May 22, 2024 | Volume 14 - Issue 1
Darius A. Green, Katharine R. Sperandio
Because of the long history of anti-drug policing in the United States and the criminalization of substance use, clients who use substances are vulnerable to direct and vicarious experiences of police violence. Consequently, those who use substances may face a greater risk of experiencing symptoms of trauma that counselors should address in treatment. We recommend the use of a trauma-informed and abolitionist praxis in clinical and social justice practices as a framework to support clients who use substances and have histories of exposure to police violence.
Keywords: substance use, police violence, trauma, abolitionist, social justice
Policing in the United States has received increased scrutiny in recent years with renewed attention resulting from the Black Lives Matter protests in 2020. Specifically, policing has been critiqued by prison–industrial complex abolitionists—activists who advocate toward an end to systems of policing, prisons, and related carceral systems in favor of systems and practices that promote accountability, justice, healing, and transformation—as being inherently violent, meaning that it relies on the use of behavior that is considered violent in any context (Cullors, 2019; A. Y. Davis et al., 2022; Green, 2022; Kaba, 2021; Klukoff et al., 2021). Violence is defined as “the intentional use of physical force or power, threatened or actual, against oneself, another person or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation” (Krug et al., 2002, p. 5). Thus, we define police violence as the inherently violent uses of force by police officers. According to the World Health Organization, there are four types of violence that can be used to categorize police violence: physical (e.g., arrests and the use of weapons), sexual (e.g., strip searching and sexual assault), psychological (e.g., intimidation and verbal threats), and neglect (e.g., failing to provide support to medical and mental health needs; DeVylder et al., 2017; Krug et al., 2002).
Current data suggests that 58.3 million U.S. residents over the age of 16 experienced contact from police officers in 2020 with roughly 1 million experiencing or being threatened with non-fatal force (Tapp & Davis, 2022). Moreover, of the 82 million arrests reported by the Federal Bureau of Investigation (FBI; 2022) between 2011 and 2021, substance use violations were the second most common arrests, accounting for 14% of arrests. Oftentimes, counselors may work with clients who have been court-ordered to treatment as part of diversion programs that seek to route individuals away from incarceration and toward treatment for criminalized behaviors, such as substance use (Scott, 2020). Given that substance use–related offenses are among the most common offenses leading to violence through an arrest (FBI, 2022), it is essential for substance use counselors to prepare to address experiences of police violence that may result from anti-drug policing—the use of police violence as a response to individuals who use substances. Although anti-drug policing impacts both those who use substances and those who traffic them, our discussion on anti-drug policing will focus on populations who use substances.
Research on counselor preparation suggests that most counselors receive no training regarding clinical practice and advocacy to address matters of police violence despite a recent study that found that 68.2% of counselors reported working with clients who had experienced police violence (Green & Evans, 2021). Moreover, Bride et al. (2009) found that most substance use counselors do not learn about treating psychological trauma in their academic programs and instead predominantly rely on continuing education. Given the vulnerable nature of those who use substances and evidence suggesting that gaps exist in training counselors in treating police violence and trauma, we will explore approaches to clinical practice, social justice, and advocacy to best support substance use clients who experience police violence because of anti-drug policing. Specifically, the purpose of this article is to provide a sociopolitical analysis of anti-drug policing in the United States that informs our proposal for substance use counselors to adopt and integrate an abolitionist praxis into their practice of counseling with clients who use substances.
Sociopolitical Context of Anti-Drug Policing in the United States
Initiated by President Richard Nixon in 1971 and escalated by President Ronald Reagan in 1982, the war on drugs increased and incentivized anti-drug policing and enforcement, intensified legal penalties associated with drug-related crimes, and demonized individuals, particularly those who were part of marginalized communities and struggled with substance use disorders (Benson et al., 1995; Cooper, 2015; Koram, 2022; Park et al., 2019). Cooper (2015) and Saleem (1997) noted that contemporary anti-drug policing practices, such as stop-and-frisk and police drug raids, have been permitted through court cases such as Terry v. Ohio, Whren v. United States, and Illinois v. Wardlow and have eroded the Fourth Amendment and 1878 Posse Comitatus Act protections against unreasonable searches, seizures, and militarization of policing. Specifically, these court cases have permitted frisking for reasonable suspicion, allowed police to conduct stops in which police may stop individuals for suspicion of drugs under the pretext of other minor criminalized violations, and expanded the definition of suspicious behavior that may warrant being stopped by police (Cooper, 2015; Saleem, 1997). Although several anti-drug policing reforms have been made, such as the development of drug courts and the decriminalization of substances in various states (Klukoff et al., 2021; Scott, 2020), anti-drug policing practices have persisted, expanded, and received legislative support. For example, despite stop-and-frisk searches being declared unconstitutional in 2013 with the decision in Ligon v. City of New York, the practice was reduced by 98% by 2017 as opposed to ceasing entirely (New York Civil Liberties Union, n.d., 2019). Despite this decrease, racial disparities were maintained in these stop-and-frisk practices between 2014 and 2017, as 53% of targets were Black and 28% were Latino (New York Civil Liberties Union, 2019). Lastly, President Donald Trump voiced support for greater anti-drug policing efforts, while President Joseph Biden’s Safer America Plan seeks reform that simultaneously increases funding for policing and substance use treatment resources (Kaba & Ritchie, 2022; Koram, 2022; The White House, 2022). Although these systemic supports for reform from the executive branch may be aimed at drug trafficking, individuals who use substances may be at continued risk of being impacted by anti-drug policing with the increased support for and reliance on carceral approaches.
Although reforms related to criminalized behaviors may reduce harm through their trauma-informed focus, abolitionist authors and activists have critiqued such reforms as counter-productive when they expand the power and legitimacy of policing, maintain the criminalization of substance use, and perpetuate harm and violence toward those who use substances (Klukoff et al., 2021; Purnell, 2021a). For example, according to Fazel et al. (2017), 24% of the global imprisoned population meets the criteria for alcohol use disorder, compared to the less than 2% of the general population (Global Burden of Disease Network, 2016). Similarly, 30% of male prisoners and 51% of female prisoners meet the criteria for illicit drug use disorder, while less than 1% of the global population meets the criteria (Global Burden of Disease Network, 2016). Moreover, as stated earlier, substance use violations are the second most common arrest reason in the United States (FBI, 2022). Lastly, some authors have concluded that mixed results exist on the effectiveness of diversion programs for offenses associated with mental illness and substance use regarding recidivism and subsequent arrests (Klukoff et al., 2021; Scott, 2020). These data highlight a prevalent connection between policing, incarceration, and substance use in the United States and around the world despite contemporary reforms to anti-drug policing established through the war on drugs.
Policing functions to maintain social order and provide security by enforcing laws, policies, and social norms (Bureau of Justice Statistics, 2021; Giovengo, 2016). Moreover, police are ordained to investigate, arrest, and enact force upon those deemed as, or suspected to be, threatening to the safety and interests of dominant communities. Thus, the criminalization of substance use has been conceptualized as exerting control over and oppressing minoritized groups (Dollar, 2019; Purnell, 2021b). Marginalized communities have been hit especially hard by these zero tolerance policies, which drastically increased community members’ run-ins with police (Cooper, 2015). For example, the influx of stop-and-frisk procedures, a method that permitted police officers to detain an individual suspected of illegal activity and physically search them, led to minoritized individuals being racially profiled and targeted for searches without specific cause (Cooper, 2015). In fact, anti-drug policing has resulted in a shift from Black people accounting for 22% of those arrested in 1976 to 40% in 1992, despite making up 12% of the U.S. population (Cooper, 2015; Tonry, 1994). Thus, instead of eliminating substance use in communities, these crackdowns have only further increased the prevalence of police brutality, traumatized communities and individuals, and increased violence within communities (Cooper, 2015; Rhodes et al., 2006; Werb et al., 2011).
Structural Violence and Trauma From Anti-Drug Policing
Given the confiscation of an individual’s bodily autonomy, resulting in the infringement of the individual’s basic and constitutional rights and liberties, as well as the possibility for physical harm to take place during searches, anti-drug policing, which can involve violence, harassment, and killings, can place significant psychological stress and turmoil on targeted individuals (Park et al., 2019; Sarang et al., 2010). It is essential to analyze the long-term consequences of police violence perpetuated upon impacted individuals, including the possibility of traumatization and death (Bryant-Davis et al., 2017; Cooper, 2015; Krieger et al., 2015). Emerging research has demonstrated connections between being stopped by police and symptoms of anxiety and post-traumatic stress disorder (PTSD), particularly when the experience is perceived as intrusive and unjustified (Geller et al., 2014); suicide attempts (DeVylder et al., 2017); and symptoms of manic and depressive episodes (Meade et al., 2017). Likewise, vicarious traumatization from watching or learning of another individual experiencing police violence is also a concern given the high proportion of individuals living with substance use disorders who have both experienced trauma and witnessed police violence (El-Bassel et al., 2011; Park et al., 2019; Shaw et al., 2016). Research on those who witness police violence has often emphasized the unique impact on Black people. This research has demonstrated associations with vicarious exposure and poor mental health (Bor et al., 2018), distress from anticipated exposure following media consumption (Green et al., 2024), and psychological distress among Black mothers (Joe et al., 2019). Galovski et al. (2016) demonstrated that community protests following instances of police violence may result in symptoms of depression and PTSD among community members. Additionally, recent research has demonstrated a connection between vicarious exposure and increased cannabis use among Black Americans (Motley et al., 2022). Taken together, these findings suggest that directly and vicariously experiencing police violence may promote greater risk of traumatization.
Literature suggests that these encounters with police may end in violence beyond psychological distress because of the influence of stigmatization and prejudice against people who use substances (Cooper et al., 2005; Hayashi et al., 2013; Lunze et al., 2015; Wood et al., 2017). Officers may also confiscate civilians’ syringes during stop-and-frisk encounters, increasing the prevalence of syringe sharing, a known risk factor for HIV and HCV transmission (Beletsky et al., 2010; Park et al., 2019; Small et al., 2007). Detainment for substance use is also associated with increased risk of death following release because of withdrawal and increased risk of overdose (Chang et al., 2015; Fazel et al., 2017; Kinner et al., 2012; Pratt et al., 2010). Stress and traumatization experienced from anti-drug policing is also associated with high-risk behaviors, including drug injection, among addicted individuals (Maher, 2004; Shannon et al., 2008; Volkmann et al., 2011). Moreover, in one study, individuals needing treatment for substance use disorders were 2.74 times more likely to experience arrest and physical assault from police (Werb et al., 2016). Additionally, Werb et al. (2016) found that 27.5% of police encounters occurred within 500 meters of a substance use treatment facility. Similarly, Park et al. (2019) found in a sample of people who inject drugs in Baltimore that 7% experienced physical police violence and one in four knew someone else who had experienced physical police violence, fueling a deep mistrust of the system. Fear of potential retaliation by the police may also discourage individuals, particularly those with marginalized identities, from going to the police during a crisis or emergency situation, such as in cases of overdose. This mistrust of the system negatively impacts individuals’ willingness to pursue treatment services, especially when they are in fear of being detained or harmed by police officers (Alang et al., 2017; Cooper, 2015; Park et al., 2019). For example, a qualitative study described the impact of increased surveillance from police as both threatening and interfering with harm reduction practices (Cooper et al., 2005). Treatment centers are typically more centralized in areas where there is a higher drug activity which means that, because policing has a significant presence in these parts of communities, individuals may be hesitant to seek out help and support to avoid police encounters, negatively impacting social and health outcomes (Werb et al., 2016). Additionally, these crackdowns are associated with reductions in syringe exchange programs, drug treatment, and HIV testing accessibility (C. S. Davis et al., 2005; Park et al., 2019; Ti et al., 2013). These findings highlight how anti-drug policing actively inhibits access to safe and needed care.
A Case for Abolition in Substance Use Counseling
Because of the increased risk of experiencing police violence and the subsequent risk for traumatization from police violence, it is essential for counselors to address encounters stemming from anti-drug policing in treatment and develop practices that divest from policing practices and systems. Trauma-informed practice is a “fundamental obligation” (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014, p. 5) for counselors who work with clients at the intersections of substance use and police violence to reduce or mitigate the adverse impacts of trauma on individuals’ physical, emotional, psychological, and spiritual well-being and to prevent further systemic (re)traumatization. Trauma-informed practice is that which recognizes and understands the impact and salience of trauma, effectively responding to it in ways that do not retraumatize and further perpetuate traumatic stress while also recognizing that marginalized groups are at greater risk of experiencing trauma and its effects (SAMHSA, 2014; Sweeney & Taggart, 2018). There are four assumptions that ground trauma-informed practices (adapted from SAMHSA, 2014): 1) a realization of the potentially long-lasting effects of trauma on individuals, communities, groups, families, and systems and that trauma can be perpetuated by systems like the criminal legal system, resulting in a significant impact on continued substance use and mental health; 2) the importance of recognizing the signs of trauma and refraining from pathologizing these responses; 3) the crucial need for a system or organization to respond supportively by applying the six principles of a trauma-informed approach; and 4) resisting the potential to retraumatize individuals who are accessing supports and care. Moreover, SAMHSA (2014) identified six principles of trauma-informed practices that are intended to serve as the fundamental spirit of trauma-informed care: 1) safety; 2) trustworthiness and transparency; 3) peer support; 4) collaboration and mutuality; 5) empowerment, voice, and choice; and 6) cultural, historical, and gender issues.
By SAMHSA’s description, current substance use treatment falls short of being trauma-informed when it occurs under systemic conditions in which anti-drug policing and police violence are part of the historical and current response in the treatment and care of individuals who struggle with substance use. As outlined above, anti-drug policing practices can result in police violence that includes stop-and-frisk, arrests, and an intimidating presence that may negatively interfere in treatment accessibility for individuals who are fearful of potential run-ins and harassment (Werb et al., 2016). Anti-drug policing and the broader criminalization of substance use may disrupt safety, retraumatize substance use clients, and diminish trust and transparency in accessing substance use treatment. Moreover, incarceration for using substances may inhibit the potential for peer support and collaborative approaches to treatment. Lastly, the existing racial disparities in anti-drug policing practices demonstrate a history of systemic racism that may disproportionately create a barrier to accessing trauma-informed care for racially marginalized groups, particularly Black Americans. Thus, we contend that an abolitionist praxis that opposes anti-drug policing and divests from carceral approaches to responding to individuals who use substances is needed to fully realize trauma-informed practice with clients who use substances.
Abolitionist Praxis for Substance Use Counseling
Abolition is a social justice praxis that is commonly referenced as a necessary solution to policing and its impact (A. Y. Davis et al., 2022; Kaba, 2021). Abolition refers to the broad movement of divesting from and eliminating carceral systems, such as law enforcement and prison systems, and carceral logics that seek to legitimize the use of punishment, retribution, and vengeance through carceral systems. Rooted in the efforts of Black feminist thought, advocacy, and organizing, abolition calls for a critical analysis of the ways in which policing has functioned to enact the violence of overlapping systems of oppression (Kaba & Ritchie, 2022). Kaba and Ritchie (2022) identified three objectives of abolitionist praxis. First, abolitionist praxis seeks to create collective safety from community violence and the violence of policing and related carceral systems that reinforce systems of oppression, such as White supremacy, patriarchy, and capitalism (Kaba, 2021; Kaba & Ritchie, 2022; Purnell, 2021a). Second, abolitionist praxis seeks to end violence from carceral systems through eliminating those systems as opposed to seeking reforms that preserve the inherent violence of policing and incarceration (Kaba & Ritchie, 2022; Klukoff et al., 2021). This second objective extends beyond institutions of policing and incarceration and extends to the ways in which carceral logic and behaviors of policing are embedded in other systems, institutions, and communities and often internalized by individuals (Kaba & Ritchie, 2022). Lastly, to achieve collective safety, abolitionist praxis necessitates a simultaneous transformation from reliance on the violence of policing and related carceral systems toward cultivating cultures, systems, communities, and ways of being that are centered around care, healing, justice, and accountability (Kaba & Ritchie, 2022).
Abolition exists beyond a theoretical and conceptual framework. It is an iterative process that combines theorizing, action, and reflection upon efforts that divest from and dismantle carceral systems and logics while simultaneously brainstorming solutions to community violence that promote safety, healing, and justice (Cullors, 2019; A. Y. Davis et al., 2022; Kaba & Ritchie, 2022; Klukoff et al., 2021). Abolitionist praxis often utilizes a transformative justice framework to achieve its objective of eliminating carceral systems while creating new systems and ways of being that foster safety, healing, and justice. Transformative justice aligns with abolitionist praxis in that it is a liberatory strategy that seeks to transform systems and structures that create the conditions for violence (Afuape & Kerry Oldham, 2022). While policing and incarceration focus on retributive justice that assigns inherently violent punishment as a mechanism for change regardless of the harm it causes, transformative justice through abolitionist praxis seeks to create processes of accountability for harm caused interpersonally from criminalized behaviors and systemically from policing and related carceral systems. As a result, abolitionist praxis utilizes transformative justice to create new systems, institutions, communities, strategies, and internalized ways of being that value safety, healing, and justice that are needed to cultivate trauma-informed care and practices for substance use clients.
Regarding substance use counseling, an abolitionist praxis seeks to reduce and eliminate violence as a response to substance use, decriminalize all substance use, and eliminate contact between substance use clients, police, and the broader criminal legal system. Similarly, an abolitionist praxis to substance use counseling challenges the logic that criminalization is a needed step in treatment for substance use. For example, in 2001, the Portuguese government enacted nationwide laws to decriminalize all substances, resulting in a decrease in the prevalence of drug use and overdose rates (Castelpietra et al., 2022; James et al., 2020; Pombo & da Costa, 2016; Smiley-McDonald et al., 2023). In 2021, Oregon decriminalized low-level drug possessions and subsequently increased options for substance use disorder treatment and harm reduction programs (Good et al., 2023; Smiley-McDonald et al., 2023). In their study, Smiley-McDonald et al. (2023) found that the Oregon legislation resulted in a decrease in the number of interactions between police officers and individuals who use drugs. Thus, the abolitionist goal of decriminalizing substance use while implementing harm reduction programs may function to both minimize inherently violent contact with police and reduce the prevalence of substance use.
Abolitionist praxis would also call for the development of accountability for interpersonal and community harm caused by client substance use that does not rely on legal punishment, or the threat of it, from the criminal legal system (Cullors, 2021). Accountability for harm caused under abolitionist theory entails a developed recognition of wrongdoing and harm, both interpersonally and as mediated by social, economic, and political context, and sustained effort toward intrapersonal, interpersonal, and institutional change that repairs harm (Cullors, 2021; Kaba, 2021). Counselors must re-envision both their clinical practice and engagement in advocacy toward abolition to holistically care for clients who use substances.
Clinical and Advocacy Recommendations
Given the previously outlined mental health outcomes that are associated with direct and vicarious experiences of police violence that suggest its traumatic impact (DeVylder et al., 2017; Galovski et al., 2016; Geller et al., 2014; Green et al., 2024; Joe et al., 2019; Meade et al., 2017; Motley et al., 2022), a trauma-informed approach is essential to working with those who experience police violence as a consequence of anti-drug policing. Counselors seeking to use a trauma-informed approach to treat substance use disorders must infuse abolition into their delivery of services while also engaging in advocacy beyond direct clinical work to better achieve SAMHSA’s six identified principles of trauma-informed practice. We provide an abolitionist framing of these six principles and offer abolitionist re-envisioning for substance use counseling below. Moreover, we adapted the sixth principle of cultural, historical, and gender issues to cultural competence and advocacy to emphasize the professional role of advocacy in counseling for substance use clients who experience anti-drug policing.
Safety
Ensuring safety in the therapeutic space is essential because anti-drug policing and the threat of police violence pose a safety risk to clients who use substances and are involved in or at risk of being targeted by the legal system. One step toward maximizing safety for clients is to end the use of abstinence-based treatment. Given that counselors may serve as treatment referral sources for court-mandated clients who meet criteria for diversion programs that seek to route individuals toward treatment for substance use and away from incarceration (Scott, 2020), abstinence-based treatment needs critical examination. Although such interventions can reduce engagement in substance use and mental health symptoms (Pinals et al., 2019), they do so with a looming threat of police violence and incarceration as a consequence for failure to complete the requirements of the diversion program (Scott, 2020). This poses a value conflict with counselors who are treating court-mandated clients for substance use. Counselor participation in diversion programs may require disclosures of client participation and progress in counseling that may lead to legal consequences for clients if they do not meet requirements of the diversion program. For example, counselors may be ethically obligated to document client relapses, which are more common in substance use treatment for minoritized groups and those with histories of experiencing multiple traumatic events (Farley et al., 2004; Heffner et al., 2011), which may be requested by probation officers, attorneys, or courts. In such a scenario, disclosure of client progress in treatment could produce a risk of clients experiencing police violence and incarceration. Moreover, this may produce a circumstance in which a client’s dominant motive for engaging in treatment is to avoid the consequences of police violence and incarceration. Consequently, acknowledging the intrapersonal, interpersonal, and community impact of one’s substance use and engaging in accountability are likely to become secondary motives for change and repair of any harm caused. Although the potential for incarceration may serve as motivation for change for substance use clients, substance use counselors can align with an abolitionist praxis by engaging in theorizing to develop methods and systems that motivate client accountability and transformation without the threat of violence induced by carceral systems. Moreover, alignment with an abolitionist praxis may require substance use counselors to proactively use their power to advocate for harm reduction in treatment as alternatives to approaches that risk harm through police violence and incarceration. Harm reduction approaches emphasize safe use over non-use of substances and have demonstrated evidence of both maintained and reduced substance use, reductions in harm related to substance use (e.g., less police contact and fewer arrests and emergency hospital visits), and self-reports of feeling safer (Carrico et al., 2014; Smiley-McDonald et al., 2023; Vallance et al., 2016).
Anti-drug policing views substance use as threatening and seeks to foster security through violent force and criminalization (Kaba, 2021). This security comes at the expense of the safety and well-being of those who use substances. An abolitionist re-envisioning of safety is one that seeks to ensure safety from the harm that both substance use and carceral systems cause to individuals, families, and communities. Regarding safety for substance use clients who experience anti-drug policing, Drustrup et al. (2023) offered an abolitionist approach to safety planning that counselors can adapt to fit the needs of clients mandated to substance use treatment. This approach decenters the default reliance on police in crises and emergencies and emphasizes collaboration with clients to establish methods that can maintain safety. Adapting this to clients, counselors can minimize disclosures of substance use, especially to police, probation officers, and employees of the criminal legal system. Noting the importance of building networks of care in place of carceral systems (Drustrup et al., 2023; Kaba, 2021), counselors should simultaneously collaborate with clients to identify interpersonal and community mechanisms to maintain safety and progress toward substance use–related treatment goals, particularly for when relapses occur. Consequently, this also promotes safety from the impact of substance use and client empowerment, voice, and choice in their treatment and wellness. For example, counselors could simultaneously utilize family therapy as a mechanism to support structural change associated with the development of a client’s substance use and to promote accountability for harm caused by substance use within the family system. Furthermore, when harm from substance use extends to one’s community, in collaboration with clients and those directly impacted, counseling could be used to promote reparation for harm caused (Cullors, 2019). Counselors should be mindful of the possibility that clients may not readily share experiences of police violence and substance use because of distrust fostered by carceral systems and if they have experienced invalidation, blame, or neglect regarding their experiences of police violence. Thus, counselors can enhance safety, trust, and the potential for change with clients through a consistent practice of accurate empathy and attunement to clients’ subjective experience of police violence (Miller & Rollnick, 2013).
Trustworthiness and Transparency
Trustworthiness and transparency are essential given the systemic distrust fostered by histories of collaboration between helping professions and carceral systems (Jacobs et al., 2021; Klukoff et al., 2021). Counselors need to promote an optimal level of safety and trustworthiness with their clients through nonjudgement, empathy, transparency, positive regard, validation, normalization of the client’s responses to adversity, and consistency (SAMHSA, 2014). Counselors pursuing abolition can establish trustworthiness and transparency through using the informed consent process to build rapport and establish parameters of the therapeutic relationship within a societal context that largely criminalizes substance use. While Drustrup et al. (2023) offered inspiration for abolition in the therapeutic relationship, counselors are ethically obligated to make exceptions to confidentiality when imminent risk to self and others is established. Additionally, as mentioned above, substance use counselors may be required to make exceptions to confidentiality to share progress for court-mandated clients. Informing clients of these exceptions to confidentiality is standard in helping professions; however, abolition can maximize trustworthiness and transparency by going beyond merely capturing client signatures on informed consent documents. In addition to establishing the limits of confidentiality, counselors pursuing abolition are recommended to ensure that clients fully understand these limits and the impact of these limits on their participation in the therapeutic context. For example, a substance use counselor could clearly articulate known risks of making exceptions to confidentiality of the therapeutic relationship with police and legal system employees, such as increased risk of experiencing police violence, incarceration, and state-sanctioned surveillance. Counselors pursuing abolition who are directly embedded in carceral systems as a function of their employment, such as prisons, should inform clients of any dual or conflicting interests associated with their counseling in the prison system. Additionally, counselors can use open-ended questioning to provide clients an opportunity to check their understanding of confidentiality, its limits, and the impact of needing to make exceptions to confidentiality. Moreover, counselors pursuing abolition should collaborate with clients to identify external resources to counseling that offer greater trustworthiness that can facilitate transformation and healing from substance use in situations where clients may feel a lack of trust in counseling because of the threat of carceral systems.
