Apr 1, 2026 | Volume 16 - Issue 1
Brian J. Clarke, Michael T. Hartley, Austin M. Guida
Impostor phenomenon (IP), characterized by persistent self-doubt despite objective success, is prevalent during the early stages of counselor development, often emerging as individuals transition from training into professional practice. This study examined whether self-compassion mediates relationships between IP, resilience, and mental health among 281 counselors-in-training enrolled in departments accredited by the Council for the Accreditation of Counseling and Related Educational Programs. Mediation analyses showed that self-compassion fully mediated the effects of IP on resilience and depression and partially mediated the effect on anxiety. MANOVA results indicated that higher self-compassion corresponded with lower IP, anxiety, and depression, and greater resilience, with robust effects. Findings identify self-compassion as a developmental competency that supports balanced self-evaluation, emotional regulation, and sustainable counselor well-being. Integrating self-compassion training into counselor education and supervision may help developing counselors manage impostor-related distress, strengthen resilience, and promote ethical, sustainable professional practice.
Keywords: impostor phenomenon, counselor development, self-compassion, resilience, mental health
Building resilience and prioritizing mental health are vital during the formative stages of counselor development. During the early stages of training and supervised practice, developing counselors experience the inherent emotional demands and elevated anxiety common while learning to integrate theoretical knowledge into clinical practice (Skovholt & Trotter-Mathison, 2024; Stoltenberg & McNeill, 2010). Although these feelings may diminish with increased experience, enduring self-doubt and inadequacy may signal impostor phenomenon (Clance & Lawry, 2024). Imposter phenomenon (IP), characterized by persistent feelings of fraudulence and incompetence despite evidence of success, impacts nearly all developing counselors (Clarke et al., 2025; Tigranyan et al., 2021). Those experiencing IP may struggle to internalize mastery experiences and fail to consolidate moments of success into genuine confidence (Gadsby & Hohwy, 2024; Roskowski, 2010). Individual differences in coping with IP may be partially explained by self-compassion, which may buffer IP’s negative effects on counseling self-efficacy and well-being (Clarke et al., 2025).
The persistent fear of being exposed as a fraud becomes a harmful cycle whereby individuals ruminate on perceived shortcomings, discount positive feedback, and misattribute positive outcomes to external factors (Clance & Lawry, 2024). Behaviors associated with IP include extreme perfectionism, procrastination, and/or exhausting overpreparation, which can inhibit counselor development (Clarke et al., 2025; Nguyen, 2023). Because IP is rooted in shame and feelings of inadequacy, it contributes to isolation, burnout, and compassion fatigue (Garba et al., 2024; Ojeda, 2024).
IP undermines the reflective, relational, and self-evaluative capacities that are central to counselor development. Counselors who experience chronic self-doubt may hesitate to disclose errors in supervision, question their competence, and struggle to sustain resilience, patterns that can jeopardize client care and professional longevity (Delaney, 2018; Housenecht & Swank, 2022). Given the demands of counselor training and practice, protective factors such as resilience and self-compassion may be critical for developing counselor well-being and persistence.
Resilience is a protective factor to cope with mental distress and burnout (Gerber & Anaki, 2021; Webb & Rosenbaum, 2019). Emerging from the positive psychology movement, resilience explains why some individuals behave adaptively under great stress while others do not. Beyond recovery from adversity, resilience is a process of successful adaptation and coping during challenging or threatening circumstances (Webb & Rosenbaum, 2019). Cultivating new coping mechanisms and fostering personal growth, resilience can sustain well-being and performance during difficult experiences. The limited research on resilience among developing counselors has identified self-awareness and self-compassion as critical protective factors to cope with the emotional demands of becoming a counselor (Hou & Skovholt, 2020).
As a protective factor, self-compassion can play an important role in the resilience and mental health of developing counselors, especially in the presence of IP (Clarke et al., 2025; Neff et al., 2005). Self-compassion is comprised of three interrelated dimensions: mindfulness, common humanity, and self-kindness (Neff, 2023). Mindfulness, the core of self-compassion, involves maintaining awareness of present experiences with reduced reactivity and self-judgment. The common humanity dimension refers to the acceptance that suffering is inherent to our shared human experience. By normalizing challenging experiences, this perspective helps prevent the isolation that may arise from perceiving failures as uniquely personal. Finally, self-kindness encompasses behaviors and ways of relating intrapersonally that offer support and comfort during times of suffering or setbacks. Rather than defaulting to self-criticism, overidentification with failures, or isolation, self-compassion enables understanding and resilience, reducing the impact of IP and the fear of failure during counselor development (Clarke et al., 2025; Warren et al., 2016).
The theoretical alignment between self-compassion and resilience is rooted in their shared emphasis on adaptive emotional regulation, growth through adversity, and the development of a stable and supportive inner identity (Warren et al., 2016). Self-compassion supports sustainable resilience by reducing self-criticism and perfectionism and fostering a growth mindset (Neff, 2023; Warren et al., 2016). Indeed, a recent meta-analysis indicated that self-compassion is consistently linked to positive outcomes among mental health professionals, including enhanced competence, improved therapeutic presence, and a greater willingness to seek guidance and supervision (Crego et al., 2022).
Because of its regulating effects, self-compassion may help developing counselors to tolerate the stress of IP through improved emotional self-regulation (Crego et al., 2022; Neff, 2023). In this way, self-compassion can function as an emotion-focused coping mechanism that reduces the mental distress associated with IP (Clarke, 2024; Crego et al., 2022; Gerber & Anaki, 2021). Ultimately, when individuals experience IP-related distress, self-compassionate responses (mindfulness, common humanity, self-kindness) may interrupt the IP cycle, preserving resilience and mental health (Neff et al., 2005).
The purpose of this study is to examine how self-compassion functions as a protective factor in the relationship between IP, resilience, and mental health during counselor development. Research has found self-compassion to support resilience among health care providers (Delaney, 2018), yet much less is known about the relationship between self-compassion and resilience among developing counselors who experience IP. Addressing the negative impact of IP on counselor development, this article explores how self-compassion might mitigate IP’s negative relationships with resilience and mental health (Clarke et al, 2025; Roskowski, 2010; Tigranyan et al., 2021). The guiding research questions were:
- To what extent does self-compassion mediate the relationships between IP and the outcomes of resilience and mental health?
- How do levels of self-compassion relate to variations in IP, resilience, and mental health among the sample?
We hypothesized that IP would have a significant negative relationship with resilience and mental health, and that self-compassion will significantly mediate these negative associations. Specifically, higher levels of self-compassion will relate to lower IP and improved mental health and resilience. Our findings offer valuable insights into how self-compassion can enhance resilience and promote mental health during counselor development.
Methods
Procedure
The study received IRB approval prior to the recruitment of master’s-level counseling students from across the United States. Data were collected between April and October 2023, using an online survey disseminated via email to Council for the Accreditation of Counseling and Related Educational Programs (CACREP)–accredited program liaisons. These emails described the study and outlined informed consent procedures and inclusion criteria. Eligible participants were individuals enrolled in CACREP-accredited counseling programs aged 18 or older. After consenting, participants were presented with the measures and a demographic questionnaire developed by the authors. Engagement with the study concluded once participants either completed or exited the survey.
Participants
The sample consisted of 281 counseling students attending CACREP-accredited counseling programs from 37 U.S. states and the District of Columbia. Although the present sample consisted of counselors-in-training (CITs), the term developing counselors is used throughout this paper to reflect the broader developmental continuum that spans counselor training and early professional practice (Stoltenberg & McNeill, 2010).
Consistent with the population of CITs, most participants identified as White (n = 190, 67.29%) with lower percentages identifying as Hispanic or Latinx (n = 43, 15.2 %), Asian (n = 17, 6.0%), African American or Black (n = 13, 4.6%), multiracial (n = 13, 4.6%), American Indian or Alaskan Native (n = 3, 1.1%) and Middle Eastern (n = 2, 0.7%). The majority (n = 237, 83.7%) identified as female, with 32 (11.3%) identifying as male, 6 (2.1%) as non-binary, 4 (1.4%) as genderqueer, and 2 (0.7%) choosing not to disclose their gender identity. Participants were from clinical mental health (n = 170, 60.1%), school counseling (n = 49, 17.3%), rehabilitation counseling (n = 49, 17.3%), and marriage and family counseling (n = 13, 4.6%) programs. The average participant age was 32 years (SD = 10.35), with an age range from 21 to 67 years.
Measures
Self-Compassion Scale-Short Form (SCS-SF)
The SCS-SF is a short form of the Self-Compassion Scale (Neff, 2003), consisting of 12 self-report items selected from the original scale (Raes et al., 2011). Items are rated on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Examples include “I try to see my failings as part of the human condition” and “I’m disapproving and judgmental about my own flaws and inadequacies” (Neff, 2003, p. 2). SCS-SF scores have shown good internal consistency (α = .86), with its total scores strongly correlating with those of the full version (r = .98; Raes et al., 2011). Factor analysis has confirmed that the SCS-SF shares the same factor structure as the original scale (Neff et al., 2019; Raes et al., 2011). Scores are interpreted as levels of self-compassion: low (1–2.4), moderate (2.5–3.5), and high (3.51–5). In the present study, SCS-SF scores demonstrated good internal consistency reflected in an alpha of .85, and omega of .85.
Academic Resilience Scale-6 (ARS-6)
The ARS-6 is a concise self-report scale designed to measure academic resilience, defined as the ability to manage challenges, stress, and setbacks within a learning environment (Martin & Marsh, 2006). Items include statements such as “I’m good at bouncing back from a poor grade or difficult feedback” and “I don’t let a bad grade or feedback affect my confidence.” Responses are rated on a 7-point Likert-type response scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater academic resilience. Item and factor level construct validity was supported through factor score estimates, correlation, path analysis, and cluster analysis, showing the ARS scores were closely aligned with related constructs including self-efficacy, control, planning, low anxiety, and persistence (Martin & Marsh, 2006). ARS-6 scores have demonstrated good internal consistency, with an alpha coefficient of .89 (Martin & Marsh, 2006). In the current study, the ARS-6 scores showed acceptable reliability supported by alpha and omega scores of .83.
Clance Impostor Phenomenon Scale (CIPS-10)
The CIPS-10 (Wang et al., 2022) is a condensed, 10-item version of the original 20-item Clance Impostor Phenomenon Scale (CIPS) designed to assess impostor feelings (Clance, 1985). A systematic review by Mak et al. (2019) supported the CIPS-20 as a valid (construct, criterion, and content) measure of IP. The CIPS-10 utilizes a Likert-type response scale ranging from 1 (not at all true) to 5 (very true) and includes items from the CIPS-20, such as “I’m afraid people important to me may find out that I’m not as capable as they think I am” and “I feel my success was due to some kind of luck rather than competence.” Wang et al. (2022) reported strong internal reliability for the CIPS-10 (α = .93), with total scores closely aligning with those of the CIPS-20. Construct validity was supported through factor score estimates, revealing a single-factor structure similar to the 20-item version. In this study, CIPS-10 scores were interpreted using adjusted categories from Clance (1985): few IP (less than 20), moderate IP (20–29), frequent IP (30–39), and intense IP (40–50). Within the current sample, CIPS-10 scores demonstrated good internal consistency with an alpha of .88 and omega of .90.
Patient Health Questionnaire-4 (PHQ-4)
The PHQ-4 is a 4-item, self-report assessment screening tool for depression and anxiety (Kroenke et al., 2009). The Likert-type responses are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). A total score of 3 or more, across both items, indicates the presence of moderate-to-severe symptoms (Kroenke et al., 2009). In meta-analyses, PHQ-4 scores have shown good internal consistency (α = .89) and have yielded valid and diagnostically accurate depression and anxiety scores (Khubchandani et al., 2016; Kroenke et al, 2009). Construct validity was supported using a varimax-rotated principal components analysis conducted on the four screening items (PHQ-2 and GAD-2), yielding two components that together explained 83% of the overall variance. Likewise, criterion validity was indicated by individuals diagnosed with depression or anxiety by a health care professional scoring significantly higher on the PHQ-2, GAD-2, and PHQ-4 compared to participants without a clinical diagnosis (Khubchandani et al., 2016). In the present sample, the PHQ-4 scores showed good internal consistency with an alpha score of .87 and omega of .84.
Data Analysis
Portions of this data set informed a previously published manuscript that focused on how self-compassion can mitigate IP’s negative relationship with counselor self-efficacy (Clarke et al., 2025). Although the two manuscripts share IP and self-compassion data, the current manuscript is distinct and extends this line of inquiry by its unique focus on the benefits of self-compassion for counselor resilience and mental health, despite the presence of IP.
All analyses were performed using SPSS (v29) with a p ≤ .01 benchmark to reduce the likelihood of Type I error and ensure that the most reliable effects are interpreted as statistically meaningful. Preliminary analyses were conducted to examine statistical assumptions for the mediation and MANOVA models. Normality was confirmed for all variables via Shapiro-Wilk (all p > .05). Box’s M test supported homogeneity of variance–covariance matrices (p = .021), and observations were independent. In addition to all VIF scores being < 2, no bivariate correlations exceeded r = .80, suggesting that multicollinearity was not a concern. Collectively, these results suggest that the data met all assumptions necessary for the planned analyses (Tabachnick & Fidell, 2019).
We selected a regression-based mediation analysis because of the study’s focus on specific indirect effects of self-compassion and the moderate sample size, both of which made alternative analyses less ideal (Hayes, 2022). Because the variables tested were represented by composite scores rather than latent constructs, a mediation was statistically appropriate and provided a parsimonious method to examine self-compassion as a buffer for IP. Although cross-sectional mediation cannot establish temporal precedence or causation, it can identify statistical pathways that warrant future longitudinal investigation (Fairchild & McDaniel, 2017; Hayes, 2022). The 99% confidence intervals (CI) of the effects were derived from 10,000 bootstrap samples. If the upper and lower bounds of the CI did not include zero, they were considered statistically significant.
Finally, MANOVA was used to determine how the severity of IP affected its relationships with resilience, anxiety, depression, and self-compassion. The four levels of IP used in this analysis were defined as few, moderate, frequent, and intense IP according to the CIPS author (Clance, 1985). MANOVA effect size was described using partial eta squared values of 0.01 (small), 0.059 (medium), and 0.14 (large; Richardson, 2011). Cohen’s d was used to interpret effect sizes for follow up Tukey analyses, small effect (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8; Gignac & Szodorai, 2016).
A priori power analysis for mediation effects (Fritz & MacKinnon, 2007) indicated a minimum sample of 148 participants would provide .80 power to detect medium-sized indirect effects using bias-corrected bootstrapping. For MANOVA with three groups and four dependent variables, G*Power indicated 158 participants would yield .80 power for detecting medium effects (f² = .25). Our sample of 281 exceeded both requirements.
Results
Descriptives
Pearson correlations indicated significant (< .01) bivariate relationships among self-compassion, impostor phenomenon, depression, anxiety, and academic resilience (Table 1). There were no significant differences in self-compassion, IP, resilience, anxiety, or depression across demographics or counseling program emphasis.
Table 1
Descriptive Statistics and Bivariate Correlations
|
Mean |
SD |
1 |
2 |
3 |
4 |
|
| 1. Self-Compassion |
3.06 |
0.74 |
– |
|
|
|
| 2. Impostor Phenomenon |
32.81 |
8.22 |
−.54* |
– |
|
|
| 3. Depression |
1.27 |
1.60 |
−.42* |
.35* |
– |
|
| 4. Anxiety |
2.54 |
1.78 |
−.55* |
.46* |
.59* |
– |
| 5. Academic Resilience |
27.66 |
6.51 |
.53* |
−.36* |
−.23* |
−.40* |
*p ≤ .01.
The sample included high levels of impostor phenomenon (M = 32.81, SD = 8.22), with over 65% falling in the frequent-to-intense range. IP showed strong negative correlations with self-compassion (r = −.54) and resilience (r = −.36), and strong positive correlations with anxiety (r = .46) and depression (r = .35).
Mediation Analysis
Mediation analyses were used to explore the statistical associations among IP, self-compassion, and the outcome variables of resilience, anxiety, and depression. Results indicated that self-compassion functioned as a statistical mediator in the relationships between IP and each outcome.
Figure 1
Mediation Analysis: Impostor and Resilience
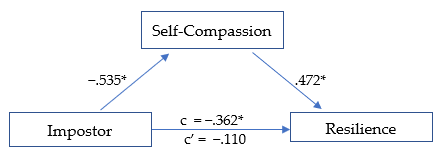
*p ≤ .01
The first model (Figure 1) was significant, R² = .290, F(1, 278) = 59.78, p < .01. The total effect (c) of IP on academic resilience was negative and significant, β = −.362, SE = .126, t = −2.868, p < .01, suggesting that higher IP scores were associated with lower resilience. When self-compassion was included in the model, the direct effect (c′) of IP on resilience was no longer significant, β = −.110, SE = .060, t = −1.838, p = .07, consistent with full statistical mediation (Hayes, 2022). The indirect pathway through self-compassion represented 69.6% of the total standardized association. IP was negatively associated with self-compassion (β = −.535, p < .01; large effect), and self-compassion was positively associated with resilience (β = .472, p < .01; large effect). The overall indirect effect was significant (β = −.252, p < .01).
Figure 2
Mediation Analysis: Impostor and Anxiety
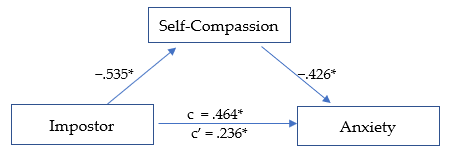
*p ≤ .01.
The second model (Figure 2) was significant, R² = .345, F(1, 278) = 73.159, p < .01. The total effect (c) of IP on anxiety was positive and significant, β = .464, SE = .053, t = 8.747, p < .01, indicating that higher IP scores were related to higher anxiety levels. After including self-compassion, the direct effect (c′) was reduced but remained significant, β = .236, SE = .057, t = 4.110, p < .01, suggesting partial statistical mediation. The indirect pathway through self-compassion accounted for 49.2% of the total standardized association. IP was negatively associated with self-compassion (β = −.535,p < .01; large effect), and self-compassion was negatively associated with anxiety (β = −.426, p < .01; medium effect). The overall indirect effect was significant, β = −.228, p < .01.
