Dec 5, 2024 | Volume 14 - Issue 3
Fei Shen, Ying Zhang, Xiafei Wang
Intimate partner violence (IPV) has consistently been shown to have deleterious effects on survivors’ interpersonal and intrapersonal relationships. Despite the negative outcomes of IPV, distress after IPV varies widely, and not all IPV survivors show a significant degree of distress. The present study examined the impact of IPV on adult attachment and self-esteem, as well as the moderating role of childhood attachment on the relationships between IPV, adult attachment, and self-esteem using path analysis. A total of 1,708 adult participants were included in this study. As hypothesized, we found that IPV survivors had significantly higher levels of anxious and avoidant adult attachment than participants without a history of IPV. Additionally, childhood attachment buffered the relationship between IPV and self-esteem. We did not find that childhood attachment moderated the relationship between IPV and adult attachment. These results provide insight on attachment-based interventions that can mitigate the negative effects of IPV on people’s perceptions of self.
Keywords: intimate partner violence, childhood attachment, adult attachment, self-esteem, moderation
More than 10 million adults experience intimate partner violence (IPV) victimization annually in the United States (Black et al., 2011); therefore, it undoubtedly remains a prominent public health concern. IPV victimization has been consistently associated with deleterious effects on survivors’ physical and mental health. It is well established that IPV survivors demonstrated increased risks for chronic pain, injury, insomnia, disabilities, post-traumatic stress disorder, depression, and suicidality (Burke et al., 2005; Gilbert et al., 2023; Matheson et al., 2015; McLaughlin et al., 2012). Historically, empirical studies on trauma and violence have focused on psychopathology and symptoms (McLaughlin et al., 2012; Sayed et al., 2015). However, there is limited research on exploring the link between IPV victimization and intrapersonal and interpersonal relationship outcomes. Attachment theory (Bowlby, 1969) not only provides a rich theoretical framework for conceptualizing an individual’s psychopathology, but also establishes a foundation for understanding the intrapersonal and relational sequelae of IPV (Levendosky et al., 2012; Sutton, 2019). IPV survivors often experience a violation of trust and a sense of betrayal in the aftermath and develop ineffective coping mechanisms (e.g., distancing themselves emotionally), which could potentially impact their new intimate relationships (St. Vil et al., 2021).
Despite the negative outcomes of IPV victimization, the levels of distress following such incidents can vary (Scott & Babcock, 2010). Although evidence has implicated numerous risk factors related to IPV victimization (e.g., childhood trauma, gender inequity; Jewkes et al., 2017; Meeker et al., 2020), limited effort has been put forth to recognize protective factors that contribute to IPV survivors’ coping and healing processes. Childhood attachment has been proposed as a potential protective factor for IPV survivors’ coping with traumatic experiences and a moderator for buffering the negative psychological outcomes of IPV (Pang & Thomas, 2020), which provides a meaningful foundation for us to further investigate childhood attachment as a moderator buffering relational outcomes. To our knowledge, no study to date has investigated the potential moderating role of childhood attachment security on the association between IPV, interpersonal outcomes (e.g., adult attachment), and intrapersonal outcomes (e.g., self-esteem) in a non-clinical sample. Understanding the moderating role of childhood attachment can potentially provide further directions toward protecting survivors from negative outcomes and creating interventions that foster healthier interpersonal relationships. In tackling the gaps in the literature, we aim to: (a) investigate the impact of IPV on adult attachment and self-esteem; and (b) examine the moderating role of childhood attachment on the relationships between IPV, adult attachment, and self-esteem.
Theoretical Framework—Attachment Theory
Attachment theory (Bowlby, 1969) offers an explanation of how the relationship between children and their primary caregiver(s) develops and how it impacts children’s subsequent developmental process. According to Bowlby (1973), children develop mental representations of themselves and others, known as internal working models, through their interactions with their primary caregiver(s). Children with secure attachment are more likely to form positive self-perceptions and relationships with others (Bowlby, 1969). In contrast, children who develop insecure attachment are more likely to struggle with coping with distress and form poor relationships with others, resulting from caregivers responding to their needs insensitively.
Although evidence suggests the continuity of attachment from childhood to adulthood (Bowlby, 1969), there are distinctions between these two variables based on individuals’ attachment needs, developmental stages, and characteristics of different relationships. As children grow into adolescents and emerging adults, they often continue to maintain connections with their primary caregivers while exploring new social roles outside of the family and forming close relationships with peers and romantic partners to develop adult attachment (Moretti & Peled, 2004). Secure adult attachment is generally characterized by flexibility, the ability to work independently and cooperatively with others, the ability to seek support from intimate partners, and the capacity to manage loss in a healthy manner (Brennan et al., 1998). Adult romantic relationships are thought to be underlined by two fundamental attachment-related dimensions: anxiety and avoidance. Adults with anxious attachment tend to experience worry and fear regarding abandonment or rejection by their partner, leading them to seek constant reassurance and validation from their partner. On the other hand, avoidant-attached individuals often feel uncomfortable with being close to their partner, which can lead them to withdraw from intimacy and emotional closeness in the relationship (Brennan et al., 1998). Thus, understanding the similarities and differences of attachment categories as well as dynamics of the attachment system is warranted (Lopez & Brennan, 2000).
Childhood Attachment, IPV Victimization, and Adult Attachment
Various researchers have extensively investigated the significant association between attachment developed with romantic partners and its involvement in IPV dynamics (Bradshaw & Garbarino, 2004; Duru et al., 2019; Levendosky et al., 2012). However, most studies explored the relationship between adult attachment and IPV perpetration (Gormley & Lopez, 2010; McClure & Parmenter, 2020). Specifically, individuals with insecure attachment present intense fear of abandonment or rejection and activate their aggressive behaviors to control their partners (Gormley & Lopez, 2010). Regarding IPV victimization circumstances, few studies have examined attachment security among IPV survivors. Specifically, simultaneously exploring attachment with primary caregivers in childhood and attachment with romantic partners in adulthood could capture the complexity of the impact of IPV victimization experiences on relational and emotional outcomes. Ponti and Tani (2019) investigated both childhood attachment and adult attachment among 60 women who experienced IPV and indicated that the attachment to the mother could influence IPV victimization both directly and indirectly through the mediation effect of adult attachment with romantic partners. In other words, attachment with the mother could serve as a protector for not entering a violent romantic relationship or healthily managing the aftermath of traumatic experiences.
Childhood attachment has been identified as a potential moderator that may contribute to the variations of the healing process among IPV survivors in a small but growing number of studies (e.g., Scott & Babcock, 2010). Pang and Thomas (2020) examined the moderating role of childhood attachment on the relationship between exposure to domestic violence in adolescence and psychological outcomes and adult life satisfaction with a sample of 351 adult college students. They found that childhood attachment moderated the relationship between IPV exposure and adult life satisfaction but not psychological outcomes. This study provides empirical support for the moderating role of childhood attachment on early IPV exposure and later adult psychological and relationship outcomes. Given the context in which IPV occurs in the intimate relationships, not addressing the association between childhood attachment and adult attachment together would not fully capture the complexity of the attachment process in the adult population. It is possible that the relationship between IPV victimization and adult attachment security would be attenuated in conditions of childhood attachment. Therefore, the moderation effect of childhood attachment in the context of IPV needs to be empirically substantiated.
Childhood Attachment, IPV Victimization, and Self-Esteem
Self-esteem generally refers to a person’s overall evaluation and attitude toward themself (Rosenberg, 1965). Experiencing IPV was found to have detrimental effects on an individual’s self-esteem; IPV survivors often have lower levels of self-esteem than non-abused individuals (Childress, 2013; Karakurt et al., 2014; Tariq, 2013). Experiencing IPV (e.g., emotional and psychological abuse) can lead to feelings of worthlessness and hopelessness, making it difficult for survivors to maintain autonomy and make decisions that are in their best interest (Tariq, 2013). IPV survivors consistently reported feeling burdened with a sense of guilt, shame, and self-blame for being victimized (Lindgren & Renck, 2008). Unfortunately, this can contribute to a vicious cycle, as survivors who have low self-esteem are less likely to take steps to leave abusive relationships (Karakurt et al., 2014), which leads to further victimization (Eddleston et al., 1998). Understanding the link between IPV victimization and self-esteem is crucial, as rebuilding self-esteem can also help survivors develop stronger relationships with others, gain strength toward ending abusive relationships, reduce risks of mental health problems, and feel more empowered to seek help and support (Karakurt et al., 2022).
The development of the self can be seen to unfold in the context of attachment and the internalization of important others’ perceptions and expectations. Numerous studies have shed some light on the association between childhood attachment and self-esteem, suggesting that secure attachment with primary caregivers can serve as a key protective factor for developing higher levels of self-esteem (Shen et al., 2021; Wilkinson, 2004). In contrast, individuals who reported insecure attachment with their primary caregivers tended to demonstrate lower levels of self-esteem (Gamble & Roberts, 2005). However, interpersonal trauma such as IPV can produce long-term dysfunctions of self (Childress, 2013). Although no study has directly explored the moderating role of childhood attachment buffering the relationship between IPV and self-esteem, several studies have indicated that parental support serves as a moderator role in the relationship between interpersonal violence and self-esteem (Duru et al., 2019). Indeed, if a person had secure attachment experiences in childhood, they may have developed a positive sense of self-worth and the belief that they deserve love and respect, which could buffer the negative effects of IPV on their self-esteem. Considering the existing literature and theoretical explanations as a whole, it seems reasonable to postulate that childhood attachment might serve as a potential moderator of the association between IPV and self-esteem.
Taken together, the literature consistently supports the significance of exploring protective factors contributing to IPV survivors’ healing process, yet no study to date has investigated the potential moderating role of childhood attachment on the association between IPV, adult attachment, and self-esteem in a non-clinical diverse sample. In tackling these gaps, we pose two research questions (RQs):
RQ1: How is IPV associated with adult attachment and self-esteem?
RQ2: How does childhood attachment moderate the relationships between IPV, adult
attachment, and self-esteem?
We hypothesized that: 1) IPV victimization is significantly positively associated with adult attachment (i.e., anxious attachment, avoidant attachment) and negatively associated with self-esteem; 2) Childhood attachment moderates the relationship between IPV victimization and adult attachment (i.e., anxious attachment, avoidant attachment); and 3) Childhood attachment moderates the relationship between IPV victimization and self-esteem.
Method
Sampling Procedures
With approval from the university IRB, research recruitment information was posted on various social media platforms (e.g., Facebook, Craigslist, university announcement boards). Individuals who were 18 years of age or older and able to fill out the questionnaire in English were eligible for the study. Participants were directed to an online Qualtrics survey to voluntarily complete the informed consent and the measures listed in the following section. At the end of the survey, participants were prompted to enter their email addresses to win one of 10 $15 e-gift cards. Their email addresses were not included for data analysis.
Participants
Of the 2,373 voluntary adult participants who took the survey, 1,708 (71.76%) individuals were retained for the final analysis, including 507 (29.68%) participants who experienced IPV in adulthood and 1,191 (69.73%) participants without a history of IPV in adulthood. We eliminated participants who either did not consent to the study (n = 36, 1.51%), were younger than 18 years old (n = 33, 1.39%), or did not complete 95% of the survey questions (n = 596, 25.11%). We examined whether those who were excluded from the sample because of missing or invalid data differed from those who were retained. There was a significant difference in age between the included sample (M = 28.89, SD = 12.38) and excluded sample (M = 32.10, SD = 13.51); t (2,255) = −3.48, p = 0.001. Therefore, excluding participants with missing data was less likely to significantly impact our results. Table 1 shows that 76.23% of the participants were female. The age range of the sample was broad, from 18 to 89 years old, with an average age of 30.
Table 1
Demographic and Key Variables Information (N = 1,708)
| Variables |
N |
Percent |
Range |
M(SD) |
| Childhood attachment |
1,708 |
100% |
1–5 |
3.34(0.92) |
| IPV status
IPV
Non-IPV |
1,698
507
1,191 |
99.41%
29.68%
69.73% |
0–1 |
|
| Self-Esteem |
1,704 |
99.77% |
3–40 |
26.98(7.46) |
| Anxious Attachment |
1,708 |
100% |
1–7 |
4.11(1.26) |
| Avoidant Attachment |
1,708 |
100% |
1–7 |
3.71(1.16) |
| Control Variables |
|
|
|
|
| Gender
Male
Female |
1,683
381
1,302 |
98.54%
22.31%
76.23% |
|
|
| Household Income
Less than $5,000
$5,000–$9,999
$10,000–$14,999
$15,000–$19,999
$20,000–$24,999
$25,000–$29,999
$30,000–$39,999
$40,000–$49,999
$50,000–$74,999
$75,000–$99,999
$100,000–$149,999
$150,000 or more |
1,514
183
96
119
83
98
78
128
141
239
143
139
67 |
88.64%
10.70%
5.60%
7.00%
4.90%
5.70%
4.60%
7.50%
8.30%
14.00%
8.40%
8.10%
3.90% |
|
|
Measures
Childhood Attachment
The parental attachment subscale of the Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987) was used to measure childhood attachment. Participants rated their attachment to their parent(s) or caregiver(s) who had the most influence on them during their childhood. The subscale consists of 25 items divided into three dimensions, including 10 items on Trust (e.g., “My mother/father trusts my judgment”), nine items on Communication (e.g., “I can count on my mother/father when I need to get something off my chest”), and six items on Alienation (e.g., “I don’t get much attention from my mother/father”). Participants rated the items using a 5-point Likert scale ranging from 1 (almost never or never true) to 5 (almost always or always true). Responses were averaged, with a higher score reflecting more secure childhood attachment. This subscale has demonstrated relatively high internal consistency, with a Cronbach’s alpha of .93 (Armsden & Greenberg, 1987), and construct validity (Cherrier et al., 2023; Gomez & McLaren, 2007). In the present study, the Cronbach’s alpha coefficient for this subscale was .96.
Intimate Partner Violence
Participants’ experiences of IPV were assessed through the question “Have you ever experienced intimate partner violence (physical, sexual, or psychological harm) by a current or former partner or spouse since the age of 18?” Responses were coded as 1 = Yes, 0 = No.
Adult Attachment
Adult attachment was measured using the Experience in Close Relationships Scale (ECR; Brennan et al., 1998). The ECR consists of 36 items with 18 items assessing each of the two dimensions: anxious attachment (e.g., “I worry about being abandoned”) and avoidant attachment (e.g., “I try to avoid getting too close to my partner/friends”). To reduce confounding factors with childhood attachment with their parent(s) or primary caregiver(s), we only assessed adult attachment with close friends and/or romantic partners. Responses were rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Two scores were computed by averaging items on each subscale, with a higher score reflecting a higher level of anxious or avoidant attachment. Two subscales demonstrated high construct validity in various studies (Gormley & Lopez, 2010; Ponti & Tani, 2019) and a relatively high consistency for anxiety (α = .91) and avoidance (α = .94; Brennan et al., 1998). Cronbach’s alpha coefficients for the present study were .93 for anxiety and .92 for avoidance.
Self-Esteem
The Rosenberg Self-Esteem Scale (RSES; Rosenberg, 1965) is a 10-item self-report measure of overall feelings of self-worth or self-acceptance (e.g., “I am satisfied with myself”). All items were coded using a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree). Items were summed, with a higher score indicating a higher level of self-esteem. RSES has been frequently used in various studies, demonstrating high reliability and validity (Brennan & Morris, 1997; Rosenberg, 1979). The Cronbach’s alpha for the present study was .89.
Control Variables
To make more accurate estimates, we included control variables that are potentially associated with IPV exposures, such as gender and household income. Gender was dummy coded as 1 = Male, 2 = Female.
Data Analysis
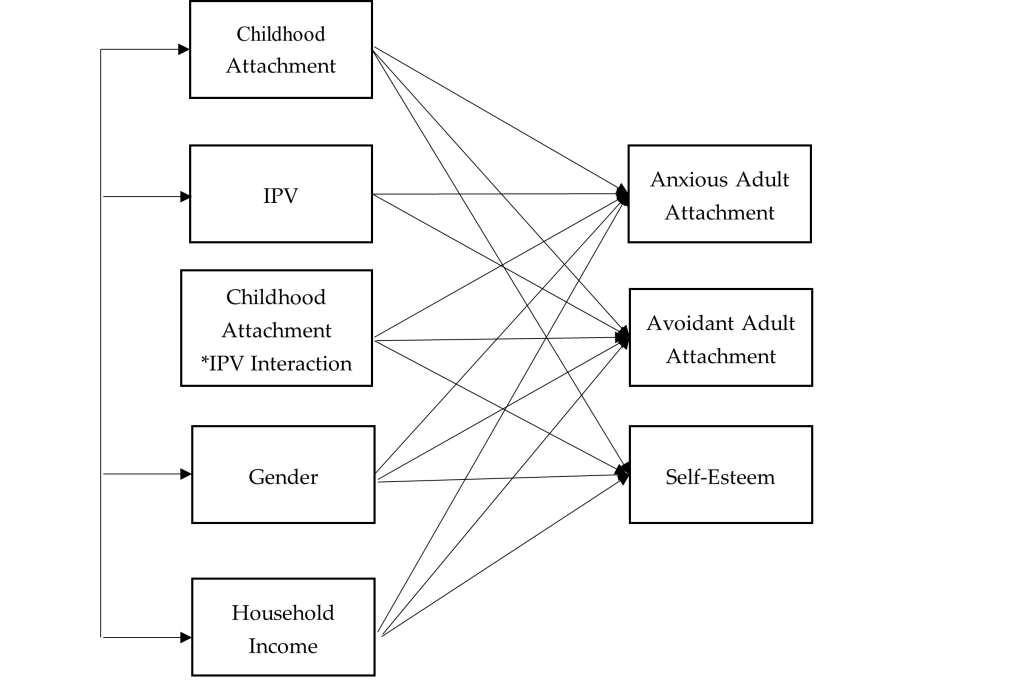
We used SPSS 27 for data preparation and Mplus 8 for data analysis. Missing data were treated with the full information maximum likelihood in Mplus as recommended (Acock, 2005). We examined all the bivariate relationships between all the variables within our study including IPV, childhood attachment, adult attachment (anxious and avoidant attachment), self-esteem, and control variables (i.e., gender and household income). We conducted path analysis to examine the moderating role of childhood attachment between IPV, self-esteem, and adult attachment (see Figure 1). We computed an interaction term by multiplying the predictor (IPV) and the moderator (childhood attachment). A moderation relationship is identified if the interaction item significantly predicts the dependent variables (Baron & Kenny, 1986). The goodness of model fit was evaluated by recommended indices with a non-significant chi-square value, RMSEA < .08, CFI > .90, TLI > .90, and SRMR < .05 (Hooper et al., 2008).
Figure 1
Path Analysis: Moderating Effect of Childhood Attachment on the Relationship Between IPV, Self-Esteem, and Adult Attachment
Results
Descriptive statistics and bivariate correlations of the study variables are demonstrated in Tables 1 and 2. Our model demonstrated good fit to the data, with χ2(4) = 41.90, p = .001, RMSEA = .07, 90% CI [.05, .08], CFI = .99, TLI = .99, SRMR = .02.
The standardized coefficients of the path model revealed that IPV survivors tended to have higher levels of anxious adult attachment (b = .67, p < .001) and avoidant adult attachment (b = .62, p < .001), and lower levels of self-esteem (b = −.29, p < .001) compared with participants without a history of IPV (see Table 3). Individuals with more secure childhood attachment tended to have lower levels of anxious adult attachment (b = −.38, p < .001) and avoidant adult attachment (b = −.31, p < .001), and higher levels of self-esteem (b = .22, p < .001). We found that childhood attachment buffered the relationship between IPV and self-esteem (b = .12, p < .001). Specifically, IPV survivors with more secure childhood attachment demonstrated higher levels of self-esteem. Although the moderation effect was statistically significant, the magnitude of the effect was small. Moreover, IPV survivors with more secure childhood attachment did not demonstrate significant differences on anxious or avoidant adult attachment compared to participants without a history of IPV.
Table 2
Bivariate Correlation Matrix of Variables
| |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
| 1. Anxious Adult Attachment |
– |
|
|
|
|
|
|
| 2. Avoidant Adult Attachment |
.40*** |
– |
|
|
|
|
|
| 3. Self-Esteem |
−.18*** |
−.15*** |
– |
|
|
|
|
| 4. Childhood Attachment |
−.45*** |
−.47*** |
.18*** |
– |
|
|
|
| 5. IPV |
.26*** |
.54*** |
−.17*** |
−.31*** |
– |
|
|
| 6. Gender |
−.10*** |
−.06** |
.14*** |
−.01 |
−.08*** |
– |
|
| 7. Household Income |
.03 |
.08*** |
−.05* |
−.08** |
−.06* |
−.01 |
– |
*p < .05 (two-tailed). **p < .01. ***p < .001.
Table 3
Unstandardized and Standardized Path Coefficients (Standard Errors) for Path Analysis
| Parameter Estimates |
|
Anxious Adult
Attachment |
Avoidant Adult
Attachment |
Self-esteem |
| Childhood Attachment |
Unstandardized |
−.37(.01)*** |
−.33(.02)*** |
.26(.04)*** |
| |
Standardized |
−.38(.01)*** |
−.31(.02)*** |
.22(.03)*** |
| IPV |
Unstandardized |
.61(.01)*** |
.62(.02)*** |
−.33(.04)*** |
| |
Standardized |
.67(.01)*** |
.62(.02)*** |
−.29(.03)*** |
| IPV*Childhood Attachment
Interaction |
Unstandardized |
.00(.00) |
.01(.01) |
.10(.02)*** |
| Standardized |
.01(.01) |
.01(.01) |
.12(.02)*** |
| Control Variables |
| Gender |
Unstandardized |
−.03(.01)** |
−.08(.03)** |
.18(.06)** |
| |
Standardized |
−.02(.01)** |
−.04(.01)** |
.07(.02)** |
| Household Income |
Unstandardized |
.01(.00)*** |
.01(.00)*** |
−.02(.01)** |
| |
Standardized |
.02(.01)*** |
.04(.01)*** |
−.06(.02)** |
*p < .05 (two-tailed). **p < .01. ***p < .001.
Female participants tended to have lower levels of anxious (b = −.02, p < .01) or avoidant adult attachment (b = −.04, p < .01), and higher levels of self-esteem (b = .07, p < .01). Individuals with higher household income reported higher levels of anxious adult attachment (b = .02, p < .001), avoidant adult attachment (b = .04, p < .001), and lower levels of self-esteem (b = −.06, p < .01).
Discussion
Although most existing literature predominantly focuses on revealing how the attachment style of the IPV perpetrators may influence their behavior (Velotti et al., 2018), our study contributes to the field by exploring the potential association between IPV victimization and adult attachment. Using a non-clinical sample, this study identified a positive association between IPV victimization and adult insecure attachment, including both anxious and avoidant dimensions. Meanwhile, a negative association was observed between IPV victimization and self-esteem. These findings concur with the tenets of attachment theory, which posits that individuals who experienced IPV would have a sense of betrayal of trust within intimate relationships. Rather than serving a secure attachment base in intimate adult relationships, IPV experience altered internal models of self as a victim and the other as perpetrator if the individuals stay in the abusive relationships for long enough (Levendosky et al., 2012). IPV survivors may adopt maladaptive coping strategies to mitigate the distress stemming from such intimate relationships. Consequently, these individuals might manifest anxious or avoidant attachment (Levendosky et al., 2012). At the same time, our results indicating reduced self-esteem among IPV victims resonates with previous studies, underscoring the detrimental effects of IPV on self-esteem (Childress, 2013; Karakurt et al., 2014). Enduring undeserved maltreatment from partners can persistently undermine an individual’s sense of self-efficacy and competency (Tariq, 2013).
Our findings do not identify childhood attachment as a significant moderating factor between IPV victimization and insecure attachment in adulthood. There is currently no study to compare with this finding, as the present study is the first to investigate the moderating role of childhood attachment on the relationship between adult IPV victimization and adult attachment.
Although previous research implied that childhood attachment can mitigate the adverse effects of IPV on psychological health and adult life satisfaction (Pang & Thomas, 2020), those studies assessed IPV experiences during an individual’s childhood. Nevertheless, we speculate that IPV targets an individual’s sense of security, which is predominantly influenced by adult romantic relationships (Dutton & White, 2012). This IPV-related sense of security distinguishes itself from childhood attachment, which primarily arises from interactions between parents and children. For instance, the fear associated with intimate relationships and feelings of betrayal, as a result of sustained physical and emotional abuse from an intimate partner, may not be readily alleviated by the sense of security instilled by one’s primary caregivers during childhood. Survivors who were abused by their partner may attempt to manage their distress by deactivating their attachment system, which would reflect more insecure working models of self and others, less self-confidence, and lack of trust in others (Kobayashi et al., 2021).
Conversely, our research determined that childhood attachment acts as a moderator between IPV victimization and self-esteem, aligning with previous studies showing parental support as a vital protective mechanism for the self-esteem of individuals subjected to interpersonal violence (Duru et al., 2019). As posited by attachment theory, secure childhood attachment fosters a robust self-concept, equipping individuals with the belief that they are valuable and deserving of love (Bowlby, 1969). This foundational belief may serve as an effective counterbalance, attenuating the damage to self-esteem precipitated by IPV. We acknowledge that although the moderating effect of childhood attachment on the relationship between IPV victimization and self-esteem was statistically significant, the magnitude standardized coefficients were fairly low. One possible explanation could be that when transitioning to adulthood, individuals expand their social relationships with their peers, romantic partners, and offspring, which may increasingly take on their attachment organizations (Allen et al., 2018; Guarnieri et al., 2015). Future studies could further explore the level of effectiveness of childhood attachment mitigating the negative impact of IPV experience on interpersonal and intrapersonal outcomes in adulthood.
Limitations and Future Directions
Although the present study adds important contributions to the literature on IPV victimization and attachment, several limitations must be acknowledged. First, the dichotomous question of IPV could not fully capture all of the complexity of IPV victimization experiences. Future research should consider other factors related to IPV, including severity of the violence, types of IPV, age of onset, frequency, and duration. Second, retrospective reporting of childhood attachment with the primary caregiver(s) may lead to bias, or distortion in the recall of traumatic events from family of origin. However, previous studies have shown that retrospective reports only have a small amount of bias and that it is not strong enough to invalidate the results for adverse childhood experiences (Hardt & Rutter, 2004).
A growing body of literature has identified adult attachment as a risk factor of IPV (Doumas et al., 2008); here, we were not able to determine the causal relationship between adult attachment and IPV. We did conduct a path analysis using childhood attachment and adult attachment to predict IPV and self-esteem, but the model did not demonstrate a good fit. It is possible that attachment and IPV do not have a simple causal relationship; other childhood trauma experiences may contribute to the complexity of the IPV (Li et al., 2019).
Finally, not knowing the types of attachment in childhood limited our exploration regarding the changes of attachment styles from childhood to adulthood. The cross-sectional design of assessing childhood attachment and adult attachment concurrently did not provide sufficient evidence to determine the cause and effect. Bowlby (1969) believed that there is a continuity between childhood attachment and adult attachment over the life course. An individual’s security in adult relationships may be a partial reflection of their experiences with primary caregivers in early childhood (Ammaniti et al., 2000). However, one of the common misconceptions about attachment theory is that attachment is always stable from infancy to adulthood (Hazan & Shaver, 1994). It is possible that adults’ attachment patterns would change if their relational experiences were disturbed by relational trauma such as IPV (West & George, 1999) or childhood trauma (Shen & Soloski, 2024), which partially explains that childhood attachment is not a significant moderator between IPV and adult attachment from our findings. Future research could conduct longitudinal studies to examine the changes of attachment and how childhood trauma and IPV influences attachment over time.
Implications
The findings of the present study provide insights that may inform clinical interventions for adult survivors who have experienced IPV to rebuild trusting interpersonal relationships and relationships with self. First, IPV experiences were significantly associated with anxious and avoidant adult attachment. During a traumatic experience, such as IPV, the attachment security system is activated, and survivors are in a surviving mode and tend to seek protection. Unfortunately, IPV involves power, control, and betrayal within an intimate relationship, which may damage internal working models of self and others if they stay for long enough (Levendosky et al., 2012). Thus, clinical interventions could focus on altering survivors’ negative internal working models to increase security within non-abusive close relationships. Close friends and family members could remain as a secure base for IPV survivors while they rebuild their personal and social lives that IPV have damaged. Additionally, therapeutic relationships could potentially serve as a secure base for survivors to explore their attachment behaviors. Survivors with avoidant attachment demonstrate deactivation attachment behaviors (Brenner et al., 2021), such as minimizing the impact of their trauma experiences, having a tendency to perceive and present themselves as strong, or avoiding discussing their trauma experiences to avoid the possible pain (Muller, 2009). Therefore, clinicians need to hold a safe space to challenge survivors with avoidant attachment to reactivate their attachment systems, such as by validating their avoidance and ambivalence or facilitating conversations to turn toward trauma-related experiences and emotions instead of turning away. Survivors with anxious attachment, on the other hand, demonstrate hyperactivation attachment behaviors, including fear of rejection and abandonment, hypersensitivity to and preoccupation with relationships and intimacy, utilization of negative emotional regulation strategies, as well as difficulties with leaving abusive relationships (Kural & Kovacs, 2022; Velotti et al., 2018). Clinicians could teach anxious-attached survivors some effective coping strategies, including self-regulation skills, creating boundaries, establishing safety plans, maintaining relationships with others, and increasing self-compassion (Rizo et al., 2017), which may help them to perceive themselves as worthy, lovable, and less dependent on others.
