Aug 10, 2022 | Volume 12 - Issue 2
Gregory T. Hatchett
This study involved a longitudinal analysis of the journal article publications accrued by counselor educators at comprehensive universities over the first 20 years since receiving their doctoral degrees. A review of electronic databases revealed these counselor educators accrued a median of three journal article publications over the first 20 years since degree completion. Faculty rank, inferred binary gender, and the date of terminal degree all predicted cumulative journal article publication counts. An analysis of sequence charts revealed that journal article publication counts are not invariant over the first 20 years since degree completion, but vary based on time, faculty rank, and inferred binary gender. The implications of this research for counselor education training are discussed.
Keywords: counselor educators, journal article publications, faculty rank, comprehensive universities, gender
The primary purpose of doctoral-level training in counselor education is to prepare program graduates for careers as counselor educators and clinical supervisors (Snow & Field, 2020). Consistent with this objective, graduates of counselor education and supervision programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP) are required to attain numerous research competencies that will equip them for making scholarly contributions to the counseling literature (CACREP, 2015). Likewise, the PhD degree, which is the terminal degree offered to graduates of nearly all these programs, has been traditionally designed to prepare graduates for research and teaching in higher education (e.g., Dill & Morrison, 1985).
Be that as it may, most graduates of counselor education and supervision programs do not become faculty members, let alone faculty at research-intensive universities (e.g., Lawrence & Hatchett, 2022; Schweiger et al., 2012; Zimpfer, 1996). For example, Lawrence and Hatchett (2022) recently investigated the occupational outcomes of 314 graduates of CACREP-accredited doctoral programs. Overall, they found that 41.4% of these graduates had some type of faculty position in higher education. However, faculty positions as assistant professors in CACREP-accredited programs were much less common (23.9% of the total sample), and assistant professor positions in CACREP-accredited counseling programs at universities classified by the Carnegie Classification System (https://carnegieclassifications.acenet.edu) as either R1 (Very high research activity) or R2 (High research activity) were relatively rare (8.3% of the total sample). Thus, fewer than 1 in 10 of these recent program graduates attained professor positions at universities that expect high levels of scholarly productivity.
At the time of this writing, 401 colleges and universities in the United States and Puerto Rico have at least one CACREP-accredited counseling program. However, only 134 (33.5%) of these institutions have a Carnegie Classification of either an R1 or R2. More common are CACREP-accredited programs at master’s degree–granting institutions designated by the Carnegie system as M1 (Larger programs), M2 (Medium programs), or M3 (Smaller programs). Many of these universities would fall under the general umbrella of what are commonly denoted as comprehensive universities. At comprehensive universities, the focus is typically on undergraduate education, and graduate education tends to be limited to master’s degrees in professional disciplines, such as education and business (Youn & Price, 2009). Compared to their colleagues at research-intensive universities, faculty at comprehensive universities tend to have high teaching loads and greater expectations for service along with substantially lower expectations for faculty scholarly productivity (Hatchett, 2021; Henderson, 2011).
Though the scholarship expectations are lower, counselor educators at comprehensive universities are still commonly expected to exhibit some level of scholarly productivity for performance evaluations as well as tenure and promotion decisions (Fairweather, 2005; Hatchett, 2020; Youn & Price, 2009). Specific to counselor education, Hatchett (2020) recently surveyed 168 counselor educators about their perceptions of the tenure process, workloads, and their annual scholarly productivity. Regarding journal article publications, these counselor educators reported accruing a median of 0.45 national or international journal article publications a year. However, there is reason to believe that this sample statistic may be an overestimate. For one, only about 20% of the counselor educators at comprehensive universities completed the survey. Secondly, the rate of journal article publications reported by this sample of counselor educators greatly exceeds estimates attained from archival research.
For example, Hatchett et al. (2020) assessed the journal article publications of a large sample (N = 821) of counselor educators employed in CACREP-accredited master’s-level counseling programs housed in comprehensive universities. To identify peer-reviewed journal articles, they searched these counselor educators’ names through three electronic databases (i.e., PsycINFO, ERIC, Academic Search Complete) for the time interval of January 1, 2008, through December 31, 2017. They found that these counselor educators had attained a median of only 1 (M = 1.99, SD = 3.46) peer-reviewed publication over this
10-year time interval; notably, nearly half of this sample (n = 381, 46.4%) did not have any journal article publications indexed in any of the three databases. Granted, these three electronic databases do not capture all the journal article publications attained by counselor educators. Nonetheless, the gap between self-report (Hatchett, 2020) and archival publication estimates (Hatchett et al., 2020) is so large that it probably cannot be explained away by publications that were not referenced in any of these databases.
A second shortcoming of the archival research by Hatchett et al. (2020) was its cross-sectional nature. A cross-section cannot directly answer the question as to whether publication rates might vary or decline over the course of counselor educators’ careers. Hatchett et al. (2020) and Lambie et al. (2014) found some evidence that journal article publications may decline over counselor educators’ careers. To better evaluate this phenomenon, Lambie et al. recommended that future researchers use a longitudinal research design that tracks publication counts across time. Not only would a longitudinal design better detect changes and trends in publication rates across time, but such a design could also better illuminate the extent to which counselor educators at comprehensive universities publish in peer-reviewed journals across their careers.
Purpose of the Present Study
Accordingly, the purpose of the current study was to use a longitudinal research design to summarize and track the rate of journal article publications by counselor educators at comprehensive universities over an extended period of time. Specifically, this study assessed the cumulative journal article publications attained by counselor educators at master’s-only counseling programs at comprehensive universities for the first 20 years since receiving their terminal degrees. A secondary objective of this study was to evaluate whether factors identified in previous research would also be useful for predicting journal article publication counts in this sample. Previous researchers have found that binary gender (Lambie et al., 2014; Newhart et al., 2020; Ramsey et al., 2002), faculty rank (Hatchett et al., 2020; Newhart et al., 2020; Ramsey et al., 2002), and year of degree completion (Hatchett et al., 2020; Lambie et al., 2014) predict journal article publication counts. Thus, these same three variables were used to predict cumulative journal article publication counts accrued by these counselor educators over the 20 years since their degree completion.
Method
Procedures and Participants
Because this study involved only the collection and analysis of publicly available data, the internal IRB determined this study was exempt from IRB oversight. As in the methodology used by Hatchett et al. (2020), a comprehensive university was operationally defined as an institution classified by the Carnegie Classification of Institutions of Higher Education as a master’s-level institution with a designation of M1 (Larger programs), M2 (Medium programs), or M3 (Smaller programs). In addition, any M1, M2, or M3 institution was excluded from this study if it did not denote at least part of its faculty with traditional academic ranks (i.e., assistant professor, associate professor, professor) or if the program also offered a doctoral degree program in counseling or counselor education. The process for collecting data involved three steps. The first step was to identify CACREP-accredited master’s programs at comprehensive universities that met the abovementioned criteria.
As a result of this search process, 157 colleges and universities were identified for potential study inclusion. At the second step, the websites of these colleges and universities were searched to identify counselor educators with the rank of either associate or full professor. In addition to the rank of at least associate professor, a minimum of 20 years must have passed since the counselor educator received their doctoral degree to be included in this study. At the end of this process, 162 counselor educators were eventually identified. For each identified counselor educator, the following information was recorded: (a) name of the counselor educator, (b) Carnegie Classification of their current university, (c) inferred binary gender based on name and any contextual information, (d) type of terminal degree (e.g., PhD, EdD), (e) academic discipline of terminal degree, and (h) date of doctoral degree. If any of this data was not available on a counseling program’s website, additional public resources were searched, such as university catalogs, Dissertations Abstracts International, Google, and LinkedIn. There were six counselor educators for whom a terminal degree date could not be identified; these counselor educators were removed from the sample, leaving a final sample size of 156.
Count of Journal Article Publications
To identify journal article publications, each counselor educator’s name was searched through three major electronic databases: PsycINFO, ERIC, and Academic Search Complete. The beginning date for each search was the year following a counselor educator’s terminal degree date and the end date of the search was 20 years later. A journal article publication was operationally defined as any authored publication in a peer-reviewed journal indexed in any of the three databases that involved theory, counseling practice, quantitative research, qualitative research, mixed method research, or published responses to other published works; for the purpose of this study, editor notes and book reviews were excluded. The number of journal article publications for each counselor educator over the first 20 years after degree completion was summed to represent journal article publication counts.
Results
Data Analysis Strategy
Prior to conducting any analyses, the dataset was screened for data entry errors, unusual values, and extreme outliers; none were identified. Prior to running the negative binomial regression analysis, the categorical predictor variables (inferred binary gender, faculty rank) were dummy coded. All screening procedures and subsequent analyses were conducted using IBM SPSS (Version 28).
To predict journal article publication counts, a negative binomial regression analysis was conducted because the criterion variable, journal article publications, represented a count variable that contained a large number of zero values and the variance of the distribution exhibited overdispersion (Fox, 2008). Power estimates for negative binomial regression models are less developed than those available for linear models. Nonetheless, traditional power estimates for general linear models (Cohen, 1988) and experimental estimates for generalized linear models (Doyle, 2009; Lyles et al., 2007) suggested that the negative binomial regression analysis likely had sufficient statistical power (> .80) to detect at least medium effect sizes. The following assumptions for negative binomial regression were examined: multicollinearity, residual plots, independence of residual errors, and the presence of any highly influential cases. No difficulties were identified.
Ideally, a time series analysis is recommended for identifying trends or changes in longitudinal data across time (Yaffee & McGee, 2000). However, it is commonly recommended that a time series analysis should be based on a minimum of 50 observation periods (e.g., Tabachnick & Fidell, 2019). Power estimates for time series analyses can become very complex, and in some cases, 100 to 250 observational periods may be needed to reliably detect trends or seasonal patterns in time series data (Yaffee & McGee, 2000). It would not be feasible to track even a minimum of 50 years of journal article publications for a sizeable sample of counselor educators. Furthermore, inferential statistics—and accompanying power analyses—are needed for making inferences from a sample to the larger population from which the sample was drawn. Aside from inaccuracies on department websites, the counselor educators in this study represent the entire population of counselor educators at master’s-only programs in comprehensive universities who received their doctoral degrees at least 20 years ago. As Garson (2019) pointed out, “having data on all the cases in the population of interest eliminates the need for a random sample and, indeed, for significance testing at all” (p. 25). Consequently, the longitudinal analysis of this data will be limited to the creation and visual analysis of sequence charts.
Characteristics of the Sample
Regarding inferred binary gender, 51.9% (n = 81) of these counselor educators appeared to identify as female, and 48.1% (n = 75) appeared to identify as male. Two-thirds (n = 104, 66.7%) held the rank of full professor, and 33.3% (n = 52) held the rank of associate professor. The years in which they earned their terminal degrees ranged from 1970 to 2000 (Mdn = 1995.00, M = 1992.70, SD = 6.48). The number of years after earning their terminal degrees ranged from 20 to 50 (Mdn = 25.00, M = 27.30, SD = 6.48). Their terminal degrees included PhDs (n = 118, 75.6%), EdDs (n = 31, 19.9%), PsyDs (n = 4, 2.6%), and other (n = 3, 1.9%). Slightly over half of these faculty members had terminal degrees in counseling/counselor education (n = 80, 51.3%), followed in frequency by counseling psychology, clinical psychology, or educational psychology (n = 47, 30.1%); education (n = 13, 8.3%); rehabilitation or rehabilitation psychology (n = 10, 6.4%); and other (n = 6, 3.8%). Almost two-thirds (n = 102, 65.4%) were faculty at public universities with the remainder (n = 54, 34.6%) being faculty at private universities. Regarding current Carnegie Classifications, over four-fifths were faculty at M1 institutions (n = 128, 82.1%), which was followed in frequency by M2 institutions (n = 20, 12.8%) and M3 institutions (n = 8, 5.1%).
Journal Article Publication Counts
At the end of the first 20 years after receiving their terminal degrees, these counselor educators had accrued a median of three (M = 5.26, SD = 6.92) journal article publications referenced in at least one of the three electronic databases. Notably, a fourth of the sample (n = 39, 25%) did not have any journal article publications indexed in any of the electronic databases. Expressed on an annual basis, the entire sample of counselor educators had accrued a median of 0.15 (M = 0.26, SD = 0.35) journal articles each year for the first 20 years after completing their terminal degrees.
Prediction of Publication Counts
Based on prior research in counselor education (e.g., Hatchett et al., 2020; Lambie et al., 2014; Newhart et al., 2020; Ramsey et al., 2002), the next set of analyses evaluated whether cumulative journal article publication counts could be predicted from faculty rank, inferred binary gender, and year of terminal degree. In fitting a negative binomial regression model to the data, the likelihood ratio chi-square statistic was statistically significant, indicating that the three combined variables were useful for predicting publication counts: χ2(3, N = 156) = 21.22, p < .001, McFadden R2 = .024. All three predictor variables made unique contributions to the prediction of journal article publication counts (see Table 1). The estimated number of publications for full professors was 1.73 times higher (95% CI [1.18, 2.53]; p = .005) than for associate professors. For reference, over the first 20 years since degree completion, associate professors had accrued an average of 3.31 (SD = 5.52) journal article publications compared to an average of 6.24 (SD = 7.36) journal article publications for full professors. The estimated number of publications for male counselor educators was 1.45 times higher (95% CI [1.02, 2.06]; p = .037) than for female counselor educators. For reference, male counselor educators had accrued a mean of 6.17 (SD = 7.89) journal article publications compared to a mean of 4.42 (SD = 5.81) for female counselor educators. Finally, with each 1-year increase in terminal degree date, the estimated number of cumulative publications increased by 4.1% (95% CI [1.01, 1.07]; p = .005).
Table 1
Prediction of Journal Article Publication Counts From Faculty Rank, Inferred Binary Gender, and Terminal Degree Date
________________________________________________________________________________
Predictors B SE Wald χ2 p
________________________________________________________________________________
Faculty Rank .55 .19 8.01 .005
Inferred Binary Gender .37 .18 4.36 .04
Year of Terminal Degree .04 .01 7.75 .005
________________________________________________________________________________
Longitudinal Analyses
As reported previously, cumulative journal article publications varied as a function of both faculty rank and inferred binary gender. Because of this, two sequence charts were created to illuminate how journal article publication trajectories varied based on faculty rank and inferred binary gender. SPSS (Version 28) was used to create two sequence charts of the average number of journal article publications accrued each year for the first 20 years since degree completion. Figure 1 represents a sequence chart for journal article publications disaggregated by faculty rank. Figure 2 represents a sequence chart for journal article publications disaggregated by inferred binary gender.
Figure 1
Average Number of Journal Article Publications for Associate and Full Professors Over 20 Years After Degree Completion
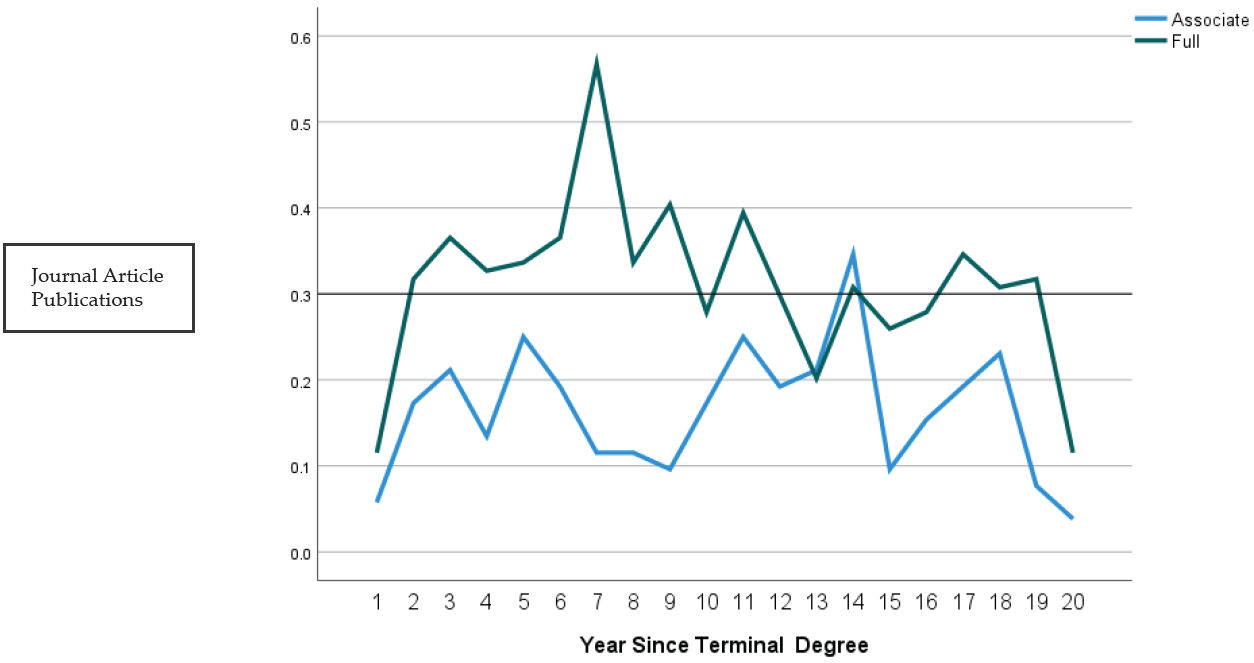
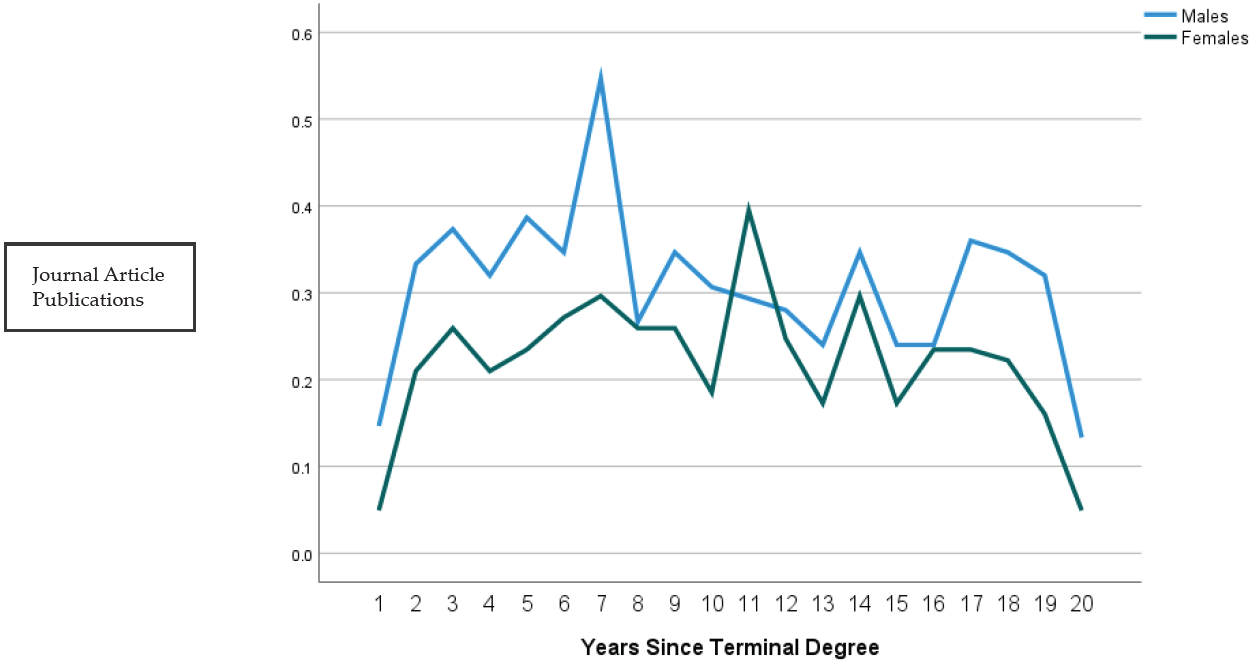
Figure 2
Average Number of Journal Article Publications for Male and Female Counselor Educators Over 20 Years After Degree Completion
Discussion
The main objective of this study was to conduct a longitudinal analysis of the journal article publications of counselor educators at comprehensive universities for the first 20 years after receiving their doctoral degrees. A secondary objective was to evaluate how well these publication counts could be predicted from faculty rank, inferred binary gender, and year of terminal degree. Parallel to the results section, summary statistics will be discussed first, followed by the results of the regression analysis, and ending with the results of the longitudinal analyses.
