy, J. (2024). Negative performance evaluation in the impostor phenomenon. Current Psychology, 43, 9300–9308. https://doi.org/10.1007/s12144-023-05030-0
Garba, R., Coleman, C., & Kelley, T. (2024). The impostor phenomenon and mental health. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 61–79). American Psychological Association.
Gerber, Z., & Anaki, D. (2021). The role of self-compassion, concern for others, and basic psychological needs in the reduction of caregiving burnout. Mindfulness, 12, 741–750. https://doi.org/10.1007/s12671-020-01540-1
Germer, C., & Neff, K. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. Guilford.
Gignac, G. E., & Szodorai, E. T. (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. https://doi.org/10.1016/j.paid.2016.06.069
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford.
Hou, J.-M., & Skovholt, T. M. (2020). Characteristics of highly resilient therapists. Journal of Counseling Psychology, 67(3), 386–400. https://doi.org/10.1037/cou0000401
Housenecht, A., & Swank, J. (2022). Motivation, belonging, and support: Examining persistence in counseling programs. Teaching and Supervision in Counseling, 4(2), Article 3. https://doi.org/10.7290/tsc04g4iv
Khubchandani, J., Brey, R., Kotecki, J., Kleinfelder, J., & Anderson, J. (2016). The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Archives of Psychiatric Nursing, 30(4), 457–462. https://doi.org/10.1016/j.apnu.2016.01.014
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Liu, S., Wei, M., & Russell, D. (2023). Effects of a brief self-compassion intervention for college students with impostor phenomenon. Journal of Counseling Psychology, 70(6), 711–724. https://doi.org/10.1037/cou0000703
Luo, X., Che, X., & Lei, Y. (2023). Characterizing the effects of self-compassion interventions on anxiety: Meta-analytic evidence from randomized controlled studies. Journal of Contextual Behavioral Science, 30, 132–141. https://doi.org/10.1016/j.jcbs.2023.10.004
Mak, K. K. L., Kleitman, S., & Abbott, M. J. (2019). Impostor phenomenon measurement scales: A systematic review. Frontiers in Psychology, 10, 671. https://doi.org/10.3389/fpsyg.2019.00671
Martin, A. J., & Marsh, H. W. (2006). Academic resilience and its psychological and educational correlates: A construct validity approach. Psychology in the Schools, 43(3), 267–281. https://doi.org/10.1002/pits.20149
Neff, K. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2023). Self-compassion: Theory, method, research, and intervention. Annual Review of Psychology, 74, 193–218. https://doi.org/10.1146/annurev-psych-032420-031047
Neff, K. D., Hsieh, Y. P., & Dejitterat, K. (2005). Self-compassion, achievement goals, and coping with academic failure. Self and Identity, 4(3), 263–287. https://doi.org/10.1080/13576500444000317
Neff, K. D., Tóth-Király, I., Yarnell, L. M., Arimitsu, K., Castilho, P., Ghorbani, N., Guo, H. X., Hirsch, J. K., Hupfeld, J., Hutz, C. S., Kotsou, I., Lee, W. K., Montero-Marin, J., Sirois, F. M., de Souza, L. K., Svendsen, J. L., Wilkinson, R. B., & Mantzios, M. (2019). Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: Support for use of a total score and six subscale scores. Psychological Assessment, 31(1), 27–45. https://doi.org/10.1037/pas0000629
Nguyen, L. T. (2023). Development and validation of the Counseling Impostor Scale (Doctoral dissertation). Texas A&M University–Corpus Christi.
Ojeda, L. (2024). Impostor phenomenon and burnout. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 81–110). American Psychological Association.
Pákozdy, C., Askew, J., Dyer, J., Gately, P., Martin, L., Mavor, K. I., & Brown, G. R. (2023). The impostor phenomenon and its relationship with self-efficacy, perfectionism, and happiness in university students. Current Psychology, 43, 1–10. https://doi.org/10.1007/s12144-023-04672-4
Patzak, A., Kollmayer, M., & Schober, B. (2017). Buffering impostor feelings with kindness: The mediating role of self-compassion between gender-role orientation and the impostor phenomenon. Frontiers in Psychology, 8, Article 1289. https://doi.org/10.3389/fpsyg.2017.01289
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Roskowski, J. C. R. (2010). Impostor phenomenon and counseling self-efficacy: The impact of impostor feelings (Doctoral dissertation). Ball State University.
Skovholt, T. M., & Trotter-Mathison, M. (2024). The elevated stressors of the novice practitioner. In T. M. Skovholt & M. Trotter-Mathison (Eds.), The resilient practitioner: Burnout and compassion fatigue prevention and self-care strategies for the helping professions (4th ed., pp. 42–68). Taylor & Francis.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Thériault, A., Gazzola, N., & Richardson, B. (2009). Feelings of incompetence in developing therapists: Consequences, coping, and correctives. Canadian Journal of Counselling, 43(2), 105–119.
Tigranyan, S., Byington, D. R., Liupakorn, D., Hicks, A., Mathis, M., & Rodolfa, E. (2021). Factors related to the impostor phenomenon in psychology doctoral students. Training and Education in Professional Psychology, 15(4), 298–305. https://doi.org/10.1037/tep0000321
Wang, B., Andrews, W., Bechtoldt, M. N., Rohrmann, S., & de Vries, R. E. (2022). Validation of the short Clance Impostor Phenomenon Scale (CIPS-10). European Journal of Psychological Assessment, 40(2), 158–168. https://doi.org/10.1027/1015-5759/a000747
Warren, R., Smeets, E., & Neff, K. (2016). Self-criticism and self-compassion: Risk and resilience. Current Psychiatry, 15(12), 18–33. https://self-compassion.org/wp-content/uploads/2016/12/Self-Criticism.pdf
Webb, R. E., & Rosenbaum, P. (2019). Resilience and thinking perpendicularly: A meditation or morning jog. Journal of College Student Psychotherapy, 33(1), 75–88. https://doi.org/10.1080/87568225.2018.1449687
Brian J. Clarke, PhD, NCC, LAC, is an assistant professor at the University of Arizona. Michael T. Hartley, PhD, CRC, is a professor at the University of Arizona. Austin M. Guida, PhD, NCC, LAC, is an assistant professor at Northern Arizona University. Correspondence may be addressed to Brian J. Clarke, Department of Disability and Psychoeducational Studies, College of Education, 1430 E. 2nd Street, Room 422, Tucson, AZ, 85721-0069, bclarke14@arizona.edu.
Apr 1, 2026 | Volume 16 - Issue 1
Darius A. Green, Kade Stanzilis, Sierra Roach-Coye, Connor Sullivan
Online racism has increasingly become a mental health concern alongside rapid advancements in digital technology and social media use. This cross-sectional study investigated the associations between exposure to online racism, racial trauma, and social connectedness among a sample of 227 adult social media users in the United States. Using regression and mediation analyses, we found that both exposure to online racism and online social connectedness predicted increased racial trauma symptoms. Additionally, results indicated that the relationship between exposure to online racism was significantly mediated by online social connectedness. These results highlight the existence of online racism as a racially traumatic stressor and the importance of enhancing social connectedness among individuals who may be exposed to online racism.
Keywords: online racism, digital technology, social media, racial trauma, social connectedness
Digital technology use has skyrocketed with advancements in and accessibility of digital technology in the United States. According to Pew Research Center (2024), smartphone ownership has increased from 35% of adults in the United States in 2011 to 91% in 2024, with 41% of adults indicating that they are constantly using the internet (Gelles-Watnick, 2024). Additionally, social media platforms such as Facebook, Instagram, and TikTok have expanded their integration into everyday lives across the globe. It is estimated that there are 4.9 billion social media users worldwide with an anticipated growth to 5.85 billion by 2027 (Wong, 2023). Although use of social media among adults may vary across platforms, estimates highlight that 83% of adults in the United States have used YouTube, and 68% of U.S. adults have used Facebook (Gottfried, 2024). Given the rapid development and expanding use of digital technology, it is essential for counselors to develop awareness of these technologies and their impact on client wellness.
Social media platforms have been the center of scrutiny for several reasons, including online aggression. Online aggression involves various problematic online behaviors such as online hate speech, harassment, and cyberbullying (Rudnicki et al., 2023). Although not a new phenomenon, online racism has emerged in research as a pervasive issue for social media users and People of the Global Majority (PGM; Bliuc et al., 2018; Keum & Miller, 2017). We use PGM to acknowledge Black, Indigenous, Asian, Southwest Asian and North African, and Latine populations that are marginalized by white supremacy despite making up most of the world’s population. Online racism has existed as a concern and stressor for PGM since the inception of the internet. Moreover, the threat of online racism for PGM requires that critical attention be paid to its impact (Keum & Miller, 2017).
