Nov 9, 2021 | Volume 11 - Issue 4
Charles F. Shepard, Darius A. Green, Karli M. Fleitas, Debbie C. Sturm
This qualitative grounded theory study is the first of its kind aimed at understanding the decision-making process of parents and guardians of transgender and gender-diverse (TGD) youth providing informed consent for their children to undergo gender-confirming endocrinological interventions (GCEI), such as hormone replacement therapy and puberty blockers. Using primarily intensive interviews supported by observational field notes and document review, this study examined the decision-making processes of a national sample of participants who identified as a parent or legal guardian of at least one TGD youth and who have given informed consent for the youth in their care to undergo GCEI. A variety of inhibiting and contributing factors were illuminated as well as a “dissonance-to-consonance” model that participants used to combine contributing factors to overcome inhibitors and grant informed consent. Implications for professional counseling practitioners are discussed, including guidance for direct services, gatekeeping, case management, and advocacy functions.
Keywords: transgender, gender-diverse, youth, decision-making, intervention
One of the more controversial topics currently addressed in professional counseling involves gender identity and access for gender-confirming interventions for transgender or otherwise gender-diverse (TGD) youth. Since academic journals began publishing studies of the experiences of people expressing what today could be considered gender expansiveness in the late 19th century (Drescher, 2010), there has been considerable struggle in Western culture to understand the constructs of gender identity and expression and the implications that these aspects of human development present for mental and physical health. In the United States, controversy around pathologizing TGD identity or normalizing and affirming it has influenced popular and professional opinions since the early 20th century (Drescher, 2010; Stryker, 2008). Within the past decade, TGD identity has been associated with pervasive patterns of mistreatment and discrimination across social, educational, occupational, legal, and health care experiences in the United States (James et al., 2016).
Transgender Health Care in the United States
TGD people have been shown to be overrepresented in populations associated with negative mental, physical, and social health outcomes, such as those suffering from suicidality and homelessness (James et al., 2016). Among transgender older adolescents and young adults, 25% to 32% have reported attempting suicide (Grossman & D’Augelli, 2007), while the national rate for attempted suicide is 4.6% (James et al., 2016). According to the Lesbian, Gay, Bisexual, and Transgender (LGBT) Homeless Youth Survey (Durso & Gates, 2012), LGBT youth comprised 40% of the populations served by 354 agencies serving homeless youth. Of the 381 youth that responded to the survey, 46% reported that they ran away from home because of family rejection of their affectional orientation or gender identity, and 43% reported that they were forced out by their parents because of their affectional orientation or gender identity.
According to the 2015 U.S. Transgender Survey, TGD people have also had their access to health care limited by stigma and discrimination by health care providers (James et al., 2016). One-third (33%) of respondents reported experiencing at least one negative experience with a health care provider in relation to their gender identity, and nearly a quarter (23%) did not seek services for fear of being mistreated. One-third (33%) did not seek health care because of an inability to afford the cost of TGD-specific or other services. These disparities are among the many motivators of the current movement to make health care, and professional counseling in particular, more affirming of TGD people (Rose et al., 2019; Vincent, 2019).
Factors Influencing Rejection and Affirmation of TGD Identity
Factors that support the pathologization of TGD identity and behavior find their roots across a variety of intersecting segments of American society. One of the more prominent influencers of these practices in the United States has been religion (Drescher, 2010; Stryker, 2008; Vines, 2014). More than 70% of the U.S. population identifies as Christian, with more than half the population practicing Christianity as members of evangelical denominations, which have been associated with traditionally rejecting attitudes toward lesbian, gay, bisexual, transgender, queer, questioning, intersex, asexual, and pansexual (LGBTQ+) people and behavior (Pew Research Center, 2014; Vines, 2014). Chronic suicidal thinking among LGBT people ages 18 to 24 has been associated with parents’ rejecting religious beliefs, and fears about being forced to leave one’s religion have been associated with a suicide attempt within a 12-month period for the same population (Gibbs & Goldbach, 2015).
Religion has been closely associated with recent changes in state legislation and federal policy that suggest that disparities in the treatment of TGD people are socially and professionally acceptable. At least four states (Arkansas, Montana, Ohio, and South Dakota) have passed legislation that has included what is known as a conscience clause that could impede access to health care for LGBTQ+ people (Dailey, 2017; Goodkind, 2021; Rose et al., 2019). These health care–related laws have allowed legal protection for health care providers, sometimes specifically addressing professional counselors, who refuse services to clients who request help in ways that conflict with the provider’s particular religious beliefs (Dailey, 2017; Rose et al., 2019). In 2018, conscience clause–type considerations were expanded to the federal level when the U.S. Department of Health and Human Services (DHHS) created the Conscience and Religious Freedom Division (CRFD) in the DHHS Office for Civil Rights (DHHS, 2018a). At the time, CRFD policy explicitly cited protections for health care practitioners who declined to provide services related to abortion and assisted suicide (DHHS, 2018b); however, some noted that the division’s loose language could have left room for health care providers to deliver sub-standard care for LGBTQ+ clients as well (Gonzalez, 2018; Rose et al., 2019). In fact, a DHHS spokesperson stated at the time that the department would not interpret prohibitions on sex discrimination in health care to cover gender identity (Gonzalez, 2018). It should be noted that federal protections of TGD individuals in health care were restored in 2021 (Shabad, 2021).
Awareness of Gender Diversity
The general beginnings of the social consciousness of gender diversity in the United States can be traced to the attention that Christine Jorgensen commanded during her transition in the 1950s (Drescher, 2010; Stryker, 2008). Jorgensen was a U.S. Army veteran who served during World War II and travelled to Europe to undergo orchiectomy and penectomy procedures. Upon her return to the United States, she underwent vaginoplasty and became a preeminent advocate for LGBTQ+ rights (Drescher, 2010; Jorgensen, 1967; Stryker, 2008). About a decade later, physician Harry Benjamin pioneered gender-confirming endocrinological interventions (GCEI) aimed at medically supporting TGD patients who wished to feminize or masculinize their bodies to be more congruent with their gender identity without surgery (Drescher, 2010; Stryker, 2008). The most popular forms of GCEI—cross-sex hormone replacement therapy and gonadotropin-releasing hormone analogues or “puberty blockers”—have been associated with positive physical and mental health outcomes (Bränström & Pachankis, 2020; Couric, 2017; Drescher, 2010; Murad et al., 2010) and have been made available to people from pre-puberty through late adulthood (E. Coleman et al., 2012; Hembree et al., 2017).
Nearly all the research regarding GCEI has been conducted on adults (Couric, 2017), and the experiences of parents of TGD youth are not well represented in the literature (Hill & Menvielle, 2009), despite the growing popularity of GCEI among TGD minors (Couric, 2017; Drescher, 2010; Pew Research Center, 2013; Rosin, 2008). In the United States, minors are almost always dependent on their parents or legal guardians to provide informed consent for GCEI (Burt, 2016; D. L. Coleman, 2019; D. L. Coleman & Rosoff, 2013) even though they are likely to be considered by the medical profession to be cognitively capable of making an informed choice to undergo hormone-related treatments (E. Coleman et al., 2012; Hembree et al., 2017). At least one study that intends to contribute to the literature on the long-term risks and benefits of GCEI on minors is ongoing but not complete as of this publication (Bunim, 2015; S. Rosenthal, personal communication, November 7, 2019). This leaves both TGD youth and their parents—who are unlikely to share their child’s gender identity—in the precarious position of making meaningful decisions about the youth’s mental and physical health in a climate dominated by legal, political, religious, and social trends and without a body of rigorous research to instill confidence in giving or denying consent for GCEI.
Role of Professional Counselors
Partially for the reasons stated above, professional counselors who work with TGD youth and their families have unique opportunities to serve their clients at the micro-, meso-, and macrolevels. With professional emphases on human development, the helping relationship, and social justice (Lawson, 2016), counselors have an ethical obligation to develop competencies related to addressing issues concerned with gender identity, spirituality, and social systems to enable the empowerment of clients through individual, group, and family counseling in addition to interprofessional consultation and advocacy (American Counseling Association [ACA], 2014; Burnes et al., 2010; Cashwell & Watts, 2010; Ratts et al., 2015; Toporek & Daniels, 2018). ACA’s stance that TGD identity is a normal part of human development and should be affirmed (Burnes et al., 2010) aligns with the positions of every major health care professional organization globally (Drescher, 2010). Professional counselors are likely to be presented with opportunities to provide psychoeducation about gender identity development and best practices regarding the affirmative care of TGD clients as well as opportunities to advocate for their clients through the writing of referral letters for GCEI (E. Coleman et al., 2012). It is not uncommon, however, for professional counselors to challenge this obligation, especially when they feel compelled to prioritize religious teachings that pathologize LGBTQ+ identity (Kaplan, 2018; Rose et al., 2019).
The Purpose of the Present Study
The purpose of this research was to explore the process by which parents or legal guardians of TGD youth develop affirmative understandings and approaches to their children’s gender identity, affirm their related transition needs, and grant informed consent for the TGD youth in their care to undergo GCEI. With that in mind, the primary research question of this grounded theory study was, How did the parents of TGD youth who have undergone GCEI decide to give informed consent? Secondarily, are there specific themes that emerge for Christian, heterosexual, cisgender parents who go through this process? Finally, what part, if any, did a professional counselor play in the process?
Method
A qualitative grounded theory method was employed because this method is used to understand how participants go about resolving a particular concern or dilemma (Charmaz, 2014; Glaser & Strauss, 1967). Unlike other forms of qualitative research, grounded theory guides the researcher with a set of general principles, guidelines, strategies, and heuristic devices rather than formulaic prescriptions to help the researcher direct, manage, and streamline data collection so that analyses and emerging theory are well grounded in the collected data (Charmaz, 2014). For the purposes of this study, we followed prescribed grounded theory protocols for data collection, analysis, and trustworthiness (Charmaz, 2014; Corbin & Strauss, 2015; Creswell, 2013; Merriam & Tisdell, 2016).
Participants
Following IRB approval, a snowball sampling method (Creswell, 2013; Merriam & Tisdell, 2016) was employed to recruit a purposive sample of adult participants who (a) self-identified as a parent and/or legal guardian of a person who self-identifies as TGD and (b) have given informed consent for their TGD child to receive GCEI. Study information and a request for assistance with identifying participants was disseminated to national organizations that advocate for TGD rights such as the Society for Affectional, Intersex, and Gender Expansive Identities (SAIGE), Parents and Friends of Lesbians and Gays (PFLAG), and Transparent USA. Prospective participants were asked to contact the researcher and forward the information to others that they believed met the study criteria. Participant screening consisted of an online Qualtrics survey that included confidentiality and informed consent information, inclusion criteria, and demographic items. Once identified, participants were asked to participate in initial intensive interviews.
Theoretical sampling (Charmaz, 2014) is the preferred strategy for grounded theory because it allows emerging themes to direct simple decisions until saturation is met (i.e., no new information is being detected). In this study, saturation was met at the 16th interview and confirmed in the 17th. Table 1 details the sociodemographic characteristics of the participants, the majority of which identified as cisgender women (n = 13), White (n = 16), married (n = 14), college educated (n = 17), and employed full-time (n = 12). Participants’ ages ranged between 32 and 61 years with a mean age of 49 (see Table 2). The participants made up a national sample (see Table 3), both in regard to region of birth and region of residence. As Table 4 shows, a near majority identified as mainline Protestant Christian (n = 8). The majority had one TGD child (n = 13), and the children’s ages at which the participants gave consent for GCEI ranged from 10 to 18 years (M = 13.93; see Table 2).
Instrumentation and Data Collection
Because the main emphasis of this study was to understand parents’ decision-making processes, intensive interviews were the main instrument of data collection. Environmental observation and document reviews were conducted when they were accessible. To protect the participants’ confidentiality, each was randomly assigned a pseudonym. Additionally, interviews—which lasted between 30 and 75 minutes—were facilitated through telehealth video conferencing software that complied with the Health Information Portability and Accountability Act of 1996 (HIPAA). Electronic recordings of interviews were stored on a HIPAA-compliant version of an internet-based file hosting service, and transcription was provided by a company that provides confidential transcription services.
Table 1
Sociodemographic Characteristics of Participants
| Demographic characteristic* n % |
| Gender |
| Cisgender Women 13 76.5 |
| Cisgender Men 4 23.5 |
| Ethnicity
White 16 94.1
Mixed-race 1 0.1 |
| Marital Status |
| Married 14 82.4 |
| Divorced 2 11.8 |
| Separated 1 5.8 |
|
| Highest level of education |
| Some college 3 17.6 |
| Associates degree 2 11.8 |
| Bachelor’s degree 5 29.4 |
| Master’s degree 3 17.6 |
| Doctoral degree 4 23.5 |
|
| Employment status |
| Employed full-time 12 70.6 |
| Employed part-time 5 29.4 |
|
| Professional identity |
| Office/clerical 1 5.8 |
| Sales/marketing 2 11.8 |
| Professional 9 52.9 |
| Mid-level management 2 11.8 |
| Upper-level management/ 1 5.8 |
| business owner |
| Other 2 11.8
Household annual income
More than $90,000 9 52.9
$60,001 to $90,000 6 35.3
$35,000 to $60,000 2 11.8 |
Note. N = 17.
*Participants were asked to identify across a variety of different gender identities, relationship statuses, educational statuses, employment statuses, professional identities, and income statuses. Only the identities or statuses selected by participants are shown. |
Table 2
Relevant Ages
|
M |
Range |
| Current age of parents |
49 |
32–61 |
| Current age of TGD child |
15.78 |
10–26 |
| Age of TGD child at time of consent |
13.93 |
10–18 |
Table 3
Participant Regions of Birth/Residence
| Region |
Place of birth |
% |
Place of residence |
% |
| Northeast |
1 |
5.8 |
0 |
0 |
| Mid-Atlantic |
6 |
35.3 |
12 |
70.6 |
| Midwest |
3 |
17.6 |
2 |
11.8 |
| Southeast |
4 |
23.5 |
1 |
5.8 |
| Southwest |
1 |
5.8 |
1 |
5.8 |
| Mountain West |
0 |
0 |
1 |
5.8 |
| Outside U.S. |
2 |
11.8 |
0 |
0 |
Note. N = 17
Table 4
Participant Religious Affiliation
| Affiliation |
n |
% |
| Christian (mainline Protestant) |
8 |
47.1 |
| Christian (Catholic) |
0 |
0 |
| Christian (Evangelical Protestant) |
0 |
0 |
| Muslim |
0 |
0 |
| Jewish |
1 |
5.8 |
| Agnostic |
2 |
11.8 |
| Atheist |
2 |
11.8 |
| Other/unaffiliated |
4 |
23.5 |
Based on Charmaz’s (2014) recommendations, the researchers developed an interview protocol (see Appendix) that was examined and confirmed for (a) its sensitivity to the experience of participants and (b) its capability for addressing the research questions at hand with two individuals who meet criteria for participation. One of the individuals was the executive director of a small, rural LGBTQ+ advocacy organization. The second was a professional counselor who works with TGD clients. Both were parents of at least one TGD child.
Analysis
The researchers used line-by-line coding of interview data and continuously compared new codes with those of previous interviews. Microsoft Excel software (version 16.44) was used for keeping track of the coding matrix. The coding matrix was reworked until a core theoretical category emerged that explained the underlying concepts inherent in the process under examination.
Trustworthiness
In qualitative research, a study’s rigor is typically measured by trustworthiness, or the consistency of the results with the data collected (Merriam & Tisdell, 2016). To support this process, we used a variety of strategies, including triangulation, member checks, and reflexivity (Corbin & Strauss, 2015; Creswell, 2013; Merriam & Tisdell, 2016). Triangulation was accomplished by the recruitment of two study auditors who conducted blind coding of data samples and reviewed the study design, procedures, and process of theory integration for accuracy (Creswell, 2013). Reflexivity involves the “critical self-reflection of the researcher regarding assumptions, worldview, biases, theoretical orientation and relationship to the study that may affect the investigation” (Merriam & Tisdell, 2016, p. 256). The first author and lead researcher, Charles F. Shepard, identifies as a White, cisgender, straight, middle-aged man who has lived his entire life in the Southeastern United States. He has been married for more than 14 years, and he is the father of two young children who were assigned female at birth. Shepard’s interest in the present topic is rooted in personal, academic, and professional experiences with conscience conflicts during the past three decades. The second author, Darius A. Green, served as an auditor and identifies as a Black, cisgender, straight, young adult man who has lived predominantly in the Southeastern United States. Green is a doctoral-level counselor educator who has conducted research and provided counseling with underrepresented populations. The third author, Karli M. Fleitas, served as the second auditor and identifies as a Japanese American, cisgender, straight, young adult woman who has lived predominantly in the Southeastern United States. Fleitas is a doctoral student in a counselor education program accredited by the Council for Accreditation of Counseling and Related Educational Programs who has clinical experience working with LGBTQ+ clients as well as certification with respect to diversity, equity, and inclusion practices. The fourth author, Debbie C. Sturm, served as the chairperson of Shepard’s dissertation committee and provided guidance to the research and reporting processes. Sturm identifies as a White, cisgender, straight, middle-aged woman who has lived between the Northeastern and Southeastern regions of the United States. She has conducted and supervised previous research relevant to LGBTQ+ concerns. We considered our identities and backgrounds throughout for their potential effect on the data collection and analysis processes.
Results
The major findings of this study included inhibitors and contributors to consent as well as a central theme, specifically how participants combined contributing factors to overcome inhibiting factors of the consent-giving process.
Inhibitors to Consent
Participants identified five major inhibitors to giving consent: (a) lack of knowledge and awareness of issues and concerns related to TGD identity, (b) fear, (c) doubt, (d) grief over a lost parenting narrative, and (e) rejection from healthcare providers (or payors) and parenting partners. To a lesser degree, lack of access to affirming care due to residential location and the cost of treatments were cited as notable experiences of participants.
