Aug 10, 2022 | Volume 12 - Issue 2
Lacey Ricks, Malti Tuttle, Sara E. Ellison
Quantitative methodology was utilized to assess factors influencing veteran school counselors’ decisions to report suspected child abuse. Veteran school counselors were defined as having 6 or more years of experience working as a school counselor within a public or private school. This study is a focused examination of the responses of veteran school counselors from a larger data set. The results of the analysis revealed that academic setting, number of students within the school, and students’ engagement in the free or reduced lunch program were significantly correlated with higher reporting among veteran school counselors. Moreover, veteran school counselors’ self-efficacy levels were moderately correlated with their decision to report. Highly rated reasons for choosing to report suspected child abuse included professional obligation, following school protocol, and concern for the safety of the child. The highest rated reason for choosing not to report was lack of evidence. Implications for training and advocacy for veteran school counselors are discussed.
Keywords: child abuse, reporting, veteran school counselors, self-efficacy, training
In 2019, approximately 4.4 million reports alleging maltreatment were made to U.S. child protective services (U.S. Department of Health & Human Services [HHS] et al., 2021). Of these reports, nearly two thirds were made by professionals who encounter children as a part of their occupation. Child maltreatment is identified as all types of abuse against a child under the age of 18 by a parent, caregiver, or person in a custodial role, and includes physical abuse, sexual abuse, emotional abuse, and neglect (Fortson et al., 2016). Public health emergencies, such as the continued COVID-19 pandemic, increase the risk for child abuse and neglect due to increased stressors (Swedo et al., 2020). Factors such as financial hardship, exacerbated mental health issues, lack of support, and loneliness may contribute to increased caregiver distress, ultimately resulting in negative outcomes for children and adolescents (Collin-Vézina et al., 2020).
The psychological impact of child abuse and neglect on victims can increase the risk of mental health disorders such as depression, anxiety, eating disorders, and post-traumatic stress disorder (Heim et al., 2010; Klassen & Hickman, 2022). Similarly, trauma experienced in childhood is associated with higher rates of long-term physical health issues when compared to individuals with less trauma; these include cancer (2.4 times more likely to develop), diabetes (3.0 times as likely to develop), and stroke (5.8 times more likely to experience; Bellis et al., 2015). Children who are victims of child abuse and neglect may also experience educational difficulties, low self-esteem, and trouble forming and maintaining relationships (Child Welfare Information Gateway, 2019).
Voluntary disclosure of childhood abuse is relatively uncommon; one study found that less than half of adults with histories of abuse reported disclosing the abuse to anyone during childhood, and only 8%–16% of those disclosures resulted in reporting to authorities (McGuire & London, 2020). For this reason, mandated reporting by professionals is an integral piece of child abuse prevention. School counselors, by virtue of their ongoing contact with children, are uniquely positioned to identify and report child abuse (Behun et al., 2019). We recognize that school-based professionals such as teachers, administrators, and other school-based staff are mandated reporters as well. However, for the purpose of this article, we specifically focus on school counselors based on their role, responsibility, and training that best equips them to fulfill this expectation. School counselors have a unique role within the school system and play a critical role in ensuring schools are a safe, caring environment for all students (American School Counselor Association [ASCA], 2017). School counselors also work to identify the impact of abuse and neglect on students as well as ensure the necessary supports for students are in place (ASCA, 2021).
Ethical and Legal Mandates for Reporting Suspected Child Abuse
Although current estimates for the reporting frequency within schools are not available, it appears likely that high numbers of school counselors encounter the decision to report suspected child abuse each year. In fact, a 2019 survey of 262 school counselors indicated that 1,494 cases of child abuse had been reported by participants over a 12-month period (Ricks et al., 2019). Despite the frequency with which it occurs, reporting can be a distressing part of school counselors’ responsibilities (Remley et al., 2017); this could be because of limited knowledge or competency in reporting procedures, unfamiliarity with the law, or potential repercussions for the child (Bryant, 2009; Bryant & Milsom, 2005; Lambie, 2005). Additionally, laws, definitions, and mandates of child abuse and neglect vary by state; therefore, confusion may arise when school counselors relocate to another area (ASCA, 2021; Hogelin, 2013; Lambie, 2005; Tuttle et al., 2019). School counselors need to identify and familiarize themselves with the unique laws in their state in addition to reviewing federal law and ethical codes.
Federally, school counselors are mandated by the Child Abuse Prevention and Treatment Act of 1974, Public Law 93-247, to report suspected abuse and neglect to proper authorities (ASCA, 2021). Failure to report suspected abuse could result in civil or criminal liability (Remley et al., 2017; White & Flynt, 2000). ASCA Ethical Standards echo this mandate, directing school counselors to report suspected child abuse and neglect while protecting the privacy of the student (ASCA, 2022a, A.12.a). School counselors should also assist students who have experienced abuse and neglect by connecting them with appropriate services (ASCA, 2022a). Moreover, school counselors should work to create a safe environment free from abuse, bullying, harassment, and other forms of violence for students while promoting autonomy and justice (ASCA, 2022a).
School Counselors as Advocates in Mandated Reporting
Barrett et al. (2011) recognized school counselors as social justice leaders based on their role to advocate for students who are underserved, disadvantaged, maltreated, or living in abusive situations. Child abuse impacts children and adolescents from every race, socioeconomic status, gender, and age (Lambie, 2005; Tillman et al., 2015). School counselors who are trained to provide culturally sustaining school counseling will work with students and families from all demographics to promote student wellness within their comprehensive school counseling program (ASCA, 2021). As leaders within the school, school counselors, and especially veteran school counselors, can work to educate all stakeholders on the implications of child abuse.
School counselors not only are legally positioned to serve as mandated reporters but also ethically positioned to train school personnel in recognizing and identifying child abuse symptoms and in reporting procedures (Hodges & McDonald, 2019). Training of school personnel, such as teachers, to identify and report suspected child abuse is essential because they are also recognized legally as mandated reporters (Hupe & Stevenson, 2019) and they interact with students daily. It is vital that school counselors advocate for ongoing comprehensive training related to child abuse because their knowledge affects many stakeholders in the school setting (ASCA, 2021; Tuttle et al., 2019).
Self-Efficacy Among Veteran School Counselors
Previous literature from this data set highlighted the reporting behaviors of early career school counselors (Ricks et al., 2019), and a framework was developed to assist new professionals in reporting (Tuttle et al., 2019). However, the child abuse reporting behaviors and needs of veteran school counselors are understudied. Therefore, this article focuses on veteran school counselors. For the purpose of this study, veteran school counselors are considered licensed school counselors having 6 or more years of experience. Professional literature has highlighted the unique needs and experiences of novice counselors as compared to veteran school counselors (Buchanan et al., 2017; Johnson et al., 2017). One study (Mishak, 2007) examined differences in instructional strategies for early career and veteran school counselors in elementary schools in Iowa. Although that study does not specifically address child abuse reporting, it does highlight differences found among the respondents based on their experience level.
One factor supporting the unique needs of veteran school counselors is self-efficacy. Self-efficacy theory posits that an individual’s expectations of mastery are strongly influenced by personal experience and indirect exposure to a phenomenon (Bandura, 1977, 1997). Veteran school counselors, based on their years of experience in a school setting, are likely to have multiple exposures to child abuse reporting. They may have filed reports themselves, spoken to peers about their reporting experiences, or assisted other professionals in the school with reporting. Bandura (1997) suggested that self-efficacy is supported when individuals not only possess the skill and ability to complete a task, but also have the confidence and motivation to execute it.
Veteran school counselors can receive ongoing training from workshops, university courses, webinars, district training, or other professional organizations that may further impact self-efficacy levels. Previous research has shown that as an individual’s knowledge of child abuse increases, their levels of self-efficacy in recognizing or reporting child abuse also increases (Balkaran, 2015; Jordan et al., 2017). However, little research linking school counselors’ self-efficacy levels to child abuse reporting has been published. Despite the paucity of research on this topic, Ricks et al. (2019) found a moderate relationship between early career school counselors’ self-efficacy and their ability to identify types of abuse. Additionally, Tang (2020) found that school counseling supervision increased school counselor self-efficacy; differences between early career and veteran school counselors were not addressed in Tang’s study. Although the positive correlation found by Tang did not directly address child abuse reporting, assisting students with crisis situations was one of the principal components of the analysis. Even though veteran school counselors have experience serving as mandated reporters, they require ongoing professional development in this area to effectively fulfill their roles as advocates in maintaining the welfare and safety of students (ASCA, 2021; Tuttle et al., 2019). Therefore, we seek to utilize this article as a form of advocacy on behalf of veteran school counselors by providing additional research and literature in the field.
Purpose of the Present Study
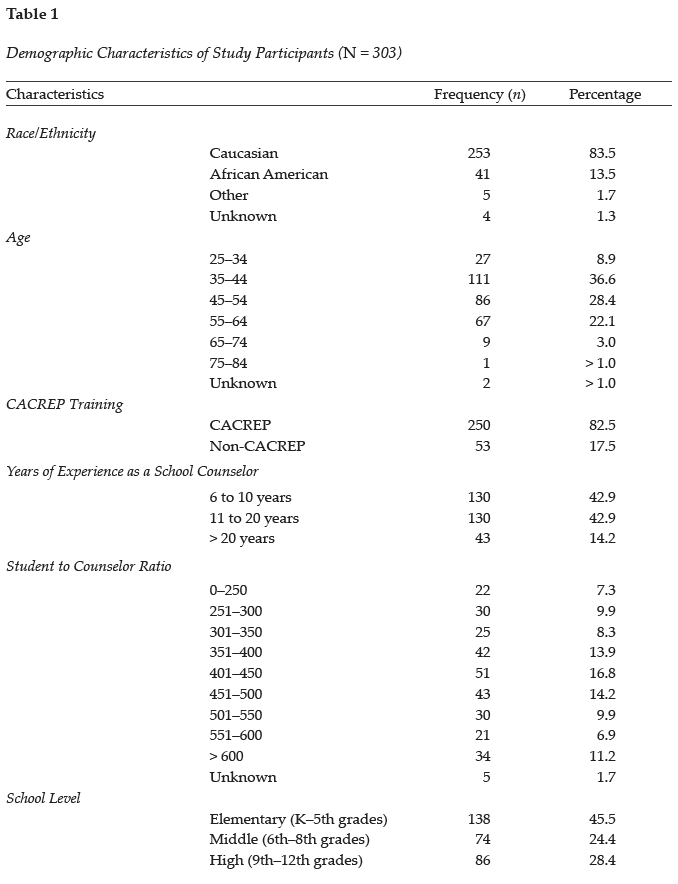
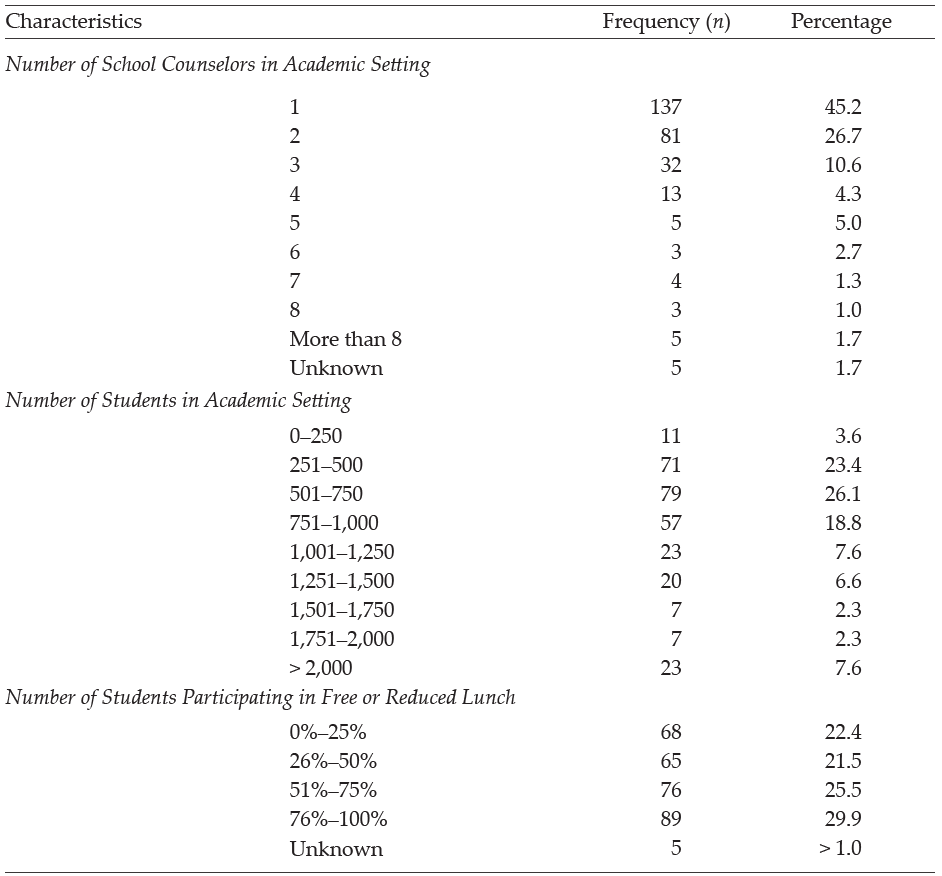
The purpose of this quantitative study is to examine (a) the prevalence of child abuse reporting by veteran school counselors within the school year; (b) the factors affecting veteran school counselors’ decisions to report or not report suspected child abuse; (c) reasons for reporting or not reporting suspected child abuse by veteran school counselors; and (d) veteran school counselors’ self-efficacy levels related to child abuse reporting. Our intent was to build upon an initial larger study to examine veteran school counselors’ knowledge of procedures and experiences with child abuse reporting. The present study is a focused examination of the data collected from veteran school counselors as part of the primary study, which solicited data from school counselors across their careers related to their experiences with child abuse reporting (see Ricks et al., 2019). Demographic variables were collected from participants to assess their impact on child abuse reporting; see Table 1 for a complete list of variables.
Methods
Multiple correlation and regression analyses were conducted to assess factors influencing veteran school counselors’ decisions to report suspected child abuse. After obtaining IRB approval, the authors recruited school counselors in the Southeastern United States (Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, South Carolina, Tennessee, Texas, Virginia, and West Virginia). Participants were recruited using a professional school counseling association membership list, a southeastern state counseling association listserv, and social media. Participants were informed that participation in the online study was voluntary and that they could withdraw from the study at any time. Participants were also informed that the survey would take between 10–15 minutes and that the information collected in the survey would remain anonymous.
Participants
A total of 848 surveys were collected from participants. Veteran school counselor data was extracted from the total sample and analyzed to assess the unique experiences of these individuals in child abuse reporting. Veteran school counselors were defined as having 6 or more years of experience working as a school counselor within a public or private school. Four hundred and twenty-eight veteran school counselors began the survey, but data from 125 participants was excluded from the analysis for incomplete responses, resulting in a final sample of 303 participants. Most participants (n = 265, 87.5%) reported being licensed/certified as a school counselor. Some participants may not have possessed a license because of working in the private school sector or working on a provisional basis. See Table 1 for all demographic frequencies and percentages related to participants in the study.
Measures
Three measures were selected and employed as part of the larger study. These included the Child Abuse Reporting Questionnaire (Bryant & Milsom, 2005), the School Counselor Self-Efficacy Scale (Bodenhorn & Skaggs, 2005), and the Knowledge of Child Abuse Reporting Questionnaire (Ricks et al., 2019). Each measure is described below as previously reported in Ricks et al. (2019).
Child Abuse Reporting Questionnaire
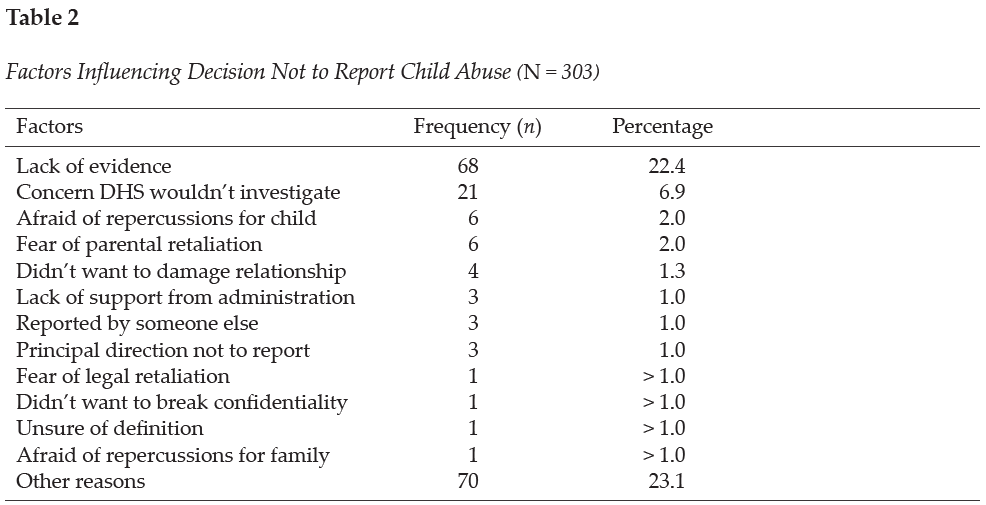
The Child Abuse Reporting Questionnaire was developed to assess three domains, including school counselor General Information, Training in Child Abuse Reporting, and Child Abuse Reporting Experience (Bryant & Milsom, 2005). In the first section of the questionnaire, Training in Child Abuse Reporting, participants were asked to list where they obtained their knowledge of child abuse reporting and to assess four different types (physical, sexual, neglect, emotional) of child abuse. In the Child Abuse Reporting Experience section, the participants were asked two questions. The first question asked participants to recall the number of suspected child abuse cases they encountered during the preceding school year and the number of child abuse cases they reported. The next question asked participants how many cases of suspected child abuse they did not report. Participants were also asked in the survey to indicate reasons for choosing not to report suspected child abuse cases based on 12 commonly reported barriers or to list other reasons for not reporting the suspected cases. See Table 2 for a complete list of the common reasons given for not reporting suspected child abuse cases. Internal consistency measures were not obtained for this questionnaire because of the demographic nature of assessing participants’ personal experiences with child abuse reporting.
School Counselor Self-Efficacy Scale
The School Counselor Self-Efficacy Scale (SCSE) was used to assess school counselors’ self-efficacy and to link their personal attributes to their career performance (Bodenhorn & Skaggs, 2005). Participants completed Likert scale questions to indicate their confidence in performing school counseling tasks for 43 scale items. An example question would ask school counselors to indicate their confidence in advocating for integration of student academic, career, and personal development into the mission of their school. A rating of 1 indicated not confident and a rating of 5 indicated highly confident. The coefficient alpha for the scale score was found to be .95 (Bodenhorn & Skaggs, 2005). The SCSE subscales include five domains: Personal and Social Development (12 items), Leadership and Assessment (9 items), Career and Academic Development (7 items), Collaboration and Consultation (11 items), and Cultural Acceptance (4 items). The correlations of the subscales ranged from .27 to .43.
