Nov 9, 2022 | Volume 12 - Issue 3
Michael T. Kalkbrenner
Conducting and publishing rigorous empirical research based on original data is essential for advancing and sustaining high-quality counseling practice. The purpose of this article is to provide a one-stop-shop for writing a rigorous quantitative Methods section in counseling and related fields. The importance of judiciously planning, implementing, and writing quantitative research methods cannot be understated, as methodological flaws can completely undermine the integrity of the results. This article includes an overview, considerations, guidelines, best practices, and recommendations for conducting and writing quantitative research designs. The author concludes with an exemplar Methods section to provide a sample of one way to apply the guidelines for writing or evaluating quantitative research methods that are detailed in this manuscript.
Keywords: empirical, quantitative, methods, counseling, writing
The findings of rigorous empirical research based on original data is crucial for promoting and maintaining high-quality counseling practice (American Counseling Association [ACA], 2014; Giordano et al., 2021; Lutz & Hill, 2009; Wester et al., 2013). Peer-reviewed publication outlets play a crucial role in ensuring the rigor of counseling research and distributing the findings to counseling practitioners. The four major sections of an original empirical study usually include: (a) Introduction/Literature Review, (b) Methods, (c) Results, and (d) Discussion (American Psychological Association [APA], 2020; Heppner et al., 2016). Although every section of a research study must be carefully planned, executed, and reported (Giordano et al., 2021), scholars have engaged in commentary about the importance of a rigorous and clearly written Methods section for decades (Korn & Bram, 1988; Lutz & Hill, 2009). The Methods section is the “conceptual epicenter of a manuscript” (Smagorinsky, 2008, p. 390) and should include clear and specific details about how the study was conducted (Heppner et al., 2016). It is essential that producers and consumers of research are aware of key methodological standards, as the quality of quantitative methods in published research can vary notably, which has serious implications for the merit of research findings (Lutz & Hill, 2009; Wester et al., 2013).
Careful planning prior to launching data collection is especially important for conducting and writing a rigorous quantitative Methods section, as it is rarely appropriate to alter quantitative methods after data collection is complete for both practical and ethical reasons (ACA, 2014; Creswell & Creswell, 2018). A well-written Methods section is also crucial for publishing research in a peer-reviewed journal; any serious methodological flaws tend to automatically trigger a decision of rejection without revisions. Accordingly, the purpose of this article is to provide both producers and consumers of quantitative research with guidelines and recommendations for writing or evaluating the rigor of a Methods section in counseling and related fields. Specifically, this manuscript includes a general overview of major quantitative methodological subsections as well as an exemplar Methods section. The recommended subsections and guidelines for writing a rigorous Methods section in this manuscript (see Appendix) are based on a synthesis of (a) the extant literature (e.g., Creswell & Creswell, 2018; Flinn & Kalkbrenner, 2021; Giordano et al., 2021); (b) the Standards for Educational and Psychological Testing (American Educational Research Association [AERA] et al., 2014), (c) the ACA Code of Ethics (ACA, 2014), and (d) the Journal Article Reporting Standards (JARS) in the APA 7 (2020) manual.
Quantitative Methods: An Overview of the Major Sections
The Methods section is typically the second major section in a research manuscript and can begin with an overview of the theoretical framework and research paradigm that ground the study (Creswell & Creswell, 2018; Leedy & Ormrod, 2019). Research paradigms and theoretical frameworks are more commonly reported in qualitative, conceptual, and dissertation studies than in quantitative studies. However, research paradigms and theoretical frameworks can be very applicable to quantitative research designs (see the exemplar Methods section below). Readers are encouraged to consult Creswell and Creswell (2018) for a clear and concise overview about the utility of a theoretical framework and a research paradigm in quantitative research.
Research Design
The research design should be clearly specified at the beginning of the Methods section. Commonly employed quantitative research designs in counseling include but are not limited to group comparisons (e.g., experimental, quasi-experimental, ex-post-facto), correlational/predictive, meta-analysis, descriptive, and single-subject designs (Creswell & Creswell, 2018; Flinn & Kalkbrenner, 2021; Leedy & Ormrod, 2019). A well-written literature review and strong research question(s) will dictate the most appropriate research design. Readers can refer to Flinn and Kalkbrenner (2021) for free (open access) commentary on and examples of conducting a literature review, formulating research questions, and selecting the most appropriate corresponding research design.
Researcher Bias and Reflexivity
Counseling researchers have an ethical responsibility to minimize their personal biases throughout the research process (ACA, 2014). A researcher’s personal beliefs, values, expectations, and attitudes create a lens or framework for how data will be collected and interpreted. Researcher reflexivity or positionality statements are well-established methodological standards in qualitative research (Hays & Singh, 2012; Heppner et al., 2016; Rovai et al., 2013). Researcher bias is rarely reported in quantitative research; however, researcher bias can be just as inherently present in quantitative as it is in qualitative studies. Being reflexive and transparent about one’s biases strengthens the rigor of the research design (Creswell & Creswell, 2018; Onwuegbuzie & Leech, 2005). Accordingly, quantitative researchers should consider reflecting on their biases in similar ways as qualitative researchers (Onwuegbuzie & Leech, 2005). For example, a researcher’s topical and methodological choices are, at least in part, based on their personal interests and experiences. To this end, quantitative researchers are encouraged to reflect on and consider reporting their beliefs, assumptions, and expectations throughout the research process.
Participants and Procedures
The major aim in the Participants and Procedures subsection of the Methods section is to provide a clear description of the study’s participants and procedures in enough detail for replication (ACA, 2014; APA, 2020; Giordano et al., 2021; Heppner et al., 2016). When working with human subjects, authors should briefly discuss research ethics including but not limited to receiving institutional review board (IRB) approval (Giordano et al., 2021; Korn & Bram, 1988). Additional considerations for the Participants and Procedures section include details about the authors’ sampling procedure, inclusion and/or exclusion criteria for participation, sample size, participant background information, location/site, and protocol for interventions (APA, 2020).
Sampling Procedure and Sample Size
Sampling procedures should be clearly stated in the Methods section. At a minimum, the description of the sampling procedure should include researcher access to prospective participants, recruitment procedures, data collection modality (e.g., online survey), and sample size considerations. Quantitative sampling approaches tend to be clustered into either probability or non-probability techniques (Creswell & Creswell, 2018; Leedy & Ormrod, 2019). The key distinguishing feature of probability sampling is random selection, in which all prospective participants in the population have an equal chance of being randomly selected to participate in the study (Leedy & Ormrod, 2019). Examples of probability sampling techniques include simple random sampling, systematic random sampling, stratified random sampling, or cluster sampling (Leedy & Ormrod, 2019).
Non-probability sampling techniques lack random selection and there is no way of determining if every member of the population had a chance of being selected to participate in the study (Leedy & Ormrod, 2019). Examples of non-probability sampling procedures include volunteer sampling, convenience sampling, purposive sampling, quota sampling, snowball sampling, and matched sampling. In quantitative research, probability sampling procedures are more rigorous in terms of generalizability (i.e., the extent to which research findings based on sample data extend or generalize to the larger population from which the sample was drawn). However, probability sampling is not always possible and non-probability sampling procedures are rigorous in their own right. Readers are encouraged to review Leedy and Ormrod’s (2019) commentary on probability and non-probability sampling procedures. Ultimately, the selection of a sampling technique should be made based on the population parameters, available resources, and the purpose and goals of the study.
A Priori Statistical Power Analysis. It is essential that quantitative researchers determine the minimum necessary sample size for computing statistical analyses before launching data collection (Balkin & Sheperis, 2011; Sink & Mvududu, 2010). An insufficient sample size substantially increases the probability of committing a Type II error, which occurs when the results of statistical testing reveal non–statistically significant findings when in reality (of which the researcher is unaware), significant findings do exist. Computing an a priori (computed before starting data collection) statistical power analysis reduces the chances of a Type II error by determining the smallest sample size that is necessary for finding statistical significance, if statistical significance exists (Balkin & Sheperis, 2011). Readers can consult Balkin and Sheperis (2011) as well as Sink and Mvududu (2010) for an overview of statistical significance, effect size, and statistical power. A number of statistical power analysis programs are available to researchers. For example, G*Power (Faul et al., 2009) is a free software program for computing a priori statistical power analyses.
Sampling Frame and Location
Counselors should report their sampling frame (total number of potential participants), response rate, raw sample (total number of participants that engaged with the study at any level, including missing and incomplete data), and the size of the final useable sample. It is also important to report the breakdown of the sample by demographic and other important participant background characteristics, for example, “XX.X% (n = XXX) of participants were first-generation college students, XX.X% (n = XXX) were second-generation . . .” The selection of demographic variables as well as inclusion and exclusion criteria should be justified in the literature review. Readers are encouraged to consult Creswell and Creswell (2018) for commentary on writing a strong literature review.
The timeframe, setting, and location during which data were collected are important methodological considerations (APA, 2020). Specific names of institutions and agencies should be masked to protect their privacy and confidentiality; however, authors can give descriptions of the setting and location (e.g., “Data were collected between April 2021 to February 2022 from clients seeking treatment for addictive disorders at an outpatient, integrated behavioral health care clinic located in the Northeastern United States.”). Authors should also report details about any interventions, curriculum, qualifications and background information for research assistants, experimental design protocol(s), and any other procedural design issues that would be necessary for replication. In instances in which describing a treatment or conditions becomes exorbitant (e.g., step-by-step manualized therapy, programs, or interventions), researchers can include footnotes, appendices, and/or references to refer the reader to more information about the intervention protocol.
Missing Data
Procedures for handling missing values (incomplete survey responses) are important considerations in quantitative data analysis. Perhaps the most straightforward option for handling missing data is to simply delete missing responses. However, depending on the percentage of data that are missing and how the data are missing (e.g., missing completely at random, missing at random, or not missing at random), data imputation techniques can be employed to recover missing values (Cook, 2021; Myers, 2011). Quantitative researchers should provide a clear rationale behind their decisions around the deletion of missing values or when using a data imputation method. Readers are encouraged to review Cook’s (2021) commentary on procedures for handling missing data in quantitative research.
Measures
Counseling and other social science researchers oftentimes use instruments and screening tools to appraise latent traits, which can be defined as variables that are inferred rather than observed (AERA et al., 2014). The purpose of the Measures (aka Instrumentation) section is to operationalize the construct(s) of measurement (Heppner et al., 2016). Specifically, the Measures subsection of the Methods in a quantitative manuscript tends to include a presentation of (a) the instrument and construct(s) of measurement, (b) reliability and validity evidence of test scores, and (c) cross-cultural fairness and norming. The Measures section might also include a Materials subsection for studies that employed data-gathering techniques or equipment besides or in addition to instruments (Heppner et al., 2016); for instance, if a research study involved the use of a biofeedback device to collect data on changes in participants’ body functions.
Instrument and Construct of Measurement
Begin the Measures section by introducing the questionnaire or screening tool, its construct(s) of measurement, number of test items, example test items, and scale points. If applicable, the Measures section can also include information on scoring procedures and cutoff criterion; for example, total score benchmarks for low, medium, and high levels of the trait. Authors might also include commentary about how test scores will be operationalized to constitute the variables in the upcoming Data Analysis section.
Reliability and Validity Evidence of Test Scores
Reliability evidence involves the degree to which test scores are stable or consistent and validity evidence refers to the extent to which scores on a test succeed in measuring what the test was designed to measure (AERA et al., 2014; Bardhoshi & Erford, 2017). Researchers should report both reliability and validity evidence of scores for each instrument they use (Wester et al., 2013). A number of forms of reliability evidence exist (e.g., internal consistency, test-retest, interrater, and alternate/parallel/equivalent forms) and the AERA standards (2014) outline five forms of validity evidence. For the purposes of this article, I will focus on internal consistency reliability, as it is the most popular and most commonly misused reliability estimate in social sciences research (Kalkbrenner, 2021a; McNeish, 2018), as well as construct validity. The psychometric properties of a test (including reliability and validity evidence) are contingent upon the scores from which they were derived. As such, no test is inherently valid or reliable; test scores are only reliable and valid for a certain purpose, at a particular time, for use with a specific sample. Accordingly, authors should discuss reliability and validity evidence in terms of scores, for example, “Stamm (2010) found reliability and validity evidence of scores on the Professional Quality of Life (ProQOL 5) with a sample of . . . ”
Internal Consistency Reliability Evidence. Internal consistency estimates are derived from associations between the test items based on one administration (Kalkbrenner, 2021a). Cronbach’s coefficient alpha (α) is indisputably the most popular internal consistency reliability estimate in counseling and throughout social sciences research in general (Kalkbrenner, 2021a; McNeish, 2018). The appropriate use of coefficient alpha is reliant on the data meeting the following statistical assumptions: (a) essential tau equivalence, (b) continuous level scale of measurement, (c) normally distributed data, (d) uncorrelated error, (e) unidimensional scale, and (f) unit-weighted scaling (Kalkbrenner, 2021a). For decades, coefficient alpha has been passed down in the instructional practice of counselor training programs. Coefficient alpha has appeared as the dominant reliability index in national counseling and psychology journals without most authors computing and reporting the necessary statistical assumption checking (Kalkbrenner, 2021a; McNeish, 2018). The psychometrically daunting practice of using alpha without assumption checking poses a threat to the veracity of counseling research, as the accuracy of coefficient alpha is threatened if the data violate one or more of the required assumptions.
Internal Consistency Reliability Indices and Their Appropriate Use. Composite reliability (CR)
internal consistency estimates are derived in similar ways as coefficient alpha; however, the proper computation of CRs is not reliant on the data meeting many of alpha’s statistical assumptions (Kalkbrenner, 2021a; McNeish, 2018). For example, McDonald’s coefficient omega (ω or ωt) is a CR estimate that is not dependent on the data meeting most of alpha’s assumptions (Kalkbrenner, 2021a). In addition, omega hierarchical (ωh) and coefficient H are CR estimates that can be more advantageous than alpha. Despite the utility of CRs, their underuse in research practice is historically, in part, because of the complex nature of computation. However, recent versions of SPSS include a breakthrough point-and-click feature for computing coefficient omega as easily as coefficient alpha. Readers can refer to the SPSS user guide for steps to compute omega.
Guidelines for Reporting Internal Consistency Reliability. In the Measures subsection of the Methods section, researchers should report existing reliability evidence of scores for their instruments. This can be done briefly by reporting the results of multiple studies in the same sentence, as in: “A number of past investigators found internal consistency reliability evidence for scores on the [name of test] with a number of different samples, including college students (α =. XX, ω =. XX; Authors et al., 20XX), clients living with chronic back pain (α =. XX, ω =. XX; Authors et al., 20XX), and adults in the United States (α = . XX, ω =. XX; Authors et al., 20XX) . . .”
Researchers should also compute and report reliability estimates of test scores with their data set in the Measures section. If a researcher is using coefficient alpha, they have a duty to complete and report assumption checking to demonstrate that the properties of their sample data were suitable for alpha (Kalkbrenner, 2021a; McNeish, 2018). Another option is to compute a CR (e.g., ω or H) instead of alpha. However, Kalkbrenner (2021a) recommended that researchers report both coefficient alpha (because of its popularity) and coefficient omega (because of the robustness of the estimate). The proper interpretation of reliability estimates of test scores is done on a case-by-case basis, as the meaning of reliability coefficients is contingent upon the construct of measurement and the stakes or consequences of the results for test takers (Kalkbrenner, 2021a). The following tentative interpretative guidelines for adults’ scores on attitudinal measures were offered by Kalkbrenner (2021b) for coefficient alpha: α < .70 = poor, α > .70 to .84 = acceptable, α > .85 = strong; and for coefficient omega: ω < .65 = poor, ω > .65 to .80 = acceptable, ω > .80 = strong. It is important to note that these thresholds are for adults’ scores on attitudinal measures; acceptable internal consistency reliability estimates of scores should be much stronger for high-stakes testing.
Construct Validity Evidence of Test Scores. Construct validity involves the test’s ability to accurately capture a theoretical or latent construct (AERA et al., 2014). Construct validity considerations are particularly important for counseling researchers who tend to investigate latent traits as outcome variables. At a minimum, counseling researchers should report construct validity evidence for both internal structure and relations with theoretically relevant constructs. Internal structure (aka factorial validity) is a source of construct validity that represents the degree to which “the relationships among test items and test components conform to the construct on which the proposed test score interpretations are based” (AERA et al., 2014, p. 16). Readers can refer to Kalkbrenner (2021b) for a free (open access publishing) overview of exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) that is written in layperson’s terms. Relations with theoretically relevant constructs (e.g., convergent and divergent validity) are another source of construct validity evidence that involves comparing scores on the test in question with scores on other reputable tests (AERA et al., 2014; Strauss & Smith, 2009).
Guidelines for Reporting Validity Evidence. Counseling researchers should report existing evidence of at least internal structure and relations with theoretically relevant constructs (e.g., convergent or divergent validity) for each instrument they use. EFA results alone are inadequate for demonstrating internal structure validity evidence of scores, as EFA is a much less rigorous test of internal structure than CFA (Kalkbrenner, 2021b). In addition, EFA results can reveal multiple retainable factor solutions, which need to be tested/confirmed via CFA before even initial internal structure validity evidence of scores can be established. Thus, both EFA and CFA are necessary for reporting/demonstrating initial evidence of internal structure of test scores. In an extension of internal structure, counselors should also report existing convergent and/or divergent validity of scores. High correlations (r > .50) demonstrate evidence of convergent validity and moderate-to-low correlations (r < .30, preferably r < .10) support divergent validity evidence of scores (Sink & Stroh, 2006; Swank & Mullen, 2017).
In an ideal situation, a researcher will have the resources to test and report the internal structure (e.g., compute CFA firsthand) of scores on the instrumentation with their sample. However, CFA requires large sample sizes (Kalkbrenner, 2021b), which oftentimes is not feasible. It might be more practical for researchers to test and report relations with theoretically relevant constructs, though adding one or more questionnaire(s) to data collection efforts can come with the cost of increasing respondent fatigue. In these instances, researchers might consider reporting other forms of validity evidence (e.g., evidence based on test content, criterion validity, or response processes; AERA et al., 2014). In instances when computing firsthand validity evidence of scores is not logistically viable, researchers should be transparent about this limitation and pay especially careful attention to presenting evidence for cross-cultural fairness and norming.
Cross-Cultural Fairness and Norming
In a psychometric context, fairness (sometimes referred to as cross-cultural fairness) is a fundamental validity issue and a complex construct to define (AERA et al., 2014; Kane, 2010; Neukrug & Fawcett, 2015). I offer the following composite definition of cross-cultural fairness for the purposes of a quantitative Measures section: the degree to which test construction, administration procedures, interpretations, and uses of results are equitable and represent an accurate depiction of a diverse group of test takers’ abilities, achievement, attitudes, perceptions, values, and/or experiences (AERA et al., 2014; Educational Testing Service [ETS], 2016; Kane, 2010; Kane & Bridgeman, 2017). Counseling researchers should consider the following central fairness issues when selecting or developing instrumentation: measurement bias, accessibility, universal design, equivalent meaning (invariance), test content, opportunity to learn, test adaptations, and comparability (AERA et al., 2014; Kane & Bridgeman, 2017). Providing a comprehensive overview of fairness is beyond the scope of this article; however, readers are encouraged to read Chapter 3 in the AERA standards (2014) on Fairness in Testing.
In the Measures section, counseling researchers should include commentary on how and in what ways cross-cultural fairness guided their selection, administration, and interpretation of procedures and test results (AERA et al., 2014; Kalkbrenner, 2021b). Cross-cultural fairness and construct validity are related constructs (AERA et al., 2014). Accordingly, citing construct validity of test scores (see the previous section) with normative samples similar to the researcher’s target population is one way to provide evidence of cross-cultural fairness. However, construct validity evidence alone might not be a sufficient indication of cross-cultural fairness, as the latent meaning of test scores are a function of test takers’ cultural context (Kalkbrenner, 2021b). To this end, when selecting instrumentation, researchers should review original psychometric studies and consider the normative sample(s) from which test scores were derived.
Commentary on the Danger of Using Self-Developed and Untested Scales
Counseling researchers have an ethical duty to “carefully consider the validity, reliability, psychometric limitations, and appropriateness of instruments when selecting assessments” (ACA, 2014, p. 11). Quantitative researchers might encounter instances in which a scale is not available to measure their desired construct of measurement (latent/inferred variable). In these cases, the first step in the line of research is oftentimes to conduct an instrument development and score validation study (AERA et al., 2014; Kalkbrenner, 2021b). Detailing the protocol for conducting psychometric research is outside the scope of this article; however, readers can refer to the MEASURE Approach to Instrument Development (Kalkbrenner, 2021c) for a free (open access publishing) overview of the steps in an instrument development and score validation study. Adapting an existing scale can be option in lieu of instrument development; however, according to the AERA standards (2014), “an index that is constructed by manipulating and combining test scores should be subjected to the same validity, reliability, and fairness investigations that are expected for the test scores that underlie the index” (p. 210). Although it is not necessary that all quantitative researchers become psychometricians and conduct full-fledged psychometric studies to validate scores on instrumentation, researchers do have a responsibility to report evidence of the reliability, validity, and cross-cultural fairness of test scores for each instrument they used. Without at least initial construct validity testing of scores (calibration), researchers cannot determine what, if anything at all, an untested instrument actually measures.
Data Analysis
Counseling researchers should report and explain the selection of their data analytic procedures (e.g., statistical analyses) in a Data Analysis (or Statistical Analysis) subsection of the Methods or Results section (Giordano et al., 2021; Leedy & Ormrod, 2019). The placement of the Data Analysis section in either the Methods or Results section can vary between publication outlets; however, this section tends to include commentary on variables, statistical models and analyses, and statistical assumption checking procedures.
Operationalizing Variables and Corresponding Statistical Analyses
Clearly outlining each variable is an important first step in selecting the most appropriate statistical analysis for answering each research question (Creswell & Creswell, 2018). Researchers should specify the independent variable(s) and corresponding levels as well as the dependent variable(s); for example, “The first independent variable, time, was composed of the three following levels: pre, middle, and post. The dependent variables were participants’ scores on the burnout and compassion satisfaction subscales of the ProQOL 5.” After articulating the variables, counseling researchers are tasked with identifying each variable’s scale of measurement (Creswell & Creswell, 2018; Field, 2018; Flinn & Kalkbrenner, 2021). Researchers can select the most appropriate statistical test(s) for answering their research question(s) based on the scale of measurement for each variable and referring to Table 8.3 on page 159 in Creswell and Creswell (2018), Figure 1 in Flinn and Kalkbrenner (2021), or the chart on page 1072 in Field (2018).
Assumption Checking
Statistical analyses used in quantitative research are derived based on a set of underlying assumptions (Field, 2018; Giordano et al., 2021). Accordingly, it is essential that quantitative researchers outline their protocol for testing their sample data for the appropriate statistical assumptions. Assumptions of common statistical tests in counseling research include normality, absence of outliers (multivariate and/or univariate), homogeneity of covariance, homogeneity of regression slopes, homoscedasticity, independence, linearity, and absence of multicollinearity (Flinn & Kalkbrenner, 2021; Giordano et al., 2021). Readers can refer to Figure 2 in Flinn and Kalkbrenner (2021) for an overview of statistical assumptions for the major statistical analyses in counseling research.
Exemplar Quantitative Methods Section
The following section includes an exemplar quantitative methods section based on a hypothetical example and a practice data set. Producers and consumers of quantitative research can refer to the following section as an example for writing their own Methods section or for evaluating the rigor of an existing Methods section. As stated previously, a well-written literature review and research question(s) are essential for grounding the study and Methods section (Flinn & Kalkbrenner, 2021). The final piece of a literature review section is typically the research question(s). Accordingly, the following research question guided the following exemplar Methods section: To what extent are there differences in anxiety severity between college students who participate in deep breathing exercises with progressive muscle relaxation, group exercise program, or both group exercise and deep breathing with progressive muscle relaxation?