Lack of Knowledge and Awareness
Of the participants, all but one (n = 16) reported that they lacked knowledge or awareness of the issues that TGD youth face when their children either came out to them, asked to participate in GCEI, or both. When asked what she knew about gender identity and/or gender expression prior to her child coming out, Jaylene (51), a White, cisgender woman divorced from her parenting partner, but remarried and living in the Southeast, stated:
Really not a lot, because I think that transgender people in the past were really colored as men who were sick and dressed like women. . . . I was kind of ignorant to it all, but I didn’t know I was ignorant is the thing.
Participants often cited their lack of knowledge as a key component of their fear over giving informed consent for their TGD child’s GCEI.
Fear
Participants reported experiencing fear on multiple levels in response to their child’s request to begin GCEI, including fear of negative future social experiences for their child, fear of the side effects of the treatments, and political fears. Of the 17 participants, 13 reported fears over negative future experiences. Hilda (50), a White, cisgender woman married to her parenting partner and residing in the Mid-Atlantic region, said, “It’s scary as hell. It’s terrifying. . . . It’s not that I’m fearful of who she is, I’m fearful of what the world is going to do to her.”
Similar to fear of future experiences for their children, 12 participants cited fear of the side effects of their child’s requested GCEI. Camilla (46), a White, cisgender woman separated from her partner and living in the Mid-Atlantic region, had similar concerns, stating that she “didn’t have a whole lot of information on how testosterone, for instance, would affect [my child] . . . . It was a concern of, ‘How does that affect the long-term health of my child?’ That’s actually a question that I still have.”
Finally, at least six participants communicated that fear related to the political climate inhibited their decision-making process. Honour (43), a White, cisgender woman divorced from her parenting partner and residing in the Mid-Atlantic region, recounted that political fears affected her and her child’s decision to request a subcutaneous implant, saying:
The physician seemed surprised and said, “Tell me more about why that’s your first choice.” And (child) says, “We have a presidential election coming up, and I don’t want to be in a situation where I start monthly or quarterly shot treatments only to have that right taken away from me. If they put a 2-year implant in my arm, they’re not going to come rip it out.”
Doubt
Although fewer than half of participants (n = 6) expressed doubt in the genuineness of their youth’s TGD identity, doubt was still considered a main inhibitor because each participant who described their doubt gave vivid descriptions thereof. Berta (48), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, provided the following example that was indicative of the sample’s experiences:
It was scary at first because everybody goes to the same place, which is scared for your child. And then, you know, maybe this is a phase? Maybe he’s confused? Maybe—you know? And so, you go through all those things.
Grief Over a Lost Parenting Narrative
The most prominent inhibiting factor not directly related to lack of knowledge leading to fear or doubt was participants’ description of grief over their lost parenting narrative. A majority of participants (n = 9) reported that the change in their expected future with their child came as a result of learning that their child identified as TGD. Adele (32), a White, cisgender woman married to her child’s father and living in the Mountain West region, described an internal conflict consistent with her peers:
There’s this creeping in of grief. . . . Even if you should be able to adapt, it’s still there. When we make these choices for hormone therapy, it’s kind of a step further in the direction of whatever could have been will definitely never be.
Rejection
A substantial subset of participants (n = 8) reported experiencing what could be considered some form of rejection, either from a parenting partner or a health care provider or payor. Of the six participants who reported that their parenting partner demonstrated signs of rejection, all were cisgender women; however, only two reported that their parenting partner maintained their rejecting stance in a way that ultimately put informed consent at risk (for legal reasons). Mellony (49), a White, cisgender woman married to her child’s father and living in the Mid-Atlantic region, recounted an experience that was more typical in the sample:
My husband was a little slower, in the beginning, to get on board. I just think he had a harder time—you know, “Is this really real? Is this a phase? Did she learn it on the internet? What’s really going on?”
Three participants described what they considered to be rejecting messages and/or behavior from health care providers. In response to a question about how a mental health professional was involved in her decision-making process, Journey (51), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, said that meeting with a counselor was one of the worst parts of the process, and they walked out of the session early:
One of the things that was concerning me at the time was, “How do I tell my younger children.” And she said, “Oh, I wouldn’t do that. He’s probably going to change his mind.” And so we said, “Well, OK, there’s a lot we don’t know, but that’s not the right answer.”
Adele described denials of reimbursement from her child’s insurance company as well as unwelcoming responses from front-desk workers at the clinic at which they were seeking treatment: “They seemed incredibly—I don’t know how to word it—off-putting in that, we were like, ‘one of those.’”
Lack of Access
A subset of participants reported a lack of access to affirming treatment. Five participants reported a lack of access due to their residential location; three reported it was due to insurmountable financial cost. Some drove several hours away and across state lines so that their child could receive treatment. Sharyn (47), a White, cisgender woman divorced from her child’s father and living in the Mid-Atlantic region, recounted that her ex-partner’s reluctance to give consent affected the cost of treatment, stating, “All we could do was a prescription to stop periods, which [was] about three or four times more expensive than hormones.”
Contributors to Consent
Participants identified four factors that contributed to giving consent: (a) parental attunement to the experiences and emotions of the youth in their care, (b) parental autonomy from their family of origin and religious communities, (c) access to affirming education about TGD issues and GCEI, (d) the presence and/or development of affirming relationships and community, and (e) affirming religious beliefs and/or community.
Parental Attunement to Youth’s Experience
The construct of parental attunement has been defined as a relational dynamic between parent and child that surpasses what is typically included in the construct of empathy. Erskine (1998) posited that attunement is a two-part process that includes (a) the ability to sense and to identify with another person’s sensations, needs, and feelings: and (b) communicating that sensitivity to the other person. A parent’s ability to attune to their child’s experience and emotional world has been prominently associated with the fostering of secure attachment and personality development (Ainsworth & Bowlby, 1991; Bowlby, 1988; Siegel, 2013; Wallin, 2007). Participants in the present study conveyed their ability to demonstrate parental attunement by describing their wishes for their TGD youth’s social and emotional well-being as a primary motivator for granting informed consent for them to undergo GCEI. Furthermore, participants implied respect for their youth’s autonomy, their recognition of their youth’s gender non-conformity, and their recognition of their youth’s mental health symptoms. Participants also recognized their own position of privilege that facilitated granting consent and a sense of their own autonomy from their families of origin or religious backgrounds.
One of the more striking examples of parental attunement in this sample was provided by Tony (61), a White, cisgender man married to his child’s mother and living in the Mid-Atlantic region, who tearfully recounted a conversation with his then–16-year-old child following a support group meeting:
I said, “You know, what would really help me is, could you write down your goals, what you want, and be honest with everything. We want to support you.” So, after we got home, within about two hours, [child] brought me something that I still have. . . . It says “Trans with the Plans.” And that was when I knew that this kid I love so much knew what they wanted, and I had to support them.
A notable subset of participants (n = 16) reported that they recognized their child’s rejection of binary gender norms prior to their child coming out to them. This recognition often came during early childhood. Hilda remembered noticing her child’s “Sunday best”:
I had [child] in her little dress shirt and tie and dress pants, and I told her to go get her dress shoes, and her little face lit up. She ran down the hall and came back in those little Cinderella shoes—so, [child] was always [child]. It just took us awhile to catch on.
Every participant recounted a recognition of and concern for their child’s mental health. Prudence (46), a mixed-race, cisgender woman married to her child’s father and living in the Southwest region, said that her child “came to us in the middle of the night, and I said, ‘Are you feeling suicidal?’ He didn’t respond verbally, but he just started crying. So I just pulled him in bed with me and I snuggled him.”
Parental Autonomy From Their Family of Origin or Religious Communities
A less frequent, but nonetheless notable, sign of parental attunement to the experience and emotions of their child was participants’ descriptions of how they prioritized the wishes and needs of their child and demonstrated autonomy from their families of origin (n = 10) or religious backgrounds (n = 4). Berta recounted planning with her partner how to break the news of their consent to extended family members:
[When] we told extended family, I was making the phone calls, but [my partner] reminded me, he said, “Remember, this is not a terminal illness.” It could be, right, if you don’t do it right, but just say, “We’re not asking permission, and we are not apologizing.” So, he kind of like, you know, held me up when we made those calls.
Brenda (48), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, described her experience within a religious community that had members that were reluctant to openly lend support and others who wanted to offer support but lacked the necessary knowledge and skill to do so. In recounting what led her and her family to leave their congregation at the time, she stated:
I did chat about it to anyone who asked and had hoped to educate and affect some positive change from within, but lots of folks just weren’t ready or willing to have these conversations. Which was interesting because this was all during the time when the [denomination] was making high-level decisions about whether or not to affirm LGBTQ folks.
Access to Affirming Community, Education, Health Care, and Parenting Partnership
All participants made at least some reference to having access to affirming (a) community of parents, professionals, colleagues, and/or friends; (b) education; (c) health care; and (d) parenting partnership. A key element of access to an affirming community was participants’ acknowledgement of possibility models. This term, which participants credited to prominent transgender actor Laverne Cox, refers to a person who identifies as TGD and has successfully gone through a medical transition, or a parent who has successfully supported their child through a medical transition. Possibility models were referenced when participants spoke about their experiences with family friends, support group members, professionals, and members of the mass media.
Participants were all members of affirming communities, and they reported that they received affirming education from group members and health care providers, including professional counselors. Adele reported the following about the support her child received from an affirming professional counselor during the process toward GCEI:
This counselor met her where she was and was using interventions geared toward just expressing herself. And I think it helped her to externalize what was happening, and then also, she was able to talk about the things that she was going through . . . because it was a space where there was no pressure.
Several participants reported that the counselors or mental health providers who wrote referral letters for their youth to begin GCEI were often closely associated with support groups they attended, completed gatekeeping procedures efficiently and without unexpected fees, had TGD-affirming staff and office procedures in place, and did not necessarily focus exclusively on gender identity.
Affirming Religious Beliefs and/or Community
Nearly half the participants (n = 8) identified as mainline Protestant Christians (i.e., members of denominations that have historically rejected fundamentalist practices) and reported that affirming religious beliefs contributed to their decision-making process. Emma (56), a White, cisgender woman married to her child’s father and living in the Midwest region, provided a response typical of the sample regarding the role of religion in her decision-making process:
Jesus said we are children of God, and he did not define what a child of God looks like. God created this world to be diverse. Look outside, and you’re going to see it. We’re just living in that reality of being children of God.
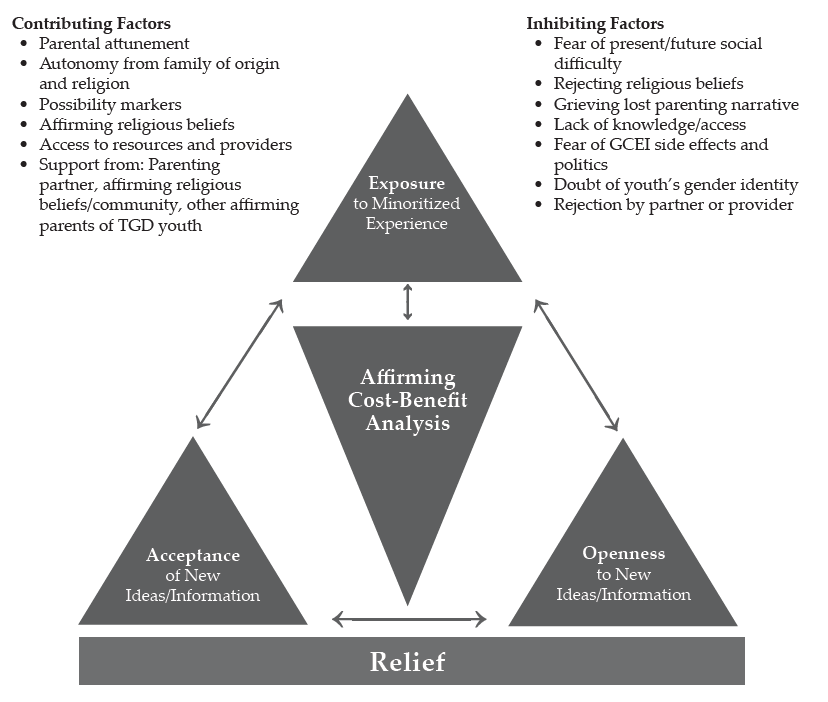
Central Theme: From Dissonance to Consonance
Each participant described an initial expectation that their youth would identify, like them, as cisgender. When they recognized that their child’s gender expression did not align with those social expectations, each participant described experiencing some level of intra- and interpersonal tension. This phenomenon may also be understood by what is commonly known as cognitive dissonance (Festinger, 1957; Myers & DeWall, 2019). Like the construct of parental attunement described previously, the construct of cognitive dissonance borrows from the physics of music, in which the term dissonance is used to describe a lack of harmony. On the other hand, consonance is the term used to describe a combination of one or more tones of different frequencies that combine and result in a musically pleasing (i.e., harmonious) sound (Errede, 2017). Festinger’s cognitive dissonance theory (1957) suggests that when faced with this type of mental tension, humans often bring their attitudes and beliefs into alignment with their actions (Myers & DeWall, 2019). The responses of the participants of this study suggest that this is an apt metaphor for their decision-making process.
Each participant described 1) an experience of exposure to some form of human diversity prior to their youth confirming a TGD identity, 2) cognitive-emotional openness to new and TGD-affirming information, and 3) acceptance of the new and affirming information presented to them, followed by the participant 4) using the affirming information available to them to make an affirming cost-benefit analysis that led to the granting of informed consent and finally 5) feeling a sense of relief that they gave informed consent for their youth to undergo GCEI. Figure 1 shows a dissonance-to-consonance model of these mutually influencing central factors.
Exposure to Historically Minoritized Experiences
Each participant described previous exposure to some type of historically minoritized experience, whether it was as personal as identifying as a woman (as in Journey’s case), a professional experience, or knowing someone within their children’s social networks. Mellony reported personal and professional exposure, stating that a former colleague had come out as trans, “so I did know someone. I also knew another mom whose child had come out a couple years earlier, so it was not completely foreign to me.”
Openness
Each participant described generally open attitudes that led to parenting decisions ranging from the toys they gave to their child to seeking education. Adele recounted that her family “did a lot of research on our own. We had other parents and kiddos that [we] were able to talk to about what they were experiencing, and we heard from families about what the process looked like for them.”
Figure 1
A Dissonance-to-Consonance Model
Acceptance
Prudence provided an example of acceptance typical of the sample in that she not only accepted that the GCEI and other affirming practices would be beneficial, but she also arrived at a place where she wished she had started them earlier:
I often say [child’s given name at birth] was the vessel, [child’s name] is the soul. If I had known that, and understood it wasn’t a phase, I probably would have pushed to start so he didn’t go through puberty as a female.
Affirming Cost-Benefit Analysis
Berta provided a description typical of the sample regarding her and her partner’s affirming cost-benefit analysis that led to granting informed consent. She highlighted her access to a supportive community as well as her recognition of the mental health implications of a non-affirmed TGD identity for her child:
A parent who had come before me said there’s really nothing that you can’t reverse. You can wear a wig if your hair falls out. . . . If you start growing facial hair and then you decide you don’t want to, you can get electrolysis. . . . If you get your breasts removed, you can get implants. But what it really comes down to is do you want a dead kid, or do you want a kid that might be slightly altered? We looked at [our child] and thought, “You’re miserable, and if this will help you not be miserable, then we will go for it.”
Relief
Each participant expressed a sense of relief that they had granted informed consent, usually because they noticed improvements in their child’s moods and general sense of happiness. Lennon (55), a White, cisgender man married to his parenting partner and living in the Midwest region, provided a statement that was typical in the sample: “His mood changed. That was the key. I think the fact that we saw [child] become happier with it, that’s the key. That’s all that really mattered.”
Discussion
The purpose of this research was to explore the process by which 17 parents of TGD youth developed affirmative understandings and approaches to their children’s gender identity, affirmed their related transition needs, and granted informed consent for the TGD youth in their care to undergo GCEI. Based upon our review of the literature, there are no studies related to the process that the parents and guardians of TGD minors go through to give informed consent for GCEI. This research appears likely to inform best practice for professional counselors and other helping professionals serving TGD youth who wish to have an endocrinologically supported transition and those charged with giving informed consent for these interventions.
Implications for Professional Counselors
First, this research provides a plausible model for practitioners to follow when presented with the challenge of supporting parents of TGD youth as they work to develop affirming attitudes and support their respective children’s medical transition. Though the dissonance-to-consonance model as presented still needs to be tested by more objective means, the interplay of exposure, openness, and acceptance as contributing factors to parents’ TGD-affirming cost-benefit analyses toward the experience of relief for themselves and their children appears to be consistent with attachment and family counseling best practices (Ainsworth & Bowlby, 1991; Bowlby, 1988; Gladding, 2019; Minuchin, 1974; Siegel, 2013; Siegel & Bryson, 2011; Wallin, 2007). The combination of these factors, especially as they relate to parents’ fears about the side effects of GCEI and doubts about the genuineness of their child’s gender identity, appeared particularly relevant to this study given the previously cited paucity of research examining the long-term effects of GCEI on developing pre-adolescent and adolescent bodies and that the consistency between gender-expansive identity development and cisgender identity development has only been published recently (Drescher, 2010; Gülgöz et al., 2019). The challenges, however, for adolescents regarding decision-making, impulse control, and executive functioning are well-documented (Siegel, 2013).
Participants in this study praised the work of the professional counselors and other mental health professionals in their life when they (a) provided credible and affirming education about gender identity development; (b) worked in connection with support groups with which participants were involved; (c) recognized that the presenting concerns for the child and/or family may not necessarily be related to gender identity; and (d) completed gatekeeping responsibilities and tasks succinctly, efficiently, and without unexpected financial costs. These factors appear to be consistent with competencies for working with transgender clients developed by SAIGE (Burnes et al., 2010). Participants lamented their experiences with professional counselors and other health care professionals when (a) the above tasks were not completed within these guidelines, (b) the professionals were dismissive of the child’s gender identity or unwilling to provide care, and (c) clinic staff gave participants an unwelcoming or non-affirming impression.
