May 2, 2025 | Volume 15 - Issue 2
Natalie M. Ricciutti, Willough Davis
Substance use disorders (SUDs) and addictions are prevalent client issues that counselors are likely to encounter. Yet, researchers have previously found that counseling journals publish articles about addiction issues at lower rates when compared to other topics. The purpose of this study was to determine recent publication rates of addiction-focused articles in 24 counseling journals between 2016 and 2023. We determined that only 174 (4%) of 4,356 articles published in counseling journals explored addictions-related issues. We conducted a multiple regression analysis and found that the publishing journal had a significant predictive relationship with the publication of addiction-focused articles, while publication year did not. We provide implications for counselors, researchers, reviewers, and journal editors to advocate for the publication of addiction-focused literature for the benefit of the counseling profession.
Keywords: substance use disorders, addictions, counseling journals, publication rates, addiction-focused articles
Addiction treatment is an important and necessary service to both individuals and communities. The 2022 National Survey on Drug Use and Health published by the Substance Abuse and Mental Health Services Administration (SAMHSA; 2024) estimated that 48.7 million people have a substance use disorder (SUD). The same survey also found that approximately 21.5 million adults in the United States have co-occurring substance use and mental health disorders. These figures indicate that SUDs and addictions are prevalent issues that counseling professionals are likely to treat. Accordingly, the U.S. Bureau of Labor Statistics (2024) estimated that the job outlook for substance abuse, behavioral disorder, and mental health counselors is expected to grow by 18% by 2032. This rate of growth is notably faster than the average career growth rate of 5% for those counseling fields. For this reason, it is important that counselors have access to resources that help them learn about addiction issues and treatment in order to better serve their clients. Research articles are one type of resource counselors and counselors-in-training use regularly (Golubovic et al., 2021; Lee, 2014).
Despite the value placed on published counseling literature (Council for the Accreditation of Counseling and Related Educational Programs [CACREP], 2024; Golubovic et al., 2021), counselors have reported difficulty finding articles written about evidence-based addiction treatment practices and research (Doumas et al., 2019; McCuistian et al., 2023; Ricciutti & Storlie, 2024; Sperandio et al., 2023). Previous researchers also found that addiction-focused articles make up a small percentage of the overall counseling literature (Moro et al., 2016; Wahesh et al., 2017). The potential lack of addiction literature in counseling journals may contribute to professionals being uninformed about evidence-based practices and techniques (Golubovic et al., 2021; Lee, 2014). The purpose of this study was to conduct a conceptual content analysis to determine: (a) the rate and frequency of addiction-focused articles that were published in counseling journals from 2016 to 2023, (b) the journals that published the most addiction-focused articles, (c) the most common type of articles published (quantitative, qualitative, mixed methods, conceptual, etc.), and (d) if publishing journal and year of publication predicted the frequency of published addiction-focused articles.
Addiction Issues in Counseling Specialty Areas
SUDs, addictions, and addiction-related issues are prevalent across a variety of populations and age groups and can be common co-occurring disorders (SAMHSA, 2021, 2024). Addictions are also considered to be a continuously growing public health crisis (Matsuzaka & Knapp, 2020; SAMHSA, 2014; Wing Lo et al., 2020). Given the scope and magnitude of addiction prevalence, counselors are likely to work with individuals with an SUD or addiction in treatment, academic, and clinical settings (Chetty et al., 2023). It is vital that counselors across all counseling specialties are informed about addiction-related issues.
One specialty area in which knowledge about SUD and addiction treatment is of the utmost importance is college counseling. According to the American College Health Association (2023), 65.9% of students reported alcohol use and 30.4% reported cannabis use in the previous 3 months. Additionally, 12.8% of the students who reported alcohol use demonstrated moderate or high risk; 20.5% of the students who reported cannabis use demonstrated moderate or high risk. Researchers have found that use of other substances such as opiates (Schulenberg et al., 2019), unprescribed medication (Sharif et al., 2021), and vaping products (National Institutes of Health, 2020) have all recently increased among college students. College students are also susceptible to developing internet addiction (Krishnamurthy & Chetapalli, 2015; Pu et al., 2023) and sex addiction (Giordano & Cashwell, 2018; Giordano et al., 2017), which are categorized as behavioral addictions (American Psychiatric Association, 2022). Counseling services have been found to have a positive impact on college student substance use (Pu et al., 2023; Zhang et al., 2020). However, students enrolled in counseling programs are not required to complete addiction counseling courses (CACREP, 2024). Some college counselors have reported that they lack the addiction counseling training and competence needed to work with students with an SUD or addiction (DePue & Hagedorn, 2015; Giordano & Cashwell, 2018). The prevalence of substance use and addiction issues in university settings suggests that college counselors may benefit from evidence-based addiction counseling literature.
Career counseling is another specialty area in which professionals may work with individuals experiencing SUDs and addictions. Addiction can impact an individual’s occupational wellness as well as their ability to secure and maintain employment (Allen & Bradley, 2015; Siu et al., 2019). Sherba et al. (2018) found that individuals with addictions experienced difficulty finding and sustaining employment. Researchers also identified that employment issues increased relapse rates for individuals in recovery (Sánchez-Hervás et al., 2012). Conversely, individuals with an SUD or addiction who received career counseling services experienced an increase in career maturity and career self-efficacy (Allen & Bradley, 2015) and a decreased risk of relapse (Kim et al., 2022). Yet, similar to college counselors, future career counselors are not required to take an addiction counseling course (CACREP, 2024). Graham (2006) found that this lack of education may cause career counselors to engage in treatment with biases that may negatively impact the therapeutic alliance. Therefore, career counselors need access to addiction counseling information, as it can be a beneficial aspect of an effective and well-rounded treatment plan and potentially decrease counselors’ biases.
Clinical mental health counselors (CMHCs) may often work with individuals with addictions. It is estimated that 7.7 million American adults have both a diagnosable mental health disorder and an SUD or addiction (Han et al., 2017; SAMHSA, 2024). Common comorbidities include mood and anxiety disorders (Kingston et al., 2017), attention-deficit hyperactivity disorder (Harstad et al., 2014), personality disorders (Medeiros & Grant, 2018; Pennay et al., 2011), and schizophrenia (Menne & Chesworth, 2020). For this reason, CMHCs are likely to work with individuals with addictions who initially seek treatment for a mental health disorder. Han et al. (2017) also found that individuals with comorbid mental health disorders and SUDs may seek out different treatment providers for each diagnosable issue. For example, clients may work with a CMHC for a mood disorder and an addiction counselor for an SUD. This dual treatment approach can be problematic because the providers may be unaware of the individual’s co-occurring disorders, and they may provide contradicting information and treatment (Han et al., 2017). Further, comorbid diagnoses have been found to be more effectively treated when one counselor uses integrated therapeutic modalities for both mental health and SUDs (Chetty et al., 2023). Thus, CMHCs must have access to research and information about SUDs and addiction issues to effectively treat individuals with comorbid disorders.
Like other specialties, marriage or couples and family counseling can be impacted by addiction-related issues. Addiction can lead to decreased trust between married or coupled partners (Molla et al., 2018) and an increased risk of marital dissolution and divorce (Torvik et al., 2013). In family systems, researchers found that having a child with an addiction was associated with lower family quality of life and lower marital satisfaction (Hamza et al., 2021). Children are more likely to experience attachment issues and mental health concerns if one or both parents have an addiction (Patton et al., 2019). Marriage or couples and family counselors must be aware of the impact SUD and addiction issues can have on their clients, as well as effective, evidence-based practices in order to support the development of healthy couple and family functioning.
School counselors also face SUD and addiction-related issues among their students and can work in the areas of intervention and prevention. Substance use at an early age may increase the risk of developing an addiction later in life (Nelson et al., 2015). According to the National Institute on Alcohol Abuse and Alcoholism (2024), 29.8% of high school students reported current alcohol use, 13.2% reported current electric vape use, and 19.8% reported current marijuana use. Some students may also be at risk of developing behavioral addictions, such as internet gaming disorder (Chibbaro et al., 2019; Sylvestro et al., 2023). Similar to marriage or couples and family counselors, school counselors may also work with students whose parents have an addiction (Bröning et al., 2012). These children are at a higher risk of experiencing mental health issues (Patton et al., 2019), experimenting with substances, and developing an addiction themselves (Järvinen, 2015; Leijdesdorff et al., 2017). School counselors play a vital role in the early intervention of substance use and the prevention of addictions because of their position as school-based helping professionals (Bröning et al., 2012). Consequently, school counselors, and all counseling professionals, must have access to accurate, peer-reviewed, evidence-based literature about general addiction issues and specific topics relevant to their specialty.
Addiction-Focused Research and Publications
Despite evidence that substance use and addiction issues are common in every area of counseling (Allen & Bradley, 2015; Han et al., 2017; Pu et al., 2023), previous researchers have found that these issues are not reflected in published research (Moro et al., 2016; Wahesh et al., 2017). In 2017, Wahesh et al. reviewed articles published in 23 counseling journals from 2005 to 2014 and found that 4.5% (210 out of 4,640) were focused on addiction-related topics. They also found that an average of 23.33 addiction-focused articles were published each year from 2005 to 2014. Wahesh et al. highlighted that many journals had the capacity to publish more addiction-focused articles but did not. For example, the Journal of Specialists in Group Work published a total of 209 articles between 2005 and 2014. Only five of those articles were focused on addictions or addiction-related issues. The researchers also analyzed changes in publication trends by year and determined that, of the 210 articles focused on addiction-related topics, most were published in 2011 (n = 30) and 2012 (n = 30), while the fewest articles were published in 2008 (n = 14) and 2009 (n = 17). Wahesh et al. concluded that their results may stem from journals rejecting addiction-focused articles and/or addiction counseling researchers submitting their work to journals in other professions (e.g., psychology, social work, public health).
Moro et al. (2016) found similar results when they explored the prevalence of addiction-related articles in four counseling journals published between 2007 and 2011. They found that the Journal of Counseling and Development (JCD) published three (5.1%) addiction-related articles, Measurement and Evaluation in Counseling and Development (MECD) published two (12.9%) articles, Counseling Outcome Research and Evaluation published four (19%) articles, and Counselor Education and Supervision (CES) did not publish any addiction-related articles. Moro et al. also analyzed the frequency of addiction counseling topics presented at the Association for Counselor Education and Supervision conferences during that time frame. Thirty-six out of 1,966 (1.8%) conference presentations discussed addictions, addiction counseling, or addiction counseling education. These results are particularly concerning because many practicing counselors obtain continuing education through reading articles and attending conferences. Counselors may not have other avenues for learning about addiction-related research and evidence-based treatment if the information is not disseminated to the profession via published literature or conference presentations (Moro et al., 2016).
This lack of published literature and conference presentations has led counselors to advocate for more information about addictions and addiction-related issues. Both Moro et al. (2016) and Wahesh et al. (2017) stressed the importance of publishing more addiction-focused articles in counseling journals. Wahesh et al. specifically advocated for research that focuses on how addictions impact diverse groups, subcommunities, and evidence-based practices. Regarding diverse groups, Chaney (2019) explored the degree to which LGBTQ+ populations were included in articles published in the Journal of Addiction and Offender Counseling (JAOC). Chaney found that five (1.78%) out of the 281 articles published since the inauguration of the journal in 1980 to 2018 were focused on LGBTQ+ individuals. Behavioral addictions are another type of addiction that counselors have reported treating (Király et al., 2020; Oka et al., 2021; Ricciutti & Storlie, 2024), yet there is a dearth of published research (Giordano, 2019; Ricciutti, 2023; Wilson & Johnson, 2013). Ricciutti & Storlie (2024) interviewed practicing counselors about their experiences working with clients with process addictions, and all of the participants indicated that they had trouble finding relevant evidence-based practices and techniques in counseling literature. Carlisle et al. (2016) called for more research about the treatment of internet gaming disorder by counselors. Chaney and Burns-Wortham (2014) advocated for more research about sex addiction among the LGBTQ+ community.
Published research is a necessity for the counseling and counselor education professions (Giordano et al., 2021; Golubovic et al., 2021; Lee, 2014). Advancement in counseling practices cannot occur without the constant publication of exemplary research. Some counseling subtopics have seen a surge in published research within the previous decade (i.e., diversity and multicultural issues). Addiction counselors, researchers, and educators have repeatedly called for more addiction counseling information to be published in counseling journals (Golubovic et al., 2021; Moro et al., 2016; Ricciutti & Storlie, 2024; Wahesh et al., 2017). At this time it is unclear if these calls have been answered and if changes have been made. If they have not, it may reflect the lack of addiction-related content being published in counseling journals.
The purpose of this research study was to update the research done by Wahesh et al. (2017) and to determine: (a) the rate and prevalence of addiction articles that have been published in counseling journals between 2016 and 2023, (b) which journals published the most addiction-focused articles, (c) the type of addiction-focused articles (e.g., quantitative, qualitative, mixed methods) published, and (d) if the publishing journal and year of publication predicted the frequency of published addiction-focused articles. We hope that this research will highlight any changes that counseling journals have made to publish more information about addictions and addiction counseling since
the Wahesh et al. review was published in 2017.
Research Questions
Four research questions guided this study:
RQ1: What was the rate and percentage of addiction-focused articles that were published in counseling journals between 2016 and 2023?
RQ2: Which journals published the most addiction-focused articles?
RQ3: What type of article was most commonly published (e.g., quantitative, qualitative, mixed methods, content analysis, literature review)?
RQ4: Did the publishing journal and the year of publication predict the frequency of published addiction-focused articles?
Methodology
We used journal websites and the library resources at the university where the study took place to answer the research questions. We followed Delve et al. (2023) and Hsieh and Shannon’s (2005) recommended guidelines for conducting a conceptual content analysis research study. These guidelines supported our choice to: (a) focus on the concept of addiction-focused counseling research, (b) identify specific words presented in text form (e.g., “addiction,” “substance use,” “addiction counseling”), (c) follow a combined deductive and inductive coding process by categorizing segments of the text that represent the focused concept, (d) take steps to address potential coder disagreements, and (e) use appropriate subjective interpretation based on our expertise.
Our research team included one professor, Natalie M. Ricciutti, and one doctoral-level graduate student, Willough Davis. Ricciutti has a degree in counselor education and supervision, with specializations in addiction counseling and addiction education, and extensive experience conducting content analysis research. At the time of the study, Davis was enrolled in a counselor education and supervision program and has a strong clinical background in addiction counseling. Davis also assisted in the study to fulfill requirements of an independent study about content analyses. We are both White females who have previously completed multiple courses in research methods. Ricciutti determined the purpose of the study, outlined the coding process, and trained Davis to identify and include relevant data prior to and throughout the study. Davis completed the initial review and categorization of the addiction counseling literature and Ricciutti provided feedback weekly.
Journal Search and Data Collection
In an attempt to update Wahesh et al.’s (2017) study with fidelity, the data collection and review processes in the current study remained the same, with a few exceptions. First, we chose a timeline of 8 inclusive years instead of 9 because 8 years had passed since Wahesh et al. ended their data collection in 2015. Second, we selected the same 23 counseling journals for our study and added the Journal of School Counseling, bringing our journal total to 24. We organized the 24 journals into a list for data collection purposes (Table 1). This list included national journals (n = 19, 79.2%), regional journals (n = 3, 12.5%), and international journals (n = 2, 8.3%). National journals included JCD, CES, JAOC, and the Professional School Counselor; regional journals included Counselor Preparation and Supervision and Teaching & Supervision in Counseling; and international journals included the International Journal for the Advancement of Counseling and the Asia Pacific Journal of Counseling & Psychotherapy. We conducted a thorough review of all the articles published in the 24 journals, which resulted in a total of 4,356 articles.
We reviewed the title, abstract, keywords, and full narrative of each of the 4,356 articles to determine whether or not each was about addiction or substance use–related issues. We labeled articles as addiction-focused if they used addiction-related terminology in the title, abstract, keywords, and/or full narrative. Common terminology included specific types of substance or behavioral addictions, addiction recovery, addiction treatment, and addiction counseling. We also included articles if they focused on addictions or addiction-related topics. Common topics included evidence-based addiction treatment practices, issues related to specific SUDs and behavioral addictions, risk and protective factors of addictions, the impact of addiction and/or substance use among specific populations, and addiction counseling education.
We collected data by categorizing each addiction-focused article’s relevant information in an Excel spreadsheet. This included the article title, the publishing journal, year of publication, the article’s keywords, type of article (e.g., original research, conceptual, literature review), and the type of research the article included (if relevant; quantitative, qualitative, mixed methods). Similar to the inclusion process, we excluded articles if they did not have an addiction-related focus, and they did not include addiction-related terminology in the title, abstract, keywords, and full narrative. Ricciutti reviewed Davis’s categorization of articles and data coding during weekly meetings to ensure coder agreement. We both reviewed articles when it was unclear if an article was focused on addiction-related content. When necessary, we discussed an article’s focus until we resolved disagreements and reached consensus on inclusion or exclusion. Lastly, we cross-referenced our collected data with the 4,356 articles to ensure that we included all of the published addiction-focused articles. We determined that no articles needed to be added or removed. The data was transferred into SPSS (Version 28) for analysis.
Data Analysis
We used descriptive statistics to answer the first research question and to determine the rate and percentage of all addiction-focused articles published in counseling journals between 2016 and 2023. For the second research question, we used descriptive statistics to determine the rate and percentage of the addiction-focused articles published in each journal. For the third research question, we used descriptive statistics to determine the rate and percentage of the type of articles and the research methodology researchers used. We also used descriptive statistics to determine the number of the type of article and type of methodology published each year (Figures 1 and 2). We conducted a multiple regression analysis to answer the final research question to determine the predictive relationship between the independent variables of publishing journal and year of publication as well as the dependent variable of frequency of published addiction-focused articles.
Table 1
Addiction-Focused Article Trends per Journal
| Journal |
Total Number of Articles |
Number of Addiction-Focused Articles |
Percentage of Addiction-Focused Articles |
| Adultspan Journal |
62 |
0 |
0% |
| Asia Pacific Journal of Counseling and Psychotherapy |
96 |
0 |
0% |
| Counseling Outcome Research and Evaluation |
79 |
4 |
5.0% |
| Counseling and Values |
107 |
2 |
1.87% |
| Counselor Education and Supervision |
178 |
1 |
0.56% |
| The Family Journal |
448 |
20 |
4.46% |
| International Journal for the Advancement of Counseling |
281 |
7 |
4.49% |
| The Journal for Specialists in Group Work |
141 |
2 |
1.42% |
| Journal of Addiction & Offender Counseling |
67 |
51 |
74.63% |
| Journal of College Counseling |
118 |
15 |
13.56% |
| Journal of Counseling & Development |
324 |
14 |
4.32% |
| Journal of Counselor Preparation and Supervision |
305 |
4 |
1.31% |
| Journal of Creativity in Mental Health |
316 |
12 |
4.11% |
| Journal of Employment Counseling |
114 |
1 |
0.89% |
| Journal of Humanistic Counseling |
117 |
3 |
2.56% |
| Journal of LGBT Issues in Counseling |
155 |
4 |
2.58% |
| Journal of Mental Health Counseling |
182 |
6 |
3.29% |
| Journal of Multicultural Counseling & Development |
148 |
2 |
1.35% |
| Journal of School Counseling |
172 |
3 |
1.74% |
| Journal of Technology in CE&S |
49 |
0 |
0% |
| Measurement and Evaluation in Counseling and Development |
167 |
6 |
3.59% |
| The Professional Counselor |
227 |
11 |
4.85% |
| Professional School Counselor |
408 |
2 |
0.98% |
| Teaching and Supervision in Counseling |
95 |
2 |
2.11% |
Note. Total number of articles is 4,356. Number of addiction-focused articles is 174.
Figure 1
Type of Addiction-Focused Articles Published per Year
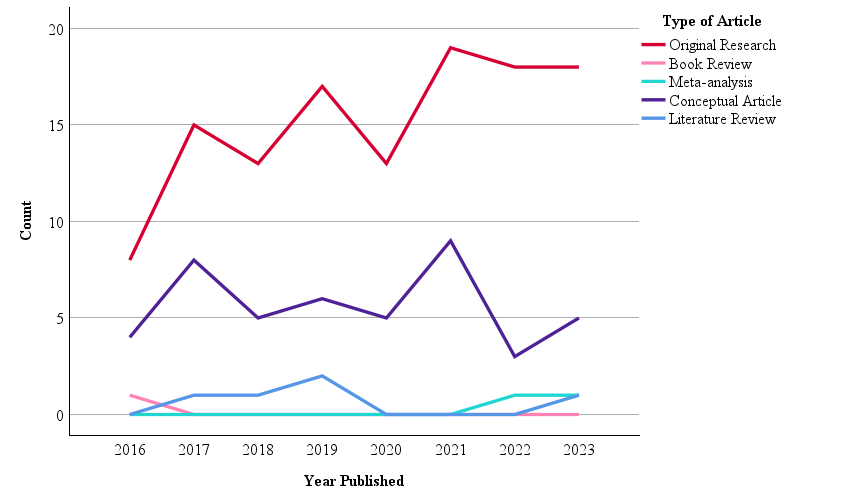
Note. N = 174.
Figure 2
Type of Research in Published Addiction-Focused Articles per Year
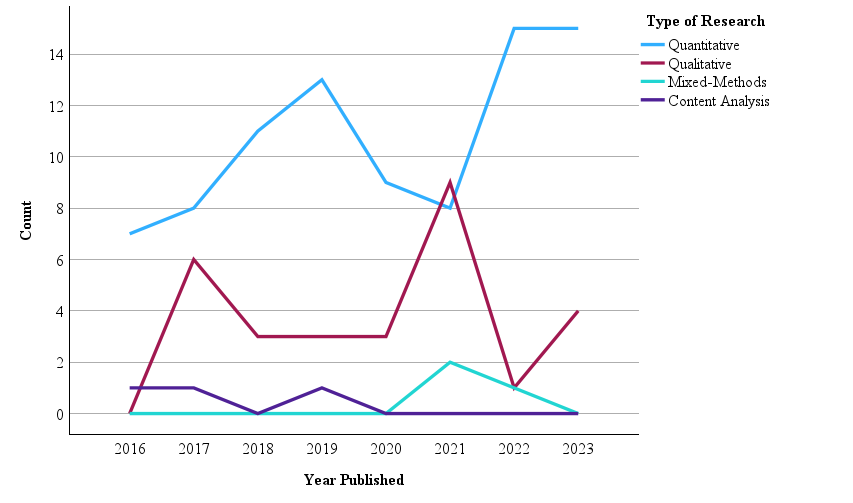
Note. N = 121.
Results
Of the 4,356 articles published in 24 counseling journals from 2016 to 2023, we identified 174 (4%) as focused on addiction counseling or other addiction-related issues (Table 1). Regarding our second research question, JAOC had the highest rate and percentage of addiction-focused articles at 74.63% (n = 51). Adultspan Journal, Asia Pacific Journal of Counseling & Psychotherapy, and Technology in CES were tied with the lowest percentage of addiction-focused articles at 0%. Regarding the third research question, the most common type of article was original research (n = 121, 69.5%). Other types of articles included conceptual pieces (n = 45, 25.9%), literature reviews (n = 5, 2.9%), meta-analyses (n = 2, 1.1%), and book reviews (n = 1, 0.6%). Figure 1 provides a description of the type of addiction-focused articles published during each year. Of the 121 original research articles, 86 (71.1%) were quantitative studies, 29 (24%) were qualitative studies, three (2.5%) were content analyses, and three (2.5%) were mixed method studies. Figure 2 provides a description of the type of research conducted in each addiction-focused published article during each year.
