May 22, 2024 | Volume 14 - Issue 1
Kaprea F. Johnson, Alexandra Gantt-Howrey, Bisola E. Duyile, Lauren B. Robins, Natese Dockery
Career counselors practicing in rural communities must understand and address social determinants of mental health (SDOMH). This conceptual article details the relationships between SDOMH domains and employment and provides evidence-based recommendations for integrating SDOMH into practice through a rural community health and well-being framework. Description of the adaptation of the framework for career counselors in rural communities, SDOMH assessment strategies and tools, and workflow adjustments are included. Conclusions suggest next steps for practice and research.
Keywords: social determinants of mental health, career counselors, rural communities, health and well-being framework, assessment
Career counselors in rural communities address standard employment needs of the population, but they also must be aware of the socioeconomic circumstances that impact their community’s mental health and, in return, employment. Such socioeconomic factors are termed the social determinants of mental health (SDOMH). SDOMH are nonclinical psychosocial and socioeconomic circumstances that contribute to mental health outcomes (Office of Disease Prevention and Health Promotion [ODPHP], n.d.). Healthy People 2030, a government initiative to promote health and well-being, describes a five-domain framework of SDOMH which includes: economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context (ODPHP, n.d.). Collectively, SDOMH can disrupt overall well-being and have a cyclical relationship with employment. For example, in rural communities, minimal access to public transportation may make sustaining employment difficult, which can then impact health insurance. Without insurance, a person loses access to health care; with unmet health care needs, a person who is unwell and without access to treatment has less opportunity for employment. Thus, understanding and addressing SDOMH is critically important for career counselors working in rural and other underserved communities (Pope, 2011). This conceptual paper will define SDOMH, introduce a theoretical framework for addressing SDOMH, provide evidence-based recommendations for assessment and treatment, and conclude with national resources to support career counselors in rural communities as they incorporate addressing SDOMH into their work.
Rural Communities, Employment, and Career Counselors
The U.S. Census Bureau considers rural communities as a group of people, counties, and housing outside of an urban area. More specifically, the Office of Management and Budget defines rural as areas with an urban core population of fewer than 50,000 people (Health Resources and Services Administration, 2017). After the 2010 Census, it was estimated that approximately 15% of the population lives in rural communities (Health Resources & Services Administration, 2017). Rural communities experience higher rates of unemployment and poverty, and residents are therefore more likely to live below the poverty line (United States Department of Agriculture [USDA], 2014). This is largely rooted in the fact that rural communities experience underdevelopment, economic decline, and neglect (Dwyer & Sanchez, 2016). Economic focus in rural environments typically centers around agriculture, rather than technological advancement (Dwyer & Sanchez, 2016). This contributes in part to a dearth of economic resources and thereby to increased unemployment and poverty and reduced health and well-being outcomes (Bradshaw, 2007; Brassington, 2011; Dwyer & Sanchez, 2016).
According to research conducted by the USDA, the unemployment rate in rural communities steadily declined for approximately 10 years prior to the COVID-19 pandemic; in September of 2019, the rural unemployment rate was 3.5% (Dobis et al., 2021). However, unemployment in rural communities reached 13.6% in April 2020, with unemployment disparately affecting those in more impoverished communities (Dobis et al., 2021). The role and goal of the career counselor is to help individuals in a specific community obtain or retain employment (Landon et al., 2019). For example, career counselors start the counseling process by systematically assessing clients’ needs, qualifications, and job aspirations. They provide career planning services and effective job search strategies. They help with résumé writing, interview preparations, skill development, and training opportunities (Amundson, 1993). Further, career counselors provide case management services by tracking and monitoring their clients’ progress. They record client information, document counseling sessions, track job applications, and survey employment outcomes (Amundson, 1993). Through tailored support, the career counselor works with the client throughout the life span to support the search for and maintaining of employment, while building client resilience and feelings of empowerment along the way.
However, rural communities have limited employment options and self-employment opportunities, which makes the role of the career counselor difficult in rural settings. Individuals in rural communities seeking employment may find it difficult to trust an outside counselor, and they may experience limited or no access to mental health services, health care practitioners, and transportation services, thereby negatively impacting their ability to participate effectively in the employment process (Landon et al., 2019). Career counselors in rural settings must develop a broader range of skills and connections to better serve their clients. These inequities experienced in rural settings reflect SDOMH and are factors which interfere with the role of the career counselor.
Social Determinants of Mental Health and Employment
SDOMH are the nonmedical factors shaped by the unequal distribution of power, privilege, and resources that influence the health outcomes of individuals and communities (World Health Organization, 2014). SDOMH concern the environmental living conditions that affect a wide range of health, functioning, and quality-of-life outcomes and risks (Centers for Disease Control and Prevention, 2020). In the Healthy People 2030 framework, the ODPHP (n.d.) defined social determinants of health (SDOH) through five primary domains: Economic Stability, Education Access and Quality, Health Care Access and Quality, Neighborhood and Built Environment, and Social and Community Context. These five domains are important to understand within the context of employment. In the Economic Stability domain, employment is the most pertinent issue (ODPHP, n.d.), as a lack of employment typically influences both mental and physical health (Norström et al., 2019). A few distinct factors related to economic stability and employment include job security, work environment, monetary factors (e.g., pay), and the demands of the job (ODPHP, n.d.). For example, in rural communities, agriculture is a significant source of employment for individuals. However, this source of income is seemingly unstable, as farming and agriculture are mostly dependent on the season (Liebman, 2010). In the Education Access and Quality domain, enrollment in higher education or holding a higher education degree has been found to have a positive impact on employment, as well as yielding more positive overall health outcomes and optimal well-being (ODPHP, n.d.; USDA, 2017). For adults living in rural communities, unemployment rates are higher for those with lower education attainment, further supporting the connection between education and employment (USDA, 2017). Regarding the Health Care Access and Quality domain—specifically in rural communities—factors such as proximity to hospitals, lack of insurance, and the overall cost of health care can reduce accessibility. Health care, especially higher-quality health care, aids in preventing disease and improving individuals’ quality of life (ODPHP, n.d.). However, inadequate health care leads to higher rates of disease, which have a direct impact on individuals’ ability to sustain employment, due to factors such as missing work because of illness or having to travel further to receive health care (Dueñas et al., 2016).
Ability to travel is also a cause for concern in rural communities and is closely related to the Neighborhood and Built Environment domain. Healthy People 2030 proposed various objectives related to neighborhood and built environment, with one being to increase access to mass transit (ODPHP, n.d.). It is apparent that a lack of reliable transportation is directly tied to unemployment, especially in rural communities due to distance and limited accessibility (U.S. Department of Transportation, 2019). Public transportation carries many noteworthy benefits, such as reducing air pollution, being inexpensive compared to purchasing a car, minimizing the cost of fuel and upkeep for personal vehicles, and increased convenience. Although these positive aspects of public transportation are ideal, individuals living in rural communities may not be able to reap these benefits due to the lack of public transportation in these areas, perhaps also limiting employment options (Shoup & Homa, 2010; U.S. Department of Transportation, 2019).
Lastly, the fifth domain, Social and Community Context, is interrelated with employment, as it tends to have a significant impact on workplace conditions, influences individuals’ overall mental and physical health, and can hinder growth and development (Norström et al., 2019). Additionally, social cohesion and adequate support in communities can be leveraged to locate and obtain employment and other helpful resources; however, this often falls short in rural communities. For example, in rural communities, the inability to secure gainful employment is notably linked to geographical disparities, such as those within the Neighborhood and Built Environment SDOH domain. Examples of such geographic disparities which affect employment include limited or nonexistent options for public transportation, a lack of available local jobs, and a lack of childcare facilities for use by working parents. Rural communities also often experience a lack of resources to improve the employment outlook and overall well-being of their population (Bradshaw, 2007; Dwyer & Sanchez, 2016). In addition, structurally, it has been observed that economic resources tend to cluster or aggregate together. For example, businesses that have been successful in a community invite and attract more businesses, thus pulling resources away from rural communities that might not have such a history of business success. Meanwhile, communities that are left behind experience economic restructuring and delays in receiving new technologies, leading to fewer employment opportunities (Bradshaw, 2007; Landon et al., 2019). Thus, providing employment or vocational services in rural America can be particularly challenging.
Furthermore, unemployment, poverty, and mental health concerns are inextricably linked. When career counselors uncover and address these factors in rural America, they must consider the surplus of needed services and resources to systemically address interrelated issues. To be intentional, career counselors practicing in rural communities should consider using a theoretical foundation that provides direction for action on the SDOMH which impact their clients’ lives and ability to be gainfully employed. The Rural Community Health and Well-Being Framework (Annis et al., 2004) is a framework that would be exceedingly helpful in this pursuit.
Theoretical Framework for Action: Rural Community Health and Well-Being Framework
Rural communities make up over 20% of the population and are often classified by a lack of necessary resources, lower levels of education, and persistent economic inequities (Hughes et al., 2019; Mohatt et al., 2006). Although they face many challenges, individuals in rural communities have been found to be resilient, especially when the proper resources are available (Annis et al., 2004). Application of a theoretical framework to practice centered on the unique needs of rural communities is important in addressing SDOMH through career counseling. The Rural Community Health and Well-Being Framework (Annis et al., 2004) strategically builds upon community resiliency and identifies economic, social, and environmental factors which are seen as essential components of health in rural communities. This framework also implores career counselors to consider how SDOMH indicators impact the community as a whole as well as individual people. For example, the framework provides specific areas for increased career counselor awareness and action: health, safety and security, economics, education, environment, community infrastructure and processes, recreation, social support and cohesion, and the overall population. These specific areas for rural communities are within the SDOMH domains, but emphasis is placed on recognition of the specific areas within the SDOMH domains that have the greatest impact on the community.
This comprehensive framework centers the needs of rural communities and provides direction for assessing and addressing SDOMH that impact employment and overall well-being. This framework will assist in uncovering employment issues and barriers faced by individuals within rural communities. Using this framework to assess SDOMH conditions (e.g., economic, social, environmental) will aid in developing employment and mental health interventions that are socially conscious and address root causes of unemployment and poor mental health. Overall, this framework provides a model for assessing and addressing SDOMH in rural communities.
Adaptation for Career Counselors
Career counselors in rural communities who wish to use the Rural Community Health and Well-Being Framework for practice should consider doing the following: (a) increasing their awareness and understanding of SDOMH and the framework, (b) increasing their understanding of the specific community needs outlined by the framework, and (c) assessing the values and needs of the community. However, because the framework is primarily focused on community-level indicators of need, career counselors will need to adapt what they learn about the community to inform their practice with individual community members. The role of the career counselor is multifaceted; thus, career counselors can engage various aspects of their role, such as listener, leader, and evaluator, in their advocacy efforts.
