Sep 16, 2016 | Article, Volume 6 - Issue 3
Jennifer Betters-Bubon, Todd Brunner, Avery Kansteiner
The American School Counselor Association (ASCA) National Model and a multi-tiered system of supports (MTSS) both provide frameworks for systematically solving problems in schools, including student behavior concerns. The authors outline a model that integrates overlapping elements of the National Model and MTSS as a support for marginalized students of color exhibiting problem behaviors. Individually, the frameworks employ data-driven decision making as well as prevention services for all students and intervention services for at-risk students. Thus, the integrated model allows schools to provide objective alternatives to exclusionary disciplinary actions (e.g., suspensions and expulsions) that are being assigned to students of color at a disproportionate rate. The manuscript outlines the steps within the integrated model and provides implications for school counselors and counselor educators.
Keywords: ASCA National Model, multi-tiered system of supports, school counselors, marginalized students, students of color
In 1957, Horace Mann stated, “Education, then, beyond all other devices of human origin, is a great equalizer of conditions of men” (p. 87). Public education was designed to bridge the inequalities of society such that experiences in schools could ensure all individuals have the opportunity to excel in school and in life. This tenet has been challenged in recent years as the achievement and opportunity gaps in our schools continue to grow. A disproportionate number of youth from culturally and linguistically diverse backgrounds are not succeeding and may be excluded from public school (Gregory, Skiba, & Noguera, 2010). In 2012, for example, African American students were 3.5 times more likely than their Caucasian peers to be suspended (U.S. Department of Education Office of Civil Rights, 2014). African American, Latino, and Native American students receive harsher punishments for more subjective reasons such as disrespect, insubordination or excessive noise (Losen & Gillespie, 2012). Further, data from the National Center on Educational Statistics show that while the gap is narrowing slightly, African American youth lag behind their Caucasian peers an average of 23–26 points in math and 21–26 points in reading assessments (Vanneman, Hamilton, Baldwin Anderson, & Rahman, 2009).
To close these achievement gaps and disparities in discipline practices, important research has linked schoolwide behavior programs and student achievement and engagement outcomes (Lassen, Steele, & Sailor, 2006; Luiselli, Putnam, Handler, & Feinberg, 2005). A recent focus has included schoolwide behavior programs that are multi-tiered in nature, including Positive Behavior Interventions and Supports (PBIS) programs. PBIS programs integrate research-based practice within a three-tier approach, including those at the primary, secondary, and tertiary levels of prevention and intervention. This multi-tiered system of supports has been supported by the American School Counselor Association (ASCA; 2014) and cited as evidence-based practices that have potential in closing the achievement gap (Benner, Kutash, Nelson, & Fisher, 2013). Recent research has focused on how to implement PBIS in culturally responsive ways (Bal, Kozleski, Schrader, Rodriguez, & Pelton, 2014; Greflund, McIntosh, Mercer, & May, 2014) to better impact disproportionality in discipline outcomes that exist in schools today.
School counselors with extensive training in data-informed student intervention and school-level systemic change can play integral roles in PBIS implementation and can serve as leaders in the process (Cressey, Whitcomb, McGilvray-Rivet, Morrison, & Shander-Reynolds, 2014; Goodman-Scott, 2014). Goodman-Scott, Betters-Bubon, and Donohue (2015) noted that PBIS programs can be integrated with comprehensive school counseling programs to enhance the role of the school counselor and better improve student outcomes. With knowledge of cultural diversity (Schulz, Hurt, & Lindo, 2014) and data-focused interventions to close the achievement gap (Hatch, 2013), school counselors are poised to ensure that these programs are implemented in ways that combat disproportionality. While literature exists on culturally responsive PBIS (Fallon, O’Keeffe, & Sugai, 2012) and the school counselor’s role in PBIS (Goodman-Scott, 2014), there does not exist research examining the school counselor’s role implementing culturally responsive PBIS programs, despite their role as multiculturally competent advocates for student equity. This article extends existing research on culturally
responsive PBIS by examining longitudinal data from one elementary school that intentionally engaged in culturally responsive practices within PBIS implementation, highlighting the leadership role of the school counselor. To better understand these potential relationships, we will first provide an overview of PBIS. Second, we will provide an overview of research linking PBIS to culturally responsive practice, focusing on how PBIS can combat disproportionality. Finally, we describe the case study in light of Vincent, Randall, Cartledge, Tobin and Swain-Bradway’s (2011) paper that outlines the main tenets of effective culturally responsive PBIS implementation.
Positive Behavior Interventions and Supports (PBIS)
PBIS is an educational program initiative that has great promise in helping schools promote positive behavior and engaged students. Grounded in the theory of applied behavior analysis, PBIS includes the application of a tiered system of support to change and improve behavior among students (Sugai & Horner, 2006). At the primary level (Tier 1) is the establishment of preventative systems of support, including the formation of schoolwide expectations and monitoring student behavioral data. The secondary level (Tier 2) includes the use of systematic and intensive behavior strategies for at-risk students, while the tertiary level (Tier 3) incorporates wraparound interventions for youth and families in crisis. At all levels of implementation, PBIS includes the use of evidence-based behavioral practices and formal and ongoing data-based decision making within schools (Sugai & Horner, 2006).
Next, PBIS includes a focus on four key elements: outcomes, practices, systems and data use (Horner, Sugai, Todd, & Lewis-Palmer, 2005). Student outcomes are at the foundation of any PBIS program, including behavior and academic success for students within a safe school environment. Practices include the use of evidence-based curricula, instructional practices, rewards, and contingencies that ultimately impact both teacher instruction and student behavior. Systems include an emphasis on sustained school change, including staffing, policy and training that impact how and what is done in any given school. Finally, data focuses on the continued use of school data to monitor program effectiveness. Data often used within PBIS studies includes academic achievement, school safety and behavioral indicators. Members of the PBIS team regularly analyze this data, which also is used to make subsequent decisions regarding both system and practice change.
In theory and practice, PBIS should facilitate a school environment that is more likely to promote feelings of safety and positive relationships as well as more effective teaching and learning. Recent randomized, controlled studies of PBIS implementation in elementary schools demonstrated the improved use of PBIS practices were related to feelings of safety and reading assessment results (Horner et al., 2009). In addition, schools that undertook specific schoolwide trainings were more positive and friendly than schools that did not (Bradshaw, Koth, Thornton, & Leaf, 2009). At the same time, the overall success of PBIS programs has come into question with the continued problem of disproportionality and perceived lack of cultural relevance.
Culturally Responsive Positive Behavior Interventions and Supports
Disproportionality
The question remains how and whether PBIS programs provide the same level of success for students from different racial and ethnic backgrounds. Recent researchers examined the relationship between PBIS implementation and disproportionality in discipline referrals that resulted in school removal of students. In an examination of a national sample of 364 elementary and middle schools engaged in PBIS implementation for one year, Skiba et al. (2011) noted that in comparison to Caucasian peers, African American students were overrepresented in referrals to the office and Hispanic students were underrepresented in elementary and overrepresented in middle schools. In addition, both groups of students were more likely to be suspended for offenses than their Caucasian peers. Other researchers have noted PBIS may reduce overall problem behavior as measured by the total number of office discipline referrals (ODRs), but disparities in discipline for students from minority cultures continue (Kaufman et al., 2010). Vincent, Swain-Bradway, Tobin, and May (2011) noted that the discipline gaps between Caucasian and African American students were smaller in schools implementing PBIS than those not implementing PBIS.
Integrating Culture in PBIS Programs
Recent articles have focused on further defining the nature of culture within PBIS systems. According to Fallon et al. (2012), “culturally and contextually relevant is used to describe and consider the unique variables, characteristics, and learning histories of students, educators, families, and community members involved in the implementation of PBIS” (p. 210). Sugai, O’Keeffe, and Fallon (2011) examined this definition in the context of behavioral analytic theory, positing that cultural miscommunications can occur when the behavior of one person (e.g., a teacher) serves as an antecedent for the behavior of another (e.g., a student). Individuals with different cultural learning histories may interpret the same behavior in different ways. For example, staff members may perceive walking as either strolling or strutting, which may be considered inappropriate in different classroom contexts. Fraczek (2010) found that without proper consideration of culture, PBIS programs could take a White approach, with teachers treating cultural differences among students as deficiencies rather than assets.
Culture and context, then, must be considered when planning, developing and teaching important PBIS concepts. Sugai et al. (2011) provided specific suggestions across different elements in implementation (e.g., provide opportunities for faculty to learn about cultural norms, develop lessons that are appropriate across cultural groups). Utley, Kozleski, Smith, and Draper (2002) recommended examining social behaviors from a cultural perspective (e.g., communication styles, interactional styles with adults, peers) within PBIS. Additional multicultural practices include the intentional engagement of families in the policies and expectations, particularly with diverse, urban youth. Bal, Thorius, and Kozleski (2012) extended these ideas with culturally responsive PBIS learning labs that include ongoing discussions of culture with a variety of school stakeholders (e.g., parents, staff, administration, students).
The few studies that have examined outcomes of culturally responsive PBIS programs demonstrate potential positive outcomes. Greflund et al. (2014) found no disproportionality for Aboriginal students in a diverse sample of K–8 students from British Columbia, due in part to the incorporation of Aboriginal values, language and voice in PBIS implementation (McIntosh, Moniz, Craft, Golby, & Steinwand-Deschambeault, 2014). Citing data from a number of schools in Illinois, Eber, Upreti, and Rose (2010) noted that engaging in difficult conversations and building relationships between students and staff, along with integrating data-based decision-making into the fabric of school discipline, led to positive outcomes for ethnic minority youth.
Vincent, Randall, et al. (2011) situate the integration of cultural responsiveness within key features of PBIS implementation, including data, practices, systems and outcomes (Figure 1). Only through culturally responsive practices and conversations can PBIS achieve intended outcomes. For example, while PBIS proposes that behavioral expectations are taught in an effort to increase behavioral success for all students, in a diverse school setting, these expectations would need to be taught in ways reflective of the cultural backgrounds of students. This case study will explore ways in which PBIS programs can include intentional integration of culturally responsive practices.
Case Study
Due to the lack of research in culturally responsive PBIS, this case study provides a model of culturally responsive practices within PBIS implementation. It situates PBIS implementation within the conceptual model of Vincent, Randall, et al. (2011), who suggest culturally responsive approaches serve as mediators between PBIS programs and desired outcomes (Figure 1). Specifically, culturally relevant PBIS programs will include systems emphasizing staff cultural knowledge and self-awareness, outcomes focusing on cultural equity, and data use that supports culturally valid decision making along with practices grounded in cultural validation and support (Figure 1). For example, to support culturally relevant staff behavior, schools must provide opportunities for staff to explore their own cultural awareness. Likewise, use of evidence-based practices must be grounded in knowledge and understanding of student cultural identities. Following a brief overview of the general PBIS implementation process, we outline specific culturally responsive practices as outlined by Vincent, Randall, et al. (2011).
Setting and Participants
This case study focuses on one elementary school (grades K–5) located in a suburb of a mid-sized Midwestern town from 2009–2014. The suburb had a population of approximately 10,000 residents. Median household income in 2009 was $75,000. The school district had approximately 4,900 students drawn from the suburb itself and a suburb located 10 miles away. The target school, one of 11 in the district, had an enrollment of approximately 500 students. A substantial shift in student population occurred during the first year of implementation due to redistricting. A population of approximately 130 Spanish-speaking bilingual students was transferred to the school in 2008, shifting the student demographics to 60% Caucasian, 28% Hispanic, 9% African American and 2% Asian American. Approximately 40% of students received free and reduced lunch at the time of observance.
Procedures
Given that the first author was engaged in PBIS implementation first as a school counselor and later as a consultant while the other authors are currently engaged in PBIS implementation, this article uses a participatory action research framework (Reason & Bradbury, 2008). Action research includes a planning and reflective process that is linked to action, all of which are influenced by an understanding of history, culture and local context (Baum, MacDougall, & Smith, 2006). Thus, the article includes a description of PBIS planning and action stages along with the reflective process that was involved in culturally responsive PBIS implementation.
Within the action research framework, data were used, including ODRs as a fidelity measure of PBIS. ODRs are a reliable and valid indicator of overall school climate levels (Irvin et al., 2006) and are commonly used in PBIS analysis. The PBIS Self-Assessment Survey (SAS) was used for initial and annual assessment of implementation quality of behavior support systems in the school. This online survey, completed by a cross-section of school staff, examines the “current status” and “need for improvement” of four behavior support systems: (a) schoolwide discipline systems, (b) non-classroom management systems (e.g., cafeteria, hallway, playground), (c) classroom management systems, and (d) systems for individual students engaging in chronic problem behaviors. Results give an overall implementation level as it pertains to PBIS, with 80% indicating full implementation (Sugai, Horner, Lewis-Palmer, & Todd, 2005).
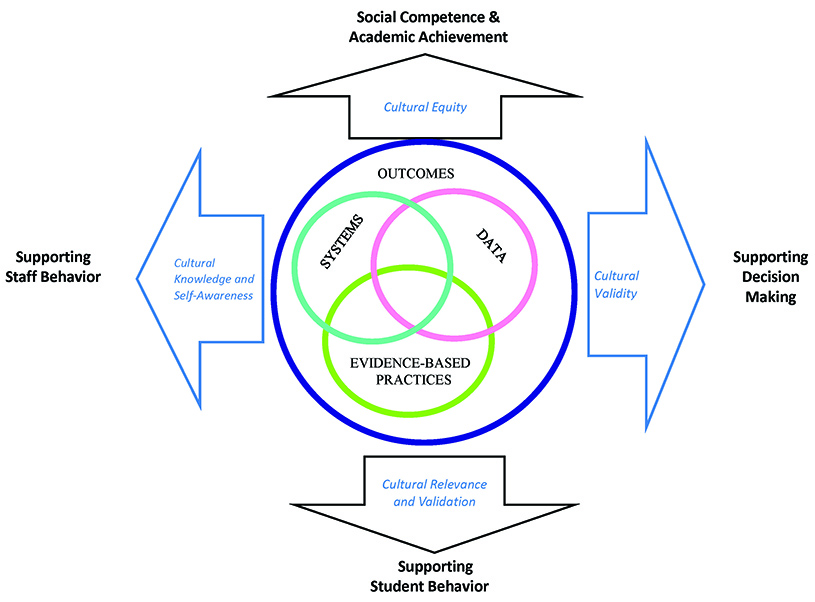
Figure 1. Integrating Schoolwide Positive Behavior Support and Culturally Responsive Practices. Reprinted from “Toward a Conceptual Integration of Cultural Responsiveness and Schoolwide Positive Behavior Support,” by C. G. Vincent, C. Randall,, G. Cartledge, T. J. Tobin, and J. Swain-Bradway, 2011, Journal of Positive Behavior Interventions, 13, 219–229.
Copyright 2011 by Sage Publishing. Reprinted with permission.
Planning: PBIS Implementation
PBIS within this school grew out of immediate concerns regarding the number of ODRs. For example, during 2006–2007, the school had 573 discipline referrals and an enrollment of 314 students. As a result of this situation, during 2007–2008 and 2008–2009 the school implemented a schoolwide goal that included the creation and implementation of a multi-component plan for integrating new students with a goal of a 50% reduction in discipline referrals. Two additional school goals focused on math and reading development. All certified staff were required to attend monthly meetings focusing on one of the goals, and results were communicated yearly to the site council, the governing body of the school and the school board.
The PBIS team formed in 2009–2010 as a way to coordinate and organize the many interventions that were attempted through the prior 2 years of work. The school counselor organized and led a summer PBIS training that included a cross-section of 25 staff members prior to the beginning of the school year.
Action: PBIS Implementation
Leadership team. At the core of the PBIS implementation process was the leadership team. The school counselor led the team along with coaches who focused on core areas of PBIS (e.g., systems, acknowledgements). The team varied in number between 15 and 25 and included a representative group of the school staff, such as classroom teachers, special teachers (e.g., music), educational assistants, special education teachers, student support staff (e.g., psychologist, social worker) and the principal. The team met on a monthly basis to discuss data, student behavior and acknowledgement. Because PBIS had not been adopted district-wide, the school hired a PBIS consultant to train and meet with the team coaches to ensure fidelity.
Behavioral expectations. The leadership team spent a considerable amount of time determining four behavioral expectations for the school at a summer workshop. The discussion included the meaning of such words as “respect” as well as the types of behaviors that would be universally expected by parents and teachers from different backgrounds. The four expectations: Be Safe, Be Kind & Respectful, Be a Problem-Solver and Be Responsible became the cornerstone behavioral expectations for the school. The team planned teacher training regarding the newly developed expectations as well as community gatherings to teach the expectations to students and families. Within this process, the school counselor played an integral role, organizing the gatherings and using expertise in social and emotional development to write the behavioral lessons known as Cool Tools. In subsequent years, the school counselor provided trainings to all new staff on PBIS.
Defining procedures. Along with expectations, the team delineated behaviors that would be handled in the classroom versus in the office (e.g., a t-chart delineating the discipline infractions that office and teaching staff respond to on a day-to-day basis). Not only were the processes outlined on paper, they were discussed in monthly staff meetings and meetings with student services staff and administration and educational assistants. For example, student services staff, including the school counselor, met with grade-level teachers each month to discuss student needs. This served as a way to reinforce key PBIS procedures. Similarly, the educational assistants who supervise students in the lunchroom, at recess and in the hallways were included as important team members through monthly meetings. These meetings, along with the monthly PBIS meeting, allowed for continuous conversation around student behavior and adult response.
Acknowledgements. Typically, PBIS programs provide a tangible, positive reinforcement system to promote appropriate behavior. These systems should include immediate feedback systems, such as verbal praise or tickets given to students demonstrating school expectations that can be turned in for prizes (e.g., pencils), as well as long-term feedback systems (e.g., quarterly schoolwide celebrations). Many staff members expressed concern about implementing an extrinsically focused ticket system, noting that this may lead to decreased intrinsic motivation. As such, a formal acknowledgement system was not immediately integrated into the PBIS program in year one. In January, the counselor had conversations with educational assistants about piloting a positive reinforcement ticket program on the playground in response to data showing an increase in ODRs. The success, measured by teacher and educational assistant perception and ODR referrals on the playground, was almost immediate. This led to staff interest in using this ticket system as a form of acknowledgement and reinforcement. Conversations at staff meetings along with printed materials, describing in detail the purpose of acknowledgements, helped the school move forward with a formal “thumbs up” ticket plan that transcended the playground to include all areas of the school. The PBIS team included student voices in the acknowledgements and leadership of PBIS, with a team of fifth-grade students assisting in the development of PBIS acknowledgement ideas in year two and beyond.
Data analysis. Data on ODRs had been collected at this school for many years. The principal sent out monthly updates on the number of discipline referrals, including referrals broken down by ethnicity. The integration of PBIS meant that the data analysis became a focus of the monthly meetings. The school counselor became actively involved in data analysis, sharing monthly updates with staff members. School staff examined types of areas of problem behavior and created plans to respond. While this data often focused on ODRs, more qualitative data also was discussed. For example, the lunchroom became an area of focus when teachers and staff shared concerns about behavior and noise. The leadership team took the qualitative data and created strategies to increase positive behavior (e.g., re-teaching, positive acknowledgement plan, community assemblies).
Family outreach. From the start, the PBIS team informed parents of the purpose of PBIS and later more fully integrated the voices of parents in the planning processes. The school counselor wrote monthly newsletters while teachers encouraged students to share their acknowledgement tickets with parents so as to share the positives happening in the school. Additionally, the team created a home behavior matrix and a Web site where parents and families could obtain additional information on PBIS at the school.
Reflection: Culturally Responsive PBIS Integration
As the team engaged in PBIS implementation, multiple situations emerged that brought culture to the forefront. Table 1 outlines several ways in which the team intentionally integrated culturally responsive practices into the PBIS program, and additional examples are illustrated below.
Table 1
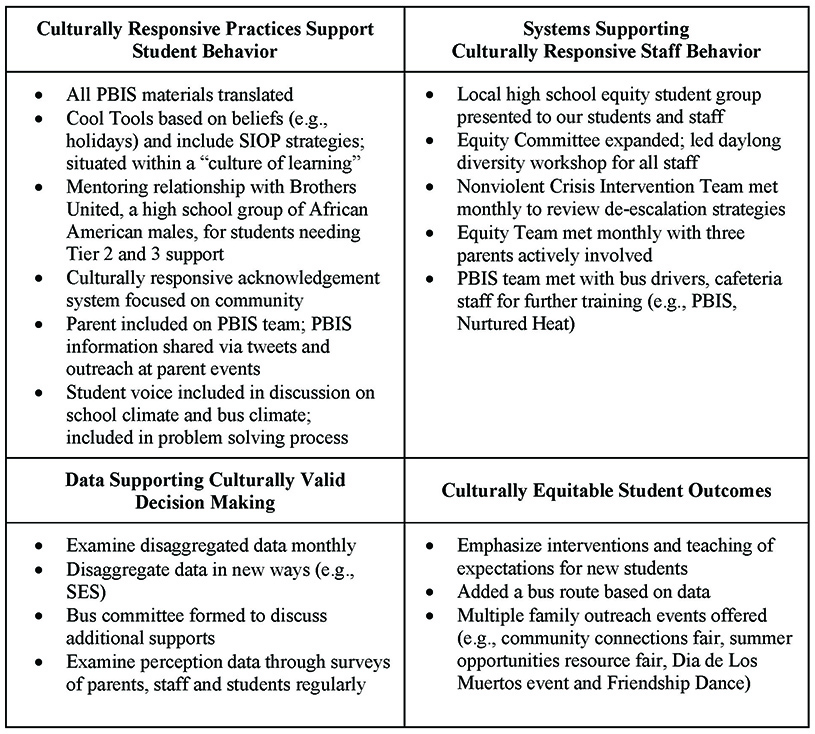
CR-PBIS Elements by Category
Systems built on cultural knowledge and awareness. From the onset of PBIS implementation, the leadership team integrated aspects of culture and cultural responsiveness into the systems. First, the PBIS team was diverse and included many different voices (e.g., bus drivers, educational assistants, bilingual and monolingual classroom teachers, special education staff). The redistricting in the first year of PBIS and the resulting change in student population led to the PBIS team having intentional discussion of important topics involving whether the expectations were culturally relevant to all students, including the Spanish-speaking students.
Further, the leadership team engaged in conversations about their own cultural biases and knowledge to inform the practices implemented within PBIS. When a team member suggested staff should teach the top 10 manners (e.g., table manners, eye contact) as part of the PBIS expectations, the team engaged in intentional conversation about whether the manners would be relevant to all students and parents. Ultimately, this team abandoned this idea due to the potential lack of cultural relevance. For example, the team discussed how eye contact during conversation may not be applicable to all families and students in the school. The principal encouraged staff learning and self-awareness that went beyond these conversations and scheduled subsequent trainings in the following years.
The team helped to create systems by which parents were informed and included in the PBIS process. For example, all information was sent to parents in multiple ways (e.g., translated) and parent voices were sought whenever possible. By year four, the leadership team included parents on the team and in year five, one of the school counselors started a Latino parent group.
The school counselor’s role changed as a result of PBIS and resource allocation was specifically addressed through the budget process at site council in the spring. Because the counselor was charged with leading the school’s PBIS efforts, the school increased the counselor full-time equivalent (FTE) from .60 to 1.20 to support this goal, thus adding a part-time bilingual counselor early in the first year of implementation.
Practices grounded in cultural validation and support. The change in school population led to more intentional conversations of culture in teaching and learning, validating the backgrounds of students and families. First and foremost, the universal practices that staff engaged in focused on community and acceptance. For example, the school principal left time in the master schedule for all classroom teachers to implement morning meetings, as recommended by the Responsive Classroom© Approach (Kriete, 2002). Daily class meetings are in line with culturally relevant practice as they lead to teachers and students knowing each other in the creation of a classroom community (Bondy, Ross, Gallingane, & Hambacher, 2007).
As the team implemented culturally responsive PBIS, the school counselor, in consultation with bilingual teaching staff, integrated Sheltered Instruction Observation Protocol (SIOP) strategies (Short, Fidelman, & Louguit, 2012) in the behavioral lessons. SIOP includes strategies in lessons that ensure that English language learners have the necessary background information to learn the material presented. As such, the team ensured that expectations were taught in culturally relevant ways. In addition, the teaching of expectations included recognition of the different backgrounds of students. For example, one of the behavioral lessons given to teachers close to winter break involved discussion of different student and staff beliefs that might be practiced over the break. Being respectful in this case transcended outside of traditional definitions of respect to include knowledge of others’ beliefs. Further, discussions among the leadership team in year three acknowledged the lack of overarching student understanding of the school expectations. For example, staff was not engaging in larger discussions about why respect can lead to success in life. As such, the team integrated the all-encompassing theme “Be A Learner” and situated the teaching of all expectations under this framework. In this way, staff, students and families could discuss how this is relevant in school and life, thus reflecting the perspectives of students and families (Swain-Bradway, Loman, & Vincent, 2014).
The PBIS team, along with school staff, discussed the inclusion of an acknowledgement system with intention. Because of the aforementioned concern about extrinsic reinforcement in the form of tickets, acknowledgement tickets were often given to groups and classrooms of students. The PBIS team placed more value on group gathering of tickets than individual. For example, each classroom had a bucket in which to collect tickets. They would bring their tickets to community gatherings to meet schoolwide goals, which would result in schoolwide celebrations focused on learning and community. For example, students would be encouraged to take part in a pajama day or be given 20 minutes on a specific day to engage in a fun activity, such as Drop Everything and Draw. These activities served to reinforce the positive behavior displayed by students.
Data that led to culturally valid decision making. The leadership team regularly used data to inform the practices taught and reinforced in the school. Total ODR data was collected each year and demonstrated decreases in overall number of referrals despite increasing enrollment (see Table 2). In addition, the school counselor regularly broke down data by grade level, socioeconomic status, race and location. This data was then discussed monthly at grade level meetings during which general problem solving could take place, whether focused on a specific student or group of students. Additionally, the data guided decisions at monthly PBIS leadership team meetings. The team regularly examined program fidelity. The SAS implementation average rose over the years, reaching fidelity of 84% in year three (see Table 3). Moreover, the PBIS leadership team used the SAS subscales to determine program strengths and weaknesses. Subscales included how well school expectations were taught and defined, and presence of a reward (or acknowledgment) system, as well as a defined way of addressing student behavior violations and infractions. In addition, the SAS included items that measured how well the team monitored areas in the building, managed the team processes and were supported at the district level. All subscales increased over the years of implementation.
Table 2
Enrollment and ODRs by Year
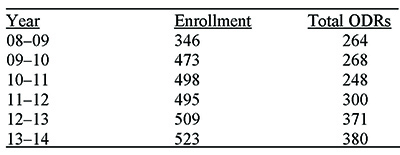
Table 3

Self-Assessment Survey (SAS) Results by Year
ODR data comparing percentage enrollment to percentage of total ODRs demonstrated variability across the years (see Figure 2). ODR trends for Hispanic students shifted from over-representation to under-representation, whereas the gap for African American students went from 14% enrollment and 55% of total ODRs to a narrower gap of 7% enrollment and 31% of total ODRs. In meetings, the leadership team went beyond examination of percentages to determine which students were having difficulty. For example, during year five the team noted that students who had moved to the school in the previous year received a high percentage of total ODRs and accounted for many of the students needing Tier 2 and 3 supports. The team integrated interventions and behavioral teaching opportunities to assist new students in that transition.
In year four, a district focus on data led to the mandated formation of school equity teams at each school site. At this school, the team was comprised of 16 staff members and four parent and community members, and focused on school climate equity and parent and community outreach. This team met monthly, and in doing so disseminated climate surveys to students and staff, examined district-wide assessments to ensure cultural fairness and planned culture nights and parent orientation nights in the community.
Outcomes that demonstrate cultural equity. The more intentional focus on data disaggregation led to the ability of the PBIS leadership team to make equitable decisions. An example occurred in
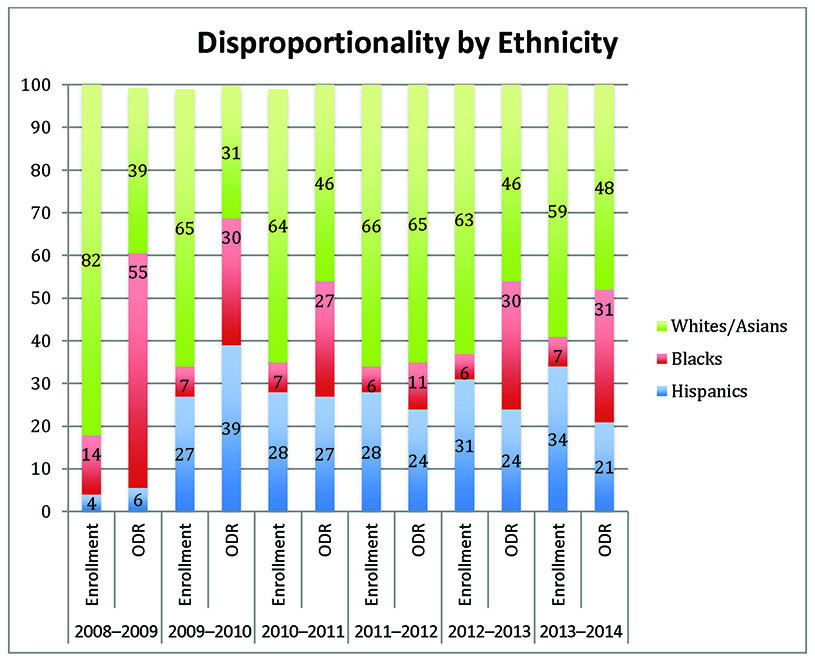
Figure 2. ODR by Ethnicity
the first year of PBIS implementation. At the start of 2009, the leadership team became concerned about behavior reported on one of the school buses. The contracted school bus driver was reporting, through written bus reports to the administration, a number of behavioral infractions on the rides to and from school. This bus included many students who received free and reduced lunch and were in racial and ethnic minority groups, traveling to and from an inner city neighborhood 10 miles away from the school. The principal worked with the general manager of the bus company and put interventions in place as part of PBIS, including meetings with the driver, principal, and translator in the cafeteria, and student–bus driver meetings, as well as letters to parents. It became apparent the problem was less about student behavior and more about equity—the bus was overcrowded. The principal shared concerns with the superintendent and the superintendent engaged in conversations with the bus company. Because the school as a whole had embraced PBIS and documenting data and steps to problem-solve, leaders at the district level were motivated to intervene. The district had funds and added a new bus route for students; bus referrals went down immediately.
Discussion
Research shows that PBIS is best implemented when considering the specific context of the school and needs of students and families (Fallon et al., 2012). The school in this case study demonstrated the intentional work that was needed to implement PBIS that was culturally responsive. The implementation of culturally responsive practices led to fewer behavioral reports for students from Hispanic backgrounds. Unfortunately, a disproportionate number of African American students received ODRs even after the implementation of culturally responsive PBIS, which is in line with previous research (Skiba et al., 2011). Thus, the intentional integration of culturally responsive PBIS practices should go beyond the examination of disaggregated data to include conversations around equity, access and success for all. The PBIS team in this school started these conversations to determine why students might not be succeeding. Because of the systems in place, staff integrated additional teaching and learning opportunities for students who were new to the school. There is still more for the team to do to reduce disproportionate representation of African American students in ODR. To that end, the leadership team recently went through PBIS Tier 2 training and the school counselors are implementing check-in/check-out, a targeted intervention program for individual students (Todd, Campbell, Meyer, & Horner, 2008) and data-driven small groups. Future research should examine whether these approaches have an impact on overall ODR data and on the continued equity conversations happening among key stakeholders in the school.