The present study suggests that when presented with the opportunity to serve TGD adults, youth, and their families, professional counselors should familiarize themselves with and develop both the SAIGE competencies and the World Professional Association for Transgender Health (WPATH) Standards of Care (E. Coleman et al., 2012). Furthermore, professional counselors should follow established informed consent guidelines and be upfront and clear about fees for services when it comes to more specialized tasks like writing a GCEI referral letter. A growing body of resources also exists for developing TGD-affirming and inclusive cultures among non-clinical staff employed by counseling practices. For example, the guidelines developed by Morenz and colleagues (2020) for developing and implementing a transgender health program include suggestions for gaining buy-in from and training for reception and administrative staff.
Finally, it appears that collegial support of counselors knowledgeable about the roles of clinicians in working with TGD individuals and families to develop competence among a wider network of providers may be necessary. This support is warranted, given the lack of access to TGD-affirming health care due to residential location, including counseling, cited as an inhibiting factor by this sample. This may support the reduction of referrals of TGD clients between counselors, a practice allowed by the ACA’s (2014) Code of Ethics in matters of limited competency but, as Kaplan (2018) has stated, is also a practice the clients may interpret as rejecting.
Limitations and Future Directions
As with all qualitative research, the results of this grounded theory study, despite the efforts made to maximize trustworthiness, need further testing using quantitative methodology to strengthen their applicability across a broader range of samples (Merriam & Tisdell, 2016). By its design, this was a study about how participants resolved their dilemma in an affirming way and therefore may not be as valuable for responding to research questions regarding dilemmas resolved in pathologizing or rejecting ways. This study was also limited demographically, with a sample heavily weighted toward the experiences of White (n = 16), cisgender women (n = 13), and married participants (n = 14). The majority of participants reported household incomes of more than $90,000, doubtlessly improving the odds that they could overcome some inhibiting factors because of greater financial ability. Finally, this research may have been limited by a sample that was heavily weighted toward participants who reside in the Mid-Atlantic region (n = 12); a sample that was more balanced across the United States may have produced different findings.
These findings lend themselves to testing with quantitative methods such as pre-test/post-test program evaluation or randomized controlled trials (RCTs). Both methods have the potential to draw larger, more representative sample sizes, thus enhancing external validity to make greater contributions to the literature. The dissonance-to-consonance model presented here could be used as a program theory for evaluation. RCTs in the vein of what has been used to test the effectiveness of specific counseling modalities, using an approach influenced by the dissonance-to-consonance model compared to a control sample using “therapy as usual” (Ramsauer et al., 2014), may also be valuable for informing best practice while avoiding the ethical dilemma presented by denying treatment. Quantitative investigation may also benefit from further qualitative exploration of the present research questions in a way that addresses the demographic limitations of this study. For example, a grounded theory study of parents who identify as Black may produce different results (Armstrong et al., 2013; Gibbons, 2019; Zheng, 2015).
Conclusion
The present study examined, for the first time, the experiences of parents of TGD youth as they decided to give informed consent for their child to undergo GCEI. They named a variety of inhibitors and contributors to this process, and a “dissonance-to-consonance” model for using contributing factors to overcome inhibitors to the process was illuminated. We found the research process to be emotionally moving and rich with guidance for both parents of TGD youth who are making decisions of considerable consequence for their children and the professional counselors working with them in supportive roles. The model appears to provide fertile ground for further study to support services that affirm and support TGD youth and their families. We relish the opportunity to continue this work and look forward to the contributions of others who advance this topic in service of TGD well-being throughout the life span.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ainsworth, M. D. S., & Bowlby, J. (1991). An ethological approach to personality development. American Psychologist, 46(4), 333–341.
American Counseling Association. (2014). ACA code of ethics. https://bit.ly/ACAcodeofethics
Armstrong, K., Putt, M., Halbert, C. H., Grande, D., Schwartz, J. S., Liao, K., Marcus, N., Demeter, M. B., & Shea, J. A. (2013). Prior experiences of racial discrimination and racial differences in health care system distrust. Medical Care, 51(2), 144–150. https://doi.org/10.1097/MLR.0b013e31827310a1
Bowlby, J. (1988). A secure base: Parent-child attachment and healthy human development. Basic Books.
Bränström, R., & Pachankis, J. E. (2020). Reduction in mental health treatment utilization among transgender individuals after gender-affirming surgeries: A total population study. The American Journal of Psychiatry, 177(8), 727–734. https://doi.org/10.1176/appi.ajp.2019.19010080
Bunim, J. (2015, August 17). First U.S. study of transgender youth funded by NIH: Four sites with dedicated transgender youth clinics to examine long-term treatment effects. UCSF News & Media. https://bit.ly/UCSFstudy
Burnes, T. R., Singh, A. A., Harper, A. J., Harper, B., Maxon-Kann, W., Pickering, D. L., Moundas, S., Scofield, T. R., Roan, A., & Hosea, J. (2010). American Counseling Association competencies for counseling with transgender clients. Journal of LGBT Issues in Counseling, 4(3–4), 135–159.
https://doi.org/10.1080/15538605.2010.524839
Burt, N. (2016). When girls play with G.I. Joes and boys play with Barbies: The path to gender reassignment in minors. Florida Law Review, 68(6), 1883–1913. https://bit.ly/3GkpSPK
Cashwell, C. S., & Watts, R. E. (2010). The new ASERVIC competencies for addressing spiritual and religious issues in counseling. Counseling and Values, 55(1), 2–5.
https://doi.org/10.1002/j.2161-007X.2010.tb00018.x
Charmaz, K. (2014). Constructing grounded theory (2nd ed.). SAGE.
Coleman, D. L. (2019). Transgender children, puberty blockers, and the law: Solutions to the problem of dissenting parents. The American Journal of Bioethics, 19(2), 82–84. https://doi.org/10.1080/15265161.2018.1557297
Coleman, D. L., & Rosoff, P. M. (2013). The legal authority of mature minors to consent to general medical treatment. Pediatrics, 131(4), 786–793. https://doi.org/10.1542/peds.2012-2470
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H. . . . Zucker, K. (2012). Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. https://doi.org/10.1080/15532739.2011.700873
Corbin, J., & Strauss, A. (2015). Basics of qualitative research: Techniques and procedures for developing grounded theory (4th ed.). SAGE.
Couric, K. (Director, Producer). (2017). Gender revolution [Documentary]. National Geographic.
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Dailey, S. F. (2017, June). Ethical & legal considerations: Complicated issues in challenging times. Presentation given at the 2017 Illuminate Symposium, Washington, D.C.
Drescher, J. (2010). Queer diagnoses: Parallels and contrasts in the history of homosexuality, gender variance, and the Diagnostic and Statistical Manual. Archives of Sexual Behavior, 39, 427–460.
https://doi.org/10.1007/s10508-009-9531-5
Durso, L. E., & Gates, G. J. (2012). Serving our youth: Findings from a national survey of services providers working with lesbian, gay, bisexual and transgender youth who are homeless or at risk of becoming homeless. The Williams Institute with True Colors Fund and The Palette Fund.
Errede, S. (2017). [Lecture notes on acoustical physics of music]. Department of Physics, University of Illinois at Urbana-Champagne, IL. https://bit.ly/3p8gh7z
Erskine, R. G. (1998). Attunement and involvement: Therapeutic responses to relational needs. International Journal of Psychotherapy, 3(3), 235–244.
Festinger, L. (1957). A theory of cognitive dissonance. Stanford University Press.
Gibbons, J. (2019). The effect of segregated cities on ethnoracial minority healthcare system distrust. City & Community, 18(1), 321–343. https://doi.org/10.1111/cico.12370
Gibbs, J. J., & Goldbach, J. (2015). Religious conflict, sexual identity, and suicidal behaviors among LGBT young adults. Archives of Suicide Research, 19(4), 472–488. https://doi.org/10.1080/13811118.2015.1004476
Gladding, S. T. (2019). Family therapy: History, theory, and practice (7th ed.). Pearson.
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory: Strategies for qualitative research. Aldine Publishing.
Gonzalez, R. (2018, January 23). How the ‘Religious Freedom Division’ threatens LGBT health—and science. Wired. https://www.wired.com/story/how-the-religious-freedom-division-threatens-lgbt-healthand-science
Goodkind, N. (2021, July 9). Ohio law allows doctors to deny health care and birth control to LGBTQ patients. Fortune. https://bit.ly/FortuneLGBTQ
Grossman, A. H., & D’Augelli, A. R. (2007). Transgender youth and life-threatening behaviors. Suicide and Life-Threatening Behavior, 37(5), 527–537. https://doi.org/10.1521/suli.2007.37.5.527
Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Chonghui, J., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116(49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Hembree, W. C., Cohen-Kettinis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine treatment of gender-dysphoric/gender-incongruent persons: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. https://doi.org/10.1210/jc.2017-01658
Hill, D. B., & Menvielle, E. (2009). “You have to give them a place where they feel protected and safe and loved”: The views of parents who have gender-variant children and adolescents. Journal of LGBT Youth, 6(2–3), 243–271. https://doi.org/10.1080/19361650903013527
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf
Jorgensen, C. (1967). Christine Jorgensen: A personal autobiography. Bantam.
Kaplan, D. M. (2018, April). Train the trainer: Delivering presentations on the 2014 ACA Code of Ethics. Presentation at the ACA 2018 Conference & Expo Pre-conference Learning Institutes, Atlanta, GA.
Lawson, G. (2016). On being a profession: A historical perspective on counselor licensure and accreditation. Journal of Counselor Leadership and Advocacy, 3(2), 71–84. https://doi.org/10.1080/2326716X.2016.1169955
Merriam, S. B., & Tisdell, E. J. (2016). Qualitative research: A guide to design and implementation (4th ed.). Jossey-Bass.
Minuchin, S. (1974). Families & family therapy (1st ed.). Harvard University Press.
Morenz, A. M., Goldhammer, H., Lambert, C. A., Hopwood, R., & Keuroghlian, A. S. (2020). A blueprint for planning and implementing a transgender health program. Annals of Family Medicine, 18(1), 73–79. https://doi.org/10.1370/afm.2473
Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta-analysis of quality of life and psychosocial outcomes. Clinical Endocrinology, 72(2), 214–231.
https://doi.org/10.1111/j.1365-2265.2009.03625.x
Myers, D. G., & DeWall, C. N. (2019). Exploring psychology in modules (11th ed.). Worth Publishers.
Pew Research Center. (2014). Religious landscape study. http://www.pewforum.org/religious-landscape-study
Ramsauer, B., Lotzin, A., Mühlhan, C., Romer, G., Nolte, T., Fonagy, P., & Powell, B. (2014). A randomized controlled trial comparing Circle of Security Intervention and treatment as usual as interventions to increase attachment security in infants of mentally ill mothers: Study protocol. BMC Psychiatry, 14(24). https://doi.org/10.1186/1471-244X-14-24
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. American Counseling Association. https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf?sfvrsn=20
Rose, J. S., Kocet, M. M., Thompson, I. A., Flores, M., McKinney, R., & Suprina, J. S. (2019). Association for Lesbian, Gay, Bisexual, and Transgender Issues in Counseling best practices in addressing conscience clause legislation in counselor education and supervision. Journal of LGBT Issues in Counseling, 13(1), 2–27. https://doi.org/10.1080/15538605.2019.1565800
Rosin, H. (2008, November). A boy’s life. The Atlantic. https://bit.ly/3lIxOCF
Shabad, R. (2021). Biden administration announces reversal of Trump-era limits on protections for transgender people in health care. NBC News. https://nbcnews.to/3drlWAr
Siegel, D. J. (2013). Brainstorm: The power and purpose of the teenage brain. Penguin.
Siegel, D. J., & Bryson, T. P. (2011). The whole-brain child: 12 revolutionary strategies to nurture your child’s developing mind. Delacorte Press.
Stryker, S. (2008). Transgender history. Seal Press.
Toporek, R. L., & Daniels, J. (2018). American Counseling Association advocacy competencies: Updated. American Counseling Association https://www.counseling.org/docs/default-source/competencies/aca-advocacy-competencies-updated-may-2020.pdf?sfvrsn=f410212c_4
U.S. Department of Health and Human Services. (2018a). HHS announces new Conscience and Religious Freedom Division. https://www.hhs.gov/about/news/2018/01/18/hhs-ocr-announces-new-conscience-and-religious-freedom-division.html
U.S. Department of Health and Human Services. (2018b). Conscience and religious freedom. https://bit.ly/3oz6p7G
Vincent, B. (2019). Breaking down barriers and binaries in trans healthcare: The validation of non-binary people. International Journal of Transgenderism, 20(2–3), 132–137. https://doi.org/10.1080/15532739.2018.1534075
Vines, M. (2014). God and the gay Christian: The biblical case in support of same-sex relationships. Convergent Books.
Wallin, D. J. (2007). Attachment in psychotherapy. Guilford.
Zheng, H. (2015). Losing confidence in medicine in an era of medical expansion? Social Science Research, 52, 701–715. https://doi.org/10.1016/j.ssresearch.2014.10.009
APPENDIX A
Interview Protocol
Beginning Questions:
- Tell me about how you came to grant informed consent for your child to receive puberty blockers or hormone replacement therapy?
- When did you first notice/realize that your child identified as transgender or gender-diverse (TGD)?
- What was that like?
Intermediate Questions:
- What, if anything, did you know about gender identity and gender expression prior to learning your child identified as TGD?
- What, if anything, did you know about gender-confirming endocrinological interventions (GCEI) prior to giving informed consent for your child to participate in them?
- How, if at all, have your thoughts and feelings changed about gender variance since learning that your child identified as TGD?
- How, if at all, have your thoughts and feelings changed about gender-confirming hormone treatments since your child indicated they wanted to receive them?
- What, if anything, inhibited your change process?
- Who, if anyone, helped you in this change process?
- How, if at all, was a professional counselor or other mental health professional involved?
- What would you say were the most helpful aspects that you experienced during your process toward giving informed consent for GCEI?
Closing Questions:
- Is there something that you might not have thought about before that occurred to you during this interview?
- Is there something else you think I should know to understand your process or experience better?
Charles F. Shepard, PhD, NCC, LPC, is a visiting faculty member at James Madison University. Darius A. Green, PhD, NCC, is the PASS Program Assistant Coordinator at James Madison University. Karli M. Fleitas, MA, is a doctoral student at James Madison University. Debbie C. Sturm, PhD, LPC, is a professor at James Madison University. Correspondence may be addressed to Charles F. Shepard, MSC 7704, James Madison University, 91 E. Grace Street, Harrisonburg, VA 22807, sheparcf@jmu.edu.
Dec 5, 2015 | Article, Volume 5 - Issue 4
Shainna Ali, Sejal Barden
Coming out is a decision-making process regarding disclosure of identity for sexual minorities. Existing literature on the coming-out process highlights a singular, linear emphasis, failing to highlight the recurring task of disclosure that sexual minorities endure. The purpose of this manuscript is to highlight the cyclical nature of the coming-out process and the importance of recognizing this cycle when counseling sexual minority clients. A case application is provided to illustrate the proposed cycle of coming out. Implications for counselors and suggestions for future research are discussed.
Keywords: sexual minority, coming-out process, identity development, decision-making, disclosure
Coming out is a pivotal process in the lives of sexual minority (e.g., lesbian, gay and bisexual) individuals. The term sexual minority is utilized in this paper to be both succinct and inclusive. Beyond the internal process of development, coming out is an interpersonal, diverse process of disclosure. During the lifetime, individuals may face various opportunities to disclose identity; each scenario may have unique implications that are essential to consider in regard to client safety. When counseling clients through the coming-out process (COP), it is essential to recognize the social context encompassing each unique occurrence in the lifelong cycle of coming out. The purpose of this manuscript is to highlight the recurring process of disclosure as we (a) address the stressors and benefits of coming out, (b) outline the social layers of coming out, (c) examine strengths and limitations of current models pertaining to coming out, (d) emphasize the importance of addressing coming out in counseling, and (e) introduce the application of a cyclical framework of the coming-out process through a case illustration.
Stressors and Benefits of Coming Out
Sexual minorities face considerable personal dilemmas regarding coming out. Coming out may be a threatening process as stigmatization and marginalization are by-products of sexual prejudice (Dermer, Smith, & Barto, 2010). Stressors include, but are not limited to, fears pertaining to acceptance, bullying, harassment, safety and oppression (Coker, Austin, & Schuster, 2010; Gay, Lesbian, and Straight Education Network [GLSEN], 2010). It is widely acknowledged that during the coming-out process, individuals may experience negative emotions (Bernal & Coolhart, 2005; Chutter, 2007; McDermott, Roen, & Scourfield, 2008). Internal discord may prompt feelings of loneliness, disconnection, confusion, grief, shame, anger, fear, vulnerability and depression that lead to potential suicidal ideations (Human Rights Campaign [HRC], 2013; Lewis, Derlega, Berndt, Morris, & Rose, 2001). Individuals facing this internal conflict may suffer from low self-esteem as low confidence and incongruence in identity prompts individuals to expend energy on suppressing identity. This stifling often prompts impulsive, negative coping mechanisms such as substance use, self-harm and engaging in risky sexual behaviors (Degges-White, Rice, & Myers, 2000; McDermott et al., 2008; Parks & Hughes, 2007).
Sexual minorities are faced with the risk that not everyone will understand or accept their identity. Individuals may react in a multitude of ways that include shock, hostility, confusion and disappointment. Reactions may reach levels of harassment and abuse. In choosing to disclose, sexual minorities must accept the risk that relationships, regardless of closeness, may permanently change. Regardless of a sexual minority’s internal awareness, acceptance and congruence, it is important to acknowledge the risk involved every time one chooses to disclose their identity, thus highlighting the cyclical, recurring decision-making process every time one reveals their identity. Therefore, it is essential for counselors to be aware of the stressors involved in the coming-out process in order to effectively aid clients.
