Sep 13, 2024 | Volume 14 - Issue 2
Eric M. Brown, Melanie Burgess, Kristy L. Carlisle, Desmond Franklin Davenport, Michelle W. Brasfield
School counselors work closely with students and are often the first point of contact regarding traumatic experiences. It is generally understood that exposure to other individuals’ trauma may lead to a reduction in compassion satisfaction and an increase in secondary traumatic stress, while long-term exposure may result in professional burnout. This study examined the role of school counselors’ (N = 240) own adverse childhood experiences (ACEs) as related to compassion satisfaction, secondary traumatic stress, and burnout. Results indicated that 50% of the professional school counselors in this convenience sample had personal histories of four or more ACEs, which is significantly higher than the general public and passes the threshold for significant risk. Results indicated that the ACEs of school counselors in the present study, as well as some demographic variables, significantly correlated with rates of compassion satisfaction, secondary traumatic stress, and burnout.
Keywords: school counselors, compassion satisfaction, secondary traumatic stress, burnout, adverse childhood experiences
As counselors in PK–12 settings, professional school counselors (PSCs) are uniquely positioned to deliver comprehensive school counseling programs that attend to all students’ academic and social/emotional needs (American School Counselor Association [ASCA], 2019). Providing these comprehensive services may lead to burnout and secondary traumatic stress, which can adversely impact PSCs’ ability to meet students’ academic and social/emotional needs (Mullen & Gutierrez, 2016). Although research has examined various factors that may contribute to burnout such as caseload, lack of administrative support, and tasks unrelated to school counseling (Bardhoshi et al., 2014; Fye, Bergen, & Baltrinic, 2020; Fye, Cook, et al., 2020), few studies have examined whether personal historical factors such as childhood adversity may be related to burnout and secondary traumatic stress. Though self-care is often encouraged in counselor education programs and promoted among practitioners (American Counseling Association [ACA], 2014; Council for the Accreditation of Counseling and Related Educational Programs [CACREP], 2015), we lack knowledge of which PSCs may be more vulnerable to burnout or secondary traumatic stress (Coaston, 2017). Therefore, it is important that we better understand whether a PSC’s own historical experiences of adversity or trauma may make them more susceptible to burnout and secondary traumatic stress, as this may impact their ability to meet students’ needs.
Adverse Childhood Experiences
Adverse childhood experiences (ACEs) encompass 10 maladaptive childhood experiences, including physical abuse, emotional abuse, sexual abuse, substance abuse, physical neglect, emotional neglect, divorce, incarcerated family member, household mental illness, and domestic abuse (Crandall et al., 2020; Felitti et al., 1998). Researchers have found that ACEs have the propensity to shape life beyond childhood, often playing a pivotal role in adult development. Several studies have outlined the dangers of multiple ACEs and negative outcomes in adulthood (Crandall et al., 2020; Felitti et al., 1998). Felitti and colleagues’ (1998) seminal study found that ACEs are common, 55.4% of the population having at least one ACE, and 6.2% reporting four or more ACEs. A growing number of subsequent studies have found that ACEs have a dose–response effect, in which a 1-point increase (using a 10-point scale) in one’s ACE score significantly increases the chance of deleterious mental and physical effects in adulthood (Boullier & Blair, 2018; Felitti et al., 1998; Merrick et al., 2017).
Scholars have found that those with four or more ACEs have a 4- to 12-fold increase in deleterious mental and physical outcomes such as depression, anxiety, addiction, and suicide attempts (Crandall et al., 2020; Crandall et al., 2019; Felitti et al., 1998). Researchers have investigated both the dose–response effect and the pervasive nature of ACEs, suggesting that they may be predictive of long-term mental health impacts. Broadly, adults who were exposed to multiple ACEs were more likely to have three or more mental health disorders such as depression, anxiety, substance addiction, suicidality, and PTSD (Atzl et al., 2019; Fellitti et al., 1998). This is especially detrimental for minoritized persons, as two large U.S. samples of over 200,000 adults have shown that Black and Latine persons, sexually minoritized individuals, and those coming from lower socioeconomic status (SES) had significantly higher levels of ACEs than White persons, heterosexual individuals, and those coming from middle- to upper-class SES backgrounds (Giano et al., 2020; Merrick et al., 2017). Giano et al. (2020) also found that women had significantly higher rates of ACEs as compared to men. Given that childhood experiences may be a critical determinant of mental health in adulthood, individuals with marginalized identities may be at greater risk for negative long-term mental health outcomes (Giano et al., 2020).
ACEs can also impact job function and satisfaction, financial stability, and increased absences (Anda et al., 2004). Of all the helping professions, researchers note that mental health professionals have some of the highest recorded rates of ACEs (Redford, 2016; Thomas, 2016); however, it is unknown how this relates specifically to the school counseling profession. PSCs serve students in a variety of ways to help students fulfill their academic and social/emotional needs (ASCA, 2019). This ability to provide services may be impacted by professional functioning. The ASCA Ethical Standards for School Counselors require PSCs to monitor their emotional and physical health while maintaining wellness to ensure effectiveness (ASCA, 2022). However, researchers note that many counselors do not routinely prioritize their own wellness (Coaston, 2017). Therefore, it is important to understand the effect ACEs have on PSCs to ensure that PSCs can meet student needs.
Burnout
Burnout can occur when a PSC feels depleted of their capacity to perform at a high level due to feelings of incompetence, fatigue, or extreme pressures from their work environment (Mullen & Gutierrez, 2016). Due to high student-to-counselor ratios, diminished counselor self-efficacy, job dissatisfaction, and non-counseling duties, PSCs run the risk of experiencing counselor burnout (Holman et al., 2019; Mullen et al., 2017; Rumsey et al., 2020). Bardhoshi et al. (2014) reported organizational factors such as lack of administrator support, the incapability to meet designated annual goals, and non-counseling duties were associated with burnout, whereas Fye, Bergen, and Baltrinic (2020) found that PSCs with fewer years of counseling experience are more prone to burnout.
Identity factors such as gender, race, and SES have been examined in relation to burnout (Fye et al., 2022); however, these factors have not been evaluated within the context of PSCs’ own personal historical experiences, such as their ACEs. Fye et al. (2022) examined demographic and organizational factors on a multidimensional model of wellness, revealing that there were no large systemic differences in wellness due to gender and race/ethnicity; however, individual elements of the wellness model were significant. One study has shown that male BIPOC counseling students report higher levels of exhaustion compared to female BIPOC counseling students (Basma et al., 2021).
Secondary Traumatic Stress
As students continue to experience traumatic events happening in and outside of school, PSCs are often immersed in the traumatic experiences of their students. This consistent exposure could have an impact on school counselors professionally. Indirect exposure to trauma stemming from students’ trauma, witnessing others’ trauma, or being exposed to graphic material is considered secondary exposure (Fye, Cook, et al., 2020; Padmanabhanunni, 2020). When PSCs attend to student trauma and become fixated, overwhelmed, or burdened, they can experience burnout and secondary traumatic stress (Rumsey et al., 2020). Yet, similar to Fye, Cook, et al.’s (2020) study on burnout, Rumsey et al. (2020) found that years of school counseling experience is negatively correlated with secondary exposure and secondary traumatic stress. School counselors with more years of experience are less likely to be affected by secondary traumatic stress (Rumsey et al., 2020). As PSCs are often the first point of contact regarding PK–12 students’ mental health in the aftermath of a traumatic event, additional research is needed regarding PSCs’ experiences of secondary traumatic stress. Presently, there is a gap in the literature regarding how demographic factors and PSCs’ own ACEs scores predict positive and negative job-related outcomes; therefore, it would be advantageous to learn how ACEs and demographic factors, such as gender, race, or SES, might influence compassion satisfaction, burnout, and secondary traumatic stress.
Compassion Satisfaction
Since the original ACEs study, researchers have turned toward identifying protective factors that may mitigate the effects of harmful childhood experiences. Firstly, compassion satisfaction, while studied limitedly, may serve as a protective factor against burnout and secondary traumatic stress (Stamm, 2010). Compassion satisfaction is defined as a psychological benefit derived from working effectively with clients/students to produce meaningful and positive change in their lives (Stamm, 2010). Researchers note the dearth of literature surrounding gender, race/ethnicity, and PSC wellness, as well as systemic gender and race/ethnicity-related barriers to wellness that exist for PSCs (Bryant & Constantine, 2006; Fye et al., 2022). Currently, the relationship between burnout, secondary traumatic stress, and compassion satisfaction in PSCs with ACEs is unclear.
Brown et al. (2022) conducted a study on ACEs, positive childhood experiences (PCEs), and compassion satisfaction, burnout, and secondary traumatic stress with a diverse national sample of 140 clinical mental health counselors (CMHCs). They found that 43% of participants had four or more ACEs and over 70% had five or more PCEs (Brown et al., 2022). Results from this study found that higher ACEs scores predicted lower compassion satisfaction, but racially minoritized CMHCs, those coming from lower childhood SES, and female CMHCs had higher rates of compassion satisfaction as compared to CMHCs who identified as White, coming from middle- or upper-class SES backgrounds, or male. Furthermore, higher ACEs scores predicted higher rates of burnout, and higher PCEs predicted less burnout (Brown et al., 2022). The relationship between PSCs’ own identity factors (e.g., gender, race/ethnicity, and childhood SES) and childhood experiences on job-related outcomes (e.g., compassion satisfaction, burnout, and secondary traumatic stress) remains unstudied.
The purpose of this study was to examine the effects of early childhood experiences on the professional quality of life of PSCs. We focused on the rates of ACEs and demographic variables of PSCs and their relationship to burnout, secondary traumatic stress, and compassion satisfaction. We aimed to answer the following research questions (RQs): 1) What are the mean rates of ACEs, compassion satisfaction, burnout, and secondary traumatic stress among PSCs? 2) To what extent do PSCs’ ACEs and demographic variables predict compassion satisfaction, burnout, and secondary traumatic stress? and 3) After separating the participants into two groups (PSCs with three or fewer ACEs and those with four or more ACEs), to what extent do PSCs’ ACEs and demographic variables predict compassion satisfaction, burnout, and secondary traumatic stress?
Method
Using a cross-sectional, non-experimental correlational design, we reported descriptive statistics (means; RQ 1) and multiple regression models (predictive relationships; RQs 2 and 3). Using G*Power 3.1.9.6, we calculated an a priori power analysis with a .05 alpha level (Cohen, 1988; 1992), a medium effect size for multiple R2 of .09 (Cohen, 1988), and a power of .80 (Cohen, 1992). This power analysis revealed a target number of participants (N = 138).
Participants
An invitation letter and informed consent document through Qualtrics outlined criteria for school counselors to participate in the study: age 18 and up who work 30 hours or more a week in the field of school counseling. Authors Eric M. Brown, Melanie Burgess, and Kristy L. Carlisle sent Qualtrics invitations to the study through social media, such as X (formerly Twitter), Facebook, and Instagram. We recruited 240 school counselors who met criteria. We could not calculate a response rate because it was impossible to track responses through social media. The majority (62.9%; n = 151) of participants identified as White. The mean age of the participants in the sample was 35 with a range of 23 to 55. Gender was split almost evenly with 50.8% (n = 122) male and 48.3% (n = 116) female. More than half (60%; n = 144) reported a childhood SES of lower or working class, while only 2.9% (n = 7) reported current lower class, and the majority (56.7%; n = 136) reported current middle class. More demographic information is included in Table 1.
Table 1
Participant Demographics
| Characteristic |
% (n) |
| Sex |
|
| Male |
50.8 (122) |
| Female |
48.3 (22) |
| Transgender or Other Gender |
0.8 (2) |
| Race/Ethnicitya |
|
| African American or Black |
7.9 (19) |
| American Indian/Native American |
2.1 (3) |
| Arab American/Middle Eastern |
1.7 (4) |
| Asian/Asian American |
1.7 (4) |
| Asian Indian |
3.3 (8) |
| Hispanic/Latinx |
23.3 (56) |
| Pacific Islander |
0.4 (1) |
| White |
62.9 (151) |
| Childhood Socioeconomic Status |
|
| Lower or Working Class |
60.0 (144) |
| Middle Class |
33.8 (81) |
| Upper Middle/Upper Class |
5.0 (12) |
Note. N = 240.
a For statistical purposes in SPSS, we grouped PSCs as Minoritized and White.
Instrumentation
In addition to a demographic questionnaire, we used instruments with strong psychometrics to measure ACEs, compassion satisfaction, burnout, and secondary traumatic stress.
Adverse Childhood Experiences (ACEs) Questionnaire
Felitti et al. (1998) developed the ACEs Questionnaire to identify instances of abuse and neglect in childhood. The 10-item questionnaire has good test–retest reliability (Dube et al., 2004) and Cronbach’s alpha coefficient of .78 in one study (Ford et al., 2014) and .90 (Mei et al., 2022) in another. Its structural validity passed invariance tests across demographics, exceeding all thresholds (CFI = .986, TLI = .985, RMSEA = .021, SRMR = .066; Mei et al., 2022). Participants self-report instances of ACEs from 0 to 10, with higher scores indicating higher risk for mental and physical ailments and prohibited quality of life. Serious risk is indicated by a score of 4 or higher (Dube et al., 2004).
Professional Quality of Life Scale (ProQOL)
Stamm (2010) created a 30-item questionnaire measuring compassion satisfaction, burnout, and secondary traumatic stress and reported Cronbach’s alpha scores of .88 for compassion satisfaction, .75 for burnout, and .81 for secondary traumatic stress. Heritage et al. (2018) found good item fit and invariance across demographics in demonstration of construct validity. The ProQOL subscales are described as being low (22 or less), moderate (23–41), or high (42 or higher). Positive feelings about helping ability (compassion satisfaction) are measured with scores of 22 or lower indicating problems. Exhaustion, frustration, and depression (burnout) are measured with scores 42 and higher showing impairment at work. Fear and trauma from work (secondary traumatic stress) are measured with scores 42 and higher indicating fear resulting from work.
As a widely used instrument, recent researchers have offered several critiques, including a four-factor structure with burnout as two latent subscales, traditional burnout and emotional well-being (Sprang & Craig, 2015), or interpreting compassion fatigue and compassion satisfaction to be on opposite ends of one spectrum (Geoffrion et al., 2019). Fleckman et al. (2022) used the ProQOL in their sample of PK–12 teachers and did not achieve a sufficient model fit; therefore, they posited that the ProQOL may be more appropriate for human service and mental health professionals compared to educators. Because PSCs are mental health professionals working in education settings, we used the instrument as it was originally designed with the three separate constructs of compassion satisfaction, burnout, and secondary traumatic stress.
Procedure
Our Institutional Review Board approved the current study. Purposeful sample methods included use of a purchased data set of 6,000 counselors’ emails as well as postings on Facebook groups for PSCs. All potential participants received an informed consent document and a Qualtrics link to the three instruments and demographic questionnaire. After data cleaning (i.e., removal of cases with incomplete responses on the instruments) produced 240 usable cases, we computed scores from the instruments and checked assumptions for multiple regression using SPSS 28. Reliability for each instrument showed Cronbach’s alpha score of .86 and an omega score of .87 for the ACEs Questionnaire and .81 Cronbach’s alpha and .82 omega scores for the ProQOL.
Data Analysis and Results
RQ 1 asked for mean scores of ACEs, compassion satisfaction, burnout, and secondary traumatic stress. We calculated a mean ACEs score of 3.68, 95% CI [3.2854, 4.0330] for PSCs, lower than the threshold of 4 and thus just below the range for significant risk. However, 50.42% of participants
(N = 121) reported an ACEs score of 4 or more. Minoritized PSCs had a particularly higher ACEs score (4.9) than White PSCs (2.96). Females had a higher ACEs score (4.14) than males (3.23). Finally, participants with lower childhood SES (low or working) had slightly lower ACEs scores (3.41) than those with higher SES (middle and upper; 3.82 and 5.04). Then we investigated mean scores of PSCs’ compassion satisfaction, burnout, and secondary traumatic stress. For compassion satisfaction, they scored 30.93, 95% CI [30.1798, 31.6785]. When we explored burnout, they scored 27.58, 95% CI [26.2399, 28.2184]. Finally, they showed a mean secondary traumatic stress score of 31.49, 95% CI [30.6610, 32.3223]. PSCs on average have moderate levels of compassion satisfaction, burnout, and secondary traumatic stress.
RQ 2 asked about predictive relationships of ACEs, gender, race/ethnicity, and SES on compassion satisfaction, burnout, and secondary traumatic stress. Three linear regression models, one for each subscale, all produced significant results. Model 1 ran a regression of compassion satisfaction on ACEs, gender, race/ethnicity, and childhood SES, explaining 27.7% of the variance in compassion satisfaction, F(5, 225) = 17.214, p < .001. Gender (β = -0.331), race/ethnicity (β = -0.125), and childhood SES (β = 0.180) significantly predicted compassion satisfaction. ACEs showed nonsignificant results in this model. Being female, being racially minoritized, and having higher childhood SES predicted higher compassion satisfaction (see Table 2).
Table 2
Regression Results: Coefficients (compassion satisfaction, burnout, secondary traumatic stress)
|
β |
Std. Error |
Beta |
T |
Sig |
| Compassion Satisfaction (Constant) |
|
26.298 |
1.682 |
— |
15.631 |
< .001 |
| ACE |
|
0.010 |
0.121 |
.006 |
0.086 |
= .931 |
|
|
|
|
|
|
|
| Gendera |
|
-3.859 |
0.704 |
-.331* |
-5.483 |
< .001* |
| Raceb |
|
-1.514 |
0.746 |
-.125* |
-2.029 |
= .044* |
| Childhood SESc
R2 = .277 (p < .001) |
|
2.149 |
0.711 |
.180* |
-3.021 |
= .003*
|
|
Burnout (Constant) |
|
27.052 |
1.583 |
— |
17.089 |
< .001 |
| ACE |
|
0.176 |
0.114 |
.107 |
1.544 |
= .124 |
|
|
|
|
|
|
|
| Gendera |
|
1.714 |
0.662 |
.169* |
2.588 |
= .010* |
| Raceb |
|
2.940 |
0.702 |
.279* |
4.189 |
< .001* |
Childhood SESc
R2 = .152 (p < .001) |
|
-0.175
|
0.669 |
-.017 |
-0.261 |
= .795
|
|
Secondary Traumatic Stress (Constant) |
|
28.695 |
2.139 |
— |
13.413 |
< .001 |
| ACE |
|
0.166 |
0.154 |
.079 |
1.081 |
= .281 |
|
|
|
|
|
|
|
| Gendera |
|
-2.068 |
0.895 |
-.159* |
-2.311 |
= .022* |
| Raceb |
|
0.502 |
0.948 |
.037 |
0.530 |
= .597 |
| Childhood SESc |
|
2.171 |
0.904 |
.163* |
2.401 |
= .017* |
| R2 = .059 (p = .017) |
|
|
|
|
|
|
Note. ACE = Adverse Childhood Experiences; SES = socioeconomic status.
aFor statistical purposes in SPSS, we grouped gender as female, male, and transgender or other gender.
ᵇFor race, we grouped PSCs as Minoritized and White.
cFor Childhood SES, we grouped PSCs as lower or working class, middle-class, or upper middle/upper class.
Model 2 ran a regression of burnout on ACEs, gender, race/ethnicity, and childhood SES, explaining 15.2% of the variance in compassion satisfaction, F(5, 225) = 8.062, p < .001. Gender (β = 0.169) and race/ethnicity (β = 0.279) significantly predicted burnout. ACEs and childhood SES showed nonsignificant results in this model. Being male and being White predicted higher burnout (see Table 2).
Model 3 ran a regression of secondary traumatic stress on ACEs, gender, race/ethnicity, and childhood SES, explaining 5.9% of the variance in secondary traumatic stress, F(5, 225) = 2.862, p = .017. Only gender (β = -0.159) and childhood SES (β = 0.163) significantly predicted secondary traumatic stress. ACEs and race/ethnicity showed nonsignificant results in this model. Being female and having higher childhood SES predicted higher secondary traumatic stress (see Table 2).
RQ 3 asked about the predictive relationship of ACEs, gender, race/ethnicity, and SES to compassion satisfaction, burnout, and secondary traumatic stress after dividing the sample into two groups: PSCs with three or fewer ACEs (n = 119) and those with four or more ACEs (n = 121). Three linear regression models for each group all produced significant results. Model 1 ran a regression of compassion satisfaction on ACEs, gender, race/ethnicity, and childhood SES. For Group 1 (three or fewer ACEs) the model explained 41.7% of the variance in compassion satisfaction, F(5, 109) 15.599, p < .001. Gender (β = -0.369), and childhood SES (β = 0.194) significantly predicted compassion satisfaction. ACEs and race/ethnicity showed nonsignificant results. Being female and having higher childhood SES predicted higher compassion satisfaction for those with three or fewer ACEs. For Group 2 (four or more ACEs), the model explained 26.6% of the variance in compassion satisfaction, F(5, 110) = 7.975, p < .001. Gender (β = -0.277) and race/ethnicity (β = -0.342) significantly predicted compassion satisfaction. ACEs and childhood SES showed nonsignificant results. Being female and being a racially minoritized person predicted higher compassion satisfaction for those with four or more ACEs (see Table 3).
Table 3
Regression Results: Coefficients (compassion satisfaction)
|
β |
Std. Error |
Beta |
T |
Sig |
| ACE < 4 (Constant) |
20.214 |
2.846 |
— |
7.102 |
< .001 |
| ACE |
-0.070 |
0.545 |
.006 |
-0.012 |
= .897 |
|
|
|
|
|
|
| Gendera |
-5.046 |
1.040 |
-.369* |
-4.852 |
< .001* |
| Raceb |
0.820 |
1.165 |
.194 |
2.307 |
= .524 |
| Childhood SESc
R2 = .417 (p < .001) |
2.688 |
1.165 |
.194* |
2.307 |
= .023*
|
|
ACE > 4 (Constant) |
29.897 |
1.990 |
— |
15.024 |
< .001 |
| ACE |
0.286 |
0.228 |
.106 |
1.253 |
= .213 |
|
|
|
|
|
|
| Gendera |
-2.702 |
0.855 |
-.277* |
-3.161 |
= .002* |
| Raceb |
-3.296 |
0.821 |
-.342* |
-4.017 |
< .001* |
| Childhood SESc
R2 = .266 (p < .001) |
0.443 |
0.866 |
.045 |
0.511 |
= .610
|
Note. ACE = Adverse Childhood Experiences; SES = socioeconomic status.
aFor statistical purposes in SPSS, we grouped gender as female, male, and transgender or other gender.
ᵇFor race, we grouped PSCs as Minoritized and White.
cFor Childhood SES, we grouped PSCs as lower or working class, middle-class, or upper middle/upper class.