To begin this process of learning about community and individual needs, Annis et al. (2004) suggested the importance of listening. For example, based on the community-level indicators of need, career counselors can assess individual clients for their unmet needs within those specific areas. By understanding how members of the community are experiencing indicators such as health, recreation, social support, transportation, and resources, career counselors will become better equipped to understand and address issues that are impacting their clients’ ability to obtain and maintain employment. Beyond the use of assessments, this framework equips career counselors to broach important conversations about social needs (Andermann, 2016) with their clients, to inform potential connection with community resources. These conversations may include explicit discussion about particular SDOMH challenges (e.g., education, safety, access to affordable childcare), as well as about the client’s sense of belonging, or lack thereof, within their community. These conversations should allow for increased understanding and rapport building through genuine listening and empathy (Annis et al., 2004; Covey, 1989).
Finally, the framework implores career counselors to advocate with and for individuals within their rural community to provide equitable employment opportunities (Crumb et al., 2019). Such advocacy may take place through connection with local rural community leaders, who may have power to alter or increase the distribution of certain resources within the community setting. For example, a career counselor may advocate on behalf of their clients to the local county board of commissioners for increased budget toward affordable transportation access within that county, thereby broadening clients’ access to job opportunities. Advocacy with local leaders outside of government might include collaboration with community college administrators for provision of additional support for working adults and parents who wish to return to school, such as more evening course options, advisor support, or readily available information on scholarships. Again, considering the aforementioned roles career counselors may have (e.g., leader, evaluator), career counselors may also consider further training in program evaluation—or collaboration with those who have such training—to better understand the efficacy of their community partnerships, referrals, and other advocacy-related efforts made toward supporting clients’ SDOMH.
Assessing and Addressing Social Determinants of Mental Health
As noted earlier, SDOMH are inextricably linked to employment, which means career counselors in rural communities must acknowledge these challenges and seek to address these issues with their clients. However, researchers have also highlighted the importance of considering both facilitators and barriers to addressing SDOMH challenges (Browne et al., 2021). In a qualitative case study of staff at a community health center and hospital, participants identified practical facilitators of SDOMH response, including community collaboration and support from leadership, as well as barriers such as time limitations and lack of resources (Browne et al., 2021). As career counselors hold similar client outcome goals as community mental health providers, they can take these findings into consideration when determining how to best respond to clients’ SDOMH challenges through attention to opportunities for collaboration with community leaders (e.g., religious leaders, politicians) and resources within the community (e.g., food banks, health care providers). Another study highlighted the importance of collaboration, partnerships with local agencies, and understanding the role of the counselor in SDOMH response (Johnson & Brookover, 2021; Robins et al., 2022). With these findings in mind, career counselors in rural communities are well positioned to assess for and address SDOMH challenges faced by their clients (Crucil & Amundson, 2017; Tang et al., 2021) through individual-level action (i.e., counseling) and systems-level advocacy action.
Systems-Level Advocacy Through Assessment
To effectively engage in systems-level advocacy, it is important for career counselors to recognize and understand the needs of their rural communities. When using the Rural Community Health and Well-Being Framework in practice, it is important to complete an assessment of the rural health of one’s community. Ryan-Nicholls and Racher (2004) purport that it is imperative to assess rural health within five categories: health status, health determinants, health behavior, health resources, and health service utilization. Counselors may consider these items when assessing the needs of their clients in rural communities, as these items provide a basis for assessment of other health factors, such as indicators of community health (e.g., environment and lifestyle) and economic well-being, and provide a foundation for systems-level advocacy and planning. This level of action focuses on improving the lives of the entire community through strategic advocacy efforts that improve population health and well-being (Ryan-Nicholls & Racher, 2004). A career counselor engaged at this level might focus their energy on advocating for increased economic development in their rural community, livable wages, universal health care, immigration issues, employment discrimination legislation, and other employment-related issues that impact the community directly or indirectly. Additionally, a career counselor may address client self-advocacy and utilize empowerment approaches to increase the voices of community members and their clients as related to work and employment needs.
In connection with this framework (Annis et al., 2004), career counselors can utilize this broader community-level assessment to inform specific points of advocacy. As an example, Annis et al. (2004) provided a sample form that may be utilized to collect community data on alcohol consumption (p. 79). Upon noting concern from individual clients on alcohol consumption, a career counselor may collaborate with public health professionals, for instance, to collect such data from the local community. Annis et al. encourage consideration of the implications for such findings, as well as opportunities for follow-up. After determining a need in the community for support regarding high alcohol consumption, the career counselor may utilize the framework to consider points of community resilience, including existing supports, attitudes about alcohol consumption, existing resources, and any actions the community is already taking in this area. Overall, assessment through the context suggested by Ryan-Nicholls and Racher (2004) may yield individual and community data to inform action to address SDOMH challenges through Annis et al.’s (2004) framework.
Individual-Level Action Through Assessment
When a client seeks services from a career counselor, the relationship centers on exploration and evaluation of the client’s education, training, work history, interests, skills, personality, and career goals. Through engaging with the Rural Community Health and Well-Being Framework, the career counselor might also examine the SDOMH facilitators and barriers that impact a client’s employment goals. To address employment and SDOMH, a career counselor must understand the community-level needs (i.e., systems approach) and the individual needs of their clients; for these goals, one strategy is to use assessments. There are various assessment tools that career counselors may find helpful, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE; National Association of Community Health Centers, 2017), an SDOH assessment tool purposed to empower professionals to not only understand their clients more holistically through assessment, but to better meet clients’ needs through the use of such information. The PRAPARE assessment tool includes questions related to four domains: Personal Characteristics, Family and Home, Money and Resources, and Social and Emotional Health. PRAPARE emphasizes the importance of assessing SDOMH needs of clients in order for providers to “define and document the complexity of their patients; transform care with integrated services and community partnerships to meet the needs of their patients; demonstrate the value they bring to patients, communities, and payers; and advocate for change in their communities” (https://prapare.org/). There are several benefits of using the PRAPARE assessment tool, such as it being free of charge, having a website linked to the tool with an “actionable toolkit and resources,’’ and being evidence-based. Barriers to using PRAPARE include that it is a long assessment tool that clients must complete in-office, which may slow workflow.
Another SDOH assessment tool is the WellRx Questionnaire (Page-Reeves et al., 2016). The WellRx Questionnaire is an 11-item screening tool that gathers information on various SDOMH, like food security, access to transportation, employment, and education. Participants are to answer “yes” or “no” to each item on the questionnaire. According to Page-Reeves and colleagues (2016), the WellRx Questionnaire provides a feasible means of assessing patients’ social needs and thereby addressing those needs. Benefits to using the WellRx include that it is free of cost, questions are at a 4th-grade reading level, and it can typically be completed by a client individually without the help of a professional. A potential barrier is that it does not assess a wide range of SDOMH challenges. Lastly, Andermann (2018) conducted a scoping review of social needs screening tools and found that the focus on such screening has increased over time. Andermann suggested that health care workers take advantage of the existing means of assessment, and made a number of specific resource recommendations, such as the Canadian Task Force on Preventive Health Care (2019) and the U.S. Preventive Services Task Force (2022).
Addressing SDOMH Through Action
Documenting and defining the needs of clients through assessment is the first step in addressing SDOMH. The next step is taking action through an integrated career counseling approach. An integrated approach may include consistent collaboration with other professionals, like medical doctors, nurse practitioners, social workers, probation officers, or case managers. Additionally, scholars like Andermann (2016) suggest integrated efforts such as ensuring social challenges are included in client records and shared with other professionals to best support care. For “particularly isolated and hard-to-reach patients . . . [actions like] assertive outreach, patient tracking and individual case managers” may be helpful (para. 19). Another practical suggestion for beginning to address clients’ SDOMH challenges is adding an SDOMH assessment tool or specific SDOMH questions to an intake form that the client completes independently or during the intake session. Selection of specific questions can be derived from the data that displays community-level needs (e.g., systems-level advocacy through assessment). For example, if a community-level assessment found that public transportation was lacking, then transportation might be an important assessment question on the SDOMH screener.
Another consideration specific for career counselors is that counselors are obligated by their code of ethics to take appropriate action based on assessment results (American Counseling Association [ACA], 2014, Section E.2.b.). Appropriate action can include consultation and collaboration with other professionals within and outside of counseling and/or advocacy to address the SDOMH need. After establishing the need through assessment, it is important for the career counselor to support the client in understanding system-level challenges and to work to address SDOMH issues while simultaneously supporting employment needs. For example, a career counselor who determines that their client is struggling with food insecurity might address this issue in several ways. At the individual level, the counselor might print resources for local food pantries, assist the client in applying for SNAP benefits, and counsel the client on resources within the community to access food. They could establish a small food pantry within the office, collaborate with local restaurants to receive pre-packaged food that might otherwise be disposed of, or consult with local food pantries and free food kitchens to establish a mobile pantry and kitchen. At the systems level, a career counselor may build partnerships with local farmers to increase locations where fresh fruits and vegetables are available for little or no cost.
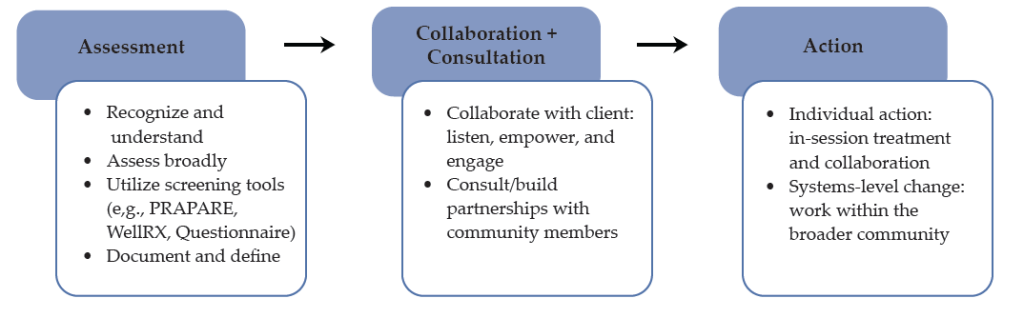
Collaboration and consultation are imperative to addressing the complex needs of clients in rural communities who are both seeking career counseling and challenged by SDOMH issues. For example, as noted earlier, health care access and quality are major disruptors of employment, and addressing these challenges will afford benefits for employment. The career counselor can consider using interprofessional collaboration and telehealth to support the health care needs of their rural clients (Johnson & Mahan, 2020). Interprofessional collaboration is a practice in which health care providers from two or more professional backgrounds interact and practice with the client at the center of care (Prentice et al., 2015). Using telehealth, the distribution of health-related services via telecommunication technologies is a useful strategy to support the health care needs of persons in rural communities. A career counselor can address health care access through telehealth in several ways, including education (e.g., introduce their client to telehealth; assist them in understanding the technology), telehealth (e.g., provide the telecommunication equipment in the office), and collaborative partnership (e.g., use a portion of the career counseling session to assist the client in connecting with health care providers using distance technology). As a collaborative partner in addressing health care access and quality, the career counselor can also use future sessions to follow up with the client on their experience with telehealth and, if needed, assist them in connecting to other health care providers. Figure 1 provides a visual for conceptualizing how career counselors may navigate the SDOMH needs of their clients, from assessment to action.