Peer Support
Providing opportunities for peer support for clients who have experienced police violence and are living with substance use disorders could also be promotive and helpful for healing because of the access to other individuals who have undergone similar experiences. Group therapy has been associated with positive mental health outcomes, particularly among individuals with PTSD and substance use disorders, due to receiving mutual support from others who have similar experiences and can provide empathy, a sense of belongingness and collectivism, and the opportunity to provide and receive feedback; build safety through interpersonal relationships; and reduce feelings of isolation and loneliness (Barrera et al., 2013; Mott et al., 2013; Schwartze et al., 2019; Sloan et al., 2013). Substance use counselors pursuing abolition can actively incorporate group therapy within the therapeutic context and help clients heal following traumatization from police violence while promoting their long-term recovery. Additionally, counselors employed in treatment centers who are pursuing abolition should be mindful of added benefits toward safety and trustworthiness that embedding peer support can offer, particularly for court-mandated clients. When a client is unable to experience enough safety and trustworthiness because of the threat and impact of carceral systems, embedded peer support that exists outside of the counselor–client relationship can provide alternate spaces for clients to be heard and validated. Abolitionist substance use counselors can advocate for the inclusion of peer mentoring for accountability and transformation akin to that which exists within 12-step groups through sponsor relationships. Although it may be conceptualized as part of a process of accountability to utilize clients who have advanced in their treatment as peer mentors, counselors pursuing abolition should also consider the feasibility of paying peer mentors to avoid replicating the occurrence of unpaid and underpaid labor that may occur in prison systems.
Collaboration and Mutuality
It is essential for counselors pursuing abolition to cultivate environments and therapeutic relationships that promote collaboration and mutuality. It would behoove substance use counselors to utilize frameworks for treatment that are inherently trauma-informed and collaborative, such as motivational interviewing, for assessing client motivation for change and structuring treatment with clients that is centered around partnership, acceptance, compassion, and evocation (Clark et al., 2014; Miller & Rollnick, 2013). These efforts may be particularly beneficial for clients who have experienced police violence as a result of anti-drug policing in that they allow greater client participation and trustworthiness to a client population that may be prone to experiencing coercion and restricted freedom and being acted upon. Abolitionist substance use counselors can foster greater collaboration and mutuality in their practice of counseling by making mutual aid foundational to their practice. Mutual aid is an intentional resistance to reliance on institutions that cause structural violence (S. W. Davis & Fayter, 2021; Jacobs et al., 2021). Instead of relying on such institutions, mutual aid seeks to establish networks of care that use community members and resources to meet the needs of others (S. W. Davis & Fayter, 2021; Jacobs et al., 2021). Establishing mutual aid in substance use counseling for clients who experience anti-drug policing requires counselors to advocate to establish and streamline connections to community resources that address underlying, unmet, or neglected needs of clients that play a role in their use of substances and experience of anti-drug policing. For example, an abolitionist substance use counselor may actively coordinate with community agencies that provide support in securing shelter to mitigate substance use and the risk of subsequent anti-drug policing that may be associated with homelessness. Integrating peer support and mentoring, as mentioned previously, within and outside of treatment facilities could function as mutual aid; however, substance use counselors working in carceral institutions may experience pushback to such efforts given that mutual aid seeks divestment from carceral systems (S. W. Davis & Fayter, 2021). Lastly, in terms of collaborative goal-setting, the counselor can work with the client to identify the client’s objectives for attending therapy. The counselor is recommended to honor the client’s voice and work with the client to establish whether the client would like to refrain from using substances in the future, engage in harm reduction practices, and/or process the trauma that the client may have experienced at the hands of police.
Empowerment, Voice, and Choice
Anti-drug policing, incarceration, drug courts, and related carceral approaches to substance use may use interventions that limit the agency of those subjected to their demands. Counselors can engage in an abolitionist praxis that is rooted in trauma-informed practice by screening and assessing for the prevalence and impact of police violence as a potentially traumatic stressor that relates to the use of substances (Green, 2022; Green & Evans, 2021). Given the importance of divesting from carceral systems and logic in abolitionist praxis, counselors need to engage in an ongoing and iterative process of reflection and change in attitudes and practices that reinforce the criminalization of substance use and practices that treat it as the moral failure of the individual. This can be achieved through screening and assessment for substance use and police violence that counteracts experiences of shame and guilt that may be fostered from interactions with police and the criminal legal system (Clark et al., 2014). Moreover, abolitionist praxis in counseling with clients who experience police violence due to anti-drug policing requires a strength- and healing-oriented approach as an act of radical resistance to the pathologizing and moralizing norm of carceral approaches (Cook et al., 2014; Moh & Sperandio, 2022). In practice, this may entail an intentional focus on a client’s progress in collaboratively defined goals and support in actualizing accountability for harm caused from substance use. Similarly, this would require a commitment to approaching clients who use substances with care and compassion, rather than criminalizing, shaming, or infantilizing the individual’s responses to trauma and violence they have endured prior to, during, or after their substance use. Lastly, abolitionist praxis in the context of substance use treatment may require counselors to provide opportunities for clients to have input regarding their needs in treatment by prioritizing individualized treatment over a standardized “one size fits all” approach to counseling. Thus, rather than prescribing a course of treatment or implementing treatment prescribed by a referring carceral system, abolitionist praxis would leverage collaboration to allow clients to have a voice in determining what they need to cope and heal from their use of substances and any traumatic experiences that precede and result from substance use.
Cultural Competence and Advocacy
Abolitionist praxis requires efforts to repair histories of structural violence (Cullors, 2019); thus, substance use counselors pursuing abolition must develop a critical understanding of the sociopolitical history of anti-drug policing toward those who use substances. This article provided a snapshot of this history as a starting point; however, counselors can delve further into learning about the intersection of anti-drug policing and race, gender, sexuality, disability, and socioeconomic status to develop more robust competence in addressing the scope of anti-drug policing. Counselors should critically reflect upon this historical knowledge to confront and actively dismantle any internalized biases they may have about substance use clients that are perpetuated by carceral systems. Counselors should specifically become aware of how the criminal legal system may perpetuate racial prejudice, particularly anti-Black racism, and how these attitudes affect the counselor’s conceptualization of their clients to avoid pathologizing or blaming the client for the structural violence they endure through anti-drug policing. To that end, counselors should actively incorporate practices that are not only trauma-informed, but also culturally responsive (SAMHSA, 2014).
Abolitionist praxis aimed at repairing historical structural violence through anti-drug policing would broadly include efforts toward the decriminalization of substance use. In addition to decriminalization efforts, counselors engaged in an abolitionist praxis might advocate with legal professionals and lawmakers for the retroactive and automatic expungement of drug-related criminal record charges for substance use clients (Adinoff & Reiman, 2019). These efforts would ensure that those with histories of substance use disorder are able to experience transformation that such records and their associated stigma may hinder. Given that abolition calls for counselors to address and promote healing from issues that underlie substance use, counselors seeking to engage in abolitionist praxis should advocate for funds that are currently and formerly used toward criminalizing substance use to be invested in transformative justice practices and trauma-informed treatment for substance use disorders (Adinoff & Reiman, 2019). For example, abolitionist praxis would call for transformative justice systems and practices to replace drug courts and related diversion programs. Although drug courts may be successful in deterring those who use substances from arrests and incarceration, Klukoff et al. (2021) highlighted the paradoxical nature of relying on carceral punishment as a motive for change because it risks police violence toward those who use substances when drug court requirements are not met. As stated earlier, this creates a value conflict for counselors who may have to disclose information regarding relapse during treatment that can be used in ways that jeopardize and harm the wellness of clients who use substances.
Limitations and Considerations
Adopting and incorporating an abolitionist praxis to counseling with clients impacted by anti-drug policing comes with challenges that counselors must critically reflect on prior to and during the implementation of this practice. First, counselors should prepare themselves to navigate pushback and resistance to social justice practices that would disrupt the status quo (S. W. Davis & Fayter, 2021). For example, it is common for individuals to criticize abolitionist praxis as utopian to inhibit the process of creatively imagining communities and systems that do not rely on carceral logics and systems (Kaba, 2021). Approaches like motivational interviewing are poised to navigate these challenges from colleagues who may be hesitant to embark upon making abolitionist change. In addition to pushback from individuals, it should be noted that, as a praxis seeking the elimination of carceral systems, barriers to the adoption of an abolitionist praxis can be expected from current carceral systems and approaches that may have existing evidence that establish them as efficacious. To counteract this expected barrier, substance use counselors need to engage in research, assessment, and program evaluation of efforts that are developed in alignment with an abolitionist praxis to establish efficacy. This would serve the purpose of ensuring that progress toward safety is achieved, that substance use clients are receiving trauma-informed care, and that other substance use counselors are introduced to new alternatives to existing carceral approaches that may increase the risk of harm to substance use clients. Additionally, counselors should critically reflect on and identify solutions to ethical, legal, and employment-related barriers if implementing an abolitionist praxis on their own. For example, making the choice as an individual counselor in a broader agency to not report substance use to a referring probation officer may be construed as fraudulent and unethical, thus jeopardizing a counselor’s employment and career. When making these decisions about whether or not to report substance use, counselors need to carefully weigh the options and consider consequences that can come from each course of action from a legal and ethical perspective, similar to what is suggested in the Forester-Miller and Davis (2016) Ethical Decision-Making Model. In the meantime, counselors can inform and educate probation officers about the nature of addiction and the potential for relapse to occur. Increasing awareness about these matters could generate a landscape shift for how probation officers and other authorities treat those struggling with addiction. Lastly, counselors should consider advocating for organizational support to adopt and implement trauma-informed and abolitionist changes to prevent such outcomes.
Conclusion
Clients who meet criteria for substance use disorders may have experienced, have witnessed, or be vulnerable to experiencing police violence. As a result, those who use substances are vulnerable to experiencing trauma that stems from exposure to police violence, which counselors must address. Counselors need to utilize abolitionist praxis to achieve a trauma-informed practice that supports healing from experiences of trauma affiliated with substance use and police violence, aim to prevent retraumatization, and create opportunities for both accountability and repair of harm caused by one’s use of substances.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adinoff, B., & Reiman, A. (2019). Implementing social justice in the transition from illicit to legal cannabis use. The American Journal of Drug and Alcohol Abuse, 45(6), 673–688. https://doi.org/10.1080/00952990.2019.1674862
Afuape, T., & Kerry Oldham, S. (2022). Beyond “solidarity” with Black Lives Matter: Drawing on liberation psychology and transformative justice to address institutional and community violence in young Black lives. Journal of Family Therapy, 44(1), 20–43. https://doi.org/10.1111/1467-6427.12369
Alang, S., McAlpine, D., McCreedy, E., & Hardeman, R. (2017). Police brutality and Black health: Setting the agenda for public health scholars. American Journal of Public Health, 107(5), 662–665. https://doi.org/10.2105/AJPH.2017.303691
Barrera, T. L., Mott, J. M., Hofstein, R. F., & Teng, E. J. (2013). A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clinical Psychology Review, 33(1), 24–32. https://doi.org/10.1016/j.cpr.2012.09.005
Beletsky, L., Grau, L. E., White, E., Bowman, S., & Heimer, R. (2010). The roles of law, client race and program visibility in shaping police interference with the operation of US syringe exchange programs. Addiction, 106(2), 357–365. https://doi.org/10.1111/j.1360-0443.2010.03149.x
Benson, B. L., Rasmussen, D. W., & Sollars, D. L. (1995). Police bureaucracies, their incentives, and the war on drugs. Public Choice, 83(1/2), 21–45. https://www.jstor.org/stable/30026940
Bor, J., Venkataramani, A. S., Williams, D. R., & Tsai, A. C. (2018). Police killings and their spillover effects on the mental health of Black Americans: A population-based, quasi-experimental study. The Lancet, 392(10144), 302–310. https://doi.org/10.1016/S0140-6736(18)31130-9
Bride, B. E., Hatcher, S. S., & Humble, M. N. (2009). Trauma training, trauma practices, and secondary traumatic stress among substance abuse counselors. Traumatology, 15(2), 96–105.
https://doi.org/10.1177/1534765609336362
Bryant-Davis, T., Adams, T., Alejandre, A., & Gray, A. A. (2017). The trauma lens of police violence against racial and ethnic minorities. Journal of Social Issues, 73(4), 852–871. https://doi.org/10.1111/josi.12251
Bureau of Justice Statistics. (2021). Law enforcement. https://bjs.ojp.gov/topics/law-enforcement
Carrico, A. W., Flentje, A., Gruber V. A., Woods, W. J., Discepola, M. V., Dilworth, S. E., Neilands, T. B., Jain, J., & Siever, M. D. (2014). Community-based harm reduction substance abuse treatment with methamphetamine-using men who have sex with men. Journal of Urban Health, 91(3), 555–567. https://doi.org/10.1007/s11524-014-9870-y
Castelpietra, G., Knudsen, A. K. S., Agardh, E. E., Armocida, B., Beghi, M., Iburg, K. M., Logroscino, G., Ma, R., Starace, F., Steel, N., Addolorato, G., Andrei, C. L., Andrei, T., Ayuso-Mateos, J. L., Banach, M., Bärnighausen, T. W., Barone-Adesi, F., Bhagavathula, A. S., Carvalho, F., . . . Monasta, L. (2022). The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990-2019: Findings from the Global Burden of Disease Study 2019. The Lancet Regional Health: Europe, 16(100341), 1–18. https://doi.org/10.1016/j.lanepe.2022.100341
Chang, Z., Lichtenstein, P., Larsson, H., & Fazel, S. (2015). Substance use disorders, psychiatric disorders, and mortality after release from prison: A nationwide longitudinal cohort study. The Lancet Psychiatry, 2(5), 422–430. https://doi.org/10.1016/S2215-0366(15)00088-7
Clark, C., Classen, C. C., Fourt, A., & Shetty, M. (2014). Treating the trauma survivor: An essential guide to trauma-informed care. Routledge. https://doi.org/10.4324/9780203070628
Cook, J. M., Newman, E., & The New Haven Trauma Competency Group. (2014). A consensus statement on trauma mental health: The New Haven Competency Conference process and major findings. Psychological Trauma: Theory, Research, Practice, and Policy, 6(4), 300–307. http://doi.org/10.1037/a0036747
Cooper, H. L. F. (2015). War on drugs policing and police brutality. Substance Use & Misuse, 50(8–9), 1188–1194. https://doi.org/10.3109/10826084.2015.1007669
Cooper, H., Moore, L., Gruskin, S., & Krieger, N. (2005). The impact of a police drug crackdown on drug injectors’ ability to practice harm reduction: A qualitative study. Social Science & Medicine, 61(3), 673–684. https://doi.org/10.1016/j.socscimed.2004.12.030
Cullors, P. (2019). Abolition and reparations: Histories of resistance, transformative justice, and accountability. Harvard Law Review, 132(6), 1684–1694. https://harvardlawreview.org/print/vol-132/abolition-and-reparations-histories-of-resistance-transformative-justice-and-accountability
Cullors, P. (2021). An abolitionist’s handbook: 12 steps to changing yourself and the world. St. Martin’s Press.
Davis, A. Y., Dent, G., Meiners, E. R., & Richie, B. E. (2022). Abolition. Feminism. Now. Haymarket Books.
Davis, C. S., Burris, S., Kraut-Becher, J., Lynch, K. G., & Metzger, D. (2005). Effects of an intensive street-level police intervention on syringe exchange program use in Philadelphia, PA. American Journal of Public Health, 95(2), 233–236. https://doi.org/10.2105/AJPH.2003.033563
Davis, S. W., & Fayter, R. (2021). Mutual aid as abolitionist praxis. Citizenship Studies, 25(2), 162–165. https://doi.org/10.1080/13621025.2020.1859190
DeVylder, J. E., Frey, J. J., Cogburn, C. D., Wilcox, H. C., Sharpe, T. L., Oh, H. Y., Nam, B., & Link, B. G. (2017). Elevated prevalence of suicide attempts among victims of police violence in the USA. Journal of Urban Health, 94, 629–636. https://doi.org/10.1007/s11524-017-0160-3
Dollar, C. B. (2019). Criminalization and drug “wars” or medicalization and health “epidemics”: How race, class, and neoliberal politics influence drug laws. Critical Criminology, 27(2), 305–327.
https://doi.org/10.1007/s10612-018-9398-7
Drustrup, D., Kivlighan, D. M., & Ali, S. R. (2023). Decentering the use of police: An abolitionist approach to safety planning in psychotherapy. Psychotherapy, 60(1), 51–62. https://doi.org/10.1037/pst0000422
El-Bassel, N., Gilbert, L., Witte, S., Wu, E., & Chang, M. (2011). Intimate partner violence and HIV among drug-involved women: Contexts linking these two epidemics—Challenges and implications for prevention and treatment. Substance Use & Misuse, 46(2–3), 295–306. https://doi.org/10.3109/10826084.2011.523296
Farley, M., Golding, J. M., Young, G., Mulligan, M., & Minkoff, J. R. (2004). Trauma history and relapse probability among patients seeking substance abuse treatment. Journal of Substance Abuse Treatment, 27(2), 161–167. https://doi.org/10.1016/j.jsat.2004.06.006
Fazel, S., Yoon, I. A., & Hayes, A. J. (2017). Substance use disorders in prisoners: An updated systematic review and meta-regression analysis in recently incarcerated men and women. Addiction, 112(10), 1725–1739. https://doi.org/10.1111/add.13877
Federal Bureau of Investigation. (2022). Crime data explorer [Data set]. https://cde.ucr.cjis.gov
Forester-Miller, H., & Davis, T. E. (2016). Practitioner’s guide to ethical decision making (Rev. ed.). http://www.counseling.org/docs/default-source/ethics/practioner’s-guide-toethical-decision-making.pdf
Galovski, T. E., Peterson, Z. D., Beagley, M. C., Strasshofer, D. R., Held, P., & Fletcher, T. D. (2016). Exposure to violence during Ferguson protests: Mental health effects for law enforcement and community members. Journal of Traumatic Stress, 29(4), 283–292. https://doi.org/10.1002/jts.22105
Geller, A., Fagan, J., Tyler, T., & Link, B. G. (2014). Aggressive policing and mental health of young urban men. American Journal of Public Health, 104(12), 2321–2327. https://doi.org/10.2105/AJPH.2014.302046
Giovengo, R. D. (2016). Training law enforcement officers. Routledge. https://doi.org/10.1201/9781315367262
Global Burden of Disease Network. (2016). Global Burden of Disease Study 2015 (GBD 2015) life expectancy, all-cause and cause-specific mortality 1980-2015 [Data set]. Institute for Health Metrics and Evaluation. https://ghdx.healthdata.org/record/ihme-data/gbd-2015-life-expectancy-all-cause-and-cause-specific-mortality-1980-2015
Good, D., Leichtling, G., & Pustejovsky, S. (2023). Oregon decriminalizes drugs: A state-level process evaluation of early implementation. Coimagine Health and Vital Strategies. https://comagine.org/resource/2466
Green, D. A. (2022, May 10). Developing competence to address undue police violence. Counseling Today. https://ctarchive.counseling.org/2022/05/developing-competence-to-address-undue-police-violence
Green, D. A., & Evans, A. M. (2021). Undue police violence toward African Americans: An analysis of professional counselors’ training and perceptions. Journal of Counseling & Development, 99(4), 363–371. https://doi.org/10.1002/jcad.12389
Green, D. A., Evans, A. M., Litam, S. D. A., Hornsby, T., Boulden, R., Shannon, J., Ford, D. J., & Landrum, D. (2024). Racial identity attitudes and vicarious traumatization from undue police violence on anticipatory traumatic reaction among Black Americans. Journal of Interpersonal Violence, 39(3–4), 848–868. https://doi.org/10.1177/08862605231198484
Hayashi, K., Ti, L., Csete, J., Kaplan, K., Suwannawong, P., Wood, E., & Kerr, T. (2013). Reports of police beating and associated harms among people who inject drugs in Bangkok, Thailand: A serial cross-sectional study. BMC Public Health, 13(1), 733.
https://doi.org/10.1186/1471-2458-13-733
Heffner, J. L., Blom, T. J., & Anthenelli, R. M. (2011). Gender differences in trauma history and symptoms as predictors of relapse to alcohol and drug use. The American Journal on Addictions, 20(4), 307–311. https://doi.org/10.1111/j.1521-0391.2011.00141.x
Jacobs, L. A., Kim, M. E., Whitfield, D. L., Gartner, R. E., Panichelli, M., Kattari, S. K., Downey, M. M., McQueen, S. S., & Mountz, S. E. (2021). Defund the police: Moving towards an anti-carceral social work. Journal of Progressive Human Services, 32(1), 37–62. https://doi.org/10.1080/10428232.2020.1852865
James, S. L., Castle, C. D., Dingels, Z. V., Fox, J. T., Hamilton, E. B., Liu, Z., Roberts, N. L. S., Sylte, D. O., Henry, N. J., LeGrand, K. E., Abdelalim, A., Abdoli, A., Abdollahpour, I., Abdulkader, R. S., Abedi, A., Abosetugn, A. E., Abushouk, A. I., Adebayo, O. M., Agudelo-Botero, M., Ahmad, T., . . . Vos, T. (2020). Global injury morbidity and mortality from 1990 to 2017: Results from the Global Burden of Disease Study 2017. Injury Prevention, 26(Supp 1), i96–i114. https://doi.org/10.1136/injuryprev-2019-043494
Joe, J. R., Shillingford-Butler, M. A., & Oh, S. (2019). The experiences of African American mothers raising sons in the context of #BlackLivesMatter. The Professional Counselor, 9(1), 67–79.
https://doi.org/10.15241/jrj.9.1.67
Kaba, M. (2021). We do this ’til we free us: Abolitionist organizing and transforming justice. Haymarket Books.
Kaba, M., & Ritchie, A. J. (2022). No more police: A case for abolition. New Press.
Kinner, S. A., Forsyth, S., & Williams, G. (2012). Systematic review of record linkage studies of mortality in ex-prisoners: Why (good) methods matter. Addiction, 108(1), 38–49. https://doi.org/10.1111/add.12010
Klukoff, H., Kanani, H., Gaglione, C., & Alexander, A. (2021). Toward an abolitionist practice of psychology: Reimagining psychology’s relationship with the criminal justice system. Journal of Humanistic Psychology, 61(4), 451–469. https://doi.org/10.1177/00221678211015755
Koram, K. (2022). Drug prohibition and the policing of warfare: The war on drugs, globalization, and the moralization of perpetual violence. Humanity, 13(1), 22–39. https://doi.org/10.1353/hum.2022.0001
Krieger, N., Chen, J. T., Waterman, P. D., Kiang, M. V., & Feldman, J. (2015). Police killings and police deaths are public health data and can be counted. PLOS Medicine, 12(12), e1001915.
https://doi.org/10.1371/journal.pmed.1001915
Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2002). The world report on violence and health. The Lancet, 360(9339), 1083–1088. https://doi.org/10.1016/S0140-6736(02)11133-0
Lunze, K., Lunze, F. I., Raj, A., & Samet, J. H. (2015). Stigma and human rights abuses against people who inject drugs in Russia—A qualitative investigation to inform policy and public health strategies. PLOS One, 10(8), e0136030. https://doi.org/10.1371/journal.pone.0136030
Maher, L. (2004). Drugs, public health and policing in Indigenous communities. Drug and Alcohol Review, 23(3), 249–251. https://doi.org/10.1080/09595230412331293306
Meade, B., Steiner, B, & Klahm, C. F., IV. (2017). The effect of police use of force on mental health problems of prisoners. Policing and Society, 27(2), 229–244. https://doi.org/10.1080/10439463.2015.1049602
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). Guilford.
Moh, Y. S., & Sperandio, K. R. (2022). The need to consider requiring trauma training in entry-level academic training programs in clinical mental health counseling. Journal of Mental Health Counseling, 44(1), 18–31. https://doi.org/10.17744/mehc.44.1.03
Motley, R. O., Jr., Byansi, W., Siddiqi, R., Bills, K. L., & Salas-Wright, C. P. (2022). Perceived racism-based police use of force and cannabis use among Black emerging adults. Addictive Behaviors Reports, 15, 100430. https://doi.org/10.1016/j.abrep.2022.100430
Mott, J. M., Sutherland, R. J., Williams, W., Lanier, S. H., Ready, D. J., & Teng, E. J. (2013). Patient perspectives on the effectiveness and tolerability of group-based exposure therapy for posttraumatic stress disorder: Preliminary self-report findings from 20 veterans. Psychological Trauma: Theory, Research, Practice, and Policy, 5(5), 453–461. https://doi.org/10.1037/a0029386
New York Civil Liberties Union. (n.d.). Ligon v. City of New York (challenging the NYPD’s aggressive patrolling of private apartment buildings). https://www.nyclu.org/en/cases/ligon-v-city-new-york-challenging-nypds-aggressive-patrolling-private-apartment-buildings
New York Civil Liberties Union. (2019, March 14). Stop-and-frisk in the de Blasio era (2019). https://www.nyclu.org/en/publications/stop-and-frisk-de-blasio-era-2019
Park, J. N., Linton, S. L., Sherman, S. G., & German, D. (2019). Police violence among people who inject drugs in Baltimore, Maryland. International Journal of Drug Policy, 64, 54–61.
https://doi.org/10.1016/j.drugpo.2018.12.005
Pinals, D. A., Gaba, A., Clary, K. M., Barber, J., Reiss, J., & Smelson, D. (2019). Implementation of MISSION–Criminal Justice in a treatment court: Preliminary outcomes among individuals with co-occurring disorders. Psychiatric Services, 70(11), 1044–1048. https://doi.org/10.1176/appi.ps.201800570
Pombo, S., & da Costa, N. F. (2016). Heroin addiction patterns of treatment-seeking patients, 1992-2013: Comparison between pre-and post-drug policy reform in Portugal. Heroin Addiction & Related Clinical Problems, 18(6), 51–60. https://dependencias.pt/images/files/HEROINA.pdf
Pratt, D., Appleby, L., Piper, M., Webb, R., & Shaw, J. (2010). Suicide in recently released prisoners: A case-control study. Psychological Medicine, 40(5), 827–835. https://doi.org/10.1017/S0033291709991048
Purnell, D. (2021a). Reforms are the master’s tools: The system is built for power, not justice. In C. Kaepernick (Ed.) Abolition for the people: The movement for a future without policing and prisons. Kaepernick Publishing.