Figure 3
Mediation Analysis: Impostor and Depression
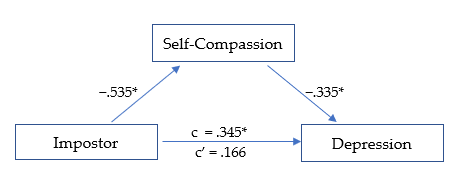
*p ≤ .01.
The third model (Figure 3) was significant, R² = .199, F(1, 278) = 34.484, p < .01. The total effect (c) of IP on depression was positive and significant, β = .345, SE = .056, t = 6.135, p < .01, indicating that higher IP scores were associated with higher depression levels. After accounting for self-compassion, the direct effect (c′) was reduced and no longer significant, β = .166, SE = .064, t = 2.611, p = .02, suggesting full statistical mediation. The indirect pathway through self-compassion represented 51.9% of the total standardized association. IP was negatively related to self-compassion (β = −.535, p < .01; large effect), and self-compassion was negatively related to depression (β = −.335, p < .01; medium effect). The overall indirect effect was significant, β = −.179, p < .01.
MANOVA
Self-compassion scores were divided into three levels (low, moderate, and high) as suggested by Neff (2003) to determine if the effect of self-compassion was consistent across each level. MANOVA analyses revealed that IP, resilience, depression, and anxiety each varied significantly based on level of self-compassion, F(8, 550) = 20.790, p < .01, Wilk’s Λ = 0.590, ηp2 = .232, indicating a large effect size.
The MANOVA results revealed that IP scores varied according to level of self-compassion, F(2, 281) = 48.807, p < .01, ηp2 = .260, with a large effect size. IP decreased significantly at each rising level of self-compassion, from low to moderate (d = 0.666, p < .01) and moderate to high (d = 0.987, p < .01), with medium and large effect sizes, respectively. The greatest decrease in IP was seen as self-compassion rose from moderate to high.
Resilience was significantly higher at each increasing level of self-compassion F(2, 281) = 39.323, p < .01, ηp2 = .221, with a large overall effect size. Resilience rose linearly across each level of self-compassion, from low to moderate (d = −0.756, p < .01), and from moderate to high (d = −0.790, p < .01), each with a medium-high effect size.
Depression scores lowered significantly as self-compassion level increased, F(2, 281) = 20.232, p < .01, ηp2 = .127, with an overall medium effect size. The decrease in depression was noted across levels of self-compassion, from low to moderate (d = 0.446, p < .01), and from moderate to high (d = 0.625, p < .01), each with a medium effect size. The largest decrease in depression was observed as self-compassion rose from moderate to high.
Anxiety scores decreased significantly as the level of self-compassion increased, F(2, 281) = 45.898, p < .01, ηp2 = .248, with a large overall effect size. Anxiety scores were lower as self-compassion rose from low to moderate (d = 0.895, p < .01), and from moderate to high (d = 0.711, p < .01), with large and medium effect sizes, respectively. The largest decrease in anxiety was noted as self-compassion increased from low to moderate.
Discussion
Our findings indicate that self-compassion is a strong protective factor and may enhance resilience and promote mental health among developing counselors, despite impostor feelings. Specifically, self-compassion fully mediated the negative relationship between IP, resilience, and depression, while partially mediating the relationship between IP and anxiety. This suggests that even when experiencing IP, higher self-compassion may help to maintain greater resilience and significantly reduced anxiety and depression. The results are promising and suggest that cultivating self-compassion may facilitate professional growth by interrupting the IP cycle. Our results offer further insights into how self-compassion can support resilience and mental health (Housenecht & Swank, 2022).
Descriptive Statistics
Descriptive analyses revealed a notably high prevalence of IP in the sample, with 96.1% (n = 270) reporting moderate to intense symptoms. Scores were skewed toward the higher end of the scale, with 65.1% of participants in the frequent-to-intense range and 21% in the highest category. Compared with earlier samples, these findings suggest that the severity of IP has increased substantially over the past 15 years (Roskowski, 2010; Tigranyan et al., 2021). For example, only 27.6% of a 2010 sample fell into the frequent-to-intense categories, compared with nearly two-thirds in the present study. Likewise, the proportion of students in the highest IP range has risen fivefold, from 4.1% in 2010 to 21% here. Although this increase may be influenced by broader cultural or educational factors, the trend underscores the importance of implementing effective coping strategies to support counselor well-being and persistence.
Consistently elevated IP scores across studies suggest that impostor feelings may be a common element of counselor development. Such feelings are often fueled by both internal and environmental pressures, particularly graduate students’ unreasonably high expectations of their performance and rapid development (Clance & Lawry, 2024). These unrealistic standards can generate unnecessary self-doubt, distorted self-assessments, and persistent self-criticism (Gadsby & Hohwy, 2024). Importantly, the current results indicate that self-compassion is a powerful counterbalance to IP. Higher self-compassion was associated with lower IP, anxiety, and depression, and with greater resilience, findings that align with previous research (Liu et al., 2023).
Mediation Models
Self-Compassion, IP, and Resilience
The first mediation analysis revealed that self-compassion fully mediated the negative relationship between IP and resilience. When accounting for self-compassion, the negative relationship between IP and resilience was rendered statistically non-significant. This outcome suggests that developing counselors with higher self-compassion may more easily adapt and recover when experiencing impostor-related distress. Self-compassion may assist key aspects of resilience, including stress management, coping with adversity, and maintaining a stable and supportive inner identity (Webb & Rosenbaum, 2019).
Although IP encourages harsh self-criticism and rumination on perceived failures, it is possible that through increased self-acceptance and soothing kindness, counselors can embody greater resilience when confronting areas of growth with less fear of failure. Additionally, a common humanity perspective can encourage acceptance of struggles as a normal part of counselor development and one shared by their peers. These soothing and normalizing aspects of self-compassion can encourage community rather than isolation when struggling, helping counselors to maintain resilience amidst adversity (Hou & Skovholt, 2020; Neff, 2023). Without effective coping practices, the challenges of counselor development can wear down resilience, creating vulnerability to mental distress, burnout, and counselor impairment (Cook et al., 2021; Gerber & Anaki, 2021).
Self-Compassion, IP, and Mental Health
Our results indicate that self-compassion is associated with less anxiety among those experiencing IP. Because anxiety is prevalent in this population and a primary emotional response to IP, efforts to increase self-compassion can have widely beneficial outcomes (Crego et al., 2022; Garba et al., 2024). The common humanity and mindfulness components of self-compassion may be critical to this outcome, as they can help limit emotional reactivity, normalize the IP experience, and reduce the isolation and fear of being exposed as an impostor (Clarke & Guida, 2025). This process involves mindfully recognizing that others share similar experiences and feelings, empowering developing counselors to seek support and reduce fear of failure (Neff, 2023). Likewise, practicing self-kindness may counter the harsh self-criticism associated with IP and encourage them to embrace the developmental process, including their imperfections (Patzak et al., 2017; Warren et al., 2016).
Anxiety and depression are closely linked and often co-occur (Beck & Alford, 2009). Though depression may not correlate as strongly with IP as anxiety does, it remains a common outcome (Garba et al., 2024). IP is persistent and sustained by cognitive distortions and misattributions, which also contribute to depressive thought patterns (Beck & Alford, 2009). However, our analysis revealed that self-compassion fully mediated the relationship between IP and depression. This suggests that a combination of mindful awareness and active self-kindness may facilitate more balanced self-assessment, countering perfectionism and harsh self-criticism commonly associated with IP (Clarke & Hartley, 2025; Pákozdy et al., 2023).
Although IP significantly predicted anxiety and depression, the buffering effect of self-compassion suggests that those with more compassionate self-perceptions may better tolerate the uncertainty and challenges common to counselor training. For example, those with a self-compassionate mindset may reinterpret failures as growth opportunities, a shift that may protect against anxious and depressive symptoms (Crego et al., 2022; Warren et al., 2016). These findings highlight the regulatory potential of self-compassion in reducing emotional reactivity to impostor-related distress.
Level of Self-Compassion in Relation to IP, Resilience, and Mental Health
MANOVA was utilized to determine whether the level of self-compassion (categorized as low, moderate, or high) was related to the level of IP, resilience, anxiety, and depression (Neff, 2003). Self-compassion had a significant positive relationship with mental health and resilience; however, the relationships varied significantly based on level of self-compassion (Figure 4). The results demonstrate that even lower levels of self-compassion were related to significantly lower IP, anxiety, and depression, as well as increased resilience. This pattern suggests that even modest improvements in self-compassion can correspond to improved well-being among developing counselors (Luo et al., 2023). For example, IP severity decreased significantly as self-compassion levels increased, revealing a linear reduction in IP from low to high self-compassion levels, with the most pronounced decrease occurring between the moderate and high categories.
Similarly, resilience scores also increased consistently across each level of self-compassion. The increase was linear, with the most substantial increase occurring when self-compassion rose from low to moderate. The steady increase in resilience across all self-compassion levels points to a possible dose-response relationship. Initial gains in self-compassion may bolster developing counselors’ ability to persevere through challenges (Neff et al., 2005), and interventions resulting in modest enhancements in self-compassion could yield significant improvements in resilience.
Figure 4
IP, Resilience, Depression, and Anxiety Across Levels of Self-Compassion
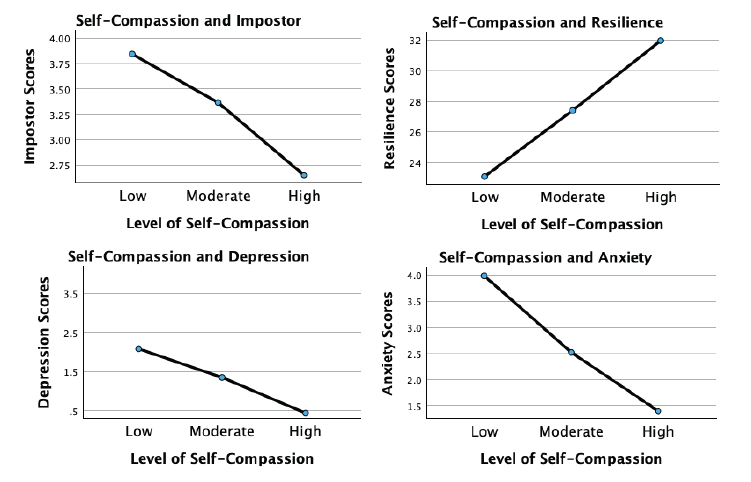
Although more variable, the association of self-compassion with anxiety and depression was similarly beneficial. Anxiety levels decreased significantly with each incremental increase in self-compassion, with the largest reduction occurring from low to moderate levels. This underscores the potential that even lower levels of self-compassion may still meaningfully alleviate anxiety. For depression, a significant decrease occurred across self-compassion levels, with the most substantial reduction noted as self-compassion increased from moderate to high. This suggests that self-compassion may interrupt the internal feedback loop of shame, self-criticism, and hopelessness that sustains depressive thinking in the context of IP.
These findings indicate that self-compassion is an important protective factor for developing counselor mental health. Contrary to expectations, even lower levels of self-compassion significantly relate to reduced IP, anxiety, and depression while increasing resilience (Luo et al., 2023). Integrating strategies to enhance self-compassion into counselor training programs could incrementally increase self-compassion, build emotional tolerance, and create a more stable internal environment from which resilience and well-being can emerge.
Implications and Future Directions for Counselor Development
Despite IP’s prevalence and association with diminished resilience and psychological distress, it remains underexamined in the counseling literature. Beyond a self-care strategy, self-compassion may build resilience and maintain mental health during and after counselor training. Integrating self-compassion into counselor education and early career development may cultivate a more supportive environment and provide counselors with evidence-based ways to manage IP and enhance resilience. Whereas, if left unaddressed, IP can lead to unnecessary distress, burnout, and professional attrition (Coaston & Lawrence, 2019; Ojeda, 2024).
Growing evidence suggests that self-compassion is vital for counselor development and ethical practice (Clarke et al., 2025; Coaston & Lawrence, 2019). The American Counseling Association (ACA) Code of Ethics (2014) emphasizes that professional counselors must engage in ongoing self-assessment and maintain their effectiveness through self-care practices. Similarly, CACREP (2023) standards require counselor education programs to integrate “self-care, self-awareness, and self-evaluation strategies for ethical and effective practice” (3.A.11.). Without meaningful coping strategies, IP can directly undermine these ethical mandates by diminishing well-being and distorting self-evaluation necessary for competent practice (Gadsby & Hohwy, 2024).
Regular engagement in reflective activities promoting balanced self-evaluation is essential to counselor development. If such exercises lack a compassionate focus, they may inadvertently reinforce impostor-related distortions by encouraging rumination and inaccurate self-critique. Matching reflective self-assessment with self-compassion practice may allow developing counselors to internalize feedback and move attention away from self-criticism and toward a growth mindset, transforming internal narratives dominated by IP (Warren et al., 2016).
Counselor educators and professional agencies can integrate self-compassion training through multiple pathways. Brief interventions, such as abbreviated versions of the Mindful Self-Compassion program (Germer & Neff, 2019), offer evidence-based approaches for enhancing counselor resilience. If limited by time and resources, supervisors and mentors can model self-compassionate practices by normalizing struggles, demonstrating constructive self-talk, and providing balanced growth-oriented feedback. The disclosure of faculty or supervisor IP experiences may be particularly powerful, reframing vulnerability and self-care as professional strengths rather than weaknesses.
Because IP is a contextual and environmentally fueled experience, counseling agencies and community mental health settings can foster organizational climates that prioritize compassion and collaboration and normalize challenges during the growth process (Coaston, 2019). When institutions reward openness, reflection, and learning from error, rather than perfection and productivity, developing counselors are more likely to engage in authentic self-assessment and seek help when struggling.
Early career peer support groups and compassion-focused initiatives can also counter the competitive, perfectionistic culture that sustains IP in professional practice (Clark et al., 2022). These approaches challenge the isolating belief that self-doubt is uniquely shameful, and foster community and belonging (Clarke & Guida, 2025; Hou & Skovholt, 2020). Future research should employ longitudinal and experimental designs to test targeted self-compassion interventions, clarifying causal relationships between self-compassion, resilience, and mental health outcomes in counselor education and professional contexts.
Clinical Supervision
Developmentally, the transition from classroom learning to applying theory and skills in clinical practice naturally provokes stress and anxiety (Skovholt & Trotter-Mathison, 2024). Although clinical supervision provides an ideal context for fostering openness and resilience (Coaston, 2019), experiencing IP may be a barrier to disclosing challenges because of emotional distress and fear of exposing perceived inadequacies (DeCandia Vitoria, 2021). Maintaining a façade of competence can compromise development and hinder the supervisory relationship (Thériault et al., 2009). These perfectionistic tendencies and IP are often motivated by context, suggesting that supervisors’ approaches may significantly alleviate these patterns.
Coaston (2019) provides a practical framework for applying self-compassion principles and philosophy in clinical supervision. Rooted in humanistic and developmental theory, this approach emphasizes that supervisors can accompany supervisees through the inevitable discomfort and vulnerability of professional growth by responding with compassion rather than judgment. By adopting a compassionate approach, the supervisory relationship can deepen, normalizing challenges and facilitating an authentic dialogue about IP-related uncertainties. In this way, clinical supervisors can address common cognitive and affective challenges.
A compassionate supervisory environment promotes balanced self-reflection and can reduce the shame-based fear of exposure that drives impostor defenses. This may allow supervisees to explore their conceptual skills openly, reframe unrealistic expectations, and persist despite challenges (Hou & Skovholt, 2020; Stoltenberg & McNeill, 2010). Future research can investigate how self-compassion contributes to the supervisory relationship, comfort with disclosure, and the integration of constructive feedback during supervised practice.
Clinical supervisors can also create a culture of shared vulnerability by modeling self-compassion and transparency about their own developmental struggles and self-doubt. This enables supervisees to internalize feedback and approach self-evaluation with less emotional reactivity. Enhancing collaboration within the alliance empowers supervisees to feel more competent in navigating their development independently (Skovholt & Trotter-Mathison, 2024). Given the potential benefits of this approach, we recommend that future research examine how embodiment and facilitation of self-compassion affect counselor development and well-being.
Limitations
Although the results of this study are encouraging, there are limitations. The cross-sectional design limits the data to a single point in time rather than showing fluctuations in self-compassion, IP, resilience, and mental health over time. Likewise, the present results do not establish causality. Replicating this study using a longitudinal approach can provide greater insight into these fluctuations. Furthermore, self-report measures introduce limitations such as social desirability bias and reliance on participant self-awareness. Likewise, individuals with a personal connection to IP may have been more likely to participate, potentially skewing results.
Participants were not asked about their matriculation status as counseling students, leaving their stage of development unknown. Future research should include clinical experience (i.e., none, practicum, internship) and matriculation status. This information would provide greater insight into how experience and counselor development interact with IP. The current study used a general IP assessment, while future research should use the Counselor Impostor Scale (CIS; Nguyen, 2023), which was published after data collection for this study was complete. The CIS is designed specifically for the counseling domain and could provide more nuanced insights. Additionally, because maladaptive coping strategies such as procrastination and perfectionism sustain IP, subsequent studies should explore these constructs, which could inform more targeted interventions.
Conclusion
The growth process during counselor training is inherently challenging and often gives rise to IP, which increases anxiety and depression while diminishing resilience. Self-compassion is a promising method for enhancing resilience and well-being, despite the presence of IP. Once learned, self-compassion is an accessible practice and relies on applying skills with which counselors are familiar, such as kindness and compassion toward themselves. The results of this study are encouraging and robust, suggesting that self-compassion can enhance resilience by supporting adaptive emotional regulation and fostering a growth-oriented mindset. Self-compassionate counselors can maintain their well-being despite experiencing IP. Importantly, the positive impact of self-compassion was consistent and significant even at lower levels, which is especially important given the prevalence and severity of IP among CITs. The findings support integrating self-compassion into counselor training and clinical supervision through modeling, training, and practice. This approach can provide effective coping for IP and improve resilience, mental health, and persistence.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default- document-library/ethics/2014-aca-code-of-ethics.pdf
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). University of Pennsylvania Press.
Council for the Accreditation of Counseling and Related Educational Programs (2023). 2024 standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Clance, P. R. (1985). Clance Impostor Phenomenon Scale (CIPS). [Database record]. APA PsycTests. https://doi.org/10.1037/t11274-000
Clance, P., & Lawry, S. (2024). Impostor phenomenon: Origins and treatment. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 17–43). American Psychological Association.
