May 10, 2023 | Volume 13 - Issue 1
Shainna Ali, John J. S. Harrichand, M. Ann Shillingford, Lea Herbert
Guyana has the highest rate of suicide in the Western Hemisphere. Despite this statistic, a wide gap exists in the literature regarding the exploration of mental wellness in this population. This article shares the first phase in a phenomenological study in which we explored the lived experiences of 30 Guyanese American individuals to understand how mental health is perceived. The analysis of the data revealed that participants initially perceived mental health as negative and then transitioned to a positive perception of mental health. We discuss how these perceptions affect the lived experience of the participants and present recommendations for counselors and counselor educators assisting Guyanese Americans in cultivating mental wellness.
Keywords: Guyanese American, mental health, phenomenological, mental wellness, perceptions
In 2014, the World Health Organization (WHO) reported Guyana as having the highest suicide rate in the world (44.2 suicides per 100,000 people; global average is 11.4 per 100,000 people). According to World Population Review (2023), within the Western Hemisphere, even after almost 10 years, Guyana remains the country with the highest rate of suicide—a concerning statistic. Responding to the WHO (2014) report, Arora and Persaud (2020) engaged in research to better understand the barriers Guyanese youth experience in relation to mental health help-seeking and suicide. Their research included 17 adult stakeholders (i.e., teachers, administrative staff, community workers) via focus groups, and 40 high school students who engaged in interviews. Arora and Persaud used a grounded theory approach and found the following themes as barriers to mental health help-seeking in Guyanese youth: shame and stigma about mental illness, fear of negative parental response to mental health help-seeking, and limited awareness and negative beliefs about mental health service. They recommended integrating culturally informed suicide prevention programs in schools and communities. In efforts to extend Arora and Persaud’s findings, we sought to further understand how Guyanese Americans define and experience mental health to better serve them in counseling.
Startled by the statistics presented by the WHO (2014) and Arora and Persaud (2020), we were compelled to focus our attention on this unique immigrant subgroup in the United States. It is important to note that between the WHO’s 2014 report and Aurora and Persaud’s research, no other studies related to Guyanese American suicidality are recorded in the literature. However, two studies on Guyanese American mental health emerged by Hosler and Kammer (2018) and Hosler et al. (2019). Our decision to conduct research on the Guyanese American community was further informed by Forte and colleagues’ (2018) review of immigrant literature in the United States, which stated that “immigrants and ethnic minorities may be at a higher risk for suicidal behavior as compared to the general population” (p. 1). Forte et al. found that immigrants, when compared with individuals in their homeland, were at an increased risk of experiencing mental health challenges like depression and other psychotic disorders. Currently, suicide is listed as the 10th leading cause of death overall in the United States (Heron, 2021). More specifically, within ages 10–34 and 35–44, suicide is the second and fourth leading cause of death, respectively. Heron’s (2021) report, referencing the Centers for Disease Control and Prevention (CDC), highlighted that in the United States, death by suicide (47,511) is 2.5 times higher than homicides (19,141). The prevalence of suicide among Guyanese people within and without the United States warranted further exploration of the experiences of this marginalized group.
The Guyanese American Experience
Comparing all countries with a population of at least 750,000 people, Guyana, a Caribbean nation, is said to have “the biggest share of its native-born population—36.4%—living abroad” due to remoteness and limited opportunities within the country to move from a lower to a higher socioeconomic status (Buchholz, 2022, para. 2). It is estimated that the United States is home to approximately 232,000 Guyanese Americans whose ancestry can be traced back to Guyana (United States Census Bureau, 2019), a country in the northeast of South America, bordered by Brazil, Venezuela, and Suriname. Although approximately 50% of all Guyanese immigrants in the United States reside in New York City alone (Indo-Caribbean Alliance, Inc., 2014), Guyanese people can be found across all 50 states and the District of Columbia (Statimetric, 2022). This draw to the United States, an English-speaking nation, might be linked to the fact that Guyana is the only country in South America that recognizes English as its official language (One World Nations Online, n.d.).
Like most immigrants, Guyanese immigrants travel to the United States seeking a better life and opportunities for themselves and their families. However, the process of transplanting can be bittersweet, in that Guyanese immigrants might be forced to relinquish their identity and customs and embrace American customs through assimilation (Arvelo, 2018; Cavalcanti & Schleef, 2001). For many Guyanese immigrants, being caught between leaving their homeland and beginning life in their adoptive home can lead to a cultural clash, resulting in problematic coping mechanisms (e.g., minimizing/hiding mental health challenges, cultural shedding [adopting American identity and losing cultural heritage]; Arvelo, 2018).
As discussed above, suicide in the Guyanese community is unquestionably a serious concern, but the community faces other challenges in the United States as well. For example, Hosler et al. (2019) found a statistically significant association between discrimination experience and major depressive symptoms in a sample of Guyanese Americans. However, Hosler et al. (2019) also found mean scores on the Everyday Discrimination Scale (EDS; Williams et al., 1997) were lower (i.e., less discriminatory experiences in everyday life) for Guyanese Americans when compared to other groups (Black, White, and Hispanic) because Guyanese Americans have a more cohesive interpersonal network. It would appear that Guyanese Americans experience lower everyday discrimination because they operate within interpersonal spaces that are more cohesive, yet their discriminatory experiences are positively associated with depression symptoms, which is a source of concern.
Another area of concern among Guyanese Americans is intimate partner violence (IPV), yet research remains lacking (Baboolal, 2016), leading us to draw directly from Guyanese literature. In Guyana, IPV is one of the most prevalent forms of violence (Parekh et al., 2012). As a country, although Guyana endorses the commitment to gender equality, women are the majority only in the tertiary sector (e.g., education, human services, clerical services, and tourism). Nicolas et al. (2021) stated that “domestic duties, marriage, and child-bearing, particularly for women between the ages of 25–29, have hindered their labor force participation” (p. 147). They documented that 1 in 6 Guyanese women, mostly from rural parts of the country, hold the belief that beating one’s wife is necessary (i.e., husbands are justified in beating their wives, resulting in domestic violence being a relevant mental health issue). In fact, suicide is identified as a public health issue for Guyanese women, who use it as a means of coping “with economic despair, poverty, and hopelessness . . . [and] to escape family turmoil, relationship issues, and domestic violence” (Nicolas et al., 2021, p. 148). However, even with access to mental health services increasing in Guyana, seeking out mental health care is uncommon due to stigma, lack of communication, inadequate financial resources, limited providers, and other barriers related to access (Nicolas et al., 2021). Within the U.S. literature, there remains a dearth of information on the experiences of this group as it relates to suicide and IPV. Most likely, this is a result of racial categorization within the United States, where, based on phenotype and racial composite, individuals are often lumped into one category, such as Black. As important as Guyanese literature on IPV is to inform the work of counselors, we believe it is equally important for us to engage in research regarding IPV and other mental health challenges on Guyanese Americans specifically. Learning about Guyanese Americans’ perceptions of mental health may facilitate closing the gap in the utilization of mental health services, warranting the current investigation.
Recognizing the noticeable research gap related to the mental health experiences of Guyanese Americans, we conducted a thorough review of the literature related to mental health and well-being. Through databases such as PsycINFO, ProQuest Central, Web of Science, MEDLINE, and SocINDEX, using the search terms “Guyanese Americans, Health and Wellbeing, Mental Health of Guyanese Americans, Access to Mental Health,” 54 search results were found. However, only two applicable studies were found to address Guyanese Americans’ mental health specifically (Hosler & Kammer, 2018; Hosler et al., 2019). The other search results were either not research manuscripts (i.e., reflections and newspaper articles) or addressed other constructs specific to the Guyanese people (e.g., family, education). The first study by Hosler and Kammer (2018) focused specifically on the health profiles of Guyanese immigrants in Schenectady, New York. This study was conducted with 1,861 residents between the ages of 18–64 years. Guyanese Americans from Schenectady were mostly from a low socioeconomic status, which resulted in them being less likely to have health insurance coverage, an identified place to receive care, and access to cancer screenings. They were also identified as being more likely to engage in alcohol binge drinking—all conditions of significant concern to us, resulting in the present study. In fact, Hosler and Kammer reported that Guyanese Americans are among the lowest group of those insured in the United States when compared with other minority groups such as Black and Latinx groups. Some researchers believe ethnocentric stereotyping, cultural incompetence by professionals, a lack of steady employment, and poor previous interactions with the health care system are barriers Guyanese immigrants experience when accessing medical and mental health services (Arvelo, 2018; Cheng & Robinson, 2013; Jackson et al., 2007).
The second study of Guyanese immigrants was conducted by Hosler et al. (2019) and explored everyday discrimination experiences and depressive symptoms in relation to urban Black, Hispanic, and White adults. This study included 180 Guyanese Americans (i.e., both citizens by birth and naturalized citizens/immigrants), all 18 years and older, from Schenectady, New York. The researchers found a significant independent association between the EDS score and major depressive symptoms for Guyanese Americans, suggesting that discrimination experiences might be an important social cause for depression within this community. Based on the reported challenges faced by Guyanese Americans, as well as our desire to contribute meaningfully to the extant body of literature on the Guyanese American community, we conducted a phenomenological inquiry. More specifically, we sought to better understand the lived experiences of Guyanese Americans pertaining to mental health (i.e., definitions, beliefs, practices), and how they access and incorporate mental health resources to mitigate the known mental health risks of this population in the United States, in the hopes of creating tailored methods for culturally responsive care.
Method
Because limited mental health research exists on this unique community, the present study, which is part of a larger research endeavor, sought to explore Guyanese Americans’ lived experiences with mental health. To lay the foundation of understanding, the present study focused on Guyanese Americans’ perceptions of mental health. Phenomenology, a constructivist approach, recognizes the existence of multiple realities and provides an understanding of participants’ lived experiences using their own voices (Haskins et al., 2022). We selected transcendental phenomenology (Moustakas, 1994) as the appropriate methodology for answering our research questions, as it is congruent with the counseling profession’s similar objective of understanding the human being. Akin to the practice of counseling, transcendental phenomenology emphasizes methods of the researcher to best set aside the potential clouds caused by bias in an effort to allow the explored phenomenon to surface. Transcendental phenomenology aligns with one of the core professional values in the American Counseling Association’s Code of Ethics (ACA, 2014), that of supporting “the worth, dignity, potential, and uniqueness of people within their social and cultural contexts” (p. 3). It also aligns with Ratts et al.’s (2015) Multicultural and Social Justice Counseling Competencies (MSJCC), specifically understanding the client’s worldview domain. Our focus on Guyanese Americans, an understudied minority group in the United States (Hosler & Kammer, 2018) originating from a country that has been identified as having the world’s highest suicide rate (WHO, 2014), led us to select this method so that we could maintain cognizance of our surroundings, hold respect for the population, and examine participants’ experiences (Haskins et al., 2022; Hays & Singh, 2012; Hays & Wood, 2011).
Participants
Before participants were recruited for the study, IRB approval was obtained from the university with whom Shainna Ali, M. Ann Shillingford, and Lea Herbert are affiliated. Purposive criterion sampling was used to recruit participants, leading to a sample of adults who self-identified as Guyanese American (i.e., either immigrated to the United States themselves or had at least one parent who was born in Guyana). Recruitment materials were shared with Guyanese Americans using counseling listservs (i.e., ACA–AMCD Connect and CESNET) and social media platforms (i.e., LinkedIn, Facebook, and Instagram). Members of the research team contacted all participants using email to share details regarding the study and the informed consent document, collect demographic data, and schedule individual interviews. According to qualitative research, sample size recommendations range from six to 12 participants (Creswell, 2013; Guest et al., 2006; Onwuegbuzie & Leech, 2007). Hence, we sought to recruit 15–20 participants to account for the possibility of attrition.
Our recruitment efforts yielded 73 individuals who expressed interest in the study, 60 of whom met all inclusion criteria and were initially contacted. Forty-three individuals were unable to complete an individual interview due to scheduling conflicts; hence, we secured a total of 30 participants who completed the study. Of this number, 17 participated in individual interviews and a total of 23 individuals participated in a one-time focus group to further clarify data from the individual interviews. It should be noted that 10 of the 23 focus group participants also participated in the individual interview. Further recruitment was deemed unnecessary, as the data analysis reached saturation with data from the individual interviews and focus group. We present demographic data on all participants who engaged in the study, both individual interviews and the focus group (N = 30), in Table 1.
Table 1
Participant Demographic Data
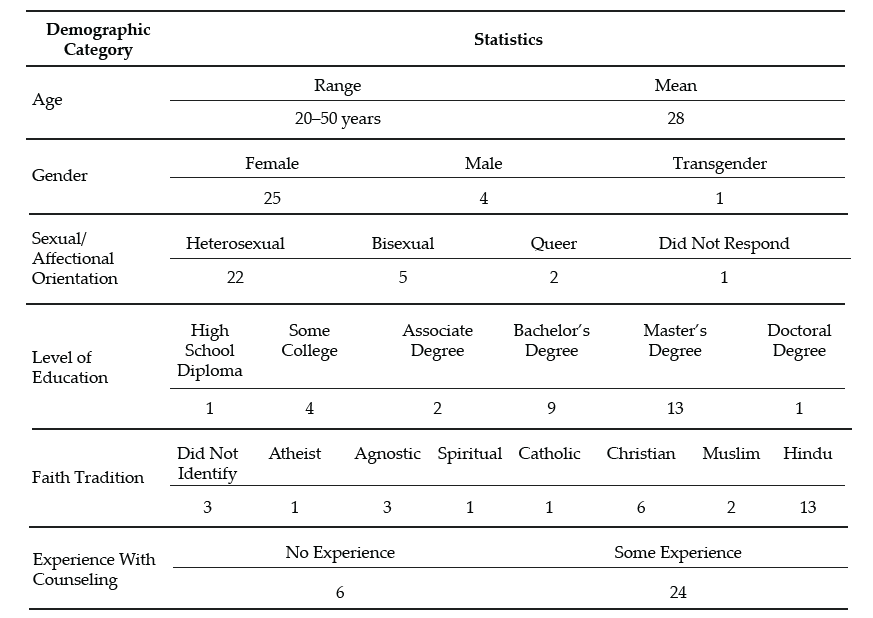
Note. This table provides a breakdown of the demographic characteristics of Guyanese American participants (N = 30).
Data Collection and Analysis
Participants engaged in a semi-structured interview lasting 30–60 minutes, conducted by Ali and Shillingford. Interviews were conducted via Zoom, audio-recorded, and transcribed verbatim. The interview protocol consisted of three primary questions, and sub-questions were used to clarify responses: 1) How do you define mental health?; 2) Who in your life has had experiences with mental health?; and 3) What experiences have you had with mental health? Prior to conducting our study, we included in our IRB documentation that data collection of individual interviews would follow saturation guidelines and that a focus group could be used for further data illumination. Following initial data analysis, we found it necessary to conduct a 1-hour follow-up focus group via Zoom to probe deeper into the data and to allow participants to clarify concepts related to emerging themes. Upon the first round of analysis, it was noted that several participants experienced a shift in perceptions regarding mental health. Focus group probes explored whether participants noticed this shift, what may have contributed to this shift, and when the shift occurred.
After all focus group and individual interviews were transcribed, we used guidelines outlined by Moustakas (1994) to analyze the data. First, we immersed ourselves in the data, reviewing each transcript individually. The transcripts were then divided equally among the four researchers, who read through each to become familiar with the data. With each transcript, we identified relevant statements reflecting participants’ lived experiences (horizontalization) as Guyanese Americans within the contexts of mental health beliefs and experiences.
Following this process, we met multiple times to review all transcripts and confer about the textural descriptions. We identified relevant codes, then synthesized the textural descriptions into themes based on commonalities, distilling the meaning expressed by participants. Then we engaged in reduction and elimination via consensus coding. This process included reading and rereading transcripts together, which followed an iterative process of reviewing the text and code, coding, rereading, and recoding, before determining which thematic content was a new horizon or new dimension of the phenomenon.
After all transcripts were analyzed following this reduction process, clustering and thematizing occurred (i.e., thematic content was clustered into core themes based on participant experiences; Hays & Singh, 2012; Moustakas, 1994). We extracted verbatim examples from the transcripts to generate a thematic and visual description of the phenomenon being examined. After completing the initial data analysis, we conducted member checking by sending each participant their individual transcript as well as the written results section. Participants were requested to provide feedback on the accuracy of their transcripts. Additionally, following the focus group and elucidation of themes all participants were offered an opportunity to member check and clarify the degree to which the results aligned with their lived experiences. The participants did not report any errors; however, clarification was offered by one participant.
Trustworthiness and Positionality
Trustworthiness is a key element of qualitative research in which the research findings accurately reflect the data (Lincoln & Guba, 1985). A critical element of maintaining research credibility is through reflexivity, wherein researchers critically examine procedures employed in relation to power, privilege, and oppression (Hunting, 2014). To safeguard against researcher bias, we worked collaboratively to establish and maintain credibility throughout data collection and analysis processes. Our research team consisted of one Indo-Guyanese American female faculty member, one Afro-Guyanese American female doctoral student, one Black female faculty member, and one Indo-Chinese-Guyanese Canadian male faculty member. All three faculty members belong to CACREP-accredited counselor education programs, and all four researchers have clinical experience working with diverse populations.
To address researcher bias, we engaged in bracketing to minimize the ways in which our experiences influence our approach to research and expectations of the outcomes of the study. Prior to data collection, we discussed our experiences in relation to Guyana, mental health in the Guyanese American community, and our roles as mental health leaders and advocates. We identified our personal experiences, acknowledged our biases, and attempted to bracket while conducting the interviews and focus group. Throughout the data collection and analysis processes, we participated in personal reflection and kept analytic memos documenting our reactions and initial thoughts about the data collected.
Before analyzing the data, we met to confirm analysis procedures, ensuring consistency. We initially analyzed data individually, then determined codes and themes as a team to reduce bias. Throughout the data analysis process, we consulted with each other, addressing questions or concerns related to the data. We also consulted with an outside researcher experienced in qualitative research to obtain critical feedback on the data analysis process and the research findings (Marshall & Rossman, 2006). Our consultant served as an external check of the research methodology and theoretical interpretation of the data.
Findings
The results of the analysis increase understanding of the lived mental health experiences of Guyanese Americans by elucidating perceptions of mental health (Creswell, 2013). All participants shared their beliefs about mental health and the direct and indirect experiences that informed their conceptualization. Three themes surfaced. The first two showed a clear divide in the data: 1) mental health being perceived as negative, stigmatized, elusive, and intimidating; and 2) mental health being perceived as positive, important, helpful, and empowering. It is important to note that these primary themes were not representative of two subsets of participants, and this extracted another theme, which centered on the tendency of participants’ beliefs to transition from negative to positive views of mental health.
The Perception of Mental Health as Negative
When exploring obstacles, subthemes emerged in which hindrances to mental health were acknowledged to exist across three levels: individual, familial, and sociocultural. In parallel, these three subthemes were echoed in the exploration of factors that participants acknowledged have contributed to their mental wellness. The following section explores the primary themes in detail by highlighting the participants’ voices in describing their lived experiences.
Mental Health Concerns Are a Sign of Weakness
All participants in the individual interviews shared that they originally believed that mental health developed out of weakness. This belief was often attributed to minimizing remarks from family members. Oftentimes these comments were paired with other suggestions of how to ameliorate symptoms such as praying more, working harder, or contributing to physical health (e.g., drinking tea). Sharon shared:
It was just like, oh no, you just need to read a book or you just need to go and do something and take your mind off of however it is you’re feeling, like there’s no reason for you to be sad, you have a roof over your head and you’re going to school and you’re doing all of these things, it doesn’t matter. There’s no reason for you to be sad or feel any type of way about anything because we provide everything for you.
Several participants noted that investment in physical wellness was preferable to mental wellness, although physical health was not genuinely prioritized. Participants shared personal and observed maladaptive coping with poor eating habits (i.e., quality and quantity) and excessive substance abuse, namely alcohol. Some participants shared that these tactics were used to manage mental health symptoms or avoidance. Christine shared, “When you’re struggling with things . . . you have nowhere to go to with them except alcohol and the bottom of a rum bottle.” Many participants recognized that coping with alcohol is normalized within the culture. Further, the commonality of these methods normalized consumption and have caused additional issues (e.g., diabetes, heart disease, alcoholism). Arjun noted:
We all have relatives that are kind of stuck on the whole drinking issue. We know a lot of them. They get together with their friends and they “lime,” as we like to call it. They drink in groups and they “gyaff,” they have fun. But it’s a completely different story when they’re by themselves and they’re drinking.
Mental Health Is Taboo
A general consensus was that all participants in the study once believed that mental health was not important and that mental health problems were shameful and not to be discussed. This consistent trend was one of the reasons that we opted to further understand responses through a focus group. Therefore, a direct probe was offered to the focus group participants to explore if they believed discussing mental health was taboo. When delving deeper into these perceptions, participants noted that these thoughts were informed by the beliefs of others and upheld in the wider cultural paradigm. All participants reported that, generally, mental health should not be talked about in order to save face and be respectful. Because mental health issues were seen to be synonymous with weakness, sharing about mental health was equated with the risk of bringing shame to oneself or to one’s family. For example, Chandra shared that “Guyanese people don’t want a kid that’s broken or a little off.” Hence, if someone opts to discuss their mental illness, it is to be done carefully, or secretly.
Most participants shared that typically, when divulging their symptoms, they went to an elder, often a parent, grandparent, or elder sibling, in an effort to keep concerns within the family system. However, many participants noted being minimized or dismissed when sharing their concerns with family members. Ramona explained her feeling that her family
is really strong about, like, don’t be selfish. And I wonder if they would categorize it under that. Like if you’re taking up too much space or time or whatever, you’re trying to center the attention on you or whatever, so that’s a self-serving thing.
A generational rule of discourse emerged from the data. Though the tendency was to keep mental health discussions within the family system, it was also atypical for a younger member to address observed issues with an elder. Several participants noted that this hidden guideline kept informed younger generations from being able to utilize their recognition of warning signs to help the given person and the family system. Arjun shared that as he’s gotten older and has learned more about mental health, he has acquired the courage to address the problems he sees with elders, including his uncle:
I said, “Uncle, what’s wrong?” And he said, “No, nothing is wrong.” But he was crying, you could see tears were streaked on his face, but he wouldn’t talk about it—he wouldn’t say anything. It’s not only one time I saw him, it’s multiple times that I’ve seen him when he has been drinking by himself, that he kind of has the same face all the time. Prior to the times that I asked him, I kind of looked at him and I kind of walked away the first couple of times. Because I was kind of like, this is not something that looked like I should butt in, as a child especially. When you’re younger, your parents tell you, “Mind your business.” Or they say, “You’re not an adult, go with the kids.” So . . . the first couple of times I saw him, I kind of avoided it.
Others Are Not To Be Trusted
Some participants noted that beyond the purpose of family protection, caution to mental health discourse was also due to lack of trust of others. Christine explained: “We had a counseling center on campus, but I was like, ‘Oh, I can’t go talk to anybody,’ because that’s what I was raised with. You don’t talk to strangers about your problems. I had to keep everything inside.” Nevertheless, some families encouraged talking to a religious leader to assist the individual in enhancing devotion and reducing mental health symptoms. Still, regarding professional mental health services, many participants believed, at least at one time, that such services are not helpful, providers are not to be trusted, assistance of that nature is for other (e.g., White) people, and succumbing to that level of desperation is a sign of weakness. When sharing about mistrust in professional mental health assistance, misconceptions and stereotypes surfaced. Ramesh shared:
Oh boy. I have to be honest with you, I feel counseling is, I’ll speak to a shrink and they’ll prescribe drugs to me, like Ritalin or . . . I was like, you know what, I’m better than that. I’m probably totally wrong about it, but that’s just the perception that I have. I’ll be laying on the couch and I’m going to speak into someone and then they’re going to prescribe drugs to me. I don’t want that. I can try to figure this out on myself by talking and trying to do things—positive behavior.
Mental Health Perceived as Positive
All participants in the individual interviews acknowledged a shift in their perceptions of mental health. Their newfound conceptualization included a holistic view of wellness in which mental wellness was seen as an important component to overall well-being and quality of life. In this newer perception, participants acknowledged the ability to consider more variables influencing mental health than they recognized in the past. For example, many participants noted a link between mind and body, versus the previously held notion that physical health is more important than mental health. A few participants noted that mental health can be influenced by genetics, while some noted that it could be influenced by personality, and others noted that it can be influenced by people and the surrounding environment.
All participants, from both the individual interviews and focus group, concurred that everyone feels mental health effects; furthermore, showing signs of a problem is not attributed to weakness. Moreover, because mental health affects everyone, a widespread belief emerged that we all have the responsibility to foster our mental wellness. Additionally, participants shared several examples of what naturally ensued without investing in strategies for mental health such as challenges with emotional regulation, coping, relationships, and worsening mental health problems.
The Transition Between Negative and Positive Perceptions
The transition between old and new conceptualizations of mental health was informed by direct and indirect experiences. All participants shared a transition in beliefs in the individual interviews, and this was explored in the focus group for further clarification. Most participants shared that their personal mental health history informed a change in their beliefs. Many of these participants noted the influence of their healing process, most notably seeking professional help. All participants, from both the individual interviews and the focus group, shared at least one example of learning about mental health by observing another person’s experience. For example, Jessie shared, “Unfortunately, I came from a home of domestic violence . . . I was around maybe six, my dad was bipolar . . . [and] he was just a wife beater. That is probably when I can recall [learning] of mental health.” Another example of learning about mental health from others is captured in Reginald’s comment:
[As] an only child . . . my parents took it upon themselves to [teach me]. . . . It wasn’t like, “Okay, sit down. Let me tell you why these things are.” It was just we’ll be talking about somebody else or going over something that happened and then they’ll explain why, but never directly for me. It was always about other people’s kids.
Many of these individuals emphasized the belief that by paying attention to others, you can learn what is helpful and unhelpful for mental health. Oftentimes this was in their own family; however, extended family and community members were also highlighted. Moreover, a few participants shared their recognition that living with someone who is struggling with their mental health may negatively impact personal wellness (e.g., be triggering). Beyond the family system, some participants noted that exposure to other cultures and perceptions of mental health informed a conceptualization of mental wellness. Seeta shared:
I had friends of other religions or like no religions. And then we would talk about a lot of different things. Like I would ask them questions like, “Oh, so how do things work in your house? Do your parents talk about your God or whatever?” And they’re like, “No.” And I’m like, “So where do your emotions come from?” And they’re like, “Well, you know, we just feel them. Some days I feel angry and some days I feel sad, some days I feel happy.” And I’m just like, “Okay, this is interesting.”
From the quote, it might appear that one’s emotions are in some way connected with God or another higher power; however, this is not something that was observed with other participants of our study. It was more common for participants to share stories of their families using religion as the solution to mental health concerns. For example, Yolanda shared:
My grandmother came when I turned 16 and she kept trying to tell my mom I was showing signs of depression. And my mom was like, “No, she’s like that all the time, like, that’s just how she is.” And my grandma was like, “That’s not normal. You should get her checked out.” And my mom kept saying, “No” and kept denying it. And then my grandma said, “You have to do something.” And then my mom replied, “Oh, I’m going to pray for her.”
In addition to personal experiences and observations of others, participants noted that improved mental health awareness and education prompted them to think critically about their mental health schemas. Ramesh shared:
My education, I always feel like this is what saved me in the end, because I was able to be around other people to know better and to come back home and be like, “Excuse me, this is not how we do things. This is not how we say things. I don’t know what it was like in Guyana.”
Some participants associated this with growing older, and others noted their personal initiative to improve mental health knowledge by following mental health pages on social media, taking a related class, and for some, becoming a part of the mental health field themselves. From this vantage point, many participants were able to equate their previously held notions with beliefs embedded in the culture such as generational rules of respect, gender differences, and the impact of colonialism. Participants, despite their gender differences, noted that within the cultural framework, the rule that mental health should not be discussed is disproportionately applicable to males. Participants shared that this is often due to the perception that it is important for men to be strong, and again, mental illness is a symptom of weakness. This was also linked to the breadwinner role and the pressure to provide for the family. However, this was only noted to have detrimental effects, as anger issues, IPV, and alcoholism were noted to arise out of this rule. Some participants noted that the survival aspect of colonialism may have contributed to the lack of privilege to focus on mental health. In addition, the history of colonialism in Guyana (i.e. slavery, indentured labor) could have informed the lack of trust in professional services.
The change in mental health conceptualization was noted to have benefits beyond the participants themselves. Some participants remarked that the shift in perception was recognized in the wider generation. Ramona reflected:
I will say that a lot of folks from my generation have been a lot more like, “Go to therapy. We should be taking care of our thoughts and our feelings or emotions.” That’s important to you in the same way that if you tore a ligament that you would need to get surgery or do whatever.