Because the results of this action research case study focus on one school’s efforts to engage in culturally responsive practice, the results should be interpreted with caution. The study is descriptive in nature and connections between the integration of culturally responsive PBIS elements and outcomes were not tested empirically. Future research should examine the relationship between intentional integration of culturally responsive PBIS components on school and student outcomes, to include outcomes beyond discipline referrals. Important work in this area is emerging and it will be imperative for school counselors to remain at the forefront of these initiatives to ensure PBIS practices take all students into consideration.
Currently, PBIS is implemented in thousands of schools in over 40 states. PBIS systems emphasize a shift from responding to problem behavior with exclusionary discipline to the use of instructional responses to problem behavior and corrective procedures to help students to identify and practice acceptable behavior instead of removing them from the classroom (McIntosh, Filter, Bennett, Ryan, & Sugai, 2010). While PBIS is an evidence-based intervention that should address disproportionality within discipline systems (Eber et al., 2010), this study and others have demonstrated that this is not always the case. As such, culture and context must be considered when planning, developing and implementing PBIS programs to make them more culturally responsive. In doing this important work, Swain-Bradway et al. (2014) recommended that school leaders systematically integrate the range of student cultural perspectives along with teacher cultural perspectives in creating disciplinary policies and practices that are nondiscriminatory. The cultural mismatch between individual teachers and students may be mitigated by the systematic implementation of school-wide systems supporting culturally responsive practices within schools. (p. 4)
Equity can only be achieved when all students and student backgrounds are considered within systemic programs implemented in a school environment and when all possible reasons for the gaps in success, including the ever increasing needs of students, disproportionate access to resources and opportunities, and mandates made on the educational system as a whole, are considered.
Conclusion and Implications
With much at stake at the national, district, school and individual levels, school counselors can play a critical role in ensuring PBIS programs are implemented with fidelity and in culturally responsive ways. School counselors can use their knowledge and recommendations (McIntosh, Girvan, Horner, Smolkowski, & Sugai, 2014) to reduce this very real problem of disproportionality in discipline practices, including implementing culturally responsive PBIS, disaggregating data and implementing accountability policies focused on discipline equity (Green et al., 2015; McIntosh, Barnes, Eliason, & Morris, 2014). Further, school counselors can use their expansive knowledge of data to extend the focus beyond just ODRs. Perception surveys focused on process rather than outcome data might be better at capturing change across time. For example, interviews with staff, parents and students examining school climate and social behavior can and should be examined within culturally responsive PBIS implementation. In that way, a clearer picture of student behavior, school climate, family perception and staff support might emerge. A recent national survey found school personnel to be supportive of the implementation of culturally and contextually responsive elements of PBIS (Fallon, O’Keeffe, Gage, & Sugai, 2015). School counselors can be champions in the process of encouraging culturally responsive practices within PBIS program implementation.
Schools play a privileged and strategic role in influencing social, emotional and academic outcomes for youth (Herman, Reinke, Parkin, Traylor, & Agarwal, 2009). School counselors can serve as leaders in conversations about equity and social justice as it pertains to student behavior and success in schools. Through continued conversations, intentional understanding of self and others, and targeted family involvement, school staff can ensure that education indeed continues to be the great equalizer for all.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
American School Counselor Association. (2014). The school counselor and multitiered system of supports. Retrieved from https://www.schoolcounselor.org/asca/media/asca/PositionStatements/PS_MultitieredSupportSystem.pdf.
Bal, A., Kozleski, E. B., Schrader, E. M., Rodriguez, E. M., & Pelton, S. (2014). Systemic transformation from the ground–up: Using learning lab to design culturally responsive schoolwide positive behavioral supports. Remedial and Special Education, 35, 327–339. doi:10.1177/0741932514536995
Bal, A., Thorius, K., & Kozleski, E. (2012). Culturally responsive Positive Behavioral Support matters. Retrieved from www.equityallianceatasu.org/sites/default/files/CRPBIS_Matters.pdf
Baum, F., MacDougall, C., & Smith, D. (2006). Participatory action research. Journal of Epidemiology & Community Health, 60, 854–857. doi:10.1136/jech.2004.028662
Benner, G. J., Kutash, K., Nelson, J. R., & Fisher, M. B. (2013). Closing the achievement gap of youth with
emotional and behavioral disorders through multi-tiered systems of support. Education and Treatment
of Children, 36(3), 15–29. doi:10.1353/etc.2013.0018
Bondy, E., Ross, D. D., Gallingane, C., & Hambacher, E. (2007). Creating environments of success and resilience:
Culturally responsive classroom management and more. Urban Education, 42, 326–348. doi:10.1177/0042085907303406
Bradshaw, C. P., Koth, C. W., Thornton, L. A., & Leaf, P. J. (2009). Altering school climate through school-wide positive behavioral interventions & supports: Findings from a group-randomized effectiveness trial. Prevention Science, 10, 100–115. doi:10.1007/s11121-008-0114-9.
Cressey, J. M., Whitcomb, S. A., McGilvray-Rivet, S. J., Morrison, R. J., & Shander-Reynolds, K. J. (2015). Handling PBIS with care: Scaling up to school-wide implementation. Professional School Counseling, 18, 90–99. doi:10.5330/prsc.18.1.g1307kql2457q668
Eber, L, Upreti, G, & Rose, J. (2010). Addressing ethnic disproportionality in school discipline through positive behavior interventions and supports (PBIS). Building Leadership, 17, 1–10.
Fallon, L. M., O’Keeffe, B. V., Gage, N. A., & Sugai, G. (2015). Brief report: Assessing attitudes toward culturally and contextually relevant schoolwide positive behavior support strategies. Behavioral Disorders, 40, 251–260. doi:10.17988/0198-7429-40.4.251
Fallon, L. M., O’Keeffe, B. V., & Sugai, G. (2012). Consideration of culture and context in school-wide positive behavior support: A review of current literature. Journal of Positive Behavior Interventions, 209–219. doi:10.1177/1098300712442242
Fraczek, M. S. (2010). Perpetuating a culture of White behavior: The experiences of non-native speaking Hispanic students in a PBIS school. (Doctoral dissertation). Retrieved from ProQuest Dissertations and Theses. (3397846)
Goodman-Scott, E. (2013). Maximizing school counselors’ efforts by implementing school-wide positive behavioral interventions and supports: A case study from the field. Professional School Counseling, 17, 111–119. doi:10.5330/prsc.17.1.518021r2x6821660
Goodman-Scott, E., Betters-Bubon, J., & Donohue, P. (2015). Aligning comprehensive school counseling programs and positive behavioral interventions and supports to maximize school counselors’ efforts.
Professional School Counseling, 19, 57–67. doi:10.5330/1096-2409-19.1.57
Green, A. L., Nese, R. N. T., McIntosh, K., Nishioka, V., Eliason, B., & Canizal Delabra, A. (2015). Key elements of policies to address discipline disproportionality: A guide for district and school teams. OSEP Technical Assistance Center on Positive Behavioral Interventions and Supports. Retrieved from https://www.pbis.org/Common/Cms/files/pbisresources/PBIS%20Disproportionality%20Policy%20Guidebook%202016-7-24.pdf
Greflund, S., McIntosh, K., Mercer, S. H., & May, S. L. (2014). Examining disproportionality in school
discipline for Aboriginal students in schools implementing PBIS. Canadian Journal of School Psychology, 29, 213–235. doi:10.1177/0829573514542214
Gregory, A., Skiba, R. J., & Noguera, P. A. (2010). The achievement gap and the discipline gap: Two sides of the same coin? Educational Researcher, 39, 59–68. doi:10.3102/0013189X09357621
Hatch, T. (2013). The use of data in school counseling. Thousand Oaks, CA: Corwin Press.
Herman, K. C., Reinke, W. M., Parkin, J., Traylor, K. B., & Agarwal, G. (2009). Childhood depression: Rethinking the role of the school. Psychology in the Schools, 46, 433–446. doi:10.1002/pits.20388
Horner, R. H., Sugai, G., Smolkowski, K., Eber, L., Nakasato, J., Todd, A. W., & Esperanza, J. (2009). A randomized, wait-list controlled effectiveness trial assessing school-wide positive behavior support in elementary schools. Journal of Positive Behavior Interventions, 11, 133–144.
Horner, R. H., Sugai, G., Todd, A. W., & Lewis-Palmer, T. (2005). School-wide positive behavior support: An alternative approach to discipline in schools. In L. M. Bambara & L. Kern (Eds.), Individualized supports for students with problem behaviors: Designing positive behavior plans (pp. 359–390). New York, NY: Guilford Press.
Irvin, L. K., Horner, R. H., Ingram, K., Todd, A.W., Sugai, G., Sampson, N. K., & Boland, J. B. (2006). Using office discipline referral data for decision making about student behavior in elementary & middle schools: An empirical evaluation of validity. Journal of Positive Behavior Interventions, 8, 10–23.
doi:10.1177/10983007060080010301
Kaufman, J. S., Jaser, S. S., Vaughan, E. L., Reynolds, J. S., Di Donato, J., Bernard, S. N., & Hernandez-Brereton, M. (2010). Patterns in office referral data by grade, race/ethnicity, and gender. Journal of Positive Behavior Interventions, 12, 44–54. doi:10.1177/1098300708329710
Kriete, R. (2002). The morning meeting book. (2nd ed.). Turners Falls, MA: Northeast Foundation for Children.
Lassen, S. R., Steele, M. M., & Sailor, W. (2006). The relationship of school-wide positive behavior support to academic achievement in an urban middle school. Psychology in the Schools, 43, 701–712.
doi:10.1002/pits.20177
Losen, D. J., & Gillespie, J. (2012). Opportunities suspended: The disparate impact of disciplinary exclusion from school. Los Angeles, CA: The Center for Civil Rights Remedies.
Luiselli, J. K., Putnam, R. F., Handler, M. W., & Feinberg, A. B. (2005). Whole-school positive behaviour
support: Effects on student discipline problems & academic performance. Educational Psychology, 25, 183–198. doi:10.1080/0144341042000301265
Mann, H. (1957). Twelfth annual report. In L. Cremin (Ed.), The republic and the school: Horace Mann on the education of free men (pp. 79–112). New York, NY: Teachers College Press.
McIntosh, K., Barnes, A., Eliason, B., & Morris, K. (2014). Using discipline data within SWPBIS to identify and
address disproportionality: A guide for school teams. OSEP Technical Assistance Center on Positive
Behavioral Interventions and Supports. Retrieved from http://www.pbis.org/Common/Cms/files/pbisresources/PBIS_Disproportionality_Data_Guidebook.pdf
McIntosh, K., Filter, K. J., Bennett, J. L., Ryan, C., & Sugai, G. (2010). Principles of sustainable prevention:
Designing scale-up of school-wide Positive Behavior Support to promote durable systems. Psychology in the Schools, 47, 5–21. doi:10.1002/pits.20448
McIntosh, K., Girvan, E. J., Horner, R. H., Smolkowski, K., & Sugai, G. (2014). Recommendations for addressing discipline disproportionality in education. OSEP Technical Assistance Center on Positive Behavior Intervention and Supports. Retrieved from https://www.pbis.org/Common/Cms/files/pbisresources/RecommendationsForAddressingDisciplineDisproportionality.pdf
McIntosh, K., Moniz, C., Craft, C. B., Golby, R., & Steinwand-Deschambeault, T. (2014). Implementing school-wide positive behavioural interventions and supports to better meet the needs of Indigenous students. Canadian Journal of School Psychology, 29, 236–257. doi:10.1177/0829573514542217
Reason, P., & Bradbury, H. (2008). The Sage handbook of action research: Participative inquiry and practice (2nd ed.)Los Angeles, CA: Sage.
Schulz, L. L., Hurt, K., & Lindo, N. (2014). My name is not Michael: Strategies for promoting cultural respon-siveness in schools. Journal of School Counseling, 12(2), 1–35.
Short, D. J., Fidelman, C. G., & Louguit, M. (2012). Developing academic language in English language learners through sheltered instruction. TESOL Quarterly, 46, 334–361. doi:10.1002/tesq.20
Skiba, R. J., Horner, R. H., Chung, C.-G., Rausch, M. K., May, S. L., & Tobin, T. (2011). Race is not neutral: A national investigation of African American and Latino disproportionality in school discipline. School Psychology Review, 40, 85–107.
Sugai, G., & Horner, R. R. (2006). A promising approach for expanding & sustaining school-wide positive behavior support. School Psychology Review, 35, 245–259.
Sugai, G., Horner, R. H., Lewis-Palmer, T., & Todd, A. (2005). School-wide positive behavior support team training manual. Eugene: Educational and Community Supports, University of Oregon.
Sugai, G., O’Keeffe, B. V., & Fallon, L. M. (2011). A contextual consideration of culture and schoolwide positive behavior support. Journal of Positive Behavior Interventions, 14, 197–208.
Swain-Bradway, J., Loman, S. L., & Vincent, C. G. (2014). Systematically addressing discipline disproportion-ality through the application of a school-wide framework. Multiple Voices for Ethnically Diverse Exceptional Learners, 14, 3–17.
Todd, A. W., Campbell, A. L., Meyer, G. G., & Horner, R. H. (2008). The effects of a targeted intervention to reduce problem behaviors: Elementary school implementation of check in—check out. Journal of Positive Behavior Interventions, 10, 46–55.
U.S. Department of Education Office of Civil Rights. (2014, March). Civil rights data collection. Washington, DC: Author. Retrieved from http://ocrdata.ed.gov/Downloads/CRDC-School-Discipline-Snapshot.pdf
Utley, C. A., Kozleski, E. B., Smith, A., & Draper, I. L. (2002). Positive behavior support: A proactive strategy for minimizing behavior problems in urban multicultural youth. Journal of Positive Behavior Interventions, 4, 196–207. doi:10.1177/10983007020040040301
Vanneman, A., Hamilton, L., Baldwin Anderson, J., & Rahman, T. (2009). Achievement gaps: How Black and White students in public schools perform in mathematics and reading on the National Assessment of Educational Progress, (NCES 2009-455). National Center for Education Statistics, Institute of Education Sciences, U.S.
Department of Education. Washington, DC. Retrieved from https://nces.ed.gov/nationsreportcard/pubs/studies/2009455.aspx
Vincent, C. G., Randall, C., Cartledge, G., Tobin, T. J., & Swain-Bradway, J. (2011). Toward a conceptual integration of cultural responsiveness and schoolwide positive behavior support. Journal of Positive Behavior Interventions, 13, 219–229. doi:10.1177/1098300711399765
Vincent, C. G., Swain-Bradway, J., Tobin, T. J., & May, S. (2011). Disciplinary referrals for culturally and linguistically diverse students with and without disabilities: Patterns resulting from school-wide positive behavior support. Exceptionality, 19, 175–190. doi:10.1080/09362835.2011.579936
Jennifer Betters-Bubon is an Assistant Professor at the University of Wisconsin-Whitewater. Todd Brunner is the Principal and Avery Kansteiner is a School Counselor at Sugar Creek Elementary School in Verona, WI. Correspondence can be addressed to Jennifer Betters-Bubon, 6039 Winther Hall, Whitewater, WI 53190, bettersj@uww.edu.
Sep 16, 2016 | Article, Volume 6 - Issue 3
Karen Harrington, Catherine Griffith, Katharine Gray, Scott Greenspan
This article provides an overview of a grant project designed to create a district-wide elementary school counseling program with a strong data-based decision-making process. Project goals included building data literacy skills among school counselors and developing the infrastructure to efficiently collect important social-emotional indicators through a revised system for recording disciplinary infractions and a new research-based behavioral component for the district’s standards-based report cards. This enhanced system for accessing and analyzing social-emotional indicators resulted in broad systemic changes in the district, including extending a number of grant initiatives to the middle and high school levels, restructuring data teams to adopt a multi-tiered system of supports, and establishing school counselors as leaders in data-driven discussions about student success.
Keywords: school counseling, data-based decision making, multi-tiered system of supports, social–emotional, elementary school
This article reports on an Elementary and Secondary School Counseling Program (ESSCP) grant project designed to build an elementary school counseling program in a district that previously had not employed school counselors at that level. The new school counseling program was organized around an innovative shift in the district’s multi-tiered system of supports (MTSS) model that expanded to integrate social-emotional and behavioral data with academic indicators. School counselors used the new social-emotional data to help answer the question of why students were struggling academically when scholastic deficiencies were not the primary cause. The grant project also focused on developing strong data literacy skills among elementary school counselors so they could serve as leaders in data-based discussions. These complementary grant goals transformed the data team process as school counselors, teachers and administrators began to use data to better understand the complex relationship between social-emotional factors and academic achievement. These practices resulted in systemic changes throughout the district as data-driven elements of the elementary school counseling program were adopted at the secondary level. The purpose of this article is to: (a) highlight the importance of engaging in data-based decision making regarding students’ social-emotional needs in schools, (b) provide an overview of the specific elements that comprised the new MTSS model in the school district as a part of this grant-funded project, and (c) underscore the importance of building human capacity to enable school-based data teams to meaningfully integrate academic and social-emotional data to promote improved student outcomes. Limitations of this project, directions for future research and implications for school counselors also are discussed.
School Counselors and Social-Emotional Data
School counselors are often advised to adopt a data-based decision-making model as part of their practice (American School Counselor Association [ASCA], 2012; Dimmitt, Carey, & Hatch, 2007). Accountability mandates require school counselors to use data to demonstrate the impact of their work and to link their interventions to academic achievement (Dahir & Stone, 2009: Isaacs, 2003; Sink & Stroh, 2003.) Moreover, data use also is central to the transformed model of school counseling, which positions school counselors as advocates in educational reform efforts such as closing the achievement gap and carrying out school improvement initiatives (Dahir, 2004; Hayes, Nelson, Tabin, Pearson, & Worthy, 2002; House & Hayes, 2002). However, institutional factors can limit the role of the school counselor in data-based decision making. Typically, data teams primarily (or even exclusively) consider academic indicators, and schools often lack the infrastructure to systematically collect the social-emotional data that more directly aligns with the work of the school counselor.
Accountability requirements of the No Child Left Behind Act of 2001 (NCLB; 2002) have strongly influenced schools’ approaches to data-based decision making (Mandinach, Honey, & Light, 2006; Marsh, Pane, & Hamilton, 2006). The pressure to demonstrate adequate yearly progress (AYP) has prioritized state standardized tests scores and other academic benchmark assessments in data-driven discussions. A tremendous amount of achievement data were routinely collected and housed by school districts to fulfill reporting demands of NCLB; these data will continue to be gathered under the new Every Student Succeeds Act (ESSA; 2015). School staff can access these data to guide instructional practices and measure student progress. However, these data are more directly linked to teachers’ work with students and primarily measure academic achievement and cognitive ability (Heckman & Rubinstein, 2001).
The role of the school counselor encompasses not only students’ academic achievement but also their social-emotional development (ASCA, 2012). Social-emotional and behavioral data are typically not collected in the same robust manner as academic achievement data and are often limited to office discipline referrals and attendance rates. These behaviors are poor proxies of student engagement and reveal little information about underlying issues that need to be addressed. Measures of motivation, perseverance, self-regulation and other factors that impact students’ ability to achieve are not present in most school districts’ data collection systems, rendering them absent also from data-driven discussions about student outcomes.
In addition, while NCLB articulated which data are considered the critical measures of academic achievement, a corresponding set of social-emotional data has not been clearly delineated. Despite growing recognition of the impact of non-cognitive factors on student achievement (Farrington et al., 2012), educators are often uncertain about which specific behaviors, attitudes and dispositions link to success in school and throughout life. Educational organizations such as The Partnership for 21st Century Skills; Collaboration for Academic, Social, and Emotional Learning (CASEL); and ASCA (2014) have suggested promoting specific mindsets, college and career-readiness skills, and prosocial behaviors, but consensus is lacking about which social-emotional or non-cognitive factors are integral to students’ academic and social skill development.
The process of data-based decision making in schools has been shaped both by a prevailing belief concerning which data are important to examine and an existing infrastructure that constrains what data are routinely collected to those of a primarily academic nature. These factors also limit the role of the school counselor in data-based discussions about student achievement. With the end of the NCLB era and the ushering in of ESSA, all educators are being asked to address non-cognitive factors and be accountable for showing gains in these areas in addition to academic areas.
A construct-based approach to school counseling. Squier, Nailor, and Carey (2014) extensively reviewed the educational and developmental psychology literature to determine what capabilities are strongly related to students’ academic achievement and later success in life. The authors intentionally chose lines of research connected to student competencies in the academic, personal/social and career domains that comprise the school counseling ASCA (2012) National Model. Squier and colleagues (2014) established four overarching constructs that explicitly link to student success: (a) motivation, the forces that compel action and direct the behavior of individuals; (b) self-knowledge, the understanding that people have about their own abilities, values, preferences and skills and a necessary precondition for effective self-regulation; (c) self-direction, being able to identify one’s own life directions, to make academic choices consistent with these directions and to connect classroom learning to life goals; and (d) relationships, the ability to establish and maintain productive, collaborative, social relationships with teachers and peers. These four constructs have been shown to be strongly associated with students’ academic achievement and well-being; they also are considered to be malleable, receptive to intervention and within the range of expertise of school counselors (Bass, Lee, Wells, Carey, & Lee, 2015).
Multi-Tiered System of Supports
Use of MTSS is the recommended process for assessing and potentially intervening with an array of academic, behavioral and social-emotional issues while promoting schoolwide systems change (Lane, Menzies, Ennis, & Bezdek, 2013). An MTSS approach aligns closely with the ASCA (2012) National Standards and the work of school counselors in implementing prevention-based initiatives at a schoolwide level while providing more targeted intervention-based supports for students in need. It should be noted that MTSS is neither overly prescriptive nor rigid and has varying implementations and utility based on school districts’ needs.
Schools use MTSS to approach issues within the student population in tiers and place students in such tiers in order to appropriately address their needs. For example, the primary tier refers to a universal intervention geared toward the general student body, whose members may not be faced with distinct difficulty, thereby focusing on prevention to reduce potential problems (Horner, Sugai, & Anderson, 2010). The secondary tier refers to interventions for at-risk students, which typically involve more small group-based and individual interventions for those students still demonstrating difficulty after receiving primary intervention and support (Horner et al., 2010). The tertiary tier refers to working with students who are faced with identified difficulties and have not responded efficiently to primary or secondary levels and are subsequently in need of significant school- and community-based supports (Horner et al., 2010).
An MTSS approach can be conceptualized as incorporating elements of Response to Intervention (RTI) and Positive Behavioral Interventions and Supports (PBIS; Sugai & Horner, 2009). While RTI brings forth opportunities for preventative approaches and early intervention for students struggling with academic skills (Sandomierski, Kincaid, & Algozzine, 2007), MTSS incorporates a broader focus on both academic and social-emotional matters. Within the PBIS framework, the primary focus is on promoting consistent behavior expectations and systems of support to incentivize behaviors of all students within a school (Bohanon, Fenning, Eber, & Flannery, 2007). Both RTI and PBIS utilize MTSS, and specifically tiered intervention delivery, to accommodate the range of student needs. These frameworks are closely aligned in regards to their prevention foci, problem solving, implementation fidelity and data-based decision making (Sugai & Horner, 2009).
Elementary and Secondary School Counseling Program Grant
The ESSCP grant was established by the U.S. Department of Education (USDOE) to provide funding for school districts that demonstrate “the greatest need for counseling services, propose the most innovative and promising approaches, and show the greatest potential for their approach to be replicated and disseminated” (Rentner & Price, 2014, p. 28). To be eligible, proposed projects must incorporate a preventative approach, and effectiveness must at least in part be measured by: (a) the reduction in school counselor-to-student ratios in the district, and (b) decreases in student discipline referrals (USDOE, 2015). Selected projects also must involve the collection, examination, and use of high-quality and timely data, including data on program participant outcomes, and improving instructional practices, policies, and student outcomes (Rentner & Price, 2014).
The current grant project was considered trailblazing in its approach to expanding the data-based decision-making process in the district through a number of initiatives, including the following: (a) identifying research-based social-emotional indicators that link to academic and behavioral school success; (b) creating a user-friendly system for routinely collecting data on these critical areas of student development; and (c) developing the data literacy skills of school counselors in order to ensure that this social-emotional data would continue to be gathered, analyzed and included in data-based discussions long after the grant project had concluded. The funds provided by the ESSCP grant to support these initiatives enhanced the existing RTI model enacted by the school district by integrating a wide range of data related to student development and thus allowed data team members to examine the relationship between social-emotional factors and academic achievement, conducive to a more effective and comprehensive MTSS approach. Through a sophisticated new data collection infrastructure, as well as school counselors’ service in a leadership role, a nuanced and more targeted system of tiered supports emerged that allows the district to respond to a wide range of non-cognitive as well as cognitive issues.
Method
The grant project, formally entitled “An Asset Building Culture,” consisted of four primary initiatives: (a) hiring school counselors in order to create more favorable counselor-to-student ratios, (b) reducing the number of disciplinary incidents, (c) establishing a robust system of strengths-based social-emotional data collection grounded in sound theory, and (d) building human capacity and the technological means to incorporate new social-emotional information in a formal data-based decision-making process. These initiatives would subsequently inform a continuum of cognitive and non-cognitive supports and services within an MTSS model. Ultimately, the goal was to create positive systemic change within the district in which school counselors serve as leaders in using data as a tool for supporting students’ social-emotional, academic and behavioral development.
Setting and Participants
The project was conducted in an urban suburb with a population of approximately 30,000, located in the Northeast region of the United States. The district served nearly 3,000 students and had four elementary schools. More than half of the students were considered low-income and 43% did not speak English as their first language, with 52% identifying as Black/African American, 17% Asian-American, 15% White/Caucasian, 12% Hispanic/Latino/a, and 4% as Multiracial. The racial diversity represented in students was not reflected in its school staff, as more than 80% identified as White/Caucasian.
The school district was awarded the ESSCP grant in 2012. The grant team, comprised of school district leadership, Unique Potential Consulting (UPC), the Ronald H. Fredrickson Center for School Counseling Outcome Research and Evaluation (CSCORE), and Sebastian Management oversaw the grant project’s objectives. UPC served as coordinator of the day-to-day operations of the grant project and provided coaching and professional development to the district’s superintendent, elementary school principals and four grant school counselors. By allocating grant resources to this coordinator position, the project had an advocate for transformed school counseling practices who kept grant priorities in focus amidst other district initiatives. As evaluator of the grant, CSCORE collected quantitative and qualitative data to measure project outcomes and provided training in evidence-based practice to school counselors and district administrators.
Improving School Counselor-to-Student Ratios
The ASCA (2012) National Standards recommend a ratio of one school counselor to every 250 students, though the national average is actually well above these recommendations at nearly 1:500 (Carey & Dimmitt, 2012). Ample research suggests that school counselors have a positive impact on students’ academic, social-emotional and behavioral outcomes (Lapan, Gysbers, & Petroski, 2001; Lapan, Gysbers, & Sun, 1997; Sink & Stroh, 2003; Webb, Brigman, & Campbell, 2005), with further research suggesting that these ratios matter a great deal in a school counseling program’s overall effectiveness (Carrell & Carrell, 2006; Lapan, Whitcomb, & Aleman, 2012). Improving these ratios is especially impactful in high-poverty school districts (Lapan, Gysbers, Stanley, & Pierce, 2012).
Prior to the ESSCP grant, the district’s elementary school staff did not include school counselors at all, resulting in very high mental health provider-to-student ratios. Hiring four school counselors at the beginning of the grant period brought the counselor caseload ratios down to 1:369. Because the district experienced economies of hiring, the grant team added a half-time school counselor in the 2013–2014 school year, further reducing the ratio of school counselor to student to 1:340 despite an increase in enrollment. Grant monies continued to fund each of the 4.5 school counseling positions in the subsequent two school years, strengthening the district’s capacity to provide a broad range of services to students and maintain ratios more closely aligned with ASCA recommendations.
Office Discipline Referral Data
Office discipline referrals (ODR) offer a measure of both individual student behavior and school climate (Clonan, McDougal, Clark, & Davison, 2007; McIntosh, Frank, & Spaulding, 2010) and convey valuable information about students’ social-emotional competencies. A primary requirement of the ESSCP grant was to reduce the number of disciplinary infractions in the district and to demonstrate this improvement through ODR data. The process of determining baseline discipline data revealed great variability in how these incidents were both defined and recorded across different schools. Collecting and using valid discipline data is essential for creating safe schools conducive to teaching and learning (USDOE, 2015), and systematic data collection offers useful information for “understanding and ameliorating individual student and school-wide disruptive behavior problems” (Rusby, Taylor, & Foster, 2007, p. 333). The grant team therefore established new protocols for collecting discipline data in the district’s elementary schools, including creating a standardized ODR form that provided detailed information about the nature and frequency of disciplinary infractions. In addition, the district moved from a paper to an electronic system of recording these data.
The revised ODR form included a comprehensive list of disciplinary infractions that teachers considered high incidence behaviors in the elementary schools. The form was divided into three tiers to delineate progressive levels of severity. Level 1 infractions, such as “failure to obey classroom rules/procedures,” were regarded as problematic behaviors to be managed within the classroom. Documenting Level 1 infractions provided a data-based mechanism for teachers to record a student’s behavioral challenges in the classroom, and this information could be used within an MTSS model to justify the need for additional support or special education services. Level 2 infractions were considered more serious and included behaviors such as “using obscene language/gestures or a repeated offense of the same Level 1 behavior.” Teachers involved the assistance of other staff, such as another teacher or the school counselor, in handling Level 2 infractions. A list of classroom management and behavioral strategies also were listed on the ODR form, and teachers were asked to indicate any strategy they employed in addressing Level 1 or Level 2 problem behaviors. Infractions at Level 3 were recognized as major offenses and warranted involvement of the building principal. Level 3 infractions were further divided into two categories so that crisis incidents demanding immediate action and state reporting, such as “possession of a weapon” or “physical attack on a student or staff,” were recorded separately. The ODR form also included name of staff making the referral, grade of student, date and time of disciplinary incident, location where infraction took place and administrative action taken. In addition, space was provided for teachers to write a brief narrative about events as they occurred, including possible motivation for observed behaviors. The ODR form was revised multiple times based on feedback from principals, teachers and school counselors and piloted during the second year of the grant project.
The Protective Factors Index
The ESSCP grant was launched at a time when district leadership was considering introducing a standards-based student report card. Standards-based report cards list specific skills and knowledge linked to learning standards in each academic subject, and classroom teachers assess a student’s proficiency in each of these areas using a rating scale instead of traditional grades (Swan, Guskey, & Jung, 2014). This shift in practice for measuring academic performance provided an opportunity to create a district-wide system for assessing students’ social-emotional development to inform a more elaborate MTSS framework. While most elementary-level report cards contain a section for behavior or deportment, these indicators may not systematically align with research on personal, social and emotional factors related to achievement and success. In addition, teachers are often asked to rate student behavior without reference to a rubric that would ensure the reliability and validity of these ratings (Squier et al., 2014). To ground the new behavioral component of the report card in the research base, the grant team used the aforementioned Construct-Based Approach to School Counseling (CBA; Squier et al., 2014).
Incorporation of CBA included the identification of four social-emotional constructs that correlate with academic achievement. The grant team broke these constructs down into 15 indicators, which they deemed protective factors. The Protective Factors Index (PFI) was created as the assessment instrument for systematically collecting social-emotional data. Furthermore, the grant team developed a number of specific and measurable competency indicators related to each construct (see Table 1). In addition to being informed by a strong research base, the grant team wanted to ensure that each indicator reflected competencies considered relevant by staff and families in the grant school district. A representative group of school counselors, teachers from each grade level, a teacher of English Language Learners, a special education teacher and the principals from each school reviewed the 15 original PFI items for developmental appropriateness and cultural sensitivity. The group expressed misgivings about two standards under the self-knowledge construct (i.e., “identifies personal feelings,” and “identifies personal strengths and abilities”). There was concern that these behaviors involved attributes valued more by the dominant culture and that benchmarking students against what families might view as culturally specific standards was not fair. These items were therefore omitted from the pilot version, leaving a total of 13 items.