Knowledge of Child Abuse Reporting Questionnaire
The Knowledge of Child Abuse Reporting Questionnaire was developed to assess respondents’ knowledge of child abuse reporting and procedures within three areas (Ricks et al., 2019). To develop the survey, the researchers and outside counselor educators reviewed the questionnaire to determine if it clearly measured the constructs. In the first section of the questionnaire, Identifying Types of Abuse, participants’ perceptions of their ability to identify the four different types of child abuse were assessed. To complete this section, participants rated their comfort level using a 4-point Likert scale. A rating of 1 indicated very uncertain and a rating of 4 indicated very certain. The coefficient alpha for the scale score was found to be .902. The Knowledge of Guidelines section assessed participants’ knowledge of the state rules, ASCA Ethical Standards, and child abuse reporting protocol within their current school and district. To complete this section, participants rated their comfort level using a 5-point Likert scale. A rating of 1 indicated not knowledgeable and a rating of 5 indicated extremely knowledgeable. The coefficient alpha for the scale score was found to be .799. Lastly, the Child Abuse Training section assessed where participants received training on general knowledge of child abuse reporting, how to make a referral, and indicators of child abuse. To complete this section, participants selected options from a dropdown menu based on commonly reported agencies or listed an organization not provided. Options included in the survey list were universities or colleges, schools or districts, conferences or workshops, colleagues, journals, professional organizations, or the state department of education.
Data Analysis
SPSS Statistics 27 was used to analyze data within this study. First, a correlation analysis was executed to assess the strength of the relationship across variables. Next, analyses of variance (ANOVAs) were performed to assess the relationship between the number of reported child abuse cases and five demographic variables, which included academic setting (elementary, middle, high); number of students participating in the school’s free or reduced lunch program; number of school counselors working in a school setting; years of experience as a school counselor; and number of students enrolled in a school setting. Lastly, regression analyses were used to determine the relationship between school counselors’ self-efficacy and their decisions to report or not report suspected child abuse cases as well as to assess the relationship between school counselors’ self-efficacy and their certainty in identifying types of abuse.
Results
Suspected and Reported Cases of Abuse
Descriptive statistics generated from the child abuse survey included the participants (N = 303) suspecting 2,289 cases of child abuse during the school year. Scores reported by participants ranged from 0 to 100 (M = 7.71, SD = 10.58). Seven participants omitted this question within the questionnaire. Participants indicated reporting a total of 2,140 cases of suspected child abuse; individual frequency ranged from 0 to 100 (M = 7.21, SD = 10.25). Physical child abuse cases (M = 4.03, SD = 7.12) were reported at a higher rate than cases of neglect (M = 2.72, SD = 5.10), emotional abuse (M = 0.56, SD = 1.52), and sexual abuse (M = 0.57, SD = 1.37).
School Demographics
The relationship between the number of reported child abuse cases and demographic variables was examined using a bivariate correlation. Results indicated a negative correlation between the number of child abuse reports and the academic level of students the school counselor works with (elementary, middle, or high school), r(293) = −.283, p < .001, with elementary school counselors reporting child abuse at a higher rate than high school counselors. An additional negative correlation was found between the number of child abuse reports and the number of school counselors working within the school, r(293) = −.164, p < .001. Results indicated a positive significant relationship between the number of reported child abuse cases and the number of students who participate in the school’s free or reduced lunch program, r(293) = .225, p < .001. Weaker negative relationships were also found between the number of child abuse reports and the participants’ years of experience as a school counselor, r(297) = −.115, p < .05, as well as how many students are enrolled in a school, r(293) = −.127, p < .06. No other significant relationships were found among the variables and reported cases.
An ANOVA was conducted to examine the relationship between the academic level of students (elementary, middle, and high) the participants worked with and the number of child abuse cases reported. Results showed a significant relationship among the variables, f(2, 290) = 13.021, p > .00. A follow-up test was used to evaluate pairwise differences among the means. Results of a Tukey HSD indicated a significant difference between elementary (M = 10.314) and high school (M = 3.58) counselors who reported child abuse. A difference was also found between elementary and middle school (M = 5.86) reporting levels. No other significant differences were found between variables.
An ANOVA was also conducted to evaluate the differences between child abuse reporting and the percentage (0%–25%, 26%–50%, 51%–75%, 76%–100%) of students who participated in free or reduced lunch. Results showed a significant relationship among the variables, f(3, 289) = 5.22, p = .002. A Tukey HSD post hoc test was used to make a pairwise comparison and statistically significant mean differences were found between the 0%–25% (M = 2.33) group and the 51%–75% (M = 7.78) group. Additionally, a difference was found between the 0%–25% group and the 76%–100% (M = 10.12) group. Lastly, a difference was found between the 26%–50% (M = 6.54) group and the 76%–100% group. No other significant differences were found between the groups.
An ANOVA was conducted to examine the relationship between how many school counselors are working in a school setting and the differences in child abuse reporting. Analysis of the ANOVA found no significant difference (p < .05) between the groups (one counselor, M = 8.26; two counselors, M = 7.81; three counselors, M = 7.69; four counselors, M = 5.00; five counselors, M = 2.80; six counselors, M = 2.25; seven counselors, M = 3.50; eight counselors, M = 2.33; more than eight counselors, M = 2.20), but a downward trend can be seen in the number of cases reported with the increase in the number of school counselors within a school.
Likewise, an ANOVA was used to examine the relationship between years of experience as a school counselor and the differences in child abuse reporting, but no significant difference (p < .05) was found between groups (6 to 10 years, M = 8.58; 11 to 20 years, M = 6.36; above 20 years, M = 5.57); however, a slight trend can be seen with participants who have less experience reporting at higher rates. A larger sample size may have yielded significant results, but additional research is needed in this area.
Lastly, an ANOVA was also executed to assess the differences in child abuse reporting and the number of students enrolled in a school setting. A significant difference was found between schools with more than 2,000 students (M = 3.00) and schools with 251–500 students (M = 8.07) as well as schools with 501–750 students (M = 8.63). This difference suggests school counselors who work in schools with more students tend to report child abuse at a lower rate than those who work in smaller schools. A downward trend can be seen in reporting of cases as student numbers increase (751–1,000 students, M = 7.62; 1,001–1,250 students, M = 7.39; 1,251–1,500 students, M = 6.68; 1,501–1,750 students, M = 6.00; 1,751–2,000 students, M = 2.57), with the exception of the 0–250 students (M = 4.82) school classification. Differences in the sample sizes of classification categories could have impacted significance outcomes. No other significant differences were found between the groups.
The Decision to Report
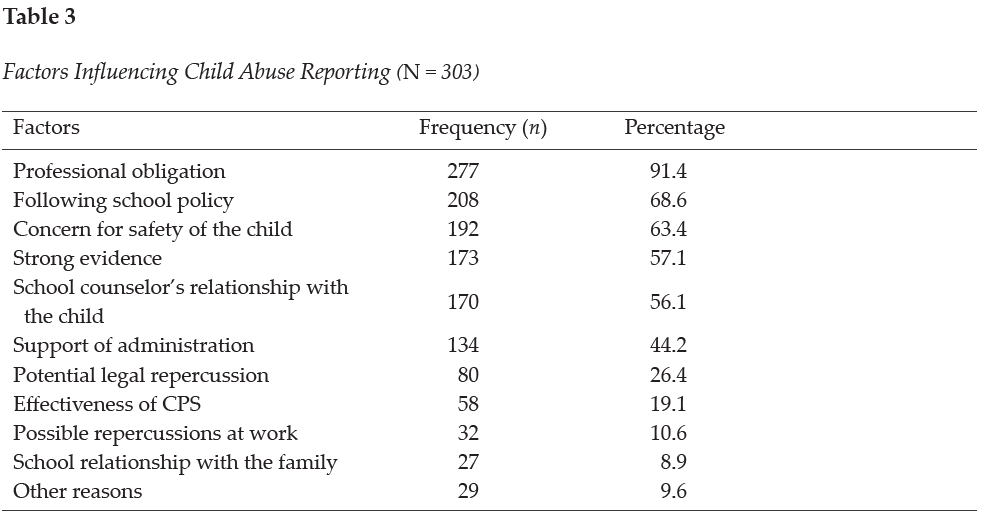
On the Child Abuse Reporting Survey, participants (N = 303) were asked to indicate what factors influenced their decision to report child abuse. Participants indicated the number one factor was following the law (professional obligation; 91.4%, n = 277). Other reasons cited by over half of school counselors included following school policy (68.6%, n = 208), concern for safety of the child (63.4%, n = 192), strong evidence that abuse had occurred (57.1%, n = 173), and the school counselor’s relationship with the child (56.1%, n = 173). See Table 3 for factors influencing child abuse reporting. Further, participants indicated reasons why they chose not to report suspected child abuse. Participants specified inadequate evidence as the primary reason for not reporting suspected child abuse (22.4%, n = 68). Another notable influence included concern that DHS would not investigate the reported case (6.9%, n = 21). See Table 2 for factors influencing the decision not to report child abuse.
Knowledge and Training
On the Knowledge of Child Abuse Reporting Questionnaire, participants were asked to rate how certain they feel about their abilities to identify types of abuse on a 4-point Likert scale with 1 indicating very uncertain and 4 indicating very certain. Participants reported most confidence in their ability to identify physical abuse (M = 3.49, Mdn = 4), followed by neglect (M = 3.30, Mdn = 3), sexual abuse (M = 3.20, Mdn = 3), and emotional abuse (M = 3.06, Mdn = 3). When participants (N = 303) were asked where they gained knowledge about child abuse, most reported receiving training from professional experiences (88.4%, n = 268), mandated reporting training at school (79.5%, n = 241), workshops (72.3%, n = 219), discussion with colleagues (61.4%, n = 186), or literature (58.1%, n = 176). Additionally, participants indicated gaining knowledge from university courses (46.5%, n = 141), media (9.2%, n = 28), or other avenues unlisted in the survey (12.2%, n = 37).
Participants were asked where they received training on how to make a referral for a child abuse case. Most of the school counselors responded that they received the training from a school/district training (87.5%, n = 265), conference/workshop (57.4%, n = 174), or university class (42.9%, n = 130). Other responses included from a colleague (38.9%, n = 118), professional organization (32.7%, n = 99), Department of Education website (20.5%, n = 62), journal (10.9%, n = 33), or other sources (11.2%, n = 34). Lastly, veteran counselors were asked where they received training about the indicators of child abuse. The majority of the respondents reported learning in a school/district training (87.1%, n = 264), conference/workshop (77.9%, n = 236), or university/college course (67.3%, n = 204). Other responses included learning from a professional organization (38%, n = 115), colleague (30%, n = 91), journal (23.4%, n = 71), Department of Education website (21.5%, n = 65), or other sources (9.9%, n = 30).
Veteran school counselors reported that 88.1% (n = 267) of schools/districts provided them with training on local abuse reporting policies. Therefore, 11.9% did not receive training from their local school system. Additionally, 60.1% (n = 182) of the school counselors reported their school/district had a handbook/resource outlining the steps for mandated reporter training within their school system. Consequently, 39.9% of the school counselors reported not having a handbook/resource to reference outlining steps for mandated reporting.
Self-Efficacy and Child Abuse Reporting
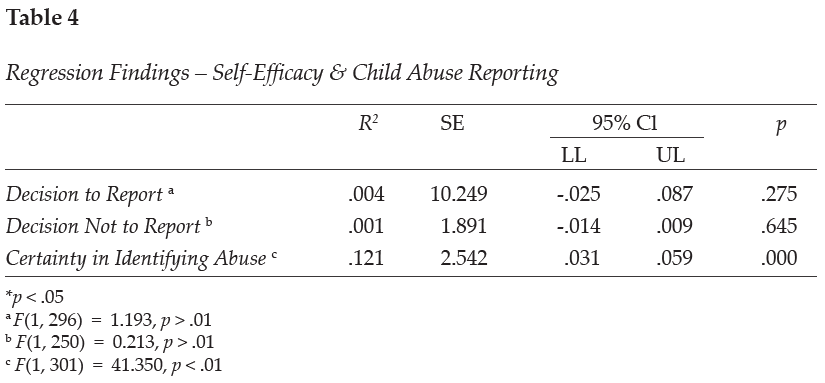
A regression analysis was used to examine the relationship between veteran school counselors’ self-efficacy and three variables, including the number of reported child abuse cases, the decision not to report suspicion of child abuse, and certainty in identifying types of child abuse. Results showed the strength of the relationship between self-efficacy and certainty in identifying types of child abuse was moderately related, F(1, 301) = 41.350, p < .01. Over 12% (r2 = 0.121) of the variance of the school counselors’ self-efficacy level was associated with certainty in identifying child abuse. No other significant results were found among the variables. See Table 4 for the regression analysis related to self-efficacy and child abuse reporting.
Discussion
Given the well-documented negative impact of child abuse on the emotional, physical, and academic well-being of children, it is essential to understand how school counselors are trained to identify and report child abuse. Understanding trends and research in child abuse reporting can help schools prepare school counselors and other staff members. It is imperative for veteran school counselors to receive ongoing training to best serve as advocates for students, maintain relevancy in their roles as mandated reporters by staying current on laws and policies, and further their ability to work within their scope of practice. Ongoing training may also help alleviate difficulties that arise because of terminology differing from state to state and district to district (ASCA, 2021; Hogelin, 2013; Lambie, 2005; Tuttle et al., 2019).
In this study, veteran school counselors’ reporting frequency is shown to differ based on various school demographics. Veteran school counselors were specifically targeted in this analysis to examine their experiences related to child abuse reporting. Although these findings may not show direct causation to child abuse reporting among veteran school counselors, they can help us better understand school and school counselor demographics that need to be evaluated further. The findings can also be used to guide professional development training needed for school counselors as well as additional training needs for counselors-in-training.
Elementary school counselors were found to report child abuse at a higher rate than middle or high school counselors; however, this is anticipated because studies show that younger children experience higher rates of maltreatment than older children (HHS et al., 2021). In fact, rates of maltreatment seem to decrease as age increases. Children who are 6 years old have victimization rates of 9.0 per 1,000 children compared to children who are 16 years of age who have a victimization rate of 5.5 per 1,000 children (HHS et al., 2021). Higher maltreatment levels in younger children may be because of increased caregiver burden (Fortson et al., 2016); as children get older, they are better able to care for themselves and avoid parental confrontation. In addition, older students may be more likely to hide abuse and more astute when dealing with disclosure protocol (Bryant & Milsom, 2005). Knowledge of the signs and symptoms of child abuse and neglect can help school counselors identify children suffering from maltreatment.
Within this study on veteran school counselors, a slight trend can be seen with participants with less experience reporting suspected child abuse at a higher rate. Differences of reporting rates by years of experience may be because of higher ego maturity in less experienced school counselors because of more recent training in their graduate programs (Lambie et al., 2011). According to Lambie et al. (2011), ego development predicts an individual’s level of ethical and legal knowledge, which has been found to be higher in counselors-in-training than the average school counselor. Ego development has also been correlated with greater degrees of self-efficacy (Singleton et al., 2021), which can impact school counselors’ actions when making decisions related to child abuse reporting. Tuttle et al. (2019) also emphasized the need for continuous training to increase school counselors’ self-efficacy as mandated reporters, although more research is needed to understand the impact of self-efficacy on school counselor action. These findings highlight the need for continued assessment of training needs for school counselors of various experience levels.
Although age has been associated with varying levels of child abuse victimization, low socioeconomic status within the home environment has also been identified as a high risk factor for child abuse (Bryant, 2009; Bryant & Milsom, 2005; Ricks et al., 2019; Sedlak et al., 2010). Specifically, the higher the percentage of students participating in the school’s free or reduced lunch program, the more child abuse cases the school counselor reported (Bryant, 2009; Bryant & Milsom, 2005; Ricks et al., 2019). Although most children in low-income families do not experience child abuse, one study estimated that 22.5 children per 1,000 in low-income families experience maltreatment as compared to 4.4 per 1,000 in more affluent families (Sedlak et al., 2010). However, it is important to note the disproportionality that exists within child welfare reporting; non-White children and children of low socioeconomic status are reported to child protective services at a higher rate than their peers (Krase, 2015; Luken et al., 2021). School counselors working in low-income schools need to be aware of the increased risk factors of low socioeconomic status as well as the racial and economic disproportionality that occurs within child maltreatment reporting as a result of possible bias. School counselors should work to be aware of potential biases they may hold with regard to over-reporting certain groups of children and under-reporting others (Tillman et al., 2015).
When examining the current practices of veteran school counselors, participants reported professional obligation as the number one reason they reported suspected child abuse. The primary reason given for failing to report suspected abuse was inadequate evidence. These findings are similar to prior research that shows lack of evidence as an influencing factor in school counselors’ decisions not to report suspected abuse (Bryant, 2009; Bryant & Milsom, 2005; Tillman et al., 2015); this is concerning because some cases of abuse may go unreported. As Tuttle et al. (2019) have stated, “the school counselor’s responsibility is to follow legal and ethical obligations as a mandated reporter by reporting all suspected child abuse” (p. 242). Although concern that DHS would not investigate is denoted as an important factor for why school counselors choose not to report, school counselors must recognize they do not have the proper resources or training to lead a child abuse investigation on their own (Tuttle et al., 2019). As a result, school counselors are ethically and legally mandated to report all suspected cases of abuse to the proper authorities defined by their state, school policies, and ethical codes. Failure to report cases could lead to legal ramifications for the school counselor (Remley et al., 2017; White & Flynt, 2000) and continued maltreatment for the student.
School counselors should strive to “understand child abuse and neglect and its impact on children’s social/emotional, physical and mental well-being” (ASCA, 2021, para. 6). Veteran school counselors completing this survey were most confident in their ability to identify physical abuse and less confident in their ability to identify emotional abuse. This finding supports the assertion that types of abuse with visible evidence are more identifiable than other types of abuse such as emotional or sexual abuse (Bryant, 2009; Bryant & Milsom, 2005). Cases of suspected abuse in which a child reports physical abuse are less likely to be reported if there is no evidence of bodily harm (Tillman et al., 2015). Although school counselors report physical abuse as the most easily identifiable type of abuse, child protective services report neglect as the most common type of maltreatment (Child Welfare Information Gateway, 2021).