Over the first 20 years since receiving their terminal degrees, the counselor educators in this sample had accrued a median of three (M = 5.26, SD = 6.62) journal article publications, which translates to a median of 0.15 (M = 0.26, SD = 0.35) journal articles published per year. Notably, a fourth (n = 39, 25%) of the sample did not have any journal article publications referenced in any of three major electronic databases. These findings are consistent with those of Hatchett et al. (2020), who investigated the journal article publications of this same population over a discrete 10-year period (2008–2017) using a similar methodology. They found that counselor educators at comprehensive universities had a median of 0.10 journal article publications each year, but a much higher proportion (46.4%) of their sample did not have any journal article publications referenced in any of the electronic databases. These differences may be the result of both the specific compositions of their samples and the timeframes for data collection. The current study examined the publication records of only associate and full professors, whereas Hatchett et al. (2020) examined the publication records of assistant, associate, and full professors of counselor education. Consistent with that expanded population, some of the counselor educators in the study by Hatchett et al. were just starting their careers and may not yet have attained many publications. There is also the possibility that some of the assistant professors in that study will be, or have been, turned down for promotion to associate professor because of inadequate scholarly productivity. Of course, it is not surprising that the current study, which examined a 20-year timeframe, uncovered a lower percentage of counselor educators without any journal article publications; after all, the counselor educators in the current study had double the time in which to accrue journal article publications.
Based on previous research in counselor education (Hatchett et al., 2020; Lambie et al., 2014; Newhart et al., 2020; Ramsey et al., 2002), this study also examined how well faculty rank, inferred binary gender, and year of terminal degree predicted journal article publication counts. Full professors had more journal article publications for the first 20 years after receiving their terminal degrees than those at the rank of associate professor. Not only would more publications be expected for a counselor educator at the rank of full professor, but other studies in counselor education have also found higher levels of scholarly productivity for full professors compared to associate professors (Hatchett et al., 2020; Ramsey et al., 2002). Although Lambie et al. (2014) found that associate professors had more journal article publications than full professors, their study included only counselor educators at doctoral-level programs and covered a discrete 6-year period of journal article publication counts. Thus, these two studies are not directly comparable. Several researchers have also found that male counselor educators attain more journal article publications than female counselor educators (Lambie et al., 2014; Newhart et al, 2020; Ramsey et al., 2002). Thus, the results from the current study are consistent with the majority of other research on this topic. Finally, in the current study, the date of terminal degree attainment had a minor impact on journal article publication counts. This is consistent with two other studies in the literature (Hatchett et al., 2020; Lambie et al., 2014). There are at least two plausible explanations for this finding. On the one hand, expectations for scholarly productivity have increased in recent years (Fairweather, 2005; Youn & Price, 2009); thus, it is not surprising that counselor educators who have attained their terminal degrees more recently have more journal article publications. From another perspective, Lambie et al. (2014) hypothesized that more recent graduates of counselor education programs may have stronger research skills than those who graduated earlier. Both explanations are speculative, so future research might better elucidate the role of time and training experiences on journal article publications.
The final objective of the study was to evaluate the extent to which journal article publication rates change over the course of counselor educators’ careers. The sequence charts presented in Figures 1 and 2 provide evidence that scholarly productivity is not invariant over the first 20 years since doctoral degree completion but tends to vary based on time, current academic rank, and inferred binary gender. There seems to be a relative peak around Year 7 for full professors and Year 14 for associate professors. The peak at Year 7 for full professors may be attributable to the typical timeframe for applying for tenure and promotion to associate professor; however, it is unclear why the associate professors exhibited a relative peak at Year 14. There also seems to be a peak around Year 7 for male counselor educators and Year 11 for female counselor educators. Again, the peak around Year 7 for male counselor educators is consistent with the typical timeframe for applying for tenure and promotion to associate professor. Though speculative, the delayed peak for female counselor educators may be the result of childbirth and early childcare responsibilities. Some research indicates that female faculty members plan childbirth around the academic calendar and tenure clock (e.g., Armenti, 2004), so perhaps a similar phenomenon occurred among the female counselor educators in this sample. More research is needed on how childbirth and childcare experiences impact the career decisions and scholarly productivity of female counselor educators (e.g., Trepal & Stinchfield, 2012). Finally, for the entire sample, there seems to be a relative decline in journal article publications near the end of the 20-year observational period. This lower level of scholarly productivity may reflect fewer institutional incentives to continue publishing, less interest in conducting original research, or a shift to other professional responsibilities, such as leadership positions on campus or in professional counseling associations.
Limitations
One clear limitation to the current study was the inability to apply a time series analysis to the data. As already mentioned, there were not enough observation periods to run a time series analysis with sufficient statistical power. In addition, the sequence charts were based on the average number of publications attained by these counselor educators on a yearly basis. The distribution of journal article publications for every observational unit was positively skewed, and the median number of publications for every observational unit was zero. Consequently, if the median number of publications each year had been plotted on the sequence charts, both graphs would have included two flat lines directly on the x-axis. Expressed differently, the typical counselor educator at a comprehensive university did not attain any journal article publications in a typical year. Thus, to some extent, the trends plotted in Figures 1 and 2 reflect only the most active researchers in this population.
It is also important to note that this study operationalized a very narrow definition of scholarly productivity: journal articles referenced in the PsycINFO, ERIC, or Academic Search Complete electronic databases. Though a highly reliable operational definition, and one used by other researchers (Barrio Minton et al., 2008; Hatchett et al., 2020; Lambie et al., 2014), this index certainly does not capture the full breadth of scholarly productivity. Counselor educators across all types of universities write book chapters and books, present at conferences, prepare reports, and secure external grant funding, among many other additional activities (e.g., Ramsey et al., 2002).
A final limitation of this study was the professional backgrounds of the counselor educators in this sample. Though all the counselor educators were faculty at CACREP-accredited programs, only about 50% had terminal degrees in counseling or counselor education. At the time of these counselor educators’ terminal degrees, CACREP did not stipulate that core faculty must have doctoral degrees in counselor education and supervision from CACREP-accredited programs. Even accounting for the grandfathering clause of 2013, a clear majority of the faculty in CACREP-accredited counseling programs now have doctoral degrees from CACREP-accredited counselor education and supervision programs (Hatchett, 2021). It is unknown whether this shift in the professional backgrounds of counselor education faculty will eventually impact the long-term trajectory of counselor educators at comprehensive universities.
Implications for Counselor Education
The results from the current study indicate that the typical counselor educator at a master’s-only counseling program at a comprehensive university will generate less than six journal article publications over the course of their career. Also, if these reported trends are stable across time, a significant minority will not attain any referenced journal article publications across their careers. These trends do not mean that counselor educators at comprehensive universities do not make meaningful contributions to the field of counseling in other ways, such as conference presentations, book chapters, grants, or evaluation reports (e.g., Ramsey et al., 2002). Also, as already mentioned, the electronic databases selected for this study and the study by Hatchett et al. (2020) do not capture all of the journals in which counselor educators publish. Nonetheless, it does reflect a relatively low level of original research published in peer-reviewed journals that is easily accessible through searching three popular electronic databases.
The results from this study—combined with the typical occupational outcomes of program graduates—should have implications for doctoral-level training in counselor education. As previously mentioned, all graduates of CACREP-accredited doctoral programs are required to acquire numerous research competencies that will equip them for making original and meaningful contributions to the counseling literature (CACREP, 2015). Yet, most graduates of these programs do not attain faculty positions in higher education, and among those who do, relatively few will be employed at research-intensive universities (e.g., Lawrence & Hatchett, 2022; Schweiger et al., 2012; Zimpfer, 1996). Furthermore, based on the distribution of CACREP programs across the Carnegie Classification System, program graduates who do secure faculty positions will be more likely to be employed at master’s-level universities than at institutions classified as R1 or R2.
It might be argued that the low rate of journal article publications produced by counselor educators at comprehensive universities is not problematic. Counselor educators at comprehensive universities spend proportionately more of their worktime on teaching and administrative tasks (Hatchett, 2021), and they often lack the institutional resources experienced by their colleagues at more research-intensive universities, such as access to research assistants (Henderson, 2011). Expecting counselor educators at comprehensive universities to do more research might be as fair as asking counselor educators at research-intensive universities to do more teaching and service (Hatchett et al., 2020). Yet, on the other hand, one should also consider what is being lost by the low levels of research found among many of the counselor educators at comprehensive universities. Many of these counselor educators are presumably not using the multitude of research competencies they developed during their doctoral-level training. The research training prescribed by CACREP is not just the means to a single end, a completed dissertation. One of the explicit training objectives of CACREP-accredited doctoral programs is to prepare program graduates to generate and disseminate new knowledge in the field of counseling (CACREP, 2015), an objective commonly discharged through publishing original research in peer-reviewed journal articles. The current study cannot resolve this conflict, but hopefully it will facilitate additional discussions on the value and role of research training in CACREP-accredited doctoral-level programs.
Recommendations for Future Research
One recommendation for future research, and one directly derived from the previous discussion, would be to investigate the extent to which graduates of CACREP-accredited doctoral programs use the skills and competencies acquired as part of their training. For example, researchers might investigate the extent to which program graduates use specific skills in teaching, research, grant work, clinical supervision, program evaluation, consultation, and clinical practice as part of their postgraduate occupations. The distributions of these actual work responsibilities could then be compared to the relative emphases of these competencies in doctoral-level training programs. Another recommendation for future research would be to replicate this study with counselor educators at universities with higher expectations of scholarly productivity, such as counselor educators at R1 or R2 universities, and those universities that offer CACREP-accredited doctoral degrees in counselor education, irrespective of Carnegie Classifications. Such research might identify trends and patterns in publication patterns for those counselor educators who are expected to produce and maintain higher levels of scholarly productivity over the entire course of their careers.
Conclusion
Consistent with the results of earlier research (Hatchett et al., 2020), the current study suggests that counselor educators at comprehensive universities—in general—publish minimal research in peer-reviewed journals. Furthermore, the journal article publications of these counselor educators exhibited a relative decline over the course of the first 20 years of the educators’ careers. These findings are somewhat in conflict with the accreditation standards delineated by CACREP and the objectives of doctoral-level training in counselor education. CACREP (2015) requires that all new core faculty have a doctoral degree in counselor education and supervision from accredited doctoral programs. These accredited doctoral programs stipulate that all program graduates attain numerous competencies in research and scholarship, irrespective of the graduates’ career plans. Yet, most graduates of CACREP-accredited doctoral programs do not attain faculty positions as counselor educators (Lawrence & Hatchett, 2022; Schweiger et al., 2012; Zimpfer, 1996), and for those who do, they are more likely to be employed at comprehensive universities at which scholarly productivity tends to be minimal than at more research-intensive universities at which high levels of scholarly productivity will be needed for promotion and tenure. Given these outcomes, counselor educators should revisit the nature of doctoral-level training and reevaluate the extent to which the curricula of CACREP-accredited programs prepare program graduates for the most common career pathways after graduation.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Armenti, C. (2004). May babies and posttenure babies: Maternal decisions of women professors. The Review of Higher Education, 27(2), 211–231. https://doi.org/10.1353/rhe.2003.0046
Barrio Minton, C. A., Fernando, D. M., & Ray, D. C. (2008). Ten years of peer-reviewed articles in counselor education: Where, what, who? Counselor Education and Supervision, 48(2), 133–143.
https://doi.org/10.1002/j.1556-6978.2008.tb00068.x
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum.
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards.
http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Dill, D. D., & Morrison, J. L. (1985). EdD and PhD research training in the field of higher education: A survey and a proposal. The Review of Higher Education, 8(2), 169–186.
Doyle, S. R. (2009). Examples of computing power for zero-inflated and overdispersed count data. Journal of Modern Applied Statistical Methods, 8(2), 360–376. https://doi.org/10.22237/jmasm/1257033720
Fairweather, J. S. (2005). Beyond the rhetoric: Trends in the relative value of teaching and research in faculty salaries. The Journal of Higher Education, 76(4), 401–422. https://doi.org/10.1353/jhe.2005.0027
Fox, J. (2008). Applied regression analysis and generalized linear models (2nd ed.). SAGE.
Garson, G. D. (2019). Multilevel modeling: Applications in STATA®, IBM® SPSS®, SAS®, R, & HLM™. SAGE.
Hatchett, G. T. (2020). Perceived tenure standards, scholarly productivity, and workloads of counselor educators at comprehensive universities. The Journal of Counselor Preparation and Supervision, 13(4).
https://digitalcommons.sacredheart.edu/jcps/vol13/iss4/9
Hatchett, G. (2021). Tenure standards, scholarly productivity, and workloads of counselor educators at doctoral and master’s-only counseling programs. The Journal of Counselor Preparation and Supervision, 14(4).
https://digitalcommons.sacredheart.edu/jcps/vol14/iss4/4
Hatchett, G. T., Sylvestro, H. M., & Coaston, S. C. (2020). Publication patterns of counselor educators at comprehensive universities. Counselor Education and Supervision, 59(1), 32–45.
https://doi.org/10.1002/ceas.12164
Henderson, B. B. (2011). Publishing patterns at state comprehensive universities: The changing nature of faculty work and the quest for status. The Journal of the Professoriate, 5(2), 35–66. http://caarpweb.org/wp-content/uploads/2016/11/5-2_Henderson_p.35.pdf
Lambie, G. W., Ascher, D. L., Sivo, S. A., & Hayes, B. G. (2014). Counselor education doctoral program faculty members’ refereed article publications. Journal of Counseling & Development, 92(3), 338–346.
https://doi.org/10.1002/j.1556-6676.2014.00161.x
Lawrence, C., & Hatchett, G. T. (2022). Academic employment prospects for counselor education doctoral candidates [Manuscript submitted for publication]. Northern Kentucky University, School of Kinesiology, Counseling, and Rehabilitative Sciences.
Lyles, R. H., Lin, H.-M., & Williamson, J. M. (2007). A practical approach to computing power for generalized linear models with nominal, count, or ordinal responses. Statistics in Medicine, 26(7), 1632–1648.
https://doi.org/10.1002/sim.2617
Newhart, S., Mullen, P. R., Blount, A. J., & Hagedorn, W. B. (2020). Factors influencing publication rates among counselor educators. Teaching and Supervision in Counseling, 2(1), 5. https://doi.org/10.7290/tsc020105
Ramsey, M., Cavallaro, M., Kiselica, M., & Zila, L. (2002). Scholarly productivity redefined in counselor education. Counselor Education and Supervision, 42(1), 40–57. https://doi.org/10.1002/j.1556-6978.2002.tb01302.x
Schweiger, W. K., Henderson, D. A., McCaskill, K., Clawson, T. W., & Collins, D. R. (2012). Counselor preparation: Programs, faculty, trends (13th ed.). Routledge.
Snow, W. H., & Field, T. A. (2020). Introduction to the special issue on doctoral counselor education. The Professional Counselor, 10(4), 406–413. https://doi.org/10.15241/whs.10.4.406
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Trepal, H. C., & Stinchfield, T. A. (2012). Experiences of motherhood in counselor education. Counselor Education and Supervision, 51(2), 112–126. https://doi.org/10.1002/j.1556-6978.2012.00008.x
Yaffee, R., & McGee, M. (2000). Introduction to time series analysis and forecasting with applications of SAS and SPSS. Academic Press.
Youn, T. I. K., & Price, T. M. (2009). Learning from the experience of others: The evolution of faculty tenure and promotion rules in comprehensive institutions. The Journal of Higher Education, 80(2), 204–237.
Zimpfer, D. G. (1996). Five-year follow-up of doctoral graduates in counseling. Counselor Education and Supervision, 35(3), 218–229. https://doi.org/10.1002/j.1556-6978.1996.tb00225.x
Gregory T. Hatchett, PhD, NCC, LPCC-S, is a professor at Northern Kentucky University. Correspondence may be addressed to Gregory T. Hatchett, MEP 211, Highland Heights, KY 41099, hatchettg@nku.edu.
Aug 10, 2022 | Volume 12 - Issue 2
Lacey Ricks, Malti Tuttle, Sara E. Ellison
Quantitative methodology was utilized to assess factors influencing veteran school counselors’ decisions to report suspected child abuse. Veteran school counselors were defined as having 6 or more years of experience working as a school counselor within a public or private school. This study is a focused examination of the responses of veteran school counselors from a larger data set. The results of the analysis revealed that academic setting, number of students within the school, and students’ engagement in the free or reduced lunch program were significantly correlated with higher reporting among veteran school counselors. Moreover, veteran school counselors’ self-efficacy levels were moderately correlated with their decision to report. Highly rated reasons for choosing to report suspected child abuse included professional obligation, following school protocol, and concern for the safety of the child. The highest rated reason for choosing not to report was lack of evidence. Implications for training and advocacy for veteran school counselors are discussed.
Keywords: child abuse, reporting, veteran school counselors, self-efficacy, training
In 2019, approximately 4.4 million reports alleging maltreatment were made to U.S. child protective services (U.S. Department of Health & Human Services [HHS] et al., 2021). Of these reports, nearly two thirds were made by professionals who encounter children as a part of their occupation. Child maltreatment is identified as all types of abuse against a child under the age of 18 by a parent, caregiver, or person in a custodial role, and includes physical abuse, sexual abuse, emotional abuse, and neglect (Fortson et al., 2016). Public health emergencies, such as the continued COVID-19 pandemic, increase the risk for child abuse and neglect due to increased stressors (Swedo et al., 2020). Factors such as financial hardship, exacerbated mental health issues, lack of support, and loneliness may contribute to increased caregiver distress, ultimately resulting in negative outcomes for children and adolescents (Collin-Vézina et al., 2020).
The psychological impact of child abuse and neglect on victims can increase the risk of mental health disorders such as depression, anxiety, eating disorders, and post-traumatic stress disorder (Heim et al., 2010; Klassen & Hickman, 2022). Similarly, trauma experienced in childhood is associated with higher rates of long-term physical health issues when compared to individuals with less trauma; these include cancer (2.4 times more likely to develop), diabetes (3.0 times as likely to develop), and stroke (5.8 times more likely to experience; Bellis et al., 2015). Children who are victims of child abuse and neglect may also experience educational difficulties, low self-esteem, and trouble forming and maintaining relationships (Child Welfare Information Gateway, 2019).
