Mar 9, 2020 | Volume 10 - Issue 1
Laura Haddock, Kristi Cannon, Earl Grey
Computer-enhanced counselor education dates as far back as 1984, and since that time counselor training programs have expanded to include instructional delivery in traditional, hybrid, and fully online programs. While traditional schools still house a majority of accredited programs, the Council for Accreditation of Counseling and Related Educational Programs (CACREP) has accredited almost 40 fully online counselor education programs. The purpose of this article is to outline the similarities and differences between CACREP-accredited online or distance education and traditional program delivery and instruction. Topics include andragogy, engagement, curriculum, instruction, assessment, and gatekeeping.
Keywords: online, distance education, counselor education, andragogy, CACREP
Online counselor education training programs have continued to be developed year after year and have grown in both popularity and effectiveness. Recent trends in graduate education reflect online instruction as part of common practice (Kumar et al., 2019). Virtual training opportunities promote access for students who might not otherwise be able to participate in advanced education, and for some students, distance learning can be the ideal method to further their education as they strive to balance enrollment with remote geography, family life, and employment commitments. However, regardless of instructional setting, all counselor training programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP) have distinct similarities. For example, CACREP-accredited programs are by nature graduate programs. There are no CACREP-accredited counselor training programs at the bachelor’s level or the doctoral level. To clarify, CACREP does offer accreditation for doctoral programs; however, most are focused on counselor education and supervision, and the curriculum is geared toward instructor and supervisor preparation versus counselor training. Thus, in every academic setting, master’s-level CACREP-accredited professional counselor training programs are simultaneously an introductory and a terminal degree. Both online and traditional programs must be prepared to design and deliver curriculum to students of various educational backgrounds that will ultimately equip graduates with the skills and dispositions needed for professional practice. As graduate students, enrollment is fully comprised of adult learners and this holds true regardless of instructional setting. Interestingly, most professional counseling literature uses the term pedagogy to reference the facilitation of learning within counselor training. For the purposes of this article, we will utilize the term andragogy, which is “the art and science of teaching adults” (Merriam-Webster, n.d.).
Counselor Education and Andragogy
Professional counseling literature related to andragogy is scarce and largely contains studies focused on meeting the needs of diverse students and preparing counselors to work with culturally diverse clients. Barrio Minton et al. (2014) conducted a 10-year content analysis of studies related to teaching and learning in counselor education, and the large majority of the studies grounded counselor preparation andragogy in counseling literature and theory as opposed to learning theories or research. Efforts to identify research specific to the andragogy of online counselor training produced minimal results, and a clear gap in the literature exists for empirical research when comparing online and traditional learning and instructional delivery. What did emerge from the research was debate regarding whether an online environment is appropriate to teach adult learners curriculum of the interpersonal nature of counseling (Lucas & Murdock, 2014). However, empirical evidence does exist to support the delivery of instruction in online academic environments as effective, although they require different andragogical methods and teaching practices (Cicco, 2013a). Additionally, studies on online education in higher education suggest that differences in student learning outcomes for traditional students and online students are not statistically significant (Buzwell et al., 2016). In fact, some evidence demonstrates superior outcomes in students enrolled in online courses (Allen et al., 2016). However, student perceptions of online learning and learning technologies outweighed pedagogy for impact on the quality of academic achievement (Ellis & Bliuc, 2019). Thus, emerging research on both method and student perceptions supports online counselor education as a viable instructional approach.
Characteristics of Online Learners
Before examining the similarities and differences in instructional practice and curriculum development between online and brick-and-mortar settings, consideration for the composition of the student body is warranted. The student body for both online and traditional programs have a higher enrollment of female versus male students and Caucasian versus other ethnicities across genders (CACREP, 2017). Because online programs are often comprised of non-traditional students who work full-time and are geographically diverse, this invites a student enrollment varied in age, race, ethnicity, physical ability, and educational background (Barril, 2017). Online training programs also demonstrate greater enrollment by learners from underrepresented populations (Buzwell et al., 2016).
Online Education Stakeholders
When we compare traditional programs and their online counterparts, the primary stakeholders for both settings include students and faculty members. In counselor training programs, the clients the graduates will serve also are stakeholders. The processes that occur in both traditional and online classrooms are aligned, with the “foci being teaching, learning, and . . . evaluation” (Cicco, 2013b, p. 1).
In 2018, Snow et al. conducted a study examining the current practices in online counselor education. The results indicated that overall, faculty instructors for online settings indicate a smaller class size with a reported mean enrollment of 15.5 students compared to traditional classroom enrollment of 25 or more. The study showed that both online and traditional programs utilize a variety of strategies for course enrollment, including both student-driven course selection and program-guided course enrollment within the learning community.
Learning Community
As previously mentioned, student perceptions of online learning emerged in the literature as a key for student academic success. However, research suggests that attrition rates for online students are much higher than those in traditional programs (Murdock & Williams, 2011). It has been suggested that elevated attrition rates in online programs could be related to students lacking a sense of connection to peers and program faculty and an insufficient learning community (Lu, 2017). Research reveals that the use of learning communities has proven successful in improving the retention rates (DiRamio & Wolverton, 2006; Kebble, 2017). The type and frequency of student-to-student and student-to-faculty interactions in online versus traditional programs are different. In both settings, scholars seek a valuable learning experience (Onodipe et al., 2016). However, while social interaction is a routine part of face-to-face learning, the online environment requires intentional effort to promote interaction between learners and faculty. Research has suggested that online learners need assignments and activities that emphasize the promotion of connection with both the material and peers and faculty (Lu, 2017). At a basic level, affirmation for a job well done on an assignment and prompt and comprehensive feedback are examples of faculty–student engagement that produce student satisfaction regardless of instructional setting (O’Shea et al., 2015). However, we contend these sorts of intentional, personalized instructional interactions are critical for online students who could otherwise feel alienated or isolated in the online learning environment. For online educators, one requirement is to persistently promote engagement for online learners, which can prove to be challenging, and require supplementary or diverse approaches to forging productive student learning communities. Simply transferring material used in traditional classrooms into an online learning management system is not adequate to promote engagement and could instead contribute to both cognitive and emotional detachment.
Instructional Practice and Curriculum Development
There is limited literature comparing the curriculum development and content delivery methods between traditional and distance education specific to counselor education, but there is a body of literature comparing the factors that influence the efficacy of traditional and distance education in general. The gap in the counselor education literature requires a comparative assessment of the deciding factors leading to different curriculum development and delivery methods for counselor education programs.
Delivery Preferences
Taylor and Baltrinic (2018) conducted a study in which they explored counselor educator course preparation and instructional practices. Unfortunately, the researchers did not include the educational delivery setting as a variable in the descriptive demographics, so it was impossible to discern whether the techniques that were identified as preferred methods of instruction were associated with online or traditional classrooms. However, it can be assumed that the preferences that were identified were geared more specifically to an in-class, face-to-face presentation. The five teaching methods that were explored for preferences in teaching content versus clinical courses included lecture, small group discussions, video presentations, case studies, and in-class modeling. Anecdotally, we assert that the reported preferences for instruction delivery would be different for online instructors and would be impacted by content delivery modality and technology. For example, if plans are disrupted in the traditional face-to-face classroom, such as internet disconnection, an instructor has the freedom to shift focus and move to a backup plan. However, an alternate instructional plan is not always available or feasible in an online environment (Marchand & Gutierrez, 2012). Delivery preferences can be influenced by the educational delivery setting in which the program was developed.
Educational Delivery Settings
Content delivery modalities determine whether a program is defined as traditional or distance (telecommunications or correspondence) in accordance with the Office of Postsecondary Education Accreditation Division of the U.S. Department of Education (2012). If a program offers 49% or less of their instruction via distance learning technologies, with the remaining 51% via in-person synchronous classroom, the Department of Education categorizes that program as traditional education. The Department of Education defines distance education as instructional delivery using technology to support “regular and substantive interaction between the students and the instructor, either synchronously or asynchronously” in courses in which the students are physically separated from their instructor (Office of Postsecondary Education Accreditation Division, 2012, p. 5). The Department of Education further clarifies that a distance education program offers at least 50% or more of their instruction via distance learning technologies that include telecommunications (Office of Postsecondary Education Accreditation Division, 2012). The Office of Federal Student Aid of the U.S. Department of Education separates distance programs between telecommunications courses and correspondence courses. A telecommunication course uses “television, audio, or computer (including the Internet)” to deliver the educational materials (Office of Federal Student Aid, 2017, p. 299). A correspondence course includes home study materials without a course or regular interactions with an instructor (Office of Federal Student Aid, 2017). Although discussing correspondence education is outside the scope of this article, including it as context for educational delivery settings is valuable to have a full view of content delivery options as defined by the Department of Education.
Through informal observations of counselor education programs, the hybrid or blended program seems to be neglected in the current educational delivery setting definitions provided by the Department of Education. Although there are variations in the definition of a hybrid or blended program, the Department of Education does not use hybrid or blended education as a category. Because most, if not all, programs integrate some level of telecommunications technology as defined above, we recommend using the word hybrid as a qualifier to the categories of educational delivery settings to more accurately categorize the unique complexity and needs of every counselor education program. We recommend defining the qualifier of hybrid as a program that offers at least 25% and no more than 75% of their instruction via a combination of distance learning telecommunication technologies and a traditional classroom. This qualifier would be added to the Department of Education’s primary definition of a traditional or distance program based on the percentage of telecommunications technologies used for content delivery. By adding this qualifier, a program may be categorized as traditional, traditional hybrid, distance hybrid, or distance education. The traditional setting uses telecommunications technologies for up to 25% of their content delivery, traditional hybrid is 26%–49%, distance hybrid is 50%–75%, and distance education has 76%–100% of their content delivered using telecommunications technologies. See Figure 1 for a visual representation of the Educational Delivery Settings Continuum.
Figure 1
Educational Content Delivery Continuum.
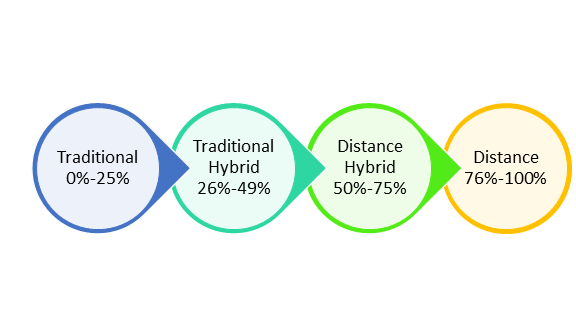
Note. This figure demonstrates the percentages of content delivered using telecommunications technologies for each setting.
When we adopt the continuum above it becomes clear that counselor education content delivery cannot be reduced to a dichotomy. Viewing counselor education program content delivery through the lens of a continuum results in valuing the unique needs, complexities, and strengths of all counselor education programs with varying degrees of technology sophistication. Further, using this continuum can more accurately highlight the similarities across counselor educator programs instead of the differences. By definition, if any program relies on email and a website to communicate information about the content of the program (e.g., submitting assignments), that program is using telecommunication technologies to some degree. The above continuum is an important context for reviewing the current state of counselor education program content delivery and curriculum development. Because the traditional educational delivery setting was the starting point for formal education, a program will inevitably have a reason, purpose, or motive for integrating technology into a traditional model.
Motivation to Integrate Learning Technologies
When we examine the history of curriculum development and delivery methods, we can use traditional education as our starting point, dating back to the Socratic method (Snow & Coker, 2020). As Snow and Coker (2020) have shared, there are two primary motivators to developing or integrating technology into content delivery—increasing access and increasing revenues. These program development motivators can be valuable when initiating curricula, as long as programs consider how technological tools will be used to promote the “regular and substantive interaction between the students and the instructor” (Office of Postsecondary Education Accreditation Division, 2012, p. 5). This requires initial planning to integrate technological tools that can both deliver content and promote a learning community. Technology in any amount is a tool requiring skillful application in order to promote an effective technologically supported learning experience (Hedén & Ahlstrom, 2016; Koehler et al., 2004). Although some might choose to debate the differences in benefit between increasing access and revenues, a more equitable comparison for motivations requires the context of the faculty’s ability to skillfully deliver course content using technology. The faculty’s instructional practices impact the application of the program development motivators.
Instructional Practice
As we consider the continuum of technology integration for counselor education programs in different settings, we must consider the level of synchronicity for content delivery. Historically, the nature of professional counseling work has been synchronous, in-person interactions. The synchronous nature of the counseling profession is often used to argue that traditional programs are more effective than distance programs. Looking at a historical read/write approach (i.e., read materials and rely on written assignments to evaluate learning) to distance education, there can be some validity to the perceived challenges for a distance counselor education program that delivered its content in a read/write format only. Often, distance counselor education programs have overcome this perceived challenge by integrating traditional components into their curriculum.
Technology advancements provide new mediums for both synchronous and asynchronous learning to prepare a counselor-in-training. Counselors’ and counselor educators’ duties require some amount of synchronous activities (i.e., in-person interactions between two or more individuals occurring at the same time). As we view the counseling profession through the lens of telecommunications, the paradigm is expanding to include asynchronous counseling activities (i.e., interactions between two or more individuals occurring at various time intervals, such as text messaging).
Because the counseling profession requires human interactions, it seems fair that synchronous components, whether in person or technologically assisted, are necessary to prepare counselors-in-training. The synchronous component of every counselor education program is that of the practicum and internship experiences. The didactic curriculum in a counselor education program can vary between synchronous and asynchronous. But when a counselor-in-training meets the practicum and internship benchmarks, synchronicity is required by virtue of program accreditation standards and professional regulations. Although there can be an expansion into the asynchronous approach to counseling field experience in the distant future, it may not be realistic to imagine a fully asynchronous field experience. Consideration of the modalities used to deliver supervision and direct counseling services as part of the practicum and internship provides great opportunity to align these experiences with the overall curriculum delivery methods of the counselor education program and promote future skills for professional counselors.
Curriculum Development Models
The curriculum development model used for the counselor education program also can impact the program’s level of synchronicity. Although there are multiple designs that can guide curriculum development, there are two models often used in counselor education—teacher-centered and subject-centered. Programs used the teacher-centered approach when the curriculum was designed with the teacher as the subject matter expert and the content was designed to guide the learner through the content by way of the guidance of the teacher (Dole et al., 2016; Pinnegar & Erickson, 2010). Programs used the subject-centered approach when the subject matter guided the organization of the content and how the learning was assessed to support consistency across instructors (Burton, 2010; Dole et al., 2016). It would be inaccurate to assign either one of the approaches to a specific setting category as each approach can be plotted along the above continuum.
Teacher-Centered Approach
The teacher-centered approach allows the teacher to own their curriculum, and the specifics of the content within the same subject can vary across teachers. The teacher-centered approach occurs when assigned faculty members develop a course from scratch. They can use information from similar courses; however, there is a great amount of flexibility and freedom to develop the course content and delivery modalities. This approach may or may not integrate curriculum across multiple sections of the course taught by different instructors. The teacher-centered approach also can have varying degrees of course curriculum connections across different courses within the program. The instructor of the course in the teacher-centered approach typically develops the course and teaches the course, so they are intimately aware of the intention and nuances behind each element of the course curriculum.
Subject-Centered Approach
The subject-centered approach often relies on a team approach and can support consistency across sections of the same course. The subject-centered approach can assign responsibilities for the development to different team members (e.g., subject matter expert, curriculum design expert, learning resource expert). Team members work collaboratively to develop curriculum that targets critical elements of knowledge, skills, or dispositions directed by the subject matter. There can be a scaffolding approach to the overarching program curriculum when using a subject-centered approach. The subjects can be linked across courses to support collective success across the program’s curriculum. Although the instructor of the subject-centered curriculum did not typically take part in the development, they are tasked with bringing the course content to life by adding additional resources, examples, and professional experiences to the course curriculum. Now that we have discussed the various educational delivery settings, the motivation for integrating technologies, impact of instructional practices, and curriculum development models, we can consider the application of learning telecommunication technologies.
Learning Telecommunication Technologies
As telecommunication technologies have advanced, the integration of asynchronous counseling and telehealth is changing the landscape of the profession. Although there are state-specific definitions of the term, in sum telehealth refers to providing technology-assisted health care from a distance (Lerman et al., 2017). These changes in the counseling profession force us to consider the needs and the impact of the level of formal integration of technology skills training or practice in a counselor education program. This alone may begin to separate counselor education programs along the educational delivery settings continuum.
Using the traditional education category as our foundational approach for counselor education, we can see the parallels between the in-person synchronous experiences in the classroom and in counseling sessions. Professional counselors of the 21st century now need to be equipped with skills using and maneuvering technologies for communicating, documenting, and billing. Technology skills have received limited attention in the current CACREP standards as only five core standards and seven specialty standards mention technology. Technology is not mentioned in the specialty standards for Addiction Counseling; Clinical Mental Health Counseling; College Counseling and Student Affairs; Marriage, Couple, and Family Counseling; or School Counseling. There is one mention of technology for the doctoral program specialty standards (CACREP, 2015). Conversely, all 50 states in the United States have laws related to practicing telehealth (Lerman et al., 2017). The limited number of program accreditation standards that include technology neglects the current and future needs of professional counselors. Professional counselors are taxed with learning the required technological skills on the job instead of while enrolled as a student in their counselor education programs.
Student Considerations
A key factor in content delivery decisions is considering the type of learner the program will serve. The motivation, synchronicity level, and design approach all guide how successful a student will be. Not all students can be successful in every type of educational delivery setting. When considering synchronicity, the teacher-centered approach often is dependent on a greater percentage of synchronicity, while the subject-centered approach has flexibility in the percentage of synchronicity needed to effectively deliver the content. The choice in curriculum design approach also relates to the type of learner that the program attempts to serve. Yukselturk and Bulut’s (2007) description of the self-regulated learner summarizes the qualities of a learner that can be more successful with a greater percentage of asynchronous work. We also need to consider the comparative processes in a counselor-in-training’s development through a program of study.
Student Development in Online Education
Assessment of Skills and Dispositions
Assessment of skills and dispositions is a critical element of any counselor training program. The assessment process ensures that students have received the necessary training to demonstrate the skills and dispositions required to work with the public. The sections below will highlight a few of the ways student assessment is currently addressed within programs with online components.
Skills
Regardless of format, the key to effectively developing clinical skills in counselor trainees begins with intention. There are many shared approaches to teaching skills and techniques to counselor trainees in both online and traditional university settings. The nuances of online skills evaluation often begin with student access. Whereas traditional training programs have direct access to students in class and often do things like role-plays, practice sessions, and mock session evaluation in person, online programs do these in differing ways. There is a heavier reliance on technology to help facilitate exposure, practice, and assessment at a distance. This is demonstrated with greater use of podcasts, video clips, and video interfaces (Cicco, 2011). Additionally, there is a stronger need for well-developed relationships between students, faculty, and supervisors (Cicco, 2012). This strengthens the communication process and allows for more familiarity between the student and evaluators. It also allows for increased positive feedback, which can help reduce student anxiety and increase skill competency among counselor trainees in an online setting (Aladağ et al., 2014).
