May 22, 2024 | Volume 14 - Issue 1
Kaprea F. Johnson, Alexandra Gantt-Howrey, Bisola E. Duyile, Lauren B. Robins, Natese Dockery
Career counselors practicing in rural communities must understand and address social determinants of mental health (SDOMH). This conceptual article details the relationships between SDOMH domains and employment and provides evidence-based recommendations for integrating SDOMH into practice through a rural community health and well-being framework. Description of the adaptation of the framework for career counselors in rural communities, SDOMH assessment strategies and tools, and workflow adjustments are included. Conclusions suggest next steps for practice and research.
Keywords: social determinants of mental health, career counselors, rural communities, health and well-being framework, assessment
Career counselors in rural communities address standard employment needs of the population, but they also must be aware of the socioeconomic circumstances that impact their community’s mental health and, in return, employment. Such socioeconomic factors are termed the social determinants of mental health (SDOMH). SDOMH are nonclinical psychosocial and socioeconomic circumstances that contribute to mental health outcomes (Office of Disease Prevention and Health Promotion [ODPHP], n.d.). Healthy People 2030, a government initiative to promote health and well-being, describes a five-domain framework of SDOMH which includes: economic stability, education access and quality, health care access and quality, neighborhood and built environment, and social and community context (ODPHP, n.d.). Collectively, SDOMH can disrupt overall well-being and have a cyclical relationship with employment. For example, in rural communities, minimal access to public transportation may make sustaining employment difficult, which can then impact health insurance. Without insurance, a person loses access to health care; with unmet health care needs, a person who is unwell and without access to treatment has less opportunity for employment. Thus, understanding and addressing SDOMH is critically important for career counselors working in rural and other underserved communities (Pope, 2011). This conceptual paper will define SDOMH, introduce a theoretical framework for addressing SDOMH, provide evidence-based recommendations for assessment and treatment, and conclude with national resources to support career counselors in rural communities as they incorporate addressing SDOMH into their work.
Rural Communities, Employment, and Career Counselors
The U.S. Census Bureau considers rural communities as a group of people, counties, and housing outside of an urban area. More specifically, the Office of Management and Budget defines rural as areas with an urban core population of fewer than 50,000 people (Health Resources and Services Administration, 2017). After the 2010 Census, it was estimated that approximately 15% of the population lives in rural communities (Health Resources & Services Administration, 2017). Rural communities experience higher rates of unemployment and poverty, and residents are therefore more likely to live below the poverty line (United States Department of Agriculture [USDA], 2014). This is largely rooted in the fact that rural communities experience underdevelopment, economic decline, and neglect (Dwyer & Sanchez, 2016). Economic focus in rural environments typically centers around agriculture, rather than technological advancement (Dwyer & Sanchez, 2016). This contributes in part to a dearth of economic resources and thereby to increased unemployment and poverty and reduced health and well-being outcomes (Bradshaw, 2007; Brassington, 2011; Dwyer & Sanchez, 2016).
According to research conducted by the USDA, the unemployment rate in rural communities steadily declined for approximately 10 years prior to the COVID-19 pandemic; in September of 2019, the rural unemployment rate was 3.5% (Dobis et al., 2021). However, unemployment in rural communities reached 13.6% in April 2020, with unemployment disparately affecting those in more impoverished communities (Dobis et al., 2021). The role and goal of the career counselor is to help individuals in a specific community obtain or retain employment (Landon et al., 2019). For example, career counselors start the counseling process by systematically assessing clients’ needs, qualifications, and job aspirations. They provide career planning services and effective job search strategies. They help with résumé writing, interview preparations, skill development, and training opportunities (Amundson, 1993). Further, career counselors provide case management services by tracking and monitoring their clients’ progress. They record client information, document counseling sessions, track job applications, and survey employment outcomes (Amundson, 1993). Through tailored support, the career counselor works with the client throughout the life span to support the search for and maintaining of employment, while building client resilience and feelings of empowerment along the way.
However, rural communities have limited employment options and self-employment opportunities, which makes the role of the career counselor difficult in rural settings. Individuals in rural communities seeking employment may find it difficult to trust an outside counselor, and they may experience limited or no access to mental health services, health care practitioners, and transportation services, thereby negatively impacting their ability to participate effectively in the employment process (Landon et al., 2019). Career counselors in rural settings must develop a broader range of skills and connections to better serve their clients. These inequities experienced in rural settings reflect SDOMH and are factors which interfere with the role of the career counselor.
Social Determinants of Mental Health and Employment
SDOMH are the nonmedical factors shaped by the unequal distribution of power, privilege, and resources that influence the health outcomes of individuals and communities (World Health Organization, 2014). SDOMH concern the environmental living conditions that affect a wide range of health, functioning, and quality-of-life outcomes and risks (Centers for Disease Control and Prevention, 2020). In the Healthy People 2030 framework, the ODPHP (n.d.) defined social determinants of health (SDOH) through five primary domains: Economic Stability, Education Access and Quality, Health Care Access and Quality, Neighborhood and Built Environment, and Social and Community Context. These five domains are important to understand within the context of employment. In the Economic Stability domain, employment is the most pertinent issue (ODPHP, n.d.), as a lack of employment typically influences both mental and physical health (Norström et al., 2019). A few distinct factors related to economic stability and employment include job security, work environment, monetary factors (e.g., pay), and the demands of the job (ODPHP, n.d.). For example, in rural communities, agriculture is a significant source of employment for individuals. However, this source of income is seemingly unstable, as farming and agriculture are mostly dependent on the season (Liebman, 2010). In the Education Access and Quality domain, enrollment in higher education or holding a higher education degree has been found to have a positive impact on employment, as well as yielding more positive overall health outcomes and optimal well-being (ODPHP, n.d.; USDA, 2017). For adults living in rural communities, unemployment rates are higher for those with lower education attainment, further supporting the connection between education and employment (USDA, 2017). Regarding the Health Care Access and Quality domain—specifically in rural communities—factors such as proximity to hospitals, lack of insurance, and the overall cost of health care can reduce accessibility. Health care, especially higher-quality health care, aids in preventing disease and improving individuals’ quality of life (ODPHP, n.d.). However, inadequate health care leads to higher rates of disease, which have a direct impact on individuals’ ability to sustain employment, due to factors such as missing work because of illness or having to travel further to receive health care (Dueñas et al., 2016).
Ability to travel is also a cause for concern in rural communities and is closely related to the Neighborhood and Built Environment domain. Healthy People 2030 proposed various objectives related to neighborhood and built environment, with one being to increase access to mass transit (ODPHP, n.d.). It is apparent that a lack of reliable transportation is directly tied to unemployment, especially in rural communities due to distance and limited accessibility (U.S. Department of Transportation, 2019). Public transportation carries many noteworthy benefits, such as reducing air pollution, being inexpensive compared to purchasing a car, minimizing the cost of fuel and upkeep for personal vehicles, and increased convenience. Although these positive aspects of public transportation are ideal, individuals living in rural communities may not be able to reap these benefits due to the lack of public transportation in these areas, perhaps also limiting employment options (Shoup & Homa, 2010; U.S. Department of Transportation, 2019).
Lastly, the fifth domain, Social and Community Context, is interrelated with employment, as it tends to have a significant impact on workplace conditions, influences individuals’ overall mental and physical health, and can hinder growth and development (Norström et al., 2019). Additionally, social cohesion and adequate support in communities can be leveraged to locate and obtain employment and other helpful resources; however, this often falls short in rural communities. For example, in rural communities, the inability to secure gainful employment is notably linked to geographical disparities, such as those within the Neighborhood and Built Environment SDOH domain. Examples of such geographic disparities which affect employment include limited or nonexistent options for public transportation, a lack of available local jobs, and a lack of childcare facilities for use by working parents. Rural communities also often experience a lack of resources to improve the employment outlook and overall well-being of their population (Bradshaw, 2007; Dwyer & Sanchez, 2016). In addition, structurally, it has been observed that economic resources tend to cluster or aggregate together. For example, businesses that have been successful in a community invite and attract more businesses, thus pulling resources away from rural communities that might not have such a history of business success. Meanwhile, communities that are left behind experience economic restructuring and delays in receiving new technologies, leading to fewer employment opportunities (Bradshaw, 2007; Landon et al., 2019). Thus, providing employment or vocational services in rural America can be particularly challenging.
Furthermore, unemployment, poverty, and mental health concerns are inextricably linked. When career counselors uncover and address these factors in rural America, they must consider the surplus of needed services and resources to systemically address interrelated issues. To be intentional, career counselors practicing in rural communities should consider using a theoretical foundation that provides direction for action on the SDOMH which impact their clients’ lives and ability to be gainfully employed. The Rural Community Health and Well-Being Framework (Annis et al., 2004) is a framework that would be exceedingly helpful in this pursuit.
Theoretical Framework for Action: Rural Community Health and Well-Being Framework
Rural communities make up over 20% of the population and are often classified by a lack of necessary resources, lower levels of education, and persistent economic inequities (Hughes et al., 2019; Mohatt et al., 2006). Although they face many challenges, individuals in rural communities have been found to be resilient, especially when the proper resources are available (Annis et al., 2004). Application of a theoretical framework to practice centered on the unique needs of rural communities is important in addressing SDOMH through career counseling. The Rural Community Health and Well-Being Framework (Annis et al., 2004) strategically builds upon community resiliency and identifies economic, social, and environmental factors which are seen as essential components of health in rural communities. This framework also implores career counselors to consider how SDOMH indicators impact the community as a whole as well as individual people. For example, the framework provides specific areas for increased career counselor awareness and action: health, safety and security, economics, education, environment, community infrastructure and processes, recreation, social support and cohesion, and the overall population. These specific areas for rural communities are within the SDOMH domains, but emphasis is placed on recognition of the specific areas within the SDOMH domains that have the greatest impact on the community.
This comprehensive framework centers the needs of rural communities and provides direction for assessing and addressing SDOMH that impact employment and overall well-being. This framework will assist in uncovering employment issues and barriers faced by individuals within rural communities. Using this framework to assess SDOMH conditions (e.g., economic, social, environmental) will aid in developing employment and mental health interventions that are socially conscious and address root causes of unemployment and poor mental health. Overall, this framework provides a model for assessing and addressing SDOMH in rural communities.
Adaptation for Career Counselors
Career counselors in rural communities who wish to use the Rural Community Health and Well-Being Framework for practice should consider doing the following: (a) increasing their awareness and understanding of SDOMH and the framework, (b) increasing their understanding of the specific community needs outlined by the framework, and (c) assessing the values and needs of the community. However, because the framework is primarily focused on community-level indicators of need, career counselors will need to adapt what they learn about the community to inform their practice with individual community members. The role of the career counselor is multifaceted; thus, career counselors can engage various aspects of their role, such as listener, leader, and evaluator, in their advocacy efforts.
To begin this process of learning about community and individual needs, Annis et al. (2004) suggested the importance of listening. For example, based on the community-level indicators of need, career counselors can assess individual clients for their unmet needs within those specific areas. By understanding how members of the community are experiencing indicators such as health, recreation, social support, transportation, and resources, career counselors will become better equipped to understand and address issues that are impacting their clients’ ability to obtain and maintain employment. Beyond the use of assessments, this framework equips career counselors to broach important conversations about social needs (Andermann, 2016) with their clients, to inform potential connection with community resources. These conversations may include explicit discussion about particular SDOMH challenges (e.g., education, safety, access to affordable childcare), as well as about the client’s sense of belonging, or lack thereof, within their community. These conversations should allow for increased understanding and rapport building through genuine listening and empathy (Annis et al., 2004; Covey, 1989).
Finally, the framework implores career counselors to advocate with and for individuals within their rural community to provide equitable employment opportunities (Crumb et al., 2019). Such advocacy may take place through connection with local rural community leaders, who may have power to alter or increase the distribution of certain resources within the community setting. For example, a career counselor may advocate on behalf of their clients to the local county board of commissioners for increased budget toward affordable transportation access within that county, thereby broadening clients’ access to job opportunities. Advocacy with local leaders outside of government might include collaboration with community college administrators for provision of additional support for working adults and parents who wish to return to school, such as more evening course options, advisor support, or readily available information on scholarships. Again, considering the aforementioned roles career counselors may have (e.g., leader, evaluator), career counselors may also consider further training in program evaluation—or collaboration with those who have such training—to better understand the efficacy of their community partnerships, referrals, and other advocacy-related efforts made toward supporting clients’ SDOMH.
Assessing and Addressing Social Determinants of Mental Health
As noted earlier, SDOMH are inextricably linked to employment, which means career counselors in rural communities must acknowledge these challenges and seek to address these issues with their clients. However, researchers have also highlighted the importance of considering both facilitators and barriers to addressing SDOMH challenges (Browne et al., 2021). In a qualitative case study of staff at a community health center and hospital, participants identified practical facilitators of SDOMH response, including community collaboration and support from leadership, as well as barriers such as time limitations and lack of resources (Browne et al., 2021). As career counselors hold similar client outcome goals as community mental health providers, they can take these findings into consideration when determining how to best respond to clients’ SDOMH challenges through attention to opportunities for collaboration with community leaders (e.g., religious leaders, politicians) and resources within the community (e.g., food banks, health care providers). Another study highlighted the importance of collaboration, partnerships with local agencies, and understanding the role of the counselor in SDOMH response (Johnson & Brookover, 2021; Robins et al., 2022). With these findings in mind, career counselors in rural communities are well positioned to assess for and address SDOMH challenges faced by their clients (Crucil & Amundson, 2017; Tang et al., 2021) through individual-level action (i.e., counseling) and systems-level advocacy action.
Systems-Level Advocacy Through Assessment
To effectively engage in systems-level advocacy, it is important for career counselors to recognize and understand the needs of their rural communities. When using the Rural Community Health and Well-Being Framework in practice, it is important to complete an assessment of the rural health of one’s community. Ryan-Nicholls and Racher (2004) purport that it is imperative to assess rural health within five categories: health status, health determinants, health behavior, health resources, and health service utilization. Counselors may consider these items when assessing the needs of their clients in rural communities, as these items provide a basis for assessment of other health factors, such as indicators of community health (e.g., environment and lifestyle) and economic well-being, and provide a foundation for systems-level advocacy and planning. This level of action focuses on improving the lives of the entire community through strategic advocacy efforts that improve population health and well-being (Ryan-Nicholls & Racher, 2004). A career counselor engaged at this level might focus their energy on advocating for increased economic development in their rural community, livable wages, universal health care, immigration issues, employment discrimination legislation, and other employment-related issues that impact the community directly or indirectly. Additionally, a career counselor may address client self-advocacy and utilize empowerment approaches to increase the voices of community members and their clients as related to work and employment needs.
In connection with this framework (Annis et al., 2004), career counselors can utilize this broader community-level assessment to inform specific points of advocacy. As an example, Annis et al. (2004) provided a sample form that may be utilized to collect community data on alcohol consumption (p. 79). Upon noting concern from individual clients on alcohol consumption, a career counselor may collaborate with public health professionals, for instance, to collect such data from the local community. Annis et al. encourage consideration of the implications for such findings, as well as opportunities for follow-up. After determining a need in the community for support regarding high alcohol consumption, the career counselor may utilize the framework to consider points of community resilience, including existing supports, attitudes about alcohol consumption, existing resources, and any actions the community is already taking in this area. Overall, assessment through the context suggested by Ryan-Nicholls and Racher (2004) may yield individual and community data to inform action to address SDOMH challenges through Annis et al.’s (2004) framework.
Individual-Level Action Through Assessment
When a client seeks services from a career counselor, the relationship centers on exploration and evaluation of the client’s education, training, work history, interests, skills, personality, and career goals. Through engaging with the Rural Community Health and Well-Being Framework, the career counselor might also examine the SDOMH facilitators and barriers that impact a client’s employment goals. To address employment and SDOMH, a career counselor must understand the community-level needs (i.e., systems approach) and the individual needs of their clients; for these goals, one strategy is to use assessments. There are various assessment tools that career counselors may find helpful, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE; National Association of Community Health Centers, 2017), an SDOH assessment tool purposed to empower professionals to not only understand their clients more holistically through assessment, but to better meet clients’ needs through the use of such information. The PRAPARE assessment tool includes questions related to four domains: Personal Characteristics, Family and Home, Money and Resources, and Social and Emotional Health. PRAPARE emphasizes the importance of assessing SDOMH needs of clients in order for providers to “define and document the complexity of their patients; transform care with integrated services and community partnerships to meet the needs of their patients; demonstrate the value they bring to patients, communities, and payers; and advocate for change in their communities” (https://prapare.org/). There are several benefits of using the PRAPARE assessment tool, such as it being free of charge, having a website linked to the tool with an “actionable toolkit and resources,’’ and being evidence-based. Barriers to using PRAPARE include that it is a long assessment tool that clients must complete in-office, which may slow workflow.
Another SDOH assessment tool is the WellRx Questionnaire (Page-Reeves et al., 2016). The WellRx Questionnaire is an 11-item screening tool that gathers information on various SDOMH, like food security, access to transportation, employment, and education. Participants are to answer “yes” or “no” to each item on the questionnaire. According to Page-Reeves and colleagues (2016), the WellRx Questionnaire provides a feasible means of assessing patients’ social needs and thereby addressing those needs. Benefits to using the WellRx include that it is free of cost, questions are at a 4th-grade reading level, and it can typically be completed by a client individually without the help of a professional. A potential barrier is that it does not assess a wide range of SDOMH challenges. Lastly, Andermann (2018) conducted a scoping review of social needs screening tools and found that the focus on such screening has increased over time. Andermann suggested that health care workers take advantage of the existing means of assessment, and made a number of specific resource recommendations, such as the Canadian Task Force on Preventive Health Care (2019) and the U.S. Preventive Services Task Force (2022).
Addressing SDOMH Through Action
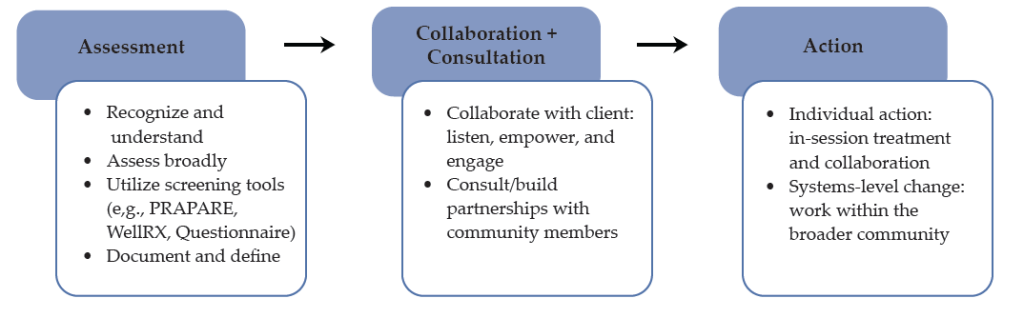
Documenting and defining the needs of clients through assessment is the first step in addressing SDOMH. The next step is taking action through an integrated career counseling approach. An integrated approach may include consistent collaboration with other professionals, like medical doctors, nurse practitioners, social workers, probation officers, or case managers. Additionally, scholars like Andermann (2016) suggest integrated efforts such as ensuring social challenges are included in client records and shared with other professionals to best support care. For “particularly isolated and hard-to-reach patients . . . [actions like] assertive outreach, patient tracking and individual case managers” may be helpful (para. 19). Another practical suggestion for beginning to address clients’ SDOMH challenges is adding an SDOMH assessment tool or specific SDOMH questions to an intake form that the client completes independently or during the intake session. Selection of specific questions can be derived from the data that displays community-level needs (e.g., systems-level advocacy through assessment). For example, if a community-level assessment found that public transportation was lacking, then transportation might be an important assessment question on the SDOMH screener.
Another consideration specific for career counselors is that counselors are obligated by their code of ethics to take appropriate action based on assessment results (American Counseling Association [ACA], 2014, Section E.2.b.). Appropriate action can include consultation and collaboration with other professionals within and outside of counseling and/or advocacy to address the SDOMH need. After establishing the need through assessment, it is important for the career counselor to support the client in understanding system-level challenges and to work to address SDOMH issues while simultaneously supporting employment needs. For example, a career counselor who determines that their client is struggling with food insecurity might address this issue in several ways. At the individual level, the counselor might print resources for local food pantries, assist the client in applying for SNAP benefits, and counsel the client on resources within the community to access food. They could establish a small food pantry within the office, collaborate with local restaurants to receive pre-packaged food that might otherwise be disposed of, or consult with local food pantries and free food kitchens to establish a mobile pantry and kitchen. At the systems level, a career counselor may build partnerships with local farmers to increase locations where fresh fruits and vegetables are available for little or no cost.
Collaboration and consultation are imperative to addressing the complex needs of clients in rural communities who are both seeking career counseling and challenged by SDOMH issues. For example, as noted earlier, health care access and quality are major disruptors of employment, and addressing these challenges will afford benefits for employment. The career counselor can consider using interprofessional collaboration and telehealth to support the health care needs of their rural clients (Johnson & Mahan, 2020). Interprofessional collaboration is a practice in which health care providers from two or more professional backgrounds interact and practice with the client at the center of care (Prentice et al., 2015). Using telehealth, the distribution of health-related services via telecommunication technologies is a useful strategy to support the health care needs of persons in rural communities. A career counselor can address health care access through telehealth in several ways, including education (e.g., introduce their client to telehealth; assist them in understanding the technology), telehealth (e.g., provide the telecommunication equipment in the office), and collaborative partnership (e.g., use a portion of the career counseling session to assist the client in connecting with health care providers using distance technology). As a collaborative partner in addressing health care access and quality, the career counselor can also use future sessions to follow up with the client on their experience with telehealth and, if needed, assist them in connecting to other health care providers. Figure 1 provides a visual for conceptualizing how career counselors may navigate the SDOMH needs of their clients, from assessment to action.
Figure 1
Working to Address Clients’ SDOMH Needs
Lastly, in the work of addressing SDOMH and employment, counselors should be aware of local, state, and national resources. Local and state resources are unique to every state but have similar purposes which include disseminating information on local resources and initiatives and providing public services that address SDOMH (e.g., food banks, public programs). National resources that are accessible to every community include 211 and the “findhelp.org” website. The Federal Communications Commission designated 211 as a national number in the United States that anyone can call for information and referrals to social services and other assistance. The services provided by 211 are confidential and free, available 24/7, and help connect people in the United States to essential community services. Moreover, the “findhelp.org” website is designed to help people search and connect with social care support based on their ZIP Code.
Integrating career counseling and social care support in rural communities is a strategy to facilitate the readiness of clients for work and the sustainability of employment for clients because basic needs are met or being addressed. While every rural community is unique, the foundation of understanding both systemic and individual SDOMH needs—and addressing those needs through strategic partnerships and individual counseling, as well as advocacy—is important in every rural community and to the success of any career counseling endeavor.
Discussion
In rural communities, career counselors hold a significant role. They are tasked with aiding individuals with employment needs; they may often address mental health concerns, and while doing so, it is important for them to be aware of and prepared to address SDOMH. Career counselors can gain more insight into issues related to SDOMH through consultation, collaboration, and advocacy, which should all be a part of the repertoire of a rural career counselor. The use of theoretical frameworks such as the Rural Community Health and Well-Being Framework (Racher et al., 2004) provides direction for career counselors seeking to understand the systemic issues impacting employment access and opportunities in the community, as well as direction for intervention. This framework will assist in identifying and minimizing barriers to employment that may exist within rural communities. More specifically, this framework will help to uncover SDOMH challenges that exist in the community and serve as barriers to well-being and employment and provide direction for advocating for resources necessary for equitable work opportunities and environments. Being that individuals in rural America experience various barriers that have huge impacts on their lives, such a guide for career counselors is essential.
Lastly, addressing SDOMH within career counseling is a social justice issue that counselors should address (ACA, 2014; Crucil & Amundson, 2017; Ratts et al., 2016). The Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) serve as a guide for counselors to address social justice issues and were endorsed by the ACA in 2015. Like the aforementioned framework and empirically based suggestions, the MSJCC includes four areas of competence: counselor self-awareness, client worldview, counseling relationship, and counseling and advocacy interventions. The authors of the MSJCC also implore counselors to consider “attitudes and beliefs, knowledge, skills, and action,” and suggest that competent counselors are aware of the experiences of marginalized clients (Ratts et al., 2016; p. 3). Thus, career counselors’ efforts to assess and address the individual and systems-based SDOMH challenges faced by their clients is social justice work that career counselors are trained and prepared to address.
Implications
Given this review, there are specific implications for career counselors practicing in rural communities, counselor educators training career counselors, and pertinent policy needs.
Practicing Career Counselors
The role of the career counselor often entails identifying employment objectives, goals, and needs for both the job seeker and employer. In addition, the career counselor is responsible for résumé development, teaching job placement and retention skills, providing self-advocacy tips, teaching organizational goal–redefining skills, and many other components (Ysasi et al., 2018). However, providing these services can be difficult when the individuals reside in rural communities because of the SDOMH disparities such as limited available resources, isolation, increased poverty, and decreased educational and employment opportunities (Temkin, 1996).
Therefore, career counselors must actively work to ensure their visibility and accessibility to individuals in rural areas who are seeking employment opportunities. Further, career counselors need to market themselves and their skills to employers and job seekers of rural communities. Consequently, marketing generally entails engaging and developing community partnerships with employers and job seekers, which involves educating individuals unfamiliar with the specific services that career counselors provide. In addition, employers are often interested in services that improve their business (e.g., increase revenue), while job seekers may be searching for skill training to achieve employment goals (Richardson et al., 2010). Therefore, career counselors can enhance service delivery and provide adequate services when they intentionally market their services to the community members.
Furthermore, job insecurity has been linked to mental health concerns like stress and anxiety, financial concerns, and fear of organizational change (Holm & Hovland, 1999). Therefore, career counselors need to be aware of the impact of job insecurity on rural communities and devise strategies to help organizations and workers manage job insecurity. Managing job insecurity of workers in rural organizations could include helping organizations to redefine their present and future goals and commitments made to employees. Organizations could also manage organizational transitions depending on the skills and resources available to affected employees (Holm & Hovland, 1999). Clearly stated organizational objectives, goals, and plans can help employees feel less insecure about their jobs and increase focus on their roles and responsibilities instead of devising means to move out of the community for a better and more secure future. In addition, career counselors in rural communities should be aware of the mental health concerns experienced by employees and job seekers and connect them to available mental health resources.
Counselor Educators
Counselor educators are responsible for the training and development of the next generation of counselors, including career counselors. It will be important for counselor educators to include training on SDOMH, interprofessional collaboration, and telehealth, as these are especially relevant for rural communities ( Johnson & Mahan, 2021; Johnson & Rehfuss, 2021). It is essential to provide adequate time to review and discuss SDOMH in all courses throughout the curriculum (Waters et al., 2022) to ensure the competence of career counselors. To ensure this continuity, counselor educators should advocate for an SDOMH module across the curriculum. This would ensure the inclusion of this content throughout the program, providing ample opportunity for the understanding of SDOMH and how they should be addressed. Career counselors must be prepared to address the complex employment and social health needs with which their clients might present. Without adequate education and training, these will seem much more difficult to address.
Policy
In addressing both SDOMH and employment needs in rural communities, advocating for policy and legislative change is imperative. Lewis et al. (2002) described counselors’ roles in sharing public information as awakening the public to macro-systemic issues related to human dignity and engaging in social/political advocacy, or “influencing public policy in a large, public arena” (p. 2). Thus, career counselors are encouraged to benefit their clients through engaging in advocacy to influence policy at the local, state, and national levels. Similarly, Crucil and Amundson (2017) implore career counselors to engage in the work of influencing politics and policy and suggest awareness as a first step to enacting change through the sharing of information and impacting policy. To develop such awareness, career counselors may begin by reading about SDOMH disparities related specifically to employment issues from reputable sources. For instance, the National Alliance on Mental Illness (NAMI; 2014) has published various reports related to such issues, including the informative publication entitled Road to Recovery: Employment and Mental Illness. NAMI (2021) also published a legislative coalition letter written in support of increased SDOH funding to Congress. Career counselors may work to build their own awareness and understanding of the social and political events and influences which impact their clients, building toward eventual action in this realm.
Moreover, regarding policy change, researchers have suggested career counselors should be aware of and actively engaged in policy efforts (Crucil & Amundson, 2017; Watts, 2000). Watts (2000) described public policy considering career development as including four distinct roles: legislation, remuneration, exhortation, and regulation. Watts described these roles in detail and implored career counselors to influence these policy processes by seeking the support of interest groups and communicating with policy makers. Again, career counselors can work individually and within their own communities to increase their awareness and knowledge of policies and their impact. They can work toward influencing policies at the state and national levels to improve the accessibility and existence of important social programs and resources.
Conclusion
Career counselors in rural communities have a responsibility to acknowledge and address SDOMH challenges that are disproportionately impacting their clients. Collaboration, consultation, counseling framed through the lens of SDOMH, and advocacy appear to be strategies to support the employment needs of individuals and the rural community. Employment services in rural communities must be framed through a socially conscious (e.g., aware of the SDOMH systemic issues), action-oriented (e.g., prepared to engage in advocacy), and resiliency-focused lens that provides tailored individual services while simultaneously addressing systemic issues.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
Amundson, N. E. (1993). Mattering: A foundation for employment counseling and training. Journal of Employment Counseling, 30(4), 146–152. https://doi.org/10.1002/j.2161-1920.1993.tb00173.x
Andermann, A. (2016). Taking action on the social determinants of health in clinical practice: A framework for health professionals. Canadian Medical Association Journal, 188(17–18), E474–E483. https://doi.org/10.1503/cmaj.160177
Andermann, A. (2018). Screening for social determinants of health in clinical care: Moving from the margins to the mainstream. Public Health Reviews, 39(1), 1–17.
https://doi.org/10.1186/s40985-018-0094-7
Annis, R. C., Racher, F., & Beattie, M. (Eds.). (2004). Rural community health and well-being: A guide to action. Rural Development Institute. https://www.researchgate.net/publication/242551842_Rural_Community_Health_and_Well-Being_A_Guide_to_Action
Bradshaw, T. K. (2007). Theories of poverty and anti-poverty programs in community development. Community Development, 38(1), 7–25. https://doi.org/10.1080/15575330709490182
Brassington, I. (2011). What’s wrong with the brain drain? Developing World Bioethics, 12(3), 113–120.
https://doi.org/10.1111/j.1471-8847.2011.00300.x
Browne, J., Mccurley, J. L., Fung, V., Levy, D. E., Clark, C. R., & Thorndike, A. N. (2021). Addressing social determinants of health identified by systematic screening in a Medicaid accountable care organization: A qualitative study. Journal of Primary Care & Community Health, 12. https://doi.org/10.1177/2150132721993651
Canadian Task Force on Preventative Health Care. (2019). Canadian task force on preventive health care.
https://canadiantaskforce.ca
Centers for Disease Control and Prevention. (2020). CDC 2020 in review. https://archive.cdc.gov/#/details?url=
https://www.cdc.gov/media/releases/2020/p1229-cdc-2020-review.html
Covey, S. (1989). The 7 habits of highly effective people: Restoring the character ethic. Simon & Schuster.
Crucil, C., & Amundson, N. (2017). Throwing a wrench in the work(s): Using multicultural and social justice competency to develop a social justice–oriented employment counseling toolbox. Journal of Employment Counseling, 54(1), 2–11. https://doi.org/10.1002/joec.12046
Crumb, L., Haskins, N., & Brown, S. (2019). Integrating social justice advocacy into mental health counseling in rural, impoverished American communities. The Professional Counselor, 9(1), 20–34. https://files.eric.ed.gov/fulltext/EJ1215753.pdf
Dobis, E. A., Krumel, T. P., Jr., Cromartie, J., Conley, K. L., Sanders, A., & Ortiz, R. (2021). Rural America at a glance: 2021 edition. U.S. Department of Agriculture. https://www.ers.usda.gov/webdocs/publications/102576/eib-230.pdf
Dueñas, M., Ojeda, B., Salazar, A., Mico, J. A., & Failde, I. (2016). A review of chronic pain impact on patients, their social environment and the health care system. Journal of Pain Research, 2016(9), 457–467. https://doi.org/10.2147/JPR.S105892
Dwyer, R. E., & Sanchez, D. (2016). Population distribution and poverty. In M. J. White (Ed.), International handbook of migration and population distribution (pp. 485–504). Springer Science & Business Media. https://doi.org/10.1007/978-94-017-7282-2
Health Resources and Services Administration. (2017). Defining rural population. https://www.hrsa.gov/rural-health/about-us/definition/index.html
Holm, S., & Hovland, J. (1999). Waiting for the other shoe to drop: Help for the job-insecure employee. Journal of Employment Counseling, 36(4), 156–166.
https://doi.org/10.1002/j.2161-1920.1999.tb01018.x
Hughes, M. C., Gorman, J. M., Ren, Y., Khalid, S., & Clayton, C. (2019). Increasing access to rural mental health care using hybrid care that includes telepsychiatry. Journal of Rural Mental Health, 43(1), 30–37. https://doi.org/10.1037/rmh0000110
Johnson, K. F., & Brookover, D. L. (2021). School counselors’ knowledge, actions, and recommendations for addressing social determinants of health with students, families, and in communities. Professional School Counseling, 25(1), 1–12. https://doi.org/10.1177/2156759X20985847
Johnson, K. F., & Mahan, L. B. (2020). Interprofessional collaboration and telehealth: Useful strategies for family counselors in rural and underserved areas. The Family Journal, 28(3), 215–224.
https://doi.org/10.1177/1066480720934378
Johnson, K. F., & Rehfuss, M. (2021). Telehealth interprofessional education: Benefits, desires, and concerns of counselor trainees. Journal of Creativity in Mental Health, 16(1), 15–30.
https://doi.org/10.1080/15401383.2020.1751766
Johnson, K. F., & Robins, L. B. (2021). Counselor educators’ experiences and techniques teaching about social-health inequities. Journal of Counselor Preparation and Supervision, 14(4), 1–25. https://digitalcommons.sacredheart.edu/jcps/vol14/iss4/7
Landon, T., Connor, A., McKnight-Lizotte, M., & Peña, J. (2019). Rehabilitation counseling in rural settings: A phenomenological study on barriers and supports. Journal of Rehabilitation, 85(2), 47–57. https://bit.ly/4cvWSoT
Lewis, J., Arnold, M. S., House, R., & Toporek, R. L. (2002). ACA advocacy competencies. http://www.counseling.org/Resources/Competencies/Advocacy_Competencies.pdf
Liebman, A. K., & Augustave, W. (2010). Agricultural health and safety: Incorporating the worker perspective. Journal of Agromedicine, 15(3), 192–199. https://doi.org/10.1080/1059924x.2010.486333
Mohatt, D. F., Bradley, M. M., Adams, S. J., & Morris, C. D. (2006). Mental health and rural America: 1994-2005. An overview and annotated bibliography. U.S. Department of Health and Human Services. https://eric.ed.gov/?id=ED591902
National Alliance on Mental Health. (2014). Road to recovery: Employment and mental illness. https://nami.org/Support-Education/Publications-Reports/Public-Policy-Reports/RoadtoRecovery
National Alliance on Mental Health. (2021, April 8). Letter to congressional leadership. https://www.nami.org/getattachment/c3b797bf-5116-457f-ada9-b6b6f1f6adfb/Letter-to-Congressional-Committee-Leadership-on-So
National Association of Community Health Centers. (2017). PRAPARE. https://www.nachc.org/research-and-data/prapare
Norström, F., Waenerlund, A.-K., Lindholm, L., Nygren, R., Sahlén, K.-G., & Brydsten, A. (2019). Does unemployment contribute to poorer health-related quality of life among Swedish adults? BMC Public Health, 19(1). https://doi.org/10.1186/s12889-019-6825-y
Office of Disease Prevention and Health Promotion. (2020). Healthy People 2030: Social determinants of health. U.S. Department of Health and Human Services. https://health.gov/healthypeople/priority-areas/social-determinants-health
Page-Reeves, J., Kaufman, W., Bleecker, M., Norris, J., McCalmont, K., Ianakieva, V., Ianakieva, D. & Kaufman, A. (2016). Addressing social determinants of health in a clinic setting: The WellRx pilot in Albuquerque, New Mexico. The Journal of the American Board of Family Medicine, 29(3), 414–418. https://doi.org/10.3122/jabfm.2016.03.150272
Pope, M. (2011). The Career Counseling With Underserved Populations model. Journal of Employment Counseling, 48(4), 153–155. https://doi.org/10.1002/j.2161-1920.2011.tb01100.x
Prentice, D., Engel, J., Taplay, K., & Stobbe, K. (2015). Interprofessional collaboration: The experience of nursing and medical students’ interprofessional education. Global Qualitative Nursing Research, 2, 1–9. https://doi.org/10.1177/2333393614560566
Racher, F., Everitt, J., Annis, R., Gfellner, B., Ryan-Nicholls, K., Beattie, M., Gibson, R., & Funk, E. (2004). Rural community health & well-being. In R. Annis, F. Racher, & M. Beattie (Eds.), Rural community health and well-being: A guide to action (pp. 18–37). Rural Development Institute.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Richardson, N., Gosnay, R. M., & Carroll, A. (2010). A quick start guide to social media marketing: High impact low-cost marketing that works. Kogan Page Publishers.
