Aug 24, 2023 | Volume 13 - Issue 2
Chloe Lancaster, Michelle W. Brasfield
The COVID-19 pandemic led to an unparalleled disruption of student learning, disengaged students from school and peers, increased exposure to trauma, and had a negative impact on students’ mental health and well-being. School counselors are the most accessible mental health care professionals in a school, providing support for all students’ social and emotional needs and academic success. This study used an exploratory survey design to investigate the perspectives of 207 school counselors in Tennessee regarding students’ COVID-19–related mental health, academic functioning, and interpersonal skills; interventions school counselors have deployed to support students; and barriers they have encountered. Results indicate that students’ mental health has significantly declined across all grade levels and is interconnected with academic, social, and behavioral problems; school counselors have provided support consistent with crisis counseling; and caseload and non-counseling duties have created significant barriers in the provision of care.
Keywords: COVID-19, school counselors, student mental health, interventions, barriers
The psychological cost of the COVID-19 pandemic has been profound and wide-reaching. Although the K–12 population has been less susceptible to the adverse physical effects of COVID-19, for many, the pandemic has left an indelible mark on their mental health (Karaman et al., 2021). Before the outbreak of COVID-19 in 2020, youth mental health had become an issue of national concern, with one in six minors struggling with mental illness (Whitney & Peterson, 2019). Research has emerged to indicate that COVID-19 has further elevated the mental health problems of K–12 students across the nation (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). The end of COVID-19 lockdown restrictions may have alleviated immediate issues associated with social isolation and online learning; however, for those students experiencing COVID-19–related trauma and crisis, symptomatology has persisted beyond school reentry (Centers for Disease Control and Prevention [CDC], 2022; Patterson, 2022). As frontline helping professionals with training in mental health and school systems, school counselors are often the first responders to students in crisis (Karaman et al., 2021; Lambie et al., 2019), yet researchers have not explored reentry problems from the school counselor’s perspective. We conducted this study to understand school counselors’ experience of COVID-19–related student issues, their strategies to assist students, and their encountered barriers. We theorized that persistent problems related to the organizational structures within which counselors work, such as large caseloads, assignment of non-counseling duties, and under-resourced schools and communities (Lambie et al., 2019), may have greatly impacted their ability to meaningfully help students in high need of mental health support.
Literature Review
Students and COVID-19–Related Distress
From the outset of the COVID-19 pandemic, scholars predicted that disruptions to schooling, COVID-19–related stress, family conflict, and frequent media exposure to the pandemic would amplify mental health problems in children and youth (Imran et al., 2020). Empirical studies published in 2020 and 2021 have substantiated this concern, with findings indicating that COVID-19 restrictions adversely affected youth in multiple ways, including the development of unhealthy eating habits, increased screen time, reduced physical activity, sleep disturbances, academic delays, social problems, and an overall escalation in mental health concerns (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). The preponderance of research focused on adolescents, particularly as extended time in social isolation disrupted their developmental reliance on peer interactions for social and emotional support (Imran et al., 2020). Multiple studies found that not feeling connected to friends, high social media usage, and general COVID-19–related fears were associated with higher levels of depression and anxiety (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021).
Although less is known about the impact of COVID-19 on younger children, evidence is emerging to indicate that the COVID-19 pandemic has elevated adverse childhood experiences (ACEs; Bryant et al., 2020). From a developmental perspective, children are less able to communicate and process their thoughts and feelings and are greatly affected by the emotional state of their caregivers (Zimmer-Gembeck & Skinner, 2011). Thus, exposure to parental anxieties related to housing, food, and economic insecurity likely exerted a destabilizing effect on children during the stay-at-home mandate and beyond (Imran et al., 2020). Further, children in poverty may be particularly vulnerable to an amplification of ACEs due to their families being disproportionately impacted by economic hardships and family mortality during the pandemic (Bryant et al., 2020).
Students’ Mental Health Pre-Pandemic
The COVID-19 pandemic increased intra-family adversity, which has long-term implications for the well-being of children and adolescents (CDC, 2022). However, in pre–COVID-19 times, with the rise in school shootings and teen suicide, the mental health of K–12 populations had already become a public health concern. According to the National Alliance on Mental Illness, one in six children aged 6–17 experienced a mental health disorder (Whitney & Peterson, 2019). Since reentry following COVID-19 shutdowns, indicators suggest the COVID-19 pandemic has worsened children’s mental health (CDC, 2022; Karaman et al., 2021), with widespread reports of student learning gaps, chronic absenteeism, declines in social skills, and increased behavior problems (CDC, 2022; Patterson, 2022). Further, previous research on children’s responses to a variety of traumatic events has found that children and adolescents can develop long-term mental illness following a traumatic experience, which is unlikely to abate without intervention (Udwin et al., 2000). For youth, the experience of mental health problems increases their risk factors in other areas, such as a decline in academic performance, poor decision-making, drug use, and high-risk sexual behaviors (CDC, 2022). In this regard, the responsiveness of schools to flex their organizational resources to address the psychological changes in their student body seems instrumental in assuaging the long-term effects of COVID-related trauma and the mitigation of adverse educational outcomes (Savitz-Romer et al., 2021).
School Counselors’ Role in Provision of Mental Health Services
Schools have long been discussed as a primary access point for mental health services, given that children spend much of their day in school, and children and adolescents in need of mental health care are more likely to receive assistance in a school as opposed to a clinical setting (Lambie et al., 2019). Conversations about students’ access to mental health care in school settings segue to the role of school counselors and students’ access to school counseling services. School counselors are the most accessible mental health care professionals in schools, with 80.7% of schools employing full-time or part-time school counselors (Lambie et al., 2019). By contrast, only 66.5% employ a school psychologist, and 41.5% employ a school social worker (National Center for Educational Statistics, 2016). Further, school counselors are trained in crisis prevention and responsive services, including individual and group counseling; consultation with administrators, teachers, parents, and professionals; and coordination of services within a multi-tiered system of supports (MTSS; Pincus et al., 2020).
Evidence to support school counselors’ work in times of crisis comes from multiple sources. Salloum and Overstreet (2008) found that a school counselor–led small group implemented after Hurricane Katrina improved PTSD symptoms among elementary school students. Similarly, Udwin and colleagues (2000) found that students who received psychological support at school following a national crisis experienced a reduction in PTSD symptomology. Additionally, scholars have proposed that school counselors utilize their skill set in assessment to administer universal mental health screenings to identify students at greater risk of having or developing mental health concerns (Lambie et al., 2019; Pincus et al., 2020).
Barriers School Counselors Face in the Provision of Services
Although school counselors have the training and skills necessary to assist students transitioning back to school from a disruption like COVID-19, they face multiple barriers to their work. Most notably, they struggle with unmanageable caseloads. The American School Counselor Association (ASCA) recommends that counselor-to-student ratios not exceed 1:250 (ASCA, 2019). Yet, the average ratio in the United States is 1:455, with Tennessee experiencing an average ratio of 1:450 (Patel & Clinedinst, 2021). Research indicates that large school counselor caseloads adversely affect student outcomes, insofar as attendance, graduation, and disciplinary problems are more prevalent in schools with high school counselor caseloads (Parzych et al., 2019). Unfortunately, minority students in under-resourced schools are disproportionately impacted by high counselor ratios (Whitney & Peterson, 2019) and are more likely to experience adverse educational outcomes, as well as unmet mental health needs (Kaffenberger & O’Rorke-Trigiani, 2013). These findings raise concern for students whose mental health and academics have declined since the emergence of COVID-19 who attend schools with overstretched counselors struggling to meet the needs of their student body. This study was conducted in part to explore if caseload correlates to school counselors’ perceived ability to attend to students’ COVID-related problems and if differences were more pronounced in schools with lower socioeconomic status (SES).
In addition to ratios, ASCA recommends that school counselors spend 80% of their time providing direct and indirect services to students. Program elements within direct service include curriculum delivery, individual student planning, and responsive services. Indirect services include referrals to other agencies and programs within and outside the school system and consultation and collaboration with stakeholders, particularly for crisis response (ASCA, 2019). Researchers have documented the favorable effects on student academics and behaviors when school counselors follow these national guidelines for time and role allocations (Cholewa et al., 2015). Nonetheless, school counselors are often assigned non-counseling duties by their campus and district administrators (Gysbers & Henderson, 2012), preventing them from fulfilling their appropriate roles. These duties include test coordination, record keeping, attendance monitoring, substitute teaching, and student discipline (ASCA, 2019). Data indicate that non-counseling duties may be more problematic at the secondary level, with high school counselors over-reporting non-counseling duties, when compared to elementary school counselors (Chandler et al., 2018). Geographic differences have also been documented, with rural school counselors reporting higher levels of non-counseling duties in comparison to urban school counselors (Chandler et al., 2018). In the current study, we were curious to understand the impact of non-counseling duties on school counselors’ response to students’ COVID-19 concerns and to explore the intersection of counselor responsiveness to COVID-19 by non-counseling duties, grade level, and geographic region (e.g., urban, suburban, rural), respectively.
School Responses to COVID-19 in Tennessee
In response to the COVID-19 pandemic, Tennessee’s governor ordered all Tennessee public schools closed from March 20 until March 31, 2020, and extended this closure through the end of the 2019–2020 school year. To complete the school year outside of the physical educational space, districts created their own plans to address student learning, often dependent on available technology and resources (Tennessee Office of the Governor, 2020). Districts made decisions for returning in the fall 2020 semester based on guidelines from the Tennessee Department of Education (DOE), which included social distancing, smaller class size, assigned seats, and alternating in-person days with distance learning (Tennessee DOE, 2020). To provide further context to our survey responses, in 2019, the state DOE (Tennessee State Board of Education, 2017) updated its school counseling policy and standards to require school counselors to spend 80% of their time in direct service to students, a specification consistent with the ASCA National Model for allocation of school counselor time. Although the policy stated counselor ratios should not exceed 1:500 in elementary and 1:350 in secondary schools, this specification falls short of the ASCA 1:250 recommendation. Further, because of the state funding formula that permits school districts to hire administrators in lieu of school counselors, depending on school needs, we expected many of the school counselors would have caseloads that exceeded DOE policy.
Purpose of Study
School counselors are uniquely positioned to assist students with their mental health, including COVID-19–related concerns, in a school context (Pincus et al., 2020). Yet, even before the COVID-19 pandemic, school counseling programs were frequently under-equipped to meet the magnitude of students’ mental health needs (DeKruyf et al., 2013). This study was conducted to understand, from the perspective of school counselors in Tennessee, the ongoing impact of COVID-19 upon students’ mental health, examine strategies they have deployed to assist students, and discover barriers encountered in providing care to meet their students’ needs. Because poor mental health manifests in a plethora of academic, behavior, and social skill adjustment issues for children and adolescents (CDC, 2022), we also examined school counselors’ perceptions of changes in those domains from pre-pandemic to current times. Given documented patterns of variability in school counselor programs, we also investigated school counselors’ perceived barriers to assisting students by location, SES, and assigned non-counseling duties. To address the aim of the study, we posited three related research questions (RQs):
| RQ1: |
How has COVID-19 affected students’ mental health, academics, and social skills in Tennessee? What issues presented the greatest concern, and how did interventions differ by grade level (elementary, middle, or high school)? |
| RQ2: |
What interventions do school counselors in Tennessee use to assist students with their COVID-19–related concerns, and how do interventions differ by grade level (elementary, middle, or high school)? |
| RQ3: |
What barriers do school counselors in Tennessee report as interfering with their ability to address students’ COVID-19 concerns? Do reported barriers differ by grade level (elementary, middle, or high), location (urban, suburban, or rural), socioeconomic status, non-counseling duties, size of caseload (small, medium, or large), or following the state guideline for spending 80% of the time in student services? |
Method
Study Design and Instrumentation
Given the absence of research examining school counselors’ perspectives of how the pandemic has affected student mental health, their response to students’ COVID-19 issues, and barriers encountered in their efforts, we employed an exploratory research design. Exploratory designs are used when there is limited prior research to warrant the examination of a directional hypothesis (Swedberg, 2020). Within the framework of an exploratory design, we developed a non-standardized instrument to answer the three research questions. Although this constitutes a limitation of the study, we endeavored to address validity concerns by following the principles of the tailored design method of survey research (Dillman, 2007). Prior to constructing the survey, we reviewed the extant literature on students’ COVID-19–related issues, school counselors’ roles, and professional issues, in addition to conducting a focus group (N = 7) with school counselors and school counseling supervisors from across the state in which the study was conducted to explore their perceptions in changes to student functioning, strategies they have deployed to assist students, and obstacles they have encountered. Focus group data were used to inform the development of survey items and ensure the instrument covered relevant content. For example, the focus group provided expert insight into the non-counseling duties that are frequently assigned to counselors in the state, as well as the nature of students’ psychological, academic, and behavioral problems witnessed since the onset of COVID-19. Before launching the survey, we piloted the survey with 19 school counselors in Tennessee to elicit feedback about the flow and coverage of the survey. Based on their responses, we added an item addressing universal intervention and edited language on multiple items to align with state-specific terminology (e.g., “MTSS coordination” was expanded to “RTI2B/MTSS/PBIS coordinator” to reflect more state-recognized school counselor titles when operating in these capacities).
The final survey consisted of 64 items in predominantly binary, checkbox, and Likert scale formats. Demographic items were informed by categories outlined by the U.S. Census, the Tennessee DOE, and inclusive practices for data collection (Fernandez et al., 2016). Twenty-one items gathered demographic data related to school counselor characteristics (e.g., age, race, gender), counseling program variables (e.g., caseload, division of time, non-counseling duties, fair-share responsibilities), and school variables (e.g., school level, Title I status, location, staffing patterns). SES was measured using a school’s designated Title I status, with response categories of “yes,” “no,” and “unsure.” Likewise, to determine if school counselors dedicated 80% of their time to direct service, we created a multiple-choice item with the options of “yes,” “no,” and “unsure.” A concise description of the state guidelines was embedded into the survey to promote accurate responses to this item. We gathered data on counselors’ perspectives of their students’ current functioning in areas of mental health, academics, social skills, and behaviors through multiple-choice items with a 5-point range of “much better” to “much worse.” For each area of functioning, school counselors were required to indicate the areas of concern via a checkbox item. Additionally, checkbox items were used to identify school counselors’ strategies to assist students, barriers encountered, and needed resources. As noted, these response categories were based on extant literature and expert input.
Cronbach’s alphas were computed to determine the reliability of the survey items in indicating overall post–COVID-19 functioning of students according to school counselors. These values indicate that these four areas were moderately related with acceptable consistency (α = .653). When making additional comparisons among the four constructs, two areas—behavior and social skills—were found to be more consistent (α = .705; Sheperis et al., 2020). Further, reliability scores likely reflect the exploratory design, which requested participants respond to conceptually related but not converging constructs (e.g., academics, mental health, social skills, and behavior). For example, a change in student academics would not necessarily signify a change in student mental health and vice versa. Thus, participant responses would not necessarily be uniform across items measuring students’ mental health, academics, and social skills, and overall instrument consistency would not be affected in turn.
Participants
We recruited a state-level sample of professional school counselors employed in K–12 public schools in Tennessee. Following the pilot study, in December 2021, we recruited participants through an anonymous Qualtrics link utilizing multiple platforms: the state school counselor association’s listserv, social media, respondent referrals, and dissemination via school counseling supervisors. Participants were eligible to complete the survey if they were currently employed in a K–12 public school in Tennessee. Upon examination of our survey data, we found 276 total responses with 220 complete for a completion rate of 79.7%. Because the survey was distributed through the above-mentioned methods, we were unable to calculate the response rate without knowing how many of the approximately 2,000 public school counselors in Tennessee received the survey. Upon further examination of the survey respondents, we removed one school counseling supervisor; four school counselors whose students were remote/hybrid; and eight school counselors in private, charter, or alternative schools to maintain focus on the experiences of traditional public school counselors working with students in person during the ongoing COVID-19 pandemic for a final sample of 207 participants. An examination of the respondents’ demographics revealed a sample that was predominantly female and White/Caucasian and worked in Title I, suburban, or rural elementary schools. The sample’s mean years serving as a school counselor was 11.7 (SD = 7.5), with mean years at current school of 6.8 (SD = 6.4). See Table 1 for more demographic information. For analysis purposes, we divided the school counselors into three groups by the size of their reported caseload. These categories were informed by a national study of school counselor ratios (National Association of College Admission Counselors, 2019) and consisted of ratios in the range of small (1:100–1:300; 14.0%, n = 29), medium (1:301–1:550; 69.6%, n = 144), and large (1:551 and higher; 15.0%, n = 31).
Table 1
Demographic Characteristics of the Sample
| Characteristic |
n |
% |
| Age |
|
|
| 18–24 years |
3 |
1.4 |
| 25–44 years |
99 |
47.8 |
| 45–64 years |
102 |
49.3 |
| 65 years plus |
3 |
1.4 |
| Race/Ethnicity |
|
|
| Black/African American |
17 |
8.2 |
| Latinx/Hispanic |
1 |
0.5 |
| White/Caucasian |
183 |
88.4 |
| American Indian/Alaskan Native |
1 |
0.5 |
| Other |
5 |
2.4 |
| Gender |
|
|
| Female |
192 |
92.8 |
| Male |
15 |
7.2 |
Note. N = 207.
Data Analysis
We ran a post hoc power analysis using the G*Power 3.1.9.7 statistical software to determine if our sample size was sufficient at the .80 power level with α = .05 and found that a minimum sample size of 100 was required for our analyses. Given our sample size of 207 participants, the power analysis indicated that our sample size was sufficient (Faul et al., 2007). We utilized SPSS version 26 to calculate the following analyses for this study: (a) descriptive statistics; (b) Fisher’s exact test for two dichotomous nominal variables; (c) an extension of Fisher’s exact test, the Freeman-Halton exact test, for one dichotomous nominal variable and one nominal variable with three levels; and (d) point-biserial correlation analysis for one nominal variable and one interval variable (Frey, 2018). We also examined effect size to determine practical importance using the following levels for examining nominal data (Rea & Parker, 1992), precedence for which has been established by complementary studies in educational research (K. Erickson & Quick, 2017; Kotrlik et al., 2011): negligible [0, .1), weak [.1, .2), moderate [.2, .4), relatively strong [.4, .6), strong [.6, .8), and very strong [.8, 1.0). Phi (ϕ) indicates the effect size for the exact tests, and the correlation is the effect size for the point-biserial correlation. We only included statistical analyses that resulted in moderate associations or higher. Three school counselors (1.4%) who reported caseloads that were unusually small (< 100) and outside our specified caseload parameters were removed from the analysis. Additionally, we excluded school counselors who indicated “unsure” in the categories of location (rural, suburban, urban), Title I status, and adherence to state policy for direct service to students. See Table 2 for school characteristics.
Results
Research Question 1
RQ1 examined school counselors’ perspectives of the impact of COVID-19 on students’ mental health, academics, and social skills as well as variation by grade level (elementary, middle, or high school). When asked about the mental health changes they have witnessed in their students post–COVID-19 pandemic, 93.7% (n = 194) of school counselors reported negative changes with 42.5% (n = 88) reporting “much worse” and 51.2% (n = 106) reporting “somewhat worse” changes. Specifically, school counselors reported issues regarding anxiety (92.8%, n = 192), depression (77.3%, n = 160), family dysfunction (71.0%, n = 147), COVID-19–related grief and loss (63.8%, n = 132), technology addiction (52.7%, n = 109), suicidality (50.7%, n = 105), fear of COVID-19 (49.8%, n = 103), substance use issues (21.7%, n = 45), and other issues (12.6%, n = 26) such as separation anxiety, self-harm, and anger. The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and depression (p < .001, ϕ = .301) with a moderate positive association, suicidality (p < .001, ϕ = .499) with a relatively strong positive association, and substance use (p < .001, ϕ = .583) with a relatively strong positive association. For depression, 90.0% (n = 54) of high school counselors and 85.7% (n = 36) of middle school counselors reported this issue as compared to 63.0% (n = 51) of elementary school counselors. For suicidality, 76.2% (n = 32) of middle school counselors and 71.7% (n = 43) of high school counselors reported this concern as compared to 23.5% (n = 19) of elementary school counselors. For substance use, 58.3% (n = 35) of high school counselors and 20.0% (n = 8) of middle school counselors reported this concern as compared to 1.2% (n = 1) of elementary school counselors. All other mental health concerns were not significant with grade level.
When queried regarding academic changes post–COVID-19, 90.3% (n = 187) of school counselors reported negative changes to students’ academics with 35.3% (n = 73) reporting “much worse” and 55.1% (n = 114) reporting “somewhat worse” changes. School counselors reported an overall decline across all subjects (80.7%, n = 167). Additionally, school counselors reported non-cognitive factors regarding lack of motivation (84.1%, n = 174), lack of parental support during the school day (75.4%, n = 156), attention issues (71.0%, n = 147), poor mental health (64.7%, n = 134), sleep deprivation (41.1%, n = 85), limited technology during virtual learning (33.3%, n = 69), lack of space to work at home during virtual learning (30.4%, n = 63), poor physical health (17.9%, n = 37), and other (3.9%, n = 8). The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and lack of motivation (p = .001, ϕ = .265), poor mental health (p = .001, ϕ = .269), and attention issues (p = .009, ϕ = .232), all with positive moderate associations. For lack of motivation, 96.7% (n = 58) of high school counselors and 88.1% (n = 37) of middle school counselors reported this issue as compared to 75.3% (n = 61) of elementary school counselors. For poor mental health, 78.3% (n = 47) of high school counselors and 69.0% (n = 29) of middle school counselors reported this outcome as compared with 49.4% (n = 40) of elementary school counselors. For attention issues, 79.0% (n = 64) of elementary school counselors and 73.8% (n = 31) of middle school counselors reported concerns as compared to 55.0% (n =33) of high school counselors.
Table 2
School/Program Characteristics
| Characteristic |
n |
% |
| Location |
|
|
| Urban |
31 |
15.0 |
| Suburban |
95 |
45.9 |
| Rural |
72 |
34.8 |
| Unsure |
9 |
4.3 |
| Title I Status |
|
|
| Yes |
121 |
58.5 |
| No |
57 |
27.5 |
| Unsure |
29 |
14.0 |
| Grade Level |
|
|
| Elementary |
81 |
39.1 |
| Middle |
42 |
20.3 |
| High |
60 |
29.0 |
| Other |
24 |
11.6 |
| Follows 80% Direct Service Guideline |
|
|
| Yes |
112 |
54.1 |
| No |
65 |
31.4 |
| Unsure |
30 |
14.5 |
| School Counselor-to-Student Ratio (caseload) |
|
|
| 1:1–1:300 |
29 |
14.0 |
| 1:301–1:550 |
144 |
69.6 |
| 1:551 and higher |
31 |
15.0 |
| Other |
3 |
1.4 |
Note. N = 207
When asked about behavioral changes, 87.4% (n = 181) of school counselors reported negative changes to behaviors with 30.4% (n = 63) reporting “much worse” and 57.0% (n = 118) reporting “moderately worse” changes. Comparably, when asked about social skills changes, 87.0% (n = 180) of school counselors reported negative changes to students’ social skills with 36.2% (n = 75) reporting “much worse” and 50.7% (n = 105) reporting “moderately worse” changes. Specifically, school counselors reported trouble socializing with peers (84.1%, n = 174), absence of social flexibility (58.0 %, n = 120), increase of physical aggression (55.1%, n = 114), increase in relational aggression (50.7%, n = 105), increase in cyberbullying (23.7%, n = 49), increase in bullying (19.3%, n = 40), and other (8.2%, n = 17) such as issues with conflict resolution and preference for technology. The Freeman-Halton exact test revealed a significant relationship between grade level (n = 183) and cyberbullying (p = .003, ϕ = .255), with a moderate positive association with 42.9% (n = 18) of middle school counselors, 23.3% (n = 14) of high school counselors, and 14.8% (n = 12) of elementary school counselors reporting an increase in this area. All other social skills changes were not significant with grade level.
Research Question 2
RQ2 examined the interventions that school counselors used in assisting students with their COVID-19–related concerns and if this differed by grade level. School counselors reported the various supports that they provided to their students who struggled with COVID-19–related issues, including individual counseling (95.7%, n = 198), consultation with parents/teachers (85.5%, n = 177), referrals (80.7%, n = 167), collaboration with other school-based helpers (77.3%, n = 160), coping skills instruction (71.5%, n = 148), group counseling (44.0%, n = 91), universal health screenings (17.9%, n = 37), and other interventions (4.3%, n = 9) such as food programs, holiday donation programs, peer support, and academic support meetings. We used the Freeman-Halton exact test to examine the relationship between grade level (n = 183) and these supports and found that small group counseling (p < .001, ϕ = .405) and coping skills instruction (p = .028, ϕ = .200) were significant, both with moderate positive association. For small group counseling, 63.0% (n = 51) of elementary school counselors and 45.2% (n = 19) of middle school counselors provided this support as compared to 16.7% (n = 10) of high school counselors. For coping skills instruction, 77.8% (n = 63) of elementary school counselors and 71.4% (n = 30) of middle school counselors reported this intervention as compared to 56.7% (n = 34) of high school counselors.
Research Question 3
RQ3 examined the barriers school counselors encountered in their ability to provide services and if this differed by grade level, SES, location, number of non-counseling duties, caseload size, and following the state guideline to spend 80% of time providing student services. When asked if they had encountered barriers to assisting their students with their COVID-19–related needs, 54.6% (n = 113) of school counselors reported that they had experienced barriers, and 45.4% (n = 94) reported that they had not. For those counselors who answered “yes,” barriers included: high caseload (44.4%, n = 92), number of non-counseling duties (20.3%, n = 42), lack of administrator support (12.1%, n = 25), being included on master schedule for guidance classes (10.1%, n = 21), lack of training to address COVID-19 needs (8.2%, n = 17), too much time coordinating the MTSS program (7.7%, n = 16), and other reasons (9.7%, n = 20). Examples of other reasons include students’ attendance, lack of resources (both space and personnel), and focus on academics over mental health. Of note, 47.3% (n = 98) of school counselors reported an increase in non-counseling duties since COVID-19, ranging from a substantial to a slight increase.
We used the Freeman-Halton exact test to examine the aforementioned barriers by grade level (n = 183) and found that being on the master schedule (p < .001, ϕ = .297) was significant with moderate positive association with 19.8% (n = 16) of elementary school counselors reporting this task as compared to 2.4 % (n = 1) of middle school counselors and 1.7% (n = 1) of high school counselors. We used point-biserial correlation analysis to examine how the number of new post–COVID-19 non-counseling duties related to the perceived barriers to providing services to students and found this to be significant (rpb = .211, p = .002) with a positive moderate association. School counselors who reported barriers to providing services had been allocated more non-counseling duties since the pandemic (n = 113, M = 1.22, SD = 1.49) than those who did not report barriers (n = 94, M = .66, SD = 1.04). We used a Freeman-Halton exact test to examine the specific barriers by caseload (n = 204) and found school counselors with a high caseload reported significantly more difficulty in addressing students’ COVID-19–related needs (p < .001, ϕ = .284), with a moderate positive association for large (58.1%, n =18) and medium (47.2%, n = 68) caseloads, as compared to those with a small (10.4%, n = 3) caseload. Investigating the state DOE guideline for 80% of time in service to students (n = 177), excluding those who were unsure, revealed that 63.3% (n = 112) followed the guideline and 36.7% did not (n = 65). We used a Fisher’s exact test to examine the relationship between following the 80% guideline and specific barriers and found that reporting too many non-counseling duties (p < .001, ϕ = -.358) was significant, with a moderate negative association for those who did not follow the guideline (41.5%, n = 27) in comparison to those who did follow the 80% guideline (10.7%, n = 12). All other barriers were not significant with grade level, SES, location, number of non-counseling duties, caseload size, and following the 80% state guideline. We used a Fisher’s exact test to examine SES by Title I (n = 178) classification and found that it was not significant with any of the barriers.
Discussion
Our results render a disturbing picture of students’ post–COVID-19 mental health functioning and school counselors’ perceived ability to effectively meet their students’ needs since a return to in-person learning, as reported by this sample of 207 school counselors in Tennessee. For RQ1, over 93% of our respondents indicated that their students’ mental health had worsened, with anxiety and depression identified as the most pronounced psychological concern, followed by family dysfunction, grief, technology addiction, and suicidality. These results confirm our predictions that the COVID-19 pandemic would exert a harmful impact on the mental health of children and adolescents (Bryant et al., 2020; Cénat & Dalexis, 2020). Depression and suicidality were significant concerns for middle and high school counselors, and substance abuse was significant at the high school level. The reported spike in diagnosable mental health problems by secondary school counselors aligns with research indicating that half of all mental health and substance use disorders begin at 14 (Quinn et al., 2016). The CDC recently reported that depression, substance abuse, and suicide have increased among adult populations since COVID-19, with young adults presenting the most significant risk (Czeisler et al., 2020). Our results provide preliminary evidence indicating that COVID-19–related trends have similarly impacted adolescents. Further, given the relationship between ACEs and substance misuse (CDC, 2022; Quinn et al., 2016), it may be reasonable to conjecture that an increase in family dysfunction, grief, fear of COVID-19, and severance of social relationships underscored a rise in substance use problems, particularly among high school students.
In addition to mental health, student academics notably declined according to school counselors in Tennessee, with 90.3% of participants reporting negative changes to students’ academics. Previous research attributed students’ COVID-19 pandemic–related academic issues to the vagaries of online instruction, a lack of parental supervision, inadequate technology, and limited workspace, among other factors (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021). Our results aligned with these findings by explicitly connecting delays in students’ academic progress to psychological factors. Of note, we found a significant relationship between grade level, lack of motivation, poor mental health, and attention issues, with middle and high school counselors reporting greater concerns in the areas of motivation and mental health, and elementary and middle school counselors identifying attention problems as the greatest concern. The developmental onset of mental health disorders (Lambie et al., 2019) likely accounts for increased student mental health problems reported by middle and high school counselors. However, motivation and attentional issues across the grades were problematic, and because both are symptomatic of depression and anxiety, they raise a red flag for the mental health of all K–12 students in Tennessee.
Alongside academics, 87.0% of school counselors reported negative changes in students’ social skills and 87.4% reported worsened behaviors among students, with trouble socializing with peers, absence of social flexibility, and an increase in physical and relational aggression being the most pronounced problems. Declines in students’ ability to get along with peers may be uniquely linked to social isolation during lockdown (Ellis et al., 2020; Karaman et al., 2021); however, of great concern is the increase in all forms of bullying, with cyberbullying being particularly problematic in middle school. Youth aggression is a long-term consequence of ACEs and has implications for overall school safety, with victimization and perpetration both positively associated with school violence (Forster et al., 2020).
RQ2 investigated what interventions school counselors used to assist students with their COVID-19–related concerns and examined interventions by grade level. The preponderance of school counselors relied on individual counseling (95.7%), consultation (85.5%), referrals (80.7%), collaboration with other school-based helpers (77.3%), and coping skills instruction (71.5%), all of which are consistent with crisis-level supports. Nonetheless, only 44% of the sample, primarily elementary school counselors, had used small group counseling, despite its proven efficacy with children exposed to trauma (Salloum & Overstreet, 2008). The underutilization of group work at the high school level presents a concern, given that group work provides context for peer support and social learning, both considered critical therapeutic factors for adolescents (Gysbers & Henderson, 2012). Nonetheless, this finding resonates with previous results that high school counselors are more apt to assume administrative roles in place of the provision of direct student services (Chandler et al., 2018). Universal assessment has been proffered as an efficient and empirically grounded method for the early identification of at-risk students in need of COVID-19–related interventions (A. Erickson & Abel, 2013; Karaman et al., 2021; Pincus et al., 2020). Unfortunately, only 17.9% of the sample reported administering universal mental health screeners, a finding aligned with other studies that indicate schools have resisted adopting mental health screeners because of inadequate resources and related concerns about following up with students identified as being at risk (Burns & Rapee, 2022).
For RQ3, we explored the school counselors’ perspectives of the barriers they have encountered in assisting their students with their COVID-19 concerns. The proliferation of barriers reported by school counselors (high caseload, non-counseling duties, lack of administrator support, being on the master schedule for guidance classes, and a lack of training) verifies our concern that school counselors in Tennessee did not receive the support instrumental to their ability to provide effective student services at this critical time. Our state-level findings resonate with studies conducted in other states that indicate school counselors’ non-counseling duties increased during the pandemic while administrator support declined (Savitz-Romer et al., 2021). Other studies have also drawn attention to widespread staffing shortages associated with COVID-related absences and a reduced pool of substitute teachers (Patterson, 2022). Although we did not examine staff resources explicitly, with almost 50% of our Tennessee sample witnessing an increase in their non-counseling duties, it would be reasonable to infer that campus administrators are deploying school counselors to triage critical gaps in staffing patterns. Interestingly, despite a widespread increase in non-counseling duties post–COVID-19, only 20.3% of counselors reported non-counseling duties as a barrier to providing care. The discrepancy between these two results may be indicative of the phenomenon of role diffusion in school counseling, a problem that emerges when school counselors begin to integrate non-counseling duties as part of their accepted role and thus do not perceive them as antithetical to their professional identity (Astramovich et al., 2013). Furthermore, neither SES (Title I) nor location (rural, suburban, urban) were significant with barriers, and although this could reflect our relatively small sample, it could also be indicative of staff shortages adversely affecting the role of school counselors across all settings, regardless of the school’s demographic status.
The most notable barrier reported by respondents was a large caseload. School counselors with large and medium-sized caseloads reported more barriers and were less likely to follow the 80% guideline. Thus, those students who were negatively impacted by large counselor caseloads before COVID-19 faced further obstacles in accessing their school counseling services despite an overall increase in their mental health and academic needs. Further, elementary school counselors listed on the master schedule for guidance classes faced additional barriers to addressing their students’ needs outside of their prevention-focused (Tier 1) activities. Classroom guidance is considered helpful in elementary school for building social skills and study habits; however, when counselors are placed on the master schedule, it can impact their ability to provide responsive student services (Gysbers & Henderson, 2012) which seemed to be the case with our respondents.
Implications for Professional Advocacy
The results of this study illustrate a decline in student functioning, pronounced in the area of mental health, and have implications for school counselor advocacy in the areas of policy and practice. Advocating for policy change takes time and is beyond the individual efforts of school counselors, who are often beholden to their principal’s limited understanding of school counselors’ appropriate role and function (Lancaster & Reiner, 2022) and subsumed by untenable caseloads in under-resourced schools (Lambie et al., 2019). We, therefore, assert that advocacy is the professional imperative for all vested school counseling professionals (state counseling associations, school counselor educators, school counseling supervisors, and school counselors), all of whom could be working in tandem to advance the profession.
At the policy level, state and national counseling associations should reconsider the important role school counselors play in supporting students’ mental well-being and re-examine policies that delineate the appropriate use of school counselors’ time. Currently, the state school counseling model (Tennessee Policy 5.103) mirrors the national model (ASCA, 2019), perennially focusing on school counselors’ role in supporting student academics and delimiting their counseling role to prevention services, crisis counseling, and referrals to other mental health professionals. For state and national counseling associations, positioning school counselors as primarily focused on student academics demonstrated their value during the No Child Left Behind Act (NCLB; 2001) era, which prioritized unidimensional outcome measures of student success, particularly in math and reading (Savitz-Romer, 2019). However, the Every Student Succeeds Act (ESSA) replaced NCLB in 2015 and emphasizes more holistic aspects of student development and school climate. Many scholars argue that the ESSA (2015) combined with the rise in mental health issues has created a policy window for school counselors, led by their state and national professional associations (Savitz-Romer, 2019), to focus on the non-cognitive aspects that undergird healthy student development and to reclaim mental health as a domain central to school counselor practice (Lambie et al., 2019).
Redefining school counselors’ role in terms of mental health would require them to receive more clinical supervision (Lambie et al., 2019). In comparison to counselors in clinical settings, school counselors receive little to no supervision for their clinical efforts, which affects their clinical identity and weakens their counseling skills over time (Lancaster & Reiner, 2022). To address this gap, symbiotic partnerships could be formed with counselor education programs, particularly those that offer doctoral degrees in counselor education and supervision, to provide clinical supervision to local school counselors. Progress in this area may be forthcoming in the state, as institutions of higher education that operate school counseling, school psychology, and school social work programs have been invited to apply for grants funded through COVID-19 relief funding to support student internships in high-need schools. In addition, funds are available to support clinical supervision experiences that extend beyond students’ graduate training programs (Tennessee DOE, 2023).
MTSS programs also offer a promising prevention and intervention framework for meeting students’ comprehensive needs, including mental health, and align to both state and national school counseling models (Goodman-Scott et al., 2019). Further, the Tennessee DOE (2018) has developed a resource guide based on a tiered model for supporting students’ differential mental health needs, which school counselors could efficiently implement within their existing MTSS programs. Of note, within the Tennessee model, Tier 1 mental health practices build a foundation for mental wellness for all students. Advanced supports at Tiers 2 and 3 provide students who are at risk because of behavioral and/or mental health concerns with access to small groups and mental health interventions. One dimension of the state’s tiered mental health model is universal screening to identify students with internalizing behavioral disorders. Although few counselors in this study utilized universal screening, we recommend school counselors and their supervisors leverage the preexisting Tennessee DOE guidelines to petition their districts to adopt universal mental health screening.
Although the state mandated reduced counselor ratios in 2017 (Policy 5.103.), the funding formula allowed for uneven adoption of this policy (Tennessee Comptroller of the Treasury, n.d.), and target ratios fell short of national recommendations (ASCA, 2019). Thus, a function of this research was to utilize results in policy contexts to advocate for ratio realignments. In partnership with the state school counselor association, we produced a one-page results summary, written in simple language, to disseminate to state politicians to illuminate the acuity of mental health issues faced by K–12 students and proposed a solution through increased school counselor access. An advocacy effort led by the state association resulted in proposed legislation TN HB0364/SB0348, which would require one licensed full-time professional school counselor position for every 250 students and is currently advancing through the state Senate and House committees. A significant takeaway from this study is the importance and potency of coordinated partnerships between researchers, state counseling associations, and school counselors—an alliance that could be replicated in other states by school counselor stakeholders to advocate for the profession.