Within the newfound conceptualization of mental wellness emerged a vow of social responsibility. All participants, from both the individual interviews and the focus group, shared their intention to help others, and some even noted it as their duty. Ways to help others included advocating for mental health awareness, access, and education; helping to challenge unhelpful cultural beliefs; breaking generational cycles; and protecting others from experiencing similar struggles (e.g., child, sibling).
Discussion
The findings from this study are enlightening, and some are the first to be documented through research, even if they were observed in practice. Initial perceptions of all participants, from both the individual interviews and the focus group, were that mental health is a taboo topic and seeking mental health services is bad. These perceptions stemmed from fear, mistrust, and limited awareness of the benefits of mental health services. This is consistent with findings from Arora and Persaud (2020), who surmised that Guyanese individuals hold negative views of mental health that significantly impact their help-seeking. Furthermore, the findings point to strong familial and sociocultural influences, such as beliefs about mental health, that swayed individual perceptions of mental health, which is in keeping with recent literature on affirming cultural strengths and incorporating familial identity in working with clients of Guyanese descent (Groh et al., 2018; Nicolas et al., 2021).
Discussing issues related to mental health was viewed as a sign of weakness, which translated to help-seeking being a taboo. It would appear that the stigma associated with mental health remains a common experience for Guyanese Americans, and when coupled with limited communication, insufficient funding, and lack of providers, we can see how Nicolas et al. (2021) found this to be concerning. Cultural clash, ethnocentric stereotyping, and cultural incompetency may also be responsible for Guyanese Americans being distrustful of the health care system, leading them to engage in maladaptive behaviors (i.e., avoidance, use of substances, IPV) and not receive the mental health attention and care they need (Arvelo, 2018; Cheng & Robinson, 2013; Jackson et al., 2007).
It appears that even in the face of discrimination and experiences of mental health challenges like alcoholism, depression (Hosler & Kammer, 2018), and IPV (Parekh et al., 2012), leaning on the support of the community serves to buffer against mental health challenges for Guyanese Americans. It also seems that changing mental health perceptions from negative to positive was significantly related to mental health literacy and exposure to other systems such as school, work, and community (i.e., cross-cultural exchange).
Findings that were not previously documented in the literature suggest that an integrated view of wellness enabled participants to augment their negative abstractions of mental health care. These findings serve as an indication that among Guyanese Americans, although mental health has been perceived as negative, weak, and a taboo, the narrative is beginning to shift to make space for mental health awareness, education, access, and functioning, thereby creating unique implications for counselors seeking to meet the needs of this immigrant subgroup.
Implications
In combination with prior literature, the results of this study provide a rationale for mental health counselors, marriage and family counselors, school counselors, and counselor educators to inspire dialogue to foster mental wellness. Based on the findings from this study, when working with Guyanese Americans, counselors should focus on three key strategies to support Guyanese American clients: (a) mental health awareness, (b) mental health education, and (c) mental health experience.
Mental Health Awareness
Participants in this study initially held limited views and awareness of the signs and symptoms of mental health. When awareness was heightened through various means, they were more open to exploring the benefits of services. Counselors can be instrumental in creating awareness by first raising their own awareness pertaining to cultural stigma and its influence on Guyanese Americans’ mental health. For example, unwillingness to attend counseling sessions may be linked to the culturally held perception that discussing mental health, especially beyond the core family system, is taboo. In acknowledging this, counselors can raise awareness of confidentiality, which can be seen as an alignment with the cultural notion that talking about mental health is taboo when it means talking to anyone, and the role of the counselor can be highlighted as a professional collaboration versus communal gossip. Counselors need to be mindful of the collectivistic nature of Guyanese American culture, which causes personal and familial illnesses alike to be perceived as personal problems. Rather than dismiss a client’s concerns about mental health, a counselor can benefit from exploring how the family members’ symptoms, perceptions about mental health, and willingness to adhere to treatment influence the client’s symptoms, perceptions, and commitment to counseling. Further, collectivism spans beyond the protective family system. On one hand, this community orientation can be used to explore a broad range of support, yet on the other hand, depending on the client’s experience, this may also be a widened range of societal pressure (e.g., judgment, criticism, shame).
Mental Health Education
Increased understanding of mental health appeared to have led participants to seek services and resources to increase their mental health literacy, with the hope of improving their well-being. Counselors and counselor educators can be instrumental in offering Guyanese Americans mental health education. To begin, all mental health professionals should demonstrate a posture of cultural humility when engaged in psychoeducation on mental health and wellness for this population. In order to raise awareness through education, mental health professionals are encouraged to model trust, respect, sensitivity, compassion, and a nonjudgmental stance. Within session, counselors should be prepared to offer information regarding early signs of mental illness, compounding factors (e.g., alcohol, suicidal ideation, domestic violence), obstacles (e.g., stigma), and resources. Additionally, counselors may need to offer psychoeducation on the family system, roles, dynamics, beliefs, experiences, and generational patterns that can influence individual mental health. In the event that a family member with mental health problems is unwilling to seek assistance, helping the client to better understand the diagnosis and cope personally can be empowering. Finally, to employ the collectivistic nature of Guyanese American culture, stigma can be confronted, and mental health education can be effectively offered by providing group counseling within this population. Group counseling can offer a variety of therapeutic factors that can benefit Guyanese Americans such as universality, hope, and corrective recapitulation of the primary family group (Yalom & Leszcz, 2005).
Beyond the counseling office, counselors and counselor educators should consider collaborating with culturally supportive organizations. Workshops and information sessions can be tailored to explore and address cultural, religious, ethnic, and generational differences in addition to offering mental health resources (e.g., signs, symptoms, treatment). Several of the participants in our study shared that access to psychology courses in school helped to improve their knowledge about mental health. In addition to these classes continuing to be offered, accessibility to such courses should be expanded. Schools and universities may benefit from offering workshops and other informational sessions to support mental health. Beyond information being offered, a follow-up may be beneficial by linking school or campus counselors in order to connect an improvement in awareness and education to action, change, and health.
Several participants shared that because of a lack of access to mental health education, their knowledge was attained through social media platforms such as Instagram and TikTok. Although the quality of mental health education was not assessed in the present study, the lack of regulation on social platforms could perpetuate misleading, confusing, and stigmatizing misinformation surrounding mental health. Counselor educators should consider their roles beyond the classroom. In addition to empowering counselor trainees to utilize the suggestions above to foster awareness and education, counselor educators can offer responsive and succinct information via social media. Whereas social media is not an appropriate platform for tailored education or services, brief information can be offered to bridge the gap between awareness, education, and access.
Mental Health Experience
Growth in awareness and knowledge around mental health resulted in participants intentionally engaging in positive experiences as a way of resisting past harmful and hurtful practices and generational patterns, reauthoring a new narrative of hope and healing. Being wellness-focused, counselors are uniquely positioned to support this community by facilitating positive experiences impacting overall mental health and well-being.
Counselors can honor clients from this community by creating safe spaces for them to share their narratives without judgment. Counselors can foster healing communities through group counseling, where clients collaboratively share each other’s mental burdens and celebrate successes (Yalom & Leszcz, 2005). Counselors can honor collectivism by encouraging clients to participate in support groups in addition to personal counseling. Counselors and counselor educators can enhance the approachability of counselors by improving their visibility in the community. Examples include a community counselor being involved in outreach with a local cultural center, a school counselor offering mentorship with student clubs, a college counselor guest-speaking at a Guyanese American student organization meeting, or a counselor educator offering tailored workshops for the community.
In addition to the aforementioned implications, we believe that in order for counselors to bridge generational gaps in counselor distrust, counselors must acknowledge the lack of representation of diversity within the profession of counseling, the predominance of Western and European cultural and psychologist-centered curriculum, and lapses in poor bioethics and power dynamics among counselors and marginalized communities (Singh et al., 2020). Next, the specific intersectional impacts suggest counselors must adapt a multicultural orientation and illuminate cultural sensitivity. When a clinician enacts cultural sensitivity in session, clients can examine their perceptions of illness and center their multiple identities (Davis et al., 2018).
Limitations and Future Research
Several limitations that arose from the research process are important to mention. All interviews were conducted virtually. Although secured virtual platforms such as Zoom are considered acceptable for research, lack of face-to-face interviewing may have excluded subtle visual cues and induced video-conferencing fatigue (Spataro, 2020). Though researchers made great attempts to increase participant comfort and review the informed consent before the interview process, it is also plausible that respondents may have censored their responses out of concern for potential breach in confidentiality. A majority of respondents are college-educated, female, first generation, and of Indo-Guyanese descent; hence, the results may not be representative of all Guyanese Americans. Additionally, aligned with phenomenological methods of exploring lived experiences, research prompts were general. Recognizing the concerning statistics surrounding suicide (WHO, 2014), a future study exploring suicidality could be beneficial. Future research might seek to explore a more diverse pool of participants, including diversity in gender, age, ethnicity, and number of years in the United States. To build on the findings from the present study, future studies should explore what factors contribute to Guyanese American mental health as well as what variables may hinder mental wellness. It may also be beneficial to include research from the perspective of children and parents to further understand the influence of family systems and cross-generational norms.
Conclusion
This study highlighted the crucial need to address the mental health literacy of Guyanese Americans. The findings illuminate Guyanese Americans’ perceptions of mental health, including the transition from negative to positive perceptions and its potential influences. Efforts should be made to promote awareness, education, and experience related to mental health awareness for Guyanese Americans. Supporting mental health may help to reduce alarming rates of mental illness in Guyanese Americans and may also have the potential to influence related groups such as Guyanese, American, and Caribbean individuals. Counselors and counselor educators have the potential to play a significant role in supporting these clients by being cognizant and informed about cultural considerations.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Arora, P. G., & Persaud, S. (2020). Suicide among Guyanese youth: Barriers to mental health help-seeking and recommendations for suicide prevention. International Journal of School & Educational Psychology, 8(1), 133–145. https://doi.org/10.1080/21683603.2019.1578313
Arvelo, S. D. (2018). Biculturalism: The lived experience of first- and second-generation Guyanese immigrants in the United States (Order No. 10749930) [Doctoral dissertation, Chicago School of Professional Psychology]. ProQuest One Academic. (2027471070).
Baboolal, A. A. (2016). Indo-Caribbean immigrant perspectives on intimate partner violence. International Journal of Criminal Justice Sciences, 11(2), 159–176. https://www.researchgate.net/publication/336926774_Indo-Caribbean_Immigrant_Perspectives_on_Intimate_Partner_Violence
Buchholz, K. (2022, November 11). The world’s biggest diasporas [Infographic]. Forbes. https://www.forbes.com/sites/katharinabuchholz/2022/11/11/the-worlds-biggest-diasporas-infographic/?sh=4185fd634bde
Cavalcanti, H. B., & Schleef, D. (2001). Cultural loss and the American dream: The immigrant experience in Barry Levinson’s Avalon. Journal of American and Comparative Cultures, 24(3–4), 11–22.
https://doi.org/10.1111/j.1537-4726.2001.2403_11.x
Cheng, T. C., & Robinson, M. A. (2013). Factors leading African Americans and Black Caribbeans to use social work services for treating mental and substance use disorders. Health & Social Work, 38(2), 99–109. https://doi.org/10.1093/hsw/hlt005
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Davis, D. E., DeBlaere, C., Owen, J., Hook, J. N., Rivera, D. P., Choe, E., Van Tongeren, D. R., Worthington, E. L., Jr., & Placeres, V. (2018). The multicultural orientation framework: A narrative review. Psychotherapy, 55(1), 89–100. https://doi.org/10.1037/pst0000160
Forte, A., Trobia, F., Gualtieri, F., Lamis, D. A., Cardamone, G., Giallonardo, V., Fiorillo, A., Girardi, P., & Pompili, M. (2018). Suicide risk among immigrants and ethnic minorities: A literature overview. International Journal of Environmental Research and Public Health, 15(7), 1–21. https://doi.org/10.3390/ijerph15071438
Groh, C. J., Anthony, M., & Gash, J. (2018). The aftermath of suicide: A qualitative study with Guyanese families. Archives of Psychiatric Nursing, 32(3), 469–474. https://doi.org/10.1016/j.apnu.2018.01.007
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data saturation and variability. Field Methods, 18(1), 59–82. https://doi.org/10.1177/1525822X05279903
Haskins, N. H., Parker, J., Hughes, K. L., & Walker, U. (2022). Phenomenological research. In S. V. Flynn (Ed.), Research design for the behavioral sciences: An applied approach (pp. 299–325). Springer.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hays, D. G., & Wood, C. (2011). Infusing qualitative traditions in counseling research designs. Journal of Counseling & Development, 89(3), 288–295. https://doi.org/10.1002/j.1556-6678.2011.tb00091.x
Heron, M. (2021). Deaths: Leading causes for 2019. National Vital Statistics Reports, 70(9), 1–113. https://doi.org/10.15620/cdc:107021
Hosler, A. S., & Kammer, J. R. (2018). A comprehensive health profile of Guyanese immigrants aged 18–64 in Schenectady, New York. Journal of Immigrant and Minority Health, 20(4), 972–980.
https://doi.org/10.1007/s10903-017-0613-5
Hosler, A. S., Kammer, J. R., & Cong, X. (2019). Everyday discrimination experience and depressive symptoms in urban Black, Guyanese, Hispanic, and White adults. Journal of the American Psychiatric Nurses Association, 25(6), 445–452. https://doi.org/10.1177/1078390318814620
Hunting, G. (2014). Intersectionality-informed qualitative research: A primer. The Institute for Intersectionality Research and Policy. https://nanopdf.com/download/intersectionality-informed-qualitative-research-a-primer-gemma-hunting_pdf
Indo-Caribbean Alliance, Inc. (2014, February 3). Population analysis of Guyanese and Trinidadians in NYC.
https://www.indocaribbean.org/blog/population-analysis-of-guyanese-and-trinidadians-in-nyc
Jackson, J. S., Neighbors, H. W., Torres, M., Martin, L. A., Williams, D., & Baser, R. (2007). Use of mental health services and subjective satisfaction with treatment among Black Caribbean immigrants: Results from the National Survey of American Life. American Journal of Public Health, 97(1), 60–67. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1716231/
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Marshall, C., & Rossman, G. B. (2006). Designing qualitative research (4th ed.). SAGE.
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Nicolas, G., Dudley-Grant, G. R., Maxie-Moreman, A., Liddell-Quintyn, E., Baussan, J., Janac, N., & McKenny, M. (2021). Psychotherapy with Caribbean women: Examples from USVI, Haiti, and Guyana. Women & Therapy, 44(1–2), 136–155. https://doi.org/10.1080/02703149.2020.1775993
One World Nations Online. (n.d.). Guyana. https://www.nationsonline.org/oneworld/guyana.htm
Onwuegbuzie, A. J., & Leech, N. L. (2007). A call for qualitative power analyses. Quality & Quantity, 41, 105–121. https://doi.org/10.1007/s11135-005-1098-1
Parekh, K. P., Russ, S., Amsalem, D. A., Rambaran, N., Langston, S., & Wright, S. W. (2012). Prevalence of intimate partner violence in patients presenting with traumatic injuries to a Guyanese emergency department. International Journal of Emergency Medicine, 5(1), 1–5. https://doi.org/10.1186/1865-1380-5-23
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. American Counseling Association. https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf
Singh, A. A., Appling, B., & Trepal, H. (2020). Using the Multicultural and Social Justice Counseling Competencies to decolonize counseling practice: The important roles of theory, power, and action. Journal of Counseling & Development, 98(3), 261–271. https://doi.org/10.1002/jcad.12321
Spataro, J. (2020). The future of work—the good, the challenging & the unknown. https://www.microsoft.com/en-us/microsoft-365/blog/2020/07/08/future-work-good-challenging-unknown/
Statimetric. (2022). Distribution of Guyanese people in the US. https://www.statimetric.com/us-ethnicity/Guyanese
United States Census Bureau. (2019). People reporting ancestry: American community survey. http://bit.ly/42RazKC
Williams, D. R., Yu, Y., Jackson, J. S., & Anderson, N. B. (1997). Racial differences in physical and mental health: Socio-economic status, stress and discrimination. Journal of Health Psychology, 2(3), 335–351.
https://doi.org/10.1177/135910539700200305
World Health Organization. (2014). First WHO report on suicide prevention. https://www.who.int/news/item/04-09-2014-first-who-report-on-suicide-prevention
World Population Review. (2023). Suicide rate by country 2023. https://worldpopulationreview.com/country-rankings/suicide-rate-by-country
Yalom, I. D., & Leszcz, M. (2005). The theory and practice of group psychotherapy (5th ed.). Basic Books.
Shainna Ali, PhD, NCC, ACS, LMHC, is the owner of Integrated Counseling Solutions. John J. S. Harrichand, PhD, NCC, ACS, CCMHC, CCTP, LMHC, LPC-S, is an assistant professor at The University of Texas at San Antonio. M. Ann Shillingford, PhD, is an associate professor at the University of Central Florida. Lea Herbert is a doctoral student at the University of Central Florida. Correspondence may be addressed to Shainna Ali, 3222 Corrine Drive, Orlando, FL 32803, hello@drshainna.com.
Nov 9, 2022 | Volume 12 - Issue 3
Melissa J. Fickling, Matthew Graden, Jodi L. Tangen
The purpose of this phenomenological study was to explore how feminist-identified counselor educators understand and experience power in counselor education. Thirteen feminist women were interviewed. We utilized a loosely structured interview protocol to elicit participant experiences with the phenomenon of power in the context of counselor education. From these data, we identified an essential theme of analysis of power. Within this theme, we identified five categories: (a) definitions and descriptions of power, (b) higher education context and culture, (c) uses and misuses of power, (d) personal development around power, and (e) considerations of potential backlash. These categories and their subcategories are illustrated through narrative synthesis and participant quotations. Findings point to a pressing need for more rigorous self-reflection among counselor educators and counseling leadership, as well as greater accountability for using power ethically.
Keywords: counselor education, power, phenomenological, feminist, women
The American Counseling Association (ACA; 2014) defined counseling, in part, as “a professional relationship that empowers” (p. 20). Empowerment is a process that begins with awareness of power dynamics (McWhirter, 1994). Power is widely recognized in counseling’s professional standards, competencies, and best practices (ACA, 2014; Association for Counselor Education and Supervision [ACES], 2011; Council for the Accreditation of Counseling and Related Educational Programs [CACREP], 2015) as something about which counselors, supervisors, counselor educators, and researchers should be aware (Bernard & Goodyear, 2014). However, little is known about how power is perceived by counselor educators who, by necessity, operate in many different professional roles with their students
(e.g., teacher, supervisor, mentor).
In public discourse, power may carry different meaning when associated with men or women. According to a Pew Research Center poll (K. Walker et al., 2018) of 4,573 Americans, people are much more likely to use the word “powerful” in a positive way to describe men (67% positive) than women (8% positive). It is possible that these associations are also present among counselors-in-training, professional counselors, and counselor educators.
Dickens and colleagues (2016) found that doctoral students in counselor education are aware of power dynamics and the role of power in their relationships with faculty. Marginalized counselor educators, too, experienced a lack of power in certain academic contexts and noted the salience of their intersecting identities as relevant to the experience of power (Thacker et al., 2021). Thus, faculty members in counselor education may have a large role to play in socializing new professional counselors in awareness of power and positive uses of power, and thus could benefit from openly exploring uses of power in their academic lives.
Feminist Theory and Power in Counseling and Counselor Education
The concept of power is explored most consistently in feminist literature (Brown, 1994; Miller, 2008). Although power is understood differently in different feminist spaces and disciplinary contexts (Lloyd, 2013), it is prominent, particularly in intersectional feminist work (Davis, 2008). In addition to examining and challenging hegemonic power structures, feminist theory also centers egalitarianism in relationships, attends to privilege and oppression along multiple axes of identity and culture, and promotes engagement in activism for social justice (Evans et al., 2005).
Most research about power in the helping professions to date has been focused on its use in clinical supervision. Green and Dekkers (2010) found discrepancies between supervisors’ and supervisees’ perceptions of power and the degree to which supervisors attend to power in supervision. Similarly, Mangione and colleagues (2011) found another discrepancy in that power was discussed by all the supervisees they interviewed, but it was mentioned by only half of the supervisors. They noted that supervisors tended to minimize the significance of power or express discomfort with the existence of power in supervision.
Whereas most researchers of power and supervision have acknowledged the supervisor’s power, Murphy and Wright (2005) found that both supervisors and supervisees have power in supervision and that when it is used appropriately and positively, power contributed to clinical growth and enhanced the supervisory relationship. Later, in an examination of self-identified feminist multicultural supervisors, Arczynski and Morrow (2017) found that anticipating and managing power was the core organizing category of their participants’ practice. All other emergent categories in their study were different strategies by which supervisors anticipated and managed power, revealing the centrality of power in feminist supervision practice. Given the utility of these findings, it seems important to extend this line of research from clinical supervision to counselor education more broadly because counselor educators can serve as models to students regarding clinical and professional behavior. Thus, understanding the nuances of power could have implications for both pedagogy and clinical practice.
Purpose of the Present Study
Given the gendered nature of perceptions of power (Rudman & Glick, 2021; K. Walker et al., 2018), and the centrality of power in feminist scholarship (Brown, 1994; Lloyd, 2013; Miller, 2008), we decided to utilize a feminist framework in the design and execution of the present study. Because power appears to be a construct that is widely acknowledged in the helping professions but rarely discussed, we hope to shed light on the meaning and experience of power for counselor educators who identify as feminist. We utilized feminist self-identification as an eligibility criterion with the intention of producing a somewhat homogenous sample of counselor educators who were likely to have thought critically about the construct of power because it figures prominently in feminist theories and models of counseling and pedagogy (Brown, 1994; Lloyd, 2013; Miller, 2008).
Method
We used a descriptive phenomenological methodology to help generate an understanding of feminist faculty members’ lived experiences of power in the context of counselor education (Moustakas, 1994; Padilla-Díaz, 2015). Phenomenological analysis examines the individual experiences of participants and derives from them, via phenomenological reduction, the most meaningful shared elements to paint a portrait of the phenomenon for a group of people (Moustakas, 1994; Starks & Trinidad, 2007). Thus, we share our findings by telling a cohesive narrative derived from the data via themes and subthemes identified by the researchers.
Sample
After receiving IRB approval, we recruited counselor educators via the CESNET listserv who were full-time faculty members (e.g., visiting, clinical, instructor, tenure-track, tenured) in a graduate-level counseling program. We asked for participants of any gender who self-reported that they integrated a feminist framework into their roles as counselor educators. Thirteen full-time counselor educators who self-identified as feminist agreed to be interviewed on the topic of power. All participants were women. Two feminist-identified men expressed initial interest in participating but did not respond to multiple requests to schedule an interview. The researchers did not systematically collect demographic data, relying instead on voluntary participant self-disclosure of relevant demographics during the interviews. All participants were tenured or tenure-track faculty members. Most were at the assistant professor rank (n = 9), a few were associate professors (n = 3), and one was a full professor who also held various administrative roles during her academic career (e.g., department chair, dean). During the interviews, several participants expressed concern over the high potential for their identification by readers due to their unique identities, locations, and experiences. Thus, participants will be described only in aggregate and only with the demographic identifiers volunteered by them during the interviews. The participants who disclosed their race all shared they were White. Nearly all participants disclosed holding at least one marginalized identity along the axes of age, disability, religion, sexual orientation, or geography.
Procedure
Once participants gave informed consent, phone interviews were scheduled. After consent to record was obtained, interviewers began the interviews, which lasted between 45–75 minutes. We utilized an unstructured interview format to avoid biasing the data collection to specific domains of counselor education while also aiming to generate the most personal and nuanced understandings of power directly from the participants’ lived experiences (Englander, 2012). As experienced interviewers, we were confident in our ability to actively and meaningfully engage in discourse with participants via the following prompt: “We are interested in understanding power in counselor education. Specifically, please speak to your personal and/or professional development regarding how you think about and use power, and how you see power being used in counselor education.” After the interviews, we all shared the task of transcribing the recordings verbatim, each transcribing several interviews. All potentially identifying information (e.g., names, institutional affiliations) was excluded from the interview transcripts.
Data Analysis
Data analysis began via horizontalization of two interview transcripts by each author (Moustakas, 1994; Starks & Trinidad, 2007). Next, we began clustering meaning units into potential categories (Moustakas, 1994). This initially revealed 21 potential categories, which we discussed in the first research team meeting. We kept research notes of our meetings, in which we summarized our ongoing data analysis processes (e.g., observations, wonderings, emerging themes). These notes helped us to revisit earlier thinking around thematic clustering and how categories interrelated. The notes did not themselves become raw data from which findings emerged. Through weekly discussions over the course of one year, the primary coders (Melissa Fickling and Matthew Graden) were able to refine the categories through dialoguing until consensus was reached, evidenced by verbal expression of mutual agreement. That is, the primary coders shared power in data analysis and sometimes tabled discussions when consensus was not reached so that each could reflect and rejoin the conversation later. As concepts were refined, early transcripts needed to be re-coded. Our attention was not on the quantification of participants or categories, but on understanding the essence of the experience of power (Englander, 2012; Moustakas, 1994). The themes and subthemes in the findings section below were a fit for all transcripts by the end of data analysis.
Researchers and Trustworthiness
Fickling and Jodi Tangen are White, cis-hetero women, and at the time of data analysis were pre-tenured counselor educators in their thirties who claimed a feminist approach in their work. Graden was a master’s student and research assistant with scholarly interests in student experiences related to gender in counseling and education. We each possess privileged and marginalized identities, which facilitate certain perspectives and blind spots when it comes to recognizing power. Thus, regular meetings before, during, and after data collection and analysis were crucial to the epoche and phenomenological reduction processes (Moustakas, 1994) in which we shared our assumptions and potential biases. Fickling and Graden met weekly throughout data collection, transcription, and analysis. After the initial research design and data collection, Tangen served primarily as auditor to the coding process by comparing raw data to emergent themes at multiple time points, reviewing the research notes written by Fickling and Graden and contributing to consensus-building dialogues when needed.
Besides remaining cognizant of the strengths and limitations of our individual positionalities with the topic and data, we shared questions and concerns with each other as they arose during data analysis. Relevant to the topic of this study, Fickling served as an administrative supervisor to Graden. This required acknowledgement of power dynamics inherent in that relationship. Graden had been a doctoral student in another discipline prior to this study and thus had firsthand context for much of what was learned about power and its presence in academia. Fickling and Graden’s relationship had not extended into the classroom or clinical supervision, providing a sort of boundary around potential complexities related to any dual relationships. To add additional trustworthiness to the findings below, we utilized thick descriptions to describe the phenomenon of interest while staying close to the data via quotations from participants. Finally, we discuss the impact and importance of the findings by highlighting implications for counselor educators.
Findings
Through the analysis process, we concluded that the essence (Moustakas, 1994)—or core theme—of the experience of power for the participants in this study is engagement in a near constant analysis of power—that of their colleagues, peers, students, as well as of their own power. Participants analyzed interactions of power within and between various contexts and roles. They shared many examples of uses of power—both observed and personally enacted—which influenced their development, as well as their teaching and supervision styles. Through the interviews, participants shared the following:
(a) definitions and descriptions of power, (b) higher education context and culture, (c) uses and misuses of power, (d) personal development around power, and (e) considerations of potential backlash. These five categories comprised the overarching theme of analysis of power and are described below with corresponding subcategories where applicable, identified in italics.
Definitions and Descriptions of Power
Participants spent much of their time defining and describing just what they meant when they discussed power. For the feminist counselor educators in this study, power is about helping. One participant, when describing power, captured this sentiment well when she said, “I think of the ability to affect change and the ability to have a meaningful impact.” Several participants shared this same idea by talking about power as the ability to have influence. Participants expressed a desire to use power to do good for others rather than to advance their personal aspirations or improve their positions. Use of power for self-promotion was referenced to a far lesser extent than using power to promote justice and equity, and any self-promotional use was generally in response to perceived personal injustice or exploitation. At times, participants described power by what it is not. One participant said, “I don’t see power as a negative. I think it can be used negatively.” Several others shared this sentiment and described power as a responsibility.
In describing power, participants identified feelings of empowerment/disempowerment (Table 1). Disempowerment was described with feeling words that captured a sense of separation and helplessness. Empowerment, on the other hand, was described as feeling energetic and connected. Not only was the language markedly different, but the shifts in vocal expression were also notable (nonverbals were not visible) when participants discussed empowerment versus disempowerment. Disempowerment sounded like defeat (e.g., breathy, monotone, low energy) whereas empowerment sounded like liveliness (e.g., resonant, full intonation, energetic).