Results from this study show that veteran school counselors reported receiving their knowledge on child abuse from professional experiences and mandated reporter training at their school; comparatively, early career school counselors reported most of their knowledge came from professional experience and university courses (Ricks et al., 2019). Reported differences were also observed between veteran school counselors and early career school counselors in terms of sources of knowledge on how to make a referral and learn about indicators of abuse (Ricks et al., 2019). Differences may exist because of variable school district policies regarding ongoing mandated reporter training frequency and practices.
When assessing training needs, participants indicated that most veteran school counselors do receive training from their school district on how to make a referral, indicators of child abuse, and local abuse reporting procedures. In fact, 25% more veteran school counselors reported receiving training from their district than early career school counselors (Ricks et al., 2019). Additionally, approximately 40% of veteran school counselors reported not having a handbook or resource to reference outlining the mandated reporting protocol for their district/school. This result is slightly lower than that reported in research on early career school counselors showing approximately half of school counselors not having a handbook/resource (Ricks et al., 2019). The lack of access to a set protocol outlined by the district is concerning because of the inconsistencies that exist within protocols across states and school districts. Confusion may arise as to timeliness and manner of reporting as well as to who must make the actual report (Kenny & McEachern, 2002). As compared to novice school counselors, veteran counselors appear to report receiving training and/or a handbook/resources related to child abuse reporting in higher numbers. Discrepancies in reported training may indicate a delay in training provided to new school counselors or that training on child abuse is not occurring annually. Although the majority of veteran school counselors did report receiving some training from their school districts, it is important to have “established protocols [to] help address concerns over quality control, fear of lawsuits, and the protection of staff in reporting cases, as well as ensure that there are effective steps for helping children” (Crosson-Tower, 2003, p. 29).
Previous research (Kenny & McEachern, 2002) has indicated that school counselors with more years of experience report less adequate pre-service training in child abuse reporting and that school counselors with in-service training in the last 12 months are less concerned about the consequences of making a report (Behun et al., 2019). This might be due to recently trained school counselors having greater awareness about current information and procedures, which supports the need for participation in continuous ongoing education on this topic. Although the veteran school counselors surveyed in this study indicated experience in child abuse reporting, continued updates to the law highlight the need for current and well-defined guidelines within each school system. Ongoing training is recommended for all school counselors to ensure they stay informed on updated protocols and research (Kenny & Abreu, 2016; Tuttle et al., 2019).
Results of the data analysis also indicated a moderately significant relationship between veteran school counselor self-efficacy and their certainty identifying types of abuse. These findings echo other research indicating that school counselors’ self-efficacy levels may influence their decisions to report suspected abuse (Ricks et al., 2019; Tuttle et al., 2019). According to Larson and Daniels (1998), counselor self-efficacy beliefs are the main factor contributing to effective counseling action. Given the impact of counselor self-efficacy on effective action, it is important to understand how self-efficacy impacts school counselors’ decision-making processes. Experience and training are two factors that have been found to increase school counselor self-efficacy (Morrison & Lent, 2018). Veteran school counselors, who already have years of experience on their side, may benefit most from additional training opportunities. Increased support should be provided to all school counselors to enhance their counseling self-efficacy (Schiele et al., 2014) and contribute to positive school counseling outcomes.
Implications
Lack of knowledge related to reporting policies has been identified as a key barrier in reporting child abuse (Kenny, 2001; Petersen et al., 2014). School counselors should advocate for standardization in reporting policies. Understanding each state’s unique child abuse prevention statutes can help school counselors best serve their clients (Remley et al., 2017). Given that laws and definitions pertaining to child abuse and neglect vary among states (ASCA, 2021), school counselors should identify collaborative relationships to navigate these legal and ethical parameters. Key collaborations may include those with the school social worker, the school district’s attorney, law enforcement, child protective services, parents/guardians, and community members (Tuttle et al., 2019). Working together, in conjunction with administration and other school stakeholders, school counselors can help establish or update written guidelines and implement ongoing professional development in mandated reporting within their school district. Additionally, developing a positive working relationship with law enforcement and child protective services can help ensure that child abuse cases are reported and documented properly, which can promote positive outcomes for students and families. Moreover, based on the findings from this research study, school counseling certification organizations (i.e., state departments of education/licensure boards) may want to increase or update current training policies for professional school counselors. An area for further study would be examining school districts’ training and protocols for child abuse reporting.
Higher reporting trends in low socioeconomic settings highlight the need for additional mental health services in low-income school districts. School counselors may need more training on the risk factors associated with poverty as well as to be reminded that abuse occurs in all types of families (Bryant, 2009; Tillman et al., 2015). Practicing school counselors working with students living in poverty are often in schools where there are significantly limited resources. School counselors report that “working in schools with high poverty means academic services and the school counseling program itself are limited” (Ricks et al., 2020, p. 61). More research is needed to assess how to support school counselors working in low-income schools; however, school counselors should remain cognizant and demonstrate cultural competency. It is also important for veteran school counselors to continue to assess self-bias as a factor in identifying and reporting suspected child abuse cases (Tillman et al., 2015). Further, it is essential that school counselors emerge as advocates for students in these low socioeconomic settings by pushing for more resources for mental health services as well as changes to policies that negatively impact students’ success. School counselors can work with a task force or advisory committee within the school to examine current practices on child abuse identification and reporting (Temkin et al., 2020). The task force could look for systemic barriers that are impacting students related to child abuse reporting and trauma support; these include current school policies, reporting procedures, teacher and staff training protocols, school counselor professional development, access to mental health services, community resources, direct and indirect school counseling protocols, and other factors impacting student identification and support.
Given the higher number of child abuse cases in the elementary grade levels, more school counselors are needed to adequately identify child abuse and provide services for these students. Despite these needs, the school counselor-to-student ratio varies in each state and is higher in elementary schools (ASCA, 2022b); the national state averages for the school counselor-to-student ratio in grades kindergarten through eighth ranges from 1:419 to 1:1,135 as compared to 1:164 to 1:347 in grades nine through 12 (ASCA, 2022b). Moreover, 20 states currently have no school counseling mandates that require school counselors to be present within the schools (ASCA, 2022c). Of the 30 states that do have mandated counseling, seven do not have mandated counseling for elementary-level students (ASCA, 2022c). School counselors should advocate for more school counselors within their districts and state. Moreover, school administrations and state departments of education should consider hiring additional school counselors to address ongoing mental health needs. Recent research has shown that as a result of the COVID-19 pandemic, students may be experiencing no motivation to do schoolwork, difficulty concentrating, concern for falling behind in school, concern for getting sick, or other stress-related factors (Styck et al., 2021), as well as an increased risk for child abuse and neglect (Swedo et al., 2020). Elementary school counselors, who are uniquely trained in child development, can implement prevention and intervention programs to address these ongoing needs (ASCA, 2019). Elementary school counselors are essential in providing early intervention and prevention services for students.
Further research is needed in understanding how self-efficacy impacts school counselors’ decision-making process. The variation of confidence in identifying abuse as well as variance in reporting patterns among school counselors with differing years of experience are indicators that further professional development and training is needed within schools. It is also important to examine how school support can increase school counselors’ self-efficacy levels (Schiele et al., 2014). Current research shows that a school counselor’s level of self-efficacy predicts quality of practice and knowledge of evidence-based practices (Schiele et al., 2014).
Limitations
Although measures were used to reduce confounding variables, limitations exist in the methodological design of the study that could impact the validity of the findings. Firstly, this study obtained a sample size from a limited geographic area (Southeastern United States). Secondly, self-reported data was used. Although participants were informed their answers would remain anonymous, they may have answered based on what they perceived as acceptable and appropriate. School counselors may not be inclined to admit they did not report suspected child abuse for fear of legal or ethical violations. Likewise, selective memory may impact participants’ ability to effectively recall events that happened over a year ago. Additionally, many of the participants were White; responses from participants of color were limited. Further research with a more diverse sample would be beneficial to gain a comprehensive understanding of school counselors’ self-efficacy in identifying and reporting child abuse.
Conclusion
School counselors are mandated to report suspected child abuse and neglect cases to authorities and are key school personnel in early detection and recognition of abuse (ASCA, 2021). In this study, differing school demographics were associated with varying reporting practices among veteran school counselors. Continued professional development training, by virtue of its ability to increase veteran school counselors’ self-efficacy and knowledge of identification and reporting protocols, represents a promising possible pathway to improving outcomes among maltreated children.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2017). The school counselor and academic development. https://www.schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Academic-Development
American School Counselor Association. (2019). The essential role of elementary school counselors. https://www.schoolcounselor.org/getmedia/1691fcb1-2dbf-49fc-9629-278610aedeaa/Why-Elem.pdf
American School Counselor Association. (2021). The school counselor and child abuse and neglect prevention. https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Child-Abuse-and-Neglect-P
American School Counselor Association. (2022a). ASCA ethical standards for school counselors. https://www.school
counselor.org/About-School-Counseling/Ethical-Legal-Responsibilities/ASCA-Ethical-Standards-for-School-Counselors-(1)
American School Counselor Association. (2022b). School counselor roles & ratios. https://www.schoolcounselor.org/About-School-Counseling/School-Counselor-Roles-Ratios
American School Counselor Association. (2022c). State school counseling mandates & legislation. https://www.school
counselor.org/About-School-Counseling/State-Requirements-Programs/State-School-Counseling-Man
dates-Legislation
Balkaran, S. (2015). Impact of child abuse education on parent’s self-efficacy: An experimental study. Walden Dissertations and Doctoral Studies, 1432.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2),
191–215. https://doi.org/10.1037/0033-295X.84.2.191
Bandura, A. (1997). Self-efficacy: The exercise of control. W. H. Freeman.
Barrett, K. M., Lester, S. V., & Durham, J. C. (2011). Child maltreatment and the advocacy role of professional school counselors. Journal for Social Action in Counseling and Psychology, 3(2), 86–103.
https://doi.org/10.33043/JSACP.3.2.86-103
Behun, R. J., Cerrito, J. A., Delmonico, D. L., & Kolbert, J. B. (2019). The influence of personal and professional characteristics on school counselors’ recognition and reporting of child sexual abuse. Journal of School Counseling, 17(13), 1–34.
Bellis, M. A., Hughes, K., Leckenby, N., Hardcastle, K. A., Perkins, C., & Lowey, H. (2015). Measuring mortality and the burden of adult disease associated with adverse childhood experiences in England: A national survey. Journal of Public Health, 37(3), 445–454. https://doi.org/10.1093/pubmed/fdu065
Bodenhorn, N., & Skaggs, G. (2005). Development of the school counselor self-efficacy scale. Measurement and Evaluation in Counseling and Development, 38(1), 14–28. https://doi.org/10.1080/07481756.2005.11909766
Bryant, J. K. (2009). School counselors and child abuse reporting: A national survey. Professional School Counseling, 12(5), 333–342. https://doi.org/10.1177/2156759X0901200501
Bryant, J., & Milsom, A. (2005). Child abuse reporting by school counselors. Professional School Counseling, 9(1), 63–71.
Buchanan, D. K., Mynatt, B. S., & Woodside, M. (2017). Novice school counselors’ experience in classroom management. The Journal of Counselor Preparation and Supervision, 9(1). https://doi.org/10.7729/91.1146
Child Welfare Information Gateway. (2019). Long-term consequences of child abuse and neglect. U.S. Department of Health and Human Services, Administration for Children and Families, Children’s Bureau. https://www.childwelfare.gov/pubpdfs/long_term_consequences.pdf
Child Welfare Information Gateway. (2021). Child maltreatment 2019: Summary of key findings. U.S. Department of Health and Human Services, Administration for Children and Families, Children’s Bureau. https://www.childwelfare.gov/pubs/factsheets/canstats
Collin-Vézina, D., Brend, D., & Beeman, I. (2020). When it counts the most: Trauma-informed care and the
COVID-19 global pandemic. Developmental Child Welfare, 2(3), 172–179.
https://doi.org/10.1177/2516103220942530
Crosson-Tower, C. (2003). The role of educators in preventing and responding to child abuse and neglect. U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, Office on Child Abuse and Neglect. https://www.childwelfare.gov/pubpdfs/educator.pdf
Fortson, B. L., Klevens, J., Merrick, M. T., Gilbert, L. K., & Alexander, S. P. (2016). Preventing child abuse and neglect: A technical package for policy, norm, and programmatic activities. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/can-prevention-technical-package.pdf
Heim, C., Shugart, M., Craighead, W. E., & Nemeroff, C. B. (2010). Neurobiological and psychiatric consequences of child abuse and neglect. Developmental Psychobiology, 52(7), 671–690. https://doi.org/10.1002/dev.20494
Hodges, L. I., & McDonald, K. (2019). An organized approach: Reporting child abuse. Journal of Professional Counseling: Practice, Theory, & Research, 46(1–2), 14–26. https://doi.org/10.1080/15566382.2019.1673093
Hogelin, J. M. (2013). To prevent and to protect: The reporting of child abuse by educators. Brigham Young University Education and Law Journal, 2013(2), 225–252. https://digitalcommons.law.byu.edu/elj/vol2013/iss2/3
Hupe, T. M., & Stevenson, M. C. (2019). Teachers’ intentions to report suspected child abuse: The influence of compassion fatigue. Journal of Child Custody, 16(4), 364–386. https://doi.org/10.1080/15379418.2019.1663334
Johnson, G., Nelson, J., & Henriksen, R. (2017). Mentoring novice school counselors: A grounded theory. In G. R. Walz & J. Bleuer (Eds.), Ideas and research you can use: VISTAS 2017 (pp. 1–16). Counseling Outfitters.
Jordan, K. S., MacKay, P., & Woods, S. J. (2017). Child maltreatment: Optimizing recognition and reporting by school nurses. NASN School Nurse, 32(3), 192–199. https://doi.org/10.1177/1942602X16675932
Kenny, M. C. (2001). Child abuse reporting: Teachers’ perceived deterrents. Child Abuse and Neglect, 25(1), 81–92. https://doi.org/10.1016/s0145(00)00218-0
Kenny, M. C, & Abreu, R. L. (2016). Mandatory reporting of child maltreatment for counselors: An innovative training program. Journal of Child and Adolescent Counseling, 2(2), 112–124.
https://doi.org/10.1080/23727810.2016.1228770
Kenny, M. C., & McEachern, A. G. (2002). Reporting suspected child abuse: A pilot comparison of middle and high school counselors and principals. Journal of Child Sexual Abuse, 11(2), 59–75.
https://doi.org/10.1300/J070v11n02_04
Klassen, S. L., & Hickman, D. L. (2022). Reporting child abuse and neglect on K-12 campuses. In A. M. Powell (Ed.), Best practices for trauma-informed school counseling. IGI Global.
https://doi.org/10.4018/978-1-7998-9785-9.ch010
Krase, K. S. (2015). Child maltreatment reporting by educational personnel: Implications for racial disproportionality in the child welfare system. Children & Schools, 37(2), 89–99.
https://doi.org/10.1093/cs/cdv005
Lambie, G. W. (2005). Child abuse and neglect: A practical guide for professional school counselors. Professional School Counseling, 8(3), 249–258. http://www.jstor.org/stable/42732466
Lambie, G. W., Ieva, K. P., Mullen, P. R., & Hayes, B. G. (2011). Ego development, ethical decision-making, and legal and ethical knowledge in school counselors. Journal of Adult Development, 18(1), 50–59.
https://doi.org/10.1007/s10804-010-9105-8
Larson, L. M., & Daniels, J. A. (1998). Review of the counseling self-efficacy literature. The Counseling Psychologist, 26(2), 179–218. https://doi.org/10.1177/0011000098262001
Luken, A., Nair, R., & Fix, R. L. (2021). On racial disparities in child abuse reports: Exploratory mapping the 2018 NCANDS. Child Maltreatment, 26(3), 267–281. https://doi.org/10.1177/10775595211001926
McGuire, K., & London, K. (2020). A retrospective approach to examining child abuse disclosure. Child Abuse and Neglect, 99, 1–16. https://doi.org/10.1016/j.chiabu.2019.104263
Mishak, D. A. (2007). An investigation of early career and veteran Iowa elementary school counselors and their classroom guidance programs (Order No. 3265967). Available from ProQuest Dissertations & Theses Global. (304858653).
Morrison, M. A., & Lent, R. W. (2018). The working alliance, beliefs about the supervisor, and counseling self-efficacy: Applying the relational efficacy model to counselor supervision. Journal of Counseling Psychology, 65(4), 512–522. https://doi.org/10.1037/cou0000267
Petersen, A. C., Joseph, J., & Feit, M. (Eds.). (2014). New directions in child abuse and neglect research. The National Academies Press.
Remley, T. P., Jr., Rock, D. W., & Reed, R. M. (2017). Ethical and legal issues in school counseling (4th ed.). American School Counselor Association.
Ricks, L., Carney, J., & Lanier, B. (2020). Attributes, attitudes, and perceived self-efficacy levels of school counselors toward poverty. Georgia School Counselors Association Journal, 27, 51–68.
Ricks, L., Tuttle, M., Land, C., & Chibbaro, J. (2019). Trends and influential factors in child abuse reporting: Implications for early career school counselors. Journal of School Counseling, 17(16). http://www.jsc.montana.edu/articles/v17n16.pdf
Schiele, B. E., Weist, M. D., Youngstrom, E. A., Stephan, S. H., & Lever, N. A. (2014). Counseling self-efficacy, quality of services and knowledge of evidence-based practices in school mental health. The Professional Counselor, 4(5), 467–480. https://doi.org/10.15241/bes.4.5.467
Sedlak, A. J., Mettenburg, J., Basena, M., Petta, I., McPherson, K., Greene, A., & Li, S. (2010). Fourth national incidence study of child abuse and neglect (NIS-4): Report to Congress. U.S. Department of Health and Human Services, Administration for Children and Families. https://www.acf.hhs.gov/sites/default/files/documents/opre/nis4_report_congress_full_pdf_jan2010.pdf
Singleton, O., Newlon, M., Fossas, A., Sharma, B., Cook-Greuter, S. R., & Lazar, S. W. (2021). Brain structure and functional connectivity correlate with psychosocial development in contemplative practitioners and controls. Brain Sciences, 11(6), 728. https://doi.org/10.3390/brainsci11060728
Styck, K. M., Malecki, C. K., Ogg, J., & Demaray, M. K. (2021). Measuring COVID-19-related stress among 4th through 12th grade students. School Psychology Review, 50(4), 530–545.
https://doi.org/10.1080/2372966X.2020.1857658
Swedo, E., Idaikkadar, N., Lemmis, R., Dias, T., Radhakrishnan, L., Stein, Z., Chen, M., Agathis, N., & Holland, K. (2020). Trends in U.S. emergency department visits related to suspected or confirmed child abuse and neglect among children and adolescents aged <18 years before and during the COVID-19 pandemic—United States, January 2019–September 2020. Morbidity and Mortality Weekly Report, 69(49), 1841–1847. https://doi.org/10.15585/mmwr.mm6949al
Tang, A. (2020). The impact of school counseling supervision on practicing school counselors’ self-efficacy in building a comprehensive school counseling program. Professional School Counseling, 23(1).
https://doi.org/10.1177/2156759X20947723
Temkin, D., Harper, K., Stratford, B., Sacks, V., Rodriguez, Y., & Bartlett, J. D. (2020). Moving policy toward a whole school, whole community, whole child approach to support children who have experienced trauma. The Journal of School Health, 90(12), 940–947. https://doi.org/10.1111/josh.12957
Tillman, K. S., Prazak, M. D., Burrier, L., Miller, S., Benezra, M., & Lynch, L. (2015). Factors influencing school counselors’ suspecting and reporting of childhood physical abuse: Investigating child, parent, school, and abuse characteristics. Professional School Counseling, 19(1), 103–115. https://doi.org/10.5330/1096-2409-19.1.103
Tuttle, M., Ricks, L., & Taylor, M. (2019). A child abuse reporting framework for early career school counselors. The Professional Counselor, 9(3), 238–251. https://doi.org/10.15241/mt.9.3.238
U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2021). Child maltreatment 2019. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2019.pdf
White, J., & Flynt, M. (2000). The school counselor’s role in prevention and remediation of child abuse. In J. Wittmer (Ed.), Managing your school counseling program: K-12 developmental strategies (pp. 149–160). Educational Media.