——-Exemplar——-
Methods
A quantitative group comparison research design was employed based on a post-positivist philosophy of science (Creswell & Creswell, 2018). Specifically, I implemented a quasi-experimental, control group pretest/posttest design to answer the research question (Leedy & Ormrod, 2019). Consistent with a post-positivist philosophy of science, I reflected on pursuing a probabilistic objective answer that is situated within the context of imperfect and fallible evidence. The rationale for the present study was grounded in Dr. David Servan-Schreiber’s (2009) theory of lifestyle practices for integrated mental and physical health. According to Servan-Schreiber, simultaneously focusing on improving one’s mental and physical health is more effective than focusing on either physical health or mental wellness in isolation. Consistent with Servan-Schreiber’s theory, the aim of the present study was to compare the utility of three different approaches for anxiety reduction: a behavioral approach alone, a physiological approach alone, and a combined behavioral approach and physiological approach.
I am in my late 30s and identify as a White man. I have a PhD in counselor education as well as an MS in clinical mental health counseling. I have a deep belief in and an active line of research on the utility of total wellness (combined mental and physical health). My research and clinical experience have informed my passion and interest in studying the utility of integrated physical and psychological health services. More specifically, my personal beliefs, values, and interest in total wellness influenced my decision to conduct the present study. I carefully followed the procedures outlined below to reduce the chances that my personal values biased the research design.
Participants and Procedures
Data collection began following approval from the IRB. Data were collected during the fall 2022 semester from undergraduate students who were at least 18 years or older and enrolled in at least one class at a land grant, research-intensive university located in the Southwestern United States. An a priori statistical power analysis was computed using G*Power (Faul et al., 2009). Results revealed that a sample size of at least 42 would provide an 80% power estimate, α = .05, with a moderate effect size, f = 0.25.
I obtained an email list from the registrar’s office of all students enrolled in a section of a Career Excellence course, which was selected to recruit students in a variety of academic majors because all undergraduate students in the College of Education are required to take this course. The focus of this study (mental and physical wellness) was also consistent with the purpose of the course (success in college). A non-probability, convenience sampling procedure was employed by sending a recruitment message to students’ email addresses via the Qualtrics online survey platform. The response rate was approximately 15%, with a total of 222 prospective participants indicating their interest in the study by clicking on the electronic recruitment link, which automatically sent them an invitation to attend an information session about the study. One hundred forty-four students showed up for the information session, 129 of which provided their voluntary informed consent to enroll in the study. Participants were given a confidential identification number to track their pretest/posttest responses, and then they completed the pretest (see the Measures section below). Respondents were randomly assigned in equal groups to either (a) deep breathing with progressive muscle relaxation condition, (b) group exercise condition, or (c) both exercise and deep breathing with progressive muscle relaxation condition.
A missing values analysis showed that less than 5% of data was missing for all cases. Expectation maximization was used to impute missing values, as Little’s Missing Completely at Random (MCAR) test revealed that the data could be treated as MCAR (p = .367). Data from five participants who did not return to complete the posttest at the end of the semester were removed, yielding a robust sample of N = 124. Participants (N = 124) ranged in age from 18 to 33 (M = 21.64, SD = 3.70). In terms of gender identity, 65.0% (n = 80) self-identified as female, 32.2% (n = 40) as male, 0.8% (n = 1) as transgender, and 2.4% (n = 3) did not specify their gender identity. For ethnic identity, 50.0% (n = 62) identified as White, 26.7% (n = 33) as Latinx, 12.1% (n = 15) as Asian, 9.6% (n = 12) as Black, 0.8% (n = 1) as Alaskan Native, and 0.8% (n = 1) did not specify their ethnic identity. In terms of generational status, 36.3% (n = 45) of participants were first-generation college students and 63.7% (n = 79) were second-generation or beyond.
Group Exercise and Deep Breathing Programs
I was awarded a small grant to offer on-campus deep breathing with progressive muscle relaxation and group exercise programs. The structure of the group exercise program was based on Patterson et al. (2021), which consisted of more than 50 available exercise classes each week (e.g., cycling, yoga, swimming, dance). There was no limit to the number of classes that participants could attend; however, attending at least one class each week was required for participation in the study. Readers can refer to Patterson et al. for more information about the group exercise programming.
Neeru et al.’s (2015) deep breathing and progressive muscle relaxation programming was used in the present study. Participants completed daily deep breathing and Jacobson Progressive Muscle Relaxation (JPMR). JPMR was selected because of its documented success with treating anxiety disorders (Neeru et al., 2015). Specifically, the program consisted of four deep breathing steps completed five times and JPMR for approximately 25 minutes daily. Participants attended a weekly deep breathing and JPMR session facilitated by a licensed professional counselor. Participants also practiced deep breathing and JPMR on their own daily and kept a log to document their practice sessions. Readers can refer to Neeru et al. for more information about JPMR and the deep breathing exercises.
Measures
Prospective participants read an informed consent statement and indicated their voluntary informed consent by clicking on a checkbox. Next, participants confirmed that they met the following inclusion criteria: (a) at least 18 years old and (b) currently enrolled in at least one undergraduate college class. The instrumentation began with demographic items regarding participants’ gender identity, ethnic identity, age, and confidential identification number to track their pretest and posttest scores. Lastly, participants completed a convergent validity measure (Mental Health Inventory – 5) and the Generalized Anxiety Disorder (GAD)-7 to measure the outcome variable (anxiety severity).
Reliability and Validity Evidence of Test Scores
Tests of internal consistency were computed to test the reliability of scores on the screening tool for appraising anxiety severity with undergraduate students in the present sample. For internal consistency reliability of scores, coefficient alpha (α) and coefficient omega (ω) were computed with the following minimum thresholds for adults’ scores on attitudinal measures: α > .70 and ω > .65, based on the recommendations of Kalkbrenner (2021b).
The Mental Health Inventory–5. Participants completed the Mental Health Inventory (MHI)-5 to test the convergent validity of undergraduate students in the present samples’ scores on the GAD-7, which was used to measure the outcome variable in this study, anxiety severity. The MHI-5 is a 5-item measure for appraising overall mental health (Berwick et al., 1991). Higher MHI-5 scores reflect better mental health. Participants responded to test items (example: “How much of the time, during the past month, have you been a very nervous person?”) on the following Likert-type scale: 0 = none of the time, 1 = a little of the time, 2 = some of the time, 3 = a good bit of the time, 4 = most of the time, or 5 = all of the time. The MHI-5 has particular utility as a convergent validity measure because of its brief nature (5 items) coupled with the myriad of support for its psychometric properties (e.g., Berwick et al., 1991; Rivera-Riquelme et al., 2019; Thorsen et al., 2013). As just a few examples, Rivera-Riquelme et al. (2019) found acceptable internal consistency reliability evidence (α = .71, ω = .78) and internal structure validity evidence of MHI-5 scores. In addition, the findings of Thorsen et al. (2013) demonstrated convergent validity evidence of MHI-5 scores. Findings in the extant literature (e.g., Foster et al., 2016; Vijayan & Joseph, 2015) established an inverse relationship between anxiety and mental health. Thus, a strong negative correlation (r > −.50; Sink & Stroh, 2006) between the MHI-5 and GAD-7 would support convergent validity evidence of scores.
The Generalized Anxiety Disorder–7. The GAD-7 is a 7-item screening tool for appraising anxiety severity (Spitzer et al., 2006). Participants respond to test items based on the following prompt: “Over the last 2 weeks, how often have you been bothered by the following problems?” and anchor definitions: 0 = not at all, 1 = several days, 2 = more than half the days, or 3 = nearly every day (Spitzer et al., 2006, p. 1739). Sample test items include “being so restless that it’s hard to sit still” and “feeling afraid as if something awful might happen.” The GAD-7 items can be summed into an interval-level composite score, with higher scores indicating greater levels of Anxiety Severity. GAD-7 scores can range from 0 to 21 and are classified as mild (0–5), moderate (6–10), moderately severe (11–15), or severe (16–21).
In the initial score validation study, Spitzer et al. (2006) found evidence for internal consistency (α = .92) and test-retest reliability (intraclass correlation = .83) of GAD-7 scores among adults in the United States who were receiving services in primary care clinics. In more recent years, a number of additional investigators found internal consistency reliability evidence for GAD-7 scores, including samples of undergraduate college students in the southern United States (α = .91; Sriken et al., 2022), Black and Latinx adults in the United States (α = .93, ω = .93; Kalkbrenner, 2022), and English-speaking college students living in Ethiopia (ω = .77; Manzar et al., 2021). Similarly, the data set in the present study displayed acceptable internal consistency reliability evidence for GAD-7 scores (α = .82, ω = .81).
Spitzer et al. (2006) used factor analysis to establish internal structure validity, correlations with established screening tools for convergent validity, and criterion validity evidence by demonstrating the capacity of GAD-7 scores for detecting likely cases of generalized anxiety disorder. A number of subsequent investigators found internal structure validity evidence of GAD-7 scores via CFA and multiple-group CFA (Kalkbrenner, 2022; Sriken et al., 2022). In addition, the findings of Sriken et al. (2022) supported both the convergent and divergent validity of GAD-7 scores with other established tests. The data set in the present study (N = 124) was not large enough for internal structure validity testing. However, a strong negative correlation (r = −.78) between the GAD-7 and MHI-5 revealed convergent validity evidence of GAD-7 scores with the present sample of undergraduate students.
In terms of norming and cross-cultural fairness, there were qualitative differences between the normative GAD-7 sample in the original score validation study (adults in the United States receiving services in primary care clinics) and the non-clinical sample of young adult college students in the present study. However, the demographic profile of the present sample is consistent with Sriken et al. (2022), who validated GAD-7 scores with a large sample (N = 414) of undergraduate college students. For example, the demographic profile of the sample in the current study for gender identity closely resembled the composition of Sriken et al.’s sample, which included 66.7% women, 33.1% men, and 0.2% transgender individuals. In terms of ethnic identity, the demographic profile of the present sample was consistent with Sriken et al. for White and Black participants, although the present sample reflected a somewhat smaller proportion of Asian students (19.6%) and a greater proportion of Latinx students (5.3%).
Data Analysis and Assumption Checking
The present study included two categorical-level independent variables and one continuous-level dependent variable. The first independent variable, program, consisted of three levels: (a) deep breathing with progressive muscle relaxation, (b) group exercise, or (c) both exercise and deep breathing with progressive muscle relaxation. The second independent variable, time, consisted of two levels: the beginning of the semester and the end of the semester. The dependent variable was participants’ interval-level score on the GAD-7. Accordingly, a 3 (program) X 2 (time) mixed-design analysis of variance (ANOVA) was the most appropriate statistical test for answering the research question (Field, 2018).
The data were examined for the following statistical assumptions for a mixed-design ANOVA: absence of outliers, normality, homogeneity of variance, and sphericity of the covariance matrix based on the recommendations of Field (2018). Standardized z-scores revealed an absence of univariate outliers (z > 3.29). A review of skewness and kurtosis values were highly consistent with a normal distribution, with the majority of values less than ± 1.0. The results of a Levene’s test demonstrated that the data met the assumption of homogeneity of variance, F(2, 121) = 0.73, p = .486. Testing the data for sphericity was not applicable in this case, as the within-subjects IV (time) only comprised two levels.
——-End Exemplar——-
Conclusion
The current article is a primer on guidelines, best practices, and recommendations for writing or evaluating the rigor of the Methods section of quantitative studies. Although the major elements of the Methods section summarized in this manuscript tend to be similar across the national peer-reviewed counseling journals, differences can exist between journals based on the content of the article and the editorial board members’ preferences. Accordingly, it can be advantageous for prospective authors to review recently published manuscripts in their target journal(s) to look for any similarities in the structure of the Methods (and other sections). For instance, in one journal, participants and procedures might be reported in a single subsection, whereas in other journals they might be reported separately. In addition, most journals post a list of guidelines for prospective authors on their websites, which can include instructions for writing the Methods section. The Methods section might be the most important section in a quantitative study, as in all likelihood methodological flaws cannot be resolved once data collection is complete, and serious methodological flaws will compromise the integrity of the entire study, rendering it unpublishable. It is also essential that consumers of quantitative research can proficiently evaluate the quality of a Methods section, as poor methods can make the results meaningless. Accordingly, the significance of carefully planning, executing, and writing a quantitative research Methods section cannot be understated.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
American Psychological Association. (2020). Publication manual of the American Psychological Association: The official guide to APA style (7th ed.).
American Educational Research Association, American Psychological Association, & National Council on Measurement in Education. (2014). The standards for educational and psychological testing.
https://www.aera.net/Publications/Books/Standards-for-Educational-Psychological-Testing-2014-Edition
Balkin, R. S., & Sheperis, C. J. (2011). Evaluating and reporting statistical power in counseling research. Journal of Counseling & Development, 89(3), 268–272. https://doi.org/10.1002/j.1556-6678.2011.tb00088.x
Bardhoshi, G., & Erford, B. T. (2017). Processes and procedures for estimating score reliability and precision. Measurement and Evaluation in Counseling and Development, 50(4), 256–263.
https://doi.org/10.1080/07481756.2017.1388680
Berwick, D. M., Murphy, J. M., Goldman, P. A., Ware, J. E., Jr., Barsky, A. J., & Weinstein, M. C. (1991). Performance of a five-item mental health screening test. Medical Care, 29(2), 169–176.
https://doi.org/10.1097/00005650-199102000-00008
Cook, R. M. (2021). Addressing missing data in quantitative counseling research. Counseling Outcome Research and Evaluation, 12(1), 43–53. https://doi.org/10.1080/21501378.2019.171103
Creswell, J. W., & Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). SAGE.
Educational Testing Service. (2016). ETS international principles for fairness review of assessments: A manual for developing locally appropriate fairness review guidelines for various countries. https://www.ets.org/content/dam/ets-org/pdfs/about/fairness-review-international.pdf
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160.
https://doi.org/10.3758/BRM.41.4.1149
Field, A. (2018). Discovering statistics using IBM SPSS Statistics (5th ed.). SAGE.
Flinn, R. E., & Kalkbrenner, M. T. (2021). Matching variables with the appropriate statistical tests in counseling research. Teaching and Supervision in Counseling, 3(3), Article 4. https://doi.org/10.7290/tsc030304
Foster, T., Steen, L., O’Ryan, L., & Nelson, J. (2016). Examining how the Adlerian life tasks predict anxiety in first-year counseling students. The Journal of Individual Psychology, 72(2), 104–120. https://doi.org/10.1353/jip.2016.0009
Giordano, A. L., Schmit, M. K., & Schmit, E. L. (2021). Best practice guidelines for publishing rigorous research in counseling. Journal of Counseling & Development, 99(2), 123–133. https://doi.org/10.1002/jcad.12360
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Heppner, P. P., Wampold, B. E., Owen, J., Wang, K. T., & Thompson, M. N. (2016). Research design in counseling (4th ed.). Cengage.
Kalkbrenner, M. T. (2021a). Alpha, omega, and H internal consistency reliability estimates: Reviewing these options and when to use them. Counseling Outcome Research and Evaluation.
https://doi.org/10.1080/21501378.2021.1940118
Kalkbrenner, M. T. (2021b). Enhancing assessment literacy in professional counseling: A practical overview of factor analysis. The Professional Counselor, 11(3), 267–284. https://doi.org/10.15241/mtk.11.3.267
Kalkbrenner, M. T. (2021c). A practical guide to instrument development and score validation in the social sciences: The MEASURE Approach. Practical Assessment, Research & Evaluation, 26(1), Article 1.
https://doi.org/10.7275/svg4-e671
Kalkbrenner, M. T. (2022). Validation of scores on the Lifestyle Practices and Health Consciousness Inventory with Black and Latinx adults in the United States: A three-dimensional model. Measurement and Evaluation in Counseling and Development, 55(2), 84–97. https://doi.org/10.1080/07481756.2021.1955214
Kane, M. (2010). Validity and fairness. Language Testing, 27(2), 177–182. https://doi.org/10.1177/0265532209349467
Kane, M., & Bridgeman, B. (2017). Research on validity theory and practice at ETS. In R. E. Bennett & M. von Davier (Eds.), Advancing human assessment: The methodological, psychological and policy contributions of ETS (pp. 489–552). Springer. https://doi.org/10.1007/978-3-319-58689-2_16
Korn, J. H., & Bram, D. R. (1988). What is missing in the Method section of APA journal articles? American Psychologist, 43(12), 1091–1092. https://doi.org/10.1037/0003-066X.43.12.1091
Leedy, P. D., & Ormrod, J. E. (2019). Practical research: Planning and design (12th ed.). Pearson.
Lutz, W., & Hill, C. E. (2009). Quantitative and qualitative methods for psychotherapy research: Introduction to special section. Psychotherapy Research, 19(4–5), 369–373. https://doi.org/10.1080/10503300902948053
Manzar, M. D., Alghadir, A. H., Anwer, S., Alqahtani, M., Salahuddin, M., Addo, H. A., Jifar, W. W., & Alasmee, N. A. (2021). Psychometric properties of the General Anxiety Disorders-7 Scale using categorical data methods: A study in a sample of university attending Ethiopian young adults. Neuropsychiatric Disease and Treatment, 17(1), 893–903. https://doi.org/10.2147/NDT.S295912
McNeish, D. (2018). Thanks coefficient alpha, we’ll take it from here. Psychological Methods, 23(3), 412–433. https://doi.org/10.1037/met0000144
Myers, T. A. (2011). Goodbye, listwise deletion: Presenting hot deck imputation as an easy and effective tool for handling missing data. Communication Methods and Measures, 5(4), 297–310.
https://doi.org/10.1080/19312458.2011.624490
Neeru, Khakha, D. C., Satapathy, S., & Dey, A. B. (2015). Impact of Jacobson Progressive Muscle Relaxation (JPMR) and deep breathing exercises on anxiety, psychological distress and quality of sleep of hospitalized older adults. Journal of Psychosocial Research, 10(2), 211–223.
Neukrug, E. S., & Fawcett, R. C. (2015). Essentials of testing and assessment: A practical guide for counselors, social workers, and psychologists (3rd ed.). Cengage.
Onwuegbuzie, A. J., & Leech, N. L. (2005). On becoming a pragmatic researcher: The importance of combining quantitative and qualitative research methodologies. International Journal of Social Research Methodology, 8(5), 375–387. https://doi.org/10.1080/13645570500402447
Patterson, M. S., Gagnon, L. R., Vukelich, A., Brown, S. E., Nelon, J. L., & Prochnow, T. (2021). Social networks, group exercise, and anxiety among college students. Journal of American College Health, 69(4), 361–369. https://doi.org/10.1080/07448481.2019.1679150
Rivera-Riquelme, M., Piqueras, J. A., & Cuijpers, P. (2019). The Revised Mental Health Inventory-5 (MHI-5) as an ultra-brief screening measure of bidimensional mental health in children and adolescents. Psychiatry Research, 247(1), 247–253. https://doi.org/10.1016/j.psychres.2019.02.045
Rovai, A. P., Baker, J. D., & Ponton, M. K. (2013). Social science research design and statistics: A practitioner’s guide to research methods and SPSS analysis. Watertree Press.
Servan-Schreiber, D. (2009). Anticancer: A new way of life (3rd ed.). Viking Publishing.
Sink, C. A., & Mvududu, N. H. (2010). Statistical power, sampling, and effect sizes: Three keys to research relevancy. Counseling Outcome Research and Evaluation, 1(2), 1–18. https://doi.org/10.1177/2150137810373613
Sink, C. A., & Stroh, H. R. (2006). Practical significance: The use of effect sizes in school counseling research. Professional School Counseling, 9(5), 401–411. https://doi.org/10.1177/2156759X0500900406
Smagorinsky, P. (2008). The method section as conceptual epicenter in constructing social science research reports. Written Communication, 25(3), 389–411. https://doi.org/10.1177/0741088308317815
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing Generalized Anxiety Disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097.
https://doi.org/10.1001/archinte.166.10.1092
Sriken, J., Johnsen, S. T., Smith, H., Sherman, M. F., & Erford, B. T. (2022). Testing the factorial validity and measurement invariance of college student scores on the Generalized Anxiety Disorder (GAD-7) Scale across gender and race. Measurement and Evaluation in Counseling and Development, 55(1), 1–16.
https://doi.org/10.1080/07481756.2021.1902239
Stamm, B. H. (2010). The Concise ProQOL Manual (2nd ed.). bit.ly/StammProQOL
Strauss, M. E., & Smith, G. T. (2009). Construct validity: Advances in theory and methodology. Annual Review of Clinical Psychology, 5, 1–25. https://doi.org/10.1146/annurev.clinpsy.032408.153639
Swank, J. M., & Mullen, P. R. (2017). Evaluating evidence for conceptually related constructs using bivariate correlations. Measurement and Evaluation in Counseling and Development, 50(4), 270–274.
https://doi.org/10.1080/07481756.2017.1339562
Thorsen, S. V., Rugulies, R., Hjarsbech, P. U., & Bjorner, J. B. (2013). The predictive value of mental health for long-term sickness absence: The Major Depression Inventory (MDI) and the Mental Health Inventory (MHI-5) compared. BMC Medical Research Methodology, 13(1), Article 115. https://doi.org/10.1186/1471-2288-13-115
Vijayan, P., & Joseph, M. I. (2015). Wellness and social interaction anxiety among adolescents. Indian Journal of Health and Wellbeing, 6(6), 637–639.
Wester, K. L., Borders, L. D., Boul, S., & Horton, E. (2013). Research quality: Critique of quantitative articles in the Journal of Counseling & Development. Journal of Counseling & Development, 91(3), 280–290.
https://doi.org/10.1002/j.1556-6676.2013.00096.x
Appendix
Outline and Brief Overview of a Quantitative Methods Section
Methods
- Research design (e.g., group comparison [experimental, quasi-experimental, ex-post-facto], correlational/predictive) and conceptual framework
- Researcher bias and reflexivity statement
Participants and Procedures
- Recruitment procedures for data collection in enough detail for replication
- Research ethics including but not limited to receiving institutional review board (IRB) approval
- Sampling procedure: Researcher access to prospective participants, recruitment procedures, and data collection modality (e.g., online survey)
- Sampling technique: Probability sampling (e.g., simple random sampling, systematic random sampling, stratified random sampling, cluster sampling) or non-probability sampling (e.g., volunteer sampling, convenience sampling, purposive sampling, quota sampling, snowball sampling, matched sampling)
- A priori statistical power analysis
- Sampling frame, response rate, raw sample, missing data, and the size of the final useable sample
- Demographic breakdown for participants
- Timeframe, setting, and location where data were collected
Measures
- Introduction of the instrument and construct(s) of measurement (include sample test items)
- Reliability and validity evidence of test scores (for each instrument):
- Existing reliability (e.g., internal consistency [coefficient alpha, coefficient omega, or coefficient H], test/retest) and validity (e.g., internal structure, convergent/divergent, criterion) evidence of scores
- *Note: At a minimum, internal structure validity evidence of scores should include both exploratory factor analysis (EFA) and confirmatory factor analysis (CFA).
- Reliability and validity evidence of test scores with the data set in the present study
- *Note: Only using coefficient alpha without completing statistical assumption checking is insufficient. Compute both coefficient omega and alpha or alpha with proper assumption checking.
- Cross-cultural fairness and norming: Commentary on how and in what ways cross-cultural fairness guided the selection, administration, and interpretation of procedures and test results
- Review and citations of original psychometric studies and normative samples
Data Analysis
- Operationalized variables and scales of measurement
- Procedures for matching variables with appropriate statistical analyses
- Assumption checking procedures
Note. This appendix is a brief summary and not a substitute for the narrative in the text of this article.
Michael T. Kalkbrenner, PhD, NCC, is an associate professor at New Mexico State University. Correspondence may be addressed to Michael T. Kalkbrenner, 1780 E. University Ave., Las Cruces, NM 88003, mkalk001@nmsu.edu.