Table 1
Empowered and Disempowered Descriptors
| Descriptors |
| Empowered |
Disempowered |
| Authentic
Free
Good
Heard
Congruent
Genuine
Selfless
Hopeful
Confident
Serene
Connected
Grounded
Energized |
Isolated
Disenfranchised
Anxious
Separated Identity
Not Accepted
Disheartened
Helpless
Small
Weak
Invisible
Wasting Energy
Tired
Powered Down |
Participants identified various types of power, including personal, positional, and institutional power. Personal power was seen as the source of the aspirational kinds of power these participants desired for themselves and others. It can exist regardless of positional or institutional power. Positional power provides the ability to influence decisions, and it is earned over time. The last type of power, institutional, is explored more through the next theme labeled higher education context and culture.
Higher Education Context and Culture
Because the focus of the study was power within counselor educators’ roles, it was impossible for participants not to discuss the context of their work environments. Thus, higher education context and culture became a salient subtheme in our findings. Higher education culture was described as “the way things are done in institutions of higher learning.” Participants referred to written/spoken and unwritten/silent rules, traditions, expectations, norms, and practices of the academic context as barriers to empowerment, though not insurmountable ones. Power was seen as intimately intertwined with difficult departmental relationships as well as the roles of rank and seniority for nearly all participants. Most also acknowledged the influence of broader sociocultural norms (i.e., local, state, national) on higher education in general, noting that institutions themselves are impacted by power dynamics.
One participant who said that untenured professors have much more power than they realize also said that “power in academia comes with rank.” This contradiction highlights the tension inherent in power, at least among those who wish to use it for the “greater good” (as stated by multiple participants) rather than for personal gain, as these participants expressed.
More than one participant described power as a form of currency in higher education. This shared experience of power as currency, either through having it or not having it, demonstrated that to gain power to do good, as described above, one must be willing or able to be seen as acceptable within the system that assigns power. Boldness was seen by participants as something that can happen once power is gained. Among non-tenured participants, this quote captures the common sentiment: “Now, once I get tenure, that can be a different conversation. I think I would feel more emboldened, more safe, if you will, to confront a colleague in that way.” The discussion of context and boldness led to the emergence of a third theme, which we titled uses and misuses of power.
Uses and Misuses of Power
Participants provided many examples of their perceptions of uses and misuses of power and linked these behaviors to their sense of ethics. Because many of the examples of uses of power were personal, unique, and potentially identifiable, participants asked that they not be shared individually in this manuscript. Ethical uses of power were described as specific ways in which participants remembered power being used for good such as intervention in unfair policies on behalf of students. Ethical uses of power shared the characteristics of being collaborative and aligned with the descriptors of “feeling empowered” (Table 1).
In contrast, misuses of power were described in terms of being unethical. These behaviors existed on a spectrum that ranged from a simple lack of awareness to a full-blown abuse of power on the most harmful end of the continuum. Lack of awareness of power, for these participants, was observed quite frequently among their counselor education colleagues and they noted that people can negatively affect others without realizing it. In some cases, they reported seeing colleagues lack cultural awareness, competence, or an awareness of privilege. Although many colleagues cognitively know about privilege and speak about it, the lack of awareness referred to here is in terms of the behavioral use of privilege to the detriment of those with less privilege. One example would be to call oneself an LGBTQ+ ally without actively demonstrating ally behavior like confronting homophobic or cis-sexist language in class. Moving along the spectrum, misuses of power were described as unfairly advantaging oneself, possibly at the expense or disadvantage of another. Misuses of power may or may not be directly or immediately harmful but still function to concentrate power rather than share it. An example shared was when faculty members insist that students behave in ways that are culturally inconsistent for that student. At the other end of the spectrum, abuses of power are those behaviors that directly cause harm. Even though abuses of power can be unintentional, participants emphasized that intentions matter less than effects. One participant described abuses of power she had observed as “people using power to make others feel small.” For example, a professor or instructor minimizing students’ knowledge or experiences serves to silence students and leads to a decreased likelihood the student shares, causing classmates to lose out on that connection and knowledge.
One participant shared a culture of ongoing misuses of power by a colleague: “And then they’re [students] all coming to me crying, you know, surreptitiously coming to me in my office, like, ‘Can I talk to you?’ I’m like, ‘Yeah, shut the door. What’d he do now?’ I’m happy to be a safe person for them, it’s an honor, but this is ridiculous.” The irony of feeling powerless to stop another’s misuses of power was not lost on the participants. One participant expressed that she wished to see more colleagues ask questions about their use of power:
We have to ask the question, “What is the impact? What is happening, what are the patterns?” We have to ask questions about access and participation and equity. . . .
And from my perspective, we have to assume that things are jacked up because we know that any system is a microcosm of the outer world, and the outer world is jacked up. So, we have to ask these questions and understand if there’s an adverse impact. And a lot of time there is on marginalized or minoritized populations. So, what are we going to do about it? It’s all well and good to see it, but what are we doing about it, you know? . . . How are you using your power for good?
Personal Development Around Power
Participants reflected deeply on their own development of their thinking about and use of power. All participants spoke early in the interviews about their training as counselors and counselor educators. Their early training was often where they first fully realized their feminist orientation and recognized a need for greater feminist multicultural dialogue and action in counseling. Participants were all cognizant of their inherent personal power but still not immune to real and perceived attempts to limit their expression of it. In general, participants felt that over time they became more able and willing to use their power in ethical ways. One participant shared the following about her change in understanding power over time:
I’ve never really been a power-focused person, and so I just don’t know that I saw it around me much before that. Which now I realize is a total construct of my privilege—that I’ve never had to see it. Then I started realizing that “Oh, there’s power all around me.” And people obsessed with power all around me. And then once I saw it, I kind of couldn’t un-see it. I think for a long time I went through a process of disillusionment, and I think I still lapse back into that sometimes where I’ll realize like, a lot of the people in positions of power around me are power-hungry or power-obsessed, and they’re using power in all the wrong ways. And maybe they don’t even have an awareness of it. You know, I don’t think everybody who’s obsessed with power knows that about themselves. It almost seems like a compulsion more than anything. And I think that’s super dangerous.
Nearly all participants reflected on their experiences of powerlessness as students and how they now attempt to empower students as a result of their experiences. Working to build a sense of safety in the classroom was a major behavior that they endorsed, often because of their own feelings of a lack of safety in learning contexts at both master’s and doctoral levels. Vulnerability and risk-taking on the part of the counselor educator were seen as evidence that efforts to create safety in the classroom were successful. Speaking about this, one participant said:
I think it’s actually very unethical and irresponsible as a counselor educator to throw students in a situation where you expect them to take all these risks and not have worked to create community and environments that are conducive to that.
Participant feelings toward power varied considerably. One said, “I think overall I feel fairly powerful. But I don’t want a lot of power. I don’t like it.” One participant shared, “I am not shy, I am not afraid to speak and so sometimes maybe I do take up too much space, and there are probably times for whatever reason I don’t take up as much space as I should,” showing both humility and a comfort with her own power. These quotes show the care with which the participants came to think about their own power as they gained it through education, position, and rank. No participants claimed to feel total ease in their relationship with their own power, though most acknowledged that with time, they had become more comfortable with acknowledging and using their power when necessary.
One participant said of her ideal expression of power: “Part of feeling powerful is being able to do what I do reasonably well, not perfect, just reasonably well. But also helping to foster the empowerment of other people is just excellent. That’s where it’s at.” This developmental place with her own power aligns with the aspirational definitions and descriptions of power shared above.
Along with their personal development around power, participants shared how their awareness of privileged and marginalized statuses raised their understanding of power. Gender and age were cited by nearly all participants as being relevant to their personal experiences with power. Namely, participants identified the intersection of their gender and young age as being used as grounds for having their contributions or critiques dismissed by their male colleagues. Older age seemed to afford some participants the confidence and power needed to speak up. One participant said:
We are talking about a profession that is three-quarters women, and we are not socialized to grab power, to take power. And so, I think all of that sometimes is something we need to be mindful of and kind of keep stretching ourselves to address.
Yet when younger participants recalled finding the courage to address power imbalances with their colleagues, the outcome was almost always denial and continued disempowerment. To this point, one participant asked, “How do we get power to matter to people who are already in the positions where they hold power and aren’t interested in doing any self-examination or critical thinking about the subject?”
Finally, power was described as permeating every part of being an educator. To practice her use of power responsibly, one participant said, “I mean every decision I make has to, at some point, consider what my power is with them [the students].” Related to the educator role, in general, participants shared their personal development with gatekeeping, such as:
I think one of the areas that I often feel in my power is around gatekeeping. And I think that is also an area where power can be grossly abused. But I think it’s just such an important part of what we do. And I think one of the ways that I feel in my power around gatekeeping is because it’s something I don’t do alone. I make a point to consult a lot because I don’t want to misuse power, and I think gatekeeping—and, really, like any use of power I think—is stronger when it’s done with others.
Again, this quote reflects the definition of power that emerged in this study as ideally being “done with others.” Gatekeeping is where participants seemed to be most aware of power and to initially have had the most anxiety around power, but also the area in which they held the most conviction about the intentional use of power. The potential cost of not responsibly using their power in gatekeeping was to future clients, so participants pushed through their discomfort to ensure competent and ethical client care. However, in many cases, participants had to seriously weigh the pros and cons of asserting their personal or positional power, as described in the next and final category.
Considerations of Potential Backlash
Participants shared about the energy they spent in weighing the potential backlash to their expressions of power, or their calling out of unethical uses of power. Anticipated backlash often resulted in participants not doing or saying something for fear of “making waves” or being labeled a “troublemaker.” Participants described feeling a need to balance confrontations of perceived misuses of power with their desire not to be seen as combative. Those participants who felt most comfortable confronting problematic behaviors cited an open and respectful workplace and self-efficacy in their ability to influence change effectively. For those who did not describe their workplaces as safe and respectful, fear was a common emotion cited when considering whether to take action to challenge a student or colleague. Many described a lack of support from colleagues when they did speak up. Some described support behind the scenes but an unwillingness of peers to be more vocal and public in their opposition to a perceived wrong. Of this, one participant said, “And so getting those voices . . . to the table seems like an uphill battle. I feel like I’m stuck in middle management, in a way.”
Discussion
For the participants in this study, analysis of power is a process of productive tension and fluidity. Participants acknowledged that power exists and a power differential in student–teacher and supervisee–supervisor relationships will almost certainly always be present. Power seemed to be described as an organizing principle in nearly all contexts—professionally, institutionally, departmentally, in the classroom, in supervision, and in personal relationships. Participants found power to be ever present but rarely named (Miller, 2008). Engaging with these data from these participants, it seems that noticing and naming power and its effects is key to facilitating personal and professional development in ways that are truly grounded in equity, multiculturalism, and social justice. Participants affirmed what is stated in guiding frameworks of counseling (ACA, 2014) and counselor education (ACES, 2011; CACREP, 2015) and went beyond a surface acknowledgement of power to a deeper and ongoing process of analysis, like Bernard and Goodyear’s (2014) treatment of power in the supervisory context.
Contemplating, reflecting on, and working with power are worthwhile efforts according to the participants in this study, which is supported by scholarly literature on the topic (Bernard & Goodyear, 2014). Participants’ personal and professional growth seemed to be catalyzed by their awareness of gender and power dynamics. Participants expressed a desire for a greater recognition of the role of power and the ways in which it is distributed in our professional contexts. For example, although mentioned by only two participants, dissatisfaction in professional associations—national, regional, and state—was shared. Specifically, there was a desire to see counselor educators with positional power make deliberate and visible efforts to bring greater diversity into professional-level decisions and discussions in permanent, rather than tokenizing, ways.
The ongoing process of self-analysis that counselors and educators purport to practice seemed not to be enough to ensure that faculty will not misuse power. Though gender and age were highly salient aspects of perceptions of power for these women, neither were clear predictors of their colleagues’ ethical or unethical use of power. Women and/or self-identified feminist counselor educators can and do use power in problematic ways at times. In fact, most participants expressed disappointment in women colleagues and leaders who were unwilling to question power or critically examine their role in status quo power relations. This is consistent with research that indicates that as individual power and status are gained, awareness of power can diminish (Keltner, 2016).
These feminist counselor educators described feelings of empowerment as those that enhance connection and collaboration rather than positionality. In fact, participants’ reports of frustration with some uses of power seemed to be linked to people in leadership positions engaging in power-over moves (Miller, 2008). Participants reported spending a significant amount of energy in deciding whether and when to challenge perceived misuses of power. Confronting leaders seemed to be the riskiest possibility, but confronting peers was also a challenge for many participants. The acknowledgement of context emerged in these data, including a recognition that power works within and between multiple socioecological levels (e.g., microsystems, mesosystems, macrosystems; Bronfenbrenner, 1979). The culture of academia and higher education also contributed to unique considerations of power in the present study, which aligns with the findings of Thacker and colleagues (2021), who noted counselor educator experiences of entrenched power norms are resistant to change.
Contextualizing these findings in current literature is difficult given the lack of work on this topic in counselor education. However, our themes are similar to those found in the supervision literature (Arczynski & Morrow, 2017; Bernard & Goodyear, 2014). The participants in our study were acutely aware of power in their relationships; however, they appeared to feel it even more when in a power-down position. This finding is similar to research in the supervision context in which supervisees felt as though power was not being addressed by their supervisors (Green & Dekkers, 2010). Further, just as the supervisors researched in Mangione et al.’s (2011) study attended to power analysis, our participants strived to examine their power with students. The distinction between positive and negative uses of power was consistent with Murphy and Wright (2005). Participants conceptualized power on a continuum, attended to the power inherent in gatekeeping decisions, managed the tension between collaboration and direction, engaged in reflection around use and misuse of power, and sought transparency in discussions around power. More than anything, though, our participants seemed to continually wrestle with the inherent complexity of power, similarly to what Arczynski and Morrow (2017) found, and how to address, manage, and work with it in a respectful, ethical manner. As opposed to these studies, though, our research addresses a gap between the profession’s acknowledgement of power as a phenomenon and actual lived experiences of power by counselor educators who claim a feminist lens in their work.
Implications
The implications of our findings are relevant across multiple roles (e.g., faculty, administration, supervision) and levels (e.g., institution, department, program) in counselor education. Power analysis at each level and each role in which counselor educators find themselves could help to uncover issues of power and its uses, both ethical and problematic. The considerable effort that participants described in weighing whether to challenge perceived misuses of power indicates the level of work needed to make power something emotionally and professionally safe to address. Thus, those who find themselves in positions of power or having earned power through tenure and seniority are potentially better situated to invite discussions of power in relatively safe settings such as program meetings or in one-on-one conversations with colleagues. Further, at each hierarchical level, individuals can engage in critical self-reflection while groups can elicit external, independent feedback from people trained to observe and name unjust power structures. Counselor educators should not assume that because they identify as feminist, social justice–oriented, or egalitarian that their professional behavior is always reflective of their aspirations. It is not enough to claim an identity; one must work to let one’s actions and words demonstrate one’s commitment to inclusion through sensitivity to and awareness of power.
Additionally, we encourage counselor educators to ask for feedback from people who will challenge them because self-identification of uses or misuses of power is likely not sufficient to create systemic or even individual change. It is important to acknowledge that power is differentially assigned but can be used well in a culture of collaboration and support. Just as we ask our students to be honest and compassionately critical of their own development, as individuals and as a profession, it seems we could be doing more to foster empowerment through support, collaboration, and honest feedback.
Limitations and Future Directions
Although not all participants disclosed all their demographic identifiers, one limitation to the current study is the relative homogeneity of the sample across racial and gender lines. The predominance of White women in the present study is of concern, and there are a few possible reasons for this. One is that White women are generally overrepresented in the counseling profession. Baggerly and colleagues (2017) found that women comprised 85% of the student body in CACREP-accredited programs but only 60% of the faculty. These numbers indicate both the high representation of women seeking counseling degrees, but also the degree to which men approach, but do not reach, parity with women in holding faculty positions. Further, in Baggerly et al.’s study, about 88% of faculty members in CACREP-accredited programs were White.
Another potential reason for the apparent racial homogeneity in the present sample is that people of color may not identify with a feminist orientation because of the racist history of feminist movements and so would not have volunteered to participate. Thus, findings must be considered in this context. Future researchers should be vocally inclusive of Black feminist thought (Collins, 1990) and Womanism (A. Walker, 1983) in their research design and recruitment processes to communicate to potential participants an awareness of the intersections of race and gender. Further, future research should explicitly invite those underrepresented here—namely, women of color and men faculty members—to share their experiences with and conceptualizations of power. This will be extremely important as counselor educators work to continue to diversify the profession of counseling in ways that are affirming and supportive for all.
Another limitation is that participants may have utilized socially desirable responses when discussing power and their own behavior. Indeed, the participants identified a lack of self-awareness as common among those who misused power. At the same time, however, the participants in this study readily shared their own missteps, lending credibility to their self-assessments. Future research that asks participants to track their interactions with power in real time via journals or repeated quantitative measures could be useful in eliciting more embodied experiences of power as they arise in vivo. Likewise, students’ experiences of power in their interactions with counselor educators would be useful, particularly as they relate to teaching or gatekeeping, because some research already exists examining power in the context of clinical supervision (Arczynski & Morrow, 2017; Green & Dekkers, 2010; Mangione et al., 2011; Murphy & Wright, 2005).
We initially embarked upon this study with a simple inquiry, wondering about others’ invisible experiences around what felt like a formidable topic. More than anything, our discussions with our participants seemed to indicate a critical need for further exploration of power across hierarchical levels and institutions. We are grateful for our participants’ willingness to share their stories, and we hope that this is just the beginning of a greater dialogue.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
Arczynski, A. V., & Morrow, S. L. (2017). The complexities of power in feminist multicultural psychotherapy supervision. Journal of Counseling Psychology, 64(2), 192–205. https://doi.org/10.1037/cou0000179
Association for Counselor Education and Supervision Taskforce on Best Practices in Clinical Supervision. (2011, April). Best practices in clinical supervision. https://acesonline.net/wp-content/uploads/2018/11/ACES-Best-Practices-in-Clinical-Supervision-2011.pdf
Baggerly, J., Tan, T. X., Pichotta, D., & Warner, A. (2017). Race, ethnicity, and gender of faculty members in APA- and CACREP-accredited programs: Changes over five decades. Journal of Multicultural Counseling and Development, 45(4), 292–303. https://doi.org/10.1002/jmcd.12079
Bernard, J. M., & Goodyear, R. K. (2014). Fundamentals of clinical supervision (5th ed.). Pearson.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
Brown, L. S. (1994). Subversive dialogues: Theory in feminist therapy. Basic Books.
Collins, P. H. (2000). Black feminist thought: Knowledge, consciousness, and the politics of empowerment (2nd ed.). Routledge.
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards
Davis, K. (2008). Intersectionality as buzzword: A sociology of science perspective on what makes a feminist theory successful. Feminist Theory, 9(1), 67–85. https://doi.org/10.1177/1464700108086364
Dickens, K. N., Ebrahim, C. H., & Herlihy, B. (2016). Counselor education doctoral students’ experiences with multiple roles and relationships. Counselor Education and Supervision, 55(4), 234–249. https://doi.org/10.1002/ceas.12051
Englander, M. (2012). The interview: Data collection in descriptive phenomenological human scientific research. Journal of Phenomenological Psychology, 43(1), 13–35. https://doi.org/10.1163/156916212X632943
Evans, K. M., Kincade, E. A., Marbley, A. F., & Seem, S. R. (2005). Feminism and feminist therapy: Lessons from the past and hopes for the future. Journal of Counseling & Development, 83(3), 269–277. https://doi.org/10.1002/j.1556-6678.2005.tb00342.x
Green, M. S., & Dekkers, T. D. (2010). Attending to power and diversity in supervision: An exploration of supervisee learning outcomes and satisfaction with supervision. Journal of Feminist Family Therapy, 22(4), 293–312. https://doi.org/10.1080/08952833.2010.528703
Keltner, D. (2016). The power paradox: How we gain and lose influence. Penguin.
Lloyd, M. (2013). Power, politics, domination, and oppression. In G. Waylen, K. Celis, J. Kantola, & S. Laurel Weldon (Eds.), The Oxford handbook of gender and politics (pp. 111–134). Oxford University Press.
Mangione, L., Mears, G., Vincent, W., & Hawes, S. (2011). The supervisory relationship when women supervise women: An exploratory study of power, reflexivity, collaboration, and authenticity. The Clinical Supervisor, 30(2), 141–171. https://doi.org/10.1080/07325223.2011.604272
McWhirter, E. H. (1994). Counseling for empowerment. American Counseling Association.
Miller, J. B. (2008). Telling the truth about power. Women & Therapy, 31(2–4), 145–161.
https://doi.org/10.1080/02703140802146282
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Murphy, M. J., & Wright, D. W. (2005). Supervisees’ perspectives of power use in supervision. Journal of Marital and Family Therapy, 31(3), 283–295.
https://doi.org/10.1111/j.1752-0606.2005.tb01569.x
Padilla-Díaz, M. (2015). Phenomenology in educational qualitative research: Philosophy as science or philosophical science? International Journal of Educational Excellence, 1(2), 101–110. https://documento.uagm.edu/cupey/ijee/ijee_padilla_diaz_1_2_101-110.pdf
Rudman, L. A., & Glick, P. (2021). The social psychology of gender: How power and intimacy shape gender relations (2nd ed.). Guilford.
Starks, H., & Trinidad, S. B. (2007). Choose your method: A comparison of phenomenology, discourse analysis, and grounded theory. Qualitative Health Research, 17(10), 1372–1380.
https://doi.org/10.1177%2F1049732307307031
Thacker, N. E., Barrio Minton, C. A., & Riley, K. B. (2021). Marginalized counselor educators’ experiences negotiating identity: A narrative inquiry. Counselor Education and Supervision, 60(2), 94–111. https://doi.org/10.1002/ceas.12198
Walker, A. (1983). In search of our mothers’ gardens: Womanist prose. Harcourt Brace.
Walker, K., Bialik, K., & van Kessel, P. (2018). Strong men, caring women: How Americans describe what society values (and doesn’t) in each gender. https://www.pewsocialtrends.org/interactives/strong-men-caring-women
Melissa J. Fickling, PhD, ACS, BC-TMH, LCPC, is an associate professor at Northern Illinois University. Matthew Graden, MSEd, is a professional school counselor. Jodi L. Tangen is an associate professor at North Dakota State University. Correspondence may be addressed to Melissa J. Fickling, 1425 W. Lincoln Hwy, Gabel 200, DeKalb, IL 60115, mfickling@niu.edu.
Feb 7, 2022 | Volume 12 - Issue 1
Diane M. Stutey, Abigail E. Solis, Kim Severn, Lori Notestine, Kodi L. Enkler, Joseph Wehrman, Molly Cammell
There is a need for mental health interventions for youth in the United States. Youth mentoring programs have proven to be successful in helping in a variety of aspects. The purpose of this phenomenological study was to gain insight into the lived experiences of participants in a therapeutic youth mentoring program. In addition to being paired 1:1 with a mentor, all of the youth had access to individual counseling with counselors-in-training throughout the program. The participants in this study were 14 youth, ages 11–15, who were considered “at-promise youth” if they were not reaching their full potential in the school setting and might be vulnerable to school dropout, substance use/misuse, and/or criminal behavior. All participants were interviewed at the beginning and end of a 12-week therapeutic mentoring program. Five themes emerged from the data: life stressors, self-awareness, trusting others, adaptability and resiliency, and hope for the future. Researchers observed an increase in participants’ self-esteem, self-efficacy, and problem-solving and coping skills. Implications for counselors, particularly those interested in adding a therapeutic component to traditional mentoring programs, are discussed along with suggestions for future research.
Keywords: mentoring programs, therapeutic, mental health interventions, at-promise youth, phenomenological
Because of a staggering dropout rate of 1.2 million students a year, as well as an increase of juvenile delinquency in the United States, there is a need for interventions that will help youth stay in school and out of the juvenile justice system (Weiler, Chesmore, et al., 2019; Weiss et al., 2019). Researchers have indicated that the absence of education, including students who do not graduate from high school, has led to an increase of youth experiencing health complications, substance abuse, social skill deficits, and premature death (Schoeneberger, 2012; Weiler, Chesmore, et al., 2019; Weiler et al., 2015; Weiss et al., 2019). In the past, youth exhibiting behaviors that might lead to juvenile delinquency were referred to as at risk. However, the term at promise is now utilized by organizations such as the California Education Code (McKenzie, 2019). The phrase at-promise youth describes youth who have the ability to reach their full potential with additional time and resources.
One way to help at-promise youth reach their full potential and feel more engaged at school might be connecting them with a young adult who understands their struggles. Youth benefit from enhanced connectedness to adults outside their immediate family to help them navigate through difficult times, and this relationship can be protective against suicidal behavior (King et al., 2018; Rhodes, 2002). Individuals within adolescent ecosystems have voiced the positive changes youth have experienced by participating in youth mentoring programs (Raposa et al., 2019). At-promise youth might benefit even more from youth mentoring programs that incorporate a therapeutic component to address mental health concerns they may be experiencing (Liang et al., 2013).
Youth Mentoring Programs
Youth mentoring is a psychosocial intervention in which a nonparental adult and a younger individual aim to develop a supportive relationship (Karcher et al., 2005; Lund et al., 2019; Sacco et al., 2014; Weiler et al., 2013). During the mentoring program, the youth mentees experience a healthy environment, which often leads to them seeking out and learning to cultivate a healthier environment beyond the youth mentoring program. This shift in environment has allowed researchers to observe improvement in self-perception, social acceptance, parent–child interaction, and academic performance of youth participating in mentoring programs (Anastasia et al., 2012). Researchers have found that mentoring programs may also buffer against the impacts of youth exposed to adverse childhood experiences and improve behavioral, social, emotional, and academic outcomes (Centers for Disease Control and Prevention, 2019; David-Ferdon et al., 2016; Durlak et al., 2010; Tolan et al., 2014). The relationship between mentor and mentee is heavily credited to the success of youth mentoring, signifying the importance of the mentee picking a mentor similar to them (e.g., appearance, culture, interests).
Researchers discovered that both mentor and mentee benefit from the dyadic relationship when there is trust and the mentor is consistent, supportive, and encouraging instead of controlling (Marshall et al., 2016; Rhodes, 2002; Weiler, Boat, & Haddock, 2019; Weiler et al., 2015; Weiss et al., 2019). A mentor should be supportive and encouraging, especially when giving advice, which helps the youth to be open to a new perspective (Lund et al., 2019; Rhodes, 2002). Youth who participated in a positive mentoring relationship had increased feelings of connectedness with a trusted adult and higher rates of pursuing purpose (Lund et al., 2019). In addition, by the end of youth mentoring programs, the majority of mentees achieved a sense of self-worth and increased levels of intimacy, communication, and trust because of the dyadic relationship they had established with their mentors (Keller & Pryce, 2012; Rhodes, 2002).
Mentors and Youth Mentees
Research on youth mentoring programs has described mentees as individuals who are at risk, may have been in the juvenile justice system, or are in danger of offending or reoffending because of a variety of variables (e.g., substance use, academic failure, absences, aggressive behavior, family stressors) present in their lives (Cavell et al., 2009; Haddock et al., 2017; Weiler et al., 2013). Weiler et al. (2013) noted that more than 60% of the youth who participated in a mentoring program in their study had acquired at least a single charge with the juvenile justice system. Numerous researchers have discussed how the role of a mentor in a mentee’s life helped the mentee with improved self-esteem, enhanced health, instilled hope for the future, and reduced reoffending behaviors (Raposa et al., 2019; Rhodes, 2002; Weiler, Boat, & Haddock, 2019; Weiss et al., 2019).
Training is required before being paired with a mentee to ensure the competency of the adult who will be mentoring the youth facing hardships. Anastasia et al. (2012) emphasized the importance of preparatory training and ongoing training so that mentors, who are not in a helping profession, will have the tools necessary to mentor an adolescent successfully. In the preparatory stage of training, mentors learn about maintaining safety, program rules, child-focused social problem–solving skills, and the activities that will be used throughout the program (Anastasia et al., 2012; Cavell et al., 2009).
At the same time, mentors may feel overwhelmed when mentees exhibit mental health issues, behavioral issues, or racial or socioeconomic differences that surpass their basic training and expertise (Marshall et al., 2016; Weiler et al., 2013). With a majority of the adolescents facing difficulties, it can be daunting for the mentor to provide adequate mentoring; therefore, ongoing training is imperative. Ongoing training is meant to help the mentor increase their effectiveness with their mentee (Anastasia et al., 2012), allowing the adult to seek guidance when they start feeling overwhelmed with their mentee’s behavior and actions (Keller & Pryce, 2012). Through ongoing training and interaction with their paired youth, the adult mentor gains a new level of insight and improved health, self-esteem, and self-awareness that they did not have before (Rhodes, 2002).