Lacey Ricks, PhD, NCC, NCSC, is an associate professor at Liberty University. Malti Tuttle, PhD, NCC, NCSC, LPC, is an associate professor at Auburn University. Sara E. Ellison, MS, NCC, LAPC, is a doctoral student at Auburn University. Correspondence may be addressed to Lacey Ricks, 1971 University Blvd, Lynchburg, VA 24515, lricks1@liberty.edu.
Aug 20, 2021 | Volume 11 - Issue 3
Alison M. Boughn, Daniel A. DeCino
This article introduces the development and implementation of the Psychological Maltreatment Inventory (PMI) assessment with child respondents receiving services because of an open child abuse and/or neglect case in the Midwest (N = 166). Sixteen items were selected based on the literature, subject matter expert refinement, and readability assessments. Results indicate the PMI has high reliability (α = .91). There was no evidence the PMI total score was influenced by demographic characteristics. A positive relationship was discovered between PMI scores and general trauma symptom scores on the Trauma Symptom Checklist for Children Screening Form (TSCC-SF; r = .78, p = .01). Evidence from this study demonstrates the need to refine the PMI for continued use with children. Implications for future research include identification of psychological maltreatment in isolation, further testing and refinement of the PMI, and exploring the potential relationship between psychological maltreatment and suicidal ideation.
Keywords: psychological maltreatment, child abuse, neglect, assessment, trauma
In 2012, the Centers for Disease Control (CDC; 2012) reported that the total cost of child maltreatment (CM) in 2008, including psychological maltreatment (PM), was $124 billion. Fang et al. (2012) estimated the lifetime burden of CM in 2008 was as high as $585 billion. The CDC (2012) characterized CM as rivaling “other high profile public health problems” (para. 1). By 2015, the National Institutes of Health reported the total cost of CM, based on substantiated incidents, was reported to be $428 billion, a 345% increase in just 7 years; the true cost was predictably much higher (Peterson et al., 2018). Using the sensitivity analysis done by Fang et al. (2012), the lifetime burden of CM in 2015 may have been as high as $2 trillion. If these trends continue unabated, the United States could expect a total cost for CM, including PM, of $5.1 trillion by 2030, with a total lifetime cost of $24 trillion. More concerning, this increase would not account for any impact from the COVID-19 pandemic.
Mental health first responders and child protection professionals may encounter PM regularly in their careers (Klika & Conte, 2017; U.S. Department of Health and Human Services [DHHS], 2018). PM experiences are defined as inappropriate emotional and psychological acts (e.g., excessive yelling, threatening language or behavior) and/or lack of appropriate acts (e.g., saying I love you) used by perpetrators of abuse and neglect to gain organizational control of their victims (American Professional Society on the Abuse of Children [APSAC], 2019; Klika & Conte, 2017; Slep et al., 2015). Victims may experience negative societal perceptions (i.e., stigma), fear of retribution from caregivers or guardians, or misdiagnosis by professional helpers (Iwaniec, 2006; López et al., 2015). They often face adverse consequences that last their entire lifetime (Spinazzola et al., 2014; Tyrka et al., 2013; Vachon et al., 2015; van der Kolk, 2014; van Harmelen et al., 2010; Zimmerman & Mercy, 2010). PM can be difficult to identify because it leaves no readily visible trace of injury (e.g., bruises, cuts, or broken bones), making it complicated to substantiate that a crime has occurred (Ahern et al., 2014; López et al., 2015). Retrospective data outlines evaluation processes for PM identification in adulthood; however, childhood PM lacks a single definition and remains difficult to assess (Tonmyr et al., 2011). These complexities in identifying PM in children may prevent mental health professionals from intervening early, providing crucial care, and referring victims for psychological health services (Marshall, 2012; Spinazzola et al., 2014). The Psychological Maltreatment Inventory (PMI) is the first instrument of its kind to address these deficits.
Child Psychological Maltreatment
Although broadly conceptualized, child PM experiences are described as literal acts, events, or experiences that create current or future symptoms that can affect a victim without immediate physical evidence (López et al., 2015). Others have extended child PM to include continued patterns of severe events that impede a child from securing basic psychological needs and convey to the child that they are worthless, flawed, or unwanted (APSAC, 2019). Unfortunately, these broad concepts lack the specificity to guide legal and mental health interventions (Ahern et al., 2014). Furthermore, legal definitions of child PM vary from jurisdiction to jurisdiction and state to state (Spinazzola et al., 2014). The lack of consistent definitions and quantifiable measures of child PM may create barriers for prosecutors and other helping professionals within the legal system as well as a limited understanding of PM in evidence-based research (American Psychiatric Association [APA], 2013; APSAC, 2019; Klika & Conte, 2017). These challenges are exacerbated by comorbidity with other forms of maltreatment.
Co-Occurring Forms of Maltreatment
According to DHHS (2018), child PM is rarely documented as occurring in isolation compared to other forms of maltreatment (i.e., physical abuse, sexual abuse, or neglect). Rather, researchers have found PM typically coexists with other forms of maltreatment (DHHS, 2018; Iwaniec, 2006; Marshall, 2012). Klika and Conte (2017) reported that perpetrators who use physical abuse, inappropriate language, and isolation facilitate conditions for PM to coexist with other forms of abuse. Van Harmelen et al. (2011) argued that neglectful acts constitute evidence of PM (e.g., seclusion; withholding medical attention; denying or limiting food, water, shelter, and other basic needs).
Consequences of PM Experienced in Childhood
Mills et al. (2013) and Greenfield and Marks (2010) noted PM experiences in early childhood might manifest in physical growth delays and require access to long-term care throughout a victim’s lifetime. Children who have experienced PM may suffer from behaviors that delay or prevent meeting developmental milestones, achieving academic success in school, engaging in healthy peer relationships, maintaining physical health and well-being, forming appropriate sexual relationships as adults, and enjoying satisfying daily living experiences (Glaser, 2002; Maguire et al., 2015). Neurological and cognitive effects of PM in childhood impact children as they transition into adulthood, including abnormalities in the amygdala and hippocampus (Tyrka at al., 2013). Brown et al. (2019) found that adults who reported experiences of CM had higher rates of negative responses to everyday stress, a larger constellation of unproductive coping skills, and earlier mortality rates (Brown et al., 2019; Felitti et al., 1998). Furthermore, adults with childhood PM experiences reported higher rates of substance abuse than those compared to control groups (Felitti et al., 1998).
Trauma-Related Symptomology. Researchers speculate that children exposed to maltreatment and crises, especially those that come without warning, are at greater risk for developing a host of trauma-related symptoms (Spinazzola et al., 2014). Developmentally, children lack the ability to process and contextualize their lived experiences. Van Harmelen et al. (2010) discovered that adults who experienced child PM had decreased prefrontal cortex mass compared to those without evidence of PM. Similarly, Field et al. (2017) found those unable to process traumatic events produced higher levels of stress hormones (i.e., cortisol, epinephrine, norepinephrine); these hormones are produced from the hypothalamic-pituitary-adrenal (HPA) and sympathetic-adrenal-medullary (SAM) regions in the brain. Some researchers speculate that elevated levels of certain hormones and hyperactive regions within the brain signal the body’s biological attempt to reduce the negative impact of PM through the fight-flight-freeze response (Porges, 2011; van der Kolk, 2014).
Purpose of Present Study
At the time of this research, there were few formal measures using child self-report to assess how children experience PM. We developed the PMI as an initial quantifiable measure of child PM for children and adolescents between the ages of 8 and 17, as modeled by Tonmyr and colleagues (2011). The PMI was developed in multiple stages, including 1) a review of the literature, 2) a content validity survey with subject matter experts (SMEs), 3) a pilot study (N = 21), and 4) a large sample study (N = 166). An additional instrument, the Trauma Symptom Checklist for Children Screening Form (TSCC-SF; Briere & Wherry, 2016), was utilized in conjunction with the PMI to explore occurrences of general trauma symptoms among respondents. The following four research questions were investigated:
- How do respondent demographics relate to PM?
- What is the rate of PM experience with respondents who are presently involved in an open CM case?
- What is the co-occurrence of PM among various forms of CM allegations?
- What is the relationship between the frequency of reported PM experiences and the frequency of general trauma symptoms?
Method
Study 1: PMI Item Development and Pilot
Following the steps of scale construction (Heppner et al., 2016), the initial version of the PMI used current literature and definitions from facilities nationwide that provide care for children who have experienced maltreatment and who are engaged with court systems, mental health agencies, or social services. Our lead researcher, Alison M. Boughn, developed a list of 20 items using category identifications from Glaser (2002) and APSAC (2019). Items were also created using Slep et al.’s (2015) proposed inclusion language for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) diagnostic codes and codes from the International Classification of Diseases, 11th edition (ICD-11) definition criteria (APA, 2013). Both Boughn and Daniel A. DeCino, our other researcher, reviewed items for consistency with the research literature and removed four redundant items. The final 16 items were reevaluated for readability for future child respondents using a web-based, age range–appropriate readability checker (Readable, n.d.) and were then presented to local SMEs in a content validity survey to determine which would be considered essential for children to report as part of a child PM assessment.
Expert Validation
A multidisciplinary team (MDT) serving as SMEs completed an online content validity survey created by Boughn. The survey was distributed by a Child Advocacy Center (CAC) manager to the MDT. Boughn used the survey results to validate the PMI’s item content relevance. Twenty respondents from the following professions completed the survey: mental health (n = 6), social services (n = 6), law enforcement (n = 3), and legal services (n = 5). The content validity ratio (CVR) was then calculated for the 16 proposed items.
Results. The content validity survey scale used a 3-point Likert-type scale: 0 = not necessary; 1 = useful, but not essential; and 2 = essential. A minimum of 15 of the 20 SMEs (75% of the sample), or a CVR ≥ .5, was required to deem an item essential (Lawshe, 1975). The significance level for each item’s content validity was set at α = .05 (Ayre & Scally, 2014). After conducting Lawshe’s (1975) CVR and applying the ratio correction developed by Ayre and Scally (2014), it was determined that eight items were essential: Item 2 (CVR = .7), Item 3 (CVR = .9), Item 4 (CVR = .6), Item 6 (CVR = .6), Item 7 (CVR = .8), Item 10 (CVR = .6), Item 15 (CVR = .5), and Item 16 (CVR = .6).
Upon further evaluation, and in an effort to ensure that the PMI items served the needs of interdisciplinary professionals, some items were rated essential for specific professions; these items still met the CVR requirements (CVR = 1) for the smaller within-group sample. These four items were unanimously endorsed by SMEs for a particular profession as essential: Item 5 (CVR Social Services = 1; CVR Law Enforcement = 1), Item 11 (CVR Law Enforcement = 1), Item 13 (CVR Law Enforcement = 1), and Item 14 (CVR Law Enforcement = 1).
Finally, an evaluation of the remaining four items was completed to explore if items were useful, but not essential. Using the minimum CVR ≥ .5, it was determined that these items should remain on the PMI: Item 1 (CVR = .9), Item 8 (CVR = .8), Item 9 (CVR = .9), and Item 12 (CVR = .9). The use of Siegle’s (2017) Reliability Calculator determined the Cronbach’s α level for the PMI to be 0.83, indicating adequate internal consistency. Additionally, a split-half (odd-even) correlation was completed with the Spearman-Brown adjustment of 0.88, indicating high reliability (Siegle, 2017).
Pilot Summary
The focus of the pilot study was to ensure effective implementation of the proposed research protocol following each respondent’s appointment at the CAC research site. The pilot was implemented to ensure research procedures did not interfere with typical appointments and standard procedures at the CAC. Participation in the PMI pilot was voluntary and no compensation was provided for respondents.
Sample. The study used a purposeful sample of children at a local, nationally accredited CAC in the Midwest; both the child and the child’s legal guardian agreed to participate. Because of the expected integration of PM with other forms of abuse, this population was selected to help create an understanding of how PM is experienced specifically with co-occurring cases of maltreatment. Respondents were children who (a) had an open CM case with social services and/or law enforcement, (b) were scheduled for an appointment at the CAC, and (c) were between the ages of 8 and 17.
Measures. The two measures implemented in this study were the developing PMI and the TSCC-SF. At the time of data collection, CAC staff implemented the TSCC-SF as a screening tool for referral services during CAC victim appointments. To ensure the research process did not interfere with chain-of-custody procedures, collected investigative testimony, or physical evidence that was obtained, the PMI was administered only after all normally scheduled CAC procedures were followed during appointments.
PMI. The current version of the PMI is a self-report measure that consists of 16 items on a 4-point Likert-type scale that mirrors the language of the TSCC-SF (0 = never to 3 = almost all the time). Respondents typically needed 5 minutes complete the PMI. Sample items from the PMI included questions like: “How often have you been told or made to feel like you are not important or unlovable?” The full instrument is not provided for use in this publication to ensure the PMI is not misused, as refinement of the PMI is still in progress.
TSCC-SF. In addition to the PMI, Boughn gathered data from the TSCC-SF (Briere & Wherry, 2016) because of its widespread use among clinicians to efficiently assess for sexual concerns, suicidal ideation frequency, and general trauma symptoms such as post-traumatic stress, depression, anger, disassociation, and anxiety (Wherry et al., 2013). The TSCC-SF measures a respondent’s frequency of perceived experiences and has been successfully implemented with children as young as 8 years old (Briere, 1996). The 20-item form uses a 4-point Likert-type scale (0 = never to 3 = almost all the time) composed of general trauma and sexual concerns subscales. The TSCC-SF has demonstrated high internal consistency and alpha values in the good to excellent ranges; it also has high intercorrelations between sexual concerns and other general trauma scales (Wherry & Dunlop, 2018).
Procedures. Respondents were recruited during their scheduled CAC appointment time. Each investigating agency (law enforcement or social services) scheduled a CAC appointment in accordance with an open maltreatment case. At the beginning of each respondent’s appointment, Boughn provided them with an introduction and description of the study. This included the IRB approvals from the hospital and university, an explanation of the informed consent and protected health information (PHI) authorization, and assent forms. Respondents aged 12 and older were asked to read and review the informed consent document with their legal guardian; respondents aged from 8 to 11 were provided an additional assent document to read. Respondents were informed they could stop the study at any time. After each respondent and legal guardian consented, respondents proceeded with their CAC appointment.
Typical CAC appointments consisted of a forensic interview, at times a medical exam, and administration of the TSCC-SF to determine referral needs. After these steps were completed, Boughn administered the PMI to those who agreed to participate in this research study. Following the completion of the TSCC-SF, respondents were verbally reminded of the study and asked if they were still willing to participate by completing the PMI. Willing respondents completed the PMI; afterward, Boughn asked respondents if they were comfortable leaving the assessment room. In the event the respondent voiced additional concerns of maltreatment during the PMI administration, Boughn made a direct report to the respondent’s investigator (i.e., law enforcement officer or social worker assigned to the respondent’s case).
Boughn accessed each respondent’s completed TSCC-SF from their electronic health record in accordance with the PHI authorization and consent after the respondent’s appointment. Data completed on the TSCC-SF allowed Boughn to gather information related to sexual concerns, suicidal ideation, and trauma symptomology. Data gathered from the TSCC-SF were examined with each respondent’s PMI responses.
Results. Respondents were 21 children (15 female, six male) with age ranges from 8 to 17 years with a median age of 12 years. Respondents described themselves as White (47.6%), Biracial (14.2%), Multiracial (14.2%), American Indian/Alaskan Native (10.0%), Black (10.0%), and Hispanic/Latino (5.0%). CM allegations for the respondents consisted of allegations of sexual abuse (86.0%), physical abuse (10.0%), and neglect (5.0%).
Every respondent’s responses were included in the analyses to ensure all maltreatment situations were considered. The reliability of the PMI observed in the pilot sample (N = 21) demonstrated high internal consistency with all 16 initial items (α = .88). The average total score on the PMI in the pilot was 13.29, with respondents’ scores ranging from 1 to 30. A Pearson correlation indicated total scores for the PMI and General Trauma Scale scores (reported on the TSCC-SF) were significantly correlated (r = .517, p < .05).
Study 2: Full Testing of the PMI
The next phase of research proceeded with the collection of a larger data sample (N = 166) to explore the item construct validity and internal reliability (Siyez et al., 2020). Study procedures, data collection, and data storage followed in the pilot study were also implemented with the larger sample. Boughn maintained tracking of respondents who did not want to participate in the study or were unable to because of cognitive functioning level, emergency situations, and emotional dysregulation concerns.
Sample
Based on a power analysis performed using the Raosoft (2004) sample size calculator, the large sample study required a minimum of 166 respondents for statistical significance (Ali, 2012; Heppner et al., 2016). The sample size was expected to account for a 10% margin of error and a 99% confidence level. The calculation of a 99% confidence interval was used to ensure the number of respondents could effectively represent the population accessed within the CAC based on the data from the CM Report (DHHS, 2018). Large sample population data was gathered between September 2018 and May 2019.
Measures
The PMI and TSCC-SF were also employed in Study 2 because of their successful implementation in the pilot. Administration of the TSCC-SF ensured a normed and standardized measure could aid in providing context to the information gathered on the PMI. No changes were made to the PMI or TSCC-SF measures following the review of procedures and analyses in the pilot.