Feb 7, 2022 | Volume 12 - Issue 1
Joshua D. Smith, Neal D. Gray
Each year TPC presents an interview with a seminal figure in counseling as part of its Lifetime Achievement in Counseling series. This year I am honored to introduce Dr. Mariaimeé Gonzalez. She is a professor of counselor education, the chair of the Clinical Mental Health Counseling Program at Antioch University Seattle, and a transformational leader and advocate. Collectivism grounds and infuses her work and her practice of mentorship as community building and a key strategy for increasing diversity in the counseling profession. I am grateful to Dr. Joshua Smith and Dr. Neal Gray for bringing the contributions and vision of Dr. Gonzalez to TPC readers. —Amie A. Manis, Editor
 Mariaimeé “Maria” Gonzalez (she/her/ella), PhD, LPC, was born in Puerto Rico and raised in the United States. She earned both her master’s and doctoral degrees from the University of Missouri–St. Louis and moved to Seattle, Washington, in 2014 to become a faculty member at Antioch University Seattle (AUS), located on the traditional land of the first people of Seattle, the Duwamish People, past and present. Dr. Gonzalez is the chair of the Master of Arts in Clinical Mental Health Program and is the co-founder of the Antioch University Latinx Mental Health & Social Justice Institute, which brings together community-engaged research, service, training, and community partnerships to promote the mental health and well-being of Latinx/e people. She truly enjoys teaching in the master’s and doctoral programs at AUS and is passionate about her work with other accomplices in liberation. She is a licensed professional counselor in the state of Missouri and an approved supervisor in the state of Washington. Dr. Gonzalez currently serves as the president of the American Counseling Association (ACA) of Washington (2020–22), chair of ACA’s International Committee (2022), president elect-elect for the Western Association for Counselor Education and Supervision (WACES), and ACA parliamentarian for 2021–22. She served as coeditor of Experiential Activities for Teaching Social Justice and Advocacy Competence in Counseling and is a board member for the WACES Journal of Technology in Counselor Education and Supervision. Her research passions are global mental health, clinical supervision, Latinx/e human rights, counselor and counselor educator professional identity development, correctional counseling, liberation psychology, social justice and advocacy counseling, and anti–human trafficking advocacy. She has been involved with global mental health and advocacy for about 15 years and served as a United Nations delegate to advocate for global mental health, especially during the COVID pandemic. Dr. Gonzalez has spent over 20 years working through the paradigm of mental liberation, which includes global community and mentorship. She is currently a WACES mentor and enjoys spending time with her loved ones and community.
Mariaimeé “Maria” Gonzalez (she/her/ella), PhD, LPC, was born in Puerto Rico and raised in the United States. She earned both her master’s and doctoral degrees from the University of Missouri–St. Louis and moved to Seattle, Washington, in 2014 to become a faculty member at Antioch University Seattle (AUS), located on the traditional land of the first people of Seattle, the Duwamish People, past and present. Dr. Gonzalez is the chair of the Master of Arts in Clinical Mental Health Program and is the co-founder of the Antioch University Latinx Mental Health & Social Justice Institute, which brings together community-engaged research, service, training, and community partnerships to promote the mental health and well-being of Latinx/e people. She truly enjoys teaching in the master’s and doctoral programs at AUS and is passionate about her work with other accomplices in liberation. She is a licensed professional counselor in the state of Missouri and an approved supervisor in the state of Washington. Dr. Gonzalez currently serves as the president of the American Counseling Association (ACA) of Washington (2020–22), chair of ACA’s International Committee (2022), president elect-elect for the Western Association for Counselor Education and Supervision (WACES), and ACA parliamentarian for 2021–22. She served as coeditor of Experiential Activities for Teaching Social Justice and Advocacy Competence in Counseling and is a board member for the WACES Journal of Technology in Counselor Education and Supervision. Her research passions are global mental health, clinical supervision, Latinx/e human rights, counselor and counselor educator professional identity development, correctional counseling, liberation psychology, social justice and advocacy counseling, and anti–human trafficking advocacy. She has been involved with global mental health and advocacy for about 15 years and served as a United Nations delegate to advocate for global mental health, especially during the COVID pandemic. Dr. Gonzalez has spent over 20 years working through the paradigm of mental liberation, which includes global community and mentorship. She is currently a WACES mentor and enjoys spending time with her loved ones and community.
In this interview, Dr. Gonzalez discusses her work as a mentor, barriers facing the Latinx/e community, and advice for future counseling professionals.
- You have recently been recognized for your work in mentorship. What is the role of a successful mentor in counselor education?
The role of mentorship in counselor education is essential for creating community and supporting the future generation of mental health professionals. The Council for Accreditation of Counseling and Related Educational Programs (CACREP) mentions mentorship in the standard section 6.B.3.i, “the role of mentoring in counselor education.” Based on its importance, I believe mentorship should be promoted more often in the counseling profession and in programs.
A successful mentor in counselor education is someone who can provide a deeper perspective to a mentee on how to navigate counselor education and counseling environments through a lens of liberation. Mentorship can be conceptualized as a form of community building that allows for the mentor and mentee to learn from one another. The mentor can be a steward of the profession and provide support for the mentee to move forward with their professional and personal goals, values, and community building.
Research suggests that women and Black, Indigenous, and People of Color (BIPOC) folx are more likely than other groups to share that mentoring was an important component of their career. It is important that counseling professionals build their village of trusted colleagues to accompany them on their journey and foster the path of liberation as a counselor and/or counselor educator. Mentors can be part of this village and provide an environment that is supportive of mentees’ growth as individuals and as members of the counseling profession. By learning from one another, we can continue to be bound in our liberation and help the counseling profession evolve toward reducing oppression, creating space for all our gifts and stories, and lifting each other up.
- What are the benefits and challenges associated with mentorship that you have experienced? How did you navigate these challenges?
The primary benefit I have experienced with mentorship is community. As someone who leans into community for strength and support, I find mentorship to be an expansion of this concept. It can be healing to have someone there to listen to or consult with us about a variety of professional issues. I have noticed over the years more students and new professionals intentionally looking for mentors because they want someone with whom they can discuss professional goals and someone who will provide a brave place for conversations about how to navigate cultural spaces and tap into their own cultural capital. More BIPOC folx and women seek out mentors to help them learn how to fully utilize their own cultural knowledge, values, and gifts in the counseling profession. Another benefit of mentorship is being present for one’s story. As a mentor, it is an honor to walk beside someone on their journey. I feel I learn so much from my mentees and get excited about ways we can continue to encourage this profession to evolve and create community for future professionals.
Mentorship, like any relationship, takes time and nurturing. I have found that it is helpful to discuss with your mentee their goals, personal expectations of the relationship, personal learning styles, cultural values, time commitment, and their support system/village. At times, mentees have had a need for personal support that was more suited for their counselor or therapist. Understanding the boundaries of the role of the mentor–mentee relationship is part of understanding our roles and being ethical professionals.
- What do you consider to be your major contribution to the development of the counseling profession and why?
My voice is part of the collective consciousness of my loved ones and my community, including my ancestors. I think we all have power in our voices, and we each bring a unique perspective to this profession. My journey through mental health counseling, social justice, and higher education took roots early in my personal life as I overcame a series of challenging life events. Transitioning from Puerto Rico to the United States as a young child, overcoming poverty, and enduring the tragic loss of a loved one were mile markers along the path that has led me toward a career focused on social justice, mental health counseling, and counselor education. From my humble origins to chairing a clinical mental health counseling program at AUS, my professional and personal journey has prepared me to be deeply engaged in a profession that has provided purpose and an opportunity to create change in my world. As a lifelong social justice advocate, I have been passionate to live a life rooted in liberation and have used different paths to implement this. Over my career, I have had the honor to teach thousands of counselors-in-training and counselor educators-in-training, work with clients from all walks of life, publish research to foster social justice and advocacy, supervise and mentor, and be involved with leadership on many levels.
In my current state and national leadership roles, I work to promote a community in which we all strive to honor one another while creating a collective bond. Within this bond, we meet at the center of compassion while implementing our individual and communal gifts, strengths, commonalities, and differences. With this collective unity, we discover what connects us as professionals so we can expand our existing journeys, thus impacting how we interact with our counseling profession. The counseling profession reflects who we are and vice versa. This includes our voices, our stories, and our truths; therefore, if we evolve, we can continue to grow as a counseling profession. I have the honor to be the co-founder and co-director of a Latinx social justice mental health institute, ACA of Washington board chair, ACA parliamentarian 2021–22, president-elect-elect of WACES, chair of a counseling program, and chair of ACA’s International Committee 2021–22. In all these roles, the goal has been to create a community in which we can provide support, resources, and opportunity for voices to be heard and for change to occur. I believe my main contributions are part of a larger story, much greater than myself. This includes honoring those who have paved the way for me and many others to be part of this profession, and as a way to keep their legacy alive, I work to co-create communities rooted in social justice within our profession and in supporting the next generation of counselors as they focus on helping the professional landscape evolve to a place of more liberated thought.
- As the co-founder and director of the Latinx Mental Health & Social Justice Institute, what current barriers do you see this population facing and what does advocacy look like in your current role?
More than 19% of the U.S. population self-identify as Hispanic or Latine/x, making people of Latin origin the nation’s largest racial/ethnic minority (Lopez et al, 2021). Approximately 1 in 10 Latine/x individuals with a mental health issue uses mental health services from a general health care provider. Current barriers impacting the Latine/x population with regard to mental health are lack of accessible health services, lack of Spanish-speaking professionals, lack of culturally responsive treatment that aligns with Latine/x values, stigma in the community around mental health, and the need for better health care policies for all Latine/x individuals, including those who are undocumented (American Psychiatric Association & Lisotto, 2017). To tackle these barriers, we need to address systemic inequities on the macro, meso, and micro levels.
Currently, my advocacy is focused on growing our Latinx Mental Health & Social Justice Institute at AUS (https://latinxinstitute.antioch.edu). The Institute provides leadership for community-engaged research and service through capacity building and authentic partnerships with community stakeholders to promote impactful improvements in the health and well-being of Latine/x communities regionally, nationally, and internationally. We hope to help address barriers by creating a community of Latine/x professionals who will be accomplices in our liberation, working together to dismantle the oppressive systems that have impacted our communities, create opportunities for change rooted in liberation, and use our cultural stories, strengths, and values to guide our practices. We offer a master’s-level certificate in Latinx mental health and social justice, workshops to learn culturally responsive practices, partnerships with different nonprofit organizations, continuing education opportunities, an annual symposium during Hispanic Heritage Month, counseling services at our university’s clinic, community building, research, mentorship, training, global engagement, and cultural justice and advocacy. All efforts and roles I participate in are based on principles of social justice, human rights, and inclusion respective to intersections of one’s cultural Latinx narrative.
- What three challenges to the counseling profession as it exists today concern you most?
In the last 20 years, the average college tuition has increased by 30%. With the rising costs of higher education, more students are taking out student loans, and this debt is a burden that weighs more heavily on today’s college graduates than any generation that came before them. Due to the financial barriers, this impacts the demographic landscape of who enters the profession, quality of life, job satisfaction, and other factors. As a profession, we need to continue working on advancing and ensuring that licensed professional counselors can have seamless portability of their licenses when moving to other states, practicing across state lines, and engaging in telecounseling. This issue was illuminated during the COVID pandemic. We need to also work toward eliminating barriers that build a wall between our profession and the needs of our communities. Specifically, we need to work on decolonizing our profession. This includes recognizing that for many BIPOC individuals, the trauma from colonization and oppression impacts the mental health of individuals, families, and communities and the process of freeing ourselves from mental and systemic oppression. And last, we need to ensure adequate and equitable reimbursement for professional counselors in all settings. This means that all professional counselors need to be included as providers under all public and private insurance plans, especially Medicare.
- What needs to change in the counseling profession for these concerns to be successfully resolved?
We need to find a way to provide financial options for students pursing degrees in counseling and counselor education. This means intentionally creating a diverse pipeline of counselors and counselor educators through offering more scholarships, setting up state funding programs for counseling programs—more grants and university initiatives—and offering more easily accessible public service student loan forgiveness. In addition to eliminating financial barriers, we need to engage in practices to decolonize our profession. This includes decolonizing counseling theories, clinical practices, training programs, policies, research practices, leadership models, financial structures, and other systemic factors that create oppressive barriers. By dismantling systems of oppression, we can move toward a place of mental liberation and support liberatory practices in collaboration with the clients and communities in which we live and serve. When I think of liberation, I lean into the words of activist, Indigenous Australian (or Murri) artist, and academic, Lilla Watson, which she presented in a speech to the UN and attributed to her work with an Aboriginal Rights group in Queensland: “If you have come here to help me, you are wasting your time. But if you have come because your liberation is bound up with mine, then let us work together” (1985). As a profession, let’s continue to work toward a place in which we are bound in our liberation, freeing ourselves from oppression, and continue to heal collectively.
For the opportunity to heal, accessibility and inclusion are important for our profession to create community and connections. Currently, ACA has a strategic plan to address the challenges of licensure portability. They are working on a Counseling Compact, which “is an interstate compact, or a contract among states, allowing professional counselors licensed and residing in a compact member state to practice in other compact member states without a need for multiple licenses” (National Center for Interstate Compacts, 2022). The Counseling Compact is to help counselors have easier access to practice across state lines, which includes telehealth options, which will also allow clients more access to a diverse range of professional mental health counselors.
ACA and NBCC have been working for years on lobbying efforts to pass legislation that would allow for licensed professional mental health counselors to be reimbursed by Medicare. ACA’s and NBCC’s Government Affairs teams are working hard to get this legislation passed, but we should also get involved. We urge counselors to contact their state senators and ask for their support on this initiative. Medicare is the nation’s largest health insurance program. Opening its access to licensed professional counselors would increase access to services for BIPOC folx, people of lower socioeconomic status, and the older population. Medicare covers more than 43 million people age 65 or older and more than 10 million Americans with disabilities. Many of these folx are in communities with limited access to mental health services and/or the services lack diversity in professionals. As professional counselors in and around these communities, we should strive to create and then join the solution to accessible health care.
- If you were advising current counseling leaders, what advice would you give them about moving the counseling profession forward?
Listen. I would advise leaders to listen to the members and stakeholders. There are many ways in which we can work toward evolving our profession, but we need to listen to one another in order to do this together. I would encourage current leaders to support and mentor leaders from communities that have been silenced or not invited to the table. As leaders, we need to think of the next generation and be thoughtful about supporting all communities, especially BIPOC leaders. As BIPOC leaders, we have many gifts to offer and need to bring our villages with us. As stated earlier, we are all bound together in liberation, so let’s collectively lead into a more inclusive future of our profession.
This concludes the seventh interview for the annual Lifetime Achievement in Counseling Series. TPC is grateful to Joshua D. Smith, PhD, NCC, LCMHC, and Neal D. Gray, PhD, LCMHC-S, for providing this interview. Joshua D. Smith is an assistant professor at the University of Mount Olive. Neal D. Gray is a professor and Chair of the School of Counseling and Human Services at Lenoir-Rhyne University. Correspondence can be emailed to Joshua Smith at jsmith@umo.edu.
References
American Psychiatric Association, & Lisotto, M. (2017). Mental health disparities: Hispanics and Latinos. Council on Minority Mental Health and Health Disparities. https://www.psychiatry.org/File%20Library/Psychiatrists/Cultural-Competency/Mental-Health-Disparities/Mental-Health-Facts-for-Hispanic-Latino.pdf
Lopez, M. H., Krogstad, J. M., & Passel , J. S. (2021, September 23). Who is Hispanic? Pew Research Center. https://www.pewresearch.org/fact-tank/2021/09/23/who-is-hispanic
National Center for Interstate Compacts. (2022, January 30). Counseling compact. https://counselingcompact.org
Watson, L. (1985, July 15–26). The World Conference to Review and Appraise the Achievements of the United Nations Decade for Women: Equality, Development and Peace 1985. United Nations.
Feb 26, 2021 | Volume 11 - Issue 1
David E. Jones, Jennifer S. Park, Katie Gamby, Taylor M. Bigelow, Tesfaye B. Mersha, Alonzo T. Folger
Epigenetics is the study of modifications to gene expression without an alteration to the DNA sequence. Currently there is limited translation of epigenetics to the counseling profession. The purpose of this article is to inform counseling practitioners and counselor educators about the potential role epigenetics plays in mental health. Current mental health epigenetic research supports that adverse psychosocial experiences are associated with mental health disorders such as schizophrenia, anxiety, depression, and addiction. There are also positive epigenetic associations with counseling interventions, including cognitive behavioral therapy, mindfulness, diet, and exercise. These mental health epigenetic findings have implications for the counseling profession such as engaging in early life span health prevention and wellness, attending to micro and macro environmental influences during assessment and treatment, collaborating with other health professionals in epigenetic research, and incorporating epigenetic findings into counselor education curricula that meet the standards of the Council for Accreditation of Counseling and Related Educational Programs (CACREP).
Keywords: epigenetics, mental health, counseling, prevention and wellness, counselor education
Epigenetics, defined as the study of chemical changes at the cellular level that alter gene expression but do not alter the genetic code (T.-Y. Zhang & Meaney, 2010), has emerging significance for the profession of counseling. Historically, people who studied abnormal behavior focused on determining whether the cause of poor mental health outcomes was either “nature or nurture” (i.e., either genetics or environmental factors). What we now understand is that both nature and nurture, or the interaction between the individual and their environment (e.g., neglect, trauma, substance abuse, diet, social support, exercise), can modify gene expression positively or negatively (Cohen et al., 2017; Suderman et al., 2014).
In the concept of nature and nurture, there is evidence that psychosocial experiences can change the landscape of epigenetic chemical tags across the genome. This change in landscape influences mental health concerns, such as addiction, anxiety, and depression, that are addressed by counseling practitioners (Lester et al., 2016; Provençal & Binder, 2015; Szyf et al., 2016). Because the field of epigenetics is evolving and there is limited attention to epigenetics in the counseling profession, our purpose is to inform counseling practitioners and educators about the role epigenetics may play in clinical mental health counseling.
Though many counselors and counselor educators may have taken a biology class that covered genetics sometime during their professional education, we provide pedagogical scaffolding from genetics to epigenetics. Care was taken to ensure accessibility of information for readers across this continuum of genetics knowledge. Much of what we offer below on genetics is putative knowledge, as we desire to establish a foundation for the reader in genetics so they may be able to have a greater understanding of epigenetics and a clearer comprehension of the implications we offer leading to application in counseling. We suggest readers review Brooker (2017) for more detailed information on genetics. We will present an overview of genetics and epigenetics, an examination of mental health epigenetics, and implications for the counseling profession.
Genetics
Genetics is the study of heredity (Brooker, 2017) and the cellular process by which parents pass on biological information via genes. The child inherits genetic coding from both parents. One can think of these parental genes as a recipe book for molecular operations such as the development of proteins, structure of neurons, and other functions across the human body. This total collection of the combination of genes in the human body is called the genome or genotype. The presentation of observable human traits (e.g., eye color, height, blood type) is called the phenotype. Phenotypes can be seen in our clinical work through behavior (e.g., self-injury, aggression, depression, anxiety, inattentiveness).
Before going further, it is important to establish a fundamental understanding of genetics by examining the varied molecular components and their relationships (Figure 1). Deoxyribonucleic acid (DNA) is a long-strand molecule that takes the famous double helix or ladder configuration. DNA is made up of four chemical bases called adenine (A), guanine (G), cytosine (C), and thymine (T). These form base pairs—A with T and C with G—creating a nucleic acid. The DNA is also wrapped around a specialized protein called a histone. The collection of DNA wrapped around multiple histones is called the chromatin. This wrapping process is essential for the DNA to fit within the cell nucleus. Finally, as this chromatin continues to grow, it develops a structure called a chromosome. Within every human cell nucleus, there are 23 chromosomes from each parent, totaling 46 chromosomes.
Figure 1
Gene Structure and Epigenetics
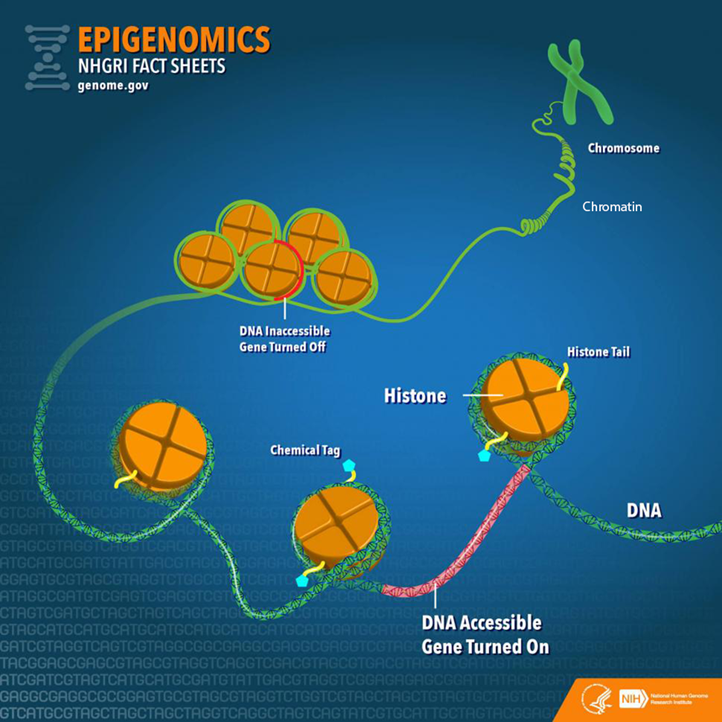
From “Epigenomics Fact Sheet,” by National Human Genome Research Institute, 2020
(https://www.genome.gov/about-genomics/fact-sheets/Epigenomics-Fact-Sheet). In the public domain.
Beyond the chromosomes, chromatin, histones, DNA, and genes, there is another key component in genetics: ribonucleic acid (RNA). RNA can be a cellular messenger that carries instructions from a DNA sequence (specific genes) to other parts of the cell (i.e., messenger RNA [mRNA]). RNA can come in several other forms as well, including transfer RNA (tRNA), microRNA (miRNA), and non-coding RNA (ncRNA). In the sections below, we elaborate on mRNA and tRNA and their impact on the genetic processes. Later in the epigenetics section, we provide fuller details on miRNA and ncRNA.
Besides the aforementioned biological aspects, it is important to understand that a child inherits genes from both parents, but they are not exactly the same genes, (i.e., alternative forms of the same gene may have differing expression). Different versions of the same gene are called alleles. Variation in an allele is one reason why we see phenotypic variation between our clients—height, weight, eye color—and this variation can contribute to mental disease susceptibility. Although there are many potential causes of poor mental health, family history is often one of the strongest risk factors because family members most closely represent the unique genetic and environmental interactions that an individual may experience. We also see this as a function of intergenerational epigenetic effects, which are covered later in this paper.
Transcription and Translation
Now that we have provided a foundation of the genetic components, we move toward the primary two-stage processes of genetics: transcription and translation (Brooker, 2017). The first step in the process of gene expression is called transcription. Transcription occurs when a sequence of DNA is copied using RNA polymerase (“ase” notes that it is an enzyme) to make mRNA for protein synthesis. We can liken transcription to the process of someone taking down information from a client’s voicemail message. In this visualization, DNA is the caller, the person writing down the message is the RNA polymerase, and the actual written message is the RNA.
A particular section of a gene, called a promotor region, is bound by the RNA polymerase (Brooker, 2017). The RNA polymerase acts like scissors to separate the double-stranded DNA helix into two strands. One of the strands, called the template, is where the RNA polymerase will read the DNA code A to T, and G to C to build mRNA. There are other modifications that must occur in eukaryotic cells such as splicing introns and exons. In short, sections of unwanted DNA, called introns, are removed by the process of splicing, and the remaining DNA codes are connected back together (exons).
Now that the mRNA has been created by the process of transcription, the next step is for the mRNA to build a protein necessary for the main functions of the body, in a process known as translation (Brooker, 2017). Here, translation is the process in which tRNA decodes or translates the mRNA into a protein in a mobile cellular factory called the ribosome. It is translating the language of a DNA sequence (gene) into the language of a protein. To do this, the tRNA uses a translation device called an anticodon. This anticodon links to the mRNA-based pairs called a codon. A codon is a trinucleotide sequence of DNA or RNA that corresponds to a specific amino acid, or building block of a protein. This process then continues to translate and connect many amino acids together until a polypeptide (a long chain of amino acids) is created. Later, these polypeptides join to form proteins. Depending on the type of cell, the protein may function in a variety of ways. For example, the neuron has several proteins for its function, and different proteins are used for memory, learning, and neuroplasticity.
Epigenetics
There is a wealth of research conducted on genetics, yet the understanding of epigenetics is more limited when focusing on mental health (Huang et al., 2017). Though the term epigenetics has been around since the 1940s, the “science” of epigenetics is in its youth. Epigenetic research in humans has grown in the last 10 years and continues to expand rapidly (Januar et al., 2015). The key concept for counselors to remember about epigenetics is that epigenetics supports the idea of coaction. Factors present in the client’s external environment (e.g., stress from caregiver neglect, foods consumed, drug intake like cigarettes) influence the expression of their genes (transcription and translation) and thus cell activity and related behavioral phenotypes. In the sections below, we will dive deeper into the understanding of epigenetic mechanisms and define key terms including epigenome, chromatin, and chemical modifications.