Once the final version was complete, teachers assessed students’ social-emotional development on each of the PFI’s indicators when grading report cards three times a year. In order to expand the consistency of the PFI and subsequently improve inter-rater reliability in data analysis, the grant team also created a scoring rubric to assist teachers in more accurately assigning ratings to these social-emotional indicators.
Creating a scoring rubric. In order to assist teachers in assessing the behaviors and attitudes that comprise the PFI within a developmental lens, the rubric was organized into three levels (K–1st, 2nd–3rd, and 4th–5th grades) to delineate the expected progression for each PFI indicator. The rubric lists specific, observable behaviors to help teachers determine whether a student was demonstrating age-appropriate skills in each domain. For example, descriptors to assess whether a kindergarten or first grade student “works collaboratively in groups of various sizes” included the descriptor “interacts appropriately with peers in group activities,” and “contributes ideas in a group.” Descriptors for second- and third-grade students included the same two behaviors as the earlier grades as well as “shows respect for others by listening to their ideas and opinions.” For fourth- and fifth-grade students “agrees or disagrees with others in a respectful manner” was added to the rubric descriptors. The rubric helped to ensure greater accuracy and consistency in scoring behaviors across classrooms and to reduce subjectivity in teachers’ ratings.
During the first year of the project, teachers requested a simple dichotomous response set for assessing PFI indicators (i.e., “struggling” or “on target”). After a successful year of piloting the new report card and accompanying rubric, teachers requested to move to a four-item response format: meets standard, progressing toward standard, emerging, and not meeting standard. The grant team expanded the original rubric, anchoring responses in degrees of support needed for a student to successfully demonstrate a behavior. Teachers were again provided concrete examples of student behavior within the rubric and were asked to assess if a student consistently and independently displayed the behavior or whether the student needed occasional, frequent or ongoing support to meet the standard.
Table 1
Summary of Primary Constructs and Indicators in the PFI
| Primary Construct |
Indicators |
| Motivation |
Engages in class activities |
|
Demonstrates an eagerness to learn |
|
Demonstrates perseverance in completing tasks |
| Self-Knowledge |
Identifies academic strengths and abilities |
|
Identifies things he/she is interested in learning |
| Self-Direction |
Demonstrates the ability to self-regulate actions and emotions |
|
Demonstrates resilience after setbacks |
|
Makes productive use of classroom time |
| Relationships |
Works collaboratively in groups of various sizes |
|
Seeks assistance when necessary |
|
Respects and accepts authority |
|
Forms respectful, equitable relationships with peers |
Building Technological and Human Capacity
Developing a more comprehensive approach to using data requires that educators have access to meaningful and useful data (Poynton & Carey, 2006). Technology is a key component to establishing effective data use, and research has demonstrated that the state of computer systems can hinder this process in schools (Mandinach, 2012; Wayman, Jimerson, & Cho, 2012) and that easy, integrated and timely access to data facilitates the data-based decision-making process (Ikemoto & Marsh, 2007; Wayman, 2005). Staff at the grant site could readily access classroom grades, state test scores and other achievement data through the district’s Student Information System (SIS). A primary objective of the grant project was to develop the infrastructure to support the same ease of access to important social-emotional indicators. The grant’s technology consultant worked with the district to interface the PFI data recorded on the new report card with the district’s SIS. Teachers, counselors and administrators could then view information about a student’s engagement in class activities or perseverance in completing tasks in the same way they could examine a student’s academic data. The technology consultant also wrote queries to extract PFI data from the SIS into user-friendly Excel reports so that school counselors could disaggregate the data by demographic variables such as gender, grade level or subsidized lunch status. Data also were aggregated at the classroom, grade or building level. The consultant then trained the school counselors to use Excel to illustrate on graphs the number of students struggling with specific PFI indicators (e.g., self-regulation, cooperation, motivation). These graphs could be organized by grade level, school site and individual students. Building strong technological capacity and functionality provides an essential foundation for effective data use. However, translating the wealth of data collected by schools into meaningful actions to support student success within an MTSS framework also requires building human capacity in data literacy skills (Ikemoto & Marsh, 2007; Mandinach, 2012; Wayman, 2005; Wayman & Stringfield, 2006). To build these competencies among school counselors, the grant team organized monthly professional development workshops in evidence-based practice, tiered interventions, data-based decision making, data analysis, and Excel charting and graphing. Counselors learned to extract the PFI data from the SIS, conduct simple analyses to determine what issues existed at various levels within the building, and create graphs to share with teachers and other educators at building-based data team meetings (see Figure 1).
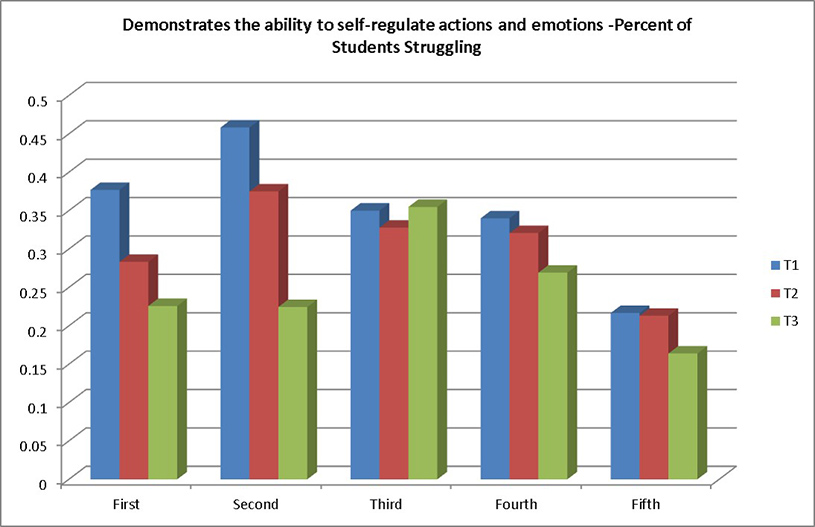
Figure 1. Sample of PFI data aggregated by a Single Indicator, Grade Level, and School Site
Results
The district’s elementary schools had previously stored hard copies of disciplinary incident forms in the principal’s office. This system did not support easy analysis of disciplinary data or examination of behavioral issues in the building. In the revised process, an administrative assistant electronically entered all information from the new ODR form into the school’s SIS database. The electronic system allowed staff to quickly determine the total number of disciplinary infractions in the building over a given period, identify patterns in the data such as a spike in infractions immediately before vacations, and disaggregate the data to determine the frequency of different problem behaviors among various subgroups of students. This streamlined method of data collection also enabled staff to identify possible trends in disciplinary infractions. If data revealed issues such as disproportionality in the district, school counselors served as advocates in establishing more equitable protocols around discipline policies. Notably, the number of disciplinary infractions dropped significantly throughout the 3-year grant program.
Data collected from the PFI provided valuable information to all stakeholders about students’ social-emotional competency development. Because teachers observe behavior and peer interactions every day, their perspective provides a keen understanding of whether a student is able to put into practice each of the indicators listed. In addition, since teachers rate students on the PFI multiple times each year through the district’s electronic report cards, educators throughout the building had access to real-time data about behavioral issues impacting individuals or groups of students. The school counseling program, which prior to this grant project had not been established, consistently reviewed these data, generated charts to determine where gaps existed in social-emotional or academic skill areas and focused their weekly classroom guidance lessons on teaching these competencies. Subsequent report card data were also analyzed to evaluate the impact of counseling lessons on students’ skill development.
Data Teams and a Multi-Tiered System of Supports
Prior to the district’s ESSCP award, data teams were operating at each elementary school and were led by the building principal. Student names were only considered for data team discussion if a teacher completed a referral form indicating a student was struggling academically in the classroom. These forms, often inconsistently completed and comprised largely of teachers’ perceptions about academic performance, served as the principal mechanism for identifying at-risk students. The only other information frequently reviewed by data teams were standardized test scores, classroom grades and serious behavioral infractions. Interventions to support students were almost exclusively academic in nature.
The grant team collaborated with staff to restructure data teams to include social-emotional data analysis. Data teams were then able to expand their RTI approach to a more expansive MTSS framework to include multi-tiered counseling interventions in addition to existing academic interventions. School counselors created graphs and charts of PFI, ODR and attendance data to illustrate such trends as common behavioral issues across grade levels or attendance patterns during certain days of the week or times of year. Data team members reviewed these graphs to identify gaps in social-emotional, behavioral or academic skill areas. Meetings shifted from an almost exclusive focus on academic data to considering multiple sources of achievement, demographic, behavioral and social-emotional variables. As teams explored the relationship across different types of data, a greater understanding began to emerge about how social-emotional factors, such as those included in the PFI, impact academic achievement. The charge of the data teams became deciding which tiered interventions (universal, targeted and intensive) were indicated to promote the development of academic competencies as well as of the protective factors to support school success for every student.
School Counselors’ Contributions to a Multi-Tiered System of Supports
Access to accurate and real-time data about student behaviors enabled school counselors to more effectively develop tiered interventions for students and environments in need of support. The PFI data were collected three times a year at the close of each marking period. Behavioral data gathered through the revised ODR form were updated in the SIS weekly. Attendance data at the elementary school sites were available daily. Access to these real-time data allowed school counselors to continuously monitor students’ social-emotional and academic progress. It also enabled counselors to easily evaluate whether their interventions were creating the desired impact. In this continuous process of data-based decision-making, the same set of data indicators, examined at different points throughout the school year, informed school counselors’ decisions about which interventions were needed and also served as outcome data to evaluate interventions at each tier.
Schoolwide, Tier 1 interventions included delivery of success classes to all students. School counselors developed a developmental guidance curriculum with 10 lessons per grade grounded in the evidence-based programs zones of regulation (Kuypers, n.d.) and second step (Low, Cook, Smolkowski, & Buntain-Ricklefs, 2015), with weekly lesson content guided by areas of improvement demonstrated in the PFI data and behavioral data represented in discipline referrals. In addition, a school counseling program “Expo” was held at the end of each year, and parents and guardians were invited to the school to see artifacts generated by students in success class. Additional schoolwide interventions included the character trait of the month project, focused on the development of positive qualities such as respect, honesty and courage, and a parent newsletter sent out by the counseling department explaining what could be done at home to enhance the development of social-emotional competencies (i.e., informing parents and guardians of the character trait of the month, suggesting a “conversation starter” about current classroom activities, and recommending related books to read with their children).
Students who were struggling academically and for whom PFI and ODR data indicated a need for additional behavioral support and social-emotional competency instruction received Tier 2 services through small group counseling sessions. School counselors facilitated groups on topics related to PFI indicators such as self-regulation, resilience and motivation throughout the year. The school counselors used discipline data, often in combination with report card indicators reflecting students’ social-emotional competencies, to determine membership in targeted small group counseling sessions and continued participation in this targeted intervention. Subsequent ODR data was reviewed to evaluate changes in students pre- to post-intervention, as these data have been demonstrated to be sensitive measures of the impact of schoolwide interventions (Irvin, Tobin, Sprague, Sugai, & Vincent, 2004; Rusby et al., 2007). School counselors also created progress monitoring tools to assess social skill development during a group cycle. As with academically focused tiered instruction, teachers were asked to briefly rate student growth so that small group instruction could be modified in a continuous formative assessment process.
The continuum of counseling services also included development of a Summer Boot Camp Transition Program. School counselors collected quantitative and qualitative survey data from sixth graders in the district about their experience in moving from elementary to middle school, which indicated that some students were anxious about this transition and wanted more support and information about the process. To proactively address these common issues, the school counselors created a series of four week-long summer boot camps that were free of charge and open to all district fifth graders. Classroom lessons and group activities for the camp were drawn from the evidence-based curricula Student Success Skills (Webb & Brigman, 2006), WhyTry (Bird, 2010) and The Real Game (Barry, n.d.) and covered topics critical to success in middle school such as perseverance, organizational skills and study strategies.
Finally, PFI, ODR and standards-based report card data also guided decisions about Tier 3 interventions. School counselors developed Behavior Improvement Plans (BIPs) for students in need of intensive behavioral support in the classroom. They also coordinated with special education or other mental health professionals when referrals were warranted.
Positive Systemic Change
The grant initiatives resulted in definitive progress and positive systemic changes throughout the district. A new policy was established which mandated that counseling groups be formed based on issues identified in the data and no longer simply by teacher request or anecdotal evidence. This more objective approach to determining which students were in need of Tier 2 social-emotional interventions ensured that students with a documented need for additional assistance received these services.
At the beginning of the grant period, the district had been declared “underperforming” by state rankings and was mandated to write an annual Accelerated Improvement Plan (AIP). Throughout the 3-year grant cycle, a number of elements from the grant project were embedded in the AIP including: (a) revising K–5 report cards to use a standards-based system, (b) integration of the PFI within the new report cards, (c) designing and delivering a developmental guidance curriculum for grades K–5, (d) collaborating with building principals to incorporate social-emotional data into data team meetings, and (e) developing tiered strategies to better address the social-emotional needs of struggling students. Officials from the State Department of Education who monitored the AIP expressed their belief that these initiatives contributed to the district’s overall improvement and began to send other struggling school systems to the grant district to learn specifically about their data-based MTSS approach and the school counselors’ role in it.
Ultimately, the success of the grant within the district can perhaps best be measured by two key administrative decisions made when grant funding ended: (a) the decision to retain the school counselors, as teachers and administrators now saw these professionals—who had not been employed at the district before the grant—as indispensable to student success; and (b) the decision to hire UPC (who had worked as project coordinator for the grant) to work to support the expansion of the grant initiatives to the middle school and high school over the next several years. At the time of this article’s publication, work was underway to identify means to collect social-emotional data at the middle and high school levels so that their multi-tiered system of supports can be as robust as that at the elementary level.
Discussion and Implications for School Counselors
Data-based decision making has become an essential component of educational practice (Mandinach, 2012). The implementation of NCLB and standards-based education have created strong pressure for schools to demonstrate improved student performance through state test scores (Ikemoto & Marsh, 2007; Marsh et al., 2006). These data often become the primary consideration of data-driven discussions as schools strive to meet state and federal requirements. Data use has the potential, however, to be more than simply a response to meeting accountability demands. The data-based decision-making process can be transformed when multiple forms of data are viewed from different professional perspectives to better describe the factors and contexts that influence student success (Mandinach, 2012). Fortunately, the new ESSA legislation stresses the importance of considering non-academic data to foster a broader vision of student success. Clearly describing what is happening for an individual or to groups of students requires “a body of relevant data, with each individual data element imparting a complementary piece of the puzzle” (National Forum on Education Statistics, 2012, p. 9).
An integrative approach to data-based decision making requires the technological capacity to organize data into user-friendly formats. It also may necessitate the collection of data beyond the scope of what is traditionally stored in district’s information systems (Poynton & Carey, 2006). Behavior in the classroom occurs within the broader context of a student’s life and developing interventions to support student success requires collecting data that reflect this context (National Forum on Education Statistics, 2012). Creating a data collection infrastructure that allows those who observe students on a daily basis (e.g., teachers) to rate social-emotional competency attainment in addition to academic competency attainment on a regular basis is a complex undertaking, but one that has very promising potential. When educators triangulate data by using multiple types and sources of data, the relationship between academic outcomes and social-emotional factors is better understood and reliance on a single data point, such as academic scores, is reduced (Marsh et al., 2006).
The grant team developed a number of initiatives designed not only to fulfill requirements of the ESSCP award, but also to create systemic changes around the culture of data use and continuum of tiered supports in the district. Each individual grant initiative aimed to improve a particular aspect of data-based decision making: incorporating research-based social-emotional indicators into the elementary school report cards, creating the infrastructure for easy and timely access to these data, developing new protocols for collecting discipline data, and building the data literacy skills of school counselors. The combined effect of each of these initiatives was a restructuring of building-based data teams that operated from a strong MTSS; these included the following: (a) coordination of schoolwide prevention efforts and systems, (b) universal screening and progress monitoring, (c) selection and use of evidence-based practices, (d) professional development that targets evidence-based practice, (e) evaluating outcomes using data-based decision making, and (f) leadership commitment from administrators and school-based teams that supports schoolwide implementation (Harn, Basaraba, Chard, & Fritz, 2015; Kame’enui, Good, & Harn, 2005; Sugai & Horner, 2009).
Notably, the grant project integrated an academic, behavioral, and social-emotional focus in the gathering of data, examined how specific behaviors and social-emotional skills impacted student achievement, and subsequently selected targeted interventions to build the competencies needed for school success. Although the majority of research and scholarly discussion has focused on using data-based decision-making models for academic concerns, researchers have proposed a similar model for social-emotional and behavioral problems (Eber, Sugai, Smith, & Scott, 2002; Fairbanks, Sugai, Guardino, & Lathrop, 2007; Gresham, 1991; Sugai, Horner, & Lewis, 2009). Though currently the majority of schools are operating these schoolwide efforts independently (McIntosh, Bohanan, & Goodman, 2010), there is a growing call for the holistic approach MTSS offers due to the known interaction of academic, behavioral and social-emotional issues in students who struggle (Mclntosh, Horner, Chard, Boland, & Good, 2006).
The grant project’s approach to adopting MTSS was also unique in the pivotal role of school counselors in the data-based decision-making process. The role of the school counselor is infrequently defined in the RTI literature (Gruman & Hoelzen, 2011) or in educational reform agendas (Dahir, 2004). School counselors have sometimes been seen as resistant to using data (Young & Kaffenberger, 2011). However, school counselors work at the intersection of the academic and social-emotional domains (ASCA, 2012) and support student development across these areas. School counselors, previously not represented on the building data teams, have now become data leaders in these schools. Because data-based decision making has focused largely on academic achievement, data use may have been seen as the charge of the classroom teacher. Through grant-based professional development workshops, the counselors developed competencies in organizing, analyzing and graphing data. These new skills have enabled the school counselors to lead data-based conversations, develop progress monitoring tools and create results reports for administrators and the school committee. Using data routinely collected through the SIS provides an efficient and timely access to not only determine which interventions are needed, but also to evaluate the impact of the schoolwide counseling curriculum, targeted small groups and other activities.
This mode of data collection represents a change from the pre/posttest method commonly employed by school counselors. Pre/posttests may provide information about whether students learned the content of a specific lesson but do not show whether students are applying these skills, attitudes or beliefs in their lives. School counselors can contribute unique insights to the data team process by going a step further and helping to determine the underlying causes for a student’s misbehavior or poor academic performance. Incorporating social-emotional indicators into data-based discussions may make the process feel more relevant to the work of the school counselor. In fact, many of the words used to describe this more comprehensive approach to data (e.g., relationships, linking, connecting, inclusion and contextualizing) sound more from the counseling lexicon than from a statistics textbook.
The overarching goal of this pilot project was to create a meaningful data-based decision-making process to promote an MTSS model based on academic and social-emotional data. Therefore, the success of this project contributes ideas as to not only what non-academic data can be analyzed, but also how to go about collecting, analyzing and incorporating findings into the planning around a continuum of supports to foster student success. Using research-based constructs, redesigning report cards, developing rubrics, identifying professional development needs, and developing human technological capacity to manage and interpret data are feasible and effective strategies to support achievement. Ultimately, discussions shifted from examining symptoms of an issue—such as disciplinary infractions, low grades and test scores, or poor attendance—to trying to unearth the underlying causes for student issues and how the school could support growth with a variety of academic and social-emotional tiered supports.
Limitations and Directions for Future Research
The grant project was not designed or implemented as an experimental study; therefore, we cannot know with certainty whether the implementation of the grant initiatives and subsequent positive outcomes share a causal relationship. Furthermore, we cannot yet know which specific elements of the grant project brought about the most positive change, or whether some elements may have been superfluous, as outcomes have been viewed as a comprehensive result of all grant-related activities. Future research involving an experimental study in which: (a) outcomes are compared to similar schools that did not received grant-funded resources; and (b) there are outcomes measures in place for each grant initiative, is recommended. Moreover, additional studies that expand these efforts to students and schools in different regions, grade levels and with a higher number of participants also is suggested.
Although the PFI is a promising new instrument for the measurement of positive social-emotional behaviors in the classroom, further research is necessary to validate its use as a universal brief screener. Bass and colleagues (2015) conducted a confirmatory factor analysis with the PFI using data gathered during the present grant project, which resulted in a three factor measurement model rather than four as hypothesized. These findings warrant further exploration with additional populations of students to determine whether they will be replicated. The PFI also relies on teacher observation, which occurs consistently at the elementary school level; therefore, it would be valuable to study its use in upper grades (i.e., middle school and high school) to verify whether the PFI is still a reliable and valid instrument in settings where teachers experience less face-to-face time with each individual student throughout the school day.
Finally, it bears noting that the research base is still emerging around social-emotional learning and which competencies best link to school success. There is not even consensus within the scholarly community on how to refer to these constructs (e.g., non-cognitive factors, non-academic skills, soft skills, grit). Further research will be necessary to determine which social-emotional learning theory or theories exhibit applicability in school settings, and the development of assessment instrumentation based on a CBA in particular is still in its early stages.
Conclusion
The ESSCP grant offered by the USDOE provides funding to establish and improve school counseling programs in high-needs school districts. The current grant project was implemented at four elementary sites in a diverse school district in an urban suburb of the Northeastern United States. Specific grant initiatives included the hiring of four full-time and one part-time school counselor in order to reduce the student-to-counselor ratio. The office discipline referral process was restructured to include greater specificity and objectivity, and the PFI was developed in order to provide an assessment tool of social-emotional competencies in the classroom. School counselors also were provided training in how to collect, analyze and include social-emotional data in the data-based decision-making process. Subsequently, the combination of a new school counseling program and data on discipline and social-emotional competencies along with existing academic data resulted in a much-improved MTSS model in the district, providing a continuum of supports for students’ needs. The study sheds light on the value of providing school counseling at the elementary level and the importance of data literacy and advocacy as a major tenet of these positions. As ESSCP grants are awarded based on their potential for replication and dissemination, the initiatives described in this manuscript represent innovative practices that hold tremendous promise at a national level.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
American School Counselor Association. (2012). The ASCA national model: A framework for school counseling programs (3rd ed.). Alexandria, VA: Author.
American School Counselor Association. (2014). Mindsets & behaviors for student success: K-12 college and career-readiness standards for every student. Alexandria, VA: Author.
Barry, B. (n.d.). The Real Game design process. Retrieved from http://www.realgame.org/process.html
Bass, G., Lee, J. H., Wells, C. W., Carey, J. C., & Lee, S. (2015). Development and factor analysis of the Protective Factors Index: A report card section related to the work of school counselors. The Professional Counselor, 5, 516–528. doi:10.15241/gb.5.4.516
Bird, B. (2010). WhyTry evaluation report 2006–2010. Churchill County Probation Report, Field Research. Retrieved from https://www.whytry.org/index.php?option=com_content&view=article&id=109
Bohanon, H., Fenning, P., Eber, L., & Flannery, B. (2007). Identifying a roadmap of support for secondary students in school-wide positive behavior support applications. International Journal of Special Education, 22, 39–52.
Carey, J., & Dimmitt, C. (2012). School counseling and student outcomes: Summary of six statewide studies. Professional School Counseling, 16, 146–153.
Carrell, S. E., & Carrell, S. A. (2006). Do lower student to counselor ratios reduce school disciplinary problems? The BE Journal of Economic Analysis & Policy, 5, 1–24.
Clonan, S. M., McDougal, J. L., Clark, K., & Davison, S. (2007). Use of office discipline referrals in school-wide decision making: A practical example. Psychology in the Schools, 44, 19–27.
Dahir, C. A. (2004). Supporting a nation of learners: The role of school counseling in educational reform. Journal of Counseling & Development, 82, 344–353. doi:10.1002/j.1556-6678.2004.tb00320.x
Dahir, C. A., & Stone, C. B. (2009). School counselor accountability: The path to social justice and systemic change. Journal of Counseling & Development, 87, 12–20. doi:10.1002/j.1556-6678.2009.tb00544.x
Dimmitt, C., Carey, J. C., & Hatch, T. (Eds.) (2007). Evidence-based school counseling: Making a difference with data-driven practices. Thousand Oaks, CA: Corwin.
Eber, L., Sugai, G., Smith, C. R., & Scott, T. M. (2002). Wraparound and positive behavioral interventions and supports in the schools. Journal of Emotional and Behavioral Disorders, 10, 171–180. doi:10.1177/10634266020100030501
Every Student Succeeds Act (2015) Pub. L. No. 114–95. Retrieved from https://www.congress.gov/bill/114th-congress/senate-bill/1177
Fairbanks, S., Sugai, G., Guardino, D., & Lathrop, M. (2007). Response to intervention: Examining classroom behavior support in second grade. Exceptional Children, 73, 288–310. doi:10.1177/001440290707300302
Farrington, C. A., Roderick, M., Allensworth, E., Nagaoka, J., Keyes, T. S., Johnson, D. W., & Beechum, N. O. (2012). Teaching adolescents to become learners – the role of noncognitive factors in shaping school performance: A critical literature review. Chicago, IL: University of Chicago Consortium on Chicago School Research.
Gresham, F. M. (1991). Conceptualizing behavior disorders in terms of resistance to intervention. School Psychology Review, 20, 23–36.
Gruman, D. H., & Hoelzen, B. (2011). Determining responsiveness to school counseling interventions using behavioral observations. Professional School Counseling, 14, 183–190.
Harn, B., Basaraba, D., Chard, D., & Fritz, R. (2015). The impact of schoolwide prevention efforts: Lessons learned from implementing independent academic and behavior support systems. Learning Disabilities: A Contemporary Journal, 13, 3–20.
Hayes, R. L., Nelson, J.-L., Tabin, M., Pearson, G., & Worthy, C. (2002). Using school-wide data to advocate for student success. Professional School Counseling, 6, 86–94.
Heckman, J. J., & Rubinstein, Y. (2001). The importance of noncognitive skills: Lessons from the GED testing program. The American Economic Review, 91, 145–149.
Horner, R. H., Sugai, G. M., & Anderson, C. M. (2010). Examining the evidence base for school-wide positive behavior support. Focus on Exceptional Children, 42(8), 1–14.
House, R. M., & Hayes, R. L. (2002). School counselors: Becoming key players in school reform. Professional School Counseling, 5, 249–256.
Ikemoto, G. S., & Marsh, J. A. (2007). Cutting through the “data-driven” mantra: Different conceptions of data-driven decision making. YSSE Yearbook of the National Society for the Study of Education, 106, 105–131. doi:10.1111/j.1744-7984.2007.00099.x
Irvin, L. K., Tobin, T. J., Sprague, J. R., Sugai, G., & Vincent, C. G. (2004). Validity of office discipline referral measures as indices of school-wide behavioral status and effects of school-wide behavioral interventions. Journal of Positive Behavior Interventions, 6, 131–147.
Isaacs, M. L. (2003). Data-driven decision making: The engine of accountability. Professional School Counseling, 6, 288–295.
Kame’enui, E. J., Good, R. G., & Harn, B. A. (2005). Beginning reading failure and the quantification of risk: Reading behavior as the supreme index. In W. L. Heward et al. (Eds.), Focus on behavior analysis in education: Achievements, challenges, and opportunities (pp. 69–89).Upper Saddle River, NJ: Prentice Hall.
Kuypers, L. (n.d.). Evidence on the Zones. Retrieved from http://www.zonesofregulation.com/research.html
Lane, K. L., Menzies, H. M., Ennis, R. P., & Bezdek, J. (2013). School-wide systems to promote positive behaviors and facilitate instruction. Journal of Curriculum and Instruction, 7, 6–31. doi:10.3776/joci.2013.v7n1pp6-31
Lapan, R. T., Gysbers, N. C., & Petroski, G. F. (2001). Helping seventh graders be safe and successful: A statewide study of the impact of comprehensive guidance and counseling programs. Journal of Counseling & Development, 79, 320–330.
Lapan, R. T., Gysbers, N. C., Stanley, B., & Pierce, M. E. (2012). Missouri professional school counselors: Ratios
matter, especially in high-poverty schools. Professional School Counseling, 16, 108–116.
Lapan, R. T., Gysbers, N. C., & Sun, Y. (1997). The impact of more fully implemented guidance programs on the school experiences of high school students: A statewide evaluation study. Journal of Counseling & Development, 75, 292–302.
Lapan, R. T., Whitcomb, S. A., & Aleman, N. M. (2012). Connecticut professional school counselors: College and career counseling services and smaller ratios benefit students. Professional School Counseling, 16, 117–124.
Low, S., Cook, C. R., Smolkowski, K., & Buntain-Ricklefs, J. (2015). Promoting social-emotional competence: An evaluation of the elementary version of Second Step. Journal of School Psychology, 53, 463–477.
Mandinach, E. B. (2012). A perfect time for data use: Using data-driven decision making to inform practice. Educational Psychologist, 47, 71–85.
Mandinach, E. B., Honey, M. & Light, D. (2006). A theoretical framework for data driven decision making. Paper presented at the annual meeting of American Educational Research Association, San Francisco, CA. Retrieved from http://cct.edc.org/sites/cct.edc.org/files/publications/DataFrame_AERA06.pdf
Marsh, J. A., Pane, J. F. & Hamilton, L. S. (2006). Making sense of data-driven decision making in education: Evidence from recent RAND research. Retrieved from http://www.rand.org/content/dam/rand/pubs/occasional_
papers/2006/RAND_OP170.pdf
McIntosh, K., Bohanan, H., & Goodman, S. (2010). Toward true integration of academic and behavior response to intervention systems: Part two—Tier 2 support. Communique, 39(3), 4–6.
McIntosh, K., Frank, J. L., & Spaulding, S. A. (2010). Establishing research-based trajectories of office discipline referrals for individual students. School Psychology Review, 39, 380–394.
McIntosh, K., Horner, R. H., Chard, D. J., Boland, J. B., & Good, R. H., III. (2006). The use of reading and behavior screening measures to predict nonresponse to school-wide positive behavior support: A longitudinal analysis. School Psychology Review, 35, 275–291.
National Forum on Education Statistics. (2012). Forum guide to taking action with education data. Washington, DC: Author.
No Child Left Behind Act of 2001. (2002). Pub. L. No. 107-110 § Title V. Retrieved from http://www2.ed.gov/
policy/elsec/leg/esea02/index.html
Poynton, T. A., & Carey, J. C., (2006). An integrative model of data-based decision making for school counseling. Professional School Counseling, 10, 121–130.
Rentner, D. S., & Price, O. A. (2014). A guide to federal education programs that can fund K-12 universal prevention and social and emotional learning activities. Center on Education Policy, 1–40.
Rusby, J. C., Taylor, T. K., & Foster, E. M. (2007). A descriptive study of school discipline referrals in first grade. Psychology in the Schools, 44, 333–350. doi:10.1002/pits.20226
Sandomierski, T., Kincaid, D., & Algozzine, B. (2007). Response to intervention and positive behavior support: Brothers from different mothers or sisters with different misters. Positive Behavioral Interventions and Supports Newsletter, 4(2), 1–4.
Sink, C. A., & Stroh, H. R. (2003). Raising achievement test scores of early elementary school students through comprehensive school counseling programs. Professional School Counseling, 6, 350–364.
Squier, K. L., Nailor, P., & Carey, J. C. (2014). Achieving excellence in school counseling through motivation, self-direction, self- knowledge, and relationships. Thousand Oaks, CA: Corwin.
