Apr 1, 2026 | Volume 16 - Issue 1
Danielle Pester Boyd, Laura K. Jones, Courtney Maier, Danica G. Hays
The intentional exploration or broaching of topics related to the social determinants of mental health (SDoMH) throughout the counseling process helps align clinical practice with the profession’s focus on multicultural and social justice counseling competency. This article identifies six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences, (e) addressing emergent needs, and (f) termination practices. These SDoMH broaching behaviors span counselor preparation, assessment, intervention, and termination, empowering counselors to address SDoMH in their work. We conclude with implications for fostering SDoMH broaching behaviors within counselor education.
Keywords: broaching, social determinants of mental health, multicultural, counseling competency, counselor education
Counselors are increasingly called upon to integrate multicultural competence and social justice advocacy into their practice, particularly when addressing systemic and environmental factors that shape client well-being. The Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) and relevant constructs, such as the social determinants–based counseling model (SDCM; Pester Boyd et al., 2025) and the multidimensional model of broaching behavior (MMBB; Day-Vines et al., 2020), provide guiding frameworks for ensuring culturally responsive care. Taken together, these models inform concrete methods for integrating discussions of systemic, environmental, and structural influences into counselor–client interactions, which create a foundation for a set of broaching behaviors focused specifically on the social determinants of mental health (SDoMH).
Social determinants of health (SDOH) refer to “the conditions in which people are born, grow, live, work, and age that shape health outcomes” (World Health Organization [WHO], 2025, para. 1). These determinants include economic stability (e.g., employment, income), health care access, education, neighborhood safety, and social relationships, all of which impact physical and mental health. The SDoMH focus specifically on the social and structural factors influencing mental health outcomes, such as exposure to discrimination, adverse childhood experiences, community violence, economic disparities, and barriers to mental health care (Compton & Shim, 2020), influences that are reflected in the MSJCC.
The SDCM is an empirically based systemic framework for addressing SDoMH across various practice settings (Pester Boyd et al., 2025). It guides counselors in identifying barriers, such as economic hardship, discrimination, and limited access to resources, and then provides a structured process for broaching these concerns in session. Beyond simple recognition, the SDCM emphasizes implementing culturally responsive interventions, including connecting clients with community supports, advocating for policy changes, or adapting treatment plans to account for systemic stressors. This systemic responsiveness communicates to clients that their external challenges are legitimate and central to their mental health care, which reinforces the therapeutic alliance by integrating advocacy with clinical practice. Given the links among the MSJCC, SDoMH, and therapeutic outcomes, it is imperative that counselors are familiar with SDoMH, understand their impact, and are prepared to broach topics related to SDoMH with clients. Therefore, integrating the SDCM with known broaching models like the MMBB can serve to operationalize these action strategies as concrete methods to demonstrate the MSJCC.
The MMBB provides a framework to explicitly explore or broach racial, ethnic, and cultural (REC) factors with clients throughout the therapeutic process (Day-Vines et al., 2020, 2021). These broaching behaviors focus on four distinct contexts: intracounseling, intraindividual, intra-REC, and inter-REC domains. Specifically, counselors acknowledge REC concerns that impact the counselor–client relationship (intracounseling), the intersections of the client’s identity (intraindividual), the client’s cultural group membership (intra-REC), and their experiences with structural inequality (inter-REC). By intentionally attending to these layers, counselors demonstrate cultural humility and multicultural competency that affirms the realities of clients’ REC concerns. Effective broaching has been linked to enhanced client trust, increased depth of client self-disclosure, higher levels of client satisfaction, and improved therapeutic outcomes, which make it a critical component of effective multicultural counseling (Depauw et al., 2025; Gantt-Howrey et al., 2024; King & Borders, 2019; Zhang & Burkard, 2008).
By integrating the SDCM with the MMBB, we developed a set of SDoMH-specific broaching behaviors. The MMBB strengthens the relational dimension of counseling through cultural engagement while the SDCM equips counselors to act on systemic barriers that influence client well-being. Together, these models ultimately foster trust, collaboration, and empowerment and establish counseling as a space where both individual experiences and broader structural inequities are acknowledged and addressed.
SDoMH Broaching Behaviors
This article describes six SDoMH broaching behaviors for counselors grounded in the MMBB and the SDCM: counselor development, client psychoeducation, contextualization, attending to differences of lived experience, addressing emergent needs, and SDoMH-informed termination practices. These SDoMH broaching behaviors represent an interactive approach in which counselors shift among the behaviors throughout their own development as well as during assessment, intervention, and termination within the counseling relationship.
Counselor Development
The first SDoMH broaching behavior is initiated during a counselor’s preparation to work with clients. In alignment with the MSJCC (Ratts et al., 2016), counselors are expected to continually foster both knowledge and self-awareness related to the multicultural and social justice issues facing their clients, including client experiences with SDoMH. In order to develop their knowledge of SDoMH scholarship, counselors can familiarize themselves with the seminal SDOH/SDoMH frameworks (e.g., Compton & Shim, 2020; Lund et al., 2018; WHO, 2025); guiding practice models related to broaching behaviors and best practices for addressing the SDoMH (e.g., MMBB, SDCM; Day-Vines et al., 2020; Pester Boyd et al., 2025); general scholarship on SDoMH application in training, practice, and research (e.g., Johnson et al., 2023; Lenz & Lemberger-Truelove, 2023; Lenz & Litam, 2023; Mason et al., 2023; Neal Keith et al., 2023; Pester et al., 2023); and, when applicable, setting-specific SDoMH resources for school counselors (e.g., Brookover, 2024; Johnson & Brookover, 2021), career counselors (Johnson et al., 2024), and family counselors (Robins et al., 2022).
Next, to facilitate self-awareness, counselors are encouraged to engage in reflective practices that identify areas of strength in addressing SDoMH with clients and areas that require skill and dispositional development. First, counselors should reflect on any personal experiences with SDoMH and how those experiences may both inform and potentially bias their work with clients. For example, counselors who have dealt with their own experiences of economic instability may need to watch for emerging countertransference with clients having similar experiences. We recommend that counselors review existing SDoMH frameworks and identify which determinants have affected them personally and interpersonally with peers, family members, and colleagues. In addition, they can consider what strategies were helpful or harmful as they personally navigated SDoMH.
Counselors should also reflect on any prior experiences working with clients who were dealing with SDoMH and how those prior professional experiences might inform and potentially bias their ability to help new clients with SDoMH. For example, counselors might view clients as resistant if they do not consistently attend counseling sessions, although those clients may be dealing with circumstances impacted by SDoMH (e.g., unstable transportation, lack of childcare, unreliable internet access). Mechanisms such as supervision or consultation can be helpful for facilitating counselor awareness and development related to being nonjudgmental, showing unconditional positive regard, and embodying congruence, which are all vital components of creating and maintaining a strong therapeutic alliance.
Additionally, counselors or counseling supervisors can administer the Addressing Client Needs with Social Determinants of Health Scale (ACN:SDH, Johnson, 2023) to more formally assess readiness for addressing SDoMH. This tool measures a provider’s SDOH competency related to knowledge, awareness, biases, skills, and preparedness. The ACN:SDH findings can be reviewed within supervision or consultation. For areas where data reflect a lack of readiness, counselors can process feelings associated with their limited readiness and brainstorm resources that may be useful for building readiness. Ultimately, as counselors focus inward to broach and support their professional development related to the SDoMH framework, they will be more prepared to implement the remaining SDoMH broaching behaviors in client interactions.
Client Psychoeducation
Client psychoeducation is the next SDoMH broaching behavior that begins during the intake and assessment process. Psychoeducation is an evidence-based intervention that integrates client education into the counseling process by connecting clinical outcomes to increased client self-awareness and skill development across many mental health presenting concerns (e.g., anxiety, depression, schizophrenia; Dolan et al., 2021; Luo et al., 2025). We suggest that counselors mindfully introduce SDoMH psychoeducation into the intake and assessment process to increase client knowledge and awareness about the potential impact of SDoMH on well-being.
Furthermore, there is growing support for universal SDoMH screening (Gantt-Howrey et al., 2024; Johnson & Brookover, 2021; Johnson et al., 2023), with many available screeners for counselors to use, including the Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences (PRAPARE; 2022); the Accountable Health Communities Health-Related Social Needs Screening Tool (Center for Medicare and Medicaid Innovation, n.d.); and the WE CARE Survey (Garg et al., 2007). These screeners can be incorporated into intake processes to establish a baseline of SDoMH data for clients. For example, the PRAPARE assessment identifies both individual areas of risk related to social determinants and an overall risk tally score. Counselors can use this data to inform both the focus of the psychoeducation intervention and the client’s treatment plan.
Many clients may not fully understand why they are being asked about these areas of their lives or be aware of how these determinants may influence well-being. Therefore, counselors should first define SDoMH and explain the overall framework using jargon-free language. For example:
Social determinants of mental health are different social and environmental factors that can positively or negatively influence our physical and mental health. These can be factors like having your basic needs of food, housing, and employment met; having access to quality education and health care; living in a safe environment free of violence and risk; and having strong social and community support. The more people are surrounded by supportive social and environmental conditions, the easier it is to improve overall health and mental health. When people do not have adequate access to these conditions, it can lead to a higher risk of health and mental health concerns. It is important for the work that we are going to do together to have a clear picture of how your environment is influencing your physical and mental health so that we can work to increase conditions that will support the positive mental health changes you are wanting to make.
Counselors can also consider using visual tools in session, such as handouts that depict SDoMH in an easily understandable format (see Figure 1 for a sample).
Counselors should then use the SDoMH data collected through the assessment process to provide data-driven psychoeducation about the specific social determinant risk areas identified in a client’s assessment, outlining the research and known physical and mental health risks and outcomes of those determinants. For example, one item on the PRAPARE assessment asks, “How often do you see or talk to people that you care about and feel close to?” If a client answers less than three times per week, they are flagged for a risk tally on this item; the counselor could provide psychoeducation on the impact of social connection and community support alongside the risks of social isolation (U.S. Department of Health and Human Services, 2023). A counselor might broach the topic by saying:
I noticed when you were asked how many times you see or talk to people you care about that you answered less than three times per week. I ask this question on the screener because at times the number and quality of our social connections can have an influence on our physical and mental health. For example, social isolation has been linked to increased risk of anxiety and depression, lower academic and job performance, greater susceptibility to viruses and respiratory illnesses, and even long-term risk of diseases such as heart disease and stroke. Healthy social connection can protect us from disease and increase our sense of safety, meaning, and resilience. Tell me more about what social connection looks like in your life.
By broaching the subject in this way, the counselor can intentionally assess the impact of a specific social determinant on the client’s overall well-being and health. In the example, the counselor would seek to understand the quantity, quality, and impact of the client’s relationships while also screening for any potential physical symptoms that might require an external referral. This practice of broaching SDoMH through client psychoeducation and assessment allows the counselor to implement data-driven practices that provide a multitiered therapeutic framework to conceptualize client concerns across various socioecological levels (e.g., individual, interpersonal, community, public policy). This in turn supports the development of a more holistic treatment plan that incorporates both individual and community interventions.
Figure 1
Visual Depiction of the Social Determinants of Mental Health for Clinical Use
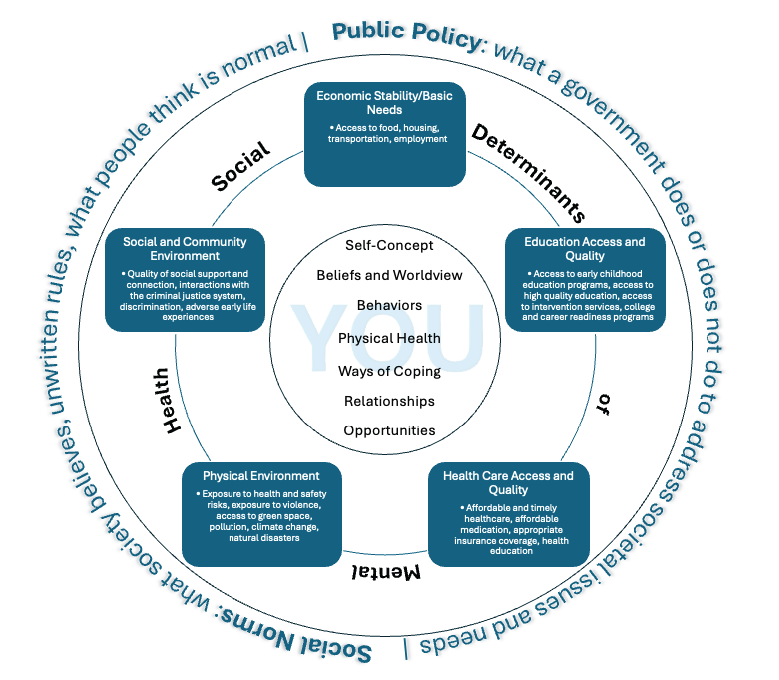
Note. Adapted from Social Determinants of Health, by Office of Disease Prevention and Health Promotion, 2025 (https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health) and “Social Determinants of Mental Health” by Compton, M. T., & Shim, R. S., 2015, Focus, 13(4), p. 420 (https://doi.org/10.1176/appi.focus.20150017).
Contextualizing SDoMH for Each Client
As a client develops understanding and awareness of the social determinants impacting their well-being, the counselor should also use broaching to contextualize that knowledge on an individual level. In this way, counselors go beyond educating clients about SDoMH in general and instead seek to collaborate with the client to understand how they are uniquely impacted by those factors. This practice of contextualizing SDoMH allows the client to make connections between their lived experiences, intrapsychic concerns, and the larger social and environmental context.
This broaching behavior aligns well with the MMBB and its intraindividual, intra-REC, and inter-REC broaching dimensions. Counselors can apply these broaching dimensions to the contextualization process. For example, intraindividual broaching can be used to acknowledge how SDoMH impact a client’s identity dimensions (e.g., race, gender, socioeconomic status, sexual orientation, immigration status). A counselor could say, “It sounds like financial strain has limited your transportation options to get to your appointments. Let’s find some free or low-cost alternatives that might better fit within your budget.” Intra-REC broaching, or the exploration of within–cultural group concerns, can help the counselor discuss any client issues impacted by SDoMH that are culture-specific. A counselor might say to the client, “I imagine it could be difficult to ask family and friends for a ride to your appointments if mental health is stigmatized in those relationships.” Finally, a counselor may apply inter-REC broaching by exploring a client’s experiences with discrimination:
Relying on public transportation resources in this city has caused you to miss important appointments and events. It sounds like these public resources don’t meet the needs of residents. I plan to write a letter to the city council explaining some of the issues. Is there anything specific that you would like me to communicate or any way that you would like to advocate for changes?
By integrating these specific broaching dimensions, counselors can help clients gain both self and situational awareness by better understanding the possible role of social determinants in their own lives. In turn, this allows the counselor and client to better address challenges by understanding the client’s unique needs in context. From the previous example, the counselor might consider the following: Does the client need help identifying additional transportation resources? Would virtual counseling sessions be a more accessible option? Can I advocate for improved public transportation in the local community by providing key context to local leaders about how unreliable transportation affects the health of their constituents? Are there self-advocacy skills that I could help the client develop? Through targeted discussions on SDoMH like these, counselors can ensure that they are providing culturally responsive care that meets their clients’ unique needs.
Broaching Differences in the Counselor–Client Relationship
As SDoMH factors are integrated into the therapeutic process, counselors must also attend to the interpersonal process of the therapeutic alliance by intentionally broaching any differences that may exist between the counselor and client. Clients from historically marginalized backgrounds may experience factors that may differ significantly from their counselor’s lived experiences, such as heightened economic instability, community violence, and health care barriers (Compton & Shim, 2015). The MMBB, through its intracounseling domain, emphasizes that a counselor must actively acknowledge and explore REC differences between the counselor and client to attend to any disruptive interpersonal processes that might impact the therapeutic relationship (Day-Vines et al., 2020). We suggest that differences in lived experience related to SDoMH be treated comparably to ensure culturally responsive and effective care.
Research suggests that counselors who fail to broach REC concerns and SDoMH-related disparities risk reinforcing dominant cultural narratives that dismiss or minimize the structural challenges clients face, potentially leading to client disengagement, cultural miscommunication, and premature termination of counseling services (Day-Vines et al., 2021; Drinane et al., 2018; Owen et al., 2014). Thus, it is incumbent upon counselors to broach these differences with cultural humility, openness, and a willingness to engage in difficult but necessary conversations (Newton & Steele, 2025). To effectively broach these conversations, a counselor should adopt a collaborative, client-centered approach by acknowledging potential differences in lived experiences while affirming the client’s perspective.
One strategy is for the counselor to invite open discussions by saying:
I recognize that my experiences may be different from yours, and I don’t want to make assumptions about the challenges that you face. I’d like to understand more about how factors like financial stress, health care access, or discrimination may be affecting your mental health. Would you be open to sharing what that has been like for you?
This type of broaching explicitly acknowledges differences in identity, privilege, and lived experience between the counselor and client while creating a nonjudgmental and validating therapeutic space for the client to share their reality (Day-Vines et al., 2021).
Another example of effective intracounseling broaching can be seen in a case where a White counselor works with a Black client who describes frequent racial discrimination in the workplace. To avoid deflecting or minimizing the client’s experience, the counselor might say, “I want to acknowledge that my lived experience may not reflect what you’re describing, but I want to understand how these challenges impact your well-being.” This affirming, non-defensive approach allows for deeper exploration of SDoMH factors such as racial stress, economic opportunity, and access to mental health care (Newton & Steele, 2025). Such intentional broaching behaviors can also help mitigate client mistrust, validate sociocultural realities, and strengthen the therapeutic alliance (Day-Vines et al., 2021).
Building rapport and trust is central to the broaching process, particularly when addressing systemic disparities. Trust building requires empathy, active listening, and a willingness to acknowledge one’s own biases (Day-Vines et al., 2021). Integrating clients’ interests, cultural values, and lived experiences into sessions makes counseling more relevant, while creating a safe space grounded in unconditional acceptance encourages openness and authenticity. Together, these broaching practices foster trust, empower clients to take an active role in the process, and strengthen the foundation for growth and change.
Broaching Emergent Needs in Session
Counselors should also be mindful to broach emergent client needs throughout the therapeutic process. Though counselors may assess clients for SDoMH at the beginning of the counseling process, that information must be viewed within a dynamic client context that requires an ongoing response rather than a one-time assessment. Therefore, counselors must remain attuned to emerging SDoMH needs throughout the therapeutic process and utilize immediacy skills to broach and address concerns as they arise.
Many clients face barriers related to income, health care access, transportation, and social support networks, all of which can create stressors that directly influence mental health outcomes because they add layers of stress that can overshadow therapeutic work (Compton & Shim, 2015). When basic needs are not met, clients may experience heightened anxiety, hopelessness, or distraction, which can limit their ability to fully engage in treatment.
Ongoing systemic barriers can also reinforce feelings of disempowerment and make it harder for clients to trust the counseling process or believe change is possible. As a result, unresolved SDoMH challenges often lead to inconsistent attendance, premature termination, or reduced treatment effectiveness. By addressing these barriers within the counseling process, counselors not only improve client retention and engagement but also enhance overall wellness by affirming that external stressors are legitimate and integral to mental health care.
For example, a client who discloses heightened anxiety over an overdue utility bill may struggle to engage in therapy until the pressing financial stressor is addressed. A counselor might broach this concern by saying, “I can see how this situation is overwhelming and I want to support you in finding a solution. Would it be helpful to take a few minutes to explore assistance programs or a payment plan?” This response validates the client’s distress while offering immediate, actionable support to address a pressing external challenge. Similarly, a client struggling with transportation barriers may benefit from a session in which the counselor helps them identify local transit options, employer benefits, or community-based ride services to ensure consistent access to mental health care. Meeting such immediate, concrete needs within the session fosters greater trust, retention, and engagement in the counseling process (Day-Vines et al., 2021; Newton & Steele, 2025). Additionally, addressing pressing SDoMH concerns in real time reinforces the message that both psychological distress and external stressors are valid therapeutic concerns. This approach ensures that counseling remains responsive and supportive of the client’s holistic well-being.
Beyond directly helping clients address pressing needs in session, the counselor can support self-advocacy and empowerment by equipping clients with the knowledge and skills to independently resolve their emergent needs. Developing self-advocacy skills enables clients to engage more effectively with health care providers, employers, and social service agencies providing skills that bridge the counseling office into everyday life (Compton & Shim, 2020). Self-advocacy intervention empowers clients to actively pursue resources, assert their rights, and confront systemic barriers with confidence. Moreover, self-advocacy skills foster resilience and equip clients to not only overcome immediate obstacles but to also sustain progress in the face of future challenges. In this way, developing self-advocacy skills is not just a counseling technique but a vital outcome that supports long-term growth and empowerment.
The counselor can facilitate the development of self-advocacy skills by helping clients identify resources, role-play difficult conversations, and anticipate potential barriers they may encounter when seeking support. For example, a client experiencing housing insecurity may feel intimidated about reaching out to a local housing agency because of past negative experiences or uncertainty about eligibility requirements. A counselor might role-play the conversation by saying, “Let’s practice how you might explain your situation when calling the housing agency. You could start by saying, ‘I’m looking for assistance with securing stable housing. Can you help me understand the eligibility requirements and next steps?’” This approach allows the client to rehearse the interaction in a supportive setting, boosting their confidence before making the actual call. Additionally, the counselor can help the client identify potential challenges, such as long wait times or required documentation, and develop strategies to navigate them, ensuring that they feel prepared and empowered when seeking resources.
Through active collaboration, counselors can help clients recognize their strengths; build resilience to adapt, recover, and grow when faced with adversity; and gain confidence in advocating for themselves in settings that may otherwise feel disempowering. This approach fosters an environment where clients feel seen, supported, and empowered to navigate both personal and systemic challenges as they arise.
Termination Considerations
Finally, SDoMH need to be broached in the context of termination because of their impact on client dropout rates and early termination of treatment (Roberts et al., 2022). Although counselors are traditionally taught that termination should be gradual and that clients should share readiness, that is not always the reality because of the influence of social determinants. For example, electricity or phone service may be terminated because of an inability to pay bills, thereby limiting the client’s access to virtual sessions; limited transportation or childcare may prevent continued session attendance. Although counselors hope that they will be able to have a final session, that is not always realistic.
Nevertheless, the termination period represents a critical phase of the clinical process and must be attended to as part of the counseling process (Baum, 2005; Goode et al., 2017; Knox et al., 2011; Lee et al., 2023; Vasquez et al., 2008). Therefore, incorporating SDoMH broaching behaviors throughout the counseling relationship lays the foundation for effective clinical termination, even if termination occurs prematurely. For example, enhancing skills such as self-advocacy and incorporating discussions of resource identification and utilization can help empower clients in the event of unexpected termination.
When a formal termination is possible, continuing to broach SDoMH throughout that process can strengthen therapeutic gains and enhance overall therapeutic outcomes. As such, a counselor may engage clients in discussions around how SDoMH have impacted their therapeutic experience and goal attainment during counseling. This conversation can extend to how SDoMH may influence goal attainment after counseling, including brainstorming potential challenges that may arise. Discussions around how to apply skills gained during counseling to navigate those challenges and address relevant social determinants can also be impactful.
Additionally, a counselor should recognize that clients who discontinue care because of SDoMH-related barriers may choose to reengage in counseling once those barriers have been resolved. Thus, using a screen door approach (Pester Boyd et al., 2025) to termination can be helpful. This may include broaching the process of how clients can return to counseling (e.g., whether a new intake is required, potential waitlist considerations), available options for returning (e.g., in person, telehealth, in-home), and factors that might warrant reengagement in counseling.
Broaching SDoMH during termination should also include providing and discussing a list of referrals and resources to support clients beyond counseling. These resources should address both immediate mental health needs and the social determinants that impact overall well-being. Clients may wish to discuss these referrals and resources further to better understand the process of accessing them. This may include empowering clients with language they can use in various settings, such as navigating legal, social services, or medical resources, or even role-playing those conversations.
Given the potential role of SDoMH in early termination, such discussions should begin early in the clinical process. For example, a counselor might say, “You mentioned concerns that you may lose your health insurance. Can we talk through what that may look like if that were to happen?” This helps the counselor address factors related to counseling and mental health while also helping the client brainstorm challenges, solutions, and resources. Using the other SDoMH broaching behaviors to sustain these conversations throughout the counseling process can lead to effective client termination, even if termination occurs unexpectedly.
SDoMH Broaching Behaviors and Counselor Education
There is a growing call within counseling and related mental health fields to enhance SDoMH training and increase counselor readiness to broach these topics in practice (Gantt-Howrey et al., 2024; Johnson & Robins, 2021; Newton & Steele, 2025; Pester Boyd et al., 2025). As such, counselor education programs at the master’s and doctoral levels should incorporate discussion and clinical practice opportunities to help counselors-in-training (CITs) build awareness of SDoMH and develop best practices for broaching and addressing their impact on client well-being. Counselor education programs can embed SDoMH broaching across coursework, supervision, and experiential learning to prepare CITs for ethical and effective practice.
Integrating SDoMH in Coursework and Supervision
SDoMH training may be integrated in a number of counselor education courses and aligns with Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2023) standards (Gantt-Howrey et al., 2024; Pester Boyd et al., 2025). For example, suggested activities per course/CACREP core area include: (a) examining ethical considerations of broaching SDoMH, including advocacy responsibilities and potential boundary issues when addressing systemic barriers (i.e., professional orientation and ethics); (b) helping CITs connect the MSJCC to SDoMH through case study analysis (i.e., social and cultural diversity); (c) highlighting how developmental outcomes are shaped by SDoMH (i.e., human growth and development); (d) addressing how economic stability, employment, and educational inequities intersect with career counseling (i.e., career development); (e) having CITs practice broaching SDoMH through role-plays to become aware of how SDoMH affects rapport, trust, and client disclosure (i.e., counseling and helping relationships); (f) integrating experiential activities in which students design psychoeducational groups focused on wellness promotion, social support, or navigating systemic barriers (i.e., group counseling and group work); (g) teaching CITs to administer and interpret SDoMH screening tools and to incorporate results into case conceptualizations (i.e., assessment and evaluation); and (h) requiring that CITs design projects to investigate the impact of SDoMH on client outcomes or evaluate community-based interventions (i.e., research and program evaluation).
In addition, practicum and internship supervision provides an important space for modeling SDoMH broaching and supporting CITs in developing cultural humility and ethical decision-making through structured activities. Supervisors might, for example, guide CITs in identifying protective factors through a strengths mapping exercise that charts client supports across individual, relational, community, and cultural identities. They can also facilitate role-plays in which CITs practice acknowledging the protective role of extended family, religious communities, cultural traditions, or neighborhood engagement. Site supervisors may also connect practicum activities to systemic issues, such as collaborating with schools or agencies on wellness or resource initiatives. Finally, reflective supervision discussions can help CITs analyze their own responses to client strengths and SDoMH barriers and notice whether they default to problem-solving or strength-building.
