Mar 26, 2019 | Volume 9 - Issue 1
Tahani Dari, John M. Laux, Yanhong Liu, Jennifer Reynolds
A gap exists in the counseling profession between research and practice. Community-based participatory research (CBPR) is one approach that could reduce this gap. The CBPR framework can serve as an additional tool for translating research findings into practical interventions for communities and counseling practitioners. Stronger community partnerships between researchers and practitioners will further improve treatment for our clients. The purpose of this study was to develop competencies that would provide the foundations for a training guideline in CBPR. Using the Delphi method, an expert panel achieved consensus on 153 competencies (knowledge, skills, attitudes, activities). Competencies are significant for the profession because they establish best practice, guidelines of service, and professional training.
Keywords: community-based participatory research, research competencies, Delphi method, community partnerships, best practices
The counseling profession has a gap between research and practice (Guiffrida, Douthit, Lynch, & Mackie, 2011; Murray, 2009; Peterson, Hall, & Buser, 2016; Wester & Borders, 2014). Thirty percent of counseling practitioners fail to use academic counseling research findings in their clinical practice (Wester & Borders, 2014). Erford et al. (2011) conducted an 8-year analysis of the Journal of Counseling & Development (JCD) author affiliation and found that the number of articles published in the JCD by non-academically affiliated authors (e.g., in private practice, K–12 schools) declined from 10% in 2002 to 5% in 2008. This decline is even more precipitous considering that 31% of the JCD’s publications between 1978 and 1993 were contributed by non-academic authors (Weinrach, Lustig, Chan & Thomas, 1998). Erford et al. suggested that this drop may be caused by a decline in collaboration between scientists and practitioners or counselors. Woolf (2008) and Wester and Borders (2014) suggested that counselors are apathetic about research because they are unprepared to translate research findings into clinical practice. Further, according to Guiffrida et al. (2011), practitioners may view research to be irrelevant to their work and their clients’ needs. Peterson et al. (2016) indicated the gap may possibly exist between the research skills highlighted in counselor education and those applied in the field. Finally, Murray (2009) noted that researchers and counselors are disconnected from one another; therefore, research findings are not clearly and quickly disseminated to field-based counselors. Although the specific reasons for the researcher–practitioner disconnection vary among authors, there is a compelling need for counseling researchers and practitioners to work toward a common goal benefiting clients.
This gap comprises a problem for the profession because research should inform counselors’ clinical interventions and supervisors’ decisions (Lilienfeld, Ammirati, & David, 2012). When they do not, the gap between academic counseling researchers and counseling practitioners puts client well-being at risk. To provide the best outcomes for clients, counseling practitioners must be aware of and make use of current evidence-based treatments identified through academic research. Likewise, counseling researchers who fail to consider the clinical zeitgeist may promulgate lines of inquiry that are difficult to translate into clinical application. One way to minimize this gap is through stronger collaborations between academic counseling researchers and counseling practitioners who already serve clients in their communities. One rationale the authors offer is that although there might be a desire to collaborate, there are currently no agreed upon standards to establish parameters of those collaborations, making setting up partnerships more challenging for counseling researchers. Efforts to incorporate community-based participatory research (CBPR) approaches could further enhance treatment for clients by strengthening researcher–practitioner partnerships (Horowitz, Robinson, & Seifer, 2009).
Community-Based Participatory Research
CBPR (Israel, Eng, Schulz, & Parker, 2013) fosters partnerships between researchers, institutions, and communities (Lachance, Quinn, & Kowalski-Dobson, 2018; Poleshuck et al., 2018; Woods-Jaeger et al., 2018). CBPR is employed in conjunction with quantitative, qualitative, or mixed methods (Minkler & Wallerstein, 2008); serves as an additional tool for translating research findings into applicable clinical practice (Lightfoot, McCleary, & Lum, 2014; Minkler & Wallerstein, 2008); and improves communication between researchers and practitioners (Poleshuck et al., 2018).
CBPR rests on nine key principles that focus on the concept of cultural humility (Israel et al., 2013). Israel, Schulz, Parker, and Becker (1998) identified the first eight, which include the following principles:
(1) recognizes the community as a unit of identity; (2) builds on strengths and resources within the community; (3) facilitates collaborative partnerships in all phases of the research;
(4) integrates knowledge and action for mutual benefit of all partners; (5) promotes a co-learning and empowering process that attends to social inequalities; (6) involves a cyclical and iterative process; (7) addresses health from both positive and ecological perspectives; and
(8) disseminates findings and knowledge gained to all partners.” (pp. 178–180)
Minkler and Wallerstein (2008) added an important ninth CBPR principle: “(9) requires a long-term process and commitment to sustainability” (p. 11). Each of these principles relies on the researcher’s dedication to the tenet of cultural humility, which is critical to building improved relationships between researchers and communities founded upon increased trust, respect, and accountability.
Hook, Davis, Owen, Worthington, and Utsey (2013) defined cultural humility as appreciating one’s limitation with respect to what can be understood about another culture. It also is described as genuine concern for others, an absence of the power and dominance dynamic, a willingness to continue learning, an understanding of our own biases, and a dedication to self-reflection. Researchers who apply cultural humility tend to develop greater levels of trust, respect, and accountability within their communities, particularly with hard-to-reach communities. For example, Mannix, Austin, Baayd, and Simonsen (2018) utilized the principles of CBPR in their work with a Native American tribe and found that cultural training was the initial step toward community integration among researchers and the formation of equalizing partnerships. Sharing in one’s role as the expert and valuing co-learning helps to reframe the community as equal partners within the collaborative research process. Nonetheless, Collins et al. (2018) advocated that the CBPR approach can be employed in collaboration with diverse types of communities, involving, for example, police officers, health care workers, and business management.
CBPR’s benefits are well documented across disciplines (e.g., Collins et al., 2018; Green, 2007; Lightfoot et al., 2014; Lindamer et al., 2008; O’Brien et al., 2018; Yuan et al., 2016). These benefits include researchers’ ability to utilize research outcomes to advocate for clients (Gray & Price, 2014; Horowitz et al., 2009; McElfish et al., 2015), advance health disciplines (O’Fallon & Dearry, 2002; Israel et al., 2013), increase participant contributions (Case et al., 2014; Wagstaff, Graham, Farrell, Larkin, & Tatham, 2018), address multifaceted client issues (Corrigan, Pickett, Kraus, Burks, & Schmidt, 2015), improve mental health services (Case et al., 2014), and foster interprofessional relationships (Hergenrather, Geishecker, Clark, & Rhodes, 2013). Despite CBPR’s acceptance as a research tool and demonstrated benefits for increasing the effectiveness of researcher–practitioner communication, the counseling literature lacks counseling research specific to CBPR competency training guidelines.
The purpose of this study was to address this paucity by developing CBPR competency training guidelines. Consistent with the profession’s approach to competency development commonly seen in the profession (e.g., Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2016), the authors organized CBPR competencies into the following areas: knowledge, skills, attitudes, and activities. The development of CBPR competencies sets the stage for counseling research to become more understandable, accessible, and applicable to counselors and their communities, thus diminishing the gap between research and practice. Competencies are significant for the profession because they establish best practice, guidelines of service, and professional trainings (Toporek, Lewis, & Crethar, 2009).
Method
The authors employed the Delphi method to identify CBPR throughout the study. The Delphi method is an empirical approach that elicits expert opinion on research results and validation of content (Garson, 2013; Jorm, 2015; Ross, Kelly, & Jorm, 2014). It is an iterative process that progresses through consecutive survey rounds. This approach provides a reliable method for gathering structured expert insight to improve professional training and typically includes a minimum of two rounds (Garson, 2013). Experts’ responses are blinded to one another. Rigor and validity of the Delphi method relies on the knowledge and experience of an expert panel (Garson, 2013). There is no set number of experts that should serve on a Delphi panel, but researchers agree that a minimum of eight to 12 experts is sufficient and appropriate for Delphi studies (Novakowski & Wellar, 2008). The authors decided upon the Delphi method because we see it as the best model for identifying additional content not reflected in the current counseling literature for use in the development of a training guideline for counselors.
An online survey platform was used to collect data. Online survey tools can provide an effective means of conducting Delphi studies (Ross et al., 2014; Weise, Fisher, & Trollor, 2016). Online data collection techniques are economical for researchers and convenient for participants, especially when experts live apart geographically. These techniques provide anonymity and facilitate the equal inclusion of expert feedback where group dynamics might preclude such participation in a face-to-face setting (Garson, 2013).
Expert Panel Formation
According to Mead and Moseley (2001), establishing expertise, and by extension experts, is a context-based process that depends on a number of criteria, which may include their position, recognition by a stakeholder community, or established specialization. The prospective panel of experts was initially identified using a review of publication records (Garson, 2013), and augmented with the recommendations. The authors required that participant experts demonstrate both knowledge of and experience with carrying out CBPR. Twenty prospective expert participants were identified and recruited with an email that explained the nature of the study and contained a link to the Delphi study. CBPR is rarely found in the counseling literature; therefore, the authors also relied upon snowball sampling to recruit CBPR expert counselor educators (Jorm, 2015). Finally, the authors extended the invitation to participate to public health professionals with evidenced CBPR expertise, identifying them through a review of public health literature, where the CBPR framework originated and is now well established (Lightfoot et al., 2014; Minkler & Wallerstein, 2008). Moreover, counselors and public health professionals are similarly committed to advancing wellness among the communities they serve (Kaplan & Gladding, 2011). Of those 20 invited experts, 17 (85%) met the study’s inclusion criteria, which centered on relevant publications and knowledge of or professional experience with CBPR. Three (15%) indicated they were not qualified to participate. Another three declined to participate. The 14 remaining experts completed all facets of the Delphi study. Nine participants (64.3%) were identified through their publication records. The final five (35.7%) came from peers’ recommendations.
Eleven experts (78.6%) reported experience with CBPR in a university setting, eight (57.1%) in a non-profit organization, four (28.6%) in an agency setting, four (28.6%) in a health system (e.g., hospital, clinic), four (28.6%) in a K–12 school setting, one (7.1%) in a community-wide setting, and one (7.1%) in international projects. One expert (7.1%) did not identify a work setting. Five (35.7%) experts reported having more than 10 years of experience conducting CBPR research, including four with 18–21 years and one with 11 years of experience. Three (21.4%) stated that they had 4–5 years of experience, and another four (28.6%) reported 2–4 years of experience. One (7.1%) expert did not respond to the question. Thirteen experts (92.9%) listed their highest educational level as a PhD, and one expert (7.1%) indicated the highest degree was a master’s degree. Participants’ ages ranged from 30 to over 60 years. Four experts (28.6%) reported their age to be 30–39, two (14.3%) 40–49, seven (50%) 50–59, and one (7.1%) over 60. When asked to report their racial affiliation, 10 (71.4%) identified as European American, one (7.1%) as Hispanic, one (7.1%) as Asian/Pacific Islander, and two (14.3%) selected Other/Mixed. Finally, 10 identified as female (71.4%) and four identified as male (28.6%).
Procedure
Stage 1: Preparing items for the questionnaire. The authors conducted a literature review to compile content statements (Sivell, Lidstone, Taubert, Thompson, & Nelson, 2015) about the knowledge, skills, attitudes, and activities (competency domains) commonly used in CBPR. These content statements were used to create an online questionnaire for the Delphi study’s first round (Ross et al., 2014; Sivell et al., 2015; Weise et al., 2016).
Stage 2: Administer Round 1. The authors sent an email to the identified experts with a URL link to the study (Sivell et al., 2015). Experts then used a 5-point Likert scale response range to assess participants’ degree of agreement with each CBPR competency statement (Sivell et al., 2015; Vázquez-Ramos, Leahy, & Hernández, 2007). Additionally, experts provided their own answers to four open-ended survey questions that reflected the coding frame (i.e., competency domains) used in this study. Additional questions included: (1) What knowledge is required for counseling researchers to effectively carry out community-based participatory research? (2) What skills are considered essential for counseling researchers to carry out community-based participatory research? (3) What attitudes are essential for counseling researchers to develop community-based participatory research? and (4) What activities are necessary for counseling researchers to experience when engaging in community-based participatory research?
Stage 3: Prepare and administer Round 2. Next, the authors employed the qualitative content analysis software program, NVivo, to analyze the 161 statements that participants contributed. Statements about which the experts did not agree were removed. Round 2’s statements (n = 112) were solely those that were contributed to the open-ended questions posed to the experts in Round 1. The experts evaluated the revised questionnaire in the same manner as in Round 1.
Stage 4: Finalize competencies. The authors compiled the final list of competencies based on expert consensus. In accordance with other Delphi study practices (Keeney, Hasson, & McKenna, 2011; Weise et al., 2016), consensus was achieved when at least 70% of the experts either agreed or strongly agreed with the statement and the statement’s median score was 2.5 or lower. The authors chose to further strengthen consensus results by ensuring that a given statement also achieved an interquartile range (IQR) of less than or equal to 1 (Wester & Borders, 2014). Following Ross et al.’s (2014) suggestion, we sent a follow-up email with a final draft of the competencies to each participant. The email contained each of the final 153 statements (Appendix). The authors asked the participants to offer their final remarks about the statements and requested that they respond within a week and received no modifications.
Data Analysis
Descriptive quantitative analysis. The review of the Delphi process started upon the experts’ completion of Round 1 and was completed following Round 2. One part of the analysis involved quantitative feedback. SPSS was used to measure expert consensus. The data included frequency outputs on the percentage of overall responses to each statement, median, and IQR. According to Dalkey and Helmer (1963), the median response for each statement is a central statistic involved in Delphi processes. IQR is a measure of variability that is less susceptible to outliers than the range. IQR allowed the authors to further increase objectivity and rigor in the validating process to determine final expert statements (Wester & Borders, 2014). IQR also allowed researchers to assess the variability in responses. An IQR of less than or equal to 1 on a 5-point Likert scale indicates a low variability in responses, whereas a score greater than 1 signifies a higher range of variability.
Content analysis. Participants’ contributed statements were used to enhance the level of expert consensus with the follow-up questionnaire. The researchers conducted a qualitative content analysis (QCA) for these contributions (Weise et al., 2016). The QCA clearly and systematically categorized statements within the range of the study’s nine CBPR principles. Using NVivo, the authors coded the experts’ statements using the domains of the theoretical coding framework (Schreier, 2012): knowledge, attitudes, skills, and activities. The authors then assigned each of the frame-coded statements to one of the nine CBPR principles.
Results
The results from Round 1 and Round 2 are presented in the Appendix. A total of 64 statements were omitted between Rounds 1 and 2 because they either did not reach consensus (meeting all three criteria) or represented a repeated item. Of the final 153 competencies, 49 relate to the knowledge domain, 43 relate to the attitudes domain, 31 relate to the skills domain, and 25 relate to the activities domain. These statements were further subcategorized according to the nine CBPR principles (P1–P9) or themes that emerged from the content analysis: 15 statements were related to P1, 12 statements were related to P2, 25 statements were related to P3, 28 statements were related to P4, 18 statements were related to P5, 12 statements were related to P6 and P7, seven statements were related to P8, and 14 statements were related to P9.
Certain statements did not fit within the nine CBPR principles. Additionally, there were statements that seemed to fit within multiple categories. Some themes that the authors did not expect emerged from the open-ended responses. These included seven statements related to core traits and three statements related to mentoring, which are also presented in the Appendix. The following discussion will further describe the results.
Discussion
The aim of the study was to develop competencies that emphasize knowledge, skills, attitudes, and activities that would provide the foundations for a training guideline in CBPR for the counseling profession. A growing number of counseling researchers highlight researcher and community collaboration (Bryan, 2009; Guiffrida et al., 2011; Wester & Borders, 2014); however, comprehensive training guidelines that outline the competencies required to foster such partnerships do not exist in the counseling literature. We argue that by providing access to this emerging approach to building researcher–community partnerships within the community (particularly practitioners), the clients/communities’ well-being will be enhanced. CBPR emerged in recent years as the most promising researcher–community approach to research (Lawson, Caringi, Pyles, Jurkowski, & Bozlak, 2015; Lightfoot et al., 2014). The CBPR competencies identified through this study could provide further guidance to researchers for building these relationships in the community. Researchers that advocate for researcher–practitioner partnerships emphasize their potential for advancing treatment for clients (Teachman et al., 2012). These partnerships improve communication and allow research findings to be translated into more practical interventions. We anticipate that by offering a standardized approach for a training guide to fostering researcher–community partnerships, future counseling researchers will receive more consistent and effective training in CBPR practices.
CBPR Competencies
Consistent with previous literature, all 14 experts agreed that CBPR is about relationships and relationship building. They further allowed that a CBPR framework fosters conversations between partners within the community. The experts also endorsed CBPR as a complementary, not competing, approach to research. Although the results of this study confirm the necessary knowledge components of the CBPR framework, they move beyond making the argument that CBPR is a necessary practice, demonstrating how researchers might effectively implement such practices. Thus, we offer key insights from the remaining categories understood as necessary for competency in a given practice (Toporek et al., 2009) with the aim of identifying best practices and means of implementation for community partnerships. Competency in this framework will enhance methodological choices made by researchers and their partner communities. The following section highlights statements categorized by domain with high expert consensus (100% of the expert panel indicated they either strongly agree or agree).
Knowledge. All experts agreed that the knowledge required for counseling researchers to effectively carry out CBPR includes understanding that the term “CBPR Researchers” applies to both academic and community partners (extended to counseling practitioners). Experts also agreed that academic CBPR researchers need to know or be willing to learn about the community’s issues, concerns, and strengths. When researchers include community partners in the research process, it helps to develop trust and respect between these two groups and potentially leads to a deeper interpretation of the findings. Likewise, experts acknowledged the importance of inviting community partners to participate in dissemination of research findings. Finally, CBPR can be effective in bringing community partners together to determine priorities.
Skills. The experts agreed that practicing CBPR requires effective and reflective listening skills, group facilitation skills, and the ability to create strong partnerships (e.g., negotiating, collaborating, networking, liaising). Researchers should practice cultural humility and be willing to work across the varying needs of communities with different cultures and identities. Therefore, researchers can help community partners recognize the strengths and resources already embedded in the current structure of their own communities. Finally, the experts agreed that CBPR researchers should communicate findings in ways that make skillful use of technology and are concise, clear, and appropriate so that the community may participate in the interpretation of results.
Attitudes. The experts identified cultural humility, flexibility, and persistence as essential CBPR attitudes. This required that researchers share power—for example, implementing shared decision-making in their projects with their community partners. It is imperative that researchers recognize that every community has its own unique strengths. Likewise, CBPR researchers make a commitment to collaboration by sharing expertise, being accountable, and giving credit to their community partners for their contributions to knowledge production. This entails researchers valuing power sharing with their community partners, including shared decision-making in their projects, while still upholding scientific rigor. Moving beyond shared decision-making, CBPR researchers also recognize the importance of working together to find innovative ways of disseminating research results. At times, researchers will need to commit to building continued relationships and networks within the community beyond a particular project or funding phase.
Activities. Finally, the findings confirm that carrying out CBPR necessitates particular experiences for counseling researchers. For instance, experts agreed that in order to foster effective partnerships, they need to practice deep listening and undertake participant observation at many different stages of their research. Other activities that experts consistently agreed were integral to the CBPR approach include frequent meetings, spending in-depth time getting to know the community, and collecting and analyzing data in collaboration with community partners. Counseling researchers commit to inviting community partners to participate throughout the research process, including organizing and planning meetings, data collection, data interpretation, findings dissemination, and even training or mentoring in research methods. All of these activities require a willingness to be educated about the community by the community members during the CBPR process.
Implications for Counseling Practice and Counselor Education
The CBPR competencies developed in this study serve to foster relationships between researchers and counseling practitioners in the community. Through these relationships, researchers, practitioners, and the communities they represent can work to reduce the gap between research and practice through enhanced community–researcher communication (Teachman et al., 2012; Wagstaff et al., 2018) and the translation of research outcomes into counseling practice (Wester & Borders, 2014). One aim of identifying the CPBR competencies was to provide mentoring to community partners, particularly counseling practitioners, on how to use research results to create effective community interventions. The goal is to close the gap between research and practice to improve treatment for our clients and improve communities.
A common language for interprofessional collaboration. This study brought together experts from two key fields whose efforts resulted in 153 competency statements that reflect the knowledge, skills, attitudes, and activities necessary to successfully carry out CBPR research. These CBPR competencies provide researchers with a vehicle to facilitate interprofessional work toward a common vision of community well-being. For instance, all experts on the panel for the present study agreed that CBPR researchers understand that when the community puts forth a common effort and agrees on common goals, trusting relationships are established, leading to enhanced social networks and better use of resources. Thus, community–researcher partnership outcomes include the enhancement of access to, delivery, and quality of mental health services for communities (Collins et al., 2018), particularly hard-to-reach communities (Brookman-Frazee et al., 2016; Nieweglowski et al., 2018; O’Brien et al., 2018), and culturally appropriate interventions (Cox, 2017; Doll & Brady, 2013). Community-based research can facilitate efforts geared toward increasing the relevance of intervention methods.
Identifying competencies for training and proficiency in CBPR. The CBPR competencies identified in this study can serve as the basis for developing a training guideline for counseling practitioners, counselor–researchers, and counselors-in-training. Such a guideline allows stakeholders to maintain awareness of current and emerging research practices such as CBPR and enhances their professional responsibility (American Counseling Association, 2014, Standard C.2.f; Council for Accreditation of Counseling and Related Educational Programs, 2015, Section 6.4.d). Identifying competencies for training and proficiency is one approach to curriculum development (Mason & Schwartz, 2012) that we believe can be particularly effective. This study not only identified the necessary competencies for best practices in CBPR, but organized the competencies into meaningful categories that pertain to the four critical domains of proficiency in a given practice: knowledge, skills, attitudes, and activities. The sequence we have provided can be a useful map to the nine principles of the CBPR approach. This study lays a foundation for an effective training guideline that highlights how each CBPR domain builds upon the next. Having a CBPR training guideline will help standardize best practices in the collaborative process, thus enhancing researcher–practitioner engagement.
Promoting experiential learning opportunities for students. Counselor educators can connect emergent research and experiential learning in their curricula. The competencies highlighted by the current study may support project-based learning activities in courses that require students to approach community members and partake in a collaborative endeavor. The expectation is that the CBPR competencies would provide counselor educators and counselors-in-training with standardized guidelines for best practice in community-based research that they can apply when ready to pursue a project of their own. The emphasis in this case would be to prepare future counselors for community–researcher partnerships. The benefit of engaging students at the training level in CBPR research through the use of these competencies is that it exposes students to an awareness of the collaborative process by moving beyond knowledge components and learning the skills, attitudes, and activities necessary to initiate a partnership. This could require that a project be spread out over two or three semesters as a component in a field-based practicum or internship. The competencies can be used to structure such courses as well. For example, course objectives for one semester’s internship might include the knowledge, skills, attitudes, and actions aimed at principles one, two, and three, whereas another semester may cover principles four, five, six, and so on. Alternatively, counselor educators might choose to design their research projects through interdisciplinary or interprofessional collaborations across campus that account for CBPR principles (McElfish et al., 2015; Talley & Williams, 2018), which students may be able to join as a component of training.
Limitations of the Study
One limitation of the study reflects the emergent nature of CBPR approaches in the counseling literature, which is that some CBPR researchers may be limited in their years of formal experience with the practice. For instance, four of the expert participants reported having less than four years of experience conducting CBPR projects. Although years of experience can be an important factor in attributing expertise, several studies have also highlighted that expert status is contingent upon many contextual factors, including recognition by other experts and stakeholders (Mead & Moseley, 2001). In this case, because CBPR is still a new practice in counseling research, peer recommendation was an identifying factor.
Another limitation of this study is the number of rounds conducted. Typically, a Delphi study will include two to eight rounds, with three as the median (Garson, 2013). The aim of the third round typically involves experts providing additional feedback about the items. Although we initiated a third round of the study, experts had little to no feedback to offer, meaning that the final statements were accepted with minimum revision. Although the authors interpreted this lack of feedback as validation of the final outcomes, one might otherwise argue that the lack of feedback better reflects other factors such as expert availability and time.
Suggestions for Future Research
We suggest that future researchers apply the Rasch model to the results of the Delphi study in order to test whether or not the competencies can be quantified in a meaningful way (Bond & Fox, 2015). The main question is whether the structure of the construct is qualitative or quantitative. If quantitative, then the Rasch model will unveil the extent to which the competency statements fall on a continuum. If they do not, that does not undermine the meaningfulness of the Delphi work or the content therein; rather, it would provide evidence that the competencies have a qualitative structure, and descriptive statistics are more appropriate for summarizing responses to them.
If the competencies can form a quantitative linear variable, then validating the results from this Delphi study against further measures will help the researchers translate the competencies into an assessment tool, where it is justifiable to sum up responses, report a total score, and perform statistical analyses. This assessment tool could then be used to identify and assess the counselors’ own knowledge, skills, attitudes, and activities toward using the CBPR approach in a quantifiable way. Thus, the Rasch model is not an alternative to the Delphi study. Rather, it is a model that can test the extent to which it is justifiable to transform the statements gathered through the Delphi model into measurable variables; strengthening the efficacy of the competency statements guides instrument development to strengthen the results. Under the Rasch model, researchers can pilot the competency items to the counselors, who can be understood as the consumers of the instrument, and not to the experts who developed the competencies.
Conclusion
In conclusion, the results of the study provide an outline of evidence-based competencies derived from an empirical Delphi method that combined a wide-ranging literature review with expert feedback. This study comprises the beginning stages of the development and validation of CBPR competencies in counseling that may be utilized for training, practice, and further research. The findings of the present study provide awareness and initial competencies necessary to carry out CBPR research. Finally, the authors consider increasing the number of researcher–community partnerships to be key in bridging the gap between scientists and practitioners and advancing the profession. Ultimately, the aim is to improve the well-being of our clients and communities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author.
Bond, T. G., & Fox, C. M. (2015). Applying the Rasch Model: Fundamental measurement in the human sciences (3rd ed.). New York, NY: Routledge.
Brookman-Frazee, L., Stahmer, A., Stadnick, N., Chlebowski, C., Herschell, A., & Garland, A. F. (2016). Characterizing the use of research-community partnerships in studies of evidence-based interventions in children’s community services. Administration and Policy in Mental Health and Mental Health Services Research, 43, 93–104. doi:10.1007/s10488-014-0622-9
Bryan, J. (2009). Engaging clients, families, and communities as partners in mental health. Journal of Counseling & Development, 87, 507–511. doi:10.1002/j.1556-6678.2009.tb00138.x
Case, A. D., Byrd, R., Claggett, E., DeVeaux, S., Perkins, R., Huang, C., . . . Kaufman, J. S. (2014). Stakeholders’ perspectives on community-based participatory research to enhance mental health services. American Journal of Community Psychology, 54, 397–408.
doi:10.1007/s10464-014-9677-8
Collins, S. E., Clifasefi, S. L., Stanton, J., The LEAP Advisory Board, Straits, K. J. E., Gil-Kashiwabara, E., . . . Wallerstein, N. (2018). Community-based participatory research (CBPR): Towards equitable involvement of community in psychology research. American Psychologist, 73, 884–898. doi:10.1037/amp0000167
Corrigan, P., Pickett, S., Kraus, D., Burks, R. & Schmidt, A. (2015). Community-based participatory research examining the health care needs of African Americans who are homeless with mental illness. Journal of Health Care for the Poor and Underserved, 26, 119–133. doi:10.1353/hpu.2015.0018
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 standards for accreditation. Alexandria, VA: Author.
Cox, R. B., Jr. (2017). Promoting resilience with the ¡Unidos se puede! program: An example of translational research for Latino families. Family Relations, 66, 712–728. doi:10.1111/fare.12265
Dalkey, N. C., & Helmer, O. (1963). An experimental application of the Delphi method to the use of experts. Management Science, 9, 458–467.
Doll, J., & Brady, K. (2013). Project HOPE: Implementing sensory experiences for suicide prevention in a Native American community. Occupational Therapy in Mental Health, 29, 149–158.
doi:10.1080/0164212X.2013.788977
Erford, B. T., Miller, E. M., Schein, H., McDonald, A., Ludwig, L., & Leishear, K. (2011). Journal of Counseling & Development publication patterns: Author and article characteristics from 1994 to 2009. Journal of Counseling & Development, 89, 73–80.
doi:10.1002/j.1556-6678.2011.tb00062.x
Garson, G. D. (2013). The Delphi method in quantitative research. Asheboro, NC: Statistical Associates Publishers.
Gray, L. A., & Price, S. K. (2014). Partnering for mental health promotion: Implementing evidence based mental health services within a maternal and child home health visiting program. Clinical Social Work Journal, 42, 70–80. doi:10.1007/s10615-012-0426-x
Green, L. W. (2007). The prevention research centers models of practice-based evidence. American Journal of Preventive Medicine, 33, S6–S8. doi:10.1016/j.amepre.2007.03.012
Guiffrida, D. A., Douthit, K. Z., Lynch, M. F., & Mackie, K. L. (2011). Publishing action research in counseling journals. Journal of Counseling & Development, 89, 282–287.
doi:10.1002/j.1556-6678.2011.tb00090.x
Hergenrather, K. C., Geishecker, S., Clark, G., & Rhodes, S. D. (2013). A pilot test of the HOPE intervention to explore employment and mental health among African American gay men living with HIV/AIDS: Results from a CBPR study. AIDS Education and Prevention, 25, 405–422. doi:10.1521/aeap.2013.25.5.405
Hook, J. N., Davis, D. E., Owen, J., Worthington, E. L., & Utsey, S. O. (2013). Cultural humility: Measuring openness to culturally diverse clients. Journal of Counseling Psychology, 60, 353–366. doi:10.1037/a0032595
Horowitz, C. R., Robinson, M., & Seifer, S. (2009). Community-based participatory research from the margin to the mainstream: Are researchers prepared? Circulation, 119, 2633–2642.
doi:10.1161/CIRCULATIONAHA.107.729863
Israel, B. A., Eng, E., Schulz, A. J., & Parker, E. A. (Eds.). (2013). Methods for community-based participatory research for health (2nd ed.). San Francisco, CA: Jossey-Bass.
Israel, B. A., Schulz, A. J., Parker, E. A., & Becker, A. B. (1998). Review of community-based research: Assessing partnership approaches to improve public health. Annual Review of Public Health, 19, 173–202. doi:10.1146/annurev.publhealth.19.1.173
Jorm, A. F. (2015). Using the Delphi expert consensus method in mental health research. Australian and New Zealand Journal of Psychiatry, 49, 887–897. doi:10.1177/0004867415600891
Kaplan, D. M., & Gladding, S. T. (2011). A vision for the future of counseling: The 20/20 principles for unifying and strengthening the profession. Journal of Counseling & Development, 89, 367–372. doi:10.1002/j.1556-6678.2011.tb00101.x
Keeney, S., Hasson, F., & McKenna, H. (2011). The Delphi technique in nursing and health research. Chichester, UK: Wiley-Blackwell.
