Nov 29, 2018 | Volume 8 - Issue 4
Joshua D. Smith, Neal D. Gray
This interview is the third in the Lifetime Achievement in Counseling Series at TPC that presents an annual interview with a seminal figure who has attained outstanding achievement in counseling over a career. Many people are deserving of this recognition, but I am happy that Josh Smith and Dr. Neal Gray have interviewed a visionary in the counseling profession. I first became aware of Dr. Capuzzi over 30 years ago when I was reading his vast research and scholarship as I prepared to teach my first classes as a counselor educator. Over the years, I have been amazed at Dr. Capuzzi’s contribution to the profession and his impact on countless educators, clinicians, and supervisors. I appreciate Josh Smith and Neal Gray for accepting my editorial assignment to interview Dr. Capuzzi. What follows are thought-provoking reflections from a counseling icon and leader.
—J. Scott Hinkle, Editor
 David Capuzzi, PhD, NCC, LPC, is past President of the American Counseling Association (ACA), and past Chair of both the ACA Foundation and the ACA Insurance Trust. Currently, Dr. Capuzzi is a member of the senior core faculty in community mental health counseling at Walden University and professor emeritus at Portland State University. Previously, he served as an affiliate professor in the Department of Counselor Education, Counseling Psychology, and Rehabilitation Services at Pennsylvania State University, and as Scholar in Residence in counselor education at Johns Hopkins University.
David Capuzzi, PhD, NCC, LPC, is past President of the American Counseling Association (ACA), and past Chair of both the ACA Foundation and the ACA Insurance Trust. Currently, Dr. Capuzzi is a member of the senior core faculty in community mental health counseling at Walden University and professor emeritus at Portland State University. Previously, he served as an affiliate professor in the Department of Counselor Education, Counseling Psychology, and Rehabilitation Services at Pennsylvania State University, and as Scholar in Residence in counselor education at Johns Hopkins University.
From 1980 to 1984, Dr. Capuzzi was editor of The School Counselor. He has authored several textbook chapters and monographs on the topic of preventing adolescent suicide and is coeditor and author with Dr. Larry Golden of Helping Families Help Children: Family Interventions with School-Related Problems (1986) and Preventing Adolescent Suicide (1988). He coauthored and edited with Douglas R. Gross numerous editions of Introduction to Group Work (2010); Counseling and Psychotherapy: Theories and Interventions (2011); Introduction to the Counseling Profession (2013); and Youth at Risk: A Prevention Resource for Counselors, Teachers, and Parents (2019).
In addition to several editions of Foundations of Addictions Counseling with Dr. Mark Stauffer, he and Dr. Stauffer have published Foundations of Couples, Marriage and Family Counseling (2015); Human Growth and Development Across the Life Span: Applications for Counselors (2016); and Counseling and Psychotherapy: Theories and Interventions (2016). Other texts include Approaches to Group Work: A Handbook for Practitioners (2003), Suicide Across the Life Span (2006), and Sexuality Counseling (2002), the last coauthored and edited with Larry Burlew. Additionally, Dr. Capuzzi has authored or coauthored articles in a number of ACA division journals.
A frequent speaker at professional conferences and institutes, Dr. Capuzzi has consulted with a variety of school districts and community agencies interested in initiating prevention and intervention strategies for adolescents at risk for suicide. He has facilitated the development of suicide prevention, crisis management, and postvention programs in communities throughout the United States; provided training on the topics of at-risk youth, grief, and loss; and served as an invited adjunct faculty member at other universities as time permits.
An ACA Fellow, Dr. Capuzzi is the first recipient of ACA’s Kitty Cole Human Rights Award and also is a recipient of the Leona Tyler Award in Oregon. In 2010, he received ACA’s Gilbert and Kathleen Wrenn Award for a Humanitarian and Caring Person. In 2011, he was named to the Distinguished Alumni of the College of Education at Florida State University and, in 2016, he received the Locke/Paisley Mentorship Award from the Association for Counselor Education and Supervision. In 2018 he received the Mary Smith Arnold Anti-Oppression Award from the Counselors for Social Justice, a division of ACA, as well as the U.S. President’s Lifetime Achievement Award.
In this interview, Dr. Capuzzi responded to six questions about his career, his impact on the counseling profession, and his thoughts about the current state and future of the counseling profession.
- Counseling has made substantial progress during the time you have been a member of the profession. In your opinion, what are the three major accomplishments of the profession?
I joined ACA in 1965, when it was known as the American Personnel and Guidance Association, and there was no such thing as counselor licensure. Although there were many excellent master’s and doctoral programs, there also were many that did not require much coursework to practice as a counselor. There were some university programs that only required 15 or so semester credits as part of a master’s degree in education to be able to seek employment as a counselor. Master’s degrees in counseling were one-year programs requiring 36 to 39 semester credits. There was little standardization of coursework requirements until licensure requirements were gradually adopted state by state. Today, all 50 states have counselor licensure, which has been instrumental in the progression of the counseling profession, and I see this as a major accomplishment.
The development of the Council for Accreditation of Counseling and Related Educational Programs (CACREP) has provided the profession with assurances that graduates of CACREP-accredited programs meet standards that elevate best practices when working with clients. CACREP accreditation has assisted universities by providing them with support for curriculum revision and improvement and impacted the requirements of the state professional counselor licensing boards.
There was little interest or emphasis on the importance of the inclusion of diverse populations, personalities, lifestyles, and cultures through most of the 1980s, even though the United States has always been a melting pot for immigrants from around the world. The affirmation of differences and the richness that diverse points of view add to our country’s tapestry has been slow to develop, and ACA has made major contributions in this area.
- Which of these major accomplishments was the most difficult to achieve for the counseling profession and why?
The acceptance of diverse populations, personalities, lifestyles, and cultures was the most difficult to achieve. Quite often, over the years, members of diverse populations have not been at the forefront of the profession, not because of lack of astuteness or competence, but because they have not been able to assume elected leadership positions. I am thankful that this is changing and affirm that this development is an asset-based characteristic of the counseling profession. I am so thankful that individuals such as Thelma T. Daley, Beverly O’Bryant, Courtland Lee, Marie Wakefield, Patricia Arredondo, Thelma Duffey, Cirecie West-Olatunji, and Marcheta Evans (and others I am probably forgetting to mention) have been willing to run for and serve in the ACA presidency position because their contributions have been stellar and essential to the maturation of the profession of counseling.
- What do you consider to be your major contribution to the development of the counseling profession and why?
I am relatively certain that I was the first ACA President to establish a diversity theme for the year that I was ACA President. My theme for 1986–1987 was Human Rights and Responsibilities: Developing Human Potential, even though colleagues and friends advised me against naming it in this manner as part of my platform for fear I would lose the election. I decided I should identify a diversity agenda as part of my pre-election platform statement because I wanted members to understand what I stood for in advance of the voting process. During my ACA presidency, I contacted all the editors of our counseling journals and requested that they consider developing special editions focused on some aspect of diversity. I think there were 16 special issues of division journals during my year as immediate past president that were diversity focused. Additionally, the opening session of the annual conference focused on diversity and human rights vignettes (presented by actors) to set the tone for the conference.
Few people know that my early years living in a mining town in Western Pennsylvania provided the backdrop for my interest in diversity and its importance. Many immigrants from other countries settled in Western Pennsylvania, and I spent the first 10 years of my life hearing three or four languages being spoken daily (newcomers could get jobs in the mines and mills, prior to learning much English, and therefore support their families). When my family left the region and moved south, I was surprised to learn that the America I experienced early in life was not typical of the rest of our country. I also was shocked when some of my classmates told me their parents wanted them to check to make sure I was not Jewish (if I was, they could not be my friends), and I was questioned about why I looked so different. When I asked what that meant I was told that most people they knew were tall, blond, and tanned. This early set of life experiences made an indelible impression, precipitated my ACA theme for 1986–87, and has stayed with me to this day.
- What three challenges to the counseling profession as it exists today concern you most, and what needs to change for these three concerns to be successfully resolved?
First, there is a lack of grassroots input to the ACA President and membership of the ACA Governing Council. During recent years, the membership in the state branches and divisions of ACA has declined and there has not been the amount of input and suggestions for agenda items at meetings of the Governing Council as in the past. For a variety of reasons and from time to time, ACA staff and leaders have not always been able to garner needed input and suggestions. Every effort needs to be made to reach out to grassroots members and identify and affirm their concerns based on the philosophy that the role of an elected leader or ACA staff member is to serve the wishes of those who are depending on their leadership.
Second, there is a lack of membership growth in ACA. In 1986, there were 55,000 members of ACA and our battle cry was “60,000—yes we can.” Currently, the association still has about the same number of members. I think grassroots members need to be re-engaged and encouraged to participate in local projects as well as ACA leadership and governance so that interest and involvement, and subsequently membership, can be reinvigorated.
Lastly, the composition of the Governing Council needs changing. Currently, there are more members of ACA who do not belong to ACA divisions than members who do belong to divisions. Yet, the composition of the Governing Council is still based on a model developed several decades ago when divisional membership was very strong and those seated “around the table,” so to speak, were primarily divisional representatives. Now that the composition of the membership has changed, I think there should be a large proportion of seated representatives for the membership at large. Granted, divisions would still need to be represented and seated, but possibly several divisions could be represented by a single member of the Governing Council if collaboration could occur.
- Assuming some challenges will get resolved and others will not, what do you think the counseling profession will look like 20 years from now?
I believe a revised governance structure of ACA, including membership on the Governing Council, will emerge. Perhaps the structure comprised of state branches, regions, and divisions will no longer exist as we now know it, and another way of organizing to insure input and renewed interest in grassroots participation will replace it to increase ACA membership numbers. The continued development of licensure portability and reciprocity across states could enhance the unification of the profession and encourage more interdisciplinary collaboration.
Accreditation and CACREP standards will continue, but hopefully with more tolerance and affirmation options for adult learners seeking specialization options. Currently, there is not much leeway in decision making regarding coursework. Also related, the increased acceptance of online counselor education programs will occur, as well as more clearly articulated requirements and expectations for online counseling.
Lastly, there is increased interest in the importance of advocacy and social justice on the part of ACA and its members. Universal acceptance and affirmation of the importance of diverse populations, personalities, lifestyles, and cultures as they contribute, not only to the profession, but also to the fabric and strength of democracy in the United States, will continue to be at the forefront of what we do.
- If you were advising current counseling leaders, what advice would you give them about moving the counseling profession forward?
First, never forget that your role is to listen to those who elected or appointed you, because your role is to serve members of the counseling profession and advocate for their best interests. Second, even though those elected to represent divisions on the Governing Council have the responsibility to articulate and explain the wishes of their division, in the end, the outcome of decisions made by the Governing Council must reflect what is best for ACA and the counseling profession. Third, although it is always appropriate for those serving in elected positions within ACA to put forward their ideas for changes, initiatives, or innovations, it is never reasonable to expect such agendas to be adopted unless they truly reflect the interests and wishes of those being served through the leadership position.
This concludes the third interview for the annual Lifetime Achievement in Counseling Series. TPC is grateful to Joshua Smith, NCC, and Dr. Neal Gray for providing this interview. Joshua Smith is a doctoral student in counselor education and supervision at the University of North Carolina at Charlotte. Neal D. Gray is a professor and Chair of the School of Counseling at Lenoir-Rhyne University. Correspondence can be emailed to Joshua Smith at jsmit643@uncc.edu.
Nov 29, 2018 | Volume 8 - Issue 4
Michael T. Kalkbrenner, Edward S. Neukrug
The primary aim of this study was to cross-validate the Revised Fit, Stigma, & Value (FSV) Scale, a questionnaire for measuring barriers to counseling, using a stratified random sample of adults in the United States. Researchers also investigated the percentage of adults living in the United States that had previously attended counseling and examined demographic differences in participants’ sensitivity to barriers to counseling. The results of a confirmatory factor analysis supported the factorial validity of the three-dimensional FSV model. Results also revealed that close to one-third of adults in the United States have attended counseling, with women attending counseling at higher rates (35%) than men (28%). Implications for practice, including how professional counselors, counseling agencies, and counseling professional organizations can use the FSV Scale to appraise and reduce barriers to counseling among prospective clients are discussed.
Keywords: barriers to counseling, FSV Scale, confirmatory factor analysis, attendance in counseling, factorial validity
According to the World Health Organization (WHO), mental health disorders are widespread, with over 300 million people struggling with depressive disorders, 260 million living with anxiety disorders, and hundreds of millions having any of a number of other mental health disorders (WHO, 2017, 2018). The symptoms of anxiety and depressive disorders can be dire and include hopelessness, sadness, sleep disturbances, motivational impairment, relationship difficulties, and suicide in the most severe cases (American Psychiatric Association, 2013). Worldwide, one in four individuals will be impacted by a mental health disorder in their lifetime, which leads to over a trillion dollars in lost job productivity each year (WHO, 2018). In the United States, approximately one in five adults has a diagnosable mental illness each year, and about 20% of children and teens will develop a mental disorder that is disabling (Centers for Disease Control, 2018).
Substantial increases in mental health distress among the U.S. and global populations have impacted the clinical practice of counseling practitioners who work in a wide range of settings, including schools, social service agencies, and colleges (National Institute of Mental Health, 2017; Twenge, Joiner, Rogers, & Martin, 2017). Identifying the percentage of adults in the United States who attend counseling, as well as the reasons why many do not, can help counselors develop strategies that can make counseling more inviting and, ultimately, relieve struggles that people face. Although perceived stigma and not having health insurance have been associated with reticence to seek counseling (Han, Hedden, Lipari, Copello, & Kroutil, 2014; Norcross, 2010; University of Phoenix, 2013), the literature on barriers to counseling among people in the United States is sparse. Appraising barriers to counseling using a psychometrically sound instrument is the first step toward counteracting such barriers and making counseling more inviting for prospective clients. Evaluating barriers to counseling, with special attention to cultural differences, has the potential to help understand differences in attendance to counseling and can help develop mechanisms that promote counseling for all individuals. This is particularly important as research has shown that there are differences in help-seeking behavior as a function of gender identity and ethnicity (Hatzenbuehler, Keyes, Narrow, Grant, & Hasin, 2008).
Attendance in Counseling by Gender and Ethnicity
Previous investigations on attendance in counseling indicated that 15–38% of adults in the United States had sought counseling at some point in their lives (Han et al., 2014; University of Phoenix, 2013), with discrepancies in counselor-seeking behavior found as a function of gender and ethnicity (Han et al., 2014; Lindinger-Sternart, 2015). For instance, women are more likely to seek counseling compared to men (Abrams, 2014; J. Kim, 2017). In addition, individuals who identify as White tend to seek personal counseling at higher rates compared to those who identify with other ethnic backgrounds (Hatzenbuehler et al., 2008; Seidler, Rice, River, Oliffe, & Dhillon, 2017). Parent, Hammer, Bradstreet, Schwartz, and Jobe (2018) examined the intersection of gender, race, ethnicity, and poverty with help-seeking behavior and found the income-to-poverty ratio to be positively related to help-seeking for White males and negatively associated for African American males. In other words, as White males gained in income, they were more likely to seek counseling, whereas the opposite was true for males who identified as African American (Parent et al., 2018).
Barriers to Mental Health Treatment and Attendance in Counseling
Despite the fact that large numbers of individuals in the United States and worldwide will develop a mental disorder in their lifetime, two-thirds of them will avoid or do not have access to mental health treatment (WHO, 2018). In wealthier countries, there is one mental health worker per 2,000 people (WHO, 2015); however, in poorer countries, this drops to 1 in 100,000, and such disparities need to be addressed (Hinkle, 2014; WHO, 2015). Although the lack of attendance in counseling and related services in poorer countries is explained by lack of services, in the United States and other wealthy countries, the availability of mental health services is relatively high, and the lack of attendance is usually explained by other reasons (Neukrug, Kalkbrenner, & Griffith, 2017; WHO, 2015). Research on the lack of attendance in counseling by the general public shows adults in the United States might be reticent to seek counseling because of perceived stigma, financial burden, lack of health insurance, uncertainty about how to find a counselor, and suspicion that counseling will not be helpful (Han et al., 2014; Norcross, 2010; University of Phoenix, 2013).
Appraising Barriers to Counseling
The quantification and appraisal of barriers to counseling is a nuanced and complex construct to measure and has been previously assessed with populations of mental health professionals and with counseling students (Kalkbrenner & Neukrug, 2018; Kalkbrenner, Neukrug, & Griffith, in press; Neukrug et al., 2017). Knowing that personal counseling is a valuable self-care strategy for mental health professionals (Whitfield & Kanter, 2014), Neukrug et al. (2017) developed the original version of the Fit, Stigma, & Value (FSV) Scale, which is comprised of three latent variables, or subscales, of barriers to counseling for human service professionals: fit (the degree to which one trusts the process of counseling), stigma (hesitation to seek counseling because of feelings of embarrassment), and value (the extent to which a respondent thinks that attending personal counseling will be beneficial). Kalkbrenner et al. (in press) extended and validated a revised version of the FSV Scale with a sample of professional counselors, and Kalkbrenner and Neukrug (2018) validated the Revised FSV Scale with a sample of counselor trainees. Although the FSV Scale appears to have utility for appraising barriers to counseling among mental health professionals (Neukrug et al., 2017; Kalkbrenner et al., in press) the factorial validity of the measure has only been tested with helping professionals and counseling students. The appraisal of barriers to seeking counseling among adults in the United States is an essential first step in understanding why prospective clients do, or do not, seek counseling. If validated, researchers and practitioners can potentially use the results of the Revised FSV Scale to aid in the early identification of specific barriers and to inform the development of interventions geared toward reducing barriers to counseling among adults in the United States. Thus, we sought to answer the following research questions (RQs): RQ 1: Is the three-dimensional hypothesized model of the Revised FSV scale confirmed with a stratified random sample of adults in the United States? RQ 2: To what extent do adults in the United States attend counseling? RQ 3: Are there demographic differences to the FSV barriers among adults in the United States?
Method
The psychometric properties of the Revised FSV Scale were tested with a confirmatory factor analysis (CFA) based on structural equation modeling (RQ 1). Descriptive statistics were used to compute participants’ frequency of attendance in counseling (RQ 2). A factorial multivariate analysis of variance (MANOVA) was computed to investigate demographic differences in respondents’ sensitivity to the FSV barriers (RQ 3). A minimum sample size of 320 (10 participants for each estimated parameter) was determined to be sufficient for computing a CFA (Mvududu & Sink, 2013). An a priori power analysis was conducted using G*Power to determine the sample size for the factorial MANOVA (Faul, Erdfelder, Lang, & Buchner, 2007). Results revealed that a minimum sample size of 269 would provide an 80% power estimate (α = .05), with a moderate effect size, f 2 = 0.25 (Cohen, 1988).
Participants and Procedures
After obtaining IRB approval, an online sampling service (Qualtrics, 2018) was contracted to survey a stratified random sample (stratified by age, gender, and ethnicity) of the general U.S. population based on the 2016–2017 census data. A Qualtrics project management team generated a list of parameters and sample quota constraints for data collection. Once the researchers reviewed and confirmed these parameters, a project manager initiated the stratified random sampling procedure and data collection by sending an electronic link to the questionnaire to prospective participants. A pilot study was conducted using 41 participants and no formatting or imputation errors were found. Data collection for the main study was initiated and was completed in less than one week.
A total of 431 individuals responded to the survey. Of these, 21 responses were omitted because of missing data, yielding a useable sample of 410. Participants ranged in ages from 18 to 84 (M = 45,
SD = 15). The demographic profile included the following: 52% (n = 213) identified as female, 44%
(n = 181) as male, 0.5% (n = 2) as transgender, and 3.4% (n = 14) did not specify their gender. For ethnicity, 63% (n = 258) identified as White, 17% (n = 69) as Hispanic/Latinx, 12% (n = 49) as African American, 5% (n = 21) as Asian, 1% (n = 5) as American Indian or Alaska Native, 0.5% (n = 2) as Native Hawaiian or Pacific Islander, and 1.5% (n = 6) did not specify their ethnicity. For highest degree completed, 1% (n = 5) held a doctoral degree, 7% (n = 29) held a master’s degree, 24% (n = 98) held a bachelor’s degree, 16% (n = 65) had completed an associate degree, 49% (n = 199) had a high school diploma, and 3% (n = 14) did not specify their highest level of education. Eighty-four percent (n = 343) of participants had health insurance at the time of data collection. The demographic profile of our sample is consistent with those found in recent surveys of the general U.S. population (Lumina Foundation, 2017; U.S. Census Bureau, 2017).
Instrumentation
Using the Qualtrics e-survey platform (Qualtrics, 2018), participants were asked to respond to a series of demographic questions as well as the Revised FSV Scale.
Demographic questionnaire. Participants responded to a series of demographic items about their age, ethnicity, gender, highest level of education completed, and if they had health insurance. They also were asked to indicate if they had ever recommended counseling to another person and if they had ever participated in at least one session of counseling as defined by the American Counseling Association (ACA) in the 20/20: Consensus Definition of Counseling: “counseling is a professional relationship that empowers diverse individuals, families, and groups to accomplish mental health, wellness, education, and career goals” (2010, para. 2).
The FSV Scale. The original version of the FSV Scale contained 32 items that comprise three subscales (Fit, Stigma, and Value) for appraising barriers to counselor seeking behavior (Neukrug et al., 2017). Kalkbrenner et al. (in press) developed and validated the Revised FSV Scale by reducing the number of items to 14 (of the original 32) and confirmed the same 3-factor structure of the scale. The Revised FSV Scale (see Table 1) was used in the present study for temporal validity, as it is more current and because it is likely to reduce respondent fatigue, because it is shorter than the original. The Fit subscale appraises the degree to which one trusts the process of counseling (e.g., item 11: “I couldn’t find a counselor who would understand me.”). The Stigma subscale measures respondents’ hesitation to seek counseling because of feelings of embarrassment (e.g., item 1: “My friends would think negatively of me.”). The Value scale reflects the extent to which a respondent thinks that attending personal counseling will be beneficial (e.g., item 8: “It is not an effective use of my time.”). For each item, respondents were prompted with the stem, “I am less likely to attend counseling because . . . ” and asked to rate each item on a Likert-type scale: 1 (strongly disagree), 2 (disagree), 3 (neither agree or disagree), 4 (agree), or 5 (strongly agree). Higher scores designate a greater sensitivity to each barrier. Previous investigators demonstrated adequate to strong internal consistency reliability coefficients for the Revised FSV Scale: α = .82, α = .91, and α = .78, respectively (Kalkbrenner et al., in press) and α = .81, α = .87, and α = .77 (Kalkbrenner & Neukrug, 2018). Past investigators found validity evidence for the 3-dimensional factor structure of the original and revised versions of the FSV Scale through rigorous psychometric testing (factor analysis) with populations of human services professionals (Neukrug et al., 2017), professional counselors (Kalkbrenner et al., in press), and counseling students (Kalkbrenner & Neukrug, 2018).
Results
CFA
A review of skewness and kurtosis values (see Table 1) indicated that the 14 items on the revised FSV scale were largely within the acceptable range of a normal distribution (absolute value < 1; Field, 2013). Mahalanobis d2 indices showed no extreme multivariate outliers. An inter-item correlation matrix (see Table 2) was computed to investigate the suitability of the data for factor analysis. Inter-item correlations were favorable and ranged from r = 0.42 to r = 0.82 (see Table 2).
Table 1
Descriptive Statistics: The Revised Version of the FSV Scale (N = 410)
| Items |
M |
SD |
Skew |
Kurtosis |
| My friends would think negatively of me. (Stigma) |
2.27 |
1.18 |
0.63 |
-0.50 |
| It would suggest I am unstable. (Stigma) |
2.55 |
1.25 |
0.29 |
-0.97 |
| I would feel embarrassed. (Stigma) |
2.72 |
1.20 |
-0.02 |
-1.00 |
| It would damage my reputation. (Stigma) |
2.43 |
1.20 |
0.41 |
-0.78 |
| It would be of no benefit. (Value) |
2.46 |
1.20 |
0.39 |
-0.71 |
| I would feel badly about myself if I saw a counselor. (Stigma) |
2.35 |
1.13 |
0.45 |
-0.61 |
| The financial cost of participating is not worth the personal benefits. (Value) |
2.61 |
1.18 |
0.25 |
-0.68 |
| It is not an effective use of my time. (Value) |
2.40 |
1.16 |
0.45 |
-0.57 |
I couldn’t find a counselor with my theoretical orientation
(personal style of counseling). (Fit) |
2.42 |
1.12 |
0.62 |
-0.68 |
| I couldn’t find a counselor competent enough to work with me. (Fit) |
2.31 |
1.12 |
0.50 |
-0.47 |
| I couldn’t find a counselor who would understand me. (Fit) |
2.41 |
1.20 |
0.48 |
-0.66 |
| I don’t trust a counselor to keep my matters just between us. (Fit) |
2.50 |
1.21 |
0.33 |
-0.82 |
| Counseling is unnecessary because my problems will resolve naturally. (Value) |
2.56 |
1.31 |
0.22 |
-0.61 |
| I have had a bad experience with a previous counselor in the past. (Fit) |
2.34 |
1.17 |
0.44 |
-0.71 |
Table 2
Inter-Item Correlation Matrix
|
Q1 |
Q2 |
Q3 |
Q4 |
Q5 |
Q6 |
Q7 |
Q8 |
Q9 |
Q10 |
Q11 |
Q12 |
Q13 |
Q14 |
| Q1 |
1 |
0.70 |
0.64 |
0.72 |
0.54 |
0.63 |
0.53 |
0.57 |
0.57 |
0.60 |
0.60 |
0.53 |
0.47 |
0.53 |
| Q2 |
|
1 |
0.76 |
0.72 |
0.51 |
0.61 |
0.52 |
0.54 |
0.55 |
0.58 |
0.60 |
0.57 |
0.42 |
0.46 |
| Q3 |
|
|
1 |
0.68 |
0.51 |
0.64 |
0.54 |
0.53 |
0.53 |
0.55 |
0.58 |
0.57 |
0.50 |
0.43 |
| Q4 |
|
|
|
1 |
0.62 |
0.68 |
0.55 |
0.59 |
0.58 |
0.61 |
0.63 |
0.61 |
0.51 |
0.53 |
| Q5 |
|
|
|
|
1 |
0.67 |
0.58 |
0.69 |
0.52 |
0.59 |
0.59 |
0.48 |
0.57 |
0.49 |
| Q6 |
|
|
|
|
|
1 |
0.58 |
0.68 |
0.59 |
0.68 |
0.69 |
0.60 |
0.56 |
0.48 |
| Q7 |
|
|
|
|
|
|
1 |
0.72 |
0.60 |
0.60 |
0.57 |
0.58 |
0.59 |
0.53 |
| Q8 |
|
|
|
|
|
|
|
1 |
0.64 |
0.66 |
0.68 |
0.61 |
0.64 |
0.54 |
| Q9 |
|
|
|
|
|
|
|
|
1 |
0.71 |
0.71 |
0.61 |
0.56 |
0.57 |
| Q10 |
|
|
|
|
|
|
|
|
|
1 |
0.82 |
0.65 |
0.56 |
0.56 |
| Q11 |
|
|
|
|
|
|
|
|
|
|
1 |
0.65 |
0.52 |
0.58 |
| Q12 |
|
|
|
|
|
|
|
|
|
|
|
1 |
0.57 |
0.52 |
| Q13 |
|
|
|
|
|
|
|
|
|
|
|
|
1 |
0.44 |
| Q14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
A CFA based on structural equation modeling was computed using IBM SPSS Amos version 25 to test the psychometric properties of the revised 14-item scale with adults in the United States (RQ1). A number of goodness-of-fit (GOF) indices recommended by Byrne (2016) were investigated to determine model fit. The Chi Square CMIN absolute fit index was statistically significant: χ2 (74) = 3.54, p < 0.001. More suitable GOF indices for large sample sizes (N > 200) were examined and revealed adequate model fit: comparative fit index (CFI = .96); root mean square error of approximation (RMSEA = .07); 90% confidence interval [.06, .08]; standardized root mean square residual (SRMR = .038); incremental fit index (IFI = .96); and normed fit index (NFI = .94). Collectively, the GOF indices above demonstrated adequate model fit based on the guidelines provided by Byrne. The path model with standardized coefficients is displayed in Figure 1. Tests of internal consistency reliability (Cronbach’s Alpha) revealed strong reliability coefficients for all three FSV subscales: α = .90, α = .91, and α = .87, respectively. An investigation of the path model coefficients (see Figure 1) revealed a moderate to strong association between the FSV barriers. Consequently, researchers computed a follow-up CFA to test if a single-factor model solution for the FSV Scale was a better fit with the data. Results revealed a poor model fit for the single-factor solution, suggesting that retaining the 3-factor model was appropriate for the data.