Procedures
Recruitment and data collection/analyses processes mirrored that of the pilot study. Voluntary respondents were recruited at the CAC during their scheduled appointments. Respondents completed an informed consent, child assent, PHI authorization form, TSCC-SF, and PMI. Following the completion of data collection, Boughn completed data entry in the electronic health record to de-identify and analyze the results.
Results
Demographics
All data were analyzed using Statistical Package for the Social Sciences version 24 (SPSS-24). Initial data evaluation consisted of exploration of descriptive statistics, including demographic and criteria-based information related to respondents’ identities and case details. Respondents were between 8 to 17 years of age (M = 12.39) and primarily female (73.5%, n = 122), followed by male (25.3%, n = 42). Additionally, two respondents (n = 2) reported both male and female gender identities. Racial identities were marked by two categories: White (59.6%, n = 99) and Racially Diverse (40.4%, n = 67) respondents. The presenting maltreatment concerns and the child’s relationship to the offender are outlined in Table 1 and Table 2, respectively.
Reliability and Validity of the PMI
The reliability of the PMI observed in its implementation in Study 2 (N = 166) showed even better internal consistency with all 16 initial items (α =.91) than observed in the pilot. Using the Spearman-Brown adjustment (Warner, 2013), split-half reliability was calculated, indicating high internal reliability (.92). Internal consistencies were calculated using gender identity and age demographic variables (see Table 3).
Table 1
Child Maltreatment Allegation by Type (N = 166)
| Allegation |
f |
Rel f |
cf |
% |
| Sexual Abuse |
113 |
0.68 |
166 |
68.07 |
| Physical Abuse |
29 |
0.17 |
53 |
17.47 |
| Neglect |
14 |
0.08 |
24 |
8.43 |
| Multiple Allegations |
6 |
0.04 |
10 |
3.61 |
| Witness to Violence |
3 |
0.02 |
4 |
1.81 |
| Kidnapping |
1 |
0.01 |
1 |
0.60 |
Note. Allegation type reported at initial appointment scheduling
Table 2
Identified Offender by Relationship to Victim (N = 166)
| Offender Relationship |
f |
Rel f |
cf |
% |
| Other Known Adult |
60 |
0.36 |
166 |
36.14 |
| Parent |
48 |
0.29 |
106 |
28.92 |
| Other Known Child (≤ age 15 years) |
15 |
0.09 |
58 |
9.04 |
| Sibling-Child (≤ age 15 years) |
10 |
0.06 |
43 |
6.02 |
| Unknown Adult |
9 |
0.05 |
33 |
5.42 |
| Step-Parent |
8 |
0.05 |
24 |
4.82 |
| Multiple Offenders |
6 |
0.04 |
16 |
3.61 |
| Grandparent |
6 |
0.04 |
10 |
3.61 |
| Sibling-Adult (≥ age 16 years) |
3 |
0.02 |
4 |
1.81 |
| Unknown Child (≤ age 15 years) |
1 |
0.01 |
1 |
0.60 |
Note. Respondent knew the offender (n =156); Respondent did not know offender (n =10)
Table 3
Internal Consistency Coefficients (α) by Gender Identity and Age (N = 166)
| Gender |
n |
α |
M |
SD |
| Female |
122 |
0.90 |
13.2 |
9.1 |
| Male |
42 |
0.94 |
13.5 |
11.0 |
| Male–Female |
2 |
0.26 |
8.5 |
2.5 |
| Age |
|
|
|
|
| 8–12 |
83 |
0.92 |
12.75 |
10.06 |
| 13–17 |
83 |
0.90 |
13.69 |
9.01 |
Note. SD = Standard Deviation; M = Mean
Respondents’ Demographic Characteristics and PM Experiences
For Research Question (RQ) 1 and RQ2, descriptive data were used to generate frequencies and determine the impact of demographic characteristics on average PMI score. To explore this further in RQ1, one-way ANOVAs were completed for the variables of age, gender, racial identity, allegation type, and offender relationships. No significant correlations were found between demographic variables and the PMI items. On average, respondents reported a frequency score of 13.5 (M = 13.5, SD = 9.5) on the PMI. Eight respondents (5%) endorsed no frequency of PM while 95% (N = 158) experienced PM.
Co-Occurrence of PM With Other Forms of Maltreatment
For RQ3, frequency and descriptive data were generated, revealing average age rates of PM reported by maltreatment type. Varying sample representations were discovered in each form of maltreatment (see Table 4). Clear evidence was found that PM co-occurs with each form of maltreatment type; however, how each form of maltreatment interacts with PM is currently unclear given the multiple dimensions of each maltreatment case including, but not limited to, severity, frequency, offender, and victim characteristics.
Table 4
Descriptive and Frequency Data for Co-Occurrence of PM (N = 166)
| Allegation |
n |
M |
SD |
95% CI |
| Sexual Abuse |
113 |
13.04 |
9.01 |
[11.37, 14.72] |
| Physical Abuse |
29 |
12.45 |
10.53 |
[8.44, 16.45] |
| Neglect |
14 |
14.57 |
12.16 |
[7.55, 21.60] |
| Multiple Allegations |
5 |
17.40 |
8.88 |
[6.38, 28.42] |
| Witness to Violence |
3 |
7.67 |
5.03 |
[–4.84, 20.17] |
| Kidnapping |
1 |
n/a |
n/a |
Missing |
Note. CI = Confidence Interval; SD = Standard Deviation; M = Mean; n/a = not applicable
PM Frequency and General Trauma Symptoms
For RQ4, Pearson’s correlation was used to calculate frequency score relationships between the PMI and TSCC-SF. There was a statistically significant relationship between the PMI and total frequency of general trauma symptoms on the TSCC-SF [r(164) = .78, p < .01, r² = .61] (Sullivan & Feinn, 2012). Cohen’s d, calculated from the means for each item as well as the pooled standard deviation, indicated a small effect relationship (d = .15) between general trauma and PMI frequencies (see Figure 1).
Figure 1
Correlation Between PMI and TSCC-SF General Trauma Subscale
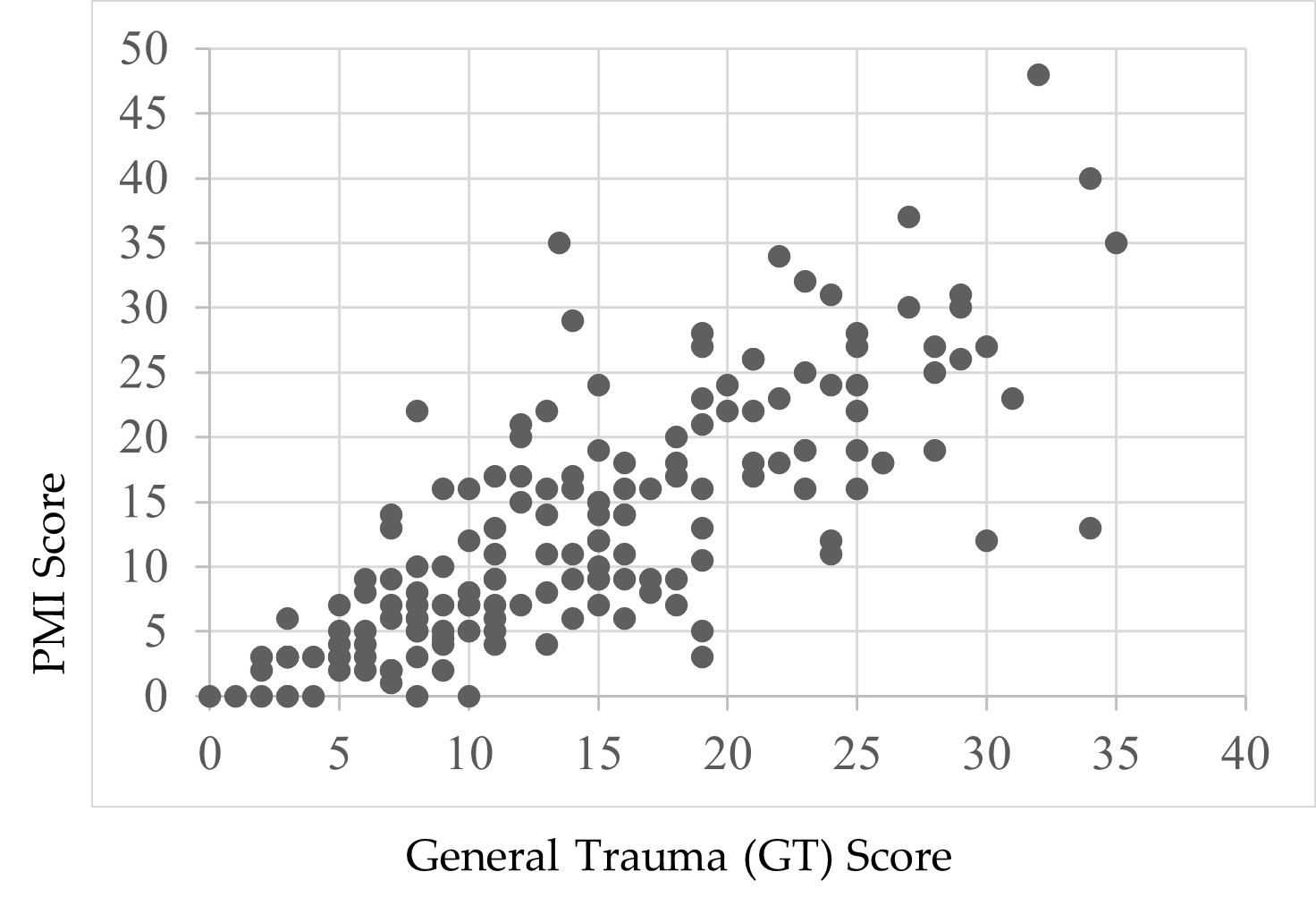
Note. Scores were endorsed by respondents’ self-reports.
Child Suicidal Ideation Reports and the PMI
Following a review of the findings of Thompson et al. (2005) and Wherry et al. (2013) that children who reported experiencing CM also experienced suicidal ideation, Boughn performed an additional two-way ANOVA that examined the effect of suicidal ideation on the PMI total score. A significant relationship—F(1, 164) = 49.52, p < .01, η2 = .23—between respondents’ PMI scores and thoughts of suicide was found. Respondents who did not report thoughts of suicide (59.0%, n = 98) indicated lower rates of PM (M = 9.37, SD = 7.97) compared to children who did report thoughts of suicide (41.0%, n = 68, M = 18.77, SD = 9.12). A preliminary review of this finding demonstrates the severity of PM’s impact on child victims.
Discussion
This study was designed with the aim of developing a tool to support accurate identification of PM among children and adolescents. Findings from its first large-scale implementation provide a foundational view to the occurrence of PM in terms of demographic characteristics, comorbidity of PM with other forms of abuse, and the relationship between PM and trauma. The analyses yielded both expected and unexpected results based on the extant research.
PM and Demographic Characteristics
Race
There was no significant effect when exploring the data related to racial demographics and PM. The respondent sample closely reflected the geographical area’s known racial demographics at the time of the study, reflecting a population approaching 80% White with residents of all other known races below 5% for each racial group (U.S. Census Bureau, 2020). Although researchers (Dakil et al., 2011) anticipated children identifying as racial minorities would be included in the representation of CM reports, evidence from this study potentially reveals a greater than expected gap in reporting for minority-race populations (Bernard & Harris, 2018; Font & Maguire-Jack, 2015). This suggests that there may be additional, unidentified barriers influencing the reporting of maltreatment among minority-race populations.
Gender
A lack of gender identity representation was evident in the data, consistent with prior research (Sivagurunathan et al., 2019). Respondents who self-identified with both male and female gender identities (1.2%) and as male (25.3%) were represented less frequently compared to female respondents (73.5%). This is not inherently a limitation of this study, as research shows that just 10% of males in the United States report their sexual abuse (Sivagurunathan et al., 2019). People who identify as male may face harmful cultural messages that enhance negative stigma for victims of abuse, causing increased feelings of weakness or vulnerability (Alaggia & Mishna, 2014). This finding may support claims that male trauma survivors feel stigmatized and report their experiences less frequently (Easton, 2012).
Additionally, children who identify outside traditional gender binary norms and definitions need more access to inclusive representation on screening assessments. Assessments like the TSCC-SF may be using antiquated gender- or biological sex–normed checkboxes, which leave certain groups underrepresented in research studies (Neukrug & Fawcett, 2015). These practices may present inaccurate findings, inadvertently reinforce discriminatory expectations, and generate inaccurate referrals. Non-binary youth encounter barriers that may compound their ability to effectively access supports in their daily life related to coming out, social violence, lack of peer and/or adult acceptance, discrimination, isolation, higher rates of suicide, and lack of representation in mainstream society (Bialer & McIntosh, 2016; Zimman, 2009). In this study, representation of non-binary respondents, specifically those who reported both male and female gender identities, was reported; this warrants further exploration to assess barriers among non-binary gender youth and their experiences with child PM (Bos et al., 2019).
Offender Relationships
Frequency data for a child’s relationship with the offender were not found to be significant either for known offenders (M = 13.35) or unknown offenders (M = 11.2). In this study, 94% of the respondents already knew their offender (n = 156). This finding is consistent with previous research that has found that although child abduction and stranger danger are real phenomena, children are more likely to experience CM as a result of relationships with familiar individuals (Walsh & Brandon, 2011).
Co-Occurrence of PM With Other Abuse
Only eight respondents (5%) endorsed no frequency of PM; the average total PM frequency rate for respondents in this study was 13.5 out of a possible 48, indicating extreme severity. In this study, we found evidence that PM is a co-occurring experience for children with open maltreatment cases, yet clinicians still lack formal, valid assessments to determine PM alone. Our findings support the National Children’s Alliance’s (NCA; 2016) call for clinicians to follow practice guidelines in accordance with state and national guidelines as they relate to mandatory reporting of CM concerns and determination of whether PM plus other forms of maltreatment may be present for child victims seeking services.
Comorbidity of PM and Trauma
PM-related experiences on the PMI and general trauma symptoms from the TSCC-SF warrant discussion. The PMI illustrated a significant relationship with the TSCC-SF general trauma subscale (Briere & Wherry, 2016). More than half (61%) of the variance on the PMI was connected to general trauma symptoms, suggesting that higher rates of PM experiences may increase trauma-related symptoms. For example, previous researchers have found adverse childhood experiences and signs of trauma-related symptoms lead to serious mental health diagnoses, early mortality, and/or significant biological health risks in children (Tyrka et al., 2013; Vachon et al., 2015; Zimmerman & Mercy, 2010). Further exploration to determine if and how PM influences other trauma-related symptoms in children throughout their life span would expand upon the results of this study.
Suicidal Ideation
Finally, our data revealed a significant effect between respondent endorsement of suicidal ideation and PMI total scores. PM experiences accounted for 23% of the variance for children who reported thoughts of suicide (41%, n = 68) compared to those who did not report thoughts of suicide (59%, n = 98). This finding is consistent with prior research exploring children’s experiences with maltreatment and suicidal thoughts (Thompson et al., 2005; Wherry et al., 2013).
Limitations
This study has several limitations. First, by developing the PMI using national definitions, some regional and localized nuances were not considered. Second, data collected for this study were from a single Midwest CAC; thus, the data are limited in geographic generalizability. Third, the majority of respondents were White, and a more diverse sample would have been more representative of the region in which data were collected. Fourth, 99% of respondents identified as either male or female and may reflect an underrepresentation of non-binary or gender fluid youth in the results of this study. Fifth, this study relied heavily on quantitative data, which limited the ability to analyze each individual’s experiences with PM as they might describe from their unique perspectives.
Implications for Research and Practice
The results of this study provide several areas for future research. While the PMI demonstrated good internal consistency across all items (α =.91), more research with diverse populations across the United States is needed. Research from other geographical locations may demonstrate how reporting patterns for PM interact with ethnicity, culture, and elements of social expectations (Spinazzola et al., 2014).
The initial results of this study indicate the PMI may be a useful tool for children to report PM experiences in CAC settings; however, future research at other CACs and similar treatment facilities is needed to determine the PMI’s true utility and scalability. Future analysis (i.e., exploratory factor analysis and confirmatory factor analysis) of the PMI may also identify factors and help refine the instrument.
More research with the PMI can expand researchers’ knowledge of PM and services needed to help children. Working with other CACs, child protection professionals, and the NCA may help bridge current gaps in interdisciplinary assessment and care and establish a stable and comprehensive understanding of PM (López et al., 2015). Furthermore, understanding how CACs are equipped to identify and handle PM cases may provide useful insights to help improve services for children in need. Although some CACs may have a variety of professionals working in specific roles, some CACs may be understaffed, causing staff to take on multiple and overlapping roles. It is important to understand if and how different combinations of trained professionals influence children reporting PM (Hart & Glaser, 2011; NCA, 2016).
More research with the PMI is needed for refinement and to ensure the instrument is not misused. Releasing the PMI at this stage to clinicians and researchers without a fully developed assessment manual may lead to inappropriate or ineffective administration of the PMI and potentially unethical practice that could place children at risk. Future research and refinement of the PMI may provide clinicians and researchers a reliable and valid tool that is grounded in consistent theory and practice.
Conclusion
The PMI was developed to assess child PM and offers researchers and clinicians useful findings. In supporting research (Arslan, 2017; Bernstein et al., 2013; Raparia et al., 2016), child PM is a serious and often harmful combination of experiences that requires professional intervention (APSAC, 2019). For children reporting PM experiences, the PMI may help mental health and other care providers determine which services are needed. Findings from this study suggest differences in demographic variables are minimal for PM. Overall PMI scores were correlated to the general trauma subscale on the TSCC-SF, and the PMI revealed higher rates of PM for children experiencing suicidal ideation. The findings are the beginning of a measure designed to illustrate the depth and frequency of PM for children. With the PMI, early PM intervention becomes possible for a once invisible form of maltreatment.
Conflict of Interest and Funding Disclosure
Data collected and content shared in this study
were part of a dissertation study, which was
awarded the 2020 Dissertation Excellence Award
by the National Board for Certified Counselors.
The Psychological Maltreatment Inventory (PMI)
items were not released in this publication to protect
victims of child maltreatment and to ensure future
publications can address comprehensive revisions
made to the PMI.
