Apr 29, 2020 | Volume 10 - Issue 2
Daniel Gutierrez, Allison Crowe, Patrick R. Mullen, Laura Pignato, Shuhui Fan
Researchers used path analysis to examine self-stigma, help seeking, and alcohol and other drug (AOD) use in a community sample of individuals (N = 406) recruited through the crowdsourcing platform MTurk. Self-stigma of help seeking contributed to AOD use and was mediated by help-seeking attitudes. We discuss the implications for advocacy and stigma reduction in substance use treatment. Counselors and counselor educators can implement and advocate for interventions and training that increase positive attitudes toward seeking help, such as providing appropriate training with supervisees and counselors-in-training, providing clients and the community with mental health literacy, and engaging in more advocacy. Moreover, they can challenge thoughts of seeking help as weakness, normalize seeking psychological help, and discuss the benefits of counseling and therapy to address the development and effects of self-stigma of help seeking for individuals with substance use issues.
Keywords: alcohol and drug use, self-stigma, help seeking, help-seeking attitudes, stigma reduction
In 2015, approximately 20.1 million people over the age of 12 suffered from an alcohol or substance use disorder (SUD) in the United States (Bose et al., 2016). However, only 3.8 million people (1 in 5) who needed treatment received any substance use counseling (Bose et al., 2016). Barriers to receiving substance use treatment include the location of the program, legal fears, peer pressure, family impact, concerns about loss of respect, and stigma (Masson et al., 2013; Stringer & Baker, 2018; Winstanley et al., 2016). Of these concerns, stigma is arguably the most complex and the least understood. In response, substance use prevention and mental health care researchers have begun to turn their attention to stigma and how it influences counseling treatment and recovery (Livingston et al., 2012; Mullen & Crowe, 2017; Stringer & Baker, 2018). Researchers have found that individuals with SUDs experience higher levels of stigma than individuals with any other health concern (Livingston et al., 2012). However, more research on the intersection of stigma, help seeking, and alcohol and other drug (AOD) use is still warranted. Thus, this article delves further into these concepts and describes a study that examined the relationships between these variables.
Stigma and Substance Use
Individuals with substance use concerns report high levels of public stigma in the form of negative labeling, discrimination, and prejudice by others (Crapanzano et al., 2019; Goffman, 1963). Prejudice against people with substance use problems is common and widespread on individual, interpersonal, and institutional levels (Barry et al., 2014). There remains a substantial public belief that those using illicit substances simply need to take responsibility for their choices (Barry et al., 2014). As a result, individuals with SUDs report experiencing judgment, mockery, inappropriate comments, overprotection, and hostility from the public (Mora-Ríos et al., 2017). Even health professionals hold negative perceptions toward patients using substances, believing them to be dangerous, violent, manipulative, irresponsible, aggressive, rude, and lazy (Ford, 2011).
People who perceive this stigma from their health or mental health professionals show a higher treatment attrition rate, less treatment satisfaction, and less perceived access to care (Barry et al., 2014). People with substance use concerns may also experience perceived stigma from the impressions they receive from society and through their own and others’ past experiences (Smith et al., 2016). Perceived stigma is also related to low self-esteem, high levels of depression and anxiety, and sleep issues (Birtel et al., 2017). Individuals who experience public stigma can develop self-stigma (i.e., stigma that is internalized), which impacts help-seeking attitudes (Vogel et al., 2007). For example, an individual could see a person struggling with alcohol use disorder portrayed in the media as being malicious, selfish, and incompetent and begin to believe those stereotypes about themselves.
Additionally, researchers have demonstrated that public stigma is a predictor of self-stigma over time (Vogel et al., 2013). Self-stigma initially develops from stereotype awareness, resulting in stereotype agreement and self-concurrence, which lead to self-esteem decrement (Schomerus et al., 2011). Self-stigma can increase maladaptive coping strategies such as avoidance that can deter seeking treatment, applying for jobs, and interacting with others in social settings (da Silveira et al., 2018). Luoma et al. (2014) also suggested that people with a higher level of self-stigma have lower levels of self-efficacy and tend to remain longer in residential substance abuse treatment.
Role of Stigma and Help Seeking in Relationship to SUDs
The role of public stigma on seeking and receiving psychological help for substance use treatment has been well established by researchers (Birtel et al., 2017; Smith et al., 2016), but the influence of negative perceptions remains less understood (Center for Behavioral Health Statistics and Quality, 2018). Researchers have asserted the importance of examining negative public attitudes toward seeking psychological help; such attitudes act as a catalyst for the development of self-stigma incurred by individuals struggling with SUDs (Vogel et al., 2013). Also, recent reports indicate that the self-stigma of seeking psychological help may be a major contributor to the treatment utilization gap (i.e., the dearth of individuals receiving substance use treatment despite substance misuse and use disorders becoming a public health crisis). The U.S. Department of Health and Human Services, Office of the Surgeon General (2018) reported that ingrained public attitudes have hindered the delivery of medications used to treat SUDs, such as methadone and buprenorphine, because of misconceptions and prejudices surrounding these medications. Other factors they found contributing to the treatment gap include the view of substance use as a moral failing rather than a disease and the belief that the person simply has a “character flaw” (p. 12). Consequently, policymakers and researchers have emphasized the importance of understanding the effect of negative public attitudes on the delivery of substance use treatment and the decision to seek psychological help for mental health concerns involving AOD (Bose et al., 2018; Corrigan, 2011).
To illustrate, the Substance Abuse and Mental Health Services Administration (SAMHSA; Bose et al., 2018) recently stated that 1.0 million (5.7%) of the 18.2 million individuals aged 12 years or older who reported experiencing an SUD perceived a need for treatment for their illicit drug or alcohol use. However, these respondents reported not seeking specialty substance use treatment because they believed getting treatment would have a negative impact on their job (20.5%) and cause their neighbors or community to have a negative opinion of them (17.2%). Additionally, out of the 4.9 million adults aged 18 or older that reported an unmet mental health service need for a serious mental illness, over a third had not received any mental health services in the previous year. Respondents gave the following reasons for avoiding seeking help: concern about being committed or having to take medicine (20.6%); the risk of it having a negative effect on their jobs (16.4%); the belief that treatment would not help (16.1%); the possibility that their neighbors or community would have negative opinions (15.7%); concern about confidentiality (15.3%); and not wanting others to find out (12.6%).
Given these responses and statistics, it is logical to infer that the commonly held public perception of seeking help for mental health concerns and substance use is still very negative and that many still experience significant fear of discrimination from others (e.g., loss of job or a negative impact on social opportunities) as a result of seeking help for AOD issues. The responses also indicate the harmful influence this public stigma has on individuals’ decisions regarding whether to seek psychological treatment for substance use. Furthermore, these findings suggest that respondents possibly internalized negative public attitudes toward seeking professional help for both mental health and substance use concerns, resulting in self-stigma. The respondents’ decision not to receive needed substance use treatment in the previous year in order to avoid negative reactions from others and their lack of belief in the utility of treatment indicate self-stigma surrounding help seeking. This corresponds to previous literature reporting the effects of self-stigma on help-seeking behaviors and attitudes (Vogel & Wade, 2009).
Purpose of the Present Study
The existing research is clear that stigma has some influence on substance use and recovery. However, there is a lack of research explicating the causal pathways that shape this influence. Another area that is unexplored is the relationship between self-stigma and AOD use, and there is no research that we know of that explores the relationship between help-seeking attitudes and AOD use. Given that self-stigma for mental illness and self-stigma for help seeking are often related in the literature (Mullen & Crowe, 2017), and that a large portion of individuals with SUDs have a co-occurring mental illness (39.1%; Center for Behavioral Health Statistics and Quality, 2015), it is reasonable to suspect that the stigma of mental illness influences help seeking in AOD users. A greater understanding of the relationships between these constructs will allow counselors and other helping professionals to develop better strategies for combatting substance abuse by addressing issues related to stigma and attitudes toward help seeking. Therefore, the aim of this study was to examine the relationships between self-stigma of mental health concerns, attitudes toward help seeking, and AOD use. Specifically, we tested the following research hypotheses: Hypothesis 1—Self-stigma toward mental health concerns will have a negative direct effect on attitudes toward help seeking and a positive indirect effect on drug and alcohol use as mediated by attitudes toward help seeking; Hypothesis 2—Self-stigma of help seeking will have a negative direct effect on attitudes toward help seeking and a positive indirect effect on drug and alcohol use as mediated by attitudes toward help seeking; and Hypothesis 3—Attitudes toward help seeking will have a negative direct effect on drug and alcohol use.
Method
Participants
We acquired 406 participants using Amazon’s Mechanical Turk (MTurk). Most of the participants were male (n = 213; 52.5%) followed by female (n = 191; 47.0%) and transgender/gender nonconforming (n = 2; 0.5%). The mean age of the participants was 34.39 years (SD = 10.02, range = 20 to 67). In addition, most participants indicated they lived in the United States at the time of the study (n = 349, 86%) with 57 (14%) participants who lived internationally. As for ethnicity, participants included American Indian or Alaska Native (n = 12; 3%), Asian (n = 79; 19.5%), Black or African American (n = 24; 5.9%), Hispanic or Latino (n = 20; 4.9%), Multiracial (n = 5; 1.2%), Other (n = 2; 0.5%), Native Hawaiian or Other Pacific Islander (n = 1; 0.2%), and White (n = 263; 64.8%). Table 1 displays additional demographic information.
Table 1
Participant Characteristics
| Demographic Characteristics |
n (%) |
| Clinical cutoff for alcohol use |
|
| Met criteria for problematic drinking |
203 (50.0%) |
| Did not meet criteria for problematic drinking |
203 (50.0%) |
| Clinical cutoff for drug use |
|
| Did not meet criteria for problematic drug use |
281 (69.2%) |
| Met criteria for problematic drug use |
125 (30.8%) |
| Individual yearly income |
|
| Less than $30,000 |
173(42.6%) |
| Between $30,000 and $50,000 |
124 (30.8%) |
| More than $50,000 |
108 (26.6%) |
| Education level |
|
| Bachelor’s degree |
169 (41.6%) |
| Some college (no degree) |
82 (20.2%) |
| Master’s degree |
59 (14.5%) |
| Associate degree |
49 (12.1%) |
| High school diploma |
34 (8.4%) |
| Doctoral degree |
8 (2.0%) |
| Some high school (no degree) |
3 (0.7%) |
| Other |
2 (0.5%) |
| Marital status |
|
| Married |
201 (49.5%) |
| Single |
139 (34.2%) |
| Cohabitation |
45 (11.1%) |
| Divorced |
17 (4.2%) |
| Widowed |
2 (0.5%) |
| Separated |
2 (0.5%) |
| Employment status |
|
| Full-time |
290 (71.4%) |
| Part-time |
53 (13.1%) |
| Unemployed (looking for work) |
18 (4.4%) |
| Full-time caregiver |
14 (3.4%) |
| Unemployed (disabled) |
10 (2.5%) |
| Student |
6 (1.5%) |
| Other |
6 (1.5%) |
| Unemployed (not looking for work) |
3 (0.7%) |
| Unemployed (volunteer work) |
1 (0.2%) |
| Note. N = 406 |
|
Procedures
Prior to starting this research investigation, approval from our Institutional Review Board was received. To collect data for a community sample, we employed the use of MTurk, which is an online crowdsourcing platform used for survey research (Follmer et al., 2017). Researchers have found evidence that supports the data quality of MTurk for studies trying to sample diverse community populations that include individuals with substance abuse concerns (Al-Khouja & Corrigan, 2017; Kim & Hodgins, 2017). We placed the consent form, measures, and demographic questions for this study in a Qualtrics survey management site. Then, we created an MTurk portfolio that linked to the Qualtrics survey. The study was advertised to all MTurk participants, and we offered a 50-cent incentive for participation. Participants were screened to allow only individuals who actively engage in the recreational use of drugs and/or alcohol. A total of 406 participants completed the study before it was closed. Participants who took the survey spent an average of 18 minutes completing it.
Measures
Self-Stigma of Mental Illness
Researchers used the Self-Stigma of Mental Illness scale (SSOMI; Tucker et al., 2013) to measure participants’ self-stigma of mental illness. The SSOMI is a self-reported, unidimensional measure consisting of 10 items on a 5-point Likert-type scale that ranges from 1 (strongly disagree) to 5 (strongly agree). Sample items include “If I had a mental illness, I would be less satisfied with myself.” We summed the items and calculated a mean score after accounting for the reverse-scored items, with higher scores indicating greater self-stigma of mental illness. Prior research has shown strong reliability with a Cronbach’s alpha of .93 on participants’ SSOMI scores collected through an online survey (Mullen & Crowe, 2017). In our study, we found good internal consistency reliability, with a Cronbach’s alpha of .91 for participants’ scores on the SSOMI.
Self-Stigma of Help Seeking
Researchers used the Self-Stigma of Help Seeking scale (SSOHS; Vogel et al., 2006) to measure participants’ self-stigma of seeking psychological help. The SSOHS is a self-reported, unidimensional measure that contains 10 items on a 5-point Likert-type scale that ranges from 1 (strongly disagree) to 5 (strongly agree). Sample items include “I would feel inadequate if I went to a therapist for psychological help.” After reverse scoring items, we summed and averaged the scores, with higher values indicating greater self-stigma of seeking psychological help. Scores on the SSOHS have indicated good internal reliability, with Cronbach’s alphas ranging from .89 to .92 in prior research (Tucker et al., 2013; Vogel et al., 2006). In our study, we found good internal consistency reliability for scores on the SSOHS, with a Cronbach’s alpha of .86.
Attitudes Toward Help Seeking
To measure attitudes toward help-seeking, researchers used the Attitudes Toward Seeking Professional Psychological Help–Short Form scale (ATSPPH-SF; Fischer & Farina, 1995). The ATSPPH is a self-reported, unidimensional measure that contains 10 items scored on a 4-point Likert-type scale from 0 (disagree) to 3 (agree). Sample items include “I might want to have psychological counseling in the future.” Participants’ total scores were calculated by summing all items together after reverse scoring items. We averaged the scores on the ATSPPH-SF to help in interpretation, with higher total scores indicating that a participant had a more positive attitude toward psychological treatment. Higher scores on the ATSPPH-SF have been associated with decreased treatment-related stigma and a higher likelihood of future help seeking (Elhai et al., 2008). Prior research has shown good internal consistency reliability for scores on the ATSPPH-SF, with Cronbach’s alphas ranging from .84 to .86 (Fischer & Farina, 1995; Karaffa & Koch, 2016). In the current study, the scores on the ATSPPH-SF provided good internal consistency reliability, with a Cronbach’s alpha of .84.
Alcohol Use
The Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993) was used to measure respondents’ alcohol use and screen for problematic drinking behaviors. The AUDIT is a 10-item, self-reported measure that gathers information on an individual’s alcohol use and provides a clinical cutoff score for harmful drinking. Participants rated their alcohol consumption and related experiences over the past year in response to a series of 3- or 5-point Likert-type scale questions. Sample items include “How often do you have a drink containing alcohol?” with a 5-point scale from 0 (never) to 4 (four or more times a week). Total scores were calculated by summing the items with scores ranging from 0 to 40. We used a total score of 8 or higher as a clinical cutoff point to identify problematic drinking (see Table 1). Prior research has reported good internal consistency reliability of the AUDIT scores with a Cronbach’s alpha value of .88 (Kim & Hodgins, 2017). For this study, the Cronbach’s alpha was .89, indicating good internal consistency reliability.
Drug Use
The Drug Abuse Screening Test (DAST-20; Skinner & Goldberg, 1986) assessed participants’ degree of drug use and potential drug abuse over the past year. The DAST-20 is a 20-item, self-reported measure that provides a total score used to calculate the severity of drug use. The DAST-20 includes 20 nominal items in which participants select Yes or No (with values of 1 and 0, respectively) to a series of questions. Sample questions include, “Can you get through the week without using drugs?” (reverse scored). Total scores were calculated by summing the participants’ item responses after reverse scoring items 4 and 5 with a range from 0 to 20. We used a cutoff score of 6 or higher to indicate problematic drug use (see Table 1). Scores on the DAST-20 have demonstrated good internal consistency reliability with Cronbach’s alphas ranging from .74 to .95 (Yudko et al., 2007). In the current study, we identified a Cronbach’s alpha of .92 for DAST-20 scores, indicating good internal consistency reliability.
Data Analysis
To address the questions in this study, we facilitated a path analysis with the data to test the a priori model with a community sample acquired through MTurk. The recommended fit indexes (Kline, 2005) used in this study included the chi-square statistics (p-value, > .05 indicates fit), comparative fit index (CFI, ≥ .90 indicates fit), standardized root mean square residual (SRMSR, ≤ .08 indicates fit), and root mean square error of approximation (RMSEA, ≤ .08 indicates fit). In addition, the Bollen-Stine bootstrapping procedure was used with 5,000 samples as an additional assessment of model fit. The path analysis was performed in AMOS (Version 24; Arbuckle, 2012) using a maximum likelihood estimation approach. The direct effects are displayed as standardized regression weights (β).
Results
Preliminary Analysis
We examined and screened the data prior to analysis. No outliers were identified, and the data met statistical assumptions associated with path analysis (e.g., multivariate normality, low multicollinearity, and linearity; Hair et al., 2006; Tabachnick & Fidell, 2007). The correlation coefficients between the variables in this path model (see Table 2) were lower than .8, meaning there was a low chance of collinearity problems. We identified no issues of multicollinearity, as the variance inflation factors for the constructs in the path model were lower than 10 (Hair et al., 2006; Tabachnick & Fidell, 2007). Table 2 also includes the means and standard deviations for the variables in this model. Various guidelines were reviewed as a means for determining the appropriate sample size for this investigation. Jackson (2003) and Kline (2005) stated that a 20:1 ratio of sample size to parameters is preferable, and our current study exceeded this recommendation.
Table 2
Correlations, Means, and Standard Deviations for the Variables in the Path Analysis
| Variables |
1 |
2 |
3 |
4 |
5 |
6 |
| Self-Stigma of Mental Illness |
– |
|
|
|
|
|
| Self-Stigma of Help Seeking |
.54** |
– |
|
|
|
|
| Attitudes Toward Help Seeking |
-.28** |
-.62 |
– |
|
|
|
| Drug Use |
-.02 |
.11 |
-.16* |
– |
|
|
| Alcohol Use |
-.01 |
.12 |
-.14* |
.68** |
– |
|
| Age |
.08 |
-.01 |
.05 |
-.27 |
-.26** |
– |
| M(SD) |
3.23(.89) |
2.74(.81) |
1.71(.61) |
4.31(5.07) |
9.79(8.01) |
34.39(9.99) |
Note. Measures used in this study include the Self-Stigma of Mental Illness Scale (SSOMI; Tucker et al., 2013), the Self-Stigma of Help Seeking Scale (SSOHS; Vogel et al., 2006), Attitudes Toward Seeking Professional Psychological Help – Short Form (ATSPPH-SF; Fischer & Farina, 1995), the Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993), and Drug Abuse Screening Test-20 (DAST-20; Skinner & Goldberg, 1986).
* = p < .01, ** = p < .001.
We examined the variables in this study (i.e., self-stigma of mental illness and help-seeking, attitudes toward help-seeking, and drug and alcohol use) to evaluate for potential control variables. Specifically, we conducted several correlations comparing the variables in this study with demographic characteristics. For dichotomous variables, we utilized point-biserial correlations. These analyses indicated that age had significant relationships with both drug and alcohol use; thus, we included age in the path analysis as a control variable.
Model Specifications
The a priori hypothesized model tested in this path analysis included a total of six observed variables that were placed in a causal directional structure that we developed from our understanding of the literature. The exogenous variables included self-stigma of mental illness (as measured by the SSOMI; Tucker et al., 2013) and self-stigma of help seeking (as measured by the SSOHS; Vogel et al., 2006). In addition, attitude toward help-seeking (as measured by the ATSPPH-SF; Fischer & Farina, 1995) was both an exogenous and endogenous variable. Lastly, alcohol use (as measured by the AUDIT; Saunders et al., 1993) and drug use (as measured by the DAST-20; Skinner & Goldberg, 1986) and were endogenous. We correlated self-stigma of mental illness and self-stigma of help seeking along with the error terms for alcohol and drug use. In the model, we examined the direct effect of self-stigma of mental illness and self-stigma of help seeking on attitudes toward help-seeking. Furthermore, we examined the direct effect of attitudes toward help seeking on drug and alcohol use. We included age in this model as a control variable as we examined its direct effect on attitudes toward help seeking, drug use, and alcohol use. A total of 5,000 bias-corrected bootstrapped samples were created (Fritz & MacKinnon, 2007) to examine the indirect effect of self-stigma of mental illness and self-stigma of help seeking on drug use and alcohol use, with attitudes toward help seeking as the mediator.
Path Analysis
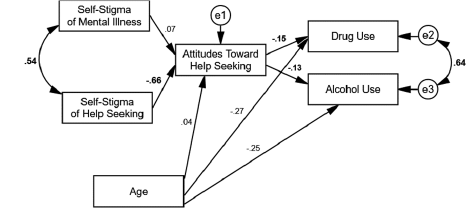
The model (see Figure 1) produced excellent fit: χ2(6, N = 406) = 6.85, p = .34; χ2/df = 1.14; CFI = .99; RMSEA = .02; SRMSR = .01, Bollen-Stine bootstrap, p = .21. Self-stigma of mental illness did not have a direct effect on attitudes toward help seeking (β = .07, SE = .03, p > .05) whereas self-stigma of help seeking did have a negative direct effect on attitudes toward help seeking (β = -.66, SE = .04, p < .001). Attitudes toward help seeking had a negative direct effect on both drug use (β = -.15, SE = .02, p < .01)
and alcohol use (β = -.13, SE = .06, p < .01). The control variable of age had a negative direct effect on drug use (β = -.27, SE = .00, p < .001) and alcohol use (β = -.25, SE = .00, p < .001) but not attitudes toward help seeking (β = .04, SE = .00, p > .05). The residuals of self-stigma of mental illness and self-stigma of help seeking had a positive correlation (r = .54, SE = .04, p < .001) along with drug and alcohol use (r = .64, SE = .01, p < .001). These findings indicated that higher self-stigma of help seeking was associated with a more negative attitude toward help seeking, and more positive attitudes toward help seeking were associated with lower drug and alcohol use. It is also important to note that the effect sizes in the model ranged from small to large (Sink & Stroh, 2006).
Figure 1
Path Model With Age as a Control Variable
The mediated path analysis results indicated that self-stigma of mental illness did not have an indirect effect on drug use (β = -.01, SE = .05, p = .14, 95% BC [-.03, .00]) nor alcohol use (β = -.01, SE = .01, p = .14, 95% BC [.-03, .00]) through attitudes toward help seeking. The mediated path analysis results also indicated that self-stigma of help seeking had an indirect effect on drug use (β = .10, SE = .03, p < .001, 95% BC [.05, .15]) and alcohol use (β = .08, SE = .03, p < .001, 95% BC [.03, .14]) through attitudes toward help seeking.
Discussion
Research has indicated the importance of decreasing stigma surrounding substance use treatment in order to address the public health issue of so many individuals lacking treatment in the United States (Bose et al., 2016; Clement et al., 2015). Although the effects of self-stigma on help-seeking behaviors (Crowe et al., 2016; Mullen & Crowe, 2017), attitudes toward seeking psychological help (Cheng et al., 2018), and AOD use (Luoma et al., 2008) have been well documented, there remains a gap in the counseling literature explicating the relationship between the above constructs. In this study, the proposed theoretical causal model (see Figure 1) suggested that self-stigma of mental illness and self-stigma of help seeking would have a direct effect on attitudes toward help seeking and a positive indirect effect on drug and alcohol use mediated by attitudes toward help seeking; moreover, it suggested that attitudes toward help seeking would have a negative direct effect on AOD use.
By using the online platform MTurk for a community sample of 406 participants, the results from a path analysis indicated an excellent fit model with significant standardized regression coefficients that revealed a complex relationship between self-stigma of mental illness, self-stigma of help-seeking, attitudes toward psychological help seeking, AOD use, and age. Although the results of the present study did not support all three initial hypotheses, the findings did show a statistically significant indirect relationship among the six variables.
The first hypothesis was not supported by data because self-stigma of mental illness did not have a direct effect on attitudes toward help seeking or an indirect effect on AOD use. However, self-stigma of mental illness did correlate with self-stigma of help seeking, which included a large effect size that indicated a strong relationship between these variables. The lack of direct effect between self-stigma of mental illness and attitudes toward help seeking may have resulted from a moderating influence caused by the direct effect of self-stigma of help seeking on attitudes toward help seeking. Based on these findings, we concluded that self-stigma of help seeking is a stronger predictor of attitudes toward help seeking when paired with self-stigma of mental illness. However, more research is needed to replicate these findings, and specifically the potential moderating effect of self-stigma of help seeking on self-stigma of mental illness.
In contrast, the results from the path analysis provided evidence for our second hypothesis. Specifically, participants who reported high levels of self-stigma of help seeking had less positive attitudes toward seeking psychological help as well as higher alcohol use or drug use. This finding is consistent with findings from prior research that revealed participants who reported high levels of stigma had decreased adaptive coping skills such as help-seeking behaviors (Crowe et al., 2016) and increased maladaptive coping skills such as drug use (Etesam et al., 2014). It is possible that participants turned to drinking or drug use as a method of coping rather than seeking formal support. However, we cannot determine if that is the case from the current study. The direct relationship of an individual’s reported stigma of help seeking with less positive attitudes toward seeking psychological help also confirms previous theoretical descriptions of the relationship between self-stigma of help seeking and attitudes toward help seeking (Tucker et al., 2013; Vogel et al., 2007; Wade et al., 2011).
Lastly, participants who reported more positive attitudes toward help seeking had significantly lower AOD use, which provided support for our third hypothesis. These findings suggest that regardless of age, participants who had a positive attitude toward seeking help reported significantly lower AOD use. In addition to the unique findings uncovered through mediation analysis, this study further supports the argument that self-stigma of mental illness and self-stigma of help seeking are two theoretically and empirically distinct constructs (Tucker et al., 2013). Moreover, the significantly direct effect of an individual’s self-stigma of help seeking on attitudes toward seeking psychological help confirms the need that treatments must address more than one component of self-stigma and that addressing self-stigma of mental illness alone may not improve attitudes toward help seeking (Tucker et al., 2013; Wade et al., 2011). The findings may also suggest the benefit of increased advocacy and health promotion as it relates to help-seeking and combatting stigma.
Implications for Counselor Education and Counselors
Given that we found an individual’s attitudes toward seeking psychological help negatively relate to AOD use, it behooves counselors to address factors that impede help seeking. Equally important, the present findings and prior evidence reporting public stigma as a predictor of the development of self-stigma over time (Vogel et al., 2013) have important implications for the advocacy work needed by counselors and counselor educators on both an individual level and a systemic level to fully address the development of self-stigma of help seeking that subsequently affects an individual’s attitudes toward seeking psychological help. On an individual level, counselors can implement and advocate for interventions that increase an individual’s positive attitudes toward seeking help that may lower the individual’s substance use through mental health literacy (Cheng et al., 2018). Moreover, they can challenge thoughts of seeking help as weakness (Wade et al., 2011), normalize seeking psychological help, and discuss the benefits of therapy to address the development and effects of self-stigma of help seeking for individuals with substance use issues. Counselors can also empower clients by cultivating awareness and reflection of internalized negative beliefs developed from experiences of discrimination and prejudice that contribute to the self-stigma of help seeking. Moreover, efforts to deliver healthier messages about help seeking for mental health concerns from the media or faith-based organizations can assist with decreasing self-stigma that still exists.
In adherence to advocacy competency standards set forth by the American Counseling Association (Lewis et al., 2003), counselors should also consider using their position of power to address, on a systemic level, the enacted and perceived stigma experienced by individuals with substance use issues as well as the detrimental impact on attitudes toward seeking psychological help. For example, counselors can disseminate information that dispels myths surrounding help seeking and substance use to the public or create multimedia materials such as public service announcements that explain the impact of stigma on those with SUDs in the United States, making sure to include affirmative language about seeking psychological help and individuals reporting AOD use (Corrigan, 2011). Counselors also can lobby to make changes to workplace policies and practices to increase mental health support for those with AOD concerns, as supportive policies and practices can also decrease the stigmas associated with AOD concerns.
Additionally, counselors and counselor educators can improve attitudes toward help seeking as well as decrease the stigma of individuals with substance use issues by intentionally using person-first language on administered surveys, academic scholarship, and provided resources to clients and the community (Tucker et al., 2013). For example, Granello and Gibbs (2016) found that participants reported higher tolerance and less stigmatized attitudes when the language on surveys was changed from “mentally ill” to “people with mental illness.” In the current study, we used person-first language in order to model correct terminology and would suggest that future researchers do the same. By disseminating knowledge and material to the public in less stigmatizing language, counselors and counselor educators can counter negative group stereotypes that lead to self-stigma of individuals with substance use issues (Al-Khouja & Corrigan, 2017; Rao et al., 2009).
For counselor educators and supervisors training beginning counselors, this study suggests the importance of increased awareness of their own attitudes toward individuals reporting AOD use because of the effects of internalized public stigma, which increases maladaptive coping skills such as treatment avoidance (Crowe et al., 2016) and AOD use (Etesam et al., 2014). To illustrate, counselor educators and supervisors may ask beginning counselors to reflect on their personal beliefs regarding seeking psychological help and individuals with substance use issues, as well as how these beliefs may have been learned based on public perceptions or knowledge of information regarding substance use. Classroom strategies that encourage reflection and increase an ethic of care may address previous findings of implicit bias, internalized negative public attitudes, or stigmatizing behaviors by health professionals that lower positive attitudes toward psychological help seeking for individuals with substance use issues (Ford, 2011). Lastly, counselor educators can further promote beginning counselors’ advocacy competencies through creative and engaging assignments that challenge students to develop ways of encouraging help seeking in the general public and dispel public myths about substance use or the stigma of seeking psychological help—for instance, the creation of fact and resource brochures distributed within the community.
