Nov 9, 2021 | Volume 11 - Issue 4
Dana L. Brookover
Access to school counseling services leads to access to college-readiness counseling initiatives, including science, technology, engineering, and mathematics (STEM) education–focused counseling for students. School counselor caseload and percentage of time spent on college-readiness counseling were analyzed in relation to longitudinal STEM postsecondary outcomes of students in a nationally representative sample. Access to school counselors who spend 21% or more of their time on college-readiness counseling predicted persistence and attainment of a STEM postsecondary degree. The current results offer implications for school counselors, counselor educators, and future researchers, including the need for STEM self-efficacy interventions, unbiased curriculum, and professional development on STEM counseling for school counselors; and the call for a more nuanced understanding of this topic.
Keywords: STEM, school counseling, college-readiness counseling, longitudinal, self-efficacy
College and career readiness are key outcome targets of school systems across the United States (Malin et al., 2017; U.S. Department of Education, 2010). Science, technology, engineering, and mathematics (STEM) initiatives are also a national priority (The White House, Office of Science and Technology Policy, National Science and Technology Council, 2018). School counselors play an integral role in their students’ college readiness through providing college-readiness counseling (Gilfillan, 2017). This includes the important role school counselors perform in educating students on the possibilities in STEM at the college level (Cabell et al., 2021; Schmidt et al., 2012).
STEM Education
STEM education has been described by Tsupros and colleagues (2009) as an interdisciplinary approach to learning science, technology, engineering, and mathematics that includes understanding and knowledge of science and math concepts, computers, and problem-solving skills. There have been long-standing calls for a more STEM-literate workforce, a more diverse STEM workforce, and more individuals interested in working in the STEM fields in general (Mohr-Schroeder et al., 2015).
STEM education attainment and persistence is an emerging topic in the career development and counseling profession, but there are differing opinions on what constitutes the “STEM crisis” (Xue & Larson, 2015). Some researchers have indicated that the demand for STEM workers in the United States will not be met because of a lack of qualified and interested individuals to step into these positions. Another viewpoint emphasizes that research has indicated there are both shortages and surpluses of STEM workers, depending on the particular job market segment (Xue & Larson, 2015). Still, the data is clear that there is a “STEM crisis” in terms of inequities in who is matriculating into and persisting in STEM majors (National Science Foundation [NSF], 2021).
Despite the great growth in traditionally underrepresented students persisting in STEM majors in college (NSF, 2021) and the potential for career development initiatives to increase retention in STEM for minority groups (Belser et al., 2018), there are still disparities in STEM college major attainment and persistence by gender, race and ethnicity, socioeconomic status (SES), and first-generation college student (FGCS) status (Chen, 2013). This is an equity issue, as the choice to enroll in a STEM postsecondary program may also lead to higher pay and the potential for positive job marketability given the projected growth in available positions (Cataldi et al., 2014; Vilorio, 2014). Hence, school counselors are called upon to address STEM education disparities in their work, as the American School Counselor Association (ASCA; 2019) emphasizes the role of the school counselor in working to ensure equitable postsecondary opportunities and outcomes for all students.
College-Readiness Counseling and STEM Education
High school counselors are in a unique position to provide career-readiness counseling, including college-readiness counseling for those students who aim to attend college after high school. College-readiness counseling involves developmentally appropriate counseling that engages students in (a) creating postsecondary goals and expectations, (b) building an awareness of interests and abilities, and (c) receiving information and support for their college access and success (Savitz-Romer, 2012). School counselors can focus on STEM education with students in each of these tasks.
Research has shown that students’ intent to pursue a STEM career already varies by populations as early as the ninth grade. Girls and students in minority racial groups, in a nationally representative sample, were less likely to expect to work in a STEM discipline at the age of 30 as compared to boys and White students (Mau & Li, 2018). Students’ SES also predicted STEM career aspirations, in that a student with higher SES was more likely to aspire to a STEM career (Mau & Li, 2018). There are multiple potential reasons for the opportunity gaps in STEM higher education, including lack of engagement in higher-level STEM coursework in high school, the time it takes to complete STEM programs, and a student’s lack of financial ability to do so, as well as attitudinal factors, such as motivation and confidence. These factors can lead to less matriculation into a STEM major and more attrition (Chen, 2013). There may also be a lack of support and encouragement and even direct discouragement from educators for underrepresented minorities and women to engage in STEM coursework, starting in adolescence (Grossman & Porche, 2014). This was echoed in a qualitative study in which high school counselors said that a barrier in their work supporting underrepresented students in STEM was a lack of anti-racist curricula in STEM classes and inconsistencies in anti-racist practice by teachers (Cabell et al., 2021). The importance of college-readiness counseling focused on STEM education is known.
Existing STEM Education–Focused College-Readiness Counseling Research
Emerging research is developing on the school counselor’s role on students’ STEM self-efficacy and students’ pursuit of postsecondary STEM education (Cabell et al., 2021; Falco, 2017; Falco & Summers, 2019; Schmidt et al., 2012). Falco (2017) provided a conceptual framework with the goal of helping school counselors better support STEM career development for all students and especially those from underrepresented groups. Falco suggested school counselors can encourage students to take advanced-level math and science courses, provide classroom instruction on the benefits of engaging in STEM, ensure balanced gender and racial/ethnic ratios in STEM classes, and organize a peer mentoring program or conduct small group counseling on relevant skills.
Cabell and colleagues (2021) interviewed high school counselors about their work with underrepresented students and STEM education. The participants were actively engaging in college-readiness counseling focused on STEM education with students, but there were barriers to their ability to support underrepresented students’ STEM interests, including lack of time, in part from administrative tasks, and large caseloads (Cabell et al., 2021). This is related to previous research suggesting that the percentage of time spent on college-readiness counseling differs by school characteristics. For example, private school counselors typically spend more time on it than public school counselors, and school counselors with more students on free-and-reduced lunch tend to spend less time (Clinedinst & Koranteng, 2017). Smaller caseloads have also been associated with school counselors spending more than half their time on college-readiness counseling (Engberg & Gilbert, 2014). Further, smaller caseloads show improved college outcomes, including higher rates of 4-year college enrollment (Engberg & Gilbert, 2014; Hurwitz & Howell, 2014).
Schmidt and colleagues (2012) also provided suggestions for school counselors to “expand their repertoire” through STEM-focused career development. Key impact areas include academic and career counseling, and leadership and advocacy. The researchers acknowledged how school climate and the large administrative demands (i.e., duties inappropriate for counselors) placed on school counselors may restrict their ability to engage in career-related and STEM course discussions with students. However, there is no data to shed light on the long-term impacts of this barrier and how their suggested key impact areas influence student outcomes.
Research has found that self-efficacy is an important pathway to students’ STEM major persistence (Lent et al., 2016; Rittmayer & Beier, 2009). Self-efficacy is an individual’s belief in their ability to influence and control the events of their life to obtain desired performances (Bandura, 1994). As an example, when students believe they can achieve desired results in science through their abilities and actions, this is considered high science self-efficacy. Researchers have detailed the results of a career group intervention that incorporated the sources of self-efficacy and addressed perceived career barriers with the goals of improving the career decision self-efficacy and STEM self-efficacy for adolescent girls (Falco & Summers, 2019). Components of the intervention included a group counseling structure, career psychoeducation, journaling, constructing a timeline of successful previous performances, progressive muscle relaxation, vicarious learning, and verbal persuasion by the leader. Results showed significantly different improvements in career decision self-efficacy and STEM self-efficacy. The results of this intervention are promising, especially as it is one of the few empirical studies on self-efficacy counseling interventions and STEM career outcomes with adolescents. The sample was all female with half of the sample identifying as Latina (Falco & Summers, 2019).
It follows that there needs to be access to school counseling services for engagement in college counseling that can effectively bolster students’ STEM aspirations. Given the potential for high school STEM interventions to make a great impact in student’s STEM self-efficacy and education outcomes, the inability of school counselors to provide college counseling, and specifically STEM-focused college counseling, is troubling (Falco & Summers, 2019). To move forward in advocating for school counseling access to promote student outcomes in the STEM pipeline, a theory-driven, longitudinal approach to investigating the impact of school counseling access on this outcome was initiated in the current study. Given the importance of considering student characteristics, environmental inputs, and self-efficacy in STEM matriculation, attainment, and persistence, social cognitive career theory (Lent et al., 1994) served as a logical base for the theoretical framework for this investigation.
Social Cognitive Career Theory
Social cognitive career theory (SCCT) was developed from Albert Bandura’s (1986) social cognitive theory to create a unifying theory of career and academic interest, choice, and performance (Lent et al., 1994). SCCT accounts for the cyclical nature of making a career choice through accounting for people receiving information from contextual influences that fuel feedback loops (Lent, 2004). These external influences can be contextual supports or barriers (Lent et al., 2000). It is also important to note that one’s perception of barriers moderates the relationship between interests and career choices (Brown & Lent, 1996). Hence, underrepresented and underserved students’ perceptions of barriers in obtaining a STEM degree can impact career choice and development. Moreover, other background environmental influences, person inputs, and behaviors interact in this feedback loop as well. One influence of utmost importance in the theory is self-efficacy. Thus, SCCT can account for external factors, otherwise known as proximal environmental influences (e.g., school counseling access), and individual characteristics (e.g., demographics and self-efficacy) within long-term career development formation.
Purpose of the Study
The current study was built upon previous SCCT school counseling and STEM attainment and persistence studies. The goal was to investigate the long-term impacts of school counseling access, in relation to student characteristics, on STEM outcomes. The research question guiding the study was: Do school counselor caseload and percentage of time spent on college-readiness counseling predict STEM major attainment and persistence?
Method
Using a multivariate, quantitative, longitudinal research design to answer the research question was well-suited to the purpose of the study. Longitudinal research designs allow for gathering and analyzing data on development over time (Lavrakas, 2008). As the research question was focused on prediction in a sample of students and the outcome was measured quantitatively, this research design was employed. I followed the process of secondary analysis of existing data (Cheng & Phillips, 2014), utilizing the High School Longitudinal Study of 2009 (HSLS:09), developed by the National Center for Education Statistics (NCES; 2020a). The HSLS:09 dataset followed a sample of high school students throughout their secondary education career into postsecondary years (NCES, 2020b).
Participants and Sampling
The HSLS:09 is a longitudinal study of over 23,000 ninth graders from 944 schools (Ingels & Dalton, 2013; NCES, 2020b). Stratified random sampling ensured a nationally representative sample. Approximately 900 high school counselors were surveyed for the study to provide information on their school counseling departments, including school counselor caseload and percentage of time spent on college-readiness counseling. School counselors in the study were not randomly selected; rather, they were either the lead counselor or the counselor deemed most knowledgeable about the ninth graders at the time of the baseline data collection (Ingels & Dalton, 2013). The baseline data was collected in 2009, then the study had a first follow-up survey with student participants in 2012; there was a brief 2013 update survey and a second follow-up in 2016 (Duprey et al., 2018).
Data Selection
Cheng and Phillips’s (2014) steps for secondary analysis of existing data under the research question–driven approach guided the data collection procedures for the current study. Thus, I determined which variables in the existing dataset to use to answer the research question. This was done through using SCCT to guide the model creation. Then, I became acquainted with the coding patterns of variables. This led to the transformation of distributions of select variables to meet assumptions of the model to be used in analysis when necessary, as detailed below.
Constructs and Variables
The HSLS:09 variables (NCES, 2020a) included in the current study both cover the research question and fit within the theoretical framework (i.e., SCCT; Lent et al., 1994). First, there are demographic variables, also known as person inputs and background environmental influences, within SCCT. Data on variables to represent self-efficacy constructs were also selected. Two variables measured school counselor caseload and school counselor percentage of time spent on college-readiness counseling. Finally, the outcome variable was STEM major attainment and persistence.
First-Generation College Student Status
The FGCS status variable was constructed as a variable detailing the highest level of education achieved by either parent/guardian in the sample member’s home in the HSLS:09 dataset. This was created from two composite variables within the dataset: highest education level of Parent 1 and highest education level of Parent 2. In its original categorical form, there are seven categories for parent highest level of education, but for the current study, it was recoded into a dichotomous/dummy variable; either the student had a parent in the home who has a bachelor’s degree or a more advanced degree, or the student did not have a parent in the home who has a bachelor’s or a more advanced degree.
Race/Ethnicity
Race/ethnicity information was provided through dichotomous race/ethnicity composites based on data from the student questionnaire, if available. If not available from the student questionnaire, they were based on, in order of preference: data from the school-provided sampling roster or data from the parent questionnaire. The designations included in the HSLS:09 and the current study are: (a) American Indian or Alaskan Native; (b) Asian; (c) Black (African American); (d) Hispanic, no race specified; (e) Hispanic, race specified; (f) more than one race; (g) Native Hawaiian/Pacific Islander; and (h) White. For the current study, the two Hispanic categories were combined.
Sex
This variable was categorical and referred to the sex of the sample member (male or female) and was provided by the student if possible, and if not, the parent or school roster. The labels male and female have held and continue to hold “powerful associations” (Lips, 2020, p. 3), and not all people identify into a gender binary of female and male (Lips, 2020). There is a gender variable assessed in the HSLS:09 study; however, it is only available in the restricted use dataset, so the sex variable was utilized in the current study.
Socioeconomic Status
SES was a composite variable consisting of five components obtained from the parent/guardian questionnaire and aligned with previous NCES longitudinal study methods for calculating SES: (a) the highest education among parents/guardians in the two-parent family of a responding student, or the education of the sole parent/guardian; (b) the education level of the other parent/guardian in the two-parent family; (c) the highest occupational prestige score among parents/guardians in the two-parent family of a responding student, or the prestige score of the sole parent/guardian; (d) the occupation prestige score of the other parent/guardian in the two-parent family; and (e) family income. This was a standardized value set to 0; hence, values ranged from −1.82 to 2.57.
Self-Efficacy Variables
This data was collected at the baseline. SCCT asserts that learning experiences and prior accomplishments are an integral part of forming self-efficacy; hence STEM grade point average (GPA) was included under self-efficacy (Lent et al., 1994). GPA information was collected at the 2013 update.
Math Self-Efficacy. Math self-efficacy is a continuous variable, with higher values representing higher math self-efficacy. The information was assessed through a scale consisting of four items (e.g., “can do excellent job on math tests”). The variable was created through principal components factor analysis and was standardized to a mean of 0 and standard deviation of 1. Only respondents who provided a full set of responses were assigned a scale value. The coefficient of reliability (demonstrated by alpha) for the scale is .65 (NCES, 2020c).
Science Self-Efficacy. Science self-efficacy is also a continuous variable, with higher values representing higher science self-efficacy, and was also created through principal components factor analysis and standardized to a mean of 0 and standard deviation of 1. There were four items on the scale (e.g., “can master skills in science course”). Only respondents who provided a full set of responses were assigned a scale value. The coefficient of reliability (indicated by alpha) for the scale is .65 (NCES, 2020c).
STEM GPA
STEM GPA, an interval variable, was computed during the 2013 update through high school transcript composites. STEM GPA values range from 0.25 to 4, in increments of 0.25.
School Counselor Caseload
Information for this continuous variable was assessed through one item on the school counselor questionnaire: “On average, what is the caseload for a counselor in this school? Students per counselor.” Students per counselor ranged from 2 to 999 (NCES, 2020c). The variable was recoded into a dichotomous variable, with 0 indicating a school counselor caseload of 250 or less, and 1 indicating a school counselor caseload of 251 or more. The ASCA-recommended caseload number for school counselors is 250:1.