Furthermore, group counseling is a powerful way to learn about trusting oneself and others and to improve interpersonal relationship skills. Clients’ attachment patterns will be activated through interactions with the group members and the facilitators. Clients with anxious attachment tend to react to group members’ rejections, while clients with avoidant attachment tend to demonstrate withdrawal behaviors (e.g., disengagement; Zorzella et al., 2014). Therefore, when working with these clients, clinicians should stimulate the change of internal working models by using the group as a secure base to foster corrective emotional exchanges that challenge group members’ maladaptive beliefs about themselves and others (Marmarosh et al., 2013).
One of the important findings of the current study is that childhood attachment with the primary caregiver(s) buffered the relationship between IPV and self-esteem. From a clinical point of view, the result may bring hope for adult survivors of interpersonal violence regarding their healing process; primary caregivers could still serve as a secure base to offer a crucial opportunity to strengthen the internal working models that would positively affect later adjustment. Counselors could assess survivors’ attachment with their primary caregivers and give them autonomy to determine if it is beneficial to get their non-abusive primary caregivers involved in the treatment to provide support. Although the moderation result from the present study was statistically significant, the magnitude of moderating effect was small. During adulthood, individuals expand their relationship networks with their peers (e.g., friends) and romantic partners, as these relationships become more central in their daily life (Guarnieri et al., 2015). Therefore, the effectiveness of childhood attachment mitigating the adverse effect of IPV in adulthood clinically needs to be further investigated.
Conclusion
The present study empirically examines the moderation role of childhood attachment on the association between IPV, adult attachment, and self-esteem. Specifically, we found that childhood attachment was a significant moderator buffering the relationship between the experience of IPV and self-esteem. A theoretical and empirical understanding of the role of attachment in the context of IPV has implications for researchers and clinicians working with survivors and their families.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Acock, A. C. (2005). Working with missing values. Journal of Marriage and Family, 67(4), 1012–1028.
https://doi.org/10.1111/j.1741-3737.2005.00191.x
Allen, J. P., Grande, L., Tan, J., & Leob, E. (2018). Parent and peer predictors of change in attachment security from adolescence to adulthood. Child Development, 89(4), 1120–1132. https://doi.org/10.1111/cdev.12840
Ammaniti, M., Van Ijzendoorn, M. H., Speranza, A. M., & Tambelli, R. (2000). Internal working models of attachment during late childhood and early adolescence: An exploration of stability and change. Attachment & Human Development, 2(3), 328–346. https://doi.org/10.1080/14616730010001587
Armsden, G. C., & Greenberg, M. T. (1987). The inventory of parent and peer attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence, 16(5), 427–454. https://doi.org/10.1007/BF02202939
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology, 51(6), 1173–1182. https://doi.org/10.1037/0022-3514.51.6.1173
Black, M. C., Basile, K. C., Breiding, M. J., Smith, S. G., Walters, M. L., Merrick, M. T., Chen, J., & Stevens, M. R. (2011). The National Intimate Partner and Sexual Violence Survey: 2010 summary report. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention.
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. Basic Books.
Bowlby, J. (1973). Attachment and loss, Vol. 2: Separation: Anxiety and anger. Basic Books.
Bradshaw, C. P., & Garbarino, J. (2004). Social cognition as a mediator of the influence of family and community violence on adolescent development: Implications for intervention. In J. Devine, J. Gilligan, K. A. Miczek, R. Shaikh, & D. Pfaff (Eds.), Youth violence: Scientific approaches to prevention (pp. 85–105). New York Academy of Sciences.
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). Guilford.
Brennan, K. A., & Morris, K. A. (1997). Attachment styles, self-esteem, and patterns of seeking feedback from romantic partners. Personality and Social Psychology Bulletin, 23(1), 23–31. https://doi.org/10.1177/0146167297231003
Brenner, I., Bachner-Melman, R., Lev-Ari, L., Levi-Ogolnic, M., Tolmacz, R., & Ben-Amitay, G. (2021). Attachment, sense of entitlement in romantic relationships, and sexual revictimization among adult CSA survivors. Journal of Interpersonal Violence, 36(19–20), NP10720–NP10743. https://doi.org/10.1177/0886260519875558
Burke, J. G., Thieman, L. K., Gielen, A. C., O’Campo, P., & McDonnell, K. A. (2005). Intimate partner violence, substance use, and HIV among low-income women: Taking a closer look. Violence Against Women, 11(9), 1140–1161. https://doi.org/10.1177/1077801205276943
Cherrier, C., Courtois, R., Rusch, E., & Potard, C. (2023). Parental attachment, self-esteem, social problem-solving, intimate partner violence victimization in emerging adulthood. The Journal of Psychology, 157(7), 451–471. https://doi.org/10.1080/00223980.2023.2242561
Childress, S. (2013). A meta-summary of qualitative findings on the lived experience among culturally diverse domestic violence survivors. Issues in Mental Health Nursing, 34(9), 693–705. https://doi.org/10.3109/01612840.2013.791735
Doumas, D. M., Pearson, C. L., Elgin, J. E., & McKinley, L. L. (2008). Adult attachment as a risk factor for intimate partner violence: The “mispairing” of partners’ attachment styles. Journal of Interpersonal Violence, 23(5), 616–634. https://doi.org/10.1177/0886260507313526
Duru, E., Balkis, M., & Turkdoğan, T. (2019). Relational violence, social support, self-esteem, depression and anxiety: A moderated mediation model. Journal of Child and Family Studies, 28, 2404–2414.
https://doi.org/10.1007/s10826-019-01509-2
Dutton, D. G., & White, K. R. (2012). Attachment insecurity and intimate partner violence. Aggression and Violent Behavior, 17(5), 475–481. https://doi.org/10.1016/j.avb.2012.07.003
Gamble, S. A., & Roberts, J. E. (2005). Adolescents’ perceptions of primary caregivers and cognitive style: The roles of attachment security and gender. Cognitive Therapy and Research, 29, 123–141. https://doi.org/10.1007/s10608-005-3160-7
Gilbert, L. K., Zhang, X., Basile, K. C., Breiding, M., & Kresnow, M. (2023). Intimate partner violence and health conditions among U. S. adults—National Intimate Partner Violence Survey, 2010–2012. Journal of Interpersonal Violence, 38(1–2), 237–261. https://doi.org/10.1177/08862605221080147
Gomez, R., & McLaren, S. (2007). The inter-relations of mother and father attachment, self-esteem and aggression during late adolescence. Aggressive Behavior, 33(2), 160–169. https://doi.org/10.1002/ab.20181
Gormley, B., & Lopez, F. G. (2010). Psychological abuse perpetration in college dating relationships: Contributions of gender, stress, and adult attachment orientations. Journal of Interpersonal Violence, 25(2), 204–218. https://doi.org/10.1177/0886260509334404
Guarnieri, S., Smorti, M., & Tani, F. (2015). Attachment relationships and life satisfaction during emerging adulthood. Social Indicators Research, 121(3), 833–847. https://doi.org/10.1007/s11205-014-0655-1
Hardt, J., & Rutter, M. (2004). Validity of adult retrospective reports of adverse childhood experiences: Review of the evidence. Journal of Child Psychology and Psychiatry, 45(2), 260–273. https://doi.org/10.1111/j.1469-7610.2004.00218.x
Hazan, C., & Shaver, P. R. (1994). Deeper into attachment theory. Psychological Inquiry, 5(1), 68–79. https://doi.org/10.1207/s15327965pli0501_15
Hooper, D., Coughlan, J., & Mullen, M. (2008). Structural equation modeling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6(1), 53–60. https://doi.org/10.21427/D7CF7R
Jewkes, R., Fulu, E., Tabassam Naved, R., Chirwa, E., Dunkle, K., Haardörfer, R., Garcia-Moreno, C., & the UN Multi-country Study on Men and Violence Study Team. (2017). Women’s and men’s reports of past-year prevalence of intimate partner violence and rape and women’s risk factors for intimate partner violence: A multicountry cross-sectional study in Asia and the Pacific. PloS Medicine, 14(9), e1002381. https://doi.org/10.1371/journal.pmed.1002381
Karakurt, G., Koç, E., Katta, P., Jones, N., & Bolen, S. D. (2022). Treatments for female victims of intimate partner violence: Systematic review and meta-analysis. Frontiers in Psychology, 13, 793021. https://doi.org/10.3389/fpsyg.2022.793021
Karakurt, G., Smith, D., & Whiting, J. (2014). Impact of intimate partner violence on women’s mental health. Journal of Family Violence, 29(7), 693–702. https://doi.org/10.1007/s10896-014-9633-2
Kobayashi, J. E., Levendosky, A. A., Bogat, G. A., & Weatherill, R. P. (2021). Romantic attachment as a mediator of the relationships between interpersonal trauma and prenatal representations. Psychology of Violence, 11(2), 133–143. https://doi.org/10.1037/vio0000361
Kural, A. I., & Kovacs, M. (2022). The role of anxious attachment in the continuation of abusive relationships: The potential for strengthening a secure attachment schema as a tool of empowerment. Acta Psychologica, 225, 103537. https://doi.org/10.1016/j.actpsy.2022.103537
Levendosky, A. A., Lannert, B., & Yalch, M. (2012). The effects of intimate partner violence on women and child survivors: An attachment perspective. Psychodynamic Psychiatry, 40(3), 397–433.
https://doi.org/10.1521/pdps.2012.40.3.397
Li, S., Zhao, F., & Yu, G. (2019). Childhood maltreatment and intimate partner violence victimization: A meta-analysis. Child Abuse & Neglect, 88, 212–224. https://doi.org/10.1016/j.chiabu.2018.11.012
Lindgren, M. S., & Renck, B. (2008). “It is still so deep-seated, the fear”: Psychological stress reactions as consequences of intimate partner violence. Journal of Psychiatric and Mental Health Nursing, 15(3), 219–228. https://doi.org/10.1111/j.1365-2850.2007.01215.x
Lopez, F. G., & Brennan, K. A. (2000). Dynamic processes underlying adult attachment organization: Toward an attachment theoretical perspective on the healthy and effective self. Journal of Counseling Psychology, 47(3), 283–300. https://doi.org/10.1037/0022-0167.47.3.283
Marmarosh, C. L., Markin, R. D., & Spiegel, E. B. (2013). Attachment in group psychotherapy. American Psychological Association. https://doi.org/10.1037/14186-000
Matheson, F. I., Daoud, N., Hamilton-Wright, S., Borenstein, H., Pedersen, C., & O’Campo, P. (2015). Where did she go? The transformation of self-esteem, self-identity, and mental well-being among women who have experienced intimate partner violence. Women’s Health Issues, 25(5), 561–569. https://doi.org/10.1016/j.whi.2015.04.006
McClure, M. M., & Parmenter, M. (2020). Childhood trauma, trait anxiety, and anxious attachment as predictors of intimate partner violence in college students. Journal of Interpersonal Violence, 35(23–24), 6067–6082. https://doi.org/10.1177/0886260517721894
McLaughlin, J., O’Carroll, R. E., & O’Connor, R. C. (2012). Intimate partner abuse and suicidality: A systemic review. Clinical Psychology Review, 32(8), 677–689. https://doi.org/10.1016/j.cpr.2012.08.002
Meeker, K. A., Hayes, B. E., Randa, R., & Saunders, J. (2020). Examining risk factors of intimate partner violence victimization in Central America: A snapshot of Guatemala and Honduras. International Journal of Offender Therapy and Comparative Criminology, 68(5), 468–487. https://doi.org/10.1177/0306624X20981049
Moretti, M. M., & Peled, M. (2004). Adolescent-parent attachment: Bonds that support healthy development. Paediatrics & Child Health, 9(8), 551–555. https://doi.org/10.1093/pch/9.8.551
Muller, R. T. (2009). Trauma and dismissing (avoidant) attachment: Intervention strategies in individual psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 46(1), 68–81. https://doi.org/10.1037/a0015135
Pang, L. H. G., & Thomas, S. J. (2020). Exposure to domestic violence during adolescence: Coping strategies and attachment styles as early moderators and their relationship to functioning during adulthood. Journal of Child & Adolescent Trauma, 13(2), 185–198. https://doi.org/10.1007/s40653-019-00279-9
Ponti, L., & Tani, F. (2019). Attachment bonds as risk factors of intimate partner violence. Journal of Child and Family Studies, 28, 1425–1432. https://doi.org/10.1007/s10826-019-01361-4
Rizo, C. F., Givens, A., & Lombardi, B. (2017). A systematic review of coping among heterosexual female IPV survivors in the United States with a focus on the conceptualization and measurement of coping. Aggression and Violent Behavior, 34, 35–50. https://doi.org/10.1016/j.avb.2017.03.006
Rosenberg, M. (1965). Society and the adolescent self-image. Princeton University Press.
Rosenberg, M. (1979). Conceiving the self. Basic Books.
Sayed, S., Iacoviello, B. M., & Charney, D. S. (2015). Risk factors for the development of psychopathology following trauma. Current Psychiatry Reports, 17, 70. https://doi.org/10.1007/s11920-015-0612-y
Scott, S., & Babcock, J. C. (2010). Attachment as a moderator between intimate partner violence and PTSD symptoms. Journal of Family Violence, 25(1), 1–9. https://doi.org/10.1007/s10896-009-9264-1
Shen, F., Liu, Y, & Brat, M. (2021). Attachment, self-esteem, and psychological distress: A multiple-mediator model. The Professional Counselor, 11(2), 129–142. https://doi.org/10.15241/fs.11.2.129
Shen, F., & Soloski, K. L. (2024). Examining the moderating role of childhood attachment for the relationship between child sexual abuse and adult attachment. Journal of Family Violence, 39, 347–357.
https://doi.org/10.1007/s10896-022-00456-9
St. Vil, N. M., Carter, T., & Johnson, S. (2021). Betrayal trauma and barriers to forming new intimate relationships among survivors of intimate partner violence. Journal of Interpersonal Violence, 36(7–8), NP3495–NP3509. https://doi.org/10.1177/0886260518779596
Sutton, T. E. (2019). Review of attachment theory: Familial predictors, continuity and change, and intrapersonal and relational outcomes. Marriage & Family Review, 55(1), 1–22. https://doi.org/10.1080/01494929.2018.1458001
Tariq, Q. (2013). Impact of intimate partner violence on self esteem of women in Pakistan. American Journal of Humanities and Social Sciences, 1(1), 25–30. https://doi.org/10.11634/232907811604271
Velotti, P., Beomonte Zobel, S., Rogier, G., & Tambelli, R. (2018). Exploring relationships: A systematic review on intimate partner violence and attachment. Frontiers in Psychology, 9, 1166. https://doi.org/10.3389/fpsyg.2018.01166
West, M., & George, C. (1999). Abuse and violence in intimate adult relationships: New perspectives from attachment theory. Attachment & Human Development, 1(2), 137–156. https://doi.org/10.1080/14616739900134201
Wilkinson, R. B. (2004). The role of parental and peer attachment in the psychological health and self-esteem of adolescents. Journal of Youth and Adolescence, 33, 479–493. https://doi.org/10.1023/B:JOYO.0000048063.59425.20
Zorzella, K. P. M., Muller, R. T., & Classen, C. C. (2014). Trauma group therapy: The role of attachment and therapeutic alliance. International Journal of Group Psychotherapy, 64(1), 24–47. https://doi.org/10.1521/ijgp.2014.64.1.24
Fei Shen, PhD, LMFT, is an assistant professor at Kean University. Ying Zhang, PhD, is an assistant professor at Clarkson University. Xiafei Wang, PhD, is an assistant professor at Syracuse University. Correspondence may be addressed to Fei Shen, 1000 Morris Ave., Union, NJ 07083, fshen@kean.edu.
Dec 5, 2024 | Volume 14 - Issue 3
Russ Curtis, Lisen C. Roberts, Paul Stonehouse, Melodie H. Frick
Tattoo art is one of the earliest forms of self-expression, but the advent of colonialism, and its accompanying religious convictions, halted the practice in many Indigenous lands and led to widespread bias against tattooed people—a bias maintained to the present. How might the counseling profession respond to this residual bias and intentionally invoke a cultural shift destigmatizing tattoos? Through an extensive literature review, this article provides a more comprehensive understanding of tattoo-related mental health correlates, biases, and theories that enhance the effectiveness of counseling and parallel trends in the counseling profession that emphasize sociocultural influences on wellness. As a result of this survey, the authors propose a new theory of tattoo motivation, the unencumbered self theory of tattoos, which advances existing tattoo theory and aligns with current counseling trends by postulating that tattoos symbolize the uniquely human desire to transcend norms and laws imposed by external influences.
Keywords: tattoo, bias, mental health, theory, counseling
Imagine you are the parent of a 13-year-old girl. While at a parent–teacher conference, you learn your daughter is struggling with disruptive behavior and angry outbursts during class. The teacher asks if you would support your daughter seeing the school counselor and adds that the counselor is in the school building and available to speak with parents. You approach the counselor’s office, gently knock, and are welcomed by a warm, feminine-presenting adult. As the counselor offers their hand to shake, you notice an entirely tattooed forearm, and as you greet their eyes, more ink is evident on their neck.
What feelings, assumptions, or concerns emerge as you put yourself in the place of the parent in the above vignette? Despite the recent popularization of tattoos, a bias remains. Current research indicates that nearly half of adults in the United States between the ages of 18–34 have at least one tattoo (Roggenkamp et al., 2017), and the tattoo business is one of the fastest-growing enterprises, producing over a billion dollars in annual revenue (Zuckerman, 2020). This trend in tattoo art transcends the United States and is evident throughout the world (Ernst et al., 2022; Khair, 2022; Roberts, 2016). Nevertheless, bias against tattooed people remains, and women and people of color receive the brunt of this discrimination (Baumann et al., 2016; Guéguen, 2013; Kaufmann & Armstrong, 2022; Khair, 2022; Roberts, 2016). Given this meteoric resurgence in tattoo art and the discrimination that clings to it, implications for counseling practice inevitably exist.
Professional questions relevant to the counseling practice include: Is there a relationship between a desire for a tattoo and mental health? What motivates a person to seek a tattoo? In what ways may a tattoo bias subconsciously shape a counselor’s interactions with a client? How might the counseling community communicate a spirit of inclusion to the tattooed? To address these questions, this article employs the following structure. First, we provide a context for this bias by briefly examining the history and cultural perspectives of tattoos. Second, to establish the importance of this issue, we empirically demonstrate the reality of tattoo bias. Third, with this history of bias in mind, we comb the literature for research that explores the relationship between mental health and tattoos. Fourth, these relationships offer a frame of reference for our survey of established tattoo motivation theories, to which we propose an additional theory, the unencumbered self theory of tattoos, and reveal its significance within a clinical setting via a case study. Fifth, before concluding the article, we demonstrate how our inquiry’s content might be applied by enumerating our argument’s implications for the counseling profession.
Historical and Cultural Perspectives of Tattoos
The word tattoo originates from the Samoan term tatau, meaning “to tap lines on the body.” The practice of tattooing is known to have existed as early as 7000 BC, as seen on Egyptian mummies (Rohith et al., 2020). Otzi the Ice Man, dating back to 3000 BC, was discovered in 1991 with tattoos on his arms and wrist that are thought to have been applied for therapeutic purposes, a potential precursor to acupuncture (Schmid, 2013). Prior to the colonization of Indigenous lands by European countries, many tribes practiced the art of tattoo to symbolize adulthood, tribal membership, and status (Dance, 2019; Thomas et al., 2005). However, with the emergence of European imperialism, colonizers taught Indigenous people that tattoos were an abomination, scripturally prohibited, and therefore immoral. For instance, in The Holy Bible (New International Version, 1978, Leviticus 19:28) and The Qur’an (2004, Surah 7:46), specific passages forbid marking the skin.
Despite these condemnations, the practice of tattooing was not eradicated. Many cultures continued their tattoo traditions, and modern culture has adopted new traditions, which are even now expanding throughout the world (Ernst et al., 2022; Khair, 2022; Roberts, 2016). Although there is much intergroup variability, cultural identity can influence the motivation for and type of preferred tattoo. In India, for instance, tattoos often depict unique patterns specific to different tribal regions in the country. Specifically, in urbanized Indian geographic areas, there is increasing integration of tribal pattern tattoos with Western-influenced designs (Rohith et al., 2020). In Samoan culture, men receive an intricate tattoo called a pe’a while women receive a malu, both to indicate maturity (Dance, 2019). Lest the cultural importance of Indigenous tattoos be doubted, their misappropriation has resulted in litigation, thereby challenging attorneys to consider the property rights of tattoo designs (Tan, 2013).
Profoundly relevant to counseling, tattoos are often representational and symbolize something of importance. In a recent qualitative study of tattooed Middle Eastern women, Khair (2022) discovered themes related to taking ownership of their bodies in a patriarchal society and symbolism of their strength and desire to break free of patriarchal rules and religious mandates. In the United States, a study of mixed-race Americans’ tattoos revealed the most common tattoo themes include animal images and text of personally meaningful messages (Sims, 2018). In yet another group, White supremacists often get swastikas, crossed hammers, Confederate flags, and embellished Celtic crosses (Southern Poverty Law Center, 2006). Similarly, in Czech Republic prisons, the skull tattoo is a symbol representing neo-Nazi extremism, which then informs prison officials of inmates potentially becoming radicalized (Vegrichtová, 2018).
Exploring the intersection of religion and tattoos, Morello’s (2021) qualitative analysis of 21 people in three South American cities revealed that tattoos were more accepted among Catholics than evangelicals. Explained below, Morello classified the types of Christian tattoos as reversal, devotional, foundational, and then a nonreligious fourth category termed relational. According to participants, reversal tattoos symbolized regaining control of disempowering events, such as when Christians historically tattooed themselves to show Roman enslavers their devotion to Christ. Devotional tattoos were comprised of images and symbols representing religious themes (e.g., a cross), often used as a source of strength and identity. Foundational tattoos represent significant moments in life, such as major life transitions (e.g., the date of one’s conversion) or mystical experiences. Morello’s last category is akin to devotional tattoos, but the relational category was created to represent devotion to loved ones, such as images or symbols of one’s children.
In a related study examining the beliefs of religious women with and without tattoos, Morello et al. (2021) identified several common themes. This mixed methods study of 48 women in a conservative Christian college indicated that tattoos were not considered taboo by their religious friends and family and that tattooed participants spent considerable time determining which tattoo to receive. Predominant reasons for obtaining tattoos included social justice, friendship, and spiritual values. Summarizing previous research, individuals primarily choose tattoos to express their identity and uniqueness or to take ownership of their bodies. However, as discussed in the following section, there exists a bias against tattooed individuals.
Tattoo Bias
Unfortunately, with any practice that diverges from dominant cultural values, there is bias (Broussard & Harton, 2018). Although evidence indicates less discrimination against tattoos in the 21st century, negative judgments still exist explicitly and implicitly (Broussard & Harton, 2018; Williams et al., 2014; Zestcott et al., 2018). For example, Kaufmann and Armstrong (2022) found that law enforcement and the medical community hold negative sentiments toward tattooed people. They found that medical professionals who expressed negative judgments about their tattooed patients were likely to have patients not return. In fact, patients reported better rapport and increased trust with medical professionals who asked about the meaning of their tattoos. In other words, negative judgment toward, and lack of acknowledgment of, tattoos were detrimental to building the trust needed to provide optimal and consistent care (Kaufmann & Armstrong, 2022).
Unjustly, women and people of color with tattoos experience more significant discrimination than men or White people (Baumann et al., 2016; Camacho & Brown, 2018; Guégen, 2013; Solanke, 2017). For example, women encounter prejudice when failing to gain employment due to having visible tattoos regardless of having excellent job qualifications (Al-Twal & Abuhassan, 2024; Henle et al., 2022). Moreover, women of color have experienced job discrimination by being questioned if they have visible or nonvisible tattoos (i.e., inkism), being forbidden from having or being required to cover tattoos regardless of cultural relevance (e.g., covering a traditional Māori tattoo), or being required to prove that they do not have tattoos—as alleged in a legal complaint against a Singaporean airline that required female attendants to wear a swimsuit and demonstrate to their employers that they did not have tattoos (Solanke, 2017, Chapter 8). Women with tattoos also experience ambivalent sexism due to rejecting the feminine apologetic (i.e., not acting or dressing in stereotypical feminine ways); they are also perceived as wanting attention and sexually promiscuous (Heckerl, 2021). For instance, Guéguen (2013) found that women on the beach displaying a lower-back butterfly tattoo were significantly more likely to be approached by men compared to women without the tattoo, and the men interviewed indicated that they thought they had a better chance of getting a date and having sex with the tattooed women than the nontattooed women (Guéguen, 2013). In other words, men in this study had the biased perception that women with tattoos were more sexually promiscuous than nontattooed women.
This bias appears within incarceration rates as well. In a study conducted by Camacho and Brown (2018), they found that arrestees with neck tattoos were more likely to receive felony charges specifically for larceny offenses. Among these groups, Black individuals with neck tattoos were more likely than others to face felony charges (Camacho & Brown, 2018). It is also noteworthy that law enforcement catalog the tattoos of arrestees in the Registry of Distinct Marks (Miranda, 2020), which is kept in their permanent record and could potentially bias future incarceration and convictions due to the criminogenic stigmatization of individuals with tattoos (Martone, 2023; Rima et al., 2023).
Neck tattoos specifically appear to elicit bias (Baumann et al., 2016). Given two sets of photos of male and female faces, with a neck tattoo and without a visible tattoo, participants were asked to choose among the photos that they would most like to have as their surgeon. In a separate condition, participants were asked to choose who they would most like to have as their car mechanic. In both experiments, participants preferred to have a nontattooed person as their surgeon or mechanic. However, the preference was more substantial for a nontattooed surgeon than a nontattooed mechanic. Female participants assessed the tattooed faces more positively than male participants, but still preferred the nontattooed faces (Baumann et al., 2016).
Roberts (2016) suggested that although tattoos are becoming more prevalent worldwide, they are not yet entirely accepted. As such, employment discrimination occurs for people with visible tattoos. Roberts (2016) suggested employers discriminate primarily because of the fear of customer complaints and the concomitant loss of business. They further suggested that small businesses in rural areas, which tend to be more conservative, may be even more likely to refuse employment to tattooed workers.
Clients’ Perception of Tattooed Counselors
To date, very few published studies examine the perceptions of tattoos within the mental health professional arena. One exception, however, is a recent publication examining the perception of potential mental health clients of psychologists with or without tattoos. Zidenberg et al. (2022) recruited 534 participants to determine if there were negative perceptions of psychologists who had tattoos. First, participants were presented with a mock profile of a fictional clinical psychologist. Each participant was randomly assigned to view one of three images of the psychologist: with no tattoo, a neutral tattoo (a flower), or a provocative tattoo (a skull with flames). Participants then rated the counselor on perceived competence and their personal feelings toward her.
Contrary to the researchers’ initial expectations, the psychologist’s photo with the provocative tattoo was rated more likable, interesting, and confident and less lazy than the psychologist with a neutral or no tattoo. Interestingly, the psychologist’s photo without a tattoo was rated as more professional, but this did not equate to participants’ believing that the psychologist would thus provide better care. The researchers speculated that while nontattooed people are viewed as more professional, they are not necessarily who clients believe will give the best mental health care. They further hypothesized that professionalism may convey a bias of being “better than” the clients and thereby might be perceived as less authentic. Moreover, participants in this study believed they would get better help from a more “authentic” psychologist, and that the provocative tattoo communicated a sense of authenticity (Zidenberg et al., 2022).
Mental Health and Tattoos
Although early studies (e.g., Grumet, 1983) concluded that tattoos were a sign of maladjustment, contemporary research indicates that tattooed people are as healthy as nontattooed people (Mortensen et al., 2019; Pajor et al., 2015). In general, today the mere presence of a tattoo is not correlated with mental or behavioral issues (Roggenkamp et al., 2017). In fact, most people in many cultures conscientiously obtain tattoos to express themselves and honor people and causes they deeply care about (Khair, 2022; Naudé et al., 2019; Shuaib, 2020). Nevertheless, in one study of a German community (N = 1,060), which sampled people aged 14–44, 40.6% who reported childhood abuse or neglect had at least one tattoo, compared to 29.4% tattooed participants who reported no significant abuse (Ernst et al., 2022). However, Ernst et al. (2022) cautioned that the mere presence of a tattoo is not perfectly correlated with childhood abuse. Aesthetic embellishment of the body is the most common reason for getting tattoos, and it should not be considered an automatic indication of childhood abuse (Ernst et al., 2022).
Evidence suggests that the number of tattoos as well as their placement and content better indicate potential maladjustment than the mere presence of an easily concealed tattoo. Specifically, Mortensen et al. (2019) found that participants (N = 2008 adults) who had four or more tattoos were 15.4% more likely to report having been diagnosed with a mental health problem compared to 5.8% of participants with only one tattoo. Further, 13.4% of the participants with visible tattoos reported having a mental health diagnosis, and 28.2% of the participants who self-reported having an offensive tattoo also reported having a mental health diagnosis. In other words, multiple and visible tattoos may be more closely correlated with mental and behavioral issues than the mere presence of tattoos. However, contrary to Mortensen et al. (2019), in their study of life satisfaction with a sample of 449 participants (16–58 years old), Pajor et al. (2015) used the Multidimensional Self-Esteem Inventory (MSEI; O’Brien & Epstein, 1988), a psychological assessment tool with 116 items graded on a 5-point scale and designed to measure various aspects of self-esteem. Results indicated that tattooed people reported significantly higher competence than nontattooed: 37.2 versus 33.6 (p < .001). Tattooed participants also scored significantly higher on a measure of personal power, 35.6 versus 33.5 (p < .01), and significantly lower scores on a measure of anxiety and insomnia, 1.50 versus 1.75 (p < .05). Thus, although numerous visible tattoos could potentially indicate mental or behavioral issues, the research is not conclusive, suggesting the need for counselors to open-mindedly assess each client’s motivations for obtaining tattoos.