Sugai, G., & Horner, R. H. (2009). Responsiveness-to-intervention and school-wide positive behavior supports: Integration of multi-tiered system approaches. Exceptionality, 17, 223–237.
Sugai, G., Horner, R., & Lewis, T. (2009). School-wide positive behavior support implementers’ blueprint and self-assessment. Eugene, OR: OSEP TA-Center on Positive Behavioral Interventions and Supports.
Swan, G. M., Guskey, T. R., & Jung, L. A. (2014). Parents’ and teachers’ perceptions of standards-based and traditional report cards. Educational Assessment, Evaluation and Accountability, 26, 289–299.
doi:10.1007/s11092-014-9191-4
Wayman, J. C. (2005). Involving teachers in data-based decision making: Using computer data systems to support teacher inquiry and reflection. Journal of Education for Students Placed at Risk, 10, 295–308. doi:10.1207/s15327671espr1003_5
Wayman, J. C, Jimerson, J. B., & Cho, V. (2012). Organizational considerations in establishing the data-informed district. School Effectiveness and School Improvement, 23, 159–178.
Wayman, J. C., & Stringfield, S. (2006). Technology-supported involvement of entire faculties in examination of student data for instructional improvement. American Journal of Education, 112, 549–571.
Webb, L. D., & Brigman, G. A. (2006). Student Success Skills: Tools and strategies for improved academic and social outcomes. Professional School Counseling, 10, 112–120.
Webb, L. D., Brigman, G. A., & Campbell, C. (2005). Linking school counselors and student success: A replication of the Student Success Skills approach targeting the academic and social competence of students. Professional School Counseling, 8, 407–413.
U.S. Department of Education. (2015). Elementary and secondary school counseling programs. Retrieved from http://www2.ed.gov/programs/elseccounseling/index.html
Young, A., & Kaffenberger, C. J. (2011). The beliefs and practices of school counselors who use data to implement comprehensive school counseling programs. Professional School Counseling, 15, 67–76.
Karen Harrington is the Assistant Director at the Center for Youth Engagement at the University of Massachusetts Amherst. Catherine Griffith is Associate Director at the Ronald H. Fredrickson Center for School Counseling Outcome Research and Evaluation and Assistant Professor at the University of Massachusetts Amherst. Katharine Gray is a leadership coach at Unique Potential Consulting and Leadership Coaching in Hopkinton, MA. Scott Greenspan is a doctoral student at the University of Massachusetts Amherst. Correspondence can be addressed to Karen Harrington, Furcolo Hall, University of Massachusetts, Amherst, MA 01003, Karen.harrington07@gmail.com.
Jul 20, 2016 | Article, Volume 6 - Issue 2
Dee C. Ray, David D. Huffman, David D. Christian, Brittany J. Wilson
The vast majority of graduate students in the social sciences, especially in mental health fields, are females (Crothers et al., 2010; Healey & Hays, 2012). In a recent report on counseling programs, an average of 76% of students admitted and graduated yearly from entry-level counseling programs were women (Schweiger, Henderson, McCaskill, Clawson, & Collins, 2012). Although counseling is one field that attracts mostly female graduate level students, a historical review indicates that males made up approximately 80% of counselor education faculties in the 1980s (Anderson & Rawlins, 1985). In recent years, as the number of females who seek doctoral degrees in counseling has increased, so has the number of female counselor educators, correlating to fewer males entering the field of counselor education. Currently, the average number of males admitted and graduated yearly from doctoral-level counseling programs has been reported at a meager 25% (Schweiger et al., 2012). As counselor educators strive to build best practices for working with diverse populations, it seems relevant to explore the experiences of male counselor educators as well as suggest practices that improve conditions for male counselor education faculty.
In the preparation of counselors, counselor educators are encouraged to build relationships with students that lead to greater self-awareness, personal development and interpersonal learning, which inform their work as counselors. Literature cites the importance of the relationships between counseling faculty and students as “paramount” (Dollarhide & Granello, 2012, p. 290), suggesting that it “stands out above all other factors” (McAuliffe, 2011, p. 32) in the education of adults. It seems reasonable to assume that if counselor educators espouse the importance of the relationship between client and counselor, they extend this value to their students, building relationships that facilitate learning. Thus, a belief that the relationship between teacher and student leads to mutual support and growth comprises the hallmark of humanistic education (Dollarhide & Granello, 2012).
Although the American Counseling Association (ACA) Code of Ethics (2014) asserted that counselor educators are restricted from sexual or romantic relationships with students, universities and counselor education programs typically do not clearly articulate boundaries when approaching the multiple roles adopted by faculty members (Owen & Zwahr-Castro, 2007). In the absence of guidelines and open discussion regarding faculty–student relationships, legal concerns can permeate the university environment. Sexual harassment suits have increased, and many universities have responded by going beyond sexual harassment policies and adding additional policies that restrict sexual or romantic consensual relationships between faculty and students (Bartlett, 2002; Kiley, 2011). Male faculty members seem especially affected by the legal environment and Nicks (1996) reported males had significantly higher concerns than females regarding unjust accusations of harassing a student. In the current environment of legality and ambiguous ethical guidelines, Kress and Dixon (2007) cautioned that counselor educators might choose to distance themselves from students to avoid the appearance of impropriety or placing themselves in complex ethical situations. However, there is a dearth of literature regarding issues of relationship dynamics based on sexuality and gender in academia over the last 20 years.
Further complicating the issue of faculty–student relationships is that female professors and students are more likely to perceive complex relationship issues as unethical when compared to their male counterparts. In a comparison between female and male counselor educators and counselor education students, Bowman, Hatley, and Bowman (1995) found that females were significantly more likely to rate activities outside the traditional student–teacher relationship as unethical. This finding has been supported in multiple studies regarding undergraduate students (Ei & Bowen, 2002; Oldenburg, 2005; Owen & Zwahr-Castro, 2007). Female undergraduate students were more likely to rate a relationship scenario as unethical when the professor was identified as a male as compared to scenarios with female professors (Oldenburg, 2005) and more likely to be negative than males about questionable scenarios such as sexual relationships, doing favors for a professor, and doing things alone with an instructor (Ei & Bowen, 2002). Owen and Zwahr-Castro (2007) found that female undergraduate students judged approximately one-third of faculty–student interaction scenarios as significantly more inappropriate than male students, identifying nonacademic-related interaction that occurred off campus as most inappropriate. Although not specifically explored, the tendency of females to find behaviors unethical when compared to the perceptions of males has been attributed in the literature to sensitivity of women to power differentials and potential for exploitation based on cultural experience (Ei & Bowen, 2002; Owen & Zwahr-Castro, 2007). In the context of current ratios in counselor education of a majority number of female faculty to a minority number of male graduate students, it is difficult to ascertain the perception of power dynamics based on gender.
The changing context of counselor education may present unique challenges for male faculty to navigate with little guidance. A review of the literature highlights a complex environment where male counselor educators engage in faculty–student relationships within a context of power differences and potential legal complications. The current study was conceived in a doctoral level clinical course in which male and female doctoral students processed their teaching experiences with master’s students. During the discussion, male doctoral students serving as instructors shared experiences regarding relationships with their students that appeared uniquely different from experiences shared by female colleagues. Concerns emerged regarding practices of male counselor educators when entering a female-prevalent field as a person in a position of power. As a result, we proposed that the following factors might influence the interactions of male counselor educators on a daily basis in their roles with students: majority of female graduate students, decreasing number of male faculty, increases in legal action, ambiguity of ethical guidelines, possible attraction between professors and students, and a contextual field that values human relationships. The purpose of this study was to discover attitudes and practices of male counselor educators regarding faculty-student relationships. Our research questions included: (a) what are the practices and attitudes of male counselor educators related to relationships with students and colleagues? and (b) what specific practices do male counselor educators employ to maintain boundaries with students?
Methodology
Participants and Data Collection
Using Schweiger et al.’s (2012) compilation of counseling program information, a member of the research team identified names typically attributed to males among listed faculty names, resulting in the identification of 330 males within the United States. The research team then matched the names with e-mails on university Web sites. An initial recruitment e-mail was sent to the identified sample asking for participation. Following the initial recruitment e-mail, 41 of the identified original sample responded as ineligible (22 contact e-mails were immediately returned as unavailable; 6 identified as female; and 13 identified as no longer working as a counselor educator or having never worked as a counselor educator). This resulted in a potential sample of 289. Two more e-mails were sent as reminders regarding participation. The final sample consisted of 163 male counselor educators who completed the survey, resulting in a response rate of 56%.
A summary of demographic characteristics of the 163 male counselor educators who completed the survey is presented in Table 1. In this sample, male counselor educators were mostly White, non-Hispanic (n=125). African American (n=14) and Hispanic (n=11) males also were represented, but only in small numbers, and Asian males (n=4) were few. Most of the sample identified as married/partnered (87%) and heterosexual (89%), with gay or bisexual males represented by approximately 10% of participants. The sample was more diverse in areas of age, rank, child status, and years as counselor educators.
Survey Development
We developed our survey in two phases. The research team brainstormed issues that emerged during discussion, such as the possible attitudes of male counselor educators, including feeling isolated or unsupported due to fewer numbers of male colleagues, or practices that might emerge in working with students of the opposite gender with the intent of ensuring a sense of safety. Based on discussion and an extensive literature review, the research team created a list of quantitative items surveying demographics, attitudes and practices of male counselor educators. We distributed the survey to a pilot group of six male counselor educators who represented diversity in age, experience, ethnicity and sexual orientation. The pilot participants reviewed each question and commented on its usefulness, acceptability and clarity. Based on pilot feedback, the research team modified the survey to include 22 demographic questions, 32 attitude and practice questions, and four open-ended questions. The survey was formatted for the Survey Research Suite (Qualtrics) and final quantitative data was transferred into SPSS for analysis.
Demographic questions included items regarding personal, family and program characteristics of the faculty members, and questions regarding the faculty members’ professional designations and teaching assignments. Attitude items (Cronbach’s α = .66) consisted of questions related to the impact of being male on both collegial and student relationships. Practice items (Cronbach’s α = .64) consisted of questions related to the participant’s actual practices in relating to students (e.g., private meetings, lunch/dinner, after class). For the full scale, Cronbach’s α was calculated at .70. Four open-ended questions addressed ethical challenges, thoughts related to being male, ways the counselor educator might act differently, and strategies used to avoid complications with students.
Table 1
Demographic Characteristics of Male Counselor Educator Participants
|
Variable
|
N
|
%
|
M
|
SD
|
Mdn
|
Range
|
| Age |
155
|
|
51.61
|
11.08
|
53
|
27–76
|
| Ethnicity |
|
|
|
|
|
|
| African American |
14
|
8.6
|
|
|
|
|
| Asian |
4
|
2.5
|
|
|
|
|
| White, Non-Hispanic |
125
|
76.7
|
|
|
|
|
| White, Hispanic |
11
|
6.7
|
|
|
|
|
| Self-Identified as Other |
8
|
4.9
|
|
|
|
|
| Relationship Status |
|
|
|
|
|
|
| Single |
14
|
8.6
|
|
|
|
|
| Married/Partnered |
142
|
87.1
|
|
|
|
|
| Divorced/Separated |
5
|
3.1
|
|
|
|
|
| Widowed |
1
|
.6
|
|
|
|
|
| Sexual Identity |
|
|
|
|
|
|
| Gay |
13
|
8.0
|
|
|
|
|
| Heterosexual |
145
|
89.0
|
|
|
|
|
| Bisexual |
3
|
1.8
|
|
|
|
|
| Status Regarding Children |
|
|
|
|
|
|
| No Children |
30
|
18.4
|
|
|
|
|
| Adult Children |
74
|
45.4
|
|
|
|
|
| Minor Children in Home |
55
|
33.7
|
|
|
|
|
| Minor Children Part Home |
1
|
.6
|
|
|
|
|
| Minor Children Not in Home |
2
|
1.2
|
|
|
|
|
| Years As Counselor Educator |
161
|
|
15.07
|
10.85
|
12
|
1–45
|
| Faculty Rank |
|
|
|
|
|
|
| Assistant |
38
|
23.3
|
|
|
|
|
| Associate |
50
|
30.7
|
|
|
|
|
| Full |
58
|
35.6
|
|
|
|
|
| Lecturer/Interim |
4
|
2.5
|
|
|
|
|
| Other |
13
|
8.0
|
|
|
|
|
| Total Number of Male Faculty |
156
|
|
4.04
|
1.81
|
4
|
1–10
|
| Total Number of Female Faculty |
155
|
|
4.27
|
2.27
|
4
|
0–13
|
| Estimated % of Male Students |
163
|
|
18.21
|
11.24
|
16
|
0–78
|
| Estimated % of Female Students |
162
|
|
77.66
|
18.55
|
80
|
0–99
|
The first three open-ended questions were used for qualitative analysis and the final question was used to create a list of strategies employed by male counselor educators to aid in their student relationships.
Analysis and Results
The research team used a parallel mixed-methods design (Teddlie & Tashakkori, 2009) to explore the experiences of male counselor educators. We utilized qualitative thematic analysis for data generated from three open-ended questions and optional comments following each quantitative survey question and quantitative statistical analysis for multiple-choice survey questions. By conducting independent quantitative and qualitative analyses in a parallel simultaneous nature, we allowed the separate analyses to inform one another and provide a more integrated understanding of the data (Teddlie & Tashakkori, 2009). Due to overlap in analysis and results consequential from a mixed-methods approach, we chose to present analyses and results categorized by method (qualitative and quantitative) in the following section.
Qualitative Analyses
Responses to the three open-ended questions and optional comments were analyzed from a perspective of transcendental phenomenology to explore the lived experiences of participants (Creswell, 2007; Moustakas, 1994). Within this qualitative tradition, we worked to bracket or set aside our own preconceptions about the phenomenon as much as possible to remain focused on the views of participants (Moerer-Urdahl & Creswell, 2004; Moustakas, 1994). The research team, consisting of two male doctoral students and one female tenured faculty member, discussed our student–teacher relationship experiences regarding gender and power differences. Through reflection and discussion, we developed greater awareness of how our experiences have influenced our views of being and working with male counselor educators. Team discussion allowed us to understand and bracket our positions in the development of data collection and analysis methods.
Because the experiences of male counselor educators have received little attention in literature and research, a phenomenological approach allowed for understanding to emerge from participants’ written reports as data was broken down into smaller units of meaning and reconstructed into broader themes that were clearly defined (Creswell, 2007; Giorgi, 1985). Following data collection, we independently coded responses to three open-ended questions, a smaller portion of the data, to identify initial concepts. Next, we met to review and compare our concepts. Silverman and Marvasti (2008) identified the appropriate use of smaller portions of data to establish preliminary categories. We discussed each unit of meaning in the text that was relevant to the focus of study (Giorgi, 1985), compared each concept to previous statements and discovered an initial list of broader themes suggesting common experiences among participants (Creswell, 2007). The research team clarified category definitions by comparing data units within each category for similarities and differences. Responses to optional comments sections in the survey were reviewed for inclusion in the text. Comments that offered information beyond the scope of the survey question referenced were included in the text for qualitative analysis. Then individual team members independently examined the entire text and coded each unit of meaning under the appropriately perceived category. Finally, we met as a group to develop consensus on final categories and to assign textural excerpts to appropriate themes. As suggested by Potrata (2010), research team members focused on exploring potential differences in coding rather than focusing on consistency when coming to consensus in order to illuminate complexities of the male counselor educator experience. Frequencies were tabulated to represent the magnitude of each category within the sample, and verbatim illustrative quotes were selected to clarify the meaning of each category. Saldaña (2013) suggested that magnitude coding adds supplemental texture to provide richer results in qualitative analysis.
Qualitative Results
In order to address our first research question regarding practices and attitudes of male counselor educators, participants were asked to respond to three open-ended questions to address their experiences and practices as male counselor educators. Seventy-one responses were recorded for the first question, “What ethical challenges, if any, are related to being male in counselor education?” One hundred responses were recorded for the second question, “What are your thoughts related to being male in counselor education?” Ninety-six responses were recorded for the third question, “What are the ways you act differently in student relationships because you are male?” We also coded additional comments of significance that followed each survey item. In all, qualitative analysis included the coding of 359 answers of varying lengths. During qualitative analysis, the research team discovered that participants’ answers appeared to be addressing similar themes across all questions. Hence, all answers were collapsed into one analysis.
The research team identified 10 distinct themes expressed by participants regarding the experiences of being a male counselor educator. We identified “modify behavior” as the most predominant theme, magnified by frequency (32%). This theme included intentional changes in action or interpersonal expression related to being male in professional relationships. Another major theme, “no difference” (frequency 23%) included beliefs and experiences that no unique relationship challenges exist in counselor education related to being male. Expressions of feeling “isolated or lonely” (frequency 11%) described participant experiences of feeling a lack of support as well as awareness of being a minority in the profession. Responses regarding “sexual attraction” (frequency 11%) involved experiences of sexual attraction in professional relationships. A theme of “perception of impropriety” (frequency 10%) included attention to the perception of others regarding appropriate behavior. Expressions of “prejudice or discrimination” (frequency 9.5%) involved experiences of negative beliefs or actions of others related to one’s gender. Additionally, qualitative data revealed themes related to participants’ “awareness” of professional relationships, “awareness of power difference” in relationships, the importance of a “caring or safe environment,” and “ethnicity or orientation” as part of one’s identity as a male counselor educator. A comprehensive presentation of all themes is included in Table 2.
Our second research question regarding specific practices of male counselor educators was addressed through our fourth open-ended survey question, which indicated participants cited over 40 different strategies they used to structure their relationships with students. In general faculty–student interactions, respondents indicated that they did not meet alone with students; only met with students on campus; interacted in groups when others were present; avoided jokes, conversations or language that could be perceived as too friendly; referred to family/significant others in class and conversation; avoided sharing too much personal information; made no physical contact; and avoided being overtly interested in students’ relationship issues. When meeting with students, respondents reported that they kept their doors open, structured meetings with an agenda, met in classrooms, ensured others were around, and avoided engaging in counseling with students. Participants also indicated that they consulted with colleagues regarding student relationships, had colleagues present for potentially problematic student interactions, addressed student relationship issues as soon as they arose, notified department chairs of any concerns and documented interactions. On a personal level, participants reported that they focused on having a balanced personal life, increased self-awareness of interactions, reminded self of boundaries, and engaged in honest and transparent interactions.
Quantitative Analyses
We used results from qualitative analysis to inform decision making regarding variables of interest for quantitative analysis. Due to the extensive data resultant from the 32-question survey of practices and attitudes and need for manuscript brevity, we narrowed survey data results to the survey items that matched qualitative theme results. We chose to explore one survey item per qualitative theme that appeared to closely match the qualitative analysis. Following final coding discussion, the research team identified five attitude and practice questions from the survey that appeared to be related to content evolving from the qualitative analysis. The qualitative theme of modifying behavior appeared most closely linked to the survey item, “I interact differently with female students than male students.” The theme represented by some respondents, that there were no differences related to being male, most closely aligned with the item, “I have unique ethical challenges related to being male in counselor education.” The item linked to the qualitative theme of avoiding the appearance of impropriety, “I structure my individual interaction with students to avoid the appearance of impropriety,” was further explored. The qualitative themes of isolation and discrimination were matched to two items: “I feel isolated in my faculty because I am male,” and “I feel discriminated against by faculty members because I am male.” Although most respondents did not agree with these final two statements, we chose to explore them further due to the distinct voices of some respondents related to ethnicity and sexual orientation within the data.
Table 2
Themes Related to Male Counselor Educators’ Experiences
| Theme |
Definition
|
Freq.
|
Responses
|
Sample Statements
|
| Modify Behavior |
Intentional changes in action or interpersonal expression related to being male |
32%
|
115
|
“. . . crucial to make sure distinct boundaries are established”“. . . have to focus on being appropriately relational”“must balance being supportive with providing clear boundaries” |
| NoDifference |
No unique challenges in counselor education related to being male |
23%
|
82
|
“No specific challenges related to my gender”“Ethics are ethics, male or female”“How I act has little to do with being male” |
| Awareness |
Indicating awareness or self-awareness regarding professional relationships |
13%
|
47
|
“. . . we need to be very aware of situations and interactions with female students”“Know one’s self”“I am now more aware of how I interact” |
| IsolatedorLonely |
Experiencing lack of support and awareness of being a minority in profession |
11%
|
39
|
“I feel a bit like an endangered species”“There are simply some things I can only talk with other men about”“I recognize males are a minority in the field” |
| Sexual Attraction |
Experiences of sexual attraction in professional relationships |
11%
|
38
|
“Dealing with feelings of attraction with students and colleagues”“I am attracted to female students but do not act on it”“I have to refocus my thoughts if I feel an attraction to a student or colleague” |
| Perception of Impropriety |
Attention to the perception of others regarding appropriate behavior |
10%
|
37
|
“. . . don’t want to give the impression of being unethical”“Avoiding any appearance of misconduct”“. . . vigilant in protecting myself from false accusations” |
| Awareness of Power Difference |
Awareness of the impact of privilege and power in relationships |
10%
|
35
|
“Being aware of my male privilege and not abusing it”“I can be male without being dominating”“I do see the same gender politics and gender roles in my profession as I see in society…” |
| PrejudiceorDiscrimination |
Experiences of negative or devaluing beliefs or actions of others related to being male |
9.5%
|
34
|
“tendency to view males as the victimizer”“. . . uniquely male issues that could arise in counseling situations are downplayed”“I sometimes experience sexism against men in the comments of my female colleagues” |
| Caringor Safe Environment |
Intention to provide support and safety to students |
6%
|
21
|
“We want to provide a caring environment”“I want students to feel comfortable around me.”“. . . do not want any female to feel anxious” |
| Ethnicityor Orientation as Part of Identity |
Influences of ethnicity and sexual identity upon male professional experiences |
4%
|
15
|
“Being a male and an ethnic minority is challenging and often lonely”“. . . being Black and male is more of a challenge than being male alone”“I feel isolated not because I am male but because I am a gay male” |
Note: Frequency = Number of participants who shared theme-related statements
Quantitative Results
Descriptive results for the five survey items are presented in Table 3. In order to explore relationships between survey items of interest, we employed Pearson product-moment correlation coefficient analyses on the five variables. There were statistically significant positive correlations between perception of unique ethical challenges and the four other variables: feeling isolated
(r = .290, n = 149, p < .001); interacting differently with female students (r = .317, n = 147, p < .001); structuring interactions to avoid appearance of impropriety (r = .190, n = 148, p = .021); and feeling discriminated against (r = .217, n = 150, p = .008). The more a male counselor educator felt there were unique ethical challenges related to being male, the more likely he was to feel isolated and discriminated against, structure interactions with students to avoid the appearance of impropriety, and interact differently with females than males. Additionally, there was a statistically significant positive correlation between feeling isolated and feeling discriminated against (r = .371, n = 149, p < .001). The more isolated a male counselor educator felt, the more likely he was to feel discriminated.
Table 3
Survey Items Related to Relationships for Male Counselor Educators
|
|
|
|
Percent of Responses
|
|
Survey Item
|
N
|
|
Σ
|
SD
1
|
D
2
|
N
3
|
A
4
|
SA
5
|
| I feel isolated in my faculty because I am male. |
149
|
1.89
|
.94
|
36.8
|
36.8
|
11.7
|
5.5
|
1.2
|
| I interact differently with female students than male students. |
147
|
2.90
|
1.02
|
6.7
|
29.4
|
21.5
|
30.7
|
1.8
|
| I structure my individual interactions with students to avoid the appearance of impropriety. |
148
|
3.76
|
.92
|
1.8
|
9.2
|
13.5
|
50.9
|
15.3
|
| I have unique ethical challenges related to being male in counselor education. |
150
|
2.79
|
1.03
|
9.2
|
30.7
|
23.9
|
26.4
|
1.8
|
| I feel discriminated against by faculty members because I am male. |
150
|
2.05
|
1.06
|
31.9
|
39.9
|
6.1
|
12.3
|
1.8
|
Note: SD=Strongly Disagree, D=Disagree, N=Neutral, A=Agree, SA=Strongly Agree
We further explored ethnicity and sexual orientation in relationship to the dependent variables of isolation and discrimination based on qualitative findings that indicated these characteristics impact the views of male counselor educators. We conducted four separate one-way between-groups analyses of variance to explore the impact of ethnicity and gender on isolation and discrimination. There was a statistically significant difference in ethnicity for isolation, F(4, 144) = 5.78, p < .001, η2 = .14. Means for ethnicity included Asian x̅ = 2.0; African American x̅ = 1.71; White/Non-Hispanic x̅ = 1.84; White/Hispanic x̅ = 1.64; Self-Identified as Other x̅ = 3.43. There was a statistically significant difference in ethnicity for discrimination, F(4, 144) = 5.25, p = .001, η2 = .13. Means for ethnicity included Asian x̅ = 2.0; African American x̅ = 2.23; White/Non-Hispanic x̅ = 1.94; White/Hispanic x̅ = 1.91; Self-Identified as Other x̅ = 3.71. There was a statistically significant difference in sexual orientation for isolation, F(2, 145) = 3.81, p = .024, η2 = .05. Means for sexual orientation included Gay x̅ = 2.58; Heterosexual x̅ = 1.83; Bisexual x̅ = 1.67. There was no statistically significant difference in sexual orientation for discrimination, F(2, 145) = .70, p = .50, η2 = .01.
Discussion
The sample in this study reasonably represents the current population of male counselor educators in CACREP-accredited programs. Although the sample reported equivalent numbers between male and female faculty, they also reported a disproportionate number of female students (78%) to male students (18%), as indicated in previous literature (Schweiger et al., 2012). The sizeable response rate to this survey, as well as its representativeness, lends credibility to findings.
Themes and Characteristics Related to Being a Male in Counselor Education
Qualitative analyses indicated that participants expressed diversity of attitudes and practices regarding the impact of being male upon professional relationships. The most predominant theme, “modify behavior,” indicated that being male influenced choices made by male counselor educators in their interactions with students. Conversely, the second dominant theme, “no difference,” indicated that some counselor educators do not feel that there is any difference in interactions with students or colleagues related to being male. A lack of consensus existed among male counselor educators regarding the influence of being male upon their professional relationships.
When male counselor educators acknowledged there were differences related to being a male in the field, qualitative analysis revealed additional themes related to isolation, discrimination, fear of appearing inappropriate, interacting differently with females than males and need for awareness. We wanted to explore characteristics related to these feelings, which prompted the correlational analyses.
Quantitative and qualitative analyses indicated that the appearance of impropriety was of considerable concern for male counselor educators. A majority of participants agreed or strongly agreed that they structured their interactions to avoid appearance of impropriety. Results revealed a statistically significant positive relationship between expressing a perception of unique ethical challenges for males and structuring interactions to avoid appearance of impropriety. Participants who perceived unique challenges as males also tended to take steps to avoid appearing inappropriate in their professional relationships. This finding supports qualitative themes of male counselor educators’ concerns regarding the appearance of impropriety and fear of the cultural myth of the lecherous professor (Bellas & Gossett, 2001).
Sexual attraction emerged as a relevant issue through qualitative analyses. A vast majority of respondents reported that they had experienced being attracted to a student, with frequency of feelings ranging from rare to a regular occurrence. Also, a majority of the sample reported experiencing a student being attracted to them. These results suggest that sexual attraction was experienced as a common phenomenon in male teacher–student relationships. However, participants often described their feelings of attraction as natural reactions that posed no threat if not acted upon.
When addressing the influence of student gender upon their behavior with students, male counselor educators reported diverse perspectives. Participants were asked if they interacted differently with female students than male students. Responses were about evenly distributed from “disagree” to “agree.” The variance in responses may reflect the larger disagreement among participants regarding the influence of gender upon professional relationships. The qualitative themes of “modify behavior” and “no difference” may provide context for understanding diverse results regarding this question. Correlational analysis revealed that the more a participant perceived unique challenges as a male counselor educator, the more he reported interacting differently with female students compared to male students.
Some participants also reported experiencing isolation related to being a male counselor educator. Qualitative data revealed unique experiences of isolation related to ethnicity and sexual orientation. Although there were a small number of participants who identified as gay, bisexual, African American, Latino, Asian, or other ethnicity, we chose to conduct quantitative analysis to further explore their voices, which were clearly articulated as unique in qualitative analyses. Further quantitative analysis indicated that participants who self-identified as “other” for ethnicity were more likely to feel isolated in comparison with other ethnicities. Likewise, gay male counselor educators also were more likely to feel isolated in the profession. However, gay males did not report higher levels of feeling discriminated against as compared to heterosexual males. Previous research indicates gay males may experience isolation related to not being out to co-workers, often motivated by fear of discrimination (Wright, Colgan, Creegany, & McKearney, 2006). Another possible interpretation could be that gay male counselor educators feel isolated due to interacting with fewer colleagues who are similar to them, but who they experience as accepting or non-discriminatory.
Linked to isolation, we also asked male counselor educators if they had faculty colleagues with whom they could discuss challenges. This point seemed especially salient due to qualitative results indicating male counselor educators rely on consultation as one intervention for dealing with student relationship issues. A majority of respondents agreed or strongly agreed to having a colleague on their faculty with whom they could discuss male-related issues. Qualitative and quantitative analyses identified ethnicity as an important contributor to the experiences of male counselor educators. Qualitative data included a small but consistent voice of African American male counselor educators who expressed increased isolation due to a combination of ethnicity and gender. Quantitative analysis also indicated that participants who identified as African American reported more frequent experiences of discrimination in their professional environment. These findings coincide with research indicating that African American males experience prejudice and discrimination in higher education due to stereotype images of African American males as underachieving, disengaged and threatening (Harper, 2009). Brooks and Steen (2010) discussed concerns related to the lack of African American male counselor educators and the obstacles they face in the academic setting. Participants who self-identified as “other” on ethnicity also showed increased experiences of discrimination as well as isolation. Correlational analysis confirmed the co-occurrence of these two themes, revealing a positive relationship between feeling isolated and feeling discriminated against. Asian males were more likely to feel isolated and structure their interactions to avoid appearances of impropriety, which reflects previous accounts of Asian professors in the literature (Culotta, 1993) in which they experienced isolation from their colleagues and increased student mentoring demands because of their minority status.
In returning to the issue of concern related to practices of male counselor educators in building humanistic and growth-inspiring relationships with students, the results of the current study provide some insight. Many male counselor educators appear to be aware and concerned that being male may influence how they are perceived by students and how they approach their relationships with students. However, results indicate that participants sought methods and strategies that allowed them to pursue relationships while also being sensitive to students’ perceptions of safety. Figure 1 provides specific strategies highlighted by participants that allow male counselor educators to engage in student–teacher relationships that recognize the power differential between student and teacher, inherent challenges with sexual attraction, and yet still allow the student and teacher to benefit from an accepting, inspiring relationship that mirrors the therapeutic relationship.
Limitations
The survey method used for this study was selected for exploratory purposes and did not involve the use of a rigorous assessment designed to interpret results through reliability and validity procedures; hence, results must be interpreted with caution. Additionally, the survey sample may not represent the views of the entire population of male counselor educators.
Figure 1.
Strategies Used by Male Counselor Educators to Build Student Relationships.
Note: General Interactions = strategies used in everyday interactions; Student Meetings = strategies used when having to meet with students individually; Interventions = strategies used when complications arise.
Due to the extensiveness of collected data, we were unable to report all findings related to the uniqueness of the sample. Respondents reported rich qualitative narratives and variations in their attitudes and practices. The variations are not fully represented in this report. The use of a one-time open-ended questionnaire precluded use of qualitative interviews that would reveal further depth of themes. Additionally, minority groups, such as specific ethnicities and those who identified as gay and bisexual, appeared to have a distinct voice in this survey. However, due to low representation, data analysis was limited in representing their experiences. We attempted to rectify this limitation by voicing those narratives in the qualitative analysis.