Regarding the fourth research question, we first calculated yearly analyses to determine the number of addiction-focused articles published in counseling journals each year (Table 2). The year 2016 had the lowest number of published addiction-focused articles (n = 13, 7.5%), while 2021 had the highest (n = 28, 16.1%). On average, 21.75 addiction-focused articles were published each year from 2016 to 2023. Next, we conducted a multiple linear regression analysis to determine if journal and year of publication had a predictive relationship with the frequency of published addiction-focused articles. This analysis resulted in a statistically significant regression model, F(2, 187) = 4.134, p = .018, R2 = 0.42. Finally, we examined the individual predictors (i.e., independent variables). We found that publishing journal had a significant predictive relationship with the frequency of published addiction-focused articles, (Beta = −.192, t(189) = −3.682, p = .008). In other words, some journals were significant predictors of being more likely to publish addiction-focused articles than others. We also found that publication year did not have a significant predictive relationship with the frequency of published addiction-focused articles (Beta = .07, t(189) = .973, p = .332).
Table 2
Addictions-Focused Articles Published Per Year
| Year |
n |
% |
| 2016 |
13 |
7.5 |
| 2017 |
24 |
13.8 |
| 2018 |
19 |
10.9 |
| 2019 |
25 |
14.4 |
| 2020 |
18 |
10.3 |
| 2021 |
28 |
16.1 |
| 2022 |
22 |
12.6 |
| 2023 |
25 |
14.4 |
Note. Total N = 174.
Discussion
The purpose of this study was to examine the frequency of addiction-focused articles published in counseling journals in recent years. We reviewed 4,356 articles published in 24 counseling journals from 2016 to 2023 to determine the frequency and percentage of addiction-focused literature in the counseling profession. The results indicate only 174 (4%) of those articles were focused on addiction counseling or other addiction-related issues. This percentage is less than previously identified by Wahesh et al. (2017), who found that 210 (4.5%) out of 4,640 articles published from 2005 to 2014 were about addiction issues. Publication year also did not have a significant, predictive relationship with publication rates. This result suggests that national and global events occurring between 2016 and 2023 (e.g., the opioid epidemic, the COVID-19 pandemic) did not statistically impact the publication of addiction-focused articles in counseling journals.
We also determined that the majority of addiction-focused articles were original research, many of which used quantitative analytic techniques. This result reflects a long-standing trend toward quantitative methodologies in the counseling and other helping professions (Berríos & Lucca, 2006; Marshall et al., 2025; Oh et al., 2017). We also found that only three of the 174 addiction-focused articles used mixed methods techniques. This number is lower than Wahesh et al.’s (2017) finding of six mixed methods studies. Researchers and professionals in counseling have called for more mixed methods research to achieve well-rounded study findings (Ponterotto et al., 2013; Wester & McKibben, 2019). Our results indicate that this change has yet to occur with addiction-focused research published in counseling journals.
It is worth noting the differences we found in publication rates by journal when considering potential reasons for the lack of addiction-focused counseling literature. The specific journal and the publication of addiction-focused articles had a significant, predictive relationship. Unsurprisingly, JAOC published the most addiction-related literature in both number and percentage. Yet, it had one of the lowest numbers of total published articles (67 from 2016 to 2023; Table 1). As discussed, counselors have reported experiencing difficulty finding relevant, evidence-based addiction counseling literature to support their practice (Chaney, 2019; Ricciutti & Storlie, 2024; Wilson & Johnson, 2013). This struggle may be because the only addiction counseling journal has one of the lowest publication rates out of the 24 journals included in this study.
Another reason for the publication rate may be a lack of addiction-focused articles being submitted to counseling journals. Instead, counseling researchers with expertise in addiction issues may be submitting their manuscripts to journals in other professions (e.g., psychology, social work, public health, etc.). We did not find a study exploring the rates of addiction-focused articles in the psychology, social work, or public health professions to compare with our findings. Yet, these professions each have many addiction and substance use–focused journals where researchers can choose to submit their work. A Google Scholar (2024) search of all addiction journals’ h5-indices (i.e., the number of articles published in the last 5 years) and h5-medians (i.e., the median number of citations for articles in the h5-index) shows that the top 20 publications at the time of this writing are the psychology journals the International Journal of Mental Health and Addiction, Drug and Alcohol Dependence, and Addictive Behaviors. JAOC was not included in that list.
The results may also be due to the small number of counseling researchers and educators with expertise in addiction issues compared to the overall profession. A number of studies have found that many counseling students leave their programs without the necessary academic experience to competently practice addiction counseling (Golubovic et al., 2021; Lee, 2014; Ricciutti & Storlie, 2024). As discussed, CACREP (2024) standards do not include addiction counseling content requirements for many of the specialty practice areas. Ricciutti & Storlie (2024) found that the lack of education caused some counselors to report that addiction counseling was not part of their professional identity. For this reason, we join Moro et al. (2016) in advocating for the inclusion of an addictions course into the counseling core curriculum. Requiring a course for all students may help future counselors incorporate addiction counseling into their professional identity. Doing so could instill future counselors with a passion for addiction issues and eventually lead to an increase in addiction-focused manuscripts submitted for publication in counseling journals.
Recommendations for Counselors, Counselor Educators, and Researchers
Addiction-focused literature published in counseling journals is highly relevant for practicing counselors, counseling researchers, and the overall profession. Substantial value is placed on published research to advance the counseling profession (CACREP, 2024; Golubovic et al., 2021). SUD and addictions are common primary and co-occurring disorders (SAMHSA, 2021, 2024) and the job outlook for addiction and substance use counselors is expected to grow rapidly (U.S. Bureau of Labor Statistics, 2024). Counselors in every specialty area need relevant, evidence-based research about SUD and addiction issues to inform their practice. Yet, we found the publication of addiction-focused articles to be low, with some journals failing to publish anything about addiction issues from 2016 to 2023. Journals may want to consider how to solicit addiction-focused content for publication to fill this research gap.
The existing prevalence rates of addiction-focused articles may, in part, stem from researchers not submitting articles about addiction issues to counseling journals. Researchers may believe that their manuscript is likely to be rejected if it is sent to a journal that has not published an addiction-related article in recent years. We encourage authors and researchers to push against this potential belief and consider submitting their addiction-focused manuscripts to journals that have not recently published articles about the topic. This practice could inform editors and reviewers about addiction-related issues in the counseling profession, as well as help authors reach new audiences who may not normally read addiction-focused articles. Counselors and researchers also can attempt to advocate for the inclusion of addiction-focused articles in the journals they frequently read. This advocacy can come in the form of writing letters to journal editors to request more addiction content. Practicing counselors can also work to conduct addiction-focused research studies through their agencies, practices, schools, or universities. The information gleaned from studies that are conducted in novel settings with diverse populations would be highly relevant to the profession and help grow the existing body of literature.
An increase in addiction-focused research studies and submitted manuscripts is only the first step toward a higher prevalence of published articles. Journal review boards and editors must be willing to expand the aims, scope, and acceptable topics to include addiction-related issues. For example, addiction issues are highly relevant in every counseling specialty area, including school counseling (Bröning et al., 2012). Yet, the Professional School Counselor published two addiction-focused articles and the Journal of School Counseling only published three (Table 1). This is despite recent evidence that substance use and addiction issues continue to be a common issue among children and adolescents in the last decade (National Institute on Drug Abuse, 2023). Editors and reviewers expanding journals’ scope and acceptable topics for consideration may allow researchers with an expertise in addiction counseling to feel more confident sending their manuscripts to counseling journals other than JAOC.
Journals can sponsor special issues that are dedicated to addiction-related topics. We urge researchers, writers, journal editors, and reviewers to consider the long-term implications and benefits of providing more addiction-focused articles to the entire counseling profession. These journal practices will help grow the existing literature over time; expand addiction-related topics to a variety of co-occurring disorders and populations; and provide new opportunities for continuing education, much of which can be obtained through reading and contributing to journal articles. For example, Chaney (2019) called for more literature about substance use and addiction among the LGBTQ+ community. The Journal of LGBT Issues in Counseling could combine both topics in a special issue. Finally, we encourage CACREP to consider adding new addiction counseling standards to their next edition at both the master’s and doctoral levels. As discussed, counselors in every specialty area are likely to work with individuals with addictions and SUDs (Bröning et al., 2012; Kim et al., 2022; Patton et al., 2019). Yet, many have reported their training and skills in this area have fallen short of competence (DePue & Hagedorn, 2015; Giordano & Cashwell, 2018; Han et al., 2017). It is necessary that all counselors receive education in addiction counseling in order to better serve their clients or students.
Limitations
This study is not without limitations. First, as with any conceptual content analysis, researcher error and subjective interpretation of the data is a potential limitation. Although we fully reviewed each of the 4,640 articles, we identified addiction-focused articles, in part, through the inclusion of addiction terminology in the title, abstract, keywords, and narrative. It is possible we unintentionally excluded relevant articles or included articles that were irrelevant because we did not use statistical measures of interrater reliability. Similarly, it is possible there was addiction-related language and terminology that we were unfamiliar with, causing us to exclude articles that should have been included. We also may have allowed our unconscious biases to impact our data inclusion process throughout the study. We worked to mitigate this potential limitation by reviewing each article in full and by following recommended guidelines for conducting a conceptual content analysis (Delve et al., 2023; Hsieh & Shannon, 2005).
Second, this study focuses on addiction articles published in 24 counseling journals from 2016 to 2023. For this reason, it is possible that our study may not accurately reflect published addiction-focused articles over a broader period of time or with different journals. We encourage future researchers to review additional counseling journals not included in this study, such as state counseling journals or local university counseling journals. Third, we only collected and analyzed data that was publicly available—published articles in counseling journals. We did not gather data on the number of addiction-focused manuscripts that were submitted to journals but not published. Future researchers may consider contacting counseling journal editors to ascertain the rate of submitted manuscripts that were not published for any reason (e.g., rejected, author pulled their manuscript). Researchers can then compare the number of submitted addiction manuscripts with the number of published articles. Doing so may incorporate data excluded from this study and determine if the small number of addiction-focused articles is due to lack of quality submissions or potential reviewer and editor bias. Researchers could also conduct a similar study with journals in other helping professions (e.g., psychology, social work, public health) to determine if our results reflect a common trend in the publication of addiction-focused articles.
Conclusion
We explored the prevalence of addiction-focused articles published in 24 counseling journals from 2016 to 2023 and found recent publication rates to be low. We reported the journals that have published addiction-focused articles during that time frame, the type of articles published, and the potential impact of journal and year of publication. We compared our findings with Wahesh et al. (2017) and determined that the prevalence and rate of addiction articles has not increased since 2005. The lack of information may make it difficult for counselors in every specialty area to learn about addiction issues relevant to their clients or students. Finally, we provided information about the importance of addiction literature in the counseling profession and the implications of journals expanding their aims and scopes to include addiction issues.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Allen, K. R., & Bradley, L. (2015). Career counseling with juvenile offenders: Effects on self-efficacy and career maturity. Journal of Addictions & Offender Counseling, 36(1), 28–42. https://doi.org/10.1002/j.2161-1874.2015.00033.x
American College Health Association. (2023). National College Health Assessment: Spring 2022 reference group executive summary. https://www.acha.org/ncha/data-results
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176/appi.books.9780890425787
Berríos, R., & Lucca, N. (2006). Qualitative methodology in counseling research: Recent contributions and challenges for a new century. Journal of Counseling & Development, 84(2), 174–186. https://doi.org/10.1002/j.1556-6678.2006.tb00393.x
Bröning, S., Kumpfer, K., Kruse, K., Sack, P.-M., Schaunig-Busch, I., Ruths, S., Moesgen, D., Pflug, E., Klein, M., & Thomasius, R. (2012). Selective prevention programs for children from substance-affected families: A comprehensive systematic review. Substance Abuse Treatment, Prevention, and Policy, 7(23), 1–17. http://www.substanceabusepolicy.com/content/7/1/23
Carlisle, K. L., Carlisle, R. M., Polychronopoulos, G. B., Goodman-Scott, E., & Kirk-Jenkins, A. (2016). Exploring internet addiction as a process addiction. Journal of Mental Health Counseling, 38(2), 170–182. https://doi.org/10.17744/mehc.38.2.07
Chaney, M. P. (2019). LGBTQ+ addiction research: An analysis of the Journal of Addictions & Offender Counseling. Journal of Addictions & Offender Counseling, 40(1), 2–16. https://doi.org/10.1002/jaoc.12053
Chaney, M. P., & Burns-Wortham, C. M. (2014). The relationship between online sexual compulsivity, dissociation, and past child abuse among men who have sex with men. Journal of LGBT Issues in Counseling, 8(2), 146–163. https://doi.org/10.1080/15538605.2014.895663
Chetty, A., Guse, T., & Malema, M. (2023). Integrated vs non-integrated treatment outcomes in dual diagnosis disorders: A systematic review. Health SA Gesondheid, 28(1), a2094. https://doi.org/10.4102/hsag.v28i0.2094
Chibbaro, J. S., Ricks, L., & Lanier, B. (2019). Digital awareness: A model for school counselors. Journal of School Counseling, 17(22). https://jsc.montana.edu/articles/v17n22.pdf
Council for the Accreditation of Counseling and Related Educational Programs. (2024). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2024/04/2024-Standards-Combined-Version-4.11.2024.pdf
Delve, Ho, L., & Limpaecher, A. (2023, January 25). What is conceptual content analysis in qualitative research? Step-by-step guide. https://delvetool.com/blog/what-is-conceptual-qualitative-content-analysis-step-by-step-guide
DePue, M. K., & Hagedorn, W. B. (2015). Facilitating college students’ recovery through the use of collegiate recovery programs. Journal of College Counseling, 18(1), 66–81. https://doi.org/10.1002/j.2161-1882.2015.00069.x
Doumas, D. M., Miller, R. M., & Esp, S. (2019). Continuing education in motivational interviewing for addiction counselors: Reducing the research-to-practice gap. Journal of Addictions & Offender Counseling, 40(1), 36–51. https://doi.org/10.1002/jaoc.12055
Giordano, A. L., & Cashwell, C. S. (2018). An examination of college counselors’ work with student sex addiction: Training, screening, and referrals. Journal of College Counseling, 21(1), 43–57. https://doi.org/10.1002/jocc.12086
Giordano, A. L., Cashwell, C. S., Lankford, C., King, K., & Henson, R. K. (2017). Collegiate sexual addiction: Exploring religious coping and attachment. Journal of Counseling & Development, 95(2), 135–144. http://doi.org/10.1002/jcad.12126
Giordano, A. L., Malacara, A., & Agarwal, S. (2019). A process addictions course for counselor training programs. Teaching and Supervision in Counseling, 1(1), 47–59. https://doi.org/10.7290/tcs010105
Giordano, A. L., Schmit, M. K., & Schmit, E. L. (2021). Best practice guidelines for publishing rigorous research in counseling. Journal of Counseling & Development, 99(2), 123–133. https://doi.org/10.1002/jcad.12360
Golubovic, N., Dew, B., Rumsey, A., Murphy, T., Dispenza, F., Tabet, S., & Lebensohn-Chialvo, F. (2021). Pedagogical practices for teaching addiction counseling courses in CACREP-accredited programs. Journal of Addictions & Offender Counseling, 42(1), 3–18. http://doi.org/10.1002/jaoc.12086
Google Scholar. (2024). Addiction – Google Scholar Metrics. https://scholar.google.com/citations?view_op=top_venues&hl=en&vq=med_addiction
Graham, M. D. (2006). Addiction, the addict, and career: Considerations for the employment counselor. Journal of Employment Counseling, 43(4), 168–178. https://doi.org/10.1002/j.2161-1920.2006.tb00016.x
Hamza, E. G. A., Gladding, S., & Moustafa, A. A. (2021). The impact of adolescent substance abuse on family quality of life, marital satisfaction, and mental health in Qatar. The Family Journal, 30(1), 85–90. https://doi.org/10.1177/10664807211000720
Han, B., Compton, W. M., Blanco, C., & Colpe, L. J. (2017). Prevalence, treatment, and unmet treatment needs of US adults with mental health and substance use disorders. Health Affairs, 36(10), 1739–1747. https://doi.org/10.1377/hlthaff.2017.0584
Harstad, E., Levy, S., & Committee on Substance Abuse. (2014). Attention-deficit/hyperactivity disorder and substance abuse. Pediatrics, 134(1), e293–e301. https://doi.org/10.1542/peds.2014-0992
Hsieh, H.-F., & Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qualitative Health Research, 15(9), 1277–1288. https://doi.org/10.1177/1049732305276687
Järvinen, M. (2015). Understanding addiction: Adult children of alcoholics describing their parents’ drinking problems. Journal of Family Issues, 36(6), 805–825. http://doi.org/10.1177/0192513X13513027
Kim, M., Byrne, A. M., & Jeon, J. (2022). The effect of vocational counseling interventions for adults with substance use disorders: A narrative review. International Journal of Environmental Research and Public Health, 19(8), 4674. https://doi.org/10.3390/ijerph19084674
Kingston, R. E. F., Marel, C., & Mills, K. L. (2017). A systematic review of the prevalence of comorbid mental health disorders in people presenting for substance use treatment in Australia. Drug and Alcohol Review, 36(4), 527–539. https://doi.org/10.1111/dar.12448
Király, O., Potenza, M. N., Stein, D. J., King, D. L., Hodgins, D. C., Saunders, J. B., Griffiths, M. D., Gjoneska, B., Billieux, J., Brand, M., Abbott, M. W., Chamberlain, S. R., Corazza, O., Burkauskas, J., Sales, C. M. D., Montag, C., Lochner, C., Grünblatt, E., Wegmann, E., . . . Demetrovics, Z. (2020). Preventing problematic internet use during the COVID-19 pandemic: Consensus guidance. Comprehensive Psychiatry, 100.
https://doi.org/10.1016/j.comppsych.2020.152180
Krishnamurthy, S., & Chetapalli, S. K. (2015). Internet addiction: Prevalence and risk factors, A cross-sectional study among college students in Bengaluru, the Silicon Valley of India. Indian Journal of Public Health, 59(2), 115–121. https://doi.org/10.4103/0019-557X.157531
Lee, T. K. (2014). Addiction education and training for counselors: A qualitative study of five experts. Journal of Addictions & Offender Counseling, 35(2), 67–80. https://doi.org/10.1002/j.2161-1874.2014.00027.x
Leijdesdorff, S., van Doesum, K., Popma, A., Klaassen, R., & van Amelsvoort, T. (2017). Prevalence of psychopathology in children of parents with mental illness and/or addiction: An up to date narrative review. Current Opinion in Psychiatry, 30(4), 312–317. https://doi.org/10.1097/YCO.0000000000000341
Marshall, D. T., Elmer, J. W., Hebert, C. C., & Barringer, K. E. (2025). Counseling research trends: A content analysis 2016–2020. Journal of Professional Counseling: Practice, Theory & Research, 52(1), 51–65. https://doi.org/10.1080/15566382.2024.2368647
Matsuzaka, S., & Knapp, M. (2020). Anti-racism and substance use treatment: Addiction does not discriminate, but do we? Journal of Ethnicity in Substance Abuse, 19(4), 567–593. https://doi.org/10.1080/15332640.2018.1548323
McCuistian, C., Fokuo, J. K., Dumoit Smith, J., Sorensen, J. L., & Arnold, E. A. (2023). Ethical dilemmas facing substance use counselors during the COVID-19 pandemic. Substance Use: Research and Treatment, 17, 1–19. https://doi.org/10.1177/11782218231158338
Medeiros, G. C., & Grant, J. E. (2018). Gambling disorder and obsessive–compulsive personality disorder: A frequent but understudied comorbidity. Journal of Behavioral Addictions, 7(2), 366–374. https://doi.org/10.1556/2006.7.2018.50
Menne, V., & Chesworth, R. (2020). Schizophrenia and drug addiction comorbidity: Recent advances in our understanding of behavioural susceptibility and neural mechanisms. Neuroanatomy and Behaviour, 2(1), e10. https://doi.org/10.35430/nab.2020.e10
Molla, E., Tadros, E., & Cappetto, M. (2018). The effects of alcohol and substance use on a couple system: A clinical case study. The Family Journal, 26(3), 341–350. https://doi.org/10.1177/1066480718795500
Moro, R. R., Wahesh, E., Likis-Werle, S. E., & Smith, J. E. (2016). Addiction topics in counselor educator professional development: A content analysis. Journal of Addictions & Offender Counseling, 37(1), 2–15. https://doi.org/10.1002/jaoc.12012
National Institute on Alcohol Abuse and Alcoholism. (2024). Underage drinking in the United States (ages 12 to 20). https://www.niaaa.nih.gov/alcohols-effects-health/alcohol-topics/alcohol-facts-and-statistics/underage-drinking-united-states-ages-12-20
National Institute on Drug Abuse. (2023, December 13). Reported drug use among adolescents continued to hold below pre-pandemic levels in 2023. https://nida.nih.gov/news-events/news-releases/2023/12/reported-drug-use-among-adolescents-continued-to-hold-below-pre-pandemic-levels-in-2023
National Institutes of Health. (2020, September 15). Vaping, marijuana use in 2019 rose in college-age adults.