Contrary to previous hypotheses, tattoos are rarely a form of self-harm (i.e., cutting, self-mutilation). For example, Aizenman and Jensen (2007) analyzed a sample of college students (N = 1,330; ages 17–39) to determine mental health differences between students who self-injure and those with tattoos. The majority of tattooed students reported receiving tattoos as a way to express their individuality, while students who self-injured were motivated by feelings of insecurity and loss of control. Participants also completed assessments measuring depression and self-esteem. In terms of general wellness, the self-injury group (no tattoos) reported higher mean depression scores compared to both the tattoo group’s score and the nontattooed (no self-injury) score. The self-injury group also reported lower mean self-esteem scores compared to both the tattooed and the nontattooed groups. Noteworthy is the fact that there was no significant difference between the tattooed and nontattooed groups in terms of depression and self-esteem, which further suggests that tattooed college students are no more likely to experience mental health issues than nontattooed college students.
In a more recent study to determine whether tattooing was a form of self-injury, Solís-Bravo et al. (2019) found that from a sample of 438 adolescent males, 11.5% reported engaging in nonsuicidal self-injury (NSSI), but only 1.8% indicated receiving a tattoo with the explicit intention of feeling pain. However, they also found that 62.5% of the students with tattoos self-injured compared to 10.6% of students without tattoos. Thus, with this small subsample of tattooed NSSI students, it was suggested that tattooed adolescents should be screened for potential mental health issues. Yet, considering that only eight students in this sample reported getting a tattoo to feel pain, further replication of this work is needed before confirming a conclusive relationship between tattoos and NSSI (Solís-Bravo et al., 2019).
Exploring the correlation between tattoos and premature mortality (e.g., violent death, drug overdose), Stephenson and Byard (2019) found that there was a trend for people with tattoos to die at a younger age and to experience an unnatural death compared to nontattooed people. However, these results were not statistically significant, indicating that there was no meaningful difference between age and cause of death between tattooed and nontattooed people.
More contemporary research examined the relationship between body image and tattoo acquisition (Jabłońska & Mirucka, 2023). Using a sample of 327 Polish tattooed women to examine a relationship between body image and tattoos, 45.26% reported acceptance of their appearance and a deep connection to their bodies. Researchers speculated that they received tattoos as a way to adorn their bodies and express their individuality. Another 36% reported an unstable body image, meaning they perceived both positive and negative aspects of their bodies. It was speculated that this group used tattoos to conceal perceived flaws. The remaining 18.65% held a negative body image. Although the majority of their sample held either positive or mixed body image estimations, the researchers’ speculation as to why subjects received tattoos makes it difficult to infer correlation between tattoos and well-being. Nevertheless, nearly half the sample reported appreciation for their bodies and a desire to accentuate their positive self-image with body art.
Relatedly, some trauma survivors get tattoos to symbolize what they experienced and how they have grown (Crompton et al., 2021). The semicolon is one example of this, indicating that while one life chapter may have been traumatic, that is not the end of the story. Using tattoos to navigate trauma is further supported by Kidron (2012), who noted that some descendants of Holocaust survivors replicated the number tattoo on their arms to illustrate the connection to their grandparent, redefining the tattoos from markers of trauma to markers of survival and expanding their interfamilial bond and cultural identity.
In summary, studies indicate that the mere presence of a tattoo is not significantly correlated with mental or behavioral issues. Counselors should avoid assuming that tattooed clients have mental health issues, even if multiple visible tattoos are sometimes linked with adverse health outcomes or behaviors. Because tattoos are so often attached to identity, body image, and important life events, counselors should thoroughly explore with clients why they obtained such tattoos and what they symbolize. In order to assist with such exploration, the next section identifies a number of recognized tattoo motivation theories.
Tattoo Motivation Theories
To determine effective strategies to reduce tattoo bias and counsel tattooed clients, it is important to understand the motivations and theoretical premises of why people get tattoos. This section describes recognized tattoo motivation theories. Recent findings in tattoo research cited within this article highlight the limitations of these theories and prompted us to propose our own, the unencumbered self theory of tattoos, which focuses on sociocultural influences. From this new perspective, we hope counselors will have a clearer understanding of the motivations behind getting a tattoo, which will in turn increase understanding of tattoo culture and what this implies about clients and counseling practice. To illustrate how these theoretical models might be of use in a clinical setting, in the subsequent section we provide a case study in which we discuss, compare, and contrast theories and exemplify the need for a new understanding of tattoo motivation.
Psychodynamic Theory of Tattoo
The first hypothesis for tattooing is rooted in psychodynamic theory. This theory posits that tattoos are an outward manifestation of intrapersonal conflict or unresolved psychological concerns (Grumet, 1983; Karacaoglan, 2012; Lane, 2014). The belief is that permanent skin marking serves as a visible mnemonic that prompts a defense mechanism that helps alleviate the anxiety caused by conflict within the id, ego, and superego. In other words, the symbolism embodied within the marking of the skin iteratively releases blocked psychic energy, causing temporary relief from various difficult symptoms.
Psychodynamic theory is problematic because it fails to address the alternative motivations for getting tattoos, namely, the aforementioned social–cultural perspective. Moreover, Freud’s psychoanalytic approach is rooted in Western civilization’s understanding of internal processes and is therefore heavily influenced by a European, White, male perspective of psychic processes, thus ignoring the effects of oppression and inequality on personal identity, mental health, and behavior. As was indicated in the previous research review, and as we will see in subsequent sections, current tattoo research does not support the notion that tattoos are merely the result of unconscious conflict.
Human Canvas and Upping the Ante Theories of Tattoo
Moving beyond the arguably deficit ideology of the psychodynamic theory of tattoos, Carmen et al. (2012) proposed two evolutionary theories of tattoo motivation that transcend obvious reasons like self-expression and group membership. The first theory, human canvas, argues that it is our innate longing to express the most authentic desires of our psyche through symbolic thought, originally on cave walls and later on our bodies. Their second theory, upping the ante, postulated that with increasing longevity and improved health care, the opportunities for attracting mates are more competitive, and people must devise new ways to stand out to attract mates, much like a peacock spreading its feathers.
The human canvas and upping the ante theories of tattoos are at least to some degree supported by current research (e.g., Wohlrab et al., 2007), and both theories advance our understanding of the motivation behind tattoos beyond psychodynamic theory. Indeed, people spend considerable time and thought choosing their tattoos for personal self-expression (Kaufmann & Armstrong, 2022) and to symbolize cultural traditions, sexual expression, and the love of art (Wohlrab et al., 2007). Although these theories advance tattoo theory, they fail to consider the even deeper meaning which suggests that tattoos are a way to regain bodily control and express displeasure with mandated values imposed by external influences. In essence, it is clear that tattoos are a form of self-expression, potentially to increase personal uniqueness and attractiveness, but this fails to explain what people are hoping to express. Thus, informed by contemporary tattoo research, we propose a new and expanded theory that attempts to explain the rationale behind tattoo acquisition through a wider societal lens.
The Unencumbered Self Theory of Tattoo
The unencumbered self theory of tattoos advances existing tattoo theory and aligns with current counseling trends by postulating that tattoos symbolize the uniquely human desire to transcend norms and laws imposed by external influences such as imperialism. After an exhaustive review of the tattoo literature, it is evident that the motivation to reclaim personal power from oppressive systems is one reason some people get tattoos, and this motivation is not explicitly stated within existing theories. While most closely aligned with the human canvas theory, the unencumbered self theory of tattoos differs in one subtle but essential way. The human canvas theory postulates that tattoos are a general form of self-expression (e.g., hobbies, memorials, identity, individuality). At the same time, the unencumbered self theory of tattoos suggests that specific individuals acquire tattoos as a deliberate assertion of autonomy and a repudiation of arbitrary societal norms. Take, for example, a client of Cherokee heritage who gets a tattoo depicting Cherokee syllabary. The human canvas theory would hold that this tattoo is motivated by the client’s desire to identify with her cultural heritage. The unencumbered self theory of tattoos acknowledges her desire to identify with her cultural heritage, but this desire is motivated by the need to disengage from the oppressive systems that successfully squelched her people’s values for so long.
Evidence supporting the unencumbered self theory of tattoos includes cross-cultural studies examining motivations behind obtaining tattoos (Atkinson, 2002; Khair, 2022; Kloẞ, 2022). Atkinson (2002) reported that Canadian women wore tattoos to challenge societal definitions of femininity, and Khair (2022) found that Middle Eastern women obtained tattoos primarily to express their uniqueness and to indicate ownership of their bodies. Khair (2022) stated, “In fact, women of the Middle East have been struggling to obtain the freedom of their identity due to various restrictive reasons that relate to religion” (p. 3). This sentiment is further supported by Stein (2011) who stated, “My data suggest that—rather than seeing themselves as capitulating to market forces—people think of their decision to get tattoos as an exceptionally deep expression of personal identity, as well as a dramatic declaration of autonomy” (p. 128).
Additionally supporting the cultural motivations behind obtaining tattoos, Kloẞ (2022) identified Hindu women having tattoos that symbolize both oppression from and resistance to patriarchy, colonialism, and orthodox religious beliefs. Relatedly, Stein (2011) stated that the motivation behind tattoos is, at least in part, “a defiance of patriarchal authority” (p. 113). This desire to live unencumbered is also evidenced in research indicating that tattooed people are less likely to be members of religious groups (Laumann & Derick, 2006); are less likely to conform to societal norms, as evidenced by lower scores on personality assessments measuring agreeableness and conscientiousness (Tate & Shelton, 2008); and are considered more authentic and relatable (Zidenberg et al., 2022).
The unencumbered self theory of tattoos also coincides with current research and theoretical advancements in the counseling profession. Integrative approaches, such as narrative, relational, and art therapies, illustrate how tattoos can be used to externalize issues and emotions onto the body and promote self-expression by re-authoring life stories that are freeing and healing (Alter-Muri, 2020; Covington, 2015). Further, there is an increasing interest in Indigenous healing practices and the counseling profession’s embrace of a more collaborative and collective approach to health and wellness. To illustrate how the unencumbered self theory of tattoos advances tattoo theory and serves the counseling profession, we compare and contrast the existing theories in the following case study.
Case Study and Discussion
In this fictional case study, Sage is a 28-year-old, cisgender, queer, able-bodied female whose mother is Eastern Band Cherokee and whose father identifies as Mexican American. Sage upholds many traditional Cherokee customs and regularly attends tribal council meetings as well as powwows where she dances in traditional native attire. Sage has several visible tattoos on her arms and one on the back of her neck, all of which symbolize her Cherokee heritage. She presented to counseling with increasing depression after quitting drugs and alcohol for the past year and reports being unhappy in her job with no meaningful relationships. Sage’s counselor does not have tattoos and identifies as White, female, and a social justice advocate who knows very little about people with tattoos or Cherokee customs.
From the psychodynamic theory of tattoo (Grumet, 1983), Sage’s tattoos would be considered an expression of inner conflict and unmet needs, and the counselor would ask questions hoping to uncover unconscious beliefs that are causing her depression. In this case, the counselor may not even mention her tattoos, but instead view them from a deficit lens indicating a personal problem to resolve.
In both the human canvas and upping the ante evolutionary theories of tattoos (Carmen et al., 2012), Sage’s tattoos could indicate her desire to express her individuality and enhance her attractiveness. With this in mind, the counselor is likely to acknowledge her tattoos and ask about their meaning. However, both theories fail to recognize that Sage’s tattoos may signify deeper underlying issues related to potential oppression and inequality she feels because of her race, ethnicity, and gender.
From the unencumbered self theory of tattoos, Sage’s tattoos could reflect her motivational factors, feelings of alienation, and desire to align her authentic self and heritage. From this perspective, the counselor might explore whether she has experienced discrimination and how the impact of societal marginalization shaped her current sense of self. For example, the counselor may ask, “Have you ever experienced feelings of alienation or disconnect from others, and if so, how do you think your tattoos relate to those experiences?” Another counselor probe could be, “What emotions or thoughts come up when you think about the stories or meanings behind your tattoos?” In addition, the counselor may inquire into cultural healing traditions that help Sage reclaim her authenticity and realign her with her Indigenous heritage. In this instance, the counselor may ask, “Are specific cultural or familial traditions associated with your tattoos, and how do they contribute to your sense of authenticity?” or “Have your tattoos played a role in helping you reconnect with or reclaim aspects of your cultural identity?” Ultimately, through understanding the unencumbered self theory of tattoos, the counselor can better assist Sage by gaining deeper insight into her experiences, her motivations, and the significance of her tattoos within the context of her identity and mental health journey.
In summary, clients’ motivations for tattoos are complex and include explicit explanations, such as self-expression and identity, and potentially implicit motivations, such as increased attractiveness and autonomy. Based upon the tattoo motivation research, we believe the unencumbered self theory of tattoos provides a more comprehensive understanding of the reasons people get tattoos, which appears to be motivated by boldly proclaiming their desire for autonomy and not merely to enhance personal attractiveness. With these findings in mind, the subsequent section describes how counselors, and the counseling profession more broadly, can enhance counseling practice with tattooed clients.
Implications for Counseling
Tattooed clients and counselors will become increasingly common, if not the norm. Consequently, there are clinical, professional, ethical, and societal considerations associated with the increasing popularity of tattoo art. This section addresses what counselors can do to adeptly navigate the increasing prevalence of tattoo culture and better serve their clients.
Counselors must reexamine their potential bias about tattooed clients and recognize that current research suggests they are not more likely to have mental and behavioral problems (e.g., Pajor et al., 2015). In fact, tattoos on a client might indicate their readiness for counseling by showing their strength and desire to break free of parental and societal expectations (e.g., Crompton et al., 2021). However, the number and placement of tattoos may better indicate potential mental health issues (Mortensen et al., 2019). With this in mind, asking clients about their tattoos early in the counseling relationship may help build rapport and provide potentially rich information about the client’s life story. Specifically, if the client’s tattoo is visible, it would be appropriate and possibly helpful to ask about it during intake (Kaufmann & Armstrong, 2022).
To foster genuine rapport and mitigate power imbalances in the therapeutic relationship, it is crucial for counselors to engage in self-reflection, cultivate cultural awareness and humility, and understand the potential cultural significance of tattoos (Day-Vines et al., 2018). Initiating conversations about clients’ tattoos early in counseling can be an effective strategy. Counselors might ask: “Tattoos often have special meanings or stories attached to them. What inspired you to get yours?” This approach demonstrates respect for the client’s personal and cultural narratives, promoting a more equitable and empathetic counseling environment. For instance, inquiring about a client’s neo-Nazi tattoos demonstrates the counselor’s desire to understand all aspects of the client. Despite the offensive nature of the tattoos, questioning could prompt the client to disclose personal experiences such as family addiction, abuse, poverty, insecurity, and fear of losing one’s identity in an increasingly multicultural society. These disclosures might not have emerged otherwise.
Counselors do not necessarily need to cover their tattoos, because they may help increase clients’ perception of the counselor’s relevance (Zidenberg et al., 2022). In fact, the counselor disclosing their tattoos may propel some clients to share more personally relevant information during sessions (Stein, 2011). Depending upon the client, a counselor with tattoos could broach the topic of how their tattoos symbolize their pursuit of authenticity in a society where the values of marginalized populations (e.g., women, non-White, LGBTQ) are too often not recognized, understood, or honored.
This example shows how a counselor could broach the topic of tattoos:
During our sessions, we have been exploring various aspects of identity and self-expression, which has led me to reflect on something personal I would like to share with you. As you may have noticed, I have some tattoos that hold particular significance. I have found that my tattoos remind me of essential experiences and values in my life. I share this with you because I believe it is vital for us to foster an environment of openness and authenticity in our therapeutic relationship. However, I want to emphasize that our sessions are about you and your journey. So, if you have any questions or concerns about my tattoos or anything else, please feel free to share them with me. I am here to create a safe and open space to discuss anything that comes up for you.
Thus, the counselor’s tattoo narrative may offer the client freedom to explore repressed aspects of themselves, which, once discovered, may allow for more self-awareness and appreciation, ultimately resulting in better mental health. Counselors can also simply discuss their tattoos with clients who express curiosity or concern. This approach allows the counselor to provide context and meaning behind their tattoos, potentially fostering a deeper connection and understanding between counselor and client.
However, some clients might be disinclined to continue services with an obviously tattooed counselor. As such, counselors may choose to cover their tattoos during sessions, especially if they anticipate that it may distract or discomfort certain clients. This approach can help maintain a professional appearance and minimize potential barriers to therapy. These kinds of tensions may lead to the strategic use of profile photographs on one’s counseling practice’s website. Depending on their client base and target demographics, counselors may opt for photographs that either prominently display or discreetly conceal their tattoos. Prioritizing the client’s comfort and preferences is essential. Counselors should gauge the client’s reactions and adjust their approach accordingly. In sum, the best advice for counselors with tattoos is to rely on their clinical intuition and discretion when deciding how to approach discussions about personal tattoos with clients. As with any counselor disclosure, discussing personal tattoos should be used intentionally with the client’s best interest in mind.
If a client inquires about the advisability of getting tattoos, it is essential to assist them in thoroughly processing this decision, as with any significant life choice. Be open with clients that biases against tattoos persist, with people of color and women being the most stigmatized. Regrettably, many individuals harbor negative perceptions of tattooed people, particularly regarding visible body art and content that might be deemed offensive. Counselors can ask probing questions about the client’s reasoning for obtaining tattoos, such as, “What does getting this tattoo mean to you, and how do you think it will impact your sense of identity or self-expression?” and “Have you considered any potential long-term implications of getting this tattoo, including how you might feel about it in the future or how it might affect your personal or professional life?”
The intersection of tattoos, mental health, and social justice represents a rich and largely unexplored area of research for counselor educators. As the prevalence of tattoos increases among both clients and counselors, we believe this presents a rich opportunity for personal exploration and the discovery of values and strengths, an area currently underexplored in the counseling profession. Future research on tattoos could examine their presence on counselors and clients, their effect on the therapeutic alliance, personality differences among tattooed individuals, and tattooed people’s likelihood of engaging in advocacy work. To advance dialogue and research in this domain, the Western Carolina University counseling program’s faculty, students, and graduates created the Intersection: Art, Mental Health, and Social Justice magazine (Mock et al., 2021). This publication aimed to enhance dialogue and understanding regarding tattoos. Readers are encouraged to peruse the online magazine to explore personal stories of tattooed counselors.
Conclusion
With the increasing popularity and prevalence of tattoos combined with continued cultural bias, body art is an area that warrants further research and discussion in the counseling profession. In summary, there does not appear to be significant relationship between tattooed people experiencing more mental health problems than nontattooed people. However, there is continued bias against tattooed people, and the reasons for obtaining tattoos are rooted more deeply than merely increasing personal attractiveness. As described in the unencumbered self theory of tattoos, the reemergence of tattoo art may be emblematic of the trends seen throughout the counseling profession to advance the discipline from its focus on intra- and interpersonal theories of health and wellness to include broader sociological perspectives on healing. The reemergence of tattoo art, then, could be an allegory for moving beyond the White, male, heteronormative standards that have traditionally dominated the profession, ushering forth an age of inclusivity where the rich and complex tapestry of all people’s values, traditions, and customs can be known and honored.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aizenman, M., & Jensen, M. A. C. (2007). Speaking through the body: The incidence of self-injury, piercing, and tattooing among college students. Journal of College Counseling, 10(1), 27–43. https://doi.org/10.1002/j.2161-1882.2007.tb00004.x
Alter-Muri, S. (2020). The body as canvas: Motivations, meanings, and therapeutic implications of tattoos. Art Therapy, 37(3), 139–146. https://doi.org/10.1080/07421656.2019.1679545
Al-Twal, A., & Abuhassan, R. (2024). Tattoos and career discrimination in a conservative culture: The case of Jordan. Current Psychology, 43, 11914–11923. https://doi.org/10.1007/s12144-023-05304-7
Atkinson, M. (2002). Pretty in ink: Conformity, resistance, and negotiation in women’s tattooing. Sex Roles, 47, 219–235. https://doi.org/10.1023/A:1021330609522
Baumann, C., Timming, A. R., & Gollan, P. J. (2016). Taboo tattoos? A study of the gendered effects of body art on consumers’ attitudes toward visibly tattooed front line staff. Journal of Retailing and Consumer Services, 29, 31–39. https://doi.org/10.1016/j.jretconser.2015.11.005
Broussard, K. A., & Harton, H. C. (2018). Tattoo or taboo? Tattoo stigma and negative attitudes toward tattooed individuals. The Journal of Social Psychology, 158(5), 521–540. https://doi.org/10.1080/00224545.2017.1373622
Camacho, J., & Brown, W. (2018). The evolution of the tattoo in defiance of the immutable definition of deviance: Current perceptions by law enforcement of tattooed arrestees. Deviant Behavior, 39(8), 1023–1041. https://doi.org/10.1080/01639625.2017.1395669
Carmen, R. A., Guitar, A. E., & Dillon, H. M. (2012). Ultimate answers to proximate questions: The evolutionary motivations behind tattoos and body piercings in popular culture. Review of General Psychology, 16(2), 134–143. https://doi.org/10.1037/a0027908
Covington, B. E. (2015). The sentence continues: Breaking silences and becoming authors through The Semicolon Project [Master’s thesis, James Madison University]. JMU Scholarly Commons. https://commons.lib.jmu.edu/master201019/47
Crompton, L., Amrami, G. P., Tsur, N., & Solomon, Z. (2021). Tattoos in the wake of trauma: Transforming personal stories of suffering into public stories of coping. Deviant Behavior, 42(10), 1242–1255. https://doi.org/10.1080/01639625.2020.1738641
Dance, A. (2019, April 6). How the Samoan tattoo survived colonialism. Scientific American. https://www.scientificamerican.com/article/how-the-samoan-tattoo-survived-colonialism
Day-Vines, N. L., Ammah, B. B., Steen, S., & Arnold, K. M. (2018). Getting comfortable with discomfort: Preparing counselor trainees to broach racial, ethic, and cultural factors with clients during counseling. International Journal for the Advancement of Counselling, 40(2), 89–104. https://doi.org/10.1007/s10447-017-9308-9
Ernst, M., Borkenhagen, A., Fegert, J. M., Brähler, E., & Plener, P. L. (2022). The association of childhood abuse and neglect with tattoos and piercings in the population: Evidence from a representative community survey. BMC Psychology, 10(105), 1–10. https://doi.org/10.1186/s40359-022-00811-x
Grumet, G. W. (1983). Psychodynamic implications of tattoos. American Journal of Orthopsychiatry, 53(3), 482–492. https://doi.org/10.1111/j.1939-0025.1983.tb03392.x
Guéguen, N. (2013). Effects of a tattoo on men’s behavior and attitudes towards women: An experimental field study. Archives of Sexual Behavior, 42(1), 1517–1524. https://doi.org/10.1007/s10508-013-0104-2
Heckerl, A. (2021). I can’t even wear my skin: The experiences visibly tattooed women have for rejecting hegemonic femininity (Publication No. 1099) [Master’s thesis, California State University, Monterey Bay]. Capstone Projects and Master’s Theses. https://digitalcommons.csumb.edu/caps_thes_all/1099
Henle, C. A., Shore, T. H., Murphy, K. R., & Marshall, A. D. (2022). Visible tattoos as a source of employment discrimination among female applicants for a supervisory position. Journal of Business and Psychology, 37, 107–125. https://doi.org/10.1007/s10869-021-09731-w
Jabłońska, K., & Mirucka, B. (2023). Mental body representations of women with tattoos in emerging adulthood—A cluster analysis. Archives of Women’s Mental Health, 26(4), 473–483. https://doi.org/10.1007/s00737-023-01326-z
Karacaoglan, U. (2012). Tattoo and taboo: On the meaning of tattoos in the analytic process. The International Journal of Psychoanalysis, 93(1), 5–28. https://doi.org/10.1111/j.1745-8315.2011.00497.x
Kaufmann, L., & Armstrong, M. L. (2022). The influences of tattoos on health care experiences. The Journal of Continuing Education in Nursing, 53(4), 178–184. http://doi.org/10.3928/00220124-20220311-08
Khair, N. (2022). Marketing of self: Using tattoos to symbolize ownership and control of one’s body. Narratives from Middle Eastern women. Sociology Compass, 16(7), 1–11. https://doi.org/10.1111/soc4.13002
Kidron, C. A. (2012). Breaching the wall of traumatic silence: Holocaust survivor and descendant person–object relations and the material transmission of the genocidal past. Journal of Material Culture, 17(1), 3–21. https://doi.org/10.1177/1359183511432989
Kloẞ, S. T. (2022). Embodying dependency: Caribbean godna (tattoos) as female subordination and resistance. The Journal of Latin American and Caribbean Anthropology, 27(4), 601–612. https://doi.org/10.1111/jlca.12644
Lane, D. C. (2014). Tat’s all folks: An analysis of tattoo literature. Sociology Compass, 8(4), 398–410. https://doi.org/10.1111/soc4.12142
Laumann, A. E., & Derick, A. J. (2006). Tattoos and body piercings in the United States: A national data set. Journal of the American Academy of Dermatology, 55(3), 413–421. https://doi.org/10.1016/j.jaad.2006.03.026
Martone, A. J. (2023). Scars, marks, and tattoos: How appearance influences rearrest and reconviction (Publication No. 31076097) [Master’s thesis, Sam Houston State University]. ProQuest Dissertations and Theses Global.
Miranda, M. D. (2020). Tattoos and tattoo inks: Forensic considerations. WIREs Forensic Science, 2(1), 1–16. https://doi.org/10.1002/wfs2.1360
Mock, C., Jones, B., Gillespie, L., & Curtis, R. (Eds.). (2021). Intersection: Art, mental health, and social justice (Issue No. 1). Western Carolina University. https://online.fliphtml5.com/pdhbe/uinm
Morello, G. (2021). I’ve got you under my skin: Tattoos and religion in three Latin American cities. Social Compass, 68(1), 61–80. https://doi.org/10.1177/0037768620962367
Morello, G., Sanchez, M., Moreno, D., Engelmann, J., & Evangel, A. (2021). Women, tattoos, and religion an exploration into women’s inner life. Religions, 12(7), 517. https://doi.org/10.3390/rel12070517
Mortensen, K., French, M. T., & Timming, A. R. (2019). Are tattoos associated with negative health-related outcomes and risky behaviors? International Journal of Dermatology, 58(7), 816–824. https://doi.org/10.1111/ijd.14372
Naudé, L., Jordaan, J., & Bergh, L. (2019). “My body is my journal, and my tattoos are my story”: South African psychology students’ reflections on tattoo practices. Current Psychology, 38, 177–186. http://doi.org/10.1007/s12144-017-9603-y
O’Brien, E. J., & Epstein, S. (1988). The Multidimensional Self-Esteem Inventory (MSEI): Professional manual. Psychological Assessment Resources, Inc. https://www.parinc.com/products/MSEI#details
Pajor, A. J., Broniarczyk-Dyła, G., & Świtalska, J. (2015). Satisfaction with life, self-esteem and evaluation of mental health in people with tattoos or piercings. Psychiatria Polska, 49(3), 559–573. https://doi.org/10.12740/PP/27266
Rima, D., Aldabergenova, N., Sharipova, A., Atakhanova, G., & Beaver, K. M. (2023). Tattoos as a stigmatizing label implicated in being processed through the criminal justice system. Deviant Behavior, 44(11), 1701–1712. https://doi.org/10.1080/01639625.2023.2230513
Roberts, D. (2016). Using dramaturgy to better understand contemporary Western tattoos. Sociology Compass, 10(9), 795–804. https://doi.org/10.1111/soc4.12400
Roggenkamp, H., Nicholls, A., & Pierre, J. M. (2017). Tattoos as a window to the psyche: How talking about skin art can inform psychiatric practice. World Journal of Psychiatry, 7(3), 148–158. https://doi.org/10.5498/wjp.v7.i3.148
Rohith, M. M., Belcher, W. R., Roy, J., Abraham, S. O., Chakraborty, P., Nandaniya, N. J., & Johnson, A. (2020). Tattoo in forensic science: An Indian perspective. Journal of Forensic and Legal Medicine, 74, 1–10. https://doi.org/10.1016/j.jflm.2020.102022
Schmid, S. (2013). Tattoos – An historical essay. Travel Medicine and Infectious Disease, 11(6), 444–447. https://doi.org/10.1016/j.tmaid.2013.10.013
Shuaib, S. O. (2020). African traditional body art and contemporary realities. International Journal of Humanitatis Theoreticus, 3(1), 127–140. https://bit.ly/Shuaib_bodyart
Sims, J. P. (2018). “It represents me”: Tattooing mixed-race identity. Sociological Spectrum, 38(4), 243–255. https://doi.org/10.1080/02732173.2018.1478351
Solanke, I. (2017). Discrimination as stigma: A theory of anti-discrimination law. Bloomsbury.