Model 2 ran a regression of burnout on ACEs gender, race/ethnicity, and childhood SES. For Group 1 (three or fewer ACEs), the model explained 14.5% of the variance in burnout, F(5, 109) = 3.692, p = .004. ACEs (β = 0.249) significantly predicted burnout. Gender, race/ethnicity, and childhood SES showed nonsignificant results. Having higher ACEs predicted higher burnout. For Group 2 (four or more ACEs), the model explained 35.9% of the variance in burnout, F(5, 110) = 12.336, p < .001. ACEs (β = 0.158), gender (β = 0.277), and race/ethnicity (β = 0.461) significantly predicted burnout. Childhood SES showed nonsignificant results. Having higher ACEs, being male, and being White predicted higher burnout (see Table 4).
Table 4
Regression Results: Coefficients (burnout)
|
β |
Std. Error |
Beta |
T |
Sig |
| ACE < 4 (Constant) |
31.882 |
2.448 |
— |
13.025 |
< .001 |
| ACE |
1.061 |
0.469 |
.249* |
2.264 |
= .026* |
|
|
|
|
|
|
| Gendera |
0.197 |
0.895 |
.020 |
0.220 |
= .827 |
| Raceb |
-0.806 |
1.104 |
-.067 |
-0.730 |
= .467 |
| Childhood SESc
R2 = .145 (p = .004) |
-1.543 |
1.002 |
-.157 |
-1.539 |
= .127
|
|
ACE > 4 (Constant) |
20.916 |
2.085 |
— |
10.103 |
< .001 |
| ACE |
0.471 |
0.237 |
.158* |
1.989 |
= .049* |
|
|
|
|
|
|
| Gendera |
2.999 |
0.887 |
.277* |
3.382 |
= .001* |
| Raceb |
4.939 |
0.852 |
.461* |
5.601 |
< .001* |
| Childhood SESc
R2 = .359 (p < .001) |
0.877 |
0.899 |
.081 |
0.975 |
= .332
|
Note. ACE = Adverse Childhood Experiences; SES = socioeconomic status.
aFor statistical purposes in SPSS, we grouped gender as female, male, and transgender or other gender.
ᵇFor race, we grouped PSCs as Minoritized and White.
cFor Childhood SES, we grouped PSCs as lower or working class, middle-class, or upper middle/upper class.
Model 3 ran a regression of secondary traumatic stress on ACEs, gender, race/ethnicity, and childhood SES. For Group 1 (three or fewer ACEs), the model explained 16.4% of the variance in secondary traumatic stress, F(5, 109) = 4.267, p = .001. Gender (β = -0.303) significantly predicted secondary traumatic stress. ACEs, race/ethnicity, and childhood SES showed nonsignificant results. Being female predicted higher secondary traumatic stress. For Group 2 (four or more ACEs), the model explained 14.5% of the variance in secondary traumatic stress, F(5.110) = 3.745, p = .004. ACEs (β = 0.288) significantly predicted secondary traumatic stress. Gender, race/ethnicity, and childhood SES showed nonsignificant results. Having higher ACEs predicted higher secondary traumatic stress (see Table 5).
Table 5
Regression Results: Coefficients (secondary traumatic stress)
|
β |
Std. Error |
Beta |
T |
Sig |
| ACE < 4 (Constant) |
26.661 |
3.813 |
— |
6.992 |
< .001 |
| ACE |
0.678 |
0.730 |
.101 |
0.929 |
= .355 |
|
|
|
|
|
|
| Gendera |
-4.640 |
1.394 |
-.303* |
-3.330 |
= .001* |
| Raceb |
-1.187 |
1.719 |
-.062 |
-0.691 |
= .491 |
| Childhood SESc
R2 = .164 (p = .001) |
1.068 |
1.561 |
.069 |
0.684 |
= .495
|
|
ACE > 4 (Constant) |
26.189 |
2.378 |
— |
11.015 |
< .001 |
| ACE |
0.858 |
0.273 |
.288* |
3.146 |
= .002* |
|
|
|
|
|
|
| Gendera |
0.268 |
1.021 |
.025 |
0.252 |
= .794 |
| Raceb |
0.916 |
0.980 |
.086 |
0.934 |
= .352 |
| Childhood SESc
R2 = .145 (p = .004) |
1.765 |
1.035 |
.163 |
1.705 |
= .091
|
Note. ACE = Adverse Childhood Experiences; SES = socioeconomic status.
aFor statistical purposes in SPSS, we grouped gender as female, male, and transgender or other gender.
ᵇFor race, we grouped PSCs as Minoritized and White.
cFor Childhood SES, we grouped PSCs as lower or working class, middle-class, or upper middle/upper class.
Discussion
The purpose of this study was to establish the average rates of ACEs, compassion satisfaction, burnout, and secondary traumatic stress in PSCs as well as determine the extent to which PSCs’ own ACEs might predict compassion satisfaction, burnout, and secondary traumatic stress in a U.S. sample of school counselors. This study is unique in that it is the first to explore PSCs’ personal historical predictors and their relationship with job-related variables, both establishing the present rates of ACEs while also examining their potential to be risk factors for PSCs. As professional organizations (ASCA, 2022) and previous literature (Padmanabhanunni, 2020) noted the importance of having PSCs monitor their own wellness to ensure that their own trauma does not influence their work, this study provides a deeper understanding of how personal adversity may influence professional responsibilities.
Minoritized PSCs in our convenience sample had significantly more ACEs than White PSCs, which is congruent with previous studies (Giano et al., 2020; Merrick et al., 2017). While Brown et al. (2022) established racial differences in ACEs for CMHCs for its sample, noting that racially minoritized CMHCs had higher ACEs scores than White CMHCs, in this study we established gender differences, in which female PSCs had higher rates of ACEs compared to male PSCs in the present study’s sample. This extends previous literature, which reported ACEs scores in aggregate for pediatric and adult populations (Boullier & Blair, 2018; Merrick et al., 2017). The most striking finding in our study was that 50.42% of PSCs in our convenience sample had four or more ACEs, which was slightly higher than the 43% that Brown et al. (2022) found in CMHCs, and significantly higher than the approximately 6% found in large U.S. and Austrian samples (Felitti et al., 1998; Riedl et al., 2020), suggesting PSCs may have a personal history that includes more ACEs than the general population. This is consistent with previous studies that have shown that those within mental health fields may tend to have higher rates of childhood adversity and trauma (Brown et al., 2022; McKim & Smith-Adcock, 2014; Thomas, 2016). Yet, despite having higher rates of ACEs, participants in our sample reported moderate levels of compassion satisfaction, burnout, and secondary traumatic stress on average, which is supported by previous research and theory related to these constructs, as PSCs’ stress and job satisfaction are mediated by burnout (Mullen et al., 2017).
Our examination of the compassion satisfaction of PSCs showed that as a whole, those who identified as female, racially minoritized persons, and those who came from higher childhood SES were more likely to experience higher compassion satisfaction. For PSCs having three or fewer ACEs, being female and having higher childhood SES predicted higher compassion satisfaction. For PSCs with four or more ACEs, being female and being racially minoritized predicted higher compassion satisfaction. We found these results, which were also congruent with Brown et al.’s (2022) study with CMHCs, to be notable. It may be expected that coming from a higher childhood SES would result in higher compassion satisfaction as higher SES may be a protective factor. Yet, female and racially minoritized PSCs reporting higher rates of compassion satisfaction despite having higher ACEs scores on average is worth noting, as this builds upon recent findings that BIPOC PSCs have elevated essential wellness
(i.e., meaning and purpose) compared to White PSCs (Fye et al., 2022).
In terms of who is more likely to suffer from burnout, in the total sample, we found that being male and being White predicted higher levels of burnout compared to PSCs who identified as being female and racially minoritized. Previous literature has shown that years of experience is negatively correlated with burnout (Fye, Cook, et al., 2020); however, our data extends this to other demographic variables. For those with fewer than three ACEs, having higher ACEs predicted higher burnout, suggesting that regardless of the ACEs threshold, as the number of ACEs increases, PSCs are more susceptible to burnout. For those with four or more ACEs, having higher rates of ACEs, being male, and being White predicted higher burnout scores. This lends further support to research showing that male counseling graduate students experience heightened levels of exhaustion compared to their female peers (Basma et al., 2021). Considering the higher rates of ACEs in the female and racially minoritized groups, it is notable that these two groups of PSCs experienced burnout less than male and White counselors.
Implications for School Counselors and Counselor Education
The results of the present study contribute to scholarship regarding PSC wellness, highlighting potential identity-related and personal historical predictors of positive and negative job-related outcomes that can impact PSCs and their work with students. These results are noteworthy for practicing school counselors, as well as counselor education programs dedicated to the continued health and longevity of the school counseling profession. Given that our sample was split in half, with PSCs self-reporting above and below the threshold for ACEs, we acknowledge that this may be reflective of those presently working in the field. This split presents two distinct profiles for PSCs, those who have ACEs scores above the threshold of four or more, and those who had ACEs scores of three or fewer. Regardless of profile, any increase in ACEs score puts a PSC at risk for being more susceptible to burnout. In monitoring their wellness, PSCs can reflect on how these risk factors could subsequently impact their professional functioning. Similarly, counselor educators can build reflective practices into their programs to increase pre-service school counselors’ self-awareness regarding their wellness.
PSCs-in-training need to be made aware of the effects of ACEs, not only due to the effects on students, but also the effects they may have on their own professional well-being. Counselor educators and supervisors may advise PSCs-in-training to seek counseling to process their ACEs prior to entering the field fully after graduation. There are several evidence-based counseling modalities that aid in the processing of trauma and acute stress (e.g., EMDR, cognitive process therapy, STAIR Narrative Therapy). Though childhood adversity is not synonymous with trauma, the high rates of ACEs of counselors as evidenced in this study and that of Brown and colleagues (2022) indicate that trauma-informed education may be necessary. The 2024 CACREP standards (CACREP, 2023) say relatively little regarding requirements to educate about trauma, yet it will be important for counselor educators to equip counselors-in-training with knowledge concerning both how to care for traumatized students and also to care for themselves.
Limitations
This study is limited by the nature of survey research such as self-reporting bias and inability to assess all factors that may be influencing the relationship, specifically external factors that previous studies have explored. It is important to note that this study did not examine organizational factors that previous research has shown to be impactful regarding PSCs’ burnout, such as school counselor caseload, PSCs’ supportive relationships (e.g., supervision, mentorship), and the role of school climate (Holman et al., 2019; Mullen et al., 2017; Rumsey et al., 2020). Research has indicated that years of experience (Rumsey et al., 2020) and organizational variables (e.g., non-counseling duties, role ambiguity, supervisor support; Fye, Bergen, & Baltrinic, 2020; Holman et al., 2019) are mitigating factors in PSCs’ experience of secondary traumatic stress. Qualitative research may provide a richer understanding of the phenomena of these outcomes for school counselors. For example, why do PSCs with higher childhood SES have higher levels of secondary traumatic stress?
Splitting the sample in half (PSCs with three or fewer ACEs and PSCs with four or more) produced two groups (n = 119 and n = 121), which individually did not meet our required power analysis (N = 138). While we believe in the potential of the results to shed light on the issue of PSCs’ compassion satisfaction, burnout, and secondary traumatic stress, further research may confirm or elaborate upon the findings. Furthermore, because the sample in the current study did not match previous samples’ reporting rate of reported ACEs scores (e.g., Felitti et al., 1998; Riedl et al., 2020), this study may be replicated on a different sample to contribute to trends in ACEs scores among the PSC population.
A significant limitation to our study included our lack of racially minoritized counselors. As a result, we combined racially minoritized counselors and compared them to White counselors, which limited our ability to distinguish between the unique strengths and struggles that may exist within a given racial group. More research needs to be conducted on counselors from various ethnic and cultural groups both within the U.S. and globally. It would be helpful to know what protective factors may exist for school counselors from racially or ethnically marginalized backgrounds around the world. We believe that the results of this study should not draw attention away from numerous studies that have shown that systemic and organizational factors such as school work environment and school counselor caseload have a significant impact on the professional resilience of PSCs (Bardhoshi et al., 2014; Holman et al., 2019; Mullen et al., 2017; Rumsey et al., 2020). The results of this study do not suggest that the problem of burnout is solely or primarily a result of the personal history of PSCs.
Future Research
Exploring more demographic variables, personal variables, and work characteristics may be beneficial in understanding the relationship between these factors and the presence of compassion satisfaction, burnout, and secondary traumatic stress. In addition to investigating the aforementioned variables, future research may focus on an experimental pre-/post-test design providing a group of school counselors training regarding secondary traumatic stress, burnout, and wellness practices. This may be particularly helpful for those who have experienced four or more ACEs due to the research that childhood trauma is linked to poor health in adulthood (Anda et al., 2002, 2004; Dube et al., 2004; Frewen et al., 2019; Gondek et al., 2021; Merrick et al., 2017; Mwachofi et al., 2020). Future research may also include an examination of PSCs’ rates of ACEs and the types of schools served. For example, scholars may examine whether PSCs with higher ACEs tend to work in schools where the rates of ACEs are higher for children. Furthermore, considering the timing of the current study with data collection occurring prior to the COVID-19 pandemic, assessing the roles of the pandemic, current economic uncertainty, and ongoing racial injustices on these variables would be informative as to how they may be related.
Conclusion
We sought to examine the rates of ACEs of PSCs and learn whether ACEs are correlated with higher rates of compassion satisfaction, burnout, and secondary traumatic stress. We found that an unusually high rate of PSCs in our sample had four or more ACEs and are therefore susceptible to factors such as burnout and secondary traumatic stress. As a result of these findings, we believe that in conjunction with calls for structural change to PSCs’ work environment (e.g., student caseload), greater attention needs to be given to ways that PSCs’ own history may factor into their susceptibility to burnout and secondary traumatic stress.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/ethics
American School Counselor Association. (2019). ASCA national model: A framework for school counseling programs.
American School Counselor Association. (2022). ASCA ethical standards for school counselors.
https://www.schoolcounselor.org/getmedia/44f30280-ffe8-4b41-9ad8-f15909c3d164/EthicalStandards.pdf
Anda, R. F., Fleisher, V. I., Felitti, V. J., Edwards, V. J., Whitfield, C. L., Dube, S. R., & Williamson, D. F. (2004). Childhood abuse, household dysfunction, and indicators of impaired adult worker performance. The Permanente Journal, 8(1), 30–38. https://doi.org/10.7812/tpp/03-089
Anda, R. F., Whitfield, C. L., Felitti, V. J., Chapman, D., Edwards, V. J., Dube, S. R., & Williamson, D. F. (2002). Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatric Services, 53(8), 1001–1009. https://doi.org/10.1176/appi.ps.53.8.1001
Atzl, V. M., Narayan, A. J., Rivera, L. M., & Lieberman, A. F. (2019). Adverse childhood experiences and prenatal mental health: Type of ACEs and age of maltreatment onset. Journal of Family Psychology, 33(3), 304–314. https://pubmed.ncbi.nlm.nih.gov/30802085
Bardhoshi, G., Schweinle, A., & Duncan, K. (2014). Understanding the impact of school factors on school counselor burnout: A mixed-methods study. The Professional Counselor, 4(5), 426–443. https://files.eric.ed.gov/fulltext/EJ1063202.pdf
Basma, D., DeDiego, A. C., & Dafoe, E. (2021). Examining wellness, burnout, and discrimination among BIPOC counseling students. Journal of Multicultural Counseling and Development, 49(2), 74–86. https://doi.org/10.1002/jmcd.12207
Boullier, M., & Blair, M. (2018). Adverse childhood experiences. Pediatrics and Child Health, 28(3), 132–137. https://doi.org/10.1016/j.paed.2017.12.008
Brown, E. M., Carlisle, K. L., Burgess, M., Clark, J., & Hutcheon, A. (2022). Adverse and positive childhood experiences of clinical mental health counselors as predictors of compassion satisfaction, burnout, and secondary traumatic stress. The Professional Counselor, 12(1), 49–64. https://doi.org/10.15241/emb.12.1.49
Bryant, R. M., & Constantine, M. G. (2006). Multiple role balance, job satisfaction, and life satisfaction in women school counselors. Professional School Counseling, 9(4), 265–271. https://doi.org/10.5330/prsc.9.4.31ht45132278x818
Coaston, S. C. (2017). Self-care through self-compassion: A balm for burnout. The Professional Counselor, 7(3), 285–297. https://files.eric.ed.gov/fulltext/EJ1165683.pdf
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Routledge.
Cohen, J. (1992). Statistical power analysis. Current Directions in Psychological Science, 1(3), 98–101. https://doi.org/10.1111/1467-8721.ep10768783
Council for the Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/for-programs/2016-cacrep-standards
Council for the Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Crandall, A., Broadbent, E., Stanfill, M., Magnusson, B. M., Novilla, M. L. B., Hanson, C. L., & Barnes, M. D. (2020). The influence of adverse and advantageous childhood experiences during adolescence on young adult health. Child Abuse & Neglect, 108, e104644. https://doi.org/10.1016/j.chiabu.2020.104644
Crandall, A., Miller, J. R., Cheung, A., Novilla, L. K., Glade, R., Novilla, M. L. B., Magnusson, B. M., Leavitt, B. L., Barnes, M. D., & Hanson, C. L. (2019). ACEs and counter-ACEs: How positive and negative childhood experiences influence adult health. Child Abuse & Neglect, 96, e104089.
https://doi.org/10.1016/j.chiabu.2019.104089
Dube, S. R., Williamson, D. F., Thompson, T., Felitti, V. J., & Anda, R. F. (2004). Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse & Neglect, 28(7), 729–737. https://doi.org/10.1016/j.chiabu.2003.08.009
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/S0749-3797(98)00017-8
Fleckman, J., M., Petrovic, L., Simon, K., Peele, H., Baker, C. N., Overstreet, S., & New Orleans Trauma-Informed Schools Learning Collaborative. (2022). Compassion satisfaction, secondary traumatic stress, and burnout: A mixed methods analysis in a sample of public-school educators working in marginalized communities. School Mental Health, 14, 933–950. https://doi.org/10.1007/s12310-022-09515-4
Ford, D. C., Merrick, M. T., Parks, S. E., Breiding, M. J., Gilbert, L. K., Edwards, V. J., Dhingra, S. S., Barile, J. P., & Thompson, W. W. (2014). Examination of the factorial structure of adverse childhood experiences and recommendations for three subscale scores. Psychology of Violence, 4(4), 432–444.
https://doi.org/10.1037/a0037723
Frewen, P., Zhu, J., & Lanius, R. (2019). Lifetime traumatic stressors and adverse childhood experiences uniquely predict concurrent PTSD, complex PTSD, and dissociative subtype of PTSD symptoms whereas recent adult non-traumatic stressors do not: Results from an online survey study. European Journal of Psychotraumatology, 10(1). https://doi.org/10.1080/20008198.2019.1606625
Fye, H. J., Bergen, S., & Baltrinic, E. R. (2020). Exploring the relationship between school counselors’ perceived ASCA National Model implementation, supervision satisfaction, and burnout. Journal of Counseling & Development, 98(1), 53–62. https://doi.org/10.1002/jcad.12299
Fye, H. J., Cook, R. M., Baltrinic, E. R., & Baylin, A. (2020). Examining individual and organizational factors of school counselor burnout. The Professional Counselor, 10(2), 235–250. https://doi.org/10.15241/hjf.10.2.235
Fye, H. J., Cook, R. M., & Baylin, A. (2022). Exploring individual and organizational predictors of school counselor wellness. Professional School Counseling, 26(1). https://doi.org/10.1177/2156759X211067959
Geoffrion, S., Lamothe, J., Morizot, J., & Giguère, C. (2019). Construct validity of the Professional Quality of Life (ProQOL) scale in a sample of child protection workers. Journal of Traumatic Stress, 32, 566–576. https://doi.org/10.1002/jts.22410
Giano, Z., Wheeler, D. L., & Hubach, R. D. (2020). The frequencies and disparities of adverse childhood experiences in the U.S. BMC Public Health, 20, 1327. https://doi.org/10.1186/s12889-020-09411-z
Gondek, D., Patalay, P., & Lacey, R. E. (2021). Adverse childhood experiences and multiple mental health outcomes through adulthood: A prospective birth cohort study. Social Science & Medicine-Mental Health, 1, 1–5. https://doi.org/10.1016/j.ssmmh.2021.100013
Heritage, B., Rees, C. S., & Hegney, D. G. (2018). The ProQOL-21: A revised version of the Professional Quality of Life (ProQOL) scale based on Rasch analysis. PLoS ONE, 13(2), e0193478. https://doi.org/10.1371/journal.pone.0193478
Holman, L. F., Nelson, J., & Watts, R. (2019). Organizational variables contributing to school counselor burnout: An opportunity for leadership, advocacy, collaboration, and systemic change. The Professional Counselor, 9(2), 126–141. https://doi.org/10.15241/lfh.9.2.126
McKim, L. L., & Smith-Adcock, S. (2014). Trauma counsellors’ quality of life. International Journal for the Advancement of Counselling, 36(1), 58–69. https://psycnet.apa.org/doi/10.1007/s10447-013-9190-z
Mei, X., Li, J., Li, Z.-S., Huang, S., Li, L.-L., Huang, Y.-H., & Lui, J. (2022). Psychometric evaluation of an adverse childhood experiences (ACEs) measurement tool: An equitable assessment or reinforcing biases? Health & Justice, 10, 34. https://doi.org/10.1186/s40352-022-00198-2
Merrick, M. T., Ports, K. A., Ford, D. C., Afifi, T. O., Gershoff, E. T., & Grogan-Kaylor, A. (2017). Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse & Neglect, 69, 10–19. https://doi.org/10.1016%2Fj.chiabu.2017.03.016
Mullen, P. R., Blount, A. J., Lambie, G. W., & Chae, N. (2017). School counselors’ perceived stress, burnout, and job satisfaction. Professional School Counseling, 21(1), 1–10. https://doi.org/10.1177/2156759X18782468
Mullen, P. R., & Gutierrez, D. (2016). Burnout, stress, and direct student services among school counselors. The Professional Counselor, 6(4), 344–359. https://doi.org/10.15241/pm.6.4.344
Mwachofi, A., Imai, S., & Bell, R. A. (2020). Adverse childhood experiences and mental health in adulthood: Evidence from North Carolina. Journal of Affective Disorders, 267, 251–257. https://doi.org/10.1016/j.jad.2020.02.021
Padmanabhanunni, A. (2020). Caring does not always cost: The role of fortitude in the association between personal trauma exposure and professional quality of life among lay trauma counselors. Traumatology, 26(4), 420–426. https://doi.org/10.1037/trm0000262
Redford, J. (Director). (2016). Resilience: The biology of stress and the science of hope [Film]. KPJR Films.