This study also further supported the use of MTurk for reliable and valid data in an accessible community sample (Kim & Hodgins, 2017). The anonymity, convenience, and incentive offered to participants via MTurk while reporting behaviors stigmatized by the general public may contribute to the gathering of reliable and valid data (Kim & Hodgins, 2017). Additionally, this study supports MTurk as a tool to identify clinical populations with alcohol use problems (Al-Khouja & Corrigan, 2017). The use of MTurk as a sampling method is currently limited in counselor education literature and may lead to more representative samples that resemble targeted community populations beyond the commonly accessed university samples by researchers.
Limitations
This study has several limitations. First, although the study used a community sample, the sample included only individuals accessible through MTurk, and research on the representativeness of samples drawn from MTurk is limited (Al-Khouja & Corrigan, 2017; Kim & Hodgins, 2017). The sample employed through MTurk was gathered widely from the community and previous studies have shown evidence of validity and reliability of MTurk as a recruiting tool with substance-using populations (Kim & Hodgins, 2017). However, because MTurk uses an online platform, it is subject to the same classic limitations associated with online data collection, such as representativeness and technical difficulties (Granello & Wheaton, 2004). Therefore, the current sample showed diversity among participants, but researchers could not confirm whether MTurk samples were representative of the populations from which they were drawn. Specifically, the sample consisted primarily of White and Asian participants, thereby limiting generalizability to people of other race/ethnicity classifications. Another limitation of this study is the absence of inattentive screening items. Additionally, this investigation used correlational data analysis methods to examine the proposed model; therefore, the findings could not indicate causality among the variables (Gall et al., 2007). Finally, although we wanted to know about stigma related to SUDs, we used scales that were designed to measure stigma in general. Although all instruments demonstrated strong psychometric properties in the current study, it is worth noting that stigma of SUDs may be different from stigma related to mental health concerns with no substance use.
Future Research
Considering the limitations, these findings provide significant implications for future research. We suggest replication of the present findings on future groups through the MTurk platform and other sampling methods (Al-Khouja & Corrigan, 2017). Additionally, researchers are encouraged to conduct experimental studies implementing potential substance use treatments that disrupt and measure the internalized negative group stereotypes that individuals with substance use issues may incorporate into their identity, substance usage, and treatment efficacy or length (Luoma et al., 2014; Tucker et al., 2013). Researchers have emphasized identity as a diagnostic moderator of self-stigma incurred by individuals with mental illness and substance use issues (Al-Khouja & Corrigan, 2017; Yanos et al., 2010), which suggests the importance of countering negative group stereotypes and public stigma for vulnerable groups such as individuals with substance use issues who report high levels of self-stigma. Further, counselor educators are encouraged to explore the relationship between identity, self-stigma of help seeking, and attitudes toward seeking psychological help with individuals reporting substance use issues as well. Lastly, counselor educators may examine the use of MTurk to gather a community sample, explore behaviors and attitudes considered socially unacceptable by the general public, and recruit individuals meeting the clinical criteria for substance use, who are often a hidden population because of enacted and perceived stigma.
Conclusion
The current study examined the complex and understudied relationship between AOD use, self-stigma of help seeking, self-stigma of mental illness, and attitudes toward seeking psychological help. The findings suggest the unique, indirect relationship between self-stigma of help seeking, a positive attitude toward seeking psychological help, and AOD use, regardless of participant age ranges. Previous conceptualization of the interdependence between self-stigma and group stereotypes (Al-Khouja & Corrigan, 2017) as well as the unique findings of the current study suggest that counselors and substance use interventions need to counter group stereotypes that individuals with substance use internalize, which decrease positive attitudes toward seeking psychological help and help-seeking behaviors for mental illness (Crowe et al., 2016; Tucker et al., 2013; Wade et al., 2011). By countering group stereotypes through methods targeting attitudes toward help seeking and the self-stigma of help seeking, counselors and counselor educators can potentially combat the negative attitudes toward seeking psychological help that become internalized treatment barriers for individuals with substance use issues (Luoma et al., 2008) and help lower AOD use.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Al-Khouja, M. A., & Corrigan, P. W. (2017). Self-stigma, identity, and co-occurring disorders. The Israel Journal of Psychiatry and Related Sciences, 54(1), 56–61.
Arbuckle, J. R. (2012). AMOS users guide version 24.0 [User manual]. IBM Corp.
Barry, C. L., McGinty, E. E., Pescosolido, B. A., & Goldman, H. H. (2014). Stigma, discrimination, treatment effectiveness, and policy: Public views about drug addiction and mental illness. Psychiatric Services, 65(10), 1269–1272. https://doi.org/10.1176/appi.ps.201400140
Birtel, M. D., Wood, L., & Kempa, N. J. (2017). Stigma and social support in substance abuse: Implications for mental health and well-being. Psychiatry Research, 252, 1–8. https://doi.org/10.1016/jpsychres.2017.01.097
Bose, J., Hedden, S. L., Lipari, R. N., & Park-Lee, E. (2018). Key substance use and mental health indicators in the United States: Results from the 2017 National Survey on Drug Use and Health (HHS Publication No. SMA 18-5068, NSUDH Series H-53). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHFFR2017/NSDUHFFR2017.pdf
Bose, J., Hedden, S. L., Lipari, R. N., Park-Lee, E., Porter, J. D., & Pemberton, M. R. (2016). Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health (HHS Publication No. SMA 16-4984, NSDUH Series H-51). https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2015/NSDUH-FFR1-2015/NSDUH-FFR1-2015.pdf
Center for Behavioral Health Statistics and Quality. (2015). Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15-4927, NSDUH Series H-50). https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf
Center for Behavioral Health Statistics and Quality. (2018). 2017 National Survey on Drug Use and Health: Methodological summary and definitions. https://www.samhsa.gov/data/report/2017-methodological-summary-and-definitions
Cheng, H.-L., Wang, C., McDermott, R. C., Kridel, M., & Rislin, J. L. (2018). Self-stigma, mental health literacy, and attitudes toward seeking psychological help. Journal of Counseling & Development, 96(1), 64–74. https://doi.org/10.1002/jcad.12178
Clement, S., Schauman, O., Graham, T., Maggioni, F., Evans-Lacko, S., Bezborodovs, N., Morgan, C., Rüsch, N.,
Brown, J. S. L., & Thornicroft, G. (2015). What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychological Medicine, 45(1), 11–27. https://doi.org/10.1017/S0033291714000129
Corrigan, P. W. (2011). Strategic stigma change (SSC): Five principles for social marketing campaigns to reduce stigma. Psychiatric Services, 62(8), 824–826. https://doi.org/10.1176/ps.62.8.pss6208_0824
Crapanzano, K. A., Hammarlund, R., Ahmad, B., Hunsinger, N., & Kullar, R. (2019). The association between perceived stigma and substance use disorder treatment outcomes: A review. Substance Abuse and Rehabilitation, 10, 1–12. https://doi.org/10.2147/SAR.S183252
Crowe, A., Averett, P., & Glass, J. S. (2016). Mental illness stigma, psychological resilience, and help seeking: What are the relationships? Mental Health & Prevention, 4(2), 63–68. https://doi.org/ 10.1016/j.mhp.2015.12.001
da Silveira, P. S., Casela, A. L. M., Monteiro, É. P., Ferreira, G. C. L., de Freitas, J. V. T., Machado, N. M., Noto, A. R., & Ronzani, T. M. (2018). Psychosocial understanding of self-stigma among people who seek treatment for drug addiction. Stigma and Health, 3(1), 42–52. https://doi.org/10.1037/sah0000069
Elhai, J. D., Schweinle, W., & Anderson, S. M. (2008). Reliability and validity of the Attitudes Toward Seeking Professional Psychological Help Scale-Short Form. Psychiatry Research, 159(3), 320–329. https://doi.org/10.1016/j.psychres.2007.04.020
Etesam, F., Assarian, F., Hosseini, H., & Ghoreishi, F. S. (2014). Stigma and its determinants among male drug dependents receiving methadone maintenance treatment. Archives of Iranian Medicine, 17(2), 108–114.
Fischer, E. H., & Farina, A. (1995). Attitudes toward seeking professional psychological help: A shortened form and considerations for research. Journal of College Student Development, 36(4), 368–373.
Follmer, D. J., Sperling, R. A., & Suen, H. K. (2017). The role of MTurk in education research: Advantages, issues, and future directions. Educational Researcher, 46(6), 329–334. https://doi.org/10.3102/0013189X17725519
Ford, R. (2011). Interpersonal challenges as a constraint on care: The experience of nurses’ care of patients who use illicit drugs. Contemporary Nurse, 37(2), 241–252. https://doi.org/10.5172/conu.2011.37.2.241
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gall, M. D., Gall, J. P., & Borg, W. R. (2007). Education research: An introduction (8th ed.). Allyn & Bacon.
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. Prentice-Hall.
Granello, D. H., & Gibbs, T. A. (2016). The power of language and labels: “The mentally ill” versus “people with mental illnesses.” Journal of Counseling & Development, 94(1), 31–40. https://doi.org/10.1002/jcad.12059
Granello, D. H., & Wheaton, J. E. (2004). Online data collection: Strategies for research. Journal of Counseling & Development, 82(4), 387–393. https://doi.org/10.1002/j.1556-6678.2004.tb00325.x
Hair, J. F., Black, W. C., Babin, B. J., Anderson, R. E., & Tatham, R. L. (2006). Multivariate data analysis (6th ed.). Pearson.
Jackson, D. L. (2003). Revisiting sample size and number of parameter estimates: Some support for the N:q hypothesis. Structural Equation Modeling, 10(1), 128–141. https://doi.org/10.1207/S15328007SEM1001_6
Karaffa, K. M., & Koch, J. M. (2016). Stigma, pluralistic ignorance, and attitudes toward seeking mental health services among police officers. Criminal Justice and Behavior, 43(6), 759–777. https://doi.org/10.1177/0093854815613103
Kim, H. S., & Hodgins, D. C. (2017). Reliability and validity of data obtained from alcohol, cannabis, and gambling populations on Amazon’s Mechanical Turk. Psychology of Addictive Behaviors, 31(1), 85–94. https://doi.org/10.1037/adb0000219
Kline, R. (2005). Principles and practice of structural equation modeling. (2nd ed.). Guilford.
Lewis, J. A., Arnold, M. S., House, R., & Toporek, R. L. (2003). ACA advocacy competencies. https://www.counseling.org/knowledge-center/competencies
Livingston, J. D., Milne, T., Fang, M. L., & Amari, E. (2012). The effectiveness of interventions for reducing stigma related to substance use disorders: A systematic review. Addiction, 107(1), 39–50. https://doi.org/10.1111/j.1360-0443.2011.03601.x
Luoma, J. B., Kohlenberg, B. S., Hayes, S. C., Bunting, K., & Rye, A. K. (2008). Reducing self-stigma in substance abuse through acceptance and commitment therapy: Model, manual development, and pilot outcomes. Addiction Research & Theory, 16(2), 149–165. https://doi.org/10.1080/16066350701850295
Luoma, J. B., Kulesza, M., Hayes, S. C., Kohlenberg, B., & Larimer, M. (2014). Stigma predicts residential treatment length for substance use disorder. The American Journal of Drug and Alcohol Abuse, 40(3), 206–212. https://doi.org/10.3109/00952990.2014.901337
Masson, C. L., Shopshire, M. S., Sen, S., Hoffman, K. A., Hengl, N. S., Bartolome, J., McCarty, D., Sorensen, J. L.,
& Iguchi, M. Y. (2013). Possible barriers to enrollment in substance abuse treatment among a diverse sample of Asian Americans and Pacific Islanders: Opinions of treatment clients. Journal of Substance Abuse Treatment, 44(3), 309–315. https://doi.org/10.1016/j.jsat.2012.08.005
Mora-Ríos, J., Ortega-Ortega, M., & Medina-Mora, M. E. (2017). Addiction-related stigma and discrimination: A qualitative study in treatment centers in Mexico City. Substance Use & Misuse, 52(5), 594–603. https://doi.org/10.1080/10826084.2016.1245744
Mullen, P. R., & Crowe, A. (2017). Self-stigma of mental illness and help seeking among school counselors. Journal of Counseling & Development, 95(4), 401–411. https://doi.org/10.1002/jcad.12155
Rao, H., Mahadevappa, H., Pillay, P., Sessay, M., Abraham, A., & Luty, J. (2009). A study of stigmatized attitudes towards people with mental health problems among health professionals. Journal of Psychiatric and Mental Health Nursing, 16(3), 279–284. https://doi.org/10.1111/j.1365-2850.2008.01369.x
Saunders, J. B., Aasland, O. G., Babor, T. F., de la Fuente, J. R., & Grant, M. (1993). Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction, 88(6), 791–804. https://doi.org/10.1111/j.1360-0443.1993.tb02093.x
Schomerus, G., Corrigan, P. W., Klauer, T., Kuwert, P., Freyberger, H. J., & Lucht, M. (2011). Self-stigma in alcohol dependence: Consequences for drinking-refusal self-efficacy. Drug and Alcohol Dependence, 114(1), 12–17. https://doi.org/10.1016/j.drugalcdep.2010.08.013
Sink, C. A., & Stroh, H. R. (2006). Practical significance: The use of effect sizes in school counseling research.
Professional School Counseling, 9(4), 401–411. https://doi.org/10.1177/2156759X0500900406
Skinner, H. A., & Goldberg, A. E. (1986). Evidence for a drug dependence syndrome among narcotic users. British Journal of Addiction, 81(4), 479–484. https://doi.org/10.1111/j.1360-0443.1986.tb00359.x
Smith, L. R., Earnshaw, V. A., Copenhaver, M. M., & Cunningham, C. O. (2016). Substance use stigma: Reliability and validity of a theory-based scale for substance-using populations. Drug and Alcohol Dependence, 162(1), 34–43. https://doi.org/10.1016/j.drugalcdep.2016.02.019
Stringer, K. L., & Baker, E. H. (2018). Stigma as a barrier to substance abuse treatment among those with unmet need: An analysis of parenthood and marital status. Journal of Family Issues, 39(1), 3–27. https://doi.org/10.1177/0192513×15581659
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Allyn and Bacon.
Tucker, J. R., Hammer, J. H., Vogel, D. L., Bitman, R. L., Wade, N. G., & Maier, E. J. (2013). Disentangling self-stigma: Are mental illness and help-seeking self-stigmas different? Journal of Counseling Psychology, 60(4), 520–531. https://doi.org/10.1037/a0033555
U.S. Department of Health and Human Services, Office of the Surgeon General. (2018). Facing addiction in America: The Surgeon General’s spotlight on opioids. https://addiction.surgeongeneral.gov/sites/default/files/Spotlight-on-Opioids_09192018.pdf
Vogel, D. L., Bitman, R. L., Hammer, J. H., & Wade, N. G. (2013). Is stigma internalized? The longitudinal impact of public stigma on self-stigma. Journal of Counseling Psychology, 60(2), 311–316. https://doi.org/10.1037/a0031889
Vogel, D. L., & Wade, N. G. (2009). Stigma and help-seeking. The Psychologist, 22, 20–23. https://thepsychologist.bps.org.uk/volume-22/edition-1/stigma-and-help-seeking
Vogel, D. L., Wade, N. G., & Haake, S. (2006). Measuring the self-stigma associated with seeking psychological help. Journal of Counseling Psychology, 53(3), 325–337. https://doi.org/10.1037/0022-0167.53.3.325
Vogel, D. L., Wade, N. G., & Hackler, A. H. (2007). Perceived public stigma and the willingness to seek counseling: The mediating roles of self-stigma and attitudes toward counseling. Journal of Counseling Psychology, 54(1), 40–50. https://doi.org/10.1037/0022-0167.54.1.40
Wade, N. G., Post, B. C., Cornish, M. A., Vogel, D. L., & Tucker, J. R.. (2011). Predictors of the change in self-stigma following a single session of group counseling. Journal of Counseling Psychology, 58(2), 170–182. https://doi.org/10.1037/a0022630
Winstanley, E. L., Clark, A., Feinberg, J., & Wilder, C. M. (2016). Barriers to implementation of opioid overdose prevention programs in Ohio. Substance Abuse, 37(1), 42–46. https://doi.org/10.1080/08897077.2015.1132294
Yanos, P. T., Roe, D., & Lysaker, P. H. (2010). The impact of illness identity on recovery from severe mental illness. American Journal of Psychiatric Rehabilitation, 13(2), 73–93. https://doi.org/10.1080/15487761003756860
Yudko, E., Lozhkina, O., & Fouts, A. (2007). A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. Journal of Substance Abuse Treatment, 32(2), 189–198. https://doi.org/10.1016/j.jsat.2006.08.002
Daniel Gutierrez, PhD, NCC, LPC, CSAC, is an assistant professor at the College of William & Mary. Allison Crowe, PhD, NCC, LPCS, is an associate professor at East Carolina University. Patrick R. Mullen, PhD, NCC, is an assistant professor at the College of William & Mary. Laura Pignato is a doctoral student at the College of William & Mary. Shuhui Fan, NCC, is a doctoral student at the College of William & Mary. Correspondence may be addressed to William & Mary, Daniel Gutierrez, School of Education, P.O. Box 8795, Williamsburg, VA 23187-8795, dgutierrez@wm.edu.
Apr 29, 2020 | Volume 10 - Issue 2
Heather J. Fye, Ryan M. Cook, Eric R. Baltrinic, Andrea Baylin
Burnout is a statistically significant phenomenon for school counselors, correlated with various individual and organizational factors, which have been studied independently. Therefore, we investigated both individual and organizational factors of burnout conceptualized as a multidimensional phenomenon with 227 school counselors. Multidimensional burnout was measured by the five subscales of the Counselor Burnout Inventory, which included Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life. Using hierarchal regression analyses, we found individual and organizational factors accounted for 66.6% of the variance explained in Negative Work Environment, 38.3% of the variance explained in Deterioration in Personal Life, 36.7% of the variance explained in Incompetence, 35.1% of the variance explained in Exhaustion, and 14.0% of the variance explained in Devaluing Clients. We discuss implications of the findings for school counselors and supervisors. Identifying the multidimensions of burnout and its correlates, addressing self-care and professional vitality goals, communicating defined school counselor roles, providing mentoring opportunities, and increasing advocacy skills may help alleviate burnout.
Keywords: stress, burnout, job satisfaction, coping processes, school counselors
In addition to providing counseling services, school counselors are charged with performing multiple non-counseling duties in their schools (Bardhoshi et al., 2014). These multiple and competing demands place them at risk for experiencing burnout (Mullen et al., 2018). Accordingly, it is important to identify factors that contribute to burnout to promote school counselors’ psychological well-being (Kim & Lambie, 2018), which in turn reinforces school counselors’ ability to support students’ well-being (Holman et al., 2019).
Burnout is a workplace-specific complex construct characterized by feelings of exhaustion, cynicism, and detachment, and a lack of accomplishment and effectiveness (Maslach & Leiter, 2017). Others have conceptualized counselor burnout as a multidimensional construct, featuring the interaction between the individual and work environment (Lee et al., 2007). Given the complex, multidimensional, and interactional nature of burnout, the Counselor Burnout Inventory (CBI) was developed to measure the construct with five subscales: Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life (Lee et al., 2007). Specific to school counselors, Kim and Lambie (2018) suggested that burnout occurs to varying degrees across individual and organizational factors. Individual factors include perceived stress (Fye et al., 2018; Mullen et al., 2018; Mullen & Gutierrez, 2016; Wilkerson, 2009; Wilkerson & Bellini, 2006) and coping processes (Fye et al., 2018; Wilkerson, 2009; Wilkerson & Bellini, 2006). Organizational factors include perceived job satisfaction (Baggerly & Osborn, 2006; Bryant & Constantine, 2006; Mullen et al., 2018) and role stress (Bardhoshi et al., 2014; Coll & Freeman, 1997; Culbreth et al., 2005).
Researchers of school counselor burnout have studied individual and organizational factors of this phenomenon using a unidimensional structure such as the CBI scale score (Mullen et al., 2018). Other researchers (e.g., Bardhoshi et al., 2014; Moyer, 2011) studied organizational factors, including caseload and administrative (non-counseling) duties, within the multidimensional structure of the CBI (Lee et al., 2007). However, researchers have not yet comprehensively studied these known individual and organizational factors within the context of a multidimensional structure of school counselor burnout. For example, Mullen et al. (2018) investigated the relationships between perceived stress, perceived job satisfaction, and school counselor burnout. However, they did not examine organizational factors such as role stress (e.g., clerical duties), which are also significant to understanding school counselor burnout (Bardhoshi et al., 2014). Thus, we sought to extend the research findings by examining several individual factors (i.e., perceived stress, coping processes) and organizational factors (i.e., perceived job satisfaction, role stress) within a multidimensional structure of school counselor burnout.
Individual Factors
Individual factors related to school counselor burnout include psychological constructs and demographic factors (Kim & Lambie, 2018). The two psychological constructs included in the current study were perceived stress (Mullen et al., 2018) and coping processes (Fye et al., 2018). Researchers have previously found contradictory results for the relationship between years of experience and school counselor burnout (Mullen et al., 2018; Wilkerson, 2009). Therefore, the factor of years of experience was included in the current study.
Perceived Stress
Perceived stress is theorized as an individual’s ability to appraise a threatening or challenging event in relation to the availability of coping resources (Lazarus & Folkman, 1984). To that end, a transactional model of stress and coping suggests that stress is a response that occurs when perceived demands exceed one’s coping abilities. For school counselors, perceived stress may occur regularly because of various factors, including non-counseling duties, excessive paperwork and administrative duties, and work overload (Bardhoshi et al., 2014).
Researchers have described a positive relationship between stress and burnout among school counselors (Mullen et al., 2018; Mullen & Gutierrez, 2016). Specifically, higher levels of stress and burnout were related to lower levels of job satisfaction and delivery of direct student services (Mullen et al., 2018; Mullen & Gutierrez, 2016). Others have reported increased emotional responses alongside increased burnout (Wilkerson & Bellini, 2006). For example, school counselors who attempted to deal with stress emotionally may be at greater risk for developing symptoms of burnout including emotional exhaustion, depersonalization, and lower levels of personal accomplishment (Wilkerson, 2009). Additionally, school counselors reported higher levels of emotional exhaustion than other mental health professionals, which can negatively impact their delivery of school counseling services (Bardhoshi et al., 2014). The correlation between stress and burnout further highlights the importance of assessing the components of stress and the ways school counselors are coping with these factors.
Coping Processes
Coping processes are defined as the cognitive and behavioral processes used to manage stressful situations (Folkman & Moskowitz, 2004). There are several coping processes, including problem-focused coping, active-emotional coping, and avoidant-emotional coping (Folkman & Lazarus, 1985). For example, problem-focused coping is defined as an action-oriented approach to stress in which one believes the stressors are controllable by personal action (Lazarus, 1993). Active-emotional coping is an adaptive response to unmanageable stressors and avoidant-emotional coping is described as a maladaptive response to those stressors (Folkman & Lazarus, 1985).
Among school counselors, Fye et al. (2018) studied the relationship between perfectionism, burnout, stress, and coping. These authors found that maladaptive perfectionists engaged more frequently in avoidant-emotional coping and relatedly experienced higher levels of burnout. Moreover, adaptive perfectionists experienced less stress and burnout and reported higher levels of problem-focused coping. Overall, for school counseling professionals, emotional-focused coping is positively related to burnout (Wilkerson, 2009). Given these findings, it is imperative for school counselors to be aware of their coping processes, including the degree to which they are affecting their levels of stress and burnout (Wilkerson, 2009).
Organizational Factors
In addition to individual factors such as stress and coping (Fye et al., 2018; Mullen et al., 2018; Wilkerson, 2009), school counseling researchers noted several organizational factors as contributing to school counselor burnout (Holman et al., 2019; Kim & Lambie, 2018). Accordingly, researchers in the current study examined organizational factors, including perceived job satisfaction and role stress (i.e., role ambiguity, role incongruity, and role conflict; Culbreth et al., 2005). Additionally, because previous researchers found a relationship between the organizational factor of school district (e.g., urban setting) and burnout (Butler & Constantine, 2005), this variable was included in the present study.
Perceived Job Satisfaction
Perceived job satisfaction refers to the degree of affective or attitudinal reactions one experiences relative to their job (Spector, 1985). Understanding the extent of school counselors’ perceived job satisfaction may be one way to buffer the effects of stress and burnout. This is because, according to Bryant and Constantine (2006), job satisfaction predicted life satisfaction for school counselors.
Perceived job satisfaction and its relationship with stress and burnout have received increased attention in the school counseling literature (Mullen et al., 2018). Among the contributing factors, higher levels of role balance and increased perceived job satisfaction resulted in greater overall life satisfaction (Bryant & Constantine, 2006). Higher perceived job satisfaction has been aligned with school counselors engaging in appropriate roles. For example, Baggerly and Osborn (2006) found that school counselors who frequently performed roles aligned with comprehensive school counseling programs were more satisfied and more committed to their careers. Similarly, higher perceived job satisfaction was directly related to the school counselor’s ability to provide direct student services within their schools (Kolodinsky et al., 2009). Conversely, school counselors who did not intend to return to their jobs the following year reported higher levels of demand and stress because of non-counseling duties, such as excessive paperwork and administrative disruptions (McCarthy et al., 2010). As a result, those who are not satisfied are at risk for disengagement (Mullen et al., 2018), while school counselors who are satisfied with their jobs may have increased student connections (Kolodinsky et al., 2009).
Role Stress
Role stress refers to the levels of role incongruity, role conflict, and role ambiguity experienced by school counselors (Culbreth et al., 2005; Freeman & Coll, 1997). Role incongruity may occur when there are structural conflicts, including inadequate resources for school counselors and engagement in ineffective tasks (Freeman & Coll, 1997). Several authors noted that inappropriate or non-counseling duties contributed to burnout, including excessive paperwork, administrative duties, and testing coordinator roles (Bardhoshi et al., 2014; Moyer, 2011, Wilkerson, 2009). Moyer (2011) found that school counselors who engaged in increased non-counseling duties also had increased feelings of exhaustion and incompetence, had decreased feelings toward work environment, and were less likely to show empathy toward students. Furthermore, school counselors who were assigned inappropriate roles reported higher levels of frustration and resentment toward the school system. Overall, authors emphasized the importance of educating administrators on the appropriate and inappropriate roles for school counselors to decrease burnout (Bardhoshi et al, 2014; Cervoni & DeLucia-Waack, 2011; Moyer, 2011).
Role conflict occurs when school counselors experience multiple external demands from different stakeholders (Holman et al., 2019). Role conflict examples for school counselors include: (a) whether school counselors should focus on the education goals or mental health needs of students first (Paisley & McMahon, 2001) and (b) whether a school counselor should engage in an actual role given by an administration or supervisor (e.g., testing coordinator) or preferred role (e.g., classroom guidance activity; Wilkerson, 2009). As such, school counselors can feel overwhelmed and often engage in inappropriate duties, according to the American School Counselor Association (ASCA) National Model (2019). In turn, school counselors experience stress and burnout (Mullen et al., 2018).
Role ambiguity is the discrepancy between actual and preferred counseling duties (Scarborough & Culbreth, 2008). Role ambiguity has been linked to burnout because of school counselors’ stress from lacking an understanding of their professional roles and being misinformed about the realities of the job (Culbreth et al., 2005). For example, school counselors face challenges of navigating mixed messages about role expectations across stakeholders (Coll & Freeman, 1997). This confusion may lead to school counselors experiencing role ambiguity (Scarborough & Culbreth, 2008). When school counselors interact with stakeholders who have conflicting ideas about their roles, it creates stress. It is especially difficult for school counselors when stakeholders’ conceptualization of their roles clashes with what school counselors learned during graduate training (Culbreth et al., 2005). When school counselors are assigned duties that conflict with their own understandings of their roles, they are not able to operate in alignment with their professional mandates (Holman et al., 2019). Overall, school counselors experiencing role ambiguity also report higher levels of stress, both of which have been linked to burnout (Kim & Lambie, 2018).
Purpose of the Present Study
Despite prevalence in the school counseling burnout literature regarding individual and organizational factors of burnout, we were unable to locate a study that holistically researched these variables. To align our findings with a theoretical understanding of school counselor burnout, we examined these phenomena as a multidimensional construct. Additionally, we controlled for years of experience (Mullen et al., 2018; Wilkerson, 2009; Wilkerson & Bellini, 2006) and school district (Butler & Constantine, 2005). Therefore, we answered the research question: What is the relationship between individual (i.e., perceived job stress, problem-focused coping, avoidant-emotional coping, and active-emotional coping) and organizational (i.e., perceived job satisfaction, role incongruity, role conflict, and role ambiguity) factors after controlling for years of experience and school district, with the subscales of school counselor burnout: (1) Exhaustion, (2) Incompetence, (3) Negative Work Environment, (4) Devaluing Clients, and (5) Deterioration in Personal Life?
Method
Sample
A total of 227 school counselors participated in the study. Ages ranged from 26 to 69 (M = 46.21; SD = 10.26; four declined to answer). The sex of participants included females (n = 166, 73.1%) and males (n = 61, 26.9%). The race and ethnicity of participants included White (n = 185, 81.5%), African American/Black (n = 20, 8.8%), Hispanic (n = 7, 3.1%), Asian/Pacific Islander (n = 3, 1.3%), American Indian/Alaskan Native (n = 1, 0.4%), and Biracial/Multiracial (n = 9, 4.0%), and two participants (0.9%) declined to answer. Participants held a master’s degree in school counseling (n = 175, 77.1%), a PhD or EdD (n = 33, 14.5%), or a master’s degree in another counseling or mental health specialty area (n = 19, 8.4%). The years of experience ranged from 2 to 41 years (M = 13.68, SD = 7.49). Participants reported working in suburban (n = 97, 42.7%), rural (n = 76, 33.5%), and urban (n = 54, 23.8%) settings. Regarding level of practice, participants worked in an elementary school (i.e., grades K–6; n = 80, 35.2%), middle school (i.e., grades 7–8; n = 14, 6.2%), high school (i.e., grades 9–12; n = 59, 26.0%), or multiple grade levels (e.g., K–8, K–12, etc.; n = 74, 32.6%). A power analysis was completed in G*Power 3.1 before beginning the study (Faul et al., 2009). The necessary sample size was determined to be at least 200, with a power of .80, assuming a moderate effect size of .15 in the multiple regression analyses, and with an error probability or alpha of .05 (J. Cohen, 1992).