Lachance, L., Quinn, M., & Kowalski-Dobson, T. (2018). The food & fitness community partnerships: Results from 9 years of local systems and policy changes to increase equitable opportunities for health. Health Promotion Practice, 19, 92S–114S. doi:10.1177/1524839918789400
Lawson, H. A., Caringi, J. C., Pyles, L., Jurkowski, J. M., & Bozlak, C. T. (2015). Participatory action research. New York, NY: Oxford University Press.
Lightfoot, E., McCleary, J. S., & Lum, T. Y. (2014). Asset mapping as a research tool for community-based participatory research in social work. Social Work Research, 38, 59–64. doi:10.1093/swr/svu001
Lilienfeld, S. O., Ammirati, R., & David, M. (2012). Distinguishing science from pseudoscience in school psychology: Science and scientific thinking as safeguards against human error. Journal of School Psychology, 50, 7–36. doi:10.1016/j.jsp.2011.09.006
Lindamer, L. A., Lebowitz, B. D., Hough, R. L., Garcia, P., Aquirre, A., Halpain, M. C., & Jeste, D. V. (2008). Public-academic partnerships: Improving care for older persons with schizophrenia through an academic-community partnership. Psychiatric Services, 59, 236–239. doi:10.1176/ps.2008.59.3.236
Mannix, T. R., Austin, S. D., Baayd, J. L., & Simonsen, S. E. (2018). A community needs assessment of urban Utah American Indians and Alaska Natives. Journal of Community Health, 43, 1217–1227.
doi:10.1007/s10900-018-0542-9
Mason, R., & Schwartz, B. (2012). Using a Delphi method to develop competencies: The case of domestic violence. Journal of Community Medicine & Health Education, 2(2), 124. doi:10.4172/2161-0711.1000124
McElfish, P. A., Kohler, P., Smith, C., Warmack, S., Buron, B., Hudson, J., . . . Rubon-Chutaro, J. (2015). Community-driven research agenda to reduce health disparities. CTS: Clinical & Translational Science, 8, 690–695. doi:10.1111/cts.12350
Mead, D., & Moseley, L. (2001). The use of Delphi as a research approach. Nurse Researcher, 8(4), 4–23. doi:10.7748/nr2001.07.8.4.4.c6162
Minkler, M., & Wallerstein, N. (Eds.). (2008). Community-based participatory research for health: From process to outcomes (2nd ed.). San Francisco, CA: Jossey-Bass.
Murray, C. E. (2009). Diffusion of innovation theory: A bridge for the research-practice gap in counseling. Journal of Counseling & Development, 87, 108–116.
doi:10.1002/j.1556-6678.2009.tb00556.x
Nieweglowski, K., Corrigan, P. W., Tyas, T., Tooley, A., Dubke, R., Lara, J., . . . The Addiction Stigma Research Team. (2018). Exploring the public stigma of substance use disorder through community-based participatory research. Addiction Research & Theory, 26, 323–329. doi:10.1080/16066359.2017.1409890
Novakowski, N., & Wellar, B. (2008). Using the Delphi technique in normative planning research: Methodological design considerations. Environmental and Planning A: Economy and Space, 40, 1485–1500. doi:10.1068/a39267
O’Brien, M. A., Lofters, A., Wall, B., Pinto, A. D., Elliott, R., Pietrusiak, M.-A., . . . Paszat, L. (2018). Better Health Durham: Community engagement in a cluster RCT of a prevention practitioner intervention in low-income neighborhoods. Journal of Global Oncology, 22s. doi:10.1200/jgo.18.53100
O’Fallon, L. R., & Dearry, A. (2002). Community-based participatory research as a tool to advance environmental health sciences. Environmental Health Perspectives, 110(S2), 155–159.
doi:10.1289/ehp.02110s2155
Peterson, C. H., Hall, S. B., & Buser, J. K. (2016). Research training needs of scientist-practitioners: Implications for counselor education. Counselor Education and Supervision, 55(2), 80–94. doi:10.1002/ceas.12034
Poleshuck, E., Mazzotta, C., Resch, K., Rogachefsky, A., Bellenger, K., Raimondi, C., . . . Cerulli, C. (2018). Development of an innovative treatment paradigm for intimate partner violence victims with depression and pain using community-based participatory research. Journal of Interpersonal Violence, 33, 2704–2724. doi:10.1177/0886260516628810
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44, 28–48. doi:10.1002/jmcd.12035
Ross, A. M., Kelly, C. M., & Jorm, A. F. (2014). Re-development of mental health first aid guidelines for suicidal ideation and behaviour: A Delphi study. BMC Psychiatry, 14, 241.
doi:10.1186/s12888-014-0241-8
Schreier, M. (2012). Qualitative content analysis in practice. London, UK: SAGE Publications.
Sivell, S., Lidstone, V., Taubert, M., Thompson, C., & Nelson, A. (2015). Identifying the key elements of an education package to up-skill multidisciplinary adult specialist palliative care teams caring for young adults with life-limiting conditions: An online Delphi study. BMJ Supportive & Palliative Care, 5, 306–315. doi:10.1136/bmjspcare-2013-000595
Talley, C. H., & Williams, K. P. (2018). Preparing future healthcare professionals for community engagement: A course-based research experience. ABNF Journal, 29(2), 33–41.
Teachman, B. A., Drabick, D. A., Hershenberg, R., Vivian, D., Wolfe, B. E., & Goldfried, M. R. (2012). Bridging the gap between clinical research and clinical practice: Introduction to the special section. Psychotherapy (Chicago, Ill.), 49(2), 97–100. doi:10.1037/a0027346
Toporek, R. L., Lewis, J. A., & Crethar, H. C. (2009). Promoting systemic change through the ACA advocacy competencies. Journal of Counseling & Development, 87, 260–268. doi:10.1002/j.1556-6678.2009.tb00105.x
Vázquez-Ramos, R., Leahy, M., & Hernández, N. E. (2007). The Delphi method in rehabilitation counseling research. Rehabilitation Counseling Bulletin, 50, 111–118. doi:10.1177/00343552070500020101
Wagstaff, C., Graham, H., Farrell, D., Larkin, M., & Tatham, L. (2018). Perspectives of cannabis use in the life experience of men with schizophrenia. International Journal of Mental Health Nursing, 27, 1099–1108. doi:10.1111/inm.12422
Weinrach, S. G., Lustig, D., Chan F., & Thomas, K. R. (1998). Publication patterns of The Personnel and Guidance Journal/Journal of Counseling & Development: 1978 to 1993. Journal of Counseling & Development, 76, 427–435. doi:10.1002/j.1556-6676.1998.tb02701.x
Weise, J., Fisher, K. R., & Trollor, J. (2016). Utility of a modified online Delphi method to define workforce competencies: Lessons from the Intellectual Disability Mental Health Core competencies project. Journal of Policy and Practice in Intellectual Disabilities, 13, 15–22. doi:10.1111/jppi.12142
Wester, K. L., & Borders, L. D. (2014). Research competencies in counseling: A Delphi study. Journal of Counseling & Development, 92, 447–458. doi:10.1002/j.1556-6676.2014.00171.x
Woods-Jaeger, B. A., Sexton, C. C., Gardner, B., Siedlik, E., Slagel, L., Tezza, V., & O’Malley, D. (2018). Development, feasibility, and refinement of a toxic stress prevention research program. Journal of Child & Family Studies, 27, 3531–3543. doi:10.1007/s10826-018-1178-1
Woolf, S. H. (2008). The meaning of translational research and why it matters. JAMA, 299, 211–213.
doi:10.1001/jama.2007.26
Yuan, N. P., Gaines, T. L., Jones, L. M., Rodriguez, L. M., Hamilton, N., & Kinnish, K. (2016). Bridging the gap between research and practice by strengthening academic-community partnerships for violence research. Psychology of Violence, 6, 27–33. doi:10.1037/vio0000026
Appendix
Final CBPR Competencies (Round 1 and Round 2 Results)
| Domain |
Sub-Category |
Statement |
% |
Md |
IQR |
|
|
Round One (Statements: Review of the Literature) |
|
|
|
| K |
P1 |
S.2 CBPR partnerships define the parameters of community |
78.6 |
2.00 |
0.50 |
| K |
P1 |
S.3 Community could be described as geographic entity, a group that shares a common vision and/or identity |
78.6 |
2.00 |
0.75 |
| A |
P1 |
S.4 CBPR is a research orientation, rather than a method, that aims at building community partnerships |
92.9 |
2.00 |
1.00 |
| A |
P1 |
S.6 CBPR researchers must recognize the limits of their knowledge about their community partners |
85.7 |
1.00 |
1.00 |
| A |
P1 |
S.7 CBPR researchers should work toward cultural competency |
85.7 |
1.00 |
1.00 |
| A |
P1 |
S.8 CBPR researchers should value cultural humility |
92.9 |
1.00 |
1.00 |
| S |
P1 |
S.9 CBPR researchers need to acquire appropriate tools and approaches for interacting with community partners |
100 |
1.00 |
1.00 |
| S |
P1 |
S.10 CBPR researchers must be capable of negotiating and consulting with potential community partners |
100 |
1.00 |
1.00 |
| S |
P1 |
S.12 CBPR researchers need to be skilled at problem solving that might arise when making decisions and negotiating |
92.9 |
2.00 |
1.00 |
| K |
P2 |
S.16 CBPR researchers strive to recognize and develop on assets and relations presently within the community |
100 |
1.00 |
1.00 |
| K |
P2 |
S.18 CBPR researchers understand that when the community puts forth a common effort and agrees on common goals, trust is established, which leads to enhanced social networks/relationships and better implementation of resources |
92.9 |
2.00 |
0.00 |
| A |
P2 |
S.19 Every community has its own unique strengths |
100 |
1.00 |
0.00 |
| A |
P2 |
S.20 CBPR frameworks foster conversations between partners within the community |
100 |
1.00 |
1.00 |
| S |
P2 |
S.21 CBPR approaches also help community partners recognize the strengths and resources already embedded within the current structure of their own community |
100 |
1.00 |
1.00 |
| S |
P2 |
S.22 CBPR researchers must acquire an ability to identify community assets within the community |
92.9 |
1.00 |
1.00 |
| AC |
P2 |
S.24 CBPR researchers will engage with the community in order to learn more about what resources are already available within the community |
92.9 |
1.00 |
0.25 |
| K |
P3 |
S.26 CBPR approaches aim to level the power differences between researchers and community partners by having them engage in an equal partnership |
92.9 |
1.00 |
1.00 |
| K |
P3 |
S.27 CBPR researchers encourage and invite community partners to engage in each research phase |
92.9 |
1.00 |
1.00 |
| K |
P3 |
S.28 Researchers and community partners should co-analyze and co-interpret research results |
100 |
2.00 |
1.00 |
| K |
P3 |
S.29 When community partners are involved in the research process, deeper interpretation of findings may occur |
100 |
1.00 |
1.00 |
| A |
P3 |
S.30 CBPR researchers make a commitment to collaboration by sharing expertise, being accountable, and giving credit to their communities’ partners for their contributions to knowledge production |
100 |
1.00 |
0.25 |
| A |
P3 |
S.31 CBPR researchers recognize the value of sharing power with community partners |
100 |
1.00 |
1.00 |
| A |
P3 |
S.32 CBPR researchers are flexible and accommodating |
92.9 |
1.00 |
1.00 |
| S |
P3 |
S.33 CBPR researchers must be persistent and tolerant, especially when faced with obstacles in the research plan or environment |
85.7 |
1.00 |
0.25 |
| S |
P3 |
S.34 CBPR researchers must be able to collaborate with community partners in the interpretation of results |
100 |
1.00 |
1.00 |
| S |
P3 |
S.35 Facilitate interpretation of results into practice |
92.9 |
1.50 |
1.00 |
| S |
P3 |
S.37 CBPR researchers must be willing to mentor community partners to develop skills in participating in the research project |
92.9 |
1.00 |
1.00 |
| AC |
P3 |
S.38 CBPR researchers create time for reflection and self-awareness |
85.7 |
1.00 |
1.00 |
| AC |
P3 |
S.39 CBPR researchers schedule meetings with community partners to converse and clarify viewpoints of stress/difficulties encountered |
100 |
1.00 |
1.00 |
| AC |
P3 |
S.40 CBPR researchers provide community partners the opportunity to be part of the research project from start to finish |
100 |
1.00 |
1.00 |
| K |
P4 |
S.41 CPBR starts with a research area that is significant to the community |
92.9 |
1.00 |
1.00 |
| K |
P4 |
S.42 The CBPR research agenda is co-developed with community partners |
92.9 |
1.00 |
1.00 |
| K |
P4 |
S.43 CBPR encourages community partners to identify local impediments/barriers and unite community assets to work toward community well-being |
92.9 |
1.50 |
1.00 |
| K |
P4 |
S.44 Including community partners in the research process helps develop trust and respect between researchers and community |
100 |
1.00 |
1.00 |
| A |
P4 |
S.45 CBPR researchers value the contributions of community partners |
100 |
1.00 |
0.00 |
| A |
P4 |
S.46 CBPR researchers encourage community partners to share vital perspectives and beliefs |
100 |
1.00 |
0.00 |
| A |
P4 |
S.47 CBPR researchers welcome shared responsibilities in the research process |
100 |
1.00 |
1.00 |
| A |
P4 |
S.48 CBPR researchers are prepared to learn about the community through the lens of the community partner |
92.9 |
1.00 |
0.00 |
| A |
P4 |
S.49 CBPR researchers respect local knowledge and cultural perspectives |
100 |
1.00 |
0.00 |
| S |
P4 |
S.50 CBPR researchers practice deep listening in order to learn from their community partner |
100 |
1.00 |
1.00 |
| S |
P4 |
S.51 Effective communication and management skills are critical to engaging with community stakeholders to form partnerships |
100 |
1.00 |
1.00 |
| S |
P4 |
S.52 CBPR researchers are willing to negotiate and make compromises with community partner |
100 |
1.00 |
1.00 |
| AC |
P4 |
S.54 CBPR researchers engage in consistent and open communication |
100 |
1.00 |
0.25 |
| AC |
P4 |
S.56 CBPR researchers educate community partners on the research process |
92.9 |
1.50 |
1.00 |
| AC |
P4 |
S.57 CBPR researchers and community partners must make a joint effort to decide upon task roles and allocate time for future meetings: a consistent two-way communication |
85.7 |
2.00 |
1.00 |
| K |
P5 |
S.58 CBPR researchers aspire to promote science while at the same time providing local interventions/strategies to attend to local matters in the community |
92.9 |
1.50 |
1.00 |
| K |
P5 |
S.59 CBPR integrates knowledge and action intending to enhance community well-being |
92.9 |
1.00 |
1.00 |
| K |
P5 |
S.60 CBPR researchers should include the interpretation of research results into practice, thus benefiting community partners |
85.7 |
1.00 |
1.00 |
| A |
P5 |
S.61 One aim of CBPR is to provide mentoring to community partners on how to use research results in order to create effective community interventions |
92.9 |
2.00 |
1.00 |
| A |
P5 |
S.62 CBPR researchers understand that this framework does not require researchers to give up scientific rigor |
100 |
1.00 |
1.00 |
| S |
P5 |
S.63 CBPR researcher must know how to demonstrate the direct benefits of the research project to community partners |
85.7 |
1.00 |
1.00 |
| AC |
P5 |
S.64 CBPR researcher will assist community partners in developing interventions/programs based on research findings |
85.7 |
1.00 |
1.00 |
| K |
P6 |
S.65 CBPR researchers attend to issues that are of importance to the community partners involved |
100 |
1.00 |
0.00 |
| K |
P6 |
S.66 The CBPR approach stresses the environmental influences that can cause health issues such as social, economic, cultural, and historical and political realms |
92.9 |
1.00 |
1.00 |
| K |
P6 |
S.68 CBPR researchers attend to physical, mental, and social well-being, taking into account individual, family, and community contexts |
92.9 |
1.00 |
1.00 |
| S |
P6 |
S.70 CBPR researchers possess advocacy skills to bring awareness to community partners and/or other stakeholders of the contributing factors of health problem |
85.7 |
2.00 |
1.00 |
| S |
P6 |
S.71 CBPR researchers gather data from multiple sources to assess community priority issues |
85.7 |
1.00 |
1.00 |
| AC |
P6 |
S.72 CBPR researchers and community partners problem-solve and take a course of action to reduce disparities in the community |
92.9 |
1.00 |
1.00 |
| K |
P7 |
S.76 CBPR can be effective in bringing community partners together to determine priorities |
100 |
1.00 |
1.00 |
| A |
P7 |
S.79 CBPR researchers are persistent and flexible |
100 |
1.50 |
1.00 |
| A |
P7 |
S.80 CBPR researchers are prepared for further collaboration than initially anticipated, depending on community needs |
100 |
2.00 |
1.00 |
| S |
P7 |
S.82 CBPR researchers apply problem-solving abilities in this process |
100 |
1.50 |
1.00 |
| AC |
P7 |
S.83 CBPR researchers continue to assess and reevaluate throughout the project rather than wait until the end of the research phase |
100 |
1.00 |
1.00 |
| K |
P8 |
S.84 CBPR encourages researchers to consider how to apply the knowledge acquired through their collaborations to directly benefit the community being studied |
100 |
1.00 |
1.00 |
| K |
P8 |
S.85 An important element of CPBR is inviting community partners in the dissemination of research findings |
100 |
1.00 |
1.00 |
| A |
P8 |
S.86 CBPR researchers recognize the importance of including community partners in sharing the results with the community |
100 |
1.00 |
1.00 |
| A |
P8 |
S.87 CPBR researchers recognize the importance of finding innovative ways in partnering with community partners in disseminating research results |
100 |
1.00 |
1.00 |
| A |
P8 |
S.88 CBPR researchers understand the importance of having research results readily available |
92.9 |
2.00 |
1.00 |
| S |
P8 |
S.89 CBPR researchers have the ability to communicate findings in a way that could be understood by the community (e.g. being concise, clear, and using appropriate language) |
100 |
1.00 |
1.00 |
| AC |
P8 |
S.90 CBPR researchers share results in community settings such as town hall meetings, presentations at local venues, community newsletters, and brochures |
92.9 |
1.00 |
1.00 |
| K |
P9 |
S.92 Sustainability in CBPR means the community must desire the project to continue |
85.7 |
2.00 |
1.00 |
| K |
P9 |
S.93 CBPR research actions produce preliminary accomplishments, which, in turn, improve community trust and create sustainability |
85.7 |
2.00 |
1.00 |
| A |
P9 |
S.95 CBPR researchers commit to continued relationships and networks within the community beyond a particular project or funding phase |
100 |
1.00 |
1.00 |
| A |
P9 |
S.96 CBPR researchers understand that the community partnership may not end when the project ends |
92.9 |
1.00 |
1.00 |
| S |
P9 |
S.97 CBPR researchers, in collaboration with community partners, have the ability to create a long-term vision |
92.9 |
1.50 |
1.00 |
| AC |
P9 |
S.99 CBPR researchers take the initiative to form and sustain trust through continuous community involvement |
92.3 |
1.00 |
1.00 |
| AC |
P9 |
S.101 CBPR researchers strive for a wide range of outcomes that may include impacting local policy, relational changes, sustainability, cultural awareness, reducing health disparities, and/or improved health outcomes |
92.9 |
1.00 |
1.00 |
|
|
Round 2 (Expert Contributed Statements) |
|
|
|
| K |
P1 |
S.1 The term “CBPR Researchers” applies to both academic and community partners |
85.7 |
1.5 |
1.00 |
| K |
P1 |
S.3 There is no one way to engage in CBPR |
92.9 |
1.00 |
1.00 |
| K |
P1 |
S.4 CBPR researchers need to know about what projects or plans have and have not worked in the past |
85.7 |
1.50 |
1.00 |
| K |
P1 |
S.5 CBPR is a philosophy that guides how a researcher engages a community in a respectful, honoring, and professional way |
100 |
1.00 |
1.00 |
| S |
P1 |
S.7 Researchers must practice cultural competence and be willing to work across different cultures, community identities, and varying needs |
100 |
1.00 |
0.25 |
| K |
P1 |
S.8 CBPR researchers need to know strategies for identifying and engaging relevant community partners |
100 |
1.00 |
1.00 |
| K |
P2 |
S.9 CBPR researchers need to know and/or be willing to learn about the community’s issues, concerns, and strengths |
100 |
1.00 |
0.25 |
| K |
P2 |
S.10 CBPR researchers need a strengths-based concept of skills |
100 |
1.00 |
1.00 |
| S |
P2 |
S.11 CBPR researchers should make skillful use of technology |
100 |
2.00 |
0.50 |
| A |
P2 |
S.12 CBPR researchers need to recognize that communities have strengths, assets, intelligence, history, wisdom, and perspectives that matter |
100 |
1.00 |
0.00 |
| A |
P2 |
S.13 CBPR researchers should be open-minded, better at listening than talking, and should know how to link project partners in meaningful ways |
100 |
1.00 |
0.25 |
| K |
P3 |
S.14 CBPR researchers need to be aware of personal biases |
100 |
1.00 |
0.25 |
| K |
P3 |
S.15 CBPR researchers need to know how to build trust and rapport with partners |
100 |
1.00 |
0.00 |
| S |
P3 |
S.16 Carrying out CBPR requires researchers to pay attention to power differentials that may emerge in the work |
100 |
1.00 |
0.00 |
| S |
P3 |
S.19 Carrying out CBPR requires researchers to be effective and reflective listeners |
100 |
1.00 |
0.25 |
| S |
P3 |
S.20 Carrying out CBPR requires researchers to have group facilitation skills |
100 |
1.00 |
1.00 |
| S |
P3 |
S.21 Researchers will demonstrate strong partnership skills (negotiating, collaborating, networking, liaising) |
100 |
1.50 |
1.00 |
| A |
P3 |
S.23 Carrying out CBPR projects requires researchers to be non-judgmental |
92.9 |
2.00 |
1.00 |
| A |
P3 |
S.24 CBPR researchers need to be willing to share power and control |
100 |
1.00 |
1.00 |
| A |
P3 |
S.25 CBPR researchers need to be honest and able to navigate academic and community settings with ease and transparency |
92.9 |
1.00 |
1.00 |
| A |
P3 |
S.26 CBPR researchers should value egalitarianism |
92.9 |
1.00 |
1.00 |
| A |
P3 |
S.27 CBPR researchers should be cognizant of systems of oppression and privilege |
100 |
1.00 |
0.25 |
| AC |
P3 |
S.29 CBPR researchers need to experience shared decision-making in their projects |
100 |
1.00 |
1.00 |
| K |
P4 |
S.30 Researchers must be knowledgeable about the principles of CBPR in order to decide with the partner community which of those principles will guide their work together |
85.7 |
2.00 |
1.00 |
| K |
P4 |
S.31 CBPR researchers need the ability to collaborate with community stakeholders by trusting them as experts in the research process |
92.9 |
1.00 |
1.00 |
| K |
P4 |
S.32 CBPR researchers need to understand that CBPR is about relationships and relationship building |
100 |
1.00 |
1.00 |
| K |
P4 |
S.33 CBPR researchers must learn about current community processes |
92.9 |
1.50 |
1.00 |
| S |
P4 |
S.34 Carrying out CBPR requires flexibility |
100 |
1.00 |
0.00 |
| S |
P4 |
S.36 CBPR projects require strong communication skills (including clarity, openness, deep listening, curiosity, cultural humility) |
100 |
1.00 |
0.25 |
| A |
P4 |
S.38 CBPR researchers must recognize what they do not know or that they may not be the most knowledgeable about the community within which they work, rather than insisting on their own expertise |
100 |
1.00 |
1.00 |
| A |
P4 |
S.39 CBPR requires valuing co-learning |
92.9 |
1.00 |
0.25 |
| A |
P4 |
S.40 CBPR requires that we leave our academic egos at the door and allow the community to fully “own” the project |
92.3 |
1.00 |
1.00 |
| AC |
P4 |
S.41 Researchers need to spend time listening to the community in which they work in order to build trust and rapport |
100 |
1.00 |
0.00 |
| AC |
P4 |
S.42 Researchers should practice deep listening as a means of gathering qualitative data from engagement activities |
100 |
1.00 |
0.00 |
| AC |
P4 |
S.43 Carrying out CBPR requires interactive community involvement |
100 |
1.00 |
0.00 |
| AC |
P4 |
S.44 Carrying out CBPR requires a willingness to be educated about community by community members |
100 |
1.00 |
1.00 |
| K |
P5 |
S.45 CBPR researchers need knowledge about participatory research |
100 |
1.00 |
1.00 |
| K |
P5 |
S.46 CBPR researchers need to know how to conduct qualitative and quantitative or mixed methods research designs |
100 |
2.00 |
1.00 |
| K |
P5 |
S.48 CBPR researchers need to know or learn how to do culturally responsive research |
100 |
1.00 |
0.25 |
| A |
P5 |
S.50 Researchers should be able to balance providing structure with knowing when to let go and let the group process prevail |
100 |
1.00 |
1.00 |
| S |
P5 |
S.52 Carrying out CBPR requires flexibility |
100 |
1.00 |
1.00 |
| S |
P5 |
S.53 CBPR projects require strong communication skills (including clarity, openness, deep listening, curiosity, cultural humility) |
100 |
1.00 |
0.25 |
| A |
P5 |
S.55 CBPR researchers must recognize what they do not know or that they may not be the most knowledgeable about the community within which they work, rather than insisting on their own expertise |
100 |
1.00 |
1.00 |
| K |
P6 |
S.62 CBPR researchers should be aware of the strengths and barriers of the community |
91.7 |
1.00 |
1.00 |
| K |
P6 |
S.63 The notion of “effective” in CBPR research is community-specific |
85.7 |
1.00 |
1.00 |
| K |
P6 |
S.65 CBPR researchers need cultural competency with respect to the community in which the research is conducted |
100 |
1.00 |
1.00 |
| S |
P6 |
S.67 Community partners should be advocates for change |
85.7 |
1.00 |
1.00 |
| A |
P6 |
S.68 Researchers need to be committed to an ecological approach |
85.7 |
1.00 |
1.00 |
| K |
P6 |
S.70 CBPR researchers need to know or learn how to do culturally responsive research |
100 |
1.00 |
0.00 |
| K |
P7 |
S.72 CBPR researchers need knowledge of the parameters of CBPR |
85.7 |
1.50 |
1.00 |
| K |
P7 |
S.73 CBPR researchers should know how to conduct nonlinear, cyclical research studies that inform policies, strengthen communities, and reduce disparities |
92.9 |
1.00 |
1.00 |
| A |
P7 |
S.74 CBPR researchers understand that process matters |
100 |
1.00 |
1.00 |
| A |
P7 |
S.75 CBPR researchers must be flexible and adaptable |
78.6 |
1.00 |
0.25 |
| AC |
P7 |
S.76 CBPR researchers need to be flexible and persistently observing |
100 |
1.00 |
0.25 |
| S |
P8 |
S.77 Successful CBPR projects will involve researchers who can communicate in lay language that a wide range of stakeholders will understand |
100 |
1.00 |
1.00 |
| S |
P8 |
S.78 CBPR researchers need to be able to translate scientific and research writing into plain language, and multiple languages if necessary |
100 |
1.00 |
1.00 |
| K |
P9 |
S.79 CBPR researchers need knowledge about how to broker the administrative aspects of CBPR (e.g., community subcontracts) |
100 |
2.00 |
1.00 |
| K |
P9 |
S.80 CBPR researchers need knowledge about academic institutional barriers to CBPR and how to overcome them |
100 |
2.00 |
1.00 |
| K |
P9 |
S.83 CBPR researchers need to know about the specifics of the CBPR process (e.g., how to form an advisory board) prior to beginning |
85.7 |
1.50 |
1.00 |
| S |
P9 |
S.86 Researchers need to be skilled in project management |
78.6 |
2.00 |
0.25 |
| AC |
P9 |
S.88 CBPR researchers need to spend in-depth time getting to know the community |
100 |
1.50 |
1.00 |
| AC |
P9 |
S.90 Carrying out CBPR projects requires organizing and planning meetings, data collection, data analysis, and training of others in research methods |
92.9 |
1.00 |
1.00 |
| AC |
P9 |
S.91 Carrying out CBPR projects requires frequent meetings and other forms of communications with partners |
92.9 |
1.50 |
1.00 |
| A |
CT |
S.93 Carrying out CBPR requires a researcher to have a positive outlook about the project |
78.6 |
2.00 |
0.50 |
| A |
CT |
S.96 Carrying out CBPR requires researchers to be flexible |
100 |
1.00 |
1.00 |
| A |
CT |
S.97 Carrying out CBPR requires researchers to be persistent |
92.9 |
2.00 |
1.00 |
| A |
CT |
S.98 Carrying out CBPR requires researchers to be patient |
92.9 |
1.00 |
1.00 |
| A |
CT |
S.100 Self-reflection is central to CBPR |
85.7 |
1.50 |
1.00 |
| A |
CT |
S.101 Humility is central to CBPR |
92.9 |
1.50 |
1.00 |
| A |
CT |
S.103 Beneficence is central to CBPR |
100 |
1.50 |
1.00 |
| K |
M |
S.104 Researchers need to acquire knowledge about how to frame CBPR work in their promotion, tenure materials, and IRB submissions |
92.9 |
1.00 |
1.00 |
| K |
M |
S.105 Researchers need knowledge about the availability of resources to support CBPR |
92.9 |
2.00 |
1.00 |
| K |
M |
S.106 Researchers would benefit from training or workshops in CBPR process |
100 |
1.00 |
1.00 |
Note. Final list of CBPR competencies only includes statements that met criteria for present study: (1) the statement had 70% of experts agree (responding ‘Agree’ or ‘Strongly Agree’); (2) the statement scored a 2.5 or less for the median; and, (3) the statement achieved an IQR of less than or equal to 1. Domain/Categories include: K = Knowledge, S = Skills, A = Attitudes, AC = Activities. Subcategories include: P1 = CBPR Principle 1; P2 = CBPR Principle 2; P3 = CBPR Principle 3; P4 = CBPR Principle 4; P5 = CBPR Principle 5; P6 = CBPR Principle 6; P7 = CBPR Principle 7; P8 = CBPR Principle 8; P9 = CBPR Principle 9; CT = Core Trait; M = Mentoring; S = Statement; Md = Median; % = Percentage; IQR = Interquartile Range.
Tahani Dari, NCC, is an assistant professor at the University of Toledo. John M. Laux is a professor and associate dean at the University of Toledo. Yanhong Liu is an assistant professor at Syracuse University. Jennifer Reynolds is an associate professor at the University of Toledo. Correspondence can be addressed to Tahani Dari, Mail Stop 119, Toledo, OH 43606, Tahani.Dari@rockets.utoledo.edu.