Riedl, D., Lampe, A., Exenberger, S., Nolte, T., Trawöger, I., & Beck, T. (2020). Prevalence of adverse childhood experiences (ACEs) and associated physical and mental health problems amongst hospital patients: Results from a cross-sectional study. General Hospital Psychiatry, 64, 80–86.
https://doi.org/10.1016/j.genhosppsych.2020.03.005
Rumsey, A. D., McCullough, R., & Chang, C. Y. (2020). Understanding the secondary exposure to trauma and professional quality of life of school counselors. Professional School Counseling¸ 24(1). https://doi.org/10.1177/2156759X20973643
Sprang, G., & Craig, C. (2015). An inter-battery exploratory factor analysis of primary and secondary traumatic stress: Determining a best practice approach to assessment. Best Practices in Mental Health, 11(1), 1–13. https://www.proquest.com/docview/1679872314?pq-origsite=gscholar&fromopenview=true&sourcetype=Scholarly%20Journals
Stamm, B. H. (2010). The concise manual for the professional quality of life scale (ProQOL). https://proqol.org/proqol-manual
Thomas, J. T. (2016). Adverse childhood experiences among MSW students. Journal of Teaching in Social Work, 36(3), 235–255. https://doi.org/10.1080/08841233.2016.1182609
Yildirim, İ. (2008). Relationships between burnout, sources of social support and sociodemographic variables. Social Behavior and Personality: An International Journal, 36(5), 603–616. https://doi.org/10.2224/sbp.2008.36.5.603
Eric M. Brown, PhD, LPC, is an assistant professor at the Chobanian & Avedisian School of Medicine at Boston University. Melanie Burgess, PhD, is an assistant professor at the University of Memphis. Kristy L. Carlisle, PhD, is an assistant professor at Old Dominion University. Desmond Franklin Davenport, MS, is a doctoral student at the University of Memphis. Michelle W. Brasfield, PhD, is an assistant professor at the University of Memphis. Correspondence may be addressed to Eric M. Brown, Boston University Chobanian & Avedisian School of Medicine, 72 E. Concord St., Boston, MA 02118, ebrown1@bu.edu.
Feb 7, 2022 | Volume 12 - Issue 1
Eric M. Brown, Kristy L. Carlisle, Melanie Burgess, Jacob Clark, Ariel Hutcheon
Despite an emphasis on self-care to avoid burnout and increase compassion satisfaction within the counseling profession, there is a dearth of research on the developmental experiences of counselors that may increase the likelihood of burnout. We examined the impact of mental health counselors’ (N = 140) experiences of adverse childhood experiences and positive childhood experiences on their present rates of compassion satisfaction, burnout, and secondary traumatic stress. We used a cross-sectional, non-experimental correlational design and reported descriptive statistics as well as results of multiple regression models. Results indicated significant relationships among counselors’ rates of adverse childhood experiences, positive childhood experiences, and compassion satisfaction and burnout. We include implications for the use of both the adverse and positive childhood experiences assessments in the training of counseling students and supervisees.
Keywords: counselors, burnout, childhood experiences, compassion satisfaction, secondary traumatic stress
Over the past 20 years, public health research on adverse childhood experiences (ACEs) and their deleterious effects on physical and mental health has proliferated and branched out to various disciplines (Campbell et al., 2016; Frampton et al., 2018). More recently, the importance of understanding the implications of ACEs for the mental health of clients has entered the counseling literature (Wheeler et al., 2021; Zyromski et al., 2020), yet the ways in which a counselor’s own experience of ACEs may affect their work have not been examined. The absence of such research is significant given the report that mental health workers have the highest rates of ACEs among those in the helping professions (Redford, 2016).
A thorough literature search of PsycINFO, ProQuest, and Google Scholar using terms including, but not limited to, adverse childhood experiences, positive childhood experiences (PCEs), compassion satisfaction (CS), burnout, secondary traumatic stress (STS), and mental health counselors (MHCs), found no peer-reviewed articles that examined the relationship between ACEs or PCEs and counselors’ rates of CS and burnout. Therefore, we chose to examine the effects of early developmental adversity, as well as early protective factors, on the professional quality of life of counselors, as measured by assessing the counselor’s levels of CS, burnout, and STS.
Adverse Childhood Experiences (ACEs)
In the mid-nineties, Felitti et al. (1998), with the support of the Centers for Disease Control, created the ACE Study Questionnaire to study early childhood trauma and deprivation experiences. The ACE Study Questionnaire consists of 10 questions related to whether a person before the age of 18 experienced emotional or physical abuse, substance addiction in the home, parental divorce or separation, a caretaker with mental illness, or emotional deprivation. Each question that is answered in the affirmative results in one “ACE,” with respondents’ scores ranging from 1 to 10. Studies have found that ACEs have a dose-response effect; therefore, every point increase can significantly raise the chance of experiencing negative mental and physical health effects into adulthood (Boullier & Blair, 2018; Campbell et al., 2016; Merrick et al., 2017). Additionally, individuals with four or more ACEs are significantly more likely to suffer from mental illness or substance addiction, be further traumatized as adults, and succumb to an early death (Anda et al., 2007; Metzler et al., 2017).
More recently, researchers have found that Black and Latinx individuals have significantly higher rates of ACEs compared to White individuals (R. D. Lee & Chen, 2017; Merrick et al., 2017; Strompolis et al., 2019). In a study involving 60,598 participants, R. D. Lee and Chen (2017) discovered not only that Black and Hispanic participants had higher rates of ACEs, but also that there was a correlation between ACEs and drinking alcohol heavily. In a sample of 214,517 participants across 23 states in the United States, Merrick et al. (2017) found that racially minoritized individuals, sexual minorities, the unemployed, those with less than a high school education, and those making less than $15,000 a year had significantly higher rates of ACEs than White individuals, heterosexuals, the employed, and those with higher education and income, respectively. Zyromski et al. (2020) noted that the preponderance of ACEs within marginalized communities, such as ethnic minority populations, make ACEs “a social justice issue” (p. 352).
There is scarce research related to the potential impact of ACEs on practitioners and graduate students in helping professions. Thomas (2016) evaluated the rates of ACEs with Master of Social Work (MSW) students, discovering that MSW students were 3.3 times more likely to have four or more ACEs compared to a general sample of university students. Similarly, counselors-in-training are not immune to the effects of childhood adversity; in fact, researchers noted that counselors-in-training may pursue a counseling degree because of personal trauma that drives their aspirations to help others (Conteh et al., 2017). Evans (1997) found that 93% of counselors-in-training reported at least one traumatic experience in their lives, while Conteh et al. (2017) discovered that 95% of counselors-in-training reported between one and eight traumas throughout their lifetime. Considering these results, researchers have suggested that practitioners with a history of trauma may be vulnerable to re-experiencing trauma with clients, which could negatively impact client care and increase the rate of counselor burnout (Conteh et al., 2017; Thomas, 2016). Because the rates of ACEs in practicing MHCs are unknown, it is difficult to determine how ACEs may play a role in impacting CS, burnout, and STS. Furthermore, we lack research on early developmental factors that may contribute to CS, burnout, and STS.
Positive Childhood Experiences (PCEs)
In recent years, childhood development researchers have explored protective factors that may reduce the harmful effects of ACEs. In 2018, Crouch et al. (2019) examined the relationship between two protective factors and their mitigating effects on individuals reporting at least four ACEs. In a sample of 7,079 respondents, the researchers discovered that individuals who reported growing up “with an adult who made them feel safe and protected were less likely to report frequent mental distress or poor health” (Crouch et al., 2019, p. 165). Bethell et al. (2019) found significant correlations between seven positive interpersonal experiences with family and friends and decreased negative effects of ACEs. They also discovered that these factors have a dose-response effect in relation to ACEs so that with each additional PCEs, the harmful effects of ACEs are lessened. The discovery of PCEs has become important in understanding developmentally protective factors that guard from the damaging effects of childhood adversity. Specifically, higher rates of PCEs decrease the chances of mental health disorders of adults, even in those with higher numbers of ACEs (Bethell et al., 2019). An examination of the rates of PCEs in MHCs may provide insight into the well-being of counselors.
Counselor Well-Being
As defined by the American Counseling Association (ACA; 2014), professional counselors work to empower diverse clients to achieve their personal goals. Specifically, MHCs provide client-driven services in agencies, hospitals, and private practices (American Mental Health Counselors Association [AMHCA], 2020). Counselors are trained to cultivate and monitor their own sense of well-being while providing their expertise and leadership to clients and students who have experienced difficulties related to trauma, injustice, abuse, loss, violence, and distress (Council for Accreditation of Counseling and Related Educational Programs [CACREP], 2015; S. M. Lee et al., 2010). Self-care, or the act of cultivating a subjectively defined state of health, is now ubiquitous in counselor education programs and promoted among practitioners (ACA, 2014; CACREP, 2015); however, scholars note that many counselors do not routinely prioritize their own sense of well-being and monitor CS, burnout, and STS (Coaston, 2017). While working closely with clients, practitioners may benefit from reflecting on how their own experiences of personal adversity may influence their work and possibly create a predisposition toward burnout.
Burnout of Counselors
Burnout is defined as the emotional and physical response to chronic stressors in the workplace that lead to substantial negative consequences (Maslach et al., 2001). Scholars have evaluated the external facets of professional counselors’ work that lead to increased burnout, such as time spent on non-counseling duties, lack of on-the-job support, and negative working environments (Thompson et al., 2014); however, internal factors that lead to burnout, such as counselors’ experiences of adversity, remain unstudied. The ubiquitous nature of trauma and its lifelong impact on clients has gained more attention over the past 20 years (Bemak & Chung, 2017; Debellis, 2001; Webber et al., 2017), yet researchers are only beginning to explore the impact of trauma on the lives and professional experiences of counselors (Conteh et al., 2017; McKim & Smith-Adcock, 2014).
Recently, scholars have sought to understand contributing factors that diminish CS and increase burnout (S. M. Lee et al., 2010). In a study of 86 counselors-in-training, Can and Watson (2019) found that a trainee’s degree of resilience and wellness predicted burnout, whereas empathy and supervisory working alliance did not. They did not assess for internal or experiential factors that may have contributed to burnout.
Cook et al. (2021) conducted a qualitative inquiry with 246 novice counselors to explore symptoms of burnout that may not be captured in commonly used assessments. The researchers found several predominant themes, including negative emotional experiences such as anxiety, depression and crying spells; fatigue and tiredness; and unfulfillment in work. Participants also reported physical illness and weight gain or loss, self-perceived ineffectiveness as a counselor, and cognitive impairment. Close to 10% of participants stated that an unhealthy environment contributed to their experience of burnout. Cook et al. did not inquire about any personal history that may have also contributed to symptoms of burnout.
Counselors and STS
Distinct from but related to burnout, STS has been discussed in the literature relating to the well-being of helping professions across numerous disciplines (Branson, 2019; Butler et al., 2017; Molnar et al., 2017). Secondary traumatic stress, also called vicarious trauma, is distinguished from burnout by its symptoms overlapping with post-traumatic stress disorder (PTSD), such as intrusive thoughts, hypervigilance, and avoidance of distressing memories (Ivicic & Motta, 2017; Molnar et al., 2017). In a study of 220 counselors, Lanier and Carney (2019) discovered that 49.5% of counselors experienced symptoms of vicarious trauma, with 85.5% reporting “I thought about my work with clients when I didn’t intend to” and 80.5% confirming that “I felt emotionally numb” (p. 339). Lakioti et al. (2020) found in a study of 163 Greek mental health practitioners that there was a significant positive correlation between burnout and STS (r = .48) and that practitioners who scored high in empathy also scored high in STS (r = .34). In their meta-analysis of 38 studies examining risk factors for STS in therapeutic work, Hensel et al. (2015) found small yet significant effect sizes for “trauma caseload volume (r = .16), caseload frequency (r = .12), caseload ratio (r = .19), and having a personal trauma history (r = .19)” in relation to STS (p. 83).
Research regarding counselors’ own personal trauma is still emerging and a consensus is not yet formed. In a recent study of 90 psychotherapy trainees, Klasen et al. (2019) indicated that secure attachments play a modifying role in limiting the severity of trauma’s expression. McKim and Smith-Adcock (2014) evaluated characteristics of trauma counselors to understand how frequent exposure to indirect trauma might influence burnout and CS, as assessed by the Professional Quality of Life Scale (ProQOL; Stamm, 2010). Their results indicated that higher levels of exposure to client trauma, in combination with less perceived control over the workplace, led to increased burnout (McKim & Smith-Adcock, 2014). Consistent with the ACA Code of Ethics (2014), counselors are expected to self-monitor for impairment issues that could impact clients such as burnout, STS, and the decrease of CS.
Compassion Satisfaction
CS has been studied nominally and may serve as a protective factor against burnout (Coaston, 2017). Compassion satisfaction is defined as a psychological benefit derived from working effectively with clients to produce meaningful and positive change in their lives (McKim & Smith-Adcock, 2014; Stamm, 2010). McKim and Smith-Adcock (2014) discovered that trauma counselors who experienced higher levels of personal trauma also exhibited higher levels of CS or fulfillment derived from their role in the helping alliance. Although these emergent results contradict older literature that demonstrates how counselors with more personal trauma have higher levels of burnout (Baird & Kracen, 2006; Nelson-Gardell & Harris, 2003), presently, the relationship between CS, burnout, and STS in counselors in relation to ACEs is still unclear.
Purpose of Study
The purpose of this study was to examine the effects of early developmental adversity as well as early protective factors on the CS, burnout, and STS of MHCs. Despite the ongoing concern for factors that contribute to the CS, burnout, and STS of counselors, there is a dearth of research on personal experiences that may predispose counselors to burnout (Conteh et al., 2017; McKim & Smith-Adcock, 2014). Considering the detrimental effects of burnout on counselors’ health and well-being, as well as the decrease in empathy that often accompanies burnout, it is imperative that we understand the various causes of burnout (Can & Watson, 2019; Cook et al., 2021; Maslach et al., 2001). This knowledge will assist clinical MHCs, supervisors, and counselor educators in knowing which professional counselors or counselors-in-training may be more susceptible to burnout, STS, and decreased CS.
Research on ACEs within the counseling profession, as proposed by the original Felitti et al. (1998) study, is scant. Zyromski et al. (2020) discovered in their content analysis of ACA and American School Counselor Association journals that only three articles contained any focus on ACEs as defined in the original study. They suggested that by incorporating such a well-defined and researched concept as ACEs, counselors will be better equipped to address the deleterious effects of early adverse experiences. In order to address the gap within the literature, we chose to focus on the rates of ACEs and PCEs of counselors and how they potentially impact CS, burnout, and STS. After conducting an exhaustive search of the literature, we found no other study that examined the potential relationship between counselors’ developmental history using the ACEs and PCEs assessments and their levels of burnout, CS, and STS.
Method
This study entailed a cross-sectional, non-experimental correlational design and reported descriptive statistics, as well as results of multiple regression models. Relationships among MHCs’ ACEs, PCEs, CS, burnout, and STS were examined. Research questions (RQs) guiding the study were: RQ1 (descriptive): What are the mean scores of MHCs for ACEs, PCEs, CS, burnout, and STS constructs? and RQ2 (regression): To what extent do MHCs’ ACEs, PCEs, gender, race, socioeconomic status, and educational level predict CS, burnout, and STS?
Power Analysis
The target number of participants for the study was at least N = 138, based on a power analysis. Researchers used G*Power 3.1.9.6 (Faul et al., 2009) to calculate an a priori power analysis with a .05 alpha level (Cohen, 1988, 1992), a medium effect size for multiple R2 of .09 (Cohen, 1988), and a power of .80 (Cohen, 1992).
Participants
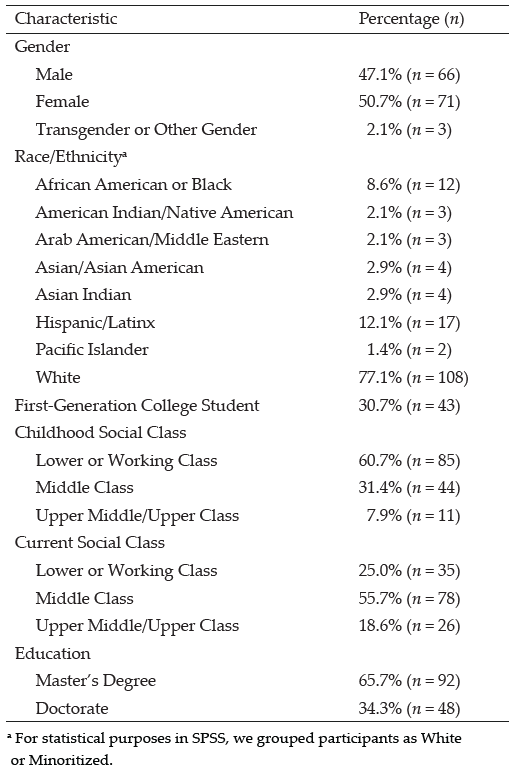
The eligibility criteria for this study were to be a clinical MHC, 18 years or older, who worked 30 hours or more per week in the field of mental health counseling. After soliciting participants nationally through emails, we collected data from 140 participants who met the criteria. MHCs ranged in age from 22 to 72 years old with an average age of 38 (SD = 11.01). Table 1 shows the diverse sample. Slightly more than half (n = 71) identified as female and a little less than half (n = 66) as male. More than three-quarters (n = 108) identified as White. The majority of participants (n = 85) reported their childhood SES as lower or working class, while more than half (n = 78) reported their current social class as middle class. Our sample with predominantly female and predominantly White participants is similar both to known counselor demographics (Norton & Tan, 2019) and to the Felitti et al. (1998) ACEs study.
Instrumentation
Three instruments with good validity and reliability were used to measure ACEs, PCEs, CS, burnout, and STS. We created a demographic questionnaire to collect information on participants’ identities (e.g., race, gender) and childhood backgrounds (e.g., ACEs, PCEs, SES).
Adverse Childhood Experiences (ACE) Study Questionnaire
The ACE Study Questionnaire (Felitti et al., 1998) is a 10-item survey of the most common examples of childhood abuse and neglect. It was developed out of research that connected childhood trauma to subsequent mental and physical ailments. Subsequent research found good test-retest reliability of the measure in an adult population (Dube et al., 2004; Frampton et al., 2018) and a Cronbach’s alpha score of .78 (Ford et al., 2014). The survey produces self-report scores between 0 and 10. The higher the score, the greater the risk for mental and physical health issues as well as decreased quality of life. Consistent research (e.g., Anda et al., 2006; Dube et al., 2004; Hughes et al., 2017) shows that a score of 4 or more indicates serious risk.
Table 1
Participant Demographics
Positive Childhood Experiences (PCE) Questionnaire
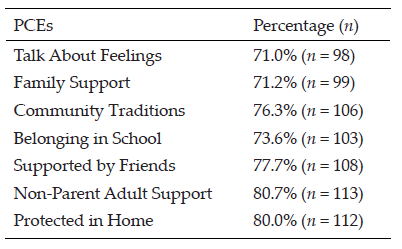
The PCE Questionnaire (Bethell et al., 2019) is a 7-item survey of PCEs (i.e., connection with family, friends, and community) that are statistically predictive of good mental health in adulthood. After accounting for ACEs, higher PCE scores reduce mental health and interpersonal problems later in life. Specifically, scores in the 6 to 7 range are most protective from harmful effects of ACEs, and scores in the 3 to 5 range are moderately protective. A Cronbach’s alpha score of .77 reported in the original 2019 study indicates good reliability.
Professional Quality of Life Scale (ProQOL)
The ProQOL (Stamm, 2010) is a 30-item survey with good construct validity measuring both positive and negative responses to the work of helping professionals. It measures three constructs: CS, which has a Cronbach’s alpha score of .88; burnout, which has a Cronbach’s alpha score of .75; and STS, which has a Cronbach’s alpha score of .81. For CS, or positive feelings about one’s ability to help, a score below 23 indicates problems at work. For burnout, or feelings of exhaustion, frustration, anger, or depression, scores below 23 indicate feeling good about work, while scores above 41 indicate feeling ineffective. For STS, or feelings of fear related to trauma in the workplace, scores above 43 indicate something frightening at work.
Procedure
After IRB approval, we used purposeful sampling methods to recruit participants. We emailed over 6,000 MHCs from a data set purchased from a national data bank. Furthermore, we posted invitations to participate on Facebook groups for MHCs. Invitations included informed consent, as well as a link to a Qualtrics survey containing all instruments and demographic questions. Researchers cleaned all collected data leading to 140 usable cases, computed instruments and transformed variables into usable form, and checked for assumptions for multiple regression. For each instrument, we assessed for reliability with Cronbach’s alpha tests. The ACEs instrument produced a Cronbach’s alpha of .89, the PCEs instrument produced .81, and the ProQOL produced .79, all within the good to excellent range. We used SPSS 28 for all analyses.
Data Analysis and Results
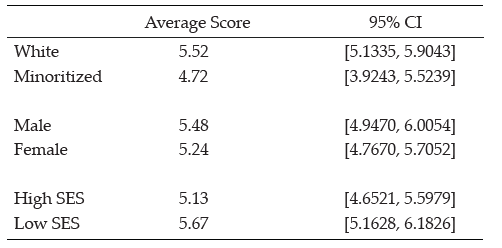
To answer our first research question, we evaluated the mean scores for ACEs, PCEs, CS, burnout, and STS. Respondents in the study had a mean ACE score of 3.42, 95% CI [2.8577, 3.9852], beneath the threshold of 4 and just below the range for significant risk. Their mean PCE score of 5.34, 95% CI [5.0006, 5.6957], was at the upper end of moderately protective. White MHCs had a lower average ACE score and higher average PCE score than minoritized MHCs. Male MHCs had higher average ACE and PCE scores than females, and MHCs with lower childhood SES had lower average ACE scores and higher average PCE scores than those with higher SES (see Tables 2 and 3).
Table 2
Average Adverse Childhood Experience Scores by Demographics
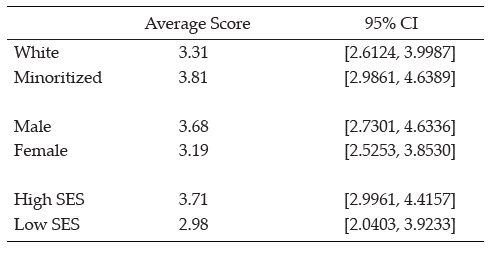
Table 3
Average Positive Childhood Experience Scores by Demographics
Type of scores are shown in percentages for each type of ACE and PCE to show what percentage of MHCs reported an adverse or protective childhood experience (see Tables 4 and 5).