Limitations
The generalizability of these findings is limited because of the use of a state-level sample and a non-standardized, self-report survey. First, self-report surveys are sensitive to respondents’ tendency to rate themselves more favorably. Thus, it would be reasonable to conjecture that school counselors overestimated their adherence to the state guideline to spend 80% of their time in service to students and underreported their non-counseling duties. Second, although the items were informed by previous research on the psychological issues faced by children and adolescents during COVID-19 (Ellis et al., 2020; Karaman et al., 2021; Magson et al., 2021) and those factors that affect school counselors’ ability to provide direct services (Kaffenberger & O’Rorke-Trigiani, 2013; Parzych et al., 2019; Whitney & Peterson, 2019), the use of an ad hoc survey precluded us from performing more robust analyses (e.g., regression analysis). Third, because we only gathered data on students’ mental health issues and academic functioning post–COVID-19 pandemic, we have no benchmark data of students’ pre–COVID-19 functioning with which to make objective comparisons.
Fourth, although the sample was large enough to find some significant results, it was a small percentage of the state’s total population of public school counselors, which is estimated to be over 2,000. A larger sample would have increased the generalizability of findings and impacted the significance levels and practical importance of the results. Fifth, our sample lacks racial and gender diversity; however, it does align with the state’s overall population of educators (Tennessee DOE, 2021). Finally, regarding data analysis, interpreting correlations on a small population sample needs to be performed cautiously because of the possibility of sampling error. Additionally, point-biserial correlation can be impacted by the dichotomous nature of one of the variables, which constrains the variability of the results (Hinkle et al., 2002). Nonetheless, correlational analyses of ordinal and nominal variables in small-scale research are consistent with our exploratory design, and the results provide evidence that the variables examined share some type of relationship and provide direction for future research.
Future Research
Given that we conducted this study in the aftermath of the COVID-19 pandemic and have utilized data and policy to advocate for expanded student access to school counseling services in Tennessee, this study design could be replicated by future researchers in the event that another pandemic or crisis of similar scale affects K–12 populations. Nonetheless, our exploratory design is an inherent limitation with the preponderance of our findings based on correlational analysis of largely non-parametric data. Future studies could explore dimensions of students’ mental health utilizing student data from empirical inventories. Rather than relying on school counselor perception data, researchers could use results from universal screenings, such as the Behavior Assessment System for Children-3rd edition (BASC-3), to better understand the nature of student issues and examine differential risk by demographic factors (e.g., age, gender, ethnicity), which could be used to inform evidence-based interventions with at-risk and high-risk populations. Further, researchers could employ quasi-experimental designs to assess outcomes of school counselor-led interventions, such as small groups, with students who have scored as being at risk based on universal screening. Studies of this nature can help build a case for the efficacy of school counselors and, in turn, protect them from role misallocation. Qualitative research could also be conducted in those schools in which school counselors implement a universal screening, intervention, and referral system to glean an implementation blueprint practical to other school counselors within and outside the state.
Conclusion
With elevated rates of depression, anxiety, substance use, and bullying, it is reasonable to conjecture that students in Tennessee have experienced COVID-19–related trauma, which according to research is unlikely to abate without intervention (CDC, 2022; Savitz-Romer et al., 2021). Although our state-level respondents indicated that they provided services consistent with crisis counseling (e.g., individual counseling, group counseling, consultation, and referrals), almost 50% of the counselors had been burdened with additional non-counseling duties, which could reduce their capacity to work with students at different levels of risk. Large caseload was a significant barrier, leaving counselors struggling to provide an appropriate level of care. This finding raises considerable concern about the risk faced by students who have experienced deterioration in their mental health and academics since the onset of COVID-19, yet attend schools in Tennessee with elevated school counselor-to-student caseloads. Nationally and at the state level, school counselors are the most prevalent mental health professionals in schools and are trained in crisis response (National Center for Education Statistics, 2016). Unfortunately, Tennessee school counselors appear to be facing barriers in the provision of student services related to high caseload and non-counseling duties, which presents cause for professional advocacy within the state and beyond.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2019). ASCA national model: A framework for school counseling programs (4th ed.).
Astramovich, R. L., Hoskins, W. J., Gutierrez, A. P., & Bartlett, K. A. (2013). Identifying role diffusion in school counseling. The Professional Counselor, 3(3), 175–184. https://doi.org/10.15241/rla.3.3.175
Bryant, D. J., Oo, M., & Damian, A. J. (2020). The rise of adverse childhood experiences during the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S193–S194.
https://doi.org/10.1037/tra0000711
Burns, J. R., & Rapee, R. M. (2022). Barriers to universal mental health screening in schools: The perspective of school psychologists. Journal of Applied School Psychology, 38(3), 1–18.
https://doi.org/10.1080/15377903.2021.1941470
Cénat, J. M., & Dalexis, R. D. (2020). The complex trauma spectrum during the COVID-19 pandemic: A threat for children and adolescents’ physical and mental health. Psychiatry Research, 293, 113473.
https://doi.org/10.1016/j.psychres.2020.113473
Centers for Disease Control and Prevention. (2022, March 31). New CDC data illuminate youth mental health threats during the COVID-19 pandemic [Press release]. https://tinyurl.com/yckv6v9d
Chandler, J. W., Burnham, J. J., Riechel, M. E. K., Dahir, C. A., Stone, C. B., Oliver, D. F., Davis, A. P., & Bledsoe, K. G. (2018). Assessing the counseling and non-counseling roles of school counselors. Journal of School Counseling, 16(7), 1–33. https://files.eric.ed.gov/fulltext/EJ1182095.pdf
Cholewa, B., Burkhardt, C. K., & Hull, M. F. (2015). Are school counselors impacting underrepresented students’ thinking about postsecondary education? A nationally representative study. Professional School Counseling, 19(1), 144–154. https://doi.org/10.5330/1096-2409-19.1.144
Czeisler, M. É., Lane, R. I., Petrosky, E., Wiley, J. F., Christensen, A., Njai, R., Weaver, M. D., Robbins, R., Facer-Childs, E. R., Barger, L. K., Czeisler, C. A., Howard, M. E., & Rajaratnam, S. M. W. (2020). Mental health, substance use, and suicidal ideation during the COVID-19 pandemic. Morbidity & Mortality Weekly Report, 69(32), 1049–1057. https://www.cdc.gov/mmwr/volumes/69/wr/mm6932a1.htm
DeKruyf, L., Auger, R. W., & Trice-Black, S. (2013). The role of school counselors in meeting students’ mental health needs: Examining issues of professional identity. Professional School Counseling, 16(5), 271–282. https://doi.org/10.1177/2156759X0001600502
Dillman, D. A. (2007). Mail and internet surveys: The tailored design method (2nd ed.). Wiley.
Ellis, W. E., Dumas, T. M., & Forbes, L. M. (2020). Physically isolated but socially connected: Psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Canadian Journal of Behavioural Science/Revue canadienne des sciences du comportement, 52(3), 177–187.
https://doi.org/10.1037/cbs0000215
Erickson, A., & Abel, N. R. (2013). A high school counselor’s leadership in providing school-wide screenings for depression and enhancing suicide awareness. Professional School Counseling, 16(5), 283–289.
https://doi.org/10.1177/2156759X1201600501
Erickson, K., & Quick, N. (2017). The profiles of students with significant cognitive disabilities and known hearing loss. The Journal of Deaf Studies & Deaf Education, 22(1), 35–48.
https://doi.org/10.1093/deafed/enw052
Every Student Succeeds Act, Pub. L. No. 114–95 § 114 Stat. 1177 (2015, Dec. 10). https://www.congress.gov/114/plaws/publ95/PLAW-114publ95.pdf
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
https://doi.org/10.3758/bf03193146
Fernandez, T., Godwin, A., Doyle, J., Verdin, D., Boone, H., Kirn, A., Benson, L., & Potvin, G. (2016). More comprehensive and inclusive approaches to demographic data collection. School of Engineering Education Graduate Student Series. Paper 60. https://tinyurl.com/2p9p2ct7
Forster, M., Gower, A. L., McMorris, B. J., & Borowsky, I. W. (2020). Adverse childhood experiences and school-based victimization and perpetration. Journal of Interpersonal Violence, 35(3–4), 662–681.
https://doi.org/10.1177/0886260517689885
Frey, B. B. (2018). The SAGE encyclopedia of educational research, measurement, and evaluation. SAGE.
Goodman-Scott, E., Betters-Bubon, J., & Donohue, P. (Eds.). (2019). The school counselor’s guide to multi-tiered systems of support. Routledge.
Gysbers, N. C., & Henderson, P. (2012). Developing and managing your school guidance and counseling program (5th ed.). American Counseling Association.
Hinkle, D. E., Wiersma, W., & Jurs, S. G. (2002). Applied statistics for the behavioral sciences (5th ed.). Houghton Mifflin Company.
Imran, N., Zeshan, M., & Pervaiz, Z. (2020). Mental health considerations for children & adolescents in COVID-19 pandemic. Pakistan Journal of Medical Sciences, 36(COVID19-S4), S67–S72.
https://doi.org/10.12669/pjms.36.COVID19-S4.2759
Kaffenberger, C. J., & O’Rorke-Trigiani, J. (2013). Addressing student mental health needs by providing direct and indirect services and building alliances in the community. Professional School Counseling, 16(5), 323–332. https://doi.org/10.1177/2156759X1201600505
Karaman, M. A., Eşici, H., Tomar, İ. H., & Aliyev, R. (2021). COVID-19: Are school counseling services ready? Students’ psychological symptoms, school counselors’ views, and solutions. Frontiers in Psychology, 12. https://doi.org/10.3389/fpsyg.2021.647740
Kotrlik, J. W., Williams, H. A., & Jabor, M. K. (2011). Reporting and interpreting effect size in quantitative agricultural education research. Journal of Agricultural Education, 52(1), 132–142.
https://doi.org/10.5032/jae.2011.01132
Lambie, G. W., Stickl Haugen, J., Borland, J. R., & Campbell, L. O. (2019). Who took “counseling” out of the role of professional school counselors in the United States? Journal of School-Based Counseling Policy and Evaluation, 1(3), 51–61. https://doi.org/10.25774/7kjb-bt85
Lancaster, C., & Reiner, S. (2022). Supervision in K–12 school settings. In A. S. Lenz & B. Flamez (Eds.), Practical approaches to clinical supervision across settings: Theory, practice, and research (pp. 223–241). Pearson.
Magson, N. R., Freeman, J. Y. A., Rapee, R. M., Richardson, C. E., Oar, E. L., & Fardouly, J. (2021). Risk and protective factors for prospective changes in adolescent mental health during the COVID-19 pandemic. Journal of Youth and Adolescence, 50(1), 44–57. https://doi.org/10.1007/s10964-020-01332-9
National Association for College Admission Counseling. (2019). State-by-state student-to-counselor ratio maps by school district: Data visualizations. https://public.tableau.com/profile/nacac.research#!
National Center for Education Statistics. (2016). National teacher and principal survey. https://nces.ed.gov/surveys/ntps
No Child Left Behind Act of 2001, Pub. L. No. 107–110, 115 Stat. 1425 (2002). https://www.congress.gov/107/plaws/publ110/PLAW-107publ110.htm
Parzych, J. L., Donohue, P., Gaesser, A., & Chiu, M. M. (2019). Measuring the impact of school counselor ratios on student outcomes. ASCA Research Report. https://tinyurl.com/3sbuk5dd
Patel, P., & Clinedinst, M. (2021). State-by-state student-to-counselor ratio maps by school district. National Association for College Admission Counseling. https://files.eric.ed.gov/fulltext/ED615227.pdf
Patterson, J. (2022, March 4). School counselors and social workers struggle to meet student needs. National Education Association Today. https://tinyurl.com/yckwhhc4
Pincus, R., Hannor-Walker, T., Wright, L., & Justice, J. (2020). COVID-19’s effect on students: How school counselors rise to the rescue. NASSP Bulletin, 104(4), 241–256. https://doi.org/10.1177/0192636520975866
Quinn, K., Boone, L., Scheidell, J. D., Mateu-Gelabert, P., McGorray, S. P., Beharie, N., Cottler, L. B., & Khan, M. R. (2016). The relationships of childhood trauma and adulthood prescription pain reliever misuse and injection drug use. Drug and Alcohol Dependence, 169, 190–198. https://doi.org/10.1016/j.drugalcdep.2016.09.021
Rea, L. M., & Parker, R. A. (1992). Designing and conducting survey research: A comprehensive guide. Jossey-Bass.
Salloum, A., & Overstreet, S. (2008). Evaluation of individual and group grief and trauma interventions for children post disaster. Journal of Clinical Child & Adolescent Psychology, 37(3), 495–507.
https://doi.org/10.1080/15374410802148194
Savitz-Romer, M. (2019). Fulfilling the promise: Reimagining school counseling to advance student success. Harvard Education Press.
Savitz-Romer, M., Rowan-Kenyon, H. T., Nicola, T. P., Alexander, E., & Carroll, S. (2021). When the kids are not alright: School counseling in the time of COVID-19. AERA Open, 7. https://doi.org/10.1177/23328584211033600
Sheperis, C., Drummond, R. J., & Jones, K. D. (2020). Assessment procedures for counselors and helping professionals (9th ed.). Pearson.
Swedberg, R. (2020). Exploratory research. In C. Elman, J. Gerring, & J. Mahoney (Eds.), The production of knowledge: Enhancing progress in social science (pp. 17–37). Cambridge University Press.
Tennessee Comptroller of the Treasury. (n.d.). Tennessee basic education program: Handbook for computation. https://tinyurl.com/twazjrut
Tennessee Department of Education. (2018). Tennessee comprehensive school-based mental health resource guide. https://tinyurl.com/2bfetw3t
Tennessee Department of Education. (2020). Reopening schools: Overview guide for LEAs. https://tinyurl.com/2hry8hs6
Tennessee Department of Education. (2021). TDOE, TERA releases 2021 Tennessee Educator Survey results. https://tinyurl.com/523b5hmn
Tennessee Department of Education. (2023). Project RAISE internship opportunities. https://web.cvent.com/event/c34c10c7-31e5-48ec-aaa2-7d343e00af77/websitePage:fa84d4fc-c565-4872-98eb-86552d79a670
Tennessee Office of the Governor. (n.d.). COVID-19 timeline. https://www.tn.gov/governor/covid-19/covid19timeline.html
Tennessee State Board of Education. (2017). School counseling model & standards policy 5.103. https://tinyurl.com/39a7jhyx
Udwin, O., Boyle, S., Yule, W., Bolton, D., & O’Ryan, D. (2000). Risk factors for long-term psychological effects of a disaster experienced in adolescence: Predictors of post traumatic stress disorder. Journal of Child Psychology & Psychiatry, 41(8), 969–979. https://doi.org/10.1111/1469-7610.00685
Whitney, D. G., & Peterson, M. D. (2019, February 11). US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatrics, 173(4), 389–391.
https://doi.org/10.1001/jamapediatrics.2018.5399
Zimmer-Gembeck, M. J., & Skinner, E. A. (2011). Review: The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development, 35(1), 1–17. https://doi.org/10.1177/0165025410384923
Chloe Lancaster, PhD, is an associate professor at the University of South Florida. Michelle W. Brasfield, EdD, LPSC, is an assistant professor at the University of Memphis. Correspondence may be addressed to Chloe Lancaster, 422 E. Fowler Ave, EDU 105, Tampa, FL 33620, clancaster2@usf.edu.
Aug 24, 2023 | Volume 13 - Issue 2
Amy Biang, Clare Merlin-Knoblich, Stella Y. Kim
Although researchers have found that patient weight bias negatively impacts health care professionals, research is limited on client weight bias toward counselors. Given that a client’s perception of their counselor impacts the therapeutic alliance, more research is needed to understand client weight bias toward counselors. To fill this research gap, we conducted a quasi-experimental study examining people’s weight bias toward a hypothetical counselor who was overweight, average weight, or underweight. Participants (N = 189) received a random assignment to a questionnaire featuring one of the three hypothetical counselors. Participants indicated their willingness to trust them, select them as a counselor, and follow their counsel. Results from a Welch ANOVA analysis showed a statistically significantly greater preference for average-weight and overweight counselors than those who are underweight. Additionally, the participants were less willing to follow counsel from overweight and underweight counselors. Implications for counselors are discussed.
Keywords: client weight bias, overweight, underweight, average weight, counselors
Body weight can inform a client’s perception of a health professional’s level of authority, trust, and competence (Hutson, 2013; Schwartz et al., 2006). Researchers have found that overweight bias toward health professionals like fitness instructors and medical physicians results in negative impressions (Hutson, 2013; Puhl et al., 2013; Puhl & Heuer, 2010). Clients may perceive lower competence, conscientiousness, personal grooming, and intrapersonal ability for overweight individuals compared to average-weight ones (Allison & Lee, 2015). When people seek mental health treatment, these perceptions may hinder their selection of a counselor who is perceived as overweight. Additionally, research on underweight bias has emerged that shows adverse outcomes toward underweight individuals (Allison & Lee, 2015; Beggan & DeAngelis, 2015; Davies et al., 2020a). Despite research on overweight and underweight bias in health professionals, limited research on either topic exists in the counseling profession.
Research on weight bias is necessary for counseling given that counselor attributes have the potential to be an integral part of a client’s decision-making and change process (Hauser & Hays, 2010). Attributes of a counselor that may affect client impressions, such as attractiveness (Grimes & Murdock, 1989) or race (Kim & Kang, 2018; Meyer & Zane, 2013), illuminate the social influence process of counseling (McKee & Smouse, 1983). Social influence is pervasive in the judgments of people everywhere. Weight bias continues to be a product of social influence and, as such, weaves stereotypes into the minds of those who consume the message of weight as a moral indiscretion (Beggan & DeAngelis, 2015). As clients search for, build trust with, and consider life changes with a counselor, weight bias ought to be explored as a potential issue for counselors.
In the past 35 years, researchers published only one study about weight perceptions toward overweight counselors (Moller & Tischner, 2019). Furthermore, there were no published studies about underweight counselors found. This gap in research is notable, as body weight can influence clients’ first impressions of a counselor and their expectations of the ensuing relationship (Moller & Tischner, 2019). Understanding how weight bias may impact this relationship is vital to building an authentic therapeutic relationship, which may otherwise be hindered by weight bias, which inaccurately frames a counselor’s competence (McKee & Smouse, 1983). Thus, we examined client weight bias toward overweight, underweight, and average-weight counselors in the current study.
Literature Review
Weight Bias
The term weight bias indicates a negative attitude about the perceived weight of an individual (Christensen, 2021). Historically, weight bias has been directed at people perceived as overweight; however, recent evidence suggests that underweight bodies generate weight bias as well (Allison & Lee, 2015; Beggan & DeAngelis, 2015; Christensen, 2021; Davies et al., 2020a, 2020b). Weight bias is pervasive throughout the United States (McHugh & Kasardo, 2012; Puhl et al., 2014). Negative stereotypes associated with being overweight include laziness, lack of motivation, psychological instability, social rejection, and incompetence in the workforce (Hinman et al., 2015; Lewis et al., 1997; Moller & Tischner, 2019). Likewise, incorrect stereotypes about underweight people include psychological instability or weakness (Marini, 2017). Body weight is not explicitly identified as an issue in the multicultural and social justice competencies (Ratts et al., 2016). However, weight bias is similar to sexism, racism, and classism in its harmful impact on people (Bucchianeri et al., 2013). It is still a common form of prejudice (McHugh & Kasardo, 2012).
Weight bias has become a social justice issue because of how it negatively impacts the lived experiences of people across social contexts (Nutter et al., 2018). Similar to other identities that elicit prejudice, weight bias impacts an individual’s opportunities in the workforce (Hutson, 2013), quality of mental health care (Puhl et al., 2014), and interpersonal relationships (Puhl & Heuer, 2010). Oppression from weight bias may deter a person from forming relationships or making connections with others out of fear of rejection or discrimination based on weight. Likewise, a person with weight bias may struggle to overlook the body of their counselor because of their worldview of weight and health. Even if the client remains in counseling, this initial bias may impede the therapeutic alliance process.
Therapeutic Alliance
The therapeutic alliance is a key variable in predicting client outcomes in counseling (Ackerman & Hilsenroth, 2001). This alliance represents the degree to which the client and counselor are engaged in collaboration, their commitment to one another, and their understanding of the counseling process (Allen et al., 2017; Lorr, 1965). Clients are as important as counselors in building this alliance, which involves their impression of and reaction to the counselor (Tudor, 2011). Disruptions in the therapeutic alliance can be generated from the client’s adverse reaction to the counselor, which thus impacts client outcomes (Ackerman & Hilsenroth, 2001). Weight can be a disruption, as some clients see a counselor being overweight as a barrier to opening up and engaging in counseling (Moller & Tischner, 2019). As the therapeutic alliance impacts clients remaining in counseling (Sharf et al., 2010), biases toward the counselor may hinder building the relationship, leading to early termination. Clients discriminating against counselors may limit capable counselors who fall outside socially acceptable weights from co-building the therapeutic alliance (McKee & Smouse, 1983).
Even with weight bias possibly diminishing the initial therapeutic relationship, Allen et al. (2017) found that communication on tasks/goals was a predictor of a strong therapeutic alliance and activation (i.e., the clients’ readiness and willingness to take on the management of their mental health care). Allen et al. found that alliance around the tasks/goals of therapy had long-term benefits, while an initial therapeutic bond was only associated with activation at the beginning of therapy. These findings suggest that despite client bias, a strong alliance may still form if there is a connection between counselor and client on their treatment goals and plan.
Despite a client and counselor’s mutual investment in a counseling relationship, research about weight bias in counseling has focused solely on counselors’ perceptions of clients’ weight and its influence on the therapeutic alliance (Kinavey & Cool, 2019; McHugh & Kasardo, 2012; Puhl et al., 2014). Thus, research has insufficiently examined how a counselor’s weight may hinder this alliance (Moller & Tischner, 2019). This gap is further concerning given that researchers have found that professionals in other disciplines identified as overweight or underweight face discrimination in the workplace (Beggan & DeAngelis, 2015; Hutson, 2013).
Overweight Bias Toward Counselors
Researchers have found that counselors are subject to weight bias from clients. Moller and Tischner (2019) examined client perceptions of counselors by specifically examining counselor weight. They conducted a qualitative story completion task with students from Great Britain aged 15–24 (N = 203) and found that participants perceived overweight counselors as incompetent. Counselors’ competence came into question because of the perception that being overweight implies a lack of emotional stability, personal discipline, and mental stability (Moller & Tischner, 2019). Participants also reported perceiving overweight counselors as distracting because of their physical appearance. Additionally, participants viewed an overweight counselor as having poor psychological health. Some participants noted that being overweight suggested an eating disorder (ED), such as bulimia or binge eating disorder. Furthermore, responses indicated that weight bias would impact the therapeutic relationship, and many participants would not want to work with an overweight counselor (Moller & Tischner, 2019).
These results are striking, and further research is needed to corroborate their value, as they point to a high level of bias toward overweight counselors. These types of inaccuracies can perpetuate prejudice and discrimination that may also hurt potential clients who would otherwise not have access to a counselor. Stereotypes and biases impact those who choose to work in this profession and could struggle to feel they belong in the helping professions.
Underweight Bias
Research geared toward overweight bias is well established in the health professions; however, evidence suggests that underweight health professionals also experience bias and discrimination (Allison & Lee, 2015; Beggan & DeAngelis, 2015; Davies et al., 2020a, 2020b). Researchers have noted stereotypes suggesting that extreme thinness may indicate a lack of wellness or the presence of a mental health issue like anorexia (Davies et al., 2020a). Furthermore, implicit bias toward underweight people may also come from the survival instinct that hunger, poverty, and war create underfed people, and we want to be with those who can help us survive (Marini, 2017).
Interestingly, scholars have noted that if being underweight is not perceived as stemming from health issues or an ED, people possess more favoritism toward underweight persons, limiting institutional discrimination toward them (Allison & Lee, 2015; Beggan & DeAngelis, 2015). In some social settings, a slender appearance of health follows socially accepted norms and may supersede the importance of actual health (Moller & Tischner, 2019). This leads to what is known as thin privilege; hence the possibility that there is enough benefit to being thin that it negates any negative attitudes or behaviors by others.
This thin privilege allows others to overstep the concept of civil inattention, which is how people are recognized appropriately in polite society. Civil inattention warrants people to be discrete in commenting on or noticing differences among those around them (e.g., those with disabilities, obesity, low socioeconomic status, or other marginalized identities). Some people believe that being underweight may invite a breakdown of civil inattention (Beggan & DeAngelis, 2015). This breakdown may lead a client to comment on a counselor’s body, such as “You are so skinny; how can you understand anything I am feeling about my body” or “If I were as thin as you, I would…” These types of comments are seen as acceptable because they infer a compliment about a socially desirable attribute. However, they can invite feelings of judgment and unease for the counselor, perpetuating a rupture in the therapeutic alliance. As we continue to understand that weight bias exists along a spectrum, counselors may feel prepared to broach the topic of weight regardless of where they fall.
One last finding that significantly impacts weight bias toward counselors comes from a qualitative study of adults (N = 18) with an average female body mass index (BMI) of 18.80 or male BMI of 21.68, both of which fall within the normal range of 18.5 to 24.9 (Centers for Disease Control and Prevention [CDC], 2022). Beggan and DeAngelis (2015) found that participants believed that underweight people lack empathy for others who struggle with weight. Such a belief would be impactful for a counselor, given that empathy is integral for a successful counseling relationship (Clark, 2010).
Empathy
Empathy is one of the six core conditions necessary for client change and contributes significantly to therapeutic outcomes. Clients can perceive empathy from counselors when counselors act in ways consistent with their frame of reference (Feller & Cottone, 2003).
Empathy is a deep understanding of the client’s circumstances. When there is weight bias, the client may not believe their counselor can understand their frame of reference if they are of differing body weights, especially if the client is coming in for body image concerns or health concerns. Even though the counselor has empathy, the client may not accept this as truth, hindering the building of a solid therapeutic alliance.
Weight as Credibility
Whether professionals are overweight or underweight, their bodies are part of their résumé. The term bodily capital describes one’s credibility as portrayed by the body and can influence how professionals are judged by their physical appearance (Hutson, 2013; Moller & Tischner, 2019). The body can be viewed as a symbolic container that indicates the investment of time and resources into health and well-being (Hutson, 2013). Previous scholars have asserted that the healthier a professional appears, the more likely clients and patients will accept their advice and trust their counsel (Hutson, 2013; Puhl et al., 2013). Health expectations are amplified for health professionals, as overweightness can be seen by some as a moral transgression and an inadequacy that may translate into their work (Beggan & DeAngelis, 2015). Some people believe that to be psychologically healthy, a person must appear to be of an appropriate weight; this indicates willpower, discipline, and self-control (Tischner, 2019). Though these ideas are inaccurate for psychological health, they may influence how clients see counselors on the far ends of the weight spectrum.
Antifat Attitudes
Antifat attitudes are a different but related construct to weight bias. An antifat attitude is “a negative attitude toward (dislike of), belief about (stereotype), or behavior against (discrimination) people perceived as being ‘fat’” (Meadows & Daníelsdóttir, 2016, p. 47). Weight bias refers to a negative attitude toward any size body (Christensen, 2021), whereas antifat attitudes describe dislike and discrimination toward people perceived as overweight (Meadows & Daníelsdóttir, 2016). Antifat attitudes have created a marginalized group that faces external stigma throughout society, with some individuals feeling internal stigma due to personal experiences.
Despite encounters with prejudice, some clients who are overweight will still prefer an average-weight counselor because of their own bias toward being overweight (Moller & Tischner, 2019) and will have similar antifat attitudes as average-weight individuals (Schwartz et al., 2006). Contingencies of self-worth encompass the domains in a person’s life that create self-esteem (Clabaugh et al., 2008). When body weight is a domain, success or failure in their ability to lose or gain weight can lead to lower self-worth. Because of weight bias, working with a counselor who mirrors the client’s undesired body weight may impact the client’s willingness to work with the counselor. Examining weight bias across the spectrum and correlating BMI with antifat attitudes will give us further insight into these findings and if they influence client bias toward counselors.
Purpose of the Study
This study examined if client weight bias influences a client’s trust in a counselor’s competence, willingness to follow a counselor’s advice, and desire to select a counselor for therapy. We further examined if a client’s antifat attitudes are associated with their weight bias toward counselors. The following research questions guided this study: 1) Does a counselor’s weight impact a client’s decision to trust, follow advice, and select the counselor? 2) Is there an association between a client’s antifat attitudes and weight bias toward counselors? 3) Are there differences in weight bias toward counselors based on the socio-demographics of the clients using their services? and 4) Do participants with eating disorders have similar perceptions of counselors due to weight bias as those without eating disorders?
Methodology
Recruitment
At the time the research was conducted, the researchers—Amy Biang, Clare Merlin-Knoblich, and Stella Kim—were affiliated with the same university; as such, IRB approval was obtained from that university before recruiting participants. People were eligible to participate in this study if they were 18 years or older and signed an electronic consent form indicating their willingness to participate. We recruited participants through purposive and snowball sampling in three ways. First, Biang emailed a compiled database of counseling professionals within their acquaintance to request they send the survey to previous clients in an effort to obtain sufficient participation from people who have received counseling. In addition, requested participation through two research boards of counseling associations (Academy of Eating Disorders and International Association of Eating Disorder Professionals) allowed us to recruit sufficient participation from previous clients with EDs, as well as other diagnoses, as we requested they send the survey to their former clients. Second, to obtain participation from people with and without experience in counseling, Biang posted calls for participation on social media accounts (i.e., Instagram and Facebook). Third, to further increase participation, Merlin-Knoblich forwarded a participation request to their university’s counseling program listserv. After 2 weeks of data collection, we sent a second follow-up call for participation and then continued data collection for an additional week.
To prevent recruitment bias and confirmation bias during data collection, we omitted the terms weight and weight bias and modified the study title to read “Counselor Attributes that Impact Client’s Selection, Trust, and Advice Following.” The call for participation informed potential participants that we were conducting a study about the attributes of a hypothetical counselor. The end of the questionnaire contained a full disclosure of the study’s purpose. Of the 255 participants who began the study questionnaire, 189 completed the study, representing a 74% completion rate. No data was collected from the 66 non-completers other than an average of 76 seconds with the survey open before ending the survey.
Participants
A sample of 189 participants from 26 states participated in the study. Table 1 presents a summary of the sample characteristics. The majority of participants were from North Carolina (n = 72, 38%),
Ohio (n = 23, 12%), California (n = 19, 10%), Utah (n = 11, 6%), and New York (n = 10, 5%). Participants primarily identified as female (n = 158, 84%). The majority of participants identified as White (n = 153, 81.4%), with other participants identifying as Asian (n = 13, 6.9%), Black/African American (n = 12, 6.4%), Latine/Hispanic (n = 5, 2.7%), and American Indian (n = 3, 1.6%). The majority of participants were over the age of 30 (n = 139, 74%), more than half had previously participated in personal counseling (n = 135, 71.8%), and just over a quarter indicated a previous ED diagnosis (n = 52, 27.7%).
Given the focus of this study, all participants were asked to indicate their height and weight but were informed that such information (like all demographic information) was optional to submit. One hundred and eighty-four participants (97%) shared their height and weight, from which we calculated their BMI—a person’s weight in kilograms divided by the square of height in meters. The mean BMI was 28 (SD = 6.8) among the participants who shared their height and weight. This BMI is designated as “overweight” by the CDC (2022).
Study Design and Instrumentation
Physician Weight Survey Revised
We used a quasi-experimental research design in this study. With permission from Puhl and colleagues (2013), we revised the Physician Weight Survey (PWS), a 44-item questionnaire designed to assess patient weight bias of physicians who are obese, overweight, or seen as average weight. The instrument measures five constructs: physician health behaviors, physician selection, physician compassion, physician trust, and adherence to physician advice. Cronbach’s alpha tests instrument reliability and the internal consistency of the questions on a scale. Alpha scores over .70 are considered acceptable (Taber, 2018). Each subscale of the PWS has demonstrated sufficient internal consistency, with a Cronbach’s alpha of at least .90 (Puhl et al., 2013).
We adapted the questionnaire to address participants’ willingness to trust, follow the advice of, and select a hypothetical counselor based on the weight of that counselor. We replaced the term, physician with counselor and added the underweight category instead of the obese category. Using the underweight category allowed for consideration that weight bias exists on both ends of the weight spectrum. Because
of differences in occupational responsibilities and limiting the dependent variables of our study, we did not use the subscales for health behaviors or compassion. The Health Behavior subscale incorporated the physicians’ use of substances, health screenings, and illness prevention. The Compassion subscale measured the physician’s bedside manner. Without those two additional subscales, our revised measure had 23 items.
Table 1
Participant Demographic Data
| Demographics |
n |
% |
| Gender |
|
|
| Female |
158 |
84.0 |
| Male |
27 |
14.4 |
| Non-Binary |
1 |
0.05 |
| Race/Ethnicity |
|
|
| White |
153 |
81.4 |
| Black/African American |
12 |
6.4 |
| Latine/Hispanic |
5 |
2.7 |
| Asian |
13 |
6.9 |
| American Indian |
3 |
1.6 |
| Age Range |
|
|
| 18–29 |
48 |
25.6 |
| 30–42 |
64 |
34.1 |
| 43 and older |
74 |
39.4 |
| Prior History of Counseling |
|
|
| Yes |
135 |
71.8 |
| No |
51 |
27.1 |
| Prior History of Eating Disorder |
|
|
| Yes |
52 |
27.7 |
| No |
134 |
74.3 |
| BMI Range |
|
|
| Underweight |
4 |
2.1 |
| Average |
64 |
34.0 |
| Overweight |
54 |
28.7 |
| Obese |
60 |
31.9 |
Note. N = 189.
The subscales of Counselor Trust and Counselor Selection align well with our study. The subscale of Advice Following may seem counterintuitive when used with the counseling profession. The term advice equates to the construct of counseling together and incorporates the concept of counselors helping clients create and follow treatment goals, exploring ideas together for change, and even assigning homework. Advice aligns with how clients perceive what counselors do rather than the skills they use. For example, counselors using motivational interviewing and questions such as “What would it take for you to go from a 2 to a 4 in your willingness to reduce your alcohol consumption?” can be seen as advising clients to reduce their alcohol consumption. We chose to use the term advice instead of counsel so all participants, regardless of their experience with counseling, would understand the questions.
Parallel to Puhl and colleagues’ (2013) study, we then created three different versions of the questionnaire. Using Qualtrics, an electronic survey platform, consenting participants received a random assignment to one of three questionnaire versions. Seventy (37%) of the study participants completed the first version of the questionnaire, which described a hypothetical counselor as an overweight counselor. Fifty-eight (31%) participants completed the second questionnaire version, which described a hypothetical counselor as having average weight. And 61 (32%) of the participants completed the third version of the questionnaire, which described a hypothetical counselor as underweight. Participants responded to all items on a Likert scale ranging from 1 (strongly disagree/extremely unlikely) to 7 (strongly agree/extremely likely), with seven questions reverse scored.
Counselor Trust Subscale. The Counselor Trust subscale of the revised PWS consisted of nine questions focused on skills and competence (e.g., “If my counselor was [overweight/underweight/average weight], I would not trust them,” and “If my counselor was [overweight/underweight/average weight], I would have doubts about their credibility”). Other questions focused on believing the counselor would listen or understand their needs (e.g., “I believe an [overweight/underweight/average weight] counselor would listen carefully to what I have to say”). The scale demonstrated good internal consistency (α = .81) with this sample. Higher scores reflect greater trust in the counselor.
Counselor Advice Following Subscale. The Advice Following subscale contained six items. These items indicated making changes to diet, losing weight, and advice in general (e.g., “In general, my counselor’s weight affects whether I listen to their advice” and “If my counselor were [overweight/underweight/average weight], I would feel embarrassed when talking about losing weight”). Though counselors are not medical doctors, many clients explore topics associated with their bodies, exercise, and overall physical health (e.g., sleep issues, pain management, substance use, and daily routines), indicating relevance to counseling for the survey questions. Higher scores suggest more willingness to follow the advice (counsel) of the counselor. Cronbach’s alpha for this scale was .83 with this sample.
Counselor Selection Subscale. The Counselor Selection subscale had seven items indicating a willingness to select the counselor based on their appearance of weight (e.g., “If I went to a new counselor, and the counselor appeared [overweight/underweight/average weight], I would change counselors,” or “If my counselor was [overweight/underweight/average weight], I would not recommend them to my friends”). Similar to the other subscales, higher scores indicate more willingness to select the counselor. For this sample, Cronbach’s alpha was .71.
Antifat Attitudes Questionnaire
In addition to the revised PWS, participants completed the Antifat Attitudes Questionnaire (AFA; Crandall, 1994). The AFA assesses participants’ beliefs about overweight people and their feelings about becoming overweight. Three subscales, Dislike (α = .84), Fear of Fat (α = .79), and Willpower (α = .66), are combined for a composite antifat attitude score. Despite the low Cronbach’s alpha coefficient for the Willpower subscale, it positively correlates with the Dislike subscale (r = .43, p < .001), whereas the Fear of Fat subscale remains uncorrelated with both subscales, suggesting discriminate validity (Lacroix et al., 2017; Ruggs et al., 2010). Both the reliability and validity of the AFA have been extensively assessed by researchers, and the AFA has been found to be a psychometrically sound measure (Ruggs et al., 2010). The Cronbach’s alpha internal consistency reliability was acceptable, with a value of .87 for the data used in the current study. Participants indicated agreement (e.g., “I really don’t like fat people much”) on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher composite scores suggesting stronger negative antifat attitudes. Higher scores may correlate to weight bias toward the overweight counselor. Scores on the Fear of Fat subscale are directed toward a personal antifat fear and not toward others.
