Sep 28, 2018 | Volume 8 - Issue 3
Anthony Hartman, Hope Schuermann, Jovanna Kenney
Despite efforts to boost mental health treatment-seeking behaviors by combat veterans, rates have improved relatively little since 2004. Previous work suggests that trust and confidence in the mental health community may be a significant factor. This study explored how professional titles may impact trust and confidence among active-duty U.S. Army soldiers (n = 32). Consistent with previous research, eight vignettes were used to solicit ordinal (ranked) trust and confidence scores for mental health professionals. Highest confidence and trust were seen in clinical psychologists and licensed professional counselors, followed by psychiatrists, licensed clinical social workers, and marriage and family therapists; however, deviations were seen for each individual vignette and the manifested symptoms depicted. Scores for trust and confidence were strongly correlated and both appear to impact soldiers’ treatment-seeking decisions.
Keywords: soldiers, mental health professionals, licensed professional counselors, trust, confidence
The U.S. Army Medical Command’s Department of Behavioral Health provides the following vision: “Our efforts in education, prevention, and early treatment are unprecedented. Our goal is to ensure that every deployed and returning soldier receives the health care they need” (U.S. Army Medical Department, 2016). In 2004, a landmark study by Hoge and colleagues found that only 13–27% of soldiers meeting screening criteria for mental health disorders sought treatment from a mental health professional in the previous year. The researchers concluded that the primary reason for such underutilization was perhaps “concern about how a soldier will be perceived by peers and by the leadership” (Hoge et al., 2004, p. 20). Subsequently, the Army has taken significant actions to reduce negative perceptions toward mental health care and increase confidentiality for those seeking treatment.
Despite substantial efforts to reduce negative stigmas, the number of soldiers seeking mental health care seems to remain significantly low. In a population of soldiers with probable post-traumatic stress disorder (PTSD) or major depression, Schell and Marshall (2008) found that “only 30 percent had received any type of minimally adequate treatment” (p. 101). Specifically, only 18% received minimally adequate talk therapy treatment. Of a sample population of National Guard and Reserve service members reporting psychological problems, Britt et al. (2011) found that only 42% had sought treatment. Most recently, Britt, Jennings, Cheung, Pury, and Zinzow (2015) found that only 40% of soldiers who acknowledged having a mental health issue sought treatment in the last year. Although the percentages of soldiers seeking treatment seem to be improving, the current literature continues to show less than half of those in need seek even a first visit with a mental health care provider. Thus, other significant deterrents to seeking treatment remain beyond the perceptions of leadership and peers.
Research studies indicate that one possible reason for this underutilization of mental health care services could be soldiers’ lack of trust or confidence in the quality of their providers or treatments. When surveyed, one in four soldiers recently returning from deployment indicated a lack of trust in mental health care practitioners (Kim, Britt, Klocko, Riviere, & Adler, 2011). Similarly, in a different sample of soldiers and Marines screening positively for mental health disorders, 38% indicated a lack of trust in mental health providers, while one in four of the same sample indicated a belief that mental health treatments were not effective (Hoge et al., 2004). Further hinting at a lack of trust for mental health care professionals and confidence in treatment, many soldiers would prefer to address their mental health issues with family, friends, or clergy (Schell & Marshall, 2008). Recently, the statement “Marines don’t trust mental health professionals” was rated as one of the top perceptions that mark barriers to care by a sample of enlisted Marine Corps leaders (VanSickle et al., 2016, p. 1022). Ultimately, there seems to be a trend of distrust and a lack of confidence in mental health care treatments and professionals among military populations.
Mental Health Practitioners and Military Treatment
Considering that there are numerous types of mental health professionals (e.g., psychiatrists, mental health counselors), it is possible that soldiers’ perceptions and knowledge of mental health professionals may vary depending on the specific type of provider. This study aims to distinguish soldiers’ perceptions between distinct mental health professionals: psychiatrists, clinical psychologists, licensed clinical social workers (LCSWs), licensed marriage and family therapists (LMFTs), and licensed professional counselors (LPCs). Psychiatrists are distinct in that they must have earned a doctorate in medicine (i.e., MD or DO) and have the nearly exclusive privilege of prescribing pharmaceutical medications for the treatment of mental disorders. Clinical psychologists also must be educated at the doctoral level (i.e., PhD or PsyD) and maintain a licensure in order to practice, but they cannot prescribe medications in most states. LCSWs, LMFTs, and LPCs are educated at least at the master’s level by an institution accredited for their respective field, and must complete respective licensing requirements that include supervised clinical experience following degree completion.
While the educational experience and licensing protocol can easily be distinguished, the mental health professions also have evolved somewhat distinct professional identities in terms of their approaches to mental health treatment. While psychiatrists are trained in various psychotherapeutic modalities, trends indicate the majority of current and future psychiatrists plan to rely more heavily on pharmacological treatments than on talk therapies (Clemens, Plakun, Lazar, & Mellman, 2014; Zisook et al., 2011). As for clinical psychologists, a review of 50 years of literature surrounding this occupation revealed trends around specializing in one particular aspect of the field (i.e., psychotherapy, assessment, research) and one or two treatment modalities (e.g., psychodynamic therapy, cognitive-behavioral therapy), and a prevalence of cognitive therapies (Norcross & Karpiak, 2012). Generally speaking, LCSWs are likely to conduct therapy from a holistic approach that heavily considers the social impacts on a person while pursing social justice and equality agendas, such as helping underprivileged groups (Bradley, Maschi, O’Brien, Morgen, & Ward, 2012). While LMFTs are often exposed to or trained in a wide variety of therapeutic paradigms and techniques, they are likely to emphasize a collective rather than individual treatment approach, often marked by working with families and couples to identify and improve systemic or transactional issues between the members (Imber-Black, 2014). As LPCs’ professional identity continues to develop and stabilize (Mellin, Hunt, & Nichols, 2011; Reiner, Dobmeier, & Hernández, 2013), professional counselors train in a variety of treatment modalities and provide a variety of services in the mental health field, including “the diagnosis and treatment of mental and emotional disorders, including addictive disorders; psychoeducational techniques aimed at the prevention of such disorders; consultation to individuals, couples, families, groups, and organizations; and research into more effective therapeutic treatment modalities” (American Counseling Association, 2011, para. 4).
Although the average client may not know or fully understand the distinctions between mental health professionals, the literature suggests clients do exhibit some bias when selecting mental health professionals. Over the past 30 years, researchers have shown a consistent trend of professional titles or education levels impacting perceptions of mental health professionals. Warner and Bradley (1991) and Wollersheim and Walsh (1993) established that both perceptions of and confidence in mental health therapies were impacted by the title and education level of the mental health professional; generally, participants in these studies indicated a lack of confidence and knowledge about clinical psychologists and a preference for treatment from counselors. In a study examining public confidence in mental health professionals, Fall, Levitov, Jennings, and Eberts (2000) found significant differences in confidence based upon their title as well as their education level (i.e., master’s vs. doctoral level); participants mostly favored doctoral-level education and preferred counselors, except when presented with “serious psychiatric disorders” (p. 122). This study was repeated in 2005 with an African American sample that provided similar findings (Fall, Levitov, Anderson, & Clay, 2005). While specific attitudes and perceptions may have changed or evolved over the past three decades, these studies show that distinct perceptions or even biases toward professional titles do exist among civilian populations. This led the researchers to question if similar trends exist in military populations, which may be influencing the treatment-seeking decisions of service members.
To summarize, soldiers’ confidence in treatment for and trust in mental health professionals might be significantly impacting treatment-seeking decisions. In multiple studies, service members have repeatedly indicated relatively low levels of trust and confidence in mental health providers and treatments. Also, researchers have consistently shown that a professional title can impact patient or public perceptions with respect to general confidence in the professional’s abilities. To date, no known research is published on military members’ perceptions and levels of confidence or trust with differing mental health professionals. Thus, the purpose of this study was to explore soldiers’ relative levels of trust for and confidence in mental health professionals based solely upon their title and a presenting issue, in an effort to better understand what may be influencing treatment-seeking decisions among U.S. Army soldiers.
Method
The researchers for this study received approval from the Institutional Review Board of their university, and the survey was approved for distribution to active-duty soldiers by Army public affairs representatives. Sample size was determined by following similar confidence in mental health professional studies that used Friedman non-parametric tests (e.g., Fall et al., 2000; Fall et al., 2005). Participants were surveyed via the online metrics program Qualtrics, ensuring anonymity.
Participants
Active-duty soldiers serving in the U.S. Army were recruited using snowball sampling initiated by public affairs representatives at various Army installations. Each potential participant received a generalized email invitation that included an information sheet about the research and a link to complete an online survey. Participants were encouraged to forward the invitation to others who also met the inclusion criteria, which limited participation to those currently serving on active duty in the U.S. Army with more than 2 years of active-duty service or the National Guard/Army Reserve equivalent. Upon completion of the survey, participants were offered the opportunity to enroll in a raffle drawing to win one of two prizes: a $100 or a $50 gift card.
The sample included 32 active-duty soldiers, 26 males and six females, between the ages of 25 and 50 years (M = 33.3, SD = 7.0). Ethnic identities included 25 non-Hispanic Whites, two Hispanic or Latinos, one African American, one Filipino, one Native American, one White/Korean, and one White/Hispanic. Most of the participants (26) were married, while three were divorced and three had never married. Nearly two-thirds of the sample indicated current responsibility for children in their homes; there was an average of 1.85 children (SD = 1.5) reported by these 20 participants. Thirteen of the soldiers had seen at least one mental health professional (MHP) prior to completing the survey; respondents had seen all five MHPs included in this study. Participants were allowed to list multiple MHPs if applicable, and the MHPs were identified as follows: clinical psychologist, seven times; psychiatrist, five times; LPC, four times; LCSW, three times; LMFT, three times; and “other” or “unsure,”five times.
Regarding military experience, the sample included 18 officers, 11 non-commissioned officers, and three junior-enlisted (i.e., rank of E1–E4) soldiers. Twenty participants had a military occupational specialty (MOS) considered as Combat Arms in the U.S. Army. In the military, not all service members are equally likely to fight in combat; certain MOSs are combat-related while others are supportive in nature (e.g., administrative personnel, mechanics, logisticians). Of our 32 qualifying participants, we had a good mix of combat and non-combat MOSs. To the reader, this may seem to be either irrelevant or not particularly noteworthy information; however, this data can be quite important when forming conclusions about the study. On average, military service was 11.4 years (SD = 7.2), with 17 months (SD = 11.5) deployed to either Iraq or Afghanistan; only two participants had not been deployed to these countries. Seventy-five percent of the sample reported direct exposure to combat, and 59% reported having never seen an MHP for even one visit throughout their life.
Materials
Demographic questionnaire. In order to provide some description of the sample population, a demographics survey of 15 questions regarding age, sex, ethnicity, marital background, parental status, military rank, deployment and combat experience, and previous experience with mental health care providers was collected from participants. Most questions were multiple-choice but offered the options to not respond or provide a unique response if desired. The remaining questions were free-response.
Vignettes. Brief vignettes were used to depict the selected mental health diagnoses or mental health issues of eight fictional soldiers recently returning from a combat deployment. The vignettes were limited in length to approximately half of a standard printed page and were written with the goal of depicting diagnostic criteria in a manner that one might see them manifested by the soldier in the vignette. Authors specifically avoided using the exact clinical terms that an MHP may use while ensuring that enough diagnostic criteria were included to suggest the intended diagnoses may be warranted.
Each vignette was followed immediately by two questions. These questions asked the participant to rank the five MHPs in order according to the participant’s preference for (1) confidence in the MHPs in providing treatment for the soldier in the vignette, and (2) their own personal trust for the professionals if they were experiencing the symptoms described in the vignette. Because both questions were worded similarly, keywords such as trust and confident were bolded or underlined in order to highlight the intent of the question.
Development and validation of the vignettes.
The vignettes and questions were originally drafted by the lead researcher to explore how soldiers may rank MHPs under the two stated conditions (i.e., confidence and trust questions). The four mental health diagnoses selected were PTSD, anxiety disorders, depression, and substance use disorders, as these were identified by Seal, Bertenthal, Miner, Sen, and Marmar (2007) to be the most prevalent for soldiers returning from Iraq. The four common issues were suicide, marital problems, parenting difficulties, and sleep problems; these were selected from the Military Health System’s “After Deployment” (2015) website because they were depicted as common problems faced by soldiers and contributed to the breadth of issues explored in the study. Vignettes were modeled after previous studies using similar metrics to measure populations’ trust of MHPs (e.g., Fall et al., 2000; Fall et al., 2005).
After review and editing within the research team, faculty with extensive clinical and teaching expertise in the area of diagnosis reviewed the vignettes. Based on their recommendations, specific diagnostic labels, such as PTSD and depression, were removed in order to reduce the impact of these labels on participants’ responses, and the keywords trust and confidence were included and bolded in the survey questions. Their input also resulted in the refining of the vignettes to more accurately depict the intended issues based upon their clinical experience and expertise.
Procedures
From January to June of 2017, surveys were administered via Qualtrics software on an electronic device of the participant’s choosing. Respondents were requested to complete the surveys at a location and time presenting minimal distractions. After being provided information about the study and consenting to continue, participants were presented with the demographics survey followed by the vignettes. The survey would not advance to the next page unless a response was recorded to all questions on the previous page. Upon completion of the demographics portion, participants advanced to the vignettes depicting soldiers facing issues upon returning from a combat deployment.
During the vignette portion of the survey, respondents ranked the list of mental health practitioners for both the confidence and trust conditions; see the Appendix for the vignettes presented to participants. The survey would not allow duplicate ranks (i.e., MHPs could not “tie”) for either condition. The vignettes were randomized, with both the trust and confidence questions presented together on the same screen, and the listed order of the MHPs was randomized for each vignette as well.
Analysis
Data analysis focused on three main themes: the mean ranks for trust of the MHPs across the vignettes, the mean ranks for confidence in the MHPs across the vignettes, and potential correlation between trust and confidence. Consistent with the Fall et al. (2005) analysis, Friedman non-parametric tests and Wilcoxon matched-pairs tests were used to determine significant findings in the mean ranks for MHPs in each vignette with respect to both the confidence and trust conditions separately. These tests were completed 16 times—once for each of the eight vignettes for both the trust and confidence questions. Afterward, the data was aggregated separately for both the trust and confidence questions to allow an overall assessment of the mean ranks for each MHP without concern for the particular vignette presented. Both the Friedman and Wilcoxon tests were completed again on the aggregated data. Finally, a Goodman and Kruskall’s gamma test was used to determine the correlation between trust and confidence ranking for each MHP.
Results
For all eight vignettes, significant differences (n = 32, df = 4, p <= .002) were found for mean rankings in both confidence and trust conditions. Subsequently, Wilcoxon matched-pairs tests identified statistically significant differences within groups for each of the 16 conditions; see Table 1 for specific results. Figures 1 and 2 display inverted mean rankings for each MHP by vignette for the confidence and trust questions respectively; higher scores indicate a more favorable ranking.
In both the confidence and trust conditions, the data from each vignette allowed for the separation of the five MHPs into either two or three distinct groups in terms of their rankings. In some instances, some MHPs could be grouped with both the higher- and lower-ranking adjacent MHP; in this case, the MHP was placed in both groups. For example, in Table 1 under the Aggregate Rank column for the confidence condition, there was no significant difference between LPCs and psychiatrists (N = 256, p = .202), or LPCs and psychologists (N = 256, p = .336), but there was a significant difference between psychologists and psychiatrists (N = 256, p = .011).
Lastly, scores from all eight vignettes were aggregated for each MHP to allow an overall measure of the MHP’s ranking for both confidence and trust. Table 1 includes the associated statistically significant grouping, and Figure 3 depicts the aggregated inverted mean ranking for both conditions for each MHP. Using a Goodman and Kruskall’s gamma test on the aggregated data, a strong positive correlation was found between confidence and trust ratings for all five MHPs with G values ranging from 0.72 to 0.88 (N = 256, p < .0005).
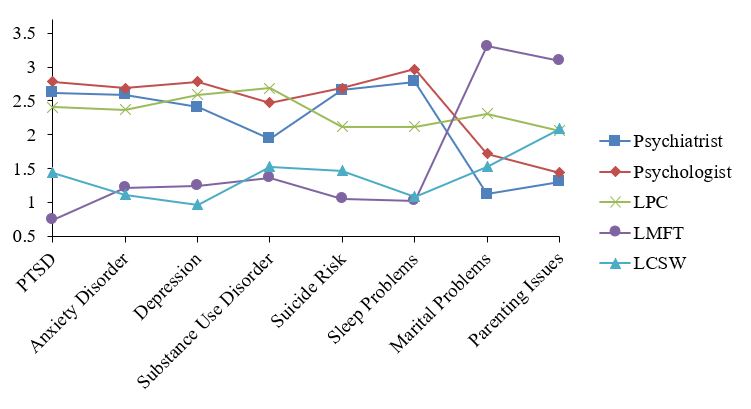
Figure 1. Inverted Mean Ranks for Confidence Question Plotted by Type of Mental Health Professional and Vignette. Higher mean rank equates to higher confidence.
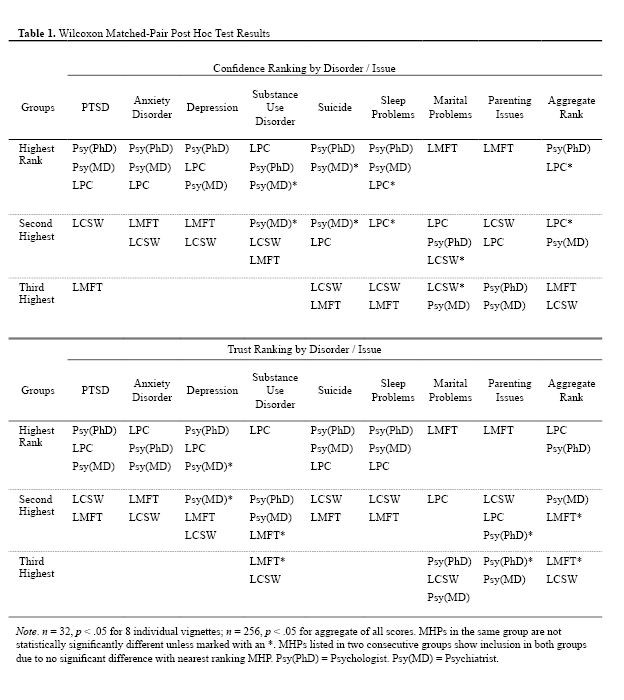
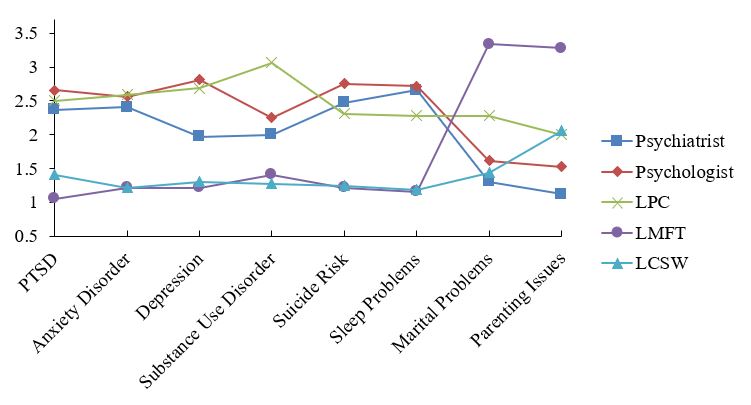
Figure 2. Inverted Mean Ranks for Trust Question Plotted by Type of Mental Health Professional and Vignette. Higher mean rank equates to higher trust.
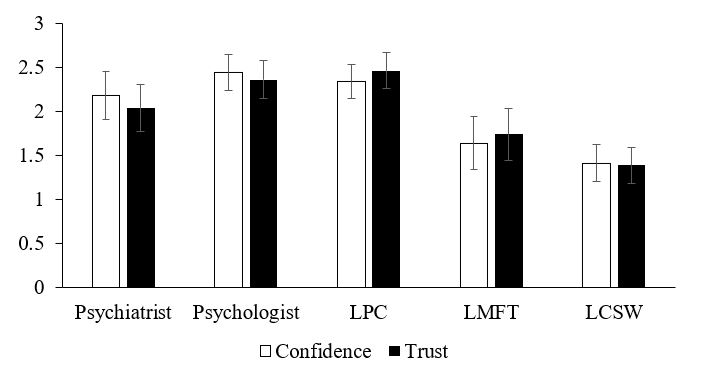
Figure 3. Aggregated Inverted Mean Ranks for Mental Health Professionals for Confidence and Trust Questions. Higher mean rank equates to higher confidence or trust. Error bars indicate standard error based on standard deviation from the mean; they do not indicate statistical significance.
Discussion
This study was designed to explore active-duty Army soldiers’ perceptions toward various mental health care providers with respect to trust and confidence in the MHP. Overall, the sample population of soldiers appears to have the highest confidence and trust in clinical psychologists and LPCs, while LCSWs and LMFTs are significantly less preferred (as seen in Table 1). Psychiatrists seem to be somewhere between each of these two groups, as they appear in both the highest and second-highest preferred groups depending on the condition (i.e., confidence or trust). The statistically significant stratification into these groups suggests that the title of available MHPs may influence a soldier’s decision to seek services. Undoubtedly, other factors are involved, but the title, and perhaps the certifications of the available professional, is likely impacting treatment-seeking behaviors in military communities.
At the heart of this study is the notion that each of the MHPs included could treat any of the soldiers in the vignettes; however, the results suggest that soldiers would seek out different professionals based on the context of the presenting symptoms rather than the type or potential efficacy of the treatment to be received. For example, the marital problems vignette (see Appendix) could arguably have been treated more effectively by a psychiatrist than an LMFT; perhaps the declining relationship was itself a symptom of biochemical issues such as vitamin or neurotransmitter deficiencies, which may be more aptly treated with medicine. Or, it also is possible that an experienced LPC or LCSW could have effectively brought to the surface some other underlying issue in the course of individual therapy rather than the marriage, couple, and family-oriented approach taken by an LMFT. Similar arguments could be made for each of the other vignettes, but the results suggest that soldiers are likely making treatment decisions based upon professional title and presumably the associated reputation. If the Army’s goal is to boost rates of treatment-seeking behaviors, professional titles and perceptions of trust and confidence should not be ignored.
Results also show a strong correlation between trust and confidence across all of the vignettes. This can best be seen by comparing the LMFTs’ rankings for the marital problems and parenting issues vignettes with their consistently lower scores on the other vignettes. The jump in scores was consistent across both conditions, demonstrating that trust and confidence for MHPs are strongly linked. Although less likely, it also is possible that the respondents might have been biased or influenced to provide similar ranks for each professional across both conditions because the survey design allowed them to see their scores for the confidence question while completing the trust question. Regardless of whether trust influences confidence or vice versa, the two should be considered in the quest to boost treatment-seeking rates among soldiers.
Implications for Service Provision
With further validating and corroborating research, the Army may be able to improve treatment-seeking rates among those in need of mental health care by adjusting services based on the perceptions of soldiers. Although LPCs were consistently favored more than LCSWs, the Army currently allows LCSWs to serve as commissioned officers in behavioral health clinics providing individual therapy to soldiers, while the LPC license does not qualify an MHP to commission and serve as an officer (U.S. Department of the Army, 2007). This means soldiers have fewer chances of seeing an LPC without some type of insurance referral because the uniformed personnel initially available will not be LPCs. This study provides evidence that LPCs may be more appropriate and effective in this role by boosting treatment-seeking rates, so it could be beneficial to make treatment with LPCs more accessible to soldiers. Likewise, incorporating the services of LMFTs following deployments could help military families, as they had the highest average trust and confidence ratings of any professional in any vignette in the study when they were the preferred MHP. Perhaps they could advocate for temporary positions following deployments or increased advertisement of their services in military communities with units returning from overseas.
Limitations and Future Research
Future research is certainly needed to further confirm the results of this study. Investigators could explore what drives trust and confidence perceptions in military communities and how prior personal experiences influence the soldiers’ views of MHPs. Studies like this one could be conducted with other branches of the military and include National Guard and Reserve forces. Exploratory qualitative research could seek to identify specific factors that build trust and confidence in the mental health community as a whole. Future studies also should continue to update the disorders or issues selected to accurately represent the issues faced by targeted populations at the time.
Limitations to this study include the sample size, delivery of the survey, and lack of consideration for gender biases. While 32 respondents can provide initial insights, a much larger sample should be surveyed before any significant policy decisions are considered. The research team also recommends administering the surveys in person rather than online with the belief that many soldiers—and people in general—may not complete the digital surveys as earnestly as a paper version following a personal interaction with the research team or a recruiter. With regards to gender, it was not considered how the names of the soldiers in the vignettes may influence the respondents’ rankings; it is possible that the scores could have varied if the soldier in the vignette was of a specific gender.
Future researchers should be cautious to ensure that voluntary participation is not influenced by environmental pressures. In military communities, the researchers recommend seeking a sample population that includes personnel from multiple units, locations, and MOSs, as culture and attitudes can be vastly different among these variables.
Although this study has limitations, the researchers believe it highlights one of the key reasons that soldiers may not seek mental health services when in need: lack of trust and confidence in the resources available. Although the military has significantly addressed other identified issues, such as the associated stigma or impact to a service member’s career, treatment-seeking rates for those in need have changed very little, which indicates other issues are contributing to the decision not to visit with an MHP. The researchers hope the results of this study are built upon and examined for alternative approaches to boost treatment-seeking rates among the military.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
After Deployment. (2015). After deployment: Wellness resources for the military community. Retrieved from
http://afterdeployment.dcoe.mil
American Counseling Association. (2011). Who are licensed professional counselors. Retrieved from
https://www.counseling.org/PublicPolicy/WhoAreLPCs.pdf
Bradley, C., Maschi, T., O’Brien, H., Morgen, K., & Ward, K. (2012). Faithful but different: Clinical social workers speak out about career motivation and professional values. Journal of Social Work Education, 48, 459–477. doi:10.5175/JSWE.2012.201000043
Britt, T. W., Bennett, E. A., Crabtree, M., Haugh, C., Oliver, K., McFadden, A., & Pury, C. L. S. (2011). The theory of planned behavior and reserve component veteran treatment seeking. Military Psychology, 23, 82–96. doi:10.1080/08995605.2011.534417
Britt, T. W., Jennings, K. S., Cheung, J. H., Pury, C. L. S., & Zinzow, H. M. (2015). The role of different stigma perceptions in treatment seeking and dropout among active duty military personnel. Psychiatric Rehabilitation Journal, 38, 142–149. doi:10.1037/prj0000120
Clemens, N. A., Plakun, E. M., Lazar, S. G., & Mellman, L. (2014). Obstacles to early career psychiatrists practicing psychotherapy. Psychodynamic Psychiatry, 42, 479–495. doi:10.1521/pdps.2014.42.3.479
Fall, K. A., Levitov, J. E., Anderson, L., & Clay, H. (2005). African Americans’ perception of mental health professions. International Journal for the Advancement of Counselling, 27, 47–56.
doi:10.1007/s10447-005-2246-y
Fall, K. A., Levitov, J. E., Jennings, M., & Eberts, S. (2000). The public perception of mental health professions: An empirical examination. Journal of Mental Health Counseling, 22, 122–134.
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., & Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. New England Journal of Medicine, 351, 13–22. doi:10.1056/NEJMoa040603
Imber-Black, E. (2014). Eschewing certainties: The creation of family therapists in the 21st century. Family Process, 53, 371–379. doi:10.1111/famp.12091
Kim, P. Y., Britt, T. W., Klocko, R. P., Riviere, L. A., & Adler, A. B. (2011). Stigma, negative attitudes about treatment, and utilization of mental health care among soldiers. Military Psychology, 23, 65–81.
doi:10.1080/08995605.2011.534415
Mellin, E. A., Hunt, B., & Nichols, L. M. (2011). Counselor professional identity: Findings and implications for counseling and interprofessional collaboration. Journal of Counseling & Development, 89, 140–147. doi:10.1002/j.1556-6678.2011.tb00071.x
Norcross, J. C., & Karpiak, C. P. (2012). Clinical psychologists in the 2010s: 50 Years of the APA Division of Clinical Psychology. Clinical Psychology: Science and Practice, 19, 1–12.
doi:10.1111/j.1468-2850.2012.01269.x
Reiner, S. M., Dobmeier, R. A., & Hernández, T. J. (2013). Perceived impact of professional counselor identity: An exploratory study. Journal of Counseling & Development, 91, 174–183.
doi:10.1002/j.1556-6676.2013.00084.x
Schell, T. L., & Marshall, G. N. (2008). Survey of individuals previously deployed for OEF/OIF. In T. Tanielian & L. H. Jaycox (Eds.), Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery (pp. 87–115). Santa Monica, CA: RAND Health Center for Military Health Policy Research.
Seal, K. H., Bertenthal, D., Miner, C. R., Sen, S., & Marmar, C. (2007). Bringing the war back home: Mental health disorders among 103,788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs facilities. Archives of Internal Medicine, 167, 476–482.
U.S. Army Medical Department. (2016). Behavioral health. Retrieved from https://armymedicine.health.mil/Behavioral-Health
U.S. Department of the Army. (2007). Army Medical Department Officer Development and Career Management: Department of the Army Pamphlet 600-4. Retrieved from http://www.apd.army.mil/epubs/DR_pubs/DR_a/pdf/web/p600_4.pdf
VanSickle, M., Werbel, A., Perera, K., Pak, K., DeYoung, K., & Ghahramanlou-Holloway, M. (2016). Perceived barriers to seeking mental health care among United States Marine Corps noncommissioned officers serving as gatekeepers for suicide prevention. Psychological Assessment, 28, 1020–1025.
doi:10.1037/pas0000212
Warner, D. L., & Bradley, J. R. (1991). Undergraduate psychology students’ views of counselors, psychiatrists, and psychologists: A challenge to academic psychologists. Professional Psychology: Research and Practice, 22, 138–140.
Wollersheim, D. M., & Walsh, J. A. (1993). Clinical psychologists: Professionals without a role? Professional Psychology: Research and Practice, 24, 171–175.
Zisook, S., McQuaid, J. R., Sciolla, A., Lanouette, N., Calabrese, C., & Dunn, L. B. (2011). Psychiatric residents’ interest in psychotherapy and training stage: A multi-site survey. American Journal of Psychotherapy, 65, 47–59.
Appendix
Vignettes Used to Depict Mental Health Diagnoses and Issues
Post-Traumatic Stress Disorder Vignette
Joe returned from deployment to Afghanistan 4 months ago. He was personally involved in combat with enemy insurgents on multiple occasions and was exposed to disfigured, dead bodies of both enemy combatants and fellow soldiers as well. He has often mentioned bad dreams about one of these times in particular and seems obviously distressed (e.g., fidgeting, faster breathing, and sometimes even sweating) whenever he speaks about it. However, when his fellow soldiers from the deployment bring up the event, he seems unwilling to participate in the conversation and has on a few occasions become angry about it. Based on these behaviors, you believe he may be struggling with traumatic experiences.
Anxiety Disorder Vignette
John returned from a combat deployment 9 months ago. Since returning, his family and coworkers have noticed changes in his behavior. He is often restless (or “on edge”), irritable, or physically tense in common, everyday situations. Plus, he has claimed poor or unsatisfying sleep for several months. These symptoms seem to be impairing his work performance and damaging personal relationships with loved ones. When asked, he hasn’t mentioned any particular traumatic events or worries that are bothering him. He simply seems much more anxious and it is affecting his well-being.
Depression Vignette
Jane returned from a combat deployment 3 months ago and has generally seemed a little bit down since coming home. Nearly every day over the past 2 weeks she has seemed to be sad or gloomy throughout the day and has shown very little interest in doing things she used to enjoy. She is clearly tired throughout the day and has mentioned feeling worthless to those around her. It seems like she is suffering greatly based on her unhappy and sad moods.
Substance Abuse Disorder Vignette
Jim returned from a combat deployment 12 months ago. Upon returning, he seemed to seamlessly reintegrate with his family, friends, and former social life. However, he soon began drinking alcohol more heavily than ever before, often binge drinking until passing out on weekdays and weekends. Although never caught in the act, he has even gone to work intoxicated and driven while drunk on multiple occasions. On two distinct occasions, he attempted to reduce his alcohol consumption but failed after only a week or two. Alcohol abuse is beginning to disrupt his work performance, family life, and physical well-being.