Figure 1
Working to Address Clients’ SDOMH Needs
Lastly, in the work of addressing SDOMH and employment, counselors should be aware of local, state, and national resources. Local and state resources are unique to every state but have similar purposes which include disseminating information on local resources and initiatives and providing public services that address SDOMH (e.g., food banks, public programs). National resources that are accessible to every community include 211 and the “findhelp.org” website. The Federal Communications Commission designated 211 as a national number in the United States that anyone can call for information and referrals to social services and other assistance. The services provided by 211 are confidential and free, available 24/7, and help connect people in the United States to essential community services. Moreover, the “findhelp.org” website is designed to help people search and connect with social care support based on their ZIP Code.
Integrating career counseling and social care support in rural communities is a strategy to facilitate the readiness of clients for work and the sustainability of employment for clients because basic needs are met or being addressed. While every rural community is unique, the foundation of understanding both systemic and individual SDOMH needs—and addressing those needs through strategic partnerships and individual counseling, as well as advocacy—is important in every rural community and to the success of any career counseling endeavor.
Discussion
In rural communities, career counselors hold a significant role. They are tasked with aiding individuals with employment needs; they may often address mental health concerns, and while doing so, it is important for them to be aware of and prepared to address SDOMH. Career counselors can gain more insight into issues related to SDOMH through consultation, collaboration, and advocacy, which should all be a part of the repertoire of a rural career counselor. The use of theoretical frameworks such as the Rural Community Health and Well-Being Framework (Racher et al., 2004) provides direction for career counselors seeking to understand the systemic issues impacting employment access and opportunities in the community, as well as direction for intervention. This framework will assist in identifying and minimizing barriers to employment that may exist within rural communities. More specifically, this framework will help to uncover SDOMH challenges that exist in the community and serve as barriers to well-being and employment and provide direction for advocating for resources necessary for equitable work opportunities and environments. Being that individuals in rural America experience various barriers that have huge impacts on their lives, such a guide for career counselors is essential.
Lastly, addressing SDOMH within career counseling is a social justice issue that counselors should address (ACA, 2014; Crucil & Amundson, 2017; Ratts et al., 2016). The Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) serve as a guide for counselors to address social justice issues and were endorsed by the ACA in 2015. Like the aforementioned framework and empirically based suggestions, the MSJCC includes four areas of competence: counselor self-awareness, client worldview, counseling relationship, and counseling and advocacy interventions. The authors of the MSJCC also implore counselors to consider “attitudes and beliefs, knowledge, skills, and action,” and suggest that competent counselors are aware of the experiences of marginalized clients (Ratts et al., 2016; p. 3). Thus, career counselors’ efforts to assess and address the individual and systems-based SDOMH challenges faced by their clients is social justice work that career counselors are trained and prepared to address.
Implications
Given this review, there are specific implications for career counselors practicing in rural communities, counselor educators training career counselors, and pertinent policy needs.
Practicing Career Counselors
The role of the career counselor often entails identifying employment objectives, goals, and needs for both the job seeker and employer. In addition, the career counselor is responsible for résumé development, teaching job placement and retention skills, providing self-advocacy tips, teaching organizational goal–redefining skills, and many other components (Ysasi et al., 2018). However, providing these services can be difficult when the individuals reside in rural communities because of the SDOMH disparities such as limited available resources, isolation, increased poverty, and decreased educational and employment opportunities (Temkin, 1996).
Therefore, career counselors must actively work to ensure their visibility and accessibility to individuals in rural areas who are seeking employment opportunities. Further, career counselors need to market themselves and their skills to employers and job seekers of rural communities. Consequently, marketing generally entails engaging and developing community partnerships with employers and job seekers, which involves educating individuals unfamiliar with the specific services that career counselors provide. In addition, employers are often interested in services that improve their business (e.g., increase revenue), while job seekers may be searching for skill training to achieve employment goals (Richardson et al., 2010). Therefore, career counselors can enhance service delivery and provide adequate services when they intentionally market their services to the community members.
Furthermore, job insecurity has been linked to mental health concerns like stress and anxiety, financial concerns, and fear of organizational change (Holm & Hovland, 1999). Therefore, career counselors need to be aware of the impact of job insecurity on rural communities and devise strategies to help organizations and workers manage job insecurity. Managing job insecurity of workers in rural organizations could include helping organizations to redefine their present and future goals and commitments made to employees. Organizations could also manage organizational transitions depending on the skills and resources available to affected employees (Holm & Hovland, 1999). Clearly stated organizational objectives, goals, and plans can help employees feel less insecure about their jobs and increase focus on their roles and responsibilities instead of devising means to move out of the community for a better and more secure future. In addition, career counselors in rural communities should be aware of the mental health concerns experienced by employees and job seekers and connect them to available mental health resources.
Counselor Educators
Counselor educators are responsible for the training and development of the next generation of counselors, including career counselors. It will be important for counselor educators to include training on SDOMH, interprofessional collaboration, and telehealth, as these are especially relevant for rural communities ( Johnson & Mahan, 2021; Johnson & Rehfuss, 2021). It is essential to provide adequate time to review and discuss SDOMH in all courses throughout the curriculum (Waters et al., 2022) to ensure the competence of career counselors. To ensure this continuity, counselor educators should advocate for an SDOMH module across the curriculum. This would ensure the inclusion of this content throughout the program, providing ample opportunity for the understanding of SDOMH and how they should be addressed. Career counselors must be prepared to address the complex employment and social health needs with which their clients might present. Without adequate education and training, these will seem much more difficult to address.
Policy
In addressing both SDOMH and employment needs in rural communities, advocating for policy and legislative change is imperative. Lewis et al. (2002) described counselors’ roles in sharing public information as awakening the public to macro-systemic issues related to human dignity and engaging in social/political advocacy, or “influencing public policy in a large, public arena” (p. 2). Thus, career counselors are encouraged to benefit their clients through engaging in advocacy to influence policy at the local, state, and national levels. Similarly, Crucil and Amundson (2017) implore career counselors to engage in the work of influencing politics and policy and suggest awareness as a first step to enacting change through the sharing of information and impacting policy. To develop such awareness, career counselors may begin by reading about SDOMH disparities related specifically to employment issues from reputable sources. For instance, the National Alliance on Mental Illness (NAMI; 2014) has published various reports related to such issues, including the informative publication entitled Road to Recovery: Employment and Mental Illness. NAMI (2021) also published a legislative coalition letter written in support of increased SDOH funding to Congress. Career counselors may work to build their own awareness and understanding of the social and political events and influences which impact their clients, building toward eventual action in this realm.
Moreover, regarding policy change, researchers have suggested career counselors should be aware of and actively engaged in policy efforts (Crucil & Amundson, 2017; Watts, 2000). Watts (2000) described public policy considering career development as including four distinct roles: legislation, remuneration, exhortation, and regulation. Watts described these roles in detail and implored career counselors to influence these policy processes by seeking the support of interest groups and communicating with policy makers. Again, career counselors can work individually and within their own communities to increase their awareness and knowledge of policies and their impact. They can work toward influencing policies at the state and national levels to improve the accessibility and existence of important social programs and resources.
Conclusion
Career counselors in rural communities have a responsibility to acknowledge and address SDOMH challenges that are disproportionately impacting their clients. Collaboration, consultation, counseling framed through the lens of SDOMH, and advocacy appear to be strategies to support the employment needs of individuals and the rural community. Employment services in rural communities must be framed through a socially conscious (e.g., aware of the SDOMH systemic issues), action-oriented (e.g., prepared to engage in advocacy), and resiliency-focused lens that provides tailored individual services while simultaneously addressing systemic issues.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
Amundson, N. E. (1993). Mattering: A foundation for employment counseling and training. Journal of Employment Counseling, 30(4), 146–152. https://doi.org/10.1002/j.2161-1920.1993.tb00173.x
Andermann, A. (2016). Taking action on the social determinants of health in clinical practice: A framework for health professionals. Canadian Medical Association Journal, 188(17–18), E474–E483. https://doi.org/10.1503/cmaj.160177
Andermann, A. (2018). Screening for social determinants of health in clinical care: Moving from the margins to the mainstream. Public Health Reviews, 39(1), 1–17.
https://doi.org/10.1186/s40985-018-0094-7
Annis, R. C., Racher, F., & Beattie, M. (Eds.). (2004). Rural community health and well-being: A guide to action. Rural Development Institute. https://www.researchgate.net/publication/242551842_Rural_Community_Health_and_Well-Being_A_Guide_to_Action
Bradshaw, T. K. (2007). Theories of poverty and anti-poverty programs in community development. Community Development, 38(1), 7–25. https://doi.org/10.1080/15575330709490182
Brassington, I. (2011). What’s wrong with the brain drain? Developing World Bioethics, 12(3), 113–120.
https://doi.org/10.1111/j.1471-8847.2011.00300.x
Browne, J., Mccurley, J. L., Fung, V., Levy, D. E., Clark, C. R., & Thorndike, A. N. (2021). Addressing social determinants of health identified by systematic screening in a Medicaid accountable care organization: A qualitative study. Journal of Primary Care & Community Health, 12. https://doi.org/10.1177/2150132721993651
Canadian Task Force on Preventative Health Care. (2019). Canadian task force on preventive health care.
https://canadiantaskforce.ca
Centers for Disease Control and Prevention. (2020). CDC 2020 in review. https://archive.cdc.gov/#/details?url=
https://www.cdc.gov/media/releases/2020/p1229-cdc-2020-review.html
Covey, S. (1989). The 7 habits of highly effective people: Restoring the character ethic. Simon & Schuster.