School Counselor Percentage of Time Spent on College-Readiness Counseling
This was assessed through one item on the school counselor questionnaire that read, “Last school year (2008–2009), what percentage of work hours did your school’s counseling staff spend assisting students with college readiness, selection, and applications?” Responses were reported according to the following categories: 5% or less, 6%–10%, 11%–20%, 21%–50%, and more than 50%. This was recoded to a dichotomous variable—20% or less time spent on college-readiness counseling or 21% or more time spent on college-readiness counseling—reflecting a cut-off of the national average of time spent on college-readiness counseling by school counselors at 21% (Clinedinst & Koranteng, 2017).
Outcome Variable: STEM Major Attainment and Persistence
This was a dichotomous variable (either Not STEM or STEM) and was collected in the second follow-up study in 2016 (i.e., approximately 3 years post–high school graduation). It referred to how the respondent declared or decided upon their degree and whether that undergraduate degree or certificate is in a STEM field of study.
Data Analysis
Continuing to follow Cheng and Phillips’s (2014) steps for secondary analysis of existing data, the first step in data analysis was to run preliminary analyses of descriptive statistics and bivariate correlations. Then, I assessed missing data patterns. When deemed necessary, the HSLS:09 developers did utilize imputation of values (Ingels & Dalton, 2013). Imputation allows the use of all study respondent records in an analysis, affording more power for statistical tests. Additionally, if the imputation procedure is effective, then the analysis results can be less biased than if there were missing data unaccounted for (Ingels & Dalton, 2013). Value imputation occurred in place of missing responses for select variables identified from the student and parent questionnaires through single-value imputation (Duprey et al., 2018; Ingels & Dalton, 2013). Further, the NCES provides analytic weighted variables and replication weights associated with those main sampling weights. The analytic weights make estimates from the sample data representative of the target population (i.e., ninth grade students in 2009–2010). These analytic weights account not only for differential selection probabilities, but also for differential patterns of response and nonresponse—in other words, nonresponse bias (Duprey et al., 2018). In addition to the analytic weight variables accounting for stratified sampling and nonresponse bias, replication weight variables address standard error concerns. Standard error calculation ensures appropriate standard errors based on the differences between the estimates of the full sample and a series of replicates (Duprey et al., 2018). These replication weights are done with the balanced repeated replication method and help account for the possibility of artificially low standard errors due to clustering in sampling (Duprey et al., 2018).
Prior to running the sequential logistic regression, assumptions testing was completed. Logistic regression analyses allow the use of criterion measures on a binary outcome (Meyers et al., 2017). The result of a logistic regression is the impact of each variable on the probability of the observed event of interest (Sperandei, 2014). Sequential logistic regression allows the researcher to specify the entry order of predictor variables into the model (Tabachnick & Fidell, 2013).
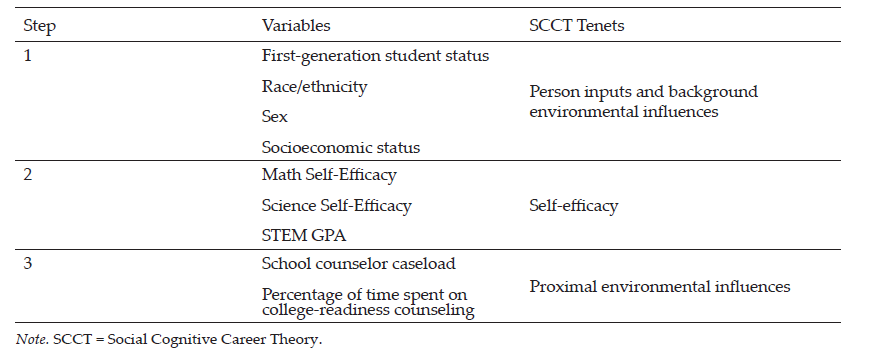
Model 1, the baseline model, represented person inputs and background environmental influences in SCCT. It included the following variables: FGCS status, race/ethnicity, sex, and SES. Model 2 represented self-efficacy, after controlling for person inputs and background environmental influences. Self-efficacy variables included math self-efficacy, science self-efficacy, and STEM GPA. Model 3 examined school counseling access, after controlling for the variables in the previous two models. School counseling access variables were school counselor caseload and school counselor percentage of time spent on college-readiness counseling. Table 1 displays the model steps and variables.
Table 1
Logistic Regression Model Steps
Results
The aim of the current study was to examine the predictors of STEM major attainment and persistence, including school counselor caseload ratio and percentage of time spent on college-readiness counseling. First, preliminary analysis included running descriptive statistics and a correlation matrix.
Preliminary Analysis
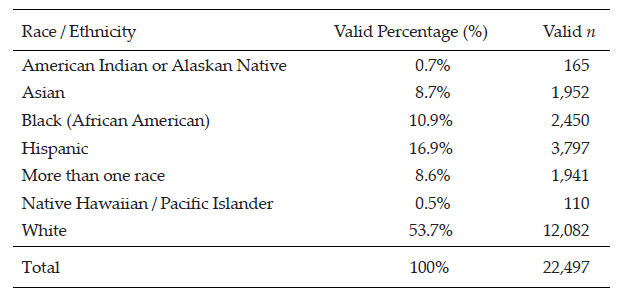
Frequencies and percentages on the variables’ unweighted, valid data (i.e., data before weights were applied and not including missing data) are reported in this section. First, descriptive statistics on person inputs and background environmental influences (i.e., student demographics) were collected. A total of 56.4% (n = 9,468) of the valid sample were FGCS, and 43.6% (n = 7,314) were non-FGCS. A total of 50.9% (n = 11,973) of the sample were identified as female, and the remaining 49% (n = 11,524) as male. The continuous SES variable ranged from −1.93 to 2.88, with a mean score of 0.05 (SD = 0.78). For information on participants’ race/ethnicity, see Table 2.
Table 2
Participant Race and Ethnicity Variable Percentages and Frequencies
Math self-efficacy scores ranged from −2.92 to 1.62 (M = 0.0421, SD = 0.96). Science self-efficacy scores ranged from −2.91 to 1.83 (M = .0372, SD = 0.99). In terms of STEM GPA, the range was 0.25 through 4.00, reported in intervals of 0.25 (M = 2.43, SD = 0.93).
The school counselor caseload in the current study had a mean score of 347.65 students (SD = 130), ranging from 2–999. The median was 350. The school counselor percentage of time spent on college-readiness counseling scores ranged from 1–5 (M = 3.37, SD = 0.95). A total of 2.3% (n = 484) chose 5% or less, and 16.2% (n = 3,389) of the sample chose 6%–10%. A total of 33.8% (n = 7,094) indicated 11%–20%, followed by 37.5% (n = 7,867) choosing 21%–50%. Finally, 10.2% (n = 2,132) of the sample chose the more than 50% option.
For the STEM major persistence and attainment variable, 23% (n = 2,658) of the valid sample were enrolled as a STEM major or had attained a STEM degree as of February 2016, and 77% (n = 8,902) were neither enrolled as a STEM major nor had attained a STEM degree as of February 2016.
Bivariate Correlations
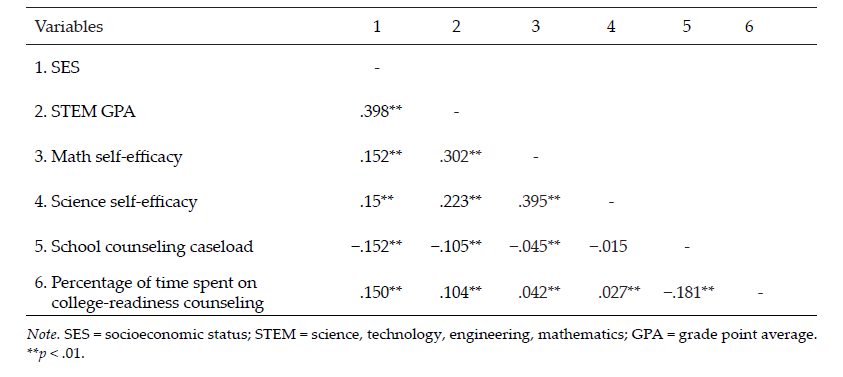
A bivariate correlational analysis of interval and ratio variables in the study allowed for preliminary examination of collinearity and provided information on relationships between the variables of interest. The bivariate correlation matrix indicated no concerns regarding multicollinearity. The correlations contain indications of relationships to school counseling access. For example, school counseling caseload and percentage of time spent on college-readiness counseling were inversely related (r = −.181, p < .01). School counselor caseload was negatively significantly correlated to SES, STEM GPA, and math self-efficacy. School counselor percentage of time spent on college-readiness counseling was positively significantly correlated with SES, STEM GPA, math self-efficacy, and science self-efficacy. See Table 3 for the full results of the bivariate correlations.
Table 3
Bivariate Correlations
Primary Analysis
Next, the results of the sequential logistic regression are presented (see Table 4). The outcome variable is a dichotomous variable of STEM major persistence and attainment and indicated if a student either is or is not enrolled as a declared STEM major in a postsecondary institution or has or has not attained a degree in a STEM field from a postsecondary institution.
Statistical assumptions of the model were assessed. Tolerance (0.26) and VIF values (mean VIF = 1.34) indicated no concerns regarding multicollinearity. The Box-Tidwell test indicated the assumption of a linear relationship between continuous predictors and the logit transform of the outcome variable was met, with nonsignificant p values. Utilizing the balanced repeated replication variance estimation method, 16,007 observations were included in the regression model, with a population size of 1,540,118 and 192 replications.
Table 4
Logistic Regression Model Predicting STEM Major Attainment and Persistence
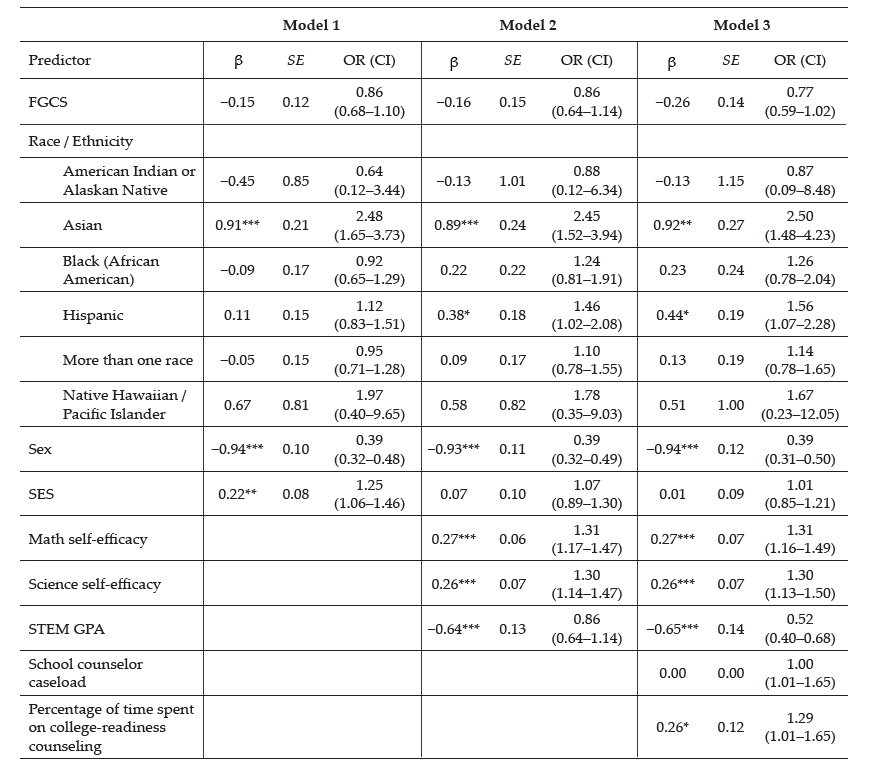
Note. Model 1 = person inputs and background environmental influences (first-generation college student [FGCS], race/ethnicity, sex, socioeconomic status [SES]), without any controls; Model 2 = person inputs and background environmental influences, and self-efficacy variables (math self-efficacy, science self-efficacy, and STEM grade point average [GPA]); Model 3 = person inputs and background environmental influences, self-efficacy variables, and proximal environmental influences (school counselor caseload and percentage of time spent on college-readiness counseling). Reference categories: FGCS = non-FGCS; Sex = male; Race/ethnicity = White; STEM GPA = 3.0–4.0; Percentage of time spent on college-readiness counseling = less than 21%.
*p < .05. **p < .01. ***p < .001.
Model 1 was significant, F(9, 189) = 12.49, p < .001. McFadden’s R Square was 0.0506, indicating that the model explains 5.06% of the variance outcomes. This model indicated that SES significantly predicted STEM major attainment and persistence (β = 0.22, p < .001). In addition, female students were less likely than males to report STEM major attainment and persistence (β = −0.94, p < .001). Asian students were significantly more likely than White students to report STEM major attainment and persistence (β = 0.91, p < .001).
Model 2 was significant, F(12, 185) = 19.03, p < 0.001, McFadden’s R Square = 0.0966. STEM GPA significantly predicted STEM major attainment and persistence, with students with GPAs ranging from 0.25–2.75 being significantly less likely to report STEM attainment and persistence compared to students with GPAs of 3.00–4.00 (β = −0.64, p < .001). Both math self-efficacy (β = 0.27, p < .001) and science self-efficacy (β = 0.26, p < .001) were significant predictors of STEM major attainment and persistence, with increases in these variables resulting in higher odds of the outcome. Female sex and Asian race identity remained significant, while SES was no longer significant.
Model 3 was significant, F(14, 178) = 15.90, p < .001, McFadden’s R Square = 0.1005. For Model 3, the Archer–Lemeshow goodness-of-fit test was not significant, and the adjusted Wald test was significant, indicating good model fit. In this model, school counselor percentage of time spent on college-readiness counseling predicted student STEM major attainment and persistence, with 21% or more time spent on college-readiness counseling being more likely to result in the outcome, compared to 20% or less time spent on college-readiness counseling (β = .26, p < .05). School counselor’s caseload was not significant. Female sex, Asian race identity, STEM GPA, math self-efficacy, and science self-efficacy all remained significant predictors in the final model. The model correctly classified 77.34% of the cases, with higher specificity (95.94%) than sensitivity (19.40%).
Discussion
A sequential logistic regression analysis provided the means for exploration of the research question: Do school counselor caseload and percentage of time spent on college-readiness counseling predict STEM major attainment and persistence? Sequential logistic regression allowed for sociocultural context to be considered in the prediction of STEM career–related performance. This is important because the structure of opportunity (e.g., SES, education access, social support), socialization of gender roles, and other societal and family norms influence abilities, self-efficacy, outcome expectations, and goals within SCCT (Lent & Brown, 1996). The first model included person inputs and background environmental influences (Lent et al., 1994), including FGCS status, race/ethnicity, sex, and SES. Students of Asian race/ethnicity had higher odds of persisting in a STEM major or attaining a degree, compared to the White student reference group, which echoes previous research (Chen, 2013; Mau, 2016). SES also predicted the outcome, with students of higher SES having higher odds of STEM persistence and attainment, which is aligned with previous research on students’ SES status and STEM outcomes (Chen, 2013). Finally, female students had lower odds of persisting in a STEM major or attaining a STEM degree than male students in the model; this gender disparity in STEM academic and career-related outcomes has also been noted in the literature (Mau, 2016).
The second model extended the investigation of predictors of STEM major attainment and persistence to include self-efficacy variables (i.e., math self-efficacy, science self-efficacy) and STEM high school GPA, in addition to still accounting for the person inputs and background environmental influences. Within this second model, Asian-identifying students and female students held the same patterns of significance as in the first model, which was that Asian-identifying students had higher odds of attaining or persisting, while female students had lower odds. When accounting for the self-efficacy variables, Hispanic-identifying students then showed significantly higher odds of persisting in a STEM major and attaining a STEM degree. Previous research does not report higher odds of Hispanic student STEM major persistence and attainment (Mau, 2016; NSF, 2021). However, this result in the model suggests that when Hispanic students have equitable math self-efficacy, science self-efficacy, and STEM GPAs, their opportunity for STEM success is increased, which has been reflected in an SCCT academic persistence model with Latinx engineering student participants (Lee et al., 2015). STEM self-efficacy is an important subject for school counselors to address with students (Falco, 2017), given its influential role in STEM outcomes (Mau & Li, 2018; Shaw & Barbuti, 2010).