SDoMH Broaching in Experiential Learning
Experiential activities provide CITs with opportunities across coursework, practicum, and internship to connect theory to practice. Experiential activities may include case analysis, role-plays, assessment practice, community engagement, and classroom discussions focused on ethical dilemmas. First, CITs can analyze case vignettes to examine how SDoMH affect individuals and families. For example, dyads might review a case through the lens of a specific determinant such as housing insecurity or underemployment, discuss the client’s presenting concerns in context, and brainstorm broaching strategies. Second, structured role-plays further allow students to develop confidence in directly addressing SDoMH with clients. For example, in triadic supervision, CITs can rotate roles as counselor, client, and observer, while peers and supervisors provide feedback on the clarity and effectiveness of broaching behaviors.
Third, assignments that incorporate SDoMH assessment tools (e.g., PRAPARE, WE CARE Survey) also prepare CITs to integrate systemic factors into case conceptualization. CITs may practice administering and interpreting screeners with hypothetical clients and then learn to translate results into simple, jargon-free explanations for use in sessions. Fourth, community engagement projects deepen this preparation by connecting CITs to the systemic realities clients face. Examples include researching local issues such as food insecurity and mapping neighborhood resources.
Ethical reflection is also a part of experiential learning. Classroom discussions may explore balancing advocacy efforts with professional boundaries or managing countertransference when counselors share similar systemic challenges with their clients. In addition, classroom dialogue can highlight positive determinants of mental health by fostering empathy and compassion. Storytelling circles or guided conversations can invite CITs to share their own lived experiences of belonging or exclusion and consider how these experiences influence their empathy and ethical decision-making.
Cultural humility is the foundation for effective SDoMH broaching. To strengthen cultural humility and responsiveness, counselor education programs can embed the abovementioned experiential learning strategies across coursework and supervision. Self-reflection exercises may include journaling prompts such as: “What identities give me privilege and how might that shape my assumptions with clients?”; “How have I responded when a client’s worldview or values conflicted with my own? What could I do differently to remain open and nonjudgmental?”; and “Recall a time you felt excluded, misunderstood, or powerless. How does that experience shape your empathy for clients navigating systemic inequities?” These reflections can be revisited across the program to track growth in self-awareness and cultural responsiveness.
Guided discussions can be facilitated through fishbowl discussions in which CITs share and listen to experiences of privilege, discrimination, or cultural differences, followed by role-plays that practice broaching these issues in counseling. Counselor educators can model effective broaching and provide feedback on student language and presence during these exercises.
Promoting Positive Social Determinants
In addition to addressing negative SDoMH (e.g., discrimination, housing insecurity, poverty, community violence), counselor educators can help CITs recognize and promote positive SDoMH that build resilience. These determinants include self-care practices, strong social support, inclusive environments, cultural affirmation, and opportunities for growth and connection. In addition, counselor educators can model and encourage strengths-based approaches that affirm client identities, such as validating cultural, gender, or spiritual expressions, during intake and treatment planning.
Wellness models and self-care planning can be integrated into coursework to benefit both CITs and future clients. For example, assignments might include creating a personal self-care plan; evaluating wellness models and interventions across cultures; or designing a client-friendly handout that translates wellness strategies (e.g., mindfulness, exercise, nutrition, social connection) into accessible, culturally responsive language.
Counselor education programs can embed advocacy projects across coursework to promote systemic conditions that support mental health equity. Examples include partnering with schools to develop anti-bullying campaigns; creating culturally inclusive mental health awareness workshops for parents and teachers; and collaborating with community agencies to expand access in areas such as housing assistance, after-school programs, health care access, or transportation services. CITs might also design stigma-reduction campaigns with public health organizations.
Service-learning projects can further immerse students in community contexts by mapping resources, conducting needs assessments, or partnering with organizations addressing issues such as refugee resettlement, food insecurity, or housing justice. As service-learning projects conclude, CITs can be asked, “What systemic barriers did you observe and how might they affect mental health?”; “How did this experience shape your understanding of your role as advocate?”; and “How might insights from this project influence how you broach SDoMH with clients in practice?”
Preparing for SDoMH Broaching Challenges
Although broaching SDoMH is a critical counseling skill, CITs may face obstacles when attempting to apply it in future practice. Agency settings may limit the time available to explore systemic issues, and some trainees may feel anxious about making missteps when discussing topics such as poverty, discrimination, or community violence. Clients themselves may hesitate to disclose experiences of marginalization out of fear of judgment or because such issues have been dismissed in past encounters with helping professionals.
Counselor educators can support student development by intentionally acknowledging these challenges within the classroom and supervision spaces. For example, they might facilitate a structured dialogue in which CITs share their concerns about broaching while the counselor educator normalizes discomfort and models language for difficult conversations. In these dialogues, they might ask CITs, “What feelings come up for you when you think about broaching SDoMH with a client?”; “What makes these conversations challenging in practice?”; or “How might you respond if a client resists or shuts down when SDoMH are introduced?” Such discussions can help trainees recognize that hesitation is common and that growth comes from practice and feedback rather than perfection.
Another way to strengthen readiness is through guided debriefing of role-plays or client simulations. After a broaching exercise, counselor educators can ask CITs to reflect on moments in which they felt stuck, explore how power dynamics may have shaped the exchange, and brainstorm alternative approaches. For instance, a CIT might role-play broaching transportation barriers with a hypothetical client who frequently misses sessions. After the role-play, other CITs within the classroom or supervision session could examine the CIT’s wording and the client’s reaction and then suggest alternative ways to frame the issue that both validate the client’s struggle and highlight systemic factors.
Counselor educators can also discuss the limitations of broaching within supervision. When reviewing case presentations, supervisors might ask CITs not only how they addressed SDoMH but also what structural limitations they encountered and how those shaped the counseling process. For example, a CIT might describe working with a client who lacked consistent childcare and therefore missed several sessions. The supervisor could guide the student to consider how systemic gaps in affordable childcare both constrained the counseling process and required exploration of advocacy or referral options. These conversations emphasize that although broaching can validate client experiences, it cannot by itself dismantle inequities, thus highlighting the importance of community collaboration and ongoing advocacy. As counselor educators intentionally and thoroughly analyze the process together, CITs can learn to approach barriers not as failures but as opportunities to deepen cultural humility.
Evaluating SDoMH Broaching Behaviors
Currently, there are no existing measures to evaluate SDoMH broaching behaviors, and future research should prioritize the development of validated tools to assess both counselor competency in SDoMH broaching and client perceptions of these efforts. Quantitative studies could focus on designing and testing new measures that assess the clarity, timing, cultural responsiveness, and impact of SDoMH broaching within the counseling relationship. Counseling researchers could utilize these instruments to conduct longitudinal studies and controlled intervention studies exploring the influence that SDoMH broaching has on client trust, client engagement in counseling, and therapeutic outcomes.
Until instruments specific to SDoMH broaching have been developed, researchers can use existing scales that independently measure broaching behaviors (e.g., Day-Vines et al., 2013; Day-Vines et al., 2024), SDoMH readiness (e.g., Johnson, 2023) and SDoMH assessment (e.g., Gantt-Howrey et al., 2024) to understand effective counseling behavior related to these constructs.
In addition to quantitative approaches, qualitative studies can help inform the impact of broaching behaviors on clients, CITs, and counselors. Studies that explore client experiences with counselors who broach SDoMH can provide contextual nuance and enhance multiculturally competent practice. For instance, interviews or focus groups with clients might uncover how broaching influences their feelings of safety, empowerment, or stigma reduction. Furthermore, researchers could conduct case studies of counselors in varied settings to examine how SDoMH broaching unfolds in practice. Data from session transcripts and client and counselor interviews could reveal additional best practices for addressing SDoMH, promoting positive social determinants, and counteracting challenges that counselors may have while broaching SDoMH.
Conclusion
Learning to effectively broach SDoMH provides an opportunity for counselors to further operationalize Ratts et al.’s (2016) MSJCC. As the cross-disciplinary call for universal SDoMH screening practices continues to grow across health professions, to remain leaders among the mental health professions, counselors must begin intentionally broaching SDoMH with clients. However, as a profession, broaching SDoMH may require reexamining the professional counselor identity, expanding advocacy roles, and reviewing ethical standards that may inadvertently create barriers to effectively addressing the impact of social determinants on clients’ lives.
Preliminary research suggests that effectively broaching SDoMH throughout the counseling process supports a number of short- and long-term benefits to clinical practice, which warrants its further integration and evaluation in the counseling profession. Counselors perceive that in the short term, broaching SDoMH strengthens the therapeutic relationship while fostering MSJCC (Pester Boyd et al., 2025). These early benefits can give way to enhanced client empowerment and improved access to interprofessional resources and services, both of which can lead to better treatment outcomes. Long-term, effectively broaching SDoMH can result in improved overall health of the client, improved community health, and decreased marginalization.
The MMBB (Day-Vines et al., 2020) and SDCM (Pester Boyd et al., 2025) provide needed frameworks to enhance these client outcomes. Using the integration of these frameworks as a foundation, we identified six SDoMH broaching behaviors for counselors: (a) counselor development, (b) client psychoeducation, (c) contextualization, (d) attending to differences of lived experience, (e) addressing emergent needs, and (f) SDoMH-informed termination practices. These broaching behaviors provide specific guidance for how to integrate SDoMH into counseling practice, which operationalizes the mandate of the MSJCC to address systemic and environmental factors impacting client mental health. We suggest that counselors integrate the identified SDoMH broaching behaviors throughout all stages of the therapeutic process to support a strong counselor–client relationship, enhanced client self-disclosure, increased client satisfaction, and improved therapeutic outcomes.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Baum, N. (2005). Correlates of clients’ emotional and behavioral responses to treatment termination. Clinical Social Work Journal, 33(3), 309–326. https://doi.org/10.1007/s10615-005-4946-5
Brookover, D. L. (2024). The career development and social determinants framework: An integrative approach. Professional School Counseling, 28(1), 1–12. https://doi.org/10.1177/2156759X241290494
Center for Medicare & Medicaid Innovation. (n.d.). The accountable health communities health-related social needs screening tool. https://innovation.cms.gov/files/worksheets/ahcm-screeningtool.pdf
Compton, M. T., & Shim, R. S. (2015). The social determinants of mental health. Focus, 13(4), 419–425. https://doi.org/10.1176/appi.focus.20150017
Compton, M. T., & Shim, R. S. (2020). Why employers must focus on the social determinants of mental health. American Journal of Health Promotion, 34(2), 215–219. https://doi.org/10.1177/0890117119896122c
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2024/04/2024-Standards-Combined-Version-4.11.2024.pdf
Day-Vines, N. L., Bryan, J., and Griffin, D. (2013). The Broaching Attitudes and Behavior Survey (BABS): An exploratory assessment of its dimensionality. Journal of Multicultural Counseling and Development, 41(4), 210–223. https://doi.org/10.1002/j.2161-1912.2013.00037.x
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., & Gubara, S. (2021). Strategies for broaching the subjects of race, ethnicity, and culture. Journal of Counseling & Development, 99(3), 348–357. https://doi.org/10.1002/jcad.12380
Day-Vines, N. L., Cluxton-Keller, F., Agorsor, C., Gubara, S., & Otabil, N. A. A. (2020). The multidimensional model of broaching behavior. Journal of Counseling & Development, 98(1), 107–118. https://doi.org/10.1002/jcad.12304
Day-Vines, N. L., Zhang, J., Cluxton-Keller, F., Hicks, D., Jones, C., Spann, R. T., Daga, D., & Agorsor, C. (2024). The development and validation of an instrument to examine clients’ perspectives about their counselors’ ability to broach racial, ethnic, and cultural concerns. Journal of Multicultural Counseling and Development, 52(3), 173–188. https://doi.org/10.1002/jmcd.12300
Depauw, H., Van Hiel, A., Talal, H., Dierckx, K., Geenen, F., Valcke, B., & De Clercq, B. (2025). The development of the Broaching Assessment Scale: A client-rated measure of therapists’ broaching behaviour in clinical counselling. Psychotherapy Research, 35(3), 424–440. https://doi.org/10.1080/10503307.2024.2301948
Dolan, N., Simmonds-Buckley, M., Kellett, S., Siddell, E., & Delgadillo, J. (2021). Effectiveness of stress control large group psychoeducation for anxiety and depression: Systematic review and meta-analysis. British Journal of Clinical Psychology, 60(3), 375–399. https://doi.org/10.1111/bjc.12288
Drinane, J. M., Owen, J., & Tao, K. W. (2018). Cultural concealment and therapy outcomes. Journal of Counseling Psychology, 65(2), 239–246. https://doi.org/10.1037/cou0000246
Gantt-Howrey, A., Lin, M., Shaikh, A., Johnson, K. F., Preston, J. W., & Wilson, L. (2024). Assessing social determinants of mental health: Client experiences and counselor practices. Journal of Counseling & Development, 102(4), 394–405. https://doi.org/10.1002/jcad.12519
Garg, A., Butz, A. M., Dworkin, P. H., Lewis, R. A., Thompson, R. E., & Serwint, J. R. (2007). Improving the management of family psychosocial problems at low-income children’s well-child care visits: The WE CARE Project. Pediatrics, 120(3), 547–558. https://doi.org/10.1542/peds.2007-0398
Goode, J., Park, J., Parkin, S., Tompkins, K. A., & Swift, J. K. (2017). A collaborative approach to psychotherapy termination. Psychotherapy, 54(1), 10–14. https://doi.org/10.1037/pst0000085
Johnson, K. F. (2023). Development and initial validation of the Addressing Client Needs with Social Determinants of Health Scale (ACN: SDH). BMC Health Services Research, 23(1), 374. https://doi.org/10.1186/s12913-023-09292-z
Johnson, K. F., & Brookover, D. L. (2021). School counselors’ knowledge, actions, and recommendations for addressing social determinants of health with students, families, and in communities. Professional School Counseling, 25(1). https://doi.org/10.1177/2156759X20985847
Johnson, K. F., Cunningham, P. D., Tirado, C., Moreno, O., Gillespie, N. N., Duyile, B., Hughes, D. C., Scott, E. G., & Brookover, D. (2023). Social determinants of mental health considerations for counseling children and adolescents. Journal of Child and Adolescent Counseling, 9(1), 21–33. https://doi.org/10.1080/23727810.2023.2169223
Johnson, K. F., Gantt-Howrey, A., Duyile, B. E., Robins, L. B., & Dockery, N. (2024). Career counselors addressing social determinants of mental health in rural communities. The Professional Counselor, 14(1), 1–14. https://doi.org/10.15241/kfj.14.1.1
Johnson, K., & Robins, L. B. (2021). Counselor educators experiences and techniques teaching about social-health inequities. Journal of Counselor Preparation and Supervision, 14(4). https://research.library.kutztown.edu/jcps/vol14/iss4/ 7
King, K. M., & Borders, L. D. (2019). An experimental investigation of White counselors broaching race and racism. Journal of Counseling & Development, 97(4), 341–351. https://doi.org/10.1002/jcad.12283
Knox, S., Adrians, N., Everson, E., Hess, S., Hill, C., & Crook-Lyon, R. (2011). Clients’ perspectives on therapy termination. Psychotherapy Research, 21(2), 154–167. https://doi.org/10.1080/10503307.2010.534509
Lee, P.-S., Wang, L.-F., & Swift, J. K. (2023). Clients’ and counselors’ termination decisions and experiences in counseling. Current Psychology, 42, 3734–3744. https://doi.org/10.1007/s12144-021-01725-4
Lenz, A. S., & Lemberger-Truelove, M. E. (2023). The social determinants of mental health and professional counseling: A call to action. Journal of Counseling & Development, 101(4), 375–380. https://doi.org/10.1002/jcad.12489
Lenz, A. S., & Litam, S. D. A. (2023). Integrating the social determinants of mental health into case conceptualization and treatment planning. Journal of Counseling & Development, 101(4), 416–428. https://doi.org/10.1002/jcad.12487
Lund, C., Brooke-Sumner, C., Baingana, F., Baron, E. C., Breuer, E., Chandra, P., Haushofer, J., Herrman, H., Jordans, M., Kieling, C., Medina-Mora, M. E., Morgan, E., Omigbodun, O., Tol, W., Patel, V., & Saxena, S. (2018). Social determinants of mental disorders and the sustainable development goals: A systematic review of reviews. The Lancet Psychiatry, 5(4), 357–369. https://doi.org/10.1016/S2215-0366(18)30060-9
Luo, H., Li, Y. L., Luo, X. J., Xia, L., Xiao, J., Xiao, H., & Chen, J. (2025). The efficacy of psychoeducation-based programs on internalized stigma in patients with schizophrenia: A systematic review and meta-analysis. Psychiatry Research, 350, 116540. https://doi.org/10.1016/j.psychres.2025.116540
Mason, S., Ragan, M., Gilbert, S. H., & Lenz, A. S. (2023). Social determinants of mental health: Implications for measurement, research, and evaluation. Journal of Counseling & Development, 101(4), 440–448. https://doi.org/10.1002/jcad.12490
Neal Keith, S., Coleman, M. L., Hicks Becton, L. Y., & Springfield, J. (2023). Assessing the social determinants of mental health in counseling practice. Journal of Counseling & Development, 101(4), 381–391. https://doi.org/10.1002/jcad.12470
Newton, C., & Steele, J. M. (2025). The broaching readiness framework: A path for psychologists to embrace cultural opportunities. Counselling Psychology Quarterly, 38(4), 1135–1152. https://doi.org/10.1080/09515070.2025.2458034
Office of Disease Prevention and Health Promotion. (2025). Social determinants of health. https://odphp.health.gov/healthypeople/objectives-and-data/social-determinants-health
Owen, J., Tao, K. W., Imel, Z. E., Wampold, B. E., & Rodolfa, E. (2014). Addressing racial and ethnic microaggressions in therapy. Professional Psychology: Research and Practice, 45(4), 283–290. https://doi.org/10.1037/a0037420
Pester, D. A., Jones, L. K., & Talib, Z. (2023). Social determinants of mental health: Informing counseling practice and professional identity. Journal of Counseling & Development, 101(4), 392–401. https://doi.org/10.1002/jcad.12473
Pester Boyd, D. A., Hays, D. G., & Jones, L. K. (2025). Assessing and addressing social determinants of mental health in counseling: A grounded theory investigation. Journal of Counseling & Development, 103(4), 469–483. https://doi.org/10.1002/jcad.70003
PRAPARE. (2022). Protocol for responding to and assessing patient assets, risks, and experiences: Implementation and action toolkit. https://prapare.org/wp-content/uploads/2022/09/Full-Toolkit_June-2022_Final.pdf
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Roberts, T., Esponda, G. M., Torre, C., Pillai, P., Cohen, A., & Burgess, R. A. (2022). Reconceptualising the treatment gap for common mental disorders: A fork in the road for global mental health? The British Journal of Psychiatry, 221(3), 553–557. https://doi.org/10.1192/bjp.2021.221
Robins, L. B., Johnson, K. F., Duyile, B., Gantt-Howrey, A., Dockery, N., Robins, S. D., & Wheeler, N. (2022). Family counselors addressing social determinants of mental health in underserved communities. The Family Journal, 31(2), 213–221. https://doi.org/10.1177/10664807221132799
U.S. Department of Health and Human Services. (2023). Our epidemic of loneliness and isolation: The U.S. Surgeon General’s advisory on the healing effects of social connection and community. https://www.hhs.gov/sites/default/files/surgeon-general-social-connection-advisory.pdf
Vasquez, M. J. T., Bingham, R. P., & Barnett, J. E. (2008). Psychotherapy termination: Clinical and ethical responsibilities. Journal of Clinical Psychology, 64(5), 653–665. https://doi.org/10.1002/jclp.20478
World Health Organization. (2025). Social determinants of health. https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1
Zhang, N., & Burkard, A. W. (2008). Client and counselor discussions of racial and ethnic differences in counseling: An exploratory investigation. Journal of Multicultural Counseling and Development, 36(2), 77–87. https://doi.org/10.1002/j.2161-1912.2008.tb00072.x
Danielle Pester Boyd, PhD, NCC, LPC (TX), RPT, is an assistant professor at Auburn University. Laura K. Jones, PhD, is an associate professor at the University of North Carolina at Asheville. Courtney Maier, MEd, NCC, APC, is a doctoral student at Auburn University. Danica G. Hays, PhD, is a dean and professor at the University of Nevada Las Vegas. Correspondence may be addressed to Danielle Pester Boyd, 345 West Samford Avenue, Suite 3188, Auburn, AL 36849, danielle.boyd@auburn.edu.
Aug 26, 2025 | Volume 15 - Issue 3
Julie C. Hill, Toni Saia, Marcus Weathers, Jr.
Ableism is often neglected in conversations about oppression and intersectionality within counselor education programs. It is vital to expand our understanding of disability as a social construct shaped by power and oppression, not a medical issue defined by diagnosis. This article is a call to action to combat ableism in counselor education. Actionable recommendations include: (a) encouraging professionals to define and discuss ableism; (b) including disability representation in course materials; (c) engaging in conversations about disability with students; (d) collaborating with, responding to, and supporting disabled people and communities; and (e) reflecting on personal biases to help dismantle ableism within counselor education. Implications for counselor educators highlight the ongoing need for more ableism content within the profession.
Keywords: ableism, disability, counselor education, representation, biases
Disability is rarely examined through intersectionality and critical consciousness, despite its deep connections to race, class, gender, and other social identities (Berne et al., 2018). As the United States becomes increasingly diverse, the need for counselors who can competently address the complex, intersecting needs of disabled people has never been more urgent (Dollarhide et al., 2020). Disabled people are the largest and fastest-growing minority group, with approximately 60 million people reporting some form of disability (Elflein, 2024). Despite this increasing prevalence, ableism, known as the systemic discrimination and exclusion of disabled people, remains persistent in our society. Slesaransky-Poe and García (2014) further discuss ableism as the belief that disability makes someone less deserving of many things, including respect, education, and access within the community.
Ableism and ableist beliefs have profoundly shaped how society perceives and interprets the disability experience. Historically, the medical model has framed disability as an inherent defect within the individual, requiring treatment, rehabilitation, or correction to restore “normal” functioning (Leonardi et al., 2006). This deficit-based perspective, reinforced by legal definitions, has shaped societal attitudes and policies, often prioritizing intervention over community integration. In contrast, the social model of disability shifts the focus from the individual to the broader societal structures, emphasizing how inaccessible environments, exclusionary policies, and ableist attitudes create disabling conditions (Bunbury, 2019; Friedman & Owen, 2017; Shakespeare, 2006). This model asserts that disability is not simply a medical issue, but a social justice concern requiring systemic change to remove barriers and promote full participation. Within counselor education programs, the biopsychosocial model is often taught as a more integrative framework that acknowledges disability as a complex interplay of biological, psychological, and social factors. Although medical interventions may be necessary for some individuals, this model emphasizes addressing environmental and attitudinal barriers contributing to marginalization. By adopting this holistic approach, counselors can better advocate for equity, inclusion, and meaningful accessibility for all.
This article provides an asset-based framework that views disability as a valuable aspect of diversity rather than a deficit or limitation. This approach recognizes the strengths, perspectives, and contributions that disabled people bring to communities and educational spaces (Olkin, 2002; Perrin, 2019). By embracing disability as an aspect of diversity, this framework challenges societal norms rooted in ableism, which often prioritize conformity and cure over anti-ableism (Bogart & Dunn, 2019). Through this lens of power and oppression, disability is celebrated as a source of innovation, creativity, and cultural richness, encouraging practices that empower disabled individuals to thrive both in the classroom and in the community. To reinforce this shift in thinking to disability as an asset, we use identity-first language, recognizing that many disabled people prefer it as a positive affirmation of their lived experiences and their connection to the disability community (Sharif et al., 2022; Taboas et al., 2023).
Intersectionality and Disability
Scholars recognize intersectionality as an analytical tool to investigate how multiple systems of oppression interact with an individual’s social identities, creating complex social inequities and unique experiences of oppression and privilege for individuals with multiple marginalized identities (Collins & Bilge, 2020; Crenshaw, 1989; Grzanka, 2020; Moradi & Grzanka, 2017; Shin et al., 2017). The topic of disability is often absent in conversations regarding power, oppression, and privilege (Ben-Moshe & Magaña, 2014; Erevelles & Minear, 2010; Frederick & Shifrer, 2018; Mueller et al., 2019; Wolbring & Nasir, 2024) despite the potential for disability to intersect with other marginalized identities (e.g., racial/ethnic identity, gender identity, socioeconomic status, religious and spiritual beliefs, citizenship/immigration status) that lead to intersectionality-based challenges that conflict with the marginalization of being disabled (Wolbring & Nasir, 2024). For example, Lewis and Brown (2018) condemned the lack of accountability in reporting on disability, race, and police violence, which often irresponsibly neglects the coexistence of disability in conversations of experienced violence. Using the framework of intersectionality responsibly in disability discourse within counselor education holds significant potential for the professional development of counselors to work toward unmasking and dismantling ableism.
Challenges and Gaps in Anti-Ableism in Counselor Education and Training
How counselor educators teach about disability is crucial to dismantling ableism, yet history reveals a troubling lack of cultural humility in educational approaches. Cultural humility is a process-oriented approach that continuously emphasizes the counselor’s openness to learn about a client’s culture and invites counselors to consistently incorporate self-reflective activities to enhance their self-awareness (Mosher et al., 2017). Although cultural humility may be well intended, it may also have a harmful impact and fall flat if inherent biases go unrecognized. For example, counselor educators heavily relied on simulation exercises to address disability in the classroom (e.g., having students blindfold themselves for an activity to simulate blindness or having them sit in a wheelchair for a short period). Simulation exercises reinforce a deeply medicalized and reductive view of disability, one rooted in fear, pity, and misconception, ultimately erasing disability as both a culture and an identity (Öksüz & Brubaker, 2020; Shakespeare & Kleine, 2013). Beatrice Wright (1980, as cited in Herbert, 2000), cautioned that simulation experiences evoke fear, aversion, and guilt. These exercises rarely foster meaningful or constructive perspectives on disability. Instead of deepening understanding, these exercises risk reinforcing harmful stereotypes, further marginalizing disabled individuals rather than empowering them. Instead of disability simulations, honor the voices and experiences of disabled individuals through their narratives, such as Being Heumann by Judy Heumann, as well as documentaries and movies like Crip Camp, Patrice, or CODA. Contact with disabled individuals has been shown to reduce stigma against disabled people (Feldner et al., 2022; Smith et al., 2011). Additionally, incorporate analyzing ableism through case studies, readings, or media, followed by a structured discussion.
Topics of multiculturalism and diversity have increased over the years; the same cannot be said for disability (Rivas, 2020). Davis (2011) poignantly asked, “Is this simply neglect, or is there something inherent in the way diversity is considered that makes it impossible to recognize disability as a valid human identity?” (p. 4). More than a decade later, this question remains painfully relevant. Atkins et al. (2023) explored this issue through a study using the Counseling Clients with Disabilities Scale to evaluate professionals’ attitudes, competencies, and preparedness when working with disabled clients. The findings underscore the critical need for education and exposure to disability-related topics in counselor training, demonstrating that such efforts improve competency, reduce biases, and foster more inclusive, equitable, and empowering support. However, disability continues to receive significantly less attention than other cultural and identity groups in professional training and discourse (Deroche et al., 2020).
