Jan 17, 2024 | Volume 13 - Issue 4
Nelson Handal, Emma Quadlander-Goff, Laura Handal Abularach, Sarah Seghrouchni, Barbara Baldwin
Understanding the overlap of symptoms between oppositional defiant disorder (ODD) and obsessive-compulsive disorder (OCD) experienced by youth is pertinent for accurate diagnosis. A quantitative, retrospective, cross-sectional design format was used to assess the relationship between ODD and OCD in addition to evaluating the difference in ODD severity and symptoms based on OCD severity. Symptoms and severity ratings of ODD and OCD were collected from youth diagnosed with ODD (N = 179). Fisher’s exact test and a Wilcoxon signed-rank test were performed. There were significant relationships between frustration related to obsessions and compulsions and the ODD symptoms of annoyance and anger. Results suggested that OCD severity predicted an increase in scores for ODD severity and symptoms.
Keywords: oppositional defiant disorder, obsessive-compulsive disorder, overlap of symptoms, youth, severity
Children and adolescents who struggle with mental health disorders experience a decline in their quality of life related to psychological, physical, and social well-being (Celebre et al., 2021). The most common disorders diagnosed in childhood and adolescence are attention-deficit/hyperactivity disorder (ADHD), generalized anxiety disorder (GAD), major depressive disorder (MDD), obsessive-compulsive disorder (OCD) and other disruptive behavior disorders such as oppositional defiant disorder (ODD) and conduct disorder (CD; Ghandour et al., 2019; Perou et al., 2013). The array of disorders diagnosed in childhood and adolescence contributes to the probability of misdiagnosis or overdiagnosis (Merten et al., 2017). Moreover, approximately 7.4% of children between the ages of 3–17 are diagnosed with a behavioral problem (Centers for Disease Control and Prevention [CDC], 2021). According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013), the prevalence of OCD in the United States is 1.2%, with the majority of cases being reported before the age of 14, while the prevalence of ODD has an average estimate of 3.3%. Behavioral problems as a result of mental health issues impact a child’s antisocial behaviors (Justicia-Arráez et al., 2021), further influencing performance at home and school.
Previous studies have documented the overlap of ODD with other mental disorders. For example, Garcia et al. (2009) found that approximately 12% of 4- to 8-year-old children who were diagnosed with OCD also presented with comorbid ODD. Furthermore, Thériault et al. (2014) suggested that irritability, a symptom affiliated with ODD, has been reported by individuals diagnosed with obsessive-compulsive behavior or OCD. A systematic review conducted by Stahnke (2021) revealed that OCD is commonly misunderstood by the general population as well as misdiagnosed by mental health professionals and primary care physicians. On the other hand, Grimmett et al. (2016) suggested that the diagnostic criterion of ODD is reflective of general child and adolescent behavior. This could result in the misdiagnosis or overdiagnosis of ODD. The interchangeable symptoms of OCD and ODD may suggest that children and adolescents are experiencing comorbidity or that they are misdiagnosed, resulting in the use of ineffective interventions and treatment for children and adolescents with OCD or ODD. The co-occurrence of ODD and OCD in youth may be attributed to the overlap of anger-related symptoms. Assessment of anger-related symptoms can provide further insight on the comorbidity of these disorders in addition to suggesting the potential for misdiagnosis.
Literature Review
Oppositional Defiant Disorder
According to Loeber et al. (2000), approximately 1%–16% of school-aged children and adolescents have been diagnosed with ODD. ODD is characterized by emotional disruptions such as anger and mood irritability in addition to behavioral issues, including argumentativeness and defiance (APA, 2013). One study suggested that ODD comprises three symptomatic components: headstrong (i.e., argumentative toward adults and defying their requests), irritable (i.e., temper dysregulation and resentfulness), and hurtful (i.e., aggression toward others; Stringaris & Goodman, 2009). ODD has demonstrated significant impairments related to emotional, social, educational, and vocational daily functioning (APA, 2013).
Pharmacological interventions that treat ODD include antipsychotics (Hood et al., 2015) and psychostimulants (Pringsheim et al., 2015). Additionally, children and adolescents diagnosed with ODD often receive therapeutic interventions such as cognitive behavioral therapy (CBT) and brief strategic family therapy (Ghosh et al., 2017). Accurate diagnosis of ODD is imperative for appropriate treatment interventions to be implemented.
Obsessive-Compulsive Disorder
OCD includes the presence of intrusive and unwanted thoughts, urges, or images that are often recurrent (obsessions) and/or repeated behaviors or mental acts that are completed as a result of obsessions (compulsions; APA, 2013). Moreover, individuals with OCD may experience intolerance of uncertainty with an emphasis on controlling their thoughts to lessen said uncertainty. A study conducted by Mancebo et al. (2008) suggested that common obsessions include contamination, catastrophic thoughts, and aligning objects to be symmetrical in addition to compulsions related to checking, repeating routine activities, and ordering or rearranging objects. Genetic, environmental, and familial factors can contribute to the severity of OCD symptoms. D. A. Geller (2006) described the average age of onset of OCD symptoms occurring between the ages of 7.5 and 12.5 years. Although the symptoms of OCD are focused on obsessions and compulsions, researchers have demonstrated that individuals with OCD experience issues with anger. For instance, Painuly et al. (2011) found that half of the participants in their study (N = 21) who were diagnosed with OCD reported anger attacks. Furthermore, individuals diagnosed with OCD (N = 48) reported increased frequency of anger along with higher anger suppression scores (Cludius et al., 2021). A third study conducted by Radomsky et al. (2007) suggested that individuals diagnosed with OCD who experience checking compulsions indicated heightened trait anger or an increased rate of anger over time. A longitudinal study that assessed children and adolescents (N = 563) demonstrated the developmental trajectories of ODD and obsessive-compulsive problems (OCP), which provided evidence that youth endorsed high scores of irritability and defiance in addition to increased scores of OCP (Ezpeleta et al., 2022). This study conceptualized OCP as a component of an OCD diagnosis. Hence, children may appear to have ODD when, in actuality, they may not be able to perform obsessions and compulsions, leading to irritability, defiance, and anger.
Pharmacological interventions for children and adolescents diagnosed with OCD include serotogenic medications (Nazeer et al., 2020) and selective serotonin reuptake inhibitors (Kotapati et al., 2019). Therapeutic interventions such as CBT and behavior therapy have demonstrated effectiveness in the treatment of OCD in children and adolescents (Avasthi et al., 2019). The differentiations in treatment approaches between OCD and ODD highlight the need for further research on the specific symptoms that lead to a diagnosis.
Comorbidity of ODD and OCD
Researchers have demonstrated that OCD is a highly comorbid disorder; approximately 80% of adults with OCD meet criteria for other conditions and 36.6% of children under the age of 17 with behavioral problems present with OCD (Ghandour et al., 2019). Moreover, a recent study by Ezpeleta et al. (2022) noted that ODD and obsessive-compulsive problems affect approximately 9.4% of children that are between the ages of 6 and 13. An additional study reported that one in five individuals experience depressive symptoms with OCD (Ghandour et al., 2019). However, there is inconclusive information regarding the comorbidity of ODD in association with OCD. Assessment tools such as the Child Behavior Checklist (Achenbach, 1991) can screen for comorbidity, including OCD, and the Children’s Yale-Brown Obsessive Compulsive Scale (Scahill et al., 1997) can evaluate the severity of obsessions and compulsions. But a thorough inventory that assesses for comorbidities in children and adolescents and considers OCD and ODD has yet to be developed. Coskun and colleagues (2012) suggested that comprehensive evaluation could screen for comorbidities with regard to OCD in children in addition to increasing understanding of severity and age of onset, as these components can vary according to coexisting disorders.
A study conducted by Storch et al. (2010) evaluated the comorbidity of disruptive behavior disorder, including adolescents diagnosed with ODD, OCD, and CD, and reported that comorbid disruptive behavior disorder is related to greater family accommodation, less symptom resistance to obsessions, and heightened OCD severity. Moreover, the DSM-5 suggested that males are more often diagnosed in childhood with OCD and ODD compared to females (APA, 2013). Although these two conditions are represented in distinct categories in the latest edition of the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; APA, 2022), clinical data and previous literature have suggested overlap. For example, one study stated that temper outbursts, which are described as behaviors such as anger outbursts, temper tantrums, and resentfulness, were two to three times more common in youth with OCD compared to those without (Krebs et al., 2013). Moreover, another study found that 53% of children diagnosed with OCD exhibited explosive anger outbursts, which were caused by perfectionism, modification to routine, or rules enforced by parents (Storch et al., 2012). Additionally, researchers have reported greater validity in OCD-diagnosed patients who exhibit increased behavioral and cognitive impulsivity (Boisseau et al., 2012). This finding has been observed and anecdotally reported by parents and teachers of youth diagnosed with OCD when compulsions cannot be acted on (Krebs et al., 2013). The influence of ODD and OCD symptoms can have lasting effects on children and adolescents, thus emphasizing the importance of mental health professionals’ accurate diagnoses and the appropriate treatment of these disorders.
The pattern of uncooperative and defiant behavior toward authority figures can pose challenges in diagnosis and assessment. Factors associated with the environment, such as externalizing behaviors secondary to trauma (Beltrán et al., 2021), psychiatric conditions that include symptoms related to aggression and defiance, and hyperactivity, can be difficult to discriminate (APA, 2013; Thériault et al., 2014). This is common in ODD-diagnosed children and adolescents who often do not comply with authority figures without reason, resulting in repetitive negative behavior patterns. Similarly, youth diagnosed with OCD might respond defiantly to their obsessive thoughts when they cannot be acted upon (J. Geller, 2022). Further, children and adolescents may experience obsessive thoughts of which parents and guardians are not aware. Ezpeleta et al. (2022) reported the coexistence of the two disorders:
The stubbornness of the oppositional child who wants to do their will and the rituals of the obsessive child who needs to do things a certain way, the low anger threshold in oppositionism and the anger attacks of the obsessive child when prevented from doing their rituals, the argumentativeness in both cases to be able to do what they want annoying others for fun or because they need to participate in the ritual, and defying rules may make the two disorders coexist. (p. 1090)
Similarly, a case study developed by Ale and Krackow (2011) described a 6-year-old boy who struggled with ritualized behaviors and avoidance that would lead to anger and aggression. The case study provided an example in which the boy feared small, round objects, and when the boy observed other children at school wearing buttons, the boy expressed his anger through name calling and kicking a peer. The distress from viewing buttons was due to an obsession that led the boy to become fearful of choking (Ale & Krackow, 2011). These explanations of anger or frustration that are an outcome of the child’s inability to engage in rituals emphasize the importance of considering the misdiagnosis and comorbidity of ODD.
Study Purpose
We hypothesized that children and adolescents diagnosed with ODD would report increased OCD severity and higher ratings of symptoms related to anger, providing further insight into the overlap in symptoms of ODD and OCD. For the purpose of this study, comorbidity was defined as the presence of two or more diagnosed disorders (Basu et al., 2018). Moreover, we hypothesized that children and adolescents would endorse higher scores on symptoms related to anger and frustration because of the inability to perform obsessions and compulsions. The research questions were:
Research Question 1: What is the relationship between ODD and OCD for youth diagnosed with ODD?
Research Question 2: Is there a difference in ODD severity and symptoms between youth that scored lower on OCD severity compared to those that had high scores of OCD severity?
Method
Design
This study followed a quantitative, retrospective, cross-sectional design format that utilized a purposive sampling technique. Purposive convenience sampling allowed for intentional selection of participants who were accessible based on location. Children and adolescents diagnosed with ODD were selected for the study in order to evaluate comorbidity with OCD. This methodological approach allowed for further insight into the overlap in symptoms experienced by children and adolescents with ODD. To answer the first research question, Fisher’s exact test was utilized, and to answer the second research question, a Wilcoxon signed-rank test was conducted.
Participants
The participants in this study (N = 179) included children and adolescents between the ages of 5 and 19 that had been referred by their parents or guardians to a mental health clinic located in the Southern region of the United States. Following the securing of IRB approval, participant documents containing diagnoses, symptoms, and severity from children and adolescents that reported to the clinic between 2017 and 2020 were retrospectively collected. Participants who were prescribed psychotropic medication or had received any other diagnosis were excluded from the study. All participants were clients at the clinic at the time of data collection. Participants gave assent through their parent or guardian’s completion of an informed consent form, which indicated that diagnostic information would be used for research purposes, including future studies that would retrospectively collect participant information while keeping their identifying information confidential. Participants did not receive any reimbursement for participation in this study.
The sample used in this study included 179 children and adolescents (121 boys and 58 girls) between 5 and 19 years of age (M = 13.34, SD = 3.56) that were diagnosed with ODD. Of the sample, 14 participants (8%) were between the ages of 5 and 8, 63 participants (35%) were between the ages of 9 and 12, 55 participants (31%) were between the ages of 13 and 16, and 47 participants (26%) were between the ages of 17 and 19. The average age of the sample was 13.34 years (SD = 3.56).
Data Collection
Measures
CliniCom™ Psychiatric Assessment Software. The CliniCom™ Psychiatric Assessment (hereafter referred to as CliniCom) is a validated and reliable web-based tool that uses algorithms based on mental health research and DSM-5 criteria to identify multiple psychiatric conditions (Handal et al., 2018). CliniCom is a self-guided measure that collects information including individual and family history, social history, responses to mental health questions, self-assessment of severity of symptoms, quality of life, and current and previous mental health treatments. Participants complete CliniCom at their own pace on a computer at a location of their preference (e.g., home, school). CliniCom assesses for 81 disorders and utilizes items from the Children’s Yale-Brown Obsessive Compulsive Scale (Scahill et al., 1997). CliniCom has undergone psychometric investigation, indicating 78% concordance in diagnosing the same disorder in test–retest analysis, including the Yale-Brown Obsessive Compulsive Scale (Y-BOCS; Goodman et al., 1989; Handal et al., 2018).
The data were retrospectively collected from participants’ charts, which included a report from CliniCom. The participants completed CliniCom prior to their initial appointment with assistance from their parent or guardian. Participants received a suggested diagnosis from the assessment. Following the completion of the CliniCom assessment, semi-structured diagnostic interviews and parent questionnaires were conducted and completed. Diagnoses were verified and confirmed by a board-certified child and adolescent psychiatrist. CliniCom and the semi-structured diagnostic interviews utilized diagnostic criteria from the DSM-5 (APA, 2013) to assess the onset, duration, frequency, and severity of mental disorders in addition to the level of impairment experienced by the client. Symptoms were conceptualized based on clinical severity, which ranges from 0–10, with 10 as the most severe presentation of the symptom and 4 or higher indicating moderate to severe symptoms. A score of 4 is the threshold to be considered positive for the symptom. The overall severity ratings for ODD and OCD are determined by the Clinical Global Impressions Scale (CGI-S). The CGI-S uses a range between 1 and 7 to indicate illness severity with 1 = normal to 7 = extremely ill (Busner & Targum, 2007).
Assessment of ODD and OCD. To determine the overlap of symptoms related to ODD and OCD for children and adolescents, the following symptoms were collected from the responses to the CliniCom items: easily annoyed, bothered, or upset by others (ODD Symptom 1), often angry or resentful (ODD Symptom 2), often spiteful or vindictive (ODD Symptom 3), and frustrated and/or angry with relation to obsessions and compulsions (OCD Symptom 1). Descriptions of symptoms can be viewed in Table 1. To respond to the ODD symptom items in the assessment, participants submitted a rating between 1 and 10. A rating of 10 represents the most severe presentation of the symptom and 4 or higher represents a moderate to severe presentation; a score of 4 is the threshold to be considered positive for the symptom. Responses to the OCD symptom item were dichotomous, wherein participants indicated “yes” or “no” if they were experiencing the symptom. OCD and ODD severity ratings for each participant were recorded.
Table 1
Description of Symptoms Collected
| Disorder Term |
Description from CliniCom™ Psychiatric Assessment |
| ODD Symptom 1 |
“Easily annoyed, bothered, or upset by others” |
| ODD Symptom 2 |
“Often angry and resentful” |
| ODD Symptom 3 |
“Often spiteful or vindictive” |
|
| OCD Symptom 1 |
“Frustrated and/or angry with relation to obsessions and compulsions” |
Data Analysis
IBM SPSS 27 software was used for data analysis. Preliminary analysis included all clients in the sample. The Kolmogorov-Smirnov test of normality was conducted to determine the numerical distribution of variables. The test of normality showed that none of the variables were normally distributed, p < .05. Spearman correlation coefficients were calculated to determine significant associations between variables.
Fisher’s exact tests were conducted to determine non-random associations between variables. Phi was used to calculate the effect size for the Fisher’s exact test. A Wilcoxon signed-rank test was performed to analyze other variables in the sample through comparison of groups. The first group included participants who endorsed a score between 1–3 on the CGI-S for OCD severity (n = 47). The second group was composed of participants who reported a score between 4–7 on the CGI-S for OCD severity (n = 132). Correlation coefficients were calculated to determine the effect sizes for the Wilcoxon signed-rank test.
Results
The mean score for the characteristics of ODD Symptom 1 was 7.79 (SD = 2.39), ODD Symptom 2 was 6.09 (SD = 3.18), and ODD Symptom 3 was 4.58 (SD = 3.49). For OCD Symptom 1, 88% (n = 159) of participants endorsed experiencing the symptom and 12% (n = 20) did not endorse the symptom. The mean score for ODD severity was 6.05 (SD = 0.996) and OCD severity was 4.61 (SD = 1.92). Descriptive statistics and Spearman correlations are reported in Table 2.