The second model demonstrated that as math self-efficacy and science self-efficacy scores increased, the odds of a student persisting in a STEM major or attaining a STEM degree increased significantly. Further, students with higher STEM GPAs in high school were more likely to persist in STEM majors or attain a STEM degree. This is aligned with SCCT, which suggests previous learning experiences and prior accomplishments have a positive effect on career-related outcomes (Lent & Brown, 1996). Previous research (Chen, 2013) has also suggested that lack of preparation in advanced STEM courses in high school leads to more STEM major attrition.
The final model included all previous variables and added the two school counseling access variables: school counselor caseload and school counselor percentage of time spent on college-readiness counseling. Variables that remained significant in the model, in the same directionality of odds of the outcome, were: Asian race/ethnicity, Hispanic race/ethnicity, sex, math self-efficacy, science self-efficacy, and high school STEM GPA. The final model showed women were less likely to persist in STEM majors or attain a STEM degree even when accounting for the access to school counseling variables. This gender disparity is unfortunately reflective of the extant literature on STEM outcomes (Chen, 2013). It also perhaps speaks to the barriers school counselors face when working with historically underrepresented students surrounding STEM (Cabell et al., 2021), such as a lack of encouragement from educators for girls to pursue STEM endeavors (Grossman & Porche, 2014).
In the current study, school counselor caseload was not significant in the model. This finding is not aligned with previous research that found the addition of each school counselor to a school’s staff was associated with a 10% increase in 4-year college-going rates (Hurwitz & Howell, 2014), which suggests the influence of caseload on student postsecondary outcomes, as typically more school counselors on staff results in lower caseloads. However, it is important to note that school counselor caseload did have a significant relationship with the percentage of time spent on college-readiness counseling in the current study, with more students on a caseload resulting in less time spent on college-readiness counseling, according to the bivariate correlation analysis.
School counselor percentage of time spent on college-readiness counseling was significant in the final model, and the results indicated that students who have a school counselor who spends at least the national average of time on college-readiness counseling (i.e., 21%) have higher odds of persisting in STEM majors or attaining a STEM degree. Students who have a school counselor who spends 21% or more of their time on college-readiness counseling have 29% higher odds of STEM major persistence and attainment 3 years post–high school graduation. This finding is novel in the literature. School counseling and STEM counseling is a relatively new area of research in the school counseling literature (Falco, 2017; Schmidt et al., 2012). The current study’s finding on the impact of school counselors’ college-readiness counseling on STEM outcomes extends existing research that has noted the importance of school counselors’ role in STEM counseling (Falco, 2017; Falco & Summers, 2019; Shillingford et al., 2017).
Implications
School counselors can use the results of this study to inform their STEM education–focused college-readiness counseling work. A promising result of the study was that school counselors’ percentage of time spent on college-readiness counseling was predictive of STEM major attainment and persistence. Although there were still inequities in which students were achieving this outcome, including female students. This is helpful information to lead school counselors to target intervention efforts with girls. For instance, girls may benefit from more STEM-focused occupational information and verbal persuasion (i.e., encouragement) from school counselors. These results indicate that school counselors should increase their knowledge and awareness of the barriers their female students are facing related to STEM and seek to correct those barriers. Barriers can include school climate, which school counselors can address through both the messages they themselves and all school staff are sending to their female students about STEM. In terms of consultation, it has been suggested school counselors should play an important role in working with STEM teachers to develop curricula that are unbiased and culturally sensitive to the needs of female and minority students, and the results of the study show the long-lasting effects of how a ninth-grade student perceives their self-efficacy in math and science, supporting this suggestion (Mau, 2016).
Additionally, high school STEM GPA was predictive of persisting and attaining a STEM degree. School counselors encourage high achievement from all students, and this result does not suggest that school counselors should focus their STEM career exploration on just those students who have higher STEM GPAs, assuming those with lower STEM GPAs will not want to enroll as STEM majors in college or cannot be successful once there. All students, regardless of STEM GPA, should receive STEM counseling opportunities. School counselors should also strive to create an environment that is inclusive for all students to be successful in STEM. Further, school counselors can connect their students to the resources to support their success in STEM coursework.
Math and science self-efficacy were important predictive factors of persistence and attainment in a STEM degree, and these areas of self-efficacy can be targeted through interventions with students; previous literature has provided suggestions on how school counselors can do so (Falco, 2017; Schmidt et al., 2012; Shillingford et al., 2017). Developing STEM self-efficacy is important, because when this was held constant, there were no students of different races/ethnicities who were at lower odds of persisting and attaining a STEM degree, nor did SES have an influence on outcomes. School counselors must remain vigilant of the structural inequalities underrepresented students face and remove these barriers (Wolniak et al., 2016).
The results of this study also emphasize the importance of counselor educators intentionally discussing STEM career development in the career counseling and other school counseling curriculum. Research has shown school counselors do not feel knowledgeable about careers in the STEM fields and desire more STEM content information to inform their work (Cabell et al., 2021; Hall et al., 2011). STEM counseling within the school counselor repertoire is a relatively new topic (Schmidt et al., 2012), and counselor educators must be aware of this counseling area and incorporate it into their curriculum. Additionally, the results of this study support the need for collaborations between university counseling programs and neighboring school districts to increase counseling access and improve underrepresented students’ STEM outcomes. Finally, both counselor educators and school counselors can use the results of this study, and the many others that have proven the effectiveness of school counseling, to advocate for lower counselor-to-student ratios and more funding for school counselors.
Limitations and Future Research
There are limitations to utilizing secondary analysis of existing data. Specifically, researchers are not privy to selection of the variables and the researchers’ bias can influence which variables are selected to study an outcome; there are many more variables in this dataset which could be included for an exploration of the research question (Cheng & Phillips, 2014). However, the use of the NCES-led HSLS:09 dataset allowed for an extensive number of variables for a massive longitudinal study (NCES, 2020a). A potential area for future exploration in this model could also be school counselors’ self-efficacy in college counseling and STEM counseling and how that impacts students’ outcomes. Further, causal inferences should not be assumed in logistic regression models; probability in correctly predicting an outcome does not mean that these variables cause the outcomes (Tabachnick & Fidell, 2013).
Future research studies could utilize multilevel modelling methods to account for school-level variables, such as staff-to-student ratio, percentage of students on free-and-reduced lunch, and geographic area. This would further investigate systemic influences on access to school counseling and student outcomes and could have the potential to increase the percentage of variance accounted for by the models. Additionally, there has recently been follow-up data added to the HSLS:09 dataset, which includes postsecondary transcripts; this study could be replicated with this data.
Research on school counselors and STEM is growing and should be continued. For instance, researchers have explored school counselors’ experiences regarding STEM and STEM counseling (Cabell et al., 2021; Shillingford et al., 2017). Quantitative research surrounding this topic is needed as well to measure differences in STEM counseling allocation and student STEM outcomes as a result of school counselors’ preparation and efficacy in this area. Finally, an understanding of how counselor education programs are and are not preparing their students to engage in college-readiness counseling and STEM counseling is warranted.
Conclusion
This study provides encouraging results regarding the impact of school counselors’ college-readiness counseling on students’ STEM major attainment and persistence. Results detailed how science and math self-efficacy had strong predictive power on STEM outcomes, which informs school counseling practice. Through increased training in college-readiness counseling and STEM counseling in school counseling training programs, and continued attention to a holistic model of college readiness, school counselors can continue to play an integral role in all students’ college and STEM readiness through providing college-readiness counseling (Gilfillan, 2017; Schmidt et al., 2012).
Conflict of Interest and Funding Disclosure
Data collected and content shared in this article
were part of a dissertation study, which was
awarded the 2021 Dissertation Excellence Award
by the National Board for Certified Counselors.
References
American School Counselor Association. (2019). The ASCA national model: A framework for school counseling programs (4th ed.).
Bandura, A. (1986). Social foundations of thought and action: A social cognitive theory. Prentice-Hall.
Bandura, A. (1994). Self-efficacy. In V. S. Ramachaudran (Ed.), Encyclopedia of human behavior (Vol. 4, pp. 71–81). Academic Press.
Belser, C. T., Shillingford, M. A., Daire, A. P., Prescod, D. J., & Dagley, M. A. (2018). Factors influencing undergraduate student retention in STEM majors: Career development, math ability, and demographics. The Professional Counselor, 8(3), 262–276. https://doi.org/10.15241/ctb.8.3.262
Brown, S. D., & Lent, R. W. (1996). A social cognitive framework for career choice counseling. The Career Development Quarterly, 44(4), 354–366. https://doi.org/10.1002/j.2161-0045.1996.tb00451.x
Cabell, A. L., Brookover, D., Livingston, A., & Cartwright, I. (2021). “It’s never too late”: High school counselors’ support of underrepresented students’ interest in STEM. The Professional Counselor, 11(2), 143–160. https://doi.org/10.15241/alc.11.2.143
Cataldi, E. F., Siegel, P., Shepherd, B., & Cooney, J. (2014). Baccalaureate and beyond: A first look at the employment experiences and lives of college graduates, 4 Years On (B&B:08/12) (NCES 2014-141). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. https://nces.ed.gov/pubs2014/2014141.pdf
Chen, X. (2013). STEM attrition: College students’ paths into and out of STEM fields (NCES 2014-001). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education.
https://nces.ed.gov/pubs2014/2014001rev.pdf
Cheng, H. G., & Phillips, M. R. (2014). Secondary analysis of existing data: Opportunities and implementation. Shanghai Archives of Psychiatry, 26(6), 371–375. https://doi.org/10.11919/j.issn.1002-0829.214171
Clinedinst, M., & Koranteng, A.-M. (2017). 2017 state of college admission. National Association for College
Admission Counseling. https://bit.ly/3BNizx8
Duprey, M. A., Pratt, D. J., Jewell, D. M., Cominole, M. B., Fritch, L. B., Ritchie, E. A., Rogers, J. E., Wescott, J. D., & Wilson, D. H. (2018). High School Longitudinal Study of 2009 (HSLS:09) base-year to second follow-up data file documentation (NCES 2018-140). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. https://nces.ed.gov/pubs2018/2018140.pdf
Engberg, M. E., & Gilbert, A. J. (2014). The counseling opportunity structure: Examining correlates of four-year college-going rates. Research in Higher Education, 55(3), 219–244.
Falco, L. D. (2017). The school counselor and STEM career development. Journal of Career Development, 44(4), 359–374. https://doi.org/10.1177/0894845316656445
Falco, L. D., & Summers, J. J. (2019). Improving career decision self-efficacy and STEM self-efficacy in high school girls: Evaluation of an intervention. Journal of Career Development, 46(1), 62–76.
https://doi.org/10.1177/0894845317721651
Gilfillan, B. H. (2017). School counselors and college readiness counseling. Professional School Counseling, 21(1). https://doi.org/10.1177/2156759X18784297
Grossman, J. M., & Porche, M. V. (2014). Perceived gender and racial/ethnic barriers to STEM success. Urban Education, 49(6), 698–727. https://doi.org/10.1177/0042085913481364
Hall, C., Dickerson, J., Batts, D., Kauffmann, P., & Bosse, M. (2011). Are we missing opportunities to encourage interest in STEM fields? Journal of Technology Education, 23(1), 32–46. https://files.eric.ed.gov/fulltext/EJ96
5337.pdf
Hurwitz, M., & Howell, J. (2014). Estimating causal impacts of school counselors with regression discontinuity designs. Journal of Counseling & Development, 92(3), 316–327. https://doi.org/10.1002/j.1556-6676.2014.00159.x
Ingels, S. J., & Dalton, B. (2013). High School Longitudinal Study of 2009 (HSLS:09) first follow-up: A first look at fall 2009 ninth graders in 2012 (NCES 2014-360). National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education. https://nces.ed.gov/pubs2014/2014360.pdf
Lavrakas, P. J. (Ed.). (2008). Encyclopedia of survey research methods (Vols. I–II). SAGE.
Lee, H.-S., Flores, L. Y., Navarro, R. L., & Kanagui-Muñoz, M. (2015). A longitudinal test of social cognitive career theory’s academic persistence model among Latino/a and White men and women engineering students. Journal of Vocational Behavior, 88, 95–103. https://doi.org/10.1016/j.jvb.2015.02.003
Lent, R. W. (2005). A social cognitive view of career development and counseling. In S. D. Brown & R. W. Lent (Eds.), Career development and counseling: Putting theory and research to work (pp. 101–127). Wiley.
Lent, R. W., & Brown, S. D. (1996). Social cognitive approach to career development: An overview. The Career Development Quarterly, 44(4), 310–321. https://doi.org/10.1002/j.2161-0045.1996.tb00448.x
Lent, R. W., Brown, S. D., & Hackett, G. (1994). Toward a unifying social cognitive theory of career and academic interest, choice, and performance. Journal of Vocational Behavior, 45(1), 79–122.
https://doi.org/10.1006/jvbe.1994.1027
Lent, R. W., Brown, S. D., & Hackett, G. (2000). Contextual supports and barriers to career choice: A social cognitive analysis. Journal of Counseling Psychology, 47(1), 36–49. https://doi.org/10.1037/0022-0167.47.1.36
Lent, R. W., Miller, M. J., Smith, P. E., Watford, B. A., Lim, R. H., & Hui, K. (2016). Social cognitive predictors of academic persistence and performance in engineering: Applicability across gender and race/ethnicity. Journal of Vocational Behavior, 94, 79–88. https://doi.org/10.1016/j.jvb.2016.02.012
Lips, H. M. (2020). Sex and gender: An introduction (7th ed.). Waveland Press.
Malin, J. R., Bragg, D. D., & Hackmann, D. G. (2017). College and career readiness and the Every Student Succeeds Act. Educational Administration Quarterly, 53(5), 809–838. https://doi.org/10.1177/0013161X17714845
Mau, W.-C. J. (2016). Characteristics of US students that pursued a STEM major and factors that predicted their persistence in degree completion. Universal Journal of Educational Research, 4(6), 1495–1500.
https://doi.org/10.13189/ujer.2016.040630 https://files.eric.ed.gov/fulltext/EJ1103170.pdf
Mau, W.-C. J., & Li, J. (2018). Factors influencing STEM career aspirations of underrepresented high school students. The Career Development Quarterly, 66(3), 246–258. https://doi.org/10.1002/cdq.12146
Meyers, L. S., Gamst, G., & Guarino, A. J. (2017). Applied multivariate research: Design and implementation
(3rd ed.). SAGE.