To start, the more formal definition of epigenetics is the differentiation of gene expression via chemical modifications upon the epigenome that do not alter the genetic code (i.e., the DNA sequence; Szyf et al., 2007). The epigenome, which is composed of chromatin (the combination of DNA and protein forming the chromosomes) and modification of DNA by chemical mechanisms (e.g., DNA methylation, histone modification), programs the process of gene expression (Szyf et al., 2007). The epigenome differs from the genome in that the chemical actions or modifications are on the outside of the genome (i.e., the DNA) or “upon” the genome. Specifically, epigenetic processes act “upon” the genome, which may open or close the chromatin to various degrees to govern access for reading DNA sequences (Figure 1). When the chromatin is opened, transcription and translation can take place; however, when the chromatin is closed, gene expression is silenced (Syzf et al., 2007).
It is important for counselors to conceptualize their client’s psychosocial environment in conjunction with the observed behavioral phenotypes, in that the client’s psychosocial environment may have partially mediated epigenetic expression (Januar et al., 2015). For example, with schizophrenia, a client’s adverse environment (e.g., early childhood trauma) influences the epigenome, or gene expression, which may contribute up to 60% of this disorder’s development (Gejman et al., 2011). Other adverse environmental influences have been associated with the development of schizophrenia, including complications during client’s prenatal development and birth, place and season of client’s birth, abuse, and parental loss (Benros et al., 2011). As we highlight below, epigenetic mechanisms (e.g., DNA methylation) may mediate between these environmental influences and genes with outcomes like schizophrenia (Cariaga-Martinez & Alelú-Paz, 2018; Tsankova et al., 2007).
Epigenetic Mechanisms
There are a variety of chemical mechanisms or tags that change the chromatin structure (either opening for expression or closing to inhibit expression). Some of the most investigated mechanisms for changes in chromatin structure are DNA methylation, histone modification, and microRNA (Benoit & Turecki, 2010; Maze & Nestler, 2011).
DNA Methylation. Methylation is the most studied epigenetic modification (Nestler et al., 2016). It occurs when a methyl group binds to a cytosine base (C) of DNA to form 5-methylcytosine. A methyl group is three hydrogens bonded to a carbon, identified as CH3. Most often, the methyl group is attached to a C followed by a G, called a CpG. These methylation changes are carried out by specific enzymes called DNA methyltransferase. These enzymes add the methyl group to the C base at the CpG site.
Methylation was initially considered irreversible, but recent research has shown that DNA methylation is more stable compared to other chemical modifications like histone modification and is therefore reversible (Nestler et al., 2016). This DNA methylation adaptability evidence is important, conceivably supporting counseling efficacy across the life span. If methylation is indeed reversible beyond 0 to 5 years of age, counseling efforts hold promise to influence mental health outcomes across the life span.
Beyond noted stability, DNA methylation is also important in that it is tissue-specific, meaning it assists in cell differentiation; it may regulate gene expression up or down and is influenced by different environmental exposures (Monk et al., 2012). For example, DNA methylation represses specific areas of a neuron’s genes, thus “turning off” their function. This stabilizes the cell by preventing any tissue-specific cell differentiation and inhibits the neuron from changing into another cell type (Szyf et al., 2016), such as becoming a lung cell later in development.
When looking at up- or downregulation, Oberlander et al. (2008) provided an example from a study using mice. When examining attachment style in mice, they found that decreased quality of mothering to offspring increased risk of anxiety, in part, because of the methylation at the glucocorticoid receptor (GR) gene and fewer GR proteins produced by the hippocampus. This change may lead to lifelong silencing or downregulation with an increased risk of anxiety to the mouse over its life span. Stevens et al. (2018) also established a link between diet, epigenetics, and DNA methylation. They found an epigenetic connection between poor dietary intake with increased risk of behavioral problems and poor mental health outcomes such as autism. The authors also remarked that further investigation is required for a clearer picture of this link and potential effects.
Histone Modification. Another process that has been extensively researched is post-translational histone modification, or changes in the histone after the translation process. The most understood histone modifications are acetylation, methylation, and phosphorylation (Nestler et al., 2016). Acetylation, the most common post-translational modification, occurs by adding an acetyl group to the histone tail, such as the amino acid lysine. The enzymes responsible for histone acetylation are histone acetyltransferases or HATs (Haggarty & Tsai, 2011). Conversely, histone deacetylases (HDACs) are enzymes that remove acetyl groups (Saavedra et al., 2016). The acetylation process promotes gene expression (Nestler et al., 2016).
Through histone methyltransferases (HMTs), histone methylation increases methylation, thereby reducing gene expression. Histone demethylases (HDMs) remove methyl groups to increase gene activity. Phosphorylation can increase or decrease gene expression. Overall, there are more than 50 known histone modifications (Nestler et al., 2016).
From a counseling perspective, it is important to note that histone modification is flexible. Unlike DNA methylation, which is more stable over a lifetime, histone modifications are more transient. To illustrate, if an acetyl group is added to a histone, it may loosen the binding between the DNA and histone, increasing transcription and thereby allowing gene expression across the life span (Nestler et al., 2016). Such acetylation processes have been found in maternal neglect to offspring (early in the life span) and mindfulness practices in adult clients (Chaix et al., 2020; Devlin et al., 2010). Yet, although histone modification can be changed across the life span (Nestler et al., 2016), it is still important for counselors to recognize the importance of early counseling interventions because of how highly active epigenetics mechanisms (e.g., DNA methylation) are in children 0 to 5 years of age.
MicroRNA. Beyond histone modification, another known mechanism is microRNA (miRNA), which is the least understood and most recently investigated epigenetic mechanism when compared to DNA methylation and histone modification (Saavedra et al., 2016). miRNA is one type of non-coding RNA (ncRNA), or RNA that is changed into proteins. Around 98% of the genome does not code for proteins, leading to a supporting hypothesis that ncRNAs play a significant role in gene expression. For example, humans and chimpanzees share 98.8% of the same DNA code. However, epigenetics and specifically ncRNA contribute to the wide phenotypic variation between the species (Zheng & Xiao, 2016). Further, Zheng and Xiao (2016) estimated that miRNA regulates up to 60% of gene expression.
miRNA has also been found to suppress and activate gene expression at the levels of transcription and translation (Saavedra et al., 2016). miRNAs affect gene expression by directly influencing mRNA. Specifically, the miRNA may attach to mRNA and “block” the mRNA from creating proteins or it may directly degrade mRNA. This then decreases the surplus of mRNA in the cell. If the miRNA binds partially with the mRNA, then it inhibits protein production; but if it binds completely, it is marked for destruction. Once the mRNA is identified for destruction, other proteins and enzymes are attracted to the mRNA, and they degrade the mRNA and eliminate it (Zheng & Xiao, 2016). Moreover, when compared to DNA methylation, which may be isolated to a single gene sequence, miRNA can target hundreds of genes (Lewis et al., 2005). Researchers have discovered that miRNA may mediate anxiety-like symptoms (Cohen et al., 2017).
Human Development and Epigenetics
Over the life of an individual, there are critical or sensitive periods in which epigenetic modifications are more heavily influenced by environmental factors (Mulligan, 2016). Early life (ages 0 to 5 years) appears to be one of the most critical time periods when epigenetics is more active. An example of this is the Dutch Famine of 1944–45, also known as the Dutch Hunger Winter (Champagne, 2010; Szyf, 2009). The Nazis occupied the Netherlands and restricted food to the country, bringing about a famine. The individual daily caloric intake estimate varied between 400 and 1800 calories at the climax of the famine. Most notably, women who gave birth during this time experienced the impact of low maternal caloric intake, which impacted their child and the child’s health outcomes into adulthood. One discovery was that male children had a higher risk of adulthood obesity if their famine exposure occurred early in gestation versus a male fetus who experienced famine in late gestation. Findings suggested that fetuses who experienced restricted caloric intake during the development of their autonomic nervous system may have an increased risk of heart disease in adulthood. The findings of epigenetic mechanisms at work between mother and child during a famine are flagrant enough, yet epigenetic researchers have also discovered that epigenetic tags carry across generations, called genomic imprinting (Arnaud, 2010; Yehuda et al., 2016; T.-Y. Zhang & Meaney, 2010).
Genomic imprinting can be defined as the passing on of certain epigenetic modifications to the fetus by parents (Arnaud, 2010). It is allele-specific, and approximately half of the imprinting an offspring receives is from the mother. The imprinting mechanism marks certain areas, or loci, of offspring’s genes as active or repressed. For instance, the loci may exhibit increased or decreased methylation.
An imprinting example is evident in the IGF-2 (insulin-like growth factor II) gene and those fetuses exposed to the Dutch Hunger Winter (Heijmans et al., 2008). Sixty years after the famine, a decrease in DNA methylation on IGF-2 was found in adults with fetal exposure during the famine compared to their older siblings. Researchers also found these intergenerational imprinting effects associated with the grandchildren of women who were pregnant during the Dutch Hunger Winter. Similar imprinting is also apparent in Holocaust survivors (Yehuda et al., 2016) and children born to mothers who experienced PTSD from the World Trade Center collapse of 9/11 (Yehuda et al., 2005). These imprinting mechanisms are important for counselors to understand in that we see the interplay between the client and the environment across generations. The client becomes the embodiment of their environment at the cellular level. This is no longer the dichotomous “nature vs. nurture” debate but the passing on of biological effects from one generation to another through the interplay of nature and nurture.
Epigenetics and Mental Health Disorders
Now we turn our focus to the influence of epigenetics on the profession of counseling. What we do know is that epigenetic mechanisms, (e.g., DNA methylation, histone modifications, miRNA) are associated with various mental health disorders. It is hypothesized that epigenetics contributes to the development of mental disorders after exposure to environmental stressors, such as traumatic life events, but it may also have positive effects based on salutary environments (Syzf, 2009; Yehuda et al., 2005). We will review only those mental health epigenetic findings that have significant implications relative to clinical disorders such as stress, anxiety, childhood maltreatment, depression, schizophrenia, and addiction. We will also offer epigenetic outcomes associated with treatment, including cognitive behavioral therapy (CBT; Roberts et al., 2015), meditation (Chaix et al., 2020), and antidepressants (Lüscher & Möhler, 2019).
Stress and Anxiety
Stress, especially during early life stages, causes long-term effects for neuronal pathways and gene expression (Lester et al., 2016; Palmisano & Pandey, 2017; Perroud et al., 2011; Roberts et al., 2015; Szyf, 2009; T.-Y. Zhang & Meaney, 2010). Currently, research supports the mediating effects of stress on epigenetics through DNA methylation, especially within the gestational environment (Lester & Marsit, 2018). DNA methylation has been associated with upregulation of the hypothalamic-pituitary-adrenal (HPA) axis, increasing anxiety symptoms (McGowan et al., 2009; Oberlander et al., 2008; Romens et al., 2015; Shimada-Sugimoto et al., 2015; Tsankova et al., 2007). DNA methylation has also been linked with increased levels of cortisol for newborns of depressed mothers. This points to an increased HPA stress response in the newborn (Oberlander et al., 2008). Ouellet-Morin et al. (2013) also looked at DNA methylation and stress. They conducted a longitudinal twin study on the effect of bullying on the serotonin transporter gene (SERT) for monozygotic twins and found increased levels of SERT DNA methylation in victims compared to their non-bullied monozygotic co-twin. Finally, Roberts et al. (2015) examined the effect of CBT on DNA methylation for children with severe anxiety, specifically testing changes in the FKBP5 gene. Although the results were not statistically significant, they may be clinically significant. Research participants with a higher DNA methylation on the FKBP5 gene had poorer response to CBT treatment.
Beyond DNA methylation, other researchers have investigated miRNA and its association with stress and anxiety. A study by Harris and Seckl (2011) found that fetal rodents with increased exposure to maternal cortisol suffered from lower birth weights and heightened anxiety. Similarly, Cohen et al. (2017) investigated anxiety in rats for a specific miRNA called miR-101a-3p. The researchers selectively bred rats, one group with low anxiety and the other with high anxiety traits. They then overexpressed miR-101a-3p in low-anxiety rats to see if that would induce greater expressions of anxiety symptomatology. The investigators observed increased anxiety behaviors when increasing the expression of miR-101a-3p in low-anxiety rats. The researchers postulated that miRNA may be a mediator of anxiety-like behaviors. Finally, paternal chronic stress in rats has been associated with intergenerational impact on offspring’s HPA axis with sperm cells having increased miRNAs, potentially indicating susceptibility of epigenetic preprogramming in male germ cells post-fertilization (Rodgers et al., 2013). The evidence suggests that paternal stress reprograms the HPA stress response during conception. This reprogramming may begin a cascading effect on the offspring’s HPA, creating dysregulation that is associated with disorders like schizophrenia, autism, and depression later in adulthood.
Though some researchers have indicated a negative association between anxiety and epigenetics, others have found positive effects between epigenetics and anxiety. A seminal study by Weaver et al. (2005) illustrated the flexibility of an offspring’s biological system to negative and positive environmental cues. Weaver et al. looked at HPA response of rodent pups who received low licking and grooming from their mother (a negative environmental effect) who exhibited higher HPA response to environmental cues in adulthood. Epigenetically, they found lower DNA methylation in a specific promotor region in these adult rodents. They hypothesized that they could reverse this hypomethylation by giving an infusion of methionine, an essential amino acid that is a methyl group donor. They discovered the ability to reverse low methylation, which improved the minimally licked and groomed adult rodents’ response to stress. This connects with counseling in that epigenetic information is not set for life but reversible through interventions such as diet.
Others have investigated mindfulness and its epigenetic effects on stress. Chaix et al. (2020) looked at DNA methylation at the genome level for differences between skilled meditators who meditated for an 8-hour interval compared to members of a control group who engaged in leisure activities for 8 hours. The control group did not have any changes in genome DNA methylation, but the skilled meditators showed 61 differentially methylated sites post-intervention. This evidence can potentially support the use of mindfulness with our clients as an intervention for treatment of stress.
Childhood Maltreatment
Childhood maltreatment includes sexual abuse, physical abuse and/or neglect, and emotional abuse and/or neglect. Through this lens, Suderman et al. (2014) examined differences in 45-year-old males’ blood samples between those who experienced abuse in childhood and those who did not, with the aim of determining whether gene promoter DNA methylation is linked with child abuse. After 30 years, the researchers found different DNA methylation patterns between abused versus non-abused individuals and that a specific hypermethylation of a gene was linked with the adults who experienced child abuse. Suderman et al. (2014) believed that adversity, such as child abuse, reorganizes biological pathways that last into adulthood. These DNA methylation differences have been associated with biological pathways leading to cancer, obesity, diabetes, and other inflammatory paths.
Other researchers have also found epigenetic interactions at CpG sites predicting depression and anxiety in participants who experienced abuse. Though these interactions were not statistically significant (Smearman et al., 2016), increased methylation at specific promoter regions was discovered (Perroud et al., 2011; Romens et al., 2015). Furthermore, in a hallmark study, McGowan et al. (2009) discovered that people with child abuse histories who completed suicide possessed hypermethylation of a particular promotor region when compared to controls. Perroud et al. (2011) noted that frequency, age of onset, and severity of maltreatment correlated positively with increased methylation in adult participants suffering from borderline personality disorder, depression, and PTSD. Yehuda et al. (2016) reported that in a smaller subset of an overall sample of Holocaust survivors, the impact of trauma was intergenerationally associated with increased DNA methylation. Continued study of these particular regions may provide evidence of DNA methylation as a predictor of risk in developing anxiety or depressive disorders.
Major Depressive Disorder
Most studies of mental illness, genetics, and depression have used stress animal models. Through these models, histone modification, chromatin remodeling, miRNA, and DNA methylation mechanisms have been found in rats and mice (Albert et al., 2019; Nestler et al., 2016). When an animal or human experiences early life stress, epigenetic biomarkers may serve to detect the development or progression of major depressive disorder (Saavedra et al., 2016). Additionally, histone modification markers may also indicate an increase in depression (Tsankova et al., 2007; Turecki, 2014). Beyond animal models, Januar et al. (2015) found that buccal tissue in older patients with major depressive disorder provided evidence that the BDNF gene modulates depression through hypermethylation of specific CpGs in promoter regions.
Lastly, certain miRNAs may serve as potential biomarkers for major depressive disorder. miRNA may be used in the pharmacologic treatment of depressive disorders (Saavedra et al., 2016). Tsankova et al. (2007) and Saavedra et al. (2016) noted that certain epigenetic mechanisms that influence gene expression may be useful as antidepressant treatments. Medication may induce neurogenesis and greater plasticity in synapses through upregulation and downregulation of miRNAs (Bocchio-Chiavetto et al., 2013; Lüscher & Möhler, 2019). This points to the potential use of epigenetic “engineering” for reducing depression progression and symptomology where a counselor could refer a client for epigenetic antidepressant treatments.
Maternal Depression
Maternal prenatal depression may program the postnatal HPA axis in infants’ responses to the caretaking environment. Such programming may result in decreased expression of certain genes associated with lesser DNA methylation in infants, depending on which trimester maternal depression was most severe, and increased HPA reactivity (Devlin et al., 2010). Further, Devlin et al. discovered that maternal depression in the second trimester affected newborns’ DNA methylation patterns. However, the authors offered key limitations in their study, namely the sample was predominantly male and depressive characteristics differed based on age. Conradt et al. (2016) reported that prenatal depression in mothers may be associated with higher DNA methylation in infants. However, maternal sensitivity (i.e., ability of mother to respond to infants’ needs positively, such as positive touch, attending to distress, and basic social-emotional needs) toward infants buffered the extent of methylation, which points to environmental influences. This finding highlights the risk of infant exposure to maternal depression in conjunction with maternal sensitivity. Yet, overall, the evidence suggests that epigenetic mechanisms are at play across critical periods—prenatal, postnatal, and beyond—that have implications for offspring. When a fetus or offspring experiences adverse conditions, such as maternal depression, there is an increased likelihood of “impaired cognitive, behavioral, and social functioning . . . [including] psychiatric disorders throughout the adult life” (Vaiserman & Koliada, 2017, p. 1). For the practicing counselor, we suggest that clinical work with expecting mothers has the potential to reduce such risk based on these epigenetic findings.
Schizophrenia
Accumulated evidence suggests that schizophrenia arises from the interaction between genetics and the client’s environment (Smigielski et al., 2020). Epigenetics is considered a mediator between a client’s genetics and environment with research showing moderate support for this position. DNA methylation, histone modifications, mRNA, and miRNA epigenetic mechanisms have been linked with schizophrenia (Boks et al., 2018; Cheah et al., 2017; Okazaki et al., 2019).
DNA methylation is a main focus in schizophrenia epigenetic research (Cariaga-Martinez & Alelú-Paz , 2018). For example, Fisher et al. (2015) conducted a longitudinal study investigating epigenetic differences between monozygotic twins who demonstrated differences in psychotic symptoms; at age 12, one twin was symptomatic and the other was asymptomatic. Fisher et al. found DNA methylation differences between these twins. The longitudinal twin study design allowed for the control of genetic contributions to the outcome as well as other internal and external threats. Further, it pointed to a stronger association between epigenetics and schizophrenia.
From a clinical perspective, Ma et al. (2018) identified a potential epigenetic biomarker for detecting schizophrenia. The authors were able to identify three specific miRNAs that may work in combination as a biomarker for the condition. According to the authors, this finding may be helpful in the future for diagnosis and monitoring treatment outcomes. We speculate that future counselors may have biomarker tests conducted as part of the diagnostic process and in monitoring treatment effectiveness with alternation in miRNA levels.
Addiction
In addictions, a diversity of epigenetic mechanisms have been identified (e.g., DNA methylation, histone acetylation, mRNA, miRNA) across various substance use disorders: cocaine, amphetamine, methamphetamine, and alcohol (Hamilton & Nestler, 2019). Moreover, these epigenetic processes have been hypothesized to contribute to the addiction process by mediating seeking behaviors via dopamine in the neurological system. Also, Hamilton and Nestler (2019) found that epigenetic mechanisms have the potential to combat addiction processes, but further research is needed.
Cadet et al. (2016) conducted a review of cocaine, methamphetamine, and epigenetics in animal models (mice and rats). Chronic cocaine use was linked with histone acetylation in the dopamine system and DNA methylation for both chronic and acute administrations. They concluded that epigenetics may be a facilitating factor for cocaine abuse. Others have supported this conclusion for cocaine specifically, in that cocaine alters the chromatin structure by increasing histone acetylation, thereby temporarily inducing addictive behaviors (Maze & Nestler, 2011; Tsankova et al., 2007). From a treatment perspective, Wright et al. (2015) reported, in a sample of rats, that an injected methyl supplementation appeared to attenuate cocaine-seeking behavior when compared to the control group associated with cocaine-induced DNA methylation.
Regarding methamphetamines, during their review, Cadet et al. (2016) discovered that there were only a few extant studies on epigenetics and methamphetamines. Numachi et al. (2004) linked extended use of methamphetamines to changes in DNA methylation patterns, which seemed to increase vulnerability to neurochemical effects. More recently, Jayanthi et al. (2014) discovered that chronic methamphetamine use in rats induced histone hypoacetylation, making it more difficult for transcription to occur and potentially supporting the addiction process. To counter this histone hypoacetylation, the authors treated the mice with valproic acid, which inhibited the histone hypoacetylation. This study may evidence potential psychopharmacological treatments in the future at the epigenetic level for methamphetamine addiction.
H. Zhang and Gelernter (2017) reviewed the literature on DNA methylation and alcohol use disorder (AUD) and found mixed results. The authors discovered that individuals with an AUD exhibited DNA hypermethylation and hypomethylation in a variety of promoter regions. They also noted generalization limitations due to small tissue samples from the same regions of postmortem brains. They suggested that DNA methylation may account for “missing heritability” (p. 510) among individuals with AUDs.
Histone deacetylation has also been connected to chromatin closing or silencing for chronic users of alcohol, which may be involved in the maintenance of an AUD. Palmisano and Pandey (2017) suggested that there are epigenetic mediating factors between comorbidity of AUDs and anxiety disorders. On a positive note, exercise has been found to have opposite epigenetic modifications when comparing a healthy exercise group to a group who experience AUDs in terms of DNA methylation at CpG sites (Chen et al., 2018). Thus, counselors may incorporate such aspects in psychoeducation when recommending exercise in goal setting and other treatment interventions.
To summarize, epigenetics has been linked to several disorders such as anxiety, stress, depression, schizophrenia, and addiction (Albert et al., 2019; Cadet et al., 2016; Lester et al., 2016; Palmisano & Pandey, 2017; Smigielski et al., 2020). DNA methylation and miRNA may have mediating effects for mental health concerns such as anxiety (Harris & Seckl, 2011; Romens et al., 2015). Additionally, epigenetic mediating effects have also been discovered in major depressive disorder, maternal depression, and addiction (Albert et al., 2019; Conradt et al., 2016; Hamilton & Nestler, 2019). Moreover, epigenetic imprinting has been associated with trauma and stress, as found in Holocaust survivors and their children (Yehuda et al., 2016). Overall, “evidence accumulates that exposure to social stressors in [childhood], puberty, adolescence, and adulthood can influence behavioral, cellular, and molecular phenotypes and . . . are mediated by epigenetic mechanisms” (Pishva et al., 2014, p. 342).
Implications
A key aim in providing a primer on epigenetics, specifically the coaction between a client’s biology and environment on gene expression, is to illuminate opportunities for counselors to prevent and intervene upon mental health concerns. This is most relevant based on the evidence that epigenetic processes change over a client’s lifetime because of environmental influences, meaning that the client is not in a fixed state per traditional gene theory (Nestler et al., 2016). Epigenetics provides an alternate view of nature and nurture, demonstrating that epigenetic tags may not only be influenced by unfavorable environmental influences (e.g., maternal depression, trauma, bullying, child abuse and neglect) but also by favorable environments and activities (e.g., mindfulness, CBT, exercise, diet, nurturing; Chaix et al., 2020; Chen et al., 2018; Conradt et al., 2016; Roberts et al., 2015; Stevens et al., 2018). Understanding the flexibility of epigenetics has the potential to engender hope for our clients and to guide our work as counselors and counselor educators, because our genetic destinies are not fixed as we once theorized in gene theory.
