Apr 29, 2020 | Volume 10 - Issue 2
Ian P. Levy, Edmund S. Adjapong
Literature on the physical design of counseling spaces suggests that calm and comfortable school counseling offices support students’ emotional disclosure. However, many counseling environment design studies fail to consider the perspectives of clients. Scholars have called for school counselors to invite youth to co-create interventions as a means to promote cultural responsiveness and honor students’ cultural knowledge. The goal of the current exploratory action research was to bring visibility to the experiences of students who participated in a classroom-based school counseling intervention in which they co-created a hip-hop studio as a social and emotional support space. Specifically, focus groups on the value of the co-creation of a hip-hop studio for urban youth were employed. Results suggested students experienced the studio as a shared space for inclusivity, comfort, and belonging; a place to make their own design choices; and a practice space to garner peer support, engage in personal self-development, and support others.
Keywords: counseling environment, urban youth, classroom-based, hip-hop, cultural responsiveness
The physical design of counseling spaces by counseling professionals has been well explored in counseling literature (Devlin et al., 2013; Liddicoat, 2010; Miwa & Hanyu, 2006; Pressly & Heesacker, 2001). Counselor office design has primarily focused on the counselor’s preference for office design and has failed to take into consideration the psychological state of clients who are in pursuit of counseling services (Sanders & Lehmann, 2019). Historically, researchers explored how counselors’ control over their office design mitigated stress and increased job satisfaction (Pressly & Heesacker, 2001). Pressly and Heesacker (2001) found that counselors who were unhappy with their office may communicate that frustration to their clients. Further, pleasant environments were found to foster creativity, a sense of well-being, and job satisfaction for practicing counselors (Ceylan et al., 2008).
More recently, school counselors reported that their creation of calm and comfortable counseling offices supported students’ emotional disclosure (Cook & Malloy, 2014). Counseling office design elements that have been found to be important for the satisfaction of counselors and clients include overall aesthetics and layout, particularly dim lighting (Liddicoat, 2015; Miwa & Hanyu, 2006; Phelps et al., 2008), as well as access to daylight and space for privacy (Huffcut, 2010). In addition, the layout of a counseling office is strongly correlated with a client’s psychological state, suggesting that environmental structure can allow clients to evoke emotions and confront discrepancies in their self-concept (Liddicoat, 2015). Goelitz and Stewart-Kahn (2008) expressed a need for counselors to consider the experiences of their clients when designing a counseling environment. Although research shows that aesthetic changes to a counseling environment can support a variety of client outcomes, a specific process for the creation of counseling offices is missing within the literature (Pearson & Wilson, 2012).
Additionally, given the current body of research, scholars note the importance of creating counseling environments that align with client preferences. A recent qualitative study conducted by Sanders and Lehmann (2019) indicated clients reported a sense of comfort when a counseling office felt more like a home or a lounge than like a traditional office space. Research has also emphasized the importance of school counselors developing an in-depth understanding of a client’s social context as well as their cultural values and differences (McMahon et al., 2014; Ratts et al., 2016), further stressing a need to understand clients’ preferences when designing emotionally supportive environments.
Client-Centered Office Design
Considering office design, Benton and Overtree (2012) posited that an understanding of clients’ cultural differences was imperative for making design choices. Similarly, Devlin et al. (2013) found that counselors who displayed artwork from different cultures in their office were perceived by clients as being more culturally competent. Decisions to hang artwork might be based on Ponterotto and Austin’s (2005) multicultural competence checklist, which suggested that “the physical surroundings of the program area reflect an appreciation of cultural diversity (e.g., artwork, posters, paintings, languages heard)” (p. 31). Beyond this checklist, however, Benton and Overtree (2012) suggested “no research or detailed guidelines on the critical physical elements to consider in designing a multiculturally friendly office” were available (p. 266). Although not in office design research explicitly, L. Smith and Chambers (2015) recommended school counselors invite youth to co-create counseling interventions as a means to promote cultural responsiveness and honor the cultural knowledge youth bring into counseling sessions. School counselors are also responsible for understanding students in the context of their own environments, in an effort to deploy culturally sensitive interventions (Hansen et al., 2014).
School Counselor Collaboration
When determining how school counselors might best employ culturally sensitive interventions, collaborative efforts are of particular value. The American School Counselor Association (ASCA; 2015) released a position statement suggesting that “school counselors demonstrate cultural responsiveness by collaborating with stakeholders to create a school and community climate that embraces cultural diversity and helps to promote the academic, career and social/emotional success for all students” (p. 24). Ratts and Greenleaf (2018) argued for school counselors to use multicultural and social justice approaches to combat threats to their students’ academic, career, and personal/social development. Using these approaches requires that school counselors create school–family–community partnerships to collaborate with all stakeholders in support of equitable and socially just school counseling interventions (Bryan et al., 2019). However, an ASCA (2019a) national dataset suggested student-to-counselor ratios in the United States are 455 students to one school counselor, far higher than the recommended 250-to-1 ratio. These results are not surprising given prior research demonstrating that school counselors are often inundated with large caseloads and non–school counseling duties, which hinders their ability to engage in direct academic, career, and personal/social development services (Kim & Lambie, 2018; Mau et al., 2016).
In response to caseload issues, school counselors are encouraged to collaborate with teachers to provide indirect services to all students (Cholewa et al., 2016). Researchers noted the success of social skills–based classroom counseling to support students’ social, personal, and academic concerns (Bostick & Anderson, 2009). A study on classroom emotional climate suggested that classroom environments that promote students’ autonomy and expression of ideas are predictive of increased academic achievement (Reyes et al., 2012). School counselors are also urged to act as consultants, supporting teachers in developing interventions within their classrooms to address identified social and emotional needs (ASCA, 2019b). Researchers have recommended that school counselors collaborate with principals on school-wide initiatives that support all stakeholders in delivering the counseling curriculum, noting principal–counselor collaboration as significantly correlated with positive school climate (Rock et al., 2017).
In the implementation of a comprehensive school counseling program, school counselors are urged to use interventions like advisory councils (composed of representatives from all stakeholders, including students) to support student outcomes (ASCA, 2019b). However, the implementation of school-wide school counselor–led interventions lacks a specific focus on cultural responsiveness (Betters-Bubon et al., 2016). Therefore, in order to adequately support the academic, career, and personal/social development of all students within a school, school counselors are encouraged to collaborate with ancillary staff who can carry out interventions that meet these developmental outcomes (ASCA, 2019b). In fact, in the current study, a collaboration is explored to support a school counselor—who had a 700-to-1 caseload—with the indirect implementation of a classroom-based school counseling intervention to aid students’ social and emotional development.
Counselor–Advocate–Scholar Model
This study strategically drew upon the counselor–advocate–scholar (CAS) model to engage various school-based stakeholders in the deployment of a culturally sensitive classroom-based school counseling intervention. The CAS model is built on the presumption that counselors who solely use office-bound interventions are unfit to address issues of social injustice (Ratts, 2009). In other words, the issues that Black and Brown youth and other marginalized groups bring into session are not solely internal and are likely symptomatic of larger societal ills that need to be addressed through outside-of-office interventions. Therefore, building upon research that suggests community-based counseling practices are particularly useful in supporting historically marginalized groups (Bailey et al., 2007), Ratts (2009) posited that counselors must hold alternative counseling roles and use interventions outside of the office.
The CAS model indicates counselors should have three roles: 1) the counselor, 2) the advocate, and
3) the scholar. The counselor role entails the use of culturally responsive approaches to in-office counseling, which assists clients in analyzing emotional experiences (Ratts & Greenleaf, 2018). Ratts and Pedersen (2014) defined the role of an advocate as leaving the four walls of the counseling office to advocate for interventions that transcend talk therapy and address larger systemic concerns. They described the scholar role as the ability to research and evaluate one’s own interventions to inform the development of best practices that support clients and their own advocacy efforts. Together these three roles form multicultural–social justice praxis, a reminder that counselors must transition between these roles to support clients in navigating internal and external forms of oppression (Ratts & Pedersen, 2014).
Hip-Hop Culture
In pursuit of using multicultural practice in schools, recent researchers have demonstrated that urban inner-city youth identify as part of hip-hop culture and have explored the use of hip-hop pedagogy (Adjapong, 2017; Adjapong & Emdin, 2015). Given the importance of school counselors honoring their students’ cultural knowledge (Hannon & Vereen, 2016), a hip-hop–based school counseling framework can be intentionally used to guide the implementation of the CAS model. Hip-hop culture is rooted in the corralling of a community to combat social inequities (Chang, 2005). The emergence of hip-hop culture was in direct response to the systemic and structural changes in the 1970s South Bronx (Caro, 1975; Chang, 2005). In the midst of an economic crisis, hip-hop culture was conceived by youth who critiqued and commented on social issues facing inner-city communities (Forman, 2002). To support the practice of hip-hop culture, hip-hop often exists within physical spaces, such as block parties, concerts, or recording studios (Harkness, 2014).
Hip-Hop and Spoken Word Therapy
Because of the growing influence of hip-hop culture, many scholars and practitioners have explored the power and potential of hip-hop lyric writing, analysis, and discussion as culturally responsive interventions in the counseling process (Kobin & Tyson, 2006; Travis & Deepak, 2011; Tyson, 2002; Washington, 2018). This research engendered hip-hop and spoken word therapy (HHSWT), a culturally responsive counseling process whereby students engage in previously validated counseling interventions through the process of writing, recording, and performing hip-hop music (Levy, 2012; Levy & Keum, 2014). The development of HHSWT over time has thoroughly examined varying hip-hop cultural processes and how those might be used inside counseling offices. For instance, HHSWT offers clinicians a set of hip-hop–centered tools that they can use in the counseling process to support youth in exploring difficult thoughts and feelings. These tools include the hip-hop cypher to support group process and sharing (Levy, Emdin, & Adjapong, 2018), creating emotionally themed mixtapes (Levy, Cook, & Emdin, 2018), lyric writing as emotive journaling, and dyadic song collaboration as role-play (Levy, 2019). Each of these HHSWT techniques offers a culturally salient process in which youth of color can disclose and process difficult thoughts and feelings with their counselor. Levy (2019) found a school counselors’ use of HHSWT in group counseling inside of a school hip-hop recording studio positively supported students’ social and emotional development.
The Hip-Hop Recording Studio
When aiming to design culturally responsive counseling environments, it is important to note that the hip-hop recording studio also has held an important place in hip-hop culture and is largely unexplored in counseling literature. Harkness (2014) defined the hip-hop recording studio as a symbolic space or “a zone in which identity and meaning are shaped by social exchanges that occur within a culturally specific location” (p. 85). Harkness locates these studios as “sites for legitimization and personal transformation” where artists convene to collaborate on music as a “means of identity construction and development” (p. 85). Home-studios mark a shift of power into the hands of youth, who have easy access to technology and online media to create and release their own content and shape hip-hop music and culture (Harkness, 2014). Harkness conducted a content analysis of interviews with rappers and producers wherein they describe the value of studios as adapted home environments and places for self-discovery and authenticity. His findings offer insight into how hip-hop practices might be used in the design of culturally responsive environments for urban youth.
Harkness (2014) illuminated that studios are often built wherever they can fit, like inside of a rapper’s room, basement, living room, or bathroom. Rappers described the need to have studios be aesthetically pleasing, with foam padding on the walls and dim lighting. For many artists, entering a recording booth to rhyme legitimized their thoughts and feelings and generated “an identity shift where they began to define themselves” (Harkness, 2014, p. 91). Although participants in the Harkness study certainly enjoyed being in recording studios, they were adamant about labeling studios as places where serious work and emotional labor occurred. Inside studios, artists felt required to display authentic reflections of their lived experiences in their music and their environment. Overall, the creation of studio spaces is not about how prestigious they look, but more about whether or not the aesthetics of the environment enable artists to carry out the hard work and emotional labor necessary for the discovery of one’s true self.
Purpose of the Present Study
Given that (a) a limited number of studies have explored clients’ opinions and perspectives on changes made by school counselors to a school counseling space, (b) most studies focus on designing counseling environments outside of schools, and (c) the school counseling profession lacks research on multicultural office design, there is a need for research exploring the processes by which students themselves engage in the construction of culturally salient school counseling spaces. Consequently, the purpose of this exploratory action research was to illuminate the experiences of urban youth of color who were part of a classroom-based school counseling intervention in which they co-created a space for social and emotional reflection in an inner-city urban high school. Specifically, this study drew on HHSWT and the CAS model as a culturally sensitive counseling intervention designed to increase understanding of the value of the co-creation of a hip-hop studio as an environment conducive to social and emotional development. The research question that guided the study was: What do students report experiencing while co-creating the school studio? Reponses from student focus group interviews were used to assess answers to this question, with an interpretative phenomenological analysis (IPA) framework guiding interview development, data collection procedures, and data analysis.
Method
Sample
This study was conducted in an inner-city urban high school in a densely populated city in the northeastern United States. The pseudonym for the high school is Liberty High School (LHS). A teacher at LHS consulted with the principal investigator (PI) of this study, given that he is a school counselor educator and a former school counselor with noted experience in the use of HHSWT and the studio creation process. Specifically, the teacher was interested in integrating interventions into a hip-hop lyric writing elective class that could support students’ social and emotional development. The teacher felt the lack of school counselors at LHS created a gap in social and emotional supports and saw students in their classroom struggle academically as a result of unprocessed emotional experiences.
After an initial planning meeting, the PI and the teacher agreed to guide students through a collaborative hip-hop studio construction process as a space to supplement social and emotional support. To garner additional support for this classroom-based intervention, the PI and the teacher attempted to collaborate with LHS’ only school counselor, who declined to participate given their large caseload and being understandably inundated. The school counselor’s inability to participate further justified the need for the PI to support the teacher and their students. In this sense, a collaborative and indirect approach was explored in which the PI/counselor educator supported a classroom teacher in the implementation of a classroom-based school counseling intervention.
Participants were recruited from a hip-hop lyric writing class where they worked with their course instructor on the co-creation of a school studio following approval from the school district’s Institutional Review Board. Students had selected this course from a range of options to fulfill an elective music course credit, a graduation requirement in the northeastern state where this study took place. There were 15 high school students ranging between 14–18 years of age who participated in this study. Neither the course instructor nor the PI had any influence on student enrollment in the class. Prior to their enrollment in this course, the teacher collected all informed consent and/or assent forms from students and parents/guardians. All 15 students agreed to participate in a post-course focus group regarding their experiences co-creating the school studio.
The racial demographic of students at LHS is: 66% Hispanic, 32% Black, 1% Asian, 1% White, and 1% Other. Like many urban high schools in this particular school district, LHS is one of three schools within a larger school’s campus. This setup inherently limits the amount of physical space and resources available to students in each school and in many instances forces them to share. LHS is a Title 1 school, and all students qualify for free or reduced lunch. LHS has 700 students and one school counselor.
Measures
Data collection measures in the present study consisted of two post-intervention focus groups, with seven to eight students in each. The PI facilitated each focus group with the aim of exploring participant experiences during the studio creation as well as assessing how they believed the studio creation process impacted them and might support them moving forward. The PI and the teacher were interested in understanding participants’ lived experiences through action research, so an IPA framework was used for interview guide development, data collection procedures, and data analysis. IPA was selected by the PI as an approach to action research that allows researchers to play a role in guiding a process that leads to development of theoretical and practical knowledge (Zuber-Skerritt & Fletcher, 2007).
The difficulty of action research in this regard is for the researchers to limit their subjectivity, which is why the PI chose not to participate in the intervention and instead facilitated the focus groups. Generally, qualitative methods are most appropriate when engaging in phenomenological research with the PI positioned outside of the intervention (Breen, 2007; Zuber-Skerritt & Fletcher, 2007). Therefore, a focus group interview guide was developed by the PI to prompt discussion around participant experiences, including perceptions of what they learned in the process as well as what they identified as important to them. However, consistent with IPA standards (J. A. Smith et al., 2009), the semi-structured interview guides were flexible enough to allow participants the opportunity to lead the discussion. The two focus groups both lasted 30 minutes and took place within the recording studio at LHS.
Design
The studio construction process occurred over a 3-month period (September to December 2018) as a classroom-based intervention during a hip-hop lyric writing course taught by the teacher. The course met twice a week for 90 minutes each time. Because of school holidays, the class met for a total of 10 sessions for studio construction. The PI met with the teacher twice in late August of 2018, prior to the launch of the class, to order necessary equipment. Further, the PI met with the teacher once a month over the course of the 3-month study to provide curricular support. The studio construction process was designed to be entirely student driven. Based on research suggesting the cultural importance of the hip-hop studio (Harkness, 2014), the need for client voice in counseling office design (Pearson & Wilson, 2012), and cultural competence literature requiring the co-designing of interventions (L. Smith & Chambers, 2015), the PI believed it was necessary to provide students with total ownership over the studio creation process.
Implementing the CAS Model
The studio construction process was guided by the CAS model, which targeted the systemic concern of school counselor availability and subsequently sought to support students in designing an ancillary space for social and emotional services. Drawing from the advocate role of the CAS model, the PI and the teacher collaboratively advocated for financial support through a GoFundMe campaign on Facebook. This crowdsourced campaign garnered $900 for school studio equipment. Next, the teacher met with their school principal to advocate for a location where the class could construct a studio. In line with the scholar role, the teacher and the principal were interested in understanding the impact this classroom-based intervention had on their student body. The PI agreed to assist the teacher and the principal in analyzing evaluation data.