As a chronic stressor rooted in racism, it is essential to analyze the connections between exposure to online racism and traumatic stress in order to develop recommendations for clinical practice (Hemmings & Evans, 2018). Moreover, it is essential to examine factors that contribute to the traumatic impact of online racism in our digital era (Keum & Miller, 2017). Notably, social connectedness is of particular interest given the emergence of digital resistance via online counterspaces as tools to combat online racism and its deleterious impact (Gomez & Cabrera, 2025; Hill, 2018; Mosley et al., 2021). Our study seeks to expand upon this growing literature base by examining the connection between exposure to online racism and racial trauma. Moreover, we examine the role of sense of social connectedness in the relationship between online racism and racial trauma.
Online Racism
Online racism refers to the use of electronic and digital communication and media that denigrate and discriminate against PGM because of their racial and ethnic identity (Bliuc et al., 2017; Volpe et al., 2021). Like offline racism, online racism creates a hierarchy of white supremacy (Volpe et al., 2021). Although online and offline racism have common roots, there are notable ways in which online racism is unique. For example, Keum and Miller (2017) noted that online racism is pervasive, permanent, and constantly evolving. Additionally, although PGM may often be the explicit targets of racism, social media allows for a broader audience, including members of a dominant racial identity, to be vicariously impacted by racist content. Moreover, algorithms and artificial intelligence may play a role in disseminating racist content to social media users, which can lead to widespread exposure (Fulmer, 2024; Volpe et al., 2021). As a result of these unique characteristics, the prevalence and impact of online racism may be wide-ranging, particularly as it relates to mental health.
Regarding the impact of online racism on mental health, several studies have documented a connection to a range of mental health symptoms. Most research on the topic has centered on children and adolescents, highlighting associations with anxiety, depression, stress- and trauma-related symptoms, as well as psychological distress (Del Toro & Wang, 2023; Thomas et al., 2023; Tynes et al., 2012). Emerging research on the mental health impact of online racism among adults has demonstrated connections to psychological distress and well-being (Cavalhieri et al., 2024; Keum & Hearns, 2021), substance use (Keum & Ahn, 2021; Keum & Cano, 2021; Keum et al., 2023), suicidal ideation (Keum, 2022), anxiety and depression (Cano et al., 2021; Layug et al., 2022), and trauma (Evans et al., 2024) among adults who experience online racism.
Racial Trauma
Given that racism is a chronic stressor with mental health implications, it is essential to consider the relevance of racial trauma. Racial trauma refers to the psychologically, emotionally, and physically injurious impacts resulting from exposure to racism that may be both directly and vicariously experienced (Carter, 2007; Comas-Díaz et al., 2019; Wright et al., 2023). Following exposure to threatening events, injury, or violence that are racist in nature, individuals may experience symptoms of intrusion, avoidance, altered cognition and mood, as well as impacted arousal and reactivity (American Psychiatric Association, 2022; Williams et al., 2022). Symptoms of racial trauma can also expand beyond these symptoms traditionally associated with post-traumatic stress disorder (PTSD; Williams et al., 2022). For example, some psychological instruments identify depression, intrusion, anger, hypervigilance, physical symptoms, self-esteem, and avoidance as core symptoms to focus on when assessing racial trauma (Carter et al., 2013; Carter, Kirkinis, & Johnson, 2020). Additionally, racial trauma may diverge from this limited categorization of symptoms to encapsulate the cumulative impact of racial discrimination (Williams et al., 2018). Moreover, the impact of racial trauma is also conceptualized as transgenerational (Comas-Díaz et al., 2019; Williams et al., 2018). It must also be noted that emerging research has highlighted that White individuals may endorse symptoms of racial trauma following exposure to racism (Carter & Kirkinis, 2021; Carter, Roberson, & Johnson, 2020). Notably for White individuals, less mature White racial identity attitudes may contribute to how racism and subsequent racial trauma symptoms are experienced (Carter, Roberson, & Johnson, 2020). Additionally, Carter and Kirkinis (2021) found vicarious exposure to racism to be the most frequently reported exposure to racism among White participants. This framing of racial trauma is essential to consider when dissecting how exposure to online racism may produce it.
Technological advancements in social media and digital technology allow for traumatic stress to occur from various manifestations of online racism. Akin to offline racism, online racism may include interpersonal encounters such as microaggressions and cyberbullying (Evans et al., 2024; Green et al., 2023; Keum, 2017). Racially traumatizing stressors may also include exposure to audiovisual media that depicts racialized violence. For example, exposure to police brutality toward Black Americans or imagery from the genocide of Palestinian people in Gaza may result in racial trauma (Green et al., 2024; Keum, 2017; Nasereddin, 2023). To date, there is a paucity of research that connects exposure to online racism and traumatic stress. A study examining race-related online traumatic events in a sample of Black and Latinx adolescents found that online exposure was related to increased PTSD symptoms (Tynes et al., 2019). Emerging research in a sample of young Black adults has also demonstrated connections between exposure to online racism and symptoms of trauma (Maxie-Moreman & Tynes, 2022). Additionally, a study with a sample of Black American adults found evidence of anticipatory traumatic reaction across audiovisual exposure, news reports, and imagined exposure to police violence (Green et al., 2024). Lastly, a study on cyberbullying victimization among PGM adults found that participants experienced racial discrimination that resulted in traumatic stress in alignment with racial trauma (Evans et al., 2024). These studies highlight that traumatic responses to online racism may result in experiences such as traditional symptoms of PTSD, a heightened sense of anticipated vulnerability to racialized violence, and attempts at suppressing the traumatic impact of online racism (Evans et al., 2024; Green et al., 2024; Maxie-Moreman & Tynes, 2022; Tynes et al., 2019). While these studies document the relationship between online racism and traumatic stress, it is important to note that the relationship between racial trauma and online racism has not yet been investigated.
Social Connectedness
French et al. (2020) proposed the psychology of radical healing as a liberatory and multicultural counseling framework for supporting healing from the traumatic impact of racism. This framework emphasizes resisting oppression and envisioning collective liberation despite the pervasive nature of oppressive systems like white supremacy (Adames et al., 2023; French et al., 2020). Moreover, the psychology of the radical healing framework identifies critical consciousness, cultural authenticity and self-knowledge, radical hope, collectivism, and strength and resistance as the foundations of radical healing (Adames et al., 2023; French et al., 2020). Based on the salience of community and social relationships in this framework (French et al., 2020; Mosley et al., 2020), we identified social connectedness as a relevant construct for exploration. Social connectedness is an aspect of sense of belonging and refers to the perceived emotional distance between oneself and others (Lee & Robbins, 1995). Social and peer connectedness are essential resources for coping with and alleviating racial trauma (Holmes et al., 2024). Conversely, having limited social connectedness that fosters radical healing may increase the likelihood of internalizing racist messages communicated online (Adames et al., 2023).
Existing data on offline experiences have indicated that the harmful impact of discrimination may be buffered by social connectedness and related variables. For example, increased social connectedness significantly moderated the relationship between discrimination and post-traumatic cognition among forcibly displaced Muslims (Sheikh et al. 2022). Specifically, lower levels of social connectedness moderated this relationship (Sheikh et al., 2022). In the context of online racism, it is possible that experiencing or witnessing online racism may result in greater emotional distance and disconnection. For example, a study on online racism among professional counselors found that greater exposure to online racism predicted decreased perception of inclusion (Green et al., 2023). Alternatively, seeking counterspaces, such as online communities and interactions that are characterized by cultural affirmation, sense of community and belonging, knowledge sharing, empowerment, resistance, and critical consciousness are theorized to be facilitative of social connectedness and wellness (Case & Hunter, 2012; Gomez & Cabrera, 2025; Hill, 2018; Lopez-Leon & Casanova, 2023). For example, participating with others in counterspaces may provide a sense of connectedness despite the isolating impact of experiencing racial microaggressions (Ong et al., 2018). Relatedly, social connectedness in these counterspaces may enhance radical healing through deconstructing racist narratives and countering self-blame (Adames et al., 2023). Emerging literature on radical healing and its overlap with online counterspaces highlights the importance of investigating how online connectedness might mediate racial trauma associated with online racism.