Bioecological Conceptualization: Proximal and Distal Impact and Interventions
The impact of epigenetics on the counseling profession can be understood using Bronfenbrenner’s (1979) bioecological model. The bioecological model conceptualizes a client’s function over time based on the coaction between the client and their environment (Broderick & Blewitt, 2015; Jones & Tang, 2015). The client’s environment can have both beneficial and deleterious proximal and distal effects. These effects are like concentric rings around the client, which Bronfenbrenner called “subsystems.” The most proximate subsystem is the microsystem, the environment that has a direct influence on the client, such as parents, teachers, classmates, coworkers, relatives, etc. The next level is the mesosystem, in which the micro entities interact with one another or intersect with influence on the client (e.g., school and home intersect to influence client’s thinking and behavior). The next system, called the exosystem, begins the level of indirect influence. This may include neighborhood factors such as the availability of fresh produce, safe neighborhoods, social safety net programs, and employment opportunities. The last subsystem is the macrosystem. This system consists of the cultural norms, values, and biases that influence all other systems. The final aspect of this model, called the chronosystem, takes into account development over time. The chronosystem directs the counselor’s attention to developmental periods that have differing risks and opportunities, or what can be called “critical” developmental periods.
Below we conceptualize epigenetic counseling implications using Bronfenbrenner’s model but simplify it by grouping systems: proximal effects (micro/meso level) labeled as micro effects and distal effects (exo/macro level) labeled as macro effects. We will also apply the chronosystem by focusing on critical developmental periods that are salient when applying epigenetics to counseling. Ultimately, our central focus is the client and the concentric influences of micro and macro effects. To begin, we will first focus on the important contribution of epigenetics during the critical developmental period of 0 to 5 years of age with implications at the micro and macro levels.
Epigenetics Supports Early Life Span Interventions
Though the evidence does support epigenetic flexibility across a client’s life span, we know that early adverse life events may alter a child’s epigenome with mediating effects on development and behavior (Lester & Marsit, 2018). We also know that epigenetic processes are most active in the first 5 years of life (Mulligan, 2016; Syzf et al., 2016). These early insults to the genome may elicit poor mental health into adulthood such as anxiety, depression, schizophrenia, and addiction. For example, a client who grew up in an urban environment with a traditionally marginalized group status and parents who experienced drug dependence has an increased risk for schizophrenia above and beyond the genetic, inherited risk. These adverse childhood experiences have the potential to modify the epigenome, increasing the likelihood of developing mental health concerns, including schizophrenia (Cariaga-Martinez & Alelú-Paz, 2018).
At the micro level, the caregiver can be a salutary effect against adverse environmental conditions (Oberlander et al. 2008; Weaver et al., 2005). Prenatally, counseling can work with parents before birth to generate healthy coping strategies (e.g., reduce substance abuse), flexible and adaptive caregiver functioning, and effective parenting strategies. An example of this is to use parent–child interactive therapy (PCIT) pre-clinically, or before the child evidences a disorder (Lieneman et al., 2017). Preventive services using PCIT have been documented as effective with externalizing behaviors, child maltreatment, and developmental delays. Additional micro-level interventions can be found in the use of home-visiting programs to improve child outcomes prenatally to 5 years of age where positive parenting and other combined interventions are utilized to improve the health of mother, father, and child (Every Child Succeeds, 2019; Healthy Families New York, 2021).
Clinically, epigenetics points to earlier care and treatment to prevent the emergence of mental disorders (e.g., major depressive disorder, schizophrenia). Also, epigenetic research has provided evidence that environmental change can be equally important as client change. Regarding treatment planning, examining the client’s individual level factors or microsystem (e.g., physical health, mental status, education, race, gender) as well as their macrosystem (e.g., social stigma, poverty, housing quality, green space, pollution) may be crucial before considering what kind of modifications and/or interventions are most appropriate. For example, if a 9-year-old White female presents to a counselor for behavioral concerns in school, it is important for the counselor to gather a holistic life history to build an informed picture of the many variables collectively impacting the child’s behavior at each level. At the micro level, a counselor will evaluate for childhood maltreatment, but from an epigenetic lens, other proximal environmental factors could be important to screen for such as poverty, maternal depression, nutrition, classroom dynamics, and exercise (McEwen & McEwen, 2017; Mulligan, 2016). If the 9-year-old child is experiencing parental neglect and food insecurity, the clinician can treat the client’s individual needs at the micro level (i.e., working with the family system to overcome any neglect by using treatments such as PCIT, and direct referral to social workers and other agencies to provide food and shelter to meet basic needs).
The science of epigenetics may also inform action taken during assessment and case conceptualization based on the coaction of environment with a client over time. Although intervention at 0–5 years of age is most preventative, it is not practical in all cases. Using assessments that collect information on an adult client’s early life may help inform case conceptualization and allow the integration of epigenetics into counseling theories to better understand the etiology of a client’s presenting problem(s). For example, using an adverse childhood experiences assessment may help identify individuals at higher risk of epigenetic concerns. Epigenetics highlights the impact of client–environment interaction and its influence (positive or negative) on overall health. Additionally, early life adversity increases the likelihood of poor health outcomes such as heart disease, anxiety, and depression. However, these poor consequences could be mediated by talking with clients about the importance of exercise and its benefit on epigenetics and, by extension, mental health.
At the macro level, examples could include the reduction of hostile environments (e.g., institutional racism, neighborhood violence, limited employment opportunities, low wages, air pollutants, water pollutants), advocacy for statutes, regulations to decrease instability such as unfair housing in low-income neighborhoods, establishing partnerships in the development of community-based and school-based prevention programs, and applying early interventions such as mindfulness to reduce the effects of stress (Chaix et al., 2020). To illustrate, postnatal depression symptom severity has been associated with residential stability (Jones et al., 2018). By developing policies that would increase housing security, a reduction in maternal depression symptom severity could potentially reduce the DNA methylation that is associated with upregulation of the HPA and child reactivity, but this would need to be investigated further for confirmation. According to Rutten et al. (2013), this change may also increase the resiliency of children by reducing their experience of chronic stress, as sustained maternal depression severity often impacts caregiving because of unstable housing.
Although members of the counseling profession have known the significance of early intervention for years, this epigenetic understanding confirms why human growth and development is a core component of our counseling professional identity (Remley & Herlihy, 2020) and provides a supporting rationale for our efforts. Additionally, epigenetic tags have the potential to cross generations via the process of imprinting (Yehuda et al., 2016). This has potential implications across the life span.
In summary, critical developmental periods must be a focal point for counseling interventions, necessitating upstream action rather than our current dominant approach of downstream activities and a shift toward primary prevention over predominantly tertiary prevention. Such primary prevention would reduce stress and trauma for children before signs and symptoms become apparent and attend to the development and sustainability of healthy environments that would increase both client and community wellness.
Epigenetics Supports Counseling Advocacy and Social Justice Efforts
When reflecting on the implications of epigenetics, it is apparent that place, context, and the client’s environment are critical factors for best positioning them for healthy outcomes, engendering a push for advocacy and social justice for clients. Because environments have no boundaries, it is important to think of advocacy across many systems: towns, counties, states, countries, and the world. This reinforces the call for counselors and counselor educators to move beyond the walls of their workplaces in order to collaborate within the larger mental health field (e.g., clinical mental health, school, marriage and family, addiction, rehabilitation). Additionally, said knowledge compels connection with other professions—such as social workers, physicians, psychologists, engineers, housing developers, public health administrators, and members of nonprofit and faith-based organizations, etc.—to enact change on a wider scale and to improve the conditions for clients at a systemic level.
This collaboration also calls for engaging at local and international levels. Global human rights issues such as sex trafficking cross countries, regions, and local communities and necessitate collaboration to ameliorate these practices and the associated trauma. For starters, the American Counseling Association and the International Association for Counseling could partner with other organizations such as the Child Defense Fund to assist in meeting their mission to level the playing field for all children in the United States. At the local level, counselors and counselor educators could collaborate with local children’s hospitals and configure a plan to meet common goals to improve children’s health and wellness.
Counseling Research and Epigenetics
Research primarily affects clients on a macro level but can trickle down to directly engage clients within our clinical work and practice. Counselors and counselor educators can partner with members of other disciplines to further the work with epigenetic biomarkers (e.g., depression and DNA methylation). Counseling researchers can also investigate how talk therapy and other adjuncts, such as diet and exercise, may improve our clients’ treatment outcomes. As counseling researchers, we can develop research agendas around intervention and prevention for those 0–5 years of age and create and evaluate programs for this age group while also creating community partnerships as noted above. An example of this partnership is The John Hopkins Center for Prevention and Early Intervention. The creators of this program developed sustainable partnerships with public schools, mental health systems, state-level educational programs, universities, and federal programs to focus on early interventions that are school-based and beyond. They collaborated to develop, evaluate, and deliver a variety of programs and research activities to improve outcomes for children and adolescents. They have created dozens of publications based on these efforts that help move the discipline forward. In one such publication, Guintivano et al. (2014) looked at epigenetic and genetic biomarkers for predicting suicide.
Counselor Education, CACREP, and Epigenetics
The counselor educational system affects clients distally but also holds implications for the work counselors conduct at the client level. Counselor educators can provide a more robust understanding of epigenetics to counseling students across the counselor education curriculum. These efforts can include introducing epigenetics in theories, diagnosis, treatment, human and family development, practicum and internship, assessment, professional orientation, and social and cultural foundations courses. By assisting counseling students to comprehend the relationship between client and environment, as well as the importance of prevention, educators will increase their students’ ability to carry out a holistic approach with clients and attend to the foundational emphases of the counseling profession on wellness and prevention. Moreover, by learning to include epigenetics in case conceptualization, students can gain a more robust understanding of the determinants of symptomology, potential etiology at the cellular level, and epigenetically supported treatments such as CBT and mindfulness.
It is fairly simple to integrate epigenetics education into programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015). To begin, counselor educators can integrate epigenetics education into professional counseling orientation and ethical practice courses. As counselor educators discuss the history and philosophy of the counseling profession, particularly from a wellness and prevention lens (CACREP, 2015, 2.F.1.a), counselor educators can discuss the connection between epigenetics and wellness. Wellness is a foundational value for the counseling profession and is a part of the definition of counseling (Kaplan et al., 2014). Many wellness models (both theoretical and evidence-based) are rooted in the promotion of a holistic balance of the client in a variety of facets and contexts (Myers & Sweeney, 2011). We can continue to support these findings by integrating epigenetics within our conversations about wellness, as we have epigenetic evidence that the positive or negative coaction between the individual and their environment can impact a person toward increased or decreased wellness.
Counselor educators can also integrate epigenetics education into Social and Cultural Diversity and Human Growth and Development courses. Within Social and Cultural Diversity courses, counselor educators can address how negative environmental conditions have negative influences on offspring. This is evidenced by the discrimination against Jews and its imprinting that crosses generations (Yehuda et al., 2016). Counselor educators can discuss how discrimination and barriers to positive environmental conditions can impact someone at the epigenetic level (CACREP, 2015, 2.F.2.h). Within Human Growth and Development, counselor educators can discuss how the study of epigenetics provides us a biological theory to understand how development is influenced by environment across the life span (CACREP, 2015, 2.F.3.a, c, d, f). In particular, it can provide an etiology of how negative factors change epigenetic tags, which are correlated with negative mental health that may become full-blown mental health disorders later in adulthood (CACREP, 2015, 2.F.3.c, d, e, g).
Additionally, counselor educators can integrate epigenetic education within specialty counseling areas. Several studies (Maze & Nestler, 2011; Palmisano & Pandey, 2017; Tsankova et al., 2007; Wong et al., 2011; H. Zhang & Gelernter, 2017) have noted how epigenetic mechanisms may support the addiction process and counselor educators can interweave this information when discussing theories and models of addiction and mental health problems (CACREP, 2015, 5.A.1.b; 5.C.1.d; 5.C.2.g). Counselor educators can also discuss epigenetics as it applies to counseling practice. Because epigenetics research supports treatments like CBT, mindfulness, nutrition, and exercise (Chaix et al., 2020; Chen et al., 2018; Roberts et al., 2015; Stevens et al., 2018), counselor educators can address these topics in courses when discussing techniques and interventions that work toward prevention and treatment of mental health issues (CACREP, 2015, 5.C.3.b).
Generally, CACREP (2015) standards support programs that infuse counseling-related research into the curriculum (2.E). We support the integration of articles, books, websites, and videos that will engender an understanding of epigenetics across the curriculum, so long as the integration supports student learning and practice.
Conclusion and Future Directions
In summary, there are numerous epigenetic processes at work in the symptoms we attend to as counselors. We have provided information that illustrates how epigenetics may mediate outcomes such as depression, anxiety, schizophrenia, and addiction. We have also illustrated how CBT, exercise, diet, and meditation may have positive epigenetic influences supporting our craft. We have discovered that epigenetic processes are most malleable in early life. This information offers incremental evidence for our actions as professional counselors, educators, and researchers, leading to a potential examination of our efforts in areas of prevention, social justice, clinical practice, and counseling program development. However, we must note that epigenetics as a science is relatively new and much of the research is correlational.
Based on the current limits of epigenetic science and a lack of investigation of mental health epigenetics in professional counseling, one of our first recommendations for future research efforts is to collaborate across professions with other researchers such as geneticists, as we did for this manuscript. From this partnership, our profession’s connection to epigenetics is elucidated. Interdisciplinary collaboration allows the professional counselor to offer their expertise in mental health and the geneticist their deep understanding of epigenetics and the tools to examine the nature and nurture relationships in mental health outcomes. We can also make efforts to look at our wellness-based preventions and interventions to document changes at the epigenetic level in our clients and communities. Ideally, as the science of epigenetics advances, we will have epigenetic research in our profession of counseling that is beyond correlation and evidences the effectiveness of our work down to the cellular level.
Conflict of Interest and Funding Disclosure
The development of this manuscript was supported
in part by a Cincinnati Children’s Hospital Medical
Center Trustee Award and by a grant from the
National Heart, Lung, and Blood Institute (HL132344).
The authors reported no conflict of interest.
References
Albert, P. R., Le François, B., & Vahid-Ansari, F. (2019). Genetic, epigenetic and posttranscriptional mechanisms for treatment of major depression: The 5-HT1A receptor gene as a paradigm. Journal of Psychiatry & Neuroscience, 44(3), 164–176. https://doi.org/10.1503/jpn.180209
Arnaud, P. (2010). Genomic imprinting in germ cells: Imprints are under control. Reproduction, 140(3), 411–423. https://doi.org/10.1530/REP-10-0173
Benoit, L., & Turecki, G. (2010). The epigenetics of suicide: Explaining the biological effects of early life environmental adversity. Archives of Suicide Research, 14(4), 291–310.
https://doi.org/10.1080/13811118.2010.524025
Benros, M. E., Nielsen, P. R., Nordentoft, M., Eaton, W. W., Dalton, S. O., & Mortensen, P. B. (2011). Autoimmune diseases and severe infections as risk factors for schizophrenia: A 30-year population-based register study. The American Journal of Psychiatry, 168(12), 1303–1310. https://doi.org/10.1176/appi.ajp.2011.11030516
Bocchio-Chiavetto, L., Maffioletti, E., Bettinsoli, P., Giovannini, C., Bignotti, S., Tardito, D., Corrada, D., Milanesi, L., & Gennarelli, M. (2013). Blood microRNA changes in depressed patients during antidepressant treatment. European Neuropsychopharmacology, 23(7), 602–611. https://doi.org/10.1016/j.euroneuro.2012.06.013
Boks, M. P., Houtepen, L. C., Xu, Z., He, Y., Ursini, G., Maihofer, A. X., Rajarajan, P., Yu, Q., Xu, H., Wu, Y., Wang, S., Shi, J. P., Hulshoff Pol, H. E., Strengman, E., Rutten, B. P. F., Jaffe, A. E., Kleinman, J. E., Baker, D. G., Hol, E. M., . . . Kahn, R. S. (2018). Genetic vulnerability to DUSP22 promoter hypermethylation is involved in the relation between in utero famine exposure and schizophrenia. Nature Partner Journals Schizophrenia, 4(1), 1–8. https://doi.org/10.1038/s41537-018-0058-4
Broderick, P. C., & Blewitt, P. (2015). The life span: Human development for helping professionals (4th ed.). Pearson.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
Brooker, R. J. (2017). Genetics: Analysis and principles (6th ed.). McGraw-Hill.
Cadet, J. L., McCoy, M. T., & Jayanthi, S. (2016). Epigenetics and addiction. Clinical Pharmacology & Therapeutics, 99(5), 502–511. https://doi.org/10.1002/cpt.345
Cariaga-Martinez, A., & Alelú-Paz, R. (2018). Epigenetic and schizophrenia. In F. Durbano (Ed.), Psychotic disorders – An update (pp. 147–162). IntechOpen. https://doi.org/10.5772/intechopen.73242
Chaix, R., Fagny, M., Cosin-Tomás, M., Alvarez-López, M., Lemee, L., Regnault, B., Davidson, R. J., Lutz, A., & Kaliman, P. (2020). Differential DNA methylation in experienced meditators after an intensive day of mindfulness-based practice: Implications for immune-related pathways. Brain, Behavior, and Immunity, 84, 36–44. https://doi.org/10.1016/j.bbi.2019.11.003
Champagne, F. A. (2010). Early adversity and developmental outcomes: Interaction between genetics, epigenetics, and social experiences across the life span. Perspectives on Psychological Science, 5(5), 564–574.
https://doi.org/10.1177/1745691610383494
Cheah, S.-Y., Lawford, B. R., Young, R. M., Morris, C. P., & Voisey, J. (2017). mRNA expression and DNA methylation analysis of serotonin receptor 2A (HTR2A) in the human schizophrenic brain. Genes, 8(1), 1–11. https://doi.org/10.3390/genes8010014
Chen, J., Hutchinson, K. E., Bryan, A. D., Filbey, F. M., Calhoun, V. D., Claus, E. D., Lin, D., Sui, J., Du, Y., & Liu, J. (2018). Opposite epigenetic associations with alcohol use and exercise intervention. Frontiers in Psychiatry, 9(594), 1–12. https://doi.org/10.3389/fpsyt.2018.00594
Cohen, J. L., Jackson, N. L., Ballestas, M. E., Webb, W. M., Lubin, F. D., & Clinton, S. M. (2017). miR-101a-3p and Ezh2 modulate anxiety-like behavior in high-responder rats. European Journal of Neuroscience, 46(7), 2241–2252.
Conradt, E., Hawes, K., Guerin, D., Armstrong, D. A., Marsit, C. J., Tronick, E., & Lester, B. M. (2016). The contributions of maternal sensitivity and maternal depressive symptoms to epigenetic processes and neuroendocrine functioning. Child Development, 87(1), 73–85. https://doi.org/10.1111/cdev.12483
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Devlin, A. M., Brain, U., Austin, J., & Oberlander, T. F. (2010). Prenatal exposure to maternal depressed mood and the MTHFR C677T variant affect SLC6A4 methylation in infants at birth. PloS ONE, 5(8), e12201.
https://doi.org/10.1371/journal.pone.0012201
Every Child Succeeds. (2019). 2019 report to the community. https://static1.squarespace.com/static/5df9251a492
ba56bc96bc96f/t/5e73b2a333e8127c09daabf2/1584640684722/Final2019Report.pdf
Fisher, H. L., Murphy, T. M., Arseneault, L., Caspi, A., Moffitt, T. E., Viana, J., Hannon, E., Pidsley, R., Burrage, J., Dempster, E. L., Wong, C. C. Y., Pariante, C. M., & Mill, J. (2015). Methylomic analysis of monozygotic twins discordant for childhood psychotic symptoms. Epigenetics, 10(11), 1014–1023.
https://doi.org/10.1080/15592294.2015.1099797
Gejman, P. V., Sanders, A. R., & Kendler, K. S. (2011). Genetics of schizophrenia: New findings and challenges. Annual Review of Genomics and Human Genetics, 12, 121–144.
https://doi.org/10.1146/annurev-genom-082410-101459
Guintivano, J., Brown, T., Newcomer, A., Jones, M., Cox, O., Maher, B. S., Eaton, W. W., Payne, J. L., Wilcox, H. C., & Kaminsky, Z. A. (2014). Identification and replication of a combined epigenetic and genetic biomarker predicting suicide and suicidal behaviors. The American Journal of Psychiatry, 171(12), 1287–1296.
https://doi.org/10.1176/appi.ajp.2014.14010008
Haggarty, S. J., & Tsai, L.-H. (2011). Probing the role of HDACs and mechanisms of chromatin-mediated neuroplasticity. Neurobiology of Learning and Memory, 96(1), 41–52. https://doi.org/10.1016/j.nlm.2011.04.009
Hamilton, P. J., & Nestler, E. J. (2019). Epigenetics and addiction. Current Opinion in Neurobiology, 59, 128–136. https://doi.org/10.1016/j.conb.2019.05.005
Harris, A., & Seckl, J. (2011). Glucocorticoids, prenatal stress and the programming of disease. Hormones and Behavior, 59(3), 279–289. https://doi.org/10.1016/j.yhbeh.2010.06.007
Healthy Families New York. (2021, January 4). [Website.] https://www.healthyfamiliesnewyork.org
Heijmans, B. T., Tobi, E. W., Stein, A. D., Putter, H., Blauw, G. J., Susser, E. S., Slagboom, P. E., & Lumey, L. H. (2008). Persistent epigenetic differences associated with prenatal exposure to famine in humans. Proceedings of the National Academy of Sciences, 105(44), 17046–17049. https://doi.org/10.1073/pnas.0806560105
Huang, W.-C., Ferris, E., Cheng, T., Hörndli, C. S., Gleason, K., Tamminga, C., Wagner, J. D., Boucher, K. M., Christian, J. L., & Gregg, C. (2017). Diverse non-genetic, allele-specific expression effects shape genetic architecture at the cellular level in the mammalian brain. Neuron, 93(5), 1094–1109.e7.
https://doi.org/10.1016/j.neuron.2017.01.033
Januar, V., Ancelin, M.-L., Ritchie, K., Saffery, R., & Ryan, J. (2015). BDNF promoter methylation and genetic variation in late-life depression. Translational Psychiatry, 5, e619. https://doi.org/10.1038/tp.2015.114
Jayanthi, S., McCoy, M. T., Chen, B., Britt, J. P., Kourrich, S., Yau, H.-J., Ladenheim, B., Krasnova, I. N., Bonci, A., & Cadet, J. L. (2014). Methamphetamine downregulates striatal glutamate receptors via diverse epigenetic mechanisms. Biological Psychiatry, 76(1), 47–56. https://doi.org/10.1016/j.biopsych.2013.09.034
Jones, D. E., & Tang, M. (2015). Health inequality: What counselors need to know to act. In Ideas and research you can use: VISTAS 2015. https://www.counseling.org/docs/default-source/vistas/article_60785a22f16116603abcacff0000bee5e7.pdf?sfvrsn=4
Jones, D. E., Tang, M., Folger, A., Ammerman, R. T., Hossain, M. M., Short, J. A., & Van Ginkel, J. B. (2018). Neighborhood effects on PND symptom severity for women enrolled in a home visiting program. Community Mental Health Journal, 54(4), 420–428. https://doi.org/10.1007/s10597-017-0175-y
Kaplan, D. M., Tarvydas, V. M., & Gladding, S. T. (2014). 20/20: A vision for the future of counseling: The new consensus definition of counseling. Journaling of Counseling & Development, 92, 366–372. https://www.counseling.org/docs/default-source/20-20/2020-jcd-article-consensus-definition.pdf?sfvrsn=76017f2c_2
Lester, B. M., Conradt, E., & Marsit, C. (2016). Introduction to the special section on epigenetics. Child Development, 87(1), 29–37. https://doi.org/10.1111/cdev.12489
Lester, B. M., & Marsit, C. J. (2018). Epigenetic mechanisms in the placenta related to infant neurodevelopment. Epigenomics, 10(3), 321–333. https://doi.org/10.2217/epi-2016-0171
Lewis, B. P., Burge, C. B., & Bartel, D. P. (2005). Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell, 120(1), 15–20.
https://doi.org/10.1016/j.cell.2004.12.035
Lieneman, C. C., Brabson, L. A., Highlander, A., Wallace, N. M., & McNeil, C. B. (2017). Parent–child interaction therapy: Current perspectives. Psychology Research and Behavior Management, 10, 239–256.