The CAS model suggests the importance of culturally sensitive counseling processes. Pulling from HHSWT, a culturally responsive, process-based counseling framework (Levy, 2012), the teacher functioned as a group facilitator who sought to keep the class focused on their group goal of creating the studio. For example, each session began with a group conversation about the plans for that day, asking group members to agree on varying roles they would take during construction. Halfway through each session, the facilitator would bring the group back into a circle to discuss work done, evaluate progress toward the group goal, and finalize what building would occur for the remainder of the session. Each session would close with a checkout in which the group reflected on how they felt having completed the work, and what changes or additions they wanted to make during the following session. Exploratory activities were also used to allow students to reflect on environments that make them comfortable, spark conversation, and work toward studio completion. As a signature assignment, the teacher pulled from the HHSWT framework and offered students the chance to create a “Where I’m From” song to support students in exploring who they are and what makes them comfortable, to ultimately inform their studio design decisions. Once the studio was developed, students requested assistance in learning how to use studio equipment for recording purposes. Advocating for students’ requests, the teacher asked the PI (as a stand-in for the school counselor) to visit and work with students to support their preparation toward recording their lyrics and teach other students how to record their peers.
Data Analysis
The qualitative data collected in the present study were analyzed using the IPA framework, a qualitative research approach designed to facilitate understanding of the participants’ worlds and subjective experiences, typically as they relate to a specific event or phenomenon common to all participants being interviewed (Chapman & Smith, 2002). The recorded focus group was transcribed verbatim using InqScribe technology (Inquirium, LLC, 2013). To begin the analysis, the PI read and re-read the focus group interview transcript to build familiarity with the data. Once familiar with the transcript, the PI started with microanalysis, which included making descriptive, linguistic, and conceptual comments in the right margin of the transcripts (J. A. Smith et al., 2009). J. A. Smith et al. (2009) suggested that descriptive comments are those that are focused on the content of the communication, and linguistic comments are those that consider the tone and use of language throughout the transcript. Conceptual comments are interpreted first through a descriptive lens, and linguistic comments are then considered together alongside the interpretation of the transcript by the researcher. Once microanalysis was completed for the entire transcript, the PI reviewed the notations that had been made to identify initial emergent themes throughout the interview, which were noted in the left margin of the document.
The initial emergent themes for each interview were then compared across individual participants to identify the lower-order themes, which were then combined to inform the identification of the higher-order themes (J. A. Smith et al., 2009). In the final stages of data analysis, emergent themes that represented the lived experiences of participants in the group were situated within the extant literature to offer an interpretation of the experiences through existing theoretical frameworks, a hallmark process of IPA research (J. A. Smith et al., 2009). Transcripts were then sent to the second author, who had not been involved in the data collection, to audit identified themes. When discrepancies existed (e.g., different themes were found), researchers engaged in discussion until consensus was reached.
Trustworthiness
To safeguard the trustworthiness of the data, authors engaged in two intentional strategies identified as important for improving the credibility and reliability of the data (Morrow, 2005). First, to ensure the credibility of the data, prior to engaging in data analysis, the PI who conducted the interview engaged in a reflexive process to examine preconceptions about the data in order to bracket those ideas and focus on understanding the lived experiences of the participants. Additionally, to allow for transferability of the research process and results, the authors provided a rich description of the research processes (i.e., methods) as well as the findings that emerged through data analysis (i.e., results).
To improve the dependability of the results, two strategies were employed. First, to improve recall for the participants, they were encouraged to review the video montage of their work building the studio. Additionally, to minimize the impact of individual bias, the marked transcript was sent to an additional colleague who acted as an outside auditor. Through the aforementioned processes, the researchers believe trustworthiness consistent with standards in qualitative inquiry was achieved (Thomas & Magilvy, 2011).
Results
The findings of this study are organized by higher- and lower-order themes in accordance with IPA (J. A. Smith, 1996). To elaborate on higher- and lower-order themes, exemplary moments from transcripts that reflect students who participated in co-creation of the school studio were identified. The first higher-order theme was school studio as shared space. The lower-order themes that constituted this theme included feeling comfort and belonging and wanting inclusivity. The second higher-order theme was student design choices. The lower-order themes contained within this theme included designing an authentic studio, needing ownership, and thinking independently. The third and final higher-order theme was studio as practice space/lab. The lower-order themes that comprised this theme included peer support, opportunity, and supporting others. Selected student quotes with student pseudonyms are provided below to illustrate each theme.
School Studio as Shared Space
The first higher-order theme, school studio as shared space, generally suggested that students experienced the hip-hop studio as a place within the school that they wanted to share with others. An example of a quote that fell within this category is: “So you get to be surrounded by rappers and a community that knows what you’re doing, and you get to be upheld by everybody else and you get to share this space with everyone.” This higher-order theme, school studio as shared space, contained two lower-order themes, which indicated that students experienced (a) feeling comfort and belonging and (b) wanting inclusivity.
Feeling Comfort and Belonging
The emergence of the first lower-order theme, feeling comfort and belonging, indicated that students felt heard and connected to others while creating the school studio. For example, when students were asked to discuss what it was like to co-create the school studio, a student named Jayda responded, “We’re just like a little group. A little family. A little rap family.” In this example, the student compares their level of connection with her peers to that of a family. When students were asked what it meant to have a studio in their school, Jordan shared, “In my personal opinion, I feel like what it means to me is being able to communicate with others and letting other people hear your voice.” Here the student highlights the school studio as an environment where they have the chance to share their “voice” and message.
Wanting Inclusivity
The emergence of the second lower-order theme, wanting inclusivity, indicated that students saw the need to create a space that was inclusive of others and that did not revolve solely around their needs and wants. Carlos shared:
I’m still overthinking about what should we do because I feel like different people have certain styles. I don’t want to make it all about me. I don’t want to make it all about other people. I want to make it about the whole school and what they think about. Because we’re not gonna be the only ones in this rap studio. I want to know what they think about and I want to know their perspectives and how they want to do it.
This student recognized that other students from LHS might also want to access the school studio; therefore, they wanted to gain the perspectives of others, beyond their peers who were co-constructing the studio, regarding what should be included. In this sense, students discouraged individual choices because that approach would not create an inclusive space. Another student, Tasha, stated that “for the wall, it was hard to know what everybody likes and the whole school and put it into just one small wall.” Again, students who had the opportunity to co-construct a school studio were thinking about ways to create a space that reflected, represented, and was inclusive of the entire school.
Student Design Choices
The second higher-order theme, student design choices, suggested that students experienced being able to make their own design choices during the co-construction process. For example, a particular student quote read:
We just came in here and it was like, everything messed around so we came in with an idea of like, where we think stuff should go, and that’s how we came up with that. Put it on the corner where the studio gonna be.
The student design choices theme contained three lower-order themes which indicated that students experienced (a) designing an authentic studio, (b) needing ownership, and (c) thinking independently.
Designing an Authentic Studio
Within the second higher-order theme, the first lower-order theme of designing an authentic studio illuminated that students made design choices in alignment with what they defined to be a professional or culturally appropriate studio environment. One example of a student quote that demonstrates this theme came while a student detailed the process of co-constructing the school studio. Specifically, Jay commented that “it makes it feel like a real studio. When you see rappers in a studio, you see all these lights and it looks professional and stuff, so I think it would make it look like the mood of that.” The installation of colorful LED lights within the school studio supported the students’ feeling that the studio was real or professional. The professional aesthetic that students established with the studio enabled the creation of a particular “mood” that also made the school studio space and experience feel culturally authentic.
Students also chose to infuse their school colors into the design of the studio, reporting that design element as an authentic representation of their school. When discussing the design process, Devante shared: “Yeah, and then like, [the foam pads] matched with our school colors like the purple and the green in the middle represents our school.” Finally, when sharing about the process, Alexandra detailed her most and least favorite moments: “My favorite moment: actually being able to build the studio, the checkered over there, the foam. The most challenging part: missing one day then being lost.” For Alexandra, the foam also functioned as an indicator of an authentic studio space. She also added that missing school made her feel lost or disconnected from the studio construction process, and that was particularly challenging.
Needing Ownership
The second lower-order theme, needing ownership, highlighted that students experienced needing ownership of the studio space. When discussing their design process, Gabriel said, “yeah, basically I said like, you put the ‘L’ so whoever comes in here know that Liberty was here first. We created this place. And that was our main point of putting that big ‘L’ right there.” In this quote, Gabriel spoke to the importance of design choices in letting the surrounding community know who was responsible for the studio’s creation. This statement and the theme of needing ownership more broadly suggests that students wanted to feel properly valued and credited for their work and that they also had ownership over their choices and felt able to make their own decisions. This sentiment is further supported by a quote from Rachael:
I know it made me feel like the room was built in our hands. Later on, when everything is done, when people come in, whatever they see is what we all thought of together. We could’ve had this over there, but we decided to put it over here. It just makes us feel . . . well, it makes me feel like, yeah.
Adding support to Gabriel’s statement, Rachael appears to be feeling a sense of pride in laying claim to the thoughts, feelings, and physical work that went into the creation of the school studio.
Thinking Independently
The third lower-order theme, thinking independently, highlighted that students had opportunities to think amongst themselves and to troubleshoot and find solutions to problems without relying on the direction of an adult. Carlos reported that “without the adults, I feel like we really had to bring our creative ideas straight from our thoughts on how to make the studio.” Carlos believed that without adults walking them through the process of creating a school studio, they were able to showcase their “creative ideas” and pull from knowledge and thoughts they already possessed. Additionally, Alexandra shared:
Well, I’m always used to being told what to do because you would give me an assignment and I’ll do it. I can’t just think for myself. As you can see, I’m still having difficulty thinking for myself with the wall.
Alexandra highlights that within the traditional classroom lessons, students are always given an assignment that offers directions on how to complete it. When students were given the task of co-constructing a school studio, there were many tasks that could be approached differently, and students were encouraged as experts to think in ways that were independent of adults and pull from within to address their task.
Studio as Practice Space/Lab
The third higher-order theme, studio as practice space/lab, suggested that students experienced the hip-hop studio as a place where they could learn to feel more prepared. Student quotes within this higher-order theme included statements like: “If we invite other people from the other school or people in other classes to see us, we’re gonna have more . . . prepared. We’re gonna be more prepared to do it.” This higher-order theme contained four lower-order themes, which indicated that students experienced (a) peer support, and (b) opportunity, (c) self-discovery, and (d) supporting others.
Peer Support
The first lower-order theme, peer support, suggested that students felt as if the school studio was a location in which they could receive feedback, support, and opportunities for personal preparation from their peers. When responding to a question regarding what students felt they might have learned throughout the co-creation process, Vicki claimed: “This small space is not gonna help me stand up in front of 400 people but bringing little by little people into here while we’re rapping or anything, would help me build up more confidence.” Although Vicki still felt there was work to do in order to feel ready to share her lyrics with a large number of people, she posited that the studio space could function as a preparation space for larger group sharing, where peers could help others and boost their confidence. Another student, John, spoke to the experience of individuals who rap within the school studio, reporting that:
The nice thing, after the person’s done with the rap, he makes somebody ask what they heard about that person, about learning about that person, that’s gonna put confidence in you. Like, they were actually listening. And that makes you want to rap more so people can actually acknowledge your bars.
In this quote, John spoke to the process of sharing lyrics. Specifically, when people share lyrics, John imagined that others would listen carefully to them and then willingly engage in a discussion about what they heard. John believes the experience of sharing lyrics would make people feel acknowledged and have an increased sense of self-confidence.
Opportunity
The second lower-order theme of opportunity evidenced that students experienced the school studio as an environment that could offer opportunities for personal advancement in life. When discussing how this school studio might be used within the school, Devante said:
It’s hard to find a place to rap. That’s 1. 2, they cost too much. And 3, you know people say you can buy a microphone and you can do this, that and the third in your own household. Not a lot of people have money, many people they use the money and give it to their parents, and then if you ask your parents, they’re gonna tell you the same thing that they tell every other kid when they want to pursue a hobby: “This is not gonna get you anywhere.” ’Cause my parents tell me that all the time.
In this statement, Devante appreciates free access to space where he can pursue his hobby. Within the school studio, there is a perceived potential among students to work toward their own dreams without waiting on financial support or support from anyone other than themselves. Statements like this one suggest that access to the school studio provided students with an opportunity to consider their career on their own terms. A second student, Melissa, builds on this notion of opportunity, suggesting:
So apart from someone finding out their identity with this studio, they could also put their work out there knowing they have a chance to get somewhere. To be very honest, in this decade, everyone has a chance to get somewhere. It doesn’t matter if you’re good at rapping, bad at rapping, you suck, you great, you can get somewhere. It’s all about other people’s opinions, it’s all about what they like, and if you’re liked by the public, then you’re gonna get until as far as you can reach.
In this quote, Melissa indicated how a student could use the school studio to garner support from the public to “get somewhere.” Within the school studio, students suggested that there is an opportunity for a unique level of access and self-advancement. Further aiding the idea that using the school studio was the desired opportunity for youth, Jay said: “I hate that we only come down here once a week.”
Supporting Others
The final lower-order theme, supporting others, demonstrated students’ intentions and goals of supporting others outside of their class who attended LHS. Jordan shared, “I want to learn how to use all this equipment. So that in the future other students will be able to be taught how to be using the mixer or putting beats into tracks.” Jordan wanted to be able to support other students outside of his class by teaching the skills that he plans on developing, which included “using the mixer” and “putting beats into tracks.” This expression demonstrated an understanding of the importance of teaching others how to utilize the school studio, which will contribute to the longevity of the space. Gabriel reported that “You teaching them how to rap, how to use the mic, the laptop and all that, that’s just gonna inspire their friends to come. They teach their friends and the cycle just continues like that.” Believing in how beneficial the studio was for them, Gabriel mentioned wanting to support his peers by sharing skills that were needed to effectively run the school studio so it could continue to be used. Gabriel also highlights that teaching others to make use of the school studio space will create a cycle that theoretically will allow students to bring their friends to engage as well. Therefore, not only is the school studio intriguing to students, but it will support their development of skills to maintain its use.
Discussion
This study was designed to increase understanding of the experiences of students partaking in a classroom-based school counseling intervention in which they co-constructed a hip-hop studio. Counseling environment data has suggested that counselors often take the lead on the creation of environments for clients (Pearson & Wilson, 2012), whereas we encourage school counselors to partner with youth in the creation of their own counseling spaces (L. Smith & Chambers, 2015). Broadly, results support the co-construction of school studios as culturally relevant environments that promote social and emotional development, addressing a need in the literature for research exploring multicultural counseling office design (Benton & Overtree, 2012). Further, the use of the CAS model enabled a collaboration in which a classroom teacher deployed an indirect and culturally responsive school counseling intervention to support students’ personal/social development (ASCA, 2019b; Ratts & Greenleaf, 2018).
Student Experiences
Results of this exploratory action research demonstrated that students experienced a sense of comfort and belonging inside the school studio. Similarly, Sanders and Lehmann (2019) indicated that clients felt a sense of comfort when the counseling office felt like a home or a lounge rather than a traditional office space. Further, data from the current study showed that the studio creation process empowered students to advocate for inclusivity in the use of this space for their entire school campus community. This outcome is ideal given that school counselors are charged with activating the entire school community in the deployment of school-wide interventions that support students’ academic, career, and personal/social development (Bryan et al., 2019). In specific comments, youth stated that they would want to locate peers who are in need of help and bring them to the school studio to develop personal/social skills. These statements suggest that after participating in the school counseling intervention, youth voiced that making the studio available to all students would improve the school counseling program at their school. This finding gives credence to the use of advisory councils at schools, with student members, to offer youth a platform to ensure that school counselors and their school counseling programs are serving all students (ASCA, 2019b). Additionally, a bevy of studies emphasized supporting youth in the development of skills as change agents in promoting peace, youth voice, and healing (Allan & Duckworth, 2018; Conner & Cosner, 2016; Levy, Emdin et al., 2018). Overall, the findings are important in that they support the use of studio co-creation as a classroom-based counseling intervention, which research suggests can result in school-wide impact (Bostik & Anderson, 2009).
Another notable finding of this study was students’ decisions in creating their authentic and professional school studio. For example, the students’ choice to install LED lights provided them with a professional aesthetic and a particular “mood” that also made the school studio space and experience feel authentic. The aesthetics of a counseling environment, particularly interior design choices such as dim lighting, are reported to positively impact clients in session (Miwa & Hanyu, 2006). Similarly, professional hip-hop artists report needing studios to be aesthetically pleasing, pointing to foam padding on walls and dim lighting. For many artists, entering an aesthetically pleasing studio environment was conducive to “an identity shift where they began to define themselves” (Harkness, 2014, p. 91). Student reports regarding the importance of aesthetics in establishing authentic studio spaces are in line with what counseling research suggests is necessary for effective counseling environments both inside and outside of schools (Ceylan et al., 2008; Cook & Malloy, 2014; Huffcut, 2010), as well as what the larger hip-hop community suggests is necessary for personal transformation (Harkness, 2014). Further, scholars have called for school counselors to tailor their interventions to the cultural knowledge and environments of their students (Hansen et al., 2014; L. Smith & Chambers, 2015), particularly when attempting to design multicultural counseling environments (Benton & Overtree, 2012). Evidence from students that the physical space constructed in this study felt like an authentic hip-hop studio suggests that through the use of a classroom-based school counseling intervention, students were able to channel their cultural knowledge and values into the design of a culturally responsive environment that could support their social and emotional development.
An additional finding highlights that youth felt the studio space would allow them to receive peer support that could be generative of improvements in confidence and self-efficacy. Similarly, a systematic review of peer support interventions found that peer educators were particularly effective in facilitating improvements in knowledge, beliefs, and attitudes as well as subsequent behavior change (Ramchand et al., 2017). Findings in the current study aid this supposition, providing evidence of the use of school studios as spaces for peer support.
When reflecting on their engagement in the studio co-construction process, youth reported feeling as if they had been given a valuable opportunity for personal advancement. This finding is particularly important to consider within the context of career counseling work in schools. Lent (2013) encourages counselors to adapt to work in the digital world by preparing individuals for a range of career opportunities. Fostering students’ career development is also an expected role of the school counselor and of school counseling interventions (ASCA, 2019b). Students’ need for opportunity and career–life preparedness requires counselors to promote students’ “alertness to resources and opportunities on which one can capitalize. Most important, preparedness can lead to the use of proactive strategies to manage barriers, build supports, and otherwise advocate for one’s own career–life future” (Lent, 2013, p. 7). Further, youth felt an opportunity for personal identity development, aiding Harkness’ (2014) argument that studios were spaces for hip-hop–identifying individuals to cultivate a deepening understanding of themselves, and Liddicoat’s (2015) position that counseling environments could allow for the positive development of a client’s self-concept.