Voluntary disclosure of childhood abuse is relatively uncommon; one study found that less than half of adults with histories of abuse reported disclosing the abuse to anyone during childhood, and only 8%–16% of those disclosures resulted in reporting to authorities (McGuire & London, 2020). For this reason, mandated reporting by professionals is an integral piece of child abuse prevention. School counselors, by virtue of their ongoing contact with children, are uniquely positioned to identify and report child abuse (Behun et al., 2019). We recognize that school-based professionals such as teachers, administrators, and other school-based staff are mandated reporters as well. However, for the purpose of this article, we specifically focus on school counselors based on their role, responsibility, and training that best equips them to fulfill this expectation. School counselors have a unique role within the school system and play a critical role in ensuring schools are a safe, caring environment for all students (American School Counselor Association [ASCA], 2017). School counselors also work to identify the impact of abuse and neglect on students as well as ensure the necessary supports for students are in place (ASCA, 2021).
Ethical and Legal Mandates for Reporting Suspected Child Abuse
Although current estimates for the reporting frequency within schools are not available, it appears likely that high numbers of school counselors encounter the decision to report suspected child abuse each year. In fact, a 2019 survey of 262 school counselors indicated that 1,494 cases of child abuse had been reported by participants over a 12-month period (Ricks et al., 2019). Despite the frequency with which it occurs, reporting can be a distressing part of school counselors’ responsibilities (Remley et al., 2017); this could be because of limited knowledge or competency in reporting procedures, unfamiliarity with the law, or potential repercussions for the child (Bryant, 2009; Bryant & Milsom, 2005; Lambie, 2005). Additionally, laws, definitions, and mandates of child abuse and neglect vary by state; therefore, confusion may arise when school counselors relocate to another area (ASCA, 2021; Hogelin, 2013; Lambie, 2005; Tuttle et al., 2019). School counselors need to identify and familiarize themselves with the unique laws in their state in addition to reviewing federal law and ethical codes.
Federally, school counselors are mandated by the Child Abuse Prevention and Treatment Act of 1974, Public Law 93-247, to report suspected abuse and neglect to proper authorities (ASCA, 2021). Failure to report suspected abuse could result in civil or criminal liability (Remley et al., 2017; White & Flynt, 2000). ASCA Ethical Standards echo this mandate, directing school counselors to report suspected child abuse and neglect while protecting the privacy of the student (ASCA, 2022a, A.12.a). School counselors should also assist students who have experienced abuse and neglect by connecting them with appropriate services (ASCA, 2022a). Moreover, school counselors should work to create a safe environment free from abuse, bullying, harassment, and other forms of violence for students while promoting autonomy and justice (ASCA, 2022a).
School Counselors as Advocates in Mandated Reporting
Barrett et al. (2011) recognized school counselors as social justice leaders based on their role to advocate for students who are underserved, disadvantaged, maltreated, or living in abusive situations. Child abuse impacts children and adolescents from every race, socioeconomic status, gender, and age (Lambie, 2005; Tillman et al., 2015). School counselors who are trained to provide culturally sustaining school counseling will work with students and families from all demographics to promote student wellness within their comprehensive school counseling program (ASCA, 2021). As leaders within the school, school counselors, and especially veteran school counselors, can work to educate all stakeholders on the implications of child abuse.
School counselors not only are legally positioned to serve as mandated reporters but also ethically positioned to train school personnel in recognizing and identifying child abuse symptoms and in reporting procedures (Hodges & McDonald, 2019). Training of school personnel, such as teachers, to identify and report suspected child abuse is essential because they are also recognized legally as mandated reporters (Hupe & Stevenson, 2019) and they interact with students daily. It is vital that school counselors advocate for ongoing comprehensive training related to child abuse because their knowledge affects many stakeholders in the school setting (ASCA, 2021; Tuttle et al., 2019).
Self-Efficacy Among Veteran School Counselors
Previous literature from this data set highlighted the reporting behaviors of early career school counselors (Ricks et al., 2019), and a framework was developed to assist new professionals in reporting (Tuttle et al., 2019). However, the child abuse reporting behaviors and needs of veteran school counselors are understudied. Therefore, this article focuses on veteran school counselors. For the purpose of this study, veteran school counselors are considered licensed school counselors having 6 or more years of experience. Professional literature has highlighted the unique needs and experiences of novice counselors as compared to veteran school counselors (Buchanan et al., 2017; Johnson et al., 2017). One study (Mishak, 2007) examined differences in instructional strategies for early career and veteran school counselors in elementary schools in Iowa. Although that study does not specifically address child abuse reporting, it does highlight differences found among the respondents based on their experience level.
One factor supporting the unique needs of veteran school counselors is self-efficacy. Self-efficacy theory posits that an individual’s expectations of mastery are strongly influenced by personal experience and indirect exposure to a phenomenon (Bandura, 1977, 1997). Veteran school counselors, based on their years of experience in a school setting, are likely to have multiple exposures to child abuse reporting. They may have filed reports themselves, spoken to peers about their reporting experiences, or assisted other professionals in the school with reporting. Bandura (1997) suggested that self-efficacy is supported when individuals not only possess the skill and ability to complete a task, but also have the confidence and motivation to execute it.
Veteran school counselors can receive ongoing training from workshops, university courses, webinars, district training, or other professional organizations that may further impact self-efficacy levels. Previous research has shown that as an individual’s knowledge of child abuse increases, their levels of self-efficacy in recognizing or reporting child abuse also increases (Balkaran, 2015; Jordan et al., 2017). However, little research linking school counselors’ self-efficacy levels to child abuse reporting has been published. Despite the paucity of research on this topic, Ricks et al. (2019) found a moderate relationship between early career school counselors’ self-efficacy and their ability to identify types of abuse. Additionally, Tang (2020) found that school counseling supervision increased school counselor self-efficacy; differences between early career and veteran school counselors were not addressed in Tang’s study. Although the positive correlation found by Tang did not directly address child abuse reporting, assisting students with crisis situations was one of the principal components of the analysis. Even though veteran school counselors have experience serving as mandated reporters, they require ongoing professional development in this area to effectively fulfill their roles as advocates in maintaining the welfare and safety of students (ASCA, 2021; Tuttle et al., 2019). Therefore, we seek to utilize this article as a form of advocacy on behalf of veteran school counselors by providing additional research and literature in the field.
Purpose of the Present Study
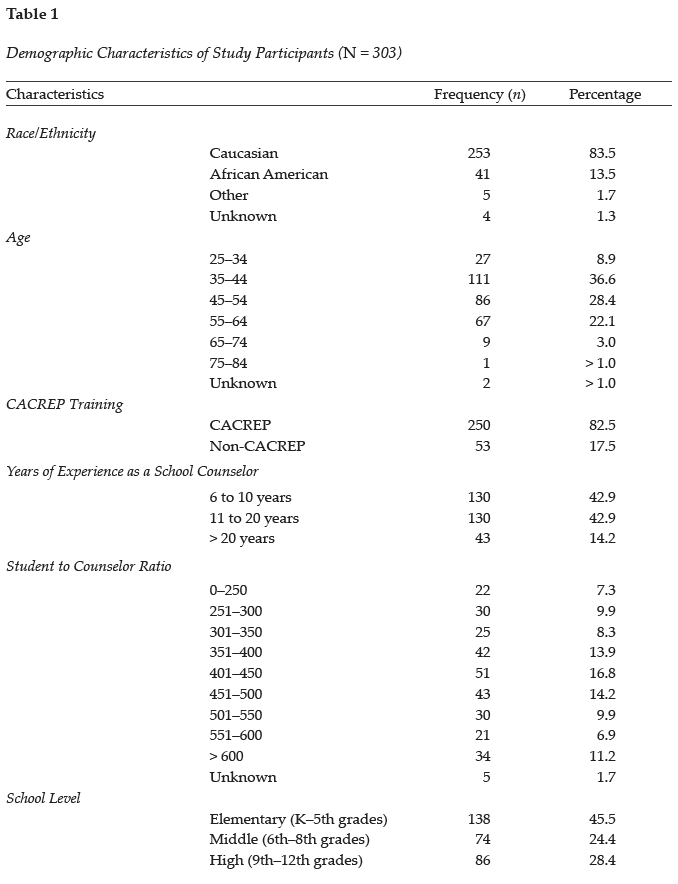
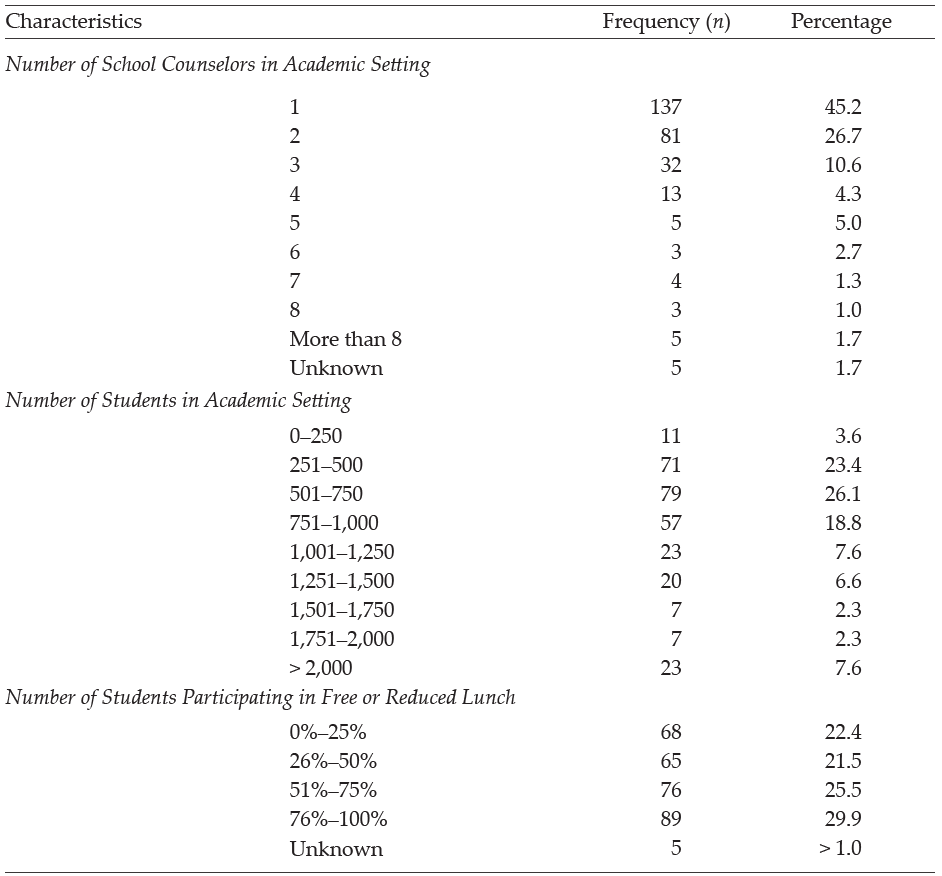
The purpose of this quantitative study is to examine (a) the prevalence of child abuse reporting by veteran school counselors within the school year; (b) the factors affecting veteran school counselors’ decisions to report or not report suspected child abuse; (c) reasons for reporting or not reporting suspected child abuse by veteran school counselors; and (d) veteran school counselors’ self-efficacy levels related to child abuse reporting. Our intent was to build upon an initial larger study to examine veteran school counselors’ knowledge of procedures and experiences with child abuse reporting. The present study is a focused examination of the data collected from veteran school counselors as part of the primary study, which solicited data from school counselors across their careers related to their experiences with child abuse reporting (see Ricks et al., 2019). Demographic variables were collected from participants to assess their impact on child abuse reporting; see Table 1 for a complete list of variables.
Methods
Multiple correlation and regression analyses were conducted to assess factors influencing veteran school counselors’ decisions to report suspected child abuse. After obtaining IRB approval, the authors recruited school counselors in the Southeastern United States (Alabama, Arkansas, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, South Carolina, Tennessee, Texas, Virginia, and West Virginia). Participants were recruited using a professional school counseling association membership list, a southeastern state counseling association listserv, and social media. Participants were informed that participation in the online study was voluntary and that they could withdraw from the study at any time. Participants were also informed that the survey would take between 10–15 minutes and that the information collected in the survey would remain anonymous.
Participants
A total of 848 surveys were collected from participants. Veteran school counselor data was extracted from the total sample and analyzed to assess the unique experiences of these individuals in child abuse reporting. Veteran school counselors were defined as having 6 or more years of experience working as a school counselor within a public or private school. Four hundred and twenty-eight veteran school counselors began the survey, but data from 125 participants was excluded from the analysis for incomplete responses, resulting in a final sample of 303 participants. Most participants (n = 265, 87.5%) reported being licensed/certified as a school counselor. Some participants may not have possessed a license because of working in the private school sector or working on a provisional basis. See Table 1 for all demographic frequencies and percentages related to participants in the study.
Measures
Three measures were selected and employed as part of the larger study. These included the Child Abuse Reporting Questionnaire (Bryant & Milsom, 2005), the School Counselor Self-Efficacy Scale (Bodenhorn & Skaggs, 2005), and the Knowledge of Child Abuse Reporting Questionnaire (Ricks et al., 2019). Each measure is described below as previously reported in Ricks et al. (2019).
Child Abuse Reporting Questionnaire
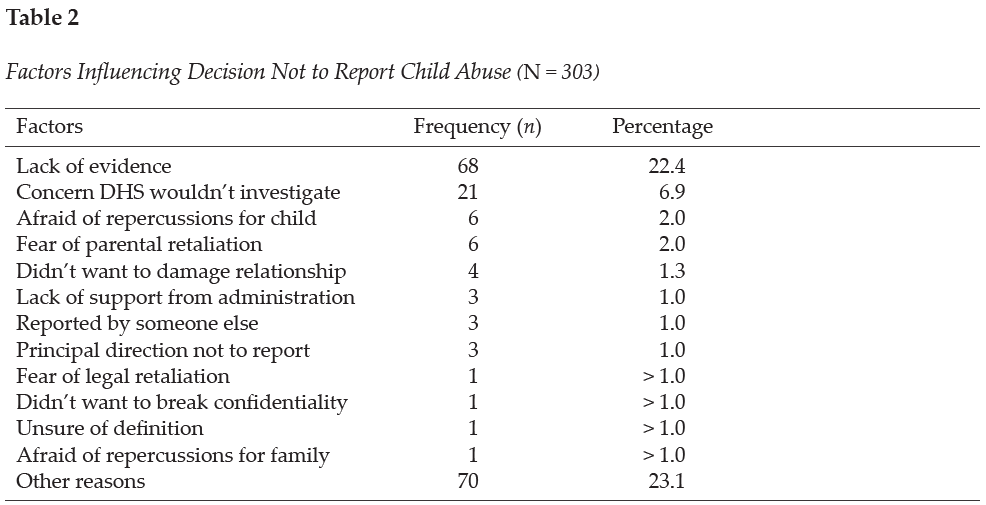
The Child Abuse Reporting Questionnaire was developed to assess three domains, including school counselor General Information, Training in Child Abuse Reporting, and Child Abuse Reporting Experience (Bryant & Milsom, 2005). In the first section of the questionnaire, Training in Child Abuse Reporting, participants were asked to list where they obtained their knowledge of child abuse reporting and to assess four different types (physical, sexual, neglect, emotional) of child abuse. In the Child Abuse Reporting Experience section, the participants were asked two questions. The first question asked participants to recall the number of suspected child abuse cases they encountered during the preceding school year and the number of child abuse cases they reported. The next question asked participants how many cases of suspected child abuse they did not report. Participants were also asked in the survey to indicate reasons for choosing not to report suspected child abuse cases based on 12 commonly reported barriers or to list other reasons for not reporting the suspected cases. See Table 2 for a complete list of the common reasons given for not reporting suspected child abuse cases. Internal consistency measures were not obtained for this questionnaire because of the demographic nature of assessing participants’ personal experiences with child abuse reporting.
School Counselor Self-Efficacy Scale
The School Counselor Self-Efficacy Scale (SCSE) was used to assess school counselors’ self-efficacy and to link their personal attributes to their career performance (Bodenhorn & Skaggs, 2005). Participants completed Likert scale questions to indicate their confidence in performing school counseling tasks for 43 scale items. An example question would ask school counselors to indicate their confidence in advocating for integration of student academic, career, and personal development into the mission of their school. A rating of 1 indicated not confident and a rating of 5 indicated highly confident. The coefficient alpha for the scale score was found to be .95 (Bodenhorn & Skaggs, 2005). The SCSE subscales include five domains: Personal and Social Development (12 items), Leadership and Assessment (9 items), Career and Academic Development (7 items), Collaboration and Consultation (11 items), and Cultural Acceptance (4 items). The correlations of the subscales ranged from .27 to .43.
Knowledge of Child Abuse Reporting Questionnaire
The Knowledge of Child Abuse Reporting Questionnaire was developed to assess respondents’ knowledge of child abuse reporting and procedures within three areas (Ricks et al., 2019). To develop the survey, the researchers and outside counselor educators reviewed the questionnaire to determine if it clearly measured the constructs. In the first section of the questionnaire, Identifying Types of Abuse, participants’ perceptions of their ability to identify the four different types of child abuse were assessed. To complete this section, participants rated their comfort level using a 4-point Likert scale. A rating of 1 indicated very uncertain and a rating of 4 indicated very certain. The coefficient alpha for the scale score was found to be .902. The Knowledge of Guidelines section assessed participants’ knowledge of the state rules, ASCA Ethical Standards, and child abuse reporting protocol within their current school and district. To complete this section, participants rated their comfort level using a 5-point Likert scale. A rating of 1 indicated not knowledgeable and a rating of 5 indicated extremely knowledgeable. The coefficient alpha for the scale score was found to be .799. Lastly, the Child Abuse Training section assessed where participants received training on general knowledge of child abuse reporting, how to make a referral, and indicators of child abuse. To complete this section, participants selected options from a dropdown menu based on commonly reported agencies or listed an organization not provided. Options included in the survey list were universities or colleges, schools or districts, conferences or workshops, colleagues, journals, professional organizations, or the state department of education.
Data Analysis
SPSS Statistics 27 was used to analyze data within this study. First, a correlation analysis was executed to assess the strength of the relationship across variables. Next, analyses of variance (ANOVAs) were performed to assess the relationship between the number of reported child abuse cases and five demographic variables, which included academic setting (elementary, middle, high); number of students participating in the school’s free or reduced lunch program; number of school counselors working in a school setting; years of experience as a school counselor; and number of students enrolled in a school setting. Lastly, regression analyses were used to determine the relationship between school counselors’ self-efficacy and their decisions to report or not report suspected child abuse cases as well as to assess the relationship between school counselors’ self-efficacy and their certainty in identifying types of abuse.
Results
Suspected and Reported Cases of Abuse
Descriptive statistics generated from the child abuse survey included the participants (N = 303) suspecting 2,289 cases of child abuse during the school year. Scores reported by participants ranged from 0 to 100 (M = 7.71, SD = 10.58). Seven participants omitted this question within the questionnaire. Participants indicated reporting a total of 2,140 cases of suspected child abuse; individual frequency ranged from 0 to 100 (M = 7.21, SD = 10.25). Physical child abuse cases (M = 4.03, SD = 7.12) were reported at a higher rate than cases of neglect (M = 2.72, SD = 5.10), emotional abuse (M = 0.56, SD = 1.52), and sexual abuse (M = 0.57, SD = 1.37).