Mar 26, 2019 | Volume 9 - Issue 1
Loni Crumb, Natoya Haskins, Shanita Brown
This phenomenological study explored the experiences of 15 professional counselors who work with clients living in impoverished communities in rural America. Researchers used individual semi-structured interviews to gather data and identified four themes that represented the counselors’ experiences using the Multicultural and Social Justice Counseling Competencies as the conceptual framework to identify the incorporation of social justice and advocacy-oriented counseling practices. The themes representing the counselors’ experiences were: (1) appreciating clients’ worldviews and life experiences, (2) counseling relationships influencing service delivery, (3) engaging in individual and systems advocacy, and (4) utilizing professional support. The counselors’ experiences convey the need to alter traditional counseling session delivery formats, practices, and roles to account for clients’ life experiences and contextual factors that influence mental health care in rural, impoverished communities. Approaches that counselors use to engage in social justice advocacy with and on behalf of rural, impoverished clients are discussed.
Keywords: rural, impoverished communities, advocacy, social justice, multicultural
Approximately 41.3 million Americans live in poverty (Semega, Fontenot, & Kollar, 2017) and consistently face multiple chronic stressors (e.g., food and housing insecurities, social isolation, inability to access adequate physical and mental health care) that impact their quality of life (Fifield & Oliver, 2016; Hill, Cantrell, Edwards, & Dalton, 2016). Nevertheless, the scope of mental health concerns of individuals and families residing in persistently poor, rural communities remains under-researched and overlooked by the public, scholars, and policymakers (Tickamyer, Sherman, & Warlick, 2017). Furthermore, advocacy efforts that foster social and economic justice and support the mental health of persons living in rural poverty warrant further advancement.
Scarce availability of mental health care services, ineffective modes of treatment and interventions, and mistrust of mental health care professionals contribute to the low utilization of mental health care services among persons living in rural poverty (Fifield & Oliver, 2016; Imig, 2014). Consequently, there are few evidence-supported culturally relevant mental health interventions tailored to address the specific needs of people living in rural poverty, particularly with a focus on social justice advocacy (Bradley, Werth, Hastings, & Pierce, 2012; Imig, 2014). Counselors practicing in rural, impoverished areas must be prepared to address systems of oppression, discrimination, marginalized statuses, and the impact these factors have on counseling services and clients’ well-being (Grimes, Haskins, & Paisley, 2013; Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2016). Moreover, according to the 2016 Code of Ethics from the National Board for Certified Counselors (NBCC) and the 2014 ACA Code of Ethics from the American Counseling Association, counselors are expected to take actions to prevent harm and help eradicate the social structures and processes that reproduce mental health disparities in vulnerable communities (ACA, 2014; NBCC, 2016). In recognition of this expectation, the Multicultural and Social Justice Counseling Competencies (MSJCCs) were developed to guide mental health counselors toward practicing culturally responsive counseling and incorporating social justice advocacy initiatives into the process (Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2015). Thus, the MSJCCs’ framework undergirds our examination of counselors’ experiences and clinical practices that support the mental health and well-being of clients living in poverty in rural America.
Understanding Rural Poverty and Mental Health Care
When discussing literature pertaining to rural poverty, it is important to first define relevant terms. The U.S. Department of Agriculture’s Economic Research Service (USDA; 2017) defines poverty as having an income below the federally determined poverty threshold. For example, the 2017 poverty threshold for an individual under 65 years of age was $12,752, and the poverty threshold was $16,895 for a household with two adults under age 65, with one child under 18 years of age (USDA, 2017). Persistently poor areas are defined as communities in which 20% or more of the population has lived below the poverty threshold over the last 30 years with low populations (fewer than 2,500 people; USDA, 2017). The majority of persistently poor communities are located in rural Southern regions of the United States (USDA, 2017). Rural communities that experience persistent poverty have had little diversification of employment, are underserved by mental health care providers, and lack affordable housing and economic development (Tickamyer et al., 2017). For the purposes of this study, the definitions described above were used to define and understand rurality and poverty.
Mental Health Care in Rural, Impoverished America
An abundance of literature exists that identifies concerns related to mental health care for people who live in rural poverty (Reed & Smith, 2014; Tickamyer et al., 2017). For example, Snell-Rood and colleagues (2017) conducted a qualitative study that explored the sociocultural factors that influence treatment-seeking behavior among rural, low-income women. Participants reported that the quality of counseling in their rural settings was unsatisfactory because of counselors recommending coping strategies that were “inconsistent” with daily routines and beliefs (Snell-Rood et al., 2017). Alang (2015) conducted a quantitative study that investigated the sociodemographic disparities of unmet health care needs and found that men in rural areas were more likely to forgo mental health treatment because of gender stereotypes. Specifically, Alang found that men were encouraged to ignore mental health concerns and avoid help-seeking behaviors. Furthermore, children living in rural poverty have fewer protective resources and less access to services that can address their needs and are subsequently exposed to increased violence, hunger, and poor health (Curtin, Schweitzer, Tuxbury, & D’Aoust, 2016).
Adults and children living in rural poverty often have lower mental health literacy (i.e., the ability to recognize a mental health concern when it arises and how to cope with one when it occurs; Rural Health Information Hub, 2017). For example, researchers (Pillay, Gibson, Lu, & Fulton, 2018) examined the experiences of the rural Appalachian clients who utilized mental health services and found that clients were ambivalent about diagnoses and suspicious when providers suggested psychotropic medications to support treatment. Likewise, Haynes et al. (2017) conducted focus group interviews that included persons living with a mental illness, health care providers, and clergy living in rural, impoverished communities in the Southern United States, and reported a general lack of awareness about mental illness. The researchers suggested that individuals have less knowledge of what mental illness looks like, how to recognize it, and how to identify warning signs of crises in Southern rural, impoverished communities (Haynes et al., 2017). As a result of less mental health literacy, people in rural low-income communities may delay seeking counseling treatment until symptoms have intensified and face a greater likelihood of hospitalization related to mental health challenges (Neese, Abraham, & Buckwalter, 1999; Stewart, Jameson, & Curtin, 2015).
Counselor Competence and Poverty Beliefs
Researchers have indicated that mental health professionals practicing in rural, economically deprived areas are not properly trained to address the multiple needs of this population (Bradley et al., 2012; Fifield & Oliver, 2016; Grimes, Haskins, Bergin, & Tribble, 2015). Fifield and Oliver (2016) surveyed 107 rural clinicians, exploring their perceived training-related needs and the pros and cons of rural counseling practice. The researchers found that many counselors did not receive adequate training to work with the population they served, and the counselors did not feel properly prepared to address the host of issues that may arise in their rural practice.
Moreover, mental health professionals continue to hold negative poverty beliefs and social class biases (Bray & Schommer-Aikins, 2015; Grimes et al., 2015; Smith, Li, Dykema, Hamlet, & Shellman, 2013) that negatively impact the quality of services provided. Researchers have shown that some counselors are less willing to work with clients of lower socioeconomic statuses because of communication barriers, having less knowledge of and exposure to the poverty culture, and possessing negative stereotypes about poor, rural populations (e.g., uneducated, dirty, violent, lazy; Bray & Schommer-Aikins, 2015; Smith et al., 2013). Consequently, clients from lower socioeconomic statuses receive more serious mental health diagnoses or are often misdiagnosed, which may be attributed to the professional’s negative biases, as well as lack of adequate multicultural training (Clark, Moe, & Hays, 2017).
Multicultural Counseling Competence
Increased training in multicultural counseling competence has a significant impact on counselors’ poverty beliefs (Clark et al., 2017; Toporek & Pope-Davis, 2005). In a quantitative study examining the relationship between multicultural counseling competence and poverty beliefs using a sample of 251 counselors, Clark et al. (2017) identified that higher levels of multicultural competence and training decreased poverty biases and helped counselors to understand the structural causes of poverty. Similarly, Bray and Schommer-Aikins’ (2015) survey of 513 school counselors found that counselors with training through multicultural courses recognized the external factors that contribute to poverty; however, the study did not focus on effective interventions that counselors utilized with this population.
Although these studies identified that multicultural knowledge and awareness increased counselors’ understanding of the culture of poverty, more research is necessary to explore how this information is applied to provide counseling professionals with evidence-based illustrations of social justice advocacy in practice (Ratts & Greenleaf, 2018). Accordingly, the purpose of this study was to (1) develop an understanding of the experiences of mental health counselors who work in rural, persistently poor communities and (2) identify ways that counselors incorporate social justice advocacy into counseling using the lens of the MSJCCs. The research question guiding this study was: What are the lived experiences of mental health counselors working in rural, persistently poor communities?
Conceptual Framework
The MSJCCs, a revision of the Multicultural Counseling Competencies (Sue, Arredondo, & McDavis, 1992), offer a framework to incorporate culturally responsive counseling and social justice advocacy initiatives into counseling practices, research, and curricula (Ratts et al., 2015). Established in a socioecological framework, the MSJCCs help counselors examine personal biases, skills, and the dynamics of marginalized and privileged identities in relation to multiculturalism and social justice counseling competence and advocacy. Additionally, the MSJCCs assist counselors in acknowledging clients’ intersecting identities, which bestow various aspects of power, privilege, and oppression that may impact their growth and development.
The developmental domains of the MSJCCs—(a) counselor self-awareness, (b) client worldview,
(c) counseling relationship, and (d) counseling and advocacy interventions—help counselors understand social inequalities that are perpetuated by institutional oppression in order to better serve historically marginalized clients (Ratts et al., 2015). Likewise, aspirational competencies espoused in the MSJCCs—namely (a) attitudes and beliefs, (b) knowledge, (c) skills, and (d) action—serve as objectives for multicultural, social justice competence and advocacy interventions (Ratts et al., 2015, 2016). Although the MSJCCs have been identified as goals for all counselors, limited research exists that illuminates the MSJCCs as a framework for understanding social justice applications within rural, high-poverty areas. Therefore, in considering the four distinct developmental domains and aspirational competencies, the authors utilized the MSJCCs as a basis to understand counselors’ experiences in rural, high-poverty communities. For the purposes of this study, social justice advocacy is understood as interventions and skills that counselors utilize to address inequitable social, political, or economic conditions that impede the personal and social development of individuals, families, and communities (Lewis, Ratts, Paladino,
& Toporek, 2011).
Method
University institutional review board approval was granted for this study. We used a descriptive phenomenological qualitative research design, which is suitable for scholars to examine the lived experiences of individuals within their sociocultural context (Creswell & Creswell, 2018; Giorgi, 2009). In descriptive phenomenological studies, researchers use participants’ responses to describe common experiences that capture the “intentionality” (perception, thought, memory, imagination, and emotion) related to the phenomenon under study (Giorgi, 2009). Furthermore, using qualitative research methods allows researchers to provide an in-depth exploration of lived experiences and helps multiculturally competent counselor–researchers highlight gaps in counseling literature and inequities in counseling practices in order to advocate for systemic changes in the counseling profession (Hays & Singh, 2012; Ratts et al., 2015).
Role of the Researchers
We recognize the possibility of bias in empirical research and acknowledge our social locations, identities, and professional experiences in relation to the current research study. All three authors identify as African American women from low socioeconomic backgrounds. We identify as counselor–advocate–scholars (Ratts & Greenleaf, 2018) and incorporate advocacy for underserved populations into our counseling practices, research, supervision, and teaching (Ratts et al., 2015). We bracketed personal thoughts and feelings and discussed biases that may possibly influence the data throughout the study. For example, the frequent criminalization of poverty was a difficult finding to discuss with the participants and we met to express our thoughts regarding this finding. A graduate research assistant (middle class, European American female) was selected to assist in data collection and analysis to increase objectivity in the research process, as she was less familiar with underserved populations, but trained extensively in qualitative research techniques. We acknowledge that we used the developmental domains and aspirational competencies espoused in the MSJCCs to conceptualize this research study, analyze the data, and present the findings and implications to foster positive changes in mental health care for people living in rural, poor communities. Furthermore, it is our view that the data did not emerge independently, but that as researchers we used a rigorous process such as the use of thick descriptions to analyze and identify nuances and commonalities in the data while also accounting for our assumptions and biases (Hays & Singh, 2012; Lincoln & Guba, 1986). Our position as counselor–advocate–scholars helps to bring expertise to our scholarship and practices (Hays & Singh, 2012; Ratts & Greenleaf, 2018).
Participants
Fifteen participants (N = 15; 13 women, two men) were selected for the study using purposeful criterion sampling (Patton, 2014). Participants’ ages ranged from 28 to 67 years (M = 40). Twelve participants identified as European American and three as African American. Twelve participants were licensed professional counselors and three were licensed professional counselor associates. Two participants had doctoral degrees in counseling. Participants practiced counseling in various settings such as private practices, colleges, secondary schools, and community counseling centers. Participants also had additional credentials: three were licensed professional counselor supervisors, seven were licensed clinical addiction specialists, one was a certified clinical trauma professional, and one was a registered play therapist. Years of work experience as a professional counselor ranged from 2 to 20 (M = 6.7).
Data Collection and Analysis
Recruitment solicitation flyers were distributed to various mental health agencies located in rural counties designated as persistently poor (USDA, 2017) in one state in the Southeastern United States. The mental health agencies were identified by searching public information websites for counseling and psychological support resources within these counties. Potential participants completed a telephone eligibility screening and a demographic questionnaire. The demographic questionnaire included questions asking potential participants to identify a pseudonym, their age, ethnicity, employment status and location, and professional credentials. Participants who met inclusion criteria (i.e., licensed mental health clinicians currently employed in persistently poor rural locales) were selected to participate in the study. There is no required sample size for phenomenological studies; rather, authors (Creswell & Creswell, 2018; Hays & Singh, 2012) recommended researchers consider the purpose of the research and depth of the data. We continued to recruit participants until saturation was achieved by seeing a recurrence in the data (Creswell & Creswell, 2018; Hays & Singh, 2012). After completing Interview 15, we did not identify novel data and agreed that a sufficient amount of data was collected to provide a comprehensive understanding of the phenomenon under investigation.
The researcher is the key instrument for data collection in qualitative research (Creswell & Creswell, 2018). A graduate assistant and the first author collected all study data by the use of qualitative interviews using an open-ended, semi-structured interview protocol (Hays & Singh, 2012). Each participant completed individual, one-phase, open-ended, semi-structured, face-to-face or live video interviews, lasting approximately 60–90 minutes. We audio-recorded all interviews, and they were transcribed by a professional transcription service.
The 12 interview questions that guided the study were framed by the MSJCCs’ constructs in extant literature related to the experiences of mental health counselors and clients in rural, poor communities (Bradley et al., 2012; Clark et al., 2017; Grimes et al., 2015; Grimes et al., 2013; Kim & Cardemil, 2012) and specific multicultural and social justice counseling constructs espoused in the MSJCCs (Ratts et al., 2015; Ratts et al., 2016). Six questions focused on understanding the participants’ knowledge of rural, poor communities and their experiences. Examples of these questions were: “Can you tell me the influence that persistent poverty has on the services you provide in a rural setting? What personal and client factors or experiences are influential to your work?” and “What is needed for you to competently provide counseling services to this population, if anything?” An additional six questions, also informed by the MSJCCs, sought to further explore the participant’s beliefs, skills, and actions related to multicultural competence, social justice advocacy, and counseling, such as “Can you share with me your definition and understanding of social justice advocacy in counseling? Can you share ways (if any) you incorporate social justice advocacy into your work as a counselor in a rural, economically deprived area?” and “Please share any perceived barriers to engaging in social justice advocacy and counseling in rural, economically deprived areas.”
Analysis of the data was informed by Giorgi’s (2009) and Giorgi, Giorgi, and Morley’s (2017) process for descriptive phenomenological data analysis. Specifically, we adhered to five steps in the data analysis process. First, we assumed a phenomenological attitude, in which we bracketed suppositions that could potentially influence the data and research process, such as our frustrations with perpetual deficit ideology in research related to marginalized populations. Second, after each interview was completed, we individually read each transcript to get a sense of the whole experience (i.e., native descriptions) and wrote brief notes in the margins to pinpoint any significant descriptive statements and expressions (Hays & Singh, 2012). For instance, we notated participants describing specific counseling practices that they believed were related to social justice advocacy as significant descriptive statements. We sent participants a copy of their transcript for member checking. Third, we re-read transcripts to demarcate data into multiple meaning units by clustering the invariant descriptions of participants’ experiences.
Initially, we also used a priori codes based on the MSJCCs to begin to identify units of meaning. For example, codes such as systems, advocacy, self-awareness, community, and collaboration helped us to infuse the MSJCCs’ framework and focus the findings toward understanding social justice experiences. As an example, the recognition and appreciation of a client’s ability to ascertain needed resources despite having less access and the participants’ willingness to assist in resource allocation were two invariant descriptions of experiences. The analysis process yielded 46 initial units of meaning. Participants’ quotes and definitions related to meaning units were contained in a research notebook to manage data and establish consensus coding (Hays & Singh, 2012). We held multiple meetings to discuss if and how these meaning units related to the developmental domains of the MSJCCs. For example, we discussed how one meaning unit, idiosyncrasies in the support system, closely related to the MSJCCs’ client worldview domain and reached a consensus in understanding that the participants’ ability to recognize that their clients had often strained their natural support systems exemplified that the counselor possessed knowledge of how their clients’ economic status and limited support systems shaped their attitudes and engagement in mental health treatment. In our fourth step, we reviewed the data to transform the meaning units into sensitive descriptive expressions that highlighted the psychological meaning of participants’ descriptions. We used free imaginative variation to determine the essence of the phenomenal structures of the participants’ experiences (Giorgi, 2009; Giorgi et al., 2017). We discussed any differences in understanding participants’ invariant experiences. For example, we discussed if the participants’ recognition of their need for a professional consultation to address underdeveloped counseling skills and biases related to the MSJCCs’ counselor self-awareness domain. Finally, we negotiated the interconnections and essential meanings of the meaning units, coalesced the data, and identified four essential structures that represented the descriptions of participants’ experiences and assigned them a descriptive thematic label.
Strategies for Trustworthiness
It is vital that researchers establish criteria for trustworthiness in qualitative research studies (Morrow, 2005). We demonstrated credibility through the use of bracketing, triangulation of the data sources, member checking, and peer debriefing (Morrow, 2005). Participants were provided with a copy of their transcriptions and case displays to review for member checking. We employed triangulation of data by crosschecking data (Hays & Singh, 2012) with the existing empirical studies related to rural poverty and mental health counseling. Data collection and analysis occurred concurrently in order to triangulate findings (Hays & Singh, 2012).
Findings
Using an MSJCCs lens, we identified four themes that represented the experiences of counselors who work with clients in rural poverty: (1) appreciating clients’ worldviews and life experiences, (2) counseling relationships influencing service delivery, (3) engaging in individual and systems advocacy, and (4) utilizing professional support. The findings are explicated using participants’ quotes to illustrate the meaning of each theme.
Appreciating Clients’ Worldviews and Life Experiences
Participants in the study described how they developed an appreciation for their clients’ worldviews and life experiences, even if they were different from their own. For example, Jade shared how she gained insight into and showed an appreciation for her clients’ worldviews by “showing empathy, being curious, and asking questions about what it was like for them in certain situations.” Jade expressed that seeking to understand clients’ worldviews was vital when working with African Americans living in rural poverty because she did not have the same experiences. Shelly also conveyed an appreciation for her clients’ worldviews and experiences and the impact on her clinical skills, sharing that she acquired a “different perspective” in her approach by gaining knowledge of her clients’ family structures and listening to their history.
Nine participants described that working in rural, impoverished communities entailed understanding the impact that limited resources have on providing adequate mental health services and recognizing the idiosyncrasies in clients’ support systems. Three participants described how their clients had often “burned” or “exhausted” their natural support system (i.e., personal relationships with other people that enhance the quality of one’s life), which made it difficult for participants to identify persons who would be supportive of their clients in the mental health treatment process. Addie described her counseling experiences in rural, poor communities, stating, “People have so little to fall back on, if they’re chronically mentally ill or they have a family member who is, they’re just out of resources, and they’ve maybe even burned their natural supports.” Addie further elaborated on her experiences, explaining that family members would often not return her phone calls after a client was admitted for inpatient mental health treatment.
Five participants expressed the importance of considering how low mental health literacy and mental illness stigma influenced clients’ knowledge, attitudes, and beliefs toward mental health treatment. Lola explained that she observed low mental health literacy in rural, poor communities: “There is a very low level of understanding with regard to symptoms associated with mental illness.” Lola discussed the prevalence of stigma toward clients with diagnosed mental health disorders as well as toward clients that had not been formally diagnosed because of the limited understanding of mental illness. Likewise Julian, a school-based counselor, expressed the impact of low mental health literacy in rural, high-poverty communities. Julian shared that the majority of her youth clientele were being raised by their grandparents, who had less knowledge of mental health symptoms and treatment; therefore, grandparents were often hesitant to seek mental health treatment services for their grandchildren.
Many (n = 11) of the participants indicated that in understanding the clients’ experiences and worldviews they were able to see how clients managed to be resourceful and resilient when faced with hardships. In illustration, Lola stated, “They are some of the most resourceful and resilient people that I’ve ever met; they have a knack for finding ways to achieve what needs to happen despite not having the typical resources . . . that’s very admirable.” Sue and Brenda expressed similar sentiments, also describing their clients as “resourceful.” In essence, participants explicated their attitudes and dispositions (e.g., recognizing and appreciating clients’ resourcefulness, possessing curiosity, learning about family structure and support systems) in working with clients in rural, impoverished communities. In accordance with the MSJCCs, participants expressed the importance of recognizing how the worldviews and life experiences of their marginalized clients are influenced by the context of rural poverty, such as how low mental health literacy and stigma impact the utilization of mental health treatment for this population.
Counseling Relationships Influencing Service Delivery
Participants (n = 10) described the importance of having a strong counseling relationship when working with marginalized individuals and families living in rural poverty. This solid relationship motivated participants to alter the mode of service delivery or intentionally focus more on client-centered services. Reflecting on her experiences providing home-based counseling services, Sue expressed the importance of building trust and empowerment in counseling relationships, especially when clients were involved with professionals from other agencies (e.g., probation officers) who also visited their homes. Sue described how she reinforced trust and empowerment by telling her clients, “This is about you and I’m walking alongside this path with you, I’m not going to make decisions for you.” Sue expressed that reinforcing empowerment was an essential part of counseling in rural, poor communities because clients often felt as if their power has been taken away.
Other participants shared that many of their clients came to counseling sessions without their basic needs met (e.g., food, housing, and safety) and that a solid counseling relationship allowed for more trust and openness. In return, participants expressed that clients were more willing to express their need for basic necessities without feeling ashamed, and that they often altered their services to assist clients in ascertaining immediate resources. For example, Heather noted that the poverty level was so low in her community that many of her youth clients’ basic needs were not being met and they would ask her to stop and purchase them meals. Heather disclosed that she often responded by stating, “Okay, we’re going to have to change where we’re providing therapy today, or maybe how therapy’s going to look today” to accommodate their needs. Similarly, Sadie shared, “It’s hard to see your clients going without things that you would consider basic.” Sadie described circumstances in which she arranged for food to be dropped off to the school and picked up by her clients.
Che and eight other participants acknowledged that having strong counseling relationships with clients living in rural poverty increased their willingness to extend their services beyond traditional counseling roles and settings. The participants described various cases in which they assisted clients in securing food or housing, or navigating Medicaid and other entities. For example, Che shared that she attended a mental health disability hearing with her client in which she was allowed to speak on the behalf of a client who experienced severe social anxiety. Additional participants described ways they broadened their roles to include consulting and case management and provided examples of ways they altered counseling sessions (e.g., including children because clients had no childcare) or offered incentives for attendance (e.g., bus passes and toiletries) to support clients’ continuity in treatment as well as using these as a means to help meet clients’ imminent needs. Overall, participants conveyed that their counseling relationships allowed for trust and flexibility that enabled them to use ancillary skills and knowledge when working in rural, persistently poor communities, such as skills in crisis management or intentionally building resource networks with medical professionals, churches, social service providers, law enforcement, and community organizations to help meet clients’ basic needs.
Engaging in Individual and Systems Advocacy
All participants reported engaging in various individual and systems advocacy interventions when working in rural, impoverished communities. Participants shared that engaging in advocacy was necessary, ranging from their initial sessions with their clients until termination and follow-up. George shared that he started advocacy initiatives in the initial assessment by “not jumping to assumptions” and spending more time observing clients and exploring their history. He stated that he acknowledged if clients were already taking steps toward positive change to encourage self-advocacy. George explained, “I think the most direct thing that I can do is to empower people to recognize their strengths and their rights.” Similarly, Jade shared, “I use motivational interviewing with clients to help them become better advocates for themselves.” Other participants expressed that promoting self-advocacy was vital for this specific population because of the high probability that a client would not return to counseling because of barriers related to transportation, finances, and stigma. Seven participants shared that it is important to have personal knowledge of systems that affect the client in order to inform advocacy interventions. Renee mentioned, “With all the Medicaid changes . . . I’ve got to take every client into a financial conversation. . . . So keeping myself educated . . . I can be a voice of support to them and have an understanding if they come to me.”
Additionally, participants reported various situations in which they engaged in advocacy interventions outside of the office setting. Two participants shared that they engaged in advocacy with and on behalf of clients to help them navigate the criminal justice system. For example, Jade advocated on behalf of a teenage client to law enforcement officials to request the removal of her client’s ankle monitor, which she believed was not necessary. Heather shared that she wrote letters to the courts on behalf of her clients.
Participants also discussed their involvement with helping clients sustain housing. Che shared, “I’ve spoken up for my clients against landlords who were trying to railroad several of my clients with their rent, and one in particular was trying to charge my client double the rent.” Similarly, Jade shared, “I was able to advocate to my supervisors to get funds to help pay the past bills so [clients] could move into a new location and not lose housing.”
Four participants conducted trainings in schools and within the community to inform others of culturally responsive practices with people living in rural poverty. Sadie shared that she provided educational workshops to school counselors, administrators, and teachers to help them understand the life experiences of individuals and families living in rural poverty. Sadie explained that she educated her colleagues on the effects of generational poverty and helped them to explore ways they could use various educational strategies for clients in these circumstances. Overall, counselors recognized clients’ needs and engaged in an array of advocacy interventions individually with clients, as well as in the community to support clients’ continuation in treatment, link clients to services, or help clients allocate resources in rural, poor communities.
Utilizing Professional Support
Some participants (n = 6) were the only mental health providers in the communities in which they worked. Thus, they spoke of instances of feeling frustrated because of the lack of resources for clients, role overload, and inability to connect with other counselors. Participants expressed that support from other professionals in the behavioral health field was helpful to alleviate frustrations. With this awareness, participants shared that conversations, consultations, and formalized supervision sessions were useful to explore their biases and feelings of hopelessness, to address compassion fatigue, and to learn new clinical interventions. For example, Blaze shared that formalized supervision was beneficial to increase his knowledge and improve his attitude about working in rural, impoverished communities. He stated, “The people who have supervised me understand that I’m coming from a different area and this is all kind of a learning curve. They’ve been good about helping me acclimate to the area.” Similarly, eight participants shared that ongoing supervision was helpful to abate adopting negative stereotypes and to address de-sensitization to clients’ needs, particularly when seeing clients who perpetually faced hardships. Lola discussed the benefits of having a professional support system among her colleagues to manage the demands of counseling in rural poverty. She stated, “We support each other personally when professional issues begin to impact our personal lives.” Furthermore, Lola described that ongoing supervision was “very helpful and necessary” as it provided her the opportunity to “check in” with herself and assess how she was managing the demands of her work.
Seven participants shared that receiving professional support reinforced ongoing self-awareness. For example, Sadie stated, “I think [it’s important] being willing to recognize that I’m not perfect . . . being willing to say here’s a place where I need to improve.” Sadie also expressed that it was important for her to seek supervision or personal mental health services to not allow her personal frustrations to “bleed over” into her client sessions. Likewise, Jade explained that supervision and taking continuing education credits regarding cultural differences were optimal to her success. In alignment with the constructs in the MSJCCs, the participants acknowledged the importance of engaging in critical self-reflection to take an inventory of their skills, beliefs, and attitudes (Ratts et al., 2016) that impact the services they provided to marginalized clients living in rural poverty. Overall, seeking ongoing supervision and engaging in professional development activities were necessary to prevent adopting stereotypes and to continue advocacy efforts.
Using participants’ voices and the lens of the MSJCCs, we illuminated the essence of providing mental health counseling in rural, persistently poor communities. The participants described the importance of showing an appreciation for clients’ worldviews and life experiences and how their counseling services encompassed varied approaches to service delivery and non-traditional counseling methods to engage rural, impoverished clients in the treatment process. Participants frequently engaged in individual and systems advocacy with and on behalf of their clients and described how having professional support was necessary to provide culturally responsive mental health counseling in rural, persistently poor communities. The findings serve as the basis for the following discussion.
Discussion
This study explored the experiences of mental health counselors working in rural, impoverished communities and identified ways counselors incorporated social justice advocacy using the lens of the MSJCCs to identify advocacy skills and interventions. We found that counselors who work with clients in rural poverty appreciate their clients’ worldviews and life experiences, value their counseling relationships, alter service delivery formats, engage in advocacy, and seek ongoing professional support and development opportunities. Specifically, the first theme captured how counselors in the study expressed an appreciation for their clients’ worldviews and life experiences, as described in the MSJCCs’ client worldview domain. Counselors recognized that various contextual factors, such as family structure, nuances in the natural support systems, less access to resources, as well as how race and social class status shaped their clients’ worldviews, influenced their utilization of mental health treatment. This finding lends support to previous literature associated with examining how economic disadvantages and rurality influence mental health care services and literacy (Deen & Bridges, 2011; Kim & Cardemil, 2012). Consistent with the MSJCCs’ (Ratts et al., 2015) client worldview domain, the counselors explored and appreciated clients’ history and life experiences, and acknowledged the clients’ “resourcefulness” as a strength.
Furthermore, counselors in the study expressed a willingness to engage in their clients’ personal communities, which aligns with the suggestion in the client worldview domain that counselors should immerse themselves in the communities in which they work to learn from and about their clients (Ratts et al., 2015). The findings from the study correspond to previous research that examines how counselors with increased exposure to individuals living in poverty have enhanced multicultural competence and are able to critically examine systemic or structural factors that contribute to the underutilization of mental health services in high-poverty communities (Clark et al., 2017).
The second theme, counseling relationships influencing service delivery, reflected the MSJCCs’ counseling relationship domain. Participants recognized that their clients’ ability to engage in the traditional therapeutic process was often thwarted because many of their clients’ basic needs were not met. As implied in the counseling relationship domain, counselors are advised to utilize culturally competent assessment and analytical and cross-cultural communication skills that allow them to effectively determine clients’ needs and employ collaborative, action-oriented strategies to strengthen the counseling relationship (Ratts et al., 2015).
Reflective of this domain, counselors in the study often altered service delivery formats and assumed alternative roles to meet clients’ needs. The current findings offer support for research that advances increasing flexibility in counseling roles and culturally competent assessments when working in marginalized communities (Fifield & Oliver, 2016).