Fully online programs and some hybrid models often include synchronous activities, such as weekly course practice sessions, whereby students will meet via video technology and practice in front of the class or through a recorded session that can be viewed by the instructor at a later date. Feedback is an important part of this process and often includes both peer feedback, in the form of observation notes or class discussion, as well as notes or scaled assessments or rubrics provided to the student by the instructor (Cicco, 2011). This type of feedback is generally formative, which allows counselor trainees the opportunity to practice skills that are required by the program with a high level of frequency and relatively low stakes. Final course or summative evaluations often reflect a student’s combined skills practice demonstration and growth across the term.
Another frequently utilized form of skills assessment in online education is a residency model. In this training format, students gather in person with program faculty for a designated time (often 5–7 days) to complete specific skills-related training. Here, students may receive a combination of skills-based practice, faculty demonstrations, and skills- and content-based lectures. Within this format, skill development is specifically highlighted and opportunities to practice and receive real-time formative feedback are included. These in-person experiences are often evaluated in a summative manner at the conclusion of the experience with some form of established skills evaluation form. Determinations for additional skills training or remediation are often made at this point as well.
Dispositions
Much like skills assessment, dispositional assessment is a key function of counselor training programs and a requirement in the 2016 CACREP standards (CACREP, 2015). However, while skills are more behavior-based and observable, dispositional assessment often requires faculty and administrators to make judgments on student characteristics that are more abstract and difficult to define (Eells & Rockland-Miller, 2010; Homrich, 2009). Coupled with this is the fact that within the counseling profession, there are currently no specifically designed dispositional competencies (Homrich et al., 2014; Rapp et al., 2018). The result is that residence-based programs, as well as those online, are faced with the challenge of generating and operationalizing key dispositional characteristics within their counseling programs and in determining solid methods for assessment.
While challenging to establish, there have been programs that have made their disposition development process available to the broader counseling profession (Spurgeon et al., 2012). Additionally, Homrich et al. (2014) conducted a study with 82 counselor educators and supervisors from CACREP-accredited programs to better determine what dispositional characteristics are most valued in the counseling profession. Their results indicated three primary clusters of behavior specific to counselor disposition: (a) professional behaviors, (b) interpersonal behaviors, and (c) intrapersonal behaviors, with an emphasis on things like maintaining confidentiality, respecting the values of others, demonstrating cultural competence, and having an awareness of how personal beliefs impact performance. Similarly, Brown (2013) proposed the domains of (a) professional responsibility, (b) professional competence, (c) professional maturity, and (d) professional integrity, with associated behaviors within each domain. Many of these behaviors are indicated in the Counseling Competencies Scale, which has a specific section on counselor disposition (Swank et al., 2012). Having this psychometrically tested and sound assessment certainly aids in the process of assessing dispositions, whether online or in a traditional university setting.
Despite having some degree of guidance on dispositions and how to assess them, the unique elements of online education similarly reflect what was noted in the skills section—a lack of direct access to students, which alters the ability to assess formally and informally on already abstract concepts. While obvious or visibly present in a traditional classroom, interaction can be hidden behind a computer screen in the online setting. As a result, online-based programs often get around this limitation by creating opportunities to challenge students’ thinking and belief systems as well as enhancing awareness of key triggers and blind spots. Within the classroom, specific efforts can be made to create assignments in which students will face dilemmas and varied cultural experiences. Similarly, students can be asked to role-play certain characters or serve as the counselor to clients who may be perceived as controversial. These types of activities allow online counselor educators to first evaluate the responses students have, as well as to gauge openness to feedback if concerns arise in the initial response. Residency or other synchronous experiences, like video-based synchronous classrooms, afford faculty the chance to see and work with students on an interpersonal level. They also allow students to interact with one another and in some cases receive feedback from one another. Much like in the classroom, faculty members are then able to assess students on the interactions as well as on how students respond to specific feedback.
One area that is unique to online education and dispositional assessment is that of cyber incivility. De Gagne et al. (2016) defined cyber incivility as “a direct and indirect interpersonal violation involving disrespectful, insensitive, or disruptive behavior of an individual in an electronic environment that interferes with another person’s personal, professional, or social well-being, as well as student learning” (p. 240). Because online education programs rely so heavily on written electronic communication, both in the classroom and through email, there is a growing need for evaluation of interpersonal interactions in written online formats. Students who would otherwise never come into their faculty member’s office and disparage them face-to-face, or speak offensively to another student in a traditional classroom, might not struggle to do so when online. As a result, online education programs need to fine-tune the way they operationalize certain dispositional characteristics and otherwise make more formal evaluations of things like tone and messaging in written communication and interpersonal interactions. Recommendations to best address this include heightening students’ awareness of cyber incivility in both the curriculum and programmatic policies and communication (De Gagne et al., 2016), and assessing for cyber incivility as part of a dispositional evaluation. These types of assessment practices ultimately help online programs in the broader area of professional gatekeeping.
Gatekeeping
Gatekeeping is a fundamental part of the counselor training process and is mandated by section F.6.b. of the American Counseling Association’s ACA Code of Ethics (2014). As defined by the ACA Code of Ethics, gatekeeping is “the initial and ongoing academic, skill, and dispositional assessment of students’ competency for professional practice, including remediation and termination as appropriate” (2014, p. 20). It therefore includes both the assessment and evaluation process of each counselor trainee, but also the need for appropriate remediation, support, and dismissal by the programs that support them. In addition to the ethical mandate for gatekeeping, significant litigation in counseling programs (Hutchens et al., 2013) and a greater emphasis on assessment and gatekeeping in the CACREP 2016 standards (CACREP, 2015) have fostered a real need for programs of all types to firm up the gatekeeping process.
Gatekeeping is well addressed in the counseling literature, including the need for programs to create transparent performance assessment policies and practices that are explicitly communicated to students and to which students can respond (Brown-Rice & Furr, 2016; Foster & McAdams, 2009; Rapp et al., 2018). Ziomek-Daigle and Christensen (2010) proposed that there are four phases to the gatekeeping process: (a) preadmission screening, in which potential students are evaluated on key metrics prior to admission; (b) postadmission screening, in which actively enrolled students are evaluated and monitored on academic aptitude as well as interpersonal reactions; (c) remediation plan, in which students requiring remediation are provided intensified supervision and personal development; and (d) remediation outcome, in which students are evaluated on their remediation efforts and determined to be successful or not. The value of these proposed frameworks and theories is that they can be adapted and used to support the gatekeeping process of all counseling programs, regardless of the format. This is particularly valuable when as many as 10% of students in counseling programs may be deficient in skills, abilities, or dispositions and ill-suited for the profession (Brown-Rice & Furr, 2016).
In online education, the process of gatekeeping can look very similar to traditional programs, but it often requires a specific or altered set of practices to support its students. First, though not always the case, many online programs have an open- or broad-access admissions policy. This means that while certain minimal requirements have to be met (e.g., GPA, letters of recommendation, goal statement) at the preadmissions phase, other more traditional prescreening steps, such as student interviews (Swank & Smith-Adcock, 2014; Ziomek-Daigle & Christensen, 2010), may not be included. The byproduct of this may mean that there is a heightened level of gatekeeping required at the other phases: postadmission screening, remediation plan, and remediation outcome (Ziomek-Daigle & Christensen, 2010). This often results in the need for more faculty support related to the remediation process itself, as well as the need for very clear policies and practices related to remediation and dismissal that are consistently applied across a larger group of students.
While there is a call for all programs to make explicit policies and practices related to the gatekeeping process (Hutchens et al., 2013), online education programs have a heightened responsibility to overly communicate these practices. Students in online programs often are required to do much of their coursework on their own as well as attend and complete orientations and information sessions via electronic formats. The lack of direct contact with students means that online programs need to be more overt with policy messaging and provide repeated exposure to gatekeeping practices so that students stay informed. Often this is done via classroom announcements, email messaging, and course- or program-based requirements in which they must sign statements or acknowledgement forms indicating they have read and understand specific policies.
As remediation needs develop through the gatekeeping process, one of the fundamental needs of distance-based programs is strong collaboration and consultation among faculty and administration. Faculty with student concerns need the outlet and opportunity to connect with their colleagues to address potential issues and determine if issues are isolated. This is not unlike what occurs in traditional programs; however, the mechanisms for communication can differ, requiring more phone calls, tracking of email communication, and increased documentation in shared electronic records platforms. Problematic behaviors can be hard to parse out (Brown, 2013; Brown-Rice & Furr, 2016) regardless of setting, but can be increasingly challenging to identify online. Having these types of opportunities to connect with colleagues and track student issues is imperative to good remediation in an online setting.
Similarly, there is often the need for remediation committees in online programs. These committees generally include faculty and leadership within the program that work specifically to address the remediation needs of identified students. They can be content-specific—focusing solely on skills remediation or dispositional remediation—or they can serve both functions. While some traditional counseling programs have remediation committees (Brown, 2013), online programs often serve a significant number of students, which can translate to a higher number of students requiring remediation and support. Having a formalized process in place that is guided by a remediation or student support committee can be invaluable to this type of load.
Conclusion
When comparing program delivery and instructional variance between CACREP-accredited online and traditional counselor training programs, it is clear there are distinct similarities and differences. While the literature included debate regarding the appropriateness of an online environment for training counselors, research supports online counselor education training as effective for skill and professional identity development, despite requiring different instructional practices than traditional classrooms. Similarities between both settings also include a student body made up of adults, with a higher enrollment of Caucasian female students. However, online programs show greater diversity within their student body with higher numbers of non-traditional and underserved populations. One significant difference in online and traditional settings was attrition rates, which were higher for online programs, and research suggests that the social interaction that is a routine part of traditional training could hold a key to successful program completion for online learners. Future implications for counselor education are the expansion of empirically based curriculum development approaches that not only engage students but promote increased connection with the material, faculty, and peer learning communities. Another critical future direction of the counseling profession that has implications for both educational environments is the formal integration of technology skills training into the curriculum. While the academic core content areas are aligned for both settings, telehealth is rapidly changing the required skill sets for counselors to include communicating, documenting, and billing clients through electronic means.
Online counseling programs are growing in number and type, with many traditional programs now offering courses or full-program offerings at a distance. The increasing demand for this delivery model ultimately means more students will be trained at a distance, with an ever-increasing need to ensure appropriate assessment and gatekeeping practices. Faculty and administrators must be mindful of developing strong processes around admissions, student developmental assessment, remediation, and, where necessary, dismissal. Visual technology and simulation experiences are already being used by many online programs and will continue to grow and diversify as students seek new ways and opportunities to train at a distance. As more programs adopt online courses or curriculum, it is important that those programs, and the larger university systems that support them, are equipped to provide necessary training in the most effective and meaningful ways, while ensuring appropriate assessment and gatekeeping.
Finally, while conducting the review of literature for the analysis of similarities and differences between online and traditional programs, we revealed some gaps in existing research. Suggestions for future research include an investigation of instructional practices within online settings inclusive of delivery methods specific to asynchronous learning. Research indicates that attrition rates are higher for online programs, but it would be useful for researchers to investigate variables that contribute to attrition in online counseling students. Similarly, a meta-analysis of remediation practices as well as a qualitative inquiry of successful remediation efforts from both the faculty and student perspective may provide useful information in closing the gap for degree completion between online and traditional students. Finally, with the growing demand for technology literacy, the development of technology competencies for professional counselors could prove very useful for both curriculum development and counselor supervisors in facilitating success in developing professionals.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aladağ, M., Yaka, B., & Koç, İ. (2014). Opinions of counselor candidates regarding counseling skills training. Educational Sciences: Theory & Practice, 14, 879–886. https://doi.org/10.12738/estp.2014.3.1958
Allen, I. E., Seaman, J., Poulin, R. & Straut, T. T. (2016). Online report card: Tracking online education in the United States. Babson Survey Research Group. https://onlinelearningsurvey.com/reports/onlinereportcard.pdf
American Counseling Association. (2014). ACA code of ethics.
Barril, L. (2017). The influence of student characteristics on the preferred ways of learning of online college students: An examination of cultural constructs. https://digitalrepository.unm.edu/oils_etds/41
Barrio Minton, C. A., Wachter-Morris, C. A., & Yaites, L. D. (2014). Pedagogy in counselor education: A 10-year content analysis of journals. Counselor Education & Supervision, 53, 162–177.
https://doi.org/10.1002/j.1556-6978.2014.00055.x
Brown, M. (2013). A content analysis of problematic behavior in counselor education programs. Counselor Education & Supervision, 52(3), 179–192. https://doi.org/10.1002/j.1556-6978.2013.00036.x
Brown-Rice, K. A., & Furr, S. (2016). Counselor educators and students with problems of professional competence: A survey and discussion. The Professional Counselor, 6, 134–146. https://doi.org/10.15241/kbr.6.2.134
Burton, L. D. (2010). Subject-centered curriculum. In C. Kridel (Ed.), Encyclopedia of curriculum studies (pp. 824–825). SAGE.
Buzwell, S., Farrugia, M., & Williams, J. (2016). Students’ voice regarding important characteristics of online and face-to-face higher education. Sensoria: A Journal of Mind, Brain & Culture, 12, 38–49. https://doi.org/10.7790/sa.v12i1.430
Cicco, G. (2011). Assessment in online courses: How are counseling skills evaluated? i-manager’s Journal of Educational Technology, 8(2), 9–15. https://files.eric.ed.gov/fulltext/EJ1102103.pdf
Cicco, G. (2012). Counseling instruction in the online classroom: A survey of student and faculty perceptions. i-manager’s Journal on School Educational Technology, 8(2), 1–10. https://files.eric.ed.gov/fulltext/EJ1101712.pdf
Cicco, G. (2013a). Online course effectiveness: A model for innovative research in counselor education. i-manager’s Journal on School Educational Technology, 9, 10–16.
Cicco, G. (2013b). Strategic lesson planning in online courses: Suggestions for counselor educators. i-manager’s Journal on School Educational Technology, 8(3), 1–8.
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2018). CACREP vital statistics 2017: Results from a national survey of accredited programs.
De Gagne, J. C., Choi, M., Ledbetter, L., Kang, H. S., & Clark, C. M. (2016). An integrative review of cybercivility in health professions education. Nurse Educator, 41, 239–245. https://doi.org/10.1097/NNE.0000000000000264
DiRamio D., & Wolverton, M. (2006). Integrating learning communities and distance education: Possibility or pipedream? Innovative Higher Education, 31(2), 99–113. https://doi.org/10.1007/s10755-006-9011-y
Dole, S., Bloom, L., & Kowalske, K. (2016). Transforming pedagogy: Changing perspectives from teacher-centered to learner-centered. Interdisciplinary Journal of Problem-Based Learning, 10(1).
https://doi.org/10.7771/1541-5015.1538
Eells, G. T., & Rockland-Miller, H. S. (2010). Assessing and responding to disturbed and disturbing students: Understanding the role of administrative teams in institutions of higher education. Journal of College Student Psychotherapy, 25, 8–23. https://doi.org/10.1080/87568225.2011.532470
Ellis, R. A., & Bliuc, A.-M. (2019). Exploring new elements of the student approaches to learning framework: The role of online learning technologies in student learning. Active Learning in Higher Education, 20, 11–24. https://doi.org/10.1177/1469787417721384
Lerman, A. F., Kim, D., & Ozinal, F. (2017). 50-State survey of telemental/telebehavioral health. https://www.ebglaw.com/telehealth-telemedicine/news/telemental-and-telebehavioral-health-considerations-a-50-state-analysis-on-the-development-of-telehealth-policy/
Foster, V. A., & McAdams, C. R., III. (2009). A framework for creating a climate of transparency for professional performance assessment: Fostering student investment in gatekeeping. Counselor Education and Supervision, 48(4), 271–284. https://doi.org/10.1002/j.1556-6978.2009.tb00080.x
Hedén, L., & Ahlstrom, L. (2016). Individual response technology to promote active learning within the caring sciences: An experimental research study. Nurse Education Today, 36, 202–206. https://doi.org/10.1016/j.nedt.2015.10.010
Homrich, A. (2009). Gatekeeping for personal and professional competence in graduate counseling programs. Counseling and Human Development, 41, 1–24.
Homrich, A. M., DeLorenzi, L. D., Bloom, Z. D., & Godbee, B. (2014). Making the case for standards of conduct in clinical training. Counselor Education and Supervision, 53(2), 126–144.
https://doi.org/10.1002/j.1556-6978.2014.00053.x
Hutchens, N., Block, J., & Young, M. (2013). Counselor educators’ gatekeeping responsibilities and students’ first amendment rights. Counselor Education and Supervision, 52(2), 82–95.
https://doi.org/10.1002/j.1556-6978.2013.00030.x
Kebble, P. G. (2017). Assessing online asynchronous communication strategies designed to enhance large student cohort engagement and foster a community of learning. Journal of Education and Training Studies, 5(8), 92–100. https://doi.org/10.11114/jets.v5i8.2539
Koehler, M. J., Mishra, P., Hershey, K., & Peruski, L. (2004). With a little help from your students: A new model for faculty development and online course design. Journal of Technology and Teacher Education, 12, 25–55.
Kumar, P., Kumar, A., Palvia, S., & Verma, S. (2019). Online business education research: Systematic analysis and a conceptual model. The International Journal of Management in Education, 17, 26–35. https://doi.org/10.1016/j.ijme.2018.11.002
Lu, H. (2017). How can effective online interactions be cultivated? Journal of Modern Education Review, 7, 557–567. https://doi.org/10.15341/jmer(2155-7993)/08.07.2017/003
Lucas, K., & Murdock, J. (2014). Developing an online counseling skills course. International Journal of Online Pedagogy and Course Design, 4(2), 46–63. https://doi.org/10.4018/ijopcd.2014040104
Marchand, G. C., & Gutierrez, A. P. (2012). The role of emotion in the learning process: Comparisons between online and face-to-face learning settings. The Internet and Higher Education, 15(3), 150–160. https://doi.org/10.1016/j.iheduc.2011.10.001
Merriam-Webster. (n.d.). Andragogy. In Merriam-Webster.com dictionary. https://www.merriam-webster.com/dictiona
ry/andragogy
Murdock, J. L., & Williams, A. M. (2011). Creating an online learning community: Is it possible? Innovative Higher Education, 36, 305–316. https://doi.org/10.1007/s10755-011-9188-6
Office of Federal Student Aid. (2017). Federal student aid handbook. U.S. Department of Education.
Office of Postsecondary Education Accreditation Division. (2012). Guidelines for preparing/reviewing petitions and compliance reports. U.S. Department of Education. https://www.asccc.org/sites/default/files/USDE%20_agency-guidelines.pdf
Onodipe, G. O., Ayadi, M. F., & Marquez, R. (2016). The efficient design of an online course: Principles of economics. Journal of Economics and Economic Education Research, 17, 39–50.
O’Shea, S., Stone, C., & Delahunty, J. (2015). “I ‘feel’ like I am at university even though I am online.” Exploring how students narrate their engagement with higher education institutions in an online learning environment. Distance Education, 36, 41–58. https://doi.org/10.1080/01587919.2015.1019970
Pinnegar, S., & Erickson, L. (2010). Teacher-centered curriculum. In C. Kridel (Ed.), Encyclopedia of Curriculum Studies (pp. 848–849). SAGE.