Clark, P., Holden, C., Russell, M., & Downs, H. (2022). The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy, 44(2), 185–197. https://doi.org/10.1007/s10591-021-09580-y
Clarke, B. J. (2024). Emerging adult life satisfaction and mental health: The mediating role of self-compassion and social support. Emerging Adulthood, 12(6), 1137–1147. https://doi.org/10.1177/21676968241279490
Clarke, B. J., & Guida, A. M. (2025). Self-compassion to community: The mediating effect of belonging on college student mental health and life satisfaction. Journal of College Student Mental Health. Advance online publication. https://doi.org/10.1080/28367138.2025.2552484
Clarke, B. J., & Hartley, M. T. (2025). Contemplative dispositions and mental health: The supportive role of self-compassion and mindfulness on college students’ resilience. Journal of College Student Mental Health, 39(1), 142–164. https://doi.org/10.1080/28367138.2024.2331931
Clarke, B. J., Hartley, M. T., & Button, C. (2025). Impostor phenomenon and counselor development: The critical role of self-compassion. Journal of Counseling & Development, 103(2), 149–160. https://doi.org/10.1002/jcad.12544
Coaston, S. C. (2019). Cultivating self-compassion within the supervision relationship. The Clinical Supervisor, 38(1), 79–96. https://doi.org/10.1080/07325223.2018.1525596
Coaston, S. C., & Lawrence, C. (2019). Integrating self-compassion across the counselor education curriculum. Journal of Creativity in Mental Health, 14(3), 292–305. https://doi.org/10.1080/15401383.2019.1610536
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in developing professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Crego, A., Yela, J. R., Riesco-Matías, P., Gómez-Martínez, M. Á., & Vicente-Arruebarrena, A. (2022). The benefits of self-compassion in mental health professionals: A systematic review of empirical research. Psychology Research and Behavior Management, 15, 2599–2620. https://doi.org/10.2147/PRBM.S359382
DeCandia Vitoria, A. (2021). Experiential supervision: Healing impostor phenomenon from the inside out. The Clinical Supervisor, 40(2), 200–217. https://doi.org/10.1080/07325223.2020.1830215
Delaney, M. C. (2018). Caring for the caregivers: Evaluation of the effect of an eight-week pilot Mindful Self-Compassion (MSC) training program on nurses’ compassion fatigue and resilience. PLoS ONE, 13(11), e0207261. https://doi.org/10.1371/journal.pone.0207261
Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gadsby, S., & Hohwy, J. (2024). Negative performance evaluation in the impostor phenomenon. Current Psychology, 43, 9300–9308. https://doi.org/10.1007/s12144-023-05030-0
Garba, R., Coleman, C., & Kelley, T. (2024). The impostor phenomenon and mental health. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 61–79). American Psychological Association.
Gerber, Z., & Anaki, D. (2021). The role of self-compassion, concern for others, and basic psychological needs in the reduction of caregiving burnout. Mindfulness, 12, 741–750. https://doi.org/10.1007/s12671-020-01540-1
Germer, C., & Neff, K. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. Guilford.
Gignac, G. E., & Szodorai, E. T. (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. https://doi.org/10.1016/j.paid.2016.06.069
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford.
Hou, J.-M., & Skovholt, T. M. (2020). Characteristics of highly resilient therapists. Journal of Counseling Psychology, 67(3), 386–400. https://doi.org/10.1037/cou0000401
Housenecht, A., & Swank, J. (2022). Motivation, belonging, and support: Examining persistence in counseling programs. Teaching and Supervision in Counseling, 4(2), Article 3. https://doi.org/10.7290/tsc04g4iv
Khubchandani, J., Brey, R., Kotecki, J., Kleinfelder, J., & Anderson, J. (2016). The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Archives of Psychiatric Nursing, 30(4), 457–462. https://doi.org/10.1016/j.apnu.2016.01.014
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Liu, S., Wei, M., & Russell, D. (2023). Effects of a brief self-compassion intervention for college students with impostor phenomenon. Journal of Counseling Psychology, 70(6), 711–724. https://doi.org/10.1037/cou0000703
Luo, X., Che, X., & Lei, Y. (2023). Characterizing the effects of self-compassion interventions on anxiety: Meta-analytic evidence from randomized controlled studies. Journal of Contextual Behavioral Science, 30, 132–141. https://doi.org/10.1016/j.jcbs.2023.10.004
Mak, K. K. L., Kleitman, S., & Abbott, M. J. (2019). Impostor phenomenon measurement scales: A systematic review. Frontiers in Psychology, 10, 671. https://doi.org/10.3389/fpsyg.2019.00671
Martin, A. J., & Marsh, H. W. (2006). Academic resilience and its psychological and educational correlates: A construct validity approach. Psychology in the Schools, 43(3), 267–281. https://doi.org/10.1002/pits.20149
Neff, K. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2023). Self-compassion: Theory, method, research, and intervention. Annual Review of Psychology, 74, 193–218. https://doi.org/10.1146/annurev-psych-032420-031047
Neff, K. D., Hsieh, Y. P., & Dejitterat, K. (2005). Self-compassion, achievement goals, and coping with academic failure. Self and Identity, 4(3), 263–287. https://doi.org/10.1080/13576500444000317
Neff, K. D., Tóth-Király, I., Yarnell, L. M., Arimitsu, K., Castilho, P., Ghorbani, N., Guo, H. X., Hirsch, J. K., Hupfeld, J., Hutz, C. S., Kotsou, I., Lee, W. K., Montero-Marin, J., Sirois, F. M., de Souza, L. K., Svendsen, J. L., Wilkinson, R. B., & Mantzios, M. (2019). Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: Support for use of a total score and six subscale scores. Psychological Assessment, 31(1), 27–45. https://doi.org/10.1037/pas0000629
Nguyen, L. T. (2023). Development and validation of the Counseling Impostor Scale (Doctoral dissertation). Texas A&M University–Corpus Christi.
Ojeda, L. (2024). Impostor phenomenon and burnout. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 81–110). American Psychological Association.
Pákozdy, C., Askew, J., Dyer, J., Gately, P., Martin, L., Mavor, K. I., & Brown, G. R. (2023). The impostor phenomenon and its relationship with self-efficacy, perfectionism, and happiness in university students. Current Psychology, 43, 1–10. https://doi.org/10.1007/s12144-023-04672-4
Patzak, A., Kollmayer, M., & Schober, B. (2017). Buffering impostor feelings with kindness: The mediating role of self-compassion between gender-role orientation and the impostor phenomenon. Frontiers in Psychology, 8, Article 1289. https://doi.org/10.3389/fpsyg.2017.01289
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Roskowski, J. C. R. (2010). Impostor phenomenon and counseling self-efficacy: The impact of impostor feelings (Doctoral dissertation). Ball State University.
Skovholt, T. M., & Trotter-Mathison, M. (2024). The elevated stressors of the novice practitioner. In T. M. Skovholt & M. Trotter-Mathison (Eds.), The resilient practitioner: Burnout and compassion fatigue prevention and self-care strategies for the helping professions (4th ed., pp. 42–68). Taylor & Francis.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Thériault, A., Gazzola, N., & Richardson, B. (2009). Feelings of incompetence in developing therapists: Consequences, coping, and correctives. Canadian Journal of Counselling, 43(2), 105–119.
Tigranyan, S., Byington, D. R., Liupakorn, D., Hicks, A., Mathis, M., & Rodolfa, E. (2021). Factors related to the impostor phenomenon in psychology doctoral students. Training and Education in Professional Psychology, 15(4), 298–305. https://doi.org/10.1037/tep0000321
Wang, B., Andrews, W., Bechtoldt, M. N., Rohrmann, S., & de Vries, R. E. (2022). Validation of the short Clance Impostor Phenomenon Scale (CIPS-10). European Journal of Psychological Assessment, 40(2), 158–168. https://doi.org/10.1027/1015-5759/a000747
Warren, R., Smeets, E., & Neff, K. (2016). Self-criticism and self-compassion: Risk and resilience. Current Psychiatry, 15(12), 18–33. https://self-compassion.org/wp-content/uploads/2016/12/Self-Criticism.pdf
Webb, R. E., & Rosenbaum, P. (2019). Resilience and thinking perpendicularly: A meditation or morning jog. Journal of College Student Psychotherapy, 33(1), 75–88. https://doi.org/10.1080/87568225.2018.1449687
Brian J. Clarke, PhD, NCC, LAC, is an assistant professor at the University of Arizona. Michael T. Hartley, PhD, CRC, is a professor at the University of Arizona. Austin M. Guida, PhD, NCC, LAC, is an assistant professor at Northern Arizona University. Correspondence may be addressed to Brian J. Clarke, Department of Disability and Psychoeducational Studies, College of Education, 1430 E. 2nd Street, Room 422, Tucson, AZ, 85721-0069, bclarke14@arizona.edu.
Jul 25, 2025 | Volume 15 - Issue 2
Kelly Emelianchik-Key, Adriana C. Labarta, Clara Bossie, Carman S. Gill
Self-compassion, or the ability to show oneself kindness in challenging situations, has various advantages for mental well-being and psychological health, encompassing three interrelated elements: self-kindness, common humanity, and mindfulness. Mothers are an often-overlooked population who face numerous mental health challenges because of socially constructed ideals of motherhood. Therefore, mothers may encounter obstacles in developing self-compassion amid the demands of motherhood, related societal pressures, and other contextual factors, such as the COVID-19 pandemic. This research study utilized a photovoice methodology to investigate how mothers with children ages 5 to 12 experience self-compassion post–COVID-19 pandemic. The findings revealed four main themes with 13 subthemes, illustrating the distinct challenges and benefits associated with self-compassion for mothers. The authors conclude with implications for counseling, including the need for interventions that promote self-compassion and wellness for mothers from culturally and racially diverse communities.
Keywords: mothers, motherhood, self-compassion, photovoice, wellness
Intensive mothering, a term coined by Hays (1996), refers to the socially constructed expectation of motherhood that a mother must meet unrealistic standards to be deemed a good mother. Although societal roles have evolved over the past 30 years, with many mothers working full-time, the unrealistic ideal of motherhood has remained unchanged (Chae, 2014; Forbes et al., 2020; Lamar et al., 2019; Prikhidko & Swank, 2018). Intensive mothering demands that mothers be the central, self-sacrificing caregivers who devote extensive time, energy, and resources to their children’s needs (Hays, 1996). Forbes et al. (2021) asserted that the fact that “the expectations of mothers remain primarily unchanged despite advances made in gender equality in the U.S. as a result of feminist critiques suggests the expectations of mothers are deeply engrained in the fabric of society” (p. 271).
Research indicates that mothers from diverse backgrounds (e.g., race, ethnicity, social class, job status) endorse unrealistic beliefs about intensive mothering (Forbes et al., 2020), though cultural ideals, lack of resources, and structural barriers could impact the extent to which diverse communities endorse intensive mothering (Lankes, 2022). Living up to intensive mothering standards causes mothers to put children (and often the whole family) before their own mental and physical health (Elliot et al., 2015). Mothers who cannot live up to this ideal often face physical and mental health consequences, such as exhaustion, overwhelming anxiety, feelings of isolation and inadequacy, identity challenges and loss of self, self-criticism, and shame and guilt (Forbes et al., 2021; Prikhidko & Swank, 2018). They are also more likely to experience depression, anxiety, and decreased life satisfaction (Forbes et al., 2020; Prikhidko & Swank, 2018).
These pressures may lead mothers to engage in counseling to seek support, build realistic expectations, develop coping skills, and create a working family system that relies on more than one person to meet the needs of a child. Wellness, a cornerstone for effective counseling practice, focuses on the optimal health and well-being of the mind, body, and spirit, allowing individuals to live life more fully (Myers & Sweeney, 2004; Neff & Germer, 2013). Relatedly, maternal health strategies help support the physical, emotional, and mental health of mothers (Mitchell et al., 2018). Research suggests that mothers may benefit from focusing less on developing coping skills and more on developing maternal wellness strategies, such as having a plan and asking for help, which can impact the overall family system and functioning (Currie, 2018). The body of research on maternal wellness promotion in the counseling literature is not extensive, and there is a notable gap in empirical studies investigating how mothers’ well-being has been affected in the aftermath of the COVID-19 pandemic.
Dual Roles of Motherhood Post-Pandemic
The COVID-19 outbreak was declared a pandemic in early March 2020. In late 2021, the World Health Organization (WHO) reported approximately 4.5 million deaths, with over 650,000 deaths in the United States alone (WHO, 2021). The COVID-19 pandemic’s impact ranged from being a manageable inconvenience for some to causing severe loss of lives and livelihoods for others, cutting across class, ethnic, and national boundaries (Park, 2021). As the COVID-19 pandemic became an inevitable daily reality, it increasingly highlighted pre-existing social disparities, including limited access to health care and education, which disproportionately affect marginalized communities. This was evident in the higher rates of cases, hospitalizations, and deaths among these groups (Centers for Disease Control and Prevention [CDC], 2020).
In a society already emphasizing intensive mothering, COVID-19 worsened gender inequalities, forcing women to take on additional home and childcare responsibilities, including homeschooling. More women left jobs because of these role changes (Alon et al., 2020; Bureau of Labor Statistics, 2021) and experienced higher rates of exhaustion, anxiety, and depression (Davenport et al., 2020; Grose, 2021). According to Grose’s (2021) article in The New York Times, 69% of mothers reported adverse health effects from COVID-19 pandemic–related stress, compared to 51% of fathers. The pandemic also intensified job disparities, with women facing more job losses and slower recovery than men, pre– and post–COVID-19 pandemic (Lofton et al., 2021). In dual-income households, mothers assumed greater childcare responsibilities than fathers, a trend that persisted throughout the COVID-19 pandemic (Zamarro et al., 2020). Hupkau and Petrongolo (2020) predicted that an unequal division of labor will perpetuate inequalities in parental roles. Although remote work allows women to balance work and family, it can dilute their workplace presence and negatively impact their careers. Increased domestic labor has led to worsening emotional and financial health for U.S. mothers (Bahn et al., 2020; Ruppanner et al., 2021). Therefore, addressing the intersection of motherhood and mental health is crucial for effectively addressing the post–COVID-19 pandemic impact.
Self-Compassion and Motherhood
Given the prevalent challenges that mothers faced before, during, and after the COVID-19 pandemic, counselors need evidence-based approaches to promote wellness in community and clinical settings. Self-compassion comprises three dichotomous yet related components: mindfulness versus overidentification, common humanity versus isolation, and self-kindness versus self-judgment (Neff & Germer, 2013). Mindfulness is an evidence-based approach that entails nonjudgment and accepting one’s experiences rather than overidentifying or suppressing emotions (Neff, 2011). Common humanity describes the interconnectedness of the human experience and allows individuals to recognize pain and failure as universal struggles. Finally, self-kindness requires treating oneself with kindness, support, and understanding rather than engaging in self-criticism in response to life’s challenges (Neff, 2011).
Research has consistently linked lower levels of self-compassion with a range of mental health issues, including depression and anxiety (Han & Kim, 2023; Neff, 2011). As such, self-compassion may represent a powerful wellness construct because of its effectiveness in treating mental health concerns like anxiety, depression, stress, eating concerns, rumination, and self-criticism (Ferrari et al., 2019). Self-compassion may also represent an effective coping mechanism for mothers experiencing post-traumatic stress symptoms after childbirth (Mitchell et al., 2018), postpartum depression (Fonseca & Canavarro, 2018), and insecure attachment and parenting stress (Moreira et al., 2015; Neff, 2011). Furthermore, self-compassion may help mothers increase mental health, mindful parenting (Moreira et al., 2015; Neff, 2011), and the “ability to respond to the challenges of parenting in ways that are more sensitive and resilient” (Psychogiou et al., 2016, p. 897). Beyond individual benefits, emerging research has considered the intergenerational impacts of self-compassion (Carbonneau et al., 2020; Lathren et al., 2020). Mothers with greater self-compassion may better tolerate difficult emotions through kindness and nonjudgment, thereby better supporting their children in navigating distressing emotional experiences (Lathren et al., 2020).
Present Study
Because of the potential for new roles, increased responsibilities, and decreased support during and post–COVID-19 pandemic, mothers are at greater risk for mental health concerns (Bahn et al., 2020; Ruppanner et al., 2021). We believe that self-compassion is a promising tool for wellness-based counseling with mothers. Although the previous examples presented in our literature review reflected a few benefits of this practice, we sought to further explore the role and impact of self-compassion in mothers’ lives post–COVID-19 pandemic. In this study, we utilized photovoice, a method within community-based participatory research (CBPR) that draws on feminist theory, in order to better understand, empower, raise consciousness, create dialogue, and produce social change on behalf of mothers struggling with mental health and wellness post–COVID-19 pandemic (Wang, 1999; Wang & Burris, 1997).
Method
Grounded in feminism, critical pedagogy, and photography (Wang & Burris, 1997), photovoice is one of several qualitative research methods in CBPR that allows individuals to express their beliefs about community and social issues using photos and personal descriptions. This robust methodology promotes social action, diversity, and advocacy within communities (Smith et al., 2010; Wang & Burris, 1997). Photovoice assumes that participants are the experts in their own lives, with the research process involving three unique components: (a) facilitating a partnership within the community, developing a research question, and training; (b) reflecting on the images, adhering to critical pedagogy while using a structured analytical framework consisting of five questions, called SHOWeD, to guide the analysis and promote meaningful change; and (c) disseminating the findings within the community (Wang & Burris, 1997).
In counseling, photovoice has the power to promote critical ideologies and reflective dialogue that allows for the constructivist creation of meaning around a social construct, promoting social justice and advocacy within the community (Sackett & Jenkins, 2015; Wester et al., 2021). Additionally, research demonstrates that photovoice fosters team building, social skills, self-efficacy, social connectedness, friendship, empowerment, and a sense of community (Wang & Burris, 1997; Wilson et al., 2007). Scholars in the counseling profession have called for the use of photovoice to promote community and advocacy and investigate interventions for issues that inhibit client growth (Sackett & Jenkins, 2015). Because of this call, the strong ties to critical pedagogy, and the underpinnings of feminist theory, we used a photovoice methodology to explore the following research question: How do mothers in our community understand, experience, and enact self-compassion in their daily lives in a post–COVID-19 pandemic world?