School Demographics
The relationship between the number of reported child abuse cases and demographic variables was examined using a bivariate correlation. Results indicated a negative correlation between the number of child abuse reports and the academic level of students the school counselor works with (elementary, middle, or high school), r(293) = −.283, p < .001, with elementary school counselors reporting child abuse at a higher rate than high school counselors. An additional negative correlation was found between the number of child abuse reports and the number of school counselors working within the school, r(293) = −.164, p < .001. Results indicated a positive significant relationship between the number of reported child abuse cases and the number of students who participate in the school’s free or reduced lunch program, r(293) = .225, p < .001. Weaker negative relationships were also found between the number of child abuse reports and the participants’ years of experience as a school counselor, r(297) = −.115, p < .05, as well as how many students are enrolled in a school, r(293) = −.127, p < .06. No other significant relationships were found among the variables and reported cases.
An ANOVA was conducted to examine the relationship between the academic level of students (elementary, middle, and high) the participants worked with and the number of child abuse cases reported. Results showed a significant relationship among the variables, f(2, 290) = 13.021, p > .00. A follow-up test was used to evaluate pairwise differences among the means. Results of a Tukey HSD indicated a significant difference between elementary (M = 10.314) and high school (M = 3.58) counselors who reported child abuse. A difference was also found between elementary and middle school (M = 5.86) reporting levels. No other significant differences were found between variables.
An ANOVA was also conducted to evaluate the differences between child abuse reporting and the percentage (0%–25%, 26%–50%, 51%–75%, 76%–100%) of students who participated in free or reduced lunch. Results showed a significant relationship among the variables, f(3, 289) = 5.22, p = .002. A Tukey HSD post hoc test was used to make a pairwise comparison and statistically significant mean differences were found between the 0%–25% (M = 2.33) group and the 51%–75% (M = 7.78) group. Additionally, a difference was found between the 0%–25% group and the 76%–100% (M = 10.12) group. Lastly, a difference was found between the 26%–50% (M = 6.54) group and the 76%–100% group. No other significant differences were found between the groups.
An ANOVA was conducted to examine the relationship between how many school counselors are working in a school setting and the differences in child abuse reporting. Analysis of the ANOVA found no significant difference (p < .05) between the groups (one counselor, M = 8.26; two counselors, M = 7.81; three counselors, M = 7.69; four counselors, M = 5.00; five counselors, M = 2.80; six counselors, M = 2.25; seven counselors, M = 3.50; eight counselors, M = 2.33; more than eight counselors, M = 2.20), but a downward trend can be seen in the number of cases reported with the increase in the number of school counselors within a school.
Likewise, an ANOVA was used to examine the relationship between years of experience as a school counselor and the differences in child abuse reporting, but no significant difference (p < .05) was found between groups (6 to 10 years, M = 8.58; 11 to 20 years, M = 6.36; above 20 years, M = 5.57); however, a slight trend can be seen with participants who have less experience reporting at higher rates. A larger sample size may have yielded significant results, but additional research is needed in this area.
Lastly, an ANOVA was also executed to assess the differences in child abuse reporting and the number of students enrolled in a school setting. A significant difference was found between schools with more than 2,000 students (M = 3.00) and schools with 251–500 students (M = 8.07) as well as schools with 501–750 students (M = 8.63). This difference suggests school counselors who work in schools with more students tend to report child abuse at a lower rate than those who work in smaller schools. A downward trend can be seen in reporting of cases as student numbers increase (751–1,000 students, M = 7.62; 1,001–1,250 students, M = 7.39; 1,251–1,500 students, M = 6.68; 1,501–1,750 students, M = 6.00; 1,751–2,000 students, M = 2.57), with the exception of the 0–250 students (M = 4.82) school classification. Differences in the sample sizes of classification categories could have impacted significance outcomes. No other significant differences were found between the groups.
The Decision to Report
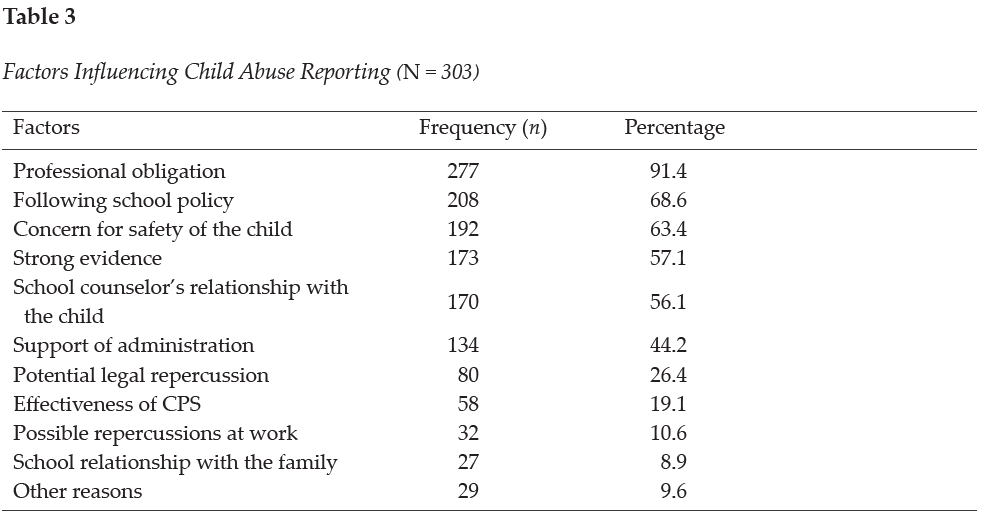
On the Child Abuse Reporting Survey, participants (N = 303) were asked to indicate what factors influenced their decision to report child abuse. Participants indicated the number one factor was following the law (professional obligation; 91.4%, n = 277). Other reasons cited by over half of school counselors included following school policy (68.6%, n = 208), concern for safety of the child (63.4%, n = 192), strong evidence that abuse had occurred (57.1%, n = 173), and the school counselor’s relationship with the child (56.1%, n = 173). See Table 3 for factors influencing child abuse reporting. Further, participants indicated reasons why they chose not to report suspected child abuse. Participants specified inadequate evidence as the primary reason for not reporting suspected child abuse (22.4%, n = 68). Another notable influence included concern that DHS would not investigate the reported case (6.9%, n = 21). See Table 2 for factors influencing the decision not to report child abuse.
Knowledge and Training
On the Knowledge of Child Abuse Reporting Questionnaire, participants were asked to rate how certain they feel about their abilities to identify types of abuse on a 4-point Likert scale with 1 indicating very uncertain and 4 indicating very certain. Participants reported most confidence in their ability to identify physical abuse (M = 3.49, Mdn = 4), followed by neglect (M = 3.30, Mdn = 3), sexual abuse (M = 3.20, Mdn = 3), and emotional abuse (M = 3.06, Mdn = 3). When participants (N = 303) were asked where they gained knowledge about child abuse, most reported receiving training from professional experiences (88.4%, n = 268), mandated reporting training at school (79.5%, n = 241), workshops (72.3%, n = 219), discussion with colleagues (61.4%, n = 186), or literature (58.1%, n = 176). Additionally, participants indicated gaining knowledge from university courses (46.5%, n = 141), media (9.2%, n = 28), or other avenues unlisted in the survey (12.2%, n = 37).
Participants were asked where they received training on how to make a referral for a child abuse case. Most of the school counselors responded that they received the training from a school/district training (87.5%, n = 265), conference/workshop (57.4%, n = 174), or university class (42.9%, n = 130). Other responses included from a colleague (38.9%, n = 118), professional organization (32.7%, n = 99), Department of Education website (20.5%, n = 62), journal (10.9%, n = 33), or other sources (11.2%, n = 34). Lastly, veteran counselors were asked where they received training about the indicators of child abuse. The majority of the respondents reported learning in a school/district training (87.1%, n = 264), conference/workshop (77.9%, n = 236), or university/college course (67.3%, n = 204). Other responses included learning from a professional organization (38%, n = 115), colleague (30%, n = 91), journal (23.4%, n = 71), Department of Education website (21.5%, n = 65), or other sources (9.9%, n = 30).
Veteran school counselors reported that 88.1% (n = 267) of schools/districts provided them with training on local abuse reporting policies. Therefore, 11.9% did not receive training from their local school system. Additionally, 60.1% (n = 182) of the school counselors reported their school/district had a handbook/resource outlining the steps for mandated reporter training within their school system. Consequently, 39.9% of the school counselors reported not having a handbook/resource to reference outlining steps for mandated reporting.
Self-Efficacy and Child Abuse Reporting
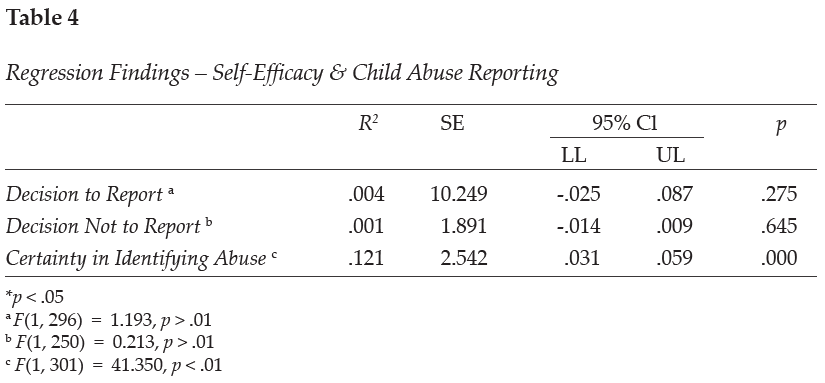
A regression analysis was used to examine the relationship between veteran school counselors’ self-efficacy and three variables, including the number of reported child abuse cases, the decision not to report suspicion of child abuse, and certainty in identifying types of child abuse. Results showed the strength of the relationship between self-efficacy and certainty in identifying types of child abuse was moderately related, F(1, 301) = 41.350, p < .01. Over 12% (r2 = 0.121) of the variance of the school counselors’ self-efficacy level was associated with certainty in identifying child abuse. No other significant results were found among the variables. See Table 4 for the regression analysis related to self-efficacy and child abuse reporting.
Discussion
Given the well-documented negative impact of child abuse on the emotional, physical, and academic well-being of children, it is essential to understand how school counselors are trained to identify and report child abuse. Understanding trends and research in child abuse reporting can help schools prepare school counselors and other staff members. It is imperative for veteran school counselors to receive ongoing training to best serve as advocates for students, maintain relevancy in their roles as mandated reporters by staying current on laws and policies, and further their ability to work within their scope of practice. Ongoing training may also help alleviate difficulties that arise because of terminology differing from state to state and district to district (ASCA, 2021; Hogelin, 2013; Lambie, 2005; Tuttle et al., 2019).
In this study, veteran school counselors’ reporting frequency is shown to differ based on various school demographics. Veteran school counselors were specifically targeted in this analysis to examine their experiences related to child abuse reporting. Although these findings may not show direct causation to child abuse reporting among veteran school counselors, they can help us better understand school and school counselor demographics that need to be evaluated further. The findings can also be used to guide professional development training needed for school counselors as well as additional training needs for counselors-in-training.
Elementary school counselors were found to report child abuse at a higher rate than middle or high school counselors; however, this is anticipated because studies show that younger children experience higher rates of maltreatment than older children (HHS et al., 2021). In fact, rates of maltreatment seem to decrease as age increases. Children who are 6 years old have victimization rates of 9.0 per 1,000 children compared to children who are 16 years of age who have a victimization rate of 5.5 per 1,000 children (HHS et al., 2021). Higher maltreatment levels in younger children may be because of increased caregiver burden (Fortson et al., 2016); as children get older, they are better able to care for themselves and avoid parental confrontation. In addition, older students may be more likely to hide abuse and more astute when dealing with disclosure protocol (Bryant & Milsom, 2005). Knowledge of the signs and symptoms of child abuse and neglect can help school counselors identify children suffering from maltreatment.
Within this study on veteran school counselors, a slight trend can be seen with participants with less experience reporting suspected child abuse at a higher rate. Differences of reporting rates by years of experience may be because of higher ego maturity in less experienced school counselors because of more recent training in their graduate programs (Lambie et al., 2011). According to Lambie et al. (2011), ego development predicts an individual’s level of ethical and legal knowledge, which has been found to be higher in counselors-in-training than the average school counselor. Ego development has also been correlated with greater degrees of self-efficacy (Singleton et al., 2021), which can impact school counselors’ actions when making decisions related to child abuse reporting. Tuttle et al. (2019) also emphasized the need for continuous training to increase school counselors’ self-efficacy as mandated reporters, although more research is needed to understand the impact of self-efficacy on school counselor action. These findings highlight the need for continued assessment of training needs for school counselors of various experience levels.
Although age has been associated with varying levels of child abuse victimization, low socioeconomic status within the home environment has also been identified as a high risk factor for child abuse (Bryant, 2009; Bryant & Milsom, 2005; Ricks et al., 2019; Sedlak et al., 2010). Specifically, the higher the percentage of students participating in the school’s free or reduced lunch program, the more child abuse cases the school counselor reported (Bryant, 2009; Bryant & Milsom, 2005; Ricks et al., 2019). Although most children in low-income families do not experience child abuse, one study estimated that 22.5 children per 1,000 in low-income families experience maltreatment as compared to 4.4 per 1,000 in more affluent families (Sedlak et al., 2010). However, it is important to note the disproportionality that exists within child welfare reporting; non-White children and children of low socioeconomic status are reported to child protective services at a higher rate than their peers (Krase, 2015; Luken et al., 2021). School counselors working in low-income schools need to be aware of the increased risk factors of low socioeconomic status as well as the racial and economic disproportionality that occurs within child maltreatment reporting as a result of possible bias. School counselors should work to be aware of potential biases they may hold with regard to over-reporting certain groups of children and under-reporting others (Tillman et al., 2015).
When examining the current practices of veteran school counselors, participants reported professional obligation as the number one reason they reported suspected child abuse. The primary reason given for failing to report suspected abuse was inadequate evidence. These findings are similar to prior research that shows lack of evidence as an influencing factor in school counselors’ decisions not to report suspected abuse (Bryant, 2009; Bryant & Milsom, 2005; Tillman et al., 2015); this is concerning because some cases of abuse may go unreported. As Tuttle et al. (2019) have stated, “the school counselor’s responsibility is to follow legal and ethical obligations as a mandated reporter by reporting all suspected child abuse” (p. 242). Although concern that DHS would not investigate is denoted as an important factor for why school counselors choose not to report, school counselors must recognize they do not have the proper resources or training to lead a child abuse investigation on their own (Tuttle et al., 2019). As a result, school counselors are ethically and legally mandated to report all suspected cases of abuse to the proper authorities defined by their state, school policies, and ethical codes. Failure to report cases could lead to legal ramifications for the school counselor (Remley et al., 2017; White & Flynt, 2000) and continued maltreatment for the student.
School counselors should strive to “understand child abuse and neglect and its impact on children’s social/emotional, physical and mental well-being” (ASCA, 2021, para. 6). Veteran school counselors completing this survey were most confident in their ability to identify physical abuse and less confident in their ability to identify emotional abuse. This finding supports the assertion that types of abuse with visible evidence are more identifiable than other types of abuse such as emotional or sexual abuse (Bryant, 2009; Bryant & Milsom, 2005). Cases of suspected abuse in which a child reports physical abuse are less likely to be reported if there is no evidence of bodily harm (Tillman et al., 2015). Although school counselors report physical abuse as the most easily identifiable type of abuse, child protective services report neglect as the most common type of maltreatment (Child Welfare Information Gateway, 2021).
Results from this study show that veteran school counselors reported receiving their knowledge on child abuse from professional experiences and mandated reporter training at their school; comparatively, early career school counselors reported most of their knowledge came from professional experience and university courses (Ricks et al., 2019). Reported differences were also observed between veteran school counselors and early career school counselors in terms of sources of knowledge on how to make a referral and learn about indicators of abuse (Ricks et al., 2019). Differences may exist because of variable school district policies regarding ongoing mandated reporter training frequency and practices.
When assessing training needs, participants indicated that most veteran school counselors do receive training from their school district on how to make a referral, indicators of child abuse, and local abuse reporting procedures. In fact, 25% more veteran school counselors reported receiving training from their district than early career school counselors (Ricks et al., 2019). Additionally, approximately 40% of veteran school counselors reported not having a handbook or resource to reference outlining the mandated reporting protocol for their district/school. This result is slightly lower than that reported in research on early career school counselors showing approximately half of school counselors not having a handbook/resource (Ricks et al., 2019). The lack of access to a set protocol outlined by the district is concerning because of the inconsistencies that exist within protocols across states and school districts. Confusion may arise as to timeliness and manner of reporting as well as to who must make the actual report (Kenny & McEachern, 2002). As compared to novice school counselors, veteran counselors appear to report receiving training and/or a handbook/resources related to child abuse reporting in higher numbers. Discrepancies in reported training may indicate a delay in training provided to new school counselors or that training on child abuse is not occurring annually. Although the majority of veteran school counselors did report receiving some training from their school districts, it is important to have “established protocols [to] help address concerns over quality control, fear of lawsuits, and the protection of staff in reporting cases, as well as ensure that there are effective steps for helping children” (Crosson-Tower, 2003, p. 29).
Previous research (Kenny & McEachern, 2002) has indicated that school counselors with more years of experience report less adequate pre-service training in child abuse reporting and that school counselors with in-service training in the last 12 months are less concerned about the consequences of making a report (Behun et al., 2019). This might be due to recently trained school counselors having greater awareness about current information and procedures, which supports the need for participation in continuous ongoing education on this topic. Although the veteran school counselors surveyed in this study indicated experience in child abuse reporting, continued updates to the law highlight the need for current and well-defined guidelines within each school system. Ongoing training is recommended for all school counselors to ensure they stay informed on updated protocols and research (Kenny & Abreu, 2016; Tuttle et al., 2019).
Results of the data analysis also indicated a moderately significant relationship between veteran school counselor self-efficacy and their certainty identifying types of abuse. These findings echo other research indicating that school counselors’ self-efficacy levels may influence their decisions to report suspected abuse (Ricks et al., 2019; Tuttle et al., 2019). According to Larson and Daniels (1998), counselor self-efficacy beliefs are the main factor contributing to effective counseling action. Given the impact of counselor self-efficacy on effective action, it is important to understand how self-efficacy impacts school counselors’ decision-making processes. Experience and training are two factors that have been found to increase school counselor self-efficacy (Morrison & Lent, 2018). Veteran school counselors, who already have years of experience on their side, may benefit most from additional training opportunities. Increased support should be provided to all school counselors to enhance their counseling self-efficacy (Schiele et al., 2014) and contribute to positive school counseling outcomes.