Crucil, C., & Amundson, N. (2017). Throwing a wrench in the work(s): Using multicultural and social justice competency to develop a social justice–oriented employment counseling toolbox. Journal of Employment Counseling, 54(1), 2–11. https://doi.org/10.1002/joec.12046
Crumb, L., Haskins, N., & Brown, S. (2019). Integrating social justice advocacy into mental health counseling in rural, impoverished American communities. The Professional Counselor, 9(1), 20–34. https://files.eric.ed.gov/fulltext/EJ1215753.pdf
Dobis, E. A., Krumel, T. P., Jr., Cromartie, J., Conley, K. L., Sanders, A., & Ortiz, R. (2021). Rural America at a glance: 2021 edition. U.S. Department of Agriculture. https://www.ers.usda.gov/webdocs/publications/102576/eib-230.pdf
Dueñas, M., Ojeda, B., Salazar, A., Mico, J. A., & Failde, I. (2016). A review of chronic pain impact on patients, their social environment and the health care system. Journal of Pain Research, 2016(9), 457–467. https://doi.org/10.2147/JPR.S105892
Dwyer, R. E., & Sanchez, D. (2016). Population distribution and poverty. In M. J. White (Ed.), International handbook of migration and population distribution (pp. 485–504). Springer Science & Business Media. https://doi.org/10.1007/978-94-017-7282-2
Health Resources and Services Administration. (2017). Defining rural population. https://www.hrsa.gov/rural-health/about-us/definition/index.html
Holm, S., & Hovland, J. (1999). Waiting for the other shoe to drop: Help for the job-insecure employee. Journal of Employment Counseling, 36(4), 156–166.
https://doi.org/10.1002/j.2161-1920.1999.tb01018.x
Hughes, M. C., Gorman, J. M., Ren, Y., Khalid, S., & Clayton, C. (2019). Increasing access to rural mental health care using hybrid care that includes telepsychiatry. Journal of Rural Mental Health, 43(1), 30–37. https://doi.org/10.1037/rmh0000110
Johnson, K. F., & Brookover, D. L. (2021). School counselors’ knowledge, actions, and recommendations for addressing social determinants of health with students, families, and in communities. Professional School Counseling, 25(1), 1–12. https://doi.org/10.1177/2156759X20985847
Johnson, K. F., & Mahan, L. B. (2020). Interprofessional collaboration and telehealth: Useful strategies for family counselors in rural and underserved areas. The Family Journal, 28(3), 215–224.
https://doi.org/10.1177/1066480720934378
Johnson, K. F., & Rehfuss, M. (2021). Telehealth interprofessional education: Benefits, desires, and concerns of counselor trainees. Journal of Creativity in Mental Health, 16(1), 15–30.
https://doi.org/10.1080/15401383.2020.1751766
Johnson, K. F., & Robins, L. B. (2021). Counselor educators’ experiences and techniques teaching about social-health inequities. Journal of Counselor Preparation and Supervision, 14(4), 1–25. https://digitalcommons.sacredheart.edu/jcps/vol14/iss4/7
Landon, T., Connor, A., McKnight-Lizotte, M., & Peña, J. (2019). Rehabilitation counseling in rural settings: A phenomenological study on barriers and supports. Journal of Rehabilitation, 85(2), 47–57. https://bit.ly/4cvWSoT
Lewis, J., Arnold, M. S., House, R., & Toporek, R. L. (2002). ACA advocacy competencies. http://www.counseling.org/Resources/Competencies/Advocacy_Competencies.pdf
Liebman, A. K., & Augustave, W. (2010). Agricultural health and safety: Incorporating the worker perspective. Journal of Agromedicine, 15(3), 192–199. https://doi.org/10.1080/1059924x.2010.486333
Mohatt, D. F., Bradley, M. M., Adams, S. J., & Morris, C. D. (2006). Mental health and rural America: 1994-2005. An overview and annotated bibliography. U.S. Department of Health and Human Services. https://eric.ed.gov/?id=ED591902
National Alliance on Mental Health. (2014). Road to recovery: Employment and mental illness. https://nami.org/Support-Education/Publications-Reports/Public-Policy-Reports/RoadtoRecovery
National Alliance on Mental Health. (2021, April 8). Letter to congressional leadership. https://www.nami.org/getattachment/c3b797bf-5116-457f-ada9-b6b6f1f6adfb/Letter-to-Congressional-Committee-Leadership-on-So
National Association of Community Health Centers. (2017). PRAPARE. https://www.nachc.org/research-and-data/prapare
Norström, F., Waenerlund, A.-K., Lindholm, L., Nygren, R., Sahlén, K.-G., & Brydsten, A. (2019). Does unemployment contribute to poorer health-related quality of life among Swedish adults? BMC Public Health, 19(1). https://doi.org/10.1186/s12889-019-6825-y
Office of Disease Prevention and Health Promotion. (2020). Healthy People 2030: Social determinants of health. U.S. Department of Health and Human Services. https://health.gov/healthypeople/priority-areas/social-determinants-health
Page-Reeves, J., Kaufman, W., Bleecker, M., Norris, J., McCalmont, K., Ianakieva, V., Ianakieva, D. & Kaufman, A. (2016). Addressing social determinants of health in a clinic setting: The WellRx pilot in Albuquerque, New Mexico. The Journal of the American Board of Family Medicine, 29(3), 414–418. https://doi.org/10.3122/jabfm.2016.03.150272
Pope, M. (2011). The Career Counseling With Underserved Populations model. Journal of Employment Counseling, 48(4), 153–155. https://doi.org/10.1002/j.2161-1920.2011.tb01100.x
Prentice, D., Engel, J., Taplay, K., & Stobbe, K. (2015). Interprofessional collaboration: The experience of nursing and medical students’ interprofessional education. Global Qualitative Nursing Research, 2, 1–9. https://doi.org/10.1177/2333393614560566
Racher, F., Everitt, J., Annis, R., Gfellner, B., Ryan-Nicholls, K., Beattie, M., Gibson, R., & Funk, E. (2004). Rural community health & well-being. In R. Annis, F. Racher, & M. Beattie (Eds.), Rural community health and well-being: A guide to action (pp. 18–37). Rural Development Institute.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Richardson, N., Gosnay, R. M., & Carroll, A. (2010). A quick start guide to social media marketing: High impact low-cost marketing that works. Kogan Page Publishers.
Robins, L. B., Johnson, K. F., Duyile, B., Gantt-Howrey, A., Dockery, N., Robins, S., & Wheeler, N. (2022). Family counselors addressing social determinants of mental health in underserved communities. The Family Journal, 31(2), 213–221. https://doi.org/10.1177/10664807221132799
Ryan-Nicholls, K. D., & Racher, F. E. (2004). Investigating the health of rural communities: Toward framework development. Rural and Remote Health, 4(1), 1–10.
https://search.informit.org/doi/abs/10.3316/informit.613919155641626
Shoup, L., & Homa, B. (2010). Principles for improving transportation options in rural and small town communities. https://t4america.org/wp-content/uploads/2010/03/T4-Whitepaper-Rural-and-Small-Town-Communities.pdf
Tang, M., Montgomery, M. L. T., Collins, B., and Jenkins, K. (2021). Integrating career and mental health counseling: Necessity and strategies. Journal of Employment Counseling, 58, 23–35.
https://doi.org/10.1002/joec.12155
Temkin, A. (1996). Creative options for rural employment: A beginning. In N. L. Arnold (Ed.), Self-employment in vocational rehabilitation: Building on lessons from rural America (pp. 61–64). Research and Training Center on Rural Rehabilitation Services.
United States Census Bureau. (2014). 2010-2014 ACS 5-year estimates. https://www.census.gov/programs-surveys/acs/technical-documentation/table-and-geography-changes/2014/5-year.html
United States Department of Agriculture. (2014). Rural America at a glance: 2014 edition. https://www.ers.usda.gov/publications/pub-details/?pubid=42897
United States Department of Agriculture. (2017). Rural education at a glance, 2017 edition. https://www.ers.usda.gov/webdocs/publications/83078/eib-171.pdf
United States Preventive Services Taskforce. (2022). US preventative services taskforce. https://www.uspreventiveservicestaskforce.org/uspstf
U.S. Department of Transportation. (2019). Rural public transportation systems. https://www.transportation.gov/mission/health/Rural-Public-Transportation-Systems
Waters, J. M., Gantt, A., Worth, A., Duyile, B., Johnson, K. F., & Mariotto, D. (2022). Motivated but challenged: Counselor educators’ experiences teaching about social determinants of health. Journal of Counselor Preparation and Supervision, 15(2), 1–30. https://digitalcommons.sacredheart.edu/jcps/vol15/iss2/6
Watts, A. G. (2000). Career development and public policy. Journal of Employment Counseling, 37(2), 62–75. https://doi.org/10.1002/j.2161-1920.2000.tb00824.x
World Health Organization. (2014). Social determinants of mental health. https://apps.who.int/iris/bitstream/handle/10665/112828/9789241506809_eng.pdf
Ysasi, N. A., Tiro, L., Sprong, M. E., & Kim, B. J. (2018). Marketing vocational rehabilitation services in rural communities. In D. A. Harley, N. A. Ysasi, M. L. Bishop, & A. R. Fleming (Eds.), Disability and vocational rehabilitation in rural settings: Challenges to service delivery (pp. 545–552). Springer.
Kaprea F. Johnson, PhD, LPC, is a professor and Associate Vice Provost for Faculty Development & Recognition at The Ohio State University. Alexandra Gantt-Howrey, PhD, LPC (ID), is an assistant professor at Idaho State University. Bisola E. Duyile, PhD, LPC, CRC, is an assistant professor at Montclair State University. Lauren B. Robins, PhD, is a clinical assistant professor and distance learning coordinator at Old Dominion University. Natese Dockery, MS, NCC, LPC, CSAM, is a licensed professional counselor and doctoral student. Correspondence may be addressed to Kaprea F. Johnson, The Ohio State University, 1945 N. High Street, Columbus, OH 43210, johnson.9545@osu.edu.
May 20, 2016 | Article, Volume 6 - Issue 2
Melissa J. Fickling
Advocacy with and on behalf of clients is a major way in which counselors fulfill their core professional value of promoting social justice. Career counselors have a unique vantage point regarding social justice due to the economic and social nature of work and can offer useful insights. Q methodology is a mixed methodology that was used to capture the perspectives of 19 career counselors regarding the relative importance of advocacy interventions. A two-factor solution was reached that accounted for 60% of the variance in perspectives on advocacy behaviors. One factor, labeled focus on clients, emphasized the importance of empowering individual clients and teaching self-advocacy. Another factor, labeled focus on multiple roles, highlighted the variety of skills and interventions career counselors use in their work. Interview data revealed that participants desired additional conversations and counselor training concerning advocacy.
Keywords: social justice, advocacy, career counselors, Q methodology, counselor training
The terms advocacy and social justice often are used without clear distinction. Advocacy is the active component of a social justice paradigm. It is a direct intervention or action and is the primary expression of social justice work (Fickling & Gonzalez, 2016; Ratts, Lewis, & Toporek, 2010; Toporek, Lewis, & Crethar, 2009). Despite the fact that counselors have more tools than ever to help them develop advocacy and social justice competence, such as the ACA Advocacy Competencies (Lewis, Arnold, House, & Toporek, 2002) and the Multicultural and Social Justice Counseling Competencies (Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2015), little is known about practitioners’ perspectives on the use of advocacy interventions.