Another distinctive finding of this study was encompassed in the third theme, which captured the MSJCCs’ counseling and advocacy interventions domain, and illuminated the participants’ use of strategies to promote continuation of services (e.g., home-based counseling, group formats with the inclusion of childcare, and distributing incentives) as well as advocacy interventions to address clients’ imminent needs. Expanding previous research that illuminated the role of self-advocacy (Singh, Meng, & Hansen, 2013), the participants expressed the importance of engaging in intrapersonal, interpersonal, and institutional advocacy interventions with and on behalf of clients, such as assisting clients in securing or maintaining housing, acquiring supportive educational resources in school settings, rebuilding familial relationships, and preventing the criminalization of poverty. Although these findings are similar to previous researchers’ perspectives that suggest that counseling in rural poverty requires counselors to engage in various advocacy roles (Kim & Cardemil, 2012; Reed & Smith, 2014), this study answers the call to provide practical examples of incorporating social justice advocacy into counseling with historically marginalized populations (Ratts & Greenleaf, 2018).
The final theme identified in our study involved the participants’ use of professional support networks and seeking professional development opportunities to address areas of professional incompetence. Accordingly, this theme aligns with aspects in the MSJCCs’ self-awareness domain. As articulated in this domain, multiculturally competent counselors are expected to have an awareness of their social group statuses, power, privilege, and oppression, as well as acknowledge how their biases, attitudes, strengths, and limitations may influence clients’ well-being (Ratts et al., 2015). The counselors in our study engaged in both informal and formal action-oriented strategies, such as consultations and ongoing supervision with other mental health professionals, that helped them examine prejudicial beliefs, prevent the development of additional biases, and explore other areas of vulnerability and skills deficiencies as designated in the MSJCCs’ counselor self-awareness domain. This finding supports past research (Bowen & Caron, 2016; Reed & Smith, 2014) that indicated that because of the limited resources and remoteness in rural, impoverished areas, professional support is vital to assuage frustrations because of consistently seeing poor, rural clients navigate difficult life circumstances. However, this finding expands current understanding by focusing on the counselors’ ability to identify their own limitations and readily seek out additional supports.
Implications for Counseling Practice, Advocacy, and Training
Foremost, in order to offer culturally competent mental health counseling, it is important for counselors to appreciate their clients’ worldviews and life experiences and understand the unique oppressions that clients from rural, impoverished communities experience. For example, participants acknowledged that various contextual factors, such as family structure, mental illness stigma, and nuances in the natural support systems, shaped their clients’ worldviews and influenced their utilization of mental health treatment. Viewing clients’ concerns from a socioecological lens may strengthen the counselor–client relationship (Ratts et al., 2016) and decrease stigma related to mental health treatment (Stewart et al., 2015).
Counselors also must be flexible and recognize that altering the format of session delivery is often necessary to engage with clients in rural poverty. Individuals living in rural poverty face immense financial barriers that impede the utilization of mental health treatment (e.g., transportation issues), and there is a general lack of awareness about mental illness in rural, poor communities (Haynes et al., 2017). Thus, counseling in rural poverty should extend beyond office-bound interventions to include community-based interventions (Ratts & Greenleaf, 2018) and account for barriers that influence treatment utilization. For instance, the findings indicated that participants had a greater appreciation for clients’ worldviews and expanded their roles to include consulting, advocacy, and case management when they became more engaged in their clients’ personal environment and community.
Furthermore, counselors in this study collaborated with and on behalf of clients in advocacy efforts in various areas such as housing, criminal justice, social services, and school systems. Engaging in individual- and systems-level advocacy interventions (Ratts et al., 2016) when working in rural, impoverished communities is vital to promote equity and positive systemic changes (Reed & Smith, 2014). Given these findings, counselors should become comfortable with professionals in these areas as well as going into the respective environments. Thus, it warrants counselors to network with community partners, schools, faith communities, and law enforcement entities to establish relationships to enhance support networks. In addition, writing letters to federal and state legislators regarding national issues such as Medicaid funding is critical to address policies that benefit rural, impoverished communities.
Finally, multicultural and social justice competence is a developmental process, and professional counselors as well as counselors-in-training need opportunities for ongoing self-reflection to examine their personal assumptions and biases and enhance their skills when working with rural, impoverished communities. Clinical supervision grounded in a social justice framework can help counselors and supervisors process their biases and assumptions, develop a social justice lens of understanding clients from rural poverty, and cultivate advocacy skills (Smith et al., 2013). The MSJCCs should be facilitated throughout counseling program curricula versus one foundation course in multicultural counseling and development. Some possibilities for incorporating the MSJCCs into student learning across all courses include experiential activities, group work, and role-plays that cover topics such as worldviews, intersecting identities, power, privilege, and social class. For example, audiovisual materials found on the Rural Health Information Hub website (www.ruralhealthinfo.org) can help students visualize the experiences of rural and impoverished communities. Additionally, encouraging or requiring counselors-in-training to engage in rural, economically disadvantaged communities for their practicum and internship experiences can be incorporated into the clinical sequence in counselor preparation programs
Recommendations for Future Research
There are several pathways to advance research pertaining to mental health counseling and social justice advocacy in rural poverty. Rural, impoverished areas continue to experience low mental health literacy, which perpetuates stigma. Thus, investigations about stigma in rural poverty can provide insights into the underutilization of mental health treatment in rural communities. Research of various designs regarding the lived experiences of poor women, men, and children in rural communities can inform culturally responsive counseling practices. For example, empirical studies about the experiences of grandparents raising grandchildren in rural poverty can offer unique perspectives for ways to enhance mental health literacy and increase utilization of mental health services. Additional studies are also needed to explore social justice advocacy interventions that are necessary to test the efficacy of the MSJCCs.
Finally, a primary limitation of this study was that the participants had varied professional license levels, areas of specialization, years of professional experience, and provided counseling services to diverse clientele in various settings. The data in the current study did not allow us to assess if variances in the noted areas had a differential impact on the participants’ counseling experiences in rural poverty. Consequently, additional qualitative studies that allow researchers to examine these differences more pointedly are needed to fully understand the experiences of counselors from varied backgrounds and experience levels. Furthermore, readers should exercise caution when generalizing the experiences of the 15 participants in this sample to other counselors working in rural, impoverished communities. The experiences of participants in this sample may not capture the experiences of all counselors working in these communities; however, readers can make decisions regarding the degree to which the findings of the study are applicable to the settings in which they live and work (Hays & Singh, 2012).
Conclusion
Poverty significantly impacts the mental health of children and adults living in rural communities, resulting in having limited access to resources and services that can promote healthy development and well-being. Therefore, mental health counselors working in rural, poor communities must often incorporate social justice advocacy within the context of clients’ experiences of oppression in their counseling practices to provide culturally responsive services. The MSJCCs provided a lens to explore the knowledge, skills, beliefs, and overall practices of 15 professional counselors working in rural, impoverished communities. By examining the experiences of these counselors, we identified how counseling professionals working in rural, impoverished communities acknowledged and appreciated their clients’ worldviews and life experiences, created strong therapeutic alliances, altered counseling service delivery, engaged in advocacy, and sought professional support to sustain their ability to provide culturally responsive counseling services. Multiculturally competent counselors should continually explore ways to amend their current practices to address the various sociocultural barriers that impede the mental health and well-being of rural, poor children and adults. It is our hope that counselors will utilize the findings from this study to further the discourse on rural poverty and create positive change in these communities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alang, S. M. (2015). Sociodemographic disparities associated with perceived causes of unmet need for mental health care. Psychiatric Rehabilitation Journal, 38, 293–299. doi:10.1037/prj0000113
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author.
Bowen, J. M., & Caron, S. L. (2016). A qualitative analysis of home-based counselors’ experiences in a rural setting. Journal of Counseling & Development, 94, 129–140. doi:10.1002/jcad.12070
Bradley, J. M., Werth, J. L., Jr., Hastings, S. L., & Pierce, T. W. (2012). A qualitative study of rural mental health practitioners regarding the potential professional consequences of social justice advocacy. Professional Psychology: Research and Practice, 43, 356–363. doi:10.1037/a0027744
Bray, S. S., & Schommer-Aikins, M. (2015). School counselors’ ways of knowing and social orientation in relationship to poverty beliefs. Journal of Counseling & Development, 93, 312–320. doi:10.1002/jcad.12029
Clark, M., Moe, J., & Hays, D. G. (2017). The relationship between counselors’ multicultural counseling competence and poverty beliefs. Counselor Education and Supervision, 56, 259–273. doi:10.1002/ceas.12084
Creswell, J. W., & Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). Thousand Oaks, CA: Sage.
Curtin, K. A., Schweitzer, A., Tuxbury, K., & D’Aoust, J. A. (2016). Investigating the factors of resiliency among exceptional youth living in rural underserved communities. Rural Special Education Quarterly, 35(2), 3–9. doi:10.1177/875687051603500202
Deen, T. L., & Bridges, A. J. (2011). Depression literacy: Rates and relation to perceived need and mental health service utilization in a rural American sample. Rural and Remote Health, 11(4), 1–13.
Fifield, A. O., & Oliver, K. J. (2016). Enhancing the perceived competence and training of rural mental health practitioners. Journal of Rural Mental Health, 40, 77–83. doi:10.1037/rmh0000040
Giorgi, A. (2009). The descriptive phenomenological method in psychology: A modified Husserlian approach. Pittsburgh, PA: Duquesne University Press.
Giorgi, A., Giorgi, B., & Morley, J. (2017). The descriptive phenomenological psychological method. In C. Willig & W. S. Rogers (Eds.), The SAGE handbook of qualitative research in psychology (2nd ed., pp.176–192). Thousand Oaks, CA: Sage.
Grimes, L. E., Haskins, N. H., Bergin, J., & Tribble, L. L. (2015). School counselor candidates’ shared beliefs and experiences regarding the rural setting. In Ideas and research you can use: VISTAS 2015. Retrieved from https://www.counseling.org/docs/default-source/vistas/school-counselor-candidates.pdf?sfvrsn=fedb432c_4
Grimes, L. E., Haskins, N. H., & Paisley, P. O. (2013). “So I went there”: A phenomenological study on the experiences of rural school counselor social justice advocates. Professional School Counseling, 17, 40–51. doi:10.5330/PSC.n.2013-17.40
Haynes, T. F., Cheney, A. M., Sullivan, J. G., Bryant, K., Curran, G. M., Olson, M., . . . Reaves, C. (2017).
Addressing mental health needs: Perspectives of African Americans living in the rural south. Psychiatric
Services, 68, 573–578. doi:10.1176/appi.ps.201600208
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. New York, NY: Guilford Press.
Hill, S. K., Cantrell, P., Edwards, J., & Dalton, W. (2016). Factors influencing mental health screening and treatment among women in a rural south central Appalachian primary care clinic. The Journal of Rural Health, 32, 82–91. doi:10.1111/jrh.12134
Imig, A. (2014). Small but mighty: Perspectives of rural mental health counselors. The Professional Counselor, 4, 404–412. doi:10.15241/aii.4.4.404
Kim, S., & Cardemil, E. (2012). Effective psychotherapy with low-income clients: The importance of attending to social class. Journal of Contemporary Psychotherapy, 42, 27–35. doi:10.1007/s10879-011-9194-0
Lewis, J. A., Ratts, M. J., Paladino, D. A., & Toporek, R. L. (2011). Social justice counseling and advocacy: Developing new leadership roles and competencies. Journal for Social Action in Counseling & Psychology, 3, 5–16.
Lincoln, Y. S., & Guba, E. G. (1986). But is it rigorous? Trustworthiness and authenticity in naturalistic
evaluation. New Directions for Program Evaluation, 1986(30), 73–84. doi:10.1002/ev.1427
Morrow, S. L. (2005). Quality and trustworthiness in qualitative research in counseling psychology. Journal of Counseling Psychology, 52, 250–260. doi:10.1037/0022-0167.52.2.250
National Board for Certified Counselors. (2016). NBCC code of ethics. Greensboro, NC: Author.
Neese, J. B., Abraham, I. L., & Buckwalter, K. C. (1999). Utilization of mental health services among rural elderly. Archives of Psychiatric Nursing, 13, 30–40. doi:10.1016/S0883-9417(99)80015-6
Patton, M. Q. (2014). Qualitative research and evaluation methods (4th ed.). Thousand Oaks, CA: Sage.
Pillay, Y., Gibson, S., Lu, H. T., & Fulton, B. (2018). The experiences of north-central rural Appalachian clients
who utilize mental health services. Journal of Rural Mental Health, 42(3–4), 196–204.
doi:10.1037/rmh0000100
Ratts, M. J., & Greenleaf, A. T. (2018). Counselor–advocate–scholar model: Changing the dominant discourse in counseling. Journal of Multicultural Counseling and Development, 46(2), 78–96. doi:10.1002/jmcd.12094
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and
social justice counseling competencies. Retrieved from https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf?sfvrsn=20
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44, 28–48. doi:10.1002/jmcd.12035
Reed, R., & Smith, L. (2014). A social justice perspective on counseling and poverty. In M. J. Ratts & P. Pedersen (Eds.), Counseling for multiculturalism and social justice: Integration, theory, and application (4th ed., pp. 259–273). Alexandria, VA: American Counseling Association.
Rural Health Information Hub. (2017, March 23). Rural mental health. Retrieved from https://www.ruralhealth info.org/topics/mental-health
Semega, J. L., Fontenot, K. R., & Kollar, M. A. (2017). Income and poverty in the United States: 2016: Current population reports (Report No. P60-256). Washington, DC: U.S. Census Bureau. Retrieved from https://www.census.gov/content/dam/Census/library/publications/2017/demo/P60-259.pdf
Singh, A. A., Meng, S., & Hansen, A. (2013). “It’s already hard enough being a student”: Developing affirming college environments for trans youth. Journal of LGBT Youth, 10, 208–223.
doi:10.1080/19361653.2013.800770
Smith, L., Li, V., Dykema, S., Hamlet, D., & Shellman, A. (2013). “Honoring somebody that society doesn’t honor”: Therapists working in the context of poverty. Journal of Clinical Psychology, 69, 138–151. doi:10.1002/jclp.21953
Snell-Rood, C., Hauenstein, E., Leukefeld, C., Feltner, F., Marcum, A., & Schoenberg, N. (2017). Mental health treatment seeking patterns and preferences of Appalachian women with depression. American Journal of Orthopsychiatry, 87, 233–241. doi:10.1037/ort0000193
Stewart, H., Jameson, J. P., & Curtin, L. (2015). The relationship between stigma and self-reported willingness to use mental health services among rural and urban older adults. Psychological Services, 12, 141–148. doi:10.1037/a0038651
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Multicultural Counseling and Development, 20(2), 64–88. doi:10.1002/j.2161-1912.1992.tb00563.x
Tickamyer, A. R., Sherman, J., & Warlick, J. L. (2017). Rural poverty in the United States. New York, NY: Columbia University Press. doi:10.7312/tick17222
Toporek, R. L., & Pope-Davis, D. B. (2005). Exploring the relationships between multicultural training, racial attitudes, and attributions of poverty among graduate counseling trainees. Cultural Diversity and Ethnic Minority Psychology, 11, 259–271. doi:10.1037/1099-9809.11.3.259
U.S. Department of Agriculture, Economic Research Service. (2017). U.S. state fact sheets. ASI 1546-6. Retrieved from
https://www.ers.usda.gov/data-products/state-fact-sheets/
Loni Crumb is an assistant professor at East Carolina University. Natoya Haskins is an associate professor at the College of William and Mary. Shanita Brown is an instructor at East Carolina University. Correspondence can be addressed to Loni Crumb, 213B Ragsdale Hall, Mail Stop: 121, Greenville, NC 27858, crumbL15@ecu.edu.
Mar 26, 2019 | Volume 9 - Issue 1
Ricardo Phipps, Stephen Thorne
This article proposes a model for an intervention designed to mitigate cultural trauma in African American children and adolescents using trauma-focused cognitive behavioral therapy (TF-CBT), an evidence-based practice for treating post-traumatic stress in children and adolescents. There is a paucity of approaches to treat cultural trauma in African American youth and the negative effects cultural trauma can have on academic performance and social interactions. This proposed intervention includes a mentoring program focused on the use of TF-CBT to help African American children and adolescents and their families in constructing positive self-images that support resilience and empowerment.
Keywords: cultural trauma, trauma-focused cognitive behavioral therapy, African American, children, empowerment
The complexity of traumatic experiences and their influence on psychological well-being expand far beyond the current diagnostic nomenclature and symptom descriptions available in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013; Burstow, 2005). Researchers and practitioners acknowledge that post-traumatic stress disorder (PTSD) has been observed in individuals not directly affected by narrowly defined traumatic experiences, creating the occasion for the study of such phenomena as vicarious traumatization or secondary traumatization, particularly when associated with mental health providers and caretakers who show PTSD symptoms because of their exposure to the stories of clients (Pearlman & Saakvitne, 1995). Beyond this concept of vicarious traumatization, researchers and practitioners also note the experience of intrafamilial PTSD symptoms driven by the display of symptoms in one or more family members. When this phenomenon involves the effects of trauma extending to other generations in the same family beyond the generation of the person experiencing primary trauma, mental health professionals have labeled this transgenerational trauma or intergenerational trauma (Danieli, 1985).
Transgenerational transmission of trauma was first documented in the literature in reference to Holocaust survivor families, with an emphasis on the psychological states of the second generation of survivor families (Danieli, 1985). The children of individuals who survived concentration camps displayed muted emotions and other symptoms of grief, loss, and depression. Researchers are currently focusing on better understanding transgenerational trauma in families affected by a variety of traumatic contexts, including child sexual abuse (Frazier, West-Olatunji, St. Juste, & Goodman, 2009), natural disasters such as Hurricane Katrina (Goodman & West-Olatunji, 2008), and immigration trauma (Phipps & Degges-White, 2014). In addition to the study of transgenerational transmission of trauma within family systems, there also is a growing scholarly interest in the effects of collective traumatic experience upon groups of people and how the traumatic experience affects subsequent generations. The term historical trauma has been used to describe the traumatization of Native American peoples at the hands of European colonizers, resulting in mass genocide and geographic displacement (BraveHeart & DeBruyn, 1998; Whitbeck, Adams, Hoyt, & Chen, 2004). Distinctly, but similarly, the construct of cultural trauma has been identified in reference to the enslavement of peoples of African descent in the United States and the subsequent oppression through “Jim Crow” practices that occurred post-emancipation (Eyerman, 2004). Cultural trauma is linked to the psychosocial outcomes that have resulted from the cultural wounds left by the experience of chattel slavery, which refers to the usually permanent holding of another human being as personal property with no rights (Eyerman, 2004; Stamm, Stamm, Hudnall, & Higson-Smith, 2004). DeGruy (2005) has referred to this phenomenon as post-traumatic slave syndrome. Vontress, Woodland, and Epp (2007) have described the psychological after-effects of enslavement and subsequent oppression and discrimination of African Americans as cultural dysthymia, suggesting that African Americans often experience a low-grade depression, or dysthymia, as a result of systemic oppression, which can affect academic, occupational, and social functioning, but do not meet other criteria for more severe depression diagnoses. Smith (2004) coined the term racial battle fatigue to depict the psychological and physiological stressors and subsequent behavioral responses some African Americans experience in reaction to repeated, cumulative racial discrimination.
Historical and cultural trauma has been recognized to be a part of the experiences of various marginalized, indigenous groups throughout the world who have undergone mass atrocities at the hands of colonizers, such as Japanese American survivors of internment camps (Nagata & Cheng, 2003), Palestinian youth (Giacaman, Abu-Rmeileh, Husseini, Saab, & Boyce, 2007), victims of the Rwandan genocide (Schaal & Elbert, 2006), and Mexican and Mexican American immigrants (Phipps & Degges-White, 2014). In the immediate and long-term aftermath of traumatic experiences, individuals have exhibited similar internalized and externalized behaviors that are characteristic of post-traumatic stress disorder and that are seen as responses to the collectively experienced trauma. Although some of the aforementioned groups underwent traumatic experiences that spanned a period of a few months or years and occurred within the last century, the history of the enslavement of African peoples in the Americas and their subsequent oppression and discrimination originated centuries ago and has endured since the first Africans were brought to the Americas. Given such prolonged exposure, the symptoms of historical and cultural trauma are highly pronounced in those African Americans who lack the protective factors needed to counter the disempowering effects of enslavement and oppression (Vontress et al., 2007).
A Brief Overview of Cultural Trauma
DeGruy (2005) and Reid, Mims, and Higginbottom (2004) proposed that African Americans have sustained traumatic psychological and emotional injury because of enslavement, exacerbated by social and institutional inequality, racism, and oppression. The effects are thought to be linked even to physical health disparities, which place African Americans at higher risk for certain medical conditions (Sotero, 2006). Wilkins, Whiting, Watson, Russon, and Moncrief (2013) and DeGruy (2005) asserted that the restrictions of slavery prompted enslaved African American parents to stress to their children the necessity of not confronting Whites, resulting in frustration with life in an oppressive system in which individuals were not permitted to question injustice. In the generations since the emancipation of slaves and the enactment of Civil Rights legislation passed to eliminate racial discrimination and unequal treatment, African Americans in large numbers continue to experience political disenfranchisement (Barnes, 2016), economic struggle (Croll, 2018), social marginalization (Benner & Wang, 2014), workplace discrimination (Hagelskamp & Hughes, 2014), housing segregation (Roscigno, Karafin, & Tester, 2009), and academic disparities (Morris & Perry, 2016). Sztompka (2000) characterized the aforementioned historical phenomena as limited collective agency, which refers to a sociocultural tendency of a group to be inhibited in positively transforming its own oppressed condition both because of external barriers and because of internalized hopelessness. Internalized responses to this limited collective agency influence self-esteem, relationships, occupational functioning, and overall psychological well-being. Linked to this are higher rates of depression and anxiety than seen in other ethnic groups, higher rates of exposure to individual and community violence, and higher rates of psychosis and other psychiatric challenges (Vontress et al., 2007).
Just as all individuals who are exposed to traumatic experience do not display symptoms of PTSD, not all African Americans display overt symptoms of cultural trauma or display them to the same degree. Rasmussen, Rosenfeld, Reeves, and Keller (2007) argued that the subjective interpretation by individuals of traumatic experience largely dictates whether their response will be pathological or whether adaptation and resiliency mechanisms will enable them to self-stabilize. Varying degrees of perceptions of limited agency, because of a plethora of factors, such as socioeconomics, educational achievement levels, family attachment and protective dynamics, and even skin tone dynamics, lead to a wide range of responses to the residual social milieu left behind by enslavement, “Jim Crow” practices, and current-day racially motivated injustice.
In a now dated publication, Pouissant and Atkinson (1972) linked exhibited feelings of rage and passivity among some African Americans to intrapsychic functioning learned during slavery as a survival mechanism. They further explained that this dynamic of rage and passivity was adopted in response to witnessing the brutality faced by enslaved peers who did challenge slave owners. Tatum (2002) postulated that this reaction to historical oppression has morphed into a number of responses to social injustice today, namely assimilation, crime, delinquency, or protest. This cultural trauma affecting African Americans has particularly and directly impacted the well-being of African American children and adolescents.
Assimilation, along with internalized racism, is no more evident than in the original and duplicate “doll studies” first launched by Clark and Clark in 1939. African American children showed preference for White dolls over Black dolls when asked to identify which were beautiful and good. Subsequent critique of the research methodology used by the Clarks and replicated and expanded studies have highlighted inattention to such details as how the skin tone of Black dolls shown to participants or developmental stage would influence their racial self-identification (Jordan & Hernandez-Reif, 2009). However, the study still demonstrates that one of the effects of cultural trauma is a preference for majority culture and characteristics over one’s own.
In terms of crime and delinquency, a long-standing trend of disproportionate numbers of African American men in the U.S. criminal justice system is paralleled by disproportionate numbers of African American males receiving disciplinary measures in schools (Monroe, 2006; Noguera, 2003). It can be argued that these statistical trends are connected to stereotyping and targeting of African American males as offenders. Alternatively, Conger et al. (2002) asserted that higher levels of externalizing symptoms and problematic behaviors in African American children and adolescents are correlated with systemic oppression and economic distress. These attitudes and behaviors, though not prevalent in the experience of all African Americans, indicate a pervasive stress that does not seem to mitigate over time and across generations. This pervasive stress has had a significant effect on the academic performance and school behavior of African American students. Thompson and Massat (2005) found in a sample of African American sixth graders attending inner-city Chicago public schools that academic achievement was significantly related to post-traumatic stress, family violence, and witnessing violence.
Cholewa and West-Olatunji (2008) have framed the academic performance divide that separates out some African American children as cultural discontinuity, highlighting a preference for Eurocentric ways of communicating, relating, and behaving in American schools. Cholewa and West-Olatunji asserted that those whose cultural background does not align with this preferred European style often find themselves marginalized in school environments, which can affect their access to academic instruction. Morris and Perry (2016) furthered this discussion by highlighting the existence of higher suspension rates of African American students and identifying the negative impact that this disparity has on African American students’ academic performance. Using data from the National Longitudinal Study of Adolescent Health, Benner and Wang (2014) concluded that segregation of students into schools in certain areas based on race and socioeconomics resulted in lower academic performance. Although researchers have not explicitly investigated the impact of cultural trauma as a complex construct on the academic performance of African American youth, the aforementioned studies indicate considerable support for the influence of various components of cultural trauma on academic performance, such as the pressure to change one’s communication style to fit a preferred Eurocentric model or the experience of being confined to a school environment with limited resources. Just as the external factors of cultural trauma and the related stressors caused by cultural trauma have perpetuated achievement divides between African American students and other groups, we propose that intentional, external interventions are needed to mitigate the effects of cultural trauma.
Interventions in Response to Cultural and Historical Trauma
Culturally sensitive curricula and character-building programs have been designed to stimulate learning and positive self-image in students of color (Vontress et al., 2007). Jarjoura (2013) adamantly maintained that such programs must be relational and address exposure to various types of traumatic experience. Jaycox (2004) created the Cognitive Behavioral Intervention for Trauma in Schools (CBITS) program as a model for working in inner-city school settings with children and adolescents of ethnically diverse backgrounds who exhibited symptoms of post-traumatic stress. The overall objective of CBITS is to reduce behavioral problems and optimize social and academic performance in students with trauma histories. Successful utilization of CBITS with Native American school children has been documented by Morsette et al. (2009). Honoring Children, Mending the Circle (HC-MC) is a structured program designed to address traumatic symptomatology in Native American children through a blending of evidence-based, trauma-focused cognitive behavioral therapy and culturally appropriate indigenous practices (BigFoot & Schmidt, 2010). BigFoot and Schmidt (2010) sought to provide an intervention in HC-MC that addressed both the high rates of exposure to traumatic events as well as the pervasive cultural, historical, and intergenerational trauma experienced by Native American children and youth, commonly referred to by BraveHeart and DeBruyn (1998) and Whitbeck et al. (2004) as historical trauma.
With the specific needs of African American children in mind, the Celebrating the Strengths of Black Youth (CSBY) program was developed as a strengths-based, small-group approach to building positive racial identity and nurturing self-esteem among African American children. CSBY focuses on teaching students skills to handle the typical challenges that Black students face related to race (Okeke-Adeyanju et al., 2014). President Barack Obama (2014) initiated My Brother’s Keeper as a mentorship program for boys of color to provide a space for accountability, guidance, and support, recognizing the need for culturally relevant approaches to help boys of color transcend barriers created by external stressors and internalized racism. Educators in various parts of the United States have designed schools and curricula around these same mentorship ideals, such as Urban Preparatory High School in Chicago (King, 2011) or Gesu School in Philadelphia (Thorne, 2015). At the core of their mission is a recognition of the need to diminish the “cultural gap” that exists between those who educate children, and the children and their families themselves. Part of bridging this cultural gap involves acknowledgment and understanding of past and present traumatic experience endured by African American people across generations. It is not only educators who need support in developing heightened awareness of these historical and current phenomena; children and their families sometimes need assistance in understanding the historical context for the current divide that often disadvantages African American children.
As models are continuously developed to address historical and cultural trauma, there is growing awareness of the need for culturally sensitive programs that target African American children and youth affected by cultural trauma and are rooted in evidence-based practice. With this in mind, we propose an approach to diminishing the effects of historical and cultural trauma in African American children and adolescents that utilizes the principles of trauma-focused cognitive behavioral therapy (TF-CBT) and key aspects of African American racial identity development and Afrocentric values and strengths.
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT)
Cohen, Mannarino, and Deblinger (2006) developed Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) as a relatively short-term, integrated approach aimed at the reduction of negative affective responses, distorted cognitions, and maladaptive behaviors that can arise from trauma exposure. TF-CBT utilizes gradual exposure to reminders of the traumatic experience and supports participants in constructing trauma narratives that focus on strengths and empowerment. Clinicians utilizing TF-CBT work to engage parents so that their support of their children is maximized. TF-CBT has proven successful with children and adolescents between the ages of 3 and 18.
The core components of TF-CBT include Psychoeducation and Parenting Skills, Relaxation, Affect Regulation, Cognitive Restructuring, Trauma Narrative, In Vivo Exposure, Conjoint Parent–Child Sessions, and Enhancing Safety Planning. The acronym P-R-A-C-T-I-C-E provides a shorthand reminder of these core components (Cohen et al., 2006). The Psychoeducation and Parenting Skills component focuses upon discussion and education about child abuse in general and the typical emotional and behavioral reactions to physical, emotional, and sexual abuse. This component helps both clients and parents understand that their reactions to trauma experience are typical and that there are evidence-based, effective responses to these behaviors.
Clinicians teach relaxation techniques as a precursor to exposure interventions. Techniques, such as focused breathing, progressive muscle relaxation, and visual imagery, help child and adolescent clients cope with overwhelming, negative emotions that can accompany trauma exposure so that they do not abandon the exposure therapy part of healing because it is distressing. The Cognitive Restructuring component involves clinicians helping their clients and parents better understand how thoughts, feelings, and behaviors are interrelated and how to identify and restructure distorted ways of thinking (Cohen et al., 2006).
The construction of a trauma narrative involves gradual exposure exercises, inviting clients to communicate about the traumatic experience and eventually create a verbal, written, symbolic, or artistic account of the traumatic experience. This provides an opportunity for the clinician to further identify any distorted cognitions related to self-blaming or guilt held by clients and to help with restructuring them into more realistic and empowering ways of thinking (Cohen et al., 2006).
Through in vivo exposure, clinicians introduce gradual reminders of the trauma in environments that are in the everyday experience of the clients or that are significant to the traumatic experience. The relaxation techniques learned earlier in therapy are then utilized to facilitate reduction of distress when clients are reintroduced to settings that trigger traumatic memories. Clinicians facilitate enhanced communication through conjoint parent–child sessions, particularly assisting parents in offering needed support in the home when traumatic memories are triggered. Lastly, clinicians focus upon offering education and skills building related to maintaining personal safety, boundaries, and healthy interpersonal relationships so that clients feel empowered to advocate for themselves more effectively when future stressors arise in life (Cohen et al., 2006).