Procedures
Institutional Review Board approval was obtained prior to beginning the study. The first author sent recruitment emails to 4,000 school counselors who were professional members of the ASCA online membership directory. Specifically, approximately 20% of school counselors in each of the 50 states and District of Columbia were chosen from the membership directory to receive the recruitment emails. The emails included a brief introduction to the study and an anonymous link that took potential participants to the online survey portal in Qualtrics. Potential participants first reviewed the informed consent. Once they consented to the survey, participants completed the demographics questionnaire and instruments. A convenience sample was obtained based upon voluntary responses to the survey (Dimitrov, 2009).
Instruments
The first author constructed a brief demographics survey to gather information about the participants (e.g., age, sex, race and ethnicity, degree, and years of experience) and their work environment (e.g., school district, grade level). The Perceived Stress Scale (PSS; S. Cohen et al., 1983) and Brief COPE (Carver, 1997) were used to measure individual factors. The Job Satisfaction Survey (JSS; Spector, 1985) and Role Questionnaire (RQ; Rizzo et al., 1970) were used to measure organizational factors. The CBI (Lee et al., 2007) was used to measure the dimensions of school counselor burnout.
Perceived Stress Scale (PSS)
The PSS (S. Cohen et al., 1983) is a 14-item inventory designed to measure an individual’s perceived stress within the past month. In the present study, we used the PSS-4, which is a subset of items from the original 14-item scale. The PSS was normed on a large sample of individuals from across the United States (S. Cohen et al., 1983). Participants responded to a 5-point Likert-type scale ranging from 0 (never) to 4 (very often). Scores on the PSS-4 ranged from 0 to 20. An example question of the PSS-4 is: “In the past month, how often have you felt difficulties were piling up so high that you could not overcome them?” The PSS-4 was determined to be a suitable brief measure of stress perceptions, based upon adequate factor structure and predictive validity (S. Cohen & Williamson, 1988). Reliability has been upheld (e.g., S. Cohen & Williamson, 1988) with test-retest reliability at .85 after 2 days (S. Cohen et al., 1983). For the present study, the internal consistency reliability was calculated at α = .76. Correlations between the perceived stress total score and CBI subscales ranged from r = .19 to .55.
Brief COPE
The Brief COPE (Carver, 1997) is a 28-item inventory designed to measure coping responses or processes and includes 14 subscales. We followed previous researchers’ (e.g., Deatherage et al., 2014) grouping of the 14 subscales into three coping processes (i.e., problem-focused, active-emotional, and avoidant-emotional). Therefore, problem-focused coping contained the Active Coping, Planning, Instrumental Support, and Religion subscales. Active-emotional coping contained the Venting, Positive Reframing, Humor, Acceptance, and Emotional Support subscales. Avoidant-emotional coping contained the Self-Distraction, Denial, Behavioral Disengagement, and Self-Blame subscales. For the present study, the items pertaining to participants’ alcohol and illegal drug use as coping responses were omitted because of their sensitive nature. Therefore, 26 items were included in the present study. The inventory uses a 4-point Likert-type scale with scores ranging from 0 (I haven’t been doing this at all) to 3 (I’ve been doing this a lot). A sample item on the Brief COPE is “I’ve been turning to work or other activities to take my mind off things.” Construct validity has been upheld with the three coping processes (e.g., Deatherage et al., 2014). Test-retest reliability for the three subscale groups has been upheld over a year timespan (Cooper et al., 2008). For the present study, the internal consistency reliability was calculated for problem-focused coping at α = .84, avoidant-emotional coping at α = .70, and active-emotional coping at α = .81. Correlations between problem-focused coping and the CBI subscales ranged from r = .00 to .13, correlations between avoidant-emotional coping and CBI subscales ranged from r = .20 to .48, and correlations between active-emotional coping and CBI subscales ranged from r = .01 to .16.
Job Satisfaction Survey (JSS)
The JSS (Spector, 1985) is a 36-item inventory intended to measure an individual’s perceived job satisfaction or attitudes and aspects of the job. The JSS contains nine subscales: Pay, Promotion, Supervision, Fringe Benefits, Contingent Rewards, Operating Procedures, Coworkers, Nature of Work, and Communication. The inventory uses a 6-point Likert-type scale with scores ranging from 1 (disagree very much) to 6 (agree very much). Total scores range from 36 to 216 with the higher the score, the higher job satisfaction experienced. An example item on the JSS is “My job is enjoyable” (Spector, 1985, p. 711). The JSS was constructed for, and normed on, social service, education, and mental health professionals (Spector, 1985, 2011). Spector (1985) established convergent validity with the Job Descriptive Index (Smith et al., 1969), and produced scores ranging from .61 to .80. Strong reliability has been established for the JSS, including a Cronbach coefficient alpha of .91 for all factors combined, and at 18 months, the test-retest reliability score was .71 (Spector, 1985). For the present study, the internal consistency reliability was calculated for the total scores at α = .91. Correlations between the perceived job satisfaction total score and CBI subscales ranged from r = -.13 to -.75.
Role Questionnaire (RQ)
The RQ (Rizzo et al., 1970) is a 14-item inventory designed to measure the level of role conflict and role ambiguity an individual has about a job. The RQ has been factor analyzed with school counselors (Freeman & Coll, 1997) and found to have three distinct factors (i.e., role incongruity, role conflict, and role ambiguity). The inventory uses a 7-point Likert-type scale with scores ranging from 1 (very false) to 7 (very true). Role incongruity refers to conflicts with the structure of the system and allocation of resources (Freeman & Coll, 1997). The role incongruity factor comprises items 1–4. Total scores range from 8 to 32, with the higher the score, the higher role incongruity experienced. A sample item for role incongruity is “I receive an assignment without adequate resources and materials to execute it.” Role conflict refers to the contradictory requests of work expectations with varying groups (Freeman & Coll, 1997). The role conflict factor comprises items 5–8. The higher the score, the higher role conflict experienced, which can range from 8 to 32. A sample item for role conflict is “I receive incompatible requests from two or more people.” The role ambiguity factor, which measures a lack of clarity on the job, is negatively worded; therefore, the lower the score, the higher the role ambiguity experienced. The role ambiguity factor comprises items 9–14, and total scores range from 6 to 42. A sample item for role ambiguity is “Explanation is clear of what has to be done.” Construct validity for the three factors with school counselors was established by Freeman and Coll (1997). Reliability of the three factors have been upheld for school counselor participants (Culbreth et al., 2005; Wilkerson, 2009; Wilkerson & Bellini, 2006). For the present study, the internal consistency reliability was calculated for role incongruity at α = .82, role conflict at α = .79, and role ambiguity at α = .90. Correlations between role incongruity and CBI subscales ranged from r = .14 to .65, correlations between role conflict and CBI subscales ranged from r = .14 to .53, and correlations between role ambiguity and CBI subscales ranged from r = -.22 to -.56.
Counselor Burnout Inventory (CBI)
The CBI (Lee et al., 2007) is a 20-item inventory designed to measure counselors’ burnout levels. The CBI includes five subscales, with four questions for each subscale: Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life. The CBI uses a 5-point Likert-type scale ranging from 1 (never true) to 5 (always true). Total scores on each subscale range from 5 to 20, with the higher the score, the higher level of burnout. A sample item from the Exhaustion subscale is “Due to my job as a counselor, I feel tired most of the time.” A sample item from the Incompetence subscale is “I am not confident in my counseling skills.” A sample item from the Negative Work Environment subscale is “I am treated unfairly in my workplace.” A sample item from the Devaluing Clients subscale is “I am not interested in my clients and their problems.” A sample item from the Deterioration in Personal Life subscale is “I feel I have poor boundaries between work and my personal life.” Two independent samples composed of counselors from a variety of settings across the United States were used to explore and confirm the factor structure (Lee et al., 2007). Gnilka et al. (2015) upheld the CBI five-factor structure with a confirmatory factor analysis in a sample of school counselors. Cronbach’s alpha for the total CBI was .88, with scores ranging from .73 to .85 for the subscales (Lee et al., 2007). For the present study, internal consistency reliability for the CBI subscales were calculated and ranged from α = .78 to .89.
Results
Prior to conducting the primary analyses, we used SPSS (Version 25.0) to clean the data, impute missing data values, and test the assumptions of the primary analyses (i.e., hierarchal regressions), as recommended by Tabachnick and Fidell (2013). We used expectation-maximization (EM) to impute missing data (Cook, 2020), after we tested the randomness of the missing values with Little’s missing completely at random (MCAR). All missing values were determined to be MCAR, except for the active-emotional coping of the Brief COPE and the JSS: χ2(40, N = 227) = 79.13, p = .000, and χ2(671, N = 227) = 836.57, p = .000, respectively. Because the missing values for the active-emotional coping and JSS were less than 1%, expectation-maximization was an appropriate imputation method (Cook, 2020). Less than 5% of values were imputed for the PSS-4, the factors of the RQ (role ambiguity, role incongruity, and role conflict), and the five subscales of the CBI (Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life), and less than 1% of the values were imputed for the problem-focused and avoidant-emotional processes of the Brief COPE.
To answer the research question, we used three-step hierarchical regression models to analyze the individual and cumulative contributions for demographic, individual, and organizational factors with each subscale of the CBI. Qualities of the instruments are provided in Table 1. In Step 1, we entered the demographic factors (i.e., years of experience and school district). In Step 2, we entered the individual factors (i.e., perceived stress, problem-focused coping, avoidant-emotional coping, and active-emotional coping). In Step 3, we entered the organizational factors (i.e., perceived job satisfaction, role incongruity, role conflict, and role ambiguity). Completed assumption checks showed no outliers or influential data points, as concluded by an examination of the Q-Q plots, histograms, scatterplots, and Mahalanobis distance. We checked multicollinearity and found it to be an issue for school district (tolerance < .01). Therefore, we removed the school district variable and reentered years of experience in Step 1. To control for Type I error, we used the Bonferroni method to adjust the family-wise alpha (Darlington & Hayes, 2017), which resulted in .01 as the cutoff for statistical significance for Step 2 (i.e., individual factors) and .0056 as the cutoff for statistical significance for Step 3 (i.e., organizational factors). Results for each of these models are presented in Table 2.
Table 1
Qualities of Instrumentation
| Instrumentation |
Scores |
M |
SD |
α |
| Perceived Stress Scale-4 Total Score
Problem-Focused Coping
Avoidant-Emotional Coping
Active-Emotional Coping
Job Satisfaction Scale Total Score
Role Ambiguity
Role Incongruity
Role Conflict
Exhaustion
Incompetence
Negative Work Environment
Devaluing Client
Deterioration in Personal Life |
4–19
8–32
8–24
10–38
82–204
7–42
4–28
4–26
4–20
4–17
4–20
4–13
4–19 |
8.24
22.55
12.48
25.74
143.25
29.67
15.47
15.18
11.54
8.77
9.87
5.61
8.65 |
2.86
5.29
3.03
5.56
25.28
7.25
5.77
5.58
3.97
2.96
3.75
2.08
3.32 |
.76
.84
.70
.81
.91
.90
.82
.79
.89
.78
.85
.80
.78 |
Table 2
Results of Hierarchal Regression Analyses of School Counselor Burnout
|
Exhaustion |
Incompetence |
Negative Work Environment |
Devaluing Clients |
Deterioration in Personal Life |
| Step 1 |
|
|
|
|
| Years of Experience |
-.038 |
-.233* |
-.072 |
-.190* |
-.047 |
|
|
|
|
|
|
| R2 |
.001 |
.054 |
.005 |
.036 |
.002 |
| F |
.323 |
12.89** |
1.17 |
8.46* |
.500 |
| Step 2 |
|
|
|
|
|
| Years of Experience |
.030 |
-.151** |
-.042 |
-.155 |
.001 |
| Perceived Stress |
.392** |
.184 |
.283** |
.093 |
.491** |
| Avoidant-Emotional Coping |
.160 |
.360** |
.025 |
.180 |
.103 |
| Active-Emotional Coping |
.030 |
.087 |
.026 |
.131 |
.151 |
| Problem-Focused Coping |
-.043 |
-.151 |
.081 |
-.229** |
-.105 |
|
|
|
|
|
|
| R2 |
.240 |
.284 |
.109 |
.116 |
.323 |
| Δ R2 |
.239 |
.229 |
.104 |
.080 |
.321 |
| ΔF |
17.34** |
17.69** |
6.43** |
4.98** |
26.24** |
| Step 3 |
|
|
|
|
|
| Years of Experience |
.056 |
-.097 |
.052 |
-.125 |
.025 |
| Perceived Stress |
.303† |
.150 |
.057 |
.070 |
.437† |
| Avoidant-Emotional Coping |
.170 |
.338† |
.025 |
.165 |
.077 |
| Active-Emotional Coping |
.034 |
.126 |
.050 |
.151 |
.155 |
| Problem-Focused Coping |
-.064 |
-.180 |
.042 |
-.243† |
-.127 |
| Perceived Job Satisfaction |
-.198 |
.080 |
-.489† |
.032 |
.029 |
| Role Ambiguity |
.014 |
-.276† |
-.122 |
-.147 |
-.029 |
| Role Incongruity |
.207 |
.190 |
.220† |
.069 |
.172 |
| Role Conflict |
-.014 |
-.096 |
.106 |
-.018 |
.188 |
|
|
|
|
|
|
| R2 |
.351 |
.367 |
.666 |
.140 |
.383 |
| Δ R2 |
.111 |
.092 |
.652 |
.024 |
.060 |
| ΔF |
9.29** |
8.03** |
90.43** |
1.51 |
5.26** |
Note. N = 227
* p < .05. ** p < .01. † p < .0056. |
Exhaustion
The hierarchical regression model for Exhaustion revealed that years of experience was not statistically significant: F(1, 225) = .323, p > .05. Introducing individual factors explained 23.9% of the variation in Exhaustion, and this change in R2 was significant: F(5, 221) = 13.96, p < .001. The inclusion of organizational factors explained an additional 11.1% of the variation in Exhaustion, and this change in R2 was significant: F(9, 217) = 13.05, p < .001. However, the β values revealed that the only statistically significant factor of Exhaustion was perceived stress (β = .303, p < .001). Together the independent variables accounted for 35.1% of the variance in Exhaustion.
Incompetence
For Incompetence, years of experience explained 5.4% of its variation and was significant: F(1, 225) = 12.89, p < .001. Adding individual factors explained an additional 22.9% of the variation in Incompetence, and this change in R2 was significant: F(5, 221) = 17.50, p < .001. Including organizational factors explained an additional 9.2% of the variation in Incompetence, and this change in R2 was significant: F(9, 217) = 14.53, p < .001. The statistically significant factors of Incompetence were avoidant-emotional coping (β = .338, p < .001) and role ambiguity (β = -.276, p < .001). Together the independent variables accounted for 36.7% of the variance in Incompetence.
Negative Work Environment
For Negative Work Environment, years of experience was not statistically significant: F(1,225) = 1.17, p > .05, R2 = .005. Adding individual factors explained 10.9% of the variation in Negative Work Environment, and this change in R2 was significant: F(5, 221) = 5.40, p < .001. Including organizational factors explained an additional 65.2% of the variation in Negative Work Environment, and this change in R2 was significant: F(9, 217) = 48.05, p < .001. In the final model, perceived job satisfaction (β = -.489, p = .000) and role incongruity (β = .220, p = .000) significantly explained Negative Work Environment. Together the independent variables accounted for 66.6% of the variance in Negative Work Environment.
Devaluing Clients
For Devaluing Clients, years of experience contributed significantly to the model and accounted for 3.6% of its variation: F(1, 225) = 8.46, p < .05. Including individual factors explained an additional 8.0% of the variation in Devaluing Clients, and this change in R2 was significant: F(5, 221) = 5.80, p < .01. Adding the organizational factors in the third step was significant: F(9, 217) = 3.92, p < .001, R2 = .140. However, the inclusion of the organizational variables did not explain a significantly different equation: ΔF(4, 217) = 1.51, p > .05, ΔR2 = .024. Therefore, we interpreted the β values of the second step, and the statistically significant factor of Devaluing Clients was problem-focused coping (β = -.229, p = .009).
Deterioration in Personal Life
Finally, for Deterioration in Personal Life, years of experience was not significant: F(1, 225) = .500,
p > .05, R2 = .002. Including individual factors explained 32.1% of the variation in Deterioration in Personal Life, and the change in R2 was significant: F(5, 221) = 21.14, p < .001. Including the organizational factors explained an additional 6.0% of the variation in Deterioration in Personal Life, and this change in R2 was significant: F(9, 217) = 14.98, p < .001. An examination of the β values revealed that only perceived stress was a statistically significant variable for Deterioration in Personal Life (β = .437, p = .000). Together the independent variables accounted for 38.3% of the variance in Deterioration in Personal Life.
Discussion
The present study illustrates an expanded understanding of individual and organizational factors associated with the subscales of school counselor burnout (i.e., Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life; Lee et al., 2007). We intended to control for years of experience but found that before adding the individual and organizational factors, it was a statistically significant variable and negatively related with Incompetence and Devaluing Clients. School counselor researchers have reported contradictory findings between years of experience and burnout. Similar to our findings, Wilkerson and Bellini (2006) and Mullen et al. (2018) reported a negative relationship between years of experience and burnout—essentially describing that those earlier in their careers have a higher risk of experiencing burnout. In contrast, Butler and Constantine (2005) and Wilkerson (2009) reported burnout happening over time (i.e., a positive relationship between years of experience and burnout). Our study underscores the vulnerability school counselors may experience earlier in their careers (Mullen et al., 2018). Our results also provide a unique finding in that fewer years of experience as a school counselor is associated with the burnout dimensions of Incompetence and Devaluing Clients.
In the present study, we found individual factors (i.e., perceived stress, problem-focused coping, and avoidant-emotional coping) significantly related to Exhaustion, Incompetence, Devaluing Clients, and Deterioration in Personal Life. School counselor scholars (e.g., Mullen et al., 2018; Mullen & Gutierrez, 2016) reported a statistically significant positive relationship between school counselors’ perceived stress and burnout. Our results provide unique findings in that stress was positively related with the Exhaustion and Deterioration in Personal Life dimensions of burnout. Other school counselor scholars (e.g., Bardhoshi et al., 2014; Moyer, 2011) found the stress-related variable of engagement in non-counseling duties was significantly related to Exhaustion and Deterioration in Personal Life.
For the coping processes, avoidant-emotional coping was positively related to Incompetence and problem-focused coping was negatively related to Devaluing Clients. These findings provide two distinct understandings of school counselor burnout. First, and notably, school counselor participants who were experiencing Incompetence were also engaging in increased avoidant-emotional coping. This finding is similar to those of Fye et al. (2018), who found maladaptive perfectionists were more frequently engaging in avoidant-coping processes. We did not research perfectionism in the present study; however, our findings may expand an understanding of a positive relationship between avoidant-emotional coping and burnout dimensions for school counselors regardless of perfectionism types. Second, we discovered school counselor participants’ problem-focused coping was negatively related to Devaluing Clients. This is a promising finding from our study because participants were likely to incorporate increased problem-focused coping alongside valuing students. As previously discussed, it appears that these school counselor participants were maintaining high levels of positive regard and empathy for students (Gnilka et al., 2015; Mullen & Gutierrez, 2016). Engaging in problem-focused coping may be beneficial to their engagement in student care and maintaining professional vitality.
The organizational factors of role ambiguity, role incongruity, and perceived job satisfaction were significantly related to the Incompetence and Negative Work Environment dimensions of burnout. Specifically, role ambiguity was positively related to Incompetence. Our results confirm that when school counselors’ roles are increasingly unclear, they are experiencing higher levels of burnout (Mullen et al., 2018), and specifically Incompetence. Perceived job satisfaction was negatively related to Negative Work Environment, while role incongruity was positively related to Negative Work Environment. Consistent with previous research, our findings support the significant relationships between organizational factors (i.e., administrative and clerical duties contributing to role stress) and Negative Work Environment (Bardhoshi et al., 2014). Other scholars have studied perceived job satisfaction as an outcome and potential preclusion to school counselor burnout (Baggerly & Osborn, 2006; Bryant & Constantine, 2006). School counseling scholars have found that burnout mediated the relationship between perceived stress and perceived job satisfaction (Mullen et al., 2018). In the present study, the perceived job satisfaction factor had the highest β at -.489. It appears that perceived job satisfaction is an important factor alongside school counselors’ specific experiences of Negative Work Environments. Perceived stress was a statistically significant factor in Step 2 with Negative Work Environment, but insignificant in the context of the organizational variables. This is an important finding because burnout, by definition, is a function of one’s work context (Lee et al., 2007; Maslach & Leiter, 2017), and we found that organizational factors explained a large amount of the variance (i.e., 65.2%) for the Negative Work Environment dimension of burnout. Overall, our findings support the complex and multidimensional nature of school counselor burnout.
Limitations and Future Research
We attempted to research multidimensional burnout with a nationally representative and diverse sample of ASCA member school counselors. Despite our efforts, the response rate was 5.68%. The majority of our participants identified as White and female, which is similar to the reported demographics of professional school counselor members (ASCA, 2018). However, caution may be warranted when generalizing our findings to all school counselors. Expanding research efforts (i.e., qualitative methods) to increase understanding of the burnout experiences of school counselors unrepresented by our participant sample is warranted. Last, it is unknown whether or not participants answered sensitive questions, such as those about burnout, in a socially desirable manner.
Future research should seek to understand additional individual and organizational variables related to the burnout dimensions for school counselors (Lee et al., 2007). For example, the Devaluing Clients dimension has been viewed by school counseling scholars as a complicated construct that has functioned differently from the other dimensions of burnout (Bardhoshi et al., 2014; Mullen & Gutierrez, 2016). Additional research is needed to understand this burnout dimension with school counselors. Kim and Lambie (2018) discussed the need for research to focus on burnout interventions. We concur and believe the distinction of individual and organizational factors within the dimensions of school counselor burnout should be considered when constructing these interventions, which may be important because burnout may not be an end state; instead, it may be a mediator of other important outcomes, such as work and health (Maslach & Leiter, 2017). It may be helpful to expand research that studies relationships between school counselor burnout and physical and mental health outcomes.
Implications for the School Counseling Profession
Our findings have implications for school counselors, school counselors-in-training, and counselor educators and supervisors. They illustrate the importance of conceptualizing the ecological relationship between individual and organizational factors with school counselor burnout. School counselors may have more control over individual factors, and supervisors may have more control over organizational factors. Despite these considerations, it is important to share the responsibility of burnout prevention within the school system. This is important because despite one’s efforts to increase helpful coping, self-care, or wellness practices, it appears that continued exposure to negative work environments will continue to place school counselors at risk for burnout.
Because school counselors are responsible for providing counseling services that align with professional and ethical standards (Kim & Lambie, 2018), it is imperative for them to recognize, monitor, and address their symptoms of burnout (ASCA, 2016). Therefore, it may be helpful for school counselors and supervisors to identify and understand the dimensions of burnout experienced and their relationships with individual and organizational factors. By using the instruments from this study, school counselors can identify contributions of individual and organizational factors with their burnout scores. This would allow supervisees to understand the relationships between these factors and burnout dimensions. During supervision, time could be dedicated to setting personal goals for maintaining self-care and professional vitality. This may be important, especially in identifying and decreasing avoidant-emotional coping, alongside increasing problem-focused coping processes. In general, school counselors should monitor their own self-care in relation to work context stressors and perceived job satisfaction. Our results may provide support to the potential limitations that wellness practices have on decreasing burnout within the Negative Work Environment (Puig et al., 2012)—meaning, wellness practices may be important in alleviating the individual factors related to burnout (i.e., high perceived stress, coping responses) but may have limited ability to decrease factors out of school counselors’ control (i.e., work context practices and policies).
Despite best practice guidelines, the reality remains that school counselors engage in various non-counseling duties (Bardhoshi et al., 2014; Gutierrez & Mullen, 2016), which contributes to role stress. To lessen organizational stressors, as early as graduate school, counselor educators and supervisors should allow space in the learning process for students to learn the various counseling and related duties expected of school counselors within the school environment. Providing learning contexts for graduate students to explore these various roles may set the stage for lessened role stress. Specifically, assignments should be included in the curriculum that allow graduate students to explore school counselors’ professional identity and the real and ideal roles of the school counselor. These discussions should be engaged in along with conversations of how these varying roles can affect burnout (specifically role incongruity and role ambiguity), especially for those earlier in their careers. These dialogues should be reinforced during the practicum and internship experiences and include personal sources of perceived job satisfaction. In schools, supervisors can help to facilitate school counselors’ competence by clearly defining expectations through measurable outcomes. For example, school counselors and supervisors can use the ASCA National Model’s (ASCA, 2019) Annual Administrative Conference Template (p. 60) and Annual Calendar Template (p. 70) to open communication between the school counselors and their supervisors and document their duties. This discussion may additionally open communication regarding the adequacy of funding, resources, materials, and staff available to school counselors (Freeman & Coll, 1997). If inadequate, school counselors may use the opportunity to advocate for increased support from supervisors and administrators.
It is important to note that in the present study, school counselors earlier in their careers reported higher levels of Incompetence and Devaluing Clients. School counselor supervisors should understand these relationships. Mentoring of school counselors who are earlier in their careers by those with significant experience may help the younger professionals build their professional identities and student-focused work. Last, recognizing dimensions of burnout in relation to individual and organizational factors may not be enough to maintain professional vitality. The school counseling profession may find it helpful to train school counselors and graduate students in advocacy skills. Trusty and Brown (2005) outlined advocacy competencies for school counselors, which include dispositional statements, knowledge, and skills necessary to becoming effective advocates. The self-advocacy model prepares school counselors to have the communication (oral and written) necessary to maintain effective advocacy roles.
Conclusion
In conclusion, our results provide an expansion of findings related to relative contributions for individual and organizational factors with school counselor multidimensional burnout. In short, burnout dimensions are uniquely related to personal and work context factors. It is difficult to conceive of burnout absent its relationship to some aspect of the work setting. School counselors and supervisors can use our results to conceptualize burnout from a multidimensional perspective, which may in turn help them find new ways to remain professionally vital to themselves, their students, and their school community.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2016). ASCA ethical standards for school counselors. https://www.schoolcounselor.org/asca/media/asca/Ethics/EthicalStandards2016.pdf
American School Counselor Association. (2018). ASCA membership demographics. https://www.schoolcounselor.org/asca/media/asca/home/Member-Demographics.pdf
American School Counselor Association. (2019). The ASCA national model: A framework for school counseling programs (4th ed.).
Baggerly, J., & Osborn, D. (2006). School counselors’ career satisfaction and commitment: Correlates and predictors. Professional School Counseling, 9(3), 197–205. https://doi.org/10.1177/2156759X0500900304
Bardhoshi, G., Schweinle, A., & Duncan, K. (2014). Understanding the impact of school factors on school counselor burnout: A mixed-methods study. The Professional Counselor, 4(5), 426–443. https://doi.org/10.15241/gb.4.5.426
Bryant, R. M., & Constantine, M. G. (2006). Multiple role balance, job satisfaction, and life satisfaction in women school counselors. Professional School Counseling, 9(4), 265–271. https://doi.org/10.1177/2156759X0500900403
Butler, S. K., & Constantine, M. G. (2005). Collective self-esteem and burnout in professional school counselors. Professional School Counseling, 9(1), 55–62. https://doi.org/10.1177/2156759X0500900107
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100. https://doi.org/10.1207/s15327558ijbm0401_6
Cervoni, A., & DeLucia-Waack, J. (2011). Role conflict and ambiguity as predictors of job satisfaction in high school counselors. Journal of School Counseling, 9(1), 1–30. http://www.jsc.montana.edu/articles/v9n1.pdf
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health: The Claremont symposium on applied social psychology (2nd ed., pp. 31–67). SAGE.
Coll, K. M., & Freeman, B. (1997). Role conflict among elementary school counselors: A national comparison with middle and secondary school counselors. Elementary School Guidance & Counseling, 31(4), 251–261.
Cook, R. M. (2020). Addressing missing data in quantitative counseling research. Counseling Outcome Research and Evaluation. https://doi.org/10.1080/21501378.2019.1711037
Cooper, C., Katona, C., & Livingston, G. (2008). Validity and reliability of the Brief COPE in carers of people with dementia: The LASER-AD Study. The Journal of Nervous and Mental Disease, 196(11), 838–843. https://doi.org/10.1097/NMD.0b013e31818b504c
Culbreth, J. R., Scarborough, J. L., Banks-Johnson, A., & Solomon, S. (2005). Role stress among practicing school counselors. Counselor Education and Supervision, 45(1), 58–71. https://doi.org/10.1002/j.1556-6978.2005.tb00130.x
Darlington, R. B., & Hayes, A. F. (2017). Regression analysis and linear models: Concepts, applications, and implementation (1st ed.). Guilford.