Mohr-Schroeder, M. J., Cavalcanti, M., & Blyman, K. (2015). STEM education: Understanding the changing landscape. In A. Sahin (Ed.), A practice-based model of STEM teaching: STEM Students on the Stage (SOS) (pp. 3–14). Sense. https://doi.org/10.1007/978-94-6300-019-2
National Center for Education Statistics. (2020a). High School Longitudinal Study of 2009 (HSLS:09) [Data set]. Institute of Education Sciences. https://nces.ed.gov/surveys/hsls09/hsls09_data.asp
National Center for Education Statistics. (2020b). High School Longitudinal Study of 2009 (HSLS:09). https://nce
s.ed.gov/surveys/hsls09/index.asp
National Center for Education Statistics. (2020c). College enrollment rates. Institute of Education Sciences.
https://nces.ed.gov/programs/coe/indicator_cpb.asp
National Science Foundation. (2021). Women, minorities, and persons with disabilities in science and engineering: 2021. National Center for Science and Engineering Statistics Special Report NSF 19-304. https://www.ns
f.gov/statistics/wmpd
Rittmayer, A. D., & Beier, M. E. (2009). Self-efficacy in STEM. In B. Bogue & E. Cady (Eds.), Applying research to practice (ARP) Resources. http://aweonline.org/selfefficacy_002.html
Savitz-Romer, M. (2012). The gap between influence and efficacy: College readiness training, urban school counselors, and the promotion of equity. Counselor Education and Supervision, 51(2), 98–111, 158.
https://doi.org/10.1002/j.1556-6978.2012.00007.x
Schmidt, C. D., Hardinge, G. B., & Rokutani, L. J. (2012). Expanding the school counselor repertoire through STEM-focused career development. The Career Development Quarterly, 60(1), 25–35.
https://doi.org/10.1002/j.2161-0045.2012.00003.x
Shaw, E. J., & Barbuti, S. (2010). Patterns of persistence in intended college major with a focus on STEM majors. NACADA Journal, 30(2), 19–34. https://doi.org/10.12930/0271-9517-30.2.19
Shillingford, M. A., Oh, S., & Finnell, L. R. (2017). Promoting STEM career development among students and parents of color: Are school counselors leading the charge? Professional School Counseling, 21(1b), 1–11. https://doi.org/10.1177/2156759X18773599
Sperandei, S. (2014). Understanding logistic regression analysis. Biochemia Medica, 24(1), 12–18.
https://doi.org/10.11613/BM.2014.003
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Pearson.
Tsupros, N., Kohler, R., & Hallinen, J. (2009). STEM education: A project to identify the missing components [Summary report]. Intermediate Unit 1: Center for STEM Education and Leonard Gelfand Center for Service Learning and Outreach, Carnegie Mellon University, Pennsylvania.
U.S. Department of Education. (2010). A blueprint for reform: The reauthorization of the Elementary and Secondary Education Act. Office of Planning, Evaluation and Policy Development. https://www.ets.org/s/education
_topics/ESEA_Blueprint.pdf
Vilorio, D. (2014). STEM 101: Intro to tomorrow’s jobs. Occupational Outlook Quarterly, Spring, 58, 3–12.
https://www.bls.gov/careeroutlook/2014/spring/art01.pdf
The White House, Office of Science and Technology Policy, National Science and Technology Council. (2018). Charting a course for success: America’s strategy for STEM education. Office of Science and Technology Policy. https://www.energy.gov/sites/default/files/2019/05/f62/STEM-Education-Strategic-Plan-2018.pdf
Wolniak, G. C., Wells, R. S., Engberg, M. E., & Manly, C. A. (2016). College enhancement strategies and socioeconomic inequality. Research in Higher Education, 57(3), 310–334.
https://doi.org/10.1007/s11162-015-9389-4
Xue, Y., & Larson, R. C. (2015). STEM crisis or STEM surplus? Yes and yes. Monthly Labor Review. U.S. Bureau of
Labor Statistics. https://doi.org/10.21916/mlr.2015.14
Dana L. Brookover, PhD, NCC, is a licensed school counselor and an assistant professor at the University of Scranton. Correspondence may be addressed to Dana L. Brookover, McGurrin Hall Room 435, McGurrin Hall, The University of Scranton, Scranton, PA 18510, brookoverdl@gmail.com.
Nov 9, 2021 | Volume 11 - Issue 4
Stacey Diane Arañez Litam, Christian D. Chan
A grounded theory study was employed to identify the conditions contributing to the core phenomenon of Asian American activists (N = 25) mobilizing toward thick solidarity with the Black Lives Matter (BLM) movement in 2020. The findings indicate achieving a collective oppressed identity was necessary to mobilize in thick solidarity with the BLM movement and occurred because of causal conditions: (a) experiences of COVID-19–related anti-Asian discrimination, and (b) George Floyd’s murder. Non-action, performative or unhelpful action, and action toward thick solidarity were influenced by contextual factors: (a) alignment with personal and community values, (b) awareness and knowledge, and (c) perspectives of oppression. Mobilization was also influenced by intervening factors, which included affective responses, intergenerational conflict, conditioning of “privileges” afforded by White supremacy, and the presence of organized communities. Mental health professionals and social justice advocates can apply these findings to promote engagement in the community organizing efforts of Asian American and Pacific Islander communities with the BLM movement, denounce anti-Blackness, and uphold a culpability toward supporting the Black community.
Keywords: Asian American, solidarity, social justice, Black Lives Matter, grounded theory
Trayvon Martin’s death in 2012 reignited conversations about the underlying sentiments of White supremacy that remain deeply entrenched in American society (Khan-Cullors & Bandele, 2017; Taylor, 2016). Shortly thereafter, the #BlackLivesMatter (BLM) movement was launched to address acts of police brutality on Black and Brown people and challenge the systemic oppression within the justice system (Lebron, 2017). Following the murder of George Floyd in 2020, the role of silence in perpetuating complicity resurfaced, and the familiar narratives and gut-wrenching images of non-Black police officers harming Black bodies once again found a place in the limelight (Chang, 2020; Elias et al., 2021). However, this time there was something noticeably different; one of the non-Black officers was Asian American.
Tou Thao’s role in sanctioning George Floyd’s murder illuminated the complex history of anti-Blackness within Asian American and Pacific Islander (AAPI) communities; created momentum for conversations about race, discrimination, and oppression; and echoed earlier support for the BLM movement among AAPIs (J. Ho, 2021; Merseth, 2018; Tran et al., 2018). These discussions may have been traditionally avoided, given the narrative invoked by racial and colonial notions that diminishes critical consciousness about racial histories and relations in AAPI communities (Chang, 2020; David et al., 2019). Because of the structural conditions of White supremacy and colonialism, AAPI communities have been forced to adopt Whiteness as a pathway to success, minimize salient cultural values, and trivialize manifestations of anti-Blackness (J. Ho, 2021; Poon et al., 2016). Erasing critical consciousness among AAPI communities has served as an insidious attempt to maintain a racial hierarchy that neither supports AAPI visibility nor eradicates racial tensions (Chou & Feagin, 2016; David et al., 2019). The invisibility of AAPI history absolves the United States from long-standing histories of anti-Asian racial violence (Li & Nicholson, 2021) and endorses complacency of White supremacy (Museus, 2021; Poon et al., 2019). Although this contention exists, a greater number of AAPI voices have begun to mobilize in solidarity with the BLM movement and the Black community in recent years (Anand & Hsu, 2020; Lee et al., 2020; Merseth, 2018; Tran et al., 2018).
Despite a complex racialized history of White supremacists weaponizing communities of color against each other (Nicholson et al., 2020; Poon et al., 2016), AAPI individuals have a long-standing history of pursuing thick solidarity and activism with the Black community and supporting Black civil rights (J. Ho, 2021). These racial coalitions have been evidenced through the Third World Liberation Front Strikes and the tireless efforts of activists like Grace Lee Boggs, Yuri Kochiyama, and Richard Aoki (W. Liu, 2018; Sharma, 2018). Thick solidarity is achieved when racial differences are acknowledged while emphasizing the specificity, irreducibility, and incommensurability of racialized experiences (W. Liu, 2018). Although understanding the factors that influence AAPIs to mobilize with the Black community represents a critical step toward thick solidarity (Tran et al., 2018), previous studies investigating the phenomenon have been limited to quantitative methods (Merseth, 2018; Yoo et al., 2021) or focused solely on Southeast Asian American populations (Lee et al., 2020).
The following sections outline the histories of racialized oppression faced by Asian American and Black communities and provide a brief overview of the extant research linking Asian American solidarity with the BLM movement. A grounded theory that identifies the emergent process that contributed to Asian American activists mobilizing toward thick solidarity with the BLM movement in 2020 is additionally presented.
The Racialized Experiences of Asian Americans and Black Communities in America
Prior to engaging in a grounded theory, researchers must build upon preexisting processes, theories, and perspectives documented in extant research (Charmaz, 2017). Thus, one cannot explore the processes that contributed to Asian American activists mobilizing toward thick solidarity with the BLM movement in 2020 without first addressing the nuanced and racialized experiences of AAPI and Black communities in America. Tran et al. (2018) asserted that navigating an oppressive system embedded in White supremacy has forced communities of color to make historical adaptations that leave AAPI voices out of the BLM movement. The following section provides a brief description of the complexity in which AAPI and Black identities are juxtaposed and elaborates on the model minority myth, racial triangulation, and historical anti-Blackness in AAPI communities as processes that may complicate the process of achieving thick solidarity.
Racial Triangulation
According to Kim (1999), racial triangulation theory refers to a “field of racial positions” (p. 106) that was proposed to extend the conceptualization of racial discourse beyond the Black and White narrative. The field of racial positions is mapped onto two dimensions. The superior/inferior axis represents the process of relative valorization, whereby Whites valorize Asian Americans relative to Black Americans in ways that maintain White privilege and White supremacy (Kim, 1999). The second dimension, an insider/foreigner axis, refers to the process of civic ostracism, in which Whites position Asian Americans as foreign, unassimilable, and outsiders (Kim, 1999; Xu & Lee, 2013). Although Asian Americans may be afforded social and economic benefits due to their proximity to Whiteness, this social location functions as an incomplete portrayal that conceals inequities, treats Asian Americans as perpetual foreigners, and maintains the status of White supremacy over communities of color (Bonilla-Silva, 2004; Nicholson et al., 2020). As a result, members of Asian American communities may be racialized to be White-adjacent and create an illusion of success with a conditional set of privileges (Kim, 1999; Museus, 2021).
One example of racial triangulation is the model minority myth, which essentializes Asian Americans by portraying them as a monolithic group with universal educational and occupational success (Chou & Feagin, 2016; Yi et al., 2020). According to Poon et al. (2016), scholars must acknowledge the model minority myth’s history to challenge processes of racial triangulation and deficit thinking. The model minority myth creates barriers to social justice efforts and racial coalitions by pitting communities of color against one another (Chang, 2020), invalidating experiences of systemic oppression and discrimination (Nicholson et al., 2020; Pendakur & Pendakur, 2016), and maintaining “a global system of racial hierarchies and White supremacy” (Poon et al., 2016, p. 6). When contextualizing the model minority myth through the lens of critical race theory, Asian Americans may be conceptualized as a “middleman minority” (Poon et al., 2016, p. 5). Originally coined by Blalock (1967) and later expanded upon by Bonacich (1973), middleman minorities are foreigners who buffer the power struggles between two major groups in a host society. Similar to other historical middleman minority groups, the minority model myth exploits Asian Americans by granting economic privileges while denying political or social power (Poon et al., 2016). As a more egregious consequence, the model minority myth can lead communities of color to harbor feelings of resentment toward Asian American communities, especially Asian immigrants who may feel pressured to prove their loyalty to American values (J. Ho, 2021) and embrace the submissive, hardworking qualities espoused by the model minority myth (Poon et al., 2019).
The complex relationship between AAPI and Black communities becomes even more complex as communities of color, including Black Americans, continue to define the boundaries of inclusion about “who belongs in communities of Color” (Tran et al., 2018, p. 78). As a result, Asian Americans are rarely included in race dialogues; may not be identified as “of color” by other groups; and are forced to navigate their weaponized, conditional identities as racialized in some spaces and White-adjacent in others (C. D. Chan & Litam, 2021; Litam & Chan, 2021; Museus, 2021; Poon et al., 2016).
Understanding Anti-Blackness in Asian American Communities
The denigration of Black identities and the desire to be viewed as distinct from Black Americans are evidenced across the histories of several Asian American ethnic subgroups. For example, in the mid-20th century, access to U.S. citizenship was limited to free White persons and persons of African descent (Pavlenko, 2002). At the time, the system was not set up to accommodate Asian Americans or other racialized groups, as evidenced by the landmark cases of Takao Ozawa and Bhagat Singh Thind (Chou & Feagin, 2016; Haney López, 2006). After living in the United States for over 20 years and articulating his relationship to White racial groups because of his light skin, Takao Ozawa, a Japanese man, was judged to be a race other than those able to obtain citizenship and deemed ineligible for naturalization (S. Chan, 1991; Yamashita & Park, 1985). Bhagat Singh Thind, an Asian Indian man, attempted to align specifically with the use of “Caucasian” and White racial ideologies, but was also denied citizenship by the U.S. Supreme Court (Haney López, 2006). Following the United States v. Bagat Singh Thind ruling, nearly 50% of Asian Indian Americans had their U.S. citizenship revoked (Haney López, 2006). Despite attempts to prove their loyalty to Whiteness, both cases reified how Asian Americans are placed in a vexing situation that provides an illusion of privileges but excludes them from fully participating as U.S. citizens (Haney López, 2006; Nicholson et al., 2020). Both cases also exemplified early instances of Asian American individuals who were pressured by prevailing racial ideologies to eschew Blackness and assimilate into dominant norms of White supremacy.
Examples of anti-Black sentiments are deeply rooted in people of Filipino descent who may endorse colonial mentality, an internalized form of oppression characterized by a preference for Western attitudes and the denigration of Filipino culture following years of colonization by the United States (David & Okazaki, 2006a, 2006b). For example, internalized anti-Black sentiments in Filipino culture are evidenced by the systematic discrimination against the dark-skinned Ati people, who are indigenous to the Aklan region (Petrola et al., 2020). As a result of the mining, logging, and tourism industries, the Ati have been forced to relocate onto smaller plots of land, face physical violence, and are denied various human rights (Petrola et al., 2020). Other insidious anti-Black attitudes that permeate the Filipino worldview include White-centered beauty notions that venerate straight hair and light skin over textured locks and dark skin (Nadal, 2021; Rafael, 2000). Despite their documented toxic and dangerous consequences, skin whitening products in the Philippines are a billion-dollar industry (Mendoza, 2014). These examples relay cultural and economic implications that are predicated on histories of global imperialism and colonialism, which root out indigeneity in favor of Eurocentric values and White norms (Fanon, 1952). Examples of anti-Black sentiments in Filipino communities are a sample of the ways in which colonialist movements mapped anti-Blackness onto Filipino communities and culture by occupation of the land, terrorism, and brutality (David, 2013; Nadal, 2021).
History of anti-Black attitudes may also exist in Korean Americans following the 1992 Los Angeles riots. After White officers were exonerated in the beating of Rodney King and a Korean store owner fatally shot 15-year-old Latasha Harlins, tension erupted between the Black and Korean American communities due to the lack of accountability for the killing of a Black person. Media reports of widespread rioting, theft, injuries, and damage to businesses were attributed to poor race relations between African American and Korean communities and larger issues of systemic racism were disregarded (Oh, 2010; Sharma, 2018). Despite calls to law enforcement for help, Korean voices were overlooked by the police (Yoon, 1997), which potentially illustrates how the law enforcement system reacts in favor of White interests. Once again, White media highlighted the undercurrent of racial tension between ethnic and racial groups as noteworthy and masked preexisting racial coalitions between Black and Asian American communities. These news stories deterred Asian American and Black communities from looking outward and acknowledging the larger issues of ongoing police brutality and inequitable justice systems (F. Ho & Mullen, 2008).
Chinese Americans may harbor anti-Black notions following the conviction of Peter Liang, who fatally shot Akai Gurley in New York City (W. Liu, 2018). Although he was the first officer indicted for killing an unarmed and innocent Black man, Liang’s conviction resulted in conflict between Chinese American and Black American communities (R. Liu & Shange, 2018; W. Liu, 2018). Many individuals within Asian American communities argued for the fair sentencing and punishment of Liang (Tran et al., 2018), but others protested the charge and believed the courts used him as a scapegoat to detract from BLM activists who called for police reform (R. Liu & Shange, 2018; W. Liu, 2018).
Challenging Historical Anti-Blackness in Asian American Communities
Challenging anti-Blackness in Asian American communities underscores a cultural paradox. On one hand, Asian American individuals, especially East Asian subgroups, benefit from social and economic privileges because of their proximity to Whiteness and identities as non-Black minorities (Bonilla-Silva, 2018; Poon et al., 2016). Thus, some Asian American individuals endorse aspects of the model minority myth because of the privilege it affords (Kim, 1999), even at the expense of maintaining a racially triangulated identity (Bonilla-Silva, 2004; Poon et al., 2019; Yi et al., 2020). Anti-Blackness therefore moves beyond prejudicial attitudes against Blacks and encompasses a performance of Whiteness (W. Liu, 2018).