Present Study
Our study seeks to expand the contemporary literature of racial trauma to online contexts. Specifically, our study seeks answers to the following research questions: 1) What is the relationship between online exposure to racism, social connectedness, and racial trauma symptoms? and 2) Does social connectedness mediate the relationship between exposure to online racism and racial trauma? We hypothesize that 1) exposure to online racism will significantly predict racial trauma symptoms, 2) social connectedness will significantly predict racial trauma symptoms, and 3) social connectedness will significantly mediate the relationship between online racism and racial trauma symptoms.
Methods
Procedures
After receiving IRB approval, participants were recruited to participate in our cross-sectional study using convenience sampling using the MTurk platform. Inclusion criteria included being a U.S. resident, being at least 18 years old, and self-identifying as using social media. A total of 518 participants accessed our online survey. We implemented a racial identity quota to ensure representation of PGM participants. The racial identity quota limited the number of White participants to 170 to prevent oversampling. We chose 170 as a target in an attempt to achieve a final sample comprising approximately 60% White participants to reflect the population of the United States in 2020 (Jones et al., 2021). As a result, a total of 292 participants completed the online survey. Participant responses were screened to remove participants who failed two validity check items, resulting in the removal of 18 participant responses. We took a conservative approach and removed an additional 47 responses from the dataset that were flagged by Qualtrics as potential duplicate responses, leaving a total of 227 participant responses. Participants who completed the online survey were compensated $8.
Participants
Participant age ranged from 19 to 70 years (M = 33.33; SD = 9.04). Regarding race, 19 (8.37%) were Asian, 26 (11.45%) were Black, one (0.44%) was Latinx, one (0.44%) was Middle Eastern and North African, five (2.20%) were Native or Indigenous American, 170 (74.89%) were White, three (1.32%) were multiracial, and two (0.88%) did not indicate their race. As for gender, 164 (72.57%) identified as cisgender men and 62 (27.43%) identified as cisgender women. One (0.44%) had less than a high school diploma or equivalent, seven (3.08%) were high school graduates, seven (3.08%) had some college experience with no degree, 13 (5.73%) had an associate degree, 160 (70.48%) had a bachelor’s degree, 36 (15.68%) had a master’s degree, and three (1.32%) had a doctoral degree. Regarding social media use, one (0.44%) reported never using social media, 13 (5.73%) reported using social media once a week, 44 (19.38%) used social media 2–3 times per week, 24 (10.57%) used social media 4–6 times per week, and 145 (63.88%) used social media daily. Of specific social media platforms, 30 (13.22%) used Discord, 197 (86.78%) used Facebook, 201 (88.55%) used Instagram, 67 (29.52%) used LinkedIn, 49 (21.59%) used Reddit, 41 (20.70%) used Threads, 107 (47.14%) used TikTok, nine (3.96%) used Tumblr, 128 (56.39%) used Twitter/X, and 193 (85.02%) used YouTube.
Measures
Perceived Online Racism
We used the 15-item Perceived Online Racism-Short Form (PORS-SF) to measure experiences of and exposure to online racist interactions and content (Keum, 2021; Keum & Miller, 2017). Participant scores ranged from 1 (not at all) to 4 (extremely). Sample items from the PORS-SF include items such as “received racist insults regarding my online profile (e.g., profile pictures, user ID)” and “seen online videos (e.g., YouTube) that portray my racial/ethnic group negatively” (Keum, 2021; Keum & Miller, 2017). Cronbach’s α for the PORS-SF ranged from .91 to .93 in its validation and was .93 in the current sample (Keum, 2021).
Social Connectedness
The 8-item Social Connectedness Scale (Lee & Robbins, 1995) was used to measure social connectedness in offline and online environments. Scores range from 1 (agree) to 6 (disagree) and were summed to compute a total score. Scores on the scale correspond to the sense of social disconnectedness and detachment experienced, with higher scores indicating greater disconnectedness and detachment (Lee & Robbins, 1995). Reliability for the Social Connectedness Scale was α = .91 in a sample of university students (Lee & Robbins, 1995). To distinguish between offline and online social connectedness, participants completed two versions of the Social Connectedness Scale, one with instructions to focus on offline relationships and another with instructions to focus on online relationships. Example items included, “I feel disconnected from the world around me” and “I catch myself losing all sense of connectedness with society.” Cronbach’s α on the Social Connectedness Scale for the current sample was .94 for both offline and online scores.
Racial Trauma
The 30-item Racial Trauma Scale (Williams et al., 2022) was used to measure participants’ experiences and symptoms of racial trauma. Specifically, the Racial Trauma Scale measures experiences related to impact on safety, negative cognition, and difficulty in coping. Participant responses ranged on each item from 1 (not at all) to 4 (extremely) and were summed for a total score. Sample items included, “thinking the world is unsafe,” “having difficulties connecting with other people,” and “having nightmares about discrimination.” White participants were included in the development of the Racial Trauma Scale and were found to report fewer symptoms of racial trauma compared to PGM (Williams et al., 2022). Internal consistency from three diverse samples of MTurk users for the Racial Trauma Scale ranged from α = .96 to .97. Cronbach’s α for the Racial Trauma Scale in the current sample was .97.
Analytic Plan
Preliminary and regression analyses were conducted using Stata (Version 18.5). We conducted a multiple regression analysis to examine the relationship between perceived online racism and social connectedness on racial trauma. Additionally, we conducted a mediation analysis to determine the mediating role of social connectedness on the relationship between perceived online racism and racial trauma. We used a significance level of α = .05 and pairwise exclusion for each of the analyses. Assumptions for normality, linearity, homoscedasticity, and multicollinearity were tested. Visual inspection of residuals demonstrated no evidence of violations of assumptions of normality, linearity, or homoscedasticity. Participant data showed no evidence of multicollinearity as evidenced by variation inflation factor values being below 10 and tolerance values being above .1; however, offline social connectedness was removed from multiple regression analyses because of the high correlation with online social connectedness (r = .91) as shown in Table 1 (Cohen et al., 2003; Tabachnick & Fidell, 2019).
Table 1
Correlations of Variables
| Variable |
M |
SD |
1 |
2 |
3 |
| 1. Online Social Connectedness |
32.48 |
9.20 |
|
|
|
| 2. Offline Social Connectedness |
32.32 |
9.67 |
.91*** |
|
|
| 3. Online Racism |
51.78 |
11.29 |
.61*** |
.60*** |
|
| 4. Racial Trauma |
77.96 |
20.65 |
.71*** |
.68*** |
.72*** |
Note. N = 186.
*p < .05; **p < .01; ***p < .001.
Results
Descriptive Analysis
Prior to our primary analyses, we conducted a descriptive analysis for participant responses on the PORS-SF, the Racial Trauma Scale, and the Social Connectedness Scale. For the PORS-SF, participants’ scores ranged from 15 to 69 with a mean of 51.88 and standard deviation of 10.94. Participant scores on the Racial Trauma Scale ranged from 30 to 120 with a mean of 78.40 and standard deviation of 20.63. Participant scores on the Social Connectedness Scale ranged from 8 to 47 with a mean of 32.55 and a standard deviation of 9.28.
Regression Analyses
We used regression analyses to answer our first research question: What is the relationship between online exposure to racism, social connectedness, and racial trauma symptoms? We hypothesized that 1) online racism exposure and 2) social connectedness would significantly predict racial trauma symptoms. Results from the hierarchical multiple regression model analyzing the impact of social connectedness and exposure to online racism on racial trauma symptoms while controlling for race, gender, education, age, and frequency of social media use are presented in Table 2. Among the control variables, age (β = −.19, p = .010) and frequency of social media use (β = −.35, p < .001) significantly predicted less racial trauma in the first step of the model. Race, gender, and education did not significantly predict racial trauma symptoms. There was a significant increase when adding social connectedness and online racism in the second step of the model for predicting racial trauma, F(7, 178) = 47.81, p < .001, ΔR2 = .44. Online social connectedness (β = .38, p < .001) and online racism (ꞵ = .45, p < .001) predicted greater racial trauma symptoms. Step 2 accounted for 66% of variance in racial trauma symptoms with the addition of perceived online racism and online social connectedness accounting for a 44% increase in explained variance. Results from the regression analyses demonstrated support for our first two hypotheses that online exposure to racism and social connectedness would significantly predict racial trauma symptoms.