Table 2
Spearman Correlation Coefficients (p Values), Mean, and Standard Deviations of Variables
| Measure |
M |
SD |
1 |
2 |
3 |
4 |
5 |
6 |
| 1. Age |
13.34 |
3.56 |
– |
|
|
|
|
|
| 2. ODD Severity |
6.05 |
0.996 |
−0.102 |
– |
|
|
|
|
| 3. OCD Severity |
4.61 |
1.92 |
−0.004 |
.286** |
– |
|
|
|
| 4. ODD Symptom 1 |
7.79 |
2.39 |
0.026 |
.246** |
0.112 |
– |
|
|
| 5. ODD Symptom 2 |
6.09 |
3.18 |
0.025 |
.240** |
0.172* |
.645** |
– |
|
| 6. ODD Symptom 3 |
4.58 |
3.49 |
0 |
.220** |
0.152* |
.522** |
.715** |
– |
*p < .05. **p < .01.
Fisher’s exact test was used to determine if there was a significant association between the OCD and ODD variables. There was no statistical significance between ODD Severity and OCD Symptom 1 (two-tailed, p = .196) or between OCD Symptom 1 and ODD Symptom 3 (two-tailed, p = .015). However, there was a strong positive relationship between OCD Symptom 1 and ODD Symptom 1
(ϕ = .43; two-tailed, p < .001) as well as a strong positive significant association between OCD Symptom 1 and ODD Symptom 2 (ϕ = .53; two-tailed, p < .001).
A Wilcoxon signed-rank test revealed a statistically significant difference between ODD Severity and OCD Severity (z = −8.803, p < .001) with a medium effect size (r = .60). The median score increased from 5 to 6 when ODD Severity was considered with OCD Severity, suggesting that OCD Severity scores predicted a significant increase in ODD Severity scores. Analysis indicated a statistically significant difference between OCD Severity and ODD Symptom 1 (z = −9.834, p < .001) with a large effect size (r = .735), suggesting that the median score of ODD Symptom 1 increased from 8 to 9 when OCD Severity was included. ODD Symptom 1 predicted a significant increase in OCD Severity scores. The results revealed a statistically significant difference between OCD Severity and ODD Symptom 2 (z = −5.114, p < .001) with a small effect size (r = .382). The median score for ODD Symptom 2 increased from 5 to 7 when OCD Severity was included. Results did not reveal a statistically significant difference between OCD Severity and ODD Symptom 3 (z = −.266, p = .790). The median score remained the same (Mdn = 5) when OCD Severity was considered with ODD Symptom 3. Results of the Wilcoxon signed-rank test are depicted in Table 3.
Table 3
Wilcoxon Signed-Rank Test for OCD Severity
| Measure |
Ranks |
Mean Rank |
Sum of
Rank |
Z |
p |
| ODD Severity |
Negative Ranks |
47.64 |
667.00 |
−8.083 |
< 0.001 |
|
Positive Ranks |
64.94 |
7208.00 |
|
|
| ODD Symptom 1 |
Negative Ranks |
61.72 |
987.50 |
−9.834 |
< 0.001 |
|
Positive Ranks |
88.51 |
13718.50 |
|
|
| ODD Symptom 2 |
Negative Ranks |
76.86 |
3766.00 |
−5.114 |
< 0.001 |
|
Positive Ranks |
86.28 |
10095.00 |
|
|
| ODD Symptom 3 |
Negative Ranks |
85.56 |
7700.50 |
−0.266 |
0.790 |
|
Positive Ranks |
88.56 |
7350.50 |
|
|
Discussion
The objective of the present study was to identify and assess children and adolescents for overlap in symptoms and severity of ODD and OCD to determine potential comorbidity and suggest misdiagnosis. The aim of this study was to better understand the potential for children and adolescents to be misdiagnosed with ODD rather than OCD based on the premise that OCD-diagnosed children and adolescents experience symptoms that mimic ODD, such as anger and frustration, because of the inability to perform compulsions.
According to the results of this study, there was a significant relationship between OCD Symptom 1 and ODD Symptom 1. This finding suggested that youth diagnosed with ODD demonstrated significant associations with anger/frustration related to obsessions, compulsions, and annoyance. Additionally, the results suggested a significant relationship between OCD Symptom 1 (feels very frustrated and or angry with relation to obsession and compulsions) and ODD Symptom 2 (often angry and resentful). These results are similar to the prior research conducted by Ezpeleta et al. (2022), which revealed that children with OCP and ODD experienced heightened severity with relation to irritability and defiance, which may be due to the inability to act on a compulsion or perform a ritual. Moreover, researchers have conceptualized that the inability to complete compulsions may result in defiance or temper/anger outbursts (Ale & Krackow, 2011; Krebs et al., 2013; Painuly et al., 2011). Perhaps the children and adolescents in this study were diagnosed with ODD because of the endorsement of symptoms associated with frustration and anger; however, these symptoms might be a result of the inability to complete compulsions.
Findings from this study suggested that ODD Severity, ODD Symptom 1 (easily annoyed, bothered, or upset by others), and ODD Symptom 2 (often angry and resentful) increased when OCD Severity was considered. The heightened severity and symptoms of ODD when OCD Severity was included in the analysis demonstrated the potential for comorbidity. These results are similar to the findings of Storch et al. (2010), who found that youth diagnosed with ODD and OCD (N = 192) reported increased OCD severity. Moreover, in a similar study, Coskun et al. (2012) found that 48% (n = 12) of children and adolescents who were diagnosed with OCD had comorbidity with ODD. Understanding the co-occurrence of these disorders is crucial because they have shown to be predictors of OCD in young adulthood (Bloch et al., 2009).
Implications
Clinical assessment is imperative to accurately diagnose children and adolescents who exhibit anger and frustration. The results of this study are imperative to understanding the potential for misdiagnosis and comorbidity among OCD and ODD. It is also important to note the overdiagnosis of ODD, which could contribute to the lack of consideration of OCD and misdiagnosis of ODD in children and adolescents. According to Grimmett et al. (2016), the DSM-5 criteria for ODD appear to be too general, which may make it more of a convenient diagnosis rather than an accurate one. Moreover, Merten et al. (2017) noted that misdiagnosis and overdiagnosis of mental disorders for children and adolescents could be due to the methods implemented in evaluation, reports of symptoms by parents or guardians, and differences in perspectives of diagnostic criteria. Consequently, clients may receive a fast and inadequate evaluation for ODD without a thorough consideration of the possibility of coexisting conditions, such as OCD. Clinicians can utilize this information by thoroughly evaluating the underlying cause or origin of the anger or frustration experienced by children and adolescents in order to engage in accurate conceptualization and planning of treatment modalities. We suggest that clinicians ask their clients about their cognitive thought processes prior to experiencing anger to determine if unwanted, intrusive, or upsetting thoughts (i.e., obsessions) are occurring prior to experiencing anger. To accurately diagnose, clinicians should ask if the client is engaging in compulsions in various environments to which the repetitive behaviors can be freely acted on and if the client experiences anger and frustration in all environments. Likewise, if the client reports experiencing anger or frustration mostly in the presence of authority figures, clinicians will be better able to rule out OCD. Additionally, clinicians should consider the onset of these disorders because ODD symptoms typically appear in preschool and OCD has an average onset of 19.5 years (APA, 2013). The assessment of both mental disorders can assist in the development of preventative efforts to better support emotional regulation of youth in the school and home settings (Ezpeleta et al., 2022). Lastly, Ale and Krackow (2011) touched on the importance of clinicians providing behavioral training to parents or guardians of children diagnosed with OCD and ODD that focused on differentiating defiant behaviors and anxiety-related behaviors. The American Academy of Children and Adolescent Psychiatry (AACAP; 2023) hosts the Oppositional Defiant Disorder Resource Center and the Obsessive-Compulsive Disorder Resource Center. These resource centers include psychoeducation on mental disorders and information on medications and treatment options (AACAP, 2023). Moreover, parents or guardians can find information, prevention, and intervention through government agencies, including the U.S. Department of Health and Human Services (2023) and state departments of mental health. Lastly, parents or guardians can seek information from nonprofit organizations, including the National Federation of Families (2023), the International OCD Foundation (2023), and the Child Mind Institute (2023).
Limitations and Future Research
This study has a few limitations. First, with relation to the CliniCom, only one symptom of OCD was collected. Future studies should consider collecting more information on OCD when evaluating for overlap in symptoms. Second, the study relied on self-report data completed by the participants and their guardians, although a semi-structured diagnostic interview was completed by a board-certified psychiatrist to verify and confirm the diagnosis. Third, the sample size for the study was small, which limited the power of the data analysis, and comprised far more boys than girls, limiting the generalizability of the results. However, this gender compilation was expected as more males are diagnosed with ODD compared to females (APA, 2013; Ezpeleta et al., 2022).
Despite limitations, this study contributes further evidence of the overlap in symptoms between ODD and OCD in addition to highlighting the challenges of accurate diagnosis. The findings of this study demonstrated that further research must be conducted to understand how frustration or anger related to obsessions and compulsions may be misinterpreted as symptoms of ODD for children and adolescents.
Conclusion
This study sought to assess the associations in symptoms and severity between ODD and OCD as reported by children and adolescents. Specifically, we examined anger and frustration with relation to obsessions and compulsions to further understand the overlap in these disorders. The premise of this study was that the inability to act on obsessions and compulsions may lead to increases in anger and frustration. The inconclusive information regarding the overlap in symptoms related to anger for youth experiencing symptoms of OCD demonstrates the need for further research. Identifying the source of defiance (i.e., anger, annoyance, resentfulness) should be considered in the development of comprehensive assessments. This will further impact accurate diagnosis and treatment planning. The associations between anger or frustration related to obsessions and compulsions with the ODD symptoms of annoyance and anger/resentfulness indicate the need for further assessment regarding comorbidity and additional consideration of misdiagnosis or overdiagnosis. Furthermore, the increases in ODD symptoms and severity when OCD severity was considered further suggest that clinicians should recognize the impact of one diagnosis on another. Accurate diagnosis of these disorders is pertinent to providing effective treatment, which will influence the daily functioning of youth diagnosed with these disorders.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Achenbach, T. M. (1991). Manual for the Child Behavior Checklist/4-18 and the 1991 profile. Department of Psychiatry, University of Vermont.
Ale, C. M., & Krackow, E. (2011). Concurrent treatment of early childhood OCD and ODD: A case illustration. Clinical Case Studies, 10(4), 312–323. https://doi.org/10.1177/1534650111420283
American Academy of Child and Adolescent Psychiatry. (2023). Resource centers. https://www.aacap.org/AACAP/Families_and_Youth/Resource_Centers/Home.aspx
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). https://doi.org/10.1176.appi.books.9780890425787
Avasthi, A., Sharma, A., & Grover, S. (2019). Clinical practice guidelines for the management of obsessive-compulsive disorder in children and adolescents. Indian Journal of Psychiatry, 61(2), 306–316. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_554_18
Basu, D., Basu, A., & Ghosh, A. (2018). Assessment of clinical co-morbidities. Indian Journal of Psychiatry, 60(4), 457–465. https://doi.org/10.4103/psychiatry.IndianJPsychiatry_13_18
Beltrán, S., Sit, L., & Ginsburg, K. R. (2021). A call to revise the diagnosis of oppositional defiant disorder—Diagnoses are for helping, not harming. JAMA Psychiatry, 78(11), 1181–1182. https://doi.org/10.1001/jamapsychiatry.2021.2127
Bloch, M. H., Craiglow, B. G., Landeros-Weisenberger, A., Dombrowski, P. A., Panza, K. E., Peterson, B. S., & Leckman, J. F. (2009). Predictors of early adult outcomes in pediatric-onset obsessive-compulsive disorder. Pediatrics, 124(4), 1085–1093. https://doi.org/10.1542/peds.2009-0015
Boisseau, C. L., Thompson-Brenner, H., Caldwell-Harris, C., Pratt, E., Farchione, T., & Barlow, D. H. (2012). Behavioral and cognitive impulsivity in obsessive–compulsive disorder and eating disorders. Psychiatry Research, 200(2–3), 1062–1066. https://doi.org/10.1016/j.psychres.2012.06.010
Busner, J., & Targum, S. D. (2007). The Clinical Global Impressions Scale: Applying a research tool in clinical practice. Psychiatry, 4(7), 28–37. PMID: 20526405
Celebre, A., Stewart, S. L., Theall, L., & Lapshina, N. (2021). An examination of correlates of quality of life in children and youth with mental health issues. Frontiers in Psychiatry, 12. https://doi.org/10.3389/fpsyt.2021.709516
Centers for Disease Control and Prevention. (2023, March 8). Children’s mental health: Data and statistics.
https://www.cdc.gov/childrensmentalhealth/data.html
Child Mind Institute. (2023, March). Complete guide to OCD. https://www.childmind.org/guide/parents-guide-to-ocd/
Cludius, B., Mannsfeld, A. K., Schmidt, A. F., & Jelinek, L. (2021). Anger and aggressiveness in obsessive-compulsive disorder (OCD) and the mediating role of responsibility, non-acceptance of emotions, and social desirability. European Archives of Psychiatry and Clinical Neuroscience, 271, 1179–1191.
https://doi.org/10.1007/s00406-020-01199-8
Coskun, M., Zoroglu, S., & Ozturk, M. (2012). Phenomenology, psychiatric comorbidity and family history in referred preschool children with obsessive-compulsive disorder. Child and Adolescent Psychiatry and Mental Health, 6. https://doi.org/10.1186/1753-2000-6-36
Ezpeleta, L., Penelo, E., Navarro, J. B., de la Osa, N., & Trepat, E. (2022). Irritability, defiant and obsessive-compulsive problems development from childhood to adolescence. Journal of Youth and Adolescence, 51, 1089–1105. https://doi.org/10.1007/s10964-021-01528-7
Garcia, A. M., Freeman, J. B., Himle, M. B., Berman, N. C., Ogata, A. K., Ng, J., Choate-Summers, M. L., & Leonard, H. (2009). Phenomenology of early childhood onset obsessive compulsive disorder. Journal of Psychopathology and Behavioral Assessment, 31, 104–111. https://doi.org/10.1007/s10862-008-9094-0
Geller, D. A. (2006). Obsessive-compulsive and spectrum disorders in children and adolescents. Psychiatric Clinics of North America, 29(2), 353–370. https://doi.org/10.1016/j.psc.2006.02.012
Geller, J. (2022, October). What is obsessive-compulsive disorder? American Psychiatric Association. https://www.psychiatry.org/patients-families/obsessive-compulsive-disorder/what-is-obsessive-compulsive-disorder
Ghandour, R. M., Sherman, L. J., Vladutiu, C. J., Ali, M. M., Lynch, S. E., Bitsko, R. H., & Blumberg, S. J. (2019). Prevalence and treatment of depression, anxiety, and conduct problems in US children. The Journal of Pediatrics, 206, 256–267. https://doi.org/10.1016/j.jpeds.2018.09.021
Ghosh, A., Ray, A., & Basu, A. (2017). Oppositional defiant disorder: Current insight. Psychology Research and Behavior Management, 2017(10), 353–367. https://doi.org/10.2147/PRBM.S120582
Goodman, W. K., Price, L. H., Rasmussen, S. A., Mazure, C., Fleischmann, R. L., Hill, C. L., Heninger, G. R., & Charney, D. S. (1989). The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Archives of General Psychiatry, 46(11), 1006–1011. https://doi.org/10.1001/archpsyc.1989.01810110048007
Grimmett, M. A., Dunbar, A. S., Williams, T., Clark, C., Prioleau, B., & Miller, J. S. (2016). The process and implications of diagnosing oppositional defiant disorder in African American males. The Professional Counselor, 6(2), 147–160. https://doi.org/10.15241/mg.6.2.147
Handal, N., LePage, J., Dayley, P., Baldwin, B., Roeser, A., Kay, J., Theobald, H. A., Nellamattathil, M., Drotar, S., Weir, C., Tindell, N., & Tice, K. (2018). Validation, reliability, and specificity of Clinicom™ psychiatric assessment software. Psychiatry Research, 265, 334–340.
https://doi.org/10.1016/j.psychres.2018.05.029
Hood, B. S., Elrod, M. G., & DeWine, D. B. (2015). Treatment of childhood oppositional defiant disorder. Current Treatment Options in Pediatrics, 1, 155–167. https://doi.org/10.1007/s40746-015-0015-7
International OCD Foundation. (2023). For parents and families. https://kids.iocdf.org/for-parents/
Justicia-Arráez, A., Pichardo, M. C., Romero-López, M., & Alba, G. (2021). Can we manage behavioral problems through the development of children’s social-emotional regulated behavior? Longitudinal study of a preschool program. International Journal of Environmental Research Public Health, 18(16), 8447. https://doi.org/10.3390/ijerph18168447
Kotapati, V. P., Khan, A. M., Dar, S., Begum, G., Bachu, R., Adnan, M., Zubair, A., & Ahmed, R. A. (2019). The effectiveness of selective serotonin reuptake inhibitors for treatment of obsessive-compulsive disorder in adolescents and children: A systematic review and meta-analysis. Frontiers in Psychiatry, 10(523). https://doi.org/10.3389/fpsyt.2019.00523
Krebs, G., Bolhuis, K., Heyman, I., Mataix-Cols, D., Turner, C., & Stringaris, A. (2013). Temper outbursts in pediatric obsessive-compulsive disorder and their association with depressed mood and treatment outcome. Journal of Child Psychology and Psychiatry, 54(3), 313–322.