Participants
For the present study, the inclusion criteria indicated that participants must (a) be 18 years of age or older, (b) have no history of a personality disorder diagnosis and no severe symptoms of mental illness (e.g., suicidal ideation or psychosis), and (c) have at least one child in the home between the ages of 5 and 12. The rationale for selecting this age range was based on neurological data demonstrating differences in brain development for children over 5 (van der Kolk, 2014) and in Erikson’s psychosocial stages of development that document differences in individuals over 12 (Orenstein & Lewis, 2021). Our target sample size was eight to 12 participants, which was determined based on the standard for photovoice methodology (Wang & Burris, 1997), but additionally, the goal was to capture the depth and breadth of each individual analysis.
After excluding participants who did not complete the study or follow the study guidelines, the final sample consisted of eight women aged 30 to 42 (M = 37.25). Seven participants self-identified as White/Caucasian; one identified as Asian and White/Caucasian. All eight participants indicated that they were married. Participants were asked about their employment status and were given the option to select all applicable options. Five participants selected part-time employment, three marked stay-at-home parent, one indicated being employed full-time, and one indicated being self-employed. Regarding education level, four participants reported earning a bachelor’s degree or higher, two reported completing some college, one reported completing trade school, and one declined to respond. Lastly, concerning mental health concerns, two participants reported struggling with anxiety and depression, one reported struggling with attention-deficit hyperactivity disorder symptoms, three declined to respond, and two denied any mental health concerns.
Procedure
After receiving IRB approval, we collaborated with two local community mental health agencies, including one nonprofit agency and one for-profit agency. These community-based mental health agencies allowed us to advertise and recruit mothers who met the criteria and demonstrated interest in this research. We shared electronic flyers via social media with the study information, including the design, purpose, and participant expectations (i.e., taking photos and discussing the meaning behind them in focus groups). We also provided a small allotment to compensate for participants’ costs, such as internet or cell phone data use. The for-profit agency also offered free self-compassion books to all participants who completed the study. Participants could receive this resource by providing their email addresses after their final interview.
After completing an informed consent form, each participant participated in a 45–60-minute psychoeducational focus group led by one or more members of our research team, where they learned the basic components of self-compassion (i.e., self-kindness, common humanity, and mindfulness) and engaged in discussions about self-compassion with other group members. These psychoeducational groups consisted of two to four participants because of the scheduling needs of participants. Our overarching research question for the study was shared and we engaged in dialogue about changes experienced because of the COVID-19 pandemic. At the end of the session, we provided participants with information about taking photos, directions, and information to assist in maintaining confidentiality (e.g., avoid taking photos of self or others to protect confidentiality). The participants had 10 days to take or select photos to visually describe self-compassion in their own lives. Following, each participant was asked to caption them with a title, respond to the SHOWeD questions, which are unique to the methodology, and send them to us via email. The SHOWeD questions consisted of the following: 1) What do you see in the photo? 2) What is happening in your photograph? 3) How does this photo capture self-compassion in your own life? 4) Why does this photo contribute to the challenge, concern, or strengths that exist in self-compassion? and 5) What can mental health professionals or others do to help foster and support self-compassion in mothers? (Wang & Burris, 1997).
Each participant completed a follow-up photovoice session in which we placed participants’ top two selected photos on a slideshow with their corresponding captions. We followed outlined guidelines for the second photovoice session (Wang & Burris, 1997; Wester et al., 2021) while focusing on the two photos each participant selected, which were used to establish themes. Most of the second photovoice sessions were held individually to give mothers more scheduling flexibility and prevent further attrition. Although these in-depth, semi-structured interviews were individual, participants were encouraged to engage in dialogue with our research team regarding other participants’ photos and captions in order to create shared meaning. Once the meeting ended, we transcribed the entire discussion while focusing on the participants’ meaning of the photos.
Data Analysis
This study used photovoice, a methodology within CBPR (Wang, 1999; Wang & Burris, 1997), and interpretative phenomenological analysis (IPA) to explore participants’ experiences within interview transcripts and photographs (Burton et al., 2017; Griffin & May, 2012). The study emphasized collaboration between researchers and community members throughout the research process, from defining research questions to disseminating findings. This approach ensured the research was relevant to and beneficial for the community it aimed to serve. The feminist framework underpinned the entire process, influencing the focus on gender issues and power dynamics, emphasizing participants’ voices and lived experiences, and promoting social change and empowerment (Wang, 1999). IPA was utilized as the primary analytical approach, aligning with the study’s aim to explore how participants make sense of their experiences (Burton et al., 2017). Participants were viewed as experts in their own experiences, and the analysis focused on understanding their perspectives.
Following the IPA procedures of Griffin and May (2012), the analysis began with thorough familiarization with the data, followed by initial coding, developing emergent themes, searching for connections, and looking for patterns across cases. Recurring patterns and key concepts were identified in each transcript, photo, and responses to the SHOWeD questions. Relationships between themes found in the written dialogue and patterns in photos were extracted, always keeping in mind the true meaning expressed by the participants. We engaged in a double hermeneutic process, interpreting the participants’ interpretations of their experiences. Interpretive themes were developed to analyze deeper meaning. All four of us met weekly during the coding process to discuss each step and reach a consensus before moving on to each next step (Larkin & Thompson, 2011).
Role of the Researcher and Trustworthiness
Trustworthiness is critical in qualitative research. To promote transparency as the research team, we identified our backgrounds and identities, which could impact the study (Creswell, 2020). Our team consisted of four members: three coders and one auditor. Kelly Emelianchik-Key (associate professor), Adriana C. Labarta (assistant professor), and Carman S. Gill (full professor) served as coders and were all counselor educators at Florida Atlantic University during the research process. They are each licensed mental health counselors, National Certified Counselors, and Approved Clinical Supervisors; Emelianchik-Key is also a licensed marriage and family therapist. Emelianchik-Key and Gill identify as White females and Labarta identifies as Latina. Emelianchik-Key also identifies as a mother, which was a critical piece of the study and important to consider to prevent bias. The auditor, Clara Bossie, is a White female and a counselor education doctoral student at Florida Atlantic University; she is a licensed marriage and family therapist with specialized training in dialectical behavioral therapy and as a Mindful Self-Compassion (MSC) teacher. She is also the owner and clinical director of a private practice.
Emelianchik-Key, Labarta, and Gill have extensive experience in qualitative research and coded the data, while Bossie served as an external auditor because of her specialized MSC training in order to provide additional perspectives and feedback, enhancing trustworthiness (Creswell & Báez, 2020). As a team, we discussed biases and assumptions throughout the research and data analysis process, maintaining an audit trail. Peer validation was used to promote trustworthiness (Larkin & Thompson, 2011) while noting intersectionality and privilege within the team. Member checking was conducted after developing the final themes, with participants providing feedback. No objections were raised, and two of the participants responded noting they agreed with the results.
Results
The findings that emerged from the discussion of the SHOWeD questions, participant photos, and corresponding captions included four overarching themes with 13 subthemes. Theme 1, Challenges With Self-Compassion, included subthemes Permission and Justification, Making Time, Self-Worth, and Understanding Self-Compassion. Theme 2, Isolation Versus Common Humanity, included subthemes Social Media, Desire for Connection, and Self-Criticism. Theme 3, Awareness and Education, included the subthemes Self-Awareness, Acknowledgment From Self and Others, and Psychoeducation. Theme 4, Mindfulness, included subthemes Open Awareness, One-Pointed Awareness, and Tactile Experiences.
Theme 1: Challenges With Self-Compassion
The initial theme revolved around mothers’ obstacles and difficulties with integrating self-compassion into their daily lives. These challenges encompassed permission giving, allocating time, grappling with feelings of self-worth, and distinguishing between self-compassion and self-care. The subtheme of Permission and Justification encompassed the hurdles mothers encounter when attempting to incorporate self-compassion into their lives. A common rationale for practicing self-compassion was the significant impact it may have on their children and families. Mothers expressed challenges with practicing self-compassion “just because” and sought justifications for their practice. The second subtheme of Making Time underscored the challenge of making time for self-compassion amid juggling various roles and responsibilities as a mother. Moreover, this subtheme emerged during our study because of the difficulty in finding mothers to participate amidst their many demands. Rather than making time for themselves, mothers described examples of wedging acts of self-compassion into everyday activities, such as morning coffee and reflective moments in the car during Little League practice.
The third subtheme of Self-Worth underscored mothers’ difficulties in recognizing their value, particularly as they navigate societal and familial expectations of the “perfect” mother. Participants expressed sentiments of needing to validate or “prove” their worthiness. The last subtheme of Understanding Self-Compassion shed light on the difficulty of discerning between self-care and self-compassion. Participants frequently equated self-care activities with self-compassion, failing to distinguish between them and often neglecting their needs. The self-compassion practices described by participants were not entirely directed toward their well-being, as evidenced by self-care activities and compassion practices that primarily sought to extend warmth and kindness to others rather than focusing on themselves. Examples from these subthemes are in Table 1.
Table 1
Participant Quotes Related to Subthemes of Theme 1: Challenges With Self-Compassion
| Subthemes |
Participant Quote |
| Permission and Justification |
Participant 3: “It’s been really important for me to find time for myself to do things that I want to do. But then I feel like sometimes, as a mom, you feel like everything revolves around your family, and then, when you take time away from that, it’s like you’re being selfish.” |
| Making Time |
Participant 2: “It’s hard to remember sometimes when you’re on autopilot. Yeah, or things happen like one after another, and then you don’t have that awareness right away sometimes.” |
| Self-Worth |
Participant 3: “I feel like I’m always trying to prove that what I do is important. And it’s not only proving that to other people, but I need to feel it myself.” |
| Understanding Self-Compassion |
Participant 1: “I think even like understanding self-compassion can be kind of strange, because nowadays it’s self-care. Everyone calls it ‛self-care.’ It seems like just everyone is getting their nails done or paying for expensive facials, or whatever, because it’s self-care. I think that’s kind of more of like a superficial thing, where self-compassion is more internal . . . you have to like, you know, be self-aware to know how to be self-compassionate.” |
Theme 2: Isolation Versus Common Humanity
The second theme highlighted one of the central components of the self-compassion model: Isolation Versus Common Humanity (Germer & Neff, 2019; Neff & Germer, 2013). This theme showcased the contrast between participants’ longing for connection while engaging in behaviors that fostered disconnection. The first subtheme was Social Media, including its positive and negative impacts. A significant aspect was the experience of social comparisons, which either provided participants with understanding and validation or left them feeling isolated and separate from others, resulting in self-criticism. Social media had both helpful and harmful influences on participants’ well-being.
The second subtheme of Desire for Connection reflected participants’ deep longing to connect with others and to feel heard, valued, and acknowledged for their efforts. This is especially true when navigating parenting challenges to avoid feelings of isolation. The last subtheme was Self-Criticism. Self-criticism captured instances in which mothers engaged in or exhibited self-critical language. Participants frequently engaged in cognitive distortions such as overgeneralizing, ruminating on “should haves,” and making self-judgments. This tendency toward self-criticism often led to narratives and expressions of isolation or feeling excluded from a group or family. Participant quotes for each of these subthemes are found in Table 2.
Table 2
Participant Quotes Related to Subthemes of Theme 2: Isolation Versus Common Humanity
| Subthemes |
Participant Quote |
| Social Media |
Participant 2: “I think the reason self-compassion isn’t as popular is because a lot of the mainstream help we easily come across makes a profit on people feeling like they’re not good enough. Self-compassion doesn’t count on people needing to take a big action to make a change in their lives.” |
| Desire for Connection |
Participant 5: “The overall experience was good. . . . It’s always nice to hear that you’re not the only person juggling a thousand things and trying to make sense of it.” |
| Self-Criticism |
Participant 6: “Sometimes we all feel like we’re alone in the things that we’re doing and the things that we’re dealing with because we can’t feel like we can talk about it cause then we’re a failure. And that’s like one of the biggest things for moms.” |
Theme 3: Awareness and Education
The third theme encapsulated participants’ journey toward cultivating heightened self-awareness regarding the importance of self-compassion, alongside a plea for counselors to provide enhanced education and incorporate strengths-based, empowering approaches for mothers. The first subtheme of Self-Awareness involved participants recognizing the significance of self-compassion and their ability to prioritize time for engaging in self-compassion and self-care. Participants acknowledged that seeking help is permissible and that the shaming associated with being unable to manage everything should not occur. The second subtheme of Acknowledgment From Self and Others centered around the desire to be recognized and valued for their many roles as mothers, spouses, breadwinners, etc., while embracing self-kindness and self-validation. The last subtheme of Psychoeducation emerged as participants emphasized the necessity for greater awareness and understanding of self-compassion and its relevance in daily life. Specifically, they stressed the importance of making this knowledge more accessible for mothers and the need for others to be educated about the challenges mothers face. Example quotes from these subthemes are in Table 3.
Theme 4: Mindfulness
The fourth theme explored the various methods by which participants incorporated mindfulness activities as part of their practice of self-compassion. The first subtheme, Open Awareness, addressed the specific ways participants engaged in mindfulness activities that allowed them to become more aware of the entire environment. Some participants participated in mindfulness activities that heightened their awareness of their surroundings, although this engagement focused more on relationship mindfulness than self-compassion. The second subtheme of One-Pointed Awareness described participants’ mindfulness practices with focused awareness, concentrating solely on one aspect of the present moment. They fully immersed themselves in the mindfulness practice, recognizing it as a means of personal growth. The last subtheme of Tactile Experiences illustrated participants’ self-soothing or grounding practices involving multiple senses, particularly touch, sensation, smell, and profound observation. These practices typically occurred in the morning and often included enjoying coffee, gardening, or immersing oneself in nature. A sample quote from each subtheme is in Table 4.
Table 3
Participant Quotes Related to Subthemes of Theme 3: Awareness and Education
| Subthemes |
Participant Quote |
| Self-Awareness
|
Participant 7: “We’d taken a picture of my daughter’s little emotion dolls, or like some animals . . . I’m like, ‛well, that’s perfect.’ Because you know, we all have these emotions. . . . So that really stood out to me, because that’s something that I’ve really learned becoming a parent and a mom . . . we are going to have these emotions. It’s okay to have emotions and that’s something I’ve been, you know, trying to teach my kids to a lot of the time . . . that was a big self-compassion thing that stood out to me was, you know, letting myself feel like, you know, anger or frustration, or all the other ones that were lined up in that picture.” |
Acknowledgment From
Self and Others |
Participant 3: “I think, that just hearing like, ‛Hey, I see you. I see that you’re working hard, and you’re doing great,’ you know. So I think that that’s what moms need to hear.” |
| Psychoeducation |
Participant 8: “Just educating mothers more on like the postpartum journey and normalizing, you know, postpartum depression and postpartum anxiety. . . . I don’t necessarily feel like I was properly educated while I was pregnant, and then postpartum on, you know, how much you, your hormones and everything, it affects you mentally, especially in this world with social media. And you know, everyone’s perfect. And you know, everyone wakes up the next day after, you know, not sleeping with a newborn all night and being exhausted. And you’re supposed to look perfect and act perfect. And you know, I just wish there was more acceptance and kind of education and normalizing the raw journey of postpartum.” |
Table 4
Participant Quotes Related to Subthemes of Theme 4: Mindfulness
| Subthemes |
Participant Quote |
| Open Awareness |
Participant 8: “I do struggle a lot with my body image as a woman. And just, you know, after you have children and your body changes. So, for me, this photo is also really powerful in that aspect, because I’ve been doing a lot of work with that as well as just not being as hard on myself. And you know, normally, I would be like super uncomfortable at the beach, and especially because it was like a packed day. It was Mother’s Day, wearing a bathing suit, and I just didn’t give a shit, and it was really cool. And I just, I think, because I was just so immersed with my family and being present.” |
| One-Pointed Awareness |
Participant 2: “Just paying attention to your body. And if I feel I’m breathing a little shallow, sometimes I notice I’m holding my breath, and sometimes I notice that my shoulders are up here, and that’s usually my little sign to like, okay . . . this doesn’t feel good. Let’s fix this for a minute. Do something.” |
| Tactile Experiences |
Participant 4: “We just moved into this house 6 months ago, and I love flowers. And you know, I missed my old house with like my garden, so I had to start over. . . . That’s like my thing. I literally go out there and do that every single morning. I mean, sometimes it’s 3 minutes, sometimes it’s 15 minutes, but mainly it’s 5 minutes. But that’s where I was like, yeah, that’s my time. You know, where I don’t bring the phone out there with me.” |
Data Presentation to Stakeholders
Consistent with CBPR goals and photovoice procedures (Wang & Burris, 1997; Wester et al., 2021), we sought to promote change and advocate for mothers by sharing our findings with stakeholders. The stakeholders included the nonprofit community-based agency and private practice that helped recruit participants, and a group of local counselors affiliated with a large community agency who could further increase awareness, co-create meaning, and facilitate change. The study participants were invited to join our meeting with stakeholders who participated in a presentation of the findings, including PowerPoint slides illustrating the primary themes and participant photos. The last question of the SHOWeD method was especially considered: “What can mental health professionals or others do to help foster and support self-compassion in mothers?” We engaged in a collaborative dialogue on implementing the study’s findings into practice, which are further elaborated in the discussion section of this manuscript.
Discussion
Mothers, often serving as the backbone of their families, face silent battles with mental health and identity, heightened by sociocultural ideals and other contextual factors like the recent COVID-19 pandemic’s isolating conditions (Chae, 2014; Davenport et al., 2020; Grose, 2021; Neff, 2011; Prikhidko & Swank, 2018). Mothers’ quiet struggles illuminate an alarming need for more mental health support tailored to the unique experiences of motherhood. Our study explored mothers’ experiences post–COVID-19 pandemic with cultivating self-compassion using photovoice, revealing four overarching themes: (a) Challenges With Self-Compassion, (b) Isolation Versus Common Humanity, (c) Awareness and Education, and (d) Mindfulness.
The first theme suggests that mothers’ challenges with self-compassion are deeply entangled in the daily realities of motherhood and exacerbated by societal ideals. These difficulties extend beyond finding time (which was extremely limited) for self-care; instead, they reflect more profound issues of how mothers perceive and treat themselves amid overwhelming external expectations, often compromising their well-being and prioritizing their children and families (Forbes et al., 2021; Lamar et al., 2019). Feminist theory recognizes how gendered expectations of motherhood create structural time poverty, but the lack of self-compassionate practices calls attention to the systemic issues about women’s unpaid labor and societal expectations. The subtheme of Permission and Justification manifested itself through the notion of self-compassion to “model it” for their children rather than themselves, which aligns with previous research (Lathren et al., 2020). A complex interplay of self-neglect and societal pressures led mothers to conflate the concept of self-care with self-compassion. Consequently, mothers frequently and erroneously equate self-care activities with self-compassion. This misunderstanding underscores the need for psychoeducation on self-compassion in counseling. Although self-care is essential to address one’s immediate needs, self-compassion embodies a more profound, forgiving, and accepting approach to our limitations and failures (Neff, 2011).