However, even with ongoing training, mentees may exhibit mental health needs that are beyond the average mentor’s training and skill set. Liang et al. (2013) highlighted that mentees might benefit from receiving traditional therapy to help with their hardships. Therefore, some mentoring programs have added a therapeutic component incorporating trained mental health personnel to positively support both mentors and mentees (Weiler et al., 2013).
Therapeutic Component to Mentoring
Mental health professionals (e.g., counselors, social workers, psychologists) learn through their education how to be culturally competent, preserve client autonomy, and maintain an unbiased perspective that is crucial when trying to develop a mentoring relationship (Anastasia et al., 2012). Liang and colleagues (2013) emphasized how youth with therapeutic needs benefit from the way therapeutic guidance and a mentoring program complement each other. For instance, if a child is stressed about how to pay for college, then a mentor can help their mentee find resources, while a therapist could focus on teaching healthier coping skills to manage stress (Liang et al., 2013). Working in tandem allows for a two-dimensional approach, a noteworthy difference between therapeutic mentoring and traditional mentoring programs (Sacco et al., 2014).
Some therapeutic mentoring programs select mentors from a helping profession and provide additional training and supervision from trained mental health clinicians to create a more therapeutic setting for mentees (Johnson & Pryce, 2013). Other youth mentoring programs include a therapeutic component by incorporating additional staff consisting of mental health professionals, such as counselors-in-training (CITs), to directly address the mental health needs of mentees and support mentors (Sacco et al., 2014; Stark et al., 2021; Weiler et al., 2013). Therapeutic mentoring programs function as an intervention for youth who are engaging in risky behavior or have experienced trauma and other developmental issues (Johnson & Pryce, 2013; Sacco et al., 2014).
Litam and Hipolito-Delgado (2021) discussed how COVID-19 highlighted that communities of color have limited access to health care and education. Marginalized youth and their families may not seek mental health services at all or may be more prone to accept help from non–mental health professionals such as mentors (Dashiff et al., 2009). Therefore, an ideal youth mentoring program might have trained mentors from a helping profession who are supervised by mental health professionals, such as counselors, who are also available to meet with youth throughout the mentoring sessions. However, many mentoring programs are volunteer-based and this may limit access to mental health professionals. In addition, there is a shortage of mental health professionals prepared to work with youth (Dashiff et al., 2009) and there is a treatment gap for mental disorders in children (Patel et al., 2013).
Often youth have access to counselors in their schools, but researchers have found that school counselors report that they have limited time to address ongoing mental health needs (Carlson & Kees, 2013). Litam and Hipolito-Delgado (2021) encouraged counselors to use creative strategies such as reduced or no-cost services when working with communities of color. Dashiff and colleagues (2009) stressed that “innovative strategies of service delivery are needed” when working with youth who may come from poverty or areas with limited access to mental health services (p. 29). Partnering with a university, with a plethora of CITs needing supervised client hours, is an innovative and low- or no-cost approach. In this scenario, the mentor takes on a therapeutic role with their mentee, but the CIT is available to address and process ongoing mental health concerns. Incorporating CITs in a youth mentoring program allows both mentor and CIT to work together to create an environment in which youth feel safe, encompassing a secure attachment to the therapeutic program (Sacco et al., 2014).
The CIT’s position facilitates insight and awareness for the youth while offering tools that will help them reach their therapeutic goals (Johnson & Pryce, 2013; Sacco et al., 2014). The role of the mentor is to serve as a role model and advocate while maintaining open communication with the CIT to facilitate necessary therapeutic modifications (Sacco et al., 2014). Some researchers have found that as the mentor models healthy behavior, the youth will eventually begin to display a healthier interpersonal and intrapersonal self (Johnson & Pryce, 2013; Sacco et al., 2014). Overall, mentoring programs appear to be an effective intervention for youth that could also benefit from the incorporation of a therapeutic component.
Despite the amount of research being done to understand the relationship between mentor and mentee from different perspectives, there is less data that examines the participants’ lived experiences of a therapeutic youth mentoring program that includes CITs. The purpose of this study was to examine and gain further insight into participants’ lived experiences with a therapeutic youth mentoring program—specifically, a therapeutic youth mentoring program in which the mentors had additional training and supervision in mental health areas and additional support was provided by CITs while under supervision. The overarching question for this study was: What were participants’ lived experiences prior to and after participating in a therapeutic youth mentoring program?
Methodology
Phenomenology was utilized in this study to gather and analyze data in order to better understand participants’ lived experiences in a therapeutic youth mentoring program. According to Trusty (2011), “if little is known about a research area or target population, it is likely that a qualitative study would be needed first” (p. 262). Although some research has been conducted with participant perceptions of youth mentoring programs, there is less research with therapeutic mentoring programs; therefore, a qualitative approach was deemed appropriate.
Therapeutic Youth Mentoring Program
The therapeutic youth mentoring program in this study was at a university in the Rocky Mountain region of the United States and utilized the theoretical framework of Campus Corps (Weiler et al., 2013, 2014), now called Campus Connections (CC). CC is an innovative licensed program combining practices from mentoring, after-school programming, and integrated mental health. CC mentors were recruited and selected from a variety of undergraduate disciplines across campus, with more than half being from counseling and human services, psychology, or education majors. All mentors attended an orientation and background screening prior to being accepted for the program. The mentors who were selected spent the first 3 weeks of the semester in intensive training with counselor educators, who were also licensed professional counselors, to learn about child abuse reporting, ethics of working with minors, crises and trauma, and basic counseling skills. Potential mentees were referred by local school counselors and attended an intake with their guardians to go over the format of the program. Mentors created profiles about themselves that were utilized during the intake so that mentees could select their mentor based on preferences.
Once mentees were paired with mentors, the faculty and staff looked at the information provided by caregivers and counselors, demographics, and other relevant information to create diverse mentor families. Each mentor family consisted of approximately three mentor/mentee pairs. In this study, there were a total of three mentor families and each family was assigned a mentor coach. The mentor coaches were graduate-level counseling students who provided their mentor family with support throughout the semester. In addition, four graduate-level CITs were selected to provide ongoing counseling to mentees throughout the therapeutic mentoring program. All CITs were in their last semester of graduate studies and met weekly with counselor educators for supervision. Two counselor educators and supervisors, also licensed professional counselors, were also present each evening of CC to support mentees, mentors, and CITs.
All youth participated in the 12-week CC therapeutic youth mentoring program that met on the university campus, once a week for 4 hours. This therapeutic youth mentoring program was designed to bring youth to a college campus to help them become more comfortable and familiar with future college and career goals. Youth followed a schedule that consisted of:
- working for 60 minutes with their mentor on academic and study skills.
- going on a 30-minute “walk and talk” to learn about different locations on the university campus each week.
- participating in a 30-minute family-style meal at the dining hall with their mentor family.
- choosing two 45-minute prosocial or social justice activities.
The prosocial and social justice activities were directed at helping youth learn skills and concepts such as resiliency, coping, inclusiveness, and empathy. These activities were adapted from a manual created by the founders of CC. Each evening, two 45-minute lessons were facilitated by our graduate assistants and CITs and covered topics around the “Big 8” identities (i.e., gender/sex, race, class/socioeconomic status, sexual orientation, ethnicity, religion, age, and ability). Some examples of the activities included: Backpack, an activity adopted from Peggy Mcintosh’s (2003) The Knapsack, that examines privilege and societal benefits; Build a House, an activity designed to illustrate the differences in resources that people have based on socioeconomic status; and Pink, Blue and Purple, an activity designed to discuss assumptions made about gender.
At any point throughout their time on campus, mentors or mentees could request for the youth to have time to meet with a CIT. CITs also routinely set up check-ins with all mentees and were present throughout the entire process. Often the CITs would help with the after-dinner activities if youth weren’t requesting to meet 1:1. The participants in this study engaged in a total of 720 minutes of counseling with the average youth receiving 50 minutes of individual counseling.
Participants
This was a purposeful sample of at-promise youth participating in the same CC therapeutic youth mentoring program in the spring of 2019. Of the 18 youth enrolled in CC, 14 youth agreed to participate in the research study. The participants in this study consisted of 14 youth, ages 11–15, with the following demographics: 71% male, 21% female, and 7% transgender/gender-expansive; 57% White, 29% Black/African American, 21% Hispanic/Latino, 14% American Indian/Alaska Native, and 7% Asian; and approximately half on free and reduced lunch. School district partners were asked to consider and recommend at-promise youth if they were not reaching their full potential and might be vulnerable to school dropout, substance use/misuse, and/or criminal behavior. Local school counselors submitted referrals based on this criterion for youth to participate in CC. Participation was voluntary and participants could remove themselves from the study at any time throughout the process.
Procedures
At-promise youth are considered a vulnerable population and therefore researchers must contemplate ethical considerations. Our research team went through a full IRB process to ensure youth participants were being treated with the highest ethical considerations. After obtaining IRB approval, informed consent and assent was secured and two audiotaped interviews were conducted with all participants—one at the beginning of the 12-week mentoring program and one 12 weeks later at the end. Semistructured interviews are progressive in design (Merriam, 1998); they allow the researcher to formulate questions ahead of time and adjust the questions based on the participants’ responses (Guba & Lincoln, 1989). Participants were asked a series of open-ended questions that were similar across interviews, such as how a mentor has helped them, their feelings about being on a college campus, and thoughts on meeting with a CIT (see Appendix for a complete list of interview questions). The final interview allowed the participants to describe their experience working with a mentor and CIT and their perceptions of meeting on a university campus each week for 12 weeks.
Our research team consisted of three PhD-level counselor educators, Diane Stutey, Lori Notestine, and Joseph Wehrman; one counselor education doctoral student, Kim Severn; one staff member in master’s-level student affairs and higher education, Molly Cammell; and two graduate students in counseling, Abigail E. Solis and Kodi L. Enkler. All members of the research team were present throughout the 12-week therapeutic youth mentoring program. We met on a regular basis to discuss the research protocol and any potential conflicts of interest or ethical concerns, ensuring trustworthiness of the study.
Data Analysis and Trustworthiness
All data were collected by the research team and Solis transcribed all the interviews. Data were analyzed and independently coded by Stutey, Solis, and Severn, utilizing Merriam’s (1998) two-level approach. After each researcher independently coded all the transcripts, we met to discuss and agree upon emerging themes. After data was further analyzed and organized to support each of the themes, we met again to come to consensus on the themes. Any disagreement of themes or supporting data was discussed until consensus was reached.
Several techniques were used to ensure the trustworthiness and rigor of data collection and analysis (Guba & Lincoln, 1989; Merriam, 1998). Stutey, Solis, and Severn independently coded the data and each kept their own researcher journal. To establish dependability and conformability, an audit trail was created (Lincoln & Guba, 1985). Notestine and Enkler served as peer reviewers and assisted Stutey, Solis, and Severn by providing feedback at various points. Peer reviewers were given access to initial emerging themes, final themes, researchers’ journals, and coding documentation to inform the feedback provided to Stutey, Solis, and Severn throughout the data collection and analysis process.
We also used bridling to establish trustworthiness and acknowledge the researchers’ prior and current experiences. Often qualitative researchers will use bracketing in an attempt to manage their understanding of or experience with a phenomenon. However, bridling encourages ongoing researcher reflexivity and is meant to be more intentional, with researchers maintaining openness and revisiting assumptions throughout the research process (Dahlberg, 2006; Vagle, 2009). Stutey et al. (2020) described bridling as “an ongoing reflective practice that takes place before, during, and after data collection” (p. 124). Bridling was chosen over bracketing because the researchers had personal and professional experiences with at-promise youth, making it unlikely to put aside all biases and assumptions. Development of a researcher’s stance and review of researchers’ journals were utilized throughout the data collection and analysis to bridle and manage researchers’ biases and assumptions.
Findings
In total, five themes emerged from the participant interview data: life stressors, self-awareness, trusting others, adaptability and resiliency, and hope for the future. In order to be considered a theme, at least seven out of the 14 participants had to endorse the theme. Within each theme, there were two to three aspects that were discussed by participants. Each of the themes is discussed in this section, and a sample of participant quotes is provided as evidence of each aspect of the theme. Participants all chose pseudonyms that were used throughout the research study.
Figure 1
Summary of Themes
| Themes |
Aspects of Themes |
| Life Stressors |
· School
· Peers/Bullying
· Mental Health |
| Self-Awareness |
· Positive Self-Image
· Accomplishments |
| Trusting Others |
· Qualities of a Trusted Mentor/Adult
· Feeling Understood or Heard |
| Adaptability and Resiliency |
· Social-Emotional Growth
· Coping Skills |
| Hope for the Future |
· Realistic Goals for School
· Future Careers
· Impact on Others |
Life Stressors
The first theme of life stressors was endorsed by all 14 participants. This theme was defined as participants’ lived experiences of how stressors in their lives were negatively impacting them. Many of the participants shared in the first interview that they were overwhelmed and a bit confused about being on a college campus. Participants were not sure why they were selected for the therapeutic mentoring program or what they might need help with beyond academics. Participants endorsed three aspects of life stressors in the areas of school, peers/bullying, and mental health.
School
In the initial interview, participants discussed wanting to get straight As and that math was a particularly tough subject area for them. Ball stated, “I really struggle with math. I don’t know why it’s always been something that’s really hard for me.” JT shared that they “have to get straight As” and indicated that if they did not, they would “get kicked out.” Tristonion said, “Right now, I really don’t have the motivation to try in school.”
Other participants struggled with certain teachers, behavior at school, or homework. Josh Billups shared, “Sometimes I’m afraid to talk to my teachers . . . talking to adults is kind of hard.” Drift King stated that they had problems in several areas, such as “not studying, not getting most of the work done, not understanding the work, too afraid to ask teachers, raise my hand, or [ask] questions.” Many participants said that they “don’t like homework” and that they also struggle in school because they “talk too much,” are “not turning in assignments,” and find it “really hard . . . to focus.” School and academic success were important to the majority of the participants in this study.
Peers/Bullying
Besides academic stressors at schools, participants shared that they sometimes struggled with bullies and many shared having a lack of peer or other support in school. Bam shared that they struggle at school because of “getting bullied and having nobody to talk to . . . somebody told me to go commit suicide.” Isabel stated that there is a lot of “drama . . . and getting bullied” at their school. Isaiah shared feelings of isolation: “Kids were being mean and stuff so I just went and sat [alone].” Others shared that they have been called “a snitch,” “Bible head,” and “God” by students in their schools that they perceive as bullies. Participants felt they could discuss these matters with their mentors and/or CIT and seek their advice.
Mental Health
Participants also discussed areas of stress that impact them at school such as learning difficulties and specific physical and mental health issues. DTS shared, “I have ADHD . . . and it’s hard getting back on the schedule taking pills every day.” Several participants mentioned struggling with symptoms associated with depression. Isabel stated, “I’ve had a lot of surgeries and I have really bad anxiety and depression.” Isaiah discussed that “everyone is mean to me” and shared that they “don’t have a good memory.” Many participants mentioned that they were using the mental health services of their school counselor and/or the CIT provided through CC but sometimes felt just as comfortable talking to their mentor.
Self-Awareness
The second theme that emerged from this study was self-awareness. This theme was endorsed by 13 of the 14 participants and is defined as participants’ lived experiences of becoming more self-aware after participating in the 12-week therapeutic mentoring program. When asked about how others perceived them, participants tended to initially interpret that teachers and caregivers might have negative views; often these views were opposite of those that they held about themselves or they perceived peers had about them. After participating in the therapeutic mentoring program, youth seemed more open to talking about their strengths and shared more positive comments about themselves and their accomplishments. Participants endorsed two aspects of self-awareness: positive self-image and awareness of accomplishments.
Positive Self-Image
Many of the participants shared a negative self-image in the initial interview. After spending time in the therapeutic mentoring program, they viewed themselves, and perceived that others also viewed them, in a more positive light. Andrew shared, “I learned you don’t have to be bad to get where you need to be. You don’t have to be dangerous for people to like you.” Jeffy stated, “I’ve been focusing on my schoolwork instead of messing around all the time. And [I’m] thinking before I do something . . . less getting in trouble.” Josh discussed how their image had changed since participating: “Back then I was kind of mean, but [the program] kind of helped me change that . . . I have a lot more friends now.” Several participants shared that they were getting along better with others and being “more social now,” were “able to talk and interact with other people,” and were “opening up to more people.” Several participants attributed this shift in their self-image to having a mentor and/or CIT who unconditionally accepted them.
Accomplishments
Along with viewing themselves in more positive ways, many participants shared what they had accomplished during this semester. Andrew stated, “I used to fight a lot and now we [mentor and me] have a goal not to fight. I haven’t fought since.” Drift King shared, “I know that I’ve got to take it [school] seriously. There’s a lot more stuff that I can accomplish in life.” Isaiah discussed that their grades had improved and “I just got accepted to be a web leader.” In fact, many participants shared improvement in their overall well-being, grades, and relationships with peers: “I’ve been more happy,” “Now I have three As and four Bs,” and “I would describe myself as really helpful and caring about other people.” Participants seemed proud to share these accomplishments and were often smiling during the final interview as they discussed ways they had seen improvement.
Trusting Others
The third theme to emerge was trusting others. This theme was endorsed by 12 of the 14 participants and is defined as participants’ lived experiences with learning to trust others, especially adults. In the initial interview, the participants were unsure of some of their relationships and especially expressed a disconnect with adults. Many participants said that they did not always ask for help or they had some past negative experiences with adults and peers. After participating in the therapeutic youth mentoring program, many participants reported having a trusting relationship with their mentor, and a few with other adults supporting the program, such as mentor coaches and CITs. There also seemed to be some shift in participants having better relationships with peers and other adults outside of the therapeutic youth mentoring program. Participants shared two aspects of trusting others: qualities of a trusted mentor/adult and feeling understood or heard.
Qualities of a Trusted Mentor/Adult
Many participants shared that they perceived their mentors as someone who will “always be there for you.” Andrew shared, “We had a lot in common. So, I can talk to her and she’ll know the answer.” Ball shared, “I just get someone to talk to other than my parents and friends . . . [he’s] a helpful person that gets you through bad times.” Drift King stated, “They help you with anything I need: anger management, class, social skills, school, someone to talk to like a counselor.” Participants described mentors as “cool,” “funny,” “nice,” “friendly,” “chill,” and “helpful.”
Participants were also asked about their perceptions of meeting with a counselor before and after participating in the therapeutic mentoring program. The majority of the participants shared positive experiences they have had with counselors both at school and during the therapeutic mentoring program, stating they helped “when I’m having a bad day,” “after my Grandpa died,” and “when I was being bullied.” Only one participant, Isabel, mentioned that she trusted the CIT more than her mentor: “She’s super there for me, and I only want to talk to her about my problems, because I don’t feel like I really know any other counselors.” Andrew seemed confused about the roles of the different adults at the therapeutic mentoring program: “I thought they were all like mentor and mentor coaches.” After clarification, he shared that the CITs “bring you up . . . if you are feeling down or unhappy.” Although there may have been some initial confusion about the difference between the CITs and coaches, it seemed that most participants felt comfortable seeking counseling support as needed.
Feeling Understood or Heard
In addition to sharing qualities that they appreciated about their mentors, participants shared that a mentor is someone who understands them and makes them feel heard. Drift King shared, “I feel like they’ve been through it too, tough times and they succeed . . . I feel they can help you.” Jeffy stated, “We’re really similar, he’s kind of like me. They talk about your weekend . . . and make you feel happier if you had a bad day.” Rene discussed how her mentor “supports me, like if I have a really bad day she helps me out to have a better rest of my day.”
Adaptability and Resiliency
The fourth theme that emerged was adaptability and resiliency. This theme was endorsed by 10 out of the 14 participants and is defined as participants’ lived experiences of the ways in which they were adapting to some of the stressors that they had shared in the first interview. Participants discussed what they had learned in the therapeutic mentoring program, and often the new resiliency skills seemed connected to experiences with their individual mentor. Participants endorsed two major aspects of this theme: social-emotional growth and coping skills.
Social-Emotional Growth
Participants shared ways in which they had grown socially and emotionally over the semester. DTS shared, “I made some new friends.” Isaiah stated, “I open up to new people.” Bam discussed how their mentor helped them “get through rough times.” Many participants shared that working with their mentors helped them “deal with stress,” “learn how to socialize,” and “make the right decisions.” Several participants were hesitant to even attend CC initially and by the end, they expressed that they were sad to leave because of the social and emotional connections.
Coping Skills
Participants also perceived they had better coping skills and strategies for how to approach a variety of problems. Andrew stated, “Yesterday there was a fight, and I didn’t go . . . [my mentor] said, ‘You can always walk away.’” Josh shared that they learned various coping skills such as better “communication skills and knowing people who will help me and be respectful . . . it’s helped me be able to talk and interact with other people.” Tristonion added, “Well, this place teaches us to calm down.” Participants shared that they also “started focusing,” “doing good deeds,” and “hang[ing] with other people.” Several participants shared that the coping skills they were using they had learned either from their mentor or the CITs during 1:1 time or in prosocial activity time.
Hope for the Future
The fifth and final theme that emerged was hope for the future. This theme was endorsed by 13 of the 14 participants and is defined as participants’ lived experiences surrounding their future hopes and plans. Many participants in the initial interview had lofty goals that did not always seem realistic (e.g., become an NBA or NFL player). Participants also emphasized the importance of having perfect grades and that this is how they would know they were successful. After participating in the therapeutic mentoring program, participants shared what they had learned and their hopes for the future. The three aspects of this theme centered around setting realistic goals for school, the importance of future careers, and the impact they could have on others.
Realistic Goals for School
At the end of this study, many participants reported improvement in grades but were not stressing about perfection as much. Participants were setting more realistic goals for themselves with school. Drift King shared they were planning ahead for high school and would “take it more seriously than middle school . . . to get the credit to actually graduate.” Super J stated about meeting with his mentor, “It’s probably going to help me be successful at college because they show you how important it is to not give up.” JT discussed how doing well in school would allow them to continue to wrestle and “get first place again.” Many participants seemed to have learned from their mentor and/or CIT more about the college process and what they needed to do now in order to reach future goals.
Future Careers
Participants were also more interested in what it might take for them to meet their future career goals. Isabel stated, “In September I’m getting my first job . . . and once I graduate high school, I want to be a lawyer in the Air Force.” Josh stated, “I want to get the highest grades I can so I can do activities and get into higher classes to set myself on the right foot for the future.” Josh mentioned the importance of “getting a good education . . . going to college and get[ting] a job.” This youth was considering a variety of occupations such as construction worker or firefighter. Some of the participants even mentioned that after working with their mentor they wanted to “go to college here” and realized that college might help them “be able to have a good job and a good house.” Participants seemed to be making the connection between college and career based on conversations with their mentor and/or CIT.
Impact on Others
At the same time that participants were discussing their hopes for the future, there were many who also wanted to have an impact on others. Isaiah knew that they wanted to help people and discussed a variety of ways they might do this by being a “teacher, nurse, or school counselor.” Rene was not sure if they wanted to help people or animals, so they were considering “being a veterinarian or a doctor.” Finally, Super J shared, “I kind of want to help other kids—like to be an orthodontist and help kids and fix their teeth.” It is important to note that the majority of the undergraduate mentors are in human services and helping degrees so this may have influenced their mentees on some level.
Discussion
The overarching question for this study was: What were participants’ lived experiences prior to and after participating in a therapeutic youth mentoring program? In this section, the findings are discussed as they relate to answering this overarching question. Furthermore, a discussion of how these findings support and add to the literature on therapeutic mentoring programs is provided.
Consistent with prior research studies on mentoring programs, the participants in this study shared that having a mentor had a positive impact on their overall behavior (DuBois et al., 2011; Tolan et al., 2014; Weiler et al., 2015). Specifically, participants indicated more adaptive and resilient thinking after participating in the youth mentoring program. Lee et al. (2012) indicated that resilience is not fixed but can be learned and fostered through the protective factors in a child or adolescent’s life. Being able to walk away from a fight or potentially violent situation and asking adults for help were two of the outcomes participants described. A few participants even cited the therapeutic youth mentoring program as the reason why they have developed better coping strategies to better handle the stress they feel in their daily lives.
Another finding consistent with the research on mentoring programs was that participants acknowledged the significance of the primary mentoring relationship (Weiler et al., 2015; Weiss et al., 2019). One significant finding between the initial and final interview was the participants’ shared perspective that they trusted their mentor and the other adults supporting the youth mentoring program (e.g., mentor coaches and counselors). Griffith and Larson (2015) stated that when youth have trusting relationships with adults they become “deliberate agents of their own development” (p. 791). Mentors and CITs supporting the youth mentoring program helped to facilitate this development of trust by being present, participating in dialogue, and leading prosocial activities with the youth.
Many participants also described that because of the trust they developed with their mentor, they were able to also trust other adults in their lives, specifically parents, counselors, and teachers. When adolescents have a trusting relationship with at least one adult in their life, help-seeking behavior increases for the youth as well as their immediate peer group (DeLay et al., 2016). Although the majority of the participants shared the positive impact of having a therapeutic component to this youth mentoring program, five of the 14 participants still shared in the final interview that they were hesitant to meet with a counselor (either at school or at the therapeutic mentoring program). Haddock and colleagues (2017) posited that youth who participated in CC might be embarrassed to share about their experiences with counselors. It is important to note that some of the youth participants also did not make the distinction between CITs and mentor coaches. So, more clarity on the role of CITs in youth mentoring programs may be needed.
However, the mentors in the CC therapeutic mentoring program do learn some basic counseling skills and are also trained in crisis intervention. Although development of the relationship with the counselor may be an area of further examination with therapeutic mentoring programs, it seemed that many of the participants felt comfortable discussing mental health issues with their mentors who were being supported by counseling professionals.
Researchers have discovered that when mentees do develop a positive perception of support, this can lead to an increase in academic attitudes and self-esteem, lower frequencies of problem behaviors, and thinking more positively about the future (Chan et al., 2013; Haddock et al., 2017; Raposa et al., 2019; Weiler et al., 2014). In this current study, not only did participants indicate that their grades improved, but they also began to develop a more balanced outlook concerning school and their future college and career goals. Similarly, Weiss and colleagues (2019) discovered that positive academic mentoring relationships help youth find hope for the future and instill a belief that college and career goals can be reached.
In the initial interview, many participants discussed their perceived barriers and stressors to academic and life success, such as learning and mental health challenges. Haft and colleagues (2019) discovered that participation in a peer-mentoring program resulted in reduced depressive symptoms and increased self-esteem in youth with ADHD and learning disabilities. Relatedly, participants in our current study talked more openly about their strengths and hopes in the final interviews, demonstrating more self-awareness, fewer depressive indicators, and a higher sense of self. Perhaps gaining more hope and a higher sense of self led the participants to also focus on ways in which they might positively impact others. This finding is interesting considering that Briggs et al. (2007) posited that some youth might seek out opportunities to volunteer to help others in order to increase their self-worth.
Implications
There are a number of implications of these findings for counselors, particularly those interested in adding a therapeutic component to traditional mentoring programs. First, although many youth mentoring programs have historically focused on the connection between mentor and mentee (Marshall et al., 2016; Rhodes, 2002; Weiss et al., 2019), the results of this study indicate a significant benefit related to the additional attention to the mental health needs of mentees. Throughout the 12-week period, mentees had the opportunity to engage with mental health professionals in a non-threatening context. This added therapeutic component appeared to provide an additional support toward the connections the youth developed with trusted adults.
Another important implication emerging from the results points to the increase in self-esteem and self-efficacy in the context of the variety of relationships and settings available to the youth mentees. A number of youth reported they could envision themselves going to college in the future after having spent time on a college campus and being exposed to a wider variety of career options. Mentoring programs may find value in creating pathways to career and college exposure supported by trusted adults, such as mental health counselors.
An increase in problem-solving and coping skills is an additional finding with significant implications for youth mentoring programs. Most of the youth interviewed shared varied experiences in the program that resulted in developing new ways of adapting to life stressors. This theme emerged in various ways for the youth, indicating that it may be effective for other programs to integrate a variety of experiences, such as psychoeducational and therapeutic components, that focus on adaptive and resiliency skills.
Mentoring programs are important in aiding struggling youth but often fall short because of a lack of resources and consistency and an inability to address the mental health needs of mentees (Weiler et al., 2013). Including counselors and incorporating a therapeutic component in youth mentoring programs may be beneficial to both youth and their mentors. The implications of adding a therapeutic component in youth mentoring programs and psychoeducational activities on a college campus are extensive and indicate that further development and research are imperative.
Limitations and Future Research
There are several limitations within this current study. One limitation is that youth reported initial reluctance to participate in the research portion of the program. For many youth, participating in an individual qualitative interview was a novel experience and establishing rapport was often contingent on the overall volume of engagement. It may be helpful to allow the youth to have their mentors present during the interview because they are a trusted adult.