Robins, L. B., Johnson, K. F., Duyile, B., Gantt-Howrey, A., Dockery, N., Robins, S., & Wheeler, N. (2022). Family counselors addressing social determinants of mental health in underserved communities. The Family Journal, 31(2), 213–221. https://doi.org/10.1177/10664807221132799
Ryan-Nicholls, K. D., & Racher, F. E. (2004). Investigating the health of rural communities: Toward framework development. Rural and Remote Health, 4(1), 1–10.
https://search.informit.org/doi/abs/10.3316/informit.613919155641626
Shoup, L., & Homa, B. (2010). Principles for improving transportation options in rural and small town communities. https://t4america.org/wp-content/uploads/2010/03/T4-Whitepaper-Rural-and-Small-Town-Communities.pdf
Tang, M., Montgomery, M. L. T., Collins, B., and Jenkins, K. (2021). Integrating career and mental health counseling: Necessity and strategies. Journal of Employment Counseling, 58, 23–35.
https://doi.org/10.1002/joec.12155
Temkin, A. (1996). Creative options for rural employment: A beginning. In N. L. Arnold (Ed.), Self-employment in vocational rehabilitation: Building on lessons from rural America (pp. 61–64). Research and Training Center on Rural Rehabilitation Services.
United States Census Bureau. (2014). 2010-2014 ACS 5-year estimates. https://www.census.gov/programs-surveys/acs/technical-documentation/table-and-geography-changes/2014/5-year.html
United States Department of Agriculture. (2014). Rural America at a glance: 2014 edition. https://www.ers.usda.gov/publications/pub-details/?pubid=42897
United States Department of Agriculture. (2017). Rural education at a glance, 2017 edition. https://www.ers.usda.gov/webdocs/publications/83078/eib-171.pdf
United States Preventive Services Taskforce. (2022). US preventative services taskforce. https://www.uspreventiveservicestaskforce.org/uspstf
U.S. Department of Transportation. (2019). Rural public transportation systems. https://www.transportation.gov/mission/health/Rural-Public-Transportation-Systems
Waters, J. M., Gantt, A., Worth, A., Duyile, B., Johnson, K. F., & Mariotto, D. (2022). Motivated but challenged: Counselor educators’ experiences teaching about social determinants of health. Journal of Counselor Preparation and Supervision, 15(2), 1–30. https://digitalcommons.sacredheart.edu/jcps/vol15/iss2/6
Watts, A. G. (2000). Career development and public policy. Journal of Employment Counseling, 37(2), 62–75. https://doi.org/10.1002/j.2161-1920.2000.tb00824.x
World Health Organization. (2014). Social determinants of mental health. https://apps.who.int/iris/bitstream/handle/10665/112828/9789241506809_eng.pdf
Ysasi, N. A., Tiro, L., Sprong, M. E., & Kim, B. J. (2018). Marketing vocational rehabilitation services in rural communities. In D. A. Harley, N. A. Ysasi, M. L. Bishop, & A. R. Fleming (Eds.), Disability and vocational rehabilitation in rural settings: Challenges to service delivery (pp. 545–552). Springer.
Kaprea F. Johnson, PhD, LPC, is a professor and Associate Vice Provost for Faculty Development & Recognition at The Ohio State University. Alexandra Gantt-Howrey, PhD, LPC (ID), is an assistant professor at Idaho State University. Bisola E. Duyile, PhD, LPC, CRC, is an assistant professor at Montclair State University. Lauren B. Robins, PhD, is a clinical assistant professor and distance learning coordinator at Old Dominion University. Natese Dockery, MS, NCC, LPC, CSAM, is a licensed professional counselor and doctoral student. Correspondence may be addressed to Kaprea F. Johnson, The Ohio State University, 1945 N. High Street, Columbus, OH 43210, johnson.9545@osu.edu.
May 22, 2024 | Volume 14 - Issue 1
William B. Lane, Jr., Timothy J. Hakenewerth, Camille D. Frank, Tessa B. Davis-Price, David M. Kleist, Steven J. Moody
Interpretative phenomenological analysis was used to explore the simultaneous supervision experiences of counselors-in-training. Simultaneous supervision is when a supervisee receives clinical supervision from multiple supervisors. Sometimes this supervision includes a university supervisor and a site supervisor. Other times this supervision occurs when a student has multiple sites in one semester and receives supervision at each site. Counselors-in-training described their experiences with simultaneous supervision during the course of their education. Four superordinate themes emerged: making sense of multiple perspectives, orchestrating the process, supervisory relationship dynamics, and personal dispositions and characteristics. Results indicated that counselors-in-training experienced compounded benefits and challenges. Implications for supervisors, supervisees, and counselor education programs are provided.
Keywords: clinical supervision, simultaneous supervision, counselors-in-training, interpretative phenomenological analysis, counselor education
Supervision is a key component of counselor education in programs accredited by the Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2015) and an ethical requirement in the ACA Code of Ethics (American Counseling Association, 2014). Supervision of counselors-in-training (CITs) serves the purpose of guiding counselor development, gatekeeping, and, ultimately, ensuring competent client care (Borders et al., 2014). For the present study, we defined simultaneous supervision as a pre-licensure CIT receiving weekly individual or triadic supervision from more than one supervisor over the same time period. At the time of the study, the 2016 CACREP standards required that internship and practicum students receive individual and/or triadic supervision averaging 1 hour per week throughout their clinical experience (Standards 3.L. & 3.H.). Some CITs may gain field experience at multiple clinical sites requiring individual site supervision at each site. Many programs require students to engage in faculty advising meetings (Choate & Granello, 2006), which may take a form analogous to formal supervision. Additionally, supervisees may have clinical supervision, focused on supervisee development and client welfare, as well as administrative supervision, focused on functionality and logistics within an agency; these roles may be fulfilled by the same person or at times by two separate supervisors (Kreider, 2014; Tromski-Klingshirn & Davis, 2007). Consequently, although simultaneous supervision is not required in and of itself, it often occurs in counselor education practice.
Supervision Foundations
Counseling supervision research has increased significantly in the last few decades (Borders et al., 2014). Borders and colleagues (2014) developed best practices for effective supervision, including emphasis on the supervision contract, social justice considerations, ethical guidelines, documentation management, and relational dynamics. Previous research has overwhelmingly demonstrated that a strong supervisory alliance is the bedrock of effective supervision (Bernard & Goodyear, 2019). Sterner (2009) further studied the supervisory relationship as a mediator for supervisee work satisfaction and stress. Lambie and colleagues (2018) developed a CIT clinical evaluation to be used in supervision, with strength in assessing personal dispositions in addition to clinical skills. A review of the supervision literature revealed that a strong supervisory relationship based in goal congruence, empathic rapport, and transparent feedback processes (Bernard & Goodyear, 2019; Borders et al., 2014; Sterner, 2009) generate mutual growth between supervisor and supervisee, enhancing clinical work. Additionally, CACREP mandates that faculty and site supervisors foster CIT professional counselor identity through the supervisory process (Borders, 2006; CACREP, 2015).
Counselor development is also a crucial factor in clinical supervision. An entire category of supervision models centralizes the professional development of supervisees in their approach (Bernard & Goodyear, 2019). One of the most widely known models, the Integrative Developmental Model, plots learning, emotion, and cognitive factors across multiple stages of therapist development (Stoltenberg & McNeill, 2010). By focusing on overarching themes of self–other awareness, autonomy, and motivation, the Integrative Developmental Model (Stoltenberg & McNeill, 2010) illuminates how supervisees fluctuate and grow in their anxiety, self-efficacy, reliance on structure, and independence. All these factors may have substantial impact when considering the complexity that simultaneous supervision brings. Furthermore, professional dispositions of openness to feedback and flexibility and adaptability (Lambie et al., 2018) may have additional developmental implications when considering the complexity of simultaneous supervision.
Ethics similarly serve as a foundation of supervisory experiences. Multiple standards and principles of the ACA Code of Ethics (2014) may be complicated by simultaneous supervision and require special attention. Veracity may be of particular interest given the commonality of supervisee nondisclosure (Kreider, 2014), multiplied by the added number of supervisors in one time period. Furthermore, specific standards in Section D: Relationships With Other Professionals may be implicated by obligations in working with multiple professionals; multiple standards in Section F: Supervision, Training, and Teaching may be indicated because of the convergence of both teaching and clinical supervision in counselor training programs; and, finally, reconciling the additional complexities of simultaneous supervision not explicitly identified elsewhere in the 2014 Code of Ethics may elicit a need to carefully consider Section I: Resolving Ethical Issues. With more parties involved, greater nuance would be expected in ethical decision-making.
Much of the foundational research and reviewed contextual factors have either focused specifically on sole supervision or do not differentiate between sole and simultaneous supervision. When considering best supervision practices, the phenomenon of simultaneous supervision presents distinct practical concerns. Exploration is needed to better understand how supervisees might navigate different but related supervisory relationships, how goals and tasks can be congruent across separate supervisory experiences, and how supervisees would make meaning of multiple sources of feedback. Despite the apparent use of simultaneous supervision in counselor education programs, few researchers have explored these dynamic concerns.
Multiple Supervisors and Multiple Roles
Early researchers began to conceptualize the challenges and strengths inherent in simultaneous supervision in both counseling (Davis & Arvey, 1978) and clinical psychology (Dodds, 1986; Duryee et al., 1996; Nestler, 1990), with mixed results overall. Nestler (1990) identified the difficulties in receiving contradictory feedback from multiple supervisors, reflective of fundamental differences in the supervisors’ approaches. Dodds (1986) similarly identified multiple potential stressors in having concurrent supervisors at agency and training settings. Dodds argued that although the general goals to teach and serve clients overlapped, each had inherent differences in their primary institutional goals and structures. Duryee and colleagues (1996) described a beneficial view of simultaneous supervision, in which supervisees overcome conflicts with site supervisors via support and empowerment from academic program coordinators. Davis and Arvey (1978) presented a case study in which supervisees, in a raw comparison, more highly favored the dual supervision overall. These findings highlight the dynamics that occur in the context of simultaneous supervision and connect with recent findings.
Recent researchers have focused on dual-role supervision, defined as one individual supervisor serving as both a clinical and administrative supervisor to one or more supervisees (Kreider, 2014). Kreider (2014) investigated supervisee self-disclosure as related to three factors: supervisor role (dual role or single role), supervisor training level, and supervisor disclosure. Level of supervisor disclosure was found to be significant in explaining differences in supervisee self-disclosure and was hypothesized as a mitigating factor in supervisor role differences (Kreider, 2014). Tromski-Klingshirn and Davis (2007) surveyed the challenges and benefits unique to dual-role supervision for post-degree supervisees. Most supervisees reported neutral to positive outcomes from a dual-role supervisor, but a minority of supervisees noted power dynamics and fear of disclosure as primarily problematic (Tromski-Klingshirn & Davis, 2007), similar to the earlier hypotheses of Nestler (1990) and Dodds (1986). The small amount of existing research solidifies the prevalence of simultaneous supervision and the challenges and benefits for the supervisees. A missing link emerges in understanding how CITs come to understand their experience in simultaneous supervision from a qualitative perspective.
The distinct focused phenomenon of simultaneous supervision is limited in counseling literature. The few conceptual examinations of simultaneous supervision in the mental health literature have indicated confusion and role ambiguity (Nestler, 1990), while at other times simultaneous supervision has been noted to improve comprehensive learning (Duryee et al., 1996). Our study addresses the gap in the literature regarding current simultaneous supervision in counselor education utilizing qualitative analysis.
Method
Given the limited research on simultaneous supervision and its prevalence within the profession, we decided to explore this phenomenon qualitatively. Our research question was “What is the experience of CITs receiving simultaneous supervision from multiple supervisors?” We used interpretative phenomenological analysis (IPA) to explore this question because of its utility with counseling research, grounded methods of analysis, and emphasis on both contextual individual experiences with the phenomenon and general themes (Miller et al., 2018).
Research Team
At the time of the study, the research team consisted of four doctoral students—William B. Lane, Jr., Timothy J. Hakenewerth, Camille D. Frank, and Tessa B. Davis-Price—who each had previous experience with simultaneous supervision as supervisees and supervisors. The team’s perspective of this phenomenon from both roles informed their interest in and analysis of the phenomenon. The fifth member of the team, David M. Kleist, was our doctoral faculty research advisor. The sixth author, Steven J. Moody, provided support in the writing process.
Participants and Procedure
Our participants were four CITs from CACREP-accredited graduate programs accruing internship hours. Smith et al. (2009) suggested seeking three to six participants for IPA, as this allows researchers to explore the phenomenon with individual participants at a deeper level. All four participants specialized in either addiction, school, or clinical mental health counseling, and identified as White, female CITs ranging from 23 to 37 years old. Additionally, each participant reported receiving supervision from at least two supervisors to include university-affiliated supervisors and site supervisors. Each participant came from a different university representing the Rocky Mountain and North Central regions of the Association for Counselor Education and Supervision. To protect confidentiality, each participant selected a pseudonym for the study.
After securing approval from our university’s review board, we recruited participants through purposive convenience sampling. We posted a recruitment email to the CESNET listserv, an informational listserv for counselor educators and supervisors. This listserv was selected as an initial step of convenience sampling to increase the potential to reach a broad range of counseling programs. Nine individuals responded to the call to participate in the research by taking a participant screening survey that helped us determine suitability for the study. After removing individuals from research consideration because of potential dual relationships, nonresponse, or not meeting inclusion criteria, four individuals were selected as participants. We further planned to engage in serial interviewing to gain richer details of the phenomenon and achieve greater depth with the four participants (Murray et al., 2009; Read, 2018). Prior to data collection, the researchers completed a brief phone screening with each participant to review the interview protocol and explain the phenomenological approach guiding the questions. A $40 gift card was provided as a research incentive to participants. Our selection criteria included (a) being a master’s student within a CACREP counseling program, (b) currently accruing internship hours, and (c) receiving simultaneous supervision. We selected participants in internship only because homogenous sampling helps produce applicable results for a given demographical experience (Smith et al., 2009).
Data Collection
Consistent with the recommendations of Smith et al. (2009), we conducted two semi-structured interviews with each participant lasting between 45–90 minutes. We utilized the online videoconferencing platform Zoom to conduct and record the interviews. First-round interviews consisted of four open-ended questions (see Appendix) that allowed participants to explore the experience of simultaneous supervision in detail (Pietkiewicz & Smith, 2014). These questions were open-ended to allow participants to explore the how of the phenomenon (Miller et al., 2018). The final interview questions were developed through initial generation based off research and personal experiences with the phenomenon, refinement in consultation with the research advisor, and interview piloting with volunteer students who did not participate in the study. Research participants were asked about their overall experience with having multiple supervisors, benefits and detriments of simultaneous supervision, and the meaning they made as a result of experiencing simultaneous supervision. Second-round interview questions were developed based on participant responses to first-round interview questions. After two rounds of interviews and analysis, we conducted a final member check to confirm themes. All participants expressed that the developed themes were illustrative of their lived experiences with simultaneous supervision.
Data Analysis
We followed IPA’s 6-step analysis process as outlined by Smith et al. (2009) and added a seventh step with the use of the U-heuristic analysis for group research teams (Koltz et al., 2010). Our process consisted of first coding and contextualizing the data individually, followed by group analysis, triangulated with the fifth author, Kleist, as research advisor. We completed this process for each participant and then analyzed themes across participants as suggested by Smith et al. We reached consensus that four superordinate themes emerged with 11 subthemes across the two rounds of interviews. All participants endorsed agreement with the themes from their experiences in simultaneous supervision during the member check process.
Trustworthiness
We integrated Lincoln and Guba’s (1985) framework in conducting multiple procedures for establishing trustworthiness and credibility. We demonstrated prolonged engagement and persistent observation through consistent coding meetings over the span of 1 year. Additionally, we adapted the U-heuristic analysis process during data analysis to analyze data individually and collectively to strengthen the credibility of our findings (Koltz et al., 2010). Finally, after we developed the themes, we triangulated the results with participants via a member check, ensuring the individual and group themes matched their idiographic experiences.
We bridled our personal experiences with simultaneous supervision throughout the research process. Bridling recognizes that researchers have had close personal experiences with the phenomenon and that bias is best managed by recognition rather than elimination (Stutey et al., 2020). The four principal investigators, Lane, Hakenewerth, Frank, and Davis-Price, individually engaged in memo writing, discussed personal reactions to the data, and participated in group discussions regarding meaning-making of the phenomenon with Kleist serving as research advisor.
Results
Our data analysis produced four superordinate themes identified across all cases. These themes were (a) making sense of multiple perspectives, (b) orchestrating the process, (c) supervisory relationship dynamics, and (d) personal dispositions and characteristics. In the sections that follow, each theme is described in further detail and exemplar quotes are given to support their development.
Making Sense of Multiple Perspectives
Making sense of multiple perspectives was defined as the receipt and conceptualization of supervisory feedback from multiple supervisors during the same academic semester. Supervisees identified their supervisors as having differing professional orientations. At times, these differing backgrounds led to supervisors providing differing opinions for the same client.
Participants used metaphors to make meaning of the distinct offerings of their supervisors’ feedback. An example of capturing multiple perspectives was one participant, Emma, utilizing the ancient Indian parable of “The Blind Men and the Elephant” (Saxe, 1868): “The point of the story is all the world religions might have a piece of the picture of God, you know. And so between all of us [clinicians and supervisors] together, maybe we have a perspective of truth.” Through retelling of the Indian fable, this participant was able to vividly capture her personal perspective of differing viewpoints through an integrative lens as opposed to a conflict of ideas. Within this superordinate theme, the two subthemes of supervisee framing and safety net vs. minefield emerged.
Supervisee Framing
Supervisee framing focused on the participant’s personal view of hearing multiple perspectives from supervisors within simultaneous supervision. Some participants described hearing varying perspectives as being helpful and valuable, providing support, and increasing confidence. They typically framed the idea of receiving various feedback as a way to gain ideas and then make their own informed decisions. Molly shared this positive perspective when she stated, “I like coming to [my differing supervisors] with different issues I have with different clients because I feel like they both have valuable experience, but in different ways.” In contrast, Hailey identified multiple perspectives as being “really difficult,” and Diana noted they were “more frustrating than beneficial” and confusing. Similarly, Hailey stated, “My supervisors are all very different, so they give me different feedback, and a lot of times it conflicts with what the other one has said.” The supervisee’s framing of discrepant feedback impacted their overall perceptions with simultaneous supervision. Supervisees either valued or were confused by the feedback. Generally, participants spoke of times when multiple perspectives were beneficial and difficult, but it appeared all participants were left with the task of making sense of multiple perspectives while receiving simultaneous supervision.
Safety Net vs. Minefield
Making sense of multiple perspectives was described as creating a safety net of support, while others found the experience to be a minefield that increased confusion, ambiguity, and isolation. Emma and Molly characterized their experience as providing support in an often overwhelming profession. Molly articulated, “I feel like if I didn’t have that good support, that good foundation, I don’t think I could do it because it’s just so much.” She later added, “I feel like getting those different perspectives, getting that support, getting those encouragers is beneficial because I don’t feel as overwhelmed, even though it’s overwhelming.”
Participants also perceived their simultaneous supervision as a minefield wherein they believed they were in double binds. Hailey reflected on an experience when her supervisors contradicted each other and expressed, “It just sucked because I was doing what my supervisor told me to do and suggested I do, and then I was told everything I did was wrong.” Diana echoed that discrepant feedback felt like a constant dilemma needing to be managed “carefully.” In reflecting on contradicting supervision, Diana said, “It’s hard because everybody has their own thing. . . . You just kind of have to appease everyone.” In the face of conflict, it was easier to placate than resolve. Participants’ cognitive framing was a major element of the phenomenon. Whereas making sense of multiple perspectives focused on the cognitive elements of receiving feedback from different supervisors, the next theme focused on the behavioral elements.
Orchestrating the Process
Another theme that emerged in our data analysis was that of supervisees orchestrating the process of simultaneous supervision. This theme revolved around action-oriented steps in supervision. The essence of this theme was captured when Hailey acknowledged the need for “checking her motives” on what she shared with different supervisors. She asked herself, “Am I sharing this with this [supervisor] because I feel like they’re going to answer in the way that I feel like . . . they should answer, because it’s easier for me?” Hailey acknowledged the difficulty in this, countering with, “Or am I just going to them because it’s that person that I’m supposed to see?” Hailey recognized that having options when it came to approaching supervisors meant that disclosure needed to be intentional rather than straightforward as it is when CITs only have one choice. Participants were aware of their process as they picked and chose what to share with whom, through seeking out a preferred supervisor and through managing the practical aspects of having multiple supervisors. The subthemes of picking and choosing, seeking a preferred perspective, and managing practical considerations were a part of orchestrating the process.
Picking and Choosing
The subtheme of picking and choosing emerged in how our participants described what they would share in supervision and the course of action taken in their counseling practice. This subtheme was labeled as an in vivo code, derived from Hailey’s quote: “So I definitely pick and choose what I talk to about each one. Because—this sounds terrible—but I respect the one [supervisor] more.” Hailey also described feelings of vulnerability and self-efficacy from week to week, related to her reactions from feedback: “I knew after having such a hard supervision last week showing tape, I was like, ‘I cannot be super vulnerable right now. I need to choose something that’s more surface level.’” Molly experienced picking and choosing as a means of proactively managing the repetitive nature of supervision: “I think just bringing different things to different supervisors is really helpful, and not constantly talking about the same client or the same situation, because that gets obnoxious and repetitive, and you’re gonna get a hundred different opinions.”
After receiving feedback, participants had varying perspectives on how to integrate and transfer constructs into action. Some participants viewed discrepant feedback as mutually exclusive, whereas others had a more integrative perspective. Molly expressed frustration in choosing between differing feedback from multiple supervisors: “Sometimes I don’t really know which I should go with, which I should choose, and which would be best for the client. . . . It’s like a double-edged sword, like it’s good at some points, but then bad at others.” Diana, who expressed similar frustration in choosing between perspectives, relieved this tension by resolving that, “I have to live with myself at the end of the day, so as long as it’s not unethical, I don’t worry about it too much. And as far as the stuff that I’m told that needs to be done, I do what I can.” Other participants espoused a much more integrative perspective. Emma stated, “I think the thing I like the best about it is actually when [my supervisors] have different advice . . . because then I feel like between the two, I can kind of find what I really like.” All participants spoke about selecting what to share with supervisors and choosing how to integrate feedback into action.
Seeking a Preferred Perspective
Coinciding with picking and choosing, participants also sought a preferred perspective in the process of receiving simultaneous supervision and orchestrating the process. Some reported the decision to go to one supervisor over another was situationally based and determined by clinical skill or specialty of the supervisor. Diana captured this as follows, “Well, I can have a conversation with either. I just get very different answers. If it’s the technical stuff of what has to be done—her. If it’s ‘how would you approach the situation?’ I do tend to talk to him.” Diana also likened seeking a preferred perspective to a child searching for a desired answer: “It’s like, who do I want to talk to? It’s almost like, talk to the person you want for the answer you want. It’s like, ‘Well, if Mom doesn’t have the right answer, go talk to Dad.’”
Managing Practical Considerations
All participants spoke to the practicality of meeting with multiple supervisors. Even though some participants strongly valued having multiple supervisors, all participants spoke to the larger time commitment needed in having simultaneous supervision. Molly captured how simultaneous supervision felt overwhelming, adding to the many other sources of feedback she received: “I already have two group supervisions. I’ve heard opinions about this, and I’m hearing other perspectives of my classmates, of my coworkers. Now I have to have triadic and hear their opinions and have individual. . . . It’s just a lot.” Emma framed this time commitment as detracting from her other obligations: “It just starts adding up. Like, my whole Tuesday evenings are gone, and that’s time I could be seeing clients.” Hailey expressed frustration about the obligatory nature and placating to the program’s requirement to see multiple supervisors: “Honestly, I just give the other supervisor little things because I know I have to talk to him . . . and it’s more, like, checking a box.” Finally, Emma captured how this time commitment was epitomized in documentation: “And the paperwork got exhausting, too, because I had to do everything in triplicate sometimes.” She further talked about the additional mental labor: “And now what are we gonna talk about since I just talked about all of this with [a different supervisor] and feel like I found good solutions, you know?” Supervisees had to manage their time and fit more supervision into their schedules. Simultaneous supervision added complexity, and participants needed to orchestrate this process to manage it efficiently and effectively.
Supervisory Relationship Dynamics
Supervisory relationship dynamics was determined to be a superordinate theme as it reflected on the connecting and disconnecting elements of the supervisory relationship. This theme was broken into three subthemes. The subthemes of vulnerability, power dynamics, and systems of supervision illustrated the relational dynamics within simultaneous supervision.
Vulnerability
In supervisory relationships, feelings of safety and vulnerability influenced interactions with different supervisors. To illustrate, Hailey noted:
There are certain supervisors I feel more safe with. And so those are the ones that I share more with . . . versus some of them I feel less safe with . . . I don’t share as much with them that is vulnerable, or that makes me vulnerable.
Participant experiences highlighted how vulnerability dictated what and how elements were shared in simultaneous supervision.
Power Dynamics
The determination of safety occurred within power dynamics. Diana commented that multiple supervisors serving as evaluators and gatekeepers can create “this weird relationship where you don’t want to be too vulnerable because this person is also your boss and can decide if you are going to stay in that position or not.” Diana and Hailey noted feeling disempowered and disengaged from supervision, referring to supervisors as “bosses” throughout their interviews. When participants perceived their supervision as a firmly directive process, discrepant directives were especially distressing. Diana rephrased this sentiment: “I guess the best thing to compare it to would be if you have more than one boss, but they all give you a different, ‘I want this, I want this, I want this.’” Emma’s experience was more accordant, and she specifically expressed at one time, “None of [my supervisors] are really super bossy either.” Participants identified power dynamics as salient aspects of how they experienced supervision and with whom they connected. Working with more than one supervisor sometimes resulted in characterization of “good” and “bad” supervisors, making individual supervisory relationship dynamics crucial.
Systems of Supervision
Participants conceptualized the phenomenon as broader systems of supervision in which individual supervisors were interacting with each other. Emma noted, “The two faculty supervisors work very closely together and I assume talk all the time.” Emma and Molly provided multiple examples of supervisors working together to best serve clients, thus bolstering supervision through their combined expertise. Molly stated, “It was nice because [my two supervisors] were in agreement and I felt comfortable going into session with [my client].” Even negative experiences contributed to systems of supervision. Hailey reported seeking out additional support when her assigned supervisory relationships did not meet her needs, widening the reach of simultaneous supervision even more: “By not being a good supervisor, he helps me seek out other resources and figure it out for myself.” Finally, Molly noted that supervisor coordination was primarily for evaluation at the end of the semester and only if problems arose. However, she imagined what it would be like if they were more collaborative:
They would have had a better understanding of the way I work in a counseling room. . . . Because my site supervisor really understood how I approached things and the way I would interact with my clients, but I feel like my university supervisor didn’t really, like, she had little snippets of what I was like in a counseling room.
Power, vulnerability, and systems in the supervisory relationship impacted supervisees from multiple levels in their clinical journey.
Personal Dispositions and Characteristics
Personal dispositions and characteristics resulted from participants speaking about the phenomenon as well as what they said about their supervisors. Three dispositions that emerged as relevant were tolerance for ambiguity, curiosity, and availability. The first two subthemes were identified as they spoke about the phenomenon and the third subtheme was a characteristic present because of the nature of simultaneous supervision.
Tolerance for Ambiguity
Tolerance for ambiguity was found to be a critical disposition. This disposition allowed participants to see differences in opinion as helpful. Emma shared that she “very rarely” saw people as giving her “conflicting information.” She said that she saw it as everybody having their own perspective. This connected to her ability to view multiple perspectives as “pieces of the puzzle,” as she expressed earlier in her retelling of the Indian fable. Although participants sometimes expressed concern about direction, Diana shared, “You can ask questions and you can not know and it’s okay.” This disposition directly related to how they reconciled and then reacted to multiple perspectives of simultaneous supervisors.
Curiosity
Curiosity also manifested more implicitly with supervisees. Participants showed curiosity by taking interest in what supervisors had to say, seeking more information, or staying open to difficult feedback. Hailey shared that simultaneous supervision “definitely requires a lot of continuing to look inward and examining your motives and yourself and what the supervisors have said.” In speaking more broadly, Emma shared, “So I don’t think I’ll ever give [simultaneous supervision] up now that I’ve kind of experienced how valuable it is to get another professional opinion.” Curiosity manifested itself as a transient characteristic for other participants. Diana experienced transference with one of her supervisors, which was a barrier to her ability to exhibit this helpful disposition. One of her supervisors suggested that she try and work things out with another supervisor she was having difficulty with, to which Diana said, “No. Who is gonna walk into their supervisor and be like, ‘Okay, so my problem with you is you’re a bitch. You remind me of my abusive ex.’ . . . But at the same time, I have to work with her.” This was an example of Diana demonstrating a closing off to feedback. Both tolerance for ambiguity and curiosity manifested and impacted their experience of multiple perspectives.
Availability
An important disposition was emotional and physical availability. Emma expressed that “there’s always somebody I can get a hold of.” Hailey expressed that she had “more coverage just in general,” but also questioned her supervisors’ true availability: “Do I even need to bring this to supervision or can I work on this on my own? Because sometimes I feel like I annoy them.” All participants expressed that availability was important to their experience, although physical availability did not always translate to being available to discuss what the supervisee wanted. Those participants who identified supervisors within simultaneous supervision as being more available had more positive thoughts regarding simultaneous supervision.
Discussion
All four participants identified the complex position of CITs receiving supervision from more than one supervisor. The results align with the growing body of literature affirming the importance of a positive working relationship between CITs and supervisors (Bernard & Goodyear, 2019; Borders et al., 2014; Sterner, 2009) as well as significant differences between faculty and site supervision (Borders, 2006; Dodds, 1986). The results parallel supervision literature detailing the multiple roles of supervisees (Bernard & Goodyear, 2019) who, unlike supervisors, are not required to have specific education in supervision. The theme of personal dispositions has been studied extensively in counselor education, resulting in prominent placement in clinical assessment instruments (Lambie et al., 2018). The presented themes diverge from the current research base in their construction of a clear model of simultaneous supervision. The subthemes of picking and choosing, seeking a preferred perspective, and systems of supervision illustrate the interpersonal dynamics of simultaneous supervision that is distinct from sole supervision, an underrepresented phenomenon in the supervision literature. Participants in this study reported mixed feelings with simultaneous supervision. Four primary themes emerged from this study: making sense of multiple perspectives, orchestrating the process, supervisory relationship dynamics, and personal dispositions and characteristics. These four themes encompass many areas of the supervisory experience while illuminating guidelines for supervisors engaging in simultaneous supervision.
Implications
Results from this study reinforce the complex levels of integration CITs experience when receiving supervision from multiple supervisors. This process of integration can lead to confusion, ambiguity, and also deeper understanding. The results indicate that the perceived benefit of simultaneous supervision was often based on the relationship between the supervisor and CIT, ability and support to organize the process, and the personal dispositions of the CIT. The implications for this research target three populations.
Supervisors
The findings of this study indicate several implications for supervisors working with clinicians receiving simultaneous supervision. First and foremost, the critical importance of the supervisory relationship to supervision in general (Bernard & Goodyear, 2019) was further substantiated as a foundation for effective simultaneous supervision. Questionable supervisee behaviors such as intentional nondisclosure via seeking a preferred perspective or picking and choosing can be avoided through purposefully fostering trust in the relationship. Similarly, supervisors may support the perspective of simultaneous supervision as a safety net if support for vulnerability is established and the relationship is actively attended to. Supervisors should be mindful of their availability to CITs and periodically check in to see if they are meeting the needs of the supervisee.
Supervisors who are aware of the themes developed from this research may be better equipped to capitalize on benefits and mitigate challenges. One benefit was that simultaneous supervision allowed participants to receive multiple synergistic perspectives regarding their work with clients. Depending on the developmental level of the supervisee and the demeanor of the supervisor, however, these multiple perspectives may present challenges. Supervisors can apply their knowledge of developmental models to tailor their interventions. Supervisors might anticipate that CITs earlier in development (e.g., in practicum) may require structured support in simultaneous supervision to avoid performance anxiety and frustration from rigid applications of multiple perspectives consistent with this stage (Stoltenberg & McNeill, 2010). Supervisors may also wish to focus supervision on interventions that actively facilitate development of these dispositions, such as employing constructivism to elicit greater cognitive flexibility (Bernard & Goodyear, 2019).
Some early-stage supervisees may experience challenges when navigating varying perspectives and feedback provided to them by multiple supervisors. Challenges can be mitigated when supervisors broach the topic of simultaneous supervision with supervisees early. Additionally, when supervisors ensure they respect other supervisors and create collaborative relationships, supervisee difficulty with simultaneous supervision may decrease. When a supervisor learns of a differing opinion of another supervisor, it is important that it is broached as a variance in approach rather than an incorrect practice. Supervisees experiencing difficulties with simultaneous supervision may also benefit from supervisors checking in with them regarding the variable feedback they are receiving. A collaborative supervisory system may strengthen supervisee development and integration of counseling constructs. Counseling programs can play a key role in setting systemic expectations for supervisors and supervisees.
Counselor Education Programs
Accredited counselor education programs have autonomy in how they meet various CACREP (2015) supervision and clinical requirements. Programs may choose to require simultaneous supervision, may require multiple clinical sites, and may utilize faculty advising as supplementary clinical supervision. In unique situations such as students completing two tracks or receiving additional supervision for gatekeeping reasons, how programs manage simultaneous supervision can become complex. Best practice guidelines, policies, and procedures regarding simultaneous supervision can be made clear in clinical handbooks, with clinical coordinators, and in material for site supervisors. This would help to address the supervisee confusion from the programmatic side. Another important implication with simultaneous supervision is to consider the supervisory process through a systemic lens. When simultaneous supervision is utilized, there will be many interactions occurring outside of the dyad or triad apparent to one individual supervisor. When supervisors collaborate and communicate, supervisees may be more likely to receive congruent feedback, understand gatekeeping action, and receive consistent expectations. In particular, communication between academic and clinical supervisors can bridge the gap between idealism and practicality (Bernard & Goodyear, 2019; Choate & Granello, 2006). Programmatically mandated, semesterly site visits and opportunities for regular check-ins could fulfill this purpose.