Sleep Problems Vignette
Joan returned from a combat deployment 4 months ago. She seems to have reintegrated very successfully into her family, social, and work environments. However, her sleep patterns have become very irregular and unsatisfactory. She rarely gets more than 4 hours of sleep consecutively and often uses her weekends to recover from a week of sleepless nights. Although her family and coworkers haven’t noticed anything wrong, Joan fears her sleep problems will soon begin disrupting her life.
Suicide Risk Vignette
James returned from a combat deployment 6 months ago. Since returning, he has outwardly seemed to have successfully reintegrated into his family, work, and social life. Although he appears to have been changed by his combat experiences, he does not seem to be generally troubled in any way (e.g., depressed, anxious, abusing drugs). However, he has jokingly mentioned “blowing his brains out” to colleagues at work and mentioned a specific plan to take his own life with his pistol. During a conversation with two friends, he has mentioned “ending it all” because he is feeling hopeless. You think James may be at risk for suicide.
Marital Problems Vignette
Jon returned from a combat deployment 5 months ago. He has rejoined his wife of 6 years, but their relationship has changed. While they used to feel very close and connected, they now both feel very distant. They do not enjoy activities together which they used to, such as hiking and dancing. They rarely hold good conversations with each other and are also less physically intimate. Jon and his wife both want their marriage to work but fear that they are nearing divorce. They are facing the most significant period of marital problems they have ever experienced.
Parenting Issues Vignette
Jerry returned from a combat deployment 10 months ago. He rejoined his wife of 16 years, their 13-year-old daughter, and their 5-year-old son. Since returning, Jerry has experienced some difficulty reassuming his role as a parent. His daughter seems to want very little to do with him. Although he thinks this is typical of a 13-year-old, it still causes him distress and he complains that he doesn’t feel like he has any influence in her life. With their son, Jerry often disagrees with his wife on discipline issues, and he can’t seem to find ways to connect with the 5-year-old. His son seems to have little interest in playing anything besides video games and always runs to his mother when Jerry attempts to discipline him. These parenting issues are significantly affecting Jerry’s mental and emotional well-being.
Anthony Hartman is a medical student at UT-Health San Antonio. Hope Schuermann is a clinical assistant professor at the University of Florida. Jovanna Kenney is a therapist at Genesis Psychiatric Center in San Antonio, TX. Correspondence can be addressed to Anthony Hartman, 7703 Floyd Curl Drive, San Antonio, TX 78229, hartmanaj@livemail.uthscsa.edu.
Sep 28, 2018 | Volume 8 - Issue 3
Jennifer L. Rogers, Dennis D. Gilbride, Brian J. Dew
This conceptual article provides a counselor-oriented overview of the origins and consequences of the current opioid epidemic in the United States. After a thorough review of Bronfenbrenner’s ecological perspective on human development, this article presents a case conceptualization model aimed at providing counselors with a tool and strategy to better understand how systemic complexities impact opioid-dependent clients and their communities. A detailed composite case study is used to demonstrate the influence of multiple ecological variables on a specific client. Individual, micro-, meso-, exo-, macro-, and chronosystem stimuli are explored, and the role of advocacy as inherent in systemic conceptualization and treatment planning is discussed.
Keywords: opioid epidemic, ecological, Bronfenbrenner, opioid-dependent, case conceptualization
Alarming national headlines related to opioid addiction highlight a public and mental health emergency across America. Overdoses and opioid-related deaths are skyrocketing (Rudd, Seth, David, & Scholl, 2016; Skolnick, 2018; Suzuki & El-Haddad, 2017), and the lifespan of many Americans, especially in rural areas, is declining for the first time in generations due in part to maladaptive use of narcotics (Katz, 2017a). Opioid painkillers are the most frequently prescribed class of drugs in the United States (Skolnick, 2018). Misuse of these drugs often leads to the use of heroin, a cheaper and more potent alternative to prescription painkillers (Skolnick, 2018). Heroin is increasingly cut with the synthetic opioid fentanyl (50–100 times stronger than morphine) and its various analogs, such as carfentanil (a veterinary drug used to rapidly immobilize wild animals; Suzuki & El-Haddad, 2017), contributing to the recent dramatic rise in overdose deaths (Katz, 2017b; Suzuki & El-Haddad, 2017). The opioid epidemic also is associated with increases in a host of other negative outcomes, including rates of HIV and hepatitis C, arrests and incarcerations, and neonatal abstinence syndrome (Skolnick, 2018).
Addictions, mental health, rehabilitation, and school counselors are challenged to find better ways to understand and assist users, families, and communities being ravaged by this public health crisis. Clinicians and researchers have developed multiple individual and community-based strategies to assist clients with substance abuse, but current circumstances have underscored the need for members of the counseling profession to take a more comprehensive and ecological approach to both understanding and addressing the needs of people struggling with opioid addiction (Dasgupta, Beletsky, & Ciccarone, 2018; Hewell, Vasquez, & Rivkin, 2017; Keyes, Cerdá, Brady, Havens, & Galea, 2014; Kolodny et al., 2015). In subsequent sections, details of this public and mental health crisis are described, and an ecological case conceptualization model that utilizes eco-mapping to assist counselors in better understanding and developing systemic treatment plans is presented. A case study allowing for the application of the model is provided, and implications for counselors are explored.
An Opioid Overview
Mental and public health officials have long recognized the popularity and uniquely addictive potential of substances classified as opioids. Use of opium and morphine first became a problem in America during the late 1800s (Kolodny et al., 2015). Morphine was used to treat a variety of chronic and acute ailments, including diarrhea and injuries sustained in battle. Smoking opium recreationally became popular in some circles, and physicians also inadvertently addicted their patients by prescribing opioid treatments. As medicine and public health advanced, more diseases could be avoided, cured, or treated without the use of highly addictive opioids, and their use fell out of favor by 1919 (Kolodny et al., 2015). In the second half of the 20th century, heroin addiction intermittently rose to epidemic levels among disadvantaged urban populations, especially in the large cities of the northeast and west coast of the United States (Kolodny et al., 2015; McCoy, McGuire, Curtis, & Spunt, 2005). More recently, the introduction of synthetic prescription opiates (e.g., Vicodin, Percocet) in the 1980s and the approval of sustained-release oxycodone (brand name OxyContin) in 1996 brought pain relief to millions of users, but has contributed to high levels of abuse and dependence nationwide (Van Zee, 2009).
Opioid Effects
To understand the addictive nature of opioids, counselors must account for the acute effects of their use (e.g., relief from physical and psychological pain), unique side effects (e.g., opioid-induced pain sensitivity, painful withdrawal symptoms), ease and speed with which tolerance is established, and potential resulting impairments in daily functioning (Kosten & George, 2002). When opiates bind with neural opioid receptors in the brain, spinal cord, gastrointestinal tract, and other organs, they inhibit the release of pain signals, blocking the user from experiencing both physical and emotional suffering. Some people are naturally more vulnerable to developing opioid tolerance (taking more drug for the same effect) and dependence (drug required to avoid withdrawal; Kosten & George, 2002). Susceptibility is influenced by a variety of biopsychosocial factors (e.g., brain structures, cellular differences, context of use, stress). In a study examining opioid prescribing patterns, 25% of patients who had a new opioid prescription progressed to receiving additional prescriptions episodically or chronically (Hooten, St. Sauver, McGree, Jacobson, & Warner, 2015). Nicotine addiction, overall poor health, psychiatric diagnosis, and history of substance abuse were found to increase the likelihood of ongoing opioid use. Withdrawal symptoms lasting three to five days—including nausea, muscle cramping, body aches, anxiety, and inability to sleep—can compel users to obtain immediate symptom relief via the use of additional opioids (Kosten & George, 2002). In an attempt to avoid debilitating withdrawal symptoms, users become reliant on the drug to function at a normative, baseline state.
Current Opioid Epidemic
Although the pathway to opioid abuse and addiction is not new, a culmination of ecological factors over the last 20 years has led to what is now commonly referred to as a national epidemic (Kolodny et al., 2015; Skolnick, 2018). These factors include changes in prescribing patterns, increased supply, rampant growth of illicit use, the progression to intravenous heroin use among chronic users, and the lethal contamination of heroin and fake prescription pills with highly potent synthetic opioids like fentanyl, as well as broader systemic variables such as poverty and access to health care (Dasgupta et al., 2018).
The dramatic increase in the availability of prescription opioids in the early 21st century stemmed, in part, from changes in medical attitudes and policies (Kolodny et al., 2015; Skolnick, 2018). Spearheaded by the American Pain Society’s advocacy efforts to have pain recognized as a fifth vital sign (along with temperature, pulse, respiration rate, and blood pressure) in the mid-1990s, the Joint Commission and the Veterans Health Administration formally endorsed patients’ rights to pain assessment management in 2000 (Kolodny et al., 2015; Skolnick, 2018). Helping patients avoid physical pain thus became a primary focus of medical care. During the same time period, Purdue Pharma provided financial contributions to multiple medical and patient organizations (e.g., the American Pain Society, the Joint Commission, the Federation of State Medical Boards) and lobbied to allay concerns regarding long-term use of prescription opioids in the treatment of chronic non-cancer pain (Kolodny et al., 2015). Methodologically questionable research studies were widely cited to minimize the perceived risks associated with long-term use and addiction. Sales of Purdue Pharma’s doggedly promoted, non-generic OxyContin grew from $48 million in sales in 1996 (316,000 prescriptions) to almost $3 billion (more than 14 million prescriptions) in 2001–2002 (Van Zee, 2009). Though the time-release formula was touted as a deterrent for misuse, users discovered the pills could be crushed and then snorted or injected. In 2000, Purdue released a 160 milligram tablet (up from the previous high dose of 80 milligrams) approved for use by patients who had developed opioid tolerance, further increasing OxyContin’s draw as a drug of abuse (Van Zee, 2009).
An increase in opioid supply via both unwitting and unscrupulous prescribers was quickly followed by the rapid acceleration of opiate abuse across the country (Van Zee, 2009). Unlike other illicit substances (e.g., cocaine, methamphetamine, ecstasy), these pain-killing medications were prescribed by medical professionals and therefore assumed to be safe. Prescription opiates were accessible through doctors, family, friends, the internet, and on the black market. Long-term use of prescription opiates can lead to tolerance and eventual physical dependence, requiring a continuous supply of drugs and financial resources to purchase them. Users of prescription opiates have increasingly turned to heroin (Skolnick, 2018) as a cheaper, more readily available option to keep painful withdrawal symptoms at bay. With increased availability and visibility, many people now report that their opioid use started with heroin rather than prescription drugs (Dasgupta et al., 2018).
The rise of the presence of illegally manufactured fentanyl in opioids available on the illicit market has had increasingly deadly consequences, with fentanyl-related deaths in the United States up 540% between 2013 and 2016 (Katz, 2017b). Average life expectancy is now declining among some segments of the population—unusual except in times of war (Dasgupta et al., 2018). Unlike other U.S. drug use crises that have disproportionately affected minority populations (e.g., crack cocaine), there has been a focus in this crisis on over-prescribing as the root cause, rather than the moral failings of individual users. This broader view may help destigmatize the current situation, but it is imperative to recognize that complex factors lead to susceptibility to all such crises. For instance, in areas particularly affected by the opioid crisis, mortality associated with alcoholism, drug overdoses, and suicide (known as “diseases of despair”) has increased as local economies have declined (Dasgupta et al., 2018).
The devastation of individual lives, families, and communities resulting from this epidemic is clear, and the complexity of the issues it has engendered requires counselors to expand treatment strategies and interventions. In the next section, we review Bronfenbrenner’s (1979, 1994) ecological systems theory and present a strategy designed to help counselors both understand and intervene with clients and communities battling this challenge.
Ecological Perspective
Bronfenbrenner’s foundational work, The Ecology of Human Development (1979), described how a child develops within a series of interrelated systems. He posited that human development processes are influenced by individual characteristics, as well as features in one’s immediate and more distant environments. Over the course of a lifetime, development progresses through a series of increasingly complex and reciprocal interactions between an individual and the people, things, and symbols in their environment. Research designed to investigate this developmental progression is described as aligning with a process-person-context model (Bronfenbrenner, 1994) and is endemic in our current understanding of psychological health and illness.
Drawing upon Lewin’s (1935) theory of psychological fields (as cited in Bronfenbrenner, 1979), the ecology of a developing person is described as a set of nested structures, one inside the other (see Figure 1). The innermost system, called the microsystem, was defined by Bronfenbrenner as the pattern of personal interactions and activities that occur face-to-face with a person in their immediate environment (Bronfenbrenner, 1979, 1994). These interactions include an individual’s family, friends, schoolmates, teachers, neighbors, and colleagues. The proximal processes occurring between family members in the microsystem are among the most frequently studied in the psychological literature (Bronfenbrenner, 1994). These close relationships have extraordinary power to normalize or stigmatize behaviors and to support or hinder optimal individual development. Examples of behaviors that may be supported or discouraged within a microsystem include child-rearing practices, therapeutic or recreational use of prescription medication, pursuit of educational or occupational goals, religious practices, and encouragement of relationships with persons or groups outside the immediate microsystem.
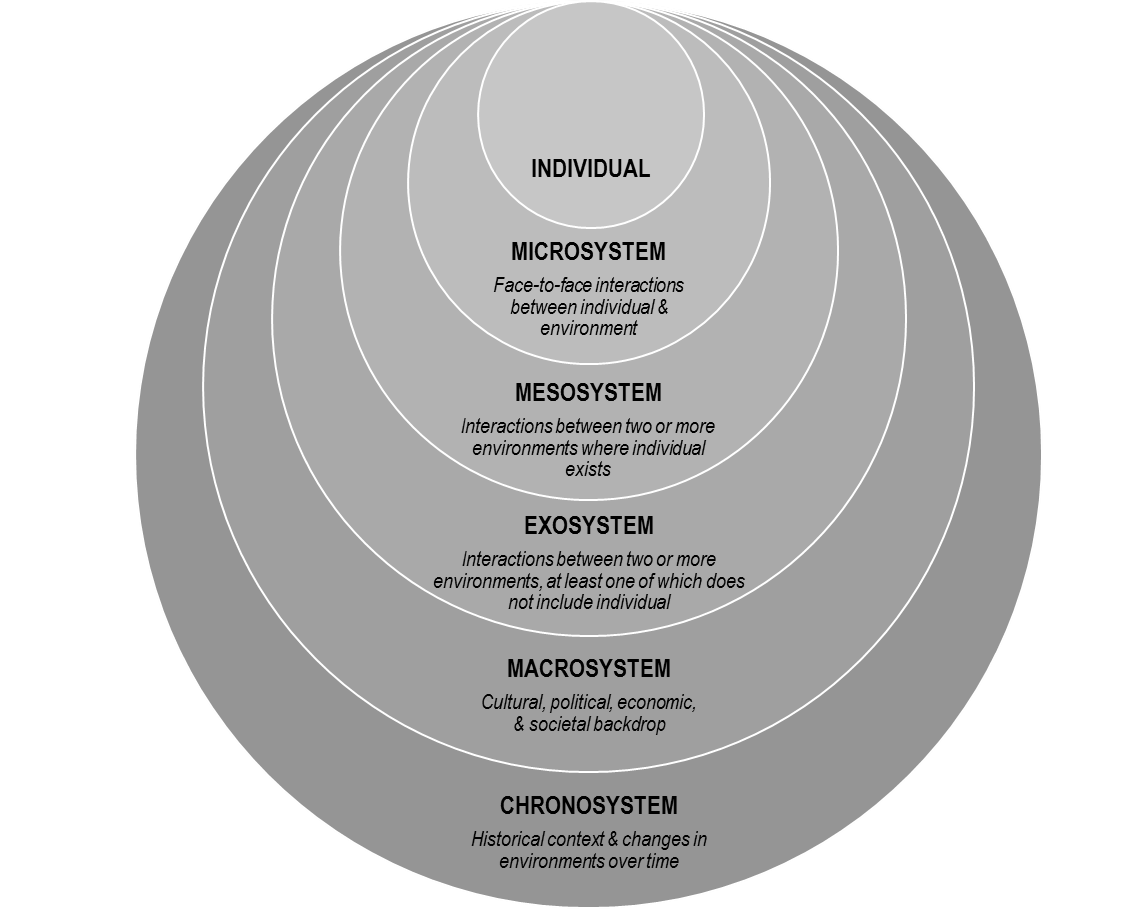
Figure 1. Bronfenbrenner’s Ecological Model
The mesosystem includes the processes and connections occurring between two or more environments in which an individual exists, or the system of microsystems in a person’s life (Bronfenbrenner, 1979, 1994). Interactions between a person’s home, school, workplace, neighborhood, place of worship, or medical providers are described as occurring within the mesosystem. Examples of mesosystem processes include how the closing of a manufacturing plant where an individual was employed could lead to a decline in the condition of his or her neighborhood, or how patients of a local physician who frequently prescribes pain medication may experience an increase in the off-market availability of such medication within his or her neighborhood, family, or peer group.
The exosystem is comprised of processes occurring between two or more environments, at least one of which does not include the individual of interest (Bronfenbrenner, 1979, 1994). Even though a person may not exist within a certain setting, outside events can indirectly influence that person’s immediate environment. Examples of exosystem processes include how a new local company’s practice of only hiring college-educated workers influences less educated workers in a nearby neighborhood, or how decisions by legislators regarding health care policy influence local hospitals and family decisions about medical care.
The macrosystem represents the patterns, policies, laws, values, and trends that comprise the broad cultural, political, economic, and societal/environmental backdrop of an individual’s life (Bronfenbrenner, 1979, 1994). Macrosystems include mega factors such as advances in technology and the rapid transition into the information age, the precipitous move away from manufacturing in the United States, the increasing need for a college education to obtain a salary that can sustain a middle-class lifestyle, changes in how health care is funded and delivered, the decline in membership in organized religious institutions, and a growing cultural emphasis on individualism. Other trends include changes in how information is delivered and consumed, and the increasing gulf between rural and urban communities.
The chronosystem describes changes in an environment over time related to each of the other systems (Bronfenbrenner, 1994)—the normal growth and development of a person or family, the effect of a move or migrations of families or groups, and the effects of large historic events such as wars, natural disasters, and recessions. The chronosystem highlights that along with living within nested or interacting systems, a person also lives within the history of their own life—as well as within the history of their family, community, state, nation, and world (Bronfenbrenner, 1994).
Ungar, Ghazinour, and Richter (2013) expanded Bronfenbrenner’s model in their studies of resilience to include a focus on the success of individuals and groups to secure resources leading to healthy development, even in adverse circumstances. Ungar and colleagues’ model describes systems as reciprocal rather than hierarchical. The effect of a systemic variable is not just related to its proximity to an individual (per Bronfenbrenner’s nested model as described above and in Figure 1), but rather on its importance to a particular person at a specific point in time. For example, a war and its related geo-politics (a macrosystem issue) may be much more salient than school (a mesosystem issue) for a particular child living under siege in Syria.
An Ecological Conceptualization of Opioid Addiction
A social-ecological perspective is tacit in many popular journalistic efforts focused upon the opioid use epidemic, including books (e.g., Hillbilly Elegy; Vance, 2016), documentaries (e.g., Warning: This Drug May Kill You; Peltz, 2017), and investigative news reports (e.g., Talbot, 2017). In these long-form examinations, a multitude of distal and proximal variables influencing opioid use patterns among individuals are described. Recent scholarly publications outside of the counseling literature have utilized implied (Dasgupta et al., 2018; Kolodny et al., 2015) and overt ecological (Hewell et al., 2017; Keyes et al., 2014) lenses to examine this problem. Keyes and colleagues (2014) undertook a large ecological synthesis of the extant empirical literature related to the opioid crisis in rural America. They identified the following risks in their analyses: (1) increased availability and access; (2) lower perceptions of harm; (3) self-medicating for pain; (4) more increased availability in rural rather than urban areas; (5) out-migration of young people (rural economic declines, and via selection effect, young adults remaining in economically depressed areas may have a greater number of risk factors); (6) differences between urban and rural social and kinship networks (importance of community investment, family ties, work over education, and local social capital in rural areas); and (7) structural stressors of modern rural living (unemployment and economic deprivation).
In their qualitative inquiry about systemic and individual factors in medication-assisted treatment for opioid abuse, Hewell and colleagues (2017) reported findings supporting the construct of recovery capital (including personal recovery capital, family and social recovery capital, and community recovery capital), as well as suggesting the interactional relationship of such resources. They advised practitioners to be educated about multiple ecological influences and to be flexible in their approaches so as to utilize ever-changing sources of recovery capital available to their clients.
Ecological Conceptualization and Treatment Planning
The proposed counseling, teaching, and intervention strategies are an extension and elaboration of the eco-webbing model proposed by Williams, McMahon, and Goodman (2015). The authors described a strategy designed to facilitate more critical consciousness thinking in their students by creating visual representations of the factors and forces that may be affecting a client’s life and situation. Concept mapping strategies have been found to be powerful tools in creating visual representations of key factors affecting a client’s health and treatment needs (Gul & Boman, 2006) and in enhancing critical thinking.
In Phase 1 of Williams and colleagues’ (2015) model, they ask counseling students to brainstorm all the variables related to a client’s problem. In the present model, we expand and structure this phase to include a systematic analysis of each of the system levels identified by Bronfenbrenner (1979, 1994) in order to create an eco-map. Phase 2 of the Williams’ et al. model (2015) involves the distillation of information and themes. We address this phase by utilizing Ungar et al.’s (2013) concept of differential impact. Ungar and colleagues assert that although Bronfenbrenner’s systemic levels are often visually represented as nested and hierarchal (i.e., levels closer to the center where the individual is more important), this structuring is merely a heuristic device, and that it is more useful to understand various systems and subsystems as reciprocal, having differential impacts at various moments and in various contexts. In the present model, we address Phase 2 by visually prioritizing different systemic issues and factors. As indicated in Figure 2, key factors from each of Bronfenbrenner’s systemic levels are illustrated by circles in the eco-map rather than in the traditionally nested manner. Based upon the client and counselor’s joint evaluation, many variables are included in the eco-map, with their current importance to the client represented by both relative size and distance from the center of the map.
The final phase of the eco-webbing process, as described by Williams and colleagues (2015), calls for reflection upon the central issue and the multiple eco-systemic factors, and how these may inform the counseling process. Reflection upon the eco-webbing process itself is also encouraged. Our model expands upon these steps by using the information visually represented in the eco-map to structure and develop a formal treatment plan including both individual and systemic variables in the order and priority of their current effect on the client. Over the course of counseling, the eco-map can be revisited and restructured to represent the shifting centrality of various factors. For example, in an initial eco-map, access to a detox treatment center may be largest and at the center, while 6 months later, labor market or family relationship issues may enlarge and move toward the center.
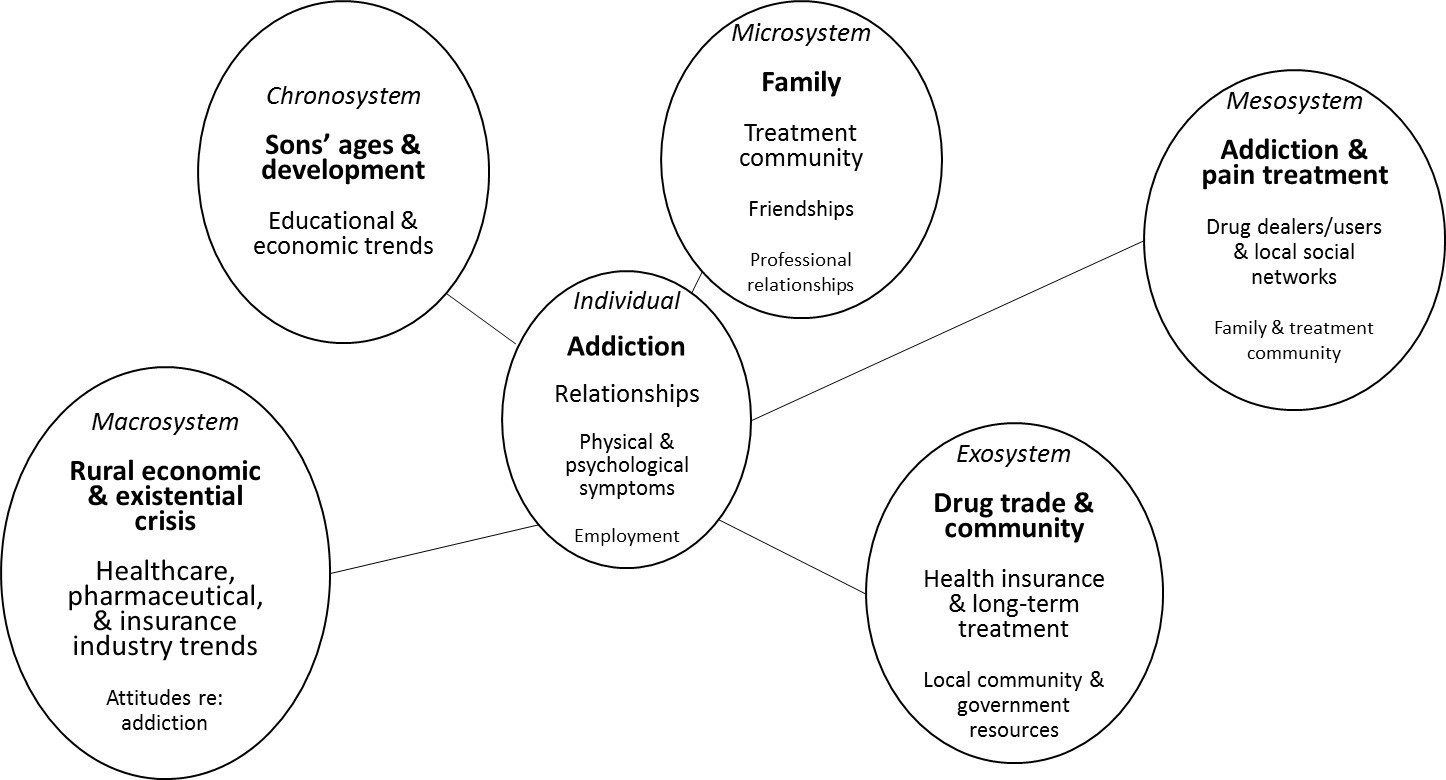
Figure 2. Eco-map for Jason
In the following sections, we present a client case study, suggest an ecological approach to understanding our client, and offer treatment strategies based upon our ecological conceptualization.
Case Study: Jason
Jason is a 37-year-old White male who lives in a southwest West Virginia town with a population of 30,000. Jason’s father and grandfather were both coal miners who worked hard, made a good living, and were active in the local community as church members and volunteer firemen. Jason had a happy childhood with no remarkable adverse events. He was a star of the high school football team. Having seen his grandfather die from black lung disease and his father suffer from emphysema, Jason vowed to never work in the mines. By the time he graduated high school, there were few mining jobs available. Jason began work for a concrete company, pouring concrete for residential and commercial projects. He was popular among his coworkers and relished working outdoors. At age 21 he married a young woman he had known since childhood and within 3 years they had two sons.
After 10 years on the job, Jason was laid off because of the lack of new development in his town. Jason moved his young family to a larger town in Ohio to do concrete work for a commercial construction company. The working environment was very different, and Jason was required to take orders from contractors, rather than being in charge of each job as he had become accustomed to back home. Jason’s wife was very unhappy living away from their friends and family. After a few months, she and the children moved back to live with her parents. Jason visited on the weekends, but the arrangement strained their marriage, and within 2 years his wife filed for divorce. Around the same time, his father died from lung cancer.
Jason had a number of back injuries over the years while working, but when he fell at home while moving a piece of heavy furniture, he herniated three discs and was restricted from many physical activities because of continuous pain. Because this debilitating injury occurred at home, Jason did not qualify for worker’s compensation benefits. He had surgery on his back and returned home with a prescription for narcotic pain medication. He did not comply with his doctor’s orders regarding physical therapy because as an hourly laborer, he could not afford any more time off work. Though the surgery did alleviate some of his pain initially, after a year it was clear that the operation did not fully repair his spine, and his pain again became unbearable. His doctor prescribed Percocet for him to take in the evenings when his pain was the worst, but over time, the medication became less effective. He visited a pain clinic near his apartment and received a prescription for OxyContin, which was stronger and long-acting. Jason noticed he felt less lonely and discouraged after taking the pills, which he began to do more often. Soon, Jason was not himself at work—making mistakes, forgetting things, and having conflicts with his supervisors. He was fired from his job.
With no savings, outstanding medical bills, and being unable to work in his field, Jason returned home to live in a small house on his mother’s property. He applied for disability benefits and began receiving prescription opioids through a pain clinic in town. As his tolerance for opioids increased, he tried various strategies to avoid the horrific withdrawal symptoms he experienced when his supply of opiates ran out: crushing and snorting pills for a stronger effect, “borrowing” medication from family and friends, and buying additional pills from dealers. Nine months ago, the high street cost of pills led Jason to begin snorting heroin, which was cheaper, but more potent. Within 2 months, he began using heroin intravenously on a daily basis. Acquiring and using heroin became his primary endeavor, increasingly isolating him from his family and his group of lifelong friends. After showing up to church several times late and disheveled, Jason’s mother told him he was no longer welcome to join her in the family’s regular pew on Sundays. Last Friday, he met his ex-wife and younger son to attend his elder son’s first varsity football game as a family. In an effort to avoid becoming ill during the long game, Jason shot heroin in the parking lot and was visibly high when he entered the stadium. The evening ended with his ex-wife enraged, his younger son in tears, and his elder son saying he could not wait to go far away to college and never see Jason again. Two days ago, Jason’s mother found him unresponsive in his truck and called 911. EMTs administered naloxone (branded as Narcan), which restored his breathing after an accidental heroin/fentanyl overdose. He was taken to the hospital and referred to an outpatient community addiction and mental health clinic upon release. With no one in his family willing to pick him up from the hospital, and his mother saying she is unsure if she wants him to continue living on her property, Jason used a hospital bus pass to travel directly to a local substance abuse treatment facility.
Treatment Planning Implications by Ecological Level: The Case of Jason
Individual: Traditional treatment focus. Assuming a disease model of addiction, a counselor would view Jason’s opioid dependence as primary, chronic, progressive, and potentially fatal (Angres & Bettinardi-Angres, 2008). As such, many substance abuse professionals would advocate that Jason’s addiction is the primary presenting problem and must be addressed first, before tackling other concerns and challenges. A treatment plan including goals and objectives focused upon enhancing his ability to remain abstinent from opioids and all other mood-altering substances should be developed, implemented, and monitored from the outset of treatment.
It is essential for Jason to reduce his isolation by developing a social network supportive of his recovery efforts. Specific objectives to meet this goal might include attending daily 12-step meetings for a minimum of 90 days, obtaining a sponsor who has a minimum of 5 years in recovery, and reestablishing relationships with non-using childhood friends.
An additional individual-level concern that must be addressed is Jason’s chronic pain from multiple herniated disks. During the first week of substance abuse treatment, Jason’s plan should include a complete physical examination with an emphasis on assessing pain level and spinal functioning, as well as HIV and hepatitis screening. Throughout his substance abuse treatment, Jason should receive psychoeducation via group work, lectures, reading materials, and videos or other media in order to enhance his understanding of the cyclic nature of pain disorders and opioid addiction. Jason also should make an appointment and establish a relationship with a medical specialist who is knowledgeable in both pain management and addictive disorders. Jason and this medical professional can develop an action plan to address his chronic back pain while minimizing his risk of opiate relapse.
Acute fiscal concerns and the accompanying stress associated with lack of financial resources were identified as primary risk factors for relapse. Individual-level interventions should include connecting Jason with vocational rehabilitation counselors who will assist him in identifying personal and employment strengths, acknowledging limitations in the current job market, and assisting him in finding employment. Finally, in order to enhance the likelihood of success in his recovery, Jason should address issues of shame resulting from his drug use and loss of family, employment, health, and identity. While in treatment, he should receive extensive psychoeducation as to the meaning and significance of shame in the recovery process. Jason should be encouraged to discuss, in individual and group counseling, the complex nature of his drug use and related intra- and interpersonal consequences.
Microsystem: Face-to-face interactions between individual and environment. Primary face- to-face interactions impacted by Jason’s addiction to opiates include communications with his ex-wife, sons, and mother. Although Jason’s marriage was negatively impacted by the family’s moving to Ohio, his use of prescription opioids following the move hurt his ability to communicate, restricted his interactions with his wife and children through gradual withdrawal from family events, and transferred parenting responsibilities to his wife. These changes in functioning within his nuclear family caused further alienation from others, including but not limited to his mother, friends, neighbors, fellow church members, and extended family. As a result of his opiate use, he no longer attended parent–teacher conferences at school and only sporadically appeared at his children’s baseball and football games.