One life domain in which social inequity can be vividly observed is that of work. The economic recession that began in 2007 has had a lasting impact on the labor market in the United States. Long-term unemployment is still worse than before the recession (Bureau of Labor Statistics, U.S. Department of Labor, 2016a). Further, in the United States, racial bias appears to impact workers and job seekers, as evidenced in part by the fact that the unemployment rate for Black workers is consistently about double that of White workers (e.g., 4.1% White unemployment and 8.2% Black unemployment as of May 2016; Bureau of Labor Statistics, U.S. Department of Labor, 2016b). Recent meta-analyses indicate that unemployment has a direct and causal negative impact on mental health, leading to greater rates of depression and suicide (Milner, Page, & LaMontagne, 2013; Paul & Moser, 2009). Clearly, the worker role is one that carries significant meaning and consequences for people who work or want to work (Blustein, 2006).
The rate at which the work world continues to change has led some to argue that worker adaptability is a key 21st century skill (Niles, Amundson, & Neault, 2010; Savickas, 1997), but encouraging clients to adapt to unjust conditions without also acknowledging the role of unequal social structures is inconsistent with a social justice paradigm (Stead & Perry, 2012). Career counselors, particularly those who work with the long-term unemployed and underemployed, witness the economic and psychological impact of unfair social arrangements on individuals, families and communities. In turn, they have a unique vantage point when it comes to social justice and a significant platform from which to advocate (Chope, 2010; Herr & Niles, 1998; Pope, Briddick, & Wilson, 2013; Pope & Pangelinan, 2010; Prilleltensky & Stead, 2012).
It appears that although career counselors value social justice and are aware of the effects of injustice on clients’ lives, they are acting primarily at the individual rather than the systemic level (Cook, Heppner, & O’Brien, 2005; McMahon, Arthur, & Collins, 2008b; Prilleltensky & Stead, 2012; Sampson, Dozier, & Colvin, 2011). Some research has emerged that focuses on practitioners’ use of advocacy in counseling practice (Arthur, Collins, Marshall, & McMahon, 2013; Arthur, Collins, McMahon, & Marshall, 2009; McMahon et al., 2008b; Singh, Urbano, Haston, & McMahan, 2010). Overall, this research indicates that advocacy is challenging and multifaceted and is viewed as a central component of good counseling work; however, more research is needed if we are to fully understand how valuing social justice translates to use of advocacy interventions in career counseling practice. This study aims to fill this theory–practice gap by illuminating the perceptions of advocacy behaviors from career counselors as they reflect upon their own counseling work.
Methodology
Through the use of Q methodology, insight into the decisions, motivations and thought processes of participants can be obtained by capturing their subjective points of view. When considering whether to undertake a Q study, Watts and Stenner (2012) encouraged researchers to consider whether revealing what a population thinks about an issue really matters and can make a real difference. Given the ongoing inequality in the labor market, increased attention and energy around matters of social justice in the counseling profession, the lack of knowledge regarding practitioners’ points of view on advocacy, and career counselors’ proximity to social and economic concerns of clients, the answer for the present study is most certainly yes.
Q methodology is fundamentally different from other quantitative research methodologies in the social sciences. It uses both quantitative and qualitative data to construct narratives of distinct perspectives. The term Q was coined to distinguish this methodology from R; Q measures correlations between persons, whereas R measures trait correlations (Brown, 1980). Rather than subjecting a sample of research participants to a collection of measures as in R methodology, Q methodology subjects a sample of items (i.e., the Q sample) to measurement by a collection of individuals through a ranking procedure known as the Q sort (see Figure 1; Watts & Stenner, 2012). Individuals are the variables in Q methodology, and factor analysis is used to reduce the number of points of view into a smaller number of shared perspectives. Then interviews are conducted to allow participants to provide additional data regarding their rankings of the Q sample items. In this study, career counselors were asked to sort a set of advocacy behaviors according to how important they were to their everyday practice of career counseling. Importance to practice was used as the measure of psychological significance since career counselors’ perspectives on advocacy interventions were of interest, rather than self-reported frequency or competence, for example.
Q Sample
The Q sample can be considered the instrumentation in Q methodology. The Q sample is a subset of statements drawn from the concourse of communication, which is defined as the entire population of statements about any given topic (McKeown & Thomas, 2013). The goal when creating the Q sample is to provide a comprehensive but manageable representation of the concourse from which it is taken. For this study, the concourse was that of counselor advocacy behaviors.
The Q sampling approach used for this study was indirect, naturalistic and structured-inductive. Researchers should draw their Q sample from a population of 100 to 300 statements (Webler, Danielson, & Tuler, 2009). For this study, I compiled a list of 180 counselor social justice and advocacy behaviors from a variety of sources including the ACA Advocacy Competencies (Lewis et al., 2002), the Social Justice Advocacy Scale (SJAS; Dean, 2009), the National Career Development Association (NCDA) Minimum Competencies (2009), the Council for Accreditation of Counseling and Related Educational Programs (CACREP) Standards (2009), and key articles in counseling scholarly and trade publications.
Consistent with a structured-inductive sampling strategy, these 180 statements were analyzed to identify categories representing different kinds of advocacy behaviors. By removing duplicates and those items that were more aligned with awareness, knowledge or skill rather than behavior, I was able to narrow the list from 180 to 43 statements. These statements were sorted into five domains that were aligned with the four scales of the SJAS (Dean, 2009) and a fifth added domain. The final domains were: Client Empowerment, Collaborative Action, Community Advocacy, Social/Political Advocacy, and Advocacy with Other Professionals. Aligning the Q sample with existing domains was appropriate since advocacy had been previously operationalized in the counseling literature.
Expert reviewers were used to check for researcher bias in the construction of the Q sample, including the addition of the fifth advocacy domain. Three expert reviewers who were faculty members and published on the topic of social justice in career counseling were asked to review the potential Q sample for breadth, coverage, omissions, clarity of phrasing and the appropriateness of the five domains of advocacy. Two agreed to participate and offered their feedback via a Qualtrics survey, leading to a refined Q sample of 25 counselor advocacy behaviors (see Table 1). Five statements were retained in each of the five domains. Finally, the Q sample and Q sorting procedure were piloted with two career counselors, leading to changes in instructions but not in the Q sample itself. Pilot data were not used in the final analysis.
Participants
In Q methodology, participant sampling should be theoretical and include the intentional selection of participants who are likely to have an opinion about the topic of interest (McKeown & Thomas, 2013; Watts & Stenner, 2012). It also is important to invite participants who represent a range of viewpoints and who are demographically diverse. For the current study, the following criteria were required for participant inclusion: (a) holds a master’s degree or higher in counseling and (b) has worked as a career counselor for at least one year full-time in the past two years. For this study, career counselor was defined as having career- or work-related issues as the primary focus of counseling in at least half of the counselor’s case load. Regarding the number of participants in a Q study, emphasis is placed on having enough participants to establish the existence of particular viewpoints, not simply having a large sample since generalizability is not a goal of Q methodology (Brown, 1980). In Q methodology, it also is important to have fewer participants than Q sample items (Watts & Stenner, 2012; Webler et al., 2009).
Participants were recruited by theoretical sampling of my professional network of practitioners, and one participant was recruited through snowball sampling. Nineteen career counselors participated in the present study from six states in the Southeast, West and Midwest regions of the United States. The participant sample was 68% female (n = 13) and 32% male (n = 6); the sample was 84% White and included two Black participants and one multi-racial participant. One participant was an immigrant to the United States and was a non-native English speaker. The participant sample was 95% heterosexual with one participant identifying as gay. Sixty-three percent of participants worked in four-year institutions of higher education and one worked in a community college. Thirty-two percent (n = 6) provided career counseling in non-profit agencies. The average age was 43 (SD = 12) and the average number of years of post-master’s counseling experience was eight (SD = 7); ages ranged from 28 to 66, and years of post-master’s experience ranged from one and a half to 31 years.
Q Sorting Procedure
The Q sort is a method of data collection in which participants rank the Q sample statements according to a condition of instruction along a forced quasi-normal distribution (see Figure 1). There is no time limit to the sorting task and participants are able to move the statements around the distribution until they are satisfied with their final configuration. The function of the forced distribution is to encourage active decision making and comparison of the Q sample items to one another (Brown, 1980).
Figure 1
Sample Q Sort Distribution

The condition of instruction for this study was, “Sort the following counselor advocacy behaviors according to how important or unimportant they are to your career counseling work.” The two poles of the distribution were most important and most unimportant. Poles range from most to most so that the ends of the distribution represent the areas that hold the greatest degree of psychological significance to the participant, and the middle of the distribution represents items that hold relatively little meaning or are more neutral in importance (Watts & Stenner, 2012).
The Q sorts for this study were conducted both in person and via phone or video chat (i.e., Google Hangouts, Skype). Once informed consent was obtained, I facilitated the Q sorting procedure by reading the condition of instruction, observing the sorting process, and conducting the post-sort interview. Once each participant felt satisfied with his or her sort, the distribution of statements was recorded onto a response sheet for later data entry.
Post-Sort Interview
Immediately following the Q sort, I conducted a semistructured interview with each participant in order to gain a greater understanding of the meaning of the items and their placement, as well as his or her broader understanding of the topic at hand (Watts & Stenner, 2012). The information gathered during the interview is used when interpreting the final emergent factors. Items in the middle of the distribution are not neglected and are specifically asked about during the post-sort interview so that the researcher can gain an understanding of the entire Q sort for each participant. Although the interview data are crucial to a complete and rigorous factor interpretation and should be conducted with every participant in every Q study, the data analysis process is guided by the quantitative criteria for factor analysis and factor extraction. The qualitative interview data, as well as the demographic data, are meant to help the researcher better understand the results of the quantitative analysis.
Data Analysis
Data were entered into the PQMethod program (Schmolck, 2014) and Pearson product moment correlations were calculated for each set of Q sorts. Inspection of the correlation matrix revealed that all sorts (i.e., all participants) were positively correlated with one another, some of them significantly so. This indicated a high degree of consensus among the participants regarding the role of advocacy in career counseling, which was further explored through factor analysis.
I used centroid factor analysis and Watts and Stenner’s (2012) recommendation of beginning by extracting one factor for every six Q sorts. Centroid factor analysis is the method of choice among Q methodologists because it allows for a fuller exploration of the data than a principal components analysis (McKeown & Thomas, 2013; Watts & Stenner, 2012). Next, I calculated the significance level at p < .01, which was .516 for this 25-item Q sample.