Figure 1. Confirmatory Factor Analysis Path Model (N = 410)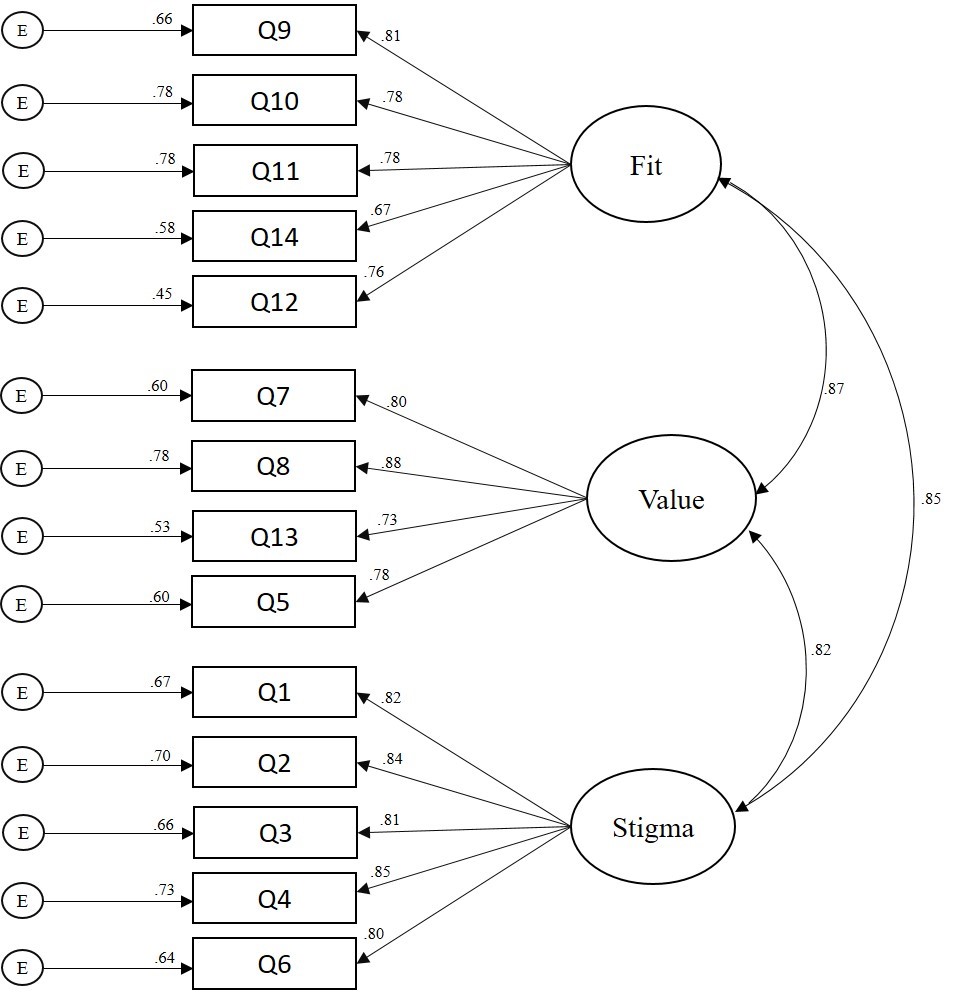
Figure 1. Confirmatory Factor Analysis Path Model (N = 410)
Frequency and Multivariate Analyses
Of the 374 participants who responded to the item regarding whether they had previously attended counseling, 32% (n = 121) indicated they had. A total of 362 participants specified both their gender and past attendance in counseling. Females’ (n = 199) rate of attendance in counseling was 35% (n = 70) and males’ (n = 163) rate of attendance in counseling was 28% (n = 45). Eleven percent
(n = 45) of participants were attending counseling at the time of data collection.
A factorial 2 (gender) X 2 (attendance in counseling) X 2 (ethnicity) MANOVA was computed to examine demographic differences in participants’ sensitivity to barriers to counseling. All three independent variables had two levels: gender (male or female), attendance in counseling (no previous attendance in counseling or previous attendance in counseling), and ethnicity (White or non-White). Based on the recommendations of Kaneshiro, Geling, Gellert, and Millar (2011), the second level of the ethnicity independent variable, non-White, was aggregated by merging all participants who did not identify as White; this ensured comparable groups for statistical analyses. The dependent variables consisted of respondents’ composite scores on each of the three FSV barriers. Because we were interested in investigating all significant main effects and interaction effects across the univariate and multivariate nature of the data, both MANOVA and follow-up univariate ANOVAs were computed (Field, 2013). Bonferroni corrections were applied to control for the familywise error rate.
A significant main effect emerged for gender: F = (7, 354) = 4.73, p = 0.003, Wilks’ Λ = 0.96, η2p = 0.04. The univariate ANOVAs (see Table 3) revealed significant main effects for all three FSV barriers:
Fit: [F = (7, 354) = 6.26, p = 0.013, η2p = 0.02]; Stigma: [F = (7, 354) = 13.71, p < 0.001, η2p = .04]; and
Value: [F = (7, 354) = 5.52, p = 0.02, η2p = .02]. Males (M = 2.56, M = 2.73, M = 2.60) scored higher than females (M = 2.25, M = 2.24, M = 2.23) on Fit, Stigma, and Value, respectively. A significant multivariate main effect also emerged for attendance in counseling: F = (7, 354) = 3.80, p = 0.01, Wilks’ Λ = 0.97, η2p = 0.031. The univariate ANOVA revealed that participants who had not attended counseling (M = 2.60) scored higher than participants who had attended counseling (M = 2.30) on the Value barrier: F = (7, 354) = 4.65, p = 0.03, η2p = 0.01. There were no other statistically significant main effects or any interaction effects (see Table 3). That is, there were no other significant group differences in respondents’ sensitivity to the FSV barriers by gender, attendance in counseling, or ethnicity.
Discussion
The primary aim of the present study was to validate the revised version of the FSV Scale with adults in the United States. Researchers also investigated the percentage of adults that have attended counseling and examined demographic differences in participants’ sensitivity to barriers to counseling. Frequency analyses revealed that 32% of our sample had attended at least one session of personal counseling, and among those who did, females reported a higher rate of attendance (35%) than males (28%). At the time of data collection, 11% of participants were seeing a counselor. Our findings are largely consistent with previous investigations that suggested 15–38% of adults in the United States had sought counseling at some point in their lives (Hann et al., 2014; University of Phoenix, 2013).
Table 3
Demographic Differences in Sensitivity to Barriers to Counseling
2 (gender) X 2 (attendance in counseling) X 2 (ethnicity) Analysis of Variance
| Independent Variable Barrier |
F |
Sig. |
Partial Eta Squared |
| Gender |
*Fit |
6.26 |
0.01 |
0.02 |
|
|
| **Stigma |
13.71 |
0.00 |
0.04 |
|
|
| *Value |
5.52 |
0.02 |
0.02 |
|
|
| Ethnicity |
Fit |
0.34 |
0.56 |
0.00 |
|
|
| Stigma |
0.00 |
0.96 |
0.00 |
|
|
| Value |
0.11 |
0.74 |
0.00 |
|
|
| Attendance in Counseling |
Fit |
0.69 |
0.41 |
0.00 |
|
|
| Stigma |
0.01 |
0.93 |
0.00 |
|
|
| *Value |
4.65 |
0.03 |
0.01 |
|
|
| Gender X Ethnicity |
Fit |
0.00 |
0.96 |
0.00 |
|
|
| Stigma |
0.12 |
0.73 |
0.00 |
|
|
| Value |
0.14 |
0.71 |
0.01 |
|
|
| Gender X Counseling |
Fit |
1.38 |
0.24 |
0.01 |
|
|
| Stigma |
3.00 |
0.08 |
0.01 |
|
|
| Value |
1.32 |
0.25 |
0.00 |
|
|
| Ethnicity X Counseling |
Fit |
0.07 |
0.79 |
0.00 |
|
|
| Stigma |
0.00 |
0.98 |
0.00 |
|
|
| Value |
0.21 |
0.65 |
0.00 |
|
|
| Gender X Ethnicity X Counseling |
Fit |
0.81 |
0.37 |
0.00 |
|
|
| Stigma |
1.19 |
0.28 |
0.00 |
|
|
| Value |
0.24 |
0.62 |
0.00 |
|
|
df = (1, 354) Note: 0.00 denotes values < 0.01. *Indicates statistical significance at the p < 0.05 level (2-tailed). ** Indicates statistical significance at the p < 0.01 level (2-tailed).
Similar to previous literature on attendance in counseling and congruent with gender theory (Levant, Wimer, & Williams, 2011; Seidler et al., 2017; Vogel, Heimerdinger-Edwards, Hammer, & Hubbard, 2011), we found that males were less likely to seek counseling and were particularly susceptible to the Stigma, Fit, and Value barriers when compared to females. Susceptibility to the Stigma barrier suggests that men might be less likely to attend counseling because of feelings of shame or embarrassment (Cheng, Kwan, & Sevig, 2013; Cheng, Wang, McDermott, Kridel, & Rislin, 2018; J. E. Kim, Saw, & Zane, 2015). Males also reported a higher sensitivity to the Fit and Value barriers as compared to women, suggesting they might place less worth on the anticipated benefits of counseling, and if they were to enter counseling, they may be particularly concerned about finding a counselor with whom they are compatible. It is possible that men’s sensitivity to all FSV barriers may simply be related to their underutilization of counseling services when compared to women, although other explanations also might be plausible.
Consistent with Kalkbrenner et al. (in press), we found that independent of gender, participants who had not attended at least one session of personal counseling placed less value on its potential benefits as compared to those who had attended counseling. This finding suggests that to some extent, attendance in personal counseling might moderate the aforementioned gender differences in participants’ sensitivity to the Value barrier. It is possible that attendance in counseling accounts for a more meaningful amount of the variance in sensitivity to the Value barrier to counseling than gender. Also, consistent with the findings of Kalkbrenner et al. (in press) and Kalkbrenner and Neukrug (2018), we found psychometric support for the factorial validity of the revised version of the FSV scale. Similar to these previous investigations (Kalkbrenner & Neukrug, 2018; Kalkbrenner et al., in press), tests of internal consistency revealed strong reliability coefficients for all three FSV scales. The findings of the present investigators add to the growing body of literature on Fit, Stigma, and Value as three primary barriers to seeking counseling among a variety of populations, including human services professionals (Neukrug et al., 2017), professional counselors (Kalkbrenner et al., in press), counselor trainees (Kalkbrenner & Neukrug, 2018), and now with members of the general U.S. population.
An investigation of the path model coefficients (see Figure 1) revealed moderate to strong associations between the FSV barriers, higher compared to past investigations (Kalkbrenner & Neukrug, 2018; Kalkbrenner et al., in press). A follow-up CFA was computed to test if a single-factor model (aggregated FSV barriers into a single scale) was a better factor solution for the data. However, the follow-up CFA revealed poor model fit for the single factor solution, suggesting that Fit, Stigma, and Value comprise three separate dimensions of a related construct. The differences in the strength of association between the FSV scales in the present study and in the studies by Kalkbrenner et al. (in press) and Kalkbrenner and Neukrug (2018) might be explained by differences between the samples. These investigators validated the FSV barriers with populations of professional counselors and counseling students. It is possible that professional counselors and counseling students were better able to discriminate between different types of barriers to counseling compared to members of the general U.S. population because of the clinical nature of their training. In addition, minor discrepancies are expected in any psychometric study in which authors are attempting to confirm the dimensionality of an attitudinal measure with a new sample (Hendrick, Fischer, Tobi, & Frewer, 2013).
To summarize, the results of internal consistency reliability and CFA indicated that the Revised FSV Scale and its dimensions were estimated adequately with a stratified random sample of adults in the United States. We found close to one-third of our sample had attended counseling, 11% were in counseling at the time of data collection, and there were demographic differences in participants’ sensitivity to barriers to counseling by gender and past attendance in counseling. A number of implications for enhancing counseling practice have emerged from these findings.
Implications for Counseling Practice
With 20% of individuals in the general U.S. population living with a mental disorder, 11% in counseling, 32% having attended counseling, and others wanting counseling but wary of attending, counselors, counseling programs, and counseling organizations can all play a part in reducing the barriers that the public faces when deciding whether or not they should attend counseling. Professional counselors can become leaders in reducing barriers to attending counseling among the general U.S. population through outreach and advocacy. The implications of the following strategies for outreach and advocacy are discussed in the subsequent sub-sections: connecting prospective clients with counselors, interprofessional communication, mobile health, and reducing stigma toward seeking counseling.
Connecting Prospective Clients With Counselors
Nationally, counseling organizations can operate campaigns aimed at reducing the stigma associated with counseling and speaking to its value. The National Board for Certified Counselors (NBCC) advocates for the development and implementation of grassroots community mental health approaches for supporting the accessibility of mental health services on both national and international levels (Hinkle, 2014). Like NBCC, other professional organizations (e.g., ACA and the American Mental Health Counselors Association) might include a directory of professional counselors on their website, along with their specialty areas, who work in a variety of geographic locations to help connect prospective clients with services. On a local level, it is recommended that professional counselors engage in outreach with members of their community to identify the potential unique mental health needs of people in their community and learn about potential barriers to counseling in their local area. Specifically, professional counselors can attend town board meetings and other public events to briefly introduce themselves and use their active listening skills to better understand the needs of the local community. The Revised FSV Scale is one potential tool that professional counselors might use when engaging in outreach with members of their community to gain a better understanding about local barriers to counseling.
We found that participants who had previously attended at least one session of personal counseling reported a higher perceived value of the benefits of counseling compared to those who did not attend counseling. It is possible that individuals’ attendance in counseling is related to their attributing a higher value to the anticipated benefits of counseling. Thus, we suggest community mental health counselors consider offering one free counseling session to promote prospective clients’ attendance in counseling. Just one free session might have the benefit of adding value to a client’s perceived worth of the counseling relationship and increase the likelihood of continued attendance in counseling. Offering one free session may be particularly important for men and minorities, who have traditionally attended counseling at lower rates (Hatzenbuehler et al., 2008; Seidler et al., 2017).
Interprofessional Communication
The flourishing of integrated behavioral health and interprofessional practice across the health care system might provide professional counselors with an opportunity to identify and reduce barriers to seeking counseling among the general U.S. population. In particular, integrated behavioral health involves infusing the delivery of physical and mental health care through interprofessional collaborations or teamwork among a variety of different professionals, thus providing a more holistic model for the patient (Johnson, Sparkman-Key, & Kalkbrenner, 2017). Professional counselors can collaborate with primary care physicians and consider the utility of administering the FSV Scale to patients while they are in the waiting room, as the FSV Scale can be accessed electronically via a tablet or smart phone. We recommend that counseling practitioners reach out to local primary care physicians to discuss the utility of integrated behavioral health and make themselves available to physicians for consultation on how to recognize and refer patients to counseling.
Mobile Health (mHealth)
mHealth refers to the delivery of interventions geared toward promoting physical or mental health by means of a cellular phone (Johnson & Kalkbrenner, 2017). Professional counselors can use mHealth to provide prospective clients with a brief overview of counseling, address prominent barriers to counseling faced by students, and provide mental health resources that are available to students. mHealth might be particularly useful for college and school counselors as academic institutions typically have access to students’ cell phone numbers, and students “appear to be open and responsive to the utilization of mHealth” (Johnson & Kalkbrenner, 2017, p. 323). The campus counseling center is underutilized on some college campuses because of stigma (Rosenthal & Wilson, 2016) and students’ unawareness of the services that are available at the counseling center (Dobmeier, Kalkbrenner, Hill, & Hernández, 2013). College counselors might consider using mHealth as a platform for both reducing stigma toward counselor-seeking behavior and for spreading students’ awareness of the services that are available to them for reduced or no fees at the counseling center.
Reducing Stigma Toward Seeking Counseling
Our results are consistent with the body of evidence indicating that when compared to women, men are less likely to attend counseling, more susceptible to barriers to attending counseling, and more likely to terminate counseling early (Levant et al., 2011; Seidler et al., 2017). Consistent with Vogel et al. (2011), we found that stigma was a predominant barrier to counseling among male participants. It is recommended that counseling practitioners focus on normalizing common presenting concerns that men are facing and find venues (e.g., barber shops, sports arenas) where they can reach out to men and lessen their concerns about attending counseling (Neukrug, Britton, & Crews, 2013).
Professional counselors can become leaders in reducing stigma toward help-seeking among men by normalizing common presenting concerns. As one example, the stress, anxiety, and depression men face when given a diagnosis of prostate cancer can potentially be reduced by counselors and their professional associations. By developing ways for the public to understand prostate cancer and its related mental health concerns, counselors and their professional associations can lessen the stigma of the disease. Promoting public awareness also can increase men’s likelihood of talking about a diagnosis of prostate cancer with friends, loved ones, and counselors, in a similar way that a diagnosis of breast cancer has been destigmatized over the past few decades. Professional counselors should consider other strategies that can be utilized to enhance the likelihood for men to attend counseling, such as group counseling or an informal setting.
Limitations and Future Research
Because causal attributions cannot be inferred from a cross-sectional survey research design, future researchers can extend the line of research on the FSV barriers using an experimental design by administering the scale to clients prior to and following attendance in counseling. Results might provide evidence of how counseling lessens one’s sensitivity to some barriers. Consistent with the U.S. Census Bureau (2017), the ethnic identity of the majority of participants in our sample was White. Thus, future research should replicate the present study using a more ethnically diverse sample, especially because individuals who identify with ethnicities other than White tend to seek counseling at lower rates (Hatzenbuehler et al., 2008; Vogel et al., 2011). In addition, despite having used a rigorous stratified random sampling procedure, it is possible that because of the sample size, this sample is not representative of adults in the United States. In addition, self-report bias is a limitation of the present study.
Our findings, coupled with existing findings in the literature (Kalkbrenner & Neukrug, 2018; Kalkbrenner et al., in press), suggest that the psychometric properties of the revised version of the FSV Scale are adequate for appraising barriers to seeking counseling among mental health professionals and adults in the United States. The next step in this line of research is to confirm the 3-factor structure of the FSV Scale with populations that are susceptible to mental health disorders and who might be reticent to seek counseling (e.g., veterans, high school students, non-White populations, and the older adult population; Akanwa, 2015; American Public Health Association, 2014; Bartels et al., 2003). Because we did not place any restrictions on sampling based on prospective participants’ history of mental illness, it is possible that the mean differences between participants’ sensitivity to the FSV barriers were influenced by the extent to which they were living with clinical problems at the time of data collection. Thus, future researchers should validate the FSV barriers with participants who are living with psychiatric conditions. Future researchers might also investigate the extent to which there might be differences in participants’ sensitivity to the FSV barriers based on the amount of time they have been in counseling (e.g., the number of sessions).
Because of the global increase in mental distress (WHO, 2018), future researchers should consider confirming the psychometric properties of the FSV Scale with international populations. In addition, we found that when gender, ethnicity, and previous attendance in counseling were entered into the MANOVA as independent variables, significant differences in the Value barrier only emerged for attendance in counseling. Therefore, previous attendance in counseling might account for a more substantial portion of the variance in barriers to counseling than gender and ethnicity. Future researchers can test this hypothesis using a path analysis.
Summary and Conclusion
Attendance in counseling among members of the general U.S. population has become increasingly important because of the frequency and complexity of mental disorders within the U.S. and global populations (WHO, 2017). The primary aim of the present study was to test the psychometric properties of the Revised FSV Scale, a questionnaire for measuring barriers to counseling using a stratified random sample of U.S. adults. The results of a CFA indicated that the Revised FSV Scale and its dimensions were estimated adequately with a stratified random sample of adults in the United States. The appraisal of barriers to seeking counseling is an essential first step in understanding why prospective clients do or do not seek counseling. At this stage of development, the Revised FSV Scale appears to have utility for screening sensitivity to three primary barriers (Fit, Stigma, and Value) to seeking counseling among mental health professionals and adults in the United States. Further, the Revised FSV Scale can be used tentatively by counseling practitioners who work in a variety of settings as one way to measure and potentially reduce barriers associated with counseling among prospective clients.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest or funding contributions for the development of this manuscript.
References
Abrams, A. (2014). Women more likely than men to seek mental health help, study finds. TIME Health. Retrieved from
http://time.com/2928046/mental-health-services-women/
Akanwa, E. E. (2015). International students in Western developed countries: History, challenges, and
prospects. Journal of International Students, 5, 271–284.
American Counseling Association. (2010). 20/20: Consensus definition of counseling. Retrieved from https://www.counseling.org/knowledge-center/20-20-a-vision-for-the-future-of-counseling/consensus-definition-of-counseling
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
American Public Health Association. (2014). Removing barriers to mental health services for veterans. Retrieved from https://www.apha.org/policies-and-advocacy/public-health-policy-statements/policy-database/2015/01/28/14/51/removing-barriers-to-mental-health-services-for-veterans
Bartels, S. J., Dums, A. R., Oxman, T. E., Schneider, L. S., Areán, P. A., Alexopoulos, G. S., & Jeste, D. V. (2003). Evidence-based practices in geriatric mental health care: An overview of systematic reviews and meta-analyses. Psychiatric Clinics of North America, 26, 971–990, x–xi. doi:10.1016/S0193-953X(03)00072-8
Byrne, B. M. (2016). Structural equation modeling with AMOS: Basic concepts, applications, and programming (3rd ed.). New York, NY: Routledge.
Centers for Disease Control and Prevention. (2018). Learn about mental health. Retrieved from https://www.cdc.gov/mentalhealth/learn/index.htm
Cheng, H.-L., Kwan, K.-L. K., & Sevig, T. (2013). Racial and ethnic minority college students’ stigma associated with seeking psychological help: Examining psychocultural correlates. Journal of Counseling Psychology, 60, 98–111. doi:10.1037/a0031169
Cheng, H.-L., Wang, C., McDermott, R. C., Kridel, M., & Rislin, J. L. (2018). Self-stigma, mental health literacy, and attitudes toward seeking psychological help. Journal of Counseling & Development, 96, 64–74. doi:10.1002/jcad.12178
Cohen, J. E. (1988). Statistical power analysis for the behavioral sciences. Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Dobmeier, R. A., Kalkbrenner, M. T., Hill, T. L., & Hernández, T. J. (2013). Residential community college student awareness of mental health problems and resources. New York Journal of Student Affairs, 13(2), 15–28.
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191.
Field, A. (2013). Discovering statistics using IBM SPSS Statistics (4th ed.). Thousand Oaks, CA: Sage.
Han, B., Hedden, S. L., Lipari, R., Copello, E. A. P., & Kroutil, L. A. (2014). Receipt of services for behavioral health problems: Results from the 2014 National Survey on Drug Use and Health. Retrieved from https://www.samh sa.gov/data/sites/default/files/NSDUH-DR-FRR3-2014/NSDUH-DR-FRR3-2014/NSDUH-DR-FRR3-2014.htm
Hatzenbuehler, M. L., Keyes, K. M., Narrow, W. E., Grant, B. F., &, Hasin, D. S. (2008). Racial/ethnic disparities in service utilization for individuals with co-occurring mental health and substance use disorders in the general population: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. The Journal of Clinical Psychiatry, 69, 1112–1121.
Hendrick, T. A. M., Fischer, A. R. H., Tobi, H., & Frewer, L. J. (2013). Self-reported attitude scales: Current practice in adequate assessment of reliability, validity, and dimensionality. Journal of Applied Social Psychology, 43, 1538–1552. doi:10.1111/jasp.12147
Hinkle, J. S. (2014). Population-based mental health facilitation (MHF): A grassroots strategy that works. The Professional Counselor, 4, 1–18. doi:10.15241/jsh.4.1.1
Johnson, K. F., & Kalkbrenner, M. T. (2017). The utilization of technological innovations to support college student mental health: Mobile health communication. Journal of Technology in Human Services, 35(4), 1–26. doi:10.1080/15228835.2017.1368428
Johnson, K. F., Sparkman-Key, N., & Kalkbrenner, M. T. (2017). Human service students’ and professionals’ knowledge and experiences of interprofessionalism: Implications for education. Journal of Human Services, 37, 5–13.
Kalkbrenner, M. T., & Neukrug, E. S. (2018). A confirmatory factor analysis of the Revised FSV Scale with counselor trainees. Manuscript submitted for publication.
Kalkbrenner, M. T., Neukrug, E. S., & Griffith, S. A. (in press). Barriers to counselors seeking counseling: Cross validation and predictive validity of the Fit, Stigma, & Value (FSV) Scale. Journal of Mental Health Counseling.
Kaneshiro, B., Geling, O., Gellert, K., & Millar, L. (2011). The challenges of collecting data on race and ethnicity in a diverse, multiethnic state. Hawai’i Medical Journal, 70(8), 168–171.
Kim, J. (2017, January 30). Why I think all men need therapy: A good read for women too. Psychology Today. Retrieved from https://www.psychologytoday.com/us/blog/the-angry-therapist/201701/why-i-think-all-men-need-therapy
Kim, J. E., Saw, A., & Zane, N. (2015). The influence of psychological symptoms on mental health literacy of college students. American Journal of Orthopsychiatry, 85, 620–630. doi:10.1037/ort0000074
Levant, R. F., Wimer, D. J., & Williams, C. M. (2011). An evaluation of the Health Behavior Inventory-20 (HBI-20) and its relationship to masculinity and attitudes towards seeking psychological help among college men. Psychology of Men & Masculinity, 12, 26–41. doi:10.1037/a0021014
Lindinger-Sternart, S. (2015). Help-seeking behaviors of men for mental health and the impact of diverse cultural backgrounds. International Journal of Social Science Studies, 3, 1–6. doi:10.11114/ijsss.v3i1.519
Lumina Foundation. (2017). A stronger nation: Learning beyond high schools builds American talent. Retrieved from http://strongernation.luminafoundation.org/report/2018/#nation
Mvududu, N. H., & Sink, C. A. (2013). Factor analysis in counseling research and practice. Counseling Outcome Research and Evaluation, 4(2), 75–98. doi:10.1177/2150137813494766
National Institute of Mental Health. (2017). Mental Illnesses. Retrieved from https://www.nimh.nih.gov/health/statistics/mental-illness.shtml#part_154787
Neukrug, E., Britton, B. S., & Crews, R. C. (2013). Common health-related concerns of men: Implications for counselors. Journal of Counseling & Development, 91, 390–397. doi:10.1002/j.1556-6676.2013.00109
Neukrug, E., Kalkbrenner, M. T., & Griffith, S. A. (2017). Barriers to counseling among human service professionals: The development and validation of the Fit, Stigma, & Value Scale. Journal of Human Services, 37, 27–40.
Norcross, A. E. (2010). A case for personal therapy in counselor education. Counseling Today, 53(2), 40–42.
Parent, M. C., Hammer, J. H., Bradstreet, T. C., Schwartz, E. N., & Jobe, T. (2018). Men’s mental health help-seeking behaviors: An intersectional analysis. American Journal of Men’s Health, 12, 64–73. doi:10.1177/1557988315625776
Qualtrics [Online survey platform software]. (2018). Provo, UT. Retrieved from https://www.qualtrics.com/
Qualtrics Sample Services [Online sampling service service]. (2018). Provo, UT. Retrieved from https://www.qualtrics.com/online-sample/
Rosenthal, B. S., & Wilson, W. C. (2016). Psychosocial dynamics of college students’ use of mental health services. Journal of College Counseling, 19(3), 194–204. doi:10.1002/jocc.12043
Seidler, Z. E., Rice, S. M., River, J., Oliffe, J. L., & Dhillon, H. M. (2017). Men’s mental health services: The case for a masculinities model. Journal of Men’s Studies, 25, 92–104. doi:10.1177/1060826517729406
Twenge, J. M., Joiner, T. E., Rogers, M. L., & Martin, G. N. (2017). Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clinical Psychological Science, Advanced online publication. doi:10.1177/2167702617723376
University of Phoenix. (2013). University of Phoenix survey reveals 38 percent of individuals who seek mental health counseling experience barriers. Retrieved from http://www.phoenix.edu/news/releases/2013/05/university-of-phoenix-survey-reveals-38-percent-of-individuals-who-seek-mental-health-counseling-experience-barriers.html
U.S. Census Bureau. (2017). Population estimates, July 1, 2017. Retrieved from https://www.census.gov/quick facts/fact/table/US/PST045216
Vogel, D. L., Heimerdinger-Edwards, S. R., Hammer, J. H., & Hubbard, A. (2011). “Boys don’t cry”: Examination of the links between endorsement of masculine norms, self-stigma, and help-seeking attitudes for men from diverse backgrounds. Journal of Counseling Psychology, 58, 368–382.
doi:10.1037/a0023688
Whitfield, N., & Kanter, D. (2014). Helpers in distress: Preventing secondary trauma. Reclaiming Children and Youth, 22(4), 59–61.