Rapp, M. C., Moody, S. J., & Stewart, L. A. (2018). Becoming a gatekeeper: Recommendations for preparing doctoral students in counselor education. The Professional Counselor, 8, 190–199. https://doi.org/10.15241/mcr.8.2.190
Snow, W. H., & Coker, J. K. (2020). Distance counselor education: Past, present, and future. The Professional Counselor, 10, 40–56. https://doi.org/10.15241/whs.10.1.40
Snow, W. H., Lamar, M., Hinkle, J. S., & Speciale, M. (2018). Current practices in online counselor education. The Professional Counselor, 8, 131–145. https://doi.org/10.15241/whs.8.2.131
Spurgeon, S. L., Gibbons, M. M., & Cochran, J. L. (2012). Creating personal dispositions for a professional counseling program. Counseling and Values, 57, 96–108. https://doi.org/10.1002/j.2161-007X.2012.00011.x
Swank, J. M., Lambie, G. W., & Witta, E. L. (2012). An exploratory investigation of the Counseling Competencies Scale: A measure of counseling skills, dispositions, and behaviors. Counselor Education and Supervision, 51(3), 189–206. https://doi.org/10.1002/j.1556-6978.2012.00014.x
Swank, J. M., & Smith-Adcock, S. (2014). Gatekeeping during admissions: A survey of counselor education programs. Counselor Education & Supervision, 53, 47–61. https://doi.org/10.1002/j.1556-6978.2014.00048.x
Taylor, J. Z., & Baltrinic, E. R. (2018). Teacher preparation, teaching practice, and teaching evaluation in counselor education: Exploring andragogy in counseling. Wisconsin Counseling Journal, 31, 25–38.
Yükseltürk, E., & Bulut, S. (2007). Predictors for student success in an online course. Educational Technology & Society, 10(2), 71–83.
Ziomek-Daigle, J., & Christensen, T. M. (2010). An emergent theory of gatekeeping practices in counselor education. Journal of Counseling & Development, 88, 407–415. https://doi.org/10.1002/j.1556-6678.2010.tb00040.x
Laura Haddock, PhD, NCC, ACS, LPC-S, is a clinical faculty member at Southern New Hampshire University. Kristi Cannon, PhD, NCC, LPC, is a clinical faculty member at Southern New Hampshire University. Earl Grey, PhD, NCC, CCMHC, ACS, BC-TMH, LMHC, LPC, is an associate dean at Southern New Hampshire University. Correspondence can be addressed to Laura Haddock, 3100 Oakleigh Lane, Germantown, TN 38138, l.haddock@snhu.edu.
Mar 9, 2020 | Volume 10 - Issue 1
Donna S. Sheperis, Ann Ordway, Margaret Lamar
Counselor education has moved firmly into the online space with multiple accredited programs available to students and potential faculty. These programs can cross state lines, either by location of training, placement of faculty, or both. As such, there are legal and ethical considerations that are outside of those that are typically considered. This article addresses some of the more common legal and ethical considerations in counselor education, such as vicarious liability and cybersecurity, and how they differ in the online education environment. Licensure and other laws and obligations for educators are explored. Opportunities for gatekeeping are discussed through the lens of a case study. A second case study with guiding questions is provided to raise visibility of state differences in practice laws. Finally, helpful resources for navigating online counselor education from a legal and ethical perspective are offered.
Keywords: counselor education, online, legal, ethical, gatekeeping
There are many reasons to consider online education when becoming a counselor or choosing a career as a counselor educator. Convenience, accessibility, and opportunities to interface with colleagues across the country and around the world are common attractions of an online environment. As of the beginning of 2020, 79 online programs were accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2020). As many opportunities as there are in this educational space, legal and ethical challenges also exist. Although these challenges may be unique to the online world, they are certainly navigable. This article tackles some of the experiences distinctive to faculty and students in counselor education who choose an online environment for training.
Considerations for Online Counselor Educators
Counselor education is a distinct professional identity geared toward the preparation of professional counselors across disciplines (e.g., clinical mental health counselor, professional school counselor, substance abuse counselor). Counselor educators who teach in CACREP-accredited programs are required to have terminal degrees in counselor education and supervision, as opposed to psychology or another helping profession, as well as active involvement and participation in the counseling profession (Calley & Hawley, 2008). These educators receive training in five core areas, including counseling, supervision, teaching, research and scholarship, and leadership and advocacy, making them uniquely qualified to prepare master’s-level clinicians in counseling (CACREP, 2015).
Prior to the publication of the 2016 CACREP Standards, counselor educators may or may not have received training specific to online counselor education. And yet as of 2014, at least 67% of students in public universities took an online course (Allen et al., 2016). To attend to this emerging trend, CACREP recognized the need for all counselor educators to understand “effective approaches for online instruction” (CACREP, 2015, p. 35). Whether fully online or fully in person, most counselor education programs contain some online elements in their instructional pedagogy. Thus, the opportunities to teach and learn counseling in an online format are present regardless of whether the program is considered an online program.
For the purposes of this article, an online counselor educator is a person who provides some or all of their teaching via a distance education format (Stanford University Teaching Commons, n.d.). Most universities offer some form of training to assist the educator in moving to online education (Dimeo, 2017), but that training is not specific to the content of counselor education. With this in mind, some of the inherent opportunities and challenges in online teaching, specifically as they relate to legal and ethical concerns, including vicarious liability and supervision in online education settings, will be discussed.
Vicarious Liability as a Counselor Educator
The counselor education literature is replete with research related to vicarious liability in supervision (Mikkelson et al., 2013; Pearson, 2000; Sheperis et al., 2016). Essentially, vicarious liability refers to a situation in which one person is held responsible for the actions or inactions of another person (Bell, 2013). In counseling, we see this term most commonly used in relation to a clinical supervisor having some responsibility for the care of the clients of a supervisee.
This definition of vicarious liability does not make concessions for the manner in which clinical oversight is provided. In other words, online or not, clinical supervisors continue to carry vicarious liability for the clinicians they supervise. By extension, counselor educators serving as practicum and internship supervisors would also be held responsible for the services provided by students under the terms of vicarious liability. According to one popular provider of malpractice insurance for counselors, CPH & Associates (2019), liability insurance covers the holder for incidences of negligence, misrepresentation, violation of good faith, and inaccurate advice. The key term to consider is inaccurate advice, as that is how supervision could be characterized in a lawsuit.
The Counselor Educator as Supervisor and Gatekeeper
Slovenko (1980), in his seminal article on the topic of supervisor responsibility to the client, stated “litigation against supervisors may be called the ‘suit of the future’” (p. 468). Over the years, we have not seen that prophecy come to fruition in counselor education, but the caution remains that counselor educators who serve as supervisors must be mindful of their potential vicarious liability. With regard to the provision of online counselor education, the opportunities to supervise students who are seeing clients that are in different cities, states, or countries exist. Although this is an exciting development in terms of working with a variety of students, it is daunting to consider the legal implications.
Counselor educators may assume that only teaching didactic classes online and not supervising practicum and internship students will reduce their overall liability. But the reality is that all counselor educators have a responsibility to gatekeeping that extends to protecting potential future clients of the students we train. To that end, we must maintain an approach to our work that keeps the concept of vicarious liability in mind.
For example, in fully online programs, there is often a residency model. The residency is a period of time in which students gather for in-person training and observation, often of clinical skills (Holstun, 2018). Walden University, which trains counselors in a fully online format, describes residency as a time to “conceptualize and develop research that contributes to positive social change; establish networks of professionals who support and practice scholarly endeavors; [and] develop and refine practice skills essential to your profession” (2019, Mission and Vision section). That may occur at the university campusor a neutral destination depending on the type of institution. These residencies are opportunities to be physically present with students, uncover any clinical or dispositional concerns, and allow for multiple faculty to relate to students. Although some of this is clearly possible in a fully online format, the majority of online programs opt for at least one in-person experience with the students they serve (Holstun, 2018).
While an online class may involve some interaction and evidence of interpersonal ability, a residency increases the opportunities for faculty to make a more accurate assessment of skills and dispositions. Thus, program administrators may be apprised of gatekeeping and supervisory issues observed in this setting.
Case Study
Malkha chose an online counselor education master’s program because she lives in a remote area, over 75 miles from the nearest CACREP-accredited campus program. She works full-time at her holistic health practice where she practices Reiki, acupuncture, and holistic health coaching, including dietetics and nutrition. She is certified as a Reiki practitioner, licensed in her state as an acupuncturist, and has recently begun offering the coaching option for her clients who need additional care. Malkha has an emotional support animal that accompanies her to sessions, and she hopes to eventually be able to provide appropriate documentation to her clients that will allow them to have emotional support animals as well.
Malkha has several academic gifts. She writes well and generally does well on course assignments. She does have a pattern of asking for last-minute extensions as she often needs more time than is allotted to complete her assignments. Faculty have also noted that Malkha occasionally engages students in the discussion board in inflammatory ways. She uses her background and training to offer advice to fellow students in ways that are not always helpful nor appropriate to the context of an academic forum. She argues with those who do not utilize alternative, holistic approaches in their own theoretical orientations, calling them “shortsighted” and “old-fashioned.” Students seem to like Malkha but have complained that she comes on too strong.
At her first residency, Malkha shares a room with two other students and her emotional support dog. Unfortunately, one of the roommates is allergic and alleges that Malkha did not disclose that the dog would be attending residency. There is conflict between the roommates about handling the payment for the room that spills over into their work as a group. Malkha also brings her animal to residency, which is allowed, but she continually talks to the dog throughout the faculty lecture and group work. While working on skills, for example, Malkha asks her dog what his opinion is, how she should proceed, and then appears to listen for a response.
A large part of the time at residency is spent in clinical skills training. Faculty spend a lot of time redirecting Malkha from giving advice and offering treatment solutions during the early phases of therapy. She continually moves away from the person-centered approach she states she is practicing and becomes more prescriptive as the practice times continue.
Faculty teaching Malkha at residency bring the concerns about her distracting interactions with her emotional support animal as well as her skills to the attention of the training director. Questions to consider underscore potentially unique dimensions of practice for online faculty and academic leadership with respect to programming, policies, and gatekeeping. For example:
- Are there ethical or gatekeeping concerns that need to be addressed? If so, what are they?
- How do those concerns fit with the American Counseling Association’s ACA Code of Ethics
(2014) and any gatekeeping procedures established by your program?
- What are some potential next steps to take with Malkha and/or faculty?
- What, if anything, could have prevented the problems that arose at residency?
While these questions are fundamental to counselor educators, they point to the importance of established policies and procedures for face-to-face residencies, effective communication of policies and expectations to online students, and preparedness to apply ethical decision-making models in navigating the ethical and legal challenges that may arise in online counselor education.
Considerations for Online Counselor Education Students
For the purposes of this article, an online counseling student is a person who receives some or all of their training via a distance education format. With this in mind, some of the inherent opportunities and challenges in this format, specifically as they relate to legal and ethical concerns, will be considered. A more comprehensive analysis of the experience of the online counseling student is addressed in another article in this special section (Sheperis et al., 2020).
Opportunities and Challenges
Opportunities for students in online programs include flexibility to accommodate life, work, and school. Online students may not be able to attend a graduate program in another format because of geographical, employment, or family considerations. Online students also have the opportunity to learn from faculty and fellow students from around the United States and the world.
Yet as appealing as this can sound, being an online student is challenging. Students are faced with the need to self-regulate, and, depending on the amount of instructor interaction, this may include deciding when to enter the class, turn in assignments, and engage with their peers (Wong et al., 2019) There can be a sense of isolation and loss of social community in virtual learning that is not present in a physical classroom (Phirangee & Malec, 2017). When looking at successful online students, it is recommended that they possess time-management skills, are self-regulated learners, and are self-motivated to complete tasks when compared to their traditional face-to-face classroom counterparts (Vineyard, 2019).
Legal and Ethical Considerations
As an online student, the ethical considerations are very similar to those experienced by on-campus students. There are gatekeeping considerations, concerns about fitness to practice, and general academic expectations regardless of the mechanism of education (CACREP, 2015). However, there are additional legal considerations that online students should be apprised of.
Each state, province, and territory has its own licensure law for professional counselors (Sheperis et al., 2016). Campus-based faculty become familiar with the state in which they offer education and may not be as familiar with licensure laws outside of that state. It will be incumbent upon the online students to familiarize themselves with state regulations so that they can ensure that their training will meet the standards for the educational component of licensure. For many states, graduation from a CACREP-accredited program is an acceptable standard of training. However, there can be exceptions even for CACREP-accredited programs. For example, the state of Georgia requires practicum and internship supervisors to have three years of postlicensure experience (State of Georgia, 2019), which is more than the CACREP standard.
In addition, not all online programs are able to provide training in every state. Applicants to online counselor education programs need to be well-educated consumers. In addition, enrollment services staff, program leaders, and counselor educators involved in admissions decisions need to be apprised of various state requirements. For example, the state of North Carolina requires that online programs, including those in private, out-of-state institutions, be approved by the University of North Carolina Board of Governors before they can engage in postsecondary degree activity in North Carolina
(University of North Carolina System, 2017).
Considerations for Cybersecurity in Counselor Education
With the rate of technology innovation, counselor education programs may find it challenging to keep up with how specific technology aligns with laws or ethics. When it comes to online counselor education and technology, student privacy and client confidentiality are of utmost importance and are often tricky to navigate with new technological development. In this section, we examine the two primary regulations and how to maintain compliance when using technology.
The Family Educational Rights and Privacy Act (FERPA)
FERPA (1974) is a regulation that protects the privacy of a student’s educational record. All programs, regardless of their delivery format, need to be aware of how FERPA impacts them and the technology they utilize. For instance, programs using online providers to help track internship hours, supervisor evaluations, and other paperwork need to be in line with FERPA best practices. The Department of Education, through their Privacy Technical Assistance Center (PTAC), provides resources for programs, including what to look for in a terms-of-service document (PTAC, 2016) and best practices (PTAC, 2014). Online programs using videoconferencing software need to be aware of the limitations on the use of videos created in a classroom or supervision setting.
Under FERPA, a photo or video of a student is considered an educational record when it is directly related to the student and is maintained by the program (Student Privacy Policy Office, n.d., para. 1). A video of a class is considered to be directly related to the student if they are visible doing a class presentation or even asking questions. The use of videoconferencing software is new enough to leave some ambiguity in the regulations surrounding recording of classes or supervision sessions. We will address supervision sessions in the section on the Health Insurance Portability and Accountability Act of 1996, which follows. Relative to teaching, there are a number of university recommendations suggesting that faculty record only themselves in class and do not include images of students in the recording. If a faculty member wants to release a recording of a class that directly relates to a student, they must gain signed consent from the student to do so. In practical terms, the faculty should gain consent from all members of the class if they appear in the recording of the class.
FERPA regulations require that institutions use “reasonable methods” to safeguard student information (PTAC, 2015). The law does not include specific requirements for firewalls, security monitoring, or response methods, but leaves that to universities to determine. It is also recommended that programs have a plan in place should a security breach occur.
Although counselor educators may use the term confidentiality when referring to a student’s experience, dispositional issues, or educational record, it is important to note that a student does not have the same rights of confidentiality as a counseling client. In fact, FERPA allows faculty and programs to share student educational records (including disciplinary records) with other faculty and other institutions where a student may be transferring. If a counseling student is dismissed for causing harm to clients, it is within the bounds of FERPA for program faculty to share that information with faculty where the student is applying for admission.
The Health Insurance Portability and Accountability Act of 1996 (HIPAA)
It is important for online counselor educators to be fully informed on HIPAA regulations as they relate to technology. These regulations provide protections for confidential and protected health information and are commonly referenced in the modern health care lexicon. With relation to training, online counselor education students and faculty frequently use various forms of software or other communication technology to communicate about client issues in practicum or internship classes and supervision sessions. It is not within the scope of this article to cover every aspect of technology and client personal health information (PHI) as defined by HIPAA. This section will focus specifically on the utilization of videoconferencing software (e.g., FaceTime, Skype, Zoom) to hold class and supervision sessions, which are often the primary ways distance faculty, supervisors, and students meet.
First, a key principle to understand in any discussion of HIPAA is that the user (e.g., faculty, supervisor, student counselor) is responsible to maintain compliance with HIPAA regulations. Videoconference software companies that counselor educators and supervisors choose to use could be considered business associates. Business associates are contractors who handle PHI of clients and have agreed to uphold HIPAA regulations.
There is no clear guidance on the need for business associate agreements for videoconferencing software. Some researchers have said that it is necessary for videoconferencing providers to have business agreements (Rousmaniere et al., 2016). Others have suggested that videoconferencing software falls under the HIPAA conduit exception (Caldwell, 2019). The conduit exception allows service providers to transmit or transport PHI without entering into a business agreement (Office for Civil Rights, 2016). To be eligible as a conduit, software providers must not store the data and may only transmit it (Taylor, 2015). Generally, videoconferencing software companies do not store any transmissions on their servers (Caldwell, 2019). FaceTime, Skype, and Zoom, for example, provide end-to-end encryption to create a peer-to-peer connection. It is not possible for them to decrypt the data as it goes from the device of the supervisor to the student. Therefore, given that no data from a supervision session or class is being recorded, the argument has been made that a business associate agreement is not necessary to use these platforms (Caldwell, 2019; Taylor, 2015). Recordings of supervision sessions or classes should not be saved to cloud services unless there is a business agreement in place, as now the company will be potentially storing PHI. As a reminder, it is still up to the faculty and student to be HIPAA-compliant when they use technological tools. Talking about a client over Facetime while in a coffee shop is still not considered HIPAA-compliant.
Technology moves swiftly. For example, Amazon has recently equipped their Alexa devices to handle PHI and has begun signing business agreements with select health care providers (Jiang, 2019). But there is little in terms of policy, law, or ethics to address anecdotal reports that the Amazon Alexa device is recording conversations in homes and therefore likely in offices where it is used. For the online educator and student, that could mean that a piece of technology intended to make home life easier creates a HIPAA or FERPA violation if portions of classes or client sessions are recorded. We anticipate this technology, and thus the policies, laws, and ethics that govern its use, will continue to develop. At this point, it is recommended that these devices not be in homes or offices where counselor education or supervision occurs.
Counselor Education Across State Lines
In general, teaching students who all live in the same state or who live in a variety of states is fairly similar. Counseling theory in Michigan is going to be the same as counseling theory in Alabama, and educational practices will be similar. However, there are some considerations unique to the online educator. As described, many of those relate to practicum, internship, and licensure. Because faculty will often be the first line of inquiry for students, online faculty need to be aware that codes of ethics and laws related to client care vary from state to state. Although the content of theory classes may stay the same across states, conversations about what to do when a client reveals something in session that may require duty to warn or other action may change from state to state. Being prepared to navigate those conversations is essential to success as an online faculty member. It would benefit the online counselor educator to become familiar with the main state licensure board challenges confronted by the department. For example, specific curricular requirements and variations in state laws that impact abuse reporting are common considerations. While faculty members cannot be experts on all state, province, and territory law, it is helpful to have a solid understanding of the primary issues impacting students.
Online programs are often part of institutional efforts to recruit international students (Lee & Bligh, 2019). In addition to differences in state regulations, program faculty then must have an awareness of international counseling practice. Many countries have no formal licensing of counselors, so a comparison of licensure laws cannot be done. The lack of laws related to the practice of many forms of counseling outside of the United States makes it impossible to declare any uniform statements about such practice. Students who are outside of the United States and the faculty who train them need to be especially vigilant in investigating standards and laws that impact training and practice.