Implications
Lack of knowledge related to reporting policies has been identified as a key barrier in reporting child abuse (Kenny, 2001; Petersen et al., 2014). School counselors should advocate for standardization in reporting policies. Understanding each state’s unique child abuse prevention statutes can help school counselors best serve their clients (Remley et al., 2017). Given that laws and definitions pertaining to child abuse and neglect vary among states (ASCA, 2021), school counselors should identify collaborative relationships to navigate these legal and ethical parameters. Key collaborations may include those with the school social worker, the school district’s attorney, law enforcement, child protective services, parents/guardians, and community members (Tuttle et al., 2019). Working together, in conjunction with administration and other school stakeholders, school counselors can help establish or update written guidelines and implement ongoing professional development in mandated reporting within their school district. Additionally, developing a positive working relationship with law enforcement and child protective services can help ensure that child abuse cases are reported and documented properly, which can promote positive outcomes for students and families. Moreover, based on the findings from this research study, school counseling certification organizations (i.e., state departments of education/licensure boards) may want to increase or update current training policies for professional school counselors. An area for further study would be examining school districts’ training and protocols for child abuse reporting.
Higher reporting trends in low socioeconomic settings highlight the need for additional mental health services in low-income school districts. School counselors may need more training on the risk factors associated with poverty as well as to be reminded that abuse occurs in all types of families (Bryant, 2009; Tillman et al., 2015). Practicing school counselors working with students living in poverty are often in schools where there are significantly limited resources. School counselors report that “working in schools with high poverty means academic services and the school counseling program itself are limited” (Ricks et al., 2020, p. 61). More research is needed to assess how to support school counselors working in low-income schools; however, school counselors should remain cognizant and demonstrate cultural competency. It is also important for veteran school counselors to continue to assess self-bias as a factor in identifying and reporting suspected child abuse cases (Tillman et al., 2015). Further, it is essential that school counselors emerge as advocates for students in these low socioeconomic settings by pushing for more resources for mental health services as well as changes to policies that negatively impact students’ success. School counselors can work with a task force or advisory committee within the school to examine current practices on child abuse identification and reporting (Temkin et al., 2020). The task force could look for systemic barriers that are impacting students related to child abuse reporting and trauma support; these include current school policies, reporting procedures, teacher and staff training protocols, school counselor professional development, access to mental health services, community resources, direct and indirect school counseling protocols, and other factors impacting student identification and support.
Given the higher number of child abuse cases in the elementary grade levels, more school counselors are needed to adequately identify child abuse and provide services for these students. Despite these needs, the school counselor-to-student ratio varies in each state and is higher in elementary schools (ASCA, 2022b); the national state averages for the school counselor-to-student ratio in grades kindergarten through eighth ranges from 1:419 to 1:1,135 as compared to 1:164 to 1:347 in grades nine through 12 (ASCA, 2022b). Moreover, 20 states currently have no school counseling mandates that require school counselors to be present within the schools (ASCA, 2022c). Of the 30 states that do have mandated counseling, seven do not have mandated counseling for elementary-level students (ASCA, 2022c). School counselors should advocate for more school counselors within their districts and state. Moreover, school administrations and state departments of education should consider hiring additional school counselors to address ongoing mental health needs. Recent research has shown that as a result of the COVID-19 pandemic, students may be experiencing no motivation to do schoolwork, difficulty concentrating, concern for falling behind in school, concern for getting sick, or other stress-related factors (Styck et al., 2021), as well as an increased risk for child abuse and neglect (Swedo et al., 2020). Elementary school counselors, who are uniquely trained in child development, can implement prevention and intervention programs to address these ongoing needs (ASCA, 2019). Elementary school counselors are essential in providing early intervention and prevention services for students.
Further research is needed in understanding how self-efficacy impacts school counselors’ decision-making process. The variation of confidence in identifying abuse as well as variance in reporting patterns among school counselors with differing years of experience are indicators that further professional development and training is needed within schools. It is also important to examine how school support can increase school counselors’ self-efficacy levels (Schiele et al., 2014). Current research shows that a school counselor’s level of self-efficacy predicts quality of practice and knowledge of evidence-based practices (Schiele et al., 2014).
Limitations
Although measures were used to reduce confounding variables, limitations exist in the methodological design of the study that could impact the validity of the findings. Firstly, this study obtained a sample size from a limited geographic area (Southeastern United States). Secondly, self-reported data was used. Although participants were informed their answers would remain anonymous, they may have answered based on what they perceived as acceptable and appropriate. School counselors may not be inclined to admit they did not report suspected child abuse for fear of legal or ethical violations. Likewise, selective memory may impact participants’ ability to effectively recall events that happened over a year ago. Additionally, many of the participants were White; responses from participants of color were limited. Further research with a more diverse sample would be beneficial to gain a comprehensive understanding of school counselors’ self-efficacy in identifying and reporting child abuse.
Conclusion
School counselors are mandated to report suspected child abuse and neglect cases to authorities and are key school personnel in early detection and recognition of abuse (ASCA, 2021). In this study, differing school demographics were associated with varying reporting practices among veteran school counselors. Continued professional development training, by virtue of its ability to increase veteran school counselors’ self-efficacy and knowledge of identification and reporting protocols, represents a promising possible pathway to improving outcomes among maltreated children.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2017). The school counselor and academic development. https://www.schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Academic-Development
American School Counselor Association. (2019). The essential role of elementary school counselors. https://www.schoolcounselor.org/getmedia/1691fcb1-2dbf-49fc-9629-278610aedeaa/Why-Elem.pdf
American School Counselor Association. (2021). The school counselor and child abuse and neglect prevention. https://schoolcounselor.org/Standards-Positions/Position-Statements/ASCA-Position-Statements/The-School-Counselor-and-Child-Abuse-and-Neglect-P
American School Counselor Association. (2022a). ASCA ethical standards for school counselors. https://www.school
counselor.org/About-School-Counseling/Ethical-Legal-Responsibilities/ASCA-Ethical-Standards-for-School-Counselors-(1)
American School Counselor Association. (2022b). School counselor roles & ratios. https://www.schoolcounselor.org/About-School-Counseling/School-Counselor-Roles-Ratios
American School Counselor Association. (2022c). State school counseling mandates & legislation. https://www.school
counselor.org/About-School-Counseling/State-Requirements-Programs/State-School-Counseling-Man
dates-Legislation
Balkaran, S. (2015). Impact of child abuse education on parent’s self-efficacy: An experimental study. Walden Dissertations and Doctoral Studies, 1432.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychological Review, 84(2),
191–215. https://doi.org/10.1037/0033-295X.84.2.191
Bandura, A. (1997). Self-efficacy: The exercise of control. W. H. Freeman.
Barrett, K. M., Lester, S. V., & Durham, J. C. (2011). Child maltreatment and the advocacy role of professional school counselors. Journal for Social Action in Counseling and Psychology, 3(2), 86–103.
https://doi.org/10.33043/JSACP.3.2.86-103
Behun, R. J., Cerrito, J. A., Delmonico, D. L., & Kolbert, J. B. (2019). The influence of personal and professional characteristics on school counselors’ recognition and reporting of child sexual abuse. Journal of School Counseling, 17(13), 1–34.
Bellis, M. A., Hughes, K., Leckenby, N., Hardcastle, K. A., Perkins, C., & Lowey, H. (2015). Measuring mortality and the burden of adult disease associated with adverse childhood experiences in England: A national survey. Journal of Public Health, 37(3), 445–454. https://doi.org/10.1093/pubmed/fdu065
Bodenhorn, N., & Skaggs, G. (2005). Development of the school counselor self-efficacy scale. Measurement and Evaluation in Counseling and Development, 38(1), 14–28. https://doi.org/10.1080/07481756.2005.11909766
Bryant, J. K. (2009). School counselors and child abuse reporting: A national survey. Professional School Counseling, 12(5), 333–342. https://doi.org/10.1177/2156759X0901200501
Bryant, J., & Milsom, A. (2005). Child abuse reporting by school counselors. Professional School Counseling, 9(1), 63–71.
Buchanan, D. K., Mynatt, B. S., & Woodside, M. (2017). Novice school counselors’ experience in classroom management. The Journal of Counselor Preparation and Supervision, 9(1). https://doi.org/10.7729/91.1146
Child Welfare Information Gateway. (2019). Long-term consequences of child abuse and neglect. U.S. Department of Health and Human Services, Administration for Children and Families, Children’s Bureau. https://www.childwelfare.gov/pubpdfs/long_term_consequences.pdf
Child Welfare Information Gateway. (2021). Child maltreatment 2019: Summary of key findings. U.S. Department of Health and Human Services, Administration for Children and Families, Children’s Bureau. https://www.childwelfare.gov/pubs/factsheets/canstats
Collin-Vézina, D., Brend, D., & Beeman, I. (2020). When it counts the most: Trauma-informed care and the
COVID-19 global pandemic. Developmental Child Welfare, 2(3), 172–179.
https://doi.org/10.1177/2516103220942530
Crosson-Tower, C. (2003). The role of educators in preventing and responding to child abuse and neglect. U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, Office on Child Abuse and Neglect. https://www.childwelfare.gov/pubpdfs/educator.pdf
Fortson, B. L., Klevens, J., Merrick, M. T., Gilbert, L. K., & Alexander, S. P. (2016). Preventing child abuse and neglect: A technical package for policy, norm, and programmatic activities. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/can-prevention-technical-package.pdf
Heim, C., Shugart, M., Craighead, W. E., & Nemeroff, C. B. (2010). Neurobiological and psychiatric consequences of child abuse and neglect. Developmental Psychobiology, 52(7), 671–690. https://doi.org/10.1002/dev.20494
Hodges, L. I., & McDonald, K. (2019). An organized approach: Reporting child abuse. Journal of Professional Counseling: Practice, Theory, & Research, 46(1–2), 14–26. https://doi.org/10.1080/15566382.2019.1673093
Hogelin, J. M. (2013). To prevent and to protect: The reporting of child abuse by educators. Brigham Young University Education and Law Journal, 2013(2), 225–252. https://digitalcommons.law.byu.edu/elj/vol2013/iss2/3
Hupe, T. M., & Stevenson, M. C. (2019). Teachers’ intentions to report suspected child abuse: The influence of compassion fatigue. Journal of Child Custody, 16(4), 364–386. https://doi.org/10.1080/15379418.2019.1663334
Johnson, G., Nelson, J., & Henriksen, R. (2017). Mentoring novice school counselors: A grounded theory. In G. R. Walz & J. Bleuer (Eds.), Ideas and research you can use: VISTAS 2017 (pp. 1–16). Counseling Outfitters.
Jordan, K. S., MacKay, P., & Woods, S. J. (2017). Child maltreatment: Optimizing recognition and reporting by school nurses. NASN School Nurse, 32(3), 192–199. https://doi.org/10.1177/1942602X16675932
Kenny, M. C. (2001). Child abuse reporting: Teachers’ perceived deterrents. Child Abuse and Neglect, 25(1), 81–92. https://doi.org/10.1016/s0145(00)00218-0
Kenny, M. C, & Abreu, R. L. (2016). Mandatory reporting of child maltreatment for counselors: An innovative training program. Journal of Child and Adolescent Counseling, 2(2), 112–124.
https://doi.org/10.1080/23727810.2016.1228770
Kenny, M. C., & McEachern, A. G. (2002). Reporting suspected child abuse: A pilot comparison of middle and high school counselors and principals. Journal of Child Sexual Abuse, 11(2), 59–75.
https://doi.org/10.1300/J070v11n02_04
Klassen, S. L., & Hickman, D. L. (2022). Reporting child abuse and neglect on K-12 campuses. In A. M. Powell (Ed.), Best practices for trauma-informed school counseling. IGI Global.
https://doi.org/10.4018/978-1-7998-9785-9.ch010
Krase, K. S. (2015). Child maltreatment reporting by educational personnel: Implications for racial disproportionality in the child welfare system. Children & Schools, 37(2), 89–99.
https://doi.org/10.1093/cs/cdv005
Lambie, G. W. (2005). Child abuse and neglect: A practical guide for professional school counselors. Professional School Counseling, 8(3), 249–258. http://www.jstor.org/stable/42732466
Lambie, G. W., Ieva, K. P., Mullen, P. R., & Hayes, B. G. (2011). Ego development, ethical decision-making, and legal and ethical knowledge in school counselors. Journal of Adult Development, 18(1), 50–59.
https://doi.org/10.1007/s10804-010-9105-8
Larson, L. M., & Daniels, J. A. (1998). Review of the counseling self-efficacy literature. The Counseling Psychologist, 26(2), 179–218. https://doi.org/10.1177/0011000098262001
Luken, A., Nair, R., & Fix, R. L. (2021). On racial disparities in child abuse reports: Exploratory mapping the 2018 NCANDS. Child Maltreatment, 26(3), 267–281. https://doi.org/10.1177/10775595211001926
McGuire, K., & London, K. (2020). A retrospective approach to examining child abuse disclosure. Child Abuse and Neglect, 99, 1–16. https://doi.org/10.1016/j.chiabu.2019.104263
Mishak, D. A. (2007). An investigation of early career and veteran Iowa elementary school counselors and their classroom guidance programs (Order No. 3265967). Available from ProQuest Dissertations & Theses Global. (304858653).
Morrison, M. A., & Lent, R. W. (2018). The working alliance, beliefs about the supervisor, and counseling self-efficacy: Applying the relational efficacy model to counselor supervision. Journal of Counseling Psychology, 65(4), 512–522. https://doi.org/10.1037/cou0000267
Petersen, A. C., Joseph, J., & Feit, M. (Eds.). (2014). New directions in child abuse and neglect research. The National Academies Press.
Remley, T. P., Jr., Rock, D. W., & Reed, R. M. (2017). Ethical and legal issues in school counseling (4th ed.). American School Counselor Association.
Ricks, L., Carney, J., & Lanier, B. (2020). Attributes, attitudes, and perceived self-efficacy levels of school counselors toward poverty. Georgia School Counselors Association Journal, 27, 51–68.
Ricks, L., Tuttle, M., Land, C., & Chibbaro, J. (2019). Trends and influential factors in child abuse reporting: Implications for early career school counselors. Journal of School Counseling, 17(16). http://www.jsc.montana.edu/articles/v17n16.pdf
Schiele, B. E., Weist, M. D., Youngstrom, E. A., Stephan, S. H., & Lever, N. A. (2014). Counseling self-efficacy, quality of services and knowledge of evidence-based practices in school mental health. The Professional Counselor, 4(5), 467–480. https://doi.org/10.15241/bes.4.5.467
Sedlak, A. J., Mettenburg, J., Basena, M., Petta, I., McPherson, K., Greene, A., & Li, S. (2010). Fourth national incidence study of child abuse and neglect (NIS-4): Report to Congress. U.S. Department of Health and Human Services, Administration for Children and Families. https://www.acf.hhs.gov/sites/default/files/documents/opre/nis4_report_congress_full_pdf_jan2010.pdf
Singleton, O., Newlon, M., Fossas, A., Sharma, B., Cook-Greuter, S. R., & Lazar, S. W. (2021). Brain structure and functional connectivity correlate with psychosocial development in contemplative practitioners and controls. Brain Sciences, 11(6), 728. https://doi.org/10.3390/brainsci11060728
Styck, K. M., Malecki, C. K., Ogg, J., & Demaray, M. K. (2021). Measuring COVID-19-related stress among 4th through 12th grade students. School Psychology Review, 50(4), 530–545.
https://doi.org/10.1080/2372966X.2020.1857658
Swedo, E., Idaikkadar, N., Lemmis, R., Dias, T., Radhakrishnan, L., Stein, Z., Chen, M., Agathis, N., & Holland, K. (2020). Trends in U.S. emergency department visits related to suspected or confirmed child abuse and neglect among children and adolescents aged <18 years before and during the COVID-19 pandemic—United States, January 2019–September 2020. Morbidity and Mortality Weekly Report, 69(49), 1841–1847. https://doi.org/10.15585/mmwr.mm6949al
Tang, A. (2020). The impact of school counseling supervision on practicing school counselors’ self-efficacy in building a comprehensive school counseling program. Professional School Counseling, 23(1).
https://doi.org/10.1177/2156759X20947723
Temkin, D., Harper, K., Stratford, B., Sacks, V., Rodriguez, Y., & Bartlett, J. D. (2020). Moving policy toward a whole school, whole community, whole child approach to support children who have experienced trauma. The Journal of School Health, 90(12), 940–947. https://doi.org/10.1111/josh.12957
Tillman, K. S., Prazak, M. D., Burrier, L., Miller, S., Benezra, M., & Lynch, L. (2015). Factors influencing school counselors’ suspecting and reporting of childhood physical abuse: Investigating child, parent, school, and abuse characteristics. Professional School Counseling, 19(1), 103–115. https://doi.org/10.5330/1096-2409-19.1.103
Tuttle, M., Ricks, L., & Taylor, M. (2019). A child abuse reporting framework for early career school counselors. The Professional Counselor, 9(3), 238–251. https://doi.org/10.15241/mt.9.3.238
U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2021). Child maltreatment 2019. https://www.acf.hhs.gov/sites/default/files/documents/cb/cm2019.pdf
White, J., & Flynt, M. (2000). The school counselor’s role in prevention and remediation of child abuse. In J. Wittmer (Ed.), Managing your school counseling program: K-12 developmental strategies (pp. 149–160). Educational Media.
Lacey Ricks, PhD, NCC, NCSC, is an associate professor at Liberty University. Malti Tuttle, PhD, NCC, NCSC, LPC, is an associate professor at Auburn University. Sara E. Ellison, MS, NCC, LAPC, is a doctoral student at Auburn University. Correspondence may be addressed to Lacey Ricks, 1971 University Blvd, Lynchburg, VA 24515, lricks1@liberty.edu.
Aug 10, 2022 | Author Videos, Volume 12 - Issue 2
Dan Li
Supervisee development is integral to counselor training. Despite the general acknowledgement that supervisors adopt different styles when supervising counselor trainees at varying levels, there is a paucity of studies that (a) measure supervisee levels using reliable and valid psychometric instruments, other than a broad categorization of supervisees based on their training progression (e.g., master’s level vs. doctoral level, practicum vs. internship, counselor trainee vs. postgraduate); and (b) empirically document how the matching of supervisory styles and supervisee levels relates to supervision processes and/or outcomes. The supervisory working alliance is key to the supervision process and outcome. To test the hypothesized moderation effects of supervisee levels on the relationship between supervisory styles and the supervisory working alliance, the author performed a series (n = 16) of moderation analyses with a sample (N = 113) of master’s- and doctoral-level counseling trainees and practitioners. Results suggested that supervisee levels and their three indicators (self and other awareness, motivation, and autonomy) were statistically significant moderators under different contexts. These findings (a) revealed extra intricacies of the relationships among the study variables, (b) shed light on future research directions concerning supervisee development, and (c) encouraged supervisors to adopt a composite of styles to varying degrees to better foster supervisee growth.
Keywords: supervisee development, supervisory styles, supervisory working alliance, supervisee levels, moderation analyses
Clinical supervision is integral to promoting counseling supervisees’ learning (Goodyear, 2014), safeguarding the quality of professional services offered to supervisees’ clients, and gatekeeping the counseling profession (Bernard & Goodyear, 2019). Because supervisors and supervisees are two parties of the tripartite entity of supervision, literature has extensively documented supervisor characteristics (e.g., supervisory styles, self-disclosure, cultural humility), supervisee characteristics (e.g., professional development levels), and the relationship between the two (e.g., supervisory working alliance) as related to supervision processes and outcomes (King et al., 2020; Ladany, Walker, & Melincoff, 2001; Stoltenberg & McNeill, 2010).