Although stressors exist, the decision to disclose one’s sexual minority identity may be enticing and empowering. From enduring the process, individuals may experience coming-out growth (Vaughan & Waehler, 2010). Researchers often have discussed that coming out may improve the quality of one’s life (Floyd & Stein, 2002; Mohr & Fassinger, 2003; Morris, Waldo, & Rothblum, 2001; Oswald, 2000; Rosario, Hunter, Maguen, Gwadz, & Smith, 2001). Moreover, studies have shown relationships between disclosing identity and reduced levels of distress. Rosario and colleagues (2001) learned that positive attitudes towards identity were related to lower anxiety and depression among sexual minority youth. Similarly, in a study of 2,401 lesbian and bisexual women, Morris and colleagues (2001) found that coming out reduces psychological distress. Furthermore, identity disclosure also has been associated with positive and strengthened identity, which often improves resilience and overall mental health (Floyd & Stein, 2002; Mohr & Fassinger, 2003; Oswald, 2000)
The interpersonal process of sharing a piece of one’s self may prompt an individual to feel more honest, open and authentic with others; thus, coming out may enhance social skills and functioning (Savin-Williams, 2001; Stevens, 2004). Disclosing identity may help to form new relationships or to deepen existing relationships (Oswald, 2000; Savin-Williams, 2001). Coming out may be related to closeness for individuals who disclose in a relationship (Berger, 1990). The presence or absence of support following identity disclosure may help individuals to determine how to create healthier boundaries (LaSala, 2000; Oswald, 2000). Beyond personal relationships, outness may be linked to interest and involvement in advocacy. Individuals who have disclosed report an increased interest in changing judgmental, biased attitudes of individuals who may display prejudice (Oswald, 2000). Coming out has the potential to provide an array of benefits from individual to societal levels. Counselors who are informed and prepared have the potential to support clients who are coming out and assist in facilitating such benefits.
Layers of the Coming-Out Process
Sexual minorities may experience multiple layers when coming out, which may include factors of disclosing to family members, friends, various communities and professional colleagues throughout the lifespan (Datti, 2009; Espelage, Aragon, Birkett, & Koenig, 2008; Joos & Broad, 2007; Rickards & Wuest, 2006; Treyger, Ehlers, Zajicek, & Trepper, 2007; Waitt & Gorman-Murray, 2011). Therefore, the COP is better conceptualized as a cycle of coming out that includes several processes throughout an individual’s lifetime. Familial disclosure is typically a salient layer, as reactions from family to identity disclosure exist on a spectrum of happiness and acceptance to anger and abandonment (Lewis, 2011; Pearson, 2003). The stressors of coming out have the potential to divide a family as some members may ascribe to heterosexist beliefs and not be accepting of the individual (Gorman-Murray, 2008). Sexual minority youth must consider the potential ramifications of disclosing their sexual identity, particularly in conservative households. Due to differences in beliefs and consequential conflicts, sexual minority youth are often beaten, disowned and kicked out of their homes (Bernal & Coolhart, 2005). According to Hilton and Szymanski (2011), the entire familial unit is affected by the disclosure. Siblings may feel concerned for the sexual minority sibling, angry or disappointed with parental reactions, consider the changes that would need to occur for themselves, and prepare to deal with the challenge of heterosexism. Children of sexual minorities also are affected by disclosure. According to Joos and Broad (2007), adult children reported experiencing feelings of fear, terror and secrecy. It is suggested that the family as a whole endures a process of coming out that includes elements of embracing identity, integrating as a family, building social networks and experiencing social awakening (Baptist & Allen, 2008).
Another layer of the cycle of coming out (CCO) that is important to consider is peer disclosure. When sexual minorities choose to acknowledge their identity publicly and reveal to their peers, they often are met with threats, assaults, harassment and hostility (Alderson, 2003; Chutter, 2007; Degges-White & Myers, 2005). A 2010 report by the GLSEN revealed that almost 90% of sexual minority students heard the term “gay” used negatively, 61% felt unsafe at school due to identity, almost 85% experienced verbal harassment, and 40% experienced physical harassment. Given that peer groups are constantly evolving, sexual minorities must face disclosure to multiple peer groups over the course of their lifetime and hence the coinciding reactions, effects and consequence are important to consider and validate.
In addition to family and peer groups, societal messages highlight the marginalized status given to individuals who identify outside of the heterosexist binary established in Western society. This marginalization provides the foundation for the unique, complex process of identity development and disclosure for sexual minorities (Cooper, 2008; Dermer et al., 2010; Israel & Selvidge, 2003). For example, sexual minorities must consider disclosure toward those within their inner social circles (e.g., family, friends) as well as to individuals who are outside of this intimate realm (e.g., colleagues, employers, neighbors, strangers). With each decision, sexual minorities may experience persistent emotions, thoughts and behaviors associated with previous instances of coming out, highlighting the importance of acknowledging the recurring experience of sexual minority status that reaches beyond the scope of a pivotal one-time occurrence.
Need for Counselor Preparation
Counselors’ competence in working with sexual minority clients requires counselors to be affirmative, open, supportive and utilize holistic approaches in assisting clients through the COP (Bidell, 2005; Cooper, 2008; Israel, Ketz, Detrie, Burke, & Shulman, 2003; Rutter, Estrada, Ferguson, & Diggs, 2008). Within this spectrum, a variety of topics have been considered as aspects to contribute to counselor preparedness such as ethical issues, terminology, awareness of current issues and willingness to advocate. Israel and colleagues (2003) conducted a modified Delphi study in an effort to better understand sexual minority counseling competencies. They surveyed professional experts who had published at least one book, book chapter, or article on lesbian, gay, and/or bisexual (LGB) clients as well as sexual minority clients who had experiences in counseling. Results indicated that out of 31 highlighted skills, the ability to assist clients through coming out was ranked as the third most important skill for working with sexual minority clients by professional experts and fourth most important skill by sexual minority experts. Although coming out is ranked highly as an important skill in assisting LGB individuals, clients are consistently dissatisfied with counselors’ abilities to assist in counseling. Nadal and colleagues (2011) conducted a qualitative study of 26 LGB clients. Participants noted several concerns with their counselors such as discomfort or disapproval, use of heterosexist language, assumption of pathology or abnormality, assumption of a universal LGB experience, exoticization and threatening. Similarly, Shelton and Delgado-Romero’s (2013) study noted similar issues such as avoidance or minimization of identity, making stereotypical assumptions about identity, assumption that sexual orientation is the cause of presenting issues, and expressions of heterosexist bias.
In addition to client dissatisfaction, counselors have noted their own lack of confidence in helping sexual minority clients (Bidell, 2005; Israel & Selvidge, 2003). Oftentimes counselors have high awareness pertaining to sexual minority concerns; however, there is a lack of knowledge and subsequent skill (Bidell 2005; Farmer, Welfare, & Burge, 2013 Grove, 2009; Rutter et al., 2008). Experts have suggested methods to increase counselor competence such as assessing for social desirability in students, increasing positive attitudes and utilizing roleplay (Dillon & Worthington, 2003; Israel & Selvidge, 2003; Kocarek & Pelling, 2003). It is essential for counselors to be competent in order to be ethical and effective with sexual and gender minority clients (American Counseling Association [ACA], 2014; American Mental Health Counselors Association [AMHCA], 2010; Association of Lesbian, Gay, Bisexual, and Transgender Issues in Counseling [ALGBTIC], 2013). In an effort to increase counselor awareness, knowledge, skills and overall effectiveness in assisting sexual minority clients, we propose that particular attention should be given to understanding the factors of coming out. The proposed cycle of coming out may assist in better preparing counselors to assist sexual minority clients and may thus contribute to an increase in sexual minority competence overall.
Conceptualization: Past and Present
Since the 1970s, several researchers have acknowledged the importance of the COP and have created models to describe it (Alderson, 2003; Cass, 1979, 1984; Cooper, 2008; Degges-White & Myers, 2005; McCarn & Fassinger, 1996; Troiden, 1989). Although considerable research has been targeted toward understanding the COP, models vary considerably and encompass factors such as awareness, disclosure, community membership and intimate experiences. Researchers often place coming out within the overarching process of sexual minority identity development (e.g., Cass, 1979; Coleman, 1982). Additionally, coming out is commonly noted as a singular event that occurs as a stage within sexual minority identity development (Cass, 1979; Chapman & Brannock, 1987; Coleman, 1982; Minton & McDonald, 1983; Troiden, 1989). Common stage approaches assert a stepwise method to coming out (Cass, 1979; Fassinger & Miller, 1996; Minton & McDonald, 1983; Troiden, 1989), failing to demonstrate the complexity of coming out.
Eli Coleman’s (1982) “Developmental Stages of the Coming Out Process” denotes potential age ranges in which coming out should occur; however, recent findings contradict this limited scope and critique the rigidity of such models (Degges-White & Myers, 2005; Dunlap, 2014; Floyd & Stein, 2002; Guittar, 2013). In a study examining milestone events of sexual minority individuals ages 16 to 27, Floyd and Stein (2002) found that some experienced coming out “early” (n = 29) while others experienced coming out beyond age 18 (n = 43). Contrary to the age implications suggested in early developmental models, coming out occurs well into adulthood as studies have explored the coming-out process for adults disclosing throughout the lifespan (Fruhauf, Orel, & Jenkins, 2009; Treyger et al., 2008).
Another concern with linear models is that research does not support the sequential transition from stage to stage. In 2000, Degges-White, Rice, and Myers conducted a qualitative study of 12 lesbian women. Results indicated that not all participants aligned with Vivienne Cass’ Homosexual Identity Formation Model (1979). Cass’ six stages include (1) identity confusion, (2) identity comparison, (3) identity tolerance, (4) identity acceptance, (5) identity pride and (6) identity synthesis. Although all 12 participants experienced the initial stage of confusion and fourth stage of acceptance, the remaining four stages were not experienced by all participants. Further, the stage of identity pride, which is associated with visible demonstration of identity in the community, was only experienced by five women. The lack of alignment between participants’ experiences and Cass’ (1979) original model may be partially explained by the model being based on the experiences of adult white males. Some researchers acknowledge the rigidity of stages and propose phases instead; however, the stepwise approach is predominant in existing models on coming out (Fassinger & Miller, 1996; McCarn & Fassinger, 1996).
Models of coming out emphasize the internal process of identity awareness (e.g., Cass, 1979; Chapman & Brannock, 1987; Coleman, 1982). Although the internal process does require attention, the emphasis on this aspect causes the external process of disclosure to lose attention. Researchers utilize constructivist perspective to acknowledge the social factors at play in the coming-out process (Cox & Gallois, 1996; Fassinger & Miller, 1996); however, the process in which an individual evaluates disclosure for multiple interpersonal encounters and relationships is not thoroughly addressed in a manner that may assist counselors in helping sexual minority clients. In an effort to expand the conceptualization of the coming-out process, Fassinger and Miller (1996) proposed a phase model of coming out that acknowledged both a personal and social process; however, the social aspect addresses the individual joining the sexual minority community rather than the interpersonal task of disclosure to individuals at large. In 1983, Minton and McDonald noted the need to highlight the cyclical nature of disclosure that includes a cost-benefit analysis and changing life situations; however, no current model emphasizes the cyclical process of disclosure in which an individual, regardless of personal awareness, acceptance, and comfort, is continually confronted with the decision to disclose identity throughout the lifespan. Thus far, research has focused on confirming conceptual models rather than clarifying the pure reality of coming out for sexual minority individuals.
Therefore, we conceptualize the COP as a task that is related to the internal process of identity development; however, we highlight the interpersonal process of disclosure. Regardless of identity security, sexual minority individuals are faced with the task of disclosure throughout the lifespan (Chutter, 2007; McCarn & Fassinger, 1996; McDermott et al., 2008). Coming out is a decision-making process in which social situations activate an individual’s awareness of the opportunity to disclose identity and the subsequent process of assessment and potential disclosure that ensues. Identity disclosure is an anxiety-provoking and potentially dangerous process in which counselors must acknowledge and be prepared to assist clients within counseling. We attempt to contribute to filling the gap in counselor preparedness by proposing a cyclical framework to assist clients through the COP.
The Cycle of Coming Out
The process of coming out is recurring and is influenced by a variety of factors (e.g., society, family, peers) that may overlap or interchange. Moreover, the cycle of coming out is a lifelong journey that influences the daily lives of sexual minorities (ALGBTIC, 2013; Chutter, 2007; Cooper, 2008; Cox, Dewaele, Van Houtte, & Vincke, 2011; Floyd & Stein, 2002; HRC, 2013; Hunter & Hickerson, 2003; Klein, Holtby, Cook, & Travers, 2015; McCarn & Fassinger, 1996). The cycle of coming out is a framework developed to assist counselors in understanding, recognizing, conceptualizing and helping clients through the process of coming out. This framework supports the idea that individuals may experience instances of awareness, assessment and disclosure in phases rather than stages during the COP. Unlike stages that imply a sequential, linear trajectory of the process of coming out, phases embody the fluidity in which an individual may navigate through the process (i.e., variance in order, skipping a phase, simultaneous occurrence of phases, return to previously endured phases).
The coming-out cycle recognizes that a main factor contributing to the variability among sexual minorities is the external process of disclosure. Disclosure is the core concept in this cyclical process; therefore, this framework emphasizes the necessity of counselor awareness in order to validate and aid sexual minority clients through their COP. The following sections outline the three phases in the cycle of coming out: (a) awareness phase, (b) assessment phase, and (c) decision phase.
Awareness Phase
In the overarching process of sexual identity development, awareness entails an individual’s recognition of sexual identity and external process in which an individual recognizes an opportunity for identity disclosure. Although triggers vary, common examples may include meeting a new person for the first time, being questioned about identity, or the desire to be open and honest in relationships with others. Awareness may be associated with confusion and contemplation (Alderson, 2003; Cass, 1984; McCarn & Fassinger, 1996; Riley, 2010).
An individual may be aware, congruent and grounded in sexual minority identity; however, societal contexts pose triggers that spark the social disclosure process. For example, an individual may identify as homosexual and his or her family and close friends may be aware of identity; however, being asked about family by a coworker may prompt him or her to consider whether or not he or she would or should disclose identity (Datti, 2009). Therefore, stressors may prompt individuals to re-experience their COP regardless of sexual minority identity development. New, unfamiliar situations raise the question of whether or not an individual should choose to disclose identity. When this prompt is posed, individuals may relive stressful risks related to coming out such as feelings of anxiety, depression, isolation, frustration and anger (Cass, 1984; McCarn & Fassinger, 1996; Pearson, 2003). In this process, individuals are at risk for negative coping mechanisms associated with coming out such as promiscuity, substance use and destructive behaviors at large (Chutter, 2007; Degges-White et al., 2000; McDermott et al., 2008; Parks & Hughes, 2007).
Assessment Phase
The assessment phase is characterized by the analysis of whether or not it is appropriate, necessary or warranted to disclose. Exploration of alternatives regarding action or inaction is often displayed. In the assessment phase, energy is expended on planning and considering potential outcomes. Regardless of how long an individual has openly identified as a sexual minority, assessment may be influenced by past experiences in the coming-out cycle. Worries prompted with the awareness phase increase as actions are planned; hence, risks during the awareness phase, such as anxiety and depression, have the potential to be exacerbated. If an individual has had a positive experience with disclosure, the assessment phase may not be a difficult process. However, if an individual has endured negative reactions to disclosure, the assessment phase may include more hesitance, anxiety and overall analysis (Joos & Broad, 2007). An individual needs to re-address the pros and cons related to coming out within the given context. Therefore, although an individual may have previously chosen disclosure, that does not necessitate the automatic disclosure in future circumstances.
In this phase, it is important to ensure that the client is internally prepared to handle the decision-making process. A counselor should aid the client in recognizing outside influences that may affect the decision-making process such as health concerns or situations of grief. The assessment phase may elicit negative emotions related to stress, anxiety and depression that prompt the need to cope. Establishing a positive support system is an essential component in preparing the client during the assessment phase. Support systems may include individuals who have positively experienced the client’s disclosure process, support groups, peer mentors or community agencies.
During the assessment phase the counselor needs to have the safety of the client in mind at all times (Cooper, 2008). Counselors should assist clients in determining a safety plan within the cost-benefit analysis related to disclosure (Floyd & Stein, 2002). Main aspects of safety planning in the assessment phase include fostering positive self-esteem, exploring appropriate methods for coping and establishing social supports (Bernal & Coolhart, 2005; Chutter, 2007; Degges-White et al., 2000; Grove, 2009). Safety planning should consider dangers at intrapersonal and interpersonal levels. Through assessment, the counselor may be able to recognize that a client may be in a situation in which disclosure may be unsafe, although that client may be unaware. For example, a sexual minority youth who is deciding to disclose identity to a conservative parent or legal guardian should consider the danger ahead in the event that the disclosed identity is not accepted positively. The counselor should assist in thoroughly processing the client’s action plan and potential consequences (Lewis, 2011). For example, possible repercussions of disclosure may include physical abuse, homelessness, neglect and excommunication from family members. Contrastingly, a client is not free from consequences if the decision to not disclose is chosen; instead, the client may be at risk for internal discord such as feelings of sadness, isolation, confusion, anger, shame and depression. Subsequently, such sentiments could cause the client to turn to self-harm or suicide (Almeida, Johnson, Corliss, Molnar, & Azrael, 2009; McDermott et al., 2008). Counselors should collaborate with the client to create a safety plan that considers the potential consequences of the client’s choice. This safety plan is essential in assuring safety as the client transitions into the decision phase.
Decision Phase
The decision phase encompasses an individual’s commitment to disclosing or withholding identity (McCarn & Fassinger, 1996; McDermott et al., 2008; Troiden, 1989). Commitment to a decision may provide the client with feelings of self-acceptance, fulfillment, synthesis, pride, resilience, happiness, strength, courage and overall improved quality of life (Floyd & Stein, 2002; McCarn & Fassinger, 1996; McDermott et al., 2008; Troiden, 1989; Vaughan & Waehler, 2010). However, the decision phase may be influenced by feelings of fear, confusion, vulnerability and uncertainty (HRC, 2013). Due to these risks, it is beneficial for the client to follow the previously established safety plan. The previously developed plan from the assessment phase is followed through in the decision phase. Clients may battle with conflicting emotions and concerns with congruence; however, it is important to recognize risks and the various layers involved in the decision to disclose.