Ethics Across State Lines
Just as there is no universal licensure law across states, there is no universal adoption of a code of ethics across states. The code of ethics provided by ACA is the most commonly used single code in the United States; however, only 19 of the 52 jurisdictions with licensure laws have adopted the ACA Code of Ethics into their rules and regulations (ACA, 2015). As you can imagine, it can be challenging for educators and students to navigate all of the complexities of the various codes. Students are guided to consult state laws to better understand the code of ethics under which they will fall.
Although codes of ethics are generally more alike than conflictual, there are a number of differences. The ACA Code of Ethics (2014) empowers counselors to warn identified others when there is a threat of serious and foreseeable harm. That code is historically rooted in the famous Tarasoff ruling in which the clinician provided information to the police, but not to the identified person that the client was threatening (Sheperis et al., 2016). However, the Texas code of ethics requires counselors to report only to authorities and not to warn the identified third party (Texas State Board of Examiners of Professional Counselors, 2011). Another example is that counselors are ethically allowed to barter under the ACA Code of Ethics. However, Texas code prohibits bartering (Texas State Board of Examiners of Professional Counselors, 2009). Thus, students and educators need to be able to assess those differences as they proceed with training across states.
Laws Across State Lines
Just as ethical codes vary from state to state, laws also vary. Few laws that govern the practice of counseling are enacted at the federal level. Instead, each state is empowered to determine what is best for their population in terms of developing laws that govern scope of practice for counselors. Licensure laws are the first areas that counseling students and counselor educators should familiarize themselves with. In addition to licensure law differences, there are other challenges that may exist.
One area of difference occurs within mandated reporting laws. Each state specifically sets out the definitions of abuse and neglect while also outlining who is considered a mandated reporter. In Mississippi, any person who knows about or has reason to suspect abuse or neglect of a child by a parent, legal custodian, caregiver, or other person(s) responsible for the child’s care is required by law to make a report (Mississippi Department of Child Protection Services, 2019). In other states, such as Pennsylvania, only mandated reporters have this requirement (State of Pennsylvania, n.d.). Mandated reporters typically include professionals expected to encounter children such as school personnel, medical professionals, and counselors. Counselors will always be required to report, but some states give that designation to any and every person, which can make a difference in working with clients who may have reason to suspect abuse.
Another distinction is found in laws related to warning identified third parties about an intent to harm. In the ethics classes of counselor training programs, we highlight the Tarasoff v. the Regents of the University of California (1974) case and subsequent rulings as the way to handle duty to warn any identified third parties. After multiple court and state supreme court rulings in California, where the Tarasoff case occurred, many states have elected to follow this case law and allow or even require counselors to report the intent to harm to the identified potential victim as well as the authorities (Sheperis et al., 2016). However, some state laws are silent on this matter. In Georgia, there is only a small mention in the code for psychologists and nothing to guide counselors (State of Georgia, 2020). Texas has a law related to Tarasoff, but it goes counter to the laws in the vast majority of states. The Texas Health and Safety Code (2005) states that counselors are not allowed to notify the identified victim:
A professional may disclose confidential information only to medical or law enforcement personnel if the professional determines that there is a probability of imminent physical injury by the patient to the patient or others or there is a probability of immediate mental or emotional injury to the patient. (p. 4,182)
In practice, this means that two students from different states in the same ethics course could respond to a case involving a threat to harm an identified party in vastly different ways and still be correct.
Gatekeeping Across State Lines
The gatekeeping aspect of counseling pertains both to the obligation of counselor educators to ensure the competency of students entering the profession and the responsibility of practicing professionals to confront and address the unethical practice of colleagues when it comes to their attention. The gatekeeping responsibility has become so much more complex because of the evolution of distance counseling and distance counselor education. Distance practices raise questions about how well a professional in one location can monitor the behavior of another located in an entirely different place. The implications, which require familiarity with federal laws such as HIPAA and FERPA, state statutes and regulations for local licensing, and other local laws pertaining to the plethora of issues a counselor may encounter in therapy with clients, are nothing short of overwhelming. The responsibility is vast when considering the overabundance of variations of rules and consequences for not following them.
Lawsuits, Inconsistent Laws, and Varying Codes of Ethics
As mentioned, the practice of counseling is not federally regulated for the most part. Each state or territory has a degree of autonomy over the regulation of professional licensure, and therefore there is a significant disparity from jurisdiction to jurisdiction. Federal laws impose uniformity and create a reliability regarding the rules and regulations for any area governed by the federal government. For example, in 2015 the U.S. Supreme Court ruled that same-sex marriage would be a legal right across the United States. The impact of the ruling was that the 14 states that had bans on same-sex marriage could no longer prevent same-sex couples from legally marrying in their individual jurisdiction. However, the application of federal laws are sometimes locally compromised, such as when a specific religious denomination refuses to perform marriage ceremonies for same-sex couples by asserting freedom of religion and the separation of church and state. The religious argument is not that the same-sex couple cannot marry in that state, but rather that the couple simply cannot marry in a religious ceremony in that church. This example sets the stage for recent legislation that impacts counselor education.
The state of Tennessee implemented legislation in 2014 that allowed counselors to refuse to provide services to someone on the basis of “strongly held personal beliefs,” thus allowing professional counselors to impose their own values as a lens for whether or not they would work with particular clients. The mere existence of this legislation led to ACA moving the annual conference in 2017 from Nashville, Tennessee, where it was scheduled to be held, to San Francisco, California. The ACA Code of Ethics (2014) calls for counselors to refrain from imposing their values on clients. As of 2015, the ACA Code of Ethics is used by 19 states, ironically with Tennessee being among them. In other words, the licensing statute in Tennessee incorporates the language of the ACA Code of Ethics, while there is a separate law indicating that a counselor cannot suffer loss of license when that code is violated through the refusal of services to someone because of what the counselor personally believes. It is noteworthy that, while the LGBT population was the likely intended target of the new law, the language would allow for a further and widespread regression to blatantly discriminatory practices under the justification that the practice is rooted in what the individual believes.
Case Study
Carolyn is a student pursuing her doctoral degree in professional counseling. She is 35 years old and her best option for pursuing her education was through a distance-based program. Accordingly, though she lives in a rural community outside Nashville, Tennessee, she is enrolled in a graduate program at Towaco University based in Chula Vista, California. Throughout her enrollment, she has attended three residencies in California, and she is presently in the field experience segment of her education. Carolyn is employed full-time as a counselor at a Christian counseling center. She has her master’s degree and she is licensed. She arranges her practicum hours at a local inpatient addictions recovery center around the requirements of her full-time job so that she is usually working at her practicum site on nights and weekends.
As a student at Towaco, she was asked to sign a statement as a condition of enrollment committing to follow the ACA Code of Ethics. She has always abided by the provisions of the code in the context of her role as a student. However, at her primary place of employment, Carolyn and her coworkers do not treat individuals who are part of the LGBT community.
This week, Carolyn has been assigned a new client at the addictions center. Dominic is a 28-year-old gay male who has been married to James for 8 years. They have a 4-year-old son. The relationship is solid. Dominic was admitted to treatment because he became addicted to pain medication following a serious car accident. James is very supportive, visits Dominic as frequently as is allowed, and attends family therapy sessions. Carolyn is assigned to work with Dominic both individually and as a facilitator of the family group. As a conservative Christian, Carolyn is uncomfortable working with a gay couple. She has never had to do so at her full-time job. In Tennessee, there is a law that allows a licensed professional counselor to refuse to provide services to anyone based upon “strongly held personal beliefs.” Carolyn tells her supervisor that she declines to work with Dominic and his husband and requests that the client be reassigned. The site supervisor suspends Carolyn and contacts her university supervisor in California.
Given Carolyn’s enrollment in an online counselor education program located in another state, this raises a number of questions when considering next steps. For example:
- Which law or guideline is the primary guide for Carolyn’s conduct as a practicum student at the addictions center?
2. What relevance is there to the fact that Carolyn is already a licensed professional counselor in Tennessee but only a student at the university in California?
3. What if any implications will there be if Carolyn similarly refuses to see a client who is gay at her full-time job?
4. Is Carolyn bound by the ACA Code of Ethics if she is not a member of the American
Counseling Association?
These questions illustrate some of the complex terrain to be navigated by online counselor educators.
Other Legal Considerations
Ward v. Wilbanks (2010), though not the first case of its kind and certainly not the last, garnered significant attention in the profession through the focus on a student-driven lawsuit against a counseling program at Eastern Michigan University and the individual faculty members. The plaintiff, Julea Ward, was enrolled in a practicum course and providing counseling services under supervision at the in-house clinic at Eastern Michigan University. She was assigned a client who presented with depression and issues related to a same-sex relationship. Ms. Ward sought to refer the client, citing a conflict with her personal religious beliefs, and she was expelled from the program, which she cited as a violation of her rights. A lower court recognized the importance of the right of educational programs to self-regulate. However, a higher court found in favor of Ms. Ward, and the Ward v. Wilbanks case became critical in the further evolution of the ACA Code of Ethics (2014), through which clarification came in terms of referrals that are rooted in competency and referrals that are rooted in the imposition of values and judgment.
Thus, in the prior case study, Carolyn could be allowed to refer in an educational program and in her state, but may not be allowed to refer under the same circumstances outside of her state. Because most states follow the ACA Code of Ethics, anyone functioning as a counselor could be held to those standards regardless of ACA membership status (Sheperis et al., 2016).
Discussion
The aforementioned examples serve to underscore the complications that arise just by virtue of the differences among the laws and regulations on like issues from state to state. With students being trained in the same program but living in different states and being trained by faculty who are also living in different states, opportunities for legal and ethical challenges abound. As counselor educators, we are trained to develop competent, ethical clinicians to serve clients, yet modern-day training, especially across state lines, requires the educator be informed of legal, ethical, and other challenges impacting the profession and students they serve.
Currently, counselor educators teaching through distance learning platforms cannot teach solely based upon licensing requirements in one state. In fact, the educator might be located in one state, while the student is in another, and the university is in yet another. The counselor educator, who might live and be licensed in Texas, is bound to follow the regulations in that state—but those regulations might not be relevant to (and might even be blatantly in conflict with) the regulations that apply to the student who resides in Tennessee. Moreover, the same professor can have 10 students in one class from 10 different states. The university, in California, will be bound by both federal and state regulations pertaining to higher education, including FERPA, but also by any relevant laws that might pertain to the different subject matters taught through that university. For example, in Alaska, if someone assists another in the act of suicide, that person can be charged with manslaughter. However, in California if that person is a medical doctor and assists another in ending their own life, the assistance could be considered a medical treatment under the End of Life Options Act (State of California, 2015).
Legal differences such as these call into question what can be taught about the professional handling of certain issues. Significant variations in law exist around confidentiality and mandatory reporting, counseling with minors and parental consent, and the nuances of licensing. Thus, it is incumbent upon counselor educators to be alert in their practice and prepared for the complex considerations that coexist with the accessibility of online counselor education.
Implications
Navigating the online space in a legal and ethical manner means staying up to date on current trends, resources, and laws. There are some resources counselor educators will find helpful in knowing licensure laws such as Licensure Requirements for Professional Counselors, A State by State Report (ACA, 2016). Also available from ACA is Licensure & Certification: State Professional Counselor Licensure Boards (2020), which links to all state requirements and is updated regularly. Other resources are more helpful for general legal concepts such as The Counselor and the Law, by Wheeler and Bertram (2019), currently in its 8th edition. For more state-specific considerations, counselor educators will want to look for resources like Caldwell’s Basics of California Law for LMFTs, LPCCs, and LCSWs (2019).
Conclusion
The myriad of legal and ethical complications inherent in online counselor education is navigable. For all of the complications of online learning, the benefits can outweigh the disadvantages. The opportunity to learn across state and national borders, interface with colleagues across the country and around the world, and develop one’s identity and practice as a professional counselor or counselor educator within this space is replete with rewards for all parties. Realistically, education is moving more and more to this format, and for counselor education, it is simply a matter of being cognizant of the legal and ethical dilemmas in order to meet them head-on.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Allen, I. E., & Seaman, J., Poulin, R., & Straut, T. T. (2016). Online report card: Tracking online education in the United States. Babson Survey Research Group. Retrieved from https://onlinelearningsurvey.com/reports/onlinereportcard.pdf
American Counseling Association. (2014). ACA code of ethics.
American Counseling Association. (2015). State licensure boards that have adopted the ACA code of ethics. https://www.counseling.org/docs/default-source/licensure/state-licensure-boards-that-have-adopted-the-aca-code-of-ethics-(pdf).pdf?sfvrsn=9331cb46_2
American Counseling Association. (2016). Licensure requirements for professional counselors, a state by state report. https://www.counseling.org/knowledge-center/licensure-requirements
American Counseling Association. (2020). Licensure & certification: State professional counselor licensure boards. https://www.counseling.org/knowledge-center/licensure-requirements/state-professional-counselor-licensure-boards
Bell, J. (2013). The basis of vicarious liability. The Cambridge Law Journal, 72, 17–20. https://doi.org/10.1017/S0008197313000238
Caldwell, B. E. (2019). Basics of California law for LMFTs, LPCCs, and LCSWs (6th ed.). Ben Caldwell Labs.
Calley, N. G., & Hawley, L. D. (2008). The professional identity of counselor educators. Clinical Supervisor, 27, 3–16. https://doi.org/10.1080/07325220802221454
Council for the Accreditation of Counseling and Related Educational Programs. (2015). CACREP 2016 standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Council for the Accreditation of Counseling and Related Educational Programs. (2020). Find a program. https://www.cacrep.org/directory
CPH & Associates. (2019). What is professional liability insurance for mental health providers? https://www.cphins.com/what-is-professional-liability-insurance-for-mental-health-providers/
Dimeo, J. (2017). How colleges train instructors to teach online courses. Inside Higher Education. https://www.insidehighered.com/print/digital-learning/article/2017/10/11/how-colleges-train-instructors-teach-online-courses
Family Educational Rights and Privacy Act of 1974, 20 U.S.C. § 1232g. (1974). https://www.law.cornell.edu/uscode/text/20/1232g
The Health Insurance Portability and Accountability Act (HIPAA) of 1996. Pub. L. 104-191. Stat. 1936. (2004).
Holstun, V. (2018). Perceptions of feedback and the relationship with self-efficacy in residency counselor education settings [ProQuest Information & Learning]. In Dissertation Abstracts International: Section B: The Sciences and Engineering (Vol. 79, Issue 10–B(E)).
Jiang, R. (2019). Introducing new Alexa healthcare skills. https://developer.amazon.com/blogs/alexa/post/ff33dbc7-6cf5-4db8-b203-99144a251a21/introducing-new-alexa-healthcare-skills
Lee, K., & Bligh, B. (2019). Four narratives about online international students: A critical literature review. Distance Education, 40(2), 153–169. https://doi.org/10.1080/01587919.2019.1600363
Mikkelson, S., Moorhead, H. J. H., & Levitt, D. H. (2013). Counselor supervision. In D. H. Levitt & H. J. H. Moorhead (Eds.), Values and ethics in counseling: Real-life ethical decision making (pp. 169–173). Routledge/Taylor & Francis Group.
Mississippi Department of Child Protection Services. (2019). Report child abuse/neglect. https://www.mdcps.ms.gov/report-child-abuse-neglect/
Office for Civil Rights. (2016). Can a CSP be considered to be a “conduit” like the postal service, and, therefore, not a business associate that must comply with the HIPAA rules? U.S. Department of Health & Human Services. https://www.hhs.gov/hipaa/for-professionals/faq/2077/can-a-csp-be-considered-to-be-a-conduit-like-the-postal-service-and-therefore-not-a-business%20associate-that-must-comply-with-the-hipaa-rules/index.html#_edn1
Pearson, Q. M. (2000). Opportunities and challenges in the supervisory relationship: Implications for counselor supervision. Journal of Mental Health Counseling, 22(4), 283–294.
Phirangee, K., & Malec, A. (2017). Othering in online learning: An examination of social presence, identity, and sense of community. Distance Education, 38(2), 160–172. https://doi.org/10.1080/01587919.2017.1322457
Privacy Technical Assistance Center. (2014, February). Protecting student privacy while using online educational services: Requirements and best practices. https://studentprivacy.ed.gov/sites/def
ault/files/resource_document/file/Student%20Privacy%20and%20Online%20Educational%20Services%20%28February%202014%29_0.pdf
Privacy Technical Assistance Center. (2015, July). Frequently asked questions – Cloud computing. U.S. Department of Education. https://studentprivacy.ed.gov/sites/default/files/resource_document/file/FAQ_Cloud_Computing_0.pdf
Privacy Technical Assistance Center. (2016). Protecting student privacy while using online educational services: Model terms of service. U.S. Department of Education. https://studentprivacy.ed.gov/sites/default/files/resource_document/file/TOS_Guidance_Mar2016.pdf
Rousmaniere, T., Renfro-Michel, E., & Huggins, R. (2016). Regulatory and legal issues related to the use of technology in clinical supervision. In T. Rousmaniere & E. Renfro-Michel (Eds.), Using technology to enhance clinical supervision (pp. 19–30). American Counseling Association.
Sheperis, D. S., & Coker, J.K. (2020). Online counselor education: A student-faculty collaboration. The Professional Counselor, 10, 133–143. https://doi.org/10.15241/dss.10.1.133
Sheperis, D. S., Henning, S., & Kocet, M. (2016). Ethical decision making for the 21st century counselor. Thousand Oaks, CA: SAGE.
Slovenko, R. (1980). Legal issues in psychotherapy supervision. In A. K. Hess (Ed.), Psychotherapy supervision: Theory, research and practice (pp. 453–473). John Wiley & Sons.
Stanford University Teaching Commons. (n.d.). Fully online. https://teachingcommons.stanford.edu/gallery/fully-online
State of California. (2015). End of Life Options Act (California Health and Safety Code 442.5.). https://codes.findlaw.com/ca/health-and-safety-code/hsc-sect-442-5.html
State of Georgia. (2019). Rules and regulations of the state of Georgia. http://rules.sos.ga.gov/gac/135-5
State of Georgia. (2020). Code of Ethics of the State Board of Examiners of Psychologists Ch. 510-4-.02§ 4.05. http://rules.sos.ga.gov/search.aspx?sortby=&search=yes&searchWithin=&wc=
&query=Code%20of%20Ethics%20of%20the%20State%20Board%20of%20Examiners%20of%20Psychologists&fid=1&docId=9725&hierarchysearch=yes&searchvalue=Chapter%20510-4.%20CODE%20OF%20ETHICS&NextDoclimit=2&p=1
State of Pennsylvania. (n.d.). Pennsylvania Professional and Vocational Standards, 49 Pa. Code § 42.42. https://casetext.com/regulation/pennsylvania-code-rules-and-regulations/title-49-professional-and-vocational-standards/part-i-department-of-state/subpart-a-professional-and-occupational-affairs/chapter-42-state-board-of-occupational-therapy-education-and-
State of Texas. (2005). The Texas health and safety code. https://statutes.capitol.texas.gov/Docs/SDocs/HEALTHANDSAFETYCODE.pdf
Student Privacy Policy Office. (n.d.). FAQs on photos and videos under FERPA. U.S. Department of Education. https://studentprivacy.ed.gov/faq/faqs-photos-and-videos-under-ferpa
Tarasoff v. Board of Regents of the University of California, 13 Cal.3d 177, 529 P.2d 533 (1974), vacated, 17 Cal.3r 425, 551 P.2d 334 (1976).