The AFA was also used to test the equivalence of groups and any effect of social desirability. Lastly, participants completed a voluntary 8-item demographic questionnaire describing their race/ethnicity, age, gender, height, weight, and experience with receiving counseling or having an ED.
Data Analysis
We conducted all analyses using SPSS Version 27. The first analysis had the four dependent variables of Counselor Trust, Counselor Selection, Advice Following, and Weight Bias, with the independent variable of Weight (overweight, underweight, and average weight). We conducted a series of assumption-checking procedures to draw valid interpretations of the findings. Engaging the Shapiro-Wilk test as a test of normality yielded a significant result (W = 0.92, p < .001) for the overweight counselor, indicating the sample was not normally distributed. After removing outliers, the sample for the overweight survey condition did not meet the assumption of normality. A test for homogeneity of variance yielded a statistically significant Levine’s score of F(2, 168) = .46, p = .013; degrees of freedom were adjusted due to unequal sample sizes for each survey condition.
Conducting a MANOVA yielded statistically significant results; however, not meeting the assumptions of multivariate normality and homogeneity of variance required, we used the Welch ANOVA, which is recommended for non-normal distributions. Using a Welch ANOVA is also a best practice when the homogeneity of variances test fails; it controls the type I error and gives more power in many instances (Liu, 2015). Although a parametric test such as a typical ANOVA or MANOVA is known to be more powerful than a non-parametric test (e.g., Welch ANOVA), it can lead to erroneous results if required assumptions are not satisfactorily met (Zar, 1998). Considering unequal variances and sample sizes across groups, we used Games-Howell for post hoc testing. We used G*Power version 3.1.9.7 (Faul et al., 2007) to perform the power analysis. For the Welch ANOVA test, the minimum sample size was 157, with a medium effect size of .25, a desired statistical power level of .8, and an alpha level of .05. Lastly, we measured the effect size using partial eta squared (ꞃ²), showing the strength of association as a proportion of variance in the dependent variable explained by group membership (Coladarci et al., 2011).
Table 2
Descriptive Statistics for Outcome Variables
|
n |
Mean |
Std.
Deviation |
Std. Error |
95% Confidence Interval for Mean |
Minimum |
Maximum |
| Lower Bound |
Upper Bound |
| Trust |
OW |
70 |
49.70 |
9.89 |
1.18 |
47.34 |
52.06 |
16.00 |
63.00 |
| UW |
59 |
41.15 |
10.72 |
1.40 |
38.36 |
43.95 |
17.00 |
63.00 |
| AW |
60 |
47.48 |
7.75 |
1.00 |
45.48 |
49.49 |
29.00 |
63.00 |
| Total |
189 |
46.33 |
10.16 |
0.74 |
44.87 |
47.79 |
16.00 |
63.00 |
| Selection |
OW |
70 |
32.41 |
5.40 |
0.64 |
31.13 |
33.70 |
19.00 |
40.00 |
| UW |
59 |
30.00 |
5.12 |
0.67 |
28.67 |
31.33 |
21.00 |
40.00 |
| AW |
60 |
31.42 |
4.92 |
0.63 |
30.15 |
32.69 |
16.00 |
40.00 |
| Total |
189 |
31.34 |
5.23 |
0.38 |
30.59 |
32.09 |
16.00 |
40.00 |
| Advice |
OW |
70 |
25.76 |
8.72 |
1.04 |
23.68 |
27.84 |
8.00 |
42.00 |
| UW |
59 |
24.73 |
7.33 |
0.95 |
22.82 |
26.64 |
8.00 |
42.00 |
| AW |
60 |
31.93 |
4.64 |
0.60 |
30.73 |
33.13 |
23.00 |
42.00 |
| Total |
189 |
27.40 |
7.81 |
0.57 |
26.28 |
28.52 |
8.00 |
42.00 |
| Note. OW = overweight; UW = underweight; AW = average weight. |
In the second data analysis, we used the Pearson correlation to assess an association between data sets from the AFA and Composite Weight Bias. Composite Weight Bias was calculated by summing the scales of the revised PWS. Before computing a correlation, we examined the scatter plot between the independent and dependent variables to check the linearity between the two variables and the existence of outliers. We found less than three outliers on all four graphs and identified negative linearity. Using G*Power (Faul et al., 2007), we obtained the estimated sample size necessary to run the correlation analysis, which was 64 with a medium effect size of .3, an alpha level of .05, and power of .8. Lastly, we explored the relationships between demographics and weight bias toward counselors using a one-way ANOVA or an independent t-test. We selected statistical methods based on the number of categories of each demographic variable. See Table 2 for descriptive statistics of the outcome variables.
Results
Areas of Trust, Advice, and Selection
We found significantly different levels of trust, advice following, and counselor selection behaviors among participants assigned to hypothetical counselors of different weights.
Welch ANOVA test results indicated a statistical significance in all three areas between groups, F(2, 120.60) = 12.89, p < .001 with a medium effect size (ꞃ² = .11). Post hoc comparisons using Games-Howell showed the following results at the significance level of α = .05. Counselor Trust for average-weight counselors (M = 47.48, SD = 7.75) was significantly higher than Counselor Trust for underweight counselors (M = 41.15, SD = 10.72) at p = .001. Counselor Trust of overweight counselors (M = 49.70, SD = 9.89) was also significantly higher than Counselor Trust for underweight counselors at p < .001. There was no statistical significance for Counselor Trust between average and overweight counselors. Advice Following for average-weight counselors (M = 31.93, SD = 4.65) was significantly higher than Advice Following for underweight counselors (M = 24.72, SD = 7.28) and Advice Following for overweight counselors (M = 25.75, SD = 8.72) at p < .001 for both. Finally, Counselor Selection for an overweight counselor (M = 32.41, SD = 5.73) was statistically higher than Counselor Selection for an underweight counselor (M = 30.00, SD = 5.59) with p = .028. There was no statistical significance in the Counselor Selection of average-weight counselors (M = 31.41, SD = 4.91) compared to overweight or underweight counselors. See Table 3 and Figures 1–3.
Next, we conducted a Welch ANOVA between overall composite scores and the three weight groups (see Table 4). Again, Welch test results indicated a statistical significance between groups, F(2, 118.73) = 11.71, p < .001 with a medium effect size (² = .10). Post hoc comparisons using Games-Howell showed statistical significance between overweight counselors (M = 107.87, SD = 21.68) and underweight counselors (M = 95.88, SD = 20.00). Underweight counselors were also significantly lower on the overall composite than average-weight counselors (M = 110.83, SD = 19.97). There was no statistical significance between overweight and average-weight counselors for their overall composite scores, which include all three variables.
Figure 1
Willingness to Trust Counselor
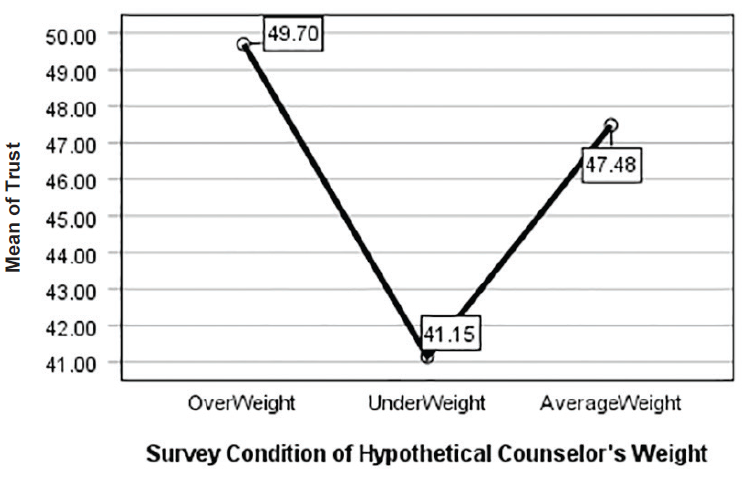
Figure 2
Willingness to Select Counselor
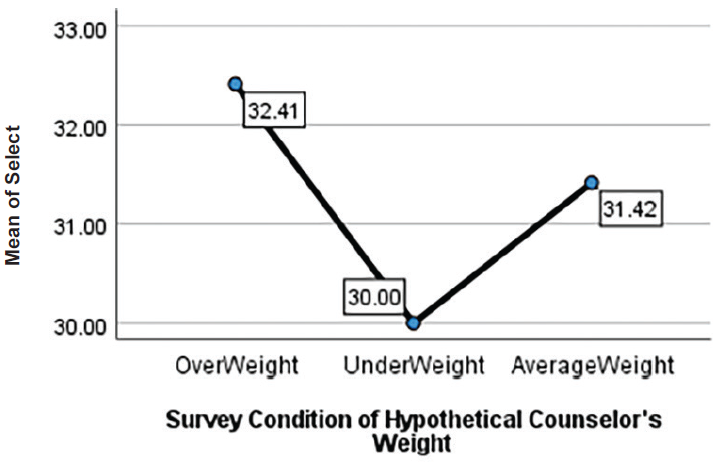
Figure 3
Following Counselor Advice
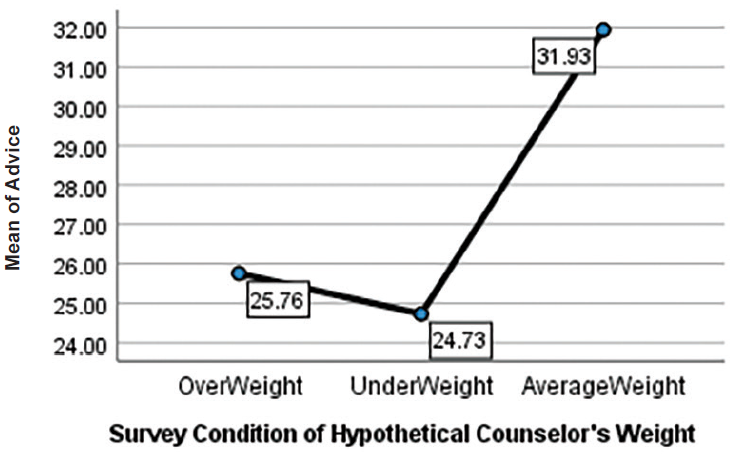
Table 3
Post Hoc Outcome Variables
|
| Dependent Variable |
Mean Difference (I-J) |
Std. Error |
Sig. |
95% Confidence Interval |
| Lower Bound |
Upper Bound |
| Trust |
OW |
UW |
8.547a |
1.829 |
0.00 |
4.206 |
12.888 |
| AW |
2.216 |
1.548 |
0.32 |
−1.456 |
5.889 |
| UW |
OW |
−8.547a |
1.829 |
0.00 |
−12.888 |
−4.206 |
| AW |
−6.330a |
1.717 |
0.00 |
−10.414 |
−2.247 |
| AW |
OW |
−2.216 |
1.548 |
0.32 |
−5.889 |
1.456 |
| UW |
6.330a |
1.717 |
0.00 |
2.247 |
10.414 |
| Selection |
OW |
UW |
2.414a |
0.927 |
0.02 |
0.215 |
4.613 |
| AW |
0.997 |
0.904 |
0.51 |
−1.144 |
3.143 |
| UW |
OW |
−2.414a |
0.927 |
0.02 |
−4.613 |
−0.215 |
| AW |
−1.416 |
0.920 |
0.27 |
−3.601 |
0.767 |
| AW |
OW |
−0.997 |
0.904 |
0.51 |
−3.143 |
1.148 |
| UW |
1.416 |
0.920 |
0.27 |
−0.767 |
3.601 |
| Advice |
OW |
UW |
1.028 |
1.413 |
0.74 |
−2.323 |
4.379 |
| AW |
−6.176a |
1.202 |
0.00 |
−9.034 |
−3.313 |
| UW |
OW |
−1.028 |
1.413 |
0.74 |
−4.379 |
2.323 |
| AW |
−7.204a |
1.126 |
0.00 |
−9.885 |
−4.523 |
| AW |
OW |
6.176a |
1.202 |
0.00 |
3.318 |
9.034 |
| UW |
7.204a |
1.126 |
0.00 |
4.523 |
9.885 |
| Note. The mean difference is significant at the 0.05 level. OW = overweight; UW = underweight; AW = average weight. Welch’s ANOVAs with Games-Howell post hoc tests were run owing to violations of the equality of variances assumption. |
Table 4
Post Hoc Composite Weight Bias
|
| (I) Group |
Mean Difference (I-J) |
Std. Error |
Sig. |
95% Confidence Interval |
| Lower Bound |
Upper Bound |
| OW |
UW |
11.99a |
3.67 |
0.004 |
3.28 |
20.70 |
| AW |
−2.96 |
3.09 |
0.604 |
−10.29 |
4.36 |
| UW |
OW |
−11.99a |
3.67 |
0.004 |
−20.70 |
−3.28 |
| AW |
−14.95a |
3.10 |
0.000 |
−22.32 |
−7.58 |
| AW |
OW |
2.96 |
3.09 |
0.604 |
−4.36 |
10.29 |
| UW |
14.95a |
3.10 |
0.000 |
7.58 |
22.32 |
| Note. The mean difference is significant at the 0.05 level. OW = overweight; UW = underweight; AW = average weight. Welch’s ANOVAs with Games-Howell post hoc tests were run owing to violations of the equality of variances assumption. |
|
In addition to statistical significance, we also examined effect size to quantify the significance found. Results indicated that Advice Following showed a large effect of association with the independent variable of Weight (² = .16). Counselor Trust had a medium effect size (² = .13), and Counselor Selection yielded a small effect size (² = .04). These results suggest that the weight of a counselor has a high association with clients following counselor advice, with average-weight counselors faring the best. Additionally, participants indicated they would trust average and overweight counselors more than underweight counselors. Lastly, overweight counselors were more favorable in Counselor Selection than underweight counselors.
Antifat Attitudes and a Correlation With Counselor Trust, Advice Following, and Counselor Selection
We used Pearson correlations to examine associations between antifat attitudes and weight bias toward counselors (see Table 5). To do so, we examined data from participants assigned to all three counselor conditions in the study. Each group showed a significant relationship between antifat attitudes and weight bias toward counselors; thus, we combined data to attain a larger sample size. The Pearson correlations between the independent variable of antifat attitudes and dependent variables of Counselor Trust, Advice Following, Counselor Selection, and Composite Weight Bias score were significant at α = .05. We found positive correlations between antifat attitudes and Counselor Selection, r(186) = .400, p < .001, and Counselor Trust, r(186) = .211, p = .004. These results indicate that as antifat attitudes increase, participants’ trust in and selection of a counselor based on weight also increase. We found no significant correlation between Advice Following and Composite Weight Bias score with antifat attitudes.
Table 5
Correlation of AFA With Outcome Variables |
|
|
|
|
|
|
AFA |
Trust |
Selection |
| AFA |
Pearson Correlation |
1.000 |
0.211** |
0.400** |
| Sig. |
|
0.004 |
0.000 |
| N |
188.000 |
188.000 |
188.000 |
| Trust |
Pearson Correlation |
0.211** |
1.000 |
0.349** |
| Sig. |
0.004 |
|
0.000 |
| N |
188.000 |
188.000 |
188.000 |
| Selection |
Pearson Correlation |
0.400** |
0.349** |
1.000 |
| Sig. |
0.000 |
0.000 |
|
| N |
188.000 |
188.000 |
188.000 |
Note. AFA = Antifat Attitude. Advice was not statistically significantly correlated with AFA. One participant of the total study sample (N = 189) did not complete this portion and is not included in the table.
*Correlation is significant at the 0.01 level (two-tailed). |
Socio-Demographic Categories
We found no statistically significant differences in weight bias toward counselors based on ethnicity F(4, 181) = .037, p = .997; age F(4, 181) = 1.71, p = .149; BMI F(4, 177) = .193, p = .942; counseling status t(184) = .798, p = .426; eating disorder t(184) = 1.055. p = .137; or gender F(2, 183) = 1.423, p = .426. Additionally, we tested for Pearson correlations between BMI and antifat attitudes. Results indicated that BMI and antifat attitudes had no significant correlation, r(N = 187) = .004, p = .958.
Antifat Attitudes by Survey Condition
To test for undue influence from survey design or responses that stem from social desirability, we ran an ANOVA comparing participants in each questionnaire condition (i.e., underweight, average weight, and overweight counselor) and their scores on the AFA. We found no statistically significant differences between the three groups, F(2, 181) = 2.74, p = .067. For the AFA scores, M = 40.22 and SD = 12.57. However, with the results of the AFA correlation with Counselor Trust and Counselor Selection, these findings may indicate that there was social desirability across all three survey conditions.
Discussion
Contrary to previous research from McKee and Smouse (1983) that suggested counselors of any weight could address personal concerns, our study results indicated that clients might use weight to select a counselor, trust the counselors’ skills, and follow their counsel. When asked about weight, participants in this study slightly preferred to select and trust the average-weight and overweight counselors, with weight bias directed mainly at the underweight counselor. Like previous research about weight bias toward physicians (Puhl et al., 2013) and personal trainers (Hutson, 2013), our results showed some weight bias toward overweight counselors when following advice. For underweight counselors, weight bias was present in all three subscales and mirrored findings that underweight persons are not immune to weight discrimination (Beggan & DeAngelis, 2015).
Overweight Counselors
Our results yielded only one finding that supported the theme from Moller and Tischner’s (2019) study that “fat counselors cannot help” (p. 14). Statistically significant results from the present study showed less willingness to follow the advice of overweight counselors. Similar to the findings from Puhl et al. (2013), taking advice or counsel from an overweight health care professional may prove more difficult than trusting they can perform their job or being willing to work with them. With two-thirds of adults in the United States considered overweight or obese (CDC, 2022), these findings may reflect cause for concern that some clients may not perceive competence in counselors who are overweight.
The correlation between the AFA with Counselor Trust and Counselor Selection can give insight into the findings. The positive correlation between AFA and Counselor Trust was low but significant. With 60% of participants in the overweight-to-obese category, there could be an underlying factor that needs further exploration. There was no correlation between BMI and AFA. However, as Schwartz et al. (2006) suggested, overweight people have similar antifat attitudes as average-weight individuals. The slight correlation potentially relates to most participants having larger bodies and knowing that being in larger bodies does not equate to untrustworthiness. Likewise, for Counselor Selection, we should consider the concept of similar attraction. This concept posits that people associate with those perceived as similar to them and who have similar physical attributes (Montoya & Horton, 2013). Relating to this concept of similar attraction, the positive correlation between AFA and Counselor Selection could be attributed to the high percentage of larger-body participants feeling more comfortable selecting the overweight counselor.
Unlike findings from other studies (Moller & Tischner, 2019; Puhl et al., 2013), our results did not indicate that Counselor Trust or Counselor Selection were negatively related to being overweight. However, when looking at the Advice Following subscale, there was a marked difference in the scores. The hypothetical overweight counselor had higher mean scores than underweight counselors on all three subscales and overall composite scores. On the upside, weight may not be an issue for many clients seeking counseling. Despite continued weight bias and stigma in social media and society, people might recognize that overweight counselors’ skills and knowledge are more important than perceived body weight. On the downside, clients may hesitate to follow counsel associated with issues concerning their own physical well-being from a perceived overweight counselor. To combat this, counselors need to be willing to broach the issue of weight if they feel it is hindering the therapeutic alliance. Similar to other multicultural topics, differences in body weight between the counselor and client may be a potential barrier for the free expression of client concerns. The willingness of the counselor to explore this topic may put the client at ease and make them able to further explore their concerns in a nonjudgmental, therapeutic manner.
Underweight Counselors
We found surprising results suggesting that participants in our study would prefer an overweight or average-weight counselor to an underweight counselor. Participants scored counselors perceived as underweight significantly lower on a client’s willingness to select, trust, and follow a counselor’s advice than average-weight and overweight counselors. These results supported the decision to add this variable to our study and indicate the need for more research on weight bias toward underweight professionals.
The underweight variable yielded results that complement previous research on weight bias, indicating that people can be biased against underweight professionals (Allison & Lee, 2015; Davies et al., 2020b). Because of the persistent social desirability to be thin or underweight, research indicates that people may be pro-underweight on an explicit level; however, they implicitly prefer an average-weight person (Marini, 2017). In our findings, participants somewhat preferred to select an overweight counselor instead of an underweight counselor, upholding the notion that people do not necessarily trust those who are underweight despite the social pressure to be thin. This result highlights a striking mismatch in thought: people may prefer to be underweight because of social pressures but not fully trust an underweight counselor. It could indicate that societal pressures to be underweight are not as strong as once thought or it may suggest that people possess complicated views on being underweight in general.
These results reflect those found by Marini (2017), in which individuals implicitly preferred an overweight individual over an underweight individual, implying maladaptive behaviors and dangerous consequences. Additionally, with body positivity and body acceptance movements, underweight persons may be overlooked as recipients of negative weight bias (Beggan & DeAngelis, 2015). These results may give underweight counselors pause about how clients perceive them in session and the notion that experiences of thin privilege may not transfer into their professional identity. In response to these possible perceptions from clients, underweight counselors may benefit from seeking professional supervision or consulting with colleagues about the topic.
Antifat Attitudes
The AFA results indicated that as a person’s negative attitudes toward overweight people decrease, they disregard weight as a factor for selecting and trusting the skills of counselors. Currently, there is no measure for anti-thin attitudes to analyze whether this bias would yield similar results. Despite the lack of an anti-thin measure, these results reiterate the belief that we judge others based on what attributes are important to us or differentiate us from others (Cermák et al., 1993). When body weight is not an attribute of self-judgment, a person may not use it as a criterion toward others or in working with professionals. As a profession, we must continue supporting movements that promote acceptance of all bodies and destigmatize weight. With strong social media campaigns against weight bias, we can dispel the stereotypes about those who fall outside socially acceptable standards and replace them with acceptance.
Demographics
In addition to antifat attitudes, we chose to study socio-demographics because weight bias may fluctuate based on various group identities. Our results showed no statistically significant differences in age, gender, ethnicity, or BMI. These findings are relevant as they imply that weight bias may exist throughout all groups. However, we interpret these results cautiously, as the sample population was predominantly female, with fewer ethnically diverse participants, and more participation from people over 30. Notably, results for ethnicity were similar to previous research indicating that Black and White women had the same bias and weight stigma toward others who were overweight and underweight (Davies et al., 2020b).
Eating Disorder Consideration
Because of the nature of EDs, we added this category to the study to explore if a counselor’s weight would impact participants with an ED more. As counselors working with EDs often explore issues around weight, exercise, and eating concerns, we hypothesized that these participants might have a higher bias toward underweight and overweight counselors. We found that participants with EDs were not significantly different from participants without EDs in weight bias toward counselors in any of the variables. This finding is favorable information for counselors in this specialty, as it does not align with the findings from Moller and Tischner (2019) that suggest that the weight of a counselor is a barrier to treatment.
Experience of Counseling
A final surprising finding revealed in our results was that people with previous counseling experience had similar levels of weight bias to those who had not worked with a counselor. Participants who previously participated in counseling may recognize attributes, such as expertise, empathy, and compassion of a counselor, as more valuable in their relationship than weight. Because attributes such as genuineness, empathy, unconditional positive regard (Nienhuis et al., 2018) build the therapeutic relationship, it is feasible to see counselor weight as a non-factor. However, we found that prior experience in counseling did not mediate the weight bias participants demonstrated. This result gives room for concern that weight bias may diminish the initial value of core conditions and counselor attributes studied in the past. Perhaps weight bias is pervasive in the decision to work with a counselor.
Implications
Despite years of education and experience, weight bias may rule out competent counselors. Professionals who fall outside the average body weight are hyper-visible (Beggan & DeAngelis, 2015) and prone to judgment of their weight. This study fills a gap in the research pertaining to the way weight bias influences a client’s willingness to trust, follow counselor advice, and select their counselors. Knowing how weight bias impacts the counseling profession can help counselors become aware of an issue that may affect the therapeutic alliance. In response to the study results, we identified two key implications for the counseling profession.
First, the results are indicative of a multicultural issue. Many people see weight as a medical concern instead of a social justice issue (Christensen, 2021). This idea limits the amount of education and training counseling graduate students receive on the topic of weight, leading to the request to address weight in multicultural courses as a core topic. Weight becomes intersectional among identities, and counselors must train to be sensitive to and inclusive of the topic of weight. Broaching weight may feel uncomfortable but be necessary to strengthen the therapeutic relationship.
Second, recognizing that weight bias may impact a client’s willingness to select, follow the counsel of, or trust a counselor reiterates the importance of knowing the factors influencing the counseling relationship. Counselors should acknowledge that stereotypes, discrimination, and oppression influence the counseling relationship (Ratts et al., 2016). Counselors should not ignore weight bias as a possible stereotype and should be comfortable discussing it with their clients. Additionally, the multicultural competencies note that “Counselors know when to initiate discussions with regard to the influences of identity development, power, privilege, and oppression within the counseling relationship” (Ratts et al., 2016, p. 41). As society continues to push the thin ideal while simultaneously pushing body acceptance at any size, these contradictory messages will keep weight bias at the forefront of how others are judged.
Until weight bias is erased, counselors must be vigilant in understanding how they show up in the session, what message a client may perceive by their body weight, and how to broach the topic to strengthen the therapeutic alliance. If counselors seek to help reduce weight bias in society, they may benefit from reflecting on their own biases, privileges, and experiences with oppression in this area. They also may consider challenging potential biases through professional development, group or individual counseling supervision, or literature about weight bias in society.
Limitations
Like all studies, this study contains limitations. One limitation is the subjectivity of weight. Without guidelines for what constitutes overweight and underweight, this study heavily relied on participants’ perceptions of these variables, which may be inconsistent across participants. Not specifying these variables opened interpretation for the overlapping areas of overweight versus obese or underweight versus extremely thin. Participants in each treatment condition may have visualized different hypothetical counselors than peers in the same treatment group. Using images may improve the specificity of the variable in future studies.
Additionally, there was no identified gender for the hypothetical counselors in each treatment condition, allowing participants to visualize any gender of counselor they chose. This lack of specificity may have created a moderating variable. Women represent higher numbers in the counseling profession. Women experience more discrimination than men (McHugh & Kasardo, 2012; Roehling et al., 2007), and it is unknown if people who identify as gender non-binary experience more or less weight bias. By not distinguishing the gender of the counselor, our ability to make inferences across genders is limited. Creating a study that specifies multiple genders may yield more representative results.
Another limitation is that a non-parametric test (e.g., Welch’s ANOVA) was used instead of parametric tests with more statistical power. The decision to use the non-parametric test was unavoidable because of violating the required assumptions. At the same time, future research may corroborate our findings using a parametric test if data allow. Future research may also replicate this study using multivariate ANOVA (MANOVA), which considers correlations of dependent variables.
Lastly, social desirability and self-reporting may have impacted responses. While completing the questionnaire, feelings about weight bias may have occurred outside of participants’ awareness, causing cognitive dissonance. To resolve this dissonance, responses may have overtly favored accepting the overweight counselor or selecting fewer negative answers on the AFA. Participants also reported their own weight bias, which may have presented a self-report limitation. The results of overweight counselors having higher mean scores on Trust and Selection than average-weight counselors give room for consideration that social desirability may have influenced some of the participants’ answers. Future studies may benefit from including a test for social desirability or implicit association tests to increase the study’s validity.
Future Considerations
Future considerations for research encompassing weight bias across the spectrum would require developing an anti-thin attitude measure to identify weight attitudes toward underweight individuals accurately. This measure would be beneficial for bringing more awareness to underweight discrimination and measuring its impact on professionals and members of society. As society continues to push the thin ideal, people will strive to fit that ideal. However, as our results suggest, underweight counselors may face significant weight bias from clients. Consequently, counselors would benefit from a measure created to address underweight bias.
The counseling profession lacks extensive, meaningful research regarding the physical and educational factors that clients find most important in selecting, trusting, and following the advice of a counselor. Another factor to incorporate in future research is a counselor’s level of education and expertise. Clients may more favorably evaluate an average weight counselor with a specialist or doctoral degree than an underweight or overweight colleague with the same credentials. If weight bias influences these variables despite the skill level of the counselor, clients may miss receiving help from highly trained and educated people. Additionally, directly exploring the role that empathy, congruence, and strengths-based counseling have compared to weight bias may yield significant findings.
A final consideration for future research involves focusing on counselors who work in the ED field, a specialty that deals with eating, weight, body image, and exercise. Though we did not find significant differences in this study between those with and without an ED, our hypothetical counselor was not an ED counselor. These counselors may experience more judgment and assumptions of lifestyle choices by their clients, as they are considered specialists in EDs. Studies show that being underweight may indicate an ED, such as anorexia or binge eating disorder (Davies et al., 2020a; Marini, 2017). It is unknown if clients would replicate the results found in this study regarding counselors in the ED field.
Conclusion
This study examined participants’ weight bias toward hypothetical counselors of different weights. Our results highlight the existence of weight bias toward counselors on both ends of the weight spectrum. Even with strengthening the counseling relationship through empathy, congruence, and unconditional positive regard, counselors may benefit from reflecting on potential client weight bias and its impact on their therapeutic alliance. Additionally, weight as a multicultural issue increases counselors’ competence in addressing the prejudice and stereotypes that may limit their client’s willingness to trust them, follow their advice, or select them as their counselor.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ackerman, S. J., & Hilsenroth, M. J. (2001). A review of therapist characteristics and techniques negatively impacting the therapeutic alliance. Psychotherapy: Theory, Research, Practice, Training, 38(2), 171–185.
https://doi.org/10.1037/0033-3204.38.2.171
Allen, M. L., Cook, B. L., Carson, N., Interian, A., La Roche, M., & Alegría, M. (2017). Patient-provider therapeutic alliance contributes to patient activation in community mental health clinics. Administration and Policy in Mental Health and Mental Health Services Research, 44(4), 431–440. https://doi.org/10.1007/s10488-015-0655-8
Allison, M., & Lee, C. (2015). Too fat too thin: Understanding bias against overweight and underweight in an Australian female university student sample. Psychology & Health, 30(2), 189–202.
https://doi.org/10.1080/08870446.2014.954575
Beggan, J. K., & DeAngelis, M. (2015). “Oh, my God, I hate you”: The felt experience of being othered for being thin. Symbolic Interaction, 38(3), 371–392. https://doi.org/10.1002/SYMB.162
Bucchianeri, M. M., Eisenberg, M. E., & Neumark-Sztainer, D. (2013). Weightism, racism, classism, and sexism: Shared forms of harassment in adolescents. Journal of Adolescent Health, 53(1), 47–53.
https://doi.org/10.1016/j.jadohealth.2013.01.006
Centers for Disease Control and Prevention. (2022, June 3). Defining adult overweight & obesity. https://www.cdc.gov/obesity/basics/adult-defining.html
Cermák, I., Osecká, L., Rehulková, O., & Blatný, M. (1993). Judging others according to yourself: II. Interpersonal characteristics of personality and the structure of interpersonal attributions. Studia Psychologica, 35(2), 185. https://librarylink.uncc.edu/login?url=https://www.proquest.com/scholarly-journals/judging-others-according-yourself-ii/docview/1306142557/se-2?accountid=14605
Christensen, K. N. (2021). Factors related to weight-bias among counselors (Order No. 28541740). Available from Dissertations & Theses @ University of North Carolina Charlotte. (2562239518).
Clabaugh, A., Karpinski, A., & Griffin, K. (2008). Body weight contingency of self-worth. Self and Identity, 7(4), 337–359. https://doi.org/10.1080/15298860701665032
Clark, A. J. (2010). Empathy: An integral model in the counseling process. Journal of Counseling & Development, 88(3), 348–356. https://doi.org/10.1002/j.1556-6678.2010.tb00032.x
Coladarci, T., Cobb, C. D., Minium, E. W., & Clarke, R. B. (2011). Fundamentals of statistical reasoning in education (3rd ed.). Wiley.
Crandall, C. S. (1994). Prejudice against fat people: Ideology and self-interest. Journal of Personality and Social Psychology, 66(5), 882–894. https://doi.org/10.1037/0022-3514.66.5.882
Davies, A., Burnette, C. B., & Mazzeo, S. E. (2020a). Real women have (just the right) curves: Investigating anti-thin bias in college women. Eating and Weight Disorders, 25, 1711–1718.
https://doi.org/10.1007/s40519-019-00812-7
Davies, A., Burnette, C. B., & Mazzeo, S. (2020b). Black and White women’s attributions of women with underweight. Eating Behaviors, 39, 101446. https://doi.org/10.1016/j.eatbeh.2020.101446
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
https://doi.org/10.3758/BF03193146
Feller, C. P., & Cottone, R. R. (2003). The importance of empathy in the therapeutic alliance. The Journal of Humanistic Counseling, Education and Development, 42(1), 53–61.
https://doi.org/10.1002/j.2164-490x.2003.tb00168.x
Grimes, W. R., & Murdock, N. L. (1989). Social influence revisited: Effects of counselor influence on outcome variables. Psychotherapy: Theory, Research, Practice, Training, 26(4), 469–474. https://doi.org/10.1037/h0085465
Hauser, M., & Hays, D. G. (2010). The slaying of a beautiful hypothesis: The efficacy of counseling and the therapeutic process. The Journal of Humanistic Counseling, Education and Development, 49(1), 32–44.
https://doi.org/10.1002/j.2161-1939.2010.tb00085.x
Hinman, N. G., Burmeister, J. M., Kiefner, A. E., Borushok, J., & Carels, R. A. (2015). Stereotypical portrayals of obesity and the expression of implicit weight bias. Body Image, 12, 32–35.
https://doi.org/10.1016/j.bodyim.2014.09.002
Hutson, D. J. (2013). “Your body is your business card”: Bodily capital and health authority in the fitness industry. Social Science & Medicine, 90, 63–71. https://doi.org/10.1016/j.socscimed.2013.05.003
Kim, E., & Kang, M. (2018). The effects of client–counselor racial matching on therapeutic outcome. Asia Pacific Education Review, 19(1), 103–110. https://doi.org/10.1007/s12564-018-9518-9
Kinavey, H., & Cool, C. (2019). The broken lens: How anti-fat bias in psychotherapy is harming our clients and what to do about it. Women & Therapy, 42(1–2), 116–130. https://doi.org/10.1080/02703149.2018.1524070
Lacroix, E., Alberga, A., Russell-Mathew, S., McLaren, L., & von Ranson, K. (2017). Weight bias: A systematic review of characteristics and psychometric properties of self-report questionnaires. Obesity Facts, 10(3), 223–237. https://doi.org/10.1159/000475716
Lewis, R. J., Cash, T. F., & Bubb-Lewis, C. (1997). Prejudice toward fat people: The development and validation of the Antifat Attitudes Test. Obesity Research, 5(4), 297–307. https://doi.org/10.1002/j.1550-8528.1997.tb00555.x
Liu, H. (2015). Comparing Welch ANOVA, a Kruskal-Wallis test, and traditional ANOVA in case of heterogeneity of variance. https://doi.org/10.25772/BWFP-YE95
Lorr, M. (1965). Client perceptions of therapists: A study of the therapeutic relation. Journal of Consulting Psychology, 29(2), 146–149. https://doi.org/10.1037/h0021924
Marini, M. (2017). Underweight vs. overweight/obese: Which weight category do we prefer? Dissociation of weight-related preferences at the explicit and implicit level. Obesity Science & Practice, 3(4), 390–398. https://doi.org/10.1002/osp4.136
McHugh, M. C., & Kasardo, A. E. (2012). Anti-fat prejudice: The role of psychology in explication, education and eradication. Sex Roles, 66(9–10), 617–627. https://doi.org/10.1007/s11199-011-0099-x
McKee, K., & Smouse, A. D. (1983). Clients’ perceptions of counselor expertness, attractiveness, and trustworthiness: Initial impact of counselor status and weight. Journal of Counseling Psychology, 30(3),
332–338. https://doi.org/10.1037/0022-0167.30.3.332
Meadows, A., & Daníelsdóttir, S. (2016). What’s in a word? On weight stigma and terminology. Frontiers in Psychology, 7, 1527. https://doi.org/10.3389/fpsyg.2016.01527
Meyer, O. L., & Zane, N. (2013). The influence of race and ethnicity in clients’ experiences of mental health treatment. Journal of Community Psychology, 41(7), 884–901. https://doi.org/10.1002/jcop.21580
Moller, N., & Tischner, I. (2019). Young people’s perceptions of fat counsellors: “How can THAT help me?” Qualitative Research in Psychology, 16(1), 34–53. https://doi.org/10.1080/14780887.2018.1536384
Montoya, R. M., & Horton, R. S. (2013). A meta-analytic investigation of the processes underlying the similarity-attraction effect. Journal of Social and Personal Relationships, 30(1), 64–94.
https://doi.org/10.1177/0265407512452989
Nienhuis, J. B., Owen, J., Valentine, J. C., Winkeljohn Black, S., Halford, T. C., Parazak, S. E., Budge, S., & Hilsenroth, M. (2018). Therapeutic alliance, empathy, and genuineness in individual adult psychotherapy: A meta-analytic review. Psychotherapy Research, 28(4), 593–605. https://doi.org/10.1080/10503307.2016.1204023
Nutter, S., Russell-Mayhew, S., Arthur, N., & Ellard, J. H. (2018). Weight bias and social justice: Implications for education and practice. International Journal for the Advancement of Counselling, 40(3), 213–226.
https://doi.org/10.1007/s10447-018-9320-8
Puhl, R. M., Gold, J. A., Luedicke, J., & DePierre, J. A. (2013). The effect of physicians’ body weight on patient attitudes: Implications for physician selection, trust and adherence to medical advice. International Journal of Obesity, 37(11), 1415–1421. https://doi.org/10.1038/ijo.2013.33
Puhl, R. M., & Heuer, C. A. (2010). Obesity stigma: Important considerations for public health. American Journal of Public Health, 100, 1019–1028. https://doi.org/10.2105/AJPH.2009.159491
Puhl, R. M., Latner, J. D., King, K. M., & Luedicke, J. (2014). Weight bias among professionals treating eating disorders: Attitudes about treatment and perceived patient outcomes. International Journal of Eating Disorders, 47(1), 65–75. https://doi.org/10.1002/eat.22186
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Roehling, M. V., Roehling, P. V., & Pichler, S. (2007). The relationship between body weight and perceived weight-related employment discrimination: The role of sex and race. Journal of Vocational Behavior, 71(2), 300–318. https://doi.org/10.1016/j.jvb.2007.04.008
Ruggs, E. N., King, E. B., Hebl, M., & Fitzsimmons, M. (2010). Assessment of weight stigma. Obesity Facts, 3(1), 60–69. https://doi.org/10.1159/000273208
Schwartz, M. B., Vartanian, L. R., Nosek, B. A., & Brownell, K. D. (2006). The influence of one’s own body weight on implicit and explicit anti-fat bias. Obesity, 14(3), 440–447. https://doi.org/10.1038/oby.2006.58
Sharf, J., Primavera, L. H., & Diener, M. J. (2010). Dropout and therapeutic alliance: A meta-analysis of adult individual psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 47(4), 637–645.
https://doi.org/10.1037/a0021175
Taber, K. S. (2018). The use of Cronbach’s alpha when developing and reporting research instruments in science education. Research in Science Education, 48, 1273–1296. https://doi.org/10.1007/s11165-016-9602-2
Tischner, I. (2019). Tomorrow is the start of the rest of their life—so who cares about health? Exploring constructions of weight-loss motivations and health using story completion. Qualitative Research in Psychology, 16(1), 54–73. https://doi.org/10.1080/14780887.2018.1536385
Tudor, K. (2011). Rogers’ therapeutic conditions: A relational conceptualization. Person-Centered & Experiential Psychotherapies, 10(3), 165–180. https://doi.org/10.1080/14779757.2011.599513
Zar, J. H. (1998). Biostatistical analysis (4th ed.). Prentice Hall.
