May 22, 2024 | Volume 14 - Issue 1
Ashley Ascherl Pechek, Kristin A. Vincenzes, Kellie Forziat-Pytel, Stephen Nowakowski, Leandrea Romero-Lucero
In counselor education programs, students acquire clinical experience through both practicum and internship; this time frequently marks students’ first counseling experiences working with suicide in a clinical context. Often, students in practicum or internship working with clients who may be experiencing suicidal ideations do not feel properly equipped to deal with suicide. This study aimed to develop a practice model for online counselor education programs that increases counseling students’ self-efficacy to work with clients who may present with suicidal ideations. Sixty online graduate-level clinical mental health counseling students completed a pre- and posttest self-efficacy assessment. Findings showed that students’ self-efficacy increased due to taking the online basic counseling skills class that included teaching activities related to suicide screening, assessment, and intervention.
Keywords: self-efficacy, suicide, assessment and intervention, online counselor education, practice model
Despite a growing body of research and evidence-based interventions, suicide remains the 11th leading cause of death in the United States (Centers for Disease Control and Prevention [CDC], 2021). A 2014 World Health Organization report (WHO; 2014) estimated that more lives were lost to suicide than to war, conflict, and natural disasters combined. More recently, the American Foundation for Suicide Prevention (AFSP; 2023) estimated that in 2021 there were 1.7 million suicide attempts; more than 48,000 Americans died by suicide. In 2023, trends showed about 130 suicides per day (AFSP, 2023).
To address the ongoing concern of suicide risk, counselor education programs are expected to prepare students for work with diverse clients who experience suicidal ideations (Wachter Morris & Barrio Minton, 2012). Specifically, the Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2023) requires counseling programs to provide counselors-in-training (CITs) with skills in crisis intervention, suicide prevention, and response models and strategies, as well as proper assessment and management of suicidal ideations. There are no consistent suicide prevention or intervention training standards or models among counselor education programs. Organizations such as the American Association of Suicidology have recommended that suicide knowledge and assessment be at the forefront of health care by having (a) graduate programs require suicide knowledge and skills acquisition in their curriculum, (b) state licensure boards require suicide-specific education for renewal of licenses, (c) government-funded health care systems and hospitals require staff training in suicide assessment and management, and (d) staff appropriately trained to assess, manage, or treat patients who experience suicidal thoughts (Schmitz et al., 2012).
The current study aimed to determine if a practice model used in an online basic counseling skills course was effective at increasing counseling students’ self-efficacy when working with clients who present with suicidal ideations. Results from the study were used to determine if the skills-based online course effectively taught suicide assessment and intervention skills to graduate students. Discussion and implications regarding the need to establish best practices in prevention and intervention training for CITs are included. Additional considerations are given for both online and brick-and-mortar counseling programs.
Competencies and Principles
To assist counselor educators with how to best address the ongoing concern of suicide risk in clients, the Suicide Prevention Resource Center (2006) identified several core competencies and skills needed to assess and manage individuals at risk for suicide. These competencies can be used as a framework for extensive suicide training (Granello, 2010). Other models, such as a core competency–based training workshop in suicide screening, assessment, and management, have been developed to assess the effectiveness of suicide training, including pre- and post-workshop self-assessments, evidence-based instruction, role-playing, expert demonstration, group discussions, and video-recorded risk assessments of trainees intended to provide feedback (Cramer et al., 2017). Together, these competencies and principles can be used to develop a practice model in graduate counselor education programs and to better assist CITs in preparing to work with a client experiencing suicidal thoughts.
Despite the Suicide Prevention Resource Center (2006) identifying core competencies and skills needed to properly assess and manage individuals for risk of suicide, the research from counseling graduate programs on the implementation of suicide training remains sparse (Wasylko & Stickley, 2007). Therefore, we looked at other graduate programs of similar disciplines (e.g., social work, school psychology, and school counseling) to gain a better idea of best practices in related fields. Unfortunately, literature related to best practices within graduate programs of similar disciplines also demonstrates a lack of training in suicide risk assessment and intervention (Becnel et al., 2021; LeCloux, 2021; Liebling-Boccio & Jennings, 2013). This expanded look into other mental health professions further supports the notion that limited research exists regarding training in suicide screening, assessment, and intervention at the graduate level; thus, more attention is needed in these areas.
Suicide Training in Graduate Programs
Graduates of other counseling programs have indicated that there were limitations in the suicide prevention training that they received (Wakai et al., 2020). In a national sample of American School Counselor Association members, Becnel et al. (2021) found that 38% of school counselors (N = 226) did not receive suicide prevention training during their graduate programs and 37% received no training in crisis intervention. Similar results were found in a study of 193 professional counselors; over a third reported no classroom training in crisis preparation, and 30% reported no or minimal preparation in suicide assessment (Wachter Morris & Barrio Minton, 2012).
Schmidt (2016) evaluated the confidence and preparedness of 339 mental health practitioners (i.e., professional counselors, school counselors, social workers, psychologists). Results indicated that 52% of participants had graduate course work in suicide intervention and assessment, but 19% reported feeling not very confident in working with clients who had suicidal ideations. Conversely, Binkley and Leibert (2015) found that students who received training before their practicum working with clients who experience suicidal thoughts had lower anxiety and a greater level of confidence in addressing those issues compared to those who did not receive training.
The results of these studies look at counselor training and confidence or preparedness, to support the need for additional training in this area and research on best practices in preparing CITs to work with clients who present with suicidal ideation. Studies report training levels associated with practice outcomes (e.g., confidence), but there is a lack of literature explaining how suicide assessment and intervention training occurs in counselor education programs. Although there is literature that demonstrates that self-efficacy directly influences a counselor’s development (Barbee et al., 2003; Barnes, 2004; Kozina et al., 2010; Lent et al., 2003; Pechek, 2018; Vincenzes et al., 2023), literature that specifically addresses self-efficacy as it relates to working with a client who experiences suicidal ideation is sparse. However, the literature supports that additional training is needed on this topic and that self-efficacy is an important concept to consider when developing training protocols for CITs.
Self-Efficacy
Self-efficacy is dynamic and plays a significant role in counselor training and skill development. Bandura (1986) first introduced self-efficacy as an individual’s judgment on their capabilities to execute an action to achieve a certain performance or goal. Later the term was linked to behavioral motivation in the academic setting and was defined as a student’s belief in their ability to accomplish and succeed on an academic-related task (Bandura, 1989). Bandura (1997) also found that self-efficacy beliefs can be altered through four primary sources: (a) personal performance accomplishments, (b) vicarious learning, (c) social persuasion, and (d) physiological and affective states. While self-efficacy is dynamic (Lent, 2020) and can be impacted by personal interpretation of these primary sources (Lent & Brown, 2006), research has found that self-efficacy is an important factor in counselor competency (Barbee et al., 2003; Barnes, 2004; Kozina et al., 2010; Pechek, 2018; Vincenzes et al., 2023). More specifically, Lent et al. (2003) found that CITs’ initial clinical work and experience with more difficult skills (e.g., managing a session, handling the role of the counselor) increased counselor self-efficacy (Kozina et al., 2010).
Self-Efficacy in Suicide Training
Counselors who lack self-efficacy in their ability to work with a client who is experiencing suicidal thoughts may conduct suicide screening, assessments, and interventions ineffectively (Douglas & Wachter Morris, 2015; Jahn et al., 2016). In addition, counselors with low self-efficacy are more likely to subconsciously choose not to see suicide warning signs (Douglas & Wachter Morris, 2015) or avoid the topic of suicide altogether (Jahn et al., 2016). It is important that CITs are exposed to the topic of suicide and that they gain more counseling experience involving this issue during their training so that they will feel more confident working with a client experiencing suicidal thoughts. More exposure to this topic leaves CITs feeling better equipped to address suicide in sessions and is also likely to increase their self-efficacy (Elliott & Henninger, 2020; Pechek, 2018; Sawyer et al., 2013; Shea & Barney, 2015).
Clear evidence of the positive effects of including training on suicide within counselor education programs has been documented, demonstrating a reduction of fear and more success in helping clients manage suicide-related issues (Jahn et al., 2016). CITs who had prior training in suicide experienced lower levels of anxiety and higher levels of confidence in working with a client with suicidal thoughts (Binkley & Leibert, 2015). Similarly, professional counselors who expressed confidence in their academic training on suicide experienced lower levels of fear related to negative client outcomes and had higher levels of confidence in their skills and abilities (Jahn et al., 2016).
Self-Efficacy in Suicide Training for Online Learning. Although the topic of self-efficacy in counselor education has been studied (Barbee et al., 2003; Barnes, 2004; Conteh et al., 2018; Fakhro et al., 2023; Kozina et al., 2010; Pechek, 2018; Suh et al., 2018; Vincenzes et al., 2023), the literature does not focus on how best to teach for improved self-efficacy related to suicide assessment and intervention in the online setting. Specifically, it is not clear how counselor educators can best teach suicide screening, assessment, or intervention skills online. Two recent studies in counselor education programs have tried to better explain self-efficacy in suicide training during online learning (Elliott & Henninger, 2020; Gallo et al., 2019).
Elliott and Henninger (2020) showed that different online teaching strategies (e.g., a combination of a written module, role-plays/observations, and a facilitated discussion) in an online counselor education program showed no between-group differences, while all teaching strategies showed significant improvements in self-efficacy of CITs. Another study found that a 15-hour youth suicide prevention course that included didactic and experiential activities in a master’s counseling program increased participants’ knowledge and perceived ability to help clients who experienced suicidal ideations, as well as increased their self-efficacy in screening, assessment, and intervention (Gallo et al., 2019).
Purpose of the Study
With the influx of online counselor education programs, it is essential to determine how to improve suicide training and intervention skills (Allen & Seaman, 2014) so that CITs are better prepared to address the topic of suicide. The current quantitative study examined the influence of an online counseling practice model on CITs’ self-efficacy when it came to the utilization of suicide assessment and intervention with clients. The research question was: Do CITs’ perceived levels of self-efficacy in suicide assessment and intervention change because of practicing these skills through role-plays in an online counseling course? By better understanding these findings, implications can be made for how counselor educators can teach suicide screening, assessment, and intervention skills online.
Method
Procedures
Prior to beginning this study, our research team received full approval from the IRB. Participants were then recruited from an online clinical mental health counseling program. Only students enrolled in the online basic counseling skills course were recruited to ensure that all participants were at the same place in the program regarding knowledge and skills learned. An electronic announcement was posted in the 10 online basic skill course shells. The announcement included a hyperlink directing participants to an informed consent document, which detailed their requirements and rights and allowed them to indicate their consent to participate. Before completing any survey questions, the participants created a username for data comparison in the pre- and posttests, which was also an avenue for dropping participants if they requested to leave the study. After providing their username, participants completed a brief demographic questionnaire and the Counselor Suicide Assessment Efficacy Survey (CSAES; Douglas & Wachter Morris, 2015). To protect participant anonymity, no additional identifying information was collected.
Structure of the Basic Skills Class
Once students completed the pretest consent form, demographic questionnaire, and assessment, the counselor educators (i.e., faculty) started the class by providing participants with a variety of technology-assisted counseling experiences and activities (e.g., role-play demonstrations, best practices in telemental health counseling, lecture videos on specific counseling skills, guidelines for a preferred topic for the role-plays). To ensure consistency of content across courses, the faculty made sure to include the same teaching resources in each section of the class and continuously consulted each other to make sure that the classes were taught as similarly as possible. In addition, they decided that all students should receive the same training and teaching activities, ensuring that they were equally prepared to address the topic of suicide during their clinical courses and after graduation.
The topic of self-care was addressed with participants, as this was the first opportunity students had to practice counseling skills within the program. This focus on self-care was an important step toward decreasing the potential of significant deep-rooted issues surfacing without sufficient time or training to properly address them. Students would learn about a new basic counseling skill each week and were instructed to incorporate that skill into the week’s role-play. In addition to reading about the skill in the course textbook, students were required to view weekly lecture videos and role-plays that specifically explained and demonstrated the skill that the students would be practicing that week during their role-play. For role-plays, participants were randomly paired with other participants within the same basic counseling skills course to practice basic foundational counseling skills. Each pair of students participated in five weekly role-plays as both the counselor and the client. Two of these role-plays occurred during class and three occurred outside of class. Each role-play occurred via Zoom and lasted approximately 10–15 minutes during class or 30 minutes when completed outside of class. For in-class role-plays, participants utilized breakout rooms in Zoom. Faculty provided each participant in the counselor role with feedback at the end of each role-play. Role-plays outside of the class required participants to send their partner a Zoom link and password. The role-plays were recorded in Zoom. Participants identified one role-play to submit to the instructor for formal assessment of their basic counseling skills and to provide formative feedback to each participant when acting in the counselor role.
Preparation for Suicidal Ideation Role-Plays
After the initial five role-plays were completed, participants prepared for role-plays that focused on crisis counseling. They read a chapter from their textbook on crisis counseling and various supplemental articles on working with a client with suicidal ideations. In addition, they viewed pre-recorded role-plays on suicide assessment created by faculty in the program. Participants remained in the same randomly assigned pairs from earlier in the semester and then completed an additional five role-plays (one weekly), which allowed for them to gain experience working with a client with suicidal ideations.
Suicidal Ideation Role-Plays
Prior to beginning the role-plays, participants were provided with a brief synopsis for the topic of suicide and were also given the instructor’s phone number in case they needed immediate support or guidance. Like the previous role-plays, each of these lasted approximately 10–15 minutes during online classes or 30 minutes outside of class. Again, role-plays completed outside of class were recorded so that faculty could provide detailed feedback to students. The first in-class role-play was completed in a fishbowl format, allowing students in the class to observe. Instead of utilizing multiple breakout rooms, students remained in one room and observed one role-play at a time. This allowed students to learn vicariously from one another and to observe the ways that suicide screening, assessment, and intervention skills were demonstrated. The initial role-play also served as a way for participants in the counselor role to gain experience completing a suicide assessment while practicing other basic counseling skills. Four additional role-plays occurred and offered an opportunity for participants to continually reassess the risk of suicide of their partners, develop a safety plan, establish treatment goals, and practice other basic counseling skills. During the last role-play, participants in the counselor role conducted a termination session in which the counselor reviewed the client’s safety and treatment plans. Additionally, they reviewed the client’s goals and objectives and provided time for the client to reflect on the counseling experience.
Faculty Supervision and Learning Activities
During the semester, faculty supervision was an essential component of the process. If additional support or guidance was needed for participants, faculty were available via phone between 8 am–8 pm, Monday through Friday. Faculty were available to all role-play participants regardless of their role (i.e., counselor, client, or observer). While supervision can look different for each instructor, the counselor educators in this study regularly consulted with one another to ensure that they were conveying the same expectations to the students enrolled in the courses. This extended to making sure they discussed similar topics at the same time during the course; included the same teaching activities, readings, and assignments; and consulted with one another when a concern arose that may have changed course plans.
In addition to completing the virtual role-plays during the semester, participants completed a variety of activities and assignments that were intended to prepare them for realistic experiences needed upon graduation. For example, participants completed components of a treatment plan after each counseling session which were submitted to the instructor immediately following the role-play. Additionally, they submitted video tapes of role-plays for faculty feedback. Finally, participants transcribed one 30-minute role-play. This assignment allowed them to identify and reflect on specific foundational skills that they used when working with a client reporting suicidal ideations. At the conclusion of the semester, participants were asked to complete the posttest using the same username they created at the beginning of the semester. The posttest included the same assessment as the pretest (CSAES).