Taylor, J. (2015, May 20). Is FaceTime HIPAA compliant? https://www.linkedin.com/pulse/facetime-hipaa-compliant-jon-taylor/
Texas State Board of Examiners of Professional Counselors. (2011). Texas Administrative Code Subchapter C. Code of ethics. www.dshs.texas.gov/counselor/CodeOfEthicsPDF.pdf
Texas State Board of Examiners of Professional Counselors. (2009). What to expect from your licensed professional counselor. www.dshs.state.tx.us/counselor/lpc_brochure.pdf
University of North Carolina System. (2017). State authorization. https://www.northcarolina.edu/stateauthorization
Vineyard, T. E. (2019). The use of an online readiness assessment to determine necessary skills, aptitude, and propensities for successful completion in a secondary online credit course [ProQuest Information & Learning]. In Dissertation Abstracts International Section A: Humanities and Social Sciences (Vol. 80, Issue 2–A(E)).
Walden University. (2019). Academic residencies: Mission and vision. https://academicguides.waldenu.edu/residencies/about
Ward v. Wilbanks. (2010). No. 09-CV-112 37, 2010 U.S. Dist. WL 3026428 (E.D. Michigan, July 26, 2010).
Wheeler, A. M., & Bertram, B. (2019). The counselor and the law: A guide to legal and ethical practice (8th ed). American Counseling Association.
Wong, J., Baars, M., Davis, D., Van Der Zee, T., Houben, G.-J., & Paas, F. (2019). Supporting self-regulated learning in online learning environments and MOOCs: A systematic review. International Journal of Human–Computer Interaction, 35, 356–373. https://doi.org/10.1080/10447318.2018.1543084
Donna S. Sheperis, PhD, NCC, CCMHC, ACS, LPC, is an associate professor at Palo Alto University. Ann Ordway, JD, PhD, NCC, is a core faculty member at the University of Phoenix. Margaret Lamar, PhD, LPC, is an assistant professor at Palo Alto University. Correspondence may be addressed to Donna Sheperis, 5151 El Camino Real, Los Altos, CA 94022, dsheperis@paloaltou.edu.
Mar 9, 2020 | Volume 10 - Issue 1
Szu-Yu Chen, Dareen Basma, Jennie Ju, Kok-Mun Ng
Distance counselor education has expanded educational opportunities for diverse groups of students. To effectively train and support global students in counseling programs, the authors explore some unique challenges and opportunities that counselor educators may encounter when integrating technology in the multicultural counseling curriculum. The authors discuss pedagogical strategies that can enhance distance learners’ multicultural and social justice counseling competencies. Through an intersectional, social construction pedagogy, counselor educators can decolonize traditional multicultural counseling curricula and foster an international distance learning environment. Additional innovative approaches and resources, such as online multiculturally oriented student services, online student-centered multiculturally based organizations and workshops, and office hours for mentoring online international students and supporting distance learners’ needs, are described.
Keywords: distance counselor education, multicultural, international, online education, social justice
The growth in distance learning has led to an integration of technology in the curriculum over the past two decades (Allen et al., 2016). Counselor educators now can deliver distance learning courses internationally via videoconference systems, such as two-way audio and video software programs, for students to attend classes either synchronously or asynchronously (Snow et al., 2018), and many programs are moving toward distance education (Benshoff & Gibbons, 2011; Reicherzer et al., 2009). This shift in educational platforms allows both domestic and international students to receive counselor education and training remotely without having to commute or leave their home countries. For example, the counselor education program at the institution of the first three authors currently has over 300 students from the five most populous continents in various stages of counselor preparation. Distance education has expanded educational opportunities, targeted underserved groups of students, and given space for the formation of a more globally diverse student body (Columbaro, 2009; Gillies, 2008).
With the dramatic increase of diversity and attention to racism and other forms of human oppression in the United States, by the early 2000s, the issues of multiculturalism and social justice had come to the center of the counseling profession (Arredondo, 1999) and were recognized as two sides of the same coin (Ratts, 2011). As a result, multicultural education in the profession has been aimed at enhancing students’ awareness of cultural diversity and social justice in counseling relationships and implementation of advocacy competencies as they grapple with power, privilege, and oppression at the individual and systemic levels (Ratts et al., 2015). More recently, the Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2015) has integrated a social justice and advocacy component into the framework of multicultural counseling competencies developed in 1992 by Sue, Arredondo, and McDavis, and highlighted the intersection of identities and the role power, privilege, and oppression play in the counseling relationship. The American Counseling Association (ACA; 2014) has also asserted that “counselor educators actively infuse multicultural/diversity competency in their training and supervision practices. They actively train students to gain awareness, knowledge, and skills in the competencies of multicultural practice” (F.11.c). Yet there seems to be a lack of attention in the literature to how online training programs can address global students’ multicultural and social justice counseling competencies given their non-traditional modes of learning delivery. With the emphasis on the helping relationship in the counseling profession, instructors who teach online face additional challenges because of a lack of in-person contact with students and may feel skeptical about the effectiveness of creating a safe and interactive space virtually, especially in relation to addressing challenging and complex topics (Hall et al., 2010).
It is worth noting that many counselor educators have not received formal pedagogical education and training on integrating technology into their curriculum and developing effective online courses (Cicco, 2012). This impacts educators’ feelings of discomfort or lack of preparedness when developing and delivering an online international multicultural counseling course, as well as facilitating discussions about multicultural issues and developing global students’ multicultural and social justice counseling training and competencies through an online medium. Consequently, when considering the development of an online multicultural counseling course, educators have to not only grapple with the complexity of designing a nuanced curriculum, but also negotiate delivery of a curriculum on an evolving learning platform in which international students who do not reside in the United States are integrated into the learning experience. As such, there are several opportunities and challenges to consider when facilitating multicultural and social justice counseling training on an online platform.
To effectively retain and support global students with diverse backgrounds and learning styles in distance counseling programs, herein we explore challenges and opportunities that counselor educators encounter when integrating technology in the multicultural and social justice counseling curriculum. Specifically, we want to discuss pedagogical strategies that we have found valuable to enhancing global learners’ multicultural and social justice counseling competencies. With the movement toward internationalizing the counseling profession, we believe that counselor educators can decolonize the traditional multicultural counseling curriculum and promote global students’ multicultural and social justice advocacy competencies through an intersectional and social construction online pedagogy and further cultivate an inclusive global learning environment. Additionally, we want to share innovative approaches counselor educators can use to support global students’ needs and enhance student retention in online counseling programs.
Internationalization of Multicultural Counseling Education in the Virtual Classroom
In international distance education, each student may differ in experiences of culture, cultural identities, and developmental level of multicultural counseling and social justice competencies. To address the increase in a globally diverse student body, the counseling profession is transforming from a Western-based to a global-based practice (Lorelle et al., 2012). Historically, textbooks and journal articles in the United States regarding diversity are typically monoculture in nature, focusing primarily on social identities such as race, ethnicity, gender, and social class that are commonly found in U.S.-based diversity discourse (Case, 2017). Students who live abroad may find these materials and foci disconnected from their contexts and not applicable to their practice. Consequently, these students can become less engaged in the learning experience.
The movement toward internationalizing the counseling profession over the past two decades has highlighted the need to extend multicultural competencies in ways that are relevant to mental health services beyond U.S. borders. Relatedly, Harley and Stansbury (2011) asserted that the multicultural movement needs to take place at two levels. On the first level, it requires our diligence to recognize, learn about, and appreciate the cultural diversity that exists on U.S. soil. The second level requires us to develop a global perspective that recognizes other cultures and sociopolitical forces that impact the lived experiences of people in other countries. Other scholars (e.g., Bhat & McMahon, 2016; Knight, 2004; Ng et al., 2012) also acknowledge these two dimensions in efforts to internationalize the counseling profession and emphasize the need to address the underdevelopment of cross-national multicultural competencies.
To date, systematic discourse related to international students’ learning experiences and perspectives in online training programs remains limited. To respond to this shift in distance counselor education, we propose adding a third dimension—the internationalization of counselor education—to the two levels of multicultural education proposed by Harley and Stansbury (2011). This third multicultural dimension requires a conceptualization of cultures and ways of being into a counseling curriculum that maintains a global and international perspective. Thus, learning is comprised of training activities and programs designed to prepare students to provide culturally responsive counseling services and advocacy that are simultaneously informed by both a local and global perspective.
Counselor educators are aware of the enormity of some of the challenges associated with the movement toward internationalizing counselor education. There have been encouraging but limited developments by the National Board for Certified Counselors (NBCC), ACA, and the Association for Counselor Education and Supervision (ACES) toward this cause. For example, to advance global mental health training and services, NBCC trains and collaborates with international counseling organizations to promote counselor professionalism as they develop their training requirements to the needs of their specific populations. ACA and ACES offer international counseling students and faculty interest networks in which counselors and counselor educators have space to facilitate discussions about challenges and solutions when providing global counseling services and preparing culturally responsive training curricula for students. However, the effect of these advocacies on internationalizing counselor education has not been widely evaluated yet. It appears that the counseling profession recognizes the benefits of this endeavor but is sorting out opportunities as well as resources necessary for implementation. We view contributing to the dialogue on internationalizing multicultural counseling training through an intersectional and social construction online pedagogy as a privilege.
Intersectional and Social Construction Online Pedagogy
An area of dissonance for international counseling students involves differences in cultural worldview. Marsella and Pederson (2004) posited that “Western psychology is rooted in an ideology of individualism, rationality, and empiricism that has little resonance in many of the more than 5,000 cultures found in today’s world” (p. 414). Ng and Smith’s study (2009) highlighted that international students, particularly those from non-Western nations, may struggle with integrating Eurocentric theories and concepts into the world they know. Their findings indicated that international trainees tend to experience more difficulties in areas related to clinical training and worldview conflicts in understanding mental health treatment compared to their domestic peers. International students can find that materials learned in Western-based counselor education have little relevance and applicability to the local demographics in which they work (Ng et al., 2012).
Ng and colleagues (2012) indicated that the goals of internationalizing counseling preparation curricula are to better equip students with required knowledge, awareness, skills, beliefs, and attitudes and to train students to become social change agents who actively resolve global mental health issues and inequalities. Herein lies the opportunity for counselor educators to intentionally search for appropriate pedagogies and to critically present readings and other media that help inculcate a multicultural perspective (Goodman et al., 2015) that is relevant to local contexts while appreciating a global perspective of lived experience and civilization. Social constructionism demands that we take a critical stance toward ways of understanding the world (Burr, 2015). It emphasizes the need to acknowledge the context and extent of subjectivity infused into what we know and invites us to critically examine the knowledge we have gained based on the culture and society surrounding the time period in which we exist. This lens helps us recognize that our knowledge is rooted in historical and cultural relativity and is socially created (Young & Collin, 2004). We need to be mindful that the knowledge created in the classroom has a social, cultural, and political impact on society. Thus, to internationalize distance counselor education, we consider it crucial for academics to recognize the social construction of the knowledge they carry and communicate in the virtual classroom setting, including the construction of their teaching methods for delivering knowledge (hooks, 1994).
Over 30 years ago, Crenshaw (1989) and hooks (1984) postulated that individuals hold a set of multiple and simultaneous identities. Crenshaw introduced the term intersectionality to describe individuals’ complex identities as opposed to categorical generalizations. Traditionally, multicultural courses tend to focus on one aspect of social identity and related oppressions separately from other social identities. The intersecting complexities among social identities and structural oppressions and privileges are often neglected. Collins (2000) provided a pedagogic conceptual framework to include both advantaged and disadvantaged identities. Although the intersectionality theory has been integrated within multiple disciplines, such as women’s studies, sociology, psychology, and law, instructors often do not incorporate intersectionality into diversity courses (Dill, 2009). Scholars, therefore, have called for an intersectional approach to transform higher education (Berger & Guidroz, 2009) and move beyond single-axis models.
To move beyond the individual and monocultural level, Case (2017) proposed that educators and students can address issues of culture, diversity, and advocacy in a diverse classroom through an intersectional pedagogy. Case emphasized an effective intersectional pedagogy that includes the following main tenets: Instructors (a) conceptualize intersectionality as a complex analysis of privileged and oppressed social identities; (b) teach intersectionality across a wide range of institutional oppression; (c) aim to explore invisible intersections; (d) include aspects of privilege and analyze power when teaching about intersectionality theory; (e) encourage students reflection about their own intersecting identities; (f) reflect the impact of educators’ social identities, biases, and assumptions on the learning community; (g) promote social action; (h) value the voice of marginalized students; and (i) infuse intersectional studies across the curriculum.
We believe that using an intersectional perspective that couples with a social construction perspective in multicultural education curriculum development can be valuable in the context of distance international counselor education, particularly in multicultural and international online education that contains a globally diverse student body. By implementing an intersectional and social construction pedagogical design in multicultural and social justice online counseling courses, instructors focus on examinations of social locations concerning privilege and oppression (Cole, 2009) and avoid overemphasizing any single characteristic of individual identities (Dill & Zambrana, 2009). This approach also provides instructors and worldwide students with a critical framework for analyzing structural power and oppression, examining the complexity of identities, and discussing action plans for empowerment and advocacy (Dill & Zambrana, 2009; Rios et al., 2017). Chan et al. (2018) also supported embodying an intersectional framework in developing multicultural and social justice courses within the counselor education curriculum. Counselor educators who teach beyond multicultural counseling knowledge and skills can enhance students’ critical thinking, case conceptualization skills (Chan et al., 2018), and cultural empathy (Davis, 2014) toward marginalized groups. Moreover, students are likely to see beyond the prescriptive counseling approach that addresses a limited set of cultural values (Chan et al., 2018). This perspective also can engage students in analyzing issues of privilege, power, and global oppression, and systematically reflecting on their own experiences.
Wise and Case (2013) noted that intersectional pedagogy is an inclusive approach that helps students reduce resistance when engaging in examining privileged and oppressed identities. This approach validates worldwide students’ various experiences and includes exploration of invisible interactions when discussing personal privilege. Considering that issues related to multiculturalism can evoke various emotions in the classroom, such as frustration, shame, guilt, and defensiveness, intersectional pedagogy provides an outlet to engage all students in this learning process (Banks et al., 2013; Wise & Case, 2013). Creating a safe space for learners in virtual classrooms to bravely experience and address these challenges requires thoughtful learning strategies. Accordingly, we illustrate intersectional and social construction pedagogy and strategies that counselor educators can consider integrating into online curricula to facilitate and assess global students’ multicultural and social justice counseling competencies, as well as provide supports for students in a diverse online learning environment.
Internationalizing an Online Multicultural Counseling Course
The master’s counseling program at the first three authors’ institution offers online or residential format options. The online counseling program provides domestic students and international students who live abroad opportunities to receive counselor education and training. Given the high ratio of international students and students with diverse backgrounds at the authors’ institutions, we believe that structuring the virtual multicultural counseling course from a global perspective and grounding it in a socially constructed, intersectional framework can facilitate student understanding and appreciation of multiculturalism, diversity, and social justice. Additionally, a successful integration of technology entails careful consideration of course content, the instructor’s role in the teaching and learning process, and students’ access to and comfort with the technology (Zhu et al., 2011). The following is an example of how an online master’s-level multicultural counseling course is delivered through an intersectional and social construction pedagogy that includes an international perspective, and how global students’ multicultural and social justice counseling competencies are assessed.
Our online multicultural counseling course focuses on creating a critical space where students can actively and transparently deconstruct their socially constructed knowledge, beliefs, and biases about differences and others. Rather than focusing on attending to specific cultural groups, which historically has been the norm for multicultural counseling classes, we focus on internationalizing the counseling profession and emphasize the need to address cross-national multicultural competencies. This course aims to develop students’ consciousness about the system of oppression that significantly impacts both dominant and marginalized groups’ well-being. Thus, the intersectional and MSJCC frameworks are used to structure our online multicultural counseling course in that knowledge, awareness, skills, and advocacy are at the core of each of the assignments, readings, and synchronized and asynchronized discussions.
Readings assigned for the class include both a clinical counseling textbook that attends to assessment, counseling, and diagnosis from a multicultural lens, and supplementary readings from the fields of multicultural and social justice education. Instructors use a learning management system to facilitate asynchronized online discussion board activities and readings and provide written, audio, or video feedback on students’ assignments. In addition to asynchronized learning, instructors and students meet in an interactive synchronized virtual classroom weekly for 1.5 hours over an 11-week course. Research shows that online models can be effective, with synchronous online programs being the most promising (Siemens et al., 2015). Students also have opportunities to do live multicultural role-plays in which instructors provide immediate feedback.
Instructors can face unique challenges in teaching and discussing some sensitive and controversial issues with students, which is an inherent part of multicultural and social justice advocacy training. It is recommended that educators foster positive relationships with students and establish a safe and trusting learning environment to engage students in constructive conversations and self-reflection (Brooks et al., 2017). Yet teaching a multicultural counseling class in a virtual setting can add additional barriers to fostering a safe learning environment. For example, in a virtual classroom, instructors are only able to see a student’s face amidst many other digital faces. As a result, some of the challenges of teaching this course virtually include effectively noting students’ nonverbal communications, sensing their emotive responses or reactions to the discussion content, and attending to topics that students may be having a difficult time speaking about in front of a large group. Moreover, many videoconferencing platforms allow students to engage in both private and public conversations with other students via chat boxes. Consequently, establishing virtual classroom ground rules is essential. Examples of ground rules and strategies that ensure a safe and respectful online learning environment may include: (a) turning on the camera to allow instructors and classmates to observe others’ nonverbal communication and address immediacy, (b) using headphones to respect classmates’ sharing, (c) turning off the private chat setting to avoid side conversations among students, and (d) providing options for students to share their thoughts and feelings in the chat box. It also is important to facilitate a discussion with students about ways to share their airtime with classmates in a virtual classroom and provide their classmates with understanding and support by observing virtual verbal and nonverbal communication.
To assess global students’ cross-national multicultural and social justice counseling competencies, we developed three major assignments and assessments for this class. Virtual classroom discussion is an essential assessment. To socially construct students’ knowledge of power, privilege, and oppression and reflect students’ learning experience, students are encouraged to actively share their reactions to the learning materials and how these materials are related to personal experience and counseling implications in their countries. Students’ level of participation and self- and other-awareness can be assessed in breakout rooms as well as in a large discussion group. However, considering students may have various ways to engage with the materials, instructors encourage students who struggle with verbally participating in the virtual classroom to collaboratively identify alternative concrete methods to evidence participation with instructors, such as reflective journals.