The second theme, Isolation Versus Common Humanity, highlights one of the primary components of the self-compassion model (Germer & Neff, 2019; Neff & Germer, 2013) and extends prior research on the impact of social comparison and media on mothers (Chae, 2014; Prikhidko & Swank, 2018). Participants described a dichotomy between the desire to connect with others while grappling with social comparison, thus leading to feelings of inadequacy and isolation. Participants acknowledged the benefits of social media (e.g., accessibility) while simultaneously struggling with the overwhelmingly “positive” and “happy” images in contrast to content addressing the challenges of motherhood. Mothers sought authentic, meaningful connections beyond social media and surface-level interactions. This finding underscores the need for counselors to foster nonjudgmental and compassionate spaces for mothers to connect on their shared experiences and struggles. Additionally, intentional engagement in mindfulness is critical for feelings of isolation that stem from social media usage. This approach can encourage mothers to become more aware of the images they engage with and facilitate the positive benefits of social media. Feminist frameworks emphasize the importance of recognizing personal struggles as connected to broader social patterns, so difficulties connecting with common humanity may also reflect the individualistic messaging mothers receive about “doing it all.”
Awareness and Education, the third theme of our study, was at the forefront of our interviews with participants. Mothers expressed excitement about the construct of self-compassion, leading to critical discussions on the need for more psychoeducation on this practice. Given the abundant research that supports self-compassion as a means of developing mental health and wellness (Ferrari et al., 2019; Fonseca & Canavarro, 2018; Lathren et al., 2020; Mitchell et al., 2018; Moreira et al., 2015), greater access to treatment and resources is crucial to mitigate mothers’ challenges to practicing self-compassion, particularly at the community level. For instance, counselors can use social media platforms to provide psychoeducation on self-compassion, share helpful resources, and foster supportive communities that challenge the “illusion of perfection” (Neff, 2011, p. 70).
The fourth theme underscores how Mindfulness and Self-Compassion are inextricably linked (Neff, 2011; Neff & Germer, 2013). Regardless of how mothers practiced mindfulness (e.g., Open Awareness, One-Pointed Awareness, or Tactile Experiences), it allows them to connect more deeply with their experiences by accepting difficult emotions, becoming more aware of their environment, or engaging the senses. However, it is essential to note that mindfulness and self-compassion do not automatically co-occur. Neff and Dahm (2015) indicated:
It is possible to be mindfully aware of painful thoughts and feelings without actively soothing and comforting oneself or remembering that these feelings are part of the shared human experience. Sometimes it takes an extra intentional effort to be compassionate toward our own suffering, especially when our painful thoughts and emotions involve self-judgments and feelings of inadequacy. (p. 130)
Neff and Dahm’s assertion highlights that while mindfulness fosters awareness, self-compassion requires additional intentionality, particularly in the face of self-judgment. Building on this, counselors play a vital role in educating mothers on the all-encompassing practice of self-compassion, which goes beyond mindful awareness to include self-kindness and a recognition of common humanity. This is especially important in addressing societal and cultural expectations that are contrary to “slowing down,” being kind to oneself, and recognizing one’s connection with others.
Implications for Counselors
The findings of this study illuminate the need for a multifaceted approach to helping mothers cultivate self-compassion and wellness. Although most participants’ narratives did not explicitly address self-compassion practices and connection to the COVID-19 pandemic, counselors should carefully consider how the additional responsibilities and stressors that emerged during this period may have become normalized and integrated into mothers’ daily lives. The minimal direct pandemic references in participants’ responses may be telling, suggesting that what began as temporary adaptations to crisis have potentially evolved into enduring expectations and workload increases for mothers. This has important implications for how counselors conceptualize and address maternal stress, role strain, and work–life integration in their practice.
Counselors must establish trust, safety, and rapport with mothers to discuss challenging topics such as self-doubt, isolation, and self-worth. Counselors can demonstrate the differences between self-compassion and self-care. For example, although self-care may help to temporarily disconnect after a difficult day (e.g., watching an entertaining television series), self-compassion encourages mothers to become curious about their inner emotional experiences (mindfulness), utilize sources of support (common humanity), and respond to uncomfortable emotions with acceptance and warmth (self-kindness). Counselors may consider various approaches to integrating self-compassion into their work and communities, from offering courses as an MSC-trained teacher (Germer & Neff, 2019) to utilizing The Mindful Self Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive (Neff & Germer, 2018) and online resources available through the Center for Mindful Self-Compassion. MSC integrates the practice of mindfulness with the nurturing qualities of self-compassion, creating a potent approach for cultivating emotional resilience. MSC combines mindfulness with nurturing self-compassion to build emotional resilience, improving overall physical wellness while reducing anxiety, depression, and burnout (Germer & Neff, 2019), making it especially valuable for mothers with limited mental health access.
Therapeutic modalities that explore underlying factors contributing to mothers’ reluctance or hesitation to engage in self-compassion practices, such as past experiences, societal expectations, or cultural influences, may increase the effectiveness of programs like MSC. Our participants indicated deeply ingrained negative beliefs about themselves, which can hinder their ability to practice self-compassion. Counselors can help mothers identify and challenge these beliefs, encouraging them to develop more compassionate and realistic self-perceptions through insight-oriented practices, such as Socratic questioning, motivational interviewing, and self-reflective practices.
Though MSC offers therapeutic benefits, it’s not therapy itself. Unlike our study participants who were prepared for vulnerability, counselors must recognize that mothers come with varying needs. Germer and Neff (2019) emphasized that effective MSC delivery depends on a client’s tolerance zone, which includes being in a safe, challenged, or overwhelmed state, with optimal learning occurring in safe or challenged states where clients can progress through acceptance stages while maintaining emotional regulation. Opening oneself to self-compassion may lead to “backdraft,” when individuals encounter previously suppressed painful emotions (Germer & Neff, 2019). Although most mothers can embrace self-compassion practices immediately, some in clinical populations may need deeper therapeutic work as preparation (Neff & Germer, 2018). In addition to the challenges and pressures of motherhood, mothers may arrive with various co-occurring issues such as grief, mental health concerns, complex trauma, or other shame-invoking experiences lying just below the surface (Neff, 2011). It is important that counselors are prepared to utilize evidence-based treatment approaches to help mothers fully access self-compassion practices and handle potential backdrafts.
Theoretical Integration
Integrating a self-compassion–informed approach into counseling is greatly enhanced by drawing from evidence-based approaches that align with the construct of self-compassion, such as acceptance and commitment therapy (ACT), compassion-focused therapy (CFT), mindfulness-based cognitive therapy (MBCT), dialectical behavior therapy (DBT), and Adlerian theory. These therapeutic models support the development of self-compassion, a key aspect of MSC, by promoting emotional resilience, self-awareness, and adaptive coping mechanisms. Gilbert (2014) developed CFT to explicitly target
self-criticism and shame while promoting the cultivation of self-compassion through exercises designed to enhance compassionate self-awareness. CFT provides structured techniques to cultivate a kind and understanding inner voice, benefiting clients with harsh self-judgment. Similarly, Adlerian theory’s holistic social perspective emphasizes social connectedness and community feeling (Adler, 1938), aligning with MSC’s principle of common humanity that recognizes suffering as a shared human experience. By fostering a sense of belonging and encouraging clients to develop self-compassion within the context of their social relationships, Adlerian theory enhances the application of MSC in promoting overall well-being. Moreover, third-wave cognitive-behavioral models are widely praised for integrating validation, mindfulness, and self-acceptance that support self-compassion–informed counseling. ACT’s emphasis on mindfulness and acceptance aligns with self-compassion by encouraging clients to accept their thoughts and feelings without judgment and commit to values-based actions (Hayes et al., 2006). This approach promotes a compassionate stance toward oneself, central to Germer and Neff’s (2019) MSC program. By fostering curiosity and kindness toward internal experiences, ACT helps integrate self-compassion practices into daily life (Hayes et al., 2006). MBCT combines cognitive strategies with mindfulness practices, making it a natural ally to MSC. By teaching clients to recognize and break free from patterns of depressive rumination, MBCT enhances clients’ ability to respond to difficult emotions with mindfulness and self-compassion (Segal et al., 2018). This supports clients in emotional balance and resilience, essential components of MSC (Segal et al., 2018). Lastly, DBT and MSC share core principles. DBT’s mindfulness emphasis and dialectical approach of balancing acceptance with change aligns with MSC, offering robust tools for navigating emotional turbulence through self-acceptance and compassion (Linehan, 2014).
Multicultural Considerations and Future Implications
One important consideration is that we recruited participants from local mental health agencies, with the final sample being predominantly White. Participation challenges arose primarily for women of color recruited via social media, including declining participation and dropout because of time constraints. Forbes et al. (2020) noted that the experience of intensive mothering was consistent across various maternal demographics (i.e., race, ethnicity, social class upbringing, relationship status, number of children, and job status). However, Lankes (2022) distinguished that the significance and impact of intensive mothering can vary depending on cultural ideals, resource availability, and structural barriers. This means that mothers from marginalized or underserved communities who face heightened societal stressors and systemic barriers may experience impediments to engaging in self-care practices and accessing mental health resources. Thus, the compounding effects of racism, discrimination, and the unique pressures associated with motherhood can exacerbate mental health challenges and diminish opportunities for cultivating self-compassion and well-being (Condon et al., 2022). Counselors must provide culturally responsive care that acknowledges their clients’ unique, intersectional identities and the historical and current context of oppression and marginalization. Overall, counselors can advocate for policies and systemic changes for underserved mothers, such as by offering self-compassion workshops for mothers in the community, thus increasing access to services.
Community Conversations
After completing the study, we sought expert validation by presenting our findings to a local community agency through a research presentation and interactive dialogue. We invited clinicians with expertise in self-compassion, family counseling, parenting, women’s issues, and vulnerable populations to share their reactions based on clinical experiences and to offer recommendations. The attending clinicians validated the four overarching themes of our study, sharing stories of motherhood marked by self-criticism, judgment, and expectation. Participants were also invited to this meeting as part of our CBPR methodology. Clinicians who identified as professionals and mothers resonated with the study’s themes, sharing personal narratives that aligned strongly with our findings. They discussed strategies to help their clients, particularly mothers, practice self-compassion, including curating social media feeds (e.g., Instagram) to avoid disempowering content that perpetuates comparison and self-criticism. Additionally, they emphasized the importance of psychoeducation from a systems perspective, suggesting mindfulness and self-compassion as powerful tools for family wellness, and acknowledged the challenges and strengths of mothers. Although no participants opted to attend because of scheduling challenges (finding time was an overarching challenge for participants throughout the study), final thoughts and comments on how this information can impact our work was discussed with community clinicians. Overall, these discussions affirmed the study’s findings and support the need for ongoing research and advocacy initiatives to raise awareness and increase access to self-compassion practices for mothers.
Following expert validation, a nationally recognized treatment center invited us to co-host an experiential seminar open to counselors and community members. The seminar, held in an underserved community, provided an overview of the study’s findings, self-compassion principles, and experiential exercises. We distributed learning materials to participants, and we offered recommendations for integrating self-compassion into daily life, family relationships, and clinical practice. As part of our ongoing efforts to disseminate the findings and advance community advocacy, the research team presented the results at a national conference, which sparked further conscious conversations, reinforcing our commitment to supporting mothers in underserved communities.
Limitations and Future Research
The present study is not without limitations. Although the nature of photovoice calls for focus groups (Wang & Burris, 1997; Wilson et al., 2007), we decided to meet with participants in smaller groups or individually to accommodate busy schedules. Although the format provided flexibility, the individual interviews can limit dialogue and community building. Additionally, our participants were too busy to attend our community meetings—a crucial component of CBPR. Future research can replicate our study using focus groups, which may provide additional insights into mothers’ self-compassion practices. Researchers may want to consider providing childcare to assist with finding time. Another limitation was a lack of racial and ethnic diversity, as our sample mainly included White women connected to counseling communities. Future research can explore the experiences of mothers with diverse racial, sexual, affectional, and marital backgrounds with self-compassion through photovoice. Mothers with intersecting identities face additional challenges, such as discrimination and systemic inequities, further impacting mental health and parenting stress (Condon et al., 2022). Wellness interventions, like self-compassion skills, could help bridge health disparities for diverse mothers.
Conclusion
Self-compassion is essential for psychological well-being. Mothers face numerous mental health challenges due to societal expectations and contextual factors, such as post–COVID-19 pandemic shifts in work–life balance, and may encounter obstacles in cultivating self-compassion. The findings reveal the unique challenges and benefits of self-compassion for mothers and the mismatch between the understanding of self-compassion and its practice in daily life. A comprehensive and multidimensional approach is necessary to assist mothers in developing self-compassion and promoting their overall well-being. Counselors must find ways to educate clients and foster this critical skill in mothers, who can often be overlooked, overburdened, and unintentionally undervalued.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
for the development of this manuscript.
Florida Atlantic University provided a small
grant to the researchers for community-engaged
research projects.
References
Adler, A. (1938). Social interest: A challenge to mankind. Faber & Faber.
Alon, T., Doepke, M., Olmstead-Rumsey, J., & Tertilt, M. (2020). The impact of COVID-19 on gender equality (Working Paper 26947). National Bureau of Economic Research. https://doi.org/10.3386/w26947
Bahn, K., Cohen, J., & van der Meulen Rodgers, Y. (2020). A feminist perspective on COVID-19 and the value of care work globally. Gender, Work, & Organization, 27(5), 695–699. https://doi.org/10.1111/gwao.12459
Bureau of Labor Statistics. (2021). The employment situation—January 2021 (Publication No. USDL-21-0142).
https://www.bls.gov/news.release/archives/empsit_02052021.pdf
Burton, A., Hughes, M., & Dempsey, R. C. (2017). Quality of life research: A case for combining photo-elicitation with interpretative phenomenological analysis. Qualitative Research in Psychology, 14(4), 375–393.
https://doi.org/10.1080/14780887.2017.1322650
Carbonneau, N., Goodman, L. C., Roberts, L. T., Bégin, C., Lussier, Y., & Musher-Eizenman, D. R. (2020). A look at the intergenerational associations between self-compassion, body esteem, and emotional eating within dyads of mothers and their adult daughters. Body Image, 33, 106–114.
https://doi.org/10.1016/j.bodyim.2020.02.007
Centers for Disease Control and Prevention. (2020). COVID-19 hospitalization and death by race/ethnicity.
https://stacks.cdc.gov/view/cdc/97937
Chae, J. (2014). “Am I a better mother than you?” Media and 21st-century motherhood in the context of the social comparison theory. Communication Research, 42(4), 503–525. https://doi.org/10.1177/0093650214534969
Condon, E. M., Barcelona, V., Ibrahim, B. B., Crusto, C. A., & Taylor, J. Y. (2022). Racial discrimination, mental health, and parenting among African American mothers of preschool-aged children. Journal of the American Academy of Child & Adolescent Psychiatry, 61(3), 402–412. https://doi.org/10.1016/j.jaac.2021.05.023
Creswell, J. W., & Báez, J. C. (2020). 30 essential skills for the qualitative researcher. SAGE.
Currie, J. L. (2018). Managing motherhood: A new wellness perspective. Springer.
Davenport, M. H., Meyer, S., Meah, V. L., Strynadka, M. C., & Khurana, R. (2020). Moms are not ok: COVID-19 and maternal mental health. Frontiers in Global Women’s Health, 1. https://doi.org/10.3389/fgwh.2020.00001
Elliott, S., Powell, R., & Brenton, J. (2015). Being a good mom: Low-income, Black single mothers negotiate intensive mothering. Journal of Family Issues, 36(3), 351–370. https://doi.org/10.1177/0192513X13490279
Ferrari, M., Hunt, C., Harrysunker, A., Abbott, M. J., Beath, A. P., & Einstein, D. A. (2019). Self-compassion interventions and psychosocial outcomes: A meta-analysis of RCTs. Mindfulness, 10(8), 1455–1473.
https://doi.org/10.1007/s12671-019-01134-6
Fonseca, A., & Canavarro, M. C. (2018). Exploring the paths between dysfunctional attitudes towards motherhood and postpartum depressive symptoms: The moderating role of self-compassion. Clinical Psychology & Psychotherapy, 25(1), e96–e106. https://doi.org/10.1002/cpp.2145
Forbes, L. K., Donovan, C., & Lamar, M. R. (2020). Differences in intensive parenting attitudes and gender norms among U.S. mothers. The Family Journal, 28(1), 63–71. https://doi.org/10.1177/1066480719893964
Forbes, L. K., Lamar, M. R., & Bornstein, R. S. (2021). Working mothers’ experiences in an intensive mothering culture: A phenomenological qualitative study. Journal of Feminist Family Therapy, 33(3), 270–294.
https://doi.org/10.1080/08952833.2020.1798200
Germer, C. K., & Neff, K. (2019). Teaching the mindful self-compassion program: A guide for professionals. Guilford.
Gilbert, P. (2014). The origins and nature of compassion focused therapy. British Journal of Clinical Psychology, 53(1), 6–41. https://doi.org/10.1111/bjc.12043
Griffin, A., & May, V. (2012). Narrative analysis and interpretative phenomenological analysis. In C. Seale (Ed.), Researching society and culture (3rd ed., pp. 441–458). SAGE.
Grose, J. (2021, February 4). America’s mothers are in crisis. The New York Times. https://www.nytimes.com/spotlight/working-moms-coronavirus
Han, A., & Kim, T. H. (2023). Effects of self-compassion interventions on reducing depressive symptoms, anxiety, and stress: A meta-analysis. Mindfulness, 14, 1553–1581. https://doi.org/10.1007/s12671-023-02148-x
Hayes, S. C., Luoma, J. B., Bond, F. W., Masuda, A., & Lillis, J. (2006). Acceptance and commitment therapy: Model, processes and outcomes. Behaviour Research and Therapy, 44(1), 1–25. https://doi.org/10.1016/j.brat.2005.06.006
Hays, S. (1996). The cultural contradictions of motherhood. Yale University Press.