Participants
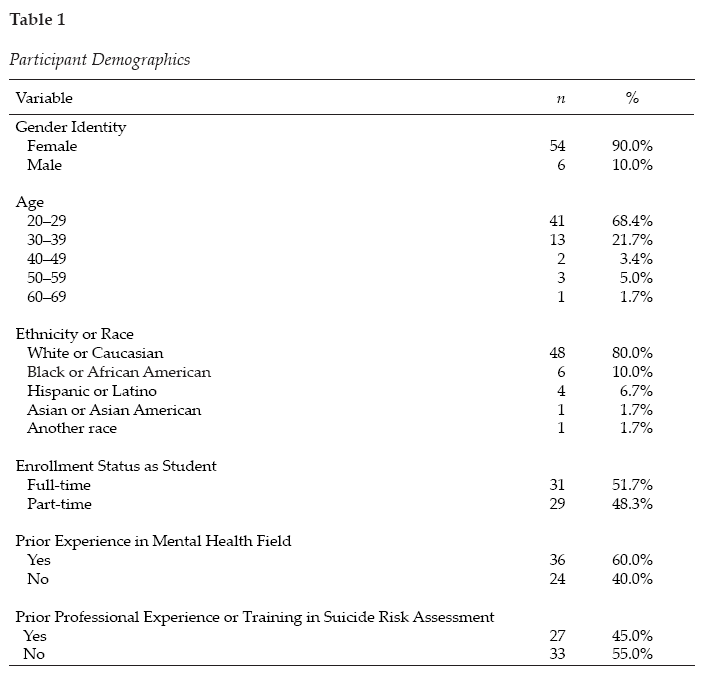
A convenience sample was used for this study. Master’s-level counseling students enrolled in the spring 2021 and spring 2022 counseling skills courses (10 sections total) in an online clinical mental health counseling graduate program were recruited via news announcements and emails to participate in this study. A total of 120 students were invited to participate in the study; however, only 60 were included because they completed both the pretest and posttest self-efficacy assessment. Included students’ ages ranged from 21–61 years old. The average age of participants was 29.03 (SD = 8.49). The sample consisted of the following racial identities: 80.0% White or Caucasian (n = 48), 10.0% Black or African American (n = 6), 6.7% Hispanic or Latino (n = 4), 1.7% Asian or Asian American (n = 1), and 1.7% did not indicate their racial identities (n = 1). Most participants identified as female (90%, n = 54) and were enrolled in the mental health counseling program full-time (51.7%, n = 31). When asked about prior experience in the mental health field, 60% (n = 36) had this experience; however, only 45% (n = 27) had prior professional experience or training in suicide risk assessment. Table 1 contains all participant demographics.
Measure
The study participants completed the CSAES (Douglas & Wachter Morris, 2015). The CSAES measures self-efficacy in suicide assessment and intervention. According to the developers (Douglas & Wachter Morris, 2015), the CSAES is comprised of 25 items that may make suicide assessment or intervention difficult for a counselor. These items are rated on a confidence scale that ranges from 1 (not confident) to 5 (highly confident). The confidence items are organized into four subscales:
- General Suicide Assessment, which has seven items and a maximum score of 35
- Assessment of Personal Characteristics, which has 10 items and a maximum score of 50
- Assessment of Suicide History, which has three items and a maximum score of 15
- Suicide Intervention, which has five items and a maximum score of 25
Sample items include the following: Q1 “I can effectively inquire if a student has had thoughts of killing oneself” (General Suicide Assessment); Q11 “I can effectively ask a student about his or her history of mental illness” (Assessment of Personal Characteristics); Q18 “I can effectively ask a student about his or her previous suicide attempts” (Assessment of Suicide History); and Q25 “I can appropriately intervene if a student is at imminent risk for suicide” (Suicide Intervention).
Table 1
Participant Demographics
The total score for the scale is 125, with higher scores representing higher levels of self-efficacy associated with suicide assessment and intervention (Douglas & Wachter Morris, 2015). The CSAES can be scored two ways. First, the assessment can be scored individually for a more detailed understanding of what differences, if any, in self-efficacy exist between differing aspects of suicide assessment. The second way is to calculate the total sum of the assessment-related subscales and the intervention subscale. In doing so, each subscale would have a mean for the individual scale (Douglas & Wachter Morris, 2015).
The assessment developers have reported internal reliability for the CSAES as a calculation for each of the four subscales and the second-order factor of Suicide Assessment using Cronbach’s α: General Suicide Assessment α = .882, Assessment of Personal Characteristics α = .88, Assessment of Suicide History α = .81, Suicide Intervention α = .83, and Suicide Assessment α = .93 (Douglas & Wachter Morris, 2015).
The CSAES was noted for showing “structural aspects of validity and sensitivity to detect differing levels of self-efficacy” (Douglas & Wachter Morris, 2015) based on the utilization of a four-factor model that was cross-validated. The scale was validated with a total of 324 participants. Of the participants, 258 (79.63%) were female. Unfortunately, a limitation of the instrument is that the diversity of participants was unknown due to ethnicity inadvertently being left off the demographic questionnaire while it was being developed (Douglas & Wachter Morris, 2015).
The current study assessed the internal reliability of the CSAES using Cronbach’s α and omega (ω) using test-retest reliability because the measure of consistency was between two measurements of the same construct to the same group at two different times. The overall CSAES has strong reliability (α = .978; ω = .978), and each subscale had the following reliability scores: General Suicide Assessment (α = .943; ω = .946); Assessment of Personal Characteristics (α = .947; ω = .947); Assessment of Suicide History (α = .896; ω = .890); and Suicide Intervention (α = .920; ω = .915). All subscale reliability coefficients were high when looking at both α and ω, meaning that good internal consistency was found among items of the scale (Green & Salkind, 2014).
Data Analysis
Before running any analyses, we screened the data using SPSS version 26.0.0.1 software to check for (a) missing data, (b) average expected scores per the outcome variables, (c) standard deviations within range, and (d) normality of data (Green & Salkind, 2014). The initial sample included 108 surveys; however, only 60 of these could be paired with posttest data, using the username data point. Therefore, individuals with their missing pair were deleted along with any others that included missing data (i.e., listwise deletion). The final sample included 60 respondents. A power analysis using a statistical power analysis program (G*Power 3.1) for paired t-test showed an N of 54 was needed for 95% power with an alpha level of .05 and a moderate effect size of .5. Next, scales were computed, and univariate testing occurred. Data met all assumptions for conducting a paired t-test (i.e., dependent variable was continuous, normally distributed, and without outliers and the observations were independent of one another). The paired t-test was used to test the effectiveness of training for suicide assessment and intervention in a basic skills class using a single-group (pretest/posttest) design, including demographics and the CSAES. To ensure that all students received the same teaching activities and assignments, we decided not to utilize a control group. We wanted to ensure that all students were equally prepared and trained to address the topic of suicide upon entering their clinical courses and upon graduation.
Results
The purpose of the study was to compare counseling students’ pretest and posttest self-efficacy assessments when taking a basic skills course that highly emphasized skills related to suicide training and assessment. The results of a paired-samples t-test on the General Suicide Assessment subscale indicate that on average, students scored significantly higher (Mpost = 28.57, SD = 4.80) after taking the basic skills class (Mpre = 21.20, SD = 7.80), t(59) = −9.15, p < .001. A large effect was found (d = 1.182, 95% CI [−1.51, −.85]). The results of a paired-samples t-test on the Assessment of Personal Characteristics subscale indicate that on average, students scored significantly higher (Mpost = 41.17, SD = 6.59) after taking the basic skills class (Mpre = 33.80, SD = 8.75), t(59) = −8.77, p < .001. A large effect was found (d = 1.133, 95% CI [−1.46, −.81]). The results of a paired-samples t-test on the Suicide History Assessment subscale indicate that on average, students scored significantly higher (Mpost = 13.07, SD = 2.22) after taking the basic skills class (Mpre = 9.95, SD = 3.33), t(59) = −8.38, p < .001. A large effect was found (d = 1.081, 95% CI [−1.40, −.76]). The results of a paired-samples t-test on the Suicide Intervention subscale indicate that on average, students scored significantly higher (Mpost = 19.00, SD = 4.32) after taking the basic skills class (Mpre = 14.63, SD = 5.46), t(59) = −7.21, p < .001. A large effect was found (d = .931, 95% CI [−1.23, −.63]). In summary, students’ level of self-efficacy related to suicide assessment and intervention increased in all areas as a result of taking the basic counseling skills class.
Because this study had a small sample size, the risk increases that at least one test is statistically significant just by chance. Therefore, a Bonferroni correction was applied to adjust the significance levels: Bonferroni correction = .05/4 = .0125 (.05 = acceptable significance level; 4 = number of subscales of CSAES). Therefore, the familywise error value is .0125. Because the above results are looking at significance at the p <.001 value, all results remain significant.
Discussion
The initial research question was: Do CITs’ perceived levels of self-efficacy in suicide assessment and intervention change because of practicing these skills through role-plays in an online counseling course? According to the results of the current study, on average, students felt significantly more prepared and confident in their ability to counsel someone experiencing suicidal ideations after practicing the skills in their basic counseling skills online course. Prior research indicated that many students were either not taught these skills (Becnel et al., 2021) or did not feel prepared to address these issues in counseling (Schmidt, 2016). The current study points to the vitality of both teaching students about suicide screening and assessment, as well as providing them with a safe space to practice the skills. By offering students opportunities to practice suicide screening, assessment, and intervention skills, instructors could help reduce their students’ anxiety in addressing the topic during their clinical courses, which Binkley and Leibert (2015) found to be a significant student concern.
Furthermore, it is important for counselor educators to observe and provide students with feedback regarding these essential skills. Past research points to the concern that students are not adequately conducting suicide screening, assessments, and interventions (Jahn et al., 2016); therefore, it would behoove counselor educators to infuse various opportunities throughout the curriculum to strengthen these skills. In turn, feedback and practice opportunities combined may help to enhance students’ levels of self-efficacy (Elliott & Henninger, 2020; Gallo et al., 2019), thus helping them to address the issues with clients in a timely and direct manner.
Implications for Training
While CACREP (2023) requires counselor educators to prepare students to work with clients who present with suicidal ideations, there is no clear criteria as to the best way of preparing students to work with these clients. Research on the topic is limited; however, the results of this study can provide a framework for helping to inform key training areas in counselor education and future research.
As counselor educators continue to expand on the didactic knowledge of suicide screening, assessment, and intervention, more intentional efforts need to be embedded throughout the curriculum to continuously expose students to experiential opportunities for practicing these skills. This idea coincides with the recommendation from the American Association of Suicidology that proposes suicide knowledge and assessment be at the forefront of graduate program curricula (Schmitz et al., 2012). First, in foundational courses, students could become more comfortable with the topic of suicide. These courses could help break down barriers and possibly calm nerves that tend to surround the topic of suicide. In assessment courses, students could role-play giving a partner various suicide screenings and assessments and gain experience interpreting the results. These role-plays could occur during class or be recorded for faculty feedback. In skills courses, students could practice suicide intervention by broaching the topic with their classmate-clients to help them feel more comfortable with directly asking clients if they are experiencing suicidal ideations. In addition, it may be helpful if a trauma and crisis counseling course was required within the core curriculum. This course could have content devoted to suicide screening, assessment, and intervention, including both didactic and experiential opportunities. By offering these opportunities throughout the curriculum, similar to ethical and cultural considerations, students may feel more comfortable and confident as they enter their clinicals (Binkley & Leibert, 2015; Guillot Miller et al., 2013). This intentional, consistent exposure to practicing these skills could help more students gain foundational knowledge and experience with this topic. In turn, as their self-efficacy and comfort levels increase, they may be more confident addressing this topic with clients. Ultimately, this may increase client welfare by ensuring effective assessment and treatment of client needs.
Implications for Counselor Education Training Research
The topic of suicide screening, assessment, and intervention in counselor education and supervision could benefit significantly from continued outcome-based research. For example, longitudinal studies could track students’ perceived levels of self-efficacy on suicide screening, assessment, and intervention as they go through a counseling program. This may help educators become more intentional about when and how the topic is infused within the curriculum. In addition, research could compare different types of teaching methods (e.g., role-play versus lecture) that expose students to the topic and assess which methods are more influential in building students’ skills and self-efficacy. Finally, researchers could interview current mental health therapists to identify knowledge and skill gaps to help educators teach students about crisis counseling more intentionally.
Limitations
There are a few limitations to the current study that are important to discuss. First is the variability in teaching and supervision styles across different instructors, which may impact the students’ overall feelings of self-efficacy. Although the same procedures were followed, educators inevitably have different styles of giving feedback. How the feedback is perceived by the student may impact their confidence in using the acquired skills.
Another limitation involves the notion of social desirability bias. The participants in the current study were students in the program; therefore, they may have felt pressured to identify increases in their self-efficacy around suicide assessment and intervention. This pressure may have been experienced because some of their current professors also served as researchers in the study and the students may have wanted to gain favor with them.
With regard to external validity, there are a few limitations. First, our research team did not account for prior experience in suicide screening, assessment, or intervention; thus, the results could have been impacted by external experiences versus the sole experience of the course activities. Additionally, there was a large portion of the data that could not be used because the pre- and post- surveys could not be aligned. Although the current study had 60 viable pre- and post- surveys, the data could have been more reliable and generalizable with a larger dataset. Furthermore, there was a lack of diversity in the research sample. Because the participants were primarily White females, the results may be limited in its generalizability to other cultures and genders.
Future studies should attempt to better isolate these variables (i.e., teaching styles, feedback, participant recruitment, prior experience in suicide training, cultural background) and find ways to improve response rates. In addition, it would be beneficial to have a comparison course or data from other counseling programs’ basic skills classes to further determine if this practice-based model was effective. Results could be linked to more general self-efficacy increases because of growing more comfortable with learning and using interviewing skills (Holladay & Quiñones, 2003).
One final limitation worth noting is the effect size estimates of the pre- and posttest scores. All effect sizes are large. Some reasons why the effect sizes may be large in the paired-samples t-tests include: (a) large differences between paired observations (the mean scores between the pre- and posttest scores were extremely different), and (b) small within-group variability (if the within-group variability is small, then even small differences between the paired observations could result in a large effect size).
Conclusion
As counselor educators prepare students for the profession, intentional inclusion of suicide screening, assessment, and intervention skills is vital to increasing students’ confidence and preparation to address this topic with their future clients. But it is not enough for students to learn about screening, assessment, and interventions; they need experiential opportunities to practice and develop these skills. In turn, feedback and practice will increase their comfort levels to directly and adequately support their clients’ needs.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Allen, I. E., & Seaman, J. (2014). Grade change: Tracking online education in the United States. The Sloan Consortium. Sloan-C. http://www.onlinelearningsurvey.com/reports/gradechange.pdf
American Foundation for Suicide Prevention. (2023). Suicide statistics. https://afsp.org/suicide-statistics
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Prentice-Hall.
Bandura, A. (1989). Human agency in social cognitive theory. American Psychologist, 44(9), 1175–1184. https://doi.org/10.1037/0003-066X.44.9.1175
Bandura, A. (1997). Self-efficacy: The exercise of control. W. H. Freeman.