https://doi.org/10.2147/PRBM.S91200
Lüscher, B., & Möhler, H. (2019). Brexanolone, a neurosteroid antidepressant, vindicates the GABAergic deficit hypothesis of depression and may foster resilience. F1000Research, 8(May), 1–14.
https://doi.org/10.12688/f1000research.18758.1
Ma, J., Shang, S., Wang, J., Zhang, T., Nie, F., Song, X., Zhao, H., Zhu, C., Zhang, R., & Hao, D. (2018). Identification of miR-22-3p, miR-92a-3p, and miR-137 in peripheral blood as biomarker for schizophrenia. Psychiatry Research, 265, 70–76. https://doi.org/10.1016/j.psychres.2018.03.080
Maze, I., & Nestler, E. J. (2011). The epigenetic landscape of addiction. Annals of the New York Academy of Sciences, 1216(1), 99–113. https://doi.org/10.1111/j.1749-6632.2010.05893.x
McEwen, C. A., & McEwen, B. S. (2017). Social structure, adversity, toxic stress, and intergenerational poverty: An early childhood model. Annual Review of Sociology, 43, 445–472.
https://doi.org/10.1146/annurev-soc-060116-053252
McGowan, P. O., Sasaki, A., D’Alessio, A. C., Dymov, S., Labonté, B., Szyf, M., Turecki, G., & Meaney, M. J. (2009). Epigenetic regulation of the glucocorticoid receptor in human brain associates with childhood abuse. Nature Neuroscience, 12(3), 342–348. https://doi.org/10.1038/nn.2270
Monk, C., Spicer, J., & Champagne, F. A. (2012). Linking prenatal maternal adversity to developmental outcomes in infants: The role of epigenetic pathways. Development and Psychopathology, 24(4), 1361–1376.
https://doi.org/10.1017/S0954579412000764
Mulligan, C. J. (2016). Early environments, stress, and the epigenetics of human health. Annual Review of Anthropology, 45(1), 233–249. https://doi.org/10.1146/annurev-anthro-102215-095954
Myers, J. E., & Sweeney, T. J. (2011). Wellness counseling: The evidence base for practice. Journal of Counseling & Development, 86(4), 482–493. https://doi.org/10.1002/j.1556-6678.2008.tb00536.x
National Human Genome Research Institute. (2020). Epigenomics fact sheet. https://www.genome.gov/about-genomics/fact-sheets/Epigenomics-Fact-Sheet
Nestler, E. J., Peña, C. J., Kundakovic, M., Mitchell, A., & Akbarian, S. (2016). Epigenetic basis of mental illness. The Neuroscientist, 22(5), 447–463. https://doi.org/10.1177/1073858415608147
Numachi, Y., Yoshida, S., Yamashita, M., Fujiyama, K., Naka, M., Matsuoka, H., Sato, M., & Sora, I. (2004). Psychostimulant alters expression of DNA methlytransferase mRNA in the rat brain. Annals of the New York Academy of Sciences, 1025(1), 102–109. https://doi.org/10.1196/annals.1316.013
Oberlander, T. F., Weinberg, J., Papsdorf, M., Grunau, R., Misri, S., & Devlin, A. M. (2008). Prenatal exposure to maternal depression, neonatal methylation of human glucocorticoid receptor gene (NR3C1) and infant cortisol stress responses. Epigenetics, 3(2), 97–106. https://doi.org/10.4161/epi.3.2.6034
Okazaki, S., Otsuka, I., Numata, S., Horai, T., Mouri, K., Boku, S., Ohmori, T., Sora, I., & Hishimoto, A. (2019). Epigenetic clock analysis of blood samples from Japanese schizophrenia patients. npj Schizophrenia, 5(9), 1–7. https://doi.org/10.1038/s41537-019-0072-1
Ouellet-Morin, I., Wong, C. C. Y., Danese, A., Pariante, C. M., Papadopoulos, A. S., Mill, J., & Arseneault, L. (2013). Increased serotonin transporter gene (SERT) DNA methylation is associated with bullying victimization and blunted cortisol response to stress in childhood: A longitudinal study of discordant monozygotic twins. Psychology of Medicine, 43(9), 1813–1823. https://doi.org/10.107/S0033291712002784
Palmisano, M., & Pandey, S. C. (2017). Epigenetic mechanisms of alcoholism and stress-related disorders. Alcohol, 60, 7–18. https://doi.org/10.1016/j.alcohol.2017.01.001
Perroud, N., Paoloni-Giacobino, A., Prada, P., Olié, E., Salzmann, A., Nicastro, R., Guillaume, S., Mouthon, D.,
Stouder, C., Dieben, K., Huguelet, P., Courtet, P., & Malafosse, A. (2011). Increased methylation of glucocorticoid receptor gene (NR3C1) in adults with a history of childhood maltreatment: A link with the severity and type of trauma. Translational Psychiatry, 1, e59. https://doi.org/10.1038/tp.2011.60
Pishva, E., Kenis, G., van den Hove, D., Lesch, K.-P., Boks, M. P. M., van Os, J., & Rutten, B. P. F. (2014). The epigenome and postnatal environmental influences in psychotic disorders. Social Psychiatry and Psychiatric Epidemiology, 49, 337–348. https://doi.org/10.1007/s00127-014-0831-2
Provençal, N., & Binder, E. B. (2015). The effects of early life stress on the epigenome: From the womb to adulthood and even before. Experimental Neurology, 268, 10–20. https://doi.org/10.1016/j.expneurol.2014.09.001
Remley, T. P., Jr., & Herlihy, B. (2020). Ethical, legal, and professional issues in counseling (6th ed.). Pearson.
Roberts, S., Keers, R., Lester, K. J., Coleman, J. R. I., Breen, G., Arendt, K., Blatter-Meunier, J., Cooper, P., Creswell, C., Fjermestad, K., Havik, O. E., Herren, C., Hogendoorn, S. M., Hudson, J. L., Krause, K., Lyneham, H. J., Morris, T., Nauta, M., Rapee, R. M., . . . Wong, C. C. Y. (2015). HPA axis related genes and response to psychological therapies: Genetics and epigenetics. Depression and Anxiety, 32(12), 861–870.
https://doi.org/10.1002/da.22430
Rodgers, A. B., Morgan, C. P., Bronson, S. L., Revello, S., & Bale, T. L. (2013). Paternal stress exposure alters sperm microRNA content and reprograms offspring HPA stress axis regulation. Journal of Neuroscience, 33(21), 9003–9012. https://doi.org/10.1523/JNEUROSCI.0914-13.2013
Romens, S. E., McDonald, J., Svaren, J., & Pollak, S. D. (2015). Associations between early life stress and gene methylation in children. Child Development, 86(1), 303–309. https://doi.org/10.1111/cdev.12270
Rutten, B. P. F., Hammels, C., Geschwind, N., Menne-Lothmann, C., Pishva, E., Schruers, K., van den Hove, D.,
Kenis, G., van Os, J., & Wichers, M. (2013). Resilence in mental health: Linking psychological and neurobiological perspectives. Acta Psychiatrica Scandinavica, 128(1), 3–20. https://doi.org/10.1111/acps.12095
Saavedra, K., Molina-Márquez, A. M., Saavedra, N., Zambrano, T., & Salazar, L. A. (2016). Epigenetic modifications of major depressive disorder. International Journal of Molecular Sciences, 17(8), 1279.
https://doi.org/10.3390/ijms17081279
Shimada-Sugimoto, M., Otowa, T., & Hettema, J. M. (2015). Genetics of anxiety disorders: Genetic epidemiological and molecular studies in humans. Psychiatry and Clinical Neurosciences, 69(7), 388–401.
https://doi.org/10.1111/pcn.12291
Smearman, E. L., Almli, L. M., Conneely, K. N., Brody, G. H., Sales, J. M., Bradley, B., Ressler, K. J., & Smith, A. K.
(2016). Oxytocin receptor genetic and epigenetic variations: Association with child abuse and adult psychiatric symptoms. Child Development, 87(1), 122–134. https://doi.org/10.1111/cdev.12493
Smigielski, L., Jagannath, V., Rössler, W., Walitza, S., & Grünblatt, E. (2020). Epigenetic mechanisms in schizophrenia and other psychotic disorders: A systematic review of empirical human findings. Molecular Psychiatry, 25, 1718–1748. https://doi.org/10.1038/s41380-019-0601-3
Stevens, A. J., Rucklidge, J. J., & Kennedy, M. A. (2018). Epigenetics, nutrition and mental health: Is there a relationship? Nutritional Neuroscience, 21(9), 602–613. https://doi.org/10.1080/1028415X.2017.1331524
Suderman, M., Borghol, N., Pappas, J. J., Pinto Pereira, S. M., Pembrey, M., Hertzman, C., Power, C., & Szyf, M. (2014). Childhood abuse is associated with methylation of multiple loci in adult DNA. BMC Medical Genomics, 7, 1–12. https://doi.org/10.1186/1755-8794-7-13
Szyf, M. (2009). The early life environment and the epigenome. Biochimica et Biophysica Acta, 1790(9), 878–885. https://doi.org/10.1016/j.bbagen.2009.01.009
Szyf, M., Tang, Y.-Y., Hill, K. G., & Musci, R. (2016). The dynamic epigenome and its implications for behavioral interventions: A role for epigenetics to inform disorder prevention and health promotion. Translational Behavioral Medicine, 6(1), 55–62. https://doi.org/10.1007/s13142-016-0387-7
Szyf, M., Weaver, I., & Meaney, M. (2007). Maternal care, the epigenome and phenotypic differences in behavior. Reproductive Toxicology, 24(1), 9–19. https://doi.org/10.1016/j.reprotox.2007.05.001
Tsankova, N., Renthal, W., Kumar, A., & Nestler, E. J. (2007). Epigenetic regulation in psychiatric disorders. Nature Reviews Neuroscience, 8, 355–367. https://doi.org/10.1038/nrn2132
Turecki, G. (2014). Epigenetics and suicidal behavior research pathways. American Journal of Preventive Medicine, 47(3), S144–S151. https://doi.org/10.1016/j.amepre.2014.06.011
Vaiserman, A. M., & Koliada, A. K. (2017). Early-life adversity and long-term neurobehavioral outcomes: Epigenome as a bridge? Human Genomics, 11(34), 1–15. https://doi.org/10.1186/s40246-017-0129-z
Weaver, I. C. G., Champagne, F. A., Brown, S. E., Dymov, S., Sharma, S., Meaney, M. J., & Szyf, M. (2005). Reversal of maternal programming of stress responses in adult offspring through methyl supplementation: Altering epigenetic marking later in life. Journal of Neuroscience, 25(47), 11045–11054.
https://doi.org/10.1523/JNEUROSCI.3652-05.2005
Wong, C. C. Y., Mill, J., & Fernandes, C. (2011). Drugs and addiction: An introduction to epigenetics. Addiction, 106(3), 480–489. https://doi.org/10.1111/j.1360-0443.2010.03321.x
Wright, K. N., Hollis, F., Duclot, F., Dossat, A. M., Strong, C. E., Francis, T. C., Mercer, R., Feng, J., Dietz, D. M., Lobo, M. K., Nestler, E. J., & Kabbaj, M. (2015). Methyl supplementation attenuates cocaine-seeking behaviors and cocaine-induced c-Fos activation in a DNA methylation-dependent manner. The Journal of Neuroscience, 35(23), 8948–8958. https://doi.org/10.1523/JNEUROSCI.5227-14.2015
Yehuda, R., Daskalakis, N. P., Bierer, L. M., Bader, H. N., Klengel, T., Holsboer, F., & Binder, E. B. (2016). Holocaust exposure induced intergenerational effects on FKBP5 methylation. Biological Psychiatry, 80, 372–380. https://doi.org/10.1016/j.biopsych.2015.08.005
Yehuda, R., Engel, S. M., Brand, S. R., Seckl, J., Marcus, S. M., & Berkowitz, G. S. (2005). Transgenerational effects of posttraumatic stress disorder in babies of mothers exposed to the World Trade Center attacks during pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(7), 4115–4118.
https://doi.org/10.1210/jc.2005-0550
Zhang, H., & Gelernter, J. (2017). Review: DNA methylation and alcohol use disorders: Progress and challenges. The American Journal on Addictions, 26(5), 502–515. https://doi.org/10.1111/ajad.12465
Zhang, T.-Y., & Meaney, M. J. (2010). Epigenetics and the environmental regulation of the genome and its function. Annual Review of Psychology, 61, 439–466. https://doi.org/10.1146/annurev.psych.60.110707.163625
Zheng, J., & Xiao, X. (2016). Epigenetic modifications and developmental origin of health and diseases (DOHaD). In Y. Dincer (Ed.), Epigenetics: Mechanisms and clinical perspectives (pp. 1–14). Nova Biomedical.
David E. Jones, EdD, NCC, LPC, is an assistant professor at Liberty University. Jennifer S. Park, PhD, NCC, ACS, LPC, is an assistant professor at Colorado Christian University. Katie Gamby, PhD, LPC, CWC, is an assistant professor at Malone University. Taylor M. Bigelow, PhD, is an assistant professor at the University of New Haven. Tesfaye B. Mersha, PhD, is an associate professor at the Cincinnati Children’s Hospital Medical Center (CCMHC), University of Cincinnati College of Medicine. Alonzo T. Folger, PhD, MS, is an assistant professor at the CCMHC, University of Cincinnati College of Medicine. Correspondence may be addressed to David E. Jones, 1971 University Blvd., Lynchburg, VA 24515, dejones14@liberty.edu.
Mar 10, 2015 | Article, Volume 5 - Issue 2
Edward Franc Hudspeth
When conceptualizing this special issue, we had a basic idea of what might be included; however, as submissions arrived, it was evident that our basic definition of special needs was limited and could include much more when broadened. Therefore, the issue was reconceptualized as “Children with Special Needs and Circumstances.” It is my hope that when practitioners, researchers and faculty read this issue, each begins to see that the term special needs encompasses more than we think, because anything that hinders the optimal growth and development of a child constitutes a special need. In this issue, readers will find articles concerning fears, trauma, sensory processing disorder, foreign adoption, cystic fibrosis, spina bifida, homelessness, special education and parent–child interaction therapy.
Keywords: counseling, children, special needs, complex trauma
To set the stage for this special issue, to provide a foundation for understanding and to link the various articles, I encourage readers to conceptualize the impact of a special need through a complex trauma or developmental lens. Over the past 15 years, countless articles have reported and described the impact of chronic stress and adverse childhood experiences (Anda et al., 2006; Edwards et al., 2005) and the subsequent development of complex trauma. Complex and Developmental TraumaThe National Child Traumatic Stress Network (n.d.-a) has defined complex trauma as a series of traumatic experiences that are usually interpersonal in nature and lead to numerous long-term adverse effects on health and well-being. Similarly, van der Kolk, Roth, Pelcovitz, Sunday and Spinazzola (2005) described experiencing repeated traumatic events during childhood as developmental trauma. The duration and intensity of the traumatic experiences, as well as the age of onset of these experiences, can determine the outcome of both complex trauma and developmental trauma. Neuroscience research provides ample evidence of neurochemical and brain structural changes caused by complex trauma that result in affective and behavioral dysregulation (Lanius, Bluhm, & Frewen, 2011). Though the terms developmental trauma and complex trauma were originally used to represent repeated abuse or an accumulation of traumatic experiences, recent neuroscience research has extended these terms to other conditions and experiences. Copeland, Keeler, Angold, and Costello (2007) noted that a long-term physical illness may lead to complex trauma, while D’Andrea, Ford, Stolbach, Spinazzola, and van der Kolk (2012) and Finkelhor, Ormrod, and Turner (2007) reported that bullying also may lead to similar outcomes. Courtois (n.d.), as well as Ford and Courtois (2009), Vogt, King, and King (2007), and the National Child Traumatic Stress Network (n.d.-b), offered a more descriptive explanation and extensive list when they stated the following: Cumulative adversities faced by many persons, communities, ethno-cultural, religious, political, and sexual minority groups, and societies around the globe can also constitute forms of complex trauma. Some occur over the life course beginning in childhood and have some of the same developmental impacts described above. Others, occurring later in life, are often traumatic or potentially traumatic and can worsen the impact of early life complex trauma and cause the development of complex traumatic stress reactions. These adversities can include but are not limited to:
- Poverty and ongoing economic challenge and lack of essentials or other resources
- Community violence and the inability to escape/relocate
- Homelessness
- Disenfranchised ethno-racial, religious, and/or sexual minority status and repercussions
- Incarceration and residential placement and ongoing threat and assault
- Ongoing sexual and physical re-victimization and re-traumatization in the family or other contexts, including prostitution and sexual slavery
- Human rights violations including political repression, genocide/“ethnic cleansing,” and torture
- Displacement, refugee status, and relocation
- War and combat involvement or exposure
- Developmental, intellectual, physical health, mental health/psychiatric, and age-related limitations, impairments, and challenges
- Exposure to death, dying, and the grotesque in emergency response work (para. 7)
Cook et al. (2005) stated that as a result of complex trauma, individuals experience impairments in (a) attachment, (b) affect regulation, (c) behavioral control, (d) cognition, (e) self-concept, and (f) sensory and motor development. Treatment recommendations include (a) being developmentally sensitive, (b) building on the safety and security of caregivers and community (e.g., teachers), and (c) addressing affective and behavioral dysregulation. Special Issue: Children with Special Needs and Circumstances The articles in this special issue provide implications for counselors and ways that specific special needs and circumstances may be addressed with individuals, families, schools and communities. In order to support the educational and emotional development of children and youth experiencing homelessness, Havlik and Bryan indicate that school counselors must first identify which students are experiencing homelessness in their school and then determine their specific needs. Some of these needs, to name a few, include violence, abuse, neglect, mental and physical health issues, and mobility issues. The authors note that once homeless children and their individual needs are identified, school counselors should engage the students within their schools and assist with collaborative efforts between school and community resources. Havlik and Bryan challenge schools counselors to seek out and participate in professional development regarding the policies related to individual needs of homeless students. Geddes Hall states that less than half of school counselor preparation programs include content related to special education in their training. Geddes Hall encourages school counselors to have a comprehensive knowledge of the specific needs of those receiving special education services, and she offers precise recommendations for how counselor educators can infuse special education content throughout a school counseling curriculum. She reflects that it is in the best interest of future school counselors, as well as the special students they will serve, to receive support and supervision during such experiences as they complete their programs. Buss, Warren, and Horton provide in-depth coverage of the short- and long-term impact of trauma on the physical, mental, emotional and social development of traumatized children that includes associated trajectories to adult mental and physical health conditions. The authors indicate that early intervention and treatment can minimize the social and emotional impact of a child’s exposure to a traumatic event. The authors also discuss the advantages of numerous evidence-based treatment strategies as well as the realistic limitations of these strategies. Across treatment methods, factors such as safety and attachment are paramount. Liu and Hazler delineate differences noted among adoptees from various countries. These differences include behavioral, social and emotional characteristics, as well as the adoptees’ proclivity to form an attachment with a primary caregiver. The authors demonstrate that pre-adoption characteristics are associated with smooth transitions during the adoption process as well as post-adoption integration. Liu and Hazler discuss ways that counselors may emphasize adoptee–parent relationships in which trust is a fundamental element. They provide specific recommendations for counselors and adoptive parents that ease the transition and support successful attachme Sheperis and colleagues acknowledge that counselors, whether working with children who have disruptive behavior or providing parenting training to families, should be knowledgeable of the application of various behavioral techniques in order to utilize them effectively and to teach them to parents. In their article, the authors review a wealth of research information related to one evidence-based method and demonstrate how this method may be useful when working with children with special needs. Sheperis and colleagues describe a session-by-session application of this model as well as report contemporary research about the model’s application to working with children with special needs. Leppma, Szente, and Brosch provide an overview of the current landscape of children’s fears to help delineate a contemporary, adaptive and holistic approach to treatment. The authors convey an image of fear and anxiety development that can be physically and mentally paralyzing for individuals who experience these states. In their treatment section, the authors outline an approach that addresses affect regulation and development of positive emotions, as well as inoculating the client against stress and supporting the development of resilience. They report on several studies that demonstrate the value of play in the development of self-efficacy, optimism and positive affect. Despite the fact that few within the world of counseling have written about the subject, Goodman-Scott and Lambert pull together many resources to conceptualize the special needs of children with sensory processing disorder (SPD). The authors provide a detailed description of the disorder and its subtypes and describe in detail appropriate assessment of the disorder. Goodman-Scott and Lambert recommend that counselors collaborate with occupational therapists in order to address the unique needs of children with SPD. They report that counselors can provide individual, group and family counseling modalities using solution-focused and cognitive-behavioral techniques to address children’s mental health needs and co-occurring disorders. Storlie and Baltrinic’s article illuminates the impact of a chronic disease on the individual, the caregivers and the counselors working with the family. They indicate that counselors working with children and families affected by cystic fibrosis (CF) should consider the physical and psychosocial challenges facing this special-needs population. The authors encourage counselors to be knowledgeable about CF so that they will be sensitive to the traumatic impact of this life-shortening disease on the child or adolescent with CF and caregivers. Storlie and Baltrinic offer suggestions for compassionate counseling as well as for avoiding compassion fatigue. In a personal account of rearing a child with spina bifida, Richmond-Frank expresses both the successes and shortcomings that she has experienced over nearly 3 decades. The author provides a thorough account of her experience as a parent of a child with special needs, as well as what she has to teach others who may be working with a child with special needs. As a professional counselor, as well as a parent of a special-needs child, Richmond-Frank provides readers with specific and realistic suggestions. She shares that a systemic, strengths-based counseling model respects the inherent worth of the child with a disability by not presuming that he or she is the identified patient. Conclusion From the special issue editor’s point of view, issues that are prolonged, intense and cumulative, and vary over developmental periods should be conceptualized through lenses that address the complexity of intermingled systems. By failing to see this complexity and all of its aspects, we fail to fully address the complexity of children with special needs and circumstances. Conflict of Interest and Funding Disclosure The author reported no conflict of interest or funding contributions for the development of this manuscript. References Anda, R. F., Felitti, V. J., Walker, J., Whitfield, C. L., Bremner, J. D., Perry, B. D., . . . Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neurosciences, 256, 174–186. doi:10.1007/s00406-005-06244 Cook, A., Spinazzola, J., Ford, J., Lanktree, C., Blaustein, M., Cloitre, M., . . . van der Kolk, B. (2005). Complex trauma in children and adolescents. Psychiatric Annals, 35, 390–398. Copeland, W., Keeler, G., Angold, A., & Costello, J. (2007). Traumatic events and posttraumatic stress in childhood. Archives of General Psychiatry, 64, 577–584. Courtois, C. A. (n.d.). Understanding complex trauma, complex reactions, and treatment approaches. Retrieved from http://www.giftfromwithin.org/html/cptsd-understanding-treatment.html D’Andrea, W. D., Ford, J., Stolbach, B., Spinazzola, J., & van der Kolk, B. A. (2012). Understanding interpersonal trauma in children: Why we need a developmentally appropriate trauma diagnosis. American Journal of Orthopsychiatry, 82, 187–200. doi:10.1111/j.1939-0025.2012.01154.x Edwards, V. J., Anda, R. F., Dube, S. R., Dong, M., Chapman, D. F., & Felitti, V. J. (2005). The wide-ranging health consequences of adverse childhood experiences. In K. A. Kendall-Tackett & S. M. Giacomoni (Eds.), Child victimization: Maltreatment, bullying, and dating violence prevention and intervention (pp. 8-1–8-12). Kingston, NJ: Civic Research Institute. Finkelhor, D., Ormrod, R. K., & Turner, H. A. (2007). Poly-victimization: A neglect component in child victimization. Child Abuse and Neglect, 31, 7–26. doi:10.1016/j.chiabu.2006.06.008 Ford, J. D., & Courtois, C. A. (2009). Defining and understanding complex trauma and complex traumatic stress disorders. In C. A. Courtois & J. D. Ford (Eds.), Treating complex traumatic stress disorders: An evidence-based guide (pp.13–30). New York, NY: Guilford Press. Lanius, R. A., Bluhm, R. L., & Frewen, P. A. (2011). How understanding the neurobiology of complex post-traumatic stress disorder can inform clinical practice. A social cognitive and affective neuroscience approach. Acta Psychiatrica Scandinavica, 124, 331–348. doi:10.1111/j.1600-0447.2011.01755.x The National Child Traumatic Stress Network. (n.d.-a). Complex trauma. Retrieved from http://www.nctsn.org/trauma-types/complex-trauma The National Child Traumatic Stress Network. (n.d.-b). Types of traumatic stress. Retrieved from http://www.nctsn.org/trauma-types#q2 van der Kolk, B. A., Roth, S., Pelcovitz, D., Sunday, S., & Spinazzola, J. (2005). Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. Journal of Traumatic Stress, 18, 389–399. Vogt, D. S., King, D. W., & King, L. A. (2007). Risk pathways for PTSD: Making sense of the literature. In M. J. Friedman, T. M. Keane, & P. A. Resick (Eds.), Handbook of PTSD: Science and practice (pp. 99–115). New York, NY: Guilford Press. Edward Franc Hudspeth, NCC, is an Assistant Professor of Counselor Education at Henderson State University and served as the guest editor for the special issue of The Professional Counselor on children with special needs and circumstances. Correspondence can be addressed to Edward Franc Hudspeth, Department of Counselor Education, Henderson State University, 1100 Henderson Street, Arkadelphia, AR 71999, franchudspeth@gmail.com
Feb 9, 2015 | Article, Volume 5 - Issue 1
Joel A. Lane
Today’s emerging adults (i.e., individuals between the ages of 18 and 29) in industrialized nations navigate multiple significant life transitions (e.g., entering career life), and do so in a rapidly changing society. While these transitions pose psychological difficulties, a growing body of research has identified attachment and social support as two notably salient protective factors in emerging adulthood. The purpose of the present article is to explore the counseling of emerging adult clients, particularly those in the midst of one or more transitions. The concept of emerging adulthood represents a relatively recent phenomenon that the counseling community has been slow to acknowledge. Specifically, this author reviews literature pertaining to emerging adulthood, attachment and social support, and uses this literature to provide clinicians with practical recommendations for counseling emerging adults.