Hupkau, C., & Petrongolo, B. (2020). Work, care and gender during the COVID-19 crisis. Fiscal Studies, 41(3), 623–651. https://doi.org/10.1111/1475-5890.12245
Lamar, M. R., Forbes, L. K., & Capasso, L. A. (2019). Helping working mothers face the challenges of an intensive mothering culture. Journal of Mental Health Counseling, 41(3), 203–220. https://doi.org/10.17744/mehc.41.3.02
Lankes, J. (2022). Negotiating “impossible” ideals: Latent classes of intensive mothering in the United States. Gender & Society, 36(5), 677–703. https://doi.org/10.1177/08912432221114873
Larkin, M., & Thompson, A. R. (2011). Interpretative phenomenological analysis in mental health and psychotherapy research. In D. Harper & A. R. Thompson (Eds.), Qualitative research methods in mental health and psychotherapy: A guide for students and practitioners (pp. 99–116). Wiley.
Lathren, C., Bluth, K., & Zvara, B. (2020). Parent self-compassion and supportive responses to child difficult emotion: An intergenerational theoretical model rooted in attachment. Journal of Family Theory & Review, 12(3), 368–381. https://doi.org/10.1111/jftr.12388
Linehan, M. M. (2014). DBT® skills training manual. Guilford.
Lofton, O., Petrosky-Nadeau, N., & Seitelman, L. (2021). Parents in a pandemic labor market (Working Paper No. 2021-04). Federal Reserve Bank of San Francisco. https://doi.org/10.24148/wp2021-04
Mitchell, A. E., Whittingham, K., Steindl, S., & Kirby, J. (2018). Feasibility and acceptability of a brief online self-compassion intervention for mothers of infants. Archives of Women’s Mental Health, 21, 553–561.
https://doi.org/10.1007/s00737-018-0829-y
Moreira, H., Gouveia, M. J., Carona, C., Silva, N., & Canavarro, M. C. (2015). Maternal attachment and children’s quality of life: The mediating role of self-compassion and parenting stress. Journal of Child and Family Studies, 24, 2332–2344. https://doi.org/10.1007/s10826-014-0036-z
Myers, J. E., & Sweeney, T. J. (2004). The indivisible self: An evidence-based model of wellness. Journal of Individual Psychology, 60(3), 234–245. https://core.ac.uk/download/pdf/149232976.pdf
Neff, K. (2011). Self-compassion: The proven power of being kind to yourself. HarperCollins.
Neff, K. D., & Dahm, K. A. (2015). Self-compassion: What it is, what it does, and how it relates to mindfulness. In B. D. Ostafin, M. D. Robinson, & B. P. Meier (Eds.), Handbook of mindfulness and self-regulation (pp. 121–137). Springer. https://doi.org/10.1007/978-1-4939-2263-5_10
Neff, K. D., & Germer, C. K. (2013). A pilot study and randomized controlled trial of the mindful self-compassion program. Journal of Clinical Psychology, 69(1), 28–44. https://doi.org/10.1002/jclp.21923
Neff, K., & Germer, C. (2018). The mindful self-compassion workbook: A proven way to accept yourself, build inner strength, and thrive. Guilford.
Orenstein, G. A. & Lewis, L. (2021). Erikson’s stages of psychosocial development. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK556096
Park, J. (2021). Who is hardest hit by a pandemic? Racial disparities in COVID-19 hardship in the U.S. International Journal of Urban Sciences, 25(2), 149–177. https://doi.org/10.1080/12265934.2021.1877566
Prikhidko, A., & Swank, J. M. (2018). Motherhood experiences and expectations: A qualitative exploration of mothers of toddlers. The Family Journal, 26(3), 278–284. https://doi.org/10.1177/1066480718795116
Psychogiou, L., Legge, K., Parry, E., Mann, J., Nath, S., Ford, T., & Kuyken, W. (2016). Self-compassion and parenting in mothers and fathers with depression. Mindfulness, 7, 896–908.
https://doi.org/10.1007/s12671-016-0528-6
Ruppanner, L., Tan, X., Carson, A., & Ratcliff, S. (2021). Emotional and financial health during COVID-19: The role of housework, employment and childcare in Australia and the United States. Gender, Work, & Organization, 28(5), 1937–1955. https://doi.org/10.1111/gwao.12727
Sackett, C. R., & Jenkins, A. M. (2015). Photovoice: Fulfilling the call for advocacy in the counseling field. Journal of Creativity in Mental Health, 10(3), 376–385. https://doi.org/10.1080/15401383.2015.1025173
Segal, Z., Williams, M., & Teasdale, J. (2018). Mindfulness-based cognitive therapy for depression (2nd ed). Guilford.
Smith, L., Davis, K., & Bhowmik, M. (2010). Youth participatory action research groups as school counseling interventions. Professional School Counseling, 14(2), 174–182. http://www.jstor.org/stable/42732946
van der Kolk, B. A. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin.
Wang, C. C. (1999). Photovoice: A participatory action research strategy applied to women’s health. Journal of Women’s Health, 8(2), 185–192. https://doi.org/10.1089/jwh.1999.8.185
Wang, C., & Burris, M. A. (1997). Photovoice: Concept, methodology, and use for participatory needs assessment. Health Education & Behavior, 24(3), 369–387. https://doi.org/10.1177/109019819702400309
Wester, K. L., Wachter Morris, C. A., Trustey, C. E., Cory, J. S., & Grossman, L. M. (2021). Promoting rigorous research using innovative qualitative approaches. Journal of Counseling & Development, 99(2), 189–199. https://doi.org/10.1002/jcad.12366
Wilson, N., Dasho, S., Martin, A. C., Wallerstein, N., Wang, C. C., & Minkler, M. (2007). Engaging young adolescents in social action through photovoice: The Youth Empowerment Strategies (YES!) Project. The Journal of Early Adolescence, 27(2), 241–261. https://doi.org/10.1177/0272431606294834
World Health Organization. (2021, May). The true death toll of COVID-19: Estimating global excess mortality.
https://www.who.int/data/stories/the-true-death-toll-of-covid-19-estimating-global-excess-mortality
Zamarro, G., Perez-Arce, F., & Jose Prados, M. (2020). Gender differences in the impact of COVID-19. Center for Economic and Social Research, University of Southern California. https://www.ktla.com/wp-content/uploads/sites/4/2020/06/ZamarroGenderDiffImpactCOVID-19_061820-2.pdf
Kelly Emelianchik-Key, PhD, NCC, ACS, LMFT, LMHC-QS, is an associate professor at Florida Atlantic University. Adriana C. Labarta, PhD, NCC, ACS, LMHC, is an assistant professor at Florida Atlantic University. Clara Bossie, MS, ACS, LMFT-QS, is a doctoral candidate at Florida Atlantic University and Owner and Clinical Director of Wisely Wellness LLC. Carman S. Gill, NCC, ACS, LCMHC, is a professor and department chair at Florida Atlantic University. Correspondence may be addressed to Kelly Emelianchik-Key, Department of Counselor Education, Florida Atlantic University, 777 Glades Rd. Bldg. 47, Rm. 275, Boca Raton, FL 33431-0991, Kemelian@fau.edu.
Apr 18, 2017 | Volume 7 - Issue 3
Susannah C. Coaston
Counselors are routinely exposed to painful situations and overwhelming emotions that can, over time, result in burnout. Although counselors routinely promote self-care, many struggle to practice such wellness regularly, putting themselves at increased risk for burning out. Compassion is essential to the helper’s role, as it allows counselors to develop the therapeutic relationship vital for change; however, it is often difficult to direct this compassion inward. Developing an attitude of self-compassion and mindfulness in the context of a self-care plan can create space for an authentic, kind response to the challenges inherent in counseling. This article expands beyond the aspirational aspects of self-compassion and suggests a variety of practices for the mind, body, and spirit, with the intention of supporting the development of an individualized self-care plan for counselors.
Keywords: self-care, self-compassion, burnout, mindfulness, wellness
Wellness, prevention, and human development compose the core of a counselor’s professional identity (Mellin, Hunt, & Nichols, 2011). This fundamental grounding is emphasized within the American Counseling Association’s (ACA) Code of Ethics (ACA, 2014), as well as by the Council for Accreditation of Counseling & Related Education Programs (CACREP; 2016). To fulfill their role in the change process, counselors depend heavily upon compassion, a key component of the therapeutic relationship that—paradoxically—counselors may seldom apply to themselves (Patsiopoulos & Buchanan, 2011). Whereas compassion means being with others in their suffering (Pollack, Pedulla, & Siegel, 2014), self-compassion can be understood as “being touched by and open to one’s own suffering, not avoiding or disconnecting from it, generating the desire to alleviate one’s suffering and to heal oneself with kindness” (Neff, 2003, p. 87). Higher levels of self-compassion can serve as a buffer against burnout (Barnard & Curry, 2011). Therefore, cultivating an attitude of self-compassion may assist counselors in employing self-care practices to refresh, rejuvenate, and recharge their bodies, minds, and souls. The purpose of this manuscript is to reimagine self-care as regular acts of self-compassion that benefit both clients and counselors.
Self-Compassion
Self-compassion, a construct from Buddhist thought, consists of self-kindness, common humanity, and mindfulness, and is characterized by gentleness with oneself when faced with a perceived sense of inadequacy or failure (Neff, 2003). Self-compassion is not based on an evaluation of the self; self-compassion becomes the path to positively relating to oneself (Neff & Costigan, 2014). The concept of self-compassion is consistent with the idea of self-acceptance in the humanistic tradition (Neff, 2003). Carl Rogers (1961) described a successful outcome of psychotherapy as an increase in positive attitudes toward self: “The client not only accepts himself . . . he actually comes to like himself. This is not a bragging or self-assertive liking; it is a rather quiet pleasure in being one’s self” (p. 87). The practice of self-compassion calls for a mindful awareness of emotions, and painful emotions are met with a sense of understanding, connection to our common humanity, and self-kindness (Neff, 2003). Neff and Costigan (2014) described self-compassion’s relationship with pain thusly: “Self-compassion does not avoid pain, but rather embraces it with kindness and goodwill that is rooted in the experience of being fully human” (p. 114). Self-compassion practices have been found to improve psychological functioning in both clinical and non-clinical settings (Neff, Kirkpatrick, & Rude, 2007; Schanche, Stiles, McCullough, Svartberg, & Nielsen, 2011).
Mindfulness is one of the core components of self-compassion and is critical for the awareness of suffering that precedes compassion (Germer & Neff, 2015). Mindfulness is the focusing on the awareness of pain in the present moment, and self-compassion becomes the act of taking that awareness and encouraging kindness toward oneself. The common humanity component of self-compassion becomes one of acknowledgment that, as humans, we are imperfect and make mistakes; recognizing our flawed condition allows for a broader perspective toward our difficulties (Neff, 2003). Adopting such a view of pain reduces the chance of over-identification or getting so wrapped up in one’s emotions that they become exaggerated (Neff & Costigan, 2014). When an individual can recognize pain as a universal occurrence, such a viewpoint then fosters a sense of connection with others who have felt suffering. Pain becomes an uncomfortable but acknowledged part of the human condition. When practicing self-compassion, the self-directed kindness is not done to change the circumstance of suffering, but done because there is suffering. The practitioner asks “What do I need now?” The individual then acts accordingly to provide comfort when experiencing the pain of inadequacy or failure (Germer & Neff, 2015). Learning self-compassion becomes a gift for both clients and the practitioner (Barnett, Baker, Elman, & Schoener, 2007). Making time for one’s self is one way counselors can practice self-care (Patsiopoulos & Buchana, 2011). That self-acceptance can prove vital for counselors, whose work often puts them at a risk for burnout (Yager & Tovar-Blank, 2007).
Counselor Burnout
Burnout is a multidimensional experience consisting of exhaustion, cynicism, and reduced professional efficacy that can result from dissatisfaction with the organizational context of the job position (Maslach, Schaufeli, & Leiter, 2001). Burnout can affect individuals in a variety of ways, with anxiety, irritability, fatigue, withdrawal, and demoralization as major examples (Schaufeli & Enzmann, 1998). Burnout can affect individuals at any point in their career and can hamper productivity and creativity, resulting in a reduction of compassion toward themselves and clients (Grosch & Olsen, 1994). “It is when counseling seems to have little effect that counselors reach despair because their raison d’être for choosing this work—to make a difference in human life—is threatened” (Skovholt, Grier, & Hanson, 2001, p. 171). Caring for others and caring for oneself becomes a difficult balance to achieve for both new and seasoned counselors alike. Carl Rogers (1980) wrote, “I have always been better at caring for and looking after others than I have in caring for myself. But in these later years, I made progress” (p. 80). Self-compassion can serve as a protective factor against such potentially debilitating effects of work-related burnout.
Historically, researchers examined the causes of burnout relating to demographic, personality, or attitudinal differences between individuals (Maslach et al., 2001). Today, burnout is viewed from an organizational standpoint and is concerned with the relationship, or fit, between the person and his or her environment, wherein mismatches can result in burnout over time (Maslach, Leiter, & Jackson, 2012). An individual’s perceptions have a reciprocal relationship with the work environment; how counselors make meaning of their work impacts their satisfaction, commitment, and performance in the workplace (Lindholm, 2003). Counselors experiencing work-related stress and burnout will construct meaning differently and require a tailored self-care plan that reflects their individual assessment of their own fit within their work environment.
Counselor Self-Care
Self-care can be defined as an activity to “refill and refuel oneself in healthy ways” (Gentry, 2002, p. 48). Self-care is vital if we are to remain effective in our role and avoid burnout; however, many counselors do not regularly implement the techniques they recommend to clients in their own lives (O’Halloran & Linton, 2000; Skovholt et al., 2001). Although self-care is widely promoted within the counseling literature, this author contends that inherent in many self-care plans and workplace improvement efforts is the idea that overwhelming work-related stress reflects an inadequacy of the individual. The message in the literature often reflects the view that a counselor’s distress hinges upon inadequate coping resources, poor health practices, or other kinds of personal failing, such as lacking assertiveness or not taking enough time off from work (Bradley, Whisenhunt, Adamson, & Kress, 2013; Killian, 2008; O’Halloran & Linton, 2000). As a result, self-care plans tend to take on the air of a New Year’s resolution, a strategy to get better. This narrow focus reflects the historical view of burnout that focused primarily on its individual dimension, without taking into consideration the organizational, interpersonal, or societal perspectives (Schaufeli & Enzmann, 1998). When self-care plans are written like self-improvement plans, the opportunities for criticism and judgment abound, particularly for new counselors who struggle with anxiety and self-doubt (Skovholt, 2012). When counselors are suffering, experiencing symptoms of burnout, struggling to maintain healthy professional boundaries (i.e., under- or over-involvement), or feeling as though they are not caring for themselves effectively, shame may cause them to be less likely to seek assistance (Graff, 2008). Some counselors may fear negative repercussions as a result of disclosure, such as being perceived as impaired or having professional competency problems (Rust, Raskin, & Hill, 2013).
Self-care is an ethical imperative (ACA, 2014), because utilizing self-care strategies reduces the likelihood of impairment (ACA, 2010). Issues in a counselor’s personal life, burnout in the workplace, mental or physical disability, or substance abuse can result in impairment (ACA, 2010). Sadly, in a survey completed in 2004, nearly two-thirds of participants knew a counselor that they would identify as impaired (ACA, 2010). Counselors who better manage their self-care needs are more likely to set appropriate boundaries with clients and less likely to use clients to meet their own personal or professional needs (Nielsen, 1988). Self-care education has been integrated into the accreditation standards for counselor training (CACREP, 2016), and there are multiple articles discussing how to incorporate the value of wellness and self-care into counselor education programs (Witmer & Young, 1996; Yager & Tovar-Blank, 2007). For counselor educators and supervisors, monitoring counselors-in-training for possible impairment is an important part of the responsibility of gatekeeping (Frame & Stevens-Smith, 1995). However, despite this attention, both students and practicing professional counselors still struggle to implement self-care (Skovholt et al., 2001; E. Thompson, Frick, & Trice-Black, 2011).
Bradley and colleagues (2013) suggested that many of the self-care suggestions in the literature are too general, focusing mainly on general health practices, such as eating healthily and getting enough sleep, or professional recommendations regarding seeking support from colleagues. A case can be made that a counselor would be better served by employing an overall approach to efforts that are based in a self-compassionate mindset. Therefore, actively seeking awareness of one’s own signs and symptoms that indicate suffering can not only help counselors recognize burnout, it also can provide clues toward the first step in soothing.
Mindfulness represents one possible means of increasing such awareness. Mindfulness allows the practitioner to be present in the moment non-judgmentally (Kabat-Zinn, 1994). To practice self-compassion, a counselor needs to be willing to attend to feelings of discomfort, pain, or suffering and acknowledge the experience without self-recrimination (Germer & Neff, 2015). Consider the experience of having a regular client stop attending sessions and returning calls or abruptly discontinuing services. Although common, the ambiguous loss of a connection with a client can be a source of stress and pain (Skovholt et al., 2001). It also can provide an opportunity. Covey (2010) shared the following quote that is often misattributed to Viktor Frankl: “Between stimulus and response there is a space. In that space is our power to choose our response. In our response lies our growth and our freedom” (p. VI). The space Covey describes is our opportunity to be mindful of the stimulus and choose to offer ourselves compassion in response. Choosing to deny, suppress, or distract to avoid these feelings may cause the counselor to miss the trigger to practice self-care. When such feelings are recognized, the counselor may act compassionately toward himself or herself by normalizing or validating the experience. Within self-compassion, the concept of common humanity becomes crucial to precluding the often-automatic tendency to become self-critical for experiencing discomfort (Neff, 2003). Thoughts such as, “I shouldn’t feel this way,” “Just snap out of it; it’s not so bad,” or “What’s wrong with me?” invalidate the sufferer and may cause the counselor to feel as though self-care is an act of indulgence rather than an essential, self-directed gift of kindness. Expressing kindness through self-care acknowledges that counseling can be both difficult and rewarding, a duality representative of the human condition.
When counselors choose to practice self-care, they enhance themselves and their practice. One participant in a narrative inquiry on self-compassion in counseling stated: “What’s so important about self-compassion? Three words: Avoidance of burnout” (Patsiopoulos & Buchanan, 2011, p. 305). Another participant noted, “When we come from a self-compassionate place, self-care is no longer about these sporadic one-time events that you do when you feel burned out and exhausted. Self-care is something you can do all the time” (Patsiopoulos & Buchanan, 2011, p. 305). The consequence of our job as counselors is working compassionately with suffering, and in doing so we suffer (Figley, 2002).