World Health Organization. (2015). Global health workforce, finances remain low for mental health. Retrieved from http://www.who.int/mediacentre/news/notes/2015/finances-mental-health/en/
World Health Organization. (2017). World mental health day, 2017: Mental health in the workplace. Retrieved from http://www.who.int/mental_health/world-mental-health-day/2017/en/
World Health Organization. (2018). World health report: Mental disorders affect one in four people. Retrieved from http://www.who.int/whr/2001/media_centre/press_release/en/
Nov 13, 2018 | Volume 8 - Issue 4
Jessica Gonzalez, Sejal M. Barden, Julia Sharp
Exploring client outcomes is a primary goal for counselors; however, gaps in empirical research exist related to the relationship between client outcomes, the working alliance, and counselor characteristics. Thus, the purpose of this investigation was to explore the relationship between the effects of multicultural competence and the working alliance on client outcomes from both client (n = 119) and counselor-in-training (n = 72) perspectives, while controlling for social desirability. Hierarchical regression results indicated counselors-in-training’s perceptions of multicultural competence and client outcome pretest scores were a significant predictor of client outcomes, after controlling for social desirability. Linear mixed effects modeling indicated significant differences in perceptions between both clients and counselors on the working alliance and multicultural competence. Findings highlight the importance of exploring what has already been working for clients before coming to counseling. Additionally, counselors are encouraged to self-reflect and explore how their clients view the relationship between the working alliance and multicultural competence.
Keywords: client outcomes, multicultural competence, working alliance, social desirability, client perspective
The past three decades of research have identified the therapeutic relationship between client and counselor as the most important predictor of change in counseling for clients (Ardito & Rabellino, 2011; Horvath & Bedi, 2002; Norcross, 2002); however, there is limited research on the associations between the working alliance and multicultural competence. Cultivating multicultural competence for counselor trainees has been the focus of considerable empirical research (Horvath & Bedi, 2002), yet the majority of studies have focused on trainees’ self-report of multicultural competence, failing to account for clients’ perceptions of trainees’ competencies (Constantine, 2001; Fuertes et al., 2006). Specifically, more research is needed exploring the influence of multicultural competence as perceived by both clients and counselors-in-training (CITs) on client outcomes (Hays & Erford, 2017; Katz & Hoyt, 2014).
Working Alliance and Client Outcomes
The working alliance is a collaborative approach that refers to the extent of agreement between clients and counselors on the goals, tasks (how to accomplish goals), and bond (development of personal bond between client and counselor) in counseling (Horvath & Greenberg, 1989). The working alliance has been identified as a key factor in positive client outcomes, despite choice of treatment modality or counseling setting (Bachelor, 2013; Baldwin, Wampold, & Imel, 2007). Considerable research has been conducted on the working alliance in relation to clients’ and CITs’ perceptions and client outcomes. Research has shown consistent similarities and differences between clients’ and counselors’ perceptions of the working alliance (Bachelor, 2013; Fitzpatrick, Iwakabe, & Stalikas, 2005; Hatcher & Barends, 1996). For example, Huppert et al. (2014) looked at the effect of counselor characteristics and the therapeutic alliance on client outcomes for clients receiving cognitive behavioral therapy for panic disorder with agoraphobia. The working alliance was measured in Sessions 3 and 9. Multilevel modeling indicated that counselors’ involvement in the alliance predicted attrition. However, client perspective of the working alliance predicted both client outcomes and attrition in counseling.
Studies such as Huppert et al. (2014) highlight the important role that the working alliance has in client outcomes in counseling. However, Drisko (2013) acknowledged that the therapeutic relationship is not the sole predictor of client outcomes and highlighted that additional factors in counseling, combined with a strong therapeutic relationship, can influence outcomes. Other common factors can include client motivation and counselor characteristics such as multicultural competence. Collins and Arthur (2010) described the working alliance as the cornerstone in the counseling process that facilitates a transformative collaborative approach in helping clients explore and understand their cultural self-awareness.
Multicultural Competence and Client Outcomes
In 1992, Sue, Arredondo, and McDavis developed the Multicultural Counseling Competencies, and in 1996 Arredondo and colleagues presented a paper outlining the Tripartite Model of Multicultural Counseling that categorized multicultural competence into three factors: awareness, knowledge, and skills. More recently, the Association for Multicultural Counseling and Development and the American Counseling Association (ACA) have endorsed a set of updated competencies, including a social justice framework entitled the Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts, Singh, Nassar-McMillan, Butler, & McCullough, 2015). Research supports positive associations between clients’ perceptions of their counselors’ multicultural competence and (a) client outcomes (Owen, Leach, Wampold, & Rodolfa, 2011); (b) the counseling relationship (Fuertes & Brobst, 2002; Fuertes et al., 2006; Li & Kim, 2004; Pope-Davis et al., 2002); and (c) satisfaction with counseling (Constantine, 2002; Fuertes & Brobst, 2002). These associations show how influential clients’ perceptions of their counselors’ multicultural competence are based on a variety of aspects of the counseling process. However, the majority of studies have focused on exploring counselors’ multicultural competence from only the counselor’s perspective (Worthington, Soth-McNett, & Moreno, 2007).
Self-report multicultural measures have been criticized for being prone to participants responding in a socially desirable manner and having a tendency to measure anticipated behaviors of multicultural competence rather than actual behaviors and attitudes of multicultural competence (Constantine & Ladany, 2000; Worthington, Mobley, Franks, & Tan, 2000). In addition, counselors’ ratings of their multicultural competence can differ from ratings from an observer (e.g., supervisor; Worthington et al., 2000) or their client (Smith & Trimble, 2016). Social desirability is a response bias in which research participants attempt to make a good impression when completing research studies by answering in an overly positive manner (Crowne & Marlowe, 1960). One way researchers can minimize the potential threat of social desirability is to input a social desirability scale (Drisko, 2013) and to control for social desirability, which can improve the accuracy of the research design (McKibben & Silvia, 2016).
In addition to the majority of studies only looking at counselors’ perspectives, there is a need for further research on how CITs’ multicultural competence associates with client outcomes (D’Andrea & Heckman, 2008). For example, Soto, Smith, Griner, Rodríguez, and Bernal (2018) conducted a meta-analysis looking at how many studies have explored how client outcomes are related to their counselors’ level of multicultural competence. Only 15 studies were found that explored client outcomes and counselors’ multicultural competence. From the 15 studies, 73% appeared since 2010, including several unpublished dissertations (40%). The fact that only 15 studies were identified that met inclusion criteria for this study and were found several decades after the multicultural competencies have emerged suggests the need for further investigation on this topic (Soto et al., 2018). Two specific studies, Owen et al. (2011) and Tao, Owen, Pace, and Imel (2015), explored the relationships between multicultural competence and the counseling process. Owen and colleagues’ findings indicated a positive association between clients’ ratings of their counselors’ multicultural competence and client outcomes. Tao and colleagues’ meta-analysis comparing the correlations and effect sizes between quantitative studies (between the years of 2002–2014) of multicultural competence and other measures of the clinical process indicated that clients ratings of their counselors’ multicultural competence accounted for 37% of the variance in the working alliance. Owen et al.’s and Tao et al.’s findings highlight the need to further explore the dynamics between clients’ and counselors’ perceptions of multicultural competence and the working alliance.
Overall, the lack of multicultural competence outcome research may be a hindrance to counselors being able to fulfill the ACA Code of Ethics because of a lack of empirical justification (D’Andrea & Heckman, 2008). In order for multicultural competence scholarship to further advance, professional counseling organizations and scholars (ACA, 2014; Bachelor, 2013; Council for Accreditation of Counseling and Related Educational Programs, 2016; Owen et al., 2011) recommend exploring how multicultural competence may influence client outcomes. Additionally, research is needed exploring the similarities and differences between clients’ and counselors’ views on the working alliance and multicultural competence. Further, in self-report counseling investigations, researchers can minimize potential threat to the study by using a social desirability scale as a control variable (Drisko, 2013; McKibben & Silvia, 2016). Thus, the purpose of this investigation was to explore the relationship between the effects of multicultural competence and the working alliance on client outcomes from both client and CIT perspectives, while controlling for social desirability.
As such, we aimed to answer three research questions: (a) Do CITs’ multicultural competence and the working alliance (as perceived by clients) predict client outcomes, while controlling for social desirability from the client’s perspective? (b) Do CITs’ multicultural competence and the working alliance (as perceived by counselors) predict client outcomes, while controlling for social desirability from the CIT’s perspective? and (c) What differences exist between clients’ and CITs’ perceptions of CITs’ multicultural competence and the working alliance, while controlling for social desirability?
Method
Participants
This investigation was conducted at a university-based community counseling research center located in the southeastern region of the United States. The primary investigator worked in the clinic in which the research study was conducted; thus, convenience sampling was used. CITs’ criteria to participate in this study was that the student had to be enrolled in their first or second semester of practicum in a master’s-level counselor education program. In addition, client criteria to participate was that they had to be an adult (over the age of 18) receiving counseling services from the CITs at the counseling research center. A total of 146 adult clients and 85 CITs participated in this study. Missing values and clients who completed the assessments more than twice were removed, yielding a response rate of 82% for clients and 84% for CITs.
Client participants self-identified as female (n = 71, 59.7%) and male (n = 48, 40.3%). The number of clients by age range was: 18–30 (n = 56, 47.1%), 31–40 (n = 27, 47.1%), 41–50 (n = 22, 18.5%), 51–60 (n = 12, 10.1%), and 61–65 (n = 2, 1.7%). Lastly, clients identified as White (n = 64, 53.8%), African American/Black (non-Hispanic, n = 21, 17.6%), Hispanic/Latino (n = 20, 16.8%), Biracial/Multiracial (n = 7, 5.9%), American Indian (n = 2, 1.7%), Asian (n = 1, 8%), and Other (n = 4, 3.4%). CIT participants self-identified as female (n = 61, 84.7%) and as male (n = 11, 15.3%). A majority of counselors were between the ages of 21–26 (n = 54, 75%), followed by 27–37 (n = 18, 25%). CITs identified as White (n = 48, 66.7%), African American/Black (non-Hispanic, n = 7, 9.7%), Hispanic/Latino (n = 7, 9.7%), Biracial/Multiracial (n = 8, 11.1%), Asian (n = 1, 1.4%), and Other (n = 1, 1.4%).
Procedure
Approval to conduct the study was obtained from the university’s institutional review board and the clinical director of the counseling research center. First, the researcher administered the consent for research during CITs’ practicum orientation and explained the purpose and voluntary nature of the study. CITs received instructions on how to administer consent for research to clients. Counselors received small tokens (a mechanical pencil and a small piece of candy) from the researcher during the practicum orientation as an incentive to complete the surveys and provide them to clients. Clinic services where the research was conducted include free counseling. Clients were already receiving free counseling services, and if they chose not to participate in this study, they would still continue to receive free counseling.
The researcher instructed CITs to provide clients with the explanation of research at the start of their first counseling session. If clients chose to participate, the CIT administered the Outcome Questionnaire 45.2 (OQ45.2; Lambert et al., 1996) assessment at the end of their first and third sessions in the counseling room. In addition, clients and CITs were instructed to complete the demographic questionnaire, the Cross-Cultural Counseling Inventory-Revised (CCCI-R; LaFromboise, Coleman, & Hernandez, 1991), the Working Alliance Inventory-Short Form (WAI-S; Horvath & Greenberg, 1989; Tracey & Kokotovic, 1989), and the Reynolds Marlowe-Crown Social Desirability Scale-Short Form A (SDS; Reynolds, 1982) after their third session was completed. Data were collected after completion of the third counseling session based on preliminary analysis on adult client retention rates at the counseling research center indicating that after the fourth counseling session, client retention rate drops by 60%. In addition, the working alliance is generally measured between the first and fifth sessions (Horvath & Bedi, 2002; Norcross, 2002).
Data were entered and then analyzed by SPSS. Prior to beginning analysis, several preliminary analyses were conducted to explore relationships among variables. Assumptions for normality, homogeneity of variance, linearity, and multicollinearity were met. To reduce the likelihood of violating the assumption of independence, clients were used as a static variable, or a variable that only has one independent observation. Utilizing static variables was important due to the possibility for the same client to have received counseling services during the two semesters in which the researcher collected the data, increasing the potential violation for the assumption of independence. Thus, if the same client had multiple ratings on assessments, they were removed from the data set, resulting in the removal of three clients. Researchers used correlation analysis, hierarchical regression, and linear mixed-effects modeling to explore their research questions.
Measures
The CCCI-R (LaFromboise et al., 1991) was used to measure client and counselor perceptions of CIT multicultural counseling competence in this investigation. The CCCI-R was developed based on the multicultural competencies defined by the Education and Training Committee of Division 17 of the American Psychological Association (Sue et al., 1982). The CCCI-R is a 20-item assessment, rated on a 6-point Likert scale intended for observer report of a counselor’s level of cultural awareness, knowledge, and skill. LaFromboise and colleagues (1991) reported an overall internal consistency coefficient alpha of .95, with an inter-item correlation between .18 and .73. Although the CCCI-R was developed to be completed by supervisors, it has been adapted for use with counselors and clients (e.g., Client: My counselor is aware of his or her own cultural heritage; Counselor: I am aware of my own cultural heritage; Fuertes et al., 2006; Owen et al., 2011). The CCCI-R is scored utilizing total scores, with higher scores indicating more perceived multicultural competence. Cronbach’s alpha results for this study were .92 for clients and .85 for CITs (Lafromboise et al., 1991).
The WAI-S (Horvath & Greenberg, 1989; Tracey & Kokotovic, 1989) was used to measure client and CIT perceptions about the strength of the working alliance relationship in counseling. The WAI-S is a 12-item assessment rated on a 7-point Likert scale ranging from 1 to 7 (1 = never to 7 = always), intended to measure the strength of the therapeutic relationship as perceived by client and counselor (e.g., Client: I am confident in my counselor’s ability to help me; Counselor: I am confident in my ability to help my client; Bachelor, 2013; Fitzpatrick et al., 2005; Hatcher & Barends, 1996). Tracey and Kokotovic (1989) indicated strong internal consistency for both the client version (α = .98) and the counselor version (α = .95) of the WAI-S. The WAI-S total score is the summation of three subscales (task, bond, and goal), with higher scores indicating a stronger therapeutic relationship. Cronbach’s alpha results for this study were .82 for clients and .81 for CITs.
The SDS (Reynolds,1982) was used to measure social desirability in this study. The SDS is a shortened version of the original Marlow Crowne Social Desirability Scale (MCSDS; Crowne & Marlow, 1960). The SDS is an 11-item dichotomous (i.e., 0 = True, 1 = False) scale designed to assess whether participants are responding truthfully in response to assessments or answering in a biased way to put forward a more socially desirable self-image (e.g., I’m always willing to admit when I make a mistake). Scoring ranges from 0–11, with a higher score indicating participant likelihood of answering in a socially desirable manner to avoid disapproval from others. Reliability for the shortened social desirability scales has been adequate (Reynolds, 1982). Cronbach’s alpha results for this study were .68 for clients and .73 for CITs. Clients’ SDS Cronbach’s alpha levels were slightly lower than the CITs’ levels; however, some authors, such as Aiken (2000), have indicated that a Cronbach’s alpha between .60 and .70 is adequate, and Streiner (2003) has indicated that the reliability on a scale of clinical samples such as the clients in this study can be different than those measured on the general population.
The OQ 45.2 (Lambert et al., 1996) contains 45 items rated on a 5-point Likert scale ranging from 0–4 (0 = almost always to 4 = never) and intended to measure clients’ distress status (e.g., I feel blue; I feel lonely). The OQ 45.2 has been used in various settings, including community clinics in a university setting similar to the one in this investigation (e.g., Wolgast, Lambert, & Puschner, 2004). The OQ 45.2 total score consists of the sum of scores of three subscales (i.e., symptomatic distress, interpersonal relationships, and social roles) and the reverse scores of nine items, with higher scores indicating more distress among clients. The total score cut off is set at 63, indicating that scores above 63 are of clinical significance (Lambert et al., 1996). Reported overall internal consistency for OQ total score (α = 93) and three subscales (α = .70) is strong (Lambert et al., 1996). Cronbach’s alpha results for this study were .82 for the OQ 45.2 pretest and .83 for the OQ 45.2 posttest.
Results
Average total scores for clients on the OQ 45.2 pretest, completed on the first session, were M = 69.37 and SD = 25.009. Average OQ 45.2 posttest scores, completed on the third session, were M = 63.73 and SD = 27.56. Average total SDS scores for clients were M = 5.74 and SD = 2.27, and average scores for CITs were M = 5.71 and SD = 2.66. Average total score of clients’ CCCI-R ratings of their CITs’ multicultural competence after completion of the third counseling session were M = 102.81 and SD = 10.42. CITs’ ratings of their own multicultural competence were M = 96.98 and SD = 7.66. Lastly, average total WAI-S scores for clients were M = 64.63 and SD = 8.0, and CITs’ scores were M = 59.40 and SD = 7.61.
A Pearson product two-tailed correlation identified four significant relationships between the variables with effect sizes ranging from small to large (Cohen, 1992). Positive relationships were indicated between clients’ perceptions of CITs’ multicultural competence and the working alliance (r =.571, p <.05), as well as CITs’ perceptions of their multicultural competence and the working alliance (r = .623, p < .05), and between the OQ 45.2 pre- and posttest scores (r = .884, p < .05). Further, a positive relationship was found between clients’ and counselors’ perceptions of the working alliance (r = .199, p < .05) and between social desirability scores on CITs’ CCCI-R responses (r = .233, p < .05); however, the effect sizes were small. The positive relationships indicate that the direction of one construct is associated with the direction of the other. For example, how a client rates their CIT’s multicultural competence is associated with the strength (high or low) of the working alliance. Lastly, a negative relationship was found between clients’ social desirability scores with both client outcome OQ 45.2 pretest scores (r = -.233, p < .05) and OQ 45.2 posttest scores (r = -.277, p < .05). This negative relationship means that higher scores on one instrument are associated with lower scores on another.
Predictors of Client Outcomes
In order to assess whether multicultural competence or the working alliance predicted client outcomes, the third-session OQ 45.2 posttest score was the dependent variable and the pretest score of the OQ 45.2 was the control variable. A hierarchical regression is used when the researcher has a theoretical basis to specify the order in which the independent variables are entered into the model (Tabachnick & Fidell, 2013). In the following analyses, social desirability and OQ 45.2 first-session scores were used as control variables. It is common practice within social sciences to use pretest scores as a control variable and posttest scores as a dependent measure in order to reduce error variance and create more powerful tests for data analysis (Tabachnick & Fidell, 2013). Also, social desirability was used as a control variable because of the relationships indicated in the correlation analysis with SDS, OQ 45.2, and CITs’ CCCI-R responses. Further, SDS scores were used as a control variable to minimize potential threat to the study (Drisko, 2013), which can improve the accuracy of the research design (McKibben & Silvia, 2016), because self-report measures have been shown to have a strong likelihood of participants responding in a socially desirable manner (DeVellis, 2003; Gall, Gall, & Borg, 2007).
Hierarchical multiple regression analysis was used to explore whether CITs’ multicultural competence (CCCI-R) and working alliance (WAI-S; as perceived by clients) predicted client outcome (OQ 45.2 pretest), while controlling for social desirability (SDS) from clients’ perspective and clients’ outcome pretest scores (OQ 45.2 posttest). Client outcome OQ 45.2 pretest scores and SDS scores were entered in the first block, explaining 78.6% [F (2, 116) = 213.3, p < .05] of the variance in client outcome OQ 45.2 posttest scores. After entry of clients’ CCCI-R and WAI-S total scores in the second block, the total variance explained by the model as a whole was 78.9%, [F (4, 114) = 106.80 p < .05]. The introduction of clients’ CCCI-R and WAI-S scores only explained an additional variance of 0.3%, after controlling for client pretest scores and social desirability [R2 change = .003, F (2, 114) = .851, p > .05]. In the final model, only one of the four predictor variables was statistically significant, client outcome pretest score (b = .859, p < .05; see Table 1). The final model indicated a large effect size (R2 = .789; Cohen, 1992). Close to 79% of the variance in posttest scores was accounted for by OQ 45.2 first-session scores on client outcomes, after controlling for social desirability response.
Table 1
Hierarchical Regression Client Perspective
|
B |
SE b |
β
|
R2
|
ΔR2 |
| Step 1: Control Variables
Client Outcome Pretest
Client Social Desirability
|
.954
-.913 |
.049
.534 |
.866*
-.076 |
.786
|
.786*
|
| Step 2: Client Perspective
Client Outcome Pretest
Client Social Desirability
Client CCCI-R
Client WAI-S |
.947
-.991
.183
-.119 |
.049
.547
.140
.152 |
.859*
-.082
.069
-.041
|
.789
|
.003
|
Note. N = 119 clients; CCCI-R Counselor Multicultural Competence; WAI-S Working Alliance. *p < .05.
Dependent Variable: Client Outcome Posttest.
Another hierarchical multiple regression analysis was used to explore whether CITs’ multicultural competence (CCCI-R) and working alliance (WAI-S; as perceived by counselors) predicted client outcomes (OQ 45.2 pretest), while controlling for social desirability (SDS) from the CITs’ perspective (OQ 45.2 posttest). Client outcome pretest score and CITs’ SDS total scores were entered in the first block, explaining 78.1% of the variance [F (2,116) = 206.60, p < .05] in client outcome OQ 45.2 posttest scores. After entry of counselors’ CCCI-R and WAI-S total scores in the second block, the total variance explained by the model as a whole was 79.6% [F (4,114) = 111.38, p < .05]. The introduction of counselors’ CCCI-R and WAI-S scores explained an additional variance of 1.5%, after controlling for client pretest score and social desirability [R2 change = .015, F (2, 114) = 4.32, p < .05]. In the final model, two of the four predictor variables were statistically significant: client outcome pretest score (b = .894, p < .05) and counselors’ CCCI-R (b = -.157, p < .05; see Table 2). The final model indicated a large effect size (R2 =.796; Cohen, 1992). In this model, 80% of the variance in posttest scores was accounted for by OQ 45.2 first session scores on client outcomes and CITs’ multicultural competence, after controlling for social desirability response.
The final research question explored the differences that exist between clients’ and counselors’ perceptions of CITs’ multicultural competence and the working alliance, while controlling for social desirability. In order to resolve the possibility of non-independence in this data set (West, Welch, & Galecki, 2007), a linear mixed-effects model was used to compare clients and counselors (fixed effect) for the dependent variables of multicultural competence and the working alliance. Thus, accounting for client observations nested within counselors (i.e., some CITs had several clients). There was a significant difference between counselor and client perceptions of CITs’ multicultural competence while controlling for social desirability: [F (1,174.38) = 30.43, p < 0.05]. The average CCCI-R score for clients was 5.91 more than the average for CITs, after controlling for social desirability. Similarly, there was a significant difference between counselor and client perceptions of the working alliance (WAI-S): [F (1, 176.20) = 79.98, p < 0.05]. The average WAI-S score for clients was 9.85 more than the average for CITs, controlling for social desirability. Thus, clients rated CITs’ multicultural competence and the working alliance higher than CITs rated themselves.
Table 2
Hierarchical Regression Counselor Perspective
|
B |
SE b |
β
|
R2 |
ΔR2 |
| Step 1: Control Variables
Client Outcome Pretest
Counselor Social Desirability |
.974
.012 |
.048
.450 |
.884
.001 |
.781
|
.781*
|
| Step 2: Counselor Perspective
Client Outcome Pretest
Counselor Social Desirability
Counselor CCCI-R
Counselor WAI-S
|
.985
.282
-.563
.192 |
.047
.451
.198
.167 |
.894*
.027
-.157*
.062 |
.796
|
.015*
|
Note. N = 72 clients; CCCI-R Counselor Multicultural Competence; WAI-S Working Alliance. *p <.05.
Dependent Variable: Client Outcome Posttest.
Discussion
The aim of this investigation was to explore the relationship between client outcomes, counselors’ multicultural competence, the working alliance, and social desirability from both clients’ and CITs’ perspectives. Hierarchical regression results indicated that clients’ perspectives of their CITs’ multicultural competence and the working alliance did not predict client outcomes, although CITs’ perceptions of their multicultural competence did, modestly, after controlling for counselors’ social desirability scores. In a related investigation, Owen et al. (2011) compared differences in perceptions of counselors’ multicultural competence between clients and CITs. Results from their intra-class correlation (ICC) analysis indicated that CITs’ perceptions accounted for 8.5% (ICC = .085) of the variance in client outcomes, although clients’ perceptions of CITs’ multicultural competence were not related to clients’ counseling outcomes, which is consistent with the findings from this investigation. In contrast, results from this investigation on the working alliance and lack of predictive ability on client outcomes are incongruent with previous research that indicates a strong association between the working alliance and client outcomes (Horvath, Del Re, Flückiger, & Symonds, 2011; Norcross, 2011). Although results from one hierarchical regression did not indicate significant predictability of the working alliance on client outcomes, a Pearson product correlation conducted before regression analysis supported the positive associations between clients’ perceptions of CITs’ multicultural competence and the working alliance, as well as CITs’ perceptions of their multicultural competence and the working alliance. Further, correlational results indicated a small association between clients’ and CITs’ perceptions of the working alliance, and between CITs’ social desirability scores and CCCI-R responses.
Potential explanations for some of the insignificant findings in this investigation include the cross-sectional research design on the constructs of multicultural competence and the working alliance. In a cross-sectional research design, the researcher looks at a snapshot of constructs at one point in time (Gall et al., 2007). In this investigation, multicultural competence and the working alliance were assessed after the third session for both clients and counselors. Thus, assessing multicultural competence and the working alliance after the third session may not have been enough time for clients to evaluate their counseling relationship or their CITs’ multicultural competence. For example, Fitzpatrick et al. (2005) explored clients’ perceptions of the working alliance utilizing the WAI-S over three phases of counseling (e.g., early: 2–4 sessions; middle: midpoint; late: fourth, third, or second to last). Fitzpatrick and colleagues (2005) conducted a MANOVA with two within-subject design factors. The two factors were phases of counseling (i.e., early, middle, late) and WAI subscales (i.e., task, bond, goal). Results indicated as a whole, client-rated alliance increased over time. Therefore, results of this analysis may have been different if multicultural competence and the working alliance were measured over time.
Linear modeling results indicated significant differences between client and CIT perceptions of the working alliance and counselors’ multicultural competence after controlling for social desirability. In addition, upon inspection of the mean scores between clients and CITs, clients rated their CITs’ multicultural competence and the working alliance higher than CITs rated their multicultural competence and the working alliance. Similar to this investigation, Depue, Lambie, Liu, and Gonzalez (2016) found significant differences on client and CIT ratings of the working alliance, with clients rating the working alliance higher than counselors. Contrastingly, Fuertes and colleagues (2006) found no significant differences between the working alliance for clients or CITs and significant differences between perceptions of counselors’ multicultural competence, with CITs’ ratings being higher than clients, highlighting mixed research findings.
A factor that may influence the perceptions of clients and CITs is the way clients and counselors would define counseling terms. First, clients and CITs may differ in their definition of what a quality therapeutic relationship or what a culturally responsive CIT looks like. For example, counselors may view the strength of the therapeutic relationship based on client progress (Bachelor & Horvath, 1999), while clients may view the quality of the relationship based on how much unconditional positive regard they sense from their counselors (Norcross, 2011). Similarly, with multicultural competence, Pope-Davis et al. (2002) suggested that clients may not perceive multicultural competence in the same way as counselors. A common theme found in Pope-Davis et al.’s (2002) qualitative investigation on client perceptions of culturally relevant components in counseling indicated that the need for integration of culture in counseling was only relevant if the client self-identified their culture as a core value in their life. On the other hand, counselors may view their level of multicultural competence based on how much knowledge they have about their clients’ cultures.