Further, a few participants expressed confusion regarding the difference in roles between the mentors, CITs, and mentor coaches. Youth and their caregivers do go through a formal intake process, but perhaps further psychoeducation or an orientation for youth on the different roles, in particular of the CITs, would be helpful. In addition, youth only participated in an average of 50 minutes of 1:1 counseling across the 12 weeks. However, there were many times they were interacting with CITs in small groups and large classroom guidance, similar to school counseling. Future studies with therapeutic mentoring programs could provide better clarification on the role of CITs and perhaps provide more structured weekly 1:1 counseling time with all participants.
Additionally, follow-up interviews with youth participants could help determine if identified change behaviors and attitudes continue to persist over time. In particular, it would be interesting to see if youth were more likely to reach out to their school counselor and/or counselors in the community after participating in a therapeutic youth mentoring program. Several participants mentioned they had never met with their school counselor and/or an outside counselor and that meeting with the CIT at CC was their first experience with individual counseling.
Lastly, future research regarding the experiences of mentors, parents, and key stakeholders in participants’ lives (e.g., teachers, parole officers, case workers, school counselors) could provide greater validity and confirmation of universal themes and experiences generated by the therapeutic youth mentoring program. A follow-up quantitative or mixed methods study could confirm and further validate key findings.
Conclusion
Mentoring programs are an effective mental health intervention for at-promise youth, and the addition of a therapeutic component might further enhance this intervention. A qualitative study was conducted to analyze youth’s lived experiences before and after participating in a therapeutic youth mentoring program. The participants in this study consisted of a diverse group of youth who were interviewed at the beginning and end of a 12-week therapeutic mentoring program. In addition to being paired 1:1 with a mentor, all of the youth had access to individual counseling with CITs throughout the program. The five themes that emerged from the data were life stressors, self-awareness, trusting others, adaptability and resiliency, and hope for the future. Some aspects discussed within these themes included peers/bullying, positive self-image, feeling heard or understood, social-emotional skills, and future careers. Researchers observed an increase in self-esteem, self-efficacy, and problem-solving and coping skills in the youth. Finally, youth participating in the therapeutic mentoring program perceived a benefit of having additional attention given to their mental health needs.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Anastasia, T. T., Skinner, R. L., & Mundhenk, S. E. (2012). Youth mentoring: Program and mentor best practices. Journal of Family & Consumer Sciences, 104(2), 38–44. https://extension.colostate.edu/docs/4h/youth-mentor-practice.pdf
Briggs, E., Landry, T., & Wood, C. (2007). Beyond just being there: An examination of the impact of attitudes, materialism, and self-esteem on the quality of helping behavior in youth volunteers. Journal of Nonprofit & Public Sector Marketing, 18(2), 27–45. https://doi.org/10.1300/J054v18n02_02
Carlson, L. A., & Kees, N. L. (2013). Mental health services in public schools: A preliminary study of school counselor perceptions. Professional School Counseling, 16(4), 211–221. https://doi.org/10.1177/2156759X150160401
Cavell, T. A., Elledge, L. C., Malcolm, K. T., Faith, M. A., & Hughes, J. N. (2009). Relationship quality and the mentoring of aggressive, high-risk children. Journal of Clinical Child & Adolescent Psychology, 38(2), 185–198. https://doi.org/10.1080/15374410802698420
Centers for Disease Control and Prevention. (2019). Preventing adverse childhood experiences: Leveraging the best available evidence. National Center for Injury Prevention and Control.
Chan, C. S., Rhodes, J. E., Howard, W. J., Lowe, S. R., Schwartz, S. E. O., & Herrera, C. (2013). Pathways of influence in school-based mentoring: The mediating role of parent and teacher relationships. Journal of School Psychology, 51(1), 129–142. https://doi.org/10.1016/j.jsp.2012.10.001
Dahlberg, K. (2006). The essence of essences: The search for meaning structures in phenomenological analysis of lifeworld phenomena. International Journal of Qualitative Studies on Health and Well-Being, 1(1), 11–19. https://doi.org/10.1080/17482620500478405
Dashiff, C., DiMicco, W., Myers, B., & Sheppard, K. (2009). Poverty and adolescent mental health. Journal of Child and Adolescent Psychiatric Nursing, 22(1), 23–32. https://doi.org/10.1111/j.1744-6171.2008.00166.x
David-Ferdon, C., Vivolo-Kantor, A. M., Dahlberg, L. L., Marshall, K. J., Rainford, N. & Hall, J. E. (2016). A comprehensive technical package for the prevention of youth violence and associated risk behaviors. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. https://www.cdc.gov/violenceprevention/pdf/yv-technicalpackage.pdf
DeLay, D., Ha, T., Van Ryzin, M., Winter, C., & Dishion, T. (2016). Changing friend selection in middle school: A social network analysis of a randomized intervention study designed to prevent adolescent problem behavior. Prevention Science, 17, 285–294. https://doi.org/10.1007/s11121-015-0605-4
DuBois, D. L., Portillo, N., Rhodes, J. E., Silverthorn, N., & Valentine, J. C. (2011). How effective are mentoring programs for youth? A systematic assessment of the evidence. Psychological Science in the Public Interest, 12(2), 57–91. https://doi.org/10.1177/1529100611414806
Durlak, J. A., Weissberg, R. P., & Pachan, M. (2010). A meta-analysis of after-school programs that seek to promote personal and social skills in children and adolescents. American Journal of Community Psychology, 45(3–4), 294–309. https://doi.org/10.1007/s10464-010-9300-6
Griffith, A. N., & Larson, R. W. (2015). Why trust matters: How confidence in leaders transforms what adolescents gain from youth programs. Journal of Research on Adolescence, 26(4), 790–804. https://doi.org/10.1111/jora.12230
Guba, E. G., & Lincoln, Y. S. (1989). Fourth generation evaluation. SAGE.
Haddock, S., Weiler, L., Krafchick, J., Zimmerman, T. S., McLure, M., & Rudisill, S. (2013). Campus Corps therapeutic mentoring: Making a difference for mentors. Journal of Higher Education Outreach and Engagement, 17(4), 225–256. https://files.eric.ed.gov/fulltext/EJ1018626.pdf
Haddock, S. A., Zimmerman, T. S., Thomas, A. G., Weiler, L. M., Krafchick, J., & Fredrickson, G. J. (2017). A qualitative analysis of mentee experiences in a campus-based mentoring program. Journal of Youth Development, 12(4), 61–80. https://doi.org/10.5195/jyd.2017.496
Haft, S. L., Chen, T., LeBlanc, C., Tencza, F., & Hoeft, F. (2019). Impact of mentoring on socio-emotional and mental health outcomes of youth with learning disabilities and attention-deficit hyperactivity disorder. Child and Adolescent Mental Health, 24(4), 318–328. https://doi.org/10.1111/camh.12331
Johnson, S. B., & Pryce, J. M. (2013). Therapeutic mentoring: Reducing the impact of trauma for foster youth. Child Welfare, 92(3), 9–25.
Karcher, M. J., Nakkula, M. J., & Harris, J. (2005). Developmental mentoring match characteristics: Correspondence between mentors’ and mentees’ assessments of relationship quality. Journal of Primary Prevention, 26(2), 93–110. https://doi.org/10.1007/s10935-005-1847-x
Keller, T. E., & Pryce, J. M. (2012). Different roles and different results: How activity orientations correspond to relationship quality and student outcomes in school-based mentoring. The Journal of Primary Prevention, 33(1), 47–64. https://doi.org/10.1007/s10935-012-0264-1
King, C. A., Gipson, P. Y., Arango, A., Foster, C. E., Clark, M., Ghaziuddin, N., & Stone, D. (2018). LET’s CONNECT community mentorship program for youths with peer social problems: Preliminary findings from a randomized effectiveness trial. Journal of Community Psychology, 46(7), 885–902. https://doi.org/10.1002/jcop.21979
Lee, J. H., Nam, S. K., Kim, A.-R., Kim, B., Lee, M. Y., & Lee, S. M. (2012). Resilience: A meta-analytic approach. Journal of Counseling & Development, 91(3), 269–279. https://doi.org/10.1002/j.1556-6676.2013.00095.x
Liang, B., Spencer, R., West, J., & Rappaport, N. (2013). Expanding the reach of youth mentoring: Partnering with youth for personal growth and social change. Journal of Adolescence, 36(2), 257–267. https://doi.org/10.1016/j.adolescence.2012.10.002
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Litam, S. D. A., & Hipolito-Delgado, C. P. (2021). When being “essential” illuminates disparities: Counseling clients affected by COVID-19. Journal of Counseling & Development, 99(1), 3–10. https://doi.org/10.1002/jcad.12349
Lund, T. J., Liang, B., Konowitz, L., White, A. E., & DeSilva Mousseau, A. (2019). Quality over quantity?: Mentoring relationships and purpose development among college students. Psychology in the Schools, 56(9), 1472–1481. https://doi.org/10.1002/pits.22284
Marshall, J. H., Davis, M. C., Lawrence, E. C., Peugh, J. L., & Toland, M. D. (2016). Mentors’ perceived program support scale: Development and initial validation. Journal of Community Psychology, 44(3), 342–357.
McIntosh, P. (2003). White privilege: Unpacking the invisible knapsack. In S. Plous (Ed.), Understanding prejudice and discrimination (pp. 191–196). McGraw-Hill.
McKenzie, L. (2019). No more ‘at-risk’ students in California. Inside Higher Ed. https://bit.ly/InsideHigherEdatrisk
Merriam, S. B. (1998). Qualitative research and case study applications in education (1st ed.). Jossey-Bass.
Patel, V., Kieling, C., Maulik, P. K., & Divan, G. (2013). Improving access to care for children with mental disorders: A global perspective. Archives of Disease in Childhood, 98(5), 323–327. https://doi.org/10.1136/archdischild-2012-302079
Raposa, E. B., Rhodes, J., Stams, G. J. J. M., Card, N., Burton, S., Schwartz, S., Yoviene Sykes, L. A., Kanchewa, S., Kupersmidt, J., & Hussain, S. (2019). The effects of youth mentoring programs: A meta-analysis of outcome studies. Journal of Youth and Adolescence, 48(3), 423–443. https://doi.org/10.1007/s10964-019-00982-8
Rhodes, J. E. (2002). Stand by me: The risks and rewards of mentoring today’s youth. Harvard University Press.
Sacco, F., Jr., Pike, N., & Bourque, J. L. (2014). Therapeutic mentoring: Mentalization training in the community. International Journal of Applied Psychoanalytic Studies, 11(2), 138–150. https://doi.org/10.1002/aps.1405
Schoeneberger, J. A. (2012). Longitudinal attendance patterns: Developing high school dropouts. The Clearing House, 85(1), 7–14.
Stark, C., Wehrman, J., Stutey, D. M., Solis, A., Severn, K., Cammell, M., Gloden, H., Enkler, K., Notestine, L., & Palacios, A. (2021). Therapeutic mentoring for at-promise youth: A grounded theory study of mentors’ adaptation during the COVID-19 crisis. Journal of Human Services: Special Interdisciplinary Issue, 40(2), 116–132.
Stutey, D. M., Givens, J., Cureton, J. L., & Henderson, A. J. (2020). The practice of bridling: Maintaining openness in phenomenological research. Journal of Humanistic Counseling, 59(2), 144–156. https://doi.org/10.1002/johc.12135
Tolan, P. H., Henry, D. B., Schoeny, M. S., Lovegrove, P., & Nichols, E. (2014). Mentoring programs to affect delinquency and associated outcomes of youth at risk: A comprehensive meta-analytic review. Journal of Experimental Criminology, 10, 179–206. https://doi.org/10.1007/s11292-013-9181-4
Trusty, J. (2011). Quantitative articles: Developing studies for publication in counseling journals. Journal of Counseling & Development, 89(3), 261–267. https://doi.org/10.1002/j.1556-6678.2011.tb00087.x
Vagle, M. D. (2009). Validity as intended: ‘Bursting forth toward’ bridling in phenomenological research. International Journal of Qualitative Studies in Education, 22(5), 585–605. https://doi.org/10.1080/09518390903048784
Weiler, L. M., Boat, A. A., & Haddock, S. A. (2019). Youth risk and mentoring relationship quality: The moderating effect of program experiences. American Journal of Community Psychology, 63(1–2), 73–87. https://doi.org/10.1002/ajcp.12304
Weiler, L. M., Chesmore, A. A., Pryce, J., Haddock, S. A., & Rhodes, T. (2019). Mentor response to youth academic support–seeking behavior: Does attunement matter? Youth & Society, 51(4), 548–569. https://doi.org/10.1177/0044118X17697235
Weiler, L. M., Haddock, S. A., Zimmerman, T. S., Henry, K. L., Krafchick, J. L., & Youngblade, L. M. (2015). Time-limited, structured youth mentoring and adolescent problem behaviors. Applied Developmental Science, 19(4), 196–205. https://doi.org/10.1080/10888691.2015.1014484
Weiler, L., Haddock, S., Zimmerman, T. S., Krafchick, J., Henry, K., & Rudisill, S. (2013). Benefits derived by college students from mentoring at-risk youth in a service-learning course. American Journal of Community Psychology, 52(3–4), 236–248. https://doi.org/10.1007/s10464-013-9589-z
Weiler, L. M., Zarich, K. J., Haddock, S. A., Krafchick, J. L., & Zimmerman, T. S. (2014). A comprehensive model of mentor experiences: Perceptions, strategies, and outcomes. Journal of Community Psychology, 42(5), 593–608. https://doi.org/10.1002/jcop.21640
Weiss, S., Harder, J., Bratiotis, C., & Nguyen, E. (2019). Youth perceptions of a school-based mentoring program. Education and Urban Society, 51(3), 423–437. https://doi.org/10.1177/0013124517722830
Appendix
Pre Semi-Structured Interview
- Tell me what you already know about Campus Connections or having a mentor.
- Describe a typical day or week at school.
- What do you enjoy?
- What is something you struggle with?
- What are some ways you think having a mentor could help you (at school, home, in life)?
- What are your future goals or plans?
- For middle school
- High school
- After high school
- What is something that is preventing you from achieving your goals or future plans?
- How could your mentor help you with these challenges?
- Tell me about your thoughts/feelings about being on a college campus.
- What kind of jobs or careers are you thinking about?
- What are your thoughts on meeting with a counselor?
- Can you describe a time when a counselor helped you?
- How do you think people would describe you?
- Teachers?
- Parent or guardians?
- Peers?
- How would you describe yourself?
- What is something you wish people knew about you?
Post Semi-Structured Interview
** Remind the student of the pseudonym they chose and ask if they want to keep or change this.
- Tell me what you now know about Campus Connections and having a mentor.
- How would you describe your mentor?
- Tell me a story about your favorite thing about Campus Connections? Least favorite?
- Describe a typical day or week at school.
- What do you enjoy?
- What is something you struggle with?
- What are some ways you think having a mentor and participating in Campus Connections helped you?
- At school
- At home
- In life
- What are your future goals or plans?
- For middle school
- High school
- After high school
- What is something that has been preventing you from achieving your goals or future plans?
- Describe how your mentor helped you with these challenges.
- Tell me about your thoughts/feelings about being on a college campus.
- What kind of jobs or careers are you thinking about?
- What are your thoughts on meeting with a counselor?
- Can you describe a time when a counselor helped you?
- How do you think people would describe you?
- Teachers?
- Parent or guardians?
- Peers?
- Mentor?
- Counselor?
- How would you describe yourself?
- Are there things about you that you think have changed/improved since joining Campus Connections?
- What is something you wish people knew about you?
- What else would you like me or others to know about Campus Connections?
Diane M. Stutey, PhD, NCC, LPC, RPT-S, is an assistant professor and department chair at the University of Colorado Colorado Springs. Abigail E. Solis, MA, is a clinical mental health counselor at Colorado Motion. Kim Severn, MA, LPC, is an instructor at the University of Colorado Colorado Springs. Lori Notestine, PhD, LPC, is an instructor and program coordinator at the University of Colorado Colorado Springs. Kodi L. Enkler is a licensed school counselor at Swigert Aerospace Academy. Joseph Wehrman, PhD, LPC, is a professor at the University of Colorado Colorado Springs. Molly Cammell, MA, is Campus Connections program manager at the University of Colorado Colorado Springs. Correspondence may be addressed to Diane M. Stutey, 1420 Austin Bluffs Parkway, Colorado Springs, CO 80918, dstutey@uccs.edu.
Nov 9, 2021 | Volume 11 - Issue 4
J. Claire Gregory, Claudia G. Interiano-Shiverdecker
Using Moustakas’s modification of Van Kaam’s systematic procedures for conducting transcendental phenomenological research, we explored ballet culture and identity and their impact on ballet dancers’ mental health. Participants included four current professional ballet dancers and four previous professionals. Four main themes emerged: (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) counseling and advocacy—“the dance population is unique.” Suggestions for counselors when working with professional ballet dancers and professional athletes, such as fostering awareness about ballet culture and its impact on ballet dancers’ identity and mental health, are provided. We also discuss recommendations to develop future research focusing on mental health treatment for this population.
Keywords: ballet dancers, culture, identity, phenomenological, mental health
“Dancers are the athletes of God.”—Albert Einstein
Professional ballet dancers’ mental health experiences are sparse within research literature (Clark et al., 2014; van Staden et al., 2009) and absent from the counseling literature. Most research including ballet dancers focuses primarily on eating disorders, performance enhancement (Clark et al., 2014), and injuries (Moola & Krahn, 2018). Although these topics are crucial to dancers’ wellness, explorations of ballet dancers’ mental health that do not primarily focus on eating disorders are also important. Increasing professional ballet dancer and athlete mental health research could provide counselors with deeper awareness of the populations’ needs. Further, counselors have access to the American Counseling Association’s (ACA; 2014) Code of Ethics, which is relevant for all clients, including athletic populations. However, the counseling profession lacks specific sports/athletic counseling ethical codes, competencies, and teaching guidelines (Hebard & Lamberson, 2017). The only mention of “athletic counseling guidelines” appears in a 1985 article from the Association for Counselor Education and Supervision (Hebard & Lamberson, 2017). In their initiative to increase counselor response to the need for athletic counseling, Hebard and Lamberson (2017) implored counselors to advocate for athletes’ mental health. Further, the researchers stated that it is common to view athletes as privileged and idolize them for their physical endurance; however, this perception may leave athletes vulnerable to mental health concerns. Recent examples of mental health difficulties experienced by formidable professional athletes include tennis player Naomi Osaka choosing to decline after-match news conferences to safeguard her mental health and gymnast Simone Biles removing herself from some events at the Tokyo 2020 Olympics in order to protect her mental health.
Moreover, scholars have been increasingly devoted to understanding the cultures within which performing artists are trained and developed and recognizing their role in supporting the health and well-being of the artist (Lewton-Brain, 2012; Wulff, 2008). For counselors, the ACA Code of Ethics (2014) promotes gaining knowledge, personal awareness, sensitivity, and skills pertinent to working with a diverse client population (C.2.a). However, this is difficult with limited current data or research seeking to advance knowledge of the culture of performing institutions and how they relate to artists’ mental health experiences. Therefore, an exploration of ballet culture and identity and their impact on ballet dancers’ mental health experiences could help inform counselors and counselor educators about the counseling needs of this population.
Mental Health Among Elite Athletes and Performing Artists
Because of the scant literature focusing directly on professional ballet dancers’ mental health, we included research findings from articles examining mental health among athletes and performing artists. Although differences exist between professional ballet dancers, elite athletes, and performing artists, a professional ballet dancer straddles multiple environments. For example, an elite athlete trains to win a national title or medal, possesses more than two years of experience, and trains daily to develop talent (Swann et al., 2015). Rouse and Rouse (2004) suggested that performing artists’ goals or outcomes are to create art and achieve a high performance level with audience satisfaction. Similar to these groups, a professional ballet dancer trains almost every day, which requires extreme dedication. They must comply with high physical and mental demands to develop their ballet technique for performing and entertaining audiences.
Scholars have discovered that elite athletes experience a high prevalence of anxiety, eating disorders, and depression compared to the general population (Åkesdotter et al., 2020; Gorczynski et al., 2017). At the same time, eating disorders are overrepresented in elite athlete studies because of the requirement that elite athletes maintain a specific stature for their profession (Åkesdotter et al., 2020). Interestingly, few elite athletes reported anxiety disorders even though they scored in the moderate range on the General Anxiety Disorder-7 (GAD-7; Åkesdotter et al., 2020). This could indicate that elite athletes normalize their anxiety and eating concerns, even at a clinical level. Likewise, performing artists display disproportionately high reporting rates for mental health disorders, such as depression, anxiety, and stress, when compared to the general population (Van den Eynde et al., 2016; van Rens & Heritage, 2021). Given professional ballet dancers’ emotionally demanding performance levels as performing artists and their physicality as athletes, they may share similar mental health experiences with elite athletes and performing artists, yet these experiences remain unknown.
Ballet Culture and Professional Dancers’ Mental Health
Literature exploring ballet dancers has focused on culture (Wulff, 2008), development (Pickard, 2012), emotional harm (Moola & Krahn, 2018), injury prevention (Biernacki et al., 2021), and disordered eating (Arcelus et al., 2014). Ballet, with origins in the Italian and French courts, is an age-old culture that fuses beauty and athleticism (Kirstein, 1970; Wulff, 2008). Influenced by social and cultural forces in the Western world (Kirstein, 1970), ballet culture is synonymous with tradition and hierarchy (Wulff, 2008). Ballet culture holds steadfast to idealistic tenets in which dispositions (e.g., tenacity), perceptions of an ideal body, and actions (e.g., constant rehearsals) provide dancers the ability to illustrate a story through movements (Wulff, 2008). Exquisite sets, costumes, and movements create a unique experience and can produce a visceral reaction in the audience (Moola & Krahn, 2018).
Yet a strong commitment to the art form requires ballet dancers to work with their bodies for hours, sustain injuries, and work through chronic pain (Pickard, 2012), often leading to emotional distress (Moola & Krahn, 2018). Physical requirements also make dancers three times more vulnerable, compared to non-dancers, to suffer from eating disorders, particularly anorexia nervosa and those labeled by the Diagnostic and Statistical Manual of Mental Disorders as eating disorders not otherwise specified (Arcelus et al., 2014). van Staden et al. (2009) focused directly on ballet dancers’ mental health, finding that professional ballet dancers also experience mental health concerns due to negative body image and stress. The vast majority of these studies originated from countries outside the United States, including South Africa (van Staden et al., 2009), the United Kingdom (Pickard, 2012), and Canada (Moola & Krahn, 2018). The scarcity of scholarly attention on professional ballet dancers’ mental health within the United States is concerning given the evidence of emotional distress in similar populations. Counselors may be less than effective without a clear understanding of this population’s mental health needs. Understanding the cultural context and its impact on ballet dancers’ mental health in the United States, therefore, requires further exploration.
Purpose of the Present Study
The purpose of this study was to explore ballet culture and identity and their impact on ballet dancers’ mental health experiences. The guiding research questions were (a) How do professional ballet dancers define ballet culture and identity? (b) What are the mental health experiences of professional ballet dancers? and (c) What are professional ballet dancers’ suggestions for counseling and advocating with this population?
Method
Given the purpose of this study, we chose a transcendental phenomenological approach as an appropriate method to discover and describe the essence of participants’ lived experiences. Both van Staden et al. (2009) and Moola and Krahn (2018) utilized phenomenological approaches to explore ballet dancers’ mental health and experiences of emotional harm. Originally introduced by Husserl (1970), this approach positions researchers to focus on the individual experience while also identifying commonalities across participants (Hays & Singh, 2012). Further, in transcendental phenomenology, researchers set aside preconceived ideas, seeking to add depth and breadth to people’s conscious experiences of their lives and the wider world. In Moustakas’s (1994) modification of Van Kaam’s method of transcendental phenomenology, researchers aim to collect the experiences of participants while consistently assessing and addressing their biases to produce a purer and transcended description of the researched phenomena. Because our lead author, J. Claire Gregory, possesses a background as a professional ballet dancer, the framework of transcendental phenomenology provided the needed structure for identification of biases and preconceived notions, allowing us to evaluate our positionality to the data.
Research Team Positionality
Our research team consisted of Gregory, a doctoral candidate and licensed professional counselor, and Claudia Interiano-Shiverdecker, an assistant professor in counselor education and supervision in a CACREP-accredited counselor education program. Gregory is a Caucasian female and was a professional ballet dancer for 7 years. Interiano-Shiverdecker is a Honduran female with extensive experience conducting qualitative research and clinical experience primarily focused on trauma, crisis, and grief. We have a combined 13 years in clinical practice. Moustakas implored researchers to uphold epoché, “a Greek word meaning to refrain from judgment, to abstain from or stay away from everyday, ordinary ways of perceiving things” (1994, p. 85), by bracketing their own opinions, theories, and expectations. Bracketing is a defining characteristic of transcendental phenomenology in which researchers set aside their own assumptions, to the extent possible, to allow individual experiences to emerge and inform a new perspective on the phenomenon (Moustakas, 1994). Given the composition of the research team and the methodology employed, it was vital to engage in ongoing conversations about our collaboration, data collection and analysis, participants, and the data. Therefore, we addressed specific biases by engaging in virtual weekly bracketing meetings for over a year. Before meetings, Gregory would log memos about thoughts during data collection and analysis. Interiano-Shiverdecker would serve as a consultant to address biases. The biases discussed included a desire to not focus on mental health disorders typically discussed in the literature (e.g., eating disorders) and a desire to highlight professional ballet dancers’ strengths to balance out negative stereotypes. Throughout data analysis, we noted that participants discussed other presenting mental health issues and the connection of ballet culture to the development of those issues, including eating disorders. We operated from a social constructivist research paradigm in which multiple realities of a phenomenon exist (ontology), researchers and participants co-construct knowledge (epistemology), and context is valuable (axiology; Hays & Singh, 2012). This approach primarily focused on reflecting the participants’ voices while recognizing our roles as researchers, so we intentionally did not incorporate a theoretical framework to analyze our data.
Sampling Procedures and Participants
The transcendental phenomenological research procedures we followed included (a) determining the phenomenon of interest, (b) bracketing researcher assumptions, and (c) collecting data from individuals who have directly experienced the phenomenon. Therefore, after receiving approval from our university’s IRB, we used purposive and snowball sampling to recruit professional ballet dancers in the spring and summer of 2020.
Purposive sampling allowed us to select participants for the amount of detail they could provide about the phenomenon (Hays & Singh, 2012). We intentionally recruited individuals who identified as a professional ballet dancer currently or in the past and were 18 years or older, aiming for a sample of at least five participants (Creswell, 2012). The parameters for “professional ballet dancer” were being a dancer with a professional ballet company and receiving financial payment. Gregory emailed potential participants, contacted professional ballet organizations to request distribution of the recruitment flyer among their members, and posted on Facebook groups used by professional ballet dancers. This email and post included an invitation to participate, a link to a demographic form, and an informed consent form. A total of seven eligible volunteers responded to recruitment emails and posts on Facebook groups. Through snowball sampling, we recruited one more participant. Seven of the dancers had worked with the same professional ballet company as Gregory, but only two had danced concurrently with her, which occurred 10 years prior to data collection.
All participants who contacted us about the study stayed enrolled and completed the interview session. Table 1 outlines the demographic information of each participant, with the use of pseudonyms. Five of the eight participants lived in a southern region of the United States, while three participants lived in northwest and eastern regions. All participants identified as Caucasian. Two participants currently worked as professional ballet dancers attached to a company; the other six were ballet teachers, office employees, freelance dancers, students, or nurses.
Data Collection Procedures
Moustakas (1994) recommended lengthy and in-depth interactions with participants in transcendental phenomenology in order to understand participants’ experiences of the phenomenon and the contexts that influence those experiences. Participation required professional ballet dancers to complete a demographic questionnaire, take a picture that represented their perspective on mental health while dancing professionally, and complete an individual semi-structured interview. We chose to include the picture to include creative expression, a vital element in ballet culture. The use of pictures during the interview process facilitated a representative and safe discussion around mental health. Although we did not directly analyze the pictures, they served as catalysts for interview questions. In qualitative research, photography can supplement primary data collection methods when participants struggle to utilize words alone to capture an experience (Hays & Singh, 2012).
