Apr 1, 2021 | Volume 11 - Issue 2
Melissa J. Sitton, Tina Du Rocher Schudlich, Christina Byrne
A psychosocial approach to predicting self-injurious behavior (SIB) may allow for more accurate predictions and enhance intervention for individuals who engage in SIB. We examined psychosocial predictors of SIB within and between two populations: individuals with traits of borderline personality disorder (BPD; N = 60) and college students (N = 116). All participants met the inclusion criteria of engaging in SIB at least once in the past year. All participants completed measures of psychological distress, social functioning, and SIB. Methods of SIB did not vary across samples, but SIB rates did. Psychological distress and population type (BPD or student) predicted SIB, whereas social factors did not. Additionally, we found a significant interaction wherein psychological distress was more related to SIB in individuals with traits of BPD. Accordingly, we recommend that counselors consider population and psychological distress when assessing SIB risk in clients.
Keywords: self-injurious behavior, borderline personality disorder, college students, psychological distress, social functioning
Self-injurious behavior (SIB), the deliberate act of self-inflicted bodily harm, is of growing concern to counselors and clinicians. According to Nock (2010), SIB is a broad concept encompassing self-injury completed with suicidal intent (i.e., suicide attempts), without suicidal intent (i.e., nonsuicidal self-injury), or with ambivalence toward life (i.e., ambivalent, meaning neither strictly suicidal nor nonsuicidal). In other words, an individual can engage in SIB with differing goals that vary in intent from harming themselves to dying. The American Psychiatric Association (2013) considers suicide behavior disorder and nonsuicidal self-injury to be “conditions for further study” (p. 801). Individuals who engage in SIB over time are likely to do so with greater frequency, more methods, and increasing lethality (Andrews et al., 2013). Therefore, there is a great need for counselors and clinicians to assess their clients for SIB.
Although there are differing theories of the development and maintenance of SIB based on intent, particularly regarding the development of suicidal and nonsuicidal SIB, there are similar intrapersonal and interpersonal themes across theories. For instance, in their four-function model of nonsuicidal SIB, Nock and Prinstein (2004, 2005) proposed that intrapersonal (e.g., affective) and interpersonal (e.g., help-seeking) factors act as positive and negative reinforcers of nonsuicidal SIB. Similarly, in their renowned interpersonal–psychological theory of suicide, Joiner and colleagues (Joiner, 2005; Van Orden et al., 2010) proposed that individuals who attempt suicide are characterized both by a desire to die (i.e., interpersonal factors of perceived burdensomeness and thwarted belongingness) and the acquired capability to attempt (i.e., intrapersonal factors such as past SIB).
Notably, there is no specific theory to date regarding ambivalent SIB. Researchers and clinicians often differentiate SIB into two categories (Nock, 2010). In the first category, there is no explicit intent to die, and therefore it is considered nonsuicidal SIB. In the second category, there is no clear lack of suicidal intent, and therefore it is considered suicidal SIB. Thus, ambivalent SIB is often categorized as suicidal SIB, rather than as a unique experience. Regardless of how ambivalent SIB is classified, it is likely that both intrapersonal and interpersonal factors relate to ambivalent SIB given that both are relevant to suicidal and nonsuicidal SIB. Furthermore, individuals who engage in SIB often report multiple intents behind their past SIB (Andover et al., 2012; Klonsky & Olino, 2008). Because of these similarities and the clinical significance of each, we examined intrapersonal (i.e., psychological distress) and interpersonal (i.e., social functioning) predictors of SIB in the current study.
Predicting SIB With Psychosocial Functioning
The relations between psychological distress and SIB are well established in the literature. Researchers have found positive associations between SIB and depression (Andover et al., 2005; Kirkcaldy et al., 2007), anxiety (Andover et al., 2005; Klonsky & Olino, 2008), obsessive-compulsion (Kirkcaldy et al., 2007), and interpersonal sensitivity (Kim et al., 2015; Kirkcaldy et al., 2007). These studies and others examined specific experiences of psychological distress as it relates to SIB in adults and adolescents and in community and inpatient samples.
Previous studies have also demonstrated relations between social functioning and SIB. For instance, SIB is associated with less social support from family and friends (Rotolone & Martin, 2012; Tuisku et al., 2014). Similarly, SIB is related to more negative interactions or negative relational dynamics with family (Halstead et al., 2014; Van Orden et al., 2010) and friends (Adrian et al., 2011).
Predicting SIB in Different Populations
Some individuals may be at greater risk for developing SIB. In particular, SIB is especially prevalent in individuals with borderline personality disorder (BPD). According to the American Psychiatric Association (2013), BPD is characterized by “marked impulsivity” along with “a pervasive pattern of instability of interpersonal relationships, self-image, and affects” (p. 663). Notably, one diagnostic criterion of BPD is “recurrent suicidal behavior, gestures, threats, or self-mutilating behavior” (p. 663). Additionally, some risk factors for developing BPD (e.g., high emotion dysregulation, trauma exposure, etc.; Crowell et al., 2009) are also risk factors for engaging in SIB (Nock, 2009, 2010). Although lifetime rates of SIB in individuals with BPD vary, one study found that 92.2% of individuals who sought outpatient treatment for symptoms of BPD had engaged in nonsuicidal SIB within the past 2 months (Andión et al., 2012). Additionally, up to 75% of individuals with BPD reported at least one instance of suicidal SIB (Black et al., 2004). Furthermore, there appear to be differences in SIB engagement when comparing individuals with BPD to a community sample. For example, adults with BPD reported engaging in nonsuicidal SIB more recently and frequently, using more varied methods, and causing more physically severe injuries that require medical attention, compared to individuals without BPD who engaged in nonsuicidal SIB (Turner et al., 2015).
Although the rates and severity of SIB are higher in individuals with BPD than in the general population (Bentley et al., 2015), SIB is considered relatively common in other populations, including nonsuicidal SIB among college students (e.g., Whitlock et al., 2006, 2013). College students are thought to engage in SIB more than the general population (as suggested by Wilcox et al., 2012) with approximately 17%–41% of college students participating in nonsuicidal SIB (Whitlock et al., 2006) compared to 5.9% of adults in the general population (Klonsky, 2011). Most college students are also in the highest risk age group for nonsuicidal SIB (Rodham & Hawton, 2009), and suicide is the second leading cause of death during this period (18–25 years old; Centers for Disease Control and Prevention, 2017). Notably, college students and non–college students of the same age (i.e., 16–24 years old) do not appear to differ in rates of SIB (McManus & Gunnell, 2020).
Current Study
A wealth of research has identified important psychological and social factors that may be associated with the occurrence of SIB. However, it remains unclear how these factors intersect to predict SIB. Additionally, as Turner et al. (2015) suggested, most research on SIB has considered either individuals with BPD or nonclinical samples (e.g., college students) without considering potential differences in predictors between these populations.
The current study used a comprehensive psychosocial approach to examine psychological distress and social functioning in two samples: a high-risk, treatment-seeking sample of individuals with traits of BPD and a sample of college students. This allowed us to characterize how key factors may intersect in predicting SIB. Our objectives were to (a) examine SIB within and between the two populations, (b) evaluate which psychosocial factors predicted total lifetime SIB for both populations, and (c) determine whether the predictors of total lifetime SIB varied by population (i.e., test for an interaction between psychosocial predictors and sample).
Method
Participants and Procedure
This study included a sample of individuals with BPD traits and a college student sample. For both samples, our inclusion criteria required that participants have a history of SIB with at least one self-reported episode of SIB (i.e., SIB of any intent) in the past year. We required recent SIB so that the measures of current psychological and social functioning would be appropriate predictors, rather than examining current functioning with a retrospective report of SIB after several years.
Sample 1: Individuals With Traits of BPD
The first sample consisted of data from a larger study on dialectical behavior therapy (DBT) in teens and adults (Sitton et al., 2020). Participants sought treatment for BPD symptoms from community-based counselors, although not all participants had formal diagnoses of BPD. The counselors obtained informed consent from participants and collaborated with a local university for this larger IRB-approved study. Of the 62 participants in this larger study, 96.8% (n = 60) reported engaging in SIB in the past year and constituted the BPD-Tx sample.
BPD-Tx participants (n = 60) were mostly young adults (M = 23.53 years, SD = 6.85 years, range = 18–48 years old). Based on self-reports, there were 49 females (81.7%), eight males (13.3%), and three participants who identified as non-binary or androgynous (5%). This sample was mostly White/European American (83.1%), followed by multiracial (10.2%), Asian American (1.7%), and Hispanic/Latinx (1.7%), with an additional 3.4% identifying as “other” or not reporting. Most (80%) reported no counseling experience prior to receiving DBT from the community counselors (i.e., at the time of recruitment). Data on sexual orientation was not available for this sample.
Sample 2: Undergraduate College Students
The second sample consisted of undergraduate students in introductory psychology courses at a university in the Pacific Northwest. We recruited students to participate in a study called “Emotional and Behavioral Responses to Stress” and informed all participants that they might experience distress as part of the study. After giving their informed consent, participants completed the measures online in a campus computer lab so any questions or concerns could be immediately addressed by a research assistant trained in suicide prevention. Debriefing included an extensive form that included on- and off-campus mental health resources.
Of the 536 students who completed the survey, 43.8% reported engaging in SIB during their lifetime, and 116 students (21.6%) met the inclusion criteria of engaging in SIB in the past year. This proportion of students is high compared to some student samples (e.g., Whitlock et al., 2006; Wilcox et al., 2012), but it is comparable to the lifetime rate from at least one other university sample (Gratz et al., 2002).
Student participants included in this study (n = 116) were mostly young adults (M = 19.62 years, SD = 1.58 years, range = 18–27 years old). Based on self-reports, there were 89 females (78.4%), 23 males (19.8%), and four participants who identified as non-binary or androgynous (4%). This sample was mostly White/European American (69%), followed by multiracial (19.8%), Asian American (6%), and Hispanic/Latinx (4.3%). Participants’ sexual orientations were as follows: 60.3% heterosexual, 18.1% bisexual, 7.8% pansexual, 6.9% homosexual, 1.7% asexual, and 1.8% who identified as “other.” Most (77.6%) reported previous counseling experiences, with about one-fifth currently seeing a counselor (22.4%). Other studies have found rates of prior experience with counseling services to be closer to 55% in college students (e.g., Niegocki & Ægisdóttir, 2019). Most student participants reported seeking counseling services for stress- and mood-related symptoms, and none reported seeking treatment specifically for BPD.
Measures
Self-Injurious Behavior (SIB)
We used the Lifetime Suicide Attempt Self-Injury Interview (LSASI; Linehan & Comtois, 1996) to assess participants’ history of SIB, including frequency, method, and intent. This 20-item measure asks about the dates of the most recent and most severe SIB act (e.g., “When was the most recent time that you intentionally injured yourself?”) and assesses the total lifetime frequency for 11 methods of SIB, as well as the separate intent(s) of each SIB act (suicidal, nonsuicidal, or ambivalent). Higher scores indicate more SIB acts.
Internal consistency was adequate for both samples (BPD-Tx sample, Cronbach’s α = .75; student sample, Cronbach’s α = .73). Notably, the LSASI was created for clinical use rather than research use; therefore, there are no known studies of its reliability or validity. However, the LSASI was already in use by the counselors in the larger study of DBT described, and they chose to use it to assess SIB in the BPD-Tx sample. We used it for the student sample to be consistent with the existing sample data. Following Linehan and Comtois’s (1996) scoring instructions, we calculated a total lifetime frequency for each participant by summing all SIB of any intent.
Psychological Distress
The Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1975) is a broad-spectrum psychiatric symptom checklist. Participants rate their distress level in the past week on a Likert-type scale from 0 (not at all) to 4 (extremely) for each of 90 items (e.g., “How much were you distressed by feeling critical of others?”). This measure assesses nine factors of psychological distress. For this study, we were interested in the factors of Depression, Anxiety, Obsessive-Compulsion, and Interpersonal Sensitivity. The internal consistency of this measure was very high in the BPD-Tx sample (α = .97).
To reduce participant burden, we used the Brief Symptom Inventory (BSI; Derogatis & Spencer, 1982), a 53-item version of the SCL-90-R, for student participants. The internal consistency was very high in the student sample (α = .96).
To assess the comparability of the SCL-90-R and the BSI for subsequent analysis, we separately averaged all items for the factors of Anxiety, Depression, Obsessive-Compulsion, and Interpersonal Sensitivity to determine BPD-Tx participants’ scores of psychological distress using these two measures. We found strong correlations between the SCL-90-R factors and the BSI factors (Depression: r = .92, p < .001; Anxiety: r = .97, p < .001; Obsessive-Compulsion: r = .95, p < .001; Interpersonal Sensitivity: r = .90, p < .001; and Average Psychological Distress: r = .98, p < .001). Following Derogatis (1993), who found no significant difference in validity between the SCL-90-R and the BSI, we used only the BSI items to create symptom factors for both samples. The internal consistency of the BSI items for the
BPD-Tx sample was very high (α = .95).
Social Functioning
The Network of Relationships Inventory-Behavioral Systems Version (NRI; Furman & Buhrmester, 2009) is a 33-item self-report measure of social support and negative interactions in various relationships (i.e., one’s mother, father, friends, and romantic partner). Participants rate the frequency of positive support or negative interactions on a Likert-scale from 1 (little or none) to 5 (the most). The Positive Support scale includes five subscales: Seeks Secure Base, Provides Secure Base, Seeks Safe Haven, Provides Safe Haven, and Companionship. The Negative Interactions scale includes three subscales: Conflict, Antagonism, and Criticism. Higher scores indicate more of each factor. The internal consistency was high for both samples (BPD-Tx, α = .93; student sample, α = .94).
We calculated the mean score of the Positive Support subscales, including Seeks Secure Base, Seeks Safe Haven, and Companionship. We did not include Provides Secure Base or Provides Safe Haven because Furman and Buhrmester (2009) described these as “caretaking” factors rather than “attachment” or “affiliation” factors. We also calculated the mean score of all three Negative Interactions subscales.
Data Analysis Plan
To begin, we tested for the assumptions of analysis, following guidelines proposed by Tabachnick and Fidell (2019). We defined outliers as data points beyond three standard deviations from the mean. We evaluated outliers within each group and replaced them with the value that was three standard deviations above the group mean. We chose this more liberal approach to outliers to maximize variability in the data. It was especially important to maintain variability in the outcome variable of total SIB given that higher levels of SIB have great clinical significance. For skewness and kurtosis of the composite variables, we used ±2 as our acceptable range of values. We transformed variables that did not meet our criteria for normality. We also utilized the missing completely at random test and found no systematic patterns to missing data, and thus used the group means to replace missing values for analysis.
To assess SIB in the two samples, we examined the intent of SIB acts separately for each sample and analyzed if SIB rates differed based on demographic information. To examine psychosocial predictors of SIB, we conducted a multiple linear regression. We used total SIB (including suicidal, nonsuicidal, and ambivalent SIB) as the outcome variable. We also examined differences in predictors of total SIB between the BPD-Tx and student samples by including interaction terms (e.g., psychological distress x sample). Statistically significant interactions were graphed to aid interpretation (Howell, 2013).
For the multiple linear regression analysis, we used effect coding for sample type (Daly et al., 2016), which allows comparison of a sample mean to the overall mean instead of using one sample as a reference group. Additionally, we centered the predictor variables around the grand mean for the whole sample to reduce the risk of multicollinearity. We inspected the tolerance and variance inflation factors, and used multiple sources (e.g., correlations between variables, p-values, and the standard error of the regression coefficients) to determine if multicollinearity was an issue.
Results
We used SPSS 24.0 to analyze the data. Using one-way analysis of variance (ANOVA), we found no differences between the samples based on gender or ethnicity (all p values > .05). However, using an independent samples t-test, we found that the BPD-Tx sample (M = 23.53, SD = 6.85) was older on average than the student sample: M = 19.62, SD = 1.58, t(173) = 5.85, p < .001. Additionally, the BPD-Tx sample (13.3%) reported prior experience with counseling (dichotomous variable) less often than the student sample (77.6%) on average: χ2(1) = 59.39, p < .001.
Sample Differences in SIB
We conducted descriptive analyses for all SIB variables. See Table 1 for descriptive statistics of the different intents of SIB (nonsuicidal, ambivalent, and suicidal), total SIB (including the untransformed total score), and the reported number of SIB methods. Table 1 also includes difference scores of SIB acts based on independent sample t-tests in consideration of the two samples. Individuals in the BPD-Tx sample engaged in more nonsuicidal, ambivalent, and total SIB in their lifetime compared to the student sample. Although there appeared to be no difference between samples in suicidal SIB, it is worth noting that this variable did not meet our criteria for normality in either sample even after transformation.
Table 1
Means (With Standard Deviations) and Difference Scores for Self-Injurious Behavior (SIB) by Sample
| Variable |
BPD-Tx
(N = 60) |
Student
(N = 116) |
t(df) |
p |
| Nonsuicidal SIB |
3.13 (1.81) |
2.34 (1.55) |
t(174) = 3.01 |
.003 |
| Ambivalent SIB |
1.92 (2.02) |
1.07 (1.33) |
t(86.25) = 2.94 |
.004 |
| Suicidal SIB |
0.66 (0.90) |
0.45 (0.81) |
t(174) = 1.61 |
.110 |
| Total SIB |
3.87 (1.84) |
2.86 (1.43) |
t(96.56) = 3.73 |
< .001 |
| Total SIB (untransformed) |
166.31 (268.69) |
44.10 (75.60) |
t(63.88) = 3.45 |
.001 |
| Number of SIB methods |
3.28 (1.53) |
3.28 (2.11) |
t(174) = -0.004 |
.997 |
Note. BPD-Tx = participants with traits of borderline personality disorder; Total SIB (untransformed) =
untransformed values after adjusting the outliers in the raw reported values. Significant p values are in bold.
Although the normality of suicidal SIB was improved using a transformation, we were unable to meet our
acceptable range of ±2 for kurtosis (BPD-Tx kurtosis = 4.22; student kurtosis = 2.71).
In the BPD-Tx sample, we found no differences in SIB frequency based on gender, age, ethnicity, or counseling experience using one-way ANOVA. In the student sample, we found no differences in SIB frequency based on age, ethnicity, living situation, or counseling experience using one-way ANOVA. However, SIB frequency differed by gender such that those who identified as non-binary (M = 4.64, SD = 1.35) reported significantly higher rates of SIB than both males (M = 2.80, SD = 1.31) and females (M = 2.95, SD = 1.20). There were no differences in SIB frequency or severity based on sexual orientation in the student sample.
Psychosocial Predictors of SIB
We compared the two samples on the predictor variables first by using independent sample t-tests. We found that BPD-Tx participants reported less psychological distress (M = 2.21, SD = 0.78) than student participants: M = 2.78, SD = 0.89, t(174) = −4.16, p < .001. The BPD-Tx participants (M = 3.25, SD = 0.49) also reported less positive social support than student participants: M = 3.44, SD = 0.54, t(174) = −2.26, p = .025. Lastly, BPD-Tx participants (M = 1.22, SD = 0.43) reported more negative interactions than student participants: M = 1.07, SD = 0.43, t(174) = 2.15, p = .033.
We conducted bivariate correlations between all predictor variables and the outcome variable for each sample. In the BPD-Tx sample, total SIB was positively correlated with average psychological distress (r = .37, p = .004). In the student sample, total SIB was negatively correlated with positive social support (r = −.18, p = .049). In both samples, average psychological distress was positively associated with negative interactions (BPD-Tx: r = .36, p = .005; student: r = .24, p = .008). No other variables were significantly correlated in either sample.
Next, we conducted a multiple linear regression using total SIB as the outcome variable for both samples together. We entered seven predictors simultaneously: psychological distress, positive social support, negative interactions, sample type, and the interactions between sample type and the three other predictors. Together, these seven variables significantly predicted total SIB: F(7,168) = 5.01, p < .001, MSE = 2.33, r2 = .17. As shown in Table 2, psychological distress (sr2 = .06), sample type (sr2 = .12), and the interaction between psychological distress and sample type (sr2 = .03) were each significant unique predictors of total SIB. Specifically, based on the positive β weights, more psychological distress and being in the BPD-Tx sample were both associated with higher lifetime rates of SIB. Notably, multicollinearity did not appear to be an issue in this regression given the moderate to low correlations between factors, sufficiently high tolerance values, acceptable variance inflation factor values (ranging from 1.25–1.55), and the low standard error of regression coefficients relative to their scale.