References
Ahern, E. C., Hershkowitz, I., Lamb, M. E., Blasbalg, U., & Winstanley, A. (2014). Support and reluctance in the pre-substantive phase of alleged child abuse victim investigative interviews: Revised versus standard NICHD protocols. Behavioral Sciences & the Law, 32(6), 762–774. https://doi.org/10.1002/bsl.2149
Alaggia, R., & Mishna, F. (2014). Self psychology and male child sexual abuse: Healing relational betrayal. Clinical Social Work Journal, 42(1), 41–48. https://doi.org/10.1007/s10615-013-0453-2
Ali, S. A. (2012). Sample size calculation and sampling techniques. Journal of the Pakistan Medical Association, 62(6), 624–626. https://jpma.org.pk/PdfDownload/3482
American Professional Society on the Abuse of Children. (2019). APSAC practice guidelines: The investigation and determination of suspected psychological maltreatment of children and adolescents. https://bit.ly/3jI7AhJ
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Arslan, G. (2017). Psychological maltreatment, coping strategies, and mental health problems: A brief and effective measure of psychological maltreatment in adolescents. Child Abuse & Neglect, 68, 96–106. https://doi.org/10.1016/j.chiabu.2017.03.023
Ayre, C., & Scally, A. J. (2014). Critical values for Lawshe’s content validity ratio: Revisiting the original methods of calculation. Measurement and Evaluation in Counseling and Development, 47(1), 79–86. https://doi.org/10.1177%2F0748175613513808
Bernard, C., & Harris, P. (2018). Serious case reviews: The lived experience of Black children. Child & Family Social Work, 24(2), 256–263. https://doi.org/10.1111/cfs.12610
Bernstein, R. E., Measelle, J. R., Laurent, H. K., Musser, E. D., & Ablow, J. C. (2013). Sticks and stones may break my bones but words relate to adult physiology? Child abuse experience and women’s sympathetic nervous system response while self-reporting trauma. Journal of Aggression, Maltreatment & Trauma, 22(10), 1117–1136. https://doi.org/10.1080/10926771.2013.850138
Bialer, P. A., & McIntosh, C. A. (2016). Discrimination, stigma, and hate: The impact on the mental health and well-being of LGBT people. Journal of Gay & Lesbian Mental Health, 20(4), 297–298. https://doi.org/10.1080/19359705.2016.1211887
Bos, H., de Haas, S., & Kuyper, L. (2019). Lesbian, gay, and bisexual adults: Childhood gender nonconformity, childhood trauma, and sexual victimization. Journal of Interpersonal Violence, 34(3), 496–515. https://doi.org/10.1177%2F0886260516641285
Briere, J. (1996). Trauma Symptom Checklist for Children (TSCC), professional manual. Psychological Assessment Resources.
Briere, J., & Wherry, J. (2016). Development and validation of the TSCC Screening Form (TSCC-SF) and TSCYC Screening Form (TSCYC-SF). Psychological Assessment Resources.
Brown, S. M., Bender, K., Orsi, R., McCrae, J. S., Phillips, J. D., & Rienks, S. (2019). Adverse childhood experiences and their relationship to complex health profiles among child welfare–involved children: A classification and regression tree analysis. Health Services Research, 54(4), 902–911. https://doi.org/10.1111/1475-6773.13166
Centers for Disease Control. (2012). Child abuse and neglect cost the United States $124 billion [Press release]. https://bit.ly/3jYbpAF
Dakil, S. R., Cox, M., Lin, H., & Flores, G. (2011). Racial and ethnic disparities in physical abuse reporting and Child Protective Services interventions in the United States. Journal of the National Medical Association, 103(9–10), 926–931. https://doi.org/10.1016/S0027-9684(15)30449-1
Easton, S. D. (2012). Disclosure of child sexual abuse among adult male survivors. Clinical Social Work Journal, 41, 344–355. https://doi.org/10.1007/s10615-012-0420-3
Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect, 36(2), 156–165. https://doi.org/10.1016/j.chiabu.2011.10.006
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Field, T. A., Jones, L. K., & Russell-Chapin, L. A. (Eds.). (2017). Neurocounseling: Brain-based clinical approaches. American Counseling Association.
Font, S. A., & Maguire-Jack, K. (2015). Decision-making in Child Protective Services: Influences at multiple levels of the social ecology. Child Abuse & Neglect, 47, 70–82. https://doi.org/10.1016/j.chiabu.2015.02.005
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment): A conceptual framework. Child Abuse & Neglect, 26(6–7), 697–714. https://doi.org/10.1016/S0145-2134(02)00342-3
Greenfield, E. A., & Marks, N. F. (2010). Identifying experiences of physical and psychological violence in childhood that jeopardize mental health in adulthood. Child Abuse & Neglect, 34(3), 161–171. https://doi.org/10.1016/j.chiabu.2009.08.012
Hart, S. N., & Glaser, D. (2011). Psychological maltreatment – Maltreatment of the mind: A catalyst for advancing child protection toward proactive primary prevention and promotion of personal well-being. Child Abuse & Neglect, 35(10), 758–766. https://doi.org/10.1016/j.chiabu.2011.06.002
Heppner, P. P., Wampold, B. E., Owen, J., Thompson, M. N., & Wang, K. T. (2016). Research design in counseling (4th ed.). Cengage.
Iwaniec, D. (2006). The emotionally abused and neglected child: Identification, assessment and intervention: A practice handbook (2nd ed.). Wiley.
Klika, J. B., & Conte, J. R. (Eds.). (2017). The APSAC handbook on child maltreatment (4th ed.). SAGE.
Lawshe, C. H. (1975). A quantitative approach to content validity. Personnel Psychology, 28(4), 563–575. https://doi.org/10.1111/j.1744-6570.1975.tb01393.x
López, M., Fluke, J. D., Benbenishty, R., & Knorth, E. J. (2015). Commentary on decision-making and judgments in child maltreatment prevention and response: An overview. Child Abuse & Neglect, 49, 1–11. https://doi.org/10.1016/j.chiabu.2015.08.013
Maguire, S. A., Williams, B., Naughton, A. M., Cowley, L. E., Tempest, V., Mann, M. K., Teague, M., & Kemp, A. M. (2015). A systematic review of the emotional, behavioural and cognitive features exhibited by school-aged children experiencing neglect or emotional abuse. Child: Care, Health and Development, 41(5), 641–653. https://doi.org/10.1111/cch.12227
Marshall, N. A. (2012). A clinician’s guide to recognizing and reporting parental psychological maltreatment of children. Professional Psychology: Research and Practice, 43(2), 73–79. https://doi.org/10.1037/a0026677
Mills, R., Scott, J., Alati, R., O’Callaghan, M., Najman, J. M., & Strathearn, L. (2013). Child maltreatment and adolescent mental health problems in a large birth cohort. Child Abuse & Neglect, 37(5), 292–302. https://doi.org/10.1016/j.chiabu.2012.11.008
National Children’s Alliance. (2016). Putting standards into practice: A guide to implementing the 2017 standards for accredited members (revised 2016). http://www.nationalchildrensalliance.org/wp-content/uploads/2015/06/NCA2017-StandardsIntoPractice-web.pdf
Neukrug, E. S., & Fawcett, R. C. (2015). The essentials of testing and assessment: A practical guide for counselors, social workers, and psychologies, enhanced (3rd ed.). Cengage.
Peterson, C., Florence, C., & Klevens, J. (2018). The economic burden of child maltreatment in the United States, 2015. Child Abuse & Neglect, 86, 178–183.
https://doi.org/10.1016/j.chiabu.2018.09.018
Porges, S. W. (2011). The polyvagal theory: Neurophysiological foundations of emotions, attachment, communication, and self-regulation. W. W. Norton.
Raosoft. (2004). Sample size calculator. http://www.raosoft.com/samplesize.html
Raparia, E., Coplan, J. D., Abdallah, C. G., Hof, P. R., Mao, X., Mathew, S. J., & Shungu, D. C. (2016). Impact of childhood emotional abuse on neocortical neurometabolites and complex emotional processing in patients with generalized anxiety disorder. Journal of Affective Disorders, 190, 414–423. https://doi.org/10.1016/j.jad.2015.09.019
Readable. (n.d.). https://readable.com
Siegle, R. (2017). Educational research basics: Excel spreadsheet to calculate instrument reliability estimates. https://researchbasics.education.uconn.edu/excel-spreadsheet-to-calculate-instrument-reliability-estimates
Sivagurunathan, M., Orchard, T., & Evans, M. (2019). Barriers to utilization of mental health services amongst male child sexual abuse survivors: Service providers’ perspective. Journal of Child Sexual Abuse, 28(7), 819–839. https://doi.org/10.1080/10538712.2019.1610823
Siyez, D. M., Esen, E., Seymenler, S., & Öztürk, B. (2020). Development of wellness scale for emerging adults: Validity and reliability study. Current Psychology.
https://doi.org/10.1007/s12144-020-00672-w
Slep, A. M. S., Heyman, R. E., & Foran, H. M. (2015). Child maltreatment in DSM-5 and ICD-11. Family Process, 54(1), 17–32. https://doi.org/10.1111/famp.12131
Spinazzola, J., Hodgdon, H., Liang, L.-J., Ford, J. D., Layne, C. M., Pynoos, R., Briggs, E. C., Stolbach, B., & Kisiel, C. (2014). Unseen wounds: The contribution of psychological maltreatment to child and adolescent mental health and risk outcomes. Psychological Trauma: Theory, Research, Practice, and Policy, 6(Suppl 1), S18–S28. https://doi.org/10.1037/a0037766
Sullivan, G. M., & Feinn, R. (2012). Using effect size—or why the p value is not enough. Journal of Graduate Medical Education, 4(3), 279–282. https://doi.org/10.4300/JGME-D-12-00156.1
Thompson, R., Briggs, E., English, D. J., Dubowitz, H., Lee, L.-C., Brody, K., Everson, M. D., & Hunter, W. M. (2005). Suicidal ideation among 8-year-olds who are maltreated and at risk: Findings from the LONGSCAN studies. Child Maltreatment, 10(1), 26–36. https://doi.org/10.1177%2F1077559504271271
Tonmyr, L., Draca, J., Crain, J., & MacMillian, H. L. (2011). Measurement of emotional/psychological child maltreatment: A review. Child Abuse & Neglect, 35(10), 767–782.
https://doi.org/10.1016/j.chiabu.2011.04.011
Tyrka, A. R., Burgers, D. E., Philip, N. S., Price, L. H., & Carpenter, L. L. (2013). The neurobiological correlates of childhood adversity and implications for treatment. Acta Psychiatrica Scandinavica, 128(6), 434–447. https://doi.org/10.1111/acps.12143
U.S. Census Bureau. (2020). Quick facts. https://www.census.gov
U.S. Department of Health & Human Services. (2018). Child maltreatment 2016 (27th ed.). https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2016.pdf
Vachon, D. D., Krueger, R. F., Rogosch, F. A., & Cicchetti, D. (2015). Assessment of the harmful psychiatric and behavioral effects of different forms of child maltreatment. JAMA Psychiatry, 72(11), 1135–1142. https://doi.org/10.1001/jamapsychiatry.2015.1792
van der Kolk, B. (2014). The body keeps the score: Brain, mind, and body in the healing of trauma. Penguin Books.
van Harmelen, A.-L., Elzinga, B. M., Kievit, R. A., & Spinhoven, P. (2011). Intrusions of autobiographical memories in individuals reporting childhood emotional maltreatment. European Journal of Psychotraumatology, 2(1), 7336. https://doi.org/10.3402/ejpt.v2i0.7336
van Harmelen, A.-L., van Tol, M.-J., van der Wee, N. J. A., Veltman, D. J., Aleman, A., Spinhoven, P., van Buchem, M. A., Zitman, F. G., Penninx, B. W. J. H., & Elzinga, B. M. (2010). Reduced medial prefrontal cortex volume in adults reporting childhood emotional maltreatment. Biological Psychiatry, 68(9), 832–838. https://doi.org/10.1016/j.biopsych.2010.06.011
Walsh, K., & Brandon, L. (2011). Their children’s first educators: Parents’ views about child sexual abuse prevention education. Journal of Child and Family Studies, 21, 734–746.
https://doi.org/10.1007/s10826-011-9526-4
Warner, R. M. (2013). Applied statistics: From bivariate through multivariate techniques (2nd ed.). SAGE.
Wherry, J. N., Baldwin, S., Junco, K., & Floyd, B. (2013). Suicidal thoughts/behaviors in sexually abused children. Journal of Child Sexual Abuse, 22(5), 534–551. https://doi.org/10.1080/10538712.2013.800938
Wherry, J. N., & Dunlop, C. E. (2018). TSCC and TSCYC screening forms in a clinical sample: Reliability, validity, and creating local clinical norms. Child Maltreatment, 23(1), 74–84.
https://doi.org/10.1177%2F1077559517725207
Zimman, L. (2009). ‘The other kind of coming out’: Transgender people and the coming out narrative genre. Gender and Language, 3(1), 53–80. https://doi.org/10.1558/genl.v3i1.53
Zimmerman, F., & Mercy, J. (2010). A better start: Child maltreatment prevention as a public
health priority. Zero to Three, 30(5), 4–10.
Alison M. Boughn, PhD, NCC, LIMHP (NE), LMHC (IA), LPC-MH (SD), ATR-BC, QMHP, TF-CBT, is an assistant professor and counseling department chair at Wayne State College. Daniel A. DeCino, PhD, NCC, LPC, is an assistant professor and Interim Program Coordinator at the University of South Dakota. Correspondence may be addressed to Alison M. Boughn, Wayne State College, 1111 Main Street, Wayne, NE 68787, albough1@wsc.edu.
Sep 1, 2019 | Volume 9 - Issue 3
Malti Tuttle, Lacey Ricks, Margie Taylor
School counselors experience various emotions, such as anxiety, when in the role of mandated reporter of child abuse. This manuscript addresses how early career school counselors might experience distress because of the lack of established child abuse reporting procedures, fear of repercussions for the school counselor or student, and limited training in identifying types of abuse. Based on the previous literature, the authors discuss the imperative role early career school counselors have as mandated reporters and provide a framework to assist in the child abuse reporting process. The framework, specifically designed for school counselors, is collaborative in nature and emphasizes maintaining ethical and legal standards, obtaining continual professional development, and following best practices for mandated child abuse reporting.
Keywords: child abuse, mandated reporter, early career, school counselors, framework
School counselors often experience anxiousness regarding child abuse reporting (Lambie, 2005; Sikes, 2008). Early career school counselors in particular can experience this because of the lack of established reporting procedures (Lambie, 2005), fear of repercussions for the school counselor or student (Bryant & Milsom, 2005; Kenny, 2001), and limited training on identifying types of abuse (Alvarez, Kenny, Donohue, & Carpin, 2004; Kenny, 2001). Because of these factors, early career school counselors seek and request support to assist them with the child abuse reporting process and clarification on these procedures (Bryant & Baldwin, 2010; Ricks, Tuttle, Land, & Chibbaro, 2019). Therefore, we propose a child abuse reporting framework designed to assist early career school counselors, who are ethically and legally mandated to report child abuse, in the child abuse reporting process (American School Counselor Association, 2016; Sikes, Remley, & Hays, 2010). This manuscript is different from previous literature (e.g., Alvarez et al., 2004; Bryant & Milsom, 2005; Kenny, 2001; Lambie, 2005; Sikes, 2008) because it focuses specifically on the concerns and needs of early career school counselors, as well as expands on previous literature. For the purpose of this article, child abuse and neglect are defined by the Child Abuse Prevention and Treatment Act Reauthorization Act of 2010 (2010) as “any recent act or failure to act on the part of a parent or caretaker which results in death, serious harm, sexual abuse, or exploitation, or an act or failure to act which presents an imminent risk of serious harm” (p. 6).
Child maltreatment can have lasting harmful effects on victims. Maltreatment includes “medical neglect, neglect or deprivation of necessities, physical abuse, psychological or emotional maltreatment, sexual abuse, and other forms included in state law” (U.S. Department of Health & Human Services [USDHHS], Administration for Children, Youth and Families, & Children’s Bureau, 2019, p. 108). Minimum standards for what constitutes child abuse are defined by federal law and further stipulated under state law (ASCA, 2015; Stone, 2013). Laws and definitions of child abuse can vary across each state, and ASCA (2019b) provides information on Child Protective Services (CPS), laws, and statutes for different states. Furthermore, ASCA’s (2015) position statement, The School Counselor and Child Abuse and Neglect Prevention, states: “It is the school counselor’s legal, ethical and moral responsibility to report suspected cases of child abuse and neglect to the proper authorities” (p. 7).
Mandated reporting is among the many responsibilities school counselors perform within the school setting. School counselors are required by the Child Abuse Prevention and Treatment Act (CAPTA) of 1974 to report suspected cases of child abuse to the appropriate authorities. School counselors need to become familiar with federal guidelines, their state laws, and school policies regarding child abuse and mandated reporting laws and procedures. ASCA (2016) speaks to the role of the school counselor in child abuse reporting by stating that school counselors are ethically and legally responsible for reporting suspected cases of child abuse to appropriate agencies. These agencies include, but are not limited to, CPS, law enforcement agencies, attorneys, social workers, and case managers assigned to open cases (Bryant, 2009; Hinkelman & Bruno, 2008).
It is essential for school counselors to have knowledge and an understanding of the ethical standards and legal statutes that apply to child abuse reporting (Corey, Corey, & Callanan, 2011). Two sections from the ASCA Ethical Standards for School Counselors (2016) specifically address child abuse reporting. The “Serious and Foreseeable Harm to Self and Others” (A.9.) section speaks to ensuring the welfare and safety of students by making appropriate reports to CPS, parents and guardians, and agencies and authorities regarding the abuse. The “Bullying, Harassment and Child Abuse” section (A.11.) highlights the ethical mandates school counselors must follow when reporting suspected child abuse (ASCA, 2016).
Froeschle and Crews (2010) echoed the vital role ethics and legalities play as well as the challenges presented in working with students. Because school counselors serve as an integral part of protecting the health and well-being of children by performing in the role of responsible mandated reporters, it is imperative that school counselors recognize the importance of maintaining student welfare when making decisions pertaining to suspected child abuse. Research regarding school counselors’ ethical and legal competency is limited; however, it has been noted that knowledge of ethical and legal parameters around child abuse reporting has increased in coursework and trainings (Lambie, Ieva, & Mullen, 2013). This necessitates the call for school counselors to have additional knowledge and training in detecting signs and symptoms of abuse and a general understanding of how to report child abuse.
Although the ethical and legal responsibilities of school counselors in the role of reporting child abuse and maltreatment has been recognized (Kenny & Abreu, 2016), counselors might not have received adequate training in identifying and reporting child abuse. Therefore, the authors of this article further recognized the dutiful call to provide a framework for early career school counselors to assist with the process of reporting child abuse. The purpose of this manuscript is to develop an effective mandated reporting framework for school counselors. The development of the framework within this manuscript was guided by the ASCA Ethical Standards for School Counselors (2016), recommendations by early career school counselors (Ricks et al., 2019), previous literature and research studies (Bryant & Baldwin, 2010; Lambie, 2005; Sikes, 2008), and current mandated reporter procedures (Hogelin, 2013). However, it is imperative to acknowledge that within any such framework, state and school policy must be followed and considered.