https://doi.org/10.1111/j.1469-7610.2012.02605.x
Loeber, R., Burke, J. D., Lahey, B. B., Winters, A., & Zera, M. (2000). Oppositional defiant and conduct disorder: A review of the past 10 years, part I. Journal of the American Academy of Child and Adolescent Psychiatry, 39(12), 1468–1484. https://doi.org/10.1097/00004583-200012000-00007
Mancebo, M. C., Garcia, A. M., Pinto, A., Freeman, J. B., Przeworski, A., Stout, R., Kane, J. S., Eisen, J. L., & Rasmussen, S. A. (2008). Juvenile-onset OCD: Clinical features in children, adolescents and adults. Acta Psychiatrica Scandinavica, 118(2), 149–159. https://doi.org/10.1111/j.1600-0447.2008.01224.x
Merten, E. C., Cwik, J. C., Margraf, J., & Schneider, S. (2017). Overdiagnosis of mental disorders in children and adolescents (in developed countries). Child and Adolescent Psychiatry and Mental Health, 11(5). https://doi.org/10.1186/s13034-016-0140-5
National Federation of Families. (2023). Oppositional defiant disorder resources. https://www.Ffcmh.org/esources-odd
Nazeer, A., Latif, F., Mondal, A., Azeem, M. W., & Greydanus, D. E. (2020). Obsessive-compulsive disorder in children and adolescents: Epidemiology, diagnosis and management. Translational Pediatrics, 9(1), S76–S93. https://doi.org/10.21037/tp.2019.10.02
Painuly, N. P., Grover, S., Mattoo, S. K., & Gupta, N. (2011). Anger attacks in obsessive compulsive disorder. Industrial Psychiatry Journal, 20(2), 115–119. https://doi.org/10.4103/0972-6748.102501
Perou, R., Bitsko, R. H., Blumberg, S. J., Pastor, P., Ghandour, R. M., Gfroerer, J. C., Hedden, S. L., Crosby, A. E., Visser, S. N., Schieve, L. A., Parks, S. E., Hall, J. E., Brody, D., Simile, C. M., Thompson, W. W., Baio, J., Avenevoli, S., Kogan, M. D., & Huang, L. N. (2013). Mental health surveillance among children – United States, 2005-2011. Morbidity and Mortality Weekly Report Supplements, 62(02), 1–35. PMID: 23677130
Pringsheim, T., Hirsch, L., Gardner, D., & Gorman, D. A. (2015). The pharmacological management of oppositional behaviour, conduct problems, and aggression in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, and conduct disorder: A systematic review and meta-analysis. Part 1: Psychostimulants, alpha-2 agonists, and atomoxetine. The Canadian Journal of Psychiatry, 60(2), 42–51. https://doi.org/10.1177/070674371506000202
Radomsky, A. S., Ashbaugh, A. R., & Gelfand, L. A. (2007). Relationships between anger, symptoms, and cognitive factors in OCD checkers. Behaviour Research and Therapy, 45(11), 2712–2725. https://doi.org/10.1016/j.brat.2007.07.009
Scahill, L., Riddle, M. A., McSwiggin-Hardin, M., Ort, S. I., King, R. A., Goodman, W. K., Cicchetti, D., & Leckman, J. F. (1997). Children’s Yale-Brown Obsessive Compulsive Scale: Reliability and validity. Journal of the American Academy of Child and Adolescent Psychiatry, 36(6), 844–852.
https://doi.org/10.1097/00004583-199706000-00023
Stahnke, B. (2021). A systematic review of misdiagnosis in those with obsessive-compulsive disorder. Journal of Affective Disorders Reports, 6, 1–7. https://doi.org/10.1016/j.jadr.2021.100231
Storch, E. A., Jones, A. M., Lack, C. W., Ale, C. M., Sulkowski, M. L., Lewin, A. B., De Nadai, A. S., & Murphy, T. K. (2012). Rage attacks in pediatric obsessive-compulsive disorder: Phenomenology and clinical correlates. Journal of the American Academy of Child and Adolescent Psychiatry, 51(6), 582–592. https://doi.org/10.1016/j.jaac.2012.02.016
Storch, E. A., Lewin, A. B., Geffken, G. R., Morgan, J. R., & Murphy, T. K. (2010). The role of comorbid disruptive behavior in the clinical expression of pediatric obsessive-compulsive disorder. Behaviour Research and Therapy, 48(12), 1204–1210. https://doi.org/10.1016/j.brat.2010.09.004
Stringaris, A., & Goodman, R. (2009). Longitudinal outcome of youth oppositionality: Irritable, headstrong, and hurtful behaviors have distinctive predictions. Journal of the American Academy of Child and Adolescent Psychiatry, 48(4), 404–412. https://doi.org/10.1097/CHI.0b013e3181984f30
Thériault, M.-C. G., Lespérance, P., Achim, A., Tellier, G., Diab, S., Rouleau, G. A., Chouinard, S., & Richer, F. (2014). ODD irritability is associated with obsessive–compulsive behavior and not ADHD in chronic tic disorders. Psychiatry Research, 220(1–2), 447–452. https://doi.org/10.1016/j.psychres.2014.07.039
U.S. Department of Health and Human Services. (2023). Youth mental health. https://www.hhs.gov/surgeon
general/priorities/youth-mental-health/index.html
Nelson Handal, MD, DFAPA, is Founder, Chairman, and Medical Director for Dothan Behavioral Medicine Clinic and Harmonex Neuroscience Research. Emma Quadlander-Goff, PhD, NCC, LPC, is a clinical researcher at Harmonex Neuroscience Research and an assistant professor at Troy University. Laura Handal Abularach, MD, is a researcher at Harmonex Neuroscience Research and PGY-1 Psychiatry Resident at Louisiana State University. Sarah Seghrouchni, BS, is a research assistant at Alabama College of Osteopathic Medicine. Barbara Baldwin, MS, is Director of Clinical Research at Harmonex Neuroscience Research. Correspondence may be addressed to Emma Quadlander-Goff, 408 Healthwest Dr., Dothan, AL 36303, equadlander@troy.edu.
Feb 7, 2022 | Volume 12 - Issue 1
Gregory T. Hatchett
The addition of disruptive mood dysregulation disorder (DMDD) to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) was a controversial decision in 2013 and one that continues to the present. Researchers have found that DMDD exhibits both poor interrater reliability and discriminant validity from other common childhood-onset disorders, most notably oppositional defiant disorder (ODD). Research also indicates that DMDD might be better conceptualized as a component of ODD, and consistent with such a conceptualization, experts have recommended that effective treatments for ODD be applied to youth who fit the diagnostic pattern of DMDD. The purpose of this article is to help readers understand the problematic diagnostic validity associated with DMDD and to present recommended treatment strategies for working with youth who fit this challenging symptom profile.
Keywords: disruptive mood dysregulation disorder, oppositional defiant disorder, conceptualization, diagnostic validity, youth
A pattern of emotional and behavioral dysregulation—characterized by severe irritability, temper outbursts, and aggressive behavior—is one of the most common reasons that children and adolescents are referred to mental health service providers (Axelson et al., 2012; Brotman et al., 2017; Stringaris et al., 2018) and a common antecedent to inpatient hospitalization (Chase et al., 2020; Rao, 2014). Despite the prevalence and severity of these associated symptoms, mental health professionals have often disagreed as to how children and adolescents who fit this symptom profile should be conceptualized and properly diagnosed. Over the years, chronic irritability and temper dysregulation have been conceptualized as associated features of externalizing disorders (Carlson, 1998), developmental variations of early-onset bipolar disorder (Biederman et al., 2000), and core features of an experimental research phenotype (Leibenluft et al., 2003; Rich et al., 2005; Stringaris et al., 2010).
In 2013, the American Psychiatric Association (APA) provided a new diagnostic home for youth with chronic and severe irritability in the depressive disorders chapter in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013). This new disorder—disruptive mood dysregulation disorder (DMDD)—was specifically added to the DSM-5 to prevent clinicians from overdiagnosing a bipolar and related disorder in children and adolescents who exhibited non-episodic irritability and temper outbursts. Beginning in the 1990s, there began an exponential increase in the number of children and adolescents who were diagnosed with bipolar disorder. As just one example of this pattern, Moreno et al. (2007) reported a 40-fold increase of the number of outpatient office visits for children and adolescents treated for bipolar disorder between 1995–1996 and 2002–2003. Not only was this increase unusual from an epidemiological perspective (Van Meter et al., 2011), but researchers also began to accumulate evidence that these youth did not match the profile of either youth or adults with traditional bipolar disorder (Leibenluft, 2011; Towbin et al., 2013). To better characterize children and adolescents who exhibited chronic irritability and temper outbursts, researchers at the National Institute of Mental Health (Leibenluft et al., 2003) developed a new diagnostic phenotype, severe emotional dysregulation (SMD), to differentiate this symptom pattern from traditional bipolar disorder. SMD subsequently became the foundation for the inclusion of DMDD in the DSM-5 (APA, 2013).
Many experts disagree about DMDD as a valid and coherent diagnostic category. However, there seems to be a strong consensus that many children and adolescents are severely impaired because of chronic irritability and severe temper dysregulation (Copeland et al., 2014; Rao, 2014). Although early estimates indicate that only 1%–3% of children and adolescents may meet the full diagnostic criteria for DMDD (Copeland et al., 2013), many more may present with at least subthreshold symptoms of the disorder (Baweja, Mayes, et al., 2016; Freeman et al., 2016). Thus, counselors, especially those working in clinical settings, will likely find themselves working with many children and adolescents who exhibit symptoms of DMDD, symptoms which need to be carefully evaluated as part of any differential diagnostic process. To provide the best possible services for this population, counselors need to be familiar with the current literature on both the diagnosis and treatment of DMDD. Consequently, this article summarizes these current DMDD topics and presents treatment recommendations for working with youth diagnosed with DMDD. Because it is important for counselors to understand the questionable diagnostic validity of DMDD and how these diagnostic limitations should inform the treatment planning process, this topic will be preceded by criticisms of DMDD as a valid mental disorder. Also discussed are the challenges of diagnosing youth who present with chronic emotional and behavioral dysregulation.
The Diagnosis of DMDD
The diagnostic criteria and decisional rules for DMDD in the DSM-5 (APA, 2013) are rather detailed, so only a summary will be provided here. (Readers should consult pages 156–160 in the DSM-5 for more detailed information.) The core diagnostic features for DMDD include recurrent (3 or more times a week) temper outbursts that are developmentally inappropriate, severe, and disproportionate to any identifiable stressor along with the persistence of a chronically irritable or angry mood between these temper outbursts—a disruption in mood that is noticeable by others. These symptoms must have begun before the age of 10, persist for a minimum of a year (with no more than 3 consecutive months of symptom-free periods), and be present in at least two out of three settings (i.e., home, school, peer relationships). According to the DSM-5, this diagnosis should not be made if these symptoms occur exclusively during a major depressive episode or if the symptoms are better explained by another mental disorder, such as autism spectrum disorder. Also, a diagnosis of DMDD cannot be given concurrently with oppositional defiant disorder (ODD), bipolar disorder, or intermittent explosive disorder. If a child meets the diagnostic criteria for both DMDD and ODD, only DMDD should be given. As mentioned previously, DMDD was specifically added to the DSM-5 to prevent clinicians from overdiagnosing bipolar and related disorder in children and adolescents who exhibit non-episodic irritability and temper outbursts. However, at first glance, a youth who meets the diagnostic criteria for DMDD may be suspected of having a bipolar and related disorder. Thus, it is important for counselors to recognize the fundamental differences between the two disorder classifications.
As explained above, in DMDD, a child or adolescent experiences non-episodic irritability that is punctuated by severe and disproportionate temper outbursts. This symptom presentation must occur for at least 365 days, and during the year, have no more than a 3-month period in which the child or adolescent does not experience the core features of the disorder. In contrast, youth who meet the diagnostic criteria for bipolar disorder experience distinctive episodes of mania (at least 7 days), hypomania (at least 4 days), or depression (at least 14 days). Although irritability and temper outbursts can certainly occur in the context of a manic or hypomanic episode, there are additional symptoms that must also be present. Specifically, the irritability or temper outbursts should be episodic, accompanied by an increase in goal-directed activity/energy, and include additional symptoms, such as grandiosity, decreased need for sleep, pressured speech, racing thoughts, or reckless impulsivity (APA, 2013). More information on the differential diagnosis of bipolar disorder from DMDD and other conditions can be found in Hatchett and Motley (2016).
Diagnostic Validity of DMDD
Many have argued that adding DMDD to the DSM-5 traded one problem—overdiagnosis of bipolar disorder—for another: a poorly conceptualized diagnostic construct lacking any evidence-based treatments (e.g., S. C. Evans et al., 2017; Freeman et al., 2016; Parker & Tavella, 2018). As Malhi and Bell (2019) recently observed, “more than half a decade later, the ‘creation’ of this new diagnostic entity [DMDD] has not provided any novel insights or greater understanding and is yet to demonstrate any tangible benefits” (p. 706).
Though DMDD has been criticized for its poor interrater reliability (Regier et al., 2013) and low temporal stability across time (e.g., Axelson et al., 2012), the strongest criticism of DMDD has been directed toward its standing as an independent and coherent diagnostic construct, a concern that was not only present at the time of its introduction in the DSM-5, but one that has been bolstered by subsequent research since the publication of the DSM-5 in 2013. Ironically, the evidentiary basis for including DMDD in the DSM-5 was not based on studies of children and adolescents who actually matched the specific diagnostic criteria for DMDD. Instead, the research support for DMDD was inferred from research conducted on SMD (Baweja, Mayes, et al., 2016; Bruno et al., 2019; Rao, 2014; Towbin et al., 2013). As mentioned previously, the phenotype of SMD was developed by researchers at the National Institute of Mental Health (Leibenluft et al., 2003) to provide an alternative conceptualization to bipolar disorder for youth who exhibited chronic and severe irritability, temper dysregulation, and hyperarousal. However, there are important differences between the diagnostic criteria for SMD and DMDD. Compared to the diagnostic criteria for DMDD, SMD includes different age parameters, the presence of an abnormal mood characterized by anger or sadness, different exclusion criteria, and most importantly, the presence of hyperarousal (e.g., insomnia, agitation, distractibility; Leibenluft, 2011). As S. C. Evans et al. (2017) pointed out, “Given the differences between the operationalization of SMD in the literature and the definition of DMDD, virtually no evidence regarding DMDD existed at the time of its inclusion in DSM-5” (p. 33).
Consistent with these differences, researchers have found low levels of correspondence between the two syndromes. For example, Copeland et al. (2013) reported that only 38.9% of those who met the criteria for SMD also met the diagnostic criteria for DMDD. These differences have important implications for the treatment planning process. Specifically, it is unclear whether any of the interventions that have been found to be helpful for youth with SMD (e.g., Towbin et al., 2020) will generalize to youth who match the different diagnostic profile for DMDD (Benarous et al., 2017).
Furthermore, since the publication of the DSM-5 in 2013, researchers have increasingly challenged the validity of DMDD as a stand-alone diagnostic construct (Freeman et al., 2016). For one, there is very little evidence to suggest that DMDD can be reliably differentiated from other common childhood-onset disorders (S. C. Evans et al., 2017; Malhi & Bell, 2019). Several of the core symptoms of DMDD—chronic irritability and recurrent temper outbursts—are not exclusive to DMDD, but rather represent transdiagnostic symptoms often present in many other disorders, such as ODD, generalized anxiety disorder, depression, autism spectrum disorder, bipolar disorder, and post-traumatic stress disorder (e.g., Stringaris et al., 2018). As Parker and Tavella (2018) pointed out, “Those who meet the criteria for DMDD may in fact have a conduct disorder, ODD, attention deficit hyperactivity disorder (ADHD), or any of myriad other behavioral disorders” (p. 815). However, on the one hand, the diagnostic criteria for DMDD in the DSM-5 is very extensive and detailed, especially compared to what is commonly delineated for many other disorders in the DSM-5. Clinicians who carefully follow these detailed criteria and decisional rules should, in theory, arrive at valid and reliable diagnoses of DMDD. Yet, in real practice, the diagnostic process is often plagued by careless errors and clinician biases (Garb, 1998; Lacasse, 2014). Consequently, the issue becomes how well clinicians can apply these criteria in often complex clinical situations.
More research is needed on how well counselors and other clinicians can reliably diagnose DMDD and differentiate it from other conditions in ordinary practice settings. Concerns about the diagnostic validity of DMDD have been most pronounced in the differentiation of DMDD from ODD. In the DSM-5 (APA, 2013), a diagnosis of DMDD automatically supersedes a diagnosis of ODD; thus, these two diagnoses cannot be given concurrently. However, when researchers have removed this exclusionary rule, they have found that nearly all the children and adolescents who met the diagnostic criteria for DMDD also met the diagnostic criteria for ODD (Axelson et al., 2012; Freeman et al., 2016; Mayes et al., 2016). As just one example, Mayes, Waxmonsky, et al. (2015) reported that 91% of the children who met the criteria for DMDD in their study also qualified for a diagnosis of ODD. However, the reverse is not true. Researchers have found that diagnoses of ODD commonly occur in the absence of DMDD. Approximately one-third of children and adolescents who meet diagnostic criteria for ODD do not have significant symptoms of DMDD (Mayes et al., 2016).
According to the hierarchy or parsimony principle in the DSM-5 (APA, 2013), a clinician should diagnose the most severe disorder that best captures the multitude of symptoms that a client is experiencing instead of adding on several more minor diagnoses to the diagnostic record. For example, children and adolescents who meet the diagnostic criteria for autism spectrum disorder simultaneously meet the diagnostic criteria for social communication disorder. Therefore, an additional diagnosis of social communication disorder is unnecessary. Likewise, in the DSM-5, a diagnosis of DMDD is higher on the diagnostic hierarchy than ODD, and thus many of the symptoms of ODD are subsumed under a diagnosis of DMDD. For clinicians who carefully follow the diagnostic rules of the DSM-5, both negative affectivity and oppositional behavior can be recognized and targeted as part of a treatment plan for a youth with DMDD.