The unrotated factor matrix revealed two factors with Eigenvalues near or above the commonly accepted cutoff of 1 according to the Kaiser-Guttman rule (Kaiser, 1970). Brown (1978) argued that although Eigenvalues often indicate factor strength or importance, they should not solely guide factor extraction in Q methodology since “the significance of Q factors is not defined objectively (i.e., statistically), but theoretically in terms of the social-psychological situation to which the emergent factors are functionally related” (p. 118). Since there currently is little empirical evidence of differing perspectives on advocacy among career counselors, two factors were retained for rotation.
In order to gain another perspective on the data, I used the Varimax procedure. I flagged those sorts that loaded significantly (i.e., at or above 0.516) onto only one factor after rotation. Four participants (2, 8, 9 and 17) loaded significantly onto both rotated factors and were therefore dropped from the study and excluded from further analysis (Brown, 1980; Watts & Stenner, 2012). Two rotated factors were retained, which accounted for 60% of the variance in perspectives on advocacy behaviors. Fifteen of the original 19 participants were retained in this factor solution.
Q methodology uses only orthogonal rotation techniques, meaning that all factors are zero-correlated. Even so, it is possible for factors to be significantly correlated but still justify retaining separate factors (Watts & Stenner, 2012). The two factors in this study are correlated at 0.71. This correlation indicates that the perspectives expressed by the two factor arrays share a point of view but are still distinguishable and worthy of exploration as long as the general degree of consensus is kept in mind (Watts & Stenner, 2012).
Constructing Factor Arrays
After the two rotated factors were identified, factor arrays were constructed in PQMethod. A factor array is a composite Q sort and the best possible estimate of the factor’s viewpoint using the 25 Q sample items. First, a factor weight was calculated for each of the 15 Q sorts that loaded onto a factor. Next, normalized factor scores (z scores) were calculated for each statement on each factor, which were finally converted into factor arrays (see Table 1). In Q methodology, unlike traditional factor analysis, attention is focused more on factor scores than factor loadings. Since factor scores are based on weighted averages, Q sorts with higher factor loadings contribute proportionally more to the final factor score for each item in a factor than those with relatively low factor loadings. Finally, factors were named by examining the distinguishing statements and interview data of participants that loaded onto the respective factors. Factor one was labeled focus on clients and factor two was labeled focus on multiple roles.
Factor Characteristics
Factor one was labeled focus on clients and accounted for 32% of the variance in perspectives on advocacy behaviors. It included nine participants. The demographic breakdown on this factor was: six females, three males; eight White individuals and one person who identified as multi-racial. The average age on this factor was about 51 (SD = 10.33), ranging from 37 to 66. Persons on this factor had on average 11 years of post-master’s counseling experience (SD = 8.6), ranging from one and a half to 31 years. Fifty-six percent of participants on this factor worked in 4-year colleges or universities, 33% in non-profit agencies, and one person worked at a community college.
Factor two was labeled focus on multiple roles and accounted for 28% of the variance in career counselors’ perspectives on advocacy behaviors. It included six participants. Five participants on this factor identified as female and one identified as male. Five persons were White; one was Black. The average age of participants on this factor was almost 35 (SD = 6.79), ranging from 29 to 48, and they had an average of just over seven years of post-master’s experience (SD = 3.76), ranging from three and a half to 14 years. Four worked in higher education, and two worked in non-profit settings.
Factor Interpretation
In the factor interpretation phase of data analysis, the researcher constructs a narrative for each factor by incorporating post-sort interview data with the factor arrays to communicate the rich point of view of each factor (Watts & Stenner, 2012). Each participant’s interview was considered only in conjunction with the other participants on the factor on which they loaded. I read post-sort interview transcripts, looking for shared perspectives and meaning, in order to understand each factor array and enrich each factor beyond the statements of the Q sample. Thus, the results are reported below in narrative form, incorporating direct quotes and paraphrased summaries from interview data, but structured around the corresponding factor arrays.
Table 1
Q Sample Statements, Factor Scores and Q Sort Values
|
No
|
Statement
|
Factor 1
|
Factor 2
|
|
|
Factor Score
|
QSV
|
Factor Score
|
QSV
|
| 1 |
Question intervention practices that appear inappropriate. |
0.09
|
1
|
0.54
|
1
|
| 2 |
Seek feedback regarding others’ perceptions of my advocacy efforts. |
-0.85
|
-2
|
-0.75
|
-1
|
| 3 |
Serve as a mediator between clients and institutions. |
-0.47
|
-1
|
-1.05
|
-2
|
| 4 |
Express views on proposed bills that will impact clients. |
-0.97
|
-2
|
-1.96
|
-4
|
| 5 |
Maintain open dialogue to ensure that advocacy efforts are consistent with group goals. |
-0.19
|
0
|
-0.05
|
0
|
| 6 |
Encourage clients to research the laws and policies that apply to them. |
-0.31
|
0
|
0.15
|
0
|
| 7 |
Collect data to show the need for change in institutions. |
-0.67
|
-2
|
-0.75
|
-2
|
| 8 |
Educate other professionals about the unique needs of my clients. |
0.87
|
1
|
0.86
|
2
|
| 9 |
Help clients develop needed skills. |
1.67
|
3
|
0.42
|
1
|
| 10 |
Assist clients in carrying out action plans. |
-1.31
|
3
|
1.06
|
2
|
| 11 |
Help clients overcome internalized negative stereotypes. |
1.02
|
2
|
0.89
|
2
|
| 12 |
Conduct assessments that are inclusive of community members’ perspectives. |
-1.31
|
-3
|
0.5
|
1
|
| 13 |
With allies, prepare convincing rationales for social change. |
-0.35
|
-1
|
-1.36
|
-3
|
| 14 |
Identify strengths and resources of clients. |
2.17
|
4
|
1.62
|
3
|
| 15 |
Get out of the office to educate people about how and where to get help. |
0.58
|
1
|
-0.47
|
-1
|
| 16 |
Teach colleagues to recognize sources of bias within institutions and agencies. |
-0.37
|
-1
|
-0.37
|
-1
|
| 17 |
Deal with resistance to change at the community/system level. |
-0.43
|
-1
|
-0.21
|
0
|
| 18 |
Collaborate with other professionals who are involved in disseminating public information. |
-0.33
|
0
|
-0.4
|
-1
|
| 19 |
Help clients identify the external barriers that affect their development. |
1.08
|
2
|
1.46
|
3
|
| 20 |
Use multiple sources of intervention, such as individual counseling, social advocacy and case management. |
-0.32
|
0
|
1.73
|
4
|
| 21 |
Train other counselors to develop multicultural knowledge and skills. |
0.15
|
1
|
0.19
|
0
|
| 22 |
Work to ensure that clients have access to the resources necessary to meet their needs. |
1.03
|
2
|
0.85
|
1
|
| 23 |
Work to change legislation and policy that negatively affects clients. |
-1.78
|
-4
|
-1.39
|
-3
|
| 24 |
Ask other counselors to think about what social change is. |
-0.25
|
0
|
-0.22
|
0
|
| 25 |
Communicate with my legislators regarding social issues that impact my clients. |
-1.45
|
-3
|
-1.28
|
-2
|
Note. Q sort values are -4 to 4 to correspond with the Q distribution (Figure 1) where 4 is most important
and -4 is most unimportant; QSV = Q Sort Value.
Results
Factor 1: Focus on Clients
For participants on the focus on clients factor, the most important advocacy behavior was to “identify client strengths and resources” (see Table 1). When speaking about this item, participants often discussed teaching clients self-advocacy skills, stating that this is a key way in which career counselors promote social justice. Identifying client strengths and resources was referred to as “the starting point,” “the bottom line” and even the very “definition of career counseling.” One participant said that counseling is about “empowering our clients or jobseekers, whatever we call them, to do advocacy on their own behalf and to tell their story.” In general, persons on this factor were most concerned with empowering individual clients; for example, “I would say, even when we’re doing group counseling and family counseling, ultimately it’s about helping the person in the one-to-one.” Similarly, one participant said, “Instead of fighting for the group in legislation or out in the community, I’m working with each individual to help them better advocate for themselves.” Interview data indicated that social justice was a strongly held value for persons on this factor, but they typically emphasized the need for balancing their views on social injustice with their clients’ objectives; they wanted to take care not to prioritize their own agendas over those of their clients.
Several participants on this factor perceived items related to legislation or policy change as among the least client-centered behaviors and therefore as the more unimportant advocacy behaviors in their career counseling work. Persons on this factor stated that advocacy at the systems level was neither a strength of theirs nor a preference. A few reported that there are other people in their offices or campuses whose job is to focus on policy or legislative change. There also was a level of skepticism about counselors’ power to influence social change. In regard to influencing legislative change in support of clients, one participant said, “I don’t think in my lifetime that is going to happen. Maybe someday it will. I’m just thinking about market change right now instead of legislative change.”
Interview data revealed that career counselors on this factor thought about advocacy in terms of leadership, both positively and negatively. One person felt that a lack of leadership was a barrier to career counselors doing more advocacy work. Another person indicated that leaders were the ones who publicly called for social change and that this was neither his personality nor approach to making change, preferring instead to act at the micro level. Finally, persons on this factor expressed that conversations about social change or social justice were seen as potentially divisive in their work settings. One White participant said the following:
There is a reluctance to do social justice work because—and it’s mostly White people—people really don’t understand what it means, or feel like they don’t have a right to do that, or feel like they might be overstepping. Talking about race or anything else, people are really nervous and they don’t want to offend or say something that might be wrong, so as a result they just don’t engage on that level or on that topic.
Factor 2: Focus on Multiple Roles
One distinguishing feature of the focus on multiple roles factor was the relatively high importance placed on using multiple sources of intervention (see Table 1). Participants described this as being all-encompassing of what a career counselor does and reflective of the multiple roles a career counselor may hold. One participant said, “You never know what the client is going to come in with,” arguing that career counselors have to be open to multiple sources of intervention by necessity. Another participant indicated that she wished she could rely more on multiple sources of intervention but that the specialized nature of her office constricted her ability to do so.
Participants on this factor cited a lack of awareness or skills as a barrier to their implementing more advocacy behaviors. They were quick to identify social justice as a natural concern of career counselors and one that career counselors are well qualified to address due to their ability to remain aware of personal, mental health and career-related concerns simultaneously. One participant said:
I don’t know if the profession of career counseling is really seen as being as great as it is in that most of us have counseling backgrounds and can really tackle the issues of career on a number of different levels.
In talking about the nature of career counseling, another participant said, “Social justice impacts work in so many ways. It would make sense for those external barriers to come into our conversations.”