Deatherage, S., Servaty-Seib, H. L., & Aksoz, I. (2014). Stress, coping, and internet use of college students. Journal of American College Health, 62(1), 40–46. https://doi.org/10.1080/07448481.2013.843536
Dimitrov, D. M. (2009). Quantitative research in education: Intermediate and advanced methods. Whittier.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process: Study of emotion and coping during three stages of a college examination. Journal of Personality and Social Psychology, 48(1), 150–170. https://doi.org/10.1037/0022-3514.48.1.150
Folkman, S., & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55(1), 745–774. https://doi.org/10.1146/annurev.psych.55.090902.141456
Freeman, B., & Coll, K. M. (1997). Factor structure of the Role Questionnaire (RQ): A study of high school counselors. Measurement & Evaluation in Counseling and Development, 30(1), 32–39. https://doi.org/10.1080/07481756.1997.12068915
Fye, H. J., Gnilka, P. B., & McLaulin, S. E. (2018). Perfectionism and school counselors: Differences in stress, coping, and burnout. Journal of Counseling & Development, 96(4), 349–360. https://doi.org/10.1002/jcad.12218
Gnilka, P. B., Karpinski, A. C., & Smith, H. J. (2015). Factor structure of the Counselor Burnout Inventory in a sample of professional school counselors. Measurement and Evaluation in Counseling and Development, 48(3), 177–191. https://doi.org/10.1177%2F0748175615578758
Holman, L. F., Nelson, J., & Watts, R. (2019). Organizational variables contributing to school counselor burnout: An opportunity for leadership, advocacy, collaboration, and systemic change. The Professional Counselor, 9(2), 126–141. https://doi.org/10.15241/lfh.9.2.126
Kim, N., & Lambie, G. W. (2018). Burnout and implications for professional school counselors. The Professional Counselor, 8(3), 277–294. http://doi.org/10.15241/nk.8.3.277
Kolodinsky, P., Draves, P., Schroder, V., Lindsey, C., & Zlatev, M. (2009). Reported levels of satisfaction and frustration by Arizona school counselors: A desire for greater connections with students in a data-driven era. Professional School Counseling, 12(3), 193–199. https://doi.org/10.1177%2F2156759X0901200307
Lazarus, R. S. (1993). Coping theory and research: Past, present, and future. Psychosomatic Medicine, 55(3), 234–247. https://doi.org/10.1097/00006842-199305000-00002
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., Ogle, N. T., Powell, M. L., Quinn, J. J., Wallace, S. L., & Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40(3), 142–154. https://doi.org/10.1080/07481756.2007.11909811
Maslach, C., & Leiter, M. P. (2017). Understanding burnout: New models. In C. L. Cooper & J. C. Quick (Eds.), The handbook of stress and health: A guide to research and practice (1st ed., pp. 36–56). Wiley-Blackwell.
McCarthy, C., Van Horn Kerne, V., Calfa, N. A., Lambert, R. G., & Guzmán, M. (2010). An exploration of school counselors’ demands and resources: Relationship to stress, biographic, and caseload characteristics. Professional School Counseling, 13(3), 146–158. https://doi.org/10.1177%2F2156759X1001300302
Moyer, M. (2011). Effects of non-guidance activities, supervision, and student-to-counselor ratios on school counselor burnout. Journal of School Counseling, 9(5), 1–30. http://www.jsc.montana.edu/articles/v9n5.pdf
Mullen, P. R., Blount, A. J., Lambie, G. W., & Chae, N. (2018). School counselors’ perceived stress, burnout, and job satisfaction. Professional School Counseling, 21(1), 1–10. https://doi.org/10.1177/2156759X18782468
Mullen, P. R., & Gutierrez, D. (2016). Burnout, stress and direct student services among school counselors. The Professional Counselor, 6(4), 344–359. http://doi.org/10.15241/pm.6.4.344
Paisley, P. O., & McMahon, H. G. (2001). School counseling for the 21st century: Challenges and opportunities. Professional School Counseling, 5(2), 106–115.
Puig, A., Baggs, A., Mixon, K., Park, Y. M., Kim, B. Y., & Lee, S. M. (2012). Relationship between job burnout and personal wellness in mental health professionals. Journal of Employment Counseling, 49(3), 98–109. https://doi.org/10.1002/j.2161-1920.2012.00010.x
Rizzo, J. R., House, R. J., & Lirtzman, S. I. (1970). Role conflict and ambiguity in complex organizations. Administrative Science Quarterly, 15(2), 150–163. https://doi.org/10.2307/2391486
Scarborough, J. L, & Culbreth, J. R. (2008). Examining discrepancies between actual and preferred practice of school counselors. Journal of Counseling & Development, 86(4), 446–459. https://doi.org/10.1002/j.1556-6678.2008.tb00533.x
Smith, P. C., Kendall, L. M., & Hulin, C. L. (1969). Measurement of satisfaction in work and retirement: A strategy for the study of attitudes. Rand McNally.
Spector, P. E. (1985). Measurement of human service staff satisfaction: Development of the Job Satisfaction Survey. American Journal of Community Psychology, 13(6), 693–713. https://doi.org/10.1007/bf00929796
Spector, P. E. (2011). Job Satisfaction Survey norms. https://shell.cas.usf.edu/~pspector/scales/jssnorms.html
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Pearson.
Trusty, J., & Brown, D. (2005). Advocacy competencies for professional school counselors. Professional School Counseling, 8(3), 259–265.
Wilkerson, K. (2009). An examination of burnout among school counselors guided by stress-strain-coping theory. Journal of Counseling & Development, 87(4), 428–437. https://doi.org/10.1002/j.1556-6678.2009.tb00127.x
Wilkerson, K., & Bellini, J. (2006). Intrapersonal and organizational factors associated with burnout among school counselors. Journal of Counseling & Development, 84(4), 440–450. https://doi.org/10.1002/j.1556-6678.2006.tb00428.x
Heather J. Fye, PhD, NCC, LPC, is an assistant professor at the University of Alabama and a certified PK–12 school counselor. Ryan M. Cook, ACS, LPC, is an assistant professor at the University of Alabama. Eric R. Baltrinic, LPCC-S, is an assistant professor at the University of Alabama. Andrea Baylin, NCC, PEL, is a doctoral student at the University of Alabama. Correspondence may be addressed to Heather Fye, Box 870231, Graves Hall 315B, Tuscaloosa, AL 35487, hjfye@ua.edu.
Apr 29, 2020 | Volume 10 - Issue 2
Nathaniel J. Wagner, Colleen M. L. Grunhaus, Victor E. Tuazon
According to recent research, counselors may benefit from a variety of supports offered by mental health agencies after a client dies by suicide. Research is sparse concerning how often agency supports and outreach are offered to counselors and what supports counselors find to be the most helpful after a client suicide. In this cross-sectional survey research study, the researchers recruited a sample of counselors (N = 228) who self-identified as having experienced a client suicide. The authors examined relationships between perceived organizational support, supervisory alliance, and the impact of the event on counselors. The authors also examined the use and perceived helpfulness of agency policies regarding counselor-oriented support after client suicide. Results highlight the need for more counselor training around suicide, increased empathy for counselor survivors, and the need for agency policies related to postvention.
Keywords: client suicide, supervision, agency policies, counselor survivors, postvention
According to McAdams and Foster (2000), approximately 23% of counselors are counselor survivors, meaning the counselor has had a client die by suicide. These client suicides impact counselor survivors personally and professionally. Counselors can feel sad at work and lose professional confidence in the aftermath of client suicides (Draper et al., 2014). Some counselor survivors demonstrate a fear of working with clients who present with suicidal ideations and are reluctant to accept subsequent suicidal clients (Hendin et al., 2000). Counselors also may experience various emotions, including anger, betrayal, fear of blame, grief, guilt, self-doubt, shame, and shock (Draper et al., 2014; Hendin et al., 2000). In addition, counselor survivors may become more sensitive to client suicidal ideation and experience heightened stress (e.g., Draper et al., 2014; Fairman et al., 2014; McAdams & Foster, 2000, 2002).
McAdams and Foster (2002) reported that counselor survivors found the support of a supervisor helpful in the recovery process. However, counselors further along in their professional experience, or practicing independently, might not have access to supervisory support. According to Fairman et al. (2014), after a client suicide, counselors benefitted from the following: (a) facilitated debriefing, (b) informal group support, (c) individual counseling, (d) paid leave of absence, and (e) continuing education activities. A dearth of research exists regarding how often employers offer the above supports to counselor survivors of client suicide. Considering the deleterious impact of client suicide on the personal and professional functioning of counselor survivors, researchers have implored mental health organizations to provide supportive actions to the distressed individual (e.g., Michel, 1997).
For this study, we recruited a sample of counselor survivors who identified as having a client who completed suicide during their professional career. We explored the effect of supervisory and organizational support on participants’ perception of the impact of client suicide. Participants also described the responses of their colleagues, supervisors, and agencies, and reported which responses participants viewed to be the most and least helpful for counselor survivors coping with client suicide.
Suicide is the 10th leading cause of death in the United States, and for younger populations (ages 15–24), suicide is the second leading cause of death (McIntosh & Drapeau, 2020). In a study of 5,894 deaths by suicide, Ahmedani et al. (2014) found that nearly one-third (29%) of individuals who completed suicide were enrolled in mental health services in the year prior to their death. In this same study, 45% of those who completed suicide had an appointment with a health professional resulting in a mental health diagnosis within the month prior to their completed suicide. In a national comorbidity survey (N = 5,692), Nock et al. (2010) found that 44.1% of those who attempted suicide were diagnosed with an anxiety disorder and 43% were diagnosed with a mood disorder. In total, Nock et al. estimated that 76% of people who attempt suicide have a mental disorder of some kind. Unsurprisingly, counselors are highly likely to work with clients who complete suicide. Approximately 25% of counselors will experience a client suicide (McAdams & Foster, 2002), and the vast majority of mental health professionals will encounter clients with presentations of suicidality or suicide attempts throughout the course of their career (Kleespies & Dettmer, 2000; McAdams & Foster, 2002; Rogers et al., 2001).
Counselors have some training to assess and respond to suicide risk through required trainings on models and strategies of suicide prevention as well as methods of suicide risk assessment (Council for Accreditation of Counseling and Related Educational Programs [CACREP], 2015). Despite this experience and exposure, counselor survivors often reported feeling overwhelmed and unprepared, substantial emotional distress, and reduced work performance when a client suicide occurs (Ellis & Patel, 2012). Identifying avenues of support for affected counselors is paramount to address the harmful effects to counselor well-being and effectiveness.
The Impact of Client Suicide
The profound emotions counselor survivors experience when a client dies by suicide may be moderated by the length and quality of the therapeutic relationship (Grad & Michel, 2004; Luoma et al., 2002). Researchers found that counselor survivors experienced shock, disbelief, or numbness upon learning of a client suicide (Darden & Rutter, 2011; Sanders et al., 2005). Counselor survivors described strong emotions in the context of losing control; for example, some felt angry toward a mental health system that presumably failed the deceased client along with emotions related to grief and sadness (Christianson & Everall, 2009; Knox et al., 2006). Sadness was associated both with the loss of the client and regret that the client was unable to thrive (Sanders et al., 2005). Other counselor survivors experienced fear of litigation or guilt related to holding some responsibility for the death (Christianson & Everall, 2009; Grad & Michel, 2004). Shame impacted counselor survivors’ self-conception as competent counselors and may have prevented them from admitting their fears to family and intimate partners (Darden & Rutter, 2011; Grad & Michel, 2004).
Behaviorally, counselor survivors often changed their professional practices after experiencing a client suicide. Some counselor survivors refused to see clients they perceived as potentially suicidal (Hendin et al., 2000). Knox et al. (2006) found that counselor survivors’ sensitivity to suicide risk and client suicidal ideation may be heightened after client suicide. Loss of a client can lead to increased feelings of self-doubt. Darden and Rutter (2011) determined that approximately half of counselor survivors who participated in their study experienced increased self-doubt when working with clients who presented with suicidal ideations or intent. Similarly, Sanders et al. (2005) found that counselor survivors felt like professional failures after client suicide. On the other hand, counselor growth may also accompany the loss of a client. For example, some counselor survivors indicated using the pain of the experience to grow in their understanding and approach with suicidal clients (Grad & Michel, 2004; Sanders et al., 2005). This growth included greater self-confidence in clinical instincts because of what they learned from the suicide event (Sanders et al., 2005). Counselor survivors can also grow through external supportive resources such as supervision and support groups.
Supportive Resources
Researchers found that counselor survivors often look to the professionals around them (e.g., colleagues, supervisors, mental health professionals) to provide a response, support, or assistance in processing bereavement (Grad & Michel, 2004; Knox et al., 2006; Sanders et al., 2005). Counselor survivors’ complex emotions and perception of failing as a professional can leave survivors grasping for assistance to make sense of the event. Professional responses to survivors vary and include chart audits (Grad & Michel, 2004), debriefing (Ting et al., 2006), or avoidance (Christianson & Everall, 2009; Darden & Rutter, 2011; Grad & Michel, 2004).
Organizational Support
Counselor survivors can benefit from organizational support and outreach in the wake of client suicide. Often, survivors experience frustration and isolation in unsupportive organizational contexts (Hendin et al., 2000). Counselor survivors indicated that institutional responses such as case reviews were rarely helpful and instead increased counselor survivor self-doubt and distress, particularly when these reviews included blame for the client suicide or false reassurance that the suicide was inevitable (Hendin et al., 2000).
On the other hand, supportive contexts that allow for increased social connection with colleagues and debriefing can be helpful (Ting et al., 2006). Michel (1997) suggested that debriefing sessions for the team may be beneficial for coping with client loss. Fairman et al. (2014) stated that when coping with a patient suicide, hospice clinical staff found team-based support strategies and debriefings supported counselor recovery. Alternatively, Michel reported that counselor survivors may find it difficult to disclose intimate and personal feelings to colleagues, especially in a team setting and without reassurance of confidentiality; these counselors may only disclose emotional problems to a personal therapist. Hendin et al. (2000) suggested that team-based debriefings may inhibit insight when they include platitudes such as “it’s not your fault.” Similarly, counselor survivors felt isolated by client suicide when coworkers offered empty assurances. On the other hand, counselor survivors felt supported and less isolated when coworkers shared their own experiences and demonstrated empathy (Hendin et al., 2000).
Counselor survivors may perceive organizational and collegial support as helpful, but researchers have not described the extent to which professional organizational support ameliorates the impact of the suicide event. Further research is needed to explore this interaction. In addition, further inquiry is needed to clarify what forms of organizational support are frequently offered to survivors of client suicide and which resources are most and least helpful.
Supervisory Support
Supervisors play a critical role in preparing for and responding to client suicidal behavior (Ellis & Patel, 2012). Knox et al. (2006) found that counselors-in-training who survived a client suicide appreciated when supervisors created a safe place to discuss the event, self-disclosed their experiences with client suicide, and provided reassurance that the suicide was not the fault of the counselor-in-training. Conversely, counselor survivors found conversations that were particularly critical of their actions prior to the client suicide, or insensitive to the counselors’ experience of the loss, as prohibitive to coping (Knox et al., 2006). Ellis and Patel (2012) recommended that supervisors actively guide supervisees toward self-care (e.g., support-seeking, personal counseling) and reduced workloads, rather than expecting them to know how to manage their grief and professional concerns simultaneously.
Darden and Rutter (2011) found that counselor survivors without a direct supervisor perceived lack of supervision as a barrier to recovery from the loss. Alternatively, counselor survivors in training programs can feel inhibited in fully processing grief and other emotional reactions with a supervisor who also is responsible for their professional evaluation (Gill, 2012). Counselor survivors without a strong supervisory relationship prior to the client suicide typically have limited access to effective and cathartic supervision experiences and to other professional support networks. Depending on the approach of the supervisor and the relationship between the supervisor and supervisee, supervision can be helpful or harmful. Further empirical research is needed to determine the effect of the supervisory relationship on the impact of the suicide event. In addition, more specific information related to agency and supervisory practices and policies that are helpful for counselor survivor recovery would provide further clarification.
Purpose of the Present Study
The following research questions guided our study: (a) Does the perceived support from a supervisor or an organization impact counselor survivors’ experiences of client suicide?; (b) Which policies are most frequently utilized by agencies when a counselor experiences client suicide?; and (c) What interpersonal and agency responses are perceived to be most and least helpful for counselor survivors?
Method
Participants
Prior to data collection, the researchers were granted Institutional Review Board approval to conduct the research. We utilized Qualtrics as a survey management website to conduct a web-based survey to collect data from practicing counselors. We invited 9,521 counselors to participate; however, eligible participants were only counselors who experienced a client suicide, and many invited participants did not meet this study requirement. Potential participants’ names and email addresses were accessed from the Florida licensing board and publicly available state counseling association directories, including those from Alabama, Connecticut, Georgia, Illinois, Kentucky, Maine, Missouri, New Hampshire, New Jersey, Rhode Island, Texas, and Wyoming. We distributed the survey through an initial email that provided a description of the study and included a link to the web-based survey. Potential participants who did not complete the survey and did not choose to opt out of the survey received a second email. Finally, participants who did not respond after the first two emails received a final email reminder. Emails and survey materials were developed according to the Tailored Design Method (Dillman et al., 2014). No incentive was provided for participation in this study.
Of the 9,521 potential participants contacted, 980 of the addresses provided were invalid. In addition, 172 individuals responded to the invitation and indicated that they had not experienced a client suicide. Out of the resulting 8,369 potential participants, 228 participants completed the survey (2.7% useable response rate). The response rate was low; however, only counselors who had experienced a client suicide were appropriate for the survey and it is likely that approximately 75% of those surveyed did not meet the qualifications for this survey (McAdams & Foster, 2002). Also, Dillman et al. (2014) noted that low response rates may be acceptable for niche populations that are difficult to directly access. We used an a priori power analysis (Balkin & Sheperis, 2011) with a power of .8, an alpha error probability of .05, and a .25 effect size, resulting in a required sample size of 200 for the most robust statistical test we used in our data analysis.
Our participants (N = 228) were predominately Caucasian females. Also, participants had a mean age of 49.1 (SD = 11.6, Mdn = 48) with 15.5 years of experience (SD = 10, Mdn = 14). Table 1 describes additional demographics of our participants, including their race/ethnicity, licensure status, professional orientation, and the agency type that employed them.
Table 1
Participant Demographics
| Variable |
n |
% |
| Gender |
|
|
| Female |
175 |
76.8 |
| Male |
51 |
22.4 |
| Other |
2 |
0.9 |
| Race/Ethnicity |
|
|
| Caucasian |
174 |
76.3 |
| Black or African American |
21 |
9.2 |
| Hispanic or Latino |
19 |
8.3 |
| Multiracial |
9 |
3.9 |
| Asian |
3 |
1.3 |
| Native Hawaiian or Other Pacific Islander |
1 |
0.4 |
| Other |
1 |
0.4 |
| Professional Orientation |
|
|
| Licensed professional counselors (LMHC, LPC etc.) |
159 |
69.7 |
| School counselors |
43 |
18.9 |
| Marriage and family therapists |
7 |
3.1 |
| Clinical psychologists |
8 |
3.5 |
| Social workers |
3 |
1.3 |
| Other |
8 |
3.5 |
| License Level |
|
|
| Fully licensed |
190 |
83.3 |
| Provisional license |
23 |
10.1 |
| Other |
15 |
6.6 |
| Employment setting |
|
|
| Outpatient |
58 |
25.4 |
| K–12 schools |
54 |
23.7 |
| Inpatient |
43 |
18.9 |
| Private practice |
35 |
15.4 |
| Community mental health |
8 |
3.5 |
| Corrections |
8 |
3.5 |
| College counseling |
6 |
2.6 |
| Intensive in-home |
4 |
1.7 |
| Social services |
4 |
1.7 |
| Government |
4 |
1.8 |
| Shelter and domestic violence |
2 |
0.9 |
| Telephone counseling |
1 |
0.4 |
| Religious-based counseling |
1 |
0.4 |
Note. N = 228
Measures
For the purpose of this study, three measures were utilized: (a) the Short Supervisory Relationship Questionnaire (S-SRQ; Cliffe et al., 2016), (b) the Survey of Perceived Organizational Support (SPOS; Eisenberger et al., 1986), and (c) the Impact of Event Scale–Revised (IES-R; Weiss & Marmar, 1997). We also used open-response questions to ask about client suicide experiences and perceptions of agency responses. Participants completed a demographics form that queried participants’ personal information (e.g., age, race, ethnicity, and gender) as well as professional experiences (e.g., discipline, years of experience, and agency responses).
S-SRQ
Cliffe et al. (2016) created the S-SRQ scale, which is an 18-item self-report scale to measure an individual’s perception of their supervisory relationship with their supervisor. Respondents identified their level of agreement to each item on a 7-point Likert scale that ranged from strongly disagree to strongly agree. Sample statements on the S-SRQ include “my supervisor was approachable,” “my supervisor encouraged me to reflect on my practice,” and “supervision sessions were focused.” Evidence for reliability was described by Cliffe et al., including internal consistency (α = .96), and test-retest reliability (r = .94). In the present study, the measure had excellent internal consistency as measured by Cronbach’s alpha (α = .95).
SPOS
The SPOS is a one-factor scale created by Eisenberger et al. (1986). The SPOS scale measures whether individuals believe their organizations care about their well-being. The original scale had 32 items; however, we utilized the eight-item short form self-report measure. Respondents rated their agreement to each statement on a 7-point Likert scale (strongly disagree to strongly agree). The SPOS includes statements such as “The organization values my contribution to its well-being” and “Even if I did the best job possible, the organization would fail to notice.” For scoring purposes, we reverse-scored negatively worded items and summed all items to find a final score. With the full scale, Eisenberger et al. found evidence of internal consistency (α = .97). The current sample had high internal consistency (α = .95).
IES-R
Weiss and Marmar (1997) created the IES-R scale to examine stress responses or PTSD symptoms following an event. The IES-R has 22 items and consists of three subscales, Intrusion (eight items), Avoidance (eight items), and Hyperarousal (six items). Participants responded to items asking about the degree of distress they have been experiencing in the previous 7 days. The IES consists of items such as “Other things kept making me think about it” and “I stayed away from reminders of it.” Responses are on a 5-point Likert scale from 0 (not at all) to 4 (extremely). Participants took the scale twice—once as recommended relating to current experiences (IES-Rc) and once as they remembered their experiences during the first 7 days after the client suicide happened (IES-Rp). Weiss and Marmar reported evidence for good internal consistency for Intrusion (α = .89), Avoidance (α = .84), and Hyperarousal (α = .82). The current sample resulted in Cronbach’s alphas of .90, .86, and .87 respectively. The adapted scale had similar Cronbach’s alphas to the original scale, .90, .88, and .88, respectively.
Open-Ended Responses
We used open-ended questions to assess information not captured by the previous instruments and to gain insight into factors participants believed were helpful or unhelpful in the experience. We asked four open-ended questions: (a) “At the time of your first client suicide, what was most helpful in this experience?” (b) “At the time of your first client suicide, what was least helpful in this experience?” (c) “Thinking back on your experience of your first client suicide, what more could your agency have done that you might have found helpful?” and (d) “Thinking back on your first client suicide, what would you have liked the agency to have done less of, or differently?”
Agency Policies
We asked participants to choose from a list of possible agency policies for responding to client suicide that their agency had in place at the time of the suicide. We also asked participants if they perceived these policies to be helpful in their coping with the event. Policy options included extra supervision, mandated counseling, mandated debriefing, mandated time off, additional paperwork, an option to select “other” along with a text box to explain, and an option for “no policy.” Participants were encouraged to select all options that applied.
Data Analysis
A cross-sectional research design was utilized for this study. Upon completion of data collection, numerical data was transferred to SPSS (Version 23) to conduct statistical analyses. To assess responses to the open-ended questions, we followed Brown’s (2009) method to individually code participants’ responses into categorical themes and clusters. We then compared codes and negotiated results to come to a consensus on categories (Creswell & Poth, 2018). We assessed frequencies and descriptive statistics of these themes to determine the most prevalent participant responses. We examined statistical assumptions (e.g., independence of cases, normality, and homoscedasticity; Tabachnick & Fidell, 2007) for each measure, including the Kolmogorov-Smirnov measure for normality. Data were analyzed with frequencies and descriptive statistics, Pearson’s correlations, one-way analysis of variance (ANOVA), and a simple linear regression (SLR), independent samples t-test, and chi-square goodness-of-fit and tests of independence.
Results
Our first research question examined the impact of supervision and organizational supports as moderators of the impact of client suicide on counselor survivors. More specifically, we wanted to determine whether or not the supervisory relationship (S-SRQ; Cliffe et al., 2016) and counselors’ perceptions of organizational support (SPOS; Eisenberger et al., 1986) predicted the impact of client suicide on the counselor survivor at the time of the event (IES-Rp; Weiss & Marmar, 1997) and at the present (IES-Rc; Weiss & Marmar, 1997). The findings of this research question are reported below.
Participants who reported being under supervision when they experienced a client suicide (n = 118) completed the S-SRQ (M = 96.9, SD = 25) as a measure of their supervisory relationship, and the IES-Rp (M = 45.1; SD = 15.9) and IES-Rc (M = 26.6; SD = 8.4). An SLR was calculated to predict the impact of events at the time of the event based on the counselor survivor’s supervisory relationship at the time of the event. A significant regression equation was found (F[1,116] = 6.9, p = .01) with an R2 of .06. Participants’ impact of events at the time of the event decreased .15 for each point increase in supervisory relationships. This indicates that a strong supervisory relationship at the time of a client suicide may help mitigate counselor survivors’ symptoms. An SLR was also calculated to examine the impact of events at the present with their supervisory relationship at the time of the event. However, the findings were not significant (F[1,116] = 57.53, p = .37), suggesting that any differences found between supervisory relationship and the current impact of events may be attributed to chance.
All respondents (N = 228) completed the SPOS (M = 23.9, SD = 3.5), the IES-Rp (M = 43.7, SD = 16.1), and the IES-Rc (M = 26.8, SD = 9.4). Bivariate correlations revealed a lack of significance between SPOS and either impact of events scale (p = .6 for each). We also conducted an ANOVA to examine the effect of perceived level of support based on agency type and found no significant difference in SPOS scores based on agency type (F[7, 220] = 1.084, p = .4). Contrary to expectations, SPOS did not seem to affect the counselor survivors’ experience of client suicide.
Agency Responses
Our second research question inquired about agency policies governing responses to the counselor survivor at the time of a client suicide. Possible agency policies that respondents could choose from included no policy; debriefing of the event; required paperwork; extra supervision; mandated personal counseling; mandated time off; and a final category, “other,” which allowed respondents to fill in an answer that was not listed in the choices. Respondents were provided with the opportunity to choose as many responses as applied; thus, the responses cumulatively totaled over 100%. The most frequently indicated response for agency-initiated policies was no policy (n = 118, 52%). This was followed by mandated debriefing of the event (n = 63, 28%), required paperwork (n = 57, 25%), extra supervision (n = 16, 7%), mandated counseling (n = 8, 4%), and mandated time off (n = 4, 2%). Fourteen respondents (6%) chose “other” to indicate that the agency enforced a policy not listed in the choices. Write-in responses that differed from the listed choices included group debriefing (n = 6), psychological autopsy (n = 2), notification of administrators (n = 2), crisis team intervention (n = 1), and liability review (n = 1).
We conducted a chi-square test of independence to determine if agency type differed according to the presence of an agency policy for counselor support at the time of suicide. Because of insufficient group size of some of the agency types, only participant responses from agency types that had over five participants (outpatient [n = 59], K–12 schools [n = 54], private practice [n = 34], acute psychiatric [n = 26], and residential [n = 16]) were included in the analysis. A significant difference was detected with this test (χ2 = 14.3, p < .01), which indicated that some agency types may be more likely to have a policy in place than others. We then followed up with multiple chi-square goodness-of-fit tests, which revealed that participants who worked in acute psychiatric settings (n = 26, χ2 = 5.6, p < .05) were significantly more likely to have a policy in place than other agency types, and participants who worked in private practice settings (n = 34, χ2 = 5.77, p < . 05) were significantly more likely to have no policy in place than participants who worked in other settings.
Helpfulness of Agency Responses
Regarding our third research question, participants (N = 228) were asked to rate the level of helpfulness of responses to client suicide. Of the participants who reported receiving counseling after client suicide (n = 99, 43%), 54 (55%) participants reported that this agency response was either very helpful or extremely helpful. Additionally, 28 (28%) participants reported counseling as moderately helpful, 13 (13%) reported counseling as a little helpful, and four (4%) participants reported counseling as not helpful at all.
Over one-third (n = 77, 34%) of participants reported that they took time off work after a client suicide. Most of the participants who reported taking time off reported it was very helpful or extremely helpful (n = 41, 53%). This was followed by those who found time off as moderately helpful (n = 15, 20%), a little helpful (n = 12, 16%), and not helpful at all (n = 9, 12%).
Participant responses to our questions inquiring about agency policies and mandated responses differed from responses to perceived helpfulness of agency responses. For example, only eight individuals indicated that their agency mandated personal counseling, whereas 99 individuals indicated that they engaged in personal counseling after the event and rated the perceived helpfulness of the counseling. Similarly, only four participants indicated their agency required they take time off, whereas 77 participants reported that they took time off and rated the helpfulness of this response. These discrepancies are likely due to the wording of “mandated” in the item choices related to agency policy responses, as most participants (n = 118, 52%) indicated that their agencies had no formal policy.
Participants described debriefing discussions related to the counselors’ emotional experience of the event (n = 140, 61%) and the actions of the counselor leading up to the event (n = 136, 59%). Sixty-three (45%) participants described debriefings related to the emotions of the experience as very helpful or extremely helpful. Other participants expressed that emotional debriefing was moderately helpful (n = 31, 22%), a little helpful (n = 36, 26%), or not helpful at all (n = 10, 7%). Debriefings related to the actions of the counselor were reported by 60 (44%) participants to be very helpful or extremely helpful, whereas 34 (25%) participants identified them as moderately helpful, and 42 participants indicated that debriefing of the actions of the counselor was either a little helpful (n = 26, 19%) or not helpful (n = 16, 12%).
Participants (n = 92, 40%) also described their perception of audits of the client’s chart. About half of the respondents (n = 47, 51%) described their audit experience as only a little helpful or not helpful. Fewer (n = 24, 26%) found audits to be very helpful or extremely helpful and 13 (14%) respondents indicated audits as moderately helpful.
Some participants (n = 72, 32%) reported agencies providing additional training for counselors when there was a suicide in the agency. Additional training was reported as very helpful or extremely helpful 63% of the time (n = 45). Twenty-four (33%) participants described additional training as moderately helpful, whereas three (4%) participants indicated receiving additional training as not helpful at all. Only 25% (n = 58) of participants were provided with increased supervision. Twenty-five (43%) of these participants found it very helpful or extremely helpful, 11 (19%) viewed their additional supervision as moderately helpful, and 22 participants (38%) reported increased supervision as only a little helpful or not helpful at all.