Second, counselors’ level of experience might influence the way they rate themselves. For example, novice counselors, such as the participants in this investigation, often have anxiety that can negatively influence their beliefs about their counseling performance (Rønnestad & Skovholt, 2003; Stoltenberg & McNeill, 2010). Barden and Greene (2015) explored the relationship between counselor education students’ levels of self-reported multicultural counseling competence and multicultural counseling self-efficacy, with results indicating that students who had been in graduate education longer had higher self-reported multicultural counseling competence and higher levels of multicultural knowledge, highlighting a potential explanation for lower multicultural competence ratings in the current investigation.
Implications for Counselors
In this investigation, results highlighted that clients and CITs perceive the working alliance and counselors’ multicultural competence differently. Counselors might want to give assessments such as the CCCI-R (LaFromboise et al., 1991) or the WAI-S (Tracey & Kokotovic, 1989) in session to facilitate discussions with clients. For example, if counselors see that their client strongly disagrees with the CCCI-R assessment question 20, “My counselor acknowledges and is comfortable with cultural differences,” counselors can utilize this as a discussion point to address any cultural differences that may be interfering with the counseling process. Furthermore, in this study, positive relationships were shown between clients’ and counselors’ perceptions of counselors’ multicultural competence and the working alliance. Given these associations, counselors are encouraged to self-reflect and explore how their clients view the relationship between the working alliance and multicultural competence. Slone and Owen (2015) explored the relationship between the effects of the therapeutic relationship, counselors’ level of comfort in session, and the systematic alliance on client outcomes between counselors and clients. Multilevel model analysis revealed that client outcome improved when counselors checked in with clients about how the therapeutic relationship was going, when counselors had a high comfort level in session, and when clients had perceived interpersonal networks that aligned with the goals and tasks in counseling. Thus, counselors are encouraged to check in with clients about their views at multiple times throughout the counseling process. For example, CITs can ask clients probing points early on to promote discussion on the working alliance and multicultural competence, such as, “What are you looking for in a counseling relationship?” or “Please tell me a little bit about your culture.” Moreover, counselors can check in with a client mid-session and ask, “How has our counseling relationship been going?” or “What would improve our counseling relationship?”
This study also highlighted the importance of exploring what has already been working for clients before coming to counseling. The therapeutic relationship has been shown to have the most explained variance in client outcomes (Norcross, 2011; Wampold & Imel, 2015); however, in this investigation, it was found that 80% of the variance in client outcomes after the third session was predetermined. Given that close to 80% of the variance in posttest scores were accounted for by OQ 45.2 first-session scores on client outcomes after controlling for social desirability responses, counselors are encouraged to explore what coping strategies clients are already using that have been helpful with their clients’ presenting issues during the first session. In addition, counselor educators can consider that three weeks of counseling may not be enough time to show clinically significant change in client outcomes. Furthermore, three weeks in counseling may not be enough time to show how the working alliance and CITs’ multicultural competence may influence client outcomes. Lastly, given that there was a positive relationship between CITs’ social desirability scores and their ratings of their multicultural competence, counselor educators who supervise CITs are encouraged to explore their supervisees’ expectations and comfort in discussing developing multicultural competence.
Limitations and Suggestions for Future Research
The first limitation is that the multicultural competence and working alliance assessments were collected in a cross-sectional manner, limiting the results to a singular time point. Second, the generalizability to populations other than novice counselors or clients within a university setting is low. Third, at the time data collection for this investigation was completed, there was not a validated formative assessment developed to explore the updated social justice framework based on the new MSJCC competencies, so the instrument used was based on the Multicultural Competence Tripartite Model. Despite the limitations from this investigation, the use of a social desirability scale, an emphasis on both clients’ and CITs’ perceptions, and the study’s implications contribute to the empirical research on multicultural competence and the working alliance.
There are several implications for future research that are suggested from this study. First, researchers can conduct a longitudinal design and increase data collection points for assessing client outcome (e.g., first, fifth, tenth, and fifteenth sessions) to determine if and when clinically significant change in client outcomes occurs. Second, further exploration is needed of the perceptions of counselors who have completed their training programs to see how results may differ. Third, researchers are encouraged to develop a formative assessment tool to explore the new MSJCCs (Ratts et al., 2015) and replicate a similar study. Researchers are encouraged to explore, from the clients’ perspectives, how their counselors are implementing multicultural and social justice competencies. Fourth, investigators can implement a mixed method design (e.g., qualitative and quantitative) to explore factors that influence client outcomes for brief therapy. Utilizing a qualitative component may help counselors and counselor educators gain insight into what clients perceive a culturally sensitive counselor to be or what a strong working alliance looks like. Lastly, counselor educators can continue to investigate how social desirability, if at all, influences participants’ responses on counseling assessments.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aiken, L. R. (2000). Psychological testing and assessment (10th ed.). Boston, MA: Allyn & Bacon.
American Counseling Association. (2014). ACA code of ethics. Alexandria, VA: Author.
Ardito, R. B., & Rabellino, D. (2011). Therapeutic alliance and outcome of psychotherapy: Historical excursus, measurements, and prospects for research. Frontiers in Psychology, 2, 270. doi:10.3389/fpsyg.2011.00270
Arredondo, P., Toporek, R., Brown, S. P., Jones, J., Locke, D. C., Sanchez, J., & Stadler, H. (1996). Operationalization of the multicultural counseling competencies. Journal of Multicultural Counseling and Development, 24, 42–78. doi:10.1002/j.2161-1912.1996.tb00288.x
Bachelor, A. (2013). Clients’ and therapists’ views of the therapeutic alliance: Similarities, differences and relationship to therapy outcome. Clinical Psychology & Psychotherapy, 20(2), 118–135. doi:10.1002/cpp.792
Bachelor, A., & Horvath, A. (1999). The therapeutic relationship. In M. A. Hubble, B. L. Duncan, & S. D. Miller (Eds.), The heart and soul of change: What works in therapy (pp. 133–178). Washington, DC: American Psychological Association.
Baldwin, S. A., Wampold, B. E., & Imel, Z. E. (2007). Untangling the alliance-outcome correlation: Exploring the relative importance of therapist and patient variability in the alliance. Journal of Consulting and Clinical Psychology, 75, 842–852. doi:10.1037/0022-006X.75.6.842
Barden, S. M., & Greene, J. H. (2015). An investigation of multicultural counseling competence and multicultural counseling self-efficacy for counselors-in-training. International Journal for the Advancement of Counselling, 37, 41–53. doi:10.1007/s10447-014-9224-1
Cohen, J. (1992). A power primer. Psychological Bulletin, 112, 155–159.
Collins, S., & Arthur, N. (2010). Culture-infused counselling: A model for developing multicultural competence. Counselling Psychology Quarterly, 23, 217–233. doi:10.1080/09515071003798212
Constantine, M. G. (2001). Predictors of observer ratings of multicultural counseling competence in Black, Latino, and White American trainees. Journal of Counseling Psychology, 48, 456–462.
doi:10.1037/0022-0167.48.4.456
Constantine, M. G. (2002). Predictors of satisfaction with counseling: Racial and ethnic minority clients’ attitudes toward counseling and ratings of their counselors’ general and multicultural counseling competence. Journal of Counseling Psychology, 49, 255–263. doi:10.1037/0022-0167.49.2.255
Constantine, M. G., & Ladany, N. (2000). Self-report multicultural counseling competence scales: Their relation to social desirability attitudes and multicultural case conceptualization ability. Journal of Counseling Psychology, 47, 155–164. doi:10.1037/0022-0167.47.2.155
Council for Accreditation of Counseling and Related Educational Programs. (2016). CACREP Standards. Retrieved from http://www.cacrep.org/for-programs/2016-cacrep-standards/
Crowne, D. P., & Marlowe, D. (1960). A new scale of social desirability independent of psychopathology.
Journal of Consulting Psychology, 24, 349–354. doi:10.1037/h0047358
D’Andrea, M., & Heckman, E. F. (2008). A 40-year review of multicultural counseling outcome research: Outlining a future research agenda for the multicultural counseling movement. Journal of Counseling & Development, 86, 356–363. doi:10.1002/j.1556-6678.2008.tb00520.x
DePue, M. K., Lambie, G. W., Liu, R., & Gonzalez, J. (2016). Investigating supervisory relationships and therapeutic alliances using structural equation modeling. Counselor Education and Supervision, 55, 263–277. doi:10.1002/ceas.12053
DeVellis, R. F. (2003). Scale development: Theory and applications (2nd ed.). Thousand Oaks, CA: Sage.
Drisko, J. (2013). The common factors model: Its place in clinical practice and research. Smith College Studies in Social Work, 83, 398–413. doi:10.1080/00377317.2013.833435
Fitzpatrick, M. R., Iwakabe, S., & Stalikas, A. (2005). Perspective divergence in the working alliance. Psychotherapy Research, 15(1–2), 69–80. doi:10.1080/10503300512331327056
Fuertes, J. N., & Brobst, K. (2002). Clients’ ratings of counselor multicultural competency. Cultural Diversity and Ethnic Minority Psychology, 8, 214–223. doi:10.1037/1099-9809.8.3.214
Fuertes, J. N., Stracuzzi, T. I., Bennett, J., Scheinholz, J., Mislowack, A., Mindy, H., & Cheng, D. (2006). Therapist multicultural competency: A study of therapy dyads. Psychotherapy: Theory, Research, Practice, Training, 43, 480–490. doi:10.1037/0033-3204.43.4.480
Gall, M. D., Gall J. P., & Borg, W. R. (2007). Educational research: An introduction (8th ed.). Boston, MA: Allyn & Bacon.
Hatcher, R. L., & Barends, A. W. (1996). Patients’ view of the alliance in psychotherapy: Exploratory factor analysis of three alliance measures. Journal of Consulting and Clinical Psychology, 64, 1326–1336. doi:10.1037/0022-006X.64.6.1326
Hays, D. G., & Erford, B. T. (2017). Developing multicultural counseling competence: A systems approach (3rd ed.). New York, NY: Pearson.
Horvath, A. O., & Bedi, R. P. (2002). The alliance. In J. C. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 37–70). New York, NY: Oxford University Press.
Horvath, A. O., Del Re, A. C., Flückiger, C., & Symonds, D. (2011). Alliance in individual psychotherapy. Psychotherapy: Theory, Research, Practice, Training, 48, 9–16. doi:10.1037/a0022186
Horvath, A. O., & Greenberg, L. S. (1989). Development and validation of the Working Alliance Inventory. Journal of Counseling Psychology, 36, 223–233. doi:10.1037/0022-0167.36.2.223
Huppert, J. D., Kivity, Y., Barlow, D. H., Gorman, J. M., Shear, M. K., & Woods, S. W. (2014). Therapist effects
and the outcome–alliance correlation in cognitive behavioral therapy for panic disorder with
agoraphobia. Behaviour Research and Therapy, 52, 26–34. doi:10.1016/j.brat.2013.11.001
Katz, A. D., & Hoyt, W. T. (2014). The influence of multicultural counseling competence and anti-Black prejudice on therapists’ outcome expectancies. Journal of Counseling Psychology, 61, 299–305.
doi:10.1037/a0036134
LaFromboise, T. D., Coleman, H. L. K., & Hernandez, A. (1991). Development and factor structure of the Cross-Cultural Counseling Inventory—Revised. Professional Psychology: Research and Practice, 22, 380–388. doi:10.1037/0735-7028.22.5.380
Lambert, M. J., Burlingame, G. M., Umphress, V., Hansen, N. B., Vermeersch, D. A., Clouse, G. C., & Yanchar, S. C. (1996). The reliability and validity of the Outcome Questionnaire. Clinical Psychology & Psychotherapy, 3, 249–258. doi:10.1002/(SICI)1099-0879(199612)3:4<249::AID-CPP106>3.0.CO;2-S
Li, L. C., & Kim, B. S. (2004). Effects of counseling style and client adherence to Asian cultural values on counseling process with Asian American college students. Journal of Counseling Psychology, 51(2), 158-167. doi:10.1037/0022-0167.51.2.158}
McKibben, W. B., & Silvia, P. J. (2016). Inattentive and socially desirable responding: Addressing subtle threats to validity in quantitative counseling research. Counseling Outcome Research and Evaluation, 7, 53–64. doi:10.1177/2150137815613135
Norcross, J. C. (Ed.). (2002). Psychotherapy relationships that work: Therapist contributions and responsiveness to patients. New York, NY: Oxford University Press.
Norcross, J. C. (Ed.). (2011). Psychotherapy relationships that work: Evidence-based responsiveness (2nd ed.). New York, NY: Oxford University Press.
Owen, J., Leach, M. M., Wampold, B., & Rodolfa, E. (2011). Client and therapist variability in clients’ perceptions of their therapists’ multicultural competencies. Journal of Counseling Psychology, 58, 1–9. doi:10.1037/a0021496
Pope-Davis, D. B., Toporek, R. L., Ortega-Villalobos, L., Ligiéro, D. P., Brittan-Powell, C. S., Liu, W. M., . . . & Liang, C. T. H. (2002). Client perspectives of multicultural counseling competence: A qualitative examination. The Counseling Psychologist, 30, 355–393. doi:10.1177/0011000002303001
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. Retrieved from www.counseling.org/knowledge-center/competencies
Reynolds, W. M. (1982). Development of reliable and valid short forms of the Marlowe-Crowne Social Desirability Scale. Journal of Clinical Psychology, 38, 119–25.
doi:10.1002/1097-4679(198201)38:1<119::AID-JCLP2270380118>3.0.CO;2-I
Rønnestad, M. H., & Skovholt, T. M. (2003). The journey of the counselor and therapist: Research findings and perspectives on professional development. Journal of Career Development, 30, 5–44. doi:10.1023/A:1025173508081
Slone, N. C., & Owen, J. (2015). Therapist alliance activity, therapist comfort, and systematic alliance on individual psychotherapy outcome. Journal of Psychotherapy Integration, 25, 275–288.
doi:10.1037/a0039562
Smith, T. B., & Trimble, J. E. (2016). Foundations of multicultural psychology: Research to inform effective practice. Washington, DC: American Psychological Association.
Soto, A., Smith, T. B., Griner, D., Rodríguez, M. D., & Bernal, G. (2018). Cultural adaptations and therapist multicultural competence: Two meta-analytic reviews. Journal of Clinical Psychology, 1–17.
doi:10.1002/jclp.22679
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). New York, NY: Routledge.
Streiner, D. L., (2003). Starting at the beginning: An introduction to coefficient alpha and internal consistency. Journal of Personality Assessment, 80, 99–103. doi:10.1207/S15327752JPA8001_18
Sue, D. W., Arredondo, P., & McDavis, R. J. (1992). Multicultural counseling competencies and standards: A call to the profession. Journal of Counseling & Development, 70, 477–486.
doi:10.1002/j.1556-6676.1992.tb01642.x
Sue, D. W., Bernier, J. E., Durran, A., Feinberg, L., Pedersen, P., Smith, E. J., & Vasquez-Nuttall, E. (1982). Position paper: Cross-cultural counseling competencies. The Counseling Psychologist, 10(2), 45–52. doi:10.1177/0011000082102008
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Boston, MA: Allyn & Bacon.
Tao, K. W., Owen, J., Pace, B. T., & Imel, Z. E. (2015). A meta-analysis of multicultural competencies and psychotherapy process and outcome. Journal of Counseling Psychology, 62, 337–350.
doi:10.1037/cou0000086
Tracey, J. T., & Kokotovic, A. M. (1989). Factor structure of the Working Alliance Inventory. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 1, 207–210. doi:10.1037/1040-3590.1.3.207
Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.). New York, NY: Routledge.
West, B. T., Welch, K. E., & Galecki, A. T. (2007). Linear mixed models: A practical guide using statistical software. Boca Raton, FL: Chapman-Hall/CRC.
Wolgast, B. M., Lambert, M. J., & Puschner, B. (2004). The dose-response relationship at a college counseling center. Journal of College Student Psychotherapy, 18(2), 15–29. doi:10.1300/J035v18n02_03
Worthington, R. L., Mobley, M., Franks, R. P., & Tan, J. A. (2000). Multicultural counseling competencies: Verbal content, counselor attributions, and social desirability. Journal of Counseling Psychology, 47, 460–468. doi:10.1037/0022-0167.47.4.460
Worthington, R. L., Soth-McNett, A. M., & Moreno, M. V. (2007). Multicultural counseling competencies research: A 20-year content analysis. Journal of Counseling Psychology, 54, 351–361.
doi:10.1037/0022-0167.54.4.351
Nov 12, 2018 | Volume 8 - Issue 4
Jeffrey M. Warren, Leslie A. Locklear, Nicholas A. Watson
This study explored the relationships between parenting beliefs, authoritative parenting style, and student achievement. Data were gathered from 49 parents who had school-aged children enrolled in grades K–12 regarding the manner in which they parent and their child’s school performance. Pearson product-moment correlation coefficients and multiple regression modeling were used to analyze the data. Findings suggested that parent involvement, suspension, and homework completion significantly accounted for the variance explained in grade point average. Authoritativeness was positively and significantly related to both rational and irrational parenting beliefs. Irrational parenting beliefs were positively and significantly related to homework completion. School counselors are encouraged to consider the impact of parenting on student success when developing comprehensive programming.
Keywords: student achievement, homework completion, irrational parenting beliefs, authoritative parenting, school counseling
There are many indicators of success as students matriculate through elementary, middle, and high school. Student success is generally defined by the degree to which students meet or exceed a predetermined set of competencies (York, Gibson, & Rankin, 2015). These competencies are often academic in nature and align with state curriculum. Data collected at numerous points (i.e., formal and informal assessment) throughout an academic year are used to monitor student performance. Student achievement data, including end-of-grade tests and grade point average (GPA), are key determinants of student outcomes such as promotion or retention (Schwerdt, West, & Winters, 2017). Although both are distal data points that measure achievement, GPA is a cumulative measure of student performance based on mental ability, motivation, and personality demonstrated throughout the course of a school year (Imose & Barber, 2015; Spengler, Brunner, Martin, & Lüdtke, 2016).
Numerous factors are related to and impact student achievement. According to Hatch (2014), these factors include discipline referrals, suspension, homework completion, and parental involvement. Research suggests that these factors are good indicators of distal or long-term academic success (Kalenkoski & Pabilonia, 2017; LeFevre & Shaw, 2012; Noltemeyer, Ward, & Mcloughlin, 2015; Roby, 2004). Although it is a challenge to determine student progress based on GPA alone, these variables can be monitored across the school year for a real-time snapshot of student success (Hatch, 2014).
The American School Counselor Association (ASCA; 2012) has suggested that school counselors work to promote student success by operating across three distinct areas or domains: academic, social and emotional, and career development. As such, school counselors play an integral role in developing, delivering, and evaluating programs that promote academic achievement. School counselors are challenged to determine the direct impact of services on student achievement. Student achievement–related data can be measured to understand the impact of school counseling interventions. For example, a study skills curriculum such as SOAR® (SOAR Learning Inc., 2018) may increase homework completion by 20%. School counselors can infer that the intervention will lead to increases in student achievement; literature suggests homework completion is positively correlated with GPA (Kalenkoski & Pabilonia, 2017).
Although school counselors often work directly with students, they also can engage in efforts to promote student achievement through work with parents and families. For example, Ray, Lambie, and Curry (2007) suggested school counselors can offer parenting skills training to promote positive parenting practices. Other authors have advocated to strengthen the partnerships with and involvement of parents, which are factors related to student achievement (Bryan & Henry, 2012; Epstein, 2018). In developing interventions that aim to build partnership and increase involvement, it is important for school counselors to understand the values, assumptions, beliefs, and behaviors of parents (Bryan & Henry, 2012). During the initial stages of partnering with families, school counselors should address any biases and assumptions that may impede the partnership (Warren, 2017). Furthermore, strategies and interventions should be data-driven and aim to promote student achievement (Hatch, 2014). In the current study, researchers examined the relationships between parenting beliefs, authoritative parenting style, and student achievement. School counselors who understand the relationships between these factors are best positioned to meet the needs of all students.
Parenting Beliefs
The beliefs parents maintain are especially pertinent to the overall wellness and success of their children (Warren, 2017). At times, parents may place unreasonable demands on themselves, their children, or the practice of parenting in general. For example, a parent may think, “My child should always do what I say, and I cannot stand it otherwise.” This belief can have a detrimental impact on the parent–child relationship and family unit as well as the psychosocial development of the child (Bernard, 1990).
Rational emotive behavior therapy (REBT), developed by Ellis (1962), emphasizes two main types of thoughts pertinent to the beliefs of parents: rational and irrational. Rational thoughts are flexible and preferential in nature. These thoughts lead to healthy emotions and functional behaviors. Alternatively, irrational beliefs are rigid and dogmatic and stem from demands placed on the self, others, and life. “Life should always treat me fairly and it is horrible when it does not,” is an example of an irrational belief. This belief can lead to unhealthy emotions (e.g., anger, depression) and result in unhelpful or dysfunctional behavior.
A central goal of REBT is to advance acceptance of the self, others, and life in general. In turn, individuals are encouraged to abstain from global evaluations or rating the self, others, or life as totally bad. When striving toward acceptance, individuals are happier and more successful in life (Dryden, 2014). Researchers have studied REBT and associated constructs among various populations, including children (Gonzalez et al., 2004; Sapp, 1996; Sapp, Farrell, & Durand, 1995; Warren & Hale, 2016), teachers (Warren & Dowden, 2012; Warren & Gerler, 2013), college students (McCown, Blake, & Keiser, 2012; Warren & Hale, in press), and parents (Terjesen & Kurasaki, 2009; Warren, 2017). Literature suggests a strong correlation between irrational beliefs and dysfunction, regardless of the measure used or sample under investigation.
Findings from Hamamci and Bağci (2017) have suggested that a relationship exists between family functioning and the degree to which parents hold irrational expectations about their children. Emotional support and responsiveness of parents deteriorate with an increase in irrational beliefs. Additionally, child behavior issues are more prevalent when parents think irrationally. Hojjat et al. (2016) found that children are more susceptible to substance abuse when their parents maintain irrational beliefs and unrealistic expectations. Parenting styles that advance unrealistic or irrational academic expectations may stifle academic success and promote the development of irrational beliefs and unhealthy negative emotions (e.g., anxiety) in children (Kufakunesu, 2015).
Parenting Styles
Parenting style is most often used to broadly describe how parents interact with their children. In 1966, Diana Baumrind presented three major parenting styles: authoritarian, authoritative, and permissive. Later, Maccoby and Martin (1983) identified a fourth style of parenting: neglectful. Parenting styles are defined by collections of attitudes and behaviors expressed to children by their parents (Darling & Steinberg, 1993) and are often based upon the degree of demandingness/control and responsiveness. Parents who maintain an authoritarian parenting style are highly demanding, yet emotionally unresponsive, while authoritative parents exude high demands, but are communicative and responsive (Baumrind, 1991). Permissive parents, on the other hand, are responsive, yet lack firm control of their children; neglectful parenting involves a lack of emotional support as well as little control (Pinquart, 2016).
The manner in which parents parent can impact their child’s success in school. Of the four parenting styles described, research findings suggested that models of parenting aligning with the authoritative parenting style are most closely linked to student achievement (Carlo, White, Streit, Knight, & Zeiders, 2018; Castro et al., 2015; Kenney, Lac, Hummer, Grimaldi, & LaBrie, 2015; Masud, Thurasamy, & Ahmad, 2015). Additionally, the impact of parenting style on student success seems to vary little across culture. A meta-analysis conducted by Pinquart and Kauser (2018) suggested that children across the world may benefit academically from authoritative parents. Although a plethora of evidence supporting this relationship exists, a meta-analysis conducted by Pinquart (2016) found a small effect size, suggesting the relationship between authoritative parenting and student achievement is minimal. Regardless, the manner in which parents interact with their children impacts many aspects of child development, including their ability to succeed in school.
Purpose of the Study
This article explores the relationships between parenting beliefs, styles, and student achievement. Ellis, Wolfe, and Moseley (1981) suggested parents’ behaviors stem from their thoughts and emotions. These beliefs impact the manner in which parents interact with their children. For example, parents who hold rigid or extreme beliefs may respond to their children more negatively than parents who maintain a flexible belief system. As such, parenting beliefs may impact parenting style, and therefore the success of students. However, the literature is scant when exploring the relationships between parenting beliefs, parenting style, and student achievement.
In order to work effectively with parents, it is important that school counselors understand parenting beliefs and styles and their impact on student achievement. Several research questions guided this study, including: (a) Is there a relationship between student achievement and parental involvement, homework completion, discipline referrals, and suspensions?; (b) Is authoritative parenting related to student achievement?; and (c) Are parenting beliefs related to student achievement? Based on these research questions and existing literature, the following hypotheses were generated: Hypothesis #1: A significant relationship exists between GPA and student achievement–related variables. Hypothesis #2: Rational, irrational, and global evaluation parenting beliefs are predictive of authoritative parenting. Hypothesis #3: Authoritative parenting is significantly positively related to student achievement. Hypothesis #4: Parenting beliefs are significantly related to student achievement–related variables.
Method
Participants
This study included parents living in the southeastern United States (N = 49) who self-reported having children enrolled in elementary, middle, or high school. Of the participants, 96% (n = 47) were mothers, while 4% (n = 2) were fathers. Regarding race and ethnicity, 45% (n = 22) identified as White, 41% (n = 20) identified as American Indian, 8% (n = 4) identified as African American, and 6% (n = 3) identified as Hispanic/Latino. The mean age of the participants’ children was 11 years old; ages ranged from 5 to 18. All grade levels (K–12) across elementary (n = 28), middle (n = 6), and high school (n = 15) were represented, with second grade represented most frequently.
G*Power 3.1, developed by Faul, Erdfelder, Lang, and Bucher (2007), was utilized during an a priori power analysis. The author conducted the power analysis to ascertain the minimum number of participants needed to reach statistical significance, should it exist among the variables under investigation. With statistical power set at .80 and alpha level set at .05, the analysis produced a minimum sample size of 40. This sample size was large enough to detect a medium effect size
(f2 = .35). As a result, the sample size was sufficient to explain the relationships between the predictor and criterion variables.
Instruments
The parents who participated in this study completed a demographic questionnaire and two surveys. The demographic questionnaire, developed by the first author, captured race/ethnicity and gender of the parent in addition to the level of involvement in their child’s schooling. Student achievement–related questions also were asked to capture the age of the participant’s child, grade level, GPA, homework completion percentage, and number of discipline referrals and suspensions. Participants responded to questions such as, “What percentage of your child’s homework is completed on a weekly basis?” Other surveys utilized in this study include the following.
Parental Authority Questionnaire–Revised (PAQ-R; Reitman, Rhode, Hupp, & Altobello, 2002). The PAQ-R is a 30-item self-report measure of parenting style. The PAQ-R is a revision of the Parental Authority Questionnaire (PAR; Buri, 1991) and is grounded in the work of Baumrind (1971). Three subscales, Authoritarian, Authoritative, and Permissive, comprising 10 items each, assess the degree to which parents exhibit control, demand maturity, and are responsive and communicative with their child. Participants indicate their level of agreement with statements such as, “I tell my children what they should do, but I explain why I want them to do it” using a 5-point Likert-type scale ranging from strongly disagree (1) to strongly agree (5).
Findings from a study conducted by Reitman et al. (2002) suggested that the PAQ-R is a reliable measure of authoritarian, authoritative, and permissive parenting styles when considering respondents’ demographic characteristics such as socioeconomic status or race. The Authoritarian (r = .87), Authoritative, (r = .61), and Permissive (r = .67) subscales of the PAQ-R have good test-retest reliability at one month. The Authoritarian (r = .25) and Authoritative (r = .34) subscales were positively correlated with the Communication subscale of the Parent-Child Relationship Inventory (Gerard, 1994), suggesting convergent validity. Across three distinct samples of parents, coefficient alphas ranged from .72 to .76 for Authoritarian, .56 to .77 for Authoritative, and .73 to .74 for Permissive, demonstrating internal consistency (Reitman et al., 2002).
In the current study, only the Authoritative subscale was used. The demographic characteristics of participants in Sample A in a study conducted by Reitman et al. (2002) most closely aligned with the sample in the present study. Factor loadings for Sample A were identical to the Authoritative subscale of the original PAR and therefore used in this study. For the present study, the Authoritative subscale has an internal consistency of .69.
Parent Rational and Irrational Belief Scale (PRIBS; Gavita, David, DiGiuseppe, & DelVecchio, 2011). The PRIBS was used in this study to assess participants’ beliefs related to their child’s behavior and parenting roles. The self-report instrument contains a total of 24 items; four are control items. Three subscales, Rational Beliefs (RB), Irrational Beliefs (IB), and Global Evaluation (GE), comprise the remaining 20 items. The RB subscale contains 10 items and assesses the degree to which preferential and realistic thoughts related to parenting are maintained. The IB subscale includes six items and evaluates the demands parents place on themselves and their child. The GE subscale comprises four items and assesses the degree to which parents globally rate themselves or their children.