Supervisees
Participants often spoke to the challenge of organizing simultaneous supervision effectively in relation to feedback, documentation, and case presentation material. Although a certain level of organizational skill is expected of graduate students, the coordination required in simultaneous supervision often seemed unanticipated and unwieldy for students. Preparing for the supervision experience in another course and/or an orientation in lab supervision may aid in this. All participants discussed, at varying distress levels, how having supervision scheduled too close together (e.g., same day or two days in a row) increased repetitiveness and thus made simultaneous supervision feel less efficacious. Supervisees may want to intentionally schedule supervision sessions spaciously to avoid potential repetition or redundancy. With the steady increase in virtual supervision, scheduling supervision in ideal time frames may be easier with increased access and absent travel time. Programmatic preparation, intentional scheduling, and collaborative supervision notes may aid the simultaneous supervision process.
In the areas of core dispositions, CITs who embraced ambiguity and fostered reflexivity, curiosity, and flexibility tended to navigate simultaneous supervision with more ease. Reflexivity, curiosity, and tolerance for ambiguity seemed to strengthen the ability to receive feedback from multiple sources, integrate feedback appropriately, and maintain strong supervisory relationships. A typical guiding question from participants was, “How can I apply this combined feedback to my particular site and client while still maintaining my own clinical identity?” Necessarily, students will enter a program with differing levels of core strengths, yet any student can be encouraged to strengthen their core dispositions. Supervisees are encouraged to think about simultaneous supervision with the same organization and openness required for other courses such as pre-practicum and multicultural counseling. Correspondingly, supervisors have complex responsibilities maintaining ethical competent care, organizing supervision, and fostering these core dispositions.
Ethical Implications of Simultaneous Supervision
In addition to recommendations for the three populations above, findings from this study highlight ethical considerations. Worthington et al. (2002) identified “intentional nondisclosure of important information” (p. 326) and “inappropriate methods of managing conflict with supervisors” (p. 329) as two major ethical issues that are unique to supervisees and correlate with some of the participant supervisees’ experiences of triangulating supervisors, seeking outside consultation to circumvent supervisors, or intentionally withholding information. To ensure client welfare, supervisors and supervisees may benefit from explicitly discussing ethical implications and considerations unique to this phenomenon at the outset of supervision and again when conflicts arise. Future research that addresses limitations of this study will further clarify the role of supervisors, supervisees, and programs in simultaneous supervision as well as specific ethical guidelines.
Limitations and Future Directions
Limited information was gathered about the specific counselor education programs in which our participants were enrolled, restricting the inferences able to be made about simultaneous supervision in context. We also chose a convenience sampling method using CESNET and selected four participants. The choice of indirect sampling, primarily through counselor educators redirecting calls to their students, may have limited participants. Further, all participants of this study identified as the same gender and race, which limits the diversity of experience shared. Future researchers may consider sampling more participants to get a broader exploration of the phenomenon. In doing so, researchers may be able to obtain greater representation in gender and race to increase the transferability of this study.
This study focused on the phenomenon of simultaneous supervision as experienced within individual and triadic supervision. Simultaneous supervision is embedded within the broader experience of supervision, and isolating the phenomenon required vigilance by the researchers. Future researchers would benefit from intentional follow-up questions that better focus participants on simultaneous supervision rather than individual experiences with supervisors. As our study did not explicitly ask participants to distinguish between university-affiliated and site supervisors, future researchers may pursue a qualitative study that highlights the difference. Other research may utilize grounded theory to develop a model of simultaneous supervision for supervisors and supervisees to follow or focus explicitly on supervisors’ perspectives of simultaneous supervision. Quantitative research may illuminate the frequency and use of simultaneous supervision in counselor education programs overall or identify correlations between counselor dispositions such as tolerance for ambiguity and supervision outcomes in simultaneous supervision. Because of the lack of information regarding the phenomenon of simultaneous supervision, many opportunities for research regarding the phenomenon persist.
Conclusion
Overall, the findings from this research indicate CITs valued greater support and thrived when integrating “both/and thinking” in navigating feedback from multiple supervisors. This perspective reinforces the need for systemic communication among counselor educators and supervisors. Additionally, results suggest CITs would benefit from supervisors broaching the topic of simultaneous supervision early in their clinical experience.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Borders, L. D. (2006). Snapshot of clinical supervision in counseling and counselor education: A five-year review. The Clinical Supervisor, 24(1–2), 69–113. https://doi.org/10.1300/J001v24n01_05
Borders, L. D., Glosoff, H. L., Welfare, L. E., Hays, D. G., DeKruyf, L., Fernando, D. M., & Page, B. (2014). Best practices in clinical supervision: Evolution of a counseling specialty. The Clinical Supervisor, 33(1), 26–44. https://doi.org/10.1080/07325223.2014.905225
Choate, L. H., & Granello, D. H. (2006). Promoting student cognitive development in counselor preparation: A proposed expanded role for faculty advisers. Counselor Education and Supervision, 46(2), 116–130.
https://doi.org/10.1002/j.1556-6978.2006.tb00017.x
Council for the Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards/
Davis, K. L., & Arvey, H. H. (1978). Dual supervision: A model for counseling and supervision. Counselor Education and Supervision, 17(4), 293–299. https://doi.org/10.1002/j.1556-6978.1978.tb01086.x
Dodds, J. B. (1986). Supervision of psychology trainees in field placements. Professional Psychology: Research and Practice, 17(4), 296–300. https://doi.org/10.1037/0735-7028.17.4.296
Duryee, J., Brymer, M., & Gold, K. (1996). The supervisory needs of neophyte psychotherapy trainees. Journal of Clinical Psychology, 52(6), 663–671. https://doi.org/bmp9p9
Koltz, R. L., Odegard, M. A., Provost, K. B., Smith, T., & Kleist, D. (2010). Picture perfect: Using photo-voice to explore four doctoral students’ comprehensive examination experiences. Journal of Creativity in Mental Health, 5(4), 389–411. https://doi.org/10.1080/15401383.2010.527797
Kreider, H. D. (2014). Administrative and clinical supervision: The impact of dual roles on supervisee disclosure in counseling supervision. The Clinical Supervisor, 33(2), 256–268.
https://doi.org/10.1080/07325223.2014.992292
Lambie, G. W., Mullen, P. R., Swank, J. M., & Blount, A. (2018). The Counseling Competencies Scale: Validation and refinement. Measurement and Evaluation in Counseling and Development, 51(1), 1–15.
https://doi.org/10.1080/07481756.2017.1358964
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Miller, R. M., Chan, C. D., & Farmer, L. B. (2018). Interpretative phenomenological analysis: A contemporary qualitative approach. Counselor Education and Supervision, 57(4), 240–254. https://doi.org/10.1002/ceas.12114
Murray, S. A., Kendall, M., Carduff, E., Worth, A., Harris, F. M., Lloyd, A., Cavers, D., Grant, L., & Sheikh, A. (2009). Use of serial qualitative interviews to understand patients’ evolving experiences and needs. BMJ, 339, b3702. https://doi.org/10.1136/bmj.b3702
Nestler, E. J. (1990). The case of double supervision: A resident’s perspective on common problems in psychotherapy supervision. Academic Psychiatry, 14(3), 129–136. https://doi.org/10.1007/BF03341284
Pietkiewicz, I., & Smith, J. A. (2014). A practical guide to using interpretative phenomenological analysis in qualitative research psychology. Psychological Journal, 20, 7–14. https://doi.org/10.14691/CPPJ.20.1.7
Read, B. L. (2018). Serial interviews: When and why to talk to someone more than once. International Journal of Qualitative Methods, 17(1), 1–10. https://doi.org/10.1177/1609406918783452
Saxe, J. G. (1868). The poems of John Godfrey Saxe. Ticknor and Fields.
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research (1st ed.). SAGE.
Sterner, W. (2009). Influence of the supervisory working alliance on supervisee work satisfaction and work-related stress. Journal of Mental Health Counseling, 31(3), 249–263. https://doi.org/10.17744/mehc.31.3.f3544l502401831g
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Stutey, D. M., Givens, J., Cureton, J. L., & Henderson, A. J. (2020). The practice of bridling: Maintaining openness in phenomenological research. The Journal of Humanistic Counseling, 59(2), 144–156.
https://doi.org/10.1002/johc.12135
Tromski-Klingshirn, D., & Davis, T. E. (2007). Supervisees’ perceptions of their clinical supervision: A study of the dual role of clinical and administrative supervisor. Counselor Education and Supervision, 46(4), 294–304. https://doi.org/10.1002/j.1556-6978.2007.tb00033.x
Worthington, R. L., Tan, J. A., & Poulin, K. (2002). Ethically questionable behaviors among supervisees: An exploratory investigation. Ethics & Behavior, 12(4), 323–351. https://doi.org/10.1207/S15327019EB1204_02
William B. Lane, Jr., PhD, NCC, BC-TMH, LPCC, is an assistant professor at Western New Mexico University. Timothy J. Hakenewerth, PhD, NCC, LPC, is an assistant professor at the University of Illinois Springfield. Camille D. Frank, PhD, NCC, LMHC, LPC, is an assistant professor at Eastern Washington University. Tessa B. Davis-Price, PhD, LMHC, LCPC, is an assistant professor at Saint Martin’s University. David M. Kleist, PhD, LCPC, is a professor and department chair at Idaho State University. Steven J. Moody, PhD, is a clinical professor at Adams State University. Correspondence may be addressed to William B. Lane, Jr., 1000 W College Ave, Silver City, NM 88061, william.lanejr@wnmu.edu.
Appendix
Interview Protocol
| Interview Questions |
| Round 1 |
| What has been your experience with having multiple simultaneous supervisors?
In your own experience, how has simultaneous supervision been a strength?
In your own experience, how has simultaneous supervision been challenging?
What have you learned about yourself and the counseling profession as you’ve experienced simultaneous supervision? |
| Round 2 |
| How has having simultaneous supervision been different from times when you have only had one supervisor?
What has it been like to have your supervisors interact with each other in regard to the supervision that you have received from them?
What personal dispositions (characteristics/qualities) do you think you have that influenced your experience of simultaneous supervision?
How has simultaneous supervision impacted your experience of safety or vulnerability in supervision?
What practical considerations have you needed to consider for having multiple simultaneous supervisors? |
May 22, 2024 | Volume 14 - Issue 1
Emily Horton
Body neutrality is a concept wherein individuals embody a neutral attitude toward the body that is realistic and flexible, appreciate and care for the function of the body, and acknowledge that self-worth is not defined by one’s outward appearance. Family behavior regarding body image has been related to higher levels of body dissatisfaction and unhealthy eating behavior among children and adolescents. Caregivers need knowledge and support on how to cultivate healthy body image for their children and adolescents. Limited studies explore how to parent in a way that promotes healthy relationships with one’s body, food, and exercise. I conducted a grounded theory study to explore the experiences of caregivers who integrate tenets of body neutrality. Semi-structured interviews were conducted with 10 caregivers of children and adolescents who self-identified as approaching parenting from a place of body neutrality. Through constructivist grounded theory, I discerned insights regarding how caregivers can support their children and adolescents in developing healthy relationships with their bodies and how this corresponds with self-esteem. Considerations for counselors using body neutrality to support children, adolescents, and caregivers are provided.
Keywords: body neutrality, body image, parenting, children and adolescents, self-esteem
Body image and related low self-esteem are frequently under-addressed or unaddressed in counseling children, adolescents, and their caregivers (Damiano et al., 2020). Too often, counselors may take a reactive approach to addressing unhealthy relationships with food, bodies, and exercise in the family system, such as counseling after an adolescent is diagnosed with an eating disorder (Liechty et al., 2016). Thus, counselors may benefit from considering how to take a preventative, proactive approach to supporting children’s mental health specific to their relationship with food, bodies, and movement (Siegel et al., 2021). Because the family system has tremendous impact on children’s body image and relationship with food, counselors need to consider how to provide appropriate psychoeducation and support to caregivers on how to manage food and body talk (Gutin, 2021). Positive caregiver influence on body image can prevent disordered eating, negative body image, and low self-worth, and many families need a licensed mental health professional to cultivate said positive influence (Veldhuis et al., 2020).
Researchers have found that children as young as 3 to 5 years old experience body image issues (Damiano et al., 2015; Dittmar et al., 2006). Caregivers often communicate body dissatisfaction, engage in dieting, and demonstrate a drive for thinness, messages that children can internalize (National Eating Disorders Association, 2022). Families can inadvertently pass down unhealthy ideals regarding body image to their children (Kluck, 2010). Kluck (2010) emphasized that a family’s focus on appearance was related to their child’s body image dissatisfaction, and the dissatisfaction predicted increased disordered eating. Counselors with appropriate training can play an important role in mitigating the harmful cycle before disordered thinking turns into disordered eating (Klassen, 2017). Counselors have the unique opportunity to support families in encouraging a healthy relationship with their bodies (Horton, 2023; Horton & Powers, 2024).
In this study, I sought to explore the experiences of caregivers who integrate tenets of body neutrality. Body neutrality is a concept wherein individuals embody a neutral attitude toward the body that is realistic and flexible, appreciate and care for the function of the body, and acknowledge that self-worth is not defined by one’s outward appearance (Pellizzer & Wade, 2023). Examples of body neutrality can include not describing food as healthy or unhealthy, talking about what our bodies do for us rather than what they look like, and moving for enjoyment rather than to burn calories. Because the tripartite model emphasizes that parental influence, in addition to peer and media influence, is significant for children’s body image development, I explored existing research on parental influence on body image and self-esteem (Thompson et al., 1999).
Parental Influence on Body Image and Self-Esteem
Some family members negatively impact children’s and adolescents’ body image (Pursey et al., 2021). Neumark-Sztainer et al. (2010) found that over half of the adolescents in their study experienced weight-based and appearance-based teasing from family, and these experiences correlated to higher levels of body dissatisfaction, disordered eating, and related mental health difficulties, such as depression. Parental influence on body image includes both direct (e.g., criticism about their child’s weight) and indirect (e.g., parents’ attitudes about their own bodies, food, and exercise) behaviors (Rodgers & Chabrol, 2009). Abraczinskas and colleagues (2012) conducted a study exploring parent direct influence, including weight- and eating-related comments, and modeling, including parental modeling of dieting and related behavior. In the study of over 360 participants, Abraczinskas and colleagues found that parental influence is a risk factor in the development of a drive for thinness, body shape dissatisfaction, and eating disorder symptomology.
Moreover, Wymer and colleagues (2022) emphasized the importance of parent engagement in body image and self-esteem development. Often, families recognize the importance of discussing body image with their children but do not feel confident or competent in doing so (Siegel et al., 2021). The lack of confidence and competence leads to messages about health being conflated with messages about thinness (Siegel et al., 2021). In addition, researchers highlighted that although parental influence has a significant impact on body image and self-esteem, siblings, friends, and the media are also perceived to have influence over youth’s feelings about their bodies (Ricciardelli et al., 2000). The exiguous literature on parental influence on body image repeatedly emphasizes the negative impact of parents on body image yet seldom explores preventative and therapeutic ways of promoting healthy body image (Phares et al., 2004). Thus, I sought to explore how counselors might integrate body neutrality when supporting families and provide early intervention and prevention for adverse relationships with food, body, and movement.
Body Neutrality
Body neutrality is a concept wherein individuals accept their bodies as a vessel that carries them through life, and as such, do not attach positive or negative feelings to their physicality. For example, body neutrality can entail nurturing and respecting the body, being mindful of body talk, engaging in body gratitude and functionality appreciation, and recognizing self-worth that is not focused on appearance (Pellizzer & Wade, 2023). Body neutrality is an approach taken to help with the healing of body image, particularly in the field of eating disorders (Perry et al., 2019). Body neutrality tenets appear to be integral in the prevention of body image dissatisfaction and disordered eating (Herle et al., 2020). Practicing body neutrality positively impacts body satisfaction, self-esteem, and negative affect with adults, though continued empirical research is needed on its impact with youth (Walker et al., 2021). Although counselors and other allied professionals integrate body neutrality into their clinical practice, there is minimal research on its efficacy outside of eating disorder treatment. Existing research has emphasized the need for counseling approaches with youth that highlight body neutrality tenets, such as mindful eating and awareness-building conversations about societal messaging (Klassen, 2017). However, researchers have yet to explore how body neutrality could be integrated into a parenting approach. The bulk of the limited understanding of body neutrality is treatment based, rather than prevention oriented.
Thus, the purpose of this study was to cultivate a grounded theory or an abstract theoretical understanding of body neutral parenting (Charmaz, 2014). Further insight into the experiences, challenges, and potential barriers in parenting with body neutrality can enable a deeper understanding of how parents seek to promote healthy body image and self-esteem for children and adolescents. In this study, I aimed to offer a newfound understanding to mental health professionals supporting children, adolescents, and caregivers in the areas of body, food, movement, and related mental health implications.
Method
Methodology
To address the paucity of literature, a grounded theory study was conducted to examine the following research question: How do caregivers conceptualize and actualize body neutral parenting with their children? The study derived from constructivist grounded theory (CGT; Charmaz, 2014). CGT is an interpretative, qualitative methodology that acknowledges that researchers and participants co-create the theory (Charmaz, 2014). Given a desire to understand how caregivers conceptualize and utilize body neutral parenting, CGT was deemed appropriate. The purpose of the study was to generate a new theory through inductive analysis of data gleaned from caregivers who self-identify as using body neutral parenting.
Role of the Researcher
Congruent with CGT, I maintained a position of distant expert (Charmaz, 2014). The theoretical meaning was constructed by turning participants’ experiences into digestible theoretical interpretations. While staying as true to the experiences of the participants as possible, I reconstructed the participants’ stories in the development of the grounded theory via balancing conceptual analysis of participants’ stories and creating a sense of their presence in the narrative (Mills et al., 2006). I sought to examine the impact of my privilege and preconceptions as a White, cisgender woman and professional in the field of mental health counseling, with experience supporting families navigating eating disorders and disordered eating (Charmaz, 2014). Also, as a parent who integrates body neutrality into my approach with my child, I practiced reflexive journaling and other trustworthiness strategies to bracket my biases throughout the study.
Participant Recruitment
I obtained IRB approval prior to data collection. Per the IRB, all participants verbally consented before partaking in the research study. I used purposive sampling (Patton, 2014) for participant selection. Selection criteria included: (a) being a caregiver to at least one child under the age of 18, (b) identifying as integrating body neutrality into their parenting approach, and (c) willingness to participate in an interview lasting roughly 1 hour. I circulated electronic flyers detailing the focus of the study to social media pages for caregivers and professional networks. The recruitment flyers provided examples of body neutral parenting, including not describing food as healthy or unhealthy, talking about what our bodies do for us rather than what they look like, and moving for enjoyment rather than to burn calories.
Ten participants were interviewed. Of the 10 participants, nine identified as cisgender women and one identified as nonbinary. All 10 participants described themselves as being middle class. Nine participants were married and one was single. All of the participants had graduate-level or doctorate-level educations; four had master’s degrees and six had doctoral degrees. Participants lived in seven different states and two different countries. Participants had at least one child, with the number of children ranging from 1 to 5. Table 1 provides detailed demographic data.
Table 1
Participants’ Demographic Data
| Pseudonym |
Age |
Race |
Number
of Children |
Age of Children |
Race of Children |
| Logan |
27 |
White |
1 |
20 months |
White |
| Esmeralda |
38 |
Hispanic |
2 |
8 and 5 years |
White |
| Imani |
29 |
Black, White |
2 |
6 and 3 years |
White |
| Kimberly |
33 |
White |
2 |
5 and 2 years |
White |
| Heather |
42 |
White |
2 |
3 years, 8 months |
White |
| Cassie |
45 |
White |
5 |
16, 13, 11, 9, and 7 years |
White |
| Shanice |
36 |
African American |
4 |
15, 9, and 2 years; 4 months |
African American |
| Scarlett |
36 |
White |
3 |
17, 5, and 4 years |
White |
| Leilani |
43 |
White |
1 |
9 years |
Polynesian, White |
| Jennifer |
36 |
White |
1 |
2 years |
Middle Eastern, White |
Data Collection and Analysis
As guided by Charmaz’s (2014) CGT protocol, data collection and data analysis proceeded simultaneously, and the inclusion criteria evolved to include caregivers with children of all ages. The semi-structured interviews occurred via confidential videoconferencing software and lasted between 60 and 75 minutes. Interviews were an open-ended, detailed exploration of an aspect of life in which the participants had substantial experience and considerable insight: parenting with body neutrality principles (Charmaz & Liska Belgrave, 2012). During the interviews, I inquired about caregivers’ experiences, challenges, and insights of body neutral parenting. With the emergent categories, the guide evolved to emphasize the nuances of the parenting approach in alignment with three-cycle coding or focused coding (Charmaz, 2014).
Grounded theorists try to elicit their participants’ stories and attend to whether the participants’ interpretations are theoretically plausible (Charmaz & Liska Belgrave, 2012). As such, the interview protocol began with an initial open-ended question: “Tell me about a time in which you used body neutral parenting.” Then, I asked intermediate questions, such as “How, if at all, have your thoughts and feelings about body neutral parenting changed since your child was born?” I also asked ending questions, including: “How has taking the approach with your children impacted you as a parent? As a person?” The interview questions were informed by the literature and were reviewed by another content matter expert.
In addition to the in-depth interview, I used information from other data sources to support the depth of the data and theory construction. Other triangulated data sources included field notes of observations during the interviews, a reflexive journal, literature and previous research on body neutrality, and a demographic survey. In this way, the constant comparative analysis unique to CGT increases rigor through complex coding procedures more so than other methods of qualitative data analysis (Hays & McKibben, 2021). The constant comparative analysis examines nuanced relationships between participants through negative case analysis to strengthen findings (Hays & McKibben, 2021).
Three-cycle coding and constant comparative analysis drove the data analysis process (Charmaz, 2014). Through the data analysis process, I constantly compared data (Mills et al., 2006). Inductive in nature, the constant comparison through the data analysis grounded my theories from the participants’ experiences (Mills et al., 2006). In alignment with CGT, I coded the interviews through a fluid process of initial coding, focused coding, and theoretical coding. During initial coding, I focused on “fragments of data,” such as words, lines, segments, and incidents (Charmaz, 2014, p. 109). The initial coding process not only included the transcripts, but also continued the interaction and data collection to facilitate the continuous analytical process. I also engaged with focus coding, wherein I used the most significant and frequent codes that made the most analytic sense (Charmaz, 2014). The focused codes were more theoretical than line-by-line coding practices. I engaged in theoretical coding of the data; theoretical coding is a way of “weaving the fractured story back together” (Charmaz, 2014, p. 63). In accordance with Charmaz (2014), theoretical coding involved clarifying the “general context and specific conditions” and discovering “participants’ strategies for dealing with them” (p. 63). As I moved throughout the three-cycle coding process, the number of codes, categories, and emerging core categories decreased and refined, leaving me with the final core categories described below (Khanal, 2018).
Rigor and Trustworthiness
Throughout the totality of the research process, I engaged with five strategies to ensure trustworthiness. In the data analysis process, significant care was taken to ground analytic claims in the data obtained and remain true to the raw material provided by participants (Charmaz, 2014). I fostered trustworthiness through member checking and memo-writing (Creswell & Poth, 2017). I sent the transcript and the themes to participants and had six of 10 participants verify the themes as being congruent with their experiences. The other participants did not respond to the email with the transcript. Memo-writing was critical in constructing theoretical categories (Charmaz, 2014). I stopped and analyzed my ideas about the codes and emerging categories via memo-writing. Successive memos kept me immersed in the analysis and increased the abstraction of my ideas (Charmaz, 2014). In the theory construction, I also triangulated data sources, including semi-structured interviews, field notes of observations during the interviews, memo-writing, literature and previous research on body neutrality, and a demographic survey. Charmaz (2014) emphasized the importance of “thick descriptions” (p. 14), which I captured via writing extensive field notes of observations during the interviews and compiling detailed narratives from transcribed tapes of interviews.
I also shared my memos and data analysis process with an external auditor (Hays & McKibben, 2021). The external auditor was a researcher with experience in qualitative research and content familiarity. After the external auditor reviewed the data analysis trail, including the three stages of coding, I reviewed her written feedback and we met to process the feedback. The external auditor offered several pieces of feedback regarding the analytic process, including leaning more into the theory rather than the stories and removing quotes that captured pieces outside of the theory (i.e., removing content rooted in diet culture and body positivity). Feedback was integrated to strengthen the study’s development and explication of the theory based on data.
Results
This study involved the caregivers and researcher co-constructing the parenting theory while integrating body neutrality concepts. The theory stemmed from the perspectives shared by caregivers who parent in such a way as to promote body acceptance, such as focusing on what our bodies can do for us, avoiding body talk, eating the foods we want to eat, listening to our bodies, not focusing compliments on appearance, etc. As such, the grounded theory below explains caregivers interacting and experiencing body neutral parenting (Charmaz, 2014).
The emergent core category was the balancing of internal experiences with external parenting, moving toward body neutral parenting. The emergent core category captured the essence of the theory—parents integrating body neutrality balance internal experiences (e.g., their own relationship with their bodies and food) with external parenting (e.g., their parenting skills of how to handle food in the household). Figure 1 depicts a conceptual diagram of the body neutral parenting grounded theory. The “mobile” emphasizes the movement and interconnectedness within the body neutral parenting process. At the top of the diagram, there is a seesaw balance between the external parenting skills and internal experiences, processing, and regulating. The internal and external experiences teeter and totter and inform one another as a parent integrates body neutrality. The mobile diagram showcases that if one piece moves, the other pieces move as well. To illustrate, if a parent’s external parenting skills move (e.g., a parent no longer says negative things about their body in front of their children), their internal experiences are impacted (e.g., their own unmet childhood mental health needs related to body image are addressed). The core category of balancing internal experiences with external parenting moving toward body neutral parenting included two categories: (a) De-moralizing Food, Bodies, and Movement, and (b) Reprogramming and Re-Parenting. Each of the two emergent categories has associated subcategories.
De-moralizing Food, Bodies, and Movement
The first category is De-moralizing Food, Bodies, and Movement (n = 10). Within this category, there were three subcategories: De-moralizing Food, De-moralizing Bodies, and De-moralizing Movement. The category embodied acknowledging and countering the large cultural narrative of “good” foods and “bad” foods as well as “good” bodies and “bad” bodies. Participants emphasized the impact of removing the reward and punishment that accompanies the moralization of food, bodies, and movement. As captured by Kimberly, body neutral parenting is about “giving children more of a voice”and trusting them: “When they say that they’re hurt, believing them; when they say that they’re hungry, believing them. Letting them speak for themselves and not speaking for them or for their body. Trusting that they know their body the best.”
Figure 1
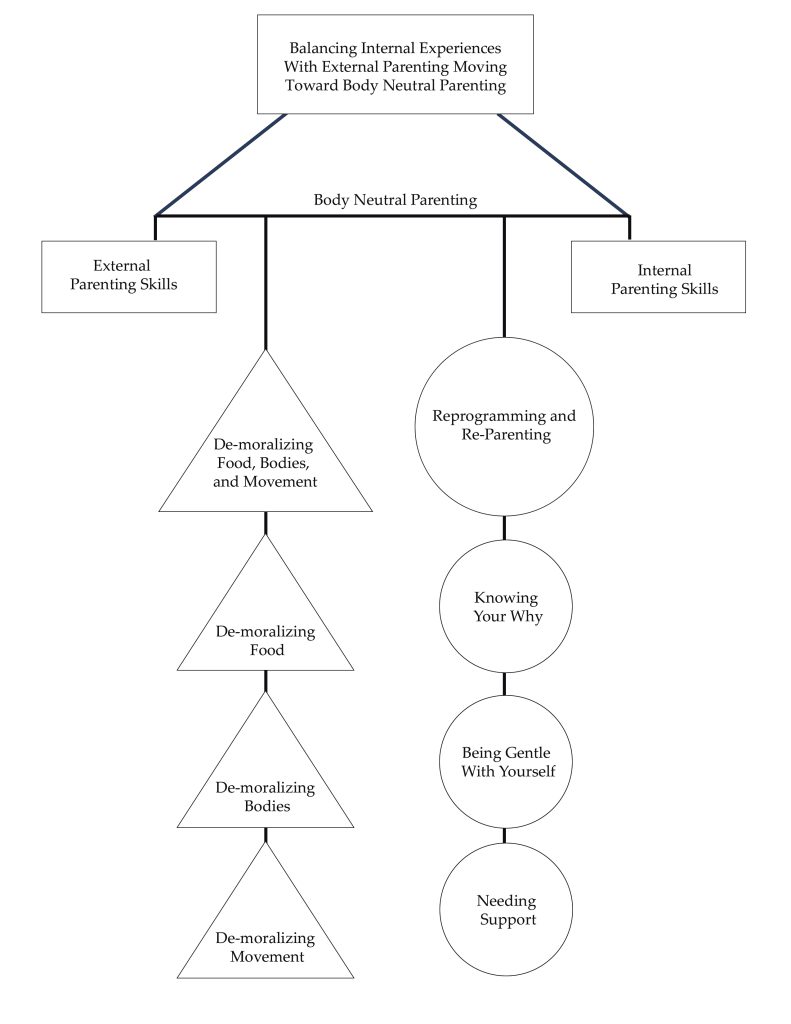
Note. This figure showcases the diagram of the body neutral parenting theory. The diagram shows a visual representation of the emergent core category, two categories, and six subcategories and their relationships (Charmaz, 2014).
De-moralizing Food
The first subcategory (n = 10) was De-moralizing Food. Participants consistently noted that food was “one of the biggest” parts of body neutral parenting—specifically, approaching food not as “good” or “bad,” not as “healthy” or “unhealthy,” but simply, neutrally, as “fuel” for the body. Cassie articulated that “A big piece is trying to take the moral piece out of it too. That it’s somehow good to have a certain body or foods are good or bad. Just trying to get away from that.”
The demoralization of food, moving toward neutrality with food, presented in numerous ways across participants’ approaches to caregiving. A primary way in which participants showcased their beliefs about food with regard to body neutrality was to present different foods in a neutral way. For example, the neutral presentation of different foods could look like desserts on the child’s plate from the beginning of the meal, rather than something to be “earned” after eating the “good” foods first. Esmeralda articulated a way in which she demoralized foods and presented them neutrally through what she coined as “Tasting Tuesdays.” She shared:
Instead of making a meal that you serve up in bowls or on plates, you basically charcuterie board the whole meal. . . . I noticed the effect it had on my kids to present a bunch of options, including desserts or traditional treats—it was all presented together. I was laying out all the foods on equal ground, lots of options. And many traditionally unhealthy foods and many traditionally healthy foods just all on the table together. There was no instruction. They just got an empty plate, and they could fill it with whatever they wanted, and I think for them there was some autonomy built into that. They could decide exactly what and how much they wanted to eat off the table. But it also, I think, inspired some adventurousness in them.
Presenting foods neutrally mitigated food judgment, created variety and exposures to food, and met the developmental needs of her children by making mealtime fun.
Another pivotal element of de-moralizing food and moving toward neutrality with food was to create space for children to practice noticing their hunger and fullness cues. Jennifer shared about her experience helping her child learn to trust their body and its cues. She explained:
Trying to trust him and listening to his body, even though he’s 2, and knowing where to intervene and where I shouldn’t intervene. If I make dinner and I put it in front of him and he touches nothing and wants to get down, the way that I was raised was you finish your plate no matter what. Reading everything that I’m reading and trying to move to this neutral space. What I want to say is “At least taste it. At least take a bite. Take one bite. Take three bites.” And what I’m choosing to do is, “Okay, you don’t have to eat right now. We’ll have a bedtime snack later.” I was conditioned to think that first thought.
While not explicitly using the language, participants spoke to helping their children with their hunger, fullness, and satiety cues. Practicing satiety looked like the children being able to say, as Scarlett’s son said, “My body is hungry for ice cream.” Also, Kimberly shared trying to instill autonomy within her children as they learn their hunger, fullness, and satiety cues:
We do defer to them a lot in terms of what they eat or when they’re eating. My daughter wanted canned cooked carrots for breakfast. It was like, well, okay, that’s not maybe socially typical, eating cooked carrots for breakfast. But if that’s what your body wants, go for it. . . . They asked her a question at school when she was graduating from preschool. What would you spend $1,000,000 on? A doughnut. So, it’s like, okay, we’re not going to demonize your doughnuts. You can have your doughnuts when you want your doughnuts.
Here, Kimberly also captured body neutral parenting’s emphasis on avoiding “healthy” vs. “unhealthy” food and other dichotomous language, stemming from diet culture.
Neutral beliefs and behaviors regarding food also manifest via portion sizes for children. Scarlett highlighted differences she noticed in how her family members wanted to portion food for her two sons: one in a larger body and one in a smaller body. She explained that her family members will “offer to my one son and not to the other” while also saying “Oh, do you need that?” to the son in a larger body. Thus, integrating body neutral parenting entails presenting food neutrally, rather than being driven by internalized societal messages about food and thin privilege (e.g., suggesting to a child in a larger body that they may not need the amount of food they are being served perhaps because of anti-fat bias). Body neutral parenting applies for children of all body types.
Moreover, caregivers practicing body neutrality with their children talked about food in a way that emphasizes how it “fuels the body” rather than being about “reward or punishment.” Esmeralda explained:
It’s like you have to basically find a whole new system of rewards. Sweet things are good motivators. They’re reward systems. And they’re also seen as the desirable food after you choke down the “healthy” food . . . these are the “good” foods you have to eat in order to get the “bad” foods that you get rewarded with after dinner. That just is such an insidious concept.
Counter to food being a “reward” or “punishment,” children get to choose rather than falling into the power struggle with food. Cassie described
taking the power out of the food situation. With little kids, everyone thinks like, “Oh, you have to control it and you have to make sure they get vegetables in and all that stuff.” Then it becomes about this power dynamic and just trying to take power out of it and then it is about letting them listen to their body and learn about their body.
Avoiding using food as a reward or as a punishment was integral to the body neutral parenting approach.
De-moralizing Bodies
The second subcategory (n = 9) was De-moralizing Bodies, wherein there are not “good” bodies and “bad” bodies. Leilani described, “In relation to size, shape, behavior, disposition, bad habits . . . everybody’s different.” Body neutral parenting conceptualizes bodies in neutral ways, emphasizing what they help people do. As Cassie explained, “You need food to do the things you want to do, and so we take care of our bodies . . . not to look pretty, but to be able to do—focus more on the doing.” Similarly, Leilani shared,
My go-to approach is to say things like “Everyone’s body is growing at its own pace” and “We have to let our bodies grow at their own pace.” I’m freaked out by stats on how many U.S. girls are dieting around age 10-ish. I’m hoping that my emphasis on letting our bodies do what they need to do will have some impact against pre-teen dieting fads taking hold in our home.
Many participants spoke about their goal for their children of “listening to their bodies.” Kimberly explained, “We tell our children a lot, ‘Listen to your body.’ So, what your body is feeling, what your body is saying, if your body is not hungry anymore, that’s fine. Or if it is hungry.” Further, participants named the impact of modeling, and not modeling, ideals about bodies. To illustrate, Imani explained,
Not talking about other people, that is a huge thing in our family, is just to not talk negatively about people that we don’t know or about people we do know. We don’t talk negatively about our own bodies in front of our kids or anybody else’s body in front of our kids. That’s honestly probably one of the more impactful things that we do.
Kimberly, too, emphasized being mindful of modeling how to think and talk about bodies:
Making sure that we model kindness to our bodies in front of them as well. So not saying things that are self-deprecating about the way that we look. Making sure that our children don’t hear us saying, “Oh my gosh, I’m just so fat,” those kinds of messages.