For an alternative point of view, some researchers have expressed the concern that a single, overruling diagnosis of DMDD will fail to adequately acknowledge the behavioral problems associated with ODD, resulting in suboptimal treatment planning decisions (S. C. Evans et al., 2017; Mayes et al., 2016). Mayes et al. (2016) pointed out that a diagnosis of DMDD fails to acknowledge many of the disruptive behavioral components of ODD that are nearly always present in children and adolescents who meet the diagnostic criteria for DMDD. Likewise, S. C. Evans et al. (2017) argued that
treating DMDD as a Depressive Disorder—and withholding a diagnosis of ODD, per DSM-5 hierarchical rules—may lead clinicians to conceptualize these youth as having a mood disorder rather than a behavior disorder. For primary care providers and pediatricians, treating DMDD as a mood disorder and removing the ODD label may both decrease referrals for behavioral interventions that are well established (e.g., parent management training) and increase the administration of psychotropic medications such as antidepressants, antipsychotics, and mood stabilizers, for which evidence is limited. (p. 39)
However, the concerns just mentioned may reveal more about problems in the correct use and application of the DSM-5 by clinicians rather than problems inherent in diagnostic rules prescribed by the DSM-5.
Because of the transdiagnostic nature of DMDD symptoms (e.g., Parker & Tavella, 2018), several experts have recommended that DMDD be recognized as either a subtype or specifier under other DSM-5 diagnoses (Mayes, Mathiowetz, et al., 2015), most often as a subtype or specifier under ODD (S. C. Evans et al., 2017; Malhi & Bell, 2019; Mayes et al., 2016; Mayes, Waxmonsky, et al., 2015). This was the approach recently taken by the World Health Organization (2019) in the 11th edition of the International Statistical Classification of Diseases and Related Health Problems (ICD-11). In the ICD-11, clinicians have the option to diagnose a youth with oppositional defiant disorder with or without chronic irritability-anger. Thus, this diagnostic code allows clinicians to concurrently recognize both symptoms of emotional dysregulation and symptoms of argumentative, oppositional, and vindictive behavior. However, at the time of this writing, the ICD-11 has not been adopted in the United States, so counselors in the United States are still using the DSM-5 (APA, 2013) and the ICD-10 (World Health Organization, 2016).
On the other hand, some have cautioned against the use of DMDD as only a subtype or specifier under ODD (e.g., Benarous et al., 2017; Stringaris et al., 2018). Brotman et al. (2017) expressed the concern that many clinicians do not record available specifiers in diagnostic records, and consequently, children and adolescents who are diagnosed with ODD under the DSM-5 might not receive targeted interventions for symptoms of severe irritability and temper outbursts. At the very least, perhaps clinicians should be allowed to diagnose DMDD and ODD concurrently.
Another concern in the differential diagnosis of DMDD is potential racial/ethnic bias. As a depressive disorder in the DSM-5 (APA, 2013), DMDD is conceptualized as an internalizing disorder, whereas ODD is conceptualized as an externalizing or disruptive behavior disorder. Researchers have found that African American youth are more likely to be diagnosed with externalizing disorders, whereas European American youth are more likely to be diagnosed with internalizing disorders (e.g., Fadus et al., 2020; Minsky et al., 2006). Though this research has not yet been replicated specifically in the diagnosis of DMDD, prior research indicates that African American youth may be less likely to be identified as having DMDD and may not receive adequate treatment for potential depressive symptoms. Furthermore, researchers have found that African Americans and other minority groups who experience higher rates of racial/ethnic discrimination also experience more mental health and psychosocial functioning difficulties compared to those with lower experienced rates of racial/ethnic discrimination (Tobler et al., 2013). Consequently, counselors should evaluate the extent to which irritability and aggression among minority youth are associated with experiences of discrimination as opposed to internal psychopathology implicit in the DSM framework (e.g., Carter et al., 2019; Mouzon et al., 2017).
Treatment Planning Strategies
Diagnostic Considerations
Certainly, the main source of information for the proper diagnosis of DMDD is the explicit diagnostic criteria and decision rules in the DSM-5 (APA, 2013). To document these diagnostic criteria, counselors might consider using one or more of the cross-cutting measures included in Section III of the DSM-5 (pp. 733–741). Outside the DSM-5, there are currently few diagnostic tools for counselors to use in confirming a diagnosis of DMDD (Baweja, Mayes, et al., 2016). The assessment tools most often used in the research literature measure general irritability, such as the Affective Reactivity Index (Stringaris et al., 2012) or the Clinician Affective Reactivity Index (Haller et al., 2020). Specific to the diagnosis of DMDD, Wiggins et al. (2016) developed a DMDD module that was used in conjunction with the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–Present and Lifetime Version (K-SADS-PL; Kaufman et al., 1997). However, this is a new module that has not undergone extensive psychometric evaluation.
In addition to confirming a diagnosis of DMDD, counselors should also assess for common comorbid mental disorders (Mayes et al., 2016). Youth who meet the diagnostic criteria for DMDD almost always have comorbid disorders, most often attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and specific learning disorders (Althoff et al., 2016; Bruno et al., 2019). Though one cannot technically diagnose DMDD and ODD concurrently under DSM-5 rules, counselors should also carefully assess and document symptoms of ODD, which will likely be appropriate targets in the treatment planning process (e.g., S. C. Evans et al., 2017).
Though there are currently not any clearly validated inventories for directly assessing DMDD, there are several inventories available for assessing the comorbid conditions that often accompany the DMDD symptom profile. In addition to the previously mentioned cross-cutting measures in Section III of the DSM-5 (APA, 2013), there are several commercially available inventories for assessing symptoms of ODD, such as the Achenbach Series (Achenbach & Rescorla, 2006) or the Child and Adolescent Disruptive Behavior Inventory (Cianchetti et al., 2013). Again, though a diagnosis of DMDD technically overrides a diagnosis of ODD, symptoms of ODD will likely be present and a major target area of a counseling plan. Administration of a validated measure of ODD will not only help counselors identify symptom severity at the beginning of the counseling process, but can also be repeatedly administered throughout the counseling process to evaluate areas of improvement and areas that need additional attention. This same assessment process could also be used for other conditions comorbid with DMDD. Counselors might use the Conner’s Rating Scales (Conners, 1999) to assess for ADHD and other associated symptoms, such as aggression and learning problems. Symptoms of depression can be evaluated through administering the Children’s Depression Inventory (Sitarenios & Kovacs, 1999) or the Beck Depression Inventory with older adolescents (Beck et al., 1996). As is often the case, an assessment and treatment protocol that targets specific symptoms may be more effective than one that tries to remediate global diagnostic constructs, such as DMDD (e.g., Weisz & Kazdin, 2017).
Evidence-Based Treatments for DMDD
This next section will review the currently available research on both the use of pharmacotherapy and psychosocial interventions in working with youth who meet the diagnostic criteria for DMDD. This will be followed by a review of evidence-based treatments for related clinical conditions and will end with a summary of general treatment recommendations for working with youth diagnosed with DMDD.
Psychopharmacology
Researchers have conducted only a few studies on the effectiveness of pharmacotherapy in reducing symptoms of DMDD. For youth diagnosed with both DMDD and ADHD, researchers have found some evidence for the effectiveness of psychostimulant monotherapy (Baweja, Belin, et al., 2016; Winters et al., 2018) as well as the combination of methylphenidate with aripiprazole (Pan et al., 2018); however, in a small (n = 12) retrospective study, Ozyurt et al. (2017) found that methylphenidate resulted in increased irritability in children diagnosed with both DMDD and ADHD. Most recently, Rice et al. (2019) found some effectiveness for the use of amantadine with a 12-year-old diagnosed with DMDD who was admitted to a psychiatric hospital. Consistent with this limited research base, there are currently not any medications that have received Food and Drug Administration approval for treating children and adolescents specifically diagnosed with DMDD.
Psychosocial Interventions
Parallel to the research on pharmacological interventions, very little research has been published on the use of psychosocial interventions with youth who meet the diagnostic criteria for DMDD. Perepletchikova et al. (2017) reported that a modified version of dialectical behavior therapy, which also included a parent training module, was more effective than treatment as usual (TAU) in improving irritability, temper outbursts, and overall functioning among youth diagnosed with DMDD. In a subsequent study, Miller et al. (2018) reported that a modified version of interpersonal psychotherapy—interpersonal psychotherapy for mood and behavior dysregulation (IPT-MBD)—was more effective than TAU in reducing irritability and angry outbursts. However, both treatment groups had equivalent scores on measures of depression and anxiety by the end of treatment. There have also been a couple of case studies published in the literature. Tudor et al. (2016) reported that cognitive behavioral therapy was effective in reducing irritability and aggression in a 9-year-old girl diagnosed with DMDD and ADHD. In another case study report, Linke et al. (2020) reported that an exposure-based, cognitive behavioral model was effective in treating an 11-year-old boy diagnosed with both DMDD and ADHD.
Interventions for Comorbid Disorders
In the absence of evidence-based treatments for DMDD, many experts have recommended that clinicians select evidence-based treatments for disorders that are often comorbid with DMDD, most commonly ODD (Baweja, Mayes, et al., 2016). As Freeman et al. (2016) recommended, “Until a better evidence base exists, clinicians should be cautious when diagnosing youth with DMDD, and treatment often might best start with using evidence-based practices for ODD” (p. 129). This recommendation is also consistent with the ICD-11, in which the core features of DMDD are conceptualized as a potential subtype of ODD. There are several evidence-based interventions for oppositional behavior in general and ODD in particular, such as cognitive therapy (Greene et al., 2004), parent management training (Costin & Chambers, 2007), and multisystemic therapy (Asscher et al., 2013). There are also several established treatments for ADHD, a condition that is also often comorbid with DMDD. Effective interventions include the use of psychostimulants (Castells et al., 2020) as well as several variations of behavior therapy (S. W. Evans et al., 2014).
Treatments for General Irritability
Another source of information for selecting potentially effective treatments for youth with DMDD may be found in research programs that have targeted transdiagnostic symptoms of irritability and aggressive behavior (Roy et al., 2014). Some evidence suggests that cognitive behavior therapy may be effective in reducing general symptoms of irritability in youth (Derella et al., 2020; S. C. Evans et al., 2020; Sukhodolsky et al., 2016). Along this line, Sukhodolsky and Scahill (2012) have published a treatment manual for working with youth and their families who struggle with anger and aggression. The competencies covered in this manual include, but are not limited to, relaxation training, emotional regulation, problem solving, and social skills training. With regard to pharmacotherapy, Tourian et al. (2015) conducted a literature review on the use of pharmacological agents in reducing symptoms of chronic irritability, aggression, and temper outbursts in children and adolescents. Based on their review, they found that methylphenidate, risperidone, and divalproex may offer some measure of effectiveness in reducing irritability and aggressive behavior.
General Treatment Recommendations
As mentioned earlier, one of the criticisms of adding DMDD to the DSM-5 was that DMDD provided clinicians with a new diagnostic label in the absence of any evidence-based treatments (e.g., Parker & Tavella, 2018). As evidenced by this review, this criticism continues to be valid. Based on the limited treatment literature for DMDD and the larger literature for disruptive behavior disorders, only a few general guidelines seem suitable at this time. For one, experts generally recommend that treatment commence with the use of cognitive behavior therapy combined with parent management training (Brotman et al., 2017; Bruno et al., 2019; Roy et al., 2014; Stringaris et al., 2018). As previously mentioned, recent research indicates that dialectical behavior therapy (Perepletchikova et al., 2017) and interpersonal therapy (Miller et al., 2018) may also be promising. Second, if there is comorbid ADHD, it is recommended that pharmacotherapy begin with the use of a psychostimulant (Blader et al., 2016; Roy et al., 2014). Mood stabilizers and atypical antipsychotics may also be considered if psychostimulants prove ineffective or in cases where there is a need for a quick reduction in severe irritability or aggressive behavior (e.g., Baweja, Mayes, et al., 2016; Roy et al., 2014). Stringaris et al. (2018) recommended that these medications should be used very cautiously:
Our recommendation is that antipsychotic prescriptions be reserved for those young people who have not responded to a series of other treatments and that the prescription be for a short period of time during which health indicators such as weight are tightly monitored. (p. 733)
Third, as mentioned previously, counselors should also consider the use of evidence-based interventions for ODD, a disorder that substantially overlaps with DMDD (e.g., Freeman et al., 2016).
Concluding Comments
The addition of DMDD to the fifth edition of the DSM was a controversial decision, a dispute that continues to the present. At the time of its inclusion in the DSM-5, there was no solid evidentiary foundation for including DMDD as a new diagnostic category (S. C. Evans et al., 2017). Evidence for the validity of DMDD was inferred from the research on SMD, a distinct phenotype (Bruno et al., 2019). Subsequent research since the publication of the DSM-5 in 2013 on the nature of DMDD has demonstrated that DMDD lacks discriminant validity from other common disorders, most notably ODD (Parker & Tavella, 2018).
As this literature has revealed, there continues to be a paucity of evidence-based treatments for children and adolescents who fit the common symptom profile of DMDD. Although evidence-based treatments for comorbid disorders offer promise, it is important that clinicians and researchers develop and validate psychosocial and pharmacological treatments that directly target the core symptoms of DMDD (Baweja, Mayes, et al., 2016). Yet, in addition to more effective remediation strategies (i.e., tertiary prevention), there is also a clear need for prevention processes that can identify and effectively help those children and adolescents who exhibit severe and chronic irritability (Stringaris & Goodman, 2009). Though research is still emerging, a diagnosis of DMDD seems to be a precursor for a lifetime of impairment. Youth with DMDD are at high risk for developing numerous mental health problems in adulthood, including major depressive disorder, persistent depressive disorder (dysthymia), and generalized anxiety disorder (Copeland et al., 2014; Stringaris et al., 2009; Stringaris & Goodman, 2009). The development and evaluation of such prevention processes should be taken up by professional counselors in both school and community settings, a responsibility that is part of our professional identity (Albee & Ryan-Finn, 1993).
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Achenbach, T. M., & Rescorla, L. A. (2006). The Achenbach System of Empirically Based Assessment. In R. P. Archer (Ed.), Forensic uses of clinical assessment instruments (pp. 229–262). Routledge.
Albee, G. W., & Ryan-Finn, K. D. (1993). An overview of primary prevention. Journal of Counseling & Development, 72(2), 115–123. https://doi.org/10.1002/j.1556-6676.1993.tb00909.x
Althoff, R. R., Crehan, E. T., He, J.-P., Burstein, M., Hudziak, J. J., & Merikangas, K. R. (2016). Disruptive mood dysregulation disorder at ages 13–18: Results from the National Comorbidity Survey—Adolescent Supplement. Journal of Child and Adolescent Psychopharmacology, 26(2), 107–113. https://doi.org/10.1089/cap.2015.0038
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Asscher, J. J., Deković, M., Manders, W. A., van der Laan, P. H., Prins, P. J. M., & Dutch MST Cost-Effectiveness Study Group. (2013). A randomized controlled trial of the effectiveness of multisystemic therapy in the Netherlands: Post-treatment changes and moderator effects. Journal of Experimental Criminology, 9, 169–187. https://doi.org/10.1007/s11292-012-9165-9
Axelson, D., Findling, R. L., Fristad, M. A., Kowatch, R. A., Youngstrom, E. A., Horwitz, S. M., Arnold, L. E., Frazier, T. W., Ryan, N., Demeter, C., Gill, M. K., Hauser-Harrington, J. C., Depew, J., Kennedy, S. M., Gron, B. A., Rowles, B. M., & Birmaher, B. (2012). Examining the proposed disruptive mood dysregulation disorder diagnosis in children in the Longitudinal Assessment of Manic Symptoms Study. The Journal of Clinical Psychiatry, 73(10), 1342–1350. https://doi.org/10.4088/JCP.12m07674
Baweja, R., Belin, P. J., Humphrey, H. H., Babocsai, L., Pariseau, M. E., Waschbusch, D. A., Hoffman, M. T., Akinnusi, O. O., Haak, J. L., Pelham, W. E., & Waxmonsky, J. G. (2016). The effectiveness and tolerability of central nervous system stimulants in school-age children with attention-deficit/hyperactivity disorder and disruptive mood dysregulation disorder across home and school. Journal of Child and Adolescent Psychopharmacology, 26(2), 154–163. https://doi.org/10.1089/cap.2015.0053
Baweja, R., Mayes, S. D., Hameed, U., & Waxmonsky, J. G. (2016). Disruptive mood dysregulation disorder: Current insights. Neuropsychiatric Disease and Treatment, 12, 2115–2124. https://doi.org/10.2147/NDT.S100312
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Manual for the Beck Depression Inventory-II (2nd ed.). Psychological Corporation.