Table 2
Multiple Regression Analysis Predicting Total Self-Injurious Behavior for the Whole Sample (N = 176)
|
|
CI |
| Variable |
B |
SE B |
β |
t |
p |
sr2 |
Lower |
Upper |
| Psych. distress |
0.57 |
0.16 |
.31 |
3.55 |
.001 |
.06 |
0.25 |
0.89 |
| Pos. social support |
−0.48 |
0.25 |
−.16 |
−1.96 |
.052 |
.02 |
−0.97 |
0.00 |
| Neg. interactions |
−0.26 |
0.30 |
−.07 |
−0.85 |
.399 |
.003 |
−0.85 |
0.34 |
| Sample type |
0.68 |
0.14 |
.39 |
4.87 |
< .001 |
.12 |
0.40 |
0.95 |
| Psych. distress x sample |
0.40 |
0.16 |
.21 |
2.46 |
.015 |
.03 |
0.08 |
0.71 |
| Pos. social support x sample |
0.00 |
0.25 |
.00 |
0.00 |
.997 |
.001 |
−0.49 |
0.49 |
| Neg. interactions x sample |
−0.08 |
0.30 |
−.02 |
−0.25 |
.801 |
.001 |
−0.67 |
0.52 |
|
|
|
|
|
|
|
|
|
|
Note. Psych. = psychological; Pos. = positive; Neg. = negative; sr2 = squared semipartial correlation. Sample type was
coded so that BPD-Tx sample = 1, student sample = -1. Significant p values are in bold.
Sample Differences in SIB Predictors
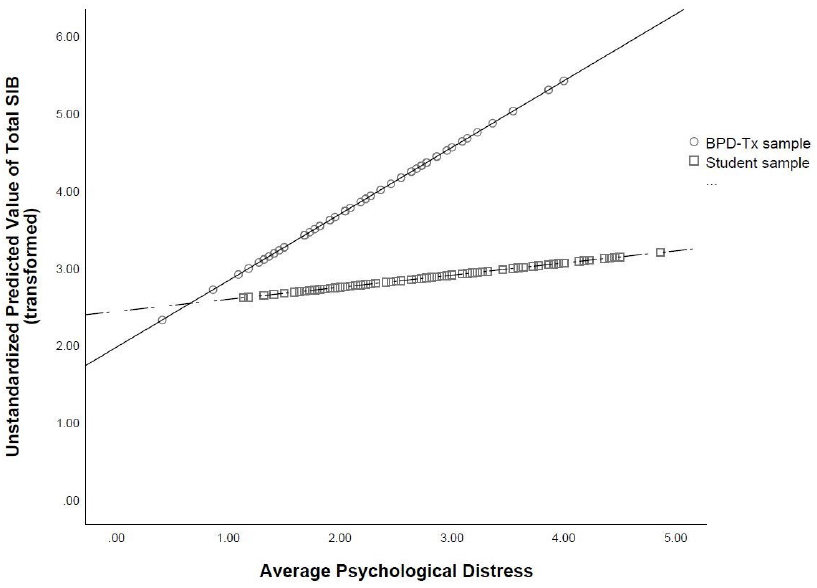
To further probe the statistically significant interaction, we plotted the regression paths for psychological distress predicting total SIB by sample type. As shown in Figure 1, more psychological distress was related to higher lifetime rates of total SIB in both samples, which supports the main effect of psychological distress found in the multiple regression analysis. However, the relation between psychological distress and total SIB was stronger in the BPD-Tx sample than in the student sample (as evidenced by the steeper slope of the regression line representing the BPD-Tx sample compared to that of the student sample).
Figure 1
Regression Lines of Average Psychological Distress Predicting Total Self-Injurious Behavior (SIB) by Sample Type
Discussion
The primary goals of the current study were to establish a more comprehensive set of predictors of SIB and to better understand how the experience of SIB varied by population (BPD-Tx vs. college students). This study was unique in its psychosocial approach to predictors. Additionally, we tested for interactions between sample type and the psychosocial predictors of SIB. This singular examination of interacting predictors has seldom been conducted in the literature, and thus is an important strength of this study.
SIB Engagement and Psychosocial Functioning
The results demonstrate a very high lifetime frequency of SIB in both samples. Although most studies do not report the lifetime frequency rates of SIB of their participants, the frequency of SIB in our student sample was comparable to that found in another study of students using the same SIB methods with nonsuicidal intent (Croyle & Waltz, 2007). The frequency rate of SIB in the BPD-Tx sample appeared to be lower than found in some other studies with individuals with BPD (e.g., Turner et al., 2015).
Additionally, we found that the lifetime frequency rates of SIB were higher in the BPD-Tx sample than in the student sample, which aligns with previous studies (e.g., Klonsky & Olino, 2008; Turner et al., 2015). This makes sense given the maladaptive behaviors often seen in individuals with BPD. Additionally, given that the BPD-Tx sample was older than student participants on average, it is also possible that their increased lifetime rates of SIB reflected a greater number of years to engage in it. Alternatively, the higher SIB frequency reported by the BPD-Tx participants may serve an interpersonal function. According to Linehan (1993), nonsuicidal SIB is commonly used by individuals with BPD to communicate with and gain attention from others.
Interestingly, despite higher rates of total SIB, BPD-Tx participants reported less psychological distress than did student participants. This was contrary to many other studies showing a strong association between psychological distress and engagement in nonsuicidal SIB for individuals with BPD (e.g., Sadeh et al., 2014; Turner et al., 2015). One possible explanation for the lower rates of psychological distress reported by BPD-Tx participants is that their baseline level of psychological distress was higher, leading these negative emotions to be considered normal and therefore not “distressing.” Additionally, given that fewer BPD-Tx participants reported prior experience with counseling than student participants, it could be that BPD-Tx participants reported less psychological distress because of a lack of emotional self-awareness. This aligns with Turner et al.’s (2015) finding that participants with BPD who engage in nonsuicidal SIB reported less awareness of their emotional states. Another explanation is that the BPD-Tx participants were recruited from a community-based clinic wherein they were preparing to start DBT. Although the data used in the current study represents pretest data gathered prior to treatment, it is possible that the BPD-Tx participants were experiencing lowered distress at the time of data collection because of the hope and positive expectations that are often associated with starting a new treatment (Dew & Bickman, 2005).
Socially, the BPD-Tx participants reported less positive support than student participants. This finding aligns with the biosocial theory of BPD (Linehan, 1993), which suggests that individuals with BPD may experience or perceive an invalidating environment. Alternatively, BPD-Tx participants may be more likely to interpret interactions with others as negative, which aligns with Peters et al.’s (2015) finding that individuals with traits of BPD often demonstrated maladaptive responses to emotional experiences, leading them to interact negatively with others.
Psychosocial Predictors of SIB
An important finding of the current study is that psychological distress predicted total SIB with a small to moderate effect size. This suggests that psychological distress (including experiences of anxiety, depression, obsessive-compulsion, and interpersonal sensitivity) is an important component of SIB of various intents. Specifically, psychological distress may act as a catalyst for SIB, wherein individuals engage in SIB to decrease their psychological distress. This explanation aligns with Nock and Prinstein’s (2004, 2005) theory of the intrapersonal negative reinforcement function of nonsuicidal SIB. Namely, that one might engage in SIB in order to reduce tension or psychological distress, particularly anxiety.
Contrary to the majority of extant literature (e.g., Wilcox et al., 2012), neither positive social support nor negative interactions predicted total SIB in the current study. We also did not find an interaction between either social variable and sample type, suggesting that social functioning might not be a direct, distinct predictor of total SIB for either population. However, it is possible that social functioning is indirectly related to total SIB. For example, we found a significant positive correlation between negative interactions and psychological distress in both samples. Given these correlations, negative interactions may contribute to experiences of psychological distress, which then predict total SIB. This proposed indirect relation is supported by Adrian et al.’s (2011) study, which found that emotion dysregulation partially mediated the relation between interpersonal problems (i.e., problems with one’s family and peers) and nonsuicidal SIB.
Another possible explanation for the lack of significant social predictors of SIB in the current study is the variability in the data that stems from inconsistent timing of social support. Specifically, it is unclear if positive support preceded SIB engagement, followed the SIB act, or both. Turner et al. (2016) found that perceived social support increased after participants disclosed their nonsuicidal SIB acts to others. However, they also found that this increased support was associated with increased nonsuicidal SIB urges and acts the following day, presumably because the SIB had achieved the desired interpersonal function. Thus, similar to Turner et al.’s (2016) study, the lack of a clear, linear relation between SIB and social support may have contributed to nonsignificant findings of social predictors in the current study.
Notably, the strongest single predictor of total SIB was sample type, with BPD-Tx participants showing greater frequency of total lifetime SIB than student participants. This aligns with Turner et al. (2015), who found that individuals with BPD traits engage in nonsuicidal SIB more often than do those without BPD traits.
Sample Differences in SIB Predictors
The relation between psychological distress and total SIB was stronger for the BPD-Tx sample than for the student sample. This finding is somewhat supported by previous literature; for example, Klonsky and Olino’s (2008) latent class analysis revealed that the group with the most nonsuicidal SIB also reported more symptoms of BPD and psychological distress and reported regularly engaging in nonsuicidal SIB to help regulate their emotions. In comparison, individuals with BPD traits in the current study reported engaging in more total SIB (as well as nonsuicidal SIB) but did not report greater levels of psychological distress than did the student participants. However, if our BPD-Tx participants used SIB for emotion regulation, too, then perhaps this strategy allowed them to experience lower levels of psychological distress day-to-day than student participants. This aligns with Sadeh et al.’s (2014) finding that BPD symptoms related to the affect-regulating function of SIB, especially nonsuicidal SIB.
Additionally, the significant interaction we found between psychological distress and sample type resembles Andover et al.’s (2005) finding that BPD symptoms accounted for the relation between anxiety and nonsuicidal SIB. However, in our study, psychological distress was a significant unique predictor of total SIB (in addition to the significant interaction between psychological distress and sample type). In other words, sample type seems to be a moderator between psychological distress and SIB in our study, as opposed to a mediator.
Counseling Implications
Our findings have several treatment implications. Many counselors will not be surprised by the high rates of SIB found in our BPD-Tx sample. However, we also found a clinically important high rate of SIB in college students. Given that past engagement in SIB is one of the strongest predictors of future SIB (including nonsuicidal and suicidal SIB; Tuisku et al., 2014), the high lifetime rates of SIB found in both samples in the current study are noteworthy for service providers. Specifically, our results suggest that universities and other institutions concerned with mental health in college students should consider utilizing SIB screening tools. Additionally, the high prevalence of students with a lifetime history of any SIB suggests the need for widespread intervention programs for student populations. For example, some research (e.g., Kannan et al., 2021) has examined the implementation of DBT skills groups in college counseling centers for students with a variety of presenting issues, including SIB. Such intervention programs could benefit a wider range of students and help improve quality of life for many, especially those struggling with SIB.
Given that psychological distress predicted total SIB, it may be beneficial for counselors to regularly assess the level of psychological distress in all clients, including those with BPD and college students. Clients with high psychological distress, including anxiety, depression, obsessive-compulsion, and interpersonal sensitivity, will likely engage in more SIB than those with low psychological distress, and thus the counselor may be able to intervene before the client escalates to a high frequency of SIB. Assessing and tracking affective distress levels may be common with suicide assessment and safety planning, but there may be less awareness about the need for this with SIB. Treatment protocols could also focus on lowering psychological distress to see if that will decrease SIB. For example, DBT, which emphasizes psychological distress tolerance, has been increasingly implemented in college campus counseling centers (see Chugani, 2015). However, given that the current study’s findings are not causal, we cannot definitively conclude that lowering psychological distress will affect SIB.
Importantly, the interaction between psychological distress and sample type is noteworthy given that it contributes to the small extant evidence of divergence between populations of individuals with symptoms of BPD and other, more community-based populations like college students. Specifically, we found differences in SIB prevalence, in lifetime frequency, and in one predictor (i.e., psychological distress) in our two samples. This aligns with Turner et al.’s (2015) findings that individuals who engaged in SIB with and without BPD differed in SIB frequency, severity, and comorbid affective symptomology.
It is also worth noting that the correlational analysis revealed a difference between these two samples in social functioning. In particular, there was a statistically significant negative correlation between total SIB and positive social support in the student sample, but not in the BPD-Tx sample. Because of this, although we only found one statistically significant interaction between psychosocial predictors and sample type, it is plausible that there are other notable differences in SIB risk factors between these two populations. Thus, when treating SIB, it may be worth assessing for other symptoms of BPD to form a more accurate representation of a client’s experience and to help form a specific treatment plan.
Limitations and Future Studies
One potential limitation of the current study is that we included only individuals who reported engaging in SIB in the past year because we wanted to examine current predictors of current SIB. However, it is possible that psychological distress and social support are more effective predictors of future SIB acts. In other words, the current study examined predictors of the frequency of SIB using current psychosocial functioning, yet the psychosocial variables might have been better at predicting whether or not an individual will engage in SIB in the future. This theory aligns with Heath et al.’s (2009) interpretation of their lack of results linking social support to lifetime rates of nonsuicidal SIB. Specifically, that social support may better relate to differences between those who will engage in SIB compared to those who will not, as opposed to the degree (i.e., frequency) of SIB. It is unclear how the results may have differed if we included a comparison group of individuals who do not engage in SIB or have never engaged in SIB.
A second limitation was the need to use specific measures to compare the student sample to the existing BPD-Tx sample data. Although the LSASI measure has the advantage of thoroughly examining SIB methods and intent, it was intended for clinical use rather than research. Additionally, the LSASI is a lifetime measure of SIB as opposed to assessing recent SIB; although our inclusion criteria required participants to have engaged in SIB at least once in the past year, it is unknown how recent or severe the SIB was in the past year relative to one’s lifetime. Because of this, a dichotomous measure of past-year engagement in SIB may have better suited our need for recent SIB assessment. Nonetheless, the LSASI provided a great depth and variability in the data that was not only valuable in the current research study, but also clinically important to the counselors with whom we collaborated in the larger DBT study.
A third limitation is that there may be other variables involved in predicting SIB that were not assessed, such as emotion regulation skills or trauma exposure. For example, SIB frequency might be more strongly related to one’s ability to regulate distress rather than the presence of distress itself. Given that emotional reactivity and trauma exposure are both risk factors for SIB (Nock, 2009, 2010) and for the development of BPD (Crowell et al., 2009), future studies may want to further explicate these relations.
It is also worth noting that the samples in the current study may include theoretically overlapping populations. Specifically, we did not screen the BPD-Tx group for current academic status, and therefore it is possible that some participants in the BPD-Tx group were also college students. We decided not to exclude BPD-Tx participants based on academic status in order to reduce barriers to study participation and so that the BPD-Tx sample would represent people who seek treatment for BPD in the community, not just those who are not college students. Additionally, although we screened the student sample for the explicit endorsement of BPD diagnosis, it is possible that some participants in the student sample had subthreshold symptoms of BPD (especially considering that SIB itself is a symptom of BPD) or simply had not received a diagnosis of BPD at the time of this study.
Future studies should continue to examine psychosocial predictors of SIB with larger and more diverse samples in order to explore the relations between psychological and social predictors. Additionally, future studies should explore other relevant factors with the psychosocial predictors (e.g., emotion regulation, trauma exposure) to determine if other factors may better explain (or mediate the relations with) SIB. Moreover, longitudinal and experience-sampling designs would allow researchers to gain better understanding of how changes in psychosocial functioning relate to decisions to engage in SIB as well as the exact sequence of events for SIB acts. Although some studies have recently begun using these techniques, a more psychosocial approach to predictors and consequences of SIB (also considering various intents) may provide more prudent information for intervention and treatment of individuals who engage in SIB.
Conclusion
The current study sought to identify psychosocial predictors of SIB in two clinically different populations and to compare predictors between these populations. We found high lifetime frequency rates of SIB in both samples, suggesting a need for more widespread assessment of SIB in young adults from different populations. We also found that population type itself was the strongest predictor of SIB—individuals with traits of BPD engaged in more SIB in their lifetimes than did college students. Additionally, psychological distress predicted SIB; however, we also found a significant interaction between population and psychological distress, which suggests that psychological distress may be more related to SIB in individuals with traits of BPD than in more community-based populations like college students. Consequently, counselors should consider population and psychological distress when assessing SIB risk in clients.
Conflict of Interest and Funding Disclosure
Data from the existing BPD sample was partially
funded by an internal grant awarded to coauthor
Christina Byrne. The authors reported no conflict
of interest or other funding for the development
of this manuscript.
References
Adrian, M., Zeman, J., Erdley, C., Lisa, L., & Sim, L. (2011). Emotional dysregulation and interpersonal difficulties as risk factors for nonsuicidal self-injury in adolescent girls. Journal of Abnormal Child Psychology, 39(3), 389–400. https://doi.org/10.1007/s10802-010-9465-3
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Andión, Ó., Ferrer, M., Matali, J., Gancedo, B., Calvo, N., Barral, C., Valero, S., Di Genova, A., Diener, M. J., Torrubia, R., & Casas, M. (2012). Effectiveness of combined individual and group dialectical behavior therapy compared to only individual dialectical behavior therapy: A preliminary study. Psychotherapy, 49(2), 241–250. https://doi.org/10.1037/a0027401
Andover, M. S., Morris, B. W., Wren, A., & Bruzzese, M. E. (2012). The co-occurrence of non-suicidal self-injury and attempted suicide among adolescents: Distinguishing risk factors and psychosocial correlates. Child and Adolescent Psychiatry and Mental Health, 6. https://doi.org/10.1186/1753-2000-6-11
Andover, M. S., Pepper, C. M., Ryabchenko, K. A., Orrico, E. G., & Gibb, B. E. (2005). Self-mutilation and symptoms of depression, anxiety, and borderline personality disorder. Suicide and Life-Threatening Behavior, 35(5), 581–591. https://doi.org/10.1521/suli.2005.35.5.581
Andrews, T., Martin, G., Hasking, P., & Page, A. (2013). Predictors of continuation and cessation of nonsuicidal self-injury. Journal of Adolescent Health, 53(1), 40–46. https://doi.org/10.1016/j.jadohealth.2013.01.009
Bentley, K. H., Cassiello-Robbins, C. F., Vittorio, L., Sauer-Zavala, S., & Barlow, D. H. (2015). The association between nonsuicidal self-injury and the emotional disorders: A meta-analytic review. Clinical Psychology Review, 37, 72–88. https://doi.org/10.1016/j.cpr.2015.02.006
Black, D. W., Blum, N., Pfohl, B., & Hale, N. (2004). Suicidal behavior in borderline personality disorder: Prevalence, risk factors, prediction, and prevention. Journal of Personality Disorders, 18(3), 226–239. https://doi.org/10.1521/pedi.18.3.226.35445
Centers for Disease Control and Prevention. (2017). Leading causes of death reports. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html
Chugani, C. D. (2015). Dialectical behavior therapy in college counseling centers: Current literature and implications for practice. Journal of College Student Psychotherapy, 29(2), 120–131.
https://doi.org/10.1080/87568225.2015.1008368
Crowell, S. E., Beauchaine, T. P., & Linehan, M. M. (2009). A biosocial developmental model of borderline personality: Elaborating and extending Linehan’s theory. Psychological Bulletin, 135(3), 495–510. https://doi.org/10.1037/a0015616
Croyle, K. L., & Waltz, J. (2007). Subclinical self-harm: Range of behaviors, extent, and associated characteristics. American Journal of Orthopsychiatry, 77(2), 332–342. https://doi.org/10.1037/0002-9432.77.2.332
Daly, A., Dekker, T., & Hess, S. (2016). Dummy coding vs effects coding for categorical variables: Clarifications and extensions. Journal of Choice Modelling, 21, 36–41. https://doi.org/10.1016/j.jocm.2016.09.005
Derogatis, L. R. (1975). The SCL-90-R. Clinical Psychometric Research.