Furthermore, ableist microaggressions continue to be a concern for disabled individuals. Cook and colleagues (2024) conducted a study looking at microaggressions experienced by disabled individuals and found four categories of microaggressions: minimization, denial of personhood, otherization, and helplessness. They also found that experiencing ableist microaggressions affected participants’ mental health and wellness. Additionally, they found that those with visible disabilities were more likely to experience ableist microaggressions than those with invisible disabilities. Given these findings, counselor educators need to be aware that ableist microaggressions exist, what those microaggressions may sound like, and how they impact disabled clients.
Concerns exist about the extent to which counselor education programs cover disability content; there is also a need to examine instructors’ preparedness for covering such content. In a survey of counselor educators in programs accredited by the Council for the Accreditation of Counseling and Related Educational Programs (CACREP), 36% of the faculty surveyed believed their program was ineffective at addressing disability topics and that programs did not address disability and ableism to the extent necessary to produce competent professionals. Only 10.6% felt their program to be “very effective” in this content area, with the belief that their students were only somewhat prepared to work with disabled people (Feather & Carlson, 2019). Notably, these oversights in education translate into inadequacy in practice. A sample of mental health professionals who all reported working with disabled clients indicated the least amount of perceived disability competence in skills, the second least competence in knowledge, and the most competence in awareness (Strike et al., 2004). Faculty self-assessment of their ability to teach disability-related content was strongly linked to their prior work or personal experience with disability. This highlights the importance of integrating exposure to and training on disability-related concepts throughout core areas (Pierce, 2024). Although separated by a decade, these studies can be tied to a unifying, persistent issue: the lack of disability competence in counseling and counselor education spaces.
The 2024 CACREP standards call for an infusion of disability competencies into counseling curricula (CACREP, 2023), meaning that counselor educators and counselors-in-training must reimagine the available literature to provide adequate professional development and growth. Pierce (2024) advised that disability competence areas be focused on the following topics: accessibility, able privilege, disability culture, and disability justice. We must seek to dismantle ableism by infusing disability into curricula in an authentic manner that highlights the societal values and attitudes in which multiple forms of oppression work in tandem to create unique, intersectional experiences for disabled people.
Training Recommendations for Counselor Education Programs
The authors aim to ensure counselor educators have tangible strategies to dismantle ableism and teach their students to do the same. Counselor educators and counselors-in-training must look inward and rid themselves of negative attitudes and biases to eradicate ableism. Part of this process includes the critical skill of self-reflection and examining and understanding biased and ableist beliefs held by individuals and perpetuated by society. Until that happens, counselors will continue to do a disservice to disabled people (Friedman, 2023). For students who have never interacted with disabled people or thought about ableism, these conversations and strategies have the very real possibility of making them uncomfortable. Discomfort is okay. Disabled people often feel awkward or out of place every day because of ableism. It is not our job as counselor educators to make students comfortable; it is our job to make them competent, informed, and ethical professionals.
The following are five tangible strategies to thoughtfully and intentionally dismantle ableism. These strategies are purposefully broad and aim to expose counseling professionals and those in training to an intersectional perspective of disability that acknowledges disability as a valid aspect of diversity, identity, and culture. Rather than siloing these discussions to disability-related training, these strategies belong in all settings within counseling. Counseling professionals must include ableism in the conversations happening in places where they learn and work to shift the way they think, view, respond to, and construct disability. To begin, counselor education programs should consider hosting a workshop or seminar focused on ableism by disabled people to ensure that all students and faculty are on the same page and are using the same terminology. Once this has been established, ableism and disability content and knowledge should be incorporated into lectures, assignments, discussions, and exams across the counselor education curriculum. Further information on this integration is described in the first strategy below.
Define Ableism
One of the factors that further perpetuates ableism is the lack of clarity on what ableism is and how it intersects with other forms of oppression. Counselor educators must share definitions of ableism that center on the perspective of the disabled community. Talia Lewis (2022) provided a working definition of ableism that disabled Black/negatively racialized communities developed:
A system of assigning value to people’s bodies and minds based on societally constructed ideas of normalcy, productivity, desirability, intelligence, excellence, and fitness. These constructed ideas are deeply rooted in eugenics, anti-Blackness, misogyny, colonialism, imperialism, and capitalism. This systemic oppression leads to people and society determining people’s value based on their culture, age, language, appearance, religion, birth or living place, “health/wellness,” and/or their ability to satisfactorily re/produce, “excel,” and “behave.” You do not have to be disabled to experience ableism. (para. 4–6)
This definition expands on the definition provided earlier of ableism as the systemic discrimination and exclusion of disabled people. It rejects the notion that ableism can be dismantled or separated from other forms of oppression (e.g., racism, sexism, and other systems of oppression). Within counseling curricula, we often use the term intersectionality, but it is impossible to address intersectionality with our students if we do not thoughtfully include ableism. We should challenge the idea that disability is a monolithic experience as we seek to build a more complex, interconnected, and whole understanding of disability (Mingus, 2011).
It is also essential to acknowledge internalized ableism, which is ableism directed inward when a disabled person consciously or unconsciously believes in the harmful messages they hear about disability. They project negative feelings onto themselves. They start to believe and internalize the message that society labels disability as inferior. They begin to accept the stereotypes. Internalized ableism occurs when individuals are so heavily influenced by stereotypes, misconceptions, and discrimination against disabled people that they start to think that their disabilities make them inferior (Presutti, 2021). For example, a disabled student may not participate in class because they believe their contributions are inferior compared to their nondisabled peers, or a disabled client may experience feeling undeserving, undesirable, and burdensome.
To effectively implement this awareness, ask students to define ableism in their own words. Coming up with their definition of ableism encourages critical thinking and allows the counselor educator to gauge students’ existing understanding. Then, introduce the Lewis (2022) definitions above to provide a more comprehensive framework. To reinforce these concepts, incorporate case studies illustrating real-world examples of ableism. Analyzing these cases in class discussions or group activities will help students identify ableist structures, challenge assumptions, and explore solutions for creating more welcoming environments. Counselors can examine ableism in societal contexts by viewing movies or television shows that feature disabled characters and analyzing how ableism is portrayed in media. Because of societal barriers to access and the taboos surrounding discussions of disability, the entertainment and news media serve as a key source for many people to form opinions about disability and disabled individuals. Unfortunately, these portrayals are limited and often spread misinformation and harmful stereotypes (Pierce, 2024). One way to help combat this could be by watching a movie or show together as a class and then having a discussion or having students watch on their own and write a short reflection followed by a class discussion. Some suggested movies include Crip Camp, Murderball, The Temple Grandin Story, Patrice, and Out of My Mind. Some suggested television shows include Speechless, Love on the Spectrum, Special, Raising Dion, Atypical, and The Healing Powers of Dude.
Include Disability Representation in Course Content
The phrase “representation matters” also applies to disability. Counselor educators should include disability and discussions of the impact of systemic ableism throughout course content, not only in a single lecture or reading on the course syllabus. Decisions about course content send powerful messages about what the counselor educator, the program, and the broader counseling profession prioritize and value. Including or excluding specific topics reflects the educator’s perspective and shapes future counselors’ professional identity and competencies. When disability is overlooked or inadequately addressed, it signals to students that it is not a central concern in counseling practice, which reinforces systemic gaps in knowledge, awareness, and advocacy. To counter this erasure and to ensure meaningful representation, intentionally incorporate guest speakers, videos, readings, memoirs, and research that center on the perspectives of disabled people. This gives students an authentic and multifaceted understanding of disability beyond theoretical discussions. Consider integrating a book or memoir that centers a disabled perspective alongside the course textbook to bridge the gap between academic content and real-life experiences. This approach not only deepens students’ engagement but also challenges ableist assumptions by highlighting the lived realities, resilience, and contributions of disabled people.
Engage in Conversation About Disability With Students
Disability is not a bad word. Counselor educators must instill this simple yet profound truth in students. Euphemisms like differently abled, handicapable, or special needs perpetuate ableism when used in place of the term disability, implying that disability is something shameful or in need of softening; they do more harm than good. Counselor educators must allow students the opportunity to engage in discussion about disability to challenge the idea that disability is taboo and move into a space where students can appreciate that disability is a natural part of life. Counselor educators must foster a safe and supportive learning community that allows students to engage in dialogue and discussion about their beliefs and experiences that have shaped their beliefs, and examine how those beliefs led to the development or perpetuation of ableist ideas and microaggressions. This allows students to learn, grow, and reshape their beliefs and understanding together. This quote sums it up best: “Disabled people are reclaiming our identities, our community, and our pride. We will no longer accept euphemisms that fracture our sense of unity as a culture: #SaytheWord” (Andrews et al., 2019, p. 6). To empower students to #SayTheWord in both classroom discussions and professional practice, dedicate time, especially during the first weeks of class, to explicitly affirm that disability is not a bad word. Normalize its use by providing historical context, sharing first-person perspectives, and emphasizing the importance of language in shaping attitudes. By reinforcing disability as an act of recognition rather than avoidance, you help students develop confidence in using identity-affirming language and challenging the stigma often associated with the term.
Collaborate, Respond, and Support Disabled People
Counselor educators, counselors, and counselors-in-training should seek opportunities to listen to, respond to, support, and collaborate with disabled counselors and other disabled scholars. Thoughtful collaborations allow for authentic exposure and conversation that support the unlearning of ableist beliefs. This approach is consistent with the disability rights mantra “nothing about us without us” (Charlton, 1998, p. 3), which implies that no change can occur without the direct input of disabled individuals. One opportunity for collaboration includes professional conferences and attending presentations by disabled academics and professionals. Other opportunities for collaboration include working with and supporting local disabled business owners and seeking out organizations such as independent living centers to bring in disabled speakers to share their lived experience and interactions with ableism and microaggressions. Be sure to compensate these individuals for their time so that the work of collaboration is mutually beneficial to all parties.
Disabled people are the experts of their experiences, not professionals. This statement is not synonymous with implementing a client-centered or person-centered approach. Instead, the focus of this statement is to make sure counselors have the tools to trust, support, uplift, and dismantle ableism with disabled clients. If it starts in the classroom, counselors-in-training will be better prepared in practice and life outside of work. As professionals know, trust in the counselor-client relationship is essential for the disabled community. It often develops when individuals feel heard, trusted, and validated, rather than being second-guessed or minimized, especially as they share about the external and internal ableism they face daily. Lund (2022) recommended consulting with both disabled psychologists and trainees to bring a “critical insider-professional perspective” (p. 582) to the profession. By consulting and bringing these disabled professionals in for training or speaking about personal experiences, we can ensure that disabled voices are heard and recognized.
Another way to amplify disabled voices is through the teaching of disability justice. The Disability Justice framework affirms that every person’s body holds inherent value, power, and uniqueness. It recognizes that identity is shaped by the interconnected influences of ability, race, gender, sexuality, class, nationality, religion, and other factors. It stresses the importance of viewing these influences together rather than separately. From this perspective, the fight for a just society must be grounded in these intertwined identities while also acknowledging Berne et al.’s (2018) critical insight that the current global system is “incompatible with life” (para. 13). Central principles of disability justice, such as centering leadership by those most impacted, fostering interdependence, ensuring collective access, building cross-disability solidarity, and pursuing collective liberation, prioritize intersectionality and cross-movement collaboration to guarantee that no one is excluded or left behind. (Pierce, 2024).
Helping students understand and internalize these ideas and principles should lead to the development of more aware and anti-ableist counselors in several ways. Rather than viewing client struggles as isolated or purely personal issues, understand that many forms of suffering, especially those faced by disabled people and people with intersecting marginalized identities, are rooted in larger social, economic, and political systems that devalue certain lives. For example, ableism, racism, and capitalism often create conditions that threaten people’s survival, whether through limited access to health care, environmental injustice, or social exclusion.
Counselors-in-training should be attuned to how multiple aspects of identity (such as disability, race, gender, and class) interact to shape each client’s lived experience. This approach moves counseling away from a one-size-fits-all perspective and helps address the unique, layered barriers that clients face. Traditional counseling and counselor preparation often focus on assisting clients to adapt to oppressive systems. The Disability Justice perspective instead calls for counselors-in-training to see their role as also advocating for systemic change, working toward environments and policies that are actually supportive of all people’s well-being. Rather than idealizing independence, disability justice values interdependence and community care. Counselors and counselors-in-training can foster this by helping clients build supportive networks and by modeling collaborative, relational approaches in practice.
Regularly Reflect on Personal Biases and Be Open to Feedback
Counselor educators often ask counselors-in-training to reflect on their own biases in terms of race, gender, and sexual orientation. However, ableism and disability are often forgotten or left out of those conversations. It is essential for these conversations about bias to include disability so that everyone has opportunities to explore and discuss their own potential biases. Embedding disability representation in the classroom allows everyone to see how they respond to disabled people, especially when that representation is in the form of case studies and client role-play. Then, everyone, including supervisors, can constructively receive feedback from a trusted figure and can change or improve their reactions and responses if necessary. Furthermore, counselor educators and counselors-in-training can keep reflective journals, seek supervision or peer discussions, and review case notes with an anti-ableist lens, which can help identify areas for growth. Additionally, counselor educators should actively solicit feedback from the disability community, welcoming their perspectives without defensiveness. When possible, attend training led by disabled professionals and the disabled community to reinforce a commitment to continuous learning and accountability.
Implications for Counselor Educators
Counselor educators are responsible for training counselors to work with all types of clients, including disabled clients. Counselors will encounter disabled clients, no matter the setting that they are working in. Disability can impact anyone and does not discriminate across gender, race, socioeconomic status, sexual orientation, or geographic location. Disability is the one minority group that anyone can become a part of at any time in their life. Most people will age into disability as they get older (Shapiro, 1994). Counselor educators need to be sure that counselors are confronting and dismantling their own ableism and ableist beliefs and that they understand that they may need to assist clients in processing their own experiences with ableism in society and interactions with others. One self-assessment for self-reflection and insight is the Systematic Ableism Scale (SAS; Friedman, 2023). The SAS has four underlying themes: individualism, recognition of continuing discrimination, empathy for disabled people, and excessive demands. The SAS is a tool that can be used to help understand how contradicting disability ideologies manifest in modern society to determine how best to counteract them. By using this assessment as a self-evaluation tool, both students and counselor educators can identify where their beliefs may be problematic or ableist and then set goals to address and improve in those areas.
We recommend that counselors intentionally occupy spaces where discussions on disability advocacy are occurring. Universities are often regarded as a primary source of knowledge production, but a common misconception is that the people themselves produce the knowledge. The reality is that not all disability content is produced by disabled individuals or organizations. Thus, we encourage counselor educators to expand access to knowledge about disability by seeking spaces outside the institution that share insider perspectives on the disability experience and organizations dedicated to empowering disabled communities. This may involve engaging with informal educational organizations such as Sins Invalid, AXIS Dance Company, and Krip Hop Nation or getting involved with formal professional organizations such as APA Division 22, the American Rehabilitation Counseling Association, or the National Rehabilitation Counseling Association. Some strategies that can be used to advocate for and in support of disabled clients include client-centered advocacy, understanding disability as a cultural identity, and building knowledge of the disability rights movement, ableism, and intersectionality, as well as integrating disability-inclusive language, avoiding ableist assumptions, and incorporating clients’ lived experiences into treatment (Chapin et al., 2018; Smart, 2015; Smith et al., 2011).
The foundation for a competent and qualified counselor begins with their training. This training can be formal education or ongoing professional development. For those responsible for educating counselors-in-training, laying the foundation for anti-ableism practices begins in the classroom. A universal design for learning (UDL) framework, developed by the Center for Applied Special Technology (CAST, 2018), aims to create accessible material and inclusive environments that are usable for all people by intentionally incorporating multiple representations of content to enhance student expression of learning and increase a variety of opportunities for engagement with the learning environment (Black et al., 2015; Dolmage, 2017; Fornauf & Erickson, 2020). UDL principles support anti-ableist practice by encouraging an ongoing partnership between students and instructors that facilitates consistent and practical feedback to promote student belongingness (Hennessey & Koch, 2007; Oswald et al., 2018). Promoting belonging and acceptance in counselor education programs requires intentional strategies that foster inclusivity, respect for diversity, and a strong sense of community. Effective techniques include: 1) Use inclusive curriculum design. Integrate diverse perspectives throughout the curriculum, with special attention paid to marginalized voices, such as disabled voices. 2) Use culturally responsive pedagogy. This includes employing a range of instructional methods to cater to diverse learning styles. Use trauma-informed practices by creating a learning environment that is sensitive to trauma, both past and present. 3) Implement community-building activities such as structuring programs around cohorts and encouraging the formation of affinity groups and peer support groups. 4) Encourage active dialogue and reflection around tough conversations such as diversity, ableism, inequality, and marginalization. This can be done both in person and online via discussion boards. Faculty can also encourage students to explore their thoughts, reflections, and experiences around issues of identity, belonging, and ableism in a reflective journal. 5) Collect feedback to guide continuous improvement. Faculty can assess students’ experiences with inclusion and ableism through climate surveys.
Additionally, the adoption of multiple methods for delivering information in alternate formats and continuous assessment of student progress reduces barriers to student engagement and expression in the learning environment, which in turn systematically challenges normative ableist practice that values a one-size-fits-all perspective that often neglects disabled thought and existence in pedagogical practices (Oswald et al., 2018). UDL strategies to disrupt ableist thought and practices may include using closed captioning on visual multimedia content (e.g., videos, PowerPoint presentations), incorporating movement breaks, creating interactive activities (e.g., role-play activities, gamification, debates on critical topics), and receiving feedback on instruction.
Hill and Delgado (2023) discussed the importance of including disability coursework and content across multiple domains to effectively address ableism in counselor education programs. Building upon their work, we suggest that the following key types of coursework and content be included. At a minimum, disability content should be integrated into the core CACREP curriculum areas: professional counseling orientation and ethical practice, social and cultural foundations, lifespan development, career development, counseling practice, group counseling, assessment and diagnosis, and research and program evaluation (CACREP, 2023).
Foundational Disability Studies
Students should explore and understand how ableism developed and its systemic nature, especially in the current political climate (Campbell, 2009; Dolmage, 2017). Additionally, students can learn about models of disability: medical, sociopolitical, functional, religious, moral, and biopsychosocial (Engel, 1977; Shakespeare, 2006; Smart, 2015). Students must also understand the concept of intersectionality, which examines how disability interacts with race, gender, sexuality, and socioeconomic status (Erevelles & Minear, 2010; Garland-Thompson, 2005).
Ethics and Multicultural Competence
Students should understand the intersection of disability and ethics by being able to apply the ACA Code of Ethics to disability issues (Chapin et al., 2018; Feather & Carlson, 2019). In either an ethics class or a multicultural class, students must learn about crucial disability-related legislation, such as the Rehabilitation Act of 1973, the Americans with Disabilities Act, the Individuals with Disabilities Education Act, and the Workforce Innovation and Opportunity Act. In the multicultural class, students need to understand disability cultural competence and receive training on disability as a cultural identity and recognizing ableism as a form of oppression (Feldner et al., 2022; Smith et al., 2011). Additionally, in the multicultural class, students should be taught about biases and microaggressions, as well as how to identify and address ableist language and behavior.
Counseling Skills and Practice
In a counseling skills class, students must learn accessible counseling techniques, such as modifying approaches for different abilities (e.g., sensory, cognitive, mobility). Students should also be presented with case studies involving disabled clients, with an emphasis on strengths-based and person-centered approaches. Additionally, students ought to receive supervision and advocacy training on how to support and advocate for clients with disabilities in clinical settings. Counselor educators can use the strategies listed here in the classroom and in practice.
Directions for Future Research
Two of the three authors of this article are disabled and bring lived experience to their teaching, writing, research, and engagement with the nondisabled world. This real-world experience informs the strategies presented and has been applied in both classroom and professional settings. However, these approaches have not yet been empirically tested through formal research. Future research could focus on empirically validating these strategies through qualitative or quantitative studies, particularly in evaluating confidence when working with disabled clients before and after implementing these strategies. Strategies include incorporating disability knowledge into the counselor education curriculum coursework (Hill & Delgado, 2023), using critical pedagogy and disability justice frameworks when teaching (Dolmage, 2017; Erevelles & Minear, 2010), providing experiential learning and opportunities for contact with disabled individuals (Smith et al., 2011), giving disability-related education and training for faculty and supervisors (Feldner et al., 2022), and encouraging the development of allyship and advocacy skills (Feldner et al., 2022; Goodman et al., 2004). Additional studies are also needed to examine ableism and confidence in teaching anti-ableist concepts and disability-related competencies by counselor educators. Finally, scales or measures to assess ableism, specifically in counselor education, could be created and validated.
Conclusion
These strategies do not aim to be an all-encompassing, definitive, or exhaustive checklist, as there are many ways to dismantle ableism. These strategies are a starting point, a reminder, a point of reflection, or an opportunity to affirm current strategies. Significantly, these strategies extend beyond counseling and are relevant across various educational and professional settings, from K–12 classrooms to higher education, social work, health care, and beyond. Wherever you land, we invite you to continue learning, growing, and committing to change with us. Alice Wong (2020) proclaimed, “There is so much that able-bodied people could learn from the wisdom that often comes with disability. However, space needs to be made. Hands need to reach out. People need to be lifted up” (p. 17). Together, we can extend our hands, challenge systemic barriers, and work to dismantle ableism in counseling settings and across all aspects of society.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Andrews, E. E., Forber-Pratt, A. J., Mona, L. R., Lund, E. M., Pilarski, C. R., & Balter, R. (2019). #SaytheWord: A disability culture commentary on the erasure of “disability.” Rehabilitation Psychology, 64(2), 111–118. https://doi.org/10.1037/rep0000258
Atkins, K. M., Bell, T., Roy-White, T., & Page, M. (2023). Recognizing ableism and practicing disability humility: Conceptualizing disability across the lifespan. Adultspan Journal, 22(1). https://doi.org/10.33470/2161-0029.1151
Ben-Moshe, L., & Magaña, S. (2014). An introduction to race, gender, and disability: Intersectionality, disability studies, and families of color. Women, Gender, and Families of Color, 2(2), 105–114. https://doi.org/10.5406/womgenfamcol.2.2.0105
Berne, P., Morales, A. L., Langstaff, D., & Invalid, S. (2018). Ten principles of disability justice. Women’s Studies Quarterly, 46(1–2), 227–230. https://doi.org/10.1353/wsq.2018.0003
Black, R. D., Weinberg, L. A., & Brodwin, M. G. (2015). Universal design for learning and instruction: Perspectives of students with disabilities in higher education. Exceptionality Education International, 25(2), 1–26.
Bogart, K. R., & Dunn, D. S. (2019). Ableism special issue introduction. Journal of Social Issues, 75(3), 650–664. https://doi.org/10.1111/josi.12354
Bunbury, S. (2019). Unconscious bias and the medical model: How the social model may hold the key to transformative thinking about disability discrimination. International Journal of Discrimination and the Law, 19(1), 26–47. https://doi.org/10.1177/1358229118820742
Campbell, F. K. (2009). Contours of ableism: The production of disability and abledness. Palgrave Macmillan.
CAST. (2018). Universal design for learning guidelines version 3.0. http://udlguidelines.cast.org
Chapin, M., McCarthy, H., Shaw, L., Bradham-Cousar, M., Chapman, R., Nosek, M., Peterson, S., Yilmaz, Z., & Ysasi, N. (2018). Disability-related counseling competencies. American Rehabilitation Counseling Association. https://www.counseling.org/docs/default-source/competencies/arca-disability-related-counseling-competencies-v51519.pdf?sfvrsn=984f4bd0_1
Charlton, J. I. (1998). Nothing about us without us: Disability oppression and empowerment. California University Press.
Collins, P. H., & Bilge, S. (2020). Intersectionality (2nd ed.). Wiley.
Cook, J. M., Deroche, M. D., & Ong, L. Z. (2024). A qualitative analysis of ableist microaggressions. The Professional Counselor, 14(1), 64–82. https://doi.org/10.15241/jmc.14.1.64
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2024/04/2024-Standards-Combined-Version-4.11.2024.pdf
Crenshaw, K. (1989). Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. University of Chicago Legal Forum, 1989(1), 139–167. https://chicagounbound.uchicago.edu/cgi/viewcontent.cgi?article=1052&context=uclf
Davis, L. J. (2011, September 25). Why is disability missing from the discourse on diversity? The Chronicle of Higher Education, 25, 38–40. https://www.chronicle.com/article/why-is-disability-missing-from-the-discourse-on-diversity
Deroche, M. D., Herlihy, B., & Lyons, M. L. (2020). Counselor trainee self-perceived disability competence: Implications for training. Counselor Education and Supervision, 59(3), 187–199. https://doi.org/10.1002/ceas.12183
Dollarhide, C. T., Rogols, J. T., Garcia, G. L., Ismail, B. I., Langenfeld, M., Walker, T. L., Wolfe, T., George, K., McCord, L., & Aras, Y. (2020). Professional development in social justice: Analysis of American Counseling Association conference programming. Journal of Counseling & Development, 98(1), 41–52. https://doi.org/10.1002/jcad.12298
Dolmage, J. T. (2017). Academic ableism: Disability and higher education. University of Michigan Press. https://doi.org/10.3998/mpub.9708722
Elflein, J. (2024, November 19). Topic: Disability in the U.S. – Statistics & facts. Statista. https://www.statista.com/topics/4380/disability-in-the-us
Engel, G. L. (1977). The need for a new medical model: A challenge for biomedicine. Science, 196(4286), 129–136. https://doi.org/10.1126/science.847460
Erevelles, N., & Minear, A. (2010). Unspeakable offenses: Untangling race and disability in discourses of intersectionality. Journal of Literary & Cultural Disability Studies, 4(2), 127–145. https://doi.org/10.3828/jlcds.2010.11
Feather, K. A., & Carlson, R. G. (2019). An initial investigation of individual instructors’ self-perceived competence and incorporation of disability content into CACREP-accredited programs: Rethinking training in counselor education. Journal of Multicultural Counseling and Development, 47(1), 19–36.
https://doi.org/10.1002/jmcd.12118
Feldner, H. A., Evans, H. D., Chamblin, K., Ellis, L. M., Harniss, M. K., Lee, D., & Woiak, J. (2022). Infusing disability equity within rehabilitation education and practice: A qualitative study of lived experiences of ableism, allyship, and healthcare partnership. Frontiers in Rehabilitation Sciences, 3, 947592.
https://doi.org/10.1080/09638288.2022.9397845
Fornauf, B. S., & Erickson, J. D. (2020). Toward an inclusive pedagogy through universal design for learning in higher education: A review of the literature. Journal of Postsecondary Education and Disability, 33(2), 183–199. https://files.eric.ed.gov/fulltext/EJ1273677.pdf
Frederick, A., & Shifrer, D. (2018). Race and disability: From analogy to intersectionality. Sociology of Race and Ethnicity, 5(2), 200–214. https://doi.org/10.1177/2332649218783480
Friedman, C. (2023). Explicit and implicit: Ableism of disability professionals. Disability and Health Journal, 16(4), 101482. https://doi.org/10.1016/j.dhjo.2023.101482
Friedman, C., & Owen, A. L. (2017). Defining disability: Understandings of and attitudes towards ableism and disability. Disability Studies Quarterly, 37(1).