Regarding collaborating with other professionals to prepare convincing rationales for social change, one participant stated that there are already enough rationales for social change; therefore, this advocacy behavior was seen as less important to her. Persons on this factor placed relatively higher importance on valuing feedback on advocacy efforts than did participants on factor one. One participant said she would like to seek feedback more often but had not thought of doing so in a while: “I did this more when I was in graduate school because you are thinking about your thinking all the time. As a practitioner, as long as social justice and advocacy are on my radar, that’s good.”
Discussion
Neither setting nor gender appeared to differentiate the factors, but age and years of post-master’s experience may have been distinguishing variables. Younger individuals and those with fewer years of post-master’s experience tended to load onto factor two. Factor one had an average age of 51 compared to 35 for factor two, and the average age for all study participants was 43. It is interesting to note that the four participants who loaded onto both factors and were therefore dropped from analysis had an average of just over two years of post-master’s counseling experience versus 11 for factor one and seven for factor two. It is possible that their more recent training regarding advocacy may account for some differences in perspective from those of more experienced counselors.
Participants on factor one (focus on clients) who emphasized the importance of individual clients tended to perceive it as more difficult to have conversations about social justice with their peers or supervisors. In contrast, participants on factor two (focus on multiple roles) were more likely to cite a lack of knowledge or skills regarding their reasons for not engaging in more advocacy behaviors beyond the client level. Factor arrays indicated that factor one participants viewed engaging at the community level as more important, whereas participants on factor two viewed conversations with colleagues and clients about social justice as more important to their work.
The broader view of persons on factor two regarding the career counselor’s role and their openness to acknowledging their own lack of awareness or skills may reflect a different kind of socialization around advocacy compared to persons on factor one. Career counselors who graduated from counseling programs prior to the emphasis on multicultural competence in the early 1990s or before the inclusion of social justice in the literature and CACREP standards in the first decade of the 21st century may have had limited exposure to thinking about contextual or social factors that impact client wellness. Persons on both factors, however, expressed interest in social justice and felt that the vast majority of advocacy behaviors were important.
In post-sort interviews, participants from both factors described a gradual shift in emphasis from a focus on the individual on the right hand (most important) side of the Q sort distribution to an emphasis on legislation on the left hand (most unimportant) side. For example, the statement identify strengths and resources of clients was one of the most important behaviors for nearly every participant. Likewise, the statement work to change legislation and policy that negatively affects clients was ranked among the most unimportant advocacy behaviors for both factors. Interestingly, the statement encourage clients to research the laws and policies that apply to them was a consensus statement with a Q sort value of 0, or the very middle of the distribution. Since this advocacy behavior is both client focused and presumably would provide clients with important self-advocacy skills, it is interesting that it was ranked lower than other items related to client self-advocacy. Some participants indicated that they considered this item a “passive” counselor behavior in that they might encourage clients to research laws but could not or would not follow up with clients on this task. One participant said she would like to encourage clients to research laws that apply to them but shared that she would first need to learn more about the laws that impact her clients in order to feel effective in using this intervention.
Participants were asked directly about potential barriers to advocacy and potential strengths of career counselors in promoting social justice. Responses are discussed below. The questions about strengths and barriers in the post-sort interview did not reference Q sample items, so participant responses are reported together below.
Barriers to Promoting Social Justice
In the post-sort interviews, lack of time was mentioned by nearly every participant as a barrier to implementing more advocacy in career counseling, and it often came in the form of little institutional support for engaging in advocacy. For example, participants indicated that while their supervisors would not stop them from doing advocacy work, they would not provide material support (e.g., time off, reduced case load) to do so. This finding is consistent with other literature that suggests that career counselors report a lack of institutional support for engaging in advocacy (Arthur et al., 2009).
Another major barrier to advocacy was a lack of skill or confidence in one’s ability as an advocate. Advocacy at the social/political level requires a unique set of skills (M. A. Lee, Smith, & Henry, 2013), which practitioners in the present study may or may not have learned during their counseling training. Pieterse, Evans, Risner-Butner, Collins, and Mason (2009) reviewed 54 syllabi from required multicultural courses in American Psychological Association (APA)- and CACREP-accredited programs and found that awareness and knowledge tended to be emphasized more than skill building or application of social justice advocacy. This seems to have been reflected in the responses from many participants in the present study.
Participants on both factors indicated that they held some negative associations to advocacy work, calling it “flag waving” or “yelling and screaming” about inequality or social issues. They expressed some concern about how they might be perceived by their peers if they were to engage in advocacy; however, involvement in this study seemed to provide participants with a new understanding of advocacy as something that happens at the individual as well as at the social level. Participants appeared to finish the data collection sessions with a more positive understanding of what advocacy is and could be.
Strengths of Career Counselors in Promoting Social Justice
In addition to discussing barriers to advocacy, participants were asked directly about strengths of career counselors in promoting social justice and were able to identify many. First and foremost, participants saw the ability to develop one-on-one relationships with clients as a strength. One participant nicely captured the essence of all responses in this area by stating, “The key thing is our work one-on-one with an individual to say that even though you’re in a bad place, you have strengths, you have resources, and you have value.” Participants indicated that social change happens through a process of empowering clients, instilling hope and seeing diversity as a strength of a client’s career identity. The ability to develop strong counseling relationships was attributed partially to participants’ counseling training and identity, as well as to their exposure to a broad range of client concerns due to the inseparable nature of work from all other aspects of clients’ lives (Herr & Niles, 1998; Tang, 2003).
Career counselors in this study served diverse populations and highly valued doing so. These participants described multicultural counseling skills and experience as central to competent career counseling and to advocacy. They felt that they possessed and valued multicultural competence, which bodes well for their potential to engage in competent and ethical advocacy work with additional training, experience and supervision (Crook, Stenger, & Gesselman, 2015; Vespia, Fitzpatrick, Fouad, Kantamneni, & Chen, 2010).
Finally, participants felt that career counseling is seen as more accessible than mental health counseling to some clients, giving career counselors unique insight into clients’ social and personal worlds. Participants reported having a broad perspective on their clients’ lives and therefore unique opportunities to advocate for social justice. Relatedly, participants noted that the more concrete and tangible nature of career counseling and its outcomes (e.g., employment) may lead policymakers to be interested in hearing career counselors’ perspectives on social issues related to work. One participant noted that “there’s a huge conversation to be had around work and social justice” and that career counselors’ key strength “is empowering clients and the broader community to understand the role of work.”
Implications for Career Counselors, Counselor Educators, and Supervisors
Nearly all participants described the sorting process as thought provoking and indicated that social justice and advocacy were topics they appreciated the opportunity to think more about. There was a strong desire among some practitioners in this study to talk more openly with colleagues about social justice and its connection to career counseling, but a lingering hesitation as well. Therefore, one implication of the present study is that practitioners should begin to engage in discussions about this topic with colleagues and leaders in the profession. If there is a shared value for advocacy beyond the individual level, but time and skills are perceived as barriers, perhaps a larger conversation about the role of career counselors is timely. Career counselors may benefit from finding like-minded colleagues with whom to talk about social justice and advocacy. Support from peers may help practitioners strategize ways to question or challenge coworkers who may be practicing career counseling in ways that hinder social justice.
To move toward greater self-awareness and ethical advocacy, practitioners and career counseling leaders must ask themselves critical and self-reflexive questions about their roles and contributions in promoting social justice (McIlveen & Patton, 2006; Prilleltensky & Stead, 2012). Some authors have indicated there is an inherent tension in considering a social justice perspective and that starting such conversations can even lead to more questions than answers (Prilleltensky & Stead, 2012; Stead & Perry, 2012). Counselors should turn their communication skills and tolerance for ambiguity inward and toward one another in order to invite open and honest conversations about their role in promoting social justice for clients and communities. The participants in this study seem eager to do so, though leadership may be required to get the process started in a constructive and meaningful way.
Counselor educators and supervisors can provide counselors-in-training increased experience with systemic-level advocacy by integrating the ACA Advocacy Competencies and the Multicultural and Social Justice Counseling Competencies into all core coursework. Even though broaching issues of social justice has been reported as challenging and potentially risky, counselor educators should integrate such frameworks and competencies in active and experiential ways (Kiselica & Robinson, 2001; M. A. Lee et al., 2013; Lopez-Baez & Paylo, 2009; Manis, 2012). Singh and colleagues (2010) found that even self-identified social justice advocates struggled at times with initiating difficult conversations with colleagues; they argued that programs should do more to help counselors-in-training develop skills “to anticipate and address the inevitable interpersonal challenges inherent in advocacy work” (p. 141). Skills in leadership, teamwork and providing constructive feedback might be beneficial to prepare future counselors for addressing injustice. Furthermore, Crook and colleagues (2015) found that advocacy training via coursework or workshops is associated with higher levels of perceived advocacy competence among school counselors, lending more support in favor of multi-level training opportunities.
Limitations
The current study is one initial step in a much-needed body of research regarding advocacy practice in career counseling. It did not measure actual counselor engagement in advocacy, which is important to fully understand the current state of advocacy practice; rather, it measured perceived relative importance of advocacy behaviors. Researcher subjectivity may be considered a limitation of this study, as researcher decisions influenced the construction of the Q sample, the factor analysis and the interpretation of the emergent factors. By integrating feedback from two expert reviewers during construction of the Q sample, I minimized the potential for bias at the design stage. Factor interpretation is open to the researcher’s unique lens and also may be considered a limitation, but if it is done well, interpretation in Q methodology should be constrained by the factor array and interview data. Although generalizability is not a goal of Q methodology, the sample size in this study is small and therefore limits the scope of the findings.
Suggestions for Future Research and Conclusion
Advocacy is central to career counseling’s relevance in the 21st century (Arthur et al., 2009; Blustein, McWhirter, & Perry, 2005; McMahon, Arthur, & Collins, 2008a), yet due to the complexity and personal nature of this work, more research is required if we are to engage in advocacy competently, ethically and effectively. There appears to be interest among career counselors in gaining additional skills and knowledge regarding advocacy, so future research could include analyzing the effects of a training curriculum on perceptions of and engagement with advocacy. Outcome research could also be beneficial to understand whether career counselors who engage in high levels of advocacy report different client outcomes than those who do not. Finally, research with directors of career counseling departments could be helpful to understand what, if any, changes to career counselors’ roles are possible if career counselors are interested in doing more advocacy work. Understanding the perspectives of these leaders could help further the conversation regarding the ideals of social justice and the reality of expectations and demands faced by career counseling offices and agencies.
This research study is among the first to capture U.S. career counselors’ perspectives on a range of advocacy behaviors rather than attitudes about social justice in general. It adds empirical support to the notion that additional conversations and training around advocacy are wanted and needed among practicing career counselors. Stead (2013) wrote that knowledge becomes accepted through discourse; it is hoped that the knowledge this study produces will add to the social justice discourse in career counseling and move the profession toward a more integrated understanding of how career counselors view the advocate role and how they can work toward making social justice a reality.