Child Abuse Trends
Mandated reporting is increasingly needed because of the extent of child abuse and neglect in the United States. In 2015, CPS agencies received approximately 4.1 million referrals for potential child abuse or neglect, which involved roughly 7.5 million children (USDHSS et al., 2019). Gullatt (1999) published a manuscript that reported the number of abused children to be astonishing. Despite decades passing since the 1990s, the number of children abused today is still considered shocking. In 2017 it was reported that 674,000 children were victims of abuse and neglect (USDHHS et al., 2019). The number of children abused increased by 2.7% from 2013 to 2017, and it is estimated that 1,720 children died from abuse and neglect in 2017, a rate of 2.32 per 100,000 children (USDHSS et al., 2019). These staggering statistics attest to the need for school counselors to become more educated and confident in reporting child abuse.
“Abuse is encountered in all socioeconomic groups, races, and religions” (Lambie, 2005, p. 250). The racial distribution for all children within the United States who experience abuse is 50.7% Caucasian, 13.7% African American, and 25.2% Hispanic (USDHHS et al., 2019). The percentages of victims are similar for both boys (48.6%) and girls (51.0%; USDHHS et al, 2019); however, rates of abuse seem to vary by socioeconomic status. According to Sedlak et al. (2010), children from households of low socioeconomic status experience some type of maltreatment at a rate more than five times higher than other children; they also were more than three times as likely to experience abuse and about seven times more likely to experience neglect. Bias has been suggested as a cause of differentiation in demographics of reported child abuse cases. When looking at school counseling reporting trends, a recent study specifically examining school counselors’ decisions found school counselors were not statistically more likely to report students based on race but were more likely to suspect abuse when students were from a middle or lower socioeconomic class (Tillman et al., 2015). However, research data suggest that the variation in the overrepresentation of low-income children is driven by the presence of increased risk factors among this population (Jonson-Reid, Drake, & Kohl, 2009).
Despite the increased need for school counselors to be proficiently trained in mandated reporting, many school counselors experience challenges with the reporting process. School counselors are frontline workers who develop trusting relationships with children, which in turn leaves school counselors with a much higher reporting rate than other professionals within the school (Bryant, 2009). A study by Bryant and Milsom (2005) found the second most reported legal issue experienced by school counselors was whether to report alleged sexual abuse. However, there are some laws that no longer give school counselors the choice. Furthermore, according to Davis (1995) and Sikes (2008), the reporting of child and sexual abuse cases are the second highest reasons for school counselors to attend court. The increase in reports of child abuse, legal issues experienced by school counselors, and the frequency of court appearances by school counselors also are valid reasons for developing a better, more effective, and easily understood framework for mandated reporting.
Challenges in Reporting Child Abuse
Reporting child abuse and neglect can often be a challenging and stressful experience for school counselors. This might be due to difficulty in collaborating with reporting agencies; the lack of training in child abuse symptomology (Alvarez et al., 2004; Kenny, 2001); unclear guidelines for reporting child abuse (Lambie, 2005), including what defines reasonable suspicion to report (Levi & Brown, 2005); and the fear of repercussions from parents and school officials (Bryant & Milsom, 2005; Kenny, 2001). A recent research study (Ricks et al., 2019) identified challenges faced by early career school counselors, which provided the impetus to further consult the literature to seek what circumstances led to these challenges and how to mitigate potential barriers to reporting child abuse. Each of these challenges are discussed in further detail.
Collaboration with reporting agencies. A review of literature on school counselors’ relationships with reporting agencies found that the relationships are disconnected and misunderstood (Bryant & Baldwin, 2010). A study conducted by Sikes et al. (2010) indicated most school counselors had negative experiences when making reports to reporting agencies. Participants in the study reported high levels of anxiety because of the concern that the report would not be investigated. Consistent with findings from the research study conducted by Ricks et al. (2019), Bryant and Baldwin (2010) found that school counselors experience frustration and irritation when the school counselor’s report did not result in an investigation from CPS. Furthermore, a study conducted by Behun, Cerrito, Delmonico, and Kolbert (2019) found that school counselors chose not to report suspected child abuse because of the belief CPS would not intervene effectively.
Furthermore, school counselors experience concern when CPS does not provide follow-up information regarding the report of alleged abuse. A study conducted by Bryant (2009) found school counselors reported 77% of alleged cases of child abuse to CPS, and only 66% of those cases were investigated by CPS. Some school counselors believe they are entitled to information about the ongoing investigation of the report made; however, because of confidentiality, CPS is not legally obligated to provide school counselors with detailed information about an ongoing investigation (Child Welfare Information Gateway, 2003; Minnesota Department of Human Services, 2016). After the initial assessment, the CPS caseworker will determine the disposition of the reported case based on state laws, agency guidelines, and gathered information (Child Welfare Information Gateway, 2003).
According to the Child Welfare Information Gateway (2003), CPS agencies use different terminology for this decision. Most states use a two-tiered system of substantiated–unsubstantiated or founded–unfounded. Some states use a three-tiered system of substantiated, indicated, or unsubstantiated. The indicated classification means evidence of abuse has been found, but not enough to substantiate the case. A school counselor can be provided information on whether the case was indicated or not indicated by CPS (Minnesota Department of Human Services, 2016; Washington State Department of Social & Health Services, 2018).
To resolve this issue, further education and collaboration with CPS and other agencies can aid school counselors’ understanding of policies, leading to less frustration for school counselors. Bryant (2009) recommended CPS provide additional training for school counselors on mandated reporting and recognition of child abuse. This training conducted by CPS with schools can improve the working relationship between CPS and school counselors.
Likewise, Hinkelman and Bruno (2008) recommended attorneys, CPS, and mental health professionals gather to discuss child abuse through in-service trainings. During such time, school administrators can review their written policies to be certain they correspond with state laws, ensuring the reporting process is both ethical and legal for school counselors. This practice would mitigate challenges to communication, consultation, and collaboration between school counselors and reporting agencies, which would be helpful.
School counselors’ knowledge of child abuse symptomology. Previous research studies indicated the most significant hindrance to reporting child abuse is the lack of knowledge in recognizing signs of child maltreatment (Kenny & Abreu, 2016). A study conducted by Bryant (2009) evaluated school counselors’ perceived ability to recognize different types of child abuse. Generally, most school counselors felt confident in their knowledge to recognize physical abuse; however, fewer counselors reported certainty in identifying sexual as well as emotional abuse (Bryant, 2009; Bryant & Baldwin, 2010; Bryant & Milsom, 2005; Kenny & Abreu, 2016).
More experienced counselors believe themselves to be competent in recognizing and reporting child abuse, while beginning school counselors with less experience perceive themselves to be less knowledgeable and in need of additional training (Tillman et al., 2015). Bryant and Baldwin (2010) also found most experienced school counselors reported more confidence in recognizing signs of physical abuse in children. Certain physical and behavioral concerns in children can serve as indicators of physical abuse (Mayo Clinic, 2015; Sikes, 2008). Behavioral changes can include isolation, change in school performance, depressed affect, sudden weight loss or gain, or inability to control emotions (Lambie, 2005; Mayo Clinic, 2015; Minnesota Department of Human Services, 2016; Sikes, 2008). School counselors spend a significant amount of time with children and can be alert to the changes in behavior of a student, or teachers can notify the school counselor of their concerns for a child (Brown, Brack, & Mullis, 2008).
Conversely, certain forms of abuse, such as sexual and emotional abuse, are not as easily recognized by school counselors (Bryant & Baldwin, 2010). Emotional abuse can be defined as the continuous use of abusive language that hurts the child’s self-esteem or well-being (Mayo Clinic, 2015). Emotional abuse includes verbal and emotional assault, and isolating, ignoring, or rejecting a child (Mayo Clinic, 2015). Lack of empathy, warmth, and understanding also are associated with emotional abuse (McEachern, Aluede, & Kenny, 2008). A study conducted by Bryant and Milsom (2005) stated three-quarters of school counselors in the study felt sure of their ability to identify child physical abuse, but less so in their ability to recognize sexual and emotional abuse. The difficulty in determining emotional abuse can lead to school counselors feeling less qualified to make a report of suspected child abuse (Valkyrie, Creamer, & Vaughn, 2008).
Further training and education on the signs and symptoms of different types of abuse are necessary for school counselors to feel more confident in making a report of suspected child abuse (Herlihy & Corey, 2015). Awareness and instruction on the symptomology of the various forms of child abuse can increase early reporting from school counselors, resulting in improved chances of children recovering from the negative effects of child abuse (Valkyrie et al., 2008).
Unclear guidelines for reporting child abuse. Although school counselors are in the role to report suspected child abuse, many still struggle to determine if a report is warranted. School counselors have voiced the issue of needing evidence to make a report of child abuse (Valkyrie et al., 2008). Past studies indicated school counselors felt more comfortable reporting abuse when they had solid evidence the abuse occurred and were more likely to hesitate to report if less evidence was present in the case (Bryant & Milsom, 2005; Tillman et al., 2015). Moreover, a study conducted by Bryant (2009) indicated that the lack of evidence was the main reason school counselors decided not to report the suspicion of abuse.
Despite these findings, it is important that school counselors recognize that it is not their responsibility to investigate the case or determine the truth of the allegation of abuse. In fact, it is not in the best interest of the child for school counselors to investigate the alleged abuse because they do not have the proper resources and it could lead to further issues for the child (Hinkelman & Bruno, 2008; Lambie, 2005; Miller, Dove, & Miller, 2007). The school counselor’s responsibility is to follow legal and ethical obligations as a mandated reporter (ASCA, 2016) by reporting all suspected child abuse. It is important for school counselors to be aware of their state laws because it can be a felony if child abuse is not reported (Child Welfare Information Gateway, 2019).
Additional education on the school counselor’s role in reporting child abuse could elevate their understanding of their role in mandated reporting. Being aware that the law does not require school counselors to investigate cases and that they will not be held liable if a report is false (Hinkelman & Bruno, 2008) may increase the reports made by school counselors. It is important for school counselors to report suspected child abuse to the appropriate agencies and authorities by following state laws and school district protocol to ensure the safety of all children.
Fear of Repercussions. Numerous studies have suggested school counselors fear the repercussions that can result from reporting suspected child abuse (Bryant, 2009; Bryant & Baldwin, 2010; Bryant & Milsom, 2005; Sikes et al., 2010). These repercussions may originate from school administration, colleagues (Bell & Singh, 2017; Kenny, 2001; Sikes et al., 2010), or the family of the student (Bryant & Baldwin, 2010; Kenny, 2001; Valkyrie et al., 2008), or impact the relationship with the student (Alvarez et al., 2004; Bryant & Baldwin, 2010; Sikes et al., 2010). Moreover, school counselors may be afraid the family of the child will file a lawsuit against the school and the counselor for making a report of suspected child abuse (Valkyrie et al., 2008). Conversely, a study conducted by Kenny, Abreu, Helpingstine, Lopez, and Mathews (2018) found that all 50 states give immunity to professionals who report alleged child abuse. The purpose of the immunity is to encourage professionals to report suspected abuse, knowing they do not have to fear the repercussions of disgruntled family members (Kenny et al., 2018). Further exposure to the law of mandated reporting can in fact reduce the anxiety of reporting and encourage more reporting of alleged abuse.
Additional education on mandated reporting and a specific plan for mandated reporting can help to alleviate the fears school counselors have when reporting abuse. If the school policy includes a specific model for mandated reporting, then school counselors may be less likely to fear repercussions and follow appropriate guidelines (Committee for Children, 2014; Oloumi-Johnson, 2016; Sinanan, 2011). If faced with disgruntled parents, school counselors can refer to their school policy within the mandated reporting model to verify to the concerned individual that school policy and procedures were followed.
Challenges of the Early Career School Counselor
Early career school counselors are often faced with tremendous challenges as they enter their new work environment. These challenges include differing expectations from site to site and district to district (Hatch, 2008). Although school counselors are designated as mandated reporters, many may struggle with identifying different types of abuse, understanding reporting procedures, and understanding their district and state policies (Bryant, 2009; Ricks et al., 2019). New school counselors may be especially vulnerable to challenges because they are still defining their roles within their new school system and learning what the expectations are for their site. Past research also has shown that school counselors’ understanding of child abuse reporting is related to past professional experiences (Bryant, 2009), and early career school counselors can be deficient in this knowledge. Additional training in child abuse reporting is needed to help school counselors become more proficient and knowledgeable in these procedures (Tillman et al., 2015). Currently, there is a lack of research and resources for early career school counselors on child abuse reporting. This proposed framework aims to aid early career school counselors in developing their understanding of child abuse reporting procedures and expectations.
Framework Foundation
The purpose of this article is to develop an effective mandated reporting framework for school counselors based on the ASCA Ethical Standards for School Counselors (2016), the research from Ricks et al. (2019), and previous literature reviews and research studies. Even though previous recommendations for collaboration have been made, we recognized the need for school counselors to have a specific framework for reporting child abuse that is collaborative and specific to school counseling.
Ricks et al. (2019) examined the experiences of child abuse reporting by early career school counselors (0 to 5 years of experience as a school counselor) in the Southeastern United States. Early career school counselors were targeted because they can be confused and frustrated regarding their roles within the school as mandated reporters (Slaten, Scalise, Gutting, & Baskin, 2013). Participants responded to a survey allowing them to share their experiences and suggestions regarding child abuse reporting using two open-ended questions (Ricks et al., 2019). The two open-ended questions asked: (1) What types of additional training do you need regarding child abuse reporting? and (2) What challenges did you or are you facing as a new SC (0–5 years) regarding mandated reporting? (Ricks et al., 2019). Findings revealed the need for help identifying types and signs of abuse; staff and faculty training; information on reporting procedures; and additional mandated report training. Additionally, the findings found challenges with mandated reporting including fear of repercussions, agency concern and collaboration, reporting policies, identifying types of abuse, and school counselor responsibilities. The responses to the open-ended questions informed the direction and development of this framework to assist early career school counselors as they navigate the child abuse reporting process.
Child Abuse Reporting Framework for Early Career School Counselors
The purpose of this framework is to provide steps for early career school counselors to ensure their school counseling program is following best practices in mandated reporting. The steps are designed based on the recommendations by the participants in the study by Ricks et al. (2019) to provide clarity in the informed decision-making process when child abuse is suspected. School counselors should adhere to all the steps identified to ensure they are knowledgeable of current research and best practices on child abuse reporting. This information is considered vital for reviewing mandated reporter guidelines and identifying resources to assist students. Additionally, early career school counselors are encouraged to continuously review guidelines and procedures to ensure execution of streamlined services; however, keeping resources is not enough. School counselors should continually update their collected information by participating in ongoing professional development to ensure they remain abreast of changes in laws, policies, agencies, and personnel.
The authors recognize that reporting child abuse is a collaborative effort within the school setting, which includes faculty, administrators, school counselors, and other mandated reporters. Therefore, a collaborative approach was deemed appropriate, especially when seeking support and understanding the gravity of reporting child abuse to the appropriate agencies and authorities. A collaborative approach is substantiated based on previous literature by Gullatt (1999), Bell and Singh (2017), and Ricks et al. (2019). Gullatt called for a collaborative approach to child abuse reporting and recommended school principals be aware and know how to identify child abuse as well as the laws for reporting.
Eight steps have been outlined in the Child Abuse Reporting Framework for Early Career School Counselors to guide early career school counselors in their role as mandated reporters: (1) become familiar with and follow state laws and district/school child abuse reporting policies, (2) become familiar with and follow the ASCA ethical standards, (3) obtain training to identify and recognize signs of child abuse, (4) identify stakeholders, (5) build collaborative partnerships, (6) provide school-based training, (7) report child abuse, and (8) perform post-reporting procedures. Each of these steps includes recommendations and considerations to assist in increasing self-efficacy for early career school counselors in the child abuse reporting process.
Step I: Become Familiar With and Follow State Laws and District/School Child Abuse Reporting Policies
State laws define the role of community members, helpers, and school officials as mandated reporters. Therefore, it is in the best interest of early career school counselors to review the laws on mandated reporting within their state of employment to understand what is expected for mandated reporters, the timeframe to report, and contact information. Knowledge and awareness of state laws is particularly imperative because state requirements to report child abuse vary for each state (Hogelin, 2013; Lambie, 2005). Not only do state laws differ, but schools within the same district can vary in their child abuse reporting policies. Early career school counselors must make familiarizing themselves with state laws and district/school child abuse reporting policies a priority. This should be done during the pre-planning period and first days on the job in order to be knowledgeable and aware of what the laws and policies state. Areas in particular to be aware of include who is to be contacted when knowledge of suspected child abuse has been identified; who officially makes the report; what the procedures are; how to make a report (e.g., electronically, phone call, in person, website); where and how to file documentation of the report; and who to inform once the report has been made.
Some schools and states require everyone who has knowledge of suspected child abuse to file a report. This would include school counselors, administrators, teachers, and school personnel. In some school districts, a designated school official is the individual to make the report. This generally is the school counselor. Therefore, it is incumbent on early career school counselors to be aware of what their role is and how it meets the legal and ethical requirements. School counselors should be aware that if the school has designated only a specific individual to file a report, this may go against the law and possibly jeopardize the school counselor’s licensure and certification. Therefore, it is important that all stakeholders in the school setting be aware of their respective state’s laws.
Step II: Become Familiar With and Follow the 2016 ASCA Ethical Standards
ASCA ethical standards A.9. and A.11. highlight the responsibilities school counselors have in reporting child abuse (ASCA, 2016). Early career school counselors have received training in their master’s programs regarding ethics; however, it is especially imperative to review the ethical standards pertaining to child abuse reporting on a regular basis. This will aid in maintaining ethical dispositions at the forefront, while leveraging the ASCA ethical decision-making process as a guide (ASCA, 2016). Additionally, the ASCA ethical standards can be used as a tool to advocate for school counseling services in reporting child abuse. This is especially useful in circumstances when there might be role confusion by administrators, school personnel, authorities, and agencies. By referencing the ethical standards, school counselors can advocate for their role in reporting child abuse and working to keep students safe.
Step III. Obtain Training to Identify and Recognize Signs of Child Abuse
It is recommended that educators consistently receive training to identify and recognize signs of child abuse (Hogelin, 2013). Kenny and Abreu (2016) recommended counselors seek continued education on child abuse reporting by attending workshops that will help them remain abreast of the changes to reporting laws and requirements. Therefore, school counselors should advocate to receive opportunities to attend professional development conferences and trainings by the district and/or local agencies (Hogelin, 2013). Advocacy is considered an integral component of the ASCA National Model (ASCA, 2012; 2019a). Although regular training is recommended, it is not guaranteed this practice occurs across states and school districts. Furthermore, it would be beneficial for early career school counselors to seek and participate in professional development because of varying types of training they have or have not received on identifying and reporting child abuse during their master’s-level school counseling programs.