The power of choice is understood to be within the client; however, in assuring the client’s safety, it is helpful for the counselor to be realistic, open, honest and genuine in aiding the client to address concerns prior to disclosure (Chutter, 2007; Degges-White et al., 2000). The essential responsibility of the counselor in the decision phase is to continue to support clients in executing their process. In addition, it is important to follow up on personal reactions, adjustments in relationships, and safety plans that may be components in the decision phase (HRC, 2013; Riggle, Gonzalez, Rostosky, & Black, 2014). Reflecting on the recurring process may assist in integrating the current process into the narrative of the client’s overall coming-out experiences. The CCO is intended to be a flexible approach that allows counselors to utilize their theoretical orientation within the awareness, assessment and decision phases. Counselors may be creative in utilizing interventions of their choice that align to phase goals. The following case provides an example of how to incorporate the cycle of coming out with a client.
Case Application
Jane is a 28-year-old middle school teacher who initiated counseling due to concerns with her increasing anxiety. Jane’s anxiety has been increasing within recent months; she also is concerned about the necessity of medication management. In the intake interview, Jane identifies as lesbian and states she has been “out” for a decade. When asked about her experience with coming out, she shares that she first disclosed her identity to her parents and has been warmly accepted since that very day. She also states that she is embraced by her friends; however, acceptance was not always the case. In high school, Jane developed feelings for her best friend of five years, Sarah. Unfortunately, Sarah did not share Jane’s feelings and took it upon herself to “out” Jane to the entire school.
In exploring the root of anxiety, social factors are considered in counseling. Jane informed the counselor that she experiences anxiety in uncertain situations, but it often subsides. She noticed her anxiety level when applying for her current job a few months ago. This is not her first job or her first time enduring anxiety with the interview process. Jane happily reports that she obtained the job and is now working as an eighth grade teacher in a new school. Although she enjoys her job, she is upset that her anxiety has not diminished since her employment.
When a cyclical perspective of coming out is shared with Jane, she is able to reflect on her experiences. Jane notes that throughout her life, regardless of her own comfort level, she has experienced at least some level of anxiety when disclosing to others. Jane clarifies that the anxiety with disclosing has been severe in some cases, such as when she disclosed to her college roommate and grandparents. Jane shares a recent incident in which a colleague made inappropriate remarks pertaining to a student who identifies as gay. Since then, Jane has noted the teacher’s homophobic jokes and believes that the instructor treats the student unfairly. Recognizing the injustice, Jane has been concerned about the student as she noticed an increase in bullying and lack of the support from the teacher. As Jane is disclosing these recent events, the counselor notices she becomes tearful, is speaking rapidly, and is having difficulty breathing. In the moment, the counselor’s first priority is to de-escalate Jane’s increased anxiety. It is important to note that her natural demonstration displays a link between the predicaments at work and her anxiety, and also shows that the situation is influential and meaningful to Jane.
Case Discussion
The case of Jane illustrates how a cyclical model of coming out can be helpful in counseling. Applying the cyclical model may begin prior to counseling itself, as with any intake process, it is essential to gather thorough, pertinent information for case conceptualization. One common mistake at this pivotal point would be to minimize Jane’s coming-out process. From the intake paperwork, we know that Jane has been open with her sexual identity for 10 years; however, we do not know what this means for Jane’s overall identity. Individuals define “out” differently; out can mean that identity is shared with individuals who are deemed important or can mean that the individual specifically discloses to individuals beyond the personal realm. Due to fear, in some cases individuals are more comfortable sharing identity with acquaintances rather than close individuals. Probing about coming out should be handled delicately, with care and respect, as the therapeutic alliance may be threatened if the client presumes that the inquiry is trivial, insensitive or thoughtless.
Awareness Phase. When Jane clarifies her experiences with coming out, it is essential to understand the importance of what Jane discloses pertaining to her previous experiences as they may have influenced her development. For one, Jane was fortunate to have a positive experience with her nuclear family; it is possible that this experience caused her to have an optimistic perspective regarding identity disclosure. The genuine respect and care from her parents is helpful for Jane overall; however, it may have caused her to presume she would certainly receive similar approval when disclosing to others. Secondly, the societal perspective of coming out as a one-time process may have caused Jane to only assess the positives and negatives of disclosure in reference to her parents and may have prompted her to undermine future disclosure. Finally, it is important to consider that disapproval from her friends and subsequent marginalization may have contributed to her previously disclosed experiences with anxiety.
Jane shares helpful information to better understand her reported anxiety. As recognized by Jane, stress in new situations, such as interviews or jobs, may prompt anxiety; however, it is important to note that this steady maintenance of anxiety is uncharacteristic. Although Jane explicitly states that she enjoys her job, it is possible that she may be reminded of her previous experience being “outed” in high school. Additionally, her new environment may have triggered her to consider identity disclosure, and, unbeknownst to Jane, she may be in the cycle of coming out. Specifically, the recent occurrence at work may have triggered Jane to re-experience the turmoil associated with her past experiences. Therefore, it may be helpful to discuss this view with Jane in order to collaborate in understanding her anxiety and planning for counseling.
Assessment Phase. It is possible that the scenario at work may have prompted Jane to the phase of assessment in which a cost-benefit analysis of disclosure is warranted. The assessment process should be gentle and collaborative; Jane should explore potential avenues as the counselor serves as the helpful facilitator. Pros and cons to the assessment phase vary per individual; however, useful variables to consider include (a) motivation, (b) importance and (c) safety. The bullied student may be at the epicenter of Jane’s motivation. On one hand, Jane has the ability to model appropriate disclosure and provide support, respect and acceptance for the student in a time of need. On the other hand, intrinsic motivation is needed in addition to advocacy as the decision should be congruent with personal values and beliefs regarding identity. For example, disclosure to colleagues may not be an important value; however, advocacy may be a strongly held value and thus eliciting such meaning may influence the decision-making process. It is important to consider perceptions of importance held by the counselor and client. For example, the counselor may believe that coming out displays congruency and assists individuals in leading fulfilling lives. However, simplifying the coming-out process to a personal decision uninfluenced by societal factors is unrealistic. A counselor may regard disclosure as a necessary decision, causing the client to ignore the assessment phase and be in a place of danger. Regardless of motivation and meaning, assessment of safety is paramount. Certain environments may be toxic for sexual minorities and disclosure may cause danger. It is important to caution minimizing lack of disclosure as “passing.” An individual can be secure in identity; however, disclosure could prompt harassment or violence. A person has the right to choose when to disclose or to withhold personal information, and this choice does not bear influence on identity synthesis. When navigating the assessment phase with Jane, it is important to assist in covering the subtopics of motivation, importance and safety while validating and supporting the process.
Decision Phase. Following a thorough evaluation of the risks and benefits of coming out and the importance of coming out for Jane’s values, Jane proceeds into the decision phase. Similar to the assessment phase, safety is a primary concern in this phase. If Jane chooses to not disclose, it is important to clarify that her identity is not influenced by her choice. When clients choose to not disclose, there are often ramifications for self-worth; however, it is helpful to delineate that disclosure is a difficult task that is not always the answer. Since coming out is cyclical, a decision to disclose does not deem future decisions, as each scenario is comprised of unique variables. Therefore, if an individual chooses to disclose in one context, that does not immediately prompt all future disclosures. Due to context, an individual can select to waiver and choose between instances of disclosing and withholding personal identity information. If Jane chooses to disclose, it would be helpful to develop a disclosure plan in which she considers her method of disclosure, potential outcomes and plans for safety. The role of the counselor in this process is to assist in developing a disclosure plan that is consistent with Jane’s wishes and values, addresses the range of outcomes, and consistently supports Jane throughout the process. Beyond counseling, Jane should be provided resources for support that may include supportive family and friends, books, Web sites, movies and LGB-affirmative centers. Counseling should provide Jane with a safe space to process her plan and overall process. Processing should validate the experience, discuss the process in relation to values, and consider plans for future COP. Since the cyclical nature of coming out is undermined in our society, counseling provides an important space to recognize the strength and resilience warranted in the process.
Implications for Counseling
It is essential for counselors to collaborate in order to utilize the client’s definition of coming out, educate their clients on the cycle of coming out, and recognize their own biases. Coming out is often conceptualized as linear not only in the field of counseling, but in the lives of clients as well. Clients may or may not recognize the implications of coming out and the cyclical nature at large; therefore, it is important for counselors to assist in exploring beyond a one-time culminating event. However, it is equally as important to not force a cyclical perspective on a client. The counselor facilitates exploration, but it is unethical to attempt to change clients’ opinions and values or impose decisions (ACA, 2014; AMHCA, 2010).
Counselors should utilize their knowledge of the recurring cycle by educating their clients of this occurrence and affirming the overall experience. Conjointly, counselors and clients can process the potential to be in the awareness phase. Table 1 displays areas to consider when counseling a client who is coming out. A counselor should be knowledgeable of the recurring process of coming out and the potential risks and associations that may surface. A client who is triggered into the awareness phase may have anxiety, confusion and stress regarding the question of disclosure. These stressors may be misdiagnosed or underrepresented clinically if there is a lack of focus on the actuality of the potential cause (Pearson, 2003). Counselors should consider the client’s current status of identity in separate forms; the counselor may collaborate with the client to understand the client’s individual definition of sexual minority identity and how the client chooses to define being “out.” Counselors should assist in acknowledging risks, recognizing experiences and validating emotions when a sexual minority client has been triggered and is in the awareness phase (Bernal & Coolhart, 2005; Chutter, 2007). This overall analysis and subsequent clinical action may aid in alleviating risks and stressors as it prompts counselors and clients to address the concern directly.
We aimed to specify the coming-out process for sexual minority clients; however, we do not wish to undermine this experience for gender minorities as well. When considering gender identity and the potential interaction with relationship orientation, the coming-out process may become more complex. Further, the primary internal process may have different implications in considering instances of disclosure. We do not wish to exclude the potential utilization of this model for gender minorities; however, we also do not wish to disrespect unique identities by suggesting a one-size-fits-all approach. It is possible that this model may be applied to gender and other minorities as well; nevertheless, we do not wish to minimize the unique experience of other minority identities. Furthermore, research is needed on the coming-out process as a cyclical occurrence for various minorities.
Table 1.
Phases of Coming Out and Areas to Explore
| Phase |
Areas to Explore |
| Awareness Phase |
Does the client identify as a sexual minority?Is the client questioning sexual minority identity?Does the client identify as “out”?Has the client disclosed sexual minority identity previously?Is there a present trigger prompting the client to consider disclosure?Is the client experiencing mental health concerns as an effect of this phase? |
| Assessment Phase |
Is the client actively considering disclosure?Is disclosure important to the client?What are the client’s motivations for disclosure?What are the client’s perceived benefits for disclosing?What are the client’s perceived consequences for disclosure?Is the client experiencing mental health concerns as an effect of this phase?Is the client’s safety at risk?
|
| Decision Phase |
Has the client assessed the benefits and consequences of disclosure?Is the client adhering to the safety plan?Who does the client have as a support system?Is the client experiencing mental health concerns as an effect of this phase? |
Conclusion
The American Counseling Association (2014) encourages counselors to support the “worth, dignity, potential, and uniqueness of people within their social and cultural contexts” (p. 3). It is essential for counselors to be aware of and acknowledge experiences of sexual minorities’ coming-out processes throughout their lives. In addition to supporting the safe, nurturing environment required for counseling during these times, a counselor has the responsibly to identify heterosexism, homophobia and prejudice that underlie the need for the multiple processes endured. A client may be clouded by his or her experience and may be unable to accurately assess the situation at hand; hence, it is the counselor’s duty to assist in understanding and shedding light on the surrounding scenario. Further, counselors need to understand the varying contextual layers applied to each unique process within the cycle in order to best assist sexual minority clients. Practitioners should be cognizant of the potential for variables to serve as catalysts or obstacles in the unique, complex cycle of coming out and to address these matters in counseling (ALGBTIC, 2013). Although the continual nature of coming out is implied in existing frameworks, it is not emphasized. Counselors should acknowledge the recurring cycle in an effort to better assist sexual minority clients (ALGBTIC, 2013; HRC, 2013). Future research is needed in order to emphasize the cycle of coming out rather than a linear, simplistic and unrealistic process. Additionally, effective clinical methods that consider the cycle of coming out as influential should be included in mental health counselor training in order to better assist minority clients in counseling.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Alderson, K. G. (2003). The ecological model of gay male identity. Canadian Journal of Human Sexuality, 12,
75–85.
Almeida, J., Johnson, R. M., Corliss, H. L., Molnar, B. E., & Azrael, D. (2009). Emotional distress among LGBT youth: The influence of perceived discrimination based on sexual orientation. Journal of Youth and Adolescence, 38, 1001–1014. doi:10.1007/s10964-009-9397-9
American Counseling Association. (2014). ACA code of ethics. Alexandria, VA: Author.
American Mental Health Counselors Association. (2010). AMHCA code of ethics. Alexandria, VA: Author.
Association of Lesbian, Gay, Bisexual, and Transgender Issues in Counseling. (2013). Association for Lesbian,
Gay, Bisexual, and Transgender Issues in Counseling competencies for counseling with lesbian, gay, bisexual,
queer, questioning, intersex,and ally individuals. Alexandria, VA: Author.
Baptist, J. A., & Allen, K. R. (2008). A family’s coming out process: Systemic change and multiple realities. Contemporary Family Therapy: An International Journal, 30, 92–110. doi:10.1007/s10591-008-9057-3
Berger, R. M. (1990). Passing: Impact on the quality of same-sex couple relationships. Social Work, 35, 328–332.
doi:10.1093/sw/35.4.328
Bernal, A. T., & Coolhart, D. (2005). Learning from sexual minorities: Adolescents and the coming out process.
Guidance &Counselling, 20, 128–138.
Bidell, M. P. (2005). The Sexual Orientation Counselor Competency Scale: Assessing attitudes, skills, and knowledge of counselors working with lesbian, gay, and bisexual clients. Counselor Education & Supervision, 44, 267–279. doi:10.1002/j.1556-6978.2005.tb01755.x
Cass, V. C. (1979). Homosexual identity formation: A theoretical model. Journal of Homosexuality, 4, 219–235.
Cass, V. C. (1984). Homosexuality identity formation: Testing a theoretical model. The Journal of Sex Research,
20, 143–167. doi:10.1080/00224498409551214
Chapman, B. E., & Brannock, J. C. (1987). Proposed model of lesbian identity development: An empirical examination. Journal of Homosexuality, 14, 69–80. doi:10.1300/J082v14n03_05
Chutter, K. (2007). Opening our awareness to heterosexist and homophobic attitudes in society. Relational Child and Youth Care Practice, 20(3), 22–27.
Coker, T. R., Austin, S. B., & Schuster, M. A. (2010). The health and health care of lesbian, gay, and bisexual
adolescents. Annual Review of Public Health, 457–477. doi:10.1146/annurev.publhealth.012809.103636
Coleman, E. (1982). Developmental stages of the coming out process. Journal of Homosexuality, 7(2–3), 31–43.
doi:10.1300/J082v07n02_06
Cooper, L. (2008). On the other side: Supporting sexual minority students. British Journal of Guidance & Counselling, 36(4), 425–440.
Cox, N., Dewaele, A., Van Houtte, M., & Vincke, J. (2011). Stress-related growth, coming out, and internalized
homonegativity in lesbian, gay, and bisexual youth. An examination of stress-related growth within the
minority stress model. Journal of Homosexuality, 58, 117–137. doi:10.1080/00918369.2011.533631
Cox, S., & Gallois, C. (1996). Gay and lesbian identity development: A social identity perspective. Journal of Homosexuality, 30(4), 1–30. doi:10.1300/J082v30n04_01
Datti, P.A. (2009). Applying social learning theory of career decision making to gay, lesbian, bisexual,
transgender, and questioning young adults. The Career Development Quarterly, 58, 54–64. doi:10.1002/j.2161-0045.2009.tb00173.x
Degges-White, S. E., & Myers, J. E. (2005). The adolescent lesbian identity formation model: Implications for counseling. The Journal of Humanistic Counseling, Education and Development, 44, 185–197.
doi:10.1002/j.2164-490X.2005.tb00030.x
Degges-White, S., Rice, B., & Myers, J. E. (2000). Revisiting Cass’ theory of sexual identity formation: A
study of lesbian development. Journal of Mental Health Counseling, 22, 318–333.
Dermer, S. B., Smith, S. D., & Barto, K. K. (2010). Identifying and correctly labeling sexual prejudice,
discrimination, and oppression. Journal of Counseling & Development, 88, 325–331. doi:10.1002/j.1556-6678.2010.tb00029.x
Dillon, F. R., & Worthington, R. L. (2003). The Lesbian, gay and bisexual affirmative counseling self-
efficacy inventory (LGB-CSI): Development, validation, and training implications. Journal of
Counseling Psychology, 50, 235–251. doi:10.1037/0022-0167.50.2.235
Dunlap, A. (2014). Coming-out narratives across generations. Journal of Gay & Lesbian Social Services, 26,
318–335. doi:10.1080/10538720.2014.924460
Espelage, D. L., Aragon, S. R., Birkett, M., & Koenig, B. W. (2008). Homophobic teasing, psychological outcomes, and sexual orientation among high school students: What influence do parents and
schools have? School Psychology Review, 37, 202–216.
Farmer, L. B., Welfare, L. E., & Burge, P. L. (2013). Counselor competence with lesbian, gay, and
bisexual clients: Differences among practice settings. Journal of Multicultural Counseling and
Development, 41(4), 194–209. doi:10.1002/j.2161-1912.2013.00036.x
Fassinger, R. E., & Miller, B. A. (1996). Validation of an inclusive model of sexual minority identity
formation on a sample of gay men. Journal of Homosexuality, 32, 53–78.