Derogatis, L. R. (1993). BSI Brief Symptom Inventory: Administration, Scoring, and Procedure Manual (4th ed.). National Computer Systems.
Derogatis, L. R., & Spencer, P. (1982). The Brief Symptom Inventory: Administration, scoring and procedures manual—1. Clinical Psychometric Research.
Dew, S. E., & Bickman, L. (2005). Client expectancies about therapy. Mental Health Services Research, 7(1), 21–33. https://doi.org/10.1007/s11020-005-1963-5
Furman, W., & Buhrmester, D. (2009). Methods and measures: The Network of Relationships Inventory: Behavioral Systems Version. International Journal of Behavioral Development, 33(5), 470–478. https://doi.org/10.1177/0165025409342634
Gratz, K. L., Conrad, S. D., & Roemer, L. (2002). Risk factors for deliberate self-harm among college students. American Journal of Orthopsychiatry, 72(1), 128–140. https://doi.org/10.1037/0002-9432.72.1.128
Halstead, R. O., Pavkov, T. W., Hecker, L. L., & Seliner, M. M. (2014). Family dynamics and self-injury behaviors: A correlation analysis. Journal of Marital and Family Therapy, 40(2), 246–259.
https://doi.org/10.1111/j.1752-0606.2012.00336.x
Heath, N. L., Ross, S., Toste, J. R., Charlebois, A., & Nedecheva, T. (2009). Retrospective analysis of social factors and nonsuicidal self-injury among young adults. Canadian Journal of Behavioural Science/Revue Canadienne des sciences du comportement, 41(3), 180–186. https://doi.org/10.1037/a0015732
Howell, D. C. (2013). Statistical methods for psychology (8th ed.). Cengage.
Joiner, T. (2005). Why people die by suicide. Harvard University Press.
Kannan, D., Chugani, C. D., Muhomba, M., & Koon, K. (2021). A qualitative analysis of college counseling center staff experiences of the utility of dialectical behavior therapy programs on campus. Journal of College Student Pychotherapy, 35(1), 1–17. https://doi.org/10.1080/87568225.2019.1620662
Kim, K. L., Cushman, G. K., Weissman, A. B., Puzia, M. E., Wegbreit, E., Tone, E. B., Spirito, A., & Dickstein, D. P. (2015). Behavioral and emotional responses to interpersonal stress: A comparison of adolescents engaged in non-suicidal self-injury to adolescent suicide attempters. Psychiatry Research, 228(3), 899–906.
https://doi.org/10.1016/j.psychres.2015.05.001
Kirkcaldy, B. D., Brown, J. M., & Siefen, G. R. (2007). Profiling adolescents attempting suicide and self-injurious behavior. International Journal on Disability and Human Development, 6(1), 75–86. https://doi.org/10.1515/IJDHD.2007.6.1.75
Klonsky, E. D. (2011). Non-suicidal self-injury in United States adults: Prevalence, sociodemographics, topography and functions. Psychological Medicine, 41(9), 1981–1986. https://doi.org/10.1017/S0033291710002497
Klonsky, E. D., & Olino, T. M. (2008). Identifying clinically distinct subgroups of self-injurers among young adults: A latent class analysis. Journal of Consulting and Clinical Psychology, 76(1), 22–27. https://doi.org/10.1037/0022-006X.76.1.22
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. Guilford.
Linehan, M. M., & Comtois, K. A. (1996). Lifetime parasuicide count. Unpublished manuscript, Department of Psychology, University of Washington, Seattle.
McManus, S., & Gunnell, D. (2020). Trends in mental health, non-suicidal self-harm and suicide attempts in 16–24-year-old students and non-students in England, 2000–2014. Social Psychiatry and Psychiatric Epidemiology, 55(1), 125–128. https://doi.org/10.1007/s00127-019-01797-5
Niegocki, K. L., & Ægisdóttir, S. (2019). College students’ coping and psychological help-seeking attitudes and intentions. Journal of Mental Health Counseling, 41(2), 144–157. https://doi.org/10.17744/mehc.41.2.04
Nock, M. K. (2009). Why do people hurt themselves? New insights into the nature and functions of self-injury. Current Directions in Psychological Science, 18(2), 78–83. https://doi.org/10.1111/j.1467-8721.2009.01613.x
Nock, M. K. (2010). Self-injury. Annual Review of Clinical Psychology, 6, 339–363.
https://doi.org/10.1146/annurev.clinpsy.121208.131258
Nock, M. K., & Prinstein, M. J. (2004). A functional approach to the assessment of self-mutilative behavior. Journal of Consulting and Clinical Psychology, 72(5), 885–890. https://doi.org/10.1037/0022-006X.72.5.885
Nock, M. K., & Prinstein, M. J. (2005). Contextual features and behavioral functions of self-mutilation among adolescents. Journal of Abnormal Psychology, 114(1), 140–146. https://doi.org/10.1037/0021-843X.114.1.140
Peters, J. R., Smart, L. M., & Baer, R. A. (2015). Dysfunctional responses to emotion mediate the cross-sectional relationship between rejection sensitivity and borderline personality features. Journal of Personality Disorders, 29(2), 231–240. https://doi.org/10.1521/pedi_2014_28_151
Rodham, K., & Hawton, K. (2009). Epidemiology and phenomenology of nonsuicidal self-injury. In M. K. Nock (Ed.), Understanding nonsuicidal self-injury: Origins, assessment, and treatment (pp. 37–62). American Psychological Association. https://doi.org/10.1037/11875-003
Rotolone, C., & Martin, G. (2012). Giving up self-injury: A comparison of everyday social and personal resources in past versus current self-injurers. Archives of Suicide Research, 16(2), 147–158.
https://doi.org/10.1080/13811118.2012.667333
Sadeh, N., Londahl-Shaller, E. A., Piatigorsky, A., Fordwood, S., Stuart, B. K., McNiel, D. E., Klonsky, E. D., Ozer, E. M., & Yaeger, A. M. (2014). Functions of non-suicidal self-injury in adolescents and young adults with borderline personality disorder symptoms. Psychiatry Research, 216(2), 217–222.
https://doi.org/10.1016/j.psychres.2014.02.018
Sitton, M., Du Rocher Schudlich, T., Byrne, C., Ochrach, C. M., & Erwin, S. E. A. (2020). Family functioning and self-injury in treatment-seeking adolescents: Implications for counselors. The Professional Counselor, 10(3), 351–364. https://doi.org/10.15241/ms.10.3.351
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Tuisku, V., Kiviruusu, O., Pelkonen, M., Karlsson, L., Strandholm, T., & Marttunen, M. (2014). Depressed adolescents as young adults: Predictors of suicide attempt and non-suicidal self-injury during an 8-year follow-up. Journal of Affective Disorders, 152, 313–319. https://doi.org/10.1016/j.jad.2013.09.031
Turner, B. J., Cobb, R. J., Gratz, K. L., & Chapman, A. L. (2016). The role of interpersonal conflict and perceived social support in nonsuicidal self-injury in daily life. Journal of Abnormal Psychology, 125(4), 588–598. https://doi.org/10.1037/abn0000141
Turner, B. J., Dixon-Gordon, K. L., Austin, S. B., Rodriguez, M. A., Rosenthal, M. Z., & Chapman, A. L. (2015). Non-suicidal self-injury with and without borderline personality disorder: Differences in self-injury and diagnostic comorbidity. Psychiatry Research, 230(1), 28–35. https://doi.org/10.1016/j.psychres.2015.07.058
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & Joiner, T. E., Jr. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575–600. https://doi.org/10.1037/a0018697
Whitlock, J., Eckenrode, J., & Silverman, D. (2006). Self-injurious behaviors in a college population. Pediatrics, 117(6), 1939–1948. https://doi.org/10.1542/peds.2005-2543
Whitlock, J., Muehlenkamp, J., Eckenrode, J., Purington, A., Baral Abrams, G., Barreira, P., & Kress, V. (2013). Nonsuicidal self-injury as a gateway to suicide in young adults. Journal of Adolescent Health, 52(4), 486–492. https://doi.org/10.1016/j.jadohealth.2012.09.010
Wilcox, H. C., Arria, A. M., Caldeira, K. M., Vincent, K. B., Pinchevsky, G. M., & O’Grady, K. E. (2012). Longitudinal predictors of past-year non-suicidal self-injury and motives among college students. Psychological Medicine, 42(4), 717–726. https://doi.org/10.1017/S0033291711001814
Melissa J. Sitton, MS, is a doctoral student at Southern Methodist University. Tina Du Rocher Schudlich, PhD, MHP, is a professor at Western Washington University. Christina Byrne, PhD, is an associate professor at Western Washington University. Correspondence may be addressed to Melissa J. Sitton, Department of Psychology, Southern Methodist University, P.O. Box 750442, Dallas, TX 75275-0442, msitton@smu.edu.
Apr 1, 2021 | Volume 11 - Issue 2
Taylor Irvine, Adriana Labarta, Kelly Emelianchik-Key
Counselor education (CE) programs are expected to provide counselors-in-training (CITs) with a diversity-infused curriculum. Throughout the CE literature, there are many available methods to accomplish this goal, yet trainees have reported a lack of self-efficacy in essential multicultural competencies before entering clinical work. Graduates of CE programs have also noted feeling unprepared when working with culturally diverse clients. The integration of culturally responsive models in CE programs is limited, and methods to decolonize current educational practices remain sparse. To address these gaps, we propose a culturally responsive and decolonizing framework grounded in the extant research that integrates relational-cultural theory (RCT) and Adlerian theory principles. The Relational-Cultural and Adlerian Multicultural Framework (RAMF) is intended to be a new pedagogical approach to enhance multicultural education across CE programs. By integrating RCT and Adlerian theory frameworks, the RAMF may offer a more comprehensive lens to view multicultural and social justice issues.
Keywords: relational-cultural theory, Adlerian theory, multicultural competencies, counselor education, decolonizing
Counselor education (CE) programs are charged with preparing counselors-in-training (CITs) to become culturally competent counselors. The Council for Accreditation of Counseling and Related Educational Programs (CACREP) and the American Counseling Association (ACA) require multicultural education training to ensure that CITs develop essential multicultural competencies needed to ethically and effectively serve diverse client populations (ACA, 2014; CACREP, 2015). The 2016 CACREP Standards define multicultural as “denoting the diversity of racial, ethnic, and cultural heritage; socioeconomic status; age; gender; sexual orientation; and religious and spiritual beliefs, as well as physical, emotional, and mental abilities” (CACREP, 2015, p. 42). CE programs must equip trainees with the knowledge and skills crucial to providing culturally responsive treatment (ACA, 2014; CACREP, 2015). We begin by defining multicultural competence as it relates to the counseling profession, followed by a review of key terms that lay the groundwork for the proposed pedagogical framework.
Multicultural Competence
Many definitions of multicultural competence exist in the literature. We operationally define multicultural competence as a counselor’s awareness and knowledge of their own culture and their clients’ cultures, which allows them to tailor counseling approaches to client cultural identities and appreciate and embrace cultural differences (Ratts et al., 2016; Sue et al., 1992). C. C. Lee (2019) also outlined three self-reflective questions to promote multicultural competence: “1) Who am I as a cultural being? . . . 2) What do I know about cultural dynamics and how they may influence my client’s worldview? . . . [and] 3) How do I promote client mental health and well-being in a culturally competent manner?” (p. 10). These reflective questions are crucial to multicultural competence development, particularly given the recent increase in cultural pluralism throughout the United States (C. C. Lee, 2019). In response to the growth in diverse client populations and the call to infuse social justice into CE, the Association for Multicultural Counseling and Development has endorsed the revised Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) to facilitate clinical competency in this domain.
The Multicultural and Social Justice Counseling Competencies (MSJCC)
The MSJCC serve to impact, influence, and broaden the scope of multicultural training in CE programs (Ratts et al., 2016). Building from Sue et al.’s (1992) seminal tripartite model, four essential competencies comprise the MSJCC and are inherent to producing culturally competent counselors: attitudes and beliefs, knowledge, skills, and action (Ratts et al., 2016). More than ever, our current sociopolitical climate tasks counselors with the ethical responsibility of cultural sensitivity and increased diversity awareness, which is central to being multiculturally competent and fundamental to the counseling relationship itself (ACA, 2014).
The MSJCC highlight the importance of social justice and advocacy by addressing mental health disparities and empowering marginalized groups (Ratts et al., 2016). Throughout the professional literature, there is a lack of consensus on defining this construct, furthering the experience of oppression for marginalized group members (C. C. Lee, 2019). For this article, we operationally define marginalized group members as historically oppressed persons and communities in society that experience discrimination and lack access to systemic benefits that privileged groups receive because of structural power advantages; this power imbalance occurs within sociopolitical, economic, and cultural dimensions (C. C. Lee, 2019; Ratts et al., 2016). Marginalized group members include a host of group identities, including but not limited to Black, Indigenous, and People of Color (BIPOC); LGBTGEQIAP+ individuals; persons with disabilities; and undocumented immigrants and refugees (C. C. Lee, 2019). Integral to the MSJCC and overall multicultural competence is an awareness of clients’ and counselors’ intersecting identities, which allows for a deeper examination of privilege, power, and oppression dynamics.
Intersecting Identities
Because culture encompasses classifications that extend beyond race and ethnicity, cultural identity can be viewed as one’s self-identification as a member of a specific group based on a connection with the group’s core beliefs and values that fit with one’s sense of self (C. C. Lee, 2019; Ratts et al., 2016; Singh et al., 2020). According to intersectionality theory, individuals who hold multiple marginalized identities may experience a greater risk of mental health concerns because of the compounding effects of various forms of discrimination and oppression (Crenshaw, 1989). Thus, CITs must understand intersecting identities (e.g., Hispanic Christian lesbian) to holistically and effectively conceptualize clients’ presenting issues and examine dynamics of identity and power within the counseling relationship (Ratts et al., 2016). Intersectionality theory also provides a framework for counselors to critically investigate Westernized counseling theories stemming from a White Eurocentric lens and move toward a decolonizing paradigm. When conducting multicultural and social justice research, Hays (2020) noted the cruciality of applying intersectionality and decolonizing practices to enhance client and training outcomes.
Decolonizing Counseling and CE
A definition of decolonization is warranted to further the discussion on dismantling oppressive systems impacting marginalized communities. In the literature, scholars have described coloniality as the dominant culture’s attempts to socialize marginalized communities into adopting Westernized ideals and values (Goodman & Gorski, 2015; Hernández-Wolfe, 2011; Singh et al., 2020). Therefore, decolonization requires critically analyzing and challenging hierarchical structures that perpetuate inequities and injustices in underrepresented groups (Hernández-Wolfe, 2011). Integration of decolonization is also crucial to informing multicultural counseling and education (Goodman & Gorski, 2015; Singh et al., 2020). Within CE programs, Singh et al. (2020) argued that social justice theories should be “taught alongside traditional counseling theories” to provide culturally responsive counseling and challenge colonizing educational practices (p. 262). Despite the persistent calls to incorporate the MSJCC and decolonizing practices into counseling and educational paradigms, scholars have continued to note deficits within multicultural education (Barden & Greene, 2015; Singh et al., 2020).
Deficits in Multicultural Education
The literature reveals gaps between the pedagogical practices, acquired skill development and theory integration, and personal awareness needed to become culturally competent and prepared to work with diverse clients (Barden & Greene, 2015; Priester et al., 2008). CITs have also indicated a lack of self-efficacy in essential multicultural competencies upon entering their practicum sequence (Flasch et al., 2011). In addition, graduates of counseling programs have reported feeling unprepared to work with culturally diverse clients (Barden et al., 2017; Bidell, 2012; Schmidt et al., 2011). This issue reflects the current deficits in multicultural education among CE programs. Many definitions of multicultural education exist in the literature. For this study, we define it as a holistic approach to critically analyzing systems of power and privilege and inequitable policies that serve to disenfranchise marginalized group members; at the same time, multicultural education centralizes matters of social justice and the decolonization of discriminatory educational practices (Gorski, 2016; Singh et al., 2020).
Across CE programs, one notable factor that influences multicultural education is educational delivery method. Swank and Houseknecht (2019) conducted a Delphi study of teaching competencies in CE, which revealed that students were twice as likely to rate a professor as effective based on their content knowledge and delivery method. Thus, educational delivery method may play a significant role in facilitating multicultural competence among CITs. As such, there is a need for more effective diversity training approaches in CE programs, with an emphasis on fostering CITs’ ability to integrate theory and therapeutic techniques to fully meet clients’ needs with diverse and deep intersectional ties (Killian & Floren, 2020).
Although studies conducted on multicultural education have increased (Chang & Rabess, 2020; Uzunboylu & Altay, 2021), there remains a paucity of available research on integrating culturally responsive models in CE programs (Pieterse et al., 2009; Shelton, 2020; Trahan & Keim, 2019). Similarly, researchers in related fields, such as teacher education, have also noted ongoing challenges pertaining to multicultural education, including minimizing or avoiding challenging conversations about race and privilege, misrepresenting the voices of marginalized group members, integrating content over equity-based practices, and underemphasizing the factors that impact the teaching practices of multicultural educators (Chouari, 2016; Gorski, 2016; Kim, 2011; McGee Banks & Banks, 1995). Relational-cultural theory (RCT) and Adlerian theory are detailed and presented as grounding for a proposed pedagogical approach to address these training limitations.
Relational-Cultural Theory (RCT)
RCT is a feminist approach rooted in Jean Baker Miller’s (1976) Toward a New Psychology of Women. In collaboration with colleagues Judith Jordan, Janet Surrey, and Irene Stiver, Miller developed RCT and challenged Westernized psychotherapy theories that portray human development as a journey from dependence to independence (Jordan, 2010). From an RCT lens, healing occurs in the context of mutually empathic, growth-fostering relationships. Rather than focusing on separation and self-sufficiency, RCT is grounded in the assertion that human beings need connection to flourish. J. B. Miller and Stiver (1997) stated that “five good things” occur when individuals engage in growth-fostering relationships: 1) a greater sense of “zest,” or vitality and energy; 2) increased self-worth; 3) a better understanding of self and others in the context of relationships; 4) elevated levels of productivity and creativity; and 5) a desire for more connection.
Conversely, isolation is perceived as a significant source of suffering (Jordan, 2018). Across the life span, relational development is highly interrelated with a person’s racial, cultural, and social identities (Pedersen et al., 2008). RCT addresses the breadth and depth that identity and power structures have within relationships and the intersectionality of culture across various contexts (Comstock et al., 2008; Schwartz, 2019). RCT also emphasizes acknowledgement of how hierarchical systems contribute to cultural oppression and social isolation for traditionally marginalized communities. Further, this theory centers contextual and relational factors that impact clients and encourages counselors to examine dynamics of privilege and oppression that perpetuate suffering and create disconnection (Jordan, 2018). Disconnection can be conceptualized as a routine part of relationships, yet when left unaddressed, the invalidated person may experience shame, withdrawal, and disempowerment. Therefore, RCT highlights the importance of attending to ruptures in relationships when they occur. By centering connection, authenticity, and mutual empowerment, humans can differentiate relational patterns and develop meaningful self and other relationships (Jordan, 2010). RCT also recognizes the ability for multiple truths within a relationship, which allows the individual’s unique experiences and perspectives to be acknowledged within the social and cultural subsystems that they are embedded within (Comstock et al., 2008; Jordan, 2018).
RCT has feminist, postmodern epistemological underpinnings that make it a suitable theoretical framework to implement in the various facets of CE. Several authors have proposed the use of RCT as a framework for pedagogy (Byers et al., 2020; K. G. Hall et al., 2014), mentorship (Lewis & Olshansky, 2016), supervision (Bradley et al., 2019), and advising students of color (Dipre & Luke, 2020). As a pedagogical model, RCT is applied in several courses, including human diversity (Byers et al., 2020), group counseling (B. S. Hall et al., 2018), and counseling theories (Lertora et al., 2020). Thus, RCT appears to be an emerging and robust framework to enhance students’ relational, multicultural, and social justice competencies.