Barbee, P. W., Scherer, D., & Combs, D. C. (2003). Prepracticum service-learning: Examining the relationship with counselor self-efficacy and anxiety. Counselor Education and Supervision, 43(2), 108–119. https://doi.org/10.1002/j.1556-6978.2003.tb01835.x
Barnes, K. L. (2004). Applying self-efficacy theory to counselor training and supervision: A comparison of two approaches. Counselor Education and Supervision, 44(1), 56–69. https://doi.org/10.1002/j.1556-6978.2004.tb01860.x
Becnel, A. T., Range, L., & Remley, T. P., Jr. (2021). School counselors’ exposure to student suicide, suicide assessment self-efficacy, and workplace anxiety: Implications for training, practice, and research. The Professional Counselor, 11(3), 327–339. https://doi.org/10.15241/atb.11.3.327
Binkley, E. E., & Leibert, T. W. (2015). Prepracticum counseling students’ perceived preparedness for suicide response. Counselor Education and Supervision, 54(2), 98–108. https://doi.org/10.1002/ceas.12007
Centers for Disease Control and Prevention. (2021, February 20). Web-based injury statistics query and reporting system (WISQARS) fatal injury reports. https://wisqars.cdc.gov/fatal-leading
Conteh, J. A., Mariska, M. A., & Huber, M. J. (2018). An examination and validation of personal counseling and its impact on self-efficacy for counselors-in-training. Journal of Counselor Practice, 9(2), 109–138.
https://www.journalofcounselorpractice.com/uploads/6/8/9/4/68949193/jac902111_jcp_vol_9_issue_2.pdf
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Cramer, R. J., Bryson, C. N., Eichorst, M. K., Keyes, L. N., & Ridge, B. E. (2017). Conceptualization and pilot testing of a core competency-based training workshop in suicide risk assessment and management: Notes from the field. Journal of Clinical Psychology, 73(3), 233–238. https://doi.org/10.1002/jclp.22329
Douglas, K. A., & Wachter Morris, C. A. (2015). Assessing counselors’ self-efficacy in suicide assessment and intervention. Counseling Outcome Research and Evaluation, 6(1), 58–69.
https://doi.org/10.1177/2150137814567471
Elliott, G. M., & Henninger, J. (2020). Online teaching and self-efficacy to work with suicidal clients. Counselor Education and Supervision, 59(4), 283–296. https://doi.org/10.1002/ceas.12189
Fakhro, D., Rujimora, J., Zeligman, M., & Mendoza, S. (2023). Counselor self-efficacy, multicultural competency, and perceived wellness among counselors in training during COVID-19: A pre- and peri-analysis. Journal of Counselor Leadership and Advocacy, 10(2), 99–111. https://doi.org/10.1080/2326716X.2023.2229323
Gallo, L. L., Doumas, D. M., Moro, R., Midgett, A., & Porchia, S. (2019). Evaluation of a youth suicide prevention course: Increasing counseling students’ knowledge, skills, and self-efficacy. Journal of Counselor Preparation and Supervision, 12(3), 1–23. https://digitalcommons.sacredheart.edu/jcps/vol12/iss3/9
Granello, D. H. (2010). The process of suicide risk assessment: Twelve core principles. Journal of Counseling & Development, 88(3), 363–370. https://doi.org/10.1002/j.1556-6678.2010.tb00034.x
Green, S. B., & Salkind, N. J. (2014). Using SPSS for Windows and Macintosh: Analyzing and understanding data (7th ed.). Pearson.
Guillot Miller, L., McGlothlin, J. M., & West, J. D. (2013). Taking the fear out of suicide assessment and intervention: A pedagogical and humanistic practice. The Journal of Humanistic Counseling, 52(1), 106–121. https://doi.org/10.1002/j.2161-1939.2013.00036.x
Holladay, C. L., & Quiñones, M. A. (2003). Practice variability and transfer of training: The role of self-efficacy generality. Journal of Applied Psychology, 88(6), 1094–1103. https://doi.org/10.1037/0021-9010.88.6.1094
Jahn, D. R., Quinnett, P., & Ries, R. (2016). The influence of training and experience on mental health practitioners’ comfort working with suicidal individuals. Professional Psychology: Research and Practice, 47(2), 130–138. https://doi.org/10.1037/pro0000070
Kozina, K., Grabovari, N., De Stefano, J., & Drapeau, M. (2010). Measuring changes in counselor self-efficacy: Further validation and implications for training and supervision. The Clinical Supervisor, 29(2), 117–127. https://doi.org/10.1080/07325223.2010.517483
LeCloux, M. (2021). Efficient, yet effective: Improvements in suicide-related knowledge, confidence, and preparedness after the deployment of a brief online module on suicide in a required MSW course. Journal of Teaching in Social Work, 41(4), 389–407. https://doi.org/10.1080/08841233.2021.1954577
Lent, R. W. (2020). Career development and counseling: A social cognitive framework. In S. D. Brown & R. W. Lent (Eds.), Career development and counseling: Putting theory and research to work (3rd ed., pp. 129–164). Wiley.
Lent, R. W., & Brown, S. D. (2006). Integrating person and situation perspectives on work satisfaction: A social-cognitive view. Journal of Vocational Behavior, 69(2), 236–247. https://doi.org/10.1016/j.jvb.2006.02.006
Lent, R. W., Hill, C. E., & Hoffman, M. A. (2003). Development and validation of the Counselor Activity Self-Efficacy Scales. Journal of Counseling Psychology, 50(1), 97–108. https://doi.org/10.1037/0022-0167.50.1.97
Liebling-Boccio, D. E., & Jennings, H. R. (2013). The current status of graduate training in suicide risk assessment. Psychology in the Schools, 50(1), 72–86. https://doi.org/10.1002/pits.21661
Pechek, A. A. (2018). Counselor education learning modalities: Do they predict counseling self-efficacy in students? (Publication No. 10785997) [Doctoral dissertation, Adams State University]. ProQuest Dissertations Publishing.
Sawyer, C., Peters, M. L., & Willis, J. (2013). Self-efficacy of beginning counselors to counsel clients in crisis. Journal of Counselor Preparation and Supervision, 5(2), 30–43. https://digitalcommons.sacredheart.edu/jcps/vol5/iss2/3/
Schmidt, R. C. (2016). Mental health practitioners’ perceived levels of preparedness, levels of confidence and methods used in the assessment of youth suicide risk. The Professional Counselor, 6(1), 76–88.
https://doi.org/10.15241/rs.6.1.76
Schmitz, W. M., Jr., Allen, M. H., Feldman, B. N., Gutin, N. J., Jahn, D. R., Kleespies, P. M., Quinnett, P., & Simpson, S. (2012). Preventing suicide through improved training in suicide risk assessment and care: An American Association of Suicidology Task Force report addressing serious gaps in U.S. mental health training. Suicide and Life-Threatening Behavior, 42(3), 292–304. https://doi.org/10.1111/j.1943-278X.2012.00090.x
Shea, S. C., & Barney, C. (2015). Teaching clinical interviewing skills using role-playing: Conveying empathy to performing a suicide assessment: A primer for individual role-playing and scripted group role-playing. Psychiatric Clinics of North America, 38(1), 147–183. https://doi.org/10.1016/j.psc.2014.10.001
Suicide Prevention Resource Center. (2006). Core competencies in the assessment and management of suicide risk.
Suh, S., Crawford, C. V., Hansing, K. K., Fox, S., Cho, M., Chang, E., Lee, S., & Lee, S. M. (2018). A cross-cultural study of the self-confidence of counselors-in-training. International Journal for the Advancement of Counselling, 40(3), 255–266. https://doi.org/10.1007/s10447-018-9324-4
Vincenzes, K., Pechek, A., & Sprong, M. (2023). Counselor trainees’ development of self-efficacy in an online skills course. Journal of Counselor Preparation and Supervision, 17(1). https://digitalcommons.sacredheart.edu/jcps/vol17/iss1/1
Wachter Morris, C. A., & Barrio Minton, C. A. (2012). Crisis in the curriculum? New counselors’ crisis preparation, experiences, and self-efficacy. Counselor Education and Supervision, 51(4), 256–269.
https://doi.org/10.1002/j.1556-6978.2012.00019.x
Wakai, S., Schilling, E. A., Aseltine, R. H., Blair, E. W., Bourbeau, J., Duarte, A., Durst, L. S., Graham, P., Hubbard, N., Hughey, K., Weidner, D., & Welsh, A. (2020). Suicide prevention skills, confidence, and training: Results from the Zero Suicide Workforce Survey of behavioral health care professionals. SAGE Open Medicine, 8, 1–12. https://doi.org/10.1177/2050312120933152
Wasylko, Y., & Stickley, T. (2007). Promoting emotional development through using drama in mental health education. In T. Stickley & T. Basset (Eds.), Teaching mental health (pp. 297–309). Wiley.
https://doi.org/10.1002/97804470713617.ch25
World Health Organization. (2014). Preventing suicide: A global imperative. https://www.who.int/publications/i/item/9789241564779
Ashley Ascherl Pechek, PhD, NCC, ACS, LPC, is an associate professor at Commonwealth University of Pennsylvania. Kristin A. Vincenzes, PhD, NCC, ACS, BC-TMH, LPC, is a professor at Commonwealth University of Pennsylvania. Kellie Forziat-Pytel, PhD, NCC, ACS, LPC, is an assistant professor at Commonwealth University of Pennsylvania. Stephen Nowakowski is a graduate student at Commonwealth University of Pennsylvania. Leandrea Romero-Lucero, PhD, ACS, LPCC, CSOTS, is an associate professor and Clinical Mental Health Counseling Program Director at Commonwealth University of Pennsylvania. Correspondence may be addressed to Ashley Ascherl Pechek, 401 N. Fairview Street, Lock Haven, PA 17745, aap402@commonwealthu.edu.
May 22, 2024 | Volume 14 - Issue 1
Joshua D. Smith, Neal D. Gray
Each year TPC presents an interview with an influential veteran in counseling as part of its Lifetime Achievement in Counseling series. This year I am honored to introduce Dr. Kathleen Brown Rice, a clinician, supervisor, and counselor educator with expertise in substance use disorders and historical trauma. In this interview, she discusses the personal and professional motivations for her work and her perspective on the future of counseling and counselor education. I am grateful to Dr. Joshua Smith and Dr. Neal Gray for highlighting the ongoing contributions of leaders in the profession for the TPC readership. —Richelle Joe, Editor
 Kathleen Brown Rice, PhD, NCC, ACS, LPC-S (TX), LPC (SD), LCMHC (NC), is a professor of counselor education in the College of Education at Sam Houston State University. She obtained her CACREP-accredited PhD in counselor education and supervision from the University of North Carolina at Charlotte and her CACREP-accredited Master of Science in counseling from South Dakota State University. Dr. Rice is a Licensed Professional Counselor-Supervisor in Texas, a Licensed Professional Counselor in South Dakota, and a Licensed Clinical Mental Health Counselor in North Carolina. Additionally, she holds the National Certified Counselor and Approved Clinical Supervisor credentials. She has worked as a professional counselor in various clinical settings and currently operates a private practice assisting clients with mental health, trauma, and substance abuse issues. Dr. Rice’s scholarly research activity focuses on counselor supervision and training with an emphasis in ethical considerations; the implications of historical and generational trauma; and the impact of substance abuse on individuals, families, and the community. She also incorporates the use of biomarkers in her research to understand emotional regulation, risky behaviors, and resiliency. As part of her extensive scholarship, she serves as an expert peer reviewer on the TPC Editorial Review Board.
Kathleen Brown Rice, PhD, NCC, ACS, LPC-S (TX), LPC (SD), LCMHC (NC), is a professor of counselor education in the College of Education at Sam Houston State University. She obtained her CACREP-accredited PhD in counselor education and supervision from the University of North Carolina at Charlotte and her CACREP-accredited Master of Science in counseling from South Dakota State University. Dr. Rice is a Licensed Professional Counselor-Supervisor in Texas, a Licensed Professional Counselor in South Dakota, and a Licensed Clinical Mental Health Counselor in North Carolina. Additionally, she holds the National Certified Counselor and Approved Clinical Supervisor credentials. She has worked as a professional counselor in various clinical settings and currently operates a private practice assisting clients with mental health, trauma, and substance abuse issues. Dr. Rice’s scholarly research activity focuses on counselor supervision and training with an emphasis in ethical considerations; the implications of historical and generational trauma; and the impact of substance abuse on individuals, families, and the community. She also incorporates the use of biomarkers in her research to understand emotional regulation, risky behaviors, and resiliency. As part of her extensive scholarship, she serves as an expert peer reviewer on the TPC Editorial Review Board.
In this interview, Dr. Rice provides her analysis of the current state of the counseling profession and the possibilities for its future, in addition to discussing the importance of social justice, access to online education, and service.
- As a counselor educator with experience in both traditional (face-to-face) and online delivery, what do you see as the benefits and challenges of both? Additionally, in your opinion, how can online delivery for skills courses ensure counselor competency?
During my master’s and doctoral studies, not one online class was offered. Things have changed immensely. According to the Council for the Accreditation of Counseling and Related Educational Programs website (CACREP; 2024), there are 12 CACREP-accredited online doctoral programs and 118 CACREP-accredited online master’s programs. I believe as telecounseling in the field increases, the number of online programs and online course offerings in face-to-face programs will also continue to grow. A 2021 Ruffalo Noel Levitz Graduate Student Recruitment Report surveyed prospective students who planned to enroll in graduate school and found that 48% preferred hybrid programs, 32% preferred fully online programs, and 20% wanted a traditional classroom program. When looking at within-group differences, doctoral students preferred traditional classroom instruction and master’s students preferred hybrid or online programs (Ruffalo Noel Levitz, 2022).
Courses and programs being offered online provide greater flexibility for our students to schedule around work and personal commitments. This can provide students with a better school–life balance. Online counseling programs can provide access to learners who would not otherwise be able to pursue their graduate education and search out specialty tracks that may not be available in their own geographical area. Online programming diversifies the learning environment by providing the opportunity for students from different backgrounds, worldviews, and cultures to engage and collaborate. While these virtual learning environments increase opportunities, there are also struggles we need to consider with this learning modality. Students in online programs may feel isolated and have fewer or qualitatively different opportunities to engage. This can result in a loss of community and feelings of being unsupported, and even have implications on their professional identity development. Given the differences in jurisdictional requirements for licensure, every program might not lead to the educational requirements for licensure where the student lives or wants to practice. There are also legal considerations related to mandatory reporting and limits of confidentiality that vary across jurisdictions. Lastly, online instruction can restrict assessment related to professional comportment issues. This can lead to students’ gate-slipping to the detriment of clients and the counseling profession.
When looking at how to best support skills courses to ensure we are training competent and ethical counselors, it is important to consider the traits of the student, faculty, and program. Vineyard (2019) recommended that a successful virtual student is one who has good time management skills, has the ability to self-regulate, and is self-motivated. Thus, we must be honest with ourselves as educators and administrators that online programming is not the right fit for every student. Additionally, to best support virtual students, educators need to think about different types of support such as providing regular live supervision of sessions and consistently reviewing recordings. Further, faculty should seek out training and continuing education to enhance their online instruction and understand gatekeeping strategies. For programs, they should be committed to providing the required online platforms and training for both students and faculty to support an online counseling training program. Also, there should be a residency component built into the program. My personal experience and the results of my research on problems of professional competency prove that having face-to-face personal contact is how most disposition problems are discovered. I believe observing how our students interact with us and each other is a crucial part of the gatekeeping process.
- Having an extensive research and publication record aimed toward understanding racial and generational trauma, particularly with Indigenous, tribal, and Native American populations, could you speak about the importance of advocacy and social justice in the counseling profession?
We have great privilege being counselors and counselor educators. Those initials behind our names have inherent power. Thus, advocacy should be embedded in everything we do from our practice, teaching, research, and mentorship. Our training and education provide us a seat at the table to promote equity and inclusion and advocate with others—and we should take full advantage. Advocacy also relates to us being engaged with the population that we are advocating for. In that, to advocate for any population, you have to know them, understand them, and ask them if and how they want your support—this is how we advocate with. Many groups that have been historically marginalized in the United States were done so under the guise of helping. One example of this relates to the Indian boarding schools.