https://www.nih.gov/news-events/news-releases/vaping-marijuana-use-2019-rose-college-age-adults
Nelson, S. E., Van Ryzin, M. J., & Dishion, T. J. (2015). Alcohol, marijuana, and tobacco use trajectories from age 12 to 24 years: Demographic correlates and young adult substance use problems. Development and Psychopathology, 27(1), 253–277. https://doi.org/10.1017/S0954579414000650
Oh, J., Stewart, A. E., & Phelps, R. E. (2017). Topics in the Journal of Counseling Psychology, 1963–2015. Journal of Counseling Psychology, 64(6), 604–615. https://doi.org/10.1037/cou0000218
Oka, T., Hamamura, T., Miyake, Y., Kobayashi, N., Honjo, M., Kawato, M., Kubo, T., & Chiba, T. (2021). Prevalence and risk factors of internet gaming disorder and problematic internet use before and during the COVID-19 pandemic: A large online survey of Japanese adults. Journal of Psychiatric Research, 142, 218–225. https://doi.org/10.1016/j.jpsychires.2021.07.054
Patton, R., Goerke, J., Fye, J., & Katafiasz, H. (2019). Does hazardous alcohol use impact individual and relational functioning among couples seeking couples therapy? The Family Journal, 27(3), 287–292. https://doi.org/10.1177/1066480719844033
Pennay, A., Cameron, J., Reichert, T., Strickland, H., Lee, N. K., Hall, K., & Lubman, D. I. (2011). A systematic review of interventions for co-occurring substance use disorder and borderline personality disorder. Journal of Substance Abuse Treatment, 41(4), 363–373. https://doi.org/10.1016/j.jsat.2011.05.004
Ponterotto, J. G., Mathew, J. T., & Raughley, B. (2013). The value of mixed methods designs to social justice research in counseling and psychology. Journal for Social Action in Counseling & Psychology, 5(2), 42–68. https://doi.org/10.33043/JSACP.5.2.42-68
Pu, Y., Liu, Y., Qi, Y., Yan, Z., Zhang, X., & He, Q. (2023). Five-week of solution-focused group counseling successfully reduces internet addiction among college students: A pilot study. Journal of Behavioral Addictions, 12(4), 964–971. https://doi.org/10.1556/2006.2023.00064
Ricciutti, N. M. (2023). Counselors’ stigma toward addictions: Increasing awareness and decreasing stigma. Journal of Counselor Preparation and Supervision, 17(3). https://digitalcommons.sacredheart.edu/jcps/vol17/iss3/6
Ricciutti, N. M. & Storlie, C. A. (2024). The experiences of clinical mental health counselors treating clients for process/behavioral addictions. Alcoholism Treatment Quarterly, 42(1), 27–44. https://doi.org/10.1080/07347324.2023.2267004
Sánchez-Hervás, E., Gómez, F. J., Villa, R. S., García-Fernández, G., García-Rodríguez, O., & Romaguera, F. Z. (2012). Psychosocial predictors of relapse in cocaine-dependent patients in treatment. The Spanish Journal of Psychology, 15(2), 748–755. https://doi.org/10.5209/rev_SJOP.2012.v15.n2.38886
Schulenberg, J. E., Johnston, L. D., O’Malley, P. M., Bachman, J. G., Miech, R. A., & Patrick, M. E. (2019). Monitoring the Future national survey results on drug use, 1975–2018: Volume 2, College students & adults ages 19–60. Institute for Social Research, The University of Michigan. https://monitoringthefuture.org/wp-content/uploads/2022/08/mtf-vol2_2018.pdf
Sharif, S., Guirguis, A., Fergus, S., & Schifano, F. (2021). The use and impact of cognitive enhancers among university students: A systematic review. Brain Sciences, 11(3), 355. https://doi.org/10.3390/brainsci11030355
Sherba, R. T., Coxe, K. A., Gersper, B. E., & Vinley, J. V. (2018). Employment services and substance abuse treatment. Journal of Substance Abuse Treatment, 87, 70–78. https://doi.org/10.1016/j.jsat.2018.01.015
Siu, A. M. H., Fung, M. S. M., Cheung, P. P. P., Shea, C. K., & Lau, B. W. M. (2019). Vocational evaluation and vocational guidance for young people with a history of drug abuse. WORK: A Journal of Prevention, Assessment & Rehabilitation, 62(2), 327–336. https://doi.org/10.3233/WOR-192867
Sperandio, K. R., Goshorn, J. R., Moh, Y. S., Gonzalez, E., & Johnson, N. G. (2023). Never ready: Addictions counselors dealing with client death. Journal of Counseling & Development, 101(1), 29–45. https://doi.org/10.1002/jcad.12440
Substance Abuse and Mental Health Services Administration. (2014). Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-48, HHS Publication No. (SMA) 14-4863.
https://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.pdf
Substance Abuse and Mental Health Services Administration. (2021). Key substance use and mental health indicators in the United States: Results from the 2020 National Survey on Drug Use and Health. http://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf
Substance Abuse and Mental Health Services Administration. (2024). 2022 National Survey on Drug Use and Health. https://www.datafiles.samhsa.gov/dataset/national-survey-drug-use-and-health-2022-nsduh-2022-ds0001
Sylvestro, H. M., Glance, D. E., Ripley, D., & Stephenson, R. (2023). Elementary school counselors’ experiences working with children affected by parental substance use. Professional School Counseling, 27(1). https://doi.org/10.1177/2156759X231182142
Torvik, F. A., Røysamb, E., Gustavson, K., Idstad, M., & Tambs, K. (2013). Discordant and concordant alcohol use in spouses as predictors of marital dissolution in the general population: Results from the Hunt Study. Alcoholism: Clinical and Experimental Research, 37(5), 877–884. https://doi.org/10.1111/acer.12029
U.S. Bureau of Labor Statistics. (2024). Substance abuse, behavioral disorder, and mental health counselors.
http://www.bls.gov/ooh/community-and-social-service/substance-abuse-behavioral-disorder-and-mental-health-counselors.htm
Wahesh, E., Likis-Werle, S. E., & Moro, R. R. (2017). Addictions content published in counseling journals: A 10-year content analysis to inform research and practice. The Professional Counselor, 7(1), 89–103. https://doi.org/10.15241/ew.7.1.89
Wester, K., & McKibben, B. (2019). Integrating mixed methods approaches in counseling outcome research. Counseling Outcome Research and Evaluation, 10(1), 1–11. http://doi.org/10.1080/21501378.2018.1531239
Wilson, A. D., & Johnson, P. (2013). Counselors’ understanding of process addiction: A blind spot in the counseling field. The Professional Counselor, 3(1), 16–22. https://doi.org/10.15241/adw.3.1.16
Wing Lo, T., Yeung, J. W. K., & Tam, C. H. L. (2020). Substance abuse and public health: A multilevel perspective and multiple responses. International Journal of Environmental Research and Public Health, 17(7), 2610. https://doi.org/10.3390/ijerph17072610
Zhang, X., Shi, X., Xu, S., Qiu, J., Turel, O., & He, Q. (2020). The effect of solution-focused group counseling intervention on college students’ internet addiction: A pilot study. International Journal of Environmental Research and Public Health, 17(7), 2519. https://doi.org/10.3390/ijerph17072519
Natalie M. Ricciutti, PhD, NCC, LPCC, LCASA, is an assistant professor at the University of North Carolina Charlotte. Willough Davis, MEd, NCC, LCMHC, LCASA, is a doctoral candidate at the University of North Carolina Charlotte. Correspondence may be addressed to Natalie M. Ricciutti, University of North Carolina Charlotte, 9201 University City Blvd., Charlotte, NC 28223, nricciut@charlotte.edu.
Oct 31, 2023 | Volume 13 - Issue 3
Alexander M. Fields, Cara M. Thompson, Kara M. Schneider, Lucas M. Perez, Kaitlyn Reaves, Kathryn Linich, Dodie Limberg
The integration of behavioral health care within primary care settings, otherwise known as integrated care, has emerged as a treatment modality for counselors to reach a wide range of clients. However, previous counseling scholars have noted the lack of integrated care representation in counseling journals. In this scoping review, we identified 27 articles within counseling journals that provide integrated care implications. These articles appeared in 10 unique counseling journals, and the publication years ranged from 2004–2023. Articles were classified as: (a) conceptual, (b) empirical, or (c) meta-analyses and systematic reviews. The data extracted from the articles focused on the implications for integrated care training and practice for the next generation of counselors, evidence-based treatment approaches, and future research directions.
Keywords: integrated care, counseling journals, scoping review, implications, research
One in five U.S. adults are living with a mental illness or substance use disorder (e.g., major depressive disorder, generalized anxiety disorder, alcohol use disorder, nicotine use disorder) and individuals with a mental illness or substance use disorder are more likely to have a chronic health condition (Substance Abuse and Mental Health Services Administration [SAMHSA], 2021). Integrated primary and behavioral health, also termed integrated care (IC), has emerged as a noted treatment strategy to meet the holistic needs of individuals with comorbid mental and physical health symptoms. Although IC has been operationalized inconsistently by scholars, most definitions describe the integration and coordination of behavioral health services within primary care settings (Giese & Waugh, 2017). The SAMHSA-HRSA (Health Resources and Services Administration) Center for Integrated Health Solutions expanded upon this definition to outline IC on a continuum of health care service delivery (Heath et al., 2013). Heath and colleagues described the progressive movement toward IC as (a) collaborative care: providers from multiple health care professions collaborating on holistic health care treatment planning at a distance;
(b) co-located care: providers from multiple health care professions sharing basic system integration, such as sharing physical proximity and more frequent collaboration; and (c) IC: providers from multiple health care professions having systematic integration (i.e., sharing electronic medical records and office space) and a high level of collaboration resulting in a unified treatment approach. Thus, health care consumers are able to receive care for their behavioral and physical health at the same time and location when an IC approach is applied, which may reduce barriers (e.g., transportation, child care, time off work) and increase access to behavioral health care (Vogel et al., 2014).
Beyond support from SAMHSA and HRSA, the IC movement has been endorsed through government legislation. The Patient Protection and Affordable Care Act (2010) paved the way for agencies and health care systems demonstrating an IC approach to receive additional funding for health care providers, as well as increased reimbursements for the services they deliver. Furthermore, the federal government has recently pledged to double the funding support for IC to be more accessible in hospitals, substance abuse treatment facilities, family care practices, school systems, and other health care settings (The White House, 2022). This may be the result of IC showing efficacy in reducing mental health symptoms (Lenz et al., 2018), saving health care expenditures (Basu et al., 2017), and promoting overall life satisfaction (Gerrity, 2016). Compared to traditional (i.e., siloed) care, IC involves simultaneous treatment from physical and mental health providers, thus providing additional access to mental health screenings and services. For example, McCall et al. (2022) concluded that a mental health counselor in an IC setting may support treatment engagement and reduce health care costs for an individual with a substance use disorder when utilizing the screening, brief intervention, and referral to treatment (SBIRT) model. However, the IC paradigm is not a novel concept; Aitken and Curtis (2004) introduced IC to counseling journals by providing emerging evidence of IC support and advocating for health care settings to recognize counselors as an asset to IC teams and for counselors to be trained in IC.
Brubaker and La Guardia (2020) noted that the Council for Accreditation of Counseling and Related Educational Programs (Section 5, Standard C.3.d; CACREP; 2015) required IC education in counselor-in-training (CIT) development. Additionally, the 2024 CACREP Task Force has also included these standards for its proposed revisions (CACREP, 2022). HRSA has funded counselor education programs to train CITs during practicum and internship experiences, funding over 4,000 new school, addiction, or mental health counselors during 2014–2022 through the Behavioral Health Workforce and Education Training (BHWET) Program (HRSA, 2022). Although IC training, education, and practice is occurring within counselor education, IC literature remains scarce in counseling journals (Fields et al., 2023). The lack of representation presents an issue for appropriate training for CITs and future research directions, which leads to sustainability concerns. Specifically, Fields et al. (2023) reported that a lack of IC literature in counseling journals creates a weak foundation to advocate for counselors to be included in the IC movement. With the understanding that nearly half of U.S. adults with poor mental health receive their mental health care in a primary care setting (Petterson et al., 2014), counselors may increase their access to additional clients when they are invited to IC settings. Furthermore, it weakens counselors’ professional identity if counselors are not trained in a standardized approach. As such, this scoping review aims to amalgamate current IC literature within counseling journals and provide CITs, counselors, and counselor educators from diverse backgrounds with a resource to inform their education, practice, and scholarship. The guiding research question for this review is: What are the publication trends (i.e., publication years and journals), study characteristics and outcomes, implications, and recommendations for future research from IC literature within counseling journals?
Method
We conducted a scoping review to identify the publication trends, key characteristics of IC studies (i.e., type of article and study outcomes), and implications for future research of IC literature published in counseling journals (Munn et al., 2018). Our methodology followed the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews; Tricco et al., 2018) checklist to 1) establish eligibility, 2) identify sources of information, 3) conduct a screening process to select included articles, 4) identify and chart data items, 5) conduct a critical appraisal of included articles, and 6) synthesize results. We searched the following databases for eligible literature: (a) Alt HealthWatch, (b) APA PsycArticles, (c) APA PsycInfo, (d) Education Source, (e) EBSCOHost, (f) Health Source: Consumer Edition, (g) Health Source: Nursing/Academic Edition, (h) MEDLINE with Full Text, (i) Science Reference Center, (j) Social Sciences Full Text (H.W. Wilson), and (k) Social Work Abstracts. We used the search terms: “Integrat* care” OR “integrat* primary and behavioral healthcare” OR “integrat* primary and behavioral care” AND “counsel* education” OR “counsel*.” Additional criteria for this search were full-text, peer-reviewed journal articles, and an English translation.
Eligibility Criteria
Eligibility criteria for articles included in this review are publication in a counseling journal, presentation of implications (i.e., recommendations for training and evidence-based counseling models or approaches) of IC practice for CITs and counselors through research methodology or conceptual themes, and discussion of future research on IC for counselor educators and counseling scholars through research methodology or conceptual themes. Eligible counseling journals included those published by divisions of the American Counseling Association (ACA), the American Mental Health Counselors Association (AMHCA), the American School Counselor Association (ASCA), the National Board for Certified Counselors (NBCC), and Chi Sigma Iota. Journals connected to international and regional divisions were also included. The initial database search resulted in 222 articles, which we reduced to 125 articles after removing duplicates. Another two articles were identified through additional sources. These additional sources included references identified through a review of an article and a social media post advertising an IC article. We reviewed titles and abstracts for inclusion criteria. This resulted in 28 articles that were fully reviewed. Research team members independently examined articles to summarize information relevant to the research question. During this process, articles were excluded if they did not provide future implications for IC in counseling or counselor education. Following this process, 27 articles were included. A visual representation of the eligibility and inclusion process can be found in Figure 1.
Data Extraction
After consensus was reached on the final 27 articles, our research team assessed the available evidence and synthesized the results. The seven-member research team comprised four doctoral students in counselor education, an undergraduate student minoring in counselor education, a clinical assistant professor in a counselor education program, and an associate professor in a counselor education program. The initial data extraction process began with identifying journal representation and organizing articles based on similar characteristics. This resulted in classifying articles as either (a) conceptual, (b) empirical, or (c) meta-analyses and systematic reviews. Conceptual articles provided an overview of available literature and identified a current gap in IC understanding for counseling or counselor education. Articles classified as conceptual did not present original data or follow research methodology. Moreover, the conceptual models typically advocated for increased counseling representation in IC settings to reach traditionally underserved groups (e.g., LGBTQ+ clients, individuals from rural communities) or a replicable model of training grounded in empirical support to prepare CITs to work in IC settings. Data from these articles were presented in accordance with the authors’ population(s) of interest, the identified research gap, implications gathered from existing literature, and recommendations for future research. Empirical articles introduced a novel research question and presented results to address that question. Data from these articles were presented in accordance with the authors’ study classification (i.e., qualitative, quantitative, or mixed methods), research methodology, the number and profile of participants, research of interest, and results from their analyses. Lastly, meta-analyses and systematic reviews organized previous empirical studies and presented big picture results across multiple studies. Data from these articles were presented in accordance with the authors’ article classification (i.e., meta-analysis or systematic review), population of interest, number of included studies and number of total participants (if applicable), results, and implications for future research. Because of the broad scope and exploratory nature of this review, a quality assessment was not performed.
Figure 1
Integrated Care Literature in Counseling and Counselor Education Flow Chart
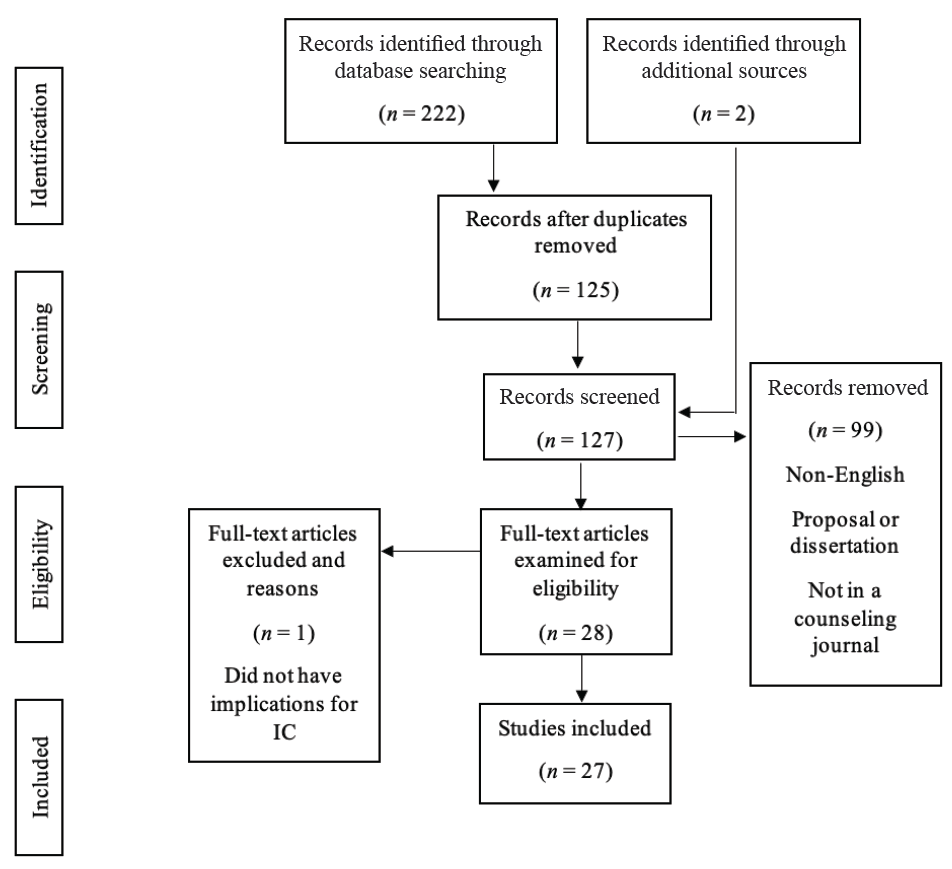
Note. This flow chart outlines the PRISMA-ScR (Tricco et al., 2018) search process.
Results
This scoping review resulted in a wide variety of articles in counseling journals that may inform the future of IC research in counseling and counselor education. Additionally, articles included in our review have ranging implications at the CIT, counselor, and client levels. The results section will begin with an overview of IC publication trends within counseling journals, detailing the publication range and specific journals. Next, results for this review were organized based on study outcomes and the classification of the article. The study outcomes sections will further detail included articles that are conceptual, empirical, or meta-analyses and systematic reviews.
Publication Trends
Articles included in this review range in publication year from 2004–2023. Articles are represented in 10 unique journals. Specifically, the following journals are represented in this review: (a) Counseling Outcome Research and Evaluation (n = 2); (b) International Journal for the Advancement of Counselling (n = 2); (c) Journal of Addictions & Offender Counseling (n = 2); (d) Journal of College Counseling (n = 1); (e) Journal of Counseling & Development (n = 7); (f) Journal of Creativity in Mental Health (n = 1); (g) Journal of LGBTQ Issues in Counseling (n = 1); (h) Journal of Mental Health Counseling (n = 9); (i) The Family Journal (n = 1); and (j) The Professional Counselor (n = 1).
Study Outcomes
Conceptual Articles
Our review included 11 conceptual articles (see Appendix A). Of these studies, five described IC as a treatment approach for underserved populations. In each of these articles, the authors described how IC provided a “one-stop-shop” treatment approach that provided increased access to a mental health provider in a traditional primary care setting, which reduced barriers to transportation, cost per service, and provider shortages. Six studies focused on current licensed counselors in primary care settings, counselor educators, CITs in a CACREP-accredited program, and counselors interested in IC. Common implications of these articles included advocacy, education, communication, networking, and teamwork.
Eight studies described how additional research could empirically investigate their IC model. The authors of these conceptual articles recommended continued investigation of the current medical model and national recognition of gaps of care for both the chronic pain and substance abuse population; integrating the interprofessional education collaborative (IPEC) into the curriculum of mental health counselors; interprofessional telehealth collaboration (IPTC) through cognitive behavioral therapy (CBT) for rural communities; treatments aligned with cultural tailoring; implementation of IC for those in the LGBTQ+ community; trauma-informed IC; and the role of counselors in an IC team treating obesity. The conceptual models reported in Table 1 highlight evidence-based approaches a counselor can apply in IC settings to assess for substance abuse and mental health disorders, brief interventions (e.g., CBT technique of challenging automatic thoughts, motivational interviewing) to encourage engagement in preventative health care, and trauma-informed practices (e.g., psychoeducation on trauma somatization). Moreover, counselors trained in the Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) can advocate for culturally tailored interventions to respect a client’s cultural identity.
Two studies highlighted different approaches to IC. Johnson and Mahan (2020) identified the IPTC model, which allows health professionals to use technology to increase access to services for rural communities. The IPTC model provides telehealth services to rural communities through an IC model to reduce negative social determinants of health, such as distance from a mental health provider. Specifically, Johnson and Mahan (2020) detailed their approach to working alongside primary care providers to deliver family counseling services and coordinate health care services to promote overall health and wellness for family systems. Goals of their family counseling sessions included increasing health literacy, enhancing a family’s coping strategies for medical conditions, and reducing family conflicts. The Chronic Care Model has been shown to improve the quality of care for clients with chronic medical conditions by increasing communication between health care professionals (Sheesley, 2016). Two articles also focused on the impact of two identified training programs. Johnson and Freeman (2014) identified the IPEC Expert Panel and their efforts to effectively train health professionals to collaborate. Lloyd-Hazlett et al. (2020) focused on the Program for the Integrated Training of Counselors in Behavioral Health (PITCH), which is a training program for master’s-level counseling students in a CACREP-accredited program aimed at training students to supply IC to rural, vulnerable, and underserved communities. These results are represented in Appendix A.
Empirical Articles
Our review resulted in 13 empirical studies using the following designs: three mixed-methods designs, three quasi-experimental designs, two cross-sectional surveys, two pre-post designs, three phenomenological studies, and one exploratory cross-case synthesis. The studies were completed in a variety of settings, such as university clinics, trauma centers, and hospitals. Participant profiles varied across studies, with nine representing CITs or practicing counselors, three representing clients, and one representing both. In addition to counselors, studies with client-level data included service providers and undergraduate students from social work, speech–language pathology, dental hygiene, nursing, and physical therapy programs. Articles that reported client-level data tested an intervention (e.g., motivational interviewing in an IC setting for a substance use disorder), compared an IC approach to treatment as usual (TAU) in silos, or explored relationships between health care indicators and client engagement in a setting applying an IC modality. Furthermore, three studies in this article used Heath et al.’s (2013) conceptualization of IC, which was the most common model cited.
Most study outcomes were reported as positive benefits for IC. For CIT and counselor-level studies, six described a theme of increased ability and desirability to work with a collaborative approach on IC teams. Participants also commonly reported an increase in professional identity and self-efficacy. Participants in studies by Agaskar et al. (2021), Alvarez et al. (2014), and Lenz and Watson (2023) further demonstrated that working with underserved populations in IC settings increased their multicultural competence, specifically around areas of acceptance, advocacy, and awareness. A gap in IC awareness among service providers and organizational constraints were noted as potential barriers to IC care. Johnson et al. (2021) found interprofessional supervision as a potential barrier to remaining within a provider’s scope of practice, because a supervisor providing supervision to a supervisee from a different professional identity may not appropriately understand roles and responsibilities. Because of this, Johnson and colleagues noted implications for future research and graduate-level training in the classroom and field experience. All four of the studies completed with client-level data were quantitative, accounting for 2,378 client participants. Results of these studies suggested improvement in holistic client functioning (i.e., reduction in pathological symptoms and increase in preventative behaviors; Ulupinar et al., 2021), a decrease in crisis events (Schmit et al., 2018), and decrease in risky drinking behaviors for individuals receiving IC trauma care (Veach et al., 2018). The self-stigma of mental illness and of seeking help had an inverse relationship with mental health literacy among patients who received treatment in an IC setting (Crowe et al., 2017). These results are represented in Appendix B.