Garland-Thomson, R. (2005). Feminist disability studies. Signs: Journal of Women in Culture and Society, 30(2), 1557–1587. https://doi.org/10.1086/423352
Goodman, L. A., Liang, B., Helms, J. E., Latta, R. E., Sparks, E., & Weintraub, S. R. (2004). Training counseling psychologists as social justice agents: Feminist and multicultural principles in action. The Counseling Psychologist, 32(6), 793–836. https://doi.org/10.1177/0011000004268802
Grzanka, P. R. (2020). From buzzword to critical psychology: An invitation to take intersectionality seriously. Women & Therapy, 43(3–4), 244–261. https://doi.org/10.1080/02703149.2020.1729473
Hennessey, M. L., & Koch, L. (2007). Universal design for instruction in rehabilitation counselor education. Rehabilitation Research, Policy, and Education, 21(3), 187–194. https://doi.org/10.1891/088970107805059689
Herbert, J. T. (2000). Simulation as a learning method to facilitate disability awareness. Journal of Experiential Education, 23(1), 5–11. https://doi.org/10.1177/105382590002300102
Hill, J. C., & Delgado, H. (2023). Incorporating disability knowledge and content into the counselor education curriculum. ACES Teaching Practice Briefs, 21(2), 18–31. https://www.researchgate.net/publication/388758290_Incorporating_Disability_Knowledge_and_Content_into_the_Counselor_Education_Curriculum
Leonardi, M., Bickenbach, J., Ustun, T. B., Kostanjsek, N., & Chatterji, S. (2006). The definition of disability: What is in a name? The Lancet, 368(9543), 1219–1221. https://doi.org/10.1016/S0140-6736(06)69498-1
Lewis, T. A. (2022, January 1). Working definition of ableism—January 2022 update. https://www.talilalewis.com/blog/working-definition-of-ableism-january-2022-update
Lewis, T. A., & Brown, L. X. Z. (2018). Accountable reporting on disability, race & police violence: A community response to the “Ruderman Foundation paper on the media coverage of use of force and disability.” https://www.talilalewis.com/blog/archives/06-2018
Lund, E. M. (2022). Valuing the insider-professional perspective of disability: A call for rehabilitation psychologists to support disabled psychologists and trainees across the profession. Rehabilitation Psychology, 67(4), 582–586. https://doi.org/10.1037/rep0000452
Mingus, M. (2010, February 12). Changing the framework: Disability justice. Leaving Evidence. https://leavingevidence.wordpress.com/2011/02/12/changing-the-framework-disability-justice
Moradi, B., & Grzanka, P. R. (2017). Using intersectionality responsibly: Toward critical epistemology, structural analysis, and social justice activism. Journal of Counseling Psychology, 64(5), 500–513. https://doi.org/10.1037/cou0000203
Mosher, D. K., Hook, J. N., Captari, L. E., Davis, D. E., DeBlaere, C., & Owen, J. (2017). Cultural humility: A therapeutic framework for engaging diverse clients. Practice Innovations, 2(4), 221–233. https://doi.org/10.1037/pri0000055
Mueller, C. O., Forber-Pratt, A. J., & Sriken, J. (2019). Disability: Missing from the conversation of violence. Journal of Social Issues, 75(3), 707–725. https://doi.org/10.1111/josi.12339
Öksüz, E., & Brubaker, M. D. (2020). Deconstructing disability training in counseling: A critical examination and call to the profession. Journal of Counselor Leadership and Advocacy, 7(2), 163–175. https://doi.org/10.1080/2326716X.2020.1820407
Olkin, R. (2002). Could you hold the door for me? Including disability in diversity. Cultural Diversity and Ethnic Minority Psychology, 8(2), 130–137. https://doi.org/10.1037/1099-9809.8.2.130
Oswald, G. R., Adams, R. D. N., & Hiles, J. A. (2018). Universal design for learning in rehabilitation education: Meeting the needs for equal access to electronic course resources and online learning. Journal of Applied Rehabilitation Counseling, 49(1), 19–22.
Perrin, P. B. (2019). Diversity and social justice in disability: The heart and soul of rehabilitation psychology. Rehabilitation Psychology, 64(2), 105–110. https://doi.org/10.1037/rep0000278
Pierce, K. L. (2024). Bridging the gap between intentions and impact: Understanding disability culture to support disability justice. The Professional Counselor, 13(4), 486–495. https://doi.org/10.15241/klp.13.4.486
Rivas, M. (2020). Disability in counselor education: Perspectives from the United States. International Journal for the Advancement of Counselling, 42, 366–381. https://doi.org/10.1007/s10447-020-09404-y
Shakespeare, T. (2006). The social model of disability. In L. J. Davis (Ed.), The Disability Studies Reader (2nd ed.; pp. 197–204). Routledge. https://disabilitystudies.nl/sites/default/files/beeld/onderwijs/lennard_davis_the_disability_studies_reader_secbookzz-org_0.pdf
Shakespeare, T., & Kleine, I. (2013). Educating health professionals about disability: A review of interventions. Health and Social Care Education, 2(2), 20–37. https://doi.org/10.11120/hsce.2013.00026
Shapiro, J. P. (1994). No pity: People with disabilities forging a new civil rights movement. Three Rivers Press.
Sharif, A., McCall, A. L., & Bolante, K. R. (2022). Should I say “disabled people” or “people with disabilities”? Language preferences of disabled people between identity- and person-first language. ASSETS ’22: Proceedings of the 24th International ACM SIGACCESS Conference on Computers and Accessibility, 1–18. https://doi.org/10.1145/3517428.3544813
Shin, R. Q., Welch, J. C., Kaya, A. E., Yeung, J. G., Obana, C., Sharma, R., Vernay, C. N., & Yee, S. (2017). The intersectionality framework and identity intersections in the Journal of Counseling Psychology and The Counseling Psychologist: A content analysis. Journal of Counseling Psychology, 64(5), 458–474. https://doi.org/10.1037/cou0000204
Slesaransky-Poe, G., & García, A. M. (2014). The social construction of difference. In D. Lawrence-Brown, M. Shapon-Shevin, & N. Erevelles (Eds.), Condition critical: Key principles for equitable and inclusive education (pp. 66–85). Teachers College, New York.
Smart, J. (2015). Disability, society, and the individual (3rd ed.). ProEd, Inc.
Smith, W. T., Roth, J. J., Okoro, O., Kimberlin, C., & Odedina, F. T. (2011). Disability in cultural competency pharmacy education. American Journal of Pharmaceutical Education, 75(2), 26. https://doi.org/10.5688/ajpe75226
Taboas, A., Doepke, K., & Zimmerman, C. (2023). Preferences for identity-first versus person-first language in a US sample of autism stakeholders. Autism, 27(2), 565–570. https://doi.org/10.1177/13623613221130845
Strike, D. L., Skovholt, T. M., & Hummel, T. J. (2004). Mental health professionals’ disability competence: Measuring self-awareness, perceived knowledge, and perceived skills. Rehabilitation Psychology, 49(4), 321–327. https://doi.org/10.1037/0090-5550.49.4.321
Wolbring, G., & Nasir, L. (2024). Intersectionality of disabled people through a disability studies, ability-based studies, and intersectional pedagogy lens: A survey and a scoping review. Societies, 14(9), 176. https://doi.org/10.3390/soc14090176
Wong, A. (Ed.). (2020). Disability visibility: First-person stories from the twenty-first century. Vintage.
Julie C. Hill, PhD, NCC, BC-TMH, LPC, CRC, is an assistant professor at the University of Arkansas. Toni Saia, PhD, CRC, is an associate professor at San Diego State University. Marcus Weathers, Jr., PhD, CRC, LPC-IT, is an assistant professor at Mississippi State University. Correspondence may be addressed to Julie C. Hill, 751 W. Maple St., Fayetteville, AR 72701, jch029@uark.edu.
Sep 13, 2024 | Volume 14 - Issue 2
Sapna B. Chopra, Rebekah Smart, Yuying Tsong, Olga L. Mejía, Eric W. Price
This mixed methods program evaluation study was designed to assist faculty in better understanding students’ multicultural and social justice training experiences, with the goal of improving program curriculum and instruction. It also offers a model for counselor educators to assess student experiences and to make changes that center social justice. A total of 139 first-semester students and advanced practicum students responded to an online survey. The Consensual Qualitative Research-Modified (CQR-M) method was used to analyze brief written narratives. The Multicultural Counseling Competence and Training Survey (MCCTS) and the Advocacy Competencies Self-Assessment Survey (ACSA) were used to triangulate the qualitative data. Qualitative findings revealed student growth in awareness, knowledge, skills, and action, particularly for advanced students, with many students reporting a desire for more social justice instruction. Some students of color reported microaggressions and concerns that training centers White students. Quantitative analyses generally supported the qualitative findings and showed advanced students reporting higher multicultural and advocacy competencies compared to beginning students. Implications for counselor education are discussed.
Keywords: social justice, program evaluation, training, multicultural counseling, counselor education
In the midst of the COVID-19 pandemic and the long-standing inequities it brought to light, many universities began examining the ways that injustice unfolds within their institutions (Mull, 2020). Arredondo et al. (2020) noted that counseling and counselor education continue to uphold white supremacy and center the experiences of White people within theories, training, and research. White supremacy culture promotes Whiteness as the norm and standard, intersects with and reinforces other forms of oppression, and shows up in institutions in both overt and covert ways, such as emphasis on individualism, avoidance of conflict, and prioritizing White comfort (Okun, 2021). Arredondo et al. (2020) called for counselor educators to engage in social justice advocacy and to unpack covert White supremacy in training programs. The present study investigated the multicultural and social justice training experiences of students in a Western United States counseling program so that counseling faculty can be empowered to uncover biases and better integrate social justice in the curriculum.
Counselor education programs are products of the larger sociopolitical environment and dominant patriarchal, cis-heteronormative, Eurocentric culture that often fails to “challenge the hegemonic views that marginalize groups of people” which “perpetuate deficit-based ideologies” (Goodman et al., 2015, p. 148). For example, the focus on the individual in traditional counseling theories can reinforce oppression by failing to address the role of systemic oppression in a client’s distress (Singh et al., 2020). Counseling theory textbooks usually provide an ancillary section at the end of each chapter focusing on multicultural issues (Cross & Reinhardt, 2017). White supremacy culture is so ubiquitous that it is typically invisible to those immersed within it (DiAngelo, 2018). It is not surprising then that counseling is often viewed as a White, middle-class endeavor, and BIPOC (Black, Indigenous, and People of Color) clients frequently perceive that they should leave their cultural identities and experiences outside the counseling session (Turner, 2018). Counselor educators have been encouraged to reflect on how Eurocentric curricula and pedagogy may marginalize students and seek liberatory teaching practices that promote critical consciousness (Sharma & Hipolito-Delgado, 2021).
Students’ Perceptions of Their Growth, Learning Process, and Critiques of Their Training
Studies of mostly White graduate students show gains in expanding awareness of their own biases and privilege, knowledge about other cultures and experiences of oppression, as well as the importance of empowering and advocating for clients (Beer et al., 2012; Collins et al., 2015; Sanabria & DeLorenzi, 2019; Singh et al., 2010). Others indicated the benefits of integrating feminist principles in treatment (Hoover & Morrow, 2016; Singh et al., 2010). Consciousness-raising and self-reflection were key parts of multicultural and social justice learning (Collins et al., 2015; Hoover & Morrow, 2016), and could be emotionally challenging. Indeed, Goodman et al. (2018) identified a theme of internal grappling reflecting students’ experiences of intellectual and emotional struggle; others noted students’ experiences of overwhelm and isolation (Singh et al., 2010), as well as resistance, such as withdrawing or dismissing information that challenged their existing belief system (Seward, 2019). Researchers have also documented student complaints about their social justice training; for example, that social justice is not well integrated or that there was inadequate coverage of skills and action (Collins et al., 2015). Kozan and Blustein (2018) found that even among programs that espouse social justice, there was a lack of training in macro level advocacy skills. Barriers to engaging in advocacy included: lack of time (Field et al., 2019; Singh et al., 2010), emotional exhaustion stemming from observations of the harms caused by systemic inequities (Sanabria & DeLorenzi, 2019), and ill-informed supervisors (Sanabria & DeLorenzi, 2019).
The studies reviewed thus relied on samples of mainly White, cisgender, heterosexual women. Some noted that education on social justice is often centered on helping White students expand their awareness (Haskins & Singh, 2015). In one study focused on challenges faced by students of color, participants expressed frustration with the lack of diversity among their professors, classmates, and curriculum (Seward, 2019). Participants also experienced marginalization and disconnection when professors and students made offensive or culturally uninformed comments and when course content focused on teaching students with privileged identities. Students from marginalized communities also face isolation in academic settings and sometimes question the multicultural competence of their professors (Haskins & Singh, 2015), which in turn contributes to the underrepresentation of students of color in counseling and psychology (Arney et al., 2019).
The Present Study
Counselor educators must critically examine their curriculum, course materials, and overall learning climate for students (Haskins & Singh, 2015). Listening to students’ experiences and perceptions of their training offers faculty an opportunity to model cultural humility, gain useful feedback, and make necessary changes. Given the increased recognition of racial trauma and societal inequities, it is critical that counseling programs engage with students of diverse backgrounds as they seek to shift their pedagogy. Historically, academic institutions have responded to student demands with performative action rather than meaningful change (Zetzer, 2021). This mixed methods study is part of a larger process of counseling faculty working to invite student feedback and question internalized assumptions and biases in order to implement real change. The goal of program evaluation is to investigate strengths and weaknesses in order to improve the program (Royse et al., 2010). According to the 2024 Council for Accreditation of Counseling and Related Educational Programs (CACREP) standards, program evaluation is essential to assess and improve the program (CACREP, 2023). Thus, the purpose of this program evaluation study was to understand students’ self-assessment and experiences with the counseling program’s curriculum in the area of multicultural and social justice advocacy, with the overarching goal of program curriculum and instruction improvement. This article offers counselor educators a model of how to assess program effectiveness in multicultural and social justice teaching and practical suggestions based on the findings. The research questions were: What are beginning and advanced students’ self-perceptions regarding their multicultural and social justice advocacy competencies? What are beginning and advanced students’ perceptions of the multicultural and social justice advocacy competencies training they are receiving in their program?
Method
We employed a mixed method, embedded design in which the quantitative data offered a supportive and secondary role to the qualitative results (Creswell et al., 2003). Qualitative and mixed methods research designs are particularly useful in program evaluation (Royse et al., 2010). Mixed method approaches also offer value in research that centers social justice advocacy, as the integration of diverse methodological techniques within a single study fosters the understanding of multiple perspectives and facilitates a deeper comprehension of intricate issues (Ponterotto et al., 2013). We used an online survey to collect written narratives (qualitative) and survey data (quantitative) from two counseling courses: a beginning counseling course in the first semester (beginning students), and an advanced practicum course, taken by those who had completed at least part of their year-long practicum (advanced students).
Participants
Participants were counseling students enrolled in a CACREP-accredited program at a large West Coast public university in the United States that is both a federally designated Hispanic-serving institution and an Asian American and Native American Pacific Islander–serving institution. Responses were collected from two courses, which included 94 beginning students (84% response rate) and 62 advanced students (71% response rate). Twelve percent of the advanced practicum students also completed the survey when they were first-semester (beginning) students. The mean age of the 139 participants was 27.7 (SD = 7.11), ranging from 20 to 58 years. Racial identifications were 40.3% White, 33.1% Latinx, 14.4% Asian, 7.2% Biracial or Multiracial, 2.9% Black, 0.7% Middle Eastern, 0.7% American Indian/Alaska Native, and 0.7% Native Hawaiian/Pacific Islander. The majority identified as women (82.0%), followed by 14.4% as men, and 2.9% as nonbinary/queer. Students self-identified as heterosexual (71.2%), bisexual (11.5%), lesbian/gay (6.5%), queer (4.3%), pansexual (1.4%), and about 1% each as asexual, heteroflexible, and unsure. About 19.4% of students were enrolled in a bilingual/bicultural (Spanish/Latinx) emphasis within the program.
Procedure
After receiving university IRB approval, graduate students enrolled in the first-semester beginning counseling course (fall 2018 and 2019) or the advanced practicum course (summer 2019 and 2020) were asked to complete an online survey through Qualtrics with both quantitative measures and open-ended questions as part of their preparation for class discussion. Students were informed that this homework would not be graded and was not intended to “test” their knowledge but rather would serve as an opportunity to reflect on their experience of the program’s multicultural and social justice training. Students were also given the option to participate in the current study by giving permission for their answers to be used. Those who consented were asked to continue to complete the demographic questionnaire. In accordance with the American Counseling Association Code of Ethics (2014), students were informed that there would be no repercussions for not participating. A faculty member outside the counseling program managed the collection of and access to the raw data in order to protect the identities of the students and ensure that their participation or lack of participation in the study could not affect their grade for the course or standing in the program. All students, regardless of participation status, were given the option to enter an opportunity drawing for a small cash prize ($20 for data collection in 2018 and 2019, $25 for 2020) through a separate link not connected to their survey responses.
Data Collection
We collected brief written qualitative data and responses to two quantitative measures from both beginning and advanced students.
Qualitative Data
The faculty developed open-ended questions that would elicit student feedback on their multicultural and social justice training. Prior to beginning the counseling program, first-semester students were asked two questions about their experiences and impressions: How would you describe your knowledge about and interest in multiculturalism/diversity and social justice from a personal and/or academic perspective? and How would you describe your initial impressions or experience of the focus on multicultural and social justice in the program so far? They were also asked, if it was relevant, to include their experience in the Latinx counseling emphasis program component. Advanced students, who were seeing clients, were asked the same questions and also asked to: Consider/describe how this experience of multiculturalism and social justice in the program may impact you personally and professionally (particularly in work with clients) in the future.
Quantitative Data
Two instruments were selected to quantitatively assess students’ perceptions of their own multicultural and advocacy competencies. The Multicultural Counseling Competence and Training Survey (MCCTS; Holcomb-McCoy & Myers, 1999) is designed to assess counselors’ perceptions of their multicultural competence and the effectiveness of their training. The survey contains 32 statements for which participants answer on a 4-point Likert scale (not competent, somewhat competent, competent, extremely competent). Sample items include: “I can discuss family therapy from a cultural/ethnic perspective” and “I am able to discuss how my culture has influenced the way I think.” The reliability coefficients for each of the five components of the MCCTS ranged from .66 to .92: Multicultural Knowledge (.92), Multicultural Awareness (.92), Definitions of Terms (.79), Knowledge of Racial Identity Development Theories (.66), and Multicultural Skills (.91; Holcomb-McCoy & Myers, 1999). In this study, the Cronbach’s alpha coefficients ranged from .75 to .96.
The Advocacy Competencies Self-Assessment Survey (ACSA; Ratts & Ford, 2010) assesses for competency and effectiveness across six domains: (a) client/student empowerment, (b) community collaboration, (c) public information, (d) client/student advocacy, (e) systems advocacy, and (f) social/political advocacy. It contains 30 statements that ask participants to respond with “almost always,” “sometimes,” or “almost never.” Sample questions include “I help clients identify external barriers that affect their development” and “I lobby legislators and policy makers to create social change.” Although Ratts and Ford (2010) did not provide psychometrics of the original ACSA, it was validated with mental health counselors (Bvunzawabaya, 2012), suggesting an adequate internal consistency for the overall measure, but not the specific domains. In this study, the Cronbach’s alpha coefficients ranged from .69 to.79 for the six domains, and .94 for the overall scale. For the purposes of this study, we were not interested in specific domains and used the overall scale to assess students’ overall social justice/advocacy competencies.
Data Analysis
Qualitative Data Analysis
To analyze the qualitative data, we used Consensual Qualitative Research-Modified (CQR-M; Spangler et al., 2012), which was based on Hill et al.’s (2005) CQR but modified for larger numbers of participants with briefer responses. In contrast to the in-depth analysis of a small number of interviews, CQR-M was ideal for our data, which consisted of brief written responses from 139 participants. CQR-M involves a consensus process rather than interrater reliability among judges, who discuss and code the narratives, and relies on a bottom-up approach, in which categories
(i.e., themes) are derived directly from the data rather than using a pre-existing thematic structure. Frequencies (i.e., how many participants were represented in each category) are then calculated. We analyzed the beginning and advanced students’ responses separately, as the questions were adjusted for their time spent in the program.
After immersing themselves in the data, the first two authors, Sapna B. Chopra and Rebekah Smart, met to outline a preliminary coding structure, then met repeatedly to revise the coding into more abstract categories and subcategories. The computer program NVivo was used to organize the coding process and determine frequencies. After all data were coded, the fifth author, Eric W. Price, served as auditor and provided feedback on the overall coding structure. Both the consensus process and use of an auditor are helpful in countering biases and preconceptions. Brief quantitative data, as used in this study, can be used effectively as a means of triangulation (Spangler et al., 2012).
Quantitative Data Analysis
To examine for significant differences in the self-perceptions of multicultural competencies and advocacy competencies between White and BIPOC students as well as between beginning and advanced students, a two-way (2×2) ANOVA was conducted with the overall MCCT as the criterion variable and student levels (beginning, advanced) and race (White, BIPOC) as the two independent variables. In addition, two (5×2) multivariate analyses of variances (MANOVAs) were conducted with the five factors of multicultural competencies (knowledge, awareness, definition of terms, racial identity, and skills) as criterion variables and with student levels (beginning, advanced) and student races (White, BIPOC) as independent variables in each analysis. Data for beginning and advanced students were analyzed separately to assess whether time in the counseling program helped to expand their interest and commitment to social justice.
Research Team
We were intentional in examining our own social identities and potential biases throughout the research process. Chopra is a second-generation South Asian American, heterosexual, cisgender woman. Smart is a White European American, heterosexual, cisgender woman. Yuying Tsong identifies as a genderqueer first-generation Taiwanese and Chinese American immigrant. Olga L. Mejía is an Indigenous-identified Mexican immigrant, bisexual, cisgender woman. Price is a White, gay, cisgender male. All have experience as counselor educators and in qualitative research methods, and all have been actively engaged in decolonizing their syllabi and incorporating multicultural and social justice into their pedagogy.
Results
The research process was guided by the overarching question: What are beginning and advanced counseling students’ perceptions of their multicultural and social justice competencies and training and how can their feedback be used to improve their counselor education program? We explore the qualitative findings first, as the primary data for the study, followed by the quantitative data.
Qualitative Findings for Beginning Counseling Students
Two higher-order categories emerged from the beginning students’ narratives: developing competencies and learning process so far.
Developing Competencies
Students’ descriptions of the competencies they were developing included themes of awareness, knowledge, and skills and action. Some students entered the program with an already heightened awareness, while others were making new discoveries. Awareness included subthemes of humility (24.5%), awareness of own privilege (6.4%), and awareness of bias (3.2%). “There’s a lot to learn” was a typical sentiment, particularly from White students. One White female student wrote: “I definitely need more and I believe that open discussions, even hard ones would be some of the best ways to go about this.” A large group expressed knowledge of oppression and systemic inequities (33%); a smaller group referenced intersectionality (3.2%). Within skills and action, some students expressed specific intentions in allyship (11.7%); a number of students expressed commitment to social action but felt unsure how to engage in social justice (11.7%).
Learning Process So Far
Central themes in this category were support for growth, concerns in training, and internal challenges. Some students felt excited and supported, while some were cautiously optimistic or concerned. Support for growth was a strong theme that reflected excited and enthusiastic to learn (22.3%); appreciation for the Latinx emphasis (18.1%); and receiving support from professors and program (17.0%). For example, one Mexican student in the Latinx emphasis who noted that mental health was rarely discussed in her family shared: “For me to see that there is a program that teaches students how to communicate to individuals who are unsure of what counseling is about, gave me a sense of happiness and relief.”
A few students were adopting a wait-and-see attitude and expressed some concerns about their training. Although the percentage for these subthemes is low, they provide an important experience that we want to amplify. This theme had multiple subthemes. The subtheme concerns from students of color included centering White students (3.2%), microaggressions (3.2%), and lack of representation (1.1%). A student who identified as a Mexican immigrant shared experiences of microaggressions, including classmates using a hurtful derogatory phrase referring to immigrants with no comment from the professor until the student raised the issue. Concerns in training also included the subtheme concerns with how material is presented in classes (7.0%). For some, the concern related to the potential for harm in classes in which White and BIPOC students were encouraged to process issues of privilege and oppression. For example, one Asian Pacific Islander student wrote that although they appreciated the emphasis on social justice, “Time always runs out and I believe it’s careless and dangerous to cut off these types of conversations in a rushed manner.” A small minority seemed to suggest a backlash to the emphasis on social justice, stating that the content was presented in ways that were too “politically correct,” “biased,” or “repetitive.”
Multiple subthemes emerged from the theme of internal challenges. Both BIPOC and White students shared feeling afraid to speak up (5.3%). BIPOC students expressed struggling with confidence or wanting to avoid conflict, while White students’ fear of speaking up was also connected to discomfort and uncertainty as a White person (2.1%). A small minority of White students did not express explicit discomfort but seemed to engage in a color-blind strategy, as indicated in the theme of people are people (2.1%): “I find people are people, regardless of any differences, and love hearing the good and bad about everybody’s experiences.” Some students of color expressed limited knowledge about cultures other than one’s own (4.3%). For example, an Asian American student stated that they had gravitated to “those who were most similar to me” growing up. Lastly, a few students shared feeling overwhelmed and exhausted (3.2%).
Qualitative Findings for Advanced Counseling Students
Four higher-order themes emerged: competencies in process, multiculturalism and diversity in the program, social justice in the program, and the learning process.
Competencies in Process
Similar to beginning students, advanced students described growing self-awareness, knowledge and awareness of others, skills, and action. Their disclosures often related to clinical work, now that they had been seeing clients. Self-awareness included strong subthemes of: humility and desire to keep learning (25.8%); increased open-mindedness, acceptance of others, and compassion (22.6%); awareness of personal privilege and oppression (17.7%); awareness of personal bias and value systems (17.7%); and awareness of personal cultural identity (14.5%). One Mexican American student wrote: “I have also gained an increased awareness of how my prejudices can impact my work with clients and learned about how to check-in with myself.”
Knowledge and awareness of others had subthemes of privilege and oppression (19.4%) and increased knowledge of culture (14.5%), with awareness of the potential impact on clients. The advanced students also had more to say about skills, which included subthemes of diversity considerations in conceptualization (29%), and in treatment (12.9%), and cultural conversations in the therapy room (21%). One White student wrote: “I have been able to have difficult conversations that once were unheard of. I have also been able to bring culture, ethnicity, and oppression into the room so that my clients can feel understood and safe.” Within the theme of action, 52% wrote about their commitment to social justice and intention to advocate. Although this strongest subtheme suggested action was still more aspirational than currently enacted, a smaller group also wrote about the experiences that they have already had with client advocacy (12.9%), community and/or political action (12.9%), and unspecified action (11.3%).
Multiculturalism and Diversity in the Program
Many students (44%) indicated that they appreciated that multicultural issues were integrated or addressed well within the program. However, with more time spent in the program, 26% felt that there was more nuance, depth, or scope needed. Some wanted more attention to specific issues, such as disability, gender identity, and religion/spirituality. One Asian American student wrote that the focus had been “basic and surface-level,” adding “I feel like it has also generally catered to the protection of White feelings and voices, which is inherently complicit in the system of White supremacy, especially in higher ed.” Others (9.7%) said more training in clinical application was needed.