From the beginning of the formation of the United States into the 19th century, a central agenda for many government officials was to acquire Indigenous lands (e.g., Indian Removal Act of 1830). By 1876, the majority of lands had been seized, and native people were forced to either relocate or live on reservations. Captain Richard H. Pratt believed that this segregation was wrong and supported better treatment for the native people. He delivered a speech at the Nineteenth Annual Conference of Charities and Correction regarding how to reeducate Native Americans/American Indians, where he proclaimed the only course was to “Kill the Indian, and Save the Man.” In that, to save the Indian, full assimilation into White European culture was required. Thereafter, the government and religious organizations established boarding schools (for more information, see this article). General Platt would have seen himself as an advocate. However, his actions led to the abuse of many children under the care of these schools, loss of cultural identity, and disruption of the parental relationship, and are seen as the prominent predecessor to many of the existing problems for some American Indians/Native Americans. Advocacy is crucial in the counseling profession. However, it needs to be done in a culturally competent and collaborative manner. I have been approached by researchers to ask for my assistance working in the Indigenous populations. However, when I ask them if they reached out to the community they want to research in, they most often say “no.” I believe it is crucial to be part of the community before you engage in research with the community. Learn what would be beneficial to the community, not just what will get the researcher published and/or grant funding.
- As a follow-up to the previous questions, where did this passion and pursuit originate for you?
For me, it has a both personal and professional origination and intersection. I am a linear descendent of the Chickasaw tribe. I grew up not knowing a lot about my heritage because my father was trying to protect our family. His lived experience was that it was not safe to let people know. So, our heritage remained closeted the majority of my life. For almost 20 years I worked as a paralegal. The majority of my work supported lawyers focusing on criminal and family law, which included federal law related to reservation crimes. I saw so many judicial problems occurring with many American Indian/Native American individuals, which made me curious about the reasons. I was repeatedly told “that is just how those people are.” Now, I knew that was not true because I was one of those people. I got frustrated with the pattern of what I was seeing and felt I was more part of the problem than the solution. At the age of 39, I decided to go back to school to pursue a different career.
During my undergraduate studies, I chose to take an American Indian/Native American history class to understand more. My father supported my quest for knowledge and started to share our heritage with me. This class helped me understand more about the historical components of the why. During my master’s studies, I first heard the term historical trauma. I began to research this concept and more parts of the why were answered for me. For my doctoral studies, I sought a program that specialized in multicultural competency to assist me in gaining more knowledge. However, I was still struggling with truly embracing my biracial identity—then fate interceded. I was the director of clinical experiences at the university where I was working. I received an email from a local reservation that they lost funding and had to let some counselors go and they wondered if we had any interns. No interns were available, so I said I would go. I was assigned a supervisor and during our first supervision session she said to me, “So, when are you going to tell me you’re Indian?” I started stumbling over excuses about how I was only part, and that I was not really raised a part of the culture. And she said two pivotal things to me: “You are not part, your Indian blood flows through all of you” and “Do you know how powerful it would be for the adolescents that you are going to work with to see someone from their people that is a counselor and doctor? How much you can encourage them?” She was right. I do this work to advocate for my people. That is my passion.
- Having a background in mental health and substance use counseling, what has been your experience navigating comorbidity? What changes have you seen socially and culturally as a result of the ever-changing landscape in our current society?
When I co-led my first substance abuse group as a practicum student 17 years ago, the focus was on the substance of abuse (i.e., consequences of use, identifying triggers, and changing behavior to not use). There was little discussion regarding trauma or other comorbid mental health disorders. All therapy work was done in group format. This did not leave space for individual counseling to assist clients with working through their own personal mental health struggles. When I was working at a large urban treatment facility, we were not allowed to engage in individual therapy. To meet the needs of my clients, I requested to conduct individual counseling with my group members who met the criteria for comorbidity. I was told that I could, but I would not be paid for the individual sessions and offered to clients pro bono. I agreed. Once I started working with my clients in both individual and group sessions, I saw so much improvement.
I have slowly been seeing a change in this perspective and clients getting counseling for both their substance use and other mental health concerns with the inclusion of holistic interventions. However, lately I have seen a focus more on mental health counseling only. In fact, through survey research by the Substance Abuse and Mental Health Services Administration (2022), it was found that of the 5.8 million adults aged 18 or older who reported a co-occurring mental health and illicit drug or alcohol use disorder in the past year, most (81.5%) received only mental health services. I think it is important that if a counselor is going to work with individuals who meet the criteria for comorbidity, they should be trained in both specialties. I know my educational training and clinical supervised experiences in both have been crucial to successful client outcomes.
The emergence of reality shows (e.g., Addicted, Intervention, Celebrity Rehab) and scripted shows (e.g., Euphoria, Mom, Nurse Jackie, Painkiller) related to addiction have changed how our society views addiction. These shows have allowed the general public to understand more about drug use, how people become addicted, and the consequences of addiction. I believe this has resulted in our society understanding that addiction is a disease and the person with the addiction needs treatment and support, not punishment and disdain. While media has brought some insight to substance use, words such as addict, alcoholic, drunk, and junkie are still being regularly utilized. Rather than these labeling words that are shame producing, person-first language (e.g., person with a substance use disorder) is critical to creating a therapeutic environment.
- It appears service is also an integral part of your counseling identity. What does service mean to you at the local, community, national, and international level?
Service for me encompasses two main concepts: 1) leaving things better than how I found them and 2) working for a cause not for applause. Active involvement in the department, college, university, profession, and community is an important component of service for me as a faculty member. However, I believe all service should first start on the local level. The analogy of putting your oxygen mask on first applies here. First give oxygen to your local stakeholders. I actively volunteer where gaps have been identified in my microsystem and work to fill these breaches to better serve clients and students. I then move onto service in the macrosystem. I strive to be strategic with the opportunities. We cannot be everything to everyone. Throughout my career, I have said no to roles because I knew that I did not have the bandwidth to do them competently. Service, to me, means making sure that I am only taking on those roles for which I have the time and energy to do well.
I have been honored to be appointed and elected to leadership roles in state and national organizations, serve on several editorial boards, and be selected to present at numerous national and international conferences. I value these opportunities and appreciate these roles and opportunities to provide service to the profession. However, I believe the most impactful service I have done relates to service that has no recognition by a title or line of my curriculum vitae (e.g., pro bono counseling, supervision for licensure, and workshops; consultation; mentorship). This also connects back to advocacy and leaving people with more than what they had, which are core values for me and how I hope to always operate as a counselor educator.
- What three challenges to the counseling profession as it exists today concern you most?
Counselors-in-training, professional counselors, and counselor educators not doing their own counseling work. I see the concept of the wounded healer being manifested more and more in our profession. In my opinion, this is strongly related to the aftermath of the COVID-19 pandemic. The pressure counselors, clinical supervisors, and educators had on them to immediately adjust to the new norm of telecounseling, online education, and the increase in individuals seeking service caused a perfect storm. In connection with the above is the predatory use of pre-licensed counselors. Given the jurisdictional differences related to the scope of practice and insurance companies’ view of pre-licensed counselors, the ability to bill or bill under a supervisor varies widely. This can lead to some agencies and practices over-scheduling pre-licensed counselors or bringing in too many supervisees to be supervised and, thus, supervision quality is compromised. The financial costs of a graduate education and the need to get those required hours results in many students and those working on their hours toward licensure being in a vulnerable position with little recourse to do anything regarding these situations. Lastly, there seems to be a lack of focus on evidence-based practices and research being conducted with clients. In the academic world, we have access to the latest peer-reviewed articles, and there is a research culture that motivates and encourages us to research and add to the literature. However, in the practice world, there may not be as much encouragement of counselor research engagement, consumption, and production. Therefore, there is a need to continue to find ways to bridge the research-to-practice gap and promote more counselors conducting research and gathering data with clients.
- What needs to change in the counseling profession for these three concerns to be successfully resolved or addressed?
As educators and supervisors, we need to do better with talking about going to counseling. I still do tune-ups with my counselor. We need to acknowledge what we do is difficult and that it is important that we continue our own self-care and our own work. I think we talk the talk about self-care; however, how often do we walk the walk? Are we providing space for our students and supervisees? Are we providing space for ourselves? Professional counselors, whether in training or practicing, need to remember counselor heal thyself first and to do their own work to avoid burnout and unethical practice. As our profession continues to grow, the need for good training sites and competent supervisors will continue to be a concern. I believe the responsibility for developing support for supervisors in the field is with counselor educators. We have resources and time allotted to us to work on strategies to better train and guide supervisors in the field and to advocate for more financial support for counselors-in-training. Lastly, in order for more practitioners in the field to gain access to the new developments in evidence-based practices, more counseling-related journals need to be open-access. We also need to find more ways to disseminate counseling research where counselors may tend to access information such as at scholarly conferences, in Counseling Today, and on social media platforms like the Mental Health Research Facebook page. Additionally, to get counselors more involved with conducting research and gathering data with their clients, more educators need to include practitioners as co-researchers on their studies. Ultimately, research to develop evidence-based practices should be seen as part of our service to our profession and advocacy for the clients we serve.
This concludes the ninth interview for the annual Lifetime Achievement in Counseling Series. TPC is grateful to Joshua D. Smith, PhD, NCC, LCMHC, and Neal D. Gray, PhD, LCMHC-S, for providing this interview. Joshua D. Smith is an assistant professor at the University of Mount Olive. Neal D. Gray is a professor at Lenoir-Rhyne University. Correspondence can be emailed to Joshua Smith at jsmith@umo.edu.
References
Council for Accreditation of Counseling and Related Educational Programs. (2024). Find a program. https://www.cacrep.org/directory
Ruffalo Noel Levitz. (2022). 2021 graduate student recruitment report. https://www.ruffalonl.com/papers-research-higher-education-fundraising/graduate-student-recruitment-report-2
Substance Abuse and Mental Health Services Administration. (2022). Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report
Vineyard, T. E. (2019). The use of an online readiness assessment to determine necessary skills, aptitude, and propensities for successful completion in a secondary online credit course [ProQuest Information & Learning]. In Dissertation Abstracts International Section A: Humanities and Social Sciences (Vol. 80, Issue 2–A(E)).
May 15, 2024 | Book Reviews
edited by James P. Sampson, Jr., Janet G. Lenz, Emily Bullock-Yowell, Debra S. Osborn, and Seth C. W. Hayden
 I don’t know how to make this choice. While working in a university career center, I have heard these words of distress countless times from students who were feeling the unbearable weight of making a decision that they saw as having the power to shape their future, their lives, and their identities in significant and lasting ways. Fortunately, during a vocational psychology course, I studied cognitive information processing (CIP) theory, the pyramid of information processing, and the CASVE cycle, which gave me the confidence and competence to navigate the complicated decision-making process with students who felt emotionally and mentally overwhelmed by academic and career choices.
I don’t know how to make this choice. While working in a university career center, I have heard these words of distress countless times from students who were feeling the unbearable weight of making a decision that they saw as having the power to shape their future, their lives, and their identities in significant and lasting ways. Fortunately, during a vocational psychology course, I studied cognitive information processing (CIP) theory, the pyramid of information processing, and the CASVE cycle, which gave me the confidence and competence to navigate the complicated decision-making process with students who felt emotionally and mentally overwhelmed by academic and career choices.
The need to make occupational decisions is universal. Cognitive Information Processing: Career Theory, Research, and Practice provides a comprehensive exploration of CIP theory, which serves as the theoretical framework for understanding the cognitive processes that affect how individuals interpret and utilize career-related information to guide their career choices.
Drawn from both cognitive and counseling psychology, CIP theory underscores the various mental processes involved in career decision making, including information gathering, self-awareness, and goal setting. As a career intervention, CIP theory is intended to assist individuals with career-related problems by enhancing their understanding of both problem solving and decision making. One tool used to accomplish this goal is the CASVE cycle. With each letter representing a step in the decision-making model, readers are guided through a structured process that helps them make informed choices. By following this model, individuals can be supported in avoiding impulsive decisions, minimizing risks, and increasing the likelihood of achieving their desired outcomes.
Published in 2023, this book focuses on integrating theory, research, and practical applications, making it an invaluable resource with applicability across a multitude of domains. Educators and researchers studying vocational behavior and aspiring to understand the future direction(s) of CIP theory would benefit from consulting Chapter 21. Likewise, practitioners seeking evidence-based career interventions and individuals navigating the complexities of career decision-making will discover instrumental guidance in the chapters dedicated to understanding occupational, educational, and training choices, as well as those exploring the psychological and developmental factors influencing an individual’s readiness to make career decisions. For employment agencies and government policymakers aiming to establish career-focused initiatives, Chapter 16 offers both a comprehensive blueprint and essential resources for developing and executing successful career services programs.
One of the book’s strengths, as stated above, is its integration of theory with practical applications. Each chapter provides insights into how CIP theory can be translated into effective career counseling interventions. The authors lay out the discussion of complex factors that affect career decisions in a straightforward and digestible manner. Practitioners and individuals will find a set of easily understandable concepts that will equip them with the knowledge and skills needed to inform effective and satisfying academic and career decision making. Through case studies, reflective exercises, practical guidelines, and summaries offered at the end of each chapter, readers will find that these skills can also be applied to a myriad of decision-making opportunities.
In addition to its theoretical and practical contributions, this book’s attention to the impact of systemic inequalities and cultural factors on career opportunities and outcomes is also notable. The authors expertly promote a culturally sensitive approach to career counseling that recognizes, respects, and affirms the diversity of individuals’ identities, values, and beliefs. They further emphasize the significance of an inclusive and empowering counseling atmosphere that fosters clients’ self-awareness and agency while making career choices. Case examples and reflective activities are presented to encourage readers to examine their own biases and assumptions that may hinder a culturally competent approach to career counseling.
Cognitive Information Processing: Career Theory, Research, and Practice is published through Florida State Open Publishing as an open-access resource. By making the book available for free, the authors have eliminated the financial barrier to accessing this invaluable asset aimed at equipping readers with theory-based knowledge of vocational behavior and career interventions. This accessibility benefits students, educators, researchers, practitioners, and anyone wanting to establish cost-effective and evidence-based career development intervention programming that helps individuals to make informed career decisions across their life span.
Sampson, J. P., Jr., Lenz, J. G., Bullock-Yowell, E., Osborn, D. S., & Hayden, S. C. W. (Eds.). (2023). Cognitive information processing: Career theory, research, and practice. Florida State Open Publishing. https://manifold.lib.fsu.edu/projects/cognitive-information-processing-career-theory-research-and-practice
Reviewed by: Nikkie Bailey, MS, LCSW
Mar 18, 2024 | Volume 13 - Issue 4
Jennifer M. Cook, Camille Y. Humes
This special issue of The Professional Counselor (TPC) is in honor of the NBCC Foundation (NBCCF)’s 2023 Bridging the Gap Symposium: Eliminating Mental Health Disparities. The theme for the 2023 Symposium, From Awareness to Action, represented the importance of attendee reflection on current issues and the need for intentional engagement in meaningful work that empowers underserved and never-served clients and communities. The event was attended by over 500 counselors and counselors-in-training who connected with peers and had the opportunity to learn from presenters of 70 sessions. Unique to this year’s Symposium was the celebration of the 10th anniversary of the Minority Fellowship Program (MFP). Members of the inaugural cohort, affectionately known as the Dream Team, came together to share memories of receiving their awards and spent time engaging in discussions about their remarkable contributions to the counseling profession over the past decade.
In this special edition of TPC, guest editors from the first and second cohorts of the MFP reviewed submissions and selected articles for publication. Keeping the 2023 Symposium theme in mind, we worked hard to ensure that the articles in this issue reflect the purpose and vision of the event. Submissions covered a wide range of topics that provided perspectives about mental health disparities across diverse populations. Our hope is that this issue, like Symposium, will provoke thought and promote action.