Implications
The purpose of this research was to reveal attitudes and practices of male counselor educators, allowing the reader an understanding of how the experience of being male influences the daily choices of male counselor educators. Implications of this research study include better understanding of the experiences of counselor educators that lead to enhanced job satisfaction for males, best practices to improve faculty–student relationships and possible areas for further investigation. Additionally, in Figure 1, we provide a list of behaviors used by male counselor educators to ensure appropriate student–teacher boundaries. This list offers male counselor educators possible strategies to address perceptions of impropriety or misconduct.
If male counselor educators experience greater job satisfaction, then more males may choose the counseling field, as they observe possible role models with whom they identify. Substantial variables identified by this study that might influence job satisfaction are feelings of isolation, discrimination, fear of appearing inappropriate and hypervigilance to behavioral interactions with students. Qualitative data revealed a desire by male counselor educators to offer a safe, caring environment, qualified by some respondents as an authentic relationship. Findings indicate that if male counselor educators feel limited by personal loneliness or concern for appearances, this will most likely interfere with their student and faculty relationships. Consultation with and support of colleagues appeared to be a process regularly utilized by many of the male counselor educators in this study. Counselor education departments would benefit from engaging in practices that promote collegiality and support among faculty members as well as formalizing mentoring processes.
Male counselor educators revealed that they take measures to modify their behaviors with students, especially female students. Our results indicate that fear of impropriety, awareness of cultural power differentials, desire to create safe relationships with students and realistic awareness of potential sexual attraction prompt male counselor educators to engage in behaviors that will provide safety for students and for themselves. These strategies reveal concrete behavioral actions taken to ensure the maintenance of boundaries with students. Kolbert, Morgan, and Brendel (2002) concluded that faculty must consider student perceptions of a relationship as the primary criterion in making decisions regarding their interactions with students. This conclusion requires considerable awareness from male counselor educators related to how they present themselves and how students perceive them. One common strategy used by male counselor educators and commonly supported in the literature (Ei & Bowen, 2002) is engaging in group activities, as opposed to one-on-one activities, in order to establish authentic relationships in a safe environment.
The most cited strategy among this sample was not being alone or out of sight from others when engaging in personal interactions with students. In a field where confidentiality is the base of intervention, this particular strategy seems incongruous, especially for professionals who value relationship in teacher–student interactions. Additionally, students may question a faculty member’s authenticity if intimacy is avoided in the relationship. However, contextual, legal and cultural considerations appear to encourage these types of restraints. Counselor education departments may benefit from discussion of these issues of behavior, relationship, philosophy and safety in an open forum among faculty and with students.
The relational experiences of male counselor educators have gone virtually unexamined in literature and research, leaving many opportunities for further inquiry. Some participants indicated that ethnicity influenced their experiences and relationships, yet sample size prevented meaningful exploration. Further research may investigate the unique experiences of African American, Latino and Asian male counselor educators. Likewise, sexual orientation emerged as a major influence for some participants. An exploration of experiences of gay male counselor educators is needed to enhance understanding of their relational experiences and the influence of gender.
Participants expressed concerns about perceptions of impropriety with students, feelings of isolation within the profession, and experiences of prejudice and discrimination in their work environments. These elements require further exploration to better understand the nature of these experiences and investigate causal factors to heighten sensitivity and identify appropriate measures for creating a safe environment for faculty and students. Participants also indicated that they alter behavior in student relationships to avoid the appearance of impropriety and maintain professional boundaries. Further research could explore the implications of those decisions for the quality of relationships with students. A study of student perspectives would greatly enhance understanding of these relational dynamics. Additionally, a study of ways in which female counselor educators approach their relationships with students, in regard to feeling restricted or limited in intimacy, is warranted.
This study provides an enhanced understanding of male counselor educators’ perceptions and experiences of their relationships with students and colleagues. Male counselor educators shared a unique voice of experience. Further research may expand understanding of male counselor educator experiences, provide insights to improve the quality of faculty–student relationships and assist in developing male role models for the future of our profession.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 American Counseling Association Code of Ethics. Retrieved from http://www.counseling.org/docs/ethics/2014-aca-code-of-ethics.pdf?sfvrsn=4
Anderson, J. A., & Rawlins, M. (1985). Availability and representation of women in counselor education with strategies for recruitment, selection, and advancement. Counselor Education and Supervision, 25, 56–65. doi:10.1002/j.1556-6978.1985.tb00512.x
Bartlett, T. (2002, April 5). The question of sex between professors and students. The Chronicle of Higher Education. Retrieved from http://chronicle.com/article/The-Question-of-Sex-Between/33174
Bellas, M. L., & Gossett, J. L. (2001). Love or the “lecherous professor”: Consensual sexual relationships between professors and students. The Sociological Quarterly, 42, 529–558. doi:10.1111/j.1533-8525.2001.tb01779.x
Bowman, V. E., Hatley, L. D., & Bowman, R. L. (1995). Faculty-student relationships: The dual
role controversy. Counselor Education and Supervision, 34, 232–242. doi:10.1002/j.1556-6978.1995.tb00245.x
Brooks, M., & Steen, S. (2010). “Brother where art thou?” African American male instructors’ perceptions of the counselor education profession. Journal of Multicultural Counseling and Development, 38, 142–153. doi:10.1002/j.2161-1912.2010.tb00122.x
Creswell, J. W. (2007). Qualitative inquiry & research design: Choosing among five approaches. Thousand
Oaks, CA: Sage.
Crothers, L. M., Hughes, T. L., Schmitt, A. J., Theodore, L. A., Lipinski, J., Bloomquist, A. J., & Altman, C. L. (2010). Has equity been achieved? Salary and promotion negotiation practices of a national sample of school psychology university faculty. The Psychologist-Manager Journal, 13, 40–59. doi:10.1080/10887150903553790
Culotta, E. (1993). Finding—and keeping—minority professors. Science, 262, 1091–1096.
doi:10.1126/science.262.5136.1091
Dollarhide, C. T., & Granello, D. H. (2012). Humanistic perspectives on counselor education and
supervision. In M. B. Scholl, A. S. McGowan, & J. T. Hansen (Eds.), Humanistic perspectives on contemporary counseling issues (pp. 277–303). New York, NY: Routledge.
Ei, S., & Bowen, A. (2002). College students’ perceptions of student-instructor relationships. Ethics & Behavior, 12, 177–190. doi:10.1207/S15327019EB1202_5
Giorgi, A. (1985). Sketch of a psychological phenomenological method. In A. Giorgi (Ed.),
Phenomenology and psychological research. Pittsburgh, PA: Duquesne University Press.
Harper, S. R. (2009). Niggers no more: A critical race counternarrative on black male student
achievement at predominately white colleges and universities. International Journal of Qualitative Studies in Education, 22, 697–712. doi:10.1080/09518390903333889
Healey, A. C., & Hays, D. G. (2012). A discriminant analysis of gender and counselor
professional identity development. Journal of Counseling & Development, 90, 55–62. doi:10.1111/j.1556-6676.2012.00008.x
Kiley, K. (2011, August 30). Relationship problems. Inside Higher Education. Retrieved from
https://www.insidehighered.com/news/2011/08/30/idaho_student_s_death_and_ties_to_former_
professor_highlights_difficulty_of_preventing_faculty_student_relationships
Kolbert, J. B., Morgan, B., & Brendel, J. M. (2002). Faculty and student perceptions of dual relationships within counselor education: A qualitative analysis. Counselor Education and Supervision, 41, 193–206. doi:10.1002/j.1556-6978.2002.tb01283.x
Kress, V. E., & Dixon, A. (2007). Consensual faculty–student sexual relationships in counselor
education: Recommendations for counselor educators’ decision making. Counselor Education and Supervision, 47, 110–122. doi:10.1002/j.1556-6978.2007.tb00042.x
McAuliffe, G. J. (2011). Guidelines for constructivist-developmental counselor education. In G. J. McAuliffe & K. P. Eriksen (Eds.), Handbook of counselor preparation: Constructivist, developmental,
and experiential approaches (pp. 31–48). Thousand Oaks, CA: Sage.
Moerer-Urdahl, T., & Creswell, J. W. (2004). Using transcendental phenomenology to explore the “ripple effect” in a leadership mentoring program. International Journal of Qualitative Methods, 3, 1–28.
Moustakas, C. (1994). Phenomenological research methods. Thousand Oaks, CA: Sage.
Nicks, S. D. (1996). Fear in academia: Concern over unmerited accusations of sexual harassment. The Journal of Psychology, 130, 79–82. doi:10.1080/00223980.1996.9914990
Oldenburg, C. M. (2005). Students’ perceptions of ethical dilemmas involving professors: Examining the impact of the professor’s gender. College Student Journal, 39, 129–140.
Owen, P. R., & Zwahr-Castro, J. (2007). Boundary issues in academia: Student perceptions of faculty–student boundary crossings. Ethics & Behavior, 17, 117–129. doi:10.1080/10508420701378065
Potrata, B. (2010). Rethinking the ethical boundaries of a grounded theory approach. Research Ethics, 6, 154–158. doi:10.1177/174701611000600408
Saldaña, J. (2013). The coding manual for qualitative researchers (2nd ed.). Thousand Oaks, CA:
Sage.
Schweiger, W. K., Henderson, D. A., McCaskill, K., Clawson, T. W., & Collins, D. R. (2012).
Counselor preparation: Programs, faculty, trends (13th ed.). New York, NY: Routledge.
Silverman, D., & Marvasti, A. (2008). Doing qualitative research: A comprehensive guide. Thousand Oaks, CA: Sage.
Teddlie, C. B., & Tashakkori, A. M. (2009). Foundations of mixed methods research: Integrating
quantitative and qualitative approaches in the social and behavioral sciences. Thousand Oaks, CA: Sage.
Wright, W., Colgan, F., Creegany, C., & McKearney, A. (2006). Lesbian, gay and bisexual workers: Equality, diversity and inclusion in the workplace. Equal Opportunities International, 25, 465–470. doi:10.1108/02610150610713782
Dee C. Ray, NCC, is a Professor at the University of North Texas. David D. Huffman is an Adjunct Professor at the University of North Texas. David. D. Christian is an Assistant Professor at the University of Arkansas. Brittany J. Wilson, NCC, is Assistant Director, Child and Family Resource Clinic, University of North Texas. Correspondence can be addressed to Dee C. Ray, University of North Texas, 1155 Union Circle, Box 310829, Denton, TX 76203, dee.ray@unt.edu.
Jul 20, 2016 | Article, Volume 6 - Issue 2
John M. Laux, Robin M. DuFresne, Allison K. Arnekrans, Sylvia Lindinger-Sternart, Christopher P. Roseman, Amy Wertenberger, Stephanie Calmes, Darren W. Love, Andrew M. Burck, Jim Schultz
The Substance Abuse Subtle Screening Inventory-3 (SASSI-3; Miller & Lazowski, 1999) is a substance use screen that uses logically derived, or obvious questions, as well as subtle, or empirically derived questions. The SASSI-3 can be completed, scored and interpreted in 15 minutes. Side one consists of 67 true–false items selected for their ability to statistically differentiate between a criterion group of persons with substance dependence and a control group of non-substance dependent persons. The 67 empirically derived items are used in an effort to defeat dissimulation and are similar in nature and purpose to items found on the MacAndrew Alcoholism Scale-Revised (MAC-R; MacAndrew, 1965). As such, these empirically derived items are useful with individuals who are either intentionally or unintentionally denying a substance use disorder (Laux, Piazza, Salyers, & Roseman, 2012). These comprise the Symptoms scale (SYM), which assesses the symptoms and consequences of drug and alcohol use; the Obvious Attributes scale (OAT), a measure of the obvious symptoms of substance dependence; the Subtle Attributes scale (SAT), an indirect measure of substance use that employs items with non-substance-related content; the Defensiveness scale (DEF), which measures denial or minimization; the Supplemental Addiction Measure scale (SAM), which discriminates general defensiveness from defensiveness related to substance use; the Family Versus Control Subjects scale (FAM), which identifies those who are likely to focus on the thoughts and feelings of others to their own neglect; the Correctional scale (COR), used to detect response patterns similar to those produced by persons with a history of criminal behaviors; and the Random Answering Pattern scale (RAP), designed to identify haphazard answering. Side one also includes questions about respondents’ marital status, employment status, education, ethnicity and income.
Side Two consists of 12 items specific to alcohol use and 14 items regarding use of other substances. Response options to these 26 items are never, once or twice, several times, and repeatedly. These 26 items comprise the Face Valid Alcohol (FVA) and Face Valid Other Drugs (FVOD) scales and are similar to items found on the Michigan Alcoholism Screening Test (MAST; Selzer, 1971) and the CAGE (Ewing, 1984). The SASSI-3 is interpreted using nine decision rules. The first five decision rules are based solely on the unique contributions of individual scales. The remaining four decision rules involve a combination of two or more scales. A decision rule is coded “yes” if the associated SASSI-3 scale or scales’ raw score is equal to or greater than the decision rule’s cut score. Otherwise, the decision rule is coded as “no.” The respondent is determined to have a “high probability of having a substance dependence disorder” if any of the decision rules are met (Miller & Lazowski, 1999, p. 10).
Not only does the SASSI-3 do a better job of identifying alcohol use disorders than the MAST, CAGE and MAC-R (Laux, Perera-Diltz, Smirnoff, & Salyers, 2005; Laux, Salyers, & Kotova, 2005), it provides the added benefit of screening for drug use other than alcohol. The most recent inquiry into substance use screens indicated that the SASSI-3 is the substance use screen most frequently used by Master Addictions Counselors certified by the National Board for Certified Counselors (Juhnke, Vacc, Curtis, Coll, & Paredes, 2003).
The SASSI-3 Manual (Miller & Lazowski, 1999) reported a sensitivity (true positive) rate of 94.6% and specificity (true negative) rate of 93.2%. Subsequent field research produced results consistent with the psychometric claims made in the SASSI-3 Manual (Burck, Laux, Harper, & Ritchie, 2010; Burck, Laux, Ritchie, & Baker, 2008; Calmes et al., 2013; Hill, Stone, & Laux, 2013; Laux, Perera-Diltz, Smirnoff, & Salyers, 2005; Laux, Salyers, & Bandfield, 2007; Laux, Salyers, & Kotova, 2005; Wright, Piazza, & Laux, 2008). Further, Laux et al. (2012) demonstrated that the SASSI-3’s empirical items and associated decision rules increased the instrument’s screening accuracy. In addition, persons’ willingness and ability to self-report having a substance use disorder as described in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR; American Psychiatric Association [APA], 2000) did not negatively affect the instrument’s sensitivity. Laux et al. (2012) found that the SASSI-3 produced high sensitivity rates across varying levels of motivation to change among persons who lost parental rights due to substance use.
APA published the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) in 2013. This most current version of the DSM brought forward major and important changes to the way the substance use disorder (SUD) chapter is conceptualized (Dailey, Gill, Karl, & Barrio Minton, 2014). Notably, the former dichotomous substance abuse and substance dependence categories have been removed and replaced with a continuum under the heading of “Substance Use Disorders” (APA, 2013, p. 483). The criterion formerly associated with the substance abuse and substance dependence disorders have been merged onto one continuum, to which craving has been added. Clients are determined to have a mild SUD if two or three criteria are met, a moderate SUD when four to five symptoms are met, and a severe SUD when six or more symptoms are endorsed.
Because previous versions of the DSM criteria were frequently used as the gold standard against which SUD screens were compared (Ashman, Schwartz, Cantor, Hibbard, & Gordon, 2004; Lazowski, Miller, Boye, & Miller, 1998), it is of interest to investigate the degree to which the SASSI-3 accurately predicts the new DSM-5 substance use diagnostic criteria. Our literature review produced two examples of empirical comparison between the SASSI-3, or its predecessors, and DSM criteria. The first (Lazowski et al., 1998) reported on the standardization efforts that produced the instrument’s third version. This research team used the data from persons whose case files had a DSM-III-R (APA, 1987) or a DSM-IV (APA, 1994) substance use diagnosis and an administration of the SASSI-3. How the participants were diagnosed was not specified. The results of this investigation found that the SASSI-3’s overall accuracy rating was 97%, the sensitivity rating was 97% and the specificity rating was 95%. A second study (Ashman et al., 2004) sought to determine the SASSI-3’s ability to screen for substance abuse among persons with traumatic brain injury. Ashman et al. (2004) used the Structured Clinical Interview for DSM-IV (First, Spitzer, Gibbon, & Williams, 1996) as the criterion variable against which the SASSI’s results were compared. These authors concluded that while the SASSI’s overall decision and FVA scale yielded “modest accuracy, sensitivity, and specificity rates” (p. 198), the FVOD scale had high sensitivity (95%) but only moderate accuracy (83%) and specificity (82%) among persons with traumatic brain injury.
The purpose of this study was to extend this line of research and examine the SASSI-3’s ability to accurately assess the presence of an SUD using DSM-5 criteria. Specifically, the authors calculated kappa statistics to estimate the degree of agreement between the SASSI-3’s overall decision rules, its individual decision rules and counselors’ DSM-5 SUD diagnoses. This analysis is important because these decision rules directly affect the SASSI-3’s final SUD classification (i.e., high probability of substance dependence disorder/low probability). Further, we examined the SASSI-3’s specificity and sensitivity using receiver operating characteristics (ROC) curves. We hypothesized that we would find good agreement between the overall SASSI-3 score and the DSM-5 SUD diagnosis. We further expected to find good agreement between the SASSI-3 face valid scales and the DSM-5 SUD diagnosis. We expected to find a moderate to low agreement between the SASSI-3 subtle scales and the DSM-5 SUD diagnosis. Additionally, we hypothesized that the ROC analysis would provide optimal cut-off scores for each of the SASSI-3 subscales that would improve those scales’ sensitivity and specificity. Study participants were selected from an inpatient SUD treatment center, an urban university, and a community mental health center that provides court-ordered outpatient treatment for clients with substance use issues. These populations were selected in order to match the populations on which the SASSI-3 was standardized (Miller & Lazowski, 1999).
Method
Participants
This study included participants (N = 241) recruited between October 2013 and May 2014. There were 114 females (47.3%) and 127 males (52.7%). The participants’ average age was 33.63 (SD = 6.83, range = 19–47). One hundred thirty-one (54.4%) were European American, 52 (21.6%) were African American, 7 (2.9%) were Hispanic, 12 (5.0%) were biracial, and 4 (1.7%) were Asian American. Thirty-five (14.5%) provided no ethnic background information. The average number of years of education completed was 12.48 (SD = 1.79, range = 7–18). Thirty-two (13.3%) were married, 156 (64.7%) were never married, 27 (11.2%) were divorced, 16 (6.6%) were separated, 4 (1.7%) were widowed, and 6 (2.5%) did not indicate a marital status. Thirty-three (13.7%) participants listed their employment as full-time, 22 (9.1%) as part-time, 91 (37.8%) as not employed, 65 (27.0%) as student, 9 (3.7%) as home maker, 13 (5.4%) were disabled, 2 (.8%) listed retired, and 6 (2.5%) listed no employment status. The sample features fewer employed, and more unemployed and student participants than the SASSI-3 normative sample (Miller & Lazowski, 1999).
Participants were recruited from three sites in Ohio. A total of 117 (48.5% of the total sample) participants were recruited from an adults-only comprehensive community mental health substance abuse treatment center. Another 61 subjects (25.3% of the total) were recruited from a private, non-profit organization specializing in court-ordered outpatient mental health treatment. Finally, 63 students (26.1% of the sample) enrolled at a large, public, urban university in Ohio were recruited to provide a sample of individuals who were less likely to be substance users. A one-way ANOVA [F(2, 233) = 24.28, p = .000, η2 = .172] showed that the college students’ mean age (M = 23.86, SD = 9.04) was significantly lower than the inpatient substance abuse clients’ (M = 35.80, SD = 11.36) and the outpatient clients’ (M = 32.80, SD = 10.88).
Procedure and Materials
The procedures involved here were approved by the sponsoring institution’s Institutional Review Board and the data collection sites, and were consistent with the American Counseling Association’s Code of Ethics (2014). Three licensed counselors who had completed two graduate courses in testing and assessment conducted standardized interviewing and administered SASSI-3s. All three counselors completed training in SUD interviewing and SASSI-3 administration and scoring prior to the study’s beginning. All persons receiving treatment at sites 1 and 2 were asked to participate. A total of 117 of the 118 (99.2%) persons at site 1 and 61 of the 64 (95.3%) persons at site 2 agreed to participate. Sixty-three of 79 students (79.8%) enrolled in one of three separate undergraduate counseling courses agreed to participate.
Each participant met individually with a researcher who used the structured SUD questionnaire to conduct an interview and administered the SASSI-3. The SASSI-3s were scored and interpreted by a fourth researcher who had no knowledge of the interviewing researchers’ diagnostic impressions. For quality control purposes, the senior author reviewed the SASSI-3 scoring and questionnaire results.
Instruments
Structured Substance Use Disorder Questionnaire. At present, no structured guide or screen exists that was developed and normed using the current DSM-5 SUD criteria. To ensure that the counselors were uniform in their substance use interviews and that their interviews were consistent with the DSM-5 criteria, we designed a 22-item questionnaire to determine whether participants would meet criteria for a DSM-5 SUD. This questionnaire was based on the 11 criteria for an SUD from the DSM-5 (APA, 2013). These items were yes/no questions corresponding to the criteria for an SUD and were divided into two sections. The first 11 items applied to alcohol use and the second 11 items applied to the use of other drugs. Consistent with the DSM-5’s SUD section, participants who responded “yes” to two or more items in either section met criteria for a DSM-5 substance use disorder.
Endorsement of two items in the first section indicated the participant met criteria for an SUD involving alcohol use; endorsement of two items in the second section indicated the participant met criteria for an SUD involving other drugs. Severity of the SUD was based on decision rules provided in the DSM-5: 2–3 symptoms indicated a mild SUD, 4–5 symptoms indicated a moderate SUD, and 6 or more symptoms indicated a severe SUD (APA, 2013). Counselors clarified the meaning of items as needed. No distinction was made between different types of drug use (marijuana, cocaine, etc.) because the SASSI-3 does not do so. The internal consistency estimates for the alcohol and other drug use sections were high ( = .94 and = .97, respectively).
Data Analysis
The authors used two methods of statistical analysis. Cohen’s kappa was used to measure the agreement between the two dichotomous DSM-5 SUD diagnosis variables (i.e., met criteria or not) and the overall score on the SASSI-3 (high probability of substance dependence disorder/low probability). Cohen’s kappa also was used to compare the DSM-5 diagnosis of either an SUD involving alcohol or one involving other drug use to the score on the SASSI-3 subscale 1 (FVA) or subscale 2 (FVOD), respectively. It was then used to measure agreement between the DSM-5 SUD diagnosis and the scores on subscales 3–9 on the SASSI-3. The value of the kappa is between 0 and 1 and is divided into 5 levels of agreement: .01 to .20 signifies slight agreement; .21 to .40 fair; .41 to .60 moderate; .61 to .80 substantial; and .81 to .99 near perfect agreement (Landis & Koch, 1977).
Unlike the kappa, ROC curve analysis is used with continuous variables. ROC analysis allows one to measure a trade-off between specificity (true positives) and sensitivity (true negatives; Youngstrom, 2014). ROC allows the investigator to determine how specificity and sensitivity change when the cut-off value of the continuous variable is changed. ROC value is expressed as an area under the ROC curve (AUROC). ROC curves are graphically represented as the relationship between an instrument’s specificity (horizontal axis) and sensitivity (vertical axis). ROC curves are interpreted by finding the point on the graph where a scale’s sensitivity and specificity are balanced. To the naked eye, this optimal point is where the curve begins to flatten out at the top. ROC analyses are performed on individual scales, but not multiple scales. As such, ROC analyses can only be performed on those SASSI-3 decision rules that involve individual scales (decision rules 1–5). Decision rules 6–9 involve input from two or more SASSI-3 scales and are therefore not subject to ROC analysis. The ROC scores are categorized as follows: ≥ .90, excellent; ≥ .80, good; ≥ .70, fair; and < .70, poor (Youngstrom, 2014).
Results
A review of the participants’ random answering profile (RAP) scores indicated that all profiles were valid. Of the 241 participants, the SASSI-3 classified 153 (63.5%) as having a high probability of having a substance dependence disorder. Raw SASSI-3 scale scores were converted to t scores using the SASSI-3 Manual’s Appendix C (Miller & Lazowski, 1999).
Table 1
SASSI-3 Scale Descriptive Data and Internal Consistency Estimates
|
SASSI-3 Scale
|
Mean t score
|
Standard Deviation
|
Range
|
Alpha
|
|
|
|
|
|
|
FVA
|
55.67
|
15.86
|
41-110
|
0.93
|
|
|
|
|
|
|
FVOD
|
70.58
|
25
|
5-116
|
0.97
|
|
|
|
|
|
|
SYM
|
63.58
|
14.68
|
36-92
|
0.81
|
|
|
|
|
|
|
OAT
|
60.23
|
12.25
|
35-85
|
0.74
|
|
|
|
|
|
|
SAT
|
58.35
|
14.78
|
24-99
|
0.52
|
|
|
|
|
|
|
DEF
|
45.33
|
10.81
|
24-73
|
0.53
|
|
|
|
|
|
|
SAM
|
62.76
|
12.09
|
30-94
|
0.63
|
|
|
|
|
|
|
FAM
|
44.1
|
12.18
|
4-76
|
0.24
|
|
|
|
|
|
|
COR
|
61.21
|
13.74
|
36-88
|
0.63
|
Note. FVA = Face Valid Alcohol scale; FVOD = Face Valid Other Drugs scale; SYM = Symptoms scale; OAT = Obvious Attributes scale; SAT = Subtle Attributes scale; DEF = Defensiveness scale; SAM = Supplemental Addiction Measure scale; FAM = Family versus Control Subjects scale; COR = Correctional scale.
Table 1 represents each SASSI-3 scale’s mean, standard deviation, range of scores and Cronbach’s alpha. These internal consistency reliability estimates were comparable with previously reported alphas (Burck, Laux, Harper, & Ritchie, 2010; Burck et al., 2008). The counselor’s interviews indicated that 188 (78.0%) of the participants met SUD criteria as specified in the DSM-5. Of these 188, 25 (13.3%) had a mild SUD, 13 (6.9%) were moderate, and 127 (67.6%) had a severe SUD. Of the 188 participants diagnosed with an SUD, 85 participants (45.2%) had an alcohol use disorder. Of these 85, 33 (38.8%) had a mild alcohol SUD, 13 (15.3%) were moderate, and 39 (45.9%) were severe. One hundred thirty-three participants (55.2%) were positive for an SUD other than alcohol. Of these 133, 10 (7.5%) had a mild disorder, 8 (6.0%) were moderate, and 115 (86.5%) were severe.
Cohen’s kappa (κ) statistic was calculated to determine the agreement between the DSM-5 diagnosis (i.e., met criteria or not) and the SASSI-3 overall score and each of the SASSI-3’s decision rules. Table 2 presents the results of these analyses as well as the number of SASSI-3 true positive, true negative, false positive and false negative classifications. The overall SASSI-3’s agreement with the counselors’ diagnostic decisions was fair (κ = .423, p = .060). The SASSI-3 results concurred with counselors’ diagnostic interviews on 182 cases and disagreed on 59 cases. The SASSI-3’s sensitivity (true positives) and specificity (true negatives) rates were .75 and .77, respectively.
Table 2
Agreement Between Counselors’ Diagnoses and SASSI-3 Individual and Total Decision Rules
|
Rule
|
True Positive
|
True Negative
|
False Positive
|
False Negative
|
Kappa
|
|
|
|
|
|
|
|
11
|
31 (12.9%)
|
151 (62.7%)
|
5 (2.1%)
|
54 (22.4%)
|
0.383***
|
|
|
|
|
|
|
|
22
|
105 (43.6%)
|
105 (43.6%)
|
3 (1.2%)
|
28 (11.6%)
|
0.745*****
|
|
|
|
|
|
|
|
3
|
91 (37.8%)
|
47 (19.5%)
|
6 (2.5%)
|
97 (40.2%)
|
0.229***
|
|
|
|
|
|
|
|
4
|
32 (13.3%)
|
53 (22.0%)
|
0 (0%)
|
156 (64.7%)
|
0.083**
|
|
|
|
|
|
|
|
5
|
38 (15.8%)
|
53 (22.0%)
|
0 (0%)
|
150 (62.2%)
|
0.100**
|
|
|
|
|
|
|
|
6
|
62 (25.7%)
|
50 (20.7%)
|
3 (1.2%)
|
126 (52.3%)
|
0.149**
|
|
|
|
|
|
|
|
7
|
107 (44.4%)
|
48 (19.9%)
|
5 (2.1%)
|
81 (34.0%)
|
0.313***
|
|
|
|
|
|
|
|
8
|
4 (1.7%)
|
52 (21.6%)
|
1 (0.4%)
|
184 (76.3%)
|
0.001*
|
|
|
|
|
|
|
|
9
|
59 (24.5%)
|
46 (19.1%)
|
7 (2.9%)
|
129 (53.5%)
|
0.100**
|
|
|
|
|
|
|
|
SASSI-3
|
141 (58.5%)
|
41 (17.0%)
|
12 (5.0%)
|
47 (19.5%)
|
0.423****
|
Note. 1 = Rule 1 kappa tested against positive for alcohol use disorder only. 2 = Rule 2 kappa tested against all substance use disorders but alcohol use. All other kappa values are calculated for each Decision Rule’s agreement a clinical diagnosis of any substance use disorder. * = less than chance agreement, ** = slight agreement, *** = fair agreement, **** = moderate agreement and ***** = substantial agreement (Landis & Koch, 1977).
A closer examination of the kappa data indicates that the SASSI-3 and its subscales’ areas of weakness were the false negative rates. That is, the SASSI-3 failed to identify persons as likely substance dependent that the counselors judged as substance dependent (i.e., met criteria or not). Based on the kappa data, the SASSI-3 overall score incorrectly categorized 47 (19.5%) of the sample as not in need of further SUD assessment. This suggests that the decision rules’ cut scores may be too high for this sample. To test this hypothesis, the researchers investigated the SASSI-3’s FVA, FVOD, SYM, OAT and SAT scales’ specificity and sensitivity using ROC analyses (Youngstrom, 2014).
The ROC analysis of the FVA scale produced an AUROC value of .861, p = .000, standard error = .026, with a 95% confidence interval range of .811 to .912. This indicates that there is a good agreement between the FVA scale and the counselors’ alcohol use disorder diagnoses (Youngstrom, 2014). A review of the coordinates of the curve (Figure 1) demonstrates that an adjusted FVA t score cut-off of 53.5 would provide the optimal balance between sensitivity (.79) and specificity (.80). A t score of 53.5 translates into an FVA raw score of approximately 6 for both sexes. Rule 1 was recalculated using a raw score of 6 for both sexes and a kappa statistic was calculated to determine the agreement rate between this new FVA cut score and the counselors’ alcohol use disorder diagnoses. The new kappa statistic was .551, p = .000. The new Rule 1 sensitivity and specificity rates were, respectively, .81 and .77. Rule 1’s false positive rate was .19 and the false negative rate was .23. Lowering the Rule 1 cut score to 6 improved the kappa statistic by .168.
Figure 1.
ROC Curve for FVA t Score Plotted Against Counselor Alcohol Use Disorder Diagnosis
Note. Diagonal segments are produced by ties.