Amy Biang, PhD, LCMHC, CEDS, is an assistant professor at Northern Arizona University. Clare Merlin-Knoblich, PhD, is an associate professor at the University of North Carolina at Charlotte. Stella Y. Kim, PhD, is an assistant professor at the University of North Carolina at Charlotte. Correspondence may be addressed to Amy Biang, 15451 N 28th Ave, Phoenix, AZ 85053, amy.biang@nau.edu.
Aug 24, 2023 | Volume 13 - Issue 2
Kelly Emelianchik-Key, Bridget Glass, Adriana C. Labarta
Teen dating violence (TDV) is an ongoing epidemic in the United States. Subsequently, gender symmetry regarding the experience and perpetration of violence continues to be a prevalent debate in American society. TDV is a clinical concern that can impact clients’ safety; therefore, counselors must be adequately trained and cognizant of any biases that may influence the assessment and treatment of survivors of abuse. We conducted a qualitative research study using case vignettes to explore how counseling students conceptualize and propose treatment of TDV with male and female clients. Six overarching categories and 19 corresponding themes emerged, with gender bias as the most notable finding of the study. We conclude by discussing the implications for counseling and providing recommendations for educational standards and best practices to reduce gender bias and promote more inclusive treatment.
Keywords: teen dating violence, abuse, counseling students, gender bias, educational standards
Teen dating violence (TDV) is an adverse childhood experience that often shapes future relationship patterns throughout adulthood (Emelianchik-Key et al., 2022; Offenhauer & Buchalter, 2011). As a result, TDV has become a significant public health concern among adolescents in the United States (Centers for Disease Control and Prevention [CDC], 2021). After a compilation of prevalence rates, dating violence victimization rates range from 20%–53% in early adolescence (Goncy et al., 2017). In 2019 alone, one in 12 high school students reported physical and sexual violence within a dating relationship (CDC, 2021). Of those who reported intimate partner violence, 11 million women and 5 million men noted experiences of TDV before age 18 (CDC, 2021). TDV is characterized by physically or sexually violent acts that one adolescent perpetrates against another whom they are dating (CDC, 2021). This is inclusive of maladaptive behaviors, such as stalking and emotional abuse. In fact, emotional abuse (e.g., stonewalling, insulting language, social isolation, name-calling, gaslighting) exceeds the expression of physical violence within most teen dating relationships (Offenhauer & Buchalter, 2011).
TDV compromises the physical and emotional safety of American youth and can potentially impair adolescent development (CDC, 2021; K. E. Hunt et al., 2022), including how young people learn emotional regulation and form healthy relationships. K. E. Hunt et al. (2022) noted that many complicated variables play a role in the development and the prevention of dating violence, with family of origin belief systems and peers contributing to social learning. This was apparent in Emelianchik-Key et al.’s (2022) qualitative study, which determined that young college-aged females consistently normalized and accepted toxic relationship behaviors as common and justified because of norms created by family, peers, and society.
Further, the consequences of TDV on an adolescent’s psychological well-being and decision-making may be severe and persist over time, causing problems later in life. For example, Temple et al. (2013) determined a significant increase in the internalization of emotions in adolescent girls who experienced TDV. Youth with pre-existing mental health conditions are also at increased risk for traumatization by a relationship partner (Temple et al., 2013). Because TDV may lead to various mental health concerns, such as substance misuse, eating disorders, antisocial behaviors, self-injury, and suicidality (Foshee et al., 2013), counselors play an integral role in TDV prevention and intervention. Many young clients may choose to initially disclose personal experiences of TDV or unhealthy relationship behaviors in a therapeutic setting, making counselor preparedness critical.
Gender Symmetry in TDV
TDV has also led to strong debates regarding the issue of gender symmetry. Several studies have found that TDV is reciprocal, with both partners exhibiting aggressive or toxic behaviors in response to each other (Eisner, 2021; Emelianchik-Key et al., 2022; K. E. Hunt et al., 2022). However, some studies indicate vastly disproportionate rates of TDV victimization among adolescent girls (Kann et al., 2018), mainly in instances of extreme physical brutality or sexual violence (Swahn et al., 2010). The inconsistent rates may be related to social perceptions of TDV as a female concern, decreased male reporting (often attributed to stigma), conceptualization and understanding of violence, and a lack of validated measures that encompass diverse cultural and gendered experiences (Eisner, 2021; Walker et al., 2020). These contradictory reports make it even more challenging for clinicians.
Counselor Preparedness
Currently, there are several gaps in the literature regarding counselor education and TDV, including training, competency, and expertise (Murray et al., 2016). In a small sample of programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP), Henriksen et al. (2010) found that graduate counseling programs minimally addressed specialty training areas, requiring graduates to acquire additional skills independently. CACREP (2015) standards do not include TDV in training criteria, thus leaving the inclusion of these topics to the discretion of faculty. Further, Wozny (2005) found that 34% of marriage and family therapy programs had a domestic violence course, compared to 4% of counselor education programs. Similarly, in a sample of practicing school counselors, only 10% reported specific domestic violence training and continuing education at their workplace in the past 2 years (Khubchandani et al., 2012). Among the participants, 19% reported no formal education or training on TDV, and 83% of the participants’ settings did not assess TDV amongst the students within their school system (Khubchandani et al., 2012). This is alarming, given that 72% of sexual harassment and 28% of dating violence incidents occur in schools (Turner et al., 2011). A lack of preparation for crisis training, intervention, and prevention may cause serious detriment and endangerment to clients and counselors (Morris & Minton, 2012).
Counselor Bias
Gender bias related to survivors of relationship abuse is prevalent among trainees and professional counselors, reflecting stigmas among the general population (Maghsoudi, 2018). Karakurt et al.’s (2013) study on counselor attitudes toward perpetrators of violence revealed that most participants believed female offenders were justified in their violent actions and were not as dangerous as their male counterparts. Results also indicated that participants expressed less empathy for male survivors and more confidence in treating male perpetrators (Karakurt et al., 2013). Counselors may perpetuate stigma regarding female survivors by over-pathologizing, minimizing their complaints, and invalidating their feelings (Maghsoudi, 2018). Maghsoudi (2018) contended that there is a lack of training, but more importantly, there are limited opportunities within the educational curriculum for trainees to explore implicit biases regarding violence among partners.
The development of counselor self-awareness regarding personally held biases and beliefs can mitigate widespread assumptions about TDV. In addition, counselor self-awareness is a focal point of counselor education programs. This study sought to examine if there were differences in how counseling students conceptualize and work with male and female survivors of TDV. Using a qualitative design, we utilized case vignettes to examine how counseling students conceptualize, assess, and treat TDV. The overarching research question was: How do counseling students conceptualize and propose treatment for the experience of TDV in both female and male clients?
Method
Data Collection
After receiving IRB approval, the primary researcher, Kelly Emelianchik-Key, recruited a convenience sample of participants over 6 months in three counselor education programs. Emails were sent to the clinical placement coordinators to request the dissemination of the study details to their students. The three clinical placement coordinators agreed and sent the email with links to a Survey Monkey for students 2 years or more into their academic studies. The students received an email containing study information, a link to the electronic consent forms, demographic questions, and a case scenario with open-response questions. After completing the consent and demographic form, participants were randomly assigned one of two client case vignettes. The scenarios were identical vignettes (located in the Appendix) containing details of a struggling teen client experiencing TDV. The only difference in cases was the identified gender of the client. One case had a male client with a female partner while the other had a female client with a male partner. Counseling students were then asked questions about the vignette to better understand their clinical impressions of the client, a diagnosis (if warranted), any concerns regarding the case, and treatment ideas and considerations. The case vignettes and written responses were collected and analyzed until saturation was achieved (Braun & Clarke, 2021). To assess data saturation, we evaluated the data for completeness and at specific intervals of the data analysis process. Data saturation was met with 45 participants, with 22 responses to the female case and 23 responses to the male case.
Participants
The inclusion criteria for this study required that participants 1) were current students in a CACREP-accredited counseling program (any specialization) and 2) had completed all program-related content coursework, with only clinical field placements remaining. Of the 45 participants, eight self-identified as male and 37 self-identified as female. The participants’ degree track specializations were as follows: clinical mental health counseling (n = 21; 51%), school counseling (n = 8; 17%), rehabilitation counseling (n = 6; 13%), marriage and family therapy (n = 2; 4%), doctoral counselor education students (n = 3; 6%), and non–degree seeking students who already held a master’s degree in counseling (n = 3; 6%). All students were either enrolled in a clinical experience or had completed their clinical experiences. Participants ranged from 21 to 52 years of age, with a mean of 26.8. We did not collect data on participants’ race/ethnicity or sexual orientation in the demographic form, as it was not a variable of consideration in our study.
Procedure
In the present study, we aimed to understand how counseling students conceptualize clients experiencing TDV while considering differences in approach based on client gender. We used a qualitative case vignette design with a deductive approach to better understand gender-based assumptions, myths, or stigmas that may affect counseling students’ conceptualization and approach to treating TDV. The vignette design allows for assessing attitudes, values, norms, and perceptions regarding sensitive social science issues in qualitative research (Hughes, 1998). It may also be beneficial in exploring topics such as gender equality, gender norms, gender discrimination, drug use, mental illness, and emotional and behavioral difficulties (de Macedo et al., 2015). The case vignettes were created using a three-phase approach to test for content validity in health care education research (St. Marie et al., 2021): 1) Developing the vignette and associated questions, 2) sending the vignette to three experts in counseling and domestic violence research, and 3) testing the revised vignette with a small group of participants that suggested edits for clarity. The Appendix contains the vignette for a female teen client. An identical vignette for a male teen client was also utilized during the study. The only difference in the cases was the identified gender of the client and their partner; names, scenarios, and all non-gendered wording remained the same.
We approached this research from a post-structural feminist theoretical lens, conceptualizing TDV as reciprocal and challenging the common sociocultural notions of women as “powerless” and men as “powerful” in a patriarchal society. For this reason, we did not specify the client’s cultural background and used binary gender identities and heterosexual relationships in the case examples. Case vignettes with varying intersecting identities may have elicited other forms of bias, such as internalized homophobia, heteronormativity, gender-normative assumptions, and ethnocentric views, further compounding the dynamics and potentially leading to misinterpretations of the qualitative findings. Our hope is that this study can provide a framework for future research to incorporate additional layers of identity and address existing gaps in the TDV literature.
Research Team Positionality
The researchers’ experiences, qualities, personalities, or histories can potentially influence qualitative research outcomes (B. Hunt, 2011). Therefore, we engaged in reflexivity throughout the research process to minimize bias during data analysis. Our research team consisted of three cisgender female faculty in counselor education. All are licensed mental health counselors and one is also a licensed marriage and family therapist. We also have diverse counseling experiences in various mental health settings, including schools, university counseling centers, residential treatment facilities, domestic violence shelters and outreach programs, and private practice. Our related research interests include TDV, intimate partner violence, gender issues, sexuality, and culturally responsive approaches to counseling and research. Consistent with the qualitative research process, we continually engaged in dialogue and a self-reflective process to examine personal beliefs and challenge biases in TDV literature to ensure that our positionality did not impede the research process.
Data Analysis and Trustworthiness
Thematic analysis is a grouping of methods that examines commonalities and differences in research. Theoretically flexible, thematic analysis is a useful and practical approach to counseling research (Clarke & Braun, 2018). In this study, we utilized reflexive thematic analysis to form themes from codes, which were also grouped by major categories based on our questions to participants (Braun & Clarke 2013, 2021). Thematic analysis can also be expansive, ranging from research with rich descriptions to research that aims to describe and summarize (Clarke & Braun, 2018). The recommended steps for a reflexive thematic analysis were followed (Braun & Clarke, 2013, 2021; Clarke & Braun, 2018). We independently reviewed all data for familiarization, which included detailed documentation of thoughts, field notes, and decisions that were made individually. We met weekly to develop initial codes that were placed into a codebook to chart the developing analysis. Per Braun and Clarke’s (2013) recommendations, we set the data into central organizing concepts or categories to communicate and develop the themes. Within each category, we further grouped data by gender of the client to assess gender normative assumptions that may be guiding counseling students’ decision-making processes. Meetings took place over 6 weeks (one category per week) to discuss and group initial overarching themes for each vignette. Once this phase was complete, the themes were refined, defined, and named; the outcome was a final report.
To promote trustworthiness, we followed Nowell et al.’s (2017) recommendations for methodological rigor within Braun and Clarke’s (2013, 2021) steps for thematic analysis. These included a review of responses at various points prior to analysis. Peer debriefing took place during the 6-week coding process, along with an audit trail of documentation and codebooks connecting themes and content. Based on consensus coding, codebook refining took place weekly (Nowell et al., 2017). As a final step, member checking took place by sending the resulting themes and subthemes to the respective programs where students were recruited. Because the participants were anonymous, the programs disseminated findings to all students, asking anyone who initially participated to check for credibility in the results and reach out via email or anonymously through a Qualtrics link if they found inaccuracies (Braun & Clarke, 2013; Nowell et al., 2017). No participants responded or objected to the findings after three rounds of email blasts.
Findings
We determined six emergent categories that spanned across both cases: (a) case conceptualization and clinical impressions, (b) diagnostic impressions, (c) relationship considerations, (d) clinical concerns, (e) treatment approaches, and (f) gender bias. Within these six categories, 19 themes emerged, which are defined below in their corresponding category.
Case Conceptualization and Clinical Impressions
The case conceptualization and clinical impressions category captured counseling students’ perceptions of the presenting problem, resulting in the two themes of interpersonal and intrapersonal concerns. Although both vignettes aimed to illustrate specific cases of TDV, counseling students presented various explanations regarding the cause of the client’s symptoms. The interpersonal theme focused on aspects outside the client’s immediate control, including limited peer support, the dating relationship, and academic concerns. For example, a counseling student responding to the male client’s case suggested that he needs “to get involved in more extracurricular activities and find things that he enjoys doing” or “extra support from school and family.” Students responding to the female case also focused on relational issues, indicating that “she needs to build better relationships with her family, friends, and partner.” Participants also considered intrapersonal factors related to the client’s mood, level of assertiveness, self-esteem, and self-confidence. For example, in responding to the male client case, counseling students indicated that the client “has poor or low self-esteem” or “should be able to stand up for himself in all areas of his life.” The female case elicited similar responses from participants, such as “she needs to stop being so codependent” and “she could get better if she wanted to.”
Diagnostic Impressions
The second category was grouped based on diagnostic criteria. Four themes emerged: mood disorders, personality disorders, stress disorders, and neurodevelopmental disorders. Three subthemes were also identified: insufficient information, no diagnoses warranted, and only symptomology. Counseling students provided various responses regarding whether a diagnosis was warranted in the case vignette. Some participants responded with multiple possible diagnoses for the client presented in the case scenario. Others prefaced the diagnosis with statements alluding to uncertainty with making a concrete diagnosis, such as “possibly is experiencing depression,” or noting a diagnosis followed by “but more information will be needed to confirm.” About half of the participants stated a concrete diagnosis while providing support and examples from the case vignette.
Although many diagnoses overlapped in both scenarios, there were differences regarding the frequency of endorsement. The most common diagnoses for the male client included adjustment disorder (n = 9) and attention-deficit/hyperactivity disorder (ADHD; n = 7). Conversely, the female client was most frequently diagnosed with a dependent personality disorder or style (n = 8). The female client was never diagnosed with ADHD and was only determined to have “attention problems.”
Dating Relationship Considerations
Participants drew attention to relational concerns in the client’s life within this category. The identified themes included unhealthy relationships, support, and dating violence. The unhealthy relationship theme was evident in both client cases. Several participants (n = 15; seven in the male client case and eight in the female client case) noted comments like “unhealthy relationship” while providing examples of unhealthy behaviors, such as the partner’s communication style and controlling behaviors. Several responses highlighted the theme of support. Participants appeared to skirt around labeling relationship violence and resorted to more general comments, such as “the client needs relationship support” or “better communication in the relationship is needed.” Additionally, one counseling student noted the lack of support in the relationship and questioned the need for such a serious relationship at this “young age,” demonstrating judgment and bias (further discussed in Category 6). This theme also captured counseling students’ recommendations for enhanced relational support (e.g., date nights).
The final theme within this category, dating violence, was evident in six responses that labeled the relationship as “violent” or mentioned “dating abuse” as a concern. In responses that noted abuse, three mentioned “emotional abuse,” and two identified “sexual abuse” in the female case. The word “sexual pressure” was also used by two counseling students that completed the female case, but it was not explicitly noted as abuse or violence. In the female case, two participants mentioned “rape” four times, whereas “rape” was never mentioned in the male case. In the male case, the only comment that slightly implied relationship violence noted: “needs to discuss relationship boundaries with his partner, so she doesn’t pressure him to advance sexually.”
Treatment Approaches
Treatment approaches were categorized and counted based on theoretical orientations. Most participants responded with similar treatment considerations for both presented cases. The five grouped themes included cognitive behavioral therapy (n = 15), solution-focused therapy (n = 11), family therapy (n = 9), couples counseling (n = 3), and other (n = 7). The other theme resulted from various suggestions that were not specific approaches for individual therapy but could support the client. These suggestions included tutoring, group therapy, and peer support. Several counseling students made referral recommendations instead of offering treatments or approaches that the counselor could directly utilize with these clients. For example, a suggestion included psychiatric evaluation or referral for the female survivor (n = 10). This suggestion was not recommended as often for the male survivor (n = 2). Additionally, one respondent suggested that the female survivor should “get a referral for a gynecologist.” In contrast, no responses indicated a medical referral for the male client.
Practice Considerations
Participants answered questions regarding any apprehension or reservations they might experience while treating the proposed clients, categorized as practice considerations. The themes that emerged were ethical and legal concerns, family concerns, and school concerns. Almost a quarter of participants (n = 11) indicated clinical concerns related to ethical or legal implications or limits of confidentiality because of the clients’ ages. Some counseling students mentioned “involving parents” or “disclosing to parents” without explaining what warranted disclosure. One participant was concerned for the client’s safety because of sexual violence (i.e., rape) and specifically mentioned reporting to authorities. Nearly half of the participants (n = 20) identified the client’s family issues as problematic, offered solutions to repair relationship ruptures within the family dynamic, and mentioned strategies for improved communication. Additionally, participants (n = 22) identified school-related difficulties, such as decreased grades, as an area of concern for the client. Examples of commentary provided by those participants included, “Jordan needs a tutor” or “Jordan needs to be evaluated educationally at school to see if there are learning challenges and get an IEP.”
Gender Bias
The sixth category was identified because of the overwhelming gender biases that emerged throughout the participants’ responses. This category was further grouped into two themes: language and judgments and myths. The researchers compared the language counseling students used to describe male and female clients. Although the counseling students described the male and female clients with similar terms (i.e., influenced, boundaries, codependence), the frequency across all responses grossly varied. For example, participants used the term “abuse” twice as many times when describing the female client’s relationship (n = 23) as opposed to the male client’s relationship (n = 11). Similarly, counseling students utilized the term “survivor” to describe the female client (n = 13), but not the male client (n = 0). The male client was often described as “withdrawn” (n = 28) and experiencing “attention” difficulties (n = 43), “adjustment” (n = 29), and “codependence” issues (n = 23). Conversely, the female client was more likely to be described as “influenced” (n = 19), “manipulative” (n = 22), and experiencing “dependency” (n = 47) concerns. Although these counts could highlight one participant using the word one or more times in a response, they illuminate the disparity and lack of discernment in the language used to describe both clients.
Within the theme of judgments and myths, the counseling students consistently referenced and discussed the female partner (perpetrator) in the male client scenario. These comments made inferences or judgments about the female partner (perpetrator) even though she was not the identified client. Counseling students made various comments about the female perpetrator, including, “she is controlling,” “nasty,” or “needy,” alluding to the fact that she is causing these issues for the male client. Counseling students also provided clinical impressions, recommendations, and diagnoses for the male client’s partner (female perpetrator). Conversely, participants who completed the female client case noted clinical recommendations for the female client’s partner (male perpetrator), such as general “relationship help” and “anger management and self-help.” These comments and recommendations were less frequent and judgmental of the female client’s partner (male perpetrator). Relatedly, no participants provided a diagnosis for the male perpetrator. Overall, counseling students frequently mentioned the female partner (perpetrator) rather than focusing on the identified client, although this was less frequent for the male partner (perpetrator).
Additionally, many judgments about the survivors arose, perpetuating myths and the stigma surrounding TDV and survivors. For example, one student noted the female survivor “could get better if she wanted to” and “she needs to express her feelings to her partner.” Another student wrote that the male survivor needed to “be more assertive in the relationship and not get walked all over” and “seems like he is a people pleaser and needs to take more control over his situation.” Furthermore, the few times relationship violence was discussed, the female client was always referred to as a “victim” or “survivor,” whereas the male client was referred to by name or “the client.”
Discussion
This study aimed to examine how counseling students conceptualize and propose treatment for the experience of TDV in both female and male clients. The results indicate that gender played a significant role in counseling students’ responses to a survivor’s clinical needs. Data were grouped using the following categories that corresponded with questions: (a) case conceptualization and clinical impressions, (b) diagnostic impressions, (c) relationship considerations, (d) practice considerations, (e) treatment approaches, and (f) gender bias. Within these categories, 19 themes emerged, which we discuss further below.
The counseling students presented similar challenges in their case conceptualizations and diagnoses for each scenario. Sperry and Sperry (2020) noted that case conceptualization is essential for counseling students to inform clients of diagnostic, treatment, and clinical formulations. Many responses demonstrated counselor bias, limitations in practical skills and case conceptualization, and minimal depth of knowledge. As found in this study, there was a misdiagnosis of the client’s presenting issue as a mental health disorder and an overemphasis on comorbid symptoms (e.g., failing grades) instead of evaluating these phenomena as a response to the trauma (i.e., TDV). This failure to conceptualize clients accurately leads to improper diagnosis and ineffective treatment.
Interestingly, although the study did not include a requirement to diagnose the fictitious clients, many of the participants still provided a diagnosis. In a systematic review of the literature, Merten et al. (2017) found that misdiagnosis and unintended overdiagnosis of mental health disorders in children and adolescents is likely more common than expected, leading to improper treatment. Qualitative research illuminates how cognitive information processing obscures diagnostic and clinical decision-making (Hays et al., 2009). This phenomenon, known as availability bias, is when clinicians determine the mental health status of clients based on personal experiences or stigma rather than the observable criterion. It is plausible that the counseling students in this qualitative study demonstrated availability bias (based on gender or age), inhibiting their future work with TDV in young clients.
Further, the study’s findings show that many counseling students are unaware of evidence-based interventions to treat TDV appropriately. Students mentioned interventions like cognitive behavioral therapy (CBT), solution-focused therapy, couples counseling, and academic tutoring to reduce client distress and increase self-esteem. Although CBT is a viable treatment approach, none of the responses suggested the implementation of trauma-informed modalities or protocols (such as STAIR; American Psychiatric Association, 2019) for teens recovering from emotional and physical abuse. Trauma-informed approaches focusing on empowerment and advocacy are incredibly powerful in healing relationship trauma (Ogbe et al., 2020). Most strikingly, the counseling students appeared to overlook many critical aspects of treating trauma survivors, including screening, risk assessment, safety planning, and psychoeducation (Ogbe et al., 2020).
A promising aspect of this study is that some counseling students suggested peer support and group therapy as appropriate treatment responses for TDV. Research indicates that school-based peer groups can decrease the rate of abuse among middle and high school–aged students (Ball et al., 2015) and reduce physical dating violence following treatment (Temple et al., 2013). Studies also reveal higher success rates for the prevention of TDV when survivors perceive consistent emotional safety. Factors like school climate, group setting, peer interactions, perspectives on abuse, and opportunities for adaptive skills-building can contribute to survivor care (Ball et al., 2015).
Regarding relationship considerations, only 15 participants noted relationship concerns related to a toxic relationship, regardless of the perpetrator’s gender. Only six of those who indicated relationship discord reported concerns related to sexual abuse or rape. The staggering implication is that novice clinicians cannot identify unhealthy relationship patterns and violence. Research also indicates that young people often misinterpret or minimize partner violence because of unrealistic or distorted relationship beliefs (Eisner, 2021; Walker et al., 2020), continuing into early adulthood with difficulty conceptualizing violence upon entering college (Emelianchik-Key et al., 2022). When clients and clinicians cannot label and conceptualize relationship violence, it leaves room for error in intervention and prevention measures. This extends to the demonstrated lack of knowledge regarding legal, ethical, and clinical responsibilities for treating TDV, particularly within the scope of mandatory reporting laws for the protection of minors. This issue extended to the appropriate disclosure of TDV to parents and caregivers, mainly because young people are more apt to discuss TDV in confidential settings (Cutter-Wilson & Richmond, 2011).
Other practice concerns in the data stemmed from a general inability to conceptualize the presented cases. Although the case vignette highlights academic and interpersonal problems, the client’s presenting problem was TDV. The counseling students neglected to recognize adolescent relationship abuse, leading to the symptomology of academic decline, lowered self-esteem, dysthymia, and isolation (Cutter-Wilson & Richmond, 2011). Recommendations to treat other problems outside of TDV to resolve trauma from abuse can lead to the revictimization of the client by the counselor (Maghsoudi, 2018). Counseling students must be cognizant of their capacity to retraumatize TDV survivors, as victims who perceive any shame or blame during their disclosure may be reluctant to seek help in the future (Maghsoudi, 2018; Walker et al., 2020). Counselor bias is often attributed to poor training at the graduate level (Maghsoudi, 2018). With more informed preparation, counseling students may shift from a pathologized response to a strengths-based approach founded on client self-efficacy and resilience.
Consistent with prior research (Karakurt et al., 2013; Machado et al., 2020; Maghsoudi, 2018; Walker et al., 2020), gender bias was prevalent across all categories and ultimately emerged as an independent category upon final analyses. Gender discrepancies were evident in clinical diagnosis, treatment planning, ethical implications, and client descriptors. Although the content presented in each scenario was identical, counseling students diagnosed the male and female survivors differently. For example, the female survivor was diagnosed with borderline personality disorder and bipolar disorder while the male survivor received depression, anxiety, and ADHD diagnoses. With many criteria for these disorders overlapping, misdiagnosis can occur (Fruzzetti, 2017; Scott, 2017). Yet, gender bias is a common factor in misdiagnosis, especially with a diagnosis of borderline personality disorder, bipolar disorder, and ADHD (Bruchmüller et al., 2012; Fruzzetti, 2017). Counselors perpetuate stigma regarding female survivors by over-pathologizing, minimizing their complaints, and invalidating their feelings (Maghsoudi, 2018).
We contend that the most alarming finding of this study was how the counseling students portrayed several gender disparities when identifying relationship abuse. The divide between gender treatment of TDV was apparent when comparing the counseling students’ view of the female client as a “survivor” and not using strengths-based terminology to identify the male client. Many statements continued to perpetuate societal stigmas about female survivors being passive while male survivors were described as needing to assert “control,” further exacerbating common notions about power and control. A recent qualitative study of male survivors explained that professionals minimized and ridiculed most participants for not being the “stereotypical victim of domestic violence” (Machado et al., 2020, p. 9). Counselors must develop the necessary skills to provide equal support and resources to populations navigating stigma concurrently with TDV (Walker et al., 2020). These findings affirm that even professional counselors are subject to the inherent and socially constructed biases regarding relationship abuse and further emphasize the importance of counselor training to increase one’s professional capacity to treat all survivors of TDV. These outcomes also support a feminist conceptualization of TDV to dismantle gender disparities in treatment and the importance of empowering survivors of all genders experiencing TDV.
Implications for Counselors and Counseling Programs
Collectively, the study’s findings point to the need for enhanced counselor training, reflexivity, and knowledge on the intersection of age, relationship status, violence, and gender issues. Counseling students must understand that relationship violence can happen at any age and has damaging, long-lasting impacts on an adolescent’s well-being, future relationships, and mental health (e.g., depression, suicidal ideation, drug use, self-injury; CDC, 2021; Kann et al., 2018). TDV has detrimental consequences on an adolescent’s psychological well-being and decision-making (CDC, 2021; K. E. Hunt et al., 2022), thus making it critical that counselors do not underestimate the impact dating violence can have on a relationship regardless of age. Because counselors may encounter the presence of relationship violence in teens within various settings (e.g., counseling centers, schools, and universities), they must be familiar with and adept at recognizing and addressing these factors for client safety and aid in ending the abuse cycle.
Although counselor education programs produce very competent and knowledgeable counselors, there remains an inability to comprehensively cover all the necessary content to prepare counselors for working with clients (Henriksen et al., 2010; Khubchandani et al., 2012). Some of these topic areas, like TDV, must be explored further in continuing education. More emphasis must be placed on trauma-informed approaches to assist all clients, including teens in a critical developmental age at which TDV threatens current and future mental health (Foshee et al., 2013; Temple et al., 2013). Strengths-based and advocacy-informed trauma approaches have been influential in healing relationship trauma (Ogbe et al., 2020) by assisting teens in preventing pervasive patterns of violence in future relationships.
At the same time, other relevant factors, such as unacknowledged biases, should be examined personally and within supervision. Counseling students, new professionals, and supervisors must be willing to broach biases and assumptions regarding gender in counseling and supervision to prevent them from affecting clients. Counselors must understand the impact of gender and age on highly stigmatized topics, such as TDV and sexuality, to prevent biases and misunderstandings from guiding assessment and treatment. Counselor educators can teach students about TDV using theoretical lenses that deconstruct stigma. For example, a feminist perspective could lend to classroom dialogue uncovering societal power differentials. At the same time, structural functionalism theory or conflict theory could offer unique lenses to discuss systemic inequities in the quality and delivery of mental health care.
Counselor education programs are essential in helping counseling students develop strong case conceptualization skills that affirm diverse clients and consider strengths-based and trauma-informed interventions. Therefore, counselor training must incorporate instruction and practice for adolescent risk assessment of TDV. Counseling students who gain experience using TDV screening tools may increase their confidence when clinical decision-making is required, such as disclosing abuse. Mandatory reporting is not always transparent for students. Instructional role plays and a review of the limitations of confidentiality may also prompt further growth and development for counseling students, in addition to reviewing state laws and any differences with our profession’s ethical guidelines. Research demonstrates that teens fear the information counselors report to their parents or caregivers from counseling sessions. In contrast, caregivers can often lack the ability to respond appropriately to this information (Black et al., 2015). Thus, counselors must understand the critical role of establishing trust and rapport with teens experiencing TDV to strengthen the therapeutic relationship and ability to work together and increase support and trust within the family system.
Limitations and Future Research Directions
Research findings must always be considered in the context of the existing limitations. One limitation was that the study included a sample of counseling students across three universities in the southern region of the United States and we did not delineate the number of students affiliated with each university. The study may have benefited from a more diverse sample across many CACREP-accredited programs. The students in the study pertained to four different tracks (school, mental health, marriage and family therapy, and rehabilitation counseling), with some non–degree-seeking students and doctoral students. Although this illuminates overarching gaps in the counseling profession, future researchers may examine differences between specializations, allowing for more in-depth assessments and recommendations for training and continuing education.
Additionally, we did not inquire about counseling students’ strategies and decision-making processes to develop their case conceptualizations and treatment decisions. This data would have been beneficial for counselor educators to address these areas early on in training. A final limitation of the study included the use of binary gender identities and heterosexual relationships in the case vignettes. Although the present research may provide a framework for future studies to build upon, it is essential to note that TDV occurs across diverse populations, including LGBTQ+ youth. As such, future research should examine counseling students’ conceptualization of TDV within diverse communities and relationships. This would further illuminate disparities and challenges in the conceptualization and treatment of TDV, shedding light on areas needing attention in counselor training.
Conclusion
Counseling students must develop self-awareness and knowledge of TDV to treat the transgenerational cycle of violence, thereby preventing or addressing potential mental health consequences. To do so, students must understand the etiology of violence, manifestations of violence in relationships, and trauma-informed conceptualization and treatment of violence. Although such training must begin in counselor education programs and continue after graduation (Murray et al., 2016; Wozny, 2005), this study revealed the importance of reflexivity and self-awareness on existing biases, assumptions, and beliefs on TDV. Counselor biases can significantly impact client treatment outcomes (Karakurt et al., 2013). Therefore, personal biases must be recognized early in training to prevent harmful and stigmatizing treatment of clients experiencing TDV.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Psychiatric Association. (2019). Treating women who have experienced intimate partner violence.
https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/IPV-Guide/APA-Guide-to-IPV-Among-Women.pdf
Ball, B., Holland, K. M., Marshall, K. J., Lippy, C., Jain, S., Souders, K., & Westby, R. P. (2015). Implementing a targeted teen dating abuse prevention program: Challenges and successes experienced by Expect Respect facilitators. Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 56(2), Supp. 2, S40–S46. https://doi.org/10.1016/j.jadohealth.2014.06.021
Black, B. M., Weisz, A. N., Preble, K. M., & Sharma, B. (2015). Parents’ awareness of and anticipated responses to their teens’ reports of dating violence. Journal of Family Social Work, 18(1), 3–20.
https://doi.org/10.1080/10522158.2014.968941
Braun, V., & Clarke, V. (2013). Successful qualitative research: A practical guide for beginners. SAGE.