We divided the articles in this issue into two sections: The first section is comprised of articles that align with the special issue theme but were not presented at Symposium. The second section is comprised of articles that were written by authors who presented at this year’s Symposium and transformed their presented work into articles.
The three articles in the first section of this issue are those that align with the Symposium’s theme. Although the authors of these articles did not present at Symposium, we think you will find what the authors share captures the Symposium’s purpose beautifully. In “‘A Learning Curve’: Counselors’ Experiences Working With Sex Trafficking,” the authors present findings from their qualitative study with clinicians who work with clients who have experienced sex trafficking to offer recommendations for working with this population. “Ableist Microaggressions, Disability Characteristics, and Nondominant Identities” reveals how ableist microaggressions manifest most frequently for people with a range of disabilities and sociocultural identities, and the authors suggest ways to better support clients with disabilities. In the third article of the issue, “Using the Cultural Formulation Interview with Afro Latinx Immigrants in Counseling: A Practical Application,” the authors utilize a case study to demonstrate how to use this assessment tool with an Afro Latinx immigrant client from Mexico.
In the second section of the issue, “Diondre Also Has Bad Days: Cannabis Use and the Criminalization of Black Youth” and “Utilizing Collective Wisdom: Ceremony-Assisted Treatment for Native and Non-Native Clients” introduce readers to communities, concepts, and skills with which they may be less familiar. The authors convey clearly that counselors must develop these skills in order to serve populations who are in need of their identity-affirming, empathetic services. In “Diondre Also Has Bad Days,” the author challenges readers to examine how they treat Black and White youth and to overcome potentially biased approaches that have traditionally served one group more affirmatively than the other. “Ceremony-Assisted Treatment for Native and Non-Native Clients” presents readers with intervention options that integrate Indigenous practices, such as smudging and drumming.
The final three articles in the second section are “Taking Action: Reflections on Forming and Facilitating a Peer-Led Social Justice Advocacy Group,” “Comorbidity of Obsessive-Compulsive Disorder in Youth Diagnosed With Oppositional Defiant Disorder,” and “Bridging the Gap Between Intentions and Impact: Understanding Disability Culture to Support Disability Justice.” In “Reflections on Forming and Facilitating a Peer-Led Social Justice Advocacy Group,” the authors provide their individual insights about their experiences as students who established a social justice advocacy group for peers in their counseling program. “Comorbidity of Obsessive-Compulsive Disorder in Youth Diagnosed With Oppositional Defiant Disorder” gives readers insight into the complexity of distinguishing between OCD and ODD in youth and the potential for misdiagnosis, while “Bridging the Gap Between Intentions and Impact” offers counseling professionals strategies for competent care and allyship for disabled clients through a disability justice framework.
As you read the articles in this issue, we hope you will accept the opportunity to discover new ways to engage in the profession and to reflect on the why behind your commitment to your work. May this special issue serve as an inspiration for lifelong learning and lasting impact in the spaces where it is needed the most.
 Jennifer M. Cook, PhD, NCC, ACS, LPC, is an associate professor in the Department of Counseling at the University of Texas at San Antonio. Dr. Cook is a multiculturally focused counselor educator who utilizes strength-based methods, culturally relevant practices, and social justice advocacy in her work and teaching. Her research focuses on counselor preparation and counselor cultural competence development, with emphasis on social class, socioeconomic status, and multiple identities. Dr. Cook has published extensively, completed over 40 national and international peer-reviewed presentations, and will publish a co-edited multicultural counseling textbook, Multicultural and Social Justice Counseling: A Systemic, Person-Centered, and Ethical Approach, later this year. Dr. Cook is a 2013 NBCC doctoral Minority Fellowship Program recipient, part of the Dream Team cohort.
Jennifer M. Cook, PhD, NCC, ACS, LPC, is an associate professor in the Department of Counseling at the University of Texas at San Antonio. Dr. Cook is a multiculturally focused counselor educator who utilizes strength-based methods, culturally relevant practices, and social justice advocacy in her work and teaching. Her research focuses on counselor preparation and counselor cultural competence development, with emphasis on social class, socioeconomic status, and multiple identities. Dr. Cook has published extensively, completed over 40 national and international peer-reviewed presentations, and will publish a co-edited multicultural counseling textbook, Multicultural and Social Justice Counseling: A Systemic, Person-Centered, and Ethical Approach, later this year. Dr. Cook is a 2013 NBCC doctoral Minority Fellowship Program recipient, part of the Dream Team cohort.
 Camille Y. Humes, EdD, NCC, LCPC (IL), LPC (MI), I/ECMH-C, is an assistant professor in the School of Counseling at Divine Mercy University in Sterling, Virginia. Dr. Humes holds an Endorsement® from the Michigan Association for Infant Mental Health, where she currently serves on the Board of Directors. For over 20 years Dr. Humes has worked as a counselor, mental health consultant, and leader in the mental health profession, advocating both nationally and internationally to inform policies that support mental health services. She is a writer, professor, and a regular grant reviewer for the United States Department of Education. Dr. Humes enjoys speaking to audiences about various topics, including the social/emotional health of young children.
Camille Y. Humes, EdD, NCC, LCPC (IL), LPC (MI), I/ECMH-C, is an assistant professor in the School of Counseling at Divine Mercy University in Sterling, Virginia. Dr. Humes holds an Endorsement® from the Michigan Association for Infant Mental Health, where she currently serves on the Board of Directors. For over 20 years Dr. Humes has worked as a counselor, mental health consultant, and leader in the mental health profession, advocating both nationally and internationally to inform policies that support mental health services. She is a writer, professor, and a regular grant reviewer for the United States Department of Education. Dr. Humes enjoys speaking to audiences about various topics, including the social/emotional health of young children.
Jan 17, 2024 | Volume 13 - Issue 4
Claudia G. Interiano-Shiverdecker, Devon E. Romero, Katherine E. McVay, Emily Satel, Kendra Smith
In this transcendental phenomenological study, we interviewed 10 counselors who have clinical experience working with sex trafficking survivors. Through in-depth individual interviews, participants discussed their lived experiences providing counseling to this population. Our analysis revealed four primary themes: (a) counselor knowledge: “learning curve,” (b) counselor skills: “creating a safe space to dive into work,” (c) counselor attitudes: “being able to listen to the client’s story,” and (d) counselor action: “more than just a counselor.” The findings indicated that counselors working with sex trafficking survivors needed to understand and address the different aspects of trauma. Our findings also demonstrate that working with sex trafficking survivors requires additional competencies such as recognizing the signs of sex trafficking, vulnerable populations, and the processes by which traffickers force people into sex trafficking. We discuss these findings in more detail and identify implications for counselor training and practice.
Keywords: sex trafficking survivors, counseling, phenomenological, trauma, competencies
Sex trafficking of any individual is a significant concern globally. In 2000, the United States government enacted the Victims of Trafficking and Violence Protection Act of 2000, which defined sex trafficking as “the recruitment, harboring, transportation, provision, or obtaining of a person for labor or services through the use of force, fraud, or coercion for the purpose of subjection to involuntary servitude, peonage, debt bondage, or slavery” or “when the person induced to perform such act has not attained 18 years of age” (§ 103). Although the United States’s efforts fully meet the minimum standards established by the Victims of Trafficking and Violence Protection Act of 2000 to eliminate severe forms of trafficking, the Department of Justice initiated a total of 210 federal human trafficking prosecutions in 2020, of which 195 involved predominantly sex trafficking (U.S. Department of State, 2021). As stated in the Trafficking in Persons Report (U.S. Department of State, 2021), all 50 states, the District of Columbia, and U.S. territories have reported all forms of human trafficking over the past 5 years. With an estimated 4.8 million people victimized by sex trafficking (International Labour Organization, 2017), it is important to understand how counselors identify, provide services to, and advocate on behalf of sex trafficking survivors within the counseling setting.
Sex Trafficking and Mental Health
As a form of human trafficking, sex trafficking exposes individuals to torture; kidnapping; and severe psychological, physical, and sexual abuse. Physical health consequences of sex trafficking include general health complications (e.g., malnutrition), reproductive health consequences (e.g., sexually transmitted diseases, unwanted pregnancies), substance abuse, and physical injuries (Grosso et al., 2018; Lutnik, 2016; Muftić & Finn, 2013). Psychological abuses are numerous and can include intimidation, threats against loved ones, lies, deception, blackmail, isolation, and forced dependency (Thompson & Haley, 2018).
Constantly experiencing atrocious physical and psychological abuses creates mental health consequences such as depression, post-traumatic stress, dissociation, irritability, suicidal ideation, self-harm, and suicide (Cole et al., 2016; O’Brien et al., 2017). Survivors of sex trafficking may exhibit severe mental illness, including schizophrenia and psychotic disorders, increased risk of compulsory psychiatric admission, and longer duration of psychiatric hospitalizations (Oram et al., 2016). Moreover, social distancing and the global economic downturn due to the COVID-19 pandemic increased online sexual exploitation and the number of individuals vulnerable to sex trafficking (U.S. Department of State, 2021).
Because of the prevalence of sex trafficking, the health consequences that result from it, and the diverse areas in which counselors practice (e.g., community clinics, private practices, behavioral health departments, college/universities, K–12 schools), counselors must be prepared to work with sex trafficking survivors (Interiano-Shiverdecker et al., 2022, 2023; Litam, 2017, 2019; Romero et al., 2021; Thompson & Haley, 2018). Standards required by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015) prepare counselors to demonstrate clinical competencies to address a variety of circumstances, including traumatic experiences, across various continuums of care (e.g., inpatient, outpatient). Clinical mental health counselors with specialization in substance abuse and marriage, couple, and family counseling can also address other comorbid issues typically encountered with sex trafficking clients such as substance abuse and relational difficulties (CACREP, 2015; Litam & Lam, 2020). Early incidence of sex trafficking (12–16 years for girls, 11–13 for boys and transgender youth; Franchino-Olsen, 2019) demands the attention of school counselors trained to promote the academic, career, and personal/social development of school-aged children (American School Counselor Association [ASCA], 2022; CACREP, 2015). Therefore, first-hand accounts of counselors providing services to this population can provide an overview of current needs, challenges, and recommendations for clinical practice and research.
Sex Trafficking Research in the Counseling Profession
A recent review of the literature showed increased attention to sex trafficking coverage in top-tier counseling journals. Conceptual pieces reviewed relevant information on sex trafficking, counselor awareness, and counseling implications (Browne-James et al., 2021; Burt, 2019; Litam, 2017; Thompson & Haley, 2018). Empirical studies explored counselors’ attitudes toward sex trafficking (Litam, 2019; Litam & Lam, 2020), assessment for the screening of sex trafficking (Interiano-Shiverdecker et al., 2022, 2023; Romero et al., 2021), mental health treatment programs and modalities for sex trafficking (Johnson, 2020; Kenny et al., 2018; Schmidt et al., 2022; Woehler & Akers, 2022), and survivors’ recovery stories (Bruhns et al., 2018). Thompson and Haley (2018) reported a need for more training and education for counselors on sex trafficking. In a study done by Litam and Lam (2020), results indicated that counselor training in sex trafficking increased awareness. As a response, Interiano-Shiverdecker et al. (2023) developed an initial list of child sex trafficking competencies for counselors.
Although these studies provide relevant information for counselors’ work with sex trafficking, they do not focus on the experience of providing care for sex trafficking victims and survivors. Exploring counselors’ experiences provides a significant breakdown of current mental health care for this population. In other words, what does providing care for this population look and feel like in reality and what competencies work when serving sex trafficking victims and survivors? Only one phenomenological study focused on this inquiry, but this study examined therapists’ experiences working with foreign-national survivors of sex trafficking in the United States (Wang & Park-Taylor, 2021). Although this study presents important findings, it explored counselors’ work with only a certain group of sex trafficking individuals. Despite incomplete records, most data indicate that U.S. citizens are equally vulnerable to sex trafficking. For example, the National Human Trafficking Hotline (n.d.), which maintains one of the most extensive data sets on human trafficking in the United States, indicates that U.S. citizens comprised approximately 40% of their callers. The current study seeks to expand on the work of Wang and Park-Taylor (2021) by obtaining first-hand accounts of counselors providing services to sex trafficking clients in the United States and providing an overview of needs, challenges, and recommendations for clinical practice and research. The guiding research question for this study was: What are the lived experiences of counselors working with sex trafficking survivors in the United States?
Method
Using transcendental phenomenological research, the researchers—Claudia G. Interiano-Shiverdecker, Devon E. Romero, Katherine E. McVay, Emily Satel, and Kendra Smith—sought to understand counselors’ experiences working with sex trafficking survivors. A transcendental phenomenological method was best suited for this study because it allowed us to provide thick descriptions of the phenomena while employing bracketing techniques to explore participants’ experiences outside of our perspectives (Hays & Singh, 2012). Utilizing Moustakas’s (1994) modification of Van Kaam’s method, we sought to explore the occurrences of counselors working with sex trafficking survivors and collectively met to address any biases that came up during data analysis.
Researchers as Instruments
At the time of the study, Interiano-Shiverdecker and Romero were counselor educators at a university in the Southern United States with recent sex trafficking publications and experience working with youth vulnerable to sex trafficking in community and school settings. McVay was a doctoral candidate and a licensed professional counselor who was practicing as a social–emotional wellness counselor at a private school. Satel and Smith were master’s students in a clinical mental health program. Our desire to explore this topic stemmed from a limited discussion of sex trafficking in the literature and sought to include the voices of counselors. As the research team, we are all involved in a research lab dedicated to understanding sex trafficking and how counselors can better serve sex trafficking survivors. As such, we had varying levels of experience with research and engagement with sex trafficking. Satel and Smith were new to research, including topics surrounding sex trafficking. Therefore, Interiano-Shiverdecker and Romero’s broader understanding of the topic could have influenced newer members. For example, Interiano-Shiverdecker assumed that codes would resemble counseling competency categories (e.g., knowledge, skills, awareness). To reduce researcher bias, we engaged in weekly debriefing meetings for approximately 5 months for ongoing discussion of our perspectives and preconceived notions throughout data analysis. We documented our biases in journals, checked in on them during meetings, and referenced participants’ quotes to prevent imposing our assumptions of the data.
Participants and Sampling
After receiving IRB approval from the university, we sought participants through purposeful sampling and snowball sampling. Purposeful sampling strategies included reaching out directly via email to counselors who fit the study criteria and sending two calls for participants on an email mailing list for counselors and counselor educators (i.e., CESNET). For direct emails, McVay created a list of individuals who fit the criteria from Interiano-Shiverdecker and Romero’s professional network and an internet search. We also engaged in snowball sampling methods through recruited participants involved in the study. Inclusion criteria included counselors over the age of 18, who had previously or were currently working with children or adults who had been sex trafficked. Participants confirmed meeting the inclusion criteria by responding to a demographic questionnaire before beginning the interview. Following the qualitative researcher’s recommendation of sample size, we sought a range between five and 25 participants for this study (Creswell, 2013; Moustakas, 1994). Counselors who agreed to participate completed the consent forms, a demographic form, and a one-time Zoom interview. Participants received a $25 gift card for their involvement in the study. We recruited for about 5 weeks after interviewing 10 counselors. After the tenth interview was completed and we concluded the first round of analysis for all interviews, we felt that data saturation was achieved when similar codes showed up throughout the data.