Solís-Bravo, M. A., Flores-Rodríguez, Y., Tapia-Guillen, L. G., Gatica-Hernández, A., Guzmán-Reséndiz, M., Salinas-Torres, L. A., Vargas-Rizo, T. L., & Albores-Gallo, L. (2019). Are tattoos an indicator of severity of non-suicidal self-injury behavior in adolescents? Psychiatry Investigation, 16(7), 504–512.
https://doi.org/10.30773/pi.2019.03.06
Southern Poverty Law Center. (2006, October 19). A look at racist skinhead symbols and tattoos. The Intelligence Report. https://www.splcenter.org/fighting-hate/intelligence-report/2006/look-racist-skinhead-symbols-and-tattoos
Stein, A. (2011). The tattooed therapist: Exposure, disclosure, transference. Psychoanalysis, Culture & Society, 16, 113–131. https://doi.org/10.1057/pcs.2010.17
Stephenson, L., & Byard, R. W. (2019). Cause, manner and age of death in a series of decedents with tattoos presenting for medicolegal autopsy. Journal of Forensic and Legal Medicine, 64(1), 49–51. https://doi.org/10.1016/j.jflm.2019.04.003
Tan, L. (2013). Intellectual property law and the globalization of indigenous cultural expressions: Māori tattoo and the Whitmill versus Warner Bros. case. Theory, Culture & Society, 30(3), 61–81. https://doi.org/10.1177/0263276412474328
Tate, J. C., & Shelton, B. L. (2008). Personality correlates of tattooing and body piercing in a college sample: The kids are alright. Personality and Individual Differences, 45(4), 281–285. https://doi.org/10.1016/j.paid.2008.04.011
The Holy Bible: New International Version. (1978). The Zondervan Corporation.
The Qur’an (M. A. S. Abdel Haleem, Trans.). (2004). Oxford University Press.
Thomas, N., Cole, A., & Douglas, B. (Eds.). (2005). Tattoo: Bodies, art and exchange in the Pacific and the West. Reaktion Books.
Vegrichtová, B. (2018). Nonverbal communication of prison subculture through criminal tattoo symbols. Academic and Applied Research in Military and Public Management Science, 17(3), 179–186. https://doi.org/10.32565/aarms.2018.3.13
Williams, D. J., Thomas, J., & Christensen, C. (2014). “You need to cover your tattoos!”: Reconsidering standards of professional appearance in social work. Social Work, 59(4), 373–375. https://doi.org/10.1093/sw/swu025
Wohlrab, S., Stahl, J., & Kappeler, P. M. (2007). Modifying the body: Motivations for getting tattooed and pierced. Body Image, 4(1), 87–95. https://doi.org/10.1016/j.bodyim.2006.12.001
Zestcott, C. A., Tompkins, T. L., Kozak Williams, M., Livesay, K., & Chan, K. L. (2018). What do you think about ink? An examination of implicit and explicit attitudes toward tattooed individuals. The Journal of Social Psychology, 158(1), 7–22. https://doi.org/10.1080/00224545.2017.1297286
Zidenberg, A. M., Dutrisac, S., & Olver, M. (2022). “No ragrets”: Public perception of tattooed mental health professionals. Professional Psychology: Research and Practice, 53(3), 304–312. https://doi.org/10.1037/pro0000441
Zuckerman, A. (2020, May 13). 38 tattoo statistics: 2020/2021 industry, trends & demographics. Compare Camp. https://comparecamp.com/tattoo-statistics/
Russ Curtis, PhD, LCMHC, is a professor at Western Carolina University. Lisen C. Roberts, PhD, is an associate professor at Western Carolina University. Paul Stonehouse, PhD, is an assistant professor at Western Carolina University. Melodie H. Frick, PhD, NCC, ACS, LPC-S, is a professor at Western Carolina University. Correspondence may be addressed to Russ Curtis, Western Carolina University, 28 Schenck Parkway, Office 214, Asheville, NC 28803, curtis@wcu.edu.
Dec 5, 2024 | Volume 14 - Issue 3
Katherine M. Hermann-Turner, Jonathan D. Wiley, Corrin N. Brown, Alyssa A. Curtis, Dessie S. Avila
The social and emotional challenges experienced by new mothers residing in rural areas are distinct from those confronted by their urban and suburban counterparts. However, the existing literature on postpartum social and emotional experiences of rural mothers is limited. To address this gap in knowledge, we conducted a phenomenological study to explore the postpartum social and emotional experiences of rural mothers. The study revealed that rural mothers experience feelings of powerlessness, thwarted help-seeking, and resilience. Findings are discussed in the context of the wider discourse on childbirth and postpartum experiences of rural mothers and have important implications for professional counselors serving rural communities.
Keywords: rural mothers, postpartum, social, emotional, rural communities
It is estimated that approximately 3.6 million women give birth in the United States annually (Osterman et al., 2023). The process of becoming a mother is a challenging and transformative experience that may bring about emotional vulnerability, radical changes in identity, and the risk of adverse psychosocial outcomes (Darvill et al., 2010). This transition can have a significant impact on a mother’s overall social and emotional well-being, including their self-efficacy, self-esteem, and sense of empowerment (Fenwick et al., 2003). For example, mothers who have reported a traumatic birth described subsequent difficulties with maternal self-efficacy and emotional disconnection from their child after delivery (Molloy et al., 2021). Furthermore, balancing family responsibilities, caring for a newborn, and focusing on career postpartum provide less available time and fewer energy resources to support self-care behaviors and to manage stress (Dugan & Barnes-Farrell, 2020), factors that have been shown to be a part of the experience of maternal postpartum depression and anxiety (Cho et al., 2022).
The purpose of this study is to explore the experiences of postpartum biological mothers residing in rural communities. Through qualitative inquiry, the study seeks to provide a comprehensive understanding of social support networks, emotional health, and the overall adjustment of mothers living in rural areas following childbirth. While we recognize that many individuals are impacted by the birth of a child (biological parents, adoptive parents, surrogate parents, grandparents, kin, and friends), that the role of a mother can be assumed by various individuals in families, and that not all individuals who give birth identify as a mother, this study specifically investigated the experiences of women who identified as biological birth mothers. By exploring the unique contexts of rural settings, we aim to uncover the nuanced factors that influence psychological well-being during the postpartum period. The findings are intended to inform clinical interventions and support strategies that will ultimately contribute to improved postpartum support and family health in rural communities.
Postpartum Social and Emotional Experiences
Social support or the absence of social support can be connected to maternal rates of depression, anxiety, self-harming behaviors, and general maladjustment (Bedaso et al., 2021; Milgrom et al., 2019). Enlander and colleagues (2022) qualitatively explored relevant themes regarding mothers’ perceptions of support as they related to perinatal distress and recovery. They found that mothers communicated themes of limited practical and emotional support, vulnerability to long-term relational or familial norms, and the relevance of sociocultural norms related to subjective feelings of perinatal distress. In addition, they found that having supportive and understanding relationships with friends and family can help protect against feelings of postpartum distress. On the other hand, a lack of such supportive relationships can reinforce unhelpful social norms related to motherhood and mental health (Enlander et al., 2022). These norms include both high expectations of new mothers and mental health stigma. Furthermore, the cumulative benefit of large support systems throughout the perinatal period can be beneficial in promoting psychological wellness (Vaezi et al., 2019).
Like the quantity of maternal social relationships, the quality of relational support is also an influential characteristic in new mothers’ social and emotional experiences. The quality of social relationships or support, including romantic and familial, can significantly minimize the maternal risk of postpartum psychosocial distress (Smorti et al., 2019). For example, the influence of new mothers having contact with other new mothers has been identified as beneficial social support in early postpartum recovery, as it promotes confidence and connection through shared history (Darvill et al., 2010; Enlander et al., 2022). Acknowledging the skills and abilities of mothers, as well as forming reliable and unconditional relationships where support is provided consistently, can not only serve as protective measures against postpartum depression, anxiety, and stress (Milgrom et al., 2019), but can also promote positive postpartum recovery (Zamani et al., 2019).
Given that social support has been found to be associated with a decreased probability of a mother developing postpartum depression (Cho et al., 2022), it can be inferred that public health guidance such as social distancing measures, neonatal visitation limitations, and reduced interpersonal contact with hospital staff during COVID-19 have had an impact on the maternal social and emotional experiences that can contribute to maternal psychosocial well-being or distress. For example, Ford and Ayers (2009) found that the support provided by hospital staff during childbirth had a more significant impact on mothers’ emotional responses to childbirth than perinatal and postpartum stressors.
Rural Postpartum Social and Emotional Experiences
Mothers who reside in rural localities have unique challenges compared to their urban and suburban counterparts. Due to the scarcity of health care providers and infrastructure in rural communities, significant differences in access to critical care obstetrics in rural and frontier areas of the United States exist (Kozhimannil et al., 2016, 2019; Kroelinger et al., 2021). Mothers in these areas often cope with challenges such as poverty, transportation barriers, and long distances to health care facilities, sometimes beyond a 50-mile radius. Hung and colleagues (2017) found that 45% of rural counties had no hospitals with obstetric services, with 9% experiencing a loss of in-county obstetric services. Rural counties that did not have hospital obstetric services tended to be smaller in geographical area; more significant gaps in service increased with the removal of hospital-based obstetric care. This evidence points to an overall decline in critical infrastructure related to childbirth and postpartum care in rural communities.
Disparities in mental health outcomes, including symptoms of depression during pregnancy and the postpartum period, have been observed in rural areas among mothers when compared to those residing in urban areas (Nidey et al., 2020). Factors associated with poor mental health outcomes outlined by Nidey and colleagues (2020) included socioeconomic barriers commonly found in rural contexts, such as limited access to services. Additionally, mothers living in rural areas were more likely to be younger, unmarried, and publicly insured and to possess lower education levels than their urban counterparts (Nidey et al., 2020).
Geographic isolation, limited resources, and the stigma associated with mental illness can cause rural residents to avoid seeking mental health care (Letvak, 2002). Within low-income rural populations, maternal distress is significantly predicted by experiences of emotional abuse, recent stressors, and discrimination (Ruyak et al., 2022). New mothers in rural communities deal with several challenges regarding limited health care services and support access. These challenges can be further complicated by a history of trauma and rejection, which may create barriers to seeking social relationships and hinder their recovery (Hine et al., 2017). Building trust with others can be difficult when social support is limited. According to a study conducted in the midwestern United States (Eapen et al., 2019), pregnant women living in rural areas received significant support from their partners and female relatives. The mothers often expressed their desire to have access to emotional support and maintain social support throughout their pregnancy from partners and social networks of relatives and friends.
Understanding Rural Mothers’ Postpartum Social and Emotional Experiences
Counseling researchers have not thoroughly explored the postpartum experiences of rural mothers. The current understanding of childbirth is limited to outdated studies related to prenatal care (Choate & Gintner, 2011) and postpartum depression (Albright, 1993; Pfost et al., 1990), with little to no understanding of the social and emotional factors contributing to these conditions. Furthermore, a lack of knowledge about rural mothers’ social and emotional experiences during the postpartum period exists, including what factors contribute to these experiences. This study sought to understand mothers’ postpartum social and emotional experiences in rural communities. We defined social experiences as the verbal, nonverbal, and interactive events that occurred between the postpartum women and individuals (e.g., friends, family, neighbors) in their community. We defined emotional experiences as events that impacted the mothers psychologically during the period after giving birth. The research question that this study aimed to address was: What are the postpartum social and emotional experiences of mothers in rural communities?
Method
We used a qualitative research approach to understand the postpartum experiences of women who identify as biological mothers in rural communities. Specifically, we selected transcendental phenomenology (Moustakas, 1994) for this study’s methodology. Drawing from a realist ontology and constructivist epistemology (Flynn et al., 2019), Moustakas’s (1994) transcendental phenomenology is congruent with this study’s purpose and research question, which desired to understand the lived experiences of postpartum mothers in rural communities. Additionally, Moustakas’s (1994) transcendental phenomenology provided a methodological context that emphasized the bracketing of prior assumptions and knowledge (i.e., epoche) among the members of the research team to distinguish, understand, and describe the particular postpartum experiences of the participants.
Participants
Institutional Review Board approval was obtained prior to recruitment from the university with whom we were affiliated at the time this study was conducted. Participants were recruited from five rural counties in the Appalachian region of the Southeastern United States. Each of the five counties identified was selected based on its classification as rural by the Federal Office of Rural Health Policy (2022). Purposive criterion sampling was used to recruit participants based on the following selection criteria: biological mothers, at least 18 years old, residing in one of the identified rural counties, and having a child under the age of 2. Recruitment materials in the form of flyers were shared (in person and via email) with various community venues within each of the five counties, such as childcare facilities, medical clinics, and public libraries. The flyers included information on the study, inclusion criteria, and notification of a $100 gift card for compensation (research was supported by a grant from the Tennessee Tech Center for Rural Innovation). Members of our research team contacted representative gatekeepers from these recruitment venues and gained permission to share the recruitment flyers with potential participants within these settings. Potential participants interested in the study could voluntarily communicate their interest in participating to the research team; a member of our research team screened each participant based on the study’s inclusion criteria.
Our recruitment strategy resulted in a sample size of 16 participants from four counties. We organized focus groups based on the geographic residency of the participants within the four counties. This approach resulted in participants from the same rural county being grouped into the same focus group. The mean composition of participants per focus group was four, with a standard deviation of 2.3 across the four focus groups. Participants ranged from 25 to 34 years of age (M = 30, SD = 2.6). Fifteen participants identified as White/Caucasian and one as multiracial/multiethnic. The total household income reported by participants included $10,000–$24,999 (n = 1), $25,000–$49,999 (n = 5), $50,000–$74,999 (n = 5), $75,000–$99,999 (n = 4), and $100,000–$149,999 (n = 1). The participants had between one and four children (M = 2.25, SD = 0.9), who at the time of the study were between the ages of 4 months to 14 years (M = 4.2, SD = 3.3). Thirteen participants reported being married, two reported being in committed relationships, and one reported being single. Five participants were high school or equivalent graduates. One engaged in some college coursework, three earned associate degrees, six earned bachelor’s degrees, and one earned a master’s degree. Ten participants reported being employed; six reported not being employed outside of the home at the time of the study. Twelve participants reported that they did not receive any postpartum professional counseling, while four participants indicated they had received some form of postpartum professional counseling services.
Data Collection and Analysis
Data was collected through focus group interviews led by Katherine M. Hermann-Turner. Discussions were held in large meeting spaces familiar to that community (e.g., library, church hall, community center). Participants provided informed consent before engaging in research activities. Participants attended one of four focus groups and engaged in a semi-structured interview designed to last 90 minutes. Focus groups were moderated by Hermann-Turner, who has extensive qualitative interviewing experience, and were conducted in person and audio recorded. At each focus group meeting, institutionally approved childcare specialists offered participants no-cost childcare in a designated area of the meeting space.
The semi-structured interview protocol consisted of three primary areas of focus related to understanding participants’ descriptions of their postpartum social and emotional experiences (e.g., What are your feelings about this experience?), processing of postpartum social and emotional experiences (e.g., What has helped you process your postpartum social and emotional experiences?), and their experiences of postpartum social and emotional meaning-making (e.g., Who have you talked to about your postpartum social and emotional experiences since you went home with [your baby]?). To increase the accuracy of participants’ recall during data collection, Hermann-Turner asked the participants to discuss their last birth experience and if they had multiple children. The research team provided each participant with contact information for mental health resources and services should they want to follow up on any topics discussed during the focus groups. The focus group audio recordings were manually transcribed by the research team to ensure the accuracy of the transcripts used for data analysis.
Hermann-Turner, Jonathan D. Wiley, and Corrin N. Brown served as the data analysis team. They worked together to analyze the data by meeting as a group and reaching a consensus during each stage of the research process. Once the focus group interviews were transcribed, the team used the guidelines Moustakas (1994) provided to analyze the data. Based on these data analysis guidelines, they selected the Stevick-Colaizzi-Keen phenomenological data analysis method. This method, completed for each focus group transcript, involved identifying salient descriptions of participants’ experiences. These descriptions were then grouped into themes that were used to create a detailed description of the meanings and essences of the participants’ experiences. They then constructed a composite textual–structural description of the meanings and essences of participants’ experiences across all the focus group transcripts, including verbatim examples from the transcripts to describe the themes reported in this study.
Trustworthiness and Positionality
Epoche—setting aside prejudgments, biases, and preconceptions throughout the research process—is essential to transcendental phenomenological research (Husserl, 1931; Moustakas, 1994). As such, we aspired to maintain epoche by employing trustworthiness strategies focused on bracketing our prejudgments, biases, and preconceptions throughout the research process. Before engaging in any research activities, we explored our subjectivity related to the phenomenon of the study by engaging in a reflective writing process to explore the connections we had with the conceptualization of the study, the phenomenon of study, the participant population, and the context of the research.
Collectively, we acknowledge how our anecdotal observations and experiences guided us to explore this topic and understand how mothers’ postpartum social and emotional experiences in rural communities can be enhanced. Although we share this unified belief, we represent a variety of backgrounds and experiences related to the present study. Specifically related to the phenomenon of inquiry, two researchers are biological mothers and have had their own postpartum social and emotional experiences. One of the researcher’s postpartum recoveries was in a non-rural context. In contrast, the other researcher’s postpartum recovery was within a rural community. The remaining three researchers have not experienced postpartum social and emotional experiences as biological parents. Concerning experience with rural communities, three of the five authors have direct experience with rurality, as they reside and serve as counselors in rural communities. The remaining two authors acknowledge limited experience related to living and working within rural communities.
We employed several trustworthiness strategies that supported the bracketing of our various experiences to the study phenomenon and context. In addition to the a priori reflective writing exercise mentioned above, all researchers engaged in weekly reflexive journaling during study formulation, recruitment, and data collection. Weekly reflexive journal entries were discussed among the research team. These group-based reflexive discussions focused on making sense of and, when necessary, bracketing the influence of prejudgments, biases, and preconceptions in relation to the study such as our personal and professional commitments to advocating for the presence of familial support, family-oriented community structures, and greater accessibility to postpartum services. As the research process transitioned to the data analysis phase, we reserved our reflexive responses and primary interpretations of the data for discussion in face-to-face meetings. Containing the data analysis process to the group milieu supported our use of analyst triangulation, providing that no one member of the data analysis team engaged in the analysis and interpretation of the data alone.
Findings
Four themes were found using Moustakas’s (1994) transcendental phenomenology methodology: powerlessness, help-seeking, recovering power, and here and now. Below, we present these themes, building on the theme of powerlessness and culminating with the participants’ empowering experience of being heard in the present moment during the focus groups. While this data is presented in a progressive sequence that seemingly indicates a transition from powerlessness to empowerment, we would like to note that we are not proposing a developmental model. Each theme is described and elaborated upon below using the participants’ words.
Powerlessness
The first theme pertains to the feelings of powerlessness experienced by participants from rural communities regarding childbirth and postpartum recovery (i.e., physical and emotional). Participants expressed feelings of powerlessness within childbirth by sharing ways this feeling impacted their delivery and how the experience of being inadequate, out of control, or powerless extended into their role as mothers and sometimes into their postpartum recovery.
In talking about childbirth, the participants recounted intense experiences where they felt that they did not have a choice or a voice when birthing their child or have autonomy over their body. One participant stated, “I could have pushed. But the doctor was busy, and I was like, this is ridiculous.” Others collectively described the limitations of epidurals: “My back looked like I had been shot with a BB gun because they kept trying to poke. And I’m like, can you please get somebody that’s going to get it right the first time at this point?” Another participant noted the disregard for knowledge of her own body:
But the epidural didn’t work for me either. I had a hot spot, so they kept trying to put it back in and there was one spot that it wasn’t working on, which I knew would happen because of my back problems.
Other participants shared their lack of voice when deciding to have a vaginal delivery or an epidural, stating:
The doctor was like, well, we’ll schedule C-section for tomorrow. I was like, oh no we will not! What’s my options here? So, I had a C-section with her at 38 weeks. When she came out, I got to see her for a minute, but they told me all kinds of things were wrong with her. And then she went to the NICU.
Another similarly recounted:
I was in labor for 4 nights with my first. Four nights, we’re talking contractions 5 minutes or less apart for 4 days and all the trauma on my body. . . . I begged for a C-section towards the end, and they just kept telling me “No.” On the fourth night, I begged, and I begged, and begged. They said, “No, no, no.” No one listened to me. And then when his heart rate started dropping, they were like, “Okay, we have to do a C-section.’’
Powerlessness within participants’ postpartum recovery was also expressed. Similar to the statements above concerning powerlessness within the birth experience, participants described continued barriers to recovery, bonding with their baby, and building memories due to external constraints (e.g., physical recovery or sleep deprivation). One participant stated, “I kind of don’t remember any of his first couple of months because I had three surgeries after he was born, and I couldn’t take care of him by myself.” Another shared, “I was so sleep deprived . . . I don’t remember their first year of life.” Participants’ ability to fully embrace the experience with their newborn was seemingly governed by secondary factors.
In addition, participants stated a lack of empowerment in their follow-up care and in making decisions regarding the care of their newborn. Two participants shared, “When I breastfed, I had no idea what I was doing. Nobody helped me,” and “I skipped my appointment because I just felt not heard. I didn’t want to go . . . I felt like it was pointless.” One participant shared, “They’re almost pushing formula . . . ‘No, you’re giving me an out. I really want to do this [breastfeed],’ like ‘Let me do this please.’ . . . They’re not hearing you at all.” Another participant expressed the weight of expectation of “having it together,” where seeking support is met with, “You got it, you’re such a super mom,” communicating a further sense of perceived abandonment.
Powerlessness in postpartum recovery also emerged through participant disclosures concerning their position as a mother. One participant stated, “We don’t get the option to walk away,” communicating the longevity and sense of direct responsibility experienced as a new mother. Another participant shared, “I remember lifting her up and the midwife was like, ‘Now you have to burp her.’ And I’m like, ‘Every time I feed her, I have to burp her?’ and I just started crying.” Another participant described a similar moment realizing that having a child is “gonna take work. And that was just the beginning.”
Experiencing powerlessness extended beyond overarching postpartum adjustment to subjective emotional aspects of recovery. Participants described a certain vulnerability to emotions that emerged, stating, “It hits you in the wildest of places. Like, I’m in Target.” And another shared, “I’d just be driving down the road in the car again . . . it’s so hard . . . babies are easy, but then it feels so hard, like in the moment.” Another participant shared her mechanism for navigating through intense emotions throughout postpartum recovery, stating, “I feel these feelings, I’ve had these thoughts run across my mind and I just shut them out” to cope in the moment.
Help-Seeking
A salient theme in the participants’ interviews relates to the disparity that they faced in effectuating requisite emotional and physiological needs. Participants identified postpartum needs such as sustaining physiological routines, emotional processing of postpartum experiences, and exploring postpartum selfhood and identity. Alternately, they also identified inconsistencies in their ability to meet these needs. Overall, the participants communicated support-seeking incongruities through their use of affective language relating fear and shame.
Participants described complexities related to sustaining the physiological routine needs of those in their care quickly after birth. Many participants described the rapid speed at which they returned to caring for their families after giving birth. For example, one participant stated, “We aren’t told to rest. We’re told to . . . have your baby and then keep going with your life.” This rapid transition to caring for their families after birth was described by several participants as a bewildering time. One participant illustrated this perplexing time by sharing, “I don’t know what I need. I don’t even know. My husband says, ‘What do you need from me?’ I don’t really know. I don’t know what I need.” This explanation describes the bewilderment many of the participants expressed.
Many participants described an interdependent relationship between meeting their and others’ physiological needs and their individual emotional experiences. For example, one participant stated, “I’m struggling physically, which is making me struggle mentally.” Many of the participants described challenging experiences related to the physical process of birth concerning the safety and livelihood of their child. Also, several participants described the postpartum period as more difficult emotionally. When asked to compare their emotional experiences of childbirth to the postpartum period, one participant answered, “That’s more postpartum, postpartum experience because that was harder for me than the births.” A few participants used words such as “debilitating” and “extreme” to characterize their postpartum emotional experience. One participant stated she “just didn’t understand how everybody else could be so normal around me, and I felt such extreme anxiety and fear.”
Another need frequently described by participants was the exploration of their postpartum identity and sense of self. Participants characterized this need as navigating the changes to their selfhood and identity due to their transition to parenthood. One participant candidly stated this need: “Like you’re still a person.” Within the context of parenthood, one participant described a process of “figuring out who you are outside of that [parenthood].” Many participants described challenges in integrating their individuality within their new role as a mother. For example, one participant explained, “It would help me to not just talk about the kids. Of course, your kids are a big chunk of your life, but actually being a person and having adult problems is a big chunk, too.” Explicitly referring to parenthood, one participant remarked, “I get resentful because I still deserve to be treated like a woman and not just like ‘mom and dad.’”
Whereas the dimensions above describe the postpartum needs of mothers for physiological routines, emotional processing, and identity exploration, most participants in the study had challenges in accessing these identified needs. These challenges were particularly noted in seeking social and emotional support. Most of the participants within this study described the accessibility they experience related to social support postpartum in affective terms; one of the most prominent affective dimensions identified was shame in seeking postpartum support. For example, one participant described their experience seeking available interpersonal and intrapersonal resources in their community: “There are resources all around me, but it’s like you feel ashamed.”
For some of the participants in this study, the experience of shame was associated with a fear of the consequences of being open and authentic with health care providers about their social and emotional experiences. One participant explained this shame and fear, stating:
You feel ashamed to say it. At one of my postpartum follow-ups, they’re like, “Oh, you feel like hurting yourself?” And, I’m thinking, “Yes, I want to die, I feel so depressed,” but you say “No” because you’re scared they’re gonna take your child away or they’re gonna call the police, they’re going to hospitalize you.
Several participants described similar patterns of desiring to be honest with health care providers but instead choosing to refrain from sharing their social and emotional experiences. Most of the participants described these types of inconsistencies in self-advocating for social and emotional support postpartum, given the acceptability of mental health within their specific rural communities. In response to discussion of providers’ preferred responses when seeking emotional support, one participant declared she would prefer a provider said, “‘Let’s go to counseling. Let’s have another follow-up appointment.’ Instead of, ‘Maybe we should call DCS’ and assuming she’s harming these kids or herself. It’s not that type of situation.” The discrepancy between self-identified needs and the potential repercussions of sharing their need for support, particularly emotional and mental health support, was a common theme across participants.
Recovering Power
Participants shared their processes of recovering their sense of power within the postpartum period. One participant explained their process of carving out personal time while navigating the challenges of the day:
Nursing her this whole time, I think has really helped with processing because I have to stop and sit down and breathe. So, I think it’s really helped having that 30–40 minutes of just sitting down because I don’t sit down when I’m home. I’m up cleaning and running, but yeah, nursing has really helped me process this birth a lot.
Other participants shared experiences of recovering their sense of power through personal growth and adapting to life’s challenges as new mothers. One participant stated:
I think you find yourself in motherhood. Not to say that women aren’t their true selves before they’re a mother. Who you are as a mother is who you are, you don’t have to be different or go back to who you were. It’s a growing experience and it’s hard, definitely.
Another participant shared how the experiences of childbirth and postpartum recovery helped shape her capacity for self-advocacy, stating, “I think through all of it, I learned to stand up for myself more than I ever have.”
Lastly, participants illustrated the moments of acceptance with their new roles as mothers and the decision to exercise gratitude for the profound changes associated with postpartum recovery. One participant recognized the position of mothers in providing care and support to their children with little acknowledgment or reciprocation, sharing, “You give so much, because you chose them, they owe you nothing in return. I think you come to terms with that too when you have babies because what are they going to give you?” Another participant shared the complexity of varied comfort levels of motherhood while recognizing the swiftness of childhood development, stating, “Postpartum is really hard for me. I’m just not good at it. But luckily, it’s such like a small time, I think just seeing them grow and knowing you’re doing it for a reason,” leading to assumed acceptance within the postpartum recovery process for many participants and that their efforts are not without meaning.
Here and Now
In addition to the themes presented about the birthing and postpartum period, throughout the interview processes, we became aware of the connectedness among the participants. The participants spoke about their here-and-now experiences, feeling supported in the focus group setting. Participants commented about the experience of being together, expressed support and empathy, and described hopes for ongoing opportunities to connect.
We were aware of the vulnerability of the participants as they found a safe place to share their stories. One participant described how she felt that the group was different from her previous group experiences, stating, “I hate group therapy. I do not speak in group therapy, but obviously, I can’t shut up. It just came out so openly because there’s a comfort here; there’s no uppity.” Another participant playfully shared, “I’m sharing a lot. Don’t judge me,” identifying how she felt comfortable talking about herself in the focus group setting.
The ability to be open was likely encouraged by the experience of being in a group of mothers who shared similar histories. One participant stated, “It’s nice knowing that you’re not alone like, you know, whenever you feel sad or upset or whatever, like, knowing other moms feel that too,” which was a similar sentiment to a participant of another group who said, “You know, it makes you feel so much better. It’s like, man, [you’re] going through it too, I’m not crazy.” The mothers also appreciated one another’s support, stating, “Yeah, it’s nice for someone to say, ‘Yeah, I get it.’”
The participants’ willingness to be vulnerable could result from the expression of support and empathy among the participants. The participants made frequent comments like, “That’s right. That’s how I feel too,” “Oh, that’s a good idea. I never thought about that,” “I didn’t even realize it till you just said that,” and “You’ve done a great job!” Sometimes, these expressions were minimal encouragers as the participants supported one another with ongoing head nods, mm-hmms, and the occasional expression of “Oh my gosh!” or “It really is!” At other times, the expression of support was more overt, as in statements like, “I don’t blame you for not having any more [children] after everything you went through. I’d be done, too.” The participants seemed to connect even when there were differences in their experiences, such as one participant describing respect for the participants who had C-sections: “Y’all are the women having C-sections that terrifies me. They said something about the C-section, and I was like [gasp!] no, I will get her out. . . . y’all are amazing for doing that.”