Of these relationships, research has consistently revealed a positive correlation between supervisory styles and the supervisory working alliance (Efstation et al., 1990; Heppner & Handley, 1981; Ladany & Lehrman-Waterman, 1999; Ladany, Walker, & Melincoff, 2001). Although such direct positive correlation is theoretically appealing and statistically compelling, there is limited research that further investigates the intricacy of this association, if at all (e.g., whether the direction or strength of this relationship may alter in different contexts). Particularly, abundant supervision literature (Friedlander & Ward, 1984; Li et al., 2018; Li et al., 2019; Li, Duys, & Granello, 2020; Li, Duys, & Vispoel, 2020; Stoltenberg & McNeill, 2010) suggested the adoption of different supervision approaches when working with supervisees at various levels of professional development. Therefore, supervisee levels present as a potential context to examine how supervisory styles relate to the supervisory working alliance.
However, supervisee levels are frequently conceptualized based on supervisees’ training progression (e.g., master’s level vs. doctoral level, practicum vs. internship, counselor trainee vs. postgraduate), which may not accurately approximate where supervisees are. As such, I adopted the Supervisee Levels Questionnaire-Revised (SLQ-R; McNeill et al., 1992), a reliable and valid psychometric instrument, to measure supervisee levels (collectively as an overall assessment and separately with their three indicators) in this study.
Supervisory Styles
Supervisory styles embody a constellation of behavior patterns that supervisors exhibit in establishing a working relationship with supervisees (Hunt, 1971) and are related to the interactional pattern that is fostered by supervisors in a direct or indirect manner (Munson, 1993). Specifically, supervisory styles encompass supervisors’ consistent focus in supervision, the manner in articulating their theoretical orientation, as well as the philosophy of practice and supervision and how it is communicated to supervisees (Munson, 1993). Friedlander and Ward (1984) identified three distinctive factors that correspond to three supervisory styles—attractive, interpersonally sensitive, and task-oriented—as measured by the Supervisory Styles Inventory (SSI) used in the present study. Attractive style supervisors appear to be warm, supportive, friendly, open, and flexible, denoting the collegial dimension of supervision; the interpersonally sensitive style is a relationship-oriented approach, and supervisors of this style tend to be invested, committed, therapeutic, and perceptive; and task-oriented supervisors are content-focused, goal-oriented, thorough, focused, practical, and structured (Friedlander & Ward, 1984). These styles resonate with the consultant, counselor, and teacher roles of the supervisor, respectively, in Bernard’s (1997) discrimination model.
Of the three styles, the interpersonally sensitive and task-oriented styles appear to be empirically distinct from one another and distinct from the attractive style (Shaffer & Friedlander, 2017). For instance, Li, Duys, and Vispoel (2020) studied 34 supervisory dyads and found the interpersonally sensitive style was the only discriminant variable, based on which supervisory dyads exhibited statistically different state-transitional patterns (i.e., movement patterns across six common supervision states). Earlier, Fernando and Hulse-Killacky (2005) also found this same style was the only predictor that uniquely and significantly explained supervisees’ satisfaction with supervision, but the task-oriented style was the only significant predictor in explaining supervisees’ perceived self-efficacy.
Supervisory Working Alliance
Park et al.’s (2019) meta-analysis indicated that the supervisory working alliance was positively related to supervision outcome variables. Bordin (1983) first coined the concept of the supervisory working alliance as a parallel concept to the therapeutic working alliance and introduced the three aspects of the therapeutic working alliance to the alliance in supervision—mutual agreements on the goals, tasks, and bond—which laid the foundation for the adapted Working Alliance Inventory (WAI; Bahrick, 1989) for both supervisors and supervisees. Efstation et al. (1990) instead used three supervisor factors (client focus, rapport, and identification) and two supervisee factors (rapport and client focus) to conceptualize the supervisory working alliance in their Supervisory Working Alliance Inventory (SWAI). In view of the collinearity issue for the goal and task dimensions in the WAI (Hatcher et al., 2020), I adopted the SWAI in the present study.
The working alliance is one of the most robust predictors of outcome in psychotherapy (Norcross, 2011). Although such robust prediction cannot be directly replicated in supervision between the supervisory working alliance and supervision outcome (Goodyear, 2014), scholars (DePue et al., 2016; DePue et al., 2022) have found the supervisory working alliance to be related to the therapeutic working alliance. Specifically, supervisees’ perception of the supervisory working alliance was positively related to their perception of the therapeutic alliance (DePue et al., 2016). However, supervisees’ perception of the supervisory working alliance did not significantly contribute to clients’ perception of the therapeutic working alliance (DePue et al., 2016).
Supervisory Styles and the Supervisory Working Alliance
Extensive research has documented a close relationship between supervisory styles and the supervisory working alliance (Efstation et al., 1990; Heppner & Handley, 1981; Ladany, Walker, & Melincoff, 2001; Shaffer & Friedlander, 2017). Broadly, as supervisees perceived a greater mixture of supervisory styles in their supervisors (i.e., higher ratings on all three styles; Ladany, Marotta, & Muse-Burke, 2001), supervisees were more likely to report a stronger supervisory working alliance (Li et al., 2021). Despite this global positive correlation, when scholars examined each style independently in relation to each dimension of the supervisory working alliance, such statistical significance was not consistent (Ladany, Walker, & Melincoff, 2001). For instance, in Ladany, Walker, and Melincoff’s (2001) study, participants’ perceptions of an attractive style uniquely and significantly accounted for their perceptions of the bond dimension in alliance, whereas both the interpersonally sensitive and task-oriented styles had this unique and significant association with the task dimension in alliance.
The Moderating Role of Supervisee Levels
It is not uncommon for a counselor supervisor to start supervision with an expectation of a supervisory style to use (Hart & Nance, 2003). But supervisors have to decide what to address with the supervisee and adopt the most functional style (Bernard, 1997), which could be subject to a myriad of factors, such as contextual factors (Holloway, 1995), cultural considerations (Li et al., 2018), and supervisees’ developmental levels and needs (Friedlander & Ward, 1984; Stoltenberg & McNeill, 2010), among others. Particularly, in Friedlander and Ward’s (1984) study, supervisory styles were differentially related to supervisees’ experience levels. For example, supervisors reported that they were more task-oriented with practicum students but more attractive and interpersonally sensitive with internship students. This interaction effect was also echoed by practicum students’ higher ratings on the task-oriented style but lower ratings on the interpersonally sensitive style, compared to their internship counterparts (Friedlander & Ward, 1984). Similarly, in the study conducted by Li, Duys, and Granello (2020), supervisory dyads with less experienced supervisees tended to be more preoccupied with foundational competencies (e.g., counseling skills and theories, maintenance of standards of service) than dyads with more experienced supervisees. Consistently, more experienced supervisees in Li et al.’s (2019) study were more likely to display positive social emotional behaviors (e.g., self-disclosure, empathy, reflection of feelings, expanding on supervisors’ ideas, praise) in response to supervisors’ opinions, which in turn were more likely to elicit supervisors’ opinions that helped facilitate supervisees’ growth.
However, supervisees’ developmental levels were not always significantly associated with supervision processes or outcomes. For instance, in Bucky et al.’s (2010) study, doctoral-level supervisees did not rate their supervisor characteristics as related to the supervisory working alliance differently based on their developmental levels. Nevertheless, researchers in that study (Bucky et al., 2010) gauged supervisees’ developmental levels based on supervisees’ training progression (i.e., the current level or year level) as commonly practiced (e.g., practicum vs. internship), which may not accurately capture the actual developmental levels of supervisees. Or supervisee levels may not be strikingly distinct in doctoral programs, at least in that sample. In this study, supervisee levels were conceptualized not only as an overall assessment of where supervisees are but with three dimensions (self and other awareness, motivation, and autonomy) aligned with Stoltenberg and McNeill’s (2010) integrative developmental model (IDM) using the Supervisee Levels Questionnaire-Revised (SLQ-R; McNeill et al., 1992).
Statement of Purpose
Although literature evidenced the overall positive correlation between supervisory styles and the supervisory working alliance, the direction and strength of such a relationship in different contexts warrants additional attention. Particularly, supervisees’ developmental progression entails a flexible mixture of different supervisory styles as suggested theoretically and empirically, but whether and how the relationship between supervisory styles and the supervisory working alliance may vary across different supervisee levels calls for further investigation. To this end, the purpose of the current study was to test the potential moderation effects of supervisee levels on the relationship between supervisory styles and the supervisory working alliance.
Given that supervisees at earlier stages of professional development may need more guidance and support from supervisors, which necessitates a variety of supervision styles that are critical to their perception of the working alliance with their supervisors, I hypothesized that the positive relationship between supervisory styles and the supervisory working alliance would be more sensitive for supervisees at earlier stages of development, compared to their more experienced counterparts. In other words, the positive relationship would be stronger for supervisees at lower levels of professional development and weaker for supervisees at higher levels of professional development.
Method
Participants
The data set of this study is part of a larger national quantitative study with a cross-sectional sample (Li et al., 2021). Yet, researchers have not examined supervisee levels that are crucial to measuring supervisee development using a robust psychometric instrument. The current sample comprised 113 participants (see Table 1), with the majority as master’s-level (n = 54, 47.79%) or doctoral-level students (n = 46, 40.71%). Approximately 17% of participants (n = 19) identified themselves as post-master’s or post-doctoral practitioners or other. Some participants reported both their training and practicing levels (e.g., both as a doctoral student and a post-master’s practitioner), which caused the sample size to be larger than 113 if simply adding the frequencies across the three categories together. Most participants reported their specialty areas in clinical mental health counseling (n = 53, 46.90%), school counseling (n = 43, 38.05%), and counselor education and supervision (n = 27, 23.89%). Because some participants indicated more than one specialty area, the total percentage did not add up to 100.
In this sample, approximately 80% were female (n = 90) and 23 were male (20.35%). At the time of filling out the questionnaire, most of them fell in the 21–30 age range (n = 72, 63.72%), with 19 in the 31–40 range (16.81%), 13 in the 41–50 range (11.50%), and nine beyond 50 years old (7.96%). Participants in this sample predominantly identified themselves as White (n = 97; 85.84%), with eight as Asian (7.08%), five as Black or African American (4.42%), one as American Indian and Alaska Native (0.88%), one as biracial or multiracial (0.88%), and one indicating other (0.88%). Most participants reported their counseling experience as 1 year or less (n = 44, 38.94%) or longer than 3 years (n = 37; 32.74%), with the rest reporting in between (n = 32, 28.31%). See Table 1 for more detailed demographic information.
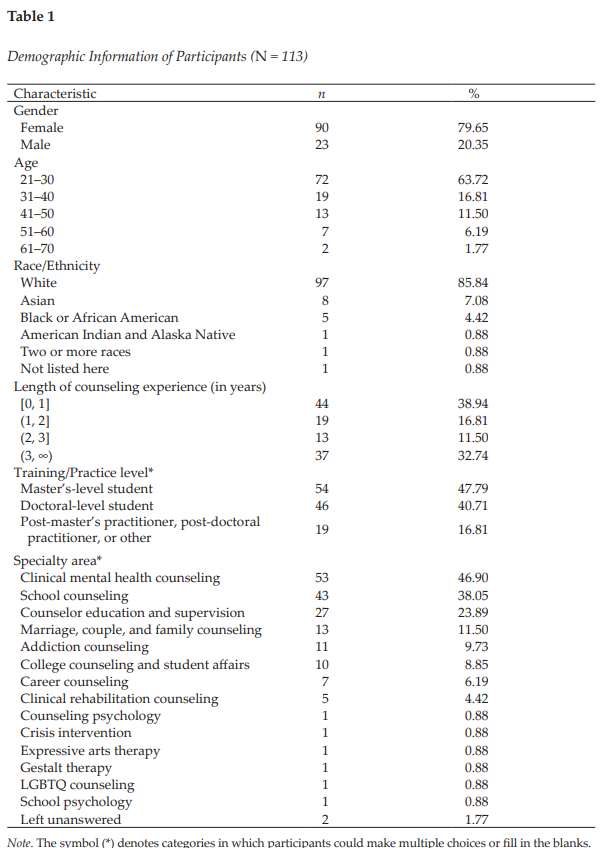
Procedure
Upon receiving IRB approval, I started collecting data online through Qualtrics in 2017–2018. The recruitment criteria included (a) one is at least 18 years of age by the time of filling out the survey; and (b) one is a student or a practitioner who had supervision experience in the counseling field. I disseminated the recruitment post through several professional networks, including the Counselor Education and Supervision Network-Listserv (CESNET-L) and American Counseling Association (ACA) Connect. In addition to this convenience sampling, I also used snowball sampling because participants were encouraged to share the recruitment post with anyone who they thought might be eligible to participate in the study. The recruitment post contained a survey link that directed potential participants to the informed consent webpage and then a compiled questionnaire webpage.
Instruments
Demographic Questionnaire
The purpose of including this self-constructed Demographic Questionnaire was to report the basic demographic information of participants. Specifically, the questionnaire included the gender, age, race/ethnicity, length of counseling-related work experience, training/practicing level, and training or specialty area of participants.
Supervisory Styles Inventory
The SSI (Friedlander & Ward, 1984) is a 33-item instrument used to measure the degree to which one endorses descriptors representative of each of the three dimensions of supervisory style: Attractive (7 items), Interpersonally Sensitive (8 items), and Task-Oriented (10 items), with the remainder as the filler items (8 items). Participants rate each item along a 7-point Likert scale from 1 (not very) to 7 (very). Higher scores in each dimension mean that one endorses descriptors of a certain supervisory style to a larger extent. Sample items for the Attractive, Interpersonally Sensitive, and Task-Oriented subscales are “supportive,” “perceptive,” and “didactic,” respectively.
Friedlander and Ward (1984) reported the Cronbach’s alphas of the three subscales separately and combined ranged from .76 to .93 (Ns ranging from 105 to 202). Additionally, the item–scale correlations ranged from .70 to .88 for the Attractive subscale, from .51 to .82 for the Interpersonally Sensitive style, and from .38 to .76 for the Task-Oriented scale (N1 = 202, N2 = 183; Friedlander & Ward, 1984). The test-retest reliability (N = 32) for the combined scale was .92; they were .94, .91, and .78 for the Attractive, Interpersonally Sensitive, and Task-Oriented subscales, respectively (Friedlander & Ward, 1984). They also reported the convergent validity based on moderate to high positive relationships (ps < .001) between the SSI and Stenack and Dye’s (1982) measure of supervisor roles (i.e., consultant, counselor, and teacher; N = 90). In the present study, the Cronbach’s alpha was .96 for the Attractive style, .94 for the Interpersonally Sensitive style, .92 for the Task-Oriented style, and .96 for the entire measure.
Supervisory Working Alliance Inventory
The SWAI (Efstation et al., 1990) is used to measure the relationship in counselor supervision. It has both the supervisor and supervisee forms. The supervisee form applied to the current study includes two scales: Rapport (12 items) and Client Focus (7 items). Supervisees indicate the extent to which the behavior described in each item seems characteristic of their work with their supervisors on a 7-point Likert scale, with 1 being almost never and 7 being almost always. Higher scores in the Rapport scale indicate a stronger perceived rapport with their supervisor, and higher scores in the Client Focus scale suggest more attention to issues related to the client in supervision. A sample item for the Rapport scale is “I feel free to mention to my supervisor any troublesome feelings I might have about him/her.” A sample item for the Client Focus scale is “I work with my supervisor on specific goals in the supervisory session.”
Efstation et al. (1990) reported that the alpha coefficient was .90 for Rapport and .77 for Client Focus (N = 178) for the supervisee form. Moreover, the item–scale correlations ranged from .44 to .77 for Rapport, and from .37 to .53 for Client Focus. They used the SSI to obtain initial estimates of convergent and divergent validity for the SWAI (Efstation et al., 1990). As expected, the Client Focus dimension of the SWAI showed moderate correlation (r = .52) with the Task-Oriented style in the SSI supervisee’s form, but low correlation (r = .04) with the Attractive style and low correlation (r = .21) with the Interpersonally Sensitive style. The Rapport dimension from the SWAI had low correlation (r < .00) with the Task-Oriented style of the SSI. In the present study, the Cronbach’s alpha was .95 for Rapport, .90 for Client Focus, and .96 for the entire scale.
Supervisee Levels Questionnaire-Revised
The Supervisee Levels Questionnaire-Revised (SLQ-R; McNeill et al., 1992) is used to measure supervisees’ developmental levels (Stoltenberg & Delworth, 1987). It has 30 items developed around three dimensions: Self and Other Awareness (12 items), Motivation (8 items), and Dependency-Autonomy (10 items). Supervisees can indicate their current behavior along a 7-point Likert scale, with 1 representing never, 2 rarely, 3 sometimes, 4 half the time, 5 often, 6 most of the time, and 7 always. Higher scores (after reverse-scoring for some of the items) in these dimensions reflect higher levels of supervisee development in Self and Other Awareness, Motivation, and Autonomy, respectively. A sample item for the Self and Other Awareness dimension is “I feel genuinely relaxed and comfortable in my counseling/therapy sessions”; a sample item (reverse-scoring) for the Motivation dimension is “The overall quality of my work fluctuates; on some days I do well, on other days, I do poorly”; and a sample item for the Dependency-Autonomy dimension is “I am able to critique counseling tapes and gain insights with minimum help from my supervisor.”
McNeill et al. (1992) reported that the Cronbach alpha coefficients of the SLQ-R (N = 105) were .83, .74, and .64 for the three subscales, respectively, and .88 for the total scores. To assess the construct validity of the SLQ-R, they examined the differences in subscale and total scores across the beginning, intermediate, and advanced groups. Hotelling’s test of significance indicated that the three groups differed significantly both on the total SLQ-R scores, F(2, 102) = 7.37, p < .001, and on a linear combination of SLQ-R subscale scores, F(6, 198) = 2.45, p < .026. In the present study, the Cronbach’s alpha was .89 for Self and Other Awareness, .85 for Motivation, .57 for Autonomy, and .91 for the entire measure.
Data Analysis
To thoroughly test the potential moderation effects of supervisee levels on the relationship between supervisory styles and the supervisory working alliance, I carried out three rounds of moderation analysis in which the supervisory working alliance was always the outcome variable. In the first round (n = 1), supervisory styles as a whole were the predictor, and supervisee levels as a whole were the moderator. The second round (n = 6) involved two series of analyses. In the first series (n = 3), each supervisory style was the predictor, and supervisee levels as a whole were the moderator. In the second series (n = 3), supervisory styles as a whole were the predictor, and each indicator of supervisee levels was the moderator. In the third round (n = 9), each supervisory style was the predictor, and each indicator of supervisee levels was the moderator. Figure 1 presents path diagrams of three rounds of tests and Table 2 lists all tested models (n = 16).