Table 4
Type of Adverse Childhood Experience Score
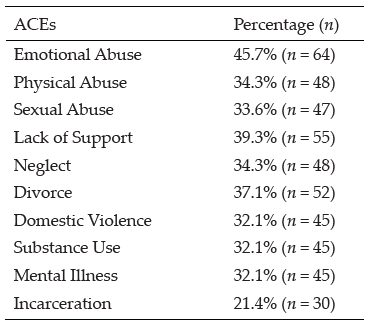
Table 5
Type of Positive Childhood Experience Score
Next, we analyzed MHCs’ scores related to CS, burnout, and STS. Participants’ mean CS score of 31.81, 95% CI [30.6005, 33.0138], was well above the threshold of 23, which indicates a positive level of CS. Their overall mean burnout score of 24.59, 95% CI [23.5793, 25.5921], was well below the threshold of 41, which indicates that the average MHC was not suffering from burnout. Their overall mean STS score of 26.37, 95% CI [25.0346, 27.7083], was also well below the threshold of 43, which indicates the average MHC was not experiencing STS.
For RQ 2, we also tested whether and to what extent MHCs’ ACEs, PCEs, and demographic variables predict CS, burnout, and STS. We ran three linear regression models to assess significant predictors of CS, burnout, and STS. In the first model, a regression of CS on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 40.5% of the variance in CS, F (5, 134) = 17.558, p < .001. Specifically, significant predictors of CS were ACEs (β = −.550), gender (β = −.218), race/ethnicity (β = −.160), and childhood SES (β = −.171). PCEs were nonsignificant in relation to CS. Items negatively related to CS were ACEs (i.e., higher ACE scores predicted lower CS), gender (i.e., being female predicted higher CS), race/ethnicity (i.e., being minoritized predicted higher CS), and childhood SES (i.e., lower levels of SES predicted higher CS; see Table 6).
In the second model, a regression of burnout on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 18.9% of the variance in burnout, F (5, 134) = 6.032, p < .001. Specifically, both ACEs and PCEs were significant predictors of burnout (β = .309 and β= −.197, respectively). Gender, race/ethnicity, and SES were nonsignificant predictors of burnout. ACEs were positively related to burnout (i.e., higher ACE scores indicated higher burnout), and PCEs were negatively related to burnout (i.e., higher PCEs indicated lower burnout; see Table 7).
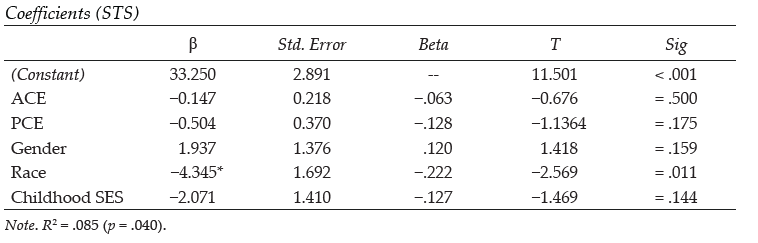
In the third model, a regression of STS on ACEs, PCEs, gender, race/ethnicity, and childhood SES explained a significant 8.5% of variance in STS, F (5, 134) = 2.402, p < .001. Only race/ethnicity was a significant predictor of STS (β= −.222; i.e., being White indicated lower STS). ACEs, PCEs, gender, and SES produced nonsignificant results related to STS (see Table 8).
Table 6
Regression Results Using Compassion Satisfaction as the Criterion
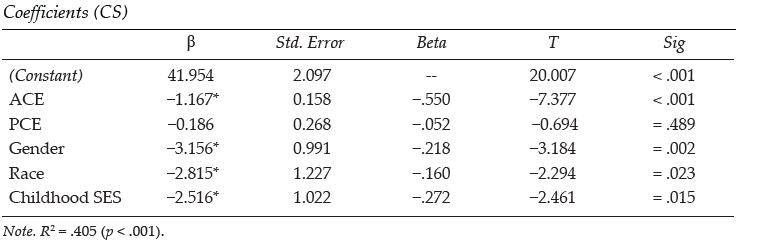
Table 7
Regression Results Using Burnout as the Criterion
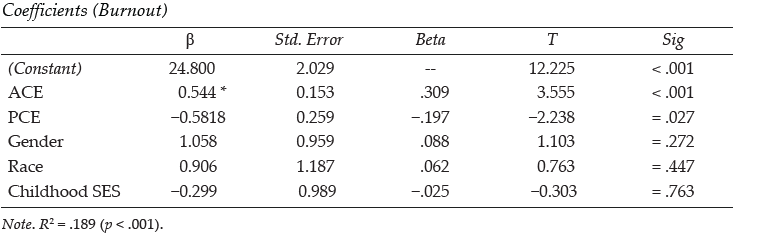
Table 8
Regression Results Using Secondary Traumatic Stress as the Criterion
Discussion
After conducting an exhaustive literature review, we found no other study that examined the relationship between a counselor’s personal history of childhood adversity and protective factors (i.e., ACEs and PCEs) and their professional experience with burnout, STS, and CS. As the counseling profession is placing a greater emphasis on counselors becoming trauma-informed (e.g., Bemak & Chung, 2017; Debellis, 2001; Webber et al., 2017), recent research has examined counselor wellness, burnout, PTSD symptoms, and possible contributing factors (Can & Watson, 2019; Cook et al., 2021; Lanier & Carney, 2019). In line with other studies, we found that some individuals drawn to the profession of counseling are more likely to have had adversity and hardship events in their personal histories (Conteh et al., 2017; McKim & Smith-Adcock, 2014). What is unique in this study is the examination of how both adverse and positive childhood experiences may impact the CS, burnout, and STS of MHCs.
Similar to Thomas (2016), who found that social work students had higher rates of ACEs than the general population, the results of this study indicated that counselor participants had higher rates of ACEs for all 10 experiences than the original Felitti et al. (1998) ACEs study. This was also aligned with Conteh and colleagues (2017), who found that counselors-in-training may have higher rates of trauma than the average population. The results also indicated that almost 43% (n = 60) of MHCs scored four or more ACEs, which placed them at high risk for mental and physical health problems (Boullier & Blair, 2018; Campbell et al., 2016; Merrick et al., 2017). As may be surmised from other studies on the deleterious effects of ACEs on emotional well-being, having higher numbers of ACEs was a significant predictor of burnout. Lower ACEs scores also significantly predicted CS with a high effect size (.55). Similarly, higher PCEs were linked to lower burnout. However, PCEs were not found to significantly predict CS.
We examined the average rates of and relationships between ACEs, PCEs, CS, burnout, and STS in a sample of MHCs. McKim and Smith-Adcock (2014) examined the burnout rates of trauma counselors, finding that counselors with more personal trauma had an increase in CS, perhaps due to personal growth. In contrast, this study found that counselors with more ACEs were more likely to experience less CS. This difference may be a result of this study utilizing the ACE Study Questionnaire (Felitti et al., 1998) whereas McKim and Smith-Adcock (2014) used Stamm’s (2008) Stressful Life Experiences – Short Form to assess for experiences that may have happened in adulthood or to someone outside of the family. Developmentally, painful childhood experiences may be harder to process, which may in turn produce further-reaching negative outcomes. McKim and Smith-Adcock also found that having a sense of control in the workplace and the number of years of experience as a counselor also positively correlated with CS. The results from our analysis indicated that greater attention needs to be given to the traumatic experiences of counselors and how these events may impact professional resilience.
This study may also be the first to examine the demographic factors of counselors, including gender, racial identity, and childhood SES, as potential predictive factors of burnout, STS, and CS. All three demographic variables were found to be predictive of CS, but none were predictive of burnout. The results from our analysis indicated that greater attention needs to be given to the traumatic experiences of counselors and how these events may impact CS, burnout, and STS.
It should be noted that ethnically minoritized counselors had higher rates of CS than their White peers. Given that higher ACEs scores had a negative relationship with CS with a high effect size, and that minoritized counselors had higher average rates of ACEs and lower average rates of PCEs when compared to White counselors, we expected minoritized counselors to experience lower CS. However, the current study found that being a minoritized counselor actually predicted higher CS and lower burnout. It may encourage all counselors to know that greater CS among minoritized counselors indicates that ACEs and PCEs are not determinative of whether a person experiences burnout or satisfaction.
Our findings that female counselors were more likely to have higher CS than their male peers, and that counselors from low-income or working-class SES had higher CS than those from middle and upper classes, are also noteworthy. It is possible that the more collectivist tendencies of minoritized individuals in general, and of female counselors regardless of race, may help foster greater professional resilience or quality of life (Graham et al., 2020; Jordan, 2017). Counselors from lower- or working-class childhood SES may also maintain the collectivist orientation of their upbringing. This proposition is supported by previous research, which indicates that social support is a significant factor that promotes CS in therapists (Ducharme et al., 2008). This may also relate to Crouch et al.’s (2019) finding that the most significant PCE that mitigates the effects of ACEs is having a safe relationship with an adult. These results are further supported by research indicating that secure attachments in adulthood moderate the effect of childhood adversity (Klasen et al., 2019). Despite a limited sample size, Conteh et al. (2017) found that 95% of their sample of 86 counselors-in-training reported having experienced at least one trauma. Although male participants in Conteh’s study were significantly more likely to report more traumas than women—4.93 to 3.46 respectively—women reported more post-traumatic growth than men. Similar to our findings, this may indicate why female counselors were more likely to experience greater CS than male counselors.
Although close to half of our participants (42.9%) met the critical threshold of four ACEs, it is encouraging that the average participant indicated that they were not experiencing burnout. This may be the result of more than half of our participants having five or more PCEs, with PCEs predicting lower burnout. It should also be noted that in this study, ACEs were not significantly correlated with STS, which may be counterintuitive as one may assume that childhood adversity may leave one more susceptible to STS. The strongest findings in the current study, as demonstrated by high effect sizes, are that lower ACE scores predict higher CS and lower burnout. However, the potentially mitigating influence of PCEs only predicted burnout, not CS, with a lower effect size.
Limitations
Threats to internal and external validity are unavoidable in descriptive studies. As such, one limitation of this study is that it focused on descriptive and predictive relationships and therefore does not describe causation. Furthermore, this study used self-report data which may threaten internal validity. Finally, selection bias may be a risk to generalizability. However, the sample in this study is demographically similar to other studies examining the counseling population, so this risk may be minimal.
Implications
Both professional organizations (e.g., ACA, AMHCA) and CACREP can promote counselor wellness by putting policies in place recognizing that individuals going into the counseling profession are likely to have personal histories shaped by adverse experiences. These policies may include a more systemic understanding of wellness strategies for counselors. Self-care is often conceptualized as a personal endeavor achieved outside of work hours, yet policies may be put in place to promote organizational wellness by providing space and emotional support for counselor wellness. For example, far too often grants require caseloads that are too heavy to foster and maintain the well-being of counselors.
The results of this study may also have implications for counselor education. Given that 42% of our participants had four or more ACEs, it may be likely that close to half of students within counseling programs have also suffered from a significant amount of childhood adversity. This may have implications for how we educate counselors to work with trauma. Trauma-informed training generally focuses on the effects of trauma on the life of clients and supports evidence-based practices that aid in recovery, resilience, and improved quality of life. Training that is trauma-attuned may focus more on the counselor’s awareness of how their own history of adversity may shape their professional stamina. This may also lead to more research on trauma-attuned supervision.
Considering the substantial percentage of MHCs who may have four or more ACEs, it is possible that many clinical supervisors have also been greatly affected by their personal histories. Trauma-attuned supervisors will continually reflect on how their past adversity may be influencing the supervisory relationship while also monitoring both their own as well as their supervisee’s levels of burnout and emotional reactivity toward clients.
As Zyromski et al. (2020) posited, the use of ACEs as a construct can provide clarity and focus to the harmful experiences that may impede the healthy development of a client. Likewise, knowledge about ACEs and PCEs can help supervisors and counselor educators train counselors who are at greater risk for burnout. It is important that the privacy of the counselor’s childhood experiences be protected, but trainees can be given the ACE and PCE assessments and told of the risk factors that high ACE and low PCE scores have with regard to burnout and CS. Furthermore, clinical and faculty supervisors can provide assessments for CS and burnout at key points during a trainee’s internship or first few years of postgraduate experience. Counselor educators and supervisors may then help trainees develop a self-care plan that will help to foster CS.
Directions for Future Research
Future studies may further examine the difference between demographic groups based on gender, race, and education in relation to potential protective factors that female and minoritized MHCs have that may decrease the likelihood they will experience burnout. Further research may also examine which ACEs, if any, may have higher correlations with burnout and which PCEs are more likely to serve as protective factors. Furthermore, our results indicate a need to study the CS and burnout of minoritized counselors, female counselors, and those coming from lower childhood SES. Examination of potential cultural and protective factors of these groups may contribute significantly to the literature on burnout prevention.
Given the percentage of counselors who have ACE scores that fall within the range of concern, future research may examine potential differences of counselors who are trauma-attuned and not simply trauma-informed. As stated above, ACEs were not significantly correlated with STS. It may be helpful for future researchers to use different measurements of secondary stress to further assess whether there is any correlation between ACEs and STS.
Conclusion
The purpose of this study was to examine personal factors in the developmental history of clinical MHCs that may influence their likelihood of experiencing professional burnout. This is the first known study we can identify using the ACE Study Questionnaire as a measure to inquire about a potential relationship between the counselors’ developmental adversity and their rates of burnout, CS, and STS. Results indicated that higher ACE scores correlate positively with burnout, and yet PCEs may serve as protective factors. Finally, we found that women and minoritized counselors were more likely to experience compassion satisfaction than males and White counselors. This was true for minoritized counselors despite their having slightly higher rates of ACEs and lower rates of PCEs. We recommend that counselors become aware of how their own experiences of ACEs and PCEs may be impacting their current practice.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf
American Mental Health Counselors Association. (2020). AMHCA code of ethics. https://bit.ly/AMHCAcodeofethics
Anda, R. F., Brown, D. W., Felitti, V. J., Bremner, J. D., Dube, S. R., & Giles, W. H. (2007). Adverse childhood experiences and prescribed psychotropic medications in adults. American Journal of Preventive Medicine, 32(5), 389–394. https://doi.org/10.1016/j.amepre.2007.01.005
Anda, R. F., Felitti, V. J., Bremner, J. D., Walker, J. D., Whitfield, C., Perry, B. D., Dube, S. R., & Giles, W. H. (2006). The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience, 256, 174–186. https://doi.org/10.1007/s00406-005-0624-4
Baird, K., & Kracen, A. C. (2006). Vicarious traumatization and secondary traumatic stress: A research synthesis. Counselling Psychology Quarterly, 19(2), 181–188. https://doi.org/10.1080/09515070600811899
Bemak, F., & Chung, R. C.-Y. (2017). Refugee trauma: Culturally responsive counseling interventions. Journal of Counseling & Development, 95(3), 299–308. https://doi.org/10.1002/jcad.12144
Bethell, C., Jones, J., Gombojav, N., Linkenbach, J., & Sege, R. (2019). Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatrics, 173(11), e193007. https://doi.org/10.1001/jamapediatrics.2019.3007
Boullier, M., & Blair, M. (2018). Adverse childhood experiences. Pediatrics and Child Health, 28(3), 132–137. https://doi.org/10.1016/j.paed.2017.12.008
Branson, D. C. (2019). Vicarious trauma, themes in research, and terminology: A review of literature. Traumatology, 25(1), 2–10. https://doi.org/10.1037/trm0000161
Butler, L. D., Carello, J., & Maguin, E. (2017). Trauma, stress, and self-care in clinical training: Predictors of burnout, decline in health status, secondary traumatic stress symptoms, and compassion satisfaction. Psychological Trauma: Theory, Research, Practice, and Policy, 9(4), 416–424. https://doi.org/10.1037/tra0000187
Campbell, J. A., Walker, R. J., & Egede, L. E. (2016). Associations between adverse childhood experiences, high- risk behaviors, and morbidity in adulthood. American Journal of Preventive Medicine, 50(3), 344–352. https://doi.org/10.1016/j.amepre.2015.07.022
Can, N., & Watson, J. C. (2019). Individual and relational predictors of compassion fatigue among counselors-in-training. The Professional Counselor, 9(4), 285–297. https://doi.org/10.15241/nc.9.4.285
Coaston, S. C. (2017). Self-care through self-compassion: A balm for burnout. The Professional Counselor, 7(3), 285–297. https://doi.org/10.15241/scc.7.3.285
Cohen, J. (1988). Statistical power analysis for the behavioral sciences. (2nd ed.) Routledge.
Cohen, J. (1992). Statistical power analysis. Current Directions in Psychological Science, 1(3), 98–101. https://doi.org/10.1111/1467-8721.ep10768783
Conteh, J. A., Huber, M. J., & Bashir, H. A. (2017). Examining the relationship between traumatic experiences and posttraumatic growth among counselors-in-training. The Practitioner Scholar: Journal of Counseling and Professional Psychology, 6, 32–36.
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in novice professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2018/05/2016-Standards-with-Glossary-5.3.2018.pdf
Crouch, E., Radcliff, E., Strompolis, M., & Srivastav, A. (2019). Safe, stable, and nurtured: Protective factors against poor physical and mental health outcomes following exposure to adverse childhood experiences (ACEs). Journal of Child & Adolescent Trauma, 12, 165–173. https://doi.org/10.1007/s40653-018-0217-9
Debellis, M. D. (2001). Developmental traumatology: the psychobiological development of maltreated children and its implications for research, treatment, and policy. Development and Psychopathology, 13(3), 539–564. https://doi.org/10.1017/s0954579401003078
Dube, S. R., Williamson, D. F., Thompson, T., Felitti, V. J., & Anda, R. F. (2004). Assessing the reliability of retrospective reports of adverse childhood experiences among adult HMO members attending a primary care clinic. Child Abuse & Neglect, 28(7), 729–737. https://doi.org/10.1016/j.chiabu.2003.08.009
Ducharme, L. J., Knudsen, H. K., & Roman, P. M. (2008). Emotional exhaustion and turnover intention in human service occupations: The protective role of coworker support. Sociological Spectrum, 28(1), 81–104. https://doi.org/10.1080/02732170701675268
Evans, J. H. (1997). Trauma and post-traumatic growth among graduate level counselor education students: What is their relative incidence and what relationships do they share? (Order No. 9732654) [Doctoral dissertation, Ohio University]. ProQuest Dissertations & Theses Global.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/brm.41.4.1149
Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., Koss, M. P., & Marks, J. S. (1998). Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine, 14(4), 245–258. https://doi.org/10.1016/s0749-3797(98)00017-8
Ford, D. C., Merrick, M. T., Parks, S. E., Breiding, M. J., Gilbert, L. K., Edwards, V. J., Dhingra, S. S., Barile, J. P., & Thompson, W. W. (2014). Examination of the factorial structure of adverse childhood experiences and recommendations for three subscale scores. Psychology of Violence, 4(4), 432–444. https://doi.org/10.1037/a0037723
Frampton, N. M. A., Poole, J. C., Dobson, K. S., & Pusch, D. (2018). The effects of adult depression on the recollection of adverse childhood experiences. Child Abuse & Neglect, 86, 45–54. https://doi.org/10.1016/j.chiabu.2018.09.006
Graham, C., Chun, Y., Grinstein-Weiss, M., & Roll, S. (2020, June 24). Well-being and mental health amid COVID-19: Differences in resilience across minorities and whites. Brookings. https://www.brookings.edu/research/well-being-and-mental-health-amid-covid-19-differences-in-resilience-across-minorities-and-whites
Hensel, J. M., Ruiz, C., Finney, C., & Dewa, C. S. (2015). Meta-analysis of risk factors for secondary traumatic stress in therapeutic work with trauma victims. Journal of Traumatic Stress, 28(2), 83–91. https://doi.org/10.1002/jts.21998
Hughes, K., Bellis, M. A., Hardcastle, K. A., Sethi, D., Butchart, A., Mikton, C., Jones, L., & Dunne, M. P. (2017). The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. The Lancet Public Health, 2(8), 356–366. https://doi.org/10.1016/S2468-2667(17)30118-4
Ivicic, R., & Motta, R. (2017). Variables associated with secondary traumatic stress among mental health professionals. Traumatology, 23(2), 196–204. https://doi.org/10.1037/trm0000065
Jordan, J. V. (2017). Relational–cultural theory: The power of connection to transform our lives. The Journal of Humanistic Counseling, 56(3), 228–243. https://doi.org/10.1002/johc.12055
Klasen, J., Nolte, T., Möller, H., & Taubner, S. (2019). Aversive kindheitserfahrungen, bindungsrepräsentationen und mentalisierungsfähigkeit von psychotherapeuten in ausbildung [Adverse childhood experiences, attachment representations and mentalizing capacity of psychotherapists in training]. Zeitschrift für Psychosomatische Medizin und Psychotherapie, 65(4), 353–371. https://doi.org/10.13109/zptm.2019.65.4.353
Lakioti, A., Stalikas, A., & Pezirkianidis, C. (2020). The role of personal, professional, and psychological factors in therapists’ resilience. Professional Psychology: Research and Practice, 51(6), 560–570. https://doi.org/10.1037/pro0000306
Lanier, B. A., & Carney, J. S. (2019). Practicing counselors, vicarious trauma, and subthreshold PTSD: Implications for counselor educators. The Professional Counselor, 9(4), 334–346. https://doi.org/10.15241/bal.9.4.334
Lee, R. D., & Chen, J. (2017). Adverse childhood experiences, mental health, and excessive alcohol use: Examination of race/ethnicity and sex differences. Child Abuse & Neglect, 69, 40–48. https://doi.org/10.1016/j.chiabu.2017.04.004
Lee, S. M., Cho, S. H., Kissinger, D., & Ogle, N. T. (2010). A typology of burnout in professional counselors. Journal of Counseling & Development, 88(2), 131–138. https://doi.org/10.1002/j.1556-6678.2010.tb00001.x
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. https://doi.org/10.1146/annurev.psych.52.1.397
McKim, L. L., & Smith-Adcock, S. (2014). Trauma counsellors’ quality of life. International Journal for the Advancement of Counselling, 36, 58–69. https://doi.org/10.1007/s10447-013-9190-z
Merrick, M. T., Ports, K. A., Ford, D. C., Afifi, T. O., Gershoff, E. T., & Grogan-Kaylor, A. (2017). Unpacking the impact of adverse childhood experiences on adult mental health. Child Abuse & Neglect, 69, 10–19. https://doi.org/10.1016/j.chiabu.2017.03.016
Metzler, M., Merrick, M. T., Klevens, J., Ports, K. A., & Ford, D. C. (2017). Adverse childhood experiences and life opportunities: Shifting the narrative. Children and Youth Services Review, 72, 141–149.