Social Justice in the Program
Students expressed a variety of opinions. The largest number (29%) were satisfied that social justice issues were well integrated into the program. Although more students were satisfied than not, many (24%) noted that social justice is addressed but not demonstrated. Similarly, 24% noted minimal attention, specifically that social justice was not addressed much beyond the one course focused on culture, and 24% noted a desire for more opportunities within the program to engage in advocacy. Some suggested requiring social justice work rather than leaving it as an optional activity. Others (13%), mostly from 2020, noted the relevance of current events and sociopolitical climate. One White student shared about a presentation on Black Lives Matter: “This project opened my eyes to my limited knowledge of systemic oppression in the U.S. and impacted me in ways that I will NEVER be the same.” A small number of students (3%) reported that there was no need or room for more training in social justice. One White student wrote that they felt “frustrated” and that the social justice “agenda is so in my face all the time,” adding “sometimes I feel like I am being trained to be an advocate and an activist, which is/are a different job.”
The Learning Process
Three central themes emerged: enrichment experienced, challenges, and suggestions for change. Many students were appreciative of their experience. A strong subtheme within enrichment experienced was professors’ encouragement and modeling (24%). Others commented on how much came from learning from peers (21%). Some shared feeling personally empowered (14.5%). For example, a student who identified as coming from an Asian culture wrote about the hesitancy to be an activist, stating, “There is an underlying belief that our voices will not really ever be heard which is strongly tied to systemic oppression and racism throughout history. Consequently, I appreciate this challenge to grow more in social justice issues.” Others shared ways that the program prompted them to engage in social justice outside the classroom (11.3%). For example, one student wrote: “This program gave me the knowledge and education I needed to make sure that when I did speak out I wasn’t just talking to talk. I would actually have facts, stats, evidence-based research to back up my argument.” A number of students noted the unique benefits of the Latinx program (9.7%). One Mexican American student reflected that they had learned about diversity within Latinx cultures, and that, “As a result, I feel more confident in being able to serve clients from various Latinx cultures or at least know where to obtain relevant information when needed.” Many students expressed a sense of belonging (8.1%).
Challenges. Nearly 10% wrote about struggling to make time [for social justice] and 6.5% noted the emotional impact. For example, one White student wrote: “It was a rude and brutal awakening, to say the least. It was riddled with emotion and heartache but was worth the process.” A few had conflicted or mixed feelings (8.1%)—they felt appreciative but wanted more. A few noted possible harm to marginalized students (6.5%). One Asian American student wrote that faculty should be “calling out microaggressions . . . otherwise, their stance on social justice feels more performative and about protecting their own liability rather than caring for their students of color.” A smaller number (4.8%) struggled with peers and colleagues who seemed uninformed.
Suggestions for Change. Students offered suggestions for improvement, with a strong theme to develop more diverse representation (16.1%), including more representation in faculty, students, case examples, and class discussions. Some comments were specifically about needed attention to Black experiences; one concerned teaching about resiliencies and strengths in the face of oppression. Almost 15% suggested making changes to courses or curriculum. One White student wrote: “If it were me running the program (lol) I would . . . remove the culture class and have all those topics embedded into the fabric of each class because culture and diversity are in all those topics.” A few suggested that faculty require social justice assignments (8.1%), adding that many students will not act unless required. A few also suggested that the program provide more education of White students (8.1%).
Quantitative Findings
Quantitative analyses were conducted to provide triangulation for the qualitative findings and a different view of the data, including possible differences between BIPOC and White students and beginning and advanced students. Table 1 includes descriptive statistics providing an overview of beginning and advanced students’ self-perception of their multicultural and social justice competencies.
Table 1
Descriptive Statistics of Competencies
|
|
|
Multicultural |
Social Justice/Advocacy |
|
|
N |
Mean |
SD |
Mean |
SD |
| White |
Beginning |
35 |
2.58 |
.50 |
62.97 |
24.23 |
| Advanced |
27 |
3.09 |
.38 |
76.07 |
19.11 |
| Total |
62 |
2.80 |
.52 |
68.68 |
22.93 |
| BIPOC |
Beginning |
59 |
2.66 |
.56 |
63.05 |
29.30 |
| Advanced |
35 |
3.01 |
.30 |
77.14 |
20.71 |
| Total |
94 |
2.79 |
.51 |
68.30 |
27.19 |
| Total |
Beginning |
94 |
2.63 |
.54 |
63.02 |
27.39 |
| Advanced |
62 |
3.05 |
.34 |
76.68 |
19.87 |
| Total |
156 |
2.80 |
.51 |
68.45 |
25.51 |
To examine if there were discernable differences between the beginning and advanced students’ perceptions of their competencies, and if there were differences between White and BIPOC students, a two-way (2×2) ANOVA was conducted with the overall MCCT as the criterion variable and student levels (beginning, advanced) and race (White, BIPOC) as the two independent variables. Results indicated that although there were no interaction effects between race and student levels, there were significant differences in overall multicultural competencies between beginning and advanced students, F(1, 152) = 30.54, p < .001, indicating that advanced practicum students reported significantly higher overall multicultural competencies than beginning students. There were no statistically significant differences between White and BIPOC students in their overall multicultural competencies. Two (5×2) MANOVAs were conducted with the five factors of multicultural competencies as criterion variables (knowledge, awareness, definition of terms, racial identity, and skills). Student levels (beginning, advanced) and student race (White, BIPOC) were independent variables. Results indicated that there were significant differences between beginning and advanced students in at least one of the multicultural competencies components, Wilks’ Lambda = .72, F(5, 150) = 11.97, p < .001. More specifically, follow-up univariate ANOVAs indicated that advanced students reported significantly higher multicultural competencies in their knowledge, F(1, 154) = 43.74, p < .001, µ2 = .22; awareness, F(1, 154) = 6.20, p = .014, µ2 = .04; and racial identity, F(1, 154) = 43.17, p < .001, µ2 = .21. However, there were no significant differences in definitions of terms or skills. Even though there were no significant differences between White and BIPOC students in their overall multicultural competencies, the results of the 5×2 MANOVA indicated that there were significant differences in at least one of the components, Wilks’ Lambda = .87, F(5, 150) = 4.49, p = .001. Follow-up univariate ANOVAs indicated that White students reported higher multicultural competencies in racial identity than BIPOC students in this study, F(1, 154) = 4.51, p = .035, µ2 = .03. There were no differences in the other areas.
A two-way (2×2) ANOVA was conducted with the overall ACSA as the criterion variable and student levels (beginning, advanced) and race (White, BIPOC) as the two independent variables. Results indicated that while there were no interaction effects between race and student levels, there were significant differences in overall advocacy competencies between beginning and advanced students, F(1, 152) = 10.78, p = .001, indicating that advanced students reported significantly higher overall advocacy competencies (M = 76.68) than beginning students (M = 63.02). There were no statistically significant differences between White and BIPOC students in their overall advocacy competencies.
Discussion
This study was designed to examine students’ experiences of their multicultural and social justice training as an aspect of program evaluation, specifically to assist faculty in improving curriculum and instruction with regard to multicultural and advocacy competencies; the study also offers a unique contribution to existing literature by including a more racially diverse (60% BIPOC) sample. Students reported growth in the core areas of multicultural and social justice competency as outlined by Ratts et al. (2016): awareness, knowledge, skills, and action. Consistent with Field et al.’s (2019) findings, students reported more growth in awareness and knowledge than in social justice action, with some differences as students moved through the program. Although beginning students identified personal biases, the theme of self-awareness was more complex for them later in the program. This suggests that a longer time spent in the program contributed to personal growth; although this seems expected, these outcomes have not necessarily been examined before and confirm that the programs’ increasing effort on multiculturalism and social justice are showing gains. The advanced students wrote about clinical application as well and made overt statements of their commitment to social justice. The quantitative results supported these qualitative findings, with advanced students reporting higher multicultural competencies in knowledge, awareness, and racial identity and higher overall advocacy competencies compared to beginning students. With one exception, there were no significant differences between White and BIPOC students in their self-assessment of multicultural or advocacy competencies. Across racial groups, students expressed humility and desire to learn more.
Although students expressed mixed opinions about their experience of the multicultural and social justice training, a greater number of advanced students reported that they thought multicultural (44%) and social justice issues (30%) were well integrated into the program compared to the number of students with critiques. Students reported that support from faculty and peers facilitated their growth and learning, consistent with previous research (e.g., Beer et al., 2012; Keum & Miller, 2020). Some students noted a sense of belonging, particularly those in the Latinx emphasis.
Similar to other researchers, we found that many students wanted social justice issues to be integrated across the curriculum rather than into one course (Beer et al., 2012; Collins et al., 2015); they also wanted more focus on skills and action (Collins et al., 2015; Kozan & Blustein, 2018). Students’ scores on the ACSA advocacy competencies scale reflect this gap in training as well. Though fewer students offered critiques of their training, these responses are important to amplify because some of these concerns are rarely solicited or acknowledged. For example, BIPOC students echoed the challenges faced by students in Seward’s (2019) study, including lack of representation in their faculty, classmates, and curriculum as well as feelings of marginalization when microaggressions in the classroom went unchecked and when instruction centered the needs of White students. Additionally, a few advanced students from 2020, during a time of significant racial-sociopolitical uprising in the United States, expressed concern that class discussions potentially caused harm to students from marginalized communities. Though more students expressed a desire for greater in-depth training, a small minority of mostly White students indicated that they did not want more social justice training and would rather focus solely on traditional counseling skills. These different student perspectives point to the challenges of teaching social justice amidst diverse political and ideological backgrounds and the need to increase community and collaboration.
Listening to Student Feedback and Implications for Decolonizing Program Curriculum
This study’s findings support the benefits of listening to students’ voices related to multicultural and social justice to inform counselor educators on program strengths and areas for growth. Although student feedback was not the sole impetus for making program changes, accessing this more detailed response was helpful in refining our purpose and direction, as well as highlighting weaknesses. Perhaps more important was the faculty’s willingness to engage in this self-reflective process and to take necessary actions. Rather than waiting for exit interview feedback from graduating students, counselor educators can conduct ongoing program evaluations through anonymous online surveys as well as town hall meetings that invite students to share their process of learning, perceptions of the cultural climate, and experiences of microaggressions. We have a growing understanding that during such evaluations great care needs to be taken for building safety, so as not to retraumatize students from marginalized communities. Based on the results and a series of Zoom town hall meetings, we have implemented changes, such as more consistent integration of social justice across the curriculum; training and day-long retreats focused on increasing faculty competence; faculty participation in Academics for Black Survival and Wellness, an intensive training led by Dr. Della Mosely and Pearis Bellamy; accountability support groups in social justice work; and decolonizing syllabi and class content (e.g., including BIPOC voices and non–APA-style writing assignments). Faculty have also made significant modifications to course materials. For example, beginning students complete weekly modules that include readings and exercises from The Racial Healing Handbook (Singh, 2019), and students study Liberation Psychology during the first week of theories class so they can consider ways to decolonize more traditional models throughout the semester. These strategies have been helpful in preparing students for more difficult conversations surrounding anti-racism in more advanced courses throughout the program. Forming faculty accountability partners or small groups is helpful so that faculty can support each other as a part of their ongoing development in addressing internalized White supremacy and avoiding harm to students.
Student feedback also called attention to the need for self-care, which our program continues to explore. Consistent with previous research (Collins et al., 2015; L. A. Goodman et al., 2018; Hoover & Morrow, 2016; Singh et al., 2010), students reported that their multicultural and social justice learning was often accompanied by moments of overwhelm, hopelessness, and despair. Without tools to manage these emotions, some students may retreat into defensiveness and withdrawal (Seward, 2019), and some may experience activist burnout (Gorski, 2019). Sustainability is necessary for effective social change efforts (Toporek & Ahluwalia, 2021). Counseling programs can offer resources and guidance for students to practice self-care with counselor educators modeling self-care behavior. For example, the Psychology of Radical Healing Collective (Chen et al., 2019) offered strategies to practice radical self-care, including making space for one’s own healing, finding joy and a sense of belonging, and engaging in advocacy at the local community level. Mindfulness practices can be integrated into social justice education to help students and counselor educators manage difficult emotions, increase their ability to be present, and strengthen compassion and curiosity (Berila, 2016). In addition to individual self-care practices, counselor educators can advocate for community care by tending to the community’s needs and drawing on collective experience and wisdom (Gorski, 2019).
The findings point to the need for counselor educators to better address Whiteness and White supremacy, as well as to center the experiences of students from marginalized communities. Counselor educators may be able to mobilize and direct White students’ feelings of guilt into racial consciousness and action by helping them explore Whiteness, White privilege, and what it means to them while allowing and confronting feelings that arise (Grzanka et al., 2019). It may be helpful for educators to read and assign books on White fragility and ways to address it (DiAngelo, 2018; Helms, 2020; Saad, 2020), so that they can assist White students in managing these emotions. It is important that educators explicitly name and recognize White supremacy as it shows up in counseling theory and practice, and to include a shift from the primary focus on the individual to understanding and dismantling oppressive systems. Counselor educators must also attend to the ways in which they center the comfort of White students over the needs of BIPOC students, so that they do not perpetuate harm and trauma (Galán et al., 2021). Although students with privileged identities may learn powerful lessons about oppression from their classmates, it is important that such learning does not occur at the expense of students with marginalized identities. Offering spaces for White students, especially those who are new to conversations about race and racism, to process their feelings may be helpful to avoid harm to BIPOC students who have experienced racial trauma. Similarly, BIPOC students may benefit from spaces in which they can talk freely and support each other as they unpack their own experiences of microaggressions and trauma (Galán et al., 2021).
Based on the finding that support from faculty was important in facilitating student growth and learning, counselor educators may benefit from implementing strategies informed by relational pedagogy and relational–cultural theory (Dorn-Medeiros et al., 2020). Relational pedagogy centers the relationship between teachers and students and posits that all learning takes place in relationships. Relational–cultural theory emphasizes mutual empathy and empowerment and is rooted in feminist multicultural principles. Practices grounded in these approaches include professors’ use of self-disclosure to model openness, vulnerability, and self-reflection; and their work to reduce power imbalances and invite student feedback at multiple points in time through anonymous surveys and one-on-one meetings. Counselor educators can uplift students as the experts of their experience (Sharma & Hipolito-Delgado, 2021).
Limitations and Future Research
The results of this study must be considered in light of a number of limitations. The use of the online survey meant that we were not able to follow up with students for further discussion or clarification of their responses. Adding focus groups or interviews to this methodology would likely provide a more thorough picture. In spite of assurances to the contrary, some students may have been hesitant to be honest out of concern that their own professors would be reading their feedback. It is possible that different themes would have emerged if all students had participated. In addition, 12% of the advanced students had participated as beginning students and therefore were previously exposed to the survey materials. Although this could have impacted their later responses, we suspect that given the nearly 2-year time lapse this may not have been meaningful. Nevertheless, future research and program evaluation would be strengthened with longitudinal analyses. Lastly, the reliability for the ACSA was relatively low, so conclusions are tentative; however, the results support the qualitative data. Despite these limitations, this study offers a model for assessing students’ learning and experiences with the goal of program improvement. The process of counselor educators humbling themselves and inviting and integrating student feedback is an important step in decolonizing counselor education and better serving students and the clients and communities that they will serve.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/ethics/2014-aca-code-of-ethics.pdf?sfvrsn=55ab73d0_1
Arney, E. N., Lee, S. Y., Printz, D. M. B., Stewart, C. E., & Shuttleworth, S. P. (2019). Strategies for increased racial diversity and inclusion in graduate psychology programs. In M. T. Williams, D. C. Rosen, & J. W. Kanter (Eds.), Eliminating race-based mental health disparities: Promoting equity and culturally responsive care across settings (pp. 227–242). Context Press.
Arredondo, P., D’Andrea, M., & Lee, C. (2020). Unmasking White supremacy and racism in the counseling profession. Counseling Today. https://ctarchive.counseling.org/2020/09/unmasking-white-supremacy-and-racism-in-the-counseling-profession
Beer, A. M., Spanierman, L. B., Greene, J. C., & Todd, N. R. (2012). Counseling psychology trainees’ perceptions of training and commitments to social justice. Journal of Counseling Psychology, 59(1), 120–133. https://doi.org/10.1037/a0026325
Berila, B. (2016). Integrating mindfulness into anti-oppression pedagogy: Social justice in higher education. Routledge.
Bvunzawabaya, B. (2012). Social justice counseling: Establishing psychometric properties for the Advocacy Competencies Self-Assessment Survey (Doctoral dissertation, Auburn University). https://etd.auburn.edu/handle/10415/3369
Chen, G. A., Neville, H. A., Lewis, J. A., Adames, H. Y., Chavez-Dueñas, N. Y., Mosley, D. V., & French, B. H. (2019). Radical self-care in the face of mounting racial stress: Cultivating hope through acts of affirmation. Psychology Today. https://www.psychologytoday.com/us/blog/healing-through-social-justice/201911/radical-self-care-in-the-face-mounting-racial-stress
Collins, S., Arthur, N., Brown, C., & Kennedy, B. (2015). Student perspectives: Graduate education facilitation of multicultural counseling and social justice competency. Training and Education in Professional Psychology, 9(2), 153–160. https://doi.org/10.1037/tep0000070
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards.
https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Creswell, J. W., Plano Clark, V. L., Gutmann, M. L., & Hanson, W. E. (2003). Advanced mixed methods research designs. In A. Tashakkori & C. Teddlie (Eds.), SAGE handbook of mixed methods in social and behavioral research (1st ed.; pp. 209–240). SAGE.
Cross, W. E., Jr., & Reinhardt, J. S. (2017). Whiteness and serendipity. The Counseling Psychologist, 45(5), 697–705. https://doi.org/10.1177/0011000017719551
DiAngelo, R. (2018). White fragility: Why it’s so hard for White people to talk about racism. Beacon Press.
Dorn-Medeiros, C. M., Christensen, J. K., Lértora, I. M., & Croffie, A. L. (2020). Relational strategies for teaching multicultural courses in counselor education. Journal of Multicultural Counseling and Development, 48(3), 149–160. https://doi.org/10.1002/jmcd.12174
Field, T. A., Ghoston, M. R., Grimes, T. O., Sturm, D. C., Kaur, M., Aninditya, A., & Toomey, M. (2019). Trainee counselor development of social justice counseling competencies. Journal for Social Action in Counseling and Psychology, 11(1), 33–50. https://doi.org/10.33043/JSACP.11.1.33-50
Galán, C. A., Bekele, B., Boness, C., Bowdring, M., Call, C., Hails, K., McPhee, J., Mendes, S. H., Moses, J., Northrup, J., Rupert, P., Savell, S., Sequeira, S., Tervo-Clemmens, B., Tung, I., Vanwoerden, S., Womack, S., & Yilmaz, B. (2021). Editorial: A call to action for an antiracist clinical science. Journal of Clinical Child and Adolescent Psychology, 50(1), 12–57. https://doi.org/10.1080/15374416.2020.1860066
Goodman, L. A., Wilson, J. M., Helms, J. E., Greenstein, N., & Medzhitova, J. (2018). Becoming an advocate: Processes and outcomes of a relationship-centered advocacy training model. The Counseling Psychologist, 46(2), 122–153. https://doi.org/10.1177/0011000018757168
Goodman, R. D., Williams, J. M., Chung, R. C.-Y., Talleyrand, R. M., Douglass, A. M., McMahon, H. G., & Bemak, F. (2015). Decolonizing traditional pedagogies and practices in counseling and psychology education: A move towards social justice and action. In R. D. Goodman & P. C. Gorski (Eds.), Decolonizing “multicultural” counseling through social justice (pp. 147–164). Springer.
Gorski, P. C. (2019). Fighting racism, battling burnout: Causes of activist burnout in US racial justice activists. Ethnic and Racial Studies, 42(5), 667–687. https://doi.org/10.1080/01419870.2018.1439981
Grzanka, P. R., Gonzalez, K. A., & Spanierman, L. B. (2019). White supremacy and counseling psychology: A critical–conceptual framework. The Counseling Psychologist, 47(4), 478–529. https://doi.org/10.1177/0011000019880843
Haskins, N. H., & Singh, A. (2015). Critical race theory and counselor education pedagogy: Creating equitable training. Counselor Education and Supervision, 54(4), 288–301. https://doi.org/10.1002/ceas.12027
Helms, J. E. (2020). A race is a nice thing to have: A guide to being a White person or understanding the White persons in your life (3rd ed.). Cognella.
Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A., & Ladany, N. (2005). Consensual qualitative research: An update. Journal of Counseling Psychology, 52(2), 196–205. https://doi.org/10.1037/0022-0167.52.2.196
Holcomb-McCoy, C. C., & Myers, J. E. (1999). Multicultural competence and counselor training: A national survey. Journal of Counseling & Development, 77(3), 294–302. https://doi.org/10.1002/j.1556-6676.1999.tb02452.x
Hoover, S. M., & Morrow, S. L. (2016). A qualitative study of feminist multicultural trainees’ social justice development. Journal of Counseling & Development, 94(3), 306–318. https://doi.org/10.1002/jcad.12087
Keum, B. T., & Miller, M. J. (2020). Social justice interdependence among students in counseling psychology training programs: Group actor-partner interdependence model of social justice attitudes, training program norms, advocacy intentions, and peer relationships. Journal of Counseling Psychology, 67(2), 141–155. https://doi.org/10.1037/cou0000390
Kozan, S., & Blustein, D. L. (2018). Implementing social change: A qualitative analysis of counseling psychologists’ engagement in advocacy. The Counseling Psychologist, 46(2), 154–189. https://doi.org/10.1177/0011000018756882
Mull, R. C. (2020). Colleges are in for a racial reckoning. The Chronicle of Higher Education. https://www.chronicle.com/article/colleges-are-in-for-a-racial-reckoning
Okun, T. (2021). White supremacy culture – Still here. https://drive.google.com/file/d/1XR_7M_9qa64zZ00_JyFVTAjmjVU-uSz8/view
Ponterotto, J. G., Mathew, J. T., & Raughley, B. (2013). The value of mixed methods designs to social justice research in counseling and psychology. Journal for Social Action in Counseling and Psychology, 5(2), 42–68. https://doi.org/10.33043/JSACP.5.2.42-68
Ratts, M. J., & Ford, A. (2010). Advocacy Competencies Self-Assessment (ACSA) Survey©: A tool for measuring advocacy competence. In M. J. Ratts, R. L. Toporek, & J. A. Lewis (Eds.), ACA advocacy competencies: A social justice framework for counselors (pp. 21–26). American Counseling Association.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Royse, D., Thyer, B. A., & Padgett, D. K. (2010). Program evaluation: An introduction (5th ed.). Cengage.
Saad, L. F. (2020). Me and White supremacy: Combat racism, change the world, and become a good ancestor. Sourcebooks.
Sanabria, S., & DeLorenzi, L. (2019). Social justice pre-practicum: Enhancing social justice identity through experiential learning. Journal for Social Action in Counseling and Psychology, 11(2), 35–53. https://doi.org/10.33043/JSACP.11.2.35-53
Seward, D. X. (2019). Multicultural training resistances: Critical incidents for students of color. Counselor Education and Supervision, 58(1), 33–48. https://doi.org/10.1002/ceas.12122
Sharma, J., & Hipolito-Delgado, C. P. (2021). Promoting anti-racism and critical consciousness through a critical counseling theories course. Teaching and Supervision in Counseling, 3(2), 15–25. https://doi.org/10.7290/tsc030203
Singh, A. A. (2019). The racial healing handbook: Practical activities to help you challenge privilege, confront systemic racism, and engage in collective healing. New Harbinger.
Singh, A. A., Appling, B., & Trepal, H. (2020). Using the multicultural and social justice counseling competencies to decolonize counseling practice: The important roles of theory, power, and action. Journal of Counseling & Development, 98(3), 261–271. https://doi.org/10.1002/jcad.12321
Singh, A. A., Hofsess, C. D., Boyer, E. M., Kwong, A., Lau, A. S. M., McLain, M., & Haggins, K. L. (2010). Social justice and counseling psychology: Listening to the voices of doctoral trainees. The Counseling Psychologist, 38(6), 766–795. https://doi.org/10.1177/0011000010362559
Spangler, P. T., Liu, J., & Hill, C. E. (2012). Consensual qualitative research for simple qualitative data: An introduction to CQR-M. In C. E. Hill (Ed.), Consensual qualitative research: A practical resource for investigating social science phenomena (pp. 269–283). American Psychological Association.
Toporek, R. L., & Ahluwalia, M. K. (2021). Taking action: Creating social change through strength, solidarity, strategy, and sustainability. Cognella Press.
Turner, D. (2018). “You shall not replace us!” White supremacy, psychotherapy and decolonisation. Journal of Critical Psychology, Counselling and Psychotherapy, 18(1), 1–12. https://cris.brighton.ac.uk/ws/portalfiles/portal/495044/JCPCP+18-1+-+Turner+article.pdf
Zetzer, H. A. (2021). Decolonizing the curriculum in health service psychology. Association of Psychology Training Clinics Bulletin: Practicum Education & Training, 20–22. https://aptc.org/images/File/newsletter/APTC_Bulletin_PET_2021_Spring%20FINAL.pdf
Sapna B. Chopra, PhD, is an associate professor at California State University, Fullerton. Rebekah Smart, PhD, is a professor at California State University, Fullerton. Yuying Tsong, PhD, is a professor and Associate Vice President for Student Academic Support at California State University, Fullerton. Olga L. Mejía, PhD, is a licensed psychologist and an associate professor at California State University, Fullerton. Eric W. Price, PhD, is an associate professor at California State University, Fullerton. Correspondence may be addressed to Sapna B. Chopra, Department of Human Services, California State University, Fullerton, P.O. Box 6868, Fullerton, CA 92834-6868, sapnachopra@fullerton.edu.
Sep 13, 2024 | Volume 14 - Issue 2
Taylor J. Irvine, Adriana C. Labarta
Eating disorders (EDs) are increasingly prevalent and pose significant public health challenges. Yet, deficits exist in counselor education programs regarding ED assessment, conceptualization, and treatment. Consequently, counselors report feeling incompetent and distressed when working with ED clients. We propose a conceptual framework, the 3 Cs of ED Education and Training, to enhance trainee development. The 3 Cs are: (a) cultivating trainee self-awareness through reflexivity and deliberate skill practice, (b) capturing contextual and sociocultural factors with culturally responsive approaches, and (c) collaborating with interdisciplinary ED professionals while strengthening counselor professional identity. Implications for counselor educators include incorporating activities aligned with this framework into curriculum and experiential training in order to facilitate trainee competence in ED assessment and treatment.