Table 1
Participant Demographic Information
| Pseudonym |
Gender |
Age |
Race |
Professional Status |
| Abby |
F |
31 |
Caucasian |
Former Professional |
| Cleo |
F |
28 |
Caucasian |
Current Professional |
| Luna |
F |
35 |
Caucasian |
Former Professional |
| Mica |
F |
30 |
Caucasian |
Former Professional |
| Monica |
F |
37 |
Caucasian |
Former Professional |
| Paul |
M |
25 |
Caucasian |
Current Professional (Freelance) |
| Sophie |
F |
33 |
Caucasian |
Current Professional |
| Zelda |
F |
25 |
Caucasian |
Current Professional (Freelance) |
We developed a 9-item open-ended interview protocol (see Appendix) intended to explore participants’ experiences with mental health, counseling, and advocacy. Gregory conducted all interviews, which lasted from 30 to 60 minutes with an average of 40 minutes, and transcribed each interview verbatim afterward. Three interviews were in person, while six interviews occurred over the phone because of the COVID-19 pandemic. During development, we decided to begin with a simple question to help the dancer feel more at ease. In the next five questions, we utilized their picture to discuss mental health. Because the term “mental health” may or may not be known to the dancers, or it may hold stigma, we felt the picture could produce more insight and depth of the concept. Question 6 asked the dancers to consider their social context and its relation to their mental health. We also chose to include a question asking about ballet dancers’ strengths, as this seems to be rare within performing artist and athlete literature. Next, we directly asked the dancers how counselors could help and then asked a final question that created space for any other relevant thoughts. Through these interviews with eight (seven female, one male) professional ballet dancers, we reached data saturation, meaning that no new information emerged in the data creating redundancy.
Data Analysis
We followed Moustakas’s (1994) modification of Van Kaam’s steps for data analysis, which included (a) developing clusters of meaning, (b) using significant statements and themes to write a description of what participants experienced (textural description) and how they experienced it (structural description), and (c) describing the essence of participant experience from the textural and structural descriptions. First, Gregory engaged in member checking by emailing each participant their interview transcript to ensure accuracy and provide an opportunity to redact any statements. No participant changed their transcript.
Gregory then reviewed each transcript independently, highlighting significant statements or quotes that conveyed participants’ experience. This process is known as horizontalization (Moustakas, 1994). Then, we discussed each identified statement and assigned meaning to similar statements (i.e., clusters of meaning). We used NVivo software for data analysis to ensure consistency, transparency, and accuracy. NVivo, a qualitative data analysis software, aids researchers with consistency in assigning codes to similar topics and allows the research team to cross-check codes for accuracy.
We then determined the invariant constituents, or the final code list, from redundant and ancillary information through a process of reduction and elimination. For example, we eliminated codes that did not illustrate participants’ lived experiences in relation to the purpose of this study. Through the process of reduction, we merged codes if their meaning was similar. These processes allowed us to have a final list of codes that were not repetitive and aligned with the purpose of the study. Using the final codebook, we began the recursive coding process to recode every interview and reach final consensus. Recursive coding, a qualitative data analysis technique, is very useful when analyzing interview data, allowing researchers to compact the data into different categories and illuminating patterns within the data not otherwise apparent (Hays & Singh, 2012). For example, we noticed several codes that illustrated traditions or customs, both positive and negative, that ballet dancers embraced, so we decided to categorize codes about traditions and customs, in both negative and positive categories, to illustrate ballet culture.
Following this initial coding, we explored the latent meanings and clustered invariant constituents into themes, ensuring that all themes were representative of the participants’ experiences. We then synthesized themes into textural descriptions of participants’ experiences, including verbatim quotes and emotional, social, and cultural connections to create a textural-structural description of meanings and essences of experience (Moustakas, 1994). Using the individual textural-structural descriptions, we proceeded to create composite textural and structural descriptions of reoccurring and prominent themes. Finally, Gregory engaged in the member-checking process for a second time by sending the final themes to all participants via email. Four participants responded, all supporting the final themes.
Strategies for Trustworthiness
To ensure quality, we engaged in multiple strategies to meet trustworthiness criteria, such as transferability, confirmability, dependability, and credibility. Specific strategies included using researcher triangulation, member checking, in-depth description of the analyses, and thick description of the data (Hays & Singh, 2012). Weekly meetings for a year helped reduce researcher bias through openly challenging each other with any conclusions. We also engaged in two rounds of member checking for dependability and confirmability. In addition, we utilized an external auditor with previous experience in qualitative research who was unfamiliar with ballet traditions and culture to aid in establishing confirmability of the results and credibility of our data analysis process (Hays & Singh, 2012). The auditor reviewed our NVivo file for data analysis and notes, and the final presentation of the results in a Microsoft Word document. Although the external auditor provided us with APA suggestions, she had no critical feedback regarding our analysis. Instead, she supported our findings on ballet culture that provided a new insight for counselors. Finally, we used thick description when reporting the study findings to increase trustworthiness. Utilizing thick description allowed us to depict deeper meaning and context of the data instead of only reporting the basic facts (Hays & Singh, 2012).
Results
We identified four prevalent themes about professional ballet dancers’ mental health experiences: (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) recommendations for counseling and advocacy—“the dance population is unique.”
Ballet Culture—“It’s Not All Tutus and Tiaras”
All eight participants described ballet as a unique culture with its own set of customs and ingrained traditions. One of the participants, Monica, further elucidated this point: “The traditions of ballet are very old-fashioned, but it’s beautiful when something endures and exists after hundreds of years.” Throughout their narratives, dancers mentioned patterns of “good” and “bad” sides to ballet culture. “It’s not all tutus and tiaras or the perfect life. There is so much beneath the surface,” explained Cleo. To clarify this theme, we divided it into two subthemes: negative aspects of ballet culture and positive aspects of ballet culture. Although we present this theme in two opposing subthemes for simplicity, dancers’ experiences existed along a continuum.
Negative Aspects of Ballet Culture
All of the participants shared that customs of ballet culture focused primarily on requirements indispensable to successfully performing a job that was emotionally and physically demanding. The dancers’ comments centered around physical body requirements and arduous training, highlighting the need for extreme physical athleticism to perform at a professional level. Monica explained, “They [ballet dancers] have obvious physical strength, stamina, endurance, and mind over matter for what they need to do.” “We’re a very underrated athlete,” echoed Abby. Zelda added, “I would compare us to what the world knows a little bit better as gymnastics for the Olympics.”
Although no interview questions specifically asked about the negative side to ballet, participants shared feeling constant stress, pushing their bodies and minds to their limits, worrying about body image and injuries, and feeling pressure to find and keep employment. It was commonplace for participants to experience a sense of pressure and stress from internal and external forces. For example, Paul stated, “I think about my ballet career, and I think how I was tired all the time, because I would wake up and do so much.” Echoing this feeling, Zelda shared, “I was half thriving, half dying inside.” Other participant statements emphasized feeling mentally broken with the lack of time for any outside hobby and having no power as a dancer. Abby stated, “In ballet, everything was just so competitive and mind twisting. I was raised with the idea that every day is an audition.” She added, “This could be your day, or if you don’t work hard today then 3 months from now it is going to creep up on you. So, it’s this weird, like, permanence that is doomed upon us.” According to Abby, there was a daily pressure to achieve greatness, which at times caused injury. For Cleo, a current professional ballet dancer, employment pressure and injury were prevalent: “I actually had an injury where I was not able to dance for a year. . . . I managed to sprain my ankle in three places. I had spent the entire summer rehabbing and keeping it in a boot.” Yet she explained that because she was “scared [of not being asked to return to the dance school], I danced on it for weeks after the initial injury.” Cleo also saw her peers struggling with the same issue:
My friend had food poisoning yesterday. She is still sick today and they told her she has to come in because they were setting the Adagio scene . . . she literally left class to throw up and then came back to class and the whole time was trying not to throw up.
Other professional dancers echoed these fears of financial stress and employment stability, which justified their reasons to push their minds and bodies to the limit, despite physical or mental injuries. Despite perceptions of glamour, Paul highlighted the financial strain that most ballet dancers experience by detailing how he made only “$100 a week and lived in a place that charged me $250 a month.” Even with their efforts, three participants had lost their dancing jobs. Luna believed it was her weight that got her fired, while Paul shared, “I would work super hard all day, back to the gym at night, eat super healthy, and I was still fired for not being good enough, according to my old boss.”
Positive Aspects of Ballet Culture
Despite these intense demands, all participants also discussed positive qualities of ballet culture. These included connection to others, learned adaptability, and creating a story for the audience. Paul highlighted, “Even with the bad parts, there’s a lot more good than there was bad. . . . It’s one of those things, you’re like, I love it so I’ll do it for whatever money.” Monica reflected on her career, saying, “I see fond memories and really good times.” Several participants shared how long training hours and a common goal created a unique connection to others that was difficult to experience elsewhere. Monica passionately stated that “dancers thrive in the sense of community. When you are in a company you are exactly that—part of the greater company and you work together.” Mica shared, “You aren’t really your own person when you are dancing in a professional setting.” “It helps create friends and that was the beauty behind it, you had a support system,” added Luna. Three of the dancers shared their enjoyment of creating an onstage story for the audience. Mica enjoyed how ballet “uses the body to give meaning to stories, more so than other forms of dance.” Luna shared, “We were giving back to the community and being a part of the arts. That was great. I loved that.”
Professional Ballet Dancers’ Identity—“It Is a Part of Me”
All dancers either directly or indirectly attested to a ballet identity and how it influenced their development. To display the range of experiences, we described this theme in two subthemes: ballet dancer traits and connections to their ballet dancer identities. The first subtheme illustrates aspects that ballet dancers might share, while the second theme discusses how participants connected these traits to their personal identity.
Ballet Dancer Traits
All participants shared traits they felt were central to life as a professional dancer, such as tenacity and grit, that influenced their identity during and after dancing. Luna, Mica, Sophie, and Zelda mentioned the discipline a dancer must possess for a successful ballet career. “The level of discipline, I think, is unmatched,” Mica fervently stated. Sophie, Mica, Zelda, and Paul mentioned that their determination for continuous improvement represented their role on stage and ability to maintain their jobs. Sophie expressed, “Your determination, your artistic expression, all of those things include the whole person.” The dancers expressed an ability to push through any odds knowing that, eventually, their hard work would pay off. Sophie shared:
Delayed gratification I feel is a big one [strength], especially in a society with everything now being instant and we are always on our phones, but to work on something slowly over time and be patient. Just trust that hard work pays off.
Dancers indicated a connection between their transformation as dancers and their development as adults. Cleo shared, “If you make it to a professional, you are one of the few that had a hard road, and it makes you have a very thick skin that can help in all matters of life.”
Connection to Their Ballet Dancer Identities
All dancers expressed both positive and negative emotions about their ballet identity, ranging from gratitude to contempt. Four participants expressed that dancing was not just something they did, it was who they were. For them, ballet, and the culture of ballet, were integral parts of their identity. During her interview, Zelda paused after a question about why she continues to dance and simply stated, “It is a part of me.” Sophie shared, “Over the years, I think I stuck with it because it became wrapped up in my identity a bit. This is who I am, this is what I do, this is what makes me special.” Additionally, Cleo and Sophie identified the power and connection they felt while dancing on stage. This connection gave meaning to their dance career. Sophie shared, “Somehow dance felt like it gave me the most ability to participate in music in a way I really wanted to and a kind of level of expression I never really had.”
Yet four participants also felt that their identity had evolved past ballet. “It’s a picture that represented me at a point in time, but I don’t feel it represents me anymore,” shared Mica. Paul, a freelance professional, shared, “I feel like it definitely was how I viewed myself. But I’m not 100% sure if I do or don’t feel that way now.” Monica, a former professional, explained:
Our identity is who we were and what we had, but that is not my core identity. I know who I am in my identity, and it is in Christ who made me, and also just me as a person is more than what I did and what I do on my days at a job.
Mental Health Experiences—“You Have to Compartmentalize”
Utilizing pictures to discuss mental health attended to participants’ preferred form of expression. As Zelda stated early in her interview, “I don’t know how to put it into words. It’s hard.” Despite their dedication and passion, all dancers spoke of the demanding nature of professional dancing and its impact on their mental health. Their conversation around mental health focused on two areas: perfectionism and the perfect body and compartmentalization.
Perfectionism and the Perfect Body
All dancers felt they needed an additional picture to represent the darker side of ballet or related this darker side to imperfections within the picture. Figure 1 displays Paul’s picture of artwork, which the dancer felt represented the outward appearance of perfection but included lumps of paint (i.e., imperfections), a representation of his mental health.
Figure 1
Paul’s Picture of His Mental Health Experience as a Professional Ballet Dancer

Despite there being no interview questions about their body image, seven of the eight dancers shared thoughts about body image concerns or pressure to develop a certain physique. Throughout their dancing career came numerous hours of practice in front of mirrors. Abby’s chosen picture displayed part of a bathroom mirror: “When I look into the mirror, a lot of judgments come back in, and ballet is all based off of opinions and judgments that really mess with your head.” She added, “Everything revolved around the mirror, and if the mirror said it was ok, then my brain said it was ok . . . with ballet and mental health, I feel like a lot of my mental health was based off the reflection.” Paul also shared, “I was going to the gym every single day and was in really good shape but was still told I was not in ballet shape.” Monica shared another company dancer’s experience: “Even though she was a gorgeous dancer and had the most incredible feet and legs, she was told she was overweight, and she did not know, in those days, how to deal with it.” Luna spoke openly about feelings of depression when she gained weight: “When I got fired, I would go into periods where I gained 20 pounds because of my depression. The whole reason I was fired was because I got too big.” She later added, “I started losing it when I got hired back but was not allowed to be in productions because I was too big. . . . The depression made me eat and go into a dark place.” However, Luna also spoke about current cultural changes regarding the “ideal” body shape for ballet dancers in the United States: “Nowadays I feel that they [ballet companies] have embraced differences in dancers.”
Although participants recognized the benefits of an unbreakable determination, discipline, and rigor toward their professional career, they also noted the emotional consequences of their dedicated work. Cleo best illustrated this point: “It just felt like it didn’t matter how hard I worked, it just took a toll. . . . I thought it [ballet] was beautiful, and 13 years ago I believed this, but then things started to turn darker mentally for me.” Mica shared, “I would say a lot of us, we have anxiety and depression, but we are also crazily mentally strong . . . like me, for example, I was told I was too fat from the age of 12.” With this constant stress, the dancers felt their mental health fluctuated with external forces (i.e., thoughts about not being good enough). Zelda stated, “I had constant anxiety of not being good enough.”
Compartmentalization
Another prominent subtheme for all of the dancers was compartmentalization. The dancers described compartmentalization of thoughts and feelings as a healthy coping mechanism for some and a hindrance for others. Abby and Sophie spoke about their need to separate from their feelings and thoughts to perform well. Abby told herself, “Do not think that way. You work really hard and you can put all those thoughts into a little box and hopefully, eventually, get rid of it.” She added that “when the thoughts creep up, I try to put them into my little mental box and try not to open it.” Sophie also spoke in depth about how she maintained her mental health and navigated her negative feelings:
I have to separate myself from my feelings sometimes. I have to remember that my feelings aren’t me. . . . You have to believe you can make it happen and it’s going to work out and be resilient enough to take rejection and injuries, and the uncertainty of finances. You have to hold on and believe it will happen for you. . . . Over time I have become more resilient or grounded. My mental health is very dependent on how I take care of the situations I am in.
However, several dancers also explained how this compartmentalization fostered a negative approach toward mental health, silenced their voice, and led them to bottle up their feelings. Abby described, “If you are sad and can’t handle it, then the director is going to see that, and consequences will happen . . . then it’s the worst . . . we are conditioned to accept whatever is given to us.” Cleo added, “You have to compartmentalize, to hold it in and aren’t allowed to talk about it . . . you’re not allowed to feel the validation of ‘I’m bothered by this.’ It’s almost wrong to feel bothered by this.” When analyzing the data, we noticed that the four participants who were former professional dancers noted an improvement in their mental health after their life in ballet. Sophie also illustrated changes in dancers’ mental health: “It is able to grow and change and be cultivated. So, I do not think mental health as a dancer is fixed.”
Recommendations for Counseling and Advocacy—“The Dance Population Is Unique”
As the conversation turned toward mental health experiences, all participants expressed recommendations in two areas: counseling and society’s view of ballet dancers and advocacy.
Counseling
All participants discussed recommendations for counseling when working with professional ballet dancers. Regarding counseling, Mica shared, “The dance population is unique in itself. A counselor being able to counsel to this is very important.” She further explained, “It’s not the same as advising someone who’s on a basketball team, nor is it the same as advising someone who’s on a theatre crew. It’s just different. It’s an athlete and it’s an artist.”
Abby also urged counselors to recognize trauma among this population: “I think counselors should be aware of emotional abuse and treat dancers as such.” Monica described how ballet dancers joined voices with the MeToo movement: “It just seemed like the movement of women being able to finally express what had happened to them and the abuse they had been enduring was very empowering.” At the same time, she indicated that a lot of people responded with “well that’s just what ballet is.”
Participants highlighted dancers’ absence of mental health services in their work contracts. “Just having someone to talk to would be nice. I know it’s not covered on a lot of health insurances or dancers’ insurance,” said Cleo. “It would be really cool if it were in the context of the studio and dancers could have one session a month at least . . . individual session, group sessions . . . I think a lot of people would jump at the opportunity,” stated Abby. Monica further explained how a counselor could “do a lot to sustain dancers and maybe help their careers because they might be less prone to injury if they aren’t sad and depressed or feeling alone or pushing themselves beyond their breaking point.” She added how counselors may support company staff: “I think there is a lot on the shoulders of the artistic director or one of the ballet mistresses or ballet masters to be an emotional shoulder or a listening ear.”
Another prevalent tenet woven throughout the dancers’ interviews was counselors’ awareness of ballet culture. Three dancers specifically mentioned that if counselors increased their awareness of dance careers, it might help dancers open up to counselors. Paul stated, “I think about when I was dancing, if someone had just been like ‘oh well, you don’t have to be super skinny to dance.’ I’d be like, you don’t know anything, ya know?” Another dancer shared:
Counselors may not need dance experience, but it would be helpful for the dancers if counselors at least have an idea of what a rehearsal day is . . . how many hours we are dancing, how many dancers have second jobs, how often we perform, it adds context . . . having an understanding of the rigors and demands from within the profession.
Society’s View of Ballet Dancers and Advocacy
At some point in their interviews, all participants described ballet dancers’ mental health as hidden or unknown to society, and therefore believed that the first step for advocacy required awareness. Participants explained that when people go to the theatre to watch The Nutcracker around the holiday season or attend Romeo and Juliet, they see a story, a real-time depiction of magic and narrative. Yet participants felt that this led society to view dancers as having “glamourous lifestyles” or, because of Hollywood, believe that dancers “are frail individuals that do not have a real job, throw their friends down the stairs, and steal husbands.” Cleo openly spoke about the hidden side of the ballet world when sharing her picture:
The idea is that it’s so glamorous and they have this perfect life, it’s like the same way they [society] perceive celebrities and they have these glamourous lives and everything is perfect when you see the surface and the smile you are forced to put on, but they do not see everything that goes on underneath. That’s why I love this photo: you don’t know what the person is actually feeling. . . . On the outside I am a very bubbly person, and people don’t know anything going on behind, I guess behind the curtain.
Along these same lines, participants advocated for gender equality within the profession. Although no interview questions asked about gender differences, three dancers pointed out this discrepancy by sharing that women are under extreme pressure to maintain their dance careers. Cleo and Abby also identified how most directors were male. Abby expressed this always “trying to appease the person in charge, who is almost always a man.” For five of the participants, the company director played a vital role in how they viewed themselves. Although some dancers noted overall societal changes and awareness that dancers did not have to fit “this anorexic ballerina” stereotype, some felt that overcoming long-lasting traditions in ballet culture of “skinny equals better” required significant change.
Discussion
The purpose of this qualitative study was to provide a better understanding of ballet culture and its impact on dancers’ identity and mental health. More specifically, we sought to explore different facets of professional ballet dancers’ mental health, while also providing cultural context to professional ballet dancers’ lived experiences. Our attention to cultural context is parallel to trends over the past decade reflecting scholars’ increased focus on performing artists’ training environments to understand their experiences (Lewton-Brain, 2012). Using this perspective allowed us to offer recommendations for counseling and advocacy directly inspired by the ballet dancers’ viewpoints.
The findings from this study resemble descriptions of belief systems and practices entrenched in ballet culture previously discussed in the literature (Wulff, 1998, 2008). One overarching premise presented by the dancers was their need to acquire physical strength, stamina, and a “mind over matter” attitude to have successful ballet careers. The positive and negative qualities of ballet culture created a constant push and pull; however, the participants kept dancing. They recognized their hardships and yet believed enduring them was necessary to live their dreams. The ethos of ballet culture made going through hardships—restricting eating, dancing with injuries, and other stressors—worthwhile. Without providing a justification for these physical and emotional injuries, these new findings provide context to understand ballet dancers’ ideas on body, mind, and health. As some dancers shared, ballet was more than a career to them; it was a part of them, and life without it was hard to imagine.
Participant narratives revealed the ballet dancers’ numerous strengths, such as tenacity, grit, learned adaptability, and unbreakable discipline and rigor. At the same time, participants discussed several mental health hardships. To live up to their ballet dancing goals, dancers focused on their most highly used attribute—their bodies. Because of this, body concerns were prevalent in the findings. The dancers also relayed mental struggles and with them a will to succeed and compartmentalize, to carry on for the performance and the art despite physical and/or emotional pain and at times unsupportive or even abusive environments. Their experiences seemed to align with similar concerns shared by tennis player Naomi Osaka and gymnast Simone Biles. To illustrate, Biles withdrew from part of the 2021 Olympics because of a mind and body disconnect. Her decision earned criticism from the public. She later shared her struggles with mental health concerns (i.e., depression) and how stepping down from competition allowed her to prioritize her mental health and protect her body from potential serious injury.
Our findings also aligned with similar results found with elite athletes and performing artists (Åkesdotter et al., 2020; Gorczynski et al., 2017) and ballet literature in other countries that underscore concerns with disordered eating and body image issues that run deep within ballet culture (Clark et al., 2014; van Staden et al., 2009). Participants discussed anxiety, depression, trauma, abuse, and perfectionism. Their discussions indicated a connection, with anxiety and depression feeding into restrictive eating or other types of eating disorders, and an emotional turmoil following when they were unable to have control. Comorbidity between these mental health disorders and eating disorders is prevalent in the literature, and the present findings elucidate a similar connection among professional ballet dancers.
The findings from this study add to our understanding of professional ballet dancers’ mental health across the world by presenting, to the best of our knowledge, the only study within the United States to fully focus on a qualitative exploration of professional ballet dancer mental health experiences. Our findings expand on and reinforce Hebard and Lamberson (2017), whose work implored counselors to advocate for athletes’ mental health awareness. They stressed that athletes are idolized for their physical endurance, and this perception may leave them specifically vulnerable to mental health issues. Our participants expressed a similar concern and desired counseling services integrated into their schedule and provided by a counselor possessing an understanding of the ballet culture and its specific stressors. They believed that mental health services could not only address their mental health struggles and provide trained support, but also reduce physical injuries often caused by repressed feelings of sadness, loneliness, or insecurity. Participants expressed that advocating for this population should focus on increased access to mental health service providers with an awareness of ballet culture.
Lastly, these findings elucidate a need to evaluate aspects of ballet culture ingrained in tradition that can lead to physical and emotional injuries. Conversations about ballet culture and the emphasis on “petite ballerina dancers” are slowly becoming a part of current efforts to dismantle established perceptions of beauty, athleticism, and inclusion. As Pickard (2012) stated about herself as a dancer, “My body is ballet” (p. 25), and participants expressed that for counselors to advocate for and counsel this population, building awareness about this ongoing conversation while acknowledging the impact of ballet culture on professional ballet dancers’ mindset should be a requirement.
Implications for Counseling
Because of ballet culture and traditions, ballet dancers experience intense physical and mental demands. Counselors must attempt to understand ballet culture as well as its impact on dancer identity and mental health. Counselors need to remain aware of ballet culture when broaching the topic of weight and body identity influences, requirements for a successful ballet dancer, and the relationship between ballet standards and mental health disorders. From the dancers’ perspective, their physical form is directly related to their mental state or how they view themselves. Dancers’ identities intertwine with their bodies from a young age. Although this creates many positive experiences for the dancers, they also expressed how this can lead to depression, anxiety, and other mental health disorders. Considering these experiences, we encourage counselors to support dancers with a client-centered approach and to create an atmosphere of understanding about the dancers’ physical form as integral to their identity and their profession. Utilizing a client-centered approach would allow counselors to inquire about the dancers’ professional experience and help them build an understanding of the professional demands of ballet. Additionally, we encourage counselors to help professional ballet dancers explore their internal self-talk around comparing themselves to others and their relationship with their body.
Although not as prevalent in the data, the dancer statements about abuse are just as vital for counselor awareness. As Monica stated, ballet is a culture with centuries-old traditions and, according to five of the dancers, artist leadership tends to be authoritative in nature. Ballet requires certain physical attributes and training to achieve professional status, which can manifest as abusive relationships and power struggles. We suggest that counselors help professional dancers learn when certain demands may be perceived as abuse by the world outside of the studio. Providing psychoeducation of abuse (e.g., different forms of abuse, power and control wheel) can help ballet dancers differentiate these behaviors and seek help, when needed.
Although many dancers in this study expressed wanting counseling, it seems as though they feared counselors would not understand them or why they committed to such an intense lifestyle. The central need, according to the dancers, is for counselors to be aware of the unique ballet culture. For many dancers, ballet was a part of them, their identity, and something they felt drawn to always be improving. It is not a sport or a hobby, though there seem to be some commonalities between professional ballet dancers and elite athletes. According to the literature (Åkesdotter et al., 2020; Gorczynski et al., 2017), elite athletes experience intense physical demands and elevated anxiety. Our current findings from the dancers are comparable to these features. Therefore, counselors working with dancers may find some similarities with sports counseling. However, counselors should remain aware that sports are for competition and winning, whereas ballet is an art that seeks to provide the audience enjoyment and entertainment.
Limitations and Suggestions for Future Research
As with all research, limitations exist because of many factors. For example, this study engaged a small, homogenous sample of ballet dancers with limited opportunity to dive deeply into within-group differences. All participants identified as Caucasian and many of the dancers had resided in the same geographical location at one point. We recognize that racial and geographical differences, among others, can significantly impact participants’ mental health experiences.
In addition, seven of the eight participants had experienced a prior dance connection with Gregory. Although this may have contributed to trust and more candid interviews, it is also possible that this resulted in biases despite our measures to ensure trustworthiness (e.g., weekly research meetings in order to bracket).
Another limitation is the ballet dancers’ subjective representation of their own mental health. Their illustrations of their experiences provide an inner look at their mental health yet do not guarantee an accurate or clinical representation of their experiences.
Because of the limited research examining professional ballet dancer mental health experiences, many opportunities remain open for future research. One recommendation is for future researchers to consider within-group differences (e.g., race, gender) through recruitment of a heterogenous sample. Also, considering the study’s participants all identified as Caucasian, we recommend future researchers explore the mental health experiences of minority ballet dancers, as they tend to be underrepresented in professional ballet companies in the United States. Additionally, this study included both former and current professional ballet dancers. Researchers may discover insightful data using a longitudinal study, as this could display information about the career transition period from professional dancer to former professional dancer. Other recommendations for future research include quantitative studies focusing on counseling interventions or prevention. Finally, some participants discussed instances of trauma, depression, and anxiety. Future researchers could examine specific mental health disorders and their comorbidity among ballet dancers by using the GAD-7 (Spitzer et al., 2006) for assessing anxiety and the BDI-II (Beck et al., 1996) for depression.
Conclusion
This qualitative study explored ballet culture and identity and their impact on professional ballet dancers’ mental health experiences, which resulted in the four themes of (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) counseling and advocacy—“the dance population is unique.” A distinct culture exists for professional ballet dancers that includes traditions passed down since the 14th century. Hence, tradition, dedication, and commitment to their profession shape professional ballet dancers’ identities. Further, their identities straddle the environments of performing artists and elite athletes, creating contextually distinctive experiences. For counselors to adequately support professional ballet dancers, they must first build their awareness of ballet culture and the unique mental health needs and resiliencies of dancers.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Åkesdotter, C., Kenttä, G., Eloranta, S., & Franck, J. (2020). The prevalence of mental health problems in elite athletes. Journal of Science and Medicine in Sport, 23(4), 329–335. https://doi.org/10.1016/j.jsams.2019.10.022
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Arcelus, J., Witcomb, G. L., & Mitchell, A. (2014). Prevalence of eating disorders amongst dancers: A systemic review and meta-analysis. European Eating Disorders Review, 22(2), 92–101. https://doi.org/10.1002/erv.2271
Beck, A. T., Steer, R. A., & Brown, G. (1996). Beck Depression Inventory–II [Database record]. APA PsycTests. https://doi.org/10.1037/t00742-000
Biernacki, J. L., Stracciolini, A. S., Fraser, J., Micheli, L. J., & Sugimoto, D. (2021). Risk factors for lower-extremity injuries in female ballet dancers: A systematic review. Clinical Journal of Sports Medicine, 31(2), e64–e79.