Braun, V., & Clarke, V. (2021). To saturate or not to saturate? Questioning data saturation as a useful concept for thematic analysis and sample-size rationales. Qualitative Research in Sport, Exercise and Health, 13(2), 201–216. https://doi.org/10.1080/2159676X.2019.1704846
Bruchmüller, K., Margraf, J., & Schneider, S. (2012). Is ADHD diagnosed in accord with diagnostic criteria? Overdiagnosis and influence of client gender on diagnosis. Journal of Consulting and Clinical Psychology, 80(1), 128–138. https://doi.org/10.1037/a0026582
Centers for Disease Control and Prevention. (2021). Fast facts: Preventing teen dating violence. https://www.cdc.gov/violenceprevention/intimatepartnerviolence/teendatingviolence/fastfact.html
Clarke, V., & Braun, V. (2018). Using thematic analysis in counselling and psychotherapy research: A critical reflection. Counselling and Psychotherapy Research, 18(2), 107–110. https://doi.org/10.1002/capr.12165
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Cutter-Wilson, E., & Richmond, T. (2011). Understanding teen dating violence: Practical screening and intervention strategies for pediatric and adolescent healthcare providers. Current Opinion in Pediatrics, 23(4), 379–383. https://doi.org/10.1097/MOP.0b013e32834875d5
de Macedo, J. Q., Khanlou, N., & Luis, M. A. V. (2015). Use of vignettes in qualitative research on drug use: Scoping review and case example from Brazil. International Journal of Mental Health and Addiction, 13(5), 549–562. https://doi.org/10.1007/s11469-015-9543-4
Eisner, M. (2021). The gender symmetry problem in physical teen dating violence: A commentary and suggestions for a research agenda. New Directions for Child and Adolescent Development, 2021(178), 157–168. https://doi.org/10.1002/cad.20443
Emelianchik-Key, K., Byrd, R., & Gill, C. S. (2022). Dating violence and the impact of technology: Examining the lived experiences of sorority members. Violence Against Women, 28(1), 73–92.
https://doi.org/10.1177/1077801221998799
Foshee, V. A., McNaughton Reyes, H. L., Gottfredson, N. C., Chang, L.-Y., & Ennett, S. T. (2013). A longitudinal examination of psychological, behavioral, academic, and relationship consequences of dating abuse victimization among a primarily rural sample of adolescents. Journal of Adolescent Health, 53(6), 723–729. https://doi.org/10.1016/j.jadohealth.2013.06.016
Fruzzetti, A. E. (2017, October 3). Why borderline personality disorder is misdiagnosed. National Alliance on Mental Illness. https://www.nami.org/Blogs/NAMI-Blog/October-2017/Why-Borderline-Personality-Disorder-is-Misdiagnose
Goncy, E. A., Sullivan, T. N., Farrell, A. D., Mehari, K. R., & Garthe, R. C. (2017). Identification of patterns of dating aggression and victimization among urban early adolescents and their relations to mental health symptoms. Psychology of Violence, 7(1), 58–68. https://doi.org/10.1037/vio0000039
Hays, D. G., McLeod, A. L., & Prosek, E. (2009). Diagnostic variance among counselors and counselor trainees. Measurement and Evaluation in Counseling and Development, 42(1), 3–14.
https://doi.org/10.1177/0748175609333559
Henriksen, R. C., Jr., Nelson, J., & Watts, R. E. (2010). Specialty training in counselor education programs: An exploratory study. Journal of Professional Counseling: Practice, Theory & Research, 38(1), 39–51.
https://doi.org/10.1080/15566382.2010.12033865
Hughes, R. (1998). Considering the vignette technique and its application to a study of drug injecting and HIV risk and safer behaviour. Sociology of Health & Illness, 20(3), 381–400. https://doi.org/10.1111/1467-9566.00107
Hunt, B. (2011). Publishing qualitative research in counseling journals. Journal of Counseling & Development, 89(3), 296–300. https://doi.org/10.1002/j.1556-6678.2011.tb00092.x
Hunt, K. E., Robinson, L. E., Valido, A., Espelage, D. L., & Hong, J. S. (2022). Teen dating violence victimization: Associations among peer justification, attitudes toward gender inequality, sexual activity, and peer
victimization. Journal of Interpersonal Violence, 37(9–10), 5914–5936. https://doi.org/10.1177/08862605221085015
Kann, L., McManus, T., Harris, W. A., Shanklin, S. L., Flint, K. H., Queen, B., Lowry, R., Chyen, D., Whittle, L., Thornton, J., Lim, C., Bradford, D., Yamakawa, Y., Leon, M., Brener, N., & Ethier, K. A. (2018). Youth Risk Behavior Surveillance – United States, 2017. Morbidity and Mortality Weekly Report Surveillance Summaries, 67(8), 1–114. https://doi.org/10.15585/mmwr.ss6708a1
Karakurt, G., Dial, S., Korkow, H., Mansfield, T., & Banford, A. (2013). Experiences of marriage and family therapists working with intimate partner violence. Journal of Family Psychotherapy, 24(1), 1–16.
https://doi.org/10.1080/08975353.2013.762864
Khubchandani, J., Price, J. H., Thompson, A., Dake, J. A., Wiblishauser, M., & Telljohann, S. K. (2012). Adolescent dating violence: A national assessment of school counselors’ perceptions and practices. Pediatrics, 130(2), 202–210. https://doi.org/10.1542/peds.2011-3130
Machado, A., Hines, D., & Douglas, E. M. (2020). Male victims of female-perpetrated partner violence: A qualitative analysis of men’s experiences, the impact of violence, and perceptions of their worth. Psychology of Men & Masculinities, 21(4), 612–621. https://doi.org/10.1037/men0000285
Maghsoudi, M. (2018). Addressing counselor stigma in working with female intimate partner violence survivors. Journal of Professional Counseling: Practice, Theory & Research, 45(1), 33–44.
https://doi.org/10.1080/15566382.2019.1603015
Merten, E. C., Cwik, J. C., Margraf, J., & Schneider, S. (2017). Overdiagnosis of mental disorders in children and adolescents (in developed countries). Child and Adolescent Psychiatry and Mental Health, 11(5), 1–11.
https://doi.org/10.1186/s13034-016-0140-5
Morris, C. A. W., & Minton, C. A. B. (2012). Crisis in the curriculum? New counselors’ crisis preparation, experiences, and self-efficacy. Counselor Education and Supervision, 51(4), 256–269.
https://doi.org/10.1002/j.1556-6978.2012.00019.x
Murray, C. E., King, K., & Crowe, A. (2016). Understanding and addressing teen dating violence: Implications for family counselors. The Family Journal, 24(1), 52–59. https://doi.org/10.1177/1066480715615668
Nowell, L. S., Norris, J. M., White, D. E., & Moules, N. J. (2017). Thematic analysis: Striving to meet the
trustworthiness criteria. International Journal of Qualitative Methods, 16(1), 1–13.
https://doi.org/10.1609406917733847
Offenhauer, P., & Buchalter, A. (2011). Teen dating violence: A literature review and annotated bibliography. Library of Congress, Federal Research Division. https://www.ojp.gov/pdffiles1/nij/grants/235368.pdf
Ogbe, E., Harmon, S., Van den Bergh, R., & Degomme, O. (2020). A systematic review of intimate partner violence interventions focused on improving social support and mental health outcomes of survivors. PLOS ONE, 15(6), e0235177. https://doi.org/10.1371/journal.pone.0235177
Scott, N. P. (2017). Misdiagnosis or comorbidity: Borderline personality disorder in a patient diagnosed with bipolar disorder. The American Journal of Psychiatry Residents’ Journal, 12(10), 4–5.
https://doi.org/10.1176/appi.ajp-rj.2017.121002
Sperry, L., & Sperry, J. (2020). Case conceptualization: Mastering this competency with ease and confidence. Routledge.
St. Marie, B., Jimmerson, A., Perkhounkova, Y., & Herr, K. (2021). Developing and establishing content validity of vignettes for health care education and research. Western Journal of Nursing Research, 43(7), 677–685. https://doi.org/10.1177/0193945920969693
Swahn, M. H., Alemdar, M., & Whitaker, D. J. (2010). Nonreciprocal and reciprocal dating violence and injury occurrence among urban youth. Western Journal of Emergency Medicine, 11(3), 264–268.
Temple, J. R., Le, V. D., Muir, A., Goforth, L., & McElhany, A. L. (2013). The need for school-based teen dating violence prevention. Journal of Applied Research on Children: Informing Policy for Children at Risk, 4(1), 1–11. https://doi.org/10.58464/2155-5834.1136
Turner, H. A., Finkelhor, D., Hamby, S. L., Shattuck, A., & Ormrod, R. K. (2011). Specifying type and location of peer victimization in a national sample of children and youth. Journal of Youth and Adolescence, 40, 1052–1067. https://doi.org/10.1007/s10964-011-9639-5
Walker, A., Lyall, K., Silva, D., Craigie, G., Mayshak, R., Costa, B., Hyder, S., & Bentley, A. (2020). Male victims of female-perpetrated intimate partner violence, help-seeking, and reporting behaviors: A qualitative study. Psychology of Men & Masculinities, 21(2), 213–223. https://doi.org/10.1037/men0000222
Wozny, D. A. (2005). The prevalence of suicide and violence assessment/intervention courses in CACREP and COAMFTE-accredited counseling curriculums. In G. R. Waltz and R. Yep (Eds.), VISTAS: Compelling perspectives on counseling 2005 (pp. 271–274). American Counseling Association.
Appendix
Female Case Vignette
Jordan is a 17-year-old female in her junior year of high school. Her teacher referred her for assistance from the school counselor after she began struggling academically. Jordan’s parents had also become concerned when Jordan’s grades dropped from As and Bs to Cs and a D in less than one school year, and she had begun isolating herself from her friends, even quitting the basketball team that she had loved.
During her initial session with her school’s guidance counselor, Jordan discussed being increasingly distracted in class and being unable to complete her assignments on time. Jordan also discussed being happy and in her first serious relationship with a boyfriend during this past year but reports that she hasn’t quite felt like herself lately. Jordan disclosed that she quit the basketball team to spend more time with her boyfriend because she wanted to prove her love to him, as he would become anxious whenever she was without him. She states they love each other very much and proves this by spending as much time as she can with him and sharing everything, including the passwords for all her social media accounts. Jordan notes that her boyfriend was more physically experienced with relationships, and her past boyfriends “strayed,” so these were things she wanted to do to make him feel “safe and secure.” She also stated that she had past relationships, but nothing serious or that went beyond kissing. The couple recently advanced in their sexual relationship because her boyfriend said he couldn’t date someone who wasn’t physically and emotionally close to him. Jordan didn’t want to lose him and went ahead with what she called the “next step” in their sexual relationship so he would not break up with her.
Jordan wasn’t sure why her grades were slipping but said things were fine at home, and she loved having a boyfriend. She appears to discuss her friends and basketball teammates fondly, but says her relationship is better without them. When Jordan was in basketball, her boyfriend would call and text her 20 plus times after practice let out until he heard back. She said quitting helped with his anxiety and her stress of dealing with all the calls. She stated that she had no energy to commit to basketball or hanging out with friends. Her focus was on school and her boyfriend.
Jordan appeared willing to try to improve her grades and said her boyfriend and parents supported these efforts. She reports her boyfriend has been tutoring her and helping her study when they are together because he told her he doesn’t want a “stupid girlfriend.” Jordan reports this as “playful teasing” and his “way to motivate” her. Jordan wants to go to college, but she is concerned that her recent drop in grades will affect her school admission. She is unsure why she cannot concentrate. She has been tired lately and said she’s just “in a funk” that she needs to shake off.
Her parents reported wanting her grades to improve, and Jordan seems preoccupied lately. Her parents don’t know how to improve her focus in school and at home but seem supportive. They said they appreciate her boyfriend’s “tutoring” as Jordan refers to it. Jordan was cooperative and pleasant in the session.
Note. The case vignette presented here is that of a female teen client. An identical vignette for a male teen client was also utilized during the study. The only difference in cases was the identified gender of the client and their partner; names, scenarios, and all non-gendered wording remained the same.
Questions
- Provide a brief case conceptualization for this client. Be as specific as possible and note any clinical impressions.
- What is your diagnosis (if you feel one is warranted) or any diagnostic impressions related to Jordan’s behaviors? Please be specific and include any V codes if you believe they are justified.
- What would be your treatment approach when working with Jordan, and what areas would be your treatment goals for Jordan?
- Are there any relationship considerations to incorporate in your work with Jordan?
- Are there any additional clinical or practice concerns you might have in working with Jordan?
- Is there anything else you would like to share about working with Jordan that has not been mentioned elsewhere?
Kelly Emelianchik-Key, PhD, NCC, ACS, LMFT, LMHC, is an associate professor at Florida Atlantic University. Bridget Glass, PhD, LMHC, is an assistant professor at South University. Adriana C. Labarta, PhD, LMHC, is an assistant professor at Florida Atlantic University. Correspondence may be addressed to Kelly Emelianchik-Key, 777 Glades Road, Bldg 47, Room 275, Boca Raton, FL 33431, Kemelian@fau.edu.
Aug 24, 2023 | Volume 13 - Issue 2
Kyoung Mi Choi, Jung H. Hyun
This study, using a transcendental phenomenological approach, explored the perceptions and experiences of school counselor trainees participating in a self-care course grounded in mindfulness and social–emotional learning. Seven students who enrolled in a master’s-level school counseling program and completed a summer self-care course shared their experiences, leading to the identification of five key themes: (a) recognizing the importance and need for self-care, (b) cultivating a nonjudgmental mindset toward challenging emotions, (c) integrating self-care into both personal and professional settings, (d) an increase in compassion and empowerment, and (e) a commitment to ongoing learning and advocacy. The school counselor trainees’ narratives highlight the importance of self-care as a way to reclaim power within themselves and become change agents in their school communities.
Keywords: school counselor trainees, self-care, mindfulness, social–emotional learning, advocacy
The COVID-19 pandemic has dramatically changed the way we live, work, learn, and interact on a daily basis, making self-care a crucial topic of discussion in both schools and workplaces (Harrichand et al., 2021; Norcross & Phillips, 2020). Many K–12 students are facing increased emotional distress and mental health issues, such as high levels of anxiety, depression, and post-traumatic symptoms (Chen et al., 2020; Marques de Miranda et al., 2020; Prime et al., 2020). At the same time, school counselors are also struggling with issues such as fatigue, burnout, and even vicarious trauma (Parker & Henfield, 2012), along with other challenges like high workloads, uncertainty about their role, and a lack of perceived support and professional development opportunities (Savitz-Romer et al., 2021). This makes self-care for school counselors and trainees more critical now than ever before (Harrichand et al., 2021).
Self-care refers to engaging in activities or behaviors that promote one’s overall wellness and prevent burnout (Christopher et al., 2016). This concept can also be expanded to include a larger sense of self-care that encompasses embracing one’s humanity; increasing awareness of internalized negative cultural messages; and fostering a positive cultural identity that embraces one’s heritage and community strengths, assets, traditions, and legacy (Duncan-Andrade & Morrell, 2008). Some scholars view self-care as the start of personal power (hooks, 1994) and a process of humanization in education that is reciprocal, anti-oppressive, and supportive of collective well-being (Paris & Winn, 2013). Additionally, many educators and scholars believe that dismantling oppressive ideologies and power structures is an important objective in the transformative process of self-care, which involves critical self-reflection, recognition of dehumanization, and reclaiming agency (Berila, 2016; Freire, 1970/2000; hooks, 1994; Litam & Hipolito-Delgado, 2021).
The significance of self-care has led to it being viewed not just as an individual responsibility, but also a professional one. Leading counseling organizations, such as the American Counseling Association (ACA) and the Council for the Accreditation of Counseling and Related Educational Programs (CACREP), consider self-care to be a crucial aspect of a mental health professional’s duties. The ACA Code of Ethics (2014) states that “counselors engage in self-care activities to maintain and promote their own emotional, physical, mental, and spiritual well-being to best meet their professional responsibilities” (p. 8). The CACREP (2015) standards, under the Professional Counseling Identity section, include standards for counselor education programs that emphasize self-care strategies appropriate to the counselor role (Section 2.F.1.i). The American School Counselor Association (ASCA; 2019) promotes the monitoring of “emotional and physical health and practice wellness to ensure optimal professional effectiveness” for school counselors (p. 7).
However, despite the recognition of self-care as an ethical responsibility, most counseling training programs do not incorporate it as part of their curriculum (Chen et al., 2020; Christopher & Maris, 2010; Shapiro et al., 2007). Lack of time, academic pressure, and the absence of guidance and faculty role models are cited as barriers (Campbell & Christopher, 2012; Christopher & Maris, 2010; Nelson et al., 2018). Nevertheless, there is a pressing need for self-care strategies to be included in counselor training and curriculum (Mitchell & Binkley, 2021). This study utilized transcendental phenomenology to investigate the essence of self-care experiences among school counseling trainees who participated in a 10-session seminar course that focused on mindfulness and social–emotional learning (SEL).
Literature Review
Mindfulness as Humanizing Process in Self-Care
The integration of mindfulness as a self-care practice into counseling training and programs has been widely adopted over the past three decades (Bohecker & Horn, 2016; Bohecker et al., 2016; Campbell & Christopher, 2012; Christopher & Maris, 2010; Shapiro et al., 2007). Research has shown that mindfulness can lead to numerous benefits, including reduced levels of anxiety and depression, enhanced life satisfaction, increased social connection, optimism, tolerance, empathy, and self-efficacy (Bohecker & Horn, 2016; Bohecker et al., 2016; Brown & Ryan, 2003). Christopher and Maris (2010) asserted that incorporating mindfulness practices into counselor training programs could help reduce burnout, compassion fatigue, and other stress-related physical and psychological symptoms by providing education in self-care and stress management. Furthermore, Shapiro and his team (2007) found that Mindfulness-Based Stress Reduction training had a significant impact, decreasing stress levels, negative affect, rumination, and anxiety, and boosting positive affect and self-compassion.
Moreover, mindfulness is more than just a form of relaxation, but a transformative and proactive approach to self-care. It involves increased awareness of internalized negative cultural messages and the cultivation of a positive cultural identity (Duncan-Andrade & Morrell, 2008). The practice of mindfulness can lead to critical self-reflection and bring to the surface issues of power and privilege, and through deep reflection and honest dialogue, can support the process of humanization and the dismantling of oppressive ideologies (Berila, 2016; del Carmen Salazar, 2013).
Given the high levels of stress and burnout that school counselors commonly experience, prioritizing self-care practices is crucial for maintaining their personal and professional well-being. Mindfulness-based self-care has emerged as a promising approach for addressing these challenges and provides a unique opportunity for school counselors to reflect on their identities within societal and cultural contexts. Additionally, the SEL framework can be helpful in self-care training by outlining specific skills essential for managing stress, fostering well-being, and developing advocacy in both personal and professional contexts.
Social–Emotional Learning
SEL is defined as “the process in which children enhance their ability to integrate thinking, feelings, and behaving to achieve important life tasks” (Zins et al., 2007, p. 194). The Collaborative for Academic, Social, and Emotional Learning (CASEL) outlines five core competencies of SEL: self-awareness, self-management, social awareness, relationship skills, and responsible decision-making (CASEL, 2023a). CASEL’s mission is to make SEL a fundamental aspect of every child’s education through offering training and educational opportunities to advance scientific research, assessment, and implementation of effective SEL practices in schools (CASEL, 2023b). Numerous studies have demonstrated the positive impact of SEL programs on students’ growth (Carrell & Carrell, 2006; Durlak & DuPre, 2008; Lapan & Harrington, 2009).
Despite the positive effects of SEL in education, its traditional definition has faced numerous criticisms for its inadequacy in addressing equity and justice issues in classrooms and the educational system in light of recent racial and gender awareness. Higheagle Strong and McMain (2020) argued that the traditional SEL approach reinforces oppressive ideologies by valuing White, middle-class knowledge systems above others, portraying marginalized students as troubled and incompetent, and perpetuating injustice. With a growing emphasis on cultural responsiveness in the SEL definition (Higheagle Strong & McMain, 2020; Jagers et al., 2019), a critical question arises: “Are we teaching individual students to manage their emotions and behaviors simply for the sake of upward mobility or recognize and reclaim their emotions and relationships as fuel for social and cultural healing and transformation?” (Camangian & Cariaga, 2021, p. 16).
CASEL subsequently revised their definition of SEL and introduced a new concept of transformative SEL, defined as “a process whereby students and teachers build strong, respectful relationships founded on an appreciation of similarities and differences; learn to critically examine root causes of inequity; and develop collaborative solutions to community and social problems” (Jagers et al., 2018, p. 2). This updated definition acknowledges existing educational disparities and places an emphasis on authentic partnerships between schools, families, and communities. It also calls for a re-examination of the curriculum, instructional methods, and evaluation systems. Educators are encouraged to adopt an equity-focused lens when assessing the five core SEL competencies, asking questions such as “What are the social dynamics among students from different backgrounds in your class? Do you view these differences as a liability or an asset?”, “How do you create an inclusive and safe learning environment for all your students?”, and “Are there policies or practices in your school that prevent your students from receiving the quality education they deserve?”
Overall, the principles of SEL are closely aligned with the goals of school counseling, particularly in developing the skills necessary for promoting the social, emotional, and cognitive development of their students and promoting equity, social justice, and cultural competence necessary for supporting diverse student populations. School counselors can leverage SEL strategies to create a welcoming and inclusive environment that fosters learning, resilience, and well-being among students. Van Velsor (2009) emphasized the role of school counselors as SEL consultants, empowering students to achieve their personal goals and promoting prosocial behaviors, with the ultimate aim of improving the well-being of both the school and society.
Self-care has been integrated into the ethical standards of school counselor preparation programs (Christopher et al., 2016; Nelson et al., 2018), and mindfulness is often taught and studied in these programs (Campbell & Christopher, 2012; Christopher & Maris, 2010). However, there has been a lack of research investigating the experiences of school counselor trainees when learning and practicing self-care alongside mindfulness and SEL competencies in counselor education. In this study, we created and implemented a self-care curriculum for school counseling trainees and examined how this curriculum impacted their personal and professional lives through the use of transcendental phenomenology. The goal was to delve into the experiences of master’s students who took part in a summer course on self-care that was grounded in both mindfulness and SEL.
Methodology
The transcendental phenomenological investigation is often used in research to explore individuals’ subjective experiences and perceptions of a particular phenomenon (Giorgi, 2009; Moustakas, 1994). Using this approach, we aimed to explore the school counseling trainees’ thoughts, feelings, and behaviors of the personal and professional changes in the areas of self-awareness, self-management, social awareness, relationship skills, and responsible decision-making. The umbrella research question that guided this study was “What is the essence of the lived experiences of self-care of school counseling trainees who took 10 seminar sessions grounded in mindfulness and SEL in a master’s-level counseling program over a 5-week period?” Semi-structured interview questions were used to explore the participants’ experiences in their own words, which are detailed in Appendix A. After the approval from the IRB, we invited counseling trainees to participate in the study and followed the three steps of Moustakas’s (1994) transcendental approach: (a) the epoche, (b) the eidetic reduction, and (c) the transcendental reduction in data analysis.
Participants
The purposive sampling method outlined by Glesne (2011) was utilized to select participants for the study. Invitations were extended to all 15 students who had completed the EDCO 298 Seminar in Professional Counseling during the summer course. Based on the guidelines set by Polkinghorne (1989), a sample size of 5–25 individuals is recommended for a phenomenological study. Seven participants, who were female graduate students in the counselor education program, agreed to take part in the study through in-depth interviews. The participants were between the ages of 21 and 45 and attended a single, midsized, public university designated as a Hispanic-Serving Institution in Northern California, United States. Five of the participants identified as Hispanic, Mexican, or Latinx, while two identified as White.
Data Collection
The data for this study was collected through qualitative interviews with individuals who had completed a summer course, EDCO 298 Seminar in Professional Counseling, taught by Kyoung Mi Choi. To ensure impartiality and minimize the impact of the professor’s influence, three precautions were taken: (a) participants were contacted at least 14 days after the course had ended and their grades were posted, (b) they were informed that participation in the study was voluntary, and (c) all interviews were conducted by Jung Hee Hyun, who had no association with the program and held no power over the students’ grades.
Description of the Course
In summer 2020, Choi created an online 5-week course called EDCO 298 Seminar in Professional Counseling, which is detailed in Appendix B. The focus of the course was on self-care, combining six mindfulness core values (such as presence, gratitude, and compassion) and the five SEL competencies framework (self-awareness, self-management, social awareness, relationship skills, and responsible decision-making). The course was attended by 15 master’s-level school counseling students. The aim of the class was to encourage and inspire the students to make a deeper connection with their thoughts, emotions, and physical well-being.
The objectives of the course were to (a) explore the five SEL competencies, (b) explore the mindfulness-based self-care and SEL interventions for counseling and personal growth, (c) understand the effectiveness of the SEL tools and practice mindfulness in daily life, and (d) create a workshop that serves the community the student hopes to serve. The instructor’s role was to create a supportive and safe environment in which students could share their personal narratives and experiences, including their strengths, cultural assets, resilience, privilege, discrimination, and oppression. Throughout the course, various mindfulness practices were utilized, such as collective breathing, body scan, mindful walking, mindful eating, mindful speaking, journaling, storytelling, visualization, and meditation.
Individual Interviews
After the summer session was over, Choi’s counselor education department gave permission to announce the research project via email. Those who showed interest in participating were given a research packet containing details of the study, informed consent, and a demographic sheet, as well as contact information for further inquiries. At every stage of the recruitment and research process, it was emphasized that participation or non-participation in the study would not affect the participants’ course credit or final grade. To be eligible for the study, participants had to meet the following criteria: (a) enrolled in the counselor education program, (b) completed the summer seminar, (c) successfully finished the entire course, and (d) willing to participate in a voluntary lengthy interview.
Once students agreed to participate in the study and submitted their informed consent, contact information, and demographic questionnaire (including a pseudonym, gender, age, self-identified ethnicity, and specialization), they were individually interviewed by Hyun through Zoom. The interviews lasted for approximately an hour and followed a semi-structured format consisting of 16 open-ended questions asked in a consistent order (see Appendix A). The interviews were recorded in their entirety and then transcribed by a graduate student who was not affiliated with the study. After being reviewed by the participants and analyzed by the researchers, the audio recordings were deleted. To maintain the confidentiality of the participants, only pseudonyms were used in all written materials.
Data Analysis
The research methodology employed by the team was transcendental phenomenology (Moustakas, 1994), aimed at uncovering the fundamental nature of human experience (Moerer-Urdahl & Creswell, 2004). NVivo12, a qualitative data analysis software by QSR International (2018), was utilized for data storage, coding, and retrieval. To analyze the data, we followed Moustakas’s (1994) steps for data analysis, which involved the following process: (a) the researchers reflected on and recorded their own experiences of self-care, mindfulness, and critical consciousness before, during, and after data collection; (b) the transcripts were imported into NVivo12, and key statements that provided insight into the participants’ experiences of self-care were highlighted (horizontalization); (c) themes were formed by summarizing these significant statements (cluster of meanings); (d) the significant statements and themes were used to describe the participants’ experiences as a collective whole (textural description); (e) the context that influenced the participants’ experiences of self-care was described using the significant statements and themes (imaginative variation/structural description); and (f) a synthesis of the meanings and essence of the experience was provided by integrating all of the textual and structural descriptions into a universal description.
Reflexivity Statement
Choi is a professor and holds a master’s degree in school counseling and international relations, as well as a doctorate in counselor education and supervision. She has been teaching at the master’s level for over a decade and has received extensive training in mindfulness, yoga, and SEL. Hyun is an associate professor specializing in school counseling and holds a master’s degree in school counseling and a doctorate in counselor education. She provides counseling and consultation to children and parents using play therapy and multicultural counseling interventions. Choi taught the course that the study is based on, while Hyun conducted the participant interviews. Both Choi and Hyun have prior experience in qualitative research and are dedicated to promoting multiculturalism and social justice in counselor education.
In our research, we utilized the epoche technique, which involves temporarily setting aside our preconceived beliefs and assumptions about self-care to approach the research with an open mindset. Throughout the research process, we made a conscious effort to examine and clarify our assumptions to avoid potential biases. We also practiced reflexivity by reflecting on our own positionality and how it could affect our assumptions and interpretations of the data. This approach helped us to ensure that our findings were based on the actual experiences and perspectives of the participants, rather than on our own assumptions. Our assumptions about self-care included the following: (a) the importance for counselors to be responsible about self-care; (b) the impact of self-care practice on both personal and professional life; (c) the necessity for counseling programs to provide specific tools and strategies to support students in developing the knowledge and skills for self-care; (d) the holistic approach of self-care, encompassing cognitive, emotional, physical, interpersonal, and spiritual well-being; (e) the gradual development and continual practice required for self-care ability; (f) the possibility of self-care looking different based on individual and cultural backgrounds; and (g) the transformation process of self-care, facilitating the humanization process, increasing awareness of internalized oppressive messages and cultural identities and leading to individual and collective liberation.
Establishing Trustworthiness
In order to enhance the reliability and validity of the study, we employed the use of an external auditor and member checking (Glesne, 2011; Hays & Wood, 2011; Lincoln & Guba, 1985). The external auditor, a research assistant with previous experience in phenomenological approaches but no prior knowledge of self-care or mindfulness research, was appointed to assist in increasing the credibility of the study. The external auditor reviewed the research process, examined the interview process for potential biases, and verified the interpretations of the data. Additionally, we utilized member checking, in which we presented emergent themes and interview content to the participants to ensure their agreement with the written comments and to check for any additional information or edits.
Findings
We identified five themes that reflect the perceptions and experiences of school counseling trainees regarding self-care grounded on mindfulness and SEL: (a) recognizing the importance and need for self-care, (b) cultivating a nonjudgmental mindset toward challenging emotions, (c) integrating self-care into both personal and professional settings, (d) an increase in compassion and empowerment, and (e) a commitment to ongoing learning and advocacy. These themes, which capture the essence of the participants’ experiences, are contextualized as follows.
Theme One: Recognizing the Importance and Need for Self-Care
Participants in a summer course focused on self-care were aware of their motivations and inspiration for registering for the course. They reported their experiences of struggle and challenges in their lives, particularly during the COVID-19 pandemic. Elizabeth stated, “I was facing personal challenges. This course arrived just when I needed it the most.” Sophia added, “I was struggling with intense emotions during the lockdown period and had doubts about myself. But after taking the first class, I felt that it was meant for me.”
Despite the eagerness of all participants to gain knowledge on self-care, they lacked a clear understanding of the concept. The term “self-care” had been mentioned in other classes within the counseling program, but the application of self-care through mindfulness and SEL was unfamiliar to most of them. Daisy expressed:
I never truly comprehended the meaning of connecting with oneself, which requires dedicating time for personal reflection within daily activities and establishing a connection with one’s body and emotions. This was a new idea for me, as I had not previously implemented or even recognized its significance before participating in the course.
The participants were amazed to discover the relationship between their body, mind, emotions, and nature when they made time for self-reflection and self-care. Stacy expressed, “I never considered the idea of self-care before. This class has shown me that some of the things I already do actually fall under the category of self-care.” Sophia also said, “Self-compassion, I did hear about it or read about it, but I never truly dedicated myself to practicing it.” Furthermore, Stacy added, “I never realized the importance of having a complete connection between the body and nature.”
Theme Two: Cultivating a Nonjudgmental Mindset Toward Challenging Emotions
The participants shared their difficulties in managing emotions such as anxiety, depression, anger, disappointment, uncertainty, and shame. They found learning practical mindfulness strategies to recognize and process these emotions without judgment to be helpful. Elizabeth shared how she connected with her body and was able to understand the physical and emotional cues signaling her needs through increased self-awareness:
I have always been constantly on the move and never took the time to acknowledge my physical and emotional well-being. This class taught me the importance of paying attention to my body’s signals, both physical and mental, signaling the need to slow down. I learned to recognize signs, such as backaches, sore muscles, and headaches, and to listen to what they are trying to tell me about my overall well-being.
Sara echoed, saying, “Self-awareness is about embracing and loving myself.” Veronica, who identified as an immigrant, shared her insight on the impact of self-compassion and a shift in perspective:
As an English learner, I often get nervous during public speaking or classroom presentations because I self-doubt. That’s where self-compassion has played a crucial role for me. Instead of viewing myself as someone who doesn’t speak perfect English, I see myself as someone who has accomplished much despite being an immigrant. I used to struggle with low self-confidence, but after being introduced to self-compassion, it has opened my eyes to see everything as a growth opportunity rather than a potential failure. It’s about focusing on what you have, rather than what you lack, and viewing yourself as a human being like any other. This shift in perspective has been healing.
Carol explained how the class aided her in processing challenging emotions, saying “I learned to create space between myself and my emotions, have more control over impulsive emotions, and take breaks to have fun or engage in self-care.” Daisy summarized her approach to dealing with challenging emotions by saying, “The course taught me that it’s okay to accept my feelings, allowing myself to experience them without judgment. I understand that they are temporary and by processing them, I am able to let them go.”
Theme Three: Integrating Self-Care Into Both Personal and Professional Settings
A strong connection between understanding the importance of self-care and its practical application in daily life was evident in the narratives of all participants. They explored, experimented with, and reinforced a variety of self-care strategies both in and outside of class. Sophia stated, “The class helped me to become more patient, and I now practice those techniques daily.” Elizabeth also spoke of the impact of the class and her daily self-care practices:
I realized the enormous benefits of taking time for myself, both in the morning to start my day and in the evening to relax. Practicing mindfulness and self-care, such as staying aware of my body’s signals through yoga, stretching, and breathing, has been incredibly helpful. My physical healing has become a path to emotional healing. I’m making a conscious effort to care for myself. The class was the perfect introduction to this.
Veronica echoed similar experiences in implementing what she learned from the course.
I feel like I gained a lot from this course because we were able to put what we learned into practice. This class provided a deeper understanding of the subject through reading and trying different practices such as meditation and deep breathing. I’ve made a conscious effort to practice mindfulness daily, instead of only when I felt the need. Currently, I’ve been more consistent and practice it at least five times a week.
Positive and affirmative perspectives toward oneself transformed the participants’ relationship with themselves. Sophia described this transformation by saying, “Since taking the class, I have become a different person. By different, I mean that I approach things differently and I don’t feel stressed out as much. I am able to identify and process my emotions, and accept them.” She explained how her 5-minute mindfulness practice changed her challenging relationship:
Mindfulness allows me to connect with myself, to disconnect from external distractions. I only need 5 minutes of silent meditation to feel that inner connection. If I have an issue or conflict with someone in my family, I take those 5 minutes to disconnect from the story, reflect, and become more relaxed.
Theme Four: An Increase in Compassion and Empowerment
The participants, who exuded confidence and a newfound sense of self-care, expressed their eagerness to assist others in their own self-care journeys. They saw their role as school counselors as being further strengthened, and they showed a keen interest in exploring effective mindfulness and self-care techniques. Veronica stated, “I am confident that offering emotional support online will be just as impactful as in person. I now have a wider range of tools and activities to support my students.” Sophia also shared how her newfound sense of empowerment has made her more compassionate toward her students, saying:
I have changed. Our learning has taught me that my students are the most important individuals sitting in front of me in my counseling offices . . . my goal in supporting them is to acknowledge their opinions, feelings, and emotions. I care about all that they are experiencing, not just their issues but also their emotions. I have gained more empathy for them and strive to provide them with the best support I can.
Elizabeth stated, “As a future school counselor, I am confident that incorporating mindfulness practices into my work will have a positive impact on my interactions with students, staff, and teachers. I have learned these techniques in class and am eager to put them into practice.” Daisy shared her engagement with her students, saying:
At times, I can feel overwhelmed by the volume of students I see in a day and the diverse range of topics discussed. However, by taking the time to connect with myself and acknowledge my emotions, I find that I am more grounded after a workday. This has also helped me form stronger connections with my students.
Carol also expressed that mindfulness can rejuvenate one’s energy and foster positive relationships with oneself and others:
When you have a student who requires a lot of your energy, and you find yourself feeling depleted afterwards, it can be challenging to give your best to the next student. I think it’s important to learn how to recharge quickly so that each student receives the best version of you. With the pandemic, it’s even more crucial to meet the students’ needs academically, emotionally, and for career and college planning. What I have found is that students especially need emotional support because of the stress caused by COVID-19.
Theme Five: A Commitment to Ongoing Learning and Advocacy
The participants recognized the significance of self-care and appreciated their capacity to support others with openness, curiosity, and empathy without any judgments. They viewed self-care and mindfulness as a never-ending journey of learning and personal growth. They expressed their determination to continue their mindfulness-based self-care journey. Elizabeth described the process of healing as like a domino effect, in which one positive change can lead to a chain of similar changes in other areas of life: “Healing one aspect of my life has a positive impact on other parts as well. I’m excited to attend workshops and read more to further my mindfulness journey.” Daisy spoke of her strengthened connection with her students, saying “I feel like I am able to better communicate with my students. I strive to offer them a warm and caring presence, and I am being transparent and accepting of their diverse cultural backgrounds.”
Sara explained her practice with her family, saying, “I have been continuing to study and practice throughout the summer and have been sharing and discussing with my family members. This has been a really healing experience for our family.” Sophia also emphasized the importance of continuing her practice, stating:
Healing is a process, and it doesn’t happen overnight. However, it does help us become better people, improve our connections with others, become better listeners, judge less, and listen more to ourselves. This class has had a truly positive impact on me, and I plan to continue my mindfulness practices.
Advocacy is seen as a natural progression. Stacy also expressed her commitment to practicing alongside her students, saying, “It’s important to understand the importance of congruence in both teaching and life. If I just tell my students what to do, they won’t listen. But if I practice alongside them, it’s more effective.” Sophia spoke about the power of sharing mindfulness practices and their impacts with others, stating,
As a counselor and advocate for these techniques, I want to bring them into the K–12 education system at an early age. I hope to introduce these practices wherever I go and to our students, as I believe everyone can benefit from them.
Discussion
The five themes embody the significance and definition of self-care grounded in mindfulness and SEL for graduate students in counseling who took a summer self-care course. Participants reported a new experience in self-discovery through the practice. Despite the difficulties brought by the COVID-19 pandemic and the shift to online education, learning about self-care helped them cope with daily stress. By participating in a group, they discovered their personal and professional understanding of self-care. They learned how to connect with their emotions, physical sensations, thoughts, and others in their relationships. Particularly, they emphasized the importance of embracing difficult emotions. The self-care grounded in mindfulness and SEL taught in the course enabled them to face emotions such as anger, disappointment, anxiety, uncertainty, and shame with nonjudgment and acceptance. The students connected their understanding of self-care with their daily practices both in and outside of the class. The consistent and dedicated practice demonstrated a true embodiment of self-care among the participants.
Along with displaying great confidence in themselves and their self-care practices, the participants strongly expressed their desire to help others in their communities. Their professional identity as school counselors was enhanced, and the participants developed agency to empower underserved students and communities by introducing self-care strategies and mindfulness practices. After completing the course, the participants expressed their intention to continue the practice and viewed self-care and mindfulness as a lifelong journey.
These findings align with previous qualitative studies (Baker, 2016; Bohecker & Horn, 2016; Campbell & Christopher, 2012; Christopher et al., 2011, 2016; Christopher & Maris, 2010) on the experiences of master’s-level students in mindfulness self-care courses. Across these studies, a common theme is that students reported substantial changes in both their personal and professional lives. This included increased confidence in their professional and interpersonal relationships, a greater appreciation for their physical well-being, healthier lifestyle choices, and the ability to handle challenging situations more effectively.
Furthermore, the significance of the current study is to confirm that self-care is imperative for counselor training. As the participants expressed their sense of empowerment and desire to engage in creating and providing workshops for their families, schools, and communities, they demonstrated self-care as part of social and cultural advocacy. There was a clear shift from a deficit- to a strengths-based self-identity regarding linguistic ability, emotional availability, and a healing-focused process. This is consistent with the role of school counselors, as system change agents need to critically examine dominant culture and its impact on their own racial identity development, power, privilege, and oppression in educational settings (Mitchell & Binkley, 2021). Before disrupting and dismantling the oppression and power in the system, school counselors will need to embrace themselves wholly and consider using themselves as a tool in advocating for those in need. When serving diverse students and communities, self-care goes beyond relaxation and self-awareness of one’s own thoughts and emotions. It also involves reclaiming power within oneself—physically, emotionally, spiritually, and culturally.
Implications
The study’s results have significant implications for counselor educators. First, student readiness is crucial for the maximum impact of self-care courses. What is noticeable in the findings is that the students were ready to change as they chose the course and had a strong desire to learn more about self-care. When students are prepared, the impact can be powerful. Additionally, students who accepted themselves, both strengths and weaknesses, and experienced the mind–body–spirit connection had a greater awareness of themselves and felt more prepared to serve others. The study suggests that self-reflection is essential to maintaining an ethical practice when working with people of different identities, values, and cultures. The participants in this study emphasized their humanity by accepting their identities, processing challenging feelings, practicing self-compassion, and sharing their experiences and knowledge to empower others.