Table 2
Regression Coefficients of Variables on Racial Trauma
| Variable |
Step 1 |
Step 2 |
| B (SE) |
β |
B (SE) |
β |
| Age |
−0.40 (0.15) |
−.19** |
−0.14 (0.10) |
−.07 |
| Race |
|
|
|
|
| White (ref) |
|
|
|
|
| PGM |
3.49 (3.22) |
.08 |
0.98 (2.15) |
.02 |
| Gender |
|
|
|
|
| Cisgender Man (ref) |
|
|
|
|
| Cisgender Woman |
−3.66 (3.24) |
−.08 |
1.28 (2.18) |
.03 |
| Education |
|
|
|
|
| > Bachelors (ref) |
|
|
|
|
| < Bachelors |
3.22 (4.47) |
.05 |
−2.62 (3.02) |
−.04 |
| Social Media Use |
|
|
|
|
| > Daily (ref) |
|
|
|
|
| Daily |
−15.20 (3.01) |
−.35*** |
−5.07 (2.11) |
−.12* |
| Online Social Connectedness |
|
|
0.86 (0.13) |
.38*** |
| Online Racism |
|
|
0.83 (0.11) |
.45*** |
|
|
|
|
|
| R2 |
.21*** |
|
.65*** |
|
| ΔR2 |
|
.44*** |
Note. N = 185.
*p < .05; **p < .01; ***p < .001.
Mediation Analysis
We conducted a simple mediation analysis using Hayes (2018) PROCESS macro (Version 5.0) in RStudio (Version 4.5) to answer our second research question: Does social connectedness mediate the relationship between exposure to online racism and racial trauma? Results from the mediation analysis are presented in Table 3 and depicted in Figure 1. The total effect of online racism exposure on racial trauma was significant, b = 1.32, β = .72, SE = .09, 95% CI [1.13, 1.50], R2 = .52. The indirect effect of exposure to online racism on racial trauma through online social connectedness was significant, b = .47, β = .26, SE = .13, bootstrapped 95% CI [0.24, 0.73]. Confirming our third hypothesis, these results indicate that online social connectedness significantly mediated the relationship between online racism and racial trauma among participants.
Table 3
Results of Mediation Analysis
| Path |
b |
SE |
β |
t |
R2 |
95% CI |
| LL |
UL |
| Online racism → Social connectedness (a) |
0.50 |
.05 |
.61*** |
10.44 |
.37 |
0.40 |
0.59 |
| Social connectedness → Racial trauma (b) |
0.95 |
.13 |
.70*** |
7.49 |
|
0.70 |
1.20 |
| Online racism → Racial trauma (c’) |
0.85 |
.10 |
.72*** |
8.25 |
|
0.65 |
1.05 |
| Total Effect |
1.32 |
.09 |
.72*** |
14.18 |
.52 |
1.14 |
1.50 |
| Indirect Effect |
0.47 |
.13 |
.26 |
|
|
0.13 |
0.40 |
Note. N = 185. The indirect effect was estimated using 10,000 bootstrap samples.
***p < .001.
Figure 1
Mediation Model of Relationships Between Online Racism, Online Social Connectedness, and Racial Trauma
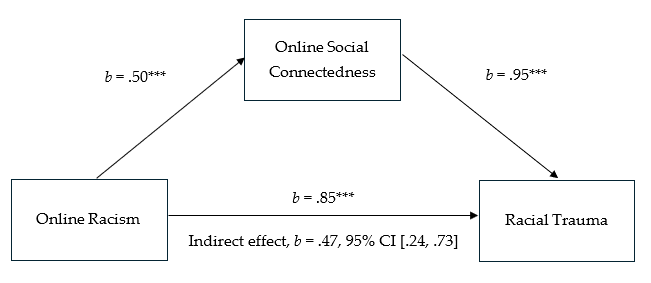
Note. Coefficients presented are unstandardized regression coefficients of direct effects. Confidence interval for the indirect effect is a bootstrapped confidence interval using 10,000 samples.
***p < .001.
Discussion
Prior and emerging literature has documented the significant impact of online racism on mental health and wellness, such as anxiety, depression, stress- and trauma-related symptoms, and psychological distress among children and adolescents (Del Toro & Wang, 2023; Thomas et al., 2023; Tynes et al., 2012) as well as emerging findings of psychological distress, substance use, suicidal ideation, anxiety, and depression among adults (Cano et al., 2021; Cavalhieri et al., 2024; Keum, 2022; Keum & Ahn, 2021; Keum & Cano, 2021; Keum et al., 2023; Keum & Hearns, 2021; Layug et al., 2022). This study sought to build upon these findings to determine if online racism exists as a racially traumatic stressor that may lead to the development of symptoms of racial trauma. Confirming our first hypothesis, the results of our study demonstrated that exposure to online racism was associated with increased racial trauma symptoms among participants. Thus, our findings indicate that such exposure contributes to emotional and psychological injury upon individuals’ racial identity. Our study aligns with emerging research on adults that has demonstrated exposure to racism via online communication and media as a traumatic stressor (Evans et al., 2024; Green et al., 2024; Maxie-Moreman & Tynes, 2022).
Our study builds upon existing research by highlighting that exposure to online racism may be experienced as racially traumatizing by PGM as well as by White individuals. Although not part of our primary research question and analysis, our regression analysis found no statistically significant difference in racial trauma between White and PGM participants. This finding should be interpreted with nuance given that White individuals do not experience racism as a function of white supremacy. Echoing findings from Carter, Roberson, and Johnson (2020) and Carter and Kirkinis (2021), White individuals’ quantitative endorsement of racial trauma from vicarious exposure to racism may be qualitatively different from experiences of PGM. Specifically, racial identity attitudes may play a role in how White individuals perceive racism and experience subsequent distress (Carter, Roberson, & Johnson, 2020). Prior research highlights that White individuals with greater racial awareness endorse fewer racial trauma symptoms despite reporting vicarious exposure to racism (Carter, Roberson, & Johnson, 2020). Moreover, White individuals with color-evasive racial attitudes may view White individuals as targets of online racism (Green et al., 2023). Thus, this finding may be best understood as being connected to racial attitudes that impact measurement of racial trauma symptoms rather than equating White and PGM participant experiences.
Our study also sought to examine the relationship and mediating role of social connectedness with online racism and racial trauma. Confirming our second hypothesis, we found that online social connectedness both significantly predicted racial trauma in our regression model and significantly mediated the relationship between online racism and racial trauma. These findings suggest that feeling disconnected in online contexts following exposure to online racism may relate to increased symptoms of racial trauma. Additionally, individuals who experience challenges in finding and maintaining connectedness and supportive communities with others may be at greater risk of developing racial trauma symptoms. This aligns with findings of suppression and social withdrawal following experiences of racialized cybervictimization (Evans et al., 2024). Conversely, our findings highlight that stronger social connectedness after exposure to online racism may relate to decreased racial trauma symptoms. These findings emphasize the value of resources like online counterspaces that may foster racial identity affirmation, sense of community, social support, and resistance to online racism (Case & Hunter, 2012; Gomez & Cabrera, 2025; Lopez-Leon & Casanova, 2023). In summary, this study highlights the important roles of online interactions, relationships, and communities as they relate to the racial trauma experienced following exposure to online racism.
Clinical Implications and Future Research
As discussed above, our study contributes to existing literature on online racism and symptoms of mental health and wellness. Findings from our study indicate that online racism may be experienced as a racially traumatic stressor. This is noted in participant scores for racial trauma (M = 78.40; SD = 20.63) being above the established clinical cut-off score of 48 (Williams et al., 2022). Thus, counselors should integrate experiences of online racism into assessment and interventions with adult clients, particularly at times when online racist content may be prevalent. This assessment and acknowledgement can incentivize counselors to focus on processing these traumatic experiences. For example, a counselor naming a client’s response as part of racial trauma can support validating their experiences following exposure. Moreover, this may also support client healing by attributing their intrapsychic racial trauma symptoms as responses to external racism while reducing the odds of internalizing racism (Adames et al., 2023). Likewise, counselors can focus on enhancing client social connectedness as a potential protective factor that may support reducing client experiences of self-blame and social withdrawal (Adames et al., 2023; Evans et al., 2024). Counselors may also consider supporting clients in developing digital hygiene to optimize self-care in their therapeutic work.
Considering the significance of social connectedness as a protective factor, counselors can advocate for clients experiencing racial trauma from online racism to actively participate in digital counterspaces that foster social connectedness (Gomez & Cabrera, 2025; Mosley et al., 2021). This may occur through traditional modalities of counseling such as group counseling via telehealth or other community-developed groups across social media platforms. Counselors may encourage client participation in such digital counterspaces during treatment to empower them to engage in community care as a compliment to self-care behaviors. Additionally, these client recommendations may aid in developing critical consciousness, a sense of belonging with others, and in developing resistance strategies despite experiences of online racism (Case & Hunter, 2012; Gomez & Cabrera, 2025; Lopez-Leon & Casanova, 2023). Beyond individual counseling, it is imperative that counselors engage in community-level advocacy in addressing online racism. For example, facilitating workshops, public education, and creating safe spaces in school or university settings may support vulnerable populations in building awareness around online racism and its impact. Such spaces can offer safety and validation of racial trauma experiences (Wright et al., 2023). Moreover, these spaces and events can provide critical insight toward preventing engagement in online racism and healing from its traumatic impact (Wright et al., 2023).