Benarous, X., Consoli, A., Guilé, J.-M., de La Rivière, S. G., Cohen, D., & Olliac, B. (2017). Evidence-based treatments for youths with severely dysregulated mood: A qualitative systematic review of trials for SMD and DMDD. European Child & Adolescent Psychiatry, 26, 5–23. https://doi.org/10.1007/s00787-016-0907-5
Biederman, J., Mick, E., Faraone, S. V., Spencer, T., Wilens, T. E., & Wozniak, J. (2000). Pediatric mania: A developmental subtype of bipolar disorder? Biological Psychiatry, 48(6), 458–466.
https://doi.org/10.1016/S0006-3223(00)00911-2
Blader, J. C., Pliszka, S. R., Kafantaris, V., Sauder, C., Posner, J., Foley, C. A., Carlson, G. A., Crowell, J. A., & Margulies, D. M. (2016). Prevalence and treatment outcomes of persistent negative mood among children with attention-deficit/hyperactivity disorder and aggressive behavior. Journal of Child and Adolescent Psychopharmacology, 26(2), 164–173. https://doi.org/10.1089/cap.2015.0112
Brotman, M. A., Kircanski, K., & Leibenluft, E. (2017). Irritability in children and adolescents. Annual Review of Clinical Psychology, 13, 317–341. https://doi.org/10.1146/annurev-clinpsy-032816-044941
Bruno, A., Celebre, L., Torre, G., Pandolfo, G., Mento, C., Cedro, C., Zoccali, R. A., & Muscatello, M. R. A. (2019). Focus on disruptive mood dysregulation disorder: A review of the literature. Psychiatry Research, 279, 323–330. https://doi.org/10.1016/j.psychres.2019.05.043
Carlson, G. A. (1998). Mania and ADHD: Comorbidity or confusion. Journal of Affective Disorders, 51(2), 177–187. https://doi.org/10.1016/s0165-0327(98)00179-7
Carter, S. E., Ong, M. L., Simons, R. L., Gibbons, F. X., Lei, M. K., & Beach, S. R. H. (2019). The effect of early discrimination on accelerated aging among African Americans. Health Psychology, 38(11), 1010–1013. https://doi.org/10.1037/hea0000788
Castells, X., Ramon, M., Cunill, R., Olivé, C., & Serrano, D. (2020). Relationship between treatment duration and efficacy of pharmacological treatment for ADHD: A meta-analysis and meta-regression of 87 randomized controlled clinical trials. Journal of Attention Disorders, 25(10), 1352–1361.
https://doi.org/10.1177/1087054720903372
Chase, D., Harvey, P. D., & Pogge, D. L. (2020). Disruptive mood dysregulation disorder (DMDD) in psychiatric inpatient child admissions: Prevalence among consecutive admissions and in children receiving NOS diagnoses. Neurology, Psychiatry and Brain Research, 38, 102–106. https://doi.org/10.1016/j.npbr.2020.11.001
Cianchetti, C., Pittau, A., Carta, V., Campus, G., Littarru, R., Ledda, M. G., Zuddas, A., & Fancello, G. S. (2013). Child and Adolescent Behavior Inventory (CABI): A new instrument for epidemiological studies and pre-clinical evaluation. Clinical Practice and Epidemiology in Mental Health, 9, 51–61. https://doi.org/10.2174/1745017901309010051
Conners, C. K. (1999). Conners Rating Scales-Revised. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (1st ed., pp. 467–495). Lawrence Erlbaum.
Copeland, W. E., Angold, A., Costello, E. J., & Egger, H. (2013). Prevalence, comorbidity, and correlates of DSM-5 proposed disruptive mood dysregulation disorder. The American Journal of Psychiatry, 170(2), 173–179. https://doi.org/10.1176/appi.ajp.2012.12010132
Copeland, W. E., Shanahan, L., Egger, H., Angold, A., & Costello, E. J. (2014). Adult diagnostic and functional outcomes of DSM-5 disruptive mood dysregulation disorder. American Journal of Psychiatry, 171(6), 668–674. https://doi.org/10.1176/appi.ajp.2014.13091213
Costin, J., & Chambers, S. M. (2007). Parent management training as a treatment for children with oppositional defiant disorder referred to a mental health clinic. Clinical Child Psychology and Psychiatry, 12(4), 511–524. https://doi.org/10.1177/1359104507080979
Derella, O. J., Burke, J. D., Romano-Verthelyi, A. M., Butler, E. J., & Johnston, O. G. (2020). Feasibility and acceptability of a brief cognitive-behavioral group intervention for chronic irritability in youth. Clinical Child Psychology and Psychiatry, 25(4), 778–789. https://doi.org/10.1177/1359104520918331
Evans, S. C., Burke, J. D., Roberts, M. C., Fite, P. J., Lochman, J. E., de la Pena, F. R., & Reed, G. M. (2017). Irritability in child and adolescent psychopathology: An integrative review for ICD-11. Clinical Psychology Review, 53, 29–45. https://doi.org/10.1016/j.cpr.2017.01.004
Evans, S. C., Weisz, J. R., Carvalho, A. C., Garibaldi, P. M., Bearman, S. K., Chorpita, B. F., & The Research Network on Youth Mental Health. (2020). Effects of standard and modular psychotherapies in the treatment of youth with severe irritability. Journal of Consulting and Clinical Psychology, 88(3), 255–268. https://doi.org/10.1037/ccp0000456
Evans, S. W., Owens, J. S., & Bunford, N. (2014). Evidence-based psychosocial treatments for children and adolescents with attention-deficit/hyperactivity disorder. Journal of Clinical Child & Adolescent Psychology, 43(4), 527–551. https://doi.org/10.1080/15374416.2013.850700
Fadus, M. C., Ginsburg, K. R., Sobowale, K., Halliday-Boykins, C. A., Bryant, B. E., Gray, K. M., & Squeglia, L. M. (2020). Unconscious bias and the diagnosis of disruptive behavior disorders and ADHD in African American and Hispanic youth. Academic Psychiatry, 44, 95–102. https://doi.org/10.1007/s40596-019-01127-6
Freeman, A. J., Youngstrom, E. A., Youngstrom, J. K., & Findling, R. L. (2016). Disruptive mood dysregulation disorder in a community mental health clinic: Prevalence, comorbidity and correlates. Journal of Child and Adolescent Psychopharmacology, 26(2), 123–130. https://doi.org/10.1089/cap.2015.0061
Garb, H. N. (1998). Studying the clinician: Judgment research and psychological assessment. American Psychological Association.
Greene, R. W., Ablon, J. S., Goring, J. C., Raezer-Blakely, L., Markey, J., Monuteaux, M. C., Henin, A., Edwards, G., & Rabbitt, S. (2004). Effectiveness of collaborative problem solving in affectively dysregulated children with oppositional-defiant disorder: Initial findings. Journal of Consulting and Clinical Psychology, 72(6), 1157–1164. https://doi.org/10.1037/0022-006X.72.6.1157
Haller, S. P., Kircanski, K., Stringaris, A., Clayton, M., Bui, H., Agorsor, C., Cardenas, S. I., Towbin, K. E., Pine, D. S., Leibenluft, E., & Brotman, M. A. (2020). The Clinician Affective Reactivity Index: Validity and reliability of a clinician-rated assessment of irritability. Behavior Therapy, 51(2), 283–293. https://doi.org/10.1016/j.beth.2019.10.005
Hatchett, G. T., & Motley, N. R. (2016). Bipolar and related disorders. In B. Flamez and C. J. Sheperis (Eds.), Diagnosing and treating children and adolescents: A guide for mental health professionals (pp. 177–202). Wiley.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., Williamson, D., & Ryan, N. (1997). Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of the American Academy of Child & Adolescent Psychiatry, 36(7), 980–988. https://doi.org/10.1097/00004583-199707000-00021
Lacasse, J. R. (2014). After DSM-5: A critical mental health research agenda for the 21st century. Research on Social Work Practice, 24(1), 5–10. https://doi.org/10.1177/1049731513510048
Leibenluft, E. (2011). Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths. The American Journal of Psychiatry, 168(2), 129–142. https://doi.org/10.1176/appi.ajp.2010.10050766
Leibenluft, E., Charney, D. S., Towbin, K. E., Bhangoo, R. K., & Pine, D. S. (2003). Defining clinical phenotypes of juvenile mania. The American Journal of Psychiatry, 160(3), 430–437. https://doi.org/10.1176/appi.ajp.160.3.430
Linke, J., Kircanski, K., Brooks, J., Perhamus, G., Gold, A. L., & Brotman, M. A. (2020). Exposure-based cognitive-behavioral therapy for disruptive mood dysregulation disorder: An evidence-based case study. Behavior Therapy, 51(2), 320–333. https://doi.org/10.1016/j.beth.2019.05.007
Malhi, G. S., & Bell, E. (2019). Fake views: DMDD, indeed! Australian & New Zealand Journal of Psychiatry, 53(7), 706–710. https://doi.org/10.1177/0004867419863162
Mayes, S. D., Mathiowetz, C., Kokotovich, C., Waxmonsky, J., Baweja, R., Calhoun, S. L., & Bixler, E. O. (2015). Stability of disruptive mood dysregulation disorder symptoms (irritable-angry mood and temper outbursts) throughout childhood and adolescence in a general population sample. Journal of Abnormal Child Psychology, 43, 1543–1549. https://doi.org/10.1007/s10802-015-0033-8
Mayes, S. D., Waxmonsky, J. D., Calhoun, S. L., & Bixler, E. O. (2016). Disruptive mood dysregulation disorder symptoms and association with oppositional defiant and other disorders in a general population child sample. Journal of Child and Adolescent Psychopharmacology, 26(2), 101–106. https://doi.org/10.1089/cap.2015.0074
Mayes, S. D., Waxmonsky, J., Calhoun, S. L., Kokotovich, C., Mathiowetz, C., & Baweja, R. (2015). Disruptive mood dysregulation disorder (DMDD) symptoms in children with autism, ADHD, and neurotypical development and impact of co-occurring ODD, depression, and anxiety. Research in Autism Spectrum Disorders, 18, 64–72. https://doi.org/10.1016/j.rasd.2015.07.003
Miller, L., Hlastala, S. A., Mufson, L., Leibenluft, E., Yenokyan, G., & Riddle, M. (2018). Interpersonal psychotherapy for mood and behavior dysregulation: Pilot randomized trial. Depression and Anxiety, 35(6), 574–582. https://doi.org/10.1002/da.22761
Minsky, S., Petti, T., Gara, M., Vega, W., Lu, W., & Kiely, G. (2006). Ethnicity and clinical psychiatric diagnosis in childhood. Administration and Policy in Mental Health and Mental Health Services Research, 33, 558–567. https://doi.org/10.1007/s10488-006-0069-8
Moreno, C., Laje, G., Blanco, C., Jiang, H., Schmidt, A. B., & Olfson, M. (2007). National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Archives of General Psychiatry, 64(9), 1032–1039. https://doi.org/10.1001/archpsyc.64.9.1032
Mouzon, D. M., Taylor, R. J., Woodward, A. T., & Chatters, L. M. (2017). Everyday racial discrimination, everyday non-racial discrimination, and physical health among African-Americans. Journal of Ethnic & Cultural Diversity in Social Work, 26(1–2), 68–80. https://doi.org/10.1080/15313204.2016.1187103
Ozyurt, G., Emiroglu, N., Baykara, B., & Akay Pekcanlar, A. (2017). Effectiveness and adverse effects of methylphenidate treatment in children diagnosed with disruptive mood dysregulation disorder and attention-deficit hyperactivity disorder: A preliminary report. Psychiatry and Clinical Psychopharmacology, 27(1), 99–100. https://doi.org/10.1080/24750573.2017.1293252
Pan, P.-Y., Fu, A.-T., & Yeh, C.-B. (2018). Aripiprazole/methylphenidate combination in children and adolescents with disruptive mood dysregulation disorder and attention-deficit/hyperactivity disorder: An open-label study. Journal of Child and Adolescent Psychopharmacology, 28(10), 682–689. https://doi.org/10.1089/cap.2018.0068
Parker, G., & Tavella, G. (2018). Disruptive mood dysregulation disorder: A critical perspective. The Canadian Journal of Psychiatry, 63(12), 813–815. https://doi.org/10.1177/0706743718789900
Perepletchikova, F., Nathanson, D., Axelrod, S. R., Merrill, C., Walker, A., Grossman, M., Rebeta, J., Scahill, L., Kaufman, J., Flye, B., Mauer, E., & Walkup, J. (2017). Randomized clinical trial of dialectical behavior therapy for preadolescent children with disruptive mood dysregulation disorder: Feasibility and outcomes. Journal of the American Academy of Child & Adolescent Psychiatry, 56(10), 832–840. https://doi.org/10.1016/j.jaac.2017.07.789
Rao, U. (2014). DSM-5: Disruptive mood dysregulation disorder. Asian Journal of Psychiatry, 11, 119–123. https://doi.org/10.1016/j.ajp.2014.03.002
Regier, D. A., Narrow, W. E., Clarke, D. E., Kraemer, H. C., Kuramoto, S. J., Kuhl, E. A., & Kupfer, D. J. (2013). DSM-5 field trials in the United States and Canada, part II: Test-retest reliability of selected categorical diagnoses. The American Journal of Psychiatry, 170(1), 59–70. https://doi.org/10.1176/appi.ajp.2012.12070999
Rice, T., Simon, H., Barcak, D., Maiyuran, H., Chan, V., Hassan, Y., Tatum, J., & Coffey, B. J. (2019). Amantadine for treatment of disruptive mood dysregulation disorder symptoms. Journal of Child and Adolescent Psychopharmacology, 29(8), 642–646. https://doi.org/10.1089/cap.2019.29172.bjc
Rich, B. A., Bhangoo, R. K., Vinton, D. T., Berghorst, L. H., Dickstein, D. P., Grillon, C., Davidson, R. J., & Leibenluft, E. (2005). Using affect-modulated startle to study phenotypes of pediatric bipolar disorder. Bipolar Disorders, 7(6), 536–545. https://doi.org/10.1111/j.1399-5618.2005.00265.x
Roy, A. K., Lopes, V., & Klein, R. G. (2014). Disruptive mood dysregulation disorder: A new diagnostic approach to chronic irritability in youth. American Journal of Psychiatry, 171(9), 918–924.
https://doi.org/10.1176/appi.ajp.2014.13101301
Sitarenios, G., & Kovacs, M. (1999). Use of the Children’s Depression Inventory. In M. E. Maruish (Ed.), The use of psychological testing for treatment planning and outcomes assessment (1st ed., pp. 267–298). Lawrence Erlbaum.
Stringaris, A., Baroni, A., Haimm, C., Brotman, M., Lowe, C. H., Myers, F., Rustgi, E., Wheeler, W., Kayser, R., Towbin, K., & Leibenluft, E. (2010). Pediatric bipolar disorder versus severe mood dysregulation: Risk for manic episodes on follow-up. Journal of the American Academy of Child & Adolescent Psychiatry, 49(4), 397–405. https://doi.org/10.1016/j.jaac.2010.01.013
Stringaris, A., Cohen, P., Pine, D. S., & Leibenluft, E. (2009). Adult outcomes of youth irritability: A 20-year prospective community-based study. The American Journal of Psychiatry, 166(9), 1048–1054.
https://doi.org/10.1176/appi.ajp.2009.08121849
Stringaris, A., & Goodman, R. (2009). Longitudinal outcome of youth oppositionality: Irritable, headstrong, and hurtful behaviors have distinctive predictions. Journal of the American Academy of Child & Adolescent Psychiatry, 48(4), 404–412. https://doi.org/10.1097/CHI.0b013e3181984f30
Stringaris, A., Goodman, R., Ferdinando, S., Razdan, V., Muhrer, E., Leibenluft, E., & Brotman, M. A. (2012). The Affective Reactivity Index: A concise irritability scale for clinical and research settings. Journal of Child Psychology and Psychiatry, 53(11), 1109–1117. https://doi.org/10.1111/j.1469-7610.2012.02561.x
Stringaris, A., Vidal-Ribas, P., Brotman, M. A., & Leibenluft, E. (2018). Practitioner review: Definition, recognition, and treatment challenges of irritability in young people. Journal of Child Psychology and Psychiatry, 59(7), 721–739. https://doi.org/10.1111/jcpp.12823
Sukhodolsky, D. G., & Scahill, L. (2012). Cognitive-behavioral therapy for anger and aggression in children. Guilford.
Sukhodolsky, D. G., Smith, S. D., McCauley, S. A., Ibrahim, K., & Piasecka, J. B. (2016). Behavioral interventions for anger, irritability, and aggression in children and adolescents. Journal of Child and Adolescent Psychopharmacology, 26(1), 58–64. https://doi.org/10.1089/cap.2015.0120
Tobler, A. L., Maldonado-Molina, M. M., Staras, S. A. S., O’Mara, R. J., Livingston, M. D., & Komro, K. A. (2013). Perceived racial/ethnic discrimination, problem behaviors, and mental health among minority urban youth. Ethnicity & Health, 18(4), 337–349. https://doi.org/10.1080/13557858.2012.730609
Tourian, L., LeBoeuf, A., Breton, J.-J., Cohen, D., Gignac, M., Labelle, R., Guile, J.-M., & Renaud, J. (2015). Treatment options for the cardinal symptoms of disruptive mood dysregulation disorder. Journal of the Canadian Academy of Child and Adolescent Psychiatry, 24(1), 41–54.
Towbin, K., Axelson, D., Leibenluft, E., & Birmaher, B. (2013). Differentiating bipolar disorder–not otherwise specified and severe mood dysregulation. Journal of the American Academy of Child & Adolescent Psychiatry, 52(5), 466–481. https://doi.org/10.1016/j.jaac.2013.02.006
Towbin, K., Vidal-Ribas, P., Brotman, M. A., Pickles, A., Miller, K. V., Kaiser, A., Vitale, A. D., Engel, C., Overman, G. P., Davis, M., Lee, B., McNeil, C., Wheeler, W., Yokum, C. H., Haring, C. T., Roule, A., Wambach, C. G., Sharif-Askary, B., Pine, D. S, . . . Stringaris, A. (2020). A double-blind randomized placebo-controlled trial of citalopram adjunctive to stimulant medication in youth with chronic severe irritability. Journal of the American Academy of Child & Adolescent Psychiatry, 59(3), 350–361. https://doi.org/10.1016/j.jaac.2019.05.015
Tudor, M. E., Ibrahim, K., Bertschinger, E., Piasecka, J., & Sukhodolsky, D. G. (2016). Cognitive-behavioral therapy for a 9-year-old girl with disruptive mood dysregulation disorder. Clinical Case Studies, 15(6), 459–475. https://doi.org/10.1177/1534650116669431
Van Meter, A. R., Moreira, A. L. R., & Youngstrom, E. A. (2011). Meta-analysis of epidemiologic studies of pediatric bipolar disorder. The Journal of Clinical Psychiatry, 72(9), 1250–1256. https://doi.org/10.4088/JCP.10m06290
Weisz, J. R., & Kazdin, A. E. (Eds.). (2017). Evidence-based psychotherapies for children and adolescents (3rd ed.). Guilford.