Movements initiated by younger Asian American generations that challenge anti-Black sentiments (e.g., #Asians4BlackLives) are gaining traction (Anand & Hsu, 2020; Lee et al., 2020) and can help Asian immigrants move beyond their own unacknowledged pain and racial trauma to appreciate the challenges of other marginalized communities (David et al., 2019; Tran et al., 2018). For example, Letters for Black Lives is a crowdsourcing project that empowers communities of color to have conversations about anti-Blackness with older generations (R. Liu & Shange, 2018) who may endorse anti-Black attitudes following injustices against Asian people (e.g., Peter Liang) or anti-Asian historical events (e.g., the LA riots). These letters help younger Asian American communities describe ambiguous and complex issues related to social justice, racism, and systemic oppression with their families and have been helpful in promoting support for the BLM movement (Arora & Stout, 2019).
Extant Research on Racial Coalitions
Extant research posits how experiences of ingroup discrimination cultivate increased empathy, positive attitudes, and a collective sense of community (Craig & Richeson, 2012; Tajfel & Turner, 1979). As rates of anti-Asian discrimination have substantially increased following the COVID-19 pandemic and negatively affected the psychological well-being of Asian American communities (C. D. Chan & Litam, 2021; Jeung & Nham, 2020; Litam, 2020; Litam & Oh, 2020, 2021; Litam et al., 2021), the Common Ingroup Identity Model (CIIM; Gaertner & Dovidio, 2000) may help explain the increasing number of Asian American voices in support of BLM. According to the CIIM, experiences of racial discrimination toward one’s own racial group may lead to a shared disadvantaged racial minority identity that engenders positive attitudes and feelings of closeness toward other racial minorities. Compared to White, male, high-status groups, racialized minorities (e.g., Asian Americans) may be more likely to experience feelings of solidarity and affiliation with other communities of color believed to share experiences of racial discrimination (Brewer, 2000; Gaertner & Dovidio, 2000).
Preliminary support for the CIIM may be evidenced by a quantitative study conducted by Merseth (2018). Using a nationally representative sample of data, Merseth determined AAPIs who supported BLM were more likely to perceive anti-Black discrimination in the United States and identify race-based linked fates. A recent ethnography that examined AAPI support for the BLM movement identified the importance of community-based educational spaces as paramount to engaging in antiracist work and cultivating cross-racial coalitions among Southeast Asian Americans (Lee et al., 2020). Lee and colleagues’ (2020) results illuminated the importance of educational institutions that provide the foundation and language needed to challenge anti-Blackness among Southeast Asian communities. Combined with these studies, a more recent investigation by Yoo et al. (2021) involved a quantitative measurement of racial groups and their support for the BLM movement. Although this crucial study revealed the implications of solidarity among several racial groups with the BLM movement, the Yoo et al. study only involved a convenience sample of college students and did not necessarily account for the nuances within participants’ social identities, their motivations for support, or historical and political contexts. In the context of increased anti-Asian racial discrimination in the wake of COVID-19, shared experiences of anti-Asian discrimination may result in “a common ground of solidarity that Asian Americans and African Americans can forge against White supremacy” (Anand & Hsu, 2020, p. 194).
Purpose of the Present Study
The centralization of police brutality on Black and Brown people has reignited conversations about systemic oppression and has illuminated the need for civil rights, racial equity, and the dismantling of White supremacy (Elias et al., 2021; R. Liu & Shange, 2018; W. Liu, 2018; Tran et al., 2018). Although AAPIs may face discrimination in the wake of COVID-19 in ways that may result in solidarity with the BLM movement (Chang, 2020; J. Ho, 2021), a qualitative study that underscores this process with diverse Asian American voices can further contextualize meaningful opportunities for racial coalitions. Given the historical presence of anti-Blackness in Asian American communities (W. Liu, 2018; Tran et al., 2018), generating an emergent process that outlines the path of Asian American activists mobilizing toward thick solidarity with the BLM movement is of paramount importance to continue bolstering efforts toward racial coalitions (Lee et al., 2020; Merseth, 2018). To address the paucity of literature, a grounded theory was conducted to examine the following research question: What is the process that mobilizes Asian American activists to pursue thick solidarity with the BLM movement in 2020?
Method
Qualitative methods are appropriate when researchers seek to develop a complex or detailed understanding of an experience (Creswell & Poth, 2018). Specifically, grounded theory is a qualitative method used to generate a theory grounded in the data from participants who have experienced the process under inquiry and focuses on maximizing numerous perspectives constructed over phases of time (Charmaz, 2017). Given our desire to understand the process of action through which Asian American activists mobilize toward thick solidarity with the BLM movement, a grounded theory approach was deemed appropriate. To this end, the grounded theory focused on what participants experience and how the process of mobilizing in solidarity for BLM unfolds.
This study was implemented using a social constructionist paradigm to complement Charmaz’s (2014) constructivist grounded theory. Social constructionist researchers recognize the presence of multiple, processual, and constructed realities while acknowledging the role and importance of the researchers’ and participants’ positionality (Charmaz, 2014; Clarke, 2012). Social constructionism augments three overarching themes: (a) critiquing the neutrality of participants’ and researchers’ values by locating perspectives within social contexts (e.g., time, culture); (b) revealing language as a vehicle for shaping representation within particular communities; and (c) introducing different perspectives to unsettle social conditions and co-create new knowledge (K. J. Gergen, 2020; M. Gergen, 2020).
Procedure and Participants
Internal Review Board approval was obtained before beginning the study. Participants in this study were selected through the use of purposive and theoretical sampling (Timonen et al., 2018). The first and second authors, Stacey Diane Arañez Litam and Christian D. Chan, used purposive sampling to disseminate recruitment materials to key social media groups and community networks focused on AAPI community organizing. In the initial stages, Litam interviewed the first group of participants and ascertained their social identities. Next, theoretical sampling was employed. To introduce additional perspectives after the first group, Litam focused on soliciting more participants to expand the sample based on region, gender, and ethnic identities. Prospective participants could participate if they (a) self-identified as a member of the Asian American community and (b) identified as being engaged in ongoing support of the BLM movement. Prospective participants were recruited by posting on social media pages frequented by Asian American individuals actively involved in BLM activism. Prospective participants were asked to email Litam and were given more information describing the study’s purpose, design, and research questions. Eligible participants were informed that participation was voluntary, the research would not directly benefit them, and no compensation would be offered. A consent form was completed before participation occurred. Interviews were held on a HIPAA-compliant Zoom account.
This study consisted of interviews with 25 AAPI individuals who were actively engaged with the BLM movement. To protect confidentiality, participants were given pseudonyms. Participants reported a diversity of identities that increased the heterogeneity of the sample. Participants’ ages ranged from 25 to 73, and ethnic identities of participants included Filipino (n = 10), Korean (n = 5), Chinese (n = 2), Japanese (n = 1), Vietnamese (n = 1), Chamorro (n = 1), and multiracial (n = 5) descent. The gender identities of participants included women (n = 17), men (n = 5), and non-binary (n = 3). Most participants reported being a U.S. citizen and one participant identified as Canadian. Four participants identified as transracial adoptees.
Data Collection
Data collection occurred between June and July 2020. Semi-structured interviews lasted an average of 90 minutes. Participants responded to the following questions: (a) What are your experiences regarding how Asian Americans have historically supported, or are currently supporting, the Black Lives Matter movement? (b) Which contexts or situations have influenced your desire to support the Black Lives Matter movement? and (c) Which contributing factors influenced your development toward a social justice–oriented mindset? Follow-up questions developed organically. Participants provided consent for the interview to be recorded and were informed they could end the recording or the interview at any time. Only the audio file of the interview was saved, and the file was not uploaded to any cloud-based servers so as to promote participant confidentiality. Litam transcribed all interviews. Following the interview, participants completed two 15-minute member-check meetings—first to confirm the accuracy of researchers’ themes, and second to reflect on the final grounded theory.
Throughout the interview, Litam restated the major points after each response. Clarification was obtained through follow-up questions when participants described new concepts that had not been described by previous participants. Litam did not move onto the next question until each of the major points described by the participant were accurately identified and reflected. At the end of the interview, Litam summarized the conversation and restated the major points to confirm understanding of the participants’ statements. Follow-up questions, member checks, restatements, analytic memo writing, and constant comparative method were used to analyze the data.
Data Analysis
The data collection and analysis process reflected a concurrent process and a recursive process, which informed one another and led to the development of an emerging grounded theory (Charmaz, 2017). Throughout the data analysis process, concurrent analytic techniques of induction, deduction, and verification were used to develop an emergent theory (Charmaz, 2014). Litam immersed herself in the raw data by transcribing, reading, and listening to the audio transcripts. Transcription was completed within 24 hours of the interview, and member checks with participants to confirm themes were completed within 72 hours of the interview. New data were compared to existing data following the completion of each transcribed interview. Initial codes and analytic memos were used throughout the process to create an audit trail. Data were closely examined for disconfirming evidence, and two external auditors were used throughout the data analysis process to understand how our assumptions could influence the coding and findings.
Two external auditors were used between open and focused coding to confirm emergent findings, discuss the accuracy of emerging themes, and triangulate across perspectives (Saldaña, 2021). Both external auditors identified as members of the AAPI community and endorsed a strong commitment to AAPI concerns, research, and mental health. The second external auditor also carried in-depth training in qualitative methodologies. Data were coded with labels that categorized, summarized, or accounted for each piece of data (Charmaz, 2014; Saldaña, 2021) and analytic memos were used to help scrutinize the data (Miles et al., 2020). Each participant confirmed the accuracy of themes and reported feeling energized by the theory, a phenomenon known as catalytic validity (Guba & Lincoln, 1989).
We engaged in reflective commentary throughout the interview and data analysis process by using bracketing and ongoing evaluation. Peer scrutiny was employed by inviting three AAPI colleagues who were familiar with the phenomenon to offer feedback and fresh perspectives on the findings as they continued to emerge and become saturated. The first colleague identifies as a transnational Chinese woman and is an associate professor. The second colleague identifies as a Chinese woman who specializes in counseling AAPI communities. The third colleague identifies as a Filipino, Chinese, and Malaysian man and works as a counselor educator. Interviews were conducted until saturation occurred and fresh data no longer sparked new theoretical insights or properties of the generated grounded theory, its categories, or its concepts.
Researcher Reflexivity
A researcher’s social location, biases, theoretical lens, and epistemological beliefs must be established to increase the trustworthiness of results (Saldaña, 2021). Litam identifies as a foreign-born Filipina and Chinese American woman. She is a counselor educator, an assistant professor, and a licensed professional clinical counselor and a supervisor. She conducts research on topics related to human sexuality, human trafficking, trauma, race, diversity, and AAPI issues. Litam has overcome her own internalized colonial mentality as a Filipina American woman and endorses a strong commitment toward issues of social justice and racial equity. She is dedicated to engaging in work that dismantles the forces of White supremacy that oppress all racialized groups.
Chan is a queer person of color and a second-generation Asian American of Filipino, Chinese, and Malaysian heritage. As an assistant professor, he invests primarily in scholarship on intersectionality, social justice, activism, multiculturalism, career development, and communication of culture and socialization in couple, family, and group modalities. He actively works toward racial coalitions that interrogate structures of White supremacy and organizes intentional community initiatives for solidarity. Many of his perspectives, especially toward the inquiry at hand, attend to social structures and histories that underpin ideologies of White supremacy.
Trustworthiness
Grounded theory requires standards of quality and trustworthiness, including credibility, originality, resonance, and usefulness (Charmaz, 2014; Creswell & Poth, 2018). To promote trustworthiness, constant comparison was employed by using open codes, a codebook, and data to inform, analyze, and compare new data sources (Charmaz, 2014). Any new data were consistently checked and compared to the emerging theory. Member checks were completed twice by connecting with participants over Zoom for approximately 15 minutes each. We also used peer scrutiny with three AAPI colleagues and two AAPI external auditors to challenge assumptions and biases, triangulate findings, and engage in dialogue about clusters of meaning and themes as they emerged. These strategies were used to ensure the theory was data-driven rather than reflective of our own beliefs, values, and assumptions (Hays & Singh, 2012). Analytic memos were written after each round of coding, which elaborated emotions, thoughts, and personal reactions to the data. This information strengthened the tracking of the data and our influence as we shared the audit trail with both external auditors. Thus, multiple measures of trustworthiness were used to account for positionality that could influence the data and theory development.
Findings
We sought to examine the following research question: What is the process that mobilizes Asian American activists to pursue thick solidarity with the BLM movement in 2020? The results of the grounded theory analysis describe the process through which causal conditions, contextual factors, and intervening conditions affect actions and foster pathways to consequences following the core category of the phenomena of interest (see Figure 1).
Figure 1
Grounded Theory Outlining AAPI Process of Mobilizing in Thick Solidarity With BLM in 2020
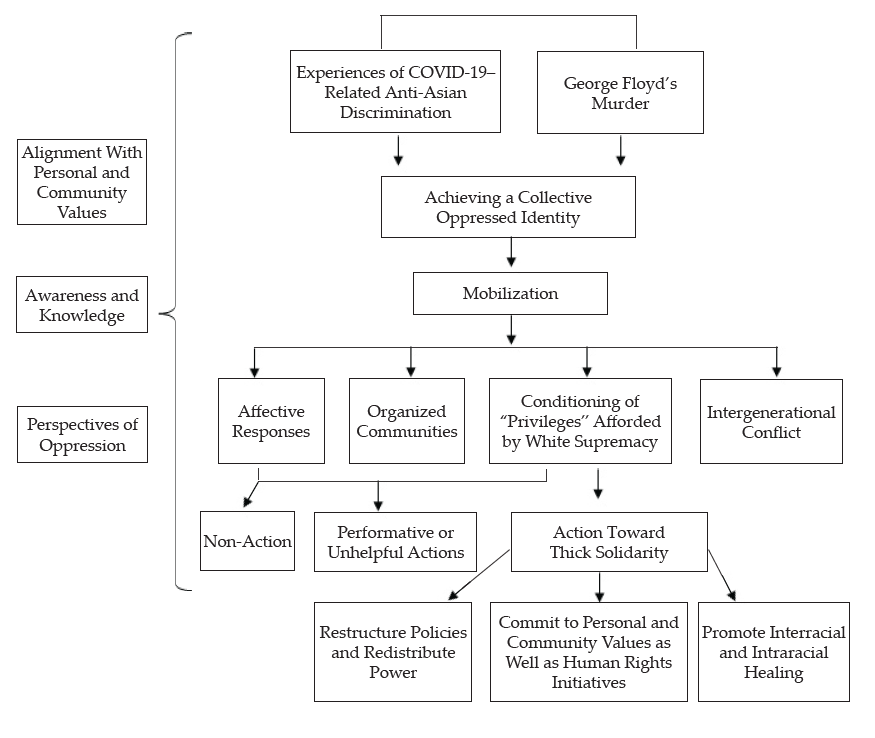
Causal Conditions
Based on perspectives from participants, two causal conditions led participants to mobilize toward solidarity for BLM in 2020.
George Floyd’s Murder
Exposure to George Floyd’s murder through social media and news outlets was the first causal condition. For each of the participants, this event represented the “breaking point,” “threshold,” “spark,” or “tipping point” that illuminated the need to “act,” “pursue justice,” “make change,” and “fight back.” As stated by Gemma, a Filipina woman in her mid-30s:
When George Floyd died . . . I just refused to be silent about what happened to him. I just kept thinking, well, what the hell have I been doing that it didn’t impact enough change [so] that this man could have lived? This man died because we have not done enough. He died calling out for his mom. What I could not handle was if I had been born with a particular fear, and I died that way. This man was born and lived knowing that he could be murdered by the police. And that’s how he died. I refuse that. And I am personally responsible that the narrative has not changed in this country. I am responsible and I hold my communities responsible. We have not done enough so that man could have lived.