Strategies to Improve Agency Responses
We asked participants open-ended questions regarding agency responses that should be improved, changed, or reduced to improve care of future counselor survivors and categorized these into themes. The most frequent response, which occurred in 29% (n = 94) of responses, indicated that increased empathy and acknowledgement of the traumatic nature of the experience would be most helpful. Sample statements from participants included “more focus on the emotional impact on the clinicians,” “reacted to me as a person and as someone who was also grieving instead of just someone who needed to do their job,” “given me some attention and validation for my distress,” “the school I was at never asked about my wellness,” and “I felt like the suicide was viewed as an unfortunate part of being a counselor.” Some participants (n = 51, 18%) described a need for more thorough debriefing and discussion of the event (e.g., “provide a more thorough debriefing,” “been more open to processing the issue”).
Many participants (n = 37, 11%) indicated feeling unprepared to deal with client suicide and recommended further training and resources so that they would be better prepared if they or others were to face a similar situation again. Similarly, participants reported that it would be helpful if their employers had clearer policies and procedures about how to handle client suicide. Participants expressed a desire for agencies to provide policies and procedures (n = 34, 11%) and indicated that these policies should not focus solely on “pointing the finger” or assigning blame (n = 17, 5%) but on the emotional impact of the death on counselor wellness.
Discussion
Client suicide is a painful personal and professional experience for counselors (Ellis & Patel, 2012). Unfortunately, client suicide is not a rare occurrence for counselors (McAdams & Foster, 2000). For the purpose of our study, we examined how organizational and supervisory support might mitigate the impact of the client suicide on counselor well-being. We also examined the supports offered in various work environments and the perceived helpfulness of this outreach in counselor survivor coping.
Supervisory Support
Our first research question was related to the effect of supervisor and organizational support on the impact of client suicide on the counselor survivor. Based on our findings, stronger supervisor relationships seemed to help participants process their experience of client suicide. This may align with Knox et al. (2006), who suggested that negative interactions with supervisors can prohibit the counselor’s coping. Conversely, supportive supervisory interactions, such as those actions that address counselor survivors’ grief and loss experiences (e.g., accepting responses, openly discussing the loss and trauma, creation of a safe environment), could have a lasting impact on the counselor survivors’ recovery (Ellis & Patel, 2012). According to Broadbent (2013), supportive supervision assisted grieving counselors in experiencing greater empathy and connectedness within their future therapeutic relationships. Effective supervision included developing a safe place in which supervisees felt “heard and witnessed” and affirmed (Broadbent, 2013, p. 268).
We did not find supervisory relationships to have a significant impact on participants’ experience at the present. We suspect that one reason for the lack of impact of supervisory relationships on the current impact of events was that the grief and trauma may have changed and lessened over time, as evidenced by a dramatic reduction in mean scores between IES-Rp and IES-Rc (45 and 27 respectively). Similarly, other life events may have influenced the counselor survivors between the suicide of their client and the present which could serve to diminish the impact of the supervisory relationship on how participants perceived client suicide.
Implications for Mental Health Organizations
Surprisingly, we found no effect of organizational support and the impact of the event on counselor survivors. A number of questions from the SPOS were focused on the employee’s contribution, accomplishments, and effort. However, when coping with client suicide participants reported a desire for emotional care and support. Based on our quantitative data, the support participants perceived from agencies did not influence the IES scores, but participants’ qualitative responses revealed they valued agency responses that demonstrated support for the counselor as a person (e.g., additional counseling, empathy, debriefings related to the counselor’s experience).
Participants expressed a desire for agencies to treat them more holistically, and to recognize that they had experienced a trauma. Other researchers also indicated need for empathic support for the clinician following a client suicide. For example, Ellis and Patel (2012) expressed that “clinicians and supervisors should recognize the right (and responsibility) to engage in self-care activities following a client’s suicide” (p. 285). In contrast, our participants reported finding administrative responses focused on agency liability (e.g., chart audit, debriefings related to the actions of the counselor survivor) as unhelpful.
Nearly half of participants indicated that debriefings were helpful. Participant responses to open-ended questions indicated that debriefings were helpful when focused on the emotional experience of the event. In practice, agencies can work to enhance the debriefing procedures they use. The authors encourage agencies to carefully avoid blaming or finger pointing within debriefing procedures, as these responses often have deleterious effects on counselor survivors. Instead, agencies can provide an environment in which the client suicide can be discussed safely and openly, and offer an opportunity for learning and growth.
Despite relatively infrequent agency utilization, counselor survivors who received trainings related to suicide prevention reported these trainings as one of the most helpful responses to client suicide. Many participants reported not feeling prepared for a client suicide and a desire that their agency would have provided additional trainings that could have prepared them for the loss or helped them better respond to the suicidal client. Trainings may include a wide variety of topics such as factors to look for to recognize suicidal ideation, development of a concrete method of responding to expressions of suicidal ideation/intent, discussion of consultation practices, possible steps that a counselor may take when facing client suicidal ideation, when to explore hospitalization, and how to increase the network of people who know about the client’s suicidal ideations. Participants reported that increased trainings would heighten their self-efficacy in working with clients experiencing suicidal ideation, intent, and planning. Additional training may help counselors feel more prepared to work with suicidal clients and thereby reduce client suicide while also increasing the counselor’s feelings of competence (e.g., Ellis & Patel, 2012).
Training should not only include knowledge and skills, but also the development of appropriate attitudes around client suicide (Ellis & Patel, 2012; Michel, 1997). Considering the lack of self-efficacy identified by our participants in response to client suicide, when developing additional trainings, we suggest consideration of Bandura’s theory of self-efficacy which holds that mastery experiences, vicarious experiences, and verbal persuasion can be used to increase confidence (Bandura, 1986). Trainings developed with bolstering self-efficacy in mind can help counselors develop beliefs that they can effectively work with suicidal clients. Best practice indicates that trainings should occur after the counselor survivor has time to recover, whereas supportive resources to assist with grief reactions can be offered immediately following the event (Dransart et al., 2017).
Agencies and supervisors must develop a realistic sense of the extent and limits of a clinician’s responsibilities regarding client suicide (Ellis & Patel, 2012), but they must do so in an empathic manner. Our participants often reported feeling ill-prepared for client suicide, and then blamed, questioned, or challenged about their treatment of the client; this unempathetic response was prohibitive to counselor coping. Agencies and supervisors can instead offer more helpful supportive resources such as emotional debriefing, time off, and personal counseling, and then implement suicide prevention trainings to bolster self-efficacy after the counselor survivor has stabilized. Suicide prevention training is effective in preventing suicide and in reducing self-doubt and questioning when a suicide occurs (Dransart et al., 2017).
Suicide Response Policy
Over 50% of respondents shared that their agency did not have a formal policy of response to the counselor survivor. Although we found no effect of this lack of protocol on participants’ IES scores, participants from this study, along with researchers in other studies, have suggested that agency responses can be valuable supports to counselor survivors (e.g., Hendin et al., 2000; Michel, 1997; Ting et al., 2006). Counselor survivors in our study reported that organized and empathic agency responses were helpful for their recovery. We found that organizations that predominantly treat higher acuity cases (i.e., acute psychiatric) may be more likely to have a policy in place, perhaps because of the frequency of suicide. However, even agencies less likely to experience client suicide would benefit from a pre-planned agency response policy.
Although organizations and supervisors may have informal responses to counselor survivors and clinical teams, researchers (e.g., Michel, 1997; Ting et al., 2006) have argued that a formal policy can have some beneficial effects. Postvention is an organized response that provides “psychological support, crisis intervention and other forms of assistance” to survivors of suicide (Higher Education Mental Health Alliance, 2018, p. 6). Based on our findings, helpful formal postvention policies include debriefing of the counselor survivor’s emotional experience, suggested time off for self-care and personal counseling, and recommended follow-up trainings for handling future suicidality in clients.
Larger mental health treatment teams such as community mental health agencies or university counseling centers may develop a postvention team that creates a hierarchy and communication chain for informing appropriate parties (including the counselor survivor) in a timely and sensitive manner. Michel (1997) suggested this postvention should include tiered plans specific to staff levels (e.g., therapists, supervisors, administration) that take into consideration confidentiality and the professional closeness of the employee to the client. Thus, responses to those who work closely with the client (e.g., counselor survivors) may be different than to those who are more removed from the client (e.g., administration).
Beyond simply having an action plan, based on our findings and our literature review (e.g., Dransart et al., 2017), we believe that agencies should specifically focus on trainings conducted as preventative measures. Some trainings should include information on how to recognize factors that increase suicide risk among clients. Additional needed trainings may address how to respond to high-risk clients and clients who report suicidal ideations or intent.
Limitations and Future Research
Our study was a cross-sectional survey study; as such, we were only able to examine one point in time. We asked participants to reflect on their experiences of client suicide and how it impacted them at the time, as well as how they currently experienced the impact. The passage of time likely influenced participants’ memories of their traumatic experience and might have impacted our results. Because of these limitations, future longitudinal examination of the experience of client suicide may be warranted. Our low response rate, though acceptable based on the niche population (Dillman et al., 2014), and our use of convenience sampling inherently reduces the generalizability of our findings. We cannot claim that the counselors we found through this method are representative of all counselor survivors. As such, future research that can reach a more representative sample of counselors who have experienced a client suicide could be valuable in reproducing our findings.
There also may be some limitations with our scales. The IES-R scale was originally created to account for the impact of events as perceived within the last 7 days (Weiss & Marmar, 1997) and our use of the IES for recalling past experiences has limited supporting evidence. In addition, the SPOS scale may have been focused more on the organizational structure as opposed to the immediate working environment the counselor survivors faced. Although our findings are generally consistent with previous researchers (e.g., Ellis & Patel, 2012; Michel, 1997), they should be considered in light of these limitations.
Summary and Implications for Counseling
Our findings highlight client suicide as a traumatic event for counselor survivors and their subsequent desire for emotional support in the aftermath. Our results inform counselors and mental health agencies of ways they can provide an active and emotionally aware response that recognizes the impact of the event and the myriad of emotions the counselor survivor might be experiencing. Our findings especially indicate the need for counselors to receive supportive supervision (e.g., that supervisors are approachable, respectful, non-judgmental, and collaborative; Cliffe et al., 2016), as this seems to impact counselor survivors’ experience of client suicide. Our findings support the need for counselors to continue to take care of themselves, find support from others, and pursue their own counseling.
For community agencies, administrators, and supervisors, having an action plan detailing how the agency will respond to crises such as client suicide may increase the thoroughness of agency responses to affected individuals including the counselor survivor. The development of a crisis plan increases sensitivity and awareness, and contributes to the development of an institutional culture in which postvention after a client suicide is common practice. Considering the potential benefits of having an action plan, the number of respondents who suggested the agency where they are employed has no protocol or plan in place in the event of a client suicide is concerning. Recommended agency policies may include encouraging the counselor survivor to engage in personal counseling or take time off, or facilitating empathic debriefings and future suicide prevention trainings.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ahmedani, B. K., Simon, G. E., Stewart, C., Beck, A., Waitzfelder, B. E., Rossom, R., Lynch, F., Owen-Smith, A., Hunkeler, E. M., Whiteside, U., Operskalski, B. H., Coffey, M. J., & Solberg, L. I. (2014). Health care contacts in the year before suicide death. Journal of General Internal Medicine, 29(6), 870–877. https://doi.org/10.1007/s11606-014-2767-3
Balkin, R. S., & Sheperis, C. J. (2011). Evaluating and reporting statistical power in counseling research. Journal of Counseling & Development, 89(3), 268–272. https://doi.org/10.1002/j.1556-6678.2011.tb00088.x
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Prentice Hall.
Broadbent, J. R. (2013). ‘The bereaved therapist speaks.’ An interpretative phenomenological analysis of humanistic therapists’ experiences of a significant personal bereavement and its impact upon their therapeutic practice: An exploratory study. Counselling and Psychotherapy Research, 13(4), 263–271. https://doi.org/10.1080/14733145.2013.768285
Brown, J. D. (2009). Open-response items in questionnaires. In J. Heigham & R. A. Croker (Eds.), Qualitative research in applied linguistics: A practical introduction (pp. 200–219). Palgrave MacMillan.
Christianson, C. L., & Everall, R. D. (2009). Breaking the silence: School counsellors’ experiences of client suicide. British Journal of Guidance & Counselling, 37(2), 157–168. https://doi.org/10.1080/03069880902728580
Cliffe, T., Beinart, H., & Cooper, M. (2016). Development and validation of a short version of the Supervisory Relationship Questionnaire. Clinical Psychology & Psychotherapy, 23(1), 77–86. https://doi.org/10.1002/cpp.1935
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Creswell, J. W., & Poth, C. N. (2018). Qualitative inquiry and research design: Choosing among five approaches (4th ed.). SAGE.
Darden, A. J., & Rutter, P. A. (2011). Psychologists’ experiences of grief after client suicide: A qualitative study. Omega: Journal of Death and Dying, 63(4), 317–342. https://doi.org/10.2190/OM.63.4.b
Dillman, D. A., Smyth, J. D., & Christian, L. M. (2014). Internet, phone, mail, and mixed-mode surveys: The tailored design method (4th ed.). Wiley.
Dransart, D. A. C., Treven, M., Grad, O. T., & Adriessen, K. (2017). Impact of client suicide on health and mental health professionals. In K. Andriessen, K. Krysinska, & O. T. Grad (Eds.), Postvention in action: The international handbook of suicide bereavement support (pp. 245–254). Hogrefe.
Draper, B., Kōlves, K., De Leo, D., & Snowdon, J. (2014). The impact of patient suicide and sudden death on health care professionals. General Hospital Psychiatry, 36(6), 721–725. https://doi.org/10.1016/j.genhosppsych.2014.09.011
Eisenberger, R., Huntington, R., Hutchison, S., & Sowa, D. (1986). Perceived organizational support. Journal of Applied Psychology, 71(3), 500–507. https://doi.org/10.1037/0021-9010.71.3.500
Ellis, T. E., & Patel, A. B. (2012). Client suicide: What now? Cognitive and Behavioral Practice, 19(2), 277–287. https://doi.org/10.1016/j.cbpra.2010.12.004
Fairman, N., Thomas, L. P. M., Whitmore, S., Meier, E. A., & Irwin, S. A. (2014). What did I miss? A qualitative assessment of the impact of patient suicide on hospice clinical staff. Journal of Palliative Medicine, 17(7), 832–836. https://doi.org/10.1089/jpm.2013.0391
Gill, I. J. (2012). An identity theory perspective on how trainee clinical psychologists experience the death of a client by suicide. Training and Education in Professional Psychology, 6(3), 151–159. https://doi.org/10.1037/a0029666
Grad, O. T., & Michel, K. (2004). Therapists as client suicide survivors. Women & Therapy, 28(1), 71–81. https://doi.org/10.1300/J015v28n01_06
Hendin, H., Lipschitz, A., Maltsberger, J. T., Haas, A. P., & Wynecoop, S. (2000). Therapists’ reactions to patients’ suicides. The American Journal of Psychiatry, 157(12), 2022–2027. https://doi.org/10.1176/appi.ajp.157.12.2022
Higher Education Mental Health Alliance. (2018). Postvention: A guide for response to suicide on college campuses. http://hemha.org/wp-content/uploads/2018/06/jed-hemha-postvention-guide.pdf
Kleespies, P. M., & Dettmer, E. L. (2000). An evidence-based approach to evaluating and managing suicidal emergencies. Journal of Clinical Psychology, 56(9), 1109–1130.
Knox, S., Burkard, A. W., Jackson, J. A., Schaack, A. M., & Hess, S. A. (2006). Therapists-in-training who experience a client suicide: Implications for supervision. Professional Psychology: Research & Practice, 37(5), 547–557. https://doi.org/10.1037/0735-7028.37.5.547
Luoma, J. B., Martin, C. E., & Pearson, J. L. (2002). Contact with mental health and primary care providers before suicide: A review of the evidence. American Journal of Psychiatry, 159(6), 909–916. https://doi.org/10.1176/appi.ajp.159.6.909
McAdams, C. R., III, & Foster, V. A. (2000). Client suicide: Its frequency and impact on counselors. Journal of Mental Health Counseling, 22(2), 107–121.
McAdams, C. R., III, & Foster, V. A. (2002). An assessment of resources for counselor coping and recovery in the aftermath of client suicide. The Journal of Humanistic Counseling, Education and Development, 41(2), 232–241. https://doi.org/10.1002/j.2164-490X.2002.tb00145.x
McIntosh, J. L., & Drapeau, C. W. (2020). U.S.A. suicide 2018: Official final data. American Association of Suicidology. https://suicidology.org/wp-content/uploads/2020/02/2018datapgsv2_Final.pdf
Michel, K. (1997). After suicide: Who counsels the therapist? Crisis, 18(3), 128–130. https://doi.org/10.1027/0227-5910.18.3.128
Nock, M. K., Hwang, I., Sampson, N. A., & Kessler, R. C. (2010). Mental disorders, comorbidity and suicidal behavior: Results from the National Comorbidity Survey Replication. Molecular Psychiatry, 15(8), 868–876. https://doi.org/10.1038/mp.2009.29
Rogers, J. R., Gueulette, C. M., Abbey-Hines, J., Carney, J. V., & Werth, J. L. (2001). Rational suicide: An empirical investigation of counselor attitudes. Journal of Counseling & Development, 79(3), 365–372. https://doi.org/10.1002/j.1556-6676.2001.tb01982.x
Sanders, S., Jacobson, J., & Ting, L. (2005). Reactions of mental health social workers following a client suicide completion: A qualitative investigation. Omega: Journal of Death and Dying, 51(3), 197–216. https://doi.org/10.2190/D3KH-EBX6-Y70P-TUGN
Tabachnick, B. G., & Fidell, L. S. (2007). Using multivariate statistics (5th ed.). Allyn & Bacon.
Ting, L., Sanders, S., Jacobson, J. M., & Power, J. R. (2006). Dealing with the aftermath: A qualitative analysis of mental health social workers’ reactions after a client suicide. Social Work, 51(4), 329–341. https://doi.org/10.1093/sw/51.4.329
Weiss, D. S., & Marmar, C. R. (1997). The Impact of Event Scale—Revised. In J. P. Wilson & T. M. Keane (Eds.), Assessing psychological trauma and PTSD (pp. 399–411). Guilford.
Nathaniel J. Wagner, PhD, LMHC, is an assistant professor at Indiana State University. Colleen M. L. Grunhaus, PhD, NCC, ACS, LPC, is an assistant professor at the University of the Cumberlands. Victor E. Tuazon, PhD, NCC, LPC, is an assistant professor at New Jersey City University. Correspondence may be addressed to Nathaniel Wagner, 401 N. 7th Street, Terre Haute, IN 47809, nathaniel.wagner@indstate.edu.
Apr 29, 2020 | Volume 10 - Issue 2
Ian P. Levy, Edmund S. Adjapong
Literature on the physical design of counseling spaces suggests that calm and comfortable school counseling offices support students’ emotional disclosure. However, many counseling environment design studies fail to consider the perspectives of clients. Scholars have called for school counselors to invite youth to co-create interventions as a means to promote cultural responsiveness and honor students’ cultural knowledge. The goal of the current exploratory action research was to bring visibility to the experiences of students who participated in a classroom-based school counseling intervention in which they co-created a hip-hop studio as a social and emotional support space. Specifically, focus groups on the value of the co-creation of a hip-hop studio for urban youth were employed. Results suggested students experienced the studio as a shared space for inclusivity, comfort, and belonging; a place to make their own design choices; and a practice space to garner peer support, engage in personal self-development, and support others.
Keywords: counseling environment, urban youth, classroom-based, hip-hop, cultural responsiveness
The physical design of counseling spaces by counseling professionals has been well explored in counseling literature (Devlin et al., 2013; Liddicoat, 2010; Miwa & Hanyu, 2006; Pressly & Heesacker, 2001). Counselor office design has primarily focused on the counselor’s preference for office design and has failed to take into consideration the psychological state of clients who are in pursuit of counseling services (Sanders & Lehmann, 2019). Historically, researchers explored how counselors’ control over their office design mitigated stress and increased job satisfaction (Pressly & Heesacker, 2001). Pressly and Heesacker (2001) found that counselors who were unhappy with their office may communicate that frustration to their clients. Further, pleasant environments were found to foster creativity, a sense of well-being, and job satisfaction for practicing counselors (Ceylan et al., 2008).
More recently, school counselors reported that their creation of calm and comfortable counseling offices supported students’ emotional disclosure (Cook & Malloy, 2014). Counseling office design elements that have been found to be important for the satisfaction of counselors and clients include overall aesthetics and layout, particularly dim lighting (Liddicoat, 2015; Miwa & Hanyu, 2006; Phelps et al., 2008), as well as access to daylight and space for privacy (Huffcut, 2010). In addition, the layout of a counseling office is strongly correlated with a client’s psychological state, suggesting that environmental structure can allow clients to evoke emotions and confront discrepancies in their self-concept (Liddicoat, 2015). Goelitz and Stewart-Kahn (2008) expressed a need for counselors to consider the experiences of their clients when designing a counseling environment. Although research shows that aesthetic changes to a counseling environment can support a variety of client outcomes, a specific process for the creation of counseling offices is missing within the literature (Pearson & Wilson, 2012).
Additionally, given the current body of research, scholars note the importance of creating counseling environments that align with client preferences. A recent qualitative study conducted by Sanders and Lehmann (2019) indicated clients reported a sense of comfort when a counseling office felt more like a home or a lounge than like a traditional office space. Research has also emphasized the importance of school counselors developing an in-depth understanding of a client’s social context as well as their cultural values and differences (McMahon et al., 2014; Ratts et al., 2016), further stressing a need to understand clients’ preferences when designing emotionally supportive environments.
Client-Centered Office Design
Considering office design, Benton and Overtree (2012) posited that an understanding of clients’ cultural differences was imperative for making design choices. Similarly, Devlin et al. (2013) found that counselors who displayed artwork from different cultures in their office were perceived by clients as being more culturally competent. Decisions to hang artwork might be based on Ponterotto and Austin’s (2005) multicultural competence checklist, which suggested that “the physical surroundings of the program area reflect an appreciation of cultural diversity (e.g., artwork, posters, paintings, languages heard)” (p. 31). Beyond this checklist, however, Benton and Overtree (2012) suggested “no research or detailed guidelines on the critical physical elements to consider in designing a multiculturally friendly office” were available (p. 266). Although not in office design research explicitly, L. Smith and Chambers (2015) recommended school counselors invite youth to co-create counseling interventions as a means to promote cultural responsiveness and honor the cultural knowledge youth bring into counseling sessions. School counselors are also responsible for understanding students in the context of their own environments, in an effort to deploy culturally sensitive interventions (Hansen et al., 2014).
School Counselor Collaboration
When determining how school counselors might best employ culturally sensitive interventions, collaborative efforts are of particular value. The American School Counselor Association (ASCA; 2015) released a position statement suggesting that “school counselors demonstrate cultural responsiveness by collaborating with stakeholders to create a school and community climate that embraces cultural diversity and helps to promote the academic, career and social/emotional success for all students” (p. 24). Ratts and Greenleaf (2018) argued for school counselors to use multicultural and social justice approaches to combat threats to their students’ academic, career, and personal/social development. Using these approaches requires that school counselors create school–family–community partnerships to collaborate with all stakeholders in support of equitable and socially just school counseling interventions (Bryan et al., 2019). However, an ASCA (2019a) national dataset suggested student-to-counselor ratios in the United States are 455 students to one school counselor, far higher than the recommended 250-to-1 ratio. These results are not surprising given prior research demonstrating that school counselors are often inundated with large caseloads and non–school counseling duties, which hinders their ability to engage in direct academic, career, and personal/social development services (Kim & Lambie, 2018; Mau et al., 2016).
In response to caseload issues, school counselors are encouraged to collaborate with teachers to provide indirect services to all students (Cholewa et al., 2016). Researchers noted the success of social skills–based classroom counseling to support students’ social, personal, and academic concerns (Bostick & Anderson, 2009). A study on classroom emotional climate suggested that classroom environments that promote students’ autonomy and expression of ideas are predictive of increased academic achievement (Reyes et al., 2012). School counselors are also urged to act as consultants, supporting teachers in developing interventions within their classrooms to address identified social and emotional needs (ASCA, 2019b). Researchers have recommended that school counselors collaborate with principals on school-wide initiatives that support all stakeholders in delivering the counseling curriculum, noting principal–counselor collaboration as significantly correlated with positive school climate (Rock et al., 2017).
In the implementation of a comprehensive school counseling program, school counselors are urged to use interventions like advisory councils (composed of representatives from all stakeholders, including students) to support student outcomes (ASCA, 2019b). However, the implementation of school-wide school counselor–led interventions lacks a specific focus on cultural responsiveness (Betters-Bubon et al., 2016). Therefore, in order to adequately support the academic, career, and personal/social development of all students within a school, school counselors are encouraged to collaborate with ancillary staff who can carry out interventions that meet these developmental outcomes (ASCA, 2019b). In fact, in the current study, a collaboration is explored to support a school counselor—who had a 700-to-1 caseload—with the indirect implementation of a classroom-based school counseling intervention to aid students’ social and emotional development.
Counselor–Advocate–Scholar Model
This study strategically drew upon the counselor–advocate–scholar (CAS) model to engage various school-based stakeholders in the deployment of a culturally sensitive classroom-based school counseling intervention. The CAS model is built on the presumption that counselors who solely use office-bound interventions are unfit to address issues of social injustice (Ratts, 2009). In other words, the issues that Black and Brown youth and other marginalized groups bring into session are not solely internal and are likely symptomatic of larger societal ills that need to be addressed through outside-of-office interventions. Therefore, building upon research that suggests community-based counseling practices are particularly useful in supporting historically marginalized groups (Bailey et al., 2007), Ratts (2009) posited that counselors must hold alternative counseling roles and use interventions outside of the office.
The CAS model indicates counselors should have three roles: 1) the counselor, 2) the advocate, and
3) the scholar. The counselor role entails the use of culturally responsive approaches to in-office counseling, which assists clients in analyzing emotional experiences (Ratts & Greenleaf, 2018). Ratts and Pedersen (2014) defined the role of an advocate as leaving the four walls of the counseling office to advocate for interventions that transcend talk therapy and address larger systemic concerns. They described the scholar role as the ability to research and evaluate one’s own interventions to inform the development of best practices that support clients and their own advocacy efforts. Together these three roles form multicultural–social justice praxis, a reminder that counselors must transition between these roles to support clients in navigating internal and external forms of oppression (Ratts & Pedersen, 2014).
Hip-Hop Culture
In pursuit of using multicultural practice in schools, recent researchers have demonstrated that urban inner-city youth identify as part of hip-hop culture and have explored the use of hip-hop pedagogy (Adjapong, 2017; Adjapong & Emdin, 2015). Given the importance of school counselors honoring their students’ cultural knowledge (Hannon & Vereen, 2016), a hip-hop–based school counseling framework can be intentionally used to guide the implementation of the CAS model. Hip-hop culture is rooted in the corralling of a community to combat social inequities (Chang, 2005). The emergence of hip-hop culture was in direct response to the systemic and structural changes in the 1970s South Bronx (Caro, 1975; Chang, 2005). In the midst of an economic crisis, hip-hop culture was conceived by youth who critiqued and commented on social issues facing inner-city communities (Forman, 2002). To support the practice of hip-hop culture, hip-hop often exists within physical spaces, such as block parties, concerts, or recording studios (Harkness, 2014).
Hip-Hop and Spoken Word Therapy
Because of the growing influence of hip-hop culture, many scholars and practitioners have explored the power and potential of hip-hop lyric writing, analysis, and discussion as culturally responsive interventions in the counseling process (Kobin & Tyson, 2006; Travis & Deepak, 2011; Tyson, 2002; Washington, 2018). This research engendered hip-hop and spoken word therapy (HHSWT), a culturally responsive counseling process whereby students engage in previously validated counseling interventions through the process of writing, recording, and performing hip-hop music (Levy, 2012; Levy & Keum, 2014). The development of HHSWT over time has thoroughly examined varying hip-hop cultural processes and how those might be used inside counseling offices. For instance, HHSWT offers clinicians a set of hip-hop–centered tools that they can use in the counseling process to support youth in exploring difficult thoughts and feelings. These tools include the hip-hop cypher to support group process and sharing (Levy, Emdin, & Adjapong, 2018), creating emotionally themed mixtapes (Levy, Cook, & Emdin, 2018), lyric writing as emotive journaling, and dyadic song collaboration as role-play (Levy, 2019). Each of these HHSWT techniques offers a culturally salient process in which youth of color can disclose and process difficult thoughts and feelings with their counselor. Levy (2019) found a school counselors’ use of HHSWT in group counseling inside of a school hip-hop recording studio positively supported students’ social and emotional development.
The Hip-Hop Recording Studio
When aiming to design culturally responsive counseling environments, it is important to note that the hip-hop recording studio also has held an important place in hip-hop culture and is largely unexplored in counseling literature. Harkness (2014) defined the hip-hop recording studio as a symbolic space or “a zone in which identity and meaning are shaped by social exchanges that occur within a culturally specific location” (p. 85). Harkness locates these studios as “sites for legitimization and personal transformation” where artists convene to collaborate on music as a “means of identity construction and development” (p. 85). Home-studios mark a shift of power into the hands of youth, who have easy access to technology and online media to create and release their own content and shape hip-hop music and culture (Harkness, 2014). Harkness conducted a content analysis of interviews with rappers and producers wherein they describe the value of studios as adapted home environments and places for self-discovery and authenticity. His findings offer insight into how hip-hop practices might be used in the design of culturally responsive environments for urban youth.