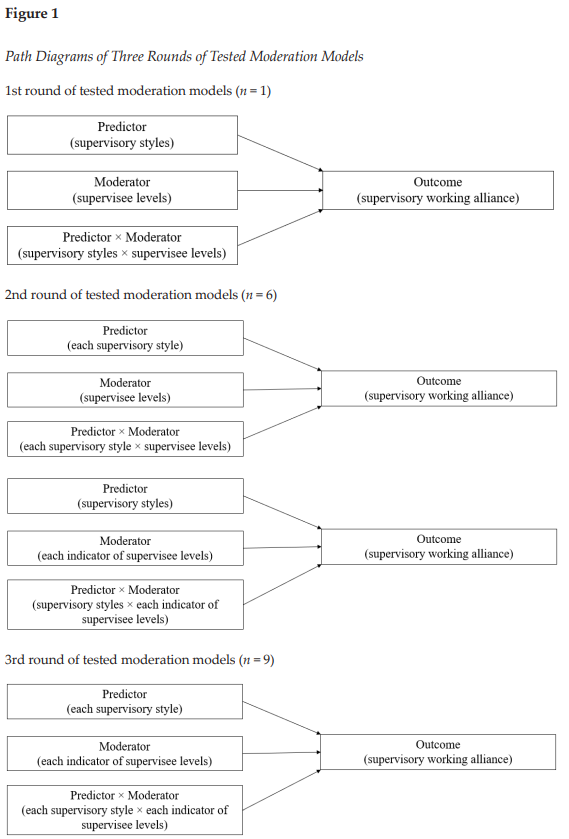
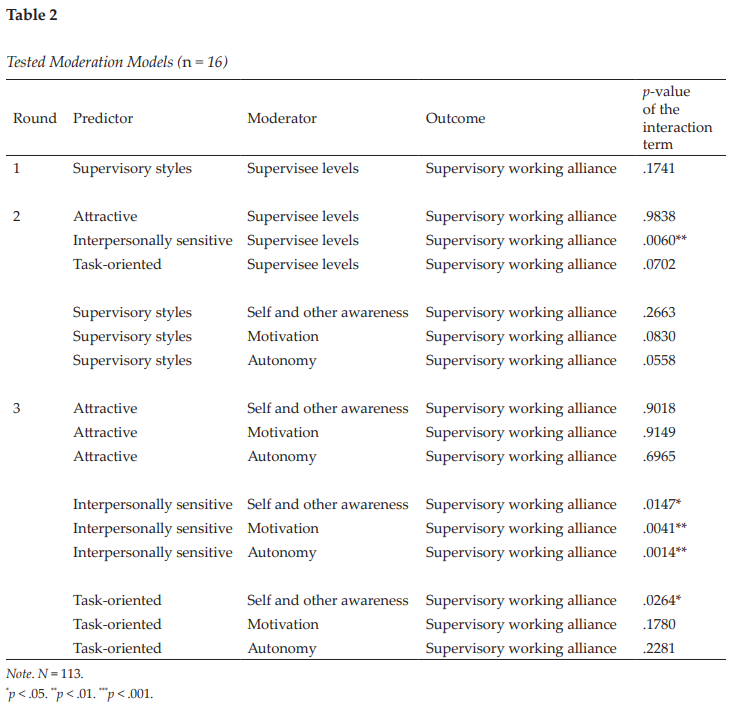
I followed up each significant moderation effect (n = 5) with a simple slopes analysis (Aiken & West, 1991) to interpret the nature of the interaction effect. The PROCESS v4.0 tool in SPSS was employed to perform all these analyses. A total of 166 potential participants accessed the survey, but only 113 of them completed all the study instruments (SSI, SWAI, and SLQ-R) in the present study. To alleviate the impact of significantly incomplete responses, I removed the 53 respondents who left at least one instrument unanswered. The a priori power analysis via G*Power 3.1.9.7 indicated that the minimum sample size would be 55 to detect an interaction effect with a medium effect size (f 2 = .15), given the desired statistical power level of .80 and type I error rate of .05. As such, the ultimate sample size of 113 meets this requirement.
I made the linearity and homoscedasticity assumptions using the zpred vs. zresid plot, which did not show a systematic relationship between the predicted values and the errors in the model (Field, 2017). Provided that participants independently filled out the study survey, I held the assumption of independence that the errors in the model were not dependent on each other. Further screening detected 12 missing values scattered across the three scales, which accounted for 0.13% of the entire 9,266 possible values. To determine the nature of these missing values, I performed the Little’s test (1988), and the results signified that these values were missing completely at random (MCAR; χ2 = 884.185, df = 890, p = .549). Because multiple imputation (MI; Schafer, 1999) can provide unbiased and valid estimates of associations based on information from the available data and can handle MCAR (Pedersen et al., 2017), I adopted MI to replace the missing values before performing further analyses in this study.
Results
Results of this study in part supported my broad hypothesis that the positive relationship between supervisory styles and the supervisory working alliance would be more sensitive for supervisees at earlier stages of development, compared to their more experienced counterparts. Examining each supervisory style and each indicator of supervisee levels independently revealed the intricacy of the relationship between the two constructs.
There were two groups of major findings. First, supervisee levels as a whole were a significant moderator between the interpersonally sensitive style and the supervisory working alliance according to supervisees’ perceptions, ΔR2 = .0272, F(1, 109) = 7.8551, p = .006, with a small to medium effect size
(f 2 = .07; Lorah & Wong, 2018). Specifically, the strength of the relationship between the interpersonally sensitive style and the supervisory working alliance differed based on supervisee levels (see Table 3).
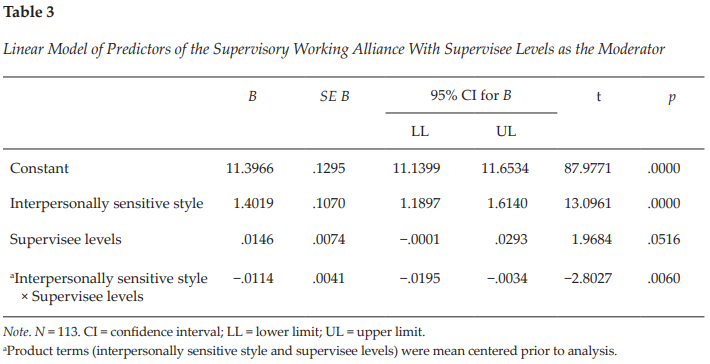
In view of this significant moderation effect, I conducted a simple slopes analysis as a follow-up, which indicated that the simple slopes for 1 standard deviation (SD) below the mean, at the mean, and 1 SD above the mean of supervisee levels were 1.6185, 1.4019, and 1.1853, respectively (see Figure 2). In other words, the interpersonally sensitive style and the supervisory working alliance were positively associated (B = 1.4019, p < .001), but the strength of this correlation decreased as supervisees reported higher levels of professional development. It is worth noting that supervisees at higher developmental levels tended to report a stronger supervisory working alliance in general, compared to those at lower levels. The linear model of the interpersonally sensitive style, supervisee levels, and the product of the two (interpersonally sensitive style × supervisee levels) explained 62.31% (p < .001) of the variance in the supervisory working alliance. A further look into the moderation effect of supervisee levels indicated that statistical significance consistently persisted as each indicator of supervisee levels (self and other awareness, motivation, and autonomy) was independently tested as a moderator between the interpersonally sensitive style and the supervisory working alliance (see Round 3 in Table 2).
Figure 2
Moderation Effect of Supervisee Levels With the Interpersonally Sensitive Style on the Supervisory Working Alliance
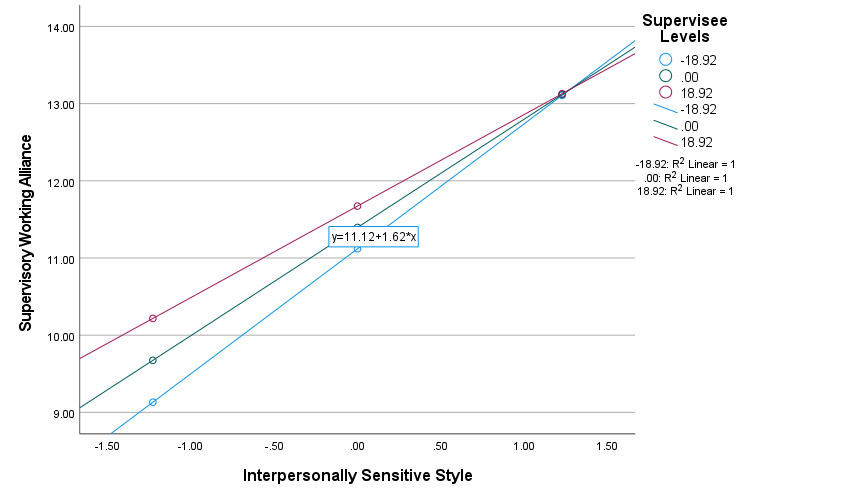
Note. N = 113. Predictor = Interpersonally Sensitive Style; Moderator = Supervisee Levels; Outcome = Supervisory Working Alliance. The three lines of color represent three regressions with the interpersonally sensitive style as predictor and the supervisory working alliance as outcome at different supervisee levels. The blue regression line denotes the group in which supervisee levels were one standard deviation (SD) below the mean, the green denotes the group in which supervisee levels were at the mean, and the pink denotes the group in which supervisee levels were one SD above the mean.
The second major finding was about the task-oriented supervisory style. When the three indicators of supervisee levels were independently examined as moderators, it was found that self and other awareness moderated the relationship between the task-oriented style and the supervisory working alliance, ΔR2 = .0311, F(1, 109) = 5.0639, p = .0264, with a small to medium effect size (f 2 = .05; Lorah & Wong, 2018). Similar to the first group of findings, the strength of the relationship between the task-oriented style and the supervisory working alliance varied based on the level of supervisee self and other awareness (one indicator of supervisee levels; see Table 4). A simple slopes analysis signified a consistent pattern—the task-oriented style and the supervisory working alliance were positively correlated, but the strength of this relationship decreased as supervisees rated higher on self and other awareness (see Figure 3). Specifically, the simple slopes for one SD below the mean, at the mean, and one SD above the mean of supervisee self and other awareness were 1.2620, 0.9540, and 0.6460, respectively. The area below the moderator (self and other awareness) value of 13.3857 constituted a region of significance in which the relationship between the task-oriented style and the supervisory working alliance was significant (p < .05; Johnson & Neyman, 1936). The linear model of the task-oriented style, supervisee self and other awareness, and the product of the two (task-oriented style × self and other awareness) accounted for 33.13% (p < .001) of the variance in the supervisory working alliance.
Discussion
Findings of the present study corroborated the positive correlation between supervisory styles and the supervisory working alliance that has been consistently identified in the existing literature (Efstation et al., 1990; Heppner & Handley, 1981; Ladany & Lehrman-Waterman, 1999; Ladany, Walker, & Melincoff, 2001). The intricacy of this relationship was further explored, and the current study confirmed that the strength of such correlation varied across different contexts. Supervisee levels and their three indicators turned out to be significant moderators in five models out of the 16 tested. Explicitly, the positive correlation between the interpersonally sensitive style and the supervisory working alliance was stronger for supervisees at lower levels of professional development but weaker for supervisees at higher levels. Furthermore, this significant moderation effect existed not only when supervisee levels were viewed as an overarching construct but when each indicator of supervisee levels was independently examined. Moreover, this moderation pattern was echoed by the positive association between the task-oriented style and the supervisory working alliance, wherein the correlation was stronger for supervisees at lower levels of self and other awareness (one indicator of supervisee levels) but weaker for those at higher levels of self and other awareness. Notably, supervisees at higher developmental levels (including indicators of supervisee levels) in all models with significant moderation effects reported a stronger supervisory working alliance than did their counterparts at lower levels.
According to developmental theories of supervision, supervisees broadly progress through a series of qualitatively different levels in the process of becoming effective counselors, despite myriad individual idiosyncrasies (Chagnon & Russell, 1995; Stoltenberg & McNeill, 2010). Entry-level supervisees typically focus on their own anxiety, their lack of skills and knowledge, and the likelihood that they are being regularly evaluated (Stoltenberg & McNeill, 2010). Accordingly, beginning supervisees identified supervisor care and concern as one of the most important supervisor variables to allow supervisees to take risks and grow (Jordan, 2007). As such, interpersonally sensitive supervisors who are invested, committed, therapeutic, and perceptive (Friedlander & Ward, 1984) would be easily perceived as relationship-oriented and helpful in rapport building (one indicator of the supervisory working alliance) for supervisees early on in their training. Similarly, task-oriented supervisors are content-focused, goal-oriented, thorough, focused, practical, and structured (Friedlander & Ward, 1984).
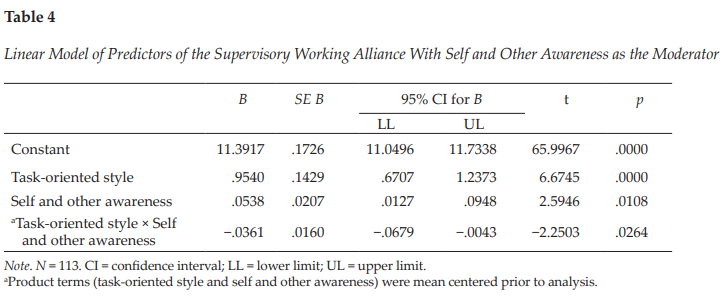
Figure 3
Moderation Effect of Self and Other Awareness With the Task-Oriented Style on the Supervisory Working Alliance
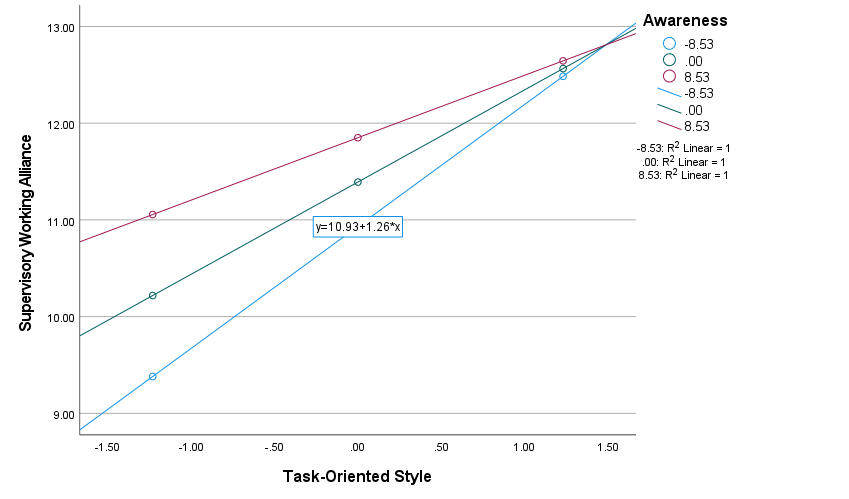
Note. N = 113. Predictor = Task-Oriented Style; Moderator = Self and Other Awareness; Outcome = Supervisory Working Alliance. The three lines of color represent three regressions with the task-oriented style as predictor and the supervisory working alliance as outcome at different levels of self and other awareness (one indicator of supervisee levels). The blue regression line denotes the group in which supervisee self and other awareness was one standard deviation (SD) below the mean, the green denotes the group in which supervisee self and other awareness was at the mean, and the pink denotes the group in which supervisee self and other awareness was one SD above the mean.
Task-oriented supervisors can be perceived as particularly helpful and informative with client focus (a second indicator of the supervisory working alliance) for beginning supervisees (as indicated by their lower self and other awareness) who commonly experience substantial anxiety or fear pertaining to their lack of confidence in knowing what to do, being able to do it, and being evaluated by their clients or supervisors (Stoltenberg & McNeill, 2010).
Therefore, supervisees at lower levels of professional development were more likely to report a stronger supervisory working alliance as they perceived more interpersonally sensitive or task-oriented supervisor characteristics. As they progress to higher levels of development with accumulated knowledge, skills, and competencies, supervisees become more aware of clients and themselves, intrinsically and consistently motivated, and autonomous as practitioners (Stoltenberg & McNeill, 2010), which may in part explain why their ratings of the supervisory working alliance were less related to their perceptions of supervisor characteristics but generally higher than supervisees at lower levels of development.
In the present study, the moderator of supervisee levels as a composite score was only significant when the interpersonally sensitive style was the predictor; the moderator of self and other awareness (one indicator of supervisee levels) was also significant when the task-oriented style was the predictor. These findings resonated with the existing literature in that compared to the attractive style, the interpersonally sensitive and task-oriented styles tend to have stronger discriminating effects (Friedlander & Ward, 1984). For instance, practicum and internship students differed significantly in rating the task-oriented and interpersonally sensitive styles of their supervisors, but their perceptions about the attractive style were similar at both levels (Friedlander & Ward, 1984). Li, Duys, and Vispoel (2020) also found that supervisory state–transitional patterns differed significantly only based on the interpersonally sensitive style but not the other two styles.
Implications for Clinical Supervision
The supervisory working alliance is inextricably intertwined with supervisees’ willingness to disclose (Ladany et al., 1996), supervisee satisfaction with clinical supervision (Cheon et al., 2009; Ladany, Ellis, & Friedlander, 1999), supervisee work satisfaction and work-related stress (Sterner, 2009), and therapeutic working alliance (DePue et al., 2016; DePue et al., 2022), among others. Nelson et al. (2001) proposed that a key task in early supervision is to build a strong supervisory working alliance that serves as a foundation to manage future potential dilemmas in supervision, and the ongoing maintenance of this working alliance should be the supervisor’s responsibility throughout the supervisory relationship. Although the three supervisory styles appear to be clear-cut with distinguishable characteristics and roles (Friedlander & Ward, 1984), supervisors are encouraged to adopt a composite of different styles to varying degrees to better serve supervisees’ needs. As revealed by the present study, and also the extant literature (Efstation et al., 1990; Ladany, Walker, & Melincoff, 2001; Li et al., 2021), supervisees were more likely to report a stronger supervisory working alliance as they perceived their supervisors to adopt a mixture of three supervisory styles (i.e., higher overall ratings of supervisory styles).
Particularly, beginning supervisees are characteristic of a strong focus on self, extrinsic motivation, and high dependency on supervisors (Stoltenberg & McNeill, 2010). Supervisors’ emphases on relationship-building (interpersonally sensitive style) and task focus (task-oriented style) would help build a safe, predictable supervision environment and enhance the working alliance with supervisees. Notably, although the strengths of the correlation between the interpersonally sensitive or task-oriented style and the supervisory working alliance were stronger for beginning supervisees, they did not suggest that these styles would not be effective in augmenting the alliance for supervisees at higher levels of professional development. The positive correlations still existed, albeit smoother, for more advanced supervisees, and they reported higher levels of supervisory working alliance in general, which may imply that these styles help maintain the working alliance that has been established early on in supervision.
Another point that is worth noting is that although no significant moderator was detected between the attractive style and the supervisory working alliance in the present study, the attractive style explained the most variance (68.1%, p < .001) in the supervisory working alliance, compared to the interpersonally sensitive (55.9%, p < .001) and task-oriented styles (24.1%, p < .001). This finding made it clear that the warm, supportive, friendly, open, and flexible features of attractive style supervisors are foundational to building and maintaining the supervisory working alliance, which does not differentiate across different levels of supervisees. As such, supervisors are encouraged to bring these qualities to their supervision and make them perceived by supervisees.