Also, participants emphasized integrating body neutrality into clothing approaches with their children. Scarlett described being mindful of the language she uses regarding clothes and bodies: “You’re too big for that versus those clothes don’t fit your body, or you’re too small for that versus that doesn’t really look like it’s comfortable on your body. Let’s find something that works best for you.”
De-moralizing Movement
The last subcategory (n = 7) was De-moralizing Movement, which included engaging in movement for fun and being mindful of how we speak about exercise. Imani explained:
And so I think that for us, we really try to keep those things [exercise, body image, and food] disconnected. If you’re doing gymnastics, it’s because you’re interested in it and you think it’s a fun thing, not because it’s going to impact your body, not because you know it’s going to make you thin. It’s because you think it’s fun.
Cassie conceptualized movement as being fun, not for compensation, as well: “Being excited about things our bodies are doing and not just kind of the emphasis on like, well, if it’s fun, let’s do it. But if it’s not fun, then we’re not going to push ourselves or torture ourselves.” Moreover, Scarlett emphasized the importance of being conscientious of language used to describe her children’s bodies:
How big they are. We use that term especially with male children. But you are such a big boy is always the thing. You’re such a big boy . . . instead trying to just say things like, “Oh, hey, that’s really awesome that you can do X, Y, and Z.” Trying to make it very concrete, it’s very cool that your body allows you to run around and play.
When it came to De-moralizing Food, Bodies, and Movement, a theme of removing the “shoulds” prevailed across participants. Kimberly described trying to “stay neutral with foods so that we don’t end up so much down the should line of what they should be eating or what they should be doing in terms of physical activity or those kinds of things.” Taking out the “should” entailed avoiding dictating what children “should be eating, “should look like,” or how they “should be exercising.” In summary, as poignantly articulated by Logan, “just focusing on the objectivity of what’s there without having the positive or negative associations.”
Reprogramming and Re-Parenting
The second category (n = 10) was Reprogramming and Re-Parenting. Beyond the skills of body neutral parenting, a key tenet of the approach was ample self-reflection. Caregivers engaged in deep reflection of their own relationship with food, their body, and movement while supporting their children in their body image development. The self-reflection process entailed identifying, rewiring, and, often, re-parenting oneself through the sociocultural messages that have permeated one’s life span. Scarlett shared that body neutral parenting “makes me reflect on myself and why I’m saying the things I’m saying and why I feel the way I’m feeling.” Subcategories of Reprogramming and Re-Parenting included: Knowing Your Why, Being Gentle With Yourself, and Needing Support.
To illustrate, Leilani increased her awareness of her history with disordered eating and exercising for compensation and shared the impact her daughter has had on rewiring her way of thinking:
If I had a child who was very thin, it would have reinforced that dysfunction for me, because then I’m someone who produced a very thin child, and that makes me even better. . . . And then when you have a kid who’s really big and she’s pretty chubby, that you have to make such a hard shift to undo. Being the skinniest person in the room isn’t your greatest value in life and really reestablishing that personal value system. That’s been a massive kind of change for me.
This is a tangible example of the rewiring that happened for Leilani, though all of the parents spoke to their rewiring process and need to re-parent themselves alongside their children.
Knowing Your Why
The first subcategory (n = 10) of Reprogramming and Re-Parenting was Knowing Your Why. Participants acknowledged the value they put into the parenting approach. Jennifer captured common collective values of body neutral parenting when she shared:
Number one, reducing shame. Number two, increasing quality of life and self-confidence . . . that would probably eventually help with any mental health issues or any relationship issues because he’ll have the self-confidence to say where his boundaries are and trust his body. And at the same time listen to other people and be empathetic.
Similarly, Kimberly emphasized how much it means to be parenting without shame: “I love that we know we’re not parenting with shame . . . as the hidden motivator. That’s why you don’t eat that extra food you might be hungry for.”
A significant challenge for many participants was the “internalized messaging” they experienced regarding their body image, food, and movement. Almost all of the participants (n = 8) directly spoke to their experiences with an eating disorder or disordered eating driving their desire to parent from a body neutral stance. Cassie, for example, cited her eating disorder recovery as sparking her passion for body neutral parenting:
Right when my husband and I got married, I went into treatment for an eating disorder, and so that shaped me a lot. . . . I was using all of the things that I had learned and trying to really instill it in them. How we talk about food, how we talk about bodies. It was such an integral part of my parenting.
Being Gentle With Yourself
The second subcategory was Being Gentle With Yourself. Each participant (n = 10) criticized themselves in some fashion about not perfectly integrating body neutrality into their parenting approach. They were quick to highlight their failures and slow to honor their successes. Body neutral parenting, given its emphasis on countering long-standing sociocultural messaging, requires offering oneself a great deal of grace. Body neutral parenting entails tremendous learning, and that learning starts with reminding caregivers that they are doing the best that they can with the knowledge, support, and resources that they have. Imani spoke to how she navigated thoughts from these internalized messages and filtered them:
I think about things like, “She’s thinning out.” . . . It’s so ingrained, it’s hard not to think those things. And so then even if that’s something that goes across my mind or I think about the things that they’re eating and how that might impact their body or their physical health, just stopping that conversation with me and not actually talking about that with them, it’s not something that they need to hear. So, I think that it’s just as much what we don’t say as much as what we do say to them.
Having thoughts stemming from diet culture and stumbling and saying the “wrong” thing is inevitable when rewiring these deeply embedded messages. Not only are those moments of “messing up” normal, but they also create space for beautiful moments to repair. Scarlett explained her process of repairing the inevitable ruptures:
Which all sounds well and good and wonderful until you are running around with a 4-year-old and a 5-year-old on your day to day. I will also balance that, it’s also trying to catch myself when I say things that I’ve just internalized from society in my own childhood and being like, “Hey, isn’t that interesting.” Just talking out loud to them. Saying, “Isn’t it interesting that I said X, Y, and Z? Is that really maybe the best way to talk about our bodies?” Trying to just be reflective and knowing that I’m not always going to be body neutral but trying to be intentional about noticing when I’m not.
The participants reflected that parenting is an imperfect, human process.
Needing Support
The third subcategory was Needing Support. All of the caregivers in the study (n = 10) spoke to the importance of feeling support in their parenting approach. Support looked different for each family; some received support through social media, and others described finding support from their partner or other like-minded caregivers. Every participant described the role that social media had in their body neutral parenting approach. Many described learning about the approach via social media and experiencing continued support through certain social media pages. For example, common social media pages referenced by participants included Feeding Littles, Our Mama Village, Dr. Becky, and Kids Eat in Color. Most participants recommended that caregivers interested in starting body neutral parenting seek out social media for knowledge and support.
Additionally, participants emphasized the importance of being on the same page with other primary caregivers. Consistently, participants accentuated the need to talk through how to navigate situations in advance, to be on the same page for how to handle them. To illustrate, Scarlett described how to navigate their child “wanting ice cream after not eating all of their dinner” and how she and her partner talked through how to approach that situation. Esmeralda emphasized a need for support that she felt she was not getting:
I don’t think I’ve really found a group of parents or moms where we can talk through these things or troubleshoot together. I feel like I’m a consumer of some social media on the topic, and then I’m just sort of alone.
Feeling supported appeared to be integral to body neutral parenting.
Discussion
This co-created grounded theory on body neutral parenting is a valuable addition to the literature, given the gaps in understanding how counselors can help guardians support healthy body image amongst children (Klassen, 2017). Given the significant familial influence on body image development, counselors can consider this study’s findings through a preventative lens (Liechty et al., 2016). The findings align with the scant literature on body neutrality, suggesting the need for continued exploration of how to support children, adolescents, and their families in their conceptualizations of body, food, and movement (Gutin, 2021). Mental health counselors can consider body neutral parenting as an avenue to foster positive familial influence in body image development. Positive familial influence on body image and related self-worth can prevent disordered eating, negative body image, and low self-worth (Veldhuis et al., 2020). Thus, body neutral parenting appears to have the potential to have significant impact on the mental health and self-efficacy of children, as well as their caregivers.
Based on the findings of this study, critical tenets of body neutral parenting include de-moralizing food, bodies, and movement, and reprogramming and re-parenting. The co-created parenting theory constructed in this study can be utilized as a way of conceptualizing a parenting practice that facilitates healthy body image development for families. Specifically, counselors can help families learn that food is not “healthy” or “unhealthy” and there are not “good” or “bad” bodies. In addition, the co-created theory emphasizes the need for counselors to help family members heal from internalized messages and misconceptions about health that can perpetuate body image dissatisfaction and disordered eating across generations.
Implications for Counselors and Caregivers
Counselors and caregivers are uniquely positioned to use the findings of this study to inform how they support children and their body image development. In this study, parents offered their approach to integrating body neutral parenting with their children. The co-created theory of body neutral parenting offers a baseline for counselors and parents to consider, and future research on the theory is needed. Thus, counselors and parents can consider learning about body neutrality and integrating the principles in supporting the mental health of families.
Counselors
Body neutral parenting gives families and counselors alike a framework of how to navigate conversations of body, food, and movement to promote a healthy relationship with body image. Families need the language, including specific scripts of what to say and do, and what to avoid saying and doing, to support their children in their body image development. It appears that many families would be interested in shifting the larger sociocultural narrative, including diet culture, with their approach to raising their children, if they had the appropriate psychoeducation and support (Siegel et al., 2021). Clinical mental health counselors can meet that need. The co-created grounded theory in this study and further research can provide a launching pad for counselors who want to take a more preventative approach to body image and related mental health support for youth. Counselors can teach families about de-moralizing food, bodies, and movement in their household, for example, as part of the counseling process for children and adolescents who are at risk for disordered eating and body image concerns.
Counselors can consider how to be of support to families with an interest in integrating body neutrality into their childrearing approach. Mental health professionals can consider how to be of support through the arduous, though meaningful, process of simultaneously parenting one’s children and re-parenting oneself. Some ways in which mental health counselors can support families include normalizing and validating how difficult body neutrality can be and offering specific scripts of what to avoid saying and what to say instead. To illustrate, a counselor might provide psychoeducation to a parent on how to talk to their child about food. Rather than saying “Apples are good for you,” the caregiver could say, “Red food gives you a strong heart” (Kids Eat in Color, 2022). Moreover, families will need support as they navigate the tremendous amount of rewiring involved for body neutral parenting. Counselors can keep in mind the larger overarching goal to drive their clinical decisions in supporting families through body neutral parenting and avoid the negative experience of shame (Ruckstaetter et al., 2017). Counselors can support families in realizing that parenting is an imperfect, human process. Reminding caregivers that imperfect moments will happen, and how to be gentle with themselves, is critical for caregivers continuing the body neutral lifestyle.
As practicing counselors, we must engage in deep reflective practice ourselves to support families and children with body neutrality. In order to be culturally responsive and meet the needs of diverse families, we must “gain knowledge, personal awareness, sensitivity, dispositions, and skills” specific to body neutrality (ACA, 2014, C.2.a). All people have internalized messages and “shoulds” about food, bodies, and exercise, and those internalized biases can hinder the counselor’s ability to support the intricate needs of diverse families healing their relationships with food, bodies, and exercise. Thus, it is an ethical imperative for counselors to engage in self-reflective work about their internalized messages and how those biases might impact the body image needs of children. To illustrate, a counselor might have thin privilege and internalized messages of fat phobia and unknowingly perpetuate the social justice issue of sizeism. Similarly, a parent might make negative comments about the larger body individuals on a TV show. When working with a client in a larger body, a counselor might congratulate the client on their weight loss, when the client might actually be struggling with restricting food and exercising for compensation. It remains an ethical and social justice requirement to engage in both self-reflective work and learning new skills, such as de-moralizing food, to be a culturally responsive, ethical counselor.
Parents and Caregivers
Relatedly, parents and caregivers can consider body neutrality when supporting their children with their body image development. For example, parents might consider the findings of this study and consider what de-moralizing food, bodies, and movement might look like in their home as well as reflect on their own healing process related to reprogramming and re-parenting. Parents might first identify how they engage in power struggles with food; use food as a reward; or use moralized language around food, bodies, and movement. Then, they might work toward identified areas for growth that can help move toward a more neutral relationship with food, bodies, and movement in their home.
Parents might be intentional about their use of language related to food, bodies, and movement with their children. For example, parents might avoid using the terms “healthy” and “unhealthy” related to food, but rather, emphasize the nutrients in the food, how the body feels after food, and other concepts congruent with intuitive and mindful eating. Further, in this study, many parents prefer the term “movement” over “exercise,” as it more accurately captures the relationship with moving the body. “Exercise” has a connotation for many clients as being punitive, exhausting, or for compensation, as opposed to “movement” embodying the mindful moving of the body for fun concepts aligned with body neutrality. In addition to language considerations, parents might consider how they maneuver mealtimes and integrate suggestions from the findings of this study, such as offering sweet foods at the same time as the meal, rather than having the dessert afterward as something to be earned.
Parents might also engage in their own healing and reflective practices, such as identifying their own food rules and reprogramming their internalized messages about food. Parents can model body neutrality with their own body by avoiding negative body talk, such as “I am so fat” or “I am bad for eating that, now I need to walk off those calories,” and replacing those comments with more body neutral statements. Similarly, caregivers can be mindful of how they talk about others’ bodies, such as avoiding negative comments about the larger body individuals on a TV show. Examples of body neutral statements might be: “My body is hungry for” and “I love that my body allows me to give you big hugs.”
Limitations
The sampling procedure is a limitation of this study. Onwuegbuzie and Collins (2007) suggested an ideal sample size between 12 and 15 for a grounded theory investigation using interviews. Although the study met theoretical saturation, the sample size was slightly under some recommended sources for a grounded theory investigation with 10 interviews. Moreover, although attempts were made to have a diverse sample and a geographically diverse sample was acquired, the study primarily captured the experiences of highly educated, middle-class mothers.
In addition, another primary limitation is the self-report from parents. Although parents self-reported as enacting body neutral parenting practices, I did not confirm if their self-report aligned with their actual parenting practices. As such, this study was not able to confirm how or in what way the participants’ parenting was effective. Moreover, research has not yet confirmed that body neutral parenting practices are helpful for children, necessitating further outcome research.
Future Research
Future studies could cast a more comprehensive, representative net and capture the experiences of other caregivers of more diverse gender, socioeconomic, and educational backgrounds. Researchers could explore the nuances of caregivers integrating body neutrality into their approach caring for their children, such as specific developmental considerations. Research exploring current counseling practices, including how counselors support families through body neutral parenting, would also be a helpful addition to a scant literature base.
Conclusion
This study uncovered body neutral practices that caregivers and mental health professionals alike can use to support the body image development of children and adolescents. In particular, findings emphasized the importance of the caregiver’s reflective work and de-moralizing food, bodies, and movement. Body neutrality as an approach to parenting appears to underpin the healthy development of body image and related self-esteem in children and adolescents.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Abraczinskas, M., Fisak, B., Jr., & Barnes, R. D. (2012). The relation between parental influence, body image, and eating behaviors in a nonclinical female sample. Body Image, 9(1), 93–100.
https://doi.org/10.1016/j.bodyim.2011.10.005
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/Resources/aca-code-of-ethics.pdf
Charmaz, K. (2014). Constructing grounded theory: A practical guide through qualitative analysis (2nd ed.). SAGE.
Charmaz, K., & Liska Belgrave, L. (2012). Qualitative interviewing and grounded theory analysis. In J. F. Gubrium, J. A. Holstein, A. B. Marvasti, & K. D. McKinney (Eds.), The SAGE handbook of interview research: The complexity of the craft (2nd ed., pp. 347–365). SAGE.
Creswell, J. W., & Poth, C. N. (2017). Qualitative inquiry and research design: Choosing among five approaches (5th ed.). SAGE.
Damiano, S. R., Gregg, K. J., Spiel, E. C., McLean, S. A., Wertheim, E. H., & Paxton, S. J. (2015). Relationships between body size attitudes and body image of 4-year-old boys and girls, and attitudes of their fathers and mothers. Journal of Eating Disorders, 3(1), 1–10. https://doi.org/10.1186/s40337-015-0048-0
Damiano, S. R., McLean, S. A., Nguyen, L., Yager, Z., & Paxton, S. J. (2020). Do we cause harm? Understanding the impact of research with young children about their body image. Body Image, 34, 59–66.
https://doi.org/10.1016/j.bodyim.2020.05.008
Dittmar, H., Halliwell, E., & Ive, S. (2006). Does Barbie make girls want to be thin? The effect of experimental exposure to images of dolls on the body image of 5- to 8-year-old girls. Developmental Psychology, 42(2), 283–292. https://doi.org/10.1037/0012-1649.42.2.283
Gutin, I. (2021). Body mass index is just a number: Conflating riskiness and unhealthiness in discourse on body size. Sociology of Health & Illness, 43(6), 1437–1453. https://doi.org/10.1111/1467-9566.13309
Hays, D. G., & McKibben, W. B. (2021). Promoting rigorous research: Generalizability and qualitative research. Journal of Counseling & Development, 99(2), 178–188. https://doi.org/10.1002/jcad.12365
Herle, M., De Stavola, B., Hübel, C., Abdulkadir, M., Ferreira, D. S., Loos, R. J. F., Bryant-Waugh, R., Bulik, C. M., & Micali, N. (2020). A longitudinal study of eating behaviours in childhood and later eating disorder behaviours and diagnoses. The British Journal of Psychiatry, 216(2), 113–119. https://doi.org/10.1192/bjp.2019.174
Horton, E. (2023). “I want different for my child”: An interpretative phenomenological analysis of mothers’ histories of disordered eating and the impact on their parenting approach. The Family Journal, 31(2), 314–321. https://doi.org/10.1177/10664807221151171
Horton, E., & Powers, M. (2024). Demoralizing food, bodies, and movement: A phenomenological exploration of caregivers’ experience in a body neutral parenting support group. The Family Journal.
https://doi.org/10.1177/10664807231226232
Khanal, K. P. (2018). Constructivist grounded theory practice in accountability research. Journal of Education and Research, 8(1), 61–88. https://doi.org/10.3126/jer.v8i1.25480
Kids Eat in Color [@kids.eat.in.color]. (2022, April 21). How to talk: May not help, may help a lot [Photograph]. Instagram. https://www.instagram.com/p/Ccnn7CMr2D5/?utm_source=ig_web_copy_link
Klassen, S. (2017). Free to be: Developing a mindfulness-based eating disorder prevention program for preteens. Journal of Child and Adolescent Counseling, 3(2), 75–87. https://doi.org/10.1080/23727810.2017.1294918
Kluck, A. S. (2010). Family influence on disordered eating: The role of body image dissatisfaction. Body Image, 7(1), 8–14. https://doi.org/10.1016/j.bodyim.2009.09.009
Liechty, J. M., Clarke, S., Birky, J. P., & Harrison, K. (2016). Perceptions of early body image socialization in families: Exploring knowledge, beliefs, and strategies among mothers of preschoolers. Body Image, 19, 68–78. https://doi.org/10.1016/j.bodyim.2016.08.010
Mills, J., Bonner, A., & Francis, K. (2006). The development of constructivist grounded theory. International Journal of Qualitative Methods, 5(1), 25–35. https://doi.org/10.1177/160940690600500103
National Eating Disorders Association. (2022). Body image. https://www.nationaleatingdisorders.org/body-image
Neumark-Sztainer, D., Bauer, K. W., Friend, S., Hannan, P. J., Story, M., & Berge, J. M. (2010). Family weight talk and dieting: How much do they matter for body dissatisfaction and disordered eating behaviors in adolescent girls? Journal of Adolescent Health, 47(3), 270–276. https://doi.org/10.1016/j.jadohealth.2010.02.001
Onwuegbuzie, A. J., & Collins, K. M. T. (2007). A typology of mixed methods sampling designs in social science research. The Qualitative Report, 12(2), 281–316. https://doi.org/10.46743/2160-3715/2007.1638
Patton, M. Q. (2014). Qualitative research and evaluation methods: Integrating theory and practice. SAGE.
Pellizzer, M. L., & Wade, T. D. (2023). Developing a definition of body neutrality and strategies for an intervention. Body Image, 46, 434–442. https://doi.org/10.1016/j.bodyim.2023.07.006
Perry, M., Watson, L., Hayden, L., & Inwards-Breland, D. (2019). Using body neutrality to inform eating disorder management in a gender diverse world. Child and Adolescent Health, 3(9), 597–598.
https://doi.org/10.1016/s2352-4642(19)30237-8
Phares, V., Steinberg, A. R., & Thompson, J. K. (2004). Gender differences in peer and parental influences: Body image disturbance, self-worth, and psychological functioning in preadolescent children. Journal of Youth and Adolescence, 33(5), 421–429. https://doi.org/10.1023/B:JOYO.0000037634.18749.20
Pursey, K. M., Burrows, T. L., Barker, D., Hart, M., & Paxton, S. J. (2021). Disordered eating, body image concerns, and weight control behaviors in primary school aged children: A systematic review and meta-analysis of universal–selective prevention interventions. International Journal of Eating Disorders, 54(10), 1730–1765. https://doi.org/10.1002/eat.23571
Ricciardelli, L. A., McCabe, M. P., & Banfield, S. (2000). Body image and body change methods in adolescent boys: Role of parents, friends and the media. Journal of Psychosomatic Research, 49(3), 189–197.
https://doi.org/10.1016/S0022-3999(00)00159-8
Rodgers, R., & Chabrol, H. (2009). Parental attitudes, body image disturbance and disordered eating amongst adolescents and young adults: A review. European Eating Disorders Review, 17(2), 137–151. https://doi.org/10.1002/erv.907
Ruckstaetter, J., Sells, J., Newmeyer, M. D., & Zink, D. (2017). Parental apologies, empathy, shame, guilt, and attachment: A path analysis. Journal of Counseling & Development, 95(4), 389–400.
https://doi.org/10.1002/jcad.12154
Sharpe, H., Patalay, P., Choo, T.-H., Wall, M., Mason, S. M., Goldschmidt, A. B., & Neumark-Sztainer, D. (2018). Bidirectional associations between body dissatisfaction and depressive symptoms from adolescence through early adulthood. Development and Psychopathology, 30(4), 1447–1458. https://doi.org/10.1017/S0954579417001663
Siegel, J. A., Ramseyer Winter, V., & Cook, M. (2021). “It really presents a struggle for females, especially my little girl”: Exploring fathers’ experiences discussing body image with their young daughters. Body Image, 36, 84–94. https://doi.org/10.1016/j.bodyim.2020.11.001
Thompson, J. K., Heinberg, L. J., Altabe, M., & Tantleff-Dunn, S. (1999). Exacting beauty: Theory, assessment, and treatment of body image disturbance (1st ed.). American Psychological Association.
https://doi.org/10.1037/10312-000
Veldhuis, J., Alleva, J. M., Bij de Vaate, A. J. D., Keijer, M., & Konijn, E. A. (2020). Me, my selfie, and I: The relations between selfie behaviors, body image, self-objectification, and self-esteem in young women. Psychology of Popular Media, 9(1), 3–13. https://doi.org/10.1037/ppm0000206
Walker, D. C., Gorrell, S., Hildebrandt, T., & Anderson, D. A. (2021). Consequences of repeated critical versus neutral body checking in women with high shape or weight concern. Behavior Therapy, 52(4), 830–846. https://doi.org/10.1016/j.beth.2020.10.005
Wymer, B., Swartz, M. R., Boyd, L., Zankman, M., & Swisher, S. (2022). A content analysis of empirical parent engagement literature. Journal of Child and Adolescent Counseling, 8(1), 16–30. https://doi.org/10.1080/23727810.2022.2037987
Emily Horton, PhD, LPC, RPT, is an assistant professor at the University of Houston–Clear Lake. Correspondence may be addressed to Emily Horton, 2700 Bay Area Boulevard, Houston, TX 77058, horton@uhcl.edu.
May 22, 2024 | Volume 14 - Issue 1
Darius A. Green, Katharine R. Sperandio
Because of the long history of anti-drug policing in the United States and the criminalization of substance use, clients who use substances are vulnerable to direct and vicarious experiences of police violence. Consequently, those who use substances may face a greater risk of experiencing symptoms of trauma that counselors should address in treatment. We recommend the use of a trauma-informed and abolitionist praxis in clinical and social justice practices as a framework to support clients who use substances and have histories of exposure to police violence.
Keywords: substance use, police violence, trauma, abolitionist, social justice
Policing in the United States has received increased scrutiny in recent years with renewed attention resulting from the Black Lives Matter protests in 2020. Specifically, policing has been critiqued by prison–industrial complex abolitionists—activists who advocate toward an end to systems of policing, prisons, and related carceral systems in favor of systems and practices that promote accountability, justice, healing, and transformation—as being inherently violent, meaning that it relies on the use of behavior that is considered violent in any context (Cullors, 2019; A. Y. Davis et al., 2022; Green, 2022; Kaba, 2021; Klukoff et al., 2021). Violence is defined as “the intentional use of physical force or power, threatened or actual, against oneself, another person or against a group or community that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation” (Krug et al., 2002, p. 5). Thus, we define police violence as the inherently violent uses of force by police officers. According to the World Health Organization, there are four types of violence that can be used to categorize police violence: physical (e.g., arrests and the use of weapons), sexual (e.g., strip searching and sexual assault), psychological (e.g., intimidation and verbal threats), and neglect (e.g., failing to provide support to medical and mental health needs; DeVylder et al., 2017; Krug et al., 2002).
Current data suggests that 58.3 million U.S. residents over the age of 16 experienced contact from police officers in 2020 with roughly 1 million experiencing or being threatened with non-fatal force (Tapp & Davis, 2022). Moreover, of the 82 million arrests reported by the Federal Bureau of Investigation (FBI; 2022) between 2011 and 2021, substance use violations were the second most common arrests, accounting for 14% of arrests. Oftentimes, counselors may work with clients who have been court-ordered to treatment as part of diversion programs that seek to route individuals away from incarceration and toward treatment for criminalized behaviors, such as substance use (Scott, 2020). Given that substance use–related offenses are among the most common offenses leading to violence through an arrest (FBI, 2022), it is essential for substance use counselors to prepare to address experiences of police violence that may result from anti-drug policing—the use of police violence as a response to individuals who use substances. Although anti-drug policing impacts both those who use substances and those who traffic them, our discussion on anti-drug policing will focus on populations who use substances.
Research on counselor preparation suggests that most counselors receive no training regarding clinical practice and advocacy to address matters of police violence despite a recent study that found that 68.2% of counselors reported working with clients who had experienced police violence (Green & Evans, 2021). Moreover, Bride et al. (2009) found that most substance use counselors do not learn about treating psychological trauma in their academic programs and instead predominantly rely on continuing education. Given the vulnerable nature of those who use substances and evidence suggesting that gaps exist in training counselors in treating police violence and trauma, we will explore approaches to clinical practice, social justice, and advocacy to best support substance use clients who experience police violence because of anti-drug policing. Specifically, the purpose of this article is to provide a sociopolitical analysis of anti-drug policing in the United States that informs our proposal for substance use counselors to adopt and integrate an abolitionist praxis into their practice of counseling with clients who use substances.
Sociopolitical Context of Anti-Drug Policing in the United States
Initiated by President Richard Nixon in 1971 and escalated by President Ronald Reagan in 1982, the war on drugs increased and incentivized anti-drug policing and enforcement, intensified legal penalties associated with drug-related crimes, and demonized individuals, particularly those who were part of marginalized communities and struggled with substance use disorders (Benson et al., 1995; Cooper, 2015; Koram, 2022; Park et al., 2019). Cooper (2015) and Saleem (1997) noted that contemporary anti-drug policing practices, such as stop-and-frisk and police drug raids, have been permitted through court cases such as Terry v. Ohio, Whren v. United States, and Illinois v. Wardlow and have eroded the Fourth Amendment and 1878 Posse Comitatus Act protections against unreasonable searches, seizures, and militarization of policing. Specifically, these court cases have permitted frisking for reasonable suspicion, allowed police to conduct stops in which police may stop individuals for suspicion of drugs under the pretext of other minor criminalized violations, and expanded the definition of suspicious behavior that may warrant being stopped by police (Cooper, 2015; Saleem, 1997). Although several anti-drug policing reforms have been made, such as the development of drug courts and the decriminalization of substances in various states (Klukoff et al., 2021; Scott, 2020), anti-drug policing practices have persisted, expanded, and received legislative support. For example, despite stop-and-frisk searches being declared unconstitutional in 2013 with the decision in Ligon v. City of New York, the practice was reduced by 98% by 2017 as opposed to ceasing entirely (New York Civil Liberties Union, n.d., 2019). Despite this decrease, racial disparities were maintained in these stop-and-frisk practices between 2014 and 2017, as 53% of targets were Black and 28% were Latino (New York Civil Liberties Union, 2019). Lastly, President Donald Trump voiced support for greater anti-drug policing efforts, while President Joseph Biden’s Safer America Plan seeks reform that simultaneously increases funding for policing and substance use treatment resources (Kaba & Ritchie, 2022; Koram, 2022; The White House, 2022). Although these systemic supports for reform from the executive branch may be aimed at drug trafficking, individuals who use substances may be at continued risk of being impacted by anti-drug policing with the increased support for and reliance on carceral approaches.
Although reforms related to criminalized behaviors may reduce harm through their trauma-informed focus, abolitionist authors and activists have critiqued such reforms as counter-productive when they expand the power and legitimacy of policing, maintain the criminalization of substance use, and perpetuate harm and violence toward those who use substances (Klukoff et al., 2021; Purnell, 2021a). For example, according to Fazel et al. (2017), 24% of the global imprisoned population meets the criteria for alcohol use disorder, compared to the less than 2% of the general population (Global Burden of Disease Network, 2016). Similarly, 30% of male prisoners and 51% of female prisoners meet the criteria for illicit drug use disorder, while less than 1% of the global population meets the criteria (Global Burden of Disease Network, 2016). Moreover, as stated earlier, substance use violations are the second most common arrest reason in the United States (FBI, 2022). Lastly, some authors have concluded that mixed results exist on the effectiveness of diversion programs for offenses associated with mental illness and substance use regarding recidivism and subsequent arrests (Klukoff et al., 2021; Scott, 2020). These data highlight a prevalent connection between policing, incarceration, and substance use in the United States and around the world despite contemporary reforms to anti-drug policing established through the war on drugs.
Policing functions to maintain social order and provide security by enforcing laws, policies, and social norms (Bureau of Justice Statistics, 2021; Giovengo, 2016). Moreover, police are ordained to investigate, arrest, and enact force upon those deemed as, or suspected to be, threatening to the safety and interests of dominant communities. Thus, the criminalization of substance use has been conceptualized as exerting control over and oppressing minoritized groups (Dollar, 2019; Purnell, 2021b). Marginalized communities have been hit especially hard by these zero tolerance policies, which drastically increased community members’ run-ins with police (Cooper, 2015). For example, the influx of stop-and-frisk procedures, a method that permitted police officers to detain an individual suspected of illegal activity and physically search them, led to minoritized individuals being racially profiled and targeted for searches without specific cause (Cooper, 2015). In fact, anti-drug policing has resulted in a shift from Black people accounting for 22% of those arrested in 1976 to 40% in 1992, despite making up 12% of the U.S. population (Cooper, 2015; Tonry, 1994). Thus, instead of eliminating substance use in communities, these crackdowns have only further increased the prevalence of police brutality, traumatized communities and individuals, and increased violence within communities (Cooper, 2015; Rhodes et al., 2006; Werb et al., 2011).
Structural Violence and Trauma From Anti-Drug Policing
Given the confiscation of an individual’s bodily autonomy, resulting in the infringement of the individual’s basic and constitutional rights and liberties, as well as the possibility for physical harm to take place during searches, anti-drug policing, which can involve violence, harassment, and killings, can place significant psychological stress and turmoil on targeted individuals (Park et al., 2019; Sarang et al., 2010). It is essential to analyze the long-term consequences of police violence perpetuated upon impacted individuals, including the possibility of traumatization and death (Bryant-Davis et al., 2017; Cooper, 2015; Krieger et al., 2015). Emerging research has demonstrated connections between being stopped by police and symptoms of anxiety and post-traumatic stress disorder (PTSD), particularly when the experience is perceived as intrusive and unjustified (Geller et al., 2014); suicide attempts (DeVylder et al., 2017); and symptoms of manic and depressive episodes (Meade et al., 2017). Likewise, vicarious traumatization from watching or learning of another individual experiencing police violence is also a concern given the high proportion of individuals living with substance use disorders who have both experienced trauma and witnessed police violence (El-Bassel et al., 2011; Park et al., 2019; Shaw et al., 2016). Research on those who witness police violence has often emphasized the unique impact on Black people. This research has demonstrated associations with vicarious exposure and poor mental health (Bor et al., 2018), distress from anticipated exposure following media consumption (Green et al., 2024), and psychological distress among Black mothers (Joe et al., 2019). Galovski et al. (2016) demonstrated that community protests following instances of police violence may result in symptoms of depression and PTSD among community members. Additionally, recent research has demonstrated a connection between vicarious exposure and increased cannabis use among Black Americans (Motley et al., 2022). Taken together, these findings suggest that directly and vicariously experiencing police violence may promote greater risk of traumatization.
Literature suggests that these encounters with police may end in violence beyond psychological distress because of the influence of stigmatization and prejudice against people who use substances (Cooper et al., 2005; Hayashi et al., 2013; Lunze et al., 2015; Wood et al., 2017). Officers may also confiscate civilians’ syringes during stop-and-frisk encounters, increasing the prevalence of syringe sharing, a known risk factor for HIV and HCV transmission (Beletsky et al., 2010; Park et al., 2019; Small et al., 2007). Detainment for substance use is also associated with increased risk of death following release because of withdrawal and increased risk of overdose (Chang et al., 2015; Fazel et al., 2017; Kinner et al., 2012; Pratt et al., 2010). Stress and traumatization experienced from anti-drug policing is also associated with high-risk behaviors, including drug injection, among addicted individuals (Maher, 2004; Shannon et al., 2008; Volkmann et al., 2011). Moreover, in one study, individuals needing treatment for substance use disorders were 2.74 times more likely to experience arrest and physical assault from police (Werb et al., 2016). Additionally, Werb et al. (2016) found that 27.5% of police encounters occurred within 500 meters of a substance use treatment facility. Similarly, Park et al. (2019) found in a sample of people who inject drugs in Baltimore that 7% experienced physical police violence and one in four knew someone else who had experienced physical police violence, fueling a deep mistrust of the system. Fear of potential retaliation by the police may also discourage individuals, particularly those with marginalized identities, from going to the police during a crisis or emergency situation, such as in cases of overdose. This mistrust of the system negatively impacts individuals’ willingness to pursue treatment services, especially when they are in fear of being detained or harmed by police officers (Alang et al., 2017; Cooper, 2015; Park et al., 2019). For example, a qualitative study described the impact of increased surveillance from police as both threatening and interfering with harm reduction practices (Cooper et al., 2005). Treatment centers are typically more centralized in areas where there is a higher drug activity which means that, because policing has a significant presence in these parts of communities, individuals may be hesitant to seek out help and support to avoid police encounters, negatively impacting social and health outcomes (Werb et al., 2016). Additionally, these crackdowns are associated with reductions in syringe exchange programs, drug treatment, and HIV testing accessibility (C. S. Davis et al., 2005; Park et al., 2019; Ti et al., 2013). These findings highlight how anti-drug policing actively inhibits access to safe and needed care.