Second, the study recommends that counselor education programs incorporate a self-care course or workshop into their curriculum, as it has been shown to have a positive impact on pre-service counselors (Harrichand et al., 2021). Students’ strong desire to learn more about mindfulness and self-care is consistent with the literature (Baker, 2016) and shows the urgency of incorporating mindfulness practice, SEL, and self-care practice in the school counseling curriculum. The participants recommended offering the course every year and an advanced level later in the program. Because of logistical difficulties, it may be more practical to integrate self-care knowledge and practice into existing coursework and programs rather than adding an extra course.
Lastly, many studies on mindfulness, SEL, or self-care do not give enough importance to humanization, agency, inclusion, and equity in the individual and collective self-care process (Mitchell & Binkley, 2021). This study suggests that it is essential to include mindfulness in personal as well as social and cultural transformative processes. Participants expressed increased agency and advocacy during and after learning and practicing self-care. The self-care course can cultivate and strengthen the capacity to imagine a world beyond the current social conditions with confidence in the ability to bring change through individual and collective efforts (Pyles, 2020).
Limitations and Future Research
The authors of the study acknowledge that self-selection may have contributed to biases in the findings, as participants who enrolled voluntarily in the summer elective course showed strong interest in the research topic (Lavrakas, 2008). They also volunteered to share their experiences, which could have resulted in them focusing on positive and socially desirable narratives. The authors of the study also acknowledge that factors such as the class format, selected activities, and instructor’s teaching styles may have contributed to the participants’ experiences, which may not be generalizable to other school counseling trainees and programs. For future research, a study exploring how master’s students with different placements (i.e., pre/post-practicum, internship) or cultural identities (ethnicity, sexual and gender identity, religion, generation) experience and practice self-care could provide valuable insights to counselor educators. Additionally, a quantitative study using pre- and post-surveys to assess progress in the five SEL competencies can provide useful data for counselor educators and researchers to understand students’ social–emotional development.
Conclusion
This study examined the experiences of school counselor trainees in a self-care course based on mindfulness and SEL, consisting of 10 seminar sessions over 5 weeks. The findings revealed information about the transformation process, the importance of self-care in counseling preparation programs, and the empowering effects on graduate students becoming agents of change. Participants experienced a transformation leading to a change in their relationship with their mind, body, and emotions, and this transformation extended to their relationships with family, friends, students, and colleagues, empowering them to be more engaged with their communities and society. They embodied Carl Rogers’s (1980) core conditions for change, including unconditional positive regard, genuineness, and empathy (Campbell & Christopher, 2012), both personally and professionally, describing the experience as encountering a new self through fresh eyes.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
American School Counselor Association. (2019). The ASCA national model: A framework for school counseling programs (4th ed.). https://www.schoolcounselor.org/About-School-Counseling/ASCA-National-Model-for-School-Counseling-Programs
Baker, S. (2016). Working in the present moment: The impact of mindfulness on trainee psychotherapists’ experience of relational depth. Counselling and Psychotherapy Research, 16(1), 5–14.
https://doi.org/10.1002/capr.12038
Berila, B. (2016). Mindfulness as a healing, liberatory practice in queer anti-oppression pedagogy. Social Alternatives, 35(3), 5–10. https://socialalternatives.com/wp-content/uploads/2021/02/berila_soc_alt_vol_35_3.pdf
Bohecker, L., & Horn, E. A. D. (2016). Increasing students’ empathy and counseling self-efficacy through a mindfulness experiential small group. The Journal for Specialists in Group Work, 41(4), 312–333.
https://doi.org/10.1080/01933922.2016.1232322
Bohecker, L., Vereen, L. G., Wells, P. C., & Wathen, C. C. (2016). A mindfulness experiential small group to help students tolerate ambiguity. Counselor Education and Supervision, 55(1), 16–30.
https://doi.org/10.1002/ceas.12030
Brown, K. W., & Ryan, R. M. (2003). The benefits of being present: Mindfulness and its role in psychological well-being. Journal of Personality and Social Psychology, 84(4), 822–848. https://doi.org/10.1037/0022-3514.84.4.822
Camangian, P., & Cariaga, S. (2021). Social and emotional learning is hegemonic miseducation: Students deserve humanization instead. Race Ethnicity and Education, 25(7), 901–921.
https://doi.org/10.1080/13613324.2020.1798374
Campbell, J., & Christopher, J. (2012). Teaching mindfulness to create effective counselors. Journal of Mental Health Counseling, 34(3), 213–226. https://doi.org/10.17744/mehc.34.3.j75658520157258l
Carrell, S. E., & Carrell, S. A. (2006). Do lower student to counselor ratios reduce school disciplinary problems? Contributions to Economic Analysis & Policy, 5(1), 1–24. https://www.schoolcounselor-ca.org/files/Advocacy/Lower%20Counselor%20Ratios%20Equal%20Less%20Discipline.pdf
Chen, S., Cheng, Z., & Wu, J. (2020). Risk factors for adolescents’ mental health during the COVID-19 pandemic: A comparison between Wuhan and other urban areas in China. Globalization and Health, 16(1).
https://doi.org/10.1186/s12992-020-00627-7
Christopher, J. C., Chrisman, J. A., Trotter-Mathison, M. J., Schure, M. B., Dahlen, P., & Christopher, S. B. (2011). Perceptions of the long-term influence of mindfulness training on counselors and psychotherapists: A qualitative inquiry. Journal of Humanistic Psychology, 51(3), 318–349.
https://doi.org/10.1177/0022167810381471
Christopher, J. C., Christopher, S. E., Dunnagan, T., & Schure, M. (2016). Teaching self-care through mindfulness practices: The application of yoga, meditation, and qigong to counselor training. Journal of Humanistic Psychology, 46(4), 494–509. https://doi.org/10.1177/0022167806290215
Christopher, J. C., & Maris, J. A. (2010). Integrating mindfulness as self-care into counselling and psychotherapy training. Counselling and Psychotherapy Research, 10(2), 114–125. https://doi.org/10.1080/14733141003750285
Collaborative for Academic, Social, and Emotional Learning. (2023a). What is the CASEL framework? https://casel.org/fundamentals-of-sel/what-is-the-casel-framework
Collaborative for Academic, Social, and Emotional Learning. (2023b). Our mission and work. https://casel.org/about-us/our-mission-work
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
del Carmen Salazar, M. (2013). A humanizing pedagogy: Reinventing the principles and practice of education as a journey toward liberation. Review of Research in Education, 37(1), 121–148.
https://doi.org/10.3102/0091732X12464032
Duncan-Andrade, J. M. R., & Morrell, E. (2008). The art of critical pedagogy: Possibilities for moving from theory to practice in urban schools. Peter Lang.
Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41(3–4), 327–350. https://doi.org/10.1007/s10464-008-9165-0
Freire, P. (2000). Pedagogy of the oppressed. Continuum. (Original work published 1970)
Giorgi, A. (2009). The descriptive phenomenological method in psychology: A modified Husserlian approach. Duquesne University Press.
Glesne, C. (2011). Becoming qualitative researchers: An introduction (4th ed.). Pearson.
Harrichand, J. J. S., Litam, S. D. A., & Ausloos, C. D. (2021). Infusing self-care and wellness into CACREP curricula: Pedagogical recommendations for counselor educators and counselors during COVID-19. International Journal for the Advancement of Counselling, 43(3), 372–385. https://doi.org/10.1007/s10447-021-09423-3
Hays, D. G., & Wood, C. (2011). Infusing qualitative traditions in counseling research designs. Journal of Counseling & Development, 89(3), 288–295. https://doi.org/10.1002/j.1556-6678.2011.tb00091.x
Higheagle Strong, Z., & McMain, E. M. (2020). Social emotional learning for social emotional justice: A conceptual framework for education in the midst of pandemics. Northwest Journal of Teacher Education, 15(2).
https://doi.org/10.15760/nwjte.2020.15.2.6
hooks, b. (1994). Teaching to transgress: Education as the practice of freedom. Routledge.
Jagers, R., Rivas-Drake, D., & Borowski, T. (2018). Toward transformative social and emotional learning: Using an equity lens. https://measuringsel.casel.org/wp-content/uploads/2018/11/Framework_EquitySummary-.pdf
Jagers, R. J., Rivas-Drake, D., & Williams, B. (2019). Transformative social and emotional learning (SEL): Toward SEL in service of educational equity and excellence. Educational Psychologist, 54(3), 162–184.
https://doi.org/10.1080/00461520.2019.1623032
Lapan, R. T., & Harrington, K. M. (2009). Paving the road to college: How school counselors help students succeed. Center for School Counseling Outcome Research.
Lavrakas, P. J. (2008). Encyclopedia of survey research methods. SAGE. https://doi.org/10.4135/9781412963947
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Litam, S. D. A., & Hipolito-Delgado, C. P. (2021). When being “essential” illuminates disparities: Counseling clients affected by COVID-19. Journal of Counseling & Development, 99(1), 3–10. https://doi.org/10.1002/jcad.12349
Marques de Miranda, D., da Silva Athanasio, B., Sena Oliveira, A. C., & Simoes-e-Silva, A. C. (2020). How is COVID-19 pandemic impacting mental health of children and adolescents? International Journal of Disaster Risk Reduction, 51, 101845. https://doi.org/10.1016/j.ijdrr.2020.101845
Mitchell, M., & Binkley, E. (2021). Self-care: An ethical imperative for anti-racist counselor training. Teaching and Supervision in Counseling, 3(2), Article 5. https://doi.org/10.7290/tsc030205
Moerer-Urdahl, T., & Creswell, J. W. (2004). Using transcendental phenomenology to explore the “ripple effect” in a leadership mentoring program. International Journal of Qualitative Methods, 3(2), 19–35.
https://doi.org/10.1177/160940690400300202
Moustakas, C. E. (1994). Phenomenological research methods. SAGE.
Nelson, J. R., Hall, B. S., Anderson, J. L., Birtles, C., & Hemming, L. (2018). Self–compassion as self-care: A simple and effective tool for counselor educators and counseling students. Journal of Creativity in Mental Health, 13(1), 121–133. https://doi.org/10.1080/15401383.2017.1328292
Norcross, J. C., & Phillips, C. M. (2020). Psychologist self-care during the pandemic: Now more than ever. Journal of Health Service Psychology, 46(2), 59–63. https://doi.org/10.1007/s42843-020-00010-5
Paris, D., & Winn, M. T. (Eds.). (2013). Humanizing research: Decolonizing qualitative inquiry with youth and communities. SAGE.
Parker, M., & Henfield, M. S. (2012). Exploring school counselors’ perceptions of vicarious trauma: A qualitative study. The Professional Counselor, 2(2), 134–142. https://doi.org/10.15241/mpp.2.2.134
Polkinghorne, D. E. (1989). Phenomenological research methods. In R. S. Valle & S. Halling (Eds.), Existential-phenomenological perspectives in psychology: Exploring the breadth of human experience (pp. 41–60). Plenum Press.
Prime, H., Wade, M., & Browne, D. T. (2020). Risk and resilience in family well-being during the COVID-19 pandemic. American Psychologist, 75(5), 631–643. https://doi.org/10.1037/amp0000660
Pyles, L. (2020). Healing justice, transformative justice, and holistic self-care for social workers. Social Work, 65(2), 178–187. https://doi.org/10.1093/sw/swaa013
QSR International Pty Ltd. (2018). NVivo (Version 12) [Software]. https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home
Rogers, C. R. (1980). A way of being. Houghton Mifflin.
Savitz-Romer, M., Rowan-Kenyon, H. T., Nicola, T. P., Alexander, E., & Carroll, S. (2021). When the kids are not alright: School counseling in the time of COVID-19. AERA Open, 7.
https://doi.org/10.1177/23328584211033600
Shapiro, S. L., Brown, K. W., & Biegel, G. M. (2007). Teaching self-care to caregivers: Effects of mindfulness-based stress reduction on the mental health of therapists in training. Training and Education in Professional Psychology, 1(2), 105–115. https://doi.org/10.1037/1931-3918.1.2.105
Van Velsor, P. (2009). School counselors as social-emotional learning consultants: Where do we begin? Professional School Counseling, 13(1), 50–58. https://www.jstor.org/stable/42732919
Zins, J. E., Bloodworth, M. R., Weissberg, R. P., & Walberg, H. J. (2007). The scientific base linking social and emotional learning to school success. Journal of Educational and Psychological Consultation, 17(2–3), 191–210. https://doi.org/10.1080/10474410701413145
Appendix A
Semi-Structured Interview Protocol
Title of the Study: School Counselor Trainees’ Perceptions and Experiences on Self-Care Grounded in Mindfulness and Social–Emotional Learning (SEL)
To be consistent with the goal of qualitative research, all participants will be described through their own viewpoints and in their own words. All questions are open-ended, and these semi-structured interview protocols will guide the researcher throughout the interviews. However, it is not expected that the remaining questions will be asked sequentially, that all questions will be asked of all participants, or that the list of provided questions is exhaustive. Rather, we offer the questions below as representing possible directions in which we anticipate the interviews may proceed.
Introduction
We want to thank you for your willingness to participate in this study. Recently, you completed the course EDCO 298-01 Seminar in Professional Counseling. Today, we would like to take some time to collect information on your perceptions, thoughts, reactions, and follow-up response to your mindfulness-based self-care and SEL practice. If at any time you feel uncomfortable or do not desire to answer a question, please let me know.
Semi-Structured Interview Questions
- What are the most important things you learned regarding mindfulness-based self-care and SEL?
- How have your knowledge and practice of SEL affected your personal and professional life in the area of self-awareness, self-management, responsible decision-making, relationship skills, and social awareness?
- Do you attribute these changes to the class?
- Have these changes stayed with you since you took the class? What has changed?
- Describe the history of your self-care practices.
- What self-care practices do you currently practice? How often for each?
- How did the class influence these practices?
- Describe how your mindfulness-based self-care affects your personal and professional life.
- In what ways do your own practice of mindfulness and self-care change how you think about students’ or clients’ issues or problems? How have your ideas about what is therapeutic, or healing, changed since taking the class? Do you see mindfulness techniques as healing? How?
- Have the mindfulness practices influenced who you are as a counselor, advisor, educator, or therapist or what it’s like for you to be in the role of the counselor, advisor, educator, or therapist? How?
- Have you tried to introduce mindfulness concepts/techniques with a client/student? Which techniques? What was your level of comfort with introducing the mindfulness techniques?
- What are consequences/outcomes from mindfulness-based self-care practices? (elaborate)
General Questions & Feedback
Is there anything you would like to say about your experiences in relation to the course that we have overlooked? What suggestions do you have to make this course a better experience?
Ending
We want to thank you for your participation in this project.
Appendix B
Course Content and Activities
| Week |
Module |
Mindful Theme |
SEL Competencies |
Class Activities |
| One |
1 |
Presence |
Self-Awareness |
Course Overview: Review syllabus, expectations, course
requirements, and online resourcesWhat’s Social and Emotional Learning (SEL)?
Three Collective Breaths
Why Aren’t We Teaching Mindfulness: TED Video
Pre-Training Survey
Small Group with Accountability and Support |
| 2 |
Self-Connection Practice
Mindful Listening and Speaking
Brave Zone
Trauma-Informed Practice: Grounding, Orienting, and Centering
“Seven Up” Film
My Seven Up Writing
Body Scan
Weekly Journal Entry |
| Two |
3 |
Gratitude |
Self-Management |
Setting Intentions
Mind–Body Connection
Non-Violent Communication
Empathy Practice
Appreciation Circle |
| 4 |
Non-Violent Communication Tools: Mourn/Celebrate/Learn (MCL)
Exploring Identities: “I Am”
Thankful Thoughts
Negative Bias
Weekly Journal Entry |
| Three |
5 |
Creativity |
Relationship Skills |
Play Therapy: Foundations and Techniques (1)
Creative Arts
Additional Readings |
| 6 |
Play Therapy: Foundations and Techniques (2)
My Relationships
Community Circle: Appreciation Practice
Weekly Journal Entry |
| Four |
7 |
Compassion |
Social Awareness |
Check-In: Daily Practice
Compassionate Self-Talk
Neuroplasticity
“Into Light” Video
My Life and Vision: Milestones |
| 8 |
Courageous Conversations
Mindful Eating
Sound Healing
Capstone Preparation
Weekly Journal Entry |
| Five |
9 |
Equity & Inclusion |
Responsible Decision-Making |
Giving and Receiving Loving-Kindness
Transformative SEL: Advocacy
Gender Identities and Pronouns
Mindful Breathing
Silent Mindfulness Practice
Yoga and Mindfulness |
| 10 |
Capstone Presentations
Celebration: A Closing Ceremony
Post-Training Survey
Final Journal Entry |
Kyoung Mi Choi, PhD, NCC, is a professor at San José State University. Jung H. Hyun, PhD, NCC, is an associate professor at Nova Southeastern University. Correspondence may be addressed to Kyoung Mi Choi, One Washington Square, San José, CA 95192, kyoungmi.choi@sjsu.edu.
Aug 24, 2023 | Volume 13 - Issue 2
Marissa Meyer, Elizabeth Wiggins, Gregory M. Elliott
In this transcendental phenomenological study, we interviewed seven adult adoptees regarding their lived experiences of growing up as an adoptee and how this shaped their perception of loss, grief, and counseling in relation to their adoption. Our analysis revealed an overarching concept of the level and manner with which the participants integrated their adoption story into their life narrative and whether loss, grief, and working with a counselor were significant integration factors. As a result, six themes emerged, including ambivalence toward loss and grief, how one’s adoption story was impactful, issues with connection, identity curiosity, relational distrust, and involvement with counseling. We discuss these findings and identify implications for counselors working with adoptees.
Keywords: adoption, loss, grief, integration, ambivalence
There is a growing recognition that the adjustment of adoptees is an important area for further research (Cashen & Grotevant, 2020; Liu et al., 2019). It is estimated that over 100 million Americans are connected to adoption in some manner (Jones & Placek, 2017). Miller, Fan, Christensen et al. (2000) have suggested that higher numbers of adopted persons seek counseling than non-adopted persons. Research also shows that adult adoptees value counseling experiences that address adoption-related topics (Baden et al., 2017). Yet, little is known about the adult adoptee’s experience with counseling, loss, and grief (Côté & Lalumière, 2020). Given the rise of adoption in the United States and counseling needs of adoptees, counselors are likely to encounter an adult adoptee during their career. Gaining a deeper grasp of the impact of adoption on adult adoptees’ mental health and potential distress in adulthood is an important consideration for counselors (Côté & Lalumière, 2020; Liu et al., 2019; Miller, Fan, Grotevant et al., 2000).
One important aspect of exploring adult adoptees’ experiences with mental health and counseling is understanding how they experience and process feelings of loss and grief related to their adoption. When addressing the topic of loss, at a rudimentary level, it can represent familial and relational loss due to separation from one’s biological roots. For some, this occurs not long after birth, which can influence how one adapts psychologically (Cai et al., 2020). For years, researchers have explored the impact of adoption, notably during childhood and adolescence, with an emphasis on psychological adjustment and mental health compared to non-adoptees (Melero & Sánchez-Sandoval, 2017; Miller, Fan, Christensen et al., 2000). Yet, research is limited concerning lived experiences from adult adoptees’ perspectives on how they progressed from a psychosocial standpoint over time (Melero & Sánchez-Sandoval, 2017), in addition to how the distinctive loss(es) they incurred impacted their lives. In one study addressing how adult adoptees navigated adulthood developmental tasks, the researchers acknowledged loss as a predominant theme and recognized it might not be well understood until middle adulthood (Penny et al., 2007). Neil (2012) similarly validated the notion that loss may be too complex for children to comprehend wholly. As adoptees developmentally transition from childhood through adolescence and then into adulthood, their perception of adoption and their identity formation likewise evolve. Researchers have suggested the integration of what it means to be adopted is continual for adoptees over their lifetime (Field & Pond, 2018). This is another reason why considering the perspectives of adult adoptees is important, as adults may have a more mature ability to process and understand the concept of loss on a meaningful level.
For this study, our operational definition of loss was separation from one’s family of origin, including absence of knowledge about, and relationships with, birth parents and families. This may result in a grief response toward these losses, manifested via sadness, anger, denial, depression, and other complex emotions. Each person’s story is unique and for some adult adoptees, loss is a central theme due to the obvious separation, which may disrupt their capacity to connect, leaving them susceptible to relational difficulties (Field & Pond, 2018; Liu et al., 2019). However, some adult adoptees perceive this loss ambiguously because of an atypical separation, meaning the exposure to loss was experienced under abnormal or non-ideal circumstances. Examples of these atypical separations with the birth parent(s)/family could include socioeconomic status, educational level, complicated dynamics (e.g., inability to handle another child, rape), or being in the public care system (O’Leary Wiley & Baden, 2005). Notwithstanding the reason(s) a birth parent(s) decides not to raise their biological child, an obvious loss occurs due to separation from at least two primary, biological relatives. In Westernized culture, tangible losses are naturally recognized, such as death to illness (Brodzinsky, 2011), whereas less concrete losses, or intangible losses, go unacknowledged (Wright, 2009). Intangible losses can produce a feeling of disenfranchised grief, particularly for adoptees. Intangible loss is typically overshadowed by what a person has retained or gained, and in the case of an adoptee, the gain is a family, with associated feelings of permanence and security (Brodzinsky, 2011).
Because the processing of loss can be a central theme in a person’s adoption narrative and throughout the natural life span, it is likely this can surface for an adult adoptee within the therapeutic setting. Loss of biological parents and genealogical continuity are just two elements tied to an increased risk for psychological disorders (Côté & Lalumière, 2020). Additionally, qualitative studies exploring the lived experience of adult adoptees, such as this study, shed light on participants’ perception of loss, the handling or dismissal of grief, and whether counseling has been, or could be, a source of support.
Impact of Adoption
It is not surprising that adoption impacts a person’s life on multiple levels, merely because of the complexity of relationships and human nature. Recognition of both positive and negative facets of adoption is important because denial of grief and the inherent aspect of discontinuity with this life event can interfere with the generation of a healthy life narrative (Wright, 2009). According to Soares et al. (2019), adoptees experience both gains and losses/difficulties. A significant gain is what the researchers referred to as family experience, meaning the adoptee was provided an opportunity to have parents and maybe siblings, whereas the dominant difficulties were discomfort around conversations about adoption and adapting to the adoptive family relationships (Soares et al., 2019). This information highlights the intricacies of how adoption can affect both connection and disconnection among relationships for adoptees. Anderson et al. (2015) highlighted how varying views (i.e., acknowledgment, rejection, or discrepant) regarding the significance of communication around ethnic differences among international adoptive families impacts the level of engagement and familial cohesiveness. On another note, Soares et al. (2019) examined perceived losses in child research participants, with results showing only 32.4% of children interviewed as identifying with birth family loss. The researchers noted that even in positively viewed adoption experiences, there needs to be recognition that children may not be in an environment in which they can acknowledge and grieve their losses (Soares et al., 2019). That study, however, did not extend its results into the realm of adulthood by observing how adults experience the impact of adoption losses and subsequently grieve those losses.
Mental Health
Another common topic concerning adoption is mental health, and Lehto et al. (2020) studied the relationship between being adopted as a child and the mental health of adoptees in adulthood, with respect to phenotypic (genes plus environment) and genetic factors. The results pertaining to phenotype, or observable characteristics, revealed no significant differences between adoptees and non-adoptees regarding general life and relational satisfaction, although their data also suggested adoptees were more susceptible to depression, schizophrenia, and neuroticism compared to their counterparts (Lehto et al., 2020). In an earlier article, Brodzinsky (2011) shared clinical case scenarios of child adoptees and their respective parents to examine identity and psychological adjustment issues that arise, including both pre-placement factors (e.g., genetics, unfavorable birth parent conditions) and how adoptive parents navigate conversations about adoption. Yet, within this research, there was a dearth of qualitative, lived experience research data concerning mental health issues present in adult adoptees, including any possible instances of unidentified loss and, in turn, unresolved grief.
Ambiguous Loss
In adoption, loss(es) ranges from separation from one’s biological family to losing one’s cultural heritage and identity. Boss (2010) explored the notion of two types of ambiguous loss—one tied to a physical absence, and one tied to a psychological absence that precluded closure for adoptees. For example, it is considered common knowledge that some adoptees have likely created a fantasy of their biological parent(s), but if they lack information about their genealogy (due to closed adoption or no contact with birth relatives), what remains are assumptions and questions. Thus, adoption is an example of ambiguous loss, with symptomatology that can include depression, anxiety, and feelings of ambivalence due to the scarcity or absence of information and potential for closure (Boss, 2010). Although this research explored symptoms of ambiguous loss tied to adoption, it did not address adoptees’ experience with loss and grief work in counseling.
Although there is adoption research exploring the topic of loss, there is minimal literature incorporating the lived experiences of adult adoptees. For adult adoptees, loss is distinctly a part of their life story, including hypothetical aspects of one’s identity, sense of control, and possible sadness over not being biologically linked to their adoptive family, all of which may be presented in counseling (Corder, 2012). Corder’s (2012) research was to assist counselors in their work with adoptees, including briefly addressing loss and grief, yet it did not delve into the lived experiences of adult adoptees concerning these topics.
Purpose of the Study
In summary, there is a recognition of the need for more research on the counseling needs of adults who were adopted as children because of both the growing number of Americans who have been touched by adoption and the underrepresentation of the needs of adult adoptees in the research literature (Cashen & Grotevant, 2020; Côté & Lalumière, 2020). Therefore, we set out to explore the lived experiences of adult adoptees regarding their perspectives of loss and grief resulting from their adoption, including any involvement with counseling. In a comprehensive content analysis of adoption articles in counseling journals, Liu et al. (2019) found 45 articles on the topic spanning 30 years, and only 10 of those articles (22%) investigated adults who were adopted as children. Literature on adoptees has largely focused on children and adolescents, specifically regarding their psychological adjustment and mental health compared to non-adoptees (Miller, Fan, Christensen et al., 2000; Soares et al., 2019). Researchers have suggested that loss is an important aspect of the adoption experience needing more exploration (Corder, 2012; Liu et al., 2019; Neil, 2012; Penny et al., 2007), but to date the research on loss as part of the adoption experience has largely been explored quantitatively (Field & Pond, 2018). Despite the assertion that grief is a significant aspect of a child’s adoption story that extends into adulthood (Wright, 2009), we found a minimal amount of qualitative published literature exploring the impact of adoption and associated feelings of loss and grief on adult adoptees.
Method
Our study was guided by our research question: What was the lived experience of adult adoptees regarding loss, grief, and counseling as it related to their adoption experience? We implemented a descriptive, qualitative research design utilizing a transcendental phenomenological methodology to explore these topics from an inquisitive standpoint. Transcendental phenomenology encourages researchers to suspend preconceived judgments about a subject and adopt epoche or intentional bracketing (Moustakas, 1994). This phenomenological concept has researchers bracket presumptions about the phenomenon being studied, which allows for transparent reflection and an ability to view the research data with a fresh perspective (Moustakas, 1994). By utilizing this approach, the reality of the participants’ lived experience of adoption, loss, grief, and counseling could be deeply surveyed to produce a true meaning of the phenomenon. In this qualitative approach, there is a correlation between the what, or the noema, of the experience, and how something is experienced, or the noesis (Sloan & Bowe, 2014).
Research Team
The research team consisted of one full-time counselor, Marissa Meyer, who identifies as Latina, and two full-time counselor educators, Elizabeth Wiggins and Gregory M. Elliott, who identify as European American. Meyer is an adoptee, Wiggins has no affiliation with adoption, and Elliott’s first child is a child by adoption.
Procedure
We submitted the study protocols through the IRB of the university where we were all engaged, as either a student or professor. Once approval was granted by our institution’s IRB, we transitioned into the participation selection process. Inclusion criteria were that participants be adults who experienced adoption as children and were willing to share their perspective of loss and grief pertaining to their adoption experience. Additionally, we vetted adoption-competent counselors as referrals to provide to participants, in the event they were triggered.
We utilized a purposeful, snowball sampling procedure to select participants. We advertised the study regionally to Colorado adoption agencies and counseling centers offering services to adoptees. Potential participants were referred to the study by current participants. Prospective participants who responded to the advertising contacted Meyer by email and were subsequently scheduled for screening. Our initial contact with the potential participants was conducted via email, which included the invitation to participate and a link to a brief survey. The survey included criterion questions to capture the participants’ demographic data and perceived level of loss and grief via a 5-point Likert scale (see Table 1).
Table 1
Participant Information
|
No. |
% |
| Gender Expression |
|
|
| Female |
3 |
42.86 |
| Male |
4 |
57.14 |
| Race |
|
|
| Asian American |
1 |
14.28 |
| White |
3 |
42.86 |
| Hispanic/Latino(a) |
3 |
42.86 |
| Current Age |
|
|
| 20–29 |
3 |
42.86 |
| 40–49 |
1 |
14.28 |
| 50–59 |
1 |
14.29 |
| 60–69 |
2 |
28.57 |
| Age at Adoption |
|
|
| 0–9 Months |
6 |
85.71 |
| After 9 Months |
1 |
14.29 |
| Adoption Circumstances |
|
|
| Initially Placed in Foster Care |
4 |
57.14 |
| Learned Was Adopted as a Kid |
7 |
100.00 |
| Domestic |
6 |
85.71 |
| International |
1 |
14.29 |
| Reunion Status |
|
|
| Contact With Birth Family |
4 |
57.14 |
| No Contact With Birth Family |
3 |
42.86 |
| 5-Point Likert Scale Ratings of Loss/Grief Toward Adoption w/ 1 (minimal)–5 (extreme) |
|
|
| Rating 1 |
2 |
28.57 |
| Rating 2 |
1 |
14.29 |
| Rating 3 |
0 |
0.00 |
| Rating 4 |
2 |
28.57 |
| Rating 5 |
2 |
28.57 |
Participants
Nine prospective participants responded to study advertisements and during the initial screening the final pool was narrowed to seven, with one respondent not meeting the inclusion criteria and another one withdrawing from communication with the research team. The final seven respondents accepted the invitation to participate and were emailed the informed consent form to formalize their participation status. The participant sample included four males and three females, and the ethnicity/race breakdown identified by each participant was: one Asian American, three White, and three Hispanic/Latino(a). Six of the adoptions were domestic and one was international (see Table 1). Smaller sample sizes and lack of randomization are common with phenomenological studies because of the level of data analysis and the need for participants to share a common experience (Nicholls, 2009). We assigned participants pseudonyms for confidentiality (Sheperis et al., 2017), which were used in the analysis and writing processes.
The goal of transcendental phenomenology is to describe the essential structures of the participants’ lived experiences around a particular phenomenon (Barnes, 2003) as opposed to analyzing data for the purpose of generalization to broader populations. It can be conceptualized as a “science of examples” (Van den Berg, 1955, as cited in Farrell, 2020, p. 5). Therefore, recruitment of participants is based on finding diverse participants whose lived experiences illustrate the phenomenon being studied. Published studies utilizing a phenomenological methodology have utilized samples ranging from three (Pretorius & Hull, 2005), to six (McCaig et al., 2012), to many more. We felt we achieved saturation with the seven participants given the breadth and diversity of their adoption experiences.
Data Collection Measures
Qualitative research inquiries are emergent, making interviews and semi-structured interviews common methods of data collection (Levitt et al., 2021). We developed four foundational interview prompts to frame our interviews based on our initial meetings to develop the research protocols and on our literature review. The foundational interview prompts were designed to ground the interviews in the phenomenon of study and to allow space for semi-structured exploration based on participants’ responses. Prior to beginning interviews with our participants, we engaged in an epoche process (Moustakas, 1994), by having Meyer (an adoptee herself) answer the foundational interview prompts. Meyer’s responses were analyzed and referenced throughout the data analysis process. We then conducted phenomenological semi-structured interviews individually with each participant. The four foundational interview prompts were: 1) describe your experience with adoption and how it has played out in your life, 2) recount your experiences with counseling related to adoption, 3) tell me how your adoption narrative has influenced your perceptions of loss and grief, and 4) share how you feel your grief has been or not been expressed over your adoption-related losses. The semi-structured interviews supported flexibility and helped ensure the participants could fully share their stories (Levitt et al., 2021). Thus, the semi-structured interviews helped us understand the participants’ adoption stories and their experiences with grief, loss, and counseling.
We conducted and recorded interviews via Zoom video conferencing technology. Then we manually transcribed the recorded interviews into transcripts via Microsoft Word. For participant anonymity, the assigned pseudonyms were used during the transcription process. After the transcription and data analysis, all video recordings were destroyed to protect participant confidentiality, and only the pseudonyms were utilized in the manuscript.
Data Analysis
We initiated thematic analysis by following Moustakas’s (1994) process of phenomenological reduction to analyze the data. Thus, we each explored and analyzed our unique experiences with adoption that allowed us to transcend any presumptions regarding the phenomenon being studied by implementing the concept of epoche (Moustakas, 1994). As noted earlier and regarding closeness with adoption, Meyer was adopted as an infant, Elliott has adopted a child, and Wiggins has no experience with adoption. Therefore, the thematic analysis and epoche process included Meyer’s answers to the research questions. Lastly, the examination of our experiences with the phenomenon were considered in the research findings as part of the transcendental phenomenology view of researchers and participants working together as “co-researchers” (Creswell, 2013; Moustakas, 1994).
We transcribed the interviews and analyzed the participant phrases via an Excel spreadsheet to ascertain themes. Then, we engaged in an initial holistic reading of each interview transcript to allow ourselves to be attuned to each participant’s words. Next, we performed a line-by-line reading and formulated a list of “significant” statements and grouped them into “meaning units” (Creswell, 2013). Transcendental phenomenology seeks to find meaning units that provide a textual description of what was experienced by the participants, as well as an imaginative variation describing how it was experienced (Moustakas, 1994). With each distinguishable reading of the data, we searched for phrases shared by the participants that illustrated a description of what they experienced and how it was perceived. Ultimately, through a process of consensus coding, the integration of the textual description and the imaginative variation yielded a composite of essential themes.
After we analyzed and narrowed down the dominant themes via the final transcription phase, we emailed the participants these preliminary findings. We asked the participants to reflect and provide feedback on whether the final themes represented their experiences with adoption-related loss and grief, as well as their experiences with counseling related to adoption, as a form of member checking (Creswell, 2013). The participants confirmed that the findings adequately expressed their experiences with adoption-related loss, grief, and counseling.
Trustworthiness
Qualitative researchers promote trustworthiness in their work by safeguarding the credibility and confirmability of their methods and findings (Cope, 2014). Credibility is viewed as the direct connection between the participants’ words and the findings of the study (Cope, 2014). Confirmability is the level to which interpretation of the texts are representative of the participants’ meanings rather than the researchers’ preconceptions or bias alone (Cope, 2014). In this study, we ensured credibility and confirmability through immersion in the texts and by developing a spreadsheet that we utilized to track the analysis process of transforming the participants’ words into themes. This audit trail allowed us to revisit the data when questions of interpretation arose and as we worked toward consensus in our interpretation, as opposed to relying on any one researcher’s sole interpretation (Hill et al., 2005). In addition, we utilized member checking to test the goodness of fit of the findings and interpretations of the participants’ lived experiences to minimize researcher bias (Cope, 2014; Sheperis et al., 2017).
Findings
Our analysis brought to our awareness the concept of integration regarding the participants’ adoption stories, meaning to what depth the participants’ adoption experiences impacted their perceptions of loss, grief, and their involvement with counseling. Expanding on this and in alignment with the initial participants’ survey results regarding the perceived level of loss and grief toward their adoption (see Table 1), it was clear the prominent theme was that of ambivalence of whether loss and grief were significant aspects of their adoption story. Under this notion of integration, we identified six themes that expressed our participants’ experiences. The central theme was ambivalence toward loss and grief, followed by identity curiosity, the impact of one’s adoption story, connection, relational distrust, and involvement with counseling.
Ambivalence Toward Loss and Grief
This first theme regarding uncertainty toward loss and grief was significant, as it closely touched on the study’s research question and the participants’ perception of these two topics in relation to their adoption. Thus, it established the degree to which loss and grief were associated with and/or processed in the context of being adopted. Some of the participants indicated they did not feel they had undergone measurable loss and grief explicitly tied to their adoption experience. For example, Martin stated that he is “not an emotional person, [so] I really don’t have a huge amount of grief.” Similarly, Teresa stated, “I think the reason that I don’t personally feel, and haven’t really ever felt, a ton of loss is because of the strategies my mom used.” Teresa explained that her adoptive mother’s intentionality regarding her processing and normalizing her adoption story helped Teresa not struggle emotionally with her adoptee status.
However, most participants relayed a personal story of loss and grief that they initially believed did or did not relate to their adoption, which iterated the sense of ambivalence from the participants when asked about loss and grief in association with their adoption experience. For example, even though Martin expressed not having feelings of loss and grief related to his adoption, when he discussed the loss of his adoptive parents, he was struck with a sudden, profound feeling of emptiness: “After my [adoptive] parents passed away, it was like, okay, now I need to fill that void to see where I really come from.”
In contrast, Tonya saw how her feelings of loss and grief were directly related to her adoption: “I guess I just experienced loss at a younger age than most people probably would. Because I had to learn how to let go of something I didn’t even know. Someone I didn’t even know.” Mike echoed Tonya’s feelings about the immense ache of missing a person he had never known, his birth mother. The realization that he was grieving the loss of his birth mother initially hit him when he was processing the loss of a romantic relationship:
I think that mother aspect was really something that was powerful in that moment. . . . That moment stayed with me. Because I realized that was the night that I finally started to grieve the loss of my [birth] mom. And I started to realize, it’s OK. She’s out there, and you’re out here, and you’re OK with being sad for her, and finally, someone opened the door for me to do that.