Conflict of Interest and Funding Disclosure
The author conducted this research with the assistance of grants awarded by the National Career Development Association, the North Carolina Career Development Association, and the Southern Association for Counselor Education and Supervision.
References
American Counseling Association. (2014). 2014 ACA Code of Ethics. Alexandria, VA: Author. Retrieved from http://www.counseling.org/Resources/aca-code-of-ethics.pdf
Arthur, N., Collins, S., Marshall, C., & McMahon, M. (2013). Social justice competencies and career development practices. Canadian Journal of Counselling and Psychotherapy, 47, 136–154.
Arthur, N., Collins, S., McMahon, M., & Marshall, C. (2009). Career practitioners’ views of social justice and barriers for practice. Canadian Journal of Career Development, 8, 22–31.
Blustein, D. L. (2006). The psychology of working. Mahwah, NJ: Erlbaum.
Blustein, D. L., McWhirter, E. H., & Perry, J. C. (2005). An emancipatory communitarian approach to vocational development theory, research, and practice. The Counseling Psychologist, 33, 141–179. doi:10.1177/0011000004272268
Brown, S. R. (1978). The importance of factors in Q methodology: Statistical and theoretical considerations. Operant Subjectivity, 1, 117–124.
Brown, S. R. (1980). Political subjectivity: Applications of Q methodology in political science. New Haven, CT: Yale University Press.
Bureau of Labor Statistics, U.S. Department of Labor. (2016a). Charting the labor market: Data from the Current Population Survey (CPS). Retrieved from http://www.bls.gov/web/empsit/cps_charts.pdf
Bureau of Labor Statistics, U.S. Department of Labor. (2016b). The employment situation – May 2016. Retrieved from http://www.bls.gov/news.release/pdf/empsit.pdf
Chope, R. C. (2010). Applying the ACA advocacy competencies in employment counseling. In M. J. Ratts, R. L. Toporek, & J. A. Lewis (Eds.), ACA advocacy competencies: A social justice framework for counselors (pp. 225–236). Alexandria, VA: American Counseling Association.
Cook, E. P., Heppner, M. J., & O’Brien, K. M. (2005). Multicultural and gender influences in women’s career development: An ecological perspective. Journal of Multicultural Counseling and Development, 33, 165–179. doi:10.1002/j.2161-1912.2005.tb00014.x
Council for Accreditation of Counseling and Related Educational Programs. (2009). 2009 standards. Retrieved from http://www.cacrep.org/wp-content/uploads/2013/12/2009-Standards.pdf
Crook, T. M., Stenger, S., & Gesselman, A. (2015). Exploring perceptions of social justice advocacy competence among school counselors. Journal of Counselor Leadership and Advocacy, 2, 65–79.
Dean, J. K. (2009). Quantifying social justice advocacy competency: Development of the social justice advocacy scale
(Doctoral dissertation). Retrieved from http://scholarworks.gsu.edu/cgi/viewcontent.cgi?article=10
39&context=cps_diss
Fickling, M. J., & Gonzalez, L. M. (2016). Linking multicultural counseling and social justice through advocacy. Journal of Counselor Leadership and Advocacy. doi:10.1080/2326716X.2015.1124814
Herr, E. L., & Niles, S. G. (1998). Career: Social action on behalf of purpose, productivity, and hope. In C. C. Lee & G. R. Walz (Eds.), Social action: A mandate for counselors (pp. 117–136). Alexandria, VA: American Counseling Association.
Kaiser, H. F. (1970). A second generation little jiffy. Psychometrika, 35, 401–415. doi:10.1007/BF02291817
Kiselica, M. S., & Robinson, M. (2001). Bringing advocacy counseling to life: The history, issues, and human dramas of social justice work in counseling. Journal of Counseling & Development, 79, 387–397. doi:10.1002/j.1556-6676.2001.tb01985.x
Lee, C. C., & Hipolito-Delgado, C. P. (2007). Introduction: Counselors as agents of social justice. In C. C. Lee
(Ed.), Counseling for social justice (2nd ed., pp. xiii–xxviii). Alexandria, VA: American Counseling Association.
Lee, M. A., Smith, T. J., & Henry, R. G. (2013). Power politics: Advocacy to activism in social justice counseling. Journal for Social Action in Counseling and Psychology, 5, 70–94. Retrieved from http://www.psysr.org/jsacp/Lee-V5n3-13_70-94.pdf
Lewis, J. A., Arnold, M. S., House, R., & Toporek, R. L. (2002). ACA advocacy competencies. American Counseling Association. Retrieved from https://www.counseling.org/docs/default-source/competencies/advocacy_competencies.pdf?sfvrsn=9
Lopez-Baez, S. I., & Paylo, M. J. (2009). Social justice advocacy: Community collaboration and systems advocacy. Journal of Counseling & Development, 87, 276–283. doi:10.1002/j.1556-6678.2009.tb00107.x
Manis, A. A. (2012). A review of the literature on promoting cultural competence and social justice agency among students and counselor trainees: Piecing the evidence together to advance pedagogy and research. The Professional Counselor, 2, 48–57. doi:10.15241/aam.2.1.48
McIlveen, P., & Patton, W. (2006). A critical reflection on career development. International Journal for Educational and Vocational Guidance, 6, 15–27. doi:10.1007/s10775-006-0005-1
McKeown, B., & Thomas, D. B. (2013). Q methodology (2nd ed.). Thousand Oaks, CA: Sage.
McMahon, M., Arthur, N., & Collins, S. (2008a). Social justice and career development: Looking back, looking forward. Australian Journal of Career Development, 17, 21–29. doi:10.1177/103841620801700205
McMahon, M., Arthur, N., & Collins, S. (2008b). Social justice and career development: Views and experiences of Australian career development practitioners. Australian Journal of Career Development, 17(3), 15–25. doi:10.1177/103841620801700305
Milner, A., Page, A., & LaMontagne, A. D. (2013). Long-term unemployment and suicide: a systematic review and meta-analysis. PLoS ONE, 8, e51333. doi:10.1371/journal.pone.0051333
National Career Development Association. (2009). Minimum competencies for multicultural career counseling and development. Retrieved from http://ncda.org/aws/NCDA/pt/sp/guidelines
Niles, S. G., Amundson, N. E., & Neault, R. A. (2010). Career flow: A hope-centered approach to career development. Boston, MA: Pearson Education.
Paul, K. I., & Moser, K. (2009). Unemployment impairs mental health: Meta-analyses. Journal of Vocational Behavior, 74, 264–282. doi:10.1016/j.jvb.2009.01.001
Pieterse, A. L., Evans, S. A., Risner-Butner, A., Collins, N. M., & Mason, L. B. (2009). Multicultural competence and social justice training in counseling psychology and counselor education: A review and analysis of a sample of multicultural course syllabi. The Counseling Psychologist, 37, 93–115. doi:10.1177/0011000008319986
Pope, M., Briddick, W. C., & Wilson, F. (2013). The historical importance of social justice in the founding of the National Career Development Association. The Career Development Quarterly, 61, 368–373.
doi:10.1002/j.2161-0045.2013.00063.x
Pope, M., & Pangelinan, J. S. (2010). Using the ACA advocacy competencies in career counseling. In M. J. Ratts, R. L. Toporek, & J. A. Lewis (Eds.), ACA advocacy competencies: A social justice framework for counselors (pp. 209–223). Alexandria, VA: American Counseling Association.
Prilleltensky, I., & Stead, G. B. (2012). Critical psychology and career development: Unpacking the adjust–challenge dilemma. Journal of Career Development, 39, 321–340. doi:10.1177/0894845310384403
Ratts, M. J., Lewis, J. A., & Toporek, R. L. (2010). Advocacy and social justice: A helping paradigm for the 21st century. In M. J. Ratts, R. L. Toporek, & J. A. Lewis (Eds.), ACA advocacy competencies: A social justice framework for counselors (pp. 3–10). Alexandria, VA: American Counseling Association.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. Retrieved from http://www.counseling.org/knowledge-center/competencies
Sampson, J. P., Jr., Dozier, V. C., & Colvin, G. P. (2011). Translating career theory to practice: The risk of unintentional social injustice. Journal of Counseling & Development, 89, 326–337.
doi:10.1002/j.1556-6678.2011.tb00097.x
Savickas, M. L. (1997). Career adaptability: An integrative construct for life-span, life-space theory. The Career Development Quarterly, 45, 247–259. doi:10.1002/j.2161-0045.1997.tb00469.x
Schmolck, P. (2014). PQMethod 2.35 with PQROT 2.0 [Computer software and manual]. Retrieved from
http://schmolck.userweb.mwn.de/qmethod
Singh, A. A., Urbano, A., Haston, M., & McMahan, E. (2010). School counselors’ strategies for social justice change: A grounded theory of what works in the real world. Professional School Counseling, 13, 135–145. doi:10.5330/PSC.n.2010-13.135
Stead, G. S. (2013). Social constructionist thought and working. In D. L. Blustein (Ed.), The Oxford handbook of the psychology of working (pp. 37–48). New York, NY: Oxford University Press.
Stead, G. B., & Perry, J. C. (2012). Toward critical psychology perspectives of work-based transitions. Journal of Career Development, 39, 315–320. doi:10.1177/0894845311405661
Tang, M. (2003). Career counseling in the future: Constructing, collaborating, advocating. The Career Development Quarterly, 52, 61–69. doi:10.1002/j.2161-0045.2003.tb00628.x
Toporek, R. L., Lewis, J. A., & Crethar, H. C. (2009). Promoting systemic change through the ACA advocacy competencies. Journal of Counseling & Development, 87, 260–268. doi:10.1002/j.1556-6678.2009.tb00105.x
Vespia, K. M., Fitzpatrick, M. E., Fouad, N. A., Kantamneni, N., & Chen, Y.-L. (2010). Multicultural career counseling: A national survey of competencies and practices. The Career Development Quarterly, 59, 54–71. doi:10.1002/j.2161-0045.2010.tb00130.x
Watts, S., & Stenner, P. (2012). Doing q methodological research: Theory, method and interpretation. Thousand Oaks, CA: Sage.
Webler, T., Danielson, S., & Tuler, S. (2009). Using Q method to reveal social perspectives in environmental research.
Greenfield, MA: Social and Environmental Research Institute. Retrieved from
http://seri-us.org/sites/default/files/Qprimer.pdf
Melissa J. Fickling, NCC, is an Assistant Professor at the University of Memphis. Correspondence can be addressed to Melissa J. Fickling, University of Memphis, Ball Hall 100, Memphis, TN 38152, mfckling@memphis.edu.