A Case for Abolition in Substance Use Counseling
Because of the increased risk of experiencing police violence and the subsequent risk for traumatization from police violence, it is essential for counselors to address encounters stemming from anti-drug policing in treatment and develop practices that divest from policing practices and systems. Trauma-informed practice is a “fundamental obligation” (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014, p. 5) for counselors who work with clients at the intersections of substance use and police violence to reduce or mitigate the adverse impacts of trauma on individuals’ physical, emotional, psychological, and spiritual well-being and to prevent further systemic (re)traumatization. Trauma-informed practice is that which recognizes and understands the impact and salience of trauma, effectively responding to it in ways that do not retraumatize and further perpetuate traumatic stress while also recognizing that marginalized groups are at greater risk of experiencing trauma and its effects (SAMHSA, 2014; Sweeney & Taggart, 2018). There are four assumptions that ground trauma-informed practices (adapted from SAMHSA, 2014): 1) a realization of the potentially long-lasting effects of trauma on individuals, communities, groups, families, and systems and that trauma can be perpetuated by systems like the criminal legal system, resulting in a significant impact on continued substance use and mental health; 2) the importance of recognizing the signs of trauma and refraining from pathologizing these responses; 3) the crucial need for a system or organization to respond supportively by applying the six principles of a trauma-informed approach; and 4) resisting the potential to retraumatize individuals who are accessing supports and care. Moreover, SAMHSA (2014) identified six principles of trauma-informed practices that are intended to serve as the fundamental spirit of trauma-informed care: 1) safety; 2) trustworthiness and transparency; 3) peer support; 4) collaboration and mutuality; 5) empowerment, voice, and choice; and 6) cultural, historical, and gender issues.
By SAMHSA’s description, current substance use treatment falls short of being trauma-informed when it occurs under systemic conditions in which anti-drug policing and police violence are part of the historical and current response in the treatment and care of individuals who struggle with substance use. As outlined above, anti-drug policing practices can result in police violence that includes stop-and-frisk, arrests, and an intimidating presence that may negatively interfere in treatment accessibility for individuals who are fearful of potential run-ins and harassment (Werb et al., 2016). Anti-drug policing and the broader criminalization of substance use may disrupt safety, retraumatize substance use clients, and diminish trust and transparency in accessing substance use treatment. Moreover, incarceration for using substances may inhibit the potential for peer support and collaborative approaches to treatment. Lastly, the existing racial disparities in anti-drug policing practices demonstrate a history of systemic racism that may disproportionately create a barrier to accessing trauma-informed care for racially marginalized groups, particularly Black Americans. Thus, we contend that an abolitionist praxis that opposes anti-drug policing and divests from carceral approaches to responding to individuals who use substances is needed to fully realize trauma-informed practice with clients who use substances.
Abolitionist Praxis for Substance Use Counseling
Abolition is a social justice praxis that is commonly referenced as a necessary solution to policing and its impact (A. Y. Davis et al., 2022; Kaba, 2021). Abolition refers to the broad movement of divesting from and eliminating carceral systems, such as law enforcement and prison systems, and carceral logics that seek to legitimize the use of punishment, retribution, and vengeance through carceral systems. Rooted in the efforts of Black feminist thought, advocacy, and organizing, abolition calls for a critical analysis of the ways in which policing has functioned to enact the violence of overlapping systems of oppression (Kaba & Ritchie, 2022). Kaba and Ritchie (2022) identified three objectives of abolitionist praxis. First, abolitionist praxis seeks to create collective safety from community violence and the violence of policing and related carceral systems that reinforce systems of oppression, such as White supremacy, patriarchy, and capitalism (Kaba, 2021; Kaba & Ritchie, 2022; Purnell, 2021a). Second, abolitionist praxis seeks to end violence from carceral systems through eliminating those systems as opposed to seeking reforms that preserve the inherent violence of policing and incarceration (Kaba & Ritchie, 2022; Klukoff et al., 2021). This second objective extends beyond institutions of policing and incarceration and extends to the ways in which carceral logic and behaviors of policing are embedded in other systems, institutions, and communities and often internalized by individuals (Kaba & Ritchie, 2022). Lastly, to achieve collective safety, abolitionist praxis necessitates a simultaneous transformation from reliance on the violence of policing and related carceral systems toward cultivating cultures, systems, communities, and ways of being that are centered around care, healing, justice, and accountability (Kaba & Ritchie, 2022).
Abolition exists beyond a theoretical and conceptual framework. It is an iterative process that combines theorizing, action, and reflection upon efforts that divest from and dismantle carceral systems and logics while simultaneously brainstorming solutions to community violence that promote safety, healing, and justice (Cullors, 2019; A. Y. Davis et al., 2022; Kaba & Ritchie, 2022; Klukoff et al., 2021). Abolitionist praxis often utilizes a transformative justice framework to achieve its objective of eliminating carceral systems while creating new systems and ways of being that foster safety, healing, and justice. Transformative justice aligns with abolitionist praxis in that it is a liberatory strategy that seeks to transform systems and structures that create the conditions for violence (Afuape & Kerry Oldham, 2022). While policing and incarceration focus on retributive justice that assigns inherently violent punishment as a mechanism for change regardless of the harm it causes, transformative justice through abolitionist praxis seeks to create processes of accountability for harm caused interpersonally from criminalized behaviors and systemically from policing and related carceral systems. As a result, abolitionist praxis utilizes transformative justice to create new systems, institutions, communities, strategies, and internalized ways of being that value safety, healing, and justice that are needed to cultivate trauma-informed care and practices for substance use clients.
Regarding substance use counseling, an abolitionist praxis seeks to reduce and eliminate violence as a response to substance use, decriminalize all substance use, and eliminate contact between substance use clients, police, and the broader criminal legal system. Similarly, an abolitionist praxis to substance use counseling challenges the logic that criminalization is a needed step in treatment for substance use. For example, in 2001, the Portuguese government enacted nationwide laws to decriminalize all substances, resulting in a decrease in the prevalence of drug use and overdose rates (Castelpietra et al., 2022; James et al., 2020; Pombo & da Costa, 2016; Smiley-McDonald et al., 2023). In 2021, Oregon decriminalized low-level drug possessions and subsequently increased options for substance use disorder treatment and harm reduction programs (Good et al., 2023; Smiley-McDonald et al., 2023). In their study, Smiley-McDonald et al. (2023) found that the Oregon legislation resulted in a decrease in the number of interactions between police officers and individuals who use drugs. Thus, the abolitionist goal of decriminalizing substance use while implementing harm reduction programs may function to both minimize inherently violent contact with police and reduce the prevalence of substance use.
Abolitionist praxis would also call for the development of accountability for interpersonal and community harm caused by client substance use that does not rely on legal punishment, or the threat of it, from the criminal legal system (Cullors, 2021). Accountability for harm caused under abolitionist theory entails a developed recognition of wrongdoing and harm, both interpersonally and as mediated by social, economic, and political context, and sustained effort toward intrapersonal, interpersonal, and institutional change that repairs harm (Cullors, 2021; Kaba, 2021). Counselors must re-envision both their clinical practice and engagement in advocacy toward abolition to holistically care for clients who use substances.
Clinical and Advocacy Recommendations
Given the previously outlined mental health outcomes that are associated with direct and vicarious experiences of police violence that suggest its traumatic impact (DeVylder et al., 2017; Galovski et al., 2016; Geller et al., 2014; Green et al., 2024; Joe et al., 2019; Meade et al., 2017; Motley et al., 2022), a trauma-informed approach is essential to working with those who experience police violence as a consequence of anti-drug policing. Counselors seeking to use a trauma-informed approach to treat substance use disorders must infuse abolition into their delivery of services while also engaging in advocacy beyond direct clinical work to better achieve SAMHSA’s six identified principles of trauma-informed practice. We provide an abolitionist framing of these six principles and offer abolitionist re-envisioning for substance use counseling below. Moreover, we adapted the sixth principle of cultural, historical, and gender issues to cultural competence and advocacy to emphasize the professional role of advocacy in counseling for substance use clients who experience anti-drug policing.
Safety
Ensuring safety in the therapeutic space is essential because anti-drug policing and the threat of police violence pose a safety risk to clients who use substances and are involved in or at risk of being targeted by the legal system. One step toward maximizing safety for clients is to end the use of abstinence-based treatment. Given that counselors may serve as treatment referral sources for court-mandated clients who meet criteria for diversion programs that seek to route individuals toward treatment for substance use and away from incarceration (Scott, 2020), abstinence-based treatment needs critical examination. Although such interventions can reduce engagement in substance use and mental health symptoms (Pinals et al., 2019), they do so with a looming threat of police violence and incarceration as a consequence for failure to complete the requirements of the diversion program (Scott, 2020). This poses a value conflict with counselors who are treating court-mandated clients for substance use. Counselor participation in diversion programs may require disclosures of client participation and progress in counseling that may lead to legal consequences for clients if they do not meet requirements of the diversion program. For example, counselors may be ethically obligated to document client relapses, which are more common in substance use treatment for minoritized groups and those with histories of experiencing multiple traumatic events (Farley et al., 2004; Heffner et al., 2011), which may be requested by probation officers, attorneys, or courts. In such a scenario, disclosure of client progress in treatment could produce a risk of clients experiencing police violence and incarceration. Moreover, this may produce a circumstance in which a client’s dominant motive for engaging in treatment is to avoid the consequences of police violence and incarceration. Consequently, acknowledging the intrapersonal, interpersonal, and community impact of one’s substance use and engaging in accountability are likely to become secondary motives for change and repair of any harm caused. Although the potential for incarceration may serve as motivation for change for substance use clients, substance use counselors can align with an abolitionist praxis by engaging in theorizing to develop methods and systems that motivate client accountability and transformation without the threat of violence induced by carceral systems. Moreover, alignment with an abolitionist praxis may require substance use counselors to proactively use their power to advocate for harm reduction in treatment as alternatives to approaches that risk harm through police violence and incarceration. Harm reduction approaches emphasize safe use over non-use of substances and have demonstrated evidence of both maintained and reduced substance use, reductions in harm related to substance use (e.g., less police contact and fewer arrests and emergency hospital visits), and self-reports of feeling safer (Carrico et al., 2014; Smiley-McDonald et al., 2023; Vallance et al., 2016).
Anti-drug policing views substance use as threatening and seeks to foster security through violent force and criminalization (Kaba, 2021). This security comes at the expense of the safety and well-being of those who use substances. An abolitionist re-envisioning of safety is one that seeks to ensure safety from the harm that both substance use and carceral systems cause to individuals, families, and communities. Regarding safety for substance use clients who experience anti-drug policing, Drustrup et al. (2023) offered an abolitionist approach to safety planning that counselors can adapt to fit the needs of clients mandated to substance use treatment. This approach decenters the default reliance on police in crises and emergencies and emphasizes collaboration with clients to establish methods that can maintain safety. Adapting this to clients, counselors can minimize disclosures of substance use, especially to police, probation officers, and employees of the criminal legal system. Noting the importance of building networks of care in place of carceral systems (Drustrup et al., 2023; Kaba, 2021), counselors should simultaneously collaborate with clients to identify interpersonal and community mechanisms to maintain safety and progress toward substance use–related treatment goals, particularly for when relapses occur. Consequently, this also promotes safety from the impact of substance use and client empowerment, voice, and choice in their treatment and wellness. For example, counselors could simultaneously utilize family therapy as a mechanism to support structural change associated with the development of a client’s substance use and to promote accountability for harm caused by substance use within the family system. Furthermore, when harm from substance use extends to one’s community, in collaboration with clients and those directly impacted, counseling could be used to promote reparation for harm caused (Cullors, 2019). Counselors should be mindful of the possibility that clients may not readily share experiences of police violence and substance use because of distrust fostered by carceral systems and if they have experienced invalidation, blame, or neglect regarding their experiences of police violence. Thus, counselors can enhance safety, trust, and the potential for change with clients through a consistent practice of accurate empathy and attunement to clients’ subjective experience of police violence (Miller & Rollnick, 2013).
Trustworthiness and Transparency
Trustworthiness and transparency are essential given the systemic distrust fostered by histories of collaboration between helping professions and carceral systems (Jacobs et al., 2021; Klukoff et al., 2021). Counselors need to promote an optimal level of safety and trustworthiness with their clients through nonjudgement, empathy, transparency, positive regard, validation, normalization of the client’s responses to adversity, and consistency (SAMHSA, 2014). Counselors pursuing abolition can establish trustworthiness and transparency through using the informed consent process to build rapport and establish parameters of the therapeutic relationship within a societal context that largely criminalizes substance use. While Drustrup et al. (2023) offered inspiration for abolition in the therapeutic relationship, counselors are ethically obligated to make exceptions to confidentiality when imminent risk to self and others is established. Additionally, as mentioned above, substance use counselors may be required to make exceptions to confidentiality to share progress for court-mandated clients. Informing clients of these exceptions to confidentiality is standard in helping professions; however, abolition can maximize trustworthiness and transparency by going beyond merely capturing client signatures on informed consent documents. In addition to establishing the limits of confidentiality, counselors pursuing abolition are recommended to ensure that clients fully understand these limits and the impact of these limits on their participation in the therapeutic context. For example, a substance use counselor could clearly articulate known risks of making exceptions to confidentiality of the therapeutic relationship with police and legal system employees, such as increased risk of experiencing police violence, incarceration, and state-sanctioned surveillance. Counselors pursuing abolition who are directly embedded in carceral systems as a function of their employment, such as prisons, should inform clients of any dual or conflicting interests associated with their counseling in the prison system. Additionally, counselors can use open-ended questioning to provide clients an opportunity to check their understanding of confidentiality, its limits, and the impact of needing to make exceptions to confidentiality. Moreover, counselors pursuing abolition should collaborate with clients to identify external resources to counseling that offer greater trustworthiness that can facilitate transformation and healing from substance use in situations where clients may feel a lack of trust in counseling because of the threat of carceral systems.
Peer Support
Providing opportunities for peer support for clients who have experienced police violence and are living with substance use disorders could also be promotive and helpful for healing because of the access to other individuals who have undergone similar experiences. Group therapy has been associated with positive mental health outcomes, particularly among individuals with PTSD and substance use disorders, due to receiving mutual support from others who have similar experiences and can provide empathy, a sense of belongingness and collectivism, and the opportunity to provide and receive feedback; build safety through interpersonal relationships; and reduce feelings of isolation and loneliness (Barrera et al., 2013; Mott et al., 2013; Schwartze et al., 2019; Sloan et al., 2013). Substance use counselors pursuing abolition can actively incorporate group therapy within the therapeutic context and help clients heal following traumatization from police violence while promoting their long-term recovery. Additionally, counselors employed in treatment centers who are pursuing abolition should be mindful of added benefits toward safety and trustworthiness that embedding peer support can offer, particularly for court-mandated clients. When a client is unable to experience enough safety and trustworthiness because of the threat and impact of carceral systems, embedded peer support that exists outside of the counselor–client relationship can provide alternate spaces for clients to be heard and validated. Abolitionist substance use counselors can advocate for the inclusion of peer mentoring for accountability and transformation akin to that which exists within 12-step groups through sponsor relationships. Although it may be conceptualized as part of a process of accountability to utilize clients who have advanced in their treatment as peer mentors, counselors pursuing abolition should also consider the feasibility of paying peer mentors to avoid replicating the occurrence of unpaid and underpaid labor that may occur in prison systems.
Collaboration and Mutuality
It is essential for counselors pursuing abolition to cultivate environments and therapeutic relationships that promote collaboration and mutuality. It would behoove substance use counselors to utilize frameworks for treatment that are inherently trauma-informed and collaborative, such as motivational interviewing, for assessing client motivation for change and structuring treatment with clients that is centered around partnership, acceptance, compassion, and evocation (Clark et al., 2014; Miller & Rollnick, 2013). These efforts may be particularly beneficial for clients who have experienced police violence as a result of anti-drug policing in that they allow greater client participation and trustworthiness to a client population that may be prone to experiencing coercion and restricted freedom and being acted upon. Abolitionist substance use counselors can foster greater collaboration and mutuality in their practice of counseling by making mutual aid foundational to their practice. Mutual aid is an intentional resistance to reliance on institutions that cause structural violence (S. W. Davis & Fayter, 2021; Jacobs et al., 2021). Instead of relying on such institutions, mutual aid seeks to establish networks of care that use community members and resources to meet the needs of others (S. W. Davis & Fayter, 2021; Jacobs et al., 2021). Establishing mutual aid in substance use counseling for clients who experience anti-drug policing requires counselors to advocate to establish and streamline connections to community resources that address underlying, unmet, or neglected needs of clients that play a role in their use of substances and experience of anti-drug policing. For example, an abolitionist substance use counselor may actively coordinate with community agencies that provide support in securing shelter to mitigate substance use and the risk of subsequent anti-drug policing that may be associated with homelessness. Integrating peer support and mentoring, as mentioned previously, within and outside of treatment facilities could function as mutual aid; however, substance use counselors working in carceral institutions may experience pushback to such efforts given that mutual aid seeks divestment from carceral systems (S. W. Davis & Fayter, 2021). Lastly, in terms of collaborative goal-setting, the counselor can work with the client to identify the client’s objectives for attending therapy. The counselor is recommended to honor the client’s voice and work with the client to establish whether the client would like to refrain from using substances in the future, engage in harm reduction practices, and/or process the trauma that the client may have experienced at the hands of police.
Empowerment, Voice, and Choice
Anti-drug policing, incarceration, drug courts, and related carceral approaches to substance use may use interventions that limit the agency of those subjected to their demands. Counselors can engage in an abolitionist praxis that is rooted in trauma-informed practice by screening and assessing for the prevalence and impact of police violence as a potentially traumatic stressor that relates to the use of substances (Green, 2022; Green & Evans, 2021). Given the importance of divesting from carceral systems and logic in abolitionist praxis, counselors need to engage in an ongoing and iterative process of reflection and change in attitudes and practices that reinforce the criminalization of substance use and practices that treat it as the moral failure of the individual. This can be achieved through screening and assessment for substance use and police violence that counteracts experiences of shame and guilt that may be fostered from interactions with police and the criminal legal system (Clark et al., 2014). Moreover, abolitionist praxis in counseling with clients who experience police violence due to anti-drug policing requires a strength- and healing-oriented approach as an act of radical resistance to the pathologizing and moralizing norm of carceral approaches (Cook et al., 2014; Moh & Sperandio, 2022). In practice, this may entail an intentional focus on a client’s progress in collaboratively defined goals and support in actualizing accountability for harm caused from substance use. Similarly, this would require a commitment to approaching clients who use substances with care and compassion, rather than criminalizing, shaming, or infantilizing the individual’s responses to trauma and violence they have endured prior to, during, or after their substance use. Lastly, abolitionist praxis in the context of substance use treatment may require counselors to provide opportunities for clients to have input regarding their needs in treatment by prioritizing individualized treatment over a standardized “one size fits all” approach to counseling. Thus, rather than prescribing a course of treatment or implementing treatment prescribed by a referring carceral system, abolitionist praxis would leverage collaboration to allow clients to have a voice in determining what they need to cope and heal from their use of substances and any traumatic experiences that precede and result from substance use.
Cultural Competence and Advocacy
Abolitionist praxis requires efforts to repair histories of structural violence (Cullors, 2019); thus, substance use counselors pursuing abolition must develop a critical understanding of the sociopolitical history of anti-drug policing toward those who use substances. This article provided a snapshot of this history as a starting point; however, counselors can delve further into learning about the intersection of anti-drug policing and race, gender, sexuality, disability, and socioeconomic status to develop more robust competence in addressing the scope of anti-drug policing. Counselors should critically reflect upon this historical knowledge to confront and actively dismantle any internalized biases they may have about substance use clients that are perpetuated by carceral systems. Counselors should specifically become aware of how the criminal legal system may perpetuate racial prejudice, particularly anti-Black racism, and how these attitudes affect the counselor’s conceptualization of their clients to avoid pathologizing or blaming the client for the structural violence they endure through anti-drug policing. To that end, counselors should actively incorporate practices that are not only trauma-informed, but also culturally responsive (SAMHSA, 2014).
Abolitionist praxis aimed at repairing historical structural violence through anti-drug policing would broadly include efforts toward the decriminalization of substance use. In addition to decriminalization efforts, counselors engaged in an abolitionist praxis might advocate with legal professionals and lawmakers for the retroactive and automatic expungement of drug-related criminal record charges for substance use clients (Adinoff & Reiman, 2019). These efforts would ensure that those with histories of substance use disorder are able to experience transformation that such records and their associated stigma may hinder. Given that abolition calls for counselors to address and promote healing from issues that underlie substance use, counselors seeking to engage in abolitionist praxis should advocate for funds that are currently and formerly used toward criminalizing substance use to be invested in transformative justice practices and trauma-informed treatment for substance use disorders (Adinoff & Reiman, 2019). For example, abolitionist praxis would call for transformative justice systems and practices to replace drug courts and related diversion programs. Although drug courts may be successful in deterring those who use substances from arrests and incarceration, Klukoff et al. (2021) highlighted the paradoxical nature of relying on carceral punishment as a motive for change because it risks police violence toward those who use substances when drug court requirements are not met. As stated earlier, this creates a value conflict for counselors who may have to disclose information regarding relapse during treatment that can be used in ways that jeopardize and harm the wellness of clients who use substances.
Limitations and Considerations
Adopting and incorporating an abolitionist praxis to counseling with clients impacted by anti-drug policing comes with challenges that counselors must critically reflect on prior to and during the implementation of this practice. First, counselors should prepare themselves to navigate pushback and resistance to social justice practices that would disrupt the status quo (S. W. Davis & Fayter, 2021). For example, it is common for individuals to criticize abolitionist praxis as utopian to inhibit the process of creatively imagining communities and systems that do not rely on carceral logics and systems (Kaba, 2021). Approaches like motivational interviewing are poised to navigate these challenges from colleagues who may be hesitant to embark upon making abolitionist change. In addition to pushback from individuals, it should be noted that, as a praxis seeking the elimination of carceral systems, barriers to the adoption of an abolitionist praxis can be expected from current carceral systems and approaches that may have existing evidence that establish them as efficacious. To counteract this expected barrier, substance use counselors need to engage in research, assessment, and program evaluation of efforts that are developed in alignment with an abolitionist praxis to establish efficacy. This would serve the purpose of ensuring that progress toward safety is achieved, that substance use clients are receiving trauma-informed care, and that other substance use counselors are introduced to new alternatives to existing carceral approaches that may increase the risk of harm to substance use clients. Additionally, counselors should critically reflect on and identify solutions to ethical, legal, and employment-related barriers if implementing an abolitionist praxis on their own. For example, making the choice as an individual counselor in a broader agency to not report substance use to a referring probation officer may be construed as fraudulent and unethical, thus jeopardizing a counselor’s employment and career. When making these decisions about whether or not to report substance use, counselors need to carefully weigh the options and consider consequences that can come from each course of action from a legal and ethical perspective, similar to what is suggested in the Forester-Miller and Davis (2016) Ethical Decision-Making Model. In the meantime, counselors can inform and educate probation officers about the nature of addiction and the potential for relapse to occur. Increasing awareness about these matters could generate a landscape shift for how probation officers and other authorities treat those struggling with addiction. Lastly, counselors should consider advocating for organizational support to adopt and implement trauma-informed and abolitionist changes to prevent such outcomes.
Conclusion
Clients who meet criteria for substance use disorders may have experienced, have witnessed, or be vulnerable to experiencing police violence. As a result, those who use substances are vulnerable to experiencing trauma that stems from exposure to police violence, which counselors must address. Counselors need to utilize abolitionist praxis to achieve a trauma-informed practice that supports healing from experiences of trauma affiliated with substance use and police violence, aim to prevent retraumatization, and create opportunities for both accountability and repair of harm caused by one’s use of substances.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Adinoff, B., & Reiman, A. (2019). Implementing social justice in the transition from illicit to legal cannabis use. The American Journal of Drug and Alcohol Abuse, 45(6), 673–688. https://doi.org/10.1080/00952990.2019.1674862
Afuape, T., & Kerry Oldham, S. (2022). Beyond “solidarity” with Black Lives Matter: Drawing on liberation psychology and transformative justice to address institutional and community violence in young Black lives. Journal of Family Therapy, 44(1), 20–43. https://doi.org/10.1111/1467-6427.12369
Alang, S., McAlpine, D., McCreedy, E., & Hardeman, R. (2017). Police brutality and Black health: Setting the agenda for public health scholars. American Journal of Public Health, 107(5), 662–665. https://doi.org/10.2105/AJPH.2017.303691
Barrera, T. L., Mott, J. M., Hofstein, R. F., & Teng, E. J. (2013). A meta-analytic review of exposure in group cognitive behavioral therapy for posttraumatic stress disorder. Clinical Psychology Review, 33(1), 24–32. https://doi.org/10.1016/j.cpr.2012.09.005
Beletsky, L., Grau, L. E., White, E., Bowman, S., & Heimer, R. (2010). The roles of law, client race and program visibility in shaping police interference with the operation of US syringe exchange programs. Addiction, 106(2), 357–365. https://doi.org/10.1111/j.1360-0443.2010.03149.x
Benson, B. L., Rasmussen, D. W., & Sollars, D. L. (1995). Police bureaucracies, their incentives, and the war on drugs. Public Choice, 83(1/2), 21–45. https://www.jstor.org/stable/30026940
Bor, J., Venkataramani, A. S., Williams, D. R., & Tsai, A. C. (2018). Police killings and their spillover effects on the mental health of Black Americans: A population-based, quasi-experimental study. The Lancet, 392(10144), 302–310. https://doi.org/10.1016/S0140-6736(18)31130-9
Bride, B. E., Hatcher, S. S., & Humble, M. N. (2009). Trauma training, trauma practices, and secondary traumatic stress among substance abuse counselors. Traumatology, 15(2), 96–105.
https://doi.org/10.1177/1534765609336362
Bryant-Davis, T., Adams, T., Alejandre, A., & Gray, A. A. (2017). The trauma lens of police violence against racial and ethnic minorities. Journal of Social Issues, 73(4), 852–871. https://doi.org/10.1111/josi.12251
Bureau of Justice Statistics. (2021). Law enforcement. https://bjs.ojp.gov/topics/law-enforcement
Carrico, A. W., Flentje, A., Gruber V. A., Woods, W. J., Discepola, M. V., Dilworth, S. E., Neilands, T. B., Jain, J., & Siever, M. D. (2014). Community-based harm reduction substance abuse treatment with methamphetamine-using men who have sex with men. Journal of Urban Health, 91(3), 555–567. https://doi.org/10.1007/s11524-014-9870-y
Castelpietra, G., Knudsen, A. K. S., Agardh, E. E., Armocida, B., Beghi, M., Iburg, K. M., Logroscino, G., Ma, R., Starace, F., Steel, N., Addolorato, G., Andrei, C. L., Andrei, T., Ayuso-Mateos, J. L., Banach, M., Bärnighausen, T. W., Barone-Adesi, F., Bhagavathula, A. S., Carvalho, F., . . . Monasta, L. (2022). The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990-2019: Findings from the Global Burden of Disease Study 2019. The Lancet Regional Health: Europe, 16(100341), 1–18. https://doi.org/10.1016/j.lanepe.2022.100341
Chang, Z., Lichtenstein, P., Larsson, H., & Fazel, S. (2015). Substance use disorders, psychiatric disorders, and mortality after release from prison: A nationwide longitudinal cohort study. The Lancet Psychiatry, 2(5), 422–430. https://doi.org/10.1016/S2215-0366(15)00088-7
Clark, C., Classen, C. C., Fourt, A., & Shetty, M. (2014). Treating the trauma survivor: An essential guide to trauma-informed care. Routledge. https://doi.org/10.4324/9780203070628
Cook, J. M., Newman, E., & The New Haven Trauma Competency Group. (2014). A consensus statement on trauma mental health: The New Haven Competency Conference process and major findings. Psychological Trauma: Theory, Research, Practice, and Policy, 6(4), 300–307. http://doi.org/10.1037/a0036747
Cooper, H. L. F. (2015). War on drugs policing and police brutality. Substance Use & Misuse, 50(8–9), 1188–1194. https://doi.org/10.3109/10826084.2015.1007669
Cooper, H., Moore, L., Gruskin, S., & Krieger, N. (2005). The impact of a police drug crackdown on drug injectors’ ability to practice harm reduction: A qualitative study. Social Science & Medicine, 61(3), 673–684. https://doi.org/10.1016/j.socscimed.2004.12.030
Cullors, P. (2019). Abolition and reparations: Histories of resistance, transformative justice, and accountability. Harvard Law Review, 132(6), 1684–1694. https://harvardlawreview.org/print/vol-132/abolition-and-reparations-histories-of-resistance-transformative-justice-and-accountability
Cullors, P. (2021). An abolitionist’s handbook: 12 steps to changing yourself and the world. St. Martin’s Press.
Davis, A. Y., Dent, G., Meiners, E. R., & Richie, B. E. (2022). Abolition. Feminism. Now. Haymarket Books.
Davis, C. S., Burris, S., Kraut-Becher, J., Lynch, K. G., & Metzger, D. (2005). Effects of an intensive street-level police intervention on syringe exchange program use in Philadelphia, PA. American Journal of Public Health, 95(2), 233–236. https://doi.org/10.2105/AJPH.2003.033563
Davis, S. W., & Fayter, R. (2021). Mutual aid as abolitionist praxis. Citizenship Studies, 25(2), 162–165. https://doi.org/10.1080/13621025.2020.1859190
DeVylder, J. E., Frey, J. J., Cogburn, C. D., Wilcox, H. C., Sharpe, T. L., Oh, H. Y., Nam, B., & Link, B. G. (2017). Elevated prevalence of suicide attempts among victims of police violence in the USA. Journal of Urban Health, 94, 629–636. https://doi.org/10.1007/s11524-017-0160-3
Dollar, C. B. (2019). Criminalization and drug “wars” or medicalization and health “epidemics”: How race, class, and neoliberal politics influence drug laws. Critical Criminology, 27(2), 305–327.
https://doi.org/10.1007/s10612-018-9398-7
Drustrup, D., Kivlighan, D. M., & Ali, S. R. (2023). Decentering the use of police: An abolitionist approach to safety planning in psychotherapy. Psychotherapy, 60(1), 51–62. https://doi.org/10.1037/pst0000422
El-Bassel, N., Gilbert, L., Witte, S., Wu, E., & Chang, M. (2011). Intimate partner violence and HIV among drug-involved women: Contexts linking these two epidemics—Challenges and implications for prevention and treatment. Substance Use & Misuse, 46(2–3), 295–306. https://doi.org/10.3109/10826084.2011.523296
Farley, M., Golding, J. M., Young, G., Mulligan, M., & Minkoff, J. R. (2004). Trauma history and relapse probability among patients seeking substance abuse treatment. Journal of Substance Abuse Treatment, 27(2), 161–167. https://doi.org/10.1016/j.jsat.2004.06.006
Fazel, S., Yoon, I. A., & Hayes, A. J. (2017). Substance use disorders in prisoners: An updated systematic review and meta-regression analysis in recently incarcerated men and women. Addiction, 112(10), 1725–1739. https://doi.org/10.1111/add.13877
Federal Bureau of Investigation. (2022). Crime data explorer [Data set]. https://cde.ucr.cjis.gov
Forester-Miller, H., & Davis, T. E. (2016). Practitioner’s guide to ethical decision making (Rev. ed.). http://www.counseling.org/docs/default-source/ethics/practioner’s-guide-toethical-decision-making.pdf
Galovski, T. E., Peterson, Z. D., Beagley, M. C., Strasshofer, D. R., Held, P., & Fletcher, T. D. (2016). Exposure to violence during Ferguson protests: Mental health effects for law enforcement and community members. Journal of Traumatic Stress, 29(4), 283–292. https://doi.org/10.1002/jts.22105
Geller, A., Fagan, J., Tyler, T., & Link, B. G. (2014). Aggressive policing and mental health of young urban men. American Journal of Public Health, 104(12), 2321–2327. https://doi.org/10.2105/AJPH.2014.302046
Giovengo, R. D. (2016). Training law enforcement officers. Routledge. https://doi.org/10.1201/9781315367262
Global Burden of Disease Network. (2016). Global Burden of Disease Study 2015 (GBD 2015) life expectancy, all-cause and cause-specific mortality 1980-2015 [Data set]. Institute for Health Metrics and Evaluation. https://ghdx.healthdata.org/record/ihme-data/gbd-2015-life-expectancy-all-cause-and-cause-specific-mortality-1980-2015
Good, D., Leichtling, G., & Pustejovsky, S. (2023). Oregon decriminalizes drugs: A state-level process evaluation of early implementation. Coimagine Health and Vital Strategies. https://comagine.org/resource/2466
Green, D. A. (2022, May 10). Developing competence to address undue police violence. Counseling Today. https://ctarchive.counseling.org/2022/05/developing-competence-to-address-undue-police-violence
Green, D. A., & Evans, A. M. (2021). Undue police violence toward African Americans: An analysis of professional counselors’ training and perceptions. Journal of Counseling & Development, 99(4), 363–371. https://doi.org/10.1002/jcad.12389
Green, D. A., Evans, A. M., Litam, S. D. A., Hornsby, T., Boulden, R., Shannon, J., Ford, D. J., & Landrum, D. (2024). Racial identity attitudes and vicarious traumatization from undue police violence on anticipatory traumatic reaction among Black Americans. Journal of Interpersonal Violence, 39(3–4), 848–868. https://doi.org/10.1177/08862605231198484
Hayashi, K., Ti, L., Csete, J., Kaplan, K., Suwannawong, P., Wood, E., & Kerr, T. (2013). Reports of police beating and associated harms among people who inject drugs in Bangkok, Thailand: A serial cross-sectional study. BMC Public Health, 13(1), 733.
https://doi.org/10.1186/1471-2458-13-733
Heffner, J. L., Blom, T. J., & Anthenelli, R. M. (2011). Gender differences in trauma history and symptoms as predictors of relapse to alcohol and drug use. The American Journal on Addictions, 20(4), 307–311. https://doi.org/10.1111/j.1521-0391.2011.00141.x
Jacobs, L. A., Kim, M. E., Whitfield, D. L., Gartner, R. E., Panichelli, M., Kattari, S. K., Downey, M. M., McQueen, S. S., & Mountz, S. E. (2021). Defund the police: Moving towards an anti-carceral social work. Journal of Progressive Human Services, 32(1), 37–62. https://doi.org/10.1080/10428232.2020.1852865
James, S. L., Castle, C. D., Dingels, Z. V., Fox, J. T., Hamilton, E. B., Liu, Z., Roberts, N. L. S., Sylte, D. O., Henry, N. J., LeGrand, K. E., Abdelalim, A., Abdoli, A., Abdollahpour, I., Abdulkader, R. S., Abedi, A., Abosetugn, A. E., Abushouk, A. I., Adebayo, O. M., Agudelo-Botero, M., Ahmad, T., . . . Vos, T. (2020). Global injury morbidity and mortality from 1990 to 2017: Results from the Global Burden of Disease Study 2017. Injury Prevention, 26(Supp 1), i96–i114. https://doi.org/10.1136/injuryprev-2019-043494
Joe, J. R., Shillingford-Butler, M. A., & Oh, S. (2019). The experiences of African American mothers raising sons in the context of #BlackLivesMatter. The Professional Counselor, 9(1), 67–79.
https://doi.org/10.15241/jrj.9.1.67
Kaba, M. (2021). We do this ’til we free us: Abolitionist organizing and transforming justice. Haymarket Books.
Kaba, M., & Ritchie, A. J. (2022). No more police: A case for abolition. New Press.