Molnar, B. E., Sprang, G., Killian, K. D., Gottfried, R., Emery, V., & Bride, B. E. (2017). Advancing science and practice for vicarious traumatization/secondary traumatic stress: A research agenda. Traumatology, 23(2), 129–142. https://doi.org/10.1037/trm0000122
Nelson-Gardell, D., & Harris, D. (2003). Childhood abuse history, secondary traumatic stress, and child welfare workers. Child Welfare, 82(1), 5–26.
Norton, A. L., & Tan, T. X. (2019). The relationship between licensed mental health counselors’ political ideology and counseling theory preference. American Journal of Orthopsychiatry, 89(1), 86–94. https://doi.org/10.1037/ort0000339
Redford, J. (Director). (2016). Resilience: The biology of stress and the science of hope [Film]. KPJR Films. https://kpjrfilms.co/resilience/
Stamm, B. H. (2008). Design theory and psychometrics of the stressful life experiences screening (SLES). https://bit.ly/StammSLES
Stamm, B. H. (2010). The concise manual for the professional quality of life scale (ProQOL). https://proqol.org/proqol-manual
Strompolis, M., Tucker, W., Crouch, E., & Radcliff, E. (2019). The intersectionality of adverse childhood experiences, race/ethnicity, and income: Implications for policy. Journal of Prevention & Intervention in the Community, 47(4), 310–324. https://doi.org/10.1080/10852352.2019.1617387
Thomas, J. T. (2016). Adverse childhood experiences among MSW students. Journal of Teaching in Social Work, 36(3), 235–255. https://doi.org/10.1080/08841233.2016.1182609
Thompson, I., Amatea, E., & Thompson, E. (2014). Personal and contextual predictors of mental health counselors’ compassion fatigue and burnout. Journal of Mental Health Counseling, 36(1), 58–77. https://doi.org/10.17744/mehc.36.1.p61m73373m4617r3
Webber, J. M., Kitzinger, R., Runte, J. K., Smith, C. M., & Mascari, J. B. (2017). Traumatology trends: A content analysis of three counseling journals from 1994 to 2014. Journal of Counseling & Development, 95(3), 249–259. https://doi.org/10.1002/jcad.12139
Wheeler, N. J., Regal, R. A., Griffith, S.-A. M., & Barden, S. M. (2021). Dyadic influence of adverse childhood experiences: Counseling implications for mental and relational health. Journal of Counseling & Development, 99(1), 24–36. https://doi.org/10.1002/jcad.12351
Zyromski, B., Baker, E., Betters-Bubon, J., Dollarhide, C. T., & Antonides, J. (2020). Adverse childhood experiences: A 20-year content analysis of American Counseling Association and American School Counselor Association journals. Journal of Counseling & Development, 98(4), 351–362. https://doi.org/10.1002/jcad.12338
Eric M. Brown, PhD, LPC, is an assistant professor at DePaul University. Kristy L. Carlisle, PhD, is an assistant professor at Old Dominion University. Melanie Burgess, PhD, is an assistant professor at the University of Memphis. Jacob Clark, BS, is a graduate student at Old Dominion University. Ariel Hutcheon, MA, is a doctoral student at Old Dominion University. Correspondence may be addressed to Eric M. Brown, 2247 N. Halsted St., Chicago, IL 60614, ebrow107@depaul.edu.
Feb 26, 2021 | Volume 11 - Issue 1
Ryan M. Cook, Heather J. Fye, Janelle L. Jones, Eric R. Baltrinic
This study explored the self-reported symptoms of burnout in a sample of 246 novice professional counselors. The authors inductively analyzed 1,205 discrete units using content analysis, yielding 12 categories and related subcategories. Many emergent categories aligned with existing conceptualizations of burnout, while other categories offered new insights into how burnout manifested for novice professional counselors. Informed by these findings, the authors implore counseling scholars to consider, in their conceptualization of counselor burnout, a wide range of burnout symptoms, including those that were frequently endorsed symptoms (e.g., negative emotional experience, fatigue and tiredness, unfulfilled in counseling work) as well as less commonly endorsed symptoms (e.g., negative coping strategies, questions of one’s career choice, psychological distress). Implications for novice professional counselors and supervisors are offered, including a discussion about counselors’ experiences of burnout to ensure they are providing ethical services to their clients.
Keywords: novice professional counselors, burnout, content analysis, conceptualization, symptoms
The term high-touch professions refers to the fields that require professionals to provide ongoing and intense emotional services to clients (Maslach & Leiter, 2016). Although such work can be highly rewarding, these professionals are also at risk for burnout (Bardhoshi et al., 2019). In counseling, professionals are called to provide ongoing and intensive mental health services to clients with trauma histories (Foreman, 2018) and complicated needs (Freadling & Foss-Kelly, 2014). The risk of burnout is exacerbated by the fact that counselors often work in professional environments that are highly demanding and lack resources to serve their clients (Freadling & Foss-Kelly, 2014; Maslach & Leiter, 2016).
The consequences of burnout for counselors and clients can be considerable (Bardhoshi et al., 2019). Potential impacts include a decline in counselors’ self-care, strain of personal relationships, and damage to their overall emotional health (Bardhoshi et al., 2019; Cook et al., 2020; Maslach & Leiter, 2016). Unaddressed burnout might also lead to more serious professional issues like impairment (e.g., substance use, mental illness, personal crisis, or illness; Lawson et al., 2007). Thus, self-monitoring symptoms of burnout is of the utmost importance for counselors to ensure they are providing ethical services to their clients (American Counseling Association [ACA], 2014).
Although burnout is an occupational risk to all counselors (e.g., Bardhoshi et al., 2019; J. Lee et al., 2011; S. M. Lee et al., 2007), novice professional counselors may be especially vulnerable to burnout (Thompson et al., 2014; Westwood et al., 2017; Yang & Hayes, 2020). In the current study, we define novice professional counselors as those who are currently engaged in supervision for licensure in their respective states. Novice professional counselors face a multitude of challenges, such as managing large caseloads, working long hours for low wages, and receiving limited financial support for client care (Freadling & Foss-Kelly, 2014). Even though their professional competencies are still developing (Freadling & Foss-Kelly, 2014; Rønnestad & Skovholt, 2013), these counselors receive minimal direct oversight from a supervisor (Cook & Sackett, 2018). However, to date, no study has exclusively examined novice professional counselors’ descriptions of their experiences of burnout. Input from these counselors is important to understand their specific issues of counselor burnout. Other helping professionals have studied a rich context of practitioners’ burnout experiences. For example, Warren et al. (2012) examined open-ended text responses of people who treated clients with eating disorders and found nuanced contributors to burnout among these providers, including patient descriptors (e.g., personality, engagement in treatment), work-related descriptors (e.g., excessive work hours, inadequate resources), and therapist descriptors (e.g., negative emotional response, self-care). Accordingly, we employed a similar approach to examine the open-ended qualitative responses of 246 novice professional counselors’ self-reported symptoms of burnout.
Conceptual Framework of Burnout
Burnout is defined as “a psychological syndrome emerging as a prolonged response to chronic interpersonal stressors on the job” (Maslach & Leiter, 2016, p. 103). Although there are multiple conceptual frameworks of burnout (e.g., Kristensen et al., 2005; S. M. Lee et al., 2007; Maslach & Jackson, 1981; Shirom & Melamed, 2006; Stamm, 2010), the predominant model used to study burnout is the one developed by Maslach and Jackson (1981), which is measured by the Maslach Burnout Inventory (MBI). Informed by qualitative research, Maslach and Jackson (1981) developed the MBI and conceptualized burnout for all human service professionals as a three-dimensional model consisting of Exhaustion, Depersonalization, and Decreased Personal Accomplishment. Exhaustion is signaled by emotional fatigue, loss of energy, or feeling drained. Depersonalization is characterized by cynicism or negative attitudes toward clients, while Decreased Personal Accomplishment is indicated by a lack of fulfillment in one’s work or feeling ineffective. This conceptualization of burnout has been used to develop several versions of the MBI that are targeted for different professions (e.g., human services, education) and for professionals in general.
Despite the prominence of the MBI model in the burnout literature (Koutsimani et al., 2019), other scholars (e.g., Kristensen et al., 2005; Shirom & Melamed, 2006) have argued for a different conceptualization of burnout, noting several shortcomings of Maslach and Jackson’s (1981) three-dimensional model. Shirom and Melamed (2006) criticized the lack of theoretical framework of the MBI and noted that the factors were derived via factor analysis. They developed the Shirom-Melamed Burnout Measure (Shirom & Melamed, 2006), a measure informed by the Conservation of Resources theory (Hobfoll, 1989), which measures burnout as a depletion of physical, emotional, and cognitive resources using two subscales: Physical Fatigue and Cognitive Weariness.
Kristensen et al. (2005) also criticized the utility of the MBI for numerous reasons, including the lack of theoretical underpinnings of the instrument. Therefore, they developed the Copenhagen Burnout Inventory to capture burnout in professionals across disciplines, most notably human service professionals. From Kristensen et al.’s perspective, the underlying cause of burnout is physical and psychological exhaustion, which occurs across three domains: Personal Burnout (i.e., burnout that is attributable to the person themselves), Work-Related Burnout (i.e., burnout that is attributable to the workplace), and Client-Related Burnout (i.e., burnout that is attributable to their work with clients; Kristensen et al., 2005).
Stamm (2010) conceptualized the construct of professional quality of life for helping professionals, which included three dimensions: Compassion Satisfaction, Burnout, and Secondary Traumatic Stress. Burnout, as theorized by Stamm, is marked by feelings of hopelessness, frustration, and anger, as well as a belief that one’s own work is unhelpful to others, which results in a decline in professional performance. The experience of burnout may also be caused by an overburdening workload or working in an unsupportive environment (Stamm, 2010). Stamm’s model is reflected in the Professional Quality of Life Scale (ProQOL), and this instrument has been used by counseling scholars (e.g., Lambert & Lawson, 2013; Thompson et al., 2014).
A reason for variations in the conceptualization of burnout is that it manifests differently across professions (Maslach & Leiter, 2016). The only counseling-specific model of burnout is conceptualized by S. M. Lee et al. (2007), who developed the Counselor Burnout Inventory (CBI). The CBI was informed by the three dimensions of the MBI and additionally captured the unique work environment of professional counselors and its impact on their personal lives. As such, the CBI poses a five-dimensional model consisting of Exhaustion, Incompetence, Negative Work Environment, Devaluing Client, and Deterioration in Personal Life. In recent years, the CBI has been the instrument predominantly used by researchers to study counselor burnout (e.g., Bardhoshi et al., 2019; Fye et al., 2020; J. Lee et al., 2011).
The Current Study
J. Lee et al. (2011) noted the challenges of studying counselor burnout across diverse samples. They encouraged scholars to examine burnout within homogenous samples of counselors in order to offer more nuanced implications for each group. Prior scholarship (e.g., Freadling & Foss-Kelly, 2014; Thompson et al., 2014) suggested that novice professional counselors may be at risk of burnout, and despite the aforesaid vulnerabilities (e.g., low wages, work with high need clients, professional competency limitations), their self-reported manifestation of burnout symptoms have yet to be studied.
We acknowledge the critical importance of studying burnout in the profession of counseling. However, repeatedly relying on data from similar instruments to measure burnout may fail to capture new or relevant information about the phenomenon (Kristensen et al., 2005) for human service professionals (e.g., Maslach & Jackson, 1981) or professional counselors (e.g., S. M. Lee et al., 2007). Alternatively, content analysis, which focuses on the analysis of open-ended qualitative text (Krippendorff, 2013), may better capture the intricacies of burnout that could not be measured using quantitative instruments (e.g., Warren et al., 2012). Thus, we aimed to address the following research question: What are novice professional counselors’ self-reported symptoms of burnout?
Methodology
Participants
Participants in the current study were 246 postgraduate counselors who were currently receiving supervision for licensure. The age of participants ranged from 23 to 69, averaging 36.91 (SD = 10.15) years. The majority of participants identified as female (n = 195, 79.3%), while 22 participants identified as male (8.9%), four identified as non-binary (1.6%), nine indicated that they did not want to disclose their gender (3.7%), and 16 participants did not respond to the item (6.5%). The participants’ race/ethnicity was reported as follows: White (n = 186; 75.6%), Multiracial (n = 15, 6.1%), Latino/Hispanic (n = 7, 3.3%), Black (n = 6, 2.4%), Asian (n = 6, 2.4%), American Indian or Alaska Native (n = 3, 0.8%), Native Hawaiian or Pacific Islander (n = 1, 0.4%), and Other (n = 7, 3.3%), while 15 participants declined to respond to the item (6.1%). The self-reported race/ethnicity demographic information is comparable to all counselors in the profession, based on DataUSA (2018). The participants’ client caseload ranged from 1 to 650 (M = 41.88; Mdn = 30.0; SD = 53.74). On average, participants had worked as counselors for 5 years (Mdn = 3.3; SD = 4.87). The provided percentages may not total to 100 percent because of rounding and because participants were afforded the option to select more than one response.
Procedure
To answer our research question, we used data from a larger study of novice professional counselor burnout, which included both quantitative and qualitative data. After receiving IRB approval, we obtained lists of names and email addresses of counselors engaged in supervision for licensure from the licensing boards in seven states: Florida, Nebraska, New Mexico, Oregon, Utah, Washington, and Wisconsin. We aimed to recruit a nationally representative sample by purposefully choosing at least one state from each of the ACA regions. In addition, states were selected based upon our ability to obtain a list of counselors who were engaged in supervision for licensure from the respective licensure boards. We were able to survey at least one state from each ACA region except the North Atlantic Region. After removing invalid email addresses, we invited 6,874 potential participants by email to complete an online survey in Qualtrics. This survey was completed by 560 counselors, yielding a response rate of 8.15%. This response rate is consistent with other studies that employed a similar design (Gonzalez et al., 2020). All participants were asked, Do you believe you are currently experiencing symptoms of burnout?, to which participants responded (a) yes or (b) no. Participants who responded yes were then prompted with the direction, Describe your symptoms of burnout, using an open-ended text box, which did not have a character limit. A total of 246 participants (43.9%) responded yes and qualitatively described their symptoms of burnout. On average, participants provided 30.31 words (SD = 36.30). We answered our research question for the current study using only the qualitative data, which aligns with the American Psychological Association’s Journal Article Reporting Standards for Qualitative Research (JARS-Qual; Levitt et al., 2018).
Data Analysis
To answer our research question, we analyzed participants’ open-ended responses using content analysis, which allows for systematic and contextualized review of text data (Krippendorff, 2013). As recommended by Krippendorff (2013), we followed the steps of conducting content analysis: unitizing, sampling, recording, and reducing. We first separated the responses of the 246 participants into discrete units. For example, “feeling exhausted and back pain” was coded as two units: (a) feeling exhausted and (b) back pain. This process resulted in a total of 1,205 discrete units. We reduced our data into categories using an inductive approach, which allowed for new categories to emerge from the data without an a priori theory (Krippendorff, 2013). Although there are multiple conceptualizations of burnout (Maslach & Jackson, 1981; S. M. Lee et al., 2007) that could have informed our analysis (i.e., deductive approach; Krippendorff, 2013), we chose an inductive approach to capture the conceptualization of burnout for novice professional counselors—generating categories based on participants’ explanations of their own symptoms of burnout (Kondracki et al., 2002).
To that end, we developed a codebook by randomly selecting roughly 10% of the discrete units to code as a pretest. Our first and third authors, Ryan M. Cook and Janelle L. Jones, independently reviewed the discrete units, met to discuss and develop categories and corresponding definitions, and coded the pretest data together to enhance reliability. This process yielded a codebook that consisted of 12 categories. Cook and Jones then used the codebook (categories and definitions) to independently code the remaining 90% of the data across three rounds (i.e., 30% increments). After each round, Cook and Jones met to discuss discrepancies and to reach consensus on the final codes. The overall agreement between Cook and Jones was 97% and the interrater reliability was acceptable (Krippendorff α = .80; Krippendorff, 2013), which was calculated using ReCal2 (Freelon, 2013). At the end of the coding process, Cook and Jones reviewed their notes for each code and further organized them into subcategories based on commonalities. The second author, Heather J. Fye, served as the auditor (see Researcher Trustworthiness section) and reviewed the entire coding process.
Researcher Trustworthiness
The research team consisted of four members, three counselor educators and one counselor education and supervision doctoral student. The first and third authors, Cook and Jones, served as coders, while the second author, Fye, served as the auditor and the fourth author, Eric R. Baltrinic, served as a qualitative consultant. The counseling experience of the four authors ranged from 4 to 18 years, and the supervision experience of the authors ranged from 3 to 9 years. Cook, Fye, and Baltrinic are licensed professional counselors and three of the authors are credentialed as either a National Certified Counselor or Approved Clinical Supervisor.
We all acknowledged our personal experiences of burnout to some degree as practicing counselors as well as observing the consequences of burnout to our students and supervisees. All members of the research team had prior experience studying counselor burnout. Although these collective experiences enriched our understanding of the subject matter, we also attempted to bracket our assumptions and biases throughout the research process. To increase the trustworthiness of the coding process, the auditor, Fye, reviewed the codebook, categories and subcategories, discreteness, and two coders’ notes coding process after the pretest and rounds of coding. Fye provided feedback on the category definitions, coding process, and coding decisions during the analysis process.
Results
Using an inductive approach, 12 categories and related subcategories emerged from the 1,205 discrete self-reported symptoms of burnout. Full results, including the 12 categories and subcategories, as well as the frequencies of the categories and subcategories, are presented in the Appendix. We discuss each category in detail and provide illustrative examples of each category using direct participant quotes (Levitt et al., 2018).
Negative Emotional Experience
Of the 1,205 coded units, 218 units (18.1%) were coded into the category negative emotional experience. This category reflected participants’ descriptions of experiencing negative feelings related to their work as counselors (e.g., anxiety, depression, irritability) or unwanted negative emotions (e.g., crying spells). This category included 15 subcategories, and the units coded into these subcategories reflected the participants’ descriptions of a wide range of negative feelings. For example, one participant reported she was “struggling to feel happy,” while another participant shared that she “is carrying a heavy burden [that] no one understands or is aware of.” Some participants also reported crying spells. One participant shared she “has fits of crying,” while another reported she “[cries] in the bathroom at work.”
Fatigue and Tiredness
The category fatigue and tiredness was coded 195 times (16.2%) and included four subcategories. This category captured participants’ descriptions of feeling exhausted, fatigued, or tired. Units coded into this category included the participants’ indications that they feel exhausted, despite sleeping well. For example, one participant described feeling perpetually exhausted—“nothing recharges my batteries”— while another participant stated that her fatigue worsened as the week progressed: “[I feel] more and more exhausted throughout the week.”
Unfulfilled in Counseling Work
The category unfulfilled in counseling work captured the participants’ descriptions of no longer deriving joy at work, dread in going to work or completing work-related responsibilities, or lacking motivation to do work. This category was coded 140 times (11.6%) and subcategories included five subcategories. Avoidance of burdensome administrative responsibilities (e.g., paperwork) were commonly reported units that were captured in this category. For example, a participant noted “putting off doing notes.” Units also captured in this category reflected participants’ self-report of no longer feeling motivated or deriving joy from their work, which ultimately led some participants to stop seeking training. For instance, a participant described herself as “going through the motions at work,” and another added that she was no longer “motivated to improve [her] skills.”
Unhealthy Work Environment
Across all coded units, 128 units (10.6%) were coded in the category unhealthy work environment, which included 15 subcategories. This category captured participants’ descriptions of their work environment that contribute to a counselor experiencing burnout. For example, units captured in this category commonly described participants’ reports of working long hours with few or no breaks throughout the day, and participants feeling pressured to take on additional clients. Some participants described managing large client caseloads or caseloads with “high risk or high needs” clients. The units reflecting participants’ perceived lack of supervisor support were also coded into this category. For example, a participant noted that she was “scared to make a mistake or ask questions about doing my job,” while another participant described a supervisor as not “supportive or trustworthy.” Finally, units that signaled participants’ feelings of being inadequately compensated were coded into this category, such as this participant’s response: “I do not get paid enough for the work that I do.”
Physical Symptoms
The category physical symptoms reflected participants’ descriptions of physical ailments, physical manifestations of burnout (e.g., soreness, pain), physical illnesses, or physical descriptors (e.g., weight gain, weight loss). There were 107 coded units (8.9%) that referenced physical symptoms. The seven subcategories captured in this category reflected a wide range of physical ailments. The most commonly coded units were participants’ descriptions of headaches, illnesses, and weight changes, although some less commonly coded units reflected more serious physical and medical issues. For example, a participant noted, “I have TMJ [temporomandibular joint dysfunction] pain most days from clenching my jaw,” while another participant stated that she “recently began to have debilitating stomach symptoms, which were identified as small ulcerations.”
Negative Impact on Personal Interest or Self-Care
Across all coded units, 101 units (8.4%) were coded in the category negative impact on personal interest or self-care, which included eight subcategories. This category reflected the participants’ descriptions of reduced self-care or inability to engage in self-perceived healthy behaviors (e.g., cannot fall asleep), or lacking personal interest. Units coded in this category most commonly reflected participants’ experience of sleep issues—difficulty either falling asleep or staying asleep. Other units reflected participants’ lessening desire to engage in once-enjoyable activities. For example, one participant noted, “I find myself knowing that I need more time for play, rest, recovery, socializing, and personal interests, but [I am] feeling confused about how to fit that in.” Another participant described her self-care as unconstructive: “It often feels like no amount of self-care is helpful, which makes it more difficult to engage in any self-care.”
Self-Perceived Ineffectiveness as a Counselor
We coded 127 units (10.5%) into the category self-perceived ineffectiveness as a counselor, which included six subcategories. This category reflected the participants’ descriptions of their self-perceived decrease in self-efficacy as a counselor, difficulty in developing or maintaining therapeutic relationships with clients, decreased empathy toward clients, or questioning of their own abilities as counselors (e.g., ability to facilitate change). For example, one participant noted that she did not “have as much empathy for clients as before,” while another participant expressed, “I often feel like clients are being demanding and trying to waste my time.” Units coded into this category also reflected participants’ feelings of inadequacy or struggles to develop a meaningful professional relationship with clients. One participant stated that she must “reach very deep every morning for the presence of mind and spirit to pay close attention and to care deeply for each of these people.” Although less frequently coded, some units described participants’ feelings of compassion satisfaction or self-reported secondary traumatic stress. For example, one participant shared that she was “personally disturbed” by her work.
Cognitive Impairment
Across all coded units, 75 units (6.2%) were coded in the category cognitive impairment, and this category included seven subcategories. The units coded into this category reflected the participants’ descriptions of their cognitive abilities being negatively impacted in different ways. For example, one participant described “feeling like I am in a fog at work,” while another participant shared that she found it “hard to concentrate at work.” Some units captured in this category reflected participants’ rumination of clients or work; for example, one participant noted “shifting my attention to ruminating about dropouts at times, when I need to be present with a [current] client.”