Purnell, D. (2021b). Becoming abolitionists: Police, protests, and the pursuit of freedom. Astra House.
Rhodes, T., Platt, L., Sarang, A., Vlasov, A., Mikhailova, L., & Monaghan, G. (2006). Street policing, injecting drug use and harm reduction in a Russian city: A qualitative study of police perspectives. Journal of Urban Health, 83(5), 911–925. https://doi.org/10.1007/s11524-006-9085-y
Saleem, O. (1997). The age of unreason: The impact of reasonableness, increased police force, and colorblindness on Terry “Stop and Frisk.” Oklahoma Law Review, 50(4), 451–493. https://core.ac.uk/download/pdf/323046413.pdf
Sarang, A., Rhodes, T., Sheon, N., & Page, K. (2010). Policing drug users in Russia: Risk, fear, and structural violence. Substance Use & Misuse, 45(6), 813–864. https://doi.org/10.3109/10826081003590938
Schwartze, D., Barkowski, S., Strauss, B., Knaevelsrud, C., & Rosendahl, J. (2019). Efficacy of group psychotherapy for posttraumatic stress disorder: Systematic review and meta-analysis of randomized controlled trials. Psychotherapy Research, 29(4), 415–431. https://doi.org/10.1080/10503307.2017.1405168
Scott, C. L. (2020). Jail diversion: A practical primer. CNS Spectrums, 25(5), 651–658. https://doi.org/10.1017/S1092852919001834
Shannon, K., Rusch, M., Shoveller, J., Alexson, D., Gibson, K., & Tyndall, M. W. (2008). Mapping violence and policing as an environmental–structural barrier to health service and syringe availability among substance-using women in street-level sex work. International Journal of Drug Policy, 19(2), 140–147. https://doi.org/10.1016/j.drugpo.2007.11.024
Shaw, S. A., El-Bassel, N., Gilbert, L., Terlikbayeva, A., Hunt, T., Primbetova, S., Rozental, Y., & Chang, M. (2016). Depression among people who inject drugs and their intimate partners in Kazakhstan. Community Mental Health Journal, 52, 1047–1056. https://doi.org/10.1007/s10597-015-9883-3
Sloan, D. M., Feinstein, B. A., Gallagher, M. W., Beck, J. G., & Keane, T. M. (2013). Efficacy of group treatment for posttraumatic stress disorder symptoms: A meta-analysis. Psychological Trauma: Theory, Research, Practice, and Policy, 5(2), 176–183. https://doi.org/10.1037/a0026291
Small, W., Rhodes, T., Wood, E., & Kerr, T. (2007). Public injection settings in Vancouver: Physical environment, social context and risk. International Journal of Drug Policy, 18(1), 27–36.
https://doi.org/10.1016/j.drugpo.2006.11.019
Smiley-McDonald, H. M., Attaway, P. R., Wenger, L. D., Greenwell, K., Lambdin, B. H., & Kral, A. H. (2023). “All carrots and no stick”: Perceived impacts, changes in practices, and attitudes among law enforcement following drug decriminalization in Oregon State, USA. International Journal of Drug Policy, 118, 1–10. https://doi.org/10.1016/j.drugpo.2023.104100
Substance Abuse and Mental Health Services Administration. (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach. https://store.samhsa.gov/product/SAMHSA-s-Concept-of-Trauma-and-Guidance-for-a-Trauma-Informed-Approach/SMA14-4884
Sweeney, A., & Taggart, D. (2018). (Mis)understanding trauma-informed approaches in mental health. Journal of Mental Health, 27(5), 383–387. https://doi.org/10.1080/09638237.2018.1520973
Tapp, S. N., & Davis, E. (2022). Contacts between police and the public, 2020. (BJS Publication No. NCJ 304527). Bureau of Justice Statistics. https://bjs.ojp.gov/library/publications/contacts-between-police-and-public-2020
Ti, L., Hayashi, K., Kaplan, K., Suwannawong, P., Wood, E., Montaner, J., & Kerr, T. (2013). HIV test avoidance among people who inject drugs in Thailand. AIDS and Behavior, 17, 2474–2478.
https://doi.org/10.1007/s10461-012-0347-2
Tonry, M. (1994). Racial politics, racial disparities, and the war on crime. Crime & Delinquency, 40(4), 475–494. https://doi.org/10.1177/0011128794040004001
Vallance, K., Stockwell, T., Pauly, B., Chow, C., Gray, E., Krysowaty, B., Perkin, K., & Zhao, J. (2016). Do managed alcohol programs change patterns of alcohol consumption and reduce related harm? A pilot study. Harm Reduction Journal, 13(1), 13. https://doi.org/10.1186/s12954-016-0103-4
Volkmann, T., Lozada, R., Anderson, C. M., Patterson, T. L., Vera, A., & Strathdee, S. A. (2011). Factors associated with drug-related harms related to policing in Tijuana, Mexico. Harm Reduction Journal, 8, 7. https://doi.org/10.1186/1477-7517-8-7
Werb, D., Rowell, G., Guyatt, G., Kerr, T., Montaner, J., & Wood, E. (2011). Effect of drug law enforcement on drug market violence: A systematic review. International Journal of Drug Policy, 22(2), 87–94. https://doi.org/10.1016/j.drugpo.2011.02.002
Werb, D., Strathdee, S. A., Vera, A., Arredondo, J., Beletsky, L., Gonzalez-Zuniga, P., & Gaines, T. (2016). Spatial patterns of arrests, police assault and addiction treatment center locations in Tijuana, Mexico. Addiction, 111(7), 1246–1256. https://doi.org/10.1111/add.13350
The White House. (2022, August 1). Fact sheet: President Biden’s Safer America Plan. https://www.whitehouse.gov/briefing-room/statements-releases/2022/08/01/fact-sheet-president-bidens-safer-america-plan-2
Wood, E. F., Werb, D., Beletsky, L., Rangel, G., Mota, J. C., Garfein, R. S., Strathdee, S. A., & Wagner, K. D. (2017). Differential experiences of Mexican policing by people who inject drugs residing in Tijuana and San Diego. International Journal of Drug Policy, 41, 132–139. https://doi.org/10.1016/j.drugpo.2016.12.010
Darius A. Green, PhD, NCC, is an assistant professor at the University of Colorado Colorado Springs. Katharine R. Sperandio, PhD, NCC, ACS, LPC, is an assistant professor and a CACREP-accreditation coordinator at Saint Joseph’s University. Correspondence may be addressed to Darius A. Green, 1420 Austin Bluffs Pkwy, Colorado Springs, CO 80918, dgreen20@uccs.edu.
Jan 17, 2024 | Volume 13 - Issue 4
Claudia G. Interiano-Shiverdecker, Devon E. Romero, Katherine E. McVay, Emily Satel, Kendra Smith
In this transcendental phenomenological study, we interviewed 10 counselors who have clinical experience working with sex trafficking survivors. Through in-depth individual interviews, participants discussed their lived experiences providing counseling to this population. Our analysis revealed four primary themes: (a) counselor knowledge: “learning curve,” (b) counselor skills: “creating a safe space to dive into work,” (c) counselor attitudes: “being able to listen to the client’s story,” and (d) counselor action: “more than just a counselor.” The findings indicated that counselors working with sex trafficking survivors needed to understand and address the different aspects of trauma. Our findings also demonstrate that working with sex trafficking survivors requires additional competencies such as recognizing the signs of sex trafficking, vulnerable populations, and the processes by which traffickers force people into sex trafficking. We discuss these findings in more detail and identify implications for counselor training and practice.
Keywords: sex trafficking survivors, counseling, phenomenological, trauma, competencies
Sex trafficking of any individual is a significant concern globally. In 2000, the United States government enacted the Victims of Trafficking and Violence Protection Act of 2000, which defined sex trafficking as “the recruitment, harboring, transportation, provision, or obtaining of a person for labor or services through the use of force, fraud, or coercion for the purpose of subjection to involuntary servitude, peonage, debt bondage, or slavery” or “when the person induced to perform such act has not attained 18 years of age” (§ 103). Although the United States’s efforts fully meet the minimum standards established by the Victims of Trafficking and Violence Protection Act of 2000 to eliminate severe forms of trafficking, the Department of Justice initiated a total of 210 federal human trafficking prosecutions in 2020, of which 195 involved predominantly sex trafficking (U.S. Department of State, 2021). As stated in the Trafficking in Persons Report (U.S. Department of State, 2021), all 50 states, the District of Columbia, and U.S. territories have reported all forms of human trafficking over the past 5 years. With an estimated 4.8 million people victimized by sex trafficking (International Labour Organization, 2017), it is important to understand how counselors identify, provide services to, and advocate on behalf of sex trafficking survivors within the counseling setting.
Sex Trafficking and Mental Health
As a form of human trafficking, sex trafficking exposes individuals to torture; kidnapping; and severe psychological, physical, and sexual abuse. Physical health consequences of sex trafficking include general health complications (e.g., malnutrition), reproductive health consequences (e.g., sexually transmitted diseases, unwanted pregnancies), substance abuse, and physical injuries (Grosso et al., 2018; Lutnik, 2016; Muftić & Finn, 2013). Psychological abuses are numerous and can include intimidation, threats against loved ones, lies, deception, blackmail, isolation, and forced dependency (Thompson & Haley, 2018).
Constantly experiencing atrocious physical and psychological abuses creates mental health consequences such as depression, post-traumatic stress, dissociation, irritability, suicidal ideation, self-harm, and suicide (Cole et al., 2016; O’Brien et al., 2017). Survivors of sex trafficking may exhibit severe mental illness, including schizophrenia and psychotic disorders, increased risk of compulsory psychiatric admission, and longer duration of psychiatric hospitalizations (Oram et al., 2016). Moreover, social distancing and the global economic downturn due to the COVID-19 pandemic increased online sexual exploitation and the number of individuals vulnerable to sex trafficking (U.S. Department of State, 2021).
Because of the prevalence of sex trafficking, the health consequences that result from it, and the diverse areas in which counselors practice (e.g., community clinics, private practices, behavioral health departments, college/universities, K–12 schools), counselors must be prepared to work with sex trafficking survivors (Interiano-Shiverdecker et al., 2022, 2023; Litam, 2017, 2019; Romero et al., 2021; Thompson & Haley, 2018). Standards required by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015) prepare counselors to demonstrate clinical competencies to address a variety of circumstances, including traumatic experiences, across various continuums of care (e.g., inpatient, outpatient). Clinical mental health counselors with specialization in substance abuse and marriage, couple, and family counseling can also address other comorbid issues typically encountered with sex trafficking clients such as substance abuse and relational difficulties (CACREP, 2015; Litam & Lam, 2020). Early incidence of sex trafficking (12–16 years for girls, 11–13 for boys and transgender youth; Franchino-Olsen, 2019) demands the attention of school counselors trained to promote the academic, career, and personal/social development of school-aged children (American School Counselor Association [ASCA], 2022; CACREP, 2015). Therefore, first-hand accounts of counselors providing services to this population can provide an overview of current needs, challenges, and recommendations for clinical practice and research.
Sex Trafficking Research in the Counseling Profession
A recent review of the literature showed increased attention to sex trafficking coverage in top-tier counseling journals. Conceptual pieces reviewed relevant information on sex trafficking, counselor awareness, and counseling implications (Browne-James et al., 2021; Burt, 2019; Litam, 2017; Thompson & Haley, 2018). Empirical studies explored counselors’ attitudes toward sex trafficking (Litam, 2019; Litam & Lam, 2020), assessment for the screening of sex trafficking (Interiano-Shiverdecker et al., 2022, 2023; Romero et al., 2021), mental health treatment programs and modalities for sex trafficking (Johnson, 2020; Kenny et al., 2018; Schmidt et al., 2022; Woehler & Akers, 2022), and survivors’ recovery stories (Bruhns et al., 2018). Thompson and Haley (2018) reported a need for more training and education for counselors on sex trafficking. In a study done by Litam and Lam (2020), results indicated that counselor training in sex trafficking increased awareness. As a response, Interiano-Shiverdecker et al. (2023) developed an initial list of child sex trafficking competencies for counselors.
Although these studies provide relevant information for counselors’ work with sex trafficking, they do not focus on the experience of providing care for sex trafficking victims and survivors. Exploring counselors’ experiences provides a significant breakdown of current mental health care for this population. In other words, what does providing care for this population look and feel like in reality and what competencies work when serving sex trafficking victims and survivors? Only one phenomenological study focused on this inquiry, but this study examined therapists’ experiences working with foreign-national survivors of sex trafficking in the United States (Wang & Park-Taylor, 2021). Although this study presents important findings, it explored counselors’ work with only a certain group of sex trafficking individuals. Despite incomplete records, most data indicate that U.S. citizens are equally vulnerable to sex trafficking. For example, the National Human Trafficking Hotline (n.d.), which maintains one of the most extensive data sets on human trafficking in the United States, indicates that U.S. citizens comprised approximately 40% of their callers. The current study seeks to expand on the work of Wang and Park-Taylor (2021) by obtaining first-hand accounts of counselors providing services to sex trafficking clients in the United States and providing an overview of needs, challenges, and recommendations for clinical practice and research. The guiding research question for this study was: What are the lived experiences of counselors working with sex trafficking survivors in the United States?
Method
Using transcendental phenomenological research, the researchers—Claudia G. Interiano-Shiverdecker, Devon E. Romero, Katherine E. McVay, Emily Satel, and Kendra Smith—sought to understand counselors’ experiences working with sex trafficking survivors. A transcendental phenomenological method was best suited for this study because it allowed us to provide thick descriptions of the phenomena while employing bracketing techniques to explore participants’ experiences outside of our perspectives (Hays & Singh, 2012). Utilizing Moustakas’s (1994) modification of Van Kaam’s method, we sought to explore the occurrences of counselors working with sex trafficking survivors and collectively met to address any biases that came up during data analysis.
Researchers as Instruments
At the time of the study, Interiano-Shiverdecker and Romero were counselor educators at a university in the Southern United States with recent sex trafficking publications and experience working with youth vulnerable to sex trafficking in community and school settings. McVay was a doctoral candidate and a licensed professional counselor who was practicing as a social–emotional wellness counselor at a private school. Satel and Smith were master’s students in a clinical mental health program. Our desire to explore this topic stemmed from a limited discussion of sex trafficking in the literature and sought to include the voices of counselors. As the research team, we are all involved in a research lab dedicated to understanding sex trafficking and how counselors can better serve sex trafficking survivors. As such, we had varying levels of experience with research and engagement with sex trafficking. Satel and Smith were new to research, including topics surrounding sex trafficking. Therefore, Interiano-Shiverdecker and Romero’s broader understanding of the topic could have influenced newer members. For example, Interiano-Shiverdecker assumed that codes would resemble counseling competency categories (e.g., knowledge, skills, awareness). To reduce researcher bias, we engaged in weekly debriefing meetings for approximately 5 months for ongoing discussion of our perspectives and preconceived notions throughout data analysis. We documented our biases in journals, checked in on them during meetings, and referenced participants’ quotes to prevent imposing our assumptions of the data.
Participants and Sampling
After receiving IRB approval from the university, we sought participants through purposeful sampling and snowball sampling. Purposeful sampling strategies included reaching out directly via email to counselors who fit the study criteria and sending two calls for participants on an email mailing list for counselors and counselor educators (i.e., CESNET). For direct emails, McVay created a list of individuals who fit the criteria from Interiano-Shiverdecker and Romero’s professional network and an internet search. We also engaged in snowball sampling methods through recruited participants involved in the study. Inclusion criteria included counselors over the age of 18, who had previously or were currently working with children or adults who had been sex trafficked. Participants confirmed meeting the inclusion criteria by responding to a demographic questionnaire before beginning the interview. Following the qualitative researcher’s recommendation of sample size, we sought a range between five and 25 participants for this study (Creswell, 2013; Moustakas, 1994). Counselors who agreed to participate completed the consent forms, a demographic form, and a one-time Zoom interview. Participants received a $25 gift card for their involvement in the study. We recruited for about 5 weeks after interviewing 10 counselors. After the tenth interview was completed and we concluded the first round of analysis for all interviews, we felt that data saturation was achieved when similar codes showed up throughout the data.
The resulting participant pool consisted of 10 counselors (nine female and one male) ranging in age from 27 to 61 years (M = 40.7, Mdn = 38.5, SD = 11.1). Seven participants identified as White, two participants identified as Hispanic, and one participant identified as Asian. The participants also identified their employment setting: university (n = 1), agency (n = 3), and private practice (n = 6). Participants disclosed providing services in one or several states such as Alabama (n = 1), Florida (n = 1), Missouri (n = 1), Nevada (n = 1), North Carolina (n = 1), and Texas (n = 7). One participant also reported providing services to sex trafficking survivors in the United Kingdom. Years working with survivors of sex trafficking ranged from 1 to 13+ years, with a range of three to 50+ clients who disclosed their sex trafficking experience. One participant (Alejandra) who had worked primarily with survivors of sexual abuse did not indicate their number “since a lot of clients I have worked with do not readily admit to being sex trafficked, I’m not sure.” Table 1 outlines participant demographics in more detail.
Table 1
Participant Demographics
| Pseudonym |
Age |
Gender |
Race/Ethnicity |
Work Setting |
Years of Service |
# ST Clients |
CACREP |
| Kimberly |
48 |
Female |
White |
Private Practice |
11 |
30 |
Yes |
| John |
38 |
Male |
White |
University |
11 |
5 |
Yes |
| Stacy |
33 |
Female |
White |
Private Practice |
8 |
3+ |
Yes |
| Alejandra |
54 |
Female |
Hispanic |
Agency |
Unsure |
Most of career |
No |
| Fen |
39 |
Female |
Asian |
Private Practice |
5 |
4 |
Yes |
| Cassandra |
33 |
Female |
White |
Private Practice |
5 |
50+ |
Yes |
| Tiffany |
27 |
Female |
White |
Private Practice |
1 |
25 |
Yes |
| Amanda |
29 |
Female |
White |
Private Practice |
4 |
5 |
Yes |
| Ana |
61 |
Female |
Hispanic |
Agency |
13+ |
20 |
Yes |
| Cristina |
45 |
Female |
White |
Agency |
3 |
10+ |
No |
Note. Years of Service = Years providing services to ST survivors; ST = Sex trafficking; CACREP = Program accredited by the Council for Accreditation of Counseling and Related Educational Programs.
Data Collection Procedures
To follow phenomenological research methods, Interiano-Shiverdecker trained the doctoral student (McVay) in conducting semi-structured interviews. The researchers developed interview questions based on the purpose of the study and from a review of the literature. Interiano-Shiverdecker and McVay completed the interviews. Following Moustakas’s (1994) recommendations, the interview protocol consisted of 12 semi-structured, open-ended questions that invited an in-depth discussion of their experiences. To create our interview protocol, we reviewed current literature in counseling on sex trafficking, particularly qualitative studies (Browne-James et al., 2021; Bruhns et al., 2018; Johnson, 2020; Wang & Park-Taylor, 2021; Woehler & Akers, 2022). Based on this review and Interiano-Shiverdecker’s experience in qualitative research, we decided to focus not only on counselors’ experiences with working with this population but also on their perspectives on the identification, prevention, and impact of sex trafficking on their clients. The complete interview protocol can be found in the Appendix. Interviews lasted from 26 to 69 minutes in length and occurred via Zoom because data collection occurred in 2021 and it was the most appropriate medium to respect social distancing and obtain a national sample. According to our IRB approval, our data collection presented no more than minimal risks for the participants. All interview questions followed a respectful disposition using open-ended questions to engage participants. However, McVay explained before beginning the interviews that participants could stop, pause, or opt out of the interview if the questions brought too much emotional distress. No participant requested the interview to be stopped or paused. During the interviews, we used counseling skills to facilitate the conversation and to build upon the experiences discussed. We recorded and de-identified all interviews for verbatim transcription.
Participants also completed a demographic questionnaire before the interview to confirm their eligibility for the interview and obtain information on their age, gender, race/ethnicity, work setting, CACREP accreditation and degree, years working with sex trafficking survivors, and the number of clients they worked with who identified as trafficked.
Data Analysis
Utilizing Moustakas’s (1994) modification of Van Kaam’s data analysis, the research team engaged in the seven steps proposed by this approach. Data analysis and management relied on the use of NVivo software (Version 12). Interiano-Shiverdecker provided training in data analysis to McVay, Satel, and Smith. Interiano-Shiverdecker, McVay, Satel, and Smith engaged in the first step by individually analyzing transcripts and engaging in horizontalization of meaning units (Hays & Singh, 2012) to create in vivo codes for all nonrepetitive, nonoverlapping statements (meaning units). Second, we merged all files to determine the invariant constituents through a process of reduction and elimination. This first process of reduction allowed us to determine what was necessary and sufficient data to understand the phenomenon (Moustakas, 1994). The team then assigned themes or clusters of meaning to similar statements (third step). From the clusters of meaning, we created an initial codebook based on the discussions and findings from individual data analysis. We used the initial codebook to examine the themes against the dataset, ensuring that it was representative of participants’ experiences (fourth and fifth steps). As a team, we discussed any disagreements and worked on the data until we achieved a consensus. We worked out disagreements by discussing any opposing views and voting as a group on the best decision. We subsequently created textural descriptions through participants’ verbatim quotes, as well as created structural descriptions by examining the emotional, social, and cultural connections between what participants said (sixth step). Finally, we created composite textural-structural descriptions that outlined the reoccurring and prominent themes across all participants by organizing the themes into subthemes and ensuring that they represented all (if not most) participants’ experiences. After this analysis, we felt we achieved data saturation. After the completion of the initial analysis, Romero reviewed the data as a peer reviewer and offered suggestions. The entire research team reviewed the suggestions and came together to incorporate them until we reached a consensus and developed the final codebook.
Strategies for Trustworthiness
To limit the effects of researcher bias, we employed several strategies for trustworthiness. These included reflexive journals, triangulation of researchers, peer debriefers, an external auditor, member checking, and thick descriptions to ensure ethical validation, credibility, transferability, confirmability, sampling adequacy, and authenticity of our analysis (Hays & Singh, 2012). We engaged in reflexive journaling and weekly bracketing meetings during our individual and group data analysis to discuss codes, potential themes, and our assumptions shadowing the participants’ words. Researchers on the team brought varying levels of experience with research and the topic of sex trafficking, which we believe helped balance our subjective analysis of the data. We engaged in two rounds of member checking with the participants, one occurring after the transcription of the interviews and the second one after we wrote the themes. No participants changed the transcription of their interview or disagreed with the presentation of the themes. After the formulation of the themes from the original coding team, Romero served as a peer debriefer and reviewed the themes, key terms, and raw data, allowing participants to make recommendations on the content presented. This division in the research team allowed for another check outside of the original designated research team. An external auditor, a counselor educator with experience in conducting qualitative research, also reviewed the NVivo file and the write-up of the findings. The external auditor agreed with our data analysis procedures and presentation of the findings. He did provide suggestions to reduce the repetition of our first and second themes, which we implemented. Finally, we provide thick descriptions of our data collection and analysis procedures and present our results with direct quotes to ground our work.
Results
We identified four prevalent themes about mental health counselors’ experiences with sex trafficking survivors: (a) counselor knowledge: “learning curve,” (b) counselor skills: “creating a safe space to dive into work,” (c) counselor attitudes: “being able to listen to the client’s story,” and (d) counselor action: “more than just a counselor.” We use pseudonyms to present our results.
Counselor Knowledge: “Learning Curve”
All participants emphasized the importance not only of understanding trauma but also of gaining sex trafficking–specific knowledge throughout their work with survivors. Tiffany noted a “learning curve” when working with this population, despite working with trauma for most of her career. We categorized this theme into two subthemes: (a) understanding trauma work and (b) understanding sex trafficking and survivors.
Understanding Trauma Work
To work with sex trafficking, all counselors spoke about the importance of having general knowledge of trauma work. The most prominent topics included multicultural, legal, and ethical considerations. Important multicultural considerations for counselors involve understanding group differences between their clients (e.g., gender, race, age) and working from a culturally sensitive framework. Kimberly emphasized that “we really need people to not only have cultural sensitivity but also encourage those who are of other races to counsel these girls,” adding that “they need someone that’s like them from the same culture . . . to relate culturally to somebody.” Legal implications included understanding consent, informing clients of their limits of confidentiality when assessing for risk, and their role as mandated reporters. In reference to ethical practices, consultation and supervision arose as with any other trauma work. Stacy noted that it was “important for us to talk to one another if something’s going awry.”