The ROC analysis of the FVOD scale produced an AUROC value of .965, p = .000, standard error = .013, with a 95% confidence interval range of .940 to .990. This indicates that there is an excellent agreement between the FVOD scale and the counselors’ SUD other than alcohol dependence diagnoses (Youngstrom, 2014). A review of the coordinates of the curve (Figure 2) argued against making any adjustments to the current FVOD score cut-offs for Rule 2.
Figure 2.
ROC Curve for FVOD t Score Plotted Against Counselor SUD Diagnosis
Note. Diagonal segments are produced by ties.
The ROC analysis of the SYM scale produced an AUROC value of .803, p = .000, standard error = .035, with a 95% confidence interval range of .735 to .871. This indicates that there is a good agreement between the SYM scale and the counselors’ SUD diagnoses (Youngstrom, 2014). A review of the coordinates of the curve (Figure 3) demonstrates that an adjusted SYM t score cut-off of 56.5 would provide the optimal balance between sensitivity (.761) and specificity (.774). A t score of 56.5 translates into an SYM raw score of approximately 5 for males and 4 for females. Rule 3 was recalculated using these new raw scores and a kappa statistic was calculated to determine the agreement rate between this new SYM cut score and the counselors’ overall SUD diagnoses. The kappa statistic was .437, p = .000. The new Rule 3 sensitivity and specificity rates were, respectively, .76 and .77. Rule 3’s false positive rate was .23 and the false negative rate was .24. Lowering the Rule 3 cut score to 6 improved the kappa statistic by .208.
Figure 3.
ROC Curve for SYM, OAT and SAT t Scores Plotted Against Counselor SUD Diagnosis
Note. Diagonal segments are produced by ties.
The ROC analysis of the OAT scale produced an AUROC value of .717, p = .000, standard error = .038, with a 95% confidence interval range of .643 to .791 (Figure 3). This indicates that there is fair agreement between the OAT scale and the counselors’ SUD diagnoses (Youngstrom, 2014). It was not possible to adjust the OAT t score to produce an optimal cut-off score such that a balance between sensitivity and specificity could be obtained. For example, to attain a sensitivity rating of .82, the
t score cut-off would have to be lowered to 48.5, which would produce a specificity rating of .634.
The ROC analysis of the SAT scale produced an AUROC value of .654, p = .001, standard error = .037, with a 95% confidence interval range of .582 to .727 (Figure 3). This indicates that there is poor agreement between the SAT scale and the counselors’ SUD diagnoses (Youngstrom, 2014). As with the OAT scale, no cut-off score could be determined that would provide an optimal balance between sensitivity and specificity.
The SASSI-3’s overall decision was recalculated using the lowered Rule 1 and Rule 3 cut scores. This process resulted in a total of 188 persons being classified as likely dependent on the SASSI-3, or a change in the total number of classifications by 28. A follow-up analysis comparing the SASSI-3 final decision using the adjusted scores for Rules 1 and 3 and the original cut scores for Rules 2 and 4–9 with the counselors’ decisions produced a kappa of .457 (p = .000). This kappa is slightly higher than the kappa produced using unadjusted Rule 1 and 3 cut-offs (κ = .423). The adjusted process identified 161 of the 181 (sensitivity = .89) participants whom the counselors classified as having an SUD. However, this increased sensitivity came at the cost of decreased specificity. The adjusted process identified only 33 (specificity = .55) of those participants whom the counselors determined did not have an SUD. The false positive rate and the false negative rate for this adjusted process were, respectively .45 and .11. In sum, this process increased the number of true positives by 20, decreased the number of true negatives by 8, increased the number of false positives by 8, and decreased the number of false negatives by 20. As one might expect, lowering the cut scores on these two rules increased the instrument’s ability to detect the presence of problems, but did so at the cost of possibly overdiagnosing 8 (3%) additional participants while reducing the false negative classifications by 20 (8.3%).
Discussion
The DSM-5 section on SUDs includes significant changes. Chief among these changes is the movement away from an abuse/dependence dichotomy to an SUD continuum that includes all of the criteria previously unique to abuse and dependence disorders as well as the addition of a craving criterion. The present study examined the SASSI-3’s utility in predicting counselors’ diagnostic classifications using the new DSM-5 SUD criteria. The results provided a mixed picture. The SASSI-3’s agreement with the counselors’ diagnoses was moderate. This finding prompted us to conduct a similar series of kappa analyses for each of the SASSI-3’s decision rules and ROC analyses for the first five SASSI-3 decision rules. The last four decision rules could not be analyzed with the ROC as they are each composed of more than one scale of the SASSI-3. The decision rules’ agreement with the counselors’ diagnoses varied considerably. The kappa values presented in Table 1 are below what would be expected based on previously published agreement statistics using previous versions of the DSM (Miller & Lazowski, 1999). The SASSI-3 and its decision rules’ false negative values suggested that the instrument’s modest agreement with the counselors may have been a consequence of unnecessarily high raw score cut-off points. Consistent with Clements’ (2002) findings related to adjusting cut scores, the ROC score analyses presented mixed results. The ROC analyses provided evidence that lowered FVA and SYM cut scores improved these scales’ respective sensitivity and specificity estimates. The FVOD scale’s current cut score produced high sensitivity and specificity and did not need to be improved. The OAT and SAT cut scores could not be adjusted without unwanted compromises to either scale’s associated decision rules’ sensitivity and specificity. The SASSI-3’s overall decision was recalculated using the lowered Rule 1 and Rule 3 cut scores. This process resulted in an improvement in sensitivity with a slight decrease in specificity. The net result was an improvement in the SASSI-3’s overall agreement with licensed counselors’ SUD determinations. Our FVOD scale’s sensitivity and specificity findings are consistent with those of First et al. (1997) and Lazowski et al. (1998), and suggest that the FVOD scale is useful in predicting DSM-IV-TR and DSM-5 non-alcohol SUDs. Our FVA scale findings are consistent with those of First et al. (1997) but differ from those of Lazowski et al. (1998). There are no other SASSI-3 ROC analyses available for comparison.
These results elicit deliberation about whether SUD counselors would be better served by an SUD screening instrument that over- or under-predicts SUD diagnoses. In the case of a scoring method that produces higher sensitivity but lower specificity, resource allocation might be a concern. A counselor’s diagnostic time might be unnecessarily spent ruling out clients, and clients might be unnecessarily inconvenienced by participating in a full SUD assessment. Alternatively, counselors using a scoring method with lower sensitivity but higher specificity would have fewer clients unnecessarily inconvenienced and spend less time assessing persons who do not need SUD treatment. The unfortunate trade-off is that persons with an SUD who might benefit from assessment and treatment would otherwise be sent home without an appropriate recommendation.
The health, social, psychological and legal implications of misdiagnosing clients with SUDs have been documented (Brown, Suppes, Adinoff, & Thomas, 2001; Horrigan, Piazza, & Weinstein, 1996; McMillan et al., 2008). Therefore, SUD counselors would benefit from a screening instrument with high sensitivity and specificity (Tiet, Finney, & Moos, 2008). When that goal cannot be achieved, SUD counselors and agencies may want to consider which of these two is more important.
Counselors and their agencies might consider their patient population and setting. Among populations likely to have an SUD, specificity might be less important than sensitivity. Conversely, a counselor working at a community mental health agency or college counseling center may benefit from a highly sensitive instrument to identify clients with dual diagnosis treatment needs. In sum, this study represents the first investigation of the SASSI-3’s agreement with the new DSM-5 SUD criteria. Past research (e.g., Laux et al., 2012) has demonstrated that the SASSI-3’s subtle scales improve the instrument’s diagnostic accuracy over that which is obtained using face valid approaches only. As such, we are cautious about drawing strong conclusions about the SASSI-3’s agreement with the DSM-5 criteria until a larger sample of research is available.
Limitations and Suggestions for Future Research
ROC curve analysis allows for the examination of one scale at a time. Consequently, we were unable to use these methods to examine the SASSI-3 decision rules that use more than one scale (Rules 6, 7, 8 and 9). These decision rules include data from the instrument’s subtle and obvious questions and are important contributors to the overall instrument’s sensitivity and specificity. Thus, the inability to examine these decision rules excludes results that may impact the SASSI-3 sensitivity and specificity.
This study collected data from three different locations: a university campus, an inpatient SUD treatment center and an outpatient mental health counseling center. The participants from the college sample were significantly younger, by 9 and 11 years respectively, than those from the other collection sites. Because SUDs are progressive in nature, we recommend that subsequent researchers conduct sample-specific SASSI-3 analyses to determine whether or not population-specific, rather than universal, cut-offs would be useful. Additionally, because there were very few persons in this sample whose use of drugs other than alcohol was categorized as mild, it is not clear whether the FVOD’s lower kappa value was due to the instrument itself or the sample’s homogeneity.
Finally, the DSM-5’s SUD diagnosis is on a continuum and includes severity specifiers (mild, moderate or severe). It may be more diagnostically useful to expand the SASSI-3 to address these specifiers, rather than rely solely on the current dichotomous likely/not likely dependent conclusion. Future researchers are encouraged to determine what decision rule cut scores would be associated with each of the three levels of SUD severity.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 American Counseling Association Code of Ethics. Alexandria, VA: Author.
American Psychiatric Association. (1987). Diagnostic and statistical manual of mental disorders (3rd ed., revised). Washington, DC: Author.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Ashman, T. A., Schwartz, M. E., Cantor, J. B., Hibbard, M. R., & Gordon, W. A. (2004). Screening for substance abuse in individuals with traumatic brain injury. Brain Injury, 18, 191–202. doi:10.1080/0269905031000149506
Brown, E. S., Suppes, T., Adinoff, B., & Thomas, N. R. (2001). Drug abuse and bipolar disorder: Comorbidity or misdiagnosis? Journal of Affective Disorders, 65, 105–115. doi:10.1016/S0165-0327(00)00169-5
Burck, A. M., Laux, J. M., Harper, H. L., & Ritchie, M. (2010). Detecting faking good and faking bad with the Substance Abuse Subtle Screening Inventory—3 in a college student sample. Journal of College Counseling, 12, 63–72. doi:10.1002/j.2161-1882.2010.tb00048.x
Burck, A. M., Laux, J. M., Ritchie, M., & Baker, D. (2008). An examination of the Substance Abuse Subtle Screening Inventory-3 Correctional scale in a college student population. Journal of Addictions & Offender Counseling, 29, 49–61. doi:10.1002/j.2161-1874.2008.tb00043.x
Calmes, S. M., Laux, J. M., Scott, H., Reynolds, J. L., Roseman, C. P., & Piazza, N. J. (2013). Childhood psychological trauma and its role in first-year college students’ substance dependence. Journal of Addiction and Offender Counseling, 34, 70–80. doi:10.1002/j.2161-1874.2013.00016.x
Clements, R. (2002). Psychometric properties of the Substance Abuse Subtle Screening Inventory-3. Journal of Substance Abuse Treatment, 23, 419–423. doi:10.1016/S0740-5472(02)00279-9
Dailey, S. F., Gill, C. S., Karl, S. L., & Barrio Minton, C. A. (2014). Historical underpinnings, structural alterations, and philosophical changes: Counseling practice implications of the DSM-5. The Professional Counselor, 4, 166–178. doi:10.15241/sfd.4.3.166
Ewing, J. A. (1984). Detecting alcoholism: The CAGE Questionnaire. Journal of the American Medical Association, 252, 1905–1907. doi:10.1001/jama.1984.03350140051025
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W. (1996) Structured Clinical Interview for DSM-IV Axis I Disorders, Clinician Version (SCID-CV). Washington, DC: American Psychiatric Press, Inc.
Hill, T., Stone. G., & Laux, J. M. (2013). A psychometric review of the Substance Abuse Subtle Screening Inventory-3: Using Rasch analysis. Journal of Addictions and Offender Counseling, 34, 40–50.
doi:10.1002/j.2161-1874.2013.00013.x
Horrigan, T. J., Piazza, N. J., & Weinstein, L. (1996). The Substance Abuse Subtle Screening Inventory is more cost effective and has better selectivity than urine toxicology for the detection of substance abuse in pregnancy. Journal of Perinatology, 16, 326–330.
Juhnke, G. A., Vacc, N. A., Curtis, R. C., Coll, K. M., & Paredes, D. M (2003). Assessment instruments used by addictions counselors. Journal of Addictions & Offender Counseling, 23, 66–72.
doi:10.1002/j.2161-1874.2003.tb00171.x
Landis, J. R., & Koch, G. G. (1977). The measurement of observer agreement for categorical data.
Biometrics, 33, 159–174.
Laux, J. M., Perera-Diltz, D., Smirnoff, J. B., & Salyers, K. M. (2005). The SASSI-3 Face Valid Other Drugs scale: A psychometric investigation. Journal of Addictions & Offender Counseling, 26, 15–21.
doi:10.1002/j.2161-1874.2005.tb00003.x
Laux, J. M., Piazza, N. J., Salyers, K. M., & Roseman, C. P. (2012). The Substance Abuse Subtle Screening Inventory-3 and stages of change: A screening validity study. Journal of Addictions & Offender Counseling, 33, 82–92. doi:10.1002/j.2161-1874.2012.00006.x
Laux, J. M., Salyers, K. M., & Bandfield, A. (2007). Defensiveness in female college students and its impact on their MAST and CAGE scores. Journal of Addictions and Offender Counseling, 28, 21–30. doi:10.1002/j.2161-1874.2007.tb00029.x
Laux, J. M., Salyers, K. M., & Kotova, E. (2005). A psychometric evaluation of the SASSI-3 in a college sample. Journal of College Counseling, 8, 41–51. doi:10.1002/j.2161-1882.2005.tb00071.x
Lazowski, L. E., Miller, F. G., Boye, M. W., & Miller, G. A. (1998). Efficacy of the Substance Abuse Subtle Screening Inventory-3 (SASSI-3) in identifying substance dependence disorders in clinical settings. Journal of Personality Assessment, 71, 114–128.
MacAndrew, C. (1965). The differentiation of male alcoholic outpatients from nonalcoholic psychiatric outpatients by means of the MMPI. Quarterly Journal of the Study of Alcohol, 26, 238–246.
McMillan, G. P., Timken, D. S., Lapidus, J., C’de Baca, J., Lapham, S. C., & McNeal, M. (2008). Underdiagnosis of comorbid mental illness in repeat DUI offenders mandated to treatment. Journal of Substance Abuse Treatment, 34, 320–325. doi:10.1016/j.jsat.2007.04.012
Miller, F. G., & Lazowski, L. E. (1999). The Substance Abuse Subtle Screening Inventory-3 (SASSI-3) manual. Springville, IN: The SASSI Institute.
Selzer, M. L. (1971). The Michigan Alcoholism Screening Test (MAST): The quest for a new diagnostic instrument. American Journal of Psychiatry, 127, 1653–1658.
Tiet, Q. Q., Finney, J. W., & Moos, R. H. (2008). Screening psychiatric patients for illicit drug use disorders and problems. Clinical Psychology Review, 28, 578–591. doi:10.1016/j.cpr.2007.08.002
Wright, E. E., II, Piazza, N. J., & Laux, J. M. (2008). The utility of the SASSI-3 in early detection of substance use disorders in not guilty by reason of insanity acquittees: An exploratory study. Journal of Addictions & Offender Counseling, 28, 119–127. doi:10.1002/j.2161-1874.2008.tb00037.x
Youngstrom, E. A. (2014). A primer on receiver operating characteristic analysis and diagnostic efficiency
statistics for pediatric psychology: We are ready to ROC. Journal of Pediatric Psychology, 39, 204–221. doi:10.1093/jpepsy/jst062
John M. Laux is a Professor at The University of Toledo. Robin M. DuFresne is a practicing clinical counselor at the Zepf Center in Toledo, Ohio. Allison K. Arnekrans is an Assistant Professor at Central Michigan University. Sylvia Lindinger-Sternart is an Assistant Professor at the University of Great Falls. Christopher P. Roseman is an Associate Professor at The University of Toledo. Amy Wertenberger is a doctoral candidate at The University of Toledo. Stephanie Calmes is a professional counselor at Harbor Behavioral Health in Toledo, Ohio. Darren W. Love is the Treatment Program Manager at Court Diagnostic and Treatment Center in Toledo, Ohio. Andrew M. Burck is an Assistant Professor at Marshall University. Jim Schultz is a mental health counselor at Harbor Behavioral Health in Toledo, Ohio. Correspondence may be addressed to John M. Laux, MS 119, 2801 W. Bancroft St., Toledo, Ohio, 43606, John.Laux@utoledo.edu.
Jul 20, 2016 | Article, Volume 6 - Issue 2
Kathleen Brown-Rice, Susan Furr
It has been found that 10% of counselors-in-training are ill-suited for the profession (Gaubatz & Vera, 2002). In that, they have problems of professional competence (PPC) that impede their ability to function as professional counselors (Elman & Forrest, 2007). These PPC include skill competencies, ethical behaviors and appropriate personal functioning (Kaslow et al., 2007). To evaluate students in terms of professional competence and prevent those with inadequate skills and dispositions from entering the profession, gatekeeping is utilized. Counselor educators are required to be transparent in their gatekeeping procedures with students. Students are to be informed of “the levels of competency expected, appraisal methods, and timing of evaluations for both didactic and clinical competencies” and be provided “ongoing feedback” (American Counseling Association [ACA], 2014, p. 15). There has been significant research to provide counselor educators with information to establish gatekeeping and remediation procedures (Gaubatz & Vera, 2002; Homrich, DeLorenzi, Bloom, & Godbee, 2014; Hutchens, Block, & Young, 2013; Kerl, Garcia, McCullough, & Maxwell, 2002; McAdams, Foster, & Ward, 2007; Pease-Carter & Barrio Minton, 2012; Vacha-Haase, Davenport, & Kerewsky, 2004; Zoimek-Daigle & Christensen, 2010). However, little research has been done to examine the impact on counselor educators when interacting with students who have PPC and the roadblocks that impede educators’ ability to gatekeep.
Gatekeeping Procedures
Gatekeeping is a mechanism for counselor educators to determine the fitness of students to enter the counseling profession (Vacha-Haase et al., 2004). Gatekeeping begins as part of the admission process of a counseling program (Kerl & Eichler, 2007). During the admission process, counselor educators do not allow entry to prospective students who show traits, qualities or behaviors that would result in them not being able to meet professional competencies or who lack the prescribed academic requirements (Lumadue & Duffey, 1999; Swank & Smith-Adcock, 2013). However, gatekeeping is not just part of the admission process. Ziomek-Daigle and Christensen (2010) found that gatekeeping is a progressive activity that includes four phases, including preadmission screening, postadmission screening, remediation plan and remediation outcome.
Informing Students of Program Expectations
The American Counseling Association Code of Ethics (2014) provides that counseling students be aware of what type and degree of skill and knowledge will be required of them to be successful in the program, specific training goals and objectives, what students’ evaluations are based on, and the policies and procedures for students’ evaluations. One of the most important methods of ensuring understanding of expectations is informing students of the program’s expectations at the beginning of the program. Once clearly defined behaviors are established, sharing these expectations with students can result in fewer problematic situations (Kerl et al., 2002; McAdams et al., 2007). Furthermore, not providing students with clear expectations for conduct may be viewed as unfair to those wanting to become counselors (Homrich et al., 2014).
It is recommended that professional standards be made clear to students and applied consistently (Hutchens et al., 2013). Using multiple methods of distributing information is desired by students who have stated they want information shared both orally and in written form, and want the information presented throughout the program (Pease-Carter & Barrio Minton, 2012). Pease-Carter and Barrio Minton (2012) found that students desired information not only about academic expectations but also wanted to know about self-disclosure, reflection, personal growth and student rights.
Assessing Students’ PPC Behaviors
Individual programs have developed standards for evaluating students on professional competencies and use these evaluations to provide formative feedback (Kerl et al., 2002). Historically, the most commonly cited problematic behaviors have been inadequate clinical skills, defensiveness in supervision and deficient interpersonal skills (Vacha-Haase et al., 2004). Efforts to identify criteria for evaluating students in terms of professional behaviors, interpersonal behaviors and intrapersonal behaviors have recently been undertaken (Homrich et al., 2014), and these criteria provide a platform for developing clear expectations for counseling trainees.
Roadblocks to Gatekeeping
There are a variety of reasons that counselor educators do not engage in the gatekeeping process. Gateslipping rates have been reported as higher in programs where faculty members reported that their colleagues were concerned about being sued or receiving less than favorable teaching evaluations (Gaubatz & Vera, 2002; Jacobs et al., 2011). In some settings, colleagues and administration provide support for engaging in gatekeeping; however, lack of clear evidence and bias toward leniency lead to gateslippage (Brear & Dorrian, 2010). Absence of well-defined program policies may make it difficult to initiate gatekeeping conversations with a student as well (Jacobs et al., 2011).
Gatekeeping demands a great amount of time and energy, and situations involving PPC often seem unending (Gizara & Forrest, 2004). Not only do PPC have to be identified and communicated to the student, remediation plans need to be developed. Such plans may include helping the counselor-in-training obtain remedial assistance, providing intensified supervision, documenting the activities of the plan and ensuring the student understands due process options (Ziomek-Daigle & Christensen, 2010). When remediation plans are not successful, decisions about dismissal must be made, and the actions taken must be transparent (Kaslow et al., 2007).
There may be occasions where the gatekeeping responsibility is diffused among different entities. In a review of ethical issues around professional competence problems (Johnson et al., 2008), Johnson labeled this issue as the “hot potato game” (p. 589), where the last entity engaged with the problematic student is stuck with the issue. If a student is allowed to gateslip through the graduate program, then the training facility and licensing board now become involved. Rather than address the issue when it is first recognized, the student may be allowed to move to the next stage of training with the hope that the problem disappears or that that it is addressed at the next level. Addressing issues early in the training may help avoid more serious issues, like the empathy veil, later when students go to clinical sites.
The Empathy Veil
This term was coined by Brown-Rice and Furr (2014) and refers to the counselor educator’s need to empathize with the counselor-in-training, which can result in reluctance to engage in gatekeeping activities. Role tension may be one factor in developing an empathy veil. This term evolved from work by Sue and Sue (2012) where a person’s worldview is seen as having an invisible veil that is created by cultural conditioning and is believed to operate outside of consciousness. Forrest et al. (2013) found that empathy may contribute to avoiding confronting student issues for fear of damaging the relationship. Because of the role that faculty play in fostering growth and development, which often involves compassion and support, it may become difficult to provide accurate summative evaluations of trainees’ behaviors (Johnson et al., 2008). Given that many faculty members also are professional counselors, they may view their role as assisting the student in behavior change and thus work with the student to address interpersonal issues that interfere with developing counseling skills (Kerl et al., 2002). This empathy can be both a support and a challenge when difficult conversations about problematic professional, interpersonal and intrapersonal behaviors need to take place (Jacobs et al., 2011). Although empathy can create a safe environment in which to discuss difficulties, an educator’s empathy also can lead to overprotective behaviors that may actually interfere with the student’s development (Gizara & Forrest, 2004).
Role of Diversity
Another important area of consideration is how cultural differences intersect with PPC. When there is a cross-cultural student PPC situation, a complex power differential arises that not only is associated with the faculty–student relationship, but also related to cultural differences (Goodrich & Shin, 2013). Kaslow et al. (2007) proposed that consideration should be given to the impact of beliefs, values and attitudes when assessing competence problems. Fear of appearing biased may complicate identifying trainees with PPC and how decisions are made regarding students (Shen-Miller, Forrest, & Elman, 2009). The counselor educator’s own cultural background may influence how counselors-in-training are evaluated, and it is recommended that cultural dynamics be assessed when addressing PPC (Rust, Raskin, & Hill, 2013). Shen-Miller, Forrest, and Burt (2012) identified two approaches that often are used by faculty in assessing students—culture-attentive (i.e., approaches that include attention to aspects of diversity) or colorblind (i.e., inattention or minimization of differences associated with diversity). These views represent two ends of a “continuum of conceptualizing intersections between diversity and professional standards” (Shen-Miller et al., 2012, p. 1207). In trying to find a place on this continuum to address PPC, do counselor educators underidentify PPC because of fear of being biased? Or, are counselor educators more prone to overidentify PPC because of not examining contextual factors that influence competence? In this study, an attempt is made to examine counselor educators’ views of what interferes with their ability to address issues of counselor education student PPC.
Other Barriers
Previous research has found that educators believe that they have not been provided with sufficient training related to gatekeeping and remediation procedures, and they do not feel supported by their agency and colleagues (Gizara & Forrest, 2004; Vacha-Haase et al., 2004). Additionally, counselor educators may be reluctant to dismiss a student for dread of potential litigation and personal recrimination (Crawford & Gilroy, 2012; Hutchens et al., 2013) and receiving poor teaching evaluations (Gaubatz & Vera, 2002). Recent court cases have increased awareness about the legal consequences of gatekeeping. The Ward and Keeton cases have highlighted the need for counseling programs to establish clear statements about student expectations (Herlihy, Hermann, & Greden, 2014). Other cases have taught faculty members the importance of providing regular process evaluations and thorough documentation (McAdams & Foster, 2007). Reflection on the results of facing a court challenge includes the significance of having a measure of performance that helps faculty retain objectivity and the importance of adhering to established procedures (McAdams et al., 2007).
The purpose of this study was to answer the following research questions: (a) What types of master’s students’ PPC do Council for Accreditation of Counseling and Related Educational Programs (CACREP) counselor educators perceive have the greatest impact on them as educators? (b) What do CACREP counselor educators perceive are roadblocks that interfere with their ability to engage in the gatekeeping of master’s students with PPC? and (c) What is CACREP counselor educators’ knowledge of their programs’ protocol for addressing a student with PPC? In this study, student refers to a master’s student enrolled in the participant’s counseling program, colleague is another counselor educator teaching in the participant’s counseling program, and impact means to have a strong effect. PPC refers to attitudes and behaviors that could interfere with the professional competence of a counselor-in-training, including: (a) a lack of ability or opposition to acquire and integrate professional standards into one’s professional counseling behavior; (b) a lack of ability to attain professional skills and reach an acceptable level of competency; (c) a lack of ability to manage one’s stress, psychological dysfunction or emotional responses that may impact professional performance; or (d) engagement in unethical behavior (Falender, Collins, & Shafranske, 2009).
Methods
Participants and Procedures
Prior to initiating the study, institutional review board approval was obtained. Recruitment of participants was conducted by an e-mail to all faculty employed at CACREP-accredited programs in the United States. The researchers of this study obtained a list of accredited programs from the official CACREP Web site and then visited each program’s Web site to obtain the e-mail addresses of the program’s counselor educators. Seven programs did not list faculty e-mails on their university Web sites. The exact number of educators teaching in CACREP-accredited programs is not known, as the programs’ Web sites might have imprecise or out-of-date information. Based upon the e-mail addresses gathered from the university Web sites, a list of 1,584 faculty members was created. Thereafter, one e-mail solicitation was sent to all identified faculty that directed participants to an online survey entitled, Problems of Professional Competency Survey – Counselor Educator Version (PPCS-CE), which was located on Psychdata.com. Of the 1,584 e-mails that were sent, 71 were undeliverable due to lacking a valid address or security issues, 15 were returned with automatic responses that the faculty member was absent (e.g., on sabbatical, no longer at university, ill, professor emeritus), and five responses indicated that the receiver of the e-mail was not a counselor educator. This left a total sample size of 1,493 CACREP counselor educators. For a population of 1,500, a sample size of 306 is adequate to generalize with a confidence interval of 95% (Gay, Mills, & Airasian, 2009). A total of 382 participants completed the survey; however, respondents with missing or invalid data (n = 12, less than 4%) were eliminated via listwise deletion, leaving a total number of 370 participants included in this study. This resulted in an adequate sample size of 370 participants and a final response rate of 25%. Frequencies and percentages of the demographic variables in this study are reported in Table 1.
| Table 1 Numbers and Percentages of Demographic Variables |
| Variable |
Number |
Percentage |
| Gender: |
|
|
| Female |
213
|
58
|
| Male |
157
|
42
|
| Background: |
|
|
| Caucasian |
310
|
84
|
| African American |
24
|
6
|
| Hispanic/Latino |
12
|
3
|
| Multi-Racial |
15
|
4
|
| Asian/Pacific Islander |
8
|
2
|
| Native American |
1
|
1
|
| Age: |
|
|
| 20 years to 29 years |
7
|
2
|
| 30 years to 39 years |
77
|
21
|
| 40 years to 49 years |
97
|
26
|
| 50 years to 59 years |
76
|
21
|
| 60 years or older |
113
|
31
|
| Sexual Orientation: |
|
|
| Heterosexual |
331
|
90
|
| Bisexual |
9
|
2
|
| Gay or Lesbian |
30
|
8
|
|
|
|
| Description of Program: |
|
|
| Predominantly on Campus |
318
|
86
|
| Predominantly Online |
7
|
2
|
| Hybrid of Online/on Campus |
45
|
12
|
|
|
|
| Location of Program: |
|
|
| South |
146
|
40
|
| Northeast |
93
|
25
|
| Midwest |
74
|
20
|
| West |
57
|
15
|
| Highest Degree: |
|
|
| PhD – CACREP Program |
201
|
54
|
| PhD – Non-CACREP Program |
38
|
10
|
| EdS in Counseling |
10
|
3
|
| PhD – Counseling Psychology |
31
|
8
|
| PhD – Clinical Psychology |
4
|
1
|
| Other (doctoral in another discipline ormaster’s in counseling or related field) |
86
|
23
|
| Academic Rank: |
|
|
| Assistant Professor |
145
|
39
|
| Associate Professor |
102
|
28
|
| Professor |
92
|
25
|
| Clinical Instructor |
8
|
2
|
| Adjunct Instructor |
6
|
.2
|
| Other |
17
|
5
|
|
|
|
| Years Teaching in a CACREP-Accredited Program: |
|
|
| Less than 2 years |
59
|
16
|
| 2 to 5 years |
84
|
23
|
| 6 to 10 years |
90
|
24
|
| 11 to 15 years |
66
|
18
|
| 16 to 20 years |
28
|
8
|
| Over 20 years |
43
|
12
|
| Licenses and Certifications Held: |
|
|
| Licensed Professional Counselor |
201
|
55
|
| Licensed Alcohol and Drug Counselor |
21
|
6
|
| Provisionally Licensed Professional Counselor |
14
|
4
|
| Licensed Marriage & Family Counselor |
33
|
9
|
| Licensed Psychologist |
37
|
10
|
| Licensed Social Worker |
7
|
2
|
| Certified School Counselor |
95
|
26
|
| National Certified Counselor |
199
|
54
|
Instrument
The survey for this present study was designed based upon the Problems of Professional Competency Survey – Master Student Version (PPCS-MS) developed by Brown-Rice and Furr (2013), related to determining master’s students’ enrolled in CACREP-accredited programs knowledge of classmates with PPC. The PPCS-MS was constructed based upon the literature regarding PPC in psychology, counseling and social work. To establish content validity and reliability, the PPCS-MS underwent an expert review process and two pilot studies to provide clarity and conciseness of the survey questions. Additionally, a principal components analysis created components representative of what the review of the literature provided on these issues (Brown-Rice & Furr, 2013). The questions and format of the PPCS-MS were used and adjusted to create a self-report survey entitled the Problems of Professional Competency Survey – Counselor Educator Version (PPCS-CE). This instrument was divided into three parts: Part I – Demographic Information, Part II – Counselor Educators and Students with PPC, and Part III – Counselor Educators’ Knowledge of Colleagues’ PPC (removed from this analysis). Part II included three sections. Section I, Counselor Educators’ Knowledge of Students’ Problems of Professional Competency, included one question to determine whether participants have observed students with PPC and two questions to determine participants’ knowledge of the type of students’ PPC and the impact of the problematic behavior. Each PPC was rank ordered from 1 being the most common and 9 being the least common observed behavior, and the impact of having a student with PPC was ranked ordered with 1 having the most impact and 9 having the least impact. Chi square analyses of each of the rank ordered items led to a rejection of the null hypotheses of the categories of the item occurring with equal probabilities.