Having grown up in a small town, Jason was well known and well liked by many in his community. While working at the local concrete company in his home town, he had developed a tight-knit group of close friends, many of whom he knew from childhood. Upon his return to West Virginia following his loss of employment and injury while in Ohio, Jason no longer reached out to this group of friends. Instead, his primary focus became finding, paying for, and using opioids in order to avoid painful withdrawal symptoms. His social circle was nearly replaced by his drug dealer and occasional fellow heroin users with whom he would shoot up and share needles.
It should be noted that all of the individual-level treatment concerns involve microsystem-level interactions between Jason and his environment. Jason’s counselor should be aware that achieving these goals will depend upon Jason’s pursuit or avoidance of interactions with various individuals, groups, and settings (i.e., the microsystem). This ecological awareness will increase the counselor’s understanding of the magnitude of Jason’s task, allowing for both deeper empathy and better planning. By highlighting the microsystem interactions required to pursue treatment goals, the counselor can help Jason become aware of the many variables in the environment he may not be able to control, thus emphasizing the importance of remaining steadfast regarding those elements of his treatment and life in which he does have power and choice.
Mesosystem: Interactions between two or more environments where an individual exists. In Jason’s West Virginia and Ohio communities, there were several changes in economic and medical systems that impacted his use of opiates. The shutting down of coal mines and businesses associated with the coal industry (housing, rail transportation, and facility maintenance provision) made a significant economic impact on communities and extended to multiple industries outside of mining. New houses were not being constructed, and local small businesses began to struggle and disappear. As a result, the need for concrete diminished and Jason’s boss was forced to lay off workers. Families like Jason’s were faced with a difficult choice: remain in a community in which they and multiple generations before them had lived and hope jobs would one day return or uproot their families in search of employment opportunities elsewhere. Many families chose the latter—which left the small town void of human resources and an adequate tax base from which to provide municipal and human services.
Jason’s long-term treatment provider should take into account employment opportunities within the community and assess if Jason has adequate training for today’s workforce. Vocational rehabilitation counseling is recommended to assess his skills and to determine if further education is needed. All of the local helping service providers (e.g., medical, addictions, mental health, vocational, and school professionals) in Jason’s town are overwhelmed because of high needs and dwindling financial resources. As such, Jason’s counselor must be aware of mesosystem-level obstacles; these interactions between microsystems may be fraught because of the challenges being experienced in each system. For example, the process of one facility making a referral to another can be difficult because of high demand and a lack of resources in either system. For clients like Jason, already struggling with shame and disenfranchisement, a mesosystem-level challenge might be taken personally and be potentially triggering. A counselor working with Jason through an ecological lens could engage with him regarding such an obstacle, and draw parallels to other system-to-system interactions that have affected him (e.g., how decline of coal is impacting other economic opportunities in his town; how the influx of cheap heroin is impacting hospitals, treatment centers, and neighborhoods). As mentioned above, increasing a client’s awareness as a person in a system may help create more accurate assessments of the forces at play within the respective environments.
Exosystem: Interactions between two or more environments, at least one of which does not include the individual. In addition to the economic shifts noted in the previous section, important changes in the way pharmaceutical companies marketed prescription opioids to both consumers and medical providers impacted the availability of these narcotics in the communities where Jason lived. Jason was told by physicians that the drugs he was prescribed carried a very low risk of addiction and was given documentation supporting the effective and safe use of Oxycontin as a treatment for pain (Van Zee, 2009). Jason was not aware that his physician had attended an all-expenses-paid pain management conference at a Florida resort, hosted by Purdue Pharma, or that his doctor had been invited to become a speaker for the company. He also was not aware that his physician was being tracked by Purdue as a frequent prescriber of OxyContin and thus receiving increased attention and gifts from their regional sales representative, who was eagerly pursuing an annual sales bonus that could more than double her salary.
These distal variables had a profound effect on Jason as an individual, along with many other examples in the mesosystem: his Ohio boss’s enforcement of company policies regarding drug use and addiction; health care policies about prescription opiates, addictions treatment (including medication-assisted therapies), and insurance for people with pre-existing conditions; drug traffickers contaminating heroin with fentanyl and pushing an influx of heroin into Jason’s vulnerable community; and state and local policy regarding the availability and administration of naloxone—which likely saved Jason’s life. If Jason’s counselor views Jason and the helping process through an ecological lens including such variables, both counselor and client will be better prepared to co-construct a treatment narrative around the past, present, and future that draws upon Jason’s strengths and recognizes his limitations within the realities of a complex system.
Macrosystem: Cultural, political, economic, societal backdrop. Jason’s current circumstances have unfolded against a multifaceted socio-political backdrop, influencing many clinically salient factors in his treatment. The economic decline of his hometown is not isolated, but rather part of global trends related to the urbanization of wealth and resources. There has been a marked decline in well-paying blue-collar jobs with benefits, overall economic dislocation due to automation, and an increasing need for advanced education in order to be competitive for open positions. Technology has increased the breadth and depth of information available to the average American, and those who cannot afford access to technology fall further and further behind. With access to information about opportunities available elsewhere, young adults from small rural communities increasingly leave areas their families may have resided in for multiple generations. Religious authority and institutions have declined, and the purpose and services churches traditionally provided in rural areas have also eroded. State- and federal-level health care policy, pharmaceutical industry regulations, scientific progress in the fields of pain management and addiction, and changing norms in our cultural understanding of addiction, treatment, and outcomes are all at play in the macrosystem.
As part of Jason’s long-term treatment, psychoeducation and client-centered processing regarding these and other macrosystem variables can support multiple treatment goals, particularly those related to issues of shame. Placed within a broad ecological context, Jason’s feelings of anger and shame can be normalized while facilitating a shift from a personalized focus (e.g., “I am bad,”) to a broader perspective (e.g., “These are difficult times, and new skills I never had the chance to learn before are needed for survival”).
Chronosystem: Historical context and changes in environments over time. In developing a comprehensive treatment plan, along with the systems already outlined, the ecologically sensitive counselor should help Jason plan for challenges that are likely to occur over time as a result of his developmental process, along with the historical moment in which Jason lives. He is 37 years old and still in the first half of his working life. He has adolescent children who will be growing into young adulthood; they may look toward him for guidance or choose to challenge and reject him. This moment in time is a developmentally critical one for Jason’s family.
At the time of writing this article, the United States is in the midst of a number of policy debates that will have an enormous effect on Jason’s life and health (Kessler, 2018). Long-term funding and access to health care is a contentious and unsettled issue. Ecologically aware counselors should both monitor and engage in the unfolding policy debates related to the funding of substance abuse treatment and other ongoing services Jason and clients like him need now and in the future. Furthermore, economic trends toward clean energy, globalization, technology, urbanization, and higher education continue to accelerate; the world is already a different place than when Jason first started working, or when he first started using drugs as a means to cope with pain. Jason and those seeking to help him must have accurate, up-to-date knowledge of how industry trends are impacting local and regional sectors, and devise strategies to engage and compete in the current economic environment.
Although vital, it is not enough for Jason’s counselor to help him survive only in the present moment. The counselor should anticipate future challenges Jason will confront and assist him in mapping out a sustainable, long-term plan. Such a plan will normalize the influence of both individual- and systems-level variables, emphasizing the importance of multiple sources of support, maintenance of his sobriety, and the inevitability of confronting both developmental and historical challenges. Just as a person with progressive multiple sclerosis needs to anticipate their future medical and assistive technology needs, so does Jason need to identify and plan for his future health, wellness, and economic needs within our rapidly changing society. An ecologically sensitive counselor understands both Jason’s personal development and larger historical trends, and is thus able to advocate for Jason’s preparation to survive and thrive over time.
Advocacy as an Inherent Element of Ecologically Informed Treatment
Over the past few decades, the counseling profession has increasingly recognized that advocacy is a vital component of the counselor’s role (Chang, Barrio Minton, Dixon, Myers, & Sweeney, 2012; Ratts, Toporek, & Lewis, 2010). Counselors are ethically required to understand their clients in a deeply contextualized manner and have a responsibility to try and reduce social and ecological barriers that may be blocking their clients’ growth, development, and flourishing, and exacerbating their clients’ mental and physical health challenges. Understanding the pivotal role ecological factors play in clients’ health, relationships, and careers has long been central to the field of rehabilitation counseling (Parker & Patterson, 2012). Issues such as accessibility and universal design were recognized as central to the success of people with disabilities, just like evidence-based treatments. For example, if a client who uses a wheelchair is seeking to participate in a program or obtain a job requiring access to a particular building, and that building lacks accessible parking or public transportation, curb cuts, and an accessible entrance and bathroom, the client is likely going to be blocked from reaching goals. Such systemic, advocacy-oriented thinking can be applied to the current opioid crisis.
As described in the previous sections, using Bronfenbrenner’s ecological model and creating an eco-map as a tool in the client conceptualization process led to the identification of a wide range of variables related to Jason’s treatment and recovery. Counselors need both awareness of and knowledge about factors affecting their clients at multiple systemic levels. Advocacy as understood within this model includes understanding labor market trends and participating in public policy discussions concerning support for workers displaced by globalization and automation. It means working to obtain more medical resources and treatment centers for clients struggling with addiction, striving to change laws to emphasize treatment over incarceration, and providing more access to life-saving medications such as naloxone. In short, the pursuit of social justice and counselors’ roles as advocates are intrinsic in this model of conceptualization and intervention, highlighting the clinical and societal relevance of a broad range of systemic variables and public policy debates.
One area in which counselors can advocate for the improved access to services for those struggling with opioid use is through supporting programs, such as the Mental Health Facilitator program (Hinkle, 2014), aimed at training laypersons with the basic skills to identify, briefly intervene with, and refer people in their communities who are experiencing a mental health crisis. The increased presence of persons with such skills in the microsystem—in schools, hospitals, faith communities, businesses, and neighborhoods—creates opportunities for detection, referrals to treatment, and life-saving emergency interventions, particularly among underserved populations. Mental Health First Aid is an international, evidence-based, 8-hour training course that teaches community members steps they can take if they encounter a person who is having an emergency, such as having suicidal ideation, a panic attack, or an overdose. Mental Health First Aid has recently added opioid-specific overdose training and naloxone administration to their curriculum (Pellitt, 2018).
Conclusion
Ecological thinking is a powerful skill, and one we argue is necessary for clinically competent counseling. The ecological conceptualization and treatment planning process outlined in this article is designed to provide a structured and systematic template for helping counselors identify clients’ complex needs, as well as the many influential variables at play in the past, present, and future. Engaging from an ecological perspective requires counselors to understand their clients as embedded in multiple systems. Further, it calls upon counselors to develop a deep understanding of the social, economic, and political contexts in which their clients live, and to develop systemic intervention skills. Utilizing this model in clinical settings could enrich the lives of clients, who may come to embrace a more nuanced and inclusive way of conceptualizing themselves and their environment.
Counselors-as-advocates are inherent in this model, and those professionals who espouse ecological thinking cannot ignore the multitude of powerful forces that either enhance or impede our clients’ well-being. Clinicians who understand and engage with their clients through this lens may find that ecological psychoeducation can lead to clients-as-advocates as well. Clients who come to understand themselves and others as people in environments may find their individual-level goals are supported and enhanced by goals associated with learning about and eventually acting upon systems-level variables in their lives, thus increasing the recovery capital (Hewell et al., 2017) available to them within their own environments. Attention to the American opioid epidemic is increasing based on advocacy by citizens, journalists, public servants, and health professionals. As focus and resources are directed to this complex problem, ecologically informed interventions by stakeholders in all of the interconnected systems are advised to both save and improve lives now and in the future.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Angres, D. H., & Bettinardi-Angres, K. (2008). The disease of addiction: Origins, treatment, and
recovery. Disease-a-Month, 54, 696–721. doi:10.1016/j.disamonth.2008.07.002
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U. (1994). Ecological models of human development. In M. Gauvain & M. Cole (Eds.), Readings on the development of children (2nd ed., pp. 37–43). New York: Freeman.
Chang, C. Y., Barrio Minton, C. A., Dixon, A. L., Myers, J. E., & Sweeney, T. J. (Eds.). (2012).
Professional counseling excellence through leadership and advocacy. New York, NY: Routledge.
Dasgupta, N., Beletsky, L., & Ciccarone, D. (2018). Opioid crisis: No easy fix to its social and economic determinants. American Journal of Public Health, 108, 182–186. doi:10.2105/AJPH.2017.304187
Gul, R. B., & Boman, J. A. (2006). Concept mapping: A strategy for teaching and evaluation in nursing education. Nurse Education in Practice, 6, 199–206. doi:10.1016/j.nepr.2006.01.001
Hewell, V. M., Vasquez, A. R., & Rivkin, I. D. (2017). Systemic and individual factors in the
buprenorphine treatment-seeking process: A qualitative study. Substance Abuse Treatment, Prevention, and Policy, 12(3), 1–10. doi:10.1186/s13011-016-0085-y
Hinkle, J. S. (2014). Population-based mental health facilitation (MHF): A grassroots strategy that works. The Professional Counselor, 4, 1–18. doi:10.15241/jsh.4.1.1
Hooten, W. M., St. Sauver, J. L., McGree, M. E., Jacobson, D. J., & Warner, D. O. (2015). Incidence and risk factors for progression from short-term to episodic or long-term opioid prescribing: A population-based study. Mayo Clinic Proceedings, 90, 850–856. doi:10.1016/j.mayocp.2015.04.012
Katz, J. (2017a, June 5). Drug deaths in America are rising faster than ever. The New York Times. Retrieved from https://www.nytimes.com/interactive/2017/06/05/upshot/opioid-epidemic-drug-overdose-deaths-are-rising-faster-than-ever.html
Katz, J. (2017b, September 2). The first count of fentanyl deaths in 2016: Up 540% in three years. The New York Times. Retrieved from https://www.nytimes.com/interactive/2017/
09/02/upshot/fentanyl-drug-overdose-deaths.html
Kessler, D. A. (2018, January 10). How to fight the opioid crisis. The New York Times. Retrieved from https://www.nytimes.com/2018/01/10/opinion/fight-opioid-crisis.html
Keyes, K. M., Cerdá, M., Brady, J. E., Havens, J. R., & Galea, S. (2014). Understanding the rural–urban differences in nonmedical prescription opioid use and abuse in the United States. American Journal of Public Health, 104(2), e52–e59. doi:10.2105/AJPH.2013.301709
Kolodny, A., Courtwright, D. T., Hwang, C. S., Kreiner, P., Eadie, J. L., Clark, T. W., & Alexander, G. C. (2015). The prescription opioid and heroin crisis: A public health approach to an epidemic of addiction. Annual Review of Public Health, 36, 559–574.
doi:10.1146/annurev-publhealth-031914-122957
Kosten, T. R., & George, T. P. (2002). The neurobiology of opioid dependence: Implications for treatment. Science & Practice Perspectives, 1, 13–20.
McCoy, K., McGuire, J., Curtis, R., & Spunt, B. (2005). White chicks on dope: Heroin and identity dynamics in New York in the 1990s. Journal of Drug Issues, 35, 817–841. doi:10.1177/002204260503500408
Parker, R. M., & Patterson, J. B. (Eds.). (2012). Rehabilitation counseling: Basics and beyond (5th ed.). Austin, TX: Pro Ed.
Pellitt, S. (2018, May 10). Briefing showcases Mental Health First Aid and opioid epidemic [Web log post]. Retrieved from https://www.thenationalcouncil.org/capitol-connector/2018/05/briefing-showcases-mental-health-first-aid-and-opioid-epidemic/
Peltz, P. (Director). (2017). Warning: This drug may kill you. [Motion picture]. United States: HBO Documentary Films.
Ratts, M. J., Toporek, R. L., & Lewis, J. A. (2010). ACA advocacy competencies: A social justice
framework for counselors. Alexandria, VA: American Counseling Association.
Rudd, R. A., Seth, P., David, F., & Scholl, L. (2016). Increases in drug and opioid-involved overdose deaths—United States, 2010–2015. Morbidity and Mortality Weekly Report, 65, 1445–1452.
Skolnick, P. (2018). The opioid epidemic: Crisis and solutions. Annual Review of Pharmacology and Toxicology, 58, 143–159. doi:10.1146/annurev-pharmtox-010617-052534
Suzuki, J., & El-Haddad, S. (2017). A review: Fentanyl and non-pharmaceutical fentanyls. Drug & Alcohol Dependence, 171, 107–116. doi:10.1016/j.drugalcdep.2016.11.033
Talbot, M. (2017, June 5). The addicts next door. The New Yorker. Retrieved from https://www.newyorker.com/magazine/2017/06/05/the-addicts-next-door
Ungar, M., Ghazinour, M., & Richter, J. (2013). Annual research review: What is resilience within the social ecology of human development? Journal of Child Psychology and Psychiatry, 54, 348–366. doi:10.1111/jcpp.12025
Vance, J. D. (2016). Hillbilly elegy: A memoir of a family and culture in crisis. New York, NY:
Harper.
Van Zee, A. (2009). The promotion and marketing of OxyContin: Commercial triumph, public health tragedy. American Journal of Public Health, 99, 221–227. doi:10.2105/AJPH.2007.131714
Williams, J. M., McMahon, H. G., & Goodman, R. D. (2015). Eco-webbing: A teaching strategy to facilitate critical consciousness and agency. Counselor Education and Supervision, 54(2), 82–97. doi:10.1002/ceas.12006
Jennifer L. Rogers, NCC, is an assistant professor at Wake Forest University. Dennis D. Gilbride is a professor at Georgia State University. Brian J. Dew, NCC, is an associate professor at Georgia State University. Correspondence can be addressed to Jennifer Rogers, P.O. Box 7406, Winston-Salem, NC 27109, rogersjl@wfu.edu.
Sep 28, 2018 | Volume 8 - Issue 3
M. Ann Shillingford, Seungbin Oh, Amanda DiLorenzo
Natural disasters over the past few decades have necessitated mass migration of Haitian immigrants to the United States. Haitians residing in the United States have experienced significant cultural and social challenges. Recent political deportation mandates have increased the systemic challenges that Haitian students and their families are currently facing in the United States. These systemic barriers have fostered an increase in stressors affecting the mental wellness of Haitian students and their families. This article introduces school counselors to the culturally focused, multiphase model of psychotherapy, counseling, human rights, and social justice as a framework to assist Haitian students and their families.
Keywords: Haiti, immigrant, school counseling, human rights, social justice
There has been a growing trend in the counseling profession to provide culturally relevant services to all clients. In fact, most recently, Ratts, Singh, Nassar-McMillan, Butler, and McCullough (2016) proposed the Multicultural and Social Justice Counseling Competencies to support the evolving need for multiculturally competent counselors to support today’s diverse populations and their varying mental health needs. One diverse group that has caught the attention of counseling professionals is the Haitian population. A long history of political unrest, coupled with grievous damage from natural disasters over the past few decades, has snowballed the migration of Haitian families into the United States. With mass migrations come challenges with cultural identity, social and academic obstacles, and psychological impairment. This article highlights the role of school counselors as social justice advocates and introduces the multiphase model of psychotherapy, school counseling, human rights, and social justice as a framework for offering services to Haitian students and their families. The authors present literature underlining the experiences of the Haitian population both within the context of their home country and also as immigrants in the United States.
Effects of Natural Disasters on Haitian Migration
Over the past few decades, the small nation of Haiti has suffered tremendously from natural disasters. In January 2010, a major 7.1-magnitude earthquake shook the island’s core, killing close to 300,000 men, women, and children. An equal number of individuals were injured and at least 1.5 million were displaced. Among the damage and destruction were almost 4,000 schools (CNN, 2017). Six years later, Hurricane Matthew swept through the south side of the island, killing over 900 citizens and leaving severe devastation in its tracks (BBC News, 2016). A year after that, Haiti, already crippled economically by previous natural disasters, was hit by Hurricane Irma, a Category 5 storm. Cook (2017) reported that homes, bridges, and housing already weakened by previous disasters were destroyed. Not only were homes destroyed, but the country’s ability to rebuild also was diminished.
Each natural disaster in Haiti has meant a struggle for regrowth. Between 2015 and 2016, it was reported that the economic growth in Haiti was down to a staggering 2% (U.S. Department of State, 2018). Damage from natural disasters, drought conditions, governmental unrest, and a significant decrease in the country’s currency were identified as contributors to the financial stagnation (U.S. Department of State, 2018). Migration trends portrayed a parallel between decreased stability in Haiti and increased migration to the United States and other more secure territories. In fact, over the years, the United States has been the recipient of thousands of immigrants seeking security and a better future for their families. Stepick and Stepick (2002) reported that in the 20th century, the number of Haitian immigrants to the United States reached an all-time high. By 2010, there were approximately 587,000 Haitians living in the United States, and that number rose to almost 700,000 by 2015 (Migration Policy Institute, 2017). The distribution of Haitian immigrants varies from state to state, with Florida having the largest population (46%), followed by New York (25%), New Jersey (8%), Massachusetts (7%), Georgia (2%), and Maryland (2%). These numbers may continue to rise as the outlook for the island of Haiti remains bleak.
Prior to the January 2010 earthquake, Haitian migration to the United States was considered high due to unemployment, low socioeconomic stability, poverty, violence, and political instability on the island (Cone, Buxton, Lee, & Mahotiere, 2014). Presently, Haiti is considered the economically poorest country in the Western hemisphere (Coupeau, 2008; Mendelson-Forman, 2006). Haiti also has been notorious for its high number of orphans, with at least 380,000 before the earthquake and a significantly increased number of displaced and homeless children after the earthquake (Little, 2010). Concern exists for the well-being of Haiti’s survivors of natural disasters, particularly the children. According to Potocky (1996), in the past years many Haitian children and their families who fled Haiti due to hardships and entered the United States as refugees often suffered from post-traumatic stress disorder (PTSD; Potocky, 1996).
The U.S. Department of State (2018) estimated that Haiti has received nearly $5.1 billion in aid from the United States since the earthquake. Assistance offered included increasing the number of officers on the police force to increase security, increasing basic health care through development of new clinics, construction of a mega power plant to provide electricity, and support for farmers to increase crop development. Even so, Haitians continue to struggle and have sought immigration support from the United States. Reports have suggested that as many as 55,000 Haitians applied and have been granted visas to the United States since the earthquake, and as many as 500 orphaned children have been allowed travel documents for adoption by U.S. families (Zissis, 2010).
To support Haiti over the past decade, U.S. Homeland Security has offered Temporary Protected Status (TPS) to large numbers of Haitians affected by the debilitating conditions caused by natural disasters as well as political unrest. TPS is offered to individuals from foreign countries where it may be unsafe or where resources are inadequate to support the citizens. TPS may be granted to individuals who are already in the United States or those still in their native country. TPS allows recipients to remain in the United States and secure travel and employment authorization (U.S. Department of State, 2018). As such, TPS has been granted to an estimated 60,000 Haitian citizens following the destruction from the 2010 earthquake. Outside of Haitians who have entered the United States through the TPS program, it has been reported that at least 40,000 more Haitians have entered the United States seeking refuge following Hurricane Matthew (Fifield, 2016). It appears that with each natural disaster the number of Haitian immigrants in the United States has increased.
Impact of Migration on Haitian Students and Families
Migration to a new country may come with difficulties for families, particularly children. Haitian children experience multiple layers of challenges in the American educational system and society at large. To better support Haitian students, counselors need to understand the impact of these hardships on various aspects of Haitian students’ lives and needs. The following sections provide a review on the complications facing these students and their unique needs.
Research suggests that traumatic events affect the physiological, psychological, and social welfare of immigrant students (Bean, Derluyn, Eurelings-Bontekoe, Broekaert, & Spinhoven, 2006). Haitian families may experience household stress due to separation of family members between the United States and their homeland (Desrosiers & St. Fleurose, 2002). Additional stressors include cultural misunderstanding and isolation in the school setting (Chhuon, Hudley, Brenner, & Macias, 2010); differences in educational policies, pedagogical practices, and teaching styles; and overall differences in school culture and climate (Cone et al., 2014). These challenges, particularly in the school setting, may be problematic for Haitian students and parents trying to acculturate to the American system.
Haitian students experience significant social difficulties. In a study exploring stressors experienced by immigrants to the United States, Haitian parents and children reported the highest number of stressors among immigrants from the Caribbean islands (Levitt, Lane, & Levitt, 2009). In addition, it has been reported that Haitian immigrants have a 20–30% higher chance of living in poverty-stricken conditions in the United States than people who are White (Hernandez, Denton, & Mcartney 2009). Douyon, Marcelin, Jean-Gilles, and Page (2005) indicated that students in highly populated Haitian communities—such as the Miami-Dade, Florida, area—may be surviving in not only poor health conditions, but also hostile territories where education appears to be futile and a life of crime is more appealing. Those social problems may add stress to the Haitian household, which may compound existing economic problems (Chierici, 2004). Indeed, migration disrupts the familial and social networks as well as the behavioral norms and cultural values of new immigrants. It places responsibility on counselors and other educators to meet the needs of these students academically, socially, and culturally (Asner-Self & Marotta, 2005). Thus, it is imperative for schools to help provide both supportive relationships to foster resiliency and additional resources for Haitian immigrant students.
Social and Cultural Needs
Haitian students face potential cultural difficulties, such as language barriers, cultural identity, and acculturation, particularly in the school setting. Haitian students and their families may primarily speak Haitian Creole, yet few interpreters are available to assist with standardized test explanations (Kretsedemas, 2005), student code of conduct reviews, and other pertinent information that may affect students’ academic functioning. In comparison to Spanish, which is taught in American schools, Haitian Creole is spoken only within the Haitian culture (Phelps & Johnson, 2004). Although Haitian Creole is based on the French language, it has syntactical influences from West African languages. It should be noted that it is not a dialect of French, but is its own independent language (Solano-Flores & Li, 2006).
Along with sensitivity to language barriers, Haitian students may encounter challenges in developing their cultural identity. As reported by Doucet (2005), Haitian students who may be struggling between their own cultural identity and the American culture might encounter school-related problems such as suspensions, truancy, academic failure, and eventual school dropout. Cone and colleagues (2014) reported the results of a qualitative study and emphasized the difficulty in identity formation that Haitian students experience in the United States. Identity formation was influenced by three factors: differences in pedagogical approaches to teaching between Haiti and the United States; differences in disciplinary approaches between teacher groups; and pressure from peers to become Americanized. To counter the stigma associated with being and looking different, Cone and colleagues noted that Haitian students may accede to their peers and hide any indication of their Haitian heritage. Consequently, these practices may foster added stress within the family network and community at large. Struggles with cultural identity formation can cause Haitian students to feel anxiety, confusion, fear, helplessness, and homesickness (Bachay, 1998), which may ultimately lead to increased risk of PTSD.
To further compound psychological distress experienced by Haitian families living in the United States, in November 2017, U.S. President Donald Trump declared an end to TPS for Haiti and several other countries (Park, 2018). This means that at least 60,000 Haitians currently residing legally in the United States through TPS can be deported by January 2019 (Daugherty, 2018). Additionally, deportation holds on Haitian citizens activated following the 2010 earthquake are being released, increasing the number of Haitians being deported. Deportation is destructive to family units, especially children. Children are affected by the knowledge of deportation of individuals within their community, even when that individual is unrelated to them. When a family member is deported, the rest of the family, including children, may suffer from poverty, reduced access to food and health care, and limited educational opportunities (Wiley, 2013). Thus, the already fragile academic, social, and cultural experiences of some Haitian students and families currently residing in the United States might be further aggravated by political mandates and changing policies. Therefore, culturally relevant support is warranted from those who serve this population, including school counselors and other stakeholders.
School Counselors’ Role in Supporting the Haitian Students
According to the American School Counselor Association (ASCA; 2012) National Model, professional school counselors are to develop a comprehensive school counseling program that addresses the social, personal, academic, and career needs of students. Several approaches have been introduced to provide school counselors a pathway to supporting immigrant students, including parenting workshops for Jamaican parents (Morrison, Smith, Bryan, & Steele, 2016); community outreach programs on college preparation for first-generation Latinx students, families, and friends (Tello & Lonn, 2017); and a comprehensive, multilevel system of support that includes school–family–community partnerships for adolescent immigrants (Suárez-Orozco, Onaga, & de Lardemelle, 2010). A thorough search of the literature, particularly school counseling literature, yielded a dearth of information on working with Haitian students and their families. In light of the numerous challenges that this population faces, the scarcity of research support is disappointing. Therefore, the authors provide a guideline for school counselors to support their Haitian clients by using the Multiphase Model of Psychotherapy, Counseling, Human Rights, and Social Justice (MPM; Chung & Bemak, 2012). The MPM was developed by counselor educators as a culturally responsive intervention to support individuals from marginalized groups. The MPM is psychoeducational in nature and consists of “affective, behavioral, and cognitive interventions and prevention strategies that are rooted in cultural foundations and relate to social and community process and change” (Chung & Bemak, 2012, p. 2).
Multiphase Model of Psychotherapy, Counseling, Human Rights, and Social Justice (MPM)
The MPM was developed by Chung and Bemak (2012), who expertly recognized the need for a culturally sensitive approach to supporting refugees globally. Chung and Bemak indicated that an effective counselor is one who understands the importance of refugees’ historical, sociopolitical, cultural, and psychological context when dealing with displacement, loss, and trauma. The MPM was constructed as a trauma-based model that integrates humanistic trauma therapy, exposure therapy, stress inoculation approach, and cognitive behavior therapy, and is framed by the multicultural counseling competencies (Arredondo et al. 1996). According to Chung and Bemak, the MPM includes five phases: (a) mental health education; (b) group, family, and individual psychotherapy; (c) cultural empowerment; (d) indigenous healing; and (e) social justice and human rights. Each phase can be used independently of the other and can be adjusted based on the needs of the client. The following section expands on the five phases and incorporates practical interventions for school counselors.
Phase One: Mental Health Education
Mental health education focuses on defining the counseling process for the client. Haitian immigrant students might not have had exposure to counseling in the past; therefore, it is important for school counselors to thoroughly explain what counseling is about, what the expectations are, and the expected outcomes of counseling. Chung and Bemak (2012) also noted the importance of discussing the meaning of confidentiality in both the context of the U.S. counseling community and in the client’s native community. Confidentiality is an ethical consideration supported by ASCA as an obligation for school counselors (ASCA, 2014). Lazovsky (2008) remarked on the fact that laws and regulations regarding confidentiality may differ internationally, so it is important for the counselor to explain the meaning and objectives of using confidentiality as it relates to family and school. During this phase, school counselors should pay close attention to the experiences of marginalization and trauma that these students and their families may have faced and the psychological distress related to potential deportation. Mistrust of Americans may be an essential part of the Haitian family’s survival mechanism (Stepick, Stepick, & Kretsedemas, 2018); therefore, school counselors should be cautious in this phase to be culturally sensitive to the fears and anxiety that the student and family may be experiencing.
Phase Two: Group, Family, and Individual Psychotherapy
The second phase is focused on providing culturally relevant counseling techniques and strategies. To do so, the school counselor needs to understand the contextual background of the student. What have their experiences been either while in Haiti or within the United States? How has that student and the family been affected by natural disasters and sociopolitical experiences? Based on this information, the school counselor needs to decide on the most appropriate culturally relevant interventions for the student. Surveys and questionnaires are an ideal format for gathering information about the experiences of Haitian students and their families (Ekstrom, Elmore, Schafer, Trotter, & Webster, 2004). However, school counselors should be mindful of language barriers and provide surveys that have been translated in both English and Haitian Creole. Additionally, individual and group counseling sessions need to be adapted to meet the cultural needs of the Haitian student. For instance, singing, dancing, and spiritual guidance are an integral part of the Haitian culture (Marcus, 2010). School counselors should consider the collectivist cultures of the Haitian population, which may influence their decision to engage the students in small groups as opposed to individual counseling. By utilizing culturally relevant counseling approaches, school counselors might find small group expressive techniques to be beneficial for developing trust, while assessing the psychological needs of the student.