Teresa, whose potential struggles with loss and grief were alleviated by her adoptive parents’ openness in talking about her adoption story, shared some sadness related to her adoption. She stated that she mostly thought about the parent who gave her up. She wondered about the impact on her biological mom, sharing “What if it was really hard for my mom? Or what if I had a sister out there who misses me? Or a brother or something?” Her expression of grief and loss was more around the questions to which she did not have answers.
All the participants were able to discuss aspects of loss and grief, as would be expected, because they are existential elements of the human experience. In interviewing the participants and reviewing their transcribed stories, it appeared that some of them had potentially never processed the idea that they could have experienced sensations of loss and grief related to their adoption, and the research interview was the first time they had been confronted with the idea explicitly. However, most of the participants were ultimately able to connect some loss and grief feelings to their adoption status or experience.
Identity Curiosity
Another notable theme was an expressed desire for the participants to understand who they are as human beings—to clarify their identity since being adopted. The seven participants varied in the amount and timing of the information they had about their adoptions as children. One participant, Teresa, poignantly shared how her adoptive mother would tell Teresa’s adoption story at bedtime, including being adopted from Korea without identifying information of her birth family. In contrast, Luke relayed that his adoption was revealed to him by a vindictive cousin. However, regardless of the amount of information the participants knew about their adoptions as children, as adults, most of them made some reference to intentionally working toward discovering and understanding who they are.
For example, Mike reflected on where some of his personality and emotional traits stemmed from:
I saw things that my dad would do, or my mom would do, and I would do the exact opposite of what they were both doing. [And I would be] like, “where am I getting this from?” You know, I don’t pick this up from either of them . . . I’m not part of them, so where’d I get this stuff that I do?
Carla expressed sadness that when her adoptive parents died, she lost the possibility to learn more about her birth circumstances and identity. She expressed still feeling curiosity surrounding her identity as well as regret and bitterness associated with losing any potential of having questions answered by the people who were there when she was adopted.
I had four parents I guess, and they’re all gone, and that just hit me as incredibly sad that I will never know. I’d always hoped she [adoptive mother] would come forth and be honest about what it was, what happened. I don’t know if she didn’t know, or if she just blocked it, or she was refusing. I don’t know, but with her died my story.
The participants largely positioned their identity curiosity as a response of being an adoptee with an implicit assumption that if they were not adopted, some sense of self-identity would have been granted to them by their birth parents.
Impact of Adoption Story
This theme acknowledged that all the participants expressed in at least one way how their adoption story impacted their overall life narrative. The level of impact varied between the participants, but they all recognized their status as an adoptee was a significant component of their personhood. Ivan expressed that despite knowing his whole life he was adopted, he never had a desire to connect with his birth parents and never considered his adoptive parents to be anything other than his “real” parents. Even with these views, Ivan related a compelling adoption story of his birth mother being talked out of aborting him during a smoke break while she was waiting at the abortion clinic. Ivan felt this brush with almost having his life terminated had put a special meaning on his existence.
The fact that I was minutes away from being aborted just always placed some sort of significance in my life where I say “I can’t waste my life.” . . . It’s given me a proponent to excel in life because if I was saved for a reason, I have that mentality in the back of my head because I know that story.
Tonya also expressed a tumultuous adoption story that involved several years in which she tried to contact her biological mother. Tonya indicated that her adoptive parents “had always told me that I was adopted, but I don’t really think I understood when I was little what that all meant.” However, the knowledge of her status as an adopted child did eventually impact Tonya’s relationship with her adoptive mother as she grew up. She experienced anger toward her adoptive mom, stating that she had thoughts of her “not being my real mom.” But she is grateful that they were able to carve out a close relationship over time.
Participants roughly characterized if they felt their adoption had been smooth or difficult. However, whether the participants felt positively or negatively about their adoption, they all acknowledged the experience of being an adoptee has been an important aspect of coming to terms with their identity. Overall, they felt it was an essential component of their life story.
Connection
Several of the participants recognized they had difficulties connecting with others, and they attributed these difficulties to being adopted. Some participants expressed struggles among immediate family members, such as their own biological children, while for others, issues were localized to social situations. Yet, on a larger scale, some participants’ struggles were characterized as being global. For example, Luke stated, “I certainly always have, more often than not, viewed myself negatively . . . lots of self-doubts in terms of self-worth, very negative feelings, just not good enough. And super-sensitive to the perceptions and judgments of others, and particularly rejection.” These feelings led him to allow boundary violations and being taken advantage of in order to “please, placate, and satisfy the needs of others.”
Like Luke, Carla expressed difficulties with connection and relationships that had persisted for most of her life. Carla spoke poignantly of her difficulties with “attaching” to anyone or anything, except for her own biological children:
I’ve always been kind of a searcher . . . I’m searching for a home, searching for a place, searching for a person, searching for something. Though I’ve moved around the country, I’ve moved from house to house, I’ve moved from apartment to apartment, I’ve moved from boyfriend to boyfriend, I’ve moved from husband to husband, and I’ve moved all over trying to find something, which I never did. And I always kind of explained it like a piece of floating chain in the air and all the posts are standing on the sidewalk down below, but I’m not attached to any of them . . . even when I had my own children, I just kind of added their link onto mine, so then we were just free-floating a couple of links instead of by myself. I never had anything to attach to.
Teresa discussed how social connection specifically was complicated for her growing up because being an international infant adoptee raised by White parents meant she was racially different than her family:
I remember being really self-conscious in high school about, you know, I would see a lot of people [of my race] who had recently immigrated to [the state where I lived]. And I clearly didn’t fit in there. And then I had all of these very White people, and I was like, “I don’t know if I fit in with them either.” And so, it was like this awkward, “where do I fit?” kind of situation. But I think part of why I didn’t try immersing myself more in [my birth] culture was because I wanted to be more in the mainstream White, American culture; that’s kind of how I identified as culturally. I know racially I wasn’t.
As illustrated by Luke, Carla, and Teresa, the participants possessed a deep desire for connection with others, but factors related to their adoption made this challenging at times.
Relational Distrust
Because of the occurrence of some participants noting that they continually struggle to trust others in relationships and certain social circumstances, this theme was notable. In our analysis, we recognized some overlap between this theme and the theme of connection, but we felt there were enough specific mentions of distrust to position it as its own theme. Luke reflected on this theme of not being able to trust others when he processed his feelings of low self-worth, which he attributed to his adoption circumstances:
You can go through all kinds of rationalizations, and probably a lot of true thinking about the realities of what led to this, and at the end of the day, you come back to that same conclusion—someone didn’t love me, someone didn’t want me, I was rejected, I’m unlovable, you know, you come back to that. And you sit in that, and that’s what you believe. And no one’s going to tell you any different.
It is worth noting that Luke was one of the few participants who stated that his adoptive parents were not honest with him about his status as an adoptee from early on in his life. Luke related first being told he was adopted by a cousin who was taunting him, and Luke’s processing of his identity included some significant challenges to obtain valid information about the circumstances of his birth and adoption. In further discussing this with Luke, he expressed, “Here’s another dead end, or another misinformation, or whatever it is, and I just kind of gave up on that. I will tell you, that creates anger and resentment and loss, and it’s a real double-bind.”
In exploring his adoption story, Ivan also reflected on distrust and noted that “When you feel some sort of deception or some sort of awkwardness, that’s what tends to, at least for me, want to dig more and see if there’s something that they’re hiding or something underneath that.” Some of the participants adopted an investigative role in trying to track down information on their birth and adoption. For the participants who related this mission of exploring their roots, the theme of relational distrust occasionally presented itself in the frustrations of pursuing false leads and overcoming dead ends in the search for their origin stories.
For Tonya, however, the theme of relational distrust showed up as not trusting that she could be accepted or loved if she didn’t perform perfectly. She struggled with accepting Bs in middle and high school, having to remind herself that “B doesn’t mean bad.” Admittedly, she had to work on her self-esteem. She shared that she felt insecure and that she had to “prove [she] was worth something.” For Tonya, her sense of distrust was seemingly rooted in a self-concept of inadequacy, a feeling that was echoed by Luke, Mike, and other participants.
Involvement With Counseling
Participants in this study also explored their experience with counseling. These contacts ranged from intense, long-term therapeutic work to a psychological interview prior to being allowed access to adoption records. Although there was significant variation in how much benefit the participants ascribed to this therapeutic contact, the fact that all seven of the adoptees had initiated work with a mental health professional was notable.
The participants’ varied responses when asked about counseling as it related to their adoption brought to our awareness this theme that depicts the perceived applicability of engagement with therapeutic services. We discovered that all participants had some level of involvement in working with a counselor.
Carla was one of the participants who sought out counseling with multiple clinicians over the course of several years. She summarized her attempts to connect with a counselor this way:
I’ve done a fair amount of counseling over the years. Most of it was not with anybody who was adoption savvy. . . . And it really hasn’t stuck until 4 years ago when I started the adoption group and the therapist there is an adoptee as well.
Tonya reflected on her experience with counseling as eventually being beneficial. She shared how she began her experience with therapy at a young age and how she eventually received her diagnosis through the counseling process. She expressed that having a good counselor was important to her and recalled one counselor that she just “clicked with right away.”
Luke’s experience with counseling started later in life. He shared that the impetus for seeking out a counselor was not specifically geared toward his adoption. Instead, he found himself seeking counseling related to his “whole person,” noting that although it wasn’t specifically related to adoption, he recognizes that it is “part of the story, and that’s part of what informed so much of my self-perception.” In contrast, Martin relayed that counseling has not been necessary, stating “I haven’t had any major issues, so I haven’t needed counseling.” He limited his exposure to counseling to a 1-hour interview with a psychologist after requesting adoption records.
As shown by some participants, therapeutic involvements were distinct and ranged in need, intensity, adoption relevancy, and perceived benefit. Additionally, several participants indicated a preference for a counselor who was competent in matters of adoption to be sure they were properly cared for and understood in the therapeutic environment. Although mental health professionals are trained in multicultural competencies to be able to provide help and support to clients who are different from the counselor in demographic characteristics and lifetime experiences, the inclusion of adoption experiences should be considered within this realm.
Discussion
This study revealed if and/or how the participants integrated aspects of their adoption story into their perception of loss and grief, and whether counseling played a role in this process. Ambiguity toward loss and grief was of utmost significance given the impetus for our research study. When posing questions to our study participants regarding their experiences about grief and loss, they relayed mixed responses or ambiguous feelings. Interestingly, Powell and Afifi (2005) define adoption as an ambiguous loss, stating that adoption is associated with the physical loss of the birth parents’ presence in an adoptee’s life, but that there remains a psychological presence that can cause ambiguity in an adoptee’s life. Mitchell (2018) suggested ambiguous loss can be the most traumatic type of loss because the grieving process is often overlooked. Unacknowledged grief may be why our participants experienced ongoing ambiguity around the topics of grief and loss.
The themes of identity curiosity and impact of one’s adoption experience were complementary to one another, which was apparent when our participants shared how they have viewed these topics both in the past and now as adults. Chatham-Carpenter (2012) conducted a study on the impact of an adoption narrative on Chinese adopted children, stating that “As human beings, our identity, or sense of who we are and what our place is in the world, is formed through the telling of narratives or stories” (p. 159). The same seemed to be true of our participants, as they were impacted by positive and negative narratives, as well as by the way they were told about their adoption. Our participants, like those in the Chatham-Carpenter study, were also curious about their identity. Erikson (1968) researched the development of one’s identity and posited that this occurs in stages. A significant life event, such as adoption, during an early stage of development can lead to an unhealthy or underdeveloped sense of self.
There was a moderate overlap between the themes of connection and relational distrust, which afforded us a deeper understanding of the participants’ adoption narrative. For example, our participants revealed struggles connecting with others, supporting existing research that shows people who have been adopted often struggle to form relationships (DeLuca et al., 2019), and that the quality of relationships with adoptive families is an influential component of the ability of adoptees to form healthy connections with others (Melero & Sánchez-Sandoval, 2017). As it pertains to relational distrust, our findings were similar to the Shahab et al. (2021) study, which found that adults with a history of childhood maltreatment are more likely to experience distrust; feel distant from others; and develop an insecure attachment style, which may also affect relationship quality.
Our final theme concerning involvement with counseling connected to the notion of adoptees potentially experiencing ambivalence regarding how they feel toward their adoption experience. Our participants expressed a wide range of information regarding their reasons for seeking out counseling, as well as the prominence of the topic of adoption within the therapeutic setting. Thankfully, the need for adoption-competent counselors has been the subject of numerous studies (Baden et al., 2017; Evan B. Donaldson Adoption Institute, 2010; Freundlich, 2006; Lenerz et al., 2006), and our participants echoed this need for someone who could understand their experiences and help them explore the impact adoption had on their lives. Baden et al. (2017) found that adoptees in counseling reported greater satisfaction in proportion to the amount of attention the therapist paid to the topic of adoption.
Implications
This study explored the experiences of adoptees with counseling, loss, and grief, leading to important implications for professional counselors. Counselors should recognize that adoptees value mental health professionals who address the topic of adoption and are competent in working with clients who are adoptees. Counselors working with adoptees may benefit from treating a client’s adoptee status as an area of multicultural diversity and studying the relevant literature to help develop competence (Remley & Herlihy, 2020). Being more aware of the challenges adoptees experience integrating loss and grief into their life narrative could help a counselor successfully engage with such clients. An ability to address these intricacies through a relationally oriented counseling technique such as existential therapy’s here-and-now processing approach (Yalom, 2002) might be warranted. Additionally, it is important to recognize that grief is a unique process for everyone, including every adoptee. Grief that arises from a recognition and acceptance process when coming to terms with one’s adoption is likely to be complex and interwoven with accepting the fact and circumstances of one’s adoption. A narrative therapy approach could offer clients an opportunity to re-author both their adoption story (unique and alternate outcomes) and the future story they want to have (White & Epston, 1990). Kessler (2019) suggested that a sixth stage of grief (added to the traditional stages of denial, anger, bargaining, depression, and acceptance) is finding meaning, and this additional stage would appear to be resonant in the lives of virtually all of our study’s participants.
Limitations
The findings and discussion of this study should be considered within the context of its limitations. One limitation is the sample used by the researchers. The study included seven purposefully selected participants to represent adult adoptees, including four males and three females, and more minorities than White participants. The U.S. Department of Health and Human Services (2020) reported that White children (50%) are adopted at approximately the same rate as other ethnicities, and male children (51%) are adopted slightly more frequently than female children (49%). Although this study’s sample is representative of the current racial and gender makeup of adoptees, expanding on the diversity of participants could make for a more robust description of the lived experiences of adult adoptees.
Another study limitation is the use of self-report interviews for data collection. Using interviews alone, participants may be influenced by social desirability, which may impact the credibility and dependability of the data collected (Heppner et al., 2008). At each interview, the researchers encouraged participants to share their unique experiences. Yet, participants may have felt compelled to respond in ways viewed as desirable to the researchers, society, or the profession of counseling. In the future, this limitation could be addressed by increasing persistent observations. This would allow for the researchers to determine if the responses to the interview protocol remained consistent over time, thus increasing the study’s dependability.
Recommendations for Further Research
Further research around the notion of integration of one’s adoption story into a person’s life narrative by exploring our six identified themes via the lived experiences of adult adoptees could benefit the profession of counseling. We recommend continuing research in this area while expanding the diversity of participants being studied. One possibility could be a grounded theory study that explores the process of identity development for adoptees. Although this study identified themes of deep curiosity about oneself and being impacted (either positively or negatively) by adoption, we were not able to establish causal relationships between the status as an adoptee and these intrapersonal traits. A larger, quantitative study might be able to further explore these issues and determine a causal link between adoption and the development of these intrapersonal characteristics.
Another identified theme was adult adoptees’ involvement with counseling and what each participant’s situation entailed. Although the interviews contained questions that explored the participants’ counseling experiences, this study did not specifically focus on what adoptees valued in counselors. Further research could utilize more explicit questions regarding this topic, including interventions that counselors draw from to build a strong therapeutic alliance with clients who have been adopted.
Finally, creating a research design to further explore the themes of connection and relational distrust is important in understanding the relational impacts of adoption on adoptees. Research on these topics may lead to more effective counseling techniques and goals for adoptees and families, along with common challenges for families considering adoption.
Conclusion
We explored the lived experiences of adult adoptees to grasp and understand their perceptions of loss, grief, and their involvement with counseling in relation to being adopted. Our findings suggested a common theme of ambivalence around loss and grief in connection to our participants’ adoption stories. This data suggested that loss and grief may not have been processed or integrated in relation to the participants’ adoption. These findings encourage professional counselors to treat adoption status as a form of multicultural diversity and to approach counseling with adoptees with a willingness to provide ample focus on the client’s adoption story. Counselors trained in adoption issues are assets to this population, as unresolved grief can result in connection, developmental, and relational issues throughout the life span.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Anderson, K. N., Rueter, M. A., & Lee, R. M. (2015). Discussions about racial and ethnic differences in internationally adoptive families: Links with family engagement, warmth, & control. Journal of Family Communication, 15(4), 289–308. https://doi.org/10.1080/15267431.2015.1076420
Baden, A. L., Kitchen, A., Mazza, J. R., Harrington, E. S., & White, E. E. (2017). Addressing adoption in counseling: A study of adult adoptees’ counseling satisfaction. Families in Society: The Journal of Contemporary Social Services, 98(3), 209–216. https://doi.org/10.1606/1044-3894.2017.98.26
Barnes, J. (2003). Phenomenological intentionality meets an ego-less state. Indo-Pacific Journal of Phenomenology, 3(1), 1–17. https://doi.org/10.1080/20797222.2003.11433880
Boss, P. (2010). The trauma and complicated grief of ambiguous loss. Pastoral Psychology, 59(2), 137–145. https://doi.org/10.1007/s11089-009-0264-0
Brodzinsky, D. M. (2011). Children’s understanding of adoption: Developmental and clinical implications. Professional Psychology: Research and Practice, 42(2), 200–207. https://doi.org/10.1037/a0022415
Cai, J., Kim, A. Y., & Lee, R. M. (2020). Psychological correlates of interest in genetic testing among Korean American adoptees and their parents. Journal of Genetic Counseling, 29(3), 460–470.
https://doi.org/10.1002/jgc4.1237
Cashen, K. K., & Grotevant, H. D. (2020). Relational competence in emerging adult adoptees: Conceptualizing competence in close relationships. Journal of Adult Development, 27, 83–94.
https://doi.org/10.1007/s10804-019-09328-x
Chatham-Carpenter, A. (2012). “It was like this, I think”: Constructing an adoption narrative for Chinese adopted children. Adoption Quarterly, 15(3), 157–184. https://doi.org/10.1080/10926755.2012.698404
Cope, D. G. (2014). Methods and meanings: Credibility and trustworthiness of qualitative research. Oncology Nursing Forum, 41(1), 89–91. https://doi.org/10.1188/14.onf.89-91
Corder, K. (2012). Counseling adult adoptees. The Family Journal, 20(4), 448–452. https://doi.org/10.1177/1066480712452088
Côté, K., & Lalumière, M. L. (2020). Psychological adjustment of domestic adult adoptees. Journal of Adult Development, 27, 118–134. https://doi.org/10.1007/s10804-019-09337-w
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
DeLuca, H. K., Claxton, S. E., & van Dulmen, M. H. M. (2019). The peer relationships of those who have experienced adoption or foster care: A meta-analysis. Journal of Research on Adolescence, 29(4), 796–813. https://doi.org/10.1111/jora.12421
Erikson, E. H. (1968). Identity: Youth and crisis. W. W. Norton.
Evan B. Donaldson Adoption Institute. (2010). Keeping the promise: The critical need for post-adoption services to enable children and families to succeed.
Farrell, E. (2020). Researching lived experience in education: Misunderstood or missed opportunity? International Journal of Qualitative Methods, 19, 1–8. https://doi.org/10.1177/1609406920942066
Field, J., & Pond, R. (2018). How adoption affects the experience of adult intimate relationships and parenthood. New Zealand Journal of Counselling, 38(2), 24–55. https://nzac.org.nz/document/7049/2.-How-adoption-affects-the-experience-of-adult-intimate-relationships-and-parenthood.pdf
Freundlich, M. (2006). Where do we go from here? Implications of current research findings for policy, program and practice in post-adoption services. In M. M. Dore (Ed.), The postadoption experience: Adoptive families’ service needs and service outcomes (pp. 283–298). CWLA Press.
Heppner, P. P., Wampold, B. E., & Kivlighan, D. M. (2008). Research design in counseling (3rd ed.). Brooks/Cole.
Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A., & Ladany, N. (2005). Consensual qualitative research: An update. Journal of Counseling Psychology, 52(2), 196–205.
https://doi.org/10.1037/0022-0167.52.2.196
Jones, J., & Placek, P. (2017). Adoption by the numbers: A comprehensive report of U.S. adoption statistics. National Council for Adoption. https://www.indianaadoptionprogram.org/wp-content/uploads/2021/11/Adoption-by-the-Numbers-NACAC-2017.pdf
Kessler, D. (2019). Finding meaning: The sixth stage of grief. Scribner.
Lehto, K., Hägg, S., Lu, D., Karlsson, R., Pedersen, N. L., & Mosing, M. A. (2020). Childhood adoption and mental health in adulthood: The role of gene-environment correlations and interactions in the UK biobank. Biological Psychiatry, 87(8), 708–716. https://doi.org/10.1016/j.biopsych.2019.10.016
Lenerz, K., Gibbs, D., & Barth, R. P. (2006). Postadoption services: A study of program participants, services, and outcomes. In M. M. Dore (Ed.), The postadoption experience: Adoptive families’ service needs and service outcomes (pp. 95–110). CWLA Press.
Levitt, H. M., Morrill, Z., Collins, K. M., & Rizo, J. L. (2021). The methodological integrity of critical qualitative research: Principles to support design and research review. Journal of Counseling Psychology, 68(3), 357–370. https://doi.org/10.1037/cou0000523
Liu, Y., Jacoby, R. P., Jang, H., & Li, D. (2019). A content analysis of adoption articles in counseling journals: A 30-year review. The Family Journal, 27(1), 67–74. https://doi.org/10.1177/1066480718809424
McCaig, M., Waugh, A., Duffy, T., & Martin, C. R. (2012). The lived experience of older people using assistive technology. Working with Older People, 16(4), 170–174. https://doi.org/10.1108/13663661211286693
Melero, S., & Sánchez-Sandoval, Y. (2017). Mental health and psychological adjustment in adults who were adopted during their childhood: A systematic review. Children and Youth Services Review, 77, 188–196. https://doi.org/10.1016/j.childyouth.2017.05.006
Miller, B. C., Fan, X., Christensen, M., Grotevant, H. D., & Van Dulmen, M. (2000). Comparisons of adopted and nonadopted adolescents in a large, nationally representative sample. Child Development, 71(5), 1458–1473. https://doi.org/10.1111/1467-8624.00239
Miller, B. C., Fan, X., Grotevant, H. G., Christensen, M., Coyl, D., & Van Dulmen, M. (2000). Adopted adolescents’ overrepresentation in mental health counseling: Adoptees’ problems or parents’ lower threshold for referral? Journal of the American Academy of Child & Adolescent Psychiatry, 39(12), 1504–1511.
https://doi.org/10.1097/00004583-200012000-00011
Mitchell, M. B. (2018). “No one acknowledged my loss and hurt”: Non-death loss, grief, and trauma in foster care. Child and Adolescent Social Work Journal, 35(1), 1–9. https://doi.org/10.1007/s10560-017-0502-8
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Neil, E. (2012). Making sense of adoption: Integration and differentiation from the perspective of adopted children in middle childhood. Children and Youth Services Review, 34(2), 409–416.
https://doi.org/10.1016/j.childyouth.2011.11.011
Nicholls, D. (2009). Qualitative research: Part three – methods. International Journal of Therapy and Rehabilitation, 16(12), 638–647. https://doi.org/10.12968/ijtr.2009.16.12.45433
O’Leary Wiley, M., & Baden, A. L. (2005). Birth parents in adoption: Research, practice, and counseling psychology. The Counseling Psychologist, 33(1), 13–50. https://doi.org/10.1177/0011000004265961
Penny, J., Borders, L. D., & Portnoy, F. (2007). Reconstruction of adoption issues: Delineation of five phases among adult adoptees. Journal of Counseling & Development, 85(1), 30–41.
https://doi.org/10.1002/j.1556-6678.2007.tb00441.x
Powell, K. A., & Afifi, T. D. (2005). Uncertainty management and adoptees’ ambiguous loss of their birth parents. Journal of Social and Personal Relationships, 22(1), 129–151. https://doi.org/10.1177/0265407505049325
Pretorius, H. G., & Hull, R. M. (2005). The experience of male rape in non-institutionalised settings. Indo-Pacific Journal of Phenomenology, 5(2), 1–11. https://doi.org/10.1080/20797222.2005.11433902
Remley, T. P., Jr., & Herlihy, B. (2020). Ethical, legal, and professional issues in counseling (6th ed.). Pearson.
Shahab, M. K., de Ridder, J. A., Spinhoven, P., Penninx, B. W. J. H., Mook-Kanamori, D. O., & Elzinga, B. M. (2021). A tangled start: The link between childhood maltreatment, psychopathology, and relationships in adulthood. Child Abuse & Neglect, 121. https://doi.org/10.1016/j.chiabu.2021.105228
Sheperis, C. J., Young, J. S., & Daniels, M. H. (2017). Counseling research: Quantitative, qualitative, and mixed methods (2nd ed.). Pearson.
Sloan, A., & Bowe, B. (2014). Phenomenology and hermeneutic phenomenology: The philosophy, the methodologies, and using hermeneutic phenomenology to investigate lecturers’ experiences of curriculum design. Quality & Quantity, 48(3), 1291–1303. https://doi.org/10.1007/s11135-013-9835-3
Soares, J., Ralha, S., Barbosa-Ducharne, M., & Palacios, J. (2019). Adoption-related gains, losses and difficulties: The adopted child’s perspective. Child and Adolescent Social Work Journal, 36(3), 259–268.
https://doi.org/10.1007/s10560-018-0582-0
U.S. Department of Health and Human Services. (2020, June). The AFCARS report. https://www.acf.hhs.gov/sites/default/files/documents/cb/afcarsreport27.pdf
White, M., & Epston, D. (1990). Narrative means to therapeutic ends. W. W. Norton.
Wright, J. L. (2009). The princess has to die: Representing rupture and grief in the narrative of adoption. The Psychoanalytic Study of the Child, 64, 75–91. https://doi.org/10.1080/00797308.2009.11800815
Yalom, I. D. (2002). The gift of therapy: An open letter to a new generation of therapists and their patients. Harper Perennial.
Marissa Meyer, MA, LPC, is Manager of Navigation at the Jefferson Center for Mental Health. Elizabeth Wiggins, PhD, LPC, LSC, is an assistant professor and the director of the Master of Arts in School Counseling program at Colorado Christian University. Gregory M. Elliott, PhD, LPC (CO), LMHC (IA), is an associate professor at Colorado Christian University. Correspondence may be addressed to Marissa Meyer, 4851 Independence St., Wheat Ridge, CO 80033, marissameyer73@gmail.com.
Aug 24, 2023 | Volume 13 - Issue 2
Corrine R. Sackett, Heather L. Mack, Jyotsana Sharma, Ryan M. Cook, Jardin Dogan-Dixon
Microaggressions can and do occur in the counseling process, yet there is a dearth of literature about how counselors-in-training (CITs) experience this phenomenon from clients or how they may respond to clients who perpetuate microaggressions against them in a therapeutic setting. Therefore, in this constructivist phenomenological study, we explored CITs’ experiences of microaggressions from clients in the counseling process. Two interviews with six participants of various marginalized identities revealed the following themes: (a) internal reactions, (b) attempts to contextualize, (c) prevalence of microaggressions, (d) navigating microaggressions, and (e) seeking support. Findings and implications for CITs and counselor educators and supervisors are discussed.
Keywords: microaggressions, constructivist phenomenology, counseling process, counselors-in-training, counselor educators
Microaggressions have been defined as intentional or unintentional ongoing verbal or nonverbal offensives experienced by individuals of a marginalized group (Ratts et al., 2016) and as “subtle and stunning” daily racial offenses that impact the health and well-being of individuals (Pierce, 1970). Counselors and counselors-in-training (CITs) of marginalized identities are often uncertain of whether or how to respond to microaggressions in counseling sessions while keeping the counseling relationship intact (Branco & Bayne, 2020). As such, counseling researchers have the opportunity and responsibility to explore the experiences of counselors or CITs who are the target of microaggressions from clients. Scholarship around this topic can help the counseling profession, and counselor education specifically, in developing competencies to help guide CITs and counselors in these situations.
Given the reality that there are clients from privileged groups receiving counseling from CITs from marginalized groups (Haskins et al., 2015; Ratts et al., 2016) and that the counseling process is an intersection of cultural identities between the client and CIT (Ratts et al., 2016), there is potential for microaggressions to occur in this relationship. Various studies have explored microaggressions within the counseling setting as experienced by clients who identify as racial/ethnic minorities (Constantine, 2007; Crawford, 2011; Morton, 2011; Owen et al., 2011, 2014); however, much less is known about counselors’ and CITs’ experiences with clients who may perpetuate microaggressions against them (Branco & Bayne, 2020). Given the dearth of literature focusing on how CITs can and do handle microaggressions from clients, we aimed to help fill this gap in the literature by exploring CITs’ experiences of microaggressions from clients.
In the 1970s, Harvard-trained Black psychiatrist Chester M. Pierce coined the term “microaggression” to describe the insults that he witnessed Black Americans encounter daily (Pierce, 1970). His work has been seminal in laying a foundation for understanding the damage that negative interracial interactions have on Black Americans’ health. Decades later, Sue and colleagues (2007) continued Pierce’s research on microaggressions and expanded its definition to include experiences of cultural bias, prejudice, and power imbalance. Literature about microaggressions in the counseling profession highlights the negative impact of counselors being the offender, or the person who perpetuates microaggressions, toward a racially/ethnically marginalized client in session (Constantine, 2007; Owen et al., 2011).
Although racial microaggressions toward racially/ethnically marginalized people have been studied extensively, microaggressions can also target gender, sexual orientation, ability status, class, religion, and other visible and invisible identities (Chan et al., 2018). The consequences of microaggressions on the counselor–client relationship have been studied in the context of gender (Owen et al., 2010) and sexual orientation (Shelton & Delgado-Romero, 2013). As such, there is a need for more research to explore microaggressions as a phenomenon that affects various identities. When individuals identify with multiple salient identities, they are more likely to experience privilege and oppression. For instance, a person can experience White privilege while simultaneously experiencing marginalization from identifying as queer—this person can belong to both oppressive and oppressed groups. Because one identity can be stigmatized while another is privileged, there is complexity in understanding one’s whole identity rather than only its parts. The Multicultural and Social Justice Counseling Competencies (MSJCC) include a quadrant to represent a privileged client and a marginalized counselor (Ratts et al., 2016) that can be used to conceptualize the dynamic of microaggressions experienced by counselors from clients. It is possible, of course, for counselors and clients to identify with being in more than one quadrant simultaneously as members of both privileged and marginalized groups. Further, the intersectionality of race, gender, sexual orientation, and other identities may increase the frequency and impact of microaggressions (Williams et al., 2021). Microaggressions toward intersecting marginalized identities compound their harmful impact (Nadal et al., 2015).
Oppression on an individual level in the form of microaggressions, regardless of whether they are intentional or unintentional, can have a devastating impact on individuals’ physical and mental health (Pierce, 1970; Ratts et al., 2016). Depression, anxiety, and post-traumatic stress have been reported by researchers as being associated with microaggressions (Williams et al., 2021). Thus, it is feasible that CITs would experience these same mental and physical reactions to microaggressions within the counseling relationship (Branco & Bayne, 2020), which in turn seems likely to influence their work with current and future clients.
Purpose of the Study
Branco and Bayne (2020) asserted that counselor educators are called to provide training for counselors from marginalized identities to work with clients from privileged identities, and the counselor education field is lacking in this area. Because the cultural experiences and backgrounds of clients and counselors impact the counseling relationship (Constantine, 2007; Crawford, 2011; Morton, 2011; Owen et al., 2011, 2014), counseling process, treatment selection, and outcomes, it is critical that counseling researchers expand inquiry in this area (Hays, 2020). Specifically, counseling researchers need to inquire more about counselors’ experiences with social injustice and how those affect the counseling process. As established, the MSJCC framework allows for counselors and clients from many intersecting privileged and marginalized identities (Ratts et al., 2016). Although previous studies have focused exclusively on racial microaggressions from clients, Branco and Bayne (2020) called for a broader examination to include counselors or CITs who identify with a marginalized status outside of race and ethnicity. As such, the purpose of the current study was to explore CITs’ experiences of microaggressions from clients, regardless of the one or more marginalized identities they carried, through van Manen’s (2016) constructivist hermeneutic phenomenological approach. This is a reflective process focused on the lived experiences of participants. By specifically focusing on CITs’ experiences of microaggressions from clients, we gain insight into how to better provide supervision and training in this area. Thus, the research question that guided this investigation was: “What are CITs’ experiences of microaggressions from clients in the counseling process?”
Method
Research Design Overview
We chose van Manen’s (2016) constructivist hermeneutic phenomenological approach for this inquiry of CITs’ experiences of microaggressions from clients, as it aims to increase thoughtfulness, grasp essential meaning, and come into closer contact with the world while providing thought-provoking data that are ideal for clinical practice (Sackett & Cook, 2021). van Manen described hermeneutic phenomenological research as choosing a phenomenon of serious interest, investigating the lived experience of the phenomenon, reflecting on its essential themes, describing the phenomenon through writing and rewriting, remaining in pedagogical relationship, and balancing the parts of the whole of the research.
Researcher Reflexivity
Following van Manen’s (2016) advisement that researchers be aware of and transparent about their own experience of the phenomenon under investigation and the influence of their own values, beliefs, and experiences, we describe our positionality here for transparency. At the time of the study, authors Corrine R. Sackett, Jyotsana Sharma, and Ryan M. Cook were faculty members in counselor education programs at research universities—Sackett was an associate professor and Sharma and Cook were assistant professors. Heather L. Mack and Jardin Dogan-Dixon were graduates of a CACREP-accredited program specializing in clinical mental health counseling; Mack was practicing in agency and private practice settings and Dogan-Dixon was a correctional psychologist. Sackett, Mack, Sharma, and Dogan-Dixon identify as heterosexual and cisgender women, and Cook as a heterosexual and cisgender man. Sackett, Mack, and Cook identify as White, Sharma identifies as Asian Indian and international, and Dogan-Dixon identifies as Black and from a Christian background.
Sackett was drawn to this line of inquiry after a supervision session in which a supervisee disclosed a microaggression from a client related to gender. The supervisee’s site supervisor (a male counselor) was in the session as a co-counselor. Following the session, the CIT and site supervisor processed the event. Although the site supervisor was supportive, he advised the CIT not to address the microaggression with the client because it was not related to the client’s counseling goals. The CIT described feeling dismissed by her site supervisor’s response. She also described uncertainty in how to continue a meaningful counseling relationship with the client afterward without addressing the microaggression. This experience led Sackett to seek guidance from the literature on CITs’ or counselors’ handling of microaggressions from clients, but she found limited scholarly resources. Sackett was influenced by this experience in her conceptualization of the current study, and in analyzing and writing the findings. Further, while recognizing her privileged identities, Sackett has experienced gender microaggressions that have impacted her and the way she views this topic area. Mack, while also recognizing her privileged identities, has experienced gender microaggressions from clients and a site supervisor. Sharma identifies as an international scholar of Asian Indian descent. As an international woman of color, Sharma has experienced many microaggressions since moving to the United States. She has experienced microaggressions from clients, colleagues, and supervisors. Cook has wondered how supportive or unintentionally unsupportive he has been as a supervisor and faculty member with CITs’ experiences of microaggressions. Dogan-Dixon has experienced gendered racial microaggressions from clients, peers, and supervisors in various counseling settings across her training. She initially struggled to address microaggressions in the moment because of potential rejection and backlash; with practice, however, she has learned to address microaggressions in multiple ways, including caring confrontation. She now educates others on how to navigate microaggressions in personal and professional settings. In harnessing the interpretive nature of van Manen’s (2016) approach, instead of bracketing these biases, we embraced them as part of the process (Prosek & Gibson, 2021).
Participants
Participants included six CITs from CACREP-accredited counselor education programs in the United States. Sampling was purposive for the phenomenon under investigation (Prosek & Gibson, 2021), and all participants met the eligibility criteria of being enrolled in a CACREP-accredited master’s program with a specialty in clinical mental health or school counseling, being enrolled in or completed practicum or internship in their program, and having lived experience of microaggressions from clients in the counseling process. Constructivist qualitative studies tend to have smaller sample sizes that allow for more depth of understanding and intriguing findings (Boddy, 2016). Though we recruited from across the United States, our resulting sample consisted of participants from the Southern region of counselor education programs. Participant ages ranged from 26–30 years. Self-named gender identity included one female, two cisgender female, two cisgender male, and one participant who did not specify gender. Self-named sexual orientation included one straight, one lesbian, two bisexual, and two who did not specify. Participants self-identified their racial/ethnic identities as Hispanic (one), Hispanic/Latina (one), Black/Afro Latino (one), Caucasian (one), and White (two). Those who answered the question of other relevant identities named student or partnership status. Participants were entered into a drawing for one of three $15 Starbucks gift cards after completion of the second interview as a token of appreciation for their time.