The resulting participant pool consisted of 10 counselors (nine female and one male) ranging in age from 27 to 61 years (M = 40.7, Mdn = 38.5, SD = 11.1). Seven participants identified as White, two participants identified as Hispanic, and one participant identified as Asian. The participants also identified their employment setting: university (n = 1), agency (n = 3), and private practice (n = 6). Participants disclosed providing services in one or several states such as Alabama (n = 1), Florida (n = 1), Missouri (n = 1), Nevada (n = 1), North Carolina (n = 1), and Texas (n = 7). One participant also reported providing services to sex trafficking survivors in the United Kingdom. Years working with survivors of sex trafficking ranged from 1 to 13+ years, with a range of three to 50+ clients who disclosed their sex trafficking experience. One participant (Alejandra) who had worked primarily with survivors of sexual abuse did not indicate their number “since a lot of clients I have worked with do not readily admit to being sex trafficked, I’m not sure.” Table 1 outlines participant demographics in more detail.
Table 1
Participant Demographics
| Pseudonym |
Age |
Gender |
Race/Ethnicity |
Work Setting |
Years of Service |
# ST Clients |
CACREP |
| Kimberly |
48 |
Female |
White |
Private Practice |
11 |
30 |
Yes |
| John |
38 |
Male |
White |
University |
11 |
5 |
Yes |
| Stacy |
33 |
Female |
White |
Private Practice |
8 |
3+ |
Yes |
| Alejandra |
54 |
Female |
Hispanic |
Agency |
Unsure |
Most of career |
No |
| Fen |
39 |
Female |
Asian |
Private Practice |
5 |
4 |
Yes |
| Cassandra |
33 |
Female |
White |
Private Practice |
5 |
50+ |
Yes |
| Tiffany |
27 |
Female |
White |
Private Practice |
1 |
25 |
Yes |
| Amanda |
29 |
Female |
White |
Private Practice |
4 |
5 |
Yes |
| Ana |
61 |
Female |
Hispanic |
Agency |
13+ |
20 |
Yes |
| Cristina |
45 |
Female |
White |
Agency |
3 |
10+ |
No |
Note. Years of Service = Years providing services to ST survivors; ST = Sex trafficking; CACREP = Program accredited by the Council for Accreditation of Counseling and Related Educational Programs.
Data Collection Procedures
To follow phenomenological research methods, Interiano-Shiverdecker trained the doctoral student (McVay) in conducting semi-structured interviews. The researchers developed interview questions based on the purpose of the study and from a review of the literature. Interiano-Shiverdecker and McVay completed the interviews. Following Moustakas’s (1994) recommendations, the interview protocol consisted of 12 semi-structured, open-ended questions that invited an in-depth discussion of their experiences. To create our interview protocol, we reviewed current literature in counseling on sex trafficking, particularly qualitative studies (Browne-James et al., 2021; Bruhns et al., 2018; Johnson, 2020; Wang & Park-Taylor, 2021; Woehler & Akers, 2022). Based on this review and Interiano-Shiverdecker’s experience in qualitative research, we decided to focus not only on counselors’ experiences with working with this population but also on their perspectives on the identification, prevention, and impact of sex trafficking on their clients. The complete interview protocol can be found in the Appendix. Interviews lasted from 26 to 69 minutes in length and occurred via Zoom because data collection occurred in 2021 and it was the most appropriate medium to respect social distancing and obtain a national sample. According to our IRB approval, our data collection presented no more than minimal risks for the participants. All interview questions followed a respectful disposition using open-ended questions to engage participants. However, McVay explained before beginning the interviews that participants could stop, pause, or opt out of the interview if the questions brought too much emotional distress. No participant requested the interview to be stopped or paused. During the interviews, we used counseling skills to facilitate the conversation and to build upon the experiences discussed. We recorded and de-identified all interviews for verbatim transcription.
Participants also completed a demographic questionnaire before the interview to confirm their eligibility for the interview and obtain information on their age, gender, race/ethnicity, work setting, CACREP accreditation and degree, years working with sex trafficking survivors, and the number of clients they worked with who identified as trafficked.
Data Analysis
Utilizing Moustakas’s (1994) modification of Van Kaam’s data analysis, the research team engaged in the seven steps proposed by this approach. Data analysis and management relied on the use of NVivo software (Version 12). Interiano-Shiverdecker provided training in data analysis to McVay, Satel, and Smith. Interiano-Shiverdecker, McVay, Satel, and Smith engaged in the first step by individually analyzing transcripts and engaging in horizontalization of meaning units (Hays & Singh, 2012) to create in vivo codes for all nonrepetitive, nonoverlapping statements (meaning units). Second, we merged all files to determine the invariant constituents through a process of reduction and elimination. This first process of reduction allowed us to determine what was necessary and sufficient data to understand the phenomenon (Moustakas, 1994). The team then assigned themes or clusters of meaning to similar statements (third step). From the clusters of meaning, we created an initial codebook based on the discussions and findings from individual data analysis. We used the initial codebook to examine the themes against the dataset, ensuring that it was representative of participants’ experiences (fourth and fifth steps). As a team, we discussed any disagreements and worked on the data until we achieved a consensus. We worked out disagreements by discussing any opposing views and voting as a group on the best decision. We subsequently created textural descriptions through participants’ verbatim quotes, as well as created structural descriptions by examining the emotional, social, and cultural connections between what participants said (sixth step). Finally, we created composite textural-structural descriptions that outlined the reoccurring and prominent themes across all participants by organizing the themes into subthemes and ensuring that they represented all (if not most) participants’ experiences. After this analysis, we felt we achieved data saturation. After the completion of the initial analysis, Romero reviewed the data as a peer reviewer and offered suggestions. The entire research team reviewed the suggestions and came together to incorporate them until we reached a consensus and developed the final codebook.
Strategies for Trustworthiness
To limit the effects of researcher bias, we employed several strategies for trustworthiness. These included reflexive journals, triangulation of researchers, peer debriefers, an external auditor, member checking, and thick descriptions to ensure ethical validation, credibility, transferability, confirmability, sampling adequacy, and authenticity of our analysis (Hays & Singh, 2012). We engaged in reflexive journaling and weekly bracketing meetings during our individual and group data analysis to discuss codes, potential themes, and our assumptions shadowing the participants’ words. Researchers on the team brought varying levels of experience with research and the topic of sex trafficking, which we believe helped balance our subjective analysis of the data. We engaged in two rounds of member checking with the participants, one occurring after the transcription of the interviews and the second one after we wrote the themes. No participants changed the transcription of their interview or disagreed with the presentation of the themes. After the formulation of the themes from the original coding team, Romero served as a peer debriefer and reviewed the themes, key terms, and raw data, allowing participants to make recommendations on the content presented. This division in the research team allowed for another check outside of the original designated research team. An external auditor, a counselor educator with experience in conducting qualitative research, also reviewed the NVivo file and the write-up of the findings. The external auditor agreed with our data analysis procedures and presentation of the findings. He did provide suggestions to reduce the repetition of our first and second themes, which we implemented. Finally, we provide thick descriptions of our data collection and analysis procedures and present our results with direct quotes to ground our work.
Results
We identified four prevalent themes about mental health counselors’ experiences with sex trafficking survivors: (a) counselor knowledge: “learning curve,” (b) counselor skills: “creating a safe space to dive into work,” (c) counselor attitudes: “being able to listen to the client’s story,” and (d) counselor action: “more than just a counselor.” We use pseudonyms to present our results.
Counselor Knowledge: “Learning Curve”
All participants emphasized the importance not only of understanding trauma but also of gaining sex trafficking–specific knowledge throughout their work with survivors. Tiffany noted a “learning curve” when working with this population, despite working with trauma for most of her career. We categorized this theme into two subthemes: (a) understanding trauma work and (b) understanding sex trafficking and survivors.
Understanding Trauma Work
To work with sex trafficking, all counselors spoke about the importance of having general knowledge of trauma work. The most prominent topics included multicultural, legal, and ethical considerations. Important multicultural considerations for counselors involve understanding group differences between their clients (e.g., gender, race, age) and working from a culturally sensitive framework. Kimberly emphasized that “we really need people to not only have cultural sensitivity but also encourage those who are of other races to counsel these girls,” adding that “they need someone that’s like them from the same culture . . . to relate culturally to somebody.” Legal implications included understanding consent, informing clients of their limits of confidentiality when assessing for risk, and their role as mandated reporters. In reference to ethical practices, consultation and supervision arose as with any other trauma work. Stacy noted that it was “important for us to talk to one another if something’s going awry.”
Many participants conveyed how crucial it was for them to understand healing and its complexities. Cristina shared that clients are “going to have their ups and downs,” with Amanda echoing that there are “so many layers to the healing process.” Kimberly felt it important to remind herself that “you’re probably not going to see the seeds that you plant develop a lot of times.” Another important aspect of healing trauma, mentioned by half of the sample, was understanding clients’ stages of change. Stacy shared that one of her clients “went back to her hometown and relapsed immediately. And that’s also a hard thing to deal with—to know that I felt like we had some good sessions . . . and then it’s, ‘Wait a minute. You went back to the relapse [sex trafficking].’” Cristina noted that “especially [when they’re] first out and they’re not quite sure, that pre-contemplation if they want to leave or stay” was very important.
Another important aspect of their work included boundaries and self-care. All participants acknowledged that at some point in their careers, it was challenging to practice healthy boundaries. Cassandra acknowledged the following when working with individuals forced into sexual acts, “I wish I could take all the ladies I’ve ever worked [with], that have danced on stripper poles for money, unwillingly, and just like put clothes on them and wrap them up and hug them.” She added,
[It] can get really tricky when we start answering our phone because it’s an emergency all the time . . . and it’ll wear you out, your batteries will wear out, and you’ll end up having this dual relationship that will end up hurting her because . . . you’re not her friend.
It was helpful for Cassandra to remind herself that she was not the client’s parent. Rather, she shared, “when I hear things like that, I have to remind them that this is my job, this is what I do for a living.” Implementing healthy professional boundaries reduced burnout and facilitated self-care. Participants highlighted activities such as meditating, doing yoga, or taking the occasional day off. The counselors heeded that self-care also included managing their caseload to limit emotionally heavy clients or seeing a personal counselor themselves, as Cassandra and Amanda respectively noted. Amanda said, “you definitely have to secure your oxygen before you can secure other people’s.”
Understanding Sex Trafficking and Survivors
All participants explained that working with this population required them “to understand what sex trafficking is and . . . the many different ways that it looks,” as stated by John. He elaborated that “it takes many different forms and shapes,” some of which may not be immediately recognized as trafficking. Participants agreed that sex trafficking can often be much more discreet than one might anticipate. Tiffany commented on media portrayals like the film Taken, stating that the real experience is often much less dramatic: “Listening to their stories, it’s very, very subtle . . . like, if you do this then I’ll pay for your college tuition . . . and then from there it gets bigger.” Similarly, Cassandra noted that sex trafficking “can be, like, a bunch of underaged females, thrown in the back of a truck and trafficked across the United States” or people that “have their own residences, that don’t actually live with the trafficker, or they live with a family member that’s trafficking them.”
Counselors learned that although anyone can be trafficked, some populations are more vulnerable. According to Fen, these populations include clients with cognitive disabilities, immigrants, emotional abuse survivors, clients with PTSD, and clients with addictions. Other populations mentioned included the LGBTQ+ population, people recently released from jail/juvenile detention centers, college students with debt, and people in financial need.
The participants’ work also required them to learn how clients were recruited and what kept them from leaving sex trafficking. John and Amanda noted that many survivors knew their traffickers or were introduced to them by family, friends, or a romantic partner. Ana explained that traffickers may kidnap people from big sporting events or from opposing gang(s) or may train survivors to recruit and groom for them. She also worked with women recruited online from abroad and trafficked once they arrived in the United States. Counselors also learned about the numerous tactics used by traffickers, including the trauma bond, coercion, and control. John noted that traffickers often use manipulation: “The common theme was ‘If you do this, you’d really be helping me out. You wanna see me be okay?’ or ‘You don’t want me to go to jail, do you?’” Cassandra reported working with a client whose parents used “an odd twist on Christianity” and the principle of “respect your elders” to traffic her. Other tactics mentioned were threats of violence against survivors and their families, branding or tattooing survivors, stalking, taking survivors’ IDs, gaslighting, and fear. Cassandra also observed that trafficking was “so alluring . . . there’s a lot of money in that . . . so much about leaving sex trafficking is starting from zero and creating something new.” Amanda recalled a client who “was very upscale and so they lived kind of a lavish lifestyle, and I could see and understand, really emphasize the struggle to like give that up,” particularly when they were worried about providing for their families. Factors that forced individuals into sex trafficking were multilayered. Amanda continued, “so many other facets and like layers to this. It’s like an onion.”
As a result, counselors learned about the overall impact of sex trafficking on survivors’ mindsets, behaviors, and presenting symptomology. As noted by Kimberly, sex trafficking impacted every aspect of survivors’ lives. Tiffany noticed that many of her clients were initially very fragile and mistrusting of everyone, while Cristina and Stacy shared that it was common for their clients to display guarded and closed-off body language. John’s work taught him that sex trafficking “affects [clients] in terms of intimacy and trust, and that trickles into their relationships, whether it’s with family, roommates, or romantic partners.” The counselors’ work with sex trafficking survivors included clients with an array of presenting concerns. Cassandra observed clients with complex PTSD, substance use issues, self-harm behaviors, suicidal ideation, self-hatred, self-blame, feelings of insecurity, an inability to trust, and eating disorders. Ana also noted that clients presented with anxiety, depression, paranoia, and physical concerns such as sexually transmitted diseases (STDs) and sleep problems.
Counselor Skills: “Creating a Safe Space to Dive Into Work”
All participants recognized that because of the nature of their work and their clients, they needed to “create a safe space to dive into work,” as stated by Tiffany. To do so, they needed to build skills in two main categories: (a) assessment and ensuring safety and (b) processing trauma. Amanda explained, “I think all of that stuff [assessment and ensuring safety] really has to come first before we can do any really heavy work and therapy. . . They have to be stable before they can really dig into whatever they want to dig into.” Although this separation provides clarity, counselors’ experiences were also more fluid, at times requiring them to use skills particular to ensuring safety while processing trauma and vice versa.
Assessment and Ensuring Safety
All counselors’ experiences of assessment and ensuring safety consisted of effectively engaging with their clients during the intake interview, assessing risk, applying crisis skills, and formulating personalized treatment plans. Based on her experiences, Cristina spoke about the importance of building rapport during that initial interview: “When I do our initial assessment with them . . . I have the assessment, but I’m having a conversation with them.” She also learned to discuss confidentiality and mandated reporting with her clients to explain her role as the counselor while also giving them a choice: “I tell them straight out, like, ‘Hey, you tell me this, I have to report it, I have to call law enforcement . . . so how do you want to do it?’” Cassandra found that obtaining a thorough history of the client was a critical part of the process:
When addressing trauma, I don’t just go back to when the trafficking started. I go all the way back, make sure that I have that thorough history, because 99 times out of a 100, from my experience, that was not the first trauma that person experienced.
Seven participants spoke about learning the signs of sex trafficking and knowing what questions to ask to obtain more information and determine a person’s exposure to sex trafficking. Amanda explained, “I don’t think I’ve ever had somebody start off within an intake session be, like, ‘Hiya, so I was trafficked.’” Participants learned to ask about phone use and the number of phones owned, the extent of drug use, sexually transmitted diseases, wanted and unwanted pregnancies, boyfriends and their ages, and sexual behaviors such as the use of a condom. When assessing, Alejandra learned to “ask questions that minimize you coming across as being shaming or judging.” At the same time, some counselors spoke about the lack of sex trafficking assessments that could facilitate this part of their work. Alejandra explained that she “did an assessment at work yesterday, and there, there are no questions about sex trafficking. . . . There are questions about abuse, but it is inferring more [about] sexual abuse, physical abuse, emotional abuse versus sex trafficking.” Fen echoed this sentiment by wishing there was a more rigorous psychosocial interview that assessed risks associated with sex trafficking because “at times people do hide and at times people don’t disclose.”