Phase Three: Cultural Empowerment
Cultural empowerment extends support for client needs beyond the counseling setting to community resources. This phase incorporates collaborating with multiple agencies. Examples of such agencies include housing services, social services, and health services. The school counselor can choose to develop a team approach with the school’s social worker and other school stakeholders and serve as the facilitator of services. The objective during this phase is to serve as an advocate and guide for the student and their family to reduce their levels of stress and anxiety as well as meet their basic needs. In fact, Chung and Bemak (2012) surmised that cultural empowerment goes beyond in-office counseling to the greater community, with helpers rallying for services and resources to meet the families’ basic needs. Finally, cultural empowerment may mean providing adequate interpretation services for students and families (Kretsedemas, 2005) so that all stakeholders fully understand each other and the processes that are at work. In fact, school counselors and educators have a civic obligation to provide interpretive services to students and parents with limited English proficiency (Office for Civil Rights, 2015).
Phase Four: Indigenous Healing
From the American viewpoint, counseling, therapy, medicine, and health care are considered important aspects of holistic healing. However, within the Haitian culture, indigenous healing has been noted as a longstanding cultural practice. It is not uncommon for individuals from the Haitian population to seek help from spiritual healers, herbal specialists, and midwives rather than more formalized Westernized therapy. In fact, many Haitians hold extreme faith in natural healing and may be hesitant to pursue counseling in the context of the United States. Furthermore, Haitian individuals often believe that illness is caused by supernatural forces (Nicolas, DeSilva, Grey, & Gonzalez-Eastep, 2006); therefore, it is not unusual for families to pursue help from family healers, spiritual healers, or folk medicine in seeking the supernatural cause of illnesses. Nicolas and colleagues (2006) noted that common beliefs may attribute illnesses to evil spirits, a poor relationship with God, or offending the Lwa, a deity associated with the voodoo religion. Although not all Haitians hold these indigenous views, there may be a general mistrust of mental health services. Counselors working with Haitian clients should be cautious to embrace culturally sensitive practices that combine Westernized practices with indigenous healing. Seeking consultation from a Haitian spiritual healer might be a first step in formulating an effective counseling approach. Nicolas and colleagues (2006) suggested seeking these healers through Haitian community centers and through communication with family members of the clients. Counselors should avoid assumptions and initiate conversations with Haitian clients to understand their beliefs and practices.
Phase Five: Social Justice and Human Rights
The final phase of the multiphase model focuses on counselors advocating for the rights of their clients. Haitian immigrants in the United States experience political discrimination. For example, recent threats of deportation and the termination of TPS protection can be discriminatory. At this phase, it is vital that counselors examine their own worldviews, community relations, and the role of politics and political policies in counseling, as well as the impact of social injustices (e.g., discrimination, oppression, racism) on the well-being of their clients (Chung & Bemak, 2012). Griffin and Steen (2011) mentioned nine steps that school counselors can employ as social justice advocates: develop cultural competence; use data to support work, particularly educational inequalities; gain allies, recognizing that the work cannot be done alone; speak up at school, at town hall meetings, and at board meetings, and write to state legislators; educate and empower parents and families; stay politically engaged and know what is happening in the current political environment; be bold and confident in beliefs; be persistent, understanding that systemic barriers may stand in the way of progress; and conduct research to demonstrate the needs for justice, equity, equality, and fairness. School counselors are inundated with multiple roles and as such may not have the time and/or resources to cover all nine steps mentioned. However, knowledge of these practical strategies may be helpful in their ethical decision making and development of a culturally sensitive, comprehensive school counseling program. Essentially, school counselors should be leading agents of change, seeking to provide culturally relevant services to their immigrant students.
Summary
Haitian children face various systemic challenges adjusting to the U.S. educational system and society. Given their unique challenges and needs, Haitian children require specialized, culturally responsive school counseling programs. To provide such programs, school counselors need practical strategies on how to provide culturally appropriate interventions that address the multiple systemic challenges to Haitian students’ well-being. However, school counselors may find it difficult to find such information given the dearth of school counseling literature concerning Haitian students. Therefore, this article provides practical guidelines using the MPM that may strengthen school counselors’ approach to providing culturally responsive services to Haitian students and their families.
Using the MPM, school counselors will be in a better position to explore the benefits of counseling with their Haitian families. The model encourages school counselors to assess the unique needs of the children and families within a cultural context. Moreover, by using this model, school counselors are encouraged to actively engage in collaborative partnerships with multiple agencies and professionals to meet the practical needs of Haitian families. Lastly, school counselors need to work beyond the structure of the office setting and integrate social justice advocacy work for systemic changes to maximize therapeutic changes for Haitian students and their families. The authors hope that this guideline will help school counselors to better understand the multiple layers of challenges for Haitian students, as well as how to provide culturally relevant support.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
American School Counselor Association. (2012). The ASCA National Model: A framework for school counseling programs (2nd ed.). Alexandria, VA: Author.
American School Counselor Association. (2014). The school counselor and confidentiality. Retrieved from https://www.schoolcounselor.org/asca/media/asca/PositionStatements/PS_Confidentiality.pdf
Arredondo, P., Toporek, R., Brown, S. P., Jones, J., Locke, D. C., Sanchez, J., & Stadler, H. (1996). Operationalizing of the multicultural counseling competencies. Journal of Multicultural Counseling and Development, 24, 42–78.
Asner-Self, K. K., & Marotta, S. K. (2005). Development indices among Central American immigrants exposed to war-related trauma: Clinical implications for counselors. Journal of Counseling & Development, 83, 162–171. doi:10.1002/j.1556-6678.2005.tb00593.x
Bachay, J. (1998). Ethnic identity development and urban Haitian adolescents. Journal of Multicultural Counseling and Development, 26(2), 96–109. doi:10.1002/j.2161-1912.1998.tb00190.x
BBC News. (2016, October 8). Hurricane Matthew: Haiti south ‘90% destroyed.’ Retrieved from https://www.bbc.com/news/world-latin-america-37596222
Bean, T., Derluyn, I., Eurelings-Bontekoe, E., Broekaert, E., & Spinhoven, P. (2006). Validation of the multiple language versions of the reaction of adolescents to traumatic stress questionnaires. Journal of Traumatic Stress, 19, 241–255. doi:10.1002/jts.20093
Chhuon, V., Hudley, C., Brenner, M. E., & Macias, R. (2010). The multiple worlds of successful Cambodian American students. Urban Education, 45, 30–57. doi:10.1177/0042085909352583
Chierici, R. (2004). Caribbean migration in the age of globalization: Transnationalism, race, and ethnic identity. Reviews in Anthropology, 33, 43–59. doi:10.1080/713649339
Chung, R. C.-Y., & Bemak, F. P. (2012). Social justice counseling: The next steps beyond multiculturalism. Thousand
Oaks, CA: Sage.
CNN. (2017). Haiti earthquake fast facts. Retrieved from https://www.cnn.com/2013/12/12/world/haiti-earthquak
e-fast-facts/index.html
Cone, N., Buxton, C., Lee, O., & Mahotiere, M. (2014). Negotiating a sense of identity in a foreign land: Navigating public school structures and practices that often conflict with Haitian culture and values. Urban Education, 49, 263–296. doi:10.1177/0042085913478619
Cook, J. (2017). 7 years after Haiti’s earthquake, millions still need aid. Retrieved from Huffington Post, https://www.huffingtonpost.com/entry/haiti-earthquakeanniversary_us_5875108de4b02b5f858b3f9c
Coupeau, S. (2008). The history of Haiti. Westport, CT: Greenwood Press.
Daugherty, A. (2018). TPS solution for Haitians not a priority in high-stakes immigration debate. Retrieved from http://www.miamiherald.com/news/politics-government/article198879294.html
Desrosiers, A., & St. Fleurose, S. (2002). Treating Haitian patients: Key cultural aspects. American Journal of Psychotherapy, 56, 508–521.
Doucet, F. (2005). Divergent realities: The home and school lives of Haitian immigrant youth. Journal of Youth Ministries, 3(2), 37–65.
Douyon, R., Marcelin, L .H., Jean-Gilles, M., & Page, J. B. (2005). Response to trauma in Haitian youth at risk. Journal of Ethnicity in Substance Abuse, 4(2), 115–138. doi:10.1300/J233v04n02_06
Ekstrom, R. B., Elmore, P. B., Schafer, W. D., Trotter, T. V., & Webster, B. (2004). A survey of assessment and evaluation activities of school counselors. Professional School Counseling, 8, 24–30.
Fifield, J. (2016). After Hurricane Matthew, Haitians hope for change in US policy. Retrieved from The Pew Charitable Trusts: http://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2016/10/21/after-hurricane-matthew-haitians-hope-for-change-in-us-policy
Griffin, D., & Steen, S. (2011). A social justice approach to school counseling. Journal for Social Action in Counseling & Psychology, 3, 74–85.
Hernandez, D. J., Denton, N. A., & Mcartney, S. E. (2009). School-age children in immigrant families: Challenges and opportunities for America’s schools. Teachers College Record, 111, 616–658.
Kretsedemas, P. (2005). Language barriers and perceptions of bias: Ethnic differences in immigrant encounters with the welfare system. The Journal of Sociology & Social Welfare, 32(4), 109–123.
Lazovsky, R. (2008). Maintaining confidentiality with minors: Dilemmas of school counselors. Professional School Counseling, 11, 335–346.
Levitt, M. J., Lane, J. D., & Levitt, J. (2009). Immigration stress, social support, and adjustment in the first postmigration year: An intergenerational analysis. Research in Human Development, 2, 159–177.
Little, C. (2010). Immigration reform needed for U.S. economy and for Haiti. CNN Opinion. Retrieved from http://www.cnn.com/2010/OPINION/05/07/little.haiti.immigrants/index.html
Marcus, E. (2010). PTSD manifests differently in Haitian patients, says researcher. Retrieved from The Huffington Post: https://www.huffingtonpost.com/erin-marcus/ptsd-manifests-differentl_b_580825.html
Mendelson-Forman, J. (2006). Security sector reform in Haiti. International Peacekeeping, 13, 14–27. doi:10.1080/13533310500424629
Migration Policy Institute. (2017). Haitian immigrants in the United States. Retrieved from https://www.migration
policy.org/article/haitian-immigrants-united-states/
Morrison, S. S., Smith, D. E., Bryan, J. A., & Steele, J. M. (2016). An exploratory study of the child disciplinary practices of Jamaican immigrant parents in the United States: Implications for school counselors. Journal of School Counseling, 14(5). Retrieved from http://jsc.montana.edu/articles/v14n5.pdf
Nicolas, G., DeSilva, A. M., Grey, K. S., & Gonzalez-Eastep, D. (2006). Using a multicultural lens to understand illnesses among Haitians living in America. Professional Psychology: Research and Practice, 37, 702–707. doi:10.1037/0735-7028.37.6.702
Office for Civil Rights. (2015). Schools’ civil rights obligations to English learner students and limited English proficient parents. Retrieved from https://www2.ed.gov/about/offices/list/ocr/ellresources.html
Park, M. (2018). Trump administration ended protected status for 250,000 Salvadorans. These immigrants might be next. Retrieved from CNN Politics: https://www.cnn.com/2018/01/09/politics/temporary-protected-status-countries/index.html
Phelps, L. D., & Johnson, K. E. (2004). Developing local public health capacity in cultural competency: A case study with Haitians in a rural community. Journal of Community Health Nursing, 21, 203–215. doi:10.1207/s15327655jchn2104_1
Potocky, M. (1996). Refugee children: How are they faring economically as adults? Social Work, 41, 364–373.
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44, 28–48. doi:10.1002/jmcd.12035
Solano-Flores, G., & Li, M. (2006). The use of generalizability (G) theory in the testing of linguistic minorities. Educational Measurement: Issues and Practice, 25, 13–22. doi:10.1111/j.1745-3992.2006.00048.x
Stepick, A., & Stepick, C. D. (2002). Becoming American, constructing ethnicity: Immigrant youth and civic engagement. Applied Developmental Science, 6, 246–257. doi:10.1207/S1532480XADS0604_12
Stepick, A., Stepick, C. D., & Kretsedemas, P. (2018). Civic engagement of Haitian immigrants and Haitian Americans in Miami-Dade County. Retrieved from https://www.researchgate.net/publication/268441078_Civic_Engagement_of
_Haitian_Immigrants_and_Haitian_Americans_in_Miami-Dade_County
Suárez-Orozco, C., Onaga, M., & de Lardemelle, C. (2010). Promoting academic engagement among immigrant adolescents through school-family-community collaboration. Professional School Counseling, 14, 15–26.
Tello, A. M., & Lonn, M. R. (2017). The role of high school and college counselors in supporting the psychosocial and emotional needs of Latinx first-generation college students. The Professional Counselor, 7, 349–359. doi:10.15241/amt.7.4.349
U.S. Department of State. (2018). U.S. relations with Haiti. Retrieved from https://www.state.gov/r/pa/ei/bgn/198
2.htm
Wiley, D. (2013, June 13). New study findings on mixed-status immigrant families: Threat of family separation affects health of the children. Retrieved from https://ccf.georgetown.edu/2013/06/13/new-study-findings-on-mixed-status-immigrant-families-threat-of-family-separation-affects-health-of-the-children/
Zissis, C. (2010). The Haitian immigration debate. Council of the Americas. Retrieved from https://www.as-oa.org/
articles/haitian-migration-debate
- M. Ann Shillingford is an associate professor at the University of Central Florida. Seungbin Oh, NCC, is a doctoral candidate at the University of Central Florida. Amanda DiLorenzo is a doctoral student at the University of Central Florida. Correspondence can be addressed to M. Ann Shillingford, P.O. Box 161250, Orlando, FL 32816, Dr-S@ucf.edu.
Sep 28, 2018 | Volume 8 - Issue 3
Nancy E. Thacker, Jillian M. Blueford
Counselors are becoming more involved with clients pursuing physician-assisted death (PAD) as legislation for legalization increases. PAD may present complex values-based conflicts that can challenge counselors to maintain ethical practice in counseling. When conflicts arise, counselors must engage in ethical decision making that considers systemic influences on personally held beliefs and values. The authors merge ecological systems theory with the counselor values-based conflict model to offer a holistic approach to resolving values-based conflicts surrounding PAD. In this article, the authors review PAD and counselors’ roles in the hastened death process, discuss sources and impacts of personal and professional values through an ecological systems lens, and provide an applied method of managing values-based conflicts with PAD through a case illustration.
Keywords: physician-assisted death, hastened death, values-based conflict, ethical decision making, ecological systems
Individuals with terminal illnesses encounter difficult end-of-life decisions amidst experiencing physical and emotional distress (Daneker, 2006). Currently in six U.S. states and Washington, DC, terminally ill individuals have a legal right to end their lives via physician-assisted death (PAD). As legislation for legalization of PAD increases, more terminally ill patients can consider PAD as an option (Miller, Hedlund, & Soule, 2006). As a result, the need for mental health professionals to assist individuals dealing with these end-of-life decisions is on the rise.
The topic of death presents complex questions about the meaning of life and death and evokes reflections on one’s personal beliefs and values surrounding death and dying (Yalom, 2009). Terminally ill individuals may confront their personal beliefs about a morally just or good death, explore feelings about the process of dying, and consider their levels of personal control or power in their processes of dying (Laakkonen, Pitkala, & Strandberg, 2004; Yalom, 2008). Religion and spirituality often contribute to terminally ill individuals’ beliefs and values surrounding death and dying and can influence end-of-life decisions (Reiner, 2007). Each personal belief and value is influenced by systemic factors, cultural experiences, and cultural customs or expectations that play a role in end-of-life decision making (Laakkonen et al., 2004; Neimeyer, Klass, & Dennis, 2014).
Counselors will confront their beliefs and values about death and dying as terminally ill individuals who are contemplating PAD (PAD clients) seek counseling to explore end-of-life decisions (Werth & Crow, 2009). If counselors’ beliefs and values conflict with PAD clients’ beliefs and values, or PAD itself, then it may present an ethical dilemma that challenges the quality of care counselors provide (Heller Levitt & Hartwig Moorhead, 2013). Although not all counselors may experience a value conflict related to PAD, those who do experience a conflict may look to the American Counseling Association’s (ACA) Code of Ethics (2014) and an ethical decision-making model that accurately addresses the values-based nature of the ethical dilemma at hand.
Multiple scholars have discussed the need to explore values related to personal conflicts to maintain ethical practice in counseling (Cottone & Tarvydas, 2016). However, few sources have yet to provide direction for counselors on how to resolve personal values-based conflicts regarding PAD. There is an added layer of difficulty with PAD clients because of the multifaceted nature of personal and professional values at play. Counselors are grounded on the ethical principles of promoting client autonomy and respecting cultural differences in decisions (ACA, 2014), but hastening death conflicts with the counseling profession’s inherent stance to “first do no harm” and to maintain client safety and preserve life when clients desire to end their lives (Cohen, 2001). Even though hastening death is legal in certain states, values surrounding the decision to end life do not simply cease because there is justified reasoning for a decision. Thus, counselors face a challenging dichotomy between law and values in their practice with PAD clients.
Recent changes in the counseling profession’s ethical code also contribute to the potential challenge of maintaining ethical practice with PAD clients. The ACA Code of Ethics (2005) included codes that addressed counseling practice with clients considering end-of-life options. Section A.9 in the ACA Code of Ethics (2005) provided guidelines about the quality of care counselors should uphold for clients facing the end of their life, including the counselor’s role in assisting clients with end-of-life decisions. Counselors were tasked with the responsibility to reflect upon personal values and morals regarding end-of-life to ensure competent and ethical care. Although the revised ACA Code of Ethics (2014) includes considerations for confidentiality, legal concerns, and client safety during end-of-life care, there is no longer a designated section for the end-of-life care of terminally ill clients, and explicit codes regarding PAD are absent. The ACA Code of Ethics (2014) included guidelines for counselors regarding methods to maintain client autonomy and seek continuing education to address the holistic needs of clients, along with giving clients the tools necessary to make the most appropriate decisions for their care. However, lack of explicit codes about PAD and few guidelines related to end-of-life care might cause ambiguity when values-based ethical dilemmas about PAD arise.
In summary, consideration for counselors’ personal and professional values, along with the ethical and legal implications at hand, creates unique potential for a values-based conflict surrounding PAD unlike other sources of values-based conflicts. Values are influenced by numerous factors in multiple settings and contexts (Heller Levitt & Hartwig Moorhead, 2013). Therefore, resolving value conflicts related to PAD warrants a unique systemic perspective that considers the multiple influential sources that shape values about death and grief in personal and professional realms (Neimeyer et al., 2014).
The authors of this article review PAD, counselors’ roles in the hastened death process, and an applied method of managing values-based conflicts with PAD through a values-based ethical decision-making model and ethical bracketing. The impacts of personal and professional values will be described through an ecological systems lens. It is important for counselors to understand PAD in the context of various systems, as individuals’ decisions concerning PAD are influenced by multiple sources that contribute to their beliefs and values related to death and dying.
Physician-Assisted Death
PAD is currently legal in six U.S. states: California, Colorado, Montana (by court ruling), Oregon, Vermont, and Washington, as well as Washington, DC (Death with Dignity, 2018). Hawaii will become the seventh state to legalize PAD when their legal statute takes effect in January 2019 (Death with Dignity, 2018). PAD has been a topic of debate throughout American society and health care for decades (Werth & Holdwick, 2000). Many have voiced opposition to PAD as a legalized option (Werth & Holdwick, 2000), and previous “standards of mental health practice [have treated] all suicides as products of mental illness” (Cohen, 2001, p. 279). However, health care advocates of PAD, such as Dr. Jack Kevorkian, have fought for individual rights to choose dignified death when faced with terminal illness (Kevorkian, 1991). As the legalization of PAD emerged in the aforementioned states, the topic of debate shifted from the right to choose hastened death toward the policies that guide health care professionals to assist terminally ill individuals in hastening their deaths (Werth & Holdwick, 2000).
Language within each state statute slightly varies, but requirements to legally hasten death are similar across states. There are no formal requirements for PAD in Montana, because a law permitting PAD does not exist in that state; however, there is a legal precedent that protects physicians from prosecution as long as there is written consent from the patient (Baxter v. Montana, 2009). For all other states, patients must be over the age of 18, permanent residents of the state, have been determined by an attending and consulting physician to be suffering from a terminal illness, and carry a life expectancy of under 6 months to be eligible to legally hasten their deaths. Patients must voluntarily express their wishes to die orally, make a written request for medication to end their lives in a humane and dignified manner, and be deemed mentally competent to make end-of-life decisions by a licensed psychiatrist or psychologist. In addition, there is typically a 15-day waiting period between the initial request and when the physician provides a written prescription for medication to end life (Death with Dignity, 2018).
In the legal requirements of each state and district statute, there is no mandate for counseling services beyond an assessment of competency. However, PAD clients and their families often work with mental health professionals throughout the process of considering hastened death and implementing PAD (Fulmer, 2014). As more states move toward legislation to legalize PAD, counselors are becoming more involved in the interdisciplinary teams of health professionals working to meet the needs of this population. Interdisciplinary teams may be comprised of medical physicians, psychiatrists, psychologists, social workers, palliative care nurses and specialists, occupational therapists, and mental health counselors (O’Connor & Fisher, 2011). Clients pursuing PAD have physical, social, emotional, spiritual, and practical needs as they deal with the process and experience of dying (Daneker, 2006). Helping professionals’ roles can be blurred as the interdisciplinary team works together to meet PAD clients’ needs (O’Connor & Fisher, 2011). Physical needs include keeping clients comfortable in their final months of life when all other treatment options are exhausted. Practical needs include making arrangements for after death and navigating the legal processes to hasten death, including the competency assessment a psychiatrist or psychologist must conduct to ensure that PAD clients are stable and well-informed enough to decide to hasten their death (O’Connor & Fisher, 2011). Clients’ social, emotional, and spiritual needs will vary depending on the nature of the terminal illness, individual contexts, and familial and cultural contexts; counselors are trained to address such biopsychosocial needs within clients’ individual and cultural contexts (Peruzzi, Canapary, & Bongar, 1996; Werth & Crow, 2009).
A counselor’s primary role is to address how clients’ medical diagnoses are impacting their biopsychosocial well-being, including their decision-making processes to hasten death (O’Connor & Fisher, 2011; Peruzzi et al., 1996; Werth & Crow, 2009). Counselors build a unique therapeutic relationship that provides professional emotional support, and they help clients reflect on the factors that have led them to make this life-ending decision. They may explore what hastened death means to clients’ families or communities. Counselors also seek to understand how clients’ spiritual beliefs and emotional needs influence their well-being and decision making. Counselors recognize that spirituality and religious practices can be significant to clients when discussing dying, death, and grief (Altmaier, 2011). Addressing these factors allows counselors to be intentional in creating a safe setting for difficult discussions.
Standards of Counseling Practice With Dying Clients
The ACA Code of Ethics (2014) not only serves as a guide to ethical practice in counseling, but also provides an understanding of the goals and mission of the counseling profession. Counselors are committed to engaging in “a professional relationship that empowers diverse individuals, families, and groups to accomplish mental health [and] wellness” (ACA, 2014, p. 3). In order to engage in such a relationship with ethical integrity, counselors consider the six principles of ethical behavior: autonomy, nonmaleficence, beneficence, justice, fidelity, and veracity (ACA, 2014). These principles are foundational to the ways in which counselors practice ethically across diverse client groups and settings. Counselors working with PAD clients should review relevant ethical codes concerning end-of-life issues, personal value conflicts, and confidentiality concerns pertinent to fulfilling the needs of terminally ill clients. Of these relevant issues, one specific code includes guidance in managing personal values in counseling:
Counselors are aware of—and avoid imposing—their own values, attitudes, beliefs, and behaviors.
Counselors respect the diversity of clients . . . and seek training in areas in which they are at risk
of imposing their values onto clients, especially when the counselor’s values are inconsistent with
the client’s goals or are discriminatory in nature. (ACA, 2014, A.4.b)
As counselors confront the socioemotional and spiritual needs of PAD clients, regulating personal values related to PAD is of utmost importance for the well-being of a dying client (Werth, 1999).
Values and PAD
Personal values exist at individual, professional, and societal levels. Counselors develop and mold their values in multiple contexts and through various experiences in their lifetime. Thus, counselors’ values surrounding death, dying, and PAD are multifaceted and influenced by multiple factors. Counselors’ views and values surrounding death may be impacted by age, race, gender, religion or spiritual beliefs, phase of life, family structure and influence, cultural identity (e.g., individualistic vs. collectivistic), and education (Bevacqua & Kurpius, 2013; Harrawood, Doughty, & Wilde, 2011; Kemmelmeier, Wieczorkowska, Erb, & Burnstein, 2002). How these factors are interwoven into personal views and values depends on counselors’ perceptions of their experiences and influences from their surrounding environments.
Because personal values are constructed and influenced by a multitude of factors and environments (Heller Levitt & Hartwig Moorhead, 2013), a systemic perspective can be used to appropriately explore and understand how personal values may form and influence counselors. Bronfenbrenner (1979) established the ecological model to describe an individual’s development within four ecosystems: the microsystem, mesosystem, exosystem, and macrosystem. In 1994, Bronfenbrenner revised the ecological model to include the chronosystem, which considers the influence of time and history as individuals develop. Each ecosystem interacts with the others and influences how each ecosystem forms and impacts the developing individual. The ecosystems can be understood as “a set of nested structures, each inside the next, like a set of Russian dolls” (Bronfenbrenner, 1979, p. 3). Next to the chronosystem, the outermost system, the macrosystem encompasses one’s culture, societal norms, and traditions. The exosystem lies within the macrosystem and represents the interactions between environments that may or may not directly affect an individual’s daily interactions. An example of this system would be a parent having trouble at work, and that stressor then affecting the relationship with the child. Within the exosystem is the mesosystem. The mesosystem includes the interactions between the individual’s microsystem and has direct effects on the individual. Lastly, the microsystem involves the individual’s immediate settings and relationships. Relationships can include family and caregivers among others in the environment. Each of these ecosystems and the interactions between them impact the developing individual’s behaviors (Bronfenbrenner, 1979).
Within a systemic ecological perspective, beliefs and values can be viewed as forming and ensuing through layers of influence first from the macrosystem and filtered down through the exosystem, mesosystem, and microsystem (Bronfenbrenner, 1979). The chronosystem includes a history of culture that influences development over time, but the cultural expressions of such influence play out in the macrosystem (Bronfenbrenner, 1994). The macrosystem, the most external of systemic influence, can include societal norms of death and dying and a religious or spiritual belief system. These norms and belief systems influence the exosystem, where laws and regulations exist (e.g., the right for individuals to hasten death in legalized states). Events that occur in the exosystem might not directly include counselors, but they impact the ways in which counselors interact with their lower systems (e.g., news reports of terminally ill patients miraculously overcoming illness).
Through the mesosystem structure, counselors directly engage with multiple settings that influence their beliefs surrounding death and dying (e.g., work and family). Counselors’ interactions with two settings, such as workplace and family, will shed light onto how beliefs, values, and behaviors about death and dying are experienced in each setting. Counselors’ values are subsequently influenced by the interactions between the two settings. Finally, direct experiences in counselors’ immediate settings, the microsystem, impact the unique views and values counselors espouse. Although values filter through larger systems with influence from external factors that impact multiple people, counselors will form distinct perceptions of their experiences that inform their intrapersonal reactions to death and dying (Werth & Crow, 2009).
As counselors consider each layer of the surrounding environment that informs their personal values, they face the values of the counseling profession in the mesosystem. The ACA Code of Ethics (2014) highlighted five fundamental professional values:
- enhancing human development throughout the lifespan;
- honoring diversity and embracing a multicultural approach in support of the worth, dignity,
potential, and uniqueness of people within their social and cultural contexts;
- promoting social justice;
- safeguarding the integrity of the counselor–client relationship; and
- practicing in a competent and ethical manner. (p. 3)
These values provide a foundation for counselors’ ethical behaviors and decisions and inform the collective identity of the counseling profession.
Counselors first encounter professional values in their training programs and are continually exposed to new expressions of professional values throughout their careers. Counselors are nurtured throughout their development to integrate their personal attributes with professional factors as they form an identity congruent with the counseling profession (D. M. Gibson, Dollarhide, & Moss, 2010; Post & Wade, 2009). The ways in which counselors integrate professional values and develop their identities depends on the culture of their training programs, professional work settings, experiences in those settings, and individual perceptions that form from those experiences (Francis & Dugger, 2014). As a result, counselors may vary in their level of support for PAD, personal conflicts related to PAD, and general beliefs and values about death and dying. Therefore, counselors must evaluate their values at a personal and professional level as they work through value conflicts and ethical dilemmas with PAD clients (Johnson, Hayes, & Wade, 2007).
Ethical Decision Making and Bracketing
Counselors’ abilities to resolve value conflicts are determined through ethical decision making (Cottone & Tarvydas, 2016; Kocet & Herlihy, 2014). The ACA Code of Ethics (2014) serves as a guide to counselors to uphold equitable standards of care across client populations when ethical dilemmas and value conflicts arise. According to ACA:
When counselors are faced with ethical dilemmas that are difficult to resolve, they are expected to
engage in a carefully considered ethical decision-making process, consulting available resources as
needed. Counselors acknowledge that resolving ethical issues is a process; ethical reasoning
includes consideration of professional values, professional ethical principles, and ethical
standards. (ACA, 2014, p. 3)
Becoming an ethical decision maker is most effectively done through practice in intentional decision-making processes (P. A. Gibson, 2008). There are many ethical decision-making models that are relevant to maintaining ethical integrity during a variety of dilemmas (Cottone & Tarvydas, 2016). Counselors most often use practice-derived models that are produced from counselors’ experiences and are intended to provide a step-by-step guide for practice (Cottone & Tarvydas, 2016). Although each model is distinct in its step-by-step process, there are common elements throughout them that highlight a standard of practice for ethical decision making. Significant commonalities include gathering information; considering the context of the situation; reviewing codes, standards, and laws; evaluating the counselor’s values or biases; consultation; developing a plan; and executing the plan. For counselors working with PAD clients, their decision-making processes will require a more in-depth exploration of the context of the situation, counselors’ values and biases, and the counseling profession’s values (Heller Levitt & Hartwig Moorhead, 2013; Kurt & Piazza, 2012). Thus, a decision-making model that carefully considers values-based conflicts is needed.
Using a practice-derived framework, Kocet and Herlihy (2014) developed the counselor values-based conflict model (CVCM) to specifically address ethical dilemmas stemming from value conflicts. The model includes five steps: (1) determine nature of values-based conflict (personal or professional); (2) explore core issues and potential barriers to providing appropriate standard of care; (3) seek assistance/remediation for providing appropriate standard of care; (4) determine and evaluate possible courses of action; and (5) ensure that proposed actions promote client welfare (Kocet & Herlihy, 2014). Each step includes consideration for potential personal and professional values that may arise for counselors.
A key part of resolving values-based conflicts is avoiding imposing one’s values onto the client. To address this key issue, Kocet and Herlihy (2014) also introduced the term ethical bracketing. Ethical bracketing in qualitative research is “a reflexive process [that] enables [researchers] to bracket or set aside their own experiences and assumptions when they interact with their participants and thus accurately capture their participants’ voices” (Kocet & Herlihy, 2014, p. 182). To apply this concept to counseling, Kocet and Herlihy stated that ethical bracketing
is defined as the intentional separating of a counselor’s personal values from his or her
professional values or the intentional setting aside of the counselor’s personal values in order to
provide ethical and appropriate counseling to all clients, especially those whose worldviews,
values, belief systems, and decisions differ significantly from those of the counselor. (p. 182)
Counselors can engage in ethical bracketing by seeking supervision, consultation, continuing education, and personal counseling (Kocet & Herlihy, 2014). This bracketing technique allows counselors to confront their values and establish awareness of how their values may be impacting their views and interactions with clients. Counselors may more easily recognize the unique worldviews of clients through this process, thereby respecting the diversity of clients in their cultural contexts. Such recognition protects the welfare of clients as counselors strive to work from the client’s worldview rather than their own (ACA, 2014). The CVCM, along with ethical bracketing, can be used as a guiding ethical decision-making framework for counselors to explore the systemic nature of their values and resolve values-based conflicts with PAD.
Values-Based Ethical Decisions and Bracketing With PAD
The CVCM is designed to assist counselors in managing personal conflicts related to values that may arise when working with clients (Kocet & Herlihy, 2014). The model begins with a prompt for counselors to determine if the nature of the conflict is personal or professional and ensues with steps that align with the nature of the conflict. However, considering the systemic makeup of individual values, particularly related to PAD, counselors must be mindful of the influences that stem from the profession’s values in the formation and modification of their personal values. Personal and professional values are interwoven and will consequently impact the ethical decision-making process related to values-based conflicts with PAD (Heller Levitt & Hartwig Moorhead, 2013). As a result, adding a systemic lens to the process of resolving values-based conflicts using the CVCM and ethical bracketing is important to maintaining ethical practice with PAD clients.