Lastly, counselors might consider ways to support the wellness of White clients who experience distress related to online racism. Counselors should emphasize development in White racial identity and coping practices to navigate vicarious exposure to racism online. This might include supporting White clients in reshaping their cognition of their adverse reactions toward a more critical understanding of white supremacy (Carter, Roberson, & Johnson, 2020). Counselors are encouraged to address color-evasive racial attitudes expressed by White clients during sessions to enhance critical consciousness in alignment with theory on radical healing (Adames et al., 2023; French et al., 2020; Green et al., 2023). Counselors should also encourage White clients who are struggling with their adverse reactions to online racism to build relationships with other White individuals to enhance social connectedness as it pertains to critical consciousness raising. Supporting White clients in appropriately attributing their adverse experiences may also aid in reducing online racism toward PGM. For example, a White client who experiences online backlash from engaging in online racism may attribute their adverse experience to reverse racism, resulting in further engagement in online racism (Green et al., 2023).
Future research may build upon our study by more specifically investigating the role of counterspaces as they relate to mental health, wellness, and exposure to online racism and other forms of online hate. Such research should consider the significance of qualitative methodologies to better understand the lived experiences of coping and resisting through social resources that may reduce the impact of online racism. Further quantitative research on the racial trauma of online racism might compare differences in coping between White and PGM populations to better understand ways for counselors to enhance support for those impacted by online racism. Additionally, it is important to examine online racism experienced by online racial justice activists who may be prone to such exposure. Such research might compare racial trauma symptoms experienced because of online and offline exposure to racism to identify ways in which counselors can support the wellness of those who engage in racial justice efforts via social media and other forms of digital technology. Lastly, future research might examine the impact of long-term exposure to racially traumatizing online content on mental health and wellness in order to better understand the transgenerational impact of online racism alongside advancements in digital technology. Such research might specifically study social, cognitive, and behavioral changes across the lifespan, particularly for parents of PGM children, adolescents, and emerging adults.
Limitations
One limitation of this study lies in its cross-sectional nature. Although the use of mediation analysis was used to better understand how exposure to online racism may result in decreased social connectedness that in turn increases racial trauma symptoms, the cross-sectional design does not allow for causal conclusions. As a result, it is unknown if lower or greater social connectedness reported by participants was preexisting or the result of exposure to online racism. Another limitation of the study lies in the sampling method. First, the use of MTurk as a platform to recruit participants likely introduced bias, particularly given the financial incentive for participants to complete the study. We attempted to mitigate some bias through use of two validity check items in the online survey; however, this may not have counteracted the potential for bias to influence participant data. In addition to the use of convenience sampling with monetary incentive, the use of a quota system introduced a bias in the results for White participants who completed the survey early on while PGM participants did not experience restrictions or any subsequent bias in participation. Although the quota was intended to limit the overrepresentation of White participants that may have occurred through sampling via MTurk, it also introduced uncontrolled bias into the results. Moreover, we did not include exposure to online racism or experiences of racial trauma as criteria in the recruitment process. Using a narrower sample would have been more consistent with the underlying theory of racial trauma and could produce different results. As a result, caution should be taken in generalizing this study’s findings. Future research might mitigate such bias by sampling from multiple sources, such as directly recruiting from social media platform users and groups, to better prevent issues of oversampling as it relates to racial identity.
Conclusion
Our study sought to expand emerging research on exposure to online racism by examining how it relates to racial trauma among adults. Moreover, our study contributed to this emerging research by highlighting the significance of online social connectedness as a mediating variable in the relationship between online racism and racial trauma. Our study indicates that online racism may exist as a racially traumatic stressor that is essential for counselors to attend to in clinical practice for clients who may be vulnerable to such exposure. Lastly, our findings suggest that enhancing sense of connectedness may be an avenue for supporting client wellness among those who experience racial trauma from online racism exposure.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adames, H. Y., Chavez-Dueñas, N. Y., Lewis, J. A., Neville, H. A., French, B. H., Chen, G. A., & Mosley, D. V. (2023). Radical healing in psychotherapy: Addressing the wounds of racism-related stress and trauma. Psychotherapy, 60(1), 39–50. https://doi.org/10.1037/pst0000435
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.).
Bliuc, A-M., Faulkner, N., Jakubowicz, A., & McGarty, C. (2018). Online networks of racial hate: A systematic review of 10 years of research on cyber-racism. Computers in Human Behavior, 87, 75–86.
https://doi.org/10.1016/j.chb.2018.05.026
Cano, M. Á., Schwartz, S. J., MacKinnon, D. P., Keum, B. T., Prado, G., Marsiglia, F. F., Salas-Wright, C. P., Cobb, C. L., Garcini, L. M., De La Rosa, M., Sánchez, M., Rahman, A., Acosta, L. M., Roncancio, A. M., & de Dios, M. A. (2021). Exposure to ethnic discrimination in social media and symptoms of anxiety and depression among Hispanic emerging adults: Examining the moderating role of gender. Journal of Clinical Psychology, 77(3), 571–586. https://doi.org/10.1002/jclp.23050
Carter, R. T. (2007). Racism and psychological and emotional injury: Recognizing and assessing race-based traumatic stress. The Counseling Psychologist, 35(1), 13–105. https://doi.org/10.1177/0011000006292033
Carter, R. T., & Kirkinis, K. (2021). Differences in emotional responses to race-based trauma among Black and White Americans. Journal of Aggression, Maltreatment, & Trauma, 30(7), 889–906.
https://doi.org/10.1080/10926771.2020.1759745
Carter, R. T., Kirkinis, K., & Johnson, V. E. (2020). Relationships between trauma symptoms and race-based traumatic stress. Traumatology, 26(1), 11–18. https://doi.org/10.1037/trm0000217
Carter, R. T., Mazzula, S., Victoria, R., Vazquez, R., Hall, S., Smith, S., Sant-Barket, S., Forsyth, J., Bazelais, K., & Williams, B. (2013). Initial development of the Race-Based Traumatic Stress Symptom Scale: Assessing the emotional impact of racism. Psychological Trauma: Theory, Research, Practice, and Policy, 5(1), 1–9. https://doi.org/10.1037/a0025911
Carter, R. T., Roberson, K., & Johnson, V. E. (2020). Race-based stress in White adults: Exploring the role of White racial identity status attitudes and type of racial events. Journal of Multicultural Counseling & Development, 48(2), 95–107. https://doi.org/10.1002/jmcd.12168
Case, A. D., & Hunter, C. D. (2012). Counterspaces: A unit of analysis for understanding the role of settings in marginalized individuals’ adaptive responses to oppression. American Journal of Community Psychology, 50(1–2), 257–270. https://doi.org/10.1007/s10464-012-9497-7
Cavalhieri, K. E., Greer, T. M., Hawkins, D., Choi, H., Hardy, C., & Heavner, E. (2024). The effects of online and institutional racism on the mental health of African Americans. Cultural Diversity & Ethnic Minority Psychology, 30(3), 476–486. https://doi.org/10.1037/cdp0000585
Cohen, J., Cohen, P., West, S. G., & Aiken, L. S. (2003). Applied multiple regression/correlation analysis for the behavioral sciences (3rd ed). Lawrence Erlbaum.
Comas-Díaz, L., Hall, G. N., & Neville, H. A. (2019). Racial trauma: Theory, research, and healing: Introduction to the special issue. American Psychologist, 74(1), 1–5. https://doi.org/10.1037/amp0000442
Del Toro, J., & Wang, M.-T. (2023). Online racism and mental health among Black American adolescents in 2020. Journal of the American Academy of Child & Adolescent Psychiatry, 62(1), 25–36. https://doi.org/10.1016/j.jaac.2022.07.004
Evans, A. M., Chalk, S., Green, D., Hornsby, T., Ramsay-Seaner, K., & Haskins, R. (2024). Cyberbullying as a method of discrimination among people of color: An interpretative phenomenological analysis. Wisconsin Counseling Journal, 37, 26–46.