Keywords: eating disorders, 3 Cs of ED Education and Training, framework, counselor education, trainee development
Eating disorders (EDs) remain one of the most lethal mental health illnesses, contributing to roughly 3 million deaths globally each year (van Hoeken & Hoek, 2020) and impacting 29 million or 9% of Americans over their lifetime (Deloitte Consumer Report, 2020). In the United States alone, EDs directly result in 10,200 deaths annually, averaging one death every hour (Deloitte Access Economics, 2020). The steady rise of EDs across genders and countries is of increasing concern, with scholars noting in their systematic literature review that rates have doubled from 3.5% in 2000–2006 to 7.8% in 2013–2018 (Galmiche et al., 2019). EDs also exact a significant economic toll in the United States. In the 2018–2019 fiscal year, Streatfeild et al. (2021) found that EDs generated financial costs of nearly $65 billion, averaging about $11,000 per affected individual. Moreover, their study estimated an additional $326.5 billion in non-financial costs due to reduced well-being among those with EDs. Given their associated comorbidities with other mental health illnesses (Ulfvebrand et al., 2015), enduring somatic issues (Galmiche et al., 2019), and facilitation of psychological distress (Kärkkäinen et al., 2018), EDs pose significant public health and economic threats that necessitate further consideration. However, the literature lacks meaningful attention to ED prevention and treatment (van Hoeken & Hoek, 2020), an oversight that needs to be redressed within counselor education (CE) graduate training programs. A failure to examine this clinical issue threatens the maintenance of quality assurance and ethical standards within the profession, enabling short- and long-term client harm.
Challenges and Gaps in ED Education and Training
Given the steady rise in the prevalence of EDs and their associated consequences, counseling trainees must be equipped with comprehensive training in order to effectively conceptualize and treat these complex conditions. However, across the decades, research has illuminated ED education and training deficits, particularly in graduate programs (Biang et al., 2024; Labarta et al., 2023; Levitt, 2006; Thompson-Brenner et al., 2012). For instance, Labarta et al.’s (2023) recent study examined clinician attitudes toward treating EDs, revealing challenges related to the lack of specialized graduate training. Among surveyed respondents, only 25.7% reported that their programs offered a specialized course on EDs, while approximately half of the sample (41.3%) divulged that their program dedicated only 1–5 hours of ED-related instruction throughout the curricula. Furthermore, one participant indicated that ED education is “rarely more than one lecture at the master’s level” (Labarta et al., 2023, p. 21). This is particularly concerning as research shows that trainees are not only very likely to encounter a client battling an ED at some point in their professional career (Levitt, 2006) but are also going to be less prepared and effective in treating such clients without specialized ED training in graduate programs (Biang et al., 2024; Labarta et al., 2023).
As a result of this lack of ED education, scholars have noted negative implications for helping professions, contributing to clinician incompetence, increased burnout, and diminished self-efficacy when working with ED clients (Labarta et al., 2023; Levitt, 2006; Thompson-Brenner et al., 2012). Clinician competence is a necessary vehicle to not only promote individual accountability but to also ensure the integrity of the broader counseling profession. However, holistic competency development is threatened without adequate, targeted ED training, increasing the likelihood that counselors-in-training (CITs) will encounter recurring treatment failures when working with clients struggling with an ED (Williams & Haverkamp, 2010). Williams and Haverkamp (2010) echoed this sentiment, stating that the field risks the occurrence of “iatrogenesis . . . particularly when the practitioner has a poor understanding of EDs, the negative reactions that eating disordered clients can evoke in the clinician are not managed, and/or there are specific types of process and relationship errors made in therapy” (p. 92). For example, although a school counselor may not serve as the primary treatment provider for an adolescent with bulimia nervosa, their understanding of warning signs and symptoms, supportive collaboration with students and families, and knowledge of specialized community referrals are invaluable to the counseling process (Carney & Scott, 2012). As such, counselor educators must assist CITs with developing essential competencies for treating EDs during graduate training programs, ultimately working toward bridging this gap and improving the quality of care.
Addressing the deficit of multicultural research in the field of EDs is of paramount importance, as it directly impacts the practice and education of counselors. Accrediting and professional bodies expect counselor educators to impart multicultural knowledge and skills to CITs, including a focus on diverse cultural and social identities (American Counseling Association [ACA], 2014; Council for the Accreditation of Counseling and Related Educational Programs [CACREP], 2023). Furthermore, Levitt (2006) emphasized that the significant consequences and growing prevalence of EDs across diverse cultural groups necessitate that clinicians “gain exposure to the etiology, manifestation, and treatment of eating disorders within multiple contexts” (p. 95). This assertion underscores the critical need for a more inclusive and culturally competent approach to assessing, treating, and educating about EDs, emphasizing the urgency of addressing the existing gaps in research. Ultimately, the absence of targeted ED research and training, notably conceptualization and assessment strategies, poses ethical concerns for safeguarding clients’ welfare, rendering trainees ill-equipped to address milder presentations of these disorders, let alone complex cases with more severe symptoms, such as heightened suicidality, enduring medical complications, and acute psychological distress (Kärkkäinen et al., 2018).
Research concerning client experiences is also imperative when assessing education and training needs for effective ED treatment. Babb et al. (2022) conducted a meta-synthesis of qualitative research on ED clients’ experiences in ED treatment, illuminating important themes on clinicians’ roles in supporting clients. Several clients reported that some staff perpetuated stereotypes about EDs (e.g., viewing the client as an illness versus a person) and tried to fit clients into specific theoretical frameworks. Clients attributed this lack of awareness and sensitivity to the providers’ lack of specialized training in EDs. Conversely, clients in this study felt empowered when providers were empathic and provided individualized approaches to treatment. These participants noted that “being seen as an individual” facilitated motivation for treatment, with the therapeutic alliance as an essential factor in this process (Babb et al., 2022, p. 1289). These client perspectives provide valuable insights that should inform the development of CE training programs to better prepare CITs for working with individuals with EDs.
Training Recommendations for Counselor Education Programs
Collectively, the findings cited above underscore the importance of comprehensive ED training for counselors to be able to effectively and compassionately serve diverse clients with EDs. However, accessibility to such education and training remains a challenge to both the graduate students and practitioners (Biang et al., 2024; Labarta et al., 2023). Furthermore, despite the efficiency of manualized approaches, Babb et al.’s (2022) study emphasized the need for both flexibility and avoiding a one-size-fits-all approach to ED treatment, particularly given the diversity of clients with EDs, including those from traditionally underrepresented backgrounds (Schaumberg et al., 2017). Clients’ lived experiences corroborate these gaps, reporting instances of stereotyping, rigid adherence to theoretical frameworks, and a lack of empathy stemming from inadequate specialized training (Babb et al., 2022). These findings highlight the pressing need for training strategies that ensure competence and uphold ethical standards within the treatment of EDs, including ongoing education for new practitioners entering the field.
The following section offers competency-based recommendations for CE programs to incorporate into their curricula and experiential training. We propose a conceptual model that we call the 3 Cs of ED Education and Training. The 3 Cs are: (a) cultivating trainee self-awareness, (b) capturing contextual and sociocultural factors, and (c) collaborating with interdisciplinary professionals (see Figure 1). We also provide an overview of recommended activities and associated reflective prompts that can be used in a special topics course on EDs (see Appendix A), as well as suggested adaptations for integration across counseling curricula. By integrating these teaching strategies, CE programs can enhance competency-based education for EDs (Williams & Haverkamp, 2010), which may empower CITs to provide compassionate, empirically supported services to this vulnerable population.
Figure 1
The 3 Cs of ED Education and Training
Cultivating Trainee Self-Awareness
Cultivating trainee self-awareness is essential to ethical and multiculturally competent ED treatment. As espoused in our ethical codes (ACA, 2014), counselors are expected to examine their own beliefs, attitudes, and emotional responses when working with clients. Without such conscious examination, clinicians risk projecting their personal biases onto their clients or responding in ways that might inadvertently cause harm. For instance, the pervasive weight stigma embedded in our society can unconsciously influence counselors and may result in microaggressions, victim blaming, or the dismissal of symptoms, particularly when working with clients in larger bodies (Veillette et al., 2018). Counselors may also experience countertransference reactions triggered by ED behaviors or other challenging treatment components, such as high relapse rates, resistance to treatment, or insurance coverage issues (Labarta et al., 2023; Warren et al., 2013), negatively influencing the therapeutic relationship (Graham et al., 2020). Reflexive exercises, paired with targeted deliberate skill practice, are valuable mechanisms for facilitating conscious self-examination and building relevant knowledge and skills for effective ED treatment.
Encouraging Reflexivity and Deliberate Practice
Reflexivity, defined as “a practice of observing and locating one’s self as a knower within certain cultural and socio-historical contexts,” allows CITs to engage with courses on cognitive, affective, and experiential levels (Sinacore et al., 1999, p. 267). The integration of reflexive exercises and critical discussions into ED curricula is essential for cultivating self-awareness and, in effect, mitigating potential client harm. Such practices create opportunities for trainees to identify and address any unconscious biases or beliefs, which, if unaddressed, can undermine the quality of care provided. By establishing a habit of mindful self-inquiry, educators can take the first critical step in preparing ethically conscientious counselors attuned to ED clients’ diverse needs (Labarta et al., 2023).
This intentional practice of reflexivity should be paired with deliberate practice strategies focused specifically on promoting skill development for treating EDs. Deliberate practice is a systematic and intentional training method that targets skill development in order to attain expert performance in a given area or domain (Ericsson, 2006; Irvine et al., 2021). Research shows that integrating deliberate practice strategies early in CE training promotes competency development (Chow et al., 2015). Ericsson (2006) developed five crucial tasks of deliberate practice: self-assessment, skill repetition, formative feedback, stretch goals, and progress monitoring. The first task is a necessary step in increasing trainee self-awareness, which is particularly crucial when working with vulnerable populations, such as those struggling with EDs. Deliberate practice empowers trainees to refine their skills and continuously evolve as competent, empathic, and effective counselors. Thus, deliberate self-reflection on personal assumptions is key, as examining one’s relationship with food and body is imperative to prevent issues like value imposition and orient the focus of treatment to the client’s healing process.
Integrating reflexivity and deliberate skill practice early in CE training is vital to promoting lasting competency. CITs often overestimate their competence at the end of their training, necessitating that CE programs systematically monitor the congruence between CITs’ self-assessments and counselor educators’ assessments of CITs’ competency and skill development (Gonsalvez et al., 2023). Routine reflexive exercises can illuminate areas for growth, while deliberate practice strategies provide structured mechanisms for targeted skill refinement. As trainees embark on their professional journeys, ongoing and intentional efforts to self-reflect and evolve through skill refinement will empower them to provide safe, ethical, and effective ED treatment.
Capturing Contextual and Sociocultural Factors
It has been well-documented that EDs impact individuals across social and cultural identities despite the misconception that only thin, White, affluent, cisgender women are affected (Schaumberg et al., 2017). Indeed, scholars have pointed to the need for intersectional, social justice–informed research that addresses the unique ways that context and culture influence EDs and body image concerns (Burke et al., 2020; Halbeisen et al., 2022). The prevalence of EDs and pervasive body image issues is alarming in today’s sociocultural landscape. For instance, the recent increase in gender-affirming care bans and anti-LGBTQ+ legislation poses profound and detrimental effects on individuals battling an ED (Arcelus et al., 2017), as these restrictive policies exacerbate the mental and emotional distress already experienced by LGBTQ+ individuals, further isolating them and undermining their access to critical health care services (Canady, 2023). As a result, members of this community are more apt to experience intensified body dysphoria, heightening the risk of developing or worsening an ED in an attempt to conform to societal norms (Arcelus et al., 2017).
In the wake of the COVID-19 pandemic, the world has experienced a collective trauma that triggered a series of physical and mental health consequences that will linger for years to come, including rising rates of disordered eating and body-related concerns. Termorshuizen et al. (2020) surveyed 1,021 individuals across the United States and the Netherlands, revealing that ED diagnoses increased at a rate of roughly 60%, with respondents noting increased binge episodes (30%) and restriction behaviors (62%) during this time. Scholars have also shown the deleterious effects of the pandemic on body image perception. For instance, in one study of 7,878 respondents, 61% of surveyed adults and 66% of surveyed children (17 and under) disclosed frequent negative feelings regarding their body image, with 53% of adults and 58% of children reporting that the pandemic has significantly exacerbated these feelings (House of Commons, 2021). Unfortunately, weight stigma was also pervasive in the media, with concerns regarding quarantine weight gain (e.g., “Quarantine-15”) contributing to eating and body image challenges (Schneider et al., 2023). Amidst the multifaceted challenges presented by recent sociopolitical events and the intersecting struggles faced by diverse individuals with EDs, it is essential that counselors implement culturally responsive approaches to treatment and advocacy efforts.
Centering Culturally Responsive Approaches
Given the diversity of clients who struggle with eating and body image concerns (Schaumberg et al., 2017), CE programs must integrate culturally sensitive theories into the curriculum to ensure that CITs possess the necessary competencies to explore relevant cultural factors and effectively treat diverse clients with EDs (Williams & Haverkamp, 2010). Two theories that fostered the development of the Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016) are intersectionality theory and relational–cultural theory (Singh et al., 2020). Intersectionality is a framework for comprehensively understanding the interaction of systemic inequalities and oppression that significantly affect marginalized community members (Burke et al., 2020; Crenshaw, 1991). This theoretical paradigm deepens our understanding of factors such as age, race, ethnicity, sexual orientation, ability status, body size, and gender identity and how these factors influence an individual’s lived experience. Intersectionality is vital for promoting social justice and culturally responsive treatment while also serving as a tool to dismantle oppression and colonizing practices within the profession (Chan et al., 2018; Singh et al., 2020). Intersectionality-informed practice may assist researchers and counselors with considering risk and protective factors for EDs; however, the lack of attention to the intersecting roles and identities of ED clients (e.g., a Catholic, bisexual, Latina) remains a concern, which is crucial for informing culturally competent counseling and training practices (Burke et al., 2020).
Relational–cultural therapy (RCT; Jordan, 2009) is another promising theory that may decolonize dominant counseling approaches (Singh et al., 2020). Due to its emphasis on relational connection, social justice, and empowerment, RCT has been applied to the treatment of EDs (Labarta & Bendit, 2024; Trepal et al., 2015). Infusing RCT into practice may help counselors understand sociocultural influences that maintain ED (e.g., diet culture, weight stigma, acculturation) and perpetuate feelings of disconnection for individuals who do not conform to prevailing body or appearance standards. RCT also aligns well with counseling’s wellness orientation due to its relational and strengths-based focus, emphasizing resilience over pathology in the treatment of ED (Labarta & Bendit, 2024). Counselor educators can expand beyond traditional ED treatment approaches by integrating culturally responsive theories like intersectionality and RCT into course curricula, thus highlighting the intrapersonal, interpersonal, and systemic components that impact clients with EDs.
Collaborating With Interdisciplinary Professionals
The counseling profession has recognized the importance of interdisciplinary practice, encouraging counselors to participate in “decisions that affect the well-being of clients by drawing on the perspectives, values, and experiences of the counseling profession and those of colleagues from other disciplines” (ACA, 2014, Code D.1.c, p. 10). The CACREP Standards (2023) also emphasize the need for counseling students to learn about collaboration, consultation, and community outreach as part of interprofessional teams (Section 3.A.3). Indeed, interdisciplinary collaboration provides an opportunity for individual and systems-level advocacy (Myers et al., 2002). The challenge remains in how counselors can balance establishing a distinct professional identity while simultaneously fostering a sense of community among various helping professions (Klein & Beeson, 2022). Researchers have underscored common experiences of counselors within interdisciplinary teams, including challenges with building legitimacy and credibility, especially among more well-established helping professions such as psychiatry or psychology (Klein & Beeson, 2022; Ng et al., 2023). Given that multidisciplinary collaboration is also crucial to ED treatment (Crone et al., 2023; Williams & Haverkamp, 2010), counselor educators must prepare CITs to effectively work within interdisciplinary treatment teams while utilizing their counseling values and training to best serve their clients and advocate for the inclusion of counselors across ED treatment settings (Labarta et al., 2023).
Strengthening Counselor Professional Identity
Given that EDs are biopsychosocial in nature, effective treatment commonly involves collaboration among various health professions (e.g., medicine, psychiatry, counseling, psychology, dietetics) to ensure holistic, comprehensive client care (Crone et al., 2023). Counselors’ developmental, preventive, and wellness-based perspectives can help provide a strengths-based approach to interdisciplinary collaborations (Labarta et al., 2023). For example, a psychiatrist at a residential facility may focus on assessing a client’s pathology, comorbidity, and changes in symptoms throughout treatment. Although counselors can also focus on assessing client symptoms, their training allows them to provide insight into protective factors that foster client resilience in their recovery process (e.g., social support and cognitive flexibility). Both professionals bring unique expertise, knowledge, and skill sets that provide a distinct conceptualization of the client’s concerns with food or with their body. However, the ultimate goal of the treatment team is to ensure ethical and competent care for the client.
Outside of intensive ED treatment, counselors in school settings and community agencies can offer prevention-based approaches to mitigate risk factors leading to the development of EDs. Prevention-based efforts, such as community programs and workshops, are essential to the field of ED, given the alarmingly low rates of help-seeking in adults with lifetime EDs (34.5% for anorexia nervosa, 62.6% for bulimia nervosa, and 49.0% for binge eating disorder), which are even more pronounced among marginalized communities (Coffino et al., 2019). As such, counselors and other helping professionals can collaborate on ways to increase accessibility to mental health services for underserved groups with increased risk of eating or body image concerns (e.g., LGBTQ+; Nagata et al., 2020). Regardless of the settings within which CITs will work, students can benefit from developing teamwork, leadership, and advocacy skills, as well as a systemic conceptualization of client care (Ng et al., 2023). Ultimately, counselor educators can encourage the exploration of shared goals across helping professions and the utilization of counseling values and training to enhance interdisciplinary work for diverse clients and communities recovering from EDs (Klein & Beeson, 2022; Labarta et al., 2023; Ng et al., 2023).
Implications for Counselor Educators
The 3 Cs for ED Education and Training pose several implications for counselor educators and counseling programs. Although intended for ED treatment, this framework captures essential competencies across counseling specialties, such as counselor self-awareness, cultural and diversity issues, and interdisciplinary practice (CACREP, 2023). As such, integrating these foci into the counseling curriculum can help reinforce competencies regardless of the settings within which students will work. Counselor educators teaching about EDs should also consider ways to incorporate other ED counseling competencies, such as relevant ethical issues, assessment and screening, and evidence-based treatments into coursework (Williams & Haverkamp, 2010). These topics can be integrated into the 3 Cs for ED Education and Training in several ways. For instance, ethical issues and scenarios, such as determining when a client may need a higher level of care, can be presented to students as a standard component of collaborating with interdisciplinary professionals. Counselor educators can also review common ED assessments and encourage students to critically evaluate gaps in the diagnostic process that impact underrepresented populations (e.g., men with EDs), capturing contextual and sociocultural factors and enhancing culturally responsive care (see Appendix B for more examples.)
We also recognize the potential challenges of implementing the 3 Cs of ED Education and Training, as a stand-alone, special topics course on EDs may not be possible for all counseling programs. However, counselor educators can adapt and incorporate the suggested activities in Appendix A into various CACREP core courses to enhance ED education across the curriculum. CE programs can also utilize their Chi Sigma Iota chapters to host events on EDs, such as an interdisciplinary panel discussion followed by a group discussion on professional counseling identity and advocacy (Labarta et al., 2023). Opening these events to the local community could encourage continuing education, collaboration, and advocacy.
Directions for Future Research
Given that the 3 Cs of ED Education and Training is a conceptual framework, there are several directions for future research. Counselor educators and researchers may consider developing a stand-alone course to test the effects of this framework on CITs’ competence in treating EDs. To our knowledge, limited ED competency measures exist, especially for counselors. As such, researchers could explore developing an instrument that measures ED competency areas that include the 3 Cs of ED Education and Training. Such a tool would be helpful for research, clinical, and teaching purposes. An ED competency tool may also enhance CITs’ and counselors’ deliberate practice efforts, promoting quality care for clients across ED treatment settings. Additionally, one theoretical framework educators can modify to help enhance trainees’ clinical competencies in treating EDs is Irvine and colleagues’ (2021) Deliberate Practice Coaching Framework (DPCF), given its structured guidance for skill refinement through individualized coaching and feedback. The development and future testing of an adapted DPCF for EDs may further enhance reflexive and deliberate practice efforts for CITs and counselors working with this population.
Conclusion
In this article, we have proposed our 3 Cs of ED Education and Training to address current gaps in ED education and enhance trainee preparedness across CE programs. Informed by existing literature, this framework incorporates essential elements of comprehensive ED treatment, including counselor self-awareness, cultural and contextual factors, and interdisciplinary practice. The flexibility of this framework allows educators to adapt current curricula to strengthen ED training in CE programs and to meet the needs of their students. Further research that tests a stand-alone course incorporating this framework is needed. The 3 Cs of ED Education and Training offer a path forward in remedying the salient gaps in ED education, ultimately advocating for more compassionate, ethical, and inclusive care across counseling settings.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/ethics/2014-aca-code-of-ethics.pdf?sfvrsn=55ab73d0_1
Arcelus, J., Fernández-Aranda, F., & Bouman, W. P. (2017). Eating disorders and disordered eating in the LGBTQ population. In L. K. Anderson, S. B. Murray, & W. H. Kaye (Eds.), Clinical handbook of complex and atypical eating disorders (pp. 327–343). Oxford University Press.
https://doi.org/10.1093/med-psych/9780190630409.003.0019
Babb, C., Jones, C. R. G., & Fox, J. R. E. (2022). Investigating service users’ perspectives of eating disorder services: A meta-synthesis. Clinical Psychology and Psychotherapy, 29(4), 1276–1296. https://doi.org/10.1002/cpp.2723
Biang, A., Merlin-Knoblich, C., & Lim, J. H. (2024). An exploration of counselors of color working in the eating disorder field. Journal of Counseling & Development, 102(4), 482–494. https://doi.org/10.1002/jcad.12532
Burke, N. L., Schaefer, L. M., Hazzard, V. M., & Rodgers, R. F. (2020). Where identities converge: The importance of intersectionality in eating disorders research. International Journal of Eating Disorders, 53(10), 1605–1609. https://doi.org/10.1002/eat.23371
Canady, V. A. (2023). Mounting anti-LGBTQ+ bills impact mental health of youths. Mental Health Weekly, 33(15), 1–6. https://doi.org/10.1002/mhw.33603
Carney, J. M., & Scott, H. L. (2012). Eating issues in schools: Detection, management, and consultation with allied professionals. Journal of Counseling & Development, 90(3), 290–297. https://doi.org/10.1002/j.1556-6676.2012.00037.x
Chan, C. D., Cor, D. N., & Band, M. P. (2018). Privilege and oppression in counselor education: An intersectionality framework. Journal of Multicultural Counseling and Development, 46(1), 58–73. https://doi.org/10.1002/jmcd.12092
Chow, D. L., Miller, S. D., Seidel, J. A., Kane, R. T., Thornton, J. A., & Andrews, W. P. (2015). The role of deliberate practice in the development of highly effective psychotherapists. Psychotherapy, 52(3), 337–345. https://doi.org/10.1037/pst0000015
Coffino, J. A., Udo, T., & Grilo, C. M. (2019). Rates of help-seeking in US adults with lifetime DSM-5 eating disorders: Prevalence across diagnoses and differences by sex and ethnicity/race. Mayo Clinic Proceedings, 94(8), 1415–1426. https://doi.org/10.1016/j.mayocp.2019.02.030
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/for-programs/2024-cacrep-standards
Crandall, C. S. (1994). Prejudice against fat people: Ideology and self-interest. Journal of Personality and Social Psychology, 66(5), 882–894. https://doi.org/10.1037/0022-3514.66.5.882
Crenshaw, K. (1991). Mapping the margins: Intersectionality, identity politics, and violence against women of color. Stanford Law Review, 43(6), 1241–1299. https://doi.org/10.2307/1229039
Crone, C., Fochtmann, L. J., Attia, E., Boland, R., Escobar, J., Fornari, V., Golden, N., Guarda, A., Jackson-Triche, M., Manzo, L., Mascolo, M., Pierce, K., Riddle, M., Seritan, A., Uniacke, B., Zucker, N., Yager, J., Craig, T. J., Hong, S.-H., & Medicus, J. (2023). The American Psychiatric Association practice guideline for the treatment of patients with eating disorders. The American Journal of Psychiatry, 180(2), 167–171. https://doi.org/10.1176/appi.ajp.23180001
Deloitte Access Economics. (2020, June). Social and economic cost of eating disorders in the United States [Infographic]. https://www.hsph.harvard.edu/striped/report-economic-costs-of-eating-disorders
Ericsson, K. A. (2006). The influence of experience and deliberate practice on the development of superior expert performance. In K. A. Ericsson, N. Charness, P. J. Feltovich, & R. R. Hoffman (Eds.), The Cambridge handbook of expertise and expert performance (1st ed., pp. 683–704). Cambridge University Press.
Galmiche, M., Déchelotte, P., Lambert, G., & Tavolacci, M. P. (2019). Prevalence of eating disorders over the 2000–2018 period: A systematic literature review. The American Journal of Clinical Nutrition, 109(5), 1402–1413. https://doi.org/10.1093/ajcn/nqy342
Gonsalvez, C. J., Riebel, T., Nolan, L. J., Pohlman, S., & Bartik, W. (2023). Supervisor versus self-assessment of trainee competence: Differences across developmental stages and competency domains. Journal of Clinical Psychology, 79(12), 2959–2973. https://doi.org/10.1002/jclp.23590
Graham, M. R., Tierney, S., Chisholm, A., & Fox, J. R. E. (2020). The lived experience of working with people with eating disorders: A meta-ethnography. International Journal of Eating Disorders, 53(3), 422–441. https://doi.org/10.1002/eat.23215
Halbeisen, G., Brandt, G., & Paslakis, G. (2022). A plea for diversity in eating disorders research. Frontiers in Psychiatry, 13, 820043. https://doi.org/10.3389/fpsyt.2022.820043
House of Commons Women and Equalities Committee. (2021). Changing the perfect picture: An inquiry into body image. https://committees.parliament.uk/publications/5357/documents/53751/default
Irvine, T., Fullilove, C., Osman, A., Farmanara, L., & Emelianchik-Key, K. (2021). Enhancing clinical competencies in counselor education: The Deliberate Practice and Coaching Framework. Journal of Counselor Preparation and Supervision, 14(4). https://digitalcommons.sacredheart.edu/jcps/vol14/iss4/5
Jordan, J. V. (2009). Relational–cultural therapy. American Psychological Association.