The systemic sources of values related to PAD are important to consider in the second step of the CVCM; this step includes a prompt for counselors to “explore core issues and potential barriers to providing appropriate standard[s] of care” (Kocet & Herlihy, 2014, p. 184). Gathering awareness about counselors’ personal views related to death, dying, and PAD is the crux of working through this step in the model. As previously discussed, counselors must engage in reflective practice to examine influential factors throughout each ecosystem. Each system contributes to counselors’ personal views and beliefs, and reflecting will bring awareness to not only the sources of counselors’ values, but also potential barriers to overcoming values-based conflicts (Bronfenbrenner, 1979; Cottone & Tarvydas, 2016; Kocet & Herlihy, 2014).
Beginning with the macrosystem, societal norms and religious and spiritual views of death and dying will influence the exosystem. Legislation that gives clients legal freedom in certain states to decide to end their lives is situated in the exosystem. As the decision to engage in PAD is legalized, it then trickles down into the mesosystem where groups, such as work colleagues and family, hold beliefs and values about PAD. These beliefs and values influence counselors in new ways and impact the intrapersonal reactions counselors have in their microsystem of experience. Counselors must examine the interactions between settings and the messages they receive in those settings. Then, they may more readily discover how their values and beliefs about PAD are formed and either reinforced or undermined. Increased awareness will help counselors identify the ecosystem that is the most salient source of their value conflict with PAD (Bronfenbrenner, 1979). Identifying the salient source may then lead to increased potential for counselors to be more specific in the ways they strategize to bracket their values.
As counselors foster awareness about the sources of their value conflicts, they can move into the third step and engage in ethical bracketing as a strategy to seek necessary assistance to resolve value conflicts. In addition to referring to the ACA Code of Ethics (2014), counselors may consult with other counselors to explore individualized strategies to engage with PAD clients without imposing personal beliefs and value systems. Consultation with other professionals will shed light onto professional standards of care for PAD clients, while also serving as a mirror for further self-exploration about the sources and nature of value conflicts with PAD. It is important to note that counselors should “identify ways to maintain personal/religious/moral beliefs while still providing effective counseling” (Kocet & Herlihy, 2014, p. 184). Ethical bracketing is not designed to push counselors to give up their beliefs or values; rather, counselors simply “set aside their own experiences and assumptions” to effectively step into the client’s worldview (Kocet & Herlihy, 2014, p. 182). Seeking supervision, consultation, and personal counseling can provide guidance for counselors to determine their needs to maintain their personal beliefs and deliver ethical care for PAD clients (Cottone & Tarvydas, 2016; Kocet & Herlihy, 2014).
Next, counselors shift into the fourth step to “determine and evaluate possible courses of action” (Kocet & Herlihy, 2014, p. 184). Using ethical bracketing as a strategy may provide distinct options to consider in this step. Once counselors are aware of the intricacies of their values-based conflict with PAD, they may be more readily able to bracket their values. The guidelines for use of the CVCM in the fourth step note client referral; however, counselors may only refer when they “lack the competence to be of professional assistance to clients,” and their rationale is not the result of personal bias (ACA, 2014, A.11.a.). If counselors lack competence, they may seek appropriate continuing education and supervision to expand their competency in the future. However, in the case of personal value conflicts, referral is not ethical. There is no statement in the ACA Code of Ethics (2014) “that [indicates] referral can be made on the basis of counselor values” (Kaplan, 2014, p. 144). Self-evaluation and consultation is essential to maintain ethical practice surrounding this topic. Once a course of action has been determined as ethical and effective, counselors engage in the fifth step to “ensure that proposed actions promote client welfare” (Kocet & Herlihy, 2014, p. 184). In order to more fully conceptualize resolving values-based conflicts with PAD through this model, a specific example is provided in the following section.
Case Study Application
The following case study explores a counselor’s values-based conflict related to PAD for illustrative purposes. Although many sources may contribute to potential values-based conflicts, personally held religious beliefs are often influential to views and values about PAD (Bevacqua & Kurpius, 2013; Burdette, Hill, & Moulton, 2005; Reiner, 2007). Therefore, personal religious beliefs are explored for the purposes of this case study. Considering a systemic view of counselors’ values, the CVCM and ethical bracketing are used to generate potential conflict resolutions that ensure ethical practice and protect the welfare of the client.
Vignette
Amy is a licensed professional counselor in the state of Washington. She works for an agency that receives referrals from a local hospital. Amy identifies as a religious person and has connections and support through her religious community. Her personal religious views do not endorse hastening one’s death, even under extreme circumstances like a terminal illness. Amy also has two young children.
Amy has been meeting with Frankie, a 40-year-old woman, for about four months. Frankie was diagnosed with leukemia about six months ago and began treatment shortly thereafter. Frankie recently found out that the leukemia is not responding to treatment and her treatment options are exhausted. Frankie’s oncologist has estimated a five- to six-month life expectancy. Frankie has expressed to Amy that she wants to pursue PAD so that she does not have to be in pain for 6 more months. Frankie has a husband and 6-year-old daughter.
Amy is initially shocked to hear Frankie’s desire to hasten her death. Amy is unsure how to proceed in her work with Frankie because she feels Frankie’s decision conflicts with her religious beliefs. Amy also is wondering if Frankie has considered how her family feels and if they would be okay with Frankie’s decision. Recognizing she needs to process her thoughts and feelings, Amy seeks out a helpful colleague in order to proceed in her work with Frankie.
Discussion
Beginning with the first step of the CVCM, Amy appears to be dealing with a complex values-based conflict. The nature of Amy’s conflict is primarily personal, but she is faced with some professional conflicts as well. Amy’s religious beliefs and values are personally driven, but the countertransference she is experiencing related to Frankie’s seeming lack of concern for her family can become a professional issue if Amy considers making professional decisions that emphasize family values over Frankie’s requests (Heller Levitt & Hartwig Moorhead, 2013). Furthermore, Amy’s personal religiously driven value conflict intertwines with the counseling profession’s value and ethical standard to respect clients’ worldviews and not impose personal beliefs onto clients (ACA, 2014, A.4.b). Understanding both personal and professional implications allows counselors to move into the second step of the CVCM.
The development and context of Amy’s values may be explored through a systemic ecological lens in the second step. Beginning with the macrosystem, Amy may consider how her religious culture views death and what messages she has internalized to form her understanding of morality and autonomy (Burdette et al., 2005; Johnson et al., 2007). She also could explore how society at large influences her religious beliefs and practices and subsequently how she believes her religion views the practice of hastened death. The interaction between Amy’s religious culture and society is situated in the exosystem. Amy’s interactions with her religious community, which are a part of her mesosystem, also will play a role in her beliefs and actions. She might think about how her immediate community impacts her beliefs and influences her perceptions of hastened death; Amy’s individual perceptions and direct engagement with her religious practices play out in her microsystem. As each ecosystem is explored, Amy can develop a clear understanding of the sources of her value conflict. The same process should be repeated for her values-based conflict about Frankie’s family. Amy may value collective family decisions and could potentially struggle to meet Frankie with acceptance if she believes an isolated decision is improper.
Once Amy has explored the systemic sources of her values, she is ready to seek assistance to ethically move forward with Frankie in the third step of the CVCM. Using ethical bracketing, Amy can reach out to her colleagues to consult about the issues at hand. Exploring her values with a trusted professional may enable her to bracket her values to approach Frankie’s differing beliefs and values. Amy must review the ACA Code of Ethics (2014) before creating a plan of action. Again, Code A.4.b, regarding personal values and biases, is central to an ethical course of action; the profession’s value of client autonomy and Code A.1.a, to protect the welfare of the client, also are important to consider here (ACA, 2014). Attending to legal implications, Amy should keep in mind that Frankie has a legal right in the state of Washington to decide to hasten her death. Lastly, Amy should consider ways she can maintain her own values without compromise while still providing effective care and assistance to Frankie in her decision-making process (Kocet & Herlihy, 2014). Amy may pursue personal counseling or supervision and connect with trusted individuals in her religious community to maintain her personal beliefs and values while providing ethical care (Cottone & Tarvydas, 2016; Johnson et al., 2007).
Moving into the fourth step of the CVCM, referral is an option only if Amy lacks competence to provide Frankie with effective care. According to the CVCM, when a counselor is determining action plans, the choice to refer a client is decided after careful consideration of ethical guidelines, rationale for the referral, and in-depth consultation (Kocet & Herlihy, 2014). Referral based on personal values is not ethical according to the ACA Code of Ethics (2014); therefore, Amy cannot ethically refer Frankie, considering the source of her conflict is related to personal values.
Finally, in the fifth step, Amy can ensure her constructed course of action considers both legal and ethical implications. The rationale for Amy’s action plan should be based on professional competency, not personal bias (ACA, 2014, A.11.a). Amy’s ability to effectively bracket her values will be dependent on her depth of self-exploration, understanding of ethical practice in counseling, willingness to consult and seek appropriate resources, and ability to ensure client welfare as the priority. It is essential for Amy to seek consultation from her professional peers, who can provide insight into maintaining ethical boundaries with clients. Also, Amy can receive permission to speak with Frankie’s lawyer and the primary doctors involved with her decision to hasten her death. By increasing involvement with Frankie’s interdisciplinary team, Amy is ensuring holistic care and attending to the systemic nature of end-of-life decision making surrounding PAD.
Implications for Counseling Practice
The interplay between PAD and the values of counselors and the counseling profession is complex and warrants depth of exploration for counselors to effectively meet the needs of this population. Values-based conflicts do not occur in isolation; instead, multiple systems that impact individuals in varying ways influence the formation and expression of such conflicts (Heller Levitt & Hartwig Moorhead, 2013). No one specific cultural identity, belief, or value can predict a counselor’s conflicts with PAD, but it is crucial to explore values through a systemic lens to successfully manage values-based conflicts with PAD. The CVCM, along with ethical bracketing, can serve as an appropriate framework to confront and resolve values-based conflicts with PAD. Counselors will be better equipped to provide care to PAD clients as they willingly and openly explore their values related to death, dying, and hastening death through an ethical decision-making model (ACA, 2014). Counselors’ effectiveness in self-reflection and ethical practice is reliant in part on counselor education.
Counselor Education
As state laws change, counselor educators need to recognize that counselors will play a larger role in caring for potential PAD clients. It can be beneficial to learn about the role of value bracketing in regard to discussing the possibility of a client exploring the option of PAD. It is difficult for counselor educators to prepare counselors-in-training (CITs) for every potential ethical dilemma. However, with a better understanding of PAD, novice counselors can feel more equipped to effectively address concerns their clients may have without interference of their personal beliefs and values. PAD is a topic that will continue to expand. Introducing PAD during training may allow counselors to feel more prepared should a value conflict arise. As counselor educators facilitate conversations with CITs about their personal and professional beliefs toward PAD, CITs can implement their value bracketing skills under the supervision of their faculty. Being in a safe environment can encourage CITs to explore their authentic feelings concerning PAD and evaluate their value bracketing skillset. Addressing concerns and potential red flags during training can prevent harm to future clients and unethical clinical judgment and behaviors.
There is a potential challenge in maintaining consistency in training about end-of-life issues, including PAD, because of the nature of accreditation standards for counseling programs. There is no specific standard of learning in the 2016 Council for Accreditation of Counseling and Related Educational Programs (CACREP) standards regarding end-of-life counseling issues (CACREP, 2016). Counselor educators are tasked to meet learning standards related to human growth and development “across the lifespan,” but they have discretion over what they include and highlight throughout their curriculum (CACREP, 2016, p. 10). Counselor educators should consider the importance and advantages of including specific instruction on end-of-life issues in their curriculum (Servaty-Seib & Tedrick Parikh, 2014).
In addition to educating CITs, more research is needed to further understand counselors’ developing roles with clients pursuing PAD. With more states legalizing this procedure, it is only a matter of time before counselors are face-to-face with a client that needs a counselor’s experience and competency to assist with this life-changing decision. Although data is available concerning grief and loss counseling, literature directly related to counselors’ roles in working with PAD is sparse. Future research should incorporate counselors’ emerging roles with PAD clients and needs for training to prepare CITs. With stronger research in this area, counselor educators may feel more equipped to teach and support CITs
to become aware of and potentially bracket their values about death, dying, and PAD.
Conclusion
Counselors must be knowledgeable about the legal and ethical standards surrounding PAD in order to work effectively and ethically with PAD clients. Counselors also need to be aware of their personal beliefs and values about death and dying and be able to manage values-based conflicts. This article highlighted personal and professional values relevant to counselors working with PAD clients through an ecological systems lens. Considering the values at play, counselors can use the CVCM with ethical bracketing as an integrated method to resolve value conflicts with PAD (Kocet & Herlihy, 2014). Increased knowledge regarding ethical decision making surrounding PAD can encourage counselors to provide care for PAD clients with competence and confidence. Further research on counselors’ roles with PAD clients and needs for training may enhance counselors’ knowledge and competency with this client population.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
Altmaier, E. M. (2011). Best practices in counseling grief and loss: Finding benefit from trauma. Journal of Mental Health Counseling, 33, 33–45. doi:10.17744/mehc.33.1.tu9wx5w3t2145122
American Counseling Association. (2005). 2005 code of ethics. Retrieved from https://www.counseling.org/docs/default-source/library-archives/archived-code-of-ethics/codeethics05.pdf
American Counseling Association. (2014). 2014 code of ethics. Retrieved from https://www.counseling.org/resou rces/aca-code-of-ethics.pdf
Baxter v. Montana, 224 P.3d 1211 (Mont. 2009).
Bevacqua, F., & Kurpius, S. (2013). Counseling students’ personal values and attitudes toward euthanasia. Journal of Mental Health Counseling, 35, 172–188. doi:10.17744/mehc.35.2.101095424625024p
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Cambridge, MA: Harvard University Press.
Bronfenbrenner, U. (1994). Ecological models of human development. In International Encyclopedia of Education (Vol. 3, 2nd ed.). Oxford, UK: Elsevier.
Burdette, A. M., Hill, T. D., & Moulton, B. E. (2005). Religion and attitudes toward physician-assisted suicide and terminal palliative care. Journal for the Scientific Study of Religion, 44, 79–93.
doi:10.1111/j.1468-5906.2005.00266.x
Cohen, E. D. (2001). Permitted suicide: Model rules for mental health counseling. Journal of Mental Health Counseling, 23, 279–294.
Cottone, R. R., & Tarvydas, V. (2016). Ethics and decision making in counseling and psychotherapy (4th ed.). New York, NY: Springer.
Council for Accreditation of Counseling and Related Educational Programs (2016). 2016 CACREP standards. Retrieved from http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Daneker, D. (2006). Counselors working with the terminally ill. In VISTAS 2006 (pp. 1–13). Retrieved from https://www.counseling.org/Resources/Library/VISTAS/vistas06_online-only/Daneker.pdf
Death with Dignity. (2018). Death with dignity acts. Retrieved from https://www.deathwithdignity.org/learn/death-with-dignity-acts/
Francis, P. C., & Dugger, S. M. (2014). Professionalism, ethics, and value-based conflicts in counseling: An introduction to the special section. Journal of Counseling & Development, 92, 131–134.
doi:10.1002/j.1556-6676.2014.00138.x
Fulmer, R. (2014). Physician-assisted suicide, euthanasia, and counseling ethics. In Ideas and research you can
use: VISTAS 2014. Retrieved from https://www.counseling.org/docs/default-source/vistas/article_53.
pdf?sfvrsn=5677d2c_10
Gibson, D. M., Dollarhide, C. T., & Moss, J. M. (2010). Professional identity development: A grounded
theory of transformational tasks of new counselors. Counselor Education and Supervision, 50, 21–37.
doi:10.1002/j.1556-6978.2010.tb00106.x
Gibson, P. A. (2008). Teaching ethical decision making: Designing a personal value portrait to ignite creativity and promote personal engagement in case method analysis. Ethics & Behavior, 18, 340–352. doi:10.1080/10508420701713022
Harrawood, L. K., Doughty, E. A., & Wilde, B. (2011). Death education and attitudes of counselors-in-training toward death: An exploratory study. Counseling and Values, 56, 83–95.
doi:10.1002/j.2161-007X.2011.tb01033.x
Heller Levitt, D., & Hartwig Moorhead, H. J. (2013). Values and ethics in counseling: Real-life ethical decision making. New York, NY: Routledge.
Johnson, C. V., Hayes, J. A., & Wade, N. G. (2007). Psychotherapy with troubled spirits: A qualitative investigation. Psychotherapy Research, 17, 450–460. doi:10.1080/10503300600953520
Kaplan, D. M. (2014). Ethical implications of a critical legal case for the counseling profession: Ward v. Wilbanks. Journal of Counseling & Development, 92, 142–146. doi:10.1002/j.1556-6676.2014.00140.x
Kemmelmeier, M., Wieczorkowska, G., Erb, H.-P., & Burnstein, E. (2002). Individualism, authoritarianism, and attitudes toward assisted death: Cross-cultural, cross-regional, and experimental evidence. Journal of Applied Social Psychology, 32, 60–85. doi:10.1111/j.1559-1816.2002.tb01420.x
Kevorkian, J. (1991). Prescription: Medicide, the goodness of planned death. Amherst, NY: Prometheus Books.
Kocet, M. M., & Herlihy, B. J. (2014). Addressing value-based conflicts within the counseling relationship: A decision-making model. Journal of Counseling & Development, 92, 180–186.
doi:10.1002/j.1556-6676.2014.00146.x
Kurt, L. J., & Piazza, N. J. (2012). Ethical guidelines for counselors when working with clients with terminal illness requesting physician aid in dying. Adultspan Journal, 11, 89–96.
doi:10.1002/j.2161-0029.2012.00008.x
Laakkonen, M. L., Pitkala, K. H., & Strandberg, T. E. (2004). Terminally ill elderly patient’s experiences, attitudes, and needs: A qualitative study. Omega: Journal of Death & Dying, 49, 117–129.
doi:10.2190/KVM3-ULM7-0RUH-KVQH
Miller, P. J., Hedlund, S. C., & Soule, A. B. (2006). Conversations at the end of life: The challenge to support patients who consider death with dignity in Oregon. Journal of Social Work in End-of-Life & Palliative Care, 2, 25–43. doi:10.1300/J457v02n02_03
Neimeyer, R. A., Klass, D., & Dennis, M. R. (2014). A social constructionist account of grief: Loss and the narration of meaning. Death Studies, 38, 485–498. doi:10.1080/07481187.2014.913454
O’Connor, M., & Fisher, C. (2011). Exploring the dynamics of interdisciplinary palliative care teams in providing psychosocial care: “Everybody thinks that everybody can do it and they can’t.” Journal of Palliative Medicine, 14, 191–196. doi:10.1089/jpm.2010.0229
Peruzzi, N., Canapary, A., & Bongar, B. (1996). Physician-assisted suicide: The role of mental health professionals. Ethics & Behavior, 6, 353–366. doi:10.1207/s15327019eb0604_6
Post, B. C., & Wade, N. G. (2009). Religion and spirituality in psychotherapy: A practice-friendly review of research. Journal of Clinical Psychology, 65, 131–146. doi:10.1002/jclp.20563
Reiner, S. M. (2007). Religious and spiritual beliefs: An avenue to explore end-of-life issues. Adultspan Journal, 6, 111–118. doi:10.1002/j.2161-0029.2007.tb00036.x
Servaty-Seib, H. L., & Tedrick Parikh, S. J. (2014). Using service-learning to integrate death education into counselor preparation. Death Studies, 38, 194–202. doi:10.1080/07481187.2012.738774
Werth, J. L., Jr. (1999). Mental health professionals and assisted death: Perceived ethical obligations and proposed guidelines for practice. Ethics & Behavior, 9, 159–183. doi:10.1207/s15327019eb0902_6
Werth, J. L., Jr., & Crow, L. (2009). End-of-life care: An overview for professional counselors. Journal of Counseling & Development, 87, 194–202. doi:10.1002/j.1556-6678.2009.tb00567.x
Werth, J. L., Jr., & Holdwick, D. J., Jr. (2000). A primer on rational suicide and other forms of hastened death. The Counseling Psychologist, 28, 511–539. doi:10.1177/0011000000284003
Yalom, I. D. (2008). Staring at the sun: Overcoming the terror of death. San Francisco, CA: Jossey-Bass.
Yalom, I. D. (2009). The gift of therapy: An open letter to a new generation of therapists and their patients. New York, NY: HarperCollins.
Nancy E. Thacker, NCC, is a doctoral candidate at the University of Tennessee, Knoxville. Jillian M. Blueford, NCC, is a doctoral candidate at the University of Tennessee, Knoxville. Correspondence can be addressed to Nancy Thacker, 501 BEC, 1122 Volunteer Blvd, Knoxville, TN 37996-3452, nthacke2@vols.utk.edu.
Sep 27, 2018 | Volume 8 - Issue 3
Christopher T. Belser, M. Ann Shillingford, Andrew P. Daire, Diandra J. Prescod, Melissa A. Dagley
The United States is facing a crisis with respect to filling job vacancies within science, technology, engineering, and math (STEM) industries and with students completing STEM undergraduate degrees. In addition, disparities exist for females and ethnic minorities within STEM fields. Whereas prior research has centered on disparities in STEM fields, retention rates, and some intervention programs, researchers have not given much attention to the role of career development initiatives within STEM recruitment and retention programming. The purpose of the present study was to incorporate demographic variables, math performance, and career development–related factors into predictive models of STEM retention with a sample of undergraduate students within a STEM recruitment and retention program. The resulting two models accurately predicted first-year to second-year retention with 73.4% of the cases and accurately predicted first-year to third-year retention with 70.0% of the cases. Based on the results, the researchers provide a rationale for STEM career programming in K–12 and higher education settings and for the inclusion of career development and career counseling in STEM education programming.
Keywords: STEM, retention, career development, career counseling, undergraduate student
The United States lacks an adequate number of workers to keep up with the demand for trained workers in science, technology, engineering, and mathematics (STEM) fields (National Center for Science and Engineering Statistics [NCSES], 2017; National Science Board, 2018; Sithole et al., 2017). Researchers have pointed to the overall stagnancy of undergraduate students declaring and completing STEM degrees (Carnevale, Smith, & Melton, 2011; Doerschuk et al., 2016; Sithole et al., 2017). Additionally, underrepresentation is a problem for racial and ethnic minorities and females in STEM fields (NCSES, 2017). Because of these disparities, universities have developed programs centered on recruitment and retention of STEM undergraduates (Bouwma-Gearhart, Perry, & Presley, 2014; Dagley et al., 2016; Schneider, Bickel, & Morrison-Shetlar, 2015) and both government and private entities invest billions of dollars annually toward STEM initiatives at the K–12 and higher education levels (Carnevale et al., 2011). However, many of these endeavors have failed to incorporate components centered on career development or career planning.
The National Career Development Association (2015) defined career development as “the sequence of career-related choices and transitions made over the life span” (p. 4) and career planning as a structured process through which a person makes decisions and plans for a future career. Career development activities, such as structured career planning courses, have shown efficacy with general undergraduate populations (Osborn, Howard, & Leierer, 2007; Reardon, Melvin, McClain, Peterson, & Bowman, 2015) but have been studied less commonly with STEM-specific undergraduate populations (Belser, Prescod, Daire, Dagley, & Young, 2017, 2018; Prescod, Daire, Young, Dagley, & Georgiopoulos, in press). In the present study, researchers examined a STEM recruitment and retention program that did include a career planning course. More specifically, the research team sought to investigate relationships between demographics (e.g., gender, ethnicity), math scores, and various aspects of the undergraduate STEM program and student retention in the first 2 years of college.
Gender, Ethnicity, and STEM
Gender disparities are a common sight within STEM degree programs and the larger STEM workforce (NCSES, 2017). Females who are interested in math and science are more likely to be tracked into non-diagnosing health practitioner fields, such as nursing (ACT, 2018; NCSES, 2017). Some researchers have pointed to the K–12 arena as the root of these gender disparities that permeate undergraduate programs and STEM professions (Mansfield, Welton, & Grogan, 2014), whereas others have identified specific problems, such as differences in math and science course completion over time (Chen & Soldner, 2013; Riegle-Crumb, King, Grodsky, & Muller, 2012), stereotype threat (Beasley & Fischer, 2012), and STEM confidence (Litzler, Samuelson, & Lorah, 2014). As a result, existing predictive models typically indicate a lower likelihood of females completing a STEM degree compared to male students (Cundiff, Vescio, Loken, & Lo, 2013; Gayles & Ampaw, 2014).
Similarly, disparities in STEM degree completion and STEM job attainment exist between ethnic groups (NCSES, 2017; Palmer, Maramba, & Dancy, 2011). Although progress has been made in degree attainment in certain STEM areas, other areas have stagnated or are declining in participation by ethnic minority students (Chen & Soldner, 2013; NCSES, 2017). Foltz, Gannon, and Kirschmann (2014) identified protective factors for minority students in STEM, such as receiving college-going expectations from home, establishing connections with STEM faculty members (particularly those of color), and developing connections with other minority students in STEM majors; however, the disparities in STEM programs help perpetuate a cycle of many students not being exposed to these protective factors. The intersectionality of ethnicity and gender in STEM fields has become a topic producing interesting findings (Riegle-Crumb & King, 2010). In addition to observing disparities across ethnic groups, researchers have observed disparities within ethnic groups based on gender (Beasley & Fischer, 2012; Cundiff et al., 2013; Riegle-Crumb & King, 2010). Specifically with males of color, predictive models have been inconclusive, with some showing a higher likelihood of completing a STEM degree (Riegle-Crumb & King, 2010) and others showing a lower likelihood (Cundiff et al., 2013; Gayles & Ampaw, 2014).
Mathematics and STEM
The SAT is one of the most widely used college admissions tests (CollegeBoard, 2018). Researchers have correlated the math sub-score with undergraduate math and science classes within the first year, indicating that higher SAT math scores indicate a higher probability of higher course grades in math and science courses (Wyatt, Remigio, & Camara, 2012). Additionally, researchers have identified SAT scores as predictors of academic success and university retention (Crisp, Nora, & Taggart, 2009; Le, Robbins, & Westrick, 2014; Mattern & Patterson, 2013; Rohr, 2012). Despite its wide use in higher education admissions, the SAT may not be free from bias. Numerous scholars have highlighted potential test bias, particularly against ethnic minorities (Dixon-Román, Everson, & McArdle, 2013; Lawlor, Richman, & Richman, 1997; Toldson & McGee, 2014). Nevertheless, its wide use makes it a prime instrument for research.
In addition to the SAT scores, researchers also have demonstrated that taking higher-level math courses and having higher math self-efficacy translate to better outcomes within STEM majors (Carnevale et al., 2011; Chen & Soldner, 2013; Nosek & Smyth, 2011). Specifically, taking calculus-based courses in high school correlated with retention in STEM majors (Chen & Soldner, 2013). Nosek and Smyth (2011) found connections between gender and internalized math variables, such as warmth for math, identification with math, and self-efficacy; females across the life span showed lower levels of each of these variables, but the authors did not test these against retention outcomes in STEM majors. However, one could hypothesize that having lower levels of warmth toward math and not being able to identify with math would likely impact one’s career decisions, particularly related to math and science fields.
Career Interventions and STEM
Career theory can provide for understanding one’s interest in STEM fields (Holland, 1973), one’s exposure to STEM fields (Gottfredson, 1981), and one’s beliefs or expectations about the process of choosing a STEM field (Lent, Brown, & Hackett, 2002; Peterson, Sampson, Lenz, & Reardon, 2002). However, career interventions, such as a career planning class, are more likely to make a direct impact on career outcomes with undergraduates. In one review of research on undergraduate career planning courses, more than 90% of the courses produced some measurable positive result for students, such as increased likelihood of completing a major, decreased negative career thinking, and increased career self-efficacy (Reardon & Fiore, 2014). Other researchers have reported similar results with generic undergraduate career planning courses (Osborn et al., 2007; Saunders, Peterson, Sampson, & Reardon, 2000).
Researchers have studied structured career planning courses specific to STEM majors with much less frequency. In one such study, Prescod and colleagues (in press) found that students who took a STEM-focused career planning course scored lower on a measure of negative career thinking at the end of the semester. In a similar study, STEM-interested students in a STEM-focused career planning course had lower posttest scores on a measure of negative career thinking than declared STEM majors at the end of the same semester (Belser et al., 2018). Additionally, in a pilot study, Belser and colleagues (2017) found that greater reductions in negative career thinking predicted higher odds of being retained in a STEM major from the first to second year of college; in this same study, the authors found that students who participated in a STEM-focused career planning course were more likely to be retained in a STEM major than students in an alternative STEM course. Researchers have not given ample attention to determining how career planning and other career variables fit into predictive models of retention in STEM majors.
Statement of the Problem and Hypotheses
As previously noted, prior researchers have paid limited attention to developing predictive models that incorporate career development variables along with demographics and math performance. Developing effective predictive models has implications for researchers, career practitioners, higher education professionals, and the STEM workforce. To this end, the researchers intend to test two such models related to retention in STEM majors using the following hypotheses:
Hypothesis 1: First-year to second-year undergraduate retention in STEM majors can be predicted by ethnicity, gender, initial major, math placement–algebra scores, SAT math scores, STEM course participation, and Career Thoughts Inventory (CTI) change scores.
Hypothesis 2: First-year to third-year undergraduate retention in STEM majors can be predicted by ethnicity, gender, initial major, math placement–algebra scores, SAT math scores, STEM course participation, and CTI change scores.
Methods
In this study, researchers examined multi-year retention data for students in a STEM recruitment and retention program at a large research university in the Southeastern United States and utilized a quasi-experimental design with non-equivalent comparison groups (Campbell & Stanley, 1963; Gall, Gall, & Borg, 2007). Because this study was part of a larger research project, Institutional Review Board approval was already in place.
The COMPASS Program
The COMPASS Program (Convincing Outstanding Math-Potential Admits to Succeed in STEM; Dagley et al., 2016) is a National Science Foundation–funded project that seeks to recruit and retain undergraduate students in STEM majors. To enter the program, students must have a minimum SAT math score of 550, an undeclared major at the time of applying to the university and program, and an expressed interest in potentially pursuing a STEM degree. However, some students accepted to the COMPASS Program declare a STEM major between the time that they are accepted into the COMPASS Program and the first day of class, creating a second track of students who were initially uncommitted to a major at the time of application. Students in both tracks have access to math and science tutoring in a program-specific center on campus, are matched with undergraduate mentors from STEM majors, have access to cohort math classes for students within the program, and can choose to live in a residence hall area designated for COMPASS participants. Depending on which COMPASS track students are in, they either take a STEM-focused career planning course or a STEM seminar course during their first semester.
COMPASS participants who started college without a declared major take a STEM-focused career planning class in their first semester. The activities of this course include a battery of career assessments and opportunities to hear career presentations from STEM professionals, visit STEM research labs, and attend structured career planning activities (e.g., developing a career action plan, résumé and cover letter writing, small group discussions). The first author and fourth author served as instructors for this course, and both were counselor education doctoral students at the time.
Participants who had declared a STEM major between the time they were accepted into the COMPASS Program and the first day of class took a STEM seminar course instead of the career planning class. The structure of this course included activities designed to help students engage with and be successful in their selected STEM majors, including presentations on learning styles and strategies, time management, study skills, professional experiences appropriate for STEM majors, and strategies for engaging in undergraduate research. Guest speakers for the class focused more on providing students with information about how to be successful as a STEM student. The course did not include career planning or career decision-making activities specifically geared toward helping students decide on a major or career field. A science education doctoral student served as the instructor of record for the course, with graduate students from various STEM fields serving as teaching assistants.
Participants
The university’s Institutional Knowledge Management Office provided demographic data on program participants. Table 1 displays descriptive data for participants, organized by second-year retention data (i.e., retention from the first year of college to the second year of college, for Hypothesis 1) and third-year retention data (i.e., retention from the first year of college to the third year of college, for Hypothesis 2). The frequencies for the subcategories were smaller for the third-year retention data (Hypothesis 2) because fewer participants had matriculated this far during the life of the project. Table 1 also breaks down each subset of the data based on which students were retained in a STEM major and which were not retained.