Floyd, F. J., & Stein, T. S. (2002). Sexual orientation identity formation among gay, lesbian, and bisexual youths: Multiple patterns of milestone experiences. Journal of Research on Adolescence, 12, 167–191. doi:10.1111/1532-7795.00030
Fruhauf, C. A., Orel, N. A., & Jenkins, D. A. (2009). The coming-out process of gay grandfathers:
Perceptions of their adult children’s influence. Journal of GLBT Family Studies, 5, 99–118.
doi:10.1080/15504280802595402
Gay, Lesbian, and Straight Education Network. (2010). The 2009 national school climate survey. Retrieved from
https://www.glsen.org/download/file/NDIyMw==
Gorman-Murray, A. (2008). Reconciling self: Gay men and lesbians using domestic materiality for
identity management. Social & Cultural Geography, 9, 283–301. doi:10.1080/14649360801990504
Grove, J. (2009). How competent are trainee and newly qualified counsellors to work with lesbian, gay,
and bisexual clients and what do they perceive as their most effective learning experiences?
Counselling & Psychotherapy Research, 9, 78–85. doi:10.1080/14733140802490622
Guittar, N. A. (2013). The queer apologetic: Explaining the use of bisexuality as a transitional identity.
Journal of Bisexuality, 13(2), 166–190. doi:10.1080/15299716.2013.781975
Hilton, A. N., & Szymanski, D. M. (2011). Family dynamics and changes in sibling of origin relationship after lesbian and gay sexual orientation disclosure. Contemporary Family Therapy: An International Journal, 33, 291–309.
Human Rights Campaign. (2013). Coming out as a straight supporter. Retrieved from
http://www.hrc.org/resources/entry/straight-guide-to-lgbt-americans
Hunter, S. & Hickerson, J. (2003). Affirmative practice: Understanding and working with lesbian, gay, bisexual, and
transgender persons. Washington, D.C.: NASW Press.
Israel, T., Ketz, K., Detrie, P. M., Burke, M. C., & Shulman, J. L. (2003). Identifying counselor competencies for working with lesbian, gay, and bisexual clients. Journal of Gay & Lesbian Psychotherapy, 7(4), 3–21. doi:10.1300/J236v07n04_02
Israel, T., & Selvidge, M. (2003). Contributions of multicultural counseling to counselor competence with lesbian, gay, and bisexual clients. Journal of Multicultural Counseling and Development, 31(2), 84–98.
Joos, K. E., & Broad, K. L. (2007). Coming out of the family closet: Stories of adult women with LGBTQ Parent(s). Qualitative Sociology, 30, 275–295. doi:10.1007/s11133-007-9064-y
Klein, K., Holtby, A., Cook, K., & Travers, R. (2015). Complicating the coming out narrative: becoming oneself in a heterosexist and cissexist world. Journal of Homosexuality, 62, 297–326. doi:10.1080/00918369.2014.970829
Kocarek, C. E., & Pelling, N. J. (2003). Beyond knowledge and awareness: Enhancing counselor skills for work with gay, lesbian, and bisexual clients. Journal of Multicultural Counseling and Development, 31, 99–112. doi:10.1002/j.2161-1912.2003.tb00536.x
LaSala, M. C. (2000). Gay male couples: The importance of coming out and being out to parents. Journal of Homosexuality, 39(2), 47–71. doi:10.1300/J082v39n02_03
Lewis, G. B. (2011). The friends and family plan: Contact with gays and support for gay rights. Policy Studies Journal, 39, 217–238. doi:10.1111/j.1541-0072.2011.00405.x
Lewis, R. J., Derlega, V. J., Berndt, A., Morris, L. M., & Rose, S. (2001). An empirical analysis of stressors for gay men and lesbians. Journal of Homosexuality, 42, 63–88.
McCarn, S. R., & Fassinger, R. E. (1996). Revisioning sexual minority identity formation: A new model of lesbian identity and its implications for counseling and research. The Counseling Psychologist, 24,
508–534. doi:10.1177/0011000096243011
McDermott, E., Roen, K., & Scourfield, J. (2008). Avoiding shame: Young LGBT people, homophobia and self-destructive behaviours. Culture, Health & Sexuality, 10, 815–829. doi:10.1080/13691050802380974
Minton, H. L., & McDonald, G. J. (1983). Homosexual identity formation as a developmental process. Journal of Homosexuality, 9, 91–104.
Mohr, J. J., & Fassinger, R. E. (2003). Outness Inventory. Journal of Counseling Psychology, 50,482-495.
Morris, J. F., Waldo, C. R., & Rothblum, E. D. (2001). A model of predictors and outcomes of outness among
lesbian and bisexual women. American Journal of Orthopsychiatry, 71, 61–71.
doi:10.1037/0002-9432.71.1.61
Nadal, K. L., Issa, M., Leon, J., Meterko, V., Wideman, M., & Wong, Y. (2011). Sexual orientation microaggressions: “Death by a thousand cuts” for lesbian, gay, and bisexual youth. Journal of LGBT Youth, 8, 234–259. doi:10.1080/19361653.2011.584204
Oswald, R. E. (2000). Family and friendship relationships after young women come out as bisexual or lesbian. Journal of Homosexuality, 38(3), 65–83.
Parks, C. A., & Hughes, T. L. (2007). Age differences in lesbian identity development and drinking. Substance Use & Misuse, 42, 361–380.
Pearson, Q. M. (2003). Breaking the silence in the counselor education classroom: A training seminar on counseling sexual minority clients. Journal of Counseling & Development, 81, 292–300.
Rickards, T., & Wuest, J. (2006). The process of losing and regaining credibility when coming-out at midlife. Health Care for Women International, 27, 530–547. doi:10.1080/07399330600770254
Riggle, E. D. B., Gonzalez, K. A., Rostosky, S. S., & Black, W. W. (2014). Cultivating positive LGBTQA identities: An intervention study with college students. Journal of LGBT Issues in Counseling, 8, 264–281. doi:10.1080/15538605.2014.933468
Riley, B. H. (2010). GLB adolescent’s “coming out.” Journal of Child and Adolescent Psychiatric Nursing, 23, 3–10. doi:10.1111/j.1744-6171.2009.00210.x
Rosario, M., Hunter, J., Maguen, S., Gwadz, M., & Smith, R. (2001). The coming-out process and its adaptational and health-related associations among gay, lesbian, and bisexual youths: Stipulation and exploration of a model. American Journal of Community Psychology, 29, 113–160. doi:10.1023/A:1005205630978
Rutter, P. A., Estrada, D., Ferguson, L. K., & Diggs, G. A. (2008). Sexual orientation and counselor competency: The impact of training on enhancing awareness, knowledge and skills. Journal of LGBT Issues in Counseling, 2, 109–125. doi:10.1080/15538600802125472
Savin-Williams, R. (2001). Mom, Dad. I’m gay. How families negotiate coming out. Washington, DC: American Psychological Association.
Shelton, K., & Delgado-Romero, E. A. (2013). Sexual orientation microaggressions: The experience of lesbian, gay, bisexual, and queer clients in psychotherapy. Psychology of Sexual Orientation and Gender Diversity, 1(S), 59–70. doi:10.1037/2329-0382.1.S.59
Stevens, R. A. (2004). Understanding gay identity development within the college environment. Journal of College Student Development, 45, 185–206.
Treyger, S., Ehlers, N., Zajicek, L., & Trepper, T. (2008). Helping spouses cope with partners coming out:
A solution-focused approach. The American Journal of Family Therapy, 36, 30–47. doi:10.1080/01926180601057549
Troiden, R. R. (1989). The formation of homosexual identities. Journal of Homosexuality, 17, 43–74.
doi:10.1300/J082v17n01_02
Vaughan, M. D., & Waehler, C. A. (2010). Coming out growth: Conceptualizing and measuring stress-related growth associated with coming out to others as a sexual minority. Journal of Adult Development, 17,
94–109. doi:10.1007/s10804-009-9084-9
Waitt, G., & Gorman-Murray, A. (2011). “It’s about time you came out”: Sexualities, mobility and home. Antipode, 43, 1380–1403. doi:10.1111/j.1467-8330.2011.00876.x
Shainna Ali is a doctoral candidate at the University of Central Florida. Sejal Barden is an Assistant Professor at the University of Central Florida. Correspondence can be addressed to Shainna Ali, The University of Central Florida, 12494 University Blvd., Education Complex Suite 322, Orlando, FL 32816, ShainnaAli@knights.ucf.edu.
Feb 9, 2015 | Article, Volume 5 - Issue 1
Heather Barto, Simone Lambert, Pamelia Brott
Career adaptability, resiliency and perceived obstacles to career development of adolescent mothers were examined using a proposed conceptual framework that combined resiliency and career adaptability. The goals of this study were to gauge the current state of the career development and resiliency of adolescent mothers, including areas of strength and weakness, and to better understand the interactions between the three components of career adaptability (i.e., planfulness, exploration, decision-making), resiliency and perceived obstacles. Adolescent mothers were similar to nonparenting peers on the planfulness and decision-making dimensions of career adaptability, yet lower on career exploration. While adolescent mothers’ traits of personal resiliency and emotional reactivity were comparable to those of their peers, their relational resiliency was lower. Based on the findings of the study, proposed strategies to further the three components of career adaptability and the resiliency of adolescent mothers are suggested.
Keywords: adolescent mothers, career development, career adaptability, resiliency, decision-making
In the United States, becoming a parent during adolescence has been described as a premature and nonnormative life event that can present lifelong challenges and growth opportunities in the career development of adolescent mothers (Gruber, 2012; Zachry, 2005). Taylor (2009) reported the most prevalent negative outcomes associated with adolescent parenthood as lowered high school graduation rates, limited educational opportunities after high school, and difficulty achieving stable work and financial independence. These are important career development considerations for this population given the national statistics on adolescent motherhood, previous research findings on the impact of parenting programs on the long-term career outcomes for adolescent mothers, and the viability of the proposed theoretical framework of the integration of career adaptability and resiliency (Barto, Lambert, & Brott, in press).
The national statistics on adolescent mothers indicate a disparity between racial groups with 8.3% of Latina, 6.5% of African American and 2.7% of Caucasian (non-Hispanic) adolescent females becoming mothers (Guttmacher Institute, 2010). Race and ethnicity may influence how an adolescent pregnancy is perceived by the adolescent mother and those around her, further contributing to the mother’s obstacles to and opportunities for career development (McAdoo, 2007; Santiago-Rivera, Arredondo, & Gallardo-Cooper, 2002). Support from families has been shown to be a positive factor in furthering the career development of adolescent mothers (Brosh, Weigel, & Evans, 2009). Although both African American and Latino families may be disappointed by adolescent pregnancies, these families tend to discourage pregnancy termination or adoption, instead offering assistance to adolescent mothers (McAdoo, 2007; Santiago-Rivera et al., 2002). Conversely, Caucasian adolescent mothers have the highest rates of formal adoptions outside the family; thus, family support for attempting to combine motherhood and career development may be lower for Caucasian adolescent mothers than for adolescent mothers in other racial or ethnic groups (Low, Moely, & Willis, 1989).
Adolescent mothers typically report more challenges with life planning when compared to nonparenting peers (Spear, 2004). Related issues can be viewed through the lens of obstacles to and opportunities for career development for adolescent mothers. These obstacles may include completing an education, finding employment and experiencing increased financial strain. Conversely, becoming a mother during adolescence may stimulate resiliency and growth opportunities in the working role (Zachry, 2005). These opportunities could foster the desire to provide financially for self and child, positive attitudes toward the future after becoming a mother (Brubaker & Wright, 2006), and a greater sense of maturity and purpose about the future (Rosengard, Pollock, Weitzen, Meers, & Phipps, 2006). Therefore, adolescent parenting can be simultaneously stressful and meaningful (Perrin & Dorman, 2003) while impacting all areas of life, particularly the working role.
Career development can be viewed as a holistic, dynamic and lifelong process, whereby individuals construct meaning and determine the most appropriate expression of their life roles (Savickas et al., 2009). Life roles are conceptualized as a constellation of interacting enactments that have relative importance to the individual within the context that these roles occur (Brown & Associates, 2002). For adolescent mothers, the addition of the parenting role can influence the dynamics between life roles and affect the perceived importance of the working role (Savickas, 1997).
In both school (Kaplan, Blinn-Pike, Wittstruck, Berger, & Leigh, 2002) and community settings (Gruber, 2012; Sarri & Phillips, 2004), programs and services are designed to meet the unique needs of adolescent mothers. Adolescent mothers have reported that parenting programs are moderately helpful in providing information relevant to their parenting role, such as medically related advice to improve the health of child and mother (Sarri & Phillips, 2004). However, these programs typically do not address finding employment and educational training opportunities (Kaplan et al., 2002, Sarri & Phillips, 2004).
Longitudinal studies investigating the career outcomes (i.e., being employed and self-supporting adults) for adolescent mothers participating in parenting programs have produced mixed results. Horwitz, Klerman, Kuo, and Jekel (1991) reported that 82% of the mothers who participated in an adolescent parenting program were financially self-supporting 20 years later. However, Taylor (2009) reported that when compared with nonparenting peers, adolescent parents had lower incomes and less prestigious occupations 20 years later. Neither Horwitz et al. (1991) nor Taylor (2009) indicated which program components helped or hindered participants’ career outcomes. Research is needed to derive evidenced-based intervention strategies and programs for improving career development outcomes of adolescent mothers (Brindis & Philliber, 2003). In the current study, career adaptability and resiliency were used to better understand career development of adolescent mothers as they adjust to their new role as a parent in relation to other life roles, especially the role of worker. Career adaptability includes the dimensions of planning, exploring and decision-making about one’s future (Savickas, 1997). Resiliency includes the attributes to develop personal and relational strengths in the process of overcoming adversity (Prince-Embury, 2006). In the current study, attention was given to the unique obstacles in the adolescent mother’s career development, as she constructs meaningful expression of her working role (Klaw, 2008; Savickas et al., 2009). The goals of this study were to gauge the current state of the career development and resiliency of adolescent mothers, including areas of strength and weakness; and to better understand the interactions between the components of career adaptability, resiliency and perceived obstacles.
Conceptual Framework
Limited research has focused specifically on the career development and adaptability of adolescent mothers (e.g., Brosh et al., 2009). From a review of the literature, the current authors (in press) found the following impediments to career development of adolescent mothers: pressing immediate needs (e.g., housing, transportation, childcare), limited career development skills (e.g., decision-making skills) and lack of career-related knowledge (e.g., occupational information). Based on the existing literature, a career resiliency model has been suggested to promote career adaptability among high-risk individuals who are experiencing a dramatic life event, such as adolescent mothers (Rickwood, 2002; Rickwood, Roberts, Batten, Marshall, & Massie, 2004). The proposed conceptual framework for the career development of adolescent mothers combines resiliency and career adaptability and (a) addresses challenges (e.g., obstacles), (b) capitalizes on opportunities and strengths (e.g., increased sense of maturity/responsibility), and (c) develops positive intervention strategies and programs to better the long-term outcomes of adolescent mothers. Constructs that support this framework are career adaptability and resiliency, as previously combined by Rickwood (2002) and Rickwood et al. (2004).
Career Adaptability
Career adaptability is a central construct in adolescent career development (Hirschi, 2009) and is defined as the ability to adjust oneself to fit new and changed circumstances in one’s career by planning, exploring and making decisions about one’s future (Brown & Associates, 2002; Savickas, 1997). Planfulness is a learned skill that allows individuals to develop a future orientation to increase adaptability (Savickas, 1997). Exploration encompasses the understanding of relationships between individual differences and contextual factors that influence career development (Blustein, 1997). In the current conceptual framework, decision-making is expanded beyond the traditional models of career development to consider the multiple alternatives and objectives that are present in the career decision-making process (Phillips, 1997).
Career adaptability is currently used as a theoretical basis for both (a) the assessment of career-related skills and knowledge, and (b) the development and implementation of intervention strategies for adolescents (Creed, Fallon, & Hood, 2009; Hirschi, 2009). The concept of career adaptability is applicable to adolescent mothers, as it focuses on developing skills to address the individual and contextual factors associated with career development (Savickas et al., 2009). These career adaptability skills (i.e., planning, exploring, decision-making) are most relevant to the working role, but can be generalized and utilized easily in considering other life roles (e.g., parenting).
Resiliency
Resiliency has been defined as one’s ability to overcome adversity and be successful (Greene, Galambos, & Lee, 2004). This concept represents a paradigm shift from looking at risk factors associated with problematic situations to searching for more strengths-based personal attributes that help individuals overcome adverse or stressful situations (Richardson, 2002). Some researchers believe that resiliency is a combination of protective factors (i.e., personal characteristics and relationships) and areas of vulnerability (i.e., ability to self-regulate through adversity; Prince-Embury, 2006; Richardson, 2002; Zachry, 2005). In the current study, mastery (i.e., internalized personal characteristics of optimism, self-efficacy and adaptability) is referred to as personal resiliency. Relatedness (i.e., social and relational experience concerning trust, support, comfort and tolerance) is referred to as relational resiliency, and emotional reactivity (i.e., level of sensitivity, recovery and impairment to self-regulation in response to adverse events or circumstances) is referred to as emotional vulnerability (Prince-Embury, 2006; Richardson, 2002). These three resiliency constructs are helpful in understanding the attributes that are displayed by resilient individuals who are able to adapt to difficult or stressful situations (Prince-Embury, 2006; Richardson, 2002).
Researchers have measured the resiliency of adolescent mothers in various ways. For example, resiliency has been paired with the assessment of risks to better understand both the risks and protective factors that promote resiliency, thus moderating the negative effect of adolescent motherhood (Kennedy, 2005). Black and Ford-Gilboe (2004) used resiliency to validate and predict theoretical relationships among variables associated with creating a healthy family environment for adolescent mothers. Furstenberg, Brooks-Gunn, and Morgan (1987) found that a substantial portion of adolescent mothers demonstrated resiliency by overcoming the challenges of adolescent parenthood through maintaining regular employment and establishing financial stability without the need for public assistance (as cited in Kennedy, 2005). In summary, resiliency is thought to be one of the factors influencing the degree of success that adolescent mothers experience as adults (e.g., Schilling, 2008).