Many participants conveyed how crucial it was for them to understand healing and its complexities. Cristina shared that clients are “going to have their ups and downs,” with Amanda echoing that there are “so many layers to the healing process.” Kimberly felt it important to remind herself that “you’re probably not going to see the seeds that you plant develop a lot of times.” Another important aspect of healing trauma, mentioned by half of the sample, was understanding clients’ stages of change. Stacy shared that one of her clients “went back to her hometown and relapsed immediately. And that’s also a hard thing to deal with—to know that I felt like we had some good sessions . . . and then it’s, ‘Wait a minute. You went back to the relapse [sex trafficking].’” Cristina noted that “especially [when they’re] first out and they’re not quite sure, that pre-contemplation if they want to leave or stay” was very important.
Another important aspect of their work included boundaries and self-care. All participants acknowledged that at some point in their careers, it was challenging to practice healthy boundaries. Cassandra acknowledged the following when working with individuals forced into sexual acts, “I wish I could take all the ladies I’ve ever worked [with], that have danced on stripper poles for money, unwillingly, and just like put clothes on them and wrap them up and hug them.” She added,
[It] can get really tricky when we start answering our phone because it’s an emergency all the time . . . and it’ll wear you out, your batteries will wear out, and you’ll end up having this dual relationship that will end up hurting her because . . . you’re not her friend.
It was helpful for Cassandra to remind herself that she was not the client’s parent. Rather, she shared, “when I hear things like that, I have to remind them that this is my job, this is what I do for a living.” Implementing healthy professional boundaries reduced burnout and facilitated self-care. Participants highlighted activities such as meditating, doing yoga, or taking the occasional day off. The counselors heeded that self-care also included managing their caseload to limit emotionally heavy clients or seeing a personal counselor themselves, as Cassandra and Amanda respectively noted. Amanda said, “you definitely have to secure your oxygen before you can secure other people’s.”
Understanding Sex Trafficking and Survivors
All participants explained that working with this population required them “to understand what sex trafficking is and . . . the many different ways that it looks,” as stated by John. He elaborated that “it takes many different forms and shapes,” some of which may not be immediately recognized as trafficking. Participants agreed that sex trafficking can often be much more discreet than one might anticipate. Tiffany commented on media portrayals like the film Taken, stating that the real experience is often much less dramatic: “Listening to their stories, it’s very, very subtle . . . like, if you do this then I’ll pay for your college tuition . . . and then from there it gets bigger.” Similarly, Cassandra noted that sex trafficking “can be, like, a bunch of underaged females, thrown in the back of a truck and trafficked across the United States” or people that “have their own residences, that don’t actually live with the trafficker, or they live with a family member that’s trafficking them.”
Counselors learned that although anyone can be trafficked, some populations are more vulnerable. According to Fen, these populations include clients with cognitive disabilities, immigrants, emotional abuse survivors, clients with PTSD, and clients with addictions. Other populations mentioned included the LGBTQ+ population, people recently released from jail/juvenile detention centers, college students with debt, and people in financial need.
The participants’ work also required them to learn how clients were recruited and what kept them from leaving sex trafficking. John and Amanda noted that many survivors knew their traffickers or were introduced to them by family, friends, or a romantic partner. Ana explained that traffickers may kidnap people from big sporting events or from opposing gang(s) or may train survivors to recruit and groom for them. She also worked with women recruited online from abroad and trafficked once they arrived in the United States. Counselors also learned about the numerous tactics used by traffickers, including the trauma bond, coercion, and control. John noted that traffickers often use manipulation: “The common theme was ‘If you do this, you’d really be helping me out. You wanna see me be okay?’ or ‘You don’t want me to go to jail, do you?’” Cassandra reported working with a client whose parents used “an odd twist on Christianity” and the principle of “respect your elders” to traffic her. Other tactics mentioned were threats of violence against survivors and their families, branding or tattooing survivors, stalking, taking survivors’ IDs, gaslighting, and fear. Cassandra also observed that trafficking was “so alluring . . . there’s a lot of money in that . . . so much about leaving sex trafficking is starting from zero and creating something new.” Amanda recalled a client who “was very upscale and so they lived kind of a lavish lifestyle, and I could see and understand, really emphasize the struggle to like give that up,” particularly when they were worried about providing for their families. Factors that forced individuals into sex trafficking were multilayered. Amanda continued, “so many other facets and like layers to this. It’s like an onion.”
As a result, counselors learned about the overall impact of sex trafficking on survivors’ mindsets, behaviors, and presenting symptomology. As noted by Kimberly, sex trafficking impacted every aspect of survivors’ lives. Tiffany noticed that many of her clients were initially very fragile and mistrusting of everyone, while Cristina and Stacy shared that it was common for their clients to display guarded and closed-off body language. John’s work taught him that sex trafficking “affects [clients] in terms of intimacy and trust, and that trickles into their relationships, whether it’s with family, roommates, or romantic partners.” The counselors’ work with sex trafficking survivors included clients with an array of presenting concerns. Cassandra observed clients with complex PTSD, substance use issues, self-harm behaviors, suicidal ideation, self-hatred, self-blame, feelings of insecurity, an inability to trust, and eating disorders. Ana also noted that clients presented with anxiety, depression, paranoia, and physical concerns such as sexually transmitted diseases (STDs) and sleep problems.
Counselor Skills: “Creating a Safe Space to Dive Into Work”
All participants recognized that because of the nature of their work and their clients, they needed to “create a safe space to dive into work,” as stated by Tiffany. To do so, they needed to build skills in two main categories: (a) assessment and ensuring safety and (b) processing trauma. Amanda explained, “I think all of that stuff [assessment and ensuring safety] really has to come first before we can do any really heavy work and therapy. . . They have to be stable before they can really dig into whatever they want to dig into.” Although this separation provides clarity, counselors’ experiences were also more fluid, at times requiring them to use skills particular to ensuring safety while processing trauma and vice versa.
Assessment and Ensuring Safety
All counselors’ experiences of assessment and ensuring safety consisted of effectively engaging with their clients during the intake interview, assessing risk, applying crisis skills, and formulating personalized treatment plans. Based on her experiences, Cristina spoke about the importance of building rapport during that initial interview: “When I do our initial assessment with them . . . I have the assessment, but I’m having a conversation with them.” She also learned to discuss confidentiality and mandated reporting with her clients to explain her role as the counselor while also giving them a choice: “I tell them straight out, like, ‘Hey, you tell me this, I have to report it, I have to call law enforcement . . . so how do you want to do it?’” Cassandra found that obtaining a thorough history of the client was a critical part of the process:
When addressing trauma, I don’t just go back to when the trafficking started. I go all the way back, make sure that I have that thorough history, because 99 times out of a 100, from my experience, that was not the first trauma that person experienced.
Seven participants spoke about learning the signs of sex trafficking and knowing what questions to ask to obtain more information and determine a person’s exposure to sex trafficking. Amanda explained, “I don’t think I’ve ever had somebody start off within an intake session be, like, ‘Hiya, so I was trafficked.’” Participants learned to ask about phone use and the number of phones owned, the extent of drug use, sexually transmitted diseases, wanted and unwanted pregnancies, boyfriends and their ages, and sexual behaviors such as the use of a condom. When assessing, Alejandra learned to “ask questions that minimize you coming across as being shaming or judging.” At the same time, some counselors spoke about the lack of sex trafficking assessments that could facilitate this part of their work. Alejandra explained that she “did an assessment at work yesterday, and there, there are no questions about sex trafficking. . . . There are questions about abuse, but it is inferring more [about] sexual abuse, physical abuse, emotional abuse versus sex trafficking.” Fen echoed this sentiment by wishing there was a more rigorous psychosocial interview that assessed risks associated with sex trafficking because “at times people do hide and at times people don’t disclose.”
All counselors agreed that a significant aspect of ensuring safety for their clients was collaborating with clients on safety plans. Counselors took the time to develop a “well thought out” safety plan with their clients, as stated by Alejandra. Stacy explained how she helped the client brainstorm ways to feel safer, including leaving town for a while or taking steps to “create a new account, changing her look a little bit . . . getting [a] new phone number.” Collaboration was not only utilized to respect clients’ autonomy but also to instill hope—“Hope that you know that you have a future,” stated Cristina. Ana elaborated, “seeing what they want for themselves and their lives, like, where do you want to go with your life . . . if you didn’t have this going on, you know, what is it you would like to do for yourself?”
Processing Trauma
To process trauma, all counselors listed skills, interventions, and therapies they found helpful with this population. Utilizing foundational skills (e.g., reflection, open-ended questions, appropriate self-disclosure) to build rapport was the most referenced code in this section, addressed by all participants. Cristina saw the benefit of learning how “to connect very quickly.” Stacy added, “I would definitely start relying a lot more on the rapport when I work with trauma.” Counselors also found it helpful to have a toolbox that included creative approaches and interventions that helped clients reclaim power, develop a support system, improve self-esteem, build and discover resiliency, and utilize the client’s strengths. Psychoeducation, mentioned by nine participants, included teaching their clients about sex trafficking because as John explained, “clients don’t always know that they are being trafficked.” Psychoeducation of sex trafficking requires explaining fraud, force, and manipulation. Kimberly explained how a client did not think she was trafficked because her partner did not have her “locked in a closet. I don’t got chains around me. I’m not his slave . . . I get up and get myself dressed. I go out there and meet these guys . . . I cooperate when he’s taking pictures of me.” To help her client reevaluate her situation, Kimberly utilized motivational interviewing–based questions such as “Would you let your sister do this?” or “What would be the benefits of leaving your situation?”
Although most counselors felt that an integrative approach to counseling worked best with sex trafficking clients, the therapies most mentioned included dialectical behavioral therapy, narrative therapy, and eye movement desensitization and reprocessing therapy. Counselors recommended individual treatment to process trauma, although four participants also mentioned family and group counseling. Fen found family therapy helpful “if the family wants to get involved in the practice” and “if there are family members who are ready to support them and come with them and who are aware of this.” Other participants mentioned the benefits of providing group counseling for sex trafficking survivors. Cassandra recalled how members of a support group she facilitated “connect with each other, they know that they’re not alone, they give each other honest feedback. . . . It has been super empowering.” Yet Alejandra, Fen, and Tiffany found that group counseling may not be well suited for all clients. “Group therapy doesn’t work really well because you know every survivor is different, and they don’t want to open up in front of others until they have worked through the process for a long time,” explained Fen.
Because of the nature of their work, counselors recognized that an essential skill to processing trauma was learning how to manage countertransference. Cristina spoke about how as “clinicians, we want to save all of them.” For this reason, Kimberly recognized that it was important for her to understand her attachment style. Cassandra recalled nights when she would go home and “worry about [if] I am going to see this client again.” Ana left sessions “shaking sometimes from those places . . . ’cause the stories I would hear.” Stacy highlighted that it was also difficult at times to manage the lies. She explained, “I was a little frustrated because I knew that she was hiding things . . . obviously it just wasn’t that time and that’s okay.” As a result, counselors found it essential to process their emotions. Kimberly explained that “if you haven’t emptied your cup of all the sad, mad, bad before you come into that office with them . . . you’re going to flip your lid whether it’s in front of them or behind closed doors.”
Counselor Attitudes: “Being Able to Listen to the Client’s Story”
All participant interviews illuminated thought patterns and beliefs they needed “to listen to the client’s story,” as stated by John. Counselors learned to personify certain attitudes by (a) valuing empathy and validation and (b) embodying a sense of safety.
Valuing Empathy and Validation
All participants highlighted the importance of embracing a philosophy of empathy and validation in their work with clients by being warm, genuine, open-minded, patient, and nonjudgmental. Participant interviews described various mechanisms to embody these attitudes. For instance, a consistent approach they took was to respect and empower the clients’ choices and, ultimately, believe in and provide client autonomy through supportive and nonjudgmental means. Ana emphasized, “I think that’s huge for those whose choices were taken away. . . . It’s offering them a choice, and I think that’s very empowering for them.” Fen echoed this message stating, “You can’t push—you can definitely motivate—but you cannot just push.” Kimberly learned to be patient: “You’ll end up getting there eventually, just take your time. . . . You have to build that rapport and trust.” Cassandra stated, “Another thing I would say is don’t make any assumptions. . . . Everybody’s experiences, although there are similarities, every experience is so different.” Cristina described the shock value of hearing survivors’ stories and how essential it was for her to remain nonjudgmental and aware of her biases. Amanda embodied “those Rogerian qualities, like that open-mindedness, empathy, warmth, genuineness, authenticity—those things are all really important to utilize when meeting with that population, or any population.” Cristina provided an example of how she conveyed this to a client by saying, “I’m here if you need me. . . . There’s no judgment happening, I’m just glad you’re here.”
Counselors also shared a philosophy that validated clients’ experiences. Fen believed in “just making clients feel normal,” while Cassandra noted how helpful it was for her to approach clients’ behaviors as “normal reactions to abnormal situations.” An important attitude communicated by John was that “they are survivors.” Even though others and possibly even the client themselves might use the word victim, he found it helpful to have “the conversation about being a survivor versus a victim.” Tiffany further explained, “I’ve noticed just in working with sex trafficking survivors . . . it seems very hard for them to say the word ‘abuse’ or view themselves as anything other than a victim.” She found value in seeing the client as “a survivor” and teaching this perspective to the client.
Embodying a Sense of Safety
All participants embraced attitudes that created and maintained a safe environment for their clients. Fen explained that as the counselor, “you’re the only safety net for that person” who provides safety and trust. Cristina reflected on a client who was still in “the life” and returned for help and services when needed. She stated, “she knows that I’m a safe person” and “this [shelter name] is her home, this is where she felt safe. But [she] knew she couldn’t get out of this life yet because she wasn’t ready to.” Fen explained that “there is shame, there is guilt, there is fear, and apprehension of being caught . . . so, one has to make them feel safe.” Some participants communicated and provided safety by creating a “homier and safer” office space or by buying a client’s favorite snacks and beverages, as described by Cassandra. Alejandra spoke of establishing “an environment where it’s safe to talk about taboo subjects” such as “having been a mule or whatever they did, you know, whatever sexual acts.”
Six of the participants also spoke of attitudes that promoted consistency and predictability. Kimberly stated, “That’s something they’ve never had in their life; you know, so while you’re doing all this other stuff, be consistent.” Several participants noted how difficult it was for their clients to have continuity with counselors. Kimberly shared:
Counseling someone who’s had this kind of trauma takes a long time . . . once you leave and can’t continue that counseling process, the likelihood of them going back to the counseling is very slim to none. . . . Even though they were resistant to building that rapport with you at the same time, deep down inside they’re connecting with you.
Similarly, a few participants learned to be consistent in their messages shared with clients and accessibility to clients. For instance, Stacy spoke of the need for congruency between actions and words when working with these individuals: “Trust is such a fleeting word . . . it has to be action, sometimes, speaks louder than the words.”
Counselor Action: “More Than Just a Counselor”
All participants realized that working with this population required them to reevaluate their role as the counselor. They learned that clients required “more than just a counselor,” as stated by Kimberly. Therefore, the fourth theme elucidated actions that counselors found necessary to help clients recover from their experiences. We categorized counselor action into two subthemes: (a) client advocacy and (b) engaging with social work/workers.
Client Advocacy
Over half of our participants spoke about the importance of advocating for clients. Cristina talked about how some clients did not have a caseworker and needed someone “that’s in their corner.” Counselors spoke about specific needs they advocated on behalf of clients in the life or in recovery. Kimberly spoke about advocating for prison reform, particularly for minority women who went to prison for some of the things they got involved in while being trafficked. Cristina advocated for “easier access to get into drug treatment.” She explained that this was necessary because certain insurances did not pay for certain drug treatments, or it would take too long to get clients into treatment. Although clients would sometimes agree to treatment, it would take several days “to get everything going. . . . by then the kids change their minds, or they run. . . .The obstacles shouldn’t be that hard.” Other forms of advocacy focused on working with and educating police officers to best work with this population. Tiffany explained how many women didn’t trust law enforcement. She believed it was crucial to bridge these services because law enforcement could “get them out of that lifestyle, but then on the other hand, they’re very much like, ‘Don’t trust them.’” Stacy also spoke about advocating for shelters specific to sex trafficking. She remembered a client who visited a shelter once a month and loved it because “she felt safe there versus just, like, a domestic violence clinic . . . they had the awareness of sex trafficking versus just, like, you know, an overnight shelter type of place.”
Participants also taught clients how to advocate for themselves while also respecting their choices. Stacy explained, “It’s not my job to fix what they’re going through, but it is my job to be as supportive as I can.” She understood that she needed to “advocate for them but also having the respect that if they don’t want me to advocate for them, then that’s the place that they’re at too.” Stacy also clarified that at times she does not “really know exactly 100% how I would want to advocate” for clients who had been trafficked. Yet as she continued to reflect, she realized her desire to “seek out more education about it because I do think that it needs to be navigated in a specific way.”
Engaging With Social Work/Workers
The call for advocacy led all counselors to speak about how their work required them to expand their roles to connect clients to resources and collaborate with social workers. Kimberly explained that this population requires “more than just a counselor while they’re in session . . . you’ve really got to start with building a community around them before you get into the deep trauma work.” Counselors provided resources to obtain transportation, financial assistance, government assistance, their GED or college degree, food, employment, stable housing, legal support, childcare, hygiene products, substance treatment, and medical care. Amanda explained that this population requires that their basic-level needs be met to help them feel like they “can function in society and be comfortable,” and Kimberly elaborated:
As a counselor, I used to have a huge list of resources that I could give them, but they also needed guidance from outside of the counseling office. . . . I have, like, eight people with one survivor, that’s how much it took us ’cause it’s so much work for one person. You’re talking about every aspect, everything that you learned as a child growing up. . . . If you want counseling to be successful, they have to have that outside component to help them . . . a counselor can’t do all of that.
Ana partnered up with organizations already doing this work. She particularly spoke about an organization that not only focused on “educating people but also helping these women with resources.” She added that “the residential places they were able to stay in, they were able to finish their education and get an education there, and they also helped them with finding jobs, which was really important for them, too.” She explained that this was particularly important because many of the women she worked with had a violent criminal history. Many company insurances refused to hire women with criminal records, preventing their clients from a second chance at improving their lives. However, John learned to support clients with resources. “I don’t think it’s sufficient to just say ‘Here you go, here’s the resource guide. They have lots of options in there. Good luck.’ . . . Our job doesn’t end with giving the resources,” he explained.
An important point to make is that although some counselors spoke about collaborating with social workers, it seemed that most believe their work resembled “a little more of that, like, case management–type stuff to make sure that they have the resources if and when they want out,” added Cassandra. Kimberly elaborated, “You’re the one that’s helping to get them to [a] place where they can have a relatively stable life . . . but without the resources that come alongside that, they’re gonna go nowhere, [they’re] going to hit a wall every time.”
Discussion
We sought to understand counselors’ experiences working with sex trafficking survivors through a phenomenological analysis. The participants in our study needed to understand and address the different aspects of trauma. Because of clients’ traumatic experiences that resulted in psychological injuries (Cole et al., 2016; Grosso et al., 2018; Lutnik, 2016; Muftić & Finn, 2013; O’Brien et al., 2017), counselors benefited from respecting the process of healing, addressing stages of change, and building a safe and trusting relationship. Counselors overall possessed knowledge of the development of post-trauma responses over time. They knew what to look for and how to best treat traumatic symptoms that permeated all aspects of their client’s lives, particularly sex trafficking survivors’ ability to trust others. Counselors believed that having a trauma-informed approach could reduce instances of re-victimization. Counselors also recognized the importance of self-awareness such as assessment of personal trauma, self-care, restorative practice, and biases regarding how youth are trafficked and by whom.
Yet, our findings demonstrate that working with sex trafficking survivors requires additional competencies as illustrated in previous research (Interiano-Shiverdecker et al., 2023). The participants discussed the need to become educated in recognizing the signs of sex trafficking, vulnerable populations, and the processes by which traffickers force people into sex trafficking to obtain a deeper understanding of the client’s worldview and provide appropriate support (Interiano-Shiverdecker et al., 2023). Participants addressed components—namely force, fraud, coercion, exploitation, power, grooming, and solicitation—commonly used in sex trafficking literature (Bruhns et al., 2018). When asked about the nature of their work, their focus naturally divided into sections that focused on assessing risk and safety planning, processing trauma, and helping the client re-establish their life and their identity. Our findings align with CACREP (2015) recommendations for clinical crisis skills and knowledge while also elucidating their application to sex trafficking survivors. Participants learned to assess for specific sex trafficking signs (e.g., phone usage, boyfriends and their ages, sexual behaviors) and to ask questions that differentiated sex trafficking from other forms of abuse.
Counselors must also understand the differences between sex work (i.e., the voluntary exchange of sexual services for compensation) and sex trafficking (i.e., subjection to the exchange of sexual services due to force, fraud, or coercion or from any person under the age of 18). As Ana shared, most counselors felt that the notion to detect was on their end “because I don’t always think it’s the responsibility of the client to be able to say ‘Hey, I’ve been trafficked.’” Thus, participants indicated that possessing these competencies could help increase the identification of sex trafficking. As such, some counselors may desire more guidance on specific sex trafficking assessments, which scholars have previously noted (Interiano-Shiverdecker et al., 2022; Romero et al., 2021). A content analysis on sex trafficking instruments (Interiano-Shiverdecker et al., 2022) illustrated the importance of asking specific questions to assess for control, confinement, threat, and isolation, as these are the main indicators of sex trafficking. Example items included: “Have you ever felt you could not leave the place where you worked [or did other activities]?” (confinement; Simich et al., 2014, p. 20); “Are you kept from contacting your friends and/or family whenever you would like?” (isolation; Mumma et al., 2017, p. 619); “Do you have to ask permission to eat, sleep, use the bathroom, or go to the doctor?” (control; Mumma et al., 2017, p. 619); and “Has anyone threatened your family?” (threat; Mumma et al., 2017, p. 619).
Moreover, for some sex trafficking victims, the relationship with their traffickers represented an affirming, reliable, and secure relationship in their lives, later used to coerce or force them into sexual, violent, or illegal behavior. Therefore, participants realized that processing trauma would require attitudes and skills that provided emotional safety, patience, and a nonjudgmental process. Survivors’ lack of choice throughout their sex trafficking experience fomented counselors’ abilities to empower clients over their bodies, boundaries, and choices, and help clients reintegrate into society (Interiano-Shiverdecker et al., 2023; Thompson & Haley, 2018). Participants seemed to emphasize that without all the elements mentioned, clients might not disclose their situation or trust the counselor enough to open up, and they might even terminate counseling abruptly.
This last point is connected to our fourth finding, counselor action. Aligned with the Multicultural and Social Justice Counseling Competencies (Ratts et al., 2016), the participants in our study recognized the need to engage in work that advocated for clients within and outside of the session. Despite their dedicated work with clients to process the emotional repercussions of sex trafficking and rebuild their lives, their efforts did not seem enough to support clients in their recovery. So much of what ailed their clients fell on systemic or external forces (e.g., poverty, employment, lack of resources). Although that existed outside of the counselor’s role and verged into another profession, our participants embraced these responsibilities or connected with other professionals. They believed that otherwise, clients would not succeed in their recovery. Our findings present an important reminder that sex trafficking, a modern form of human slavery, is an act of social injustice affecting individuals vulnerable to historical and systemic oppression.
Implications
Our themes add to the existing research with implications for counseling practice, supervision, and education. Scholars (Romero et al., 2021; Thompson & Haley, 2018) have identified counselors as first-hand responders to the early detection and prevention of sex trafficking. Although each trafficking scenario is unique, counselors need to refer to sex trafficking indicators, recruitment and grooming tactics, and manipulative dynamics that prevent individuals from disclosing or leaving sex trafficking. It is important for counselors to dispel common myths of sex trafficking and understand that sex trafficking may appear differently than one may expect. Amanda alluded to clients who defined their experience as a “lavish lifestyle” and were lured by the financial benefits of sex trafficking. We caution counselors not to misinterpret sex trafficking as a “lifestyle,” as this implies choice. There may be a myriad of invisible factors contributing to their circumstances such as trauma bonding and financial instability.
Participants agreed that an integrative approach with interventions that addressed complex trauma (e.g., dialectical behavior therapy, eye movement desensitization and reprocessing therapy) worked best when working with sex trafficking. We encourage counselors to not only become familiar with such modalities but also to conceptualize any treatment modality through a trauma-focused lens that considers how sex trafficking impacts all aspects of a client’s life and how they will interact in session. Participant narratives indicated that clients could present with defiant behaviors, distrust, angry or irritable mood, and refusal to comply with treatment. These themes underscore the importance of a counselor’s ability to create safe, trusting, and empathic relationships that allow the client to disclose risk and eventually process trauma. Counselors should also integrate a strong rapport with sex trafficking clients by demonstrating unconditional positive regard, authenticity, and empathy with any treatment modality chosen. Although counselors establish a strong therapeutic relationship, they can integrate other counseling goals, including psychoeducation, assessing for risk, supporting clients through the stages of personal change, and helping the client rebuild and reintegrate into society. Based on the nature of their work, managing countertransference and self-care represents an essential instrument to maintain balance while engaging in emotionally draining clinical work. We encourage counselors to seek supervision, connect with colleagues, and practice regular self-care routines to avoid experiencing burnout, secondary trauma, and countertransference. Additionally, counselors should connect clients to services that provide basic needs (e.g., safe and stable housing, food). When clients lack basic physiological needs, they may struggle to focus on higher-order needs such as developing a safety plan or emotion regulation. Counselors can engage in legislative advocacy by writing letters to judges, sharing clinical experiences with senators, and providing training on sex trafficking victim identification and treatment. It is important for counselors to build constituency groups with education, governmental task forces, and legislators to lobby for bills that benefit clients, as sex trafficking exists in an ecosystem of community and social contexts (Farrell & Barrio Minton, 2019). Our findings also underscore the limitations of intake interviews when assessing for sex trafficking risk. Although identification and screening tools exist (Interiano-Shiverdecker et al., 2022; Romero et al., 2021), counselors are not always in a setting where a formal assessment is appropriate or accessible.