CAS Model to Support School Studio Construction
The findings in this exploratory action research support the implementation of the CAS model as a guide for school counseling interventions. In the current study, with the help of the PI, the course instructor held the counselor role in the use of Levy’s (2019) HHSWT framework by facilitating a group process in which students constructed a hip-hop recording studio. Similar to research indicating that school counselors are often inundated with large caseloads and non-counseling duties that strip them of their ability to engage in direct counseling (Kim & Lambie, 2018; Mau et al., 2016), the school counselor at LHS was unable to support the studio co-construction process. However, to facilitate a comprehensive school counseling program, school counselors are expected to collaborate with teachers to indirectly address students’ academic, career, and personal/social needs (Cholewa et al., 2016). Therefore, the current study expands upon the implementation of the CAS model by considering the role of collaboration in the school counselor’s work, and the activation of the teacher as a key stakeholder (under the guidance of a counselor educator) in facilitating a classroom-based counseling intervention in which youth co-created a school space to support social and emotional services. The teacher and the PI also held the roles of advocates for the successful deployment of the school counseling intervention (studio co-creation). The teacher met with their principal and contacted a counselor educator (the PI), and together with the PI garnered crowdsourced funding for this project. Finally, the scholar role was also maintained by the teacher, who wished to support students’ social and emotional needs by creating a school studio, and thus called on the PI to use qualitative measures to evaluate students’ experiences during this process.
Limitations
There are a series of limitations to the current study. The limited availability of the school counselor to participate in this study is a limitation, despite the conscious use of collaboration in the deployment of an indirect classroom-based school counseling intervention. The use of the CAS model without a formal school counselor was difficult, albeit consistent with existing research surrounding the lack of time for school counselors to engage in multi-session group counseling work (Kim & Lambie, 2018). Consequently, the findings of the current study fail to offer support for counselors in the use of a direct school counseling intervention. Further, student reports of their experience in the studio co-construction process are subjective in nature. Had LHS provided an intervention to a larger sample of students and administered quantitative assessments, those findings could potentially have aided this study’s qualitative conclusions. The small sample size (N = 15) of this study is a limitation, as results lack generalizability. Additionally, LHS is an urban school whose demographic information suggests the majority of youth identified as Black and/or Hispanic. Given that the present study examined a sample of mostly non-White urban youth, it is difficult to generalize findings to suburban and rural schools as well as to youth who do not identify as Black and/or Hispanic. Further, each focus group lasted 30 minutes, which could have limited the ability of the seven or eight participants to offer in-depth data. Lastly, the interactive nature of focus groups could have impacted the authenticity of responses from focus group participants (Smithson, 2000).
Implications
There are a number of implications for both practice and research that can be drawn from the current study. The findings in the current study align with the ASCA National Model and hold promise for engaging teachers and students in school-based interventions that promote social and emotional development and are culturally relevant. The ASCA National Model (2019b) calls for school counselors to use indirect approaches to counseling, often those including collaboration with a teacher, to provide supports to all students across the school. This study exemplifies the importance of activating teachers in the use of indirect classroom-based school counseling interventions, particularly when school counselors themselves are not available. The PI’s involvement in supporting the classroom teacher in implementation and evaluation of a classroom-based school counseling intervention serves as a call for school counselors to consider partnering with faculty at local colleges/universities to bolster their comprehensive school counseling programs. If available, school counselors themselves are encouraged to collaborate with teachers in the development, implementation, and evaluation of classroom-based interventions that support students’ social and emotional development.
The current study used a culturally responsive classroom-based intervention that honored students’ cultural knowledge and trusted youth to guide the studio construction process. Youth reported on the importance of the opportunity to use the hip-hop studio to positively impact their school, their peers, and themselves. Counselors need to design social and emotional development supports within their schools that adhere to the cultural realities of their clients (Ponterotto & Austin, 2005) and are thus encouraged to utilize the studio co-creation approach. Beyond hip-hop, however, the current study suggests that youth-driven construction of an ancillary social and emotional support space should be considered for all students from marginalized populations, including youth identifying as LGBTQ.
Implications for direct school counseling practice exist as well. For example, Levy (2019) demonstrated effectiveness of a series of hip-hop–based cognitive behavioral and person-centered counseling interventions on students’ social and emotional development. However, few studies have detailed the cultural importance of the hip-hop studio and how its creation might support the future use of culturally competent interventions. Although this study did not explore the use of lyric writing, recording, or performing to address counseling outcomes, students participating in the studio construction process reported wanting to use the school studio to support their peers and their own personal self-development. These findings suggested it is important for schools to consider co-creating school studios as places for school counselors to deploy hip-hop–based interventions for group and individual counseling with urban youth.
The findings in this study can be expanded upon with future mixed methods research that examines a larger sample of students. Quantitative analysis of students’ social and emotional development (examining variables like stress, emotional regulation, and executive functioning) during the studio co-construction process is recommended as a direction for future research. Qualitative researchers should consider case studies of students and counselors who engage in the construction of hip-hop studios and small-group work within counseling studies, using more in-depth interviews (lasting longer than 30 minutes) to ensure rich data is collected. There is also value in exploring the multicultural and social justice competence development of both school counselors and teachers who engage in hip-hop–based school counseling interventions.
Conclusion
The goal of this exploratory action research was to illuminate the experiences of urban youth of color who were part of a classroom-based school counseling intervention in which they co-created their own space for social and emotional support in an inner-city urban high school. As described in this article, a limited number of studies have explored clients’ opinions and perspectives on changes made by school counselors to a counseling environment (Pearson & Wilson, 2012). Additionally, most studies focus on designing counseling environments outside of schools, and the school counseling profession lacks research on multicultural office design (Benton & Overtree, 2012). Furthermore, ASCA (2019b) advocates for the use of indirect counseling interventions to support the needs of all students, while others urge school counselors to use multicultural and social justice–oriented interventions to identify and address barriers to student development (Ratts & Greenleaf, 2018). This article highlights the value in using hip-hop studio construction as an innovative approach to a culturally sensitive, indirect, classroom-based school counseling intervention in which students themselves engaged in the construction of an ancillary space to support their social and emotional development.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adjapong, E. S. (2017). Bridging theory and practice in the urban science classroom: A framework for hip-hop pedagogy in STEM. Critical Education, 8(15). https://doi.org/10.14288/ce.v8i15.186248
Adjapong, E. S., & Emdin, C. (2015). Rethinking pedagogy in urban spaces: Implementing hip-hop pedagogy in the urban science classroom. Journal of Urban Learning, Teaching, and Research, 11, 66–77.
Allan, D., & Duckworth, V. (2018). Voices of disaffection: Disengaged and disruptive youths or agents of change and self-empowerment? British Journal of Special Education, 45(1), 43–60. https://doi.org/10.1111/1467-8578.12201
American School Counselor Association. (2015). The school counselor and cultural diversity. https://www.schoolcounselor.org/asca/media/asca/PositionStatements/PS_CulturalDiversity.pdf
American School Counselor Association. (2019a). Student-to-school-counselor ratio 2016-2017. https://www.schoolcounselor.org/asca/media/asca/home/Ratios16-17.pdf
American School Counselor Association. (2019b). The ASCA national model: A framework for school counseling programs (4th ed.).
Bailey, D. F., Getch, Y. Q., & Chen-Hayes, S. F. (2007). Achievement advocacy for all students through transformative school counseling programs. In B. T. Erford (Ed.), Transforming the school counseling profession (2nd ed., pp. 98–120). Pearson.
Benton, J. M., & Overtree, C. E. (2012). Multicultural office design: A case example. Professional Psychology: Research and Practice, 43(3), 265–269. https://doi.org/10.1037/a0027443
Betters-Bubon, J., Brunner, T., & Kansteiner, A. (2016). Success for all? The role of the school counselor in creating and sustaining culturally responsive positive behavior interventions and supports programs. The Professional Counselor, 6(3), 263–277. https://doi.org/10.15241/jbb.6.3.263
Bostick, D., & Anderson, R. (2009). Evaluating a small-group counseling program—A model for program planning and improvement in the elementary setting. Professional School Counseling, 12(6), 428–433. https://doi.org/10.1177/2156759X0901200602
Breen, L. (2007). The researcher ‘in the middle’: Negotiating the insider/outsider dichotomy. The Australian Community Psychologist, 19(1), 163–174. http://hdl.handle.net/20.500.11937/22045
Bryan, J., Griffin, D., Kim, J., Griffin, D. M., & Young, A. (2019). School counselor leadership in school-family-community partnerships: An equity-focused partnership process model for moving the field forward. In S. B. Sheldon & T. A. Turner-Vorbeck (Eds.), The Wiley handbook of family, school, and community relationships in education (pp. 265–287). Wiley.
Caro, R. A. (1975). The power broker: Robert Moses and the fall of New York. Alfred A. Knopf.
Ceylan, C., Dul, J., & Aytac, S. (2008). Can the office environment stimulate a manager’s creativity? Human Factors and Ergonomics in Manufacturing & Service Industries, 18(6), 589–602. https://doi.org/10.1002/hfm.20128
Chang, J. (2005). Can’t stop, won’t stop: A history of the hip-hop generation. St. Martin’s Press.
Chapman, E., & Smith, J. A. (2002). Interpretative phenomenological analysis and the new genetics. Journal of Health Psychology, 7(2), 125–130. https://doi.org/10.1177/1359105302007002397
Cholewa, B., Goodman-Scott, E., Thomas, A., & Cook, J. (2016). Teachers’ perceptions and experiences consulting with school counselors: A qualitative study. Professional School Counseling, 20(1), 77–88. https://doi.org/10.5330/1096-2409-20.1.77
Conner, J. O., & Cosner, K. (2016). Youth change agents: Comparing the sociopolitical identities of youth organizers and youth commissioners. Democracy and Education, 24(1). https://democracyeducationjournal.org/home/vol24/iss1/2
Cook, K., & Malloy, L. (2014). School counseling office design: Creating safe space. Journal of Creativity in Mental Health, 9(3), 436–443. https://doi.org/10.1080/15401383.2014.890557
Devlin, A. S., Borenstein, B., Finch, C., Hassan, M., Iannotti, E., & Koufopoulos, J. (2013). Multicultural art in the therapy office: Community and student perceptions of the therapist. Professional Psychology: Research and Practice, 44(3), 168–176. https://doi.org/10.1037/a0031925
Forman, M. (2002). “Keeping it real”?: African youth identities and hip hop. In R. A. Young (Ed.), Music, popular culture, identities (pp. 89–118). Brill.
Goelitz, A., & Stewart-Kahn, A. S. (2008). Therapeutic use of space: One agency’s transformation project. Journal of Creativity in Mental Health, 2(4), 31–44. https://doi.org/10.1300/J456v02n04_04
Hannon, M. D., & Vereen, L. G. (2016). Irreducibility of Black male clients: Considerations for culturally competent counseling. The Journal of Humanistic Counseling, 55(3), 234–245. https://doi.org/10.1002/johc.12036
Hansen, J. T., Speciale, M., & Lemberger, M. E. (2014). Humanism: The foundation and future of professional counseling. The Journal of Humanistic Counseling, 53(3), 170–190. https://doi.org/10.1002/j.2161-1939.2014.00055.x
Harkness, G. (2014). Get on the mic: Recording studios as symbolic spaces in rap music. Journal of Popular Music Studies, 26(1), 82–100. https://doi.org/10.1111/jpms.12061
Huffcut, J. C. (2010). Can design promote healing? Behavioral Healthcare, 30(9), 33–35.
Inquirium, LLC (2013). InqScribe [Computer software]. https://www.inqscribe.com
Kim, N., & Lambie, G. W. (2018). Burnout and implications for professional school counselors. The Professional Counselor, 8(3), 277–294. https://doi.org/10.15241/nk.8.3.277
Kobin, C., & Tyson, E. (2006). Thematic analysis of hip-hop music: Can hip-hop in therapy facilitate empathic connections when working with clients in urban settings? The Arts in Psychotherapy, 33(4), 343–356. https://doi.org/10.1016/j.aip.2006.05.001
Lent, R. W. (2013). Career-life preparedness: Revisiting career planning and adjustment in the new workplace. The Career Development Quarterly, 61(1), 2–14. https://doi.org/10.1002/j.2161-0045.2013.00031.x
Levy, I. (2012). Hip hop and spoken word therapy with urban youth. Journal of Poetry Therapy, 25, 219–224. https://doi.org/10.1080/08893675.2012.736182
Levy, I. (2019). Hip-hop and spoken word therapy in urban school counseling. Professional School Counseling, 22(1b). https://doi.org/10.1177/2156759X19834436.
Levy, I. P., Cook, A. L., & Emdin, C. (2018). Remixing the school counselor’s tool kit: Hip-hop spoken word therapy and YPAR. Professional School Counseling, 22(1). https://doi.org/10.1177/2156759X18800285
Levy, I., Emdin, C., & Adjapong, E. S. (2018). Hip-hop cypher in group work. Social Work with Groups, 41(1–2), 103–110. https://doi.org/10.1080/01609513.2016.1275265
Levy, I., & Keum, B. T. (2014). Hip-hop emotional exploration in men. Journal of Poetry Therapy, 27(4), 217–223. https://doi.org/10.1080/08893675.2014.949528
Liddicoat, S. (2010). Counselling workspace design and therapeutic practice. In J. Zuo, L. Daniel, & V. Soebarto (Eds.), Fifty years later: Revisiting the role of architectural science in design and practice: 50th International Conference of the Architectural Science Association (pp. 69–78). The Architectural Science Association and The University of Adelaide. http://anzasca.net/paper/counselling-workspace-design-and-therapeutic-practice
Liddicoat, S. (2015). Exploring relations between body, communication and agency in therapeutic space. In R. H. Crawford, & A. Stephan (Eds.), Living and Learning: Research for a Better Built Environment: 49th International Conference of the Architectural Science Association (pp. 123–132). The Architectural Science Association and The University of Melbourne. http://anzasca.net/wp-content/uploads/2015/12/012_Liddicoat_ASA2015.pdf
Mau, W.-C. J., Li, J., & Hoetmer, K. (2016). Transforming high school counseling: Counselors’ roles,
practices, and expectations for students’ success. Administrative Issues Journal: Connecting Education, Practice, and Research, 6(2), 83–95. https://doi.org/10.5929/2016.6.2.5
McMahon, H. G., Mason, E. C. M., Daluga-Guenther, N., & Ruiz, A. (2014). An ecological model of professional school counseling. Journal of Counseling & Development, 92(4), 459–471. https://doi.org/10.1002/j.1556-6676.2014.00172.x
Miwa, Y., & Hanyu, K. (2006). The effects of interior design on communication and impressions of a counselor
in a counseling room. Environment and Behavior, 38(4), 484–502. https://doi.org/10.1177/0013916505280084
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52(2), 250–260. https://doi.org/10.1037/0022-0167.52.2.250
Pearson, M., & Wilson, H. (2012). Soothing spaces and healing places: Is there an ideal counselling room design? Psychotherapy in Australia, 18(3), 46–53.
Phelps, C., Horrigan, D., Protheroe, L. K., Hopkin, J., Jones, W., & Murray, A. (2008). “I wouldn’t classify myself as a patient”: The importance of a “well-being” environment for individuals receiving counseling about familial cancer risk. Journal of Genetic Counseling, 17(4), 394–405. https://doi.org/10.1007/s10897-008-9158-z
Ponterotto, J. G., & Austin, R. (2005). Emerging approaches to training psychologists to be culturally competent. In R. T. Carter (Ed.), Handbook of racial-cultural psychology and counseling (pp. 19–25). Wiley.
Pressly, P. K., & Heesacker, M. (2001). The physical environment and counseling: A review of theory and research. Journal of Counseling & Development, 79(2), 148–160. https://doi.org/10.1002/j.1556-6676.2001.tb01954.x
Ramchand, R., Ahluwalia, S. C., Xenakis, L., Apaydin, E., Raaen, L., & Grimm, G. (2017). A systematic review of peer-supported interventions for health promotion and disease prevention. Preventive Medicine, 101, 156–170. https://doi.org/10.1016/j.ypmed.2017.06.008
Ratts, M. J. (2009). Social justice counseling: Toward the development of a fifth force among counseling paradigms. The Journal of Humanistic Counseling, Education and Development, 48(2), 160–172. https://doi.org/10.1002/j.2161-1939.2009.tb00076.x
Ratts, M. J., & Greenleaf, A. T. (2018). Counselor–advocate–scholar model: Changing the dominant discourse in counseling. Journal of Multicultural Counseling and Development, 46(2), 78–96. https://doi.org/10.1002/jmcd.12094
Ratts, M. J., & Pedersen, P. B. (2014). Counseling for multiculturalism and social justice: Integration, theory, and application (4th ed.). American Counseling Association.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and Social Justice Counseling Competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Reyes, M. R., Brackett, M. A., Rivers, S. E., White, M., & Salovey, P. (2012). Classroom emotional climate, student engagement, and academic achievement. Journal of Educational Psychology, 104(3), 700–712. https://doi.org/10.1037/a0027268
Rock, W. D., Remley, T. P., & Range, L. M. (2017). Principal-counselor collaboration and school climate. NASSP Bulletin, 101(1), 23–35. https://doi.org/10.1177/0192636517698037
Sanders, R., & Lehmann, J. (2019). An exploratory study of clients’ experiences and preferences for counselling room space and design. Counselling and Psychotherapy Research, 19(1), 57–65. https://doi.org/10.1002/capr.12202
Smith, J. A. (1996). Beyond the divide between cognition and discourse: Using interpretative phenomenological analysis in health psychology. Psychology & Health, 11(2), 261–271. https://doi.org/10.1080/08870449608400256
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research. SAGE.