Harkness (2014) illuminated that studios are often built wherever they can fit, like inside of a rapper’s room, basement, living room, or bathroom. Rappers described the need to have studios be aesthetically pleasing, with foam padding on the walls and dim lighting. For many artists, entering a recording booth to rhyme legitimized their thoughts and feelings and generated “an identity shift where they began to define themselves” (Harkness, 2014, p. 91). Although participants in the Harkness study certainly enjoyed being in recording studios, they were adamant about labeling studios as places where serious work and emotional labor occurred. Inside studios, artists felt required to display authentic reflections of their lived experiences in their music and their environment. Overall, the creation of studio spaces is not about how prestigious they look, but more about whether or not the aesthetics of the environment enable artists to carry out the hard work and emotional labor necessary for the discovery of one’s true self.
Purpose of the Present Study
Given that (a) a limited number of studies have explored clients’ opinions and perspectives on changes made by school counselors to a school counseling space, (b) most studies focus on designing counseling environments outside of schools, and (c) the school counseling profession lacks research on multicultural office design, there is a need for research exploring the processes by which students themselves engage in the construction of culturally salient school counseling spaces. Consequently, the purpose of this exploratory action research was to illuminate the experiences of urban youth of color who were part of a classroom-based school counseling intervention in which they co-created a space for social and emotional reflection in an inner-city urban high school. Specifically, this study drew on HHSWT and the CAS model as a culturally sensitive counseling intervention designed to increase understanding of the value of the co-creation of a hip-hop studio as an environment conducive to social and emotional development. The research question that guided the study was: What do students report experiencing while co-creating the school studio? Reponses from student focus group interviews were used to assess answers to this question, with an interpretative phenomenological analysis (IPA) framework guiding interview development, data collection procedures, and data analysis.
Method
Sample
This study was conducted in an inner-city urban high school in a densely populated city in the northeastern United States. The pseudonym for the high school is Liberty High School (LHS). A teacher at LHS consulted with the principal investigator (PI) of this study, given that he is a school counselor educator and a former school counselor with noted experience in the use of HHSWT and the studio creation process. Specifically, the teacher was interested in integrating interventions into a hip-hop lyric writing elective class that could support students’ social and emotional development. The teacher felt the lack of school counselors at LHS created a gap in social and emotional supports and saw students in their classroom struggle academically as a result of unprocessed emotional experiences.
After an initial planning meeting, the PI and the teacher agreed to guide students through a collaborative hip-hop studio construction process as a space to supplement social and emotional support. To garner additional support for this classroom-based intervention, the PI and the teacher attempted to collaborate with LHS’ only school counselor, who declined to participate given their large caseload and being understandably inundated. The school counselor’s inability to participate further justified the need for the PI to support the teacher and their students. In this sense, a collaborative and indirect approach was explored in which the PI/counselor educator supported a classroom teacher in the implementation of a classroom-based school counseling intervention.
Participants were recruited from a hip-hop lyric writing class where they worked with their course instructor on the co-creation of a school studio following approval from the school district’s Institutional Review Board. Students had selected this course from a range of options to fulfill an elective music course credit, a graduation requirement in the northeastern state where this study took place. There were 15 high school students ranging between 14–18 years of age who participated in this study. Neither the course instructor nor the PI had any influence on student enrollment in the class. Prior to their enrollment in this course, the teacher collected all informed consent and/or assent forms from students and parents/guardians. All 15 students agreed to participate in a post-course focus group regarding their experiences co-creating the school studio.
The racial demographic of students at LHS is: 66% Hispanic, 32% Black, 1% Asian, 1% White, and 1% Other. Like many urban high schools in this particular school district, LHS is one of three schools within a larger school’s campus. This setup inherently limits the amount of physical space and resources available to students in each school and in many instances forces them to share. LHS is a Title 1 school, and all students qualify for free or reduced lunch. LHS has 700 students and one school counselor.
Measures
Data collection measures in the present study consisted of two post-intervention focus groups, with seven to eight students in each. The PI facilitated each focus group with the aim of exploring participant experiences during the studio creation as well as assessing how they believed the studio creation process impacted them and might support them moving forward. The PI and the teacher were interested in understanding participants’ lived experiences through action research, so an IPA framework was used for interview guide development, data collection procedures, and data analysis. IPA was selected by the PI as an approach to action research that allows researchers to play a role in guiding a process that leads to development of theoretical and practical knowledge (Zuber-Skerritt & Fletcher, 2007).
The difficulty of action research in this regard is for the researchers to limit their subjectivity, which is why the PI chose not to participate in the intervention and instead facilitated the focus groups. Generally, qualitative methods are most appropriate when engaging in phenomenological research with the PI positioned outside of the intervention (Breen, 2007; Zuber-Skerritt & Fletcher, 2007). Therefore, a focus group interview guide was developed by the PI to prompt discussion around participant experiences, including perceptions of what they learned in the process as well as what they identified as important to them. However, consistent with IPA standards (J. A. Smith et al., 2009), the semi-structured interview guides were flexible enough to allow participants the opportunity to lead the discussion. The two focus groups both lasted 30 minutes and took place within the recording studio at LHS.
Design
The studio construction process occurred over a 3-month period (September to December 2018) as a classroom-based intervention during a hip-hop lyric writing course taught by the teacher. The course met twice a week for 90 minutes each time. Because of school holidays, the class met for a total of 10 sessions for studio construction. The PI met with the teacher twice in late August of 2018, prior to the launch of the class, to order necessary equipment. Further, the PI met with the teacher once a month over the course of the 3-month study to provide curricular support. The studio construction process was designed to be entirely student driven. Based on research suggesting the cultural importance of the hip-hop studio (Harkness, 2014), the need for client voice in counseling office design (Pearson & Wilson, 2012), and cultural competence literature requiring the co-designing of interventions (L. Smith & Chambers, 2015), the PI believed it was necessary to provide students with total ownership over the studio creation process.
Implementing the CAS Model
The studio construction process was guided by the CAS model, which targeted the systemic concern of school counselor availability and subsequently sought to support students in designing an ancillary space for social and emotional services. Drawing from the advocate role of the CAS model, the PI and the teacher collaboratively advocated for financial support through a GoFundMe campaign on Facebook. This crowdsourced campaign garnered $900 for school studio equipment. Next, the teacher met with their school principal to advocate for a location where the class could construct a studio. In line with the scholar role, the teacher and the principal were interested in understanding the impact this classroom-based intervention had on their student body. The PI agreed to assist the teacher and the principal in analyzing evaluation data.
The CAS model suggests the importance of culturally sensitive counseling processes. Pulling from HHSWT, a culturally responsive, process-based counseling framework (Levy, 2012), the teacher functioned as a group facilitator who sought to keep the class focused on their group goal of creating the studio. For example, each session began with a group conversation about the plans for that day, asking group members to agree on varying roles they would take during construction. Halfway through each session, the facilitator would bring the group back into a circle to discuss work done, evaluate progress toward the group goal, and finalize what building would occur for the remainder of the session. Each session would close with a checkout in which the group reflected on how they felt having completed the work, and what changes or additions they wanted to make during the following session. Exploratory activities were also used to allow students to reflect on environments that make them comfortable, spark conversation, and work toward studio completion. As a signature assignment, the teacher pulled from the HHSWT framework and offered students the chance to create a “Where I’m From” song to support students in exploring who they are and what makes them comfortable, to ultimately inform their studio design decisions. Once the studio was developed, students requested assistance in learning how to use studio equipment for recording purposes. Advocating for students’ requests, the teacher asked the PI (as a stand-in for the school counselor) to visit and work with students to support their preparation toward recording their lyrics and teach other students how to record their peers.
Data Analysis
The qualitative data collected in the present study were analyzed using the IPA framework, a qualitative research approach designed to facilitate understanding of the participants’ worlds and subjective experiences, typically as they relate to a specific event or phenomenon common to all participants being interviewed (Chapman & Smith, 2002). The recorded focus group was transcribed verbatim using InqScribe technology (Inquirium, LLC, 2013). To begin the analysis, the PI read and re-read the focus group interview transcript to build familiarity with the data. Once familiar with the transcript, the PI started with microanalysis, which included making descriptive, linguistic, and conceptual comments in the right margin of the transcripts (J. A. Smith et al., 2009). J. A. Smith et al. (2009) suggested that descriptive comments are those that are focused on the content of the communication, and linguistic comments are those that consider the tone and use of language throughout the transcript. Conceptual comments are interpreted first through a descriptive lens, and linguistic comments are then considered together alongside the interpretation of the transcript by the researcher. Once microanalysis was completed for the entire transcript, the PI reviewed the notations that had been made to identify initial emergent themes throughout the interview, which were noted in the left margin of the document.
The initial emergent themes for each interview were then compared across individual participants to identify the lower-order themes, which were then combined to inform the identification of the higher-order themes (J. A. Smith et al., 2009). In the final stages of data analysis, emergent themes that represented the lived experiences of participants in the group were situated within the extant literature to offer an interpretation of the experiences through existing theoretical frameworks, a hallmark process of IPA research (J. A. Smith et al., 2009). Transcripts were then sent to the second author, who had not been involved in the data collection, to audit identified themes. When discrepancies existed (e.g., different themes were found), researchers engaged in discussion until consensus was reached.
Trustworthiness
To safeguard the trustworthiness of the data, authors engaged in two intentional strategies identified as important for improving the credibility and reliability of the data (Morrow, 2005). First, to ensure the credibility of the data, prior to engaging in data analysis, the PI who conducted the interview engaged in a reflexive process to examine preconceptions about the data in order to bracket those ideas and focus on understanding the lived experiences of the participants. Additionally, to allow for transferability of the research process and results, the authors provided a rich description of the research processes (i.e., methods) as well as the findings that emerged through data analysis (i.e., results).
To improve the dependability of the results, two strategies were employed. First, to improve recall for the participants, they were encouraged to review the video montage of their work building the studio. Additionally, to minimize the impact of individual bias, the marked transcript was sent to an additional colleague who acted as an outside auditor. Through the aforementioned processes, the researchers believe trustworthiness consistent with standards in qualitative inquiry was achieved (Thomas & Magilvy, 2011).
Results
The findings of this study are organized by higher- and lower-order themes in accordance with IPA (J. A. Smith, 1996). To elaborate on higher- and lower-order themes, exemplary moments from transcripts that reflect students who participated in co-creation of the school studio were identified. The first higher-order theme was school studio as shared space. The lower-order themes that constituted this theme included feeling comfort and belonging and wanting inclusivity. The second higher-order theme was student design choices. The lower-order themes contained within this theme included designing an authentic studio, needing ownership, and thinking independently. The third and final higher-order theme was studio as practice space/lab. The lower-order themes that comprised this theme included peer support, opportunity, and supporting others. Selected student quotes with student pseudonyms are provided below to illustrate each theme.
School Studio as Shared Space
The first higher-order theme, school studio as shared space, generally suggested that students experienced the hip-hop studio as a place within the school that they wanted to share with others. An example of a quote that fell within this category is: “So you get to be surrounded by rappers and a community that knows what you’re doing, and you get to be upheld by everybody else and you get to share this space with everyone.” This higher-order theme, school studio as shared space, contained two lower-order themes, which indicated that students experienced (a) feeling comfort and belonging and (b) wanting inclusivity.
Feeling Comfort and Belonging
The emergence of the first lower-order theme, feeling comfort and belonging, indicated that students felt heard and connected to others while creating the school studio. For example, when students were asked to discuss what it was like to co-create the school studio, a student named Jayda responded, “We’re just like a little group. A little family. A little rap family.” In this example, the student compares their level of connection with her peers to that of a family. When students were asked what it meant to have a studio in their school, Jordan shared, “In my personal opinion, I feel like what it means to me is being able to communicate with others and letting other people hear your voice.” Here the student highlights the school studio as an environment where they have the chance to share their “voice” and message.
Wanting Inclusivity
The emergence of the second lower-order theme, wanting inclusivity, indicated that students saw the need to create a space that was inclusive of others and that did not revolve solely around their needs and wants. Carlos shared:
I’m still overthinking about what should we do because I feel like different people have certain styles. I don’t want to make it all about me. I don’t want to make it all about other people. I want to make it about the whole school and what they think about. Because we’re not gonna be the only ones in this rap studio. I want to know what they think about and I want to know their perspectives and how they want to do it.
This student recognized that other students from LHS might also want to access the school studio; therefore, they wanted to gain the perspectives of others, beyond their peers who were co-constructing the studio, regarding what should be included. In this sense, students discouraged individual choices because that approach would not create an inclusive space. Another student, Tasha, stated that “for the wall, it was hard to know what everybody likes and the whole school and put it into just one small wall.” Again, students who had the opportunity to co-construct a school studio were thinking about ways to create a space that reflected, represented, and was inclusive of the entire school.
Student Design Choices
The second higher-order theme, student design choices, suggested that students experienced being able to make their own design choices during the co-construction process. For example, a particular student quote read:
We just came in here and it was like, everything messed around so we came in with an idea of like, where we think stuff should go, and that’s how we came up with that. Put it on the corner where the studio gonna be.
The student design choices theme contained three lower-order themes which indicated that students experienced (a) designing an authentic studio, (b) needing ownership, and (c) thinking independently.
Designing an Authentic Studio
Within the second higher-order theme, the first lower-order theme of designing an authentic studio illuminated that students made design choices in alignment with what they defined to be a professional or culturally appropriate studio environment. One example of a student quote that demonstrates this theme came while a student detailed the process of co-constructing the school studio. Specifically, Jay commented that “it makes it feel like a real studio. When you see rappers in a studio, you see all these lights and it looks professional and stuff, so I think it would make it look like the mood of that.” The installation of colorful LED lights within the school studio supported the students’ feeling that the studio was real or professional. The professional aesthetic that students established with the studio enabled the creation of a particular “mood” that also made the school studio space and experience feel culturally authentic.
Students also chose to infuse their school colors into the design of the studio, reporting that design element as an authentic representation of their school. When discussing the design process, Devante shared: “Yeah, and then like, [the foam pads] matched with our school colors like the purple and the green in the middle represents our school.” Finally, when sharing about the process, Alexandra detailed her most and least favorite moments: “My favorite moment: actually being able to build the studio, the checkered over there, the foam. The most challenging part: missing one day then being lost.” For Alexandra, the foam also functioned as an indicator of an authentic studio space. She also added that missing school made her feel lost or disconnected from the studio construction process, and that was particularly challenging.
Needing Ownership
The second lower-order theme, needing ownership, highlighted that students experienced needing ownership of the studio space. When discussing their design process, Gabriel said, “yeah, basically I said like, you put the ‘L’ so whoever comes in here know that Liberty was here first. We created this place. And that was our main point of putting that big ‘L’ right there.” In this quote, Gabriel spoke to the importance of design choices in letting the surrounding community know who was responsible for the studio’s creation. This statement and the theme of needing ownership more broadly suggests that students wanted to feel properly valued and credited for their work and that they also had ownership over their choices and felt able to make their own decisions. This sentiment is further supported by a quote from Rachael:
I know it made me feel like the room was built in our hands. Later on, when everything is done, when people come in, whatever they see is what we all thought of together. We could’ve had this over there, but we decided to put it over here. It just makes us feel . . . well, it makes me feel like, yeah.
Adding support to Gabriel’s statement, Rachael appears to be feeling a sense of pride in laying claim to the thoughts, feelings, and physical work that went into the creation of the school studio.
Thinking Independently
The third lower-order theme, thinking independently, highlighted that students had opportunities to think amongst themselves and to troubleshoot and find solutions to problems without relying on the direction of an adult. Carlos reported that “without the adults, I feel like we really had to bring our creative ideas straight from our thoughts on how to make the studio.” Carlos believed that without adults walking them through the process of creating a school studio, they were able to showcase their “creative ideas” and pull from knowledge and thoughts they already possessed. Additionally, Alexandra shared:
Well, I’m always used to being told what to do because you would give me an assignment and I’ll do it. I can’t just think for myself. As you can see, I’m still having difficulty thinking for myself with the wall.
Alexandra highlights that within the traditional classroom lessons, students are always given an assignment that offers directions on how to complete it. When students were given the task of co-constructing a school studio, there were many tasks that could be approached differently, and students were encouraged as experts to think in ways that were independent of adults and pull from within to address their task.
Studio as Practice Space/Lab
The third higher-order theme, studio as practice space/lab, suggested that students experienced the hip-hop studio as a place where they could learn to feel more prepared. Student quotes within this higher-order theme included statements like: “If we invite other people from the other school or people in other classes to see us, we’re gonna have more . . . prepared. We’re gonna be more prepared to do it.” This higher-order theme contained four lower-order themes, which indicated that students experienced (a) peer support, and (b) opportunity, (c) self-discovery, and (d) supporting others.
Peer Support
The first lower-order theme, peer support, suggested that students felt as if the school studio was a location in which they could receive feedback, support, and opportunities for personal preparation from their peers. When responding to a question regarding what students felt they might have learned throughout the co-creation process, Vicki claimed: “This small space is not gonna help me stand up in front of 400 people but bringing little by little people into here while we’re rapping or anything, would help me build up more confidence.” Although Vicki still felt there was work to do in order to feel ready to share her lyrics with a large number of people, she posited that the studio space could function as a preparation space for larger group sharing, where peers could help others and boost their confidence. Another student, John, spoke to the experience of individuals who rap within the school studio, reporting that:
The nice thing, after the person’s done with the rap, he makes somebody ask what they heard about that person, about learning about that person, that’s gonna put confidence in you. Like, they were actually listening. And that makes you want to rap more so people can actually acknowledge your bars.
In this quote, John spoke to the process of sharing lyrics. Specifically, when people share lyrics, John imagined that others would listen carefully to them and then willingly engage in a discussion about what they heard. John believes the experience of sharing lyrics would make people feel acknowledged and have an increased sense of self-confidence.
Opportunity
The second lower-order theme of opportunity evidenced that students experienced the school studio as an environment that could offer opportunities for personal advancement in life. When discussing how this school studio might be used within the school, Devante said:
It’s hard to find a place to rap. That’s 1. 2, they cost too much. And 3, you know people say you can buy a microphone and you can do this, that and the third in your own household. Not a lot of people have money, many people they use the money and give it to their parents, and then if you ask your parents, they’re gonna tell you the same thing that they tell every other kid when they want to pursue a hobby: “This is not gonna get you anywhere.” ’Cause my parents tell me that all the time.
In this statement, Devante appreciates free access to space where he can pursue his hobby. Within the school studio, there is a perceived potential among students to work toward their own dreams without waiting on financial support or support from anyone other than themselves. Statements like this one suggest that access to the school studio provided students with an opportunity to consider their career on their own terms. A second student, Melissa, builds on this notion of opportunity, suggesting:
So apart from someone finding out their identity with this studio, they could also put their work out there knowing they have a chance to get somewhere. To be very honest, in this decade, everyone has a chance to get somewhere. It doesn’t matter if you’re good at rapping, bad at rapping, you suck, you great, you can get somewhere. It’s all about other people’s opinions, it’s all about what they like, and if you’re liked by the public, then you’re gonna get until as far as you can reach.
In this quote, Melissa indicated how a student could use the school studio to garner support from the public to “get somewhere.” Within the school studio, students suggested that there is an opportunity for a unique level of access and self-advancement. Further aiding the idea that using the school studio was the desired opportunity for youth, Jay said: “I hate that we only come down here once a week.”
Supporting Others
The final lower-order theme, supporting others, demonstrated students’ intentions and goals of supporting others outside of their class who attended LHS. Jordan shared, “I want to learn how to use all this equipment. So that in the future other students will be able to be taught how to be using the mixer or putting beats into tracks.” Jordan wanted to be able to support other students outside of his class by teaching the skills that he plans on developing, which included “using the mixer” and “putting beats into tracks.” This expression demonstrated an understanding of the importance of teaching others how to utilize the school studio, which will contribute to the longevity of the space. Gabriel reported that “You teaching them how to rap, how to use the mic, the laptop and all that, that’s just gonna inspire their friends to come. They teach their friends and the cycle just continues like that.” Believing in how beneficial the studio was for them, Gabriel mentioned wanting to support his peers by sharing skills that were needed to effectively run the school studio so it could continue to be used. Gabriel also highlights that teaching others to make use of the school studio space will create a cycle that theoretically will allow students to bring their friends to engage as well. Therefore, not only is the school studio intriguing to students, but it will support their development of skills to maintain its use.
Discussion
This study was designed to increase understanding of the experiences of students partaking in a classroom-based school counseling intervention in which they co-constructed a hip-hop studio. Counseling environment data has suggested that counselors often take the lead on the creation of environments for clients (Pearson & Wilson, 2012), whereas we encourage school counselors to partner with youth in the creation of their own counseling spaces (L. Smith & Chambers, 2015). Broadly, results support the co-construction of school studios as culturally relevant environments that promote social and emotional development, addressing a need in the literature for research exploring multicultural counseling office design (Benton & Overtree, 2012). Further, the use of the CAS model enabled a collaboration in which a classroom teacher deployed an indirect and culturally responsive school counseling intervention to support students’ personal/social development (ASCA, 2019b; Ratts & Greenleaf, 2018).
Student Experiences
Results of this exploratory action research demonstrated that students experienced a sense of comfort and belonging inside the school studio. Similarly, Sanders and Lehmann (2019) indicated that clients felt a sense of comfort when the counseling office felt like a home or a lounge rather than a traditional office space. Further, data from the current study showed that the studio creation process empowered students to advocate for inclusivity in the use of this space for their entire school campus community. This outcome is ideal given that school counselors are charged with activating the entire school community in the deployment of school-wide interventions that support students’ academic, career, and personal/social development (Bryan et al., 2019). In specific comments, youth stated that they would want to locate peers who are in need of help and bring them to the school studio to develop personal/social skills. These statements suggest that after participating in the school counseling intervention, youth voiced that making the studio available to all students would improve the school counseling program at their school. This finding gives credence to the use of advisory councils at schools, with student members, to offer youth a platform to ensure that school counselors and their school counseling programs are serving all students (ASCA, 2019b). Additionally, a bevy of studies emphasized supporting youth in the development of skills as change agents in promoting peace, youth voice, and healing (Allan & Duckworth, 2018; Conner & Cosner, 2016; Levy, Emdin et al., 2018). Overall, the findings are important in that they support the use of studio co-creation as a classroom-based counseling intervention, which research suggests can result in school-wide impact (Bostik & Anderson, 2009).
Another notable finding of this study was students’ decisions in creating their authentic and professional school studio. For example, the students’ choice to install LED lights provided them with a professional aesthetic and a particular “mood” that also made the school studio space and experience feel authentic. The aesthetics of a counseling environment, particularly interior design choices such as dim lighting, are reported to positively impact clients in session (Miwa & Hanyu, 2006). Similarly, professional hip-hop artists report needing studios to be aesthetically pleasing, pointing to foam padding on walls and dim lighting. For many artists, entering an aesthetically pleasing studio environment was conducive to “an identity shift where they began to define themselves” (Harkness, 2014, p. 91). Student reports regarding the importance of aesthetics in establishing authentic studio spaces are in line with what counseling research suggests is necessary for effective counseling environments both inside and outside of schools (Ceylan et al., 2008; Cook & Malloy, 2014; Huffcut, 2010), as well as what the larger hip-hop community suggests is necessary for personal transformation (Harkness, 2014). Further, scholars have called for school counselors to tailor their interventions to the cultural knowledge and environments of their students (Hansen et al., 2014; L. Smith & Chambers, 2015), particularly when attempting to design multicultural counseling environments (Benton & Overtree, 2012). Evidence from students that the physical space constructed in this study felt like an authentic hip-hop studio suggests that through the use of a classroom-based school counseling intervention, students were able to channel their cultural knowledge and values into the design of a culturally responsive environment that could support their social and emotional development.
An additional finding highlights that youth felt the studio space would allow them to receive peer support that could be generative of improvements in confidence and self-efficacy. Similarly, a systematic review of peer support interventions found that peer educators were particularly effective in facilitating improvements in knowledge, beliefs, and attitudes as well as subsequent behavior change (Ramchand et al., 2017). Findings in the current study aid this supposition, providing evidence of the use of school studios as spaces for peer support.
When reflecting on their engagement in the studio co-construction process, youth reported feeling as if they had been given a valuable opportunity for personal advancement. This finding is particularly important to consider within the context of career counseling work in schools. Lent (2013) encourages counselors to adapt to work in the digital world by preparing individuals for a range of career opportunities. Fostering students’ career development is also an expected role of the school counselor and of school counseling interventions (ASCA, 2019b). Students’ need for opportunity and career–life preparedness requires counselors to promote students’ “alertness to resources and opportunities on which one can capitalize. Most important, preparedness can lead to the use of proactive strategies to manage barriers, build supports, and otherwise advocate for one’s own career–life future” (Lent, 2013, p. 7). Further, youth felt an opportunity for personal identity development, aiding Harkness’ (2014) argument that studios were spaces for hip-hop–identifying individuals to cultivate a deepening understanding of themselves, and Liddicoat’s (2015) position that counseling environments could allow for the positive development of a client’s self-concept.
CAS Model to Support School Studio Construction
The findings in this exploratory action research support the implementation of the CAS model as a guide for school counseling interventions. In the current study, with the help of the PI, the course instructor held the counselor role in the use of Levy’s (2019) HHSWT framework by facilitating a group process in which students constructed a hip-hop recording studio. Similar to research indicating that school counselors are often inundated with large caseloads and non-counseling duties that strip them of their ability to engage in direct counseling (Kim & Lambie, 2018; Mau et al., 2016), the school counselor at LHS was unable to support the studio co-construction process. However, to facilitate a comprehensive school counseling program, school counselors are expected to collaborate with teachers to indirectly address students’ academic, career, and personal/social needs (Cholewa et al., 2016). Therefore, the current study expands upon the implementation of the CAS model by considering the role of collaboration in the school counselor’s work, and the activation of the teacher as a key stakeholder (under the guidance of a counselor educator) in facilitating a classroom-based counseling intervention in which youth co-created a school space to support social and emotional services. The teacher and the PI also held the roles of advocates for the successful deployment of the school counseling intervention (studio co-creation). The teacher met with their principal and contacted a counselor educator (the PI), and together with the PI garnered crowdsourced funding for this project. Finally, the scholar role was also maintained by the teacher, who wished to support students’ social and emotional needs by creating a school studio, and thus called on the PI to use qualitative measures to evaluate students’ experiences during this process.
Limitations
There are a series of limitations to the current study. The limited availability of the school counselor to participate in this study is a limitation, despite the conscious use of collaboration in the deployment of an indirect classroom-based school counseling intervention. The use of the CAS model without a formal school counselor was difficult, albeit consistent with existing research surrounding the lack of time for school counselors to engage in multi-session group counseling work (Kim & Lambie, 2018). Consequently, the findings of the current study fail to offer support for counselors in the use of a direct school counseling intervention. Further, student reports of their experience in the studio co-construction process are subjective in nature. Had LHS provided an intervention to a larger sample of students and administered quantitative assessments, those findings could potentially have aided this study’s qualitative conclusions. The small sample size (N = 15) of this study is a limitation, as results lack generalizability. Additionally, LHS is an urban school whose demographic information suggests the majority of youth identified as Black and/or Hispanic. Given that the present study examined a sample of mostly non-White urban youth, it is difficult to generalize findings to suburban and rural schools as well as to youth who do not identify as Black and/or Hispanic. Further, each focus group lasted 30 minutes, which could have limited the ability of the seven or eight participants to offer in-depth data. Lastly, the interactive nature of focus groups could have impacted the authenticity of responses from focus group participants (Smithson, 2000).
Implications
There are a number of implications for both practice and research that can be drawn from the current study. The findings in the current study align with the ASCA National Model and hold promise for engaging teachers and students in school-based interventions that promote social and emotional development and are culturally relevant. The ASCA National Model (2019b) calls for school counselors to use indirect approaches to counseling, often those including collaboration with a teacher, to provide supports to all students across the school. This study exemplifies the importance of activating teachers in the use of indirect classroom-based school counseling interventions, particularly when school counselors themselves are not available. The PI’s involvement in supporting the classroom teacher in implementation and evaluation of a classroom-based school counseling intervention serves as a call for school counselors to consider partnering with faculty at local colleges/universities to bolster their comprehensive school counseling programs. If available, school counselors themselves are encouraged to collaborate with teachers in the development, implementation, and evaluation of classroom-based interventions that support students’ social and emotional development.
The current study used a culturally responsive classroom-based intervention that honored students’ cultural knowledge and trusted youth to guide the studio construction process. Youth reported on the importance of the opportunity to use the hip-hop studio to positively impact their school, their peers, and themselves. Counselors need to design social and emotional development supports within their schools that adhere to the cultural realities of their clients (Ponterotto & Austin, 2005) and are thus encouraged to utilize the studio co-creation approach. Beyond hip-hop, however, the current study suggests that youth-driven construction of an ancillary social and emotional support space should be considered for all students from marginalized populations, including youth identifying as LGBTQ.
Implications for direct school counseling practice exist as well. For example, Levy (2019) demonstrated effectiveness of a series of hip-hop–based cognitive behavioral and person-centered counseling interventions on students’ social and emotional development. However, few studies have detailed the cultural importance of the hip-hop studio and how its creation might support the future use of culturally competent interventions. Although this study did not explore the use of lyric writing, recording, or performing to address counseling outcomes, students participating in the studio construction process reported wanting to use the school studio to support their peers and their own personal self-development. These findings suggested it is important for schools to consider co-creating school studios as places for school counselors to deploy hip-hop–based interventions for group and individual counseling with urban youth.
The findings in this study can be expanded upon with future mixed methods research that examines a larger sample of students. Quantitative analysis of students’ social and emotional development (examining variables like stress, emotional regulation, and executive functioning) during the studio co-construction process is recommended as a direction for future research. Qualitative researchers should consider case studies of students and counselors who engage in the construction of hip-hop studios and small-group work within counseling studies, using more in-depth interviews (lasting longer than 30 minutes) to ensure rich data is collected. There is also value in exploring the multicultural and social justice competence development of both school counselors and teachers who engage in hip-hop–based school counseling interventions.