A 5-point Likert-type scale ranging from strongly disagree (1) to strongly agree (5) is used to respond to items such as, “My child must absolutely respect and obey me.” Scores on the PRIBS generally range from 39 (very low) to 60 (very high). The PRIBS and its subscales are significantly correlated with other measures of irrationality and negative emotion, including the General Attitudes and Beliefs Scale-Short Form (Lindner, Kirkby, Wertheim, & Birch, 1999) and the Parental Stress Scale (Berry & Jones, 1995). Gavita et al. (2011) suggested the PRIBS is a reliable measure of parent irrationality; test-retest reliability (r = .78) for the full scale was acceptable after two months. Internal consistency for the PRIBS was .73. The coefficient alphas for RB, IB, and GE were .83, .78, and .71, respectively. For the current study, an internal consistency coefficient of .46 was found for the PRIBS. Additionally, coefficient alphas for the subscales are .62 (RB), .80 (IB), and .43 (GE). All PRIBS subscales were used in this study.
Procedure
A review of literature was conducted in an effort to identify the measures for use in this study. Additionally, a brief demographic instrument was developed to obtain relevant parent and child demographic information. Qualtrics survey software was utilized to prepare the survey packet (i.e., informed consent, demographic questionnaire, and surveys) for electronic dissemination. An application to complete the study then was submitted for review to the institutional review board (IRB) at the researchers’ university. Upon IRB approval, the researchers disseminated an electronic message containing a link to the research packet via a graduate counseling student listserv. An email also was distributed to staff who worked in the School of Education at the researchers’ university. The email contained a request for parents of K–12 students to participate in the study; recipients also were asked to forward the email to family, friends, and colleagues. The email was disseminated on three occasions across two weeks. Participants who completed the study were entered into a drawing for a chance to win $50.
Results
Preliminary Analyses
In order to gain a better understanding of the student achievement–related data collected during this study, initial analyses were conducted. Prior to analysis, GPA was calculated using a letter grade–GPA conversion table; parents reported letter grades on the survey. As such, grades of A+, A, and A- equated to GPAs of 4.33, 4.0, and 3.67, respectively. The student achievement–related variables included in the initial analyses were parental involvement, discipline referrals, suspensions, and homework completion.
Pearson product-moment correlation coefficients and multiple regression analyses were used to test the hypothesis that GPA is related to and predicted by these student achievement–related variables. The degree of parental involvement and homework completion were positively and significantly related to GPA. Suspensions were negatively and significantly related to GPA. Discipline referrals were not significantly related to GPA. The descriptive statistics and correlations for these variables are offered in Table 1.
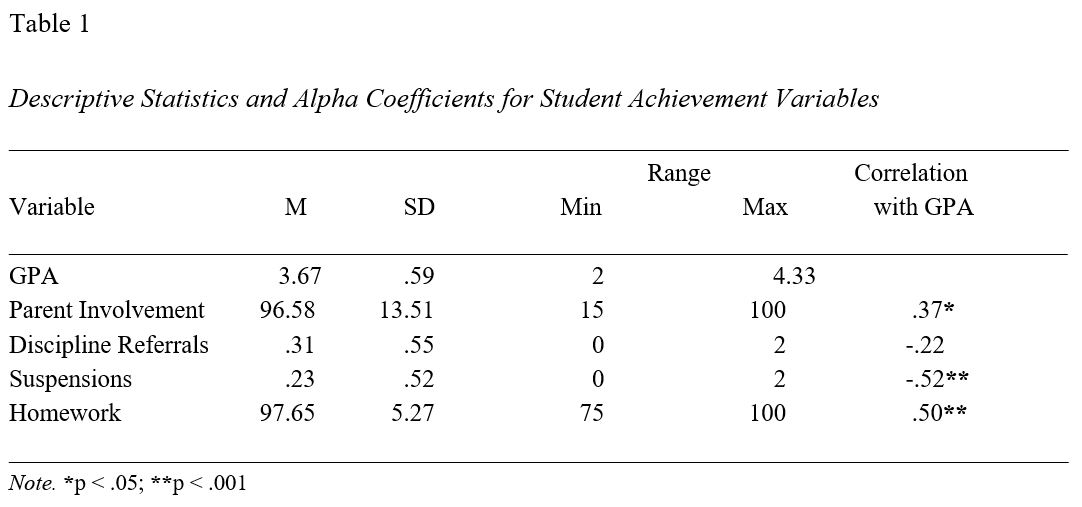
Prior to additional analysis, basic assumptions of multiple regression analysis were tested and satisfied. Standardized residual plots and Q-Q plots were inspected; bivariate correlations also were examined. Next, a multiple regression analysis including parent involvement, suspensions, and homework completion as predictors was conducted with GPA as the criterion variable. Discipline referrals were not included in the regression analysis. A significant regression equation was found: F(3, 45) = 11.539, p < .001. The model with these three predictors explained a significant amount of the variance in GPA (R2 = .435). Significant contributions were made to the model by each of the three predictor variables: parent involvement (β = .284, p < .05), suspensions (β = -.369, p < .05), and homework completion (β = .273, p < .05).
Main Analyses
A multiple linear regression was used to test the hypothesis that authoritative parenting is predicted by parenting beliefs. Authoritative parenting served as the criterion variable. RB, IB, and GE were predictor variables. A combination of these predictor variables yielded a significant regression equation: F(3, 38) = 14.536, p < .000. The model explained a significant portion of variance (53%) in authoritative parenting (see Table 2). Additionally, RB (β = .38, p < .05) was positively and significantly related to authoritative parenting. IB (β = .46, p < .001) also was positively and significantly correlated with authoritative parenting. GE did not contribute significantly to the model (β = -.25 p > .05).
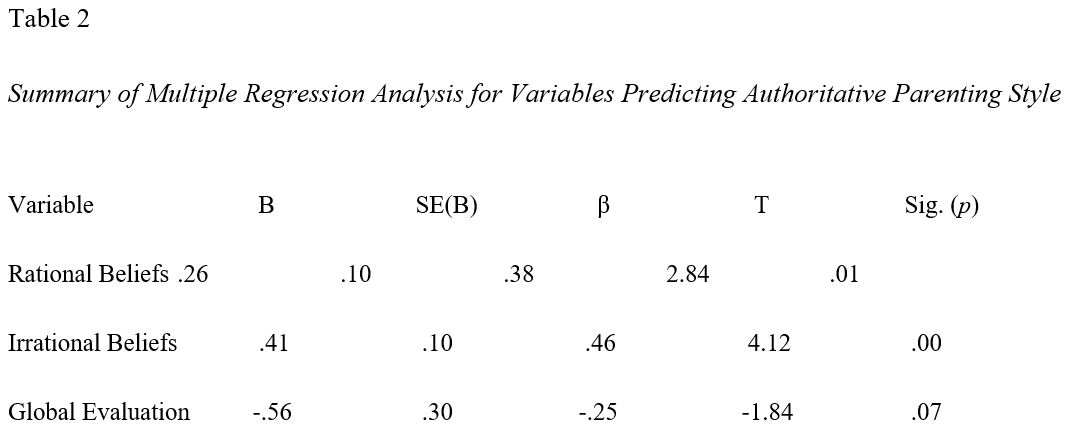
A simple linear regression was performed to test the hypothesis that authoritative parenting predicts student achievement. Based on prior research findings that suggest authoritative parenting is related to positive student achievement, authoritative parenting served as a predictor variable; the criterion variable was GPA. Output from the analysis revealed that authoritative parenting did not predict GPA for this sample of parents: F(1, 40) = .642, p > .05.
Finally, the hypothesis that parenting beliefs predict student achievement–related variables was tested using multiple linear regression modeling. IB, RB, and GE were predictor variables and parent involvement, suspension, and homework completion were criterion variables. A combination of these predictor variables yielded a non-significant regression equation when parental involvement was the criterion variable: F(3, 37) = 1.773, p = .169. Suspensions were not predicted by RB, IB, or GE: F(3, 37) = 1.232, p = .312. Finally, a combination of these predictor variables yielded a non-significant regression equation when homework completion was the criterion variable: F(3, 37) = 2.382, p = .085. Although this model did not explain variance in homework completion, IB was positively and significantly related to homework completion: t(39) = 2.34, p = .025; β = .357.
Discussion
The hypotheses put forth based on previous research and literature were supported and refuted in various instances based on the analyses of the data collected. In regard to the first hypothesis, all student achievement–related factors except discipline referrals were significantly related to GPA. This finding is consistent with research that explores the relationships of proximal student achievement–related factors and distal student achievement outcomes. Parental involvement in their child’s schooling, homework completion, and suspensions are predictors of GPA. Each of these variables contributed to the overall model for predicting student achievement. This finding demonstrates the value of parental involvement and homework completion in the success of students. Additionally, the negative impact of suspension on the academic achievement of students is highlighted. This outcome signals the importance of fostering safe and inviting schools and establishing policies that offer alternatives to suspension unless absolutely necessary.
The second hypothesis purported that authoritative parenting is significantly related to RB, IB, and GE. This hypothesis was supported; combined, RB, IB, and GE predicted authoritative parenting. Research findings suggest that authoritative parenting is related to student achievement, so it is counterintuitive that both RB and IB are positively related to authoritativeness. IB typically lead to dysfunction rather than positive outcomes such as student achievement (Terjesen & Kurasaki, 2009). However, according to Reitman et al. (2002) and others, authoritative parents are demanding, yet supportive of their children. The demandingness described in this parenting style may be a derivative of irrational thinking, as evidenced by the significant contribution of IB to the model. As suggested by Bernard (1990), parents who place rigid demands on their children may be less supportive; effective communication also may fluctuate. It is likely that an acceptable balance of demands, free of unrealistic, rigid expectations, coupled with support, is most effective when considering the role of authoritative parenting on student achievement. Excessive or unrealistic demands may lead to increases in student achievement, but at the expense of the parent–child relationship as well as mental health. In turn, these demands may serve as a barrier to home and school success (Terjesen & Kurasaki, 2009; Warren, 2017).
Closely tied to the second hypothesis, the third hypothesis suggested that authoritative parenting is significantly positively related to student achievement. Based on the data set analyzed, this hypothesis was not supported. This finding is inconsistent with previous research, which stated that the authoritative parenting style correlates to positive student achievement. In a meta-analysis conducted by Pinquart (2016), a small effect size was found in the relationship between authoritativeness and student achievement. It is possible that a significant relationship exists, yet was not found in this study because of a small sample size. Alternatively, authoritative parenting was not related to student achievement, a finding contrary to Pinquart (2016). Demographic variables such as race/ethnicity of participants (e.g., 40.8% American Indian) were not accounted for in this study and also may have implications for the findings.
The final hypothesis indicated that parenting beliefs are significantly related to student achievement–related variables; this hypothesis was partially supported. Although parenting beliefs were not predictive of parental involvement or suspensions, IB were significantly related to homework completion. Students who consistently complete their homework appear to have parents who maintain IB. Although homework completion is important and leads to academic achievement (Kalenkoski & Pabilonia, 2017), according to REBT, irrational thinking is unproductive and leads to unhealthy negative emotion and dysfunctional behaviors (Dryden, 2014). In some instances, it is possible that parents model unhelpful psychosocial processes (e.g., irrational thinking, anger, yelling) when facilitating the completion of their child’s homework. This may lead to rifts in the parent–child relationship and a general disdain for doing homework, especially that which is difficult or challenging. As such, it is important for parents to set realistic, high expectations for homework completion. These expectations should be based on the child’s strengths and weaknesses, clearly communicated, and consistently followed. Parents are encouraged to hold their children accountable without placing demands on themselves, their child, or the homework process in general (Warren, 2017).
Overall the data from this study presented interesting findings related to authoritative parenting style, beliefs, and student achievement. Certain factors such as homework completion and parental involvement were positively related to GPA; school suspension had a negative impact on GPA. Although these findings are not novel, consideration for the relationships between authoritativeness, parent beliefs, and student achievement in this investigation is noteworthy. Although homework completion was positively related to GPA, it also was correlated with IB. In combination, these findings provide an interesting perspective on the ways in which authoritativeness is related to parenting beliefs, which, in turn, appear to influence homework completion, a key determinant of positive distal student achievement outcomes. Although limitations exist, this study can help to facilitate the development of additional research and offers practical implications for school counselors.
Limitations
As suggested, there are several limitations of this study. When considering the generalizability of these results and potential implications for practice, readers should account for the method of data collection and the sample used in this study. First, data were gathered using self-report measures. Because of the nature of the questions asked on the survey, parents participating in this study may have provided socially desirable responses rather than indicating their actual parenting beliefs and behaviors. Additionally, the sample size was small, yet it was sufficiently sized to detect moderate effects. A convenience sample was used and likely is not representative of the general population. Students and faculty affiliated with a university listserv were contacted and asked to participate and disseminate the study information to their family and friends. A larger sample size would have increased the generalizability of these results and yielded greater power, including the ability to detect smaller effect sizes among the variables.
Future Research
Research investigating parenting styles, beliefs, and student achievement variables such as discipline referrals, suspension, and homework completion is sparse. This study offers a foundation for future empirical and action-based research in this area. Researchers initially are encouraged to replicate this study using a larger, more representative sample of parents with school-aged children. Replication may shed additional light on the strengths of the relationships of the variables explored in this study. Given the achievement gap, including the disproportionate suspension rates that exist in K–12 schools among students of color, it is especially important for researchers to explore the impact of parenting styles and beliefs on the achievement of students from historically underrepresented backgrounds. The American Indian population, specifically, is largely absent in research that explores factors of K–12 student success, yet over 500,000 American Indian students are enrolled in schools across the nation (Snyder, de Brey, & Dillow, 2018). This lack of research is a barrier for school counselors and other educators who seek to better support and understand American Indian families and students. Research that explores these relationships within and across specific racial/ethnic groups, including African American, Hispanic/Latino, and American Indian, can serve as a catalyst for school counselors to enhance service delivery and meet the needs of all students.
Researchers also are encouraged to explore the effects of targeted parenting interventions, such as rational emotive-social behavioral (RE-SB) consultation (Warren, 2017) on parenting and student achievement. School counselors can implement large group, small group, or individual RE-SB consultation with parents to address IB and promote student success (Warren, 2017). School counselors, in collaboration with researchers, can play a central role in the development, delivery, and evaluation of parenting interventions that aim to promote student success; these efforts also can further establish evidence-based practice in school counseling.
Implications for School Counselors
According to the ASCA National Model (ASCA, 2012), school counselors play an integral role in supporting the academic, social-emotional, and career development of all students through work with various stakeholders, including students, teachers, and parents. The findings of this study offer insight into the connection between parenting and student success. Operating in the academic domain, school counselors can deliver direct and indirect services to support the success of all students. The recommendations provided below serve to guide school counselors in identifying and delivering targeted programming that yields positive student outcomes.
A broad strategy for promoting academic success involves the establishment of a comprehensive school counseling program that includes interventions that aim to increase homework completion, decrease suspension rates, and increase parental involvement. As the findings of this study suggest, these factors have a direct impact on student achievement. Therefore, school counselors should leverage their roles as leaders, advocates, and consultants to ensure students are adequately supported by parents and positioned by their teachers to meet the daily expectations of school.
As educational leaders, school counselors are encouraged to engage parents, teachers, administrators, and students in ongoing, critical discussion about the relationships between student achievement–related factors and GPA. Classroom guidance, staff development sessions, and parent workshops are viable opportunities to disseminate this information and engage stakeholders. School counselors can involve teachers and administrators in discussions surrounding classroom and school policies and procedures that impact homework completion, suspension, and parent involvement. Leveraging student and school data during these conversations are more likely to lead to classroom and school policy revisions that accommodate all students and their families. When school counselors collaborate with teachers and administrators, innovative strategies and support structures to promote homework completion and alternatives to suspension will emerge.
School counselors also can use the findings of this study to increase their awareness of the values and beliefs of parents. Used within the context of culture, these findings can offer school counselors additional insights that may be useful when working with parents. For instance, when working with American Indian families, school counselors should consider how customs and traditions impact the manner in which parents engage with their children (Castagno & Brayboy, 2008). By understanding the culture of students and families while considering parenting styles and beliefs, school counselors can partner with parents in intentional ways in an effort to promote student achievement. It is especially important to consider strategies to engage parents who may experience barriers to visiting school. School counselors can seek community resources and partnerships that can be leveraged to increase parental involvement. Using asset mapping as promoted by Griffin and Farris (2010), school counselors can help parents connect to school via the workplace, church, or community centers.
School counselors are encouraged to work closely with parents to establish programming that best supports parents’ efforts to help their children succeed. RE-SB consultation, as described by Warren (2017), is a viable service to educate parents about parenting styles and the impact of their thoughts on emotions and behaviors. For example, school counselors can hold a workshop for parents during a PTA event to promote rational thinking. “Rational reminders” disseminated via the school’s social media account also can be useful for parents not familiar with REBT who are attempting to set realistic expectations and provide optimal support to their children. Interventions such as these can increase parents’ self-awareness of the influence they have on their children and lead to positive student outcomes.
Finally, school counselors should explore strategies that foster social-emotional development for all students and especially those with little parental support. Establishing support systems among students can increase their academic success (Sedlacek, 2017). Mentoring programs that resemble or simulate the parent–child relationship and model rational thinking may yield academic success, given the findings of this study. School counselors also can develop programming that aligns with non-cognitive factors as promoted by Warren and Hale (2016). Students who have a positive self-concept, realistically appraise themselves, are involved in the community, take on leadership roles, have experience in a specific field, and have a support network are better positioned to succeed in school and in life (Sedlacek, 2017). These efforts may position students for school success by neutralizing or reducing the negative impact a lack of parental involvement has on achievement.
Conclusion
School counselors play a critical role in today’s schools. Serving as leaders, advocates, collaborators, and consultants with an aim of promoting student success, school counselors work with many stakeholders, including teachers, administrators, and students and their parents. This study sheds light on the impact of suspension, homework completion, and parental involvement on student achievement. The relationships between parent beliefs and authoritativeness and student achievement also are explored. The authors hope the findings of this study foster awareness and lead school counselors to further consider the impact parents have on student achievement. An understanding of parenting style and beliefs and their impact on student achievement affords school counselors the opportunity to develop targeted programs that increase parent involvement, strengthen the school–parent partnership, and promote academic success.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2012). ASCA national model: A framework for school counseling programs
(3rd ed.). Alexandria, VA: Author.
Baumrind, D. (1966). Effects of authoritative parental control on child behavior. Child Development, 37, 887–907. doi:10.2307/1126611
Baumrind, D. (1971). Current patterns of parental authority. Developmental Psychology, 4, 1–103.
doi:10.1037/h0030372
Baumrind, D. (1991). Effective parenting during the early adolescent transition. In P. A. Cowan & E. M. Hetherington (Eds.), Advances in Family Research Series. Family Transitions (pp. 111–163). Hillsdale, NJ: Lawrence Erlbaum Associates.
Bernard, M. E. (1990). Rational-emotive therapy with children and adolescents: Treatment strategies. School Psychology Review, 19, 294–303.
Berry, J. O., & Jones, W. H. (1995). The parental stress scale: Initial psychometric evidence. Journal of Social and Personal Relationships, 12, 463–472. doi:10.1177/0265407595123009
Bryan, J., & Henry, L. (2012). A model for building school–family–community partnerships: Principles and process. Journal of Counseling & Development, 90, 408–420. doi:10.1002/j.1556-6676.2012.00052.x
Buri, J. R. (1991). Parental authority questionnaire. Journal of Personality Assessment, 57, 110–119.
doi:10.1207/s15327752jpa5701_13
Carlo, G., White, R. M., Streit, C., Knight, G. P., & Zeiders, K. H. (2018). Longitudinal relations among
parenting styles, prosocial behaviors, and academic outcomes in U.S. Mexican adolescents. Child
Development, 89, 577–592. doi:10.1111/cdev.12761
Castagno, A. E., & Brayboy, B. M. J. (2008). Culturally responsive schooling for Indigenous youth: A review of the literature. Review of Educational Research, 78, 941–993. doi:10.3102/0034654308323036
Castro, M., Expósito-Casas, E., López-Martín, E., Lizasoain, L., Navarro-Asencio, E., & Gaviria, J. L. (2015). Parental involvement on student academic achievement: A meta-analysis. Educational Research Review, 14, 33–46. doi:10.1016/j.edurev.2015.01.002
Darling, N., & Steinberg, L. (1993). Parenting style as context: An integrative model. Psychological Bulletin, 113, 487–496. doi:10.1037/0033-2909.113.3.487
Dryden, W. (2014). Rational emotive behaviour therapy: Distinctive features. London, UK: Routledge.
Ellis, A. (1962). Reason and emotion in psychotherapy: A new and comprehensive method of treating human disturbance.
Secaucus, NJ: Citadel.
Ellis, A., Wolfe, J. L., & Moseley, S. (1981). How to raise an emotionally healthy, happy child. Carlsbad, CA: Borden.
Epstein, J. L. (2018). School, family, and community partnerships: Preparing educators and improving schools. New York, NY: Routledge.
Faul, F., Erdfelder, E., Lang, A.-G., & Bucher, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191. doi:10.3758/BF03193146
Gavita, O. A., David, D., DiGiuseppe, R., & DelVecchio, T. (2011). The development and validation of the Parent Rational and Irrational Beliefs Scale. Procedia – Social and Behavioral Sciences, 30, 2305–2311. doi:10.1016/j.sbspro.2011.10.449
Gerard, A. B. (1994). Parent-child relationship inventory. Los Angeles, CA: Western Psychological Services.
Gonzalez, J. E., Nelson, J. R., Gutkin, T. B., Saunders, A., Galloway, A., & Shwery, C. S. (2004). Rational emotive therapy with children and adolescents: A meta-analysis. Journal of Emotional and Behavioral Disorders, 12, 222–235. doi:10.1177/10634266040120040301
Griffin, D., & Farris, A. (2010). School counselors and collaboration: Finding resources through community asset mapping. Professional School Counseling, 13, 248–256. doi:10.1177/2156759X1001300501
Hamamci, Z., & Bağci, C. (2017). Analyzing the relationship between parent’s irrational beliefs and their children’s behavioral problems and family function. Gaziantep University Journal of Social Sciences, 16, 733–740. doi:10.21547/jss.292722
Hatch, T. (2014). The use of data in school counseling: Hatching results for students, programs, and the profession. Thousand Oaks, CA: Corwin.
Hojjat, S. K., Golmakanie, E., Khalili, M. N., Smaili, H., Hamidi, M., & Akaberi, A. (2016). Personality traits and irrational beliefs in parents of substance-dependent adolescents: A comparative study. Journal of Child & Adolescent Substance Abuse, 25, 340–347. doi:10.1080/1067828X.2015.1012612
Imose, R., & Barber, L. K. (2015). Using undergraduate grade point average as a selection tool: A synthesis of the literature. The Psychologist-Manager Journal, 18, 1–11. doi:10.1037/mgr0000025
Kalenkoski, C. M., & Pabilonia, S. W. (2017). Does high school homework increase academic achievement? Education Economics, 25, 45–59. doi:10.1080/09645292.2016.1178213
Kenney, S. R., Lac, A., Hummer, J. F., Grimaldi, E. M., & LaBrie, J. W. (2015). Pathways of parenting style on adolescents’ college adjustment, academic achievement, and alcohol risk. Journal of College Student Retention: Research, Theory & Practice, 17, 186–203. doi:10.1177/1521025115578232
Kufakunesu, M. (2015). The influence of irrational beliefs on the mathematics achievement of secondary school learners in Zimbabwe. Retrieved from University of South Africa Institutional Repository (http://hdl.handle.net/10500/20072).
LeFevre, A. L., & Shaw, T. V. (2012). Latino parent involvement and school success: Longitudinal effects of formal and informal support. Education and Urban Society, 44, 707–723. doi:10.1177/0013124511406719
Lindner, H., Kirkby, R., Wertheim, E., & Birch, P. (1999). A brief assessment of irrational thinking: The
shortened General Attitude and Belief Scale. Cognitive Therapy and Research, 23, 651–663.
doi:10.1023/A:1018741009293
Maccoby, E. E., & Martin, J. A. (1983). Socialization in the context of the family: Parent-child interaction. In E.
M. Hetherington (Ed.), Mussen Manual of Child Psychology (Vol. 4, 4th ed., pp. 1–102). New York, NY:
Wiley.
Masud, H., Thurasamy, R., & Ahmad, M. S. (2015). Parenting styles and academic achievement of young adolescents: A systematic literature review. Quality & Quantity, 49, 2411–2433.
doi:10.1007/s11135-014-0120-x
McCown, B., Blake, I. K., & Keiser, R. (2012). Content analyses of the beliefs of academic procrastinators.
Journal of Rational-Emotive & Cognitive-Behavior Therapy, 30, 213–222. doi:10.1007/s10942-012-0148-6
Noltemeyer, A. L., Ward, R. M., & Mcloughlin, C. (2015). Relationship between school suspension and student outcomes: A meta-analysis. School Psychology Review, 44, 224–240. doi:10.17105/spr-14-0008.1
Pinquart, M. (2016). Associations of parenting styles and dimensions with academic achievement in children and adolescents: A meta-analysis. Educational Psychology Review, 28, 475–493. doi:10.1007/s10648-015-9338-y
Pinquart, M., & Kauser, R. (2018). Do the associations of parenting styles with behavior problems and academic achievement vary by culture? Results from a meta-analysis. Cultural Diversity and Ethnic Minority Psychology, 24, 75–100. doi:10.1037/cdp0000149
Ray, S. L., Lambie, G., & Curry, J. (2007). Building caring schools: Implications for professional school counselors. Journal of School Counseling, 5(14). Retrieved from http://jsc.montana.edu/articles/v5n14.pdf
Reitman, D., Rhode, P. C., Hupp, S. D. A., & Altobello, C. (2002). Development and validation of the Parental Authority Questionnaire–Revised. Journal of Psychopathology and Behavioral Assessment, 24(2), 119–127. doi:10.1023/A:1015344909518
Roby, D. E. (2004). Research on school attendance and student achievement: A study of Ohio schools. Educational Research Quarterly, 28, 3–14.
Sapp, M. (1996). Irrational beliefs that can lead to academic failure for African American middle school students who are academically at-risk. Journal of Rational-Emotive & Cognitive-Behavior Therapy, 14, 123–134. doi:10.1007/BF02238186
Sapp, M., Farrell, W., & Durand, H. (1995). Cognitive-behavioral therapy: Applications for African American middle school at-risk students. Journal of Instructional Psychology, 22(2), 169–177.
Schwerdt, G., West, M. R., & Winters, M. A. (2017). The effects of test-based retention on student outcomes over time: Regression discontinuity evidence from Florida. Journal of Public Economics, 152, 154–169. doi:10.1016/j.jpubeco.2017.06.004
Sedlacek, W. E. (2017). Measuring noncognitive variables: Improving admissions, success and retention for underrepresented students. Herndon, VA: Stylus.
Snyder, T. D., de Brey, C., & Dillow, S. A. (2018). Digest of Education Statistics 2016 (NCES 2017-094). Washington, DC: National Center for Education Statistics, Institute of Education Sciences, U.S. Department of Education.
SOAR Learning Inc. (2018). SOAR® Learning & Soft Skills Curriculum for College & Career Readiness. Retrieved from https://studyskills.com
Spengler, M., Brunner, M., Martin, R., & Lüdtke, O. (2016). The role of personality in predicting (change in) students’ academic success across four years of secondary school. European Journal of Psychological Assessment, 32, 95–103. doi:10.1027/1015-5759/a000330
Terjesen, M. D., & Kurasaki, R. (2009). Rational emotive behavior therapy: Applications for working with parents and teachers. Estudos de Psicologia (Campinas), 26, 3–14. doi:10.1590/S0103-166X2009000100001
Warren, J. M. (2017). School consultation for student success: A cognitive behavioral approach. New York, NY: Springer.