For someone to develop genuine compassion toward others, first he or she must have a basis upon which to cultivate compassion, and that basis is the ability to connect to one’s own feelings and to care for one’s own welfare. . . . Caring for others requires caring for oneself. (Germer & Neff, 2015, p. 48) Self-care, then, is a vital part of a counselor’s responsibilities to clients and to one’s self.
It is important to remember that counseling can be emotionally demanding for counselors in different ways (O’Halloran & Linton, 2000). Self-compassion encourages remembering the shared human experience (Neff, 2003), as the experience of being a professional counselor can be quite isolating, especially for those working in more independent environments (e.g., school counselors, private practitioners; Freadling & Foss-Kelly, 2014; Matthes, 1992). Using mindfulness, counselors can maintain an objective stance that can allow the counselor to view one’s work circumstances with a non-judgmental lens (Newsome, Waldo, & Gruszka, 2012), then act kindly to intervene with a self-care practice that is revitalizing to mind, body, and spirit. Using self-compassion tenets as a guide, self-care plans can be created that are authentic and kind, connect us to the human experience, and reflect a balanced state of self-awareness.
Creating a Self-Compassion–Infused Self-Care Plan
In wellness counseling, optimal functioning of the mind, body, and spirit is the goal for holistic wellness (Myers, Sweeney, & Witmer, 2001). The physical dimension is the most common focus for wellness intervention (Carney, 2007); however, this is quite limiting in a profession that is often sedentary, with long hours and pressure to meet productivity demands (Franco, 2016; Freadling & Foss-Kelly, 2014; Ohrt, Prosek, Ener, & Lindo, 2015). Maintaining one’s health is important but may not be enough to assuage the emotional demands of a high-touch profession in which a strong professional relationship is combined with the often-conflicting pressures of reimbursement; short-term, diagnosis-focused treatment; and behaviorally based outcomes associated with managed care (Cushman & Gilford, 2000; Freadling & Foss-Kelly, 2014). Developing a collaborative treatment plan is a common practice in counseling; it allows the counselor and the client to determine the possible direction and outcomes for their work together (Kress & Paylo, 2015). In the best case, this plan is individualized, specific, and open to revision when necessary. A good self-care plan can follow the same formula.
What follows are specific suggestions regarding self-care practices that stretch beyond the “should,” the “ought to,” and the New Year’s resolution language. When reading the interventions, consider the question Linder, Miller, and Johnson (2000) suggested for clients when encouraging self-care: “How do you reassure yourself?” (p. 4). The suggestions are organized into mind, body, and spirit; however, these are artificial divisions and some interventions may satisfy in multiple ways.
Interventions for the Mind
Mindfulness is a component of self-compassion, but it can also be used intentionally as a regular practice for self-care. Mindfulness can be described as a dispositional trait, a state of being and a practice (Brown, Ryan, & Creswell, 2007). The use of mindfulness has been integrated into many facets of counseling practice (I. Thompson, Amatea, & Thompson, 2014). For those attracted to the practice of mindfulness for self-care, non-judgmental awareness can be integrated as a practice (e.g., a set time for engagement in a particular mindfulness exercise) or as a way of being during particular activities within the day. Exercises such as mindful eating, maintaining sensory awareness while washing dishes, or mindful walking can be helpful for those who are looking for brief, everyday opportunities for self-care. Researchers I. Thompson and colleagues (2014) found that higher levels of mindfulness corresponded with lower levels of burnout. Mindfulness has been suggested as a beneficial way to teach self-care in counselor training (Christopher, Christopher, Dunnagan, & Schure, 2006), and also as a way to reduce stress and increase self-compassion in students training to be in helping professions (Newsome et al., 2012). For any number of reasons, not all counselors may find benefit in mindfulness practices; therefore, some may choose methods of self-care that are more mentally invigorating.
Intellectual stimulation in any endeavor is important to maintain engagement, interest, and enjoyment, but such motivation can be particularly helpful when a work position contains routine, mundane, or downright boring tasks. To create a stimulating work life, seasoned professionals find active ways to continue their professional development, which can decrease the boredom that can lead to burnout (Skovholt et al., 2001). Activities for growth and development can include learning something new within counseling or outside the profession, such as learning a new language, or how to make sushi, write code, or play a strategy game such as the ancient board game, Go.
The role of a counselor involves exposure to circumstances of human suffering, painful emotions, and heartbreaking situations, which increases the risk of burnout due to absorption of the clients’ pain (Ruysschaert, 2009). Finding a way to keep and maintain positive memories, cards and notes, compliments or successes—what this author terms warm and fuzzies—either personally or professionally, in a box, folder, jar, or bulletin board, can be a helpful response. Bradley and colleagues (2013) suggested tracking small changes made by clients when discouraged and sharing the progress with co-workers.
Writing can be a powerful intervention in a counseling setting and can benefit both mental and physical health (Pennebaker & Seagal, 1999; Riordan, 1996). Counselors can use the medium of writing in a multitude of ways. Whether through journaling, narrative, poetry, musical lyrics, or letters, the act of writing can reduce emotional inhibition (Connolly Baker & Mazza, 2004). Creative writing can be used to access the healing benefits of writing without worry about form or audience (Warren, Morgan, Morris, & Morris, 2010).
Warren et al.’s (2010) The Writing Workout is a way to express, validate, and externalize painful emotions. This wellness approach illustrates how creative writing for self-care can cultivate compassion. Narrative writing strategies can allow the writer to change the outcome of a lived experience or reframe a life experience (Connelly Baker & Mazza, 2004). Creating a narrative of an event can help the storyteller organize details and events, reflect and process thoughts and feelings, and derive meaning from experiences (Pennebaker & Seagal, 1999). A creative, mindful writing intervention could be used to examine a clinical situation that may not have gone as the counselor had hoped, or to creatively explore life lessons derived from a clinical encounter. For some clinicians, writing gives voice to emotions too raw to easily speak aloud (Wright, 2003).
Traditional journaling can allow for self-reflection, increased self-awareness, and growth (Lent, 2009; Utley & Garza, 2011). Journal writing can be inherently self-compassionate. Linder et al. (2000) discussed the use of a non-judgmental journaling practice in which there are no wrong words and writers are encouraged to use random sentences and words that do not make sense. Through almost nonsensical form, journaling offers a sense of safety and freedom, while creating a trusting relationship with the journal. Linder et al. (2000) stated, “Journaling finds the meaning in meaninglessness and negates the emptiness through creating writing from the heart. It is an outlet to tell the truth without being judged” (p. 7).
Beyond the traditional journal, counselors may find alternative ways to use journaling for emotional expression, such as use of bullet journaling or a personal blog online. Bullet journaling uses a rapid-logging approach, or a visual code, to represents tasks, events, and notes in a physical notebook (Bullet Journal, 2017). Keeping a bullet journal is a clever way of managing multiple arenas of one’s life in a single place, and the events and notes categories can be particularly helpful in the practice of journaling for self-care. Events are to be written down briefly and objectively despite the degree of emotional content they carry (Bullet Journal, 2017), offering an opportunity to practice the non-reactive skill of mindfulness (Kabat-Zinn, 1994). Once an event has been entered, the counselor can respond mindfully to it by writing at length on the following page. The notes category for bullet journaling consists of ideas, thoughts, or observations (Bullet Journal, 2017), which could include inspirational quotes, eureka moments, or other insights worth reviewing at a later date. The author can use signifiers (i.e., symbols) to create a legend to provide additional context for an event, note, or task. The bullet journal approach for self-expression exemplifies a creative twist on an old concept to better fit the preferences of the writer. Similarly, scrapbook journaling can be used to accommodate the types of expressive media that resonate with the counselor’s personal style or interests (Bradley et al., 2013). Counselors can use photos, poems, song lyrics, and quotes to reflect their emotional state, and then reflect on the emotional patterns or themes that arise. For counselors who prefer to share their thoughts on the Internet, an online blog can be a cost-effective, accessible medium to express oneself emotionally and share thoughts, feelings, and experiences with others (Lent, 2009). Counselors should consider the risks associated with the use of the Internet and maintenance of confidentiality in an online medium in accordance with the ACA Code of Ethics (2014).
Finally, a simple self-care intervention can involve writing oneself a permission slip or prescription for something. This could be the permission to be imperfect, to take a mental health day, or to run through a sprinkler on a hot day. A writing assignment of this sort expresses kindness in providing the very thing that is needed for an emotional recharge. In some cases, this may involve taking a quiet moment to allow one’s mind to wander. This can occur during a warm bath or shower at the end of the day or while savoring a warm cup of coffee or tea in the afternoon. Although mind-wandering can be a threat to effectiveness and productivity when it occurs at inopportune times, taking time for mind-wandering can relieve boredom, stimulate creative thoughts, and facilitate future planning (Smallwood & Schooler, 2015).
Interventions for the Body
Many self-care plans begin and end with a strong concentration on physical self-care, typically involving making nutritional changes and increasing physical activity (Bradley et al., 2013; E. Thompson et al., 2011). These therapeutic lifestyle changes (TLCs) can have a huge impact on health and well-being (Walsh, 2011). Although the mental health benefits of these types of changes are well documented (Walsh, 2011), a myopic focus on physiological wellness may be limiting, and self-care should include a broader range of ways to cope (E. Thompson et al., 2011). For individuals wishing to focus specifically on such changes, using the imagery of caring for oneself as one does a plant may increase self-awareness of bodily self-care needs (Bradley et al., 2013). Considering one’s needs in this metaphorical way may help counselors increase their own self-compassion by considering their unique needs and the changes they are ready and willing to make. A counselor may indicate they require shade from the sun, which could represent reducing over-stimulating environments; good spacing from other plants, indicating healthy boundaries or alone time; and water and nutrients, which may remind the counselor to keep a pitcher of water on the desk and a bag of almonds in a drawer. Externalizing in this way can be particularly helpful when learning self-compassion because often counselors find it easier to care for others than themselves (Patsiopoulos & Buchanan, 2011).
Although exercise has clear mental health benefits (Callaghan, 2004), for some the concept of exercise may lack appeal or may prove difficult to prioritize within a daily work schedule. The use of stretching, walking, or yoga for a short amount of time may be more easily integrated into a hectic schedule. Yoga has been found to be equivalent to exercise in many mental and physical health domains, but not all types of yoga have been found to improve overall physical fitness as compared to more rigorous exercise (Ross & Thomas, 2010). The practice of yoga has been found to increase acceptance of self and others and reduce self-criticism (Valente & Marotta, 2005). Further, the regular practice of yoga can “provide therapists with a discipline capable of fostering a greater sense of self-awareness and helping to develop a lifestyle that is conducive to their own personal growth and the goals of their profession” (Valente & Marotta, 2005, p. 79).
The benefits of movement go beyond improvements in cardiac and musculoskeletal health, while serving to benefit the mind and the spirit. Dance has been used for centuries as a healing practice (Koch, Kunz, Lykou, & Cruz, 2014) and reduces stress, increases stress tolerance, and improves well-being (Bräuninger, 2012). Marich and Howell (2015) developed the practice of dancing mindfulness, which utilizes dance as the medium for practicing meditation. Dancing mindfulness participants report improvement in emotional and spiritual domains, greater acceptance of self, and an increased ability to use mindfulness in everyday life (Marich & Howell, 2015). However, caring for oneself requires more than just nutrition and movement; self-care plans should metaphorically consider the environment.
Skovholt et al. (2001; Skovholt, 2012) uses the concept of a greenhouse to describe the characteristics for a healthy work environment. Plants flourish within a nurturing greenhouse environment. Likewise, counselors thrive within a work environment that is characterized by a sense of autonomy and fairness; growth-promoting and meaningful work; reasonable expectations and remuneration; and trust, support, and respect among colleagues (Skovholt, 2012). The metaphorical work “greenhouse” contains individualized supports and resources that allow for growth and rejuvenation, but can protect the counselor from the harshness that could characterize their work. Examining and adjusting factors that may be under the counselor’s control, such as breaks between clients; scheduling of clients engaged in trauma work; number of assessments, intakes, or group sessions in one day; or other malleable elements can help create a work day that best meets the needs of the counselor. Strategic planning and focused intentionality allows the counselor to engage fully in each client encounter.
Interventions for the Spirit
Religion and spirituality are important factors within the lives of many clients (Cashwell, Bentley, & Bigbee, 2007). Within the United States, 77% of adults identify with some religious faith (Masci & Lipka, 2016). However, the United States is growing in those who identify as spiritual, with 59% of adults reporting a regular “deep sense of ‘spiritual peace and well-being’” (Masci & Lipka, 2016, para. 2). To attend appropriately and fully to clients’ religious and spiritual needs, counselors also need to care for their own spiritual selves.
Humanistic counselors engage fully with clients to create a genuine connection and are most effective as helpers in areas in which they themselves are stronger and more grounded (Baldwin, 2013). Therefore, when addressing the spiritual concerns of a client, counselors need to be aware of where they are on their own spiritual path. Otherwise, there is no assurance their own religious or spiritual concerns will not create an obstacle for their client’s growth (Sori, Biank, & Helmeke, 2006). A counselor’s spiritual concerns can influence the therapeutic alliance in many ways. Influences can include increased reactivity to the spiritual concerns of the client, decreased recognition of how the client values personal spirituality, or inattention to how the client’s spirituality may be a therapeutic resource or contributing factor to distress (Sori et al., 2006). Sori and colleagues (2006) concluded that failure to be aware of spirituality as an aspect of the human condition can create potential boundary issues, limit a counselor’s understanding of the client due to unexamined beliefs rooted in one’s own spiritual background, and result in difficulty managing the emotional uncertainty and pain of clients due to the counselor’s own struggles with faith. Therefore, engaging in reflection, exploration, or a regular spiritual practice can benefit both the counselor and the client.
Spirituality in counseling has been defined as “the capacity and tendency present in all human beings to find and construct meaning about life and existence and to move toward personal growth, responsibility, and relationship with others” (Myers & Williard, 2003, p. 149). This definition conceptualizes spirituality as a central component of wellness that shapes one’s functioning physically, psychologically, and emotionally, not as separate parts of the whole being (Myers & Williard, 2003). Valente and Marotta (2005) asserted that a healthy spiritual life can be emotionally nourishing and keep burnout at bay. Further, greater self-awareness of one’s spirituality may allow practitioners to be more present with their own suffering and that of their clients. Chandler, Miner Holden, and Kolander (1992) stated that attending to spiritual health when making personal change toward wellness will increase the likelihood of self-transformation and greater balance in life. Because there are many expressions of spirituality, individuals wishing to incorporate spirituality into their self-care plan should consider choosing activities that align with personal goals and are consistent with their values (Cashwell et al., 2007).
A spiritual self-care practice can create an inner refuge (Linder et al., 2000) that can offer sanctuary for a counselor when overwhelmed by personal or professional suffering (Sori et al., 2006). Particularly for those in the exploration phase of their own spirituality, but beneficial for all, conducting a moral inventory can assess how individuals are living in accordance with personal beliefs and values (Sori, et al., 2006). Following the moral inventory, a counselor may create a short list of principles to live by (i.e., a distilled list of values consistent with religious and spiritual ideas that are particularly personally valuable; V. Pope, personal communication, August, 2016). Individual research or joining a spiritual community can be helpful for education, support, and guidance in learning more about a particular religious or spiritual tradition (Cashwell et al., 2007). Some religious traditions, such as Seventh-Day Adventists, offer guidelines for physical and mental exercises, as well as nutritional advice that can be translated into intentional counselor self-care practices. Seventh-Day Adventists have a strong focus on wellness and advocate a vegetarian diet and avoidance of tobacco, alcohol, and mind-altering substances (General Conference of Seventh-Day Adventist World Church, 2016). Further, self-reflection may be regularly incorporated into rituals associated with an important time of year such as Lent or the Days of Awe.
For many, prayer can be a powerful practice for connecting with a higher power. Prayer is an integral part of a variety of spiritual traditions and has been associated with a variety of improvements in health and well-being (Granello, 2013). Spending time in communion with a higher power can be integrated into a regular routine for the purpose of self-care. Meditation also can be a spiritual practice and has a long history of applications and associations with health improvement (Granello, 2013). Broadly speaking, there are two types of meditation: concentration, which involves focusing attention (e.g., repeating a mantra, counting, or attending to one’s breath), and mindfulness, which non-judgmentally expands attention to thoughts, sensations, or emotions present at the time (Ivanovski & Malhi, 2007). These quiet practices can allow the participant moments of silence to achieve various ends, such as relaxation, acceptance, or centering.
Connecting with the earth or nature also can be a practice of spiritual self-care. Grounding exercises such as massage, Tai Chi, or gardening can be helpful to encourage a reconnection with the body and the earth (Chandler, et al., 1992). Furthermore, spending time in nature has been found to be rejuvenating both mentally and spiritually (Reese & Myers, 2012).
Engaging in a creative, expressive art activity for the purposes of spiritual practice and healing can be incredibly powerful to heal mind, body, and soul (Lane, 2005). Novelist John Updike has said, “What art offers is space—a certain breathing room for the spirit” (Demakis, 2012, p. 23). Art can come in many forms. Expressive arts can be a powerful tool of self-expression (Snyder, 1997; Wikström, 2005) and provide many options that can easily be used as self-care interventions. Sometimes the inner critic, need for approval, fear of failure, or a fear of the unknown can create barriers to exploring one’s creative energy (N. Rogers, 1993). Maintaining a self-compassionate attitude can allow counselors to create a safe environment to practice self-care free of judgment.
Use of dance, music, art, photography, and other media can be used intentionally for holistic healing. Through the use of clay, paint, charcoal, or other media, the creator can become in touch with feelings, gain insight, release energy, and discover alternative spiritual dimensions of the self, as well as experience another level of consciousness (N. Rogers, 1993). Music has been found to be both therapeutic and transcendental (Knight & Rickard, 2001; Lipe, 2002; Yob, 2010). There are various ways to incorporate music into a self-care plan depending on interest, access, and preference. In many cultures, music and spirituality are integrally linked (Frame & Williams, 1996). Listening to a favorite hymn, gospel music, or other type of liturgical music can be one way to revitalize the spirit during the workday. Relaxing music has been found to prevent physiological responses to stress and subjective experience of anxiety in one study of undergraduates (Knight & Rickard, 2001). Singing is another way of expressing thoughts and feelings, and for some it can provide a vehicle for self-actualization, connection to a higher power, and self-expression (Chong, 2010). After a long day, singing in the office, in the car, or while cooking dinner can be particularly cathartic.