Conclusion
The goal of this exploratory action research was to illuminate the experiences of urban youth of color who were part of a classroom-based school counseling intervention in which they co-created their own space for social and emotional support in an inner-city urban high school. As described in this article, a limited number of studies have explored clients’ opinions and perspectives on changes made by school counselors to a counseling environment (Pearson & Wilson, 2012). Additionally, most studies focus on designing counseling environments outside of schools, and the school counseling profession lacks research on multicultural office design (Benton & Overtree, 2012). Furthermore, ASCA (2019b) advocates for the use of indirect counseling interventions to support the needs of all students, while others urge school counselors to use multicultural and social justice–oriented interventions to identify and address barriers to student development (Ratts & Greenleaf, 2018). This article highlights the value in using hip-hop studio construction as an innovative approach to a culturally sensitive, indirect, classroom-based school counseling intervention in which students themselves engaged in the construction of an ancillary space to support their social and emotional development.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adjapong, E. S. (2017). Bridging theory and practice in the urban science classroom: A framework for hip-hop pedagogy in STEM. Critical Education, 8(15). https://doi.org/10.14288/ce.v8i15.186248
Adjapong, E. S., & Emdin, C. (2015). Rethinking pedagogy in urban spaces: Implementing hip-hop pedagogy in the urban science classroom. Journal of Urban Learning, Teaching, and Research, 11, 66–77.
Allan, D., & Duckworth, V. (2018). Voices of disaffection: Disengaged and disruptive youths or agents of change and self-empowerment? British Journal of Special Education, 45(1), 43–60. https://doi.org/10.1111/1467-8578.12201
American School Counselor Association. (2015). The school counselor and cultural diversity. https://www.schoolcounselor.org/asca/media/asca/PositionStatements/PS_CulturalDiversity.pdf
American School Counselor Association. (2019a). Student-to-school-counselor ratio 2016-2017. https://www.schoolcounselor.org/asca/media/asca/home/Ratios16-17.pdf
American School Counselor Association. (2019b). The ASCA national model: A framework for school counseling programs (4th ed.).
Bailey, D. F., Getch, Y. Q., & Chen-Hayes, S. F. (2007). Achievement advocacy for all students through transformative school counseling programs. In B. T. Erford (Ed.), Transforming the school counseling profession (2nd ed., pp. 98–120). Pearson.
Benton, J. M., & Overtree, C. E. (2012). Multicultural office design: A case example. Professional Psychology: Research and Practice, 43(3), 265–269. https://doi.org/10.1037/a0027443
Betters-Bubon, J., Brunner, T., & Kansteiner, A. (2016). Success for all? The role of the school counselor in creating and sustaining culturally responsive positive behavior interventions and supports programs. The Professional Counselor, 6(3), 263–277. https://doi.org/10.15241/jbb.6.3.263
Bostick, D., & Anderson, R. (2009). Evaluating a small-group counseling program—A model for program planning and improvement in the elementary setting. Professional School Counseling, 12(6), 428–433. https://doi.org/10.1177/2156759X0901200602
Breen, L. (2007). The researcher ‘in the middle’: Negotiating the insider/outsider dichotomy. The Australian Community Psychologist, 19(1), 163–174. http://hdl.handle.net/20.500.11937/22045
Bryan, J., Griffin, D., Kim, J., Griffin, D. M., & Young, A. (2019). School counselor leadership in school-family-community partnerships: An equity-focused partnership process model for moving the field forward. In S. B. Sheldon & T. A. Turner-Vorbeck (Eds.), The Wiley handbook of family, school, and community relationships in education (pp. 265–287). Wiley.
Caro, R. A. (1975). The power broker: Robert Moses and the fall of New York. Alfred A. Knopf.
Ceylan, C., Dul, J., & Aytac, S. (2008). Can the office environment stimulate a manager’s creativity? Human Factors and Ergonomics in Manufacturing & Service Industries, 18(6), 589–602. https://doi.org/10.1002/hfm.20128
Chang, J. (2005). Can’t stop, won’t stop: A history of the hip-hop generation. St. Martin’s Press.
Chapman, E., & Smith, J. A. (2002). Interpretative phenomenological analysis and the new genetics. Journal of Health Psychology, 7(2), 125–130. https://doi.org/10.1177/1359105302007002397
Cholewa, B., Goodman-Scott, E., Thomas, A., & Cook, J. (2016). Teachers’ perceptions and experiences consulting with school counselors: A qualitative study. Professional School Counseling, 20(1), 77–88. https://doi.org/10.5330/1096-2409-20.1.77
Conner, J. O., & Cosner, K. (2016). Youth change agents: Comparing the sociopolitical identities of youth organizers and youth commissioners. Democracy and Education, 24(1). https://democracyeducationjournal.org/home/vol24/iss1/2
Cook, K., & Malloy, L. (2014). School counseling office design: Creating safe space. Journal of Creativity in Mental Health, 9(3), 436–443. https://doi.org/10.1080/15401383.2014.890557
Devlin, A. S., Borenstein, B., Finch, C., Hassan, M., Iannotti, E., & Koufopoulos, J. (2013). Multicultural art in the therapy office: Community and student perceptions of the therapist. Professional Psychology: Research and Practice, 44(3), 168–176. https://doi.org/10.1037/a0031925
Forman, M. (2002). “Keeping it real”?: African youth identities and hip hop. In R. A. Young (Ed.), Music, popular culture, identities (pp. 89–118). Brill.
Goelitz, A., & Stewart-Kahn, A. S. (2008). Therapeutic use of space: One agency’s transformation project. Journal of Creativity in Mental Health, 2(4), 31–44. https://doi.org/10.1300/J456v02n04_04
Hannon, M. D., & Vereen, L. G. (2016). Irreducibility of Black male clients: Considerations for culturally competent counseling. The Journal of Humanistic Counseling, 55(3), 234–245. https://doi.org/10.1002/johc.12036
Hansen, J. T., Speciale, M., & Lemberger, M. E. (2014). Humanism: The foundation and future of professional counseling. The Journal of Humanistic Counseling, 53(3), 170–190. https://doi.org/10.1002/j.2161-1939.2014.00055.x
Harkness, G. (2014). Get on the mic: Recording studios as symbolic spaces in rap music. Journal of Popular Music Studies, 26(1), 82–100. https://doi.org/10.1111/jpms.12061
Huffcut, J. C. (2010). Can design promote healing? Behavioral Healthcare, 30(9), 33–35.
Inquirium, LLC (2013). InqScribe [Computer software]. https://www.inqscribe.com
Kim, N., & Lambie, G. W. (2018). Burnout and implications for professional school counselors. The Professional Counselor, 8(3), 277–294. https://doi.org/10.15241/nk.8.3.277
Kobin, C., & Tyson, E. (2006). Thematic analysis of hip-hop music: Can hip-hop in therapy facilitate empathic connections when working with clients in urban settings? The Arts in Psychotherapy, 33(4), 343–356. https://doi.org/10.1016/j.aip.2006.05.001
Lent, R. W. (2013). Career-life preparedness: Revisiting career planning and adjustment in the new workplace. The Career Development Quarterly, 61(1), 2–14. https://doi.org/10.1002/j.2161-0045.2013.00031.x
Levy, I. (2012). Hip hop and spoken word therapy with urban youth. Journal of Poetry Therapy, 25, 219–224. https://doi.org/10.1080/08893675.2012.736182
Levy, I. (2019). Hip-hop and spoken word therapy in urban school counseling. Professional School Counseling, 22(1b). https://doi.org/10.1177/2156759X19834436.
Levy, I. P., Cook, A. L., & Emdin, C. (2018). Remixing the school counselor’s tool kit: Hip-hop spoken word therapy and YPAR. Professional School Counseling, 22(1). https://doi.org/10.1177/2156759X18800285
Levy, I., Emdin, C., & Adjapong, E. S. (2018). Hip-hop cypher in group work. Social Work with Groups, 41(1–2), 103–110. https://doi.org/10.1080/01609513.2016.1275265
Levy, I., & Keum, B. T. (2014). Hip-hop emotional exploration in men. Journal of Poetry Therapy, 27(4), 217–223. https://doi.org/10.1080/08893675.2014.949528
Liddicoat, S. (2010). Counselling workspace design and therapeutic practice. In J. Zuo, L. Daniel, & V. Soebarto (Eds.), Fifty years later: Revisiting the role of architectural science in design and practice: 50th International Conference of the Architectural Science Association (pp. 69–78). The Architectural Science Association and The University of Adelaide. http://anzasca.net/paper/counselling-workspace-design-and-therapeutic-practice
Liddicoat, S. (2015). Exploring relations between body, communication and agency in therapeutic space. In R. H. Crawford, & A. Stephan (Eds.), Living and Learning: Research for a Better Built Environment: 49th International Conference of the Architectural Science Association (pp. 123–132). The Architectural Science Association and The University of Melbourne. http://anzasca.net/wp-content/uploads/2015/12/012_Liddicoat_ASA2015.pdf
Mau, W.-C. J., Li, J., & Hoetmer, K. (2016). Transforming high school counseling: Counselors’ roles,
practices, and expectations for students’ success. Administrative Issues Journal: Connecting Education, Practice, and Research, 6(2), 83–95. https://doi.org/10.5929/2016.6.2.5
McMahon, H. G., Mason, E. C. M., Daluga-Guenther, N., & Ruiz, A. (2014). An ecological model of professional school counseling. Journal of Counseling & Development, 92(4), 459–471. https://doi.org/10.1002/j.1556-6676.2014.00172.x
Miwa, Y., & Hanyu, K. (2006). The effects of interior design on communication and impressions of a counselor
in a counseling room. Environment and Behavior, 38(4), 484–502. https://doi.org/10.1177/0013916505280084
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52(2), 250–260. https://doi.org/10.1037/0022-0167.52.2.250
Pearson, M., & Wilson, H. (2012). Soothing spaces and healing places: Is there an ideal counselling room design? Psychotherapy in Australia, 18(3), 46–53.
Phelps, C., Horrigan, D., Protheroe, L. K., Hopkin, J., Jones, W., & Murray, A. (2008). “I wouldn’t classify myself as a patient”: The importance of a “well-being” environment for individuals receiving counseling about familial cancer risk. Journal of Genetic Counseling, 17(4), 394–405. https://doi.org/10.1007/s10897-008-9158-z
Ponterotto, J. G., & Austin, R. (2005). Emerging approaches to training psychologists to be culturally competent. In R. T. Carter (Ed.), Handbook of racial-cultural psychology and counseling (pp. 19–25). Wiley.
Pressly, P. K., & Heesacker, M. (2001). The physical environment and counseling: A review of theory and research. Journal of Counseling & Development, 79(2), 148–160. https://doi.org/10.1002/j.1556-6676.2001.tb01954.x
Ramchand, R., Ahluwalia, S. C., Xenakis, L., Apaydin, E., Raaen, L., & Grimm, G. (2017). A systematic review of peer-supported interventions for health promotion and disease prevention. Preventive Medicine, 101, 156–170. https://doi.org/10.1016/j.ypmed.2017.06.008
Ratts, M. J. (2009). Social justice counseling: Toward the development of a fifth force among counseling paradigms. The Journal of Humanistic Counseling, Education and Development, 48(2), 160–172. https://doi.org/10.1002/j.2161-1939.2009.tb00076.x
Ratts, M. J., & Greenleaf, A. T. (2018). Counselor–advocate–scholar model: Changing the dominant discourse in counseling. Journal of Multicultural Counseling and Development, 46(2), 78–96. https://doi.org/10.1002/jmcd.12094
Ratts, M. J., & Pedersen, P. B. (2014). Counseling for multiculturalism and social justice: Integration, theory, and application (4th ed.). American Counseling Association.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and Social Justice Counseling Competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Reyes, M. R., Brackett, M. A., Rivers, S. E., White, M., & Salovey, P. (2012). Classroom emotional climate, student engagement, and academic achievement. Journal of Educational Psychology, 104(3), 700–712. https://doi.org/10.1037/a0027268
Rock, W. D., Remley, T. P., & Range, L. M. (2017). Principal-counselor collaboration and school climate. NASSP Bulletin, 101(1), 23–35. https://doi.org/10.1177/0192636517698037
Sanders, R., & Lehmann, J. (2019). An exploratory study of clients’ experiences and preferences for counselling room space and design. Counselling and Psychotherapy Research, 19(1), 57–65. https://doi.org/10.1002/capr.12202
Smith, J. A. (1996). Beyond the divide between cognition and discourse: Using interpretative phenomenological analysis in health psychology. Psychology & Health, 11(2), 261–271. https://doi.org/10.1080/08870449608400256
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research. SAGE.
Smith, L., & Chambers, C. (2015). Decolonizing psychological practice in the context of poverty. In R. D. Goodman & P. C. Gorski (Eds.), Decolonizing “multicultural” counseling through social justice (pp. 73–84). Springer.
Smithson, J. (2000). Using and analyzing focus groups: limitations and possibilities. International Journal of Social Research Methodology, 3(2), 103–119. https://doi.org/10.1080/136455700405172
Thomas, E., & Magilvy, J. K. (2011). Qualitative rigor or research validity in qualitative research. Journal for Specialists in Pediatric Nursing, 16(2), 151–155. https://doi.org/10.1111/j.1744-6155.2011.00283.x
Travis, R., Jr., & Deepak, A. (2011). Empowerment in context: Lessons from hip-hop culture for social work practice. Journal of Ethnic & Cultural Diversity in Social Work, 20(3), 203–222. https://doi.org/10.1080/15313204.2011.594993
Tyson, E. H. (2002). Hip hop therapy: An exploratory study of a rap music intervention with at-risk and delinquent youth. Journal of Poetry Therapy, 15(3), 131–144. https://doi.org/10.1023/A:1019795911358
Washington, A. R. (2018). Integrating hip-hop culture and rap music into social justice counseling with Black males. Journal of Counseling & Development, 96(1), 97–105. https://doi.org/10.1002/jcad.12181
Zuber-Skerritt, O., & Fletcher, M. (2007). The quality of an action research thesis in the social sciences. Quality Assurance in Education, 15(4), 413–436. https://doi.org/10.1108/09684880710829983
Ian P. Levy, EdD, is an assistant professor at Manhattan College. Edmund S. Adjapong, PhD, is an assistant professor at Seton Hall University. Correspondence may be addressed to Ian Levy, 4513 Manhattan College Pkwy, The Bronx, NY 10471, ilevy01@manhattan.edu.
Apr 29, 2020 | Volume 10 - Issue 2
TeShaunda Hannor-Walker, Lynn Bohecker, Lacey Ricks, Sarah Kitchens
Literature does little to explore the perceptions of Black adolescents with depression or their perspective of treatment effectiveness. Studies are usually from urban areas and there is a dearth of research with Black adolescents from rural areas. This study explored the unique personal experiences of Black adolescents located in the rural southeastern United States, with the purpose of gaining a clearer understanding when working with this population. An interpretative qualitative method was used to explore 10 participants’ interpretation of their experiences to gain insight in how they make meaning of those experiences. Five significant categories were found to capture participant themes: (a) definition of depression, (b) seeking treatment, (c) coping and problem solving strategies, (d) types of emotional support, and (e) contributing factors to depression. Specific recommendations and interventions are suggested for mental health clinicians to become more educated and aware when working with Black adolescents.
Keywords: Black adolescents, depression, treatment effectiveness, rural, contributing factors
Depression is a leading cause of disability worldwide (World Health Organization, 2020). The World Federation for Mental Health (2012) estimated that by 2030, more people will be impacted by depression than any other health problem. In the United States, approximately 13.3% of adolescents, or 3.2 million, had at least one major depressive episode and 9.5% were Black (National Institute of Mental Health [NIMH], 2013). Black people have experienced more severe forms of mental health conditions than individuals of other races because of unmet needs and other barriers (NIMH, 2013). In fact, Black people were reported to be 10% more likely to experience serious mental health problems than the general population (Shushansky, 2017), and Black children have a suicide rate that is almost two times higher than that of their White counterparts (Bridge et al., 2018).
Weaver et al. (2015) noted that although 90% of rural Black people live in the southeastern part of the United States, there are only two studies that specifically examined depression among rural Black people using national data (i.e., Probst et al., 2006; Willis et al., 2003). Most studies of depression that include Black youth are based on data from urban communities (Al-Khattab et al., 2016; Conner & Yeh, 2018; Ofonedu et al., 2013; Robinson et al., 2015). This suggests there is a dearth of research exploring Black adolescent experiences of depression in rural communities, and there is even less research focusing on Black youth who live in the rural southeastern United States (Smokowski et al., 2015: Weaver et al., 2015). The goal of this study was to explore the unique experiences of Black adolescents living in the rural southeastern United States who had been diagnosed with depression.
Contributing Factors to Depression in Black Adolescents
Adolescents who suffer from depression may experience substantial negative health and social consequences in late adolescence and adulthood (Lu, 2019). Black adolescents are particularly vulnerable to these consequences because they are more likely to live in low-resource neighborhoods and because they contend with the negative psychological impacts of racial discrimination (Robinson et al., 2015). Choi et al. (2006) found that ethnic minorities have higher scores on social stress and mental distress and lower scores on coping, self-esteem, and family cohesion. The depressive symptoms experienced by Black adolescents are often socially and culturally based (Lu et al., 2017). Therefore, it is essential for counselors, school personnel, and related professionals to remain abreast of the current research on depressive signs and symptoms, beliefs about treatment, and specific needs of Black adolescents.
Choi et al. (2006) discovered that Black, Hispanic, and Asian adolescents in the United States have consistently higher levels of social stress beginning in childhood compared to their White counterparts. Breland-Noble et al. (2010) found that relationship problems, academic problems, bereavement, and stress were primary triggers for depressive symptoms among Black adolescents. Ofonedu et al. (2013) determined in their study of Black adolescents that life events in the home, school, and community contributed to depressive symptoms. These factors included (a) a stressful home life, (b) stressful life circumstances and unique life experiences at school, and (c) the experience of high levels of violent crimes in neighborhoods. Stress is clearly a contributing factor to the depressive symptoms of Black adolescents.
Symptoms of Depression in Black Adolescents
Although understanding national trends and contributing factors can help practitioners identify adolescents suffering from depression, it is also important to understand potential racial and ethnic differences in the expression of adolescent depression (Lu, 2019). The manifestations of depressive symptoms vary in Black youth and affect all dimensions of physical, psychological, interpersonal, and social being (Ofonedu et al., 2013). In the Black community, mental health conditions have often been unacknowledged, misunderstood, and misdiagnosed (Shushansky, 2017; Vontress et al., 2007). According to Vontress et al. (2007), Black people often experience cultural dysthymia and mental health symptoms such as low-grade depression; feelings of sadness, hopelessness, and anger; aggression; and self-destructive behaviors. Vontress et al. (2007) characterized these symptoms as a “psychosocial condition” grounded in external societal experiences of discrimination and oppression that often go unrecognized (p. 131). Additional studies are needed to show how to better identify individuals suffering from depression and thereby increase the effectiveness of treatment for Black adolescents (Ofonedu et al., 2013).
As in adults, unrecognized or undiagnosed dysthymia or symptoms of low-grade depression in adolescents can contribute to poor health and problematic behaviors (Saluja et al., 2004). Researchers discovered that untreated dysthymia elevates the risk of disruptive behaviors, anxiety, substance abuse, unsafe sexual practices, involvement in fights, lower achievement on tests, lower teacher-rated grades, and poorer peer relationships (Saluja et al., 2004). Auger (2005) discovered that the many signs and symptoms of adolescent depression were overlooked not only by parents but also by school systems, administrators, counselors, and teachers who daily were in a very unique position to identify those at risk of depression. Many cases of adolescent depression, particularly among minorities, have gone undiagnosed, misdiagnosed, and untreated (Cook et al., 2017; Shushansky, 2017). A better understanding of the unique experiences of Black adolescents diagnosed with depression would help improve symptom recognition, which may in turn reduce misdiagnosis and increase treatment effectiveness.
An understanding of the cultural implications and influence that oppression, prejudice, and various forms of discrimination have on Black people’s mental health in the United States is helpful in contextualizing and normalizing symptoms of depression and reducing instances of misdiagnosis. Hope et al. (2017) posited that discrimination remains a common experience for Black adolescents that can impact not only the onset of depression but also the quality of and access to mental health services. Furthermore, according to Liang et al. (2016), racial disparities exist, as Black youth are more likely to be misdiagnosed as having psychotic and disruptive behavior problems compared to mood (i.e., depression) and substance abuse disorders.
Lu et al. (2017) echoed these sentiments, stating that depression presents differently for Black adolescents. It is essential for Black adolescents to use their own language when describing their depressive symptoms. Additionally, it is important for clinical and school counseling professionals to be aware of gender differences in Black adolescents’ expression of depression, specifically in terms of internalizing and externalizing symptoms. The findings of Breland-Noble et al. (2010) indicated that female Black adolescents seem to internalize behaviors (e.g., becoming withdrawn, exhibiting visible sadness), while male Black adolescents seem to externalize behaviors (e.g., becoming angry or acting out). Lu et al. (2017) further highlighted that “adolescents develop [symptoms] as a means of coping in response to environmental factors” (p. 614). More research is needed to understand how depressed Black adolescents describe their symptoms and assign meaning to their experiences of depression.
Coping Strategies of Black Adolescents
In addition to presenting different symptoms than individuals of other racial groups, Black adolescents have the lowest coping skills scores compared to their peers (Conner & Yeh, 2018). Recent studies suggest that adolescents who live in low-resourced neighborhoods feel like they have limited options in how to respond to stressful and anxiety-provoking situations because of limited or ineffective coping skills (Robinson et al., 2017; Robinson et al., 2015). There are indications that Black adolescents cope with depression in a variety of contexts. Some Black adolescents describe depression as a way of life, noting that everybody becomes depressed one way or another (Ofonedu et al., 2013). Researchers have shown that some Black adolescents conceal their feelings of depression because they are uncertain of how others would perceive them (Al-Khattab et al., 2016; Ofonedu et al., 2013). For instance, some Black adolescents reported trying to manage their depression independently and only going to an adult as a last resort (Breland-Noble et al., 2010). Black adolescents have been shown to manage their depression by strong will and spiritual beliefs (Ofonedu et al., 2013). Conner and Yeh (2018) highlighted how Black adolescents cope with depression in spiritual and creative ways such as listening to music, dancing, and writing.
In 2016, Al-Khattab et al. discovered that Black adolescents controlled their depression through their interactions with other people. Al-Khattab et al. identified five typology interaction models, which include hiding feelings of depression, lashing out verbally or physically toward others, seeking help from others to address emotional feelings, joining with others in social activities, and having others approach them about behavioral and mood changes. Therefore, it is critical for Black adolescents to better understand their experiences with depression and how interactions with others may influence their symptoms.
Treatment of Depression in Black Adolescents
Cook et al. (2017) noted that there are barriers to accessing mental health services and quality of care, which include stigma associated with mental illness, distrust of the health care system, lack of providers from diverse racial/ethnic backgrounds, lack of culturally competent providers, and lack of insurance or underinsurance. Often these barriers cause Black people to be unable or reluctant to seek help (Shushansky, 2017). Although Black adolescents may feel that treatment can be effective, many are reluctant to attend therapy because of the stigma and possible misdiagnosis of their symptoms, much of which has been influenced by their culture (Al-Khattab et al., 2016; Lindsey et al., 2010; Ofonedu et al., 2013). Positive results have been seen when using family-centered prevention programs to address depressive symptoms in Black adolescents (Brody et al., 2012). Jacob et al. (2013) determined that behavioral activation was effective for decreasing depressive symptoms and impairments for the Black adolescents who participated in their study.
As highlighted by a study of Black adults from a rural faith community, Black people living in rural communities suffering from depression face additional barriers to treatment such as (a) a lack of medical resources, (b) insufficient education about depression, and (c) stigma (Bryant et al., 2013). Sullivan et al. (2017) learned that terminology was crucial when discussing treatment with rural Black adults on a stigmatized topic such as mental illness. Parental concerns about marginalization because of having a child with a mental health diagnosis and some primary care providers’ characterization of mental health symptoms as a “phase” have been found to be barriers to treatment for Black children living in rural communities (Murry et al., 2011). Working with Black children who live in poverty, Graves (2017) identified cultural and macro-level barriers that influence the process of seeking treatment.
Treatment of mental health disorders extends from diagnoses. Considering the differences in symptoms and frequency of misdiagnosis, it is not surprising that treatment options for Black adolescents have shown varied outcomes across the literature. Additionally, some researchers suggested that new measures need to be developed for accurately identifying depression in diverse populations, which would then inform modifications in treatment (Ofonedu et al., 2013). Having a better understanding of the unique and complex experiences of Black adolescents may help parents, therapists, schools, and counseling professionals understand and identify those most at risk for depression. Planey et al. (2019) discovered that Black youth viewed seeking mental health treatment as a contextual and relational process rather than an event. What is clear is that more culturally diverse training for therapists, schools, and counseling professionals is needed to prevent, detect, and implement interventions for minorities experiencing depression during the disease’s earlier stages. Likewise, research exploring Black adolescents’ unique experiences of symptoms, environmental factors, and coping strategies remains necessary in order to inform effective treatment.
Purpose of the Present Study
The review of the literature captured symptoms and coping strategies unique to Black adolescents. Studies highlight that environmental factors contribute to depressive symptoms in this population. Furthermore, disparities exist in mental health care for adolescents, specifically for minorities (Alegria et al., 2010; Brenner, 2019; Lake & Turner, 2017). This clear gap in the literature indicates insufficient knowledge regarding the personal experiences of Black adolescents with depression. Most of the studies in the extant literature took place in urban areas; little is known about rural experiences and even less is known about experiences in the southeastern United States. This qualitative study was designed to help fill that gap. It posed an overarching research question to Black adolescents living in the rural southeastern United States: “What is your experience with depression?” This study was designed to offer human services professionals a clearer understanding of the unique experiences of Black adolescents in this geographical region who had been diagnosed with depression, with the hope of informing clinical practices.
Method
The goal of this study was to explore the unique experiences of Black adolescents living in the rural southeastern United States who had been diagnosed with depression. The research design for the study was a basic interpretive qualitative method, as described by Merriam (2009). The purpose of this method is to understand the perspectives of the participants involved by uncovering and interpreting their meanings (Everall et al., 2006). This purpose was well-suited to the overall objective of this study, which was to gain a clearer understanding of the unique personal experiences of Black adolescents living with depression in the rural southeastern United States.
According to Merriam (2009), interpretive qualitative research is founded on the idea that people and their interactions with their world, or reality, socially construct meaning. Researchers using this method are interested in how individuals “interpret” their experiences, “construct their worlds,” and assign “meanings” to their experiences (Merriam, 2009, p. 38). Moreover, Merriam asserted that interpretive qualitative research has multiple meanings and is a complex phenomenon ideal for attempting to understand and treat Black adolescents with depression. Using Merriam’s (2009) model, researchers “strive to understand the meanings individuals construct regarding their world and their experiences” in a natural setting (p. 4). Another characteristic is that the researcher serves as the primary instrument for both collecting and analyzing data. The research process is inductive rather than deductive, which means that the researcher gathers data in an effort to “build concepts, hypotheses, or theories” in the forms of themes and categories (Merriam, 2009, p. 5). A final characteristic of this model is that interpretive qualitative research is richly descriptive and includes details about the context, the participants involved, and quotations and interview excerpts (Merriam, 2009).
Merriam (2009) noted that certain elements of the basic interpretive qualitative design may overlap with other designs, particularly when concepts of cultural values are discussed and explored. Merriam’s design does not require researchers to give a full sociocultural interpretation of the data, as is done in ethnography. Indeed, this study does not provide a full sociocultural interpretation. However, the data were analyzed using Patton’s (1987) content analysis model because the model provides a rigorous, systemic, and ethical procedure for analyzing data. Merriam’s model for collecting data and Patton’s model for analyzing data form a rich methodological combination that enhances the trustworthiness of the research study and improves the transferability of its findings.
Participants and Procedure
The university IRB granted approval for this study. Purposive sampling was used to identify 10 Black adolescents living in the rural southeastern United States who were being treated for depression. The southeastern part of the United States was selected because it contains fewer metropolitan areas that have been studied specifically. Each of the participants met the following criteria: (a) self-identified as Black, (b) was between the ages of 13 and 17, (c) was willing to participate, (d) had secured a signed informed consent form from their parents, (e) had signed a participant assent form, and (f) was currently under the care of a counselor either in or out of school for depression. The participants ranged in age from 13 to 17 years old and were in grades seven through 12. Six participants were female and four were male.
Approval was obtained in advance from a public school system located in the rural southeastern United States. The public school system administrator agreed to send the letter of invitation along with the consent and assent forms to the parents and potential participants. In addition, the first author sent a packet of information to a counseling agency; school professionals, including professional school counselors and school psychologists; and social workers. The packet contained an invitation letter requesting that the packet be shared with potential participants and their parents; it also contained consent and assent forms. The informed consent form described the study and the efforts that would be taken to protect the confidentiality of the participants’ information. The informed consent form stated that the risk of participating was the normal discomfort of sharing one’s experiences with depression and that if a participant felt uncomfortable, they could withdraw from the study at any time.
Parents and participants signed the consent and assent forms, respectively, and returned them to either the local counseling agency or school professionals, who forwarded the forms to the first author. The first author then contacted the parents, with the participants present, to schedule a 45- to 90-minute, face-to-face interview with the participant. The informed consent form was verbally reviewed, ensuring that the parents and participants understood that a second interview to review and correct the interpretation would be optional. Interviews took place either during the day in a private room at the school or outside of school hours in the first author’s office. Because adolescent depression is considered a sensitive topic, participants were instructed to follow up with their counselor if they experienced adverse feelings as a result of participating in the study.
Data Collection and Analysis
The first author met with each of the 10 participants for a single semi-structured interview that lasted between 45 and 90 minutes. In phenomenological research, the researcher follows the essence of participants’ responses (van Manen, 1997). The first author spent time establishing rapport with the participants. Once the first author believed a participant was comfortable, she asked the participant the overarching question, “What is your experience with depression?” Follow-up questions specific to each participant were used to probe the participants’ responses regarding their experience as Black adolescents living with depression in the rural southeastern United States. Several participants expressed a reluctance to fully disclose or discuss their experiences with depression; however, no participants withdrew from the study, and all participants completed the first interview. At the end of the first interview, the participants were notified that they would be contacted for a second interview to review the transcript of the first interview and verify its accuracy and trustworthiness.