Warren, J. M., & Dowden, A. R. (2012). Elementary school teachers’ beliefs and emotions: Implications for school counselors and counselor educators. Journal of School Counseling, 10(19). Retrieved from https://files.eric.ed.gov/fulltext/EJ981200.pdf
Warren, J. M., & Gerler, E. R., Jr. (2013). Effects of school counselors’ cognitive behavioral consultation on irrational and efficacy beliefs of elementary school teachers. The Professional Counselor, 3, 6–15. doi:10.15241/jmw.3.1.6
Warren, J. M., & Hale, R. W. (2016). Fostering non-cognitive development of underrepresented students through rational emotive behavior therapy: Recommendations for school counselor practice. The Professional Counselor, 6, 89–106. doi:10.15241/jw.6.1.89
Warren, J. M., & Hale, R. W. (in press). Predicting grit and resilience: Exploring college students’ academic rational beliefs. Journal of College Counseling.
York, T. T., Gibson, C., & Rankin, S. (2015). Defining and measuring academic success. Practical Assessment, Research & Evaluation, 20(5), 1–20.
Jeffrey M. Warren, NCC, is an associate professor and Chair of the Counseling Department at the University of North Carolina at Pembroke. Leslie A. Locklear is the FATE Director at the University of North Carolina at Pembroke. Nicholas A. Watson is a graduate student at the University of North Carolina at Pembroke. Correspondence can be addressed to Jeffrey Warren, 1 University Drive, Pembroke, NC 28372, jeffrey.warren@uncp.edu.
Nov 10, 2018 | Volume 8 - Issue 4
Zachary D. Bloom, Victoria A. McNeil, Paulina Flasch, Faith Sanders
Empathy plays an integral role in the facilitation of therapeutic relationships and promotion of positive client outcomes. Researchers and scholars agree that some components of empathy might be dispositional in nature and that empathy can be developed through empathy training. However, although empathy is an essential part of the counseling process, literature reviewing the development of counseling students’ empathy is limited. Thus, we examined empathy and sympathy scores in counselors-in-training (CITs) in comparison to students from other academic disciplines (N = 868) to determine if CITs possess greater levels of empathy than their non-counseling academic peers. We conducted a MANOVA and failed to identify differences in levels of empathy or sympathy across participants regardless of academic discipline, potentially indicating that counselor education programs might be missing opportunities to further develop empathy in their CITs. We call for counselor education training programs to promote empathy development in their CITs.
Keywords: empathy, sympathy, counselor education, counselors-in-training, therapeutic relationships
Empathy is considered an essential component of the human experience as it relates to how individuals socially and emotionally connect to one another (Goleman, 1995; Szalavitz & Perry, 2010). Although empathy can be difficult to define (Konrath, O’Brien, & Hsing, 2011; Spreng, McKinnon, Mar, & Levine, 2009), within the counseling profession there is agreement that empathy includes both cognitive and affective components (Clark, 2004; Davis, 1980, 1983). When discussing the difference between affective and cognitive empathy, Vossen, Piotrowski, and Valkenburg (2015) described that “whereas the affective component pertains to the experience of another person’s emotional state, the cognitive component refers to the comprehension of another person’s emotions” (p. 66). Regardless of specific nuances among researchers’ definitions of empathy, most appear to agree that “empathy-related responding is believed to influence whether or not, as well as whom, individuals help or hurt” (Eisenberg, Eggum, & Di Giunta, 2010, p. 144). Furthermore, empathy can be viewed as a motivating factor of altruistic behavior (Batson & Shaw, 1991) and is essential to clients’ experiences of care (Flasch et al., in press). As such, empathy is foundational to interpersonal relationships (Siegel, 2010; Szalavitz & Perry, 2010), including the relationships facilitated in a counseling setting (Norcross, 2011; Rogers, 1957).
Rogers (1957) intuitively understood the necessity of empathy in a counseling relationship, which has been verified by the understanding of the physiology of the brain (Badenoch, 2008; Decety & Ickes, 2009; Siegel, 2010) and validated in the counseling literature (Elliott, Bohart, Watson, & Greenberg, 2011). In a clinical context, empathy can be described as both a personal characteristic and a clinical skill (Clark, 2010; Elliott et al., 2011; Rogers, 1957) that contributes to positive client outcomes (Norcross, 2011; Watson, Steckley, & McMullen, 2014). For example, empathy has been identified as a factor that leads to changes in clients’ attachment styles, treatment of self (Watson et al., 2014), and self-esteem development (McWhirter, Besett-Alesch, Horibata, & Gat, 2002). Moreover, researchers regularly identify empathy as a fundamental component of helpful responses to clients’ experiences (Beder, 2004; Flasch et al., in press; Kirchberg, Neimeyer, & James, 1998).
Although empathy is lauded and encouraged in the counseling profession, empathy development is not necessarily an explicit focus or even a mandated component of clinical training programs. The Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2016) identifies diverse training standards for content knowledge and practice among master’s-level and doctoral-level counselors-in-training (CITs), but does not mention the word empathy in its manual for counseling programs. One of the reasons for this could be that empathy is often understood and taught as a microskill (e.g., reflection of feeling and meaning) rather than as its own construct (Bayne & Jangha, 2016). Yet empathy is more than a component of a skillset, and CITs might benefit from a programmatic development of empathy to enhance their work with future clients (DePue & Lambie, 2014).
The application of empathy, or a counselor’s use of empathy-based responses in a therapeutic relationship, requires skill and practice (Barrett-Lennard, 1986; Truax & Carkhuff, 1967). Clark (2010) cautioned, for example, that counselors’ empathic responses need to be congruent with the client’s experience, and that the misapplication of sympathetic responses as empathic responses can interfere in the counseling relationship. In regard to sympathy, Eisenberg and colleagues (2010) explained, “sympathy, like empathy, involves an understanding of another’s emotion and includes an emotional response, but it consists of feelings of sorrow or concern for the distressed or needy other rather than merely feeling the same emotion” (p. 145). Thus, researchers call for counselor educators to do more than increase CITs’ affective or cognitive understanding of another’s experience, and to assist them in differentiating between empathic responses and sympathetic responses in order to better convey empathic understanding and relating (Bloom & Lambie, in press; Clark, 2010).
With the understanding that a counselor’s misuse of sympathetic responses might interrupt a therapeutic dialogue and that empathy is vital to the therapeutic alliance, researchers call for counselor educators to promote empathy development in CITs (Bloom & Lambie, in press; DePue & Lambie, 2014). Although there is evidence that some aspects of empathy are dispositional in nature (Badenoch, 2008; Konrath et al., 2011), which might make the counseling profession a strong fit for empathic individuals, empathy training in counseling programs can increase students’ levels of empathy (Ivey, 1971). However, the specific empathy-promoting components of empathy training are less understood (Teding van Berkhout & Malouff, 2016). Overall, empathy is an essential component of the counseling relationship, counselor competency, and the promotion of client outcomes (DePue & Lambie, 2014; Norcross, 2011). However, little is known about the training aspect of empathy and whether or not counselor training programs are effective in enhancing empathy or reducing sympathy among CITs. Thus, the following question guided this research investigation: Are CITs’ levels of empathy or sympathy different from their academic peers? Specifically, do CITs possess greater levels of empathy or sympathy than students from other academic majors?
Empathy in Counseling
Researchers have established continuous support for the importance of the therapeutic relationship in the facilitation of positive client outcomes (Lambert & Bergin, 1994; Norcross, 2011; Norcross & Lambert, 2011). In fact, the therapeutic relationship is predictive of positive client outcomes (Connors, Carroll, DiClemente, Longabaugh, & Donovan, 1997; Krupnick et al., 1996), accounting for about 30% of the variance (Lambert & Barley, 2001). That is, clients who perceive the counseling relationship to be meaningful will have more positive treatment outcomes (Bell, Hagedorn, & Robinson, 2016; Norcross & Lambert, 2011). One of the key factors in the establishment of a strong therapeutic relationship is a counselor’s ability to experience and communicate empathy. Researchers estimate that empathy alone may account for as much as 7–10% of overall treatment outcomes (Bohart, Elliott, Greenberg, & Watson, 2002; Sachse & Elliott, 2002), making it an important construct to foster in counselors.
Despite the importance of empathy in the counseling process, much of the literature on empathy training in counseling is outdated. Thus, little is known about the training aspect of empathy; that is, how is empathy taught to and learned by counselors? Nevertheless, early scholars (Barrett-Lennard, 1986; Ivey, 1971; Ivey, Normington, Miller, Morrill, & Haase, 1968; Truax & Carkhuff, 1967) posited that counselor empathy is a clinical skill that may be practiced and learned, and there is supporting evidence that empathy training may be efficacious.
In one seminal study, Truax and Lister (1971) conducted a 40-hour empathy training program with 12 counselor participants and identified statistically significant increases in participants’ levels of empathy. In their investigation, the researchers employed methods in which (a) the facilitator modeled empathy, warmth, and genuineness throughout the training program; (b) therapeutic groups were used to integrate empathy skills with personal values; and (c) researchers coded three of participants’ 4-minute counseling clips using scales of accurate empathy and non-possessive warmth (Truax & Carkhuff, 1967). Despite identifying statistically significant changes in participants’ scores of empathy, it is necessary to note that participants who initially demonstrated low levels of empathy remained lower than participants who initially scored high on the empathy measures. In a later study modeled after the Truax and Lister study, Silva (2001) utilized a combination of didactic, experiential, and practice components in her empathy training program, and found that counselor trainee participants (N = 45) improved their overall empathy scores on Truax’s Accurate Empathy Scale (Truax & Carkhuff, 1967). These findings contribute to the idea that empathy increases as a result of empathy training.
More recent researchers (Lam, Kolomitro, & Alamparambil, 2011; Ridley, Kelly, & Mollen, 2011) have identified the most common methods in empathy training programs as experiential training, didactic (lecture), skills training, and other mixed methods such as role play and reflection. In their meta-analysis, Teding van Berkhout and Malouff (2016) examined the effect of empathy training programs across various populations (e.g., university students, health professionals, patients, other adults, teens, and children) using the training methods identified above. The researchers investigated the effect of cognitive, affective, and behavioral empathy training and found a statistically significant medium effect size overall (g ranged from 0.51 to 0.73). The effect size was larger in health professionals and university students compared to other groups such as teenagers and adult community members. Though empathy increased as a result of empathy training studies, the specific mechanisms that facilitated positive outcomes remain largely unknown.
Although research indicates that empathy training can be effective, specific empathy-fostering skills are still not fully understood. Programmatically, empathy is taught to counselors within basic counseling skills (Bayne & Jangha, 2016), specifically because empathy is believed to lie in the accurate reflection of feeling and meaning (Truax & Carkhuff, 1967). But scholars argue that there is more to empathy than the verbal communication of understanding (Davis, 1980; Vossen et al., 2015). For example, in a more recent study, DePue and Lambie (2014) reported that counselor trainees’ scores on the Empathic Concern subscale of the Interpersonal Reactivity Index (IRI; Davis, 1980) increased as a result of engaging in counseling practicum experience under live supervision in a university-based clinical counseling and research center. In their study, the researchers did not actively engage in empathy training. Rather, they measured counseling students’ pre- and post-scores on an empathy measure as a result of students’ engagement in supervised counseling work to foster general counseling skills. Implications of these findings mirror those described by Teding van Berkhout and Malouff (2016), namely that it is difficult to identify specific empathy-promoting mechanisms. In other words, it appears that empathy training, when employed, produces successful outcomes in CITs. However, counseling students’ empathy also increases in the absence of specific empathy-promoting programs. This begs the question: Are counseling programs successfully training their counselors to be empathic, and is there a difference between CITs’ empathy or sympathy levels compared to students in other academic majors? Thus, the purpose of the present study was to (a) examine differences in empathy (i.e., affective empathy and cognitive empathy) and sympathy levels among emerging adult college students, and (b) determine whether CITs had different levels of empathy and sympathy when compared to their academic peers.
Methods
Participants
We identified master’s-level CITs as the population of interest in this investigation. We intended to compare CITs to other graduate and undergraduate college student populations. Thus, we utilized a convenience sample from a larger data set that included emerging adult college students between the ages of 18 and 29 who were enrolled in at least one undergraduate- or graduate-level course at nine colleges and universities throughout the United States. Participants were included regardless of demographic variables (e.g., gender, race, ethnicity).
Participants were recruited from three sources: online survey distribution (n = 448; 51.6%), face-to-face data collection (n = 361; 41.6%), and email solicitation (n = 34; 3.9%). In total, 10,157 potential participants had access to participate in the investigation by online survey distribution through the psychology department at a large Southeastern university; however, the automated system limited responses to 999 participants. We and our contacts (i.e., faculty at other institutions) distributed an additional 800 physical data collection packets to potential participants, and 105 additional potential participants were solicited by email. Overall, 1,713 data packets were completed, resulting in a sample of 1,598 participants after data cleaning. However, in order to conduct the analyses for this study, it was necessary to limit our sample to groups of approximately equal sizes (Hair, Black, Babin, & Anderson, 2010). Therefore, we were limited to the use of a subsample of 868 participants. Our sample appeared similar to other samples included in investigations exploring empathy with emerging adult college students (e.g., White, heterosexual, female; Konrath et al., 2011).
The participants included in this investigation were enrolled in one of six majors and programs of study, including Athletic Training/Health Sciences (n = 115; 13.2%); Biology/Biomedical Sciences/Preclinical Health Sciences (n = 167; 19.2%); Communication (n = 163; 18.8%); Counseling (n = 153; 17.6%); Nursing (n = 128; 14.7%); and Psychology (n = 142; 16.4%). It is necessary to note that students self-identified their major rather than selecting it from a preexisting prompt. Therefore, the researchers examined responses and categorized similar responses to one uniform title. For example, responses of psych were included with psychology. Further, in order to attain homogeneity among group sizes, we included multiple tracks within one program. For example, counseling included participants enrolled in either clinical mental health counseling (n = 115), marriage and family counseling (n = 24), or school counseling (n = 14) tracks. Table 1 presents additional demographic information (e.g., age, race, ethnicity, graduate-level status). It is necessary to note that, because of the constraints of the dataset, counseling students consisted of master’s-level graduate students, whereas all other groups consisted of undergraduate students.
Table 1
Participants’ Demographic Characteristics
| Characteristic |
|
n
|
Total %
|
|
| Age |
18–19 |
460
|
52.4
|
|
|
20–21 |
155
|
17.9
|
|
|
22–23 |
130
|
15.0
|
|
|
24–25 |
58
|
6.7
|
|
|
26–27 |
36
|
4.1
|
|
|
28–29 |
27
|
3.1
|
|
| Gender |
Female |
692
|
79.7
|
|
|
Male |
167
|
19.2
|
|
|
Other |
8
|
0.9
|
|
| Racial |
Caucasian |
624
|
71.9
|
|
| Background |
African American/African/Black |
101
|
11.6
|
|
|
Biracial/Multiracial |
65
|
7.5
|
|
|
Asian/Asian American |
40
|
4.6
|
|
|
Native American |
3
|
0.3
|
|
|
Other |
25
|
2.9
|
|
| Ethnicity |
Hispanic |
172
|
19.8
|
|
|
Non-Hispanic |
689
|
79.4
|
|
| Academic |
Undergraduate |
709
|
81.7
|
|
| Enrollment |
Graduate |
152
|
17.5
|
|
|
Other |
5
|
0.6
|
|
| Academic Major |
Athletic Training/Health Sciences |
115
|
13.2
|
|
|
Biology/Biomedical Sciences/Preclinical Health Sciences |
167
|
19.2
|
|
|
Counseling |
153
|
17.6
|
|
|
Communication |
163
|
18.8
|
|
|
Nursing |
128
|
14.7
|
|
|
Psychology |
142
|
16.4
|
|
Note. N
= 868.
Procedure
The data utilized in this study were collected as part of a larger study that was approved by the authors’ institutional review board (IRB) as well as additional university IRBs where data was collected, as requested. We followed the Tailored Design Method (Dillman, Smyth, & Christian, 2009), a series of recommendations for conducting survey research to increase participant motivation and decrease attrition, throughout the data collection process for both web-based survey and face-to-face administration. Participants received informed consent, assuring potential participants that their responses would be confidential and their anonymity would be protected. We also made the survey convenient and accessible to potential participants by making it available either in person or online, and by avoiding the use of technical language (Dillman et al., 2009).
We received approval from the authors of the Adolescent Measure of Empathy and Sympathy (AMES; Vossen et al., 2015; personal communication with H. G. M. Vossen, July 10, 2015) to use the instrument and converted the data collection packet (e.g., demographic questionnaire, AMES) into Qualtrics (2013) for survey distribution. We solicited feedback from 10 colleagues regarding the legibility and parsimony of the physical data collection packets and the accuracy of the survey links. We implemented all recommendations and changes (e.g., clarifying directions on the demographic questionnaire) prior to data collection.
All completed data collection packets were assigned a unique ID, and we entered the data into the IBM SPSS software package for Windows, Version 22. No identifying information was collected (e.g., participants’ names). Having collected data both in person and online via web-based survey, we applied rigorous data collection procedures to increase response rates, reduce attrition, and to mitigate the potential influence of external confounding factors that might contribute to measurement error.
Data Instrumentation
Demographics profile. We included a general demographic questionnaire to facilitate a comprehensive understanding of the participants in our study. We included items related to various demographic variables (e.g., age, race, ethnicity). Regarding participants’ identified academic program, participants were prompted to respond to an open-ended question asking “What is your major area of study?”
AMES. Multiple assessments exist to measure empathy (e.g., the IRI, Davis, 1980, 1983; The Basic Empathy Scale [BES], Jolliffe & Farrington, 2006), but each is limited by several shortcomings (Carré, Stefaniak, D’Ambrosio, Bensalah, & Besche-Richard, 2013). First, many scales measure empathy as a single construct without distinguishing cognitive empathy from affective empathy (Vossen et al., 2015). Moreover, the wording used in most scales is ambiguous, such as items from other assessments that use words like “swept up” or “touched by” (Vossen et al., 2015), and few scales differentiate empathy from sympathy. Therefore, Vossen and colleagues designed the AMES as an empathy assessment that addresses problems related to ambiguous wording and differentiates empathy from sympathy.
The AMES is a 12-item empathy assessment with three factors: (a) Cognitive Empathy, (b) Affective Empathy, and (c) Sympathy. Each factor consists of four items rated on a 5-point Likert scale with ratings of 1 (never), 2 (almost never), 3 (sometimes), 4 (often), and 5 (always). Higher AMES scores indicate greater levels of cognitive empathy (e.g., “I can tell when someone acts happy, when they actually are not”), affective empathy (e.g., “When my friend is sad, I become sad too”), and sympathy (e.g., “I feel concerned for other people who are sick”). The AMES was developed in two studies with Dutch adolescents (Vossen et al., 2015). The researchers identified a 3-factor model with acceptable to good internal consistency per factor: (a) Cognitive Empathy (α = 0.86), (b) Affective Empathy (α = 0.75), and (c) Sympathy (α = 0.76). Further, Vossen et al. (2015) established evidence of strong test-retest reliability, construct validity, and discriminant validity when using the AMES to measure scores of empathy and sympathy with their samples. Despite being normed with samples of Dutch adolescents, Vossen and colleagues suggested the AMES might be an effective measure of empathy and sympathy with alternate samples as well.
Bloom and Lambie (in press) examined the factor structure and internal consistency of the AMES with a sample of emerging adult college students in the United States (N = 1,598) and identified a 3-factor model fitted to nine items that demonstrated strong psychometric properties and accounted for over 60% of the variance explained (Hair et al., 2010). The modified 3-factor model included the same three factors as the original AMES. Therefore, we followed Bloom and Lambie’s modifications for our use of the instrument.
Data Screening
Before running the main analysis on the variables of interest, we assessed the data for meeting the assumptions necessary to conduct a one-way between-subjects MANOVA. First, we conducted a series of tests to evaluate the presence of patterns in missing data and determined that data were missing completely at random (MCAR) and ignorable (e.g., < 5%; Kline, 2011). Because of the robust size of these data (e.g., > 20 observations per cell) and the minimal amount of missing data, we determined listwise deletion to be best practice to conduct a MANOVA and to maintain fidelity to the data (Hair et al., 2010; Osborne, 2013).
Next, we utilized histograms, Q-Q plots, and boxplots to assess for normality and identified non-normal data patterns. However, MANOVA is considered “robust” to violations of normality with a sample size of at least 20 in each cell (Tabachnick & Fidell, 2013). Thus, with our smallest cell size possessing a sample size of 115, we considered our data robust to this violation. Following this, we assumed our data violated the assumption for multivariate normality. However, Hair et al. (2010) stated “violations of this assumption have little impact with larger sample sizes” (p. 366) and cautioned that our data might have problems achieving a non-significant score for Box’s M Test. Indeed, our data violated the assumption of homogeneity of variance-covariance matrices (p < .01). However, this was not a concern with these data because “a violation of this assumption has minimal impact if the groups are of approximately equal size (i.e., largest group size ÷ smallest group size < 1.5)” (Hair et al., 2010, p. 365).
It is necessary to note that MANOVA is sensitive to outlier values. To mitigate against the negative effects of extreme scores, we removed values (n = 3) with standardized z-scores greater than +4 or less than -4 (Hair et al., 2010). This resulted in a final sample size of 868 participants.
We also utilized scatterplots to detect the patterns of non-linear relationships between the dependent variables and failed to identify evidence of non-linearity. Therefore, we proceeded with the assumption that our data shared linear relationships. We also evaluated the data for multicollinearity. Participants’ scores of Affective Empathy shared statistically significant and appropriate relationships with their scores of Cognitive Empathy (r = .24) and Sympathy (r = .43). Similarly, participants’ scores of Cognitive Empathy were appropriately related to their scores of Sympathy (r = .36; p < .01). Overall, we determined these data to be appropriate to conduct a MANOVA. Table 2 presents participants’ scores by academic discipline.
Table 2
AMES Scores by Academic Major
|
Scale
|
Mean (M)
|
SD
|
Range
|
| Athletic Training |
|
|
|
|
Affective Empathy
|
3.20
|
0.80
|
4.00 |
|
Cognitive Empathy
|
3.80
|
0.62
|
3.33 |
|
Sympathy
|
4.34
|
0.55
|
2.67 |
| Biomedical Sciences |
|
|
|
|
Affective Empathy
|
3.12
|
0.76
|
4.00 |
|
Cognitive Empathy
|
3.66
|
0.59
|
3.00 |
|
Sympathy
|
4.30
|
0.61
|
2.00 |
| Communication |
|
|
|
|
Affective Empathy
|
3.18
|
0.87
|
4.00 |
|
Cognitive Empathy
|
3.80
|
0.62
|
2.67 |
|
Sympathy
|
4.27
|
0.69
|
3.00 |
| Counseling |
|
|
|
|
Affective Empathy
|
3.32
|
0.60
|
3.33 |
|
Cognitive Empathy
|
3.83
|
0.48
|
4.00 |
|
Sympathy
|
4.32
|
0.54
|
2.00 |
| Nursing |
|
|
|
|
Affective Empathy
|
3.37
|
0.71
|
3.67 |
|
Cognitive Empathy
|
3.80
|
0.59
|
2.67 |
|
Sympathy
|
4.46
|
0.49
|
2.00 |
| Psychology |
|
|
|
|
Affective Empathy
|
3.28
|
0.78
|
4.00 |
|
Cognitive Empathy
|
3.86
|
0.59
|
2.67 |
|
Sympathy
|
4.35
|
0.65
|
2.67 |
Note. N
= 868.
Results
Participants’ scores on the AMES were used to measure participants’ levels of empathy and sympathy. Descriptive statistics were used to compare empathy and sympathy levels between counseling students and emerging college students from other disciplines. CITs recorded the second highest levels of affective empathy (M = 3.32, SD = .60) and cognitive empathy (M = 3.83, SD = 0.48), and the fourth highest levels of sympathy (M = 4.32, SD = 0.54) when compared to students from other disciplines. Nursing students demonstrated the highest levels of affective empathy (M = 3.37, SD = .71) and sympathy (M = 4.46, SD = .49), and psychology students recorded the highest levels of cognitive empathy (M = 3.86, SD = 0.59) when compared to students from other disciplines. The internal consistency values for each empathy and sympathy subscale on the AMES were as follows: Cognitive Empathy (α = 0.86), Affective Empathy (α = 0.75), and Sympathy (α = 0.76).
We performed a MANOVA to examine differences in empathy and sympathy in emerging adult college students by academic major, including counseling. Three dependent variables were included: affective empathy, cognitive empathy, and sympathy. The predictor for the MANOVA was the 6-level categorical “academic major” variable. The criterion variables for the MANOVA were the levels of affective empathy (M = 3.24, SD = .76), cognitive empathy (M = 3.80, SD = .58), and sympathy
(M = 4.34, SD = .60), respectively. The multivariate effect of major was statistically non-significant:
p = .062, Wilks’s lambda = .972, F (15, 2374.483) = 1.615, η2 = .009. Furthermore, the univariate F scores for affective empathy (p = .139), cognitive empathy (p = .074), and sympathy (p = .113) were statistically non-significant. That is, there was no difference in levels of affective empathy, cognitive empathy, or sympathy based on academic major, including counseling. Thus, these data indicated that CITs were no more empathic or sympathetic than students in other majors, as measured by the AMES.
We also examined these data for differences in affective empathy, cognitive empathy, and sympathy based on data collection method and educational level. However, we failed to identify a statistically significant difference between groups in empathy or sympathy based on data collection method
(e.g., online survey distribution, face-to-face data collection, email solicitation) or by educational level (e.g., master’s level or undergraduate status). Thus, these data indicate that data collection methods and participants’ educational level did not influence our results.
Discussion
The purpose of the present study was to (a) examine differences in empathy (i.e., affective empathy and cognitive empathy) and sympathy levels among emerging adult college students, and (b) determine whether CITs demonstrate different levels of empathy and sympathy when compared to their academic peers. We hypothesized that CITs would record greater levels of empathy and lower levels of sympathy when compared to their non-counseling peers, because of either their clinical training from their counselor education program or the possibility that the counseling profession might attract individuals with strong levels of dispositional empathy. Participants’ scores on the AMES were used to measure participants’ levels of empathy and sympathy. We conducted a MANOVA to determine if participants’ levels of empathy and sympathy differed when grouped by academic majors. CITs did not exhibit statistically significant differences in levels of empathy or sympathy when compared to students from other academic programs. In fact, CITs recorded levels of empathy that appeared comparable to students from other academic disciplines. This finding is consistent with literature indicating that even if empathy training is effective, counselor education programs might not be emphasizing empathy development in CITs or employing empathy training sufficiently. We also failed to identify statistically significant differences in participants’ AMES scores when grouping data by collection method or participants’ educational level. Thus, we believe our results were not influenced by our data collection method or by participants’ educational level.
Implications for Counselor Educators
The results from this investigation indicated that there was not a statistically significant difference in participants’ levels of cognitive or affective empathy or sympathy regardless of academic program, suggesting that CITs do not possess more or less empathy or sympathy than their academic peers. This was true for students in all majors under investigation (i.e., athletic training/health sciences, biology/biomedical sciences/preclinical health sciences, communication, counseling, nursing, and psychology), regardless of age and whether or not they belonged to professions considered helping professions (i.e., counseling, nursing, psychology). Although students in helping professions tended to have higher scores on the AMES than their peers, these differences were not statistically significant.
One might hypothesize that students in helping professions (especially in professions in which individuals have direct contact with clients or patients, such as counseling) would have significantly higher levels of empathy. However, counseling programs may not attract individuals who possess greater levels of trait empathy, or training programs might not be as effective in training their students as previously thought. Although microskills are taught in counselor preparation programs (e.g., reflection of content, reflection of feeling), microskill training might not overlap with material that is taught as part of an empathy training or enhance such training. Thus, microskill training might not be any more impactful for CITs’ development of empathy and sympathy than material included in training programs of other academic disciplines (e.g., athletic training, nursing).
Another potential reason for the lack of recorded differences between CITs and their non-counseling peers could be that counseling students are inherently anxious, skill-focused, self-focused, or have limited self-other awareness (Stoltenberg, 1981; Stoltenberg & McNeill, 2010). We wonder if CITs might not be focused on utilizing relationship-building approaches as much as they are on doing work that promotes introspection and reflection. Another inquiry for consideration is whether CITs potentially possess a greater understanding of empathy as a construct that inadvertently leads CITs to rate themselves lower in empathy than their non-counseling peers. Further, it is possible that CITs potentially minimize their own levels of empathy in an effort to demonstrate modesty, a phenomenon related to altruism and understood as the modesty bias (McGuire, 2003). Future research would be helpful to better understand various mitigating factors. Nevertheless, we suggest that counseling programs might be able to do more to foster empathy-facilitating experiences in counselors by being more proactive and effective in promoting empathy development in CITs. Through a review of the literature, we found support that empathy training is possible, and we wonder if there is a missed opportunity to effectively train counselors if counselor education programs do not intentionally facilitate empathy development in their CITs.