Negative Impact on Personal Relationships
The category negative impact on personal relationships captured 63 coded units (5.2%). Participants’ descriptions of strained relationships as a result of their self-reported burnout were coded into this category, which included three subcategories. For example, one participant described “not [feeling] available for emotional connects with others in my personal life,” while another participant said that they “lashed out sometimes at family members after a stressful day of work.” Another example of the negative impact on personal relationships was a participant’s description of “struggling to find joy at home with my wife and two kids.”
Negative Coping Strategies
We coded 22 units (1.8%) into the category negative coping strategies. This category included five subcategories that captured participants’ descriptions of using unhealthy or negative coping strategies to cope with burnout. Units coded into this category described participants’ use of a variety of negative coping strategies. For example, participants noted an increase in “alcohol consumption” or “smoking.” Relatedly, a participant expressed one of her coping strategies was “the excessive use of Netflix,” while another participant stated that she was “not eating or eating way too much.”
Questioning of One’s Career Choice
Units that reflected participants’ descriptions of the questioning of one’s career choice and potential or planned desire to leave the profession were coded into the category questioning of one’s career choice. There were 21 coded units (1.7%) for this category, which included two subcategories. An example of units coded into this category is a participant who stated that she has “thoughts that I have made a mistake in pursuing this line of work.” Another participant shared feelings of “wanting to quit [my] job.” Some units coded into this category captured participants who were already making plans to leave their jobs or the field. For example, one participant shared that she “recently put in [my] notice at agency,” while another participant stated plans to leave the profession “within one year.”
Psychological Distress
The least number of units were coded into the category psychological distress, which was coded eight times (0.7%) and included two subcategories. This category captured the participants’ discussions of a mental health diagnosis, which they attributed as a symptom of burnout, or suicidal ideations. For example, one participant shared, “I have been diagnosed with major depressive disorder and my job is a factor,” while another participant stated, “I sought therapy for myself and I had to increase my anti-depressant medication.” Finally, two participants endorsed experiencing suicidal ideations at some previous point related to their burnout.
Discussion
The content analysis yielded insights of self-reported burnout symptoms by capturing the phenomenon in novice professional counselors’ own words. Many of the 12 categories that emerged from the data generally aligned with prior conceptualizations of burnout for human service professionals (e.g., Maslach & Jackson, 1981) and counselors (S. M. Lee et al., 2007), while some categories provided novel insights into how burnout manifested in this sample. Further, we observed trends in common self-reported descriptors of burnout for novice professional counselors (negative emotional experiences) to the least commonly endorsed descriptors (psychological distress). We assert that these findings enrich the scholarly understanding of the burnout phenomenon in novice professional counselors.
Discussion of the Conceptual Framework of Burnout
Maslach and Jackson (1981) emphasized in their earlier work that exhaustion and fatigue are core features of burnout, and the category of fatigue and tiredness was the second most commonly coded category (16.2% of all coded units) in our study. Our findings reaffirm exhaustion (or fatigue or tiredness) as a central feature of burnout, and specifically self-reported symptoms of burnout in novice professional counselors. Scholars (e.g., Kristensen et al., 2005; Maslach & Jackson, 1981; Shirom & Melamed, 2006) have conceptualized that the interconnectedness between the emotional, physical, and psychological fatigue of burnout is different. Shirom and Melamed (2006) distinguished emotional, physical, and cognitive resources, while Kristensen et al. (2005) made no distinction between physical and psychological exhaustion. Stamm (2010) also viewed exhaustion as a feature of burnout but did not specify how this exhaustion manifested in human service professionals. In the current study, we chose to distinguish emotional, physical, and cognitive symptoms to best capture the participants’ experiences in their own words (Kondracki et al., 2002). However, we found supportive evidence that novice professional counselors’ burnout included emotional, physical, and cognitive symptoms. Our findings suggest that all three components should be examined to adequately capture this phenomenon.
The category negative emotional experience, which reflected participants’ reports of experiencing negative feelings associated with their work as counselors, was the most commonly endorsed symptom of burnout (18.1% of all coded units). In other models of burnout (e.g., Kristensen et al., 2005; Shirom & Melamed, 2006), feelings or emotions are most often conceptualized as emotional exhaustion, emotional fatigue, or emotional distress. However, the participants in the current study richly described their negative emotional experiences, as captured in the subcategories, with irritability, anxiety, depression, and stress being the most commonly endorsed negative emotions. These findings most closely align with Stamm’s (2010) conceptualization of burnout, which suggested that feelings of hopelessness, anger, frustration, and depression are evidence of burnout. Relatedly, a similar content analysis performed with eating disorder treatment professionals also found that their participants most frequently described emotional distress (61% of their sample, n = 94) as a way in which their worry for clients impacts their personal and professional lives (Warren et al., 2012). Scholars (e.g., Maslach & Leiter, 2016) have postulated about the relationship between workplace burnout and affectional distress (e.g., depression, anxiety, stress); however, such an investigation has yet to be conducted in the profession of counseling. Our findings suggest that novice professional counselors commonly describe their manifestation of burnout as an emotional experience, and as such, this represents a gap in the current conceptualization of counselor burnout.
Two other categories captured in the current study were physical symptoms and cognitive impairment symptoms. Physical symptoms were coded for 8.9% of the 1,205 units coded, while cognitive symptoms were coded for 6.1% of all coded units. In the existing burnout literature (e.g., Maslach & Jackson, 1981; Shirom & Melamed, 2006), physical symptoms of burnout often paralleled or referenced fatigue or exhaustion. For example, in Shirom and Melamed’s (2006) model, physical symptoms were reflective of feeling physically tired. However, in the current study, participants most commonly described their physical symptoms as back pain, illnesses, and headaches. This finding aligns with Kaeding et al. (2017), who found that counseling and clinical psychology trainees attributed their back and neck pain to sitting for long periods of time. We assert that specific physical symptoms may have been inadequately captured by the existing models of burnout.
Relatedly, Shirom and Melamed (2006) suggested that psychological fatigue or psychological manifestations of burnout should be distinguished from those of emotional and physical symptoms, while Kristensen et al. (2005) made no such distinctions. The participants in the current study described numerous cognitive manifestations of burnout, and the most commonly coded subcategories included concentration or focus, rumination, and forgetfulness. These self-reported symptoms closely align with the model of Shirom and Melamed, which describes psychological fatigue as an inability to think clearly and difficulty processing one’s own thoughts. Further, Kristensen et al. described one symptom of personal burnout as being at risk of becoming ill. However, no items of cognitive impairment or worsening cognitive abilities are included in the CBI. Informed by our findings, descriptors of cognitive impairment should be considered to understand burnout in novice professional counselors.
Two of the three dimensions of burnout as conceptualized by Maslach and Jackson (1981) were Depersonalization (i.e., cynicism or negative attitudes toward clients) and Decreased Personal Accomplishment (i.e., diminished fulfillment in one’s work or feeling ineffective in their work). These two dimensions are similar to Stamm’s (2010) conceptualization of burnout for human service professionals, which included the features of perceiving that one’s own work is unhelpful and no longer enjoying the work. In the current study, two of the categories that emerged closely aligned with these conceptualizations of burnout: unfulfilled in counseling work (11.6% of all coded units) and self-perceived ineffectiveness as a counselor (10.5% of all coded units). Collectively, these two categories and related subcategories provide rich descriptors of how novice professional counselors experience their own depersonalization and diminished personal accomplishment (Maslach & Jackson, 1981).
Our findings align with qualitative studies of novice professional counselors’ experiences (e.g., Freadling & Foss-Kelly, 2014; Rønnestad & Skovholt, 2013). For example, Freadling and Foss-Kelly (2014) found that novice professional counselors sometimes question if their graduate training adequately prepared them for their current positions. As such, questioning of one’s clinical abilities by counselors at this developmental level was also a common experience by participants in our study (Freadling & Foss-Kelly, 2014).
Our findings were consistent with the counselor-specific burnout model in which S. M. Lee et al. (2007) noted the importance of including the unique work environment of counselors and related impact on their personal life. Our findings support the burnout conceptualization with novice professional counselors. For example, participants in the current study described an unhealthy work environment (10.6% of all coded units). The most commonly coded subcategories included unsupportive employer or supervisor, frustrated with system, burdened by documentation, and overburdened by amount of work or multiple roles.
In terms of the impact of counseling work on their personal lives (S. M. Lee et al., 2007), evidence of this dimension was captured in the current study in two categories: negative impact on personal interest or self-care and negative impact on personal relationships. There is a high degree of interconnectedness between burnout and self-care (Maslach & Leiter, 2016; Warren et al., 2012). Thus, it is unsurprising that participants reported a decrease in their self-care; however, some of the specific self-care behaviors that are affected as a result of novice professional counselors experiencing burnout are less understood. In the current study, the most commonly coded subcategory was difficulty falling asleep or staying asleep, followed by lack of interest in hobbies, poor work/life balance, and general decrease in self-care. As defined in the CBI, lack of time for personal interest and poor work/life balance are both indicators of Deterioration in Personal Life. While sleep onset and maintenance issues are associated with burnout (Yang & Hayes, 2020), counselors’ experiences with sleep issues appears to be a novel finding. Another indicator of deterioration in counselors’ personal lives as theorized by S. M. Lee et al. was a lack of time to spend with friends, which was also observed in our study. Relatedly, some participants indicated that they isolated from their social support system. Other participants described strained personal relationships (i.e., conflict in personal relationships, poor emotional connection with others), which are unique findings.
Counselor Burnout Versus Counselor Impairment
Although uncommonly reported, some participants in the current study described using negative coping strategies (1.8% of all coded units) and psychological distress (0.7% of all coded units) as evidence of their self-reported burnout. Examples of negative coping strategies reported by participants included increased substance use (e.g., alcohol, caffeine, nicotine) and overeating or skipping meals, while examples of psychological distress included having received a psychological diagnosis and experiencing increased suicidal ideations, which participants attributed to burnout. These self-reported symptoms of burnout align more closely with the definition of counselor impairment (Lawson et al., 2007) as opposed to the definition of counselor burnout. Our findings are significant for two reasons. First, any study of counselor burnout that utilized one of the commonly used instruments of burnout (e.g., CBI, MBI) would have failed to capture these participants’ experiences. Second, these findings suggest that a small number of counselors may be experiencing significant impairment in their personal and professional lives, despite being early in their professional careers. Finally, another infrequently coded category was questioning of one’s career choice (1.7% of all coded units). Coded units in this category indicated that some counselors were wondering if counseling was a good professional fit for them, while others expressed their intention to seek employment in another profession. It is possible that prolonged disengagement from one’s professional work (i.e., cynicism; Maslach & Jackson, 1981) could result in counselors wanting to explore other career options.
Limitations
There are limitations of this study which we must address. The purpose of content analysis is not to generalize findings, so our findings may only reflect the experiences of burnout for the participants in the current study. Their experiences may be influenced by developmental levels, experiences in their specific state, or other reasons that we did not capture.
Another limitation is our response rate of 8.15%. A possible reason for our low response rate is self-selection bias—counselors who were currently experiencing burnout responded to the open-ended items as opposed to those who were not feeling burnout. Future research is needed to see how burnout presents in larger or different populations of counselors. It might also be important to study the career-sustaining behaviors and work environments of those counselors who did not endorse burnout. The final limitation is that this study was descriptive in nature. Future researchers are encouraged to explore the factors that may predict burnout while also considering the novel findings generated from this study.
Implications
Our findings offer implications for counseling researchers, counselors, and supervisors. Although many of the findings from the current study align with prior research, there appears to be some degree of discrepancy between how burnout is conceptualized by scholars and how novice professional counselors describe symptoms of burnout. We implore scholars to further examine the specific descriptors of burnout as reported by participants in this study and to see if the frequency of these self-reported symptoms can be duplicated. Specifically, scholars should focus on the emotional experience of novice professional counselors, fatigue and tiredness, and feeling unfulfilled in their work, which were the most commonly reported symptoms. It also seems critically important to explore the less commonly reported descriptors of burnout, like negative coping strategies, questioning of one’s career choice, and psychological distress. Each of these categories could signal counselor impairment and would have been otherwise missed by scholars who relied exclusively on existing Likert-type burnout inventories.
Novice professional counselors sometimes experience self-doubt about their counseling skills or even the profession (Rønnestad & Skovholt, 2013), given the difficult work conditions in which these counselors practice (e.g., low wages, long hours; Freadling & Foss-Kelly, 2014). Novice professional counselors should understand that experiences of burnout appear to be commonly occurring. The illumination of these descriptors may encourage other novice professional counselors to seek guidance from their supervisors on how best to manage these feelings. For those novice professional counselors who are experiencing more serious personal and professional issues associated with burnout (e.g., using negative coping strategies and psychological distress), they should consider whether they are presently able to provide counseling services to clients and seek consultation from a supervisor (ACA, 2014).
Our findings have implications for supervisors. For example, supervisors should be willing to openly discuss burnout with their supervisees. Our results can provide supervisors with descriptors that capture novice professional counselors’ experiences of burnout. Supervisors might find it helpful to disclose some of their own experiences of burnout (or mitigating burnout) with their supervisees, which can normalize the supervisees’ experiences (Knox et al., 2011). Finally, to the extent that supervisors are able, they should protect novice professional counselors from experiencing an unhealthy work environment or potentially harmful behaviors. For example, in response to supervisees’ self-reported symptoms of burnout, supervisors could limit caseloads, allow counselors time to complete documentation, or mandate regular breaks throughout the day (including lunchtime).
Conclusion
There are many novice professional counselors experiencing a wide range of symptoms of burnout. A career in counseling can be rewarding, but prolonged burnout can lead to both personal and professional consequences, as evidenced by the findings from this study. Counselors must attend to their own symptoms of burnout in order to provide quality care to their clients and lead a fulfilling personal life. Supervisors and educators can support these counselors by discussing the experiences of burnout, and future scholars can better understand the experiences of counselor burnout by studying the phenomenon using definitions and symptoms in the words of counselors as opposed to generic definitions.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
Bardhoshi, G., Erford, B. T., & Jang, H. (2019). Psychometric synthesis of the Counselor Burnout Inventory. Journal of Counseling & Development, 97(2), 195–208. https://doi.org/10.1002/jcad.12250
Cook, R. M., Fye, H. J., & Wind, S. A. (2020). An examination of the Counselor Burnout Inventory using item response theory in early career post-master’s counselors. Measurement and Evaluation in Counseling and Development. Advance online publication. https://doi.org/10.1080/07481756.2020.1827439
Cook, R. M., & Sackett, C. R. (2018). Exploration of prelicensed counselors’ experiences prioritizing information for clinical supervision. Journal of Counseling & Development, 96(4), 449–460. https://doi.org/10.1002/jcad.12226
DataUSA. (2018). Counselors. https://datausa.io/profile/soc/counselors#demographics
Foreman, T. (2018). Wellness, exposure to trauma, and vicarious traumatization: A pilot study. Journal of Mental Health Counseling, 40(2), 142–155. https://doi.org/10.17744/mehc.40.2.04
Freadling, A. H., & Foss-Kelly, L. L. (2014). New counselors’ experiences of community health centers. Counselor Education and Supervision, 53(3), 219–232. https://doi.org/10.1002/j.1556-6978.2014.00059.x
Freelon, D. (2013). ReCal OIR: Ordinal, interval, and ratio intercoder reliability as a web service. International Journal of Internet Science, 8(1), 10–16.
Fye, H. J., Cook, R. M., Baltrinic, E. R., & Baylin, A. (2020). Examining individual and organizational factors of school counselor burnout. The Professional Counselor, 10(2), 235–250. https://doi.org/10.15241/hjf.10.2.235
Gonzalez, E., Sperandio, K. R., Mullen, P. R., & Tuazon, V. E. (2020). Development and initial testing of the Multidimensional Cultural Humility Scale. Measurement and Evaluation in Counseling and Development, 54(1), 56–70. https://doi.org/10.1080/07481756.2020.1745648
Hobfoll, S. E. (1989). Conservation of resources: A new attempt at conceptualizing stress. American Psychologist, 44(3), 513–524. https://doi.org/10.1037/0003-066X.44.3.513
Kaeding, A., Sougleris, C., Reid, C., van Vreeswijk, M. F., Hayes, C., Dorrian, J., & Simpson, S. (2017). Professional burnout, early maladaptive schemas, and physical health in clinical and counselling psychology trainees. Journal of Clinical Psychology, 73(12), 1782–1796. https://doi.org/10.1002/jclp.22485
Knox, S., Edwards, L. M., Hess, S. A., & Hill, C. E. (2011). Supervisor self-disclosure: Supervisees’ experiences and perspectives. Psychotherapy, 48(4), 336–341. https://doi.org/10.1037/a0022067
Kondracki, N. L., Wellman, N. S., & Amundson, D. R. (2002). Content analysis: Review of methods and their applications in nutrition education. Journal of Nutrition Education and Behavior, 34(4), 224–230.
https://doi.org/10.1016/S1499-4046(06)60097-3
Koutsimani, P., Montgomery, A., & Georganta, K. (2019). The relationship between burnout, depression, and anxiety: A systemic review and meta-analysis. Frontiers in Psychology, 10(284), 1–19.
https://doi.org/10.3389/fpsyg.2019.00284
Krippendorff, K. (2013). Content analysis: An introduction to its methodology (3rd ed.). SAGE.
Kristensen, T. S., Hannerz, H., Høgh, A., & Borg, V. (2005). The Copenhagen Psychosocial Questionnaire: A tool for the assessment and improvement of the psychosocial work environment. Scandinavian Journal of Work, Environment & Health, 31(6), 438–449. https://doi.org/10.5271/sjweh.948
Lambert, S. F., & Lawson, G. (2013). Resilience of professional counselors following Hurricanes Katrina and Rita. Journal of Counseling & Development, 91(3), 261–268. https://doi.org/10.1002/j.1556-6676.2013.00094.x
Lawson, G., Venart, E., Hazler, R. J., & Kottler, J. A. (2007). Toward a culture of counselor wellness. Journal of Humanistic Counseling, 46(1), 5–19. https://doi.org/10.1002/j.2161-1939.2007.tb00022.x
Lee, J., Lim, N., Yang, E., & Lee, S. M. (2011). Antecedents and consequences of three dimensions of burnout in psychotherapists: A meta-analysis. Professional Psychology: Research and Practice, 42(3), 252–258.
https://doi.org/10.1037/a0023319
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., Ogle, N. T., Powell, M. L., Quinn, J. J., Wallace, S. L., & Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40(3), 142–154.
https://doi.org/10.1080/07481756.2007.11909811
Levitt, H. M., Bamberg, M., Creswell, J. W., Frost, D. M., Josselson, R., & Suárez-Orozco, C. (2018). Journal article reporting standards for qualitative primary, qualitative meta-analytic, and mixed methods research in psychology: The APA Publication and Communications Board task force report. American Psychologist, 73(1), 26–46. https://doi.org/10.1037/amp0000151
Maslach, C., & Jackson, S. E. (1981). The measurement of experienced burnout. Journal of Organizational Behavior, 2(2), 99–113. https://doi.org/10.1002/job.4030020205
Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. https://doi.org/10.1002/wps.20311
Rønnestad, M. H., & Skovholt, T. M. (2013). The developing practitioner: Growth and stagnation of therapists and counselors. Routledge.
Shirom, A., & Melamed, S. (2006). A comparison of the construct validity of two burnout measures in two groups of professionals. International Journal of Stress Management, 13(2), 176–200.
https://doi.org/10.1037/1072-5245.13.2.176
Stamm, B. H. (2010). Professional Quality of Life: Compassion Satisfaction and Fatigue Version 5 (ProQOL).
http://www.proqol.org.
Thompson, I., Amatea, E., & Thompson, E. (2014). Personal and contextual predictors of mental health counselors’ compassion fatigue and burnout. Journal of Mental Health Counseling, 36(1), 58–77.
https://doi.org/10.17744/mehc.36.1.p61m73373m4617r3
Warren, C. S., Schafer, K. J., Crowley, M. E., & Olivardia, R. (2012). A qualitative analysis of job burnout in eating disorder treatment providers. Eating Disorders, 20(3), 175–195.
https://doi.org/10.1080/10640266.2012.668476
Westwood, S., Morison, L., Allt, J., & Holmes, N. (2017). Predictors of emotional exhaustion, disengagement and burnout among improving access to psychological therapies (IAPT) practitioners. Journal of Mental Health, 26(2), 172–179. https://doi.org/10.1080/09638237.2016.1276540
Yang, Y., & Hayes, J. A. (2020). Causes and consequences of burnout among mental health professionals: A practice-oriented review of recent empirical literature. Psychotherapy, 57(3), 426–463.
https://doi.org/10.1037/pst0000317
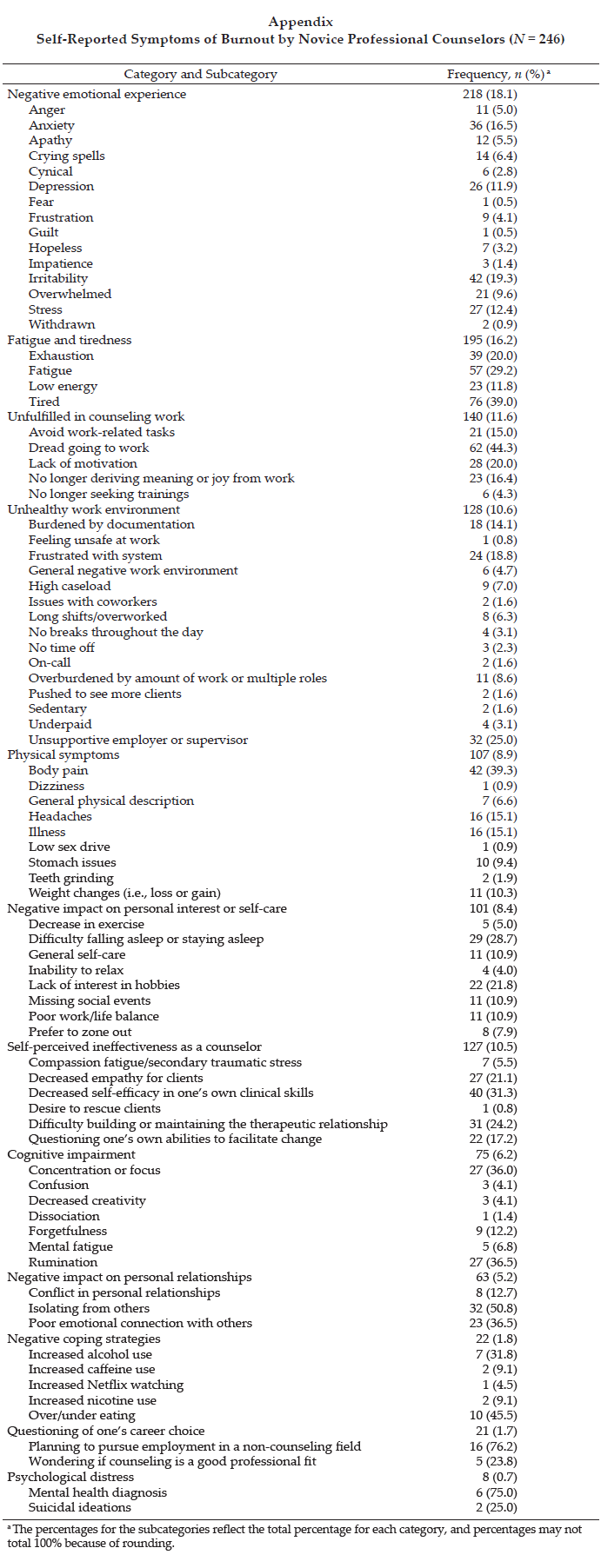
Ryan M. Cook, PhD, ACS, LPC, is an assistant professor at the University of Alabama. Heather J. Fye, PhD, NCC, LPC, is an assistant professor at the University of Alabama. Janelle L. Jones, MS, NCC, is a doctoral student at the University of Alabama. Eric R. Baltrinic, PhD, LPCC-S (OH), is an assistant professor at the University of Alabama. Correspondence may be addressed to Ryan M. Cook, 310A Graves Hall, Box 870231, Tuscaloosa, AL 35475, rmcook@ua.edu.