Kinner, S. A., Forsyth, S., & Williams, G. (2012). Systematic review of record linkage studies of mortality in ex-prisoners: Why (good) methods matter. Addiction, 108(1), 38–49. https://doi.org/10.1111/add.12010
Klukoff, H., Kanani, H., Gaglione, C., & Alexander, A. (2021). Toward an abolitionist practice of psychology: Reimagining psychology’s relationship with the criminal justice system. Journal of Humanistic Psychology, 61(4), 451–469. https://doi.org/10.1177/00221678211015755
Koram, K. (2022). Drug prohibition and the policing of warfare: The war on drugs, globalization, and the moralization of perpetual violence. Humanity, 13(1), 22–39. https://doi.org/10.1353/hum.2022.0001
Krieger, N., Chen, J. T., Waterman, P. D., Kiang, M. V., & Feldman, J. (2015). Police killings and police deaths are public health data and can be counted. PLOS Medicine, 12(12), e1001915.
https://doi.org/10.1371/journal.pmed.1001915
Krug, E. G., Mercy, J. A., Dahlberg, L. L., & Zwi, A. B. (2002). The world report on violence and health. The Lancet, 360(9339), 1083–1088. https://doi.org/10.1016/S0140-6736(02)11133-0
Lunze, K., Lunze, F. I., Raj, A., & Samet, J. H. (2015). Stigma and human rights abuses against people who inject drugs in Russia—A qualitative investigation to inform policy and public health strategies. PLOS One, 10(8), e0136030. https://doi.org/10.1371/journal.pone.0136030
Maher, L. (2004). Drugs, public health and policing in Indigenous communities. Drug and Alcohol Review, 23(3), 249–251. https://doi.org/10.1080/09595230412331293306
Meade, B., Steiner, B, & Klahm, C. F., IV. (2017). The effect of police use of force on mental health problems of prisoners. Policing and Society, 27(2), 229–244. https://doi.org/10.1080/10439463.2015.1049602
Miller, W. R., & Rollnick, S. (2013). Motivational interviewing: Helping people change (3rd ed.). Guilford.
Moh, Y. S., & Sperandio, K. R. (2022). The need to consider requiring trauma training in entry-level academic training programs in clinical mental health counseling. Journal of Mental Health Counseling, 44(1), 18–31. https://doi.org/10.17744/mehc.44.1.03
Motley, R. O., Jr., Byansi, W., Siddiqi, R., Bills, K. L., & Salas-Wright, C. P. (2022). Perceived racism-based police use of force and cannabis use among Black emerging adults. Addictive Behaviors Reports, 15, 100430. https://doi.org/10.1016/j.abrep.2022.100430
Mott, J. M., Sutherland, R. J., Williams, W., Lanier, S. H., Ready, D. J., & Teng, E. J. (2013). Patient perspectives on the effectiveness and tolerability of group-based exposure therapy for posttraumatic stress disorder: Preliminary self-report findings from 20 veterans. Psychological Trauma: Theory, Research, Practice, and Policy, 5(5), 453–461. https://doi.org/10.1037/a0029386
New York Civil Liberties Union. (n.d.). Ligon v. City of New York (challenging the NYPD’s aggressive patrolling of private apartment buildings). https://www.nyclu.org/en/cases/ligon-v-city-new-york-challenging-nypds-aggressive-patrolling-private-apartment-buildings
New York Civil Liberties Union. (2019, March 14). Stop-and-frisk in the de Blasio era (2019). https://www.nyclu.org/en/publications/stop-and-frisk-de-blasio-era-2019
Park, J. N., Linton, S. L., Sherman, S. G., & German, D. (2019). Police violence among people who inject drugs in Baltimore, Maryland. International Journal of Drug Policy, 64, 54–61.
https://doi.org/10.1016/j.drugpo.2018.12.005
Pinals, D. A., Gaba, A., Clary, K. M., Barber, J., Reiss, J., & Smelson, D. (2019). Implementation of MISSION–Criminal Justice in a treatment court: Preliminary outcomes among individuals with co-occurring disorders. Psychiatric Services, 70(11), 1044–1048. https://doi.org/10.1176/appi.ps.201800570
Pombo, S., & da Costa, N. F. (2016). Heroin addiction patterns of treatment-seeking patients, 1992-2013: Comparison between pre-and post-drug policy reform in Portugal. Heroin Addiction & Related Clinical Problems, 18(6), 51–60. https://dependencias.pt/images/files/HEROINA.pdf
Pratt, D., Appleby, L., Piper, M., Webb, R., & Shaw, J. (2010). Suicide in recently released prisoners: A case-control study. Psychological Medicine, 40(5), 827–835. https://doi.org/10.1017/S0033291709991048
Purnell, D. (2021a). Reforms are the master’s tools: The system is built for power, not justice. In C. Kaepernick (Ed.) Abolition for the people: The movement for a future without policing and prisons. Kaepernick Publishing.
Purnell, D. (2021b). Becoming abolitionists: Police, protests, and the pursuit of freedom. Astra House.
Rhodes, T., Platt, L., Sarang, A., Vlasov, A., Mikhailova, L., & Monaghan, G. (2006). Street policing, injecting drug use and harm reduction in a Russian city: A qualitative study of police perspectives. Journal of Urban Health, 83(5), 911–925. https://doi.org/10.1007/s11524-006-9085-y
Saleem, O. (1997). The age of unreason: The impact of reasonableness, increased police force, and colorblindness on Terry “Stop and Frisk.” Oklahoma Law Review, 50(4), 451–493. https://core.ac.uk/download/pdf/323046413.pdf
Sarang, A., Rhodes, T., Sheon, N., & Page, K. (2010). Policing drug users in Russia: Risk, fear, and structural violence. Substance Use & Misuse, 45(6), 813–864. https://doi.org/10.3109/10826081003590938
Schwartze, D., Barkowski, S., Strauss, B., Knaevelsrud, C., & Rosendahl, J. (2019). Efficacy of group psychotherapy for posttraumatic stress disorder: Systematic review and meta-analysis of randomized controlled trials. Psychotherapy Research, 29(4), 415–431. https://doi.org/10.1080/10503307.2017.1405168
Scott, C. L. (2020). Jail diversion: A practical primer. CNS Spectrums, 25(5), 651–658. https://doi.org/10.1017/S1092852919001834
Shannon, K., Rusch, M., Shoveller, J., Alexson, D., Gibson, K., & Tyndall, M. W. (2008). Mapping violence and policing as an environmental–structural barrier to health service and syringe availability among substance-using women in street-level sex work. International Journal of Drug Policy, 19(2), 140–147. https://doi.org/10.1016/j.drugpo.2007.11.024
Shaw, S. A., El-Bassel, N., Gilbert, L., Terlikbayeva, A., Hunt, T., Primbetova, S., Rozental, Y., & Chang, M. (2016). Depression among people who inject drugs and their intimate partners in Kazakhstan. Community Mental Health Journal, 52, 1047–1056. https://doi.org/10.1007/s10597-015-9883-3
Sloan, D. M., Feinstein, B. A., Gallagher, M. W., Beck, J. G., & Keane, T. M. (2013). Efficacy of group treatment for posttraumatic stress disorder symptoms: A meta-analysis. Psychological Trauma: Theory, Research, Practice, and Policy, 5(2), 176–183. https://doi.org/10.1037/a0026291
Small, W., Rhodes, T., Wood, E., & Kerr, T. (2007). Public injection settings in Vancouver: Physical environment, social context and risk. International Journal of Drug Policy, 18(1), 27–36.
https://doi.org/10.1016/j.drugpo.2006.11.019
Smiley-McDonald, H. M., Attaway, P. R., Wenger, L. D., Greenwell, K., Lambdin, B. H., & Kral, A. H. (2023). “All carrots and no stick”: Perceived impacts, changes in practices, and attitudes among law enforcement following drug decriminalization in Oregon State, USA. International Journal of Drug Policy, 118, 1–10. https://doi.org/10.1016/j.drugpo.2023.104100
Substance Abuse and Mental Health Services Administration. (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach. https://store.samhsa.gov/product/SAMHSA-s-Concept-of-Trauma-and-Guidance-for-a-Trauma-Informed-Approach/SMA14-4884
Sweeney, A., & Taggart, D. (2018). (Mis)understanding trauma-informed approaches in mental health. Journal of Mental Health, 27(5), 383–387. https://doi.org/10.1080/09638237.2018.1520973
Tapp, S. N., & Davis, E. (2022). Contacts between police and the public, 2020. (BJS Publication No. NCJ 304527). Bureau of Justice Statistics. https://bjs.ojp.gov/library/publications/contacts-between-police-and-public-2020
Ti, L., Hayashi, K., Kaplan, K., Suwannawong, P., Wood, E., Montaner, J., & Kerr, T. (2013). HIV test avoidance among people who inject drugs in Thailand. AIDS and Behavior, 17, 2474–2478.
https://doi.org/10.1007/s10461-012-0347-2
Tonry, M. (1994). Racial politics, racial disparities, and the war on crime. Crime & Delinquency, 40(4), 475–494. https://doi.org/10.1177/0011128794040004001
Vallance, K., Stockwell, T., Pauly, B., Chow, C., Gray, E., Krysowaty, B., Perkin, K., & Zhao, J. (2016). Do managed alcohol programs change patterns of alcohol consumption and reduce related harm? A pilot study. Harm Reduction Journal, 13(1), 13. https://doi.org/10.1186/s12954-016-0103-4
Volkmann, T., Lozada, R., Anderson, C. M., Patterson, T. L., Vera, A., & Strathdee, S. A. (2011). Factors associated with drug-related harms related to policing in Tijuana, Mexico. Harm Reduction Journal, 8, 7. https://doi.org/10.1186/1477-7517-8-7
Werb, D., Rowell, G., Guyatt, G., Kerr, T., Montaner, J., & Wood, E. (2011). Effect of drug law enforcement on drug market violence: A systematic review. International Journal of Drug Policy, 22(2), 87–94. https://doi.org/10.1016/j.drugpo.2011.02.002
Werb, D., Strathdee, S. A., Vera, A., Arredondo, J., Beletsky, L., Gonzalez-Zuniga, P., & Gaines, T. (2016). Spatial patterns of arrests, police assault and addiction treatment center locations in Tijuana, Mexico. Addiction, 111(7), 1246–1256. https://doi.org/10.1111/add.13350
The White House. (2022, August 1). Fact sheet: President Biden’s Safer America Plan. https://www.whitehouse.gov/briefing-room/statements-releases/2022/08/01/fact-sheet-president-bidens-safer-america-plan-2
Wood, E. F., Werb, D., Beletsky, L., Rangel, G., Mota, J. C., Garfein, R. S., Strathdee, S. A., & Wagner, K. D. (2017). Differential experiences of Mexican policing by people who inject drugs residing in Tijuana and San Diego. International Journal of Drug Policy, 41, 132–139. https://doi.org/10.1016/j.drugpo.2016.12.010
Darius A. Green, PhD, NCC, is an assistant professor at the University of Colorado Colorado Springs. Katharine R. Sperandio, PhD, NCC, ACS, LPC, is an assistant professor and a CACREP-accreditation coordinator at Saint Joseph’s University. Correspondence may be addressed to Darius A. Green, 1420 Austin Bluffs Pkwy, Colorado Springs, CO 80918, dgreen20@uccs.edu.
May 22, 2024 | Volume 14 - Issue 1
Jennifer M. Cook, Melissa D. Deroche, Lee Za Ong
The phenomenon of microaggressions is well established within the counseling literature, particularly as it relates to race, ethnicity, gender, and affectual orientation. However, research related to disability or ableist microaggressions is still in its infancy, so counseling professionals have limited information about experiences of disability and ableist microaggressions. The purpose of this qualitative content analysis was to describe participants’ self-reported experiences with ableist microaggressions. Participants (N = 90) had a diagnosed disability and the majority (91.11%) identified as having two or more nondominant identities beyond their disability. We report two categories and 10 themes. While participants were part of the general population, we position our discussion and implications within the context of professional counseling to increase counseling professionals’ awareness and knowledge so counselors can avoid ableist microaggressions and provide affirmative counseling services to persons with disabilities.
Keywords: disability, ableist microaggressions, professional counseling, nondominant identities, affirmative counseling
Day by day, what you choose, what you think, and what you do is who you become.
—Heraclitus, pre-Socratic philosopher
Each person is a complex makeup of dominant and nondominant sociocultural identities. Individuals with dominant cultural identities (e.g., able-bodied, White, middle social class) experience societal privilege, have more sociocultural influence, and have unencumbered access to resources. People with nondominant identities, including people with disabilities (PWD), people of color, and people in lower social class, frequently have less influence and experience structural and interpersonal inequities, limitations, and discrimination (Sue & Spanierman, 2020). As such, people with nondominant identities often experience microaggressions. Microaggressions are unintentional or deliberate verbal, nonverbal, and/or environmental messages that convey disapproval, distaste, and condemnation of an individual based on their nondominant identity (Sue et al., 2007).
Professional counselors are aware and knowledgeable that their identity constellation and their
experiences with microaggressions, as well as those of their clients, impact their worldviews, experiences, and—importantly—the counseling relationship (Ratts et al., 2016). While microaggressions associated with several cultural identities have been well-researched within counseling (e.g., race, ethnicity, gender, affectual orientation), others, like ableist microaggressions, have been examined far less frequently (Deroche et al., 2024). The purpose of this article is to describe the microaggression experiences that PWD (N = 90) encounter. Our intention is to increase counseling professionals’ awareness and knowledge about ableist microaggressions so they can examine their beliefs about disability, identify how they may have participated in ableist microaggressions and, ultimately, provide affirmative counseling services to PWD.
Literature Review
Although the term microaggressions was coined by Pierce in the 1970s, it was not until 2007 that it took hold within the allied helping professions (Sue et al., 2007). Initially, the term was used to describe experiences based on race, yet the term has been applied more broadly to the dismissive experiences people with other nondominant identities (e.g., gender, affectual/sexual orientation) encounter (Sue & Spanierman, 2020). In 2010, Keller and Galgay initiated foundational research about the microaggressions that PWD experience. Through their qualitative study, they identified eight microaggression domains experienced by PWD and described their harmful effects on the psychological and emotional well-being of PWD. Those eight domains are: (a) denial of identity, (b) denial of privacy, (c) helplessness, (d) secondary gain, (e) spread effect, (f) patronization, (g) second-class citizenship, and (h) desexualization (i.e., ignoring or avoiding the sexual needs, wants, or desires of PWD). This study marked the beginning of ableist microaggressions research that led scholars not only to naming (e.g., Dávila, 2015) and measuring (e.g., Conover et al., 2017a) specific microaggressions toward PWD, but also describing experiences with ableist microaggressions within specific disability groups (e.g., Coalson et al., 2022; Eisenman et al., 2020) and exploring the impact for specific cultural groups of PWD (e.g., Miller & Smith, 2021).
Before continuing further, it is important for us to explain our use of the term ableist microaggressions, rather than the term disability microaggressions, because it deviates from the typical convention used to name microaggressions (e.g., racial microaggressions, gender microaggressions). While some authors have used the term disability microaggressions (e.g., Dávila, 2015), we believe that this term undercuts and minimizes PWD’s microaggression experiences, as it fails to explicitly communicate that these microaggressions are forms of ableism. Therefore, to validate PWD’s experiences and to align with the disability movement’s philosophy of diversity and social justice, we use the term ableist microaggressions (Perrin, 2019).
The qualitative ableist microaggression studies we reviewed all utilized and endorsed the themes Keller and Galgay (2010) found in their qualitative study, while adding nuance and new information about ableist microaggressions. For instance, Olkin et al.’s (2019) focus group research with women who had both hidden and apparent disabilities (N = 30) supported Keller and Galgay’s eight themes while identifying two others: medical professionals not believing PWD’s symptoms and experiences of having their disability discounted based on appearing young and/or healthy. Similarly, Coalson et al. (2022), who utilized focus groups with adults who stutter (N = 7), endorsed six of Keller and Galgay’s themes and identified participants’ perceptions of microaggressive behaviors (i.e., Exonerated the Listener, Benefit of the Doubt, Focusing on Benefits, and Aggression Viewed as Microaggression) while noting that some participants had minimal or no microaggression experiences.
Although Eisenman et al. (2020) endorsed five of Keller and Galgay’s (2010) themes, they took a different approach to how they analyzed and organized their findings by using Sue et al.’s (2007) microaggression taxonomy. Of note, these researchers were the first to identify and establish microaffirmations within disability microaggressions research. According to Rolón-Dow and Davison (2018) microaffirmations are:
behaviors, verbal remarks or environmental cues experienced by individuals from minoritized racial groups in the course of their everyday lives that affirm their racial identities, acknowledge their racialized realities, resist racism or advance cultural and ideological norms of racial justice. (p. 1)
Like microaggressions, microaffirmations may be intentional or unintentional, but they have a positive rather than a negative impact on people with nondominant racial identities. Eisenman et al. (2020) found all four race-related microaffirmation types identified by Rolón-Dow and Davison (2021)—Microrecognitions, Microvalidations, Microtransformations, and Microprotections—with their sample of people with intellectual disabilities.
Finally, Miller and Smith (2021) conducted individual interviews (N = 25) with undergraduate and graduate students who identified as members of the LGBTQ community with a disability. They, too, found Keller and Galgay’s (2010) domains present in their study and identified eight additional categories. Five categories captured cultural components in addition to disability (i.e., Biphobia, Intersectionality Microaggression, Queer Passing/Disclosure, Racism, and Sexism), while the remaining three were specific to ableist microaggression–focused data: Ableism Avoidance, Faculty Accommodations, and Structural Ableism/Inaccessibility.
The purpose of our study is to add to the burgeoning disability and microaggressions discourse by analyzing participants’ responses to a qualitative prompt offered to them after they completed the Ableist Microaggression Scale (AMS; Conover et al., 2017b). We corroborate prior research findings while adding novel findings that increase professional knowledge about ableist microaggressions and their impact.
Methodology
To ensure compliance with Section 508 of the Rehabilitation Act, the federal law that requires PWD to have access to electronic information equivalent to that available to nondisabled individuals, we utilized digital accessibility tools on the internet platform used for this study (Qualtrics) and recruited PWD to test the accessibility of the study survey and questions. The data analyzed and reported in this article were part of a larger, IRB-approved study (N = 201) in which we investigated participants’ ableist microaggression experiences quantitatively using the AMS (Conover et al., 2017b) to uncover whether participants’ AMS scores were impacted by visibility of disability, type of disability, and their other nondominant identities (Deroche et al., 2024). After participants completed the survey, they were invited to provide a written response to the open-ended question: “What, if any, information do you think would be helpful for us to know about your personal experiences regarding ableist microaggressions?” Ninety participants (44.77% of the overall sample) responded with rich data that warranted analysis and reporting in an independent article. Because the open-ended question occurred after participants completed the AMS, we agreed that the survey likely influenced their responses, so we chose to conduct a content analysis using an a priori codebook grounded in the AMS subscales (Minimization, Denial of Personhood, Otherization, and Helplessness; Conover et al., 2017b), with additional coding categories for data that did not fit the a priori codes (i.e., Fortitude/Resilience/Coping, Contextual Factors, Impact of Microaggressions/Ableism on Mental Health/Wellness, Microaggression Experiences Are Different Depending on Visibility of Disability, Internalized Ableism, and Microaggressions Include Identities Other Than Disability).
Procedure
Using online data collection via Qualtrics survey, we recruited participants nationally by contacting disability organizations, listservs, social media, and professional contacts who work with organizations that serve PWD. The recruitment included a description of the research; inclusion criteria; and a confidential, anonymized survey link. The survey was Section 508–compliant and optimized to be taken on a computer or mobile device. Data were collected over a 3-month period.
Inclusion Criteria and Participants
To participate in the study, individuals (a) were at least 18 years of age, (b) had earned a high school diploma or GED, and (c) had a diagnosed disability. Under the Americans with Disabilities Act (ADA), the term disability is defined within the context of a person’s significant limitations to engage in major life activities. Different agencies and organizations such as the World Health Organization and the U.S. Social Security Administration define disability differently (Patel & Brown, 2017). For this study, we categorized disability as (a) physical disability (i.e., mobility-related disability), (b) sensory disability (i.e., seeing- or hearing-related disability), (c) psychiatric/mental disability (e.g., bipolar disorder, depression, post-traumatic stress disorder), or (d) neurodevelopmental disability (e.g., autism spectrum disorder, learning disability, or ADHD). Participants’ disabilities were apparent/visible (i.e., recognizable by others without the person disclosing they have a disability) or hidden (i.e., others are unlikely to know the individual has a disability, so the person must disclose they have a disability for it to be known), and they could identify with one or more disability categories listed above. Ninety individuals provided usable responses. Table 1 details participant demographics. The bulk of the sample, 84.43%, identified as having two (36.66%), three (26.66%), or four (21.11%) nondominant cultural identities out of the six identities the study targeted, while the rest of the sample comprised individuals who noted six (n = 2; 2.22%), five (n = 4; 4.4%), one (n = 7; 7.77%), or no (n = 1; 1.11%) nondominant identities.
Of note, a higher percentage of participants with hidden or both apparent and hidden disabilities participated in the qualitative portion of the study compared to those who completed only the quantitative portion (45.5% compared to 41.8% and 33.3% compared to 27.4%, respectively). Similarly, there was a lower response rate from participants who earned a high school diploma or GED (5.6%), completed an associate degree or trade school (7.8%), completed some college (7.8%), or earned a doctoral degree (10%). There was an increase in responses from participants who earned a bachelor’s degree (26.7% compared to 21.9% in the quantitative portion) or a master’s degree (42.2% compared to 35.8%, respectively).
Data Analysis
We analyzed data for this study using MacQueen et al.’s (1998) framework to create a codebook to promote coder consistency. We established six codes, four of which were definitionally congruent with the AMS subscales (i.e., Helplessness, Minimization, Denial of Personhood, and Otherization; Conover et al., 2017a). While we used Conover et al.’s definitions as the foundation, we utilized Keller and Galgay’s (2010) definitions to add additional nuance. The next code, Other Data, was an a priori code reserved for data that did not fit the AMS subscale codes. After completing the pilot, we added a sixth code, Fortitude/Resilience/Coping, to capture data that demonstrated ways in which participants developed strengths, dealt with adversity and microaggressions, and persevered despite their microaggressive experiences. Identifying PWD’s fortitude/resilience/coping abilities is indicative of a strengths-based framework that promotes inclusion, equity, and higher quality of life. Research has shown that resilience in PWD such as improved well-being, higher social role satisfaction, and lower mental health symptoms are correlated with positive psychological and employment outcomes (Ordway et al., 2020; Norwood et al., 2022). Once this code was established, the Other Data code was used for any data that did not fit the five a priori codes. After the pilot, we added to the codebook definitions for clarity—though no codes were changed. All codes we established had substantial representation in the data and are reported as themes in the results section. The auditor (second author Melissa D. Deroche) gave feedback on the codebook and confirmed the codebook was sound prior to analysis.
Table 1
Demographic Characteristics of Participants (N = 90)
| Variable |
n |
% |
| Disability Type |
|
|
|
Single Type: Physical |
21 |
23.33 |
|
Single Type: Sensory |
17 |
18.88 |
|
Single Type: Neurodevelopmental |
6 |
6.66 |
|
Single Type: Psychiatric/Mental Health |
6 |
6.66 |
|
Combination (2): Physical and Psychiatric/Mental Health |
8 |
8.88 |
|
Combination (2): Neurodevelopmental and Psychiatric/Mental Health |
6 |
6.66 |
|
Combination (2): Sensory and Psychiatric/Mental Health |
5 |
5.55 |
|
Combination (2): Sensory and Physical |
4 |
4.44 |
|
Combination (2): Neurodevelopmental and Physical |
2 |
2.22 |
|
Combination (2): Sensory and Neurodevelopmental |
2 |
2.22 |
|
Combination (3): Physical, Psychiatric/Mental Health, Neurodevelopmental |
4 |
4.44 |
|
Combination (3): Physical, Sensory, Neurodevelopmental |
4 |
4.44 |
|
Combination (3): Sensory, Psychiatric/Mental Health, Neurodevelopmental |
2 |
2.22 |
|
Combination (3): Physical, Sensory, Psychiatric/Mental Health |
1 |
1.11 |
|
Combination (4): Physical, Sensory, Psychiatric/Mental Health,
Neurodevelopmental |
2 |
2.22 |
| Visibility of Disability |
|
|
|
Visible/Apparent |
19 |
21.11 |
|
Hidden/Concealed |
41 |
45.55 |
|
Both |
30 |
33.33 |
| Biological Sex/Sex Assigned at Birth |
|
|
|
Female |
74 |
82.22 |
|
Male |
16 |
17.77 |
| Gender Identity |
|
|
|
Gender Fluid/Gender Queer |
6 |
6.66 |
|
Man |
16 |
17.77 |
|
Woman |
68 |
75.55 |
| Affectual/Sexual Orientation |
|
|
|
Asexual |
2 |
2.22 |
|
Bisexual |
9 |
10.00 |
|
Gay |
2 |
2.22 |
|
Heterosexual |
68 |
75.55 |
|
Lesbian |
3 |
3.33 |
|
Pansexual |
4 |
4.44 |
|
Queer |
1 |
1.11 |
|
Questioning |
1 |
1.11 |
| Racial/Ethnic Identity |
|
|
|
African American/Black |
4 |
4.44 |
|
Asian or Pacific Islander |
3 |
3.33 |
|
Biracial |
2 |
2.22 |
|
Euro-American/White |
69 |
76.66 |
|
Indigenous |
1 |
1.11 |
|
Jewish |
5 |
5.55 |
|
Latino/a or Hispanic |
3 |
3.33 |
|
Middle Eastern |
1 |
1.11 |
|
Multiracial |
2 |
2.22 |
| Religious/Spiritual Identity |
|
|
|
Atheist |
8 |
8.88 |
|
Catholic |
12 |
13.3 |
|
Jewish |
4 |
4.44 |
|
Not Religious |
1 |
1.11 |
|
Pagan |
1 |
1.11 |
|
Protestant |
36 |
40.00 |
|
Questioning |
2 |
2.22 |
|
Spiritual Not Religious |
5 |
5.55 |
|
Unitarian Universalist |
2 |
2.22 |
|
Self-Identify in Another Way |
19 |
21.11 |
| Highest Level of Education |
|
|
|
High School Diploma or GED |
5 |
5.55 |
|
Associate or Trade School Degree |
7 |
7.77 |
|
Some College, No Degree |
7 |
7.77 |
|
Bachelor’s Degree |
24 |
26.66 |
|
Master’s Degree |
38 |
42.22 |
|
PhD, EdD, JD, MD, etc. |
9 |
10.00 |
|
No Response |
1 |
1.11 |
| Employment Status |
|
|
|
Full-Time |
40 |
44.44 |
|
Part-Time |
16 |
17.77 |
|
Retired |
9 |
10.00 |
|
Student |
11 |
12.22 |
|
Unemployed |
14 |
15.55 |
| Employment Compared to Training and Skills |
|
|
|
Training/Education/Skills are lower than job responsibilities/position |
2 |
2.22 |
|
Training/Education/Skills are on par with job responsibilities/position |
42 |
46.66 |
|
Training/Education/Skills exceed job responsibilities/position |
24 |
26.66 |
|
Not applicable |
22 |
24.44 |
|
|
|
|
|
We began analysis by piloting 10% of the data (n = 9) using the initial codebook (Boyatzis, 1998). Two researchers (first and third authors Jennifer M. Cook and Lee Za Ong) coded data independently and then worked together to reach consensus. Once the pilot analysis was complete, we coded the remaining data and recoded pilot data to ensure they fit the revised coding frame. After all data were coded, we further coded the data that were assigned to Other Data using in vivo codes to establish codes that best captured the data. We identified five codes within Other Data: Contextual Factors, Impact of Microaggressions/Ableism on Mental Health/Wellness, Microaggression Experiences Are Different Depending on Visibility of Disability, Internalized Ableism, and Microaggressions Include Identities Other Than Disability.
Trustworthiness
Cook and Ong coded all data independently and then met to reach consensus. Prior to coding commencement, we identified our beliefs and potential biases about the data and discussed how they might impact coding; we continued these conversations throughout analysis. For the pilot coding phase, independent coder agreement prior to consensus was 40%. Independent coder agreement prior to consensus during regular coding was 56%, and 69% for Other Data independent coding. We reached consensus for all coded data through a team meetings consensus process (Boyatzis, 1998). Finally, we utilized an auditor (Deroche). Deroche reviewed all consensus findings during all analysis stages. The coding team met with the auditor to resolve questions and discrepancies, such as a few instances in which data were misassigned to a code.
Research Team
The research team comprised three cisgender women between the ages of 45 and 55 who are all licensed professional counselors and work as counselor educators. Cook and Deroche identify as White and hold PhDs in counselor education, while Ong holds a PhD in rehabilitation psychology and is Asian American of Chinese descent and an immigrant from Malaysia. Deroche identifies as a person with a disability, Deroche and Ong have worked extensively with PWD, and all three authors have conducted research about PWD. Cook has abundant publications in qualitative research designs related to multicultural counseling. Finally, all three authors have extensive research training and experience in qualitative and quantitative research designs.
Findings
The findings described below are organized into two categories: findings that align with the AMS subscales and unique findings that are independent of the AMS subscales. Themes are listed in their appropriate category with participants’ quotes to illustrate and substantiate each theme (see Table 2). When we provide participant quotes, we refer to them by their randomly assigned participant numbers (e.g., P105, P109).
Table 2
Categories and Themes
| Category/Theme |
n |
% of Sample |
| Category 1: Findings That Align With the AMS Subscales |
|
|
|
Minimization |
35 |
38.88 |
|
Denial of Personhood |
26 |
28.88 |
|
Otherization |
17 |
18.88 |
|
Helplessness |
16 |
17.77 |
| Category 2: Unique Findings Independent of the AMS Subscales |
|
|
|
Fortitude/Resilience/Coping |
27 |
30.00 |
|
Contextual Factors |
17 |
18.88 |
|
Impact of Microaggressions/Ableism on Mental Health/Wellness |
10 |
9.00 |
|
Microaggression Experiences Are Different Depending on Visibility of Disability |
6 |
6.66 |
|
Internalized Ableism |
4 |
4.44 |
|
Microaggressions Include Identities Other Than Disability |
4 |
4.44 |
Note. N = 90.
Category 1: Findings That Align With the AMS Subscales
Our analysis revealed that the AMS a priori codes fit the study data. As such, the codes were transitioned to themes: Minimization (n = 35), Denial of Personhood (n = 26), Otherization (n = 17), and Helplessness (n = 16). The quotes selected for each theme illustrate the lived experiences of the theme definitions and add context and nuance about the impact of ableist microaggressions.
Minimization
Conover et al. (2017a) defined Minimization as microaggression experiences demonstrating the belief that PWD are “overstating their impairment or needs” and that “individuals with a disability could be able-bodied if they wanted to be or that they are actually able-bodied” (p. 581). Thirty-five of the 90 participants’ responses (33.33%) indicated instances of Minimization.
For example, P105 described incidents from their formative years that highlight the belief that PWD are, in fact, able-bodied and overstating their impairment:
As a child, children and adults alike would test the limits of my blindness. My piers [sic] would ask me how many fingers they were holding up. And in one instance, teachers lined a hallway with chairs to see if I’d run into them. Spoiler alert, I did.
P109 spoke to their interactions with family that highlight how disbelief about a person’s disability can result in Minimization:
Family is really bad. They still don’t believe me. I was asked (when I couldn’t climb stairs into a restaurant) are you trying to make a point? My visible disability has gotten worse over 40 years. I think because they saw me before I started using a cane, they just won’t believe me.
P158 illuminated a fallacy that can result in Minimization: “Because my disability is invisible people assume I need no help, [and] when I do, they discount my disability. I hear, ‘you don’t look like you have a disability‚’ ‘don’t sell yourself short.’”
Finally, P137 spoke to the blame that underlies Minimization:
On[e] of the most frequent microaggressions encountered living with my particular invisible disability (type 1 diabetes) is the ableist idea that health is entirely a personal responsibility. There is this assumption that whatever problems we face with our health are a direct result of poor choices (dietary, financial) completely ignoring the systematic problems with for-profit health care in this country.
Denial of Personhood
Denial of Personhood is characterized by PWD being “treated with the assumption that a physical disability indicates decreased mental capacity and therefore, being reduced to one’s physicality” (Conover et al., 2017a, p. 581); such microaggressions can occur “when any aspect of a person’s identity other than disability is ignored or denied” (Keller & Galgay, 2010, p. 249). Twenty-six participants (28.88%) endorsed this theme. For example, P142 described their experiences in the workplace that illustrate the erroneous belief that PWD have diminished mental capacity: “All my life I was pushed out of jobs for not hearing. People would actually tell me, ‘if you can’t hear—how can you do anything’ even though all my performance reviews exceeded expectations.” P123 spoke to a similar sentiment: “[I] am often asked ‘what’s wrong with you?’ ‘how did you get through college?’” Finally, P173 summarized the belief that seemingly underlies Denial of Personhood microaggressions and issued a corrective action:
Disabled doesn’t mean stupid. We can figure out most things for ourselves and if we can’t we know to ask for help. Don’t tell us how to live our lives or say we don’t deserve love, happiness and children. If you don’t know the level of someone’s disability you shouldn’t have the right to judge them about such things.
Otherization
Seventeen participants (18.88%) described Otherization as part of their narrative responses. Otherization microaggressions are those in which PWD are “treated as abnormal, an oddity, or nonhuman, and imply people with disabilities are or should be outside the natural order” (Conover et al., 2017a, p. 581) and that their “rights to equality are denied” (Keller & Galgay, 2010, p. 249). Participants shared several examples of these types of microaggressions. For instance, P140 shared:
When we (PWD) ask for simple things (e.g., can you turn on the captioning) and people grumble, say they can’t, etc. it just reinforces that we’re not on equal footing and at least for me it eats away a little bit every time.
P185 indicated another manifestation of Otherization: “As a deaf person, I get frustrated when whoever I’m talking to stops listening when someone else (non-deaf person) speaks verbally, leaving me mid-sentence.” P108 shared that they have been “prayed for in public without asking,” while P106 expressed, “I hate when people compliment me on how well I push my chair or say I must have super strong arms. I just have normal arms not athletic looking or anything.”
Helplessness
Helplessness microaggressions are those in which PWD are “treated as if they are incapable, useless, dependent, or broken, and imply they are unable to perform any activity without assistance” (Conover et al., 2017a, p. 581). Sixteen participants (17.77%) described Helplessness microaggressions. For P174, the most common Helplessness microaggression they experience is when “people speak to the person I am with instead of to me. Drives me crazy! Worse is when the person I’m with answers for me.” P126 corroborated the “devastating” nature of when “people make decisions for you.” P129 shared that, “As a person with an invisible disability, I most often encounter microaggressions in the form of unsolicited advice when I disclose my disability.” Similarly, P134 noted:
Although my disability is not apparent, if people know about it, they often just act on my behalf without asking me for input or feedback. That is very frustrating and often does not change even if I bring it up to the individual who does it.
This final quote from P134 is powerful because it, like P174’s experience, demonstrates how people without disabilities participate in perpetuating ableism even when they were not the ones who initiated it.
Category 2: Unique Findings Independent of the AMS Subscales
As we indicated earlier, we separated data that did not fit into AMS codes and coded them using in vivo codes. This analysis resulted in six novel themes (i.e., Fortitude/Resilience/Coping, Contextual Factors, Impact of Microaggressions/Ableism on Mental Health/Wellness, Microaggression Experiences Are Different Depending on Visibility of Disability, Internalized Ableism, and Microaggressions Include Identities Other Than Disability) that are independent from the AMS-driven themes discussed in the prior section, yet are interrelated because they add unique insights and helpful context for understanding ableist microaggressions within the lived experiences of PWD.
Fortitude/Resilience/Coping
We defined Fortitude/Resilience/Coping as ways in which participants have developed strength, dealt with adversity/microaggressions, and persevered despite their microaggressive experiences. Thirty percent (n = 27) of participants disclosed a wide range of attitudinal and experiential tactics related to this theme. P103 shared, “I maintain what I call a healthy sense of humor about my own body and being disabled,” while P145 demonstrated a sense of humor as they shared how they cope:
I just have to remind them and myself that my brain works differently and that I am just as competent as anyone else. I have learned not to beat myself up when I forget something or can’t get my paperwork done correctly for the tenth time. (I really hate paperwork.)