The participants not only supported one another in the conversations related to the group, but they also expressed warmth toward one another’s children. As described in the methodology section, the participants’ children were in the same large room with caregivers provided by the study. In the instances where a child was drawing their mother’s attention, the participants were open to the children, such as the comment by one mother normalizing the behavior: “The one thing we know about being a mom is that kids are unpredictable.” The participants also frequently complimented one another’s family with statements about the other children like, “You’re so cute” or “They’re lovely, beautiful.” The participants seemed to accept one another wholeheartedly without judgment.
Another consistent occurrence at the end of the groups was the participants’ gratitude for the experience of being together and a desire to continue meeting. For instance, one participant stated, “It would be nice if there were a mom group here because I’m not aware of that, some kind of a meetup or something.” Another mother brainstormed, “We could take the kids to the park. That way, they could play, and we can talk.” Overall, the feeling was consistent among the participants. Being with other moms was enjoyable, as shown in the statement, “I could do this all day, every day. Like, let’s talk everything babies” and “I do love talking about birth with other people. The same as you. I’ve never met another person with experience like I have. This is really great.” Overall, while the participants described many personal struggles, they also demonstrated their individual strength and empathic ability to support one another.
Discussion
Overall, this study extends the understanding of rural mothers’ postpartum social and emotional experiences, which have been overlooked in the professional counseling literature. The present study provides a focused insight into the rurality and postpartum social and emotional experiences related to the broader category of childbirth experiences. Although there have been important and recent contributions to the literature related to counselors’ perceptions of rural women clients (Leagjeld et al., 2021), our study provides an even more focused account of a specific dimension of rural mothers’ postpartum social and emotional experiences. While the authors anticipated themes related to multigenerational support, postpartum family support, and community support due to the rurality of the setting, we were surprised to uncover more universal themes related to motherhood.
Perhaps the most compelling finding is how participants experienced social and emotional powerlessness, which directly impacted their postpartum recovery. As mentioned in the literature review, a mother’s sense of self-efficacy, self-esteem, and empowerment has been found to impact maternal mental health (Fenwick et al., 2003; Molloy et al., 2021). Given the importance of autonomy as one of the fundamental principles of ethical behavior, according to the National Board for Certified Counselors (NBCC; 2023) and the American Counseling Association (ACA; 2014), the findings of this study highlight an important area of advocacy for the counseling profession. Participants in this study described proximal and systemic factors that impacted their experience of social and emotional powerlessness.
Participants referenced these proximal factors through the way they described not having a choice or voice regarding their care during and after childbirth. Across the participants in this study, the experiences during and immediately after childbirth seemed to set a tone for their postpartum recovery, with powerlessness at birth serving as a precursor to powerlessness postpartum. Some of the participants hinted at what has been referred to in the anthropological literature as a technocratic model of birth whereby the birth experience is characterized by mechanistic separation and control, reducing mothers’ autonomy during birth (Davis-Floyd, 2004). Although this reference to this technocratic model pertains specifically to childbirth, the initial childbirth experiences of participants described as mechanical, separate, and informed by external control in this study point to the development of longer-term postpartum social and emotional powerlessness. This social and emotional powerlessness and autonomy might be related to the development of postpartum anxiety and depression. Although social support has been found to decrease the probability of a mother developing postpartum depression (Cho et al., 2022), it is possible, therefore, that social and emotional powerlessness may also contribute to the development of postpartum anxiety and depression. Although this relationship can be surmised through the findings of this study, additional explanatory (i.e., causal) analyses are needed to further confirm the social and emotional determinants of postpartum distress, such as powerlessness.
Another important finding is that rural mothers desired and expressed an active openness to support their postpartum social and emotional experiences. Participants identified postpartum needs such as sustaining physiological routines, emotional processing of postpartum experiences, and exploring postpartum selfhood and identity. However, the participants in this study described experiencing barriers to supporting their postpartum social and emotional experience due to systemic barriers that impacted their ability to realize this desired support. The help-seeking theme reported in this study highlights that participants desired social and emotional help-seeking that was ultimately thwarted based on a variety of sociocultural factors such as geographic isolation, mental health stigma, and cultural norms of help-seeking behavior in addition to the reduced availability and accessibility of postpartum social and emotional supports in rural localities. This finding is consistent with previous studies that indicate an overall decline in critical structure related to childbirth and postpartum care in rural communities (Hung et al., 2017; Kozhimannil et al., 2016, 2019; Kroelinger et al., 2021). However, the findings of this present study provide localized insight into the demand side of postpartum social and emotional help-seeking. Although the supply of postpartum social and emotional support, in addition to critical health care infrastructure, was lacking, the rural mothers who participated in this study readily identified and desired needed social and emotional support.
Implications
The study’s results have various implications for counselors, particularly those working in rural communities or with a perinatal population. While there is a precedence for targeted interventions to support postpartum women through mental health programs (Geller et al., 2018), traumatic birth recovery support (Miller et al., 2021), and postpartum post-traumatic stress disorder recovery (P-PTSD; Cirino & Knapp, 2019), we did not observe these practices being implemented in any of the rural communities studied. The participants frequently described impactful, possibly traumatic, birth experiences and identified a lack of support during delivery and after being released from the hospital. Counselors, especially in rural communities, would benefit from establishing systems for support for postpartum mothers.
The participants also described a desire to feel supported by the medical community. Although they described crafting birth plans, they often felt that these were disregarded or ignored during childbirth, which contradicts recommendations to use birth plans to create security for women (Greenfield et al., 2019). The women also expressed apprehension toward assessment for postpartum depression by their doctor. Creating an environment where mothers feel safe with an emphasis on both depression and a holistic understanding of life’s current difficulties provides a more effective assessment (Corrigan et al., 2015). Counselors could benefit from providing psychoeducation to the medical community, particularly nurses in OBGYN clinics, or those having a role in supporting mothers within a medical setting.
A final implication for counselors is to help new mothers find social support and connections in their community. While literature supports the need for social support in rural communities (Letvak, 2002) and for postpartum mothers (Geller et al., 2018), throughout the groups, the mothers frequently identified the desire to stay connected yet being unable to find mothers’ groups. However, they identified a lack of opportunities within the community (e.g., no community meeting space and parks that are inaccessible in winter months) and not having the time, energy, or knowledge to form a group themselves. As a result, counselors can help by advocating for community spaces and creating postpartum support groups, which would greatly benefit the rural communities we studied.
Recommendations for Professional Counselors
Given the findings of this study, we propose the following strategies for professional counselors to employ in supporting the social, emotional, and overall mental wellness of postpartum mothers in rural areas:
- Empowerment practices: In the context of postpartum mothers, it is crucial for counselors to address feelings of powerlessness that can impact mental health. Counselors should focus on empowering practices such as positive self-talk, affirmations, and promoting self-care to counteract external factors that diminish autonomy and control.
- Client autonomy: Autonomy is a fundamental ethical principle, and counselors must recognize the systemic relationship between clients’ life experiences and the support they can offer. Building a strong therapeutic alliance and emphasizing foundational counseling skills and relational dimensions can help establish a sense of safety and comfort in the therapeutic relationship.
- Support and counseling groups: We recommend providing support and counseling groups for postpartum mothers, as participants in this study responded positively to the group format. These groups can provide safe spaces for mothers to share their experiences and connect with one another. Counselors specializing in this area should facilitate the development of these groups to leverage the therapeutic benefits of group counseling.
- Telemental health infrastructure: The challenges related to the availability and accessibility of counseling services in rural areas have been well-documented. A commonly proposed solution is telemental health counseling, which enables facilitating support groups, conducting individual counseling, and working with postpartum mothers in remote communities. Professional counselors must advocate for improving physical infrastructure in rural areas in order to enhance telemental health services, including better internet access to facilitate the provision of these services.
- Continuing education and training: When providing telemental health counseling in rural areas, it is important to consider cultural competencies and approach differences with humility. Counselors not located in the same geographical areas as their clients may need more clarification on the specific context of their rural clients. Continuing education and training opportunities should be provided to counselors in rural communities, and they should be encouraged to share their work at state- and national-level conferences.
- Integrated primary and mental health care: Advocacy for counselors includes encouraging the integration of primary and mental health care services. This integration is critical in rural areas where the accessibility and availability of primary and mental health care is limited. Therefore, we suggest that counselors reach out to physical health professionals in their communities in order to find ways to integrate services and to address the physical and mental aspects of wellness for clients in rural areas.
Limitations and Future Research
A robust research methodology is incomplete without recognizing limitations, and we identify minor limits in recruitment, sampling, and interviewing. We intentionally selected a focus group format to create a sense of community and facilitate memory recall. Due to the rural environment, participants often had preexisting relationships. We speculated that the relationships among participants could affect their interactions, leading to either selective sharing or a sense of comfort with disclosure. We felt that the latter context was present, as the participants supported one another in vulnerable moments with empathy and self-disclosure.
Before collecting data, we identified an ideal group size of four to six participants; nevertheless, the four groups had significant variation as they had two, three, three, and eight participants. We held a fifth focus group, but because there was only one attendee, the data was not used for this study, as we felt the difference in setting was too great from the intended study. We also selected focus group times to accommodate mothers of young children (i.e., not offered during nap times or mealtimes). However, morning meeting times could have prevented mothers who worked during the day or outside of the home from attending. We also felt engagement in the community could have facilitated trust and recruitment, yet we did not have a preexisting connection to the communities. We considered that individual interviews could better accommodate participants’ schedules.
In addition, one participant was a mother of twins, which we recognize could lead to different experiences from the mothers of singletons, but at the time of the group, we felt creating a culture of inclusiveness outweighed the need for homogeneity. In retrospect, we felt the participant was a valuable contributor, and the decision toward inclusivity was correct. We recommend that future research on this population similarly create a climate of openness and community. Finally, we recognize that while using incentives is an accepted practice, the $100 gift cards may have not only motivated participants but also captured a specific demographic that was financially driven.
Additional research should pinpoint the specific challenges faced by new mothers and identify impactful support practices, especially for mothers in rural areas. Future research replicating this study in other rural areas could also strengthen the understanding of the population. As described in this study, every rural area is unique, so additional data from rural communities could further confirm this study’s understanding of women’s postpartum experiences. A final recommendation is the exploration of the impact of children in the family system as a source of postpartum support. One participant described her preteen daughter’s expression of curiosity about childbirth as a loving, supportive context where she could share developmentally appropriate information about her experience, and we wondered if this opportunity for processing is helpful for other postpartum women.
Conclusion
This study highlights the urgent need to address the disparities in postpartum support for mothers living in rural areas. The findings describe rural mothers’ social and emotional experiences, including feelings of powerlessness, a desire to seek help, and their resilience in the face of difficulties. By advocating for expansion of the overall infrastructure for care during childbirth and postpartum, counselors can enhance their support of rural mothers’ social and emotional needs. Counselors can play a vital role in developing this kind of support by being knowledgeable about the experiences of rural mothers and advocating for a holistic response to this identified need.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
in the development of this manuscript.
The research for this study was supported
by a grant from the Center for Rural
Innovation at Tennessee Tech University.
References
Albright, A. (1993). Postpartum depression: An overview. Journal of Counseling & Development, 71(3), 316–320. https://doi.org/10.1002/j.1556-6676.1993.tb02219.x
American Counseling Association. (2014). ACA code of ethics. https://bit.ly/acacodeofethics
Bedaso, A., Adams, J., Peng, W., & Sibbritt, D. (2021). The relationship between social support and mental health problems during pregnancy: A systematic review and meta-analysis. Reproductive Health, 18, 1–23. https://www.doi.org/10.1186/s12978-021-01209-5
Cho, H., Lee, K., Choi, E., Cho, H. N., Park, B., Suh, M., Rhee, Y., & Choi, K. S. (2022). Association between social support and postpartum depression. Scientific Reports, 12, 3128. https://www.doi.org/10.1038/s41598-022-07248-7
Choate, L. H., & Gintner, G. G. (2011). Prenatal depression: Best practice guidelines for diagnosis and treatment. Journal of Counseling & Development, 89(3), 373–381. https://doi.org/10.1002/j.1556-6678.2011.tb00102.x
Cirino, N. H., & Knapp, J. M. (2019). Perinatal posttraumatic stress disorder: A review of risk factors, diagnosis, and treatment. Obstetrical & Gynecological Survey, 74(6), 369–376. https://doi.org/10.1097/OGX.0000000000000680
Corrigan, C. P., Kwasky, A. N., & Groh, C. J. (2015). Social support, postpartum depression, and professional assistance: A survey of mothers in the Midwestern United States. The Journal of Perinatal Education, 24(1), 48–60. https://www.doi.org/10.1891/1058-1243.24.1.48
Darvill, R., Skirton, H., & Farrand, P. (2010). Psychological factors that impact on women’s experiences of first-time motherhood: A qualitative study of the transition. Midwifery, 26(3), 357–366. https://www.doi.org/10.1016/j.midw.2008.07.006
Davis-Floyd, R. (2004). Birth as an American rite of passage. University of California Press.
Dugan, A. G., & Barnes-Farrell, J. L. (2020). Working mothers’ second shift, personal resources, and self-care. Community, Work & Family, 23(1), 62–79. https://doi.org/10.1080/13668803.2018.1449732
Eapen, D. J., Wambach, K., & Domian, E. W. (2019). A qualitative description of pregnancy-related social support experiences of low-income women with low birth weight infants in the Midwestern United States. Maternal and Child Health Journal, 23, 1473–1481. https://www.doi.org/10.1007/s10995-019-02789-2
Enlander, A., Simonds, L., & Hanna, P. (2022). “I want you to help me, you’re family”: A relational approach to women’s experience of distress and recovery in the perinatal period. Feminism & Psychology, 32(1), 62–80. https://www.doi.org/10.1177/09593535211047792
Federal Office of Rural Health Policy. (2022). List of rural counties and designated eligible census tracts in metropolitan counties. https://data.hrsa.gov/Content/Documents/tools/rural-health/forhpeligibleareas.pdf
Fenwick, J., Gamble, J., & Mawson, J. (2003). Women’s experiences of Caesarean section and vaginal birth after Caesarian: A birthrites initiative. International Journal of Nursing Practice, 9(1), 10–17. https://doi.org/10.1046/j.1440-172X.2003.00397.x
Flynn, S. V., Korcuska, J. S., Brady, N. V., & Hays, D. G. (2019). A 15-year content analysis of three qualitative research traditions. Counselor Education and Supervision, 58(1), 49–63. https://doi.org/10.1002/ceas.12123
Ford, E., & Ayers, S. (2009). Stressful events and support during birth: The effect on anxiety, mood and perceived control. Journal of Anxiety Disorders, 23(2), 260–268. https://doi.org/10.1016/j.janxdis.2008.07.009
Geller, P. A., Posmontier, B., Horowitz, J. A., Bonacquisti, A., & Chiarello, L. A. (2018). Introducing Mother Baby Connections: A model of intensive perinatal mental health outpatient programming. Journal of Behavioral Medicine, 41(5), 600–613. https://doi.org/10.1007/s10865-018-9974-z
Greenfield, M., Jomeen, J., & Glover, L. (2019). “It can’t be like last time” – Choices made in early pregnancy by women who have previously experienced a traumatic birth. Frontiers in Psychology, 10, 56. https://doi.org/10.3389/fpsyg.2019.00056
Hine, R. H., Maybery, D., & Goodyear, M. J. (2017). Challenges of connectedness in personal recovery for rural mothers with mental illness. International Journal of Mental Health Nursing, 27(2), 672–682. https://doi.org/10.1111/inm.12353
Hung, P., Henning-Smith, C. E., Casey, M. M., & Kozhimannil, K. B. (2017). Access to obstetric services in rural counties still declining, with 9 percent losing services, 2004–14. Health Affairs, 36(9), 1663–1671. https://www.doi.org/10.1377/hlthaff.2017.0338
Husserl, E. (1931). Ideas: General introduction to pure phenomenology (W. R. B. Gibson, Trans). Macmillan.
Kozhimannil, K. B., Casey, M. M., Hung, P., Prasad, S., & Moscovice, I. S. (2016). Location of childbirth for rural women: Implications for maternal levels of care. American Journal of Obstetrics and Gynecology, 214(5), 661.E1–661.E10. https://www.doi.org/10.1016/j.ajog.2015.11.030
Kozhimannil, K. B., Interrante, J. D., Henning-Smith, C., & Admon, L. K. (2019). Rural-urban differences in severe maternal morbidity and mortality in the US, 2007–15. Health Affairs, 38(12), 2077–2085. https://www.doi.org/10.1377/hlthaff.2019.00805
Kroelinger, C. D., Brantley, M. D., Fuller, T. R., Okoroh, E. M., Monsour, M. J., Cox, S., & Barfield, W. D. (2021). Geographic access to critical care obstetrics for women of reproductive age by race and ethnicity. American Journal of Obstetrics and Gynecology, 224(3), 304.E1–304.E11.
https://www.doi.org/10.1016/j.ajog.2020.08.042
Leagjeld, L. A., Waalkes, P. L., & Jorgensen, M. F. (2021). Mental health counselors’ perceptions of rural women clients. The Professional Counselor, 11(1), 86–101. https://doi.org/10.15241/lal.11.1.86
Letvak, S. (2002). The importance of social support for rural mental health. Issues in Mental Health Nursing, 23(3), 249–261. https://doi.org/10.1080/016128402753542992
Milgrom, J., Hirshler, Y., Reece, J., Holt, C., & Gemmill, A. W. (2019). Social support—A protective factor for depressed perinatal women? International Journal of Environmental Research and Public Health, 16(8), 1426. https://www.doi.org/10.3390/ijerph16081426
Miller, P. G. T., Sinclair, M., Gillen, P., McCullough, J. E. M., Miller, P. W., Farrell, D. P., Slater, P. F., Shapiro, E., & Klaus, P. (2021). Early psychological interventions for prevention and treatment of post-traumatic stress disorder (PTSD) and post-traumatic stress symptoms in post-partum women: A systematic review and meta-analysis. PloS ONE, 16(11), e0258170–e0258170.
https://doi.org/10.1371/journal.pone.0258170
Molloy, E., Biggerstaff, D. L., & Sidebotham, P. (2021). A phenomenological exploration of parenting after birth trauma: Mothers perceptions of the first year. Women and Birth, 34(3), 278–287. https://doi.org/10.1016/j.wombi.2020.03.004
Moustakas, C. E. (1994). Phenomenological research methods. SAGE.
National Board for Certified Counselors. (2023). NBCC code of ethics. https://bit.ly/NBCCCodeofEthics
Nidey, N., Tabb, K. M., Carter, K. D., Bao, W., Strathearn, L., Rohlman, D. S., Wehby, G., & Ryckman, K. (2020). Rurality and risk of perinatal depression among women in the United States. The Journal of Rural Health, 36(1), 9–16. https://doi.org/10.1111/jrh.12401
Osterman, M. J. K., Hamilton, B. E., Martin, J. A., Driscoll, A. K., & Valenzuela, C. P. (2023). Births: Final data for 2021. National Vital Statistics Reports, 72(1), 1–52. https://www.cdc.gov/nchs/data/nvsr/nvsr72/nvsr72-01.pdf
Pfost, K. S., Stevens, M. J., & Matejcak, A. J., Jr. (1990). A counselor’s primer on postpartum depression. Journal of Counseling & Development, 69(2), 148–151. https://doi.org/10.1002/j.1556-6676.1990.tb01476.x
Ruyak, S. L., Boursaw, B., & Cacari Stone, L. (2022). The social determinants of perinatal maternal distress. Journal of Rural Mental Health, 46(4), 277–284. https://www.doi.org/10/1037/rmh0000212
Smorti, M., Ponti, L., & Pancetti, F. (2019). A comprehensive analysis of post-partum depression risk factors: The role of socio-demographic, individual, relational, and delivery characteristics. Frontiers in Public Health, 7. https://doi.org/10.3389/fpubh.2019.00295
Vaezi, A., Soojoodi, F., Banihashemi, A. T., & Nojomi, M. (2019). The association between social support and postpartum depression in women: A cross-sectional study. Women and Birth, 32(2), e238–e242. https://www.doi.org/10.1016/j.wombi.2018.07.014
Zamani, P., Ziaie, T., Lakeh, N. M., & Leili, E. K. (2019). The correlation between perceived social support and childbirth experience in pregnant women. Midwifery, 75, 146–151. https://www.doi.org/10.1016/j.midw.2019.05.002
Katherine M. Hermann-Turner, PhD, NCC, BC-TMH, LPC (TN), is an associate professor at Tennessee Tech University. Jonathan D. Wiley, PhD, NCC, LPC (VA), is an assistant professor at Tennessee Tech University. Corrin N. Brown, EdS, NCC, LPC-MHSP-Temp. (TN), is a doctoral candidate at Tennessee Tech University. Alyssa A. Curtis, MS, MA, is a graduate of Tennessee Tech University. Dessie S. Avila, MA, LPC-MHSP (TN), is a doctoral candidate at Tennessee Tech University. Correspondence may be addressed to Katherine M. Hermann-Turner, Tennessee Tech University, Box 5031, Cookeville, TN 38505, khturner@tntech.edu.
Dec 5, 2024 | Volume 14 - Issue 3
Crystal M. Morris, Priscilla Rose Prasath
This study explored the effects of the 8-week Mindfulness-Based Strengths Practice program on relationship satisfaction, mindfulness traits, and overall well-being in female survivors of military sexual trauma. Conducted via Zoom with 24 participants organized into three groups, the quasi-experimental design included pre- and post-intervention assessments. Although no statistically significant differences were found in relationship satisfaction, dispositional mindfulness, or overall well-being, a notable positive correlation emerged between gains in relationship satisfaction and mindfulness, as well as between well-being and relationship satisfaction during the intervention. The study suggests practical insights for trauma treatment using a non-pathological counseling approach, emphasizing the need for further research and offering implications for clinical application, group practice, counselor education, and future studies in the field.
Keywords: mindfulness, military sexual trauma, Mindfulness-Based Strengths Practice, relationship satisfaction, well-being
The global spotlight on violence against women, particularly sexual assault and harassment, has garnered substantial attention in recent years. The World Health Organization found sexual violence to be a major public health problem and a violation of women’s human rights (WHO; 2021). WHO estimated that 27% of women aged 15–49 years worldwide have reported being subjected to some form of sexual violence.
When trauma is prevalent among women such as female service members, particularly in the context of military sexual trauma (MST), it can often hinder the development of meaningful relationships (Department of Veterans Affairs, 2021; Wilson, 2018). The #IamVanessaGuillen movement, which gained traction in 2020, further underscored the problem. Guillen’s death was connected to sexual harassment and assault while she served in the military, sparking numerous accounts from veterans and active-duty service members who faced similar experiences (Meinert & Wentz, 2024). Despite the Department of Veterans Affairs mandating MST screening, 67% of female survivors do not report their traumatic experiences (Wilson, 2018).
Military culture, marked by language, norms, and beliefs, presents challenges in seeking mental health treatment despite the recognition of heightened risks for MST survivors (Burek, 2018; Litz, 2014). Understanding the interplay between military culture and mental health treatment is crucial, especially for female veterans facing barriers to care-seeking (Kintzle et al., 2015). MST has garnered attention, with the Veterans Health Administration providing counseling services since 1992. However, research indicates that women in the military experience higher rates of sexual assault than men in the military, emphasizing the need for multi-level interventions (Blais, 2019; Brownstone et al., 2018). Brownstone et al. (2018) underscored the factors contributing to MST and advocated for supportive and validating responses to survivors.
MST survivors face heightened risks of psychological, social, physical, and employment-related difficulties (Costello, 2022). Female MST survivors commonly experience issues such as declining sexual functioning, social support challenges, maladaptive coping mechanisms, post-traumatic stress disorder (PTSD) symptoms, and reduced relationship satisfaction (Blais, 2020; Georgia et al., 2018). Psychological trauma, triggered by such distressing events, can lead to fear, nightmares, helplessness, and difficulties in relationships (American Psychiatric Association, 2013). PTSD, a challenging diagnosis for trauma survivors, involves exposure to traumatic events and intrusive symptoms impacting intimate relationships (Campbell & Renshaw, 2018). Women who experience trauma are more susceptible to PTSD and may require exploration of the ramifications of PTSD on their relationships (W. J. Brown et al., 2021).
Relationship satisfaction is a critical outcome for trauma survivors, with positive psychology interventions addressing disparities in social functioning for survivors of MST as an option (Morris, 2022; Blais, 2020). Positive psychology has foundations rooted in ancient traditions. Concepts of human flourishing, character strengths, virtue, and well-being have shaped spiritual and philosophical thought across cultures (Peterson & Seligman, 2004; Seligman & Csikszentmihalyi, 2000). It is built on the idea that, rather than solely focusing on pathology or mental illness, psychology should explore and promote aspects of human life that contribute to happiness, fulfillment, and meaning (Peterson & Seligman, 2004; Seligman & Csikszentmihalyi, 2000). The five elements of Seligman’s PERMA model (positive emotion, engagement, relationships, meaning, and accomplishments) and character strengths, including wisdom, courage, humanity, justice, temperance, and transcendence, play a pivotal role in enhancing well-being (Seligman, 2012; VIA Institute on Character, 2019; Wagner et al., 2020). A non-pathological wellness approach, incorporating positive psychology interventions like the VIA Character Strengths (Niemiec, 2013, 2014) and mindfulness practices, have emerged as a promising intervention for trauma survivors (Carrola & Corbin-Burdick, 2015; Cebolla et al., 2017; Niemiec, 2014; Seligman & Csikszentmihalyi, 2000; Wingert et al., 2022).
Mindfulness, which has proven effective in reducing PTSD symptoms, is integrated with character strengths in the Mindfulness-Based Strengths Practice (MBSP) program (Niemiec, 2014; Zhu et al., 2019). The 8-week program combining mindfulness and character strengths practices has shown positive effects on well-being and relationship satisfaction (Ivtzan et al., 2016; Pang & Ruch, 2019). Exploring the potential of MBSP in addressing relationship satisfaction, mindfulness practices, and overall well-being for MST survivors is crucial.
Theory of Well-Being—PERMA Model
Seligman’s PERMA model and theory of well-being incorporates the hedonic (i.e., connecting with feelings of pleasure) and eudaimonic (i.e., experiences of meaning and purpose) perspectives of well-being and poses that these two components are necessary for optimal well-being (Seligman, 2012). Seligman’s PERMA model measures each element, utilizing a subjective and objective approach in the form of positive psychology interventions (Goodman et al., 2018). Furthermore, Thompson et al. (2016) reported that using both subjective and objective well-being constructs with veterans may be appropriate. The PERMA-Profiler (Butler & Kern, 2016), a multidimensional scale that assesses the five pillars of well-being, has good reliability and acceptable levels of convergent, divergent, and criterion-related validity with student veterans (Umucu et al., 2020). The PERMA-Profiler may help researchers and counselors assess the well-being of individuals, including veterans, by providing an alternative path to conceptualizing psychological interventions (Umucu et al., 2020).
Aim of the Study and Research Questions
The primary objective of the present investigation was to assess the efficacy of the MBSP program concerning its impact on the levels of relationship satisfaction, mindfulness, and overall well-being among female survivors of MST. Simultaneously, this study sought to furnish valuable insights into the implementation of practical techniques rooted in mindfulness and character strengths that can facilitate the cultivation of robust and healthy relationships in this specific population. The research questions and hypotheses that guided the study were:
RQ1. Is there a positive relationship between the use of the MBSP program and relationship satisfaction in females who experienced MST as measured by the Relationship Assessment Scale (RAS)?
H1: There will be a positive effect on relationship satisfaction of female survivors of MST after completing the MBSP program.
RQ2. Will the MBSP program improve dispositional (trait) mindfulness as measured by the Mindful Attention Awareness Scale (MAAS) in female survivors of MST?
H2: The MBSP program will improve dispositional (trait) mindfulness in female survivors of MST.
RQ3. What is the effect of the MBSP program on overall well-being in female survivors of MST as measured by the PERMA-Profiler?
H3: The MBSP program will improve overall well-being in female survivors of MST.
Method
Recruitment and Screening Procedures
In this research, a multifaceted recruitment strategy was employed, encompassing recruitment flyers, letters, referrals, and social media channels. Targeted areas included military behavioral clinics, the U.S. Department of Veterans Affairs, the Steven A. Cohen Military Family Clinic, private practices, and social media counseling groups. Word-of-mouth referrals were also completed. A pre-screening phase, conducted by phone or online, featured two questions related to MST experiences, aligning with VA-MST criteria. Upon meeting the inclusion criteria (i.e., female, 18 years of age or older, veteran or active-duty service member, has experienced sexual harassment or sexual assault while serving in the U.S. military), participants then submitted demographic information online. A counselor-in-training (CIT) and Crystal M. Morris (first author and researcher) managed the pre-screening. Qualified individuals underwent a comprehensive trauma history and psychosocial interview led by Morris and the CIT as part of the screening process.