Kärkkäinen, U., Mustelin, L., Raevuori, A., Kaprio, J., & Keski-Rahkonen, A. (2018). Do disordered eating behaviours have long-term health-related consequences? European Eating Disorders Review, 26(1), 22–28. https://doi.org/10.1002/erv.2568
Kerl-McClain, S. B., Dorn-Medeiros, C. M., & McMurray, K. (2022). Addressing anti-fat bias: A crash course for counselors and counselors-in-training. Journal of Counselor Preparation and Supervision, 15(4). https://digitalcommons.sacredheart.edu/jcps/vol15/iss4/3
Klein, J. L., & Beeson, E. T. (2022). An exploration of clinical mental health counselors’ attitudes toward professional identity and interprofessionalism. Journal of Mental Health Counseling, 44(1), 68–81. https://doi.org/10.17744/mehc.44.1.06
Labarta, A. C., & Bendit, A. (2024). Culturally responsive and compassionate eating disorder treatment: Serving marginalized communities with a relational-cultural and self-compassion approach. Journal of Creativity in Mental Health, 19(2), 251–261. https://doi.org/10.1080/15401383.2023.2174629
Labarta, A. C., Irvine, T., & Peluso, P. R. (2023). Exploring clinician attitudes towards treating eating disorders: Bridging counselor training gaps. Journal of Counselor Preparation and Supervision, 17(1). https://digitalcommons.sacredheart.edu/jcps/vol17/iss1/2
Levitt, D. H. (2006). Eating disorders training and counselor preparation: A survey of graduate programs. The Journal of Humanistic Counseling, Education and Development, 45(1), 95–107. https://doi.org/10.1002/j.2161-1939.2006.tb00008.x
Myers, J. E., Sweeney, T. J., & White, V. E. (2002). Advocacy for counseling and counselors: A professional imperative. Journal of Counseling & Development, 80(4), 394–402. https://doi.org/10.1002/j.1556-6678.2002.tb00205.x
Nagata, J. M., Ganson, K. T., & Austin, S. B. (2020). Emerging trends in eating disorders among sexual and gender minorities. Current Opinion in Psychiatry, 33(6), 562–567. https://doi.org/10.1097/YCO.0000000000000645
Ng, K.-M., Harrichand, J. J. S., Litherland, G., Ewe, E., Kayij-Wint, K. D., Maurya, R., & Schulthes, G. (2023). Interdisciplinary collaboration challenges faced by counselors in places where professional counseling is nascent. International Journal for the Advancement of Counselling, 45(1), 155–169.
https://doi.org/10.1007/s10447-022-09492-y
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Schaumberg, K., Welch, E., Breithaupt, L., Hübel, C., Baker, J. H., Munn-Chernoff, M. A., Yilmaz, Z., Ehrlich, S., Mustelin, L., Ghaderi, A., Hardaway, A. J., Bulik-Sullivan, E. C., Hedman, A. M., Jangmo, A., Nilsson, I. A. K., Wiklund, C., Yao, S., Seidel, M., & Bulik, C. M. (2017). The science behind the Academy for Eating Disorders’ nine truths about eating disorders. European Eating Disorders Review, 25(6), 432–450.
https://doi.org/10.1002/erv.2553
Schneider, J., Pegram, G., Gibson, B., Talamonti, D., Tinoco, A., Craddock, N., Matheson, E., & Forshaw, M. (2023). A mixed-studies systematic review of the experiences of body image, disordered eating, and eating disorders during the COVID-19 pandemic. International Journal of Eating Disorders, 56(1), 26–67. https://doi.org/10.1002/eat.23706
Sinacore, A. L., Blaisure, K. R., Justin, M., Healy, P., & Brawer, S. (1999). Promoting reflexivity in the classroom. Teaching of Psychology, 26(4), 267–270. https://doi.org/10.1207/S15328023TOP260405
Singh, A. A., Appling, B., & Trepal, H. (2020). Using the Multicultural and Social Justice Counseling Competencies to decolonize counseling practice: The important roles of theory, power, and action. Journal of Counseling & Development, 98(3), 261–271. https://doi.org/10.1002/jcad.12321
Streatfeild, J., Hickson, J., Austin, S. B., Hutcheson, R., Kandel, J. S., Lampert, J. G., Myers, E. M., Richmond, T. K., Samnaliev, M., Velasquez, K., Weissman, R. S., & Pezzullo, L. (2021). Social and economic cost of eating disorders in the United States: Evidence to inform policy action. International Journal of Eating Disorders, 54(5), 851–868. https://doi.org/10.1002/eat.23486
Termorshuizen, J. D., Watson, H. J., Thornton, L. M., Borg, S., Flatt, R. E., MacDermod, C. M., Harper, L. E., van Furth, E. F., Peat, C. M., & Bulik, C. M. (2020). Early impact of COVID-19 on individuals with eating disorders: A survey of ~1000 individuals in the United States and the Netherlands. International Journal of Eating Disorders, 53(11), 1780–1790. https://doi.org/10.1002/eat.23353
Thompson-Brenner, H., Satir, D. A., Franko, D. L., & Herzog, D. B. (2012). Clinician reactions to patients with eating disorders: A review of the literature. Psychiatric Services, 63(1), 73–78. https://doi.org/10.1176/appi.ps.201100050
Trepal, H., Boie, I., Kress, V., & Hammer, T. (2015). A relational-cultural approach to working with clients with eating disorders. In L. H. Choate (Ed.), Eating disorders and obesity: A counselor’s guide to prevention and treatment (pp. 261–276). https://doi.org/10.1002/9781119221708.ch18
Ulfvebrand, S., Birgegård, A., Norring, C., Högdahl, L., & von Hausswolff-Juhlin, Y. (2015). Psychiatric comorbidity in women and men with eating disorders results from a large clinical database. Psychiatry Research, 230(2), 294–299. https://doi.org/10.1016/j.psychres.2015.09.008
van Hoeken, D., & Hoek, H. W. (2020). Review of the burden of eating disorders: Mortality, disability, costs, quality of life, and family burden. Current Opinion in Psychiatry, 33(6), 521–527. https://doi.org/10.1097/YCO.0000000000000641
Veillette, L. A. S., Serrano, J. M., & Brochu, P. M. (2018). What’s weight got to do with it? Mental health trainees’ perceptions of a client with anorexia nervosa symptoms. Frontiers in Psychology, 9, 2574. https://doi.org/10.3389/fpsyg.2018.02574
Warren, C. S., Schafer, K. J., Crowley, M. E. J., & Olivardia, R. (2013). Demographic and work-related correlates of job burnout in professional eating disorder treatment providers. Psychotherapy, 50(4), 553–564. https://doi.org/10.1037/a0028783
Williams, M., & Haverkamp, B. E. (2010). Identifying critical competencies for psychotherapeutic practice with eating disordered clients: A Delphi study. Eating Disorders, 18(2), 91–109. https://doi.org/10.1080/10640260903585524
Appendix A
The 3 Cs of ED Education and Training: Suggested Activities and Reflective Prompts
| 3 Cs of ED Education & Training |
Suggested
Activities |
Activity Sample
Reflective Prompts |
Adaptations for Integration Across Counseling Curricula |
|
Cultivating Trainee
Self-Awareness |
Reflexive Journaling:
Have CITs maintain a journal, reflecting on their experiences (e.g., biases, assumptions, insights, challenges) throughout the course.
Instructors can provide suggested weekly prompts based on the content or topic area discussed.
Deliberate Practice:
During the first week, CITs will read Williams and Haverkamp’s (2010) article on ED counseling competencies.
CITs then write a reflection paper identifying 2–3 targeted, actionable areas for development and growth.
Revisit these competencies at the end of the course to assess CIT growth and ongoing development areas. |
Reflexive Journaling Prompts:
Reflect on your beliefs, values, and attitudes about counseling ED clients. What would you like to learn? What challenges do you anticipate?
How might cultural factors impact how counselors work with ED clients? Consider how your cultural and social identities shape your relationship with food and body image.
Complete the Anti-fat Attitudes Questionnaire (Crandall, 1994) and interpret your score. What insights did you gain? Why might self-assessment in this domain be an important tool for counselors? (Kerl-McClain et al., 2022)
Deliberate Practice Prompts:
Using a Likert scale of 1 (not confident) to 5 (very confident), how confident do you feel to treat clients with EDs?
Using a Likert scale of 1 (not prepared) to 5 (very prepared), how prepared do you feel to treat clients with EDs?
Identify 2–3 areas of personal or professional development and growth.
Identify 2–3 actionable steps for this semester and beyond.
|
Psychopathology and Diagnosis Courses:
Before teaching ED diagnoses, facilitate a brief activity to promote reflexive practice (see suggested prompts).
Follow up with a class discussion on CITs’ reflections, reactions, insights, and the possible impact of biases or assumptions on the diagnosis and treatment process for ED clients.
Practicum and Internship Courses:
CITs working in ED treatment settings can use the deliberate practice prompts to continually assess strengths and growth areas.
Encourage CITs to complete the self-assessment on ED knowledge and skills. Based on the identified gaps, campus instructors can invite guest lecturers to discuss topics of interest. |
| 3 Cs of ED Education & Training |
Suggested
Activities |
Activity Sample
Reflective Prompts |
Adaptations for Integration Across Counseling Curricula |
|
Capturing Contextual
and
Sociocultural Factors |
Media Critique:
Have CITs select and analyze a form of media (e.g., movies, TV series, social media).
CITs can then consider the messages conveyed about EDs and body image.
Class Discussion:
Engage in a class discussion on CITs’ observations, noted themes, and implications for counseling practice.
Educators may also initiate a discussion on media literacy and how to broach similar discussions with clients and colleagues.
|
Individual Reflection Prompts:
How were EDs and/or body image concerns portrayed explicitly and implicitly?
How do sociocultural factors (e.g., race, ethnicity, gender, etc.) influence media portrayals and messages about EDs/body image?
How might these portrayals or messages influence one’s beliefs about EDs?
Class Discussion Prompts:
What were the overarching themes or messages across the various media?
How can culturally responsive theories (e.g., RCT, intersectionality) inform how we conceptualize the impact of media on EDs and body image concerns?
How can counselors work with clients impacted by harmful media ideals?
How can counselors advocate for more culturally inclusive and responsible ED portrayals in media? |
Social and Cultural Diversity Course:
Facilitate a discussion on CITs’ observations of ED media portrayals, considering the impact of limited representation on mental health access.
Provide a case study of a client with intersecting minoritized identities and encourage CITs to identify culturally responsive treatment approaches and theories that can benefit the client’s recovery. |
| 3 Cs of ED Education & Training |
Suggested
Activities |
Activity Sample
Reflective Prompts |
Adaptations for Integration Across Counseling Curricula |
|
Collaborating with Interdisciplinary Professionals |
ED Expert Panel:
Invite professionals across disciplines specializing in treating EDs (e.g., M.D., psychiatrist, psychologist, dietician).
Engage the panelists in a discussion on their respective training, roles, responsibilities, and experiences working in interdisciplinary treatment teams.
Reserve Q&A time for CITs to share any thoughts, questions, and insights (Labarta et al., 2023).
Professional Identity Reflection Paper:
After the ED expert panel discussion, have CITs write a reflection paper on what they learned from the panelists.
CITs can reflect on how counselors contribute to interdisciplinary teams using their developmental, prevention-focused, and wellness-based training.
Facilitate a broader discussion with CITs during the subsequent class meeting. |
Expert Panel Discussion Prompts:
Briefly discuss your ED treatment experiences and describe your main roles and responsibilities.
Discuss the benefits and challenges of working in interdisciplinary treatment teams.
What would you say are the most prevalent issues faced by ED professionals today?
What words of wisdom can you share with CITs considering working with ED clients?
Professional Identity
Paper Prompts:
· What challenges and opportunities do you foresee as a counselor working in an interdisciplinary treatment team?
· How can counseling values inform an interdisciplinary perspective on ED treatment?
· What personal strengths could you contribute as an interdisciplinary treatment team member?
· Reflect on the MJSCC (Ratts et al., 2016), discussing how they can inform a counselor’s work with diverse clients struggling with eating and/or body image concerns. |
Introduction to Mental Health Counseling Course:
If coordinating an ED expert panel is not feasible, consider inviting other professionals across specialty areas (e.g., EDs, addictions, integrated behavioral health) to share their experiences
CITs can complete a reflection paper on their insights and reactions to the guest panelists using the professional identity paper prompts as a guide.
|
Appendix B
Educator Checklist for Integrating the 3 Cs of Eating Disorder (ED) Education and Training Into Counselor Education Curricula
|
| Cultivating Trainee Self-Awareness |
|
Increase trainee awareness by incorporating ED warning signs, risk factors, and conceptualization strategies into assessment and treatment approaches. |
|
Routinely assess student competency on ED-related knowledge and skills, evaluating for any incongruence between the students’ and educators’ scores. Additionally, assess multicultural counseling competencies related to EDs during student evaluations. Provide feedback for growth. |
|
Encourage student attendance at ED-focused workshops, webinars, and conferences to enhance deliberate practice efforts, promoting professional growth and development. |
|
Promote student exploration of their own cultural identities, values, and biases related to appearance, health, and eating behaviors. |
| Capturing Contextual and Sociocultural Factors |
|
Incorporate diverse ED case examples and vignettes that reflect a range of intersecting cultural identities and experiences. |
|
Provide training on culturally responsive ED treatment approaches like RCT and intersectionality. Be sure to cover strategies for adapting evidence-based ED treatment approaches to be culturally relevant for diverse clients. |
|
Emphasize the importance of cultivating cultural humility and client empowerment, particularly when working with ED clients from diverse or marginalized backgrounds. |
| Collaborating With Interdisciplinary Professionals |
|
Critically examine course syllabi to identify where ED content and scholarship could be incorporated or expanded (e.g., textbooks, media, articles). Include resources from interdisciplinary helping professionals. |
|
Compile a list of interdisciplinary community referrals and resources to support students working with ED clients. |
|
Provide opportunities (e.g., guest lecture, course assignment) for students to learn from ED experts in various helping disciplines. Encourage students to reflect on ways to utilize their counseling values and training within interdisciplinary treatment collaborations. |
Note. This checklist is a framework for integrating ED education into CE graduate training. Consider modifying components to align with your specific curriculum, resources, and student population. The goal is to integrate ED education in a way that provides students with foundational knowledge, skills, and practical experience to effectively support clients struggling with EDs and body image issues in their future counseling practice.
Taylor J. Irvine, PhD, NCC, ACS, LMHC, is an assistant professor at Nova Southeastern University. Adriana C. Labarta, PhD, NCC, ACS, LMHC, is an assistant professor at Florida Atlantic University. Correspondence may be addressed to Taylor J. Irvine, Department of Counseling, Nova Southeastern University, 3300 S. University Dr., Maltz Bldg., Rm. 2041, Fort Lauderdale, FL 33328-2004, ti48@nova.edu.
May 22, 2024 | Volume 14 - Issue 1
William B. Lane, Jr., Timothy J. Hakenewerth, Camille D. Frank, Tessa B. Davis-Price, David M. Kleist, Steven J. Moody
Interpretative phenomenological analysis was used to explore the simultaneous supervision experiences of counselors-in-training. Simultaneous supervision is when a supervisee receives clinical supervision from multiple supervisors. Sometimes this supervision includes a university supervisor and a site supervisor. Other times this supervision occurs when a student has multiple sites in one semester and receives supervision at each site. Counselors-in-training described their experiences with simultaneous supervision during the course of their education. Four superordinate themes emerged: making sense of multiple perspectives, orchestrating the process, supervisory relationship dynamics, and personal dispositions and characteristics. Results indicated that counselors-in-training experienced compounded benefits and challenges. Implications for supervisors, supervisees, and counselor education programs are provided.
Keywords: clinical supervision, simultaneous supervision, counselors-in-training, interpretative phenomenological analysis, counselor education
Supervision is a key component of counselor education in programs accredited by the Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2015) and an ethical requirement in the ACA Code of Ethics (American Counseling Association, 2014). Supervision of counselors-in-training (CITs) serves the purpose of guiding counselor development, gatekeeping, and, ultimately, ensuring competent client care (Borders et al., 2014). For the present study, we defined simultaneous supervision as a pre-licensure CIT receiving weekly individual or triadic supervision from more than one supervisor over the same time period. At the time of the study, the 2016 CACREP standards required that internship and practicum students receive individual and/or triadic supervision averaging 1 hour per week throughout their clinical experience (Standards 3.L. & 3.H.). Some CITs may gain field experience at multiple clinical sites requiring individual site supervision at each site. Many programs require students to engage in faculty advising meetings (Choate & Granello, 2006), which may take a form analogous to formal supervision. Additionally, supervisees may have clinical supervision, focused on supervisee development and client welfare, as well as administrative supervision, focused on functionality and logistics within an agency; these roles may be fulfilled by the same person or at times by two separate supervisors (Kreider, 2014; Tromski-Klingshirn & Davis, 2007). Consequently, although simultaneous supervision is not required in and of itself, it often occurs in counselor education practice.
Supervision Foundations
Counseling supervision research has increased significantly in the last few decades (Borders et al., 2014). Borders and colleagues (2014) developed best practices for effective supervision, including emphasis on the supervision contract, social justice considerations, ethical guidelines, documentation management, and relational dynamics. Previous research has overwhelmingly demonstrated that a strong supervisory alliance is the bedrock of effective supervision (Bernard & Goodyear, 2019). Sterner (2009) further studied the supervisory relationship as a mediator for supervisee work satisfaction and stress. Lambie and colleagues (2018) developed a CIT clinical evaluation to be used in supervision, with strength in assessing personal dispositions in addition to clinical skills. A review of the supervision literature revealed that a strong supervisory relationship based in goal congruence, empathic rapport, and transparent feedback processes (Bernard & Goodyear, 2019; Borders et al., 2014; Sterner, 2009) generate mutual growth between supervisor and supervisee, enhancing clinical work. Additionally, CACREP mandates that faculty and site supervisors foster CIT professional counselor identity through the supervisory process (Borders, 2006; CACREP, 2015).
Counselor development is also a crucial factor in clinical supervision. An entire category of supervision models centralizes the professional development of supervisees in their approach (Bernard & Goodyear, 2019). One of the most widely known models, the Integrative Developmental Model, plots learning, emotion, and cognitive factors across multiple stages of therapist development (Stoltenberg & McNeill, 2010). By focusing on overarching themes of self–other awareness, autonomy, and motivation, the Integrative Developmental Model (Stoltenberg & McNeill, 2010) illuminates how supervisees fluctuate and grow in their anxiety, self-efficacy, reliance on structure, and independence. All these factors may have substantial impact when considering the complexity that simultaneous supervision brings. Furthermore, professional dispositions of openness to feedback and flexibility and adaptability (Lambie et al., 2018) may have additional developmental implications when considering the complexity of simultaneous supervision.
Ethics similarly serve as a foundation of supervisory experiences. Multiple standards and principles of the ACA Code of Ethics (2014) may be complicated by simultaneous supervision and require special attention. Veracity may be of particular interest given the commonality of supervisee nondisclosure (Kreider, 2014), multiplied by the added number of supervisors in one time period. Furthermore, specific standards in Section D: Relationships With Other Professionals may be implicated by obligations in working with multiple professionals; multiple standards in Section F: Supervision, Training, and Teaching may be indicated because of the convergence of both teaching and clinical supervision in counselor training programs; and, finally, reconciling the additional complexities of simultaneous supervision not explicitly identified elsewhere in the 2014 Code of Ethics may elicit a need to carefully consider Section I: Resolving Ethical Issues. With more parties involved, greater nuance would be expected in ethical decision-making.
Much of the foundational research and reviewed contextual factors have either focused specifically on sole supervision or do not differentiate between sole and simultaneous supervision. When considering best supervision practices, the phenomenon of simultaneous supervision presents distinct practical concerns. Exploration is needed to better understand how supervisees might navigate different but related supervisory relationships, how goals and tasks can be congruent across separate supervisory experiences, and how supervisees would make meaning of multiple sources of feedback. Despite the apparent use of simultaneous supervision in counselor education programs, few researchers have explored these dynamic concerns.
Multiple Supervisors and Multiple Roles
Early researchers began to conceptualize the challenges and strengths inherent in simultaneous supervision in both counseling (Davis & Arvey, 1978) and clinical psychology (Dodds, 1986; Duryee et al., 1996; Nestler, 1990), with mixed results overall. Nestler (1990) identified the difficulties in receiving contradictory feedback from multiple supervisors, reflective of fundamental differences in the supervisors’ approaches. Dodds (1986) similarly identified multiple potential stressors in having concurrent supervisors at agency and training settings. Dodds argued that although the general goals to teach and serve clients overlapped, each had inherent differences in their primary institutional goals and structures. Duryee and colleagues (1996) described a beneficial view of simultaneous supervision, in which supervisees overcome conflicts with site supervisors via support and empowerment from academic program coordinators. Davis and Arvey (1978) presented a case study in which supervisees, in a raw comparison, more highly favored the dual supervision overall. These findings highlight the dynamics that occur in the context of simultaneous supervision and connect with recent findings.
Recent researchers have focused on dual-role supervision, defined as one individual supervisor serving as both a clinical and administrative supervisor to one or more supervisees (Kreider, 2014). Kreider (2014) investigated supervisee self-disclosure as related to three factors: supervisor role (dual role or single role), supervisor training level, and supervisor disclosure. Level of supervisor disclosure was found to be significant in explaining differences in supervisee self-disclosure and was hypothesized as a mitigating factor in supervisor role differences (Kreider, 2014). Tromski-Klingshirn and Davis (2007) surveyed the challenges and benefits unique to dual-role supervision for post-degree supervisees. Most supervisees reported neutral to positive outcomes from a dual-role supervisor, but a minority of supervisees noted power dynamics and fear of disclosure as primarily problematic (Tromski-Klingshirn & Davis, 2007), similar to the earlier hypotheses of Nestler (1990) and Dodds (1986). The small amount of existing research solidifies the prevalence of simultaneous supervision and the challenges and benefits for the supervisees. A missing link emerges in understanding how CITs come to understand their experience in simultaneous supervision from a qualitative perspective.
The distinct focused phenomenon of simultaneous supervision is limited in counseling literature. The few conceptual examinations of simultaneous supervision in the mental health literature have indicated confusion and role ambiguity (Nestler, 1990), while at other times simultaneous supervision has been noted to improve comprehensive learning (Duryee et al., 1996). Our study addresses the gap in the literature regarding current simultaneous supervision in counselor education utilizing qualitative analysis.
Method
Given the limited research on simultaneous supervision and its prevalence within the profession, we decided to explore this phenomenon qualitatively. Our research question was “What is the experience of CITs receiving simultaneous supervision from multiple supervisors?” We used interpretative phenomenological analysis (IPA) to explore this question because of its utility with counseling research, grounded methods of analysis, and emphasis on both contextual individual experiences with the phenomenon and general themes (Miller et al., 2018).
Research Team
At the time of the study, the research team consisted of four doctoral students—William B. Lane, Jr., Timothy J. Hakenewerth, Camille D. Frank, and Tessa B. Davis-Price—who each had previous experience with simultaneous supervision as supervisees and supervisors. The team’s perspective of this phenomenon from both roles informed their interest in and analysis of the phenomenon. The fifth member of the team, David M. Kleist, was our doctoral faculty research advisor. The sixth author, Steven J. Moody, provided support in the writing process.
Participants and Procedure
Our participants were four CITs from CACREP-accredited graduate programs accruing internship hours. Smith et al. (2009) suggested seeking three to six participants for IPA, as this allows researchers to explore the phenomenon with individual participants at a deeper level. All four participants specialized in either addiction, school, or clinical mental health counseling, and identified as White, female CITs ranging from 23 to 37 years old. Additionally, each participant reported receiving supervision from at least two supervisors to include university-affiliated supervisors and site supervisors. Each participant came from a different university representing the Rocky Mountain and North Central regions of the Association for Counselor Education and Supervision. To protect confidentiality, each participant selected a pseudonym for the study.
After securing approval from our university’s review board, we recruited participants through purposive convenience sampling. We posted a recruitment email to the CESNET listserv, an informational listserv for counselor educators and supervisors. This listserv was selected as an initial step of convenience sampling to increase the potential to reach a broad range of counseling programs. Nine individuals responded to the call to participate in the research by taking a participant screening survey that helped us determine suitability for the study. After removing individuals from research consideration because of potential dual relationships, nonresponse, or not meeting inclusion criteria, four individuals were selected as participants. We further planned to engage in serial interviewing to gain richer details of the phenomenon and achieve greater depth with the four participants (Murray et al., 2009; Read, 2018). Prior to data collection, the researchers completed a brief phone screening with each participant to review the interview protocol and explain the phenomenological approach guiding the questions. A $40 gift card was provided as a research incentive to participants. Our selection criteria included (a) being a master’s student within a CACREP counseling program, (b) currently accruing internship hours, and (c) receiving simultaneous supervision. We selected participants in internship only because homogenous sampling helps produce applicable results for a given demographical experience (Smith et al., 2009).
Data Collection
Consistent with the recommendations of Smith et al. (2009), we conducted two semi-structured interviews with each participant lasting between 45–90 minutes. We utilized the online videoconferencing platform Zoom to conduct and record the interviews. First-round interviews consisted of four open-ended questions (see Appendix) that allowed participants to explore the experience of simultaneous supervision in detail (Pietkiewicz & Smith, 2014). These questions were open-ended to allow participants to explore the how of the phenomenon (Miller et al., 2018). The final interview questions were developed through initial generation based off research and personal experiences with the phenomenon, refinement in consultation with the research advisor, and interview piloting with volunteer students who did not participate in the study. Research participants were asked about their overall experience with having multiple supervisors, benefits and detriments of simultaneous supervision, and the meaning they made as a result of experiencing simultaneous supervision. Second-round interview questions were developed based on participant responses to first-round interview questions. After two rounds of interviews and analysis, we conducted a final member check to confirm themes. All participants expressed that the developed themes were illustrative of their lived experiences with simultaneous supervision.
Data Analysis
We followed IPA’s 6-step analysis process as outlined by Smith et al. (2009) and added a seventh step with the use of the U-heuristic analysis for group research teams (Koltz et al., 2010). Our process consisted of first coding and contextualizing the data individually, followed by group analysis, triangulated with the fifth author, Kleist, as research advisor. We completed this process for each participant and then analyzed themes across participants as suggested by Smith et al. We reached consensus that four superordinate themes emerged with 11 subthemes across the two rounds of interviews. All participants endorsed agreement with the themes from their experiences in simultaneous supervision during the member check process.
Trustworthiness
We integrated Lincoln and Guba’s (1985) framework in conducting multiple procedures for establishing trustworthiness and credibility. We demonstrated prolonged engagement and persistent observation through consistent coding meetings over the span of 1 year. Additionally, we adapted the U-heuristic analysis process during data analysis to analyze data individually and collectively to strengthen the credibility of our findings (Koltz et al., 2010). Finally, after we developed the themes, we triangulated the results with participants via a member check, ensuring the individual and group themes matched their idiographic experiences.
We bridled our personal experiences with simultaneous supervision throughout the research process. Bridling recognizes that researchers have had close personal experiences with the phenomenon and that bias is best managed by recognition rather than elimination (Stutey et al., 2020). The four principal investigators, Lane, Hakenewerth, Frank, and Davis-Price, individually engaged in memo writing, discussed personal reactions to the data, and participated in group discussions regarding meaning-making of the phenomenon with Kleist serving as research advisor.
Results
Our data analysis produced four superordinate themes identified across all cases. These themes were (a) making sense of multiple perspectives, (b) orchestrating the process, (c) supervisory relationship dynamics, and (d) personal dispositions and characteristics. In the sections that follow, each theme is described in further detail and exemplar quotes are given to support their development.
Making Sense of Multiple Perspectives
Making sense of multiple perspectives was defined as the receipt and conceptualization of supervisory feedback from multiple supervisors during the same academic semester. Supervisees identified their supervisors as having differing professional orientations. At times, these differing backgrounds led to supervisors providing differing opinions for the same client.
Participants used metaphors to make meaning of the distinct offerings of their supervisors’ feedback. An example of capturing multiple perspectives was one participant, Emma, utilizing the ancient Indian parable of “The Blind Men and the Elephant” (Saxe, 1868): “The point of the story is all the world religions might have a piece of the picture of God, you know. And so between all of us [clinicians and supervisors] together, maybe we have a perspective of truth.” Through retelling of the Indian fable, this participant was able to vividly capture her personal perspective of differing viewpoints through an integrative lens as opposed to a conflict of ideas. Within this superordinate theme, the two subthemes of supervisee framing and safety net vs. minefield emerged.