All counselors agreed that a significant aspect of ensuring safety for their clients was collaborating with clients on safety plans. Counselors took the time to develop a “well thought out” safety plan with their clients, as stated by Alejandra. Stacy explained how she helped the client brainstorm ways to feel safer, including leaving town for a while or taking steps to “create a new account, changing her look a little bit . . . getting [a] new phone number.” Collaboration was not only utilized to respect clients’ autonomy but also to instill hope—“Hope that you know that you have a future,” stated Cristina. Ana elaborated, “seeing what they want for themselves and their lives, like, where do you want to go with your life . . . if you didn’t have this going on, you know, what is it you would like to do for yourself?”
Processing Trauma
To process trauma, all counselors listed skills, interventions, and therapies they found helpful with this population. Utilizing foundational skills (e.g., reflection, open-ended questions, appropriate self-disclosure) to build rapport was the most referenced code in this section, addressed by all participants. Cristina saw the benefit of learning how “to connect very quickly.” Stacy added, “I would definitely start relying a lot more on the rapport when I work with trauma.” Counselors also found it helpful to have a toolbox that included creative approaches and interventions that helped clients reclaim power, develop a support system, improve self-esteem, build and discover resiliency, and utilize the client’s strengths. Psychoeducation, mentioned by nine participants, included teaching their clients about sex trafficking because as John explained, “clients don’t always know that they are being trafficked.” Psychoeducation of sex trafficking requires explaining fraud, force, and manipulation. Kimberly explained how a client did not think she was trafficked because her partner did not have her “locked in a closet. I don’t got chains around me. I’m not his slave . . . I get up and get myself dressed. I go out there and meet these guys . . . I cooperate when he’s taking pictures of me.” To help her client reevaluate her situation, Kimberly utilized motivational interviewing–based questions such as “Would you let your sister do this?” or “What would be the benefits of leaving your situation?”
Although most counselors felt that an integrative approach to counseling worked best with sex trafficking clients, the therapies most mentioned included dialectical behavioral therapy, narrative therapy, and eye movement desensitization and reprocessing therapy. Counselors recommended individual treatment to process trauma, although four participants also mentioned family and group counseling. Fen found family therapy helpful “if the family wants to get involved in the practice” and “if there are family members who are ready to support them and come with them and who are aware of this.” Other participants mentioned the benefits of providing group counseling for sex trafficking survivors. Cassandra recalled how members of a support group she facilitated “connect with each other, they know that they’re not alone, they give each other honest feedback. . . . It has been super empowering.” Yet Alejandra, Fen, and Tiffany found that group counseling may not be well suited for all clients. “Group therapy doesn’t work really well because you know every survivor is different, and they don’t want to open up in front of others until they have worked through the process for a long time,” explained Fen.
Because of the nature of their work, counselors recognized that an essential skill to processing trauma was learning how to manage countertransference. Cristina spoke about how as “clinicians, we want to save all of them.” For this reason, Kimberly recognized that it was important for her to understand her attachment style. Cassandra recalled nights when she would go home and “worry about [if] I am going to see this client again.” Ana left sessions “shaking sometimes from those places . . . ’cause the stories I would hear.” Stacy highlighted that it was also difficult at times to manage the lies. She explained, “I was a little frustrated because I knew that she was hiding things . . . obviously it just wasn’t that time and that’s okay.” As a result, counselors found it essential to process their emotions. Kimberly explained that “if you haven’t emptied your cup of all the sad, mad, bad before you come into that office with them . . . you’re going to flip your lid whether it’s in front of them or behind closed doors.”
Counselor Attitudes: “Being Able to Listen to the Client’s Story”
All participant interviews illuminated thought patterns and beliefs they needed “to listen to the client’s story,” as stated by John. Counselors learned to personify certain attitudes by (a) valuing empathy and validation and (b) embodying a sense of safety.
Valuing Empathy and Validation
All participants highlighted the importance of embracing a philosophy of empathy and validation in their work with clients by being warm, genuine, open-minded, patient, and nonjudgmental. Participant interviews described various mechanisms to embody these attitudes. For instance, a consistent approach they took was to respect and empower the clients’ choices and, ultimately, believe in and provide client autonomy through supportive and nonjudgmental means. Ana emphasized, “I think that’s huge for those whose choices were taken away. . . . It’s offering them a choice, and I think that’s very empowering for them.” Fen echoed this message stating, “You can’t push—you can definitely motivate—but you cannot just push.” Kimberly learned to be patient: “You’ll end up getting there eventually, just take your time. . . . You have to build that rapport and trust.” Cassandra stated, “Another thing I would say is don’t make any assumptions. . . . Everybody’s experiences, although there are similarities, every experience is so different.” Cristina described the shock value of hearing survivors’ stories and how essential it was for her to remain nonjudgmental and aware of her biases. Amanda embodied “those Rogerian qualities, like that open-mindedness, empathy, warmth, genuineness, authenticity—those things are all really important to utilize when meeting with that population, or any population.” Cristina provided an example of how she conveyed this to a client by saying, “I’m here if you need me. . . . There’s no judgment happening, I’m just glad you’re here.”
Counselors also shared a philosophy that validated clients’ experiences. Fen believed in “just making clients feel normal,” while Cassandra noted how helpful it was for her to approach clients’ behaviors as “normal reactions to abnormal situations.” An important attitude communicated by John was that “they are survivors.” Even though others and possibly even the client themselves might use the word victim, he found it helpful to have “the conversation about being a survivor versus a victim.” Tiffany further explained, “I’ve noticed just in working with sex trafficking survivors . . . it seems very hard for them to say the word ‘abuse’ or view themselves as anything other than a victim.” She found value in seeing the client as “a survivor” and teaching this perspective to the client.
Embodying a Sense of Safety
All participants embraced attitudes that created and maintained a safe environment for their clients. Fen explained that as the counselor, “you’re the only safety net for that person” who provides safety and trust. Cristina reflected on a client who was still in “the life” and returned for help and services when needed. She stated, “she knows that I’m a safe person” and “this [shelter name] is her home, this is where she felt safe. But [she] knew she couldn’t get out of this life yet because she wasn’t ready to.” Fen explained that “there is shame, there is guilt, there is fear, and apprehension of being caught . . . so, one has to make them feel safe.” Some participants communicated and provided safety by creating a “homier and safer” office space or by buying a client’s favorite snacks and beverages, as described by Cassandra. Alejandra spoke of establishing “an environment where it’s safe to talk about taboo subjects” such as “having been a mule or whatever they did, you know, whatever sexual acts.”
Six of the participants also spoke of attitudes that promoted consistency and predictability. Kimberly stated, “That’s something they’ve never had in their life; you know, so while you’re doing all this other stuff, be consistent.” Several participants noted how difficult it was for their clients to have continuity with counselors. Kimberly shared:
Counseling someone who’s had this kind of trauma takes a long time . . . once you leave and can’t continue that counseling process, the likelihood of them going back to the counseling is very slim to none. . . . Even though they were resistant to building that rapport with you at the same time, deep down inside they’re connecting with you.
Similarly, a few participants learned to be consistent in their messages shared with clients and accessibility to clients. For instance, Stacy spoke of the need for congruency between actions and words when working with these individuals: “Trust is such a fleeting word . . . it has to be action, sometimes, speaks louder than the words.”
Counselor Action: “More Than Just a Counselor”
All participants realized that working with this population required them to reevaluate their role as the counselor. They learned that clients required “more than just a counselor,” as stated by Kimberly. Therefore, the fourth theme elucidated actions that counselors found necessary to help clients recover from their experiences. We categorized counselor action into two subthemes: (a) client advocacy and (b) engaging with social work/workers.
Client Advocacy
Over half of our participants spoke about the importance of advocating for clients. Cristina talked about how some clients did not have a caseworker and needed someone “that’s in their corner.” Counselors spoke about specific needs they advocated on behalf of clients in the life or in recovery. Kimberly spoke about advocating for prison reform, particularly for minority women who went to prison for some of the things they got involved in while being trafficked. Cristina advocated for “easier access to get into drug treatment.” She explained that this was necessary because certain insurances did not pay for certain drug treatments, or it would take too long to get clients into treatment. Although clients would sometimes agree to treatment, it would take several days “to get everything going. . . . by then the kids change their minds, or they run. . . .The obstacles shouldn’t be that hard.” Other forms of advocacy focused on working with and educating police officers to best work with this population. Tiffany explained how many women didn’t trust law enforcement. She believed it was crucial to bridge these services because law enforcement could “get them out of that lifestyle, but then on the other hand, they’re very much like, ‘Don’t trust them.’” Stacy also spoke about advocating for shelters specific to sex trafficking. She remembered a client who visited a shelter once a month and loved it because “she felt safe there versus just, like, a domestic violence clinic . . . they had the awareness of sex trafficking versus just, like, you know, an overnight shelter type of place.”
Participants also taught clients how to advocate for themselves while also respecting their choices. Stacy explained, “It’s not my job to fix what they’re going through, but it is my job to be as supportive as I can.” She understood that she needed to “advocate for them but also having the respect that if they don’t want me to advocate for them, then that’s the place that they’re at too.” Stacy also clarified that at times she does not “really know exactly 100% how I would want to advocate” for clients who had been trafficked. Yet as she continued to reflect, she realized her desire to “seek out more education about it because I do think that it needs to be navigated in a specific way.”
Engaging With Social Work/Workers
The call for advocacy led all counselors to speak about how their work required them to expand their roles to connect clients to resources and collaborate with social workers. Kimberly explained that this population requires “more than just a counselor while they’re in session . . . you’ve really got to start with building a community around them before you get into the deep trauma work.” Counselors provided resources to obtain transportation, financial assistance, government assistance, their GED or college degree, food, employment, stable housing, legal support, childcare, hygiene products, substance treatment, and medical care. Amanda explained that this population requires that their basic-level needs be met to help them feel like they “can function in society and be comfortable,” and Kimberly elaborated:
As a counselor, I used to have a huge list of resources that I could give them, but they also needed guidance from outside of the counseling office. . . . I have, like, eight people with one survivor, that’s how much it took us ’cause it’s so much work for one person. You’re talking about every aspect, everything that you learned as a child growing up. . . . If you want counseling to be successful, they have to have that outside component to help them . . . a counselor can’t do all of that.
Ana partnered up with organizations already doing this work. She particularly spoke about an organization that not only focused on “educating people but also helping these women with resources.” She added that “the residential places they were able to stay in, they were able to finish their education and get an education there, and they also helped them with finding jobs, which was really important for them, too.” She explained that this was particularly important because many of the women she worked with had a violent criminal history. Many company insurances refused to hire women with criminal records, preventing their clients from a second chance at improving their lives. However, John learned to support clients with resources. “I don’t think it’s sufficient to just say ‘Here you go, here’s the resource guide. They have lots of options in there. Good luck.’ . . . Our job doesn’t end with giving the resources,” he explained.
An important point to make is that although some counselors spoke about collaborating with social workers, it seemed that most believe their work resembled “a little more of that, like, case management–type stuff to make sure that they have the resources if and when they want out,” added Cassandra. Kimberly elaborated, “You’re the one that’s helping to get them to [a] place where they can have a relatively stable life . . . but without the resources that come alongside that, they’re gonna go nowhere, [they’re] going to hit a wall every time.”
Discussion
We sought to understand counselors’ experiences working with sex trafficking survivors through a phenomenological analysis. The participants in our study needed to understand and address the different aspects of trauma. Because of clients’ traumatic experiences that resulted in psychological injuries (Cole et al., 2016; Grosso et al., 2018; Lutnik, 2016; Muftić & Finn, 2013; O’Brien et al., 2017), counselors benefited from respecting the process of healing, addressing stages of change, and building a safe and trusting relationship. Counselors overall possessed knowledge of the development of post-trauma responses over time. They knew what to look for and how to best treat traumatic symptoms that permeated all aspects of their client’s lives, particularly sex trafficking survivors’ ability to trust others. Counselors believed that having a trauma-informed approach could reduce instances of re-victimization. Counselors also recognized the importance of self-awareness such as assessment of personal trauma, self-care, restorative practice, and biases regarding how youth are trafficked and by whom.
Yet, our findings demonstrate that working with sex trafficking survivors requires additional competencies as illustrated in previous research (Interiano-Shiverdecker et al., 2023). The participants discussed the need to become educated in recognizing the signs of sex trafficking, vulnerable populations, and the processes by which traffickers force people into sex trafficking to obtain a deeper understanding of the client’s worldview and provide appropriate support (Interiano-Shiverdecker et al., 2023). Participants addressed components—namely force, fraud, coercion, exploitation, power, grooming, and solicitation—commonly used in sex trafficking literature (Bruhns et al., 2018). When asked about the nature of their work, their focus naturally divided into sections that focused on assessing risk and safety planning, processing trauma, and helping the client re-establish their life and their identity. Our findings align with CACREP (2015) recommendations for clinical crisis skills and knowledge while also elucidating their application to sex trafficking survivors. Participants learned to assess for specific sex trafficking signs (e.g., phone usage, boyfriends and their ages, sexual behaviors) and to ask questions that differentiated sex trafficking from other forms of abuse.
Counselors must also understand the differences between sex work (i.e., the voluntary exchange of sexual services for compensation) and sex trafficking (i.e., subjection to the exchange of sexual services due to force, fraud, or coercion or from any person under the age of 18). As Ana shared, most counselors felt that the notion to detect was on their end “because I don’t always think it’s the responsibility of the client to be able to say ‘Hey, I’ve been trafficked.’” Thus, participants indicated that possessing these competencies could help increase the identification of sex trafficking. As such, some counselors may desire more guidance on specific sex trafficking assessments, which scholars have previously noted (Interiano-Shiverdecker et al., 2022; Romero et al., 2021). A content analysis on sex trafficking instruments (Interiano-Shiverdecker et al., 2022) illustrated the importance of asking specific questions to assess for control, confinement, threat, and isolation, as these are the main indicators of sex trafficking. Example items included: “Have you ever felt you could not leave the place where you worked [or did other activities]?” (confinement; Simich et al., 2014, p. 20); “Are you kept from contacting your friends and/or family whenever you would like?” (isolation; Mumma et al., 2017, p. 619); “Do you have to ask permission to eat, sleep, use the bathroom, or go to the doctor?” (control; Mumma et al., 2017, p. 619); and “Has anyone threatened your family?” (threat; Mumma et al., 2017, p. 619).
Moreover, for some sex trafficking victims, the relationship with their traffickers represented an affirming, reliable, and secure relationship in their lives, later used to coerce or force them into sexual, violent, or illegal behavior. Therefore, participants realized that processing trauma would require attitudes and skills that provided emotional safety, patience, and a nonjudgmental process. Survivors’ lack of choice throughout their sex trafficking experience fomented counselors’ abilities to empower clients over their bodies, boundaries, and choices, and help clients reintegrate into society (Interiano-Shiverdecker et al., 2023; Thompson & Haley, 2018). Participants seemed to emphasize that without all the elements mentioned, clients might not disclose their situation or trust the counselor enough to open up, and they might even terminate counseling abruptly.
This last point is connected to our fourth finding, counselor action. Aligned with the Multicultural and Social Justice Counseling Competencies (Ratts et al., 2016), the participants in our study recognized the need to engage in work that advocated for clients within and outside of the session. Despite their dedicated work with clients to process the emotional repercussions of sex trafficking and rebuild their lives, their efforts did not seem enough to support clients in their recovery. So much of what ailed their clients fell on systemic or external forces (e.g., poverty, employment, lack of resources). Although that existed outside of the counselor’s role and verged into another profession, our participants embraced these responsibilities or connected with other professionals. They believed that otherwise, clients would not succeed in their recovery. Our findings present an important reminder that sex trafficking, a modern form of human slavery, is an act of social injustice affecting individuals vulnerable to historical and systemic oppression.