Adlerian Theory
Individual psychology, better known as Adlerian theory, is a phenomenological framework that examines the social and contextual factors which inform a person’s reality (Bitter et al., 2009; Watts, 2013). At its core, Adlerian theorists believe in social embeddedness, or the idea that individuals are comprehensively understood within a social-relational context (R. Miller & Taylor, 2016). Additionally, this framework is rooted in the following core principles: 1) behavior is purposeful (teleological) and used to satisfy the primary need of belongingness; 2) human beings are innately creative and unique; 3) human beings are indivisible and, therefore, must be viewed holistically; 4) human beings prosper through social interest (community feeling); and 5) relational interactions are influenced by one’s lifestyle, or their cognitive worldview (Adler, 1946). Adlerian theory possesses flexible and growth-fostering tenets, making it well-suited for incorporation into a multicultural pedagogical model, such as the MSJCC.
Adlerian theory eschews fundamentally decolonizing tenets such as an either/or perspective and values a dialectical stance to view the individual and social environment as mutually interacting factors (Watts, 2003). The research literature has long documented the integration of Adlerian theoretical principles with supervision (Bornsheuer-Boswell et al., 2013), counseling (Yee et al., 2016), and school frameworks (Pryor & Tollerud, 1999). Adlerian theory has also demonstrated applications as a creative pedagogical framework for enhancing case conceptualization competency among CITs (Davis et al., 2019) and promoting student satisfaction with the learning environment and student–teacher relationships (Soheili et al., 2015).
In a clinical setting, Adlerian counselors conceptualize clients from a social-contextual perspective to gain a deeper understanding of how they perceive events. One of an Adlerian counselor’s roles is to assist the client with examining maladaptive lifestyle convictions while also encouraging engagement in cooperative and social interactions to inhibit disconnection, considered to be the root of suffering (Watts, 2013). Neuroscience findings have supported this focus on social interest as critical to improving relationships and enhancing overall mental health (R. Miller & Taylor, 2016). In addition, its social-relational orientation makes it well-suited for increasing multicultural competence among counselors. Specifically, this framework supports client examination of multicultural issues through a lens of community feeling, in which establishing equality is central to addressing challenges (Bitter et al., 2009). Key tenets and values of Adlerian theory align with pro-feminist and decolonizing values, making it inclusive of marginalized group members (Watts, 2013) through its support of social interest, equality and advocacy, egalitarian relationships, empowerment and individual choice, and a social-cultural view of issues (Bitter et al., 2009; Davis et al., 2019; Soheili et al., 2015).
The Relational-Cultural and Adlerian Multicultural Framework (RAMF)
We aim to bridge research and training gaps in multicultural education by integrating RCT with Adlerian theory. The core tenets of these two frameworks undergird the Relational-Cultural and Adlerian Multicultural Framework (RAMF), a pedagogical approach to enhance multicultural competence among CITs. In order to develop multicultural and social justice competence, trainees must first learn and understand the subtle complexities of theory before they can use and integrate it into their clinical practice. We believe that the RAMF can bolster current multicultural education practices by promoting the development of clinical competence in this domain while also modeling theoretical integration for CITs.
A Cross-Paradigm Framework for Pedagogy
In the realm of counseling, an individual conceptualization has long dominated as the primary means to conceptualize clients’ issues. In this regard, Singh et al. (2020) highlighted the need to critically examine and move beyond Westernized counseling theories:
Although traditional counseling theories certainly may be utilized in culturally competent ways, they are often situated in a paradigm that focuses on the individual when the source of difficulties may be rooted in oppressive structures within the environment that require direct advocacy. (p. 261)
The integrative nature of the RAMF may lend to improved multicultural and social justice competency among CITs and clinicians. This framework can be conceptualized as a cross-paradigm pedagogical approach, rooted in psychological and postmodern/social-constructivist paradigms, which blend techniques and tenets from both theories (Cottone, 2012). Despite RCT and Adlerian theory originating from different theoretical paradigms, these theories are complementary and have overlapping social and relational constructs. Specifically, Adlerian theory originated from the psychological paradigm of counseling and psychotherapy, as it centralizes an individual conceptualization of clients’ issues (Cottone, 2012). However, Watts (2003) noted that this theory’s unique encapsulation of cognitive constructivist and social constructionist elements make it better classified as a relational constructivist paradigm (i.e., emphasizing individual agency within a social-relational context). On the other hand, RCT is rooted in a postmodern philosophy, best categorizing this theory as belonging to the social-constructivist paradigm (Cottone, 2012), given its emphasis on the role that social-contextual factors (i.e., hierarchical systems) play in perpetuating oppression, inequity, and suffering. Moreover, Singh et al. (2020) recently recognized RCT as a social justice theory that can help counselors decolonize counseling and integrate the MSJCC in their work with clients.
The RAMF is intended to be a new decolonizing pedagogical approach to multicultural education that fosters an equitable learning environment and overall inclusive program culture. The RAMF is a unique approach that integrates the counseling profession’s core values, such as social justice, cultural competence, advocacy, and wellness (ACA, 2014). In contrast, many other theories, such as critical pedagogy, stem from educational fields and have different core values central to their professions. Combining RCT and Adlerian theory frameworks may provide a more holistic lens to view multicultural and social justice issues. Within the classroom, the RAMF centralizes growth-fostering relationships between students and professors. This outcome requires that professors be mindful of their positionality, minimize the power differential inherent in the professor–student relationship, and create mutually empowering relationships within the classroom (Walker, 2015). The RAMF also promotes practicing intentionality, incorporating experiential training strategies, and routine processing of CITs’ reactions to further develop multicultural competence. Ultimately, the RAMF seeks to address bias and inequity by promoting self-awareness, authenticity, personal responsibility, mutual empowerment, acceptance of differing worldviews, and a non-judgmental and curious attitude. Because the RAMF aims to cultivate a culture of mutual empowerment and social interest, diverse students may feel more supported and valued. In this next section, we will outline components comprising the RAMF, offer an integrative description to apply the RAMF effectively, and discuss implications for future research.
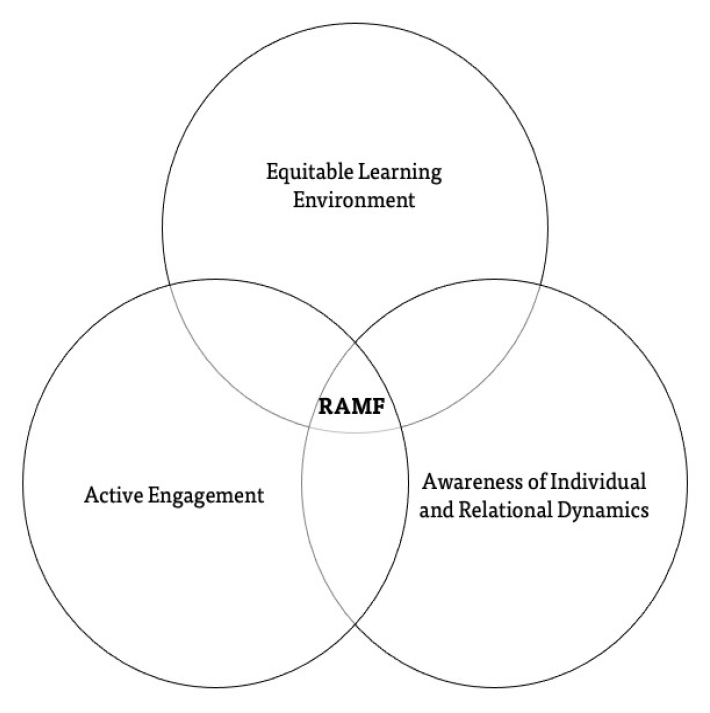
RAMF Components
The following three components found in Figure 1 are proposed as foundational to the RAMF and stem from RCT’s and Adlerian theory’s tenets: an equitable learning environment, awareness of individual and relational dynamics, and active engagement. These components and supporting research are examined in depth below.
Figure 1
RAMF Components
Equitable Learning Environment
Successful implementation of the RAMF requires an equitable learning environment to effectively assist diverse students while also fostering multicultural and social justice competence (see Figure 2). Gorski and Swalwell (2015) purported that multicultural education is grounded in social justice and equity values. Failure to ensure both equity and equality in the classroom poses detrimental implications to student professional growth and overall well-being. For instance, in a qualitative study conducted by Baker et al. (2015), marginalized doctoral students in a CE program expressed feeling excluded from class information and discussions; they also shared concerns about being misjudged because of their racial identities. These findings are consistent with previous research on the experiences of marginalized master’s-level CITs across CE programs (Henfield et al., 2013; Seward, 2014).
Figure 2
RAMF Integration Application
| RCT |
Adlerian Theory |
RAMF
Component |
Integrative Application Examples |
| Growth-fostering relationships |
Social interest |
Equitable learning environment |
Creating a safe space for all students to contribute in a way that empowers them; open discussions/exposure to diverse worldviews |
| Mutual empathy and empowerment |
Social equality and advocacy |
Active engagement |
Creating a classroom environment that mutually benefits both students and professor; collaborating on
journal article |
| Exploration of power differentials |
Egalitarian relationships |
Equitable learning environment |
Offering an outlet for students to provide anonymous feedback |
| Authenticity in relationships |
Empowerment and individual choice |
Individual and relational dynamics |
Giving yourself permission to be human; cultural humility |
| Consideration of contextual and relational factors |
Being curious about diverse perspectives; social-cultural view of issues |
Individual and relational dynamics |
Awareness of self and other cultural identity membership; role-plays, reflective journaling, classroom dialogue, etc. |
Using the RAMF, an equitable learning environment is cultivated through embracing classroom norms driven by Adlerian and RCT values. Examples include embracing a genuinely curious attitude, accepting differing worldviews, exhibiting compassion for self and others while navigating conflicts, and modeling authenticity during moments of disconnection (i.e., cultural humility). Additionally, fostering this classroom atmosphere is contingent upon incorporating decolonizing educational practices. CE programs can accomplish this task through the intentional examination of course curricula. Specific examples include things like being mindful of the language used in course content and infusing textbooks, assignments, and supplementary materials in the syllabi to address inequitable practices and discrimination against marginalized group members (e.g., current news reports, community service-learning experiences within marginalized communities, guest speakers). Thus, the RAMF encourages counselor educators to practice intentionality by diversifying curriculum and incorporating diverse scholars’ perspectives to dismantle colonized counseling and pedagogical practices.
The RAMF also stresses the importance of acknowledging the significant impact of professor interactions in fostering an equitable learning environment. Research findings have noted several factors that strengthen trainees’ experience of their learning environments, such as an emphasis on teaching and mentorship, peer support, and faculty–student connections (Henfield et al., 2013; Sheperis et al., 2020). In this regard, enhancing relational factors among professors may alleviate the power differential between professors and CITs, thereby facilitating a more equitable learning environment. Additionally, student feedback and perceptions of the teaching environment should constantly be solicited in any learning environment that aspires to be inclusive and equitable. Hopefully, if a safe and collaborative learning environment is achieved, this feedback will be provided authentically and without direct solicitation. Anonymous feedback can also be gathered in various formal and informal approaches, such as the use of specific assessments or scaling and qualitative inquiry.
Gorski (2016) noted the importance of systemic change as crucial to analyzing power and privilege in the classroom; thus, faculty support is necessary to effectively carry out this systemic endeavor. As such, it is recommended that CE programs assess their organizational climate before implementing the RAMF. A discriminatory CE program climate serves to uphold colonizing and inequitable learning practices, thereby interfering with the development of multicultural and social justice competencies. The RAMF seeks to dismantle this issue by valuing diversity and modeling equity in the classroom, directly influencing CITs’ perspectives and overall multicultural competence growth. Sanchez Bengoa et al. (2018) found that students developed multicultural competency skills faster in international teams than national teams; this finding speaks to the critical need to foster a culturally rich classroom environment where students can be exposed to diverse worldviews and engage in a cooperative learning process.
Awareness of Individual and Relational Dynamics
As a cross-paradigm approach, the RAMF acknowledges the importance of individual and relational dynamics that impact the overall learning process and program experience. Within counseling programs, CITs are encouraged to engage in ongoing self-reflection, which is essential in multicultural education. According to the MSJCC framework (Ratts et al., 2016), self-awareness is at the core of multicultural and social justice competence. Counselors must critically examine their personally held attitudes, beliefs, and biases that affect their work with diverse clients. This awareness may then contribute to counselors’ understanding of power, privilege, and oppression dynamics that impact the therapeutic relationship (Ratts et al., 2016). The RAMF takes a unique perspective on trainee self-awareness by drawing on core counseling values, such as examining the individual’s role and identity in the context of relationships. From a RAMF lens, professors can facilitate this process with CITs by modeling authentic interactions (e.g., cultural humility), which may promote personal exploration and shared disclosures in a classroom setting. In Morgan Consoli and Marin’s (2016) qualitative study on graduate students’ experiences in diversity courses, students noted the essentiality of instructor self-disclosure and viewed it as indispensable to a positive diversity course experience. Thus, valuing authenticity and cultural humility may instill the importance of multicultural competence as a lifelong process (Hook et al., 2013).
Although an individual commitment to learning and self-awareness is at the core of multicultural competence, counselors must move beyond self-reflection to foster empowering therapeutic relationships. In a descriptive content analysis of multicultural course syllabi, Pieterse et al. (2009) found that a large percentage of course syllabi focused on developing knowledge, awareness, and skills; yet, knowledge and awareness were emphasized more often, while relational skill development was not. The RAMF emphasizes relational skill development by actively addressing ruptures that may occur between professors and CITs. Although the RAMF conceptualizes conflict as a standard component of relationships, ruptures must be addressed and repaired, especially attending to feelings of disempowerment (Jordan, 2010). To address this concern, the RAMF encourages professors to model broaching, which is defined as an ongoing commitment and openness to exploring diversity and cultural issues with clients and students (Day-Vines et al., 2018). Because research has shown that broaching early on in counseling can reduce attrition and strengthen therapeutic relationships with racial and ethnic minority clients (Jones et al., 2019), CITs must have the opportunity to practice broaching within the classroom setting. Central to this practice is creating a safe space, whereby professors actively encourage students to practice vulnerability and cultural humility by leaning into challenging conversations and providing feedback to enhance both self and relational awareness.
Active Engagement
The RAMF posits that active engagement is necessary to multicultural education and effective diversity training of CITs. Ikonomopoulos et al. (2016) conducted a study that demonstrated that practicum-level CITs developed their self-efficacy by actively engaging in direct client contact and peer-group interactions. We define active engagement as the process of encouraging students to learn in a deeper context, engage in activities, and reflect upon the material in a meaningful way. Depending on the course, there is no one “correct” way to attain or measure active engagement, yet active engagement should be seen in student questions, writings, and participation. Fundamental to Adlerian theory and RCT is the belief that individuals and groups are best understood in their relationships. Using the RAMF, CITs are required to actively engage in cultural immersion experiences and service-learning projects to gain a deeper understanding of the experiences and unique challenges of marginalized group members.
Research has demonstrated the utility of service-learning experiences for CITs to develop clinical competencies (Dari et al., 2019), enhance a sense of preparedness to apply learned clinical skills (Havlik et al., 2016), deepen their understanding of human development from a social justice perspective (K. A. Lee & Kelley-Petersen, 2018), and promote social justice advocacy competency and cognitive development (K. A. Lee & McAdams, 2019). Following these experiences, scholars have noted that open dialogue about cultural and diversity matters is needed to bolster CITs’ clinical knowledge and attitudes (Celinska & Swazo, 2016; Wagner, 2015). For instance, in a study conducted by Villalba and Redmond (2008), an experiential learning exercise was incorporated in which students were exposed to a film to help facilitate multicultural competence through self-reflection. This study’s findings revealed the essentiality of open discussion on relevant social justice issues to process the experience fully. Further, Ratts et al. (2016) indicated that counselors who embody multicultural and social justice competence demonstrate cross-cultural communication skills. In using the RAMF, we emphasize classroom dialogue, such as open processing and role-plays, as a crucial part of developing these competencies in CITs. Counseling programs are tasked with preparing CITs to be future leaders and allies within the profession. This endeavor requires the exposure of CITs within culturally diverse groups by actively engaging with the community at large. In doing so, CITs stand a greater chance of developing essential multicultural and social justice competencies needed to effectively treat and conceptualize diverse client populations. The MSJCC endorses the implementation of counseling and advocacy interventions crucial to holistic diversity training; specifically, CITs must actively engage beyond intrapersonal self-reflection by considering relational, community, societal, and global interventions (Ratts et al., 2016).
Inherent to the RAMF is its focus on active engagement in social justice and advocacy initiatives to facilitate multicultural competence. Some strategies include engaging trainees in open conversations about current sociopolitical challenges and the subsequent impact on marginalized group members, promoting attendance and engagement in presentations at professional conferences, and collaborating on professional journal articles related to multicultural competence. Ultimately, the RAMF is intended to be the vehicle that translates applied multicultural knowledge and skills into active engagement. The fundamental links between RCT and Adlerian theory are social equality and relational connections. These factors are crucial not only to the active engagement component of the RAMF but also to the framework as a whole. An integrative application outlining strategy relevant to the RAMF components is illustrated in Figure 2.
Considerations and Implications for Using the RAMF in Pedagogy
The RAMF poses several implications in the realm of CE, namely enhanced clinical competency and self-efficacy with multicultural concepts. This is particularly important as graduates of counseling programs have often indicated feeling unprepared to work with culturally diverse clients (Barden et al., 2017; Bidell, 2012; Schmidt et al., 2011). They have also reported a lack of self-efficacy in key multicultural competencies when first engaging in counseling work (Flasch et al., 2011). This competency deficit among trainees may be attributed to the historical overcrowding of multicultural competencies and skills into a single-course format, which is insufficient considering multiculturalism’s depth and scope (Celinska & Swazo, 2016). The RAMF’s multimodal approach to infusing multicultural and social justice competencies across the curriculum may help bridge this gap.
Given the rise in diverse client demographics and cultural pluralism (C. C. Lee, 2019), it has become the professional responsibility of all counselors to develop essential multicultural competencies needed to provide culturally competent counseling (ACA, 2014). This need is addressed through the RAMF, which serves as an integrative vehicle to effectively transmit this knowledge to CITs. CE programs are tasked with engaging in culturally responsive gatekeeping practices to maintain professional standards, namely protecting clients from culturally incompetent trainees. Counselor educators have noted the critical importance of seeing trainees’ multicultural competence development beyond the classroom and throughout the program within their gatekeeping role (Ziomek-Daigle et al., 2016).
Directions for Future Research
The RAMF may be used to bridge the gap in multicultural competency and self-efficacy among CITs in CE programs. Currently, there is no evidence regarding the efficacy of this integrative framework as a pedagogical model. Therefore, directions for future research may include a quantitative study measuring the RAMF’s effectiveness using a pretest-posttest design. For example, pre-post of the RAMF in a course may illustrate its overall effectiveness from the beginning to the end of the semester. The RAMF can be incorporated in CITs’ practicum and internship courses, after which a posttest can be administered to measure confidence and competence upon graduating. This method will serve to address the current deficit in CITs’ multicultural competence following graduation. Future research may also include developing an instrument that measures the constructs illustrated in the RAMF. Hays (2020) noted the importance of moving beyond traditional counseling research and integrating decolonizing methodologies, such as qualitative designs, that allow for triangulation with CITs and program faculty. Thus, we suggest collecting qualitative data to learn about the individual lived experiences of CITs following their course.
Further research on implementing the RAMF into CE programs is also needed to validate its evidence base. Regarding the evaluation of multicultural competence utilizing the RAMF, we recommend that CITs take Holcomb-McCoy and Myers’ (1999) Multicultural Counseling Competence and Training Survey-Revised (MCCTS-R), which will provide insight into CITs’ perceived level of multicultural competence. This 32-item measure is grounded in the MSJCC (Barden et al., 2017) and assesses competency in three domains—multicultural knowledge, multicultural awareness, and multicultural terminology—using self-report, Likert-type questions ranging from 1 (not competent) to 4 (extremely competent; Holcomb-McCoy & Myers, 1999). To evaluate the effectiveness of the RAMF and facilitate formative feedback, we recommend administering the MCCTS-R to all CITs at the beginning and end of a course. The successful implementation of the RAMF is evidenced by CITs’ growth in the following MSJCC domains: attitudes and beliefs, knowledge, skills, and action (Ratts et al., 2016). These domains must be routinely evaluated as part of an ongoing CE program evaluation to enhance multicultural and social justice competency among CITs (Hays, 2020).