Participants
Several studies employing the MBSP program as an intervention within the general population reported individual sample sizes ranging from 20 to 126 (Hofmann et al., 2020; Ivtzan et al., 2016; Pang & Ruch, 2019; Whelan-Berry & Niemiec, 2021; Wingert et al., 2022). The sample size for the study was determined using G-Power software, adhering to Cohen’s (1998) conventions, with a medium effect size of .5, error probability of .05, and a power of .8. A priori statistical power analyses (Faul et al., 2007) indicated a sample size of 15 participants, ensuring adequate statistical power throughout the study.
A total of 24 female survivors of MST from various military branches (i.e., Army, Navy, and Air Force), both enlisted members and officers, participated in the study. After cleaning the data, participants who had greater than 20% missing data on the scale items were removed from the study (Hair et al., 2018). For the remaining participants with missing data, mean substitution was used for the Likert scale items (Hair et al., 2018). Of the 24 participants, 41.7% (n = 10) identified as Black/African American, 45.8% (n = 11) identified as White/Caucasian, and 12.5% (n = 3) identified as Latina/Hispanic. Participants were between the ages of 22 and 63, with a mean age of 43.38%. Of the participants, 54.2% served in the Army, 33.3% in the Air Force, and 12.5% in the Navy. The majority (78.3%) had an enlisted military rank and 21.7% were officers. Of the participants, 91.67% received unwanted, threatening, or repeated sexual attention while in the military; 41.67% had prior mindfulness practice experience; 79.17% received prior treatment for PTSD/trauma in therapeutic counseling; 83.33% reported no diagnosis of bipolar, schizophrenia, borderline personality disorder, or dissociative identity disorder; and 66.67% reported never being a client for PTSD/trauma with Morris.
Research Design
This study employed a quantitative quasi-experimental design, collecting data pre- and post-intervention, utilizing one-way repeated measures ANOVA, the Friedman test, and the Pearson product coefficient for analysis. The dependent variables include relationship satisfaction, mindfulness, and well-being, assessed at three time points. The independent variable was the MBSP intervention, conducted online because of COVID-19. The Relationship Assessments Scale (RAS), PERMA-Profiler, and Mindful Attention Awareness Scale (MAAS) were used as assessments. Table 1 outlines the 8-week MBSP program.
Data Collection Procedures
Data collection for this study occurred online from May 2022 to August 2022, with the approval of the University of Texas at San Antonio Institutional Review Board. All participants were provided with an IRB-approved consent form before joining the study. The research involved a pre-screening process, demographic data collection, trauma history interviews, and pretest and posttest assessments conducted at different stages (i.e., baseline, Week 4, and Week 8) of the MBSP program. Participant information was securely stored on Qualtrics. Instruments used in the study included the VA-MST screening questions (2 items), the RAS (Hendrick et al., 1998), the MAAS (Bishop et al., 2004), and the PERMA-Profiler (Butler & Kern, 2016). Those who completed the study received a $50 Amazon gift card as compensation. The MBSP sessions were conducted virtually via Zoom, with Morris, a licensed professional counselor, as the facilitator and a CIT as process observer.
Table 1
Standard Structure of MBSP Sessions and Program (Niemiec, 2014)
| Session |
Core Topic |
Mindfulness Practice Description |
Session Description |
Overall
Internal Session Structure of MBSP |
| 1 |
Mindfulness and Autopilot |
Raisin exercise
(Kabat-Zinn, 1990) |
The autopilot mind is pervasive; insights and change opportunities start with mindful attention. |
I. Opening meditation |
| 2 |
Your Signature Strengths |
You at your best (includes strength-spotting; Niemiec, 2014) |
Identify what is best in you; this can unlock potential to engage more in work and relationships and reach higher personal potential. |
II. Dyads or group discussion |
| 3 |
Obstacles are Opportunities |
Statue meditation
(Niemiec, 2014) |
The practice of mindfulness and strengths exploration leads immediately to two things—obstacles/barriers to the practice and a wider appreciation for the little things in life. |
III. Introduction to new material |
| 4 |
Strengthening Mindfulness in Everyday Life (Strong Mindfulness) |
Mindful walking |
Mindfulness helps us attend to and nourish the best, innermost qualities in everyday life in ourselves and others while reducing negative judgements of self and others; conscious use of strengths can help us deepen and maintain mindfulness practices. |
IV. Experiential–mindfulness/character strengths experience |
| 5 |
Valuing Your Relationships |
Loving-kindness/strength-exploration meditation
(Neff, 2011; Salzberg, 1995) |
Mindful attending can nourish two types of relationships: relationships with others and our relationship with ourselves. Our relationship with ourselves contributes to self-growth and can have an immediate impact on our connection with others. |
V. Debriefing or Virtue circle |
| 6 |
Mindfulness of the Golden Mean (Mindful Strengths Use) |
Character strengths 360 review and fresh start meditation |
Mindfulness helps to focus on problems directly, and character strengths help to reframe and offer different perspectives not immediately apparent. |
VI. Suggested homework exercises for next session |
| 7 |
Authenticity and Goodness |
Best possible self exercise |
It takes character (e.g., courage) to be a more authentic “you” and it takes character (e.g., hope) to create a strong future that benefits both oneself and others. Set mindfulness and character strengths goals with authenticity and goodness in the forefront of the mind. |
VII. Closing meditation (strengths Gatha)—mindfully transitioning to the next day |
| 8 |
Your Engagement with Life |
Golden nuggets exercise |
Stick with those practices that have been working well and watch for the mind’s tendency to revert to automatic habits that are deficit-based, unproductive, or that prioritize what’s wrong in you and others. Engage in an approach that fosters awareness and celebration of what is strongest in you and others. |
VIII. Reflect, assessments, close |
Note. Source: Adapted from Mindfulness-Based Strengths Practice (MBSP) Group Intervention: A Systematic Review (Prasath et al., 2021).
MBSP Program Group Intervention
In this study, the MBSP intervention was implemented using a structured curriculum from Niemiec (2014) aimed at enhancing treatment fidelity. The curriculum encompassed three main sections: an introductory portion outlining the foundational assumptions and change process in MBSP; essential information for conducting MBSP groups, including format and timing; and key reminders. The core of MBSP group sessions involved typical group dynamics, including participant interactions with themselves, fellow group members, and the group leader. Notably, the MBSP program comprises eight sessions, usually lasting 2 hours, though the duration can be adjusted based on the setting; for this study, sessions ran for 90 minutes. The MBSP program was selected for this study because it emphasizes discovering individuals’ strengths and fostering what is right within them, in contrast to focusing on deficiencies. MBSP integrates mindfulness and character strengths practices to enhance participants’ relationship satisfaction, mindfulness skills, and overall well-being (Niemiec, 2014). Morris conducted two groups per week, each accommodating 4–10 participants, over an 8-week period, with an additional group added to account for attrition, and following the standard structure outlined in Table 1.
Group Leadership
Morris has previous training in MBSP, a certification in mindfulness meditation, commitment to group work and leadership through the Association for Specialists in Group Work Leadership Institute in 2024, experience with multicultural populations, and experience living in a diverse military community, all of which equipped her for leading the MBSP program and study. Through her training to become an effective group leader, she learned to consider intersectionality, group dynamics, fostering a positive environment, promoting awareness, group cohesion, and compassion among participants sharing personal information (Corey et al., 2018).
Instruments
Demographic Questionnaire
Demographic questionnaires were given to all participants for screening purposes reporting age, ethnicity, gender, race, level of education, and military experience. Participants who met the criteria for the group (i.e., female, 18 years and older, military veteran/active-duty service member, and have experienced sexual assault or harassment while serving in the military) were assessed with a trauma history psychosocial interview.
VA-MST Screening Items
Thirty-one female veterans or service members were screened for MST with the following questions using two trichotomously scored (i.e., yes, no, decline to answer) questions: “When you were in the military: (a) Did you receive uninvited and unwanted sexual attention, such as touching, cornering, pressure for sexual favors, or verbal remarks? and (b) Did someone ever use force or threat of force to have sexual contact with you against your will?” The items may be referred to as “harassment-only MST” and “assault MST,” independently (Gibson et al., 2016). After screening, 31 participants met the criteria for the study, however, 24 completed the entire study due to attrition.
PERMA-Profiler
The PERMA-Profiler scale, developed by Butler and Kern (2016), assesses the five pillars of well-being: positive emotion, engagement, relationships, meaning, and accomplishment. Comprising 23 items, with 15 items dedicated to PERMA elements and eight fillers, each domain is measured using three items on an 11-point scale, ranging from 0 (never) to 10 (always), or 0 (not at all) to 10 (completely). Butler and Kern reported Cronbach’s alpha values ranging from .71 to .89 for positive emotion, .60 to .81 for engagement, .75 to .85 for relationships, .85 to .92 for meaning, and .70 to .86 for accomplishment. Mahamid et al. (2023) validated the PERMA-Profiler in diverse populations, reporting a 5-factor solution with 85.49% cumulative variance. Their study showed a high Cronbach’s alpha (α = .93), confirming internal consistency. Ryan et al. (2019) found acceptable internal consistency (α = .80 to .93) in Australian adults and established moderate convergent validity with health outcomes (r = 0.46 to 0.68). Umucu et al. (2020) validated the instrument utilizing Pearson correlation coefficients and the Kruskal-Wallis test among student veterans, demonstrating satisfactory reliability, convergent and divergent validity, and criterion-related aspects. The current study reported well-being domain Cronbach alphas of .96 and .94 with 95% CIs [.93, .98], [.89, 97], and [.89, .97] across data collection periods, confirming the PERMA-Profiler’s robustness and effectiveness in assessing the dimensions of well-being. The omega coefficients for well-being for this study were .96 and .94 with 95% CIs [.93, .98], [.89, .97], and [.89, .97].
Relationship Assessment Scale
The RAS (Hendrick et al., 1998) is a 7-item self-report scale, designed to measure general relationship satisfaction. The RAS can be used for anyone in a relationship, whether romantic or non-romantic (Hayden et al., 1998). The brevity of the scale makes it applicable in clinical settings and for online administration (Hendrick, 1988). The estimated time of completion is 5 minutes. Furthermore, the RAS uses a Likert-type scale with 1 representing low and 5 representing high. The scores for each item are added, totaled, and then divided by 7 to produce a mean score. Higher scores indicate higher levels of relationship satisfaction. The RAS is favored, as it is concise and useful in measuring satisfaction in relationships, including non-romantic relationships. Sample items ask the respondents to “rate their level of problems in the relationship” and “the extent to which their expectations had been met.” The RAS has generated good test–retest reliability, internal consistency, item reliabilities, and validity (Fallahchai et al. 2019; Maroufizadeh et al., 2020). Emergent data also support its convergent and predictive ability (Topkaya et al., 2023).
Hendrick et al. (1998) endorsed the RAS for several settings and populations. The RAS revealed significant connections to commitment, love, sexual attraction, self-disclosure, and relationship investment. Furthermore, Hendrick (1988) also discovered an inter-item correlation of .49 and internal consistency of α = .86 in her assessment of reliability. In this study, the Cronbach alphas for the relationship satisfaction at each data collection period were .86, .92, and .96 with 95% CIs [.66, .91], [.86, .96], and [.92, .98], showing good internal consistency and reliability. The omega coefficients for relationship satisfaction for this study were .81, .92, and .96 with 95% CIs [.66, .91], [.86, .96], and [.92, .98].
Mindful Attention Awareness Scale
The MAAS (Bishop et al., 2004) is a 15-item self-report instrument assessing dispositional mindfulness. Participants rate items on a 6-point scale, measuring how frequently they experience mindfulness-related behaviors. Higher scores indicate greater dispositional mindfulness. The MAAS does not have subscales. High scores on the MAAS correlate positively with self-consciousness, positive affect, self-esteem, and optimism and correlate negatively with anxiety, depression, and negative affect (Phang et al., 2016). Dispositional mindfulness, as measured by the MAAS, reflects a general tendency to be more aware and attentive in everyday life (Bishop et al., 2004). Examples of items include “I find myself preoccupied with the future or the past” and “I find myself doing things without paying attention.” The instrument yields a mean score by averaging responses across all items. Internal consistency estimates (Cronbach’s alpha) for the MAAS in adult samples consistently exceed .80 (K. W. Brown & Ryan, 2003). Additionally, Duffy et al. (2022) demonstrated the MAAS’s reliability and validity in measuring mindfulness in veterans with PTSD. Cronbach’s alphas for the mindfulness trait in this study were .89, .84, and .90 with 95% CIs [.81, .95], [.73, .92], and [.84, .95] across data collection periods, indicating strong internal consistency. The omega coefficients for mindfulness for this study were .89, .84, and .90 with 95% CIs [.81, .95], [.73, .92], and [.84, .95].
Data Analysis Procedure
Morris used the IBM SPSS Version 28 software package to analyze the data for this study. To examine if the MBSP group intervention (i.e., treatment condition) had any effect on the three dependent variables (i.e., relationship satisfaction, dispositional [trait] mindfulness, and well-being) over time, Morris analyzed the data using repeated measures analysis of variance (RM-ANOVA). Data was entered on an Excel spreadsheet from Qualtrics and exported to SPSS for a series of repeated measures analysis of variance (RM-ANOVA) models to include non-parametric tests such as the Friedman test. The Pearson product moment correlation coefficients were calculated to examine the relationships between the gain scores for relationship satisfaction, mindfulness, and overall well-being. The researcher checked for RM-ANOVA assumptions including (a) multivariate and univariate normality, (b) linearity, (c) multicollinearity, and (d) adequate sample size (Hahs-Vaughn & Lomax, 2020).
Results
Examining the effectiveness of the MBSP program on relationship satisfaction, dispositional trait mindfulness, and well-being, an analysis was conducted and revealed there was a positive relationship between relationship satisfaction, mindfulness, and well-being. Further analysis was provided through a one-way ANOVA repeated measure, and a Friedman test (a non-parametric) for the identified variables and assessment scores. A Pearson product-moment correlation coefficient was computed to examine gain scores between dependent variables. Table 2 provides descriptive results over each time point measured at Week 1 (baseline), Week 4, and Week 8 for relationship satisfaction, mindfulness, and overall well-being.
Table 2
Pearson Correlation Among Relationship Satisfaction, Mindfulness, and Well-Being at Baseline, Week 4, and Week 8
| Variables |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
| 1. Relationship Satisfaction |
— |
|
|
|
|
|
|
|
|
| 2. Mindfulness |
0.15 |
— |
|
|
|
|
|
|
|
| 3. Well-Being |
.71* |
.53* |
— |
|
|
|
|
|
|
| 4. Relationship Satisfaction (Wk. 4) |
|
|
|
— |
|
|
|
|
|
| 5. Mindfulness (Wk. 4) |
|
|
|
.09 |
— |
|
|
|
|
| 6. Well-Being (Wk. 4) |
|
|
|
.61* |
.27 |
— |
|
|
|
| 7. Relationship Satisfaction (Wk. 8) |
|
|
|
|
|
|
— |
|
|
| 8. Mindfulness (Wk. 8) |
|
|
|
|
|
|
.52* |
— |
|
| 9. Well-Being (Wk. 8) |
|
|
|
|
|
|
.84* |
.59* |
— |
*p < .01.
Research Question 1
In answering RQ1, a one-way RM-ANOVA examined if there were significant changes in participants’ relationship satisfaction throughout the MBSP intervention program. The independence assumption was met because the study design measured each participant’s response only once at the time of the study. The normality assumption was shown to be violated, as the p-value for the Shapiro-Wilk normality test at Week 4 was statistically significant (Shapiro-Wilk = .88, p < .001). The sphericity assumption was met because Mauchly’s test of sphericity was not found to be statistically significant, 𝜒2 (2, N = 24) = 4.39, 𝑝 = .111. No significant change over time was found, F(2, 46) = 1.74, p = .187. Therefore, H1 was rejected, as data analysis failed to demonstrate a statistically significant change in pre- and post-intervention of the MBSP group intervention on relationship satisfaction. See Table 3.
Table 3
One-Way Repeated Measures ANOVA for Changes of Relationship Satisfaction Scores Over Time (RQ1)
| Source |
Measure |
SS |
df |
MS |
F |
p |
Partial Eta Squared |
| Time |
Sphericity Assumed |
52.78 |
2.00 |
26.39 |
1.74 |
0.19 |
0.07 |
|
Greenhouse-Geisser |
52.78 |
1.69 |
31.16 |
1.74 |
0.19 |
0.07 |
|
Huynh-Feldt |
52.78 |
1.81 |
29.10 |
1.74 |
0.19 |
0.07 |
|
Lower-bound |
52.78 |
1.00 |
52.78 |
1.74 |
0.20 |
0.07 |
| Error |
Sphericity Assumed |
697.89 |
46.00 |
15.17 |
|
|
|
|
Greenhouse-Geisser |
697.89 |
38.96 |
17.92 |
|
|
|
|
Huynh-Feldt |
697.89 |
41.72 |
16.73 |
|
|
|
|
Lower-bound |
697.89 |
23.00 |
30.34 |
|
|
|
Research Question 2
In answering RQ2, a one-way RM-ANOVA examined whether participants’ mindfulness scores significantly changed throughout the MBSP intervention program. The normality assumption was shown to be violated because the p-value for the Shapiro-Wilk normality test at week 8 was statistically significant (Shapiro-Wilk = .82, p < .001). The sphericity assumption was found to be met because the sphericity statistic was not found to be statistically significant, 𝜒 2 (2, N = 24) = .78, 𝑝 = .676. Because of the non-normal data, a Friedman test (a non-parametric version of a one-way ANOVA) was implemented. The Friedman test results showed no significant change in mindfulness scores 𝜒 2 (2, N = 24) = 5.32, 𝑝 = .069. Therefore, H2 was rejected, as data analysis failed to demonstrate a statistically significant change in pre- and post-intervention of the MBSP group intervention on mindfulness (traits).
Research Question 3
In answering RQ3, a one-way RM-ANOVA examined whether participants’ overall well-being scores significantly changed throughout the MBSP intervention program. The normality assumption was met because the p-values for overall well-being scores for each time period were greater than .05. The sphericity assumption was found to be met because the sphericity statistic was found to be statistically significant 𝜒 2 (2, N =24) = 6.41, 𝑝 = .041. The Greenhouse-Geisser correction was implemented due to the sphericity assumption violation. The one-way ANOVA results found no significant change over time, 𝐹(1.60, 36.72) = 2.63, 𝑝 = .096. Therefore, H3 was rejected, as data analysis failed to demonstrate a statistically significant change in pre- and post-intervention of the MBSP program for overall well-being. See Table 4.
Table 4
One-Way Repeated Measures ANOVA for Changes of Overall Well-Being Scores Over Time (RQ3)
| Source |
Measure |
SS |
df |
MS |
F |
p |
Partial Eta Squared |
| Time |
Sphericity Assumed |
3.05 |
2.00 |
1.52 |
2.63 |
0.08 |
0.10 |
|
Greenhouse-Geisser |
3.05 |
1.60 |
1.91 |
2.63 |
0.10 |
0.10 |
|
Huynh-Feldt |
3.05 |
1.70 |
1.80 |
2.63 |
0.09 |
0.10 |
|
Lower-bound |
3.05 |
1.00 |
3.05 |
2.63 |
0.12 |
0.10 |
| Error |
Sphericity Assumed |
26.68 |
46.00 |
0.58 |
|
|
|
|
Greenhouse-Geisser |
26.68 |
36.72 |
0.73 |
|
|
|
|
Huynh-Feldt |
26.68 |
39.02 |
0.68 |
|
|
|
|
Lower-bound |
26.68 |
23.00 |
1.16 |
|
|
|
A Pearson’s correlation coefficient was calculated to assess the bivariate relationships between relationship satisfaction, mindfulness, and well-being. Well-being was shown to be positively associated with relationship satisfaction (r (22) =.71, p < .001) and mindfulness (r (22) = .53, p = .007). At Week 4 of the intervention, well-being was positively associated with relationship satisfaction (r (22) =.61, p =.002). At Week 8 of the intervention, well-being was shown to be positively associated with relationship satisfaction (r (22) =.84, p < .001) and mindfulness (r (22) = .59, p =.003). Mindfulness was positively associated with relationship satisfaction (r (22) = .52, p = .009). See Table 2.
Process Observation Results
The function of process observation, as described by Yalom and Leszcz (2020), is carried out by one of the group facilitators, referred to as the process observer (i.e., CIT). The process observer’s role is to observe the interaction and behaviors of the group (Yalom & Leszcz, 2020). Because the group was online, it was recommended to have a process observer, as it can help gain insight into the interpersonal interactions of group members (Prasath et al., 2023). In this study the process observer (CIT) took notes during the MBSP group and noted processes, behaviors of members, and group dynamics. In summary, they noted that most participants shared experiences and engaged in mindfulness and strengths activities, whether meditations or character strengths exercises. Additionally, the process observer noticed that the participants started to be less distracted during the mindfulness exercises after Week 4 of the MBSP group.
Discussion
The current study investigated MBSP program effectiveness with adult female survivors of MST, examining changes in relationship satisfaction, mindfulness, and well-being. In determining the efficacy of the MBSP program on female survivors of MST, Morris made several assumptions. Some assumptions were validated, and others were not. There was some congruence between previous literature and the current study. Findings are discussed based on the hypotheses in three areas: positive relationship between relationship satisfaction and the MBSP program, improvement in mindfulness practice, and improvement in well-being because of the MBSP program.
Positive Relationship Between Relationship Satisfaction and the MBSP Program
In line with previous studies, results reveal a similar positive change in mindfulness, showing that as mindfulness practice increased, so did relationship satisfaction and well-being, as reported by the participants during some part of the group intervention. It is not surprising that participants of this study reported some increase in mindfulness as a dispositional trait at the end of the intervention, because the MBSP program regularly incorporates several mindfulness practices, particularly meditative practices (i.e., mindful listening, walking, eating, breathing, listening, speaking, and self-compassion), during the session and for homework. This is not unusual, as there is abundant literature on mindfulness practices indicating benefits for trauma survivors (Hofmann et al., 2020; Zhu et al., 2019). Mindfulness practices with individuals impacted by trauma have revealed an improvement in self-regulation of emotions, PTSD symptoms, interpersonal relationships, and overall well-being (Hofmann et al., 2020; Shankland et al., 2021; Zhu et al., 2019).
Improvement in Well-Being Because of the MBSP Program
Consistent with previous studies, the MBSP program shows positive influence on well-being (Pang & Ruch, 2019; Whelan-Berry & Niemiec, 2021; Wingert et al., 2022). In the current study, well-being was shown to be positively associated with relationship satisfaction; as one increased, so did the other. From Week 1 to Week 4, well-being increased but did not hold statistical significance throughout the study. Results also reveal that participants struggled with completing homework tasks such as strength activities because of outside priorities, which has been mentioned in a previous study (Whelan-Berry & Niemiec, 2021). Thus, the results may have been affected, with no positive outcome at the end of the intervention for well-being.
Additional Significant Results
In the context of the MBSP program, the study reveals a slight increase in participants’ relationship satisfaction, well-being, and mindfulness from baseline to 4 weeks, followed by a plateau from Week 4 to Week 8. This apparent plateau may be attributed to a ceiling effect, in which the MBSP program’s influence on these dependent variables reached a saturation point (Chyung et al., 2020). Notably, the COVID-19 pandemic introduced a unique external factor impacting the study’s results, as previous MBSP studies occurred pre-pandemic. This study was conducted online, mirroring a broader shift toward virtual counseling services (e.g., Zoom) during the pandemic, potentially influencing participant experiences and outcomes (Kadafi et al., 2021).
Implications for Counselors
In the Council for the Accreditation of Counseling and Related Educational Programs 2016 standards (CACREP; 2015), there’s a notable gap, as few programs teach non-trauma modalities like positive psychology and mindfulness-based practices to address trauma survivor symptoms. The lack of CACREP guidance on crisis, trauma, and disaster counseling has necessitated creative pedagogical approaches to present realistic clinical challenges to CITs in a supportive and safe learning environment (Greene et al., 2016). This could help counselor educators develop innovative wellness tools and support for clients seeking non-pathology–based treatment. Therefore, it is recommended that CACREP establish standards to incorporate these alternative modalities, as the current CACREP standards focus on crisis intervention, trauma-informed, community-based, and disaster mental health strategies. Additionally, counselor educators can teach the MBSP intervention to students, which incorporates mindfulness and the VIA Character Strengths, which have been shown to build strengths, help with anxiety, and increase confidence; likewise, mindfulness can be beneficial during supervision (Evans et al., 2024, Niemiec, 2014). The VIA Character Strengths survey can aid educators in guiding students toward self-awareness of emotions, identifying strength, and identifying theoretical orientations aligning with their values (Sharp & Rhinehart, 2018).
The study reveals a positive correlation between relationship satisfaction, mindfulness, and well-being scores during the intervention. Adapting the MBSP program to a shorter duration for trauma survivors may be beneficial in future interventions. Existing literature on veterans with PTSD symptoms recommends incorporating wellness-based models like positive psychology in rehabilitation, with consideration for the timing and severity of trauma experiences (Carrola & Corbin-Burdick, 2015). For participants with varying recency and types of traumas, the MBSP program’s impact varied, indicating the importance of trauma processing before non-pathological treatments. Despite statistically insignificant outcomes, the study provides valuable mindfulness skills and character strength utilization for participants, offering practical tools for improving relationships for both clients and counselors. This research contributes insights into tailoring interventions for interpersonal traumas, enabling the development of non-pathological, preventive approaches utilizing positive psychology and mindfulness techniques to enhance the well-being of trauma survivors.
Limitations and Directions for Future Research
The research study has several limitations, including the use of a quasi-experimental design that posed threats to internal and external validity. The absence of a control group and issues with the relationship satisfaction scale’s design could have impacted the study’s results. Self-report and social desirability biases may have been present, especially among the 33% of respondents who were previous clients of the researcher and first author. The small sample size due to convenience sampling (N = 24) raises concerns about generalizability and the risk of Type II errors. Participant attrition further reduced the sample size and validity. Additionally, the COVID-19 pandemic introduced confounding factors, as previous studies on the intervention were conducted under different conditions. Zoom fatigue, resulting from increased online counseling services, also may have influenced participant experiences. Despite these limitations, a slight improvement in relationship satisfaction, well-being, and mindfulness was observed, possibly due to a ceiling effect. Although addressing these limitations is crucial, the study’s findings hold potential for enhancing counseling practice and research in the field.
Miller and Le Borgne (2020) suggested that further research is needed to evaluate the MBSP program’s effectiveness for enhancing the well-being and relationship satisfaction of MST survivors. This could involve larger sample sizes, addressing social desirability biases, and extending program exposure. A tailored relationship satisfaction assessment for trauma survivors should be developed, and qualitative investigations into post-MBSP program experiences are recommended. The program’s impact on symptoms like anxiety, depression, insomnia, and PTSD should be explored, not only for MST survivors but also for those with different trauma experiences. Couple satisfaction within the program context should be studied, and alternative program formats, such as shorter, intensive sessions or in-person delivery, should be considered. Changing the clinical environment and conducting long-term follow-up assessments are also suggested to enhance the study’s validity. These steps can improve the applicability of the MBSP program for supporting the well-being and relationships of trauma survivors.
Conclusion
This study investigated the impact of the MBSP program on female survivors of MST, examining their relationship satisfaction, dispositional mindfulness, and overall well-being. A total of 31 participants were initially recruited, with 24 completing all study requirements. Data analysis involved various statistical tests. Although statistical significance was not consistently demonstrated, a significant positive correlation was found between relationship satisfaction and mindfulness, and well-being and relationship satisfaction. These findings raise questions about the suitability of the MBSP program for trauma survivors, necessitating further exploration of relevant factors in this context.
Conflict of Interest and Funding Disclosure
Data collected and content shared in this article
were part of a dissertation study, which was
awarded the 2023 Dissertation Excellence Award
in Quantitative Research by The Professional Counselor
and the National Board for Certified Counselors.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th edition). https://doi.org/10.1176/appi.books.9780890425596
Bishop, S. R., Lau, M., Shapiro, S., Carlson, L., Anderson, N. D., Carmody, J., Segal, Z. V., Abbey, S., Speca, M., Velting, D., & Devins, G. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science and Practice, 11(3), 230–241. https://doi.org/10.1093/clipsy.bph077
Blais, R. K. (2019). Lower sexual satisfaction and function mediate the association of assault military sexual trauma and relationship satisfaction in partnered female service members/veterans. Family Process, 59(2), 586–596. https://doi.org/10.1111/famp.12449
Blais, R. K. (2020). Higher anhedonia and dysphoric arousal relate to lower relationship satisfaction among trauma-exposed female service members/veterans. Journal of Clinical Psychology, 76(7), 1327–1338. https://doi.org/10.1002/jclp.22937
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. https://doi.org/10.1037/0022-3514.84.4.822
Brown, W. J., Hetzel-Riggin, M. D., Mitchell, M. A., & Bruce, S. E. (2021). Rumination mediates the relationship between negative affect and posttraumatic stress disorder symptoms in female interpersonal trauma survivors. Journal of Interpersonal Violence, 36(13–14), 6418–6439. https://doi.org/10.1177/0886260518818434
Brownstone, L. M., Holliman, B. D., Gerber, H. R., & Monteith, L. L. (2018). The phenomenology of military sexual trauma among women veterans. Psychology of Women Quarterly, 42(4), 399–413. https://doi.org/10.1177/0361684318791154
Burek, G. (2018). Military culture: Working with veterans. American Journal of Psychiatry Residents’ Journal, 13(9), 3–5. https://doi.org/10.1176/appi.ajp-rj.2018.130902
Butler, J., & Kern, M. L. (2016). The PERMA-Profiler: A brief multidimensional measure of flourishing. International Journal of Wellbeing, 6(3), 1–48. https://doi.org/10.5502/ijw.v6i3.526
Campbell, S. B., & Renshaw, K. D. (2018). Posttraumatic stress disorder and relationship functioning: A comprehensive review and organizational framework. Clinical Psychology Review, 65, 152–162. https://doi.org/10.1016/j.cpr.2018.08.003
Carrola, P., & Corbin-Burdick, M. (2015). Counseling military veterans: Advocating for culturally competent and holistic interventions. Journal of Mental Health Counseling, 37(1), 1–14. https://doi.org/10.17744/mehc.37.1.v74514163rv73274
Cebolla, A., Enrique, A., Alvear, D., Soler, J. M, & Garcia-Campayo, J. J. (2017). Contemplative positive psychology: Introducing mindfulness into positive psychology. Papeles Del Psicólogo, 38(1), 12–18. https://www.papelesdelpsicologo.es/English/2816.pdf
Chyung, S. Y., Hutchinson, D., & Shamsy, J. A. (2020). Evidence-based survey design: Ceiling effects associated with response scales. Performance Improvement, 59(6), 6–13. https://doi.org/10.1002/pfi.21920
Cohen, M. P. (1998). Determining sample sizes for surveys with data analyzed by hierarchical linear models. Journal of Official Statistics, 14(3), 267–275.