Smith, L., & Chambers, C. (2015). Decolonizing psychological practice in the context of poverty. In R. D. Goodman & P. C. Gorski (Eds.), Decolonizing “multicultural” counseling through social justice (pp. 73–84). Springer.
Smithson, J. (2000). Using and analyzing focus groups: limitations and possibilities. International Journal of Social Research Methodology, 3(2), 103–119. https://doi.org/10.1080/136455700405172
Thomas, E., & Magilvy, J. K. (2011). Qualitative rigor or research validity in qualitative research. Journal for Specialists in Pediatric Nursing, 16(2), 151–155. https://doi.org/10.1111/j.1744-6155.2011.00283.x
Travis, R., Jr., & Deepak, A. (2011). Empowerment in context: Lessons from hip-hop culture for social work practice. Journal of Ethnic & Cultural Diversity in Social Work, 20(3), 203–222. https://doi.org/10.1080/15313204.2011.594993
Tyson, E. H. (2002). Hip hop therapy: An exploratory study of a rap music intervention with at-risk and delinquent youth. Journal of Poetry Therapy, 15(3), 131–144. https://doi.org/10.1023/A:1019795911358
Washington, A. R. (2018). Integrating hip-hop culture and rap music into social justice counseling with Black males. Journal of Counseling & Development, 96(1), 97–105. https://doi.org/10.1002/jcad.12181
Zuber-Skerritt, O., & Fletcher, M. (2007). The quality of an action research thesis in the social sciences. Quality Assurance in Education, 15(4), 413–436. https://doi.org/10.1108/09684880710829983
Ian P. Levy, EdD, is an assistant professor at Manhattan College. Edmund S. Adjapong, PhD, is an assistant professor at Seton Hall University. Correspondence may be addressed to Ian Levy, 4513 Manhattan College Pkwy, The Bronx, NY 10471, ilevy01@manhattan.edu.
Apr 29, 2020 | Volume 10 - Issue 2
TeShaunda Hannor-Walker, Lynn Bohecker, Lacey Ricks, Sarah Kitchens
Literature does little to explore the perceptions of Black adolescents with depression or their perspective of treatment effectiveness. Studies are usually from urban areas and there is a dearth of research with Black adolescents from rural areas. This study explored the unique personal experiences of Black adolescents located in the rural southeastern United States, with the purpose of gaining a clearer understanding when working with this population. An interpretative qualitative method was used to explore 10 participants’ interpretation of their experiences to gain insight in how they make meaning of those experiences. Five significant categories were found to capture participant themes: (a) definition of depression, (b) seeking treatment, (c) coping and problem solving strategies, (d) types of emotional support, and (e) contributing factors to depression. Specific recommendations and interventions are suggested for mental health clinicians to become more educated and aware when working with Black adolescents.
Keywords: Black adolescents, depression, treatment effectiveness, rural, contributing factors
Depression is a leading cause of disability worldwide (World Health Organization, 2020). The World Federation for Mental Health (2012) estimated that by 2030, more people will be impacted by depression than any other health problem. In the United States, approximately 13.3% of adolescents, or 3.2 million, had at least one major depressive episode and 9.5% were Black (National Institute of Mental Health [NIMH], 2013). Black people have experienced more severe forms of mental health conditions than individuals of other races because of unmet needs and other barriers (NIMH, 2013). In fact, Black people were reported to be 10% more likely to experience serious mental health problems than the general population (Shushansky, 2017), and Black children have a suicide rate that is almost two times higher than that of their White counterparts (Bridge et al., 2018).
Weaver et al. (2015) noted that although 90% of rural Black people live in the southeastern part of the United States, there are only two studies that specifically examined depression among rural Black people using national data (i.e., Probst et al., 2006; Willis et al., 2003). Most studies of depression that include Black youth are based on data from urban communities (Al-Khattab et al., 2016; Conner & Yeh, 2018; Ofonedu et al., 2013; Robinson et al., 2015). This suggests there is a dearth of research exploring Black adolescent experiences of depression in rural communities, and there is even less research focusing on Black youth who live in the rural southeastern United States (Smokowski et al., 2015: Weaver et al., 2015). The goal of this study was to explore the unique experiences of Black adolescents living in the rural southeastern United States who had been diagnosed with depression.
Contributing Factors to Depression in Black Adolescents
Adolescents who suffer from depression may experience substantial negative health and social consequences in late adolescence and adulthood (Lu, 2019). Black adolescents are particularly vulnerable to these consequences because they are more likely to live in low-resource neighborhoods and because they contend with the negative psychological impacts of racial discrimination (Robinson et al., 2015). Choi et al. (2006) found that ethnic minorities have higher scores on social stress and mental distress and lower scores on coping, self-esteem, and family cohesion. The depressive symptoms experienced by Black adolescents are often socially and culturally based (Lu et al., 2017). Therefore, it is essential for counselors, school personnel, and related professionals to remain abreast of the current research on depressive signs and symptoms, beliefs about treatment, and specific needs of Black adolescents.
Choi et al. (2006) discovered that Black, Hispanic, and Asian adolescents in the United States have consistently higher levels of social stress beginning in childhood compared to their White counterparts. Breland-Noble et al. (2010) found that relationship problems, academic problems, bereavement, and stress were primary triggers for depressive symptoms among Black adolescents. Ofonedu et al. (2013) determined in their study of Black adolescents that life events in the home, school, and community contributed to depressive symptoms. These factors included (a) a stressful home life, (b) stressful life circumstances and unique life experiences at school, and (c) the experience of high levels of violent crimes in neighborhoods. Stress is clearly a contributing factor to the depressive symptoms of Black adolescents.
Symptoms of Depression in Black Adolescents
Although understanding national trends and contributing factors can help practitioners identify adolescents suffering from depression, it is also important to understand potential racial and ethnic differences in the expression of adolescent depression (Lu, 2019). The manifestations of depressive symptoms vary in Black youth and affect all dimensions of physical, psychological, interpersonal, and social being (Ofonedu et al., 2013). In the Black community, mental health conditions have often been unacknowledged, misunderstood, and misdiagnosed (Shushansky, 2017; Vontress et al., 2007). According to Vontress et al. (2007), Black people often experience cultural dysthymia and mental health symptoms such as low-grade depression; feelings of sadness, hopelessness, and anger; aggression; and self-destructive behaviors. Vontress et al. (2007) characterized these symptoms as a “psychosocial condition” grounded in external societal experiences of discrimination and oppression that often go unrecognized (p. 131). Additional studies are needed to show how to better identify individuals suffering from depression and thereby increase the effectiveness of treatment for Black adolescents (Ofonedu et al., 2013).
As in adults, unrecognized or undiagnosed dysthymia or symptoms of low-grade depression in adolescents can contribute to poor health and problematic behaviors (Saluja et al., 2004). Researchers discovered that untreated dysthymia elevates the risk of disruptive behaviors, anxiety, substance abuse, unsafe sexual practices, involvement in fights, lower achievement on tests, lower teacher-rated grades, and poorer peer relationships (Saluja et al., 2004). Auger (2005) discovered that the many signs and symptoms of adolescent depression were overlooked not only by parents but also by school systems, administrators, counselors, and teachers who daily were in a very unique position to identify those at risk of depression. Many cases of adolescent depression, particularly among minorities, have gone undiagnosed, misdiagnosed, and untreated (Cook et al., 2017; Shushansky, 2017). A better understanding of the unique experiences of Black adolescents diagnosed with depression would help improve symptom recognition, which may in turn reduce misdiagnosis and increase treatment effectiveness.
An understanding of the cultural implications and influence that oppression, prejudice, and various forms of discrimination have on Black people’s mental health in the United States is helpful in contextualizing and normalizing symptoms of depression and reducing instances of misdiagnosis. Hope et al. (2017) posited that discrimination remains a common experience for Black adolescents that can impact not only the onset of depression but also the quality of and access to mental health services. Furthermore, according to Liang et al. (2016), racial disparities exist, as Black youth are more likely to be misdiagnosed as having psychotic and disruptive behavior problems compared to mood (i.e., depression) and substance abuse disorders.
Lu et al. (2017) echoed these sentiments, stating that depression presents differently for Black adolescents. It is essential for Black adolescents to use their own language when describing their depressive symptoms. Additionally, it is important for clinical and school counseling professionals to be aware of gender differences in Black adolescents’ expression of depression, specifically in terms of internalizing and externalizing symptoms. The findings of Breland-Noble et al. (2010) indicated that female Black adolescents seem to internalize behaviors (e.g., becoming withdrawn, exhibiting visible sadness), while male Black adolescents seem to externalize behaviors (e.g., becoming angry or acting out). Lu et al. (2017) further highlighted that “adolescents develop [symptoms] as a means of coping in response to environmental factors” (p. 614). More research is needed to understand how depressed Black adolescents describe their symptoms and assign meaning to their experiences of depression.
Coping Strategies of Black Adolescents
In addition to presenting different symptoms than individuals of other racial groups, Black adolescents have the lowest coping skills scores compared to their peers (Conner & Yeh, 2018). Recent studies suggest that adolescents who live in low-resourced neighborhoods feel like they have limited options in how to respond to stressful and anxiety-provoking situations because of limited or ineffective coping skills (Robinson et al., 2017; Robinson et al., 2015). There are indications that Black adolescents cope with depression in a variety of contexts. Some Black adolescents describe depression as a way of life, noting that everybody becomes depressed one way or another (Ofonedu et al., 2013). Researchers have shown that some Black adolescents conceal their feelings of depression because they are uncertain of how others would perceive them (Al-Khattab et al., 2016; Ofonedu et al., 2013). For instance, some Black adolescents reported trying to manage their depression independently and only going to an adult as a last resort (Breland-Noble et al., 2010). Black adolescents have been shown to manage their depression by strong will and spiritual beliefs (Ofonedu et al., 2013). Conner and Yeh (2018) highlighted how Black adolescents cope with depression in spiritual and creative ways such as listening to music, dancing, and writing.
In 2016, Al-Khattab et al. discovered that Black adolescents controlled their depression through their interactions with other people. Al-Khattab et al. identified five typology interaction models, which include hiding feelings of depression, lashing out verbally or physically toward others, seeking help from others to address emotional feelings, joining with others in social activities, and having others approach them about behavioral and mood changes. Therefore, it is critical for Black adolescents to better understand their experiences with depression and how interactions with others may influence their symptoms.
Treatment of Depression in Black Adolescents
Cook et al. (2017) noted that there are barriers to accessing mental health services and quality of care, which include stigma associated with mental illness, distrust of the health care system, lack of providers from diverse racial/ethnic backgrounds, lack of culturally competent providers, and lack of insurance or underinsurance. Often these barriers cause Black people to be unable or reluctant to seek help (Shushansky, 2017). Although Black adolescents may feel that treatment can be effective, many are reluctant to attend therapy because of the stigma and possible misdiagnosis of their symptoms, much of which has been influenced by their culture (Al-Khattab et al., 2016; Lindsey et al., 2010; Ofonedu et al., 2013). Positive results have been seen when using family-centered prevention programs to address depressive symptoms in Black adolescents (Brody et al., 2012). Jacob et al. (2013) determined that behavioral activation was effective for decreasing depressive symptoms and impairments for the Black adolescents who participated in their study.
As highlighted by a study of Black adults from a rural faith community, Black people living in rural communities suffering from depression face additional barriers to treatment such as (a) a lack of medical resources, (b) insufficient education about depression, and (c) stigma (Bryant et al., 2013). Sullivan et al. (2017) learned that terminology was crucial when discussing treatment with rural Black adults on a stigmatized topic such as mental illness. Parental concerns about marginalization because of having a child with a mental health diagnosis and some primary care providers’ characterization of mental health symptoms as a “phase” have been found to be barriers to treatment for Black children living in rural communities (Murry et al., 2011). Working with Black children who live in poverty, Graves (2017) identified cultural and macro-level barriers that influence the process of seeking treatment.
Treatment of mental health disorders extends from diagnoses. Considering the differences in symptoms and frequency of misdiagnosis, it is not surprising that treatment options for Black adolescents have shown varied outcomes across the literature. Additionally, some researchers suggested that new measures need to be developed for accurately identifying depression in diverse populations, which would then inform modifications in treatment (Ofonedu et al., 2013). Having a better understanding of the unique and complex experiences of Black adolescents may help parents, therapists, schools, and counseling professionals understand and identify those most at risk for depression. Planey et al. (2019) discovered that Black youth viewed seeking mental health treatment as a contextual and relational process rather than an event. What is clear is that more culturally diverse training for therapists, schools, and counseling professionals is needed to prevent, detect, and implement interventions for minorities experiencing depression during the disease’s earlier stages. Likewise, research exploring Black adolescents’ unique experiences of symptoms, environmental factors, and coping strategies remains necessary in order to inform effective treatment.
Purpose of the Present Study
The review of the literature captured symptoms and coping strategies unique to Black adolescents. Studies highlight that environmental factors contribute to depressive symptoms in this population. Furthermore, disparities exist in mental health care for adolescents, specifically for minorities (Alegria et al., 2010; Brenner, 2019; Lake & Turner, 2017). This clear gap in the literature indicates insufficient knowledge regarding the personal experiences of Black adolescents with depression. Most of the studies in the extant literature took place in urban areas; little is known about rural experiences and even less is known about experiences in the southeastern United States. This qualitative study was designed to help fill that gap. It posed an overarching research question to Black adolescents living in the rural southeastern United States: “What is your experience with depression?” This study was designed to offer human services professionals a clearer understanding of the unique experiences of Black adolescents in this geographical region who had been diagnosed with depression, with the hope of informing clinical practices.
Method
The goal of this study was to explore the unique experiences of Black adolescents living in the rural southeastern United States who had been diagnosed with depression. The research design for the study was a basic interpretive qualitative method, as described by Merriam (2009). The purpose of this method is to understand the perspectives of the participants involved by uncovering and interpreting their meanings (Everall et al., 2006). This purpose was well-suited to the overall objective of this study, which was to gain a clearer understanding of the unique personal experiences of Black adolescents living with depression in the rural southeastern United States.
According to Merriam (2009), interpretive qualitative research is founded on the idea that people and their interactions with their world, or reality, socially construct meaning. Researchers using this method are interested in how individuals “interpret” their experiences, “construct their worlds,” and assign “meanings” to their experiences (Merriam, 2009, p. 38). Moreover, Merriam asserted that interpretive qualitative research has multiple meanings and is a complex phenomenon ideal for attempting to understand and treat Black adolescents with depression. Using Merriam’s (2009) model, researchers “strive to understand the meanings individuals construct regarding their world and their experiences” in a natural setting (p. 4). Another characteristic is that the researcher serves as the primary instrument for both collecting and analyzing data. The research process is inductive rather than deductive, which means that the researcher gathers data in an effort to “build concepts, hypotheses, or theories” in the forms of themes and categories (Merriam, 2009, p. 5). A final characteristic of this model is that interpretive qualitative research is richly descriptive and includes details about the context, the participants involved, and quotations and interview excerpts (Merriam, 2009).
Merriam (2009) noted that certain elements of the basic interpretive qualitative design may overlap with other designs, particularly when concepts of cultural values are discussed and explored. Merriam’s design does not require researchers to give a full sociocultural interpretation of the data, as is done in ethnography. Indeed, this study does not provide a full sociocultural interpretation. However, the data were analyzed using Patton’s (1987) content analysis model because the model provides a rigorous, systemic, and ethical procedure for analyzing data. Merriam’s model for collecting data and Patton’s model for analyzing data form a rich methodological combination that enhances the trustworthiness of the research study and improves the transferability of its findings.
Participants and Procedure
The university IRB granted approval for this study. Purposive sampling was used to identify 10 Black adolescents living in the rural southeastern United States who were being treated for depression. The southeastern part of the United States was selected because it contains fewer metropolitan areas that have been studied specifically. Each of the participants met the following criteria: (a) self-identified as Black, (b) was between the ages of 13 and 17, (c) was willing to participate, (d) had secured a signed informed consent form from their parents, (e) had signed a participant assent form, and (f) was currently under the care of a counselor either in or out of school for depression. The participants ranged in age from 13 to 17 years old and were in grades seven through 12. Six participants were female and four were male.
Approval was obtained in advance from a public school system located in the rural southeastern United States. The public school system administrator agreed to send the letter of invitation along with the consent and assent forms to the parents and potential participants. In addition, the first author sent a packet of information to a counseling agency; school professionals, including professional school counselors and school psychologists; and social workers. The packet contained an invitation letter requesting that the packet be shared with potential participants and their parents; it also contained consent and assent forms. The informed consent form described the study and the efforts that would be taken to protect the confidentiality of the participants’ information. The informed consent form stated that the risk of participating was the normal discomfort of sharing one’s experiences with depression and that if a participant felt uncomfortable, they could withdraw from the study at any time.
Parents and participants signed the consent and assent forms, respectively, and returned them to either the local counseling agency or school professionals, who forwarded the forms to the first author. The first author then contacted the parents, with the participants present, to schedule a 45- to 90-minute, face-to-face interview with the participant. The informed consent form was verbally reviewed, ensuring that the parents and participants understood that a second interview to review and correct the interpretation would be optional. Interviews took place either during the day in a private room at the school or outside of school hours in the first author’s office. Because adolescent depression is considered a sensitive topic, participants were instructed to follow up with their counselor if they experienced adverse feelings as a result of participating in the study.