We encourage educators and supervisors to emphasize the value of informal assessment methods with counselors-in-training. Counselor knowledge of signs, symptoms, and questions to ask during an intake can improve identification efforts. Our findings also hold some implications for training beyond counselor education. Because of the complexities of working with trauma and sex trafficking, counselors intending to work with this population should seek out specialized training. For instance, they may review conference programs for trauma or sex trafficking–specific education sessions. At the same time, counseling programs should evaluate their preparation for counselors to work with sex trafficking. Requiring a trauma course, including content on sex trafficking and complex trauma throughout the curriculum (e.g., trauma, grief, addiction counseling courses), inviting guest speakers, and providing training opportunities and workshops for students and community counselors are all suggestions to ensure that counselors obtain the necessary knowledge and skills to work with this population. We believe that more training opportunities can minimize any possible misunderstanding of sex trafficking, expectations on clients to disclose, and re-victimization of clients that leads to early termination of counseling.
Limitations and Future Directions
The nature of our sample holds some limitations for the interpretation and application of the themes from this study. We collected data from single data sources (i.e., individual interviews); additional interview sources (e.g., focus groups) may have contributed more information. Moreover, lack of racial and gender diversity was a limitation in this study because most participants identified as White and female. We noticed that participants did not discuss racial and gender differences in clients’ experiences of sex trafficking. This result could have originated from our interview protocol that sought to gain an overall understanding of sex trafficking experiences and therefore did not request this information. Participants’ demographic profiles may have also provided a limited perspective of the experiences of Black, Indigenous, and/or people of color. We also did not require CACREP accreditation or specific years of practice as part of our inclusion criteria. Although all our participants were licensed professional counselors, they had different degrees in mental health, a variety of clinical practice, and did not all graduate from CACREP-accredited programs. During our interviews, we did not define sex trafficking to the participants and engaged in open-ended questions that inquired about their experiences. Participants’ responses are based on their definition of sex trafficking, which can vary and might not be accurately distinguishable from sex work. As is the case with all qualitative research, counselors and scholars should consider the transferability of these findings to other client populations and with counselors. For example, the findings of this study can be applicable to professional school counselors, but the recruitment of school counselors as participants would have provided greater insight into the roles and responsibilities of counselors in schools. Furthermore, we did not include client perspectives in this study; therefore, even though our participants’ perspectives when working with sex trafficking survivors is very insightful, they may not have an accurate representation of clients’ experiences in session.
Based on these limitations, we recommend scholars explore individual and external factors that can impact counselors’ work with sex trafficking survivors. For example, we did not explore within-group differences (e.g., race, gender, sexual orientation, religion) between counselors and cross-cultural interactions between clients and counselors. These factors are important to consider and reflect on when building trust and a sense of safety for the client, particularly when considering current conversations around racial tension in the United States. A more in-depth analysis of these considerations could facilitate a better understanding of how multicultural traits play a role in counselors’ experiences when working with sex trafficking survivors. Participants’ emphasis on the need for specialized knowledge and skills to work with sex trafficking also warrants research on evidence-based interventions for sex trafficking survivors. Moreover, an examination of the client’s experiences is necessary to garner a holistic picture of the impact of sex trafficking on the client’s healing and counseling process. We also believe that researchers should consider external factors that might impact counselors’ experiences when working with sex trafficking. Considering participants’ discussion of advocacy and engaging with social work/workers, it seems necessary to consider sociopolitical and institutional elements that either hinder or support clients’ ability to leave sex trafficking and obtain access to services that allow them to heal and flourish. As such, counselors working with sex trafficking survivors must consider specific training that allows them to assess for risk, process the emotional ramifications of sex trafficking, and rebuild their lives.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2022). ASCA ethical standards for school counselors.
https://www.schoolcounselor.org/getmedia/44f30280-ffe8-4b41-9ad8-f15909c3d164/EthicalStandards.pdf
Browne-James, L., Litam, S. D. A., & McRae, L. (2021). Child sex trafficking: Strategies for identification, counseling, and advocacy. International Journal for the Advancement of Counselling, 43, 113–125.
https://doi.org/10.1007/s10447-020-09420-y
Bruhns, M. E., del Prado, A., Slezakova, J., Lapinski, A. J., Li, T., & Pizer, B. (2018). Survivors’ perspectives on recovery from commercial sexual exploitation beginning in childhood. The Counseling Psychologist, 46(4), 413–455. https://doi.org/10.1177/0011000018777544
Burt, I. (2019). Modern-day slavery in the U.S.: Human trafficking and counselor awareness. International Journal for the Advancement of Counselling, 41, 187–200. https://doi.org/10.1007/s10447-018-9366-7
Cole, J., Sprang, G., Lee, R., & Cohen, J. (2016). The trauma of commercial sexual exploitation of youth: A comparison of CSE victims to sexual abuse victims in a clinical sample. Journal of Interpersonal Violence, 31(1), 122–146. https://doi.org/10.1177/0886260514555133
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Creswell, J. W. (2013). Research design: Qualitative, quantitative, and mixed methods approaches (4th ed.). SAGE.
Farrell, I. C., & Barrio Minton, C. A. (2019). Advocacy among counseling leaders: The three-tiered legislative professional advocacy model. Journal of Counselor Leadership and Advocacy, 6(2), 144–159. https://doi.org/10.1080/2326716X.2019.1644254
Franchino-Olsen, H. (2019). Vulnerabilities relevant for commercial sexual exploitation of children/domestic minor sex trafficking: A systematic review of risk factors. Trauma, Violence & Abuse, 22(1), 99–111. https://doi.org/10.1177/1524838018821956
Grosso, A., Busch, S., Mothopeng, T., Sweitzer, S., Nkonyana, J., Mpooa, N., Taruberekera, T., & Baral, S. (2018). HIV risks and needs related to the sustainable development goals among female sex workers who were commercially sexually exploited as children in Lesotho. Journal of the International AIDS Society, 21(S1), e25042. https://doi.org/10.1002/jia2.25042
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Interiano-Shiverdecker, C. G., Romero, D. E., Anderson, A., & Castellon, N. E. (2022). A content analysis of sex trafficking instruments. International Journal for the Advancement of Counselling, 44, 373–394. https://doi.org/10.1007/s10447-021-09463-9
Interiano-Shiverdecker, C. G., Romero, D. E., & Elliot, J. (2023). Development of child sex trafficking counseling competencies in the United States: A Delphi study. Journal of Interpersonal Violence, 38(1–2), 1397–1423. https://doi.org/10.1177/08862605221090569
International Labour Organization. (2017). Global estimates of modern slavery: Forced labour and forced marriage. https://www.ilo.org/global/topics/forced-labour/publications/WCMS_854733/lang–en/index.htm
Johnson, B. C. (2020). Featured counter-trafficking program: Trauma recovery for victims of sex trafficking. Child Abuse & Neglect, 100, 104–153. https://doi.org/10.1016/j.chiabu.2019.104153
Kenny, M. C., Helpingstine, C. E., Harrington, M. C., & McEachern, A. G. (2018). A comprehensive group approach for commercially sexually exploited girls. The Journal for Specialists in Group Work, 43(4), 376–398. https://doi.org/10.1080/01933922.2018.1484540
Litam, S. D. A. (2017). Human sex trafficking in America: What counselors need to know. The Professional Counselor, 7(1), 45–61. https://doi.org/10.15241/sdal.7.1.45
Litam, S. D. A. (2019). She’s just a prostitute: The effects of labels on counselor attitudes, empathy, and rape myth acceptance. The Professional Counselor, 9(4), 396–415. https://doi.org/10.15241/sdal.9.4.396
Litam, S. D. A., & Lam, E. T. C. (2020). Sex trafficking beliefs in counselors: Establishing the need for human trafficking training in counselor education programs. International Journal for the Advancement of Counselling, 43(1), 1–18. https://doi.org/10.1007/s10447-020-09408-8
Lutnik, A. (2016). Domestic minor sex trafficking: Beyond victims and villains. Columbia University Press.
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Muftić, L. R., & Finn, M. A. (2013). Health outcomes among women trafficked for sex in the United States: A closer look. Journal of Interpersonal Violence, 28(9), 1859–1885. https://doi.org/10.1177/0886260512469102
Mumma, B. E., Scofield, M. E., Mendoza, L. P., Toofan, Y., Youngyunpipatkul, J., & Hernandez, B. (2017). Screening for victims of sex trafficking in the emergency department: A pilot program. Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health, 18(4).
https://doi.org/10.5811/westjem.2017.2.31924
National Human Trafficking Hotline. (n.d.). National statistics. https://humantraffickinghotline.org/states
O’Brien, J., Li, W., Givens, A., & Leibowitz, G. S. (2017). Domestic minor sex trafficking among adjudicated male youth: Prevalence and links to treatment. Children and Youth Services Review, 82, 392–399. https://doi.org/10.1016/j.childyouth.2017.09.026
Oram, S., Abas, M., Bick, D., Boyle, A., French, R., Jakobowitz, S., Khondoker, M., Stanley, N., Trevillion, K., Howard, L., & Zimmerman, C. (2016). Human trafficking and health: A survey of male and female survivors in England. American Journal of Public Health, 106(6), 1073–1078. https://doi.org/10.2105/AJPH.2016.303095
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Romero, D. E., Interiano-Shiverdecker, C. G., Castellon, N. E., & Strentzsch, J. (2021). A review of child sex trafficking instruments. Journal of Child and Adolescent Counseling, 7(1), 56–69. https://doi.org/10.1080/23727810.2020.1835421
Schmidt, C., Lenz, A. S., & Oliver, M. (2022). Effectiveness of TF-CBT with sex trafficking victims in a secure post-adjudication facility. Journal of Counseling & Development, 100(4), 1–13. https://doi.org/10.1002/jcad/12438
Simich, L., Goyen, L., Powell, A., & Berberich, K. (2014). Out of the shadows: A tool for the identification of victims of human trafficking. Vera Institute of Justice. https://www.vera.org/publications/out-of-the-shadows-identification-of-victims-of-human-trafficking
Thompson, J., & Haley, M. (2018). Human trafficking: Preparing counselors to work with survivors. International Journal for the Advancement of Counselling, 40(3), 298–309. https://doi.org/10.1007/s10447-018-9327-1
U.S. Department of State. (2021). Trafficking of persons report. https://www.state.gov/wp-content/uploads/2021/09/TIPR-GPA-upload-07222021.pdf
Victims of Trafficking and Violence Protection Act of 2000, Pub. L. No. 106-386, § 103, 114 Stat. 1470.
Wang, X., & Park-Taylor, J. (2021). Therapists’ experiences of counseling foreign-national sex-trafficking survivors in the U.S. and the impact of COVID-19. Traumatology, 27(4), 419–431. https://doi.org/10.1037/trm0000349
Woehler, E., & Akers, L. (2022). Repairing the trauma bonds of sex trafficking victim-survivors with animal-assisted therapy. Journal of Creativity in Mental Health, 17(4), 456–458. https://doi.org/10.1080/15401383.2021.1921646
Claudia G. Interiano-Shiverdecker, PhD, LPC-A, is an assistant professor at the University of Texas at San Antonio. Devon E. Romero, PhD, NCC, LPC, is an assistant professor at the University of Texas at San Antonio. Katherine E. McVay, PhD, LPC, is an assistant professor at Texas A&M University–Corpus Christi. Emily Satel is a graduate of the master’s program in clinical mental health counseling at the University of Texas at San Antonio. Kendra Smith is a graduate of the master’s program in clinical mental health counseling at the University of Texas at San Antonio. Correspondence may be addressed to Claudia G. Interiano-Shiverdecker, College of Education and Human Development, One UTSA Circle, San Antonio, TX 78249, claudia.interiano-shiverdecker@utsa.edu.
Appendix
Icebreaker
- Please tell me a little about yourself, your professional background, and clinical experience.
Counseling
- What is important for counselors to know when working with sex trafficking survivors?
- How can counselors best detect when individuals are being sex trafficked or are vulnerable to sex trafficking?
- How can counselors support individuals while they are being trafficked?
- How can counselors help individuals leave their traffickers?
- How can counselors support individuals from returning to their traffickers?
- What do counselors have to know about supporting sex trafficking survivors after sex trafficking?
Personal Experiences and Mental Health
- Please share, to the extent that you are comfortable, your experiences with working with sex trafficking survivors.
- What is the age range in which most of your clients experienced sex trafficking?
- How have these experiences impacted your clients?
- Emotionally and mentally?
- Physically?
- Relationships with others?
- Spiritual/religious beliefs?
- What do you believe has helped them overcome the impact of sex trafficking?
- What services or resources do you believe were most helpful to them?
- What is important about your experience that I haven’t asked you and you haven’t had the chance to tell me?
Aug 20, 2021 | Volume 11 - Issue 3
Alison M. Boughn, Daniel A. DeCino
This article introduces the development and implementation of the Psychological Maltreatment Inventory (PMI) assessment with child respondents receiving services because of an open child abuse and/or neglect case in the Midwest (N = 166). Sixteen items were selected based on the literature, subject matter expert refinement, and readability assessments. Results indicate the PMI has high reliability (α = .91). There was no evidence the PMI total score was influenced by demographic characteristics. A positive relationship was discovered between PMI scores and general trauma symptom scores on the Trauma Symptom Checklist for Children Screening Form (TSCC-SF; r = .78, p = .01). Evidence from this study demonstrates the need to refine the PMI for continued use with children. Implications for future research include identification of psychological maltreatment in isolation, further testing and refinement of the PMI, and exploring the potential relationship between psychological maltreatment and suicidal ideation.
Keywords: psychological maltreatment, child abuse, neglect, assessment, trauma
In 2012, the Centers for Disease Control (CDC; 2012) reported that the total cost of child maltreatment (CM) in 2008, including psychological maltreatment (PM), was $124 billion. Fang et al. (2012) estimated the lifetime burden of CM in 2008 was as high as $585 billion. The CDC (2012) characterized CM as rivaling “other high profile public health problems” (para. 1). By 2015, the National Institutes of Health reported the total cost of CM, based on substantiated incidents, was reported to be $428 billion, a 345% increase in just 7 years; the true cost was predictably much higher (Peterson et al., 2018). Using the sensitivity analysis done by Fang et al. (2012), the lifetime burden of CM in 2015 may have been as high as $2 trillion. If these trends continue unabated, the United States could expect a total cost for CM, including PM, of $5.1 trillion by 2030, with a total lifetime cost of $24 trillion. More concerning, this increase would not account for any impact from the COVID-19 pandemic.
Mental health first responders and child protection professionals may encounter PM regularly in their careers (Klika & Conte, 2017; U.S. Department of Health and Human Services [DHHS], 2018). PM experiences are defined as inappropriate emotional and psychological acts (e.g., excessive yelling, threatening language or behavior) and/or lack of appropriate acts (e.g., saying I love you) used by perpetrators of abuse and neglect to gain organizational control of their victims (American Professional Society on the Abuse of Children [APSAC], 2019; Klika & Conte, 2017; Slep et al., 2015). Victims may experience negative societal perceptions (i.e., stigma), fear of retribution from caregivers or guardians, or misdiagnosis by professional helpers (Iwaniec, 2006; López et al., 2015). They often face adverse consequences that last their entire lifetime (Spinazzola et al., 2014; Tyrka et al., 2013; Vachon et al., 2015; van der Kolk, 2014; van Harmelen et al., 2010; Zimmerman & Mercy, 2010). PM can be difficult to identify because it leaves no readily visible trace of injury (e.g., bruises, cuts, or broken bones), making it complicated to substantiate that a crime has occurred (Ahern et al., 2014; López et al., 2015). Retrospective data outlines evaluation processes for PM identification in adulthood; however, childhood PM lacks a single definition and remains difficult to assess (Tonmyr et al., 2011). These complexities in identifying PM in children may prevent mental health professionals from intervening early, providing crucial care, and referring victims for psychological health services (Marshall, 2012; Spinazzola et al., 2014). The Psychological Maltreatment Inventory (PMI) is the first instrument of its kind to address these deficits.
Child Psychological Maltreatment
Although broadly conceptualized, child PM experiences are described as literal acts, events, or experiences that create current or future symptoms that can affect a victim without immediate physical evidence (López et al., 2015). Others have extended child PM to include continued patterns of severe events that impede a child from securing basic psychological needs and convey to the child that they are worthless, flawed, or unwanted (APSAC, 2019). Unfortunately, these broad concepts lack the specificity to guide legal and mental health interventions (Ahern et al., 2014). Furthermore, legal definitions of child PM vary from jurisdiction to jurisdiction and state to state (Spinazzola et al., 2014). The lack of consistent definitions and quantifiable measures of child PM may create barriers for prosecutors and other helping professionals within the legal system as well as a limited understanding of PM in evidence-based research (American Psychiatric Association [APA], 2013; APSAC, 2019; Klika & Conte, 2017). These challenges are exacerbated by comorbidity with other forms of maltreatment.
Co-Occurring Forms of Maltreatment
According to DHHS (2018), child PM is rarely documented as occurring in isolation compared to other forms of maltreatment (i.e., physical abuse, sexual abuse, or neglect). Rather, researchers have found PM typically coexists with other forms of maltreatment (DHHS, 2018; Iwaniec, 2006; Marshall, 2012). Klika and Conte (2017) reported that perpetrators who use physical abuse, inappropriate language, and isolation facilitate conditions for PM to coexist with other forms of abuse. Van Harmelen et al. (2011) argued that neglectful acts constitute evidence of PM (e.g., seclusion; withholding medical attention; denying or limiting food, water, shelter, and other basic needs).
Consequences of PM Experienced in Childhood
Mills et al. (2013) and Greenfield and Marks (2010) noted PM experiences in early childhood might manifest in physical growth delays and require access to long-term care throughout a victim’s lifetime. Children who have experienced PM may suffer from behaviors that delay or prevent meeting developmental milestones, achieving academic success in school, engaging in healthy peer relationships, maintaining physical health and well-being, forming appropriate sexual relationships as adults, and enjoying satisfying daily living experiences (Glaser, 2002; Maguire et al., 2015). Neurological and cognitive effects of PM in childhood impact children as they transition into adulthood, including abnormalities in the amygdala and hippocampus (Tyrka at al., 2013). Brown et al. (2019) found that adults who reported experiences of CM had higher rates of negative responses to everyday stress, a larger constellation of unproductive coping skills, and earlier mortality rates (Brown et al., 2019; Felitti et al., 1998). Furthermore, adults with childhood PM experiences reported higher rates of substance abuse than those compared to control groups (Felitti et al., 1998).
Trauma-Related Symptomology. Researchers speculate that children exposed to maltreatment and crises, especially those that come without warning, are at greater risk for developing a host of trauma-related symptoms (Spinazzola et al., 2014). Developmentally, children lack the ability to process and contextualize their lived experiences. Van Harmelen et al. (2010) discovered that adults who experienced child PM had decreased prefrontal cortex mass compared to those without evidence of PM. Similarly, Field et al. (2017) found those unable to process traumatic events produced higher levels of stress hormones (i.e., cortisol, epinephrine, norepinephrine); these hormones are produced from the hypothalamic-pituitary-adrenal (HPA) and sympathetic-adrenal-medullary (SAM) regions in the brain. Some researchers speculate that elevated levels of certain hormones and hyperactive regions within the brain signal the body’s biological attempt to reduce the negative impact of PM through the fight-flight-freeze response (Porges, 2011; van der Kolk, 2014).
Purpose of Present Study
At the time of this research, there were few formal measures using child self-report to assess how children experience PM. We developed the PMI as an initial quantifiable measure of child PM for children and adolescents between the ages of 8 and 17, as modeled by Tonmyr and colleagues (2011). The PMI was developed in multiple stages, including 1) a review of the literature, 2) a content validity survey with subject matter experts (SMEs), 3) a pilot study (N = 21), and 4) a large sample study (N = 166). An additional instrument, the Trauma Symptom Checklist for Children Screening Form (TSCC-SF; Briere & Wherry, 2016), was utilized in conjunction with the PMI to explore occurrences of general trauma symptoms among respondents. The following four research questions were investigated:
- How do respondent demographics relate to PM?
- What is the rate of PM experience with respondents who are presently involved in an open CM case?
- What is the co-occurrence of PM among various forms of CM allegations?
- What is the relationship between the frequency of reported PM experiences and the frequency of general trauma symptoms?
Method
Study 1: PMI Item Development and Pilot
Following the steps of scale construction (Heppner et al., 2016), the initial version of the PMI used current literature and definitions from facilities nationwide that provide care for children who have experienced maltreatment and who are engaged with court systems, mental health agencies, or social services. Our lead researcher, Alison M. Boughn, developed a list of 20 items using category identifications from Glaser (2002) and APSAC (2019). Items were also created using Slep et al.’s (2015) proposed inclusion language for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) diagnostic codes and codes from the International Classification of Diseases, 11th edition (ICD-11) definition criteria (APA, 2013). Both Boughn and Daniel A. DeCino, our other researcher, reviewed items for consistency with the research literature and removed four redundant items. The final 16 items were reevaluated for readability for future child respondents using a web-based, age range–appropriate readability checker (Readable, n.d.) and were then presented to local SMEs in a content validity survey to determine which would be considered essential for children to report as part of a child PM assessment.
Expert Validation
A multidisciplinary team (MDT) serving as SMEs completed an online content validity survey created by Boughn. The survey was distributed by a Child Advocacy Center (CAC) manager to the MDT. Boughn used the survey results to validate the PMI’s item content relevance. Twenty respondents from the following professions completed the survey: mental health (n = 6), social services (n = 6), law enforcement (n = 3), and legal services (n = 5). The content validity ratio (CVR) was then calculated for the 16 proposed items.
Results. The content validity survey scale used a 3-point Likert-type scale: 0 = not necessary; 1 = useful, but not essential; and 2 = essential. A minimum of 15 of the 20 SMEs (75% of the sample), or a CVR ≥ .5, was required to deem an item essential (Lawshe, 1975). The significance level for each item’s content validity was set at α = .05 (Ayre & Scally, 2014). After conducting Lawshe’s (1975) CVR and applying the ratio correction developed by Ayre and Scally (2014), it was determined that eight items were essential: Item 2 (CVR = .7), Item 3 (CVR = .9), Item 4 (CVR = .6), Item 6 (CVR = .6), Item 7 (CVR = .8), Item 10 (CVR = .6), Item 15 (CVR = .5), and Item 16 (CVR = .6).
Upon further evaluation, and in an effort to ensure that the PMI items served the needs of interdisciplinary professionals, some items were rated essential for specific professions; these items still met the CVR requirements (CVR = 1) for the smaller within-group sample. These four items were unanimously endorsed by SMEs for a particular profession as essential: Item 5 (CVR Social Services = 1; CVR Law Enforcement = 1), Item 11 (CVR Law Enforcement = 1), Item 13 (CVR Law Enforcement = 1), and Item 14 (CVR Law Enforcement = 1).
Finally, an evaluation of the remaining four items was completed to explore if items were useful, but not essential. Using the minimum CVR ≥ .5, it was determined that these items should remain on the PMI: Item 1 (CVR = .9), Item 8 (CVR = .8), Item 9 (CVR = .9), and Item 12 (CVR = .9). The use of Siegle’s (2017) Reliability Calculator determined the Cronbach’s α level for the PMI to be 0.83, indicating adequate internal consistency. Additionally, a split-half (odd-even) correlation was completed with the Spearman-Brown adjustment of 0.88, indicating high reliability (Siegle, 2017).
Pilot Summary
The focus of the pilot study was to ensure effective implementation of the proposed research protocol following each respondent’s appointment at the CAC research site. The pilot was implemented to ensure research procedures did not interfere with typical appointments and standard procedures at the CAC. Participation in the PMI pilot was voluntary and no compensation was provided for respondents.
Sample. The study used a purposeful sample of children at a local, nationally accredited CAC in the Midwest; both the child and the child’s legal guardian agreed to participate. Because of the expected integration of PM with other forms of abuse, this population was selected to help create an understanding of how PM is experienced specifically with co-occurring cases of maltreatment. Respondents were children who (a) had an open CM case with social services and/or law enforcement, (b) were scheduled for an appointment at the CAC, and (c) were between the ages of 8 and 17.
Measures. The two measures implemented in this study were the developing PMI and the TSCC-SF. At the time of data collection, CAC staff implemented the TSCC-SF as a screening tool for referral services during CAC victim appointments. To ensure the research process did not interfere with chain-of-custody procedures, collected investigative testimony, or physical evidence that was obtained, the PMI was administered only after all normally scheduled CAC procedures were followed during appointments.
PMI. The current version of the PMI is a self-report measure that consists of 16 items on a 4-point Likert-type scale that mirrors the language of the TSCC-SF (0 = never to 3 = almost all the time). Respondents typically needed 5 minutes complete the PMI. Sample items from the PMI included questions like: “How often have you been told or made to feel like you are not important or unlovable?” The full instrument is not provided for use in this publication to ensure the PMI is not misused, as refinement of the PMI is still in progress.