Conclusion
CE programs may use the RAMF to address challenges to CITs’ self-efficacy and ability in treating culturally diverse clients, thereby potentially reducing gatekeeping concerns that stem from lack of multicultural competence. Overall, implementation of the RAMF could pose several benefits to CE programs. A limitation of this framework includes possible compassion fatigue because of its emphasis on authentic interactions and contact with difficult conversations (e.g., power and oppression, unique challenges faced by marginalized group members). However, the RAMF’s integrative approach to addressing multicultural and social justice competence throughout the curriculum may allow for CITs to develop knowledge and skills proactively rather than retroactively engaging in future remediation strategies.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adler, A. (1946). Understanding human nature. Permabooks.
American Counseling Association. (2014). ACA code of ethics.
Baker, C. A., Gaulke, K., & Smith, K. (2015). Counselor education cultural climate: Underrepresented master’s students’ experiences. Journal for Multicultural Education, 9(2), 85–97.
https://doi.org/10.1108/JME-07-2014-0032
Barden, S. M., & Greene, J. H. (2015). An investigation of multicultural counseling competence and multicultural counseling self-efficacy for counselors-in-training. International Journal for the Advancement of Counselling, 37(1), 41–53. https://doi.org/10.1007/s10447-014-9224-1
Barden, S. M., Sherrell, R. S., & Matthews, J. J. (2017). A national survey on multicultural competence for professional counselors: A replication study. Journal of Counseling & Development, 95(2), 203–212. https://doi.org/10.1002/jcad.12132
Bidell, M. P. (2012). Examining school counseling students’ multicultural and sexual orientation competencies through a cross-specialization comparison. Journal of Counseling & Development, 90(2), 200–207. https://doi.org/10.1111/j.1556-6676.2012.00025.x
Bitter, J. R., Robertson, P. E., Healey, A. C., & Cole, L. K. J. (2009). Reclaiming a pro-feminist orientation in Adlerian therapy. Journal of Individual Psychology, 65(1), 13–33.
Bornsheuer-Boswell, J. N., Polonyi, M. M., & Watts, R. E. (2013). Integrating Adlerian and integrated developmental model approaches to supervision of counseling trainees. The Journal of Individual Psychology, 69(4), 328–343.
Bradley, N., Stargell, N., Craigen, L., Whisenhunt, J., Campbell, E., & Kress, V. (2019). Creative approaches for promoting vulnerability in supervision: A relational-cultural approach. Journal of Creativity in Mental Health, 14(3), 391–404. https://doi.org/10.1080/15401383.2018.1562395
Byers, L. G., Bragg, J., & Munoz, R. (2020). Increasing diversity and oppression scale scores through Relational Cultural Theory. Journal of Teaching in Social Work, 40(1), 18–30.
https://doi.org/10.1080/08841233.2019.1685625
Celinska, D., & Swazo, R. (2016). Multicultural curriculum designs in counselor education programs: Enhancing counselors-in-training openness to diversity. The Journal of Counselor Preparation and Supervision, 8(3). https://doi.org/10.7729/83.1124
Chang, C. Y., & Rabess, A. (2020). Response to signature pedagogies: A framework for pedagogical foundations in counselor education: Through a multicultural and social justice competencies lens. Teaching and Supervision in Counseling, 2(2), 3. https://doi.org/10.7290/tsc020203
Chouari, A. (2016). Cultural diversity and the challenges of teaching multicultural classes in the twenty-first century. Arab World English Journal, 7(3), 3–17. https://doi.org/10.2139/ssrn.2859237
Comstock, D. L., Hammer, T. R., Strentzsch, J., Cannon, K., Parsons, J., & Salazar, G., II. (2008). Relational-cultural theory: A framework for bridging relational, multicultural, and social justice competencies. Journal of Counseling & Development, 86(3), 279–287. https://doi.org/10.1002/j.1556-6678.2008.tb00510.x
Cottone, R. R. (2012). Paradigms of counseling and psychotherapy. Smashwords.
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/forprograms/2016-cacrep-standards
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory and anti-racist politics. University of Chicago Legal Forum, 1989(1), 139–167.
Dari, T., Laux, J. M., Liu, Y., & Reynolds, J. (2019). Development of community-based participatory research competencies: A Delphi study identifying best practices in the collaborative process. The Professional Counselor, 9(1), 1–19. https://doi.org/10.15241/td.9.1.1
Davis, E. S., Norton, A., & Chapman, R. (2019). Using music for case conceptualization: Looking through an Adlerian lens. The Journal of Individual Psychology, 75(2), 156–170. https://doi.org/10.1353/jip.2019.0013
Day-Vines, N. L., Booker Ammah, B., Steen, S., & Arnold, K. M. (2018). Getting comfortable with discomfort: Preparing counselor trainees to broach racial, ethnic, and cultural factors with clients during counseling. International Journal for the Advancement of Counselling, 40(2), 89–104. https://doi.org/10.1007/s10447-017-9308-9
Dipre, K. A., & Luke, M. (2020). Relational cultural theory–informed advising in counselor education. The Professional Counselor, 10(4), 517–531. https://doi.org/10.15241/kad.10.4.517
Flasch, P., Bloom, Z. D., & Holladay, K. (2011). Self-efficacy of counselor trainees in pre-practicum: A phenomenological study. Journal of Counselor Practice, 7(1), 1–20. https://www.journalofcounselorpractice.com/uploads/6/8/9/4/68949193/flasch_et_al_vol7_iss1.pdf
Goodman, R. D., & Gorski, P. C. (Eds.). (2015). Decolonizing “multicultural” counseling through social justice. Springer.
Gorski, P. C. (2016). Making better multicultural and social justice teacher educators: A qualitative analysis of the professional learning and support needs of multicultural teacher education faculty. Multicultural Education Review, 8(3), 139–159. https://doi.org/10.1080/2005615X.2016.1164378
Gorski, P. C., & Swalwell, K. (2015). Equity literacy for all. Educational Leadership, 72(6), 34–40. http://edchange.org/publications/Equity-Literacy-for-All.pdf
Hall, B. S., Harper, I., & Korcuska, J. (2018). Exploring a relational cultural group trainee model for master’s level counseling students. Journal for Specialists in Group Work, 43(1), 81–104.
https://doi.org/10.1080/01933922.2017.1411410
Hall, K. G., Barden, S., & Conley, A. (2014). A relational-cultural framework: Emphasizing relational dynamics and multicultural skill development. The Professional Counselor, 4(1), 71–83. https://doi.org/10.15241/kgh.4.1.71
Havlik, S. A., Bialka, C., & Schneider, K. (2016). Theory to practice: Integrating service-learning into a pre-practicum introduction to school counseling course. The Journal of Counselor Preparation and Supervision, 8(2). https://doi.org/10.7729/82.1168
Hays, D. G. (2020). Multicultural and social justice counseling competency research: Opportunities for innovation. Journal of Counseling & Development, 98(3), 331–344. https://doi.org/10.1002/jcad.12327
Henfield, M. S., Woo, H., & Washington, A. (2013). A phenomenological investigation of African American counselor education students’ challenging experiences. Counselor Education and Supervision, 52(2), 122–136. https://doi.org/10.1002/j.1556-6978.2013.00033.x
Hernández-Wolfe, P. (2011). Decolonization and “mental” health: A mestiza’s journey in the borderlands. Women & Therapy, 34(3), 293–306. https://doi.org/10.1080/02703149.2011.580687
Holcomb-McCoy, C. C., & Myers, J. E. (1999). Multicultural competence and counselor training: A national survey. Journal of Counseling & Development, 77(3), 294–302. https://doi.org/10.1002/j.1556-6676.1999.tb02452.x
Hook, J. N., Davis, D. E., Owen, J., Worthington, E. L., Jr., & Utsey, S. O. (2013). Cultural humility: Measuring openness to culturally diverse clients. Journal of Counseling Psychology, 60(3), 353–366. https://doi.org/10.1037/a0032595
Ikonomopoulos, J., Cavazos Vela, J., Smith, W. D., & Dell’Aquila, J. (2016). Examining the practicum experience to increase counseling students’ self-efficacy. The Professional Counselor, 6(2), 161–173. https://doi.org/10.15241/ji.6.2.161
Jones, C. T., Welfare, L. E., Melchior, S., & Cash, R. M. (2019). Broaching as a strategy for intercultural understanding in clinical supervision. The Clinical Supervisor, 38(1), 1–16.
https://doi.org/10.1080/07325223.2018.1560384
Jordan, J. V. (2010). Relational-cultural therapy (1st ed.). American Psychological Association.
Jordan, J. V. (2018). Relational-cultural therapy (2nd ed.). American Psychological Association.
Killian, T., & Floren, M. (2020). Exploring the relationship between pedagogy and counselor trainees’ multicultural and social justice competence. Journal of Counseling & Development, 98(3), 295–307. https://doi.org/10.1002/jcad.12324
Kim, B. S. K. (2011). Client motivation and multicultural counseling. The Counseling Psychologist, 39(2), 267–275. https://doi.org/10.1177/0011000010375310
Lee, C. C. (2019). Multicultural issues in counseling: New approaches to diversity (5th ed.). American Counseling Association.
Lee, K. A., & Kelley-Petersen, D. J. (2018). Service learning in human development: Promoting social justice perspectives in counseling. The Professional Counselor, 8(2), 146–158. https://doi.org/10.15241/kal.8.2.146
Lee, K. A., & McAdams, C. R., III. (2019). Using service-learning to promote social justice advocacy and cognitive development during internship. The Journal of Counselor Preparation and Supervision, 12(1). https://repository.wcsu.edu/jcps/vol12/iss1/8
Lertora, I. M., Croffie, A., Dorn-Medeiros, C., & Christensen, J. (2020). Using relational cultural theory as a pedagogical approach for counselor education. Journal of Creativity in Mental Health, 15(2), 265–276. https://doi.org/10.1080/15401383.2019.1687059
Lewis, C., & Olshansky, E. (2016). Relational-cultural theory as a framework for mentoring in academia: Toward diversity and growth-fostering collaborative scholarly relationships. Mentoring & Tutoring: Partnership in Learning, 24(5), 383–398. https://doi.org/10.1080/13611267.2016.1275390
McGee Banks, C. A., & Banks, J. A. (1995). Equity pedagogy: An essential component of multicultural education. Theory Into Practice, 34(3), 152–158. https://doi.org/10.1080/00405849509543674
Miller, J. B. (1976). Toward a new psychology of women. Beacon Press.
Miller, J. B., & Stiver, I. P. (1997). The healing connection: How women form relationships in therapy and in life. Beacon Press.
Miller, R., & Taylor, D. D. (2016). Does Adlerian theory stand the test of time?: Examining individual psychology from a neuroscience perspective. The Journal of Humanistic Counseling, 55(2), 111–128. https://doi.org/10.1002/johc.12028
Morgan Consoli, M. L., & Marin, P. (2016). Teaching diversity in the graduate classroom: The instructor, the students, the classroom, or all of the above? Journal of Diversity in Higher Education, 9(2), 143–157. https://doi.org/10.1037/a0039716
Pedersen, P. B., Crethar, H. C., & Carlson, J. (2008). Inclusive cultural empathy: Making relationships central in counseling and psychotherapy. American Psychological Association.
Pieterse, A. L., Evans, S. A., Risner-Butner, A., Collins, N. M., & Mason, L. B. (2009). Multicultural competence and social justice training in counseling psychology and counselor education: A review and analysis of a sample of multicultural course syllabi. Counseling Psychologist, 37(1), 93–115. https://doi.org/10.1177/0011000008319986
Priester, P. E., Jones, J. E., Jackson-Bailey, C. M., Jana-Masri, A., Jordan, E. X., & Metz, A. J. (2008). An analysis of content and instructional strategies in multicultural counseling courses. Journal of Multicultural Counseling and Development, 36(1), 29–39. https://doi.org/10.1002/j.2161-1912.2008.tb00067.x
Pryor, D. B., & Tollerud, T. R. (1999). Applications of Adlerian principles in school settings. Professional School Counseling, 2(4), 299–304.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and Social Justice Counseling Competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Sanchez Bengoa, D., Ganassali, S., Kaufmann, H. R., Rajala, A., Trevisan, I., van Berkel, J., Zulauf, K., & Wagner, R. (2018). Shared experiences and awareness from learning in a student multicultural environment: Measuring skills’ development in intercultural intensive programs. Journal of International Education in Business, 11(1), 27–42.
https://doi.org/10.1108/JIEB-01-2017-0006
Schmidt, S. W., Glass, J. S., & Wooten, P. (2011). School counselor preparedness: Examining cultural competence regarding gay, lesbian, and bisexual issues. Journal of School Counseling, 9(11). https://files.eric.ed.gov/fulltext/EJ933177.pdf
Schwartz, H. L. (2019). Connected teaching: Relationship, power, and mattering in higher education. Stylus.
Seward, D. X. (2014). Multicultural course pedagogy: Experiences of master’s-level students of color. Counselor Education and Supervision, 53(1), 62–79.
https://doi.org/10.1002/j.1556-6978.2014.00049.x
Shelton, R. (2020). A qualitative study on understanding entry-level professional counselors experience developing and implementing multicultural and social justice advocacy competencies in professional practice (Publication No. 28259670) [Doctoral dissertation, Capella University]. ProQuest Dissertations and Theses Global.
Sheperis, D. S., Coker, J. K., Haag, E., & Salem-Pease, F. (2020). Online counselor education: A student–faculty collaboration. The Professional Counselor, 10(1), 133–143. https://doi.org/10.15241/dss.10.1.133
Singh, A. A., Appling, B., & Trepal, H. (2020). Using the Multicultural and Social Justice Counseling Competencies to decolonize counseling practice: The important roles of theory, power, and action. Journal of Counseling & Development, 98(3), 261–271. https://doi.org/10.1002/jcad.12321
Soheili, F., Alizadeh, H., Murphy, J. M., Bajestani, H. S., & Ferguson, E. D. (2015). Teachers as leaders: The impact of Adler-Dreikurs classroom management techniques on students’ perceptions of the classroom environment and on academic achievement. The Journal of Individual Psychology, 71(4), 440–461. https://doi.org/10.1353/jip.2015.0037
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Multicultural Counseling and Development, 20(2), 64–88. https://doi.org/10.1002/j.2161-1912.1992.tb00563.x
Swank, J. M., & Houseknecht, A. (2019). Teaching competencies in counselor education: A Delphi study. Counselor Education and Supervision, 58(3), 162–176. https://doi.org/10.1002/ceas.12148
Trahan, D. P., Jr., & Keim, J. (2019). Counselor educators’ teaching practices in contemporary society. The Journal of Counselor Preparation and Supervision, 12(3). https://repository.wcsu.edu/jcps/vol12/iss3/1
Uzunboylu, H., & Altay, O. (2021). State of affairs in multicultural education research: A content analysis. Compare: A Journal of Comparative and International Education, 51(2), 1–20.
https://doi.org/10.1080/03057925.2019.1622408
Villalba, J. A., & Redmond, R. E. (2008). Crash: Using a popular film as an experiential learning activity in a multicultural counseling course. Counselor Education and Supervision, 47(4), 264–276. https://doi.org/10.1002/j.1556-6978.2008.tb00056.x
Wagner, T. M. (2015). Addressing multicultural issues in the counselor education classroom: A phenomenological analysis [Doctoral dissertation, University of North Texas]. https://digital.library.unt.edu/ark:/67531/metadc822760
Walker, S. (2015). Relationship-based teaching: A relational ethics led approach to teaching social work. Ethics and Social Welfare, 9(4), 394–402. https://doi.org/10.1080/17496535.2015.1088703
Watts, R. E. (2003). Adlerian therapy as a relational constructivist approach. The Family Journal: Counseling and Therapy for Couples and Families, 11(2), 139–147. https://doi.org/10.1177/1066480702250169
Watts, R. E. (2013). Adlerian Counseling. In B. J. Irby, G. Brown, R. Lara-Alecio, & S. Jackson (Eds.), The handbook of educational theories (pp. 459–472). IAP: Information Age Publishing.
Yee, T. T. L., Stevens, C. R., & Schulz, L. L. (2016). Exploring master’s students’ social justice consciousness through experiential group: An Adlerian approach. The Journal of Individual Psychology, 72(2), 90–103. https://doi.org/10.1353/jip.2016.0008
Ziomek-Daigle, J., Goodman-Scott, E., Cavin, J., & Donohue, P. (2016). Integrating a multi-tiered system of supports with comprehensive school counseling programs. The Professional Counselor, 6(3), 220–232. https://doi.org/10.15241/jzd.6.3.220
Taylor Irvine, MEd, EdS, LMHC, is a doctoral candidate at Florida Atlantic University. Adriana Labarta, MEd, EdS, LMHC, is a doctoral candidate at Florida Atlantic University. Kelly Emelianchik-Key, PhD, NCC, ACS, LMHC, LMFT, is an associate professor at Florida Atlantic University. Correspondence may be addressed to Taylor Irvine, Florida Atlantic University, 777 Glades Rd. [ED 47], Rm. 271, Boca Raton, FL 33431, tirvine1@fau.edu.
Apr 1, 2021 | Volume 11 - Issue 2
Stacey Diane Arañez Litam, Seungbin Oh, Catherine Chang
This exploratory study examined the extent to which coping, resilience, experiences of subtle and blatant racism, and ethnic identity predicted stress-related growth in a national convenience sample of Asians and Asian Americans and Pacific Islanders (AAPIs; N = 326) who experienced COVID-19–related racial discrimination. Our analysis indicated participants with higher levels of coping, resilience, experiences of subtle and blatant racism, and ethnic identity were significantly more likely to cultivate higher levels of stress-related growth. Coping strategies such as self-blame, religion, humor, venting, substance use, denial, and behavioral disengagement significantly moderated the relationship between experiences of racism and stress-related growth. Notably, participants in the study who used mental health services following COVID-19 reported significantly higher levels of racial discrimination, resilience, coping, and stress-related growth compared to Asians and AAPIs who did not use professional mental health services. Mental health professionals are called to utilize culturally sensitive treatment modalities and challenge traditional Western notions that frame coping responses from an individualistic worldview.
Keywords: Asian, Asian American, COVID-19, racial discrimination, stress-related growth
Asians and Asian Americans and Pacific Islanders (AAPIs) represent vulnerable ethnic groups that may present with higher rates of mental health distress during COVID-19. Following the global outbreak, rates of discrimination, harassment, and violence toward Asians and AAPIs have substantially increased (Congressional Asian Pacific American Caucus, 2020; Jeung & Nham, 2020). The rise of COVID-19–fueled racism directed toward Asians and AAPI groups, especially individuals who phenotypically appear East Asian, has deleterious effects on their mental health and wellness (Litam, 2020; Litam & Oh, in press, 2020; Wen et al., 2020).
Although Asians who reside in the United States and AAPI groups are both affected by COVID-19–related racial discrimination, mental health professionals must recognize the important distinctions and challenges that exist between Asian internationals and Asian Americans (Anandavalli et al., 2020; Sue et al., 2019). Professional counselors must also consider the vast heterogeneity that characterizes Asian and AAPI ethnic subgroups (Budiman & Ruiz, 2021; Chan & Litam, 2021). Although an extensive overview of the differences between Asians and AAPI ethnic subgroups was beyond the purview of this study, mental health professionals are called to examine how the intersection of client identities (e.g., international status, nationality, ethnic identity, acculturative status, colonization history) may influence the ways in which COVID-19 racial discrimination affects Asian and AAPI clients (Chan & Litam, 2021; Litam, 2020). For the purpose of contributing to the scant literature on the effects of COVID-19 on Asian and AAPI communities, the current study assesses a national convenience sample of Asians and AAPI groups who reported discrimination experiences following the pandemic. Aggregating these distinct populations was not intended to overlook the vast heterogeneity that exists across ethnic subgroups nor to invalidate the unique challenges faced by Asian and AAPI individuals who reside in the United States. Rather, the present study combined Asian and AAPI populations to ascertain a more collective understanding of the ways in which the greater community may be affected by COVID-19–related racial discrimination.