Although a great deal of research has been conducted studying the use of TF-CBT with child and adolescent survivors of sexual abuse (Cohen, Deblinger, Mannarino, & Steer, 2004), TF-CBT also has been shown to be effective with clients who have been exposed to community violence (Voisin & Berringer, 2015), traumatic grief and loss (Cohen & Mannarino, 2004), and even natural disasters (Jaycox et al., 2010). TF-CBT has been designated as evidence-based because of the number of random control treatment studies supporting its effectiveness. de Arellano et al. (2014) documented 10 random control treatment studies that support the effectiveness of TF-CBT in various trauma exposure contexts, seven of which compared TF-CBT participants with active control groups and three compared TF-CBT participants with wait-list control groups. Five of these studies assessed the effectiveness of TF-CBT with child survivors of sexual abuse (de Arellano et al., 2014). O’Callaghan, McMullen, Shannon, Rafferty, and Black (2013) conducted a study of Congolese girls affected by war and sexual exploitation, using a single-blind, parallel design, randomized control study, and found significant reduction in symptoms in participants treated with TF-CBT. The intervention was administered to participants in a group format in this study of Congolese war survivors.
Jensen et al. (2014) conducted a randomized control study using TF-CBT in which 156 youth in a community mental health clinic, ranging in age from 10 to 18, presented with a variety of trauma histories; the results showed significantly fewer PTSD symptoms, less depression, and greater improvements in functional impairment for those treated with TF-CBT. A field trial of children in New Orleans exposed to the trauma of Hurricane Katrina who received TF-CBT treatment both in schools and in mental health clinics showed significant reduction of PTSD symptoms (Jaycox et al., 2010). Cohen, Mannarino, and Iyengar (2011) documented similar effectiveness of TF-CBT with children exposed to intimate partner violence.
Researchers are continuously expanding the trauma contexts for which TF-CBT is utilized and studied, indicating its robustness and solidifying its evidence-based quality (Cohen et al., 2011). Given the highly adaptable nature of TF-CBT in treating children and adolescents affected by traumatic experiences, we propose an approach to addressing cultural trauma in African American children and adolescents that uses TF-CBT as its basis.
TF-CBT as a Frame for Cultural and Historical Trauma Treatment
Using the major components of TF-CBT denoted in the P-R-A-C-T-I-C-E acronym, we have drafted the following intervention to address cultural trauma in African American children and youth. This intervention is tailored to early adolescents, namely middle school students (ages 12–14), and should be adjusted when used with younger or older participants. The program is a group intervention that can be utilized in an after-school setting at a school, a church, or community center. Ideally, the program spans 16 weeks, which would roughly correspond to a school semester if conducted in the school setting. Warfield (2013) advocated for the modification of TF-CBT by practitioners to fit the cultural context of clients while maintaining the integrity of the model. To foster sensitivity to the more collectivist outlook seen in African American communities, the proposed program is community-based, involving a group approach to treatment, as opposed to a more individualistic, Eurocentric approach to treatment, which might only involve the child and clinician, with sporadic parental involvement.
Psychoeducation and Parenting Skills. From the beginning, the program is family focused. Thorne (2015) maintained that parental engagement is a critical component in the building of community networks that will support the academic and social success of African American children. Given that participants will have different experiences of family and differing family structures, participants are invited to identify a support team of at least three significant persons who will constitute “family” for the purposes of the program—a strategy utilized by Boys’ Latin Charter School in Philadelphia (Thorne, 2015). This team of three is expected to attend some family sessions and will be supported in initiating regular conversations outside the program setting about the program goals.
The introductory session of the program draws participants and their team of three together for an informational presentation on cultural and historical trauma, discussing the history of the enslavement of people of African descent in the United States, the subsequent era of segregation, the ongoing Civil Rights movement, and how these historical experiences have affected the African American family today. Ongoing psychoeducation about historical trauma may take the form of group visits to museums that highlight African American history, such as the Smithsonian Museum of African American History, the Museum of Civil and Human Rights in Atlanta, or any local museum of African American history, followed by group processing of the experience.
Relaxation. Soto, Dawson-Andoh, and BeLue (2011) cited a connection between the experience of racialized stress and discrimination in African Americans with physiological reactions to stress, such as anxiety. Cultural trauma involves a pervasive, ongoing perception of racialized stress and discrimination that can be associated with restlessness, sleep disorders, muscle tension, and other symptoms. TF-CBT stresses the importance of self-soothing and coping mechanisms that stimulate relaxation in tense situations. Muscle relaxation, deep breathing exercises, and guided imagery are promoted by TF-CBT–oriented clinicians. The proposed program places similar emphasis on the teaching of these relaxation strategies.
Spirituality, prayer, and meditation are other mechanisms that are commonly used by African Americans to manage stress and cope with and challenge discrimination (Hayward & Krause, 2015). Spirituality is a very personal expression, meaning participants will likely demonstrate a large amount of variety in their attitudes toward spirituality. Without promoting any specific spiritual tradition, participants will be invited to explore their spiritual beliefs and practices and connect them to how they cope with racism and discrimination.
Affect Regulation. The TF-CBT model also highlights the significance of the development of emotional intelligence (Cohen et al., 2006), including the proper identification of emotions and the conscious choosing of appropriate and healthy emotions. In the case of cultural trauma, as participants learn more about the history of racial power dynamics in the United States, negative emotions may increasingly arise. As a strengths-based program, emotions, such as anger, frustration, and outrage, are honored and recognized but are seen as transitions to constructive approaches to eliminating unequal power dynamics.
According to Chaplin (2015), gender differences exist in how humans express emotions, best explained through a combination of biological, psychosocial developmental, and social constructionist factors. For example, adolescent girls are thought to experience symptoms of depression significantly more often than adolescent boys (Hankin & Abramson, 2001). Along racial lines, there are differences according to gender in how African Americans typically respond to the systemic oppression and discrimination associated with cultural trauma (Vontress et al., 2007). African American boys may suppress anger and dissatisfaction with school incidents, particularly those involving microaggressive behaviors targeting them or more blatant forms of discrimination (Thomas & Stevenson, 2009). Likewise, suppressed anger may be redirected into other expressions, such as hypermasculinity, which may be interpreted by instructors and school administrators as unfounded defiance.
Role play is effective in helping participants reflect upon how they express emotions and how emotional expression influences the identities that they are striving to form (Brown, 2003). Schonert-Reichl and Lawlor (2010) documented the effectiveness of a mindfulness education program in helping fourth to seventh graders develop emotional competence and in fostering positive emotions. Both mindfulness exercises and role play can be used to help participants broaden their emotional vocabulary, experiment with various methods of controlling emotional expression, and practice new ways of communicating emotions honestly and productively. Anderson and Stevenson (2019) highlighted reactions that parents of children and adolescents of color may have when they find out their sons or daughters have been exposed to discriminatory racial encounters, one of which is described as “preparation for bias.” This includes pointed conversations about how to handle potentially dangerous encounters such as racial profiling, with opportunities to allow young people to rehearse how they will respond to situations that may generate panic in the moment. Role play in this proposed program affords the opportunity for candid preparation of participants for life incidents that may be fueled by racial discrimination.
Cognitive Restructuring. Black identity development models, such as the Cross model, underscore that the beginning of racial identity development in people of color is often characterized by positive beliefs about the dominant group and negative beliefs about their own cultural group (Cross, Parham, & Helms, 1991). In the case of African American middle school students, such negative self-beliefs may present in such subtle manners that program participants are not aware and may even deny.
One approach to engaging participants in cognitive restructuring of distorted cognitions about race, self-image, and privilege and power dynamics involves teaching young people about microaggressions directed toward African Americans. Role play is beneficial in creating a space for participants to reflect upon microaggressive behaviors and to correct the stereotypes upon which they are based. Córdova and Cervantes (2010) documented the experience of within-group discrimination among Latino youth based on English proficiency, documentation status, and generational status. In both African American and Latino American communities, within-group skin tone stratification, often referred to as colorism, perpetuates internalized racism, creating a preference for skin tones seen as lighter and more European (Hunter, 2016; Maxwell, Brevard, Abrams, & Belgrave, 2015). Reflection upon within-group microaggressions and internalized racism is utilized to foster participants filtering out negative self-images that they have incorporated based on the manner in which oppressive systems have depicted African Americans as well as individuals from other racial/ethnic groups.
Trauma Narrative. As an important component of the TF-CBT model, trauma narration creates the space for deconstruction and reconstruction of the young person’s understanding of the traumatic experience (Cohen et al., 2006). The clinician monitors for cognitive distortions that might suggest the young person is still blaming self or viewing self through a lens of weakness. Trauma narration is designed to help individuals further claim their own strengths and resources.
In the context of cultural trauma of African Americans, African American children and adolescents often have mistaken views and understandings of the history of African peoples and the history of African Americans (O’Donovan, 2009). They may not be aware of how their own personal families’ histories intersect with key moments and movements in African American history, which suggests a lack of knowledge about family strengths, empowerment, and triumphs over oppressive systems.
A critical part of addressing cultural trauma is the deconstruction and reconstruction of family history. Given the dynamics of slavery, African Americans are often not able to trace their ancestry in the same way that European Americans are able to. Students engaged in cultural trauma programs will benefit from doing oral history interviews with elders in their families and communities to better understand the evolution of their families, the perspectives of the elders on family resilience and strength, and the hopes and dreams that elders have for the current generation of youth. Although there can be obstacles to tracing ancestry beyond the previous century, students can be challenged to explore possible family history scenarios based on the social contexts of African Americans living in the same geographic regions as their known ancestors.
Although the validity of DNA ancestry kits, such as Ancestry.com or 23andme, has been questioned regarding their ability to provide accurate profiles of the ethnic origins of their consumers (Duster, 2014), these tools may still point users in the direction of developing a better understanding of their family histories. In an effort to help students bridge their family histories beyond the Americas, ancestry kits may be used to give students information about African ancestry so that they may research particular countries and tie their history into how they understand their own familial contexts.
This portion of the program is necessarily collaborative in that students will have to reach out to family members for information. It is advised that students complete this with direct involvement with their support team of three significant persons. Upon completion of the project, ideally students will present their information in a spirit of pride to the whole program group with the help of their support team.
n Vivo Exposure. The TF-CBT model encourages the use of in vivo exposure of participants as reminders of the traumatic experience in order to desensitize them to anxiety-provoking reactions (Cohen et al., 2006). In vivo exposure helps to minimize avoidance of stimuli that can trigger memories of the traumatic experience. In lieu of avoidance, participants are supported in using the coping mechanisms they have learned to manage their anxiety.
One aspect of cultural trauma that can greatly influence academic performance and social relationships is low self-efficacy. Low self-efficacy can lead to avoidance of academic challenges as well as unfamiliar social interactions (Uwah, McMahon, & Furlow, 2008). Mathews, Dempsey, and Overstreet (2009), in a study of African American children ages 10–13, found an inverse relationship between exposure to community violence and the academic performance and attendance of students. According to these researchers, the experience of community violence trauma is often associated with a lack of engagement in school activity and an overall sense of powerlessness. Interventions that foster an increase in self-efficacy can enhance students’ willingness to engage in new experiences—academic, occupational, or interpersonal. In reference to cultural trauma of African American children and adolescents, deliberate exposure to opportunities to execute projects and work that can both benefit others as well as enable students to demonstrate leadership and learn new skills can build self-efficacy and result in other positive benefits.
Scales, Blyth, Berkas, and Kielsmeier (2000) concluded from a study of racially and socioeconomically diverse middle school students that service learning (experiential educational moments that revolve around action and reflection) is positively correlated with concern for others’ social welfare, frequency of talking with parents about school, and increased belief in the efficacy of helping behaviors. Stott and Jackson (2005) highlighted growth in self-awareness and self-efficacy as additional benefits for middle school students. Song, Furco, Lopez, and Maruyama (2017) concluded from research with college students from underrepresented groups, not limited to racially diverse groups, that service learning can have a positive impact on their educational outcomes. Thus, service learning opportunities are proposed to expose participants to challenges that may be apparent in their communities and to foster a sense of power in terms of being a part of positive change and community growth.
Service learning opportunities that involve collaboration between students and parents may take the form of neighborhood clean-up days in underprivileged communities, collecting or preparing food to be distributed to homeless populations, or visits to nursing homes to share personal items that have been collected for residents. Reflection time after the project offers students the space to discuss apprehensions they had, the internal processes they used to overcome those apprehensions, and the new self-images they own since the experience.
Conjoint Sessions. The responses children and adolescents receive from their parents and guardians are powerful influences in how young people attribute meaning to trauma, including cultural trauma. Frankish and Bradbury (2012) conducted a qualitative study with Black South African families about how the decision of older family members to refrain from discussing the horrors of apartheid violence with their children and grandchildren born after the end of apartheid in 1994 has often resulted in the development of inaccurate narratives about the past. The proposed program capitalizes upon the power of parental figures, family, and other significant influences to help shape a balanced picture of the past and present and a healthy image of self. The conjoint sessions are woven through the TF-CBT model, with particular emphasis on conjoint sessions after the participant has completed the trauma narrative (Cohen et al., 2006). In this proposed program outlined to address cultural trauma, conjoint sessions are also woven throughout the process. The “family” is invited to actively participate in the Psychoeducation and Parenting Skills stage, in the Trauma Narrative stage, and in the In Vivo Exposure stage. Ideally this high level of parental involvement will stimulate conversation about the themes of the program when students are at home or in other family settings. In summary, “the family” has a critical role to play in ensuring that the narrative from which participants learn to operate is an accurate one.
Enhancing Safety. In the TF-CBT model, the Enhancing Safety component is designed to help participants develop safety plans so that they feel more empowered to advocate for and protect themselves if they find themselves in positions of danger or vulnerability. This could include helping participants generate a list of trustworthy persons to whom they can reach out if uncomfortable situations arise or helping participants assemble emergency contact numbers. Rather than encouraging hypervigilance, the Enhancing Safety component sends the message to participants that they have the power and skills to protect their well-being (Cohen et al., 2006).
Anderson and Stevenson (2019) highlighted the efforts that parents of color may engage in after discovering that their children have experienced a discriminatory racial encounter, such as unfair treatment in school because of race, or after a highly publicized racially motivated assault, such as the fatal shooting of Trayvon Martin. Parents may use affirmational messages to assuage thoughts in their children that victims of discrimination are to blame. In this sense, teaching safety and protective factors is both about the protection of young people from physical attack or violation and about their protection from assault on their identity. In the context of cultural trauma, safety from the effects of cultural traumatization can be promoted through relationships with positive role models who will continue to support growth in self-esteem among student participants. Role models also can serve as accountability partners beyond the parental or family system so that students have other positive and supportive voices as they individuate from their caretakers. Enhancing safety involves teaching participants through case examples and role playing how to recognize systemic oppression and discrimination and how to solicit the support of family, church, and community to confront discrimination and oppression through appropriate administrative, community, and political channels. Helping students identify a cause about which they feel passionate and teaching them about self-advocacy through a letter-writing campaign is a practical strategy that can be used to facilitate this skill.
Conclusion
In conclusion, the potential utilization of TF-CBT as an intervention to address cultural trauma in African American youth requires a large amount of creativity and adaptation to the needs and resources of each participant group. We identify the following recommended priorities for those seeking to use the TF-CBT framework in this context.
First, the format of this program to address cultural trauma in African American middle school students ideally should take place in environments that are not reminiscent of traditional classroom spaces. We propose a program that is informative and inspiring, but not framed as an extension of usual school time. Although logistics might dictate the use of school spaces, it is suggested that efforts be made to decorate program spaces with youth-friendly and culturally relevant art and symbols, perhaps selected or created by participants when possible. If students experience traditional classrooms as a place of disempowerment, efforts are encouraged to promote a sense of ownership and positive investment in the program space by participants.
Second, program leaders—who might be school administrators, teachers, school or professional counselors, social workers, clergy, or community activists—are charged with building relationships with participants and their families to help them engage in their own within-family dialogues about the existence of cultural trauma, and also about the resources within families and communities to challenge and upset the existing power dynamic that has held African American people in a position of social disadvantage for centuries. Initial recruitment for the program as well as ongoing engagement will require program leaders to do regular check-ins to make sure participants, especially parents and guardians, understand the vision of the program and see that they are integral parts of its success. It is recommended that persons in the community who are seen as charismatic and engaging be invited to use these strengths to elicit and maintain participation.
Third, it is important that young people participating in the program feel respected and heard. In the face of conversations and discussions about very difficult and painful subject matter, such as past or present family traumas or racial violence, differing viewpoints may emerge along the lines of age and generational perspectives. Without sacrificing the effect of the wisdom and experience adults bring to the conversation, an environment that is open to the perspectives of youth participants is crucial. Program leaders should have some experience and training in active listening and facilitating difficult dialogue.
Lastly, this adaptation of TF-CBT to address cultural trauma is a time-limited program. Realistically, youth participants will need reminders and reinforcement of the lessons they learn about their family history, their cultural identities, and themselves. As they continue to develop psychosocially, new stages of growth will bring about new challenges that may cause participants to further question the manner in which the program prompted them to make sense of the world in which they live. In role model and mentorship relationships that participants are encouraged to develop, it is recommended that ongoing and long-term efforts be made to help participants continuously reflect upon and reintegrate their sense of empowerment so that it fits their reality as they progress into high school, college, and beyond. The manner in which a middle school student understands cultural trauma might be very different from the manner in which a college student conceptualizes cultural trauma.
Without denying or minimizing what has taken place and continues to persist (i.e., the historical oppression and current discrimination of African Americans on the basis of racial background), this approach to addressing cultural trauma emphasizes the adoption of an empowered sense of self and a heightened sense of collective agency that allows for creative self-transformation even in a society that continues to exhibit systemic injustice.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Washington, DC: Author.
Anderson, R. E., & Stevenson, H. C. (2019). RECASTing racial stress and trauma: Theorizing the healing
potential of racial socialization in families. American Psychologist, 74, 63–75. doi:10.1037/amp0000392
Barnes, M. L. (2016). The more things change: New moves for legitimizing racial discrimination in a post-race
world. Minnesota Law Review, 100, 2043–2102.
Benner, A. D., & Wang, Y. (2014). Demographic marginalization, social integration, and adolescents’
educational success. Journal of Youth and Adolescence, 43, 1611–1627. doi:10.1007/s10964-014-0151-6
BigFoot, D. S., & Schmidt, S. R. (2010). Honoring children, mending the circle: Cultural adaptation of trauma-
focused cognitive-behavioral therapy for American Indian and Alaska Native children. Journal of
Clinical Psychology, 66, 847–856. doi:10.1002/jclp.20707
BraveHeart, M. Y. H., & DeBruyn, L. M. (1998). The American Indian holocaust: Healing historical unresolved
grief. American Indian and Alaska Native Mental Health Research, 8(2), 60–82. doi:10.5820/aian.0802.1998.60
Brown, R. B. (2003). Emotions and behavior: Exercises in emotional intelligence. Journal of Management
Education, 27, 122–134. doi:10.1177/1052562902239251
Burstow, B. (2005). A critique of posttraumatic stress disorder and the DSM. Journal of Humanistic Psychology,
45, 429–445. doi:10.1177/0022167805280265
Chaplin, T. M. (2015). Gender and emotion expression: A developmental contextual perspective. Emotion
Review, 7, 14–21. doi:10.1177/1754073914544408
Cholewa, B., & West-Olatunji, C. (2008). Exploring the relationship among cultural discontinuity, psychological
distress, and academic outcomes with low-income, culturally diverse students. Professional School
Counseling, 12, 54–61. doi:10.1177/2156759X0801200106
Clark, K. B., & Clark, M. K. (1939). The development of consciousness of self and the emergence of racial
identification in Negro preschool children. The Journal of Social Psychology, 10, 591–599.
doi:10.1080/00224545.1939.9713394
Cohen, J. A., Deblinger, E., Mannarino, A. P., & Steer, R. A. (2004). A multisite, randomized controlled trial
for children with sexual abuse-related PTSD symptoms. Journal of the American Academy of Child &
Adolescent Psychiatry, 43, 393–402. doi:10.1097/00004583-200404000-00005
Cohen, J. A., & Mannarino, A. P. (2004). Treatment of childhood traumatic grief. Journal of Clinical Child and
Adolescent Psychology, 33, 819–831. doi:10.1207/s15374424jccp3304_17
Cohen, J. A., Mannarino, A. P., & Deblinger, E. (2006). Treating trauma and traumatic grief in children and
adolescents. New York, NY: Guilford.
Cohen, J. A., Mannarino, A. P., & Iyengar, S. (2011). Community treatment of posttraumatic stress disorder
for children exposed to intimate partner violence: A randomized controlled trial. Archives of Pediatrics
and Adolescent Medicine, 165, 16–21. doi:10.1001/archpediatrics.2010.247
Conger, R. D., Wallace, L. E., Sun, Y., Simons, R. L., McLoyd, V. C., & Brody, G. H. (2002). Economic pressure in
African American families: A replication and extension of the family stress model. Developmental
Psychology, 38, 179–193. doi:10.1037/0012-1649.38.2.179
Córdova, D., Jr., & Cervantes, R. C. (2010). Intergroup and within-group perceived discrimination among U.S.-
born and foreign-born Latino youth. Hispanic Journal of Behavioral Sciences, 32, 259–274.
doi:10.1177/0739986310362371
Croll, P. R. (2018). Economic inequality and race: No, it can’t be that bad . . . In K. Haltinner & L. Hormel (Eds.),
Teaching economic inequality and capitalism in contemporary America (pp. 213–220). New York, NY: Springer.
Cross, W. E., Jr., Parham, T. A., & Helms, J. E. (1991). The stages of Black identity development: Nigrescence
models. In R. L. Jones (Ed.), Black psychology (3rd ed., pp. 319–338). Berkeley, CA: Cobb & Henry
Publishers.
Danieli, Y. (1985). The treatment and prevention of long-term effects and intergenerational transmission of
victimization: A lesson from Holocaust survivors and their children. In C. R. Figley (Ed.), Trauma and its
wake (pp. 295–313). New York, NY: Brunner/Mazel.
de Arellano, M. A., Lyman, D. R., Jobe-Shields, L., George, P., Dougherty, R. H., Daniels, A. S., . . . Delphin-
Rittmon, M. E. (2014). Trauma-focused cognitive behavioral therapy for children and adolescents:
Assessing the evidence. Psychiatric Services, 65, 591–602. doi:10.1176/appi.ps.201300255
DeGruy, J. (2005). Post traumatic slave syndrome: America’s legacy of enduring injury and healing. Milwaukie, OR:
Uptone Press.
Duster, T. (2014). Ancestry testing and DNA: Uses, limits—and caveat emptor. In B. Prainsack, S. Schicktanz,
& G. Werner-Felmayer (Eds.), Genetics as social practice: Transdisciplinary views on science and culture (pp.
59–72). London, UK: Routledge.
Eyerman, R. (2004). The past in the present: Culture and the transmission of memory. Acta Sociologica, 47,
159–169. doi:10.1177/0001699304043853
Frankish, T., & Bradbury, J. (2012). Telling stories for the next generation: Trauma and nostalgia. Peace and
Conflict: Journal of Peace Psychology, 18, 294–306. doi:10.1037/a0029070
Frazier, K., West-Olatunji, C., St. Juste, S., & Goodman, R. D. (2009). Transgenerational trauma and child sexual
abuse: Reconceptualizing cases involving young survivors of CSA. Journal of Mental Health Counseling,
31, 22–33. doi:10.17744/mehc.31.1.u72580m253524811
Giacaman, R., Abu-Rmeileh, N. M., Husseini, A., Saab, H., & Boyce, W. (2007). Humiliation: The invisible
trauma of war for Palestinian youth. Public Health, 121, 563–571. doi:10.1016/j.puhe.2006.10.021
Goodman, R. D., & West-Olatunji, C. A. (2008). Transgenerational trauma and resilience: Improving mental
health counseling for survivors of Hurricane Katrina. Journal of Mental Health Counseling, 30(2), 121–136.
doi:10.17744/mehc.30.2.q52260n242204r84
Hagelskamp, C., & Hughes, D. L. (2014). Workplace discrimination predicting racial/ethnic socialization across
African American, Latino, and Chinese families. Cultural Diversity and Ethnic Minority Psychology, 20,
550–560. doi:10.1037/a0035321
Hankin, B. L., & Abramson, L. Y. (2001). Development of gender differences in depression: An elaborated
cognitive vulnerability–transactional stress theory. Psychological Bulletin, 127, 773–796.
doi:10.1037/0033-2909.127.6.773
Hayward, R. D., & Krause, N. (2015). Religion and strategies for coping with racial discrimination among
African Americans and Caribbean Blacks. International Journal of Stress Management, 22, 70–91.
doi:10.1037/a0038637
Hunter, M. (2016). Colorism in the classroom: How skin tone stratifies African American and Latina/o students. Theory Into Practice, 55, 54–61. doi:10.1080/00405841.2016.1119019
Jarjoura, G. R. (2013). Effective strategies for mentoring African American boys. Washington, DC: American Institutes for Research. Retrieved from https://www.air.org/sites/default/files/downloads/report/Effective%20Strategies%20for%20Mentoring%20African%20American%20Boys.pdf
Jaycox, L. (2004). Cognitive behavioral intervention for trauma in schools (CBITS). Longmont, CO: SoprisWest.
Jaycox, L. H., Cohen, J. A., Mannarino, A. P., Walker, D. W., Langley, A. K., Gegenheimer, K. L., . . . Schonlau, M. (2010). Children’s mental health care following Hurricane Katrina: A field trial of trauma-focused psychotherapies. Journal of Traumatic Stress, 23, 223–231. doi:10.1002/jts.20518
Jensen, T. K., Holt, T., Ormhaug, S. M., Egeland, K., Granly, L., Hoaas, L. C., . . . Wentzel-Larsen, T. (2014). A randomized effectiveness study comparing trauma-focused cognitive behavioral therapy with therapy as usual for youth. Journal of Clinical Child & Adolescent Psychology, 43, 356–369. doi:10.1080/15374416.2013.822307
Jordan, P., & Hernandez-Reif, M. (2009). Reexamination of young children’s racial attitudes and skin tone preferences. Journal of Black Psychology, 35, 388–403. doi:10.1177/0095798409333621
King, T. (2011). Commentary: Swords, shields, and the fight for our children: Lessons from Urban Prep. The Journal of Negro Education, 80(3), 191–192.
Mathews, T., Dempsey, M., & Overstreet, S. (2009). Effects of exposure to community violence on school functioning: The mediating role of posttraumatic stress symptoms. Behaviour Research and Therapy, 47, 586–591. doi:10.1016/j.brat.2009.04.001
Maxwell, M., Brevard, J., Abrams, J., & Belgrave, F. (2015). What’s color got to do with it? Skin color, skin color satisfaction, racial identity, and internalized racism among African American college students. Journal of Black Psychology, 41, 438–461. doi:10.1177/0095798414542299
Monroe, C. R. (2006). African American boys and the discipline gap: Balancing educators’ uneven hand. Educational Horizons, 84(2), 102–111.
Morris, E. W., & Perry, B. L. (2016). The punishment gap: School suspension and racial disparities in achievement. Social Problems, 63, 68–86. doi:10.1093/socpro/spv026
Morsette, A., Swaney, G., Stolle, D., Schuldberg, D., van den Pol, R., & Young, M. (2009). Cognitive behavioral intervention for trauma in schools (CBITS): School-based treatment on a rural American Indian reservation. Journal of Behavioral Therapy and Experimental Psychiatry, 40, 169–178. doi:10.1016/j.jbtep.2008.07.006
Nagata, D. K., & Cheng, W. J. Y. (2003). Intergenerational communication of race-related trauma by Japanese American former internees. American Journal of Orthopsychiatry, 73, 266–278.
doi:10.1037/0002-9432.73.3.266
Noguera, P. A. (2003). The trouble with Black boys: The role and influence of environmental and cultural factors on the academic performance of African American males. Urban Education, 38, 431–459.
doi:10.1177/0042085903038004005
Obama, B. (2014). My brother’s keeper. Reclaiming Children and Youth, 23, 5–8.
O’Callaghan, P., McMullen, J., Shannon, C., Rafferty, H., & Black, A. (2013). A randomized controlled
trial of trauma-focused cognitive behavioral therapy for sexually exploited, war-affected Congolese girls. Journal of the American Academy of Child & Adolescent Psychiatry, 52, 359–369. doi:10.1016/j.jaac.2013.01.013
O’Donovan, S. E. (2009). Teaching slavery in today’s classroom. OAH Magazine of History, 23(2), 7–10. doi:10.1093/maghis/23.2.7
Okeke-Adeyanju, N., Taylor, L. C., Craig, A. B., Smith, R. E., Thomas, A., Boyle, A. E., & DeRosier, M. E. (2014). Celebrating the strengths of Black youth: Increasing self-esteem and implications for prevention. The Journal of Primary Prevention, 35, 357–369. doi:10.1007/s10935-014-0356-1
Pearlman, L. A., & Saakvitne, K. W. (1995). Trauma and the therapist: Countertransference and vicarious traumatization in psychotherapy with incest survivors. New York, NY: W. W. Norton.
Phipps, R. M., & Degges-White, S. (2014). A new look at transgenerational trauma transmission: Second-generation Latino immigrant youth. Journal of Multicultural Counseling and Development, 42, 174–187.
doi:10.1002/j.2161-1912.2014.00053.x
Pouissant, A., & Atkinson, C. (1972). Black youth and motivation. In J. A. Banks & J. D. Grambs (Eds.), Black self-concept (pp. 55–70). New York, NY: McGraw-Hill Books.
Rasmussen, A., Rosenfeld, B., Reeves, K., & Keller, A. S. (2007). The subjective experience of trauma and subsequent PTSD in a sample of undocumented immigrants. The Journal of Nervous and Mental Disease, 195, 137–143. doi:10.1097/01.nmd.0000254748.38784.2f
Reid, O. G., Mims, S., & Higginbottom, L. (2004). Post traumatic slavery disorder: Definition, diagnosis and treatment. Philadelphia, PA: Xlibris Corporation.
Roscigno, V. J., Karafin, D. L., & Tester, G. (2009). The complexities and processes of racial housing discrimination. Social Problems, 56, 49–69. doi:10.1525/sp.2009.56.1.49
Scales, P. C., Blyth, D. A., Berkas, T. H., & Kielsmeier, J. C. (2000). The effects of service-learning on middle school students’ social responsibility and academic success. The Journal of Early Adolescence, 20, 332–358. doi:10.1177/0272431600020003004
Schaal, S., & Elbert, T. (2006). Ten years after the genocide: Trauma confrontation and posttraumatic stress in Rwandan adolescents. Journal of Traumatic Stress, 19, 95–105. doi:10.1002/jts.20104
Schonert-Reichl, K. A., & Lawlor, M. S. (2010). The effects of a mindfulness-based education program on pre- and early adolescents’ well-being and social and emotional competence. Mindfulness, 1, 137–151.
doi:10.1007/s12671-010-0011-8
Smith, W. A. (2004). Black faculty coping with racial battle fatigue: The campus racial climate in a post-civil rights era. In D. Cleveland (Ed.), A long way to go: Conversations about race by African American faculty and graduate students (pp. 171–190). New York, NY: Peter Lang.