Meta-Analyses and Systematic Reviews
Three articles in this review were meta-analyses or systematic reviews. Specifically, two articles were meta-analyses and one was a systematic review. Participants within these studies included adults with substance use disorders, mental health professionals receiving training to practice within IC, and individuals receiving mental health care in traditional primary care settings. All three articles described benefits of IC. Additionally, the authors differed on the number of studies and participants included in their analyses. Fields et al. (2023) completed a review of 18 articles that studied training interventions for mental health professionals to work on IC teams and concluded that training in IC promotes aspects of interprofessional collaboration, professional identity development, and self-efficacy. Balkin et al. (2019) concluded no statistical significance between IC treatment and TAU to decrease frequency of substance use. Balkin et al. also remarked that their study, including 1,545 participants, did not reach statistical power and results should be considered preliminary. Lenz et al. (2018) reported a decrease in mental health symptoms with a greater effect when a larger treatment team and number of behavioral health sessions are increased, compared to TAU. Lenz and colleagues generated their results from 14,764 participants. Lastly, Fields et al. (2023) and Lenz et al. (2018) both used Heath et al.’s (2013) model of IC for conceptualization. For all three of these studies, additional research is needed to understand IC at the client or consumer level, as well as how different variables affect the treatment process. These results are represented in Appendix C.
Discussion
Implications for Counseling Practice
The results of this scoping review have implications that may inform clinical practice for counselors and CITs. Most results suggested clinical benefits for individuals receiving counseling services through an IC setting. Clients or consumers that received IC treatment reported a reduction of mental health symptoms (Lenz et al., 2018; Ulupinar et al., 2021), mental health stigma (Crowe et al., 2018), and crisis events (Schmit et al., 2018). As almost half of individuals with poor mental health receive treatment in primary care settings (Petterson et al., 2014), integrating a counselor into a traditional primary care setting (e.g., hospital, community health care clinic) provides an additional treatment team member with specialized training to treat mental health concerns. Because of the potentially fast nature of IC settings, interested counselors are encouraged to review SAMHSA applications of SBIRT to facilitate brief meetings until more long-term services are provided. Furthermore, counselors may consider reviewing resources on evidence-based approaches, such as Ultra-Brief Cognitive Behavioral Interventions: A New Practice Model for Mental Health and Integrated Care (Sperry and Binensztok, 2019), and understanding common medical terminology, such as A Therapist’s Guide to Understanding Common Medical Conditions (Kolbasovsky, 2008).
Articles that were classified as conceptual also suggested that IC treatment has the potential to enhance service delivery for clients from diverse populations, such as LGBTQ+ and medically underserved communities (Kohn-Wood & Hooper, 2014; Moe et al., 2018). The primary rationale described by scholars is that an IC approach advocates for diverse populations to reduce social determinants of health, such as proximity barriers, communications barriers, and availability of culturally appropriate interventions. Counselors interested in working in an IC setting are strongly encouraged to review the MSJCC (Ratts et al., 2016) and be prepared to serve as an advocate for their client as they navigate the health care system. The Hays (1996) ADDRESSING model also provides counselors a conceptualization model for understanding power and privileges associated with cultural differences. Information drawn from an understanding of power and privileges may further assist the interdisciplinary team with delivering culturally appropriate care. However, Balkin et al. (2019) concluded that IC may not result in a decrease in frequency of substance misuse. As IC may not be the most ideal approach depending on the client’s presenting concern and therapeutic goals, counselors are ethically bound to continue ongoing assessments to collaborate with their client to determine the most appropriate treatment setting.
Implications for Counselor Education
In addition to counseling practice, the results of our scoping review provide implications for counselor education and ongoing counselor development. First, counselors or CITs that have received training in IC have commonly reported an increase in their professional identity development, as practicing in IC settings creates an opportunity for counselors and CITs to differentiate counseling responsibilities from related health care professionals (Brubaker & La Guardia, 2020; Johnson et al., 2015). Counselor educators and supervisors are encouraged to consider how they can create opportunities to challenge their students or supervisees to understand their role in the health care landscape. For example, Johnson and Freeman (2014) described an interdisciplinary health care delivery course to train counselors alongside students from other disciplines (e.g., nursing, physical therapy), and counselor educators may consider how they can form partnerships across departments to provide these opportunities. Counselor or CIT participants also expressed an enhanced self-efficacy for clinical practice (Brubaker & La Guardia, 2020; Lenz & Watson, 2023). As trainings and field experience for IC practice typically involve experiential components, counselors and CITs are provided additional opportunities to practice their previous clinical trainings in IC settings. Farrell et al. (2009) provided an example of how counselor educators can use standardized patients (i.e., paid actors simulating a presenting concern) to role-play a client in a primary setting. In such situations, the CIT can practice a variety of brief assessments (e.g., substance abuse, suicide, depression screenings) and interventions (e.g., motivational interviewing techniques, such as building ambivalence) in an IC setting.
With the counseling profession’s emphasis on aspects of valuing cultural differences and social justice, counselor educators and supervisors may consider how they can train counselors and CITs to reduce social determinants of health through integrated and collaborative practices that promote affirmative and proximal care. Counselors or CITs that received training to work in IC settings often reported higher understanding of multicultural counseling (Agaskar et al., 2021; Lenz et al., 2018). Thus, counselor educators and supervisors can provide their counselors and CITs with challenges to incorporate aspects of the MSJCC (Ratts et al., 2016) when delivering interdisciplinary care. All trainings in our review were administered across multiple modalities (e.g., face-to-face, hybrid, virtual, asynchronous), which gives counselor educators flexibility in how they train counselors or CITs. The variety in training administration is a promising result, as the COVID-19 pandemic highlighted the need for flexible training options for counselors and CITs. In addition, counselors and CITs in rural communities often have infrequent access to training as compared to their non-rural colleagues, and thus flexibility may enhance the accessibility of IC training (Alvarez et al., 2014). Lastly, counselors and CITs being trained in IC modalities do not need to work in IC settings to use interprofessional skills developed through trainings. Heath et al. (2013) remarked that IC is not always a feasible option, but helping professionals can still apply collaborative approaches to enhance their client’s holistic outcomes. In other words, counselors or CITs may apply IC principles of preventative health care and interdisciplinary treatment plans by collaborating with other health care professionals at a distance. Glueck (2015) corroborated this notion and described a theme that counselors who have previously worked in IC settings believe they are able to provide more holistic care because they are better equipped to collaborate with health care professionals from multiple disciplines. However, these counselors also reported that they would have been more prepared to work in IC if they received training at some point in their career.
Limitations and Recommendations for Future Research
The methodology of a scoping review has noted limitations. Because of the nature of a scoping review, the data extraction process and results section are broad (Munn et al., 2018). Articles were not systematically evaluated to assess study quality, and the reader is encouraged to review a specific study before interpreting the results. In addition to study quality, scoping reviews include articles from a variety of article classifications, so the results and implications should be considered exploratory. Thus, we caution how readers draw conclusions from results presented in the included articles. Second, the search terms and inclusion criteria may have resulted in limitations. This search focused on IC; therefore, concepts such as interprofessional collaboration and interprofessional education may have been excluded. These concepts are discussed in the Heath et al. (2013) model, but they do not directly result in IC practice. Counseling and counselor education were also search terms, which may have excluded articles written by counseling scholars in journals outside of counseling and counselor education journals. Third, this review resulted in four studies that empirically investigated IC at the client level. With limited data at the client level, there are funding and advocacy sustainability concerns for IC within counseling and counselor education. Lastly, nine studies specifically provided implications for marginalized populations and multicultural competency development through an IC lens. Although Kohn-Wood and Hooper (2014) and Vogel et al. (2014) concluded that IC is a modality that advocates for the treatment of marginalized populations that have traditionally received services at unequal rates to their White, cisgender counterparts, this topic has limited representation in counseling IC literature. As discussed by Fields et al. (2023), this review demonstrates the need for understanding how the counseling professional identity rooted in social justice and advocacy may contribute to the advancement of IC services.
In light of our limitations, this review resulted in recommendations for future research directions. Conceptual articles included in this review synthesized literature on the importance of CITs and counselors understanding applications of IC, as well as potential treatment approaches to treat a variety of marginalized communities and clinical practices. Our research team recommends that counseling scholars reviewing the included conceptual articles consider how they can use the implications and future research directions to inform future research studies. These articles can also serve as support for counseling scholars who are applying for internal and external funding. Furthermore, the empirical studies, systematic reviews, and meta-analyses included in our review present data that can inform future research. For example, Balkin et al. (2019) and Veach et al. (2018) concluded contrasting results about IC in reducing substance abuse behaviors. Future research studies can continue researching substance misuse within IC settings to better understand evidence-based approaches to treat these populations. Twenty-one articles included recommendations for continued research at the client or consumer level, specifically for clients from marginalized communities. Counseling scholars are encouraged to stay up to date with program evaluation scholarship and implement a variety of methodical procedures to document the impact of IC on clients. Lastly, counseling scholars must advocate for continued IC literature publication within counseling and counselor education journals.
Conclusion
Our scoping review identified IC literature within counseling journals. Specifically, this review followed PRISMA-ScR protocols (Tricco et al., 2018) and identified 27 articles across 10 unique counseling journals. Most articles were within national flagship journals (such as those of ACA and AMHCA) and publication years ranged from 2004–2023. The articles in this review were organized according to their classification, and were described as either conceptual, empirical, or meta-analyses and systematic reviews. Implications for CITs, counselors, and clients were represented across each classification. Overall, IC implications from each article were positive for training and practice perceptions for CITs and counselors, as well as clinical outcomes for clients. Moving forward, authors unanimously encouraged counselor educators and counseling scholars to continue studying IC. Future scholarship would benefit from a deeper understanding of client-level implications, with an emphasis on how IC can benefit marginalized communities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Note. Studies with an asterisk (*) are included in the scoping review.
*Agaskar, V. R., Lin, Y.-W. D., & Wambu, G. W. (2021). Outcomes of “integrated behavioral health” training: A pilot study. International Journal for the Advancement of Counselling, 43, 386–405.
https://doi.org/10.1007/s10447-021-09435-z
*Aitken, J. B., & Curtis, R. (2004). Integrated health care: Improving client care while providing opportunities for mental health counselors. Journal of Mental Health Counseling, 26(4), 321–331.
https://doi.org/10.17744/mehc.26.4.tp35axhd0q07r3jk
*Alvarez, K., Marroquin, Y., Sandoval, L., & Carlson, C. (2014). Integrated health care best practices and culturally and linguistically competent care: Practitioner perspectives. Journal of Mental Health Counseling, 36(2), 99–114. https://doi.org/10.17744/mehc.36.2.480168pxn63g8vkg
*Balkin, R. S., Lenz, A. S., Dell’Aquila, J., Gregory, H. M., Rines, M. N., & Swinford, K. E. (2019). Meta-analysis of integrated primary and behavioral health care interventions for treating substance use among adults. Journal of Addictions & Offender Counseling, 40(2), 84–95. https://doi.org/10.1002/jaoc.12067
Basu, S., Landon, B. E., Williams, J. W., Jr., Bitton, A., Song, Z., & Phillips, R. S. (2017). Behavioral health integration into primary care: A microsimulation of financial implications for practices. Journal of General Internal Medicine, 32(12), 1330–1341. https://doi.org/10.1007/s11606-017-4177-9
*Brubaker, M. D., & La Guardia, A. C. (2020). Mixed-design training outcomes for fellows serving at-risk youth within integrated care settings. Journal of Counseling & Development, 98(4), 446–457.
https://doi.org/10.1002/jcad.12346
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2022). 2024 CACREP standards, draft three. https://www.cacrep.org/wp-content/uploads/2022/04/Draft-3-2024-CACREP-Standards.pdf
*Crowe, A., Mullen, P. R., & Littlewood, K. (2018). Self-stigma, mental health literacy, and health outcomes in integrated care. Journal of Counseling & Development, 96(3), 267–277. https://doi.org/10.1002/jcad.12201
Farrell, M. H., Kuruvilla, P., Eskra, K. L., Christopher, S. A., & Brienza, R. S. (2009). A method to quantify and compare clinicians’ assessments of patient understanding during counseling of standardized patients. Patient Education and Counseling, 77(1), 128–135. https://doi.org/10.1016/j.pec.2009.03.013
Fields, A. M., Linich, K., Thompson, C. M., Saunders, M., Gonzales, S. K., & Limberg, D. (2023). A systematic review of training strategies to prepare counselors for integrated primary and behavioral healthcare. Counseling Outcome Research and Evaluation, 14(1), 1–14. https://doi.org/10.1080/21501378.2022.2069555
Gerrity, M. (2016). Evolving models of behavioral health integration: Evidence update 2010–2015. Milbank Memorial Fund. https://www.milbank.org/wp-content/uploads/2016/05/Evolving-Models-of-BHI.pdf
Giese, A. A., & Waugh, M. (2017). Conceptual framework for integrated care: Multiple models to achieve integrated aims. In R. E. Feinstein, J. V. Connelly, & M. S. Feinstein (Eds.), Integrating behavioral health and primary care (pp. 3–16). Oxford University Press.
*Glueck, B. P. (2015). Roles, attitudes, and training needs of behavioral health clinicians in integrated primary care. Journal of Mental Health Counseling, 37(2), 175–188. https://doi.org/10.17744/mehc.37.2.p84818638n07447r
Hays, P. A. (1996). Addressing the complexities of culture and gender in counseling. Journal of Counseling & Development, 74(4), 332–338. https://doi.org/10.1002/j.1556-6676.1996.tb01876.x
Health Resources and Services Administration. (2022). Health professions training programs. https://data.hrsa.gov/topics/health-workforce/training-programs
Heath, B., Wise-Romero, P., & Reynolds, K. A. (2013). Standard framework for levels of integrated healthcare. SAMHSA-HRSA Center for Integrated Health Solutions. https://www.thenationalcouncil.org/wp-content/uploads/2020/01/CIHS_Framework_Final_charts.pdf?daf=375ateTbd56
*Jacobson, T., & Hatchett, G. (2014). Counseling chemically dependent chronic pain patients in an integrated care setting. Journal of Addictions & Offender Counseling, 35(1), 57–61.
https://doi.org/10.1002/j.2161-1874.2014.00024.x
*Johnson, K. F., Blake, J., & Ramsey, H. E. (2021). Professional counselors’ experiences on interprofessional teams in hospital settings. Journal of Counseling & Development, 99(4), 406–417. https://doi.org/10.1002/jcad.12393
*Johnson, K. F., & Freeman, K. L. (2014). Integrating interprofessional education and collaboration competencies (IPEC) into mental health counselor education. Journal of Mental Health Counseling, 36(4), 328–344.
https://doi.org/10.17744/mehc.36.4.g47567602327j510
*Johnson, K. F., Haney, T., & Rutledge, C. (2015). Educating counselors to practice interprofessionally through creative classroom experiences. Journal of Creativity in Mental Health, 10(4), 488–506.
https://doi.org/10.1080/15401383.2015.1044683
*Johnson, K. F., & Mahan, L. B. (2020). Interprofessional collaboration and telehealth: Useful strategies for family counselors in rural and underserved areas. The Family Journal, 28(3), 215–224.
https://doi.org/10.1177/1066480720934378
*Kohn-Wood, L., & Hooper, L. (2014). Cultural competency, culturally tailored care, and the primary care setting: Possible solutions to reduce racial/ethnic disparities in mental health care. Journal of Mental Health Counseling, 36(2), 173–188. https://doi.org/10.17744/mehc.36.2.d73h217l81tg6uv3
Kolbasovsky, A. (2008). A therapist’s guide to understanding common medical conditions: Addressing a client’s mental and physical health. W. W. Norton.
*Lenz, A. S., Dell’Aquila, J., & Balkin, R. S. (2018). Effectiveness of integrated primary and behavioral healthcare. Journal of Mental Health Counseling, 40(3), 249–265. https://doi.org/10.17744/mehc.40.3.06
*Lenz, A. S., & Watson, J. C. (2023). A mixed methods evaluation of an integrated primary and behavioral health training program for counseling students. Counseling Outcome Research and Evaluation, 14(1), 28–42.
https://doi.org/10.1080/21501378.2022.2063713
*Lloyd-Hazlett, J., Knight, C., Ogbeide, S., Trepal, H., & Blessing, N. (2020). Strengthening the behavioral health workforce: Spotlight on PITCH. The Professional Counselor, 10(3), 306–317.
https://doi.org/10.15241/jlh.10.3.306
McCall, M. H., Wester, K. L., Bray, J. W., Hanchate, A. D., Veach, L. J., Smart, B. D., & Wachter Morris, C. (2022). SBIRT administered by mental health counselors for hospitalized adults with substance misuse or disordered use: Evaluating hospital utilization and costs. Journal of Substance Abuse Treatment, 132, 108510. https://doi.org/10.1016/j.jsat.2021.108510
*Moe, J., Johnson, K., Park, K., & Finnerty, P. (2018). Integrated behavioral health and counseling gender and sexual minority populations. Journal of LGBT Issues in Counseling, 12(4), 215–229.
https://doi.org/10.1080/15538605.2018.1526156
Munn, Z., Peters, M. D. J., Stern, C., Tufanaru, C., McArthur, A., & Aromataris, E. (2018). Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Medical Research Methodology, 18(1), 1–7. https://doi.org/10.1186/s12874-018-0611-x
Patient Protection and Affordable Care Act of 2010, Pub. L. No. 111-148, 124 Stat. 119 (2010).
https://www.congress.gov/111/plaws/publ148/PLAW-111publ148.pdf
Petterson, S., Miller, B. F., Payne-Murphy, J. C., & Phillips, R. L., Jr. (2014). Mental health treatment in the primary care setting: Patterns and pathways. Families, Systems, & Health, 32(2), 157–166.
https://doi.org/10.1037/fsh0000036
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
*Regal, R. A., Wheeler, N. J., Daire, A. P., & Spears, N. (2020). Childhood sexual abuse survivors undergoing cancer treatment: A case for trauma-informed integrated care. Journal of Mental Health Counseling, 42(1), 15–31. https://doi.org/10.17744/mehc.42.1.02
*Schmit, M. K., Watson, J. C., & Fernandez, M. A. (2018). Examining the effectiveness of integrated behavioral and primary health care treatment. Journal of Counseling & Development, 96(1), 3–14.
https://doi.org/10.1002/jcad.12173
*Sheesley, A. P. (2016). Counselors within the chronic care model: Supporting weight management. Journal of Counseling & Development, 94(2), 234–245. https://doi.org/10.1002/jcad.12079
Sperry, L., & Binensztok, V. (2019). Ultra-brief cognitive behavioral interventions: A new practice model for mental health and integrated care. Routledge.
Substance Abuse and Mental Health Services Administration. (2021). Key substance use and mental health indicators in the United States: Results from the 2020 National Survey on Drug Use and Health. https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf
The White House. (2022, March 1). Fact sheet: President Biden to announce strategy to address our national mental health crisis, as part of unity agenda in his first State of the Union. [Press release]. https://www.whitehouse.gov/briefing-room/statements-releases/2022/03/01/fact-sheet-president-biden-to-announce-strategy-to-address-our-national-mental-health-crisis-as-part-of-unity-agenda-in-his-first-state-of-the-union
Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., . . . Straus, S. E. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine, 169(7), 467–473. https://doi.org/10.7326/M18-0850
*Tucker, C., Sloan, S. K., Vance, M., & Brownson, C. (2008). Integrated care in college health: A case study. Journal of College Counseling, 11(2), 173–183. https://doi.org/10.1002/j.2161-1882.2008.tb00033.x
*Ulupinar, D., Zalaquett, C., Kim, S. R., & Kulikowich, J. M. (2021). Performance of mental health counselors in integrated primary and behavioral health care. Journal of Counseling & Development, 99(1), 37–46.
https://doi.org/10.1002/jcad.12352
*Veach, L. J., Moro, R. R., Miller, P., Reboussin, B. A., Ivers, N. N., Rogers, J. L., & O’Brien, M. C. (2018). Alcohol counseling in hospital trauma: Examining two brief interventions. Journal of Counseling & Development, 96(3), 243–253. https://doi.org/10.1002/jcad.12199
*Vereen, L. G., Yates, C., Hudock, D., Hill, N. R., Jemmett, M., O’Donnell, J., & Knudson, S. (2018). The phenomena of collaborative practice: The impact of interprofessional education. International Journal for the Advancement of Counselling, 40(4), 427–442. https://doi.org/10.1007/s10447-018-9335-1
*Vogel, M., Malcore, S., Illes, R., & Kirkpatrick, H. (2014). Integrated primary care: Why you should care and how to get started. Journal of Mental Health Counseling, 36(2), 130–144.