Table 1
Descriptive Statistics for Categorical Variables
|
Second-Year Retention Descriptives |
Third-Year Retention Descriptives |
| Variables |
Retained |
Not Retained |
Total |
Retained |
Not Retained |
Total |
|
n |
%a |
n |
%b |
n |
%c |
n |
%a |
n |
%b |
n |
%c |
| Gender |
|
|
|
|
|
|
|
|
|
|
|
|
| Male |
159 |
58.9 |
74 |
46.5 |
233 |
54.3 |
72 |
55.8 |
65 |
44.8 |
137 |
50.0 |
| Female |
111 |
41.1 |
85 |
53.5 |
196 |
45.7 |
57 |
44.2 |
80 |
55.2 |
137 |
50.0 |
| Total |
270 |
100.0 |
159 |
100.0 |
429 |
100.0 |
129 |
100.0 |
145 |
100.0 |
274 |
100.0 |
| Ethnicity |
|
|
|
|
|
|
|
|
|
|
|
|
| Caucasian/White |
147 |
54.4 |
100 |
62.9 |
247 |
57.6 |
66 |
51.2 |
85 |
58.6 |
151 |
55.1 |
| African Am./Black |
31 |
11.5 |
16 |
10.1 |
47 |
11.0 |
16 |
12.4 |
18 |
12.4 |
34 |
12.4 |
| Hispanic |
57 |
21.1 |
34 |
21.4 |
91 |
21.2 |
29 |
22.5 |
32 |
22.1 |
61 |
22.3 |
| Asian/Pacific Islander |
24 |
8.9 |
4 |
2.5 |
28 |
6.5 |
10 |
7.8 |
5 |
3.4 |
15 |
5.5 |
| Other |
11 |
4.1 |
5 |
3.1 |
16 |
3.7 |
8 |
6.2 |
5 |
3.4 |
13 |
4.7 |
| Total |
270 |
100.0 |
159 |
100.0 |
429 |
100.0 |
129 |
100.0 |
145 |
100.0 |
274 |
100.0 |
| Course |
|
|
|
|
|
|
|
|
|
|
|
|
| Career Planning |
137 |
50.7 |
120 |
75.5 |
257 |
59.9 |
76 |
58.9 |
112 |
77.2 |
188 |
68.6 |
| STEM Seminar |
133 |
49.3 |
39 |
24.5 |
172 |
40.1 |
53 |
41.1 |
33 |
22.8 |
86 |
31.4 |
| Total |
270 |
100.0 |
159 |
100.0 |
429 |
100.0 |
129 |
100.0 |
145 |
100.0 |
274 |
100.0 |
| Initial Major |
|
|
|
|
|
|
|
|
|
|
|
|
| Undeclared |
130 |
48.1 |
72 |
45.3 |
202 |
47.1 |
65 |
50.4 |
63 |
43.4 |
128 |
46.7 |
| STEM |
124 |
45.9 |
40 |
25.2 |
164 |
38.2 |
55 |
42.6 |
39 |
26.9 |
94 |
34.3 |
| Non-STEM |
16 |
5.9 |
47 |
29.6 |
63 |
14.7 |
9 |
7.0 |
43 |
29.7 |
52 |
19.0 |
| Total |
270 |
100.0 |
159 |
100.0 |
429 |
100.0 |
129 |
100.0 |
145 |
100.0 |
274 |
100.0 |
Note. a = percentage of the Retained group. b = percentage of the Not Retained group. c = percentage of the Total group.
Gender representation within the two samples was split relatively evenly, with female participants represented at a higher rate in the sample than in the larger population of STEM undergraduates and at a higher rate than STEM professionals in the workforce. Both samples were predominantly Caucasian/White, with no other ethnic group making up more than one-fourth of either sample individually; these ethnicity breakdowns were reflective of the university’s undergraduate population and somewhat reflective of STEM disciplines. The students who took the STEM-focused career planning course accounted for a larger percentage of both total samples and also of the not-retained groups. Regarding initial major, the largest percentage of students fell within the initially undeclared category, with the next largest group being the initially STEM-declared group (these students officially declared a STEM major but were uncommitted with their decision).
The researchers conducted an a priori power analysis using G*Power 3 (Cohen, 1992; Faul, Erdfelder, Lang, & Buchner, 2007), and the overall samples of 429 and 271 were sufficient for the binary logistic regression. With logistic regression, the ratio of cases in each of the dependent outcomes (retained or not retained) to the number of independent variable predictors must be sufficient (Agresti, 2013; Hosmer, Lemeshow, & Sturdivant, 2013; Tabachnick & Fidell, 2013). Following Peduzzi, Concato, Kemper, Holford, and Feinstein’s (1996) rule of 10 cases per outcome per predictor, the samples were sufficient for all independent variables except ethnicity, which had multiple categories with fewer than 10 cases. However, Field (2009) and Vittinghoff and McCulloch (2006) recommended having a minimum of five cases per outcome per predictor, which the sample achieved for all independent variables.
Variables and Instruments
The analysis included 10 independent variables within the logistic regression models. The university’s Institutional Knowledge Management Office (IKMO) provided data for the four categorical variables displayed in Table 1 (gender, ethnicity, course, and initial major). Four of the independent variables represented the participants’ total and subscale scores on the CTI, which students completed in either the career planning course or the STEM seminar course. The other two independent variables were participants’ scores on the SAT math subtest and the university’s Math Placement Test–Algebra subscale; the IKMO provided these data as well.
Career Thoughts Inventory (CTI). The CTI includes 48 Likert-type items and seeks to measure respondents’ levels of negative career thinking (Sampson, Peterson, Lenz, Reardon, & Saunders, 1996a, 1996b). To complete the CTI, respondents read the 48 statements about careers and indicate how much they agree using a 4-point scale (strongly disagree to strongly agree). The CTI provides a total score and scores for three subscales: (a) Decision Making Confusion (DMC); (b) Commitment Anxiety (CA); and (c) External Conflict (EC). Completing the instrument yields raw scores for the assessment total and each of the three subscales, and a conversion table printed on the test booklet allows respondents to convert raw scores to T scores. Higher raw scores and T scores indicate a higher level of problematic thinking in each respective area, with T scores at or above 50 indicating clinical significance. For the college student norm group, internal consistency alpha coefficients were .96 for the total score and ranged from .77 to .94 for the three subscales (Sampson et al., 1996a, 1996b). With the sample in the present study, the researchers found acceptable alpha coefficients that were comparable to the norm group. The researchers used CTI change scores as predictors, calculated as the change in CTI total and subscale scores from the beginning to the end of either the career planning class or the STEM seminar class.
SAT Math. High school students take the SAT as a college admissions test typically in their junior and/or senior years (CollegeBoard, 2018). Although the SAT has four subtests, the researchers only used the math subtest in the present study. The math subtest is comprised of 54 questions or tasks in the areas of basic mathematics knowledge, advanced mathematics knowledge, managing complexity, and modeling and insight (CollegeBoard, 2018; Ewing, Huff, Andrews, & King, 2005). In a validation study of the SAT, Ewing et al. (2005) found an internal consistency alpha coefficient of .92 for the math subtest and alpha coefficients ranging from .68 to .81 for the four math skill areas. The researchers were unable to analyze psychometric properties of the SAT math test with the study sample because the university’s IKMO only provided composite and subtest total scores, rather than individual item responses.
Math Placement Test–Algebra Subtest. The Math Placement Test is a university-made assessment designed to measure mathematic competence in algebra, trigonometry, and pre-calculus that helps the university place students in their first math course at the university. All first-time undergraduate students at the university are required to take the test; when data collection began, the mandatory completion policy was not yet in place, so some earlier participants had missing data in this area. The test is structured so that all respondents first take the algebra subtest and if they achieve 70% accuracy, they move to the trigonometry and pre-calculus subtests. Similar to the SAT, the researchers were unable to analyze psychometric properties of the test because the IKMO provided only composite and subtest total scores.
Procedure
Because the dependent variables (second-year retention and third-year retention) were dichotomous (i.e., retained or not retained), the researchers used the binary logistic regression procedure within SPSS Version 24 to analyze the data (Agresti, 2013; Hosmer et al., 2013; Tabachnick & Fidell, 2013). The purpose of binary logistic regression is to test predictors of the binary outcome by comparing the observed outcomes and the predicted outcomes first without any predictors and then with the chosen predictors (Hosmer et al., 2013). The researchers used a backward stepwise Wald approach, which enters all predictors into the model and removes the least significant predictors one by one until all of the remaining predictors fall within a specific p value range (Tabachnick & Fidell, 2013). The researchers chose to set the range as p ≤ .20 based on the recommendation of Hosmer et al. (2013).
Preliminary data analysis included identifying both univariate and multivariate outliers, which were removed from the data file; conducting a missing data analysis; and testing the statistical assumptions for logistic regression. There were no missing values for categorical variables, but the assessment variables (CTI, SAT, and Math Placement Test) did have missing values. Results from Little’s (1988) MCAR test in SPSS showed that these data were not missing completely at random (Chi-square = 839.606, df = 161, p < .001). The researchers chose to impute missing values using the Expectation Maximization procedure in SPSS (Dempster, Laird, & Rubin, 1977; Little & Rubin, 2002). The data met the statistical assumptions of binary logistic regression related to multicollinearity and linearity in the logit (Tabachnick & Fidell, 2013). As previously discussed, the data also sufficiently met the assumption regarding the ratio of cases to predictor variables, with the exception of the ethnicity variable; after removing outliers, the Asian/Pacific Islander subcategory in the non-retained outcome had only four cases, violating the Peduzzi et al. (1996) and Field (2009) recommendation of having at least five cases. However, because the goal was to test the ethnicity categories separately rather than collapsing them to fit the recommendation, and because Hosmer et al. (2013) noted this was a recommendation and not a rule, the researchers chose to keep the existing categories, noting the potential limitation when interpreting this variable.
Results
The sections that follow provide the results from each of the hypotheses and interpretation of the findings.
Hypothesis 1
Hypothesis 1 stated that the independent variables could predict undergraduate STEM retention from Year 1 to Year 2. As stated previously, the backward stepwise Wald approach involved including all predictors initially and then removing predictors one by one based on p value until all remaining predictors fell within the p ≤ .20 range. This process took five steps, resulting in the removal of four variables with p values greater than .20: (a) CTI Commitment Anxiety Change, (b) CTI External Conflict Change, (c) Gender, and (d) CTI Decision Making Confusion Change, respectively. The model yielded a Chi-square value of 91.011 (df = 10, p < .001), a -2 Log likelihood of 453.488, a Cox and Snell R-square value of .198, and a Nagelkerke R-square value of .270. These R-square values indicate that the model can explain between approximately 20% and 27% of the variance in the outcome. The model had a good fit with the data, as evidenced by the Hosmer and Lemeshow Goodness of Fit Test (Chi-square = 6.273, df = 8, p = .617). The final model accurately predicted 73.4% of cases across groups; however, the model predicted the retained students more accurately (89.6% of cases) than the non-retained cases (45.8% of cases).
Table 2 explains how each of the six variables retained in the model contributed to the final model. The odds ratio represents an association between a particular independent variable and a particular outcome, or for this study, the extent that the independent variables predict membership in the retained outcome group. With categorical variables, this odds ratio represents the likelihood that being in a category increases the odds of being in the retained group over the reference category (i.e., African American/Black participants were 1.779 times more likely to be in the retained group than White/Caucasian students, who served as the reference category). With continuous variables, odds ratios represent the likelihood that quantifiable changes in the independent variables predict membership in the retained group (i.e., for every unit increase in SAT math score, the odds of being in the retained group increase 1.004 times). The interpretation of odds ratios allows them to be viewed as a measure of effect size, with odds ratios closer to 1.0 having a smaller effect (Tabachnick & Fidell, 2013).
Table 2
Variables in the Equation for Hypothesis 1
|
|
|
|
|
95% C.I. for O.R. |
| Variable |
B |
S.E. |
Wald |
O.R. |
Lower |
Upper |
| Ethnicity |
|
|
10.319* |
|
|
|
| Ethnicity (African American/Black) |
.576 |
.393 |
2.148 |
1.779 |
.823 |
3.842 |
| Ethnicity (Hispanic) |
.068 |
.290 |
.054 |
1.070 |
.606 |
1.889 |
| Ethnicity (Asian/Pacific Islander) |
1.889 |
.637 |
8.803** |
6.615 |
1.899 |
23.041 |
| Ethnicity (Other) |
.258 |
.714 |
.131 |
1.295 |
.320 |
5.246 |
| Initial Major |
|
|
35.824*** |
|
|
|
| Initial Major (Declared STEM) |
.412 |
.265 |
2.422 |
1.511 |
.899 |
2.539 |
| Initial Major (Declared Non-STEM) |
-1.944 |
.375 |
26.905*** |
.143 |
.069 |
.298 |
| STEM Seminar (Non-CP) |
.850 |
.258 |
10.885** |
2.340 |
1.412 |
3.879 |
| SAT Math |
.004 |
.002 |
2.411 |
1.004 |
.999 |
1.008 |
| Math Placement–Algebra |
.002 |
.002 |
2.080 |
1.002 |
.999 |
1.005 |
| CTI Total Change |
.017 |
.007 |
5.546* |
1.017 |
1.003 |
1.032 |
| Constant |
-2.994 |
1.378 |
4.717 |
.050 |
|
|
Note: B = Coefficient for the Constant; S.E. = Standard Error; O.R. = Odds Ratio; * p < .05; ** p < .01; *** p < .001.
With logistic regression, the Wald Chi-square test allows the researcher to determine a coefficient’s significance to the model (Tabachnick & Fidell, 2013). Based on this test, Initial Major was the most significant predictor to the model (p < .001). Students in the initially Declared STEM category were 1.511 times more likely to be in the retained group than those in the initially Undeclared category (the reference category); the odds of being in the retained group decreased by a factor of .143 for students in the initially Declared Non-STEM group. The STEM course was the predictor with the second most statistical significance (p < .01), with students in the STEM seminar class being 2.340 times more likely to be in the retained outcome than those in the career planning class. The CTI Total Change score was statistically significant (p < .05), indicating that for every unit increase in CTI Total Change score (i.e., the larger the decrease in score from pretest to posttest), the odds of being in the retained group increase by a factor of 1.017. Ethnicity was a statistically significant predictor (p < .05), with each subcategory having higher odds of being in the retained group than the White/Caucasian group; however, the researchers caution the reader to read these odds ratios for ethnicity with caution because of the number of cases in some categories. SAT Math and Math Placement–Algebra were not statistically significant, but still fell within the recommended inclusion range (p < .20).
Hypothesis 2
Hypothesis 2 stated that the independent variables could predict undergraduate STEM retention from Year 1 to Year 3. As stated previously, the backward stepwise Wald approach involved including all predictors initially and then removing predictors one by one based on p value until all remaining predictors fell within the p ≤ .20 range. This process took six steps, resulting in the removal of five variables with p values greater than .20: (a) CTI Commitment Anxiety Change, (b) CTI Decision Making Confusion Change, (c) Gender, (d) CTI External Conflict Change, and (e) CTI Total Change, respectively. The model yielded a Chi-square value of 55.835 (df = 9, p < .001), a -2 Log likelihood of 307.904, a Cox and Snell R-square value of .191, and a Nagelkerke R-square value of .255. These R-square values indicate that the model can explain between approximately 19% and 26% of the variance in the outcome. The model had a good fit with the data, as evidenced by the Hosmer and Lemeshow Goodness of Fit Test (Chi-square = 9.187, df = 8, p = .327). The model accurately predicted 70.0% of cases across groups. In this analysis, the model predicted the non-retained students more accurately (72.7% of cases) than the retained cases (66.9% of cases).
Table 3 explains how the variables within the model contributed to the final model. Based on the Wald test, Initial Major was the most significant predictor to the model (p < .001). Students in the initially Declared STEM category were 1.25 times more likely to be in the retained group than those in the initially Undeclared category (the reference category); the odds of being in the retained group decreased by a factor of .167 for students in the initially Declared Non-STEM group. The Math Placement–Algebra variable was statistically significant (p < .05), and the odds ratios indicated that for every unit increase in Math Placement–Algebra test score, the odds of being in the retained group are 1.005 higher. The STEM course variable was slightly outside the statistically significant range but fell within the inclusion range, with students in the STEM seminar class being 2.340 times more likely to be in the retained outcome than students in the career planning class. SAT Math was not statistically significant but still fell within the recommended inclusion range (p < .20). Ethnicity also was not a statistically significant predictor but fell within the inclusion range, with each subcategory having higher odds of being in the retained group than the White/Caucasian group; however, the researchers caution the reader to read these odds ratios for ethnicity with caution because of the number of cases in some categories.
Table 3
Variables in the Equation for Hypothesis 2
|
|
|
|
|
95% C.I. for O.R. |
| Variable |
B |
S.E. |
Wald |
O.R. |
Lower |
Upper |
| Ethnicity |
|
|
6.445 |
|
|
|
| Ethnicity (African American/Black) |
.542 |
.448 |
1.467 |
1.719 |
.715 |
4.134 |
| Ethnicity (Hispanic) |
.243 |
.349 |
.484 |
1.275 |
.643 |
2.528 |
| Ethnicity (Asian/Pacific Islander) |
1.636 |
.698 |
5.494* |
5.137 |
1.307 |
20.185 |
| Ethnicity (Other) |
.403 |
.684 |
.347 |
1.497 |
.391 |
5.725 |
| Initial Major |
|
|
17.362** |
|
|
|
| Initial Major (Declared STEM) |
.223 |
.328 |
.460 |
1.250 |
.656 |
2.379 |
| Initial Major (Declared non-STEM) |
-1.792 |
.468 |
14.664** |
.167 |
.067 |
.417 |
| STEM Seminar (Non-CP) |
.588 |
.323 |
3.327 |
1.801 |
.957 |
3.389 |
| SAT Math |
.004 |
.003 |
2.536 |
1.004 |
.999 |
1.010 |
| Math Placement–Algebra |
.005 |
.002 |
5.449* |
1.005 |
1.001 |
1.009 |
| Constant |
-2.994 |
1.378 |
4.717 |
.050 |
|
|
Note: B = Coefficient for the Constant; S.E. = Standard Error; O.R. = Odds Ratio; * p < .05; *** p < .001.
Discussion
The researchers sought to determine the degree to which a set of demographic variables, math scores, and career-related factors could predict undergraduate retention in STEM majors. Based on descriptive statistics, the participants are remaining in STEM majors at a higher rate than other nationwide samples (Chen & Soldner, 2013; Koenig, Schen, Edwards, & Bao, 2012). The sample
in this study was quite different based on gender than what is commonly cited in the literature; approximately 46% of the study’s sample was female, whereas the NCSES (2017) reported that white females made up approximately 31% of those in STEM fields, with minority females lagging significantly behind. The present study’s sample was more in line with national statistics with regard to ethnicity (NCSES, 2017; Palmer et al., 2011).
With Hypothesis 1, the researchers sought to improve on a pilot study (Belser et al., 2017) that did not include demographics or math-related variables. Adding these additional variables did improve the overall model fit and the accuracy of predicting non-retained students, but slightly decreased the accuracy of predicting retained students, as compared to the Belser et al. (2017) model. In addition to improving the model fit, adding in additional variables reversed the claim by Belser et al. (2017) that students in the STEM-focused career planning class were more likely to be retained than the STEM seminar students. In the present study, the STEM seminar students, who declared STEM majors prior to the first day of college, were more likely to be retained in STEM majors, which is in line with prior research connecting intended persistence in a STEM major to observed retention (Le et al., 2014; Lent et al., 2016).
With Hypothesis 2, the researchers sought to expand on the Belser et al. (2017) study by also predicting retention one year farther, into the third year of college. In this endeavor, the analysis yielded a model that still fit the data well. However, this model was much more accurate in predicting the non-retained students and was slightly less accurate in predicting the retained students, with the overall percentage of correct predictions similar to Hypothesis 1. This finding indicates that the included predictors may provide a more balanced ability to predict long-term retention in STEM majors than in just the first year. The initial major and STEM course variables performed similarly as in Hypothesis 1, and as such, similarly to prior research (Le et al., 2014; Lent et al., 2016).
Although sampling issues warrant the reader to read ethnicity results with caution, ethnicity did show to be a good predictor of retention in STEM majors with both Hypotheses 1 and 2. More noteworthy, the African American/Black and Hispanic students had higher odds of being retained. This is inconsistent with most research that shows underrepresented minorities as less likely to be retained in STEM majors (Chen & Soldner, 2013; Cundiff et al., 2013; Gayles & Ampaw, 2014); however, at least one study has previously found results in which ethnic minority students were more likely to be retained in STEM majors (Riegle-Crumb & King, 2010).
Gender was removed as a predictor from both models because of its statistical non-significance. Prior research has shown that females are less likely to be retained in STEM majors (Cundiff et al., 2013; Gayles & Ampaw, 2014; Riegle-Crumb et al., 2012), which separates this sample from prior studies. However, the COMPASS sample did have a larger representation of females than typically observed. Moreover, the COMPASS Program has been mindful of prior research related to gender and took steps to address gender concerns in program development (Dagley et al., 2016).
The continuous variables retained in the models showed only a mild effect on predicting STEM retention. The SAT Math and Math Placement–Algebra scores did perform consistently with prior research, in which higher math scores related to higher odds of retention (CollegeBoard, 2012; Crisp et al., 2009; Le et al., 2014; Mattern & Patterson, 2013; Rohr, 2012). The CTI variables that were retained in the models performed in line with the Belser et al. (2017) pilot study specific to STEM majors and with prior research examining negative career thoughts in undergraduate retention in other majors (Folsom, Peterson, Reardon, & Mann, 2005; Reardon et al., 2015).
Limitations and Implications
The present study has limitations, particularly with regard to research design, sampling, and instrumentation. First, the researchers used a comparison group design rather than a control group, and as such, there were certain observable differences between the two groups. Not having a control group limits the researchers’ ability to make causal claims regarding the predictor variables or the STEM career intervention. The researchers also only included a limited number of predictors; the inclusion of additional variables may have strengthened the models. Although the sample size was sufficient based on the a priori power analysis, the low number of participants in some of the categories may have resulted in overfitting or underfitting within the models. Finally, the researchers were not able to test psychometric properties of the SAT Math subtest or the Math Placement–Algebra subtest with this sample because of not having access to the participants’ item responses for each. The researchers attempted to mitigate limitations as much as possible and acknowledge that they can and should be improved upon in future research.
Future research in this area would benefit from the inclusion of a wider variety of predictor variables, such as math and science self-efficacy, outcome expectations, and internal processes observed with gender and ethnic minority groups (e.g., stereotype threat; Cundiff et al., 2013; Litzler et al., 2014). The researchers also recommend obtaining a larger representation of ethnic minority groups to ensure an adequate number of cases to effectively run the statistical procedure. Future researchers should consider more complex statistical procedures (e.g., structural equation modeling) and research designs (e.g., randomized control trials) to determine more causal relationships between predictors and the outcome variables.
Because the results of this study indicate that a more solidified major selection is associated with higher odds of retention in STEM majors, university career professionals and higher education professionals should strive to develop programming that helps students decide on a major earlier in their undergraduate careers. Structured career development work, often overlooked in undergraduate STEM programming, may be one such appropriate strategy. Additionally, any undergraduate STEM programming must be sensitive to demographic underrepresentation in STEM majors and the STEM workforce and should take steps to provide support for students in these underrepresented groups.
Similar to work with undergraduates, this study’s results provide a rationale for school counselors to engage students in STEM career work so that they can move toward a solidified STEM major prior to enrolling in college. The industry-specific career development work discussed within this study is just as important, if not more important, for students in K–12 settings. Moreover, school counselors, through their continued access to students, can serve as an access point for researchers to learn more about the STEM career development process at an earlier stage of the STEM pipeline. All of these endeavors point to the need for counselor educators to better prepare school counselors, college counselors, and career counselors to do work specifically with STEM and to become more involved in STEM career research.
In the present study, the researchers built upon prior research in the area of STEM retention to determine which variables can act as predictors of undergraduate STEM retention. The binary logistic regression procedure yielded two models that provide insight on how these variables operate individually and within the larger model. Finally, the researchers identified some key implications for counselors practicing in various settings and for researchers who are interested in answering some of the key questions that still exist with regard to STEM career development and retention.
Conflict of Interest and Funding Disclosure
Data collected in this study was part of a dissertation study by the first author. The dissertation was awarded the 2018 Dissertation Excellence Award by the National Board for Certified Counselors.
References
ACT. (2018). The condition of STEM 2017. Retrieved from www.act.org/stemcondition
Agresti, A. (2013). Categorical data analysis (3rd ed.). Hoboken, NJ: Wiley.
Beasley, M. A., & Fischer, M. J. (2012). Why they leave: The impact of stereotype threat on the attrition of women and minorities from science, math, and engineering majors. Social Psychology of Education, 15, 427–448. doi:10.1007/s11218-012-9185-3
Belser, C. T., Prescod, D. J., Daire, A. P., Dagley, M. A., & Young, C. Y. (2017). Predicting undergraduate student retention in STEM majors based on career development factors. The Career Development Quarterly, 65, 88–93. doi:10.1002/cdq.12082
Belser, C. T., Prescod, D. J., Daire, A. P., Dagley, M. A., & Young, C. Y. (2018). The influence of career planning on career thoughts in STEM-interested undergraduates. The Career Development Quarterly, 66(2), 176–181. doi:10.1002/cdq.12131
Bouwma-Gearhart, J., Perry, K. H., & Presley, J. B. (2014). Improving postsecondary STEM education: Strategies for successful interdisciplinary collaborations and brokering engagement with education research and theory. Journal of College Science Teaching, 44, 40–47.
Campbell, D. T., & Stanley, J. C. (1963). Experimental and quasi-experimental designs for research. Chicago, IL: Rand McNally.
Carnevale, A. P., Smith, N., & Melton, M. (2011). STEM: Science, technology, engineering, mathematics. Washington, DC: Georgetown University.
Chen, X., & Soldner, M. (2013). STEM attrition: College students’ paths into and out of STEM fields. Retrieved from http://nces.ed.gov/pubs2014/2014001rev.pdf
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159. doi:10.1037/0033-2909.112.1.155
CollegeBoard. (2018). Math Test. Retrieved from https://collegereadiness.collegeboard.org/sat/inside-the-test/math
Crisp, G., Nora, A., & Taggart, A. (2009). Student characteristics, pre-college, college, and environmental factors as predictors of majoring in and earning a STEM degree: An analysis of students attending a Hispanic serving institution. American Educational Research Journal, 46, 924–942. doi:10.3102/0002831209349460
Cundiff, J. L., Vescio, T. K., Loken, E., & Lo, L. (2013). Do gender-science stereotypes predict science identification and science career aspirations among undergraduate science majors? Social Psychology of Education, 16, 541–554. doi:10.1007/s11218-013-9232-8
Dagley, M. A., Young, C. Y., Georgiopoulos, M., Daire, A. P., Parkinson, C., Prescod, D. J., & Belser, C. T. (2016). Recruiting undecided admits to pursue a STEM degree. Proceedings from the American Society for Engineering Education 123rd Annual Conference & Exposition. Retrieved from https://peer.asee.org/recruiting-undecided-admits-to-pursue-a-stem-degree
Dempster, A., Laird, N., & Rubin, D. (1977). Maximum likelihood from incomplete data via the EM algorithm. Journal of the Royal Statistical Society, Series B, 39, 1–38.
Dixon-Román, E. J., Everson, H. T., & McArdle, J. J. (2013). Race, poverty, and SAT scores: Modeling the influences of family income on black and white high school students’ SAT performance. Teachers College Record, 115, 1–33.
Doerschuk, P., Bahrim, C., Daniel, J., Kruger, J., Mann, J., & Martin, C. (2016). Closing the gaps and filling the STEM pipeline: A multidisciplinary approach. Journal of Science Education and Technology, 25, 682–695. doi:10.1007/s10956-016-9622-8
Ewing, M., Huff, K., Andrews, M., & King, K. (2005). Assessing the reliability of skills measured by the SAT (Report No. RN-24). New York, NY: CollegeBoard. Retrieved from https://files.eric.ed.gov/fulltext/ED562595.pdf
Faul, F., Erdfelder, E., Lang, A. G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London, England: Sage Publications.
Folsom, B., Peterson, G. W., Reardon, R. C., & Mann, B. A. (2005). Impact of a career planning course on academic performance and graduation rate. Journal of College Student Retention: Research, Theory & Practice, 6, 461–473. doi:10.2190/4WJ2-CJL1-V9DP-HBMF
Foltz, L. G., Gannon, S., & Kirschmann, S. L. (2014). Factors that contribute to the persistence of minority students in STEM fields. Planning for Higher Education Journal, 42(4), 46–58.
Gall, M. D., Gall, J. P., & Borg, W. R. (2007). Educational research: An introduction (8th ed.). Boston, MA: Allyn & Bacon.
Gayles, J. G., & Ampaw, F. (2014). The impact of college experiences on degree completion in STEM fields at four-year institutions: Does gender matter? The Journal of Higher Education, 85, 439–468.
doi:10.1353/jhe.2014.0022
Gottfredson, L. (1981). Circumscription and compromise: A developmental theory of occupational aspirations. Journal of Counseling Psychology, 28, 545–579. doi:10.1037/0022-0167.28.6.545
Holland, J. L. (1973). Making vocational choices: A theory of vocational personalities and work environments (2nd ed.). Upper Saddle River, NJ: Prentice Hall.
Hosmer, D. W., Jr., Lemeshow, S., & Sturdivant, R. X. (2013). Applied logistic regression (3rd ed.). Hoboken, NJ: Wiley.
Koenig, K., Schen, M., Edwards, M., & Bao, L. (2012). Addressing STEM retention through a scientific thought and methods course. Journal of College Science Teaching, 41(4), 23–29.
Lawlor, S., Richman, S., & Richman, C. L. (1997). The validity of using the SAT as a criterion for black and white students’ admission to college. College Student Journal, 31, 507–515.
Le, H., Robbins, S. B., & Westrick, P. (2014). Predicting student enrollment and persistence in college STEM fields using an expanded P-E fit framework: A large-scale multilevel study. Journal of Applied Psychology, 99, 915–947. doi:10.1037/a0035998
Lent, R. W., Brown, S. D., & Hackett, G. (2002). Social cognitive career theory. In D. Brown (Ed.), Career choice and development (4th ed., pp. 255–311). San Francisco, CA: Jossey-Bass.
Lent, R. W., Miller, M. J., Smith, P. E., Watford, B. A., Lim, R. H., & Hui, K. (2016). Social cognitive predictors of academic persistence and performance in engineering: Applicability across gender and race/ethnicity. Journal of Vocational Behavior, 94, 79–88. doi:10.1016/j.jvb.2016.02.012
Little, R. J. A. (1988). A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association, 83, 1198–1202. doi:10.2307/2290157
Little, R. J. A., & Rubin, D. B. (2002). Statistical analysis with missing data (2nd ed.). New York, NY: Wiley.
Litzler, E., Samuelson, C. C., & Lorah, J. A. (2014). Breaking it down: Engineering student STEM confidence at the intersection of race/ethnicity and gender. Research in Higher Education, 55, 810–832.
doi:10.1007/s11162-014-9333-z
Mansfield, K. C., Welton, A. D., & Grogan, M. (2014). “Truth or consequences”: A feminist critical policy analysis of the STEM crisis. International Journal of Qualitative Studies in Education, 27, 1155–1182.
doi:10.1080/09518398.2014.916006
Mattern, K. D., & Patterson, B. F. (2013). The relationship between SAT scores and retention to the second year: Replication with the 2010 SAT validity sample (College Board Statistical Report No. 2013-1). New York, NY: The College Board. Retrieved from https://files.eric.ed.gov/fulltext/ED563087.pdf
National Career Development Association. (2015). Career development theory and its application. Broken Arrow, OK: Author.
National Center for Science and Engineering Statistics. (2017). Women, minorities, and persons with disabilities in science and engineering. Retrieved from https://www.nsf.gov/statistics/2017/nsf17310/
National Science Board. (2018). Science & engineering indicators 2018. Retrieved from https://www.nsf.gov/statistics/2018/nsb20181/
Nosek, B. A., & Smyth, F. L. (2011). Implicit social cognitions predict sex differences in math engagement and achievement. American Educational Research Journal, 48, 1125–1156. doi:10.3102/0002831211410683
Osborn, D. S., Howard, D. K., & Leierer, S. (2007). The effect of a career development course on the dysfunctional career thoughts of racially and ethnically diverse college freshmen. The Career Development Quarterly, 55, 365–377. doi:10.1002/j.2161-0045.2007.tb00091.x
Palmer, R. T., Maramba, D. C., & Dancy, T. E., II (2011). A qualitative investigation of factors promoting the retention and persistence of students of color in STEM. The Journal of Negro Education, 80, 491–504.