Conclusion
Counselors are routinely exposed to painful situations, traumatic circumstances, and overwhelming emotions. Consequently, they could benefit from creating a safe place for vulnerability, especially when emotionally overwrought after a long day or a particularly difficult counseling session. To thrive as a counselor, self-care is essential, yet many struggle to care for themselves as they care for their clients. To best achieve holistic wellness, counselors must incorporate interventions for the body, mind, and spirit. Counselors can apply self-compassion principles to the creation of an individualized self-care plan, one that functions to rejuvenate flagging professional commitment and soothe potentially debilitating stress. By cultivating an attitude of self-compassion, counselors may be more attentive to their own needs, reducing the risk of developing burnout and benefitting both clients and themselves. These counselors also may be more effective in assisting clients with overcoming their own barriers to self-care. Similarly, counselors who serve as educators or supervisors can model such principles and routinely ask students and supervisees, “What do you need now?” to increase awareness and the practice of tuning in. Consequently, the self-compassionate counselor learns to create a self-care plan that becomes a balm for burnout.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
American Counseling Association. (2010). American Counseling Association’s Task Force on Counselor Wellness and Impairment. Retrieved from http://www.creating-joy.com/taskforce/tf_history.htm
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author. Retrieved from https://www.counseling.org/resources/aca-code-of-ethics.pdf
Baldwin, M. (2013). Interview with Carl Rogers on the use of the self in therapy. In M. Baldwin (Ed.), The use of self in therapy (3rd ed., pp. 28–35). New York, NY: Routledge.
Barnard, L. K., & Curry, J. F. (2011). Self-compassion: Conceptualizations, correlates, & interventions. Review of General Psychology, 15, 289–303. doi:10.1007/s11089-011-0377-0
Barnett, J. E., Baker, E. K., Elman, N. S., & Schoener, G. R. (2007). In pursuit of wellness: The self-care imperative. Professional Psychology: Research and Practice, 38, 603–612. doi:10.1037/0735-7028.38.6.603
Bradley, N., Whisenhunt, J., Adamson, N., & Kress, V. E. (2013). Creative approaches for promoting counselor self-care. Journal of Creativity in Mental Health, 8, 456–469. doi:10.1080/15401383.2013.844656
Bräuninger, I. (2012). Dance movement therapy group intervention in stress treatment: A randomized controlled trial (RCT). The Arts in Psychotherapy, 39, 443–450. doi:10.1016/j.aip.2012.07.002
Brown, K. W., Ryan, R. M., & Creswell, J. D. (2007). Mindfulness: Theoretical foundations and evidence for its salutary effects. Psychological Inquiry, 18, 211–237. doi:10.1080/10478400701598298
Bullet Journal. (2017). Getting started. Retrieved from http://bulletjournal.com/get-started/
Callaghan, P. (2004). Exercise: A neglected intervention in mental health care? Journal of Psychiatric and Mental Health Nursing, 11, 476–483. doi:10.1111/j.1365-2850.2004.00751.x
Carney, J. V. (2007). Humanistic wellness services for community mental health providers. The Journal of Humanistic Counseling, 46, 154–171. doi:10.1002/j.2161-1939.2007.tb00033.x
Cashwell, C. S., Bentley, D. P., & Bigbee, A. (2007). Spirituality and counselor wellness. The Journal of Humanistic Counseling, 46, 66–81. doi:10.1002/j.2161-1939.2007.tb00026.x
Chandler, C. K., Holden, J. M., & Kolander, C. A. (1992). Counseling for spiritual wellness: Theory and practice. Journal of Counseling & Development, 71, 168–175. doi:10.1002/j.1556-6676.1992.tb02193.x
Chong, H. J. (2010). Do we all enjoy singing? A content analysis of non-vocalists’ attitudes toward singing. The Arts in Psychotherapy, 37, 120–124. doi:10.1016/j.aip.2010.01.001
Christopher, J. C., Christopher, S. E., Dunnagan, T., & Schure, M. (2006). Teaching self-care through mindfulness practices: The application of yoga, meditation, and qigong to counselor training. Journal of Humanistic Psychology, 46, 494–509. doi:10.1177/0022167806290215
Connolly Baker, K., & Mazza, N. (2004). The healing power of writing: Applying the expressive/creative component of poetry therapy. Journal of Poetry Therapy, 17, 141–154. doi:10.1080/08893670412331311352
Council for Accreditation of Counseling & Related Educational Programs. (2016). 2016 CACREP standards. Alexandria, VA: Author. Retrieved from http://www.cacrep.org/for-programs/2016-cacrep-standards
Covey, S. R. (2010). Foreword. In A. Pattakos (Ed.), Prisoners of our thoughts: Viktor Frankl’s principles for discovering meaning in life and work (2nd ed., pp. V–XI). Oakland, CA: Berrett-Koehler Publishers.
Cushman, P., & Gilford, P. (2000). Will managed care change our way of being? American Psychologist, 55, 985–996. doi:10.1037//0003-066X.55.9.985
Demakis, J. (2012). The ultimate book of quotations. Seattle, WA: CreateSpace.
Figley, C. R. (2002). Compassion fatigue: Psychotherapists’ chronic lack of self-care. Journal of Clinical Psychology, 58, 1433–1441. doi:10.1002/jclp.10090
Frame, M. W., & Stevens-Smith, P. (1995). Out of harm’s way: Enhancing monitoring and dismissal processes in counselor education programs. Counselor Education and Supervision, 35, 118–129. doi:10.1002/j.1556-6978.1995.tb00216.x
Frame, M. W., & Williams, C. B. (1996). Counseling African Americans: Integrating spirituality in therapy. Counseling and Values, 41, 16–28. doi:10.1002/j.2161-007X.1996.tb00859.x
Franco, G. E. (2016). Productivity standards: Do they result in less productive and satisfied therapists? The Psychologist-Manager Journal, 19, 91–106. doi:10.1037/mgr0000041
Freadling, A. H., & Foss-Kelly, L. L. (2014). New counselors’ experiences of community health centers. Counselor Education and Supervision, 53, 219–232. doi:10.1002/j.1556-6978.2014.00059.x
General Conference of Seventh-Day Adventist World Church. (2016). Living a healthful life. Retrieved from https://www.adventist.org/en/vitality/health
Gentry, J. E. (2002). Compassion fatigue: A crucible of transformation. Journal of Trauma Practice, 1(3–4), 37–61. doi:10.1300/J189v01n03_03
Germer, C. K., & Neff, K. D. (2015). Cultivating self-compassion in trauma survivors. In V. M. Follette, J. Briere, D. Rozelle, J. W. Hopper, & D. I. Rome (Eds.), Mindfulness-oriented interventions for trauma: Integrating contemplative practices (pp. 43–58). New York, NY: The Guilford Press.
Graff, G. (2008). Shame in supervision. Issues in Psychoanalytic Psychology, 30, 79–94.
Granello, P. F. (2013). Wellness counseling. Upper Saddle River, NJ: Pearson Education.
Grosch, W. N. & Olsen, D. C. (1994). When helping starts to hurt: A new look at burnout among psychotherapists. New York, NY: W. W. Norton.
Ivanovski, B., & Malhi, G. S. (2007). The psychological and neurophysiological concomitants of mindfulness forms of meditation. Acta Neuropsychiatrica, 19, 76–91. doi:10.1111/j.1601-5215.2007.00175.x
Kabat-Zinn, J. (1994). Wherever you go, there you are: Mindfulness meditation in everyday life. New York, NY: Hyperion.
Killian, K. D. (2008). Helping till it hurts? A multimethod study of compassion fatigue, burnout, and self-care in clinicians working with trauma survivors. Traumatology, 14(2), 32–44. doi:10.1177/1534765608319083
Knight, W. E., & Rickard, N. S. (2001). Relaxing music prevents stress-induced increases in subjective anxiety, systolic blood pressure, and heart rate in healthy males and females. Journal of Music Therapy, 38, 254–272. doi:10.1093/jmt/38.4.254
Koch, S., Kunz, T., Lykou, S., & Cruz, R. (2014). Effects of dance movement therapy and dance on health-related psychological outcomes: A meta-analysis. The Arts in Psychotherapy, 41, 46–64.
doi:10.1016/j.aip.2013.10.004
Kress, V. E., & Paylo, M. J. (2015). Treating those with mental disorders: A comprehensive approach to case conceptualization and treatment. Upper Saddle River, NJ: Pearson Education.
Lane, M. R. (2005). Creativity and spirituality in nursing: Implementing art in healing. Holistic Nursing Practice, 19, 122–125.
Lent, J. (2009). Journaling enters the 21st century: The use of therapeutic blogs in counseling. Journal of Creativity in Mental Health, 4, 67–73. doi:10.1080/15401380802705391
Linder, S., Miller, G., & Johnson, P. (2000, March). Counseling and spirituality: The use of emptiness and the importance of timing. Paper presented at the meeting of the American Counseling Association, Washington, DC.
Lindholm, J. A. (2003). Perceived organizational fit: Nurturing the minds, hearts, and personal ambitions of university faculty. The Review of Higher Education, 27, 125–149. doi:10.1353/rhe.2003.0040
Lipe, A. W. (2002). Beyond therapy: Music, spirituality, and health in human experience: A review of literature. Journal of Music Therapy, 39, 209–240. doi:10.1093/jmt/39.3.209
Marich, J., & Howell, T. (2015). Dancing mindfulness: A phenomenological investigation of the emerging practice. EXPLORE: The Journal of Science and Healing, 11, 346–356. doi:10.1016/j.explore.2015.07.001
Masci, D., & Lipka, M. (2016, January 21). Americans may be getting less religious, but feelings of spirituality are on the rise. Washington, DC: Pew Research Center. Retrieved from http://www.pewresearch.org/fact-tank/2016/01/21/americans-spirituality
Maslach, C., Leiter, M. P., & Jackson, S. E. (2012). Making a significant difference with burnout interventions: Researcher and practitioner collaboration. Journal of Organizational Behavior, 33, 296–300. doi:10.1002/job.784
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. doi:10.1146/annurev.psych.52.1.397
Matthes, W. A. (1992). Induction of counselors into the profession. The School Counselor, 39, 245–250.
Mellin, E. A., Hunt, B., & Nichols, L. M. (2011). Counselor professional identity: Findings and implications for counseling and interprofessional collaboration. Journal of Counseling & Development, 89, 140–147. doi:10.1002/j.1556-6678.2011.tb00071.x
Myers, J. E., Sweeney, T. J., & Witmer, J. M. (2001). Optimization of behavior: Promotion of wellness. In D. C. Locke, J. E. Myers, & E. L. Herr (Eds.), The handbook of counseling (pp. 641–652). Thousand Oaks, CA: Sage.
Myers, J. E., & Williard, K. (2003). Integrating spirituality into counselor preparation: A developmental, wellness approach. Counseling and Values, 47, 142–155. doi:10.1002/j.2161-007X.2003.tb00231.x
Neff, K. D. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2, 85–101. doi:10.1080/15298860390129863
Neff, K. D., & Costigan, A. P. (2014). Self-compassion, wellbeing, and happiness. Psychologie in Österreich, 2(3), 114–119. Retrieved from http://self-compassion.org/wp-content/uploads/publications/Neff&Costigan.pdf
Neff, K. D., Kirkpatrick, K. L., & Rude, S. S. (2007). Self-compassion and adaptive psychological functioning.
Journal of Research in Personality, 41, 139–154. doi:10.1016/j.jrp.2006.03.004
Newsome, S., Waldo, M., & Gruszka, C. (2012). Mindfulness group work: Preventing stress and increasing self-compassion among helping professionals in training. The Journal for Specialists in Group Work, 37, 297–311. doi:10.1080/01933922.2012.690832
Nielsen, L. A. (1988). Substance abuse, shame and professional boundaries and ethics: Disentangling the issues. Alcoholism Treatment Quarterly, 4, 109–137. doi:10.1300/J020v04n02_08
O’Halloran, T. M., & Linton, J. M. (2000). Stress on the job: Self-care resources for counselors. Journal of Mental Health Counseling, 22, 354–364.
Ohrt, J. H., Prosek, E. A., Ener, E., & Lindo, N. (2015). The effects of a group supervision intervention to promote wellness and prevent burnout. The Journal of Humanistic Counseling, 54, 41–58.
doi:10.1002/j.2161-1939.2015.00063.x
Patsiopoulos, A. T., & Buchanan, M. J. (2011). The practice of self-compassion in counseling: A narrative inquiry. Professional Psychology: Research and Practice, 42, 301–307. doi:10.1037/a0024482
Pennebaker, J. W., & Seagal, J. D. (1999). Forming a story: The health benefits of narrative. Journal of Clinical Psychology, 55, 1243–1254. doi:10.1002/(SICI)1097-4679(199910)55:10<1243::AID-JCLP6>3.0.CO;2-N
Pollack, S. M., Pedulla, T., & Siegel, R. D. (2014). Sitting together: Essential skills for mindfulness-based psychotherapy. New York, NY: The Guilford Press.
Reese, R. F., & Myers, J. E. (2012). EcoWellness: The missing factor in holistic wellness models. Journal of Counseling & Development, 90, 400–406. doi:10.1002/j.1556-6676.2012.00050.x
Riordan, R. J. (1996). Scriptotherapy: Therapeutic writing as a counseling adjunct. Journal of Counseling and Development, 74, 263–269. doi:10.1002/j.1556-6676.1996.tb01863.x
Rogers, C. R. (1961). On becoming a person: A therapist’s view of psychotherapy. Boston, MA: Houghton Mifflin.
Rogers, C. R. (1980). A way of being. New York, NY: Houghton Mifflin Harcourt.
Rogers, N. (1993). The creative connection: Expressive arts as healing. Palo Alto, CA: Science and Behavior Books.
Ross, A., & Thomas, S. (2010). The health benefits of yoga and exercise: A review of comparison studies. The Journal of Alternative and Complementary Medicine, 16, 3–12. doi:10.1089=acm.2009.0044
Rust, J. P., Raskin, J. D., & Hill, M. S. (2013). Problems of professional competence among counselor trainees: Programmatic issues and guidelines. Counselor Education and Supervision, 52, 30–42.
doi:10.1002/j.1556-6978.2013.00026.x
Ruysschaert, N. (2009). (Self) hypnosis in the prevention of burnout and compassion fatigue for caregivers: Theory and induction. Contemporary Hypnosis, 26, 159–172. doi:10.1002/ch.382
Schanche, E., Stiles, T. C., McCullough, L., Svartberg, M., & Nielsen, G. H. (2011). The relationship between activating affects, inhibitory affects, and self-compassion in patients with Cluster C personality disorders. Psychotherapy, 48, 293–303. doi:10.1037/a0022012
Schaufeli, W., & Enzmann, D. (1998). The burnout companion to study & practice: A critical analysis. Philadelphia, PA: Taylor and Francis.
Skovholt, T. M. (2012). The counselor’s resilient self. Turkish Psychological Counseling and Guidance Journal, 4(38), 137–146. Retrieved from http://www.pegem.net/dosyalar/dokuman/138861-20140125102831-1.pdf
Skovholt, T. M., Grier, T. L., & Hanson, M. R. (2001). Career counseling for longevity: Self-care and burnout prevention strategies for counselor resilience. Journal of Career Development, 27, 167–176. doi:10.1023/A:1007830908587
Smallwood, J., & Schooler, J. W. (2015). The science of mind wandering. Annual Review of Psychology, 66, 487–518. doi:10.1146/annurev-psych-010814-015331
Snyder, B. A. (1997). Expressive art therapy techniques: Healing the soul through creativity. Journal of Humanistic Education & Development, 36, 74–82. doi:10.1002/j.2164-4683.1997.tb00375.x
Sori, C. F., Biank, N., & Helmeke, K. B. (2006). Spiritual self-care of the therapist. In K. B. Helmeke & C. F. Sori (Eds.), The therapist’s notebook for integrating spirituality in counseling: Homework, handouts, and activities for use in psychotherapy (Vol. 1, pp. 3–18). Binghamton, NY: The Haworth Press.
Thompson, E. H., Frick, M. H., & Trice-Black, S. (2011). Counselor-in-training perceptions of supervision practices related to self-care and burnout. The Professional Counselor, 1, 152–162. doi:10.15241/eht.1.3.152
Thompson, I., Amatea, E., & Thompson, E. (2014). Personal and contextual predictors of mental health counselors’ compassion fatigue and burnout. Journal of Mental Health Counseling, 36, 58–77. doi:10.17744/mehc.36.1.p61m73373m4617r3
Utley, A., & Garza, Y. (2011). The therapeutic use of journaling with adolescents. Journal of Creativity in Mental Health, 6, 29–41. doi:10.1080/15401383.2011.557312
Valente, V., & Marotta, A. (2005). The impact of yoga on the professional and personal life of the psychotherapist. Contemporary Family Therapy, 27, 65–80. doi:10.1007/s10591-004-1971-4
Walsh, R. (2011). Lifestyle and mental health. American Psychologist, 66, 579–592. doi:10.1037/a0021769
Warren, J., Morgan, M. M., Morris, L.-N. B., & Morris, T. M. (2010). Breathing words slowly: Creative writing and counselor self-care—The writing workout. Journal of Creativity in Mental Health, 5, 109–124.
doi:10.1080/15401383.2010.485074
Wikström, B. M. (2005). Communicating via expressive arts: The natural medium of self-expression for hospitalized children. Pediatric Nursing, 31, 480–485.
Witmer, J. M., & Young, M. E. (1996). Preventing counselor impairment: A wellness approach. The Journal of Humanistic Counseling, 34, 141–155. doi:10.1002/j.2164-4683.1996.tb00338.x
Wright, J. K. (2003). Writing for protection: Reflective practice as a counsellor. Journal of Poetry Therapy, 16, 191–198. doi:10.1080/0889367042000197376
Yager, G. G., & Tovar-Blank, Z. G. (2007). Wellness and counselor education. The Journal of Humanistic Counseling, 46, 142–153. doi:10.1002/j.2161-1939.2007.tb00032.x
Yob, I. M. (2010). Why is music a language of spirituality? Philosophy of Music Education Review, 18, 145–151. doi:10.2979/pme.2010.18.2.145
Susannah C. Coaston is an assistant professor at Northern Kentucky University. Correspondence can be addressed to Susannah Coaston, 1 Nunn Drive, MEP 203C, Highland Heights, KY 41099, coastons1@nku.edu.