French, B. H., Lewis, J. A., Mosley, D. V., Adames, H. Y., Chavez-Dueñas, N. Y., Chen, G. A., & Neville, H. A. (2020). Toward a psychological framework of radical healing in communities of color. The Counseling Psychologist, 48(1), 14–46. https://doi.org/10.1177/0011000019843506
Fulmer, R. (2024). A primer on how AI algorithms control you. Journal of Technology in Counselor Education and Supervision, 5(2), Article 1. https://doi.org/10.61888/2692-4129.1098
Gelles-Watnick, R. (2024). Americans’ use of mobile technology and home broadband. Pew Research Center. www.pewresearch.org/internet/2024/01/31/americans-use-of-mobile-technology-and-home-broadband
Gomez, V., & Cabrera, J. (2025). Theorizing virtual counterspaces: How Latina graduate students build community online. Race Ethnicity and Education, 28(7), 1105–1121. https://doi.org/10.1080/13613324.2023.2292509
Gottfried, J. (2024). Americans’ social media use. Pew Research Center. https://www.pewresearch.org/internet/2024/01/31/americans-social-media-use
Green, D. A., Dockery, G. N., & Williams, B. A. (2023). Cyber racism in counseling cyberspaces. Journal of Multicultural Counseling and Development, 51(3), 195–207. https://doi.org/10.1002/jmcd.12276
Green, D. A., Evans, A. M., Litam, S. D. A., Hornsby, T., Boulden, R., Shannon, J., Ford, D. J., & Landrum, D. (2024). Racial identity attitudes and vicarious traumatization from undue police violence on anticipatory traumatic reaction among Black Americans. Journal of Interpersonal Violence, 39(3–4), 848–868. https://doi.org/10.1177/08862605231198484
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2nd ed.). Guilford.
Hemmings, C., & Evans, A. M. (2018). Identifying and treating race-based trauma in counseling. Journal of Multicultural Counseling and Development, 46(1), 20–39. https://doi.org/10.1002/jmcd.12090
Hill, M. L. (2018). “Thank you, Black Twitter”: State violence, digital counterpublics, and pedagogies of resistance. Urban Education, 53(2), 286–302. https://doi.org/10.1177/0042085917747124
Holmes, S. C., Zare, M., Haeny, A. M., & Williams, M. T. (2024). Racial stress, racial trauma, and evidence-based strategies for coping and empowerment. Annual Review of Clinical Psychology, 20, 77–95.
https://doi.org/10.1146/annurev-clinpsy-081122-020235
Jones, N., Marks, R., Ramirez, R., & Ríos-Vargas, M. (2021, August 12). 2020 census illuminates racial and ethnic composition of the country. United States Census Bureau. https://www.census.gov/library/stories/2021/08/improved-race-ethnicity-measures-reveal-united-states-population-much-more-multiracial.html
Keum, B. T. (2017). Qualitative examination on the influences of the internet on racism and its online manifestation. International Journal of Cyber Behavior, Psychology and Learning, 7(3), 13–22.
https://doi.org/10.4018/IJCBPL.2017070102
Keum, B. T. (2021). Development and validation of the Perceived Online Racism Scale short form (15 items) and very brief (six items). Computers in Human Behavior Reports, 3, 100082. https://doi.org/10.1016/j.chbr.2021.100082
Keum, B. T. (2022). Impact of online racism on suicide ideation through interpersonal factors among racial minority emerging adults: The role of perceived burdensomeness and thwarted belongingness. Journal of Interpersonal Violence, 38(5–6), 4537–4561. https://doi.org/10.1177/08862605221117247
Keum, B. T., & Ahn, L. H. (2021). Impact of online racism on psychological distress and alcohol use severity: Testing ethnic-racial socialization and silence about race as moderators. Computers in Human Behaviors, 120, 106773. https://doi.org/10.1016/j.chb.2021.106773
Keum, B. T., & Cano, M. Á. (2021). Online racism, psychological distress, and alcohol use among racial minority women and men: A multi-group mediation analysis. American Journal of Orthopsychiatry, 91(4), 524–530. https://doi.org/10.1037/ort0000553
Keum, B. T., Cano, M. Á., Valdovinos, I. C., & Boland, D.-z. (2023). Impact of online and offline racism on cigarette smoking, marijuana use, and vaping via depressive/anxiety symptoms among racially minoritized emerging adults. American Journal of Orthopsychiatry, 93(5), 450–459. https://doi.org/10.1037/ort0000691
Keum, B. T., & Hearns, M. (2021). Online gaming and racism: Impact on psychological distress among Black, Asian, and Latinx emerging adults. Games and Culture, 17(3), 445–460. https://doi.org/10.1177/15554120211039082
Keum, B. T., & Miller, M. J. (2017). Racism in digital era: Development and initial validation of the Perceived Online Racism Scale (PORS v1.0). Journal of Counseling Psychology, 64(3), 310–324. http://doi.org/10.1037/cou0000205
Layug, A., Krishnamurthy, S., McKenzie, R., & Feng, B. (2022). The impacts of social media use and online racial discrimination on Asian American mental health: Cross-sectional survey in the United States during COVID-19. JMIR Formative Research, 6(9), e38589. https://doi.org/10.2196/38589
Lee, R. M., & Robbins, S. B. (1995). Measuring belongingness: The Social Connectedness and the Social Assurance scales. Journal of Counseling Psychology, 42(2), 232–241. https://doi.org/10.1037/0022-0167.42.2.232
Lopez-Leon, G., & Casanova, S. (2023). “Those are the spaces where I feel seen and fully understood”: Digital counterspaces fostering community, resistance, and intersectional identities among Latinx LGBTQ+ emerging adults. Journal of Adolescent Research, 40(2), 331–360. https://doi.org/10.1177/07435584231165993
Maxie-Moreman, A. D., & Tynes, B. M. (2022). Exposure to online racial discrimination and traumatic events online in Black adolescents and emerging adults. Journal of Research on Adolescence, 32(1), 254–269. https://doi.org/10.1111/jora.12732
Mosley, D. V., Hargons, C. N., Meiller, C., Angyal, B., Wheeler, P., Davis, C., & Stevens-Watkins, D. (2021). Critical consciousness of anti-Black racism: A practical model to prevent and resist racial trauma. Journal of Counseling Psychology, 68(1), 1–16. https://doi.org/10.1037/cou0000430
Mosley, D. V., Neville, H. A., Chavez-Dueñas, N. Y., Adames, H. Y., Lewis, J. A., & French, B. H. (2020). Radical hope in revolting times: Proposing a culturally relevant psychological framework. Social and Personality Psychology Compass, 14(1), Article e12512. https://doi.org/10.1111/spc3.12512
Nasereddin, S. (2023). Impact of social media platforms on international public opinion during the Israel war on Gaza. Global Change, Peace & Security, 35(1), 5–31. https://doi.org/10.1080/14781158.2024.2415908
Ong, M., Smith, J. M., & Ko, L. T. (2018). Counterspaces for women of color in STEM higher education: Marginal and central spaces for persistence and success. Journal of Research in Science Teaching, 55(2), 206–245. https://doi.org/10.1002/tea.21417
Pew Research Center. (2024). Mobile fact sheet. https://www.pewresearch.org/internet/fact-sheet/mobile
Rudnicki, K., Vandebosch, H., Voué, P., & Poels, K. (2023). Systematic review of determinants and consequences of bystander interventions in online hate and cyberbullying among adults. Behaviour & Information Technology, 42(5), 527–544. https://doi.org/10.1080/0144929X.2022.2027013
Sheikh, I. S., Alsubaie, M. K., Dolezal, M. L., Walker, R. S., Rosencrans, P. L., Peconga, E., Holloway, A., Bentley, J. A., & Zoellner, L. A. (2022). The role of social connectedness in buffering the effects of discrimination on post-trauma cognitions in forcibly displaced Muslims. Psychological Trauma: Theory, Research, Practice, & Policy, 14(1), 47–54. https://doi.org/10.1037/tra0001070
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed). Pearson.