Limitations and Future Research
This study is not exempt from limitations that may be addressed in future research. Although two moderators (supervisee levels, self and other awareness) were found to be significant in the present study, the effect sizes of both were small to medium (f 21 = .07 and f 22 = .05), which were lower than the speculated medium effect size (f 2 = .15) during the a priori power analysis. Provided the effect sizes of .07 and .05 for the moderation effect, to achieve the statistical power of .80 with the α error probability of .05, the required sample size would be 115 and 159, respectively. Researchers need to be more mindful when recruiting participants to ensure the sufficient sample size. Additionally, although supervisees were asked to respond to the questionnaires consistently based on their perceptions of one supervisor, a constellation of factors could have affected their perceptions—for example, the timing of a participant’s supervisee status (e.g., currently receiving supervision vs. received supervision in the past), the potential dual role that a participant may be in (e.g., a doctoral student who is both a supervisee and a supervisor), the level of supervision (e.g., practicum, internship), and the length of the supervisory relationship (e.g., 2 months vs. 2 years). Researchers in future studies could also collect more information about participants (e.g., geographic distribution) to help readers better contextualize study results. Also, the current data set was collected in 2017–2018, which would not be able to capture more recent societal, cultural, political, and economic changes (e.g., the COVID-19 pandemic) that could have affected supervisee perceptions.
In the present study, the association between supervisory styles and the supervisory working alliance was examined in the context of different supervisee levels. Indeed, this alliance could be subject to many other factors, such as discussions of cultural variables in supervision (Gatmon et al., 2001), supervisor adherence to ethical guidelines (Ladany & Lehrman-Waterman, 1999), and relational supervision strategies (Shaffer & Friedlander, 2017), among others. Scholars may include more related variables to expand the current model so as to further disentangle the complex relationships among predictors of the supervisory working alliance.
Last, although multiple moderation effects identified in the present study were statistically significant and theoretically coherent, exactly how supervisees experience the supervisory working alliance in relation to different supervisory styles as they proceed along the professional development is less known. A longitudinal track of the same sample using repeated measures or a qualitative inquiry into participants’ lived experiences of the targeted phenomenon could enrich our understanding of the study variables in this research.
Conclusion
Although the positive correlation between supervisory styles and the supervisory working alliance is well documented in the existing literature, the present study examined such relationships specifically in the context of supervisee levels. Both supervisee levels (as a whole) and self and other awareness (one indicator of supervisee levels) appeared to be significant moderators under different contexts. These findings further revealed the intricacies embedded in the broad relationship between supervisory styles and the supervisory working alliance, pointed out future research directions concerning supervisee development, and encouraged supervisors to adopt a composite of styles to varying degrees to better support supervisee growth.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. SAGE.
Bahrick, A. S. (1989). Role induction for counselor trainees: Effects on the supervisory working alliance (Order No. 9014392) [Doctoral dissertation, The Ohio State University]. ProQuest Dissertations and Theses Global.
Bernard, J. M. (1997). The discrimination model. In C. E. Watkins, Jr. (Ed.), Handbook of psychotherapy supervision (pp. 310–327). Wiley.
Bernard, J. M., & Goodyear, R. K. (2019). Fundamentals of clinical supervision (6th ed.). Pearson.
Bordin, E. S. (1983). A working alliance based model of supervision. The Counseling Psychologist, 11(1), 35–42. https://doi.org/10.1177/0011000083111007
Bucky, S. F., Marques, S., Daly, J., Alley, J., & Karp, A. (2010). Supervision characteristics related to the supervisory working alliance as rated by doctoral-level supervisees. The Clinical Supervisor, 29(2), 149–163. https://doi.org/10.1080/07325223.2010.519270
Chagnon, J., & Russell, R. K. (1995). Assessment of supervisee developmental level and supervision environment across supervisor experience. Journal of Counseling & Development, 73(5), 553–558.
https://doi.org/10.1002/j.1556-6676.1995.tb01793.x
Cheon, H.-S., Blumer, M. L. C., Shih, A.-T., Murphy, M. J., & Sato, M. (2009). The influence of supervisor and supervisee matching, role conflict, and supervisory relationship on supervisee satisfaction. Contemporary Family Therapy, 31(1), 52–67. https://doi.org/10.1007/s10591-008-9078-y
DePue, M. K., Lambie, G. W., Liu, R., & Gonzalez, J. (2016). Investigating supervisory relationships and therapeutic alliances using structural equation modeling. Counselor Education and Supervision, 55(4), 263–277. https://doi.org/10.1002/ceas.12053
DePue, M. K., Liu, R., Lambie, G. W., & Gonzalez, J. (2022). Examining the effects of the supervisory relationship and therapeutic alliance on client outcomes in novice therapists. Training and Education in Professional Psychology, 16(3), 253–262. https://doi.org/10.1037/tep0000320
Efstation, J. F., Patton, M. J., & Kardash, C. M. (1990). Measuring the working alliance in counselor supervision. Journal of Counseling Psychology, 37(3), 322–329. https://doi.org/10.1037/0022-0167.37.3.322
Fernando, D. M., & Hulse-Killacky, D. (2005). The relationship of supervisory styles to satisfaction with supervision and the perceived self-efficacy of master’s-level counseling students. Counselor Education and Supervision, 44(4), 293–304. https://doi.org/10.1002/j.1556-6978.2005.tb01757.x
Field, A. (2017). Discovering statistics using IBM SPSS statistics (5th ed.). SAGE.
Friedlander, M. L., & Ward, L. G. (1984). Development and validation of the Supervisory Styles Inventory. Journal of Counseling Psychology, 31(4), 541–557. https://doi.org/10.1037/0022-0167.31.4.541
Gatmon, D., Jackson, D., Koshkarian, L., Martos-Perry, N., Molina, A., Patel, N., & Rodolfa, E. (2001). Exploring ethnic, gender, and sexual orientation variables in supervision: Do they really matter? Journal of Multicultural Counseling and Development, 29(2), 102–113. https://doi.org/10.1002/j.2161-1912.2001.tb00508.x
Goodyear, R. K. (2014). Supervision as pedagogy: Attending to its essential instructional and learning processes. The Clinical Supervisor, 33(1), 82–99. https://doi.org/10.1080/07325223.2014.918914
Hart, G. M., & Nance, D. (2003). Styles of counselor supervision as perceived by supervisors and supervisees. Counselor Education and Supervision, 43(2), 146–158. https://doi.org/10.1002/j.1556-6978.2003.tb01838.x
Hatcher, R. L., Lindqvist, K., & Falkenström, F. (2020). Psychometric evaluation of the Working Alliance Inventory—Therapist version: Current and new short forms. Psychotherapy Research, 30(6), 706–717. https://doi.org/10.1080/10503307.2019.1677964
Heppner, P. P., & Handley, P. G. (1981). A study of the interpersonal influence process in supervision. Journal of Counseling Psychology, 28(5), 437–444. https://doi.org/10.1037/0022-0167.28.5.437
Holloway, E. (1995). Clinical supervision: A systems approach. SAGE.
Hunt, D. E. (1971). Matching models in education: The coordination of teaching methods with student characteristics. Ontario Institute for Studies in Education, Monograph, 10, 87.
Johnson, P. O., & Neyman, J. (1936). Tests of certain linear hypotheses and their application to some educational problems. Statistical Research Memoirs, 1, 57–93.
Jordan, K. (2007). Beginning supervisees’ identity: The importance of relationship variables and experience versus gender matches in the supervisee/supervisor interplay. The Clinical Supervisor, 25(1–2), 43–51.
https://doi.org/10.1300/J001v25n01_04
King, K. M., Borders, L. D., & Jones, C. T. (2020). Multicultural orientation in clinical supervision: Examining impact through dyadic data. The Clinical Supervisor, 39(2), 248–271.
https://doi.org/10.1080/07325223.2020.1763223
Ladany, N., Ellis, M. V., & Friedlander, M. L. (1999). The supervisory working alliance, trainee self-efficacy, and satisfaction. Journal of Counseling & Development, 77(4), 447–455.
https://doi.org/10.1002/j.1556-6676.1999.tb02472.x
Ladany, N., Hill, C. E., Corbett, M. M., & Nutt, E. A. (1996). Nature, extent, and importance of what psychotherapy trainees do not disclose to their supervisors. Journal of Counseling Psychology, 43(1), 10–24. https://doi.org/10.1037/0022-0167.43.1.10
Ladany, N., & Lehrman-Waterman, D. E. (1999). The content and frequency of supervisor self-disclosures and their relationship to supervisor style and the supervisory working alliance. Counselor Education and Supervision, 38(3), 143–160. https://doi.org/10.1002/j.1556-6978.1999.tb00567.x
Ladany, N., Marotta, S., & Muse-Burke, J. L. (2001). Counselor experience related to complexity of case conceptualization and supervision preference. Counselor Education and Supervision, 40(3), 203–219.
https://doi.org/10.1002/j.1556-6978.2001.tb01253.x
Ladany, N., Walker, J. A., & Melincoff, D. S. (2001). Supervisory style: Its relation to the supervisory working alliance and supervisor self-disclosure. Counselor Education and Supervision, 40(4), 263–275.
https://doi.org/10.1002/j.1556-6978.2001.tb01259.x
Li, D., Duys, D. K., & Granello, D. H. (2019). Interactional patterns of clinical supervision: Using sequential analysis. Asia Pacific Journal of Counselling and Psychotherapy, 10(1), 70–92.
https://doi.org/10.1080/21507686.2018.1553791
Li, D., Duys, D. K., & Granello, D. H. (2020). Applying Markov chain analysis to supervisory interactions. The Journal of Counselor Preparation and Supervision, 13(1), Article 6. https://digitalcommons.sacredheart.edu/cgi/viewcontent.cgi?article=1325&context=jcps
Li, D., Duys, D. K., & Liu, Y. (2021). Working alliance as a mediator between supervisory styles and supervisee satisfaction. Teaching and Supervision in Counseling, 3(3), Article 5. https://doi.org/10.7290/tsc030305
Li, D., Duys, D. K., & Vispoel, W. P. (2020). Transitional dynamics of three supervisory styles using Markov chain analysis. Journal of Counseling & Development, 98(4), 363–375. https://doi.org/10.1002/jcad.12339
Li, D., Liu, Y., & Lee, I. (2018). Supervising Asian international counseling students: Using the integrative developmental model. Journal of International Students, 8(2), 1129–1151. https://doi.org/10.32674/jis.v8i2.137
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83(404), 1198–1202. https://doi.org/10.1080/01621459.1988.10478722
Lorah, J. A., & Wong, Y. J. (2018). Contemporary applications of moderation analysis in counseling psychology. Journal of Counseling Psychology, 65(5), 629–640. https://doi.org/10.1037/cou0000290
McNeill, B. W., Stoltenberg, C. D., & Romans, J. S. (1992). The Integrated Developmental Model of supervision: Scale development and validation procedures. Professional Psychology: Research and Practice, 23(6), 504–508. https://doi.org/10.1037/0735-7028.23.6.504
Munson, C. E. (1993). Clinical social work supervision (2nd ed.). Haworth Press.
Nelson, M. L., Gray, L. A., Friedlander, M. L., Ladany, N., & Walker, J. A. (2001). Toward relationship-centered supervision: Reply to Veach (2001) and Ellis (2001). Journal of Counseling Psychology, 48(4), 407–409.
https://doi.org/10.1037/0022-0167.48.4.407
Norcross, J. C. (Ed.). (2011). Psychotherapy relationships that work: Evidence-based responsiveness (2nd ed.). Oxford University Press.
Park, E. H., Ha, G., Lee, S., Lee, Y. Y., & Lee, S. M. (2019). Relationship between the supervisory working alliance and outcomes: A meta-analysis. Journal of Counseling & Development, 97(4), 437–446.
https://doi.org/10.1002/jcad.12292
Pedersen, A. B., Mikkelsen, E. M., Cronin-Fenton, D., Kristensen, N. R., Pham, T. M., Pedersen, L., & Petersen, I. (2017). Missing data and multiple imputation in clinical epidemiological research. Clinical Epidemiology, 9, 157–166. https://doi.org/10.2147/CLEP.S129785
Schafer, J. L. (1999). Multiple imputation: A primer. Statistical Methods in Medical Research, 8(1), 3–15.
https://doi.org/10.1177/096228029900800102
Shaffer, K. S., & Friedlander, M. L. (2017). What do “interpersonally sensitive” supervisors do and how do supervisees experience a relational approach to supervision? Psychotherapy Research, 27(2), 167–178. https://doi.org/10.1080/10503307.2015.1080877
Stenack, R. J., & Dye, H. A. (1982). Behavioral descriptions of counseling supervision roles. Counselor Education and Supervision, 21(4), 295–304. https://doi.org/10.1002/j.1556-6978.1982.tb01692.x
Sterner, W. (2009). Influence of the supervisory working alliance on supervisee work satisfaction and work-related stress. Journal of Mental Health Counseling, 31(3), 249–263.
https://doi.org/10.17744/mehc.31.3.f3544l502401831g
Stoltenberg, C. D., & Delworth, U. (1987). Supervising counselors and therapists: A developmental approach. Jossey-Bass.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Dan Li, PhD, NCC, LSC (NC, K–12), is an assistant professor of counseling at the University of North Texas. Correspondence may be addressed to Dan Li, Welch Street Complex 2-112, 425 S. Welch St., Denton, TX 76201, Dan.Li@unt.edu.
Jun 27, 2022 | Book Reviews
 by Beatriz Sheldon and Albert Sheldon
by Beatriz Sheldon and Albert Sheldon
Beatriz Sheldon, MEd, and her partner, Albert Sheldon, MD, describe their novel therapeutic approach, Complex Integration of Multiple Brain Systems (CIMBS), in this new publication. Throughout the book, references are made to the Sheldons’s 20 years of working together, 15 years of clinical experience, and 10 years of training other practitioners in CIMBS therapy. The authors emphasize that they “are practical, empirical therapists” (p. xvii). The book is seeded with references to scientists who inspire the duo, especially Daniel J. Siegel, Joseph LeDoux, Antonio Domasio, and the late Jaak Panksepp. It must be noted that CIMBS therapy as laid out in this text contains no peer-reviewed qualitative or quantitative studies; instead, the authors utilize vignettes to discuss their methods.
The brain systems referred to in CIMBS are organized into sections much like those of the triune brain model, with an additional peripheral system in the heart, lungs, and intestines. What the triune brain model labels the lizard brain relates to the primary level, the mammal brain is the secondary level, and the human brain is the tertiary level. The Sheldons assign awareness, attention, authority, autonomy, and agency (the “A Team”) to the conscious tertiary level. The secondary level holds nonconscious, inhibitory systems of fear, grief, shame, and guilt. The primary level, also nonconscious, contains the systems of safe, care, connection, sensory, assertive, play, and seeking.
The patient accesses the hidden strengths of the nonconscious mind via the CIMBS therapist’s use of techniques like Transpiring Present Moment, Go the Other Way, and Initial Directed Activation. Transpiring Present Moment is reminiscent of Fritz Perls’s emphasis on the “here-and-now.” Go the Other Way asks the patient to avoid getting bogged down in traumatic memories and instead reach for personal strengths. The CIMBS therapist cultivates the therapeutic alliance using the Therapeutic Attachment Relationship, which includes physical postures that suggest safety, reminding us of Egan’s SOLER stance taught in many counseling programs. This intervention also recommends intense focus on the patient’s micro-expressions as a guide to their conscious and nonconscious processes. Ultimately, the patient will integrate all 20 brain systems effectively and reach Fail-Safe Complex Network, a new, durable neural structure generating improved mental health.
Although the authors refer several times to the text’s internal contradictions or incongruence, the writing has the same appeal as the work of the Sheldons’s mentor, Dan Siegel, who wrote the Foreword. The book asks readers to lean on their intuition, often reminding them to “trust the process.” Nicola Swaine has provided line drawings to clarify central concepts, much as Siegel uses a curled fist to describe the triune brain. The authors relate that this text was written expressly to provide an overview of the Sheldons’s 16-part CIMBS training series (recorded and live) for students and trainees, who will find the glossary and bibliography especially useful.
In the Foreword, Siegel refers to the “cross-disciplinary framework known as interpersonal neurobiology . . . [using] universal principles discovered by independent pursuits of knowledge” (p xii). It would be useful to know which principles are considered universal in this book. Psychology sits forever on the fence between hard and soft science; some declarations of fact are based on microscopic studies of physical structures, and some are useful models that are at least partly philosophical. This text contains both. Neurologists have observed neural repairs and rerouting; thus, neuroplasticity is a demonstrable fact. The Sheldons describe 20 brain systems while noting that “one could certainly make the case for more or fewer systems” (p. 26). Clearly the number and definition of these brain systems can be thought of as helpful metaphors, a bit like Marsha Linehan describes a “wise mind” that is not a physical structure existing in the brain.
Professional counselors who like eclectic methods and enjoy pulling inspiration from many sources will appreciate CIMBS and this flagship text. The authors caution practitioners not to use CIMBS for patients who struggle with borderline personality disorder or dissociative, bipolar, or psychotic disorders. Although the Sheldons encourage clinicians to practice with their highest-functioning patients, the wise professional counselor will first disclose methods and procedures to patients.
Sheldon, B., & Sheldon, A. (2021). Complex integration of multiple brain systems in therapy. W. W. Norton.
Reviewed by: Christine Sheppard, MA, LCPC, NCC
The Professional Counselor
https://tpcwordpress.azurewebsites.net
Jun 13, 2022 | TPC Outstanding Scholar




Shaywanna Harris-Pierre, Christopher T. Belser, Naomi J. Wheeler, and Andrea Dennison received the 2021 Outstanding Scholar Award for Concept/Theory for their article, “A Review of Adverse Childhood Experiences as Factors Influential to Biopsychosocial Development for Young Males of Color.”
Shaywanna Harris-Pierre, PhD, LPC, is an assistant professor of professional counseling at Texas State University. Her research centers on the psychological and physiological impact of trauma and race-based traumatic stress. Dr. Harris-Pierre serves her community through facilitating free workshops for couples where she provides psychoeducation on communication skills. Dr. Harris-Pierre also serves the counseling profession through her position as secretary for the Association for Assessment and Research in Counseling, and her role as an editorial board member for the Journal of Addictions & Offender Counseling, Counseling Outcome Research and Evaluation, and the Journal of Multicultural Counseling and Development.
Christopher T. Belser, PhD, NCC, is an assistant professor in the counselor education program at the University of New Orleans. He earned his PhD in counselor education and supervision at the University of Central Florida and his MEd in school counseling at Louisiana State University. Dr. Belser has experience in Louisiana public and charter schools as a middle school counselor and a high school career coach. His research interests include school counselor preparation/practice and interdisciplinary P–16 STEM career development initiatives. Dr. Belser has delivered dozens of presentations at local, state, national, and international conferences and has published numerous articles and book chapters on counseling and career-related topics. He is the current associate editor of the Journal of Child & Adolescent Counseling, served as Chi Sigma Iota’s 2020–2021 Edwin Herr Fellow, and previously won The Professional Counselor’s 2018 Dissertation Excellence Award.
Naomi J. Wheeler, PhD, NCC, LPC, LMHC, is an assistant professor in counselor education and supervision at Virginia Commonwealth University. Her research builds on her professional and clinical experiences to examine relationship health across the life span, including the role of early life family adversity (such as ACEs) and couple stress as contributors to health disparities. Dr. Wheeler is also the co-director for the Urban Education and Family Center at VCU, which serves as a hub for community-engaged research and program services that address educational attainment, economic mobility, and individual and family well-being for historically marginalized populations living in poverty from a two-generational approach. The Center strives to harness research to improve the quality of life for Black and Latinx families in the greater Richmond area through community-based work.
Andrea Dennison, PhD, is an assistant professor at Texas State University.
Read more about the TPC scholarship awards here.