Laws, protocols, procedures, and staff are continuously changing; therefore, early career school counselors should remain cognizant and aware of these changes. In order for knowledge to remain relevant, school counselors should engage in continued professional development on recognizing child abuse indicators and child abuse reporting. This practice allows the school counselor to remain informed while increasing their self-efficacy in reporting suspected child abuse. Additionally, each year school counselors must continue to update administration and school personnel on procedures and protocol for identifying and reporting child abuse.
Step IV. Identify Stakeholders
School counselors who seek to strengthen partnerships with administrators (e.g., principals and assistant principals) are in a position to initiate discussion on child abuse reporting procedures and protocols to ensure an understanding of the role of the school counselor as a mandated reporter. Particularly building a partnership with principals is vital to identify the key role school counselors play in the school setting. A study conducted by Bringman, Mueller, and Lee (2010) shed light on the perception principals have on the role of the school counselor. This research indicated that principals have not received prior education on the role of the school counselor; therefore, it would be beneficial to discuss the role of the school counselor with administration. This step is deemed significant because school counselors generally see themselves as more informed in recognizing and reporting child abuse than principals (Tillman et al., 2015).
Nevertheless, a study conducted by Kenny and McEachern (2002) mentioned that both school counselors and school principals report child abuse, although school counselors reported child abuse at a higher percentage than school principals. Still, it is imperative to recognize that both professions—school counselors and administrators—share the common goal of protecting children by reporting suspected child abuse (Kenny & McEachern, 2002; Tillman et al., 2015).
Early career school counselors can leverage this insight by approaching their administrators through a collaborative stance, highlighting this shared goal, and discussing how to ethically and legally report suspected child abuse. This discussion can include, but is not limited to, state laws, district policies, and district/school child abuse reporting procedures. Furthermore, school counselors and school principals who keep the safety of students at the forefront and work together need to reduce role confusion.
Step V. Build Collaborative Partnerships
CPS. This step has been included to encourage partnerships between school counselors and CPS. District school counseling supervisors can support this endeavor by extending an invitation to CPS supervisors to attend a meeting with school counselors. This meeting would be utilized as a rapport-building opportunity as well as a way to share each other’s roles, challenges, and strengths. Additionally, this would be an opportunity for CPS to provide updates, contact information, and any other pertinent information.
It also has been recommended that joint training be done with local CPS members and school counselors (Bryant & Baldwin, 2010) to ensure collaboration between agencies and to ensure all participants are exposed to consistent training. Additionally, CPS may be able to provide training to the school system and not only school counselors. “When school counselors understand the limitations inherent in receiving a report, they might, in turn, be more efficacious in their reporting of child abuse” (Bryant & Milsom, 2005, p. 70). This training should include information on the reporting process, but also on the investigative process so that school counselors develop an understanding of the reactions and behaviors of the investigators (Bryant & Baldwin, 2010). Other stakeholders, such as school psychologists, social workers, and nurses, would benefit from this training as well.
Law enforcement. Public safety is the mission of law enforcement officers. Within the school system, police officers and especially school resource officers (SROs) engage in numerous activities and perform numerous duties. One of the duties can include being a member of the school’s crisis response team (Cowan, Vaillancourt, Rossen, & Pollitt, 2013). School counselors should work to build a positive working relationship with their SRO and local law enforcement. These individuals can help assist school counselors in providing services when students are a danger to themselves or when the student is in danger. Additionally, SROs have been provided specific training on “student needs and characteristics, and the educational and custodial interests of school personnel” (Cowan et al., 2013, p. 10). Law enforcement and SROs also can help ensure the safety of everyone in the building when a threat arises.
Attorneys. School counselors should consider consulting with the school district’s attorney to ensure that their rights and the rights of their students and others are being maintained. Most schools have a school attorney that school counselors can communicate with when issues or questions arise. School counselors also must make sure they are aware of legal and ethical guidelines on confidentiality and privacy of student information. Nonetheless, if school counselors find themselves in situations where discrepancies arise, they should call their local department of children’s services or attorney (Mitchell & Rogers, 2003). Participants from a study conducted by DeCino, Waalkes, and Matos (2017) reported positive experiences with legal counsel. An attorney not only provides guidance on ethical dilemmas but also legal advice for potential court hearings.
Step VI. Provide School-Based Training
Stakeholders in the school setting, such as teachers, school nurses, coaches, paraprofessionals, custodians, lunchroom staff, and other support staff in the building, should be provided with training to identify and report child abuse (Hogelin, 2013; Lambie, 2005). It is recommended that training on child abuse identification and reporting procedures be conducted each year; this is mandatory in some states. These individuals interact with students daily and are able to recognize if a student is in distress. Despite their daily interactions with students, many teachers struggle to identify signs of abuse and have a lack of knowledge of reporting procedures (Greytak, 2009). Therefore, school counselors are in the position to schedule dates and times at the beginning of the school year, such as during pre-planning, and mid-year as a refresher to provide school personnel with the training to identify and recognize child abuse as well as inform them of their mandated reporter obligations. This involves addressing state laws, ethical requirements, and district/school policies for child abuse reporting as well as providing the procedures and contact information to make a report.
Step VII. Report Child Abuse
Child abuse reporting involves several crucial details. These details include, but are not limited to, the name of the child, name of family members (e.g., parents, siblings), individuals who reside in the home, phone number, address, previous history of abuse, academic performance, child dispositions, and concern leading to the report (Sikes, 2008). It would behoove early career school counselors to determine if their school districts have a specific form to complete while filing an abuse report. This resource would guide the process of obtaining all the details for filing a complete report. If no such resource is available, school counselors should work with key personnel to create a standardized form for abuse reporting. Furthermore, knowledge of the method to make a report is necessary. Reporting procedures for CPS vary by state. Most states prefer an oral report be made to CPS; however, some states require a written report be completed after the oral report has been made (Child Information Gateway, 2017). Because there may be a timeframe in which to call according to state policy, early career school counselors who are aware of the specific method to report will not only report in a timely manner but be more prepared and self-efficacious in their reporting skills and capabilities.
Step VIII. Perform Post-Reporting Procedures
After the child abuse report has been made, questions often arise about how to support the student who needs to be aware of the child abuse report, and how to respond to parents who inquire about the report. Early career school counselors can reach out to the caseworker to inquire as to what supports might be provided at the school, check in with the student to ensure they are safe, and seek what procedures the district has in place to address parents. When approached by parents, early career school counselors can maintain the disposition of informing parents that all child abuse reports are confidential and that they may contact the caseworker with their questions. Additionally, pamphlets on the role of mandated reporting and resources can be made available in the school counselor’s office to provide the parents with assistance in identifying supports. School counselors also can provide parents with referrals to outside agencies, such as counseling or family supports, when asked by parents who are seeking interventions.
Conclusion
Reporting child abuse is recognized as a crucial element in the role of a school counselor. Early career school counselors often are anxious about reporting child abuse because of the fear of repercussions from parents, lack of self-efficacy in identifying abuse, limited knowledge of child abuse reporting procedures, unclear reporting procedures for school counselors, and lack of collaboration with outside agencies. This article has addressed the challenges faced by early career school counselors and provides a framework to alleviate their anxiety while increasing their self-efficacy as mandated reporters.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
Alvarez, K. M., Kenny, M. C., Donohue, B., & Carpin, K. M. (2004). Why are professionals failing to initiate mandated reports of child maltreatment, and are there any empirically based training programs to assist professionals in the reporting process? Aggression and Violent Behavior, 9, 563–578. doi:10.1016/j.avb.2003.07.001
American School Counselor Association. (2012). ASCA national model: A framework for school
counseling programs. (3rd ed.). Alexandria, VA: Author.
American School Counselor Association. (2015). The school counselor and child abuse and neglect prevention. Retrieved from https://www.schoolcounselor.org/asca/media/asca/PositionStatements/PS_ChildAbuse.pdf
American School Counselor Association. (2016). ASCA ethical standards for school counselors. Alexandria, VA: Author. Retrieved from https://www.schoolcounselor.org/asca/media/asca/
Ethics/EthicalStandards2016.pdf
American School Counselor Association. (2019a). ASCA national model: A framework for school
counseling programs. (4th ed.). Alexandria, VA: Author.
American School Counselor Association. (2019b). Legal & ethical. Retrieved from https://www.schoolcounselor.org/school-counselors-members/legal-ethical
Behun, R. J., Cerrito, J. A., Delmonico, D. L., & Kolbert, J. B. (2019). The influence of personal and professional characteristics on school counselors’ recognition and reporting of child sexual abuse. Journal of School Counseling, 17(13). Retrieved from http://www.jsc.montana.edu/
articles/v17n13.pdf
Bell, M. M., & Singh, M. I. (2017). Implementing a collaborative support model for educators reporting child maltreatment. Children & Schools, 39, 7–14. doi:10.1093/cs/cdw041
Bringman, N. M., Mueller, S. M., & Lee, S. M. (2010). Educating future school principals regarding the role of professional school counselors. Journal of School Counseling, 8(3). Retrieved from http://www.jsc.montana.edu/articles/v8n3.pdf
Brown, S. D., Brack, G., & Mullis, F. Y. (2008). Traumatic symptoms in sexually abused children: Implications for school counselors. Professional School Counseling, 11, 368–379. doi:10.1177/2156759X0801100603
Bryant, J. K. (2009). School counselors and child abuse reporting: A national survey. Professional School Counseling, 12, 333–342. doi:10.1177/2156759X0901200501
Bryant, J. K., & Baldwin, P. A. (2010). School counsellors’ perceptions of mandatory reporting training and mandatory reporting experiences. Child Abuse Review, 19, 172–186. doi:10.1002/car.1099
Bryant, J., & Milsom, A. (2005). Child abuse reporting by school counselors. Professional School Counseling, 9, 63–71.
Child Abuse Prevention and Treatment Act Reauthorization Act of 2010, Pub. L. No. 111-320 (2010).
Retrieved from https://www.congress.gov/bill/111th-congress/senate-bill/3817/text
Child Welfare Information Gateway. (2003). Child protective services: A guide for caseworkers.
Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau. Retrieved from https://www.childwelfare.gov/pubPDFs/cps.pdf
Child Welfare Information Gateway. (2017). Making and screening reports of child abuse and neglect.
Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau. Retrieved
from https://www.childwelfare.gov/pubPDFs/repproc.pdf
Child Welfare Information Gateway. (2019). Penalties for failure to report and false reporting of child abuse and neglect. Washington, DC: U.S. Department of Health and Human Services, Children’s Bureau. Retrieved from https://www.childwelfare.gov/topics/systemwide/lawspolicies/statutes/report
Committee for Children. (2014). Child protection in schools: A four-part solution. Retrieved from
http://www.cfchildren.org/wp-content/uploads/programs/docs/child-protection-in-school.pdf
Corey, G., Corey, M. S., & Callanan, P. (2011). Issues and ethics in the helping professions (8th ed.). Belmont, CA: Brooks/Cole.
Cowan, K. C., Vaillancourt, K., Rossen, E., & Pollitt, K. (2013). A framework for safe and successful schools [Brief]. Bethesda, MD: National Association of School Psychologists. Retrieved from https://www.schoolcounselor.org/asca/media/asca/home/FrameworkforSafeandSuccessfulSchoolEnvironments.PDF
Davis, T. (1995). Elementary and middle level counselors’ courtroom hearing experiences. NASSP Bulletin, 79(570), 10–15. doi:10.1177/019263659507957003
DeCino, D. A., Waalkes, P. L., & Matos, C. (2017). “Be ready for it”: School counselors’ experiences with subpoena and testifying in court. Professional School Counseling, 21, 1–9. doi:10.1177/2156759X18786450
Froeschle, J. G., & Crews, C. (2010). An ethics challenge for school counselors. Journal of School Counseling, 8(14). Retrieved from http://www.jsc.montana.edu/articles/v8n14.pdf
Greytak, E. A. (2009). Are teachers prepared? Predictors of teachers’ readiness to serve as mandated reporters of child abuse (Doctoral dissertation). Retrieved from https://repository.upenn.edu/
edissertations/57
Gullatt, D. (1999). Collaborative efforts are required as schools address suspected child abuse. Contemporary Education, 71, 24–31.
Hatch, T. A. (2008). Professional challenges in school counseling: Organizational, institutional, and political. Journal of School Counseling, 6(22).
Herlihy, B., & Corey, G. (2015). ACA ethical standards casebook seventh edition. Alexandria, VA: American Counseling Association.
Hinkelman, L., & Bruno, M., (2008). Identification and reporting of child sexual abuse: The role of elementary school professionals. The Elementary School Journal, 108, 376–391. doi:10.1086/589468
Hogelin, J. M. (2013). To prevent and to protect: The reporting of child abuse by educators. Brigham Young University Education & Law Journal, 2013(2), 225–252.
Jonson-Reid, M., Drake, B., & Kohl, P. L. (2009). Is the overrepresentation of the poor in child welfare caseloads due to bias or need? Children and Youth Services Review, 31, 422–427.
Kenny, M. C. (2001). Child abuse reporting: Teachers’ perceived deterrents. Child Abuse & Neglect, 25, 81–92. doi:10.1016/S0145-2134(00)00218-0
Kenny, M. C, & Abreu, R. L. (2016). Mandatory reporting of child maltreatment for counselors: An innovative training program. Journal of Child and Adolescent Counseling, 2, 112–124.
doi:10.1080/23727810.2016.1228770
Kenny, M. C., Abreu, R. L., Helpingstine, C., Lopez, A., & Mathews, B. (2018). Counselors’ mandated responsibility to report child maltreatment: A review of U.S. laws. Journal of Counseling & Development, 96, 372–387. doi:10.1002/jcad.12220
Kenny, M. C., & McEachern, A. G. (2002). Reporting suspected child abuse: A pilot comparison of middle and high school counselors and principals. Journal of Child Sexual Abuse, 11, 59–75.
doi:10.1300/j070v11n02_04
Lambie, G. W. (2005). Child abuse and neglect: A practical guide for professional school counselors. Professional School Counseling, 8, 249–258.
Lambie, G. W., Ieva, K. P., & Mullen, P. R. (2013). Graduate counseling students’ learning, development, and retention of knowledge. Journal of the Scholarship of Teaching and Learning, 13(4), 54–67.
Levi, B. H., & Brown, G. (2005). Reasonable suspicion: A study of Pennsylvania pediatricians regarding child abuse. Pediatrics, 116, e5–512. doi:10.1542/peds.2004-2649
Mayo Clinic. (2015). Child abuse. Retrieved from https://www.mayoclinic.org/diseases-conditions/child-abuse/symptoms-causes/syc-20370864
McEachern, A. G., Aluede, O., & Kenny, M. C. (2008). Emotional abuse in the classroom: Implications and interventions for counselors. Journal of Counseling & Development, 86, 3–10.
doi:10.1002/j.1556-6678.2008.tb00619.x
Miller, K. L., Dove, M. K., & Miller, S. M. (2007, October). A counselor’s guide to child sexual abuse: Prevention, reporting and treatment strategies. Paper based on a program presented at the Association for Counselor Education and Supervision Conferences, Columbus, OH.
Minnesota Department of Human Services. (2016). Resource guide for mandated reporters of child maltreatment concerns. Retrieved from https://www.dow.org/img/Reporting%20Child%20Abuse%20and%20Neglect%201_16.pdf
Mitchell, C. W., & Rogers, R. E. (2003). Rape, statutory rape, and child abuse: Legal distinctions and counselor duties. Professional School Counseling, 6, 332–338.
Oloumi-Johnson, R. (2016). The lived experiences of middle school counselors in reporting abuse and neglect to child protective services: A phenomenological study (Doctoral Dissertation). Retrieved from ProQuest Dissertations & Theses Database. (UMI 10307713).
Ricks, L., Tuttle, M., Land, C., & Chibbaro, J. (2019). Trends and influential factors in child abuse reporting: Implications for early career school counselors. Journal of School Counseling, 17(16). Retrieved from http://www.jsc.montana.edu/articles/v17n16.pdf
Sedlak, A. J., Mettenburg, J., Basena, M., Petta, I., McPherson, K., Greene, A., & Li, S. (2010). Fourth National Incidence Study of Child Abuse and Neglect (NIS-4): Report to Congress. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families. Retrieved from https://www.acf.hhs.gov/sites/default/files/opre/nis4_report_congress_full_pdf_jan2010.pdf
Sikes, A. (2008). A school counselor’s guide to reporting child abuse and neglect. Journal of School Counseling, 6(25). Retrieved from http://www.jsc.montana.edu/articles/v6n25.pdf
Sikes, A., Remley, T., Jr., & Hays, D. G. (2010). Experiences of school counselors during and after making suspected child abuse reports. Journal of School Counseling, 8(21). Retrieved from http://www.jsc.montana.edu/articles/v8n21.pdf
Sinanan, A. N. (2011). Bridging the gap of teacher education about child abuse. Educational Foundations. Retrieved from https://files.eric.ed.gov/fulltext/EJ954988.pdf
Slaten, C. D., Scalise, D. A., Gutting, K., & Baskin, T. W. (2013). Early career school counselors’
training perspectives: Implications for school counselor educators. Journal of School Counseling,
11(20). Retrieved from http://www.jsc.montana.edu/articles/v11n20.pdf
Stone, C. (2013). School counseling principles: Ethics and law (3rd ed.). Alexandria, VA: American School Counselor Association.
Tillman, K. S., Prazak, M. D., Burrier, L., Miller, S., Benezra, M., & Lynch, L. (2015). Factors influencing school counselors’ suspecting and reporting of childhood physical abuse: Investigating child, parent, school, and abuse characteristics. Professional School Counseling, 19, 103–115. doi:10.5330/1096-2409-19.1.103
U.S. Department of Health & Human Services, Administration for Children, Youth and Families, & Children’s Bureau. (2019). Child maltreatment 2017. Retrieved from https://www.acf.hhs.gov/sites/default/files/cb/cm2017.pdf
Valkyrie, K. T., Creamer, D. A., & Vaughn, L. (2008). Mandatory reporting and school counselors: Reporting law, obstacles, and solutions. The Alabama Counseling Association Journal, 34, 18–33.
Washington State Department of Social & Health Services. (2018). Protecting the abused & neglected
child: A guide for recognizing and reporting child abuse & neglect. Retrieved from https://www.
dshs.wa.gov/sites/default/files/SESA/publications/documents/22-163.pdf
Malti Tuttle is an assistant professor and School Counseling Program Coordinator at Auburn University. Lacey Ricks is an assistant professor at Liberty University. Margie Taylor is a visiting assistant professor at Auburn University. Correspondence can be addressed to Malti Tuttle, 2084 Haley Center, Auburn, AL 36849, mst0022@auburn.edu.