Career Adaptability and Resiliency
Linking career adaptability to resiliency may be more favorable to adolescent mothers than approaches that focus on risk factors, problems associated with adolescent motherhood, and career-related skill deficiencies (Perrin & Dorman, 2003). However, even resilient mothers can find the day-to-day demands of motherhood overwhelming. Without attention to the obstacles they may encounter, adolescent mothers may be unable to attend to career adaptability skill development (Klaw, 2008). Recognizing and addressing these pressing immediate needs helps adolescent mothers gain the ability to focus attention and effort on developing their personal career adaptability (Klaw, 2008).
Furthermore, adolescent mothers need to cultivate their own personal and relational attributes in order to foster and encourage resiliency (Zippay, 1995). Personal characteristics (i.e., optimism, self-efficacy, adaptability) can influence levels of resiliency (Prince-Embury, 2006). Socially supportive relationships based on trust, support, comfort and tolerance with family members and mentors have been effective in helping further the career adaptability of adolescent mothers by providing them with career-related information and aiding them in developing career-related skills (Klaw, Rhodes, & Fitzgerald, 2003; Prince-Embury, 2006). Both career adaptability skills and higher levels of personal and relational resiliency may be helpful in overcoming the obstacles experienced by adolescent mothers.
The Current Study
In the present study, the current state of career adaptability, resiliency and potential obstacles to career development among adolescent mothers from one state in the mid-Atlantic region of the United States was examined. Data were gathered using the career planning (CP) scale from the Career Development Inventory-School Form (CDI-S; Super, Thompson, Lindeman, Jordaan, & Myers, 1979), the self-exploration and environmental exploration scales from the Career Exploration Survey (CES; Stumpf, Colarelli, & Hartman, 1983), the Career Decision-Making Self-Efficacy Scale-Short Form (CDSE-SF; Betz, Klein, & Taylor, 1996), the Resiliency Scales for Children and Adolescents (RSCA; Prince-Embury, 2006), and the Obstacle Survey (Klaw, 2008). The participants also received a demographic questionnaire. The research questions that guided the study included the following: (1) What are the relationships between the dimensions of career adaptability (i.e., planfulness, exploration, decision-making) and resiliency? (2) What are the reported obstacles to the career development of adolescent mothers? (3) Can measures of resiliency predict career adaptability in adolescent mothers?
Method
Participants
Participants in community- and school-based parenting programs were solicited for the study. The community-based parenting program is a support and self-help organization for assisting members in becoming more self-sufficient, but no specific career development component exists. The school-based parenting program addresses the unique academic, career and personal issues of parenting students, allowing attainment of a high school diploma in an alternative school setting. Study participants (N = 101) ranged in age from 15–18 years old (65%) and 19–21 years old (35%). Participants’ racial backgrounds included Hispanic, Latino or Spanish origin (74%); African American (22%); Caucasian (2%); Asian American (1%); and bi-racial (1%). Roughly half (52%) indicated that English was not the primary language used in their home. All participants had at least one child; some participants had multiple children (one mother had three children, 12 mothers had two children and 14 were currently pregnant with their second child).
Their current living situations included residing with parent or grandparent (57%), with their child(ren)’s father (20%), in foster care with their child(ren) (9%), with family of their child(ren)’s father (8%) or on their own with their child(ren) (6%). Their primary source of income support was from parents and family (38%), their child(ren)’s father or his family (32%), self (20%) or assistance programs (10%). While most participants (63%) reported not being currently employed, 53 participants indicated that they were actively looking for a job; 31 participants worked part-time and six worked full-time. Only seven participants had graduated high school and were not currently enrolled in school. The remaining participants included ninth graders (11%), tenth graders (16%), eleventh graders (26%), twelfth graders (31%) and college students (9%). Participants indicated that their educational plans included pursuing a college degree (65%), only graduating from high school (23%), unsure (7%) and at risk for not graduating from high school (4%).
Instruments
Career Development Inventory-School Form. The CDI-S has been utilized to assess the career development and adaptability of adolescents (Super et al., 1979; Thompson & Lindeman, 1981). For this study, the CDI-S’s CP scale was used, with 12 items for career-planning engagement and eight items for career knowledge. Items are rated on a five-point Likert-type scale: career-planning engagement ranges from 1 (I have not yet given thought to this) to 5 (I have made definite plans and know what to do to carry them out); career knowledge ranges from 1 (hardly any knowledge) to 5 (a great deal of information). For female students in grades 9–12 for the CP scale, CDI-S reliability alphas range from .87–.90 (Betz, 1988; Thompson & Lindeman, 1981). The reliabilities for the current study were .89 for both CP subscales and .90 for the total scale. The content validity has been demonstrated on all scales and subgroups; the factor structure was validated as the scale items appropriately loaded on the subscales (Thompson & Lindeman, 1981). Both content and construct validity have been supported (Savickas & Hartung, 1996).
Career Exploration Survey. The CES (Stumpf et al., 1983) was developed to measure aspects of the career exploration process, including reactions and beliefs (Stumpf et al., 1983). The following two subscales were used in the current study to measure career exploration behaviors: the six-item subscale on environmental exploration (e.g., learning about specific jobs and careers) and the five-item subscale on self-exploration (e.g., reflecting on future career choice based on past experiences). Frequency of career exploration behaviors are self-rated on a five-point Likert scale. The reliabilities reported for the self-exploration and environmental exploration subscales are .87 and .88, respectively (Stumpf et al., 1983). Acceptable content and construct validity have been established (Creed et al., 2009; Stumpf et al., 1983).
Career Decision-Making Self-Efficacy Scale-Short Form. The CDSE-SF (Betz et al., 1996) measures one’s confidence in making career-related decisions. The 25-item instrument measures self-reported career decision-making behaviors on five subscales: self-appraisal, occupational information, goal selection, planning and problem solving. Reported reliabilities for the subscales range from .73–.83, and reliability for the total scale is .94 (Taylor & Betz, 1983). Content, concurrent and construct validity of the CDSE-SF have been established (Betz, Klein, & Taylor, 1996; Taylor & Betz, 1983).
Resiliency Scales for Children and Adolescents. The RSCA identifies resiliency attributes in children and adolescents (Prince-Embury, 2006) using three scales: Sense of Mastery (MAS), Sense of Relatedness (REL) and Emotional Reactivity (REA). The MAS, which assesses personal resiliency, includes 20 items in three subscales (optimism, self-efficacy and adaptability). The REL assesses relational resiliency and has 24 items in four subscales (sense of trust, support, comfort and tolerance). Emotional vulnerability is measured by the REA, which includes 20 items in three subscales (sensitivity, recovery and impairment). The sum of the subscale scores became the raw score for the respective scale (MAS, REL, REA), which converts to a T score. Higher T scores on the MAS and REL scales and lower scores on the REA indicate more resiliency resources.
The RSCA reliability alphas range from .79–.90 for 15- to 18-year-old females and are considered acceptable (Prince-Embury, 2006). Convergent and divergent validity have been correlated with those of conceptually similar instruments that measure resiliency (e.g., Reynolds Bully Victimization Scale); the criterion validity was established by comparing groups of clinical samples to matched groups of nonclinical samples of children and adolescents (Prince-Embury, 2006).
Obstacle Survey. The OS (Klaw, 2008) was designed to determine the specific obstacles that adolescent mothers encounter in daily life that could potentially impede their career adaptability, such as needing childcare and facing discrimination because of race. The survey consists of 26 items that could potentially impact participants’ career adaptability. The OS is a relatively new instrument designed for use with adolescent mothers; therefore, there is little information available about psychometric properties. However, the information provided by the OS was expected to be helpful in developing a better understanding of the perceived obstacles to the career adaptability of adolescent mothers.
Demographic Questions. The demographic items were 12 questions designed to gather the following information about the participants: age, racial/ethnic identity, language used in the home, number and age(s) of children, living situation, socioeconomic status, current school status, and employment status.
Procedure
After obtaining approval from the Institutional Review Board, the first author developed relationships with the directors of one community-based and one school-based parenting program in order to recruit study participants. All adolescent mothers in both programs who met the study criteria received the opportunity to participate in the study. Given the unstructured nature of both programs, it is unclear what exact percentage of study-eligible adolescent mothers elected not to participate in the study, but informal observations from the first author suggest that almost all the study-eligible adolescent mothers completed the survey. Attendance was voluntary in the community-based program, so the number of adolescent mothers present varied from week to week, but the first author was present at a total of four meetings. For the school-based program, the first author made two scheduled visits to the school, during which she invited adolescent mothers who were present in classes specifically provided for them (e.g., life skills, support group) to participate in the study. Participants under age 18 received parental permission forms and older participants received informed consent forms. Participants completed all instruments via the computer using an online questionnaire created in Survey Monkey, with the exception of the RSCA (Prince-Embury, 2006), which they completed using a paper-and-pencil version as the publisher required. Survey completion was untimed. Participants who completed all aspects of the study received $10.00 in compensation to encourage completion. Three incomplete surveys were excluded from the statistical analysis.
Results
Career adaptability, resiliency and perceived obstacles were measured using a number of established instruments in order to generate descriptive statistics to better understand the current state of adolescent mothers’ career development. Career adaptability and resiliency were correlated to look for relationships between the two and entered into a multiple regression to determine the predictive power. Career adaptability was defined as and measured by the participants’ process of planfulness, exploration and decision-making. In the area of career planfulness, participants’ scores were slightly higher than the average score for the norm sample of female adolescents (Thompson & Lindeman, 1981): CP (M = 3.34, SD = 0.78), career-planning engagement (M = 3.15, SD = 0.93) and career knowledge (M = 3.61, SD = 0.88). This finding suggests that adolescent mothers in this study were similar to their peers in terms of career planfulness. For career exploration (M = 2.73, SD = 0.99), participants reported a moderate amount of career exploration behaviors with slightly higher self-exploration (M = 3.16, SD = 1.12) involving reflection on one’s future career and past experiences, than environmental exploration (M = 2.34, SD = 1.08) that involves investigating career possibilities. The reliabilities for the current study were .89 for both CP subscales and .90 for the total scale. In terms of career decision-making, there was little variation between the total score (M = 3.26, SD = 0.95) and each of the subscale scores, which ranged from 3.12–3.37. The subscale reliabilities ranged from .87–.90, and reliability for the total scale was .90. Thus, participants were neither strong nor weak in terms of decision-making skills related to selecting a college major, determining one’s ideal job, deciding on values related to occupations and preparing for a job search.
Regarding resiliency, participant T scores for the three scales and scaled scores for the subscales were compared to those of the female adolescent norm group (Prince-Embury, 2006). T scores over 60 are considered high, 50–59 are above average, 46–49 are average, 41–45 are below average, and below 40 are low. The reported T scores for participants were average for both the MAS (M = 48.29, SD = 7.93) and the REA (M = 49.44, SD =10.58) and below average for the REL (M = 44.47, SD = 10.11). The manual reports that scaled scores for the subscales over 16 are considered high, 13–15 are above average, 8–12 are average, 5–7 are below average, and below 5 are low. The related subscale scores for the MAS were average (M = 9.45–9.75); subscales for the REL were average (M = 8.12–8.75); and subscales for the REA were average (M = 9.80–10.39). The subscale reliabilities ranged from .57–.87 and the scale reliabilities ranged from .84–.93.
The participants rated 25 perceived obstacles using the OS (Klaw, 2008). The obstacles were organized into seven categories plus other to capture themes that have been reflected in the literature (e.g., pressing immediate needs, work-related concerns, education-related concerns). Ratings of 2 (somewhat of a concern) and 3 (a large concern) were combined and categorized for descriptive and contextual purposes. The most frequent obstacles for adolescent mothers were related to pressing immediate needs (childcare [73%] and transportation [72%]), work-related concerns (need for more job training [72%] and not many jobs available in my area [72%]), and education-related concerns (need more preparation to continue my education [71%] and need money to continue my education [68%]). Another identified obstacle was health-related concerns for mother or child (68%). Of lesser concern for these adolescent mothers was discrimination (facing discrimination because I am a woman [26%] and facing discrimination because of where I live [20%]) and relationship concerns (parents wanting me to work full-time [27%] and my baby’s father doesn’t want me to work [19%]). Deviant behaviors do not appear to be obstacles for most adolescent mothers surveyed; these behaviors include education-related concerns such as suspended/expelled from school (14%) and community concerns such as fear of community violence (21%), being in jail or in trouble with the police (14%), and being part of a gang (5%).
Relationships Between Career Adaptability and Resiliency
The mean scores for the three dimensions of career adaptability were correlated with the three resiliency scales scores (see Table 1). Within the resiliency measures, personal resiliency (as measured by the MAS scale) and relational resiliency (as measured by the REL scale) demonstrated a moderately strong positive correlation (r = 0.65), while emotional vulnerability (as measured by the REA scale) was weakly and negatively related to the other two measures (r = -0.22; r = -0.26). The relationships among career adaptability measures suggest that, while each dimension of career adaptability is a separate aspect of career adaptability, they are related. The strongest correlation was between exploration and decision-making (r = 0.70). The interrelationships among career adaptability dimensions and the three resiliency attributes were found to moderately correlate with personal (r = 0.29; r = 0.39; r = 0.49) and relational resiliency (r = 0.27; r = 0.26; r = 0.35); emotional vulnerability was not related to any of the scales for career adaptability. Decision-making demonstrated the strongest positive relationship with personal and relational resiliency (r = 0.49; r = 0.35).
Table 1
Intercorrelations between Resiliency, Dimensions of Career Adaptability, and Obstacles
|
Variable
|
1
|
2
|
3
|
4
|
5
|
6
|
| Resiliency Measuresa |
|
|
|
|
|
|
| 1. Sense of Mastery (MAS) |
(.84) |
|
|
|
|
|
| 2. Sense of Relatedness (REL) |
0.65*
|
(.93)
|
|
|
|
|
| 3. Emotional Reactivity (REA) |
-0.22*
|
-0.26*
|
(.87)
|
|
|
|
| Career Adaptability |
|
|
|
|
|
|
| 4. Career Planfulnessb |
0.29*
|
0.27*
|
-0.10
|
(.90) |
|
|
| 5. Career Explorationc |
0.39*
|
0.26*
|
-0.11
|
0.61*
|
(.93) |
|
| 6. Career Decision Makingd |
0.49*
|
0.35*
|
0.19
|
0.56*
|
0.70*
|
(.98)
|
Note. Reliability values for this study are shown diagonally (Cronbach alphas). N = 101
* p < 0.05
a RSCA (Prince-Embury, 2006)
b CDI-S (Super et al., 1979)
c CES (Stumpf, Colarelli, & Hartman, 1983)
d CDSE-SF ( Betz, Hammond, & Multon, 2005)
Predictive Power of Resiliency for Career Adaptability
Multiple regression was used to examine the predictive power in the three constructs of resiliency to the three dimensions of career adaptability (see Table 2). The three resiliency measures explained a statistically significant 25% of variance in career decision-making (F = 10.96), 15% of variance in career exploration (F = 5.84) and 9% of variance in career planfulness (F = 3.37). Personal resiliency (MAS) was the only resiliency scale that produced statistically significant results in two of the three career adaptability measures (see Table 2). The lack of statistical significance for relational resiliency is due to its high correlation with personal resiliency. Therefore, adolescent mothers who possess higher personal resiliency appear to possess higher levels of career adaptability.
Table 2
Predicting Career Adaptability by Resiliency Scores
|
b
|
t
|
p value
|
R2
|
F
|
p value
|
| Career Planfulness |
0.09
|
3.37
|
0.0217*
|
| MASRELREA |
0.191
0.139
-0.023
|
1.50
1.08
-0.23
|
0.1373
0.2840
0.8178
|
|
|
|
| Career Exploration |
0.15
|
5.84
|
0.0010**
|
| MASRELREA |
0.385
-0.001
-0.026
|
3.12
-0.01
-0.27
|
0.0024*
0.9922
0.7857
|
|
|
|
| Career Decision Making |
0.25
|
10.96
|
< 0.0001**
|
| MASRELREA |
0.455
0.035
-0.080
|
3.93
0.30
-0.88
|
0.0002**
0.7667
0.3812
|
|
|
|
| Note. N= 101. MAS = Sense of Mastery; REL = Sense of Relatedness; REA = Emotional Reactivity.*p< 0.05** p<0.001
|
Discussion
The results of this study should inform researchers and practitioners who are interested in assessing and advancing the career adaptability and resiliency of adolescent mothers while concurrently being mindful of perceived obstacles. In terms of career adaptability skills, the adolescent mother participants endorsed similar skills to their peers in both career planfulness and career decision-making, but lower scores in career exploration. Overall, participants appear to be average in their career planfulness skills, including engagement in career planning and career knowledge. This finding suggests that adolescent mothers are just as competent with respect to career planfulness as nonparenting peers in the normative sample of the CP of the CDI-S (Thompson & Lindeman, 1981).
The career exploration scores indicate that environmental exploration (e.g., gathering information about careers of interest, jobs/careers in a local geographical region, jobs/careers with specific companies, career training opportunities; making contact with professionals in career areas of interest) is the most pressing of exploration needs. The results suggest that the participants show a need for increased career exploration skills, especially regarding environmental exploration. However, Porfeli and Skorikov (2010) stressed the importance of both aspects of career exploration. Thus, developing self-exploration skills (i.e., reflecting and connecting past experiences to future career choices and plans) would be beneficial for the participants. Consistent with the findings of Creed et al. (2009), targeted exploration initiatives are recommended to develop effective environmental and self-exploration skills to help adolescent mothers improve their overall career exploration skills.
For career decision-making, participants indicated feeling the most confident in assessing their own interests and abilities, conducting career-related research on the Internet, and planning and goal setting. They indicated feeling the least confident in navigating issues related to college, preparing a résumé, clarifying values, knowing about salary and wages for specific jobs and careers, and identifying potential employers. Several of the skills about which participants felt the least confident are reflected in the lower environmental exploration scores (e.g., knowledge of specific career information, such as salary and being able to identify potential employers). Interventions with adolescent mothers surrounding career decision-making skills should be targeted at areas of reported need (Fouad, Cotter, & Kantamneni, 2009).