Counselor training programs are not charged to develop empathy in CITs; however, given the importance of empathy in the formation and maintenance of a therapeutic relationship, we propose that counseling training programs consider ways in which empathy is or is not being developed in their specific program. As such, we urge counselor educators to consider strategies to emphasize empathy development in their CITs. For example, reviewing developmental aspects of empathy in children, adolescents, and adults might fit well in a human development course, and the subject can be used to facilitate a conversation with CITs regarding their experiences of empathy development.
Similarly, because empathy consists of cognitive and affective components, CITs might benefit from work that assists them in gaining insight into areas of strengths and limitations in regard to both cognitive and affective aspects of empathy. Students who appear stronger in one area of empathy might benefit from practicing skills related to the other aspect of empathy. For example, if a student has a strong awareness of a client’s experience (i.e., cognitive empathy) but appears to have limitations in their felt sense of a client’s experience (i.e., affective empathy), a counselor educator might utilize live supervision opportunities to assist the student in recognizing present emotions or sensations in their body when working with the client or in a role play. Alternatively, to assist a student with developing a greater intellectual understanding of their client’s experience, a counselor educator might employ interpersonal process recall when reviewing their clinical work to help the student identify what their client might be experiencing as a result of their lived experience. To echo recommendations made by Bayne and Jangha (2016), we encourage counselor educators to move away from an exclusive focus on microskills for teaching empathy and to provide opportunities to teach CITs how to foster a connecting experience through creative means (e.g., improvisational skills).
Furthermore, the results from this study indicated that CITs possess higher levels of sympathy than of both cognitive and affective components of empathy. We recommend that counselor educators facilitate CITs’ understanding of the differences between empathy and sympathy and bring awareness to their use of sympathetic responses rather than empathic responses. It is our hope that CITs will possess a strong enough understanding between empathy and sympathy to be able to choose to use either response as it fits within a counseling context (Clark, 2010). We also encourage counselor educators to consider recommendations made by Bloom and Lambie (in press) to employ the AMES with CITs. The AMES could be a valuable and accessible tool to assist counselor educators in evaluating CITs’ levels of empathy and sympathy in regard to course assignments, in response to clinical situations, or as a wholesale measure of empathy development. As Bloom and Lambie encouraged, clinical training programs might benefit from using the AMES as a tool to programmatically measure CITs’ levels of empathy throughout their experience in their training program (i.e., transition points) as a way to collect programmatic data.
Limitations
Although this study produced important findings, some limitations exist. It is noted that the majority of participants from this study attended universities located within the Southeastern United States. As a result, the sample might not be representative of students nationwide. Similarly, demographic characteristics of the present study including the race, age, and gender composition of the sample limit the generalizability of the findings.
This study also is limited in that the instrument used to assess empathy and sympathy was a self-report measure. Although self-report measures have been shown to be reliable and are widely used within research, these measures might result in the under- or over-reporting of the variables of interest (Gall, Gall, & Borg, 2007). It is necessary to note that we employed the AMES, which was normed with adolescents and not undergraduate or graduate students. Although we recognize that inherent differences exist between adolescent and emerging adult populations, we believed the AMES was an effective choice to measure empathy because of Vossen and colleagues’ (2015) intentional development of the instrument to address existing weaknesses in other empathy assessment instruments. Nonetheless, it is necessary to interpret our results with caution.
Recommendations for Future Research
We recommend future researchers address some of the limitations of this study. Specifically, we recommend continuing to compare CITs’ levels of empathy with students from other academic disciplines, but to include a more diverse array of academic backgrounds. Similarly, we suggest future researchers not limit themselves to an emerging adult population, as both undergraduate and graduate populations include individuals over the age of 29. Further, researchers should aim to collect data from students across the country and to include a more demographically diverse sample in their research designs.
Additionally, it is necessary to note that limitations exist to using self-report measures (Gall et al., 2007), and measures of empathy are vulnerable to a myriad of complications (Bloom & Lambie, in press; Vossen et al., 2015). Thus, we encourage future researchers to consider using different measures of empathy that move away from a self-report format (e.g., clients’ perceptions of cognitive and affective empathy within a therapeutic relationship; Flasch et al., in press). Another area for future research is to track counseling students’ levels of empathy as they enter the counseling profession after graduation. It is possible that as they become more comfortable and competent as counselors, and as anxiety and self-focus decrease, their ability to empathize increases.
There is agreement in the counseling profession that empathy is an important characteristic for counselors to embody in order to facilitate positive client outcomes and to meet counselor competency standards (DePue & Lambie, 2014). Yet scholars have grappled with how to identify the necessary skills to foster empathy in counselor trainees and remain torn on which approaches to use. Although empathy training programs seem effective, little is known about which aspects of such programs are the effective ingredients that promote empathy-building, and we lack understanding about whether such programs are more effective than simply engaging in clinical work or having life experiences. Thus, we encourage researchers to explore if counseling programs are effective at teaching empathy to CITs and to further explore mechanisms that may or may not be valuable in empathy development.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Badenoch, B. (2008). Being a brain-wise therapist: A practical guide to interpersonal neurobiology. New York, NY:
W. W. Norton & Company, Inc.
Barrett-Lennard, G. T. (1986). The Relationship Inventory now: Issues and advances in theory, method, and use. In L. S. Greenberg & W. M. Pinsof (Eds.), The psychotherapeutic process: A research handbook (pp. 439–476). New York, NY: Guilford Press.
Batson, C. D., & Shaw, L. L. (1991). Evidence for altruism: Toward a pluralism of prosocial motives. Psychological Inquiry, 2(2), 107–122. doi:10.1207/s15327965pli0202_1
Bayne, H. B., & Jangha, A. (2016). Utilizing improvisation to teach empathy skills in counselor education. Counselor Education and Supervision, 55(4), 250–262. doi:10.1002/ceas.12052
Beder, J. (2004). Lessons about bereavement. Journal of Loss & Trauma, 9, 383–387. doi:10.1080/15325020490491014
Bell, H., Hagedorn, W. B., & Robinson, E. H. M. (2016). An exploration of supervisory and therapeutic relationships and client outcomes. Counselor Education and Supervision, 55(3), 182–197. doi:10.1002/ceas.12044
Bloom, Z. D., & Lambie, G. W. (in press). The Adolescent Measure of Empathy and Sympathy in a sample of emerging adults. Measurement and Evaluation in Counseling and Development.
Bohart, A. C., Elliott, R., Greenberg, L. S., & Watson, J. C. (2002). Empathy. In J. C. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 89–108). New York, NY: Oxford University Press.
Carré, A., Stefaniak, N., D’Ambrosio, F., Bensalah, L., & Besche-Richard, C. (2013). The Basic Empathy Scale in Adults (BES-A): Factor structure of a revised form. Psychological Assessment, 25, 679–691.
doi:10.1037/a0032297
Clark, A. J. (2004). Empathy: Implications of three ways of knowing in counseling. The Journal of Humanistic Counseling, Education & Development, 43, 141–151. doi:10.1002/j.2164-490X.2004.tb00014.x
Clark, A. J. (2010). Empathy and sympathy: Therapeutic distinctions in counseling. Journal of Mental Health Counseling, 32(2), 95–101. doi:10.17744/mehc.32.2.228n116thw397504
Connors, G. J., Carroll, K. M., DiClemente, C. C., Longabaugh, R., & Donovan, D. M. (1997). The therapeutic alliance and its relationship to alcoholism treatment participation and outcome. Journal of Consulting and Clinical Psychology, 65, 588–598. doi:10.1037/0022-006X.65.4.588
Council for Accreditation of Counseling and Related Educational Programs. (2016). 2016 Standards. Alexandria,
VA: Author.
Davis, M. H. (1980). A multidimensional approach to individual differences in empathy. JSAS Catalog of Selected Documents in Psychology, 10, 85.
Davis, M. H. (1983). Measuring individual differences in empathy: Evidence for a multidimensional approach. Journal of Personality and Social Psychology, 44, 113–126. doi:10.1037/0022-3514.44.1.113
Decety, J., & Ickes, W. (Eds.). (2009). The social neuroscience of empathy. Cambridge, MA: MIT Press.
DePue, M. K., & Lambie, G. W. (2014). Impact of a university-based practicum experience on counseling students’ levels of empathy and assessed counseling competences. Counseling Outcome Research and Evaluation, 5(2), 89–101. doi:10.1177/2150137814548509
Dillman, D. A., Smyth, J. D., & Christian, L. M. (2009). Internet, mail, and mixed-mode surveys: The tailored design method (3rd ed.). Hoboken, NJ: Wiley.
Eisenberg, N., Eggum, N. D., & Di Giunta, L. (2010). Empathy-related responding: Associations with prosocial behavior, aggression, and intergroup relations. Social Issues and Policy Review, 4, 143–180.
doi:10.1111/j.1751-2409.2010.01020.x
Elliott, R., Bohart, A. C., Watson, J. C., & Greenberg, L. S. (2011). Empathy. Psychotherapy, 48, 43–49.
doi:10.1037/a0022187
Flasch, P. S., Limberg-Ohrt, D., Fox, J., Ohrt, J., Crunk, E., & Robinson, E. (in press). Experiences of altruistic caring by clients and their counselors in the counseling session. Counseling & Values Journal.
Gall, M. D., Gall, J. P., & Borg, W. R. (2007). Educational research: An introduction (8th ed.). Boston, MA: Allyn & Bacon.
Goleman, D. (1995). Emotional intelligence: Why it can matter more than IQ for character, health and lifelong achievement. New York, NY: Bantam Books.
Hair, J. F., Jr., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data analysis (7th ed.). Upper Saddle River, NJ: Prentice Hall.
Ivey, A. E. (1971). Microcounseling: Innovations in interviewing training. Oxford, England: Charles C. Thomas.
Ivey, A. E., Normington, C. J., Miller, C. D., Morrill, W. H., & Haase, R. F. (1968). Microcounseling and attending behavior: An approach to prepracticum counselor training. Journal of Counseling Psychology, 15(5), 1–12.
Jolliffe, D., & Farrington, D. P. (2006). Development and validation of the Basic Empathy Scale. Journal of Adolescence, 29, 589–611. doi:10.1016/j.adolescence.205.08.010
Kirchberg, T. M., Neimeyer, R. A., & James, R. K. (1998). Beginning counselors’ death concerns and empathic responses to client situations involving death and grief. Death Studies, 22(2), 99–120.
Kline, R. B. (2011). Principles and practice of structural equation modeling (3rd ed.). New York, NY: Guilford Press.
Konrath, S. H., O’Brien, E. H., & Hsing, C. (2011). Changes in dispositional empathy in American college
students over time: A meta-analysis. Personality and Social Psychology Review, 15, 180–198. doi:10.1177/1088868310377395
Krupnick, J. L., Sotsky, S. M., Simmens, S., Moyer, J., Elkin, I., Watkins, J., & Pilkonis, P. A. (1996). The role of a therapeutic alliance in psychotherapy and pharmacotherapy outcome: Findings in the National Institute of Mental Health Treatment of Depression Collaborative Research Program. Journal of Consulting and Clinical Psychology, 64, 532–539.
Lam, T. C. M., Kolomitro, K., & Alamparambil, F. C. (2011). Empathy training: Methods, evaluation practices, and validity. Journal of Multidisciplinary Evaluation, 7(16), 162–200.
Lambert, M. J., & Barley, D. E. (2001). Research summary on the therapeutic relationship and psychotherapy outcome. Psychotherapy: Theory, Research, Practice, Training, 38, 357–361. doi:10.1037/0033-3204.38.4.357
Lambert, M. J., & Bergin, A. E. (1994). The effectiveness of psychotherapy. In A. E. Bergin & S. L. Garfield (Eds.), Handbook of psychotherapy and behavior change (4th ed.; pp. 143–189). Oxford, England: John Wiley & Sons.
McGuire, A. M. (2003). “It was nothing”: Extending evolutionary models of altruism by two social cognitive biases in judgment of the costs and benefits of helping. Social Cognition, 21, 363–394.
doi:10.1521/soco.21.5.363.28685
McWhirter, B. T., Besett-Alesch, T. M., Horibata, J., & Gat, I. (2002). Loneliness in high risk adolescents: The role of coping, self-esteem, and empathy. Journal of Youth Studies, 5, 69–84. doi:10.1080/13676260120111779
Norcross, J. C. (Ed.). (2011). Psychotherapy relationships that work: Evidence-based responsiveness (2nd ed.). New York, NY: Oxford University Press.
Norcross, J. C., & Lambert, M. J. (2011). Psychotherapy relationships that work II. Psychotherapy: Theory, Research, Practice, Training, 48, 4–8.
Osborne, J. W. (2013). Best practices in data cleaning: A complete guide to everything you need to do before and after collecting your data. Thousand Oaks, CA: Sage.
Qualtrics. (2013). Qualtrics software (Version 37,892) [Computer software]. Provo, UT: Qualtrics Research Suite.
Ridley, C. R., Kelly, S. M., & Mollen, D. (2011). Microskills training: Evolution, reexamination, and call for reform. The Counseling Psychologist, 39, 800–824. doi:10.1177/0011000010378438
Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change. Journal of Consulting Psychology, 21, 95–103. doi:10.1037/h0045357
Sachse, R., & Elliott, R. (2002). Process–outcome research on humanistic therapy variables. In D. J. Cain & J. Seeman (Eds.), Humanistic psychotherapies: Handbook of research and practice (pp. 83–115). Washington, DC: American Psychological Association.
Siegel, D. J. (2010). Mindsight: The new science of personal transformation. New York: Bantam.
Silva, N. W. (2001). Effect of empathy training on masters-level counseling students. (Unpublished doctoral dissertation). University of Florida, Gainesville, FL.
Spreng, R. N., McKinnon, M. C., Mar, R. A., & Levine, B. (2009). The Toronto Empathy Questionnaire: Scale development and initial validation of a factor-analytic solution to multiple empathy measures. Journal of Personality Assessment, 91, 62–71. doi:10.1080/00223890802484381
Stoltenberg, C. (1981). Approaching supervision from a developmental perspective: The counselor complexity model. Journal of Counseling Psychology, 28, 59–65. doi:10.1037/0022-0167.28.1.59
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors & therapists (3rd ed.). New York, NY: Routledge.
Szalavitz, M., & Perry, B. D. (2010). Born for love: Why empathy is essential—and endangered. New York, NY: Harper Collins.
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed). Upper Saddle River, NJ: Pearson.
Teding van Berkhout, E., & Malouff, J. M. (2016). The efficacy of empathy training: A meta-analysis of randomized controlled trials. Journal of Counseling Psychology, 63, 32–41. doi:10.1037/cou0000093
Truax, C. B., & Carkhuff, R. R. (1967). Toward effective counseling and psychotherapy: Training and practice. Chicago, IL: Aldine Publishing.
Truax, C. B., & Lister, J. L. (1971). Effects of short-term training upon accurate empathy and non-possessive warmth. Counselor Education and Supervision, 10(2), 120–125. doi:10.1002/j.1556-6978.1971.tb01430.x
Vossen, H. G. M., Piotrowski, J. T., & Valkenburg, P. M. (2015). Development of the Adolescent Measure of Empathy and Sympathy (AMES). Personality and Individual Differences, 74, 66–71.
doi:10.1016/j.paid.2014.09.040
Watson, J. C., Steckley, P. L., & McMullen, E. J. (2014). The role of empathy in promoting change. Psychotherapy Research, 24, 286–298. doi:10.1080/10503307.2013.802823
Zachary D. Bloom is an assistant professor at Northeastern Illinois University. Victoria A. McNeil is a doctoral candidate at the University of Florida. Paulina Flasch is an assistant professor at Texas State University. Faith Sanders is a mental health counselor at Neuropeace Wellness Counseling in Orlando, Florida. Correspondence can be addressed to Zachary Bloom, 5500 North St. Louis Avenue, Chicago, IL 60625, z-bloom@neiu.edu.
Nov 9, 2018 | Volume 8 - Issue 4
Jennifer Barrow, Stanley B. Baker, Lance D. Fusarelli
The purpose of this grounded theory study was to understand and explain how training and work setting experiences influence readiness of professional school counselors for serving gang members in schools. A purposeful sample consisted of secondary school counselors (n = 5) and school leaders (n = 7) in a southeastern metropolitan school district. Blended themes from the counselors and leaders were: (a) professional development attitudes, (b) actual and potential roles when working with students in gangs, and (c) counselors’ collaborative role in discipline process. The Collaborative C.A.R.E. theory that emerged from the thematic analysis highlighted the absence of collaboration between school counselors and leaders. Specific findings identified reasons for the lack of collaboration and led to recommendations for practice and further research.
Keywords: gang members, school counselors, grounded theory, Collaborative C.A.R.E, discipline
On a daily basis, professional school counselors (PSCs) are expected to engage in a variety of functions in order to enhance the academic, career, personal, and social development of all students (American School Counselor Association [ASCA], 2012b, 2014). Serving all students can be very challenging given the disproportionate number of PSCs to students in the United States and the number of non-counseling functions often imposed on PSCs (Lambie & Williamson, 2004). ASCA (2012a) recommends a counselor-to-student ratio of 1:250. Despite this recommendation, findings have indicated that the accurate ratio is closer to 1:491 (ASCA, n.d.). Responding to the “serve all students” expectation can be even more challenging when attempting to serve gang members, who are considered members of marginalized populations that are excluded from the social, economic, cultural, and political mainstream (McCluskey, Baker, & McCluskey, 2005).
Research on the PSC’s role was conducted in the late 1990s and early 2000s, and much of the research is generalized to include the role of the PSC (both perceived and actual) with little consideration for the contextual differences in jobs (e.g., elementary, middle, high school; Brott & Myers, 1999; Lambie & Williamson, 2004). A paucity of data exists in recent research examining the role of PSCs with specific groups of students based on cultural and environmental contexts, and their role since the introduction of the ASCA National Model. Gang members are students with norms related to language, rituals, and membership (Gibbs, 2000). The presence of gangs in schools reflects a need to examine the role of the PSC in serving this culturally marginalized population.
Gang members are often viewed as outsiders associated with “outlaw organizations” engaged in deviant behaviors (Gibbs, 2000, p. 73). On the other hand, from the inside, members find structure, ritual, and norms specific to their gang structure. This study was designed to attempt to fill these gaps by examining the role of the PSC with a contemporary, marginalized population.
According to the National Gang Intelligence Center (2011), there are approximately 1.4 million active gang members representing more than 33,000 gangs in the United States. This represents a 40% increase compared to data collected in 2009. The data support an assumption that there is an increasing presence of gangs in both rural and urban communities (Brinson, Kottler, & Fisher, 2004). Unfortunately, there are several negative outcomes associated with the presence of gang members in the schools, including harassment, vandalism, aggressive recruitment of new members, irregular attendance, decreased motivation to succeed in school, and criminal activities. Consequently, gang presence can adversely affect the school environment, lower levels of academic achievement, and negatively influence perceptions of safety (Brinson et al., 2004). In and of itself, gang membership is not a crime, and gang members who are enrolled in public schools are eligible for all of the services that other students are receiving, including those offered by PSCs (Kizer, 2012).
As gang membership increases nationally, the presence of gang members will continue to expand in the schools and surrounding communities (Coggeshall & Kingery, 2001; Kingery, Coggeshall, & Alford, 1998). A recent survey of 12- to 18-year-old students indicated that 18% stated there were gangs in their schools (Robers, Kemp, Truman, & Snyder, 2013). This phenomenon will increase the exposure of PSCs to gang activity (Gündüz, 2012; Skovholt & McCarthy, 1988). Because of their training, PSCs appear to be in a unique position conceptually to offer services to gang members and to the schools where gang members are present. Potential resources include individual and group counseling competencies; core curriculum programming knowledge and skills; availability for providing helpful consultations; and the overlying quest to enhance the academic, career, personal, and social development of all students (ASCA, 2012b, 2014).
The first author’s exposure to gangs increased in her role as a PSC. Perceived lack of training and preparation to work with gang members and an absence of professional literature on the role of PSCs with gangs motivated the first author to conduct a preliminary investigation. Participants in the pilot study were PSCs in a southeastern urban public school setting. The pilot study consisted of two phases of inquiry consistent with the grounded theory methodology. Grounded theory generates data based on “participant experiences” (Hays & Singh, 2012, p. 288).
The first phase of the pilot study was a focus group of PSC participants with data being transcribed by the researcher, hand-coded, and analyzed. The second phase consisted of individual interviews completed at the respective job sites of three practicing PSCs. The interviews and observations from the second phase provided further evidence, more variation, and a greater understanding of the role of the PSC working with students in gangs across elementary, middle, and high school settings.
The preliminary investigation suggested further research in the school counseling domain. The participating PSCs appeared to experience ambiguity and lack of decision-making authority related to working with students who are gang members. Decisions on professional development opportunities and the PSC’s role were influenced by school-based leaders, such as principals, whose views tended to focus on disciplinary issues rather than academic, career, personal, and social development with regard to gang members. Consequently, the pilot study revealed a need to further explore the PSC’s role in working with gang members based on perceived and ideal roles, their professional development needs, and the influence of their educational administrators and supervisors.
Although uniquely positioned to offer something of value, there are impediments to fulfilling that role. Developing and defining the role for PSCs continues to be a challenge for PSCs, their school leaders (SLs), and national professional organizations that offer recommended roles for PSCs (Foxx, Baker, & Gerler, 2017; Griffin & Farris, 2010; Shoffner & Williamson, 2000). Some SLs determine the tasks that define the role of their PSCs with little to no input from counselors (Zalaquett & Chatters, 2012). These decisions are not aligned with ASCA’s PSC role recommendations and indicate misunderstandings about how their counselors were trained and failure to collaborate on PSC role definitions (Kirchner & Setchfield, 2005). Collaboration between PSCs and SLs is essential in the development of comprehensive counseling programs designed to support the academic goals of the school (Armstrong, MacDonald, & Stillo, 2010; Foxx et al., 2017; Zalaquett & Chatters, 2012).
An additional challenge is a lack of professional development related to working with gang members after one’s graduate training program. Caldarella, Sharpnack, Loosli, and Merrell (1996) found that many PSCs do not feel adequately trained or equipped to deal with gang activity and gang members in their schools, and almost half of the sample had no training related to gangs. Relatedly, our preliminary investigation found PSCs were trained to recognize the presence of gangs yet knew very little about how to engage with gang members and offer their services. Believing that one is unprepared and not competent to deliver counseling services to gang members may cause feelings of helplessness, apathy, and little or no desire to serve them (Ibrahim, Helms, & Thompson, 1983). As a marginalized population, students in gangs compound the unique challenges PSCs face, including role ambiguity (Burnham & Jackson, 2000), constant changes in student and school characteristics and needs (Reising & Daniels, 1983), and disconnects between training and practice (Brott & Myers, 1999; Lambie & Williamson, 2004).
The purpose of the present grounded theory study was to further understand and explain how training, perceived roles, and work setting experiences (e.g., professional development, working with students in gangs) influenced the readiness of PSCs in a large urban school district to serve gang members. Given the challenges PSCs experience related to serving gang members, the following research questions were derived in order to attempt to explain a conceptual linkage via a grounded theory based on understanding perspectives of a sample of PSCs and SLs via the interplay of context, conditions, and the PSC’s role (Hays & Singh, 2012): How do PSCs and SLs describe perceived and actual roles of PSCs regarding services to gang members? How do PSCs and SLs describe previous training related to working with gang members? and How do PSCs and SLs describe circumstances that influence opportunities PSCs have for serving gang members?
Method
Participants
A total of 12 participants were included in this study. Five participants were PSCs and seven were SLs. Of the PSCs, four were female and one was male; four were White and one was African American. All of the PSCs had master’s degrees and school counseling licenses. The mean age of the PSCs was 52 (SD = 8.57), and the mean years of counseling experience was 14.8 (SD = 7.69). All of the seven SLs were male. Six were White and one was African American. Four had master’s degrees in educational leadership, one had a bachelor’s degree in science, and two had doctoral degrees in education. Two of the seven SLs were based in the school district’s central office. The mean age of the SLs was 42 (SD = 7.23), and the average years of experience was 10.4 (SD = 3.26). Each participant is represented by a pseudonym in the findings.
Consistent with grounded theory, stratified purposeful sampling was used to identify PSCs and SLs serving at the same school to voluntarily participate (Corbin & Strauss, 2008; Hays & Singh, 2012). PSCs possessed state professional licenses in their fields and were employed in secondary school settings. Specific criteria for the SLs were that they be assistant principals, principals, or central office staff members. SLs possessed state professional licenses in their fields. An additional advantage of this approach was being able to triangulate data sources by acquiring data from different perspectives, including central school office members.
Instrumentation
Demographic questionnaire. Information related to age, ethnicity, education, and experience was collected from PSC and SL participants via a brief demographic questionnaire that asked identical questions.
Interview questions for participants. Two sets of open-ended questions were developed for semi-structured individual interviews. Topical areas addressed in the current study included role perception, professional development, and barriers to serving students in gangs. The following questions were presented to the PSC participants: (a) What factors determine the role you play in your school? (b) Who is involved in determining your professional role? (c) In your opinion, what role do professional school counselors currently play in identifying gang presence and providing intervention in your school? (d) Tell me what role you think counselors may play in identifying and providing interventions for students currently involved in a gang or considering gang membership. (e) What role has the school or school district played in providing professional school counselors with training specific to gang activity in the schools? (f) During your graduate school training, were you provided any opportunities to learn about gangs in schools? (g) Since graduate school, have you been provided or sought out opportunities to learn about gangs in schools? (h) In your own words, describe your work with students in gangs. (i) What barriers exist impacting your effectiveness in working with students in gangs? (j) In what ways do you seek out information to inform your work as a professional school counselor? (k) How might the ASCA National Model support your efforts to prevent or intervene with students in gangs? and (i) Is there anything you care to add?
The following questions were presented to the SL participants: (a) What factors determine the role school counselors play in your school? (b) Who is involved in determining their professional role? (c) In your opinion, what role do professional school counselors currently play in identifying gang presence and providing intervention in your school? (d) Tell me what role you think counselors may play in identifying and providing interventions for students currently involved in a gang or considering gang membership. (e) What role has the school or school district played in providing professional school counselors and school faculty with training specific to gang activity in the schools? (f) During your graduate school training, were you provided any opportunities to learn about the role of the school counselor? (g) Since graduate school, has your perception of the role of the school counselor changed? How so? (h) In your own words, describe your work with students in gangs. (i) How might the ASCA National Model support your school’s efforts to prevent or intervene with students in gangs? and (j) Is there anything you care to add?
Interviewer/Investigator. The first author was an insider who worked for the school district as a PSC. At the time of the study, she was working full-time and was a doctoral student in a counselor education program accredited by the Council for Accreditation of Counseling and Related Educational Programs. She was a 37-year-old White female with nine years of school counseling experience. She is a licensed school counselor, licensed professional counselor, and a National Certified Counselor (NCC). She had access to data that would not be available to an outsider. An advantage was her familiarity with the participants.
Subjectivity statement. On the one hand, the first author lacked personal gang awareness and was sensitive to the participants’ lack of knowledge (Corbin & Strauss, 2008). On the other hand, she had observed disruptive incidents created by gang members in her schools and was conflicted about how to deal with gang members as a professional. This led to a preliminary literature review that suggested ideas about how PSCs may serve gang members in their schools via both responsive services and core curriculum responses. The potential biases were role ambiguity and professional development. These biases were addressed during the data collection and analysis through the use of a journal to record immediate reactions to completed interviews.
Reflectivity during data collection is a valuable tool and is “considered essential to the research process” (Corbin & Strauss, 2008, p. 31). A journal housed field notes after each interview regarding participants’ body language, physical environment, and interviewer’s immediate thoughts and impressions. Journaling allowed for the constant comparison of data, looking for more data, and initial coding of collected data (Corbin & Strauss, 2008).
Procedure
Data collection. Established university research policies for the protection of human subjects and the research policies of the school district were followed in order to gain access to schools and participants. After receiving institutional review board approval from the first author’s affiliated university and the school district’s research department, data collection was completed via interviewing participants, journaling, and reviewing documents. The primary source of data was individual semi-structured interviews using an open-ended questions approach and an interview guide (Patton, 2002). Observations of the school setting, participants, and reflections of each interview were noted by the first author/researcher in her journal (Corbin & Strauss, 2008). In addition to journaling, policy manuals and public relations documents were accessed from the school district’s website for the triangulation process (Patton, 2002). The school district’s documents informed the researcher of existing procedures and policies and potential access to related training opportunities.