Song, W., Furco, A., Lopez, I., & Maruyama, G. (2017). Examining the relationship between service-learning participation and the educational success of underrepresented students. Michigan Journal of Community Service Learning, 24, 23–37. doi:10.3998/mjcsloa.3239521.0024.103
Sotero, M. (2006). A conceptual model of historical trauma: Implications for public health practice and research. Journal of Health Disparities Research and Practice, 1, 93–108.
Soto, J. A., Dawson-Andoh, N. A., & BeLue, R. (2011). The relationship between perceived discrimination and generalized anxiety disorder among African Americans, Afro Caribbeans, and non-Hispanic Whites. Journal of Anxiety Disorders, 25, 258–265. doi:10.1016/j.janxdis.2010.09.011
Stamm, B. H., Stamm, H. E., Hudnall, A. C., & Higson-Smith, C. (2004). Considering a theory of cultural trauma and loss. Journal of Loss and Trauma, 9, 89–111. doi:10.1080/15325020490255412
Stott, K. A., & Jackson, A. P. (2005). Using service learning to achieve middle school comprehensive guidance program goals. Professional School Counseling, 9, 156–159. doi:10.1177/2156759X0500900216
Sztompka, P. (2000). Cultural trauma: The other face of social change. European Journal of Social Theory, 3, 449–466. doi:10.1177/136843100003004004
Tatum, B. (2002). The colonial model as a theoretical explanation of crime and delinquency. In S. L. Gabbidon, H. Taylor Greene, & V. D. Young (Eds.), African American classics in criminology and criminal justice (pp. 307–322). Thousand Oaks, CA: Sage.
Thomas, D. E., & Stevenson, H. (2009). Gender risks and education: The particular classroom challenges for urban low-income African American boys. Review of Research in Education, 33, 160–180. doi:10.3102/0091732X08327164
Thompson, T., Jr., & Massat, C. R. (2005). Experiences of violence, post-traumatic stress, academic achievement and behavior problems of urban African-American children. Child & Adolescent Social Work Journal, 22, 367–393. doi:10.1007/s10560-005-0018-5
Thorne, S. D. (2015). “Walk like you have somewhere to go”: A literature review of the academic, social, and cultural needs of African American adolescent males in urban schools. Catalyst: Journal of Student Research and Academic Scholarship, 2, 67–83.
Uwah, C. J., McMahon, H. G., & Furlow, C. F. (2008). School belonging, educational aspirations, and academic self-efficacy among African American male high school students: Implications for school counselors. Professional School Counseling, 11, 296–305. doi:10.1177/2156759X0801100503
Voisin, D. R., & Berringer, K. R. (2015). Interventions targeting exposure to community violence sequelae among youth: A commentary. Clinical Social Work Journal, 43, 98–108. doi:10.1007/s10615-014-0506-1
Vontress, C. E., Woodland, C. E., & Epp, L. (2007). Cultural dysthymia: An unrecognized disorder among African Americans? Journal of Multicultural Counseling and Development, 35(3), 130–141.
doi:10.1002/j.2161-1912.2007.tb00055.x
Warfield, J. R. (2013). Supervising culturally informed modified trauma-focused cognitive behavioral therapy. Journal of Cognitive Psychotherapy, 27, 51–60. doi:10.1891/0889-8391.27.1.51
Whitbeck, L. B., Adams, G. W., Hoyt, D. R., & Chen, X. (2004). Conceptualizing and measuring historical trauma among American Indian people. American Journal of Community Psychology, 33(3–4), 119–130. doi:10.1023/B:AJCP.0000027000.77357.31
Wilkins, E. J., Whiting, J. B., Watson, M. F., Russon, J. M., & Moncrief, A. M. (2013). Residual effects of slavery: What clinicians need to know. Contemporary Family Therapy, 35, 14–28.
doi:10.1007/s10591-012-9219-1
Ricardo Phipps, NCC, is Assistant Director of Student Counseling Services at Marymount University. Stephen Thorne is a chaplain and adjunct professor at Neumann University. Correspondence can be addressed to Ricardo Phipps, 2807 N. Glebe Rd., Arlington, VA 22207, rphipps@marymount.edu.
Mar 26, 2019 | Volume 9 - Issue 1
Jennifer L. Rogers, Jamie E. Crockett, Esther Suess
About one in four women will experience miscarriage of pregnancy, which can be the impetus for significant and persistent psychological distress. Because of cultural norms of silence and minimization around pregnancy loss, as well as a notable lack of scholarship on the topic, counselors may neglect this area in their clinical work. This article describes the relevance of Bronfenbrenner’s ecological systems theory for counselors seeking to account for the numerous variables that may be at play when working with clients who have lost a pregnancy. Using a detailed case example to demonstrate ecologically informed case conceptualization, the authors draw upon practically applicable clinical literature to highlight the possible developmental, relational, cultural, political, and economic impacts of miscarriage.
Keywords: miscarriage, pregnancy loss, Bronfenbrenner, ecological systems, case conceptualization
Miscarriage is defined as the premature loss of pregnancy occurring so early that the embryo or fetus is not viable outside the womb, up to about 23 weeks’ gestation (Mutiso, Murage, & Mukaindo, 2018). Miscarriage is the most common early pregnancy complication, occurring in approximately 15%–20% of known pregnancies, and is usually caused by chromosomal abnormalities in the embryo or fetus (Bardos, Hercz, Friedenthal, Missmer, & Williams, 2015). The estimated rate of loss for both known and unknown pregnancies is 20%–50% (Markin, 2017). Risk of miscarriage declines as a pregnancy progresses, with most occurring in the first 13 weeks of gestation, and 75% occurring in the first 17 weeks (Mutiso et al., 2018). Many women and couples are unaware of the high incidence of miscarriage until, or even after, they experience one (Bardos et al., 2015). In a recent survey assessing public perception of miscarriage in the United States, most participants were mistaken in their beliefs about both the prevalence and causes of miscarriage (Bardos et al., 2015). This widespread misinformation is related, at least in part, to powerful cultural norms of silence around the premature loss of a pregnancy (Markin & Zilcha-Mano, 2018). Despite societal taboo and minimization obscuring both prevalence and impact, approximately one out of every four women will experience a first trimester miscarriage (Wallace, Goodman, Freedman, Dalton, & Harris, 2010). As such, counselors are likely to work with clients who have encountered this specific type of loss.
Women vary in their responses to miscarriage (Trepal, Semivan, & Caley-Bruce, 2005). Some women feel relief upon learning that an unplanned pregnancy will not continue (Wallace et al., 2010), and others consider miscarriage a minimal obstacle to overcome (Engelhard, 2004). Bardos and colleagues (2015) reported that women who had personally experienced miscarriage and men whose partners had one endorsed feelings of guilt (47%), having done something wrong (41%), isolation (41%), and shame (28%), as well as a belief they could have done something to prevent the loss (38%).
Multiple factors influence a woman’s reactions to miscarriage, including how she experienced and ascribed meaning to the loss, her level of psychological distress prior and subsequent to the event, and variables within her environment (deMontigny, Verdon, Meunier, & Dubeau, 2017; Engelhard, 2004; Engelhard, van den Hout, & Arntz, 2001; Shreffler, Greil, & McQuillan, 2011). Many women experience grief after miscarriage (deMontigny et al., 2017; Randolph, Hruby, & Sharif, 2015; Trepal et al., 2005). Half of women grieving after pregnancy loss report clinically significant psychological distress, most commonly manifested as anxiety or depression (Randolph et al., 2015). Of the 30%–50% of women who experience severe symptoms in the 6 months after a pregnancy loss, most can still be described as grieving, and their symptoms often decrease over time (Engelhard, 2004). Identifying those women who are at high risk for intense psychological distress is important in order to facilitate assessment and treatment (Hutti et al., 2018). Predictors of acute and persistent symptoms of depression and anxiety after an early pregnancy loss include pre-existing mental health diagnoses, childlessness, and dissatisfaction with health care received (deMontigny et al., 2017). Given the prevalence of miscarriage and associated risks to psychological well-being, as well as the cultural norms that may influence both clients’ and counselors’ willingness to acknowledge this type of loss as significant enough to warrant assessment and intervention, mental health professionals are advised to seek out knowledge and strategies to inform their work when they encounter clients who are struggling after the loss of a pregnancy (Markin & Zilcha-Mano, 2018).
The aim of this article is to provide a clinically salient and practical overview of the current literature for practitioners, educators, and researchers, as well as to suggest a conceptual lens that may counter counselors’ own assumptions about miscarriage and through which multiple germane variables influencing the client can be seen. In the following sections, we: (1) highlight the dearth of counseling-specific scholarship focused upon early pregnancy loss, (2) briefly review recent practically applicable clinical literature, and (3) describe the relevance of Bronfenbrenner’s ecological model (1979, 1994) as a conceptual tool for counselors seeking to account for multiple systemic factors that may be at play when working with clients who are experiencing psychological distress after miscarriage. We then (4) apply this ecological conceptualization strategy to a case example, demonstrating how one woman’s miscarriage is an important life span event influenced by numerous variables—developmental, relational, cultural, political, and economic.
Miscarriage: Missing in the Counseling Literature
Cultural silence regarding pregnancy loss is noted by multiple authors (e.g., Engelhard, 2004; Markin & Zilcha-Mano, 2018; Randolph et al., 2015; Trepal et al., 2005), and this reticence extends to the counseling literature as well. Our search for the word “miscarriage” in 25 peer-reviewed journals specific to the counseling profession revealed only six articles published in the last 20 years (from January 1, 1998, to August 7, 2018) in which there was more than an incidental mention of the term. A recent qualitative study examined fathers’ lived experiences of miscarriage (Wagner, Vaughn, & Tuazon, 2018). Randolph and colleagues’ (2015) review focused on counseling women who had experienced pregnancy loss; they identified six themes in the literature (silence, grief, psychological distress, the role of social support, satisfaction with health care, and coping strategies) and noted the paucity of counseling scholarship on this topic. Another article discussed grief associated with pregnancy loss, particularly as related to work with infertile couples who had experienced recurrent miscarriages (Stark, Keathley, & Nelson, 2011). Betz and Thorngren (2006) explored family grief around ambiguous losses, with miscarriage mentioned multiple times as an example of such; they described a family counseling model that includes defining the loss, accessing coping resources, and creating a meaningful narrative of the event. Trepal and colleagues (2005) offered an empathy-infused overview of the topic, including conceptual and developmental perspectives and case-specific examples of diverse reactions to this type of loss. Sperry and Sperry (2004) presented a brief review of the literature as related to medical and psychological aspects of miscarriage and ectopic pregnancy, as well as a case example illustrating a therapeutic approach with a married, heterosexual couple who had experienced early pregnancy loss. It is noteworthy that four of the six miscarriage manuscripts that were selected for publication by counseling journals did not focus specifically on women clients, instead examining families (Betz & Thorngren, 2006), heterosexual couples (Sperry & Sperry, 2004; Stark et al., 2011), and male partners’ experiences as part of such a couple (Wagner et al., 2018). Only three of the six focused on miscarriage specifically (Randolph et al., 2015; Trepal et al., 2005; Wagner et al., 2018). The limited literature on this topic can be viewed as a systemic barrier to the development of clinical competence related to pregnancy loss—an isomorphic reflection of the lack of awareness, customs, conversations, and resources related to the experience of miscarriage in our culture. In the next section, we seek to begin to address this gap in the counseling literature by offering a brief review of empirical and conceptual scholarship relevant to counselors working with clients who are struggling after pregnancy loss.
What Counselors Need to Know: Women’s Reponses to Miscarriage
As previously mentioned, women vary in their responses to miscarriage, which may include relief that an unwanted pregnancy is over, resilience in the face of a setback, or deep sadness at the loss of a child (Engelhard, 2004; Trepal et al., 2005; Wallace et al., 2010). Although grief following early pregnancy loss mirrors other grief responses in intensity and duration, it is unique in its focus on the demise of an anticipated future rather than on memories of the past, leaving the griever to create a narrative of this ambiguous loss (Betz & Thorngren, 2006). Feelings of guilt, isolation, and shame are common (Bardos et al., 2015), exacerbated by cultural taboos regarding the expression of perinatal grief and related responses of minimization and dismissal by others (Markin & Zilcha-Mano, 2018). Such taboos and responses are reflected in multiple ecological systems. Historically, the ability to reproduce has been a measure of women’s worth; this, along with the fact that pregnancy loss can be a physically and psychologically disturbing event, may contribute to the long-standing taboo, silence, and a lack of scripts around miscarriage in many cultures and settings (Burnett, 2009; Engelhard, 2004). In light of this, women and couples may struggle to find both outlets to process their stories and resources for coping with the physical, mental, relational, and spiritual dimensions of their loss (Betz & Thorngren, 2006; Randolph et al., 2015; Trepal et al., 2005), highlighting the need for counselor competence in this domain.
Findings from Shreffler and colleagues (2011) support a “social constructionist approach” (p. 353) to understanding the psychological impact of pregnancy loss. Their research showed that women’s beliefs about motherhood, their fertility, and loss; their current desire for a baby; whether or not their lost pregnancy was planned; whether or not they subsequently gave birth to a child; and time since the loss were significant predictors of distress—in other words, a woman’s experience and understanding of her miscarriage within her unique environment is related to her ability to cope with her loss.
Serious and Persistent Responses to Miscarriage
There are subsets of women for whom miscarriage is the catalyst for serious and persistent mental health symptoms (deMontigny et al., 2017; Engelhard et al., 2001; Hutti et al., 2018; Shreffler et al., 2011). Markin (2017) reported that 15%–30% of women have major psychological difficulties after losing a pregnancy and that 10% of these reactions may be classified as diagnosable, including anxiety disorders, depressive disorders, acute stress disorder, substance use disorders, and post-traumatic stress disorder (PTSD). Women already struggling with mental health concerns before their miscarriage, women without living children, women who were dissatisfied with the health care they received related to their pregnancy loss, and women who were traumatized by their miscarriage can be more vulnerable to persistent symptoms (deMontigny et al., 2017; Engelhard, 2004; Engelhard et al., 2001; Shreffler et al., 2011).
The primary foci of most investigations of the psychological impact of miscarriage are depression and anxiety, and studies often do not include trauma-specific assessments (deMontigny et al., 2017; Hutti et al., 2018; Shreffler et al., 2011). Some women, however, are traumatized by the experience of miscarriage: physical pain, distressing amounts of blood and tissue, emergency medical interventions, doubts about future fertility, insufficient support within their microsystem, and the unexpected and unexplained loss of a future child (Engelhard, 2004). The experience of pregnancy loss can represent the devastating demise of a nascent primary relationship with associated destabilizing effects (Markin & Zilcha-Mano, 2018). Some women who have a miscarriage—especially those with higher neuroticism, lower emotional regulation, more negative life events, and who experience dissociative reactions to the event—may meet criteria for PTSD (Engelhard, 2004). In a prospective longitudinal study of PTSD and depression after loss in any stage of pregnancy (including both miscarriages and stillbirths, the latter of which is much rarer and holds a much greater risk for trauma), 25% of participants met criteria for PTSD one month after pregnancy loss, dropping to 7% after four months (Engelhard et al., 2001).
A study by Engelhard and colleagues (2001) is particularly noteworthy for its inclusion of qualitative, first-person participant accounts of both miscarriage and stillbirth. These descriptions offer a window into the potential traumatic nature of such experiences—shedding light on both the stories themselves and the possible origins of cultural taboos around this topic. Such stories underscore the need for timely, sensitive interventions for some women, perhaps similar to work done with individuals who have closely experienced disaster or assault. Meeting diagnostic criteria for PTSD was associated with persistent depressive symptoms after pregnancy loss (Engelhard et al., 2001). This result raises questions as to whether women who were identified as having higher than average levels of depression and anxiety in other studies were experiencing a post-traumatic response. Even when not meeting the diagnostic threshold for PTSD, women may experience trauma-specific symptoms such as re-experiencing, hyperarousal, and intrusive recollections (Engelhard et al., 2001). Diagnosis and treatment planning for women experiencing severe distress can be improved by pushing through cultural norms of silence and minimization and fully assessing clients for trauma responses.
Health Care Experiences During and After Miscarriage
The amorphous psychological vulnerabilities associated with miscarriage exist alongside concrete biological ones; the loss of a pregnancy is, at least in part, a medical event. When appropriately managed, the physical risks of miscarriage are relatively low (Wallace et al., 2010). The first stages occur inside a woman’s body without her immediate knowledge. Quickly, however, there are interpersonal and ecological variables that begin to influence a woman’s experience (Trepal et al., 2005). Bleeding or pain may be the first sign; some women present in the emergency room with these symptoms and find out about both their pregnancy and impending miscarriage at the same time (Wallace et al., 2010). Women may learn that a pregnancy is non-viable at a prenatal medical appointment, based upon routine bloodwork or ultrasound scans. Medical professionals may not receive adequate training about working with patients who are experiencing pregnancy loss. Among a sample of third-year medical students, less than 25% had observed a physician deliver news about a miscarriage during their obstetrics and gynecology rotation (Marko et al., 2015). The high cost of medical care, particularly when not openly discussed with patients, might be another source of marked distress (Ubel, Abernethy, & Zafar, 2013). Culturally condoned minimization of miscarriage can manifest in multiple interpersonal interactions, including those with health care providers, and leave women isolated and disenfranchised in efforts to cope with their loss (Markin & Zilcha-Mano, 2018).
Satisfaction with health care was identified as a theme in the literature on early pregnancy loss (Randolph et al., 2015), and dissatisfaction with the health care received during and immediately after a miscarriage predicted atypically persistent psychological distress more than 2 years after the event (deMontigny et al., 2017). This finding is particularly important for counselors, as the nature of clients’ previous interactions with health care providers may not emerge or be noticed as potentially pertinent in standard biopsychosocial assessments. Dissatisfied patients cite providers’ attitudes and failure to convey awareness, empathy, compassion, information, and suggestions for follow-up related to the emotional impact of the loss (Geller, Psaros, & Kornfield, 2010).
Despite the large number of women impacted by miscarriage and its effects, a shortage of published clinical research in this domain across disciplines has been noted (e.g., Markin, 2017; Randolph et al., 2015). Many existing studies lack empirical or theoretical rigor (e.g., exclusive focus on only certain symptoms, use of very brief interventions that may or may not be performed by trained mental health clinicians, lack of longitudinal follow-up). Our societal classification of miscarriage as primarily a medical matter contributes to a scarcity of psychologically focused scholarship regarding how to fully support women during and after the multi-faceted experience of losing a pregnancy (Markin, 2017).
Understanding Miscarriage: Clinical Application of the Ecological Model
Counselors without specific training focused on awareness of miscarriage and ways to intervene with clients experiencing distress related to it can inadvertently neglect this area in their psychotherapeutic work (Markin, 2017). Engaging in a systemically informed approach to learning about and conceptualizing this highly prevalent life span event is one way to combat cultural silence regarding pregnancy loss. Bronfenbrenner’s (1979, 1994) ecological systems model is firmly situated within the psychological and developmental canon and is a powerful foundation from which to explore and develop systemic thinking skills in students, professionals, and clients. In it, a series of ever-broadening environmental systems influence the development and functioning of individuals (see Figure 1). Some factors related to resilience and distress originate in or are exacerbated by variables in distal systems (meso-, exo-, macro-, and chronosystems); counselors who share these complexities with their clients may help lessen self-directed attribution leading to blame, shame, and guilt (Rogers, Gilbride, & Dew, 2018). Counselors who utilize an ecological approach to understanding clients are less likely to ignore or minimize the many complex and nuanced variables that may influence clients’ experiences related to miscarriage.
During a time in which she may have just begun to grapple with the physical, emotional, and existential ramifications of her pregnancy (e.g., wanting or not wanting the pregnancy, nausea, soreness, fear, joy, what it means to become a mother, plans for the future), a woman who is miscarrying is suddenly beset with biopsychosocial ramifications of loss (Engelhard et al., 2001; Trepal et al., 2005). Awareness, understanding, and exploration of the multiple systemic influences in women’s stories of miscarriage are inherent in an ecological conceptualization of this topic. Williams, McMahon, and Goodman (2015) used ecological systems (Bronfenbrenner, 1979) as the foundation for a pedagogical intervention called eco-webbing, which is intended to develop counseling students’ critical consciousness through the creation of a visual representation of systemic influences in their clients’ lives. Resilience researchers Ungar, Ghazinour, and Richter (2013) expanded upon the traditional nested ecological model through the introduction of the idea of differential impact. This concept suggests that the importance of a given variable is not predicted by its closeness to the individual at the center of Bronfenbrenner’s model; rather, variables existing in the outer levels of the ecosystem may be extremely significant to a specific person in a specific context. Drawing upon this, Rogers and colleagues (2018) proposed the use of an eco-map, a visual representation of environmental variables organized both by systemic level and current salience to the client. Clinical relevance is noted by distance to the client at the center of the map and by the size and ordering of variables within each level. The eco-map for a particular client will change over time, with different variables gaining salience while others recede. This strategy for organizing client information may be of particular use to counselors, educators, and supervisors in search of clinical and teaching tools that counter biased assumptions and capture the complexities of current environments (Rogers et al., 2018).
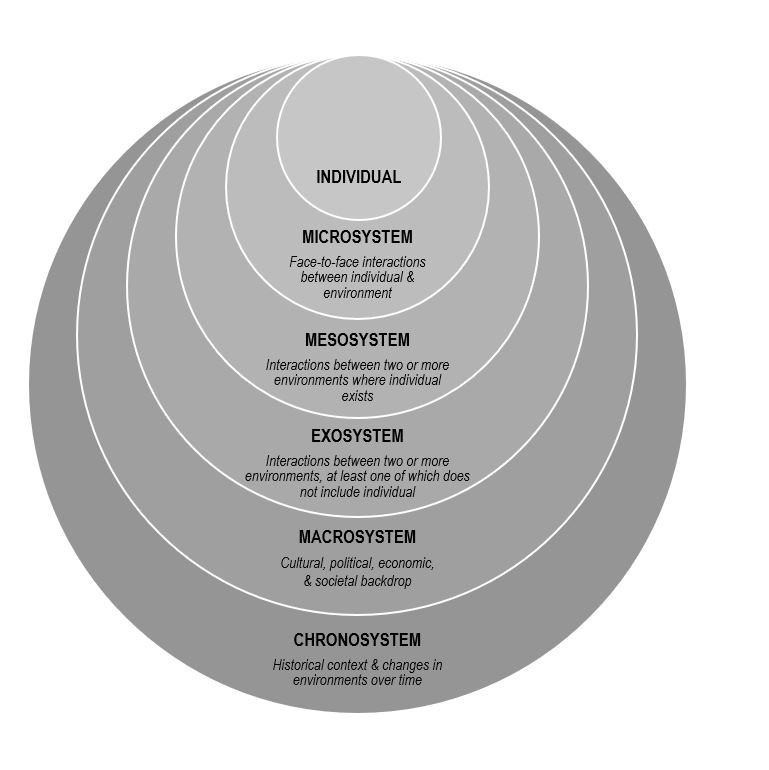
Figure 1. Bronfenbrenner’s Ecological Model.
Ecologically Informed Clinical Encounters
During clinical encounters with women who have experienced miscarriage, the importance of acknowledgment and validation is emphasized by authors working from a variety of disparate theoretical vantages (Diamond & Diamond, 2017; Markin & Zilcha-Mano, 2018; Wenzel, 2017). Narrative therapy is one recommended approach (Betz & Thorngren, 2006; Stark et al., 2011), with particular focus on clients’ reproductive story (Diamond & Diamond, 2017; Jaffe, 2017). This conceptual construct integrates exploration of the past, present, and future into work with clients who have experienced a reproductive loss, normalizing and validating both acknowledged and unacknowledged reactions to the loss, as well as making space for the client to create a hopeful narrative about the future. Therapeutic exploration of the meaning of the loss, both to the individual client and within broader relational and cultural contexts, is encouraged in order to facilitate client understanding and growth (Diamond & Diamond, 2017; Markin & Zilcha-Mano, 2018; Wenzel, 2017), supporting the utility of the ecological model as a conceptual frame. Ecological conceptualization pairs easily with a wide variety of theoretical approaches to clinical work. It can be used to facilitate a more deeply person-centered encounter, to provide context for adaptive and maladaptive relational strategies at play both in and out of the therapy room, to facilitate existential exploration, and to co-create goals and strategies tied to specific variables. Counselors can infuse ecological conceptualizations and observations into the therapeutic encounter, providing rich opportunities for reflections of meaning, re-framing, and narrative restructuring.
Following a detailed case example describing a client who has recently experienced a miscarriage, the next sections progress through each level of the ecological model (Bronfenbrenner, 1994). After explicating the level, we identify clinically relevant variables from both the literature and the case example and offer clinical implications for counselors working within an ecological framework. An eco-map summarizing ecological variables from the case example can be found in Figure 2.
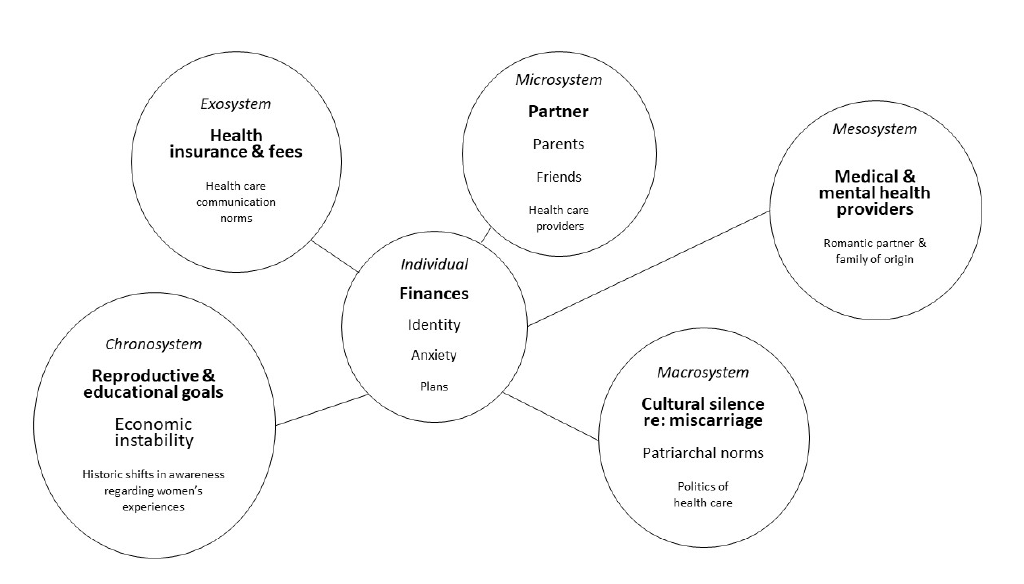
Figure 2. Eco-map of Michelle.
Case Study: Michelle
Michelle is a 27-year-old woman who lives in a mid-sized East Coast city. She resides with her boyfriend of 3 years, Jon, and is employed as a server at a high-end restaurant. She is currently applying to graduate school to be an occupational therapist. She presents for counseling at a large clinic, asks about sliding scale fees for uninsured clients, and states on her paperwork that she would prefer to see a female clinician, “middle aged or older if possible.” Intake assessments suggest mild to moderate symptoms of depression and anxiety.
During the first session, Michelle discloses that she experienced a miscarriage 4 weeks ago. She learned she was pregnant from a home pregnancy test at approximately five weeks gestation, after her menstrual period did not arrive on time. She began experiencing pregnancy symptoms (sore breasts, sensitivity to smells) the next week. When she visited a medical clinic at 9 weeks gestation, pregnancy hormone levels in her blood did not align with the dates of her last period. A transvaginal ultrasound was ordered, and results showed that the embryo had stopped developing at approximately seven weeks, with no visible heartbeat. She was told that the pregnancy was not viable, that she should prepare for “nature to take its course,” and that she should expect to begin bleeding in the coming days. She was told that if she did not spontaneously miscarry in the next week, she would need to undergo a procedure called a dilation and curettage (D&C), during which her cervix would be partially dilated and the pregnancy-related tissue would be surgically removed from her uterus in order to avoid infection and other complications.
Michelle described a growing sense of anxiety and sadness upon hearing the news that her pregnancy was not viable. Though she was initially shocked and upset about her unplanned pregnancy, she and Jon had begun to plan for their new identity as a family of three. In the days after her doctor’s appointment, Michelle had two panic attacks—something that had not happened to her since high school. Michelle experienced some painful cramping and spotting one week after her appointment. She called and reported her symptoms, and the nurse scheduled her for a D&C at an outpatient surgery center. She asked what would happen if she did not get the D&C, what to expect from the procedure, and if the D&C posed any risks for future fertility. Her male doctor offered minimal information, stating that the D&C was necessary, that she should not worry, and that the procedure would be “quick, with only mild cramping, if anything.” Jon accompanied her to the surgery center, though per facility’s policies he was not allowed to be in the room during the procedure. She experienced panic symptoms prior to and during the D&C as well as moderately severe pain, and she was reminded of the time in college when she accompanied a friend who got an abortion.
In the month since the procedure, Michelle reports a variety of distressing symptoms and situations. Though they were planning a long-term future just weeks ago, she describes a growing distance between her and Jon. He is spending more time going out with friends and does not want to talk about the pregnancy or their relationship. Michelle was unable to work for a week after the surgery, and the missed income is creating short-term financial strain. She reports this would be manageable if not for the multiple medical bills for appointments, labs, scans, and the D&C that are starting to arrive in the mail. Michelle does not currently have health insurance: She was removed from her parents’ plan on her birthday, her employer does not offer benefits, and she has been trying to save money for a few months before starting graduate school and getting a new plan through the university. So far, the bills from the surgery center alone total over $5,000. When the largest of these bills arrived in the mail, Michelle had a panic attack that included chest pain and shortness of breath. During this episode, she convinced Jon not to call an ambulance because of the cost, even though he feared she was having a heart attack. She has also been experiencing inability to sleep, loss of appetite, nightmares, and ruminations focused upon the state of her relationship with Jon, whether she still wants to go to graduate school, whether she could have done anything to prevent the miscarriage, and whether she will be able to have children in the future. She has told a few close friends about her situation, but they are confused about why she is not simply relieved to have the unplanned pregnancy no longer be a hindrance to her educational and professional aspirations. She reports that she is close with her parents but has not told them anything. They already disapprove of Michelle and Jon living together because of their religious beliefs, and she does not want to further complicate her relationship with them.
Ecological Conceptualization of Michelle
Individual. At the center of Bronfenbrenner’s model is the individual (see Figure 1). There is a great amount of variability among individual women’s experiences of miscarriage. Baseline physical and mental health, presence or absence of physical and psychological symptoms, the length of the pregnancy, whether or not the pregnancy was wanted, number of prior pregnancies, plans for the future, and the physical experience of the miscarriage are just some of the many variables that counselors should be aware of when working with clients (deMontigny et al., 2017; Shreffler et al., 2011).