Participant Recruitment
Sackett obtained human subjects research approval from her university of employment’s IRB. Sackett then recruited participants by sending two rounds of emails explaining the purpose of the study to contacts from 387 CACREP-accredited master’s programs in the United States with specialty areas in clinical mental health and school counseling. The email requested the faculty member send the recruitment email with the purpose of the study and a note about what participation entailed to their master’s students who were currently enrolled in, or had completed, practicum or internship in their program. Inclusion criteria included the experience of a microaggression from a client, regardless of marginalized identity(ies) of the CIT. The email asked CITs to contact Sackett if interested in participation. When participants contacted Sackett, she completed the informed consent process and referred them to Mack to schedule the first interview. Ten individuals contacted Sackett with interest in participating in the study. However, four of the initial 10 individuals reported not having experiences of microaggressions to share after hearing the definition of a microaggression from Mack (see Data Collection below).
Data Collection
Mack conducted two interviews over Zoom with each participant. Two interviews per participant allowed for sustained engagement with the phenomenon, and interviews were spaced from 1 to 3 weeks apart per participant to allow time for reflection between the interviews. This resulted in 12 interviews. Each participant answered demographic questions during the first interview that requested gender, age, race/ethnicity, any other relevant identities, and pseudonym. To begin each interview, Mack broached her identities with participants (Day-Vines et al., 2007) and verbally gave participants a definition of microaggressions as intentional or unintentional ongoing verbal or nonverbal offensives experienced by individuals of a marginalized group (Ratts et al., 2016). Interview questions were centered on CITs’ experiences of microaggressions from clients, in line with van Manen’s (2016) recommendation that the interview be strongly oriented to the phenomenon. Interview questions were developed by Sackett, Mack, and Sharma and were informed by extant literature of counselors’ experiences of microaggressions from clients (e.g., Branco & Bayne, 2020), multicultural counseling competencies (e.g., Ratts et al., 2016), and CITs’ prioritization of information for supervision (e.g., Cook & Welfare, 2018), coupled with the authors’ respective expertise and perspectives. Researchers used the same interview protocol for both interviews, which can be found in the Appendix. While being mindful of the differences between counseling and interviewing (Sackett & Lawson, 2016), Mack utilized counseling skills to facilitate discussion and to communicate empathy (Kleist, 2017). Interviews ranged in length from 24 to 62 minutes (M = 46.1; SD = 11.82), except for Lila’s second interview of only approximately 5 minutes, as she indicated she had nothing to add from the previous interview. Interviews were audio-recorded and later transcribed by a graduate assistant.
Analysis
We used NVivo Version 12 (QSR, 2018) software to manage the data. Operating from van Manen’s (2016) approach, we were concerned with capturing the essential meaning of the phenomenon, which involved seeing the essential meaning of each participant’s experience, reaching a reflective determination, and explaining the experience. In this process, we gave order to the research and writing by considering the phenomenon in themes. Along with van Manen’s hermeneutic phenomenological approach, we employed the First and Second Cycle coding process described by Miles et al. (2020). After listening to all participant interviews, Sackett reviewed the 12 interview transcripts while utilizing a line-by-line approach to coding (van Manen, 2016). She applied in vivo codes in her first review and then went back through the data to apply a combination of descriptive codes, process codes, emotion codes, and value codes in the First Cycle coding (Miles et al., 2020). This allowed for a way to summarize segments of data. Next, Sackett applied Second Cycle coding, or pattern coding, to group the initial codes into themes. van Manen described this theme development as giving shape to the shapeless in the data.
We followed van Manen’s (2016) recommendation that for deeper understanding, a peer may read a draft of the description of the phenomenon and share their insights of whether the description resonates with their own experience of the participants’ descriptions. As such, Mack, who had conducted the interviews, and Sharma, who listened to the recordings of the interviews, read the steps of First and Second Cycle coding Sackett employed and shared their insights of how the description of the findings reflected their experience of the participants’ accounts. Through this iterative process, we were able to examine, reinterpret, and reformulate themes while keeping in mind van Manen’s guiding question for this process of whether the phenomenon would still be the same if we were to change or delete any theme. We followed van Manen’s advisement to be mindful to capture individual experiential differences in our data analysis and writing process of the phenomenon. In this study, that meant considering the unique identities of each participant, including intersecting identities and how those may impact their experience of microaggressions from clients. We chose to structure our writing of the phenomenon thematically, one of van Manen’s suggestions for organizing the portrayal of the data. There is some overlap in the nuances of the meanings of the themes, as describing a phenomenon is bound to have a somewhat forced quality.
Methodological Integrity
As suggested by van Manen (2016), the researchers engaged with each other throughout the entire process of data collection and analysis in a collaborative way that led to deeper understanding of the phenomenon. This process strengthened our engagement with the phenomenon and transcended the limits of having a sole researcher. In doing this, we had regular phone calls, video meetings, and emails throughout the study. Sackett kept a reflective journal while listening to the interviews and conducting analysis. Further, we kept a log of each step in the process, including interview data, codes, and theme development, to show the culmination of our interpretation of the findings. Finally, we conducted two member checks through email with each participant. Member checks allowed participants to reflect on the transcripts of the interviews for further insight and to review the themes and allow for feedback on if it was an accurate description of what the experience is like (van Manen, 2016). Therefore, we conducted member checks after interviews were transcribed and after theme development. In the second member check, we invited participants into dialogue around whether the themes reflected their experience of the phenomenon.
Findings
Five themes emerged from our exploration of CITs’ experiences of microaggressions from clients in the counseling process: (a) internal reactions, (b) attempts to contextualize, (c) prevalence of microaggressions, (d) navigating microaggressions, and (e) seeking support. The first theme, internal reactions, had three subthemes: caught off guard, discomfort, and imposter phenomenon. The fourth theme, navigating microaggressions, had five subthemes: fear of responding genuinely, letting it go, attempting to redirect, directly responding, and avoiding. The final theme, seeking support, had three subthemes: site, university, and family and peers. Pseudonyms chosen by the participants are used throughout the Findings section to maintain participants’ confidentiality.
Internal Reactions
The first theme, internal reactions, embodies what was happening internally with CITs as they experienced microaggressions in the counseling process. This theme includes subthemes centered around being caught off guard, feeling discomfort, and experiencing imposter phenomenon.
Caught Off Guard
The first subtheme of internal reactions CITs experienced, caught off guard, describes the initial reaction from the microaggression and not being sure how to react outwardly. David cautiously described his reaction to a parent in a school counseling setting as “mostly just confusion and not really being sure how to respond in that particular situation to what the parent had said.” Wesley, on the other hand, also in a school counseling setting, carefully described trying to manage being caught off guard with how he responded nonverbally in the moment:
I put on my poker face. Nonverbally, eyes kind of narrow, brows furrow. . . . [if] they catch me off guard, like one eyebrow goes up. But because . . . of the mask [from the pandemic], they can’t really read my facial expression, they can only see my eyes.
Discomfort
CITs also conveyed feeling discomfort in their internal reactions to microaggressions, including anxiety, fear, hurt, sadness, and anger. Lila solemnly described her surprise and discomfort with a client making assumptions of her based on ethnicity as “not ashamed, but saddened that she made that difference between us. I didn’t think she would have done that.”
Imposter Phenomenon
The third subtheme that resonated with CITs’ experiences in terms of internal reactions was imposter phenomenon. CITs often felt microaggressions from clients made them question their competency and even confirmed doubts they already had in the counselor role, as David thoughtfully articulated:
I think this goes back a little bit to the imposter syndrome that a lot of interns feel, and that I know that I’ve certainly felt. It’s like someone seeing me for who I am and confirming all the different feelings that I have about myself. About maybe not being fully capable in the role yet. . . . very much like, “oh you’re seeing me for who I am” and feeling . . . “I agree with you. You’re seeing how I see myself in some situations.”
Attempts to Contextualize
The next theme, attempts to contextualize, captures CITs’ tendency and desire to try to make sense of the client microaggression and to understand where the client was coming from and why they may have felt that way or may have said those things. For instance, Lila rationalized—while not excusing the microaggression from her client—“I guess the moment when she said that she was ill, and she was going through a lot of issues. So, I kind of understand her, but I don’t think there was a need of saying stuff like that.” Riley came from the perspective that it is part of a counselor’s role to seek to understand the microaggression:
I see where individuals come from and . . . my job will be to understand the perspective of the other individual . . . and show that type of unconditional positive regard and that unconditional empathy toward them. And kind of look at things from their view. I try not to take things . . . too hard. Because it was just the way they were raised.
Prevalence of Microaggressions
The next theme encompasses CITs’ perspectives that microaggressions are part of their lives and ongoing experiences, and in some cases they described feeling a bit numb or resigned to microaggressions. Riley said that she “didn’t feel anything. I was just like, ‘here this guy goes again.’ I wasn’t frustrated because I didn’t feel my face getting hot. . . . Typically when I get frustrated, my ears start to burn.”
Wesley underscored the prevalence of these experiences in his world, too: “At this point, nothing really surprises me. Maybe it’s me putting on a pair of rose-colored glasses and just using the glass to filter through whatever microaggressions come at me at this point.” He expressed feeling like he had experienced enough microaggressions to “kind of become numb to it. . . . it happens, and you don’t even pay it any mind, especially living in the South.”
Navigating Microaggressions
The next theme speaks to how CITs navigated, or thought about navigating, the microaggressions with clients. These responses ranged broadly from fear of responding genuinely to letting it go, attempting to redirect, directly responding, or avoiding.
Fear of Responding Genuinely
The first subtheme captures the participants’ fear of responding genuinely to clients, even when in some cases they would have liked to. Some of this fear centered on participants’ awareness that they may be playing into stereotypes held by clients if they were to respond genuinely, as Riley richly articulated:
That really bothers me . . . I tend to find myself taking a moment to myself, and I’ll be like, “okay, you’re good” . . . “that’s okay. It’s just one thing that one person told you and maybe they were having a bad day.” So, I try to be as understanding as I can.
Riley expressed that society and the media often portray Latina women as “feisty” or “spicy,” and that she does not want to “give [someone] that satisfaction” of confirming the stereotype: “I’m not like that, you know? I’m not spicy. I’m not a food.”
Other CITs described fear of the vulnerability involved with responding genuinely to a client’s microaggression. For example, Blake explained her genuine response and surrounding fear:
And I did disclose to the client that I’m bisexual. I said, “Oh I’m, I’m bi.” But I had that like, even knowing that the client was part of LGBTQ community, I had that question of like, “Why is the client asking? Is this appropriate? What should I say? What do I do?”
Letting It Go
CITs described often letting microaggressions go for the sake of the client, the counseling, and the counseling relationship. Connecting back to the theme of attempting to contextualize the microaggression, Riley felt it was her responsibility to let it go, “because they’re [microaggressions] from clients, I understand the role as . . . as a student counselor, that I have to kind of push it aside, and bracket those feelings.” Wesley was earnest in his feeling that microaggressions from students’ parents should not get in the way of his work as a school CIT:
Yeah it’s going to take the focus off of the kid. And it’s going to make things awkward. So I’m all for teaching people, but there’s a . . . moment in time when it’s appropriate. And at this point . . . I’m just trying to get through what we’re doing so we can move on to the next parent. No . . . hard feelings, I’m not upset. I’m a little disappointed, but I’m not livid . . . let’s just move on.
Attempting to Redirect
Some CITs chose to navigate the microaggression by redirecting it back to the client or to another topic without directly addressing the microaggression. For instance, Riley spoke to her efforts to connect these incidents back to clients indirectly: “Even if it’s something said toward us, we try to find a window . . . or different backdoor type of thing to redirect whatever they are saying back to them.”
Directly Responding
There were times in the CITs’ experiences of microaggressions in counseling where there was a direct response, either by themselves, a part of the client system, or their site supervisors. CITs seemed to view these instances as reparative in the rift the microaggression created in the therapeutic relationship. For example, Wesley fondly recalled a time when a student apologized for his parent’s microaggression after the fact:
They felt that I was uncomfortable, and they felt the need to try and repair it by apologizing for their parents. So it was very validating to me as a person. And to me as a Black person, because the kid realize what their parents had [done] was out of pocket . . . I’m assuming the kid didn’t want our relationship to suffer. . . . So we talked about it. “Look it’s cool it happened, you and I are still good,” and we moved on.
In a different vein, Blake said that responding directly to a youth client questioning her sexual identity in a public area of the practice helped build trust with the client:
[If] I had hesitated, or if I had said, “oh, no, like I’m not like [that],” I think you know, I think people are perceptive and I think that would have damaged [the relationship]. Even if I’m not sure that the disclosure was an additive piece to the relationship, I think that not being forthcoming would have detracted from anything in that moment.
Avoiding
Finally, within the theme of navigating clients’ microaggressions, participants reported engaging in avoidance afterward in response. This avoidance included instances when the CIT dreaded contact with the client (or the client system) and limited contact when possible. Avoidance also showed up on behalf of the client by discontinuing work with the CIT in individual or group settings. M relayed that her site found a way to separate her and the client who microaggressed against her: “They even said . . . ‘We’re going to not put her in groups with you . . . it’s just not safe for either of you guys.’” Wesley, a school counseling CIT, somberly described parents trying to avoid him after microaggressing against him: “I’ve had a few [parents] request a different . . . counselor when they come in, because they may feel like they soured their relationship with me already. These are the parents . . . who have noticed that they . . . micro-assaulted me.”
Seeking Support
The final theme, seeking support, captures participants’ experiences (or lack thereof) of seeking and finding support from their sites, university supervisors and faculty, and family and peers.
Site
CITs often found support at their sites after experiencing microaggressions from clients. This was frequently seemingly because of physical proximity. Often CITs’ site supervisors or other counselors at the site may have witnessed the microaggression or CITs were able to debrief with someone nearby after it happened. David indicated having a quick but meaningful moment of support with his site supervisor before moving on to their next meeting. He recalled that “after the meeting my supervisor and I just kind of like gave each other a look like, ‘ooh that was kind of a strange meeting.’” M was able to debrief with her site supervisor regularly following repeated microaggressions from her client and found her guidance helpful and supportive, especially in the realm of not taking things personally. M said her supervisor encouraged her to “process it on my own, to make sure that it’s not affecting me . . . to where I can’t even use my counseling skills. Like she didn’t want me to go home at night thinking that a patient hates me.”
University
For the most part, CITs described either not taking these instances of microaggressions to university supervisors or faculty or facing unsupportive responses when they did. Blake relayed feeling shut down by a faculty member’s humor in a class discussion when she brought up how she handled a microaggression with self-disclosure:
Yeah it was a moment of . . . playful questioning of like, “Oh, that’s the decision you made?” That kind of has that implication that maybe it wasn’t the best decision without having more context, right? And I know . . . that [humor is] kind of his approach. But it was a moment, where I was . . . like, “well I don’t really feel like going further with this.”
In some cases, CITs did find helpful and supportive responses from their faculty. Riley described her professor normalizing her experience and giving her what she found to be helpful advice:
[He] told me, “Sometimes we get things like that,” and that’s when he gave me that advice of trying to redirect the question or redirect it back to the client, versus falling into the trap. Well, he called it a trap. Into that little trap they could be setting for us.
Many participants described feeling as though the microaggression was handled by themselves, at their sites, or through processing with family; thus, they felt no need to bring it up in university supervision.
Family and Peers
CITs frequently described seeking out their families, friends, and peers for support after experiencing a microaggression from a client. Lila processed her experience with her husband, who gave her advice to have more boundaries with her client and “to keep it more professional. . . . I would sometimes disclose about my personal life because she would ask. So I just stopped disclosing.” Riley expressed feeling the need to vent to friends about her experience, “like ‘What the hell was this lady thinking like telling me that?’ . . . just letting it out.”
Wesley sought support from his mother and grandmother in processing microaggressions perpetuated by students’ parents in his school counseling role. He relayed their supportive response:
It was more of a, “These things can happen, you handle it appropriately.” . . . they have had experiences with microaggressions themselves. [They] may not have known what to call them but have experienced it. And pretty much just applauded me for staying neutral, not punishing the kid for what their parents said, and not completely blasting the parent in the meeting because . . . of a joke they let out.
Discussion
In the current study, we explored six CITs’ experiences of microaggressions perpetuated by their clients in counseling settings. The findings from this study provide insight into how novice counselors experience microaggressions from their clients and choose to handle it. We hope these findings enrich the understanding of client-based microaggressions and offer important implications for CITs, counselor educators, and supervisors.
The first theme, internal reactions, reflected the ways in which participants internally processed the microaggression from their client, which is consistent with prior literature of counselors of color’s experiences with microaggressions from clients (Branco & Bayne, 2020). Interestingly, the CITs in the current study described being caught off guard—feeling confused and uncertain with how to respond—while the more seasoned counselors of color in Branco and Bayne’s (2020) study described buffering and bracing for the microaggression, as if they were prepared for it. Counselors in Branco and Bayne’s study (2020) described their readiness for microaggressions from clients was informed by their prior and extensive personal and professional experiences. Although the CITs may have experienced microaggressions in their personal lives and were used to them, as evidenced by the theme of prevalence of microaggressions, their being caught off guard may be attributable to their lack of counseling experience, and more specifically, having never experienced microaggressions from clients and having not yet learned how to navigate this issue.
The CITs further described how microaggressions from clients caused feelings of hurt, fear, anger, sadness (subtheme of discomfort), and experiences of imposter phenomenon. CITs commonly experience confusion, doubt, and worry about their own professional competencies and preparedness as counselors—sometimes internalizing issues in counseling as their own failures (Loganbill et al., 1982; McNeil & Stoltenberg, 2016). Ultimately, CITs in this study also tried to understand the microaggression from their clients’ perspectives. CITs seemed to understand that people inherit their biases from their families and ancestors and reinforce them through microaggressions, oftentimes unintentionally (Williams et al., 2021). Counselors of color in Branco and Bayne’s (2020) study expressed that they tried to make sense of the microaggression as well, and considered their clients’ worldview, racial identity development, and experiences as they evaluated how they would handle the microaggression. The degree to which CITs can consider the clients’ worldview and cultural identity development may depend on their level of professional development (McNeil & Stoltenberg, 2016) and their own identity development (Day-Vines et al., 2007; Jones et al., 2019).
The CITs in the current study described microaggressions as an ongoing part of their lives, as captured in the theme of prevalence of microaggressions. Microaggressions have been referred to as everyday racism, as they are routine and chronic for individuals of racially and ethnically marginalized populations (Williams et al., 2021). This finding is consistent with prior literature of racial microaggressions (Branco & Bayne, 2020; Haskins et al., 2015, Pierce, 1970). Our findings also extend the knowledge base about microaggressions from clients, as microaggressions can target not only race and ethnicity, but also gender, sexual orientation, age, socioeconomic class, and religion. This finding is not unexpected; as informed by the MSJCC (Ratts et al., 2016), counselors and clients possess multiple identities, both privileged and marginalized, and visible and invisible.
The CITs in this study employed a variety of strategies in navigating microaggressions from their clients. Many CITs felt discomfort in the moment, but they were fearful of responding with their genuine reactions for various reasons. Some CITs tried to redirect the microaggressive client by concentrating on the client’s presenting issue or by taking the focus of the conversation elsewhere. Some CITs directly addressed perpetrators’ microaggressions and expressed that this action helped the relationship, while others decided to forgo addressing the microaggressions altogether. In some situations, clients and CITs attempted to avoid each other following the microaggressive incident. These varying responses are not unlike those found in prior research (Branco & Bayne, 2020). A unique contribution to this study is that our participants even experienced microaggressions from clients’ parents, reflecting a larger system that may foster and perpetuate biased opinions and perspectives toward individuals with marginalized identities. When counseling children, parents play an important role in the counseling relationship, despite not being the identified client (Sackett & Cook, 2021).
The final theme, seeking support, reflected the participants’ willingness and desire to seek support for their experiences of microaggression and from whom the support was sought. CITs must decide whether to disclose an issue experienced in counseling, including microaggressions (Branco & Bayne, 2020), and with whom they trust to share this information (Cook & Welfare, 2018; Cook et al., 2019). Some counselors in Branco and Bayne’s (2020) study spoke of seeking support (i.e., coworker, friend), while others did not and chose to process the event independently. The response of the CITs in our study was also somewhat mixed in this regard, as some CITs sought guidance from professionals at their site or, less often, from university faculty or supervisors, while others sought support from individuals in their personal lives. Given that our participants were trainees, it is not unexpected that they would seek guidance from someone more experienced, like a supervisor (McNeil & Stoltenberg, 2016), though interestingly many CITs did not choose to bring these situations to a university supervisor or faculty member. Further, the participants’ satisfaction with the support that they received, especially from their university, varied greatly. Although some participants felt validated, others felt unsupported. It remains to be seen how the response of the supervisors might inform participants’ actions in the future, although Cook et al. (2019) found that CITs who disclosed a salient concern to their supervisors and felt unsupported may be less willing or unwilling to bring up similar issues in the future with the same supervisor.
The finding that CITs in this study were discussing the microaggressions with family and peers must be carefully considered, even though this finding is not entirely unexpected. Ladany et al. (1996) found that CITs commonly discussed issues withheld from their supervisors with peers and friends, although these people were most often also in the mental health field. Further, studies have found that counselors with marginalized identities value the support of others with shared identities (Branco & Bayne, 2020; Haskins et al., 2015). However, like other scholars (Ladany et al., 1996), we wonder how a CIT’s professional development or client’s care might be impacted by heeding the advice of or seeking support from someone who does not possess the necessary training or is bound to the same ethical and professional mandates as a clinical supervisor or infield peer.
Limitations
There are limitations to this study that are important to note. Although researchers recruited participants from CACREP-accredited programs from across the United States, the resulting sample consisted of only those from the Southern region. CITs’ experiences with microaggressions in this region may be different from those in other parts of the country. Next, we did not explicitly ask about participants’ targeted identities; this information was inferred from participants’ experiences. Although a plethora of existing research focuses on racial microaggressions, we acknowledge that our participants also spoke about other marginalized identities that were salient to them. Additionally, although our sample size was congruent with the constructivist philosophical stance and scope of the study (Boddy, 2016), the sample was relatively small. Counselor educators should consider the transferability to CITs with marginalized identities working with clients of privileged identities. Finally, given van Manen’s (2016) recommendation for an interpretive conversation with participants around the identified themes, scheduling a verbal conversation with each participant for the second member check may have allowed for more input from participants on the findings.
Implications for CITs, Counselor Educators, and Supervisors
Readers will need to determine, along with the researchers’ description, the naturalistic generalizability of these study findings to their contexts (Hays & McKibben, 2021). However, the findings from this study offer several notable implications for CITs. As with the participants in this study, CITs experiencing uncertainty with how to respond to microaggressions from clients should be expected, given that microaggressions can be difficult to identify and rectify because of their nebulous nature (Williams et al., 2021) and given the lack of training CITs receive on how to navigate these complex issues (Haskins et al., 2015). Further, learning how to best attend to cultural issues in the counseling relationship is a learned skill (Ratts et al., 2016) that is gained through curiosity, intentional learning, lived experience, and continued professional development (McNeil & Stoltenberg, 2016). As evidenced by findings from this study, as well as other studies (e.g., Branco & Bayne, 2020), counselors choose to respond to microaggressions from their clients in a multitude of ways, including offering no response at all. How best to respond to microaggressions is ultimately the choice of the CITs themselves, including the degree to which they discuss their experience and with whom. For example, CITs must consider their position of power in the counselor role, the impact of any decision on the counseling relationship, the intentionality of clients’ microaggressions, and their own emotional well-being
(Pierce, 1970). Given the complexity of this decision, there may be some useful strategies to help inform CITs’ decisions in how to best respond (Hernández et al., 2010; Nadal, 2011).
CITs may find it helpful to broach cultural identities with their clients at the beginning of their working relationship (Day-Vines et al., 2007). By inviting and normalizing conversations of cultural differences, it may make it easier for both parties to openly discuss microaggressions when they occur. CITs may also find it helpful to model humility in the counseling relationship by correcting their own assumptions about clients (Marbley, 2004). Broaching is a skill and a form of immediacy, or processing the here and now of the counseling relationship, which has been found meaningful in the counseling relationship and the counseling process to clients (Sackett & Lawson, 2016; Sackett et al., 2012) and CITs (Sackett et al., 2012). We believe CITs can harness the skill of immediacy (i.e., broaching) to address microaggressions with clients when they occur in counseling. But first, they need to be taught skills to disarm and dismantle microaggressions to reduce the harm and distress they may cause (Sue et al., 2019). Although the onus is not on CITs who experience microaggressions to always address them in the moment, developing a clinical skillset to educate clients on how to recognize their biases, challenge erroneous beliefs that undergird microaggressions, and develop empathy with those they have harmed is important to mitigating the risk of burnout among CITs with marginalized identities (Williams, 2020).
The findings from this study also offer important implications for counselor educators and supervisors. Fickling et al. (2019) contended that the MSJCC framework (Ratts et al., 2016) should be explicitly integrated into clinical supervision. These findings might also provide a rationale for counselor educators to consider how to infuse the MSJCC framework into their classrooms to better prepare students for microaggressions from clients. Specifically, counselor educators and supervisors can examine with CITs how a counselor holding a marginalized identity can engage with a client holding a privileged identity in a counseling relationship, including discussing or role-playing various scenarios and ways to manage microaggressions from clients (Branco & Bayne, 2020). Encouraging counselor self-care strategies (Sue et al., 2019) in processing these scenarios is critical.
Haskins and colleagues (2015) found that counselor educators acknowledged their curriculum was tailored for White students to work with White clients, even if unintentionally. Counselor education program faculty may apply critical race theory tenets to their curriculum to challenge the dominant White discourse in counselor education, as advised by Haskins and Singh (2015). Our findings highlight the value of training related to CITs’ other marginalized identities as well (e.g., gender, sexual orientation, religion, first language) when working with clients of various privileged and/or visible identities, a need identified by Branco and Bayne (2020). The absence of education on navigating microaggressions may lay the foundation for marginalized students to feel as though their experiences are misunderstood or unwelcomed by faculty or supervisors. The current study provides counselor educators and supervisors with information from CITs on how they experience the counseling process when the dynamics of clients with privileged identities and counselors with marginalized identities are present and political (Ratts et al., 2016). Our study findings fill a gap in the literature of the experiences of CITs who encounter clients who offend and perpetuate microaggressions against them while in session.
Because CITs and supervisees control what they share in supervision, fostering an environment that promotes supervisee disclosure is critical (Cook & Welfare, 2018). Studies of intentional nondisclosure (i.e., supervisees’ purposeful withholding of salient information in supervision; Cook & Welfare, 2018; Ladany et al., 1996) found that supervisors can best mitigate supervisees withholding information by attending to the supervisory relationship and demonstrating cultural humility (Cook & Welfare, 2018; Cook et al., 2020). When a CIT voices concerns related to their identities (i.e., a microaggression), counselor educators and supervisors have an opportunity to support such disclosure in a way that validates the CIT’s experience and encourages future disclosures (Cook et al., 2019). Jones et al. (2019) provided situational examples and related response prompts to guide counselor educators and supervisors on ways to broach cultural differences with their supervisees at the beginning of the supervisory relationship and appropriately attend to cultural issues throughout the relationship. Further, as multicultural competence is positively correlated to a stronger supervisory relationship from the supervisees’ perspective (Fickling et al., 2019), supervisors who work to incorporate the MSJCC framework into their supervision will benefit in their supervisory relationships, hopefully leading to increased disclosure of experienced microaggressions, and provision of appropriate support in navigating the CIT–client relationship.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Boddy, C. R. (2016). Sample size for qualitative research. Qualitative Market Research, 19(4), 426–432. https://doi.org/10.1108/QMR-06-2016-0053
Branco, S. F., & Bayne, H. B. (2020). Carrying the burden: Counselors of color’s experiences of microaggressions in counseling. Journal of Counseling & Development, 98(3), 272–282. https://doi.org/10.1002/jcad.12322
Chan, C. D., Cor, D. N., & Band, M. P. (2018). Privilege and oppression in counselor education: An intersectionality framework. Journal of Multicultural Counseling and Development, 46(1), 58–73.
https://doi.org/10.1002/jmcd.12092
Constantine, M. G. (2007). Racial microaggressions against African American clients in cross-racial counseling relationships. Journal of Counseling Psychology, 54(1), 1–16. https://doi.org/10.1037/0022-0167.54.1.1
Cook, R. M., Jones, C. T., & Welfare, L. E. (2020). Supervisor cultural humility predicts intentional nondisclosure by post-master’s counselors. Counselor Education and Supervision, 59(2), 160–167.
https://doi.org/10.1002/ceas.12173
Cook, R. M., & Welfare, L. E. (2018). Examining predictors of counselor-in-training intentional nondisclosure. Counselor Education and Supervision, 57(3), 211–226. http://doi.org/10.1002/ceas.12111
Cook, R. M., Welfare, L. E., & Sharma, J. (2019). Exploring supervisees’ in-session experiences of utilizing intentional nondisclosure. The Clinical Supervisor, 38(2), 202–221.
https://doi.org/10.1080/07325223.2019.1608344
Crawford, E. P. (2011). Stigma, racial microaggressions, and acculturation strategies as predictors of likelihood to seek counseling among Black college students. SHAREOK Repository. https://shareok.org/handle/11244/7357
Day-Vines, N. L., Wood, S. M., Grothaus, T., Craigen, L., Holman, A., Dotson-Blake, K., & Douglass, M. J. (2007). Broaching the subjects of race, ethnicity, and culture during the counseling process. Journal of Counseling & Development, 85(4), 401–409. https://doi.org/10.1002/j.1556-6678.2007.tb00608.x
Fickling, M. J., Tangen, J. L., Graden, M. W., & Grays, D. (2019). Multicultural and social justice competence in clinical supervision. Counselor Education and Supervision, 58(4), 309–316. https://doi.org/10.1002/ceas.12159
Haskins, N. H., Phelps, R. E., & Crowell, C. (2015). Critically examining Black students’ preparation to counsel White clients. The Journal of Counselor Preparation and Supervision, 7(3). https://digitalcommons.sacredheart.edu/cgi/viewcontent.cgi?article=1077&context=jcps
Haskins, N. H., & Singh, A. (2015). Critical race theory and counselor education pedagogy: Creating equitable training. Counselor Education and Supervision, 54(4), 288–301. https://doi.org/10.1002/ceas.12027
Hays, D. G. (2020). Multicultural and social justice counseling competency research: Opportunities for innovation. Journal of Counseling & Development, 98(3), 331–344. https://doi.org/10.1002/jcad.12327
Hays, D. G., & McKibben, W. B. (2021). Promoting rigorous research: Generalizability and qualitative research. Journal of Counseling & Development, 99(2), 178–188. https://doi.org/10.1002/jcad.12365
Hernández, P., Carranza, M., & Almeida, R. (2010). Mental health professionals’ adaptive responses to racial microaggressions: An exploratory study. Professional Psychology: Research and Practice, 41(3), 202–209. https://doi.org/10.1037/a0018445
Jones, C. T., Welfare, L. E., Melchior, S., & Cash, R. M. (2019). Broaching as a strategy for intercultural understanding in clinical supervision. The Clinical Supervisor, 38(1), 1–16.
https://doi.org/10.1080/07325223.2018.1560384
Kleist, D. M. (2017). Multiple perspectives on a phenomenon: The qualitative lenses. In R. S. Balkin & D. M. Kleist (Eds.), Counseling research: A practitioner-scholar approach (pp. 207–241). American Counseling Association.
Ladany, N., Hill, C. E., Corbett, M. M., & Nutt, E. A. (1996). Nature, extent, and importance of what psychotherapy trainees do not disclose to their supervisors. Journal of Counseling Psychology, 43(1), 10–24. https://doi.org/10.1037/0022-0167.43.1.10
Loganbill, C., Hardy, E., & Delworth, U. (1982). Supervision: A conceptual model. The Counseling Psychologist, 10(1), 3–42. https://doi.org/10.1177/0011000082101002
Marbley, A. F. (2004). His eye is on the sparrow: A counselor of color’s perception of facilitating groups with predominately White members. The Journal for Specialists in Group Work, 29(3), 247–258.
https://doi.org/10.1080/01933920490477002
McNeill, B. W., & Stoltenberg, C. D. (2016). Supervision essentials for the integrative developmental model. American Psychological Association.
Miles, M. B., Huberman, A. M., & Saldana, J. (2020). Qualitative data analysis: A methods sourcebook (4th ed.). SAGE.
Morton, E. (2011). The incidence of racial microaggressions in the crossracial counseling dyad. (Unpublished doctoral dissertation). Saint Louis University.
Nadal, K. L. Y. (2011). Responding to racial, gender, and sexual orientation microaggressions in the workplace. In M. A. Paludi, C. A. Paludi, Jr., & E. R. DeSouza (Eds.), Praeger handbook on understanding and preventing workplace discrimination (Vol. 2; pp. 23–32). Praeger/ABC-CLIO.
Nadal, K. L., Davidoff, K. C., Davis, L. S., Wong, Y., Marshall, D., & McKenzie, V. (2015). A qualitative approach to intersectional microaggressions: Understanding influences of race, ethnicity, gender, sexuality, and religion. Qualitative Psychology, 2(2), 147–163. https://doi.org/10.1037/qup0000026
Owen, J., Imel, Z., Tao, K. W., Wampold, B., Smith, A., & Rodolfa, E. (2011). Cultural ruptures in short-term therapy: Working alliance as a mediator between clients’ perceptions of microaggressions and therapy outcomes. Counselling & Psychotherapy Research, 11(3), 204–212. https://doi.org/10.1080/14733145.2010.491551
Owen, J., Tao, K. W., Imel, Z. E., Wampold, B. E., & Rodolfa, E. (2014). Addressing racial and ethnic microaggressions in therapy. Professional Psychology: Research and Practice, 45(4), 283–290.
https://doi.org/10.1037/a0037420
Owen, J., Tao, K., & Rodolfa, E. (2010). Microaggressions and women in short-term psychotherapy: Initial evidence. The Counseling Psychologist, 38(7), 923–946. https://doi.org/10.1177/0011000010376093
Pierce, C. (1970). Offensive mechanisms. In F. B. Barbour (Ed.), The Black seventies (pp. 265–282). Porter Sargent.
Prosek, E. A., & Gibson, D. M. (2021). Promoting rigorous research by examining lived experiences: A review of four qualitative traditions. Journal of Counseling & Development, 99(2), 167–177.
https://doi.org/10.1002/jcad.12364
QSR International Pty Ltd. (2018). NVivo (Version 12). https://lumivero.com/products/nvivo
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Sackett, C. R., & Cook, R. M. (2021). An exploration of young clients’ experiences in counseling with post-master’s counselors. Journal of Counseling & Development, 99(1), 72–83. https://doi.org/10.1002/jcad.12355
Sackett, C. R., & Lawson, G. (2016). A phenomenological inquiry of clients’ meaningful experiences in counseling with counselors-in-training. Journal of Counseling & Development, 94(1), 62–71.
https://doi.org/10.1002/jcad.12062
Sackett, C., Lawson, G., & Burge, P. L. (2012). Meaningful experiences of clients and counselors-in-training in counseling. The Professional Counselor, 2(3), 208–225. https://doi.org/10.15241/css.2.3.208
Shelton, K., & Delgado-Romero, E. A. (2013). Sexual orientation microaggressions: The experience of lesbian, gay, bisexual, and queer clients in psychotherapy. Psychology of Sexual Orientation and Gender Diversity, 1(S), 59–70. https://doi.org/10.1037/2329-0382.1.S.59
Sue, D. W., Alsaidi, S., Awad, M. N., Glaeser, E., Calle, C. Z., & Mendez, N. (2019). Disarming racial microaggressions: Microintervention strategies for targets, White allies, and bystanders. American Psychologist, 74(1), 128–142. https://doi.org/10.1037/amp0000296
Sue, D. W., Capodilupo, C. M., Torino, G. C., Bucceri, J. M., Holder, A. M. B., Nadal, K. L., & Esquilin, M. (2007). Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist, 62(4), 271–286. https://doi.org/10.1037/0003-066X.62.4.271
van Manen, M. (2016). Researching lived experience: Human science for an action sensitive pedagogy (2nd ed.). Routledge.
Williams, M. T. (2020). Microaggressions: Clarification, evidence, and impact. Perspectives on Psychological Science, 15(1), 3–26. https://doi.org/10.1177/1745691619827499
Williams, M. T., Skinta, M. D., & Martin-Willett, R. (2021). After Pierce and Sue: A revised racial microaggressions taxonomy. Perspectives on Psychological Science, 16(5), 991–1007. https://doi.org/10.1177/1745691621994247
Appendix
Interview Protocol
Tell me about your experience(s) where a client said something that felt like a microaggression toward you.
- What feelings came to you when you experienced the microaggression from your client?
- What thoughts came to you?
- How did you respond (verbally and/or nonverbally)?
- How did the client respond to your response?
- What occurred then?
- How do you feel this impacted your relationship with the client?
Did you process this experience with anyone? With whom did you share about this experience (peers, supervisors, faculty, friends, family, etc.)?
If you processed this with your supervisor(s), was this a doctoral student supervisor, faculty supervisor, or site supervisor?
- How did your supervisor(s) respond?
- How did your supervisor(s) encourage you to respond?
- How did you feel about that response from your supervisor(s)?
- How did you proceed after the feedback from your supervisor(s)?
If any further action was taken with your client following supervision:
- How did your client respond?
- How do you feel about how it went?
- How do you feel this impacted your relationship with the client?
Did you seek [additional] supervision following [remedial] interactions you may have had with your client?
- From whom?
- What was the feedback from your supervisor(s)?
How do you feel this entire experience impacted your relationship with your supervisor(s)?
Any other experiences?
Corrine R. Sackett, PhD, LMFT, is an associate professor at Clemson University. Heather L. Mack, LPC, works for The Well Center in South Carolina. Jyotsana Sharma, PhD, ACS, LCMHC(NH), is an assistant professor at Oklahoma State University. Ryan M. Cook, PhD, LPC, ACS, is an associate professor at the University of Alabama. Jardin Dogan-Dixon, PhD, is a Correctional Psychologist for the Federal Bureau of Prisons. Correspondence may be addressed to Corrine R. Sackett, 225 S. Pleasantburg Dr., Suite D-1, Greenville, SC 29607, csacket@clemson.edu.