Supervisee Framing
Supervisee framing focused on the participant’s personal view of hearing multiple perspectives from supervisors within simultaneous supervision. Some participants described hearing varying perspectives as being helpful and valuable, providing support, and increasing confidence. They typically framed the idea of receiving various feedback as a way to gain ideas and then make their own informed decisions. Molly shared this positive perspective when she stated, “I like coming to [my differing supervisors] with different issues I have with different clients because I feel like they both have valuable experience, but in different ways.” In contrast, Hailey identified multiple perspectives as being “really difficult,” and Diana noted they were “more frustrating than beneficial” and confusing. Similarly, Hailey stated, “My supervisors are all very different, so they give me different feedback, and a lot of times it conflicts with what the other one has said.” The supervisee’s framing of discrepant feedback impacted their overall perceptions with simultaneous supervision. Supervisees either valued or were confused by the feedback. Generally, participants spoke of times when multiple perspectives were beneficial and difficult, but it appeared all participants were left with the task of making sense of multiple perspectives while receiving simultaneous supervision.
Safety Net vs. Minefield
Making sense of multiple perspectives was described as creating a safety net of support, while others found the experience to be a minefield that increased confusion, ambiguity, and isolation. Emma and Molly characterized their experience as providing support in an often overwhelming profession. Molly articulated, “I feel like if I didn’t have that good support, that good foundation, I don’t think I could do it because it’s just so much.” She later added, “I feel like getting those different perspectives, getting that support, getting those encouragers is beneficial because I don’t feel as overwhelmed, even though it’s overwhelming.”
Participants also perceived their simultaneous supervision as a minefield wherein they believed they were in double binds. Hailey reflected on an experience when her supervisors contradicted each other and expressed, “It just sucked because I was doing what my supervisor told me to do and suggested I do, and then I was told everything I did was wrong.” Diana echoed that discrepant feedback felt like a constant dilemma needing to be managed “carefully.” In reflecting on contradicting supervision, Diana said, “It’s hard because everybody has their own thing. . . . You just kind of have to appease everyone.” In the face of conflict, it was easier to placate than resolve. Participants’ cognitive framing was a major element of the phenomenon. Whereas making sense of multiple perspectives focused on the cognitive elements of receiving feedback from different supervisors, the next theme focused on the behavioral elements.
Orchestrating the Process
Another theme that emerged in our data analysis was that of supervisees orchestrating the process of simultaneous supervision. This theme revolved around action-oriented steps in supervision. The essence of this theme was captured when Hailey acknowledged the need for “checking her motives” on what she shared with different supervisors. She asked herself, “Am I sharing this with this [supervisor] because I feel like they’re going to answer in the way that I feel like . . . they should answer, because it’s easier for me?” Hailey acknowledged the difficulty in this, countering with, “Or am I just going to them because it’s that person that I’m supposed to see?” Hailey recognized that having options when it came to approaching supervisors meant that disclosure needed to be intentional rather than straightforward as it is when CITs only have one choice. Participants were aware of their process as they picked and chose what to share with whom, through seeking out a preferred supervisor and through managing the practical aspects of having multiple supervisors. The subthemes of picking and choosing, seeking a preferred perspective, and managing practical considerations were a part of orchestrating the process.
Picking and Choosing
The subtheme of picking and choosing emerged in how our participants described what they would share in supervision and the course of action taken in their counseling practice. This subtheme was labeled as an in vivo code, derived from Hailey’s quote: “So I definitely pick and choose what I talk to about each one. Because—this sounds terrible—but I respect the one [supervisor] more.” Hailey also described feelings of vulnerability and self-efficacy from week to week, related to her reactions from feedback: “I knew after having such a hard supervision last week showing tape, I was like, ‘I cannot be super vulnerable right now. I need to choose something that’s more surface level.’” Molly experienced picking and choosing as a means of proactively managing the repetitive nature of supervision: “I think just bringing different things to different supervisors is really helpful, and not constantly talking about the same client or the same situation, because that gets obnoxious and repetitive, and you’re gonna get a hundred different opinions.”
After receiving feedback, participants had varying perspectives on how to integrate and transfer constructs into action. Some participants viewed discrepant feedback as mutually exclusive, whereas others had a more integrative perspective. Molly expressed frustration in choosing between differing feedback from multiple supervisors: “Sometimes I don’t really know which I should go with, which I should choose, and which would be best for the client. . . . It’s like a double-edged sword, like it’s good at some points, but then bad at others.” Diana, who expressed similar frustration in choosing between perspectives, relieved this tension by resolving that, “I have to live with myself at the end of the day, so as long as it’s not unethical, I don’t worry about it too much. And as far as the stuff that I’m told that needs to be done, I do what I can.” Other participants espoused a much more integrative perspective. Emma stated, “I think the thing I like the best about it is actually when [my supervisors] have different advice . . . because then I feel like between the two, I can kind of find what I really like.” All participants spoke about selecting what to share with supervisors and choosing how to integrate feedback into action.
Seeking a Preferred Perspective
Coinciding with picking and choosing, participants also sought a preferred perspective in the process of receiving simultaneous supervision and orchestrating the process. Some reported the decision to go to one supervisor over another was situationally based and determined by clinical skill or specialty of the supervisor. Diana captured this as follows, “Well, I can have a conversation with either. I just get very different answers. If it’s the technical stuff of what has to be done—her. If it’s ‘how would you approach the situation?’ I do tend to talk to him.” Diana also likened seeking a preferred perspective to a child searching for a desired answer: “It’s like, who do I want to talk to? It’s almost like, talk to the person you want for the answer you want. It’s like, ‘Well, if Mom doesn’t have the right answer, go talk to Dad.’”
Managing Practical Considerations
All participants spoke to the practicality of meeting with multiple supervisors. Even though some participants strongly valued having multiple supervisors, all participants spoke to the larger time commitment needed in having simultaneous supervision. Molly captured how simultaneous supervision felt overwhelming, adding to the many other sources of feedback she received: “I already have two group supervisions. I’ve heard opinions about this, and I’m hearing other perspectives of my classmates, of my coworkers. Now I have to have triadic and hear their opinions and have individual. . . . It’s just a lot.” Emma framed this time commitment as detracting from her other obligations: “It just starts adding up. Like, my whole Tuesday evenings are gone, and that’s time I could be seeing clients.” Hailey expressed frustration about the obligatory nature and placating to the program’s requirement to see multiple supervisors: “Honestly, I just give the other supervisor little things because I know I have to talk to him . . . and it’s more, like, checking a box.” Finally, Emma captured how this time commitment was epitomized in documentation: “And the paperwork got exhausting, too, because I had to do everything in triplicate sometimes.” She further talked about the additional mental labor: “And now what are we gonna talk about since I just talked about all of this with [a different supervisor] and feel like I found good solutions, you know?” Supervisees had to manage their time and fit more supervision into their schedules. Simultaneous supervision added complexity, and participants needed to orchestrate this process to manage it efficiently and effectively.
Supervisory Relationship Dynamics
Supervisory relationship dynamics was determined to be a superordinate theme as it reflected on the connecting and disconnecting elements of the supervisory relationship. This theme was broken into three subthemes. The subthemes of vulnerability, power dynamics, and systems of supervision illustrated the relational dynamics within simultaneous supervision.
Vulnerability
In supervisory relationships, feelings of safety and vulnerability influenced interactions with different supervisors. To illustrate, Hailey noted:
There are certain supervisors I feel more safe with. And so those are the ones that I share more with . . . versus some of them I feel less safe with . . . I don’t share as much with them that is vulnerable, or that makes me vulnerable.
Participant experiences highlighted how vulnerability dictated what and how elements were shared in simultaneous supervision.
Power Dynamics
The determination of safety occurred within power dynamics. Diana commented that multiple supervisors serving as evaluators and gatekeepers can create “this weird relationship where you don’t want to be too vulnerable because this person is also your boss and can decide if you are going to stay in that position or not.” Diana and Hailey noted feeling disempowered and disengaged from supervision, referring to supervisors as “bosses” throughout their interviews. When participants perceived their supervision as a firmly directive process, discrepant directives were especially distressing. Diana rephrased this sentiment: “I guess the best thing to compare it to would be if you have more than one boss, but they all give you a different, ‘I want this, I want this, I want this.’” Emma’s experience was more accordant, and she specifically expressed at one time, “None of [my supervisors] are really super bossy either.” Participants identified power dynamics as salient aspects of how they experienced supervision and with whom they connected. Working with more than one supervisor sometimes resulted in characterization of “good” and “bad” supervisors, making individual supervisory relationship dynamics crucial.
Systems of Supervision
Participants conceptualized the phenomenon as broader systems of supervision in which individual supervisors were interacting with each other. Emma noted, “The two faculty supervisors work very closely together and I assume talk all the time.” Emma and Molly provided multiple examples of supervisors working together to best serve clients, thus bolstering supervision through their combined expertise. Molly stated, “It was nice because [my two supervisors] were in agreement and I felt comfortable going into session with [my client].” Even negative experiences contributed to systems of supervision. Hailey reported seeking out additional support when her assigned supervisory relationships did not meet her needs, widening the reach of simultaneous supervision even more: “By not being a good supervisor, he helps me seek out other resources and figure it out for myself.” Finally, Molly noted that supervisor coordination was primarily for evaluation at the end of the semester and only if problems arose. However, she imagined what it would be like if they were more collaborative:
They would have had a better understanding of the way I work in a counseling room. . . . Because my site supervisor really understood how I approached things and the way I would interact with my clients, but I feel like my university supervisor didn’t really, like, she had little snippets of what I was like in a counseling room.
Power, vulnerability, and systems in the supervisory relationship impacted supervisees from multiple levels in their clinical journey.
Personal Dispositions and Characteristics
Personal dispositions and characteristics resulted from participants speaking about the phenomenon as well as what they said about their supervisors. Three dispositions that emerged as relevant were tolerance for ambiguity, curiosity, and availability. The first two subthemes were identified as they spoke about the phenomenon and the third subtheme was a characteristic present because of the nature of simultaneous supervision.
Tolerance for Ambiguity
Tolerance for ambiguity was found to be a critical disposition. This disposition allowed participants to see differences in opinion as helpful. Emma shared that she “very rarely” saw people as giving her “conflicting information.” She said that she saw it as everybody having their own perspective. This connected to her ability to view multiple perspectives as “pieces of the puzzle,” as she expressed earlier in her retelling of the Indian fable. Although participants sometimes expressed concern about direction, Diana shared, “You can ask questions and you can not know and it’s okay.” This disposition directly related to how they reconciled and then reacted to multiple perspectives of simultaneous supervisors.
Curiosity
Curiosity also manifested more implicitly with supervisees. Participants showed curiosity by taking interest in what supervisors had to say, seeking more information, or staying open to difficult feedback. Hailey shared that simultaneous supervision “definitely requires a lot of continuing to look inward and examining your motives and yourself and what the supervisors have said.” In speaking more broadly, Emma shared, “So I don’t think I’ll ever give [simultaneous supervision] up now that I’ve kind of experienced how valuable it is to get another professional opinion.” Curiosity manifested itself as a transient characteristic for other participants. Diana experienced transference with one of her supervisors, which was a barrier to her ability to exhibit this helpful disposition. One of her supervisors suggested that she try and work things out with another supervisor she was having difficulty with, to which Diana said, “No. Who is gonna walk into their supervisor and be like, ‘Okay, so my problem with you is you’re a bitch. You remind me of my abusive ex.’ . . . But at the same time, I have to work with her.” This was an example of Diana demonstrating a closing off to feedback. Both tolerance for ambiguity and curiosity manifested and impacted their experience of multiple perspectives.
Availability
An important disposition was emotional and physical availability. Emma expressed that “there’s always somebody I can get a hold of.” Hailey expressed that she had “more coverage just in general,” but also questioned her supervisors’ true availability: “Do I even need to bring this to supervision or can I work on this on my own? Because sometimes I feel like I annoy them.” All participants expressed that availability was important to their experience, although physical availability did not always translate to being available to discuss what the supervisee wanted. Those participants who identified supervisors within simultaneous supervision as being more available had more positive thoughts regarding simultaneous supervision.
Discussion
All four participants identified the complex position of CITs receiving supervision from more than one supervisor. The results align with the growing body of literature affirming the importance of a positive working relationship between CITs and supervisors (Bernard & Goodyear, 2019; Borders et al., 2014; Sterner, 2009) as well as significant differences between faculty and site supervision (Borders, 2006; Dodds, 1986). The results parallel supervision literature detailing the multiple roles of supervisees (Bernard & Goodyear, 2019) who, unlike supervisors, are not required to have specific education in supervision. The theme of personal dispositions has been studied extensively in counselor education, resulting in prominent placement in clinical assessment instruments (Lambie et al., 2018). The presented themes diverge from the current research base in their construction of a clear model of simultaneous supervision. The subthemes of picking and choosing, seeking a preferred perspective, and systems of supervision illustrate the interpersonal dynamics of simultaneous supervision that is distinct from sole supervision, an underrepresented phenomenon in the supervision literature. Participants in this study reported mixed feelings with simultaneous supervision. Four primary themes emerged from this study: making sense of multiple perspectives, orchestrating the process, supervisory relationship dynamics, and personal dispositions and characteristics. These four themes encompass many areas of the supervisory experience while illuminating guidelines for supervisors engaging in simultaneous supervision.
Implications
Results from this study reinforce the complex levels of integration CITs experience when receiving supervision from multiple supervisors. This process of integration can lead to confusion, ambiguity, and also deeper understanding. The results indicate that the perceived benefit of simultaneous supervision was often based on the relationship between the supervisor and CIT, ability and support to organize the process, and the personal dispositions of the CIT. The implications for this research target three populations.
Supervisors
The findings of this study indicate several implications for supervisors working with clinicians receiving simultaneous supervision. First and foremost, the critical importance of the supervisory relationship to supervision in general (Bernard & Goodyear, 2019) was further substantiated as a foundation for effective simultaneous supervision. Questionable supervisee behaviors such as intentional nondisclosure via seeking a preferred perspective or picking and choosing can be avoided through purposefully fostering trust in the relationship. Similarly, supervisors may support the perspective of simultaneous supervision as a safety net if support for vulnerability is established and the relationship is actively attended to. Supervisors should be mindful of their availability to CITs and periodically check in to see if they are meeting the needs of the supervisee.
Supervisors who are aware of the themes developed from this research may be better equipped to capitalize on benefits and mitigate challenges. One benefit was that simultaneous supervision allowed participants to receive multiple synergistic perspectives regarding their work with clients. Depending on the developmental level of the supervisee and the demeanor of the supervisor, however, these multiple perspectives may present challenges. Supervisors can apply their knowledge of developmental models to tailor their interventions. Supervisors might anticipate that CITs earlier in development (e.g., in practicum) may require structured support in simultaneous supervision to avoid performance anxiety and frustration from rigid applications of multiple perspectives consistent with this stage (Stoltenberg & McNeill, 2010). Supervisors may also wish to focus supervision on interventions that actively facilitate development of these dispositions, such as employing constructivism to elicit greater cognitive flexibility (Bernard & Goodyear, 2019).
Some early-stage supervisees may experience challenges when navigating varying perspectives and feedback provided to them by multiple supervisors. Challenges can be mitigated when supervisors broach the topic of simultaneous supervision with supervisees early. Additionally, when supervisors ensure they respect other supervisors and create collaborative relationships, supervisee difficulty with simultaneous supervision may decrease. When a supervisor learns of a differing opinion of another supervisor, it is important that it is broached as a variance in approach rather than an incorrect practice. Supervisees experiencing difficulties with simultaneous supervision may also benefit from supervisors checking in with them regarding the variable feedback they are receiving. A collaborative supervisory system may strengthen supervisee development and integration of counseling constructs. Counseling programs can play a key role in setting systemic expectations for supervisors and supervisees.
Counselor Education Programs
Accredited counselor education programs have autonomy in how they meet various CACREP (2015) supervision and clinical requirements. Programs may choose to require simultaneous supervision, may require multiple clinical sites, and may utilize faculty advising as supplementary clinical supervision. In unique situations such as students completing two tracks or receiving additional supervision for gatekeeping reasons, how programs manage simultaneous supervision can become complex. Best practice guidelines, policies, and procedures regarding simultaneous supervision can be made clear in clinical handbooks, with clinical coordinators, and in material for site supervisors. This would help to address the supervisee confusion from the programmatic side. Another important implication with simultaneous supervision is to consider the supervisory process through a systemic lens. When simultaneous supervision is utilized, there will be many interactions occurring outside of the dyad or triad apparent to one individual supervisor. When supervisors collaborate and communicate, supervisees may be more likely to receive congruent feedback, understand gatekeeping action, and receive consistent expectations. In particular, communication between academic and clinical supervisors can bridge the gap between idealism and practicality (Bernard & Goodyear, 2019; Choate & Granello, 2006). Programmatically mandated, semesterly site visits and opportunities for regular check-ins could fulfill this purpose.
Supervisees
Participants often spoke to the challenge of organizing simultaneous supervision effectively in relation to feedback, documentation, and case presentation material. Although a certain level of organizational skill is expected of graduate students, the coordination required in simultaneous supervision often seemed unanticipated and unwieldy for students. Preparing for the supervision experience in another course and/or an orientation in lab supervision may aid in this. All participants discussed, at varying distress levels, how having supervision scheduled too close together (e.g., same day or two days in a row) increased repetitiveness and thus made simultaneous supervision feel less efficacious. Supervisees may want to intentionally schedule supervision sessions spaciously to avoid potential repetition or redundancy. With the steady increase in virtual supervision, scheduling supervision in ideal time frames may be easier with increased access and absent travel time. Programmatic preparation, intentional scheduling, and collaborative supervision notes may aid the simultaneous supervision process.
In the areas of core dispositions, CITs who embraced ambiguity and fostered reflexivity, curiosity, and flexibility tended to navigate simultaneous supervision with more ease. Reflexivity, curiosity, and tolerance for ambiguity seemed to strengthen the ability to receive feedback from multiple sources, integrate feedback appropriately, and maintain strong supervisory relationships. A typical guiding question from participants was, “How can I apply this combined feedback to my particular site and client while still maintaining my own clinical identity?” Necessarily, students will enter a program with differing levels of core strengths, yet any student can be encouraged to strengthen their core dispositions. Supervisees are encouraged to think about simultaneous supervision with the same organization and openness required for other courses such as pre-practicum and multicultural counseling. Correspondingly, supervisors have complex responsibilities maintaining ethical competent care, organizing supervision, and fostering these core dispositions.
Ethical Implications of Simultaneous Supervision
In addition to recommendations for the three populations above, findings from this study highlight ethical considerations. Worthington et al. (2002) identified “intentional nondisclosure of important information” (p. 326) and “inappropriate methods of managing conflict with supervisors” (p. 329) as two major ethical issues that are unique to supervisees and correlate with some of the participant supervisees’ experiences of triangulating supervisors, seeking outside consultation to circumvent supervisors, or intentionally withholding information. To ensure client welfare, supervisors and supervisees may benefit from explicitly discussing ethical implications and considerations unique to this phenomenon at the outset of supervision and again when conflicts arise. Future research that addresses limitations of this study will further clarify the role of supervisors, supervisees, and programs in simultaneous supervision as well as specific ethical guidelines.
Limitations and Future Directions
Limited information was gathered about the specific counselor education programs in which our participants were enrolled, restricting the inferences able to be made about simultaneous supervision in context. We also chose a convenience sampling method using CESNET and selected four participants. The choice of indirect sampling, primarily through counselor educators redirecting calls to their students, may have limited participants. Further, all participants of this study identified as the same gender and race, which limits the diversity of experience shared. Future researchers may consider sampling more participants to get a broader exploration of the phenomenon. In doing so, researchers may be able to obtain greater representation in gender and race to increase the transferability of this study.
This study focused on the phenomenon of simultaneous supervision as experienced within individual and triadic supervision. Simultaneous supervision is embedded within the broader experience of supervision, and isolating the phenomenon required vigilance by the researchers. Future researchers would benefit from intentional follow-up questions that better focus participants on simultaneous supervision rather than individual experiences with supervisors. As our study did not explicitly ask participants to distinguish between university-affiliated and site supervisors, future researchers may pursue a qualitative study that highlights the difference. Other research may utilize grounded theory to develop a model of simultaneous supervision for supervisors and supervisees to follow or focus explicitly on supervisors’ perspectives of simultaneous supervision. Quantitative research may illuminate the frequency and use of simultaneous supervision in counselor education programs overall or identify correlations between counselor dispositions such as tolerance for ambiguity and supervision outcomes in simultaneous supervision. Because of the lack of information regarding the phenomenon of simultaneous supervision, many opportunities for research regarding the phenomenon persist.
Conclusion
Overall, the findings from this research indicate CITs valued greater support and thrived when integrating “both/and thinking” in navigating feedback from multiple supervisors. This perspective reinforces the need for systemic communication among counselor educators and supervisors. Additionally, results suggest CITs would benefit from supervisors broaching the topic of simultaneous supervision early in their clinical experience.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Borders, L. D. (2006). Snapshot of clinical supervision in counseling and counselor education: A five-year review. The Clinical Supervisor, 24(1–2), 69–113. https://doi.org/10.1300/J001v24n01_05
Borders, L. D., Glosoff, H. L., Welfare, L. E., Hays, D. G., DeKruyf, L., Fernando, D. M., & Page, B. (2014). Best practices in clinical supervision: Evolution of a counseling specialty. The Clinical Supervisor, 33(1), 26–44. https://doi.org/10.1080/07325223.2014.905225
Choate, L. H., & Granello, D. H. (2006). Promoting student cognitive development in counselor preparation: A proposed expanded role for faculty advisers. Counselor Education and Supervision, 46(2), 116–130.
https://doi.org/10.1002/j.1556-6978.2006.tb00017.x
Council for the Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards/
Davis, K. L., & Arvey, H. H. (1978). Dual supervision: A model for counseling and supervision. Counselor Education and Supervision, 17(4), 293–299. https://doi.org/10.1002/j.1556-6978.1978.tb01086.x
Dodds, J. B. (1986). Supervision of psychology trainees in field placements. Professional Psychology: Research and Practice, 17(4), 296–300. https://doi.org/10.1037/0735-7028.17.4.296
Duryee, J., Brymer, M., & Gold, K. (1996). The supervisory needs of neophyte psychotherapy trainees. Journal of Clinical Psychology, 52(6), 663–671. https://doi.org/bmp9p9
Koltz, R. L., Odegard, M. A., Provost, K. B., Smith, T., & Kleist, D. (2010). Picture perfect: Using photo-voice to explore four doctoral students’ comprehensive examination experiences. Journal of Creativity in Mental Health, 5(4), 389–411. https://doi.org/10.1080/15401383.2010.527797
Kreider, H. D. (2014). Administrative and clinical supervision: The impact of dual roles on supervisee disclosure in counseling supervision. The Clinical Supervisor, 33(2), 256–268.
https://doi.org/10.1080/07325223.2014.992292
Lambie, G. W., Mullen, P. R., Swank, J. M., & Blount, A. (2018). The Counseling Competencies Scale: Validation and refinement. Measurement and Evaluation in Counseling and Development, 51(1), 1–15.
https://doi.org/10.1080/07481756.2017.1358964
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Miller, R. M., Chan, C. D., & Farmer, L. B. (2018). Interpretative phenomenological analysis: A contemporary qualitative approach. Counselor Education and Supervision, 57(4), 240–254. https://doi.org/10.1002/ceas.12114
Murray, S. A., Kendall, M., Carduff, E., Worth, A., Harris, F. M., Lloyd, A., Cavers, D., Grant, L., & Sheikh, A. (2009). Use of serial qualitative interviews to understand patients’ evolving experiences and needs. BMJ, 339, b3702. https://doi.org/10.1136/bmj.b3702
Nestler, E. J. (1990). The case of double supervision: A resident’s perspective on common problems in psychotherapy supervision. Academic Psychiatry, 14(3), 129–136. https://doi.org/10.1007/BF03341284
Pietkiewicz, I., & Smith, J. A. (2014). A practical guide to using interpretative phenomenological analysis in qualitative research psychology. Psychological Journal, 20, 7–14. https://doi.org/10.14691/CPPJ.20.1.7
Read, B. L. (2018). Serial interviews: When and why to talk to someone more than once. International Journal of Qualitative Methods, 17(1), 1–10. https://doi.org/10.1177/1609406918783452
Saxe, J. G. (1868). The poems of John Godfrey Saxe. Ticknor and Fields.
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research (1st ed.). SAGE.
Sterner, W. (2009). Influence of the supervisory working alliance on supervisee work satisfaction and work-related stress. Journal of Mental Health Counseling, 31(3), 249–263. https://doi.org/10.17744/mehc.31.3.f3544l502401831g
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Stutey, D. M., Givens, J., Cureton, J. L., & Henderson, A. J. (2020). The practice of bridling: Maintaining openness in phenomenological research. The Journal of Humanistic Counseling, 59(2), 144–156.
https://doi.org/10.1002/johc.12135
Tromski-Klingshirn, D., & Davis, T. E. (2007). Supervisees’ perceptions of their clinical supervision: A study of the dual role of clinical and administrative supervisor. Counselor Education and Supervision, 46(4), 294–304. https://doi.org/10.1002/j.1556-6978.2007.tb00033.x
Worthington, R. L., Tan, J. A., & Poulin, K. (2002). Ethically questionable behaviors among supervisees: An exploratory investigation. Ethics & Behavior, 12(4), 323–351. https://doi.org/10.1207/S15327019EB1204_02
William B. Lane, Jr., PhD, NCC, BC-TMH, LPCC, is an assistant professor at Western New Mexico University. Timothy J. Hakenewerth, PhD, NCC, LPC, is an assistant professor at the University of Illinois Springfield. Camille D. Frank, PhD, NCC, LMHC, LPC, is an assistant professor at Eastern Washington University. Tessa B. Davis-Price, PhD, LMHC, LCPC, is an assistant professor at Saint Martin’s University. David M. Kleist, PhD, LCPC, is a professor and department chair at Idaho State University. Steven J. Moody, PhD, is a clinical professor at Adams State University. Correspondence may be addressed to William B. Lane, Jr., 1000 W College Ave, Silver City, NM 88061, william.lanejr@wnmu.edu.
Appendix
Interview Protocol
| Interview Questions |
| Round 1 |
| What has been your experience with having multiple simultaneous supervisors?
In your own experience, how has simultaneous supervision been a strength?
In your own experience, how has simultaneous supervision been challenging?
What have you learned about yourself and the counseling profession as you’ve experienced simultaneous supervision? |
| Round 2 |
| How has having simultaneous supervision been different from times when you have only had one supervisor?
What has it been like to have your supervisors interact with each other in regard to the supervision that you have received from them?
What personal dispositions (characteristics/qualities) do you think you have that influenced your experience of simultaneous supervision?
How has simultaneous supervision impacted your experience of safety or vulnerability in supervision?
What practical considerations have you needed to consider for having multiple simultaneous supervisors? |