The second assignment is a group presentation that attends to manifestations of oppression within systems. The purpose of this assignment is to increase global students’ knowledge and understanding of how racism and oppression are produced and reproduced across generations, institutions, and countries. Although oppression impacts all institutions, this project encourages student groups to focus on dynamics in eight mutually reinforcing areas: housing, education, immigration, the labor market, the criminal justice system, the media, politics, and health care. Students are also asked to create a vignette based on the presented topic and facilitate role-plays. This experiential activity facilitates students’ understanding of intersecting identities in the counseling relationship and enhances cross-national cultural empathy by attending to clients’ experience. This assignment increases global students’ awareness of the complexity of mental health issues and transgenerational trauma that can ensue as a result of systematic oppression. It also challenges unconscious biases and beliefs that students may have around marginalized populations being impacted by these systems in their countries.
The last major assignment, the resistance project, is a quarter-long individual project and targets an increase in awareness of self. For counselors, awareness of self in the context of culture is one of the more challenging parts of our work and is a process that is ongoing and constant. This assignment focuses on attending to both conscious and unconscious biases to groups of people. Initially, students are asked to identify three specific cultural groups to which they identify resistance in their countries. Students can express significant struggles around this part of the assignment indicating feelings of guilt, shame, judgment of self, denial of bias, and confusion around their biases. Normalizing and validating these feelings is crucial in fostering a space for critical reflection, as well as providing non-judgmental feedback regarding their initial explorations. The next part of our resistance project asks students to select one of the three identified groups to explore in greater detail throughout the quarter. Students are asked to begin looking for numerous academic sources, social media sources, and immersion experiences that they can engage in throughout the quarter that would encourage them to very directly examine their biases. Significant levels of discomfort appear here among students, particularly regarding individual and group experiences they have engaged in. Students are asked to reflect on and lean into that discomfort in order to better understand it. In addition, they are asked to critically examine their internal process and connect their reactions back to their identified resistance.
Supporting Globally Diverse Students Outside of the Virtual Classroom
As counselor education focuses on further developing multicultural online pedagogy, there is a need to evaluate programmatic effectiveness in demonstrating sensitivity to the concerns of globally diverse student populations. Just as it is critical for instructors to attend to creating culturally relevant curricula, program administrators need an understanding of the challenges that characterize distance students from global communities and be intentional about addressing some of those challenges. This section discusses ways that institutions can walk the walk in their application of the principles espoused in curricular pedagogy by creating an environment in which worldwide students feel welcomed and supported.
According to the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2016), approximately 32% of students enrolled in counseling programs are from racially diverse heritages. Kung (2017) reported that “in the 2015–2016 academic year, over 1 million international students were reported as studying at U.S. colleges and universities” (p. 479). Currently, there are no official statistics on the number of students enrolled in distance counselor education programs by race, ethnicity, or country of residence. Although specific data is lacking, the statistics above provide an indication of the potentially significant presence of an international student population in distance learning programs. It is critical to examine the criteria for determining a university’s effectiveness in supporting worldwide students outside the virtual classroom. “Exemplary institutions” in recruiting and retaining minority students of color have the characteristic of being successful in increasing enrollment of minority students of color and retaining students through to graduation (Rogers & Molina, 2006). While an institution’s effectiveness in providing needed support does not necessarily equate to its ability to retain students and achieve high graduation rates, one can surmise that some unsupported individuals will choose to drop out. Although there are numerous ways that an institution can provide a sustainable environment for global students outside of the virtual classroom, we will focus on six key approaches, namely technology, field experience, multiculturally oriented student support services, mentorship, student-centered multiculturally based organizations, and multiculturally based events and workshops.
Technology
In an online education format, access to reliable technology is imperative to students’ success in the program. Level of access to proper computing devices or to the internet by various social identity groups can create a digital divide, which disadvantages one group over another (Bolt & Crawford, 2000; Clark & Gorski, 2001). International students from developing and underdeveloped nations experience frequent disruption when accessing virtual class meetings and course contents because of political causes or technological deficiency in their regions. For example, a student from the Central African Republic is sometimes unable to log in to class meetings when she is unable to turn on generators in a remote village for fear that this could alert guerilla gangs and prompt additional warfare. A student in Peru who does her internship in rural areas is unable to submit her assignments on time because of a lack of internet access. Students in Beijing experience tight internet firewalls preventing them from accessing sites such as Google, Gmail, and YouTube; this problem intensifies during the week of the governmental National People’s Congress annual meetings. Therefore, Clark and Gorski (2001) urged educators to critically analyze the use of the internet as an educational medium and examine ways technology “serves to further identify social, cultural, educational ‘haves’ and ‘have-nots’” in educational settings (p. 39).
As a partial solution to the problem of Chinese students’ difficulty in accessing web-based course content, our institution has purchased a VPN with a reliable server based in Hong Kong. Given that there are approximately 30-plus China-based students in matriculation at our institution each year, this becomes an institutional business decision. Additionally, academic advisors encourage Chinese students to approach their instructors at the beginning of each term to discuss a plan for accessing course material and timely submission of assignments. Instructors and administrators also have a responsibility to be proactive in collaborating with these students in finding alternatives by inquiring and learning about students’ potential challenges regarding technology. Educators need to discuss a plan to accommodate students’ needs within reason.
Field Experience
Issues with cultural worldviews and contextual differences become prominent during students’ process of searching for practicum opportunities and experiences of participating in clinical training in their home countries. Specifically, students and educators have encountered these obstacles in three aspects. First, the philosophical understanding of the purpose of internship and supervision of interns are different. Next, the integration of Eurocentric theories and implications with their clients’ cases might not be applicable. Last, there is a lack of regulatory infrastructure to guide and oversee the helping profession. A case example is students in China, where many native organizations expect to benefit financially from placement of interns. They do not seem to consider that student interns are capable of counseling clients under proper supervision. Thus, many mental health agencies do not permit trainees to provide counseling before graduation. Supervision is considered more of a business arrangement than a supervisory and mentoring relationship.
The first three authors’ institution offers an online practicum course each academic term for students residing and doing an internship overseas. This strategy aims to provide a weekly forum where students receive additional support in applying counseling concepts and approaches to their cultural context. This also serves as a supportive distance environment in which instructors and students collaboratively conceptualize and explore treatment approaches that are culturally and contextually relevant to their client populations. The second purpose for the dedicated practicum course is to navigate students’ dual legal and ethical milieus. A lack of regulatory oversight for the counseling profession in China and other countries has created legal and ethical challenges for intern placements. This reality has added confusion and inconsistencies in what is permissible based on U.S. regulatory and accreditation boards, as well as common practices in students’ home countries.
Multiculturally Oriented Student Support Services
Student services offices in institutions generally provide a wide range of services. To meet distance learners’ needs, it is necessary to implement some student services via an online format. First, institutions provide tutoring services to help improve the English writing skills of speakers of other languages. Students from immigrant and refugee communities as well as some international students fall into this category. Students from non–English-speaking countries enrolled in counseling and related disciplines tend to experience challenges related to English proficiency (Ng, 2006). As such, one-on-one tutoring is available at our institution for students who struggle with editing and American Psychological Association (APA) style writing. This service is critical because many foreign countries do not utilize APA format, and therefore international students do not have familiarity with this style of writing.
Second, tutors at the first three authors’ institution are doctoral students from the psychology department who have opportunities to provide services for students from marginalized communities. Through collaboration between the office of student services and the counseling department, this strategy serves as an excellent service learning experience in working with individuals from globally diverse communities. With an intentional design, the writing skills tutoring service complements classroom pedagogy on multiculturalism by presenting experience with real-world problems, providing opportunities for students to grapple with their beliefs and biases and involve action-oriented solutions.
Mentorship
Mentorship is a substantive resource for supporting worldwide students from diverse communities. Rogers and Molina’s (2006) study found that nine of the 11 psychology programs and departments that were successful at recruiting and retaining students of color had established mentoring programs. In general, ethnic minority students tend to prefer and report more satisfaction with mentors who share a similar racial background (Chan et al., 2015). Figueroa and Rodriguez (2015) posited that mentoring is social justice work that “is a racially and culturally mediated experience instead of a race-neutral, objective interaction” (p. 23). It is an unfortunate reality of counselor education that there exists a significant underrepresentation of minority faculty. The disparity is prominent among Hispanic/Latinx demographics, where student enrollment (8.5%) is almost double the number of faculty (4.7%) from Hispanic/Latinx heritage among CACREP-accredited programs (CACREP, 2016). Black student enrollment is 18.3% and only 12.7% of the total faculty members in CACREP-accredited programs are Black. Chan and colleagues (2015) suggested that in the absence of same-race mentors, the presence of cross-cultural support in the form of multiculturally sensitive mentoring can be beneficial and even critical to the success of international students from diverse ethnic backgrounds.
To support the unique needs of international students in the residential and online cohort, the first author designed weekly office hours for online international students to provide advising and mentorship. The virtual office hours aim to provide a space where students and their peers can not only share challenges, struggles, and concerns about their learning experiences in the program, but also support each other. Additionally, the third author and a colleague have served as international and distance directors of clinical training, which can provide specific mentorship regarding practicum experiences for international students.
Student-Centered Multiculturally Based Organizations
The presence of student-centered organizations is another effective way to provide a sense of belonging and an environment that facilitates peer support among those with shared interests on campus (Rogers & Molina, 2006). Some culturally and social justice–based organizations active at the first three authors’ institution serve this purpose well. One of the university-wide organizations, Diaspora, serves students, staff, and faculty in the community who are interested in learning about and advocating for mental health issues relevant to the Black diaspora. Members of Diaspora aim to raise the community’s awareness of psychosocial and environmental factors that impact the Black community’s well-being. Another organization at our institution, the Latinx Task Force, was formed with a Unity grant award from our university president’s office for faculty, students, and staff to join forces across programs to implement projects that serve the Latinx/Hispanic community on and off campus (Latinx Task Force, n.d.). Furthermore, the Latinx Task Force initiated a Spanish clinician course that introduces students to essential clinical vocabulary, clinical skills, and cultural considerations required to work with Spanish-speaking clients. The Latinx Task Force also conducts a mentorship series that brings Latinx professionals in the field to offer career mentoring support to students.
Multiculturally Based Events and Workshops
Delivery of multicultural education and inclusion of diverse students should not be limited to the virtual classroom. Institutions can be intentional in hosting events and workshops that complement and reinforce classroom pedagogy on multiculturalism while actively supporting individuals from various communities. In recent years, the first three authors’ institution has hosted a rich array of workshops with topics such as “LGBT Psychology,” “Asian Americans and Suicide,” and “Risk and Resiliency Among Newcomer Immigrant Adolescents.” In addition, a “Women of Color Leaders in Psychology” event celebrates the contributions of women of color in psychology and social justice. When the workshops occur in our physical venue, they are often made accessible via videoconferencing platforms and are recorded for later viewing at a convenient time or by those in a different time zone.
Multicultural counseling education and support of the globally diverse student population are ongoing, interrelated endeavors that extend beyond the virtual classroom walls. Intentionality in hosting extracurricular events and creating a supportive environment are ways an institution makes multicultural pedagogical concepts come alive for students. They also are a way of sustaining worldwide students to graduate with a strong foundation from which to launch their counseling careers.
Discussion and Future Direction for Research
The multicultural counseling course in counselor education programs is one of the critical spaces where global students actively engage with the core components of the MSJCC. Given the complexity of teaching this course in a distance learning format, it is crucial for educators to thoroughly think through the varying foundational components, including structure, content, pedagogy, and the various challenges that can arise in virtual classrooms.
We have used our experiences in integrating technology into the multicultural counseling curriculum to discuss online pedagogical framework and virtual course development while exploring unique opportunities, challenges, and solutions. Given the movement of internationalizing the counseling profession, we postulate that multicultural counseling distance education must extend beyond U.S. borders, class meetings, and the curriculum. It is critical that counselor educators provide multicultural and social justice counseling training through systemic modeling by internationalizing the curriculum and training environment and collaborating with training programs and institutions to advocate for, attend to, and support the needs of globally diverse students in distance education.
Currently, the literature on training and online delivery of international multicultural counseling education remains limited. To explore the best online pedagogy for internationalizing multicultural counseling education, more research is needed. As such, future research could focus on examining the outcome of incorporating intersectional and social construction approaches in online counseling curricula, including global students’ multicultural and social justice counseling competencies in their home countries. Future studies also might investigate different course structures and online pedagogy to understand the best methods for multicultural distance counselor education. There is a need to explore counselor educators’ experiences of conducting online multicultural counseling education with globally diverse student populations and their perspectives on receiving multicultural counseling distance education. Supports needed for global students in the online environment may differ from traditional students. Therefore, research on how the academic support of counseling programs and institutions impacts global students’ counseling practice and retention in distance counselor education can be valuable.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Allen, I. E., Seaman, J., Poulin, R., & Straut, T. T. (2016). Online report card: Tracking online education in the United
States. https://onlinelearningsurvey.com/reports/onlinereportcard.pdf
American Counseling Association. (2014). 2014 ACA code of ethics.
Arredondo, P. (1999). Multicultural counseling competencies as tools to address oppression and racism. Journal of
Counseling & Development, 77, 102–108. https://doi.org/10.1002/j.1556-6676.1999.tb02427.x
Banks, C. A., Pliner, S. M., & Hopkins, M. B. (2013). Intersectionality and paradigms of privilege: Teaching for social
change. In K. A. Case (Ed.), Deconstructing privilege: Teaching and learning as allies in the classroom (pp. 102–
114). Routledge.
Berger, M. T., & Guidroz, K. (Eds.). (2009). The intersectional approach: Transforming the academy through race, class,
and gender. University of North Carolina Press.
Benshoff, J. M., & Gibbons, M. M. (2011). Bringing life to e-learning: Incorporating a synchronous approach to online teaching in counselor education. The Professional Counselor, 1, 21–28. https://doi.org/10.15241/jmb.1.1.21
Bhat, C. S., & McMahon, M. (2016). Internationalization at home for counseling students: Utilizing technology to expand
global and multicultural horizons. International Journal for the Advancement of Counselling, 38, 319–329.
https://doi.org/10.1007/s10447-016-9274-7
Bolt, D. B., & Crawford, R. A. K. (2000). Digital divide: Computers and our children’s future. Bantam.
Brooks, M., Alston, G. D., Townsend, C. B., & Bryan, M. (2017). Creating a healthy classroom environment in
multicultural counseling courses. Journal of Human Services: Training, Research, and Practice, 2, 1–24.
Burr, V. (2015). Social constructionism. In J. Wright (Ed.), International encyclopedia of the social & behavioral sciences (2nd ed., pp. 222–227). Elsevier. https://doi.org/10.1016/B978-0-08-097086-8.24049-X
Case, K. A. (2017). Toward an intersectional pedagogy model: Engaged learning for social justice. In K. A. Case (Ed.), Intersectional pedagogy: Complicating identity and social justice (pp. 1–24). Routledge.
Chan, A. W., Yeh, C. J., & Krumboltz, J. D. (2015). Mentoring ethnic minority counseling and clinical psychology students: A multicultural, ecological, and relational model. Journal of Counseling Psychology, 62, 592–607. https://doi.org/10.1037/cou0000079
Chan, C. D., Cor, D. N., & Band, M. P. (2018). Privilege and oppression in counselor education: An intersectionality framework. Journal of Multicultural Counseling and Development, 46, 58–73. https://doi.org/10.1002/jmcd.12092
Cicco, G. (2012). Counseling instruction in the online classroom: A survey of student and faculty perceptions. i- manager’s Journal on School Educational Technology, 8(2), 1–10. https://doi.org/10.26634/jsch.8.2.2022
Clark, C., & Gorski, P. (2001). Multicultural education and the digital divide: Focus on race, language, socioeconomic class, sex, and disability. Multicultural Perspectives, 3(3), 39–44. https://doi.org/10.1207/S15327892MCP0303_7
Cole, E. R. (2009). Intersectionality and research in psychology. American Psychologist, 64, 170–180. http://doi.org/10.1037/a0014564
Collins, P. H. (2000). Black feminist thought: Knowledge, consciousness, and the politics of empowerment (1st ed.).
Routledge.
Columbaro, N. L. (2009). E-mentoring possibilities for online doctoral students: A literature review. Adult Learning, 20(3–4), 9–15. https://doi.org/10.1177/104515950902000305
Council for Accreditation of Counseling and Related Educational Programs. (2016). CACREP annual report 2015. http://www.cacrep.org/wp-content/uploads/2019/05/CACREP-2015-Annual-Report.pdf
Crenshaw, K. W. (1989). Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics. University of Chicago Legal Forum, 1989, 139–168. https://chicagounbound.uchicago.edu/cgi/viewcontent.cgi?article=1052&context=uclf
Davis, D. N. (2014). Complexity overlooked: Enhancing cultural competency in the White lesbian counseling trainee through education and supervision. Journal of Lesbian Studies, 18, 192–201. https://doi.org/10.1080/10894160.2014.849166
Dill, B. T. (2009). Intersections, identities, and inequalities in higher education. In B. T. Dill & R. E. Zambrana (Eds.), Emerging intersections: Race, class, and gender in theory, policy, and practice (pp. 229–252). Rutgers University Press.
Dill, B. T., & Zambrana, R. E. (2009). Critical thinking about inequality: An emerging lens. In B. T. Dill & R. E. Zambrana (Eds.), Emerging intersections: Race, class, and gender in theory, policy, and practice (pp. 1–21). Rutgers University Press.
Figueroa, J. L., & Rodriguez, G. M. (2015). Critical mentoring practices to support diverse students in higher education: Chicana/Latina faculty perspectives. New Directions for Higher Education, 171, 23–33. https://doi.org/10.1002/he.20139
Gillies, D. (2008). Student perspectives on videoconferencing in teacher education at a distance. Distance Education, 29, 107–118. https://doi.org/10.1080/01587910802004878
Goodman R. D., Williams, J. M., Chung, R. C.-Y., Talleyrand, R. M., Douglass, A. M., McMahon, H. G., & Bemak, F. (2015). Decolonizing traditional pedagogies and practices in counseling and psychology education: A move towards social justice and action. In R. D. Goodman & P. C. Gorski (Eds.), Decolonizing “multicultural” counseling through social justice (pp. 147–164). Springer.
Hall, B. S., Nielsen, R. C., Nelson, J. R., & Buchholz, C. E. (2010). A humanistic framework for distance education. Journal of Humanistic Counseling, Education and Development, 49, 45–57. https://doi.org/10.1002/j.2161-1939.2010.tb00086.x
Harley, D. A., & Stansbury, K. L. (2011). Diversity counseling with African Americans. In E. Mpofu (Ed.), Counseling people of African ancestry (pp. 193–208). Cambridge University Press.
hooks, b. (1984). Feminist theory: From margin to center. South End Press.
hooks, b. (1994). Teaching to transgress: Education as the practice of freedom. Routledge.
Knight, J. (2004). Internationalization remodeled: Definition, approaches, and rationales. Journal of Studies in International Education, 8, 5–31. https://doi.org/10.1177/1028315303260832
Kung, M. (2017). Methods and strategies for working with international students learning online in the U.S. TechTrends: Linking Research and Practice to Improve Learning, 61, 479–485.