Thomas, A., Gale, A., & Golden, A. R. (2023). Online racial discrimination, critical consciousness, and psychosocial distress among Black and Latino adolescents: A moderated mediation model. Journal of Youth & Adolescence, 52(5), 967–979. https://doi.org/10.1007/s10964-022-01732-z
Tynes, B. M., Umaña-Taylor, A. J., Rose, C. A., Lin, J., & Anderson, C. J. (2012). Online racial discrimination and the protective function of ethnic identity and self-esteem for African American adolescents. Developmental Psychology, 48(2), 343–355. https://doi.org/10.1037/a0027032
Tynes, B. M., Willis, H. A., Stewart, A. M., & Hamilton, M. W. (2019). Race-related traumatic events online and mental health among adolescents of color. Journal of Adolescent Health, 65(3), 371–377.
https://doi.org/10.1016/j.jadohealth.2019.03.006
Volpe, V. V., Hoggard, L. S., Willis, H. A., & Tynes, B. M. (2021). Anti-Black structural racism goes online: A conceptual model for racial health disparities research. Ethnicity & Disease, 31(Suppl 1), 311–318.
https://ethndis.org/supplementarchive/files/ethndis-31-311.pdf
Williams, M. T., Metzger, I. W., Leins, C., & DeLapp, C. (2018). Assessing racial trauma within a DSM–5 framework: The UConn Racial/Ethnic Stress & Trauma Survey. Practice Innovations, 3(4), 242–260. https://doi.org/10.1037/pri0000076
Williams, M. T., Osman, M., Gallo, J., Pereira, D. P., Gran-Ruaz, S., Strauss, D., Lester, L., George, J. R., Edelman, J., & Litman, L. (2022). A clinical scale for the assessment of racial trauma. Practice Innovations, 7(3), 223–240. https://doi.org/10.1037/pri0000178
Wong, B. (2023). Top social media statistics and trends. Forbes Advisor. https://www.forbes.com/advisor/business/social-media-statistics
Wright, W., Hatchett Stover, J., & Brown-Rice, K. (2023). Understanding racial trauma: Implications for professional counselors. The Professional Counselor, 13(1), 17–26. https://doi.org/10.15241/ww.13.1.17
Darius A. Green, PhD, NCC, LPCC, is an assistant professor at Bowie State University. Kade Stanzilis, MA, LPCC, is a graduate researcher at the University of Colorado Colorado Springs. Sierra Roach-Coye, MSW, LSW, is a doctoral candidate at Denver University. Connor Sullivan, MA, LPCC, is a graduate researcher at the University of Colorado Colorado Springs. Correspondence may be addressed to Darius A. Green, Department of Counseling and Psychological Studies, Bowie State University, 14000 Jericho Park Road, Bowie, MD, 20715, dgreen2@bowiestate.edu.
Mar 26, 2026 | Book Reviews
by Alan W. McEvoy, PhD
 There have been strong recent shifts in our culture concerning sexual assault. Individuals who have experienced sexual assault are coming forward and demanding justice for the harm done. While this is a positive change, it can leave the men in their lives unsure of what support would be most helpful. The title reviewed here explores this very topic and helps men find ways to better understand and support all victims of sexual assault, though McEvoy focuses mainly on female victims of sexual assault.
There have been strong recent shifts in our culture concerning sexual assault. Individuals who have experienced sexual assault are coming forward and demanding justice for the harm done. While this is a positive change, it can leave the men in their lives unsure of what support would be most helpful. The title reviewed here explores this very topic and helps men find ways to better understand and support all victims of sexual assault, though McEvoy focuses mainly on female victims of sexual assault.
When the Subject Is Rape explores the multiple avenues of support that can assist someone who has experienced sexual assault and imparts advice to the male support people in their lives. Author Alan W. McEvoy also outlines practical tips like conversation topics and how to handle court or medical proceedings, while also giving more abstract suggestions and challenges for inner exploration. This book also addresses male support people’s common responses and explains how they may not be helpful in certain situations. At the end of the book, the author includes contact information for different help lines and centers for sexual assault for the United States and other countries and regions. This can be a tremendous resource for so many types of male allies and support people.
A major strength of this book is the psychoeducation around sexual assault. This includes definitions of sexual assault and other medical or legal terms that an individual might encounter. Other strengths include outlining what a sexual assault victim may go through in the legal system and how a support person can assist in some of these events. The author also addresses the different responses that an individual might display after an assault and outlines the decision-making process that these individuals go through regarding next steps and protecting their safety.
While this book offers many helpful insights and much guidance, I find it would benefit from the inclusion of first-hand accounts or stories. All of the information shared with the reader is seemingly based on the author’s opinion or experience as a clinician, but this is not fully explained by the author. First-hand accounts could strengthen and validate the advice that McEvoy shares with his readers. Additionally, the author discusses many difficult dynamics within sexual assault, including hate crimes and assault by a sibling. While these topics are incredibly important to explore and address, there are some topics (assault by a parent/stepparent), that I believe could be addressed more thoroughly by the author.
This book could have strong positive impacts in counseling practice. While there are many helpful resources for clients who are the survivors of sexual assault, this title offers practical advice for men who are a part of a survivor’s support network. When these clients come into our office, it can be hard to find resources that address their unique needs. McEvoy’s book offers both clients and clinicians a road map of what to expect as they assist someone through their grief and trauma, and practical tips on what to do in certain situations. In my own practice, I would use this title as a reference for clients who care for someone who experienced sexual assault, and as a resource that a victim of sexual assault could give to a loved one so they can better assist during recovery.
Overall, When the Subject Is Rape is a helpful starting point for all types of support people, not just men. This includes mental health professionals working with victims of sexual assault and family members or friends who want to better understand and assist someone they love as they navigate the next stages of their life following sexual assault.
McEvoy, A. W. (2023). When the subject is rape: A guide for male partners, friends & family members. Square One Publishers.
Reviewed by: Amanda Condic, MA, NCC, LPC
Dec 22, 2025 | Volume 15 - Issue 4
Lotes Nelson, Clark D. Ausloos, Kirsis A. Dipre
This special issue of The Professional Counselor (TPC) celebrates the enduring legacy of the NBCC Foundation’s Minority Fellowship Program (MFP) and the remarkable contributions of its Fellows to the counseling profession. Guided by the overarching theme Bridging Gaps, Building Futures, this issue reflects how MFP scholars continue to advance equity, belonging, and healing across diverse communities through research, practice, and advocacy. Each article in this collection represents both an individual and collective commitment to closing the gap between awareness and action, transforming knowledge into meaningful and sustainable change. Building upon this collective vision, the selected works in this special issue are organized around two interwoven subthemes: Threads of Transformation and Scholarship as Bridgework. Together, these sections illuminate the dynamic ways in which counselors, counselor educators, and researchers are bridging identity, belonging, and access while advancing scholarship that heals, connects, and transforms. Collectively, these themes invite readers to consider how transformation and bridgework function as inseparable elements of professional identity—threads woven through practice, teaching, and research. In this spirit, the articles in this issue form a tapestry of insight and inspiration, reminding us that meaningful change emerges through the ongoing continuum of reflection, action, and connection that lies at the heart of the counseling profession.
Threads of Transformation
This first theme, Threads of Transformation, captures how MFP Fellows weave identity, belonging, and access into their research, teaching, and clinical practice. Across schools, families, and communities, these scholars actively transform systems of care into more inclusive, culturally responsive, and healing-centered practices. Their work reflects the commitment of MFP Fellows to bridge awareness with action and to ensure that nondominant populations are supported in spaces that have too often excluded them, including within helping professions. The studies that comprise this theme speak to the transformative power of belonging, connection, celebrating cultural identity, and fostering resilience and growth across generations and communities.
In “A Pilot Study Examining Xinachtli: A Gender-Based Culturally Responsive Group Curriculum for Chicana, Latina, and Indigenous Secondary Students,” Vanessa Placeres and colleagues explore how culturally grounded interventions can serve as restorative spaces for Chicana, Latina, and Indigenous (CLI) youth. Guided by a healing-informed and gender-responsive framework, Xinachtli—meaning “germinating seed” in Nahuatl—nurtures identity development, life skills, and a sense of belonging among middle and high school students. The study’s preliminary outcomes underscore the feasibility of implementing culturally responsive group counseling within K–12 schools and affirm the importance of integrating feminist traditions in CLI youth development.
In “Parenting Across Racial Lines: The Lived Experiences of Transracially Adoptive Parents of Black Children,” Charmaine Conner and Natalya Lindo explore transformation within the family system itself. Using a transcendental phenomenological approach grounded in the Cultural-Racial Identity Model, the authors explore how White parents raising Black children navigate cultural humility, trauma, and identity development. Participants’ reflections reveal both the challenges of transracial parenting and the transformative potential of intentional cultural socialization, advocacy, and learning. Through their process of “becoming,” these parents model transformation through love, humility, and accountability.
In “See the Girl: Girls’ Perceptions of Listening and Helpfulness in a Relational–Cultural Theory Grounded School-Based Counseling Program,” Ne’Shaun Borden and colleagues extend this theme by centering the lived experiences of African American girls in elementary school. Drawing on years of program data from See the Girl: In Elementary, findings reveal that authentic presence, empathy, and support were key to the girls’ sense of being heard and valued. Through the lens of Relational–Cultural Theory, this study reminds us that relational connection is itself a pathway to belonging and healing.