Effects of Racial Discrimination on Asian and AAPI Mental Health
Extant research illuminated how perceived racial discrimination among Asian and AAPI communities has adverse effects on overall mental health, coping responses, and wellness. Asians and AAPIs who faced race-based discrimination reported higher levels of psychological distress, substance use, anxiety, depression, and suicidal ideation (Choi et al., 2020; Gee et al., 2007; Hwang & Goto, 2008; Le & Ahn, 2011; Leong et al., 2013). Experiences of race-related stress in Asians and AAPIs were also associated with negative outcomes related to well-being (Iwamoto & Liu, 2010; Mossakowski, 2003), self-esteem (Liang & Fassinger, 2008), and social connectedness (Wei et al., 2012). Although the importance of understanding the effects of COVID-19–related racial discrimination on the mental health of Asians and AAPIs has been established (Asmundson & Taylor, 2020; Chan & Litam, 2021; Litam, 2020), a paucity of empirical investigations examines the mental health effects of pandemic-related discrimination among Asians and AAPIs across the life span (Litam & Oh, in press).
Ethnic Identity
Ethnic identity is the quality of an individual’s affiliation with their ethnic group and includes a sense of belongingness, self-identification, and attitudes toward one’s group (Phinney, 1990). Phinney (1992) outlined four developmental stages based on high and low levels of exploration and commitment. Whereas exploration includes activities and behaviors undertaken to understand the role of one’s ethnicity or race in one’s identity, commitment refers to the affirmation, sense of connection, and clarity about how one’s ethnic or racial identity fits into one’s life and self-concept (Phinney, 1992). Taken together, the two dimensions of exploration and commitment form four statuses of ethnic and/or racial identity development: diffused (low exploration, low commitment), foreclosed (low exploration, high commitment), moratorium (high exploration, low commitment), and achieved (high exploration, high commitment; Erikson, 1968).
The mixed effect of ethnic identity in the relationship between racial discrimination experiences and well-being has been noted across earlier studies. On one hand, existing research has noted that Asians and AAPIs who cultivated strong ethnic identities were more likely to maintain a positive sense of psychological well-being, reported a greater sense of belongingness to their ethnic communities, and responded with greater resilience when racial discrimination occurred (Lee, 2003; Lee & Davis, 2000; Lee & Yoo, 2004; Litam & Oh, in press; Phinney, 2003; Yip & Fuligni, 2002). In the United States, AAPIs with a strong sense of ethnic identity reported a better quality of life and greater levels of spousal support and harmony (Lieber et al., 2001). In one study with 187 Chinese and Chinese Americans, strong ethnic identity moderated the relationship between experiences of COVID-19 discrimination and levels of depression (Litam & Oh, 2020). Levels of exploration and commitment may additionally influence whether ethnic identity buffers or exacerbates well-being among Asians and AAPIs who experience racial discrimination. According to a meta-analysis of 51 studies, Yip and colleagues (2019) asserted that individuals high in exploration reported more negative mental health and riskier health behavior outcomes following experiences of racial discrimination. Conversely, ethnic identity was a protective factor for individuals with high levels of commitment following racial discrimination (Yip et al., 2019).
The moderating effects of ethnic identity on Asian and AAPI mental health may be framed within the context of social identity theory (Tajfel & Turner, 1979) and self-categorization theory (Turner et al., 1987). According to social identity theory (Tajfel & Turner, 1979), individuals are members of many social groups with whom they may identify (e.g., religion, race, ethnicity, gender). Once individuals have determined their social identities, they become invested in maintaining and enhancing their self-concept (Tajfel & Turner, 1979). Social identity theory therefore predicts that individuals who center their identities are better equipped to cope with identity threats to protect their overall self-concept (Tajfel & Turner, 1979). Through the lens of this theory, individuals who strongly identify with their Asian or AAPI identities may be better positioned to engage in coping strategies that buffer the harmful impact of ethnic or racial discrimination.
Self-categorization theory builds on social identity theory by recognizing that individuals can identify with several social groups simultaneously and that some social identities become more psychologically salient than others (Turner et al., 1987). When ethnic identity becomes salient and represents an important component of one’s identity, self-categorization theory predicts that ethnic and racial discrimination will have a stronger negative impact on mental health and wellness outcomes (Turner et al., 1987). Taken together, social categorization theory predicts that positive feelings toward one’s ethnic group may heighten awareness to ethnic discrimination, which may exacerbate the harmful effects of ethnic or racial discrimination (Lee, 2005), whereas social identity theory posits that high regard for one’s ethnic identity may result in a buffering effect to the deleterious effects of racial discrimination (Yip et al., 2019).
Resilience
Resilience refers to the “personal qualities that enable one to thrive in the face of adversity” (Connor & Davidson, 2003, p. 76). Although responding with resilience in times of stress has been reported across diverse AAPI subgroups, various ethnic groups may conceptualize resilience in unique ways. As a coping strategy, resilience is not limited to how one responds to challenges but also encompasses strategies for goal achievement. For example, Hmong women demonstrated resilience in career development by adopting positive perspectives, focusing on goal achievement, and reflecting on ways to continue improving (Yang, 2014). In another study, Chinese immigrants demonstrated fortitude through the immigration process and continued to thrive in the United States despite living in poverty in a California Chinatown community (Cheng, 2013). Resilience, therefore, consists of a stress response and an enduring phenomenon. Resilience may be fostered through the presence of social support, especially among family members (Lim & Ashing-Giwa, 2013), through the promotion of cultural understanding (i.e., cultivating ethnic identity), engaging in meaningful activities, and developing mental toughness (i.e., resilience; Kim & Kim, 2013).
Coping and Stress Responses
Individuals evaluate racial discrimination experiences and cope with stressors differently based on their cultural values and beliefs (Lazarus & Folkman, 1984; Tweed & Conway, 2006). Asians and AAPIs who endorse higher levels of ethnic identity may be more likely to employ coping strategies that align with culturally embedded values (Miller & Kaiser, 2001; Miller & Major, 2000). These cultural values may assert the importance of adjusting one’s feelings to fit their environment, accepting rather than confronting problems, preserving social harmony, avoiding problem disclosure (Inman & Yeh, 2007; Tweed & Conway, 2006; Yeh et al., 2006), and evading conflict to preserve interpersonal relationships (Noh & Kaspar, 2003). These passive forms of coping may be problematic, as avoidant and emotion-focused responses may contribute to poorer mental health outcomes in AAPIs.
Other culturally congruent coping responses such as social isolation, which protects the user by avoiding the stressor (Edwards & Romero, 2008); self-blame or criticizing oneself, which maintains interpersonal harmony (Wei et al., 2010); and substance use (Pokhrel & Herzog, 2014), which momentarily helps one evade problems or adjust one’s feelings to the environment, may also be preferred by Asians and AAPIs. Following stressful events, social isolation has been strongly linked to increased symptoms of depression and anxiety, decreased feelings of self-worth, and lower levels of life satisfaction (Cacioppo & Hawkley, 2003; Cacioppo et al., 2002).
Stress-Related Growth
Individuals may respond to stressful life events, transitions, and traumatic experiences with positive psychological changes (Park et al., 1996; Tedeschi & Calhoun, 2004). Researchers posit that coping strategies (Helgeson et al., 2006; Janoff-Bulman, 2004; Tedeschi & Calhoun, 2004), higher levels of self-esteem, positive spiritual changes, and increased social support (Linley & Joseph, 2004; Tedeschi & Calhoun, 1995, 2004) may arise following experiences of stress. According to Tedeschi and Calhoun (1996, 2004), examples of stress-related growth may include pursuing new possibilities, having a greater appreciation for life, cultivating meaningful relationships, enhancing spiritual growth, and developing personal strengths. A meta-analysis of 103 studies identified the presence of coping strategies, cognitive reappraisal, religion, optimism, and social support as significant predictors for stress-related growth (Prati & Pietrantoni, 2009). A qualitative study with Korean immigrants indicated the use of coping strategies was a predictor for stress-related growth (Kim & Kim, 2013).
Tedeschi and Calhoun (1996, 2004) conceptualized stress-related growth as both a long-term outcome and a process. For instance, stress-related growth has been conceptualized as a coping strategy following traumatic events (Nolen-Hoeksema & Davis, 2004) and may occur as the result of ongoing medical conditions such as cancer (Cordova et al., 2017) and chronic pain (Rzeszutek & Gruszczyńska, 2018), wherein traumatic experiences are not time-limited. Thus, stress-related growth may result from the ongoing process of awareness, adaptation, and concern related to medical, psychological, and social consequences associated with the conditions of living (Edmondson et al., 2011). Given the precedence of emerging research that measures stress-related growth during COVID-19 (Vasquez et al., 2021), stress-related growth was included as an outcome variable in our study. This variable was of particular interest because research remains forthcoming on the contributing factors to stress-related growth among Asians and AAPIs following experiences of stress related to COVID-19.
The call to identify moderators of mental health in Asian and AAPI communities following racial discrimination has been established (Litam, 2020; Litam & Oh, in press; Nadal et al., 2015; Wong et al., 2014). It is of paramount importance to identify race-related response strategies to develop culturally sensitive and effective counseling interventions (Chan & Litam, 2021; Frazier et al., 2004; Litam & Hipolito-Delgado, 2021). The relationship between COVID-19–fueled racial discrimination, ethnic identity, resilience, and coping responses in Asian and AAPI populations remains to be seen and necessitates special consideration for mental health professionals. Understanding this relationship is crucial when considering how Asians and AAPIs tend to avoid health care services (DeVitre & Pan, 2020; Sue et al., 2019). To address this paucity of literature, this study was undertaken to examine the following research questions:
- To what extent do coping, resilience, experience of racism, and ethnic identity predict stress-related growth following COVID-19?
- To what extent does coping moderate experiences of COVID-19–related racism and stress-related growth?
- To what extent does resilience moderate experiences of COVID-19–related racism and stress-related growth?
Method
Participants
Data was collected from June to July 2020. A total of 409 Asian and AAPI individuals were recruited through AAPI listservs and community organizations (n = 10) and Amazon MTurk (n = 399). Sixty-eight respondents from Amazon MTurk completed less than 50% of the survey items, so their associated surveys were removed from the data. An additional 11 respondents from Amazon MTurk endorsed all survey items with the same response or incorrectly answered validity items, and their surveys were also eliminated from the data. Lastly, four multivariate outliers were removed (i.e., Mahalanobis distance value > 20.515 at a = .001), resulting in a final sample of 326 cases (79.7% useable response rate). The final sample (N = 326) met sufficient sample size for hierarchical multiple regression (N > 94) and a path analysis (N > 134; O’Rourke & Hatcher, 2013) at a = .01 to identify medium effect size.
Table 1
Descriptive Characteristics and Correlations
| Characteristic |
Frequency |
% |
| Gender |
|
|
| Male |
225 |
69.0% |
| Female |
101 |
31.0% |
| Education Level |
|
|
| High School Diploma or the equivalent |
6 |
1.8% |
| Associate Degree |
6 |
1.8% |
| Bachelor’s Degree |
205 |
62.9% |
| Master’s Degree |
95 |
29.1% |
| Doctorate Degree |
14 |
4.3% |
| Sexual Identity |
|
|
| Heterosexual |
220 |
67.5% |
| Gay or Lesbian |
9 |
2.8% |
| Bisexual, Pansexual, or Non-Monosexual |
91 |
27.9% |
| Other |
6 |
1.8% |
| Seeking Mental Health Service Since COVID-19 |
|
|
| Yes |
153 |
46.9% |
| No |
149 |
45.7% |
| No, but I have considered it |
24 |
7.4% |
|
|
|
|
|
|
|
|
|
| Variable |
a |
M |
SD |
1 |
2 |
3 |
4 |
5 |
| SBRS |
.91 |
27.48 |
7.28 |
– |
|
|
|
|
| SRGS |
.95 |
77.05 |
15.09 |
.510** |
– |
|
|
|
| MEIM |
.61 |
22.56 |
3.20 |
.437** |
.429** |
– |
|
|
| Resilience |
.95 |
134.92 |
20.97 |
.301** |
.703** |
.436** |
– |
|
| Coping |
.92 |
79.05 |
13.10 |
.662** |
.699** |
.521** |
.518** |
– |
|
|
|
|
|
|
|
|
|
|
|
Note. SBRS = Subtle and Blatant Racism Scale; SRG = Stress-Related Growth Scale; MEIM = Multigroup
Ethnic Identity Measure.
**p < .01
Table 1 presents details regarding descriptive characteristics of participants in this study. The average age of Asian and AAPI participants was 33.79 years (SD = 9.19), ranging from 18 to 72 years. The majority of participants identified as male (69.0%, n = 225), and a smaller group identified as female (31%; n = 101). Most participants reported having an international status (72.7%, n = 237), whereas 27.3% of participants (n = 89) identified as an American citizen or permanent U.S. resident. For one item, “Have you sought professional mental health counseling services since COVID-19?” approximately half of the participants (46.9%, n = 153) selected “Yes,” a total of 150 participants (45.7%) selected “No,” and a total of 24 participants (7.4%) indicated “No, but I’ve considered it.”
Procedures
IRB approval from relevant universities was obtained prior to data collection. Potential participants were recruited using non-probability convenience sampling with inclusion criteria. Participants who (a) self-identified as Asian or Asian American, (b) resided in the United States, and (c) had either directly or indirectly experienced COVID-19–related racism were able to participate in the study. Participants from the MTurk obtained $0.50 as an incentive for their completion of the survey. To ensure the quality of data, the survey included two validity items that asked participants to choose specific response options. Participants who chose incorrect responses were automatically excluded from participation in the survey.
Measures
Demographics and Background Form
A demographics/background information form was created to gather information regarding participants’ age, gender, highest level of education, race/ethnicity, sexual identity, income level, occupation, international status, religion, and generational status. Additional survey items assessed English proficiency and how rates of discrimination evidenced through verbal, covert, online, and physical harassment may have changed following COVID-19. Participants were provided with the option to input text describing additional forms of racial discrimination experienced since COVID-19.
Multigroup Ethnic Identity Measure – Revised (MEIM-R)
The Multigroup Ethnic Identity Measure (MEIM; Phinney, 1992) is a 14-item scale that assesses three aspects of ethnic identity: positive ethnic attitudes and a sense of belonging (five items), ethnic identity achievement (seven items), and ethnic behaviors or practices (two items). The measure is scored by reversing negatively worded items, summing the scores across each item, and obtaining the mean. Scores range from 4 (high ethnic identity) to 1 (low ethnic identity). Overall reliability was .90 in a college sample, and the results of a principal axis factor analysis using squared multiple correlations supported the presence of two factors, ethnic identity and other-group group orientation, accounting for 30.8% and 11.4% in college samples, respectively (Phinney, 1992). The MEIM was shortened into a six-item scale that measures two subscales, Identity Exploration and Identity Commitment (MEIM-R; Brown et al., 2014). Example items include “I have spent time trying to find out more about my own ethnic group, such as its history, traditions, and customs” and “I think a lot about how my life will be affected by my ethnic group membership.” The MEIM-R demonstrated adequate internal consistency for the overall scale and two subscales with all Cronbach alpha values near or above .70 (Brown et al., 2014). Based on the results of multiple-groups confirmatory factor analyses, the MEIM-R demonstrated evidence of measurement invariance, had good psychometric properties, and is an appropriate measure of ethnic identity across diverse Asian subgroups (Brown et al., 2014).
Resilience Scale (RS)
The Resilience Scale (RS; Wagnild & Young, 1993) is a 25-item measure that uses a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). Example items include “I usually manage one way or another” and “I feel that I can handle many things at a time.” The RS demonstrated a coefficient alpha of .91 with item-to-total correlations ranging from .37 to .75. The concurrent validity of the RS was also robust and was strongly associated with measures of life satisfaction, morale, and depression. The results of a factor analysis indicated the RS is a reliable measure that demonstrated good internal consistency reliability, concurrent validity, and preliminary construct validity (Wagnild & Young, 1993).
Subtle and Blatant Racism Scale for Asian Americans Revised (SABRA-A2)
The Subtle and Blatant Racism Scale for Asian Americans Revised (SABRA-A2; Yoo et al., 2010) is an 8-item measure that uses a 5-point Likert-type scale from 1 (almost never) to 5 (almost always) to assess the presence of subtle and blatant forms of racial discrimination. The total score is obtained by summing the responses across each of the items, with higher scores indicating greater perceived racism. Example items include “In America, I am faced with barriers in society because I’m Asian” and “In America, I have been physically assaulted because I’m Asian.” Support for the two-subscale structure was confirmed through an exploratory and confirmatory factor analysis with evidence of good internal reliability and stability over 2 weeks (Yoo et al., 2010). The SABRA-A2 also demonstrated good discriminant validity as evidenced by no correlations with color-blind racial attitudes (Yoo et al., 2010).
Brief COPE
The Brief COPE (Carver, 1997) is a 28-item measure and uses a 4-item Likert-type scale to measure the extent to which participants report using various coping strategies. The measurement has 14 subscales that include two items each. Available responses are 1 (I haven’t been doing this at all), 2 (I’ve been doing this a little bit), 3 (I’ve been doing this a medium amount), and 4 (I’ve been doing this a lot). Example items include “I’ve been concentrating my efforts on doing something about the situation I’m in” and “I’ve been criticizing myself.” The Brief COPE has demonstrated acceptable psychometric properties and has been used with Asian populations (Sue et al., 2019). Cronbach’s alpha for the entire scale is .92 in the current study. Cronbach’s alpha for each of the 14 subscales ranged from .34 to .65. Given the poor reliability for the subscales, the present study utilized the total score for the entire scale.
Stress-Related Growth Scale Revised (SRGS-R)
The Stress-Related Growth Scale Revised (SRGS-R; Boals & Schuler, 2018), is a 15-item measure that assesses the extent to which participants experience change following a negative event. The scale uses a bipolar 7-point Likert-type scale from −3 (a very negative change) to +3 (a very positive change), and example items include “I experienced a change in the extent to which I listen when others talk to me” and “I experienced a change in my belief that I have something of value to teach others about life.” The SRGS-R demonstrated acceptable measures of convergent validity and stronger associations with outcome measures of mental health, including depression, anxiety, global distress, and post-traumatic symptoms (Boals & Schuler, 2018). Compared to other measures, the SRGS-R may be a more accurate measure for human resiliency as evidenced by the neutral wording of each item and the inclusion of items that avoid measuring illusory growth (Boals & Schuler, 2018).
Data Diagnostics
Examining the proportion of missing data indicated that 88% of participants reported no missing values, and 83% of the items were not missing data for any case. The proportion of missing data for the rest of the 17% of the items ranged from 2.7% to 16.8%. The degree and pattern of missing data were examined to determine whether data were missing at random. A matrix of the estimated means with each pattern yielded no particular patterns nor severe degree of missing data, which supported evidence for proceeding with missing data replacement techniques. Missing data points were populated using multiple imputation (MI), a method to allocate missing data without causing inflated bias even when there is a large portion of missingness in the data (Osborn, 2013).
Next, the assumptions of normality, linearity, homoscedasticity, and multicollinearity were tested. The residuals were linear and did not deviate from normality as evidenced by the residuals lying reasonably in a straight, diagonal line. The assumption of homoscedasticity was also supported, as most of the residuals were concentrated along the zero point. All variance inflation factor (VIF) values were less than 10 and tolerance values were greater than .1, indicating absence of multicollinearity (Tabachnick & Fidell, 2019). Therefore, the data were deemed appropriate for hierarchical regression and path analysis (Tabachnick & Fidell, 2019).
Analytic Strategy
Hierarchical regression models of stress-related growth were employed using SPSS version 27. First, gender, age, education status, sexual identity, and help-seeking experience were entered in Model 1 as the control variables. In Model 2, the first independent variable of subtle and blatant racism was added. In Model 3, the second independent variable of ethnic identity was entered. Finally, the remaining two independent variables of resilience and coping strategy were added as key predictors that may function as potential moderators in Model 4.