TSCC-SF. In addition to the PMI, Boughn gathered data from the TSCC-SF (Briere & Wherry, 2016) because of its widespread use among clinicians to efficiently assess for sexual concerns, suicidal ideation frequency, and general trauma symptoms such as post-traumatic stress, depression, anger, disassociation, and anxiety (Wherry et al., 2013). The TSCC-SF measures a respondent’s frequency of perceived experiences and has been successfully implemented with children as young as 8 years old (Briere, 1996). The 20-item form uses a 4-point Likert-type scale (0 = never to 3 = almost all the time) composed of general trauma and sexual concerns subscales. The TSCC-SF has demonstrated high internal consistency and alpha values in the good to excellent ranges; it also has high intercorrelations between sexual concerns and other general trauma scales (Wherry & Dunlop, 2018).
Procedures. Respondents were recruited during their scheduled CAC appointment time. Each investigating agency (law enforcement or social services) scheduled a CAC appointment in accordance with an open maltreatment case. At the beginning of each respondent’s appointment, Boughn provided them with an introduction and description of the study. This included the IRB approvals from the hospital and university, an explanation of the informed consent and protected health information (PHI) authorization, and assent forms. Respondents aged 12 and older were asked to read and review the informed consent document with their legal guardian; respondents aged from 8 to 11 were provided an additional assent document to read. Respondents were informed they could stop the study at any time. After each respondent and legal guardian consented, respondents proceeded with their CAC appointment.
Typical CAC appointments consisted of a forensic interview, at times a medical exam, and administration of the TSCC-SF to determine referral needs. After these steps were completed, Boughn administered the PMI to those who agreed to participate in this research study. Following the completion of the TSCC-SF, respondents were verbally reminded of the study and asked if they were still willing to participate by completing the PMI. Willing respondents completed the PMI; afterward, Boughn asked respondents if they were comfortable leaving the assessment room. In the event the respondent voiced additional concerns of maltreatment during the PMI administration, Boughn made a direct report to the respondent’s investigator (i.e., law enforcement officer or social worker assigned to the respondent’s case).
Boughn accessed each respondent’s completed TSCC-SF from their electronic health record in accordance with the PHI authorization and consent after the respondent’s appointment. Data completed on the TSCC-SF allowed Boughn to gather information related to sexual concerns, suicidal ideation, and trauma symptomology. Data gathered from the TSCC-SF were examined with each respondent’s PMI responses.
Results. Respondents were 21 children (15 female, six male) with age ranges from 8 to 17 years with a median age of 12 years. Respondents described themselves as White (47.6%), Biracial (14.2%), Multiracial (14.2%), American Indian/Alaskan Native (10.0%), Black (10.0%), and Hispanic/Latino (5.0%). CM allegations for the respondents consisted of allegations of sexual abuse (86.0%), physical abuse (10.0%), and neglect (5.0%).
Every respondent’s responses were included in the analyses to ensure all maltreatment situations were considered. The reliability of the PMI observed in the pilot sample (N = 21) demonstrated high internal consistency with all 16 initial items (α = .88). The average total score on the PMI in the pilot was 13.29, with respondents’ scores ranging from 1 to 30. A Pearson correlation indicated total scores for the PMI and General Trauma Scale scores (reported on the TSCC-SF) were significantly correlated (r = .517, p < .05).
Study 2: Full Testing of the PMI
The next phase of research proceeded with the collection of a larger data sample (N = 166) to explore the item construct validity and internal reliability (Siyez et al., 2020). Study procedures, data collection, and data storage followed in the pilot study were also implemented with the larger sample. Boughn maintained tracking of respondents who did not want to participate in the study or were unable to because of cognitive functioning level, emergency situations, and emotional dysregulation concerns.
Sample
Based on a power analysis performed using the Raosoft (2004) sample size calculator, the large sample study required a minimum of 166 respondents for statistical significance (Ali, 2012; Heppner et al., 2016). The sample size was expected to account for a 10% margin of error and a 99% confidence level. The calculation of a 99% confidence interval was used to ensure the number of respondents could effectively represent the population accessed within the CAC based on the data from the CM Report (DHHS, 2018). Large sample population data was gathered between September 2018 and May 2019.
Measures
The PMI and TSCC-SF were also employed in Study 2 because of their successful implementation in the pilot. Administration of the TSCC-SF ensured a normed and standardized measure could aid in providing context to the information gathered on the PMI. No changes were made to the PMI or TSCC-SF measures following the review of procedures and analyses in the pilot.
Procedures
Recruitment and data collection/analyses processes mirrored that of the pilot study. Voluntary respondents were recruited at the CAC during their scheduled appointments. Respondents completed an informed consent, child assent, PHI authorization form, TSCC-SF, and PMI. Following the completion of data collection, Boughn completed data entry in the electronic health record to de-identify and analyze the results.
Results
Demographics
All data were analyzed using Statistical Package for the Social Sciences version 24 (SPSS-24). Initial data evaluation consisted of exploration of descriptive statistics, including demographic and criteria-based information related to respondents’ identities and case details. Respondents were between 8 to 17 years of age (M = 12.39) and primarily female (73.5%, n = 122), followed by male (25.3%, n = 42). Additionally, two respondents (n = 2) reported both male and female gender identities. Racial identities were marked by two categories: White (59.6%, n = 99) and Racially Diverse (40.4%, n = 67) respondents. The presenting maltreatment concerns and the child’s relationship to the offender are outlined in Table 1 and Table 2, respectively.
Reliability and Validity of the PMI
The reliability of the PMI observed in its implementation in Study 2 (N = 166) showed even better internal consistency with all 16 initial items (α =.91) than observed in the pilot. Using the Spearman-Brown adjustment (Warner, 2013), split-half reliability was calculated, indicating high internal reliability (.92). Internal consistencies were calculated using gender identity and age demographic variables (see Table 3).
Table 1
Child Maltreatment Allegation by Type (N = 166)
| Allegation |
f |
Rel f |
cf |
% |
| Sexual Abuse |
113 |
0.68 |
166 |
68.07 |
| Physical Abuse |
29 |
0.17 |
53 |
17.47 |
| Neglect |
14 |
0.08 |
24 |
8.43 |
| Multiple Allegations |
6 |
0.04 |
10 |
3.61 |
| Witness to Violence |
3 |
0.02 |
4 |
1.81 |
| Kidnapping |
1 |
0.01 |
1 |
0.60 |
Note. Allegation type reported at initial appointment scheduling
Table 2
Identified Offender by Relationship to Victim (N = 166)
| Offender Relationship |
f |
Rel f |
cf |
% |
| Other Known Adult |
60 |
0.36 |
166 |
36.14 |
| Parent |
48 |
0.29 |
106 |
28.92 |
| Other Known Child (≤ age 15 years) |
15 |
0.09 |
58 |
9.04 |
| Sibling-Child (≤ age 15 years) |
10 |
0.06 |
43 |
6.02 |
| Unknown Adult |
9 |
0.05 |
33 |
5.42 |
| Step-Parent |
8 |
0.05 |
24 |
4.82 |
| Multiple Offenders |
6 |
0.04 |
16 |
3.61 |
| Grandparent |
6 |
0.04 |
10 |
3.61 |
| Sibling-Adult (≥ age 16 years) |
3 |
0.02 |
4 |
1.81 |
| Unknown Child (≤ age 15 years) |
1 |
0.01 |
1 |
0.60 |
Note. Respondent knew the offender (n =156); Respondent did not know offender (n =10)
Table 3
Internal Consistency Coefficients (α) by Gender Identity and Age (N = 166)
| Gender |
n |
α |
M |
SD |
| Female |
122 |
0.90 |
13.2 |
9.1 |
| Male |
42 |
0.94 |
13.5 |
11.0 |
| Male–Female |
2 |
0.26 |
8.5 |
2.5 |
| Age |
|
|
|
|
| 8–12 |
83 |
0.92 |
12.75 |
10.06 |
| 13–17 |
83 |
0.90 |
13.69 |
9.01 |
Note. SD = Standard Deviation; M = Mean
Respondents’ Demographic Characteristics and PM Experiences
For Research Question (RQ) 1 and RQ2, descriptive data were used to generate frequencies and determine the impact of demographic characteristics on average PMI score. To explore this further in RQ1, one-way ANOVAs were completed for the variables of age, gender, racial identity, allegation type, and offender relationships. No significant correlations were found between demographic variables and the PMI items. On average, respondents reported a frequency score of 13.5 (M = 13.5, SD = 9.5) on the PMI. Eight respondents (5%) endorsed no frequency of PM while 95% (N = 158) experienced PM.
Co-Occurrence of PM With Other Forms of Maltreatment
For RQ3, frequency and descriptive data were generated, revealing average age rates of PM reported by maltreatment type. Varying sample representations were discovered in each form of maltreatment (see Table 4). Clear evidence was found that PM co-occurs with each form of maltreatment type; however, how each form of maltreatment interacts with PM is currently unclear given the multiple dimensions of each maltreatment case including, but not limited to, severity, frequency, offender, and victim characteristics.
Table 4
Descriptive and Frequency Data for Co-Occurrence of PM (N = 166)
| Allegation |
n |
M |
SD |
95% CI |
| Sexual Abuse |
113 |
13.04 |
9.01 |
[11.37, 14.72] |
| Physical Abuse |
29 |
12.45 |
10.53 |
[8.44, 16.45] |
| Neglect |
14 |
14.57 |
12.16 |
[7.55, 21.60] |
| Multiple Allegations |
5 |
17.40 |
8.88 |
[6.38, 28.42] |
| Witness to Violence |
3 |
7.67 |
5.03 |
[–4.84, 20.17] |
| Kidnapping |
1 |
n/a |
n/a |
Missing |
Note. CI = Confidence Interval; SD = Standard Deviation; M = Mean; n/a = not applicable
PM Frequency and General Trauma Symptoms
For RQ4, Pearson’s correlation was used to calculate frequency score relationships between the PMI and TSCC-SF. There was a statistically significant relationship between the PMI and total frequency of general trauma symptoms on the TSCC-SF [r(164) = .78, p < .01, r² = .61] (Sullivan & Feinn, 2012). Cohen’s d, calculated from the means for each item as well as the pooled standard deviation, indicated a small effect relationship (d = .15) between general trauma and PMI frequencies (see Figure 1).
Figure 1
Correlation Between PMI and TSCC-SF General Trauma Subscale
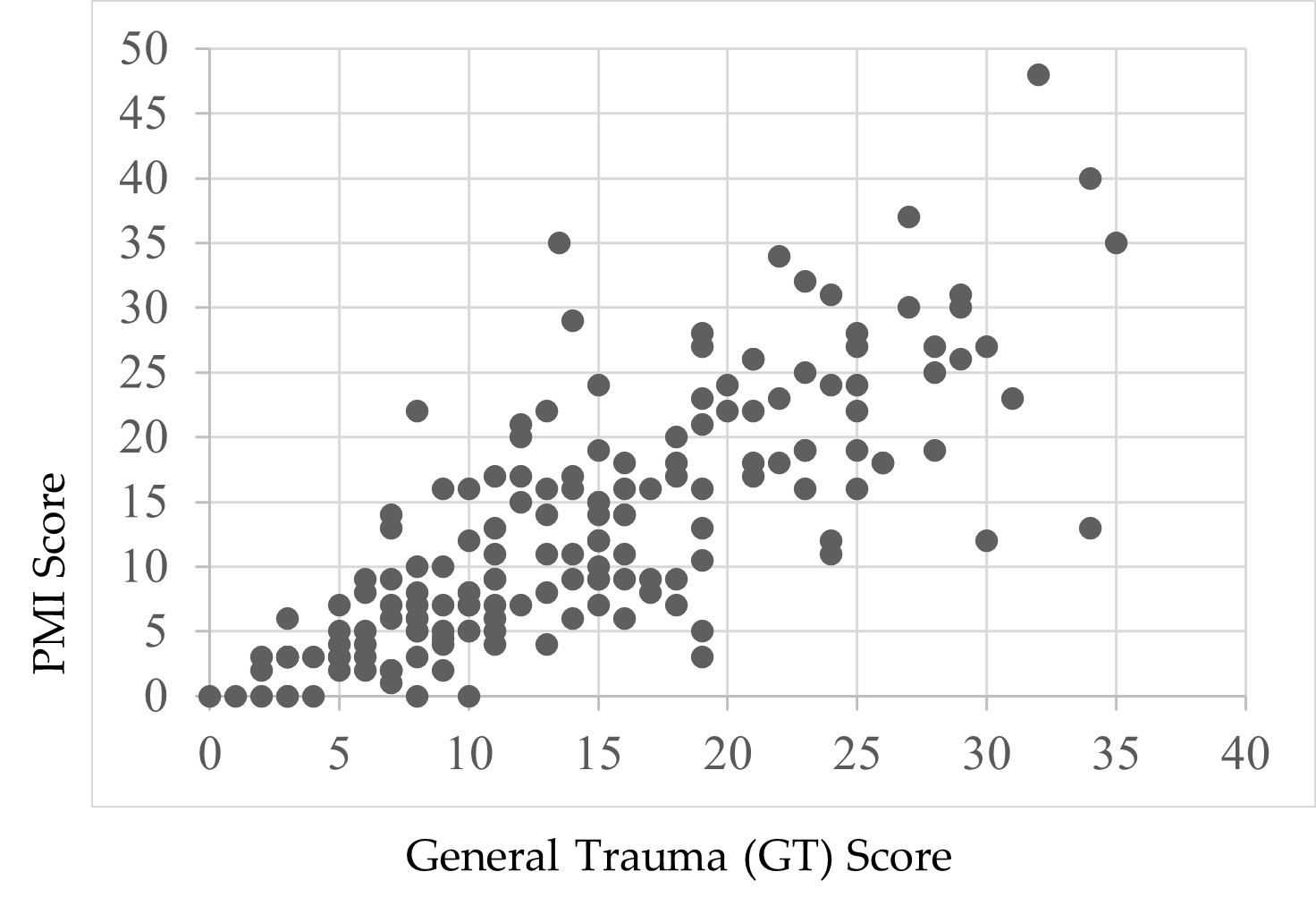
Note. Scores were endorsed by respondents’ self-reports.
Child Suicidal Ideation Reports and the PMI
Following a review of the findings of Thompson et al. (2005) and Wherry et al. (2013) that children who reported experiencing CM also experienced suicidal ideation, Boughn performed an additional two-way ANOVA that examined the effect of suicidal ideation on the PMI total score. A significant relationship—F(1, 164) = 49.52, p < .01, η2 = .23—between respondents’ PMI scores and thoughts of suicide was found. Respondents who did not report thoughts of suicide (59.0%, n = 98) indicated lower rates of PM (M = 9.37, SD = 7.97) compared to children who did report thoughts of suicide (41.0%, n = 68, M = 18.77, SD = 9.12). A preliminary review of this finding demonstrates the severity of PM’s impact on child victims.
Discussion
This study was designed with the aim of developing a tool to support accurate identification of PM among children and adolescents. Findings from its first large-scale implementation provide a foundational view to the occurrence of PM in terms of demographic characteristics, comorbidity of PM with other forms of abuse, and the relationship between PM and trauma. The analyses yielded both expected and unexpected results based on the extant research.
PM and Demographic Characteristics
Race
There was no significant effect when exploring the data related to racial demographics and PM. The respondent sample closely reflected the geographical area’s known racial demographics at the time of the study, reflecting a population approaching 80% White with residents of all other known races below 5% for each racial group (U.S. Census Bureau, 2020). Although researchers (Dakil et al., 2011) anticipated children identifying as racial minorities would be included in the representation of CM reports, evidence from this study potentially reveals a greater than expected gap in reporting for minority-race populations (Bernard & Harris, 2018; Font & Maguire-Jack, 2015). This suggests that there may be additional, unidentified barriers influencing the reporting of maltreatment among minority-race populations.
Gender
A lack of gender identity representation was evident in the data, consistent with prior research (Sivagurunathan et al., 2019). Respondents who self-identified with both male and female gender identities (1.2%) and as male (25.3%) were represented less frequently compared to female respondents (73.5%). This is not inherently a limitation of this study, as research shows that just 10% of males in the United States report their sexual abuse (Sivagurunathan et al., 2019). People who identify as male may face harmful cultural messages that enhance negative stigma for victims of abuse, causing increased feelings of weakness or vulnerability (Alaggia & Mishna, 2014). This finding may support claims that male trauma survivors feel stigmatized and report their experiences less frequently (Easton, 2012).
Additionally, children who identify outside traditional gender binary norms and definitions need more access to inclusive representation on screening assessments. Assessments like the TSCC-SF may be using antiquated gender- or biological sex–normed checkboxes, which leave certain groups underrepresented in research studies (Neukrug & Fawcett, 2015). These practices may present inaccurate findings, inadvertently reinforce discriminatory expectations, and generate inaccurate referrals. Non-binary youth encounter barriers that may compound their ability to effectively access supports in their daily life related to coming out, social violence, lack of peer and/or adult acceptance, discrimination, isolation, higher rates of suicide, and lack of representation in mainstream society (Bialer & McIntosh, 2016; Zimman, 2009). In this study, representation of non-binary respondents, specifically those who reported both male and female gender identities, was reported; this warrants further exploration to assess barriers among non-binary gender youth and their experiences with child PM (Bos et al., 2019).
Offender Relationships
Frequency data for a child’s relationship with the offender were not found to be significant either for known offenders (M = 13.35) or unknown offenders (M = 11.2). In this study, 94% of the respondents already knew their offender (n = 156). This finding is consistent with previous research that has found that although child abduction and stranger danger are real phenomena, children are more likely to experience CM as a result of relationships with familiar individuals (Walsh & Brandon, 2011).
Co-Occurrence of PM With Other Abuse
Only eight respondents (5%) endorsed no frequency of PM; the average total PM frequency rate for respondents in this study was 13.5 out of a possible 48, indicating extreme severity. In this study, we found evidence that PM is a co-occurring experience for children with open maltreatment cases, yet clinicians still lack formal, valid assessments to determine PM alone. Our findings support the National Children’s Alliance’s (NCA; 2016) call for clinicians to follow practice guidelines in accordance with state and national guidelines as they relate to mandatory reporting of CM concerns and determination of whether PM plus other forms of maltreatment may be present for child victims seeking services.
Comorbidity of PM and Trauma
PM-related experiences on the PMI and general trauma symptoms from the TSCC-SF warrant discussion. The PMI illustrated a significant relationship with the TSCC-SF general trauma subscale (Briere & Wherry, 2016). More than half (61%) of the variance on the PMI was connected to general trauma symptoms, suggesting that higher rates of PM experiences may increase trauma-related symptoms. For example, previous researchers have found adverse childhood experiences and signs of trauma-related symptoms lead to serious mental health diagnoses, early mortality, and/or significant biological health risks in children (Tyrka et al., 2013; Vachon et al., 2015; Zimmerman & Mercy, 2010). Further exploration to determine if and how PM influences other trauma-related symptoms in children throughout their life span would expand upon the results of this study.
Suicidal Ideation
Finally, our data revealed a significant effect between respondent endorsement of suicidal ideation and PMI total scores. PM experiences accounted for 23% of the variance for children who reported thoughts of suicide (41%, n = 68) compared to those who did not report thoughts of suicide (59%, n = 98). This finding is consistent with prior research exploring children’s experiences with maltreatment and suicidal thoughts (Thompson et al., 2005; Wherry et al., 2013).
Limitations
This study has several limitations. First, by developing the PMI using national definitions, some regional and localized nuances were not considered. Second, data collected for this study were from a single Midwest CAC; thus, the data are limited in geographic generalizability. Third, the majority of respondents were White, and a more diverse sample would have been more representative of the region in which data were collected. Fourth, 99% of respondents identified as either male or female and may reflect an underrepresentation of non-binary or gender fluid youth in the results of this study. Fifth, this study relied heavily on quantitative data, which limited the ability to analyze each individual’s experiences with PM as they might describe from their unique perspectives.
Implications for Research and Practice
The results of this study provide several areas for future research. While the PMI demonstrated good internal consistency across all items (α =.91), more research with diverse populations across the United States is needed. Research from other geographical locations may demonstrate how reporting patterns for PM interact with ethnicity, culture, and elements of social expectations (Spinazzola et al., 2014).
The initial results of this study indicate the PMI may be a useful tool for children to report PM experiences in CAC settings; however, future research at other CACs and similar treatment facilities is needed to determine the PMI’s true utility and scalability. Future analysis (i.e., exploratory factor analysis and confirmatory factor analysis) of the PMI may also identify factors and help refine the instrument.
More research with the PMI can expand researchers’ knowledge of PM and services needed to help children. Working with other CACs, child protection professionals, and the NCA may help bridge current gaps in interdisciplinary assessment and care and establish a stable and comprehensive understanding of PM (López et al., 2015). Furthermore, understanding how CACs are equipped to identify and handle PM cases may provide useful insights to help improve services for children in need. Although some CACs may have a variety of professionals working in specific roles, some CACs may be understaffed, causing staff to take on multiple and overlapping roles. It is important to understand if and how different combinations of trained professionals influence children reporting PM (Hart & Glaser, 2011; NCA, 2016).
More research with the PMI is needed for refinement and to ensure the instrument is not misused. Releasing the PMI at this stage to clinicians and researchers without a fully developed assessment manual may lead to inappropriate or ineffective administration of the PMI and potentially unethical practice that could place children at risk. Future research and refinement of the PMI may provide clinicians and researchers a reliable and valid tool that is grounded in consistent theory and practice.
Conclusion
The PMI was developed to assess child PM and offers researchers and clinicians useful findings. In supporting research (Arslan, 2017; Bernstein et al., 2013; Raparia et al., 2016), child PM is a serious and often harmful combination of experiences that requires professional intervention (APSAC, 2019). For children reporting PM experiences, the PMI may help mental health and other care providers determine which services are needed. Findings from this study suggest differences in demographic variables are minimal for PM. Overall PMI scores were correlated to the general trauma subscale on the TSCC-SF, and the PMI revealed higher rates of PM for children experiencing suicidal ideation. The findings are the beginning of a measure designed to illustrate the depth and frequency of PM for children. With the PMI, early PM intervention becomes possible for a once invisible form of maltreatment.
Conflict of Interest and Funding Disclosure
Data collected and content shared in this study
were part of a dissertation study, which was
awarded the 2020 Dissertation Excellence Award
by the National Board for Certified Counselors.
The Psychological Maltreatment Inventory (PMI)
items were not released in this publication to protect
victims of child maltreatment and to ensure future
publications can address comprehensive revisions
made to the PMI.
References
Ahern, E. C., Hershkowitz, I., Lamb, M. E., Blasbalg, U., & Winstanley, A. (2014). Support and reluctance in the pre-substantive phase of alleged child abuse victim investigative interviews: Revised versus standard NICHD protocols. Behavioral Sciences & the Law, 32(6), 762–774. https://doi.org/10.1002/bsl.2149
Alaggia, R., & Mishna, F. (2014). Self psychology and male child sexual abuse: Healing relational betrayal. Clinical Social Work Journal, 42(1), 41–48. https://doi.org/10.1007/s10615-013-0453-2
Ali, S. A. (2012). Sample size calculation and sampling techniques. Journal of the Pakistan Medical Association, 62(6), 624–626. https://jpma.org.pk/PdfDownload/3482
American Professional Society on the Abuse of Children. (2019). APSAC practice guidelines: The investigation and determination of suspected psychological maltreatment of children and adolescents. https://bit.ly/3jI7AhJ
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Arslan, G. (2017). Psychological maltreatment, coping strategies, and mental health problems: A brief and effective measure of psychological maltreatment in adolescents. Child Abuse & Neglect, 68, 96–106. https://doi.org/10.1016/j.chiabu.2017.03.023
Ayre, C., & Scally, A. J. (2014). Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), 79–86. https://doi.org/10.1177%2F0748175613513808
Bernard, C., & Harris, P. (2018). Serious case reviews: The lived experience of Black children. Child & Family Social Work, 24(2), 256–263. https://doi.org/10.1111/cfs.12610
Bernstein, R. E., Measelle, J. R., Laurent, H. K., Musser, E. D., & Ablow, J. C. (2013). Sticks and stones may break my bones but words relate to adult physiology? Child abuse experience and women’s sympathetic nervous system response while self-reporting trauma. Journal of Aggression, Maltreatment & Trauma, 22(10), 1117–1136. https://doi.org/10.1080/10926771.2013.850138
Bialer, P. A., & McIntosh, C. A. (2016). Discrimination, stigma, and hate: The impact on the mental health and well-being of LGBT people. Journal of Gay & Lesbian Mental Health, 20(4), 297–298. https://doi.org/10.1080/19359705.2016.1211887
Bos, H., de Haas, S., & Kuyper, L. (2019). Lesbian, gay, and bisexual adults: Childhood gender nonconformity, childhood trauma, and sexual victimization. Journal of Interpersonal Violence, 34(3), 496–515. https://doi.org/10.1177%2F0886260516641285
Briere, J. (1996). Trauma Symptom Checklist for Children (TSCC), professional manual. Psychological Assessment Resources.
Briere, J., & Wherry, J. (2016). Development and validation of the TSCC Screening Form (TSCC-SF) and TSCYC Screening Form (TSCYC-SF). Psychological Assessment Resources.
Brown, S. M., Bender, K., Orsi, R., McCrae, J. S., Phillips, J. D., & Rienks, S. (2019). Adverse childhood experiences and their relationship to complex health profiles among child welfare–involved children: A classification and regression tree analysis. Health Services Research, 54(4), 902–911. https://doi.org/10.1111/1475-6773.13166
Centers for Disease Control. (2012). Child abuse and neglect cost the United States $124 billion [Press release]. https://bit.ly/3jYbpAF
Dakil, S. R., Cox, M., Lin, H., & Flores, G. (2011). Racial and ethnic disparities in physical abuse reporting and Child Protective Services interventions in the United States. Journal of the National Medical Association, 103(9–10), 926–931. https://doi.org/10.1016/S0027-9684(15)30449-1
Easton, S. D. (2012). Disclosure of child sexual abuse among adult male survivors. Clinical Social Work Journal, 41, 344–355. https://doi.org/10.1007/s10615-012-0420-3
Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect, 36(2), 156–165. https://doi.org/10.1016/j.chiabu.2011.10.006
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Field, T. A., Jones, L. K., & Russell-Chapin, L. A. (Eds.). (2017). Neurocounseling: Brain-based clinical approaches. American Counseling Association.