Though Michelle’s pregnancy was unplanned, she demonstrated resilience and flexibility regarding the news and had begun planning for her future as a mother. She may be mourning the loss of this new life and identity (Betz & Thorngren, 2006). Her pregnancy symptoms were caused by shifting hormones; her current physical and psychological symptoms may be influenced by her hormonal levels returning to a non-pregnant state. She has a history of panic attacks from 10 years prior, and this pattern reemerged upon learning that her pregnancy was non-viable. She has undergone a series of invasive medical procedures, including transvaginal ultrasound, dilation of her cervix, and surgical removal of tissue from her uterus, as well as unexpected pain. Michelle’s surprise over her pregnancy, her adaptive response to it, the unanticipated miscarriage, and her resultant novel physiological and medical experiences have coalesced into an overwhelming intrapersonal incident. Conveyance of a caring and nonjudgmental stance around these variables, as well as normalizing her reaction to a series of physically and existentially significant life span events, is essential to creating a clinical space where she can freely explore her unique experience (Trepal et al., 2005). Knowledge on the part of the counselor around what many find to be a taboo topic may serve to both normalize the experience and highlight its uniqueness to this client at this moment in her life.
Microsystem. Per Bronfenbrenner (1979, 1994), the microsystem is made up of the person-to-person engagement that an individual experiences in their immediate environment. These interactions, and the relationships associated with them, hold tremendous sway through encouraging or discouraging an individual’s behaviors. There is a deep body of research examining the influence of relational patterns on human development and psychological functioning (Bronfenbrenner, 1994). It is within our relationships that we learn whether it is safe or unsafe to be unguarded and authentic in our environment (Ainsworth, Bell, & Stayton, 1972; Miller, 1986). As such, variables in the micro-level are of utmost importance when assessing, conceptualizing, and working with clients who have lost a pregnancy. Counselors should be aware that some clients do not tell anyone about the pregnancy, tell only a select few people in their microsystem, or share the news more broadly. Although women experience more support when loss is public (Betz & Thorngren, 2006), many are dissatisfied and distressed by others’ response to their loss (Geller et al., 2010; Randolph et al., 2015). Medical professionals may inadvertently minimize the experience (deMontigny et al., 2017; Geller et al., 2010). They and others in the client’s microsystem may project their own emotional reactions (e.g., grief, relief) or processes (e.g., minimization, spiritual bypass) onto the client.
Over the last 2 months, there has been much clinically noteworthy activity within Michelle’s microsystem. There were marked shifts in her relationship with her romantic partner: a growing intimacy with energy focused on a long-term future together, followed by a distancing that includes new behavior patterns that did not exist before her pregnancy. Though she reports closeness with her parents, she has chosen not to disclose news of her pregnancy or miscarriage to them because of her predictions regarding their reaction, suggesting a current lack of transparency in relationships that had previously been a source of support. Michelle reports a perceived lack of empathy from her close friends, who do not understand her response to the miscarriage. Similarly, her experience of pain during her surgery was not the response predicted by her physician.
Michelle’s sense of disconnection in her microsystem may be related to feelings of shame. Shame is a documented reaction to losing a pregnancy (Bardos et al., 2015). Women may feel ashamed that their body did not carry the pregnancy to term or that they are responding differently than they imagine others have responded to such a loss. Shame has been described as a sense of unworthiness to be in authentic connection with others, based upon previous experiences of disconnection or hurt in relationships (Miller, 1986), such as those that Michelle has recently experienced. Her growing sense of isolation within her microsystem is of utmost clinical importance. Her request for an older woman therapist can be understood as evidence of her resilience and ability to care for herself—she is seeking to enrich her microsystem via connection with a new person who is more likely to be empathic and validating than those currently within this sphere.
Mesosystem. The mesosystem is the system of microsystems in an individual’s life, describing interactions between environments (Bronfenbrenner 1979, 1994). Michelle describes her relationship with her parents as close, but the interactions between the system she currently lives in (Michelle and her boyfriend) and her family of origin are not without tension. She reports that her parents disapprove of her living with Jon. Based upon this, she has not told them about her pregnancy or miscarriage. Is this an example of healthy boundaries between the couple and Michelle’s parents, or are there other aspects of this system-to-system relationship in which Michelle feels torn between the norms of one system versus the other?
Questions also arise regarding the communication with and between her medical providers. Her physician minimized her concerns, and his prediction about the amount of pain she would experience during the procedure proved inaccurate. Assuming the surgical center has greater knowledge about the variability of patient responses to such procedures, could better channels of communication between the center and offices of referring physicians promote increased patient understanding regarding what they might expect? Was Michelle’s doctor aware of her history of anxiety, and was this communicated to the surgical center? If so, in what way? An ecologically informed counselor might request permission to facilitate communication between Michelle’s health care providers, so as to best serve the client and to model how advocating for such interactions might be helpful to her in the future.
Exosystem. Bronfenbrenner’s exosystem (1979, 1994) is similar to the mesosystem in that it describes interactions between two or more environments, except that the individual of interest is not present in at least one of them. This construct captures how a setting or system can have observable influence over an individual’s experience, even though a person may not ever have direct contact with it. There are multiple exosystem variables evident in Michelle’s story at intake, and more would likely emerge during the course of clinical work. For example, her current economic challenges are having a profound effect on her well-being. Michelle’s removal from her parents’ health insurance plan, her medical providers’ fees for services, and her employer’s guidelines (backed by federal and state law) regarding lack of health insurance and medical leave options for hourly employees are all examples of how the policies and actions of a seemingly distant entity can have profound consequences for an individual.
It is possible that Michelle’s physician did not receive specific training regarding communication with patients about miscarriage (Marko et al., 2015). In the absence of training and protocols that acknowledge the great variability in women’s responses to pregnancy loss, including the individual variables that influence reactions and preferences for the type of care received, medical providers may make incorrect assumptions regarding their patients’ needs and experiences. Furthermore, given the current economics of the U.S. health care system, even those providers who might like to offer a more patient-centered approach to care are pressed for both time and resources. In Michelle’s case, the information she received from her physician was likely informed by his training and the norms of the clinic where he is employed, but she experienced more physical pain during her procedure than she had been told to anticipate, exacerbating her feelings of fear and powerlessness.
Michelle is an uninsured patient who has experienced both an unplanned pregnancy and an unexpected loss; the medical organizations that have been involved in her care have not expressed awareness or concern regarding the health ramifications of their fiscal policies and procedures, a common practice in the U.S. health care system (Ubel et al., 2013). Michelle’s current distress is largely focused on her fears around her growing medical debt, which she conceptualizes as a problem that is hers alone. Sharing an ecologically informed conceptualization of this issue during the course of counseling, including the complex influence of systems on her current situation, may help broaden her view regarding both her level of personal responsibility and possible avenues for solving the problem. For instance, she may recognize that the billing department’s processes are likely automatic and choose to contact them (thus bringing them into her microsystem) in order to explain her situation and inquire about manageable payment plans and possible bill adjustments for uninsured patients.
Macrosystem. The macrosystem encompasses the societal context in which an individual exists, including elements such as laws, economics, and social norms (Bronfenbrenner 1979, 1994). The cultural environment is rich with variables that affect intra- and interpersonal experiences, and the macrosystem can hold much influence over how situations in a person’s life are understood and acted upon—even though individuals may not be aware of its effect. There are multiple influential macrosystem-level factors at play in Michelle’s situation. The cultural taboo around miscarriage—including the lack of general knowledge around causes and prevalence (Bardos et al., 2015) and the lack of traditional behaviors for both women experiencing miscarriage and those whom they tell about the loss (Trepal et al., 2005)—are woven throughout her story. Jon’s need for distance in their relationship may be a manifestation of a number of macro-level factors, including the taboo around the topic and the more general cultural expectations regarding masculine avoidance of painful emotions and the imperative for men to disguise a lack of knowing what to do in a given situation. Religion, another pervasive cultural force, influences Michelle’s parents’ conceptualization of her decision to live with her romantic partner, thus affecting microsystem relationships and the mesosystem interactions between those systems. Religious and other deeply held personal beliefs (e.g., how miscarriage should be addressed—or not addressed—per the norms of a specific culture) were likely at play in many of the interactions Michelle has experienced since the loss of her pregnancy.
Michelle’s removal from her parents’ health insurance plan upon turning 27 is deeply influential; this occurrence is one based upon laws that were enacted amidst a complex economic and political environment. Through a systemic lens, the quality and cost of her health care without insurance, as well as the cost of her upcoming graduate education, can be conceptualized not merely as facts, but rather as products of a dynamic and complex ecology. In this way, Michelle’s difficulties are not hers alone, but those of a much larger system. When ecologically framed, questions arise regarding the expectation that an individual should or even could be able to grapple with such situations in a vacuum. Through this lens, her economic anxiety may be seen as a normative and appropriate response, rather than as a symptom to overcome.
Research indicating the importance of patients’ perceptions of their health care and its relationship to ongoing distress after miscarriage (deMontigny et al., 2017) supports the notion that Michelle’s dissatisfaction with some elements of her medical care and her current mental health symptoms are not unrelated. These micro- and macrosystem interactions also occurred within a broader cultural context. In a recent exploration of the status of women physicians within the field of obstetrics and gynecology, Hughes and Bernstein (2018) noted:
Physicians are social creatures raised within a society with historical roots founded on patriarchy and a system in which men, particularly white men, have disproportionate power. People living today did not create this system, but all of us perpetuate it to some degree, usually without realizing it. (p. 365)
In Michelle’s case, the minimization of her miscarriage—including her doctor’s incorrect predictions about her pain level and a lack of assessment related to her emotional response to her pregnancy loss and related procedures—seems to have exacerbated her distress. Michelle may have benefited from expressed empathy and discussion both normalizing and educating her about the wide variety of biopsychosocial reactions to miscarriage (e.g., pain, relief, grief, guilt, anxiety, depression, trauma), as well as a collaborative conversation about her choices and the risks and benefits of her options, including costs. The lack of such discussions stems at least in part from macrosystem-level sexism that silently minimizes women’s experiences, thus placing the responsibility for the distress on the individual rather than spreading it throughout the system.
Chronosystem. The chronosystem in Bronfenbrenner’s (1994) ecological systems theory captures the role of time within environments. Specific events and developmental transitions that occur over the course of an individual’s life span and the parallel unfolding of sociocultural history are included in this level. Women’s personal histories of trauma, previous pregnancy losses, and concerns about future fertility (Engelhard, 2004; Shreffler et al., 2011) are significant variables identified in the miscarriage literature that may be understood more deeply when placed within the time-dependent chronosphere. For Michelle, her pregnancy and subsequent miscarriage occurred at a time in her life when her focus was on plans for furthering her education, not on having children. However, she quickly found herself developing a new facet of her identity—that of a future mother. This unexpected life span event may have triggered changes in her concept of self, including her assumptions about how, when, and if she might become a parent. This transition, followed by the existentially activating event of the miscarriage, has caused Michelle to question many other of her previous assumptions; she feels unable to simply return to her original plans.
Michelle’s personal experience is unfolding during a time of burgeoning national awareness regarding multiple areas of instability and injustice in our culture. Specific to Michelle at this point in both her individual life and in history are concerns about the present and future as related to economics (medical bills, upcoming costs of graduate school), health care (availability, quality, cost; her chosen future career in the health care field), and gender (her experiences of becoming pregnant, miscarrying, and exploring what it might mean to become a mother; awareness of how sexism and gender stereotypes may have influenced these experiences). An ecologically attuned counselor can utilize the construct of the chronosystem to highlight Michelle’s development as a person within the context of historic developments. Framing of her self-concerns (e.g., debt, lack of empathic responses) alongside societal-level concerns (e.g., economic instability, hostile and benevolent sexism) suggests a universality in her individual experiences and offers an explanation for the depth of her responses—her problems are not just significant within the arc of her own life, but are examples of significant events within the arc of history as well.
Discussion
Miscarriage is a highly common life span event that is shrouded by misinformation and silence regarding its prevalence, causes, and associated outcomes (Bardos et al., 2015; Wallace et al., 2010). This opacity also is evidenced in the paucity of counseling scholarship that includes mention of miscarriage, much of which focuses on the early loss of a pregnancy as a challenge experienced by heterosexual couples en route to parenthood (Sperry & Sperry, 2004; Stark et al., 2011; Wagner et al., 2018). Women’s reactions to miscarriage are varied and unique, influenced by a multitude of variables (deMontigny et al., 2017; Engelhard, 2004; Engelhard et al., 2001; Shreffler et al., 2011). Some women experience clinically significant and persistent psychological distress subsequent to miscarriage (deMontigny et al., 2017; Hutti et al., 2018). Dissatisfaction with health care among women is widely reported, and research indicates a need for improved biopsychosocial care for women after miscarriage, which would fulfill women’s stated needs regarding acknowledgment, validation, education, and resources (Geller et al., 2010). The necessity of system-to-system communication between medical and mental health services, as well as for emotional support provided by clinicians who have knowledge of the complex potential ramifications of miscarriage, is evident. Such care could improve outcomes for many women, particularly those who are vulnerable to clinically severe and persistent distress.
Counselors’ education, theoretical leanings, cultural beliefs, and personal experiences influence their understanding of clients. A lack of both societal norms and clinical training regarding helpful ways to intervene with women who have experienced miscarriage may lead to challenges for clinicians. Clients with a history of miscarriage may or may not view the experience as important in their own story, but—particularly given the documented prevalence of silence, distress, and dissatisfaction around responses to this common life span event (Randolph et al., 2015; Trepal, 2005)—its possible clinical salience for individual clients warrants both inclusion in standard counseling assessments and therapeutic attention, according to the goals and needs of the client. It is important for counselors to: (a) be aware of the possibility of serious and persistent distress related to miscarriage; (b) thoroughly assess clients around this topic, despite cultural norms of not mentioning or minimizing pregnancy loss; and (c) have knowledge of the myriad of risk and protective factors around this issue, as well as recommended strategies for working with such clients.
The counseling profession has recognized that advocacy to diminish systemic impediments to our clients’ growth is an ethical and clinical imperative (Ratts, Toporek, & Lewis, 2010). When viewed through an ecological lens, the current literature on pregnancy loss describes the influence not just of individual- and microsystem-level variables (e.g., premorbid anxiety disorder, unsatisfying interactions with medical professionals), but also the influence of distal system interactions (e.g., health care policy, cultural norms). Politics and economics are inherent in health care, both of which are deeply influenced by cultural beliefs and historical context. Awareness of ecological variables when understanding a woman’s reaction to her miscarriage—the attitudes conveyed by the individuals in her immediate sphere, as well as the practices and policies enacted by those outside it—may provide the foundation for a more complex and deeply person-centered approach to counseling.
Although the complex definitions of Bronfenbrenner’s levels (1994) may not be of use or interest to many clients, learning to think about oneself and one’s experiences as occurring within a nuanced ecology is a valuable skill. The ability to self-conceptualize ecologically can transfer to multiple domains beyond the counseling office. Counselors may choose to share elements from their ecological conceptualizations with clients directly, both to check in regarding possible salience to the client and to demonstrate systemic thinking as useful cognitive strategy.
As people become more aware of the complexity of the systems in which all experiences are embedded, issues related to social justice and advocacy will naturally emerge (Rogers et al., 2018). Ecologically attuned counselors may feel called upon to seize opportunities for systemic-level interventions, using their awareness of complex systems and relational expertise as a foundation for actions that extend beyond their work with individual clients. In turn, as clients experience authentic connection based upon being deeply understood by their counselors, they may reap therapeutic benefits by using their growing awareness of the interplay between experience, relationships, and systems to take action outside the therapy room (Miller, 1986).
Conclusion
Miscarriage is a common life span event that can be the impetus for persistent mental health concerns. Distress may be exacerbated by non-supportive cultural norms that are both internalized by the client and systemically manifested. By utilizing established models that account for the influence of variables throughout the environment in which a person exists, counselors are more likely to consider the wide variety of factors that may be affecting an individual client. Bronfenbrenner’s bioecological model (1979, 1994) places individuals within complex ecosystems and posits that even interactions between system-level variables not directly connected to a person still influence their experience and development. We propose that an ecological assessment of the variables impacting the client as related to her miscarriage can counter culturally learned avoidance and facilitate complex, nuanced conceptualizations and interventions around the unique biopsychosocial issues that may emerge related to pregnancy loss. Research is needed to further examine women’s experiences of miscarriage and the processes and outcomes of miscarriage-specific counseling interventions. An investigation of the validity and the utility of the proposed conceptual model is just one example of the many areas rich with potential for further inquiry. Future scholarly endeavors on this important topic may ultimately improve awareness, visibility, knowledge, resources, and care for the many women who endure miscarriages during their lifetimes.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ainsworth, M. D. S., Bell, S. M., & Stayton, D. J. (1972). Individual differences in the development of some attachment behaviors. Merrill-Palmer Quarterly of Behavior and Development, 18(2), 123–143.
Bardos, J., Hercz, D., Friedenthal, J., Missmer, S. A., & Williams, Z. (2015). A national survey on public
perceptions of miscarriage. Obstetrics and Gynecology, 125, 1313–1320. doi:10.1097/OG.0000000000000859
Betz, G., & Thorngren, J. M. (2006). Ambiguous loss and the family grieving process. The Family Journal, 14, 359–365. doi:10.1177/1066480706290052
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U. (1994). Ecological models of human development. In M. Gauvain & M. Cole (Eds.), Readings on the development of children (2nd ed., pp. 37–43). New York, NY: Freeman.
Burnett, J. A. (2009). Cultural considerations in counseling couples who experience infertility. Journal of Multicultural Counseling and Development, 37(3), 166–177. doi:10.1002/j.2161-1912.2009.tb00100.x
deMontigny, F., Verdon, C., Meunier, S., & Dubeau, D. (2017). Women’s persistent depressive and perinatal grief symptoms following a miscarriage: The role of childlessness and satisfaction with healthcare services. Archives of Women’s Mental Health, 20, 655–662. doi:10.1007/s00737-017-0742-9
Diamond, D. J., & Diamond, M. O. (2017). Parenthood after reproductive loss: How psychotherapy can help with postpartum adjustment and parent–infant attachment. Psychotherapy, 54, 373–379. doi:10.1037/pst0000127
Engelhard, I. M. (2004). Miscarriage as a traumatic event. Clinical Obstetrics and Gynecology, 47, 547–551. doi:10.1097/01.grf.0000129920.38874.0d
Engelhard, I. M., van den Hout, M. A., & Arntz, A. (2001). Posttraumatic stress disorder after pregnancy loss. General Hospital Psychiatry, 23(2), 62–66. doi:10.1016/S0163-8343(01)00124-4
Geller, P. A., Psaros, C., & Kornfield, S. L. (2010). Satisfaction with pregnancy loss aftercare: Are women getting what they want? Archives of Women’s Mental Health, 13(2), 111–124. doi:10.1007/s00737-010-0147-5
Hughes, F., & Bernstein, P. S. (2018). Sexism in obstetrics & gynecology: Not just a “women’s issue.” American Journal of Obstetrics & Gynecology, 219, 364–366. doi:10.1016/j.ajog.2018.07.006
Hutti, M. H., Myers, J. A., Hall, L. A., Polivka, B. J., White, S., Hill, J., . . . Kloenne, E. (2018). Predicting need for follow-up due to severe anxiety and depression symptoms after perinatal loss. Journal of Obstetric, Gynecologic & Neonatal Nursing, 47(2), 125–136. doi:10.1016/j.jogn.2018.01.003
Jaffe, J. (2017). Reproductive trauma: Psychotherapy for pregnancy loss and infertility clients from a reproductive story perspective. Psychotherapy, 54, 380–385. doi:10.1037/pst0000125
Markin, R. D. (2017). An introduction to the special section on psychotherapy for pregnancy loss: Review of issues, clinical applications, and future research direction. Psychotherapy, 54, 367–372. doi:10.1037/pst0000134
Markin, R. D., & Zilcha-Mano, S. (2018). Cultural processes in psychotherapy for perinatal loss: Breaking the cultural taboo against perinatal grief. Psychotherapy, 55, 20–26. doi:10.1037/pst0000122
Marko, E. K., Buery-Joyner, S. D., Sheridan, M. J., Nieves, K., Khoury, A. N., & Dalrymple, J. L. (2015). Structured teaching of early pregnancy loss counseling. Obstetrics & Gynecology, 126, 1S-6S. doi:10.1097/AOG.0000000000001015
Miller, J. B. (1986). Toward a new psychology of women (2nd ed). Boston, MA: Beacon Press.
Mutiso, S. K., Murage, A., & Mukaindo, A. M. (2018). Prevalence of positive depression screen among post miscarriage women—A cross sectional study. BMC Psychiatry, 18, 32. doi:10.1186/s12888-018-1619-9
Randolph, A. L., Hruby, B. T., & Sharif, S. (2015). Counseling women who have experienced pregnancy loss: A review of the literature. Adultspan Journal, 14, 2–10. doi:10.1002/j.2161-0029.2015.00032.x
Ratts, M. J., Toporek, R. L., & Lewis, J. A. (2010). ACA advocacy competencies: A social justice framework for counselors. Alexandria, VA: American Counseling Association.
Rogers, J. L., Gilbride, D. D., & Dew, B. J. (2018). Utilizing an ecological framework to enhance counselors’ understanding of the U.S. opioid epidemic. The Professional Counselor, 8, 226–239. doi:10.15241/jlr.8.3.226
Shreffler, K. M., Greil, A. L., & McQuillan, J. (2011). Pregnancy loss and distress among U.S. women. Family Relations, 60, 342–355. doi:10.1111/j.17413729.2011.00647.x
Sperry, P., & Sperry, L. (2004). The family experience of loss associated with miscarriage and ectopic pregnancy. The Family Journal, 12, 401–404. doi:10.1177/1066480704267547
Stark, M. D., Keathley, R. S., & Nelson, J. A. (2011). A developmental model for counseling infertile couples. The Family Journal, 19, 225–230. doi:10.1177/1066480711400171
Trepal, H. C., Semivan, S. G., & Caley-Bruce, M. (2005). Miscarriage: A dream interrupted. Journal of Creativity in Mental Health, 1(3–4), 155–171.
Ubel, P. A., Abernethy, A. P., & Zafar, S. Y. (2013). Full disclosure—out-of-pocket costs as side effects. New England Journal of Medicine, 369, 1484–1486. doi:10.1056/NEJMp1306826
Ungar, M., Ghazinour, M., & Richter, J. (2013). Annual research review: What is resilience within the social ecology of human development? Journal of Child Psychology and Psychiatry, 54, 348–366. doi:10.1111/jcpp.12025
Wagner, N. J., Vaughn, C. T., & Tuazon, V. E. (2018). Fathers’ lived experiences of miscarriage. The Family Journal, 26(2), 193–199. doi:10.1177/1066480718770154
Wallace, R. R., Goodman, S., Freedman, L. R., Dalton, V. K., & Harris, L. H. (2010). Counseling women with early pregnancy failure: Utilizing evidence, preserving preference. Patient Education and Counseling, 81, 454–461. doi:10.1016/j.pec.2010.10.031
Williams, J. M., McMahon, H. G., & Goodman, R. D. (2015). Eco-webbing: A teaching strategy to facilitate critical consciousness and agency. Counselor Education and Supervision, 54(2), 82–97. doi:10.1002/ceas.12006
Wenzel, A. (2017). Cognitive behavioral therapy for pregnancy loss. Psychotherapy, 54, 400–405.
doi:10.1037/pst0000132
Jennifer L. Rogers, NCC, is an assistant professor at Wake Forest University. Jamie E. Crockett, NCC, is an assistant professor at Wake Forest University. Esther Suess, NCC, is a counselor at the Mood Treatment Center in Winston-Salem, NC. Correspondence can be addressed to Jennifer Rogers, P.O. Box 7406, Winston-Salem, NC 27109, rogersjl@wfu.edu.
Mar 26, 2019 | Volume 9 - Issue 1
J. Richelle Joe, M. Ann Shillingford-Butler, Seungbin Oh
In this phenomenological study, the authors explored the lived experiences of 19 African American mothers raising boys and young men to understand how media exposure to community and state violence connects to the physical and mental health of these mothers. Analysis of semi-structured individual interviews revealed six themes: psychological distress, physical manifestations of stress, parenting behaviors, empathic isolation, coping strategies, and strengths. The analysis of the data revealed that these themes were connected such that community and state violence were forces weighing on these mothers, resulting in emotional responses, changes to parenting approaches, physical responses, and empathic isolation, while the mothers’ coping strategies and strengths served as forces to uplift. The authors present the lived experiences of the participants through a discussion of these themes and their implications for counseling African American mothers within the current social–political context.
Keywords: African American mothers, #BlackLivesMatter, community and state violence, media exposure, mental health
During the 2016 Democratic National Convention, seven African American women took the stage in solidarity to shine a light on community and state violence and the need for criminal justice reform (Drabold, 2016; Sebastian, 2016). These women, collectively referred to as the “Mothers of the Movement,” included Lesley McSpadden, Gwen Carr, and Lucy McBath, the mothers of Michael Brown, Eric Garner, and Jordan Davis, respectively—young African American males whose deaths were widely publicized as examples of gun violence (community violence) or police use of force (state violence). Sybrina Fulton also was in attendance. The death of her son, Trayvon Martin, in 2012 sparked a modern conversation about violence against African Americans and led to the creation of the #BlackLivesMatter movement (Black Lives Matter, n.d.). During their address to the convention, the “Mothers of the Movement” shared their grief publicly and spoke on behalf of their children, with Fulton emphatically stating: “This isn’t about being politically correct. This is about saving our children” (Drabold, 2016).
Sixty-one years earlier, Mamie Till had similarly allowed the world to see her grief as she wept over the open casket of her 14-year-old son, Emmett, who had been brutally murdered for being a young Black man in the Deep South (CBS News, 2016). Like the death of Trayvon Martin, Emmett Till’s death galvanized the African American community and motivated activists—including Rosa Parks—to participate in the modern civil rights movement (CBS News, 2016). By sharing the intense pain experienced by a mother’s loss of a child to violence, Mamie Till and the “Mothers of the Movement” allowed others to share in their grief.
As written by Sybrina Fulton (2014, para 9) in a letter to Lesley McSpadden, “If they refuse to hear us, we will make them feel us . . . feeling us means feeling our pain; imagining our plight as parents of slain children.” The pain experienced by these mothers was felt. Mothers of Black children extended sympathy and support to these mothers who had lost their children to community or state violence (Stewart, 2017).
One such letter, penned by university professor Melissa Harris-Perry, illustrates the emotional connection felt among women who saw their own children reflected in the faces of Michael Brown, Trayvon Martin, and Tamir Rice. According to Harris-Perry (2014, para 8), many Black mothers “felt your anguish through the screen, felt it penetrate our core and break our hearts as we bore witness to your shock and torment.” Statements such as this indicate that the public and violent losses experienced by African American mothers, both past and present, resonate within the African American community and particularly affect other African American mothers, even those who have not experienced such a loss. How African American mothers are affected by bearing witness to the public deaths of African Americans as a result of community and state violence is not fully known. Hence, the purpose of this study was to investigate the experiences of African American mothers who have been exposed to state and community violence while raising their sons to understand how this exposure connects to their physical and mental health.
The experiences communicated by the women mentioned above suggest that parenting for these women is in some way unique and shaped by the social and racial contexts in which they live. Research on parenting in general, and parenting stress specifically, has indicated that experiences and context affect the lives of parents in particular ways. Cumulative exposures to life stressors, such as those associated with limited availability of resources, can exacerbate parenting stress, mental strain, or tension related to the role of being a parent (Berry & Jones, 1995; Raphael, Zhang, Liu, & Giardino, 2010). For example, lack of financial resources aggravates parenting stress by draining parents’ emotional resources to respond empathetically to their children. Under high economic strain, parents are more likely to become preoccupied with managing finances (e.g., an overdue bill or loan default) and emotionally less available for their children, which negatively influences child development (Berk, 2013; Conger & Donnellan, 2007). Additionally, parents’ experiences with other daily stressors (e.g., work-related frustrations and burden) influence parenting behaviors and attitudes, which may create stressful home environments for children (Matjasko & Feldman, 2006).
African American mothers in low-income families have reported high rates of trauma and post-traumatic stress disorder (PTSD) symptoms, and their PTSD can predict parental distress (Cross et al., 2018). Such parental stress has been inversely related to positive parenting behaviors (Chang et al., 2004), which can result in negative outcomes for children. Stress among African American mothers exists regardless of family structure. Cain and Combs-Orme (2005) found co-caregiving with a spouse, partner, or other family member did not affect maternal stress or parenting behaviors. This research indicates that parental stress is prevalent among African American mothers whether they are single parents or co-parenting.
A contextual factor that may shed light on the experiences of parenting stress among African American mothers is race-based stress (Carter, 2007). According to Greer (2011), the negative, race-related experiences of African Americans are associated with negative psychological outcomes such as anxiety and depression. African American women in particular experience racism within the workplace, health care system, and educational settings (Greer, 2011). Racist microagressions play a key role in the psychological distress of African American women and significantly contribute to increased levels of stress and anxiety (Szymanski & Owens, 2009). Affective costs of racism among this disenfranchised group include depression, anxiety, and somatization (Pieterse, Todd, Neville, & Carter, 2012). Pieterse et al. (2012) reported trauma-like symptoms similar to PTSD among African Americans after prolonged episodes of racism.
Exposure to community and state violence exists as a particular type of race-based stress that strains the psyche of African Americans. Galovski et al. (2016) found that among community members in Ferguson, Missouri, following the killing of Michael Brown by a law enforcement officer, post-traumatic stress and depression were higher among African Americans than their White counterparts. Additionally, direct exposure to violence was not associated with distress, suggesting that media exposure or secondary exposure provided the sufficient context for mental health concerns to exist. Similarly, Bor, Venkataramani, Williams, and Tsai (2018) reported that African American residents in a state where police killings of unarmed African Americans occurred experience worse mental health following each incident. These effects were not evident for White residents in the same state, nor was there a similar effect for unarmed White residents or armed African American residents killed by police. According to Umberson (2017), exposure to violent death within the community is particularly difficult when the loss is that of a loved one. Such a loss within the African American community “launches a lifelong cascade of psychological, social, behavioral, and biological consequences that undermine other relationships, as well as health, over the life course” (Umberson, 2017, p. 407). The continued losses of young African American men to community and state violence present a collective threat and result in a sense of vulnerability within the African American community, as well as potentially contribute to an increase in health disparities among this population because of race-related stress.
African American mothers experience parenting stress as well as race-based stress, yet the extent to which race-based parenting stress exists for them is unknown. Research on African American mothers has explored their levels of stress and the relationship that parental stress has with their parenting behaviors and children’s outcomes (e.g., Cain & Combs-Orme, 2005; Chang et al., 2004; Cross et al., 2018; Kennedy, Bybee, & Greeson, 2014). However, often the research focus is on “at-risk” African American mothers such as adolescent mothers, single mothers, mothers experiencing intimate partner violence, and mothers in low-income households. Additionally, despite the abundance of research with samples of African American mothers, the exploration of their lived experiences as mothers who may be exposed to race-based stress vis-à-vis state and community violence is absent from the literature. Violence resonates through relationships and can be conceptualized as a reproductive health and social justice issue for African American women (Premkumar, Nseyo, & Jackson, 2017). Hence, this study sought to illuminate the experiences of African American women raising sons, allowing them the platform to speak their lived experiences as mothers in the current social and racial context.