Experiences of COVID-19–Related Anti-Asian Discrimination
The second causal condition was identified as experiences of COVID-19–related anti-Asian discrimination. This condition was characterized by witnessing or experiencing broad anti-Asian discrimination and exposure to “Trump’s Anti-Chinese,” “xenophobic,” and “racist messages.” Participants described how anti-Asian rhetoric touted by political leaders and experiences of anti-Asian discrimination served as “tinder” that “incited,” “enraged,” and “irritated” AAPIs in ways that “primed” them to act.
For each of the participants, witnessing and/or experiencing COVID-19–related racism was an event that led to action. Each of the 25 participants stated that exposure to anti-Asian discrimination cultivated empathy for Black Americans and illuminated how their shared experiences of racial discrimination “opened their eyes,” “woke them up,” or “pulled off the blindfold” of their racialized identity as Asian Americans. Yuri, a Chinese and Vietnamese woman in her early 30s, explained:
We have this fresh memory of discrimination in the back of our heads, and you know, it reaches a boiling point. You have the intersection of your own experiences and somebody else’s experiences and you start to connect the dots that we are not so different. And we are not so safe. We have more in common with Black lives than we do with White ones.
These sentiments were echoed by Hunter, a Korean man in his early 50s:
The pandemic created this anti-Asian reality. It really brought attention to the average Asian American [about] how much anti-Asian sentiment is still out there. You know, we all live in our little bubbles in life. And we don’t really see what’s going on. But I think, you know, seeing all these news stories about anti-Asian violence, whether we are members of the older generation reading our ethnic papers or just, you know, a member of the younger generation watching television, we see this stuff on the news and it has kind of served as the kindling to the fire to act and do more.
Evelyn, a Filipina woman in her early 40s, also described how exposure to anti-Asian rhetoric touted by political leaders primed her to act:
This particular president [Trump] is stoking the flames [and] it’s re-energizing a particular base of people who are emboldened to say and do things that are hate-centered, that are violent, that are wrong. And I think that it also touched on a particular powerlessness that Asian Americans have felt. And when you couple that within a global pandemic you are hyper aware of your mortality. You could die from this virus that’s going around, [and] we are all wearing masks. You couldn’t get more on edge, you know? We were primed to act. We were ready.
Josie, a multiracial woman in her mid-30s, explained:
Yes, we’re being harassed. We’re being called names. We’re experiencing another wave of xenophobia and racism, being told to go back to our countries, being told that we are not welcome here. I believe that Asians are saying, “Okay, yeah, we’re being threatened, but we’re not being held to the ground and choked out to the point that we’re being killed on TV.” I believe it’s awakened a lot of levels of pain and solidarity because you can’t imagine it. People can’t imagine that the world is this bad until someone’s last breaths are on TV. I think it mobilized people to become more involved because injustice does not have a place among any minority group. Injustice resonates with the Brown community, the Latinx community, the Asian community, and I believe it empowered us to move toward human empathy. Asians are realizing that if we don’t stand together, we stand alone, and nothing in this world will change.
Contextual Factors
Contextual factors were the individual traits and characteristics that affected the actions taken by participants to pursue mobilization in solidarity with BLM. Participants described three contextual factors: (a) alignment with personal and community values, (b) awareness and knowledge, and (c) perspectives of oppression.
Alignment With Personal and Community Values
The first contextual factor was defined as alignment with personal and community values. Notions of values alignment were identified in interviews when participants described how supporting the BLM movement was not a choice; rather, “protesting,” “supporting,” “fighting,” and “engaging in human rights activism” represented “values,” “moral imperatives,” and “needs.” Each of the participants described how mobilizing toward thick solidarity with the Black community reflected the direct consequence of one’s own set of values. Hunter shared the following: “Regardless of how it benefits the Asian American community, for me, it’s my sense of value. This is my own value system. I don’t feel comfortable having groups that are continuing to be oppressed.”
For some participants, notions of values alignment and the need to act had been socialized and were shared by their families of origin. José, a Filipino man in his early 30s, indicated:
I needed to act, there was no other choice. My parents taught me years ago how this whole [BLM] movement creates an obligation to speak up when injustice occurs. Our [Filipino] history has led us to learn that we always have been stronger when we all unite together because there is so much divisiveness in our society.
Evelyn described how values alignment represented a moral imperative:
For about 17 years, I have been an activist. I have always known at a very deep, personal, soul level, that issues of race are the knife on the throat of this country. This country has not resolved or has even come close to reconciling its history. And I don’t think that it [supporting BLM] was something that I decided. It wasn’t a neuron movement. It wasn’t a shift; it wasn’t something that physiologically or intellectually or cognitively shifted. It was like something else just shed, like a skin was pulled off me. It was just so plainly obvious that it was more than overdue for people to say something. We needed to act. There was no other option. It was just this plain, visceral refusal to be silent.
Participants described how alignment with personal and community values emerged because other Asian countries have been historically oppressed. Specifically, Hong Kong, Vietnam, and the Philippines were identified as countries that “silenced Asian voices” in ways that amplified participants’ desire to underscore their values in the United States. Byron, a Vietnamese and Chinese man in his late 30s, identified the following perspective on contextual factors:
I think it’s very important for us, as Asian Americans or even Asians across the world, to really be vocal on this [BLM movement]. Because, dude, America is a crazy place. It’s a beautiful country, but at the same time, the system is kind of jacked, right? And, you know, my parents being from Vietnam and really trying to get away from communists and stuff, I see what the Hong Kong people are going through right now. That to me is like a sign. Like, their battle is different from ours, but it’s still the same. We need to fight for what’s right.
Awareness and Knowledge
The second contextual factor was identified as awareness of one’s identity as a person of color and knowledge of how all communities of color are affected by systemic racism and White supremacy. Participants described how learning about Asian American history and the impact of racial triangulation, how AAPI liberation is directly tied to Black liberation, and the weaponization of the model minority myth were critical factors that contributed to their BLM activism. Rufio, a Filipino man in his late 20s, recalled the following memory:
Peter Liang, I think, was the first person that got convicted of anything. I clearly remember a street. On one side of it were Black protesters and on the other side were Asian American protesters. One side was saying, “Peter was innocent!” and the other side was like, “He deserves more of a sentence!” African American and Asian American protesters were pointing at each other when really they should have been looking outside [of] the situation and being like, the people in power set this game up so we didn’t look at them. They were making us look at each other, but we shouldn’t be looking at each other. We should be looking at them.
Participants identified the importance of achieving multiracial unity and described how the fates of communities of color are inextricably linked. Jay, a non-binary Filipinx person in their early 20s, asserted the following about multiracial unity:
When we center the most vulnerable or the most marginalized, then we are able to lift up everyone. And I think that’s why a lot of people are focusing on the term BIPOC and [are] like, trying to center Black people and Indigenous people, because Black people have been enslaved and Indigenous people [have] had so many atrocities committed to them on stolen land. Ultimately, we are all in this together and what we do for one affects us all.
Similarly, Dante, a transracially adopted Taiwanese man in his mid-20s, observed the political implications surrounding race relations in the United States:
Honestly, I think that four years of the Trump presidency is probably a big mobilizing factor. His policy towards China has been just straight-up racist on his best days and, you know, far worse on his bad days. And so one of the concerns that I had is like, he has no problem locking up kids and immigrants in detention centers. At what point is that going to start being directed at Asian people? If we don’t fight for other people of color, who’s going to fight for us when it is our turn?
Jubilee, a Chinese woman in her early 30s, described the recent AAPI support of BLM and emphasized the importance of cultivating awareness and knowledge with her community and family of origin:
I feel like this is the first time I’ve seen such solidarity from Asians to the Black community. It happened back in the 60s during the civil rights movement so like, we are not the first, but like, in my generation and in my lifetime, this is the first time I am seeing that from us as an Asian community. There are finally conversations coming up about anti-Blackness in Asian communities, you know? It has also allowed me and my brother to bring up these conversations and issues with our friends and parents. For the first time in our lives, we are having conversations about anti-Blackness and systemic racism, and they are not brushing it off. They [my friends and parents] actually take a pause and listen, and this was the first time seeing them do that. And that’s pretty cool. There’s still a long way to go, but there is definitely some change happening. I see it and I feel it around me.
Perspectives of Oppression
Participants conceptualized their experiences from two distinct perspectives of oppression that uniquely influenced the strategies used to mobilize in thick solidarity toward the BLM movement: (a) as a member of the AAPI community or (b) as a member of a greater community of minoritized groups. Participants who limited their perspective of oppression to the AAPI community tended to center Asian voices in support of the BLM movement (i.e., “Yellow Peril for BLM”). Participants in the first category tended to limit their focus to how supporting the BLM movement would benefit the Asian community. Byron explained how supporting the BLM movement better positions the greater Asian American community to engage in advocacy:
I think us mobilizing together and supporting the Black Lives movement would really help us out as a community. Not only as just Chinese, Vietnamese, and Filipino and all that, but literally, as one Asian community. I think we are learning from the Black Lives movement. Not only are we participating with them, but it’s almost like training wheels for our community to be like, we need to be louder about certain rights that we want or certain things that we want to talk about. The United States has created the perfect platform for us to express that, and we have not utilized that.
Conversely, participants who endorsed a wider perspective that recognized Asian Americans as members of one oppressed minoritized group centered the Black community and amplified Black voices. Participants in the second category were more likely to recognize how mobilizing in thick solidarity with the BLM movement would benefit the larger constellation of communities of color. June, a Korean, non-binary, transracially adopted person in their late 20s, highlighted this connection across social movements:
So many Asian people don’t want to post about anti-Asian oppression alongside Black Lives Matter. They are like, “Oh I don’t want to take away from the Black Lives Matter movement by posting about the racism that I experienced or by posting about immigration.” But I kind of see them as being connected because we all face the same oppressor. We are all dealing with White supremacy, so we need to realize all of our movements are interconnected. We need to be in solidarity with each other.
Mia, a Korean woman in her early 30s, similarly explained this relationship:
Just like how we wonder, How is discrimination affecting the greater Asian community?, I think you have to extend that exercise to, How is it affecting the Black community? Where is it [discrimination] starting from? Whose lives are affected? Instead of just being like, “These are the discrimination experiences I face in my life,” it becomes a bigger conversation about what our greater community of minorities faces.
Intervening Conditions
Intervening conditions represent the broad and general factors that influence strategies based upon action or inaction and may include time, space, culture, history, emotions, and institutions. In this study, Asian American participants described four intervening conditions that either facilitated or created barriers to mobilizing toward thick solidarity with the BLM movement. Intervening conditions were described as having a bidirectional nature with the contextual conditions and action strategies used by participants.
Affective Responses
Participants described how feelings of “fear,” “anger,” “helplessness,” “empathy,” and “compassion” intersected with George Floyd’s murder, experiences of COVID-19–related anti-Asian discrimination, alignment with personal and community values, awareness and knowledge, and perspectives of oppression. Nearly every participant identified how they had “struggled” with, “overcome,” or “witnessed” how Asian Americans become paralyzed by fears of “taking up space,” “being too privileged,” or “not sharing the same intensity of oppression as Black Americans.” June described how some AAPIs become too overwhelmed by their privilege to engage in activism:
I so often hear them [AAPIs] say, “I want to help, but I can’t do anything. I can’t, I can’t. I don’t feel it’s in my place because I’m not Black. I feel like my voice doesn’t matter in this situation because I don’t suffer in the way that they [Black Americans] do.” I’ve seen so many excuses about how their voices are too privileged to matter, and it’s not true.
Annie, a Vietnamese woman in her early 30s, explained how fear can limit action:
They [AAPIs] fear that if they stand with the Black community, they will be ousted, attacked, treated differently, and looked down upon. I’ve seen a lot of fears that family would disown them if they become more vocal about Black Lives Matter because the older generation is very stuck in their own mindset of teaching the younger generations, you know, “You keep your head down, you go to school, you make a life for yourself, you don’t make waves, because it will only ruin your life.” I’ve seen a lot of people say that they can’t be as vocal because they are only one person.
Intergenerational Conflict
Participants identified intergenerational conflict as the second intervening condition that influenced Asian American action or inaction. Each participant described how Asian Americans and Asian immigrants (especially older individuals) lacked social justice–oriented language and stressed the importance of assimilation, and how those influences affected the shifting realities between first-generation Asian Americans and subsequent generations in their support of the BLM movement. Conversely, Asian Americans who were willing to engage in discussions about racial discrimination and cultivate cross-racial relationships were more likely to mobilize toward thick solidarity with the BLM movement. Participants also described how older Asian Americans and Asian immigrants struggled to grasp the “cultural nuances” that contextualize the history of systemic oppression and police brutality on Black and Brown individuals in America. The cultural barriers for many older Asian immigrants were described by Lin, a transracially adopted Korean woman in her early 30s:
The social justice language that we use when it comes to Black Lives Matter is difficult enough for a White person who is unfamiliar with this terminology. [It’s hard] to try and communicate that across generational lines, especially because a lot of us don’t have the strength in language skills to be able to translate. From what I’ve observed in my parents, they’ve kind of just kept their head down. They stressed assimilation very strongly for their children. It’s that old-school, “don’t rock the boat” mentality. Don’t give them a reason to look at us. Don’t give them a reason to hate us, you know? Don’t do anything to jeopardize this freedom that they worked so hard to achieve [and] that we’re so lucky to have.
Participants also described how first-generation Asian American and Asian immigrants were more likely to be “encapsulated,” “avoid other racial groups,” and “keep to themselves” in ways that prevented the cultivation of meaningful cross-racial relationships and kept them from challenging historical anti-Black sentiments. The importance of connecting with other communities of color to foster empathy and challenge historical anti-Blackness among Asian Americans and Asian immigrants was described by Ira, a multiracial woman in her early 70s:
I think that when older Asians are exposed in even a small way to the African American community, they can understand. But many Asian people stay within people of their own color, and they stay within their own ethnicity and they stay within their own groups. If you stay in your own community and you never see an African American person except [for] what you see on TV, it’s hard to see the similarities and realize that we are not so different.
To complement this notion, Jenny, a multiracial woman in her early 40s, discussed this perspective:
I feel like it’s really common for Asian immigrants not to connect with these situations [of discrimination] that are happening to them, either in individual instances or in bigger systems. They’re not tying them back to racism. I think that for so long, you know, immigrants were just trying to survive. First-generation folks were just trying to keep their head down, stay out of trouble, and survive, and they couldn’t get distracted by thinking about what else was happening around them.
Conditioning of “Privileges” Afforded by White Supremacy
The third intervening condition was coded when participants described how being Asian American represented “conditional,” “unsafe,” and “hyphenated” identities and when proximity to Whiteness elicited confusion about their role in activism. For some participants, the conditioning of “privileges” afforded by White supremacy contributed to action. As described by Evelyn, Whiteness elucidated a system of different racialized experiences:
I begin to wonder how powerful is Whiteness, you know? If I’m not the one being killed in the street, but I’m also experiencing racism, where do I fit into all of this? You begin to question how Asian Americans have been inserted into this narrative. And for me, you begin to wonder like, am I a pawn in this? What is my level of responsibility here? Is there a shared oppression? Yes. Are we all tethered the same way? No.
Participants who struggled to overcome the conditioning of privileges afforded by White supremacy were more likely to vacillate between action and inaction. Monica, a transracially adopted Korean woman in her early 30s, stated the following:
I do feel like for Asians, you’re in this really interesting space. I do actually think I have a lot of privilege. And with that, potentially, some responsibility as a person that essentially has a long-standing visa or passport into Whiteness. I know the language. I know how White people think and act. I feel like I can talk to White people about racism in a way that other people don’t necessarily have access to. But also, I experience racism and I’m also really tired.