Peterson, G. W., Sampson, J. P., Jr., Lenz, J. G., & Reardon, R. C. (2002). A cognitive information processing approach to career problem solving and decision making. In D. Brown (Ed.), Career choice and development (4th ed., pp. 312–369). San Francisco, CA: Jossey-Bass.
Peduzzi, P., Concato, J., Kemper, E., Holford, T. R., & Feinstein, A. R. (1996). A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology, 49, 1373–1379. doi:10.1016/S0895-4356(96)00236-3
Prescod, D. J., Daire, A. P., Young, C. Y., Dagley, M. A., & Georgiopoulos, M. (in press). Exploring negative career thoughts between STEM declared and STEM interested students. Journal of Employment Counseling, 55(4), 166–176.
Reardon, R., & Fiore, E. (2014). College career courses and learner outputs and outcomes, 1976-2014 (Technical report No. 55). Tallahassee, FL: Center for the Study of Technology in Counseling & Career Development, Florida State University. Retrieved from http://career.fsu.edu/content/download/223105/1906289/TechRept_55_201406.pdf
Reardon, R. C., Melvin, B., McClain, M. C., Peterson, G. W., & Bowman, W. J. (2015). The career course as a factor in college graduation. Journal of College Student Retention: Research, Theory, & Practice, 17, 336–350. doi:10.1177/1521025115575913
Riegle-Crumb, C., & King, B. (2010). Questioning a white male advantage in STEM: Examining disparities
in college major by gender and race/ethnicity. Educational Researcher, 39, 656–664. doi:10.3102/0013189X10391657
Riegle-Crumb, C., King, B., Grodsky, E., & Muller, C. (2012). The more things change, the more they stay the same? Prior achievement fails to explain gender inequality in entry into STEM college majors over time. American Educational Research Journal, 49, 1048–1073. doi:10.3102/0002831211435229
Rohr, S. L. (2012). How well does the SAT and GPA predict the retention of science, technology, engineering, mathematics, and business students? Journal of College Student Retention: Research, Theory, & Practice, 14, 195–208. doi:10.2190/CS.14.2.c
Sampson, J. P., Jr., Peterson, G. W., Lenz, J. G., Reardon, R. C., & Saunders, D. E. (1996a). Career Thoughts Inventory: Professional manual. Odessa, FL: Psychological Assessment Resources.
Sampson, J. P., Jr., Peterson, G. W., Lenz, J. G., Reardon, R. C., & Saunders, D. E. (1996b). Improving your career thoughts: A workbook for the Career Thoughts Inventory. Odessa, FL: Psychological Assessment Resources.
Saunders, D. E., Peterson, G. W., Sampson, J. P., Jr., & Reardon, R. C. (2000). Relation of depression and dysfunctional career thinking to career indecision. Journal of Vocational Behavior, 56, 288–298. doi:10.1006/jvbe.1999.1715
Schneider, K. R., Bickel, A., & Morrison-Shetlar, A. (2015). Planning and implementing a comprehensive student-centered research program for first-year STEM undergraduates. Journal of College Science Teaching, 44(3), 37–43.
Sithole, A., Chiyaka, E. T., McCarthy, P., Mupinga, D. M., Bucklein, B. K., & Kibirige, J. (2017). Student attraction, persistence and retention in STEM programs: Successes and continuing challenges. Higher Education Studies, 7, 46–59. doi:10.5539/hes.v7n1p46
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Upper Saddle River, NJ: Pearson Education.
Toldson, I. A., & McGee, T. (2014). What the ACT and SAT mean for black students’ higher education prospects. The Journal of Negro Education, 83, 1–3.
Vittinghoff, E., & McCulloch, C. E. (2006). Relaxing the rule of ten events per variable in logistic and Cox regression. American Journal of Epidemiology, 165, 710–718.
Wyatt, J. N., Remigio, M., & Camara, W. J. (2012). SAT Subject Area Readiness Indicators: Reading, Writing, & STEM. Retrieved from https://files.eric.ed.gov/fulltext/ED562872.pdf
Christopher T. Belser, NCC, is an assistant professor at the University of New Orleans. M. Ann Shillingford is an associate professor at the University of Central Florida. Andrew P. Daire is a dean at Virginia Commonwealth University. Diandra J. Prescod is an assistant professor at Pennsylvania State University. Melissa A. Dagley is an executive director at the University of Central Florida. Correspondence can be addressed to Christopher Belser, 2000 Lakeshore Drive, Bicentennial Education Center Room 174, New Orleans, LA 70148, ctbelser@uno.edu.
Sep 1, 2018 | Volume 8 - Issue 3
Nayoung Kim, Glenn W. Lambie
To prevent school counselors from experiencing feelings of burnout, identifying relevant factors is important. The purpose of this article is to review studies investigating the constructs of burnout and occupational stress in school counseling samples. Eighteen published research articles fit the inclusion criteria for this review. The researchers identified external and internal variables relating to school counselor burnout, as well as protective and risk factors. The review identified that school counselors’ higher level of burnout correlated with having non-counseling duties, being assigned large caseloads, working in schools that did not meet adequate yearly progress (AYP) status, experiencing a lack of supervision, possessing greater emotion-oriented stress coping scores, providing fewer direct student services, and having greater perceived stress. In contrast, feelings of burnout among school counselors were mitigated when counselors received supervision, possessed higher task-oriented stress coping strategies, scored at higher levels of ego maturity, reported greater occupational support at their schools, had greater grit scores, and worked in schools that met AYP.
Keywords: burnout, occupational stress, school counselors, non-counseling duties, coping strategies
There are multiple definitions of burnout (e.g., Burke & Richardson, 2000; Stalker & Harvey, 2002); however, the primary consistent aspect of burnout is that it is a psychological phenomenon associated with job-related stress (Maslach, 2017). Burnout occurs when professionals are unable to meet their own needs, as well as their clients’ needs, in a high-pressure environment (Maslach, 2017). Freudenberger (1990) identified common symptoms of burnout, including negative changes in individuals’ (a) attitudes and decision making; (b) physiological states; (c) mental, emotional, and behavioral health; and (d) occupational motivation. Burnout has significant consequences, including compromised physical health, increased risk of mental health disorders (e.g., depression, substance abuse), poor job performance, absenteeism, occupational attrition, and low self-esteem (Maslach & Leiter, 2016). Burnout can also cause symptoms such as fatigue, exhaustion, and insomnia (Armon, Shirom, Shapira, & Melamed, 2008).
Burnout in School Counseling
Morse, Salyers, Rollins, Monroe-DeVita, and Pfahler (2012) identified that 21% to 67% of mental health professionals reported experiencing high levels of burnout, possibly because of dealing with high client caseloads (Ducharme, Knudsen, & Roman, 2007) or overall job effectiveness (Stalker & Harvey, 2002). In addition, Oddie and Ousley (2007) found that 21% to 48% of mental health workers reported experiencing high levels of emotional exhaustion. School counselors specifically are at risk for experiencing feelings of burnout because of their multiple job demands, including paperwork, parent conferences, school-wide testing, large caseloads, and requests from administrators (McCarthy & Lambert, 2008), and other factors such as role ambiguity and limited occupational support (Young & Lambie, 2007). The school counseling job environment, where “the demands of the work are high, but the resources to meet those demands are low” (Maslach & Goldberg, 1998, pp. 63–64), increases susceptibility to experiencing feelings of burnout (e.g., average student-to-counselor ratio being 491-to-1; National Center for Education Statistics, 2016). Stephan (2005) found that within a national sample of school counselors, 66% of middle school counselors scored at moderate to high levels of emotional exhaustion. Further, Wachter (2006) found that 20% of the school counselors in her investigation (N = 132) experienced feelings of burnout; 16% scored at moderate levels of burnout, and 4% scored at severe levels of burnout. Thus, many school counselors experience feelings of burnout that may influence their ability to provide ethical and effective counseling services to the students they serve.
School counselors may experience chronic fatigue, depersonalization, or feelings of hopelessness and leave their jobs because of the rigidity of school systems and limited support (Young & Lambie, 2007). In fact, counselors experiencing significant feelings of burnout provide reduced quality of service to their clientele because burnout relates to lower productivity, turnover intention, and a lowered level of job commitment (Maslach, Schaufeli, & Leiter, 2001). Because of the importance of preventing the burnout phenomenon, the American School Counselor Association’s (ASCA; 2016) ethical standards note that school counselors are responsible for maintaining their health, both physically and emotionally, and caring for their wellness to ensure their effective practice. The American Counseling Association’s (2014) ethical standards also state that school counselors have an ethical responsibility to monitor their feelings of burnout and remediate when their feelings potentially influence their ability to provide quality services to their stakeholders. To monitor burnout, counselors need to understand the symptoms of burnout and prevent it from happening, while maintaining their psychological well-being.
School counselors face challenges with their significant job demands (McCarthy, Van Horn Kerne, Calfa, Lambert, & Guzmán, 2010), such as large caseloads (Lambie, 2007) and extreme amounts of non-counseling duties (Moyer, 2011). In fact, school counselors report job stress and dissatisfaction when they are required to complete non-counseling duties, hindering their ability to work with their students (McCarthy et al., 2010). Examples of non-counseling duties include clerical tasks, such as scheduling students for classes; fair share, such as coordinating the standardized testing program; and administrative duties, such as substitute teaching (Scarborough, 2005). School counselors with large caseloads and high student-to-counselor ratios are more likely to experience increased feelings of burnout (Bardhoshi, Schweinle, & Duncan, 2014). Although ASCA (2015) recommends a student-to-counselor ratio of 250-to-1, the U.S. average student-to-counselor ratio is almost double the recommended proportion (491-to-1; National Center for Education Statistics, 2016).
Insufficient resources for school counselors and negative job perception increase their likelihood of experiencing feelings of burnout. Lower levels of principal support and lack of clinical supervision raise school counselors’ occupational stress (Bardhoshi et al., 2014; Moyer, 2011). For instance, school counselors with higher levels of role ambiguity are likely to experience burnout (Wilkerson & Bellini, 2006). School counselors experience role ambiguity when their responsibilities or the expected level of performance is not clearly identified (Coll & Freeman, 1997). As a result, school counselors report increased levels of stress (Culbreth, Scarborough, Banks-Johnson, & Solomon, 2005), leading to burnout and attrition from the profession (Wilkerson & Bellini, 2006). ASCA (2016) dictated that school counselors’ responsibilities include providing counseling services to students to support their development, which distinguishes them from other school personnel. With the importance of preventing burnout in school counseling, the purpose of this review is twofold: (a) to present identified factors influencing school counselors’ levels of burnout and (b) to offer strategies to assist school counselors in mitigating the feelings of burnout.
Research Examining Burnout in School Counseling
We began by conducting a formal search of electronic databases—PsycINFO, ERIC (EBSCOhost), and Academic Search Premiere—relating to school counselor burnout. The search term burnout was first used to analyze the research trend in the field. Both the search terms burnout and school counselors OR school counseling were used to collect any articles on the topic of school counselor burnout published between 2000 and 2018. An additional search was conducted with the terms occupational stress and school counselors OR school counseling to identify potential studies related to the topic in the same type of literature.
The following inclusion criteria were applied for our review: (a) investigations of school counselor burnout and occupational stress, (b) sample participants were school counselors in the United States, (c) the primary topic of the investigation was burnout and/or occupational stress, (d) articles were written in English, (e) articles were published in refereed journals, and (f) articles were published between 2000 and 2018. In addition, our review excluded literature reviews, editorials, and rejoinders. The abstracts of the articles meeting the criteria were examined and confirmed in order to be included in our review.
Our literature search based on the inclusion criteria produced 51 articles. As not all articles from the search satisfied the criteria, the articles were reviewed manually to evaluate whether they met the criteria, resulting in 35 articles not meeting criteria (e.g., conceptual articles, studies related to teachers) and 16 articles meeting all criteria. An additional literature search yielded two more studies meeting the inclusion criteria, identifying 18 studies in total. None of the identified research articles examined prevention or treatment interventions for burnout in school counselors. The 18 investigations had school counselor burnout or occupational stress as the constructs of interest. The research findings identified the positive relationships between school counselors’ burnout or occupational stress scores and the following factors: (a) non-counseling duties, (b) large caseloads, (c) not meeting adequate yearly progress (AYP) status (i.e., the expected amount of students’ academic growth per year based on the No Child Left Behind mandate [Minnesota House of Representatives, 2003]), (d) lack of supervision, (e) emotion-oriented stress coping scores, (f) grit, and (g) perceived stress.
Fourteen out of 18 articles provided information related to school counselor burnout (see Table 1 for quantitative studies and Table 2 for qualitative studies), and the other four studies investigated school counselors’ occupational stress (see Table 3). Occupational stress refers to the strain a person experiences when the perceived stress in a workplace outweighs their ability to cope (Decker & Borgen, 1993). Quantitative research methods were employed in 15 of the investigations, two used mixed-methods, and one study utilized a qualitative approach. For all 18 articles, the participants were current school counselors, and the number of participants ranged from 3 to 926. Effect sizes were categorized depending on the analysis into three groups (i.e., small, medium, and large) based on the effect size matrix from Sink and Stroh (2006), offering a better understanding of the results. Specifically, the effect size from independent samples t-test (2 groups; Cohen’s d) is interpreted as small for 0.2, medium for 0.5, and large for 0.8. For the effect size of other analyses listed in this review, including paired-samples t-tests (η2), multiple regression (R2), and analysis of variance (ANOVA; η2), 0.01 is considered as small, 0.06 as medium, and 0.14 as large.
Table 1
Summary of Quantitative/Mixed Studies Related to Professional School Counselor (PSC) Burnout
| Study |
Sample |
Variables |
Findings |
| Bain, Rueda, Mata-Villarreal, & Mundy (2011) |
PSCs in rural districts of South Texas
(N = 27)
Convenient Sampling |
Mental health awareness, the amount of time spent on academic advising
|
Feelings of burnout were reported by the majority of the PSCs (89%) in the study and many of them spent the greatest amount of time on administrative duties and the least on counseling. |
| Bardhoshi, Schweinle, & Duncan (2014) |
PSCs
(N = 212)
Random Sampling |
Non-counselor duties, school factors, five subscales of the CBI |
Non-counseling duties and school factors were associated with PSC burnout. Non-counseling duties explained the variance of the three burnout subscales: Exhaustion (11%; medium effect size), NWE (6%; medium effect size), and DPL (8%; medium effect size). Non-counseling duties and other factors (e.g., caseload, principal support) explained the variance of the four burnout subscales: Exhaustion (21%; large effect size), Incompetence (9%; medium effect size), NWE (49%; large effect size), and DPL (17%; large effect size). |
| Butler & Constantine (2005) |
PSCs
(N = 533)
Random Sampling |
Collective self-esteem, burnout, demographics |
Collective self-esteem explained 3% of the variance of PSC burnout (small effect size). In particular, PRCS (2%) and PUCS (1%) accounted for PA (both small effect sizes), and IICS explained 1% of feelings of DP and PA (both small effect sizes). Higher collective self-esteem was associated with lower PSC burnout. PSCs working in urban settings tended to have higher levels of burnout than the counterparts in other environmental settings. PSCs with experience of 20–29 years reported higher levels of burnout than the counterparts with 0–9 years of experience. PSCs with experience of 30 or more years reported higher levels of burnout than those with less experience. |
| Gnilka, Karpinski, & Smith (2015) |
PSCs
(N = 269)
Convenient Sampling |
Five subscales on the CBI |
Effect size differences were found between PSCs and other professionals in the counseling fields (Exhaustion, d = .26, small effect size; DC, d = -.50, medium effect size). Effect size differences were noted between PSCs and sexual offender and sexual abuse therapists (Exhaustion, d = .27, small effect size; DPL, d = -.23, small effect size; DC, d = -.82, large effect size). |
| Lambie (2007) |
PSCs
(N = 218)
Random Sampling
|
Ego maturity, three subscales on the MBI-HSS
|
PSCs with greater levels of ego maturity tended to have a higher level of PA than those with lower ego maturity. Ego maturity predicted PA (3.3%; small effect size). Occupational support and the subscales of burnout were correlated. Reported occupational support predicted EE (16%; large effect size), DP (12%; medium effect size), and PA (7.2%; medium effect size). |
| Limberg, Lambie, & Robinson (2016-2017) |
PSCs
(N = 437)
Random Sampling/
Purposive Sampling |
Altruistic motivation, altruistic behavior, burnout |
PSCs with greater levels of altruism had lower levels of EE and higher feelings of PA. PSC altruism explained 31.36% of the variance in EE (large effect size), and 29.16% of the variance in PA (large effect size). Self-Efficacy accounted for 14.4% of the variance in EE (large effect size) and 9% of the variance in PA (medium effect size). |
| Moyer (2011) |
PSCs
(N = 382)
Convenient Sampling |
Non-guidance activities, supervision, student-to-counselor ratios, five subscales of the CBI |
Non-guidance–related duties and clinical supervision were significant predictors of PSC burnout. Non-guidance duties (7.3%; medium effect size) and supervision (9%; medium effect size) predicted burnout.
|
| Mullen, Blount, Lambie, & Chae (2017) |
PSCs
(N = 750)
Random Sampling |
Perceived stress, burnout, job satisfaction |
Perceived stress predicted burnout positively (large effect size) and job satisfaction negatively (large effect size). Perceived stress and burnout predicted job satisfaction (large effect size). Burnout mediated the relationship between perceived stress and job satisfaction. |
| Mullen & Crowe (2018) |
PSCs
(N = 330)
Convenient Sampling |
Grit, stress, burnout |
Grit was negatively related to burnout (small effect size) and stress (small to medium effect size). |
| Mullen & Gutierrez (2016)
|
PSCs
(N = 926)
Random Sampling
|
Burnout, perceived stress, direct student services
|
Burnout attributed to direct counseling activities (12%; medium effect size), direct curriculum activities (5%; small to medium effect size), and percentage of time at work providing direct services to students (6%; medium effect size). |
| Wachter, Clemens, & Lewis (2008) |
PSCs
(N = 249)
Random Sampling |
Demographics, stakeholder involvement, lifestyle themes, burnout |
Burnout and lifestyle themes were associated. Perfectionism subscale was negatively related to burnout, and the Self-Esteem subscale was positively related to PSC burnout. About 15.1% of the variance in burnout was accounted for by the lifestyle themes of Self-Esteem and Perfectionism (large effect size). |
| Wilkerson & Bellini (2006)
|
PSCs in northeastern U.S.
(N = 78)
Systematic Random Sampling
|
Demographics, intrapersonal, and organizational factors; three subscales on the MBI-ES |
Demographic (age, counseling experience, supervision, and student/counselor ratio), intrapersonal, and organizational factors significantly accounted for the amount of the variance in each subscale of burnout, including EE (45%; large effect size), DP (30%; large effect size), and PA (42%; large effect size). |
| Wilkerson (2009)
|
PSCs
(N = 198)
Random Sampling |
Demographic and organizational stressors and individual coping strategies; three subscales on the MBI-ES |
Demographic factors (years of experience and student/counselor ratio), organizational stress, and coping styles explained the variance of each subscale of burnout including EE (49%; large effect size), DP (27%; large effect size), and PA (36%; large effect size).
|
Table 2
Summary of Qualitative/Mixed Studies Related to Professional School Counselor Burnout
| Study |
Sample |
Topic |
Identified Themes |
| Bain, Rueda, Mata-Villarreal, & Mundy (2011) |
PSCs in rural districts of South Texas (N = 27)
Convenient Sampling |
Helpful ways to better provide mental health services at school |
Having access to additional staff and additional education and awareness in terms of helpful ways to provide mental health services at their school. |
| Bardhoshi, Schweinle, & Duncan (2014) |
PSCs
(N = 252)
Random Sampling |
a) Their experience of burnout
b) The meaning of performing non-counseling duties |
a) Lack of time, budgetary constraints, lack of resources, lack of organizational support, etc.
b) Adverse personal/professional effects, a reality of the job, reframing the duties within the context of the job. |
| Sheffield & Baker (2005) |
Female PSCs
(N = 3)
Purposive Sampling |
Burnout experience |
Important beliefs, burnout feelings, burnout attitude, (lack of) collegial support. |
Table 3
Summary of Quantitative Studies Related to Professional School Counselor Occupational Stress
| Study |
Sample |
Variables |
Findings |
| Bryant & Constantine (2006) |
Female PSCs
(N = 133)
Random Sampling |
Role balance, job satisfaction, satisfaction with life, demographics |
Multiple role balance ability and job satisfaction positively predicted overall life satisfaction. Role balance and job satisfaction explained the variance of life satisfaction (41%; large effect size). |
| Culbreth, Scarborough, Banks-Johnson, & Solomon (2005) |
PSCs
(N = 512)Stratified Random Sampling |
Role conflict, role ambiguity, role incongruence, demographics |
Perceived match between the job expectations and actual experiences predicted role-related job stress, including role conflict (7.6%; medium effect size); role incongruence (19.7%; large effect size); and role ambiguity (8.3%; medium effect size). |
| McCarthy, Van Horn Kerne, Calfa, Lambert, & Guzmán (2010) |
PSCs in Texas
(N = 227) Convenient Sampling |
Demographics, job stress, resources and demands |
Job stress was different between the resourced, balanced, and demand groups. The effect sizes were large in the differences between the demand group and the resourced group (1.62; large effect size) and the balanced group (0.70; large effect size).
|
| Rayle (2006) |
PSCs
(N = 388)Convenient Sampling |
Demographics, mattering, job-related stress |
Thirty-five percent of the variance in overall job satisfaction was explained by mattering to others at work and job-related stress (large effect size). Mattering to others (19.36%; large effect size) and job-related stress (16.81%; large effect size) explained the variance in overall job satisfaction. |
Three instruments were used to measure levels of school counselor burnout, including: (a) the Maslach Burnout Inventory (MBI; Maslach, Jackson, & Leiter, 1996), (b) the Counselor Burnout Inventory (CBI; S. M. Lee et al., 2007), and (c) the Burnout Measure Short Version (BMS; Malach-Pines, 2005). Maslach and Jackson (1981) defined burnout with three dimensions: Emotional Exhaustion (EE), Depersonalization (DP), and reduced Personal Accomplishment (PA). Emotional exhaustion is to exhaust one’s capacity to continuously involve with clients (R. T. Lee & Ashforth, 1996). Not being able to respond to clients’ needs may cause counselors to distance themselves from their job emotionally and cognitively, which is defined as depersonalization. Lastly, having a lower sense of effectiveness may reduce feelings of personal accomplishment (Maslach et al., 2001). Four studies used the MBI-Education Survey (MBI-ES), which was designed for the education population, and another study utilized the MBI-Human Services Survey (MBI-HSS), in which the word students from the MBI-ES is substituted with recipients in a third of the items (Sandoval, 1989).
Four studies used the CBI, which is a 20-item instrument with five subscales, including:
(a) Exhaustion, (b) Incompetence, (c) Negative Work Environment (NWE), (d) Devaluing Client (DC), and (e) Deterioration in Personal Life (DPL). Exhaustion is the condition of being physically and emotionally exhausted by the duties of a counselor, and incompetence focuses on counselors’ feelings of being incompetent. While negative work environment refers to the stress caused by the working environment, devaluing client is related to being unable to establish emotional connectedness with clients. Finally, deterioration in personal life assesses the level of deterioration in a counselor’s personal life. Sample items include “I feel exhausted due to my work as a counselor,” and “I feel I have poor boundaries between work and my personal life.” The internal consistency of the CBI ranged from .73 to .85 (S. M. Lee et al., 2007). In addition, three studies used the BMS (Malach-Pines, 2005), a 10-item scale in which participants rate their answers to the question “When you think about your work overall, how often do you feel the following?” in seven prompts, including: “Trapped,” “Hopeless,” and “Helpless.” The BMS is adapted from the original version of the Burnout Measure (Pines & Aronson, 1988). The internal consistency of the BMS ranged from .85 to .87 (Malach-Pines, 2005).
Researchers investigated different factors relating to school counselor burnout within the 18 published articles. One of the studies provided descriptive statistics of school counselor burnout, comparing school counselors to other mental health professionals and showing how burnout symptoms may emerge (N = 269; Gnilka, Karpinski, & Smith, 2015). School counselors had greater levels of Exhaustion (d = .26; small effect size) and lower levels of DC (d = -.50; medium effect size) than mental health professional participants. Furthermore, school counselors had greater levels of Exhaustion (d = .27; small effect size) and lower levels of DC (d = -.82; large effect size) compared to the mental health professional participants working with sex offenders and clients that have been sexually abused. Therefore, school counselors score higher in exhaustion as compared to other mental health professionals and score lower on devaluing their clients.
Individual Factors Related to Burnout
The two categories of individual factors relating to school counselor burnout were (a) psychological constructs and (b) demographic factors. The psychological constructs included ego maturity (Lambie, 2007), collective self-esteem (Butler & Constantine, 2005), altruism (Limberg, Lambie, & Robinson, 20162017), lifestyle themes (Wachter, Clemens, & Lewis, 2008), coping styles (Wilkerson, 2009), perceived stress (Mullen, Blount, Lambie, & Chae, 2017), and grit (Mullen & Crowe, 2018). The definitions of these psychological constructs related to school counselor burnout follow.
Ego maturity refers to the fundamental element of an individual’s personality, encompassing components of self, social, cognitive, character, and moral development (Loevinger, 1976). When individuals’ egos develop, they become more individualistic, autonomous, and highly aware of themselves (Loevinger, 1976). Collective self-esteem is individuals’ perception of their identification with the social group they belong to (Bettencourt & Dorr, 1997). Altruism is the behavior driven by values or goals individuals possess or their concerns for others, aside from external rewards (Eisenberg et al., 1999). A lifestyle is an individual’s way of perceiving self, others, and the world (Mosak & Maniacci, 2000), and lifestyle themes refer to common patterns people possess in relation to their lifestyles (Mosak, 1971). Coping is defined as cognitive and behavioral efforts to deal with specific demands that take up or exceed individuals’ resources (Lazarus & Folkman, 1984), and coping styles refer to individuals’ relatively stable patterns in handling stress (Heszen-Niejodek, 1997). Perceived stress represents the extent to which individuals evaluate their situations as stressful (Cohen, 1986). Grit is “perseverance and passion for long-term goals” (Duckworth, Peterson, Matthews, & Kelly, 2007, p. 1087). Specifically, grit refers to efforts to achieve a goal despite challenges. In addition to psychological constructs, the demographic factors category included years of experience in school counseling (Butler & Constantine, 2005; Wilkerson, 2009; Wilkerson & Bellini, 2006) and age (Wilkerson & Bellini, 2006).
Psychological constructs. Seven studies identified that psychological constructs relate to school counselors’ feelings of burnout. Five of seven factors had large effect sizes, including ego maturity, altruism, lifestyle themes, coping styles, and grit, and three of the factors with large effect sizes were associated with Emotional Exhaustion (EE) among the MBI (Maslach et al., 1996) subscale scores (i.e., ego maturity, altruism, and coping styles).
Specifically, Lambie (2007) examined the directional relationship between school counselors’
(N = 218) burnout and ego maturity, identifying that those counselors with higher levels of ego maturity were likely to have greater feelings of Personal Accomplishment (PA; R2 = .033). The researcher also investigated the relationship between the school counselors’ reported occupational support and their MBI burnout subscales scores (Maslach & Jackson, 1996), identifying that each MBI subscale relates to the participants’ levels of reported occupational support; EE (large effect size; R2 = .167); DP (medium effect size; R2 = .120); and PA (medium effect size; R2 = .072). The results indicated that school counselors scoring at higher ego maturity levels had lower feelings of burnout, and counselors experiencing high levels of occupational support had significantly lower burnout scores.
The relationship between burnout and collective self-esteem was investigated within a sample of school counselors (N = 533; Butler & Constantine, 2005). The Collective Self-Esteem Scale has four subscales (Luhtanen & Crocker, 1992), including (a) Private Collective Self-Esteem (PRCS), (b) Public Collective Self-Esteem (PUCS), (c) Membership Collective Self-Esteem (MCS), and (d) Importance to Identity Collective Self-Esteem (IICS). These subscales measure individuals’ perception of social groups they belong to, including how they feel about the group (PRCS), how they perceive others feel about the group (PUCS), how they perceive themselves being a good member of the group (MCS), and how important their social group is to their self-concept (IICS). These four Collective Self-Esteem Scale subscales explained 3% of the variance in the burnout subscales (Pillai’s trace = .08, F [12, 1584] = 3.48, p < .001, η2M = .03; Maslach & Jackson, 1986).
In general, higher collective self-esteem relates to lower levels of burnout, and different dimensions of collective self-esteem relate to different components of burnout. Higher PRCS was associated with higher feelings of PA (η2 = .02), and higher PUCS was related to lower levels of EE (η2 = .01). The school counselors’ IICS subscale scores were related to their lower feelings of DP (η2 = .01) and greater feelings of PA (η2 = .01). Although a small amount of variance in burnout scores (.01–.02) was explained by the components of collective self-esteem, the positive relationship between higher PRCS and higher feelings of PA identified that positive perceptions of the group school counselors belong to might reduce their feelings of burnout. For instance, having a sense of pride as a school counselor by observing other school counselors’ hard work and good relationships with students may promote their sense of PRCS, which may lead to higher feelings of PA. Taken together, promoting school counselors’ collective self-esteem may decrease their feelings of burnout.
Limberg and colleagues (2016–2017) investigated the directional relationship between school counselors’ (N = 437) levels of altruism and burnout. The school counselors with greater levels of altruism had lower levels of EE and higher feelings of PA. Specifically, the altruism subscales of Positive Future Expectation (PFE) and Self-Efficacy from the Self-Report Altruism Scale (Rushton, Chrisjohn, & Fekken, 1981) and two subscales of burnout (MBI) correlated (χ2 = 403.611, df = 216, χ2 ratio = 1.869, p < .001). PFE and Self-Efficacy accounted for 31.36% of the variance in the EE subscale (large effect size), and 29.16% of the variance in the PA subscale (large effect size). The Self-Efficacy subscale, which involves individuals’ perceived competence in a certain skill, explained 14.4% of the variance in EE subscale scores (large effect size), and 9% of the variance in PA subscale scores (medium effect size). Therefore, the results identified that school counselors’ levels of altruism negatively contribute to their burnout scores.
Burnout was related to lifestyle themes among school counselors (N = 249; Wachter et al., 2008). Two subscales of lifestyle themes from the Kern Lifestyle Scale (Kern, 1996), Self-Esteem and Perfectionism, accounted for 15.1% of the variance in burnout (large effect size; R2 = .151). Specifically, the Perfectionism subscale was negatively related to school counselor burnout scores (Burnout Measure: Short Version; BMS; Malach-Pines, 2005), and the Self-Esteem subscale was positively related to school counselor burnout. As a result, these findings identified school counselors’ personality factors relating to their risk of burnout, supporting that higher levels of perfectionism and lower levels of self-esteem may increase the likelihood of experiencing burnout.
Two studies employed hierarchical regression analyses to examine what factors may predict burnout subscale scores of the MBI, and one of the predicting variables was coping styles (Wilkerson, 2009; Wilkerson & Bellini, 2006). Wilkerson (2009) used four-step hierarchical regression models that included demographics, organizational stressors, and coping strategies, such as task-oriented, emotion-oriented, and avoidance-oriented coping (N = 198). The models with large effect sizes explained all three MBI burnout subscales. Specifically, 49% of the variance in the EE subscale was explained (large effect size; R2 = .49); 27% of the variance in the DP subscale was accounted for (large effect size; R2 = .27); and 36% of the variance of the PA subscale was explained (large effect size; R2 = .36). The results identified school counselors’ stressor scores both at the individual and organizational levels; intrapersonal coping strategies contributed to feelings of burnout with large effect sizes in the final model. In other words, demographic factors (e.g., more school counseling experience), coping styles (e.g., more emotion-oriented and less task-oriented coping strategies), and organizational variables (e.g., lack of decision-making authority, role ambiguity, role incongruity, and role conflict) positively predicted the level of burnout among school counselors.