Interviews were recorded and transcribed verbatim by both the first author and a professional transcriber. The transcripts were coded and analyzed for themes related to the research question of this study. The first author utilized Patton’s (1987) content analysis model as a process of bringing order to the data by organizing the data into major themes, categories, and case examples. The first author consulted with two experts in qualitative research in the human services field and used three levels of coding: open, axial, and selective. Open coding included reading the transcribed interviews several times and coding phrases, from one word to portions of paragraphs. Based on input from the consultants, the first author enhanced the coding process by entering the data into the NVivo QSR software program, which facilitated organization and analysis. The first author then condensed the data into five categories. Axial coding enabled the first author to organize, link, and cluster codes, while selective coding allowed the first author to analyze the words, sentences, and themes from the interviews. Data analysis via coding was a back and forth process, and staying close to the transcripts was essential. The labeling and coding allowed the first author to interpret and classify the data and themes into five categories that were supported with direct quotations from the participants.
Trustworthiness
Trustworthiness is an important aspect of qualitative research (Hays & Singh, 2012). The generally candid nature of each participant in relating even the most difficult experiences, such as rape, would suggest a high degree of trustworthiness in their responses. Member checking was offered to all participants in the form of a follow-up interview. When contacted by the first author to schedule this interview, however, none of the participants felt that it was necessary. Rather, all of the participants stated they were satisfied with their responses in the first interview. In addition to offering member checking, the first author used rich data, prolonged engagement, respondent validation, a search for discrepant data, and peer review to ensure trustworthiness. A peer review of the method was conducted by doctoral-level professors in human services who specialized in qualitative research in order to enhance internal validity (Lincoln & Guba, 1985; Merriam, 2009). The first author used an audit trail by engaging in memo-writing to express thoughts, perspectives, observations, and reactions to interviews, transcriptions, and coding. An audit trail is a strategy in which a researcher explains as best as possible how they arrived at the results of the study by documenting how the data were collected, how categories were developed, and how findings were interpreted throughout the study (Lincoln & Guba, 1985). An audit trail thus improves the quality of a study. The information and details from this study may be generalizable to other groups and may contribute to the knowledge base of best practices when working with this population in counseling.
Results
Through data analysis, the researcher identified five significant thematic categories: (a) definitions of depression, (b) seeking treatment, (c) coping and problem-solving strategies, (d) types of emotional support, and (e) contributing factors to depression. These five thematic categories were broken down into their constituent contents. Each thematic category was addressed with the invariant constituents that make up that category, including elaboration on any significant constituent patterns (such as high and low frequency of occurrence). Quotations from the participants are included in the text as examples to elucidate the invariant constituents and thematic categories. For reasons of confidentiality, some identifying information was excluded. All participants identified as Black and lived in the rural southeastern United States.
At the time of the study, the participants were living in a southeastern U.S. community in one of the lowest socioeconomic brackets of the country. In the participants’ community, the majority of the population was Black and participated in the school’s free or reduced-fee lunch program. Because of the homogeneous nature of the community, the participants did not speak of any adverse social or political circumstances, and the researcher avoided broaching the topic in an effort to do no harm. The researcher believed that overlooking the social and political climate of the community increased the trustworthiness of the participants’ responses, as the participants were not influenced by the discussion of the climate nor did they voluntarily express its relevance to their experience. As a Black adult, the researcher, who is first author, was aware of how the social and political climate played into their experience. However, because the participants were adolescents experiencing emotional pain, the first researcher attempted to instill hope in them as part of their experiences of this study. To maintain confidentiality, specific details about the contextual factors in the participants’ community have been omitted.
Definitions of Depression
Data analysis identified 18 codes that were relevant to the category regarding how participants defined depression. Of these codes, three emerged with significantly higher prevalence than the others: (a) sadness; (b) isolation, social withdrawal, or loneliness; and (c) permanent or persistent. Nine out of the 10 participants (90%) indicated that they experienced the feelings associated with these three codes. For example, in response to how he defined depression, Participant 5 noted that he became “sad, mad, and very frustrated.” Participant 1 defined depression in terms of social withdrawal, saying, “Usually I stay in my room and I don’t talk to anybody, I just stay in there, and that is about it.” Participant 4 provided an example of the theme of permanent or persistent experiences by stating, “I don’t think it could just go away, especially when it’s very serious.” Participant 3 provided an example that captured the overall essence of this category when he stated:
I have been sad a whole lot, without reason; and so, I think that is why I was depressed . . . when I am around people for too long, I get sad; but when I am alone, I am happier. I feel safe when I am by myself. When it [depression] comes on, it comes on strong. It is really bad. Because I feel really, really sad, and my thoughts aren’t, you know, normal. Sometimes they are violent . . . like I don’t have any hope at all. I don’t think like I normally would. Sometimes I don’t think at all. Sometimes when I get really sad or angry, I think about hurting people. So, I have to withdraw further. I have to push it further down into my mind so that I won’t act on it.
It is interesting to note that the next most frequently found codes were stress-related and frustration, each with a prevalence of 60%, and more common in young Black girls, which had a prevalence of 50%. Alternatively, only one participant mentioned each of the following codes with regard to defining depression: suicidal thoughts or attempts, more common in young Black boys, and feeling sick.
Seeking Treatment
The category of seeking treatment contained 10 codes. Participants expressed contradictory feelings about the effectiveness of treatment and the barriers to seeking treatment. For example, 90% of participants expressed that they felt that therapeutic treatment was effective in mitigating or curing depression, including Participant 7: “To me, to talk to my therapist was like a relief to me, because he was the only person that I can be able to tell my thoughts, get my thoughts together why I was in there.” Simultaneously, 30% of participants noted that they felt that therapy was not effective as a treatment. This overlap and apparent incompatibility in the data helped reveal the full breadth of Black adolescents’ opinions and feelings about depression and seeking treatment, as participants expressed both positive and negative experiences.
This overlapping trend was seen elsewhere in this thematic category. For example, there were codes of medication is effective (50%) and medication is not effective (30%). This apparent contradiction was highlighted not only between participants but also within a single participant. Participant 10 directly stated she believed medication to be effective; she then revealed that she had been given medication that sent her into a coma. She reported taking her medication as prescribed but “after that I passed out, and I didn’t remember nothing, all I knew I woke up in the hospital.” Three codes were identified as directly related to seeking treatment. Significant barriers to therapeutic treatment were negative connotation of mental illness (80%), uncomfortable issues brought up in treatment (80%), and lack of trust (70%). The code negative connotation of mental illness was grounded in external perceptions, as many participants indicated that they did not want other people to know that they were in treatment.
For example, Participant 2 stated, “I don’t tell them. I don’t want them to know,” when referring to his friends. Participant 3 provided an example of the code of uncomfortable issues, noting, “I don’t like to talk about it much. You know, it is kind of aggravating. It makes me feel weak when I talk to people about my problems.” Regarding the code lack of trust, Participant 6 noted, “I have very weak trust issues. Sometimes they can be strong but mostly weak.”
Three minor codes emerged relating to seeking treatment. Two were trouble expressing self in therapy (40%) and treatment was not necessary (40%). Participant 3 stated, “I have a lot of trouble expressing myself. You know, when I get into the office, I just forget what to say.” Three of the 10 participants openly discussed lack of Black people’s knowledge or education about depression as a specific barrier to treatment. They shared their perceptions of the lack of education and discussion about depression within their own community, which they felt presented a specific barrier to treatment for them. Participant 6 stated, “I can’t overly generalize it, but some people need to know more, ’cause they don’t understand, because sometimes you just need that time and people they don’t understand that you need it.” However, taking these and the other barriers in this thematic category into account, the prevalence of participants who reported that treatment was effective was three times greater than the prevalence of participants who thought that treatment was ineffective.
Coping and Problem-Solving Strategies
The third thematic category contained 29 different codes related to problem-solving strategies and behaviors or activities the participants used to cope with depressive symptoms. The participants described various strategies to cope with depression, but the most prevalent was suppressing/hiding thoughts/feelings. There were seven strategies that more than half of the participants reported using as problem-solving strategies and strategies to cope with depression. The positive problem-solving strategies were listening to music, turning to religion/going to church/praying, and talking/spending time with family. The problematic coping strategies reported were using illegal drugs, engaging in self-harm, having sex, and isolating. See Table 1 for codes and results.
It is encouraging that 18 out of the 29 codes could be characterized as neutral or positive coping strategies. The other 11 are areas of concern, even if only one participant reported engaging in the behavior. Participant responses overlapped and participants reported coping and problem-solving strategies that might be characterized as both positive and negative. In addition to contrasts in the specific codes and types of behaviors, contrasts in the percentages of participants who reported negative behaviors compared to positive behaviors were noted. For example, participants reporting the negative problem-solving strategy of engaging in self-harm as a way to cope often went into detailed narrative descriptions. This strategy was more frequently reported than any of the positive or neutral coping and problem-solving strategies.
Types of Emotional Support
This thematic category addressed the types of emotional support that the participants received during their experiences with depression. Four distinct subthemes of codes were identified: peers; family; school (teachers); and helping professionals such as hospitals, managed care facilities, and therapists. Each of the four subthemes contained codes that were sorted as either positive or negative. A lack of support or refusal of support was considered a negative, and similar to other categories, participants shared multiple overlapping experiences. Negative support from peers was the only theme to have 100% prevalence; every participant mentioned that peers had negatively affected them through a lack of emotional support during their experience with depression, including Participant 2: “They didn’t believe me at first, but later they just seem like they don’t care.” Half of the participants expressed that they had also received positive emotional support from their peers during their experience with depression. In the family group, equal percentages of participants (60%) reported receiving positive support from family and experiencing a lack of support from family. The participants were similarly split regarding their perceptions of receiving positive (50%) and negative (50%) emotional support from teachers at school. The greatest proportional difference in negative and positive emotional support was within the category of helping professionals. In this subtheme, four times as many participants (40%) reported that they had had positive emotional support from mental health care providers in a hospital, halfway house, or therapeutic community than participants reporting negative emotional support from mental health care providers (10%).
Table 1
Coping and Problem-Solving Strategies
| Strategy |
Percent of Respondents
(N = 10) |
| Positive or Neutral
Coping Strategies |
Listening to music |
70% |
| Turning to religion / going to church / praying |
70% |
| Talking / spending time with family |
60% |
| Attending therapy |
40% |
| Writing |
40% |
| Creating art |
30% |
| Playing video games |
30% |
| Watching TV |
30% |
| Crying |
30% |
| Taking prescription drugs |
20% |
| Eating food |
20% |
| Reading |
20% |
| Talking / spending time with friends |
20% |
| Distracting self |
20% |
| Laughing |
20% |
| Joining clubs |
10% |
| Working out |
10% |
| Researching |
10% |
| Problematic
Coping Strategies |
Suppressing / hiding thoughts / feelings |
90% |
| Using illegal drugs |
70% |
| Engaging in self-harm |
60% |
| Having sex |
60% |
| Isolating |
60% |
| Attempting suicide |
40% |
| Engaging in violence |
40% |
| Running away |
30% |
| Yelling / shouting |
10% |
| Having violent thoughts |
10% |
| Avoiding responsibilities / rebelling |
10% |
Contributing Factors to Depression
This theme of contributing factors to depression appeared to be the most salient to the central research question of how Black adolescents living in the rural southeastern United States described their experiences with depression. The previous themes captured definitions of depression, seeking treatment, coping and problem-solving strategies, and types of emotional support. This theme provided a description of the participants’ lives in terms of their context and environment, which the participants identified as contributing factors to their experiences of depression. When asked about contributing factors to their depression, the three most noted by the participants were verbal abuse (70%), differences from other people and being bullied (70%), and parental or family problems (70%). Participants also reported sexual abuse (40%) and physical abuse (30%) as contributing factors. Participant 6 made the following statement, which captures the essence of this theme:
My depression started really kicking in when I was around 13 . . . it runs in my family. My mom has it and when I was little, I was sexually abused . . . and I’ve been made fun of all my life . . . my weight . . . a scalp infection. People make fun of stuff like that. And that’s been going on since I was little.
The least prevalent factors mentioned by participants were foster care (20%), stress of schoolwork (20%), and a scary book (10%). Verbal abuse was reported 30% more frequently than sexual abuse and 40% more frequently than physical abuse. However, it is interesting to note that Participant 2 considered foster care to be a cause of depression and not a solution. Most participants identified a combination of these factors as contributing to the onset of their depressive symptoms.
Discussion and Implications
This study sought to examine the unique experiences of Black adolescents diagnosed with depression living in a rural community located in the southeastern part of the United States. Five themes emerged when examining the participants’ narratives with depression. These themes included definitions of depression, seeking treatment, coping and problem-solving strategies, types of emotional support, and contributing factors to depression. In defining depression, 90% of the participants in this study cited sadness, isolation, and depression’s ongoing nature. This is not surprising, as these codes fit within the diagnostic criteria for depression. It was surprising, however, that participants defined depression as stress-related, as stress is not one of the diagnostic criteria. At the same time, the idea of depression as stress-related is supported in other studies (Breland-Noble et al., 2010; Bryant et al., 2013; Choi et al., 2006; Ofonedu et al., 2013; Robinson et al., 2015). The mental health community would do well to acknowledge the differences in how Black adolescents from rural U.S. communities may define depression. When working with Black adolescent clients, practitioners may wish to inquire about stressors and consider their relation to depression in order to inform treatment plans and interventions.
Most participants who sought treatment for depression indicated that treatment was effective; however, 30% of participants expressed that therapy was ineffective. Additionally, only 50% of participants indicated that medication was an effective form of treatment. Participants also identified barriers to seeking treatment, which included negative connotations associated with mental illness and discomfort discussing issues in treatment. Barriers identified included a lack of trust, problems with self-expression, the belief that therapy was not needed, and a lack of knowledge about depression in the Black culture. These results are consistent with prior research (Al-Khattab et al., 2016; Bryant et al., 2013; Lindsey et al., 2010; Ofonedu et al., 2013; Sullivan et al., 2017), indicating that mental health conditions are often misunderstood, misdiagnosed, or unacknowledged within the Black community (Graves, 2017; Murry et al., 2011; Shushansky, 2017).
Prior research has also highlighted the stigma of mental illness in the Black community (Cook et al., 2017). This stigma helps to explain previous research showing that Black people often seek help as a last resort (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013; Vontress et al., 2007). It is essential that counselors acknowledge the stigma associated with mental illness and reluctance to seek treatment within the Black community. More practitioners who are aware of and sensitive to the mental health needs of Black communities are needed. It is imperative that clinicians take it upon themselves to become competent when working with this population. To address the stigma, practitioners might offer training in evidence-based practices related to Black adolescents’ mental health at churches, schools, and various community organizations in the Black community. These types of trainings could be particularly effective in rural communities where participants are likely to communicate to others about the trainings, thereby validating the information and possibly reducing the stigma. One of the codes from this study was related to the effectiveness of medication for reducing depressive symptoms. More research is needed to explore factors that may contribute to this experience. Additionally, more research is needed to understand the unique traits of Black adolescents seeking treatment in other regions of the United States.
There were a few positive strategies for coping with depression that the participants identified, including listening to music, engaging in spiritual practices, and spending time with family. These positive coping strategies supported the constructs of spiritual beliefs and relationships with others, which were established in prior studies (Al-Khattab et al., 2016; Conner & Yeh, 2018; Ofonedu et al., 2013). The theme of coping and problem-solving strategies was dominated by the most common strategy: participants hiding their thoughts and feelings as a way of managing their depressive symptoms. This result corroborates the findings of prior studies that show Black adolescents conceal their feelings and symptoms of depression (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013; Vontress et al., 2007). As previous studies have suggested, hiding thoughts and feelings may be due to the stigma associated with mental illness and limited options in how to respond to stressful and anxiety-provoking situations (Robinson et al., 2017; Robinson et al., 2015). The finding that the participants hide thoughts and feelings also supports previous research that Black adolescents may be fearful of how others will react to them and isolate themselves as a result (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013). Participants also reported engaging in unhealthy coping behaviors such as self-harm, sexual intercourse, and isolation. These harmful strategies may be due to the limited coping skills of Black adolescents that have been identified in prior research studies (Robinson et al., 2017; Robinson et al., 2015). Again, these findings highlight the need for culturally specific training regarding mental health in Black communities.
The theme of emotional support resonated with all participants in this study, suggesting the significance of relationships (Breland-Noble et al., 2010). When examining emotional support, positive and negative experiences emerged. Positive emotional supports were found in family members (60%), teachers (50%), and mental health professionals (40%). Yet all participants indicated being negatively impacted by a lack of support among their peers. Participants reported feeling invalidated or not believed by their peers. They also reported that their peers did not seem to show concern. These experiences may have exacerbated the participants’ symptoms. Only half of the participants indicated receiving positive peer support when seeking help for depressive symptoms. These findings are concerning because of the heavy emphasis placed on relationships within Black communities (Breland-Noble et al., 2010).
Relationships were identified as significant to all participants in this study, indicating that healthy relationships may be a protective factor and may increase emotional and mental health. Counseling professionals in private practice and in schools are thus encouraged to inquire about a wide range of relationships when working with their Black adolescent clients. For example, a counseling professional might ask a client to complete a detailed relationship profile for each significant person in their life. This would help to uncover significant relationships that could support the client’s current challenges and to identify those individuals who might not be providing support. Counseling professionals might also conceptualize client symptoms as connected to these relationships. Family or systemic interventions may be incorporated into treatment planning to decrease depressive symptoms.
The theme of contributing factors encompassed a surprisingly high number of significant adverse and traumatic experiences. When examining the factors contributing to the development of depression in Black adolescents, most participants in this study cited verbal abuse, differences from others/bullying, and family-related issues as salient factors. Other contributing factors included sexual and physical abuse. Participants reported verbal abuse (70%), sexual abuse (40%), and physical abuse (30%) as contributing factors of depression. However, participants did not identify one single factor but rather described multiple and overlapping factors that contributed to their depressive symptoms. The connection between adverse and traumatic experiences and depressive symptoms specifically within the Black adolescent population appears to be underreported in the literature.
It is important to note the high prevalence of abuse indicated within the study. The lack of existing studies exploring the relationship among Black adolescents, depression, and adverse childhood experiences indicates that additional research is needed. An implication of this study is that when working with Black adolescent clients who are presenting with symptoms of depression, counseling professionals might incorporate an adverse childhood experience screening tool. Assessing clients for adverse childhood experiences as a matter of regular practice may better inform preventative measures and treatment. As this study highlights, it is essential for clinical and school professionals working with Black adolescents to understand that abuse can contribute to depressive symptoms.
Overall, many of the symptoms described by participants could be associated with a diagnosis of
dysthymia as a result of oppression, supporting the work of Vontress et al. (2007). However, the participants did not use the word “oppression” and may not have recognized the systemic aspects of their experiences (Vontress et al., 2007). It may be that the participants’ adverse experiences of abuse overshadowed any cultural or historical factors that may also have been present. The current study highlighted the overlooked and undertreated experiences of Black adolescents with depression. Counseling professionals may choose to gain a preliminary understanding of Black adolescent depression and dysthymia symptoms “within the context of their legacy of discrimination and oppression” (Vontress et al., 2007, p. 132).
Limitations
Overall, these findings need to be considered in light of some specific limitations. First, the interview questions were semi-structured. This means that the researcher used open-ended questions followed by discussion. As a result, the interviewer may not have covered the exact same content with each participant. Furthermore, because of the nature of the study, some participants may have been more forthcoming about their personal experiences. Thirdly, although the participants were asked about past events, the memories of those events may have been compromised because of the passage of time or because of received or ongoing treatment. Lastly, given the limited number of participants interviewed, more research is needed to understand the mental health needs and experiences of Black adolescents who are experiencing depression.
Conclusion
In this qualitative study of 10 Black adolescents living in a rural community, the authors provided space for the participants to use their own terms and language to define depression. It is clear through this and other research that contextual factors are often involved in the onset of depression in Black adolescents, and there is not enough active therapeutic and medical treatment for Black adolescents living with depression. There is a stigma associated with mental illness and reluctance to seek treatment within the Black community, particularly in rural areas. As a result, counselors and mental health providers need to become more educated and aware when working with Black adolescents who live in rural communities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alegria, M., Vallas, M., & Pumariega, A. J. (2010). Racial and ethnic disparities in pediatric mental health. Child and Adolescent Psychiatric Clinics of North America, 19(4), 759–774. https://doi.org/10.1016/j.chc.2010.07.001
Al-Khattab, H., Oruche, U., Perkins, D., & Draucker, C. (2016). How African American adolescents manage depression: Being with others. Journal of the American Psychiatric Nurses Association, 22(5), 387–400. https://doi.org/10.1177/1078390316657391
Auger, R. W. (2005). School-based interventions for students with depressive disorders. Professional School Counseling, 8(4), 344–352.
Breland-Noble, A. M., Burriss, A., & Poole, H. K. (2010). Engaging depressed African American adolescents in treatment: Lessons from the AAKOMA PROJECT. Journal of Clinical Psychology, 66(8), 868–879. https://doi.org/10.1002/jclp.20708
Brenner, E. (2019). The crisis of youth mental health. Stanford Social Innovation Review. https://ssir.org/articles/entry/the_crisis_of_youth_mental_health#
Bridge, J. A., Horowitz, L. M., Fontanella, C. A., Sheftall, A. H., Greenhouse, J., Kelleher, K. J., & Campo, J. V. (2018). Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatrics, 172(7), 697–699. https://doi.org/10.1001/jamapediatrics.2018.0399
Brody, G. H., Chen, Y.-F., Kogan, S. M., Yu, T., Molgaard, V. K., DiClemente, R. J., & Wingood, G. M. (2012). Family-centered program deters substance use, conduct problems, and depressive symptoms in Black adolescents. Pediatrics, 129(1), 108–115. https://doi.org/10.1542/peds.2011-0623
Bryant, K., Greer-Williams, N., Willis, N., & Hartwig, M. (2013). Barriers to diagnosis and treatment of depression: Voices from a rural African-American faith community. Journal of National Black Nurses’ Association: JNBNA, 24(1), 31–38.
Choi, H., Meininger, J. C., & Roberts, R. E. (2006). Ethnic differences in adolescents’ mental distress, social stress, and resources. Adolescence, 41(162), 263–283.
Conner, L. C., & Yeh, C. J. (2018). Stress, coping, and depression among Black urban adolescents: Implications for school counseling. Journal of School Counseling, 16(15), 1–31.
Cook, B. L., Trinh, N.-H., Li, Z., Hou, S. S.-Y., & Progovac, A. M. (2017). Trends in racial–ethnic disparities in access to mental health care, 2004–2012. Psychiatric Services, 68(1), 9–16. https://doi.org/10.1176/appi.ps.201500453
Everall, R. D., Altrows, J., & Paulson, B. L. (2006). Creating a future: A study of resilience in suicidal female adolescents. Journal of Counseling & Development, 84(4), 461–471. https://doi.org/10.1002/j.1556-6678.2006.tb00430.x
Graves, L. (2017). Filters of influence: The help-seeking process of African American single mothers living in poverty seeking mental health services for their children. Child & Youth Services, 38(1), 69–90. https://doi.org/10.1080/0145935X.2016.1251836.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hope, M. O., Assari, S., Cole-Lewis, Y. C., & Caldwell, C. H. (2017). Religious social support, discrimination, and psychiatric disorders among Black adolescents. Race and Social Problems, 9(2), 102–114. https://doi.org/10.1007/s12552-016-9192-7
Jacob, M., Keeley, M. L., Ritschel, L., & Craighead, W. E. (2013). Behavioural activation for the treatment of low-income, African American adolescents with major depressive disorder: A case series. Clinical Psychology & Psychotherapy, 20(1), 87–96. https://doi.org/10.1002/cpp.774
Lake, J., & Turner, M. S. (2017). Urgent need for improved mental health care and a more collaborative model of care. Permanente Journal, 21, 17–24. https://doi.org/10.7812/TPP/17-024
Liang, J., Matheson, B. E., & Douglas, J. M. (2016). Mental health diagnostic considerations in racial/ethnic minority youth. Journal of Child and Family Studies, 25(6), 1926–1940. https://doi.org/10.1007/s10826-015-0351-z
Lindsey, M. A., Joe, S., & Nebbitt, V. (2010). Family matters: The role of mental health stigma and social support on depressive symptoms and subsequent help seeking among African American boys. Journal of Black Psychology, 36(4), 458–482. https://doi.org/10.1177/0095798409355796
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Lu, W. (2019). Adolescent depression: National trends, risk factors, and healthcare disparities. American Journal of Health Behavior, 43(1), 181–194. https://doi.org/10.5993/AJHB.43.1.15
Lu, W., Lindsey, M. A., Irsheid, S., & Nebbitt, V. E. (2017). Psychometric properties of the CES-D among Black adolescents in public housing. Journal for the Society for Social Work and Research, 8(4), 595–619. https://doi.org/10.1086/694791
Merriam, S. B. (2009). Qualitative research: A guide to design and implementation (3rd ed.). Jossey-Bass.
Murry, V. M., Heflinger, C. A., Suiter, S. V., & Brody, G. H. (2011). Examining perceptions about mental health care and help-seeking among rural African American families of adolescents. Journal of Youth and Adolescence, 40(9), 1118–1131.
https://doi.org/ 10.1007/s10964-010-9627-1
National Institute of Mental Health. (2013). Major depression. https://www.nimh.nih.gov/health/statistics/major-depression.shtml
Ofonedu, M. E., Percy, W. H., Harris-Britt, A., & Belcher, H. M. E. (2013). Depression in inner city African American youth: A phenomenological study. Journal of Child and Family Studies, 22(1), 96–106. https://doi.org/10.1007/s10826-012-9583-3
Patton, M. Q. (1987). How to use qualitative methods in evaluation (2nd ed.). SAGE.
Planey, A. M., Smith, S. M., Moore, S., & Walker, T. D. (2019). Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Children and Youth Services Review, 101, 190–200. https://doi.org/10.1016/j.childyouth.2019.04.001
Probst, J. C., Laditka, S. B., Moore, C. G., Harun, N., Powell, M. P., & Baxley, E. G. (2006). Rural-urban differences in depression prevalence: implications for family medicine. Family Medicine Kansas City, 38(9), 653–660.
Robinson, W. L., Brown, M., Beasley, C. R., & Jason, L. A. (2017). Advancing prevention intervention from theory to application: Challenges and contributions of community psychology. In M. A. Bond, I. Serrano-García, C. B. Keys, & M. Shinn (Eds.), APA handbook in psychology. APA handbook of community psychology: Methods for community research and action for diverse groups and issues (pp. 193–213). American Psychological Association.
Robinson, W. L., Droege, J. R., Case, M. H., & Jason, L. A. (2015). Reducing stress and preventing anxiety in African American adolescents: A culturally-grounded approach. Global Journal of Community Psychology Practice, 6(2). https://doi.org/10.7728/0602201503
Saluja, G., Iachan, R., Scheidt, P. C., Overpeck, M. D., Sun, W., & Giedd, J. N. (2004). Prevalence of and risk factors for depressive symptoms among young adolescents. Archives of Pediatrics and Adolescent Medicine, 158(8), 760–765. https://doi.org/10.1001/archpedi.158.8.760
Shushansky, L. (2017, July 31). Disparities within minority mental health care [Blog post]. National Alliance on Mental Illness. https://www.nami.org/Blogs/NAMI-Blog/July-2017/Disparities-Within-Minority-Mental-Health-Care
Smokowski, P. R., Bacallao, M. L., Cotter, K. L., & Evans, C. B. R. (2015). The effects of positive and negative parenting practices on adolescent mental health outcomes in a multicultural sample of rural youth. Child Psychiatry & Human Development, 46(3), 333–345. https://doi.org/10.1007/s10578-014-0474-2
Sullivan, G., Cheney, A., Olson, M., Haynes, T., Bryant, K., Cottoms, N., Reaves, C., & Curran, G. (2017). Rural African Americans’ perspectives on mental health: Comparing focus groups and deliberative democracy forums. Journal of Health Care for the Poor and Underserved, 28(1), 548–565. https://doi.org/10.1353/hpu.2017.0039
van Manen, M. (1997). Researching lived experience: Human science for an action sensitive pedagogy. (2nd ed.). Althouse.
Vontress, C. E., Woodland, C. E., & Epp, L. (2007). Cultural dysthymia: An unrecognized disorder among African Americans? Journal of Multicultural Counseling and Development, 35(3), 130–141. https://doi.org/10.1002/j.2161-1912.2007.tb00055.x
Weaver, A., Himle, J. A., Taylor, R. J., Matusko, N. N., & Abelson, J. M. (2015). Urban vs. rural residence and the prevalence of depression and mood disorder among African American women and non-Hispanic white women. JAMA Psychiatry, 72(6), 576–583. https://doi.org/10.1001/jamapsychiatry.2015.10
Willis, L. A., Coombs, D. W., Drentea, P., & Cockerham, W. C. (2003). Uncovering the mystery: Factors of African American suicide. Suicide and Life-Threatening Behavior, 33(4), 412–429. https://doi.org/10.1521/suli.33.4.412.25230
World Federation for Mental Health. (2012). Depression: A global crisis. https://www.who.int/mental_health/management/depression/wfmh_paper_depression_wmhd_2012.pdf
World Health Organization. (2020). Depression. https://www.who.int/news-room/fact-sheets/detail/depression
TeShaunda Hannor-Walker, PhD, NCC, LPC, CPCS, is an assistant professor at Liberty University. Lynn Bohecker, PhD, LMFT, is an associate professor at Liberty University. Lacey Ricks, PhD, NCC, is an assistant professor at Liberty University. Sarah Kitchens, PhD, NCC, is an assistant professor at Liberty University. Correspondence may be addressed to TeShaunda Hannor-Walker, 1971 University Blvd., Lynchburg, VA 24515, thannorwalker@liberty.edu.