To examine potential moderating roles of resilience and coping strategy in the relationship between racism and stress-related growth, Hayes’ (2018) PROCESS macro version 3.5 was conducted. Specifically, 10,000 bootstrapping resampling was conducted to produce 95% percentile confidence intervals (CIs) for the moderating effect. If the CIs excluded zero, moderating effect was considered to be significant. Furthermore, the moderating effects were examined utilizing three conditional values of moderators (Hayes, 2018; Preacher et al., 2017), which included low (the mean score of the moderator −1 SD), moderate (the mean score), and high values (the mean score of the moderator +1 SD). Bodner’s (2017) formula was used to calculate effect size across moderator values. All predictors and moderators were mean-centered for more meaningful interpretation of moderating effect (Hayes, 2018).
Results
Preliminary Analyses
Descriptive characteristics are found in Table 1. Male and female participants reported similar mean scores on all measurements, except the SABRA-A2. Female participants reported experiencing significantly higher levels of racism (M = 29.10, SD = 6.25) than their male counterparts (M = 26.75, SD = 7.59), with a small effect size (d = 0.34; Cohen, 1998). Participants who had sought mental health services since COVID-19 reported significantly higher resilience scores (M = 138.78, SD = 20.59), experiences of subtle and blatant racism (M = 29.99, SD = 6.38), coping strategy (M = 84.34, SD = 12.61), and stress-related growth (M = 81.13, SD = 14.25) than participants who either did not seek professional mental health services or who considered seeking services, but had not used them.
Correlations
Correlational analyses among all study variables were conducted. Table 1 presents the correlations among the predictive and outcome variables assessed in the study as well as the mean and standard deviations for each variable and internal reliability for each measurement. As expected, ethnic identity, resilience, coping strategy, and stress-related growth were positively and moderately correlated with each other. Interestingly, subtle and blatant racism were also positively related to ethic identity, resilience, coping, and stress-related growth.
Hierarchical Regression Analyses
Results from the hierarchical regression analyses are provided in Table 2. The control variables of gender, age, education status, sexual identity, and help-seeking experience were examined in Model 1. Among the control variables, education status, sexual identity, and help-seeking experiences were significantly associated with stress-related growth for Asians and AAPIs. Specifically, participants who had earned a master’s degree or higher and identified as heterosexual had significantly lower scores of stress-related growth compared to those who did not identify as heterosexual. Moreover, participants who sought mental health services following the COVID-19 outbreak reported significantly higher scores of overall stress-related growth compared to those who did not use professional mental health services. Model 1 accounted for 11.6% of the variance in stress-related growth.
The direct effects of subtle and blatant racism on stress-related growth were examined in Model 2. Subtle and blatant racism had a significantly positive relationship with stress-related growth among Asians and AAPIs (β = .456, p < .001) after controlling for gender, age, education, sexual identity, and help-seeking experience. Thus, higher levels of subtle and blatant racism were correlated with higher levels of stress-related growth. Among the control variables, only education status was found to be significantly associated with stress-related growth. Model 2 explained 28.8% of the variance in stress-related growth. The addition of subtle and blatant racism accounted for a 17.2% increase in the explained variance in stress-related growth, which was deemed a medium effect size (Cohen, 1998).
Ethnic identity was added in Model 3. Results indicated that ethnic identity was significantly positively associated with stress-related growth for Asians and AAPIs (β = .244, p < .001) after controlling for gender, age, education, sexual identity, and help-seeking experience. Based on these results, participants in the study who endorsed stronger levels of ethnic identity were more likely to cultivate higher levels of stress-related growth. Model 3 accounted for 33.5% of the variance in stress-related growth. The addition of ethnic identity explained 4.7% of increase in the variance of stress-related growth.
Resilience and coping strategy were added and analyzed in Model 4. Both resilience and coping strategy had significantly positive associations with stress-related growth for Asians and AAPIs after controlling for gender, age, education, sexual identity, and help-seeking experience. Specifically, Asians and AAPIs who had higher levels of resilience and higher levels of coping strategy were more likely to develop higher levels of stress-related growth. Model 4 explained 66.2% of the variance in stress-related growth. The addition of resilience and coping strategy accounted for a 32.7% increase in the explained variance in stress-related growth, which represented a large effect size (Cohen, 1998).
Moderating Effect of Resilience and Coping Strategy
To examine the moderating effect of resilience and coping strategy, Hayes’ (2018) PROCESS macro (Model 1) was employed using 10,000 bootstrapping resamples. As shown in Table 3, coping strategy was significantly positively related to the slope of subtle and blatant racism on stress-related growth
(β = .017, p < .001). Based on these results, coping strategy significantly moderated (i.e., strengthened) the positive link between racism and stress-related growth. As the moderator, coping strategy explained 1.4% of the total variance (51.2%) in stress-related growth, yielding a small effect size (Cohen, 1998). The nature of the moderating effect is presented in the simple slope analyses (Figure 1). Subtle and blatant racism had a significant effect on the development of stress-related growth for Asians and AAPIs with higher levels of coping strategy (+1 SD; b = .468, 95% CI [.169, .767]), but the significant effect did not hold for those with lower levels of coping strategy (−1 SD; b = .017, 95% CI [−.224, .257]). A +2 SD increase in resilience yielded less than .001 change in the conditional effect on stress-related growth, which was small in magnitude (Bodner, 2017). Thus, resilience did not significantly moderate the link between racism and stress-related growth.
Table 2
Results From Hierarchical Multiple Regression and Moderated Path Analysis
|
Model 1 |
Model 2 |
Model 3 |
Model 4 |
| Variables |
Β (S.E.) |
β |
Β (S.E.) |
β |
Β (S.E.) |
β |
Β (S.E.) |
β |
| Gender
Female (ref) |
|
|
|
|
|
|
|
|
| Male |
−1.668
(1.718) |
−.051 |
.187
(1.559) |
.006 |
−.036
(1.510) |
−.001 |
−1.831
(1.085) |
−.056 |
| Age
> 34 (ref) |
|
|
|
|
|
|
|
|
| ≤ 34 |
−1.205
(1.623) |
−.039 |
−2.059
(1.462) |
−.067 |
−2.287
(1.417) |
−.074 |
.397
(1.027) |
.013 |
| Education
≤ Bachelor (ref) |
|
|
|
|
|
|
|
|
| ≥ Master |
−5.017
(1.698) |
−.157** |
−3.470
(1.537) |
−.109* |
−2.249
(1.510) |
−.070 |
.320
(1.090) |
.010 |
| Sexual Identity
Non-hetero (ref) |
|
|
|
|
|
|
|
|
| Heterosexuality |
−4.479
(1.697) |
−.139** |
−1.721
(1.557) |
−.109 |
−1.621
(1.508) |
−.050 |
−1.512
(1.090) |
−.047 |
| Help-Seeking
No (ref) |
|
|
|
|
|
|
|
|
| Yes |
6.796
(1.605) |
.225*** |
2.691
(1.517) |
.089 |
2.880
(1.469) |
.095 |
.452
(1.065) |
.015 |
| SBRS |
|
|
.947
(.108) |
.456*** |
.734
(.114) |
.354*** |
.220
(.095) |
.106* |
| MEIM |
|
|
|
|
1.152
(.243) |
.244*** |
−.172
(.190) |
−.037 |
| Resilience |
|
|
|
|
|
|
.357
(.029) |
.496*** |
| Coping |
|
|
|
|
|
|
.433
(.059) |
.375*** |
| R2 |
.116 |
.288 |
.335 |
.662 |
| ∆ R2 |
|
.172 |
.047 |
.327 |
|
|
|
|
|
|
|
|
|
|
Note. Β = unstandardized regression coefficients; S.E. = standard errors; β = standardized coefficients; SBRS = Subtle and Blatant Racism Scale; MEIM = Multigroup Ethnic Identity Measure; ref = reference group.
*p < .05. **p < .01. ***p < .001
Table 3
Results From Moderation Path Analysis
| Variable |
β |
SE |
LLCI |
ULCI |
| SBRS |
0.242* |
0.115 |
0.015 |
0.469 |
| Coping |
0.718*** |
0.062 |
0.596 |
0.841 |
| SBRS × Coping |
0.017** |
0.006 |
0.006 |
0.029 |
| Controlled Variables |
|
|
|
|
| Age |
−1.420 |
1.215 |
−3.811 |
0.971 |
| Gender |
−0.681 |
1.297 |
−3.232 |
1.871 |
| Education |
−1.409 |
1.287 |
−3.942 |
1.124 |
| Sexual Identity |
0.185 |
1.304 |
−2.380 |
2.750 |
| Help-Seeking |
0.070 |
1.282 |
−2.452 |
2.592 |
| SBRS |
0.577*** |
0.089 |
0.403 |
0.751 |
| Resilience |
0.443*** |
0.029 |
0.387 |
0.499 |
| SBRS × Resilience |
0.001 |
0.004 |
−0.006 |
0.009 |
| Controlled Variables |
|
|
|
|
| Age |
0.472 |
1.109 |
−1.709 |
2.654 |
| Gender |
−1.704 |
1.175 |
−4.015 |
0.607 |
| Education |
-0.084 |
1.174 |
−2.227 |
2.395 |
| Sexual Identity |
−2.569* |
1.184 |
−4.899 |
−0.239 |
| Help-Seeking |
1.542 |
1.138 |
−0.696 |
3.781 |
Note. SBRS = Subtle and Blatant Racism Scale; LLCI = lower limit of confidence interval; ULCI = upper limit
of confidence interval.
*p < .05. **p < .01. ***p < .001.
Supplementary Analyses
Because the 14 coping subscales demonstrated poor reliability, we examined which types of coping strategies moderated the link between racism and stress-related growth. Among the different types of coping responses, self-blame, religion, humor, venting, substance use, denial, and behavioral disengagement had significant moderation effects on the relation between racism and stress-related growth. On the contrary, self-distraction, active coping, use of emotional support, use of instrumental support, positive reframing, planning, and acceptance did not significantly moderate the relationship between racism and stress-related growth.
Figure 1
Coping Strategy Moderates the Effect of Subtle and Blatant Racism on Stress-Related Growth
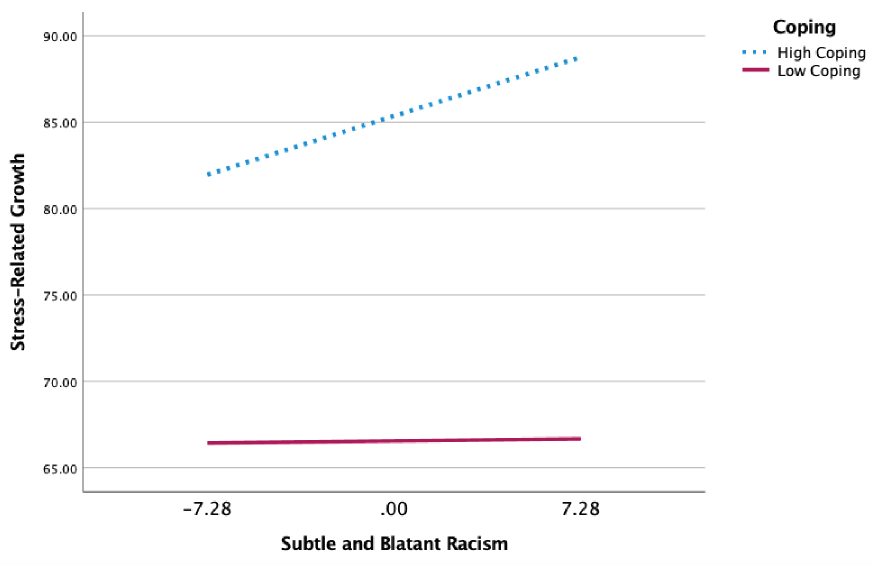
Discussion
The present study examined the extent to which coping, resilience, experiences of racism, and ethnic identity predicted stress-related growth in a national convenience sample of Asian and AAPI individuals. The results of our exploratory study provide empirical evidence for the moderating effects of coping on the relationship between racial discrimination and stress-related growth in Asians and AAPIs following the COVID-19 pandemic. In our study, ethnic identity was positively associated with stress-related growth, which further supports the current body of research linking ethnic identity to well-being (Iwamoto & Liu, 2010; Mossakowski, 2003; Yip et al., 2019). Our findings may be additionally explained through the lens of social identity theory (Tajfel & Turner, 1979), which posits that individuals who strongly identify with their social identities (i.e., ethnic and/or racial identities) are better equipped to leverage effective coping strategies that protect their overall self-concept and buffer the harmful impact of discrimination.
Participants in the study who used mental health services following COVID-19 also reported significantly higher levels of racial discrimination, resilience, coping, and stress-related growth compared to Asians and AAPIs who did not use professional mental health services. The results from our study are consistent with existing research that asserted how individuals may cultivate coping responses following traumatic experiences (Helgeson et al., 2006; Janoff-Bulman, 2004; Tedeschi & Calhoun, 2004) in ways that can strengthen the relationship between stressful experiences (i.e., racism) and stress-related growth (Park et al., 1996; Tedeschi & Calhoun, 2004). The results of our study therefore contribute to a larger body of research that establishes the relationship between stress-related growth and psychological health, optimism, positive affect, and psychological well-being (Bostock et al., 2009; Bower et al., 2009; Durkin & Joseph, 2009) while contributing nascent findings to the relationship between COVID-19 racial discrimination and stress-related growth in Asian and AAPI communities.
The results from Model 1 indicated education status, sexual identity, and help-seeking experiences were significantly associated with stress-related growth for Asians and AAPIs in the study. Specifically, participants who reported higher levels of education and identified as heterosexual or straight had lower scores of stress-related growth compared to those who did not identify as heterosexual. These findings are notable as individuals with lesbian, gay, bisexual, and other marginalized identities experience more stress and mental health issues compared to their heterosexual counterparts (Mongelli et al., 2019), resulting in greater opportunities to cultivate coping responses, build resilience, and establish meaningful social supports (Helgeson et al., 2006; Janoff-Bulman, 2004; Tedeschi & Calhoun, 2004). Participants in our study who used mental health services following the COVID-19 outbreak reported significantly higher levels of stress-related growth compared to Asians and AAPIs who did not use professional mental health services. One possible explanation for this finding may be that participants who sought mental health services already demonstrated higher levels of psychological mindedness, which may have influenced higher levels of stress-related growth following COVID-19–related racial discrimination.
In our study, the combined effects of resilience and coping explained 66.2% of the variance in Model 4, with coping strategies moderating the relationship between experiences of racism and stress-related growth. Participants in our study may have learned cognitive coping responses in the therapeutic setting that mitigated the effects of racism and cultivated stress-related growth. Our findings are consistent with the results of a meta-analysis (n = 103) that identified coping responses such as reappraisal, acceptance, and support seeking as significant predictors of stress-related growth (Prati & Pietrantoni, 2009). The specific coping responses that moderated the link between racism and stress-related growth in this study were self-blame, religion, humor, venting, substance use, denial, and disengagement. Leveraging these coping strategies in response to stressful experiences may be consistent with culturally congruent coping responses that protect Asians and AAPIs by avoiding the stressor (Edwards & Romero, 2008; Litam, 2020). Consistent with extant research on culturally congruent coping, engaging in self-blame responses may maintain interpersonal harmony (Wei et al., 2010), and humor, venting, denial, disengagement, and substance use may help one evade problems or adjust one’s feelings to the environment (Pokhrel & Herzog, 2014). The results of our study are thus consistent with research that emphasizes the influence of cultural notions on coping responses (Lazarus & Folkman, 1984; Tweed & Conway, 2006) while contributing new findings about which coping responses may contribute to stress-related growth in Asian and AAPI communities following COVID-19.
Implications for Counselors
This study highlights how experiences of racism, ethnic identity, resilience, and coping strategies may cultivate stress-related growth among Asian and AAPI individuals who experience COVID-19–related racial discrimination. Each of these variables were found to predict stress-related growth in our study. Mental health professionals working with Asian and AAPI clients who have experienced COVID-19 racism are encouraged to consider how their clients’ ethnic identity, resilience, and coping strategies may be leveraged to promote their well-being. In this exploratory study, participants with higher levels of ethnic identity experienced greater levels of stress-related growth, so it may behoove mental health professionals to embolden Asian and AAPI clients to fortify the quality of their ethnic group affiliation by pursuing cultural practices that promote a sense of group belongingness (Phinney, 1990). For example, ethnic identity can be cultivated by fostering community connection through local Asian and AAPI organizations, embracing cultural notions, and learning more about one’s culture, background, and family history (Chan & Litam, 2021; Litam, 2020). Clients who embody strong ethnic identities may be more likely to employ coping strategies that align with culturally embedded values; therefore, it is essential that mental health counselors recognize their own cultural values while remaining respectful of their client’s cultural values (Chang & O’Hara, 2013; see MSJCC, Ratts et al., 2016).
Given the importance of coping strategies and resilience on stress-related growth, mental health professionals are encouraged to identify and amplify clients’ existing coping strategies while fostering responses that cultivate resilience. Though limited, a supplementary analysis indicated that different forms of coping, such as self-blame, religion, humor, venting, substance use, denial, and disengagement, may moderate the relationship between racism and stress-related growth among Asian and AAPI communities facing racial discrimination following COVID-19. Thus, mental health professionals working with Asian and AAPI clients must assess the intention and outcome of client coping responses and challenge individualistic assumptions that minimize the value of culturally congruent coping strategies. The importance of using culturally sensitive therapeutic interventions when supporting Asian and AAPI clients during COVID-19 has been established (Litam, 2020). For example, mental health professionals must challenge assumptions that disengagement coping strategies are inherently problematic for their Asian and AAPI clients (Wong et al., 2010). Instead, mental health professionals are encouraged to focus on the usefulness of their Asian and AAPI clients’ coping strategies without imposing their own preconceived notion of what healthy and unhealthy coping entails. Of note, substance use was identified as a coping strategy used by participants in this study. Counselors are therefore called to examine the purpose and outcomes associated with client substance use with nuance to determine the extent to which ongoing substance use may contribute to mental health sequelae.
Limitations and Future Areas of Study
The results of the study must be interpreted within the context of methodological limitations. First, although all participants resided in the United States, the majority of participants held international statuses compared to U.S. citizens or permanent residents. Readers must be cautioned before generalizing these findings to AAPIs, who may endorse generational differences. Next, it is possible that participants recruited from MTurk may not be representative of the general Asian and AAPI population in the United States (Burnham et al., 2018). Future areas of research may consider incorporating various strategies to recruit more representative samples. Additional areas of investigation may also examine how generational identity may affect the extent to which coping, resilience, racism, and ethnic identity predict stress-related growth. Next, although a significant positive association was found between using professional mental health services and levels of resilience, racism, coping, and stress-related growth, it is unknown whether participants in the study already embodied higher levels of stress-related growth, coping, and resilience before seeking services. Future areas of study may examine whether these variables may actually predict help-seeking behaviors in Asians and AAPIs. For example, seeking professional mental health services is consistent with predictors of stress-related growth, including leveraging community support, engaging in cognitive responses, appraisal, and facilitating meaning making (Park & Fenster, 2004; Prati & Pietrantoni, 2009). Moreover, the validity of the findings from the supplementary analysis could be limited because of the low reliability of 14 subscales. Finally, Asians and AAPIs were aggregated in the study, which results in the loss of important within-group distinctions. Future studies are warranted that investigate the extent to which coping, resilience, racism, and ethnic identity predict stress-related growth in specific Asian and AAPI subgroups.