In “‘Deep in the Hollers’: LGBTQ+ Narratives of Addiction and Recovery in Appalachia,” Jacob Perkins and Harley Locklear amplify voices from rural queer communities navigating addiction and recovery. Through narrative inquiry, Perkins captures stories of resilience, chosen family, and the reimagining of wellness amid systemic and cultural marginalization. Participants’ narratives illuminate how isolation, stigma, and restrictive norms around identity and substance use intersect in rural regions. The article also demonstrates that recovery can emerge from solidarity and creative redefinitions of care. By positioning queer Appalachian experiences as central rather than peripheral, this work transforms dominant understandings of addiction recovery and challenges counselors to consider how regional identity, sexuality, and belonging intersect within the healing process.
Scholarship as Bridgework
The second theme, Scholarship as Bridgework, highlights how each article contributes to collective equity and healing in our profession, inviting us to center those in the margins and amplify their voices through our privileged positions as counselors, educators, supervisors and scholars.
In “Associations Between Coping and Suicide Risk Among Emerging Adults of Asian Descent,” Afroze Shaikh and colleagues use research as a tool to bridge the lack of knowledge and amplify the invisible fight with suicidality among emerging adults of Asian descent. Grounded in the Interpersonal Theory of Suicide, this quantitative study examines the associations between coping orientations (e.g., problem-focused, emotion-focused, and avoidant) and strategies (e.g., gratitude, self-compassion, and search for meaning in life) and suicide risk (e.g., perceived burdensomeness and thwarted belongingness). The findings underscore the importance of culturally responsive coping interventions as bridges toward understanding and addressing suicide risk factors, urging us to center and uplift the voices of those made invisible by dominant societal norms and expectations.
Finally, Shadin Atiyeh examines the challenges and strategies employed by counselor educators in training students to work effectively with refugee populations in “Preparing Counseling Students to Work With Refugees: A Descriptive Analysis.” Utilizing a qualitative descriptive analysis, Atiyeh has identified several barriers to effective training in CACREP-accredited master’s programs across the United States. These include (a) perceived limited relevance of the topic, (b) time constraints within courses, and (c) the complexity of addressing refugee issues. The findings call us to embrace our collective responsibility to re-envision the counseling curriculum and implement creative, forward-thinking teaching practices that transcend institutional barriers, ensuring that students are well prepared to address the distinctive mental health needs of refugee populations.
Conclusion
Collectively, MFP Fellows demonstrate that culturally responsive practice is an active reimagining of what it means to belong, to heal, and to thrive. The Threads of Transformation woven throughout these studies remind us that when counselors and educators engage with identity and belonging as foundations of wellness, they reshape the systems that define who is seen, valued, and supported in our profession. Through the lens of Scholarship as Bridgework, these articles extend that vision by building bridges between knowledge, practice, and purpose. Our shared purpose is to prepare future counselors with the knowledge and skills to support marginalized and underserved communities while integrating equity-focused content across counseling curricula to promote social justice and collective healing. As you explore this special issue, we invite you to reflect on how these perspectives can inspire your own practice, teaching, and advocacy. What bridges can you build to move from awareness to action, and how can your work contribute to the elimination of mental health disparities? Our hope is that this collection not only informs but also inspires continued commitment to equity, belonging, and transformation within the counseling profession. Together, these works remind us that by bridging gaps and building worlds, we collectively transform the future of counseling.
_________________________________________________________________________________________________________________
 Lotes Nelson (she/her/siya), PhD, NCC, ACS, LCMHC-S, is an associate professor in the counselor education and supervision program at the University of the Cumberlands and was proud to be a 2015 Mental Health Counseling Doctoral Fellow with the NBCCF Minority Fellowship Program. She remains deeply connected to the NBCC Foundation as a mentor, scholarship reviewer, journal guest co-editor, and contributor to Foundation initiatives, and she is honored to continue giving back to the program that shaped her. Dr. Nelson is co-editor of Multicultural Counseling: Responding with Cultural Humility, Empathy, & Advocacy and brings a strong commitment to uplifting marginalized and underserved communities through culturally responsive counseling, social justice advocacy, and leadership development. Her work focuses on counselor resilience, identity formation, and preparing future counselors and counselor educators to lead with equity, compassion, and purpose.
Lotes Nelson (she/her/siya), PhD, NCC, ACS, LCMHC-S, is an associate professor in the counselor education and supervision program at the University of the Cumberlands and was proud to be a 2015 Mental Health Counseling Doctoral Fellow with the NBCCF Minority Fellowship Program. She remains deeply connected to the NBCC Foundation as a mentor, scholarship reviewer, journal guest co-editor, and contributor to Foundation initiatives, and she is honored to continue giving back to the program that shaped her. Dr. Nelson is co-editor of Multicultural Counseling: Responding with Cultural Humility, Empathy, & Advocacy and brings a strong commitment to uplifting marginalized and underserved communities through culturally responsive counseling, social justice advocacy, and leadership development. Her work focuses on counselor resilience, identity formation, and preparing future counselors and counselor educators to lead with equity, compassion, and purpose.
 Clark D. Ausloos (he/him), PhD, NCC, LPC, LPCC, LSC, is an assistant professor in the counseling department at Oakland University, an NBCCF MFP Alumnus (2019 Mental Health Counseling Doctoral Fellow), and Past- Chairperson of the NBCCF MFP Advisory Council. His research interests center on supporting nondominant populations, particularly queer and trans youth, and enhancing cultural responsivity in counselor education preparation. Dr. Ausloos has authored numerous peer-reviewed manuscripts and delivered extensive conference presentations. He serves in multiple professional leadership roles, including as President-Elect of the Society for Sexual, Affectional, Intersex, and Gender Expansive Identities (SAIGE), in addition to maintaining an active clinical practice serving clients in Ohio and Michigan.
Clark D. Ausloos (he/him), PhD, NCC, LPC, LPCC, LSC, is an assistant professor in the counseling department at Oakland University, an NBCCF MFP Alumnus (2019 Mental Health Counseling Doctoral Fellow), and Past- Chairperson of the NBCCF MFP Advisory Council. His research interests center on supporting nondominant populations, particularly queer and trans youth, and enhancing cultural responsivity in counselor education preparation. Dr. Ausloos has authored numerous peer-reviewed manuscripts and delivered extensive conference presentations. He serves in multiple professional leadership roles, including as President-Elect of the Society for Sexual, Affectional, Intersex, and Gender Expansive Identities (SAIGE), in addition to maintaining an active clinical practice serving clients in Ohio and Michigan.
 Kirsis A. Dipre (she/her/ella), PhD, NCC, LPC (IL), is an assistant professor in the counselor education department at Northeastern Illinois University and a licensed professional counselor. Dr. Dipre is dedicated to supporting the development and training of culturally responsive counselors while providing mental health services to underserved populations, centering advocacy and social justice throughout the process. Her scholarly, teaching, service, mentoring, and supervisory work is collectively aimed at increasing access to mental health care, challenging structural barriers within and outside the counseling profession, and creating healing spaces that honor the intersections each of us inhabits. Grounded in liberation-focused and culturally affirming practices, Dr. Dipre’s work amplifies the voices and experiences of racialized and systemically excluded communities, particularly Latine immigrants and Afro-Latine individuals and families. Dr. Dipre was a 2020 Mental Health Counseling Doctoral Fellow with the NBCCF Minority Fellowship Program and is currently serving a second term as an Advisory Council member for the MFP–CMHC program.
Kirsis A. Dipre (she/her/ella), PhD, NCC, LPC (IL), is an assistant professor in the counselor education department at Northeastern Illinois University and a licensed professional counselor. Dr. Dipre is dedicated to supporting the development and training of culturally responsive counselors while providing mental health services to underserved populations, centering advocacy and social justice throughout the process. Her scholarly, teaching, service, mentoring, and supervisory work is collectively aimed at increasing access to mental health care, challenging structural barriers within and outside the counseling profession, and creating healing spaces that honor the intersections each of us inhabits. Grounded in liberation-focused and culturally affirming practices, Dr. Dipre’s work amplifies the voices and experiences of racialized and systemically excluded communities, particularly Latine immigrants and Afro-Latine individuals and families. Dr. Dipre was a 2020 Mental Health Counseling Doctoral Fellow with the NBCCF Minority Fellowship Program and is currently serving a second term as an Advisory Council member for the MFP–CMHC program.