Font, S. A., & Maguire-Jack, K. (2015). Decision-making in Child Protective Services: Influences at multiple levels of the social ecology. Child Abuse & Neglect, 47, 70–82. https://doi.org/10.1016/j.chiabu.2015.02.005
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment): A conceptual framework. Child Abuse & Neglect, 26(6–7), 697–714. https://doi.org/10.1016/S0145-2134(02)00342-3
Greenfield, E. A., & Marks, N. F. (2010). Identifying experiences of physical and psychological violence in childhood that jeopardize mental health in adulthood. Child Abuse & Neglect, 34(3), 161–171. https://doi.org/10.1016/j.chiabu.2009.08.012
Hart, S. N., & Glaser, D. (2011). Psychological maltreatment – Maltreatment of the mind: A catalyst for advancing child protection toward proactive primary prevention and promotion of personal well-being. Child Abuse & Neglect, 35(10), 758–766. https://doi.org/10.1016/j.chiabu.2011.06.002
Heppner, P. P., Wampold, B. E., Owen, J., Thompson, M. N., & Wang, K. T. (2016). Research design in counseling (4th ed.). Cengage.
Iwaniec, D. (2006). The emotionally abused and neglected child: Identification, assessment and intervention: A practice handbook (2nd ed.). Wiley.
Klika, J. B., & Conte, J. R. (Eds.). (2017). The APSAC handbook on child maltreatment (4th ed.). SAGE.
Lawshe, C. H. (1975). A quantitative approach to content validity. Personnel Psychology, 28(4), 563–575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x
López, M., Fluke, J. D., Benbenishty, R., & Knorth, E. J. (2015). Commentary on decision-making and judgments in child maltreatment prevention and response: An overview. Child Abuse & Neglect, 49, 1–11. https://doi.org/10.1016/j.chiabu.2015.08.013
Maguire, S. A., Williams, B., Naughton, A. M., Cowley, L. E., Tempest, V., Mann, M. K., Teague, M., & Kemp, A. M. (2015). A systematic review of the emotional, behavioural and cognitive features exhibited by school-aged children experiencing neglect or emotional abuse. Child: Care, Health and Development, 41(5), 641–653. https://doi.org/10.1111/cch.12227
Marshall, N. A. (2012). A clinician’s guide to recognizing and reporting parental psychological maltreatment of children. Professional Psychology: Research and Practice, 43(2), 73–79. https://doi.org/10.1037/a0026677
Mills, R., Scott, J., Alati, R., O’Callaghan, M., Najman, J. M., & Strathearn, L. (2013). Child maltreatment and adolescent mental health problems in a large birth cohort. Child Abuse & Neglect, 37(5), 292–302. https://doi.org/10.1016/j.chiabu.2012.11.008
National Children’s Alliance. (2016). Putting standards into practice: A guide to implementing the 2017 standards for accredited members (revised 2016). http://www.nationalchildrensalliance.org/wp-content/uploads/2015/06/NCA2017-StandardsIntoPractice-web.pdf
Neukrug, E. S., & Fawcett, R. C. (2015). The essentials of testing and assessment: A practical guide for counselors, social workers, and psychologies, enhanced (3rd ed.). Cengage.
Peterson, C., Florence, C., & Klevens, J. (2018). The economic burden of child maltreatment in the United States, 2015. Child Abuse & Neglect, 86, 178–183.
https://doi.org/10.1016/j.chiabu.2018.09.018
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
Raosoft. (2004). Sample size calculator. http://www.raosoft.com/samplesize.html
Raparia, E., Coplan, J. D., Abdallah, C. G., Hof, P. R., Mao, X., Mathew, S. J., & Shungu, D. C. (2016). Impact of childhood emotional abuse on neocortical neurometabolites and complex emotional processing in patients with generalized anxiety disorder. Journal of Affective Disorders, 190, 414–423. https://doi.org/10.1016/j.jad.2015.09.019
Readable. (n.d.). https://readable.com
Siegle, R. (2017). Educational research basics: Excel spreadsheet to calculate instrument reliability estimates. https://researchbasics.education.uconn.edu/excel-spreadsheet-to-calculate-instrument-reliability-estimates
Sivagurunathan, M., Orchard, T., & Evans, M. (2019). Barriers to utilization of mental health services amongst male child sexual abuse survivors: Service providers’ perspective. Journal of Child Sexual Abuse, 28(7), 819–839. https://doi.org/10.1080/10538712.2019.1610823
Siyez, D. M., Esen, E., Seymenler, S., & Öztürk, B. (2020). Development of wellness scale for emerging adults: Validity and reliability study. Current Psychology.
https://doi.org/10.1007/s12144-020-00672-w
Slep, A. M. S., Heyman, R. E., & Foran, H. M. (2015). Child maltreatment in DSM-5 and ICD-11. Family Process, 54(1), 17–32. https://doi.org/10.1111/famp.12131
Spinazzola, J., Hodgdon, H., Liang, L.-J., Ford, J. D., Layne, C. M., Pynoos, R., Briggs, E. C., Stolbach, B., & Kisiel, C. (2014). Unseen wounds: The contribution of psychological maltreatment to child and adolescent mental health and risk outcomes. Psychological Trauma: Theory, Research, Practice, and Policy, 6(Suppl 1), S18–S28. https://doi.org/10.1037/a0037766
Sullivan, G. M., & Feinn, R. (2012). Using effect size—or why the p value is not enough. Journal of Graduate Medical Education, 4(3), 279–282. https://doi.org/10.4300/JGME-D-12-00156.1
Thompson, R., Briggs, E., English, D. J., Dubowitz, H., Lee, L.-C., Brody, K., Everson, M. D., & Hunter, W. M. (2005). Suicidal ideation among 8-year-olds who are maltreated and at risk: Findings from the LONGSCAN studies. Child Maltreatment, 10(1), 26–36. https://doi.org/10.1177%2F1077559504271271
Tonmyr, L., Draca, J., Crain, J., & MacMillian, H. L. (2011). Measurement of emotional/psychological child maltreatment: A review. Child Abuse & Neglect, 35(10), 767–782.
https://doi.org/10.1016/j.chiabu.2011.04.011
Tyrka, A. R., Burgers, D. E., Philip, N. S., Price, L. H., & Carpenter, L. L. (2013). The neurobiological correlates of childhood adversity and implications for treatment. Acta Psychiatrica Scandinavica, 128(6), 434–447. https://doi.org/10.1111/acps.12143
U.S. Census Bureau. (2020). Quick facts. https://www.census.gov
U.S. Department of Health & Human Services. (2018). Child maltreatment 2016 (27th ed.). https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2016.pdf
Vachon, D. D., Krueger, R. F., Rogosch, F. A., & Cicchetti, D. (2015). Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry, 72(11), 1135–1142. https://doi.org/10.1001/jamapsychiatry.2015.1792
van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin Books.
van Harmelen, A.-L., Elzinga, B. M., Kievit, R. A., & Spinhoven, P. (2011). Intrusions of autobiographical memories in individuals reporting childhood emotional maltreatment. European Journal of Psychotraumatology, 2(1), 7336. https://doi.org/10.3402/ejpt.v2i0.7336
van Harmelen, A.-L., van Tol, M.-J., van der Wee, N. J. A., Veltman, D. J., Aleman, A., Spinhoven, P., van Buchem, M. A., Zitman, F. G., Penninx, B. W. J. H., & Elzinga, B. M. (2010). Reduced medial prefrontal cortex volume in adults reporting childhood emotional maltreatment. Biological Psychiatry, 68(9), 832–838. https://doi.org/10.1016/j.biopsych.2010.06.011
Walsh, K., & Brandon, L. (2011). Their children’s first educators: Parents’ views about child sexual abuse prevention education. Journal of Child and Family Studies, 21, 734–746.
https://doi.org/10.1007/s10826-011-9526-4
Warner, R. M. (2013). Applied statistics: From bivariate through multivariate techniques (2nd ed.). SAGE.
Wherry, J. N., Baldwin, S., Junco, K., & Floyd, B. (2013). Suicidal thoughts/behaviors in sexually abused children. Journal of Child Sexual Abuse, 22(5), 534–551. https://doi.org/10.1080/10538712.2013.800938
Wherry, J. N., & Dunlop, C. E. (2018). TSCC and TSCYC screening forms in a clinical sample: Reliability, validity, and creating local clinical norms. Child Maltreatment, 23(1), 74–84.
https://doi.org/10.1177%2F1077559517725207
Zimman, L. (2009). ‘The other kind of coming out’: Transgender people and the coming out narrative genre. Gender and Language, 3(1), 53–80. https://doi.org/10.1558/genl.v3i1.53
Zimmerman, F., & Mercy, J. (2010). A better start: Child maltreatment prevention as a public
health priority. Zero to Three, 30(5), 4–10.
Alison M. Boughn, PhD, NCC, LIMHP (NE), LMHC (IA), LPC-MH (SD), ATR-BC, QMHP, TF-CBT, is an assistant professor and counseling department chair at Wayne State College. Daniel A. DeCino, PhD, NCC, LPC, is an assistant professor and Interim Program Coordinator at the University of South Dakota. Correspondence may be addressed to Alison M. Boughn, Wayne State College, 1111 Main Street, Wayne, NE 68787, albough1@wsc.edu.
Mar 9, 2020 | Volume 10 - Issue 1
Kathryn Marburger, Sheri Pickover
Providing treatment to survivors of human trafficking requires mental health professionals to understand complex layers of multiple traumas. These layers include an understanding of how trafficking occurs; what gender, ages, sexual orientations, life circumstances, and ethnicities are most at risk to be trafficked; the lasting impact of trafficking on human development, mental health, and family relationships; and the stigma victims face from their own families, communities, and mental health providers. These survivors suffer from physical ailments and post-traumatic stress disorder, and they are at high risk for developing comorbid disorders such as depression and addiction disorders. Integrated treatment options to alleviate these concerns, including cognitive behavioral therapy, trauma-focused therapy, ecologically focused therapy, and family therapy, are presented.
Keywords: human trafficking, trauma, post-traumatic stress disorder, addiction disorder, sexual orientation
Human trafficking is often referred to as modern-day slavery and is found in every corner of the globe (Cecchet & Thoburn, 2014; Department of Homeland Security [DHS], n.d.; Gerassi, 2015; Hardy et al., 2013; Hodge, 2014; Litam, 2017; Polaris, n.d.-b; Sanchez & Stark, 2014; Zimmerman & Kiss, 2017). The United Nations defines trafficking as:
the recruitment, transportation, transfer, harbouring or receipt of persons, by means of the threat or
use of force or other forms of coercion, of abduction, of fraud, of deception, of the abuse of power or
of a position of vulnerability or of the giving or receiving of payments or benefits to achieve the
consent of a person having control over another person, for the purpose of exploitation. (Office of the
High Commissioner for Human Rights, 2000, article 3, para. 1)
The International Labour Office (2017) has estimated that 40.3 million people are victims of modern-day slavery throughout the world. This means that one person in every 1,000 is being victimized through modern-day slavery. Offering high rewards with minimal risk, human trafficking is a profitable and fast-growing criminal enterprise. Human trafficking profits surpass illegal arms trafficking and are second only to drug trafficking (Busch-Armendariz et al., 2014; Greer & Davidson Dyle, 2014; UNICEF USA, 2017). The International Labour Office (2014) has estimated that the profits from human trafficking are $150 billion a year, of which $99 billion comes from sexual exploitation.
The DHS reported that the crime of human trafficking is often hidden in plain sight in both legal and illegal industries; victims can be any gender, sexual orientation, age, and nationality, including documented or undocumented immigrants (DHS, n.d.; Rothman et al., 2017). However, statistics on human trafficking within the United States are lacking (DHS, n.d.; Gerassi, 2015; Miller-Perrin & Wurtele, 2017; Varma et al., 2015), and a uniform system of collecting data to identify victims currently does not exist, which increases the difficulty of obtaining accurate data (Gerassi, 2015; Miller-Perrin & Wurtele, 2017). Additional factors that contribute to the underreporting of human trafficking include legal and social services that are not readily accessible to victims, fear of punishment from traffickers, and fear or distrust of law enforcement. Moreover, some victims may not even recognize themselves as being the victims of human trafficking (De Chesnay, 2013; Miller-Perrin & Wurtele, 2017).
Human trafficking is a crime that inflicts complex layers of trauma on victims and survivors. The goal of this article is to provide mental health professionals with a systemic view of this crime from various perspectives so that they can implement wraparound-focused treatment plans. The perspectives adopted include how individuals become trafficked, sociocultural factors, the impact on the victims’ development and mental health, family relationships, and the stigma victims face from communities and their families. Having knowledge of these complex factors will allow mental health professionals to devise trauma-sensitive approaches to treat survivors of human trafficking. For the purpose of this paper, the term victims refers to individuals who are actively under the control of the trafficker, and the term survivors refers to individuals who are no longer being exploited.
Sexual exploitation and forced labor are two of the most common forms of human trafficking (Busch-Armendariz et al., 2014; De Chesnay, 2013; Greer & Davidson Dyle, 2014; Hodge, 2014; Martinez & Kelle, 2013; Miller-Perrin & Wurtele, 2017; U.S. Department of State, 2017). Human Rights First (2017) reported that 19% of human trafficking victims are trafficked for sex, and yet sex trafficking accounts for 66% of trafficking profits worldwide. Sex trafficking includes a wide variety of traditionally accepted forms of labor, including commercial sex, exotic dancing, and pornography. It is a form of oppression placing men, women, and children throughout the world at risk of sexual exploitation (Litam, 2017; Polaris, n.d.-a; Zimmerman & Kiss, 2017).
Traffickers treat victims’ bodies as resources to be used and repeatedly sold for money or goods such as pornography, cigarettes, drugs, clothing, and shelter (Busch-Armendariz et al., 2014; Greer & Davidson Dyle, 2014; Litam, 2017; Miller-Perrin & Wurtele, 2017; Sanchez & Stark, 2014). International trafficking often receives more attention; however, most trafficking occurs domestically within the same country (Martinez & Kelle, 2013; Zimmerman & Kiss, 2017). Furthermore, trafficking does not have to include crossing a state line, nor does it necessarily involve moving locations (Busch-Armendariz et al., 2014). Domestic minor sex trafficking is flourishing in every region, state, and community in the United States (Countryman-Roswurm & Bolin, 2014), with Midwestern cities showing increased rates of recruitment; such cities have access to several highways to transport victims to destination cities, including Detroit, Chicago, and Las Vegas, where demand for sexual exploitation is highest (Litam, 2017).
Sex trafficking has been linked not only to escort and massage services, strip clubs, and pornography, but also to major sporting events, entertainment venues, truck stops, business meetings, and conventions (Busch-Armendariz et al., 2014; Hardy et al., 2013; Litam, 2017). As long as demand exists, the opportunity for traffickers to sell victims is limitless. The internet increases the convenience and reduces the risk for traffickers and consumers. For instance, although Backpage.com was shut down by the U.S. government in 2017 for participating in and profiting from sex trafficking advertisements, and other websites like Craigslist began to censor and remove sex advertisements (Anthony et al., 2017; Leary, 2018; Peterson et al., 2019), numerous websites are used by traffickers not only to lure victims but also to advertise and sell to consumers. These websites include Eros.com, Bedpage.com, and social media platforms such as Instagram, Facebook, Twitter, Tinder, and Grindr (Jordan et al., 2013; Litam, 2017; Moore et al., 2017; O’Brien, 2018). The physical and psychological abuse victims experience from both traffickers and consumers leaves victims traumatized (Graham et al., 2019; Greer & Davidson Dyle, 2014; Litam, 2017; Moore et al., 2017; Zimmerman & Kiss, 2017).
The Victims of Trafficking
One out of every four victims of human trafficking is a child (International Labour Office, 2017), and these children are often found in the child welfare and juvenile justice systems, and runaway and homeless youth shelters (Moore et al., 2017; U.S. Department of State, 2017). In 2016, it was estimated that one out of six runaways was a victim of sex trafficking and 86% had been in foster care or social services when they ran away (Polaris, n.d.-a). Runaway youth are usually approached by traffickers within 48 hours of living on the street (Jordan et al., 2013). Traffickers recruit runaway or homeless children into trafficking rings, exposing them to extreme forms of abuse that result in many being killed from the violence inflicted or from diseases acquired through sexual abuse (Litam, 2017).
Sex trafficking is prevalent throughout the world, affecting men, women, children, families, and communities. Individuals also are trafficked for various other purposes, including domestic service, agricultural work, commercial fishing, the textile industry, construction, mining, factory work, and petty crime (U.S. Department of State, 2017; Zimmerman & Kiss, 2017). Although men have been confirmed to be victims in all areas of trafficking, they are disproportionately subjected to forced labor, whereas women and children account for the majority of sexually exploited victims (International Labour Office, 2017). Although trafficking occurs in all parts of the world and can affect anyone, several factors increase the risk of trafficking, including gang activity, a history of childhood abuse, and poverty. Substance abuse also plays a key role (De Chesnay, 2013; Moore et al., 2017; O’Brien, 2018).
Addiction
Substance abuse within families is a risk factor for children becoming the victims of trafficking (Hardy et al., 2013; Miller-Perrin & Wurtele, 2017). Parents or other family members with an addiction can force youth into sexual exploitation, selling or trading them to support their drug addiction (De Chesnay, 2013; Litam, 2017). Traffickers often force substance use on victims in order to control and sexually exploit them (De Chesnay, 2013; Gerassi, 2015; Hodge, 2014; Hom & Woods, 2013; Litam, 2017; Moore et al., 2017). Substance abuse also may be a way for trafficking victims to cope with the abuse they endure (Miller-Perrin & Wurtele, 2017).
Trafficking victims who engage in substance abuse usually experience detrimental personal outcomes, including an increased likelihood of engaging in high-risk behaviors (i.e., unprotected sex), infection from needles, and overdosing (Gerassi, 2015; Zimmerman et al., 2011). They often commit drug-related crimes for their trafficker and are therefore at risk of arrest and conviction for prostitution and drug offenses (Litam, 2017; Miller-Perrin & Wurtele, 2017; Zimmerman et al., 2011). Arrests, drug charges, substance abuse, and violent clients can trap trafficking victims in a vicious circle of re-traumatization by their traffickers, their potentially abusive consumers, and the criminal justice system (Gerassi, 2015; Zimmerman et al., 2011).
Impact on Physical and Mental Health
A concern for children who fall prey to sex trafficking is the impact these experiences have on their development. Not only are victims affected by educational deprivation, but trafficking also causes serious harm to their psychological, spiritual, and emotional development (Miller-Perrin & Wurtele, 2017; Rafferty, 2008; Sanchez & Stark, 2014). Child victims suffer from an increased risk of several emotional problems such as guilt, shame, anxiety, hopelessness, and loss of self-esteem (Miller-Perrin & Wurtele, 2017; Rafferty, 2008). Some of the mental health consequences for child victims include depression, dissociation, post-traumatic stress disorder (PTSD), eating disorders, somatization, poor attachment, antisocial behaviors, substance use disorders, self-harm, and suicidality (Kiss et al., 2015; Miller-Perrin & Wurtele, 2017; Rafferty, 2008). Furthermore, because of the exposure to the violence and sexual assault linked to trafficking, child victims have been found to be at higher risk of sexually transmitted infections, reproductive health problems from unsafe abortions, fractures, genital lacerations, malnutrition, and dental problems (Miller-Perrin & Wurtele, 2017).
Trafficking poses significant risk to child victims’ long-term mental health. Survivors trafficked in childhood report a high prevalence of mental health problems such as depression, anxiety, and PTSD. These mental health problems also affect adult victims (Hom & Woods, 2013; Oram et al., 2016). Among women who have survived trafficking, there are increased rates of anxiety and stress disorders, disassociation, depression, personality disorders, low self-esteem, suicidal ideation, and poor interpersonal relationships (Sanchez & Stark, 2014). Additionally, somatic symptoms such as headaches, fainting, and memory problems are commonly reported among women who are victims of trafficking (Oram et al., 2016). A high prevalence of sexually transmitted infections has been reported in both men and women (Hom & Woods, 2013; Oram et al., 2016; Sanchez & Stark, 2014). Borschmann et al. (2017) found high rates of self-harm among adult victims of human trafficking.
Pregnancy is a common occurrence for trafficked women (Bick et al., 2017; Gerassi, 2015; Hom & Woods, 2013; Oram et al., 2016; Sanchez & Stark, 2014). Several barriers to maternity services have been identified for pregnant victims, including traffickers preventing women from seeking care and the victims feeling reluctant because they might not have valid documents (Bick et al., 2017). Additionally, children and family members are often used by traffickers to threaten and coerce victims, which further isolates victims and distances them from their families (Hardy et al., 2013; Hodge, 2014; Juabsamai & Taylor, 2018; Sanchez & Stark, 2014).
Sex trafficking often involves the exploitation of victims by force, and the brutal nature of the crime can cause complex mental health problems for victims (Gerassi, 2015; Greer & Davidson Dyle, 2014; Hodge, 2014; Hom & Woods, 2013; Litam, 2017). Victims endure high levels of trauma, and survivors show increased rates of depression, anxiety, PTSD, and substance use disorders (Gerassi, 2015). The goal of traffickers is to physically and psychologically break victims down into subservience (Hodge, 2014). Not only are victims forced to engage in humiliating sexual acts and use substances, but traffickers also use recurrent beatings, rape, and even murder as tactics to control their victims (De Chesnay, 2013; Gerassi, 2015; Hodge, 2014; Hom & Woods, 2013; Litam, 2017). Victims may believe that the traffickers have their best interests in mind and develop significant bonds with their traffickers, similar to Stockholm syndrome, and may be reluctant to escape (De Chesnay, 2013; Hodge, 2014; Hom & Woods, 2013; Litam, 2017). In addition, victims of sexual exploitation have not only endured physical and emotional abuse from their traffickers, but there also is a strong correlation with childhood abuse (Gerassi, 2015; Miller-Perrin & Wurtele, 2017). However, issues of physical and mental health tend to be exacerbated by issues of economic deprivation and racial inequality. These factors may act as a catalyst for putting individuals more at risk of human trafficking (Greer, 2013).
Multicultural Considerations
Sex traffickers often target vulnerable individuals, including runaway and homeless youth; victims of domestic abuse or sexual assault; victims of war; and individuals who experience social discrimination, including gender, racial, ethnic, and socioeconomic inequality (Anthony et al., 2017; Miller-Perrin & Wurtele, 2017). For example, LGBTQ homeless youth account for 20% of the homeless youth population in the United States, yet 58.7% of homeless LGBTQ youth are victims of sex trafficking (Martinez & Kelle, 2013). Martinez and Kelle (2013) further noted that this figure is significantly higher than the 33.4% of the heterosexual homeless youth. Furthermore, LGBTQ youth are more than seven times more likely to experience acts of violence than their cisgender peers (Anthony et al., 2017). Trafficking often affects victims of poverty. Studies of sexual exploitation and domestic sex trafficking also have reported higher rates of violence against women of color, especially African American women, and undocumented immigrants (Gerassi, 2015; Zimmerman & Kiss, 2017).
Finally, individuals with intellectual disabilities are at risk because of an unfamiliarity with sexual activities and an inability to understand the nature of sexual abuse and exploitation (Reid, 2018). As a result, such individuals are at a higher risk of becoming victims of trafficking (Greer & Davidson Dyle, 2014; Hodge, 2014; Miller-Perrin & Wurtele, 2017; Reid, 2018).
Returning Home
Women who have been victims of trafficking have often been found to come from abusive households (Gerassi, 2015; Hom & Woods, 2013; O’Brien, 2018; Oram et al., 2016). As a result, once victims are free from their traffickers, they have often been found to not only lack social support but also lack basic needs such as shelter and financial support (Hom & Woods, 2013; Le, 2017; Oram et al., 2016). Reconciliation with supportive family often plays a key role for trafficking survivors; however, because of stigma, some victims are met with shame and judgment from their families and are not welcomed (Hom & Woods, 2013; Juabsamai & Taylor, 2018; McCarthy, 2018; Zimmerman & Kiss, 2017).
Unfortunately, it is not uncommon for victims to be exploited by someone they know and love. Oftentimes a trafficker is a family member, intimate partner, friend, or acquaintance (Gerassi, 2015; Hardy et al., 2013; Hom & Woods, 2013; Le, 2017; Miller-Perrin & Wurtele, 2017; Moore et al., 2017), which further complicates survivors’ ability to establish trusting relationships. Moreover, law enforcement may charge adult victims with prostitution. Not only is the victim caught in legal limbo, but they are re-victimized by law enforcement (Sanchez & Stark, 2014). Finally, female survivors who socialize with men after being freed from their traffickers have reported being triggered with memories of their abusive experiences, further affecting their ability to develop healthy, stable relationships and social support (Hom & Woods, 2013).