Method
The following research question was examined: What are the lived experiences of African American mothers who have been exposed to community and state violence while raising their sons? The research team chose a qualitative approach, specifically phenomenological methodology. As a constructivist approach, phenomenology acknowledges the existence of multiple realities and allows for an understanding of the lived experiences of participants through their own voices. This methodology is congruent with the profession of counseling (Hays & Wood, 2011), and the researchers felt using phenomenology was particularly important given the focus on African American women who experience multiple layers of marginalization at the intersection of race and gender (Crenshaw, 1989).
Participants
Prior to participant recruitment, the Institutional Review Board at the authors’ university approved the study. The participants were recruited via purposive, criterion sampling to gain a sample of African American mothers with at least one son age 25 or younger at the time of the study. Recruitment materials were shared with African American women using direct electronic mail as well as social media. Participants also referred potential participants to the research team for inclusion in the study (snowball sampling). Research team members contacted all participants via direct electronic mail to provide them with details about the study, review the informed consent document, collect demographic information, and schedule the individual interview. Sample size recommendations for qualitative research such as the present study range from six to 12 participants (Creswell, 2013; Guest, Bunce, & Johnson, 2006; Onwuegbuzie & Leech, 2007). Hence, the research team sought to recruit 20 participants to account for the possibility of attrition.
In response to recruitment efforts, 22 individuals expressed interest in the study and were initially contacted by the researchers. Two of those individuals were unable to complete an individual interview, and another individual was eliminated because of poor audio recording quality. Hence, data from 19 participants were analyzed for this study. Further recruitment was deemed unnecessary as the sample size exceeded the recommended size and the data analysis reached saturation with data from these 19 participants.
The participants ranged in age from 31 to 61, with a mean age of 44.8. Their sons ranged in age from 2 to 35, though all had at least one son under age 25. All participants were high school graduates, and most had an advanced degree (52.6%). Additionally, most participants lived in two-parent households (52.6%) at the time of the study, earned an annual household income of more than $100,000 (42.1%), and lived in a suburban setting (57.9%). Participant profiles are provided in Table 1.
Data Collection and Analysis
The researchers conducted semi-structured individual interviews with the 19 participants, each lasting 20 to 60 minutes. All interviews were conducted over the phone, audio-recorded, and transcribed verbatim. The interview protocol consisted of the following questions: (a) What have your experiences been like being a mother of an African American boy or young man? (b) There have been several violent incidents reported by the media involving African American young men. How do you feel about these incidents? (c) Was there any particular incident that affected you the most? (d) How would you describe your overall mental and physical health? and (e) What would you say are your strengths as a mother? The interviewers provided follow-up questions and clarifying statements to participants when they were deemed necessary or when participants asked for clarification.
Once the interviews were transcribed, the research team analyzed the data in accordance with methods outlined by Moustakas (1994). First, the team immersed themselves in the data by reviewing each transcript individually. They divided the 19 transcripts between the two of them and read through them to become familiar with the data. For each transcript, they identified relevant statements that reflected the participants’ lived experiences (horizontalization) as African American mothers raising boys and young men within the contexts of structural racism and community and state violence. After going through this process individually, the research team met multiple times to review all transcripts and confer about these textural descriptions. The research team identified relevant codes and then synthesized the textural descriptions into themes by examining them for commonalities to distill the meaning expressed by the participants. Verbatim examples were extracted from the transcripts and used to generate a thematic and visual description of the phenomenon being examined. Once the initial data analysis was completed, the researchers conducted member checking by sending each participant their individual transcript as well as the written results section. Participants were asked to comment on the accuracy of their transcripts as well as the alignment of the results with their lived experiences. None of the participants reported any errors or additions to the transcripts, and none provided any additions or corrections to the themes provided in the results.
Table 1. Participant Demographic Information
| Participant |
Age |
Number of Male Children in Home |
Age(s) of Male Children |
Household Composition |
Education |
| 1 |
31 |
1 |
2 |
Multi-generational |
Bachelor’s Degree |
| 2 |
45 |
3 |
15, 20, 27 |
Two-parent |
Master’s Degree |
| 3 |
50 |
1 |
19 |
Two-parent |
Master’s Degree |
| 4 |
42 |
1 |
15 |
Two-parent |
Doctoral Degree |
| 5 |
48 |
1 |
23 |
Two-parent |
Master’s Degree |
| 6 |
43 |
2 |
2, 16, 19 |
Two-parent |
Master’s Degree |
| 7 |
46 |
1 |
16 |
One-parent |
Doctoral Degree |
| 8 |
61 |
1 |
20 |
One-parent |
Some College |
| 9 |
40 |
2 |
2.5, 5 |
Two-parent |
Bachelor’s Degree |
| 10 |
56 |
0 |
19 |
One-parent |
Master’s Degree |
| 11 |
47 |
1 |
18, 26 |
Two-parent |
Bachelor’s Degree |
| 12 |
43 |
1 |
10 |
Two-parent |
Doctoral Degree |
| 13 |
43 |
1 |
18 |
One-parent |
Bachelor’s Degree |
| 14 |
36 |
2 |
2, 7 |
Two-parent |
Bachelor’s Degree |
| 15 |
41 |
1 |
17, 21, 26 |
One-parent |
Doctoral Degree |
| 16 |
45 |
1 |
16 |
One-parent |
Master’s Degree |
| 17 |
42 |
1 |
12 |
Multi-generational |
Bachelor’s Degree |
| 18 |
35 |
1 |
9 |
One-parent |
Some College |
| 19 |
57 |
1 |
22, 35 |
Two-parent |
Bachelor’s Degree |
Trustworthiness and the Research Team
Qualitative research requires credibility, a key element of trustworthiness, such that the research findings accurately reflect the data (Lincoln & Guba, 1985). Reflexivity, wherein researchers critically examine their procedures with respect to power, privilege, and oppression, is a critical element of maintaining research credibility (Hunting, 2014). To safeguard against researcher bias, the researchers worked collaboratively to establish credibility throughout data collection and analysis. The research team consisted of two African American female faculty members at a large Southeastern university. Both were core faculty in the same counselor education program and have experience working as professional school counselors. To address researcher bias, the researchers engaged in bracketing to address the ways in which their experiences influence their approach to research and expectations of the outcomes of the study. Prior to the data collection, they discussed their experiences as African American women who have experienced systemic racism and are aware of state and community violence affecting the African American community. They identified their personal experiences and acknowledged their biases, attempting to put them aside as they conducted the interviews. Throughout the data collection and analysis, they engaged in personal reflection and maintained analytic memos chronicling their reactions and initial thoughts about the data being collected.
Prior to beginning data analysis, the research team met to confirm the analysis procedures to ensure consistency. They analyzed data individually and as a team and determined codes and themes jointly to reduce bias. They also consulted throughout the data analysis process to address questions or concerns regarding the data. They consulted with an outside researcher experienced in qualitative research to get critical feedback on the data analysis process and the research findings (Marshall & Rossman, 2006). This peer review was used as an external check of the research methodology and theoretical interpretation of the data.
Results
Six themes emerged from the data to illustrate the lived experiences of African American mothers who have been exposed to community and state violence while raising their sons: (a) psychological distress, (b) physical manifestations of stress, (c) parenting behaviors, (d) empathic isolation, (e) coping strategies, and (f) strengths. The analysis of the data revealed that these themes were connected such that community and state violence were forces weighing on these mothers, resulting in emotional responses, changes to parenting approaches, physical responses, and empathic isolation, while the mothers’ coping strategies and strengths served as forces to uplift. Below is a discussion of each theme using exemplars from the data to present the experiences of these mothers in their own words.
Psychological Distress
The participants in this study described the emotions they felt regarding community and state violence, with all of them expressing various levels of fear, anger, heartbrokenness, and exhaustion. Fear or anxiety was most prominent for these mothers, many of whom thought of their own sons when they heard stories about young African American men killed by gun violence at the hands of other citizens or by law enforcement officers. Some felt fear of the unknown, as in Participant 9 who stated, “Like, what will the world do to you?” Many expressed that the fear was persistent, as they seemed to ruminate over such shootings. In Participant 10’s words, “I see the pictures of those young men daily in my mind.” The fear that these mothers described relates directly to their sons in that they have a baseline fear that their son also will become a victim of state violence. Participant 2 described living with “an underpinning of terror,” adding that “my fear is that . . . one of my sons is going to be murdered by a police officer.” In addition to fear, the participants reported feelings of anger and outrage. Participant 5 stated that she considered purchasing a gun, although she did not articulate what she would do with it. For many of the mothers, their anger was closely associated with their experience of motherhood: “Before I had kids, I didn’t realize how angry I already was about the injustice . . . it just (caused) more anger and frustration” (Participant 9).
Feelings of being heartbroken, helpless, and psychologically exhausted emerged clearly from the data. Participants expressed disbelief upon hearing about police shootings of unarmed African American men and a lack of control about what Participant 7 referred to as “a cancer on society.” Participant 1 described the experience of feeling like she had been “hit with a rubber bullet, like, you know there’s no penetration, but it hurts all the same.” A particularly poignant statement from Participant 10 indicated that participants feel helpless and almost hopeless about the possibility that a change is possible: “I don’t even know what our children have to do to convince the world that they are children . . . or even that they are human.” Additionally, the mothers are mentally exhausted by reports of community and state violence against African American young men. Participant 1 described feeling burned out, tired, and “just one tipping point message away from a breakdown.”
Part of this exhaustion seemed to stem from a sense of proximity to the events in the news because of social media and 24-hour news cycles. Participants reported that they felt like the shootings were happening right in front of them, making them more aware of the existence of community and state violence. Some reported feeling numb to the media reports and others stopped watching the news or engaging with social media sites in an attempt to try to disconnect from reports they found overwhelming.
Physical Manifestations of Stress
The mothers in this study described the ways in which the exposure to community and state violence affected them physically. Some reported reactions that sounded like responses to trauma or some anxiety-provoking experience that were manifested in their physical bodies. Participant 1 felt “sick to my stomach . . . heart, you know like adrenaline pumping . . . like a tightness in my chest.” Participant 5 stated that after hearing about a recent police shooting and out of concern for the safety of her son, she “would be physically sick.” Additionally, participants reported a loss of sleep and difficulty relaxing. A response by Participant 14 illustrates the connection that the physical effects have to the psychological effects of community and state violence for these mothers: “I cried as though this was my child that had been killed . . . I was sick to my stomach . . . I had a pit in my stomach . . . and I also . . . became overly concerned about my son.” They were psychologically affected by incidents of state and community violence and those effects manifested physically as well as in their hypervigilance regarding their sons.
Parenting Behaviors
The participants described how their mothering has been shaped by their exposure to community and state violence. They reported being hypervigilant and overprotective in their parenting behaviors in an effort to protect their sons. These parenting behaviors included hovering over their sons, micromanaging their sons’ lives, and attempting to limit their sons’ movements. Participant 5 stated that she wanted to put a camera in her son’s car so that she could have an eye on him when he was driving. Participants described their efforts to keep their sons insulated, such as Participant 13’s statement that “I just try to keep my son as far away from it as I possibly can.” Participant 10 expounded on this behavior in great detail, stating “If I could have, I would have locked him in my house and just kept him there.” The mothers seemed to have a keen awareness that their parenting had become overly protective, and they experienced some ambiguity about it. One mother acknowledged that she parents her son and daughter differently and lamented that she may be limiting his cognitive development. Similarly, Participant 4 expressed concern that being overprotective might affect her son’s social life, yet her concern for his safety outweighed that concern, as evidenced by her statement that, “I don’t want that for him, but at the same time I need him to be alive.”
The participants also stated that they regularly have conversations with their sons about how to behave and present themselves to others. They reported increasing these conversations following incidents of community and state violence in the news. The conversations they have include how to carry themselves in a respectable way in public and how to make wise decisions when outside the home. Specifically, they have talked with their sons about what to do if stopped by the police. The participants described the conversations as ones that go beyond the typical lessons that parents teach their children in that these are conversations shaped by their experiences as African American mothers of African American sons. As Participant 5 stated “we’ve had to say things to them that their White friends don’t have to say.”
Empathic Isolation
In their description of the effects community and state violence have had on their emotions, physical bodies, and parenting, the participants also described an experience that the researchers have called empathic isolation. Participants described receiving little to no empathy from others outside of the home as well as a self-imposed masking of emotions within the home in an effort to protect their sons. The lack of empathy outside of the home seemed to be connected with the perceived White privilege of coworkers and community members. Participant 5 stated of such individuals: “I want you to feel my frustration and my anger”—yet those individuals did not. Participant 3 added that the responses that she heard from others after publicized incidents of community or state violence upset her because they reflected a lack of empathy and understanding. During the trial of George Zimmerman, Participant 10 was hopeful because the jury largely consisted of women. However, she was disappointed by the outcome of the trial and felt that the women on the jury saw Trayvon Martin as a Black male adult rather than a 16-year-old boy. She wondered how and when Black children would be seen as children rather than threats. As a result of this lack of empathy, many of the mothers reported masking their emotions in public spaces. Participant 19 stated, “I have to put on my face in the morning when I go into the workplace that has every ethnicity and just be me, not be that concerned mother.”
Similarly, at home the mothers reported holding their emotions close in an attempt to protect their sons. They expressed concern about their emotions affecting their sons, so they mask their emotions. Participant 18 described having to “put on” for her son, meaning that despite her sadness or concern, she had to “put on that face that everything is okay.” A single mother participant expressed how it is particularly difficult for her to allow herself to fully experience her emotions. She described feeling as though she had no choice but to be strong even in moments in which she feels weak. Both inside and outside of the home, these mothers feel a multitude of emotions, yet they do not feel fully free to express them and receive empathy, either because of the empathic failures of others or because they want to shield their sons and keep pushing forward.
Coping Strategies
Despite the stress they feel as mothers raising African American boys and young men, participants identified multiple ways in which they cope or care for themselves in the face of adversity. Some coping strategies were internal or individual, such as maintaining a positive outlook, engaging in self-care, journaling, and prayer or meditation. Reliance on faith was evident for many participants and for at least one participant was a means to fight oppression and liberate her son (Participant 10). Participants also discussed other ways of coping that had more of an external focus, such as connecting with other African American mothers and looking to their existent social network of family and friends for support. Several participants discussed either current involvement or a desire for future involvement in community activism to address systemic racism. These participants described a type of self-care motivated by a desire to see change and manifested in action to address the systemic racism that affected their lives and the lives of their sons.
Few of the participants (n = 4) reported seeking out and utilizing professional mental health services as a coping strategy. Participants gave multiple reasons for not seeking mental health services, including pragmatic ones, such as not having time or not being able to afford services. Participants also made statements such as “I just deal with it” (Participant 7) and “I feel like I can control it” (Participant 15), which seem to relate to the experience of wearing the mask discussed above with the theme of empathic isolation. Other statements by participants indicated that they have little confidence that counseling would help. Participant 14 stated plainly that there is no use in her seeking counseling if the systems that affect her son are still in existence. Participant 10 focused on what the experience in a counseling session would be like if she were to share her experiences and feelings as an African American mother raising a son. She described the potential exhaustion she would feel as a client, stating, “In terms of talking about the anxiety around racism and concern for my children, I just did not have the energy to seek any kind of help for that.”
Strengths
In response to the question about their strengths as mothers, participants identified several internal strengths that shape their parenting as well as the outward behaviors that characterize their motherhood. Among their internal strengths were responsibility, morality, unconditional love and acceptance, integrity, thinking big, being open and honest in communication, being informed and educated, having the ability to see purpose and strengths in their children, flexibility, resourcefulness, and resilience. Participant 10 gave a particularly powerful characterization of her strengths, stating, “I think . . . as African American women to go ahead and be mothers in the world that we live in, it’s a combination of crazy and brave.” With these internal strengths, the mothers reported being active on behalf of their children by giving them as many opportunities as possible, advocating for them when necessary, teaching them skills, building a social support network, and keeping their children as a priority.
Discussion
The aim of this study was to explore the experiences of African American mothers who have been exposed to state and community violence while raising their sons to understand how this exposure connects to their physical and mental health. Six themes emerged from the data: psychological distress, physical manifestations of stress, parenting behaviors, empathic isolation, coping strategies, and strengths. From the perspectives of these participants, state and community violence weigh down on them as African American mothers, negatively impacting their psychological and physical health and altering their parenting behaviors. Additionally, the interplay between their psychological distress and the change in their parenting facilitates an experience of empathic isolation, in which these mothers mask their emotions inside their homes so as not to adversely affect their sons, and mask their emotions outside of the home (e.g., in the workplace) as they interact with others who are either incapable or unwilling to provide empathic responses to their experiences. Further, participants identified clear personal strengths and coping strategies, such as devotion to their children and involvement in community activism, which were used to uplift themselves. Interestingly, the coping strategies for most of these women did not include seeking help from a mental health professional, even when they were aware of the psychological distress associated with exposure to community and state violence.
These results are both enlightening and disheartening. African American mothers live with daily fear for their sons of all ages. This fear exists despite most of the participants reporting that their sons had not been directly involved in or exposed to violence. These mothers constantly relive psychological trauma because of media exposure of incidents of community and state violence involving African American boys and young men. The results support sentiments of Galovski et al. (2016) that African American mothers are not concerned with just a few random incidents of violence, but rather are affected by greater, continuous, and systemic experiences of psychological trauma spanning decades. These continued distressing experiences of direct and indirect violence appear to negatively impact the psychological (e.g., anger, fear, outrage) and physiological (e.g., tightness in the chest) well-being of African American mothers and likely exacerbate existing health disparities for this population. Findings support previous research regarding the experience of ongoing race-related PTSD among African American mothers (Pieterse et al., 2012). Still, despite threats to their mental and physical health, African American mothers continue to press through with the hopes of protecting and empowering their sons using a cloak of resilience and buoyancy. Additionally, African American mothers wear a mask of courage and strength to educate their children about racism, resilience, and resistance without revealing their true emotions. DePouw and Matias (2016) highlighted the concept of critical race parenting, whereby parents of color work to educate, advocate, and protect their children from cultural racism. Based on the findings of this study, African American mothers continue to fight for access to safety and equality for their children, while simultaneously attempting to shield their sons from the psychological and physical health effects that community and state violence have on them as mothers.
Implications for Counselors
The results of this study provide insight into the experiences of African American mothers raising sons in the context of #BlackLivesMatter and can inform the work of mental health professionals regarding this population. Given that many African American mothers live with fear or anxiety regarding the safety of their sons, which affects their mental and physical health and parenting behaviors, practitioners might consider culturally sensitive and responsive methods to attract and retain these mothers as clients. An ideal start would be to seek to understand the social and historical context of the experiences of African Americans and the connection with current events of violence and racism. This exploration should be done not within the confines of counseling, but in preparation for building therapeutic rapport. Participants in this study reported possessing little faith that White counselors would understand or believe their experiences. This finding underscores the need for greater cultural competence among White mental health professionals and an increase in the number of available African American counselors to serve African American women. Additionally, work with African American mothers must be strengths-based, building upon the internal and external strengths and resources that exist within the lives of these women. Specifically, the sense of determination encapsulated in the phrase “crazy and brave,” used by one of the participants to describe herself, highlights the resourcefulness of African American mothers to provide for and protect their families. Counselors are encouraged to recognize and enhance such personal assets by highlighting the positive energy that these mothers bring to the therapeutic setting through their stories. Relational cultural theory (RCT) might be an appropriate framework to use in counseling clients like the women in this study. RCT centers the cultural experiences of clients and considers how systems of oppression and marginalization affect individuals and their relationships (Comstock, et al., 2008). The mutual empathy, mutual empowerment, and authenticity that are foundational in RCT can provide a therapeutic environment in which African American mothers can explore their experiences of disconnection, such as the empathic isolation that they described in this study.
Finally, mental health professionals need to consider the importance of social justice advocacy to address the community and state violence that negatively impacts the African American community at large and African American mothers of sons specifically. This, in fact, is an ethical obligation of professional counselors who advocate on multiple levels “to address potential barriers and obstacles that inhibit access and/or the growth and development of clients” (American Counseling Association, 2014, p. 5). The results of this study clearly indicate that community and state violence can be a barrier to optimal physical and mental health of African American mothers. The #BlackLivesMatter movement has created resources for individuals seeking to engage in advocacy and encourage open dialogue around issues of community and state violence (https://blacklivesmatter.com/resources). Specifically, mental health professionals can access and utilize the #BlackLivesMatter toolkits focused on healing justice and action, as well as the toolkit titled #TalkAboutTrayvon. Such resources can be a starting place to gain knowledge and develop a strategy for advocacy.
Limitations and Future Research
This study, although rich in details of the experiences of African American mothers, is not without limitations. Although attempts were made to secure African American mothers from varying sub-groups, the resulting sample yielded mainly educated women from mostly two-parent middle-class families, most of whom were from the Southern region of the United States. A more economically and educationally diverse sample of African American mothers might have yielded differences in experiences. For instance, given that poor communities of color are often over-policed (Alexander, 2010), African American mothers in lower socioeconomic brackets might have discussed direct contact with law enforcement and increased incidents of both community and state violence. Additionally, although many of the participants were married or partnered, the researchers did not explore how their spouses or partners played a role in their experience as African American mothers. Some participants mentioned the fathers of their sons and their perspectives; however, this relational aspect needs further inquiry to fully understand its essence. It was beyond the scope of this study to examine the experiences of African American fathers raising sons in the context of #BlackLivesMatter, yet this is certainly a worthy line of research that would augment the findings of this study.
Despite the lack of heterogeneity in this sample with regards to education and income, and focus on mothers to the exclusion of their spouses, partners, or co-parents, the design of the study provided rich and in-depth data regarding a relatively unexplored yet salient topic among a unique sample. Future research can extend the knowledge base regarding African American mothers by exploring the experiences of mothers who are raising daughters in the current context in which exposure to community and state violence occurs regularly through social media. Often, conversations regarding community and state violence, particularly when police use of excessive force is involved, focus on the experiences of African American boys and men. However, Crenshaw’s (1991) work on intersectionality as well as the #SayHerName movement (2015) reminds us that African American girls and women also are victims of community and state violence. Including mothers raising daughters into this line of research will help uncover the ways in which gender influences motherhood among African Americans when #BlackLivesMatter and #SayHerName intersect. Additionally, future research should include both homogenous and heterogenous focus groups of mothers to explore, compare, and contrast the experiences of mothers of color and White mothers in terms of parental stress, mental health, and physical health. Finally, future research should focus on identifying social determinants of health that counselors, physicians, and other helpers can use to address health disparities that may be exacerbated by ongoing psychological trauma.
Conclusion
The results of this qualitative study highlight the experiences of African American mothers—“crazy and brave” women—determined to protect and provide for their sons while also contending with a lingering fear for their safety within the current social context. State and community violence, now widely broadcasted in media, affect the psychological and physical well-being of these mothers and contribute to hypervigilance in their parenting. As mental health professionals that value the enhancement of human development and the promotion of social justice, counselors have a duty to provide culturally sensitive services to support this population so that they can take off their masks and experience the empathy that is lacking in many aspects of their lives. Additionally, this duty extends beyond the counseling room as counselors serve as social justice advocates in order to address the systemic barriers to mental health and wellness for members of the African American community.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alexander, M. (2010). The new Jim Crow: Mass incarceration in the age of colorblindness. New York, NY: The
New Press.
American Counseling Association. (2014). 2014 ACA code of ethics. Retrieved from http://www.counseling.org/
Resources/aca-code-of-ethics.pdf
Berk, L. E. (2013). Child development (9th ed.). Boston, MA: Pearson.
Berry, J. O. & Jones, W. H. (1995). The Parental Stress Scale: Initial psychometric evidence. Journal of Social and Personal Relationships, 12, 463–472. doi:10.1177/0265407595123009
Black Lives Matter. (n.d.). Herstory. Retrieved from https://blacklivesmatter.com/about/herstory
Bor, J., Venkataramani, A. S., Williams, D. R., & Tsai, A. C. (2018). Police killings and their spillover effects on the mental health of black Americans: A population-based, quasi-experimental study. The Lancet, 392, 302–310. doi:10.1016/S0140-6736(18)31130-9
Cain, D. S., & Combs-Orme, T. (2005). Family structure effects on parenting stress and practices in the African American family. Journal of Sociology and Social Welfare, 32(2), 19–40.
Carter, R. T. (2007). Racism and psychological and emotional injury: Recognizing and assessing race-based traumatic stress. The Counseling Psychologist, 35, 13–105. doi:10.1177/0011000006292033
CBS News. (2016). How Emmett Till’s brutal death “ignited a movement” in America. Retrieved from https://www.cbsnews.com/news/emmett-till-murder-mamie-mobley-america-civil-rights-movement-smithsonian-museum
Chang, Y., Fine, M. A., Ispa, J., Thornburg, K. R., Sharp, E., & Wolfenstein, M. (2004). Understanding parenting stress among young, low-income, African-American, first-time mothers. Early Education and Development, 15, 265–282. doi:10.1207/s15566935eed1503_2
Comstock, D. L., Hammer, T. R., Strentzsch, J., Cannon, K., Parsons, J., & Salazar, G., II (2008). Relational-cultural theory: A framework for bridging relational, multicultural, and social justice competencies. Journal of Counseling & Development, 86, 279–287. doi:10.1002/j.1556-6678.2008.tb00510.x
Conger, R. D. & Donnellan, M. B. (2007). An interactionist perspective on the socioeconomic context of human development. Annual Review of Psychology, 58, 175–199. doi:10.1146/annurev.psych.58.110405.085551
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics. University of Chicago Legal Forum, 1989, 139–167.
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43, 1241–1299.
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). Thousand Oaks, CA: Sage.
Cross, D., Vance, L. A., Kim, Y. J., Ruchard, A. L., Fox, N., Jovanovic, T., & Bradley, B. (2018). Trauma exposure, PTSD, and parenting in a community sample of low-income, predominantly African American mothers and children. Psychological Trauma: Theory, Research, Practice, and Policy, 10, 327–335.
doi:10.1037/tra0000264
DePouw, C., & Matias, C. (2016). Critical race parenting: Understanding scholarship/activism in parenting our children. Educational Studies, 52, 237–259.
Drabold, W. (2016). Meet the mothers of the movement speaking at the Democratic Convention. Retrieved from
http://time.com/4423920/dnc-mothers-movement-speakers
Fulton, S. (2014). Trayvon Martin’s mom: “If they refuse to hear us, we will make them feel us.” Retrieved from http://time.com/3136685/travyon-sybrina-fulton-ferguson
Galovski, T. E., Peterson, Z. D., Beagley, M. C., Strasshofer, D. R., Held, P., & Fletcher, T. D. (2016). Exposure to violence during Ferguson protests: Mental health effects for law enforcement and community members. Journal of Traumatic Stress, 29, 283–292. doi:10.1002/jts.22105
Greer, T. M. (2011). Coping strategies as moderators of the relation between individual race-related stress and mental health symptoms for African American women. Psychology of Women Quarterly, 35, 215—226. doi:10.1177/0361684311399388
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data saturation and variability. Field Methods, 18, 59–82. doi:10.1177/1525822X05279903
Harris-Perry, M. (2014). A letter of sympathy to Michael Brown’s mother. Retrieved from http://www.msnbc.com/melissa-harris-perry/letter-sympathy-michael-browns-mother
Hays, D. G., & Wood, C. (2011). Infusing qualitative traditions in counseling research designs. Journal of Counseling & Development, 89, 288–295. doi:10.1002/j.1556-6678.2011.tb00091.x
Hunting, G. (2014). Intersectionality-informed qualitative research: A primer. Vancouver, British Columbia: The Institute for Intersectionality Research and Policy.
Kennedy, A. C., Bybee, D., & Greeson, M. R. (2014). Examining cumulative victimization, community violence exposure, and stigma as contributors to PTSD symptoms among high-risk young women. American Journal of Orthopsychiatry, 84, 284–294. doi:10.1037/ort0000001
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. Newbury Park, CA: Sage.
Marshall, C., & Rossman, G. B. (2006). Designing qualitative research (4th ed.). Thousand Oaks, CA: Sage.
Matjasko, J. L., & Feldman, A. F. (2006). Bringing work home: The emotional experiences of mothers and fathers. Journal of Family Psychology, 20, 47–55. doi:10.1037/0893-3200.20.1.47
Moustakas, C. (1994). Phenomenological research methods. Thousand Oaks, CA: Sage.
Onwuegbuzie, A. J., & Leech, N. L. (2007). A call for qualitative power analyses. Quality & Quantity, 41, 105–121. doi:10.1007/s11135-005-1098-1
Pieterse, A. L., Todd, N. R., Neville, H. A., & Carter, R. T. (2012). Perceived racism and mental health among Black American adults: A meta-analytic review. Journal of Counseling Psychology, 59, 1–9.
doi:10.1037/a0026208
Premkumar, A., Nseyo, O., & Jackson, A. V. (2017). Connecting police violence with reproductive health. Obstetrics and Gynecology, 129, 153–156. doi:10.1097/AOG.0000000000001731
Raphael, J. L., Zhang, Y., Liu, H., & Giardino, A. P. (2010). Parenting stress in US families: Implications for paediatric healthcare utilization. Child: Care, Health and Development, 36, 216–224.
doi:10.1111/j.1365-2214.2009.01052.x
#SayHerName Movement. (2015). #SayHerName: Resisting police brutality against Black women. Retrieved from http://aapf.org/sayhernamereport
Sebastian, M. (2016). Who are the “Mothers of the Movement” speaking at the Democratic National Convention? Retrieved from https://www.elle.com/culture/career-politics/news/a38111/who-are-mothers-of-the-movement-dnc
Stewart, F. R. (2017). The rhetoric of shared grief: An analysis of letters to the family of Michael Brown. Journal of Black Studies, 48, 355–372. doi:10.1177/0021934717696790
Szymanski, D. M., & Owens, G. P. (2009). Group-level coping as a moderator between heterosexism and sexism and psychological distress in sexual minority women. Psychology of Women Quarterly, 33, 197–205. doi:10.1111/j.1471-6402.2009.01489.x
Umberson, D. (2017). Black deaths matter: Race, relationship loss, and effects on survivors. Journal of Health and Social Behavior, 58, 405–420. doi:10.1177/0022146517739317
Richelle Joe, NCC, is an assistant professor at the University of Central Florida. M. Ann Shillingford-Butler, NCC, is an associate professor at the University of Central Florida. Seungbin Oh is an assistant professor at Merrimack College. Correspondence can be addressed to Richelle Joe, P.O. Box 161250, Orlando, FL 32816-1250, jacqueline.joe@ucf.edu.