Clark, T., Gupta, A., & Ho, C. H. (2014). Developing a dancer wellness program employing developmental evaluation. Frontiers in Psychology, 5(731), 1–9.
https://doi.org/10.3389/fpsyg.2014.00731
Creswell, J. (2012). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Gorczynski, P. F., Coyle, M., & Gibson, K. (2017). Depressive symptoms in high-performance athletes and non-athletes: A comparative meta-analysis. British Journal of Sports Medicine, 51(18), 1348–1354. https://doi.org/10.1136/bjsports-2016-096455
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hebard, S. P., & Lamberson, K. A. (2017). Enhancing the sport counseling specialty: A call for a unified identity. The Professional Counselor, 7(4), 375–384. https://doi.org/10.15241/sph.7.4.375
Husserl, E. (1970). The crisis of European sciences and transcendental phenomenology: An introduction to phenomenological philosophy. Northwestern University Press.
Kirstein, L. (1970). Dance: A short history of classic theatrical dancing. Praeger.
Lewton-Brain, P. (2012). Conversation with a clinician: William G. Hamilton, MD – Is more always more for young dancers? International Association of Dance Medicine and Science Newsletter, 19(4).
Moola, F., & Krahn, A. (2018). A dance with many secrets: The experience of emotional harm from the perspective of past professional female ballet dancers in Canada. Journal of Aggression, Maltreatment & Trauma, 27(3), 256–274. https://doi.org/10.1080/10926771.2017.1410747
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Nejedlo, R. J., Arredondo, P., & Benjamin, L. (1985). Imagine: A visionary model for counselors of tomorrow. George’s Printing.
Pickard, A. (2012). Schooling the dancer: The evolution of an identity as a ballet dancer. Research in Dance Education, 13(1), 25–46. https://doi.org/10.1080/14647893.2011.651119
Rouse, W. B., & Rouse, R. K. (2004). Teamwork in the performing arts. Proceedings of the IEEE, 92(4), 606–615. https://doi.org/10.1109/JPROC.2004.825880
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Swann, C., Moran, A., & Piggott, D. (2015). Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychology of Sport and Exercise, 16(1), 3–14.
https://doi.org/10.1016/j.psychsport.2014.07.004
Van den Eynde, J., Fisher, A., & Sonn, C. (2016). Working in the Australian entertainment industry: Final report. Entertainment Assist, 1–181. https://crewcare.org.au/images/downloads/WorkingintheAustralianEntertainmentIndustry_FinalReport_Oct16.pdf
van Rens, F. E. C. A., & Heritage, B. (2021). Mental health of circus artists: Psychological resilience, circus factors, and demographics predict depression, anxiety, stress, and flourishing. Psychology of Sport and Exercise, 53, 101850. https://doi.org/10.1016/j.psychsport.2020.101850
van Staden, A., Myburgh, C. P. H., & Poggenpoel, M. (2009). A psycho-educational model to enhance the self-development and mental health of classical dancers. Journal of Dance Medicine & Science, 13(1), 20–28.
Wulff, H. (1998). Ballet across borders: Career and culture in the world of dancers. Berg Publishers.
Wulff, H. (2008). Ethereal expression: Paradoxes of ballet as a global physical culture. Ethnography, 9(4), 518–535. https://journals.sagepub.com/doi/10.1177/1466138108096990
J. Claire Gregory, MA, NCC, LPC, LCDC, is a doctoral candidate at the University of Texas at San Antonio. Claudia G. Interiano-Shiverdecker, PhD, is an assistant professor at the University of Texas at San Antonio. Correspondence may be addressed to J. Claire Gregory, Department of Counseling, 501 W. César E. Chávez Boulevard, San Antonio, TX 78207-4415, jessica.gregory@utsa.edu.
Appendix
Interview Protocol
- Tell me a little bit about yourself.
- Tell me about the picture you took and how this represents your understanding of mental health as a professional ballet dancer.
- Is this picture representative of your mental health? If so, how?
- What do you see here when you look at your picture?
- What are you trying to convey to someone who is looking at your picture?
- Describe how this image relates to society and what prevailing ideas about your mental health are present in this picture.
- What are some strengths about being a professional ballet dancer?
- What can we as counselors do about ballet dancers’ mental health?
- Is there anything else you would like to add?
Nov 9, 2021 | Volume 11 - Issue 4
Bilal Urkmez, Chanda Pinkney, Daniel Bonnah Amparbeng, Nanang Gunawan, Jennifer Ojiambo Isiko, Brandon Tomlinson, Christine Suniti Bhat
The COVID-19 pandemic resulted in many universities moving abruptly from face-to-face to online instruction. One group of students involved in this transition was master’s-level counseling students. Their experiential group counseling training (EGCT) program started in a face-to-face format and abruptly transitioned to an online format because of COVID-19. In this phenomenological study, we examined these students’ experiences of participating and leading in six face-to-face and four online EGCT groups. Two focus groups were conducted, and three major themes emerged: positive participation attributes, participation-inhibiting attributes, and suggestions for group counseling training. The findings point to additional learning and skill development through the online group experience as well as its utility as a safe space to process the novel experience brought about by COVID-19.
Keywords: experiential group counseling training, phenomenological, COVID-19, face-to-face, online format
Most of what is known about group counseling and the training of group counselors has been learned from groups that occur in face-to-face group environments (Kozlowski & Holmes, 2014). This includes seminal works on group counseling’s therapeutic factors, such as universality, altruism, instillation of hope, cohesiveness, existential factors, interpersonal learning, self-understanding, and catharsis (Yalom & Leszcz, 2005). Researchers have found positive contributions of group therapeutic factors toward therapy outcomes (Behenck et al., 2017), and they have explored the experiences of group members in face-to-face group counseling settings, including the interpersonal and intrapersonal processes of members (Holmes & Kozlowski, 2015; Krug, 2009; Murdock et al., 2012). By contrast, there is considerably less research on online group counseling (Kozlowski & Holmes, 2014) or group counselors’ training in online modalities (Kit et al., 2014; Kozlowski & Holmes, 2017).
In this qualitative study, we utilized the phenomenological method to explore and compare master’s-level students’ experiences of participating in and leading during six face-to-face and four online experiential group counseling training (EGCT) groups as part of an introductory group counseling course. The master’s-level counseling students began their EGCT in face-to-face groups, and because of the COVID-19 pandemic, they continued to meet in four online groups after their university decided to suspend all face-to-face instruction.
Experiential Groups in Counselor Education
Group counseling training is one of the eight core areas of required training for counselors stipulated by the Council for the Accreditation of Counseling and Related Educational Programs (CACREP; 2015). In order to learn the complex group processes necessary for effective group counseling, master’s-level counseling students are required to participate in EGCT (Association for Specialists in Group Work [ASGW], 2007; CACREP, 2015). For CACREP-accredited master’s programs, at least 10 clock hours of group participation during one academic semester are required (CACREP, 2015). During this experiential training, students learn to be both group counseling participants and group counseling leaders (Ieva et al., 2009) and gain valuable experience in and insight into group dynamics, group processes, and catharsis (Ohrt et al., 2014).
Master’s-level counseling students “benefit a great deal when allowed to develop practical and relevant clinical skills” (Steen et al., 2014, p. 236). Experiential training in group counseling also promotes self-awareness, personal growth, and a greater understanding of vulnerability and self-disclosure in the learners (Yalom & Leszcz, 2005). The experiential component of group counseling training provides an environment for counseling students to experience vicarious modeling, self-disclosure, validation, and genuineness from their classmates (Kiweewa et al., 2013). Finally, these experiential opportunities promote students’ self-confidence (Ohrt et al., 2014; Shumaker et al., 2011; Steen et al., 2014).
Online Counseling
Barak and Grohol (2011) defined online counseling as “a mental health intervention between a patient (or a group of patients) and a therapist, using technology as the modality of communication” (p. 157). Counselors are increasingly using more digital modalities in their practice (Anthony, 2015; Richards & Viganó, 2013), and it is being seen as a viable alternative to support clients (Hearn et al., 2017). Since the start of the COVID-19 pandemic, counselors have begun to use more online modalities to provide counseling services (Peng et al., 2020). Online counseling began to emerge as a potential solution for mental health services when providers were forced to discontinue or scale down in-person services and adjust to virtual formats during the pandemic (Békés & Aafjes-van Doorn, 2020; Peng et al., 2020; Wind et al., 2020). Peng et al. (2020) noted the effects COVID-19 have had on the delivery of mental health services in China. They mentioned the governmental and authorities’ support for preparedness and response and the multidisciplinary enhancement of remote intervention quality for clients. They also suggested that governments should integrate the mental health interventions related to COVID-19 into existing public mental health emergency preparedness and response structures.
Because of the growing importance of online counseling, it is essential to train counseling students to conduct online counseling, including online group counseling, effectively. Understanding master’s students’ experiences in online EGCT can help identify potential challenges they may face during their training. It is also important to explore students’ experiences in face-to-face and online EGCT groups to better understand possible future training needs and help counselor educators create an educational curriculum that addresses group counseling knowledge and skills for online groups. There is currently a lack of information about how to train counseling students in the delivery of online counseling (Kozlowski & Holmes, 2014), and specifically group counseling (Kit et al., 2014).
Professional and Accreditation Bodies’ Guidance on Technology
The American Counseling Association (ACA) Code of Ethics states, “Counselors understand that the profession of counseling may no longer be limited to in-person, face-to-face interactions” (2014, p. 17). The ASGW Best Practices Guidelines require that “Group workers are aware of and responsive to technological changes as they affect society and the profession” (ASGW, 2007, p. 115, A.9). Similarly, CACREP (2015) indicates “students are to understand the impact of technology on the counseling profession” (2.F.1.j) as well as “the impact of technology on the counseling process” (2.F.5.e). CACREP also emphasized that students understand “ethical and culturally relevant strategies for establishing and maintaining in-person and technology-assisted relationships” (2.F.5.d). Additionally, the Association for Counselor Education and Supervision (ACES; 2018) provides guidelines for online instruction featuring descriptions regarding course quality, content, instructional support, faculty qualifications, course evaluation procedures and expected technology standards.
Online Group Counseling
Textbooks on group counseling have mainly approached EGCT in face-to-face formats (e.g., G. Corey, 2016; Yalom & Leszcz, 2005). Given the growing interest and demand for online counseling in recent years (Holmes & Kozlowski, 2015; Kozlowski & Holmes, 2017), COVID-19 has highlighted the need for greater awareness and understanding of online group counseling training. However, there is limited research on online group counseling and counseling students’ training in online group counseling.
Kozlowski and Holmes (2014) explored master’s-level counseling students’ experience in an online process group, reporting themes of participants’ experiences of a linear discussion, role confusion, and feelings of being disconnected, isolated, and unheard. In 2015, Holmes and Kozlowski expanded on their work with a study on master’s-level counseling students’ experiences in face-to-face and online group counseling training. They found that the online group participants felt significantly less comfortable than participants in the face-to-face group. Further, participants in the study evaluated face-to-face groups as preferable for participation, social cohesion, and security (Holmes & Kozlowski, 2015). Lopresti (2010) compared students’ group therapy experiences between face-to-face and online group counseling methods using synchronous text-based software. This research involved six master’s-level students engaging in an 8-week, 60-minute, weekly online group counseling session using the WebCT chat system. Results indicated that in the online format, some participants reported self-disclosure more easily, but they also shared that it was easy to hide behind the screen and to censor themselves.
Effectiveness of Online Group Counseling
Some researchers have observed the efficacy of online support groups (Darcy & Dooley, 2007; Freeman et al., 2008; Lieberman et al., 2010; Webb et al., 2008). Haberstroh and Moyer (2012) reported that professionally moderated online support groups could supplement face-to-face counseling, especially for clients who want regular daily support during the process of recovering from self-injury. They also found that online group interaction provided clients with opportunities to engage in healthy self-expression and reduce their sense of loneliness and isolation (Haberstroh & Moyer, 2012). King et al. (2009) examined the effectiveness of internet-based group counseling to treat clients with methadone substance abuse, reporting that internet-based group counseling could reduce resistance and non-adherence in clients. Clients expressed satisfaction with the process and reported convenience and higher levels of trust in confidentiality because they were able to participate from home.
Similarly, Gilkey et al. (2009) reported the advantages and disadvantages of synchronous videoconferencing (SVC) web-based interventions. This study involved families with children with traumatic brain injury. The results revealed that SVC had the potential for family-based therapy delivery. However, it required important factors such as client readiness to address their issues and patience with the technology’s imperfections. SVC could reduce barriers to treatment with motivated families from diverse backgrounds. Nevertheless, the online group experience is vulnerable to the impact of technology glitches, privacy issues, disruptions in connectivity, and personal detachment (Amulya, 2020). In online group therapy, Weinberg (2020) identified four obstacles: managing the frame of the treatment, the disembodied environment, the question of presence, and the transparent background.
Purpose of Study and Research Questions
In March 2020, as a result of the pandemic, our university moved most face-to-face classes to virtual environments following statewide restrictions for in-person gatherings. This sudden change led to a unique experience for first-year master’s-level counseling students enrolled in an introductory group counseling course at a CACREP-accredited program in the Midwest. It was planned that students would participate in 10 face-to-face EGCT groups of 90 minutes each to fulfill the CACREP (2015) group counseling experiential training requirements. Doctoral students facilitated the first five group counseling experiences for the counselors-in-training. The plan was for two master’s students to lead face-to-face groups under the supervision of doctoral students for the remaining five groups (6–10). However, the university closed for 2 weeks after Session 6 was completed. As a result, when classes resumed, they were online. EGCT Sessions 7 through 10 were conducted online using Microsoft Teams with master’s students leading and doctoral students supervising. Thus, in a single semester, the master’s students had the experience of participating in and leading both face-to-face and online groups. Our study was guided by the following research question: What were master students’ experiences of participating and leading in both face-to-face and online EGCT groups?
Methods
Research Design
Qualitative methodology was used to explore first-year master’s students’ experiences of participating and leading in both face-to-face and online formats of EGCT. Our aim was to build an understanding of their experience shifting to an online modality with a specific interest in their attitudes, learning, facilitating, and adaptation to these two environments. For this purpose, a phenomenological approach was appropriate for investigating students’ unique experiences in both versions of the EGCT groups. Moustakas (1994) defined phenomenology as an approach for “comprehending or having in-depth knowledge of a phenomenon or setting and . . . attained by first reflecting on one’s own experience” (p. 36). In a phenomenological study, the aim is to describe the essence of individuals’ experiences with a certain phenomenon (Creswell & Creswell, 2018).
Participants and Procedures
IRB approval was obtained, and purposive sampling was implemented with a recruitment email. All participants were recruited from a CACREP-accredited counseling program in the Midwest United States. Our inclusion criteria were that participants must be current master’s-level counseling students and must be enrolled in a group counseling course. In addition, each participant must have experienced both participating in and leading at least one EGCT session during the prior term.
The invitation to participate in a focus group was emailed to all students enrolled in the group counseling course in the prior term. It included information about the study, addressed voluntary participation, and explained the entirely separate nature of participation in the focus group from evaluation of performance in the group class that had concluded. This recruitment email was sent out a total of three times within a 3-week period before the study was conducted.
Nine students agreed to participate in the study, and written consent forms were sent to them via email to read and review. Of the nine participants, three self-identified as male and six self-identified as female. Seven participants identified as White and two identified as “other,” and the age range was 18–34 years old. Two participants were specializing in school counseling, three in clinical mental health counseling, three in clinical mental health/clinical rehabilitation counseling, and one in clinical mental health/school counseling.
Before the focus group, prospective participants were emailed a copy of the semi-structured interview questions to alleviate any anxiety or concerns about the questions that would be asked during the study. Prospective participants were also invited to ask any questions at the start of the focus group and were then invited to provide verbal consent. To secure confidentiality, participants were assigned a code consisting of letters and numbers to protect their identity. Participants’ identification codes, with corresponding names, were kept securely in the possession of the first author, Bilal Urkmez.
Focus Groups
Focus groups were used because they allow students to share their experiences with EGCT groups and compare points of view (Krueger & Casey, 2014). Two online focus groups were held—one with five participants (one male, four females) and one with four participants (two males, two females). Participants received invitation links from the focus group facilitator via Microsoft Teams. All participants were familiar with Microsoft Teams because they had used it for their experiential groups and classes after moving to online instruction. Urkmez contacted the university’s IT department regarding the protocol of recording and securing the video and audio of the focus groups on Microsoft Teams.
Our fifth and sixth authors, Jennifer Ojiambo Isiko and Brandon Tomlinson, who led and supervised the original EGCT groups, conducted the focus groups. Care was taken to ensure that master’s students were not placed in a focus group led by the same doctoral student who had previously led and supervised their 10-session EGCT groups.
We used Krueger and Casey’s (2014) guidelines to create a semi-structured focus group protocol. Open-ended questions were built in for the focus group leaders to use as prompts to facilitate discussion when necessary. The online focus groups lasted approximately 60 minutes. All the conversations were recorded and then transcribed verbatim by the designated focus group facilitator.
Authors’ Characteristics and Reflectivity
Our research team consisted of two counselor educators with experience teaching and facilitating group counseling courses and five counselor education doctoral students. All doctoral students were part of a single cohort, and all had prior experiences facilitating group counseling. The counselor educators were Urkmez, who self-identifies as a White male, and Christine Suniti Bhat, an Asian female. The doctoral students were Chanda Pinkney, an African American female; Daniel Bonnah Amparbeng, an African male; Nanang Gunawan, an Asian male; Isiko, an African female; and Tomlinson, a White male. Before data collection, we met to discuss focus group questions, explore biases and assumptions, and assign focus group leaders for the study.
Our team used multiple strategies to establish trustworthiness. As two of the researchers taught group counseling and five of the researchers had led and supervised the EGCT groups, it was necessary to discuss possible biases before and during the data analysis process to ensure that the resulting themes and subthemes emerged from participants’ responses (Bowen, 2008).
First, some of the researchers shared that they believe face-to-face group counseling is better than online group counseling because they do not personally like to take or teach online courses in their education. All research members taught, learned, and supervised EGCTs predominantly in face-to-face environments prior to the study and pandemic. Secondly, some of the researchers also mentioned their frustrations with learning and supervising online. These discussions were held to promote awareness of potential biases so as to avoid focusing on the negative experiences of the master’s students. Bracketing was implemented throughout the study to reduce researchers’ possible influence on participants of favoring face-to-face counseling environments (Chan et al., 2013). This measure helped ensure the validity of the study’s data collection and analysis by having the researchers put aside any negative experiences of online learning environments during the pandemic (Chan et al., 2013). Urkmez, Pinkney, Bonnah Amparbeng, Gunawan, Isiko, and Tomlinson analyzed the data first, fulfilling investigator triangulation (Patton, 2015). This same group then met several times to discuss their analyses of the transcripts and agree upon the significant statements and themes.
Experiential Group Counseling Training
Twenty-eight first-year master’s students were enrolled in an introductory group counseling course in the spring 2020 academic semester. The EGCT groups were a required adjunct to the didactic portion of the course. EGCT sessions for the master’s students met weekly for 90 minutes and were set up so that the master’s students were participants for Sessions 1 through 5 (led by doctoral students) and were leaders for Sessions 6 through 10 (supervised by doctoral students). All 10 sessions were planned to be face-to-face sessions. Doctoral students were enrolled in an advanced group counseling course, and their participation was a required component of the course.
During the first five sessions, doctoral students’ responsibilities as leaders included facilitating meaningful interaction among the participants, promoting member–member learning, and encouraging participants to translate insights generated during the interaction into practical actions outside the group (G. Corey, 2016). For Sessions 6–10, in the role of supervisors, doctoral students’ responsibilities were to mentor and monitor the master’s students’ group leadership skills and provide verbal feedback immediately after the session. Doctoral students also provided written feedback to both the master’s students and group counseling course instructors. Additionally, the doctoral students engaged in peer supervision with each other under the tutelage of the advanced group counseling course instructor, discussing how EGCT could be supervised more effectively.
As stated previously, two master’s students started to co-lead the EGCT groups during Session 6, which was conducted face-to-face. After Session 6, in-person classes were canceled by the university in response to COVID-19, so the remaining four sessions of EGCT were conducted online on Microsoft Teams. The online groups were conducted synchronously on the same day and time as the face-to-face groups had been conducted in the earlier part of the semester.
Session 7 was the first synchronous online session of the EGCT and deserves special mention. Prior to Session 7, the doctoral students received brief training on Microsoft Teams. The master’s students had no previous exposure to Microsoft Teams. Thus, during Session 7, the doctoral students provided support by demonstrating how Microsoft Teams worked and processing the master’s students’ thoughts, feelings, and levels of wellness in relation to the sudden pandemic. Students resumed leading the online synchronous groups for Sessions 8, 9, and 10 under doctoral students’ supervision.
Data Analysis
Isiko and Tomlinson led the two focus groups and transcribed the data collected from the participants who shared their experiences in the focus groups. We utilized the phenomenological data analysis method described by Moustakas (1994). Urkmez, Pinkney, Bonnah Amparbeng, Gunawan, Isiko, and Tomlinson conducted the data analysis while Bhat served as a peer debriefer because of her position of seniority in terms of expertise in not only qualitative methodology, but also group counseling research, as well as her experience of more than 15 years in teaching both master’s- and doctoral-level group counseling courses at the CACREP-accredited program. Her primary role was to read the transcripts, review the raw data and analysis, and scrutinize established themes to point out discrepancies (Creswell & Creswell, 2018).
Our research team (except for Bhat) met to discuss our potential biases and bracket our assumptions about the phenomenon under investigation. Then, each of us independently read all transcripts multiple times to become familiar with the data. Next, we reviewed the transcripts according to the horizontalization phase of analysis (Moustakas, 1994). Moustakas defined the horizontalization phase as the part of the analysis “in which specific statements are identified in the transcripts that provide information about the experiences of the participants” (Moustakas, 1994, p. 28). During this step, we independently reviewed each transcript and identified significant statements that reflected the participants’ interpretations of their experiences with the phenomenon. We identified these significant statements based on the number of times they were mentioned both within and across participants. From this point, we each independently created a list of significant statements.
Subsequently, we met to review our lists to establish coder consistency, create initial titles for the themes, and place data into thematic clusters (Moustakas, 1994). Each of our themes and related subthemes were similar in content and typically varied only in the titles used. Titles for themes and subthemes were discussed until consensus was obtained. We revisited the horizontalized statements and discussed our different perspectives. Next, we evaluated the most commonly occurring themes and created a composite summary of each theme from the participants’ experiences. After these steps, we arrived at a consensus about each theme’s essential meaning and decided on specific participant quotes that represented each theme.
Findings
We identified three main themes related to the participants’ experiences of taking part in and leading both face-to-face and online EGCT. The three main themes were positive participation attributes, participation-inhibiting attributes, and suggestions for group counseling training.
Positive Participation Attributes
The central theme of positive participation attributes focused on exploring master’s students’ perceptions about what helped them actively participate in both online and face-to-face EGCT groups as a group member. Five subthemes were identified in the main theme of positive participation attributes: (a) knowing other group members, (b) physical presence, (c) comfortability of online sessions, (d) cohesiveness, and (e) leadership interventions.
Knowing Other Group Members
The EGCT group involved graduate-level counseling students who knew each other for a semester before engaging in the EGCT. Study participants shared that seeing familiar faces provided a safe and supportive environment for them to participate in both face-to-face and online group sessions as a group member. One participant noted that “a part of it helped because it was many people I had already known,” and another participant stated that “it was easier to have face-to-face after we had already kind of met everybody in the semester and so I wasn’t worried about confidentiality. I wasn’t in this group with a whole bunch of strangers.” Participants noted that knowing other group members helped them to participate actively in EGCT. They reported that having familiar faces in the group made them feel comfortable and connected, and that it helped them engage more fully during the ECGT groups.
Physical Presence
Study participants shared that group members’ physical presence during the face-to-face sessions enhanced their willingness to participate. The physical presence provided access and a better ability to understand group members’ content and emotion through their body language, eye contact, vocal tone, and other nonverbal cues during sessions. As one participant shared, “I feel so much more in touch and present with people when I can see them, but just kind of feel their physical presence rather than just watching the faces online.” Furthermore, the study participants shared that being physically present during the face-to-face sessions allowed for the incorporation of more icebreaker activities by both doctoral and master’s student group leaders, enhancing their participation in groups. One participant noted that “the small icebreakers, I just remember doing those at the beginning during our face-to-face sessions; those were a lot of fun.”
Comfortability of Online Sessions
Participants reported that they felt comfortable engaging in online EGCT from their familiar surroundings at home. They appreciated the convenience of participating in ECGT groups from wherever they were. One participant reported that “people could be outside or eating or drinking or whatever, which I think is cool.” Another participant shared that before the state-issued quarantine, they already used online technology to communicate with friends, so it was easy to use Microsoft Teams for online experiential training groups. Another participant noted:
We were doing them (EGCT) from the comfort of our own home; it just increased how comfortable you were in general. We were all at home, rocking in sweatpants and not having to worry about stuff. I feel we were in our own comfortable, safe space, and that made the online easier for me.
Cohesiveness
Participants reported they felt “anxious,” “lonely,” and “isolated” and experienced other difficulties during the COVID-19 pandemic. They noted that they actively engaged in online EGCT sessions because it provided them with the opportunity to connect, share, and process their thoughts and emotions. A group participant reported, “We all had to isolate. [It] made it exciting to be able to connect with everyone again, to talk about how it (COVID-19) was affecting us, to vent out our emotions and check in with others.” Additionally, another participant reported:
When we started these sessions [online], it was at the beginning of these COVID-19 issues, and I was feeling more stressful, and there was nothing to do. It was so difficult to adjust to this environment, even staying at home. This was like an opportunity for me to connect with classmates in the group and [it] helped me to reflect on my anxiety and how other people were thinking around these COVID-19 issues.
As a result of the online EGCT groups, participants gained a means of personal interaction during isolation. The subthemes presented above capture the positive participation factors that helped participants to engage actively in both online and face-to-face sessions.
Leadership Interventions
Participants shared leadership interventions that helped them to participate during face-to-face and online sessions. The sudden transition to online groups due to COVID-19 was characterized by trial and error and uncertainty for everyone. Participants noted that while working with the new online EGCT group and different processes than what they experienced before COVID-19, doctoral students and master’s student leaders demonstrated a sense of flexibility and adaptability to the prevailing situation and could steer the groups in the changing environment. Both the doctoral and master’s student leaders were aware of the effect of COVID-19 on the participants, and they allowed the participants to get support from each other before they could get into the session plan for the group. One participant mentioned that “we kind of partly used that [the group] as a social support group . . . and reflect on how we’re feeling during social isolation.” Another participant shared that “the facilitators were flexible. So, even if they had a topic or something like that, they would allow for flexibility, to check in [with participants], and be able to kind of shift focus to what we all needed.”
Participants explicitly mentioned that the doctoral and master’s students’ leadership interventions, such as encouraging, checking in, and being present, helped them engage in the EGCT groups. Participants highlighted the strength of the group leaders’ encouragement of reflection (“I appreciated that the leader really put emphasis on encouraging us to answer questions”) and overall presence and attention (“[The leader] was attending our behavior and was really good with reflecting”). The participants also found the aspect of “checking in” by the leaders as something that enhanced their participation: “The leaders were always pretty quick to check in on someone if something seemed off.”
Group leaders’ ability to coordinate and successfully facilitate group sessions can significantly influence group outcomes (G. Corey, 2016; Gladding, 2012). Study participants shared that group facilitators demonstrated leadership skills and techniques to facilitate meaningful discussions and participation among members in both face-to-face and online sessions: “Like she [group leader] was always there to answer questions if there is silence; like she didn’t want us to rely on her to do the entire conversation, so her encouragement was beneficial for me.”
Participation-Inhibiting Attributes
For this main theme, we examined attributes that negatively influenced participation and leading in the online and face-to-face formats of the EGCT groups. Three subthemes were identified: (a) group dynamics, (b) challenges with online EGCT, and (c) technological obstacles for online EGCT. The most prominent subtheme that arose and spread across both group formats was that of the group dynamic. Friction within the group dynamic was one of the primary issues reported by participants. The remaining subthemes were related to challenges with online EGCT groups. These challenges include the importance of “being with” or physically present with the rest of the group, problems with missing nonverbal communication in the online meetings, difficulties navigating awkward silences and pauses in the group, and technical obstacles.
Group Dynamics
Study participants shared that the group dynamics dictated how much of a connection developed among group members and significantly influenced the progression to the working phase in the groups. In the words of one participant, “I feel like that was definitely something with our group dynamic. . . . There was definitely still good conversations, but I think that impacted it.”