Wiggins, J. L., Brotman, M. A., Adleman, N. E., Kim, P., Oakes, A. H., Reynolds, R. C., Chen, G., Pine, D. S., & Leibenluft, E. (2016). Neural correlates of irritability in disruptive mood dysregulation and bipolar disorders. The American Journal of Psychiatry, 173(7), 722–730. https://doi.org/10.1176/appi.ajp.2015.15060833
Winters, D. E., Fukui, S., Leibenluft, E., & Hulvershorn, L. A. (2018). Improvements in irritability with open-label methylphenidate treatment in youth with comorbid attention deficit/hyperactivity disorder and disruptive mood dysregulation disorder. Journal of Child and Adolescent Psychopharmacology, 28(5), 298–305. https://doi.org/10.1089/cap.2017.0124
World Health Organization. (2016). International statistical classification of diseases and related health problems (10th ed.). https://icd.who.int/browse10/2016/en
World Health Organization. (2019). International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int
Gregory T. Hatchett, PhD, NCC, LPCC-S, is a professor at Northern Kentucky University. Correspondence may be addressed to Gregory T. Hatchett, MEP 211, Highland Heights, KY 41099, hatchettg@nku.edu.
Nov 9, 2021 | Volume 11 - Issue 4
Charles F. Shepard, Darius A. Green, Karli M. Fleitas, Debbie C. Sturm
This qualitative grounded theory study is the first of its kind aimed at understanding the decision-making process of parents and guardians of transgender and gender-diverse (TGD) youth providing informed consent for their children to undergo gender-confirming endocrinological interventions (GCEI), such as hormone replacement therapy and puberty blockers. Using primarily intensive interviews supported by observational field notes and document review, this study examined the decision-making processes of a national sample of participants who identified as a parent or legal guardian of at least one TGD youth and who have given informed consent for the youth in their care to undergo GCEI. A variety of inhibiting and contributing factors were illuminated as well as a “dissonance-to-consonance” model that participants used to combine contributing factors to overcome inhibitors and grant informed consent. Implications for professional counseling practitioners are discussed, including guidance for direct services, gatekeeping, case management, and advocacy functions.
Keywords: transgender, gender-diverse, youth, decision-making, intervention
One of the more controversial topics currently addressed in professional counseling involves gender identity and access for gender-confirming interventions for transgender or otherwise gender-diverse (TGD) youth. Since academic journals began publishing studies of the experiences of people expressing what today could be considered gender expansiveness in the late 19th century (Drescher, 2010), there has been considerable struggle in Western culture to understand the constructs of gender identity and expression and the implications that these aspects of human development present for mental and physical health. In the United States, controversy around pathologizing TGD identity or normalizing and affirming it has influenced popular and professional opinions since the early 20th century (Drescher, 2010; Stryker, 2008). Within the past decade, TGD identity has been associated with pervasive patterns of mistreatment and discrimination across social, educational, occupational, legal, and health care experiences in the United States (James et al., 2016).
Transgender Health Care in the United States
TGD people have been shown to be overrepresented in populations associated with negative mental, physical, and social health outcomes, such as those suffering from suicidality and homelessness (James et al., 2016). Among transgender older adolescents and young adults, 25% to 32% have reported attempting suicide (Grossman & D’Augelli, 2007), while the national rate for attempted suicide is 4.6% (James et al., 2016). According to the Lesbian, Gay, Bisexual, and Transgender (LGBT) Homeless Youth Survey (Durso & Gates, 2012), LGBT youth comprised 40% of the populations served by 354 agencies serving homeless youth. Of the 381 youth that responded to the survey, 46% reported that they ran away from home because of family rejection of their affectional orientation or gender identity, and 43% reported that they were forced out by their parents because of their affectional orientation or gender identity.
According to the 2015 U.S. Transgender Survey, TGD people have also had their access to health care limited by stigma and discrimination by health care providers (James et al., 2016). One-third (33%) of respondents reported experiencing at least one negative experience with a health care provider in relation to their gender identity, and nearly a quarter (23%) did not seek services for fear of being mistreated. One-third (33%) did not seek health care because of an inability to afford the cost of TGD-specific or other services. These disparities are among the many motivators of the current movement to make health care, and professional counseling in particular, more affirming of TGD people (Rose et al., 2019; Vincent, 2019).
Factors Influencing Rejection and Affirmation of TGD Identity
Factors that support the pathologization of TGD identity and behavior find their roots across a variety of intersecting segments of American society. One of the more prominent influencers of these practices in the United States has been religion (Drescher, 2010; Stryker, 2008; Vines, 2014). More than 70% of the U.S. population identifies as Christian, with more than half the population practicing Christianity as members of evangelical denominations, which have been associated with traditionally rejecting attitudes toward lesbian, gay, bisexual, transgender, queer, questioning, intersex, asexual, and pansexual (LGBTQ+) people and behavior (Pew Research Center, 2014; Vines, 2014). Chronic suicidal thinking among LGBT people ages 18 to 24 has been associated with parents’ rejecting religious beliefs, and fears about being forced to leave one’s religion have been associated with a suicide attempt within a 12-month period for the same population (Gibbs & Goldbach, 2015).
Religion has been closely associated with recent changes in state legislation and federal policy that suggest that disparities in the treatment of TGD people are socially and professionally acceptable. At least four states (Arkansas, Montana, Ohio, and South Dakota) have passed legislation that has included what is known as a conscience clause that could impede access to health care for LGBTQ+ people (Dailey, 2017; Goodkind, 2021; Rose et al., 2019). These health care–related laws have allowed legal protection for health care providers, sometimes specifically addressing professional counselors, who refuse services to clients who request help in ways that conflict with the provider’s particular religious beliefs (Dailey, 2017; Rose et al., 2019). In 2018, conscience clause–type considerations were expanded to the federal level when the U.S. Department of Health and Human Services (DHHS) created the Conscience and Religious Freedom Division (CRFD) in the DHHS Office for Civil Rights (DHHS, 2018a). At the time, CRFD policy explicitly cited protections for health care practitioners who declined to provide services related to abortion and assisted suicide (DHHS, 2018b); however, some noted that the division’s loose language could have left room for health care providers to deliver sub-standard care for LGBTQ+ clients as well (Gonzalez, 2018; Rose et al., 2019). In fact, a DHHS spokesperson stated at the time that the department would not interpret prohibitions on sex discrimination in health care to cover gender identity (Gonzalez, 2018). It should be noted that federal protections of TGD individuals in health care were restored in 2021 (Shabad, 2021).
Awareness of Gender Diversity
The general beginnings of the social consciousness of gender diversity in the United States can be traced to the attention that Christine Jorgensen commanded during her transition in the 1950s (Drescher, 2010; Stryker, 2008). Jorgensen was a U.S. Army veteran who served during World War II and travelled to Europe to undergo orchiectomy and penectomy procedures. Upon her return to the United States, she underwent vaginoplasty and became a preeminent advocate for LGBTQ+ rights (Drescher, 2010; Jorgensen, 1967; Stryker, 2008). About a decade later, physician Harry Benjamin pioneered gender-confirming endocrinological interventions (GCEI) aimed at medically supporting TGD patients who wished to feminize or masculinize their bodies to be more congruent with their gender identity without surgery (Drescher, 2010; Stryker, 2008). The most popular forms of GCEI—cross-sex hormone replacement therapy and gonadotropin-releasing hormone analogues or “puberty blockers”—have been associated with positive physical and mental health outcomes (Bränström & Pachankis, 2020; Couric, 2017; Drescher, 2010; Murad et al., 2010) and have been made available to people from pre-puberty through late adulthood (E. Coleman et al., 2012; Hembree et al., 2017).
Nearly all the research regarding GCEI has been conducted on adults (Couric, 2017), and the experiences of parents of TGD youth are not well represented in the literature (Hill & Menvielle, 2009), despite the growing popularity of GCEI among TGD minors (Couric, 2017; Drescher, 2010; Pew Research Center, 2013; Rosin, 2008). In the United States, minors are almost always dependent on their parents or legal guardians to provide informed consent for GCEI (Burt, 2016; D. L. Coleman, 2019; D. L. Coleman & Rosoff, 2013) even though they are likely to be considered by the medical profession to be cognitively capable of making an informed choice to undergo hormone-related treatments (E. Coleman et al., 2012; Hembree et al., 2017). At least one study that intends to contribute to the literature on the long-term risks and benefits of GCEI on minors is ongoing but not complete as of this publication (Bunim, 2015; S. Rosenthal, personal communication, November 7, 2019). This leaves both TGD youth and their parents—who are unlikely to share their child’s gender identity—in the precarious position of making meaningful decisions about the youth’s mental and physical health in a climate dominated by legal, political, religious, and social trends and without a body of rigorous research to instill confidence in giving or denying consent for GCEI.
Role of Professional Counselors
Partially for the reasons stated above, professional counselors who work with TGD youth and their families have unique opportunities to serve their clients at the micro-, meso-, and macrolevels. With professional emphases on human development, the helping relationship, and social justice (Lawson, 2016), counselors have an ethical obligation to develop competencies related to addressing issues concerned with gender identity, spirituality, and social systems to enable the empowerment of clients through individual, group, and family counseling in addition to interprofessional consultation and advocacy (American Counseling Association [ACA], 2014; Burnes et al., 2010; Cashwell & Watts, 2010; Ratts et al., 2015; Toporek & Daniels, 2018). ACA’s stance that TGD identity is a normal part of human development and should be affirmed (Burnes et al., 2010) aligns with the positions of every major health care professional organization globally (Drescher, 2010). Professional counselors are likely to be presented with opportunities to provide psychoeducation about gender identity development and best practices regarding the affirmative care of TGD clients as well as opportunities to advocate for their clients through the writing of referral letters for GCEI (E. Coleman et al., 2012). It is not uncommon, however, for professional counselors to challenge this obligation, especially when they feel compelled to prioritize religious teachings that pathologize LGBTQ+ identity (Kaplan, 2018; Rose et al., 2019).
The Purpose of the Present Study
The purpose of this research was to explore the process by which parents or legal guardians of TGD youth develop affirmative understandings and approaches to their children’s gender identity, affirm their related transition needs, and grant informed consent for the TGD youth in their care to undergo GCEI. With that in mind, the primary research question of this grounded theory study was, How did the parents of TGD youth who have undergone GCEI decide to give informed consent? Secondarily, are there specific themes that emerge for Christian, heterosexual, cisgender parents who go through this process? Finally, what part, if any, did a professional counselor play in the process?
Method
A qualitative grounded theory method was employed because this method is used to understand how participants go about resolving a particular concern or dilemma (Charmaz, 2014; Glaser & Strauss, 1967). Unlike other forms of qualitative research, grounded theory guides the researcher with a set of general principles, guidelines, strategies, and heuristic devices rather than formulaic prescriptions to help the researcher direct, manage, and streamline data collection so that analyses and emerging theory are well grounded in the collected data (Charmaz, 2014). For the purposes of this study, we followed prescribed grounded theory protocols for data collection, analysis, and trustworthiness (Charmaz, 2014; Corbin & Strauss, 2015; Creswell, 2013; Merriam & Tisdell, 2016).
Participants
Following IRB approval, a snowball sampling method (Creswell, 2013; Merriam & Tisdell, 2016) was employed to recruit a purposive sample of adult participants who (a) self-identified as a parent and/or legal guardian of a person who self-identifies as TGD and (b) have given informed consent for their TGD child to receive GCEI. Study information and a request for assistance with identifying participants was disseminated to national organizations that advocate for TGD rights such as the Society for Affectional, Intersex, and Gender Expansive Identities (SAIGE), Parents and Friends of Lesbians and Gays (PFLAG), and Transparent USA. Prospective participants were asked to contact the researcher and forward the information to others that they believed met the study criteria. Participant screening consisted of an online Qualtrics survey that included confidentiality and informed consent information, inclusion criteria, and demographic items. Once identified, participants were asked to participate in initial intensive interviews.
Theoretical sampling (Charmaz, 2014) is the preferred strategy for grounded theory because it allows emerging themes to direct simple decisions until saturation is met (i.e., no new information is being detected). In this study, saturation was met at the 16th interview and confirmed in the 17th. Table 1 details the sociodemographic characteristics of the participants, the majority of which identified as cisgender women (n = 13), White (n = 16), married (n = 14), college educated (n = 17), and employed full-time (n = 12). Participants’ ages ranged between 32 and 61 years with a mean age of 49 (see Table 2). The participants made up a national sample (see Table 3), both in regard to region of birth and region of residence. As Table 4 shows, a near majority identified as mainline Protestant Christian (n = 8). The majority had one TGD child (n = 13), and the children’s ages at which the participants gave consent for GCEI ranged from 10 to 18 years (M = 13.93; see Table 2).
Instrumentation and Data Collection
Because the main emphasis of this study was to understand parents’ decision-making processes, intensive interviews were the main instrument of data collection. Environmental observation and document reviews were conducted when they were accessible. To protect the participants’ confidentiality, each was randomly assigned a pseudonym. Additionally, interviews—which lasted between 30 and 75 minutes—were facilitated through telehealth video conferencing software that complied with the Health Information Portability and Accountability Act of 1996 (HIPAA). Electronic recordings of interviews were stored on a HIPAA-compliant version of an internet-based file hosting service, and transcription was provided by a company that provides confidential transcription services.
Table 1
Sociodemographic Characteristics of Participants
| Demographic characteristic* n % |
| Gender |
| Cisgender Women 13 76.5 |
| Cisgender Men 4 23.5 |
| Ethnicity
White 16 94.1
Mixed-race 1 0.1 |
| Marital Status |
| Married 14 82.4 |
| Divorced 2 11.8 |
| Separated 1 5.8 |
|
| Highest level of education |
| Some college 3 17.6 |
| Associates degree 2 11.8 |
| Bachelor’s degree 5 29.4 |
| Master’s degree 3 17.6 |
| Doctoral degree 4 23.5 |
|
| Employment status |
| Employed full-time 12 70.6 |
| Employed part-time 5 29.4 |
|
| Professional identity |
| Office/clerical 1 5.8 |
| Sales/marketing 2 11.8 |
| Professional 9 52.9 |
| Mid-level management 2 11.8 |
| Upper-level management/ 1 5.8 |
| business owner |
| Other 2 11.8
Household annual income
More than $90,000 9 52.9
$60,001 to $90,000 6 35.3
$35,000 to $60,000 2 11.8 |
Note. N = 17.
*Participants were asked to identify across a variety of different gender identities, relationship statuses, educational statuses, employment statuses, professional identities, and income statuses. Only the identities or statuses selected by participants are shown. |
Table 2
Relevant Ages
|
M |
Range |
| Current age of parents |
49 |
32–61 |
| Current age of TGD child |
15.78 |
10–26 |
| Age of TGD child at time of consent |
13.93 |
10–18 |
Table 3
Participant Regions of Birth/Residence
| Region |
Place of birth |
% |
Place of residence |
% |
| Northeast |
1 |
5.8 |
0 |
0 |
| Mid-Atlantic |
6 |
35.3 |
12 |
70.6 |
| Midwest |
3 |
17.6 |
2 |
11.8 |
| Southeast |
4 |
23.5 |
1 |
5.8 |
| Southwest |
1 |
5.8 |
1 |
5.8 |
| Mountain West |
0 |
0 |
1 |
5.8 |
| Outside U.S. |
2 |
11.8 |
0 |
0 |
Note. N = 17
Table 4
Participant Religious Affiliation
| Affiliation |
n |
% |
| Christian (mainline Protestant) |
8 |
47.1 |
| Christian (Catholic) |
0 |
0 |
| Christian (Evangelical Protestant) |
0 |
0 |
| Muslim |
0 |
0 |
| Jewish |
1 |
5.8 |
| Agnostic |
2 |
11.8 |
| Atheist |
2 |
11.8 |
| Other/unaffiliated |
4 |
23.5 |
Based on Charmaz’s (2014) recommendations, the researchers developed an interview protocol (see Appendix) that was examined and confirmed for (a) its sensitivity to the experience of participants and (b) its capability for addressing the research questions at hand with two individuals who meet criteria for participation. One of the individuals was the executive director of a small, rural LGBTQ+ advocacy organization. The second was a professional counselor who works with TGD clients. Both were parents of at least one TGD child.
Analysis
The researchers used line-by-line coding of interview data and continuously compared new codes with those of previous interviews. Microsoft Excel software (version 16.44) was used for keeping track of the coding matrix. The coding matrix was reworked until a core theoretical category emerged that explained the underlying concepts inherent in the process under examination.
Trustworthiness
In qualitative research, a study’s rigor is typically measured by trustworthiness, or the consistency of the results with the data collected (Merriam & Tisdell, 2016). To support this process, we used a variety of strategies, including triangulation, member checks, and reflexivity (Corbin & Strauss, 2015; Creswell, 2013; Merriam & Tisdell, 2016). Triangulation was accomplished by the recruitment of two study auditors who conducted blind coding of data samples and reviewed the study design, procedures, and process of theory integration for accuracy (Creswell, 2013). Reflexivity involves the “critical self-reflection of the researcher regarding assumptions, worldview, biases, theoretical orientation and relationship to the study that may affect the investigation” (Merriam & Tisdell, 2016, p. 256). The first author and lead researcher, Charles F. Shepard, identifies as a White, cisgender, straight, middle-aged man who has lived his entire life in the Southeastern United States. He has been married for more than 14 years, and he is the father of two young children who were assigned female at birth. Shepard’s interest in the present topic is rooted in personal, academic, and professional experiences with conscience conflicts during the past three decades. The second author, Darius A. Green, served as an auditor and identifies as a Black, cisgender, straight, young adult man who has lived predominantly in the Southeastern United States. Green is a doctoral-level counselor educator who has conducted research and provided counseling with underrepresented populations. The third author, Karli M. Fleitas, served as the second auditor and identifies as a Japanese American, cisgender, straight, young adult woman who has lived predominantly in the Southeastern United States. Fleitas is a doctoral student in a counselor education program accredited by the Council for Accreditation of Counseling and Related Educational Programs who has clinical experience working with LGBTQ+ clients as well as certification with respect to diversity, equity, and inclusion practices. The fourth author, Debbie C. Sturm, served as the chairperson of Shepard’s dissertation committee and provided guidance to the research and reporting processes. Sturm identifies as a White, cisgender, straight, middle-aged woman who has lived between the Northeastern and Southeastern regions of the United States. She has conducted and supervised previous research relevant to LGBTQ+ concerns. We considered our identities and backgrounds throughout for their potential effect on the data collection and analysis processes.