Corey, M. S., Corey, G., & Corey, C. (2018). Groups: Process and practice (10th ed). Cengage.
Costello, K. (2022). Distress tolerance and institutional betrayal factors related to posttraumatic stress outcomes in military sexual trauma (MST) (Publication No. 29322504) [Doctoral dissertation, Hofstra University]. ProQuest Dissertations and Theses Global.
Council for the Accreditation of Counseling and Related Educational Programs. (2015). 2016 CAREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards
Department of Veterans Affairs. (2021). Women and military sexual trauma. https://www.research.va.gov/topics/womens_health.cfm#research6
Duffy, J. R., Thomas, M. L., Bormann, J., & Lang, A. J. (2022). Psychometric comparison of the Mindful Attention Awareness Scale and the Five Facet Mindfulness Questionnaire in veterans treated for posttraumatic stress disorder. Mindfulness, 13(9), 2202–2214. https://doi.org/10.1007/s12671-022-01948-x
Evans, A., Griffith, G. M., & Smithson, J. (2024). What do supervisors’ and supervisees’ think about mindfulness-based supervision? A grounded theory study. Mindfulness, 15, 63–79. https://doi.org/10.1007/s12671-023-02280-8
Fallahchai, R., Fallahi, M., Chahartangi, S., & Bodenmann, G. (2019). Psychometric properties and factorial validity of the Dyadic Coping Inventory–the Persian Version. Current Psychology, 38, 486–496. https://doi.org/10.1007/s12144-017-9624-6
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39(2), 175–191. https://doi.org/10.3758/BF03193146
Georgia, E. J., Roddy, M. K., & Doss, B. D. (2018). Sexual assault and dyadic relationship satisfaction: Indirect associations through intimacy and mental health. Violence Against Women, 24(8), 936–951. https://doi.org/10.1177/1077801217727371
Gibson, C. J., Gray, K. E., Katon, J. G., Simpson, T. L., & Lehavot, K. (2016). Sexual assault, sexual harassment, and physical victimization during military service across age cohorts of women veterans. Women’s Health Issues, 26(2), 225–231. https://doi.org/10.1016/j.whi.2015.09.013
Goodman, F. R., Disabato, D. J., Kashdan, T. B., & Kauffman, S. B. (2018). Measuring well-being: A comparison of subjective well-being and PERMA. The Journal of Positive Psychology, 13(4), 321–332. https://doi.org/10.1080/17439760.2017.1388434
Greene, C. A., Williams, A. E., Harris, P. N., Travis, S. P., & Kim, S. Y. (2016). Unfolding case-based practicum curriculum infusing crisis, trauma, and disaster preparation. Counselor Education and Supervision, 55(3), 216–232. https://doi.org/10.1002/ceas.12046
Hahs-Vaughn, D. L., & Lomax, R. G. (2020). Statistical concepts: A first course. Routledge.
Hair, J. F., Black, W. C., Babin, B., Anderson, R. E., & Tatham, R. (2018). Multivariate data analysis (8th ed.). Cengage.
Hayden, L. C., Schiller, M., Dickstein, S., Seifer, R., Sameroff, S., Miller, I., Keitner, G., & Rasmussen, S. (1998). Levels of family assessment: I. Family, marital, and parent–child interaction. Journal of Family Psychology, 12(1), 7–22. https://doi.org/10.1037/0893-3200.12.1.7
Hendrick, S. S. (1988). A generic measure of relationship satisfaction. Journal of Marriage and Family, 50(1), 93–98. https://doi.org/10.2307/352430
Hendrick, S. S., Dicke, A., & Hendrick, C. (1998). The Relationship Assessment Scale. Journal of Social and Personal Relationships, 15(1), 137–142. https://doi.org/10.1177/0265407598151009
Hofmann, J., Heintz, S., Pang, D., & Ruch, W. (2020). Differential relationships of light and darker forms of humor with mindfulness. Applied Research in Quality of Life, 15(2), 369–393. https://doi.org/10.1007/s11482-018-9698-9
Ivtzan, I., Niemiec, R. M., & Briscoe, C. (2016). A study investigating the effects of Mindfulness-Based Strengths Practice (MBSP) on wellbeing. International Journal of Wellbeing, 6(2), 1–13. https://doi.org/10.5502/ijw.v6i2.557
Kabat-Zinn, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Dell Publishing.
Kadafi, A., Alfaiz, A., Ramli, M., Asri, D. N., & Finayanti, J. (2021). The impact of Islamic counseling intervention towards students’ mindfulness and anxiety during the Covid-19 pandemic. Islamic Guidance and Counseling Journal, 4(1), 55–66.
Kintzle, S., Schuyler, A. C., Ray-Letourneau, D., Ozuna, S. M., Munch, C., Xintarianos, E., Hasson, A. M., & Castro, C. A. (2015). Sexual trauma in the military: Exploring PTSD and mental health care utilization in female veterans. Psychological Services, 12(4), 394–401. https://doi.org/10.1037/ser0000054
Litz, B. T. (2014). Clinical heuristics and strategies for service members and veterans with war-related PTSD. Psychoanalytic Psychology, 31(2), 192–205. https://doi.org/10.1037/a0036372
Mahamid, F., Veronese, G., & Bdier, D. (2023). The factorial structure and psychometric properties of the PERMA-Profiler Arabic version to measure well-being within a Palestinian adult population. Middle East Current Psychiatry, 30(1), 1–7. https://doi.org/10.1186/s43045-023-00282-9
Maroufizadeh, S., Omani-Samani, R., Hosseini, M., Almasi-Hashiani, A., Sepidarkish, M., & Amini, P. (2020). The Persian version of the Revised Dyadic Adjustment Scale (RDAS): A validation study in infertile patients. BMC Psychology, 8, 1–8. https://doi.org/10.1186/s40359-020-0375-z
Meinert, E. K., & Wentz, E. A. (2024). Protecting but not protected: Sexual assault in the military. Victims & Offenders, 19(4), 671–691. https://doi.org/10.1080/15564886.2023.2299007
Miller, M., & Le Borgne, A. (2020, July 7). Statistical significance: How to validate your incrementality test results. Adikteev. https://www.adikteev.com/blog/statistical-significance-how-to-validate-your-incrementality-test-results
Morris, C. M. (2022). Silent no more: Exploring the effects of mindfulness-based strengths practice on relationship satisfaction, mindfulness, and well-being in female survivors of military sexual trauma (Publication No. 30000181) [Doctoral dissertation, The University of Texas at San Antonio]. ProQuest Dissertations and Theses Global.
Neff, K. D. (2011). Self-compassion, self-esteem, and well-being. Social and Personality Psychology Compass, 5(1), 1–12. https://doi.org/10.1111/j.1751-9004.2010.00330.x
Niemiec, R. M. (2013). VIA character strengths: Research and practice (The first 10 years). In H. H. Knoop & A. Delle Fave (Eds.), Well-being and cultures: Perspectives on positive psychology (pp. 11–30). Springer.
Niemiec, R. M. (2014). Mindfulness and character strengths: A practical guide to flourishing. Hogrefe.
Pang, D., & Ruch, W. (2019). Fusing character strengths and mindfulness interventions: Benefits for job satisfaction and performance. Journal of Occupational Health Psychology, 24(1), 150–162. https://doi.org/10.1037/ocp0000144
Peterson, C., & Seligman, M. E. P. (2004). Character strengths and virtues: A handbook and classification. American Psychological Association.
Phang, C.-K., Mukhtar, F., Ibrahim, N., & Mohd. Sidik, S. (2016). Mindful Attention Awareness Scale (MAAS): Factorial validity and psychometric properties in a sample of medical students in Malaysia. The Journal of Mental Health Training, Education and Practice, 11(5), 305–316. https://doi.org/10.1108/JMHTEP-02-2015-0011
Prasath, P. R., Morris, C., & Maccombs, S. (2021). Mindfulness-Based Strengths Practice (MBSP) group intervention: A systematic review. Journal of Counselor Practice, 12(1), 1–23. https://doi.org/10.22229/asy1212021
Prasath, P. R., Xiong, Y., & Zhang, Q. (2023). A practical guide to planning, implementing, and evaluating the mindfulness-based well-being group for international students. The Journal of Humanistic Counseling, 63, 214–227. https://doi.org/10.1002/johc.12200
Ryan, J., Curtis, R., Olds, T., Edney, S., Vandelanotte, C., Plotnikoff, R., & Maher, C. (2019). Psychometric properties of the PERMA Profiler for measuring wellbeing in Australian adults. PloS ONE, 14(12), e0225932. https://doi.org/10.1371/journal.pone.0225932
Salzberg, S. (1995). Lovingkindness: The revolutionary art of happiness. Shambhala Publications.
Seligman, M. E. P. (2012). Flourish: A visionary new understanding of happiness and well-being. Simon and Schuster.
Seligman, M. E. P., & Csikszentmihalyi, M. (2000). Positive psychology: An introduction. American Psychologist, 55(1), 5–14. https://doi.org/10.1037/0003-066X.55.1.5
Shankland, R., Tessier, D., Strub, L., Gauchet, A., & Baeyens, C. (2021). Improving mental health and well-being through informal mindfulness practices: An intervention study. Applied Psychology: Health and Well-Being, 13(1), 63–83. https://doi.org/10.1111/aphw.12216
Sharp, J. E., & Rhinehart, A. J. (2018). Infusing mindfulness and character strengths in supervision to promote beginning supervisee development. Journal of Counselor Practice, 9(1), 64–80. https://www.journalofcounselorpractice.com/uploads/6/8/9/4/68949193/sharp_rhinehart_vol9_iss1.pdf
Thompson, J. M., MacLean, M. B., Roach, M. B., Banman, M., Mabior, J., & Pedlar, D. (2016). A well-being construct for veterans’ policy, programming and research (Technical Report). Research Directorate, Veterans Affairs Canada. https://cimvhr.ca/vacreports/data/reports/Thompson%202016_WellBeing%20Construct%20for%20Veterans%20policy,%20programming,%20and%20research.pdf
Topkaya, N., Şahin, E., & Mehel, F. (2023). Relationship-specific irrational beliefs and relationship satisfaction in intimate relationships. Current Psychology, 42(2), 1257–1269. https://doi.org/10.1007/s12144-021-01426-y
Umucu, E., Wu, J.-R., Sanchez, J., Brooks, J. M., Chiu, C.-Y., Tu, W.-M., & Chan, F. (2020). Psychometric validation of the PERMA-Profiler as a well-being measure for student veterans. Journal of American College Health, 68(3), 271–277. https://doi.org/10.1080/07448481.2018.1546182
VIA Institute on Character. (2019). The VIA Character Strengths Survey. https://www.viacharacter.org/survey/account/register
Wagner, L., Gander, F., Proyer, R. T., & Ruch, W. (2020). Character strengths and PERMA: Investigating the relationships of character strengths with a multidimensional framework of well-being. Applied Research in Quality of Life, 15(2), 307–328. https://doi.org/10.1007/s11482-018-9695-z
Whelan-Berry, K., & Niemiec, R. (2021). Integrating mindfulness and character strengths for improved well-being, stress, and relationships: A mixed-methods analysis of Mindfulness-Based Strengths Practice. International Journal of Wellbeing, 11(1), 38–50. https://doi.org/10.5502/ijw.v11i2.1545
Wilson, L. C. (2018). The prevalence of military sexual trauma: A meta-analysis. Trauma, Violence, & Abuse, 19(5), 584–597. https://doi.org/10.1177/1524838016683459
Wingert, J. R., Jones, J. C., Swoap, R. A., & Wingert, H. M. (2022). Mindfulness-based strengths practice improves well-being and retention in undergraduates: A preliminary randomized controlled trial. Journal of American College Health, 70(3), 783–790. https://doi.org/10.1080/07448481.2020.1764005
World Health Organization. (2021). Violence against women. https://www.who.int/news-room/fact-sheets/detail/violence-against-women
Yalom, I. D., & Leszcz, M. (2020). The theory and practice of group psychotherapy (6th ed.). Basic Books.
Zhu, J., Wekerle, C., Lanius, R., & Frewen, P. (2019). Trauma- and stressor-related history and symptoms predict distress experienced during a brief mindfulness meditation sitting: Moving toward trauma-informed care in mindfulness-based therapy. Mindfulness, 10, 1985–1996. https://doi.org/10.1007/s12671-019-01173-z
Crystal M. Morris, PhD, NCC, CSC, LPC-S, is an assistant professor at St. Mary’s University. Priscilla Rose Prasath, PhD, MBA, LPC, GCSC, is an associate professor at The University of Texas at San Antonio. Correspondence may be addressed to Crystal M. Morris, St. Mary’s University, One Camino Santa Maria, San Antonio, TX 78228, cmorris4@stmarytx.edu.
Dec 5, 2024 | Volume 14 - Issue 3
Matthew L. Nice, Arsh, Rachel A. Dingfelder, Nathan D. Faris, Jean K. Albert, Michael B. Sickels
Emerging adults (18–29 years) are at a vulnerable developmental stage for mental health issues. The counseling field has been slow to adapt to the evolving landscape of the specific needs of emerging adult clients. The purpose of this qualitative study was to investigate the experiences of professional counselors who primarily counsel emerging adult clients. Using interpretative phenomenological analysis, data was collected from 11 professional counselors to produce four major themes of their experiences working with emerging adult clients: parental pressures, self-discovery, transitions, and dating and attachment. The findings from this study provide insights regarding practices and preparation for professional counselors to work with emerging adult clients.
Keywords: emerging adults, professional counselors, experiences, phenomenological, qualitative study
Emerging adulthood (18–29 years) is a distinct human developmental stage between adolescence and adulthood. Arnett (2000) defined emerging adulthood after interviewing hundreds of young adults around the United States about their developmental experiences over several years. It is a period of life that is both theoretically and empirically different than late adolescence and early adulthood due to the psychosocial factors that young adults experience during this time in their lives (Lane, 2020). It is a time when individuals often leave their parents’ or guardians’ home, enter college or begin a career, seek romantic relationships, and begin to make decisions independently (Arnett, 2004). Emerging adults no longer experience the restrictions from their parents/guardians or teachers and they are not yet burdened with normative adult responsibilities. These freedoms allow individuals to develop qualities (e.g., self-sufficiency, new adult roles, major responsibilities) that are required during adulthood (Arnett, 2004).
As a result of this shift in human development, individuals in their twenties are marrying and starting families later, changing jobs more frequently, and pursuing higher levels of education than they were in previous decades (Arnett, 2015). Thus, the developmental factors and needs of this age group have been increasingly shifting. Although emerging adulthood is the most well-studied theory of young adult development, it is not without limitations. The most notable of these is the applicability of emerging adulthood features to young adults in all contexts. For example, the college experience offers young adults new opportunities to explore their identities and to try new things that non–college-going young adults may not experience (Mitchell & Syed, 2015). Additionally, emerging adulthood may be a Western-centric experience that young adults in other parts of the world may not experience in the same way (Hendry & Kloep, 2010).
Emerging adulthood is distinguished by its five defining features: identity exploration, sense of possibilities, self-focus, instability, and feeling in-between (Arnett, 2004, 2015). These features indicate normative developmental affordances and challenges, as well as help to define the common experiences of emerging adulthood (Nelson, 2021; Nice & Joseph, 2023). Identity exploration refers to emerging adults’ process of self-discovery in education, careers, and romantic partnerships. Sense of possibilities refers to emerging adults’ tendency to look to the future optimistically, imagining the many avenues they may take in their lives. Self-focus, not to be confused with selfishness, is the normative process in which emerging adults have the opportunity to focus on themselves without parental constraints, and before the responsibilities of marriage or parenthood. Feeling in-between is the developmental limbo between adolescence and adulthood, when emerging adults do not identify as an adolescent or an adult. Lastly, instability refers to emerging adults experiencing unstable and frequently changing life conditions, such as change in romantic partnerships, transitioning to and from college, or moving in and out of living situations (Arnett, 2015).
Experiencing these normative developmental features often results in challenges to emerging adults’ mental health (Arnett et al., 2014; Lane, 2015a; Lane et al., 2017). Navigating identity exploration and new possibilities by experimenting with anomalous life roles and experiences may lead to distress and failure (Lane, 2015b). The subjective experience of not feeling salient in adulthood but being tasked with new adult responsibilities that were not present in adolescence may cause periods of identity crisis and various psychological difficulties (Lane et al., 2017; Weiss et al., 2012). The various transitions such as entering and leaving college, starting and ending careers, or moving out of the house of a parent/guardian and moving in with roommates or living alone may contribute to instabilities and significant distress (Murphy et al., 2010; Nice & Joseph, 2023). Additionally, the salience of emerging adults’ cultural identities affects the ways in which they experience satisfaction with their lives (Nice, 2024). Although not every emerging adult will experience all of these difficulties (Buhl, 2007), many will respond with significant distress that may affect the critical juncture in mental health development that occurs during the emerging adulthood years (American Psychiatric Association [APA], 2022; Lane, 2015a). The mental health needs of emerging adults is often overlooked, as society may only see the opportunities for new growth, fun, freedom, and promise of being a young adult, and may overlook the instabilities and distress that accompany this developmental period (C. Smith et al., 2011).
Although emerging adults are some of the most vulnerable of the age groups for developing mental health issues (Cheng et al., 2015), including being particularly prone to anxiety and depression (American College Health Association, 2019), the counseling field has been slow to adapt to the evolving landscape of these individuals. Many counselors are challenged with using outdated developmental models to conceptualize their work with emerging adult clients that do not adequately address the nuances within this age group (Lane, 2015a). During high school years, school counselors are often tasked with prioritizing students for college and career readiness, but not for their upcoming transition into emerging adults (Nice et al., 2023). Given these circumstances, counselors who work with emerging adult clients are uniquely positioned to foster resilience, wellness, and navigation of various challenges during this often tumultuous stage of human development (Lane, 2015a). Understanding the experiences of professional counselors who work primarily with emerging adult clients may be necessary to assess the unique needs and support that emerging adult clients can benefit from in the counseling setting. Although other studies have examined the lived experiences of counselors working with specific clients (e.g., Wanzer et al., 2021) and other phenomena (Coll et al., 2019), no studies have examined counselors’ experiences working with emerging adults.
Given that there is little systematic research exploring how counselors experience working with emerging adult clients, qualitative research is a warranted methodological approach to understanding these social phenomena. Conceptualizing this study using the theoretical lens of emerging adulthood (Arnett, 2000, 2004, 2015) and its five features can assist in exploring the experiences of counseling emerging adults through a developmental perspective that accounts for the current circumstances of young adults. The present research addresses this by investigating the following research question: What are the perspectives and experiences of professional counselors working with emerging adult clients?
Method
The present qualitative study used interpretative phenomenological analysis (IPA) by collecting data through semi-structured interviews. The IPA approach was selected as the methodology for this study in order to reveal the experiences of counselors working with emerging adult clients because it permits an abundant level of data collection and interpretation and allows for consideration of participant accounts within a broader context/theory (Hays & Singh, 2023). During the interviews, participants were given the opportunity to discuss their experiences of working with emerging adult clients in order to give voice to their thoughts, beliefs, and attitudes surrounding these experiences.
Research Team and Reflexivity
The research team consisted of the first author and principal investigator, Matthew L. Nice; four research assistants, Arsh, Rachel A. Dingfelder, Nathan D. Faris, and Jean K. Albert; and an external auditor, Michael B. Sickels. Nice holds a PhD in counselor education and supervision and has studied and worked with emerging adults in various settings. Albert is a doctoral student in a counselor education and supervision program who has worked with emerging adults in a clinical setting. Arsh, Dingfelder, and Faris were master’s students at the time of this study who were enrolled in a clinical mental health counseling program and who indicated interest in counseling emerging adults after graduation. Arsh and Faris identified as emerging adults. Sickels served as the external auditor and is a counselor educator who holds a PhD in counselor education and supervision and has several years of clinical experience counseling emerging adult clients. Nice pursued this study as part of a research agenda that includes emerging adulthood mental health. Arsh, Dingfelder, Faris, and Albert were research assistants who worked on this study because they had communicated interest in collaborating on this topic and as part of their paid graduate assistantships. Both prior to and throughout the study, these research assistants were trained on the qualitative research process, conducting qualitative interviews, and data analysis.
We engaged in bracketing to minimize the ways in which our experiences, expectations, or any potential biases might influence the study. We discussed our experiences in relation to being or having been an emerging adult, our roles as scholars who have researched emerging adults and clinicians who have counseled emerging adults, and our overall commitment to the counseling profession. During these discussions we identified our experiences, acknowledged any biases that we may have had, and talked about ways to bracket while conducting interviews. We kept analytic memos and personal notes during the data collection and coding process. Sickels examined our reflexivity in relation to data collection and coding to provide us with critical feedback.
Participants
This study consisted of a purposive criteria sample of 11 professional counselors who met the following criteria: graduation from a CACREP-accredited counseling program, a minimum of 2 years of professional counseling experience post-graduation, and a full-time caseload of at least 60% or more emerging adults (ages 18–29) during their time as a professional counselor. Demographic data for each participant are displayed in Table 1. Pseudonyms are used for each counselor selected for the study to maintain confidentiality (American Counseling Association [ACA], 2014), along with their age, gender, race/ethnicity, highest counseling degree, years of experience as a counselor, and the type of work setting. We chose to require 2 years of counseling experience as inclusion criteria given that most states require no less than 2 years of experience to become a fully licensed professional counselor (e.g., Pennsylvania Department of State, 2024), which is a benchmark of demonstrating experience as a professional counselor. We chose not to require that participants hold licensure as a professional counselor, as we hoped to include college counselors in our study, many of whom may not seek licensure as a professional counselor, as many universities do not require counselors to hold licensure to work in counseling centers. We elected to require a full-time caseload of at least 60% of clients currently within the ages of 18–29 years to ensure that the experiences of the counselors working with this age group were substantial enough to provide generalizability.
Table 1
Participant Demographics
| Pseudonym |
Age |
Gender |
Race/Ethnicity |
Education |
Total years as a professional counselor |
Type of practice |
| Judy |
30 |
Female |
White |
MA |
5 |
Private practice |
| Lorraine |
31 |
Female |
White |
PhD |
8 |
Private practice |
| Peter |
48 |
Male |
White |
MA |
10 |
College counseling center |
| Claire |
40 |
Female |
White |
MA |
16 |
Private practice |
| Christine |
30 |
Female |
White |
MA |
5 |
College counseling center |
| Patricia |
48 |
Female |
White |
MA |
20 |
College counseling center |
| Mark |
32 |
Male |
White |
PhD |
7 |
College counseling center |
| Theresa |
30 |
Female |
White |
MA |
5 |
Outpatient practice agency |
| Emily |
39 |
Female |
White |
MA |
2 |
College counseling center |
| Stephen |
37 |
Male |
Asian |
MA |
7 |
Community mental health |
| Sarah |
27 |
Female |
Hispanic |
MA |
3.5 |
Outpatient agency & private practice |
Note. N = 11.
Procedures and Data Collection
After we obtained university Institutional Review Board approval, participants were invited to participate through convenience sampling from agencies, private practices, and university counseling centers in the northeast region of the United States. We also searched online counselor directories for counselors who fit the criteria of our study. Upon completing interviews, we also recruited participants via snowball sampling by asking initial participants for recommendations for new potential participants to interview who also met our inclusion criteria. Given that many college counselors’ clients are almost all within the emerging adult age range, they served as valuable participants in our data collection. However, these counselors only see clients in the college context and do not see non-college emerging adult clients, an important and often forgotten population of emerging adults (Nice & Joseph, 2023). To assure the study focused on professional counselors, we limited our participants who worked in college counseling centers to account for less than half of our total participants (n = 5).
Interview questions were developed by the research team by first examining the extant counseling and young and emerging adulthood literature. Nice developed questions grounded by the literature and sent the questions to the research team for their suggestions, additions, and edits. The interview questions approved by the research team were sent to Sickels, who provided feedback for creating the final interview protocol. Prior to interviews, participants signed a consent form and completed a demographics questionnaire. Participants were also provided with a document outlining the five features of emerging adulthood (Arnett, 2004, 2015) that they were asked to review prior to the interview in order to better understand and answer the interview questions pertaining to these features. We conducted semi-structured interviews lasting approximately 60 minutes via Zoom over an 8-month span. Participants were offered a $20 electronic gift card as an incentive for participation. At the start of each interview, participants were reminded that questions pertaining to their clients only pertained to their emerging adult–aged clients, within the years of 18 to 29, and not any clients outside of that age range. Each interview consisted of eight open-ended questions (see Table 2). Participants were also asked follow-up questions for clarification. These questions were guided by Arnett’s (2000) theory of emerging adulthood, a well-studied and accepted understanding of the developmental markers and features that individuals experience during young adult development.
To understand participants’ experiences of counseling young adults during this developmental phase, we asked several questions pertaining to their experience of their clients’ developmental features of emerging adulthood (i.e., identity exploration, sense of possibilities, self-focus, instability, and feeling in-between) in counseling sessions. For consistency across participants, we asked each interview question in the same order during each interview (Creswell & Creswell, 2017). The pace of each interview was determined by the participant to allow for the development of richer data (Hays & Singh, 2023), with impromptu questions asked between established questions when elaboration was needed.
Table 2
Interview Questions
| Question Number |
|
Question Content |
| 1 |
|
What is your process for working with emerging adult clients? |
| 1a |
|
Why do you choose to work with this population? |
| 2 |
|
What developmental considerations do you make when working with emerging adult clients? |
| 2a |
|
Can you provide an example or case using developmental considerations working with emerging adult clients? |
| 3 |
|
To what extent does clients’ “identity exploration” factor into your counseling of emerging adult clients? |
| 4 |
|
To what extent does clients’ “sense of possibilities” factor into your counseling of emerging adult clients? |
| 5 |
|
To what extent does clients’ “feeling in-between” factor into your counseling of emerging adult clients? |
| 6 |
|
To what extent does clients’ “instability” factor into your counseling of emerging adult clients? |
| 7 |
|
To what extent does clients’ “self-focus” factor into your counseling of emerging adult clients? |
| 8 |
|
When you look back on the process of counseling emerging adults, what other thoughts stand out which we have not discussed about the outcomes of counseling emerging adult clients? |
| 8a |
|
How have those implications affected the outcome of the counseling process with emerging adult clients? |
| 8b |
|
How did you respond to these outcomes as a counselor? |
To enhance the trustworthiness, credibility, dependability, confirmability, and transferability of the data, we enlisted several procedures during data collection (Morrow, 2005; Prosek & Gibson, 2021). Field notes, researcher observations, and experiences pertaining to each interview were expressed and processed during research team meetings, which assisted in triangulation of data by confirming interpretations of interview data (Anney, 2015). Nice used member checking by sending each participant documents that outlined summaries of the emergent findings, quotes, themes, and data (Flynn & Korcuska, 2018). Of the 11 participants, 10 responded to member checking by confirming the accuracy of the documents to the best of their knowledge or suggesting new thoughts or ideas regarding the documents. To establish the confirmability of findings, analytic memos and a reflexivity journal were used to assist with objectivity in the interpretations during data analysis (Saldaña, 2021). Analytic memos were also kept to record thoughts around the meaning behind participants’ statements.
Nice used a reflexivity journal throughout the interviews and data analysis processes and made efforts to bracket assumptions as a professional in the counseling field (Hays & Singh, 2023). The purposive sampling method of clients based on their experiences of counseling emerging adults assisted in establishing transferability of the findings of the study (Anney, 2015). The trustworthiness and dependability of the study was assisted using an external auditor and peer briefer. Sickels served as the auditor throughout the study, reviewing interview transcripts, data collection, data analysis, themes, and overall processes, procedures, and coherence of the study (Flynn & Korcuska, 2018; Hays & Singh, 2023). Nice and Sickels met face-to-face or by phone to engage in peer-debriefing during all major points of the study, including Nice’s positionality, thoughts, emotions, and reactions to the procedures of the study.