Organized Communities
The presence of social media groups; local, regional, national, and international groups; participants’ own Asian American communities; and other communities with shared group identities (e.g., the lesbian, gay, bisexual, and transgender [LGBT] community) were identified by participants as the fourth intervening condition. When organized communities were present, they either hindered or fostered mobilization. Participants who had communities that hindered mobilization described how their families and Asian American communities socialized them “not to rock the boat,” raised them to “keep their head down,” and discouraged “making waves.” Participants who lacked the presence of organized communities described feeling “burned out,” “alone,” and “unsupported.” As reported by Andi, a non-binary Korean person in their late 20s:
I have been fighting alone for years and it’s exhausting. I carry on because our activism is important, but it would be so nice to be able to meet up with other groups, share our experiences, and fill our validation cups, you know? It’s like, there is only so much I can do alone, and I don’t have the support I need to really keep going.
Participants described how communities fostered mobilization by providing the language, structure, resources, validation, and space necessary to begin talking about race and understanding the plight of other communities of color. Communities that fostered mobilization were most frequently described as college and university settings. Jackie, a Chinese and Japanese student in her mid-20s, described how her Asian American community on the university campus fosters action:
I just didn’t want to be by myself and protest alone. It feels good to learn more about why we are doing this and why it is important. Now, I felt like I have learned why it was so important that we as a group are able to rally behind the Black Lives Matter movement. I think community plays a huge part in supporting the BLM movement. It’s not just enough for us as individuals to be moving forward, it’s important that we have an Asian community presence in this battle.
The fostering role of communities in promoting thick solidarity was further described by Trichelle, a Chamorro woman in her late 50s:
I think the college and university experience has helped facilitate an understanding about race, generally, and experiences as Asian Americans or Pacific Islanders, secondarily. They facilitated an ability to see the connections, both the differences and the similarities of how racism has impacted AAPI communities but also how it is linked to the experiences of Black folks. The ability to have the language and to have some kind of infrastructure is critical to mobilize. Mobilization does not happen in the absence of some kind of organizational infrastructure.
Actions
To understand this larger process of action, participants in this study described non-action, performative action, or action toward thick solidarity. Participants additionally described how contextual factors, causal conditions, and intervening conditions interacted to influence the type of actions that occurred.
Non-Action
Non-action occurred when Asian American individuals were unable to challenge collectivistic notions of “not rocking the boat,” “not making waves,” and “not causing trouble.” Non-action was also more likely to occur when Asian Americans became overwhelmed by the economic and social privilege afforded to them because of their proximity to Whiteness. Upon considering the distinctness of Black oppression, participants described recognition of how Asian Americans may feel “unable,” “unsupported,” “guilty,” or “ineffective” to engage in action because of burnout; lack of community, validation, support, or resources; or feelings of “privilege guilt.” Participants also described how non-action may occur in older generations and Asian immigrants who may have internalized model minority traits, emphasized the importance of assimilation, remained encapsulated within the Asian American community, or lacked an understanding of systemic racism and social justice language.
Performative or Unhelpful Action
Performative or unhelpful action occurred when Asian American individuals either felt compelled to act to avoid being perceived as anti-Black or because supporting the BLM movement was “trending.” Unhelpful action occurred when Asian American individuals centered their issues in ways that disenfranchised Black issues or centered AAPI voices over Black voices (i.e., Asians4BlackLives). June described an example of how Asian American individuals may engage in performative action: “They’ll say one or two things online, and they’ll be like, ‛Oh, I did my part. I posted #BlackLivesMatter. Look at my profile picture. Look at my Instagram. Look, I posted a couple links for donations.’”
They also explained how centering AAPI voices constituted unhelpful action:
When someone posts “Yellow Peril Stands for Black Lives,” you’re actually overshadowing Black Lives Matter. Taking our title, our movement, and placing it in front of BLM says, “Hey, we’re here. We’re standing with you. Look at us.” That’s not acting in solidarity. It becomes one group saying, “I AM HERE. Here’s my voice for your voice.” We need to make our voices strong for theirs. We are the chorus and they are the lead singers.
Action Toward Thick Solidarity
Action toward thick solidarity occurred when Asian American individuals were able to support the BLM movement without centering AAPI issues or focusing on their own racial trauma histories. Demonstrating a willingness to learn how to be an ally and cultivating cultural humility were effective strategies in transcending action from performative or unhelpful to action toward thick solidarity. Sari, a Chinese and Lebanese woman in her early 30s, described the process of acting toward solidarity and the importance of communities that foster mobilization:
Solidarity to me is not a noun. It is a process that you continue to refine and reflect on and add or subtract things to, and it has a lot to do with your perspective and your approach. And I think a lot of solidarity with others comes from a genuine dedication to building your own community. I think a really important piece of solidarity is that introspection and community building with your own ingroup.
José explained how acting toward thick solidarity requires Asian Americans to follow the lead of Black activists. He tells the following story of how he explained allyship to a friend:
Remember two summers ago when you asked me to help you fix your deck, and I never knew how to work with power tools? The weekend before, I went on the internet and learned basic skills like how to hold a tool and how to be safe. And then when I went to your house, I wore a hard hat. I had everything ready, and I followed your lead and your leadership. That’s how you become an ally. You educate yourself. And when you go to situations you don’t center yourself. You follow the person who has the most experience.
Phenomenon, Consequences, and Core Category
Participants in the study described the process of feeling “primed” to act because of the combined causal conditions of George Floyd’s murder and experiences of COVID-19–related anti-Asian discrimination. Participants were able to mobilize because of the contextual factors of alignment with personal and community values, awareness and knowledge, and perspectives of oppression. The phenomenon of Asian American activists mobilizing in thick solidarity with the BLM movement were influenced by intervening conditions, which included affective responses, intergenerational conflict, conditioning of “privileges” afforded by White supremacy, and organized communities. Each of these conditions and factors interacted to influence non-action, performative or unhelpful action, and action toward thick solidarity.
Participants identified the consequences of pursuing thick solidarity with the Black community as resulting in pathways that facilitate three domains: (a) to promote intraracial and interracial healing, (b) to commit to personal and community values as well as human rights initiatives, and (c) to restructure policies and redistribute power. Within this study, “achieving a collective oppressed identity” occurred most frequently in participant narratives, experiences, and practices and was identified as absolutely critical for mobilization to occur. The core category of achieving a collective oppressed identity arose as a result of George Floyd’s murder, because of experiences of COVID-19–related anti-Asian discrimination, and in the light of awareness and knowledge.
Discussion
A grounded theory analysis with 25 diverse individuals outlined an emergent process describing how contributing factors mobilized Asian American activists toward thick solidarity with the BLM movement in June and July 2020. Understanding and abstracting this theoretical process is important to embolden other Asian American individuals to engage in collective social action. Components of the emergent process are consistent with the CIIM (Gaertner & Dovidio, 2000) and supplement additional studies that explored AAPI support for the BLM movement (Lee et al., 2020; Merseth, 2018; Yoo et al., 2021). Specifically, the theoretical process that emerged from this study illuminates new findings that indicate how achieving a collective oppressed identity and contextualizing the historical relationship between the Asian American and Black communities are critical to empowering AAPI communities to form racial coalitions (Chang, 2020; J. Ho, 2021). For many participants, understanding this history and becoming more racially conscious propelled their motivations for achieving solidarity and dismantling the forces of White supremacy that oppress all racialized groups. This finding reveals numerous perspectives that value historical context and knowledge as a central factor for AAPI activism, especially in tandem with other communities of color (Museus, 2021; Nicholson et al., 2020).
Participants in the study identified how George Floyd’s murder and their experiences of anti-Asian discrimination resulted in an achieved collective oppressed identity that contributed to their mobilization toward thick solidarity with the BLM movement. This finding is consistent with extant research that hypothesized how ingroup discrimination may cultivate increased empathy, positive attitudes, and a collective sense of greater community (Craig & Richeson, 2012; Tajfel & Turner, 1979). The ways that causal conditions identified in this study led to a collective oppressed identity may further be explained through the lens of the CIIM model (Gaertner & Dovidio, 2000), which posits that experiences of racial discrimination can engender positive attitudes and feelings of closeness to other racial minorities. The findings of the study additionally complement earlier studies on AAPI support for BLM that identified race-based linked fate beliefs among Asian Americans as a predictor of BLM support (Merseth, 2018), and an ethnography that identified the importance of organized educational communities for Southeast Asian Americans engaging in activism (Lee et al., 2020). Another possibility may be that participants in the study achieved a dual identity. As explained by Gaertner and colleagues (1994), dual identity occurs when individuals perceive themselves as members of different ethnic or racial groups “playing on the same team” (p. 227)—in this case, to dismantle the forces of White supremacy that continue to oppress all communities of color. The findings from the present study further elaborate on processes that may outline how anti-Asian discrimination can create the impetus for mobilizing in thick solidarity with the Black community (Anand & Hsu, 2020; Li & Nicholson, 2021; R. Liu & Shange, 2018; W. Liu, 2018).
Implications From the Study
The findings from this study can be used by mental health professionals and counselor educators to engage in meaningful racial dialogues and foster interracial coalitions. Specifically, professional counselors can employ this grounded theory to help Asian Americans heal from their own racial and intergenerational trauma by supporting other communities of color. The process of action outlined in our study illuminates the importance of promoting awareness and knowledge about the history of Black and AAPI oppression (Chang, 2020; J. Ho, 2021), connecting AAPI individuals to supportive communities (C. D. Chan & Litam, 2021; Yi et al., 2020), and providing helpful resources (e.g., Letters for Black Lives) and strategies (e.g., exposure and connection with other communities of color) to navigate cultural barriers (Arora & Stout, 2019).
Mental health professionals and social justice advocates can apply these findings to promote engagement in community organizing efforts of AAPI communities with the BLM movement, denounce anti-Blackness, and uphold culpability in supporting the Black community. Following the COVID-19 pandemic, AAPI individuals may experience greater rates of racial discrimination and anti-Asian rhetoric in ways that negatively impact their well-being (C. D. Chan & Litam, 2021; Jeung & Nham, 2020; Litam, 2020; Litam & Oh, 2020, 2021; Litam et al., 2021). Mental health professionals can validate these experiences of oppression and help clients redirect affective experiences in ways that promote awareness and knowledge (David et al., 2019; Museus, 2021), challenge proximity to Whiteness (Poon et al., 2016; Yi et al., 2020), and cultivate meaningful action in racial solidarity movements (Chang, 2020; Litam, 2021; Yoo et al., 2021). Helping Asian American individuals find communities that foster action toward thick solidarity with BLM and exploring how affective experiences influence accountability may be helpful in garnering support. For example, mental health professionals can explore whether limited perspectives of oppression and assimilation strategies may result in inaction or performative action, especially in directly challenging Whiteness (Chang, 2020; Yoon et al., 2016) or intentionally taking accountability for harboring anti-Black sentiments (Museus, 2021). This consideration is especially crucial as AAPIs build long-term solidarity as a proactive approach to Black solidarity rather than a temporary measure. Finally, mental health professionals may encourage AAPI individuals to expand their perspectives to include dual identities as AAPI people and as members of a greater group of oppressed minoritized individuals to foster racial coalitions.
Limitations
First, participants self-selected into the study with a strong working knowledge of their activist and AAPI identities. Readers must therefore be judicious about transferring these findings to AAPI individuals whose activist and/or racial identities may not be fully developed. Second, participants represented a small sample of a larger Asian American community that endorses varying views about activism, anti-Blackness, and other human rights issues. Notably, the sample only included one person with Pacific Islander heritage. Although the importance of thick solidarity continues to gain traction, readers must caution themselves against interpreting these perspectives as a monolithic viewpoint held by all AAPI individuals.
Recommendations for Future Research
The limitations of the study yield additional opportunities to build upon empirical research that illuminates racial coalitions, particularly among communities of color. With the findings of this study, it would be helpful to elucidate critical developmental points that shift AAPI communities into racial consciousness of White supremacy. This developmental point may be complex, given different histories of regions within the United States, migration histories, acculturation rates, and racial socialization within families. Similarly, White supremacy seeks to homogenize AAPI communities as a single racial group solely characterized by educational and economic success (Museus, 2021).
Built upon the premise of this study, it behooves researchers to address how anti-Blackness persists within AAPI communities (Yi et al., 2020; Yoo et al., 2021). Because only one participant had Pacific Islander heritage in the current study, researchers can further explore how Pacific Islanders may (a) endorse anti-Blackness, (b) experience the nexus of racism and colonialism, and (c) shape their commitments to solidarity with Black communities. Based on the themes underpinning the process toward thick solidarity in the study, it may be beneficial for researchers to consider the institutional conditions of their neighborhoods, communities, schools, and workplaces in promoting racial coalitions. Given that the study’s findings emphasized the importance of awareness and knowledge, it would be helpful to engage in qualitative research that further explores how educators in the P–16 system (i.e., preschool to college) map their curriculum of Asian history to include knowledge of racial coalitions, White supremacy, imperialism, and colonialism. Further research may also examine how counselor educators address the complex and racialized experiences of Asian American and Black communities within graduate coursework. Additionally, it is imperative to expand on research that illuminates Black organizers, activists, and communities in racial solidarity movements and Black-Asian racial coalitions.
Conclusion
The results of a grounded theory with diverse Asian American voices illuminated how causal conditions, contextual factors, intervening conditions, actions, and outcomes mobilized Asian Americans toward solidarity with the BLM movement in 2020. Understanding these conditions are of paramount importance to overcoming anti-Black notions embedded within AAPI ethnic subgroups and challenging systemic forms of racial oppression that impact all communities of color.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Anand, D., & Hsu, L. (2020). COVID-19 and Black Lives Matter: Examining anti-Asian racism and anti-Blackness in US education. International Journal of Multidisciplinary Perspectives in Higher Education, 5(1), 190–199. https://doi.org/10.32674/jimphe.v5i1.2656
Arora, M., & Stout, C. T. (2019). Letters for Black Lives: Co-ethnic mobilization and support for the Black Lives Matter movement. Political Research Quarterly, 72(2), 389–402. https://doi.org/10.1177/1065912918793222
Blalock, H. M., Jr. (1967). Toward a theory of minority-group relations. Wiley.
Bonacich, E. (1973). A theory of middleman minorities. American Sociological Review, 38(5), 583–594. https://doi.org/10.2307/2094409
Bonilla-Silva, E. (2004). From bi-racial to tri-racial: Towards a new system of racial stratification in the USA. Ethnic and Racial Studies, 27(6), 931–950. https://doi.org/10.1080/0141987042000268530
Bonilla-Silva, E. (2018). Racism without racists: Color-blind racism and the persistence of racial inequality in America (5th ed.). Rowman & Littlefield.
Brewer, M. B. (2000). Reducing prejudice through cross-categorization: Effects of multiple social identities. In S. Oskamp (Ed.), Reducing prejudice and discrimination (pp. 165–183). Erlbaum.
Chan, C. D., & Litam, S. D. A. (2021). Mental health equity of Filipino communities in COVID-19: A framework for practice and advocacy. The Professional Counselor, 11(1), 73–85. https://doi.org/10.15241/cdc.11.1.73
Chan, S. (1991). Asian Americans: An interpretive history. Twayne.
Chang, B. (2020). From ‘illmatic’ to ‘kung flu’: Black and Asian solidarity, activism, and pedagogies in the COVID-19 era. Postdigital Science and Education, 2(3), 741–756. https://doi.org/10.1007/s42438-020-00183-8
Charmaz, K. (2014). Constructing grounded theory (2nd ed.). SAGE.