Latinx Task Force. (n.d.). Welcome to Palo Alto University Latinx task force. https://www.ltf.paloaltou.edu
Lorelle, S., Byrd, R. J., & Crockett, S. (2012). Globalization and counseling: Professional issues for counselors. The Professional Counselor, 2, 115–123. https://doi.org/10.15241/sll.2.2.115
Marsella, A. J., & Pedersen, P. (2004). Internationalizing the counseling psychology curriculum: Toward new values, competencies, and directions. Counselling Psychology Quarterly, 17, 413–423. https://doi.org/10.1080.09515070412331331246
Ng, K.-M. (2006). Counselor educators’ perceptions of and experiences with international students. International Journal for the Advancement of Counselling, 28, 1–19. https://doi.org/10.1007/s10447-005-8492-1
Ng, K.-M., Choudhuri, D. D., Noonan, B. M., & Ceballos, P. (2012). An internationalization competency checklist for American counseling training programs. International Journal for the Advancement of Counselling, 34, 19–38. https://doi.org/10.1007/s10447-011-9141-5
Ng, K.-M., & Smith, S. D. (2009). Perceptions and experiences of international trainees in counseling and related programs. International Journal for the Advancement of Counselling, 31, 57–70.
https://doi.org/10.1007/s10447-008-9068-7
Ratts, M. J. (2011). Multiculturalism and social justice: Two sides of the same coin. Journal of Multicultural Counseling and Development, 39, 24–37. https://doi.org/10.1002/j.2161-1912.2011.tb00137.x
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf?sfvrsn=20
Reicherzer, S., Dixon-Saxon, S., & Trippany, R. (2009). Quality counselor training in a distance environment. Counseling Today, 51(12), 46–47.
Rios, D., Bowling, M., & Harris, J. (2017). Decentering student “uniqueness” in lessons about intersectionality. In K. A. Case (Ed.), Intersectionality pedagogy: Complicating identity and social justice (pp. 194–213). Routledge.
Rogers, M. R., & Molina, L. E. (2006). Exemplary efforts in psychology to recruit and retain graduate students of color. American Psychologist, 61, 143–156.https://doi.org/10.1037/0003-066X.61.2.143
Siemens, G., Gašević, D., & Dawson, S. (2015). Preparing for the digital university: A review of the history and current state of distance, blended, and online learning. Massive Open Online Course Research Initiative.
Snow, W. H., Lamar, M. R., Hinkle, J. S., & Speciale, M. (2018). Current practices in online counselor education. The Professional Counselor, 8, 131–145. https://doi.org/10.15241/whs.8.2.131
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Multicultural Counseling and Development, 20(2), 64–88. https://doi.org/10.1002/j.2161-1912.1992.tb00563.x
Wise, T., Case, K. A. (2013). Pedagogy for the privileged: Addressing inequality and injustice without shame or blame. In K. A. Case (Ed.), Deconstructing privilege: Teaching and learning as allies in the classroom (pp. 17–33). Routledge.
Young, R., & Collin, A. (2004). Introduction: Constructivism and social constructionism in the career field. Journal of Vocational Behavior, 64, 373–388. https://doi.org/10.1016/j.jvb.2003.12.005
Zhu, E., Kaplan, M., & Dershimer, C. (2011). Engaging faculty in effective use of instructional technology. In C. E. Cook
& M. Kaplan (Eds.), Advancing the culture of teaching on campus: How a teaching center can make a difference (pp. 151–166). Stylus Publishing.
Szu-Yu Chen, PhD, NCC, LPC, RPT, is an assistant professor at Palo Alto University. Dareen Basma, PhD, LPC-MHSP, is a core faculty member at Palo Alto University. Jennie Ju, PhD, LPC, is a core faculty member at Palo Alto University. Kok-Mun Ng, PhD, NCC, ACS, LPC, is a professor at Oregon State University. Correspondence can be mailed to Szu-Yu Chen, 1791 Arastradero Drive, Palo Alto, CA 94304, dchen@paloaltou.edu.
Mar 9, 2020 | Volume 10 - Issue 1
Donna S. Sheperis, J. Kelly Coker, Elizabeth Haag, Fatma Salem-Pease
Online counselor education has been studied extensively since its inception, but the experiences of students within these programs have received limited attention. This collaborative view from faculty and students of online counselor education was developed to share the stories of students who have engaged in both synchronous and asynchronous distance counselor education programs at the master’s and doctoral level. Students talked about finding online programs to be viable options to work flexibly within their adult lives. In addition, they shared that they were more satisfied when there were efforts to foster connection through synchronous or other means found in a community of inquiry. Finally, their reports illuminate potential directions for research in exploring the experience of students in online counselor education programs.
Keywords: online programs, counselor education, synchronous, community of inquiry, students
Online counselor education has been a reality since the late 1990s, yet little is known about the training experiences of students in these programs. At the time of this writing, there are approximately 79 master’s and doctoral online counseling programs accredited by the Council for the Accreditation of Counseling and Related Educational Programs (CACREP; n.d.) and several other distance counseling programs without CACREP accreditation. Potential students have many options to consider in the online counselor education environment, and distance programs continue to strive to differentiate themselves from an ever-growing landscape of educational offerings. What is it that students and recent graduates of different online programs reported were the experiences that fostered their growth as professional counselors and counselor educators? Who supported them and their growth (e.g., peers, faculty, supervisors)? How did they stay engaged, motivated, and focused on their goals in a distance environment?
The aim of this article was to explore these questions with students and graduates of distance counseling and counselor education programs. Current students and recent graduates of distance counseling and counselor education programs were invited to bring voice to their experiences through informal interviews and this collaborative account. Program faculty contacted the students and graduates who volunteered to share their perspectives about the programs and agreed to have their responses used in this article. Two of the students who provided their opinion also served as coauthors. This effort was not designed to create generalizable or transferable knowledge; thus, there was no formal sampling strategy in place. It should also be noted that because the goal was not to generate generalizable or transferable knowledge, these interviews did not fall under the purview of IRB review. Thus, student responses are not anonymized and are cited as personal communications, with the students’ permission.
To gather a broad range of information, we reached out to students from programs with a variety of characteristics, including both CACREP- and non–CACREP-accredited counselor education programs; private for-profit and private nonprofit programs; faith-based and secular programs; and programs employing a continuum of distance delivery methods ranging from asynchronous, to hybrid, to synchronous. However, the information provided is not exhaustive in terms of the types of programs available. Instead, we were interested in the views of students across diverse online counselor education programs. Throughout the article, we include direct quotes from students as well as references from the literature that relate to those experiences.
For our small group of students and graduates who shared their perspectives for this article, the average age was 41.4, with all contributors in their 40s except one. Given that distance education learners tend to fall into the category of “adult learner,” an exploration of motivators for choosing online education among this group was germane. In a survey of adult learners, the Education Activities Board (2019) indicated that today’s adult learners are “savvy, digital consumers who approach their education with a consumer-like mindset” (p. 2).
As indicated by Snow and Coker (2020), one might expect there would be a plethora of literature to assist in understanding experiences of students in distance education programs. Studies examining student perceptions of social presence, engagement, outcomes, and teaching strategies in online distance education have been conducted, but specific inclusion of student perceptions of distance counselor education is lacking (Bolliger & Halupa, 2018; Gering et al., 2018; Lowenthal & Dunlap, 2018; Murdock & Williams, 2011). This glimpse into the experiences of students and graduates from distance counselor education programs informs our understanding of how direct consumers view their counseling training and preparation experiences.
Choosing Online Counselor Education
It is a major decision to become a professional counselor or counselor educator. Another important decision is deciding where to train and by what learning method to receive training. To understand why a prospective student might choose a distance education program, we must first understand the characteristics of the online learner. Distance education students tend to skew older than their on-campus counterparts, and the average age of an online learner is 34 (Education and Careers, 2019).
With this fact in mind, we asked our five students to respond to the following prompt: “Provide us with a brief statement as to why you chose counseling and then online education.” Among our small group, reasons for choosing online counselor education clustered around family, work, and lifestyle. Two of our five students shared that being a single parent of one or more children with special needs was a driving factor. Another, also the parent of a child with special needs, needed the flexibility afforded by distance learning to be able to live overseas to accommodate her husband’s job. Keeping a particular job and work schedule were reasons for other students.
According to an Education Activities Board survey (2019), the number of graduate students taking online courses rose 47% between 2012 and 2017, suggesting that the appeal of flexible options for adult learners is a salient factor in their decision to pursue an online education. Amy Campos, a graduate of a large for-profit university with a CACREP-accredited program, summed it up well:
I was in my late 30s when I decided it was time to level up and begin the journey to a graduate degree. I was raising two neurodiverse children and had just entered the unfamiliar territory of single parenting! I knew I would need to find a program that not only supported my career and educational goals but blended with my personal and family needs as well. (personal communication, May 3, 2019)
Overall, students indicated that an online program offered the flexibility they needed to successfully navigate graduate training at the current stage of their lives.
Structure and Process of Online Counselor Education Programs
When we started training in online counselor education programs, there were limited options in terms of program structure and student experiences. In the early 2000s, the delivery of curriculum in counseling programs was an either–or proposition: students either enrolled in a traditional face-to-face (F2F) program or in an online program that was solely asynchronous except for an on-campus skills training component (i.e., residency). Asynchronous learning simply means that students do not attend required meetings of the class during a given week, although they likely have assignments with required dates. The early adopters of online counselor education were able to meet and achieve CACREP accreditation through a blend of asynchronous learning experiences in learning management systems such as Blackboard with asynchronous assignments, readings, and discussion posts, and F2F, on-campus training residencies to practice and demonstrate clinical skills.
Given that most early online counselor education training programs followed this same format, much of the early literature regarding the efficacy of online learning focused on the comparisons between two instructional modalities: F2F or on-campus vs. online, asynchronous instruction. In a comparison of levels of learning and perceived learning efficiency of on-campus and online learning environments, Smith et al. (2015) found that levels of learning (i.e., student participants’ perceptions of learning) between online and on-campus students were essentially the same, while the efficiency of learning outcome (i.e., student participants’ perceptions of time devoted to learning activities and achieving learning outcomes) favored the online modality.
Other studies have shown little difference in academic outcomes between on-campus and online delivery methods in psychology programs (Hickey et al., 2015) and counseling programs in Australia (Furlonger & Gencic, 2014). Examinations of blended learning models similarly have shown that students can benefit from both on-campus and distance modalities (Karam et al., 2014). More and more, teasing out the different kinds of learning opportunities across the ever-widening spectrum of distance education is becoming the focus. The use of videoconferencing, interactive media, and a blend of synchronous and asynchronous deliveries is increasingly common in counselor education (Snow et al., 2018).
Our students discussed a variety of delivery methods and structures from their online learning experiences. According to Fatma Salem-Pease, a coauthor who was also interviewed as a student at a private nonprofit university with a non–CACREP-accredited program,
some courses are lighter than others, with more focus on practicing counseling skills, and will therefore have more synchronous activities. Other courses focus on psychology and counseling fundamentals and therefore require more reading, research, and involve writing more papers. A big majority of the learning is done individually. (personal communication, April 25, 2019)
Two of the students’ programs were structured with required weekly, synchronous class meetings, and the students indicated that these components positively impacted their sense of engagement and learning. According to Michelle Fowler, a graduate of a private nonprofit university with a CACREP-accredited program, “group projects and small group breakouts through Zoom were a good way to get to know people. The best way to really get to know people was through assigned weekly meeting groups” (personal communication, April 10, 2019). Similarly, Libby Haag, a student at a private nonprofit religious university with a CACREP-accredited program, shared that the synchronous nature of her program was her favorite part (personal communication, April 16, 2019). She felt that being connected in that fashion to faculty and peers allowed her to practice the relational elements essential to becoming a competent counselor. There was a definite enthusiasm for these relationships from students whose programs offered the synchronous environment online.
Two other students interviewed for this article were in programs that followed the more traditional online format of asynchronous classes with F2F residency experiences. Interestingly, comments from one of our students who attended a program with an asynchronous learning model identified a potential need to include other modes of training and delivery in addition to asynchronous learning. Shawn Clark, a graduate of a public university with a large CACREP-accredited program, wrote:
We have to meet once a week at night as a class during the internship processes but not during any other classes. I enjoyed the interaction during these meetings because we were able to critique each other’s skills, which helped me develop professionally. If we could have met as a class online during all my classes, I believe I would be more prepared as a counselor. (personal communication, April 22, 2019)
From all of our students’ observations, a blend of formats, deliveries, and experiences seemed to benefit them most. These observations support the emerging literature concerning different deliveries of distance education. According to Harris (2018), a combination of modalities, including F2F, online, asynchronous, and synchronous, tap into a variety of learning styles and together can create a learning experience that positions students for success.
Community of Inquiry
Allen et al. (2016) suggested that about 77% of institutions with distance offerings find them critical to their long-term strategy and the future growth of their institutions. An important element in online education is the community of inquiry, which is a framework for teaching and learning that is built on aspects of constructivist pedagogy. Specifically, the community of inquiry is comprised of social presence, cognitive presence, and teaching presence (Richardson & Ice, 2010). Akyol and Garrison (2008) defined these types of presence as follows: social presence is the experience of connection in online learning, cognitive presence is the exchange of information and ideas, and teaching presence is the facilitation and shaping of the discourse. For the purpose of this article, we asked students to talk with us about how they experienced these in their interactions with peers and faculty.
Interactions With Peers
Researchers who have studied the community of inquiry model have found that a lack of interaction between online students results in an experience of loneliness and an increase in students dropping courses (Ozaydın Ozkara & Cakir, 2018). All of the students we spoke with talked about developing deeper connections during the residency component of their curriculum and how meaningful those relationships were. But there were other areas for connection provided as well. Students who were in programs with a synchronous online component commented on the use of breakout rooms in virtual platforms such as Zoom and how helpful they were to developing community. Additionally, the use of virtual groups during the group counseling course increased opportunities to interact with peers. None of the students participating in our discussion cited online discussion boards as a way to increase or improve interactions with peers, but some did share that simply seeing the same students’ names in multiple classes was helpful.
Interactions With Faculty
Within the community of inquiry, teaching presence is comprised of both the way the faculty member sets the stage for learning and the way they generate a focus for the online discourse (Walsh, 2019). Unfortunately, faculty tend to view their teaching presence more favorably than students (Blaine, 2019). As such, it was important to get the student perspective on interactions with faculty.
Students’ interaction ranged from being in the classroom to taking advantage of opportunities to connect out of class. Within the class, students found instructor videos to be helpful, sharing that in some fully asynchronous programs, students may never see their faculty members’ faces or hear their voices as lectures are developed at the institutional level and prepopulated in each course shell. Faculty members who took the use of video even further, such as using the video feedback options in the learning management system, were appreciated even more. But it was the interactions outside of the classroom that seemed to be the most impactful to students.
Students discussed having email, phone, and video chat communication with faculty and how important that was to their experience. These interactions felt personal and “helped me rebuild my self-esteem and acknowledge my self-worth” as well as student self-efficacy while serving as a professional model (F. Salem-Pease, personal communication, April 25, 2019). Students who did not have more personal interactions outside of class reported less satisfaction in this area. A clear takeaway is that the more students can interact with each other and with their faculty both in and out of the classroom, the more fulfilling their experience is with online education.
Practicum and Internship
Having taught in counselor education programs for a combined 40 years, we recognize that whether on-campus or online, the experience of practicum and internship is one of the most anxiety-provoking elements of counselor training. Whether the anxiety is about finding an appropriate site, securing sufficient direct client hours, or struggling with insecurity around skills and abilities, students entering field experience need additional support (Nease, 2013). The experience of online students is no different. Those who live in towns with a large, campus-based program reported some challenges helping sites understand their status. One student talked about needing to make a case for her program when the site was primarily accustomed to dealing with the hometown university. However, students who had lived in their hometown for a while and had good connections, or who lived in areas that are highly populated and have multiple agency opportunities, reported less stress.
Faculty connections were also found to be helpful. Just as students may come from all areas of the country or the world, so may faculty. Having faculty familiar with state requirements and who have peers in the towns where students are trying to gain a site can be helpful. All students reported a willingness to be persistent, make the necessary calls, know their program and training, and take on the hurdles of a human resource department as necessary qualities for success in finding practicum and internship sites.
Counselor Licensure
Counselor educators are well aware that state licensure requirements are not uniform, can be tricky, and are challenging to even the most seasoned licensure candidate. But students often enter counseling programs assuming that licensure is similar across states and territories (Buckley & Henning, 2016). To this end, most of the students we spoke to talked about having discussions about state licensure requirements early in their training. Students were advised to look for any challenges or deficiencies posed by their program of study:
The only concern I had with my license was from not having a human sexuality course from my university. The state of Florida requires this class. However, when I reached out to my university and told them of my dilemma, they found the course in another program and offered it to me. I will be taking it this summer. (S. Clark, personal communication, April 22, 2019)
In addition, many students reported having early assignments that required them to review their state board requirements.
We are required to research the state requirements and write several papers about them during the very first term. After that, we are constantly reminded of our state requirements, especially as we head into practicum and internship, and also when selecting elective courses. (F. Salem-Pease, personal communication, April 25, 2019).
Students seemed to benefit from programs that began the licensure discussion during admissions and kept it at the forefront throughout their training.
Motivation in Online Training
We started this paper with a premise that many learners in distance education programs need to be self-motivated to be successful. Even programs that have synchronous and on-campus portions still generally require students to engage in some amount of self-paced and self-guided learning. As early as 1986, Moore was writing about the importance of self-directed learning in distance education environments. He suggested that the self-directed or autonomous learner is motivated to “set their goals and define criteria for achievement” (Moore, 1986, p. 13).
Our students were asked to consider any strategies that have helped them remain motivated through their training program. All of the students mentioned some combination of the need to stay organized, make and keep a schedule, and set realistic goals for success. Fatma Salem-Pease offered that it is a combination of having an organized weekly schedule and self-care routines that helps to maintain motivation: “One significant aspect of my self-care has become planning ahead and giving myself the appropriate amount of time to complete an assignment well before the deadline.” She went on to say, “Self-care is an important component of any journey and is absolutely necessary to maintain stamina until the end” (personal communication, April 25, 2019). Two students discussed the roles their professors played in their ability to stay motivated. Michelle Fowler shared that “[a] big challenge was dealing with the different formats teachers used” (personal communication, April 10, 2019). Libby Haag discussed how being an independent thinker and problem solver goes hand-in-hand with being mindful and respectful of professors’ time: “I make sure my email communications are respectful, clear, and concise. I believe these relationship-focused skills have helped me to have better connections with my professors and peers in an environment that often feels isolating” (personal communication, April 16, 2019).
Other ways our students described their ability to be self-motivated in a distance learning environment included being disciplined, intrinsically driven, resourceful, dedicated, and having a sense of self-efficacy. As one student stated, “self-efficacy is an important factor that determines the student’s perception of her ability to achieve certain tasks” (F. Salem-Pease, personal communication, April 25, 2019). This observation is supported by inquiries that have examined the relationships between self-efficacy, confidence, and attainment in online formats. Watson (2012) found that students in online learning environments have higher self-efficacy beliefs than students in traditional, on-campus programs and that online learning environments may in fact increase personal motivation and self-efficacy.
A framework for understanding motivation in educational environments is self-determination theory, which makes a distinction between autonomous (self-determined) motivation and controlled (externally pressured) motivation (Ryan & Deci, 2008). Ryan and Deci (2008) posited that individuals are more likely to engage in positive change, whether in therapeutic, educational, or family settings, when there are external supports in place that promote autonomy. Autonomous motivation is achieved when the needs for autonomy, competence, and relatedness are met (Baeten et al., 2012). Learning environments that strive to create conditions where students can feel they have some level of autonomy balanced with a clearly formulated structure, as well as opportunities for involvement and engagement with faculty and peers, have a combination of factors that are conducive to student motivation (Baeten et al., 2012).