Apr 29, 2020 | Volume 10 - Issue 2
Heather J. Fye, Ryan M. Cook, Eric R. Baltrinic, Andrea Baylin
Burnout is a statistically significant phenomenon for school counselors, correlated with various individual and organizational factors, which have been studied independently. Therefore, we investigated both individual and organizational factors of burnout conceptualized as a multidimensional phenomenon with 227 school counselors. Multidimensional burnout was measured by the five subscales of the Counselor Burnout Inventory, which included Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life. Using hierarchal regression analyses, we found individual and organizational factors accounted for 66.6% of the variance explained in Negative Work Environment, 38.3% of the variance explained in Deterioration in Personal Life, 36.7% of the variance explained in Incompetence, 35.1% of the variance explained in Exhaustion, and 14.0% of the variance explained in Devaluing Clients. We discuss implications of the findings for school counselors and supervisors. Identifying the multidimensions of burnout and its correlates, addressing self-care and professional vitality goals, communicating defined school counselor roles, providing mentoring opportunities, and increasing advocacy skills may help alleviate burnout.
Keywords: stress, burnout, job satisfaction, coping processes, school counselors
In addition to providing counseling services, school counselors are charged with performing multiple non-counseling duties in their schools (Bardhoshi et al., 2014). These multiple and competing demands place them at risk for experiencing burnout (Mullen et al., 2018). Accordingly, it is important to identify factors that contribute to burnout to promote school counselors’ psychological well-being (Kim & Lambie, 2018), which in turn reinforces school counselors’ ability to support students’ well-being (Holman et al., 2019).
Burnout is a workplace-specific complex construct characterized by feelings of exhaustion, cynicism, and detachment, and a lack of accomplishment and effectiveness (Maslach & Leiter, 2017). Others have conceptualized counselor burnout as a multidimensional construct, featuring the interaction between the individual and work environment (Lee et al., 2007). Given the complex, multidimensional, and interactional nature of burnout, the Counselor Burnout Inventory (CBI) was developed to measure the construct with five subscales: Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life (Lee et al., 2007). Specific to school counselors, Kim and Lambie (2018) suggested that burnout occurs to varying degrees across individual and organizational factors. Individual factors include perceived stress (Fye et al., 2018; Mullen et al., 2018; Mullen & Gutierrez, 2016; Wilkerson, 2009; Wilkerson & Bellini, 2006) and coping processes (Fye et al., 2018; Wilkerson, 2009; Wilkerson & Bellini, 2006). Organizational factors include perceived job satisfaction (Baggerly & Osborn, 2006; Bryant & Constantine, 2006; Mullen et al., 2018) and role stress (Bardhoshi et al., 2014; Coll & Freeman, 1997; Culbreth et al., 2005).
Researchers of school counselor burnout have studied individual and organizational factors of this phenomenon using a unidimensional structure such as the CBI scale score (Mullen et al., 2018). Other researchers (e.g., Bardhoshi et al., 2014; Moyer, 2011) studied organizational factors, including caseload and administrative (non-counseling) duties, within the multidimensional structure of the CBI (Lee et al., 2007). However, researchers have not yet comprehensively studied these known individual and organizational factors within the context of a multidimensional structure of school counselor burnout. For example, Mullen et al. (2018) investigated the relationships between perceived stress, perceived job satisfaction, and school counselor burnout. However, they did not examine organizational factors such as role stress (e.g., clerical duties), which are also significant to understanding school counselor burnout (Bardhoshi et al., 2014). Thus, we sought to extend the research findings by examining several individual factors (i.e., perceived stress, coping processes) and organizational factors (i.e., perceived job satisfaction, role stress) within a multidimensional structure of school counselor burnout.
Individual Factors
Individual factors related to school counselor burnout include psychological constructs and demographic factors (Kim & Lambie, 2018). The two psychological constructs included in the current study were perceived stress (Mullen et al., 2018) and coping processes (Fye et al., 2018). Researchers have previously found contradictory results for the relationship between years of experience and school counselor burnout (Mullen et al., 2018; Wilkerson, 2009). Therefore, the factor of years of experience was included in the current study.
Perceived Stress
Perceived stress is theorized as an individual’s ability to appraise a threatening or challenging event in relation to the availability of coping resources (Lazarus & Folkman, 1984). To that end, a transactional model of stress and coping suggests that stress is a response that occurs when perceived demands exceed one’s coping abilities. For school counselors, perceived stress may occur regularly because of various factors, including non-counseling duties, excessive paperwork and administrative duties, and work overload (Bardhoshi et al., 2014).
Researchers have described a positive relationship between stress and burnout among school counselors (Mullen et al., 2018; Mullen & Gutierrez, 2016). Specifically, higher levels of stress and burnout were related to lower levels of job satisfaction and delivery of direct student services (Mullen et al., 2018; Mullen & Gutierrez, 2016). Others have reported increased emotional responses alongside increased burnout (Wilkerson & Bellini, 2006). For example, school counselors who attempted to deal with stress emotionally may be at greater risk for developing symptoms of burnout including emotional exhaustion, depersonalization, and lower levels of personal accomplishment (Wilkerson, 2009). Additionally, school counselors reported higher levels of emotional exhaustion than other mental health professionals, which can negatively impact their delivery of school counseling services (Bardhoshi et al., 2014). The correlation between stress and burnout further highlights the importance of assessing the components of stress and the ways school counselors are coping with these factors.
Coping Processes
Coping processes are defined as the cognitive and behavioral processes used to manage stressful situations (Folkman & Moskowitz, 2004). There are several coping processes, including problem-focused coping, active-emotional coping, and avoidant-emotional coping (Folkman & Lazarus, 1985). For example, problem-focused coping is defined as an action-oriented approach to stress in which one believes the stressors are controllable by personal action (Lazarus, 1993). Active-emotional coping is an adaptive response to unmanageable stressors and avoidant-emotional coping is described as a maladaptive response to those stressors (Folkman & Lazarus, 1985).
Among school counselors, Fye et al. (2018) studied the relationship between perfectionism, burnout, stress, and coping. These authors found that maladaptive perfectionists engaged more frequently in avoidant-emotional coping and relatedly experienced higher levels of burnout. Moreover, adaptive perfectionists experienced less stress and burnout and reported higher levels of problem-focused coping. Overall, for school counseling professionals, emotional-focused coping is positively related to burnout (Wilkerson, 2009). Given these findings, it is imperative for school counselors to be aware of their coping processes, including the degree to which they are affecting their levels of stress and burnout (Wilkerson, 2009).
Organizational Factors
In addition to individual factors such as stress and coping (Fye et al., 2018; Mullen et al., 2018; Wilkerson, 2009), school counseling researchers noted several organizational factors as contributing to school counselor burnout (Holman et al., 2019; Kim & Lambie, 2018). Accordingly, researchers in the current study examined organizational factors, including perceived job satisfaction and role stress (i.e., role ambiguity, role incongruity, and role conflict; Culbreth et al., 2005). Additionally, because previous researchers found a relationship between the organizational factor of school district (e.g., urban setting) and burnout (Butler & Constantine, 2005), this variable was included in the present study.
Perceived Job Satisfaction
Perceived job satisfaction refers to the degree of affective or attitudinal reactions one experiences relative to their job (Spector, 1985). Understanding the extent of school counselors’ perceived job satisfaction may be one way to buffer the effects of stress and burnout. This is because, according to Bryant and Constantine (2006), job satisfaction predicted life satisfaction for school counselors.
Perceived job satisfaction and its relationship with stress and burnout have received increased attention in the school counseling literature (Mullen et al., 2018). Among the contributing factors, higher levels of role balance and increased perceived job satisfaction resulted in greater overall life satisfaction (Bryant & Constantine, 2006). Higher perceived job satisfaction has been aligned with school counselors engaging in appropriate roles. For example, Baggerly and Osborn (2006) found that school counselors who frequently performed roles aligned with comprehensive school counseling programs were more satisfied and more committed to their careers. Similarly, higher perceived job satisfaction was directly related to the school counselor’s ability to provide direct student services within their schools (Kolodinsky et al., 2009). Conversely, school counselors who did not intend to return to their jobs the following year reported higher levels of demand and stress because of non-counseling duties, such as excessive paperwork and administrative disruptions (McCarthy et al., 2010). As a result, those who are not satisfied are at risk for disengagement (Mullen et al., 2018), while school counselors who are satisfied with their jobs may have increased student connections (Kolodinsky et al., 2009).
Role Stress
Role stress refers to the levels of role incongruity, role conflict, and role ambiguity experienced by school counselors (Culbreth et al., 2005; Freeman & Coll, 1997). Role incongruity may occur when there are structural conflicts, including inadequate resources for school counselors and engagement in ineffective tasks (Freeman & Coll, 1997). Several authors noted that inappropriate or non-counseling duties contributed to burnout, including excessive paperwork, administrative duties, and testing coordinator roles (Bardhoshi et al., 2014; Moyer, 2011, Wilkerson, 2009). Moyer (2011) found that school counselors who engaged in increased non-counseling duties also had increased feelings of exhaustion and incompetence, had decreased feelings toward work environment, and were less likely to show empathy toward students. Furthermore, school counselors who were assigned inappropriate roles reported higher levels of frustration and resentment toward the school system. Overall, authors emphasized the importance of educating administrators on the appropriate and inappropriate roles for school counselors to decrease burnout (Bardhoshi et al, 2014; Cervoni & DeLucia-Waack, 2011; Moyer, 2011).
Role conflict occurs when school counselors experience multiple external demands from different stakeholders (Holman et al., 2019). Role conflict examples for school counselors include: (a) whether school counselors should focus on the education goals or mental health needs of students first (Paisley & McMahon, 2001) and (b) whether a school counselor should engage in an actual role given by an administration or supervisor (e.g., testing coordinator) or preferred role (e.g., classroom guidance activity; Wilkerson, 2009). As such, school counselors can feel overwhelmed and often engage in inappropriate duties, according to the American School Counselor Association (ASCA) National Model (2019). In turn, school counselors experience stress and burnout (Mullen et al., 2018).
Role ambiguity is the discrepancy between actual and preferred counseling duties (Scarborough & Culbreth, 2008). Role ambiguity has been linked to burnout because of school counselors’ stress from lacking an understanding of their professional roles and being misinformed about the realities of the job (Culbreth et al., 2005). For example, school counselors face challenges of navigating mixed messages about role expectations across stakeholders (Coll & Freeman, 1997). This confusion may lead to school counselors experiencing role ambiguity (Scarborough & Culbreth, 2008). When school counselors interact with stakeholders who have conflicting ideas about their roles, it creates stress. It is especially difficult for school counselors when stakeholders’ conceptualization of their roles clashes with what school counselors learned during graduate training (Culbreth et al., 2005). When school counselors are assigned duties that conflict with their own understandings of their roles, they are not able to operate in alignment with their professional mandates (Holman et al., 2019). Overall, school counselors experiencing role ambiguity also report higher levels of stress, both of which have been linked to burnout (Kim & Lambie, 2018).
Purpose of the Present Study
Despite prevalence in the school counseling burnout literature regarding individual and organizational factors of burnout, we were unable to locate a study that holistically researched these variables. To align our findings with a theoretical understanding of school counselor burnout, we examined these phenomena as a multidimensional construct. Additionally, we controlled for years of experience (Mullen et al., 2018; Wilkerson, 2009; Wilkerson & Bellini, 2006) and school district (Butler & Constantine, 2005). Therefore, we answered the research question: What is the relationship between individual (i.e., perceived job stress, problem-focused coping, avoidant-emotional coping, and active-emotional coping) and organizational (i.e., perceived job satisfaction, role incongruity, role conflict, and role ambiguity) factors after controlling for years of experience and school district, with the subscales of school counselor burnout: (1) Exhaustion, (2) Incompetence, (3) Negative Work Environment, (4) Devaluing Clients, and (5) Deterioration in Personal Life?
Method
Sample
A total of 227 school counselors participated in the study. Ages ranged from 26 to 69 (M = 46.21; SD = 10.26; four declined to answer). The sex of participants included females (n = 166, 73.1%) and males (n = 61, 26.9%). The race and ethnicity of participants included White (n = 185, 81.5%), African American/Black (n = 20, 8.8%), Hispanic (n = 7, 3.1%), Asian/Pacific Islander (n = 3, 1.3%), American Indian/Alaskan Native (n = 1, 0.4%), and Biracial/Multiracial (n = 9, 4.0%), and two participants (0.9%) declined to answer. Participants held a master’s degree in school counseling (n = 175, 77.1%), a PhD or EdD (n = 33, 14.5%), or a master’s degree in another counseling or mental health specialty area (n = 19, 8.4%). The years of experience ranged from 2 to 41 years (M = 13.68, SD = 7.49). Participants reported working in suburban (n = 97, 42.7%), rural (n = 76, 33.5%), and urban (n = 54, 23.8%) settings. Regarding level of practice, participants worked in an elementary school (i.e., grades K–6; n = 80, 35.2%), middle school (i.e., grades 7–8; n = 14, 6.2%), high school (i.e., grades 9–12; n = 59, 26.0%), or multiple grade levels (e.g., K–8, K–12, etc.; n = 74, 32.6%). A power analysis was completed in G*Power 3.1 before beginning the study (Faul et al., 2009). The necessary sample size was determined to be at least 200, with a power of .80, assuming a moderate effect size of .15 in the multiple regression analyses, and with an error probability or alpha of .05 (J. Cohen, 1992).
Procedures
Institutional Review Board approval was obtained prior to beginning the study. The first author sent recruitment emails to 4,000 school counselors who were professional members of the ASCA online membership directory. Specifically, approximately 20% of school counselors in each of the 50 states and District of Columbia were chosen from the membership directory to receive the recruitment emails. The emails included a brief introduction to the study and an anonymous link that took potential participants to the online survey portal in Qualtrics. Potential participants first reviewed the informed consent. Once they consented to the survey, participants completed the demographics questionnaire and instruments. A convenience sample was obtained based upon voluntary responses to the survey (Dimitrov, 2009).
Instruments
The first author constructed a brief demographics survey to gather information about the participants (e.g., age, sex, race and ethnicity, degree, and years of experience) and their work environment (e.g., school district, grade level). The Perceived Stress Scale (PSS; S. Cohen et al., 1983) and Brief COPE (Carver, 1997) were used to measure individual factors. The Job Satisfaction Survey (JSS; Spector, 1985) and Role Questionnaire (RQ; Rizzo et al., 1970) were used to measure organizational factors. The CBI (Lee et al., 2007) was used to measure the dimensions of school counselor burnout.
Perceived Stress Scale (PSS)
The PSS (S. Cohen et al., 1983) is a 14-item inventory designed to measure an individual’s perceived stress within the past month. In the present study, we used the PSS-4, which is a subset of items from the original 14-item scale. The PSS was normed on a large sample of individuals from across the United States (S. Cohen et al., 1983). Participants responded to a 5-point Likert-type scale ranging from 0 (never) to 4 (very often). Scores on the PSS-4 ranged from 0 to 20. An example question of the PSS-4 is: “In the past month, how often have you felt difficulties were piling up so high that you could not overcome them?” The PSS-4 was determined to be a suitable brief measure of stress perceptions, based upon adequate factor structure and predictive validity (S. Cohen & Williamson, 1988). Reliability has been upheld (e.g., S. Cohen & Williamson, 1988) with test-retest reliability at .85 after 2 days (S. Cohen et al., 1983). For the present study, the internal consistency reliability was calculated at α = .76. Correlations between the perceived stress total score and CBI subscales ranged from r = .19 to .55.
Brief COPE
The Brief COPE (Carver, 1997) is a 28-item inventory designed to measure coping responses or processes and includes 14 subscales. We followed previous researchers’ (e.g., Deatherage et al., 2014) grouping of the 14 subscales into three coping processes (i.e., problem-focused, active-emotional, and avoidant-emotional). Therefore, problem-focused coping contained the Active Coping, Planning, Instrumental Support, and Religion subscales. Active-emotional coping contained the Venting, Positive Reframing, Humor, Acceptance, and Emotional Support subscales. Avoidant-emotional coping contained the Self-Distraction, Denial, Behavioral Disengagement, and Self-Blame subscales. For the present study, the items pertaining to participants’ alcohol and illegal drug use as coping responses were omitted because of their sensitive nature. Therefore, 26 items were included in the present study. The inventory uses a 4-point Likert-type scale with scores ranging from 0 (I haven’t been doing this at all) to 3 (I’ve been doing this a lot). A sample item on the Brief COPE is “I’ve been turning to work or other activities to take my mind off things.” Construct validity has been upheld with the three coping processes (e.g., Deatherage et al., 2014). Test-retest reliability for the three subscale groups has been upheld over a year timespan (Cooper et al., 2008). For the present study, the internal consistency reliability was calculated for problem-focused coping at α = .84, avoidant-emotional coping at α = .70, and active-emotional coping at α = .81. Correlations between problem-focused coping and the CBI subscales ranged from r = .00 to .13, correlations between avoidant-emotional coping and CBI subscales ranged from r = .20 to .48, and correlations between active-emotional coping and CBI subscales ranged from r = .01 to .16.
Job Satisfaction Survey (JSS)
The JSS (Spector, 1985) is a 36-item inventory intended to measure an individual’s perceived job satisfaction or attitudes and aspects of the job. The JSS contains nine subscales: Pay, Promotion, Supervision, Fringe Benefits, Contingent Rewards, Operating Procedures, Coworkers, Nature of Work, and Communication. The inventory uses a 6-point Likert-type scale with scores ranging from 1 (disagree very much) to 6 (agree very much). Total scores range from 36 to 216 with the higher the score, the higher job satisfaction experienced. An example item on the JSS is “My job is enjoyable” (Spector, 1985, p. 711). The JSS was constructed for, and normed on, social service, education, and mental health professionals (Spector, 1985, 2011). Spector (1985) established convergent validity with the Job Descriptive Index (Smith et al., 1969), and produced scores ranging from .61 to .80. Strong reliability has been established for the JSS, including a Cronbach coefficient alpha of .91 for all factors combined, and at 18 months, the test-retest reliability score was .71 (Spector, 1985). For the present study, the internal consistency reliability was calculated for the total scores at α = .91. Correlations between the perceived job satisfaction total score and CBI subscales ranged from r = -.13 to -.75.
Role Questionnaire (RQ)
The RQ (Rizzo et al., 1970) is a 14-item inventory designed to measure the level of role conflict and role ambiguity an individual has about a job. The RQ has been factor analyzed with school counselors (Freeman & Coll, 1997) and found to have three distinct factors (i.e., role incongruity, role conflict, and role ambiguity). The inventory uses a 7-point Likert-type scale with scores ranging from 1 (very false) to 7 (very true). Role incongruity refers to conflicts with the structure of the system and allocation of resources (Freeman & Coll, 1997). The role incongruity factor comprises items 1–4. Total scores range from 8 to 32, with the higher the score, the higher role incongruity experienced. A sample item for role incongruity is “I receive an assignment without adequate resources and materials to execute it.” Role conflict refers to the contradictory requests of work expectations with varying groups (Freeman & Coll, 1997). The role conflict factor comprises items 5–8. The higher the score, the higher role conflict experienced, which can range from 8 to 32. A sample item for role conflict is “I receive incompatible requests from two or more people.” The role ambiguity factor, which measures a lack of clarity on the job, is negatively worded; therefore, the lower the score, the higher the role ambiguity experienced. The role ambiguity factor comprises items 9–14, and total scores range from 6 to 42. A sample item for role ambiguity is “Explanation is clear of what has to be done.” Construct validity for the three factors with school counselors was established by Freeman and Coll (1997). Reliability of the three factors have been upheld for school counselor participants (Culbreth et al., 2005; Wilkerson, 2009; Wilkerson & Bellini, 2006). For the present study, the internal consistency reliability was calculated for role incongruity at α = .82, role conflict at α = .79, and role ambiguity at α = .90. Correlations between role incongruity and CBI subscales ranged from r = .14 to .65, correlations between role conflict and CBI subscales ranged from r = .14 to .53, and correlations between role ambiguity and CBI subscales ranged from r = -.22 to -.56.
Counselor Burnout Inventory (CBI)
The CBI (Lee et al., 2007) is a 20-item inventory designed to measure counselors’ burnout levels. The CBI includes five subscales, with four questions for each subscale: Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life. The CBI uses a 5-point Likert-type scale ranging from 1 (never true) to 5 (always true). Total scores on each subscale range from 5 to 20, with the higher the score, the higher level of burnout. A sample item from the Exhaustion subscale is “Due to my job as a counselor, I feel tired most of the time.” A sample item from the Incompetence subscale is “I am not confident in my counseling skills.” A sample item from the Negative Work Environment subscale is “I am treated unfairly in my workplace.” A sample item from the Devaluing Clients subscale is “I am not interested in my clients and their problems.” A sample item from the Deterioration in Personal Life subscale is “I feel I have poor boundaries between work and my personal life.” Two independent samples composed of counselors from a variety of settings across the United States were used to explore and confirm the factor structure (Lee et al., 2007). Gnilka et al. (2015) upheld the CBI five-factor structure with a confirmatory factor analysis in a sample of school counselors. Cronbach’s alpha for the total CBI was .88, with scores ranging from .73 to .85 for the subscales (Lee et al., 2007). For the present study, internal consistency reliability for the CBI subscales were calculated and ranged from α = .78 to .89.