Data Analysis
Data was analyzed by following Pietkiewicz and Smith’s (2014) guidelines of data analysis. The process involves three stages: immersion, transformation, and connection. This process began with Nice listening to recordings of each interview to review the content as a whole and to mark any additional observations. Nice and the research team manually transcribed each interview. All transcribed interviews were reviewed by Nice concurrently with recordings to ensure accuracy of the transcripts and to create a deeper immersion into the data. During this process any new insights or observations were recorded in field notes and a reflexivity journal (Pietkiewicz & Smith, 2014). The rest of the research team also engaged in this three-stage process by reviewing each team member’s recordings and processing them in team meetings. Research team members participated in consensus coding team meetings after every two or three interviews, resulting in a total of five meetings. Prior to meetings team members all examined the materials for coding and submitted them to Nice. During meetings Nice led the discussions about each participant interview and the research team discussed how and why they arrived at specific codes. Intercoder reliability was maintained by Sickels, who examined each initial coding from all research members as well as the coding results from consensus coding meetings (Cofie et al., 2022).
Following IPA qualitative methodology, Nice and the research team reviewed and interpreted their notes regarding the transcripts in order to transform them into emergent themes using both hand coding and ATLAS.ti coding software (J. A. Smith, 2024). These initial themes were linked together by their conceptual similarities, which developed a thematic hierarchy (Pietkiewicz & Smith, 2014). Finally, Nice and the research team created a narrative account of each theme, which included direct quotes from the participants. The interpretations of these emergent themes and the overall interview content were reviewed by Nice and the research team in order to reach agreement on the final, distinct themes. Afterward, Sickels conducted an independent cross-analysis on the interview transcripts, notes, and emergent and final themes to ensure the accuracy and clarity of the final themes.
Results
The data analysis process using IPA qualitative methods resulted in four distinct themes. These themes were identified and designated based on the meaning related with professional counselors’ experiences working with emerging adult clients. It should be noted that anxiety/stress was initially considered as a fifth theme; however, further coding and team meetings concluded that anxiety/stress is grounded within the other four themes and was not an independent distinct theme. Hence, the following four phenomenological themes emerged: parental pressures, self-discovery, transitions, and dating and attachment. The results of this interpretative phenomenological study are outlined in the following section.
Theme 1: Parental Pressures
This theme indicates the expectations, criticisms, and imposed beliefs that emerging adult clients often process in the counseling session. Participants expressed that much of their experiences counseling emerging adult clients involved working on their clients’ relationship with their parents. Within this theme, participants expressed that their clients struggle with meeting their parents’ expectations, criticisms, standards, and imposed beliefs. Sarah shared:
A lot of people, whether they had good or bad relationships with their families, are learning how that looks now in their adulthood, like how they incorporate their family. So like creating more boundaries and what not, boundaries is a huge thing for this.
Mark asserted: “Parents are always into the stuff [emerging adult clients] are doing and criticizing it, saying ‘no, do this or that instead.’ I think it pushes them into feeling like they are still this adolescent or kid.” Additionally, Stephen mentioned: “Clients might be going through, let’s say, gender identity. There’s this rejection of themselves from their parents when they were younger, and they struggle exploring who they want to be, because they were never fully accepted by their parents.” Participants largely expressed that although their emerging adult clients are adults, their parents still have a profound effect on them and what they bring to counseling sessions. Counselors experiencing their clients navigating their parental relationships is likely due to the individuation process (Youniss & Smollar, 1985). Individuation is an age-normative co-constructed process occurring in emerging adulthood in which young adults redefine their relationship with their parents after transitioning into emerging adulthood (Zupančič & Kavčič, 2014). This process often involves young adults’ fear of disappointing, seeking approval, and navigating parent intrusiveness (Nice & Joseph, 2023).
Theme 2: Self-Discovery
The theme self-discovery refers to counselors’ experiences of assisting emerging adult clients in finding who they are, how they fit into society, and their exploration of being an adult. Judy expressed:
I just recognize that there’s a really great impact for folks during these [emerging adult] years to explore themselves and really get to know who they are, but in a space that feels comfortable and accepting. And, hey, however, you want to show up to session, you know that the counselor there has got your back.
Similarly, Emily stated: “You know [emerging adult clients] are trying these identities possibilities on for size, you know, I could be this! What would that feel like? What would that be like?” Claire also had similar experiences working with emerging adult clients. She expressed:
Finding who they are is probably the biggest type of stress that I see [as a professional counselor]. What does it mean to be by myself? What does it mean to be outside of a family? What does it mean to be alone and not alone? But you know just kind of out there in the world.
This theme likely speaks to the features of emerging adulthood, namely identity exploration and instability (Arnett, 2000, 2004). Exploring identities can be a stressful time for young adults, especially when some identities are marginalized (Pender et al., 2023). Participants expressed the importance of being a stable and safe place for clients as they explore who they are, who they want to be, and their place in society.
Theme 3: Transitions
This theme highlights the worry and indecisiveness emerging adult clients struggle with as they transition to their new roles. Based on their experiences focusing on the transitions of emerging adult clients in therapy, participants identified and articulated the stressors and challenges to mental health experienced by clients facing frequent transitions. To this point, Theresa noted:
So there’s a lot of transitions that are happening within young adulthood that I find really helpful to not only manage within therapy, but just to help clients better understand themselves. It’s such a pivotal time to really test out the way in which they’re experiencing the world.
Judy also experienced how transitions can be difficult with some of her emerging adult clients. She shared: “I had some [emerging adult clients] who have not had a traumatic background, but the instability and chaos of all these changes and transitions really threw them for a loop.” Christine noted some specific transitions she sees in her emerging adult clients:
There’s a lot of like hopping around with sort of short timelines, especially if they’re not living at home. Their room, their dorm, their apartment, whatever it is, is changing every year. A lot of students are transferring in or transferring to other schools. Their jobs are changing. They’re getting internships. Their classes are different every semester. And so the entire emerging adult experience is pretty much based on some level of instability with transitions . . . that plays into the work that I do, because I’m trying to give them a place that is stable and consistent, and somewhere that they can go and feel safe and comfortable.
The frequent transitions and changes that occur in emerging adulthood often lead to instability and distress (Howard et al., 2010). Participants noted these transitions, their role in assisting clients with these transitions during emerging adulthood, and the importance of the counseling session providing clients with stability that they may not be receiving in other areas of their lives.
Theme 4: Dating and Attachment
This theme signifies the instability of romantic relationships and learning healthy attachment styles that emerging adult clients bring to the counseling session. When discussing some of the most prevalent concerns emerging adult clients bring to counseling sessions, Lorraine indicated:
Dating is an interesting time in early adulthood. So I pay attention to that and I spend a lot of time on psychoeducation, paying attention to healthy, unhealthy attachment styles, unhealthy and healthy relationship characteristics, and what people would identify as like red flags. And then going into attachment styles and how they’re attaching to others is serving them or not serving them.
On that note, Christine discussed a specific emerging adult client she is working with:
Someone I’m working with now is going through a breakup. She was with the same person for the past 3 years, and it recently ended. And so, a lot of the work that we’re doing now is processing who she is apart from the relationship and doing so in a way that feels safe for her.
Mark identified similar experiences working with emerging adult clients:
[Emerging adult clients say] “my dating relationships are nonexistent. So now I feel that I don’t have any worth because I know I can’t take somebody out on a date or go to the movies or whatever.” So I think that plays a huge role because it’s almost like something that clients that I work with experience. . . . like everything is just not stable.
Dating and navigating romantic relationships in therapy has been widely researched in counseling scholarship (Feiring et al., 2018). Exploring these concepts with emerging adults in therapy may be especially crucial given that emerging adulthood is the formative stage in which individuals explore romantic relationships (Shulman & Connolly, 2013). Participants indicated that they process healthy and unhealthy attachment styles with clients as they navigate dating, which may be significant given the effects of emerging adults’ attachment styles on their overall mental health (Riva Crugnola et al., 2021).
Discussion
Eleven professional counselors provided insight into their experiences and perceptions working with emerging adult clients in this study. Four phenomenological themes—parental pressures, self-discovery, transitions, and dating and attachment—were derived from participants’ perspectives. These findings support the available literature on the mental health needs of emerging adults (e.g., Cheng et al., 2015; Lane, 2015a) and extend this knowledge with increased direction.
The results of this study supported Arnett’s (2000, 2004, 2015) theory of emerging adulthood. Participants reported that their clients experience stress and anxiety from age-normative developmental experiences. The transitions and dating stress that emerging adults process in counseling can be linked to the emerging adulthood feature of instability (Arnett, 2004). The stress of self-discovery that is present in emerging adults’ counseling sessions is related to the emerging adulthood features of identity exploration, sense of possibilities, self-focus, and feeling in-between (Arnett, 2004). The parental pressure that counselors expressed are often prevalent when counseling emerging adults is consistent with individuation in emerging adulthood (Youniss & Smollar, 1985). Komidar and colleagues (2016) found that emerging adults often experience both a fear of disappointing their parents and feelings of parental intrusiveness in their lives while traversing the individuation process of redefining the parent–child relationship during emerging adulthood. The parental pressures that emerging adults process in counseling sessions is likely due to emerging adults individuating by establishing their own independence while sustaining a healthy level of connectedness with their parents (Nice & Joseph, 2023).
Participants’ experiences of their emerging adult clients expressing issues related to pressures from their parents stem from many contexts. These pressures came from parents exerting their expectations for their emerging adult children to choose specific education and careers and to perform well in them. Although emerging adults have newly entered adulthood and can explore their own belief systems, counselors still experienced their emerging adult clients feeling pressured to conform to the beliefs that their parents imposed on them. Emerging adult clients who were not meeting the specific expectations of their parents often expressed stress and anxiety from criticisms they received from their parents. These experiences are not to be confused with poor parenting. Mark reported that many parents are “helicopter parents” (Padilla-Walker & Nelson, 2012) who are overly involved in their emerging adult children’s lives; this increased involvement often results in their children experiencing stress and pressures.
The self-discovery that participants experienced their emerging adult clients undergoing was related to emerging adults not only determining who they are, but who they want to be. Given that individuals may not feel comfortable exploring their identities in the high school setting (Palkki & Caldwell, 2018), emerging adulthood may serve as a safer time for young adults to explore who they are. Discovering who they are is a formative task that is often met with much stress and instability (Arnett, 2004). Participants found that emerging adult clients often experience stress and anxiety about learning what they want in terms of careers, jobs, family roles, and communities.
Several participants used the word “scared” when describing how their emerging adult clients express their feelings about the many transitions they experience. Counselors noted that their emerging adult clients are facing many transitions, such as entering and leaving college, entering and leaving jobs, moving out of their parents’ home, moving in with roommates or romantic partners, and changing friend groups. With these transitions, counselors reported that their clients expressed a level of indecisiveness in knowing if they are following the correct path. Many of these transitions come with an increased level of new independence that counselors noted their clients had difficulty navigating. In line with prior research (Leipold et al., 2019), counselors expressed that promoting resilience and fostering coping methods during these transitions is beneficial to establishing consistency, safety, and security for emerging adults in counseling sessions.
Internet dating applications have led to emerging adults being more aware of the characteristics and criteria for who they want to date (Sprecher et al., 2019). Participants expressed that emerging adults often feel distress from the ending of relationships, conflicts with romantic partners, navigating who they want to date, and traversing internet dating applications. Several participants mentioned that their emerging adult clients’ self-worth was tied to their relationship status or who they are in a relationship. Participants reported that their clients’ attachment styles often lead to issues in dating. Participants noted that in their experiences, psychoeducation about healthy dating and attachment is often necessary to assist clients with these issues in the counseling session.
Implications for Counselor Practice and Training
The findings from this study provide valuable insights regarding counselors’ clinical experiences with emerging adult clients with several practice implications. Professional counselors can benefit from understanding the roles that emerging adults’ parental pressures, self-discovery, transitions, and dating and attachment have on their mental health. Counselors can benefit from asking about these four themes during the beginning of the counseling relationship to build rapport and immediately assist emerging adult clients with common developmental issues experienced by these clients.
To assist emerging adult clients with negative feelings regarding parental pressures, counselors can offer clients the opportunity to bring their parent(s) to therapy. Marriage and family counselors can also intentionally address and process parental pressures in applicable family systems. Attending to emerging adult clients’ issues surrounding self-discovery has potential implications for multicultural and social justice counseling (Ratts et al., 2016). For example, emerging adult clients who identify as gender diverse or as a sexual minority may be discovering themselves in new ways that can elicit transprejudice, discrimination, and stigmatization in society (Wanzer et al., 2021). Utilizing the Multicultural and Social Justice Counseling Competencies (MSJCCs; Ratts et al., 2016) in the counseling session provides a framework for emerging adults who are discovering and exploring their cultural identities (Nice, 2024). Counselors can use the MSJCCs to understand emerging adults’ specific intersections of their identities (e.g., race/ethnicity, sexual identity, gender identity, spirituality).
Counselors can assist clients with feelings of distress regarding self-discovery, identity, and fitting in by normalizing these developmental experiences and processing their values and life desires. Regarding transitions, counselors should be intentional to assure that the counseling session is a safe and stable environment for emerging adult clients. Given the stress and instability during emerging adulthood from frequently changing contexts in college, jobs, families, friends, romantic partnerships, and living situations, assuring that the counseling session remains stable and safe can provide clients with a sense of ease and security that they may be lacking in other areas of their lives.
Addressing dating and attachment in emerging adulthood can prove to be a difficult task, as some emerging adults may be seeking monogamous relationships while others may be more interested in hooking up or casual, no-strings-attached sexual encounters that are increasingly common during emerging adulthood (Stinson, 2010). Meeting clients where they are in terms of dating can be beneficial to supporting them in their specific needs. Given the relationship between dating and self-worth (Park et al., 2011), counselors may benefit from counseling modalities such as cognitive behavioral therapy to assist clients with cognitive distortions and feelings surrounding dating and their worth. Regarding attachment, counselors can consider using attachment theory (Bowlby, 1969) with emerging adult clients struggling with their attachment types in romantic relationships.
Lastly, findings demonstrated that counselors encounter unique developmental issues when counseling emerging adult clients. It may be beneficial for counselors to be instructed on these unique needs of emerging adult clients during their counselor education programs, given the vulnerability of this age group to mental health difficulties, and the needs that participants reported (Cheng et al., 2015). Counselor educators can implement case studies surrounding emerging adult clients struggling with parental pressures, self-discovery, transitions, and dating and attachment to prepare them for real-world scenarios that they are likely to encounter while working with this population. Information on Erikson’s (1968) stages of development, specifically aspects of identity achievement versus role confusion, can align with instruction on emerging adulthood. Counselor educators should also acknowledge that the majority of counselors-in-training may be within the emerging adulthood age range and consider developmental implications for these students during instruction and mentorship (Nice & Branthoover, 2024). The Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2023) standards highlight lifespan development as a foundational counseling curriculum, with lifespan development standards addressing: “1. theories of individual and family development across the lifespan” and “7. models of resilience, optimal development, and wellness in individuals and families across the lifespan.” Counselor education should include training on the unique developmental needs and issues of emerging adulthood such as the themes found within this study in order to assist in meeting these standards.
Limitations and Future Research
Given the subjective nature of qualitative research, we implemented multiple measures of trustworthiness to account for our influence and positionality on this study. Regardless, our influence should still be considered a limitation of this study (Hays et al., 2016). Although we limited the total number of professional counselors working in college counseling centers to less than half of the total sample (n = 5), those participants only experienced emerging adults within the college context and could not speak to experiences of counseling emerging adults who have never attended college, an understudied population of young adults (Seiffge-Krenke et al., 2013). The semi-structured interviews were grounded in emerging adulthood theory and asked specifically about the five features of emerging adulthood. These questions may have influenced participants’ thoughts and feelings about their experiences with this population and affected the overall findings of the study. Finally, some members of our research team were master’s students who did not have doctoral-level research design and qualitative research classes or training. To combat this limitation, several steps were taken to assure the research team members were appropriately trained for their participation in this study, such as online trainings, training from Nice, reflexivity journals, and numerous research team meetings between interviews.
The findings from the present study suggest future investigation concerning the practices for counseling emerging adults is warranted. Whereas this study provides a distinct contribution to the professional counseling and emerging adulthood literature, studies can use these findings to explore future methods for counseling emerging adults. Given that the present study is a phenomenological examination of counselors’ experiences of counseling emerging adults, future studies should use a grounded theory methodology to generate the best practices for working with emerging adults in therapy. Interviews from both professional counselors and emerging adults currently in counseling would assist in providing a complete perspective of the needs for emerging adults in therapy.
Quantitatively, the four themes from this study can be examined in relation to stress, anxiety, wellness, and life satisfaction in order to understand the levels of distress these factors have on the mental health of emerging adults. For example, survey research seeking to understand emerging adults’ levels of stress and wellness can include the Revised Dyadic Adjustment Scale (Busby et al., 1995) and the Short Version of the Individuation Test for Emerging Adults (Komidar et al., 2016) to examine dating and attachment (i.e., Theme 4) and parental relationships and pressures (i.e., Theme 1) in relation to stress and wellness scales.
Conclusion
Counseling with emerging adult clients presents professional counselors with a unique task that includes important developmental implications to address. Consistent with emerging adulthood theory (Arnett, 2000, 2004), counselors experienced their emerging adult clients demonstrating high levels of stress and anxiety from developmental phenomena exclusive to this age range. Specifically, counselors experienced their emerging adults consistently bringing issues to counseling sessions related to parental pressures, self-discovery, transitions, and dating and attachment. Applying these insights derived from professional counselors’ experiences of counseling emerging adult clients in clinical settings and counselor education training programs can support counselors to better serve the specific needs of this frequently served population and, consequently, better address the mental health of emerging adults in therapy.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American College Health Association. (2019). National college health assessment II reference group executive summary Spring 2019.
American Counseling Association. (2014). ACA code of ethics. https://bit.ly/acacodeofethics
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Anney, V. N. (2015). Ensuring the quality of the findings of qualitative research: Looking at trustworthiness criteria. Journal of Emerging Trends in Educational Research and Policy Studies, 5(2), 272–281. https://bit.ly/Anney_truthworthiness
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480. https://doi.org/10.1037/0003-066X.55.5.469
Arnett, J. J. (2004). Emerging adulthood: The winding road from the late teens through the twenties (1st ed.). Oxford University Press.
Arnett, J. J. (2015). Emerging adulthood: The winding road from the late teens through the twenties (2nd ed.). Oxford University Press.
Arnett, J. J., Žukauskienė, R., & Sugimura, K. (2014). The new life stage of emerging adulthood at ages 18–29 years: Implications for mental health. The Lancet Psychiatry, 1(7), 569–576. https://doi.org/10.1016/S2215-0366(14)00080-7
Bowlby, J. (1969). Attachment and loss, Vol. 1: Attachment. Random House.
Buhl, H. M. (2007). Well-being and the child-parent relationship at the transition from university to work life. Journal of Adolescent Research, 22(5), 550–571. https://doi.org/10.1177/0743558407305415
Busby, D. M., Christensen, C., Crane, D. R., & Larson, J. H. (1995). A revision of the Dyadic Adjustment Scale for use with distressed and nondistressed couples: Construct hierarchy and multidimensional scales. Journal of Marital and Family Therapy, 21(3), 289–308. https://doi.org/10.1111/j.1752-0606.1995.tb00163.x
Cheng, H.-L., McDermott, R. C., & Lopez, F. G. (2015). Mental health, self-stigma, and help-seeking intentions among emerging adults: An attachment perspective. The Counseling Psychologist, 43(3), 463–487. https://doi.org/10.1177/0011000014568203
Cofie, N., Braund, H., & Dalgarno, N. (2022). Eight ways to get a grip on intercoder reliability using qualitative-based measures. Canadian Medical Education Journal, 13(2), 73–76. https://doi.org/10.36834/cmej.72504
Coll, D. M., Johnson, C. F., Williams, C. U., & Halloran, M. J. (2019). Defining moment experiences of professional counselors: A phenomenological investigation. The Professional Counselor, 9(2), 142–155. https://doi.org/10.15241/dmc.9.2.142
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/for-programs/2024-cacrep-standards
Creswell, J. W., & Creswell, J. D. (2017). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). SAGE.
Erikson, E. H. (1968). Identity: Youth and crisis. W. W. Norton.
Feiring, C., Simon, V. A., & Markus, J. (2018). Narratives about specific romantic conflicts: Gender and associations with conflict beliefs and strategies. Journal of Counseling & Development, 96(3), 254–266. https://doi.org/10.1002/jcad.12200
Flynn, S. V., & Korcuska, J. S. (2018). Credible phenomenological research: A mixed-methods study. Counselor Education and Supervision, 57(1), 34–50. https://doi.org/10.1002/ceas.12092
Hays, D. G., & Singh, A. A. (2023). Qualitative research in education and social sciences (2nd ed.). Cognella Academic Publishing.
Hays, D. G., Wood, C., Dahl, H., & Kirk-Jenkins, A. (2016). Methodological rigor in Journal of Counseling & Development qualitative research articles: A 15-year review. Journal of Counseling & Development, 94(2), 172–183. https://doi.org/10.1002/jcad.12074
Hendry, L. B., & Kloep, M. (2010). How universal is emerging adulthood? An empirical example. Journal of Youth Studies, 13(2), 169–179. https://doi.org/10.1080/13676260903295067
Howard, A. L., Galambos, N. L., & Krahn, H. J. (2010). Paths to success in young adulthood from mental health and life transitions in emerging adulthood. International Journal of Behavioral Development, 34(6), 538–546. https://doi.org/10.1177/0165025410365803
Komidar, L., Zupančič, M., Puklek Levpušček, M., & Bjornsen, C. A. (2016). Development of the Short Version of the Individuation Test for Emerging Adults (ITEA–S) and its measurement invariance across Slovene and U.S. emerging adults. Journal of Personality Assessment, 98(6), 626–639.
https://doi.org/10.1080/00223891.2016.1171231
Lane, J. A. (2015a). Counseling emerging adults in transition: Practical applications of attachment and social support research. The Professional Counselor, 5(1), 30–42. https://doi.org/10.15241/jal.5.1.30
Lane, J. A. (2015b). The imposter phenomenon among emerging adults transitioning into professional life: Developing a grounded theory. Adultspan Journal, 14(2), 114–128. https://doi.org/10.1002/adsp.12009
Lane, J. A. (2020). Attachment, ego resilience, emerging adulthood, social resources, and well-being among traditional-aged college students. The Professional Counselor, 10(2), 157–169. https://doi.org/10.15241/jal.10.2.157
Lane, J. A., Leibert, T. W., & Goka-Dubose, E. (2017). The impact of life transition on emerging adult attachment, social support, and well-being: A multiple-group comparison. Journal of Counseling & Development, 95(4), 378–388. https://doi.org/10.1002/jcad.12153
Leipold, B., Munz, M., & Michéle-Malkowsky, A. (2019). Coping and resilience in the transition to adulthood. Emerging Adulthood, 7(1), 12–20. https://doi.org/10.1177/2167696817752950
Mitchell, L. L., & Syed, M. (2015). Does college matter for emerging adulthood? Comparing developmental trajectories of educational groups. Journal of Youth and Adolescence, 44(1), 2012–2027. https://doi.org/10.1007/s10964-015-0330-0
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52(2), 250–260. https://doi.org/10.1037/0022-0167.52.2.250
Murphy, K. A., Blustein, D. L., Bohlig, A. J., & Platt, M. G. (2010). The college-to-career transition: An exploration of emerging adulthood. Journal of Counseling & Development, 88(2), 174–181. https://doi.org/10.1002/j.1556-6678.2010.tb00006.x
Nelson, L. J. (2021). The theory of emerging adulthood 20 years later: A look at where it has taken us, what we know now, and where we need to go. Emerging Adulthood, 9(3), 179–188. https://doi.org/10.1177/2167696820950884286
Nice, M. L. (2024). Exploring the relationships and differences of cultural identity salience, life satisfaction, and cultural demographics among emerging adults. Adultspan Journal, 23(1), 1–13. https://doi.org/10.33470/2161-0029.1158
Nice, M. L., & Branthoover, H. (2024). Wellness and the features of emerging adulthood as predictors of counseling leadership behaviors among counselors-in-training. Journal of Counselor Leadership and Advocacy, 1–13. https://doi.org/10.1080/2326716X.2024.2361092
Nice, M. L., & Joseph, M. (2023). The features of emerging adulthood and individuation: Relations and differences by college-going status, age, and living situation. Emerging Adulthood, 11(2), 271–287. https://doi.org/10.1177/21676968221116545
Nice, M. L., Potter, P., & Hecht, C. L. (2023). The role of school counselors in preparing students for the developmental transition from adolescence to emerging adulthood. Journal of Child and Adolescent Counseling, 9(3), 260–272. https://doi.org/10.1080/23727810.2023.2183798
Padilla-Walker, L. M., & Nelson, L. J. (2012). Black hawk down?: Establishing helicopter parenting as a distinct construct from other forms of parental control during emerging adulthood. Journal of Adolescence, 35(5), 1177–1190. https://doi.org/10.1016/j.adolescence.2012.03.007
Palkki, J., & Caldwell, P. (2018). “We are often invisible”: A survey on safe space for LGBTQ students in secondary school choral programs. Research Studies in Music Education, 40(1), 28–49. https://doi.org/10.1177/1321103X17734973
Park, L. E., Sanchez, D. T., & Brynildsen, K. (2011). Maladaptive responses to relationship dissolution: The role of relationship contingent self-worth. Journal of Applied Social Psychology, 41(7), 1749–1773. https://doi.org/10.1111/j.1559-1816.2011.00769.x
Pender, K. N., Hope, E. C., & Sondel, B. (2023). Reclaiming “Mydentity”: Counterstorytelling to challenge injustice for racially and economically marginalized emerging adults. Journal of Community & Applied Social Psychology, 33(2), 300–312. https://doi.org/10.1002/casp.2662
Pennsylvania Department of State. (2024). Social workers, marriage and family therapists and professional counselors licensure guide. https://www.pa.gov/en/agencies/dos/resources/professional-licensing-resources/licensure-processing-guides-and-timelines/social-workers-guide.html
Pietkiewicz, I., & Smith, J. A. (2014). A practical guide to using interpretative phenomenological analysis in qualitative research psychology. Psychological Journal, 20(1), 7–14.
Prosek, E. A., & Gibson, D. M. (2021). Promoting rigorous research by examining lived experiences: A review of four qualitative traditions. Journal of Counseling & Development, 99(2), 167–177. https://doi.org/10.1002/jcad.12364
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Riva Crugnola, C., Bottini, M., Madeddu, F., Preti, E., & Ierardi, E. (2021). Psychological distress and attachment styles in emerging adult students attending and not attending a university counselling service. Health Psychology Open, 8(1). https://doi.org/10.1177/20551029211016120
Saldaña, J. (2021). The coding manual for qualitative researchers (4th ed.). SAGE.
Seiffge-Krenke, I., Persike, M., & Luyckx, K. (2013). Factors contributing to different agency in work and study: A view on the “forgotten half”. Emerging Adulthood, 1(4), 283–292. https://doi.org/10.1177/2167696813487337
Shulman, S., & Connolly, J. (2013). The challenge of romantic relationships in emerging adulthood: Reconceptualization of the field. Emerging Adulthood, 1(1), 27–39. https://doi.org/10.1177/2167696812467330
Smith, C., Christoffersen, K., Davidson, H., & Herzog, P. S. (2011). Lost in transition: The dark side of emerging adulthood. Oxford University Press.
Smith, J. A. (2024). Qualitative psychology: A practical guide to research methods (4th ed.). SAGE.
Sprecher, S., Econie, A., & Treger, S. (2019). Mate preferences in emerging adulthood and beyond: Age variations in mate preferences and beliefs about change in mate preferences. Journal of Social and Personal Relationships, 36(10), 3139–3158. https://doi.org/10.1177/0265407518816880
Stinson, R. D. (2010). Hooking up in young adulthood: A review of factors influencing the sexual behavior of college students. Journal of College Student Psychotherapy, 24(2), 98–115. https://doi.org/10.1080/87568220903558596
Wanzer, V. M., Gray, G. M., & Bridges, C. W. (2021). Lived experiences of professional counselors with gender diverse clients. Journal of LGBTQ Issues in Counseling, 15(2), 240–262. https://doi.org/10.1080/15538605.2021.1914274
Weiss, D., Freund, A. M., & Wiese, B. S. (2012). Mastering developmental transitions in young and middle adulthood: The interplay of openness to experience and traditional gender ideology on women’s self-efficacy and subjective well-being. Developmental Psychology, 48(6), 1774–1784. https://doi.org/10.1037/a0028893
Youniss, J., & Smollar, J. (1985). Adolescent relations with mothers, fathers, and friends. The University of Chicago Press.
Zupančič, M., & Kavčič, T. (2014). Student personality traits predicting individuation in relation to mothers and fathers. Journal of Adolescence, 37(5), 715–726. https://doi.org/10.1016/j.adolescence.2013.12.005
Matthew L. Nice, PhD, is an assistant professor at Indiana University of Pennsylvania. Arsh, MA, is a doctoral student at Indiana University of Pennsylvania. Rachel A. Dingfelder, MA, is a professional counselor and a graduate of the clinical mental health counseling program at Indiana University of Pennsylvania. Nathan D. Faris, MA, is a professional counselor and a graduate of the clinical mental health counseling program at Indiana University of Pennsylvania. Jean K. Albert, MA, is a doctoral student at Indiana University of Pennsylvania. Michael B. Sickels, PhD, is a clinical assistant professor at Duquesne University. Correspondence may be addressed to Matthew L. Nice, 400 Penn Center Boulevard, Building 4, Suite 900, Indiana University of Pennsylvania Pittsburgh East, Pittsburgh, PA 15235, Mnice@iup.edu.