Results
The major findings of this study included inhibitors and contributors to consent as well as a central theme, specifically how participants combined contributing factors to overcome inhibiting factors of the consent-giving process.
Inhibitors to Consent
Participants identified five major inhibitors to giving consent: (a) lack of knowledge and awareness of issues and concerns related to TGD identity, (b) fear, (c) doubt, (d) grief over a lost parenting narrative, and (e) rejection from healthcare providers (or payors) and parenting partners. To a lesser degree, lack of access to affirming care due to residential location and the cost of treatments were cited as notable experiences of participants.
Lack of Knowledge and Awareness
Of the participants, all but one (n = 16) reported that they lacked knowledge or awareness of the issues that TGD youth face when their children either came out to them, asked to participate in GCEI, or both. When asked what she knew about gender identity and/or gender expression prior to her child coming out, Jaylene (51), a White, cisgender woman divorced from her parenting partner, but remarried and living in the Southeast, stated:
Really not a lot, because I think that transgender people in the past were really colored as men who were sick and dressed like women. . . . I was kind of ignorant to it all, but I didn’t know I was ignorant is the thing.
Participants often cited their lack of knowledge as a key component of their fear over giving informed consent for their TGD child’s GCEI.
Fear
Participants reported experiencing fear on multiple levels in response to their child’s request to begin GCEI, including fear of negative future social experiences for their child, fear of the side effects of the treatments, and political fears. Of the 17 participants, 13 reported fears over negative future experiences. Hilda (50), a White, cisgender woman married to her parenting partner and residing in the Mid-Atlantic region, said, “It’s scary as hell. It’s terrifying. . . . It’s not that I’m fearful of who she is, I’m fearful of what the world is going to do to her.”
Similar to fear of future experiences for their children, 12 participants cited fear of the side effects of their child’s requested GCEI. Camilla (46), a White, cisgender woman separated from her partner and living in the Mid-Atlantic region, had similar concerns, stating that she “didn’t have a whole lot of information on how testosterone, for instance, would affect [my child] . . . . It was a concern of, ‘How does that affect the long-term health of my child?’ That’s actually a question that I still have.”
Finally, at least six participants communicated that fear related to the political climate inhibited their decision-making process. Honour (43), a White, cisgender woman divorced from her parenting partner and residing in the Mid-Atlantic region, recounted that political fears affected her and her child’s decision to request a subcutaneous implant, saying:
The physician seemed surprised and said, “Tell me more about why that’s your first choice.” And (child) says, “We have a presidential election coming up, and I don’t want to be in a situation where I start monthly or quarterly shot treatments only to have that right taken away from me. If they put a 2-year implant in my arm, they’re not going to come rip it out.”
Doubt
Although fewer than half of participants (n = 6) expressed doubt in the genuineness of their youth’s TGD identity, doubt was still considered a main inhibitor because each participant who described their doubt gave vivid descriptions thereof. Berta (48), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, provided the following example that was indicative of the sample’s experiences:
It was scary at first because everybody goes to the same place, which is scared for your child. And then, you know, maybe this is a phase? Maybe he’s confused? Maybe—you know? And so, you go through all those things.
Grief Over a Lost Parenting Narrative
The most prominent inhibiting factor not directly related to lack of knowledge leading to fear or doubt was participants’ description of grief over their lost parenting narrative. A majority of participants (n = 9) reported that the change in their expected future with their child came as a result of learning that their child identified as TGD. Adele (32), a White, cisgender woman married to her child’s father and living in the Mountain West region, described an internal conflict consistent with her peers:
There’s this creeping in of grief. . . . Even if you should be able to adapt, it’s still there. When we make these choices for hormone therapy, it’s kind of a step further in the direction of whatever could have been will definitely never be.
Rejection
A substantial subset of participants (n = 8) reported experiencing what could be considered some form of rejection, either from a parenting partner or a health care provider or payor. Of the six participants who reported that their parenting partner demonstrated signs of rejection, all were cisgender women; however, only two reported that their parenting partner maintained their rejecting stance in a way that ultimately put informed consent at risk (for legal reasons). Mellony (49), a White, cisgender woman married to her child’s father and living in the Mid-Atlantic region, recounted an experience that was more typical in the sample:
My husband was a little slower, in the beginning, to get on board. I just think he had a harder time—you know, “Is this really real? Is this a phase? Did she learn it on the internet? What’s really going on?”
Three participants described what they considered to be rejecting messages and/or behavior from health care providers. In response to a question about how a mental health professional was involved in her decision-making process, Journey (51), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, said that meeting with a counselor was one of the worst parts of the process, and they walked out of the session early:
One of the things that was concerning me at the time was, “How do I tell my younger children.” And she said, “Oh, I wouldn’t do that. He’s probably going to change his mind.” And so we said, “Well, OK, there’s a lot we don’t know, but that’s not the right answer.”
Adele described denials of reimbursement from her child’s insurance company as well as unwelcoming responses from front-desk workers at the clinic at which they were seeking treatment: “They seemed incredibly—I don’t know how to word it—off-putting in that, we were like, ‘one of those.’”
Lack of Access
A subset of participants reported a lack of access to affirming treatment. Five participants reported a lack of access due to their residential location; three reported it was due to insurmountable financial cost. Some drove several hours away and across state lines so that their child could receive treatment. Sharyn (47), a White, cisgender woman divorced from her child’s father and living in the Mid-Atlantic region, recounted that her ex-partner’s reluctance to give consent affected the cost of treatment, stating, “All we could do was a prescription to stop periods, which [was] about three or four times more expensive than hormones.”
Contributors to Consent
Participants identified four factors that contributed to giving consent: (a) parental attunement to the experiences and emotions of the youth in their care, (b) parental autonomy from their family of origin and religious communities, (c) access to affirming education about TGD issues and GCEI, (d) the presence and/or development of affirming relationships and community, and (e) affirming religious beliefs and/or community.
Parental Attunement to Youth’s Experience
The construct of parental attunement has been defined as a relational dynamic between parent and child that surpasses what is typically included in the construct of empathy. Erskine (1998) posited that attunement is a two-part process that includes (a) the ability to sense and to identify with another person’s sensations, needs, and feelings: and (b) communicating that sensitivity to the other person. A parent’s ability to attune to their child’s experience and emotional world has been prominently associated with the fostering of secure attachment and personality development (Ainsworth & Bowlby, 1991; Bowlby, 1988; Siegel, 2013; Wallin, 2007). Participants in the present study conveyed their ability to demonstrate parental attunement by describing their wishes for their TGD youth’s social and emotional well-being as a primary motivator for granting informed consent for them to undergo GCEI. Furthermore, participants implied respect for their youth’s autonomy, their recognition of their youth’s gender non-conformity, and their recognition of their youth’s mental health symptoms. Participants also recognized their own position of privilege that facilitated granting consent and a sense of their own autonomy from their families of origin or religious backgrounds.
One of the more striking examples of parental attunement in this sample was provided by Tony (61), a White, cisgender man married to his child’s mother and living in the Mid-Atlantic region, who tearfully recounted a conversation with his then–16-year-old child following a support group meeting:
I said, “You know, what would really help me is, could you write down your goals, what you want, and be honest with everything. We want to support you.” So, after we got home, within about two hours, [child] brought me something that I still have. . . . It says “Trans with the Plans.” And that was when I knew that this kid I love so much knew what they wanted, and I had to support them.
A notable subset of participants (n = 16) reported that they recognized their child’s rejection of binary gender norms prior to their child coming out to them. This recognition often came during early childhood. Hilda remembered noticing her child’s “Sunday best”:
I had [child] in her little dress shirt and tie and dress pants, and I told her to go get her dress shoes, and her little face lit up. She ran down the hall and came back in those little Cinderella shoes—so, [child] was always [child]. It just took us awhile to catch on.
Every participant recounted a recognition of and concern for their child’s mental health. Prudence (46), a mixed-race, cisgender woman married to her child’s father and living in the Southwest region, said that her child “came to us in the middle of the night, and I said, ‘Are you feeling suicidal?’ He didn’t respond verbally, but he just started crying. So I just pulled him in bed with me and I snuggled him.”
Parental Autonomy From Their Family of Origin or Religious Communities
A less frequent, but nonetheless notable, sign of parental attunement to the experience and emotions of their child was participants’ descriptions of how they prioritized the wishes and needs of their child and demonstrated autonomy from their families of origin (n = 10) or religious backgrounds (n = 4). Berta recounted planning with her partner how to break the news of their consent to extended family members:
[When] we told extended family, I was making the phone calls, but [my partner] reminded me, he said, “Remember, this is not a terminal illness.” It could be, right, if you don’t do it right, but just say, “We’re not asking permission, and we are not apologizing.” So, he kind of like, you know, held me up when we made those calls.
Brenda (48), a White, cisgender woman married to her parenting partner and living in the Mid-Atlantic region, described her experience within a religious community that had members that were reluctant to openly lend support and others who wanted to offer support but lacked the necessary knowledge and skill to do so. In recounting what led her and her family to leave their congregation at the time, she stated:
I did chat about it to anyone who asked and had hoped to educate and affect some positive change from within, but lots of folks just weren’t ready or willing to have these conversations. Which was interesting because this was all during the time when the [denomination] was making high-level decisions about whether or not to affirm LGBTQ folks.
Access to Affirming Community, Education, Health Care, and Parenting Partnership
All participants made at least some reference to having access to affirming (a) community of parents, professionals, colleagues, and/or friends; (b) education; (c) health care; and (d) parenting partnership. A key element of access to an affirming community was participants’ acknowledgement of possibility models. This term, which participants credited to prominent transgender actor Laverne Cox, refers to a person who identifies as TGD and has successfully gone through a medical transition, or a parent who has successfully supported their child through a medical transition. Possibility models were referenced when participants spoke about their experiences with family friends, support group members, professionals, and members of the mass media.
Participants were all members of affirming communities, and they reported that they received affirming education from group members and health care providers, including professional counselors. Adele reported the following about the support her child received from an affirming professional counselor during the process toward GCEI:
This counselor met her where she was and was using interventions geared toward just expressing herself. And I think it helped her to externalize what was happening, and then also, she was able to talk about the things that she was going through . . . because it was a space where there was no pressure.
Several participants reported that the counselors or mental health providers who wrote referral letters for their youth to begin GCEI were often closely associated with support groups they attended, completed gatekeeping procedures efficiently and without unexpected fees, had TGD-affirming staff and office procedures in place, and did not necessarily focus exclusively on gender identity.
Affirming Religious Beliefs and/or Community
Nearly half the participants (n = 8) identified as mainline Protestant Christians (i.e., members of denominations that have historically rejected fundamentalist practices) and reported that affirming religious beliefs contributed to their decision-making process. Emma (56), a White, cisgender woman married to her child’s father and living in the Midwest region, provided a response typical of the sample regarding the role of religion in her decision-making process:
Jesus said we are children of God, and he did not define what a child of God looks like. God created this world to be diverse. Look outside, and you’re going to see it. We’re just living in that reality of being children of God.
Central Theme: From Dissonance to Consonance
Each participant described an initial expectation that their youth would identify, like them, as cisgender. When they recognized that their child’s gender expression did not align with those social expectations, each participant described experiencing some level of intra- and interpersonal tension. This phenomenon may also be understood by what is commonly known as cognitive dissonance (Festinger, 1957; Myers & DeWall, 2019). Like the construct of parental attunement described previously, the construct of cognitive dissonance borrows from the physics of music, in which the term dissonance is used to describe a lack of harmony. On the other hand, consonance is the term used to describe a combination of one or more tones of different frequencies that combine and result in a musically pleasing (i.e., harmonious) sound (Errede, 2017). Festinger’s cognitive dissonance theory (1957) suggests that when faced with this type of mental tension, humans often bring their attitudes and beliefs into alignment with their actions (Myers & DeWall, 2019). The responses of the participants of this study suggest that this is an apt metaphor for their decision-making process.
Each participant described 1) an experience of exposure to some form of human diversity prior to their youth confirming a TGD identity, 2) cognitive-emotional openness to new and TGD-affirming information, and 3) acceptance of the new and affirming information presented to them, followed by the participant 4) using the affirming information available to them to make an affirming cost-benefit analysis that led to the granting of informed consent and finally 5) feeling a sense of relief that they gave informed consent for their youth to undergo GCEI. Figure 1 shows a dissonance-to-consonance model of these mutually influencing central factors.
Exposure to Historically Minoritized Experiences
Each participant described previous exposure to some type of historically minoritized experience, whether it was as personal as identifying as a woman (as in Journey’s case), a professional experience, or knowing someone within their children’s social networks. Mellony reported personal and professional exposure, stating that a former colleague had come out as trans, “so I did know someone. I also knew another mom whose child had come out a couple years earlier, so it was not completely foreign to me.”
Openness
Each participant described generally open attitudes that led to parenting decisions ranging from the toys they gave to their child to seeking education. Adele recounted that her family “did a lot of research on our own. We had other parents and kiddos that [we] were able to talk to about what they were experiencing, and we heard from families about what the process looked like for them.”
Figure 1
A Dissonance-to-Consonance Model
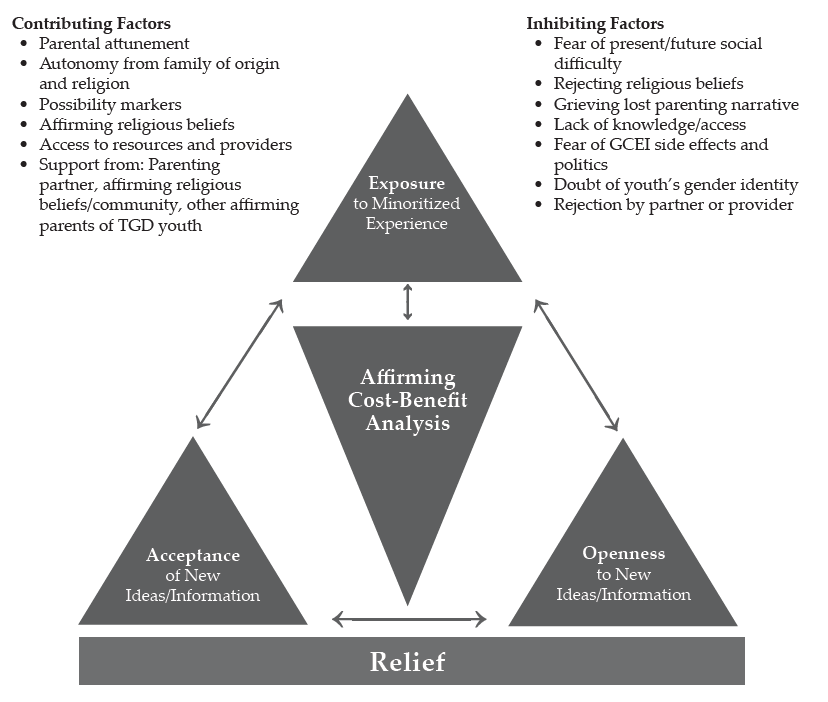
Acceptance
Prudence provided an example of acceptance typical of the sample in that she not only accepted that the GCEI and other affirming practices would be beneficial, but she also arrived at a place where she wished she had started them earlier:
I often say [child’s given name at birth] was the vessel, [child’s name] is the soul. If I had known that, and understood it wasn’t a phase, I probably would have pushed to start so he didn’t go through puberty as a female.
Affirming Cost-Benefit Analysis
Berta provided a description typical of the sample regarding her and her partner’s affirming cost-benefit analysis that led to granting informed consent. She highlighted her access to a supportive community as well as her recognition of the mental health implications of a non-affirmed TGD identity for her child:
A parent who had come before me said there’s really nothing that you can’t reverse. You can wear a wig if your hair falls out. . . . If you start growing facial hair and then you decide you don’t want to, you can get electrolysis. . . . If you get your breasts removed, you can get implants. But what it really comes down to is do you want a dead kid, or do you want a kid that might be slightly altered? We looked at [our child] and thought, “You’re miserable, and if this will help you not be miserable, then we will go for it.”
Relief
Each participant expressed a sense of relief that they had granted informed consent, usually because they noticed improvements in their child’s moods and general sense of happiness. Lennon (55), a White, cisgender man married to his parenting partner and living in the Midwest region, provided a statement that was typical in the sample: “His mood changed. That was the key. I think the fact that we saw [child] become happier with it, that’s the key. That’s all that really mattered.”
Discussion
The purpose of this research was to explore the process by which 17 parents of TGD youth developed affirmative understandings and approaches to their children’s gender identity, affirmed their related transition needs, and granted informed consent for the TGD youth in their care to undergo GCEI. Based upon our review of the literature, there are no studies related to the process that the parents and guardians of TGD minors go through to give informed consent for GCEI. This research appears likely to inform best practice for professional counselors and other helping professionals serving TGD youth who wish to have an endocrinologically supported transition and those charged with giving informed consent for these interventions.