https://doi.org/10.17744/mehc.36.2.5312041n10767k51
*Wood, A. W., Zeligman, M., Collins, B., Foulk, M., & Gonzalez-Voller, J. (2020). Health orientation and fear of cancer: Implications for counseling and integrated care. Journal of Mental Health Counseling, 42(3), 265–279. https://doi.org/10.17744/mehc.42.3.06
Appendix A
Conceptual Articles
| Author(s) |
Population(s) of Interest |
Research Gap Identified |
Implications and Future Directions |
| Aitken & Curtis, 2004 |
Counselor educators
and counselors |
Lack of IC literature in counselor education journals |
Increased training for counselors to work competently in IC. Increased advocacy efforts to be on insurance panels. Build relationships with other health care professionals. More literature is needed in counselor education journals. |
| Jacobson & Hatchett, 2014 |
Clients who are chemically dependent with chronic pain |
Lack of literature for clients who are chemically dependent with chronic pain |
Clients that have co-occurring chemical dependence and chronic pain have reported benefits when their symptoms are treated by mental and physical health providers. Additional research is needed to understand treatment strategy effectiveness. |
| Johnson & Freeman, 2014 |
Health care undergraduate and graduate students (including CITs)
learning IC strategies |
Lack of literature documenting IC training across multiple disciplines, specifically including CITs |
Provides a framework for IC training across multiple disciplines in accordance with SAMHSA IC competency standards. Additional research is needed to understand the effectiveness for each discipline and as a whole. |
| Johnson & Mahan, 2020 |
Family counselors
in rural and
underserved areas |
Family counselors leading connection between rural families and other providers
of health care services |
Emphasis on interprofessional collaboration (IPC) and use of telehealth options where family counselors use systemic training to advocate for rural, marginalized families, as well as network and connect families to health care providers when family members have unmet medical health needs or need specialized mental health care treatment. Additional research is needed to understand this phenomenon. |
| Kohn-Wood & Hooper, 2014 |
Mental health professionals working
in primary care settings |
How culturally tailoring evidence-based treatment models can reduce mental health disparities |
Cultural tailoring of treatments should be a primary factor that is evaluated in future research studies. Future researchers should consult existing literature on culturally tailoring treatment to increase engagement and improve outcomes for diverse groups. |
|
|
|
|
| Lloyd-Hazlett et al., 2020 |
CITs |
Need for a replicable model
to train CITs in IC |
The Program for the Integrated Training of Counselors in Behavioral Health (PITCH) model creates community partnerships, introduces CITs to applications of IC, and awards CITs a graduate certificate. Additional research is needed to demonstrate sustainability. |
| Moe et al., 2018 |
LGBTQ+ clients |
Lack of LGBTQ+ literature pertaining to IC |
CITs, counselors, and other health care professionals working with LGBTQ clients may benefit from additional training and supervision in collaborative care and IC. Additional research is needed to understand the impact IC has with the LGBTQ+ population. |
| Regal et al., 2020 |
Clients with cancer who are survivors of childhood sexual abuse |
Lack of trauma-informed
care literature pertaining
to IC, specifically for individuals with adverse childhood experiences (ACEs) |
IC offers opportunities for appropriate assessments to identify ACEs for holistic care, as represented in the case study. Additional research is needed to understand universal screening for ACEs and the integration of trauma-informed practices within traditional primary care settings. |
| Sheesley, 2016 |
Counselor educators, counselors, and primary care settings |
Elaborate on the role of mental health counselors within the Chronic Care Model (CCM) |
Counselors influencing the future of obesity treatment within the CCM. Additional research is needed to understand evidence-based practices for counselors within the CCM for the treatment of obesity. |
| Tucker et al., 2008 |
An international student’s experience receiving IC on a college campus |
The effect of an IC program and mindfulness-based cognitive therapy (MCBT) approach |
As reported by the multidisciplinary team, clients using medication and individual and group therapy improved from the first time they had met. The authors emphasized the use of MCBT in treatment. Additional research is needed for IC on college campuses. |
| Vogel et al., 2014 |
Counselors considering IPC |
Access issues, adherence, and the effectiveness of IPC with particular attention to culturally diverse groups |
Increased training in evidence-based culturally tailored practices. Increased education for counselors regarding IPC to help determine if primary care is a good fit. Additional research is needed on various aspects of successful IPC execution. |
Appendix B
Empirical Articles
| Author(s) |
Methodology |
N and
Participant
Profile |
Research of Interest |
Results |
Agaskar
et al., 2021 |
Mixed methods; quantitative: single-group design; qualitative: thematic analysis |
12 CITs |
The effect of an IPC and evidence-based practices curriculum to enhance students’ ability to work with at-risk youth in IC settings |
CITs reported an increase in multicultural competence and ability to work on IC teams, utilize evidence-based practices, and implement suicide interventions. |
Alvarez
et al., 2014 |
Qualitative; exploratory
cross-case synthesis |
8 service providers in an IC setting |
The experiences of IC service providers working with culturally and linguistically diverse populations |
Three themes emerged: (a) patient-centered care benefits underserved populations, (b) desirability of a multidisciplinary team, and
(c) importance of the organization to change with circumstances. |
| Brubaker & La Guardia, 2020 |
Quantitative;
single case and quasi-experimental |
11 CITs |
The effect of an IC training intervention, Serving At-Risk Youth Fellowship Experience for Counselors (SAFE-C) |
CITs reported an increase in understanding professional identity, self-efficacy, and interprofessional socialization. |
Crowe
et al., 2017 |
Quantitative;
Cross-sectional survey design |
102 clients from an IC medical facility |
To examine the relationship between mental health self-stigmas, mental health literacy, and health care outcomes |
Self-stigma of mental illness and self-stigma of seeking help had an inverse relationship with mental health literacy. |
| Glueck 2015 |
Qualitative; phenomenological |
10 mental health professionals working in IC settings |
Roles and attitudes of mental health professionals working in IC and perceived training needs |
Mental health professionals reported that they were involved in brief interventions and assessments, administrative work, and consultation and that additional graduate training is needed in classroom and field experiences. |
Johnson
et al., 2015 |
Mixed methods; qualitative: the pre- and post-survey design; qualitative: thematic analysis |
22 CITs, as well as dental hygiene, nursing, and
physical therapy students |
CITs’ attitudes toward interprofessional learning and collaboration following an interdisciplinary course on IPC |
Perceptions about learning together and collaboration improved, negative professional identity scores decreased, and higher reports of positive professional identity. |
Johnson
et al., 2021 |
Qualitative; phenomenology |
11 counselors in hospital setting |
Experiences of counselors working on interprofessional teams (IPTs) in a hospital setting |
Four themes emerged:
(a) counselors rely on common factors and foundational principles; (b) counselors must have interprofessional supervision; (c) counselors must remember their scope of practice; and (d) counselors must adhere to ethical codes and advocacy standards. |
|
|
|
|
|
| Lenz & Watson, 2023 |
Mixed-methods; quantitative: non-experimental pre- and post-test; qualitative: thematic analysis |
45 CITs |
The impact an IC training program has on CITs’ self-efficacy, interprofessional socialization, and multicultural competence, as well as barriers to student growth |
Increase in self-efficacy, interprofessional socialization, and aspects of multicultural competence. Most reported barriers were IC awareness and organizational constraints. |
Schmit
et al., 2018 |
Quantitative;
quasi-experimental |
196 clients; 98 received IC and 98 received treatment as usual (TAU) |
The effect of IC for individuals with severe mental illness compared
to TAU |
Group that received the IC intervention demonstrated an improvement in overall functioning, including a
decrease in crisis events. |
| Ulupinar et al., 2021 |
Quantitative;
quasi-experimental |
1,747 clients and 10 counselors |
To examine the therapeutic outcomes and client dropout rates of adults experiencing mental disorders in an IC center |
The addition of counselors resulted in a decrease in client symptom reports. |
Veach
et al., 2018 |
Quantitative; pre- and post-test survey |
333 clients in a trauma-based IC center |
A brief IC counseling intervention for risky alcohol behavior |
The IC counseling intervention resulted in reduced risky alcohol behaviors. |
Vereen
et al., 2018 |
Qualitative; phenomenological inquiry |
13 graduate students; five CITs and eight speech– language pathologists |
The effect of interprofessional education (IPE) on the development of collaborative practice for both CITs and speech– language pathologists-in-training |
Five themes emerged:
(a) benefits of IPE,
(b) expectations of collaborative practice, (c) benefits of experienced IC providers,
(d) challenges of IC practice, and
(e) optimization of IC practice. |
Wood
et al., 2020 |
Quantitative;
cross-sectional survey design |
155 undergraduate students studying psychology and aspects of counseling |
How factors related to prevention and wellness relate to topics that counselors are adept at addressing, such as optimism, social support, and resilience |
Results indicated that health anxiety was positively correlated with fear of cancer, but that psychosocial variables either had no relationship or were not significant moderators between health anxiety and fear of cancer. |
Appendix C
Meta-Analyses and Systematic Reviews
| Author(s) |
Article Classification |
Population of Interest |
Number
of Included Studies and Participants |
Results and Implications |
Balkin
et al., 2019 |
Meta-analysis |
Adults with substance use disorders |
8 studies with 1,545 participants;
722 received IC and 823
received alternative |
Effects of IC were small with this sample (i.e., small effect in decrease in substance use).
Authors recommended additional research to understand substance use disorders within an IC context and variables beyond use of substances. |
Fields
et al., 2023 |
Systematic review |
Mental health professionals and mental health professionals-in-training receiving education on IC |
18 studies |
Four themes emerged:
(a) HRSA-funded studies,
(b) trainee skill development, (c) enhancement of
self-efficacy, and
(d) increased understanding of interprofessional collaboration. Authors recommended more studies focusing on client-level data and more multicultural competencies. |
|
|
|
|
|
Lenz
et al., 2018 |
Meta-analysis |
Individuals receiving mental health care in traditional primary care settings |
36 studies with 14,764 participants |
Effects of IC, as compared to alternative treatments, resulted in a decrease in mental health symptoms. A greater effect is shown with a larger treatment team and number of behavioral health sessions. |
Alexander M. Fields, PhD, is an assistant professor at the University of Nebraska at Omaha. Cara M. Thompson, PhD, is an assistant professor at the University of North Carolina at Pembroke. Kara M. Schneider, MS, is a doctoral candidate at the University of South Carolina. Lucas M. Perez, MA, is a doctoral candidate at the University of South Carolina. Kaitlyn Reaves, BS, is a doctoral student at Adler University. Kathryn Linich, PhD, is a clinical assistant professor at Duquesne University. Dodie Limberg, PhD, is an associate professor at the University of South Carolina. Correspondence may be addressed to Alexander M. Fields, University of Nebraska at Omaha, College of Education, Health, and Human Services, Department of Counseling, Omaha, NE 68182, alexanderfields@unomaha.edu.
Oct 31, 2023 | Volume 13 - Issue 3
Byeolbee Um, Lindsay Woodbridge, Susannah M. Wood
This content analysis examined articles on international counseling students published in selected counseling journals between 2006 and 2021. Results of this study provide an overview of 18 articles, including publication trends, methodological designs, and content areas. We identified three major themes from multiple categories, including professional practices and development, diverse challenges, and personal and social resources. Implications for counseling researchers and counselor education programs to increase understanding and support for international counseling students are provided.
Keywords: international counseling students, counseling journals, content analysis, publication trends, counseling researchers
International counseling students (ICSs) can be defined as individuals from outside the United States who seek professional training by enrolling in counselor education programs in the United States. After graduation, they often keep contributing to the counseling field as professional counselors or counselor educators, either in the United States or their home countries (Behl et al., 2017). In 2021, non-resident international students accounted for 1.02% of master’s students and 3.81% of doctoral students in counseling programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2022). However, because these percentages do not include international students who have resident alien status in the United States (Karaman et al., 2018), the actual numbers of international students in counseling programs may be higher. Despite the underestimated number of ICSs in CACREP-accredited programs, Ng (2006) found that at least one international student was enrolled in 41% of CACREP-accredited programs, which suggested that many counselor education programs already had some degree of global cultural diversity. Considering that the number of ICSs in the United States has risen within a few decades (CACREP, 2022; Ng, 2006), additional research is needed on this population and how best to prepare them for professional practice.
Research on International Students in Counseling Programs
While in training, ICSs, like domestic students, experience pressure to perform across academic, practical, and personal contexts (Thompson et al., 2011). However, ICSs face the additional challenges of adapting to a new culture and practicing counseling in that culture (Ju et al., 2020; Kuo et al., 2021; Ng & Smith, 2009). These challenges stem from having varying levels of experience using English in an academic context, adapting to new sociocultural and interpersonal patterns, and navigating key clinical factors of counselor education such as supervision and therapeutic relationships (Jang et al., 2014; C. Li et al., 2018; Y. Mori et al., 2009). Researchers have found that ICSs perceive more barriers and concerns regarding their training, such as academic problems and role ambiguity in supervision (Akkurt et al., 2018; Ng & Smith, 2009).
Regarding the experiences of ICSs, researchers have paid scholarly attention to the concept of acculturation, which is the assimilation process an individual experiences in response to the psychological, social, and cultural forces they are exposed to in a new dominant culture (C. Li et al., 2018; Ng & Smith, 2012). According to counseling studies, ICSs’ levels of acculturation and acculturative stress were associated with several variables related to their professional development, including counseling self-efficacy, language anxiety, and diverse academic and life needs (Behl et al., 2017; Interiano-Shiverdecker et al., 2019; C. Li et al., 2018). For example, Interiano-Shiverdecker et al. (2019) found that two domains of acculturation—ethnic identity and individualistic values—were positively associated with counseling self-efficacy for international counseling master’s students. Researchers have also uncovered the potential issues ICSs can experience related to a lack of acculturation: Behl et al. (2017) found that students’ acculturative stress was positively associated with their academic, social, cultural, and language needs.
With goals of uncovering effective coping strategies and identifying characteristics of high-quality training environments, researchers have investigated the personal and academic experiences of ICSs (Lau & Ng, 2012; Nilsson & Wang, 2008; Park et al., 2017; Woo et al., 2015). Woo and colleagues (2015) identified several coping tools of ICSs. These tools included self-directed strategies such as engaging in reflection and keeping up with the latest literature, support from mentors, and networking among international students and graduates (Woo et al., 2015). Researchers have attended to strategies that support ICSs’ development of cultural competence and commitment to social justice (Delgado-Romero & Wu, 2010; Karaman et al., 2018; Ng & Smith, 2012). For example, Delgado-Romero and Wu (2010) piloted a social justice group intervention with six Asian ICS participants and found the intervention to be a useful way to empower students and enhance their critical consciousness about inequity.
Supervision has been another area of focus in ICS research. Through interviews and surveys of ICSs, researchers have identified supervision strategies that support ICSs’ developing cultural competence, professional development, and self-efficacy (Mori et al., 2009; Ng & Smith, 2012; Park et al., 2017). A shared theme across these studies is the importance of clear communication. Findings of two studies (Mori et al., 2009; Ng & Smith, 2012) support supervisors engaging ICS supervisees in communication about critical topics such as cultural differences and the purpose and expectations of supervision. Based on a consensual qualitative analysis of interviews with 10 ICS participants, Park et al. (2017) recommended that programs and supervisors make sure to share basic information about systems of counseling, health care, and social welfare in the United States.
Necessity of ICS Research
Across academic units, there has been a growing attention to international graduate students (Anandavalli et al., 2021; Vakkai et al., 2020). Given the increasing representation of international students in counseling programs, researchers have called for academic and practical strategies to support ICSs’ success in training (Lertora & Croffie, 2020; Woo et al., 2015). These calls are aligned with the values of professional counseling organizations. Specifically, the American Counseling Association (ACA; 2014) endorsed respect for diversity and multiculturalism as elements of counselor competence. This value is reflected in the ACA Code of Ethics, including Standard F.11.b, which urges counselor educators to value a diverse student body in counseling programs. Similarly, the CACREP standards have identified counseling programs as responsible for working to include “a diverse group of students and to create and support an inclusive learning community” (CACREP, 2015, p. 6). Because counselors must have a profound comprehension of and commitment to diversity, experiences with multiculturalism during professional training programs are essential (O’Hara et al., 2021; Ratts et al., 2016). In this vein, the presence of international students in counseling programs can be beneficial for both domestic and international students by enhancing trainees’ understanding of diversity and multicultural counseling competencies (Behl et al., 2017; Luo & Jamieson-Drake, 2013). Given that there is a substantially increasing need for addressing multiculturalism, diversity, and social justice in the counseling profession, counseling programs’ efforts to recruit various minority student groups, including ICSs, will contribute to not only counselor training but also client outcomes in the long term.
However, despite the importance of the topic, researchers have consistently indicated that research on ICSs has been quite limited (Behl et al., 2017; Lau et al., 2019). In counseling research, there is a history of researchers using content analysis to provide a comprehensive overview of topics that are underrepresented but have growing importance. For example, Singh and Shelton (2011) published a content analysis of qualitative research related to counseling lesbian, gay, bisexual, transgender, and queer clients. Involving the summarization of findings from a body of literature into a few key categories or content areas (Stemler, 2001), content analysis is a useful methodology for expanding the field’s knowledge and understanding of the topic. Considering ICSs’ unique challenges and their potential contributions to enriching diversity in counseling programs and in the profession (Park et al., 2017), a comprehensive understanding of the current ICS literature is needed. This content analysis can identify how the research on ICSs has progressed and what remains unexplored or underexplored, which can provide meaningful implications for researchers interested in conducting ICS research in the future.
Purpose of the Study
The purpose of this study is to identify major findings in literature recently published on ICSs in the United States and to draw useful implications for counseling researchers and counseling programs seeking to better understand and support international students in counseling programs. Our content analysis, which focused on ICS research published between 2006 and 2021 in selected counseling journals, was driven by the following research questions: 1) What are the publication trends in ICS research, such as prevalence, publication outlets, authorship, methodological design, and sample size and characteristics?; and 2) What is the content of the ICS research published in counseling journals? Based on the findings, this study aimed to suggest recommendations for counseling researchers to fill the scholarly gap in ICS research and for counselor education programs to provide more effective training experiences to their international trainees.
Method
Content analysis is a useful methodology to expand our knowledge and understanding of the field through an overview of the current literature (Stemler, 2001). This approach makes it possible to effectively summarize a large amount of data using a few categories or content areas. In counseling research, content analysis has been used to provide an overview of a profession that is underrepresented but with growing importance (e.g., LGBTQ; Singh & Shelton, 2011), which is aligned with the aim of this study. This study employed both quantitative and qualitative content analysis to provide an overview of ICS research. Quantitative content analysis refers to analyzing the data in mathematical ways and applying predetermined categories that do not derive from the data (Forman & Damschroder, 2007). After reviewing existing content analysis articles in the counseling field, Byeolbee Um and Susannah M. Wood determined the scope of our quantitative analysis as: (a) journal and authorship, (b) research design, (c) participant characteristics, and (d) data collection methods.
Research Team
The research team consisted of two doctoral candidates and one full professor, all of whom were affiliated with the same CACREP-accredited counselor education and supervision program at a Midwestern university. Um and Lindsay Woodbridge were doctoral candidates in counselor education and supervision when conducting this research project and are currently counselor educators. Um is an international scholar from an East Asian country. She has drawn on her experiences in quantitative and qualitative courses and research projects to engage in research of marginalized counseling students, including ICSs. Woodbridge is a domestic scholar who has taken classes and collaborated with international student peers and worked with international students in instructional and clinical capacities. She has taken quantitative and qualitative research courses and completed several research projects. The first and second authors met regularly to establish the scope of the investigation, collect data, and form a consensus on coding emerging categories and sorting them into themes. Wood, an experienced researcher and instructor, has worked as a counselor educator for more than 15 years. She has worked with international students in teaching, supervision, advising, and mentoring capacities. She audited the research process, reviewed emergent categories and themes, and provided constructive feedback at each phase of the study.
Data Collection
To identify a full list of ICS studies that satisfy the scope of this study, Um and Woodbridge independently performed electronic searches using research databases including EBSCO, PsycINFO, and ERIC. Because ICSs have attracted scholarly attention relatively recently and because Ng’s (2006) study that estimated the number of ICSs in CACREP-accredited programs was the first published research on ICSs in counselor education programs, we set 2006 as the initial year of our search. We used the following search criteria to identify candidate articles: (a) published between 2006 and 2021 in ACA division, branch, and state journals and major journals under the auspices of professional counseling organizations; (b) containing one or more of the following keywords: international students, international counseling students, international counseling trainees, international counseling programs, counselor education; and (c) involving original empirical findings from ICSs in the United States.
We conducted an extensive search of ICS research across various journals in the counselor education field and identified ICS articles from several ACA-related journals, including Counselor Education and Supervision (CES), Journal of Multicultural Counseling and Development (JMCD), The Journal of Counselor Preparation and Supervision (JCPS), The Journal for Specialists in Group Work (JSGW), and the Journal of Professional Counseling: Practice, Theory & Research (JPC). Additionally, we found ICS articles from the International Journal for the Advancement of Counselling (IJAC) and the Journal of Counselor Leadership and Advocacy (JCLA), which are associated with the International Association for Counselling and Chi Sigma Iota, respectively. Although they are not under the broader umbrella of ACA, these journals have contributed to enriching scholarship in the counseling field.
After the initial searches, Um and Woodbridge made a preliminary list of the articles identified based on the search results. Subsequently, they re-screened the articles independently. Among the 27 identified articles, we excluded five conceptual papers, three articles that examined counselors’ or counselor educators’ experiences after graduation, and one article about ICSs in Turkey. Consequently, the final data consisted of 18 articles published by seven selected counseling journals.
Data Analysis
The research team analyzed content areas of the ICS research as an extension of qualitative content analysis, which requires performing the systematical coding and identifying categories/themes (Cho & Lee, 2014). We followed a series of steps suggested by Downe-Wamboldt (1992), which included selecting the unit of analysis, developing and modifying categories, and coding data. Several methods were used to ensure the trustworthiness of this content analysis study (Kyngäs et al., 2020). For credibility, Um and Woodbridge conducted multiple rounds of review on determining an adequate unit of analysis and tracked all discussions and modifications in great detail. For dependability, we calculated interrater reliability coefficients and Wood provided feedback about the results. Um also secured confirmability by utilizing audit trails, which described the specific steps and reflections of the project. Finally, to support transferability, we carefully examined other content analysis articles, reflected core aspects in the current study, and depicted the research process transparently.
Coding Protocol
After completing the quantitative content analysis, we conducted the qualitative content analysis as Downe-Wamboldt (1992) suggested. In so doing, we applied the inductive category development process suggested by Mayring (2000), which features a systematic categorization process of identifying tentative categories, coding units, and extracting themes from established categories. Specifically, after discussing the research question and levels of abstraction for categories, Um and Woodbridge determined the preliminary categories based on the text of the 18 ICS articles. We practiced coding the data using two articles and then performed independent coding of the remaining articles. Using a constructivist approach, we agreed to add additional categories as needed. Subsequently, the categories were revised until we reached a consensus. In the final step, established categories were sorted into three themes to identify the latent meaning of qualitative materials (Cho & Lee, 2014; Forman & Damschroder, 2007). Regarding validity, the congruence between existing conceptual themes and results of data coding secures external validity, which is regarded as the purpose of content analysis (Downe-Wamboldt, 1992).
Interrater Reliability
We used various indices of interrater reliability to assess the overall congruence between the researchers who performed the qualitative analysis and ensure trustworthiness. In this study, we used the kappa statistic (κ) suggested by Cohen (1960), which shows the extent of consensus among raters for selecting an article or coding texts (Stemler, 2001). Cohen’s kappa has been used extensively across various academic fields to measure the degree of agreement between raters. More specifically, the kappa statistic was calculated in two phases: 1) after screening articles and 2) after coding the texts according to the categories. The kappa results between Um and Woodbridge were .68 for screening articles and .71 for coding the text, both of which are considered substantial (.61–.80; Stemler, 2004).
Results
Results of Quantitative Content Analysis
Based on our electronic search, we identified a total of 18 ICS articles published between 2006 and 2021 in seven selected counseling journals, including three ACA division journals, one ACA state-branch journal, one ACES regional journal, and two journals from professional counseling associations (see Table 1). Specifically, two articles were published in CES, three in JMCD, one in JCPS, one in JSGW, three in JPC, seven in IJAC, and one in JCLA. Across the 18 ICS articles, a total of 35 researchers were identified as authors or co-authors with six authoring more than one article. According to researchers’ positionality statements in qualitative articles, eight researchers reported that they were previous or current ICSs in the United States. The institutional affiliations of researchers include 22 U.S. universities and two international universities, with three institutional affiliations appearing more than once across the studies.
Table 1
Summary of International Counseling Student Research in Selected Counseling Journals Between 2006 and 2021
| Journal and Author |
Research Design |
Participants |
Data Collection |
Topic |
| Counselor Education and Supervision (CES) |
Behl et al.
(2017) |
Quantitative
(Pearson product-moment correlations) |
38 counseling master’s and doctoral students |
Online survey |
Stress related to acculturation and students’ language, academic, social, and cultural needs |
D. Li & Liu
(2020) |
Qualitative (Phenomenology) |
11 doctoral students |
Semi-structured interview |
ICSs’ experiences with teaching preparation |
| Journal of Multicultural Counseling and Development (JMCD) |
Kuo et al.
(2021) |
Qualitative (Consensual
qualitative research) |
13 doctoral students |
Semi-structured interview |
ICSs’ professional identity development influenced by their multicultural identity and experience |
Nilsson &
Dodds (2006) |
Quantitative (Exploratory factor analysis, ANOVA, and hierarchical multiple regression analysis) |
115 master’s and doctoral students in counseling and psychology |
Online survey |
Development of a scale to measure issues in supervision |
Woo et al.
(2015) |
Qualitative (Consensual qualitative research) |
8 counselor education doctoral students |
Semi-structured interview |
Coping strategies used during training in supervision |
| The Journal of Counselor Preparation and Supervision (JCPS) |
Park et al.