In terms of resiliency, the participant profiles offer some consistent information about areas of strength and concern. Participants possess similar levels of personal resiliency and emotional vulnerability as same-age and same-gender peers within the normative sample of the RSCA (Prince-Embury, 2006). However, some differences are apparent between the study sample and the norm group on relational resiliency. The adolescent mothers indicated that they had more trouble communicating with others, less effective support systems, less favorable views of interpersonal relationships, and difficulty initiating and maintaining socially supportive and healthy relationships with family and friends, which is consistent with previous research findings (Gee & Rhodes, 2007; Klaw et al., 2003). It is unclear whether the inability to develop and maintain healthy interpersonal relationships is a result of contextual factors related to adolescent pregnancy/parenthood, inadequate social skills present before the pregnancy/parenthood or a combination of factors.
The multiple regression showed that all of the resiliency measures had statistically significant power in predicting the career adaptability dimensions. Personal resiliency, a relative strength for this sample of adolescent mothers, showed the most predictive power. The relational resiliency scores demonstrated less predictive power and were lower than those of the participants’ same-age peers. Participants have difficulty initiating and maintaining interpersonal relationships that are comforting, supportive, tolerant and trusting, which is consistent with previous findings (Gee & Rhodes, 2007). This finding raises questions about the relationship between below-average relational resiliency scores and average career adaptability scores. If the relatedness scores were higher, indicating that the adolescent mothers had strong interpersonal relationships, would the career adaptability scores also be higher? Looking at the relationship between career adaptability and resiliency in larger groups of adolescents, both parenting and nonparenting, might provide more information about correlation or predictive relationships between the two variables (e.g., supportive relationships may provide adolescent mothers with more career-related skills and knowledge).
Data collected from adolescent mothers on their reported obstacles are helpful in understanding the challenges of motherhood. Consistent with Klaw’s (2008) findings, the most frequently cited challenges were pressing immediate needs (e.g., transportation, childcare, caring for the baby, healthcare). The next most mentioned obstacles were career and education-related concerns (e.g., job training and difficulty in school), also similar to Klaw’s (2008) findings. Although the obstacles were not statistically related to career adaptability and resiliency, understanding the obstacles encountered by adolescent mothers may be helpful in designing and implementing strategies to further develop career adaptability and foster resiliency.
The results indicate that the dimensions of career adaptability (i.e., planfulness, exploration, decision-making) can be quantitatively measured and used for assessment purposes to inform future intervention strategies. Additionally, the nature of career adaptability is expanding to include such attributes of resiliency (Savickas, 1997; Savickas et al., 2009). Theorists are moving away from the linear definition of career adaptability as planfulness, exploration and decision-making skills in order to create a more holistic, contextual and developmental conceptualization of career adaptability (Savickas et al., 2009).
Proposed Intervention Strategies
The following are proposed strategies to further the three components of career adaptability (i.e., planfulness, exploration, decision-making) and resiliency among adolescent mothers. Interventions to increase career-planning skills include fostering a future orientation and optimism, reinforcing positive attitudes toward planning, and teaching and providing practice in planning and goal-setting skills (Muskin, 2004; Savickas, 2005). While Muskin (2004) advocated for more generalized interventions designed to teach adolescents long- and short-term goal setting, Savickas (2005) recommended specific interventions to develop career-planning skills, like the Real Game (Jarvis & Richardt, 2001).
Interventions to help foster exploration include activities designed to help adolescents learn more about themselves (e.g., clarifying values, reflecting on past exploration experiences, assessing personal interests and abilities) and the world of work (e.g., job shadowing, volunteering, reading about various careers) with exercises designed to encourage both types of exploration (Porfeli & Skorikov, 2010). Interventions to foster decision-making must consider how differing perspectives on decision-making (e.g., collectivist or individualistic) can impact the decision-making process (Cardoso & Moreira, 2009; Shea et al., 2009). Other interventions such as assertiveness and decisional training, time and self-management skills training, and discussion groups can be used to foster career decision-making skills (Muskin, 2004; Savickas, 2005). Interventions to foster resiliency focus on building self-efficacy in order for adolescents to feel that they are strong enough to handle current and future situations and typically include role modeling, encouragement, anxiety reduction and developing problem-solving skills (Savickas, 2005).
Suggestions for Future Research and Limitations
The information gathered in this study highlights the need for assessment to accurately measure and enhance the career adaptability and resiliency of adolescent mothers. Adolescent mothers face additional obstacles that necessitate intervention strategies carefully be constructed based on both theoretical and contextual considerations. The combination of resiliency and career adaptability may provide the positive, strengths-based assessment and intervention strategies framework necessary to assist adolescent mothers in overcoming obstacles and becoming self-supporting adults.
Based on observations during data collection, two recommendations were generated for researchers and practitioners working directly with adolescent mothers in further research, assessment or intervention endeavors. First, adolescent mothers indicated that they would have preferred an interview rather than a written survey. The desire for verbal communication over written communication may provide insight into the most effective means of implementing assessment and intervention strategies. Second, many of the participants expressed immediate interest in the results of the study, both personal and overall results. These inquiries suggest that adolescent mothers are interested in and committed to developing career adaptability skills. Capitalizing on this initial enthusiasm may be a key factor in structuring assessment and intervention strategies. Delays in providing results and subsequent interventions to participants may diminish their interest in further developing career adaptability skills. Prescod and Daire (2013) noted the critical need for adolescent mothers to be involved in career development counseling services in both a time-sensitive and culturally sensitive manner for optimal results.
Given the challenges of studying this population, one limitation of the current study is that the assessment data were gathered from a purposeful sample of three programs in a limited geographical region. Yet, this sample was incredibly diverse, adding much information to the literature. Another important limitation was observed during data collection—not all of the scheduled participants attended data collection sessions. As the results of the OS (Klaw, 2008) also demonstrated, the lack of childcare and reliable transportation was evident during the data collection. Many participants brought their children to the data collection sites or were unable to get transportation to the sites.
Furthermore, research has indicated that childcare may lead to socioeconomic advancements of adolescent mothers, as they have increased available time to focus on school and work (Mollborn & Blalock, 2012). Thus, exploring childcare resources and possibly providing childcare resources while adolescent mothers partake in career development programs may be essential in their ability to focus on such efforts. The childcare challenge likely far exceeds the typical time management struggles of today’s nonparenting adolescents who are in the process of exploring careers as described by Strom, Strom, Whitten, and Kraska (2014). In the current study, program staff at community and school program sites indicated that attendance was a challenge for adolescent mothers because of these obstacles (i.e., childcare and transportation), highlighting the need for researchers and practitioners to address obstacles that more than 70% of adolescent mothers face in order to work effectively with these clients.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of
interest or funding contributions for
the development of this manuscript.
References
Barto, H. H., Lambert, S. F., & Brott, P. E. (in press). The career development of adolescent mothers: A review of 25 years of professional literature. Journal of Employment Counseling.
Betz, N. E. (1988). The assessment of career development and maturity. In W. B. Walsh & S. H. Osipow (Eds.), Career decision making (pp. 77–136). Hillsdale, NJ: Erlbaum.
Betz, N. E., Hammond, M. S., & Multon, K. D. (2005). Reliability and validity of five-level response continua for the career decision self-efficacy scale. Journal of Career Assessment, 13, 131–149. doi:10.1177/1069072704273123
Betz, N. E., & Klein, K. L. (1996). Relationships among measures of career self-efficacy, generalized self-efficacy, and global self-esteem. Journal of Career Assessment, 4, 285–298. doi:10.1177/106907279600400304
Betz, N. E., Klein, K. L., & Taylor, K. M. (1996). Evaluation of a short form of the career decision-making self-efficacy scale. Journal of Career Assessment, 4, 47–57. doi:10.1177/106907279600400103
Black, C., & Ford-Gilboe, M. (2004). Adolescent mothers: Resilience, family health work and health-promoting practices. Issues and Innovations in Nursing Practice, 11, 351–360. doi:10.1111/j.1365-2648.2004.03204.x
Blustein, D. L. (1997). A context-rich perspective of career exploration across the life roles. The Career Development Quarterly, 45, 260–274.
Brindis, C., & Philliber, S. (2003). Improving services for pregnant and parenting teens. Prevention Researcher, 10(3), 9–13.
Brosh, J., Weigel, D., & Evans, W. (2009). Assessing the supports needed to help pregnant and parenting teens reach their educational and career goals. Journal of Extension, 47. Retrieved from http://www.joe.org/joe/2009february/pdf/JOE_v47_1rb8.pdf
Brown, D., & Associates. (2002). Career choice and development (4th ed.). San Francisco, CA: Jossey-Bass.
Brubaker, S. J., & Wright, C. (2006). Identity transformation and family caregiving: Narratives of African American teen mothers. Journal of Marriage and Family, 68, 1214–1228. doi:10.1111/j.1741-3737.2006.00324.x
Cardoso, P., & Moreira, J. M. (2009). Self-efficacy beliefs and the relation between career planning and perception of barriers. International Journal for Educational and Vocational Guidance, 9, 177–188. doi:10.1007/s10775-009-9163-2
Creed, P. A., Fallon, T., & Hood, M. (2009). The relationship between career adaptability, person and situation variables, and career concerns in young adults. Journal of Vocational Behavior, 74, 219–229. doi:10.1016/j.jvb.2008.12.004
Fouad, N., Cotter, E. W., & Kantamneni, N. (2009). The effectiveness of a career decision-making course. Journal of Career Assessment, 17, 338–347. doi:10.1177/1069072708330678
Furstenberg, F. F., Jr., Brooks-Gunn, J., & Morgan, S. P. (1987). Adolescent mothers in later life. New York, NY: Cambridge University Press.
Gee, C. B., & Rhodes, J. E. (2007). A social support and social strain measure for minority adolescent mothers: A confirmatory factor analytic study. Child: Care, Health and Development, 34, 87–97. doi:10.1111/j.1365-2214.2007.00754.x
Greene, R. R., Galambos, C., & Lee, Y. (2004). Resilience theory: Theoretical and professional conceptualizations. Journal of Human Behavior in the Social Environment, 8(4), 75–91.
Gruber, K. J. (2012). A comparative assessment of early adult life status of graduates of the North Carolina adolescent parenting program. Journal of Child and Adolescent Psychiatric Nursing, 25, 75–83. doi:10.1111/j.1744-6171.2012.00324.x
Guttmacher Institute. (2010). U.S. teenage pregnancies, births and abortions: National and state trends and trends by race and ethnicity. Retrieved from http://www.guttmacher.org/pubs/USTPtrends.pdf
Hirschi, A. (2009). Career adaptability development in adolescence: Multiple predictors and effect on sense of power and life satisfaction. Journal of Vocational Behavior, 74, 145–155. doi:10.1016/j.jvb.2009.01.002
Horwitz, S. M., Klerman, L. V., Kuo, H. S., & Jekel, J. F. (1991). School-age mothers: Predictors of long-term educational and economic outcomes. Pediatrics, 87, 862–868.
Jarvis, P., & Richardt, J. (2001). The real game series: Bringing real life to career development. Retrieved from ERIC database. (ED446297)
Kaplan, M. B., Blinn-Pike, L., Wittstruck, G., Berger, T. J., & Leigh, S. (2002). Journaling for pregnant and parenting adolescents. Reclaiming Children and Youth, 11, 42–46.
Kennedy, A. C. (2005). Resilience among urban adolescent mothers living with violence. Violence Against Women, 11, 1490–1514. doi:10.1177/1077801205280274
Klaw, E. (2008). Understanding urban adolescent mothers’ visions of the future in terms of possible selves. Journal of Human Behavior in the Social Environment, 18, 441–462. doi:10.1080/10911350802486767
Klaw, E. L., Rhodes, J. E., & Fitzgerald, L. F. (2003). Natural mentors in the lives of African American adolescent mothers: Tracking relationships over time. Journal of Youth and Adolescence, 32, 223–232. doi:10.1023/A:1022551721565
Low, J. M., Moely, B. E., & Willis, A. S. (1989). The effects of perceived parental preferences and vocational goals on adoption decisions: Unmarried pregnant adolescents. Youth & Society, 20, 342–354. doi:10.1177/0044118X89020003007
McAdoo, H. P. (2007). Black families. Thousand Oaks, CA: Sage.
Mollborn, S., & Blalock, C. (2012). Consequences of teen parents’ child-care arrangements for mothers and children. Journal of Marriage and Family, 74, 846–865. doi:10.1111/j.1741-3737.2012.00988.x
Muskin, M.-B. (2004). The need for a comprehensive competency-based career guidance curriculum for teen mothers. Educational Considerations, 31(2), 41–45.
Perrin, K. M., & Dorman, K. A. (2003). Teen parents and academic success. The Journal of School Nursing, 19, 288–293. doi:10.1177/10598405030190050701
Phillips, S. D. (1997). Toward an expanded definition of adaptive decision-making. The Career Development Quarterly, 4, 275–287.
Porfeli, E. J., & Skorikov, V. B. (2010). Specific and diversive career exploration during late adolescence. Journal of Career Assessment, 18, 46–58. doi:10.1177/1069072709340528
Prescod, D. J., & Daire, A. P. (2013). Career intervention considerations for unwed young black mothers in the United States. Adultspan Journal, 12, 91–99.
Prince-Embury, S. (2006). Resiliency scales for children & adolescents: A profile of personal strengths (RSCA). San Antonio, TX: Pearson Education.
Richardson, G. E. (2002). The metatheory of resilience and resiliency. Journal of Clinical Psychology, 58, 307–321. doi:10.1002/jclp.10020
Rickwood, R. R. (2002). Enabling high-risk clients: Exploring a career resiliency model. Retrieved from http://contactpoint.ca/wp-content/uploads/2013/01/pdf-02-10.pdf
Rickwood, R. R., Roberts, J., Batten, S., Marshall, A., & Massie, K. (2004). Empowering high-risk clients to attain a better quality of life: A career resiliency framework. Journal of Employment Counseling, 41, 98–104. doi:10.1002/j.2161-1920.2004.tb00883.x
Rosengard, C., Pollock, L., Weitzen, S., Meers, A., & Phipps, M. G. (2006). Concepts of the advantages and disadvantages of teenage childbearing among pregnant adolescents: A qualitative analysis. Pediatrics, 118, 503–510. doi:10.1542/peds.2005-3058
Santiago-Rivera, A. L., Arredondo, P., & Gallardo-Cooper, M. (2002). Counseling Latinos and la familia: A practical guide. Thousand Oaks, CA: Sage.
Sarri, R., & Phillips, A. (2004). Health and social services for pregnant and parenting high risk teens. Children and Youth Service Review, 26, 537–560. doi:10.1016/j.childyouth.2004.02.010
Savickas, M. L. (1997). Career adaptability: An integrative construct for life-span, life-space theory. The Career Development Quarterly, 45, 247–259.
Savickas, M. L. (2005). The theory and practice of career construction. In S. D. Brown & R. W. Lent (Eds.), Career development and counseling: Putting theory and research to work (pp. 42–70). Hoboken, NJ: Wiley & Sons.
Savickas, M. L., & Hartung, P. J. (1996). The career development inventory in review: Psychometric and research findings. Journal of Career Assessment, 4, 171–188. doi:10.1177/106907279600400204
Savickas, M. L., Nota, L., Rossier, J., Dauwalder, J.-P., Duarte, M. E., Guichard, J., . . . van Vianen, A. E. M. (2009). Life designing: A paradigm for career construction in the 21st century. Journal of Vocational Behavior, 75, 239–250. doi:10.1016/j.jvb.2009.04.004
Schilling, T. A. (2008). An examination of resilience processes in context: The case of Tasha. The Urban Review, 40, 296–316. doi:10.1007/s11256-007-0080-8
Shea, M., Ma, P.-W. W., Yeh, C. J., Lee, S. J., & Pituc, S. T. (2009). Exploratory studies on the effects of a career exploration group for urban Chinese immigrant youth. Journal of Career Assessment, 17, 457–477. doi:10.1177/1069072709334246
Spear, H. J. (2004). A follow-up case study on teenage pregnancy: “Havin’ a baby isn’t a nightmare, but it’s really hard.” Pediatric Nursing, 30, 120–125.
Strom, P. S., Strom, R. D., Whitten, L. S., & Kraska, M. F. (2014). Adolescent identity and career exploration. NASSP Bulletin, 98, 163–179. doi:10.1177/0192636514528749
Stumpf, S. A., Colarelli, S. M., & Hartman, K. (1983). Development of the career exploration survey (CES). Journal of Vocational Behavior, 22, 191–226. doi:10.1016/0001-8791(83)90028-3
Super, D. E., Thompson, A. S., Lindeman, R. H., Jordaan, J. P., & Myers, R. A. (1979). Career development inventory-school form. Palo Alto, CA: Consulting Psychologists Press.
Taylor, J. L. (2009). Midlife impacts of adolescent parenthood. Journal of Family Issues, 30, 484–510. doi:10.1177/0192513X08329601
Taylor, K. M., & Betz, N. E. (1983). Applications of self-efficacy theory to the understanding and treatment of career indecision. Journal of Vocational Behavior, 22, 63–81. doi:10.1016/0001-8791(83)90006-4
Thompson, A. S., & Lindeman, R. H. (1981). Career Development Inventory: Volume 1: User’s Manual. Retrieved from http://www.vocopher.org/ncda2008/data/resources/CDI%20User%20Manual.pdf
Zachry, E. M. (2005). Getting my education: Teen mothers’ experiences in school before and after motherhood. Teachers College Record, 107, 2566–2598. doi:10.1111/j.1467-9620.2005.00629.x
Zippay, A. (1995). Expanding employment skills and social networks among teen mothers: Case study of a mentor program. Child and Adolescent Social Work Journal, 12, 51–69. doi:10.1007/BF01876139
Heather Barto is an Assistant Professor at Messiah University. Simone Lambert, NCC, is an Assistant Professor at Argosy University. Pamelia Brott, NCC, is an Associate Professor at Virginia Polytechnic Institute and State University. Correspondence can be addressed to Heather Barto, Suite 3052, Messiah College, One College Avenue, Mechanicsburg, PA 17055, hbarto@messiah.edu.