Section II of Part II of the survey investigated counselor educators’ reactions to students’ PPC and consisted of seven questions. The answers to all these questions were based on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Section III, Counselor Educators’ Knowledge of Counseling Program’s Protocol for Addressing Problems of Professional Competency, included questions relating to responsibility for being aware of students PPC and programs’ protocols for addressing PPC. The first nine questions were evaluated on a 5-point Likert scale. The tenth item was unstructured to provide a place for participants to provide additional information.
Results
Types and Impact of Students’ Problematic Behavior
Of the 370 participants, the majority (91%, n = 338) reported that they had observed students with PPC in their programs. Additionally, 2% (n = 8) of the respondents indicated they did not know if there were students with PPC in their programs, leaving 7% (n = 24) who had not observed any students with PPC. To answer the first research question regarding the types and impact of master’s students’ PPC observed by CACREP counselor educators, the responses for the 338 participants who reported observing a student with PPC were examined according to the rank order question regarding the types of PPC that participants most observed with counselors-in-training in their programs. The most frequently identified problematic behaviors included inadequate clinical skills (M = 2.90, SD = 1.88), inadequate interpersonal skills (M = 3.15, SD = 1.69), inadequate academic skills (M = 3.38, SD = 2.29), inability to regulate emotions (M = 4.16, SD = 1.88), and unprofessional behavior (M = 4.29, SD = 2.13). Those behaviors ranked as less impactful were unprofessional behavior (M = 4.29, SD = 2.13), unethical behavior (M = 5.63, SD = 2.03), psychological concern (M = 6.20, SD = 1.84), personality disorder (M = 7.60, SD = 1.61), and substance use disorder (M = 7.69, SD = 1.68).
The responses for the rank order question regarding the type of impact of having counselors-in-training in their program with PPC focused on the behaviors having the most impact on the faculty member. Included in this list were disrupted the classroom learning environment (M = 2.99, SD = 1.86), negatively affected other students (M = 3.26, SD = 1.52), increased participant’s workload (M = 3.29, SD = 2.05), and increased participant’s stress (M = 3.39, SD = 1.64). Additional items that were ranked as less impactful included negatively affected client care (M = 5.06, SD = 2.44), negatively affected relationship with students (M = 5.47, SD = .87), negatively affected relationship with colleagues (M = 6.59, SD = 1.42), negatively affected reputation of the program (M = 6.81, SD = 1.90), and a grievance or litigation occurred (M = 8.25, SD = 1.94).
Roadblocks to Gatekeeping
All participants (n = 370) completed Section II, Part II of the PPCS-CE, and these participants’ responses for strongly agree and agree were combined to report the subsequent findings. Each of the participants reported degree of agreement or disagreement regarding beliefs around the roadblocks that interfere with their ability to engage in the gatekeeping of master’s students with PPC. Fifty-three percent (n = 197) reporting struggling emotionally to balance being empathetic with a student demonstrating PPC and their gatekeeping duties. When looking at addressing PPC with a student who is culturally different from the participant, 38% (n = 141) stated they were reluctant to do so due to the fear they would appear culturally insensitive, and 36% (n = 137) were reluctant to do so due to the fear of allegations of discrimination. Regarding being supported by others, 13% (n = 47) provided they did not feel supported by their chair to address a student who demonstrated PPC, and 13% (n = 47) stated they did not feel supported by their colleagues to address a student who demonstrated PPC. Further, 92% (n = 339) were concerned about the counseling profession when a student with PPC was allowed to pass through the program. Additionally, 30% (n = 110) provided they were reluctant to address a student demonstrating PPC for fear of recrimination (e.g., negative teaching evaluations, legal action).
Protocol for Addressing Students with PPC
When the participants’ responses for strongly agree and agree were combined, 99% (n = 368) believed it was their responsibility to be aware of students with PPC, 91% (n = 335) believed that it was their chair’s responsibility, and 96% (n = 354) believed it was both their chair and respondents’ responsibility to be aware of students with PPC. Additionally, 94% (n = 347) were aware of their programs’ procedures regarding how to address problematic behavior, 71% (n = 263) reported their chair had discussed their programs’ procedures regarding addressing PPC with them, and 38% (n = 140) stated they had received training from their program regarding how to intervene with a student who they believe is demonstrating PPC. Further, 87% (n = 321) were aware of the appropriate intervention to take with students with PPC, 51% (n = 189) would like more information regarding how to identify students with PPC, and 61% (n = 226) of the participants would like more information on how to respond to a student with PPC.
Discussion and Implications
The PPC identified in this study as being observed most frequently are consistent with those problematic behaviors identified in other studies. Vacha-Haase et al. (2004) also identified that inadequate clinical skills and deficient interpersonal skills were most commonly cited as problematic behaviors. In a study examining a proposed set of standards for clinical training, Homrich et al. (2014) identified three categories of behaviors needed by graduate students in clinical training, which included professional behaviors, interpersonal behaviors and intrapersonal behaviors. The types of PPC counselor educators observed in this study parallel the findings of Homrich et al. (2014) in that inadequate clinical skills and unprofessional behavior are similar to their theme of professional behaviors, and the category of inadequate interpersonal skills is comparable to their theme of interpersonal behaviors. Inability to regulate emotions is analogous to their theme of intrapersonal behaviors. Because they were examining clinical training standards, there was no mention of academic skills, yet this type of PPC was cited as a concern by many of the respondents in this study.
Examination of these data leads to questions about how counseling programs admit students. Both academic skills and interpersonal skills are areas that can be addressed through the admissions process. Smaby, Maddox, Richmond, Lepkowski, and Packman (2005) found that undergraduate GPA and GRE Verbal scores could be predictive of scores on the Counselor Preparation Comprehensive Examination (CPCE), which focus on knowledge, but were not highly predictive of personal development. Given the level of concern over academic skills, using these cognitive measures is important, but expanding the way of assessing academic ability also needs to be sensitive to issues around diversity and bias in standardized measures.
In a survey on admission screening measures, training directors indicated that the personal interview was the most effective screening measure (Leverett-Main, 2004). Using creative group strategies during the admission process has been advocated to help assess academic potential as well as dispositions (Swank & Smith-Adcock, 2013). Smith, Robinson, and Young (2007) found that an assessment of wellness might uncover issues around psychological distress that could affect performance in a counseling graduate education program.
Previous research has indicated that faculty members have concerns about addressing PPC because of their desire to be supportive of students (Johnson et al., 2008; Kerl et al., 2002), which would support the concept of the empathy veil (Brown-Rice & Furr, 2014). In this study, 53% of respondents reported struggling emotionally to balance empathy with their gatekeeping duties to intercede with a counselor-in-training with PPC. When the open-ended responses were reviewed, participants’ responses supported this empathetic struggle. For example, one respondent stated, “I have heard many times how a grade should be considered through compassion for student circumstances rather than demonstrated competency.” Another participant provided, “Our empathy wants to give them another chance, but our ethics don’t necessarily allow for it. It’s a struggle for me. It is not a part of the job that I anticipated. Although I remember learning the concept in my doctoral program, I wasn’t prepared to address it.” Therefore, it would appear that these counselor educators are struggling with empathy veils.
When looking at other roadblocks (e.g., lack of peer and institutional support, diversity in gatekeeping, threat of litigation or recrimination from a counselor-in-training), there were some interesting findings. Previous research has found a lack of support for counselor educators from administration and colleagues in dealing with problematic students (Gizara & Forrest, 2004; Vacha-Haase et al., 2004). This concern has been found to be especially true for field supervisors (Bogo, Regehr, Power, & Regehr, 2007; Homonoff, 2008). However, the results of the current study found that only 13% stated they did not feel supported by their chair or colleagues to address a student who demonstrated PPC. The open-ended responses supported these findings. For example, participants stated, “We have a culture and climate of supporting our gatekeeping role in the counseling profession”; “My colleagues and I work as a team in addressing student concerns”; and “I feel supported by my chair and department when dealing with such issues. We deal with these issues as a department. No one is alone in addressing such issues.” Therefore, for this study, lack of institutional and peer support do not seem to be roadblocks. This could be due to the fact that all the participants in this study worked at programs that were accredited by CACREP. CACREP (2016) requires a procedure for addressing student professional and personal development. Counselor educators at programs that are not CACREP-accredited may report different findings. A limitation of this study is that only faculty from CACREP-accredited programs were contacted. Future research focusing on non-CACREP programs and site supervisors regarding this issue may be beneficial. Those working in the field may not have a deep understanding of the role of gatekeeping and may need to develop clear guidelines for their role as supervisors for both counselors-in-training and for counselors seeking licensure.
When the counselor-in-training was from a different cultural background than the counselor educator, 38% of the respondents expressed concern about appearing culturally insensitive, and 36% were concerned about allegations of discrimination. Because this survey was a self-report measure, there is risk that some participants provided answers they considered to be socially desirable (which is a limitation of the study). The field of counseling is committed to multicultural competence in skills, knowledge and awareness, which could make it difficult for counselor educators to acknowledge problematic behaviors in students who are different from themselves. Research has indicated that White counselors tend to favor the colorblind approach in disposition cases (Neville, Lilly, Duran, Lee, & Browne, 2000). Yet fear of responding in a way that appears insensitive may have contributed to responding in socially desirable ways on this instrument. More exploration is needed in this area. While recent literature has addressed how to be culturally responsive when intervening with counseling students’ problematic behavior (Goodrich & Shin, 2013), there is a lack of research regarding culturally responsive performance standards. Until the counseling profession establishes clear performance expectations that are culturally sensitive, the tension between colorblind and culture-attentive expectations will continue to complicate responding to PPC. For example, class performance often has an evaluation component concerning class participation. If a student is from a culture where students do not contribute unless called upon by the professor, then this student may perform poorly because of not understanding expectations. The professor needs to be sensitive to this type of difference and work with the student to develop ways of being successful.
Few participants reported involvement in a legal action related to gatekeeping and remediation with a student demonstrating PPC; however, 30% stated they were reluctant to address a student for fear of retaliation from the student. Given that counselor educators who have been involved in such cases have disclosed the emotional toll these processes take on a program and its faculty members (Dugger & Francis, 2014; McAdams et al., 2007), it seems understandable that there is concern. Therefore, support from ACA, resources in the form of consultation with other campuses and endorsement of gatekeeping processes from one’s own campus are essential in navigating this demanding process. Although legal actions are not common, developing appropriate gatekeeping procedures will help prevent negative outcomes (Dugger & Francis, 2014).
In addition, Brown-Rice and Furr (2014) provided that counselor educators and supervisors should “maintain appropriate ethical boundaries and avoid dual relationships with counselors-in-training, inform and educate themselves regarding the proper gatekeeping protocols and limit their own hypocrisy regarding acting in a competent and ethical manner” (p. 5). There has been substantial research and discussion regarding ethical boundaries, dual relationships and establishing proper gatekeeping procedures (Brown, 2013; Kolbert, Morgan, & Brendel, 2002; Morrissette & Gadbois, 2006; Ziomek-Daigle & Christensen, 2010). However, there seems to be a lack of attention to the competence of counselor educators and how counselors-in-training perceive educators’ professional and personal competence. Do students see faculty members engaging in the same attitudes, skills, behaviors and self-awareness that they are required to adhere to? Are counselor educators modeling the behaviors they want to see in their students or do they hold students to different standards?
Almost all the participants (94%) provided they were aware of their programs’ procedures regarding how to address problematic behavior, and 87% were aware of the appropriate intervention to take with students with PPC. However, only 38% stated they had received training from their program regarding how to intervene with a problematic student. In the open-ended responses, participants stated that their programs had established procedures and all faculty members were aware of them; however, they also reported that PPC were minimized or not addressed. For example, one participant provided, “while there is often a policy in place . . . I find that colleagues fail to follow that policy in practice.” Another respondent stated, “It is also up to the adviser to address the issue with the student and create a plan of improvement. Not all faculty do this and this leads to students receiving different treatment.” Additionally, a participant shared that colleagues were resistant to “address inappropriate student attitudes, dispositions, personality characteristics, and behaviors unless they reach such a critical threshold that they pose a significant threat to clients or, in some cases, faculty egos.” It also appears that how a student is addressed may be related to faculty dynamics. For example, “Political alliances among faculty play a major role in determining which students are targeted for intervention.”
Participants overwhelmingly reported they were aware of their programs’ procedures and the appropriate interventions to take when they encounter counselors-in-training with PPC. However, they also reported that they struggle with their gatekeeping duties due to empathy, diversity issues and fear of recrimination; half of the participants (51%) stated they would like more information regarding how to identify students with PPC, and 61% would like more information on how to respond to these students. Apparently, counseling programs are doing a good job developing procedures and communicating these procedures to faculty members, as recommended by Gaubatz and Vera (2002). But there remains a disconnect between knowledge about procedures and the ability to implement a response to PPC that may be related to the roadblocks identified in this study.
Counselor educators and supervisors know what they are supposed to do if a PPC has been clearly delineated; however, they struggle with identifying problematic behavior that reaches a threshold of needing to be formally addressed and taking action related to problematic student behaviors. The gap between the recognition that a student is not meeting expectations and the point where formal action is initiated may be filled with the counselor educators’ own beliefs about how they can fix the problem as well as their own anxieties related to the barriers discovered in this study. The recognition of and intervention with students with PPC can be further complicated by counselor educators having to negotiate faculty politics. It would seem that more attention is needed on assisting counselor educators in negotiating these barriers to ensure students do not gateslip.
Conclusion
The results of this current study provide insight that educators are aware of counseling students with problematic behaviors, and these behaviors are impacting the learning environment, other students in the program and personal stress. It also appears that the largest roadblock present and impacting counselor educators’ ability to engage in gatekeeping procedures relates to their empathy veils. The authors of this article perceive that there is a struggle for counselor educators between balancing compassion for students’ life circumstances and developmental level with holding them to an acceptable level of professional competence. Counselor educators know it is their responsibility to engage in ethical gatekeeping procedures; however, they do not want to be excessively critical of students. Having an understanding of the empathy veil will assist educators in finding the balance between challenging and supporting students. Counselor educators must not accept students with PPC into their programs or allow them to move on without confronting and remediating their problematic behaviors. Educators need to do their due diligence and be willing to lift their empathy veils and engage in their gatekeeping responsibilities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 American Counseling Association Code of Ethics. Alexandria, VA:
Author.
Bogo, M., Regehr, C., Power, R., & Regehr, G. (2007). When values collide: Field instructors’ experiences of providing feedback and evaluating competence. Clinical Supervisor, 26, 99–117. doi: 10.1300/J001v26n01_08
Brear, P., & Dorrian, J. (2010). Gatekeeping or gate slippage? A national survey of counseling educators in Australian undergraduate and postgraduate academic training programs. Training and Education in Professional Psychology, 4, 264–273. doi:10.1037/a0020714
Brown, M. (2013). A content analysis of problematic behavior in counselor education programs. Counselor Education and Supervision, 52, 179–192. doi:10.1002/j.1556-6978.2013.00036.x
Brown-Rice, K. A., & Furr, S. (2013). Preservice counselors’ knowledge of classmates’ problems of professional competency. Journal of Counseling & Development, 91, 224–233. doi:10.1002/j.1556-6676.2013.00089.x
Brown-Rice, K. A., & Furr, S. (2014). Lifting the empathy veil: Engaging in competent supervision. In Ideas and research you can use: VISTAS 2014. Retrieved from http://www.counseling.org/knowledge-center/vistas
Council for Accreditation of Counseling and Related Educational Programs. (2016). 2016 CACREP
Standards. Retrieved from http://www.cacrep.org/wp-content/uploads/2012/10/2016-CACREP-Standards.pdf
Crawford, M., & Gilroy, P. (2012). Professional impairment and gatekeeping: A survey of master’s-level training programs. Journal of Counselor Preparation and Supervision, 5, 28–37.
Dugger, S. M., & Francis, P. C. (2014). Surviving a lawsuit against a counseling program: Lessons learned from Ward v. Wilbanks. Journal of Counseling & Development, 92, 135–141. doi:10.1002/j.1556-6676.2014.00139.x
Elman, N. S., & Forrest, L. (2007). From trainee impairment to professional competence problems: Seeking new terminology that facilitates effective action. Professional Psychology: Research and Practice, 38, 501–509. doi:10.1037/0735-7028.38.5.501
Falender, C. A., Collins, C. J., & Shafranske, E. P. (2009). “Impairment” and performance issues in clinical supervision: After the 2008 ADA Amendments Act. Training and Education in Professional Psychology, 3, 240–249. doi:10.1037/a0017153
Forrest, L., Elman, N. S., Huprich, S. K., Veilleux, J. C., Jacobs, S. C., & Kaslow, N. J. (2013). Training directors’ perceptions of faculty behaviors when dealing with trainee competence problems: A mixed method pilot study. Training and Education in Professional Psychology, 7, 23–32. doi:10.1037/a0032068
Gaubatz, M. D., & Vera, E. M. (2002). Do formalized gatekeeping procedures increase programs’ follow-up with deficient trainees? Counselor Education and Supervision, 41, 294–305.
Gay, L. R., Mills, G. E., & Airasian, P. (2009). Educational research: Competencies for analysis and applications (9th ed.). Upper Saddle River, NJ: Pearson Education.
Gizara, S. S., & Forrest, L. M. (2004). Supervisors’ experiences of trainee impairment and incompetence at APA-accredited internship sites. Professional Psychology: Research and Practice, 35, 131–140.
doi:10.1037/0735-7028.35.2.131
Goodrich, K. M., & Shin, R. Q. (2013). A culturally responsive intervention for addressing problematic behaviors in counseling students. Counselor Education and Supervision, 52, 43–55.
doi:10.1002/j.1556-6978.2013.00027.x
Herlihy, B. J., Hermann, M. A., & Greden, L. R. (2014). Legal and ethical implications of using religious beliefs as the basis for refusing to counsel certain clients. Journal of Counseling & Development, 92, 148–153. doi:10.1002/j.1556-6676.2014.00142.x
Homonoff, E. (2008). The heart of social work: Best practitioners rise to challenges in field instruction. Clinical Supervisor, 27, 135–169, doi:10.1080/07325 220802490828
Homrich, A. M., DeLorenzi, L. D., Bloom, Z. D., & Godbee, B. (2014). Making the case for standards of conduct in clinical training. Counselor Education and Supervision, 53, 126–144. doi:10.1002/j.1556-6978.2014.00053.x
Hutchens, N., Block, J., & Young, M. (2013). Counselor educators’ gatekeeping responsibilities and students’ First Amendment rights. Counselor Education and Supervision, 52, 82–95. doi:10.1002/j.1556-6978.2013.00030.x
Jacobs, S. C., Huprich, S. K., Grus, C. L., Cage, E. A., Elman, N. S., Forrest, L., . . . Kaslow, N. J. (2011). Trainees with professional competency problems: Preparing trainers for difficult but necessary conversations. Training and Education in Professional Psychology, 5, 175–184. doi:10.1037/a0024656
Johnson, W., Elman, N. S., Forrest, L., Robiner, W. N., Rodolfa, E., & Schaffer, J. B. (2008). Addressing professional competence problems in trainees: Some ethical considerations. Professional Psychology: Research and Practice, 39, 589–599. doi:10.1037/a0014264
Kaslow, N. J., Rubin, N. J., Forrest, L., Elman, N. S., Van Horne, B. A., Jacobs, S. C., . . . Thorn, B. E. (2007). Recognizing, assessing, and intervening with problems of professional competence. Professional Psychology: Research and Practice, 38, 479–492, doi:10.1037/0735-7028.38.5.479.
Kerl, S., & Eichler, M. (2007). The loss of innocence: Emotional costs to serving as gatekeepers to the counseling profession. Journal of Creativity in Mental Health, 1, 71–88.
Kerl, S. B., Garcia, J. L., McCullough, C. S., & Maxwell, M. E. (2002). Systematic evaluation of professional performance: Legally supported procedure and process. Counselor Education and Supervision, 41, 321–332.
Kolbert, J. B., Morgan, B., & Brendel, J. M. (2002). Faculty and student perceptions of dual relationships within counselor education: A qualitative analysis. Counselor Education and Supervision, 41, 193–206. doi:10.1002/j.1556-6978.2002.tb01283.x
Leverett-Main, S. (2004). Program directors’ perceptions of admission screening measures and indicators of student success. Counselor Education and Supervision, 43, 207–219.
Lumadue, C. A., & Duffey, T. H. (1999). The role of graduate programs as gatekeepers: A model for evaluating student counselor competence. Counselor Education and Supervision, 39, 101–109.
doi:10.1002/j.1556-6978.1999.tb01221.x
McAdams, C. R., III, & Foster, V. A. (2007). A guide to just and fair remediation of counseling students with professional performance deficiencies. Counselor Education and Supervision, 47, 2–13.
McAdams, C. R., III, Foster, V. A., & Ward, T. J. (2007). Remediation and dismissal policies in counselor education: Lessons learned from a challenge in federal court. Counselor Education and Supervision, 46, 212–229.
Morrissette, P. J., & Gadbois, S. (2006). Ethical consideration of counselor education teaching strategies. Counseling and Values, 50, 131–141. doi:10.1002/j.2161-007X.2006.tb00049.x
Neville, H. A., Lilly, R. L., Duran, G., Lee, R. M., & Browne, L. (2000). Construction and initial validation of the Color-Blind Racial Attitudes Scale (CoBRAS). Journal of Counseling Psychology, 47, 59–70.
Pease-Carter, C., & Barrio Minton, C. A. (2012). Counseling programs’ informed consent practices: A survey of student preferences. Counselor Education and Supervision, 51, 308–319. doi:10.1002/j.1556-6978.2012.00023.x
Rust, J. P., Raskin, J. D., & Hill, M. S. (2013). Problems of professional competence among counselor trainees: Programmatic issues and guidelines. Counselor Education and Supervision, 52, 30–42.
doi:10.1002/j.1556-6978.2013.00026.x
Shen-Miller, D. S., Forrest, L., & Burt, M. (2012). Contextual influences on faculty diversity conceptualizations when working with trainee competence problems. The Counseling Psychologist, 40, 1181–1219. doi:10.1177/0011000011431832
Shen-Miller, D. S., Forrest, L., & Elman, N. S. (2009). Training directors’ conceptualizations of the intersections of diversity and trainee competence problems: A preliminary analysis. The Counseling Psychologist, 37, 482–518. doi:10.1177/0011000008316656
Smaby, M. H., Maddux, C. D., Richmond, A. S., Lepkowski, W. J., & Packman, J. (2005). Academic admission requirements as predictors of counseling knowledge, personal development, and counseling skills. Counselor Education and Supervision, 45, 43–57.
Smith, H. L., Robinson, E. H. M., III, & Young, M. E. (2007). The relationship among wellness, psychological distress, and social desirability of entering master’s-level counselor trainees. Counselor Education and Supervision, 47, 96–109.
Sue, D. W., & Sue, D. (2012). Counseling the culturally diverse: Theory and practice (6th ed.). New York, NY: Wiley & Sons.
Swank, J. M., & Smith-Adcock, S. (2013). Creative group strategies for interviewing applicants for counselor education programs. The Journal of Counselor Preparation and Supervision, 5, 38–48.
Vacha-Haase, T., Davenport, D. S., & Kerewsky, S. D. (2004). Problematic students: Gatekeeping practices of academic professional psychology programs. Professional Psychology: Research and Practice, 35, 115– 122. doi:10.1037/0735-7028.35.2.115
Ziomek-Daigle, J., & Christensen, T. M. (2010). An emergent theory of gatekeeping practices in counselor education. Journal of Counseling & Development, 88, 407–415.
doi:10.1002/j.1556-6678.2010.tb00040.x
Kathleen Brown-Rice, NCC, is an Assistant Professor at the University of South Dakota. Susan Furr is a Professor at the University of North Carolina Charlotte. Correspondence can be addressed to Kathleen Brown-Rice, 114E Clark Street, Vermillion, SD 57069, kathleen.rice@usd.edu.
Jul 20, 2016 | Article, Volume 6 - Issue 2
Marc A. Grimmett, Adria S. Dunbar, Teshanee Williams, Cory Clark, Brittany Prioleau, Jen S. Miller
Research studies indicate that the number of African Americans diagnosed with oppositional defiant disorder (ODD) is disproportionately higher than other demographic groups (Feisthamel & Schwartz, 2009; Schwartz & Feisthamel, 2009). One contributing factor for this disproportionality is that White American clients presenting with the same disruptive behavioral symptoms as African American clients tend to be diagnosed with adjustment disorder. Feisthamel and Schwartz (2009) concluded, “counselors perceive attention deficit, oppositional, and conduct-related problems as significantly more common among clients of color” (p. 51), and racial diagnostic bias may influence the assessment process. Racial biases in clinical decision making are explained in a conceptual pathway developed by Feisthamel and Schwartz (2007).
In the pathway, counselors who hold stereotypical beliefs about clients selectively attend to client information. The counselor’s judgment is influenced by personal bias, resulting in misdiagnosing the client. African American masculinity stereotypes of criminal mindedness, violent behavior, aggression and hostility (Spencer, 2013) held by counselors with low multicultural social justice counseling competence (Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2015; Sue, Arredondo, & McDavis, 1992) potentially foster misdiagnosis and overdiagnosis of African American males with ODD.
Studies on how African American males are diagnosed with ODD and specific implications for African American males are relatively nonexistent. McNeil, Capage, and Bennett (2002) indicated the majority of information on children diagnosed with ODD has been obtained from primarily White children and families. They recommended that counselors working with African American families consider the African American family’s unique stressors, worldviews and burdens; possible inclusion of the extended family; possible therapist biases that conflict with client’s worldview; and positive factors that lead to competency, self-reliance and health in African American culture (Lindsey & Cuellar, 2000). Thus, an appropriate ODD diagnosis in African American males requires assessment and treatment plan considerations that include other related factors.
Diagnosing Oppositional Defiant Disorder in African American Males
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5; American Psychiatric Association [APA], 2013), ODD is characterized by a pattern of behavior that includes angry and irritable mood, argumentative and defiant behavior, and/or vindictiveness. Symptoms must cause significant problems at home, school or work; must occur with at least one individual who is not a sibling; and must persist for 6 months or more (APA, 2013). The diagnostic assessment also determines that (a) these behaviors are displayed more often than is typical for peers, and (b) symptoms are not associated with other mental health disorders such as anxiety, depression, antisocial behavior and substance abuse disorders.
High rates of ODD diagnosis among African American males may occur because of low cultural competency in diagnosis and counselor bias (Guindon & Sobhany, 2001; Hays, Prosek, & McLeod, 2010; Snowden, 2003). Spencer and Oatts (1999) and Clark (2007), for example, found that health professionals misinterpreted symptoms of disruptive behavior disorders like ODD at greater rates for African American children. Misdiagnosis was common among children assessed as having symptoms of (a) obsessive compulsive disorder and response to rigid classroom rules, (b) bipolar disorder or attention-deficit/hyperactivity disorder and engagement in destructive behavior, and (c) anxiety disorder (e.g., social anxiety) and dislike for school, and defiance toward teachers. These symptoms also may result from unfair treatment and discrimination (Smith & Harper, 2015). Misdiagnosis of ODD can reasonably be expected to have potentially adverse implications for healthy psychological, emotional and social development in family and education systems.
Family Systems
Primary caregivers of children diagnosed with ODD report mild to moderate levels of depression and anxiety and severe levels of stress (Oruche et al., 2015). Caregivers report having overwhelming difficulty managing the aggressive and defiant nature of their children’s behaviors and constantly watching over their children to prevent them from hurting themselves or others (Oruche et al., 2015). The well-being of family members who are not primary caregivers (i.e., in some cases fathers, siblings, grandparents) is rarely considered in disruptive behavior research, although these family members experience many of the same stressors outlined by primary caregivers (Kilmer, Cook, Taylor, Kane, & Clark, 2008). Siblings of diagnosed adolescents have demonstrated high rates of anxiety, poor school performance and adjustment problems (Kilmer et al., 2008; Oruche et al., 2015). Children with disruptive behavior disorders whose family members participated in their treatment showed improved grade point averages and attendance and reduced drop-out rates relative to students whose family members considered themselves uninvolved (Reinke, Herman, Petras, & Ialongo, 2008). While family interventions appear helpful, an accurate diagnosis remains the first step in creating an effective treatment plan and not causing further harm to clients (e.g., school suspension, expulsion, incarceration; Smith & Harper, 2015).
Educational Systems
Students with aggressive disruptive behaviors also have higher rates of mental health risk factors, including school maladjustment, antisocial activity, substance use and early sexual activity (Schofield, Bierman, Heinrichs, & Nix, 2008). Children diagnosed with ODD experience a range of academic problems, including in-school suspensions (Reinke et al., 2008), high school drop-out (Vitaro, Brendgen, Larose, & Trembaly, 2005), and lower academic grades and achievement scores (Bub, McCartney, & Willett, 2007). ODD was not cited as a contributing factor; however, a recent report by Smith and Harper (2015) revealed that in Southern states African American males comprised 47% of student suspensions and 44% of expulsions from K–12 public schools in the United States, which was highest among all racial and ethnic groups. School administrators also were more likely to rate African American children higher on symptoms related to behavioral disorders than White American children (Epstein et al., 2005).
Finally, 50–70% of juveniles detained in the United States have a diagnosable behavioral health disorder (e.g., ODD; Schubert & Mulvey, 2014). While African American youth make up only 16% of the total youth population in the United States, they account for 37% of the detained population (National Council on Crime and Delinquency, 2007). Given the potential negative trajectory of an ODD diagnosis for some African American males, the diagnostic process warrants further consideration.
Method
Design
The purpose of this qualitative research study was to (a) help understand and explain the contextual factors, diagnostic processes and counseling outcomes associated with the diagnosis of ODD in African American males, and (b) identify, describe, and make meaning of patterns and trends in mental health care systems that may be associated with the apparent overdiagnosis of African American boys with ODD. A consensual qualitative research (CQR) design was employed in this study to identify, describe and make meaning of the diagnostic processes and outcomes related to ODD. The following components of CQR identified by Hill et al. (2005) were used in this study: (a) open-ended questions in semistructured interviews “to allow for the collection of consistent data across individuals, as well as more in-depth examination of individual experiences,” (b) research team collaboration (i.e., two judges and one auditor) throughout the data analysis process for multiple perspectives, (c) “consensus to arrive at the meaning of the data,” (d) an auditor to check the work of the two judges; and (e) “domains, core ideas, and cross-analyses in the data analysis” (p. 196).
Research Team
The research team included a counselor educator and licensed psychologist (African American male, age 42), counselor educator and licensed professional counselor (White American female, age 36), three clinical mental health graduate students (African American female, age 23; White American female, age 28; White American male, age 29) and one public administration graduate student (African American female, 34). All research team members had clinical experience (i.e., as mental health counselors, research and counseling interns, or parents of clients receiving counseling) with African American males who have been diagnosed with ODD. Training to conduct the study involved reading and discussing [Hill, Knox, Thompson, Williams, Hess, & Ladany, 2005; Hill, Thompson, & Williams, 1997]; attending in-person research team meetings to discuss, design, plan and implement the research study; and electronic communication throughout the process. Feelings and reactions (i.e., biases) related to the study were openly discussed among the research team throughout the process to minimize influences on data analysis. Research team biases included: (a) awareness of apparent disproportionality of ODD diagnosis in African American males compared to other populations, based on clinical experience, (b) potential low multicultural competence of counselors making diagnoses, and (c) difficulties for African American males with an ODD diagnosis.