Participants 138 and 127 both spoke directly to the role knowledge plays. P138 shared:
I want to put out there that knowledge & understanding are power. Knowing & understanding your rights as a person with a disability as well as knowing & understanding your unique experience with your own disability (to the best of your ability) is key to making forward strides in environments that can often times feel ableist.
P127 spoke to knowledge, too, with their belief that “most microaggressions stem from a lack of education. I am often the first person they have met with a disability and the experience makes them uncomfortable.”
Finally, P187 spoke to the power of their resilience and its impact on their life, experiences which they draw from to help others:
I’ve been physically and emotionally abused my entire life, until I took control and stopped it. I’m middle aged and it took me 40 years to forgive everything that I’ve . . . had to endure. Never from my family, or close friends, but it’s been a difficult life, and now I’m all ok with it and try to help others with disabilities that are having a hard time.
Contextual Factors
Seventeen participants (18.88%) described Contextual Factors, which are data that depict relational, situational, or environmental elements that impact participants’ experiences of ableist microaggressions.
P110 shared that “microaggressions can be hard to label because they can vary based on the relationship you have with the person.” P175 added: “Most times the microaggression I receive are by people when they don’t know me, or first meet me, as opposed to get to know me better.” P162 spoke to additional situational/relational nuances: “I have very different experiences depending on what assistive technology I’m using in a given space (basically to what degree I pass as able-bodied) and how people know me.”
P163 spoke to relational roles as well as environmental context: “The attitudes about me are distinctly divided between the power structures. A case manager, medical doctor, neighbor or family member will certainly show their attitude differently. The same goes for academic settings [versus] job placement.” For P152, “The worst comments have come from mental health therapists [who] are medical professionals who should be the most compassionate towards their patients.”
P117 and P131 both identified situational differences they have noticed. P117 shared, “I find that people have treated me differently at different ages and stages in my life, particularly when I was raising three children as a divorced mom.” P131 identified their work environment as positive: “I work in the field of vocational rehabilitation so [I] interact with more people who have a more nuanced understanding of disability than the general population.” However, P165 offered an alternate view, noting that “many microaggressions are more insidious or come from within the disabled community.”
Impact of Microaggressions/Ableism on Mental Health/Wellness
Ten participants (9%) expressed how microaggressions and ableism experiences have impacted their mental health and wellness. P172 stated, “I struggle with my mental wellness and I have been hospitalized for severe depression that manifests from a combination of my disability and situations that are overwhelming.” P157 expressed a similar combination effect of having a disability and being “ostracized” by others: “The combination is very heavy on my heart and leaves me feeling incredibly alone.”
P159 expressed feeling “pathetic and weak. Sometimes I feel useless and disgraced. Most of the time I feel dumb and stupid.” P103 added additional impacts while acknowledging the differences between their experiences and those of their colleagues of color: “None of these [microaggressions] were overt, but all contributed to stress and frustration and generalized anxiety. I have seen much worse with coworkers of color and disabled Black and Brown folks in my community.”
P126 admitted that completing the study survey “evoked difficult memories.” Additionally, this participant described the turmoil and cognitive dissonance they experience:
I’m reminded taking this survey of the inner conflict with identifying as disabled. Is my disability qualifying enough, will I be rejected? I felt hints of defensiveness emerge, like imposter syndrome. I also recognize that I desire to be abled and that keeps the conflict churning.
Microaggression Experiences Are Different Depending on Visibility of Disability
Six participants (6.6%) spoke to how individuals with hidden disabilities experience microaggressions differently than individuals with visible/apparent disabilities. P141 asserted that “because my disabilities are hidden, I don’t hear many microaggressions regarding me,” and P183 corroborated that microaggressions are “different the more severe and obvious the disabilities are.”
P146 suggested that “invisible disabilities offer up a whole different category of microaggressions than those with visible disabilities,” and P151 added that “hidden disabilities is [sic] a double edged sword,” highlighting both the privilege and the dismissiveness hidden disabilities can bring. P150 emphasized the privilege of others not knowing about their disability: “In some ways, this benefits me because I’m not associated with the stigma of a disability.”
Internalized Ableism
A small number of participants (n = 4) expressed comments that were consistent with Internalized Ableism. Internalized Ableism includes believing the stereotypes, myths, and misconceptions about PWD, such as the notion that all disabilities are visible and that PWD cannot live independently, and it can manifest as beliefs about their own disability or others’ disabilities. One manifestation of Internalized Ableism is when a PWD expresses that another’s disability is not real or true compared to their own disability. For example, P112 stated: “Every time I go out I have great difficulty finding available accessible parking. I watch & people using the spots are walking/functioning just fine. Sick of hearing about ‘hidden disability.’ I think the majority are inconsiderate lazy people.”
Another manifestation of Internalized Ableism can be when PWD deny the existence of ableist microaggressions. P183 shared:
I don’t think that most people have microaggressions toward PWD. Maybe that’s different the more severe and obvious the disabilities are. It tends to be older people like 60s or 70s that treat me differently period it seems like the younger generation just sees most of us as people not disabled people. And I also think the term ableist separates PWD and people without. If we don’t want to be labeled, we shouldn’t label them.
Microaggressions Include Identities Other Than Disability
For this final theme, four participants (4.44%) spoke to the complexity related to microaggressions when a PWD has additional nondominant cultural identities. P167 expressed the compounding effect: “I have multiple minoritized identities—the intersection leads to more biases.” P161 articulated the inherent confusion when one has multiple nondominant identities: “I do not know whether I am treated in the ways I indicated because of my disabilities or because I am a person of color.” These quotes highlight the inherent increase and subsequent impact on PWD who have more than one nondominant cultural identity.
Discussion
The purpose of our analysis was to illuminate participants’ lived experiences with ableist microaggressions that were important to them. We revealed contextual information about participants’ experiences that aligned with the AMS subscales (i.e., Minimization, Denial of Personhood, Otherization, and Helplessness). Although prior qualitative ableist microaggression studies (e.g., Coalson et al., 2022; Eisenman et al., 2020; Olkin et al., 2019) grounded their research in Keller and Galgay’s (2010) eight categories rather than in Conover et al.’s (2017a) four subscales, it is fair to say that our findings substantiate other researchers’ findings because Conover et al.’s four subscales were devised based on Keller and Galgay’s findings.
While the corroboration of prior research findings based on the AMS subscales is illustrative and essential, the crucial findings from this study lie in the unique themes that arose from the in vivo coding process (i.e., Fortitude/Resilience/Coping, Contextual Factors, Impact of Microaggressions/Ableism on Mental Health/Wellness, Microaggression Experiences Are Different Depending on Visibility of Disability, Internalized Ableism, and Microaggressions Include Identities Other Than Disability). These themes introduce both novel and less-explored aspects of disability and of ableist microaggressions.
Fortitude/Resilience/Coping is a unique theme. Participants described how they became stronger and persevered despite microaggressive experiences. Eisenman et al. (2020) were the first to identify microaffirmations within ableist microaggressions research and Coalson et al. (2022) found that their participants perceived benefits that came from microaggressive experiences; both are important contributions. However, both instances of seeming positives related to ableist microaggressions in these studies are framed within the context of how others acted toward PWD rather than the autonomous choices and personal development of the person with the disability in the face of adversity. Our findings demonstrate PWD’s abilities—both innate qualities and learned skills—that rendered life-giving fortitude, resilience, and coping in which they are personally empowered and persevere despite external stimuli; they are not dependent upon whether others act appropriately. This is a key finding for counselors because they have the ability to create a therapeutic environment in which PWD can process, develop, and refine their fortitude, resilience, and coping further, acknowledging that PWD have these skills already.
Unsurprisingly, some participants spoke to the impact of ableist microaggressions and ableism on their mental health and wellness; these impacts included depression, loneliness, stress, frustration, and feeling “pathetic and weak.” What was surprising is that only 9% of the sample spoke to this impact directly, given how well-documented the harmful mental health effects of microaggressions are (Sue & Spanierman, 2020). This seeming underrepresentation of mental health ramifications amongst participants led us to wonder, based on the high percentage of participants (30%) who endorsed Fortitude/Resilience/Coping, whether this specific sample had a uniquely high ability to cope with adversity as compared to the overall disability population or if it is possible that ableist microaggression experiences have begun to decrease. While we are unable to answer these questions directly as part of this study, we posit three considerations: (a) microaggressions continue to have a negative effect on some PWD and need to be screened for and attended to within the counseling process; (b) screening for and helping clients with disabilities name, develop, or refine coping, fortitude, and resilience can prove beneficial; and (c) it is worthwhile to continue to work to reduce microaggressive behaviors in every way possible.
Although we had an independent theme in which participants indicated the differences between apparent and hidden disabilities, the participant quotes within every theme illustrate these differences as well. For instance, within the Minimization theme, P137 highlighted that those with hidden disabilities may be told that “personal responsibility” is the cause of their disability, while P105 and P109 spoke to having to “prove” their apparent disability to others, including family. Having to prove one’s disability or not being believed tracks with several other researchers’ findings including Olkin et al. (2019), who found that medical professionals did not believe PWD’s symptoms and experiences. The Helplessness theme revealed differences such as P129 receiving unsolicited advice once people learn of their hidden disability; however, this theme revealed similarities, too. Participants with both apparent and hidden disabilities experienced others acting on their behalf without their consent.
The Microaggression Experiences Are Different Depending on Visibility of Disability theme may explain why a higher percentage of participants with hidden disabilities or those who have both hidden and apparent disabilities participated in the qualitative portion of the study than those with apparent disabilities, which was the higher percentage in the quantitative part of the study. By definition, microaggressions can leave those who experience them questioning whether what they experienced was real, and this could be compounded when PWD have hidden disabilities; these participants may have needed to express their experiences more than those with apparent disabilities. While our data demonstrate that having a hidden disability may be a protective factor from experiencing ableist microaggressions, their disability experience often can be overlooked or ignored, resulting in a form of minimization that is both congruent with and distinct from the Minimization subscale definition.
Participants made a case for how Contextual Factors, defined as relational, situational, and/or environmental components, impact microaggression experiences. Implicitly, several authors spoke to what we have named as Contextual Factors (e.g., Coalson et al., 2022; Eisenman et al., 2020; Miller & Smith, 2021), yet the specificity and nuance participants provided in this study warranted a distinct theme. Relationally, participants noted that whether the perpetrator knew them and if there was a relational power differential between them and the perpetrator (e.g., doctors or counselors vs. family member or neighbor) makes a difference. Damningly, P152 stated that “the worst comments” they have received “have come from mental health therapists.” Participants noted, too, that work environments, life stage, the type of assistive technology they are using at the time, and being part of the disability community can all be impactful in both affirming and deleterious ways. It is imperative that counselors assess and understand thoroughly each client’s specific contextual factors so they can identify ways in which clients have internal and external resources and support, as well as areas in which they may want strategies, support, resources, and, potentially, advocacy intervention.
A small number of participants (n = 4) spoke to Internalized Ableism. Although this was a less robust theme, it was important to report because it adds to professional knowledge about what some clients with disabilities might believe and express during counseling sessions. We defined Internalized Ableism as participants expressing stereotypes, myths, and misconceptions about PWD that can manifest as beliefs about their own disability or the disabilities of others. One participant expressed disdain for hidden disabilities and expressed disbelief about others’ needs to use parking for disabled persons, while another participant questioned whether most PWD experience ableist microaggressions. While our study findings are not congruent with these statements, counselors must take clients’ expressions seriously, work to understand how clients have developed these beliefs, and seek to understand their impact on the client who is stating them.
Finally, four participants indicated that Microaggressions Include Identities Other Than Disability. Given the high percentage of the sample that had multiple nondominant identities, it is curious that so few participants spoke to this phenomenon. However, we theorize that this may have to do with identity salience (Hunt et al., 2006) and the fact that this was a study about ableist microaggressions. For the participants who spoke to this theme, the important features they reported were the compounding effect of microaggressions when one has multiple nondominant identities and the inherent confusion that results from microaggressive experiences, particularly when one has multiple nondominant identities. Again, counselors must screen for and be prepared to address the complexity and the impact of ableist microaggressions based on each client’s unique identities and experiences.
Implications for Practice
The study findings illustrate the ubiquitous, troubling, and impactful nature of ableist microaggressions. These findings expose many counselors, supervisors, and educators to a world they may not know well or at all, while for others, these findings validate experiences they know all too well personally and professionally. We began this article with a quote from the pre-Socratic philosopher Heraclitus: “Day by day, what you choose, what you think, and what you do is who you become.” This quote captures the charge we are issuing to counseling professionals: It is time to take action to become counseling professionals who think as, act as, and are disability-affirming professionals. The task at hand is for each counseling professional to decide what steps to take next to strengthen their disability-affirming identity based on their current awareness, knowledge, and skill level, as well as how they can enact their disability-affirming identity based on their professional roles.
Fundamentally, disability-affirming professionals validate, support, encourage, and advocate for and with PWD consistently throughout their professional activities. For many, this begins with developing their awareness and knowledge, followed later by their skills. Based on the findings presented in this article, we suggest counseling professionals engage in self-reflexivity by examining the ways in which they have unwittingly adopted the dominant discourses about disability, what they believe about the abilities and lives of PWD, how they understand disability within the context of other nondominant identities, and the ways in which they have participated in perpetuating ableist microaggressions. Without engaging in disability self-awareness development, professionals risk conveying ableist microaggressions to clients that can result in early termination, impede the therapeutic relationship, and/or inflict additional psychological harm (Sue & Spanierman, 2020). For example, counselors may assume that clients with disabilities have diminished social–emotional learning skills compared to clients without disabilities and initiate formalized assessment based on this assumption. While counselors should be attuned to all clients’ social–emotional skills, it can be damaging to PWD’s sense of self and the counseling relationship to assume their social–emotional learning skills are deficient rather than assessing how environments are not conducive to PWD’s social–emotional needs (Lindsay et al., 2023).
Counselors’ self-reflexive process is meant to foster self-awareness; to better equip counselors to recognize ableist microaggressions in clients’ stories when they occur in personal, training, and professional environments; and for them to avoid unintentionally communicating ableist microaggressions in their practice. To start this process, we encourage counselors to question whether any of the study findings rang true, whether as someone who has experienced ableist microaggressions or as one who has perpetrated them, and to ascertain whether their attitudes and beliefs about PWD differ based on the visibility of disability. Additionally, we proffer that counselors who engage in self-reflective activities, such as the ones mentioned above, and those who learn more about PWD’s lives and experiences are more apt to create a plan to work through any negative attitudes or biases they have and, in turn, refine their skills so they are more disability-affirming in their practice. Counselors who engage in these processes will benefit those they serve, whether clients, students, or supervisees.
This study represents only a slice of the microaggression experiences of PWD. We concur with Rivas and Hill (2023) that counselors must adopt an evolving commitment to develop disability counseling effectiveness. Ways that counselors can take steps toward developing their disability-affirmative counselor identity and effectiveness include familiarizing themselves with and applying the American Rehabilitation Counseling Association (ARCA) disability competencies (Chapin et al., 2018); reading additional studies (e.g., Olkin et al., 2019; Peters et al., 2017); listening to podcasts (e.g., Swenor & Reed, n.d.); reading blogs and books (e.g., Heumann & Joiner, 2020); and watching shows and movies that highlight PWD’s experiences, microaggressive and otherwise—PWD are telling their stories and want others to learn from them.
Within the relational context, no matter one’s professional roles, it is important to be prepared to attend to the interaction of identity constellations within professional relationships and the power dynamics that are present (Ratts et al., 2016). Broaching these topics initially, including ability status and similarities and differences with our experiences, is a helpful start; however, this is the beginning of the process, not the entire process. Accordingly, clinicians must continually assess PWD’s contextual factors and their impact, lived experiences of their multiple identities, resilience, fortitude, and coping skills. To do so, clinicians must first create space for clients to process their microaggression experiences through actively listening to their stories; allowing PWD to openly express their frustrations, anger, or other emotions; and validating their experiences using advanced empathy. In other words, it is critical not to dismiss such topics nor unilaterally make them the presenting problem—balance is needed to attend to microaggression experiences appropriately. Essentially, counselors need to guide clients to discern the impact and to identify what they need rather than doing it for them, and to be ready, willing, and able to advocate with and on behalf of clients. All advocacy actions must be discussed with clients so as to center their autonomy.
Clients’ resiliencies and strengths must be fostered unceasingly. It is not uncommon for clients who have experienced ableist microaggressions to feel diminished and worthless and to question their purpose. Counselors must prioritize assisting clients in naming their strengths and telling stories about how they have developed resiliencies, and they must encourage clients to draw on both when facing adversity—particularly ableist microaggressions. While the goal is to eradicate ableist microaggressions, we must reinforce with clients that they are armed with tools to safeguard against ableist microaggressions’ impact and that they can seek trusted support when they need it.
As we move forward into the future as disability-affirming counseling professionals, counselor educators and supervisors have a specific charge to include disability status and disability/ableist microaggressions as part of their professional endeavors when working with students and supervisees. For many, the aforementioned recommendations likely apply because they, too, did not receive education about disability and disability microaggressions (Deroche et al., 2020). This is a setback, but not a limitation. Counselor educators and supervisors are continual learners who seek additional awareness, knowledge, skills, and advocacy actions to positively impact their work with counselors-in-training. Webinars, disability-specific conference sessions, and engaging with community disability organizations are helpful ways to start, and we recommend counselor educators and supervisors engage in the same self-examination strategies mentioned above to begin combating any biases they may hold about PWD. More specifically, counselor educators and supervisors can introduce and teach the ARCA disability competencies to trainees and supervisees, deliberately integrate self-exploration activities regarding disability into coursework, direct trainees and supervisees to inquire about ability status in intake and assessment procedures, and use cultural broaching behaviors to model appropriate use with clients (Deroche et al., 2020).
Limitations and Future Research
There are important limitations to consider to contextualize the study findings. The data used in this analysis were the result of one open-ended prompt as part of a larger quantitative study. Although participants offered robust and illustrative responses, it is a significant limitation that no follow-up questions were asked. Additionally, because the study utilized the AMS (Conover et al., 2017b), we analyzed data using the AMS subscales. While this was an appropriate choice given the context, it limited our ability to compare our findings with other qualitative studies that used Keller and Galgay (2010) to explain their findings.
We recommend that future research investigates the unique themes from this study in more detail to ascertain whether they are applicable to the larger PWD population. We suggest that focus groups combined with individual interviews may help to tease out nuances and could potentially lead to developing theory related to ableist microaggressions and best practices that will support PWD. Finally, we propose that more in-depth intersectionality research would benefit PWD and the professionals who serve them. The confounding nature of microaggressions combined with individuals’ unique identity compositions that often include both nondominant and dominant identities can make this type of research challenging, yet both are the reality for many PWD and this research is therefore needed.
Conclusion
Ableist microaggressions are ubiquitous and damaging to PWD. Through our analysis, we found that participants’ experiences corroborated prior researchers’ findings related to established ableist microaggression categories and added new knowledge by introducing six novel themes. We envision a disability-affirmative counseling profession and offered concrete recommendations for clinicians, supervisors, and counselor educators. Together, we can create a reality in which all PWD who seek counseling services will experience relief, validation, and empowerment as we work to create a society that provides access to all.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Boyatzis, R. E. (1998). Transforming qualitative information. SAGE.
Chapin, M., McCarthy, H., Shaw, L., Bradham-Cousar, M., Chapman, R., Nosek, M., Peterson, S., Yilmaz, Z., & Ysasi, N. (2018). Disability-related counseling competencies. American Rehabilitation Counseling Association (ARCA) Task Force on Competencies for Counseling Persons with Disabilities. https://arcaweb.org/wp-content/uploads/2023/12/ARCA-Disability-Related-Counseling-Competencies.pdf
Coalson, G. A., Crawford, A., Treleaven, S. B., Byrd, C. T., Davis, L., Dang, L., Edgerly, J., & Turk, A. (2022). Microaggression and the adult stuttering experience. Journal of Communication Disorders, 95, 106180. https://doi.org/10.1016/j.jcomdis.2021.106180
Conover, K. J., Israel, T., & Nylund-Gibson, K. (2017a). Development and validation of the Ableist Microaggressions Scale. The Counseling Psychologist, 45(4), 570–599. https://doi.org/10.1177/0011000017715317
Conover, K. J., Israel, T., & Nylund-Gibson, K. (2017b). Ableist Microaggressions Scale (AMS) [Database record]. APA PsycTESTS. https://doi.org/10.1037/t64519-000
Dávila, B. (2015). Critical race theory, disability microaggressions, and Latina/o student experiences in special education. Race, Ethnicity, and Education, 18(4), 443–468. https://doi.org/10.1080/13613324.2014.885422
Deroche, M. D., Herlihy, B., & Lyons, M. L. (2020). Counselor trainee self-perceived disability competence: Implications for training. Counselor Education and Supervision, 59(3), 187–199. https://doi.org/10.1002/ceas.12183
Deroche, M. D., Ong, L. Z., & Cook, J. M. (2024). Ableist microaggressions, disability characteristics, and nondominant identities. The Professional Counselor, 13(4), 404–417. https://doi.org/10.15241/mdd.13.4.404
Eisenman, L. T., Rolón-Dow, R., Freedman, B., Davison, A., & Yates, N. (2020). “Disabled or not, people just want to feel welcome”: Stories of microaggressions and microaffirmations from college students with intellectual disability. Critical Education, 11(17), 1–21.
Heumann, J., & Joiner, K. (2020). Being Heumann: An unrepentant memoir of a disability rights activist. Beacon Press.
Hunt, B., Matthews, C., Milsom, A., & Lammel, J. A. (2006). Lesbians with physical disabilities: A qualitative study of their experiences with counseling. Journal of Counseling & Development, 84(2), 163–173. https://doi.org/10.1002/j.1556-6678.2006.tb00392.x
Keller, R. M., & Galgay, C. E. (2010). Microaggressive experiences of people with disabilities. In D. W. Sue (Ed.), Microaggressions and marginality: Manifestation, dynamics, and impact (pp. 241–268). Wiley.
Lindsay, S., Fuentes, K., Ragunathan, S., Lamaj, L., & Dyson, J. (2023). Ableism within health care professions: A systematic review of the experiences and impact of discrimination against health care providers with disabilities. Disability and Rehabilitation, 45(17), 2715–2731. https://doi.org/10.1080/09638288.2022.2107086
MacQueen, K. M., McLellan, E., Kay, K., & Milstein, B. (1998). Codebook development for team-based qualitative analysis. Cultural Anthropology Methods, 10(2), 31–36. https://doi.org/10.1177/1525822X980100020301
Miller, R. A., & Smith, A. C. (2021). Microaggressions experienced by LGBTQ students with disabilities. Journal of Student Affairs Research and Practice, 58(5), 491–506. https://doi.org/10.1080/19496591.2020.1835669
Norwood, M. F., Lakhani, A., Hedderman, B., & Kendall, E. (2022). Does being psychologically resilient assist in optimising physical outcomes from a spinal cord injury? Findings from a systematic scoping review. Disability and Rehabilitation, 44(20), 6082–6093. https://doi.org/10.1080/09638288.2021.1952320
Olkin, R., Hayward, H., Abbene, M. S., & VanHeel, G. (2019). The experiences of microaggressions against women with visible and invisible disabilities. Journal of Social Issues, 75(3), 757–785. https://doi.org/10.1111/josi.12342
Ordway, A. R., Johnson, K. L., Amtmann, D., Bocell, F. D., Jensen, M. P., & Molton, I. R. (2020). The relationship between resilience, self-efficacy, and employment in people with physical disabilities. Rehabilitation Counseling Bulletin, 63(4), 195–205. https://doi.org/10.1177/0034355219886660
Patel, D. R., & Brown, K. A. (2017). An overview of the conceptual framework and definitions of disability. International Journal of Child Health and Human Development, 10(3), 247–252.
Perrin, P. B. (2019). Diversity and social justice in disability: The heart and soul of rehabilitation psychology. Rehabilitation Psychology, 64(2), 105–110. https://doi.org/10.1037/rep0000278
Peters, H. J., Schwenk, H. N., Ahlstrom, Z. R., & Mclalwain, L. N. (2017). Microaggressions: The experience of individuals with mental illness. Counselling Psychology Quarterly, 30(1), 86–112. https://doi.org/10.1080/09515070.2016.1164666
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Rivas, M., & Hill, N. R. (2023). A grounded theory of counselors’ post-graduation development of disability counseling effectiveness. Journal of Counselor Preparation and Supervision, 17(1). https://digitalcommons.sacredheart.edu/jcps/vol17/iss1/7
Rolón-Dow, R., & Davison, A. (2018). Racial microaffirmations: Learning from student stories of moments that matter. Diversity Discourse, 1(4), 1–9. https://udspace.udel.edu/server/api/core/bitstreams/4230ddcd-b196-4ee2-a5bf-18120b2b1f24/content
Rolón-Dow, R., & Davison, A. (2021). Theorizing racial microaffirmations: A critical race/LatCrit approach. Race Ethnicity and Education, 24(2), 245–261. https://doi.org/10.1080/13613324.2020.1798381
Sue, D. W., Capodilupo, C. M., Torino, G. C., Bucceri, J. M., Holder, A. M. B., Nadal, K. L., & Esquilin, M. (2007). Racial microaggressions in everyday life: Implications for clinical practice. American Psychologist, 62(4), 271–286. https://doi.org/10.1037/0003-066X.62.4.271
Sue, D. W., & Spanierman, L. (2020). Microaggressions in everyday life (2nd ed.). Wiley.
Swenor, B., & Reed, N. (Hosts). (n.d.). Included: The disability equity podcast [Audio podcast]. Johns Hopkins University Disability Health Research Center. https://disabilityhealth.jhu.edu/included
Jennifer M. Cook, PhD, NCC, ACS, LPC, is an associate professor at the University of Texas at San Antonio. Melissa D. Deroche, PhD, NCC, ACS, LPC-S, is an assistant professor at Tarleton State University. Lee Za Ong, PhD, LPC, CRC, is an assistant professor at Marquette University. Correspondence may be addressed to Jennifer M. Cook, University of Texas at San Antonio, Department of Counseling, 501 W. Cesar E. Chavez Blvd, San Antonio, TX 78207, jennifer.cook@utsa.edu.
May 22, 2024 | Volume 14 - Issue 1
Rebekah Cole, Christine Ward, Taqueena Quintana, Elizabeth Burgin
Military spouses face many challenges as a result of the military lifestyle. Much focus has been placed on enhancing the resilience of military spouses by both the military and civilian communities. However, no research currently exists regarding spouses’ perceptions of their resilience or how they define resilience for themselves and their community. This qualitative study explored the perceptions of eight military spouses regarding their resilience through individual semi-structured interviews. The following themes emerged: 1) shaped by service member and mission priority; 2) challenges within the military lifestyle; 3) outside expectations of spouse resilience; 4) sense of responsibility for family’s resilience; 5) individual resilience; and 6) collective resilience. We discuss ways military leadership and the counseling profession can best understand and enhance the resilience of military spouses.
Keywords: military spouses, resilience, military lifestyle, perceptions, counseling
Because of the unique stressors associated with the military lifestyle, military spouses are at an increased risk for poor mental health (Donoho et al., 2018; Mailey et al., 2018; Numbers & Bruneau, 2017). They may experience mental health concerns, such as anxiety and depression, due to a number of reasons, including separation from their deployed service member, loss of support networks after a relocation, or issues with adjusting to the uncertain and frequent changes of the military (Cole et al., 2021). Additional concerns that arise, such as employment, marital, and financial issues, can also negatively affect the military spouse’s mental health (Cole et al., 2021; Mailey et al., 2018). Dorvil (2017) reported that 51% of active-duty spouses experience more stress than normal. Furthermore, 25% of military spouses meet the criteria for generalized anxiety disorder (Blue Star Families [BSF], 2021). Depression in military spouses is also higher than the rate found within the general population (Verdeli et al., 2011). As a military spouse casts aside their own personal needs to support their service member, stressors may continue to increase, which can contribute to the rise of mental health needs of military spouses (Moustafa et al., 2020).
Resilience and Military Spouses
Nature of Resilience
Given the challenges inherent in the military lifestyle and the associated mental health risks, military spouse resilience is essential. Resilience is a complex and multifaceted construct, significant to researchers, practitioners, and policymakers across numerous disciplines, including mental health and military science. The American Psychological Association (2020) defined resilience as “the process of adapting well in the face of adversity, trauma, tragedy, threats, or even significant sources of stress” (para. 4). Within the military community, resilience has been defined as the ability to withstand, recover, and grow in the face of stressors and changing demands (Meadows et al., 2015). Importantly, determinants of resilience include the interaction of biological, psychological, social, and cultural factors in response to stressors (Southwick et al., 2014). In addition to these salient variables embedded in resilience science, resilience may be operationalized as a trait (e.g., optimism), process (e.g., adaptability in changing conditions), or outcome (e.g., mental health diagnosis, post-traumatic growth; Southwick et al., 2014).
Resilience may also vary on a continuum across domains of functioning (Pietrzak & Southwick, 2011) and change as a function of development and the interaction of systems (Masten, 2014). Accordingly, a definition and operationalization of resilience may vary by population and context (Panter-Brick, 2014). During the post-9/11 era, the resilience of service members and their families received significant attention from stakeholders, including the Department of Defense (DoD) and National Academies of Sciences, Engineering, and Medicine (NASEM), both of which expressed a commitment to conducting research and establishing programming to enhance service member and military family resilience, resulting in increased awareness of the importance of service member and family resilience throughout the military community (NASEM, 2019).
Military Family Resilience
Though military families share the characteristics and challenges of their civilian counterparts, they additionally experience the demanding, high-risk nature of military duties; frequent separation and relocation; and caregiving for injured, ill, and wounded service members and veterans (Joining Forces Interagency Policy Committee, 2021). In recognition of the constellation of military-connected experiences military families face, the Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (DCoE) commissioned a review of family resilience research and relevant DoD policies to inform a definition of resilience for appropriate application to military spouses and children (Meadows et al., 2015). Meadows and colleagues (2015) proposed family resilience may be best defined as “the ability of a family to respond positively to an adverse situation and emerge from that situation feeling strengthened, more resourceful, and more confident than its prior state” (see Simon et al., 2005, for a further exploration of family resilience). Further, Meadows and colleagues identified two groups of policies delineated at the Joint Chiefs of Staff or DoD levels, or within individual branches of the military: 1) existing programs modified to augment resilience or family readiness, and 2) new programs developed to target family resilience. Programs established by these policies support access to mental health services (e.g., DoD Instruction [DoDI] 6490.06); parenting education (e.g., New Parent Support Program, DoDI 6400.05); child welfare (e.g., Family Advocacy Program, DoD Directive 6400.1); and myriad physical, psychological, social, and spiritual resources. The well-being of military families represents a critical mission for the DoD, extending beyond provision and access for families to meet their basic needs to individual service member and unit readiness, and the performance, recruitment, and retention of military personnel (NASEM, 2019).
Military Spouse Resilience
Though service member and family resilience are critical for accomplishing the DoD’s mission, focusing on the unique nature of military spouse resilience is key for understanding and supporting this population’s resilience. Counseling, psychology, sociology, and military medical professional research related to military spouse resilience has focused primarily on characteristics associated with resilience. In a study by Sinclair et al. (2019), 333 spouse participants completed a survey regarding their resilience, mental health, and well-being. The results revealed that spouses who had children, were a non-minority, had social support, had less work–family conflict, and had a partner with better mental health were more resilient. Another survey study examined the characteristics associated with resilience in Special Operations Forces military spouses, determining that community support and support from the service member was essential for spouse resilience (Richer et al., 2022). A study conducted within the communication field also explored spouses’ communicative construction of resilience during deployments. Qualitative data analysis of interviews with 24 spouses indicated how spouses use communication to reconcile their contradictory realities, which increases their resilience (Villagran et al., 2013). This resilience has also been found to be a protective factor against depression and substance abuse during military deployments (Erbes et al., 2017). Finally, a survey study of Army spouses (N = 3,036) determined that spouses who were less resilient were at higher risk for mental health diagnoses (Sullivan et al., 2021). While these studies explored the nature of resilience demonstrated by military spouses, our searches in JSTOR, PubMed, ERIC, PsycINFO, and Google Scholar did not reveal any studies regarding spouses’ perceptions of their own resilience or how they define this resilience for themselves and their community. Our study fills that research gap by exploring active-duty spouses’ perceptions and definitions of resilience.
Methods
The purpose of this qualitative study was to explore the perceptions of active-duty spouses regarding their resilience. This study was guided by the following research questions: 1) What are military spouses’ perceptions of their own resilience? and 2) How do military spouses define “resilience?” Phenomenology seeks to present a certain phenomenon in its most authentic form (Moustakas, 1994). In order to most authentically and openly describe our participants’ experiences, we chose a qualitative transcendental phenomenological approach to frame our study. This tradition of qualitative research focuses on portraying a genuine representation of the participants’ perceptions and experiences. However, the distinct feature of transcendental phenomenology is its first step, which involves the researchers recognizing and bracketing their biases so they can analyze the data without any interference (Moerer-Urdahl & Creswell, 2004). We selected this design because each of our research team members were military spouses. We therefore recognized the need to mitigate our biases in order to give a true representation of the participants’ perceptions, free from our own preconceived notions.
Participants
The participants in this study were selected based on their status as active-duty military spouses and their willingness to participate in the study. There were no other inclusion or exclusion criteria for the participants in this study. After gaining IRB approval, we used convenience sampling to recruit eight participants. In qualitative research, convenience sampling is used to recruit participants who are closely accessible to the researchers (Andrade, 2021). Our research team emailed participants that we knew through living, working, and volunteering on military bases throughout the United States and at overseas duty stations who fit the active-duty military spouse criteria for this study and asked them if they were willing to participate in the study. Once the participants expressed interest, they were provided with an information sheet regarding the study’s purpose and the nature of their involvement in the study. Participant demographics are included in Table 1. All of the participants were female and all were between the ages of 30–40. Four branches of the U.S. military, including Army, Navy, Air Force, and Marine Corps, were represented in the sample. No reservist, Coast Guard, or Space Force military spouses participated in our study. Five of our participants were White and three were Black. Their tenure as military spouses ranged from 4 years to 17 years. Five of the spouses were married to a military officer, while three of the participants were married to an enlisted service member. After interviewing these eight participants, our research team met and determined that because of the distinct common patterns we found across each of the participants’ transcripts, we had reached saturation and did not need to recruit any additional participants for our study (Saunders et al., 2018).
Table 1
Participant Demographics
| Participant |
Age |
Ethnicity |
Gender |
Branch |
Spouse’s Rank |
Years as a Spouse |
| 1 |
33 |
Black |
Female |
Air Force |
Enlisted |
4 |
| 2 |
36 |
Black |
Female |
Navy |
Enlisted |
17 |
| 3 |
31 |
White |
Female |
Army |
Officer |
7 |
| 4 |
34 |
Black |
Female |
Navy |
Enlisted |
14 |
| 5 |
36 |
White |
Female |
Marine Corps |
Officer |
12 |
| 6 |
35 |
White |
Female |
Marine Corps |
Officer |
14 |
| 7 |
40 |
White |
Female |
Navy |
Officer |
16 |
| 8 |
34 |
White |
Female |
Navy |
Officer |
10 |
Data Collection
Our research team first developed the interview protocol for the study based on a thorough review of the literature regarding resiliency within military culture as well as the challenges of the military lifestyle for military spouses. Our research team members interviewed each of the participants for 1–2 hours. These semi-structured interviews were audio recorded and transcribed verbatim by an automated transcription service. The interview questions were open-ended and focused on the spouses’ definitions of resilience and their perceptions of their resilience within the military lifestyle and culture (see Appendix for interview protocol). In addition, probing questions such as “Can you explain that a bit more?” or “Can you give any examples of what you mean by that?” were used to gather more in-depth data throughout the interviews.