(2017) |
Qualitative (Consensual qualitative research) |
10 counseling master’s and doctoral students |
Semi-structured interview |
Practicum and internship experiences of ICSs |
| The Journal for Specialists in Group Work (JSGW) |
Delgado-Romero
& Wu (2010) |
Qualitative
(Not identified) |
6 Asian counseling graduate students |
Counseling
practice |
Social justice–focused group intervention |
| Journal of Professional Counseling: Practice, Theory & Research (JPC) |
Interiano-
Shiverdecker
et al. (2019) |
Quantitative (Hierarchical multiple regression analysis) |
94 counseling master’s and doctoral students |
Online survey |
Relationship between acculturation and self-efficacy |
| Ng (2006) |
Quantitative (Descriptive analysis) |
96 CACREP-accredited
counseling programs |
Responses via email/telephone |
Enrollment in CACREP-accredited programs |
Sangganjanavanich
& Black (2009) |
Qualitative (Phenomenology) |
4 master’s students
and 1 doctoral student
in counseling |
Semi-structured interview |
Perceptions of supervision |
|
|
|
|
|
| International Journal for the Advancement of Counselling (IJAC) |
|
|
Akkurt et al.
(2018) |
Quantitative (Moderation analysis) |
71 counseling master’s and doctoral students |
Online survey |
Relationships between acculturation, counselor self-efficacy, supervisory working alliance, and role ambiguity moderated by frequency of multicultural discussion |
Interiano & Lim
(2018) |
Qualitative (Interpretive phenomenology) |
8 foreign-born doctoral students |
Semi-structured interview |
Influence of acculturation on ICSs’ professional development |
Lertora & Croffie
(2020) |
Qualitative (Phenomenology) |
6 counseling master’s students |
Demographics survey, focus
group, and semi-structured
interview |
Lived experiences of master’s-level ICSs in counseling program, including challenges and support, cultural differences, and future career paths |
C. Li et al.
(2018) |
Quantitative
(Linear regression analysis) |
72 counseling master’s and doctoral students |
Online survey |
Influence of acculturation and foreign language anxiety on ICSs’ counseling self-efficacy |
Ng & Smith
(2009) |
Quantitative
(F-tests) |
56 international counseling students
82 domestic
counseling students |
Survey |
Perceived barriers and concerns of ICSs in their training compared to domestic counseling students |
Ng & Smith
(2012) |
Quantitative (Hierarchical regression analysis) |
71 counseling master’s and doctoral students |
Online survey |
Relationships among ICSs’ training level, acculturation, counselor self-efficacy, supervisory working alliance, role ambiguity, and multicultural discussion |
Smith & Ng
(2009) |
Mixed methods (Descriptive analysis, constant comparative method of analysis, and phenomenology) |
11 master’s students and 10 doctoral students (including 7 recent graduates) |
Online survey |
ICSs’ experiences, resources, hindrances, and recommendations regarding multicultural counseling training |
| Journal of Counselor Leadership and Advocacy (JCLA) |
Kuo et al.
(2018) |
Qualitative (Consensual qualitative research) |
13 doctoral students |
Semi-structured interview |
ICSs’ professional identity development influenced by their multicultural identity and experience |
Note. ICS = international counseling student.
In terms of research design, eight articles employed quantitative research designs with diverse statistical methods including hierarchical multiple regression analysis, ANOVA, exploratory factor analysis, descriptive analysis, linear regression analysis, and moderation analysis. Another nine articles used qualitative approaches including phenomenology and consensual qualitative research, while one article (Smith & Ng, 2009) applied mixed methods design including both quantitative and qualitative analyses. Regarding participants, eight quantitative studies reported having between 38 to 115 ICS participants, including Ng’s (2006) study in which the author collected information on ICSs from 96 CACREP-accredited counseling programs. The numbers of participants in the eight qualitative ICS articles were relatively smaller, ranging from 5 to 13, which is natural given the characteristics of quantitative and qualitative research designs. Finally, the mixed methods study included 21 ICS participants. Quantitative researchers most frequently used online surveys to collect data, although one researcher (Ng, 2006) gathered information via email or telephone. Researchers using qualitative methodologies primarily used semi-structured interviews to collect data, while Delgado-Romero and Wu (2010) performed a group counseling intervention and interpreted the results, including the feedback of group members.
Results of Qualitative Content Analysis
The content areas of the ICS research included personal and professional aspects of ICSs’ adjustment and development. These aspects were influenced by ICSs’ unique circumstances along with their needs, potential stressors, and accessible resources and strategies. During qualitative content analysis, we generated and established preliminary categories. We then developed the preliminary categories into three main themes encompassing ICS research: (a) professional practices and professional development, (b) academic, social, and cultural challenges, and (c) personal and social resources. Each theme consisted of several identified categories.
Professional Practices and Professional Development
Many studies examined ICSs’ perceptions, concerns, needs, and suggestions of professional training experiences, including practicum and internship (e.g., Lertora & Croffie, 2020; Park et al., 2017), supervision (e.g., Ng & Smith, 2012; Nilsson & Dodds, 2006), multicultural training (e.g., Akkurt et al., 2018; Smith & Ng, 2009), social justice group intervention (Delgado-Romero & Wu, 2010), and teaching preparation (D. Li & Liu, 2020) from the unique perspective of ICSs. Furthermore, in relation to the professional practices, several categories of ICSs’ professional development were identified, such as counseling self-efficacy (e.g., Interiano-Shiverdecker et al., 2019; C. Li et al., 2018), professional identity development (e.g., Kuo et al., 2018, 2021), role ambiguity (Akkurt et al., 2018; Ng & Smith, 2012), and multicultural competencies (Smith & Ng, 2009).
Academic, Social, and Cultural Challenges
The second theme included unique challenges that ICSs encountered across academic, social, and cultural domains. The most commonly identified category from 12 studies was acculturation (e.g., Behl et al., 2017; Interiano & Lim, 2018; Lertora & Croffie, 2020). In addition, ICSs faced other cultural barriers involving cultural differences (e.g., Behl et al., 2017; Woo et al., 2015), difficulties in performing teaching and supervision practices (e.g., Li & Liu, 2020; Woo et al., 2015), and struggles in understanding cultural values and U.S. culture (e.g., Kuo et al., 2021; Sangganjanavanich & Black, 2009). ICSs reported that their academic and social concerns included English proficiency (e.g., Kuo et al., 2021; Nilsson & Dodds, 2006) and experiences of language anxiety (C. Li et al., 2018); stigma, biases, and discrimination (e.g., Ng & Smith, 2009; Sangganjanavanich & Black, 2009); and interpersonal isolation (e.g., Behl et al., 2017).
Personal and Social Resources
The third theme emerged from multiple categories of personal and social resources that supported ICSs. In terms of personal resources, researchers identified several characteristics such as self-reflection, self-regulation, and self-efficacy, which contributed to ICSs’ professional development (e.g., Delgado-Romero & Wu, 2010; Interiano-Shiverdecker et al., 2019; Woo et al., 2015). Additionally, the sources of social support for ICSs included their peers and other ICSs (e.g., D. Li & Liu, 2020; Woo et al., 2015), faculty and mentors (e.g., Smith & Ng, 2009; Woo et al., 2015), department and college (e.g., Delgado-Romero & Wu, 2010; D. Li & Liu, 2020), and family (Kuo et al., 2018).
Discussion
The purpose of this content analysis was to provide an organized overview of counseling studies conducted for ICSs over the past 16 years both from quantitative and qualitative perspectives. The aggregated findings, including publication trends and content areas of ICS research, are expected to present the missing pieces in research to better understand and support ICSs and provide meaningful recommendations to better support their professional development. Specifically, we identified 18 articles published in selected counseling journals during the 16-year period from 2006 to 2021. Our findings included the journals, authorship and affiliation, research orientation, participant characteristics, data collection method, and content areas. In general, researchers from many educational institutions have conducted collaborative research focusing on ICSs, with a balance of quantitative and qualitative methodologies. Research participants were ICSs at master’s and doctoral levels, with larger participant groups for quantitative studies and smaller groups for qualitative studies. The most frequently employed methods for data collection were online surveys and semi-structured interviews. Among the 18 identified ICS articles, three main content themes emerged, with each theme consisting of several categories.
In terms of the content, counseling researchers have consistently examined the professional practices of ICSs in their programs. Our findings indicate that many researchers were interested in supervision as an essential aspect of counselor education. Supervision involves intricate dynamics between the supervisor, supervisee, and client, and it can have a substantial influence on counselor competency development (Falender & Shafranske, 2007; Nilsson & Dodds, 2006). For this reason, ICS research has focused not only on investigating the supervisory concerns, needs, and satisfaction of ICSs, but on providing an integrative supervision model for this population (Nilsson & Dodds, 2006; Park et al., 2017; Sangganjanavanich & Black, 2009). Beyond supervision, researchers have also explored other topics, including teaching preparation and social justice counseling (Delgado-Romero & Wu, 2010;
D. Li & Liu, 2020). We found that researchers have attended to ICSs’ professional competencies as well as their training processes, including counseling self-efficacy, professional identity, and multicultural and social justice competencies (Kuo et al., 2021; C. Li et al., 2018; Smith & Ng, 2009). These professional competencies and training processes are regarded as important indices of successful and effective counselor training (Center for Substance Abuse Treatment, 2014; Woo et al., 2015). As a whole, ICS research has addressed diverse student training experiences and resultant developmental outcomes, although the absolute number of studies remains limited.
Our results highlight cultural and language differences as a primary barrier for many ICSs when they initiated their study in a foreign country. This finding is consistent with previous studies, including Mori’s (2000) seminal work. Most studies we examined identified acculturation as a key construct of ICSs’ adjustment and growth in a foreign country (Interiano & Lim, 2018; Ng & Smith, 2012). Many ICS participants sought to maintain a balance between engaging in U.S. language and culture and sustaining their own cultural identity (Interiano-Shiverdecker et al., 2019; D. Li & Liu, 2020; Sangganjanavanich & Black, 2009). Specifically, ICSs reported cultural challenges in several areas, including the educational system, teaching styles, personal interactions, social justice issues, and cultural values and practices (Behl et al., 2017; Delgado-Romero & Wu, 2010; D. Li & Liu, 2020). One study found that doctoral-level ICSs experienced greater cultural adjustment problems and conflicts compared to master’s-level ICSs (Ng & Smith, 2009), which implies that differentiated understanding and approaches may be required according to ICSs’ developmental stages. Also, our findings echoed the existing literature that one of the main obstacles for international students is language proficiency (Kuo et al., 2021; C. Li et al., 2018), as ICSs who had difficulty using English reported greater academic needs and concerns than their peers (Behl et al., 2017).
A notable finding is that the cultural barriers ICSs experienced were intertwined with their social concerns. ICSs are exposed to social dangers involving stigma, discrimination, and interpersonal isolation (Behl et al., 2017; Delgado-Romero & Wu, 2010). Although several researchers explored the potential relationship between ICSs’ length of time in the United States and their stress and cultural development (Behl et al., 2017; Nilsson & Dodds, 2006), their findings did not indicate any significant relationship. This lack of an effect may imply that other risks and protective factors have more influence on the successful adjustment and achievement of ICSs regardless of the amount of time they have spent in the United States. As such, our findings have shown that ICSs face unique challenges across their professional and personal lives in acculturating to two or more cultures and satisfying counseling training requirements.
Corresponding to these challenges, various personal and social resources have been regarded as protective factors of ICS development. Specifically, in terms of social support, researchers identified the importance of support from mentors, supervisors, peers, and other international graduate students (e.g., Woo et al., 2015). Given that ICSs often experience a lack of social support, it is noteworthy that the current ICS literature highlights the need for counselor training programs to promote students’ personal strengths and social connections.
Overall, we identified patterns and trends in research on international students in counseling programs based on studies published in selected counseling journals. Despite our efforts to reflect on diverse ICS experiences, the paucity of ICS research across selected counseling journals, particularly ACA journals, is notable. Given the increasing representation of ICSs in the wider counseling student body (Ng, 2006), further studies addressing the resources and barriers of this student population are needed. Furthermore, international students were exposed to unprecedented difficulties and mental health threats during the COVID-19 pandemic (Chen et al., 2020). These challenges necessitate more scholarly attention toward supporting and advocating for ICSs, including their adjustment, professional development, and transition from training to practice.
Implications
Because members of the counseling profession have expressly emphasized the importance of enriching multiculturalism and diversity (D. Li & Liu, 2020), we expect our findings to provide meaningful implications for counselor education programs. First, counseling researchers are encouraged to conduct more ICS research given the limited available studies and the increasing representation of international students in counseling programs. Even though they attempted to examine diverse training experiences and competency development of ICSs, many areas are understudied, such as their teaching and social justice practices. The existing ICS research mostly concentrated on identifying factors that influence ICSs’ academic and social lives. However, given the continuous increase of ICSs in the counseling field, research about strengths and support strategies of counselor education programs having many ICSs is worth studying. Also, in future studies, researchers can try to reflect the actual voices of ICSs about what they want from their training programs, whether they feel their program is affordable, and whether their program is effective in supporting their professional development. In addition, counseling researchers can develop projects considering cultural differences of ICSs in order to better understand them not as a single group but as multiple individuals having unique cultural backgrounds. Overall, this content analysis study underscores the need for more research on this student population.
Regarding counselor education programs, programs can provide specific resources to support the professional development of ICSs. To help ICSs overcome language barriers, for instance, institutions can provide professional assistance in the use of English, such as writing centers and speaking centers. Departments can provide language support specifically relevant to counseling, including workshops and seminars about practical language tips for counseling practice and research writing. For example, Jang and colleagues (2014) recommended instituting mock supervision sessions before practicum and/or internship to further prepare international counseling trainees for their duties. Counselor education programs are expected to address the unique language and academic needs of ICSs.
Counselor education programs should also facilitate ICSs’ cultural understanding and adjustment. Counselor education programs can design and provide opportunities for ICSs to socially interact with colleagues and faculty members in the program. Existing studies that highlight the importance of mentoring (e.g., Delgado-Romero & Wu, 2010; Ng, 2006; Woo et al., 2015) are further proof that faculty members in counselor education programs can play a significant role in the personal and professional development of ICSs. Because ICSs share unique challenges and learning experiences (D. Li & Liu, 2020; Sangganjanavanich & Black, 2009), faculty members who were ICSs or have experience advising or collaborating with ICSs can serve as essential mentors for this population.
Counselor education programs might benefit from developing and employing curriculum and courses that apply the empirical findings of ICS research, including the results of this study. These studies serve as a reference for designing more effective counselor training. Programs that design their training to support the needs of ICSs may also find that they are more effective in recruiting and retaining international students. For example, faculty members can respond to ICSs’ anxiety and concerns before they enter clinical practice (Ellis et al., 2015; Nilsson & Wang, 2008). Also, ICSs are expected to benefit from synthesized results about ICS research, promoting a deeper understanding of themselves and enabling them to develop their own coping strategies and access potential resources. Furthermore, counselor education programs need to prepare different training trajectories for master’s students and doctoral students. Compared to ICSs in doctoral programs, ICSs are relatively rare at the master’s level, comprising only 1% of master’s-level counseling trainees (CACREP, 2015). Because master’s-level ICSs may feel like they belong to the minority, helping them feel connected is an essential task for counselor education programs. Therefore, programs are required to prioritize the effective delivery of knowledge and adequate practical opportunities for supervisees at the master’s level.
Finally, counselor education programs should work toward a program culture that supports diversity. Although fostering multiculturalism has emerged as a priority for counselor education programs, more work is needed to support internationally diverse perspectives. For example, Taephant and colleagues (2015) examined the experiences of U.S.-educated international counselors practicing in non-Western counseling environments. Drawing upon these findings and other relevant references, counselor educators may design a class discussing the limitations of Western-style training. As is evidenced by existing literature, open discussions about cultural differences can be effective for the psychosocial adjustment and professional development of ICSs.
Limitations and Future Research
This study includes some limitations to note. The first and most important limitation is the concerning lack of research focusing on international students in the counseling profession (D. Li & Liu, 2020; Nilsson & Dodds, 2006; Woo et al., 2015). Even though ICSs have recently begun to attract scholarly attention (Lau et al., 2019), the number of articles published recently may not be sufficient to discuss the diverse purposes and areas of focus for ICS research. Although our study specifically highlighted the need for more research on ICSs, an extensive range of discussion was not possible due to the limited number of articles. Thus, we encourage more professional counseling organizations and counseling researchers to consider ICSs’ professional development as a research topic. Also, because this study was limited to articles published in journals related to ACA and selected other professional organizations, future research with a more comprehensive search may elicit rich and diverse discussion. Finally, content analysis has a few methodological limitations, such as no existence of unified rules and a precise analytical process, and potential biases in coding, which necessitates further research on ICSs using other methodologies for more in-depth investigations.
Conclusion
ICSs can contribute to increasing program diversity and cultivating students’ multicultural counseling competency but have been understudied despite their growing representation. This study provided a comprehensive overview of ICS research across 18 articles within a 16-year period, using both quantitative and qualitative content analysis. Counseling researchers can pay more scholarly attention to the academic and social lives of ICSs from a strength-based approach. Counseling programs and counselor educators can support ICSs by providing resources for adjustment, developing curricular and extracurricular activities involving ICSs, and working toward a more multicultural and inclusive program environment.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Akkurt, M. N., Ng, K.-M., & Kolbert, J. (2018). Multicultural discussion as a moderator of counseling supervision-related constructs. International Journal for the Advancement of Counselling, 40(4), 455–468.
https://doi.org/10.1007/s10447-018-9337-z
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Anandavalli, S., Borders, L. D., & Kniffin, L. E. (2021). “I am strong. Mentally strong!”: Psychosocial strengths of international graduate students of color. The Professional Counselor, 11(2), 173–187.
https://doi.org/10.15241/sa.11.2.173
Behl, M., Laux, J. M., Roseman, C. P., Tiamiyu, M., & Spann, S. (2017). Needs and acculturative stress of international students in CACREP programs. Counselor Education and Supervision, 56(4), 305–318.
https://doi.org/10.1002/ceas.12087
Center for Substance Abuse Treatment. (2014). A treatment improvement protocol: Improving cultural competence. Substance Abuse and Mental Health Services Administration.
Chen, J. H., Li, Y., Wu, A. M. S., & Tong, K. K. (2020). The overlooked minority: Mental health of international students worldwide under the COVID-19 pandemic and beyond. Asian Journal of Psychiatry, 54, 102333. https://doi.org/10.1016/j.ajp.2020.102333
Cho, J. Y., & Lee, E.-H. (2014). Reducing confusion about grounded theory and qualitative content analysis: Similarities and differences. The Qualitative Report, 19(32), 1–20. https://doi.org/10.46743/2160-3715/2014.1028
Cohen, J. (1960). A coefficient of agreement for nominal scales. Educational and Psychological Measurement, 20(1), 37–46. https://doi.org/10.1177/001316446002000104
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2022). CACREP vital statistics 2021. https://www.cacrep.org/wp-content/uploads/2023/01/vital-statistics-report-2021.pdf
Delgado-Romero, E. A., & Wu, Y.-C. (2010). Asian international students in counseling programs: A group intervention to promote social justice. The Journal for Specialists in Group Work, 35(3), 290–298.
https://doi.org/10.1080/01933922.2010.492896
Downe-Wamboldt, B. (1992). Content analysis: Method, applications, and issues. Health Care for Women International, 13(3), 313–321. https://doi.org/10.1080/07399339209516006
Ellis, M. V., Hutman, H., & Chapin, J. (2015). Reducing supervisee anxiety: Effects of a role induction intervention for clinical supervision. Journal of Counseling Psychology, 62(4), 608–620. https://doi.org/10.1037/cou0000099
Falender, C. A., & Shafranske, E. P. (2007). Competence in competency-based supervision practice: Construct and application. Professional Psychology: Research and Practice, 38(3), 232–240.
https://doi.org/10.1037/0735-7028.38.3.232
Forman, J., & Damschroder, L. (2007). Qualitative content analysis. In L. Jacoby & L. A. Siminoff (Eds.), Empirical methods for bioethics: A primer (pp. 39–62). Elsevier.
Interiano, C. G., & Lim, J. H. (2018). A “chameleonic” identity: Foreign-born doctoral students in U.S. counselor education. International Journal for the Advancement of Counselling, 40(3), 310–325.
https://doi.org/10.1007/s10447-018-9328-0
Interiano-Shiverdecker, C. G., Foxx, S. P., & Flowers, C. (2019). Acculturation domains and counselor self-efficacy. Journal of Professional Counseling: Practice, Theory & Research, 46(1–2), 48–63.
https://doi.org/10.1080/15566382.2019.1669373
Jang, Y. J., Woo, H., & Henfield, M. S. (2014). A qualitative study of challenges faced by international doctoral students in counselor education supervision courses. Asia Pacific Education Review, 15(4), 561–572.
https://doi.org/10.1007/s12564-014-9342-9
Ju, J., Merrell-James, R., Coker, J. K., Ghoston, M., Pérez, J. F. C., & Field, T. A. (2020). Recruiting, retaining, and supporting students from underrepresented racial minority backgrounds in doctoral counselor education. The Professional Counselor, 10(4), 581–602. https://doi.org/10.15241/jj.10.4.581
Karaman, M. A., Schmit, M. K., Ulus, I. C., & Oliver, M. (2018). International counseling students’ perception of ethics. Journal of International Students, 8(2), 677–695. https://doi.org/10.5281/zenodo.1250370
Kuo, P., Washington, A., & Woo, H. (2021). Professional identity development and multicultural identity among international counselor education doctoral students. Journal of Multicultural Counseling and Development, 49(2), 116–128. https://doi.org/10.1002/jmcd.12210
Kuo, P., Woo, H., & Washington, A. (2018). Professional identity development of international counselor education doctoral students. Journal of Counselor Leadership and Advocacy, 5(2), 153–169.
https://doi.org/10.1080/2326716X.2018.1452079
Kyngäs, H., Kääriäinen, M., & Elo, S. (2020). The trustworthiness of content analysis. In H. Kyngäs, K. Mikkonen, & M. Kääriäinen (Eds), The application of content analysis in nursing science research (pp. 41–48). Springer. https://doi.org/10.1007/978-3-030-30199-6_5
Lau, J., & Ng, K.-M. (2012). Effectiveness and relevance of training for international counseling graduates: A qualitative inquiry. International Journal for the Advancement of Counselling, 34(1), 87–105.
https://doi.org/10.1007/s10447-011-9128-2
Lau, J., Su, Y.-W., Chen, C.-C., & Dai, C.-L. (2019). Using a collaborative model in supervision with international counseling students. The Journal of Humanistic Counseling, 58(2), 150–164. https://doi.org/10.1002/johc.12103
Lertora, I. M., & Croffie, A. L. (2020). The lived experiences of international students in a CACREP counseling program. International Journal for the Advancement of Counselling, 42(2), 174–190.
https://doi.org/10.1007/s10447-019-09394-6
Li, C., Lu, J., Bernstein, B., & Bang, N. M. (2018). Counseling self-efficacy of international counseling students in the U.S.: The impact of foreign language anxiety and acculturation. International Journal for the Advancement of Counselling, 40(3), 267–278. https://doi.org/10.1007/s10447-018-9325-3
Li, D., & Liu, Y. (2020). International counseling doctoral students’ teaching preparation: A phenomenological study. Counselor Education and Supervision, 59(3), 200–215. https://doi.org/10.1002/ceas.12184
Luo, J., & Jamieson-Drake, D. (2013). Examining the educational benefits of interacting with international students. Journal of International Students, 3(2), 85–101. https://files.eric.ed.gov/fulltext/EJ1056457.pdf
Mayring, P. (2000). Qualitative content analysis. Forum: Qualitative Social Research, 1(2).