Charmaz, K. (2017). Special invited paper: Continuities, contradictions, and critical inquiry in grounded theory. International Journal of Qualitative Methods, 16(1), 1–8. https://doi.org/10.1177/1609406917719350
Chou, R. S., & Feagin, J. R. (2016). The myth of the model minority: Asian Americans facing racism. Routledge. https://doi.org/10.4324/9781315636313
Clarke, A. E. (2012). Feminism, grounded theory, and situational analysis revisited. In S. N. Hesse-Biber (Ed.), Handbook of feminist research: Theory and praxis (2nd ed., pp. 388–412). SAGE.
Craig, M. A., & Richeson, J. A. (2012). Coalition or derogation? How perceived discrimination influences intraminority intergroup relations. Journal of Personality and Social Psychology, 102(4), 759–777. https://doi.org/10.1037/a0026481
Creswell, J. W., & Poth, C. N. (2018). Qualitative inquiry & research design: Choosing among five approaches (4th ed.). SAGE.
David, E. J. R. (2013). Brown skin, White minds: Filipino-/American postcolonial psychology. Information Age Publishing.
David, E. J. R., & Okazaki, S. (2006a). Colonial mentality: A review and recommendation for Filipino American psychology. Cultural Diversity and Ethnic Minority Psychology, 12(1), 1–16.
https://doi.org/10.1037/1099-9809.12.1.1
David, E. J. R., & Okazaki, S. (2006b). The Colonial Mentality Scale (CMS) for Filipino Americans: Scale construction and psychological implications. Journal of Counseling Psychology, 53(2), 241–252. https://doi.org/10.1037/0022-0167.53.2.241
David, E. J. R., Schroeder, T. M., & Fernandez, J. (2019). Internalized racism: A systematic review of the psychological literature on racism’s most insidious consequence. Journal of Social Issues, 75(4), 1057–1086. https://doi.org/10.1111/josi.12350
Elias, A., Ben, J., Mansouri, F., & Paradies, Y. (2021). Racism and nationalism during and beyond the COVID-19 pandemic. Ethnic and Racial Studies, 44(5), 783–793. https://doi.org/10.1080/01419870.2020.1851382
Fanon, F. (1952). Black skin, White masks. Grove Press.
Gaertner, S. L., & Dovidio, J. F. (2000). Reducing intergroup bias: The common ingroup identity model. Psychology Press.
Gaertner, S. L., Rust, M. C., Dovidio, J. F., Bachman, B. A., & Anastasio, P. A. (1994). The contact hypothesis: The role of a common ingroup identity on reducing intergroup bias. Small Group Research, 25(2), 224–249. https://doi.org/10.1177/1046496494252005
Gergen, K. J. (2020). Constructionist theory and the blossoming of practice. In S. McNamee, M. M. Gergen, C. Camargo-Borges, & E. F. Rasera (Eds.), The SAGE handbook of social constructionist practice (pp. 3–14). SAGE. https://doi.org/10.4135/9781529714326.n1
Gergen, M. (2020). Practices of inquiry: Invitation to innovation. In S. McNamee, M. M. Gergen, C. Camargo-Borges, & E. F. Rasera (Eds.), The SAGE handbook of social constructionist practice (pp. 17–23). SAGE. https://doi.org/10.4135/9781529714326.n2
Guba, E. G., & Lincoln, Y. S. (1989). Fourth generation evaluation. SAGE.
Haney López, I. (2006). White by law: The legal construction of race (10th ed.). New York University Press.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Ho, F., & Mullen, B. V. (Eds.). (2008). Afro Asian: Revolutionary political and cultural connections between African Americans and Asian Americans. Duke University Press.
Ho, J. (2021). Anti-Asian racism, Black Lives Matter, and COVID-19. Japan Forum, 33(1), 148–159.
https://doi.org/10.1080/09555803.2020.1821749
Jeung, R., & Nham, K. (2020). Incidents of coronavirus-related discrimination. Asian Pacific Policy & Planning Council. https://bit.ly/3bITRDE
Khan-Cullors, P., & Bandele, A. (2017). When they call you a terrorist: A Black Lives Matter memoir. St. Martin’s Publishing Company.
Kim, C. J. (1999). The racial triangulation of Asian Americans. Politics Society, 27(1), 105–138.
https://doi.org/10.1177/0032329299027001005
Lebron, C. J. (2017). The making of Black Lives Matter: A brief history of an idea. Oxford University Press.
Lee, S. J., Xiong, C. P., Pheng, L. M., & Vang, M. N. (2020). “Asians for Black Lives, not Asians for Asians”: Building Southeast Asian American and Black solidarity. Anthropology & Education Quarterly, 51(4), 405–421. https://doi.org/10.1111/aeq.12354
Li, Y., & Nicholson, H. L., Jr. (2021). When “model minorities” become “yellow peril”—Othering and the racialization of Asian Americans in the COVID-19 pandemic. Sociology Compass, 15(2), 1–13. https://doi.org/10.1111/soc4.12849
Litam, S. D. A. (2020). “Take your Kung-Flu back to Wuhan”: Counseling Asians, Asian Americans, and Pacific Islanders with race-based trauma related to COVID-19. The Professional Counselor, 10(2), 144–156. https://doi.org/10.15241/sdal.10.2.144
Litam, S. D. A. (2021). Rocking the boat: A call for Asian American and Pacific Islander counselors to make waves. Journal of Mental Health Counseling, 43(3), 273–276. https://doi.org/10.17744/mehc.43.3.09
Litam, S. D. A., & Chan, C. D. (2021). Breaking the bamboo ceiling: Practical strategies for Asian American and Pacific Islander counselor educators. Counselor Education and Supervision, 60(3), 174–189. https://doi.org/10.1002/ceas.12210
Litam, S. D. A., & Oh, S. (2020). Ethnic identity and coping strategies as moderators of COVID-19 racial discrimination experiences among Chinese Americans. Counseling Outcome Research and Evaluation. https://doi.org/10.1080/21501378.2020.1814138
Litam, S. D. A., & Oh, S. (2021). Effects of COVID-19 racial discrimination on depression and life satisfaction among young, middle, and older Chinese Americans. Adultspan Journal, 20(2), 70–84. https://doi.org/10.1002/adsp.12111
Litam, S. D. A., Oh, S., & Chang, C. (2021). Resilience and coping as moderators of stress-related growth in Asians and AAPI during COVID-19. The Professional Counselor, 11(2), 248–266.
https://doi.org/10.15241/sdal.11.2.248
Liu, R., & Shange, S. (2018). Toward thick solidarity: Theorizing empathy in social justice movements. Radical History Review, 131, 189–198. https://doi.org/10.1215/01636545-4355341
Liu, W. (2018). Complicity and resistance: Asian American body politics in Black Lives Matter. Journal of Asian American Studies, 21(3), 421–451. https://doi.org/10.1353/jaas.2018.0026
Mendoza, R. L. (2014). The skin whitening industry in the Philippines. Journal of Public Health Policy, 35, 219–238. https://doi.org/10.1057/jphp.2013.50
Merseth, J. L. (2018). Race-ing solidarity: Asian Americans and support for Black Lives Matter. Politics, Groups, and Identities, 6(3), 337–356. https://doi.org/10.1080/21565503.2018.1494015
Miles, M. B., Huberman, A. M., & Saldaña, J. (2020). Qualitative data analysis: A methods sourcebook (4th ed.). SAGE.
Museus, S. D. (2021). The centrality of critical agency: How Asian American college students develop commitments to social justice. Teachers College Record, 123(1), 1–38.
Nadal, K. L. (2021). Filipino American psychology: A handbook of theory, research, and clinical practice (2nd ed.). Wiley. https://doi.org/10.1002/9781119677109
Nicholson, H. L., Jr., Carter, J. S., & Restar, A. (2020). Strength in numbers: Perceptions of political commonality with African Americans among Asians and Asian Americans in the United States. Sociology of Race and Ethnicity, 6(1), 107–122. https://doi.org/10.1177/2332649218785648
Oh, A. E. (2010). An issue of time and place: The truth behind Korean Americans’ connection to the 1992 Los Angeles riots. Asian American Policy Review, 19, 39–48.
Pavlenko, A. (2002). ‘We have room for but one language here’: Language and national identity in the US at the turn of the 20th century. Multilingua, 21(2–3), 163–196. https://doi.org/10.1515/mult.2002.008
Pendakur, S. L., & Pendakur, V. (2016). Beyond boba tea and samosas: A call for Asian American race consciousness. In S. D. Museus, A. Agbayani, & D. M. Ching (Eds.), Focusing on the underserved: Immigrant, refugee, and Indigenous Asian American and Pacific Islanders in higher education (pp. 55–72). Information Age Publishing.
Petrola, J. P., Ledesma, J., Venturillo, C. P., Del Rosario, K. E., & Isidro, R. (2020). The will to self-determination: Understanding the life of Ati people in Aklan, Philippines. Journal of Critical Reviews, 7(11), 218–222. https://doi.org/10.31838/jcr.07.11.35
Poon, O. A., Segoshi, M. S., Tang, L., Surla, K. L., Nguyen, C., & Squire, D. D. (2019). Asian Americans, affirmative action, and the political economy of racism: A multidimensional model of raceclass frames. Harvard Educational Review, 89(2), 201–226. https://doi.org/10.17763/1943-5045-89.2.201
Poon, O., Squire, D., Kodama, C., Byrd, A., Chan, J., Manzano, L., Furr, S., & Bishundat, D. (2016). A critical review of the model minority myth in selected literature on Asian Americans and Pacific Islanders in higher education. Review of Educational Research, 86(2), 469–502. https://doi.org/10.3102/0034654315612205
Rafael, V. L. (2000). White love and other events in Filipino history. Duke University Press.
Saldaña, J. (2021). The coding manual for qualitative researchers (4th ed.). SAGE.
Sharma, N. (2018). The racial studies project: Asian American studies and the Black Lives Matter campus. In C. J. Schlund-Vials (Ed.), Flashpoints for Asian American studies (pp. 48–65). Fordham University Press.
Tajfel, H., & Turner, J. C. (1979). An integrative theory of intergroup conflict. In W. G. Austin & S. Worchel (Eds.), The social psychology of intergroup relations (pp. 33–47). Brooks Cole.
Taylor, K.-Y. (2016). From #BlackLivesMatter to Black liberation. Haymarket Books.
Timonen, V., Foley, G., & Conlon, C. (2018). Challenges when using grounded theory: A pragmatic introduction to doing GT research. International Journal of Qualitative Methods, 17(1), 1–10. https://doi.org/10.1177/1609406918758086
Tran, N., Nakamura, N., Kim, G. S., Khera, G. S., & AhnAllen, J. M. (2018). #APIsforBlackLives: Unpacking the interracial discourse on the Asian American Pacific Islander and Black communities. Community Psychology in Global Perspective, 4(2), 73–84. https://doi.org/10.1285/i24212113v4i2p73
Xu, J., & Lee, J. C. (2013). The marginalized “model” minority: An empirical examination of the racial triangulation of Asian Americans. Social Forces, 91(4), 1363–1397. https://doi.org/10.1093/sf/sot049
Yamashita, R. C., & Park, P. (1985). The politics of race: The open door, Ozawa and the case of the Japanese in America. Review of Radical Political Economics, 17(3), 135–156.
Yi, V., Mac, J., Na, V. S., Venturanza, R. J., Museus, S. D., Buenavista, T. L., & Pendakur, S. L. (2020). Toward an anti-imperialistic critical race analysis of the model minority myth. Review of Educational Research, 90(4), 542–579. https://doi.org/10.3102/0034654320933532
Yoo, H. C., Atkin, A. L., Seaton, E. K., Gabriel, A. K., & Parks, S. J. (2021). Development of a support for Black Lives Matter measure among racially–ethnically diverse college students. American Journal of Community Psychology, 68(1–2), 100–113. https://doi.org/10.1002/ajcp.12498
Yoon, I.-J. (1997). On my own: Korean businesses and race relations in America. University of Chicago Press.
Stacey Diane Arañez Litam, PhD, NCC, CCMHC, LPCC-S, is an assistant professor at Cleveland State University. Christian D. Chan, PhD, NCC, is an assistant professor at the University of North Carolina at Greensboro. Correspondence may be addressed to Stacey Litam, 2121 Euclid Ave., Cleveland, OH 44115, s.litam@csuohio.edu.
 Mariaimeé “Maria” Gonzalez (she/her/ella), PhD, LPC, was born in Puerto Rico and raised in the United States. She earned both her master’s and doctoral degrees from the University of Missouri–St. Louis and moved to Seattle, Washington, in 2014 to become a faculty member at Antioch University Seattle (AUS), located on the traditional land of the first people of Seattle, the Duwamish People, past and present. Dr. Gonzalez is the chair of the Master of Arts in Clinical Mental Health Program and is the co-founder of the Antioch University Latinx Mental Health & Social Justice Institute, which brings together community-engaged research, service, training, and community partnerships to promote the mental health and well-being of Latinx/e people. She truly enjoys teaching in the master’s and doctoral programs at AUS and is passionate about her work with other accomplices in liberation. She is a licensed professional counselor in the state of Missouri and an approved supervisor in the state of Washington. Dr. Gonzalez currently serves as the president of the American Counseling Association (ACA) of Washington (2020–22), chair of ACA’s International Committee (2022), president elect-elect for the Western Association for Counselor Education and Supervision (WACES), and ACA parliamentarian for 2021–22. She served as coeditor of Experiential Activities for Teaching Social Justice and Advocacy Competence in Counseling and is a board member for the WACES Journal of Technology in Counselor Education and Supervision. Her research passions are global mental health, clinical supervision, Latinx/e human rights, counselor and counselor educator professional identity development, correctional counseling, liberation psychology, social justice and advocacy counseling, and anti–human trafficking advocacy. She has been involved with global mental health and advocacy for about 15 years and served as a United Nations delegate to advocate for global mental health, especially during the COVID pandemic. Dr. Gonzalez has spent over 20 years working through the paradigm of mental liberation, which includes global community and mentorship. She is currently a WACES mentor and enjoys spending time with her loved ones and community.
Mariaimeé “Maria” Gonzalez (she/her/ella), PhD, LPC, was born in Puerto Rico and raised in the United States. She earned both her master’s and doctoral degrees from the University of Missouri–St. Louis and moved to Seattle, Washington, in 2014 to become a faculty member at Antioch University Seattle (AUS), located on the traditional land of the first people of Seattle, the Duwamish People, past and present. Dr. Gonzalez is the chair of the Master of Arts in Clinical Mental Health Program and is the co-founder of the Antioch University Latinx Mental Health & Social Justice Institute, which brings together community-engaged research, service, training, and community partnerships to promote the mental health and well-being of Latinx/e people. She truly enjoys teaching in the master’s and doctoral programs at AUS and is passionate about her work with other accomplices in liberation. She is a licensed professional counselor in the state of Missouri and an approved supervisor in the state of Washington. Dr. Gonzalez currently serves as the president of the American Counseling Association (ACA) of Washington (2020–22), chair of ACA’s International Committee (2022), president elect-elect for the Western Association for Counselor Education and Supervision (WACES), and ACA parliamentarian for 2021–22. She served as coeditor of Experiential Activities for Teaching Social Justice and Advocacy Competence in Counseling and is a board member for the WACES Journal of Technology in Counselor Education and Supervision. Her research passions are global mental health, clinical supervision, Latinx/e human rights, counselor and counselor educator professional identity development, correctional counseling, liberation psychology, social justice and advocacy counseling, and anti–human trafficking advocacy. She has been involved with global mental health and advocacy for about 15 years and served as a United Nations delegate to advocate for global mental health, especially during the COVID pandemic. Dr. Gonzalez has spent over 20 years working through the paradigm of mental liberation, which includes global community and mentorship. She is currently a WACES mentor and enjoys spending time with her loved ones and community.
 by Dr. Julia Bain, LPCC, NCC, CEAP
by Dr. Julia Bain, LPCC, NCC, CEAP