Watson (2012) explained that “one of the common concerns often voiced has been whether or not ‘skills-based’ or ‘techniques’ courses could be offered sufficiently online” (p. 143). This aspect is often addressed in CACREP-accredited programs through the F2F residency experience and synchronous video activities that allow students to practice counseling skills and get helpful feedback and guidance from professors (Snow et al., 2018). Online students report that course materials generally make use of a variety of videos, including full counseling session videos and those incorporating certain techniques, which fosters vicarious learning. Fatma Salem-Pease indicated that the level of attention she received while pursuing her online degree was higher and more personalized than when she was pursuing an on-campus degree. She attributed this distinction to the fact that group sizes were small and her belief that there may be a benefit to professors reviewing video recordings in the comfort of their own office or home space where they are not pressured to assess the skills of multiple individuals in one sitting.
“What I Wish I Had Known Before Starting an Online Program”
The students who shared their perspectives were asked to talk about what they wish they had known coming into an online program. Many wished they had truly understood the importance of developing relationships with faculty and fellow students. Generating groups using Facebook or other social media was suggested as a way to facilitate this. In addition, some wished they had known that developing teams to practice skills would have been helpful to the online counselor-in-training.
A primary area of consideration on this topic was the financial cost of online education. Because many online programs are housed in private institutions, it was suggested that students
look long and hard at the expense associated with the program and the entry-level jobs they will get with their degree. The amount of debt in relation to that salary can be overwhelming, and while it may prove to work out in the long run, [online private institutions] may not be the wisest choice. (S. Clark, personal communication, April 22, 2019)
Whether in private or public universities, students were pleased that the online programs allowed them to pursue the education they wanted and needed while still maintaining a full-time job.
Student Perspectives of the Literature
We offered our two student coauthors and graduate interviewees the opportunity to each identify a relevant article from the literature that resonated, in some way, with their experiences as online learners and to contribute to this article by outlining the impact of that article on their learning experience. The student authors of this manuscript found that building relationships was reflected in the literature as an essential element, just as it was in their own experiences.
Building Relationships in Online Counselor Education Programs—Libby Haag
At the essence of counseling is relationships (Hall et al., 2010). Online education can often remove the humanistic quality by an absence of F2F instruction, resulting in a lost opportunity to connect with peers, professors, and future counselors and thus lacking an essential component in personal growth. Relationship-building skills are imperative for developing effective counselors, maintaining professional integrity, and implementing gatekeeping, and online learners often can feel detached from their professors and peers. Although on-site schooling offers the humanistic relationship-building aspect, online formats have the ability to educate underserved and diverse individuals to give them the opportunity to become professional counselors (Hall et al., 2010). Online counselor education combines the best aspects of technology with traditional campus education, which may create a more accessible, relational, and humanistic approach to the development and training of counselors.
Humanistic Framework
According to Hall et al. (2010), a more effective online education for counselors is a humanistic framework that includes both technology and consistent F2F video interaction while maintaining a student-centered focus. This interactive model can effectively solve the problem of how to reach many underserved students to promote diversity in growing our profession while still teaching effective counseling skills to nurture the important humanistic, personal relationship aspect that is paramount to our profession. This humanistic framework to create a more effective and personal online experience has four principles: “the importance of viewing and valuing students holistically, the importance of maintaining meaningful relationships, an emphasis on valuing intentionality, and the recognition that people are goal oriented and creative beings” (Hall et al., 2010, p. 47).
Viewing and Valuing Students Holistically. Online educators need to view each student holistically as a distinctive individual and not use a reductionist approach (Hall et al., 2010). It is essential that the student feel important and valued while being viewed phenomenologically. A suggestion for viewing and valuing students in a more holistic manner would be to do video interviews as part of the application process. This would help establish a relationship with a professor before school even begins to create a meaningful, intentional, and relationship-driven curriculum.
Maintaining Meaningful Relationships. According to Hall et al., “a good relationship is the basis of counseling and education” (2010, p. 48). Therefore, personal relationships need to be developed in an online program for both teachers and peers. Some suggestions to foster a positive relationship begin with sending emails before class starts and encouraging an open-door policy for communication. In addition, professors can approach an online class with group counseling techniques. For example, when beginning class, the professor could have all the students introduce themselves in the video forum using an icebreaker. At the next class, they can have the students reintroduce one another. Small group projects are also encouraged with some group counseling techniques (Hall et al., 2010).
Valuing Intentionality. Intentionality, as defined by Hall et al., is “a sense of purpose in guiding and choosing one’s behavior” and “our capacity to reach out, take care of, and tend to others in purposeful ways” (2010, p. 48). Online professors could begin to guide students into becoming intentional learners, with an emphasis on self-awareness and deliberate reflection of their considerate interactions with others. This will help foster and model the connection online counseling students need for effective relationship skills in the future.
People Are Goal-Directed and Creative Beings. Personal growth is a primary characteristic of a holistic, humanistic online education. Professors need to be willing to nurture creativity, drive, and resourcefulness within the classroom. Having a personal growth-based curriculum will only increase the student’s online experience. Hall et al. (2010) asserted that opportunities for growth and intrinsic motivation exist in creating an environment that promotes self-actualization, self-realization, and self-enhancement. It is suggested that teachers use a variety of techniques to match unique learning styles of a diverse student body for fostering creativity in online counselor education.
From a Personal Perspective
In examining and analyzing Hall et al. (2010) above, Libby Haag shared that her personal experience with a humanistic online framework has helped her to become a more rounded counselor. She feels as if she thrived in this environment, which was rooted in a very CACREP-driven curriculum with an emphasis on personal and professional growth. The relationships she created with teachers, peers, and supervisors were invaluable, and the F2F interaction helped to develop better social skills and a sense of community. She indicated that she made sure to reach out and let peers and professors get to know her personally. These actions helped her to feel connected and valued in a system that can sometimes lack a human element. She found that her most influential professors were those who were very personable and patient and who used humor and modeled authenticity with a focus on fostering relationships. They were available for personal consultation and they always offered a good deal of feedback. Overall, concurrent with the literature, Libby Haag’s experience was that a relationship-focused online program was essential in creating competent counselors.
Self-Efficacy and the Online Learner—Fatma Salem-Pease
Fatma Salem-Pease discovered that the 2012 article by Watson, “Online Learning and the Development of Counseling Self-Efficacy Beliefs,” supports a lot of the viewpoints she had previously shared in her personal communications. First, the article discussed the importance of practicing learned skills in real-life F2F situations and expressed the concerns voiced by many counselor educators about the efficacy of an online program that does not incorporate F2F learning components. As discussed earlier in this article, Watson (2012) explained that “One of the common concerns often voiced has been whether or not ‘skills-based’ or ‘techniques’ courses could be offered sufficiently online” (p. 143). This aspect is often addressed through residency experiences and through synchronous video activities that allow students to practice counseling skills and receive helpful feedback and guidance from professors. Course materials also have a variety of videos, including counseling sessions and how certain techniques are used, which foster vicarious learning.
Watson (2012) noted that “academic coursework, assigned readings, classroom discussions, self-reflection, modeling, supervision and hands on experiences associated with practica and internships” are required elements to enhancing competency and perception of self-efficacy (p. 145). The study hypothesized that F2F students have higher levels of perceived counseling self-efficacy than online students. The researcher administered the Counseling Self Estimate Inventory to 373 graduate students, 207 of which were F2F students, while 166 reported having taken the core skill development courses online. The results of the study disproved the hypothesis and showed that online counseling students have stronger counseling self-efficacy than F2F students.
These results support Fatma Salem-Pease’s and other students’ thoughts that online students have the opportunity to individualize their learning to their specific needs, helping them feel more confident in what they know and more aware of what they need to work on further. Structured F2F educational programs, she believes, burden students with an extensive and specific schedule to follow daily, which leaves minimal time for students to reflect on what is being learned and how to maximize the learning experience. Online students can be more actively engaged in their learning and have more freedom to choose what to accomplish and learn with their time.
Conclusion
Although much has been written about the online learning experience in counselor education, it is rare to hear faculty and students work together to share their experiences in online education and training settings. What we have captured here first and foremost is that online counselor education provides a positive option for many students and faculty. Online counselor education allows students to blend academic pursuits into their current family and career lives in a way that is more accessible than traditional on-campus programs. When embarking on this journey, students value the connections they are able to foster with faculty and with peers, many of which occur through the synchronous parts of a program. Given that many programs are fully asynchronous, further research into the use of synchronous components would benefit the field of online counselor education.
Additionally, students strongly supported the fact that the path to success is smoother when programs attend to the various field experience and licensure requirements of their students across states. It is clear that an online counselor education program requires skills in both self-motivation and self-care to provide the maximum benefit to the student. Although this paper addressed the student experience in a non-empirical manner, a more research-driven approach to understanding student experience in distance counselor education programs is needed. Overall, online counselor education is functional, effective, and preferred by many students who are now pursuing their own careers in the profession of counseling.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Allen, I. E, Seaman, J., Poulin, R. & Straut, T. T. (2016). Online report card: Tracking online education in the United States. Babson Survey Research Group. https://onlinelearningsurvey.com/reports/onlinereportcard.pdf
Akyol, Z., & Garrison, D. R. (2008). The development of a community of inquiry over time in an online course: Understanding the progression and integration of social, cognitive and teaching presence. Journal of Asynchronous Learning Networks, 12, 3–22. https://doi.org/10.24059/olj.v12i3.72
Baeten, M., Dochy, F., & Struyven, K. (2012). The effects of different learning environments on students’ motivation for learning and their achievement. British Journal of Educational Psychology, 83, 484–501. https://doi.org/10.1111/j.2044-8279.2012.02076.x
Blaine, A. M. (2019). Interaction and presence in the virtual classroom: An analysis of the perceptions of students and teachers in online and blended Advanced Placement courses. Computers & Education, 132, 31–43. https://doi.org/10.1016/j.compedu.2019.01.004
Bolliger, D. U., & Halupa, C. (2018). Online student perceptions of engagement, transactional distance, and outcomes. Distance Education, 39, 299–316. https://doi.org/10.1080/01587919.2018.1476845
Buckley, M. R., & Henning, S. (2016). Education, credentialing, and professional development. In D. S. Sheperis & C. J. Sheperis (Eds.), Clinical mental health counseling: Fundamentals of applied practice (pp. 33–63). Pearson.
Council for Accreditation of Counseling and Related Educational Programs. (n.d.). Directory of accredited programs. Retrieved from https://www.cacrep.org/directory
Education Activities Board. (2019, January 31). 3 insights for program growth from our 2019 adult learner survey. https://www.eab.com/blogs/adult-student-marketing/2019/01/3-insights-for-graduate-and-adult-learn
er-program-growth
Education and Careers. (2019). Online student demographics infographic. https://blog.classesandcareers.com/edu
cation/infographics/student-demographics-infographic
Furlonger, B., & Gencic, E. (2014). Comparing satisfaction, life-stress, coping and academic performance of counselling students in on-campus and distance education learning environments. Australian Journal of Guidance and Counselling, 24, 76–89. https://doi.org/10.1017/jgc.2014.2
Gering, C. S., Sheppard, D. K., Adams, B. L., Renes, S. L., & Morotti, A. A. (2018). Strengths-based analysis of student success in online courses. Online Learning, 22(3), 55–85. https://doi.org/10.24059/olj.v22i3.1464
Hall, B. S., Nielsen, R. C., Nelson, J. R., & Buchholz, C. E. (2010). A humanistic framework for distance education. The Journal of Humanistic Counseling, Education and Development, 49, 45–57.
https://doi.org/10.1002/j.2161-1939.2010.tb00086.x
Harris, C. A. (2018). Student engagement and motivation in a project-based/blended learning environment (Publication No. 10827819) [Doctoral dissertation, Azusa Pacific University]. ProQuest Dissertations and Theses Global.
Hickey, C., McAleer, S. J., & Khalili, D. (2015). E-learning and traditional approaches in psychotherapy education: Comparison. Archives of Psychiatry and Psychotherapy, 4, 48–52.
Karam, E. A., Clymer, S. R., Elias, C., & Calahan, C. (2014). Together face-to-face or alone at your own pace: Comparing traditional vs. blended learning formats in couple & family relationship coursework. Journal of Instructional Psychology, 41, 85–93.
Lowenthal, P. R., & Dunlap, J. C. (2018). Investigating students’ perceptions of instructional strategies to establish social presence. Distance Education, 39, 281–298. https://doi.org/10.1080/01587919.2018.1476844
Moore, M. (1986). Self-directed learning and distance education. International Journal of E-Learning & Distance Education, 1, 7–24.
Murdock, J. L., & Williams, A. M. (2011). Creating an online learning community: Is it possible? Innovative Higher Education, 36, 305–315. https://doi.org/10.1007/s10755-011-9188-6
Nease, R. T. (2013, February 7). What’s wrong with the counseling intern picture? https://www.counseling.org/news/aca-blogs/aca-member-blogs/aca-member-blogs/2013/02/07/whats-wrong-with-the-counseling-intern-picture
Ozaydın Ozkara, B., & Cakir, H. (2018). Participation in online courses from the students’ perspective. Interactive Learning Environments, 26, 924–942. https://doi.org/10.1080/10494820.2017.1421562
Richardson, J. C., & Ice, P. (2010). Investigating students’ level of critical thinking across instructional strategies in online discussions. Internet & Higher Education, 13(1/2), 52–59. https://doi.org/10.1016/j.iheduc.2009.10.009
Ryan, R. M., & Deci, E. L. (2008). A self-determination theory approach to psychotherapy: The motivational basis for effective change. Canadian Psychology, 49(3), 186–193. https://doi.org/10.1037/a0012753
Smith, R. L., Flamez, B., Vela, J. C., Schomaker, S. A., Fernandez, M. A., & Armstrong, S. N. (2015). An exploratory investigation of levels of learning and learning efficiency between online and face-to-face instruction. Counseling Outcome Research and Evaluation, 6, 47–57. https://doi.org/10.1177/2150137815572148
Snow, W. H., & Coker, J. K. (2020). Distance counselor education: Past, present, future. The Professional Counselor, 10, 40–56. https://doi.org/10.15241.whs.10.1.40
Snow, W. H., Lamar, M. R., Hinkle, J. S., & Speciale, M. (2018). Current practices in online counselor education. The Professional Counselor, 8, 131–145. https://doi.org/10.15241/whs.8.2.131
Walsh, M. T., Jr. (2019). The influence of contextual variables on teaching, social, and cognitive presence in adult
students (Publication No. 13419397) [Doctoral dissertation, Fordham University]. ProQuest Dissertations & Theses Global.
Watson, J. C. (2012). Online learning and the development of counseling self-efficacy beliefs. The Professional Counselor, 2, 143–151. https://doi.org/10.15241/jcw.2.2.143
Donna S. Sheperis, PhD, NCC, ACS, CCMHC, LPC, is an associate professor at Palo Alto University. J. Kelly Coker, PhD, NCC, LPC, is an associate professor at Palo Alto University. Elizabeth Haag was a graduate student at the University of the Cumberlands. Fatma Salem-Pease was a graduate student at Southern New Hampshire University. Correspondence can be addressed to Donna Sheperis, 5150 El Camino Real, Los Altos, CA 94022, dsheperis@paloaltou.edu.
Jan 6, 2020 | Book Reviews
by Robert C. Reardon, Janet G. Lenz, Gary W. Peterson, & James P. Sampson, Jr.
The sixth edition of Career Development and Planning was authored in 2019 by notable career researchers, Drs. Robert Reardon, Janet Lenz, Gary Peterson, and James Sampson. This book describes the processes behind theory-based career decision-making strategies and is written for a college-level audience as a guide for clients and students when formulating and implementing career decisions. In this review, an overview of the content included in the text and a description of the strengths and limitations will be provided for prospective readers to consider.
The text is organized into three sections of five chapters, each section covering a different aspect of career decision-making and planning. The first section describes the components of cognitive information processing (CIP) theory, including metacognitions, decision-making, self-knowledge, and options knowledge. Strategies for addressing each CIP theory component are provided. Some strategies are based within the theory such as the CASVE cycle for decision-making or the exploration of positive and negative self-talk to address meta-cognitions. Other strategies incorporate key tenets from other theories, including Holland’s RIASEC hexagon for self-knowledge clarification. Section two focuses on the sociological aspects of career decision-making, including organizational culture, work and family roles, the implementation of technology, and the different ways in which people conduct their work (e.g., job sharing, flex time, telecommuting). The final section of the text discusses strategies for launching a successful career search campaign, including resumé writing, networking, and salary and benefit negotiation. Tips for a successful college-to-employment transition are also included. Updated online resources for many of the topics covered in the text can be found throughout the chapters. Additionally, activities and worksheets related to the content can be found in the appendices of the text. Instructors can request the Instructor’s Manual as a text companion, but this resource was not available to this reviewer.
The organization of the information is an aspect that improves the reader’s experience. The semi-chronological structure provides an opportunity for readers to return to the text for guidance at any point in their career path. A primary strength of this text can be found in the appendices, which provide activities that enhance the learning experience by presenting an opportunity for personal reflection on text concepts. Additionally, resources are provided for readers who wish to learn more about the more specific topics covered in each chapter. Visual aids are included to assist readers in understanding abstract concepts and illustrate theories that may be otherwise difficult to comprehend.
By providing basic information on CIP theory, readers can reflect on these concepts as more information is presented while moving toward a career path. The detailed discussion of CIP theory included within the first section is unique to this book. Whereas most texts focus on the information provided in the second and third sections of this text, the inclusion of the theory is an effective way to assist students and clients with the basic skills needed for making major decisions.
Despite providing crucial information regarding career concerns, clients and students may find the text dense and difficult to navigate on their own. Because of this, career course instructors, counselors, and career professionals may find it beneficial to guide clients and students through the content and assist with connecting the information provided to personal experiences and goals. As previously discussed, the text provides activities that personalize these concepts; however, because these activities are located in the appendices, clients may have difficulty connecting the appropriate appendix item to the relevant topic. Future editions of this book may benefit from including more activities and making more obvious connections between topics and appropriate activities in relevant chapters.
Overall, Career Development and Planning is a worthy edition to any career course or career practitioner’s professional toolbelt, specifically for the resources, activities, and worksheets provided throughout the text. Additionally, the inclusion of CIP theory as the framework for the additional information provided sets this text apart from other career course texts and enables readers to use this framework while thinking through not only current career decisions, but other major decisions made throughout the life span. However, this book is meant to be a guide rather than a self-help solution to all career concerns. Career professionals will find this text to be a useful resource for clients and students with concerns ranging from deciding on the right career trajectory to preparing for their first job.
Reardon, R. C., Lenz, J. G., Peterson, G. W., & Sampson, J. P. (2019). Career development and planning: A comprehensive approach (6th ed.). Kendall Hunt Publishing.
Reviewed by: Jessica N. Schultz, University of Southern Mississippi
The Professional Counselor
tpcjournal.nbcc.org