Mori, S. C. (2000). Addressing the mental health concerns of international students. Journal of Counseling & Development, 78(2), 137–144. https://doi.org/10.1002/j.1556-6676.2000.tb02571.x
Mori, Y., Inman, A. G., & Caskie, G. I. L. (2009). Supervising international students: Relationship between acculturation, supervisor multicultural competence, cultural discussions, and supervision satisfaction. Training and Education in Professional Psychology, 3(1), 10–18. https://doi.org/10.1037/a0013072
Nilsson, J. E., & Dodds, A. K. (2006). A pilot phase in the development of the International Student Supervision Scale. Journal of Multicultural Counseling and Development, 34(1), 50–62.
https://doi.org/10.1002/j.2161-1912.2006.tb00026.x
Nilsson, J. E., & Wang, C. (2008). Supervising international students in counseling and psychology training. In A. K. Hess, K. D. Hess, & T. H. Hess (Eds.), Psychotherapy supervision: Theory, research, and practice
(2nd ed.; pp. 70–81). Wiley.
Ng, K.-M. (2006). International students in CACREP-accredited counseling programs. Journal of Professional Counseling: Practice, Theory & Research, 34(1–2), 20–32. https://doi.org/10.1080/15566382.2006.12033821
Ng, K.-M., & Smith, S. D. (2009). Perceptions and experiences of international trainees in counseling and related programs. International Journal for the Advancement of Counselling, 31(1), 57–70.
https://doi.org/10.1007/s10447-008-9068-7
Ng, K.-M., & Smith, S. D. (2012). Training level, acculturation, role ambiguity, and multicultural discussions in training and supervising international counseling students in the United States. International Journal for the Advancement of Counselling, 34(1), 72–86. https://doi.org/10.1007/s10447-011-9130-8
O’Hara, C., Chang, C. Y., & Giordano, A. L. (2021). Multicultural competence in counseling research: The cornerstone of scholarship. Journal of Counseling & Development, 99(2), 200–209.
https://doi.org/10.1002/jcad.12367
Park, S., Lee, J. H., & Wood, S. M. (2017). Experiences of international students in practicum and internship courses: A consensus qualitative research. The Journal of Counselor Preparation and Supervision, 9(2).
https://digitalcommons.sacredheart.edu/cgi/viewcontent.cgi?article=1137&context=jcps
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Sangganjanavanich, V. F., & Black, L. L. (2009). Clinical supervision for international counselors-in-training: Implications for supervisors. Journal of Professional Counseling: Practice, Theory & Research, 37(2), 52–65. https://doi.org/10.1080/15566382.2009.12033860
Singh, A. A., & Shelton, K. (2011). A content analysis of LGBTQ qualitative research in counseling: A ten-year review. Journal of Counseling & Development, 89(2), 217–226.
https://doi.org/10.1002/j.1556-6678.2011.tb00080.x
Smith, S. D., & Ng, K.-M. (2009). International counseling trainees’ experiences and perceptions of their multicultural counseling training in the United States: A mixed method inquiry. International Journal for the Advancement of Counselling, 31(4), 271–285. https://doi.org/10.1007/s10447-009-9083-3
Stemler, S. (2001). An overview of content analysis. Practical Assessment, Research, and Evaluation, 7(17). https://doi.org/10.7275/z6fm-2e34
Stemler, S. E. (2004). A comparison of consensus, consistency, and measurement approaches to estimating interrater reliability. Practical Assessment, Research, and Evaluation, 9(1).
https://doi.org/10.7275/96jp-xz07
Taephant, N., Rubel, D., & Champe, J. (2015). A grounded theory of Western-trained Asian group leaders leading groups in Asia. The Journal for Specialists in Group Work, 40(1), 74–101.
https://doi.org/10.1080/01933922.2014.993054
Thompson, E. H., Frick, M. H., & Trice-Black, S. (2011). Counselor-in-training perceptions of supervision practices related to self-care and burnout. The Professional Counselor, 1(3), 152–162. https://doi.org/10.15241/eht.1.3.152
Vakkai, R. J. Y., Harris, K., Chaplin, K. S., Crabbe, J. J., & Reynolds, M. (2020). Sociocultural factors that impact the health status, quality of life, and academic achievement of international graduate students: A literature review. Journal of International Students, 10(3), 758–775. https://files.eric.ed.gov/fulltext/EJ1265821.pdf
Woo, H., Jang, Y. J., & Henfield, M. S. (2015). International doctoral students in counselor education: Coping strategies in supervision training. Journal of Multicultural Counseling and Development, 43(4), 288–304. https://doi.org/10.1002/jmcd.12022
Byeolbee Um, PhD, is an assistant professor at the University of Oklahoma. Lindsay Woodbridge, PhD, LMHC, LPC, is an assistant professor at the University of Wisconsin-Stout. Susannah M. Wood, PhD, NCC, is a professor at the University of Iowa. Correspondence may be addressed to Byeolbee Um, 820 Van Vleet Oval, Rm 303, Norman, OK 73019, byeolbee.um-1@ou.edu.
Aug 20, 2021 | Volume 11 - Issue 3
Hannah B. Bayne, Danica G. Hays, Luke Harness, Brianna Kane
We conducted a content analysis of counseling scholarship related to Whiteness for articles published in national peer-reviewed counseling journals within the 35-year time frame (1984–2019) following the publication of Janet Helms’s seminal work on White racial identity. We identified articles within eight counseling journals for a final sample of 63 articles—eight qualitative (12.7%), 38 quantitative (60.3%), and 17 theoretical (27.0%). Our findings outline publication characteristics and trends and present themes for key findings in this area of scholarship. They reveal patterns such as type of research methodology, sampling, correlations between White racial identity and other constructs, and limitations of White racial identity assessment. Based on this overview of extant research on Whiteness, our recommendations include future research that focuses on behavioral and clinical manifestations, anti-racism training within counselor education, and developing a better overall understanding of how White attitudes and behaviors function for self-protection.
Keywords: Whiteness, White racial identity, counseling scholarship, counseling journals, content analysis
Counselors are ethically guided to understand and address the roles that race, privilege, and oppression play in impacting both themselves and their clients (American Counseling Association [ACA], 2014). Most practitioners identify as White despite the population diversity in the United States (U.S. Census Bureau, 2020), which holds implications for understanding how Whiteness impacts culturally competent counselor training and practice (Helms, 1984, 1995, 2017). It is important, then, to understand the role of racial identity within counseling, particularly in terms of how Whiteness can be deconstructed and examined as a constant force impacting power dynamics and client progress (Helms, 1990, 2017; Malott et al., 2015). Whiteness models (i.e., Helms, 1984) describe how White people make meaning of their own and others’ racial identity as a result of personal and social experiences with race (Helms, 1984, 2017). The Helms model, along with other constructs, such as color-blindness (Frankenberg, 1993), White racial consciousness (Claney & Parker, 1989), and White fragility (DiAngelo, 2018), implicates the harmful impacts of Whiteness and invites critical reflection of how these constructs impact the counseling process.
Though much has been theorized regarding Whiteness and its impact within the helping professions, the contributions of Whiteness scholarship within professional counseling journals are unclear. An understanding of the specific professional applications and explorations of Whiteness within counseling can help identify best practices in counselor education, research, and practice to counter the harmful impacts of Whiteness and encourage growth toward anti-racist attitudes and behaviors.
White Racial Identity and Related Constructs
The Helms (1984) model of White racial identity (WRI) presents Whiteness as a developmental process centering on racial consciousness (i.e., the awareness of one’s own race), as well as awareness of attitudes and behaviors toward other racial groups (Helms, 1984, 1990, 1995, 2017). According to Helms, White people have the privilege to restrict themselves to environments and relationships that are homogenous and White-normative, thus limiting their progression through the stages (DiAngelo, 2018; Helms, 1984). The initial model (Helms, 1984) contained five stages (i.e., Contact, Disintegration, Reintegration, Pseudo-Independence, and Autonomy), each with a positive or negative response that could facilitate progression toward a more advanced stage, regression to earlier stages of the model, or stagnation at the current stage of development. Helms (1990) later added a sixth status, Immersion/Emersion, to the model as an intermediary between Pseudo-Independence and Autonomy. These final three stages of the model (i.e., Pseudo-Independence, Immersion/Emersion, Autonomy) involve increasing levels of racial acceptance and intellectual and emotional comfort with racial issues, which in turn leads to the development of a positive and anti-racist WRI (Helms, 1990, 1995).WRI requires intentional and sustained attention toward how Whiteness impacts the self and others, with progression through the stages leading to beneficial intra and interpersonal outcomes (Helms, 1990, 1995, 2017).
Since Helms (1984), several additional components of Whiteness have been introduced, primarily within psychology, counseling psychology, and sociology scholarship. White racial consciousness is distinct from the WRI model in its focus on attitudes toward racial out-groups, rather than using the White in-group as a reference point (Choney & Behrens, 1996; Claney & Parker, 1989). Race essentialism refers to the degree to which a person believes that race reflects biological differences that influence personal characteristics (Tawa, 2017). Symbolic/modern racism refers to overt attitudes of White people related to their perceived superiority (Henry & Sears, 2002; McConahay, 1986). A fourth Whiteness component, color-blind racial ideology, enables color-evasion (i.e., “I don’t see color”) and power-evasion roles (i.e., “everyone has an equal chance to succeed”), which allow White people to deny the impact of race and therefore evade a sense of responsibility for oppression (Frankenberg, 1993; Neville et al., 2013). White privilege refers to the systemic and unearned advantages provided to White people over people of color (McIntosh, 1988). There are also psychosocial costs accrued to White people as a result of racism that include (a) affective (e.g., anxiety and fear, anger, sadness, guilt and shame); (b) cognitive (i.e., distorted views of self, others, and reality in general related to race); and (c) behavioral (i.e., avoidance of cross-racial situations or loss of relationships with White people) impacts (Spanierman & Heppner, 2004). White fragility (DiAngelo, 2018) reflects defensive strategies White people use to re-establish cognitive and affective equilibrium regarding their own Whiteness and impact on others.
Whiteness concepts are thus varied, with different vantage points of how White people might engage in the consideration of power, privilege, and racism, and what potential implications these constructs might have on their development. These constructs also seem largely rooted in psychology research, and it is therefore unclear the extent to which counselor educators and researchers have examined and applied these constructs to training and practice. Such an analysis can assist in situating Whiteness within the specific contexts and professional roles of counseling and can identify areas in need of further study.
The Present Study
Because of the varied components of Whiteness, as well as its potential impact on counselor development and counseling process and outcome (Helms, 1995, 2017), there is a need to examine how these constructs have been examined and applied within counseling research. We sought to identify how and to what degree Whiteness constructs have been explored or developed within the counseling profession since the publication of the Helms (1984) model. We hope to summarize empirical and theoretical constructs related to Whiteness in national peer-reviewed counseling journals to more clearly consider implications for training and practice. Such analysis can highlight the saliency of WRI, demonstrating the need for continued focus on the influences and impacts of Whiteness within counseling. The following research questions were addressed: 1) What types of articles, topics, and major findings are published on Whiteness?; 2) What are the methodological features of articles published on Whiteness?; and 3) What are themes from key findings across these publications?
Method
We employed content analysis to identify publication patterns of national peer-reviewed counseling journals regarding counseling research on Whiteness in order to understand the scope and depth of this scholarship as it applies to fostering counselor training and practice. Content analysis is the systematic review of text in order to produce and summarize numerical data and identify patterns across data sources regarding phenomena (Neuendorf, 2017). In addition, content analysis has been used to summarize and identify patterns for specific topics, including multicultural counseling (e.g., Singh & Shelton, 2011).
Data Sources and Procedure
The sampling units for this study were journal articles on Whiteness topics published in national peer-reviewed journals (N = 24) of the ACA and its divisions, the American School Counselor Association, the American Mental Health Counselors Association, the National Board for Certified Counselors, and Chi Sigma Iota International. We used the following search terms: White supremacy, White racial identity, White privilege, White fragility, White guilt, White shame, White savior, White victimhood, color-blindness, race essentialism, anti-racism, White racism, reverse racism, White resistance, and Whiteness. We selected a 35-year review period (i.e., 1984–2019) to correspond with Helms’s (1984) foundational work on WRI.
We reviewed article abstracts to identify an initial sampling unit pool (N = 185 articles; 29 qualitative [15.6%], 56 quantitative [30.3%], and 100 theoretical [54.1%]). In pairs, we reviewed the initial pool to more closely examine each sampling unit for inclusion in analysis. We excluded 122 articles upon closer inspection (e.g., special issue introductions, personal narratives or profiles, broader focus on social justice issues, ethnic identity, multiculturalism, or primary focus on another racial group). This resulted in a final sample of 63 articles—eight qualitative (12.7%), 38 quantitative (60.3%), and 17 theoretical (27.0%; see Table 1).
Research Team
Our team consisted of four researchers: two counselor education faculty members and two counselor education doctoral students. We all identify as White. Hannah B. Bayne and Danica G. Hays hold doctorates in counselor education, and Luke Harness and Brianna Kane hold master’s degrees in school counseling and mental health counseling, respectively. We were all trained in qualitative research methods, and Bayne and Hays have conducted numerous qualitative research projects, including previous content analyses. Bayne and Hays trained Harness and Kane on content analysis through establishing coding protocols and coding together until an acceptable inter-rater threshold was met.
Table 1
Exclusion and Inclusion of Articles by Journal and Article Type
| Journal |
Excludeda |
Included |
Total
Sample |
% of
Final
Sample |
| Quant |
Qual |
Theory |
Quant |
Qual |
Theory |
| Journal of Counseling & Development |
5 |
0 |
11 |
16 |
4 |
5 |
24 |
38.1% |
Journal of Multicultural Counseling and
Development |
3 |
3 |
14 |
14 |
3 |
8 |
24 |
38.1% |
| Counselor Education and Supervision |
1 |
0 |
1 |
4 |
1 |
2 |
7 |
11.1% |
| The Journal of Humanistic Counseling |
1 |
2 |
14 |
1 |
1 |
1 |
3 |
4.8% |
| Journal of Mental Health Counseling |
0 |
0 |
2 |
1 |
0 |
3 |
2 |
3.2% |
| Counseling and Values |
0 |
0 |
0 |
1 |
0 |
0 |
1 |
1.6% |
| The Family Journal |
1 |
1 |
5 |
0 |
0 |
2 |
1 |
1.6% |
| Journal of Creativity in Mental Health |
0 |
2 |
4 |
0 |
0 |
1 |
1 |
1.6% |
| Adultspan Journal |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| The Career Development Quarterly |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Counseling Outcome Research
and Evaluation |
0 |
2 |
0 |
0 |
0 |
0 |
0 |
0% |
Journal for Social Action in Counseling
and Psychology |
0 |
0 |
3 |
0 |
0 |
0 |
0 |
0% |
| The Journal for Specialists in Group Work |
0 |
1 |
6 |
0 |
0 |
0 |
0 |
0% |
Journal of Addictions & Offender
Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| Journal of Child and Adolescent Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
| Journal of College Counseling |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Journal of Counselor Leadership
and Advocacy |
1 |
5 |
6 |
0 |
0 |
0 |
0 |
0% |
| Journal of Employment Counseling |
2 |
0 |
4 |
0 |
0 |
0 |
0 |
0% |
| Journal of LGBTQ Issues in Counseling |
0 |
1 |
2 |
0 |
0 |
0 |
0 |
0% |
Journal of Military and Government
Counseling |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0% |
Measurement and Evaluation in
Counseling and Development |
1 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
| Professional School Counseling |
0 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
| Rehabilitation Counseling Bulletin |
3 |
1 |
2 |
0 |
0 |
0 |
0 |
0% |
| The Professional Counselor |
0 |
1 |
0 |
0 |
0 |
0 |
0 |
0% |
| Professional School Counseling |
0 |
0 |
2 |
0 |
0 |
0 |
0 |
0% |
Note. Quant = quantitative research articles; Qual = qualitative research articles; Theory = theoretical articles.
aArticles were excluded from analysis if they did not directly address Whiteness or White racial identity (e.g., special issue introductions, personal narratives or profiles, broader focus on social justice issues, ethnic identity, multiculturalism, or primary focus on another racial group).
Coding Frame Development
Dimensions and categories for our coding frame included: journal outlet, publication year, author characteristics (i.e., name, institutional affiliation, ACES region), article type, sample characteristics (e.g., composition, size, gender, race/ethnicity), research components (e.g., research design, data sources or instrumentation, statistical methods, research traditions, trustworthiness strategies), topics discussed (e.g., WRI attitudes, counselor preparation models, intervention use, client outcomes, counseling process), article implications and limitations, and a brief statement of key findings. Over the course of research team meetings, we reviewed and operationalized the coding frame dimensions and categories. We then selected one empirical and one conceptual article to code together in order to refine the coding frame, which resulted in further clarification of some categories.
Data Analysis
To establish evidence of replicability (Neuendorf, 2017), we coded eight (12.7%) randomly selected cases proportionate to the sample composition (i.e., two conceptual, four quantitative, two qualitative). We analyzed the accuracy rate of coding using R data analysis software for statistical analysis (LoMartire, 2020). Across 376 possible observations for eight cases, there was an acceptable rate of coding accuracy (0.89). In addition, pairwise Pearson-product correlations among raters indicated that coding misses did not follow a systematic pattern for any variable (r = −.10 to .65), and thus there were no significant variations in coding among research team members. After pilot coding, we met to discuss areas of coding misses to ensure understanding of the final coding frame.
For the main coding phase, we worked in pairs and divided the sample equally for independent and consensus coding. Upon completion of consensus coding of the entire sample, we extracted 29 keywords describing the Whiteness topics discussed in the articles. Bayne and Hays reviewed the 29 independent topics and collapsed the topics into eight larger themes. To identify themes across the key findings, Bayne and Harness reviewed 125 independent statements based on coder summaries of article findings, and through independent and consensus coding collapsed statements to yield three main themes.
Results
Article Characteristics
We focused on several article characteristics (Research Question 1): article type (conceptual, quantitative, qualitative); number of relevant articles per journal outlet; the relationship between journal outlet and article type; and frequency of Whiteness topics within and across journal outlets. Of the 24 national peer-reviewed counseling journals, eight journals (33.3%) contained publications that met inclusion criteria (i.e., contained keywords for Whiteness from our search criteria and focused specifically on WRI). The number of publications in those journals ranged from 1 to 24 (M = 2.5; Mdn = 7.88; SD = 10.15) and are listed in order of frequency in Table 2). There was not a significant relationship between the journal outlet and article type (i.e., quantitative, qualitative, conceptual) for this topic (r = 0.04, p = .39).
Table 2
Articles Addressing Whiteness and Associated Keywords in National Peer-Reviewed Counseling Journals
| Journal |
Articles Addressing Whiteness |
Percent of Total Sample |
| Journal of Counseling & Development |
24 |
38.1% |
| Journal of Multicultural Counseling and Development |
24 |
38.1% |
| Counselor Education and Supervision |
7 |
11.1% |
| The Journal of Humanistic Counseling |
3 |
4.8% |
| Journal of Mental Health Counseling |
2 |
3.2% |
| Counseling and Values |
1 |
1.6% |
| The Family Journal |
1 |
1.6% |
| Journal of Creativity in Mental Health |
1 |
1.6% |
| Adultspan Journal |
0 |
0% |
| The Career Development Quarterly |
0 |
0% |
| Counseling Outcome Research and Evaluation |
0 |
0% |
| Journal for Social Action in Counseling and Psychology |
0 |
0% |
| The Journal for Specialists in Group Work |
0 |
0% |
| Journal of Addictions & Offender Counseling |
0 |
0% |
| Journal of Child and Adolescent Counseling |
0 |
0% |
| Journal of College Counseling |
0 |
0% |
| Journal of Counselor Leadership and Advocacy |
0 |
0% |
| Journal of Employment Counseling |
0 |
0% |
| Journal of LGBTQ Issues in Counseling |
0 |
0% |
| Journal of Military and Government Counseling |
0 |
0% |
Measurement and Evaluation in Counseling and
Development |
0 |
0% |
| Professional School Counseling |
0 |
0% |
| Rehabilitation Counseling Bulletin |
0 |
0% |
| The Professional Counselor |
0 |
0% |
| Professional School Counseling |
0 |
0% |
Additionally, we identified eight themes of topics discussed within counseling research on Whiteness (see Table 3). For qualitative research, the three most frequently addressed topics were theory development, intrapsychic variables, and multicultural counseling competency (MCC). The most frequent topics discussed in theoretical articles were theory development, counselor preparation, Whiteness and WRI expression, cultural identity development, and counseling process.
Table 3
Themes in Topics Discussed Within Whiteness and WRI Articles
| Theme |
Description |
N
% |
Quant
n / % |
Qual
n / % |
Theory
n / % |
Examples |
| Whiteness and WRI Expression |
Attitudes and knowledge related to WRI and Whiteness constructs, with some (n = 5) examining pre–posttest changes
|
43
68.3% |
32 74.4% |
3
7.0% |
8
18.6% |
WRI attitudes, color-blind racial attitudes, racism and responses, White privilege and responses, and developmental considerations
|
| Cultural Identity Development |
Cultural identities and developmental processes outside of race
|
27
42.9% |
21
77.8% |
1
3.7% |
5
18.5% |
Ethnic identity, womanist identity, cultural demographics such as gender and age
|
| Counselor Preparation |
Training implications, with some presenting training intervention findings (n = 6)
|
23
36.5% |
17
73.9% |
1
4.3% |
5
21.8% |
Pedagogy, training interventions, and supervision process and outcome
|
| Theory Development |
Development or expansion of theoretical concepts |
18
28.6% |
5
27.8% |
5
27.8% |
8
44.4% |
White racial consciousness versus WRI, prominent responses to White privilege, psychological dispositions of White racism
|
| Multicultural Counseling Competency |
Measurements of perceived multicultural counseling competency
|
12
19.0% |
10
83.3% |
2
16.7% |
0
0.0% |
Perceived competency,
link with WRI |
| Counseling Process |
Counseling process and outcome variables
|
11
17.5% |
8
72.7% |
1
9.1% |
2
18.2% |
Client perceptions, working alliance, and clinical applications
|
| Intrapsychic Variables |
Affective and cognitive components that influence Whiteness and WRI
|
11
17.5% |
8
72.7% |
2
18.2% |
1
9.1% |
Personality variables, cognitive development, ego development
|
| Assessment Characteristics |
Development and/or critique of Whiteness and WRI measurements
|
9
14.3% |
8
88.9% |
0
0.0% |
1
11.1% |
Limitations of WRI scales, development of White privilege awareness scales |
| Totala |
|
154
|
111
72.1% |
15
9.7% |
30
19.5% |
|
Note. Quant = quantitative research articles; Qual = qualitative research articles; Theory = theoretical articles.
aPercentage total exceeds 100% because of rounding and/or topic overlap between articles.
Methodological Features
To address Research Question 2, we explored the methodological features of articles. These features included sample composition, research design, data sources, and limitations as reported within each empirical article (n = 46).
Sample Composition
For the 45 studies providing information about the racial/ethnic composition of their samples, White individuals accounted for a mean of 91% of total participants (range = 55%–100%; SD = 14). An average of 14% Black (SD = 6.7), 7.1% Latinx (SD = 4.7), 5.4% Asian (SD = 2.3), and less than 5% each of multiracial, Arab, and Native American respondents were included across the samples. Of studies reporting gender (n = 44), women accounted for an average of 68% of total participants (range = 33–100; SD = 14.7), and men accounted for 31% of total samples (range = 12–67; SD = 14). The age of participants, reported in 71.7% of the empirical studies, ranged from 16 to 81 (M = 29, SD = 8.2).