Keywords: emerging adulthood, life transitions, attachment, social support, counseling
Emerging adulthood is a stage of life resulting from recent societal trends in industrialized nations, occurring between the ages of 18 and 29 (Arnett, 2000, 2004, 2007). These trends include the proliferation of college enrollment, significant delays in settling down and high unemployment compared to prior generations of young adults (Furstenberg, Rumbaut, & Settersten, 2005). Corresponding with these changes is an evolution of the psychosocial development of current emerging adults, who engage in extended identity exploration and report subjectively feeling in between adolescence and adulthood (Arnett, 2001). While the benefits and drawbacks of these changes are a source of frequent and intense debate (Arnett, 2013; Twenge, 2013), few would disagree that being twenty-something today is a drastically different experience than it was several decades ago.
Emerging adulthood presents many life transitions and significant mental health risk. In the midst of prolonged identity experimentation and subjectivity, emerging adults navigate a multitude of major life and role changes, such as leaving home, entering and leaving educational settings, and starting a career. The convergence of these factors—the subjective feeling of not being an adult and near-constant life changes propelling one toward adulthood—seems to contribute to critical periods of identity crisis and various psychological difficulties (Lane, 2013b; Lee & Gramotnev, 2007; Weiss, Freund, & Wiese, 2012). Though not all emerging adults experience difficulties during these transitions (Buhl, 2007; Galambos, Barker, & Krahn, 2006), some respond with significant distress (Murphy, Blustein, Bohlig, & Platt, 2010; Perrone & Vickers, 2003; Polach, 2004), which is problematic given that the emerging adult years are considered a critical juncture in the development of mental illness (American Psychiatric Association [APA], 2013; Ingram & Gallagher, 2010) and substance abuse (APA, 2013; Chassin, Pitts, & Prost, 2002; Ingram & Gallagher, 2010). Elevated distress also has been shown to increase impulsivity and risk-taking behaviors in emerging adulthood (Scott-Parker, Watson, King, & Hyde, 2011). The distress accompanying these transitions, therefore, poses a considerable threat to emerging adult well-being.
Despite these changes and risk factors, the counseling community has been slow to acknowledge the evolving landscapes of the late teens and twenties. Counselor training programs continue to prominently feature theories of development contending that identity development is a task completed by the end of the teenage years (i.e., Erikson, 1959/1994). It seems likely that many counselors face the challenge of using outdated developmental models to conceptualize their emerging adult clients. For counselors to work effectively with the many challenges and risks that emerging adults face, they must have an increased awareness of emerging adulthood and better understand factors that predict well-being and stability during the numerous transitions commonly experienced. To address this concern, the author provides an overview of emerging adult theory and research describing the significance of emerging adult life transitions; reviews literature examining the importance of attachment and social relationships in emerging adulthood, which appear to especially salient sources of risk resilience during this period of life; and considers implications for counseling professionals to utilize when working with emerging adults.
Emerging Adulthood
Current societal expectations regarding normative life trajectories in the early-to-mid 20s—being finished with education, marrying, acclimating to a professional setting and adjusting to life as a parent—do not seem fully applicable to today’s emerging adults in most industrialized nations. Arnett (2000) described emerging adulthood as a period of feeling “in between” (p. 471), during which individuals are no longer adolescents, but do not yet identify as adults. Thus, the normative developmental tasks for individuals in their 20s seem to have shifted from objective tasks like attaining work, settling down and becoming financially independent, to more subjective tasks like considering the question, Who am I and what do I want my life to look like? This shift is reflected in several factors that distinguish emerging adulthood from other life stages and from prior young adult generations. Of these distinctions, the three most prominent pertain to demographic instability, changes in subjective self-perceptions and extended periods of identity testing (Arnett, 2000).
Characteristics of Emerging Adulthood
One way that emerging adulthood is distinct from other life stages is with regard to demographics. The past several decades correspond with higher proportions of 18- to 25-year-olds leaving home and periodically moving back home several times (Goldscheider & Goldscheider, 1999), attending college immediately after high school (Arnett, 2004), delaying marriage and childbirth (Arnett, 2000), spending more time in college (Arnett, 2004; Mortimer, Zimmer-Gembeck, Holmes, & Shanahan, 2002) and changing careers (Wendlandt & Rochlen, 2008). In comparison to other age groups, the demographic statuses of emerging adults today vary with little predictability (Arnett, 2000; Cohen, Kasen, Chen, Hartmark, & Gordon, 2003); however, the demographic factor that is most predictable is frequent residential change (Arnett, 2000, 2007; Shulman & Nurmi, 2010). All of these trends indicate the changing demographic landscapes of today’s late teens and early 20s compared to those of prior generations.
Another changing landscape of emerging adulthood is a trend toward increasingly vague and subjective self-perceptions (Arnett, 2000; Fussell & Furstenberg, 2005). Emerging adults view their progression into adulthood as long and gradual. When a sample of emerging adults were asked if they felt they had reached adulthood, over 50% selected the answer choice “in some respects yes, in some respects no,” and fewer than 5% selected “yes” (Arnett, 2001, p. 140). Moreover, emerging adults seem to consider individual character qualities (e.g., accepting responsibility) to be more salient indicators of having reached adulthood than objective milestones, such as completing education or becoming a parent (Lopez, Chervinko, Strom, Kinney, & Bradley, 2005). In short, emerging adults perceive themselves as no longer adolescents, but also not quite adults, and report vague perceptions of what it will take to feel more like adults.
A third distinction of emerging adulthood is a prolonged period of identity exploration (Arnett, 2000; Gerstacker, 2010). Given the relative freedom from life obligations, in tandem with the long-term implications of many of the decisions that will be made during emerging adulthood, this stage of life represents an opportunity for significant identity development to occur (Gerstacker, 2010). The freedom to engage in identity exploration results in the delay of firm decisions regarding adult roles (Schulenberg, Bryant, & O’Malley, 2004). These factors also contribute to an increased self-focus during emerging adulthood (Arnett, 2004). While some researchers have interpreted these features as resulting from increased narcissism among emerging adults (e.g., Twenge, 2013), Arnett (2004) conceptualized them as temporary and developmentally normative qualities.
The three most common areas of emerging adult identity exploration are love, work and worldviews (Arnett, 2000). First, emerging adults use their freedom to explore varying levels of commitment with regard to sexual and romantic relationships (Arnett, 2004), and do so in a time period with unprecedented societal acceptance of differing sexual and romantic preferences (Garcia, Reiber, Massey, & Merriwether, 2012). Second, significant identity exploration occurs with regard to professional identity, for which evidence can be found in several college trends. Emerging adults are increasingly likely to change their majors more than once (Arnett, 2000), report negative attitudes toward graduation (Lane, 2013a, in press-a; Yazedjian, Kielaszek, & Toews, 2010), spend more time in college (Arnett, 2004) and experience more career turnover (Wendlandt & Rochlen, 2008) than prior generations. Finally, worldviews represent a third area of identity exploration. With today’s unprecedented higher education enrollment (National Center for Education Statistics, 2014; Weber, 2012), a growing number of emerging adults are gaining a more complex understanding of the world around them via higher education experiences. The impact of the college environment on moral reasoning and cross-cultural experiences is well documented (e.g., Bowman, 2010). These trends may explain the observations of several scholars that today’s emerging adults share an unprecedented passion for social justice and community well-being (e.g., Arnett, 2007), especially in urban areas.
Emerging Adult Transitions
A central feature of emerging adulthood is the frequent occurrence of significant life transitions. Each of these transitions initiates significant role changes that impact social networks, familial support and autonomy. The influence of life transition on well-being has been well documented and frequently results in periods of self-doubt, immobilization and denial (Brammer & Abrego, 1981). In contrast to common assumptions that the transitions associated with emerging adulthood (e.g., college graduation, obtaining employment) are positive life events, these transitions represent periods of loss (Vickio, 1990) that consist of considerable psychological distress for some individuals (Lane, in press-a, in press-b; Lee & Gramotnev, 2007). The proceeding section reviews a growing body of recent research suggesting that the characteristic delay in adult identity formation in emerging adulthood may increase the degree of loss and difficulty experienced during several normative transitions.
High school graduation. Conclusions are mixed regarding the assertion that high school graduation is a critical emerging adult transition. Though some have reported that graduation is associated with increased quality of parental relationships and decreased depressed mood and delinquent behaviors (Aseltine & Gore, 1993), others have reported significant differences in these trajectories as a function of race and college attendance (Gore & Aseltine, 2003). Similarly, social and institutional support predicts whether deviant behaviors increase or decrease after high school (Sampson & Laub, 1990). These findings suggest that the transition of high school graduation is a positive experience for some emerging adults, but a psychologically distressing experience for others, especially those who lack social support, do not attend college, or identify as African American or Latino.
The transition to professional life among non-college attendees. After high school, the two most common trajectories are to enter either postsecondary education or the workforce (Arnett, 2004). The transition to work can be particularly difficult for those who forgo college. These emerging adults attempt to transition into professional life without the advantage of higher education—a psychologically beneficial resource that provides important institutional and social support (Raymore, Barber, & Eccles, 2001). Among individuals with high school diplomas, unemployment rates are highest between the ages of 18 and 19, approaching 20% in 2014 (Bureau of Labor Statistics, 2014). Those who do find work are unlikely to receive a sustainable income, as mean incomes among emerging adults are drastically lower than for other adult age groups (U.S. Census Bureau, 2012). Such difficulties are particularly problematic given that unemployment and economically inadequate employment have been implicated as mental health risks (Dooley, Prause, & Ham-Rowbottom, 2000).
The freshman transition. For those emerging adults who decide to attend college, their adjustment to college life also represents a significant life transition. In particular, the first year of college is a risk factor for psychological distress. Bowman (2010) found that among first-generation college freshmen, psychological well-being significantly decreased throughout the course of the freshman academic year. Similarly, Sharma (2012) demonstrated that first-year undergraduates experienced significantly greater emotional and social difficulties than other college students. A prominent focus of first-year transition literature is the important role of attachment relationships, a construct that will be discussed in greater depth later in this article. In short, the attachment security of incoming freshmen predicts their overall well-being, as well as their social and academic adjustment (Kenny & Donaldson, 1991; Larose & Boivin, 1998).
The senior year experience. A small but growing body of recent research has identified potential difficulties for college seniors preparing to transition out of school (Lane, 2013a, in press-a). The college experience represents a period of moratorium from many adult responsibilities (Fasick, 1988) and is associated with increased leisure behaviors compared to individuals who do not attend college (Raymore, Barber, Eccles, & Godbey, 1999). Given the subjective experience among emerging adults that they have not yet reached adulthood (Arnett, 2001) and the prevailing societal expectation that college graduation is associated with adult roles (e.g., entering the workforce, settling down), it is likely that emerging adults increasingly view graduation as an important signifier of impending life changes for which they do not feel ready (Lane, 2013a). For example, ambivalence about graduating was one of the primary themes to emerge from a qualitative study of college seniors (Yazedjian et al., 2010). Other qualitative studies of college seniors have found that students are frequently anxious about graduating due to the impending changes they will experience in priorities (Overton-Healy, 2010) and the sense that they lack direction regarding the next phase of life (Allen & Taylor, 2006). Factor analyses of surveys given to college seniors uncovered domains of concern about graduation, including leaving behind the student lifestyle, the impending loss of friendships and support, the process of obtaining employment, and the process of applying to graduate school (Pistilli, Taub, & Bennett, 2003). A recent path analysis revealed significant relationships between these domains of concern and factors such as life satisfaction, psychological health and attachment security (Lane, in press-a).
Life after college. Given the psychological implications of preparing to leave the college environment, it is not surprising that the time immediately following college life often presents psychological difficulties as well. A sample of Australian college graduates voiced concerns about adjusting to life after college and to work life, referring to this period as a low point of their lives (Perrone & Vickers, 2003). Chickering and Schlossberg (1998) found that well-being suffered when emerging adult graduates encountered difficulties obtaining employment. Such findings are especially significant since they contrast overall trends toward increased well-being throughout emerging adulthood (Galambos et al., 2006). That is, while emerging adulthood is associated with upward trends in well-being, the time immediately following graduation can alter this trajectory, especially when emerging adults experience difficulties obtaining employment.
However, emerging adults who do secure postcollege employment are not exempt from transition-related distress. This transition involves significant changes in attitudes, expectations and levels of preparedness compared to college life (Polach, 2004; Wendlandt & Rochlen, 2008). Transitioning to the world of work can be particularly difficult since emerging adults are typically leaving an environment in which they felt experienced (e.g., high school, college) and becoming inexperienced professionals (Lane, in press-b). More than half of all college graduates leave their initial place of postcollege employment within two years of graduating (Wendlandt & Rochlen, 2008), and there is evidence suggesting that this turnover is due to difficulties in adjusting to professional life for the first time (Sturges & Guest, 2001). Such difficulties seem to frequently result in experiences of imposter syndrome (i.e., perceiving oneself as incompetent despite evidence of competence) among emerging adults entering professional life (Lane, in press-b). Other related difficulties include significant learning curves, less feedback and structure than afforded by the college environment, guilt about initial levels of work production, and difficulties forming new social networks (Polach, 2004). Similarly, the results of a survey conducted by Sleap and Reed (2006) suggested that most graduates possess limited awareness of the impending culture changes they will experience as a result of leaving higher education and entering the workplace. The importance of this awareness was demonstrated in a longitudinal study in which emerging adults were tested as college seniors regarding their knowledge about workplace culture, and then were subsequently tested both six months and one year after entering professional life (Gardner & Lambert, 1993). Those who had more accurate information as seniors were more likely to report job satisfaction at both subsequent intervals. Buhl (2007) conducted a similar longitudinal study, finding that the subjective quality of participant parental relationships predicted well-being trajectories during the initial three years of professional life.
In sum, it is clear that the common transitions experienced during emerging adulthood pose threats to well-being due to role confusion and psychological distress. Given the risks associated with psychological distress, it is paramount to better understand factors that might promote the maintenance of well-being during periods of transition in emerging adulthood. Accordingly, a focus of emerging adult research has been examining constructs that predict positive developmental progressions through these periods of transition. Two such constructs that have received considerable attention are attachment (e.g., Kenny & Sirin, 2006) and social support (e.g., Murphy et al., 2010). It seems that emerging adults who feel secure in their relational attachments and supported by social networks are able to face the developmental challenges of emerging adulthood with greater confidence and well-being than those who lack support and secure attachments. To better explain the impact of these constructs on emerging adult development and well-being, the proceeding sections of this article examine attachment and social support literature pertaining to emerging adulthood.
Attachment
Attachment theory contends that the early relationships people develop with their caregivers inform attitudes toward help seeking and new learning in times of distress across the lifespan (Bowlby, 1969/1982). Attachment is defined as the emotional bonds that develop between children and their caregivers beginning in infancy. Based on repeated experiences of caregiver responsiveness, infants begin to develop beliefs and expectations regarding the degree to which their physical and emotional needs will be satisfied. According to attachment theory, these beliefs become internalized as subconscious representations of self and other, which continue to increase in complexity and broadly inform social interactions throughout the lifespan. Those whose representations are based on consistent and sufficient caregiver responsiveness are considered securely attached and are likely to trust their ability to resolve future needs, either by themselves or by relying on caregivers. Insecurely attached children, on the other hand, develop expectations that their caregivers cannot be adequately relied upon in times of need; these children are likely to react to perceived threats with inappropriate levels of affect (i.e., overactivation or deactivation). These reactions interfere with the children’s development of effective emotional regulation and with the successful resolution of stressful situations, thereby continuing to reinforce such responses to future stressful situations (Guttmann-Steinmetz & Crowell, 2006).
This idea positions early attachment relationships as a likely influence on psychological health in emerging adulthood. The years of later adolescence and early emerging adulthood are a time in which attachment needs are increasingly fulfilled by peers and romantic partners, as opposed to caregivers (Fraley & Davis, 1997). Thus, the relative security of parental attachment representations is likely to inform interpersonal trust and intimacy, as well as the ability to seek the meeting of attachment needs from others (Schnyders & Lane, 2014). In fact, frequency of contact with parents during emerging adulthood is negatively associated with subjective closeness to parents (Hiester, Nordstrom, & Swenson, 2009), while geographical distance from parents is positively associated with psychological adjustment (Dubas & Petersen, 1996). Younger emerging adults are likely to begin experimenting with independence, though they often still use parents or caregivers as attachment figures in times of distress (Fraley & Davis, 1997; Kenny, 1987).
Bartholomew and Horowitz (1991) conducted what was perhaps the first study to consider the relevance of attachment to the unique needs of young adult populations. They demonstrated several trajectories in interpersonal functioning on the basis of attachment functioning. In the study, attachment was conceptualized as occurring across dimensions of self and other: secure (positive representations of self and other), anxious (negative representations of self, positive representations of other), dismissive-avoidant (positive representations of self, negative representations of other), and fearful-avoidant (negative representations of self and other). Such a conceptualization has become a standard for contemporary adult attachment research (Brennan, Clark, & Shaver, 1998). Fearful-avoidant participants seemed to struggle with interpersonal passivity. Dismissive-avoidance was “related to a lack of warmth in social interactions” (Bartholomew & Horowitz, 1991, p. 234). The interpersonal problems of anxious participants suggested control seeking or overinvolvement in the affairs of their peers. These findings corroborate more recent conceptualizations of insecure attachments in adulthood (Brennan et al., 1998; Mallinckrodt, 2000). Specifically, individuals with elevated attachment anxiety are likely to respond to distress with a hyperactivated strategy, heightening awareness of their distress and causing them to seek inappropriate levels of interpersonal dependence. Conversely, individuals with elevated attachment avoidance are likely to respond to distress with a deactivated strategy, inhibiting awareness of negative affect and preventing them from seeking support from others.
A growing body of emerging adult research supports the importance of healthy attachment functioning for various psychological outcomes during emerging adulthood. Attachment is a crucial predictor of well-being trajectories at many key emerging adult transition points (Lane, 2014), including the first year of college (Kenny & Donaldson, 1991), the last year of college (Lane, in press-a) and the postcollege years (Kenny & Sirin, 2006). For example, one study tracked Israeli males from their final year of high school through their third year away from home for compulsory military service (Scharf, Mayseless, & Kivenson-Baron, 2004). Securely attached individuals demonstrated better coping strategies and higher capacity for intimacy during their military service than those with insecure attachments. More generally, attachment security in emerging adulthood also influences self-reinforcement capacity and reassurance needs (Wei, Mallinckrodt, Larson, & Zakalik, 2005), affect regulation and resilience (Karreman & Vingerhoets, 2012), perceived self-worth (Kenny & Sirin, 2006), dysfunctional attitudes and self-esteem (Roberts, Gotlib, & Kassel, 1996), self-compassion and empathy toward others (Wei, Liao, Ku, & Shaffer, 2011), self-organization strategies (Lopez, Mitchell, & Gormley, 2002), and identification with emerging adulthood (Schnyders, 2014; Schnyders & Lane, 2014). Many of these factors illustrate the importance of attachment functioning in developing healthy and supportive interpersonal social networks.
Social Support
The construct of social support refers to social relationships or interactions that provide individuals with actual or perceived assistance (Sarason et al., 1991). Social support is psychologically beneficial in its capacity to mitigate stress during stressful situations (e.g., Ditzen et al., 2008), an idea commonly referred to as the stress buffering hypothesis (Cohen & McKay, 1984). A wealth of recent research has strongly suggested that social support is particularly salient during emerging adulthood, as this is a life period marked with numerous transitions and opportunities to experience distress. In a qualitative study of emerging adults who had recently transitioned into professional life, social support was the most prominent theme related to adjustment (Murphy et al., 2010); those who reported relational isolation also struggled with unpreparedness for new financial obligations and feeling that their expectations about life after college were left unfulfilled. Mortimer et al. (2002) reported similar findings. Wendlandt and Rochlen (2008), noting that social support is often lacking in the transition out of college and into the work force, urged college counselors to develop interventions aimed at increasing perceived support. This idea was supported in a study of college graduates who had recently relocated to a metropolitan area and were adjusting to their first year of professional life (Polach, 2004). Participants reported frustration and difficulties trying to establish new peer groups outside the college environment. They also cited the importance of a sense of belonging as the primary reason for moving to a city after graduating. Clearly, ample evidence supports the protective qualities of social support for emerging adults transitioning into professional life.
Moreover, social support also seems to be important during other emerging adult transitions. In one qualitative study, emerging adult participants described the ability to understand friendship dynamics as an important component in the subjective experience of reaching adulthood (Lopez et al., 2005). Examples of understanding friendship dynamics included the maintenance of preexisting friendships, changes in friendships based on varying maturation rates, and understanding the importance of the social network. In another study, first-year college students seemed to adjust more effectively to college life when the support they received from family members shifted from actions consistent with parental attachment to actions consistent with social support (Kenny, 1987). In a multiethnic sample of urban high school students, perceived social support predicted aspirations for career success, positive beliefs pertaining to achieving career goals and the importance of work in the future (Kenny, Blustein, Chaves, Grossman, & Gallagher, 2003).
Several longitudinal studies also have demonstrated relationships between aspects of social support and various elements of positive adjustment in emerging adulthood. A large study that tracked individuals for nearly 30 years beginning at age 7 (Masten et al., 2004) found that social quality was an aspect of resilience and predicted success in various emerging adult developmental tasks (e.g., academic attainment). Moreover, success with these tasks predicted success in postemerging adult developmental tasks (e.g., parenting quality, romantic success, work success). O’Connor et al. (2011) found perceived quality of peer relationships to predict positive development in emerging adulthood, which they conceptualized to include life satisfaction, trust and civic engagement. Galambos et al. (2006), in a longitudinal study tracking nearly 1,000 Canadian participants throughout the course of emerging adulthood, found that increases in social support were significantly correlated with increases in well-being.
These findings suggest that the degree to which emerging adults are able to develop and rely upon support networks directly impacts their ability to adapt to various normative experiences and transitions. Given the aforementioned discussion regarding emerging adult attachment, it is likely that these two constructs (attachment and social support) are of shared importance during such transitions. That is, attachment representations inform one’s capacity for positive interpersonal interactions (Mallinckrodt & Wei, 2005), and in this way, attachment and social support collectively facilitate transition processes in emerging adulthood (Lane, 2014; Larose & Boivin, 1998).