Some participants reported their initial concerns about fostering rapport with group mates chosen randomly for them. Participants expressed thoughts that personalities did not mesh well in their group and that there were issues of building good rapport. Some participants indicated that having a reserved personality made it hard to participate: “For me, it was more about a personal thing because I am an introverted personality, so I find it difficult to talk in groups anyway, so that’s what hindered my participation sometimes.” Another participant stated: “I felt like the others protect themselves by not talking, so why should I open myself and put myself into risk? I thought about that.”
Challenges With Online EGCT
Participants in this study emphasized that one of the main difficulties of the online EGCT experience that affected their participation and leadership negatively was missing body language and physical cues. Participants shared that they could use nonverbal cues and body language to know when it was a good time to speak without interrupting other group members during the face-to-face ECGT. Because these were missing in online EGCT, the students did not have immediate awareness to participate in group conversation without interrupting other group members. For example, one participant noted the difficulties of “just not being able to read body language as well and not being able to see everyone at once.” As a result of these online environment limitations, study participants indicated they had a sense of “stepping on toes” while trying to participate in online EGCT: “I think that one of the biggest challenges with doing it [EGCT] online is that you want to be respectful and make sure that you are not gonna talk over somebody else.”
Kozlowski and Holmes (2014) previously noted that the unfamiliar environment of online counseling, the time delay because of technology, and the inability to utilize group members’ body language can all create a one-dimensional or “linear” experience in online group counseling environments. These factors appeared to hinder the natural growth and development of the EGCT groups in our study as well. In an effort to reduce the perception of being rude, there were times of awkward silence as participants avoided constant interruptions during the sessions; this difficulty gave the feeling of a linear environment.
One other factor the participants noted in the online format more so than the in-person group was what students described as an awkward silence. This occurrence serves as a subtheme of missed physical cues because the participants noted that the lack of said cues complicated determining when to speak and when to wait: “Online, the silence almost felt like it was much longer than what it really would have been if it was face-to-face.” Another participant stated that they “feel pretty comfortable with silences, but it’s a lot harder to gauge that when it’s online.” This issue presented itself in several circumstances, though one group did attempt to figure out a solution, per the report of one participant: “For our group . . . to help with people talking over each other, we had people type in a smiley face in the chat when they wanted to share.”
Notably, participants in this study also mentioned that there was some physical presence that they could not describe but found to be relevant to them in their connection with the group. Although students were unable to identify it precisely, several study participants agreed on its importance. One participant said that they “enjoy the voice and the video, but I feel like when we are talking, especially in a group dynamic and group processes, especially to grasp something important, I really need to be with this person in a physical space.”
The participants emphasized the importance of physical presence, from the ability to see and greet one another to having space to do activities that got them up and moving. Many participants mentioned some intangible quality they could not name but that was missing when the groups convened electronically instead of in person. A participant shared that “you can observe the body language—what is happening in the group actually, but in online sessions, it’s like you don’t know, you are just talking.”
As noted in other sections, the group members appreciated the space for doing activities together when they were in person. Master’s student group leaders reported that they felt anxious when facilitating icebreaker activities in their online EGCT sessions because of the missing physical presence and noted the loss of face-to-face icebreakers. Study participants lamented that the online format did not allow for these bonding and icebreaking exercises, which when utilized in the usual face-to face format tended to put them in a position to feel better equipped to share with their group members, almost like a metaphorical entryway to the group process: “Some of the exercises are not possible to execute [online] because we were doing some physical things in our group, like throwing balls to each other and stuff.” Without these social warm-ups, the group flow and process suffered; according to those in the focus group, leaders needed more assistance to run activities in online EGCT sessions. One participant added a similar sentiment: “How do we lead a group online with proximity activities or icebreakers we would use? We can’t really do [that] because of the virtual interaction, [it] can’t work.”
Overall, the online EGCT environment limited the interpersonal relationships of the EGCT members and group leaders. Group members could not use their nonverbal communication skills or participate in physical group activities. Lastly, online EGCT appears to provide added pressure on group leaders to keep members engaged during the session. Master’s students had to choose topics where all members felt comfortable enough to participate with minimal encouragement, which was a challenge.
Technological Obstacles for Online EGCT
Participants reported some technological difficulties that inhibited their ability to participate and lead the online EGCT sessions. Some participants noted that when participants turned off their cameras, it exacerbated disengagement levels within the group and hampered group dynamics. Some speculated that technical difficulties might be an excuse to disengage from the group: “Like in online, I can be mute, I can turn off my camera, I can not talk, and I can accuse the technology for that.” This capacity to disengage negatively impacted the group for several of the focus group participants, who noted that they felt this closed off the group and circumvented the ability to engage with all members of the group.
The limitations of the university-sanctioned online platform used for the EGCT groups, Microsoft Teams, adversely affected engagement during the online sessions as it only allowed four members (at the time of the online EGCT sessions) to be seen on the screen at a time. As one participant stated, “I cannot see all the group members . . . my attention is not with all members. This was difficult. It was difficult to lead the group.” Several group members were vociferous in their dislike for this limitation of the platform. Further, internet connectivity issues were problematic: “Sometimes like a group member would disconnect [because of technology problems], and there would be several minutes before they could come back.” These types of interruptions were frustrating to all group members and group leaders. Master’s student group leaders had a difficult time leading with interruptions.
One focus group participant noted, and others agreed, that it was challenging to learn how to lead a group online because they were missing so many elements of the in-person process of leading a group, and they did not have previous group leadership experience in an online environment. A participant shared that “it’s hard [leading group online]. It’s maybe harder for leaders because they cannot observe what’s going on . . . like body language.”
Suggestions for Group Counseling Training
Participants were invited to share their concerns and ways to develop and improve face-to-face and online EGCT group experiences. Three subthemes were identified: (a) software issues and training, (b) identified group topics, and (c) preferred EGCT environment.
Software Issues and Training
Participants shared common concerns about the software for their online experiential training groups. Specifically, they found Microsoft Teams’ display of only four people at one time prevented them from seeing all group members on the screen. Members who were not speaking were displayed at the bottom of the computer screen with their profile picture or initials, which was not conducive to interaction. One participant suggested that they should “probably just use Zoom instead . . . I like Zoom better, seriously, because I can see absolutely everyone.” Another participant agreed, “But for the reason, at least, in Zoom, I can see everyone’s faces, not, um, not just four.”
Another participant similarly emphasized the importance of seeing everyone on one screen during their meeting: “If you don’t see the faces [at one time], you’re just clueless. I mean, have to, like, awkwardly check in with this person all the time.” Participants also brought another suggestion about training on leading online experiential training groups. Participants shared their anxiety about leading groups using online software because it is a new and unique experience. Because of the sudden onset of COVID-19, the students did not have a chance to get training on how to lead online experiential training groups. A participant mentioned that having training where students could learn how to facilitate online groups before leading weekly sessions would help alleviate anxiety and build competence: “Perhaps allowing a small period where everyone kind of gets adjusted to it and becomes more familiar with it might help facilitate [online] group sessions better.”
Identified Group Topics
Another suggestion by participants regarding their EGCT experience was using one selected topic for each group. For example, a participant shared: “I think part of what was hard about this that might be something to change is, like having the group just be all over the place in terms of topics from week to week.” Another participant added: “If the group was more, like, a little bit more specific and clearer about like, the goal, or something like that, that might be—might help it flow a little bit better.” Some participants also suggested allowing students to select which group they wanted to attend, instead of having groups pre-assigned to them. In other words, participants preferred to join a specific group based on their interests. A participant mentioned: “I think that would be like a really good option to give like a list of ten types of groups or topics in the groups.” Another participant similarly suggested “giving an opportunity to all students to choose one group. For example, like the one group would work specifically on self-esteem problems or the other one would work on grief problems.”
Some participants noted that they felt there was a lack of purpose for the group, indicating that they were not sure of the group’s goals or objectives and that this hindered their ability to participate fully. Some also shared having confusion about their role and the boundaries of the group and what they could or could not share. One participant noted: “In the first session when we were trying to set up our goals, it was difficult for us to find what the goals will be as a group leader candidate, or as a person.” The focus group participants suggested giving more concrete topics overall for the EGCT group to understand better how to participate. This notion spanned across the online and face-to-face format as a more general recommendation.
Preferred Training Environment
Lastly, participants were asked about their preference for participation in a face-to-face or online EGCT experience, if given a choice. Even though participants reported a reasonably good experience with online EGCT groups, such as comfortability and cohesiveness, most of the participants voiced a preference for face-to-face sessions if they had to do the group counseling training over again. One participant stated: “Ultimately, face-to-face will probably still be better.” Another participant added: “Face-to-face for sure. I just think as like a profession, we all enjoy working with people. We would prefer to work with someone in person.” Similarly, another participant mentioned: “I would definitely choose face-to-face, but I was thankful that we had the opportunity to do it online.”
Asking the participants about their preferred experiential training group environment garnered the most reaction during the interviews. Most of the participants shared that they preferred face-to-face groups. Even though participants had personal connections in an online setting, they wanted to have face-to-face meetings to interact better. One participant mentioned that “we are doing online sessions right now. I wish that I [could] continue to do the group lab and connect with the group members, but if I have the opportunity to take face-to-face, absolutely, I would do that.” Lastly, another participant added: “Absolutely, it’s face-to-face, but if we are in a situation like this, COVID-19 issues, sometimes the online sessions can be helpful.”
Participants offered their perspectives on learning group counseling skills during the global COVID-19 pandemic. Despite the unprecedented circumstances, the students persevered and completed the course. Group leaders and professors encouraged the group members to participate to the best of their abilities. The concerns and suggestions shared in these focus groups could help counselor educators plan and develop for EGCT in both online and face-to-face formats.
Discussion
This study investigated the experiences of master’s students in an online and face-to-face EGCT group. EGCT is an essential aspect of novice counselors’ preparation and is required by CACREP (2015) standards. In this study, participants identified positive factors related to their EGCT group participation, such as knowing other group members, group leadership skills, physical presence, and connection with other group members. They also reported participation-inhibiting factors such as the complexities of group dynamics, missing physical cues, and technological challenges. Our research findings are similar to Kozlowski and Holmes’s (2014) study on online group counseling training. Their participants reported problems with the group feeling artificial, lacking attending skills, and difficulties with achieving cohesion and connectedness.
In the current study, course instructors and student leaders did not have control over the choice of an online platform. The limitations of Microsoft Teams, which at the time of the online EGCT sessions only allowed four participants to be visible on the screen at one time, added to difficulties with engaging and feeling connected. For participants to remain engaged, leaders and instructors should have access to online platforms that allow students to see all group members simultaneously on the screen. Setting ground rules requiring that cameras remain on during sessions and utilizing the chat feature or the hand-raising feature to facilitate discussions would also help create and maintain a sense of connection. Outlining contingency plans such as the alternatives for not being able to join the group with the camera on are important for successful group outcomes.
Participants in this study appreciated the convenience of participating in online ECGT groups. This is similar to the findings of King et al. (2009) about the convenience of access to online group counseling. In the same study by King et al. (2009), the participants shared that online counseling sessions allowed them to participate from the comfort of their homes, thus improving both convenience and privacy. One of the difficulties participants reported was that of awkward silence. This experience, coupled with interruptions (“stepping on toes”), resulted in students finding that the experience online was more linear and less organic compared to face-to-face interactions. These findings are similar to those of Kozlowski and Holmes (2014). Yalom and Leszcz (2005) noted that the group leader’s role is to design the group’s path, get it going, and keep it functional to achieve effectiveness. Presence, self-confidence, the courage to take risks, belief in the group process, inventiveness, and creativity are essential leadership traits in leading groups (G. Corey, 2016). However, these traits are for in-person groups. It is possible that effectively leading online groups requires other skills that have not yet been identified. The sudden change to online training in this instance did not allow for a planful design. It is necessary for group leaders to possess specific group leadership skills and appropriately perform them to help group members participate in groups (M. S. Corey et al., 2018). However, participants appreciated that the doctoral and master’s student leaders demonstrated flexibility, allowing for additional time to check in with group members and process their experiences and emotions related to the pandemic.
One interesting finding related to how COVID-19 impacted participants’ experiences in the ECGT groups was that group participants actively engaged in the online sessions when they were allowed to process their anxiety and stress due to COVID-19, as it served as a support group. This result is dissimilar to findings of previous studies in which participants felt unsafe during online group sessions and being on online platforms impeded participants’ emotional connection and trust levels (Fletcher-Tomenius & Vossler, 2009; Haberstroh et al., 2007; Kozlowski & Holmes, 2014).
Bellafiore et al. (2003) emphasized online group leaders’ roles as “shaping the group” and “setting the tone.” They also expressed that “establishing and maintaining a leadership style is important in keeping the group going” (p. 211). In the current study, first-year master’s students, many of whom were participating in or leading groups for the first time, had the unexpected and sudden additional layer of learning how to lead online. Further, the abrupt transition from face-to-face to online groups because of COVID-19 did not allow for extensive instructor planning and preparation. Leading groups online was challenging and anxiety-provoking for members, as they lacked experience and were unsure how to proceed. Master’s students need additional training on facilitating online groups, establishing a leadership style, and managing silence. This information corresponds with Cárdenas et al.’s (2008) findings that master’s-level counseling students felt more confident to provide online counseling services after training.
Implications
Although the findings from this study are not generalizable, there may be implications for designing and leading EGCT groups that merit consideration based on the experience of the counselor trainees described in this study. Part of the group design entailed assigning different topics to focus on for each session. The rationale for having different topics for each session should be clearly explained to the participants. Any questions regarding the identified topics should be addressed early to enhance the group facilitation process for both leaders and participants. Additionally, group leaders or course instructors need to explain roles clearly, and group members should understand the group’s boundaries and how they fit with their didactic course.
With online EGCT groups, it is essential to consider how participation is influenced by a lack of natural communication signals, such as body language and physical presence. Counselor educators and EGCT student leaders need to establish ground rules about online group interactions such as having all cameras remain on during sessions, having a private and quiet space from which to participate, and minimizing distractions from pets or relatives, all of which are necessary for successful groups. Further, utilizing technology that allows all members to be seen on the screen may help build connection and cohesiveness. Utilizing methods such as using the chat to insert a symbol or using the hand-raising icon can also help facilitate participation.
Overall, students reported feeling unprepared to lead online counseling groups. However, as counselor educators, we are responsible for preparing our students to engage in online counseling successfully, especially as the COVID-19 pandemic continues into its second year and will continue to affect how much virtual counseling will take place in the future. The recent normalization of online counseling (individual and group) may persuade educators and counselors to “increase their skills in terms of development, comfortability, and flexibility in the online environment” (International OCD Foundation, 2020, p. 1). Therefore, counselor educators should cover online-specific facilitation skills in their training programs.
Limitations and Future Research Directions
This study was the first step in attempting to understand and describe master’s-level students’ experiences of participating and leading in both face-to-face and online formats of EGCT. As with all research, limitations should be considered in interpreting the findings. Further, some of the limitations point to potential research directions.
COVID-19 created a situation where the transition from face-to-face to online formats was compulsory. It is therefore not clear what the experience would have been like if the transition was planned and did not have a situation like COVID-19 in the background pushing the transition, or if the group had been entirely online. Because of unplanned adjustment, course instructors and student leaders did not have control over the choice of an online platform. Outlining contingency plans, such as alternatives when a group member cannot join the group with their camera on, are essential for successful group outcomes, and a lack of familiarity with online platforms may have prevented instructors and student leaders from providing these contingencies and therefore impacted the experience for students.
Further, the EGCT groups were conducted with master’s-level students, and participants already had preexisting relationships with each other. This may have contributed to their strong support of face-to-face groups over online groups. In future research, studies with participants who do not already know each other may help us assess the appeal of online groups to participants. Further, researchers in the future may wish to examine the efficacy of online group counseling training for counseling students compared to in-person group training by comparing two equivalent experiential groups.
The current study recruited master’s-level counseling students from a CACREP-accredited counseling program in the Midwest United States; thus, results cannot be generalized to other institutions. The sample size was small in the current study. Therefore, we caution against generalizing our findings. During the focus groups, participants shared some apprehension about how much information to disclose in group counseling, and they verbalized some confusion on group purpose, direction, or goals. For many, these EGCT groups were the students’ first experience in group counseling training, and this could contribute to them questioning if their feelings and experiences were appropriate (Ohrt et al., 2014).
There are methodological considerations to improve future studies. Focus groups were conducted to collect the data from the participants. In-depth individual interviews would enhance a deeper conversation in understating and reflecting on the challenges and needs of master’s-level students. Participants may have censored some of their true feelings, as they were aware that their group leaders were also part of the research team, even though they did not run the focus groups. We acknowledge that the students knowing each other from previous classes may have influenced how much they shared in groups. Participants in this study expressed comfort with knowing each other from a previous semester. However, it is also possible that students may have disclosed minimal personal information so as not to effect public perception of themselves or effect future professional relationships.
Another area to expand on would be investigating counselors’ self-efficacy while facilitating online counseling groups. For example, exploring positive participation attributes that increase online groups’ participation from the leader’s perspective could be useful. This may allow researchers and practitioners to identify how group counseling can best be leveraged in an online environment.
Conclusion
The purpose of this study was to explore and compare first-year master’s-level counseling students’ experiences of participating and leading in both face-to-face and online formats of EGCT. In summary, students considered that the online format was challenging because it added a layer of learning to their fledgling group work skills beyond the face-to-face setting. Technological barriers that were outside the control of participants inhibited their participation, but on the other hand, the online groups served as a safe and supportive space for students to alleviate their stress and loneliness due to COVID-19. Regardless of the teaching environment, thoughtful and well-planned EGCT groups are essential for student development in this area, and skilled group leaders can manage group dynamics and model group counseling skills. COVID-19 has necessitated a focus on teletherapy and online counseling. The group counseling profession should be proactive in addressing this training need, as conducting online group counseling sessions is likely to continue to be a much-needed skill in a post-pandemic world.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf?sfvrsn=96b532c_2
Amulya, D. S. L. (2020). An experiment with online group counseling during COVID 19. In L. S. S. Manickam (Ed.), COVID-19 pandemic: Challenges and responses of psychologists from India (pp. 182–197).
Anthony, K. (2015). Training therapists to work effectively online and offline within digital culture. British Journal of Guidance & Counselling, 43(1), 36–42. https://doi.org/10.1080/03069885.2014.924617
Association for Counselor Education and Supervision. (2018). ACES guidelines for online learning – 2017. https://acesonline.net/knowledge-base/aces-guidelines-for-online-learning-2017-2
Association for Specialists in Group Work. (2007). Association for Specialists in Group Work: Best practice guidelines. https://www.researchgate.net/publication/247784312_Association_for_Specialists_in_Group_Work_Best_Practice_Guidelines_2007_Revisions
Barak, A., & Grohol, J. M. (2011). Current and future trends in internet-supported mental health interventions. Journal of Technology in Human Services, 29(3),155–196. https://doi.org/10.1080/15228835.2011.616939
Behenck, A., Wesner, A. C., Finkler, D., & Heldt, E. (2017). Contribution of group therapeutic factors to the outcome of cognitive–behavioral therapy for patients with panic disorder. Archives of Psychiatric Nursing, 31(2), 142–146. https://doi.org/10.1016/j.apnu.2016.09.001
Békés, V., & Aafjes-van Doorn, K. (2020). Psychotherapists’ attitudes toward online therapy during the COVID-19 pandemic. Journal of Psychotherapy Integration, 30(2), 238–247. https://doi.org/10.1037/int0000214
Bellafiore, D. R., Colon, Y., & Rosenberg, P. (2003). Online counseling groups. In R. Kraus, J. Zack, & G. Stricker (Eds.), Online counseling: A handbook for mental health professionals (pp. 197–216). Academic Press.
Bowen, G. A. (2008). Naturalistic inquiry and the saturation concept: A research note. Qualitative Research, 8(1), 137–152. https://doi.org/10.1177/1468794107085301
Burlingame, G. M., McClendon, D. T., & Yang, C. (2019). Cohesion in group therapy. In J. C. Norcross & M. J. Lambert (Eds.), Psychotherapy relationships that work: Evidence-based therapist contributions (pp. 205–244). Oxford University Press.
Cárdenas, G., Serrano, B., Flores, L. A., & De la Rosa, A. (2008). Etherapy: A training program for development of clinical skills in distance psychotherapy. Journal of Technology in Human Services, 26(2–4), 470–483. https://doi.org/10.1080/15228830802102180
Chan, Z. C., Fung, Y., & Chien, W. T. (2013). Bracketing in phenomenology: Only undertaken in the data collection and analysis process. The Qualitative Report, 18(30), 1–9.
https://doi.org/10.46743/2160-3715/2013.1486
Corey, G. (2016). Theory and practice of group counseling (9th ed.). Cengage.
Corey, M. S., Corey, G., & Corey, C. (2018). Groups: Process and practice (10th ed.). Cengage.
Council for the Accreditation of Counseling and Related Educational Programs. (2015). CACREP 2016 standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Creswell, J. W., & Creswell, J. D. (2018). Research design: Qualitative, quantitative, and mixed methods approaches (5th ed.). SAGE.
Darcy, A. M., & Dooley, B. (2007). A clinical profile of participants in an online support group. European Eating Disorders Review, 15(3), 185–195. https://doi.org/10.1002/erv.775
Fletcher-Tomenius, L., & Vossler, A. (2009). Trust in online therapeutic relationships: The therapist’s experience. Counselling Psychology Review, 24(2), 24–33.
Freeman, E., Barker, C., & Pistrang, N. (2008). Outcome of an online mutual support group for college students with psychological problems. Cyberpsychology & Behavior, 11(5), 591–593.
https://doi.org/10.1089/cpb.2007.0133
Gilkey, S. L., Carey, J., & Wade, S. L. (2009). Families in crisis: Considerations for the use of web-based treatment models in family therapy. Families in Society, 90(1), 37–45. https://doi.org/10.1606/1044-3894.3843
Gladding, S. T. (2012). Groups: A counseling specialty (6th ed.). Pearson.
Haberstroh, S., Duffey, T., Evans, M. P., Gee, R., & Trepal, H. (2007). The experience of online counseling. Journal of Mental Health Counseling, 29(3), 269–282. https://doi.org/10.17744/mehc.29.3.j344651261w357v2
Haberstroh, S., & Moyer, M. (2012). Exploring an online self-injury support group: Perspectives from group members. The Journal for Specialists in Group Work, 37(2), 113–132.
https://doi.org/10.1080/01933922.2011.646088
Hearn, C. S., Donovan, C. L., Spence, S. H., & March, S. (2017). A worrying trend in social anxiety: To what degree are worry and its cognitive factors associated with youth social anxiety disorder? Journal of Affective Disorders, 208, 33–40. https://doi.org/10.1016/j.jad.2016.09.052
Holmes, C. M., & Kozlowski, K. A. (2015). A preliminary comparison of online and face-to-face process groups. Journal of Technology in Human Services, 33(3), 241–262. https://doi.org/10.1080/15228835.2015.1038376
Ieva, K. P., Ohrt, J. H., Swank, J. M., & Young, T. (2009). The impact of experiential groups on master students’ counselor and personal development: A qualitative investigation. The Journal for Specialists in Group Work, 3(4), 351–368. https://doi.org/10.1080/01933920903219078
International OCD Foundation. (2020, July 15). Teletherapy in the time of COVID-19. https://iocdf.org/covid19/teletherapy-in-the-time-of-covid-19
King, V. L., Stoller, K. B., Kidorf, M., Kindbom, K., Hursh, S., Brady, T., & Brooner, R. K. (2009). Assessing the effectiveness of an Internet-based videoconferencing platform for delivering intensified substance abuse counseling. Journal of Substance Abuse Treatment, 36(3), 331–338.
https://doi.org/10.1016/j.jsat.2008.06.011
Kit, P. L., Wong, S. S., D’Rozario, V., & Teo, C. T. (2014). Exploratory findings on novice group counselors’ initial co-facilitating experiences in in-class support groups with adjunct online support groups. The Journal for Specialists in Group Work, 39(4), 316–344. https://doi.org/10.1080/01933922.2014.954737
Kiweewa, J., Gilbride, D., Luke, M., & Seward, D. (2013). Endorsement of growth factors in experiential training groups. The Journal for Specialists in Group Work, 38(1), 68–93.
https://doi.org/10.1080/01933922.2012.745914
Kozlowski, K. A., & Holmes, C. M. (2014). Experiences in online process groups: A qualitative study. The Journal for Specialists in Group Work, 39(4), 276–300. https://doi.org/10.1080/01933922.2014.948235
Kozlowski, K. A., & Holmes, C. M. (2017). Teaching online group counseling skills in an on-campus group counseling course. Journal of Counselor Preparation and Supervision, 9(1).
Krueger, R. A., & Casey, M. (2014). Focus groups: A practical guide for applied research (5th ed.). SAGE.
Krug, O. T. (2009). James Bugental and Irvin Yalom: Two masters of existential therapy cultivate presence in the therapeutic encounter. Journal of Humanistic Psychology, 49(3), 329–354.
https://doi.org/10.1177/0022167809334001
Lieberman, M., Winzelberg, A., Golant, M., Wakahiro, M., DiMinno, M., Aminoff, M., & Christine, C. (2010). Online support groups for Parkinson’s patients: A pilot study of effectiveness. Social Work Health Care, 42(2), 23–38. https://doi.org/10.1300/J010v42n02_02
Lopresti, J. M. (2010). The process and experience of online group counseling for masters-level counseling students (Order No. 3451084). Available from ProQuest Dissertations & Theses A&I. (862058819).
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Murdock, J., Williams, A., Becker, K., Bruce, M. A., & Young, S. (2012). Online versus on-campus: A comparison study of counseling skills courses. The Journal of Human Resource and Adult Learning, 8(1), 105–118.
Ohrt, J. H., Prochenko, Y., Stulmaker, H., Huffman, D., Fernando, D., & Swan, K. (2014). An exploration of group and member development in experiential groups. The Journal for Specialists in Group Work, 39(3), 212–235. https://doi.org/10.1080/01933922.2014.919047
Patton, M. Q. (2015). Qualitative research & evaluation methods: Integrating theory and practice (4th ed.). SAGE.
Peng, D., Wang, Z., & Xu, Y. (2020). Challenges and opportunities in mental health services during the COVID-19 pandemic. General Psychiatry, 33(5). https://doi.org/10.1136/gpsych-2020-100275
Richards, D., & Viganó, N. (2013). Online counseling: A narrative and critical review of the literature. Journal of Clinical Psychology, 69(9), 994–1011. https://doi.org/10.1002/jclp.21974
Shumaker, D., Ortiz, C., & Brenninkmeyer, L. (2011). Revisiting experiential group training in counselor education: A survey of master’s-level programs. The Journal for Specialists in Group Work, 36(2), 111–128. https://doi.org/10.1080/01933922.2011.562742
Steen, S., Vasserman-Stokes, E., & Vannatta, R. (2014). Group cohesion in experiential growth groups. The Journal for Specialists in Group Work, 39(3), 236–256. https://doi.org/10.1080/01933922.2014.924343
Webb, M., Burns, J., & Collin, P. (2008). Providing online support for young people with mental health difficulties: Challenges and opportunities explored. Early Intervention in Psychiatry, 2(2), 108–113. https://doi.org/10.1111/j.1751-7893.2008.00066.x
Weinberg, H. (2020). Online group psychotherapy: Challenges and possibilities during COVID-19—A practice review. Group Dynamics: Theory, Research, and Practice, 24(3), 201–211.
https://doi.org/10.1037/gdn0000140
Wind, T. R., Rijkeboer, M., Andersson, G., & Riper, H. (2020). The COVID-19 pandemic: The ‘black swan’ for mental health care and a turning point for e-health. Internet Interventions, 20.
https://doi.org/10.1016/j.invent.2020.100317
Yalom, I. D., & Leszcz, M. (2005). The theory and practice of group psychotherapy (5th ed.). Basic
Books.
Bilal Urkmez, PhD, LPC, CRC, is an assistant professor at Ohio University. Chanda Pinkney, MA, CT, is a doctoral student at Ohio University. Daniel Bonnah Amparbeng, MEd, NCC, LPC, is a doctoral student at Ohio University. Nanang Gunawan, MA, is a doctoral student at Ohio University. Jennifer Ojiambo Isiko, MA, is a doctoral student at Ohio University. Brandon Tomlinson, MA, NCC, LPC, is a doctoral student at Ohio University. Christine Suniti Bhat, PhD, LPC, LSC, is a professor at Ohio University. Correspondence may be addressed to Bilal Urkmez, Patton Hall 432P, Athens, OH 45701, urkmezbi@ohio.edu.