Of the 61 independent samples across the articles, a majority focused on student populations, with master’s trainees (n = 20, 32.8%), undergraduate students (n = 14, 21.9%), and doctoral trainees (n = 10, 16.4%) representing over 70% of the sample. The remainder of the samples included practitioners (n = 8, 13.1%), unspecified samples (n = 3, 4.9%), university educators (n = 2, 3.3%), educational specialist trainees (n = 2, 3.3%), site supervisors (n = 1, 1.6%), and general population adult samples (n = 1, 1.6%). The target audience of the articles (N = 63) focused primarily on counselor trainees (n = 34, 49.3%) or clients in agency/practice settings (n = 12, 17.4%). Other audiences included practitioners (n = 9, 13%), researchers (n = 3, 4.3%), general population (n = 6, 8.7%), counselor educators (n = 1, 1.4%), and general university personnel (n = 1, 1.4%).
Research Design and Data Sources
Of the 38 quantitative articles, 10 (26.3%) included an intervention as part of the research design. The majority employed a correlational design (n = 27, 71.1%), with the remainder consisting of four (10.5%) descriptive, four (10.5%) quasi-experimental, one (2.6%) ex post facto/causal comparative, one (2.6%) pre-experimental, and one (2.6%) true experimental design. In recruiting and selecting samples, most researchers used convenience sampling (n = 27, 57.4%), while the rest used purposive (n = 12, 31.6%), simple random (n = 5, 10.6%), stratified (n = 2, 4.3%), and homogenous (n = 1, 2.1%) sampling methods.
Regarding study instrumentation, 37 quantitative studies utilized self-report forced-choice surveys, with one study employing a combination of forced-choice and open-ended question surveys. Across the 38 quantitative studies, 13 of 50 (26%) assessments were used more than once. The most frequently used assessment was the White Racial Identity Attitudes Scale (n = 24; Helms & Carter, 1990). The 50 assessments purported to measure the following targeted variables: race/racial identity/racism (n = 17, 34%); MCC (n = 9, 18%); cultural identity (n = 6, 12%); counseling process and outcome (n = 5, 10%); social desirability (n = 2, 4%); and other variables such as personality, anxiety, and ego development (n = 11, 22%). Finally, data analysis procedures included ANOVA/MANOVA (n = 25, 30.9%), correlation (n = 23, 28.4%), regression (n = 17, 21%), t-tests (n = 7, 8.6%), descriptive (n = 5, 6.2%), exploratory factor analysis (n = 1, 1.2%), confirmatory factor analysis (n = 1, 1.2%), SEM/path analysis (n = 1, 1.2%), and cluster analysis (n = 1, 1.2%).
We identified the research traditions of the eight qualitative studies as follows: phenomenology (n = 3, 37.5%), grounded theory (n = 2, 25%), and naturalistic inquiry (n = 1, 12.5%); two were unspecified (25%). The most common qualitative recruitment method was criterion sampling (n = 5, 62.5%), followed by convenience (n = 3, 37.5%), homogenous (n = 2, 25%), snowball/chain (n = 2, 25%), intensity (n = 2, 25%), and stratified purposeful (n = 1, 12.5%) sampling procedures. (Several studies used multiple recruitment methods, resulting in totals greater than 100%.) There were 12 data sources reported across the eight qualitative studies, falling into the following categories: individual interviews (n = 7, 58.3%), focus group interviews (n = 2, 16.7%), artifacts/documents (n = 2, 16.7%), and observations (n = 1, 8.3%). Trustworthiness strategies included prolonged engagement (n = 7, 13.7%); use of a research team (n = 6, 11.8%); researcher reflexivity, triangulation of data sources, thick description, and simultaneous data collection and analysis (n = 5 each, 9.8%); peer debriefing, audit trail, and member checking (n = 4 each, 7.8%); theory development (n = 3, 5.9%); and one each (2%) of external auditor, memos and/or field notes, and persistent observation.
Limitations Within Sampled Studies
Of the 46 empirical studies, 44 (95.7%) reported limitations. Limitations included design issues related to sampling/generalizability (n = 38, 82.6%); self-report/social desirability (n = 23, 50.0%); instrumentation (n = 20, 43.5%); research design concerns related to the ability to directly measure a variable of interest (e.g., clinical work, training activities; n = 7, 15.2%); experimenter/researcher effects (n = 3, 6.5%); use of less sophisticated statistical methods (n = 3, 6.5%); and use of an analogue design (n = 2, 4.3%). Within identified limitations, researchers most often cited limited generalizability with regard to sample composition (i.e., lack of diversity, small sample sizes, homogenous samples). Social desirability was noted as a potential limitation given the nature of the topics (i.e., racism, prejudice, privilege). Instrumentation issues pertained to weak reliability for samples, limited validity evidence, and disadvantages of self-administration. Researchers also acknowledged the difficulty of conceptualizing WRI constructs as distinct, noting the multidimensional nature of WRI and the challenge in discriminating between complex constructs.
Key Findings
There were three main categories of key findings. The largest category (i.e., 51 codes) consisted of identification of correlates and predictors of Whiteness/White racial identity. Findings related to gender and WRI were mixed, with several articles (n = 7) noting differences in WRI stages among men and women (i.e., women more frequently endorsing Contact and Pseudo-Independent stages, men more frequently endorsing Disintegration and Reintegration), and others determining gender differences were not significant in predicting WRI (n = 2). Additional findings included significant positive correlations and predictive effects between WRI, racism, MCC, personality variables (i.e., Openness linked with higher WRI and Neuroticism linked with lower WRI), and working alliance. Other constructs, such as ego defenses, emotional states, social–cognitive maturity, fear, and religious orientation, also demonstrated significant alignment with WRI stages. White guilt, the impact of personal relationships with communities of color, and lower levels of race salience (i.e., race essentialism) were also linked to Whiteness.
The next largest category (i.e., 32 codes) related to critiques of White racial identity models and measures. Most of the conceptual articles focused in some way on this category, often criticizing WRI models as subjective and lacking in complexity, or critiquing WRI measurement and previous research because of issues of reliability and validity. Several stressed caution for interpreting WRI according to existing models, suggesting a more nuanced approach of contextualizing individuals and accounting for within-group variation. Empirical articles also suggested that achieving and maintaining higher levels of WRI, particularly anti-racist identities and attitudes, may be more difficult than originally conceptualized and may require levels of engagement that are difficult to maintain in a racist society.
Training implications and impact (i.e., 24 codes), noted within empirical and conceptual studies, included tips for addressing Whiteness in counselor education (e.g., offering courses focused on Whiteness and anti-racism) and in supervision (e.g., openly discussing race, privilege, and oppression; matching supervisors and supervisees by racial identity when possible). Empirical studies noted mixed improvement in WRI stages and MCC as a result of both general progression through a counselor training program as well as specific multicultural training: Training was linked to increased White guilt and privilege awareness (n = 15), though others did not find significant effects of training (n = 2). Conceptual articles emphasized focusing training on anti-racist development. Collectively, these findings and subsequent implications encourage further research and reflection on the correlates of WRI and MCC, factors facilitating growth, and ways to improve research and measurement to enhance critical engagement with these topics.
Discussion and Implications
In this content analysis of 63 articles covering a 35-year period across eight national counseling journals, we found that a third of counseling journals featured scholarship specifically related to Whiteness, with the Journal of Counseling & Development and the Journal of Multicultural Counseling and Development accounting for more than 76% of the total sampling units. The majority of the articles were quantitative, followed by theoretical and qualitative articles. Topical focus was centered on correlates of Whiteness with variables such as racism and color-blindness, other non-racial components of cultural identity, training implications, and theory development (see Table 3). Interestingly, many Whiteness constructs discussed in the general literature (e.g., White fragility, modern racism, psychosocial costs) were not addressed in counseling scholarship; the primary constructs discussed were WRI and White privilege.
The sample composition across empirical studies was primarily White and female with a mean age in the late 20s and with undergraduate students comprising on average 22% of the article samples. In addition, practitioners, site supervisors, the general population, and EdS trainees only comprised between 1.6% and 13.1% of the samples. Schooley et al. (2019) cautioned against the overuse of undergraduate students when measuring Whiteness constructs because of the complexities and situational influences of WRI development, and this warning seems to hold relevance for counseling scholarship. Methodological selection mirrored previously found patterns in counseling research (Wester et al., 2013), with most quantitative studies relying upon convenience sampling and correlational design with ANOVA/MANOVA as the selected statistical analyses. In addition, 26.3% of the articles included an intervention. For the qualitative studies, the most frequently used tradition and method was phenomenology and individual interviews.
Overall, findings from the sample support theoretically consistent relationships with Whiteness and/or WRI, including their predictive nature of MCC, social desirability, working alliance, and lower race salience. However, findings were mixed on the role of gender and MCC in connection to a training intervention. Additionally, some studies in our sample critiqued WRI models, cautioning against oversimplification of a complex model and highlighting issues in measurement due to subjectivity and social desirability. This critique aligns with previous researchers who have suggested that WRI is more complex than previously indicated (see Helms, 1984, 1990, 2017). WRI may be highly situational and affected by within-group differences and internal and external factors that complicate accuracy in assessment and clinical application. Of particular concern in previous research is the ability to properly conceptualize and measure the Contact and Autonomy stages (Carter et al., 2004). Both stages have demonstrated difficulty in assessment due to an individual’s lack of awareness of personal racism at each stage (Carter et al., 2004; Rowe, 2006). The Autonomy status, in particular, could be impacted by what DiAngelo (2018) referred to as “progressive” or “liberal” Whiteness, in which efforts are more focused on maintaining a positive self-image than engaging with people of color in meaningful ways (Helms, 2017). Therefore, although there are some consistencies and corroborations within counseling literature and other scholarship on Whiteness, the critiques and complexities of the topic suggest further inquiry is needed.
Implications for Counseling Research
Based on our findings, we note several directions for future research. First, future studies could include greater demographic diversity as well as more participation from counselor educators, site supervisors, practitioners, and clients across the ACES regions. Including counselor educators in empirical studies can highlight aspects of Whiteness that influence their approach to training and scholarship. With regard to increasing scholarship involving site supervisors, practitioners, and clients, Hays et al. (2019) highlighted several strategies for recruiting sites to participate as co-researchers as well as obtaining clinical samples through strengthening research–practice partnerships. Additionally, recruiting more heterogenous samples—in terms of sample composition and demographics—could provide much-needed psychometrics for available measures as well as refined operationalization of Whiteness. Additional research can further explore individual correlates and predictors to enhance counselor training, supervision, and practice by identifying opportunities for assessment and development at each level of WRI.
Second, most reports of empirical studies in our sample noted concerns with sampling and generalizability, social desirability, and instrumentation. Given these concerns, researchers are to be cautious about the interpretation and application of previous study findings using the White Racial Identity Attitudes Scale (WRIAS). In particular, scholarship within counseling and related disciplines reveals substantial psychometric concerns with the WRIAS’s Contact and Autonomy stages (Behrens, 1997; Carter et al., 2004; Hays et al., 2008; Malott et al., 2015). The complex nature of assessing WRI-related behaviors that may run counter to a person’s intentions (Carter et al., 2004; DiAngelo, 2018) needs further study. Additionally, given the concerns with self-report measures due to socially desirable responses, it seems problematic that none of the current quantitative articles used performance measures, which could help to compare self-report with behaviors and client outcomes. Future research can therefore emphasize behavioral assessments and clinical outcomes to correlate findings with WRI models.
Third, the use of intervention-based research could explore core components of instruction, awareness, and experience to identify facilitative strategies for enhancing WRI in both counselor trainees and within client populations. Because White people are negatively impacted by racism and restricted racial identity, encouraging growth in WRI in both clinical and educational settings can be a means of promoting wellness for counselors and clients. Thus, research is needed that can carefully examine the complexities of WRI development and address difficulties in assessment due to defensive strategies such as White fragility and lack of insight into the various intra- and interpersonal manifestations of racism.
Finally, though the research examined within this analysis advances the application of WRI theory and practices within the counseling profession, opportunities exist for further exploration of WRI development and the intersection with multiple constructs of Whiteness discussed across the helping professions (e.g., White fragility, color-blindness, race essentialism). The articles analyzed for the present study reflect an assumption that more advanced WRI attitudes, lower color-blind attitudes, greater anti-racism attitudes, and greater awareness of White privilege can yield more positive clinical outcomes. However, given some of the aforementioned limitations, this assumption has not been empirically tested in counseling. Because clients’ and counselors’ affective, cognitive, and behavioral responses to Whiteness can affect the counseling relationship, process, and treatment selection and outcomes (Helms, 1984, 2017), it is imperative that this assumption is properly tested. Empirical and conceptual work should therefore further explore Whiteness constructs to elucidate how White attitudes and behaviors at each stage function for self-protection and move toward aspirational goals of anti-racism and ethical and competent clinical application.
Implications for Counseling Practice, Training, and Supervision
In addition to future research directions related to Whiteness and WRI, findings allow for recommendations for counseling practice, training, and supervision. For example, extant literature emphasizes the importance of racial self-awareness, including an understanding of White privilege and racism. The practice of centering discussions on the harmful impacts of Whiteness, as well as the various ways Whiteness can manifest in therapeutic spaces, allows counselors to examine racial development within and around themselves. White counselors who are able to reflect on their own racial privileges and begin the conversation (i.e., broaching) about racial differences can increase the working alliance quality with clients of color (Burkard et al., 1999; Day-Vines et al., 2007; Helms, 1990).
Furthermore, counselors should heed the themes within the key findings of our sample, following recommendations for taking a broad, contextual, and critical view when understanding and applying WRI models. Counselors can be encouraged to view WRI as Helms (2019) intended—as a broad and complex interplay of relational dynamics, connected with other Whiteness constructs, and following an intentional progression toward anti-racism and social justice. Counselors should take particular caution with viewing the Autonomy stage as a point of arrival, given conflicting findings and the possibility that White people in higher stages may engage in behaviors to assuage guilt rather than to be true allies for people of color. The Helms model associates such attitudes and actions with the Pseudo-Independence stage (Helms, 2019), yet findings cast some doubt as to whether White people who score within the Autonomy stage have actually reached that level of WRI development. Counselors should thus interpret assessment scores with caution and ensure they are also assessing their own level of development and subsequent impact on others through continued and honest reflection and positive engagement in cross-racial relationships.
Regarding training, course content focusing on exploring Whiteness, WRI, and other racial identities through use of an anti-racism training model integrated throughout the curriculum can help students become comfortable with potential cross-racial conflicts and broaching Whiteness (Malott et al., 2015). The Council for Accreditation of Counseling and Related Educational Programs (CACREP) can similarly stress these desired student outcomes when updating standards for counselor training, specifically mentioning the importance of WRI as part of multicultural preparation. It is imperative to begin conversations about race and identity development to create opportunities for growth for any student who may be challenged with their racial identity and how it might impact their clients. Furthermore, counselor educators and supervisors can ask counselors in training to brainstorm how counseling and other services might be developed or adapted in order to contribute toward anti-racist goals and outcomes.
Limitations
The current findings are to be interpreted with caution, as the scope of our study presents some limitations. First, we chose to limit inclusion criteria to national peer-reviewed counseling journals in order to focus on scholarship within professional counseling journals, and therefore our results cannot be generalized to similar disciplines, dissertation research, book chapters, or more localized outlets such as state journals. Our coding sheet was also limited in the information it collected, including sample demographics. Though not all studies included the same demographic variables, we did not capture specifics related to a sample’s political affiliation, religious orientation, ability status, socioeconomic status, diversity exposure, or other details that could have better conceptualized the samples and findings. Additionally, we limited our search to the keywords related to Whiteness that we had identified in related literature but may have missed studies employing constructs outside of our search criteria. Our own identities as White academics may also have influenced the coding process as well as the subsequent interpretation of findings.
Conclusion
This content analysis provides a snapshot of Whiteness scholarship conducted in the counseling profession during a 35-year period. Patterns of study design and analysis were noted, and key findings were summarized to provide context and comparison within the broader literature. Identified themes and relationships highlight theoretically consistent findings for some Whiteness constructs, as well as showcase research gaps that need to be addressed before counselors can apply findings to practice and training. Finally, this content analysis demonstrates the need for a greater understanding of Whiteness and related constructs in counselor education, training, and practice.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
Behrens, J. T. (1997). Does the White Racial Identity Attitude Scale measure racial identity? Journal of Counseling Psychology, 44(1), 3–12. https://doi.org/10.1037/0022-0167.44.1.3
Burkard, A. W., Ponterotto, J. G., Reynolds, A. L., & Alfonso, V. C. (1999). White counselor trainees’ racial identity and working alliance perceptions. Journal of Counseling & Development, 77(3), 324–329. https://doi.org/10.1002/j.1556-6676.1999.tb02455.x
Carter, R. T., Helms, J. E., & Juby, H. L. (2004). The relationship between racism and racial identity for White Americans: A profile analysis. Journal of Multicultural Counseling and Development, 32(1), 2–17. https://doi.org/10.1002/j.2161-1912.2004.tb00357.x
Choney, S. K., & Behrens, J. T. (1996). Development of the Oklahoma Racial Attitudes Scale Preliminary Form (ORAS-P). Multicultural Assessment in Counseling and Clinical Psychology. https://digitalcommons.unl.edu/burosbookmulticultural/10
Claney, D., & Parker, W. M. (1989). Assessing White racial consciousness and perceived comfort with Black individuals: A preliminary study. Journal of Counseling & Development, 67(8), 449–451. https://doi.org/10.1002/j.1556-6676.1989.tb02114.x
Day-Vines, N. L., Wood, S. M., Grothaus, T., Craigen, L., Holman, A., Dotson-Blake, K., & Douglass, M. J. (2007). Broaching the subjects of race, ethnicity, and culture during the counseling process. Journal of Counseling & Development, 85(4), 401–409. https://doi.org/10.1002/j.1556-6678.2007.tb00608.x
DiAngelo, R. (2018). White fragility: Why it’s so hard for White people to talk about racism. Beacon Press.
Frankenberg, R. (1993). White women, race matters: The social construction of Whiteness. University of Minnesota Press.
Hays, D. G., Bolin, T., & Chen, C.-C. (2019). Closing the gap: Fostering successful research-practice partnerships in counselor education. Counselor Education and Supervision, 58(4), 278–292. https://doi.org/10.1002/ceas.12157
Hays, D. G., Chang, C. Y., & Havice, P. (2008). White racial identity statuses as predictors of White privilege awareness. The Journal of Humanistic Counseling, Education and Development, 47(2), 234–246. https://doi.org/10.1002/j.2161-1939.2008.tb00060.x
Helms, J. E. (1984). Toward a theoretical explanation of the effects of race on counseling: A Black and White model. The Counseling Psychologist, 12(4), 153–165. https://doi.org/10.1177/0011000084124013
Helms, J. E. (Ed.) (1990). Black and White racial identity: Theory, research, and practice. Praeger.
Helms, J. E. (1995). An update of Helms’ White and people of color racial identity models. In J. G. Ponterotto, J. M. Casas, L. A. Suzuki, & C. M. Alexander (Eds.), Handbook of multicultural counseling (1st ed.; pp. 181–196). SAGE.
Helms, J. E. (2017). The challenge of making Whiteness visible: Reactions to four Whiteness articles. The Counseling Psychologist, 45(5), 717–726. https://doi.org/10.1177/0011000017718943
Helms, J. E. (2019). A race is a nice thing to have: A guide to being a White person or understanding the White persons in your life (3rd ed.). Cognella.
Helms, J. E., & Carter, R. T. (1990). Development of the White Racial Identity Inventory. In J. E. Helms (Ed.), Black and White racial identity: Theory, research, and practice (pp. 67–80). Greenwood Press.
Henry, P. J., & Sears, D. O. (2002). The Symbolic Racism 2000 Scale. Political Psychology, 23(2), 253–283. https://doi.org/10.1111/0162-895X.00281
LoMartire, R. (2020). Rel: Reliability coefficients. R package version. 1.4.1. https://cran.r-project.org
Malott, K. M., Paone, T. R., Schaefle, S., Cates, J., & Haizlip, B. (2015). Expanding White racial identity theory: A qualitative investigation of Whites engaged in antiracist action. Journal of Counseling & Development, 93(3), 333–343. https://doi.org/10.1002/jcad.12031
McConahay, J. B. (1986). Modern racism, ambivalence, and the Modern Racism Scale. In J. F. Dovidio & S. L. Gaertner (Eds.), Prejudice, discrimination, and racism (pp. 91–125). Academic Press.
McIntosh, P. (1988). White privilege and male privilege: A personal account of coming to see correspondences through work in women’s studies (Wellesley College, Center for Research on Women Working Paper, No. 189). Wellesley College. https://www.wcwonline.org/images/pdf/White_Privilege_and_Male_Privilege_Personal_Account-Peggy_McIntosh.pdf
Neuendorf, K. A. (2017). The content analysis guidebook (2nd ed.). SAGE.
Neville, H. A., Awad, G. H., Brooks, J. E., Flores, M. P., & Bleumel, J. (2013). Color-blind racial ideology: Theory, training, and measurement implications in psychology. American Psychologist, 68(6), 455–466. https://doi.org/10.1037/a0033282
Rowe, W. (2006). White racial identity: Science, faith, and pseudoscience. Journal of Multicultural Counseling & Development, 34(4), 235–243. https://doi.org/10.1002/j.2161-1912.2006.tb00042.x
Schooley, R. C., Debbiesiu, L. L., & Spanierman, L. B. (2019). Measuring Whiteness: A systematic review of instruments and call to action. The Counseling Psychologist, 47(4), 530–565. https://doi.org/10.1177/0011000019883261
Singh, A. A., & Shelton, K. (2011). A content analysis of LGBTQ qualitative research in counseling: A ten-year review. Journal of Counseling & Development, 89(2), 217–226. https://doi.org/10.1002/j.1556-6678.2011.tb00080.x
Spanierman, L. B., & Heppner, M. J. (2004). Psychosocial Costs of Racism to Whites Scale (PCRW): Construction and initial validation. Journal of Counseling Psychology, 51(2), 249–262. https://doi.org/10.1037/0022-0167.51.2.249
Tawa, J. (2017). The Beliefs About Race Scale (BARS): Dimensions of racial essentialism and their psychometric properties. Cultural Diversity and Ethnic Minority Psychology, 23(4), 516–526. https://doi.org/10.1037/cdp0000151
U.S. Census Bureau. (2020). Public Use Microdata Sample data. https://www.census.gov/programs-surveys/acs/data/pums.html
Wester, K. L., Borders, L. D., Boul, S., & Horton, E. (2013). Research quality: Critique of quantitative articles in the Journal of Counseling & Development. Journal of Counseling & Development, 91(3), 280–290. https://doi.org/10.1002/j.1556-6676.2013.00096.x
The authors would like to thank Cheolwoo Park for his invaluable assistance in this study. Hannah B. Bayne, PhD, LMHC (FL), LPC (VA), is an assistant professor at the University of Florida. Danica G. Hays, PhD, is a dean and professor at the University of Nevada Las Vegas. Luke Harness is a doctoral student at the University of Florida. Brianna Kane is a doctoral student at the University of Florida. Harness and Kane contributed equally to the project and share third authorship. Correspondence may be addressed to Hannah B. Bayne, 140 Norman Hall, Gainesville, FL 32611, hbayne@coe.ufl.edu.