Implications
Our themes add to the existing research with implications for counseling practice, supervision, and education. Scholars (Romero et al., 2021; Thompson & Haley, 2018) have identified counselors as first-hand responders to the early detection and prevention of sex trafficking. Although each trafficking scenario is unique, counselors need to refer to sex trafficking indicators, recruitment and grooming tactics, and manipulative dynamics that prevent individuals from disclosing or leaving sex trafficking. It is important for counselors to dispel common myths of sex trafficking and understand that sex trafficking may appear differently than one may expect. Amanda alluded to clients who defined their experience as a “lavish lifestyle” and were lured by the financial benefits of sex trafficking. We caution counselors not to misinterpret sex trafficking as a “lifestyle,” as this implies choice. There may be a myriad of invisible factors contributing to their circumstances such as trauma bonding and financial instability.
Participants agreed that an integrative approach with interventions that addressed complex trauma (e.g., dialectical behavior therapy, eye movement desensitization and reprocessing therapy) worked best when working with sex trafficking. We encourage counselors to not only become familiar with such modalities but also to conceptualize any treatment modality through a trauma-focused lens that considers how sex trafficking impacts all aspects of a client’s life and how they will interact in session. Participant narratives indicated that clients could present with defiant behaviors, distrust, angry or irritable mood, and refusal to comply with treatment. These themes underscore the importance of a counselor’s ability to create safe, trusting, and empathic relationships that allow the client to disclose risk and eventually process trauma. Counselors should also integrate a strong rapport with sex trafficking clients by demonstrating unconditional positive regard, authenticity, and empathy with any treatment modality chosen. Although counselors establish a strong therapeutic relationship, they can integrate other counseling goals, including psychoeducation, assessing for risk, supporting clients through the stages of personal change, and helping the client rebuild and reintegrate into society. Based on the nature of their work, managing countertransference and self-care represents an essential instrument to maintain balance while engaging in emotionally draining clinical work. We encourage counselors to seek supervision, connect with colleagues, and practice regular self-care routines to avoid experiencing burnout, secondary trauma, and countertransference. Additionally, counselors should connect clients to services that provide basic needs (e.g., safe and stable housing, food). When clients lack basic physiological needs, they may struggle to focus on higher-order needs such as developing a safety plan or emotion regulation. Counselors can engage in legislative advocacy by writing letters to judges, sharing clinical experiences with senators, and providing training on sex trafficking victim identification and treatment. It is important for counselors to build constituency groups with education, governmental task forces, and legislators to lobby for bills that benefit clients, as sex trafficking exists in an ecosystem of community and social contexts (Farrell & Barrio Minton, 2019). Our findings also underscore the limitations of intake interviews when assessing for sex trafficking risk. Although identification and screening tools exist (Interiano-Shiverdecker et al., 2022; Romero et al., 2021), counselors are not always in a setting where a formal assessment is appropriate or accessible.
We encourage educators and supervisors to emphasize the value of informal assessment methods with counselors-in-training. Counselor knowledge of signs, symptoms, and questions to ask during an intake can improve identification efforts. Our findings also hold some implications for training beyond counselor education. Because of the complexities of working with trauma and sex trafficking, counselors intending to work with this population should seek out specialized training. For instance, they may review conference programs for trauma or sex trafficking–specific education sessions. At the same time, counseling programs should evaluate their preparation for counselors to work with sex trafficking. Requiring a trauma course, including content on sex trafficking and complex trauma throughout the curriculum (e.g., trauma, grief, addiction counseling courses), inviting guest speakers, and providing training opportunities and workshops for students and community counselors are all suggestions to ensure that counselors obtain the necessary knowledge and skills to work with this population. We believe that more training opportunities can minimize any possible misunderstanding of sex trafficking, expectations on clients to disclose, and re-victimization of clients that leads to early termination of counseling.
Limitations and Future Directions
The nature of our sample holds some limitations for the interpretation and application of the themes from this study. We collected data from single data sources (i.e., individual interviews); additional interview sources (e.g., focus groups) may have contributed more information. Moreover, lack of racial and gender diversity was a limitation in this study because most participants identified as White and female. We noticed that participants did not discuss racial and gender differences in clients’ experiences of sex trafficking. This result could have originated from our interview protocol that sought to gain an overall understanding of sex trafficking experiences and therefore did not request this information. Participants’ demographic profiles may have also provided a limited perspective of the experiences of Black, Indigenous, and/or people of color. We also did not require CACREP accreditation or specific years of practice as part of our inclusion criteria. Although all our participants were licensed professional counselors, they had different degrees in mental health, a variety of clinical practice, and did not all graduate from CACREP-accredited programs. During our interviews, we did not define sex trafficking to the participants and engaged in open-ended questions that inquired about their experiences. Participants’ responses are based on their definition of sex trafficking, which can vary and might not be accurately distinguishable from sex work. As is the case with all qualitative research, counselors and scholars should consider the transferability of these findings to other client populations and with counselors. For example, the findings of this study can be applicable to professional school counselors, but the recruitment of school counselors as participants would have provided greater insight into the roles and responsibilities of counselors in schools. Furthermore, we did not include client perspectives in this study; therefore, even though our participants’ perspectives when working with sex trafficking survivors is very insightful, they may not have an accurate representation of clients’ experiences in session.
Based on these limitations, we recommend scholars explore individual and external factors that can impact counselors’ work with sex trafficking survivors. For example, we did not explore within-group differences (e.g., race, gender, sexual orientation, religion) between counselors and cross-cultural interactions between clients and counselors. These factors are important to consider and reflect on when building trust and a sense of safety for the client, particularly when considering current conversations around racial tension in the United States. A more in-depth analysis of these considerations could facilitate a better understanding of how multicultural traits play a role in counselors’ experiences when working with sex trafficking survivors. Participants’ emphasis on the need for specialized knowledge and skills to work with sex trafficking also warrants research on evidence-based interventions for sex trafficking survivors. Moreover, an examination of the client’s experiences is necessary to garner a holistic picture of the impact of sex trafficking on the client’s healing and counseling process. We also believe that researchers should consider external factors that might impact counselors’ experiences when working with sex trafficking. Considering participants’ discussion of advocacy and engaging with social work/workers, it seems necessary to consider sociopolitical and institutional elements that either hinder or support clients’ ability to leave sex trafficking and obtain access to services that allow them to heal and flourish. As such, counselors working with sex trafficking survivors must consider specific training that allows them to assess for risk, process the emotional ramifications of sex trafficking, and rebuild their lives.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2022). ASCA ethical standards for school counselors.
https://www.schoolcounselor.org/getmedia/44f30280-ffe8-4b41-9ad8-f15909c3d164/EthicalStandards.pdf
Browne-James, L., Litam, S. D. A., & McRae, L. (2021). Child sex trafficking: Strategies for identification, counseling, and advocacy. International Journal for the Advancement of Counselling, 43, 113–125.
https://doi.org/10.1007/s10447-020-09420-y
Bruhns, M. E., del Prado, A., Slezakova, J., Lapinski, A. J., Li, T., & Pizer, B. (2018). Survivors’ perspectives on recovery from commercial sexual exploitation beginning in childhood. The Counseling Psychologist, 46(4), 413–455. https://doi.org/10.1177/0011000018777544
Burt, I. (2019). Modern-day slavery in the U.S.: Human trafficking and counselor awareness. International Journal for the Advancement of Counselling, 41, 187–200. https://doi.org/10.1007/s10447-018-9366-7
Cole, J., Sprang, G., Lee, R., & Cohen, J. (2016). The trauma of commercial sexual exploitation of youth: A comparison of CSE victims to sexual abuse victims in a clinical sample. Journal of Interpersonal Violence, 31(1), 122–146. https://doi.org/10.1177/0886260514555133
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Creswell, J. W. (2013). Research design: Qualitative, quantitative, and mixed methods approaches (4th ed.). SAGE.
Farrell, I. C., & Barrio Minton, C. A. (2019). Advocacy among counseling leaders: The three-tiered legislative professional advocacy model. Journal of Counselor Leadership and Advocacy, 6(2), 144–159. https://doi.org/10.1080/2326716X.2019.1644254
Franchino-Olsen, H. (2019). Vulnerabilities relevant for commercial sexual exploitation of children/domestic minor sex trafficking: A systematic review of risk factors. Trauma, Violence & Abuse, 22(1), 99–111. https://doi.org/10.1177/1524838018821956
Grosso, A., Busch, S., Mothopeng, T., Sweitzer, S., Nkonyana, J., Mpooa, N., Taruberekera, T., & Baral, S. (2018). HIV risks and needs related to the sustainable development goals among female sex workers who were commercially sexually exploited as children in Lesotho. Journal of the International AIDS Society, 21(S1), e25042. https://doi.org/10.1002/jia2.25042
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Interiano-Shiverdecker, C. G., Romero, D. E., Anderson, A., & Castellon, N. E. (2022). A content analysis of sex trafficking instruments. International Journal for the Advancement of Counselling, 44, 373–394. https://doi.org/10.1007/s10447-021-09463-9
Interiano-Shiverdecker, C. G., Romero, D. E., & Elliot, J. (2023). Development of child sex trafficking counseling competencies in the United States: A Delphi study. Journal of Interpersonal Violence, 38(1–2), 1397–1423. https://doi.org/10.1177/08862605221090569
International Labour Organization. (2017). Global estimates of modern slavery: Forced labour and forced marriage. https://www.ilo.org/global/topics/forced-labour/publications/WCMS_854733/lang–en/index.htm
Johnson, B. C. (2020). Featured counter-trafficking program: Trauma recovery for victims of sex trafficking. Child Abuse & Neglect, 100, 104–153. https://doi.org/10.1016/j.chiabu.2019.104153
Kenny, M. C., Helpingstine, C. E., Harrington, M. C., & McEachern, A. G. (2018). A comprehensive group approach for commercially sexually exploited girls. The Journal for Specialists in Group Work, 43(4), 376–398. https://doi.org/10.1080/01933922.2018.1484540
Litam, S. D. A. (2017). Human sex trafficking in America: What counselors need to know. The Professional Counselor, 7(1), 45–61. https://doi.org/10.15241/sdal.7.1.45
Litam, S. D. A. (2019). She’s just a prostitute: The effects of labels on counselor attitudes, empathy, and rape myth acceptance. The Professional Counselor, 9(4), 396–415. https://doi.org/10.15241/sdal.9.4.396
Litam, S. D. A., & Lam, E. T. C. (2020). Sex trafficking beliefs in counselors: Establishing the need for human trafficking training in counselor education programs. International Journal for the Advancement of Counselling, 43(1), 1–18. https://doi.org/10.1007/s10447-020-09408-8
Lutnik, A. (2016). Domestic minor sex trafficking: Beyond victims and villains. Columbia University Press.
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Muftić, L. R., & Finn, M. A. (2013). Health outcomes among women trafficked for sex in the United States: A closer look. Journal of Interpersonal Violence, 28(9), 1859–1885. https://doi.org/10.1177/0886260512469102
Mumma, B. E., Scofield, M. E., Mendoza, L. P., Toofan, Y., Youngyunpipatkul, J., & Hernandez, B. (2017). Screening for victims of sex trafficking in the emergency department: A pilot program. Western Journal of Emergency Medicine: Integrating Emergency Care with Population Health, 18(4).
https://doi.org/10.5811/westjem.2017.2.31924
National Human Trafficking Hotline. (n.d.). National statistics. https://humantraffickinghotline.org/states
O’Brien, J., Li, W., Givens, A., & Leibowitz, G. S. (2017). Domestic minor sex trafficking among adjudicated male youth: Prevalence and links to treatment. Children and Youth Services Review, 82, 392–399. https://doi.org/10.1016/j.childyouth.2017.09.026
Oram, S., Abas, M., Bick, D., Boyle, A., French, R., Jakobowitz, S., Khondoker, M., Stanley, N., Trevillion, K., Howard, L., & Zimmerman, C. (2016). Human trafficking and health: A survey of male and female survivors in England. American Journal of Public Health, 106(6), 1073–1078. https://doi.org/10.2105/AJPH.2016.303095
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Romero, D. E., Interiano-Shiverdecker, C. G., Castellon, N. E., & Strentzsch, J. (2021). A review of child sex trafficking instruments. Journal of Child and Adolescent Counseling, 7(1), 56–69. https://doi.org/10.1080/23727810.2020.1835421
Schmidt, C., Lenz, A. S., & Oliver, M. (2022). Effectiveness of TF-CBT with sex trafficking victims in a secure post-adjudication facility. Journal of Counseling & Development, 100(4), 1–13. https://doi.org/10.1002/jcad/12438
Simich, L., Goyen, L., Powell, A., & Berberich, K. (2014). Out of the shadows: A tool for the identification of victims of human trafficking. Vera Institute of Justice. https://www.vera.org/publications/out-of-the-shadows-identification-of-victims-of-human-trafficking
Thompson, J., & Haley, M. (2018). Human trafficking: Preparing counselors to work with survivors. International Journal for the Advancement of Counselling, 40(3), 298–309. https://doi.org/10.1007/s10447-018-9327-1
U.S. Department of State. (2021). Trafficking of persons report. https://www.state.gov/wp-content/uploads/2021/09/TIPR-GPA-upload-07222021.pdf
Victims of Trafficking and Violence Protection Act of 2000, Pub. L. No. 106-386, § 103, 114 Stat. 1470.
Wang, X., & Park-Taylor, J. (2021). Therapists’ experiences of counseling foreign-national sex-trafficking survivors in the U.S. and the impact of COVID-19. Traumatology, 27(4), 419–431. https://doi.org/10.1037/trm0000349
Woehler, E., & Akers, L. (2022). Repairing the trauma bonds of sex trafficking victim-survivors with animal-assisted therapy. Journal of Creativity in Mental Health, 17(4), 456–458. https://doi.org/10.1080/15401383.2021.1921646
Claudia G. Interiano-Shiverdecker, PhD, LPC-A, is an assistant professor at the University of Texas at San Antonio. Devon E. Romero, PhD, NCC, LPC, is an assistant professor at the University of Texas at San Antonio. Katherine E. McVay, PhD, LPC, is an assistant professor at Texas A&M University–Corpus Christi. Emily Satel is a graduate of the master’s program in clinical mental health counseling at the University of Texas at San Antonio. Kendra Smith is a graduate of the master’s program in clinical mental health counseling at the University of Texas at San Antonio. Correspondence may be addressed to Claudia G. Interiano-Shiverdecker, College of Education and Human Development, One UTSA Circle, San Antonio, TX 78249, claudia.interiano-shiverdecker@utsa.edu.
Appendix
Icebreaker
- Please tell me a little about yourself, your professional background, and clinical experience.
Counseling
- What is important for counselors to know when working with sex trafficking survivors?
- How can counselors best detect when individuals are being sex trafficked or are vulnerable to sex trafficking?
- How can counselors support individuals while they are being trafficked?
- How can counselors help individuals leave their traffickers?
- How can counselors support individuals from returning to their traffickers?
- What do counselors have to know about supporting sex trafficking survivors after sex trafficking?
Personal Experiences and Mental Health
- Please share, to the extent that you are comfortable, your experiences with working with sex trafficking survivors.
- What is the age range in which most of your clients experienced sex trafficking?
- How have these experiences impacted your clients?
- Emotionally and mentally?
- Physically?
- Relationships with others?
- Spiritual/religious beliefs?
- What do you believe has helped them overcome the impact of sex trafficking?
- What services or resources do you believe were most helpful to them?
- What is important about your experience that I haven’t asked you and you haven’t had the chance to tell me?