Data Collection and Analysis
The first author met with each of the 10 participants for a single semi-structured interview that lasted between 45 and 90 minutes. In phenomenological research, the researcher follows the essence of participants’ responses (van Manen, 1997). The first author spent time establishing rapport with the participants. Once the first author believed a participant was comfortable, she asked the participant the overarching question, “What is your experience with depression?” Follow-up questions specific to each participant were used to probe the participants’ responses regarding their experience as Black adolescents living with depression in the rural southeastern United States. Several participants expressed a reluctance to fully disclose or discuss their experiences with depression; however, no participants withdrew from the study, and all participants completed the first interview. At the end of the first interview, the participants were notified that they would be contacted for a second interview to review the transcript of the first interview and verify its accuracy and trustworthiness.
Interviews were recorded and transcribed verbatim by both the first author and a professional transcriber. The transcripts were coded and analyzed for themes related to the research question of this study. The first author utilized Patton’s (1987) content analysis model as a process of bringing order to the data by organizing the data into major themes, categories, and case examples. The first author consulted with two experts in qualitative research in the human services field and used three levels of coding: open, axial, and selective. Open coding included reading the transcribed interviews several times and coding phrases, from one word to portions of paragraphs. Based on input from the consultants, the first author enhanced the coding process by entering the data into the NVivo QSR software program, which facilitated organization and analysis. The first author then condensed the data into five categories. Axial coding enabled the first author to organize, link, and cluster codes, while selective coding allowed the first author to analyze the words, sentences, and themes from the interviews. Data analysis via coding was a back and forth process, and staying close to the transcripts was essential. The labeling and coding allowed the first author to interpret and classify the data and themes into five categories that were supported with direct quotations from the participants.
Trustworthiness
Trustworthiness is an important aspect of qualitative research (Hays & Singh, 2012). The generally candid nature of each participant in relating even the most difficult experiences, such as rape, would suggest a high degree of trustworthiness in their responses. Member checking was offered to all participants in the form of a follow-up interview. When contacted by the first author to schedule this interview, however, none of the participants felt that it was necessary. Rather, all of the participants stated they were satisfied with their responses in the first interview. In addition to offering member checking, the first author used rich data, prolonged engagement, respondent validation, a search for discrepant data, and peer review to ensure trustworthiness. A peer review of the method was conducted by doctoral-level professors in human services who specialized in qualitative research in order to enhance internal validity (Lincoln & Guba, 1985; Merriam, 2009). The first author used an audit trail by engaging in memo-writing to express thoughts, perspectives, observations, and reactions to interviews, transcriptions, and coding. An audit trail is a strategy in which a researcher explains as best as possible how they arrived at the results of the study by documenting how the data were collected, how categories were developed, and how findings were interpreted throughout the study (Lincoln & Guba, 1985). An audit trail thus improves the quality of a study. The information and details from this study may be generalizable to other groups and may contribute to the knowledge base of best practices when working with this population in counseling.
Results
Through data analysis, the researcher identified five significant thematic categories: (a) definitions of depression, (b) seeking treatment, (c) coping and problem-solving strategies, (d) types of emotional support, and (e) contributing factors to depression. These five thematic categories were broken down into their constituent contents. Each thematic category was addressed with the invariant constituents that make up that category, including elaboration on any significant constituent patterns (such as high and low frequency of occurrence). Quotations from the participants are included in the text as examples to elucidate the invariant constituents and thematic categories. For reasons of confidentiality, some identifying information was excluded. All participants identified as Black and lived in the rural southeastern United States.
At the time of the study, the participants were living in a southeastern U.S. community in one of the lowest socioeconomic brackets of the country. In the participants’ community, the majority of the population was Black and participated in the school’s free or reduced-fee lunch program. Because of the homogeneous nature of the community, the participants did not speak of any adverse social or political circumstances, and the researcher avoided broaching the topic in an effort to do no harm. The researcher believed that overlooking the social and political climate of the community increased the trustworthiness of the participants’ responses, as the participants were not influenced by the discussion of the climate nor did they voluntarily express its relevance to their experience. As a Black adult, the researcher, who is first author, was aware of how the social and political climate played into their experience. However, because the participants were adolescents experiencing emotional pain, the first researcher attempted to instill hope in them as part of their experiences of this study. To maintain confidentiality, specific details about the contextual factors in the participants’ community have been omitted.
Definitions of Depression
Data analysis identified 18 codes that were relevant to the category regarding how participants defined depression. Of these codes, three emerged with significantly higher prevalence than the others: (a) sadness; (b) isolation, social withdrawal, or loneliness; and (c) permanent or persistent. Nine out of the 10 participants (90%) indicated that they experienced the feelings associated with these three codes. For example, in response to how he defined depression, Participant 5 noted that he became “sad, mad, and very frustrated.” Participant 1 defined depression in terms of social withdrawal, saying, “Usually I stay in my room and I don’t talk to anybody, I just stay in there, and that is about it.” Participant 4 provided an example of the theme of permanent or persistent experiences by stating, “I don’t think it could just go away, especially when it’s very serious.” Participant 3 provided an example that captured the overall essence of this category when he stated:
I have been sad a whole lot, without reason; and so, I think that is why I was depressed . . . when I am around people for too long, I get sad; but when I am alone, I am happier. I feel safe when I am by myself. When it [depression] comes on, it comes on strong. It is really bad. Because I feel really, really sad, and my thoughts aren’t, you know, normal. Sometimes they are violent . . . like I don’t have any hope at all. I don’t think like I normally would. Sometimes I don’t think at all. Sometimes when I get really sad or angry, I think about hurting people. So, I have to withdraw further. I have to push it further down into my mind so that I won’t act on it.
It is interesting to note that the next most frequently found codes were stress-related and frustration, each with a prevalence of 60%, and more common in young Black girls, which had a prevalence of 50%. Alternatively, only one participant mentioned each of the following codes with regard to defining depression: suicidal thoughts or attempts, more common in young Black boys, and feeling sick.
Seeking Treatment
The category of seeking treatment contained 10 codes. Participants expressed contradictory feelings about the effectiveness of treatment and the barriers to seeking treatment. For example, 90% of participants expressed that they felt that therapeutic treatment was effective in mitigating or curing depression, including Participant 7: “To me, to talk to my therapist was like a relief to me, because he was the only person that I can be able to tell my thoughts, get my thoughts together why I was in there.” Simultaneously, 30% of participants noted that they felt that therapy was not effective as a treatment. This overlap and apparent incompatibility in the data helped reveal the full breadth of Black adolescents’ opinions and feelings about depression and seeking treatment, as participants expressed both positive and negative experiences.
This overlapping trend was seen elsewhere in this thematic category. For example, there were codes of medication is effective (50%) and medication is not effective (30%). This apparent contradiction was highlighted not only between participants but also within a single participant. Participant 10 directly stated she believed medication to be effective; she then revealed that she had been given medication that sent her into a coma. She reported taking her medication as prescribed but “after that I passed out, and I didn’t remember nothing, all I knew I woke up in the hospital.” Three codes were identified as directly related to seeking treatment. Significant barriers to therapeutic treatment were negative connotation of mental illness (80%), uncomfortable issues brought up in treatment (80%), and lack of trust (70%). The code negative connotation of mental illness was grounded in external perceptions, as many participants indicated that they did not want other people to know that they were in treatment.
For example, Participant 2 stated, “I don’t tell them. I don’t want them to know,” when referring to his friends. Participant 3 provided an example of the code of uncomfortable issues, noting, “I don’t like to talk about it much. You know, it is kind of aggravating. It makes me feel weak when I talk to people about my problems.” Regarding the code lack of trust, Participant 6 noted, “I have very weak trust issues. Sometimes they can be strong but mostly weak.”
Three minor codes emerged relating to seeking treatment. Two were trouble expressing self in therapy (40%) and treatment was not necessary (40%). Participant 3 stated, “I have a lot of trouble expressing myself. You know, when I get into the office, I just forget what to say.” Three of the 10 participants openly discussed lack of Black people’s knowledge or education about depression as a specific barrier to treatment. They shared their perceptions of the lack of education and discussion about depression within their own community, which they felt presented a specific barrier to treatment for them. Participant 6 stated, “I can’t overly generalize it, but some people need to know more, ’cause they don’t understand, because sometimes you just need that time and people they don’t understand that you need it.” However, taking these and the other barriers in this thematic category into account, the prevalence of participants who reported that treatment was effective was three times greater than the prevalence of participants who thought that treatment was ineffective.
Coping and Problem-Solving Strategies
The third thematic category contained 29 different codes related to problem-solving strategies and behaviors or activities the participants used to cope with depressive symptoms. The participants described various strategies to cope with depression, but the most prevalent was suppressing/hiding thoughts/feelings. There were seven strategies that more than half of the participants reported using as problem-solving strategies and strategies to cope with depression. The positive problem-solving strategies were listening to music, turning to religion/going to church/praying, and talking/spending time with family. The problematic coping strategies reported were using illegal drugs, engaging in self-harm, having sex, and isolating. See Table 1 for codes and results.
It is encouraging that 18 out of the 29 codes could be characterized as neutral or positive coping strategies. The other 11 are areas of concern, even if only one participant reported engaging in the behavior. Participant responses overlapped and participants reported coping and problem-solving strategies that might be characterized as both positive and negative. In addition to contrasts in the specific codes and types of behaviors, contrasts in the percentages of participants who reported negative behaviors compared to positive behaviors were noted. For example, participants reporting the negative problem-solving strategy of engaging in self-harm as a way to cope often went into detailed narrative descriptions. This strategy was more frequently reported than any of the positive or neutral coping and problem-solving strategies.
Types of Emotional Support
This thematic category addressed the types of emotional support that the participants received during their experiences with depression. Four distinct subthemes of codes were identified: peers; family; school (teachers); and helping professionals such as hospitals, managed care facilities, and therapists. Each of the four subthemes contained codes that were sorted as either positive or negative. A lack of support or refusal of support was considered a negative, and similar to other categories, participants shared multiple overlapping experiences. Negative support from peers was the only theme to have 100% prevalence; every participant mentioned that peers had negatively affected them through a lack of emotional support during their experience with depression, including Participant 2: “They didn’t believe me at first, but later they just seem like they don’t care.” Half of the participants expressed that they had also received positive emotional support from their peers during their experience with depression. In the family group, equal percentages of participants (60%) reported receiving positive support from family and experiencing a lack of support from family. The participants were similarly split regarding their perceptions of receiving positive (50%) and negative (50%) emotional support from teachers at school. The greatest proportional difference in negative and positive emotional support was within the category of helping professionals. In this subtheme, four times as many participants (40%) reported that they had had positive emotional support from mental health care providers in a hospital, halfway house, or therapeutic community than participants reporting negative emotional support from mental health care providers (10%).
Table 1
Coping and Problem-Solving Strategies
| Strategy |
Percent of Respondents
(N = 10) |
| Positive or Neutral
Coping Strategies |
Listening to music |
70% |
| Turning to religion / going to church / praying |
70% |
| Talking / spending time with family |
60% |
| Attending therapy |
40% |
| Writing |
40% |
| Creating art |
30% |
| Playing video games |
30% |
| Watching TV |
30% |
| Crying |
30% |
| Taking prescription drugs |
20% |
| Eating food |
20% |
| Reading |
20% |
| Talking / spending time with friends |
20% |
| Distracting self |
20% |
| Laughing |
20% |
| Joining clubs |
10% |
| Working out |
10% |
| Researching |
10% |
| Problematic
Coping Strategies |
Suppressing / hiding thoughts / feelings |
90% |
| Using illegal drugs |
70% |
| Engaging in self-harm |
60% |
| Having sex |
60% |
| Isolating |
60% |
| Attempting suicide |
40% |
| Engaging in violence |
40% |
| Running away |
30% |
| Yelling / shouting |
10% |
| Having violent thoughts |
10% |
| Avoiding responsibilities / rebelling |
10% |
Contributing Factors to Depression
This theme of contributing factors to depression appeared to be the most salient to the central research question of how Black adolescents living in the rural southeastern United States described their experiences with depression. The previous themes captured definitions of depression, seeking treatment, coping and problem-solving strategies, and types of emotional support. This theme provided a description of the participants’ lives in terms of their context and environment, which the participants identified as contributing factors to their experiences of depression. When asked about contributing factors to their depression, the three most noted by the participants were verbal abuse (70%), differences from other people and being bullied (70%), and parental or family problems (70%). Participants also reported sexual abuse (40%) and physical abuse (30%) as contributing factors. Participant 6 made the following statement, which captures the essence of this theme:
My depression started really kicking in when I was around 13 . . . it runs in my family. My mom has it and when I was little, I was sexually abused . . . and I’ve been made fun of all my life . . . my weight . . . a scalp infection. People make fun of stuff like that. And that’s been going on since I was little.
The least prevalent factors mentioned by participants were foster care (20%), stress of schoolwork (20%), and a scary book (10%). Verbal abuse was reported 30% more frequently than sexual abuse and 40% more frequently than physical abuse. However, it is interesting to note that Participant 2 considered foster care to be a cause of depression and not a solution. Most participants identified a combination of these factors as contributing to the onset of their depressive symptoms.
Discussion and Implications
This study sought to examine the unique experiences of Black adolescents diagnosed with depression living in a rural community located in the southeastern part of the United States. Five themes emerged when examining the participants’ narratives with depression. These themes included definitions of depression, seeking treatment, coping and problem-solving strategies, types of emotional support, and contributing factors to depression. In defining depression, 90% of the participants in this study cited sadness, isolation, and depression’s ongoing nature. This is not surprising, as these codes fit within the diagnostic criteria for depression. It was surprising, however, that participants defined depression as stress-related, as stress is not one of the diagnostic criteria. At the same time, the idea of depression as stress-related is supported in other studies (Breland-Noble et al., 2010; Bryant et al., 2013; Choi et al., 2006; Ofonedu et al., 2013; Robinson et al., 2015). The mental health community would do well to acknowledge the differences in how Black adolescents from rural U.S. communities may define depression. When working with Black adolescent clients, practitioners may wish to inquire about stressors and consider their relation to depression in order to inform treatment plans and interventions.
Most participants who sought treatment for depression indicated that treatment was effective; however, 30% of participants expressed that therapy was ineffective. Additionally, only 50% of participants indicated that medication was an effective form of treatment. Participants also identified barriers to seeking treatment, which included negative connotations associated with mental illness and discomfort discussing issues in treatment. Barriers identified included a lack of trust, problems with self-expression, the belief that therapy was not needed, and a lack of knowledge about depression in the Black culture. These results are consistent with prior research (Al-Khattab et al., 2016; Bryant et al., 2013; Lindsey et al., 2010; Ofonedu et al., 2013; Sullivan et al., 2017), indicating that mental health conditions are often misunderstood, misdiagnosed, or unacknowledged within the Black community (Graves, 2017; Murry et al., 2011; Shushansky, 2017).
Prior research has also highlighted the stigma of mental illness in the Black community (Cook et al., 2017). This stigma helps to explain previous research showing that Black people often seek help as a last resort (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013; Vontress et al., 2007). It is essential that counselors acknowledge the stigma associated with mental illness and reluctance to seek treatment within the Black community. More practitioners who are aware of and sensitive to the mental health needs of Black communities are needed. It is imperative that clinicians take it upon themselves to become competent when working with this population. To address the stigma, practitioners might offer training in evidence-based practices related to Black adolescents’ mental health at churches, schools, and various community organizations in the Black community. These types of trainings could be particularly effective in rural communities where participants are likely to communicate to others about the trainings, thereby validating the information and possibly reducing the stigma. One of the codes from this study was related to the effectiveness of medication for reducing depressive symptoms. More research is needed to explore factors that may contribute to this experience. Additionally, more research is needed to understand the unique traits of Black adolescents seeking treatment in other regions of the United States.
There were a few positive strategies for coping with depression that the participants identified, including listening to music, engaging in spiritual practices, and spending time with family. These positive coping strategies supported the constructs of spiritual beliefs and relationships with others, which were established in prior studies (Al-Khattab et al., 2016; Conner & Yeh, 2018; Ofonedu et al., 2013). The theme of coping and problem-solving strategies was dominated by the most common strategy: participants hiding their thoughts and feelings as a way of managing their depressive symptoms. This result corroborates the findings of prior studies that show Black adolescents conceal their feelings and symptoms of depression (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013; Vontress et al., 2007). As previous studies have suggested, hiding thoughts and feelings may be due to the stigma associated with mental illness and limited options in how to respond to stressful and anxiety-provoking situations (Robinson et al., 2017; Robinson et al., 2015). The finding that the participants hide thoughts and feelings also supports previous research that Black adolescents may be fearful of how others will react to them and isolate themselves as a result (Al-Khattab et al., 2016; Breland-Noble et al., 2010; Ofonedu et al., 2013). Participants also reported engaging in unhealthy coping behaviors such as self-harm, sexual intercourse, and isolation. These harmful strategies may be due to the limited coping skills of Black adolescents that have been identified in prior research studies (Robinson et al., 2017; Robinson et al., 2015). Again, these findings highlight the need for culturally specific training regarding mental health in Black communities.
The theme of emotional support resonated with all participants in this study, suggesting the significance of relationships (Breland-Noble et al., 2010). When examining emotional support, positive and negative experiences emerged. Positive emotional supports were found in family members (60%), teachers (50%), and mental health professionals (40%). Yet all participants indicated being negatively impacted by a lack of support among their peers. Participants reported feeling invalidated or not believed by their peers. They also reported that their peers did not seem to show concern. These experiences may have exacerbated the participants’ symptoms. Only half of the participants indicated receiving positive peer support when seeking help for depressive symptoms. These findings are concerning because of the heavy emphasis placed on relationships within Black communities (Breland-Noble et al., 2010).
Relationships were identified as significant to all participants in this study, indicating that healthy relationships may be a protective factor and may increase emotional and mental health. Counseling professionals in private practice and in schools are thus encouraged to inquire about a wide range of relationships when working with their Black adolescent clients. For example, a counseling professional might ask a client to complete a detailed relationship profile for each significant person in their life. This would help to uncover significant relationships that could support the client’s current challenges and to identify those individuals who might not be providing support. Counseling professionals might also conceptualize client symptoms as connected to these relationships. Family or systemic interventions may be incorporated into treatment planning to decrease depressive symptoms.