Wilkerson and Bellini (2006) used three-step hierarchical regression models including demographic, intrapersonal, and organizational factors to examine the relationship between the variables and burnout among school counselors (N = 78). The school counselors’ demographic data (e.g., age, counseling experience, supervision, and student/counselor ratio), and intrapersonal (i.e., coping strategies) and organizational factors (e.g., role conflict, role ambiguity, and counselor occupational stress) significantly accounted for the variance in their burnout subscale scores on the MBI. Specifically, 45% of the variance in the EE subscale was explained (large effect size; R2 = .45), 30% of the variance in the DP subscale was accounted for (large effect size; R2 = .30), and 42% of the variance in the PA subscale was explained (large effect size; R2 = .42) by the final three-step model with the variables (i.e., counselor demographics, intrapersonal factors, and organizational factors). The findings indicated that school counselors’ emotion-oriented coping style predicted their three MBI subscale scores, supporting the importance of utilizing helpful strategies (i.e., task-oriented coping) to mitigate counselors’ feelings of burnout.
Another study examined how school counselors’ perceived stress and job satisfaction relate to burnout (Mullen et al., 2017). Specifically, perceived stress measured by the Perceived Stress Scale (Cohen, Kamarck, & Mermelstein, 1983) explained 52% of the variance in burnout (F (1, 749) = 808.55, p < .001; R2 = .52) and 25% of the variance in job satisfaction (F (1, 749) = 243.36, p < .001; R2 = .25). When both perceived stress and burnout were examined in order to test the relationship with job satisfaction, they explained 40% of the variance in job satisfaction (F (2, 747) = 246.48, p < .001; R2 = .40). In addition, the results indicated that burnout mediated the relationship between perceived stress and job satisfaction (z = -21.47, p < .001), and burnout (rs = .99) predicted job satisfaction better than perceived stress (rs = .79). Overall, perceived stress predicted burnout positively (large effect size) and job satisfaction negatively (large effect size). Both perceived stress and burnout predicted job satisfaction (large effect size).
Finally, Mullen and Crowe (2018) investigated the relationship between grit, burnout, and stress among school counselors (N = 330). The researchers found that grit was negatively correlated with burnout (r = -.22, p < .001) and stress (r = -.28, p < .001). Specifically, perseverance of effort, one of the subscales from the Grit-S (Duckworth & Quinn, 2009), was negatively related with burnout (r = -.12,
p < .05) and stress (r = -.19, p < .001). Therefore, school counselors’ level of grit may be a protective factor for burnout and stress.
Demographic factors. School counselors’ individual factors, such as age (Wilkerson & Bellini, 2006) and years of experience (Butler & Constantine, 2005; Wilkerson, 2009), correlate with feelings of burnout. Age was negatively correlated to the DP subscale (r = -.19, p < .05); therefore, older school counselors were less likely to experience burnout as compared to younger counselors (Wilkerson & Bellini, 2006). Nevertheless, the correlation between school counselors’ years of experience and burnout was inconsistent. Wilkerson and Bellini (2006) indicated that years of experience negatively correlated with the EE (r = -.26, p < .01), and DP (r = -.24, p < .05) subscales, while Butler and Constantine (2005) identified that school counselors with more years of experience scored at higher levels of burnout (MBI scores). Specifically, school counselors with 20–29 years of experience had greater DP subscale scores than those with 0–9 years of experience (F (3, 529) = 3.38, p < .05); and counselors with 30 years or more of experience had lower PA subscale scores than those with less than 20 years of experience (F (3, 529) = 3.39, p < .05). Furthermore, Wilkerson (2009) also reported that the years of experience positively correlated with the EE (ß = .21, p < .01) and DP (ß = .26, p < .01) MBI subscales in the hierarchical regression models whose variables included counselor demographics and organizational and intrapersonal variables to explain the variance of the burnout scores. Possible reasons behind the incongruent results may relate to school counselors’ role ambiguity, as counselors with less experience may experience or perceive large workloads compared to more experienced counselors. The conflicting results also may be related to other school counselor factors, such as the level of social support counselors experience at their schools. The findings identified the need for more inquiry to increase our understanding of the relationship between school counselors’ years of experience and their feelings of burnout.
Organizational Factors Relating to School Counselors Levels of Burnout
Eight organizational factors appear to correlate with school counselors’ levels of burnout, including (a) workplace (Butler & Constantine, 2005), (b) non-counseling duties such as administrative and clerical tasks (Bardhoshi et al., 2014; Moyer, 2011), (c) caseloads (Bardhoshi et al., 2014), (d) AYP (Bardhoshi et al., 2014), (e) level of principal support (Bardhoshi et al., 2014), (f) clinical supervision (Moyer, 2011), (g) student-to-counselor ratio (Wilkerson, 2009; Wilkerson & Bellini, 2006), (h) perceived work environment (Wilkerson & Bellini, 2006), and (i) direct student services (Mullen & Gutierrez, 2016). We categorize these organizational factors into two domains: (a) job responsibilities and
(b) work environment factors.
Job responsibilities. Two studies examined the relationship between school counselors’ non-counseling duties and their burnout scores. First, Bardhoshi and colleagues (2014) examined school counselors’ (N = 212) non-counseling duties and identified a significant relationship between three of the CBI subscales: (a) 11% of the variance in Exhaustion was explained (medium effect size; R2 = 0.11); (b) 6% of the variance in NWE was explained (medium effect size; R2 = 0.06); and (c) 8% of the variance in DPL was explained (medium effect size; R2 = 0.08). Taken together, the results identified that school counselors’ non-counseling duties positively predict their burnout scores.
Moyer (2011) examined how school counselors’ (N = 382) non-counseling duties (non-guidance duties) were correlated to their levels of burnout as measured by the CBI. School counselors’ non-counseling duties accounted for 7.3% of the variance in the burnout score (medium effect size; R2 = .073, ß = .27, p < .01). Receiving supervision accounted for additional variance in school counselors’ burnout scores after controlling the variance explained by non-counseling activities (medium effect size; R2 = .09, ß = -.14, p < .01). As a result, school counselors with more non-counseling duties and less clinical supervision had higher burnout scores. The findings identify the importance of clinical supervision to reduce burnout among school counselors, helping them improve their quality of counseling, which in turn may increase their sense of competence in the workplace.
Bain and colleagues (2011) investigated the mental health of school counselors in a rural setting and their percentage of workweek spent on counseling and administrative duties in South Texas (N = 27). Within this sample of school counselors, 89% had experienced feelings of burnout at least sometimes when trying to provide mental health services; specifically, 41% reported feelings of burnout, and 48% sometimes experienced burnout when providing mental health services to their students. School counselors also reported that they spent the greatest amount of time completing administrative duties and the least amount of time providing counseling services. About 48% of the counselors used more than 50% of their time completing administrative duties, such as organizing facts to report to administrators and preparing for assessments of knowledge and skills, and more than 70% of the participants spent less than 50% of their time providing counseling services. The sample size for this study was small; nevertheless, the results identified that approximately 90% of the school counselors experienced some levels of burnout and spent less time providing counseling services to their students and other stakeholders than completing administrative duties.
Finally, Mullen and Gutierrez (2016) investigated the relationship between burnout and direct student services of school counselors (N = 926). The results indicated that burnout negatively contributed to the frequency of direct counseling activities (ß = -.35, p < .001), direct curriculum activities (ß = -.22, p < .001), and percentage of time at work providing direct services to students (ß = -.24, p < .001). The findings suggest that school counselors experiencing feelings of burnout are likely to have lower numbers of direct counseling activities and curriculum activities, and spend less time offering direct services to students.
Work environment factors. School counselors’ levels of burnout may be different depending on the location of their workplace (Butler & Constantine, 2005). Specifically, school counselors working in urban settings scored higher on the EE subscale as compared to counselors in suburban, rural, and other settings (F (3, 529) = 24.66, p < .001). In addition, counselors in urban settings had higher DP subscale scores than those in other environmental settings (F (3, 529) = 13.67, p < .001). The results may relate to unique stressors school counselors in the urban settings face, including their expected proficiency in working with diverse students (Constantine et al., 2001). Overall, school counselors in urban settings were likely to experience greater feelings of burnout than those counselors in other settings, suggesting that more research is warranted to better understand possible contributors to these educators having higher MBI scores.
Factors relating to school counselors’ work correlating with their feelings of burnout include counselors’ caseloads, AYP status, principal support, and non-counseling duties. Specifically, school-related factors for counselors explained the variance of four burnout subscales of the CBI (Bardhoshi et al., 2014): (a) 21% of the variance in Exhaustion scores was explained (large effect size; R2 = 0.21, p < .001); (b) 9% of the variance in Incompetence scores was explained (medium effect size; R2 = 0.09, p < .01); (c) 49% of the variance in NWE scores was explained (large effect size; R2 = 0.49, p < .001); and (d) 17% of the variance in DPL scores was explained (large effect size; R2 = 0.17, p < .001). As a result, both school counselors’ work-related factors, such as caseloads and non-counseling duties, and their school environment (support from school staff and AYP status) correlate to their feelings of burnout. Therefore, providing sufficient support for school counselors, meeting the AYP, and reducing caseloads and non-counseling duties might mitigate feelings of burnout among school counselors.
Student-to-counselor ratio (Wilkerson, 2009) and perceived work environment (e.g., role conflict; Wilkerson & Bellini, 2006) were identified as predictive factors for school counselor burnout. Wilkerson (2009) found that the hierarchical regression models with variables of demographic data (e.g., years of experience), organizational stressors (e.g., counselor–teacher professional relationships), and coping strategies (e.g., task-oriented coping) explained all three subscale scores of the MBI in a sample of school counselors (N = 198): EE (R2 = .49; large effect size), DP (R2 = .27; large effect size), and PA (R2 = 36; large effect size). Similarly, Wilkerson and Bellini (2006) identified that school counselors’ demographic, intrapersonal, and organizational factors accounted for variance in all three MBI subscale scores, including the EE, DP, and PA subscales (45%, 30%, and 42%, respectively; all large effect sizes). The findings from these studies support that environmental factors relate to school counselor burnout.
Identified Themes From Qualitative Studies
One qualitative study and two mixed-methods studies explored themes relating to school counselor burnout and ways to improve their service, which may offer ways to prevent burnout. Bardhoshi and colleagues (2014) examined how school counselors experienced burnout. Specifically, the emergent themes identified for school counselors’ feelings of burnout organized around four areas including (a) lack of time, (b) budgetary constraints, (c) lack of resources, and (d) lack of organizational support. When school counselors were asked about the meaning of performing non-counseling duties, they stated adverse personal and professional effects, the realities of practice, and reframing the duties within the context of the job. One participant described burnout stating, “It means that I am no longer helpful to my students. I feel like I’m extremely tired and overworked and consequently my effectiveness as a school counselor is negatively impacted” (p. 437).
These themes aligned with existing qualitative research examining school counselors’ feelings of burnout (N = 3; Sheffield & Baker, 2005), including (a) important beliefs, (b) burnout feelings, (c) burnout attitude, and (d) lack of collegial support. One of the participants stated, “I didn’t think I was doing any good for anybody . . . I just can’t go on this way” (p. 181). Another participant stated, “You get to the point where it is no longer fun coming to work or when you are just tired [and] don’t want to deal with anyone” (p. 182). Finally, Bain and colleagues (2011) explored helpful ways to better provide mental health services at school with 27 school counselors in rural districts of South Texas. The results identified that having access to more staff and additional education and awareness of mental health services at their school was needed. Overall, these studies identified common themes of school counselors’ need for collegial support and resources, such as a school climate encouraging collaboration, and identifying gaps in the needs and realities of school counselors (Bardhoshi et al., 2014), as well as reducing the amount of stressful, non-counseling–related work they perform.
Occupational Stress
Researchers examined which factors may influence school counselors’ job stress or job satisfaction, including (a) counselors’ perceived match between job expectations and their actual experiences (Culbreth et al., 2005), (b) the amount of resources in their work environment (McCarthy et al., 2010), (c) mattering to others (Rayle, 2006), and (d) role balance ability (Bryant & Constantine, 2006). Perceived match between initial expectations of the job and actual experiences as a school counselor was the most significant predictor of lower role stress demonstrated by each subscale score of the Role Questionnaire (N = 512; Culbreth et al., 2005): role conflict (medium effect size; R2 = .076); role incongruence (large effect size; R2 = .197); and role ambiguity (medium effect size; R2 = .083). School counseling students reported not feeling trained enough because of the significant amount of non-counseling–related duties, which increased their sense of role conflict.
Graduating from a program accredited by the Council for Accreditation of Counseling and Related Educational Programs accounted for 1.2% of the variance in school counselors’ perceived readiness for the job (small effect size; r = .111, p < .05; Culbreth et al., 2005). School counselors’ balance between job demand and resources was another important factor for their job stress. Moreover, McCarthy and colleagues (2010) identified that perceived job stress and work environment in terms of demands and resources were correlated (N = 227; F (2, 206) = 44.77, p < .001). School counselors with resources, such as other counselors in general or as mentors, and support from administrators scored lower on levels of job stress. The effect size for the difference between the demand and the resourced groups was 1.62 (large effect size), and between the demand and balanced groups was 0.70 (large effect size). In other words, school counselors with more work-related resources were likely to experience lower levels of job stress.
Several factors are related to job satisfaction for school counselors. Rayle (2006) investigated the relationship between school counselors’ (N = 388) mattering to others at work scores and job-related stress scores, and their overall job satisfaction scores. The School Counselor Mattering Survey developed for this study included seven items asking participants to rate their perceived mattering to others, including their students, administrators, and the parents and teachers they worked with. School counselors’ mattering to others at work scores and job-related stress scores explained 35% of the variance in their overall job satisfaction (large effect size; ηp² = .62). Specifically, school counselors’ job satisfaction correlated with mattering to others at work scores (large effect size; r = .44, p < .001) and their job-related stress scores (large effect size; r = -.41, p < .001). In addition, school counselors’ mattering to others scores were negatively associated with their job-related stress scores (r = -.54, p < .001; large effect size). The findings suggest that school counselors’ perceived mattering to others at work and job-related stress predict their overall job satisfaction, and mattering to others at work relates to their job-related stress.
In addition, Bryant and Constantine (2006) investigated the relationship between female school counselors’ (N = 133) role balance, job satisfaction, and life satisfaction. After controlling for demographic information (age, years of school counseling experience, and location of school), role balance and job satisfaction scores correlated with their satisfaction with life scores (large effect size; R2 = .41). As a result, school counselors’ multiple role balance ability and job satisfaction scores positively predicted their overall life satisfaction scores. In sum, these findings identified factors related to school counselors’ job satisfaction, including mattering to others at work, job-related stress, and life satisfaction.
Discussion
Because of the dearth of literature examining school counselor burnout or occupational stress, we reviewed 18 investigations based on the inclusion criteria and included articles focusing on the topic that were published between 2000 and 2018 in refereed journals and identified internal and external factors relating to the phenomena. Specific factors were identified relating to school counselor burnout or stress and their environment, including responsibilities not related to counseling, large caseloads, AYP status, and role confusion. The findings suggest the importance of school counselors asserting themselves to focus on mandated tasks (i.e., counseling) in order to experience less burnout. In addition, it is imperative to train school counseling students to understand the reality of practice, such as other job responsibilities and school climates, and inform them on the necessity of counselors advocating for themselves in order to overcome role confusion and avoid large caseloads. Furthermore, several resources were identified to mitigate burnout among school counselors. Clinical supervision from a competent supervisor is essential for school counselors to get support and learn how to intervene with their clients effectively. In addition, peer supervision or consultation from colleagues may benefit school counselors in sharing their difficulties and gaining other professionals’ perspectives (Butler & Constantine, 2005). Task-oriented coping skills which can be learned in the school counseling programs were also related to a reduced level of burnout among school counselors.
Limitations
Our review needs to be interpreted with some caution, as it is limited to the 18 published studies meeting the inclusion criteria. Therefore, additional research investigating school counselor burnout is needed to further our understanding of this significant construct that may influence the services school counselors provide to their stakeholders. In addition, the reviewed studies include methodological limitations (e.g., sample size, self-report data), further supporting the need for increased research examining the construct of burnout in school counseling. Moreover, no research was identified examining interventions to possibly reduce counselor feelings of burnout.
Implications for School Counseling
Although no studies were identified that investigated treatments for school counselor burnout, research from other similar professions may provide insight for developing coping strategies for school counselors addressing their feelings of burnout. Awa, Plaumann, and Walter (2010) reviewed 25 intervention studies for burnout prevention whose participants included employees from diverse occupations. Seventeen out of 25 studies employed person-directed interventions and indicated the positive effects of the interventions, including cognitive behavioral training (Gorter, Eijkman, & Hoogstraten, 2001), psychosocial skill training (Ewers, Bradshaw, McGovern, & Ewers, 2002), and recreational music making (Bittman, Bruhn, Stevens, Westengard, & Umbach, 2003). Two studies used organization-directed interventions, and one of the studies reduced burnout by using cognitive behavioral techniques, management skill training, and social support (Halbesleben, Osburn, & Mumford, 2006). The other six investigations explored the effects of combined (person- and organization-directed) interventions in reducing burnout. The examples of combined interventions to mitigate counselors’ feeling of burnout include professional supervision (Melchior et al., 1996); work schedule reorganization and lectures (Innstrand, Espnes, & Mykletun, 2004); and participatory action research, communication, social support, and coping skills (Le Blanc, Hox, Schaufeli, Taris, & Peeters, 2007). Overall, Awa and colleagues (2010) identified positive impacts of burnout intervention programs, suggesting potential benefits of these treatment programs for school counselors.
In addition, Krasner and colleagues (2009) reported the effectiveness of their continuing medical education program for physicians to reduce burnout, which involves mindfulness, self-awareness, and communication skills. Educating for mindfulness strategies, self-awareness, and communication skills also may be helpful for school counselors. Providing a supportive environment and acknowledging school counselors’ work may help them increase their sense of matter in their workplace. Lacking empirical studies identifying treatment outcomes for burnout in school counselors, research on decreasing the level of school counselor burnout should be examined both deeply and extensively. Furthermore, intervention programs to prevent and intervene with school counselors’ burnout and occupational stress at the individual and organizational levels are warranted. The efforts to prevent burnout may lead to school counselors providing better quality of services, benefitting the counselors and the students they serve.
Our review indicated that school counselors’ responsibilities, such as non-counseling duties and dealing with large caseloads, hindered counselors from maintaining their wellness. Additionally, experiencing role conflict and employing emotion-oriented coping skills increased their feelings of burnout. Therefore, school counselor preparation programs need to incorporate into their curriculum the characteristics of their future work environment that may involve potential risk factors for burnout. Furthermore, developing school counselors’ own strategies and practicing beneficial skills such as task-oriented coping skills may be helpful for them in decreasing their likelihood of experiencing burnout.
Conclusion
Preventing and reducing school counselors’ feelings of burnout is important to ensure counselors’ ability to provide ethical and effective services to their stakeholders. Failure to address work-related stress in school counselors may cause reduced quality of their service and increased counselor attrition from the profession. Although more investigations examining burnout in school counselors are warranted, this manuscript is the first systematic review of burnout in school counseling, offering increased insight into this significant job-related psychological phenomenon.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author.
American School Counselor Association. (2015). Student-to-school-counselor ratio 2015–2016. Retrieved from https://www.schoolcounselor.org/asca/media/asca/home/Ratios15-16.pdf
American School Counselor Association. (2016). ASCA ethical standards for school counselors. Alexandria, VA: Author.
Armon, G., Shirom, A., Shapira, I., & Melamed, S. (2008). On the nature of burnout–insomnia relationships: A prospective study of employed adults. Journal of Psychosomatic Research, 65, 5–12.
doi:10.1016/j.jpsychores.2008.01.012
Awa, W. L., Plaumann, M., & Walter, U. (2010). Burnout prevention: A review of intervention programs. Patient Education and Counseling, 78, 184–190. doi:10.1016/j.pec.2009.04.008
Bain, S. F., Rueda, B., Mata-Villarreal, J., & Mundy, M.-A. (2011). Assessing mental health needs of rural schools in South Texas: Counselors’ perspectives. Research in Higher Education Journal, 14, 1–11.
Bardhoshi, G., Schweinle, A., & Duncan, K. (2014). Understanding the impact of school factors on school counselor burnout: A mixed-methods study. The Professional Counselor, 4, 426–443. doi:10.15241/gb.4.5.426
Bettencourt, B. A., & Dorr, N. (1997). Collective self-esteem as a mediator of the relationship between allocentrism and subjective well-being. Personality and Social Psychology Bulletin, 23, 955–964.
Bittman, B., Bruhn, K. T., Stevens, C., Westengard, J., & Umbach, P. O. (2003). Recreational music-making: A cost-effective group interdisciplinary strategy for reducing burnout and improving mood states in long-term care workers. Advances in Mind Body Medicine, 19(3/4), 4–15.
Bryant, R. M., & Constantine, M. G. (2006). Multiple role balance, job satisfaction, and life satisfaction in women school counselors. Professional School Counseling, 9, 265–271.
Burke, R. J., & Richardson, A. M. (2000). Psychological burnout in organizations. In R. T. Golembiewski (Ed.), Handbook of Organizational Behavior (pp. 327–368). New York, NY: Marcel Dekker, Inc.
Butler, S. K., & Constantine, M. G. (2005). Collective self-esteem and burnout in professional school counselors. Professional School Counseling, 9, 55–62.
Cohen, S. (1986). Contrasting the Hassles Scale and the Perceived Stress Scale: Who’s really measuring appraised stress? American Psychologist, 41, 716–718. doi:10.1037/0003-066X.41.6.716
Cohen, S., Kamarck, T., &Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. doi:10.2307/2136404
Coll, K. M., & Freeman, B. (1997). Role conflict among elementary school counselors: A national comparison with middle and secondary school counselors. Elementary School Guidance & Counseling, 31, 251–261.
Constantine, M. G., Arorash, T. J., Barakett, M. D., Blackmon, S. M., Donnelly, P. C., & Edles, P. A. (2001). School counselor’s universal-diverse orientation and aspects of their multicultural counseling competence. Professional School Counseling, 5, 13–18.
Culbreth, J. R., Scarborough, J. L., Banks-Johnson, A., & Solomon, S. (2005). Role stress among practicing school counselors. Counselor Education and Supervision, 45, 58–71.
doi:10.1002/j.1556-6978.2005.tb00130.x
Decker, P. J., & Borgen, F. H. (1993). Dimensions of work appraisal: Stress, strain, coping, job satisfaction, and negative affectivity. Journal of Counseling Psychology, 40, 470–478.
Ducharme, L. J., Knudsen, H. K., & Roman, P. M. (2007). Emotional exhaustion and turnover intention in human service occupations: The protective role of coworker support. Sociological Spectrum, 28, 81–104.
Duckworth, A. L., Peterson, C., Matthews, M. D., & Kelly, D. R. (2007). Grit: perseverance and passion for long-term goals. Journal of Personality and Social Psychology, 92, 1087–1101.
Duckworth, A. L., & Quinn, P. D. (2009). Development and validation of the Short Grit Scale (Grit-S). Journal of Personality Assessment, 91, 166–174. doi:10.1080/00223890802634290
Eisenberg, N., Guthrie, I. K., Murphy, B. C., Shepard, S. A., Cumberland, A., & Carlo, G. (1999). Consistency and development of prosocial dispositions: A longitudinal study. Child Development, 70, 1360–1372.
Ewers, P., Bradshaw, T., McGovern, J., & Ewers, B. (2002). Does training in psychosocial interventions reduce burnout rates in forensic nurses? Journal of Advanced Nursing, 37, 470–476.
doi:10.1046/j.1365-2648.2002.02115.x
Freudenberger, H. J. (1990). Caring for the caregiver: Recognizing and dealing with burnout. In J. Nottingham & H. Nottingham (Eds.), The professional and family caregiver—Dilemmas, rewards, and new directions (pp. 20–27). Americus, GA: Georgia Southwestern State University.
Gnilka, P. B., Karpinski, A. C., & Smith, H. J. (2015). Factor structure of the counselor burnout inventory in a sample of professional school counselors. Measurement and Evaluation in Counseling and Development, 48, 177–191. doi:10.1177/0748175615578758
Gorter, R. C., Eijkman, M. A., & Hoogstraten, J. (2001). A career counseling program for dentists: Effects on burnout. Patient Education and Counseling, 43, 23–30.
Halbesleben, J. R., Osburn, H. K., & Mumford, M. D. (2006). Action research as a burnout intervention: Reducing burnout in the Federal Fire Service. The Journal of Applied Behavioral Science, 42, 244–266. doi:10.1177/0021886305285031
Innstrand, S. T., Espnes, G. A., & Mykletun, R. (2004). Job stress, burnout and job satisfaction: An intervention study for staff working with people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 17, 119–126. doi:10.1111/j.1360-2322.2004.00189.x
Kern, R. M. (1996). Lifestyle questionnaire inventory. In D. Eckstein & L. Baruth (Eds.), The theory and practice of lifestyle assessment (pp. 243–256). Dubuque, IA: Kendall/Hunt.
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302, 1284–1293.
Lambie, G. W. (2007). The contribution of ego development level to burnout in school counselors: Implications for professional school counseling. Journal of Counseling & Development, 85, 82–88. doi:10.1002/j.1556-6678.2007.tb00447.x
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
Le Blanc, P. M., Hox, J. J., Schaufeli, W. B., Taris, T. W., & Peeters, M. C. (2007). Take care! The evaluation of a team-based burnout intervention program for oncology care providers. Journal of Applied Psychology, 92, 213–227.
Lee, R. T., & Ashforth, B. E. (1996). A meta-analytic examination of the correlates of the three dimensions of job burnout. Journal of Applied Psychology, 81, 123–133.
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., . . . Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40, 142–154. doi:10.1080/07481756.2007.11909811
Limberg, D., Lambie, G., & Robinson, E. H. (2016–2017). The contribution of school counselors’ altruism to their degree of burnout. Professional School Counseling, 20, 127–138. doi:10.5330/1096-2409-20.1.127
Loevinger, J. (1976). Ego development. San Francisco, CA: Jossey-Bass.
Luhtanen, R., & Crocker, J. (1992). A collective self-esteem scale: Self-evaluation of one’s social identity. Personality and Social Psychology Bulletin, 18, 302–318. doi:10.1177/0146167292183006
Malach-Pines, A. (2005). The burnout measure, short version. International Journal of Stress Management, 12, 78–88. doi:10.1037/1072-5245.12.1.78
Maslach, C. (2017). Finding solutions to the problem of burnout. Consulting Psychology Journal: Practice and Research, 69, 143–152. doi:10.1037/cpb0000090
Maslach, C., & Goldberg, J. (1998). Prevention of burnout: New perspectives. Applied and Preventive Psychology, 7, 63–74. doi:10.1016/S0962-1849(98)80022-X
Maslach, C., & Jackson, S. E. (1986). The Maslach Burnout Inventory (2nd ed.). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., & Jackson, S. E. (1996). Maslach Burnout Inventory–Human Service Survey (MBI-HSS). In C. Maslach, S. E. Jackson, & M. P. Leiter (Eds.), Maslach Burnout Inventory Manual (3rd ed., pp. 3–17). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). The Maslach Burnout Inventory manual (3rd ed.). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15, 103–111. doi:10.1002/wps.20311
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. doi:10.1146/annurev.psych.52.1.397
McCarthy, C. J., & Lambert, R. G. (2008). Counselor appraisal of resources and demands. Charlotte, NC: Center for Educational Measurement and Evaluation.
McCarthy, C., Van Horn Kerne, V., Calfa, N. A., Lambert, R. G., & Guzmán, M. (2010). An exploration of school counselors’ demands and resources: Relationship to stress, biographic, and caseload characteristics. Professional School Counseling, 13, 146–158.
Melchior, M. E., Phihpsen, H., Abu-Saad, H. H., Halfens, R. J., van de Berg, A. A., & Gassman, P. (1996). The effectiveness of primary nursing on burnout among psychiatric nurses in long-stay settings. Journal of Advanced Nursing, 24, 694–702.
Minnesota House of Representatives. (2003). Adequate yearly progress under the No Child Left Behind Act. House Research. Retrieved from http://www.house.leg.state.mn.us/hrd/pubs/ss/ssayp.pdf
Morse, G., Salyers, M. P., Rollins, A. L., Monroe-DeVita, M., & Pfahler, C. (2012). Burnout in mental health services: A review of the problem and its remediation. Administration and Policy in Mental Health and Mental Health Services Research, 39, 341–352. doi:10.1007/s10488-011-0352-1
Mosak, H. H. (1971). Lifestyle. In A. G. Nikelly (Ed.), Applications of Adlerian theory: Techniques for behavior change. Springfield, IL: Charles C. Thomas.
Mosak, H., & Maniacci, M. (2000). A primer of Adlerian psychology: The analytic–behavioral–cognitive psychology of Alfred Adler. Philadelphia, PA: Brunner/Mazel.
Moyer, M. (2011). Effects of non-guidance activities, supervision, and student-to-counselor ratios on school counselor burnout. Journal of School Counseling, 9(5), n5.
Mullen, P. R., Blount, A. J., Lambie, G. W., & Chae, N. (2017). School counselors’ perceived stress, burnout, and job satisfaction. Professional School Counseling, 21, 1–10. doi:10.1177/2156759X18782468
Mullen, P. R., & Crowe, A. (2018). A psychometric investigation of the short grit scale with a sample of school counselors. Measurement and Evaluation in Counseling and Development, 51, 151–162.
doi:10.1080/07481756.2018.1435194
Mullen, P. R., & Gutierrez, D. (2016). Burnout, stress and direct student services among school counselors. The Professional Counselor, 6, 344–359. doi:10.15241/pm.6.4.344
National Center for Education Statistics. (2016). Documentation to the 2014-15 Common Core of Data. Retrieved from https://nces.ed.gov/ccd/pdf/2016077_Documentation_062916.pdf
Oddie, S., & Ousley, L. (2007). Assessing burn-out and occupational stressors in a medium secure service. The British Journal of Forensic Practice, 9(2), 32–48.
Pines, A., & Aronson, E. (1988). Career burnout: Causes and cures. New York, NY: Free Press.
Rayle, A. D. (2006). Do school counselors matter? Mattering as a moderator between job stress and job satisfaction. Professional School Counseling, 9, 206–215. doi:10.1177/2156759X0500900310
Rushton, J. P., Chrisjohn, R. D., & Fekken, G. C. (1981). The altruistic personality and the self-report altruism scale. Personality and Individual Differences, 2, 293–302.
Sandoval, J. (1989). Review of the Maslach Burnout Inventory, second edition. In J. C. Conoley & J. J. Kramer (Eds.), The Tenth Mental Measurements Yearbook (pp. 475–476). Lincoln, NE: The University of Nebraska Press.
Scarborough, J. L. (2005). The school counselor activity rating scale: An instrument for gathering process data. Professional School Counseling, 8, 274–283.
Sheffield, D. S., & Baker, S. B. (2005). Themes from retrospective interviews of school counselors who experienced burnout. Hacettepe Üniversitesi Eğitim Fakültesi Dergisi, 29, 177–186.
Sink, C. A., & Stroh, H. R. (2006). Practical significance: The use of effect sizes in school counseling
research. Professional School Counseling, 9, 401–411. doi:10.5330/prsc.9.4.283746k664204023
Stalker, C., & Harvey, C. (2002). Professional burnout: A review of theory, research, and prevention. Brantford, ON, Canada: Wilfrid Laurier University.
Stephan, J. B. (2005). School environment and counselor resources: A predictive model of school counselor burnout (Doctoral dissertation). Retrieved from https://libres.uncg.edu/ir/uncg/f/umi-uncg-1060.pdf
Wachter, C. A. (2006). Crisis in the schools: Crisis, crisis intervention training, and school counselor burnout (Doctoral dissertation). Retrieved from https://libres.uncg.edu/ir/uncg/f/umi-uncg-1190.pdf
Wachter, C. A., Clemens, E. V., & Lewis, T. F. (2008). Exploring school counselor burnout and school counselor involvement of parents and administrators through an Adlerian theoretical framework. Journal of Individual Psychology, 64, 432–449.
Wilkerson, K. (2009). An examination of burnout among school counselors guided by stress-strain-coping theory. Journal of Counseling & Development, 87, 428–437. doi:10.1002/j.1556-6678.2009.tb00127.x
Wilkerson, K., & Bellini, J. (2006). Intrapersonal and organizational factors associated with burnout among school counselors. Journal of Counseling & Development, 84, 440–450.
doi:10.1002/j.1556-6678.2006.tb00428.x
Young, M. E., & Lambie, G. W. (2007). Wellness in school and mental health systems: Organizational influences. The Journal of Humanistic Counseling, Education and Development, 46, 98–113. doi:10.1002/j.2161-1939.2007.tb00028.x