Conclusion
Asians and AAPIs who employ culturally congruent coping responses may experience greater levels of stress-related growth following experiences of COVID-19–related racial discrimination. In this study, higher levels of ethnic identity, resilience, and coping responses predicted stress-related growth in a national convenience sample of Asians and AAPIs residing in the United States. Asians and AAPIs in this study who sought professional mental health services reported higher levels of racism and endorsed higher scores of resilience, coping, and stress-related growth compared to those who did not seek professional mental health services. Mental health professionals are encouraged to support Asian and AAPI clients in strengthening their ethnic identity, building resilience, and using culturally congruent coping responses to mitigate the effects of COVID-19–related racism and promote the development of stress-related growth.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Anandavalli, S., Harrichand, J. J. S., & Litam, S. D. A. (2020). Counseling international students in times of uncertainty: A critical feminist and bioecological approach. The Professional Counselor, 10(3), 365–375. https://doi.org/10.15241/sa.10.3.365
Asmundson, G. J. G., & Taylor, S. (2020). Coronaphobia: Fear and the 2019-nCoV outbreak. Journal of Anxiety Disorders, 70. https://doi.org/10.1016/j.janxdis.2020.102196
Boals, A., & Schuler, K. L. (2018). Reducing reports of illusory posttraumatic growth: A revised version of the Stress-Related Growth Scale (SRGS-R). Psychological Trauma: Theory, Research, Practice, and Policy, 10(2), 190–198. https://doi.org/10.1037/tra0000267
Bodner, T. E. (2017). Standardized effect sizes for moderated conditional fixed effects with continuous moderator variables. Frontiers in Psychology, 8, 562. https://doi.org/10.3389/fpsyg.2017.00562
Bostock, L., Sheikh, A. I., & Barton, S. (2009). Posttraumatic growth and optimism in health-related trauma: A systematic review. Journal of Clinical Psychology in Medical Settings, 16(4), 281–296. https://doi.org/10.1007/s10880-009-9175-6
Bower, J. E., Moskowitz, J. T., & Epel, E. (2009). Is benefit finding good for your health? Pathways linking positive life changes after stress and physical health outcomes. Current Directions in Psychological Science, 18(6), 337–341. https://doi.org/10.1111/j.1467-8721.2009.01663.x
Brown, S. D., Unger Hu, K. A., Mevi, A. A., Hedderson, M. M., Shan, J., Quesenberry, C. P., & Ferrara, A. (2014). The Multigroup Ethnic Identity Measure–Revised: Measurement invariance across racial and ethnic groups. Journal of Counseling Psychology, 61(1), 154–161. https://doi.org/10.1037/a0034749
Budiman, A., & Ruiz, N. G. (2021). Key facts about Asian Americans, a diverse and growing population. Pew Research Center. https://www.pewresearch.org/fact-tank/2017/09/08/key-facts-about-asian-americans
Burnham, M. J., Le, Y. K., & Piedmont, R. L. (2018). Who is MTurk? Personal characteristics and sample consistency of these online workers. Mental Health, Religion & Culture, 21(9–10), 934–944. https://doi.org/10.1080/13674676.2018.1486394
Cacioppo, J. T., & Hawkley, L. C. (2003). Social isolation and health, with an emphasis on underlying mechanisms. Perspectives in Biology and Medicine, 46(3), S39–S52. https://doi.org/10.1353/pbm.2003.0063
Cacioppo, J. T., Hawkley, L. C., Crawford, L. E., Ernst, J. M., Burleson, M. H., Kowalewski, R. B., Malarkey, W. B., Van Cauter, E., & Berntson, G. G. (2002). Loneliness and health: Potential mechanisms. Psychosomatic Medicine, 64(3), 407–417. https://doi.org/10.1097/00006842-200205000-00005
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100. https://doi.org/10.1207/s15327558ijbm0401_6
Chan, C. D., & Litam, S. D. A. (2021). Mental health equity of Filipino communities in COVID-19: A framework for practice and advocacy. The Professional Counselor, 11(1), 73–85. https://doi.org/10.15241/cdc.11.1.73
Chang, C. Y., & O’Hara, C. (2013). The initial interview with Asian American clients. Journal of Contemporary Psychotherapy, 43(1), 33–42. https://doi.org/10.1007/s10879-012-9221-9
Cheng, H.-I. (2013). “A wobbly bed still stands on three legs”: On Chinese immigrant women’s experiences with ethnic community. Women & Language, 36, 7–25.
Choi, Y., Park, M., Noh, S., Lee, J. P., & Takeuchi, D. (2020). Asian American mental health: Longitudinal trend and explanatory factors among young Filipino- and Korean Americans. SSM – Population Health, 10. https://doi.org/10.1016/j.ssmph.2020.100542
Cohen, J. (1998). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum.
Congressional Asian Pacific American Caucus. (2020, February 26). As coronavirus fears incite violence, CAPAC members urge colleagues to not stoke xenophobia. https://capac-chu.house.gov/press-release/coronavirus-fears-incite-violence-capac-members-urge-colleagues-not-stoke-xenophobia
Connor, K. M., & Davidson, J. R. T. (2003). Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depression and Anxiety, 18(2), 76–82. https://doi.org/10.1002/da.10113
Cordova, M. J., Riba, M. B., & Spiegel, D. (2017). Post-traumatic stress disorder and cancer. The Lancet Psychiatry, 4(4), 330–338. https://doi.org/10.1016/S2215-0366(17)30014-7
DeVitre, Z., & Pan, D. (2020). Asian American values and attitudes towards seeking mental health services. Journal of Asia Pacific Counseling, 10(1), 15–26. https://doi.org/10.18401/2020.10.1.2
Durkin, J., & Joseph, S. (2009). Growth following adversity and its relation with subjective well-being and psychological well-being. Journal of Loss and Trauma, 14(3), 228–234.
https://doi.org/10.1080/15325020802540561
Edmondson, D., Chaudoir, S. R., Mills, M. A., Park, C. L., Holub, J., & Bartkowiak, J. M. (2011). From shattered assumptions to weakened worldviews: Trauma symptoms signal anxiety buffer disruption. Journal of Loss and Trauma, 16(4), 358–385. https://doi.org/10.1080/15325024.2011.572030
Edwards, L. M., & Romero, A. J. (2008). Coping with discrimination among Mexican descent adolescents. Hispanic Journal of Behavioral Sciences, 30(1), 24–39. https://doi.org/10.1177/0739986307311431
Erikson, E. H. (1968). Identity: Youth and crisis. W. W. Norton.
Frazier, P. A., Tix, A. P., & Barron, K. E. (2004). Testing moderator and mediator effects in counseling psychology research. Journal of Counseling Psychology, 51(1), 115–134. https://doi.org/10.1037/0022-0167.51.1.115
Gee, G. C., Spencer, M., Chen, J., Yip, T., & Takeuchi, D. T. (2007). The association between self-reported racial discrimination and 12-month DSM-IV mental disorders among Asian Americans nationwide. Social Science & Medicine, 64(10), 1984–1996. https://doi.org/10.1016/j.socscimed.2007.02.013
Hayes, A. F. (2018). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2nd ed.). Guilford.
Helgeson, V. S., Reynolds, K. A., & Tomich, P. L. (2006). A meta-analytic review of benefit finding and growth. Journal of Consulting and Clinical Psychology, 74(5), 797–816. https://doi.org/10.1037/0022-006X.74.5.797
Hwang, W.-C., & Goto, S. (2008). The impact of perceived racial discrimination on the mental health of Asian American and Latino college students. Cultural Diversity and Ethnic Minority Psychology, 14(4), 326–335. https://doi.org/10.1037/1099-9809.14.4.326
Inman, A. G., & Yeh, C. J. (2007). Asian American stress and coping. In F. T. L. Leong, A. G. Inman, A. Ebreo, L. H. Yang, L. Kinoshita, & M. Fu (Eds.), Handbook of Asian American psychology (2nd ed., pp. 323–340). SAGE.
Iwamoto, D. K., & Liu, W. M. (2010). The impact of racial identity, ethnic identity, Asian values, and race-related stress on Asian Americans and Asian international college students’ psychological well-being. Journal of Counseling Psychology, 57(1), 79–91. https://doi.org/10.1037/a0017393
Janoff-Bulman, R. (2004). Posttraumatic growth: Three explanatory models. Psychological Inquiry, 15(1), 30–34.
Jeung, R., & Nham, K. (2020). Incidents of coronavirus-related discrimination. Asian Pacific Policy & Planning Council. http://www.asianpacificpolicyandplanningcouncil.org/wp-content/uploads/STOP_AAPI_HATE_MONTHLY_REPORT_4_23_20.pdf
Kim, J., & Kim, H. (2013). The experience of acculturative stress-related growth from immigrants’ perspectives. International Journal of Qualitative Studies on Health and Well-Being, 8(1).
https://doi.org/10.3402/qhw.v8i0.21355
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
Le, D. L., & Ahn, S. (2011). Racial discrimination and Asian mental health: A meta-analysis. The Counseling Psychologist, 39(3), 463–489. https://doi.org/10.1177/0011000010381791
Lee, R. M. (2003). Do ethnic identity and other-group orientation protect against discrimination for Asian Americans? Journal of Counseling Psychology, 50(2), 133–141. https://doi.org/10.1037/0022-0167.50.2.133
Lee, R. M. (2005). Resilience against discrimination: Ethnic identity and other-group orientation as protective factors for Korean Americans. Journal of Counseling Psychology, 52(1), 36–44.
https://doi.org/10.1037/0022-0167-52.1.36
Lee, R. M., & Davis, C., III. (2000). Cultural orientation, past multicultural experience, and a sense of belonging on campus for Asian American college students. Journal of College Student Development, 41(1), 110–115.
Lee, R. M., & Yoo, H. C. (2004). Structure and measurement of ethnic identity for Asian American college students. Journal of Counseling Psychology, 51(2), 263–269. https://doi.org/10.1037/0022-0167.51.2.263
Leong, F., Park, Y. S., & Kalibatseva, Z. (2013). Disentangling immigrant status in mental health: Psychological protective and risk factors among Latino and Asian American immigrants. American Journal of Orthopsychiatry, 83(2–3), 361–371. http://doi.org/10.1111/ajop.12020
Liang, C. T. H., & Fassinger, R. E. (2008). The role of collective self-esteem for Asian Americans experiencing racism-related stress: A test of moderator and mediator hypotheses. Cultural Diversity and Ethnic Minority Psychology, 14(1), 19–28. https://doi.org/10.1037/1099-9809.14.1.19
Lieber, E., Chin, D., Nihira, K., & Mink, I. T. (2001). Holding on and letting go: Identity and acculturation among Chinese immigrants. Cultural Diversity and Ethnic Minority Psychology, 7(3), 247–261. https://doi.org/10.1037/1099-9809.7.3.247
Lim, J., & Ashing-Giwa, K. T. (2013). Is family functioning and communication associated with health-related quality of life for Chinese- and Korean-American breast cancer survivors? Quality of Life Research, 22, 1319–1329. https://doi.org/10.1007/s11136-012-0247-y
Linley, P. A., & Joseph, S. (2004). Positive change following trauma and adversity: A review. Journal of Traumatic Stress, 17(1), 11–21. https://doi.org/10.1023/B:JOTS.0000014671.27856.7e
Litam, S. D. A. (2020). “Take your Kung Flu back to Wuhan”: Counseling Asians, Asian Americans, and Pacific Islanders with race-based trauma related to COVID-19. The Professional Counselor, 10(2), 144–156. https://doi.org/10.15241/sdal.10.2.144
Litam, S. D. A., & Hipolito-Delgado, C. P. (2021). When being “essential” illuminates disparities: Counseling clients affected by COVID-19. Journal of Counseling & Development, 99(1), 3–10.
https://doi.org/10.1002/jcad.12349
Litam, S. D. A., & Oh, S. (in press). Effects of COVID-19 racial discrimination on depression and life satisfaction among young, middle, and older Chinese Americans. Adultspan Journal.
Litam, S. D. A., & Oh, S. (2020). Ethnic identity and coping strategies as moderators of COVID-19 racial discrimination experiences among Chinese Americans. Counseling Outcome Research and Evaluation. https://doi.org/10.1080/21501378.2020.1814138
Miller, C. T., & Kaiser, C. R. (2001). A theoretical perspective on coping with stigma. Journal of Social Issues, 57(1), 73–92. https://doi.org/10.1111/0022-4537.00202
Miller, C. T., & Major, B. (2000). Coping with stigma and prejudice. In T. F. Heatherton, R. E. Kleck, M. R. Hebl, & J. G. Hull (Eds.), The social psychology of stigma (pp. 243–272). Guilford.
Mongelli, F., Perrone, D., Balducci, J., Sacchetti, A., Ferrari, S., Mattei, G., & Galeazzi, G. M. (2019). Minority stress and mental health among LGBT populations: An update on the evidence. Minerva Psychiatrica, 60(1), 27–50. https://doi.org/10.23736/S0391-1772.18.01995-7
Mossakowski, K. N. (2003). Coping with perceived discrimination: Does ethnic identity protect mental health? Journal of Health and Social Behavior, 44(3), 318–331. https://doi.org/10.2307/1519782
Nadal, K. L., Wong, Y., Sriken, J., Griffin, K., & Fujii-Doe, W. (2015). Racial microaggressions and Asian Americans: An exploratory study on within-group differences and mental health. Asian American Journal of Psychology, 6(2), 136–144. https://doi.org/10.1037/a0038058
Noh, S., & Kaspar, V. (2003). Perceived discrimination and depression: Moderating effects of coping, acculturation, and ethnic support. American Journal of Public Health, 93(2), 232–238. https://doi.org/10.2105/ajph.93.2.232
Nolen-Hoeksema, S., & Davis, C. G. (2004). Theoretical and methodological issues in the assessment and interpretation of posttraumatic growth. Psychological Inquiry, 15, 60–64.
O’Rourke, N., & Hatcher, L. (2013). A step-by-step approach to using SAS for factor analysis and structural equation modeling (2nd ed.). SAS Press.
Osborn, J. W. (2013). Best practices in data cleaning: A complete guide to everything you need to do before and after collecting your data. SAGE.
Park, C. L., Cohen, L. H., & Murch, R. L. (1996). Assessment and prediction of stress-related growth. Journal of Personality, 64(1), 71–105. https://doi.org/10.1111/j.1467-6494.1996.tb00815.x
Park, C. L., & Fenster, J. R. (2004). Stress-related growth: Predictors of occurrence and correlates with psychological adjustment. Journal of Social and Clinical Psychology, 23(2), 195–215. https://doi.org/10.1521/jscp.23.2.195.31019
Phinney, J. S. (1990). Ethnic identity in adolescents and adults: Review of research. Psychological Bulletin, 108(3), 499–514. https://doi.org/10.1037/0033-2909.108.3.499
Phinney, J. S. (1992). The Multigroup Ethnic Identity Measure: A new scale for use with diverse groups. Journal of Adolescent Research, 7(2), 156–176. https://doi.org/10.1177/074355489272003
Phinney, J. S. (2003). Ethnic identity and acculturation. In K. M. Chun, P. B. Organista, & G. Marin (Eds.), Acculturation: Advances in theory, measurement, and applied research (pp. 63–82). American Psychological Association.
Pokhrel, P., & Herzog, T. A. (2014). Historical trauma and substance use among Native Hawaiian college students. American Journal of Health Behavior, 38(3), 420–429. https://doi.org/10.5993/AJHB.38.3.11
Prati, G., & Pietrantoni, L. (2009). Optimism, social support, and coping strategies as factors contributing to posttraumatic growth: A meta-analysis. Journal of Loss and Trauma, 14(5), 364–388.
https://doi.org/10.1080/15325020902724271
Preacher, K. J., Rucker, D. D., & Hayes, A. F. (2007). Addressing moderated mediation hypothesis: Theory, methods, and prescriptions. Multivariate Behavioral Research, 42(1), 185–227.
https://doi.org/10.1080/002731707001341316
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and Social Justice Counseling Competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Rzeszutek, M., & Gruszczyńska, E. (2018). Paradoxical effect of social support among people living with HIV: A diary study investigating the buffering hypothesis. Journal of Psychosomatic Research, 109, 25–31. https://doi.org/10.1016/j.jpsychores.2018.03.006
Sue, D. W., Sue, D., Neville, H. A., & Smith, L. (2019). Counseling the culturally diverse: Theory and practice (8th ed.). Wiley.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations. Brooks Cole.
Tedeschi, R. G., & Calhoun, L. G. (1995). Trauma and transformation: Growing in the aftermath of suffering. SAGE.
Tedeschi, R. G., & Calhoun, L. G. (1996). The posttraumatic growth inventory: Measuring the positive legacy of trauma. Journal of Traumatic Stress, 9(3), 455–471. https://doi.org/10.1007/BF02103658
Tedeschi, R. G., & Calhoun, L. G. (2004). Posttraumatic growth: Conceptual foundation and empirical evidence. Psychological Inquiry, 15(1), 1–18. https://doi.org/10.1207/s15327965pli1501_01
Turner, J. C., Hogg, M. A., Oakes, P. J., Reicher, S. D., & Wetherell, M. S. (1987). Rediscovering the social group: A self-categorization theory. Basil Blackwell.
Tweed, R. G., & Conway, L. G., III. (2006). Coping strategies and culturally influenced beliefs about the world. In P. T. P. Wong & L. C. J. Wong (Eds.), Handbook of multicultural perspectives on stress and coping (pp. 133–153). Springer.
Vasquez, C., Valiente, C., García, F. E., Contreras, A., Peinado, V., Trucharte, A., & Bentall, R. P. (2021). Post-traumatic growth and stress-related responses during the COVID-19 pandemic in a national representative simple: The role of positive core beliefs about the world and others. Journal of Happiness Studies. https://doi.org/10.1007/s10902-020-00352-3
Wagnild, G. M., & Young, H. M. (1993). Development and psychometric evaluation of the Resilience Scale. Journal of Nursing Measurement, 1(2), 165–178.
Wei, M., Heppner, P. P., Ku, T.-Y., & Liao, K. Y.-H. (2010). Racial discrimination stress, coping, and depressive symptoms among Asian Americans: A moderation analysis. Asian American Journal of Psychology, 1(2), 136–150. https://doi.org/10.1037/a0020157
Wei, M., Wang, K. T., Heppner, P. P., & Du, Y. (2012). Ethnic and mainstream social connectedness, perceived racial discrimination, and posttraumatic stress symptoms. Journal of Counseling Psychology, 59(3), 486–493. https://doi.org/10.1037/a0028000
Wen, J., Aston, J., Liu, X., & Ying, T. (2020). Effects of misleading media coverage on public health crisis: A case of the 2019 novel coronavirus outbreak in China. An International Journal of Tourism and Hospitality Research, 31(2), 331–336. https://doi.org/10.1080/13032917.2020.1730621
Wong, G., Derthick, A. O., David, E. J. R., Saw, A., & Okazaki, S. (2014). The what, the why, and the how: A review of racial microaggressions research in psychology. Race and Social Problems, 6, 181–200. https://doi.org/10.1007/s12552-013-9107-9
Wong, Y. J., Kim, S.-H., & Tran, K. K. (2010). Asian Americans’ adherence to Asian values, attributions about depression, and coping strategies. Cultural Diversity and Ethnic Minority Psychology, 16(1), 1–8. https://doi.org/10.1037/a0015045
Yang, A. (2014). Themes in the career development of 1.5-generation Hmong American women. Journal of Career Development, 41(5), 402–425. https://doi.org/10.1177/0894845313507775
Yeh, C. J., Arora, A. K., & Wu, K. A. (2006). A new theoretical model of collectivistic coping. In P. T. P. Wong & L. C. J. Wong (Eds.), Handbook of multicultural perspectives on stress and coping: International and cultural psychology series (pp. 55–72). Springer.
Yip, T., & Fuligni, A. J. (2002). Daily variation in ethnic identity, ethnic behaviors, and psychological well-being among American adolescents of Chinese descent. Child Development, 73(5), 1557–1572. https://doi.org/10.1111/1467-8624.00490
Yip, T., Wang, Y., Mootoo, C., & Mirpuri, S. (2019). Moderating the association between discrimination and adjustment: A meta-analysis of ethnic/racial identity. Developmental Psychology, 55(6), 1274–1298. https://doi.org/10.1037/dev0000708
Yoo, H. C., Steger, M. F., & Lee, R. M. (2010). Validation of the Subtle and Blatant Racism Scale for Asian American College Students (SABRA-A2). Cultural Diversity and Ethnic Minority Psychology, 16(3), 323–334. https://doi.org/10.1037/a0018674
Stacey Diane Arañez Litam, PhD, NCC, CCMHC, LPCC-S, is an assistant professor at Cleveland State University. Seungbin Oh, PhD, NCC, LPC, is an assistant professor at Merrimack College. Catherine Chang, PhD, NCC, LPC, CPCS, is a professor at Georgia State University. Correspondence may be addressed to Stacey Litam, 2121 Euclid Ave., Cleveland, OH 44115, s.litam@csuohio.edu.