The theme of contributing factors encompassed a surprisingly high number of significant adverse and traumatic experiences. When examining the factors contributing to the development of depression in Black adolescents, most participants in this study cited verbal abuse, differences from others/bullying, and family-related issues as salient factors. Other contributing factors included sexual and physical abuse. Participants reported verbal abuse (70%), sexual abuse (40%), and physical abuse (30%) as contributing factors of depression. However, participants did not identify one single factor but rather described multiple and overlapping factors that contributed to their depressive symptoms. The connection between adverse and traumatic experiences and depressive symptoms specifically within the Black adolescent population appears to be underreported in the literature.
It is important to note the high prevalence of abuse indicated within the study. The lack of existing studies exploring the relationship among Black adolescents, depression, and adverse childhood experiences indicates that additional research is needed. An implication of this study is that when working with Black adolescent clients who are presenting with symptoms of depression, counseling professionals might incorporate an adverse childhood experience screening tool. Assessing clients for adverse childhood experiences as a matter of regular practice may better inform preventative measures and treatment. As this study highlights, it is essential for clinical and school professionals working with Black adolescents to understand that abuse can contribute to depressive symptoms.
Overall, many of the symptoms described by participants could be associated with a diagnosis of
dysthymia as a result of oppression, supporting the work of Vontress et al. (2007). However, the participants did not use the word “oppression” and may not have recognized the systemic aspects of their experiences (Vontress et al., 2007). It may be that the participants’ adverse experiences of abuse overshadowed any cultural or historical factors that may also have been present. The current study highlighted the overlooked and undertreated experiences of Black adolescents with depression. Counseling professionals may choose to gain a preliminary understanding of Black adolescent depression and dysthymia symptoms “within the context of their legacy of discrimination and oppression” (Vontress et al., 2007, p. 132).
Limitations
Overall, these findings need to be considered in light of some specific limitations. First, the interview questions were semi-structured. This means that the researcher used open-ended questions followed by discussion. As a result, the interviewer may not have covered the exact same content with each participant. Furthermore, because of the nature of the study, some participants may have been more forthcoming about their personal experiences. Thirdly, although the participants were asked about past events, the memories of those events may have been compromised because of the passage of time or because of received or ongoing treatment. Lastly, given the limited number of participants interviewed, more research is needed to understand the mental health needs and experiences of Black adolescents who are experiencing depression.
Conclusion
In this qualitative study of 10 Black adolescents living in a rural community, the authors provided space for the participants to use their own terms and language to define depression. It is clear through this and other research that contextual factors are often involved in the onset of depression in Black adolescents, and there is not enough active therapeutic and medical treatment for Black adolescents living with depression. There is a stigma associated with mental illness and reluctance to seek treatment within the Black community, particularly in rural areas. As a result, counselors and mental health providers need to become more educated and aware when working with Black adolescents who live in rural communities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alegria, M., Vallas, M., & Pumariega, A. J. (2010). Racial and ethnic disparities in pediatric mental health. Child and Adolescent Psychiatric Clinics of North America, 19(4), 759–774. https://doi.org/10.1016/j.chc.2010.07.001
Al-Khattab, H., Oruche, U., Perkins, D., & Draucker, C. (2016). How African American adolescents manage depression: Being with others. Journal of the American Psychiatric Nurses Association, 22(5), 387–400. https://doi.org/10.1177/1078390316657391
Auger, R. W. (2005). School-based interventions for students with depressive disorders. Professional School Counseling, 8(4), 344–352.
Breland-Noble, A. M., Burriss, A., & Poole, H. K. (2010). Engaging depressed African American adolescents in treatment: Lessons from the AAKOMA PROJECT. Journal of Clinical Psychology, 66(8), 868–879. https://doi.org/10.1002/jclp.20708
Brenner, E. (2019). The crisis of youth mental health. Stanford Social Innovation Review. https://ssir.org/articles/entry/the_crisis_of_youth_mental_health#
Bridge, J. A., Horowitz, L. M., Fontanella, C. A., Sheftall, A. H., Greenhouse, J., Kelleher, K. J., & Campo, J. V. (2018). Age-related racial disparity in suicide rates among US youths from 2001 through 2015. JAMA Pediatrics, 172(7), 697–699. https://doi.org/10.1001/jamapediatrics.2018.0399
Brody, G. H., Chen, Y.-F., Kogan, S. M., Yu, T., Molgaard, V. K., DiClemente, R. J., & Wingood, G. M. (2012). Family-centered program deters substance use, conduct problems, and depressive symptoms in Black adolescents. Pediatrics, 129(1), 108–115. https://doi.org/10.1542/peds.2011-0623
Bryant, K., Greer-Williams, N., Willis, N., & Hartwig, M. (2013). Barriers to diagnosis and treatment of depression: Voices from a rural African-American faith community. Journal of National Black Nurses’ Association: JNBNA, 24(1), 31–38.
Choi, H., Meininger, J. C., & Roberts, R. E. (2006). Ethnic differences in adolescents’ mental distress, social stress, and resources. Adolescence, 41(162), 263–283.
Conner, L. C., & Yeh, C. J. (2018). Stress, coping, and depression among Black urban adolescents: Implications for school counseling. Journal of School Counseling, 16(15), 1–31.
Cook, B. L., Trinh, N.-H., Li, Z., Hou, S. S.-Y., & Progovac, A. M. (2017). Trends in racial–ethnic disparities in access to mental health care, 2004–2012. Psychiatric Services, 68(1), 9–16. https://doi.org/10.1176/appi.ps.201500453
Everall, R. D., Altrows, J., & Paulson, B. L. (2006). Creating a future: A study of resilience in suicidal female adolescents. Journal of Counseling & Development, 84(4), 461–471. https://doi.org/10.1002/j.1556-6678.2006.tb00430.x
Graves, L. (2017). Filters of influence: The help-seeking process of African American single mothers living in poverty seeking mental health services for their children. Child & Youth Services, 38(1), 69–90. https://doi.org/10.1080/0145935X.2016.1251836.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hope, M. O., Assari, S., Cole-Lewis, Y. C., & Caldwell, C. H. (2017). Religious social support, discrimination, and psychiatric disorders among Black adolescents. Race and Social Problems, 9(2), 102–114. https://doi.org/10.1007/s12552-016-9192-7
Jacob, M., Keeley, M. L., Ritschel, L., & Craighead, W. E. (2013). Behavioural activation for the treatment of low-income, African American adolescents with major depressive disorder: A case series. Clinical Psychology & Psychotherapy, 20(1), 87–96. https://doi.org/10.1002/cpp.774
Lake, J., & Turner, M. S. (2017). Urgent need for improved mental health care and a more collaborative model of care. Permanente Journal, 21, 17–24. https://doi.org/10.7812/TPP/17-024
Liang, J., Matheson, B. E., & Douglas, J. M. (2016). Mental health diagnostic considerations in racial/ethnic minority youth. Journal of Child and Family Studies, 25(6), 1926–1940. https://doi.org/10.1007/s10826-015-0351-z
Lindsey, M. A., Joe, S., & Nebbitt, V. (2010). Family matters: The role of mental health stigma and social support on depressive symptoms and subsequent help seeking among African American boys. Journal of Black Psychology, 36(4), 458–482. https://doi.org/10.1177/0095798409355796
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Lu, W. (2019). Adolescent depression: National trends, risk factors, and healthcare disparities. American Journal of Health Behavior, 43(1), 181–194. https://doi.org/10.5993/AJHB.43.1.15
Lu, W., Lindsey, M. A., Irsheid, S., & Nebbitt, V. E. (2017). Psychometric properties of the CES-D among Black adolescents in public housing. Journal for the Society for Social Work and Research, 8(4), 595–619. https://doi.org/10.1086/694791
Merriam, S. B. (2009). Qualitative research: A guide to design and implementation (3rd ed.). Jossey-Bass.
Murry, V. M., Heflinger, C. A., Suiter, S. V., & Brody, G. H. (2011). Examining perceptions about mental health care and help-seeking among rural African American families of adolescents. Journal of Youth and Adolescence, 40(9), 1118–1131.
https://doi.org/ 10.1007/s10964-010-9627-1
National Institute of Mental Health. (2013). Major depression. https://www.nimh.nih.gov/health/statistics/major-depression.shtml
Ofonedu, M. E., Percy, W. H., Harris-Britt, A., & Belcher, H. M. E. (2013). Depression in inner city African American youth: A phenomenological study. Journal of Child and Family Studies, 22(1), 96–106. https://doi.org/10.1007/s10826-012-9583-3
Patton, M. Q. (1987). How to use qualitative methods in evaluation (2nd ed.). SAGE.
Planey, A. M., Smith, S. M., Moore, S., & Walker, T. D. (2019). Barriers and facilitators to mental health help-seeking among African American youth and their families: A systematic review study. Children and Youth Services Review, 101, 190–200. https://doi.org/10.1016/j.childyouth.2019.04.001
Probst, J. C., Laditka, S. B., Moore, C. G., Harun, N., Powell, M. P., & Baxley, E. G. (2006). Rural-urban differences in depression prevalence: implications for family medicine. Family Medicine Kansas City, 38(9), 653–660.
Robinson, W. L., Brown, M., Beasley, C. R., & Jason, L. A. (2017). Advancing prevention intervention from theory to application: Challenges and contributions of community psychology. In M. A. Bond, I. Serrano-García, C. B. Keys, & M. Shinn (Eds.), APA handbook in psychology. APA handbook of community psychology: Methods for community research and action for diverse groups and issues (pp. 193–213). American Psychological Association.
Robinson, W. L., Droege, J. R., Case, M. H., & Jason, L. A. (2015). Reducing stress and preventing anxiety in African American adolescents: A culturally-grounded approach. Global Journal of Community Psychology Practice, 6(2). https://doi.org/10.7728/0602201503
Saluja, G., Iachan, R., Scheidt, P. C., Overpeck, M. D., Sun, W., & Giedd, J. N. (2004). Prevalence of and risk factors for depressive symptoms among young adolescents. Archives of Pediatrics and Adolescent Medicine, 158(8), 760–765. https://doi.org/10.1001/archpedi.158.8.760
Shushansky, L. (2017, July 31). Disparities within minority mental health care [Blog post]. National Alliance on Mental Illness. https://www.nami.org/Blogs/NAMI-Blog/July-2017/Disparities-Within-Minority-Mental-Health-Care
Smokowski, P. R., Bacallao, M. L., Cotter, K. L., & Evans, C. B. R. (2015). The effects of positive and negative parenting practices on adolescent mental health outcomes in a multicultural sample of rural youth. Child Psychiatry & Human Development, 46(3), 333–345. https://doi.org/10.1007/s10578-014-0474-2
Sullivan, G., Cheney, A., Olson, M., Haynes, T., Bryant, K., Cottoms, N., Reaves, C., & Curran, G. (2017). Rural African Americans’ perspectives on mental health: Comparing focus groups and deliberative democracy forums. Journal of Health Care for the Poor and Underserved, 28(1), 548–565. https://doi.org/10.1353/hpu.2017.0039
van Manen, M. (1997). Researching lived experience: Human science for an action sensitive pedagogy. (2nd ed.). Althouse.
Vontress, C. E., Woodland, C. E., & Epp, L. (2007). Cultural dysthymia: An unrecognized disorder among African Americans? Journal of Multicultural Counseling and Development, 35(3), 130–141. https://doi.org/10.1002/j.2161-1912.2007.tb00055.x
Weaver, A., Himle, J. A., Taylor, R. J., Matusko, N. N., & Abelson, J. M. (2015). Urban vs. rural residence and the prevalence of depression and mood disorder among African American women and non-Hispanic white women. JAMA Psychiatry, 72(6), 576–583. https://doi.org/10.1001/jamapsychiatry.2015.10
Willis, L. A., Coombs, D. W., Drentea, P., & Cockerham, W. C. (2003). Uncovering the mystery: Factors of African American suicide. Suicide and Life-Threatening Behavior, 33(4), 412–429. https://doi.org/10.1521/suli.33.4.412.25230
World Federation for Mental Health. (2012). Depression: A global crisis. https://www.who.int/mental_health/management/depression/wfmh_paper_depression_wmhd_2012.pdf
World Health Organization. (2020). Depression. https://www.who.int/news-room/fact-sheets/detail/depression
TeShaunda Hannor-Walker, PhD, NCC, LPC, CPCS, is an assistant professor at Liberty University. Lynn Bohecker, PhD, LMFT, is an associate professor at Liberty University. Lacey Ricks, PhD, NCC, is an assistant professor at Liberty University. Sarah Kitchens, PhD, NCC, is an assistant professor at Liberty University. Correspondence may be addressed to TeShaunda Hannor-Walker, 1971 University Blvd., Lynchburg, VA 24515, thannorwalker@liberty.edu.
Apr 28, 2020 | TPC Outstanding Scholar
Stacey Diane A. Litam

Stacey Diane A. Litam received the 2019 Outstanding Scholar Award for Quantitative or Qualitative Research for her article, “She’s Just a Prostitute: The Effects of Labels on Counselor Attitudes, Empathy, and Rape Myth Acceptance.”
Stacey Diane A. Litam (she, her, hers), PhD, NCC, CCMHC, LPCC, is an assistant professor of counselor education at Cleveland State University. Dr. Litam is a researcher, counselor educator, and social justice advocate on topics related to human sexuality, sex trafficking, and the phenomenological experiences of individuals who have intersecting marginalized identities.
As a scholar, Dr. Litam’s research has been published in prestigious journals such as The Professional Counselor (TPC), Journal of Sexual Aggression, and Journal of Child Sexual Abuse. Her doctoral dissertation, An Examination of Whether Scores of Attitudes Based on Labels and Counselor Attributes Predicted Scores of Human Relations and Beliefs About Rape in Counselors, won TPC’s 2019 Dissertation Excellence Award. In addition to her two TPC awards, Dr. Litam has won numerous awards for her academic and advocacy work, including a 2016 Doctoral Minority Fellowship from the NBCC Foundation, the 2016 Outstanding Doctoral Student of the Year award from the Ohio Association for Counselor Education and Supervision, the 2017 Humanistic Advocacy and Social Justice Award from the Association for Humanistic Counselors division of the American Counseling Association, the 2018 David K. Brooks Award from Chi Sigma Iota, and a 2019 Outstanding Service to Specialized Populations Award from NBCC.
She has facilitated over 70 refereed presentations at the national, regional, and state levels and actively contributes to peer-reviewed publications in journals, books, and edited volumes. Her professional interests encompass human sexuality, human trafficking, decolonizing the model minority stereotype, and the influence of internalized racism and intra-ethnic othering on Asian American identity development.
Read more about the TPC scholarship awards here.
Apr 28, 2020 | TPC Outstanding Scholar
Jennifer L. Rogers, Jamie E. Crockett, and Esther Suess

Jennifer L. Rogers, Jamie E. Crockett, and Esther Suess received the 2019 Outstanding Scholar Award for Concept/Theory for their article, “Miscarriage: An Ecological Examination.”
Jennifer L. Rogers, PhD, NCC, is an assistant professor in the Wake Forest University Department of Counseling. She received her PhD in counseling and counselor education from Syracuse University. Her clinical and research interests are centered around relational approaches to counseling, supervision, and counselor preparation across ecologically diverse practice contexts. Her current research focuses upon how attachment and cognitive patterns among beginning counselors influence their experiences during clinical supervision.
Jamie E. Crockett, PhD, NCC, LCMHCA, is an assistant professor in the Wake Forest University Department of Counseling and a clinical mental health counselor at Triad Counseling and Clinical Services. Her clinical and research interests include human development, attachment, gender and sexuality, reproductive health, grief and loss, contemplative and breath-based approaches, emotion, wellness, religion and spirituality, ethics, feminism, and diversity and culture.
Esther Suess, MA, NCC, LPC-A, LCMHCA, is a mental health counselor at the Mood Treatment Center in Winston-Salem, North Carolina, with a specialty in the treatment of eating disorders and obsessive-compulsive disorder. She graduated with an undergraduate degree in psychology from University College Dublin in 2016 and received her master’s degree in clinical mental health counseling from Wake Forest University in 2018. Her research interests include cultural diversity and biopsychosocial factors in counseling and eating disorders.
Read more about the TPC scholarship awards here.
Mar 9, 2020 | Volume 10 - Issue 1
Michael T. Kalkbrenner
College counselors work collaboratively with professionals in a variety of disciplines in higher education to coordinate gatekeeper training to prepare university community members to recognize and refer students in mental distress to support services. This article describes the cross-validation of scores on the Mental Distress Response Scale (MDRS), a questionnaire for appraising university community members’ responses to encountering a student in mental distress, with a sample of faculty members. A confirmatory factor analysis revealed the dimensions of the MDRS were estimated adequately. Results also revealed demographic differences in faculty members’ responses to encountering a student in mental distress. The MDRS has implications for augmenting the outreach efforts of college counselors. For example, the MDRS has potential utility for enhancing campus-wide mental health screening efforts. The MDRS also has implications for supporting psychoeducation efforts, including gatekeeper training workshops, for professional counselors practicing in college settings.
Keywords: Mental Distress Response Scale, mental health, college counselors, gatekeeper, outreach
College counselors play crucial roles in supporting students’ personal, social, and academic growth, as well as students’ success (Golightly et al., 2017). Outreach and prevention programming, including campus violence prevention and supporting college student mental health, are two key elements in the practice of college counselors (Brunner et al., 2014; Golightly et al., 2017). Addressing these two key areas has become increasingly challenging in recent years because of the prevalence of campus violence incidents, including mass shootings in the most severe cases, and the frequency of mental health distress among college students, which has increased substantially since the new millennium (Auerbach et al., 2016; Barrett, 2014; Vieselmeyer et al., 2017). In fact, supporting college student mental health has become one of the greatest challenges that institutions of higher education are facing (Reynolds, 2013).