Data Analysis
We followed the steps of the transcendental phenomenological data analysis process to analyze our study’s results (Moerer-Urdahl, 2004). First, each member of our research team engaged in epoche, in which we bracketed our biases as military spouses so that our own thoughts, feelings, perceptions, and experiences did not influence our interpretation of our participants’ experiences. The next step in the process was horizontalization. During this step, each member of our research team read through the interview transcripts and noted significant statements throughout so we could better understand how the participants perceived, understood, and experienced resilience. Next, we met as a research team to discuss these significant statements and organize them into themes (Moustakas, 1994). Our research team then developed textual and structural descriptions of the themes, describing not only a list of the participants’ perceptions, but also an in-depth analysis of what their perceptions of resilience entailed and how they have experienced it throughout their tenure as military spouses (Moerer-Urdal, 2004; Moustakas, 1994). We then constructed a comprehensive description of the participants’ perceptions of resilience, encapsulating the “essence of the experience” (Moerer-Urdal, 2004, p. 31).
Research Team and Strategies to Increase Trustworthiness
Our research team consisted of four university faculty members, all of whom possessed extensive experience in conducting qualitative research. Three of our research team members possess PhDs in counseling and one research team member possesses an EdD in counseling. All team members had extensive experience conducting research with military-connected communities. In addition, all of our research team members were active-duty military spouses, with years of experience as a military spouse ranging from 1–23 years.
We used several strategies to increase the credibility of our results. First, the use of an experienced research team to collectively analyze the data resulted in diverse perspectives on the emerging themes of the study. However, because each member of our research team was a military spouse, we recognized the need to bracket our own experiences and biases so that they did not interfere with our interpretation of the data. Each team member took notes on their individual biases, and our research team discussed these biases when interpreting themes. Biases held by research team members included a predisposition to believe that spouses of special warfare service members endured greater stressors and were better supported by their military communities; a belief that spouses of higher-ranking service members possessed greater knowledge of and access to resources to support social, behavioral, and mental health needs; and personal experience within the military spouse community. These biases were challenged throughout the research process by each member of the team. As each theme was identified, the team referenced individual transcripts to ensure that the interpretation was justified. We found that our biases were rightfully challenged.
Additionally, to avoid leading questions, our research team made the conscious decision not to define resilience as part of the interview and follow-up process. The team wanted to derive an organic definition of spouse resilience that was not clouded by a formal definition. In addition, we used member checking, in which we emailed the interview transcripts to the participants and asked them to verify the data. The participants responded to our request with minimal change requests related to grammatical errors in the transcriptions and validated our data. Several offered additional insight related to their definition of resilience, which was included in our data analysis.
Results
The following themes emerged from our data: 1) shaped by service member and mission priority; 2) challenges within the military lifestyle; 3) outside expectations of spouse resilience; 4) sense of responsibility for family’s resilience; 5) individual resilience; and 6) collective resilience.
Theme 1: Shaped by Service Member and Mission Priority
Military/Service Member Definition
When discussing their definition of resiliency, the spouses first considered what resiliency meant for their active-duty spouse. The participants varied in their perceptions of what resilience meant for their active-duty service member, though all defined resilience as an active process of adapting or persevering when faced with adversity, rather than a personal trait or characteristic the service member possesses. Participant 3 noted that, for their spouse, resilience was “the ability to adapt to changes that are beyond your control . . . adapting to situations in an optimistic and positive way.” Participant 6 stated that resilience for their spouse meant an “ability to bounce back from a hardship.” One participant asked their spouse to comment specifically about their definition and provided the following definition in a follow-up with the interviewer: “Resilience is how you persevere in difficult circumstances. It’s not about how hard you fall, but how quick you can get back up from being knocked down” (Participant 2 [P2]).
Some participants cited specific notions of resilience that are embedded in the service members’ military community. One Navy spouse remarked that resilience, to their spouse, meant “Don’t give up the ship” (P8). Another Navy spouse mentioned that for their spouse, resilience was “knowing how to weather the storm” (P7). Yet another spouse noted that resilience “the Marine Corps way” meant their service member must “do their job” (P4). Other participants noted that the root of resilience for the military service member stems from a place of selfless service. Participant 8 commented that the resiliency of their spouse was “more about the man standing next to me, the family I’m fighting for at home, the country I’m fighting for at home, than about their own personal needs.”
Adapting, Overcoming, and Persevering
Like their active-duty members, spouses indicated that resilience was about adapting, overcoming, and persevering in the face of obstacles. Resilience to one spouse was “being able to rebound or to overcome an obstacle” (P1); to another, resilience meant they must “be flexible, adapt with whatever, overcome whatever it is that you’re going through” (P2). Spouses noted that resilience was not a one-time event. Instead, spouses suggested that their own resilience stemmed from continually persevering. Participant 6 stated that for them, resilience meant not just “going through something difficult and making it out on the other side,” but that they then had to “keep pushing forward.” One participant indicated that their personal definition of resilience and the notion to persevere stemmed directly from their spouse: “I’ve almost kind of adopted a bit of my husband’s thought process, I guess. You just keep going to get things done” (P8).
Mindset
Our participants indicated that resilience was a mindset that one must choose and that when faced with difficulties, they chose to focus on gratitude, positivity, and growth. For example, Participant 8 stated that, although they had faced and would continue to face challenging and stressful experiences as a result of being a military spouse, they believed that “whatever may come, we’ve been very blessed in our life and we should always be thankful for the life that we have.” Another participant noted that for them, overcoming and persevering meant adopting an optimistic attitude. Specifically, the spouse stated, “sometimes you just have to kinda look at the bright side of things, and you have to find the things that work for you at each place” (P5). One participant drew resilience from a growth mindset:
I think it [resilience] is really a mindset switch. I think it’s changing from “oh this is happening to me, how horrid” to like “how can I take this horrid situation and turn it into something good?” And I think that is a big mindset switch. (P7)
Resilience Variations
Walsh (2012) described risk and resilience as a process of balancing risk and protective factors over the life span. Participants in our study expanded on that idea by suggesting that they reacted to situational challenges along a continuum:
I think what I’m saying is there’s different levels of resilience, like sometimes you have to tap into that different part of yourself. Sometimes you have to let it go and just accept the things that come, and sometimes you just gotta pick yourself up and keep on trucking. (P8)
Likewise, Participant 3 suggested that resilience takes different forms depending on the situation:
Sometimes resiliency just means like surviving day to day and other times, it means figuring out how to continue with your passions to the best of your ability while also supporting your family and your [service member spouse]. I think it’s just super unique to every situation. (P3)
Our participants also recognized that their understanding of resilience was often focused on the here and now of their situation but that their reactions to stressors had long-term effects. One participant indicated that resilience is a learning process and recognized that the stressors they overcome now prepare them to address stressors they will face in the future: “I think being able to come out of extremely, extremely stressful situations, be able to come out on the other side and [know] I’m okay and I survived this, and now I’m kind of better prepared for next time” (P6). Participant 3 wondered about the long-term ramifications of resilience in the face of prolonged adversity, stating “I may be resilient right now in the moment, but in the long term, like, how will this affect me?”
Individualized
Finally, participants defined resilience as an individualized process, stating things such as “everybody has their own unique ways of being resilient, and I think that they do what works best for their families” (P7) and “my resiliency may look different than someone else’s resiliency” (P2). One participant elaborated on this individualized approach to resilience by recognizing that each person has different risk factors that affect their response to stressors, thus affecting the way each person demonstrates resilience. This participant stated that, when viewing resilience among military spouses as a whole, it is important to
take into consideration somebody’s upbringing and the baggage that they bring into this life. We don’t know what people have gone through as kids, and that I think would have a big impact on whether or not someone can be resilient, so I don’t think it’s a one-size-fits-all. (P6)
Theme 2: Challenges Within the Military Lifestyle
Lack of Control
The spouses described the common challenges of the military lifestyle to their resilience. First, they discussed the stress of the feeling of a lack of control in their lives. One participant described how she
just found out yesterday that my husband was getting deployed and he’s leaving Sunday. And I keep hearing people say, “You have to be resilient. You’re gonna be okay!” You’re resilient, but right now, what it feels like is how much can you endure for the sake of the mission? (P1)
Another echoed this sentiment: “I have no control if the Navy says they’re going to deploy my husband. There’s nothing I can do to change that” (P8).
Constant Changes
Another common challenge mentioned among all of the participants was the constant changes they experience in their lives, including moving, career changes, and changes within their family dynamics. Because they move every few years, the spouses described how they are constantly separated from their support systems: “Even though you meet these great people, you don’t get to stay with them . . . and you’re generally not near your family, which is very hard” (P5). Another described how “Once I have started on something and I’m like, ‘This is it, we gon’ be here for a while,’ then my husband is like ‘nope. Military said we got to shift and move again’”(P2).
These constant changes resulted in career struggles for the spouses. One asked, “How can I get this [job] if I’m never at one place for long? . . . How do I uproot everything that I know or everything that I am doing to follow my service member?” (P2). Another described how “moving, changing jobs, not being able to have a secure profession, you do it because you have to . . . but that doesn’t mean that there’s not a whole lot of emotional and mental load that goes with it” (P3).
Another challenge for military spouses was constantly changing family dynamics. One described the difficulty in constantly changing work schedules: “We have to kind of get into this routine without him and then when he comes back, because it’s different while he’s away. We gotta kind of try to fit him back into our routine when he gets back” (P4). Another discussed the challenge of transitioning to being the sole caregiver during a deployment: “If I go down with COVID, what am I going to do? Because, like, I was literally IT. No one is going to want to take my kids. . . . That was the first time I ever felt, like, fearful” (P7).
Mission Priority
In addition to constant change, the spouses also mentioned the challenges of the military’s clear prioritization of the mission above military members and their families: “If something is going on at home, we’re going to take care of our active person first and worry about your family later” (P2). The participants described how this focus on the mission is so intense that it affects service members physically, which increases the burden on military spouses to care for them: “My husband’s health suffers because the mission is most important to him” (P1).
Theme 3: Outside Expectations of Spouse Resilience
Expectation to “Suck It Up”
The spouses described others’ expectations for their resilience. First, they described the military’s expectation that they “suck it up.” One described how “you have a lot of the ‘suck-it-up’ mentality, and I would say when you have the leaders who kind of fall under that, whether it’s seeking the mental health treatment or having stigmas with that” (P6). Another explained that “there’s so much focus and emphasis on just being resilient and sucking it up” so there is often a mindset of “‘Oh well, military spouses are resilient so they signed up for this, they know what it takes and they just have to get over it’” (P3). Another spouse described how “they put so much pressure on you to be like, just make it work, that you’ve gotta figure out the way to make yourself happy, and that’s hard to do” (P5). Participant 7 summed up the military spouse mentality as a whole: “You toughen up and you make it work. You know?”
The participants felt their overall resilience would be enhanced if individuals outside the military community better understood the challenges faced by military families. One participant felt the “suck it up” mentality stemmed less from the military community itself and more from outside communities who might not understand the struggles of military family life: “So when . . . you’re going through another stress of a PCS [permanent change of station], you can’t find a house, they say, well, at least you get a house allowance, at least you get free health care” (P6). Participant 3 expanded on this idea by stating, “I just honestly think that a greater understanding of what sacrifices that military spouses make . . . would increase resiliency, because there’s just so much lack of understanding what it actually entails.” Lastly, one participant mentioned a sentiment they frequently hear from others in a civilian community, expressing that it was frustrating when friends outside the military told her, “I don’t know how you do it,” to which the participant responded, “I don’t know, you just do it!”
Pressure to Be Resilient
The spouses also expressed frustration at others’ misperceptions of the expectation that they and their families demonstrate resilience: “When we call military spouses or children resilient, it just seems like a cop out and relinquishes any type of burden . . . or feeling of guilt about a situation that may cause emotional or mental damage” (P3). Another participant echoed this frustration: “Sometimes I don’t feel like I’m being resilient. Sometimes I feel like I’m just doing what needs to be done because that’s what needs to be done” (P8). Another participant described how her friends
call me Superwoman because I have all these different things going on and I always seem like I got it together. . . . It’s like saying to me that I have to keep going, no matter what, and I think people should be able to just feel defeated sometimes. Or be able to say “that was just too much for me” or “I don’t really feel like being resilient today, I kind of want to lay in bed and just be upset or sad.” (P4)
Given these expectations, one spouse pointed out the danger of expecting military children to consistently demonstrate resilience:
It’s so easy for everyone to say that military kids are always so resilient and sometimes they’re not. Sometimes they are stressed out. They are feeling the crushing weight. They feel sad but everyone keeps telling them that they’re resilient. So it almost makes it seem like . . . they aren’t allowed to feel those hard things or talk about those things or act on those feelings and emotions. (P8)
One spouse proposed a solution to these misperceptions, emphasizing that resilience is unique for military spouses and should be defined to accurately reflect the way they uniquely overcome challenges:
I think it’s important for military spouses to reappropriate that term [resilience] so that it is not weaponized, and I would like to see some sort of guidance as to how we can be resilient but in a way that positively impacts our mental health and physical health and not having to endure all of the things and all of the frustration and uncertainty that comes with the onset of having to be resilient. (P1)
Theme 4: Sense of Responsibility for Family’s Resilience
With their partners focused on the mission, the spouses described their sense of responsibility to maintain their resilience so they can care for their children in the absence of their active-duty spouse: “We have our husband or our spouses gone so much, we need to be a solid parent at home for our kiddos or our family” (P7). Participant 4 likewise described how “I kind of see myself as holding down the fort, you know, because when my husband is not home it is just me and the kids.” Another explained how “I have three little ones that’s looking up to me and I can’t slip away, depressed, because daddy’s not home” (P2). In the end, the spouses defined resilience as an obligation to their families. Participant 3 described that “I have to be that way for my children.” Participant 4 added that “I think that’s what resilience is like, knowing that you kind of have to carry the load, you know, for your whole family to try to keep us afloat.”
The participants described how this resilience is especially obligatory when the active-duty spouse is unable to be resilient:
I’m kind of taking the lead with our kids . . . but I’ve also kind of had to pour into my husband, you know, because he has those times you know where things are really, really hard for him. I’ve also been like his counselor and his doctor sometimes. (P4)
Theme 5: Individual Resilience
In response to being unable to control many aspects of the military lifestyle, most of the spouses described how they have become independent in order to withstand the constantly changing variables within the military lifestyle. One described being “pretty independent, and I think that helps a lot because I don’t rely on my spouse to do all these things I do” (P5). Another described how being independent resulted in self-confidence and resilience:
You gotta figure out how to do all of it just because you can’t ever rely on the spouse being able to help. But I think being able to come out of extremely, extremely stressful situations, be able to come out on the other side and say “I’m okay, and I survived this, and now I’m kind of better prepared for next time.” (P6)
Another spouse described how maintaining an independent identity was key to separating herself from the stressors of the military lifestyle: “That’s a really important part of being a military spouse. It doesn’t have to be a job specifically, but just something that you can be your own person separate from your husband or your spouse’s job” (P8).
The spouses also described the importance of taking care of themselves physically and mentally in order to maintain their resilience. Many described exercise as key to their mental health and wellness: “My biggest coping mechanism is exercise. I’ve found that no matter where I go, I can exercise” (P5). Another spouse described how she “tried to find a kickball team every place we’ve been to since Okinawa because I figured out it’s a stress relief” (P6). Participant 7 echoed that “working out . . . just helps me. It lowers my stress.” One spouse explained how she defaults to exercise when facing the challenges of the military lifestyle because she knows her “ability to recover quickly is directly tied to the way in which I care for myself” (P1).
Theme 6: Collective Resilience
The participants described their reliance on the collective military spouse community for their survival. One spouse, for example, described a connection with other military spouses as the difference between “doing well and barely surviving” (P6). Another spouse described her reliance on the military spouse community: “Community is what it’s all about. I can’t get through anything without community” (P7). Another spouse echoed this survival mechanism: “This is a beautiful community. It’s an amazing place . . . we all get each other. So I think there are times where it’s really hard . . . but we survive, we get through it. We’re resilient. We got the grit” (P7). Participant 1 explained exactly how the military spouse community offers this support to help spouses survive the challenges of the military lifestyle: “When time calls for it, I think, collectively, we bring our resources together to help pull other military spouses up and try to just forewarn them about what the obstacles are and what may have worked for our family” (P1).
The military spouses also described the comfort they found in other military spouses’ understanding of the challenges they face: “I think the most important part and coping is finding your community, so making sure you’re surrounding yourself with women who are going through similar experiences, or who have gone through similar experiences and similar life stages” (P3).
In the midst of this supportive community, the spouses discussed how they actively seek to comfort each other: “You’re not the only one who’s in it who’s having this issue, I understand that you’ll get through this, that we know we’ve been there, we understand how it goes” (P5). This outreach seemed to be especially helpful from spouses who were more experienced with the military lifestyle: “Having that senior spouse example has been so good. . . . She’s always been somebody who said, ‘Hey, I’ve been through a lot. If you ever have any questions, I’m always here for you’” (P8).
In addition to relying on other spouses for their own wellness and resilience, the spouses expressed pride in their ability to contribute to the military spouse community. One described how “I feel like I am a better team player. I feel like I’m more committed to helping others than I have in the past because I know that others will do the same for me” (P7). The participants also described increased self-growth as a result of being a part of a community: “I really don’t think I would have allowed myself to receive help if I hadn’t been part of this phenomenal community that is constantly supporting each other” (P7). Participant 5 echoed this sentiment: “Learning to get that help from other people is something that I feel like you have to kind of get when you are a military spouse because, otherwise, you’re going to have to do everything and you don’t have to.”
Finally, our participants frequently indicated that they felt a “sense of pride” (P7), “connection” (P4), or “camaraderie” (P8) from belonging to a group of military spouses who understood their unique situation. When asked how the military could enhance resilience for military spouses, participants commonly indicated that peer support and fostering connections with senior spouses should be a priority for military commands. One participant noted that their ability to be resilient in difficult times was related to the “opportunities” they had “to connect with other people who are going through similar stuff and who are a part of the same small community” and recommended that the military facilitate more opportunities to connect (P7). Another participant suggested that military commands should “have someone that [the spouse] can talk to” that would “help them to understand the military life whether you are a new spouse or a seasoned spouse” (P2).
Discussion
The purpose of this study was to explore military spouses’ perceptions of their resilience and the ways in which they define resilience for their community. Our study’s results indicate that spouses’ definitions of resilience are currently shaped by service member and mission priority. Our participants also described how they often felt burdened by outside expectations of their resilience as well as by a sense of responsibility for their family’s resilience. Overall, the spouses relied on themselves and the military spouse community to overcome the challenges they faced. Participants expressed a desire for resources aimed specifically at enhancing spouse resilience and more awareness about resilience resources already in place throughout the military.
While past research has examined resilience factors in spouses such as communication skills, social support, and spousal support (Erbes et al., 2017; Richer et al., 2022; Sinclair et al., 2019; Villagran et al., 2013), our study provided new insight into military spouses’ perspectives of their resiliency. This revelation of the spouses’ worldview aids our understanding of ways to best support spouses and areas to focus on to support their resilience. Our participants’ definitions of their resilience were shaped by their relationship with their service member and the influence of the military’s mission. In addition, while past research has indicated that the military lifestyle and culture is challenging for spouses to navigate (Cole et al., 2021; DaLomba et al., 2021; Donoho et al., 2018; Mailey et al. 2018), our participants’ description of their feelings of responsibility for their family’s well-being reveals the added burden that military spouses face as they help their families navigate the military lifestyle. Finally, our participants confirmed that resiliency should be viewed as a variation and is unique to each individual (Pietrzak & Southwick, 2011). As outlined in the professional literature (Masten, 2014; Southwick et al., 2014), the participants confirmed the dynamic nature of resiliency, recognizing that sometimes they felt more resilient than at other times.
In the midst of these challenges, our participants emphasized that the military spouse community serves as a protective factor and a source of their resilience against mental health challenges. This perception of the military spouse community aligns with previous research highlighting the supportive role that spouses play for each other, so much so that it is a protective factor against suicide (Cole et al., 2021). Therefore, military leadership and the counseling community might focus on enhancing this community and connecting spouses with one another—especially more seasoned spouses with newer spouses. In addition, because military-sponsored resilience programs are often targeted to better support service member outcomes, community providers might find ways to focus on supporting the spouses and helping them to overcome the challenges they face in their daily lives.
Finally, the participants discussed how they overcame the challenges of the military lifestyle, including constant moving, deployments, and overall uncertainty, through their own individual and collective resilience. These lifestyle challenges that the participants described correspond to career struggles and shifting family dynamics that cause ongoing stress to the military spouse, both of which have been previously documented in the professional literature (Borah & Fina, 2017; Cole et al., 2021; DaLomba et al., 2021; Donoho et al., 2018; Mailey et al., 2018; Numbers & Bruneau, 2017). Currently, since the withdrawal of troops from Afghanistan, the United States is experiencing peacetime, whereas the nature of future conflicts is uncertain (Marsh & Hampton, 2022). Enhancing the resiliency of military spouses and finding solutions to ongoing stressors is key during this time of peace so that spouses are ready and able to face the stressors of future, potentially large-scale wars (Sefidan et al., 2021).
Implications for Counselors
Professional counselors are called to be trained and ready to meet the unique needs of military spouses, especially in understanding the nature of military culture and its impact on spouse mental health and well-being and enhancing spouse resilience in times of adversity (Cole, 2014). Our study echoes the continued struggles of military spouses described in the professional literature (Cole et al., 2021; Lewy et al., 2014; Runge et al., 2014), suggesting that new and innovative ways of understanding and approaching military spouse resilience is needed within the counseling community. For example, counselors might encourage spouses to explore how their resilience is shaped by the military community in order to increase self-awareness and understanding. They might also help spouses develop their independence and sense of self-efficacy while simultaneously seeking collective support within the military community. Counselors can help spouses examine their social support and help them develop their social skills so they can connect with others around them. Counselors should also help military spouses unpack their perceptions of outsiders’ expectations of their resiliency. Encouraging spouses to reflect on others’ expectations, and the ways in which these expectations impact their sense of well-being, may help define resilience for themselves and capitalize on their unique resiliencies during challenging times. Ultimately, because the military culture is so unique, counselors should seek out professional development so they can better understand how to help military spouses navigate this culture and enhance their resilience. When working with military spouses, professional counselors might explore spouses’ feelings of responsibility for their family members’ health and well-being that were described in our results. In addition, counselors can equip spouses with supportive mental health resources for their family members so they do not feel as if they need to care for them on their own. School counselors, in particular, can provide support for military-connected students at school and can connect military families with resources within both the civilian and military communities to support their mental health and resilience (Cole, 2017; Quintana & Cole, 2021).
Our participants revealed that often the expectation of resilience is burdensome for spouses, which serves as a contradiction to its purposes. Counselors are called to acknowledge the challenges of the military lifestyle and provide support for navigating these challenges, rather than expecting spouses to face these hurdles alone. In addition, counselors might focus on more holistic manifestations of resilience, recognizing that some spouses can be resilient, yet still struggle. Approaching spouses from a strengths-based perspective, rather than from a deficit perspective, can be empowering within the counseling relationship (Smith, 2006).
Limitations
Our recruitment strategy limited our sample size as we only sought participants that we knew through our military spouse networks. In addition, our sample lacked gender diversity, with all of the participants being female. Approximately 91% of active-duty service member spouses are female (DoD, 2022). However, the lack of male participants in the present study is a limitation, and the experience of male spouses is undoubtedly unique and worth exploring in greater depth. Research suggests that stressors and characteristics of resilience transcend gender categories (NASEM, 2019).
Finally, in qualitative research, the researcher’s biases may impact their interpretation of the data. As military spouses, our own experiences may have impacted the way in which we described our participants’ experiences. We took several steps to mitigate these biases, including intentionally bracketing them and engaging in peer debriefing throughout the research process.
Implications for Future Research
The participants in our study described a need for resources and programs geared specifically toward military spouses. Future research might determine how to best develop and implement these programs that will help to enhance spouse resilience. Key areas of focus may be ways to leverage the military spouse community and enhance spouse sense of self, which were two protective factors that emerged from our data. In addition, existing resilience programs within the military that are currently aimed at the active-duty population should undergo a program evaluation to determine their effectiveness with military spouses.
As a follow-up to our qualitative research, future quantitative research studies should address limitations noted previously. Specifically, future research should target a larger sample size and broader demographic of military spouses to further explore their understanding and definition of resilience. This larger and more diverse sample size would allow for greater generalizability and would assist with advocacy within the military. Finally, future qualitative research might explore the perceptions of male spouses, in particular, in order to determine their perception of resiliency and any unique areas of needed support.
Conclusion
Military spouses face a wide range of challenges as a result of the military lifestyle. They are expected to be resilient so as to overcome these challenges. However, our study reveals the often burdensome impact of these expectations on military spouses. Our results also illuminate how spouses uniquely conceptualize their own resilience, recognizing the resilience continuum and focusing on the positive impact of their protective community. Overall, the spouses took pride in themselves and their communities for their ability to overcome obstacles. These revelations are key for both the military and the counseling profession in their work to support military spouses wherever they are on this continuum and enhance their community, which is key to their well-being.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript. The opinions and assertions
expressed herein are those of the authors and
do not reflect the official policy or position of
the Uniformed Services University of the Health
Sciences or the Department of Defense.
References
American Psychological Association. (2020). Building your resilience. https://www.apa.org/topics/resilience/building-your-resilience
Andrade, C. (2021). The inconvenient truth about convenience and purposive samples. Indian Journal of Psychological Medicine, 43(1), 86–88. https://doi.org/10.1177/0253717620977000
Blue Star Families. (2021). Military Family Lifestyle Survey: 2020 comprehensive report. https://bluestarfam.org/wp-content/uploads/2021/03/BSF_MFLS_CompReport_FULL.pdf
Blue Star Families. (2023). Military Family Lifestyle Survey: 2022 comprehensive report. https://bluestarfam.org/wp-content/uploads/2023/03/BSF_MFLS_Spring23_Full_Report_Digital.pdf
Borah, E., & Fina, B. (2017). Military spouses speak up: A qualitative study of military and veteran spouses’ perspectives. Journal of Family Social Work, 20(2), 144–161. https://doi.org/10.1080/10522158.2017.1284702
Cole, R. F. (2014). Understanding military culture: A guide for professional school counselors. The Professional Counselor, 4(5), 497–504. https://doi.org/10.15241/rfc.4.5.497
Cole, R. F. (2017). Supporting students in military families during times of transition: A call for awareness and action. Professional School Counseling, 20(1), 36–43. https://doi.org/10.5330/1096-2409-20.1.36
Cole, R. F., Cowan, R. G., Dunn, H., & Lincoln, T. (2021). Military spouses’ perceptions of suicide in the military spouse community. The Professional Counselor, 11(2), 203–217.
https://doi.org/10.15241/rfc.11.2.203
DaLomba, E., Greer, M. J., Cruz, E., Harris, A., King, C., Laurel, L., McCuaig, T., & Wilder, R. (2021). The experiences of active duty military spouses with advanced degrees in maintaining and advancing their careers. Work, 68(2), 387–398. https://doi.org/10.3233/WOR-203380
Donoho, C. J., LeardMann, C., O’Malley, C. A., Walter, K. H., Riviere, L. A., Curry, J. F., & Adler, A. B. (2018). Depression among military spouses: Demographic, military, and service member psychological health risk factors. Depression and Anxiety, 35(12), 1137–1144. https://doi.org/10.1002/da.22820
Dorvil, M. (2017). 2017 survey of active-duty spouses. Office of People Analytics, U.S. Department of Defense. https://download.militaryones ource.mil/12038/MOS/Surveys/2017-Survey-of-Active-Duty-Spouses-Overview-Briefing.pdf
Erbes, C. R., Kramer, M., Arbisi, P. A., DeGarmo, D., & Polusny, M. A. (2017). Characterizing spouse/partner depression and alcohol problems over the course of military deployment. Journal of Consulting and Clinical Psychology, 85(4), 297–308. https://doi.org/10.1037/ccp0000190
Joining Forces Interagency Policy Committee. (2021). Strengthening America’s military families: Matching their devotion: Deepening our commitment to the families, caregivers, and survivors of service members and veterans. https://www.whitehouse.gov/wp-content/uploads/2021/09/Strengthening_Americas_Military_Families.pdf
Lewy, C. S., Oliver, C. M., & McFarland, B. H. (2014). Barriers to mental health treatment for military wives. Psychiatric Services, 65(9), 1170–1173. https://doi.org/10.1176/appi.ps.201300325
Mailey, E. L., Mershon, C., Joyce, J., & Irwin, B. C. (2018). “Everything else comes first”: A mixed-methods analysis of barriers to health behaviors among military spouses. BMC Public Health, 18(1013), 1–11. https://doi.org/10.1186/s12889-018-5938-z
Marsh, M. K., & Hampton, R. L. (2022). Army medicine’s critical role in large-scale combat operations: Enable the force. Military Review, 102(4), 106–113.
Masten, A. S. (2014). Global perspectives on resilience in children and youth. Child Development, 85(1), 6–20. https://doi.org/10.1111/cdev.12205
Meadows, S. O., Beckett, M. K., Bowling, K., Golinelli, D., Fisher, M. P., Martin, L. T., Meredith, L. S., & Osilla, K. C. (2015). Family resilience in the military: Definitions, models, and policies. RAND Health Quarterly, 5(3).
Moerer-Urdahl, T. & Creswell, J. W. (2004). Using transcendental phenomenology to explore the “ripple effect” in a leadership mentoring program. International Journal of Qualitative Methods, 3(2), 19–35. https://doi.org/10.1177/160940690400300202
Moustafa, A. A., Crouse, J. J., Herzallah, M. M., Salama, M., Mohamed, W., Misiak, B., Frydecka, D., Al-Dosari, N. F., Megreya, A. M., & Mattock, K. (2020). Depression following major life transitions in women: A review and theory. Psychological Reports, 123(5), 1501–1517. https://doi.org/10.1177/0033294119872209
Moustakas, C. (1994). Phenomenological research methods. SAGE.
National Academies of Sciences, Engineering, and Medicine. (2019). Strengthening the military family readiness system for a changing American society. The National Academies Press. https://doi.org/10.17226/25380
Numbers, M., & Bruneau, L. (2017). Creating connections and fostering self-growth: Gestalt group counseling for military spouses. In Ideas and Research You Can Use: VISTAS 2017.
Panter-Brick, C. (2014). Health, risk, and resilience: Interdisciplinary concepts and applications. Annual Review of Anthropology, 43, 431–448. https://doi.org/10.1146/annurev-anthro-102313-025944
Pietrzak, R. H., & Southwick, S. M. (2011). Psychological resilience in OEF-OIF veterans: Application of a novel classification approach and examination of demographic and psychosocial correlates. Journal of Affective Disorders, 133(3), 560–568.
Quintana, T. S., & Cole, R. F. (2021). Forward march: Implementing the ASCA National Model to support military-connected students. Journal of School Counseling, 19(7). http://www.jsc.montana.edu/articles/v19n7.pdf
Richer, I., Frank, C., & Guérin, E. (2022). Understanding Special Operations Forces spouses challenges and resilience: A mixed-method study. Military Behavioral Health, 10(2), 100–111.
https://doi.org/10.1080/21635781.2022.2067921
Runge, C. E., Waller, M., MacKenzie, A., & McGuire, A. C. L. (2014). Spouses of military members’ experiences and insights: Qualitative analysis of responses to an open-ended question in a survey of health and wellbeing. PloS ONE, 9(12), e114755. https://doi.org/10.1371/journal.pone.0114755
Saunders, B., Sim, J., Kingstone, T., Baker, S., Waterfield, J., Bartlam, B., Burroughs, H., & Jinks, C. (2018). Saturation in qualitative research: Exploring its conceptualization and operationalization. Quality & Quantity, 52(4), 1893–1907. https://doi.org/10.1007/s11135-017-0574-8
Sefidan, S., Pramstaller, M., La Marca, R., Wyss, T., Sadeghi-Bahmani, D., Annen, H., & Brand, S. (2021). Resilience as a protective factor in basic military training, a longitudinal study of the Swiss Armed Forces. International Journal of Environmental Research and Public Health, 18(11), 6077. https://doi.org/10.3390/ijerph18116077
Simon, J. B., Murphy, J. J., & Smith, S. M. (2005). Understanding and fostering family resilience. The Family Journal, 13(4), 427–436. https://doi.org/10.1177/1066480705278724
Sinclair, R. R., Paulson, A. L., & Riviere, L. A. (2019). The resilient spouse: Understanding factors associated with dispositional resilience among military spouses. Military Behavioral Health, 7(4), 376–390. https://doi.org/10.1080/21635781.2019.1608876
Smith, E. J. (2006). The strength-based counseling model. The Counseling Psychologist, 34(1), 13–79.
https://doi.org/10.1177/0011000005277018
Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5(1), 25338. https://doi.org/10.3402/ejpt.v5.25338
Sullivan, K. S., Hawkins, S. A., Gilreath, T. D., & Castro, C. A. (2021). Mental health outcomes associated with profiles of risk and resilience among U.S. Army spouses. Journal of Family Psychology, 35(1), 33–43. https://doi.org/10.1037/fam0000702
U.S. Department of Defense, Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy. (2022). 2021 demographics profile: Profile of the military community. https://download.militaryonesource.mil/12038/MOS/Reports/2021-demographics-report.pdf
Verdeli, H., Baily, C., Vousoura, E., Belser, A., Singla, D., & Manos, G. (2011). The case for treating depression in military spouses. Journal of Family Psychology, 25(4), 488–496. https://doi.org/10.1037/a0024525
Villagran, M., Canzona, M. R., & Ledford, C. J. W. (2013). The milspouse battle rhythm: Communicating resilience throughout the deployment cycle. Health Communication, 28(8), 778–788. https://doi.org/10.1080/10410236.2013.800441
Walsh, F. (2012). Family resilience: Strengths forged through adversity. In F. Walsh (Ed.), Normal family processes: Growing diversity and complexity (4th ed.; pp. 399–423). Guilford.
Rebekah Cole, PhD, MEd, NCC, LPC, is a research associate professor at the Uniformed Services University. Christine Ward, PhD, is an associate professor at Walsh University. Taqueena Quintana, EdD, NCC, ACS, BC-TMH, LPC, is an associate professor at Antioch University. Elizabeth Burgin, PhD, NCC, LPC, RPT, CCCPTS, is an assistant professor and program coordinator of the Military and Veterans Counseling program at William & Mary. Correspondence may be addressed to Rebekah Cole, rebekah.cole@usuhs.edu.
Appendix
Interview Protocol
- Tell me a little about your identity as a military spouse?
- What have been some of your rewarding experiences as a military spouse?
- What have been some of your stressful experiences as a military spouse?
- How have you coped with the more stressful experiences as a military spouse?
- How would you describe the military’s definition of “resilience?”
- What does the term “resilience” mean to you?
- What does the term “resilience” mean for your military partner/family?
- How would you describe the resilience of military spouses?
- In what ways have you, personally, been resilient as a military spouse?
- What would enhance the resilience of military spouses and their families, from your perspective?
- How, if at all, has your military experience enhanced your resilience?
- How, if at all, has the military’s focus on resilience presented you with challenges during your military spouse experiences?
- How, if at all, can resilience be a negative way to describe military spouses/families?
- Is there anything else about military resilience that is important to you that I did not ask about?