Participants were provided the interview questions in the moments immediately preceding the beginning of the interviews, giving them the opportunity to view questions and consider answers or emerging thoughts as needed. They were offered an opportunity to answer all questions. In order to enhance the analysis of the role of the PSC, interviews were conducted with SLs and PSCs working at the same schools. The interviews were conducted at the jobsites of the PSCs and SLs or at mutually agreeable locations. A digital voice recorder was used to record all interviews.
Data analysis. The recorded interviews were played and reviewed immediately after face-to-face interviews, allowing for constant comparisons (Schwandt, 2001). Each individual audio-recorded interview was transcribed by a professional transcriptionist. Following transcription, the interviews were read twice by the first author before themes were highlighted and noted in the margins. Interview data were individually read for all PSCs with themes noted in the margins. Then, interview data were individually read for all SLs with themes noted in the journal. Finally, interview data were reviewed for each PSC and their corresponding SL with themes of each pairing noted by the researcher. Hand-coding was used to analyze data gathered from transcribed interviews with a focus on capturing essential concepts (Bogdan & Biklen, 2007). The process of hand-coding involved deriving codes and the emerging themes to be organized into discrete categories leading to theory development (Corbin & Strauss, 2008). In the first or open coding stage, large general conceptual domains were identified in the reflective journal. Then, the researcher searched for relationships among the domains during the axial coding stage. Finally, the selective coding stage involved: (a) explaining story lines, (b) relating subsidiary categories around the core categories by means of paradigms, (c) relating categories at the dimensional levels, (d) validating the relationships against the raw data, and (e) filling in the categories that may need further development (Corbin & Strauss, 2008).
Triangulation was used as a means to increase the trustworthiness in the present study (Creswell & Miller, 2000; Patton, 2002). Four data sources were used to inform theory development: interviews with PSCs, interviews with SLs, a reflective journal, and related school district documents (e.g., discipline policies, in-service training programs). Grounded theory is built upon the cyclical and constant analysis of data (Hays & Singh, 2012). The use of multiple data sources in this study enhanced the development of codes, categories, and theory, and strengthened the trustworthiness of the study’s findings (Merriam, 2002). The transcribed interviews were reviewed by the researcher to ensure that professional jargon was accurate. A reflective research journal was kept throughout the entire study. Each participant was offered an opportunity to member check the transcribed data (Creswell & Miller, 2000). In addition, an audit was conducted to attempt to reduce the potential for personal biases influencing the data analysis. The auditor was a White female with a doctorate in educational leadership and previous work experience as a PSC. The auditing process consisted of quality control: (a) assuring ethical concerns were addressed, including the use of pseudonyms to protect participants; (b) reviewing the data to insure the study proposed and conducted matched data reported; and (c) proofreading, including clarifying professional jargon. Data saturation was achieved after the eighth interview; however, to affirm category development, complete interview pairings, and ensure triangulation of data sources, the interviews continued through 12 participants. As stated in the introduction, the purpose of the present study was to construct a grounded theory based on the data.
Findings
Grounded theory study data analyses provide central categories that bring all of the codes together (Corbin & Strauss, 2008). The central thematic categories in the present study were: (a) professional development attitudes, (b) actual and potential roles when working with students in gangs, and (c) PSCs’ collaborative role in the discipline process. An integration of the three central categories caused a Collaborative C.A.R.E. theory to emerge. Collaboration was the category both present and notably absent in the stories of the PSCs and the SLs. The C.A.R.E. acronym emerged out of the categories that developed during the axial coding process. The categories revealed a lack, or the presence, of communication with community stakeholders. The data suggested a need for PSCs working in secondary school settings to advocate for policies, procedures, programming, and educational opportunities to clarify their role in providing responsive services for students in gangs. What follows are excerpts of the data in the voices of the participants presented via the three central themes.
Professional Development Attitudes
PSCs are increasingly overwhelmed by their day-to-day responsibilities, leading them often to not engage in professional development that may take them away from campus. In addition, the interview data revealed that PSCs were not engaging in professional development related to working with gang members because of a lack of interest in working with this population, a concern for personal safety, unclear counseling roles, and the cost of professional development.
Beth (PSC) noted in her time as a PSC that different initiatives drive the training offered in the local district. She recalled a “push” four or five years previously to identify the presence of gangs at her school, but since that training she noted, “It’s not an interest of mine” and she will look to other staff members to “handle that stuff.” Beth’s response demonstrated a lack of engagement as a result of a lack of interest.
As noted, Beth expected other staff members, primarily SLs, to address the needs of students in gangs. In contrast, Sasha’s (PSC) gang awareness training at the school level had occurred in other counties. She noted that the school district in the present study “maybe has had something,” but “I don’t think the school has provided anything.” She went on to say, “I don’t think I’ve done anything in this district.” Sasha added that possessing knowledge of gangs in schools is “just not the highest on the list of priorities.”
Sasha’s supervising SL, Joe, noted the training from the district is “probably limited, to be honest.” Joe stated as an SL: “I don’t receive training for gangs or gang-related activity. Most of what I know is either self-taught or stuff that we pick up along the way because we’re placed into that position as administrators.” Joe elaborated that much of what he had picked up was reactive: “Unfortunately it’s reactive, but that’s also predicated upon the levels that we deal with here, which is not very much . . . so some of that [training] is from our SRO [school resource officer].”
Beyond having experienced awareness training, the PSCs expressed repeated concerns about their lack of intervention tools. Sasha said she was in need of “strategies” to work with gangs. She asked, “Are you working on trying to get them out of a gang or are you working on how do you cope with being part of a gang?” She followed with an insight: “it’s . . . how it’s affecting them in the school and so, generally, it leads to academics and attendance and if there are discipline issues or . . . . But it still has to have the school slant to . . . work with them.” Judy (PSC) concurred that training had “been mostly awareness and information,” and a lack of urgency to learn more left her deficient in skills and techniques to intervene.
Although awareness training appeared to be somewhat useful, specific prevention and intervention strategies were lacking in any of the training in which PSCs had previously participated. Stacey (PSC) stated that the limited training she received had been “one or two instances” consisting of “signs or signals.” Sasha noted she had not been trained to intervene, and she believed part of the problem was the nature of gangs because they may be “generational, and I don’t think anybody really knows how exactly [to] intervene. ” When speaking about the role of training, Judy quite frankly stated, “If you’re going to provide . . . training, does that imply that I then own the problem . . . if you’re training me, you’re giving me the problem and how am I supposed to solve it?”
Actual and Potential Roles When Working With Students in Gangs
The perceived and actual role of working PSCs has been studied extensively. Recommendations for serving students representing specific populations may vary (e.g., different ethnic groups, various exceptional populations, sexual minorities). On the other hand, ASCA (2014) is explicit in its petitioning provision of services to all students to address long-term goals and “demonstrate personal safety skills” (p. 2). The findings in this study suggest a possible actual role and provide ideas for a potential role for serving gang members.
Beth’s SL, Stan, said, “I would say they [PSCs] don’t really have a specific role in identifying gang presence” and “it wouldn’t be something that I would put under their job description.” Beth also noted that interactions with students in gangs were limited to an awareness that students may be involved with a gang because any intervention or interaction was something “that the assistant principals work with.” Stan’s comments mirrored those of his PSC. He stated, “If it’s a discipline issue, then it [the student issue] would stick with the administration.” Stan’s PSCs would be involved if the student needed “more of a counseling-type component where the student needs assistance or is seeking help from . . . the school.”
Sasha said she worked with students in gangs, but their gang affiliation was “not what we’re working on.” Beth agreed: “The thing is . . . if a kid is coming to you with a specific problem, you help them with that specific problem whether he’s a gang member or not.” Beth stated her actual role as a PSC limited her ability to interact because in her opinion, “if a kid was deeply entrenched in a gang, we’re not going to be able to get them out of that gang.” Derek (SL) agreed that the degree of involvement complicates the intervention because “once they reach a certain point, it is going to be very difficult—I’m not going to say impossible—but it’s going to be very difficult to get [them] back.”
Because the immediate need for a student to seek a PSC’s assistance was rarely, if ever, gang-related, Beth noted her form of intervention was about helping the students obtain their diplomas. Beth went on to say, “If he is here and attempting to get an education, behaving himself and not fighting . . . then my role would be to help him get what he needs from the school system as long as he is playing by our rules.” Her view of services for gang members seemed focused primarily on academic counseling.
PSCs’ Collaborative Role in Discipline Processes
Jake (SL) identified collaboration as a function in the PSC’s role when working with students in gangs, although he noted that the level of collaboration would be limited by the degree of the student’s gang involvement and its impact on the school environment. Jake stated, “I don’t know that they play a role in identifying gang issues unless somebody comes to them with a situation.”
Stacey, a PSC at Jake’s school, concurred with his assessment when she noted, “We don’t do a lot in identifying the gang presence . . . administration and the resource officer tend to be the ones dealing with that.” Stacey went on to say that addressing students in gangs was handled by administrators, and there was no communication with the PSCs about those students that may be involved in gangs. Communications related to students in gangs among SLs, PSCs, and teachers did not exist at Stacey’s school. She explained, “I can’t remember anyone here ever talking about making that kind of referral.”
Like Stacey, Trevor (PSC) did not expect referrals related to gang membership coming to him from teachers. The PSC participants reported that those students violating school policy were referred to administrators. Most referrals for confirmed concerns related to gang members based on attire or language were directed to the administrative teams if they came to the counseling office first. As a counterpoint, Trevor’s SL, Frank, stated, “I can’t say I’ve ever met a counselor I would trust to even give me that type of information.” He went on to say, “So I’m not very trusting of that [information coming from PSCs] at this point. I don’t think they’re [PSCs] involved.”
The degree of collaboration in the actual role of PSCs was mentioned frequently. There seemed to be a lack of collaboration and shortage of referrals from SLs to PSCs, especially when the student gang members had committed infractions leading to disciplinary consequences. When SLs disciplined gang members, there often was no follow-up with PSCs. The SLs in this sample seemed not to view PSCs as contributors to their disciplinary and safety maintenance functions. Because of their focus on safety and discipline issues when thinking about gang members, it seemed not to occur to the SLs that PSCs could contribute to the academic, career, personal, and social development of gang members via their traditional professional functions.
Limitations
Given the impact of the school calendar and its restricted timeline on data collection, it is possible the researcher was dependent upon acquiring participants from a limited population of busy professionals. Rather than relying on power analyses to determine the sample, qualitative researchers rely on evidence of data saturation, which may not have occurred in this study, to ensure sample sizes are sufficient. Further, qualitative researchers continue interviewing if repeated themes or codes are not present in the interviewing and follow emerging themes (Corbin & Strauss, 2008; Creswell & Miller, 2000; Marshall, Cardon, Poddar, & Fontenot, 2013). In the present study, the sample size was smaller than some sources recommend for grounded theory studies. Fortunately, obvious signs of saturation were noted after the eighth participant was interviewed.
Racial diversity was limited to one African American in each sub-sample. Gender diversity was not achieved in the SL sub-sample. Consequently, the voice of a female SL’s perspective was not present in this study because there were only five female site-based SLs in a district with 25 high schools. The lack of diversity might have impacted the lens by which they led or worked with marginalized populations. Meeting the age diversity selection criterion also was a challenge. The average age of the PSCs indicated that the views and experiences of younger professionals were understated. The extent of the participating PSCs’ exposure to the ASCA National Model (2012a) was not assessed in the demographic questionnaire. Consequently, recommendations promoted in the National Model such as serving all students; offering comprehensive school counseling programs; enhancing the academic, career, and personal/social development of students; and collaboration with stakeholders, may have been limited, therefore impacting their perceived and actual roles accordingly. Participants may have self-censored responses as a result of being interviewed by a school system colleague or by knowing that a colleague in their school with more power was also being interviewed. Utilizing a researcher without ties to the school district might have enhanced the responses. Having colleagues from the same school participate was an important component of the study, a limitation that had to be accepted in addition to the population and sample being limited to one school district.
Discussion
The perceived and ideal role of PSCs has been extensively studied; however, a search of the professional literature demonstrated a paucity of research on the role of PSCs with specific, marginalized student populations (e.g., exceptional children, homeless), and the present study was designed to address the work of PSCs with one such group (i.e., students in gangs). The researcher attempted to understand the participants’ perspectives related to how participating PSCs and SLs described their actual roles, their previous training, and opportunities for further training with regard to serving gang members.
Consistent with previous research (Burnham & Jackson, 2000; Ibrahim et al., 1983; Lambie & Williamson, 2004), the findings revealed a perceived role for the PSCs’ work with students in gangs as academically focused and reactive. PSC participants noted not knowing what counseling strategies to employ in order to assist students in gangs, implying there is no ideal role for PSCs within that domain. A lack of engagement in professional development, concerns for personal safety, unclear or absent roles for working with students in gangs, and, notably, a limited role imposed by SLs, negatively impacted their potential for working with gang members constructively.
Insights Based on the Circumstances That Led to the Study
As stated in the introduction, motivation to conduct the study was based on the first author’s limited previous professional experience with gang members, suggestions from a literature search, and results of a pilot study. The first author reported having observed the influence of disruptive gang members in her schools, leading to conflicted thoughts about how to serve them. Consistent with previous literature on role confusion (Burnham & Jackson, 2000; Lambie & Williamson, 2004), PSCs in the present study also seemed conflicted about serving student gang members, and SLs seemed to consider the role of PSCs from a limited perspective. The perspectives of the two sets of professionals were somewhat different because their respective broad professional goals differed. Although SLs were more likely to focus on maintaining order and ensuring safety for all students, PSCs were more likely to focus primarily on their own safety and secondarily on providing limited responsive services to gang members (Sindhi, 2013).
Consequently, when SLs considered the role of PSCs, their perspectives were narrowly focused on safety and disciplinary issues, and PSCs were not viewed as being expected or able to contribute to those goals. They were not prompted to consider the PSC’s role from a broader professional perspective, nor did they think of it (Cobb, 2014). It seemed as if most of the PSCs also responded from a safety perspective, feeling unprepared and unwilling to be involved in that kind of role, especially if it would involve discipline or attempting to get students to leave their gangs. Two PSCs (Sasha and Beth) mentioned providing limited responsive services if requested (i.e., personal issues and academic counseling) and if the students were behaving themselves. This finding also mirrored those of the pilot investigation that prompted this study.
Related contributions to the professional literature indicated dissonance about the perceived and actual roles of PSCs (Brott & Myers, 1999; Burnham & Jackson, 2000; Ibrahim et al., 1983; Lambie & Williamson, 2004). The findings in the present study were quite similar to those of Caldarella et al. (1996) almost two decades ago—that is, the PSCs did not feel adequately trained to work with gang members. And the attitudes expressed by the PSC participants in the findings mirrored the apathy about and disinterest in serving gang members reported by Ibrahim et al. (1983) over 30 years ago. Unfortunately, the findings highlighted apparently limited potential for PSCs to address the academic, career, personal, and social development needs of students in gangs in the targeted school district because of their current settings and frames of mind.
Implications for Professional School Counseling
Limited range of counselor services. Implementation of the ASCA National Model (2012b)throughout the school system represented in the present study apparently had little influence on the role PSCs played in serving gang members. Considerable interview content from PSCs and SLs seemed focused on safety and discipline issues rather than on the academic, career, personal, and social development of student gang members. Mention of providing academic services came from two of the PSCs. Limiting counseling services to academics alone does not fit into the proactive, “serve all students” framework supported by ASCA (2012b). The perception that PSCs are solely academic counselors may cause them to feel boxed in professionally, therefore limiting their ability to advocate for counseling services for students in gangs and causing them to determine over the course of their professional careers that their role is fixed and rigidly academically focused (Lambie & Williamson, 2004).
Insufficient training. Three of the PSCs reported lacking sufficient training as a barrier to their working with students in gangs. Four of the five PSCs had not received training related to working with students in gangs during their master’s degree programs. Two of the five reported attending workshops after graduate school, and the remaining three had not sought training. Training provided by the school district on gangs in schools was limited to enhancing awareness, and there was no coverage of counseling-based techniques designed to reach students in gangs. A significant obstacle to training was time away from work and the cost of attending training. Although obstacles to training were reported, there seemed to be an underlying sense of frustration about the training that had been offered. The training from the district and from professional conferences was designed to make school personnel aware of the presence of gangs in the schools. This perceived lack of training designed to intervene and engage in counseling services for students in gangs is consistent with Brott and Myers’ (1999) work noting the need for experiential learning to enhance professional autonomy. The participants reported not knowing what to do with students in gangs and wondering what the goals of the counseling relationships would be if students were involved with gangs. This limited response model appears to have negatively impacted the way that PSCs viewed gang members. Neither the PSCs nor the SLs wanted PSCs involved in a discipline-focused mode.
PSC collaboration and advocacy. The Collaborative C.A.R.E. grounded theory presented at the beginning of the findings section suggests that PSCs respond to the challenges presented above via collaborating with others in their educational communities to advocate for policies, procedures, programs, and educational opportunities designed to clarify their role in providing responsive services to students in gangs. Although PSCs will benefit from more informed policies and richer educational opportunities, they also have advocacy competencies acquired in their training programs that should be of value when serving all students, including gang members. It appears as if the best way to serve students in gangs is through targeted responsive services designed to remove barriers and promote equitable access to counseling services (Trusty & Brown, 2005). Fortunately, most PSCs will not have to work differently in order to work with students in gangs via these approaches. Therefore, it appears as if the major changes needed are attitudinal. Believing that students in gangs deserve their services and advocacy efforts and can be served through existing services and competencies is essential. Overcoming safety concerns seems to be a very important goal. Students in gangs are members of a unique cultural group and equally worthy of positive regard and empathy. Becoming familiar with the nuances of this culture also seems to be an important goal for PSCs.
PSCs are challenged to be able to approach counseling sessions with student gang members in the same way as any other student client. Sasha noted she had not been trained to intervene with gang members; however, she likely is capable of building empathic relationships and aiding in goal setting and future planning for all student clients. The challenge might be to accept gang members as they are and attempt to help them focus on something of value that they want to be in their future and attempt to help them achieve those goals.
Recommendations for Practice and Research
Training preparation recommendations. The role of the PSC is continuously evolving via numerous influences, such as changing school policies and new initiatives at the local, state, and federal levels. Over their professional careers, PSCs may see a shift in the issues their students bring to the counseling relationship. For example, 15 years ago, PSCs were not dealing with cyberbullying. Cultural and economic shifts lead to changes in the issues students are forced to address, and changes in the lives of the students challenge PSCs to expand their expertise in order to be more effective practitioners. PSCs should be offered and encouraged to attend training based on a variety of issues impacting their work with 21st-century students, including enhancing the academic, career, personal, and social development of gang members.
As PSCs prepare to respond to evolving issues and shifting demographics, graduate training programs are challenged to provide instruction to prepare future PSCs for the realities of school settings and the diverse populations served. By no means can graduate training programs prepare graduate-level students for all of the nuances of practicing in a school; however, a careful review of the populations being served in 21st-century schools may guide the development of training modules designed to work with unique populations, including students in gangs. A training module of this type also can be developed and implemented in school districts in order to provide professional development for practicing PSCs.
Research recommendations. The paucity of research related to students in gangs and school counseling provides rich opportunities for future studies that might include examining the professional development needs of PSCs, addressing personal safety concerns, and exploring the impact of school-based stakeholders on the self-efficacy of PSCs. Until PSCs feel secure in the role they were trained to fill, they may continue to accept the non-counseling roles often expected by SLs and experience low levels of self-efficacy in working with diverse populations, including students in gangs (Dahir, Burnham, & Stone, 2009).
Responsive services address the immediate needs and concerns of students and incorporate both direct and indirect service modes (ASCA, 2012b). Further research involving responsive services may address the following questions: How is role development impacted by existing procedures and policies? How is the role of PSCs different in districts with procedures for addressing the needs of students in gangs versus districts lacking the same procedures? How effective are PSCs who collaborate with their communities when working with gang members?
Of all the research needs regarding students in gangs, knowledge acquired from the gang member’s perspective seems most needed. Without gang members as participants, the voice of students in gangs will continue to be silent. Studying students in gangs in order to understand how school staff can enhance their development may provide valuable information for both responsive and core curriculum services that can be provided by PSCs.
Conclusion
ASCA’s National Model (2012b) advocates for comprehensive school counseling programs designed to serve all students. Gang members are a unique student culture to be included within the “all students” framework and can benefit from school-based counseling services designed to enhance their academic, career, personal, and social development. Unfortunately, the findings in the present study revealed that there are impediments preventing PSCs from serving gang members. It seems as if the PSCs in the present study lacked role clarity in working with students in gangs, and there was a lack of intervention-based professional development. Not serving students in gangs led PSCs to believe they have nothing to offer those students through traditional counseling services, and this lack of efficacy may impact their role as advocates. Although this study was limited to one school district, the experiences and perceptions of PSCs and SLs in this study might not be unique. PSCs are uniquely trained and strategically located in school settings to provide valuable services to gang members that can help them feel accepted for who they are at the moment, while also helping them to focus on finding a meaningful pathway to their futures.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2012a). Position statement: The school counselor and comprehensive school
counseling programs. Alexandria, VA: Author.
American School Counselor Association. (2012b). The ASCA National Model: A framework for school counseling
programs (3rd ed.). Alexandria, VA: Author.
American School Counselor Association. (2014). Mindsets and behaviors for student success: K-12 college- and
career-readiness standards for every student. Alexandria, VA: Author.
American School Counselor Association. (n.d.). Student-to-school-counselor ratio 2015-2016. Retrieved
December 18, 2018, from https://www.schoolcounselor.org/asca/media/asca/home/Ratios15-16.pdf
Armstrong, S. A., MacDonald, J. H., & Stillo, S. (2010). School counselors and principals: Different perceptions
of relationship, leadership, and training. Journal of School Counseling, 8(15), 27.
Bogdan, R. C., & Biklen, S. K. (2007). Qualitative research for education: An introduction to theory and methods (5th
ed.). New York: Allyn and Bacon.
Brinson, J. A., Kottler, J. A., & Fisher, T. A. (2004). Cross-cultural conflict resolution in the schools: Some
practical intervention strategies for counselors. Journal of Counseling & Development, 82, 294–301.
doi:10.1002/j.1556-6678.2004.tb00313.x
Brott, P. E., & Myers, J. E. (1999). Development of professional school counselor identity: A grounded theory.
Professional School Counseling, 2, 339–348.
Burnham, J. J., & Jackson, C. M. (2000). School counselor roles: Discrepancies between actual practice and
existing models. Professional School Counseling, 4, 41–49.
Caldarella, P., Sharpnack, J., Loosli, T., & Merrell, K. W. (1996). The spread of youth gangs into rural areas: A
survey of school counselors. Rural Special Education Quarterly, 15(4), 18–27.
doi:10.1177/875687059601500404
Cobb, N. (2014). Climate, culture and collaboration: The key to creating safe and supportive schools.
Techniques: Connecting Education & Careers, 89(7), 14–19.
Coggeshall, M. B., & Kingery, P. M. (2001). Cross-survey analysis of school violence and disorder. Psychology in
the Schools, 38(2), 107–116.
Corbin, J., & Strauss, A. (2008). Basics of qualitative research: Techniques and procedures for developing grounded
theory (3rd ed.). Thousand Oaks, CA: Sage.
Creswell, J. W., & Miller, D. L. (2000). Determining validity in qualitative inquiry. Theory Into Practice, 39, 124–
130. doi:10.1207/s15430421tip3903_2
Dahir, C. A., Burnham, J. J., & Stone, C. (2009). Listen to the voices: School counselors and comprehensive
school counseling programs. Professional School Counseling, 12, 182–192.
doi:10.1177/2156759X0901200304
Foxx, S. P., Baker, S. B., & Gerler, E. R., Jr. (2017). School counseling for the twenty-first century (6th ed.). New
York, NY: Routledge/Taylor & Francis Group.
Gibbs, J. T. (2000). Gangs as alternative transitional structures: Adaptations to racial and social marginality in
Los Angeles and London. Journal of Multicultural Social Work, 8(1/2), 71–99. doi:10.1300/J285v08n01_04
Griffin, D., & Farris, A. (2010). School counselors and collaboration: Finding resources through community
asset mapping. Professional School Counseling, 13, 248–256. doi:10.1177/2156759X1001300501
Gündüz, B. (2012). Self-efficacy and burnout in professional school counselors. Educational Sciences: Theory &
Practice, 12, 1761–1767.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. New York, NY: Guilford.
Ibrahim, F. A., Helms, B. J., & Thompson, D. L. (1983). Counselor role and function: An appraisal by consumers
and counselors. Personnel and Guidance Journal, 61, 597–601. doi:10.1111/j.2164-4918.1983.tb00004.X
Kingery, P. M., Coggeshall, M. B., & Alford, A. A. (1998). Violence at school: Recent evidence from four
national surveys. Psychology in the Schools, 35, 247–258.
doi:10.1002/(SICI)1520-6807(199807)35:3<247::AID-PITS5>3.0.CO;2-K
Kirchner, G. L., & Setchfield, M. S. (2005). School counselors’ and school principals’ perceptions of the school
counselor’s role. Education, 126, 10–16.
Kizer, K. (2012). Behind the guise of gang membership: Ending the unjust criminalization. DePaul Journal for
Social Justice, 5, 333–366.
Lambie, G. W., & Williamson, L. L. (2004). The challenge to change from guidance counseling to professional
school counseling: A historical proposition. Professional School Counseling, 8(2), 124–131.
Marshall, B., Cardon, P., Poddar, A., & Fontenot, R. (2013). Does sample size matter in qualitative research? A
review of qualitative interviews in IS research. Journal of Computer Information Systems, 54, 11–22.
doi:10.1080/08874417.2013.11645667
McCluskey, K. W., Baker, P. A., & McCluskey, A. L. A. (2005). Creative problem solving with marginalized
populations: Reclaiming lost prizes through in-the-trenches interventions. Gifted Child Quarterly, 49,
330–341. doi:10.1177/001698620504900406}
Merriam, S. B. (2002). Assessing and evaluating qualitative research. In S. B. Merriam (Ed.), Qualitative research
in practice: Examples for discussion and analysis (pp. 18–33). San Francisco: Jossey-Bass.
National Gang Intelligence Center. (2011). National gang threat assessment: Emerging trends. Retrieved from
https://www.fbi.gov/file-repository/stats-services-publications-2011-national-gang-threat-
assessment-2011%20national%20gang%20threat%20assessment%20%20emerging%20trends.pdf/view
Patton, M. Q. (2002). Qualitative research and evaluation methods (3rd ed.). Thousand Oaks, CA: Sage.
Reising, G. N., & Daniels, M. H. (1983). A study of Hogan’s model of counselor development and supervision.
Journal of Counseling Psychology, 30, 235–244. doi:10.1037/0022-0167.30.2.235
Robers, S., Kemp, J., Truman, J., & Snyder, T. D. (2013). Indicators of school crime and safety: 2012 (NCES No.
2013-036/NCJ No. 241446). Washington, DC: National Center for Education Statistics, U.S. Department
of Education, and Bureau of Justice Statistics, Office of Justice Programs, U.S. Department of Justice.
Schwandt, T. A. (2001). Dictionary of qualitative inquiry (2nd ed.). Thousand Oaks, CA: Sage.
Shoffner, M. F., & Williamson, R. D. (2000). Engaging preservice school counselors and principals in dialogue
and collaboration. Counselor Education and Supervision, 40(2), 128–140.
doi:10.1002/j.1556-6978.2000.tb01244.x
Sindhi, S. A. (2013). Creating safe school environment: Role of school principals. Tibet Journal, 38(1–2), 77–89.
Skovholt, T. M., & McCarthy, P. R. (1988). Critical incidents: Catalysts for counselor development. Journal of
Counseling & Development, 67, 69–72. doi:10.1002/j.1556-6676.1988.tb02016.X
Trusty, J., & Brown, D. (2005). Advocacy competencies for professional school counselors. Professional School
Counseling, 8, 259–265.
Zalaquett, C. P., & Chatters, S. J. (2012). Middle school principals’ perceptions of middle school counselors’
roles and functions. American Secondary Education, 40(2), 89–103.
Jennifer Barrow, NCC, is an assistant professor at North Carolina Central University. Stanley B. Baker is a professor at North Carolina State University. Lance D. Fusarelli is a professor at North Carolina State University. Correspondence can be addressed to Jennifer Barrow, 700 Cecil Street, Durham NC 27707, jbarrow4@nccu.edu.