Most college students suffering from mental health issues do not seek treatment (Downs & Eisenberg, 2012). In response, college counselors, student affairs professionals, and higher education administrators are working collaboratively to develop and implement mental health awareness initiatives and gatekeeper training workshops, which include training university community members (e.g., students, faculty, and staff) as referral agents to recognize and refer students who are showing warning signs for suicide or other mental health issues to support services (Albright & Schwartz, 2017; Hodges et al., 2017). Faculty members are particularly valuable referral agents, as they tend to interact with large groups of students on frequent occasions, and they generally report positive attitudes about supporting college student mental health (Albright & Schwartz, 2017; Kalkbrenner, 2016).
Despite the utility of faculty members as gatekeepers for recognizing and referring students to the university counseling center and to other resources, the results of a recent national survey indicated that a significant proportion of faculty members (63%) do not refer a student in mental distress to support services (Albright & Schwartz, 2017). The literature is lacking research on how faculty members are likely to respond to encountering a student in mental distress, including but not limited to making a faculty-to-student referral to mental health support services. The primary aim of this investigation was to confirm the psychometric properties of the Mental Distress Response Scale (MDRS), a screening tool for measuring university community members’ responses to encountering a student in mental distress. Past investigators validated the MDRS for use with 4-year university students (Kalkbrenner & Flinn, 2020) and community college students (Kalkbrenner, 2019). If found valid for use with faculty members, college counselors could find the MDRS useful for screening and promoting faculty-to-student mental health support. A review of the extant literature is provided in the following section.
Mental Health and the State of Higher Education
Active shooter incidents on college campuses are some of the most tragic events in American history (Kalkbrenner, 2016). The 2015 massacre that occurred on a college campus in Oregon received attention at the highest level of government; former President Barack Obama urged the nation to decide when voting “whether this cause of continuing death for innocent people should be a relevant factor.” (Vanderhart et al., 2015, section A, p. 1). Seung-Hui Cho was a perpetrator of another one of these tragedies at Virginia Polytechnic Institute in 2007. According to Cho’s mother, he had a history of social isolation and unresolved mental health issues (Klienfield, 2007). Without treatment, the effects of mental health disorders can be debilitating and widespread for students, including impairments in academic functioning, attrition, self-harm, social isolation, and suicide or homicide in the most serious cases (Kalkbrenner, 2016; Shuchman, 2007). The early detection and treatment of students who are at risk for mental health disorders is a harm-prevention strategy for reducing campus violence incidents and promoting college student mental health (Futo, 2011; Kalkbrenner, 2016). Consequently, the practice of college counselors involves deploying outreach and systems-level mental health support interventions (Albright & Schwartz, 2017; Brunner et al., 2014; Golightly et al., 2017).
The Role of College Counselors in Providing Systems-Level Interventions
Providing individual counseling is a key role of college counselors (Golightly et al., 2017). In recent years, however, the practice of college counselors has been extended to providing systems-level and preventative mental health interventions to meet the growing mental health needs of college student populations (Brunner et al., 2014; Golightly et al., 2017). In particular, college counselors and their constituents engage in both campus-wide and targeted prevention and outreach programs (Golightly et al., 2017; Lynch & Glass, 2019), including gatekeeper training workshops to prepare university community members as referral agents or train them to recognize and refer students at risk for suicide and other mental health issues to the university counseling center (Albright & Schwartz, 2017; Brunner et al., 2014). These collaborative, educative, and preventative efforts are particularly crucial given the increase in both the severity and complexity of mental health disorders among college students (Gallagher, 2015; Reetz et al., 2016). The findings of past investigators suggest that faculty members are particularly viable referral agents for recognizing and referring students in mental distress to the counseling center (Kalkbrenner, 2016; Margrove et al., 2014).
Faculty Members as Referral Agents
Faculty members have a propensity to serve as referral agents (i.e., recognize and refer students in mental distress to resources) because of their frequent contact with students and their generally positive attitudes and willingness to support their students’ mental and physical wellness (Albright & Schwartz, 2017). Albright and Schwartz (2017) found that approximately 95% of faculty members and staff considered connecting students in mental distress to resources as one of their roles and responsibilities. Similarly, Margrove et al. (2014) found that 64% of untrained university staff members expressed a desire to receive training to recognize warning signs of mental health disorders in students.
Past investigators extended the line of research on the utility of faculty members as gatekeepers by identifying demographic differences by gender and help-seeking history (previous attendance in counseling) in faculty members’ tendency to support college student mental health (Kalkbrenner & Carlisle, 2019; Kalkbrenner & Sink, 2018). In particular, Kalkbrenner and Sink (2018) identified gender as a significant predictor of faculty-to-student counseling referrals, with faculty who identified as female more likely to make faculty-to-student referrals to the counseling center compared to their male counterparts. Similarly, Kalkbrenner and Carlisle (2019) found that faculty members’ awareness of warning signs for mental distress in students was a significant positive predictor of faculty-to-student referrals to the counseling center. In addition, faculty members with a help-seeking history (previous attendance in counseling) were significantly more aware of warning signs for mental distress in their students compared to faculty without a help-seeking history (Kalkbrenner & Carlisle, 2019).
Faculty Members’ Responses to Encountering a Student in Mental Distress
Despite the growing body of literature on institutional agents’ participation in gatekeeper training (i.e., recognize and refer), research on the measurement and appraisal of how faculty members are likely to respond when encountering a student in mental distress is in its infancy. The results of a recent national survey of college students (N = 51,294) and faculty members (N = 14,548) were troubling, as 63% of faculty members did not refer a student in psychological distress to mental health support services (Albright & Schwartz, 2017). Making a referral to the university counseling center is one possible response of students and faculty members to encountering a peer or student in mental distress (Kalkbrenner & Sink, 2018). However, the findings of Albright and Schwartz (2017) highlight a gap in the literature regarding how university community members are likely to respond when encountering a student in mental distress, including but not limited to making a faculty-to-student referral to the college counseling center.
To begin filling this gap in the literature, Kalkbrenner and Flinn (2020) developed, validated, and cross-validated scores on the MDRS to assess 4-year university students’ responses to encountering a student in mental distress, including but not limited to making a referral to mental health support services. In a series of two major phases of psychometric analyses, Kalkbrenner and Flinn identified and confirmed two dimensions or subscales of the MDRS, including Diminish/Avoid and Approach/Encourage, with two large samples of undergraduate students. The Diminish/Avoid subscale measures adverse or inactive responses of university community members to encountering a student in mental distress (e.g., stay away from the person or warn the person that mental issues are perceived as a weakness). The Approach/Encourage subscale appraises facilitative or helpful responses of university community members when encountering a student in mental distress that are likely to help connect the person to resources (e.g., talking to a college counselor or suggesting that the person go to the campus counseling or health center). However, the psychometric properties of the MDRS have not been tested with faculty members. If found valid for such purposes, the MDRS could be a useful tool that college counselors and their constituents can use to screen and promote faculty-to-student referrals to mental health support services. In particular, the following research questions were posed: (1) Does the two-dimensional hypothesized MDRS model fit with a sample of faculty members? and (2) To what extent are there demographic differences in faculty members’ responses to encountering a student in mental distress?
Method
Participants and Procedures
Data were collected electronically from faculty members using Qualtrics, a secure e-survey platform. A nonprobability sampling procedure was used by sending a recruitment email message with an electronic link to the survey to 1,000 faculty members who were teaching at least one course at a research-intensive, mid-Atlantic public university at the time of data collection. A total of 221 faculty members clicked on the electronic link to the survey and 11 responses were omitted from the data set because of 100% missing data, resulting in a useable sample size of 210, yielding a response rate of 21%. This response rate is consistent with the response rates of other investigators (e.g., Brockelman & Scheyett, 2015; Kalkbrenner & Carlisle, 2019) who conducted survey research with faculty members. For gender, 58% (n = 122) identified as female, 41% (n = 86) as male, and 0.5% (n = 1) as non-binary or third gender, and 0.5% (n = 1) did not specify their gender. For ethnicity, 79.0% (n = 166) identified as Caucasian, 6.2% (n = 11) as African American, 3.8% (n = 8) as Hispanic or Latinx, 2.9% (n = 6) as Asian, 2.9% (n = 6) as multiethnic, 0.5% (n = 1) as Hindu, and 0.5% (n = 1) as Irish, and 5.2% (n = 11) did not specify their ethnic identity. Participants ranged in age from 31 to 78 (M = 50; SD = 11). Participants represented all of the academic colleges in the university, including 28.6% (n = 60) Arts and Letters, 22.9% (n = 48) Education, 18.1% (n = 38) Sciences, 12.9% (n = 27) Health Sciences, 9% (n = 19) Engineering and Technology, and 7.6% (n = 16) Business, while 1% (n = 2) of participants did not specify their college.
Instrumentation
Demographic questionnaire
Following informed consent, participants were asked to indicate that they met the inclusion criteria for participation, including (1) employment as a faculty member, and (2) teaching at least one course at the time of data collection. Participants then responded to a succession of demographic items about their gender, ethnicity, age, academic college, and highest level of education completed. Lastly, respondents indicated their rank and help-seeking history (previous attendance in counseling or no previous attendance in counseling) and if they had referred at least one student to mental health support services.
Mental Distress Response Scale (MDRS)
The MDRS is a screening tool comprised of two subscales (Approach/Encourage and Diminish/Avoid) for measuring university community members’ responses to encountering a student in mental distress (Kalkbrenner & Flinn, 2020). The items that mark the Approach/Encourage subscale appraise responses to mental distress that are consistent with providing support and encouragement to a student in mental distress (e.g., “suggest that they go to the health center on campus”). The Diminish/Avoid subscale measures adverse or inactive responses to encountering a student in mental distress (e.g., “try to ignore your concern”). Kalkbrenner and Flinn (2020) found adequate reliability evidence for an attitudinal measure (α > 0.70) and initial validity evidence for the MDRS in two major phases of analyses (exploratory and confirmatory factor analysis [CFA]) with two samples of college students. Kalkbrenner (2019) extended the line of research on the utility of the MDRS for use with community college students and found adequate reliability (α > 0.80) and validity evidence (single and multiple-group confirmatory analysis).
Data Analysis
A CFA based on structural equation modeling was computed using IBM SPSS Amos version 25 to cross-validate scores on the MDRS with a sample of faculty members (research question #1). Using a maximum likelihood estimation method, the following goodness-of-fit indices and thresholds for defining model fit were investigated based on the recommendations of Byrne (2016) and Hooper et al. (2008): Chi square absolute fit index (CMIN, non-significant p-value with an x2/df ratio < 3), comparative fit index (CFI > 0.95), incremental fit index (IFI > 0.95), Tucker-Lewis index (TLI > 0.95), goodness-of-fit index (GFI > 0.95), root mean square error of approximation (RMSEA < 0.07), and standardized root mean square residual (SRMR < 0.08). Based on the findings of past investigators (e.g., Kalkbrenner & Sink, 2018) regarding demographic differences in faculty members’ propensity to support college student mental health, a 2 X 2 (gender X help-seeking history) MANOVA was computed to investigate demographic differences in faculty members’ responses to encountering a student in mental distress (research question #2). The independent variables included gender (male or female) and help-seeking history (previous attendance in counseling or no previous attendance in counseling). Discriminant analysis was used as the post hoc procedure for significant findings in the MANOVA (Warne, 2014). The researcher examined both main effects and interaction effects and applied Bonferroni adjustments to control for the familywise error rate.
Results
CFA
The researcher ensured that the data set met the necessary assumptions for CFA (Byrne, 2016; Field, 2018). A missing values analysis revealed that less than 5% of data was missing for all MDRS items. Little’s Missing Completely at Random (MCAR) test revealed that the data was missing at random: χ2 (387) = 407.98, p = 0.22. Expectation maximization was used to impute missing values. Outliers were winsorized (Field, 2018) and skewness and kurtosis values for the MDRS items (see Table 1) were largely consistent with a normal distribution (+ 1; Mvududu & Sink, 2013). Inter-item correlations between the 10 items were favorable for CFA, and Mahalanobis d2 indices revealed no extreme multivariate outliers. The researcher ensured that the sample size was sufficient for CFA by following the guidelines provided by Mvududu and Sink (2013), including at least 10 participants per estimated parameter with a sample > 200.
Table 1
Descriptive Statistics for MDRS Items
| Item Content |
M |
SD |
Skew |
Kurtosis |
| 1. I would stay away from this person |
49.83 |
9.46 |
1.11 |
0.22 |
| 2. Suggest that they go to the health center on campus |
50.15 |
9.48 |
-0.60 |
-0.08 |
| 3. Try to ignore your concern |
49.74 |
9.08 |
1.07 |
1.08 |
| 4. Take them to a party |
49.21 |
3.11 |
0.70 |
0.81 |
| 5. Tell them to “tough it out” because they will feel better over time |
49.73 |
8.94 |
1.32 |
1.26 |
| 6. Suggest that they see a medical doctor on campus |
50.00 |
9.98 |
-0.24 |
-0.06 |
| 7. Avoid this person |
49.70 |
9.02 |
1.80 |
1.33 |
| 8. Suggest that they see a medical doctor in the community |
50.00 |
9.98 |
-0.49 |
-0.10 |
| 9. Warn the person that others are likely to see their mental health issues as a weakness |
49.31 |
7.14 |
1.90 |
1.59 |
| 10. Talk to a counselor about your concern |
50.00 |
9.97 |
-0.83 |
0.15 |
SEKurtosis = 0.15, SESkewness = 0.17.
Note. Values were winsorized and reported as standardized t-scores (M = 50; SD = 10).
The 10 MDRS items (see Table 1) were entered in the CFA. A strong model fit emerged based on the GFI recommended by Byrne (2016) and Hooper et al. (2008). The CMIN absolute fit index demonstrated no significant differences between the hypothesized model and the data: χ2 (34) = 42.41, p = 0.15, CMIN/df = 1.25. In addition, the CFI = 0.98, GFI = 0.96, IFI = 0.98, TLI = 0.98, RMSEA = 0.03, 90% confidence interval [<.00, .06], and SRMR = 0.05 also demonstrated a strong model fit. Internal consistency reliability analyses (Cronbach’s coefficient alpha) revealed satisfactory reliability coefficients for an attitudinal measure, Diminish/Avoid (α = 0.73) and Approach/Encourage (α = 0.70). In addition, the path model coefficient (-0.04) between factors supported the structural validity of the scales (see Figure 1).
Figure 1
Confirmatory Factor Analysis Path Diagram for the Mental Distress Response Scale
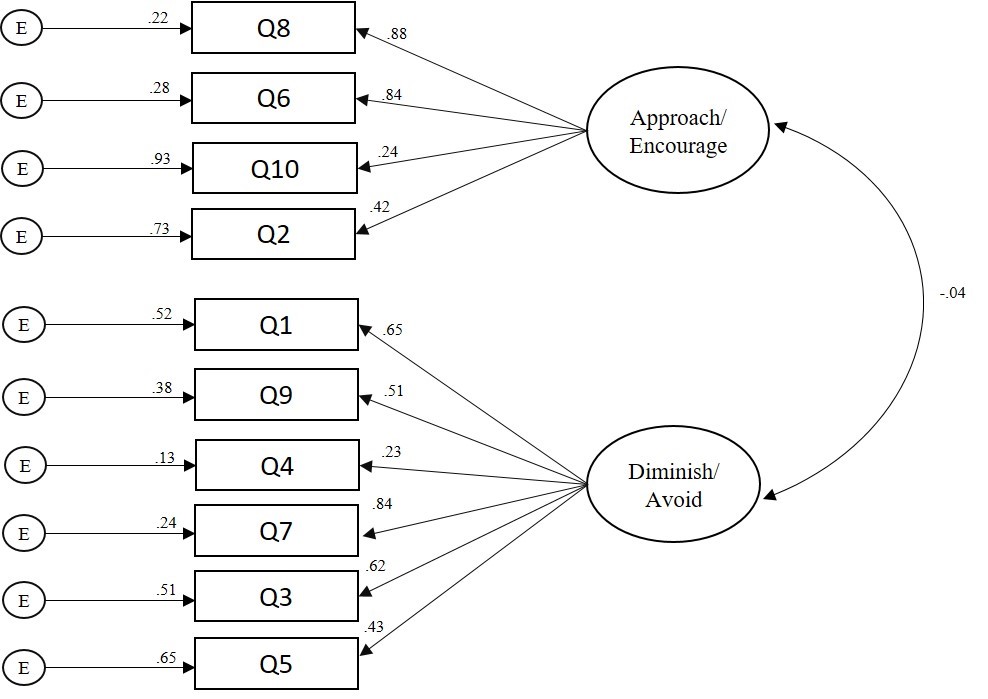
Note. CFA = confirmatory factor analysis, MDRS = Mental Distress Response Scale.
Multivariate Analysis
A 2 X 2 (gender X help-seeking history) MANOVA was computed to investigate demographic differences in faculty members’ responses to encountering a student in mental distress (research question #2). G*Power was used to conduct an a priori power analysis (Faul et al., 2007) and revealed that a minimum sample size of 151 would provide a 95% power estimate, α = .05, with a moderate effect size, F2(v) = 0.063. A significant main effect emerged for gender: F(3, 196) = 8.27, p < 0.001, Wilks’ λ = 0.92, = 0.08. The MANOVA was followed up with a post hoc discriminant analysis based on the recommendations of Warne (2014). The discriminant function significantly discriminated between groups: Wilks’ λ = 0.91, X2 = 18.85, df = 2, p < 0.001. The correlations between the latent factors and discriminant function showed that Diminish/Avoid loaded more strongly on the function (r = 0.98) than Approach/Encourage (r = 0.29), suggesting that Diminish/Avoid contributed the most to group separation in gender. The mean discriminant score on the function was -0.27 for participants who identified as female and 0.37 for participants who identified as male.