Participants
Six mental health professionals met the following criteria for participation in this study: (a) the ability to verbally describe and explain the diagnostic criteria for ODD (during the interview for data collection), (b) a minimum of 2 years’ clinical experience working with clients who have ODD as demonstrated by professional resume or curriculum vitae and explanation at the interview, and (c) a professional mental health license.
The sample consisted of diverse practitioners in identity, years of experience, professional position and places of employment. Racial/ethnic and gender identities of participants were: African American female, African American male, multiracial Arab American female, White American female (n = 2), and White American male. Participant ages ranged from: (a) 30–35 years (n = 2), (b) 35–40 years (n = 2) and (c) over 40 years (n = 2). Reported mental health licenses included: licensed professional counselor associate (n = 1), licensed professional counselor (n = 2), licensed professional counselor supervisor (n = 1), licensed clinical social worker (n = 1) and licensed psychological associate (n = 1). Years holding licensure ranged from less than one to greater than 15. The majority of participants described their professional position as a clinical supervisor and mental health counselor (n = 3), with others identifying as mental health counselors (n = 2) and multisystemic therapy program supervisor (n = 1). All participants reported working within a private organization, with two participants employed by a for-profit community mental health agency, three participants by a non-profit community mental health agency and one participant in private practice.
Procedure
The Institutional Review Board for the Use of Human Subjects in Research evaluated and approved the study. Participant recruitment involved purposeful sampling of mental health providers from local Critical Access Behavioral Health Agencies likely to meet participant criteria. Research team members contacted 10 potential participants by e-mail and follow-up phone calls to explain the study and ask for their participation. Once eligibility had been determined based on selection criteria, six mental health professionals were selected to create an intentionally diverse sample. Participants scheduled an in-person appointment to complete the informed consent process with a team member, signed the form indicating understanding and agreement to participate in the study, and engaged in an in-depth interview lasting 1 to 1.5 hours, at the office of the participants or the first author. Codes and pseudonyms protected confidential participant information and data was audio-recorded and transcribed for each interview.
Measures
Semi-structured interviews. Interview questions for the study were based on a literature review, an evaluation of the DSM-5 (APA, 2013) criteria for ODD, and pilot field interviews with mental health professionals, clients, and clinical directors experienced in providing or receiving services related to ODD. Participants were asked 12 initial questions about the process of making an ODD diagnosis for African American male clients that focused on: life circumstances that contributed to an ODD diagnosis; structural and cultural factors related to diagnosis (e.g., What are the social systems involved in the diagnosis?); post-diagnosis outcomes and implications (e.g., What happens after a client receives the diagnosis?); and treatment plan considerations (e.g., What are the benefits and/or problems of the treatment plan?).
Data Analysis
Data were analyzed using CQR beginning with a start domain list created from the initial interview questions and transcript of the first interview, where all research team members coded first interview data into domains, “topics used to group or cluster data” (Hill et al., 2005, p. 200). Next, core ideas, “summaries of the data that capture the essence of what was said in fewer words with greater clarity,” from each domain were recorded using direct quotes from participants (Hill et al., 2005, p. 200). Cross-analysis was then completed to characterize the frequency of the data: “general applies to all or all but one case; typical applies to more than half up to cutoff for general; and variant applies to two cases up to the cutoff for typical” (Hill et al., 2005, p. 203). Finally, one team member acted as the auditor and provided feedback throughout the analysis process, and most importantly, ensured “that all important material has been faithfully represented in the core ideas, that the wording of the core ideas succinctly captures the essence of the raw data, and that the cross-analysis elegantly and faithfully represents the data” (Hill et al., p. 201).
The consensus process commenced in the collaborative team design and implementation of the study and proceeded with the independent analysis of the data by the coders and auditor. Domains, core ideas and cross-analyses were then presented, discussed, debated and confirmed during in-person research team meetings, by e-mail and video conferencing. A multilayered consensus process over time contributed to the stability of the data for trustworthiness, along with: (a) consistency and documentation of data collection procedures, (b) research team description and positionality statement, (c) providing quotes that capture core ideas, and (d) using a research team of coders and an auditor to analyze data. No cases were withheld from the initial cross-analysis for the stability check of the data, as Hill et al. (2005) found it is not necessary. Rather, Hill et al. (2005) suggested presenting “evidence of trustworthiness in conducting data analysis,” as described (p. 202).
Findings
Four domains were identified related to diagnosing ODD. Categories further define each domain, supported by core ideas using direct quotes from the participants. Table 1 shows the frequency of categories within each of the domains. Hill et al. (1997) outlined the following categories: general if it applies to all (6), typical if it applies to half or more (3–5), and variant if it applies to less than half of the participants (2 up to typical; all categories applied to at least half of the participants; therefore, none were variant).
Insurance Influence
Most insurance companies require counselors to diagnose clients with a mental disorder in order to obtain payment for mental health services (Kautz, Mauch, & Smith, 2008). Many insurance companies require that a diagnosis be made during the first few counseling sessions, sometimes within the very first counseling session. All participants described the role and influence of insurance companies and managed care in the diagnostic process. One participant expressed, “the diagnosis is necessary to get paid, so you have to find something. You are not looking objectively. You are just giving them a diagnosis.” The participant continued:
We see this proportion of diagnoses [with African American males] because the insurance in managed care world drives agencies like this one and drives providers to say that an [African American] child is diagnosed a particular way . . . There is this incentive to diagnose and to diagnose in a short period of time.
| Table 1Summary of Domains From the Cross-Analysis of the Participants (N = 6) |
|
Domain and Category
|
Frequency |
|
|
| Insurance influence |
|
| Diagnosis required for payment of services |
General
|
| Reimbursement likelihood drives the type of diagnosis given |
General
|
| Insufficient assessment time allotted for proper diagnosis |
General
|
| Oppositional defiant disorder diagnostic criteria |
|
| Criteria are too general |
General
|
| Criteria provide a convenient catch-all for providers |
General
|
| Oppositional defiant disorder is stigmatized |
|
| African American males |
Typical
|
| Long-term negative implications |
Typical
|
| Assessment, diagnosis and treatment |
|
| Family, community and other contextual considerations |
General
|
| Mental health counselor bias |
Typical
|
| Cultural and contextual integration |
Typical
|
|
|
Findings suggested that the assessment time allotted by insurance companies to diagnose a mental disorder undermines the diagnostic process and invalidates the diagnosis. One participant emphasized, “the client is not going to open up to you within that time frame; this is the first time the child is ever seeing you. Those types of things progress over time.” Further structural and systemic assessment problems also were identified by another participant:
You’re allowed to do one assessment per year for the client . . . The assessor would take the previous assessment, use a majority of that information, and then just ask what has changed between then and now . . . there [are] a lot of questions that the previous assessment didn’t answer or didn’t really look into. So that piece gets missed.
Oppositional Defiant Disorder Diagnostic Criteria
The DSM-5 criteria for ODD are too general, providing a convenient catch-all for providers. Symptoms of ODD align with typical child and adolescent behavior as well as other childhood disorders (e.g., ADHD), adjustment disorder, depression and anxiety, depending on developmental context (APA, 2013). Every participant expressed the relative malleability of the ODD criteria. “It’s an easy diagnosis for most people to fit into that category, if they’re having trouble with the legal system and there’s nothing else going on,” noted one participant. Another added that ODD “serves as a holding cell for behaviors that are not understood.” Finally, one mental health counselor stated:
There are no differentials for ODD. It’s all under this blurry category of disruptive behaviors. On one hand it looks easy to diagnose, but on the other hand it’s very complicated when you are not ethically doing the right thing.
Oppositional Defiant Disorder Is Stigmatized
An ODD diagnosis carries negative social weight and judgment within and beyond the mental health fields. African American males are particularly vulnerable to diagnostic stigmatization due to multiple marginalizations that can occur when intersecting with other forms of oppression, such as racism (Arrendondo, 1999; Ratts et al., 2015). Most participants referenced long-term negative implications for these clients, including, “I think it leaves a permanent scar, with elementary kids all the way up.” One participant expressed further that:
I have had kids that have been diagnosed with [ODD] and they drop out. I have had young African American boys in my office and they say ‘You know this has been going on with me since I was a kid?’ And you know that they are telling the truth. They ask themselves, ‘Why am I still in school?’ So they drop out.
Another mental health counselor added:
I see it when we go to court even [with] an African American judge. African American boys would typically get a harsher sentence. It’s a systemic issue. We just start viewing through a lens and we automatically have an assumption to what the problem is. We have a negative interpretation of one kid’s actions versus another.
Assessment, Diagnosis and Treatment
Assessment, diagnosis and treatment do not account for family, community and other contextual problems affecting the client’s mood and behavior. One mental health counselor explained, “if the parent has been incarcerated, they are going to act out. If they are dealing with a domestic violence situation in their home, this is a way of relieving stress for them.” Another participant added:
We leave the whole family out of this process . . . That may be where the problems exist. It is person centered to a fault. To the neglect of it being family centered versus person centered or being both, because you would dare not want to intervene with a child and not involve family. Despite [that] the parents will come and say, 95% of the time, ‘I am okay—you need to fix my son or daughter.’ When treatment plans get tailored based on that premise, then everybody is in trouble.
Trauma also was identified as a contextual issue that warrants consideration in the diagnostic process.
Past trauma, living in very difficult situations, near or below poverty are not taken into account. What might be very adaptive behaviors for a kid, or might be situational dependent, are then just translated into the diagnosis.
Participants acknowledged mental health counselor bias plays a role in diagnosis as well. A mental health counselor may have a tendency to diagnose certain clients with ODD because it is a familiar and commonly used diagnosis. One mental health counselor stated, “a lot of times, particularly with new clinicians, [ODD] is a buzz word . . . like ADD was a buzz word years ago.” A different participant shared the diagnostic rationale, “it helps them, too, because it’s a relatively non-offensive diagnosis. It’s not as personal a diagnosis, so they don’t feel as bad being diagnosed oppositional defiant disorder as they would something else.”
The relative cultural competency of practitioners also was referenced by participants as potentially compromising the diagnostic process, with one indicating that:
When I think about oversight and training, it’s limited in terms of how much exposure they’ve had to diversity training or multiculturalism. What might present as disrespect or non-compliance might be very culturally appropriate . . . The assumption is made that these things are all dysfunctional for the individual as opposed to other contextual factors that are going on.
Discussion
The purpose of this study was to understand the diagnostic processes and implications associated with ODD. Findings suggest that a diagnosis of ODD can result from more factors than client symptoms fitting the diagnostic criteria. While none of the research or interview questions asked specifically about the role of insurance or managed care, every participant indicated that third party billing influenced the diagnostic process.
Specifically, the mental health counselors interviewed were keenly aware of the necessity of making a diagnosis for insurance reimbursement. It appeared that ODD is considered a reliable diagnosis for billing purposes; however, diagnostic necessity may also create an ethical dilemma for mental health counselors who want to provide quality care and need to earn a living. The possibility of racial diagnostic bias remains, even with insurance requirements, when African Americans are more likely to receive a diagnosis of ODD, while White Americans presenting with similar symptoms receive a diagnosis of adjustment disorder (Feisthamel & Schwartz, 2009; Schwartz & Feisthamel, 2009).
Professional ethical standards and best practices warrant full consideration of a diagnosis, including the purpose served and implications, as related to the health and well-being of clients (American Counseling Association [ACA], 2014). Even when a diagnosis is not warranted or conflicts with theoretical, philosophical or therapeutic approaches, mental health providers serving clients who do not pay cash for services are forced to accommodate diagnostic requirements. The use of a diagnosis as a therapeutic tool, designed to act in concert with others, has also come to serve as the gateway to mental health care services.
In the case of African American male clients, an ODD diagnosis can be particularly stigmatizing with immediate and long-term implications for marginalization and tracking (Cossu et al., 2015). Educational, judicial and incarceration data clearly demonstrate that African American males are disproportionately suspended and expelled from school compared to their peers (U.S. Department of Education Office for Civil Rights, 2014); receive harsher sentences in judicial systems for the same offenses as other defendants (Ghandnoosh, 2014; Rehavi & Starr, 2012); and are more likely to be stopped, searched, assaulted and killed by police officers than other community members (Gabrielson, Jones, & Sagara, 2014; Weatherspoon, 2004). Since ODD is categorized as a disruptive behavior disorder, it may be considered, intentionally or unintentionally, a justification, rationale or explanation for these disparate outcomes. When the diagnosis of a mental disorder is used for purposes other than helping the client, it opens the door to unintended and problematic consequences.
The assessment process is critical to making an accurate diagnosis and should not be limited to the most readily available, convenient or confirmatory information. With ODD, alternative, viable explanations for client symptoms have to be considered that may include family history and dynamics, personal trauma and social–cultural context. Guindon and Sobhany (2001) noted, “often there are discrepancies between the counselor’s perception of their clients’ mental health problems and those of the clients themselves” (p. 277). Again, there may be a tendency to diagnose African American males with perceived behavioral problems with ODD without full consideration of historical and contextual variables that may better explain mood and behavior and warrant a different diagnosis altogether (Hays et al., 2010).
Mental health counselors also have certain biases, within and beyond personal awareness, that create diagnostic tendencies, which may undermine the diagnostic process and invalidate the results of the assessment. Assessment practices and structures appear to accommodate intrinsic and individual information, more so than extrinsic and systemic variables (Hays et al., 2010). For these reasons, the gathering of client information for diagnostic purposes must be as comprehensive and inclusive as possible, notwithstanding measures to limit mental health counselor bias, such as supervision and consultation.
The ACA Code of Ethics outlines the need for even the most experienced counselors to seek supervision and consultation when necessary (ACA, 2014). One potential blind spot for many counselors experiencing bias toward African American male clients is not realizing the need for supervision and consultation when it arises. Understanding that ODD diagnoses within the African American male community have been shown to be inflated is a first step toward decreasing counselor bias. Second, recognizing the subjective nature of making an ODD diagnosis, especially since many of the behaviors and emotions listed as diagnostic criteria also “occur commonly in normally developing children and adolescents” (APA, 2013, p. 15) is another critical aspect of ensuring accurate diagnoses are made.
Counselors are trained from a multimodal approach to diagnosis based on Western medicine; therefore, diagnosing clients is a culturally-based practice (Sue & Sue, 2015). Furthermore, most research in the area of mental and behavioral health has, in large part, not included people of color (U.S. Department of Health and Human Services, 2001). Cultural discrepancies also are evident in the demographic characteristics represented within the counseling profession. Approximately 71% of counselors in the United States are women, and only 18.4% of counselors identify as Black or African American (U.S. Department of Labor, 2015); therefore, most African American male clients will likely have different cultural backgrounds from their counselors. These factors create a need for consultation and supervision to ensure that the personal and professional worldviews of counselors are not inhibiting accurate diagnosis and treatment planning for African American male clients.
In addition to supervision, another measure to limit counselor bias would be to practice reflective cultural auditing, a 13-step process for walking counselors through how culture may impact their work with clients from initial meeting through termination and follow-up. This process allows counselors to reflect on what may seem like client resistance, but may instead be a “disruption in the working alliance” (Collins, Arthur, & Wong-Wylie, 2010, p. 345) based on cultural differences. In addition to utilizing reflective audits of individual cases, it also can be helpful for counselors to review case files regularly, taking into account race and ethnic background, along with symptoms and reported diagnosis. Finding diagnostic patterns within one’s own practice can help counselors reflect on their clinical work and identify areas of bias that may exist.
Implications for Professional Counselors
Thinking through the diagnostic process and beyond the diagnosis requires the mental health counselor to consider and balance the needs of the client, provision of ethical and effective mental health services, expectations and requirements of employers, and earning a living. The following recommendations are offered to help mental health professionals balance these diagnostic considerations in light of current findings, particularly in the assessment and diagnosis of ODD.
In order to make an accurate diagnosis, billing considerations should not be a determining factor in the assessment process. We acknowledge that payment for services is a necessary component for earning a living as a mental health counselor; at the same time, there is an inherent conflict of interest between ethical diagnostic practices and billing when they are not considered as separate processes. Counselors can reference the ACA Code of Ethics (2014) regarding cultural sensitivity (Section E.5.b) as well as historical and social prejudices in the diagnosis of pathology (Section E.5.c). Additionally, counselors may reference the guidelines for informed consent in the counseling relationship (Section A.2.b), ensuring that clients are aware of how information in their client records will be used and how it may impact clients in the future. When appropriate, counselors may choose a less stigmatizing diagnosis initially (e.g., adjustment disorder), while continuing to learn more about a client’s context and cultural background before making a final diagnosis.
Consider extrinsic and external factors that may contribute to emotional and behavioral symptoms presented. It is important to keep in mind that a pattern of ODD behavior includes anger and irritability, argumentative and defiant behavior, and/or vindictiveness, which causes significant problems at work, school or home, and lasts at least 6 months. In order to qualify as ODD symptoms, these behaviors must occur with at least one person who is not a sibling, and must occur on their own (i.e., not as part of another mental health problem, such as depression, anxiety, antisocial behavior and substance abuse disorders). If family history and dynamics, personal trauma and community/contextual factors contribute to any of the above systems, a diagnosis of ODD may not be the most accurate, thereby leading to ineffective, if not harmful treatment plans and outcomes. A diagnosis of adjustment disorder may be more beneficial to ensure that the client receives adequate treatment, which would hopefully increase the client’s chances of having a positive counseling outcome.
African American males are diagnosed with ODD at a disproportionately higher rate than other social demographic groups (Feisthamel & Schwartz, 2009). Ethical and best practice standards require mental health professionals to understand personal biases that might inform their work as well as to develop strategies to reduce or eliminate negative impact (ACA, 2014; Ratts et al., 2015; Sue et al., 1992). In addition, mental health counselors need to use continuing education to remain aware of current trends in the field relevant to the populations they serve (ACA, 2014; Ratts et al., 2015). Health professionals should adhere to diagnostic criteria and integrate multicultural counseling competencies in order to avoid making decisions based on pre-defined misconceptions.
Implications for Counselor Educators and Supervisors
Included in the Council for Accreditation of Counseling and Related Educational Programs (CACREP) accreditation standards is the responsibility of counselor education programs to train students on “the effects of power and privilege for counselors and clients” (CACREP, 2016, p. 9). It is imperative that counselor educators provide specific training on racial bias among counselors, which often is automatic and hidden from conscious awareness (Abreu, 2001).
Creating a safe, comfortable, respectful classroom environment in which students are able to honestly self-reflect and ask questions is necessary to integrate and infuse multicultural and social justice counseling competence training within counselor education programs (Ratts et al., 2015). Counselors-in-training need the opportunity to think critically and experience cognitive dissonance in the classroom regarding ways African American males are portrayed and the erroneous assumptions often made by authority figures and institutions of power. In turn, counselors need to be aware of how these portrayals and assumptions potentially impact the mental health services African American males receive.
In addition to didactic teaching, experiential exercises also are critical for meaningful learning to take place (Sue & Sue, 2015). Assignments that illustrate personal and systemic prejudice can help students reflect on their own potential biases as well as build awareness of systemic influences that may impact clients of color in ways counselors-in-training previously had not considered. Reading assignments that illustrate common biases among counselors can normalize the phenomenon in ways that facilitate student openness to learning and self-reflection. In addition, using diverse theories when discussing diagnosis and treatment planning can ensure multiple perspectives are acknowledged, including the perspective that diagnoses can be both helpful and harmful to clients. Counselor educators have a responsibility to ensure students graduate with an awareness of the need to constantly monitor their own biases and prejudices toward African American males, as well as knowing when to seek supervision and consultation.
Finally, counselor educators can implement a multicultural competence approach to teaching clinical assessment and diagnosis. Guindon and Sobhany (2001) offered a conceptual framework that can be utilized in the classroom in order to achieve this goal: (a) obtain a specific and complete understanding of the client’s chief complaint, (b) be aware of discrepancies in counselor and client perceptions of clinical reality, (c) elicit clients’ clinical realities and explain counselor clinical models, (d) engage in active negotiation with the client as a therapeutic ally, (e) recognize the importance of renegotiation (of perception of presenting problem), and (f) use assessment instruments advisedly and with caution. The authors intended for this framework to be used by “counselors from any cultural background [to] assist those who are not like themselves” (Guindon & Sobhany, 2001, p. 279).
Limitations of the Study
The CQR model allowed the research team to independently and collaboratively analyze the data through a deliberate, thorough and comprehensive process over time to understand the meanings. Multiple perspectives and the relational dynamic within our team helped to check our own biases and to clearly grasp the view of our participants. The findings of this study represent an in-depth analysis of the perspectives of six licensed mental health professionals with experience diagnosing and working with clients who are diagnosed with ODD that may apply to some degree to working with similar populations and contexts. Life and professional experiences of the researchers and participants, however, naturally interact and influence our understandings of the meanings of the data. As such, different combinations of research team members, participants, or contexts could reveal similar, additional or different findings in a similar study. Finally, two graduate student members of the initial research team graduated before data analysis commenced; therefore, we had fewer coders than originally planned. Additional coders would have provided other perspectives on the data and may have further enhanced the meaning-making process.
Conclusion and Future Research
A mental health diagnosis such as ODD has destructive potential when not used properly. Professional counselors, then, have social power in their capacity to diagnose a client with a mental disorder (APA, 2013; Prilleltensky, 2008). Such power requires that counselors cultivate awareness of personal and professional biases that may influence the diagnostic process. Factors driving the diagnostic process extend beyond the mental health needs of the client and can play a critical role in assessment. Contextual explanations, including historic and systemic contexts, must be considered before a diagnosis is given. Attending to the role of counselor bias to prevent overdiagnosis is an ethical responsibility for which counselor educators and practicing counselors must hold themselves accountable.
Additional research is needed to consider whether the diagnosis–billing model is the most optimal and ethical for mental health care, particularly for preventive mental health and for African American male clients and other marginalized populations. Further study also is warranted to capture the long-term implications of an ODD diagnosis, including identifying ways in which a client‘s family can advocate for school and community resources (e.g., outpatient counseling, mentoring programs, support groups). Finally, possible relationships between an ODD diagnosis, school discipline practices and crime adjudication with marginalized groups (e.g., African American males) should be explored, given the drop-out-of-school-to-prison pipeline that is now widely recognized as a reality for many African American males (Barbarin, 2010).
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Abreu, J. M. (2001). Theory and research on stereotypes and perceptual bias: A didactic resource for multi-cultural counseling trainers. The Counseling Psychologist, 29, 487–512. doi:10.1177/0011000001294002
American Counseling Association (2014). ACA code of ethics. Alexandria, VA: Author
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author.
Arrendondo, P. (1999). Multicultural counseling competencies as tools to address oppression and racism.
Journal of Counseling & Development, 77, 102–108.
Barbarin, O. A. (2010). Halting African American boys’ progression from pre-k to prison: What families, schools, and communities can do! American Journal of Orthopsychiatry, 80, 81–88.
Bub, K. L., McCartney, K., & Willett, J. B. (2007). Behavioral problem trajectories and first-grade cognitive
ability and achievement skills: A latent growth curve analysis. Journal of Educational Psychology, 99, 653–670. doi:10.1037/0022-0663.99.3.653
Clark, E. (2007). Conduct disorders in African American adolescent males: The perceptions that lead to
overdiagnosis and placement in special programs. Alabama Counseling Association Journal, 33(2), 1–7.
Collins, S., Arthur, N., & Wong-Wylie, G. (2010). Enhancing reflective practice in multicultural counseling through cultural auditing. Journal of Counseling & Development, 88, 340–347.
doi:10.1002/j.1556-6678.2010.tb00031.x
Cossu, G., Cantone, E., Pintus, M., Cadoni, M., Pisano, A., Otten, R., . . . Carta, M. G. (2015). Integrating
children with psychiatric disorders in the classroom: A systematic review . Clinical Practice and
Epidemiology in Mental Health : CP & EMH, 11, 41–57. doi:10.2174/1745017901511010041
Council for Accreditation of Counseling and Related Educational Programs. (2016). 2016 standards for
accreditation. Alexandria, VA: Author.
Epstein, J. N., Willoughby, M., Valencia, E. Y., Tonev, S. T., Abikoff, H. B., Arnold, L. E., & Hinshaw, S. P. (2005). The role of children’s ethnicity in the relationship between teacher ratings of attention-deficit/hyperactivity disorder and observed classroom behavior. Journal of Consulting and Clinical Psychology, 73, 424–434.
Feisthamel, K. P., & Schwartz, R. C. (2007, November). Enhancing cross-cultural assessment and diagnosis in counseling. Workshop presented at the 2007 All Ohio Counselors Conference, Columbus, OH.
Feisthamel, K. P., & Schwartz, R. C. (2009). Differences in mental health counselors’ diagnoses based on client race: An investigation of adjustment, childhood, and substance-related disorders. Journal of Mental Health Counseling, 31, 47.
Gabrielson, R., Jones, R. G., & Sagara, E. (2014). Deadly force in Black and White. Retrieved from http://www.propublica.org/article/deadly-force-in-black-and-white
Ghandnoosh, N. (2014). Race and punishment: Racial perceptions of crime and support for punitive policies.
Retrieved from http://www.sentencingproject.org/wp-content/uploads/2015/11/Race-and-Punishment.pdf
Guindon, M. H., & Sobhany, M. S. (2001). Toward cultural competency in diagnosis. International Journal for the Advancement of Counseling, 23, 269–282.
Hays, D. G., Prosek, E. A., & McLeod, A. L. (2010). A mixed methodological analysis of the role of culture in the clinical decision-making process. Journal of Counseling & Development, 88, 114–121.
doi:10.1002/j.1556-6678.2010.tb00158.x
Hill, C. E., Knox, S., Thompson, B. J., Williams, E. N., Hess, S. A., & Ladany, N. (2005). Consensual qualitative research: An update. Journal of Counseling Psychology, 52, 196–205.
Hill, C. E., Thompson, B. J., & Williams, E. N. (1997). A guide to conducting consensual qualitative research. The Counseling Psychologist, 25, 517–572.
Kautz, C., Mauch, D., & Smith, S. A. (2008). Reimbursement of mental health services in primary care settings (HHS Pub. No. SMA-08-4324). Rockville, MD: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration.
Kilmer, R. P., Cook, J. R., Taylor, C., Kane, S. F., & Clark, L. Y. (2008). Siblings of children with severe emotional disturbances: Risks, resources, and adaptation. American Journal of Orthopsychiatry, 78, 1–10.
Lindsey, M. L., & Cuellar, I. (2000). Mental health assessment and treatment of African Americans: A multicultural perspective. In I. Cuellar & F. A. Paniagua (Eds.), Handbook of multicultural mental health (pp. 195–208). San Diego, CA: Academic Press.
McNeil, C. B., Capage, L. C., & Bennett, G. M. (2002). Cultural issues in the treatment of young African American children diagnosed with disruptive behavior disorders. Journal of Pediatric Psychology, 27, 339–350.
National Council on Crime and Delinquency. (2007). And justice for some: Differential treatment of youth of color in the justice system. Oakland, CA: Author.
Oruche, U. M., Draucker, C. B., Al-Khattab, H., Cravens, H. A., Lowry, B., & Lindsey, L. M. (2015). The challenges for primary caregivers of adolescents with disruptive behavior disorders. Journal of Family Nursing, 21, 149–167. doi:10.1177/1074840714562027
Prilleltensky, I. (2008). The role of power in wellness, oppression, and liberation: The promise of psychopolitical validity. Journal of Community Psychology, 36, 116–136.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. Retrieved from http://www.multiculturalcounseling.org/index.php?option=com_content&view=article&id=205:amcd-endorses-multicultural-and-social-justice-counseling-competencies&catid=1:latest&Itemid=123
Rehavi, M. M., & Starr, S. B. (2012). Racial disparity in federal criminal charging and its sentencing consequences (May 7, 2012). University of Michigan Law School, Program in Law & Economics Working Paper Series, Working Paper No. 12-002. doi:10.2139/ssrn.1985377
Reinke, W. M., Herman, K. C., Petras, H., & Ialongo, N. S. (2008). Empirically derived subtypes of child academic and behavior problems: Co-occurrence and distal outcomes. Journal of Abnormal Child Psychology, 36, 759–770.
Schofield, H. T., Bierman, K. L., Heinrichs, B., & Nix, R. L. (2008). Predicting early sexual activity with behavior problems exhibited at school entry and in early adolescence. Journal of Abnormal Child Psychology, 36, 1175–1188.
Schubert, C. A., & Mulvey, E. P. (2014, June). Behavioral health problems, treatment, and outcomes in serious youth offenders. Juvenile Justice Bulletin. U.S. Department of Justice, Office of Justice Programs, Office of Juvenile Justice Deliquency and Prevention. Retrieved from http://www.ojjdp.gov/pubs/242440.pdf
Schwartz, R. C., & Feisthamel, K. P. (2009). Disproportionate diagnosis of mental disorders among African American versus European American clients: Implications for counseling theory, research, and practice. Journal of Counseling & Development, 87, 295–301.
Smith, E. J., & Harper, S. R. (2015). Disproportionate impact of K-12 school suspension and expulsion on Black students in southern states. Philadelphia: University of Pennsylvania, Center for the Study of Race and Equity in Education. Retrieved from http://www.gse.upenn.edu/equity/sites/gse.upenn.edu.equity/files/publications/SOUTHADVANCEDDRAFT24AUG15.pdf
Snowden, L. R. (2003). Bias in mental health assessment and intervention: Theory and evidence. American Journal of Public Health, 93, 239–243. doi:10.2105/AJPH.93.2.239
Spencer, L. E., & Oatts, T. (1999). Conduct disorder vs. attention-deficit hyperactivity disorder: Diagnostic implications for African-American adolescent males. Education, 119, 514–518.
Spencer, S. Z. (2013). The sociopolitics of Black men and criminality in the media: Shaping perception, impression, and affect control. International Journal of Social Science Research and Practice, 1, 149–73. Retrieved from http://sola.vsu.edu/files/docs/sociology-criminal-justice/ijssrp.pdf
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Counseling & Development, 70, 477–486.
Sue, D. W., & Sue, D. (2015). Counseling the culturally diverse: Theory and practice. Hoboken, NJ: Wiley.
U.S. Department of Education Office for Civil Rights. (2014). Civil rights data collection: Data snapshot (School discipline). Retrieved from http://www2.ed.gov/about/offices/list/ocr/docs/crdc-discipline-snapshot.pdf
U.S. Department of Health and Human Services. (2001). Mental health: Culture, race, and ethnicity- A supplement to mental health: A report of the Surgeon General. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service, Office of the Surgeon General, Substance Abuse and Mental Health Services Administration.
U.S. Department of Labor. (2015). Bureau of Labor Statistics: Labor force statistics from the Current Population Survey. Retrieved from http://www.bls.gov/cps/cpsaat11.htm
Vitaro, F., Brendgen, M., Larose, S., & Trembaly, R. E. (2005). Kindergarten disruptive behaviors, productive factors, and educational achievement by early adulthood. Journal of Educational Psychology, 97, 617–629.
Weatherspoon, F. D. (2004). Racial profiling of African-American males: Stopped, searched, and stripped of constitutional protection. The John Marshall Law Review, 38, 439–468.
Marc A. Grimmett is an Associate Professor at North Carolina State University. Adria S. Dunbar is an Assistant Professor at North Carolina State University. Teshanee Williams and Cory Clark are doctoral students at North Carolina State University. Brittany Prioleau and Jen S. Miller are licensed professional counselors. Correspondence can be addressed to Marc. A. Grimmett, Campus Box 7801, Raleigh, NC 27695-7801, marc_grimmett@ncsu.edu.