Victims of human trafficking have often been robbed of their identities, had their self-esteem demolished, and already experienced physical and psychological abuse before they became victims of human traffickers. Once they leave their traffickers, survivors have a variety of immediate, short-, and long-term needs that must be addressed to help promote resiliency while they are reintegrating into the community (Busch-Armendariz et al., 2014; Graham et al., 2019; Hom & Woods, 2013; Le, 2017; McCarthy, 2018; O’Brien, 2018; Twigg, 2017). Immediate needs include ensuring safety; finding medical care, food, shelter, clothing, and counseling; and acquiring identification, language interpretation services, and legal and immigration assistance (Busch-Armendariz et al., 2014; Graham et al., 2019; Hom & Woods, 2013; McCarthy, 2018; Polaris, n.d.-a; Twigg, 2017). Education, employment, and establishing friendships have been identified as vital ongoing needs to successfully alleviate stress while reintegrating into the community (Hom & Woods, 2013; McCarthy, 2018; O’Brien, 2018; Polaris, n.d.-a; Twigg, 2017). However, it is important to note that survivors are often met with substantial challenges while seeking basic services. For instance, many programs may be underfunded or ill-equipped to handle the high demand for services (Polaris, n.d.-a). This reaffirms the crucial need to meet survivors with empathetic and nonjudgmental attitudes to help prevent re-victimization and a return to traffickers (Anthony et al., 2018; Hodge, 2014; Hom & Woods, 2013; McCarthy, 2018).
Family support can provide survivors with significant protection while reintegrating into the community. Reconnecting with family typically increases the likelihood of a sustainable return process (McCarthy, 2018; Twigg, 2017). However, reconciliation might require a careful approach, as the process can be met with difficulties, including stigma, dysfunctional family environments, or the family’s direct involvement with the victim’s trafficking (Le, 2017; McCarthy, 2018; Twigg, 2017; Zimmerman & Kiss, 2017). In some cases, shame within a cultural context is a prohibitive factor for many to return to their families because of the association with prostitution or having been trafficked (Hom & Woods, 2013). As a result, it is necessary to provide comprehensive, culturally sensitive interventions for trafficking survivors (Hodge, 2014; Hom & Woods, 2013; Le, 2017; McCarthy, 2018). Family continues to be essential to survivors’ sense of identity, and, upon return, cultural beliefs and values that previously formed their self-concept remain influential to survivors (Le, 2017). Many women have noted that marriage and children play an integral role in successfully reintegrating into their community and gaining acceptance from family members (McCarthy, 2018). However, issues of economic deprivation and racial inequality act as a barrier to successful community reintegration and put an individual at higher risk for trafficking (Greer, 2013).
This brief literature review has confirmed that victims of human trafficking suffer from a wide array of mental health concerns, including PTSD, depression, anxiety, and substance abuse, and from stigma associated with being victims of human trafficking. Mental health treatment should address these complex concerns and provide for comprehensive assessment and treatment planning.
Treatment Challenges
Working with trafficked clients poses a series of challenges for counselors because an intervention modality specific to sex-trafficked survivors has yet to be developed (Hopper et al., 2018; Jordan et al., 2013). Treatments are borrowed from evidence-based interventions initially developed for PTSD, domestic violence, and captivity, and a holistic approach is essential (De Chesnay, 2013; Hom & Woods, 2013; Jordan et al., 2013). Four essential practices for providers include ensuring safety and confidentiality, engagement of trauma-informed care, performing a comprehensive needs assessment, and delivery of comprehensive case management that coordinates physical and mental health and legal services. As a result of the multiple traumas trafficking victims endure, the path to restoring wellness is often long and complex, requiring additional time and patience from mental health counselors (Hodge, 2014; Hom & Woods, 2013).
Mental health counselors should conduct a needs assessment to identify the physical, emotional, and spiritual needs of trafficking survivors (Hodge, 2014; Hom & Woods, 2013). Survivors are often in need of medical treatment, as traffickers do not bother with preventative care or what they may consider minor treatment and only allow victims to seek treatment when a condition interferes with earning money (De Chesnay, 2013). Similarly, survivors are often resistant to seek help from mental health providers because of fear of physical violence or threats of retaliation from their traffickers if they disclose their circumstances (De Chesnay, 2013; Hodge, 2014; Litam, 2017). Survivor-centered approaches are recommended initially to acknowledge and validate the survivor’s experience, give the survivor control, and build a sense of safety and trust (Hodge, 2014; Hom & Woods, 2013; Twigg, 2017).
However, after months or years of abuse, trafficking survivors often need a wide array of services to meet their distinctive needs (Hodge, 2014; Hom & Woods, 2013; McCarthy, 2018; Polaris, n.d.-a). The U.S. government has enacted several policies to help victims of trafficking, including the Victims of Trafficking and Violence Protection Act of 2000, which allows victims who have been trafficked from abroad to be issued visas, enabling them to reside in the United States (Davy, 2016; Hodge, 2014). Survivors need to be met with nonjudgmental attitudes, acceptance, understanding, and genuine concern, and they should be slowly encouraged to take on risks associated with leaving their traffickers (Hodge, 2014; Hom & Woods, 2013; McCarthy, 2018). Providing survivors with emotional support and encouragement opposes the isolated world created by their trafficker. Survivors have explained that street outreach programs can play an essential role in establishing contact, allowing victims to become aware of the resources available and begin breaking down the sense of isolation (Hom & Woods, 2013). Additionally, it is vital to empower survivors so that they can understand they are in control (Anthony et al., 2018; Hodge, 2014; Hom & Woods, 2013; Twigg, 2017). Research on resiliency has found creativity, humor, flexibility, and movement are important factors in improving self-esteem, prosocial behaviors, and hope among traumatized individuals (Litam, 2017).
Evidence-Based Treatment
Counselors working with trafficking survivors should be equipped to use several trauma-sensitive interventions to assist with the individual needs of each survivor (Busch-Armendariz et al., 2014; De Chesnay, 2013; Hardy et al., 2013; Hodge, 2014; Hom & Woods, 2013; Litam, 2017; Miller-Perrin & Wurtele, 2017; Twigg, 2017). Trauma-sensitive interventions recognize safety as the foundation for working with individuals to end self-harm, develop trusting relationships, overcome obstacles, leave dangerous situations, and promote wellness (Hopper et al., 2018). Although it may be painful for trafficking survivors to verbalize their traumatic experiences, creative therapies offer alternative methods of communication and expression (De Chesnay, 2013; Litam, 2017).
Although evidence-based practices for treating sex-trafficking survivors are not widespread, counseling techniques exist that have been shown to be effective with child sex abuse victims, including trauma-focused cognitive behavioral therapy and dialectical trauma-focused cognitive behavior therapy (De Chesnay, 2013; Twigg, 2017). Similarly, participating in group counseling can empower survivors of sex trafficking and provide them with an opportunity to share their experiences, generating a sense of community and support (Hopper et al., 2018). Peer support has been noted to be a vital component of intervention, both as a motivating factor to remain in treatment and as help in the prevention of survivors returning to their traffickers (De Chesnay, 2013; Litam, 2017; Twigg, 2017). Furthermore, discussing stigmatized topics within group settings can help reduce shame, as it is common for trafficked survivors to feel that no one else has gone through similar situations (Hickle & Roe-Sepowitz, 2014; Litam, 2017). Having a setting to address the shame can help survivors recognize the commonality of their experiences and build support (Countryman-Roswurm & Bolin, 2014; Litam, 2017).
Family Therapy
As human trafficking affects individuals, families, and communities, it is necessary to adopt treatment models that engage families and communities as well as individual-based treatment models. Twigg (2017) found that survivors require and benefit from therapeutic support in order to achieve successful family and community reunification. However, like individual treatment, family therapy models specific to human trafficking survivors do not exist, but current family therapy models developed around trauma could be adapted for use with human trafficking survivors. Apsche et al. (2008) developed Family Mode Deactivation Therapy, a cognitive behavior family therapy model for use with youth and families in residential treatment that uses ongoing assessment and community skill development to reduce the behavioral symptoms associated with trauma. The researchers found this model reduced recidivism more effectively than a non–family-based approach. Hughes (2017) developed an attachment-focused family treatment for children who have experienced developmental trauma. This two-phase treatment provides therapy to a caregiver first, then transitions to joint sessions to reframe the trauma experience.
Similarly, using ecologically based family therapy with individuals involved in sex trafficking has been found to improve outcomes for sobriety and depression (Murnan et al., 2018). Agani et al. (2010) recommended the use of the linking human systems community resilience model, which is based on transgenerational and ecosystemic structural family therapies. This model focuses on identifying the strengths of community and family members, bringing them together to encourage their competency and using community leaders to solve problems. Other novel approaches to working with survivors of crime include the Family Group Project, which involves group therapy aimed at recreating a family environment to re-integrate survivors into the community (Allen et al., 2015).
A Survivor’s Story
Research provides one perspective on the plight of human trafficking victims and survivors, but a first-person account provides insight to the worldview of an actual survivor. One of the authors met with a human trafficking advocate in order to gain further perspective on the needs of survivors. The advocate, who requested that the author provide no identifying information beyond her gender, disclosed during the interview that she was a survivor who had been trafficked by her husband. Her trafficker had been blackmailing a John, a term commonly used for an exploitive consumer. She was arrested during a raid and remained in jail for 3 months because she refused to say anything. She explained that it took her a year to build up the strength and courage to testify in court because her trafficker blackmailed her. He threatened to tell her family about the exploitative acts and substance use, which he forced her to engage in. He would say, “Do you really want your family to know what you have been up to?” However, once her family was notified of her predicament, she reported that her family members provided emotional support. She explained that it was through their support she was able to come forward and testify.
Although she came forward and testified against her trafficker, she was not viewed as a victim, and she was charged with prostitution. As she explained, advocates are trying to change the legislation and work with police in her local area so that human trafficking victims are not charged with crimes. For instance, not only was she charged with prostitution, but she also had to pay the John $3,000, the money her trafficker had stolen from him. Despite never having seen the money, she was ordered to repay it and was placed on a repayment schedule. Even more disheartening, her trafficker made a plea deal and did not have to repay any money and the charges of trafficking were dropped. All these events provide an example of how the legal system can re-victimize a survivor. Although she had been the victim of trafficking, which stigmatized her, she also was told that she owed money to someone her trafficker had stolen from, thus re-victimizing her.
The charge of prostitution remained on her record and became something she had to explain to potential employers. With the support of her family and by attending therapy, she was able to rebuild her life. She had a bachelor’s degree in social work when she met her ex-husband and was able to obtain her limited license. She decided to pursue a master’s degree and was once again faced with the challenge of disclosing the charge on her record and reliving the trauma of explaining what happened. The first university she applied to denied her application, and this placed her in a deep depression; however, she was accepted at another university and after graduating became an advocate for survivors of human trafficking. She also shared that although it took time to be able to trust someone again, she has established an intimate relationship and will soon be married.
Conclusion
Counselors treating a human trafficking survivor need to develop a wide-ranging view of assessment, treatment, case management, support, advocacy, and termination from counseling. Human trafficking survivors suffer from a complex variety of developmental, mental health, and social issues that require counselors to not only engage the individual in treatment, but also to act as an advocate against stigma within their family and the community.
The myriad of issues faced by these individuals, from navigating the criminal justice system, coping with multiple layers of physical and emotional trauma, overcoming substance abuse, overcoming family and community alienation, coping with dual stigmas of human trafficking and mental health diagnoses, to finally reintegrating into daily work and life, require counselors to be vigilant in the assessment process. Counselors need to consider assessment an ongoing extensive process that should occur throughout every session and focus not just on mental health needs, but also on physical health and basic needs, and career support. Counselors will need to assess risk of the individual returning to the trafficker and have referrals ready to help the client stay safe. Human trafficking survivors will need a counselor able to quickly identify short-term crisis needs during long-term treatment.
When entering the treatment phase, counselors need to research multiple treatment modalities that may not directly relate to human trafficking but may support the client. For example, a counselor will need to navigate working with substance use, trauma, family issues, and career concerns. Counselors will need to widen their view of their role within the therapeutic relationship. Human trafficking survivors may require case management services more than long-term counseling when first entering care, yet the need to build a strong therapeutic relationship is paramount for ongoing treatment. The counselor should consider taking on the case management role as needed to promote consistency in the treatment process. As an advocate, the counselor will need to engage multiple individuals and systems into the treatment process to ensure comprehensive care. Counseling skills aimed at engaging families, law enforcement personnel, legal personnel, and medical professionals in treatment are essential for treating survivors. Counselors would also benefit from strength-based approaches with this population, as research indicates survivors most benefit from being able to identify their own qualities of self-protection and resiliency, which empowers their recovery process. This empowerment also allows for a supportive termination process, ensuring that the survivor has ongoing access to a support network in order to facilitate long-term recovery.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Agani, F., Landau, J., & Agani, N. (2010). Community-building before, during, and after times of trauma: The application of the LINC model of community resilience in Kosovo. American Journal of Orthopsychiatry, 80, 143–149. https://doi.org/10.1111/j.1939-0025.2010.01017.x
Allen, D. F., Carroll, M. A., Allen, V. S., Bethell, K. Y., & Manganello, J. A. (2015). Community resocialization via instillation of family values through a novel group therapy approach: A pilot study. Journal of Psychotherapy Integration, 25(4), 289–298. https://doi.org/10.1037/a0039563
Anthony, B., Amatullah, A. H., Anderson, J., Arias, E. F. P., N.M.B., Crisp, J. D., Crosson, L., D’Souza, H., Fasthorse, H., Hollis, J., John, D., Johnson, D., Johnson, N., Liles, T., Lipenga, F., Lundstrom, M., Marty, R., McCarty, T., Moninda, Morrissey, A., . . . Woworuntu, S. (2018). On-Ramps, intersections, and exit routes: A roadmap for systems and industries to prevent and disrupt human trafficking. https://polarisproject.org/wp-content/uploads/2018/08/A-Roadmap-for-Systems-and-Industries-to-Prevent-and-Disrupt-Human-Trafficking.pdf
Anthony, B., Penrose, J. K., Jakiel, S., Couture, T., Crowe, S., Fowler, M., Keyhan, R., Sorensen, K., Myles, B., & Badavi, M. A. (2017, March). The typology of modern slavery: Defining sex and labor trafficking in the United States. https://polarisproject.org/wp-content/uploads/2019/09/Polaris-Typology-of-Modern-Slavery-1.pdf
Apsche, J. A., Bass, C. K., & Houston, M.-A. (2008). Family mode deactivation therapy as a manualized cognitive behavioral therapy treatment. International Journal of Behavioral Consultation and Therapy, 4(2), 264–277. https://doi.org/10.1037/h0100848
Bick, D., Howard, L. M., Oram, S., & Zimmerman, C. (2017). Maternity care for trafficked women: Survivor experiences and clinicians’ perspectives in the United Kingdom’s National Health Service. PLOS ONE, 12(11), e0187856. https://doi.org/10.1371/journal.pone.0187856
Borschmann, R., Oram, S., Kinner, S. A., Dutta, R., Zimmerman, C., & Howard, L. M. (2017). Self-harm among adult victims of human trafficking who accessed secondary mental health services in England. Psychiatric Services, 68(2), 207–210. https://doi.org/10.1176/appi.ps.201500509
Busch-Armendariz, N., Nsonwu, M. B., & Heffron, L. C. (2014). A kaleidoscope: The role of the social work practitioner and the strength of social work theories and practice in meeting the complex needs of people trafficked and the professionals that work with them. International Social Work, 57, 7–18. https://doi.org/10.1177/0020872813505630
Cecchet, S. J., & Thoburn, J. (2014). The psychological experience of child and adolescent sex trafficking in the United States: Trauma and resilience in survivors. Psychological Trauma: Theory, Research, Practice, and Policy, 6, 482–493. https://doi.org/10.1037/a0035763
Countryman-Roswurm, K., & Bolin, B. L. (2014). Domestic minor sex trafficking: Assessing and reducing risk. Child and Adolescent Social Work Journal, 31, 521–538. https://doi.org/10.1007/s10560-014-0336-6
Davy, D. (2016). Anti–human trafficking interventions: How do we know if they are working? American Journal of Evaluation, 37, 486–504. https://doi.org/10.1177/1098214016630615
De Chesnay, M. (2013). Psychiatric-mental health nurses and the sex trafficking pandemic. Issues in Mental Health Nursing, 34, 901–907. https://doi.org/10.3109/01612840.2013.857200
Department of Homeland Security. (n.d.). Blue campaign: What is human trafficking? https://www.dhs.gov/blue-campaign/what-human-trafficking
Gerassi, L. (2015). From exploitation to industry: Definitions, risks, and consequences of domestic sexual exploitation and sex work among women and girls. Journal of Human Behavior in the Social Environment, 25, 591–605. https://doi.org/10.1080/10911359.2014.991055
Graham, L. M., Macy, R. J., Eckhardt, A., Rizo, C. F., & Jordan, B. L. (2019). Measures for evaluating sex trafficking aftercare and support services: A systematic review and resource compilation. Aggression and Violent Behavior, 47, 117–136. https://doi.org/10.1016/j.avb.2019.04.001
Greer, B. T. (2013). Hiding behind tribal sovereignty: Rooting out human trafficking in Indian country. The Journal of Gender, Race & Justice, 16, 453–482.
Greer, B. T., & Davidson Dyle, S. (2014). Balancing the equity of mental health injuries: Examining the “trauma exception” for sex trafficking T-VISA applicants. International Journal of Migration, Health and Social Care, 10(3), 159–191. https://doi.org/10.1108/IJMHSC-11-2013-0042
Hardy, V. L., Compton, K. D., & McPhatter, V. S. (2013). Domestic minor sex trafficking: Practice implications for mental health professionals. Affilia, 28, 8–18. https://doi.org/10.1177/0886109912475172
Hickle, K. E., & Roe-Sepowitz, D. E. (2014). Putting the pieces back together: A group intervention for sexually exploited adolescent girls. Social Work With Groups, 37(2), 99–113.
https://doi.org/10.1080/01609513.2013.823838
Hodge, D. R. (2014). Assisting victims of human trafficking: Strategies to facilitate identification, exit from trafficking, and the restoration of wellness. Social Work, 59(2), 111–118. https://doi.org/10.1093/sw/swu002
Hom, K. A., & Woods, S. J. (2013). Trauma and its aftermath for commercially sexually exploited women as told by front-line service providers. Issues in Mental Health Nursing, 34(2), 75–81.
https://doi.org/10.3109/01612840.2012.723300
Hopper, E. K., Azar, N., Bhattacharyya, S., Malebranche, D. A., & Brennan, K. E. (2018). STARS experiential group intervention: A complex trauma treatment approach for survivors of human trafficking. Journal of Evidence-Informed Social Work, 15(2), 215–241. https://doi.org/10.1080/23761407.2018.1455616
Hughes, D. (2017). Dyadic developmental psychotherapy (DDP): An attachment-focused family treatment for developmental trauma. Australian and New Zealand Journal of Family Therapy, 38, 595–605. https://doi.org/10.1002/anzf.1273
Human Rights First. (2017). Human trafficking by the numbers. http://www.humanrightsfirst.org/sites/default/files/TraffickingbytheNumbers.pdf
International Labour Office. (2014). Profits and poverty: The economics of forced labour. http://www.ilo.org/wcmsp5/groups/public/—ed_norm/—declaration/documents/publication/wcms_243391.pdf
International Labour Office. (2017). Global estimates of modern slavery: Forced labour and forced marriage. http:/www.ilo.org/wcmsp5/groups/public/@dgreports/@dcomm/documents/publication/wcms_575479.pdf
Jordan, J., Patel, B., & Rapp, L. (2013). Domestic minor sex trafficking: A social work perspective on misidentification, victims, buyers, traffickers, treatment, and reform of current practice. Journal of Human Behavior in the Social Environment, 23, 356–369. https://doi.org/10.1080/10911359.2013.764198
Juabsamai, K. J., & Taylor, I. (2018). Family separation, reunification, and intergenerational trauma in the aftermath of human trafficking in the United States. Anti-Trafficking Review, 10, 123–138. https://doi.org/10.14197/atr.201218108
Kiss, L., Yun, K., Pocock, N., & Zimmerman, C. (2015). Exploitation, violence, and suicide risk among child and adolescent survivors of human trafficking in the Greater Mekong Subregion. JAMA Pediatrics, 169(9), e152278–e152278. https://doi.org/10.1001/jamapediatrics.2015.2278
Le, P. D. (2017). “Reconstructing a sense of self”: Trauma and coping among returned women survivors of human trafficking in Vietnam. Qualitative Health Research, 27, 509–519.
https://doi.org/10.1177/1049732316646157
Leary, M. G. (2018). The indecency and injustice of section 230 of the Communications Decency Act. https://scholarship.law.edu/cgi/viewcontent.cgi?article=1990&context=scholar
Litam, S. D. A. (2017). Human sex trafficking in America: What counselors need to know. The Professional Counselor, 7, 45–61. https://doi.org/10.15241/sdal.7.1.45
Martinez, O., & Kelle, G. (2013). Sex trafficking of LGBT individuals: A call for service provision, research, and action. The International Law News, 42(4), 1–6.
McCarthy, L. A. (2018). Life after trafficking in Azerbaijan: Reintegration experiences of survivors. Anti-Trafficking Review, 10, 105–122. https://doi.org/10.14197/atr.201218107
Miller-Perrin, C., & Wurtele, S. K. (2017). Sex trafficking and the commercial sexual exploitation of children. Women & Therapy, 40, 123–151. https://doi.org/10.1080/02703149.2016.1210963
Moore, J. L., Houck, C., Hirway, P., Barron, C. E., & Goldberg, A. P. (2017). Trafficking experiences and psychosocial features of domestic minor sex trafficking victims. Journal of Interpersonal Violence. https://doi.org/10.1177/0886260517703373
Murnan, A., Wu, Q., & Slesnick, N. (2018). Effects of ecologically-based family therapy with substance-using, prostituting mothers. Journal of Family Therapy, 40, 557–583. http://doi.org/10.1111/1467-6427.12187
O’Brien, J. E. (2018). “Sometimes, somebody just needs somebody—anybody—to care:” The power of interpersonal relationships in the lives of domestic minor sex trafficking survivors. Child Abuse & Neglect, 81, 1–11. https://doi.org/10.1016/j.chiabu.2018.04.010
Office of the High Commissioner for Human Rights. (2000). Protocol to prevent, suppress and punish trafficking in persons, especially women and children, supplementing the United Nations convention against transnational organized crime. https://www.ohchr.org/Documents/ProfessionalInterest/ProtocolonTrafficking.pdf
Oram, S., Abas, M., Bick, D., Boyle, A., French, R., Jakobowitz, S., Khondoker, M., Stanley, N., Trevillion, K., Howard, L., & Zimmerman, C. (2016). Human trafficking and health: A survey of male and female survivors in England. American Journal of Public Health, 106, 1073–1078. https://doi.org/10.2105/AJPH.2016.303095
Peterson, M., Robinson, B., & Shih, E. (2019). The new virtual crackdown on sex workers’ rights: Perspectives from the United States. Anti-Trafficking Review, 12, 189–193. https://doi.org/10.14197/atr.2012191212
Polaris. (n.d.-a). Myths, facts, and statistics. https://polarisproject.org/myths-facts-and-statistics
Polaris. (n.d.-b). Human trafficking. https://polarisproject.org/human-trafficking
Rafferty, Y. (2008). The impact of trafficking on children: Psychological and social policy perspectives. Child Development Perspectives, 2, 13–18.
https://doi.org/10.1111/j.1750-8606.2008.00035.x
Reid, J. A. (2018). Sex trafficking of girls with intellectual disabilities: An exploratory mixed methods study. Sexual Abuse, 30(2), 107–131. https://doi.org/10.1177/1079063216630981
Rothman, E. F., Stoklosa, H., Baldwin, S. B., Chisolm-Straker, M., Kato Price, R., & Atkinson, H. G. (2017). Public health research priorities to address U.S. human trafficking. American Journal of Public Health, 107, 1045–1047. https://doi.org/10.2105/AJPH.2017.303858
Sanchez, R., & Stark, S. W. (2014). The hard truth about human trafficking. Nursing Management, 45, 18–23. https://doi.org/10.1097/01.NUMA.0000440630.41142.66
Twigg, N. M. (2017). Comprehensive care model for sex trafficking survivors. Journal of Nursing Scholarship, 49(3), 259–266. https://doi.org/10.1111/jnu.12285
UNICEF USA. (2017, January 13). What fuels human trafficking? https://www.unicefusa.org/stories/what-fuels-human-trafficking/31692
U.S. Department of State. (2017). Trafficking in persons report. https://www.state.gov/wp-content/uploads/2019/02/271339.pdf
Varma, S., Gillespie, S., McCracken, C., & Greenbaum, V. J. (2015). Characteristics of child commercial sexual exploitation and sex trafficking victims presenting for medical care in the United States. Child Abuse & Neglect, 44, 98–105. https://doi.org/10.1016/j.chiabu.2015.04.004
Zimmerman, C., Hossain, M., & Watts, C. (2011). Human trafficking and health: A conceptual model to inform policy, intervention and research. Social Science & Medicine, 73, 327–335.
https://doi.org/10.1016/j.socscimed.2011.05.028
Zimmerman, C., & Kiss, L. (2017). Human trafficking and exploitation: A global health concern. PLOS Medicine, 14(11), e1002437. https://doi.org/10.1371/journal.pmed.1002437
Kathryn Marburger is a graduate student at the University of Detroit Mercy. Sheri Pickover, PhD, LPC, is an associate professor at Central Michigan University. Correspondence can be addressed to Sheri Pickover, 195 Ojibway Court, Mt. Pleasant, MI 48859, picko1s@cmich.edu.