Discussion
The results of tests of internal consistency reliability (Cronbach’s coefficient alpha), CFA, and correlations between factors supported the psychometric properties of the MDRS with a sample of faculty members. The results of the CFA were promising as GFI demonstrated a strong model fit between the two-dimensional hypothesized MDRS model and a sample of faculty members (research question #1). In particular, based on one of the most conservative and rigorous absolute fit indices, the CMIN (Byrne, 2016; Credé & Harms, 2015), the researchers retained the null hypothesis—there were no significant differences between the hypothesized factor structure of the MDRS and a sample of faculty members. The strong model fit suggests that Approach/Encourage and Diminish/Avoid are two latent variables that comprise faculty members’ responses to encountering a student in mental distress. The findings of the CFA add to the extant literature about the utility of the MDRS for use with 4-year university students (Kalkbrenner & Flinn, 2020), community college students (Kalkbrenner, 2019), and now with faculty members.
An investigation of the path model coefficient between subscales (see Figure 1) revealed a small and negative association between factors, which supports the structural validity of the MDRS. In particular, the low and negative relationship between the Approach/Encourage and Diminish/Avoid subscales indicates that the dimensions of the MDRS are measuring discrete dimensions of a related construct. As expected, faculty members who scored higher on the Approach/Encourage subscale tended to score lower on the Diminish/Avoid subscale. However, the low strength of the association between factors suggests that faculty members’ responses to encountering a student in mental distress might not always be linear (e.g., a strong positive approach/encourage response might not always be associated with a strong negative diminish/avoid response). Haines et al. (2017) demonstrated that factors in the environment and temperament of a person showing signs of mental distress were significant predictors of mental health support staff’s perceptions of work safety. It is possible that under one set of circumstances faculty members might have an approach/encourage response to mental distress. However, under a difference set of circumstances, a faculty member might have a diminish/avoid response. For example, the extent to which a faculty member feels threatened or unsafe might mediate their propensity of having diminish/avoid or approach/encourage responses. Future research is needed to evaluate this possibility.
Consistent with the findings of previous researchers (Kalkbrenner & Carlisle, 2019; Kalkbrenner & Sink, 2018), the present investigators found that faculty members who identified as male were more likely to report a diminish/avoid response to encountering a student in mental distress compared to female faculty members. Similarly, Kalkbrenner and Sink (2018) found that male faculty members were less likely to make faculty-to-student referrals to the counseling center, and Kalkbrenner and Carlisle (2019) found that male faculty members were less likely to recognize warning signs of mental distress in college students. Similarly, the multivariate results of the present investigation revealed that male faculty members were more likely to report a diminish/avoid response to encountering a student in mental distress when compared to female faculty members. The synthesized findings of Kalkbrenner and Carlisle (2019), Kalkbrenner and Sink (2018), and the present investigation suggest that faculty members who identify as male might be less likely to recognize and refer a student in mental distress to mental health support services. The MDRS has valuable implications for enhancing the practice of professional counselors in college settings.
Implications for Counseling Practice
Outreach, consultation, and psychoeducation are essential components in the practice of college counselors (Brunner et al., 2014; Golightly et al., 2017). The findings of the present investigation have a number of practical implications for enhancing college counselors’ outreach and psychoeducation work—for example, gatekeeper workshops geared toward promoting faculty-to-student referrals to mental health support resources. The complex and multidimensional nature of college student mental health issues calls for interdisciplinary collaboration between college counselors and professionals in a variety of disciplinary orientations in higher education (Eells & Rockland-Miller, 2011; Hodges et al., 2017). College counselors can take leadership roles in coordinating these collaborative efforts to support college student mental health. In particular, college counselors can work with student affairs officials, higher education administrators, and their constituents, and attend new faculty orientations as well as department meetings to administer the MDRS, establish relationships with faculty, and discuss the benefits of gatekeeper training as well as supporting college student mental health. The results of the MDRS can be used to gain insight into the types of responses that faculty members are likely to have when encountering a student in mental distress. This information can be used to structure the content of gatekeeper training workshops aimed at promoting faculty-to-student referrals to mental health support services. Specifically, college counselors might consider the utility of integrating brief interventions and skills training components into gatekeeper training workshops. Motivational interviewing, for example, is an evidence-based, brief approach to counseling that includes both person-centered and directive underpinnings with utility for increasing clients’ intrinsic motivation to make positive changes in their lives (Iarussi, 2013; Resnicow & McMaster, 2012). Professional counselors who practice in higher education are already using motivational interviewing to promote college student development and mental health (Iarussi, 2013). Although future research is needed, integrating motivational interviewing principles (e.g., expressing empathy, rolling with resistance, developing discrepancies, and supporting self-efficacy; Iarussi, 2013) into gatekeeper training workshops might increase faculty members’ commitment to supporting college student mental health.
The MDRS has the potential to enhance college counselors’ outreach and mental health screening efforts (Golightly et al., 2017). College counselors can incorporate the MDRS into batteries of pretest/posttest measures (e.g., the MDRS with a referral self-efficacy measure) for evaluating the effectiveness of mental health awareness initiatives and gatekeeper training programs for faculty and other members of the campus community. If administered widely, the MDRS might have utility for assessing faculty members’ responses to students in mental distress across time and among various campus ecological systems, providing data to drive the prioritization and allocation of outreach efforts aimed at facilitating and maintaining referral networks for connecting students in mental distress to support services.
The results of the present study have policy implications related to campus violence prevention programming. The sharp increase in campus violence incidents has resulted in several universities implementing threat assessment teams as a harm-prevention measure (Eells & Rockland-Miller, 2011). Threat assessment teams involve an interdisciplinary collaboration of university faculty and staff for the purposes of recognizing and responding to students who are at risk of posing a threat to themselves or to others. College counselors can take leadership roles in establishing and supporting threat assessment teams at their universities. College counselors can administer the MDRS to faculty and staff and use the results as one way to identify potential threat assessment team members. University community members who score higher on the Approach/Encourage scale might be inclined to serve on threat assessment teams because of their propensity to support college student mental health. The brevity (10 questions) and versatility of administration (paper copy or electronically via laptop, smartphone, or tablet) of the MDRS adds to the practicality of the measure. Specifically, it might be practical for college counselors and their constituents to administer the MDRS during new faculty orientations, annual opening programs, or department meetings, or via email to faculty and staff. Results can potentially be used to recruit threat assessment team members.
Our findings indicate that when compared to their female counterparts, male faculty members might be more likely to have a diminish/avoid response when encountering a student in mental distress. College counselors might consider working collaboratively with student affairs professionals to implement gatekeeper training and mental health awareness workshops in academic departments that are comprised of high proportions of male faculty members. It is possible that male faculty members are unaware of how to identify warning signs of mental distress in their students (Kalkbrenner & Carlisle, 2019). College counselors might consider the utility of distributing psychoeducation resources for recognizing students in mental distress to faculty and staff. As just one example, the REDFLAGS model is an acronym of eight red flags or warning signs for identifying students who might be struggling with mental health issues (Kalkbrenner, 2016). Kalkbrenner and Carlisle (2019) demonstrated that the REDFLAGS model is a promising psychoeducational tool, as faculty members’ awareness of the red flags was a significant positive predictor of faculty-to-student referrals to the counseling center. The REDFLAGS model appears to be a practical resource for college counselors that can be distributed to faculty electronically or by paper copy, or posted as a flyer (Kalkbrenner, 2016; Kalkbrenner & Carlisle, 2019).
Limitations and Future Research
The findings of the present study should be considered within the context of the limitations. A number of methodological limitations (e.g., self-report bias and social desirability) can influence the validity of psychometric designs. In addition, the dichotomous nature of the faculty-to-student counseling referral variable (referred or not referred) did not provide data on the frequency of referrals. Future researchers should use a continuous variable (e.g., the number of student referrals to the counseling center in the past 2 years) to appraise faculty-to-student referrals. Future researchers can further test the psychometric properties of the MDRS through cross-validating scores on the measure with additional, unique populations of faculty members from a variety of different geographic and social locations. Invariance testing can be computed to examine the degree to which the MDRS and its dimensions maintain psychometric equivalence across different populations of faculty members. In addition, the criterion validity of the MDRS can be examined by testing the extent to which respondents’ MDRS scores are predictors of their frequency of student referrals to the counseling center and to other resources. Furthermore, future qualitative research is needed to investigate faculty members’ unique experiences around supporting college student mental health.
The low and negative association between the Approach/Encourage and Diminish/Avoid subscales suggests that faculty members might have an approach/encourage response to encountering a student in mental distress under one set of circumstances; however, they might have a diminish/avoid response under a difference set of circumstances. Future investigators might test the extent to which attitudinal variables mediate respondents’ MDRS scores—for example, the extent to which faculty members’ sense of safety predicts their MDRS scores. In addition, given the widespread public perception of individuals living with mental illness as violent and dangerous (Varshney et al., 2016), future researchers might identify demographic and background differences (particularly mental health stigma) among participants’ MDRS scores.
Summary and Conclusion
Mental health outreach and screening are essential components in the practice of college counselors, including training referral agents to recognize and refer students who might be struggling with mental health distress to support services (Golightly et al., 2017). Taken together, the results of the present study indicate that the MDRS and its dimensions were estimated sufficiently with a sample of faculty members. Our findings confirmed the two-dimensional hypothesized model for the types of responses that faculty might have when encountering a student showing signs of mental distress. In particular, the results of a CFA provided support for the MDRS and its dimensions, confirming a two-dimensional construct for the types of responses (approach/encourage and diminish/avoid) that faculty members might have when encountering a student in mental distress. Considering the utility of faculty members as gatekeepers and referral agents (Hodges et al., 2017; Kalkbrenner, 2016), researchers, practitioners, and policymakers may find the MDRS a useful screening tool for identifying the ways in which faculty members are likely to respond when encountering a student in mental distress. Results can be used to inform the content of mental health awareness initiatives and gatekeeper training programs aimed at promoting approach/encourage responses to connect students who need mental health support to the appropriate resources.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Albright, G. & Schwartz, V. (2017). Are campuses ready to support students in distress?: A survey of 65,177 faculty, staff, and students in 100+ colleges and universities. https://www.jedfoundation.org/wp-content/uploads/2017/10/Kognito-JED-Are-Campuses-Ready-to-Support-Students-in-Distress.pdf
Auerbach, R. P., Alonso, J., Axinn, W. G., Cuijpers, P., Ebert, D. D., Green, J. G., Hwang, I., Kessler, R. C., Liu, H., Mortier, P., Nock, M. K., Pinder-Amaker, S., Sampson, N. A., Aguilar-Gaxiola, S., Al-Hamzawi, A., Andrade, L. H., Benjet, C., Caldas-de-Almeida, J. M., Demyttenaere, K., . . . Bruffaerts, R. (2016). Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychological Medicine, 46, 2955–2970. https://doi.org/10.1017/S0033291716001665
Barrett, D. (2014, September 24). Mass shootings on the rise, FBI says. The Wall Street Journal. http://online.wsj.com/articles/mass-shootings-on-the-rise-fbi-says-1411574475
Brockelman, K. F., & Scheyett, A. M. (2015). Faculty perceptions of accommodations, strategies, and psychiatric advance directives for university students with mental illnesses. Psychiatric Rehabilitation Journal, 38, 342–348. https://doi.org/10.1037/prj0000143
Brunner, J. L., Wallace, D. L., Reymann, L. S., Sellers, J.-J., & McCabe, A. G. (2014). College counseling today: Contemporary students and how counseling centers meet their needs. Journal of College Student Psychotherapy, 28, 257–324. https://doi.org/10.1080/87568225.2014.948770
Byrne, B. M. (2016). Structural equation modeling with AMOS: Basic concepts, applications, and programming (3rd ed.). Routledge.
Credé, M., & Harms, P. D. (2015). 25 years of higher-order confirmatory factor analysis in the organizational sciences: A critical review and development of reporting recommendations. Journal of Organizational Behavior, 36, 845–872. https://doi.org/10.1002/job.2008
Downs, M. F., & Eisenberg, D. (2012). Help seeking and treatment use among suicidal college students. Journal of American College Health, 60, 104–114. https://doi.org/10.1080/07448481.2011.619611
Eells, G. T., & Rockland-Miller, H. S. (2011). Assessing and responding to disturbed and disturbing students: Understanding the role of administrative teams in institutions of higher education. Journal of College Student Psychotherapy, 25, 8–23. https://doi.org/10.1080/87568225.2011.532470
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191. https://doi.org/10.3758/BF03193146
Field, A. (2018). Discovering statistics using IBM SPSS Statistics (5th ed.). SAGE.
Futo, J. (2011). Dealing with mental health issues on campus starts with early recognition and intervention. Campus Law Enforcement Journal, 41, 22–23.
Gallagher, R. P. (2015). National survey of college counseling centers 2014. http://d-scholarship.pitt.edu/id/eprint/28178
Golightly, T., Thorne, K., Iglesias, A., Huebner, E., Michaelson-Chmelir, T., Yang, J., & Greco, K. (2017). Outreach as intervention: The evolution of outreach and preventive programming on college campuses. Psychological Services, 14, 451–460. https://doi.org/10.1037/ser0000198
Haines, A., Brown, A., McCabe, R., Rogerson, M., & Whittington, R. (2017). Factors impacting perceived safety among staff working on mental health wards. BJPsych Open, 3, 204–211.
https://doi.org/10.1192/bjpo.bp.117.005280
Hodges, S. J., Shelton, K., & King Lyn, M. M. (2017). The college and university counseling manual: Integrating essential services across the campus. Springer.
Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modelling: Guidelines for determining model fit. The Electronic Journal of Business Research Methods, 6, 53–60.
Iarussi, M. M. (2013). Examining how motivational interviewing may foster college student development. Journal of College Counseling, 16(2), 158–175. https://doi.org/10.1002/j.2161-1882.2013.00034.x
Kalkbrenner, M. T. (2016). Recognizing and supporting students with mental health disorders: The REDFLAGS Model. Journal of Education and Training, 3, 1–13. https://doi.org/10.5296/jet.v3i1.8141
Kalkbrenner, M. T. (2019). Peer-to-peer mental health support on community college campuses: Examining the factorial invariance of the Mental Distress Response Scale. Community College Journal of Research and Practice. https://doi.org/10.1080/10668926.2019.1645056
Kalkbrenner, M. T., & Carlisle, K. L. (2019). Faculty members and college counseling: Utility of The REDFLAGS Model. Journal of College Student Psychotherapy. https://doi.org/10.1080/87568225.2019.1621230
Kalkbrenner, M. T., & Flinn, R. F. (2020). Development, validation, and cross-validation of the Mental Distress Reaction Scale (MDRS). Journal of College Student Development.
Kalkbrenner, M. T., & Sink, C. A. (2018). Development and validation of the College Mental Health Perceived Competency Scale. The Professional Counselor, 8, 175–189. https://doi.org/10.15241/mtk.8.2.175
Kleinfield, N. R. (2007, April 22). Before deadly rage, a life consumed by a troubling silence. The New York Times. http://www.nytimes.com/2007/04/22/us/22vatech.html?pagewanted=all
Lynch, R. J., & Glass, C. R. (2019). The development of the Secondary Trauma in Student Affairs Professionals Scale (STSAP). Journal of Student Affairs Research and Practice, 56, 1–18.
https://doi.org/10.1080/19496591.2018.1474757
Margrove, K. L., Gustowska, M., & Grove, L. S. (2014). Provision of support for psychological distress by university staff, and receptiveness to mental health training. Journal of Further and Higher Education, 38, 90–106. https://doi.org/10.1080/0309877X.2012.699518
Mvududu, N. H., & Sink, C. A. (2013). Factor analysis in counseling research and practice. Counseling Outcome Research and Evaluation, 4, 75–98. https://doi.org/10.1177/2150137813494766
Reetz, D. R., Bershad, C., LeViness, P., & Whitlock, M. (2016). The Association for University and College Counseling Center Directors annual survey. https://www.aucccd.org/assets/documents/aucccd%202016%
20monograph%20-%20public.pdf
Resnicow, K., & McMaster, F. (2012). Motivational interviewing: Moving from why to how with autonomy support. International Journal of Behavioral Nutrition and Physical Activity, 9, 19.
https://doi.org/10.1186/1479-5868-9-19
Reynolds, A. L. (2013). College student concerns: Perceptions of student affairs practitioners. Journal of College Student Development, 54, 98–104. https://doi.org/ 10.1353/csd.2013.0001
Shuchman, M. (2007). Falling through the cracks—Virginia Tech and the restructuring of college mental health services. The New England Journal of Medicine, 357, 105–110. https://doi.org/10.1056/NEJMp078096
Vanderhart, D., Johnson, K., & Turkewitz, J. (2015, October 2). Oregon shooting at Umpqua College kills 10, sheriff says. The New York Times. https://www.nytimes.com/2015/10/02/us/oregon-shooting-umpqua-community-college.html?smid=pl-share
Varshney, M., Mahapatra, A., Krishnan, V., Gupta, R., & Deb, K. S. (2016). Violence and mental illness: What is the true story? Journal of Epidemiology & Community Health, 70, 223–225.
https://doi.org/10.1136/jech-2015-205546
Vieselmeyer, J., Holguin, J., & Mezulis, A. (2017). The role of resilience and gratitude in posttraumatic stress and growth following a campus shooting. Psychological Trauma: Theory, Research, Practice, and Policy, 9, 62–69. https://doi.org/10.1037/tra0000149
Warne, R. T. (2014). A primer on multivariate analysis of variance (MANOVA) for behavioral scientists. Practical Assessment, Research & Evaluation, 19(17), 1–10.
Michael T. Kalkbrenner, PhD, NCC, is an assistant professor at New Mexico State University. Correspondence can be addressed to Michael Kalkbrenner, 1220 Stewart St., OH202B, NMSU, Las Cruces, NM 88001, mkalk001@nmsu.edu.