Implications for Professional Counselors
First, this research provides a plausible model for practitioners to follow when presented with the challenge of supporting parents of TGD youth as they work to develop affirming attitudes and support their respective children’s medical transition. Though the dissonance-to-consonance model as presented still needs to be tested by more objective means, the interplay of exposure, openness, and acceptance as contributing factors to parents’ TGD-affirming cost-benefit analyses toward the experience of relief for themselves and their children appears to be consistent with attachment and family counseling best practices (Ainsworth & Bowlby, 1991; Bowlby, 1988; Gladding, 2019; Minuchin, 1974; Siegel, 2013; Siegel & Bryson, 2011; Wallin, 2007). The combination of these factors, especially as they relate to parents’ fears about the side effects of GCEI and doubts about the genuineness of their child’s gender identity, appeared particularly relevant to this study given the previously cited paucity of research examining the long-term effects of GCEI on developing pre-adolescent and adolescent bodies and that the consistency between gender-expansive identity development and cisgender identity development has only been published recently (Drescher, 2010; Gülgöz et al., 2019). The challenges, however, for adolescents regarding decision-making, impulse control, and executive functioning are well-documented (Siegel, 2013).
Participants in this study praised the work of the professional counselors and other mental health professionals in their life when they (a) provided credible and affirming education about gender identity development; (b) worked in connection with support groups with which participants were involved; (c) recognized that the presenting concerns for the child and/or family may not necessarily be related to gender identity; and (d) completed gatekeeping responsibilities and tasks succinctly, efficiently, and without unexpected financial costs. These factors appear to be consistent with competencies for working with transgender clients developed by SAIGE (Burnes et al., 2010). Participants lamented their experiences with professional counselors and other health care professionals when (a) the above tasks were not completed within these guidelines, (b) the professionals were dismissive of the child’s gender identity or unwilling to provide care, and (c) clinic staff gave participants an unwelcoming or non-affirming impression.
The present study suggests that when presented with the opportunity to serve TGD adults, youth, and their families, professional counselors should familiarize themselves with and develop both the SAIGE competencies and the World Professional Association for Transgender Health (WPATH) Standards of Care (E. Coleman et al., 2012). Furthermore, professional counselors should follow established informed consent guidelines and be upfront and clear about fees for services when it comes to more specialized tasks like writing a GCEI referral letter. A growing body of resources also exists for developing TGD-affirming and inclusive cultures among non-clinical staff employed by counseling practices. For example, the guidelines developed by Morenz and colleagues (2020) for developing and implementing a transgender health program include suggestions for gaining buy-in from and training for reception and administrative staff.
Finally, it appears that collegial support of counselors knowledgeable about the roles of clinicians in working with TGD individuals and families to develop competence among a wider network of providers may be necessary. This support is warranted, given the lack of access to TGD-affirming health care due to residential location, including counseling, cited as an inhibiting factor by this sample. This may support the reduction of referrals of TGD clients between counselors, a practice allowed by the ACA’s (2014) Code of Ethics in matters of limited competency but, as Kaplan (2018) has stated, is also a practice the clients may interpret as rejecting.
Limitations and Future Directions
As with all qualitative research, the results of this grounded theory study, despite the efforts made to maximize trustworthiness, need further testing using quantitative methodology to strengthen their applicability across a broader range of samples (Merriam & Tisdell, 2016). By its design, this was a study about how participants resolved their dilemma in an affirming way and therefore may not be as valuable for responding to research questions regarding dilemmas resolved in pathologizing or rejecting ways. This study was also limited demographically, with a sample heavily weighted toward the experiences of White (n = 16), cisgender women (n = 13), and married participants (n = 14). The majority of participants reported household incomes of more than $90,000, doubtlessly improving the odds that they could overcome some inhibiting factors because of greater financial ability. Finally, this research may have been limited by a sample that was heavily weighted toward participants who reside in the Mid-Atlantic region (n = 12); a sample that was more balanced across the United States may have produced different findings.
These findings lend themselves to testing with quantitative methods such as pre-test/post-test program evaluation or randomized controlled trials (RCTs). Both methods have the potential to draw larger, more representative sample sizes, thus enhancing external validity to make greater contributions to the literature. The dissonance-to-consonance model presented here could be used as a program theory for evaluation. RCTs in the vein of what has been used to test the effectiveness of specific counseling modalities, using an approach influenced by the dissonance-to-consonance model compared to a control sample using “therapy as usual” (Ramsauer et al., 2014), may also be valuable for informing best practice while avoiding the ethical dilemma presented by denying treatment. Quantitative investigation may also benefit from further qualitative exploration of the present research questions in a way that addresses the demographic limitations of this study. For example, a grounded theory study of parents who identify as Black may produce different results (Armstrong et al., 2013; Gibbons, 2019; Zheng, 2015).
Conclusion
The present study examined, for the first time, the experiences of parents of TGD youth as they decided to give informed consent for their child to undergo GCEI. They named a variety of inhibitors and contributors to this process, and a “dissonance-to-consonance” model for using contributing factors to overcome inhibitors to the process was illuminated. We found the research process to be emotionally moving and rich with guidance for both parents of TGD youth who are making decisions of considerable consequence for their children and the professional counselors working with them in supportive roles. The model appears to provide fertile ground for further study to support services that affirm and support TGD youth and their families. We relish the opportunity to continue this work and look forward to the contributions of others who advance this topic in service of TGD well-being throughout the life span.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ainsworth, M. D. S., & Bowlby, J. (1991). An ethological approach to personality development. American Psychologist, 46(4), 333–341.
American Counseling Association. (2014). ACA code of ethics. https://bit.ly/ACAcodeofethics
Armstrong, K., Putt, M., Halbert, C. H., Grande, D., Schwartz, J. S., Liao, K., Marcus, N., Demeter, M. B., & Shea, J. A. (2013). Prior experiences of racial discrimination and racial differences in health care system distrust. Medical Care, 51(2), 144–150. https://doi.org/10.1097/MLR.0b013e31827310a1
Bowlby, J. (1988). A secure base: Parent-child attachment and healthy human development. Basic Books.
Bränström, R., & Pachankis, J. E. (2020). Reduction in mental health treatment utilization among transgender individuals after gender-affirming surgeries: A total population study. The American Journal of Psychiatry, 177(8), 727–734. https://doi.org/10.1176/appi.ajp.2019.19010080
Bunim, J. (2015, August 17). First U.S. study of transgender youth funded by NIH: Four sites with dedicated transgender youth clinics to examine long-term treatment effects. UCSF News & Media. https://bit.ly/UCSFstudy
Burnes, T. R., Singh, A. A., Harper, A. J., Harper, B., Maxon-Kann, W., Pickering, D. L., Moundas, S., Scofield, T. R., Roan, A., & Hosea, J. (2010). American Counseling Association competencies for counseling with transgender clients. Journal of LGBT Issues in Counseling, 4(3–4), 135–159.
https://doi.org/10.1080/15538605.2010.524839
Burt, N. (2016). When girls play with G.I. Joes and boys play with Barbies: The path to gender reassignment in minors. Florida Law Review, 68(6), 1883–1913. https://bit.ly/3GkpSPK
Cashwell, C. S., & Watts, R. E. (2010). The new ASERVIC competencies for addressing spiritual and religious issues in counseling. Counseling and Values, 55(1), 2–5.
https://doi.org/10.1002/j.2161-007X.2010.tb00018.x
Charmaz, K. (2014). Constructing grounded theory (2nd ed.). SAGE.
Coleman, D. L. (2019). Transgender children, puberty blockers, and the law: Solutions to the problem of dissenting parents. The American Journal of Bioethics, 19(2), 82–84. https://doi.org/10.1080/15265161.2018.1557297
Coleman, D. L., & Rosoff, P. M. (2013). The legal authority of mature minors to consent to general medical treatment. Pediatrics, 131(4), 786–793. https://doi.org/10.1542/peds.2012-2470
Coleman, E., Bockting, W., Botzer, M., Cohen-Kettenis, P., DeCuypere, G., Feldman, J., Fraser, L., Green, J., Knudson, G., Meyer, W. J., Monstrey, S., Adler, R. K., Brown, G. R., Devor, A. H., Ehrbar, R., Ettner, R., Eyler, E., Garofalo, R., Karasic, D. H. . . . Zucker, K. (2012). Standards of Care for the Health of Transsexual, Transgender, and Gender-Nonconforming People, Version 7. International Journal of Transgenderism, 13(4), 165–232. https://doi.org/10.1080/15532739.2011.700873
Corbin, J., & Strauss, A. (2015). Basics of qualitative research: Techniques and procedures for developing grounded theory (4th ed.). SAGE.
Couric, K. (Director, Producer). (2017). Gender revolution [Documentary]. National Geographic.
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Dailey, S. F. (2017, June). Ethical & legal considerations: Complicated issues in challenging times. Presentation given at the 2017 Illuminate Symposium, Washington, D.C.
Drescher, J. (2010). Queer diagnoses: Parallels and contrasts in the history of homosexuality, gender variance, and the Diagnostic and Statistical Manual. Archives of Sexual Behavior, 39, 427–460.
https://doi.org/10.1007/s10508-009-9531-5
Durso, L. E., & Gates, G. J. (2012). Serving our youth: Findings from a national survey of services providers working with lesbian, gay, bisexual and transgender youth who are homeless or at risk of becoming homeless. The Williams Institute with True Colors Fund and The Palette Fund.
Errede, S. (2017). [Lecture notes on acoustical physics of music]. Department of Physics, University of Illinois at Urbana-Champagne, IL. https://bit.ly/3p8gh7z
Erskine, R. G. (1998). Attunement and involvement: Therapeutic responses to relational needs. International Journal of Psychotherapy, 3(3), 235–244.
Festinger, L. (1957). A theory of cognitive dissonance. Stanford University Press.
Gibbons, J. (2019). The effect of segregated cities on ethnoracial minority healthcare system distrust. City & Community, 18(1), 321–343. https://doi.org/10.1111/cico.12370
Gibbs, J. J., & Goldbach, J. (2015). Religious conflict, sexual identity, and suicidal behaviors among LGBT young adults. Archives of Suicide Research, 19(4), 472–488. https://doi.org/10.1080/13811118.2015.1004476
Gladding, S. T. (2019). Family therapy: History, theory, and practice (7th ed.). Pearson.
Glaser, B. G., & Strauss, A. L. (1967). The discovery of grounded theory: Strategies for qualitative research. Aldine Publishing.
Gonzalez, R. (2018, January 23). How the ‘Religious Freedom Division’ threatens LGBT health—and science. Wired. https://www.wired.com/story/how-the-religious-freedom-division-threatens-lgbt-healthand-science
Goodkind, N. (2021, July 9). Ohio law allows doctors to deny health care and birth control to LGBTQ patients. Fortune. https://bit.ly/FortuneLGBTQ
Grossman, A. H., & D’Augelli, A. R. (2007). Transgender youth and life-threatening behaviors. Suicide and Life-Threatening Behavior, 37(5), 527–537. https://doi.org/10.1521/suli.2007.37.5.527
Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Chonghui, J., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116(49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Hembree, W. C., Cohen-Kettinis, P. T., Gooren, L., Hannema, S. E., Meyer, W. J., Murad, M. H., Rosenthal, S. M., Safer, J. D., Tangpricha, V., & T’Sjoen, G. G. (2017). Endocrine treatment of gender-dysphoric/gender-incongruent persons: An Endocrine Society clinical practice guideline. The Journal of Clinical Endocrinology & Metabolism, 102(11), 3869–3903. https://doi.org/10.1210/jc.2017-01658
Hill, D. B., & Menvielle, E. (2009). “You have to give them a place where they feel protected and safe and loved”: The views of parents who have gender-variant children and adolescents. Journal of LGBT Youth, 6(2–3), 243–271. https://doi.org/10.1080/19361650903013527
James, S. E., Herman, J. L., Rankin, S., Keisling, M., Mottet, L., & Anafi, M. (2016). The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. https://transequality.org/sites/default/files/docs/usts/USTS-Full-Report-Dec17.pdf
Jorgensen, C. (1967). Christine Jorgensen: A personal autobiography. Bantam.
Kaplan, D. M. (2018, April). Train the trainer: Delivering presentations on the 2014 ACA Code of Ethics. Presentation at the ACA 2018 Conference & Expo Pre-conference Learning Institutes, Atlanta, GA.
Lawson, G. (2016). On being a profession: A historical perspective on counselor licensure and accreditation. Journal of Counselor Leadership and Advocacy, 3(2), 71–84. https://doi.org/10.1080/2326716X.2016.1169955
Merriam, S. B., & Tisdell, E. J. (2016). Qualitative research: A guide to design and implementation (4th ed.). Jossey-Bass.
Minuchin, S. (1974). Families & family therapy (1st ed.). Harvard University Press.
Morenz, A. M., Goldhammer, H., Lambert, C. A., Hopwood, R., & Keuroghlian, A. S. (2020). A blueprint for planning and implementing a transgender health program. Annals of Family Medicine, 18(1), 73–79. https://doi.org/10.1370/afm.2473
Murad, M. H., Elamin, M. B., Garcia, M. Z., Mullan, R. J., Murad, A., Erwin, P. J., & Montori, V. M. (2010). Hormonal therapy and sex reassignment: A systematic review and meta-analysis of quality of life and psychosocial outcomes. Clinical Endocrinology, 72(2), 214–231.
https://doi.org/10.1111/j.1365-2265.2009.03625.x
Myers, D. G., & DeWall, C. N. (2019). Exploring psychology in modules (11th ed.). Worth Publishers.
Pew Research Center. (2014). Religious landscape study. http://www.pewforum.org/religious-landscape-study
Ramsauer, B., Lotzin, A., Mühlhan, C., Romer, G., Nolte, T., Fonagy, P., & Powell, B. (2014). A randomized controlled trial comparing Circle of Security Intervention and treatment as usual as interventions to increase attachment security in infants of mentally ill mothers: Study protocol. BMC Psychiatry, 14(24). https://doi.org/10.1186/1471-244X-14-24
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. American Counseling Association. https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf?sfvrsn=20
Rose, J. S., Kocet, M. M., Thompson, I. A., Flores, M., McKinney, R., & Suprina, J. S. (2019). Association for Lesbian, Gay, Bisexual, and Transgender Issues in Counseling best practices in addressing conscience clause legislation in counselor education and supervision. Journal of LGBT Issues in Counseling, 13(1), 2–27. https://doi.org/10.1080/15538605.2019.1565800
Rosin, H. (2008, November). A boy’s life. The Atlantic. https://bit.ly/3lIxOCF
Shabad, R. (2021). Biden administration announces reversal of Trump-era limits on protections for transgender people in health care. NBC News. https://nbcnews.to/3drlWAr
Siegel, D. J. (2013). Brainstorm: The power and purpose of the teenage brain. Penguin.
Siegel, D. J., & Bryson, T. P. (2011). The whole-brain child: 12 revolutionary strategies to nurture your child’s developing mind. Delacorte Press.
Stryker, S. (2008). Transgender history. Seal Press.
Toporek, R. L., & Daniels, J. (2018). American Counseling Association advocacy competencies: Updated. American Counseling Association https://www.counseling.org/docs/default-source/competencies/aca-advocacy-competencies-updated-may-2020.pdf?sfvrsn=f410212c_4
U.S. Department of Health and Human Services. (2018a). HHS announces new Conscience and Religious Freedom Division. https://www.hhs.gov/about/news/2018/01/18/hhs-ocr-announces-new-conscience-and-religious-freedom-division.html
U.S. Department of Health and Human Services. (2018b). Conscience and religious freedom. https://bit.ly/3oz6p7G
Vincent, B. (2019). Breaking down barriers and binaries in trans healthcare: The validation of non-binary people. International Journal of Transgenderism, 20(2–3), 132–137. https://doi.org/10.1080/15532739.2018.1534075
Vines, M. (2014). God and the gay Christian: The biblical case in support of same-sex relationships. Convergent Books.
Wallin, D. J. (2007). Attachment in psychotherapy. Guilford.
Zheng, H. (2015). Losing confidence in medicine in an era of medical expansion? Social Science Research, 52, 701–715. https://doi.org/10.1016/j.ssresearch.2014.10.009
APPENDIX A
Interview Protocol
Beginning Questions:
- Tell me about how you came to grant informed consent for your child to receive puberty blockers or hormone replacement therapy?
- When did you first notice/realize that your child identified as transgender or gender-diverse (TGD)?
- What was that like?
Intermediate Questions:
- What, if anything, did you know about gender identity and gender expression prior to learning your child identified as TGD?
- What, if anything, did you know about gender-confirming endocrinological interventions (GCEI) prior to giving informed consent for your child to participate in them?
- How, if at all, have your thoughts and feelings changed about gender variance since learning that your child identified as TGD?
- How, if at all, have your thoughts and feelings changed about gender-confirming hormone treatments since your child indicated they wanted to receive them?
- What, if anything, inhibited your change process?
- Who, if anyone, helped you in this change process?
- How, if at all, was a professional counselor or other mental health professional involved?
- What would you say were the most helpful aspects that you experienced during your process toward giving informed consent for GCEI?
Closing Questions:
- Is there something that you might not have thought about before that occurred to you during this interview?
- Is there something else you think I should know to understand your process or experience better?
Charles F. Shepard, PhD, NCC, LPC, is a visiting faculty member at James Madison University. Darius A. Green, PhD, NCC, is the PASS Program Assistant Coordinator at James Madison University. Karli M. Fleitas, MA, is a doctoral student at James Madison University. Debbie C. Sturm, PhD, LPC, is a professor at James Madison University. Correspondence may be addressed to Charles F. Shepard, MSC 7704, James Madison University, 91 E. Grace Street, Harrisonburg, VA 22807, sheparcf@jmu.edu.