Implications for Counseling Emerging Adults
Counseling professionals who work in mental health or university settings are uniquely positioned to intervene with emerging adult clients and to foster resilience and well-being during this turbulent life phase. If counselors are to be effective working with the many challenges that emerging adults face, it is necessary to better understand factors that predict well-being during life transition. The aforementioned literature demonstrates the protective qualities of social support for emerging adults in transition. Emerging adults who are able to rely on positive social relationships during life transitions derive higher psychological well-being, life satisfaction and positive affect (Lane, 2014). Accordingly, counselors would be wise to assist their emerging adult clients in cultivating supportive social relationships. While counseling is a supportive relationship unto itself (Slade, 2008), the degree to which emerging adults in transition are able to derive satisfaction from a number of supportive relationships seems to directly impact the experience of well-being during transition. In this regard, counselors are encouraged to recognize the unprecedented complexity of emerging adult support networks (Arnett, 2007; Garcia et al., 2012; Manago, Taylor, & Greenfield, 2012) due to the proliferation of social media and changing attitudes toward romantic relationships.
Moreover, social support is not limited to interpersonal relationships, but also includes structural and institutional forms of support (Masten et al., 2004). Thus, possessing knowledge of community programs and resources available to emerging adults also is imperative when working with this age group. Support can be enhanced through transition-specific programs (e.g., Lane, 2013a; Yeadon, 2010) that provide information about future expectations and strengthen coping skills (Wendlandt & Rochlen, 2008). Further benefits can be derived as counselors work with their clients to rely on these support systems during times of transition.
As the literature further suggests, one’s degree of attachment security will impact the ability to develop and rely upon social support. Thus, excessive attachment anxiety or avoidance could pose challenges to working with emerging adults on support utilization. Accordingly, counselors of emerging adults should be aware of this potential therapeutic roadblock; they also should be prepared to intervene to develop corrective attachment experiences with their clients. Mallinckrodt (2000) suggested an approach in which clinicians utilize the therapeutic relationship to promote secure attachment strategies. The focus of this approach is maintaining relational boundaries through anticipating how clients might resist such boundaries. That is, because elevated attachment anxiety promotes a desire for maladaptive interpersonal dependence (Brennan et al., 1998), counselors should work to establish greater interpersonal distance than their anxiously attached clients would prefer (Mallinckrodt, 2000). Similarly, since elevated attachment avoidance promotes a desire for maladaptive interpersonal isolation, counselors should seek greater interpersonal closeness than their avoidant-attached clients would prefer. While doing so, clinicians should monitor the affective experience of their clients as a result of the therapeutic relationship, and should assist their clients in self-monitoring as well. This process can facilitate client awareness of attachment tendencies and enhance mindfulness about communicating future relational needs.
Other helpful suggestions come from a qualitative study of experienced therapists who worked toward corrective attachment experiences with their clients (Daly & Mallinckrodt, 2009). The therapists in the sample suggested that therapeutic boundaries should be reevaluated over the course of therapy. These therapists also emphasized the importance of sensitivity to client defenses early in the therapeutic relationship, and suggested several strategies for both managing boundaries and combating resistance. Such strategies included intentional disclosure of feelings toward client patterns, fostering a sense of consistency and dependability about counseling, and developing an awareness of the temporary nature of the therapeutic relationship, beginning at the onset of therapy. These considerations may aid counselors in helping emerging adult clients work past insecure attachment patterns to develop healthy social relationships that can be utilized to facilitate emerging adult transition.
More broadly, the preceding literature review speaks to the importance of counselors acknowledging the changing landscapes of young adulthood. Current trends in the media seem to advance a narrative that today’s young adults are narcissistic, entitled and lazy. While the veracity of such labels is a focus of current debate in the research community (for an overview of this debate, see Arnett, 2013 and Twenge, 2013), the narrative that these labels perpetuate is not conducive to an empathic understanding of the needs of those in this age group. Thus, counselors are encouraged to consider Arnett’s (2004) theory of emerging adulthood when conceptualizing their work with emerging adult clients. This theory indirectly encourages counselors to honor the process of emerging adulthood, during which it is normative to engage in numerous behaviors that are often negatively misconstrued. Specifically, emerging adults are likely to (a) frequently move out and back into the parental household (which could be construed as parental enmeshment), (b) engage in prolonged identity exploration (which could be construed as laziness), (c) possess vague subjective understandings regarding the realization of adult identities (which could be construed as lack of direction), (d) think optimistically about the future (which could be construed as entitlement) and (e) temporarily possess a heightened self-focus (which could be construed as narcissism). Thus, acknowledging and normalizing these characteristics, even if they might constitute relatively recent phenomena, is important for fostering empathic understanding between counselors and their emerging adult clients.
Conclusions
Emerging adults navigate many significant life and role transitions with important long-term implications. These transitions can induce great pressure and distress for some emerging adults, increasing their likelihood of experiencing many of the risks commonly associated with this age group. Thus, it is important that counselors understand the unique dynamics of emerging adulthood, especially given the myriad ways that this group has changed and evolved compared to prior young adult generations. In particular, the aforementioned literature suggests that counselors may find success with their emerging adult clients by working to enhance social support and correct potential insecure attachment behaviors, as well as by incorporating emerging adult theory to conceptualize client behaviors and perspectives. Though emerging adulthood is often a time of turmoil and instability, it is also a period rife with opportunities and possibilities, thus providing the potential for deeply rewarding and transformative counseling experiences.
Conflict of Interest and Funding Disclosure
The author reported no conflict of
interest or funding contributions for
the development of this manuscript.
References
Allen, J. K., & Taylor, K. (2006). The senior year transition: Women undergraduates search for a path. Journal of College Student Development, 47, 595–608.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55, 469–480. doi:10.1037/0003-066X.55.5.469
Arnett, J. J. (2001). Conceptions of the transition to adulthood: Perspectives from adolescence through midlife. Journal of Adult Development, 8, 133–143. doi:10.1023/A:1026450103225
Arnett, J. J. (2004). Emerging adulthood: The winding road from the late teens through the twenties. New York, NY: Oxford University Press.
Arnett, J. J. (2007). Socialization in emerging adulthood: From the family to the wider world, from socialization to self-socialization. In J. E. Grusec & P. D. Hastings (Eds.), Handbook of socialization: Theory and research (pp. 208–231). New York, NY: Guilford Press.
Arnett, J. J. (2013). The evidence for generation we and against generation me. Emerging Adulthood, 1, 5–10. doi:10.1177/2167696812466842
Aseltine, R. H., Jr., & Gore, S. (1993). Mental health and social adaptation following the transition from high school. Journal of Research on Adolescence, 3, 247–270. doi:10.1207/s15327795jra0303_3
Bartholomew, K., & Horowitz, L. M. (1991). Attachment styles among young adults: A test of a four-category model. Journal of Personality and Social Psychology, 61, 226–244. doi:10.1037//0022-3514.61.2.226
Bowlby, J. (1982). Attachment and loss: Vol. 1. Attachment. New York, NY: Basic Books. (Original work published 1969)
Bowman, N. A. (2010). The development of psychological well-being among first-year college students. Journal of College Student Development, 51, 180–200. doi:10.1353/csd.0.0118
Brammer, L. M., & Abrego, P. J. (1981). Intervention strategies for coping with transition. The Counseling Psychologist, 9, 19–36. doi:10.1177/001100008100900203
Brennan, K. A., Clark, C. L., & Shaver, P. R. (1998). Self-report measurement of adult attachment: An integrative overview. In J. A. Simpson & W. S. Rholes (Eds.), Attachment theory and close relationships (pp. 46–76). New York, NY: Guilford Press.
Buhl, H. M. (2007). Well-being and the child–parent relationship at the transition from university to work life. Journal of Adolescent Research, 22, 550–571. doi:10.1177/0743558407305415
Bureau of Labor Statistics. (2014, October). Unemployment rates by age, sex, race, and Hispanic or Latino ethnicity. Washington, DC: U.S. Department of Labor. Retrieved from http://www.bls.gov/web/empsit/cpsee_e16.htm
Chassin, L., Pitts, S. C., & Prost, J. (2002). Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: Predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology, 70, 67–78. doi:10.1037/0022-006X.70.1.67
Chickering, A. W., & Schlossberg, N. K. (1998). Moving on: Seniors as people in transition. In J. N. Gardner, G. Van der Veer, & Associates (Eds.), The senior year experience: Facilitating integration, reflection, closure, and transition (pp. 37–50). San Francisco, CA: Jossey-Bass.
Cohen, P., Kasen, S., Chen, H., Hartmark, C., & Gordon, K. (2003). Variations in patterns of developmental transitions in the emerging adulthood period. Developmental Psychology, 39, 657–669. doi:10.1037/0012-1649.39.4.657
Cohen, S., & McKay, G. (1984). Social support, stress and the buffering hypothesis: A theoretical analysis. In A. Baum, S. E. Taylor, & J. E. Singer (Eds.), Handbook of psychology and health (Vol. 4, pp. 253–267). Hillsdale, NJ: Erlbaum.
Daly, K. D., & Mallinckrodt, B. (2009). Experienced therapists’ approach to psychotherapy for adults with attachment avoidance or attachment anxiety. Journal of Counseling Psychology, 56, 549–563. doi:10.1037/a0016695
Ditzen, B., Schmidt, S., Strauss, B., Nater, U. M., Ehlert, U., & Heinrichs, M. (2008). Adult attachment and social support interact to reduce psychological but not cortisol responses to stress. Journal of Psychosomatic Research, 64, 479–486. doi:10.1016/j.jpsychores.2007.11.011.
Dooley, D., Prause, J., & Ham-Rowbottom, K. A. (2000). Underemployment and depression: Longitudinal relationships. Journal of Health and Social Behavior, 41, 421–436.
Dubas, J. S., & Petersen, A. C. (1996). Geographical distance from parents and adjustment during adolescence and young adulthood. New Directions for Child and Adolescent Development, 71, 3–19. doi:10.1002/cd.23219967103
Erikson, E. H. (1994). Identity and the life cycle. New York, NY: Norton. (Original work published 1959)
Fasick, F. A. (1988). Patterns of formal education in high school as rites de passage. Adolescence, 23, 457–468.
Fraley, R. C., & Davis, K. E. (1997). Attachment formation and transfer in young adults’ close friendships and romantic relationships. Personal Relationships, 4, 131–144. doi:10.1111/j.1475-6811.1997.tb00135.x
Furstenberg, F. F., Jr., Rumbaut, R. G., & Settersten, R. A., Jr. (2005). On the frontier of adulthood: Emerging themes and new directions. In R. A. Settersten, Jr., F. F. Furstenberg, Jr., & R. G. Rumbaut (Eds.), On the frontier of adulthood: Theory, research, and public policy (pp. 3–28). Chicago, IL: University of Chicago Press.
Fussell, E., & Furstenberg, F. F., Jr. (2005). The transition to adulthood during the twentieth century: Race, nativity and gender. In R. A. Settersten, Jr., F. F. Furstenberg, Jr., & R. G. Rumbaut (Eds.), On the frontier of adulthood: Theory, research, and public policy (pp. 29–75). Chicago, IL: University of Chicago Press.
Galambos, N. L., Barker, E. T., & Krahn, H. J. (2006). Depression, self-esteem, and anger in emerging adulthood: Seven-year trajectories. Developmental Psychology, 42, 350–365. doi:10.1037/0012-1649.42.2.350
Garcia, J. R., Reiber, C., Massey, S. G., & Merriwether, A. M. (2012). Sexual hook-up culture: A review. Review of General Psychology, 16, 161–176. doi:10.1037/a0027911
Gardner, P. D., & Lambert, S. E. (1993). It’s a hard, hard, hard, hard, hard, hard world. Journal of Career Planning and Employment, 53, 40–49.
Gerstacker, M. D. (2010). Becoming an emerging adult: Demographic and cultural factors, coping style, and coping self-efficacy as predictors of exploration and commitment during the resolution of an emerging adult’s identity crisis (Doctoral dissertation). Retrieved from repository.lib.ncsu.edu/ir/bitstream/1840.16/5134/1/etd.pdf
Goldscheider, F., & Goldscheider, C. (1999). The changing transition to adulthood: Leaving and returning home. Thousand Oaks, CA: Sage.
Gore, S., & Aseltine, R. H., Jr. (2003). Race and ethnic differences in depressed mood following the transition from high school. Journal of Health and Social Behavior, 44, 370–389.
Guttmann-Steinmetz, S., & Crowell, J. A. (2006). Attachment and externalizing disorders: A developmental psychopathology perspective. Journal of the American Academy of Child and Adolescent Psychiatry, 45, 440–451. doi:10.1097/01.chi.0000196422.42599.63
Hiester, M., Nordstrom, A., & Swenson, L. M. (2009). Stability and change in parental attachment and adjustment outcomes during the first semester transition to college life. Journal of College Student Development, 50, 521–538. doi:10.1353/csd.0.0089
Ingram, R. E., & Gallagher, M. W. (2010). The nature of adult vulnerability: History and definitions. In R. E. Ingram & J. M. Price (Eds.), Vulnerability to psychopathology: Risks across the lifespan (2nd ed., pp. 39–56). New York, NY: Guilford Press.
Karreman, A., & Vingerhoets, A. J. J. M. (2012). Attachment and well-being: The mediating role of emotion regulation and resilience. Personality and Individual Differences, 53, 821–826. doi:10.1016/j.paid.2012.06.014
Kenny, M. E. (1987). The extent and function of parental attachment among first-year college students. Journal of Youth and Adolescence, 16, 17–29. doi:10.1007/BF02141544
Kenny, M. E., Blustein, D. L., Chaves, A., Grossman, J. M., & Gallagher, L. A. (2003). The role of perceived barriers and relational support in the educational and vocational lives of urban high school students. Journal of Counseling Psychology, 50, 142–155. doi:10.1037/0022-0167.50.2.142
Kenny, M. E., & Donaldson, G. A. (1991). Contributions of parental attachment and family structure to the social and psychological functioning of first-year college students. Journal of Counseling Psychology, 38, 479–486.
Kenny, M. E., & Sirin, S. R. (2006). Parental attachment, self-worth, and depressive symptoms among emerging adults. Journal of Counseling & Development, 84, 61–71. doi:10.1002/j.1556-6678.2006.tb00380.x
Lane, J. A. (2013a). Group counseling for students transitioning out of postsecondary education: A narrative approach. Groupwork: An Interdisciplinary Journal for Working With Groups, 23, 34–55. doi:10.1921/1501230103
Lane, J. A. (2013b). The impact of attachment working models and social support on the subjective and psychological well-being of emerging adults in transition: Testing a theoretical mediation model (Unpublished doctoral dissertation). Oakland University, Rochester, MI.
Lane, J. A. (2014). Attachment, social support, and well-being during life transition in emerging adulthood. Manuscript submitted for publication.
Lane, J. A. (in press-a). Attachment, well-being, and college senior concerns about the transition out of college. Journal of College Counseling.
Lane, J. A. (in press-b). The imposter phenomenon among emerging adults transitioning into professional life. Adultspan Journal.
Larose, S., & Boivin, M. (1998). Attachment to parents, social support expectations, and socioemotional adjustment during the high school-college transition. Journal of Research on Adolescence, 8, 1–27. doi:10.1207/s15327795jra0801_1
Lee, C., & Gramotnev, H. (2007). Life transitions and mental health in a national cohort of young Australian women. Developmental Psychology, 43, 877–888. doi:10.1037/0012-1649.43.4.877
Lopez, F. G., Chervinko, S., Strom, T., Kinney, J., & Bradley, M. (2005). What does it mean to be an adult? A qualitative study of college students’ perceptions and coping processes. Journal of College and Character, 6(4), 1– 31. doi:10.2202/1940-1639.1424
Lopez, F. G., Mitchell, P., & Gormley, B. (2002). Adult attachment and college student distress: Test of a mediational model. Journal of Counseling Psychology, 49, 460–467. doi:10.1037/0022-0167.49.4.460
Mallinckrodt, B. (2000). Attachment, social competencies, social support, and interpersonal process in psychotherapy. Psychotherapy Research, 10, 239–266. doi:10.1093/ptr/10.3.239
Mallinckrodt, B., & Wei, M. (2005). Attachment, social competencies, social support, and psychological distress. Journal of Counseling Psychology, 52, 358–367. doi:10.1037/0022-0167.52.3.358
Manago, A. M., Taylor, T., & Greenfield, P. M. (2012). Me and my 400 friends: The anatomy of college students’ Facebook networks, their communication patterns, and well-being. Developmental Psychology, 48, 369–380. doi:10.1037/a0026338
Masten, A. S., Burt, K. B., Roisman, G. I., Obradović, J., Long, J. D., & Tellegen, A. (2004). Resources and resilience in the transition to adulthood: Continuity and change. Development and Psychopathology, 16, 1071–1094. doi:10.1017/S0954579404040143
Mortimer, J. T., Zimmer-Gembeck, M. J., Holmes, M., & Shanahan, M. J. (2002). The process of occupational decision making: Patterns during the transition to adulthood. Journal of Vocational Behavior, 61, 439–465. doi:10.1006/jvbe.2002.1885
Murphy, K. A., Blustein, D. L., Bohlig, A. J., & Platt, M. G. (2010). The college-to-career transition: An exploration of emerging adulthood. Journal of Counseling & Development, 88, 174–181. doi:10.1002/j.1556-6678.2010.tb00006.x
National Center for Education Statistics. (2014). Degrees conferred by sex and race. Washington, DC: U.S. Department of Education, Institute of Education Sciences. Retrieved from http://nces.ed.gov/fastfacts/display.asp?id=72
O’Connor, M., Sanson, A., Hawkins, M. T., Letcher, P., Toumbourou, J. W., Smart, D., . . . Olsson, C. A. (2011). Predictors of positive development in emerging adulthood. Journal of Youth and Adolescence, 40, 860–874. doi:10.1007/s10964-010-9593-7
Overton-Healy, J. (2010). First-generation college seniors: A phenomenological exploration of the transitional experience of the final college year (Doctoral dissertation). Retrieved from dspace.iup.edu/bitstream/handle/2069/249/Julia Overton-Healy.pdf?sequence=1
Perrone, L., & Vickers, M. H. (2003). Life after graduation as a “very uncomfortable world”: An Australian case study. Education and Training, 45, 69–78. doi:10.1108/00400910310464044
Pistilli, M. D., Taub, D. J., & Bennett, D. E. (2003). Development of the senior concerns survey: An exploratory factor analysis. Journal of the First-Year Experience, 15, 39–52.
Polach, J. L. (2004). Understanding the experience of college graduates during their first year of employment. Human Resource Development Quarterly, 15, 5–23. doi:10.1002/hrdq.1084
Raymore, L. A., Barber, B. L., & Eccles, J. S. (2001). Leaving home, attending college, partnership and parenthood: The role of life transition events in leisure pattern stability from adolescence to young adulthood. Journal of Youth and Adolescence, 30, 197–223. doi:10.1023/A:1010345825065
Raymore, L. A., Barber, B. L., Eccles, J. S., & Godbey, G. C. (1999). Leisure behavior pattern stability during the transition from adolescence to young adulthood. Journal of Youth and Adolescence, 28, 79–103. doi:10.1023/A:1021624609006
Roberts, J. E., Gotlib, I. H. & Kassel, J. D. (1996). Adult attachment security and symptoms of depression: The mediating roles of dysfunctional attitudes and low self-esteem. Journal of Personality and Social Psychology, 70, 310–320. doi:10.1037/0022-3514.70.2.310
Sampson, R. J., & Laub, J. H. (1990). Crime and deviance in the life course: The salience of adult social bonds. American Sociological Review, 55, 609–627. doi:10.2307/2095859
Sarason, B. R., Pierce, G. R., Shearin, E. N., Sarason, I. G., Waltz, J. A., & Poppe, L. (1991). Perceived social support and working models of self and actual others. Journal of Personality and Social Psychology, 60, 273–287. doi:10.1037/0022-3514.60.2.273
Scharf, M., Mayseless, O., & Kivenson-Baron, I. (2004). Adolescents’ attachment representations and developmental tasks in emerging adulthood. Developmental Psychology, 40, 430–444.
Schnyders, C. M. (2014). Parent and peer attachment as predictors of the perceived experience of emerging adulthood. Manuscript submitted for publication.
Schnyders, C. M., & Lane, J. A. (2014). Gender differences regarding attachment relationships in perceptions of early emerging adulthood experiences. Manuscript submitted for publication.
Schulenberg, J. E., Bryant, A. L., & O’Malley, P. M. (2004). Taking hold of some kind of life: How developmental tasks relate to trajectories of well-being during the transition to adulthood. Development and Psychopathology, 16, 1119–1140. doi:10.1017/S0954579404040167
Scott-Parker, B., Watson, B. C., King, M. J., & Hyde, M. K. (2011). The psychological distress of the young driver: A brief report. Injury Prevention, 17, 275–277. doi:10.1136/ip.2010.031328.
Sharma, B. (2012). Adjustment and emotional maturity among first year college students. Pakistan Journal of Social and Clinical Psychology, 9, 32–37.
Shulman, S., & Nurmi, J.-E. (2010). Dynamics of goal pursuit and personality make-up among emerging adults: Typology, change over time, and adaptation. In S. Shulman & J.-E. Nurmi (Eds.), The role of goals in navigating individual lives during emerging adulthood: New directions for child and adolescent development, number 130 (pp. 57–70). San Francisco, CA: Wiley.
Slade, A. (2008). The implications of attachment theory and research for adult psychotherapy: Research and clinical perspectives. In J. Cassidy & P. R. Shaver (Eds.), Handbook of attachment: Theory, research, and clinical applications (2nd ed., pp. 762–782). New York, NY: Guilford Press.
Sleap, M., & Reed, H. (2006). Views of sport science graduates regarding work skills developed at university. Teaching in Higher Education, 11, 47–61. doi:10.1080/13562510500400123
Sturges, J., & Guest, D. (2001). Don’t leave me this way! A qualitative study of influences on the organisational commitment and turnover intentions of graduates early in their career. British Journal of Guidance and Counselling, 29, 447–462. doi:10.1080/03069880120085992
Twenge, J. M. (2013). The evidence for generation me and against generation we. Emerging Adulthood, 1, 11–16. doi:10.1177/2167696812466548
U.S. Census Bureau. (2012, September). Table P-10. Age—people (both sexes combined) by median and mean. Washington, DC: Author. Retrieved from https://www.census.gov/hhes/www/income/data/historical/people/
Vickio, C. J. (1990). The goodbye brochure: Helping students to cope with transition and loss. Journal of Counseling & Development, 68, 575–577. doi:10.1002/j.1556-6676.1990.tb01414.x
Weber, L. (2012, June 21). Do too many young people go to college? The Wall Street Journal. Retrieved from http://online.wsj.com/article/SB10001424052970203960804577239253121093694.html
Wei, M., Liao, K. Y.-H., Ku, T.-Y., & Shaffer, P. A. (2011). Attachment, self-compassion, empathy, and subjective well-being among college students and community adults. Journal of Personality, 79, 191–221. doi:10.1111/j.1467-6494.2010.00677.x
Wei, M., Mallinckrodt, B., Larson, L. M., & Zakalik, R. A. (2005). Adult attachment, depressive symptoms, and validation from self versus others. Journal of Counseling Psychology, 52, 368–377. doi:10.1037/0022-0167.52.3.368
Weiss, D., Freund, A. M., & Wiese, B. S. (2012). Mastering developmental transitions in young and middle adulthood: The interplay of openness to experience and traditional gender ideology on women’s self-efficacy and subjective well-being. Developmental Psychology, 48, 1774–1784. doi:10.1037/a0028893
Wendlandt, N. M., & Rochlen, A. B. (2008). Addressing the college-to-work transition: Implications for university career counselors. Journal of Career Development, 35, 151–165. doi:10.1177/0894845308325646
Yazedjian, A., Kielaszek, B. J., & Toews, M. L. (2010). Students’ perceptions regarding their impending transition out of college. Journal of the First-Year Experience & Students in Transition, 22, 33–48.
Yeadon, C. (2010). College senior transition programs: Transitioning from college to the workplace. Journal of Student Affairs, 19, 44–50.
Joel A. Lane, NCC, is the recipient of the 2014 Outstanding Dissertation Award for The Professional Counselor and an Assistant Professor at Portland State University. Correspondence can be addressed to Joel A. Lane, Department of Counselor Education, Portland State University, Graduate School of Education, PO Box 751, Portland, OR 97207, lanejoel@pdx.edu.