Results
Prior to conducting the primary analyses, we used SPSS (Version 25.0) to clean the data, impute missing data values, and test the assumptions of the primary analyses (i.e., hierarchal regressions), as recommended by Tabachnick and Fidell (2013). We used expectation-maximization (EM) to impute missing data (Cook, 2020), after we tested the randomness of the missing values with Little’s missing completely at random (MCAR). All missing values were determined to be MCAR, except for the active-emotional coping of the Brief COPE and the JSS: χ2(40, N = 227) = 79.13, p = .000, and χ2(671, N = 227) = 836.57, p = .000, respectively. Because the missing values for the active-emotional coping and JSS were less than 1%, expectation-maximization was an appropriate imputation method (Cook, 2020). Less than 5% of values were imputed for the PSS-4, the factors of the RQ (role ambiguity, role incongruity, and role conflict), and the five subscales of the CBI (Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life), and less than 1% of the values were imputed for the problem-focused and avoidant-emotional processes of the Brief COPE.
To answer the research question, we used three-step hierarchical regression models to analyze the individual and cumulative contributions for demographic, individual, and organizational factors with each subscale of the CBI. Qualities of the instruments are provided in Table 1. In Step 1, we entered the demographic factors (i.e., years of experience and school district). In Step 2, we entered the individual factors (i.e., perceived stress, problem-focused coping, avoidant-emotional coping, and active-emotional coping). In Step 3, we entered the organizational factors (i.e., perceived job satisfaction, role incongruity, role conflict, and role ambiguity). Completed assumption checks showed no outliers or influential data points, as concluded by an examination of the Q-Q plots, histograms, scatterplots, and Mahalanobis distance. We checked multicollinearity and found it to be an issue for school district (tolerance < .01). Therefore, we removed the school district variable and reentered years of experience in Step 1. To control for Type I error, we used the Bonferroni method to adjust the family-wise alpha (Darlington & Hayes, 2017), which resulted in .01 as the cutoff for statistical significance for Step 2 (i.e., individual factors) and .0056 as the cutoff for statistical significance for Step 3 (i.e., organizational factors). Results for each of these models are presented in Table 2.
Table 1
Qualities of Instrumentation
| Instrumentation |
Scores |
M |
SD |
α |
| Perceived Stress Scale-4 Total Score
Problem-Focused Coping
Avoidant-Emotional Coping
Active-Emotional Coping
Job Satisfaction Scale Total Score
Role Ambiguity
Role Incongruity
Role Conflict
Exhaustion
Incompetence
Negative Work Environment
Devaluing Client
Deterioration in Personal Life |
4–19
8–32
8–24
10–38
82–204
7–42
4–28
4–26
4–20
4–17
4–20
4–13
4–19 |
8.24
22.55
12.48
25.74
143.25
29.67
15.47
15.18
11.54
8.77
9.87
5.61
8.65 |
2.86
5.29
3.03
5.56
25.28
7.25
5.77
5.58
3.97
2.96
3.75
2.08
3.32 |
.76
.84
.70
.81
.91
.90
.82
.79
.89
.78
.85
.80
.78 |
Table 2
Results of Hierarchal Regression Analyses of School Counselor Burnout
|
Exhaustion |
Incompetence |
Negative Work Environment |
Devaluing Clients |
Deterioration in Personal Life |
| Step 1 |
|
|
|
|
| Years of Experience |
-.038 |
-.233* |
-.072 |
-.190* |
-.047 |
|
|
|
|
|
|
| R2 |
.001 |
.054 |
.005 |
.036 |
.002 |
| F |
.323 |
12.89** |
1.17 |
8.46* |
.500 |
| Step 2 |
|
|
|
|
|
| Years of Experience |
.030 |
-.151** |
-.042 |
-.155 |
.001 |
| Perceived Stress |
.392** |
.184 |
.283** |
.093 |
.491** |
| Avoidant-Emotional Coping |
.160 |
.360** |
.025 |
.180 |
.103 |
| Active-Emotional Coping |
.030 |
.087 |
.026 |
.131 |
.151 |
| Problem-Focused Coping |
-.043 |
-.151 |
.081 |
-.229** |
-.105 |
|
|
|
|
|
|
| R2 |
.240 |
.284 |
.109 |
.116 |
.323 |
| Δ R2 |
.239 |
.229 |
.104 |
.080 |
.321 |
| ΔF |
17.34** |
17.69** |
6.43** |
4.98** |
26.24** |
| Step 3 |
|
|
|
|
|
| Years of Experience |
.056 |
-.097 |
.052 |
-.125 |
.025 |
| Perceived Stress |
.303† |
.150 |
.057 |
.070 |
.437† |
| Avoidant-Emotional Coping |
.170 |
.338† |
.025 |
.165 |
.077 |
| Active-Emotional Coping |
.034 |
.126 |
.050 |
.151 |
.155 |
| Problem-Focused Coping |
-.064 |
-.180 |
.042 |
-.243† |
-.127 |
| Perceived Job Satisfaction |
-.198 |
.080 |
-.489† |
.032 |
.029 |
| Role Ambiguity |
.014 |
-.276† |
-.122 |
-.147 |
-.029 |
| Role Incongruity |
.207 |
.190 |
.220† |
.069 |
.172 |
| Role Conflict |
-.014 |
-.096 |
.106 |
-.018 |
.188 |
|
|
|
|
|
|
| R2 |
.351 |
.367 |
.666 |
.140 |
.383 |
| Δ R2 |
.111 |
.092 |
.652 |
.024 |
.060 |
| ΔF |
9.29** |
8.03** |
90.43** |
1.51 |
5.26** |
Note. N = 227
* p < .05. ** p < .01. † p < .0056. |
Exhaustion
The hierarchical regression model for Exhaustion revealed that years of experience was not statistically significant: F(1, 225) = .323, p > .05. Introducing individual factors explained 23.9% of the variation in Exhaustion, and this change in R2 was significant: F(5, 221) = 13.96, p < .001. The inclusion of organizational factors explained an additional 11.1% of the variation in Exhaustion, and this change in R2 was significant: F(9, 217) = 13.05, p < .001. However, the β values revealed that the only statistically significant factor of Exhaustion was perceived stress (β = .303, p < .001). Together the independent variables accounted for 35.1% of the variance in Exhaustion.
Incompetence
For Incompetence, years of experience explained 5.4% of its variation and was significant: F(1, 225) = 12.89, p < .001. Adding individual factors explained an additional 22.9% of the variation in Incompetence, and this change in R2 was significant: F(5, 221) = 17.50, p < .001. Including organizational factors explained an additional 9.2% of the variation in Incompetence, and this change in R2 was significant: F(9, 217) = 14.53, p < .001. The statistically significant factors of Incompetence were avoidant-emotional coping (β = .338, p < .001) and role ambiguity (β = -.276, p < .001). Together the independent variables accounted for 36.7% of the variance in Incompetence.
Negative Work Environment
For Negative Work Environment, years of experience was not statistically significant: F(1,225) = 1.17, p > .05, R2 = .005. Adding individual factors explained 10.9% of the variation in Negative Work Environment, and this change in R2 was significant: F(5, 221) = 5.40, p < .001. Including organizational factors explained an additional 65.2% of the variation in Negative Work Environment, and this change in R2 was significant: F(9, 217) = 48.05, p < .001. In the final model, perceived job satisfaction (β = -.489, p = .000) and role incongruity (β = .220, p = .000) significantly explained Negative Work Environment. Together the independent variables accounted for 66.6% of the variance in Negative Work Environment.
Devaluing Clients
For Devaluing Clients, years of experience contributed significantly to the model and accounted for 3.6% of its variation: F(1, 225) = 8.46, p < .05. Including individual factors explained an additional 8.0% of the variation in Devaluing Clients, and this change in R2 was significant: F(5, 221) = 5.80, p < .01. Adding the organizational factors in the third step was significant: F(9, 217) = 3.92, p < .001, R2 = .140. However, the inclusion of the organizational variables did not explain a significantly different equation: ΔF(4, 217) = 1.51, p > .05, ΔR2 = .024. Therefore, we interpreted the β values of the second step, and the statistically significant factor of Devaluing Clients was problem-focused coping (β = -.229, p = .009).
Deterioration in Personal Life
Finally, for Deterioration in Personal Life, years of experience was not significant: F(1, 225) = .500,
p > .05, R2 = .002. Including individual factors explained 32.1% of the variation in Deterioration in Personal Life, and the change in R2 was significant: F(5, 221) = 21.14, p < .001. Including the organizational factors explained an additional 6.0% of the variation in Deterioration in Personal Life, and this change in R2 was significant: F(9, 217) = 14.98, p < .001. An examination of the β values revealed that only perceived stress was a statistically significant variable for Deterioration in Personal Life (β = .437, p = .000). Together the independent variables accounted for 38.3% of the variance in Deterioration in Personal Life.
Discussion
The present study illustrates an expanded understanding of individual and organizational factors associated with the subscales of school counselor burnout (i.e., Exhaustion, Incompetence, Negative Work Environment, Devaluing Clients, and Deterioration in Personal Life; Lee et al., 2007). We intended to control for years of experience but found that before adding the individual and organizational factors, it was a statistically significant variable and negatively related with Incompetence and Devaluing Clients. School counselor researchers have reported contradictory findings between years of experience and burnout. Similar to our findings, Wilkerson and Bellini (2006) and Mullen et al. (2018) reported a negative relationship between years of experience and burnout—essentially describing that those earlier in their careers have a higher risk of experiencing burnout. In contrast, Butler and Constantine (2005) and Wilkerson (2009) reported burnout happening over time (i.e., a positive relationship between years of experience and burnout). Our study underscores the vulnerability school counselors may experience earlier in their careers (Mullen et al., 2018). Our results also provide a unique finding in that fewer years of experience as a school counselor is associated with the burnout dimensions of Incompetence and Devaluing Clients.
In the present study, we found individual factors (i.e., perceived stress, problem-focused coping, and avoidant-emotional coping) significantly related to Exhaustion, Incompetence, Devaluing Clients, and Deterioration in Personal Life. School counselor scholars (e.g., Mullen et al., 2018; Mullen & Gutierrez, 2016) reported a statistically significant positive relationship between school counselors’ perceived stress and burnout. Our results provide unique findings in that stress was positively related with the Exhaustion and Deterioration in Personal Life dimensions of burnout. Other school counselor scholars (e.g., Bardhoshi et al., 2014; Moyer, 2011) found the stress-related variable of engagement in non-counseling duties was significantly related to Exhaustion and Deterioration in Personal Life.
For the coping processes, avoidant-emotional coping was positively related to Incompetence and problem-focused coping was negatively related to Devaluing Clients. These findings provide two distinct understandings of school counselor burnout. First, and notably, school counselor participants who were experiencing Incompetence were also engaging in increased avoidant-emotional coping. This finding is similar to those of Fye et al. (2018), who found maladaptive perfectionists were more frequently engaging in avoidant-coping processes. We did not research perfectionism in the present study; however, our findings may expand an understanding of a positive relationship between avoidant-emotional coping and burnout dimensions for school counselors regardless of perfectionism types. Second, we discovered school counselor participants’ problem-focused coping was negatively related to Devaluing Clients. This is a promising finding from our study because participants were likely to incorporate increased problem-focused coping alongside valuing students. As previously discussed, it appears that these school counselor participants were maintaining high levels of positive regard and empathy for students (Gnilka et al., 2015; Mullen & Gutierrez, 2016). Engaging in problem-focused coping may be beneficial to their engagement in student care and maintaining professional vitality.
The organizational factors of role ambiguity, role incongruity, and perceived job satisfaction were significantly related to the Incompetence and Negative Work Environment dimensions of burnout. Specifically, role ambiguity was positively related to Incompetence. Our results confirm that when school counselors’ roles are increasingly unclear, they are experiencing higher levels of burnout (Mullen et al., 2018), and specifically Incompetence. Perceived job satisfaction was negatively related to Negative Work Environment, while role incongruity was positively related to Negative Work Environment. Consistent with previous research, our findings support the significant relationships between organizational factors (i.e., administrative and clerical duties contributing to role stress) and Negative Work Environment (Bardhoshi et al., 2014). Other scholars have studied perceived job satisfaction as an outcome and potential preclusion to school counselor burnout (Baggerly & Osborn, 2006; Bryant & Constantine, 2006). School counseling scholars have found that burnout mediated the relationship between perceived stress and perceived job satisfaction (Mullen et al., 2018). In the present study, the perceived job satisfaction factor had the highest β at -.489. It appears that perceived job satisfaction is an important factor alongside school counselors’ specific experiences of Negative Work Environments. Perceived stress was a statistically significant factor in Step 2 with Negative Work Environment, but insignificant in the context of the organizational variables. This is an important finding because burnout, by definition, is a function of one’s work context (Lee et al., 2007; Maslach & Leiter, 2017), and we found that organizational factors explained a large amount of the variance (i.e., 65.2%) for the Negative Work Environment dimension of burnout. Overall, our findings support the complex and multidimensional nature of school counselor burnout.
Limitations and Future Research
We attempted to research multidimensional burnout with a nationally representative and diverse sample of ASCA member school counselors. Despite our efforts, the response rate was 5.68%. The majority of our participants identified as White and female, which is similar to the reported demographics of professional school counselor members (ASCA, 2018). However, caution may be warranted when generalizing our findings to all school counselors. Expanding research efforts (i.e., qualitative methods) to increase understanding of the burnout experiences of school counselors unrepresented by our participant sample is warranted. Last, it is unknown whether or not participants answered sensitive questions, such as those about burnout, in a socially desirable manner.
Future research should seek to understand additional individual and organizational variables related to the burnout dimensions for school counselors (Lee et al., 2007). For example, the Devaluing Clients dimension has been viewed by school counseling scholars as a complicated construct that has functioned differently from the other dimensions of burnout (Bardhoshi et al., 2014; Mullen & Gutierrez, 2016). Additional research is needed to understand this burnout dimension with school counselors. Kim and Lambie (2018) discussed the need for research to focus on burnout interventions. We concur and believe the distinction of individual and organizational factors within the dimensions of school counselor burnout should be considered when constructing these interventions, which may be important because burnout may not be an end state; instead, it may be a mediator of other important outcomes, such as work and health (Maslach & Leiter, 2017). It may be helpful to expand research that studies relationships between school counselor burnout and physical and mental health outcomes.
Implications for the School Counseling Profession
Our findings have implications for school counselors, school counselors-in-training, and counselor educators and supervisors. They illustrate the importance of conceptualizing the ecological relationship between individual and organizational factors with school counselor burnout. School counselors may have more control over individual factors, and supervisors may have more control over organizational factors. Despite these considerations, it is important to share the responsibility of burnout prevention within the school system. This is important because despite one’s efforts to increase helpful coping, self-care, or wellness practices, it appears that continued exposure to negative work environments will continue to place school counselors at risk for burnout.
Because school counselors are responsible for providing counseling services that align with professional and ethical standards (Kim & Lambie, 2018), it is imperative for them to recognize, monitor, and address their symptoms of burnout (ASCA, 2016). Therefore, it may be helpful for school counselors and supervisors to identify and understand the dimensions of burnout experienced and their relationships with individual and organizational factors. By using the instruments from this study, school counselors can identify contributions of individual and organizational factors with their burnout scores. This would allow supervisees to understand the relationships between these factors and burnout dimensions. During supervision, time could be dedicated to setting personal goals for maintaining self-care and professional vitality. This may be important, especially in identifying and decreasing avoidant-emotional coping, alongside increasing problem-focused coping processes. In general, school counselors should monitor their own self-care in relation to work context stressors and perceived job satisfaction. Our results may provide support to the potential limitations that wellness practices have on decreasing burnout within the Negative Work Environment (Puig et al., 2012)—meaning, wellness practices may be important in alleviating the individual factors related to burnout (i.e., high perceived stress, coping responses) but may have limited ability to decrease factors out of school counselors’ control (i.e., work context practices and policies).
Despite best practice guidelines, the reality remains that school counselors engage in various non-counseling duties (Bardhoshi et al., 2014; Gutierrez & Mullen, 2016), which contributes to role stress. To lessen organizational stressors, as early as graduate school, counselor educators and supervisors should allow space in the learning process for students to learn the various counseling and related duties expected of school counselors within the school environment. Providing learning contexts for graduate students to explore these various roles may set the stage for lessened role stress. Specifically, assignments should be included in the curriculum that allow graduate students to explore school counselors’ professional identity and the real and ideal roles of the school counselor. These discussions should be engaged in along with conversations of how these varying roles can affect burnout (specifically role incongruity and role ambiguity), especially for those earlier in their careers. These dialogues should be reinforced during the practicum and internship experiences and include personal sources of perceived job satisfaction. In schools, supervisors can help to facilitate school counselors’ competence by clearly defining expectations through measurable outcomes. For example, school counselors and supervisors can use the ASCA National Model’s (ASCA, 2019) Annual Administrative Conference Template (p. 60) and Annual Calendar Template (p. 70) to open communication between the school counselors and their supervisors and document their duties. This discussion may additionally open communication regarding the adequacy of funding, resources, materials, and staff available to school counselors (Freeman & Coll, 1997). If inadequate, school counselors may use the opportunity to advocate for increased support from supervisors and administrators.
It is important to note that in the present study, school counselors earlier in their careers reported higher levels of Incompetence and Devaluing Clients. School counselor supervisors should understand these relationships. Mentoring of school counselors who are earlier in their careers by those with significant experience may help the younger professionals build their professional identities and student-focused work. Last, recognizing dimensions of burnout in relation to individual and organizational factors may not be enough to maintain professional vitality. The school counseling profession may find it helpful to train school counselors and graduate students in advocacy skills. Trusty and Brown (2005) outlined advocacy competencies for school counselors, which include dispositional statements, knowledge, and skills necessary to becoming effective advocates. The self-advocacy model prepares school counselors to have the communication (oral and written) necessary to maintain effective advocacy roles.
Conclusion
In conclusion, our results provide an expansion of findings related to relative contributions for individual and organizational factors with school counselor multidimensional burnout. In short, burnout dimensions are uniquely related to personal and work context factors. It is difficult to conceive of burnout absent its relationship to some aspect of the work setting. School counselors and supervisors can use our results to conceptualize burnout from a multidimensional perspective, which may in turn help them find new ways to remain professionally vital to themselves, their students, and their school community.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American School Counselor Association. (2016). ASCA ethical standards for school counselors. https://www.schoolcounselor.org/asca/media/asca/Ethics/EthicalStandards2016.pdf
American School Counselor Association. (2018). ASCA membership demographics. https://www.schoolcounselor.org/asca/media/asca/home/Member-Demographics.pdf
American School Counselor Association. (2019). The ASCA national model: A framework for school counseling programs (4th ed.).
Baggerly, J., & Osborn, D. (2006). School counselors’ career satisfaction and commitment: Correlates and predictors. Professional School Counseling, 9(3), 197–205. https://doi.org/10.1177/2156759X0500900304
Bardhoshi, G., Schweinle, A., & Duncan, K. (2014). Understanding the impact of school factors on school counselor burnout: A mixed-methods study. The Professional Counselor, 4(5), 426–443. https://doi.org/10.15241/gb.4.5.426
Bryant, R. M., & Constantine, M. G. (2006). Multiple role balance, job satisfaction, and life satisfaction in women school counselors. Professional School Counseling, 9(4), 265–271. https://doi.org/10.1177/2156759X0500900403
Butler, S. K., & Constantine, M. G. (2005). Collective self-esteem and burnout in professional school counselors. Professional School Counseling, 9(1), 55–62. https://doi.org/10.1177/2156759X0500900107
Carver, C. S. (1997). You want to measure coping but your protocol’s too long: Consider the Brief COPE. International Journal of Behavioral Medicine, 4(1), 92–100. https://doi.org/10.1207/s15327558ijbm0401_6
Cervoni, A., & DeLucia-Waack, J. (2011). Role conflict and ambiguity as predictors of job satisfaction in high school counselors. Journal of School Counseling, 9(1), 1–30. http://www.jsc.montana.edu/articles/v9n1.pdf
Cohen, J. (1992). A power primer. Psychological Bulletin, 112(1), 155–159. https://doi.org/10.1037/0033-2909.112.1.155
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Cohen, S., & Williamson, G. (1988). Perceived stress in a probability sample of the United States. In S. Spacapan & S. Oskamp (Eds.), The social psychology of health: The Claremont symposium on applied social psychology (2nd ed., pp. 31–67). SAGE.
Coll, K. M., & Freeman, B. (1997). Role conflict among elementary school counselors: A national comparison with middle and secondary school counselors. Elementary School Guidance & Counseling, 31(4), 251–261.
Cook, R. M. (2020). Addressing missing data in quantitative counseling research. Counseling Outcome Research and Evaluation. https://doi.org/10.1080/21501378.2019.1711037
Cooper, C., Katona, C., & Livingston, G. (2008). Validity and reliability of the Brief COPE in carers of people with dementia: The LASER-AD Study. The Journal of Nervous and Mental Disease, 196(11), 838–843. https://doi.org/10.1097/NMD.0b013e31818b504c
Culbreth, J. R., Scarborough, J. L., Banks-Johnson, A., & Solomon, S. (2005). Role stress among practicing school counselors. Counselor Education and Supervision, 45(1), 58–71. https://doi.org/10.1002/j.1556-6978.2005.tb00130.x
Darlington, R. B., & Hayes, A. F. (2017). Regression analysis and linear models: Concepts, applications, and implementation (1st ed.). Guilford.
Deatherage, S., Servaty-Seib, H. L., & Aksoz, I. (2014). Stress, coping, and internet use of college students. Journal of American College Health, 62(1), 40–46. https://doi.org/10.1080/07448481.2013.843536
Dimitrov, D. M. (2009). Quantitative research in education: Intermediate and advanced methods. Whittier.
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.-G. (2009). Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods, 41(4), 1149–1160. https://doi.org/10.3758/BRM.41.4.1149
Folkman, S., & Lazarus, R. S. (1985). If it changes it must be a process: Study of emotion and coping during three stages of a college examination. Journal of Personality and Social Psychology, 48(1), 150–170. https://doi.org/10.1037/0022-3514.48.1.150
Folkman, S., & Moskowitz, J. T. (2004). Coping: Pitfalls and promise. Annual Review of Psychology, 55(1), 745–774. https://doi.org/10.1146/annurev.psych.55.090902.141456
Freeman, B., & Coll, K. M. (1997). Factor structure of the Role Questionnaire (RQ): A study of high school counselors. Measurement & Evaluation in Counseling and Development, 30(1), 32–39. https://doi.org/10.1080/07481756.1997.12068915
Fye, H. J., Gnilka, P. B., & McLaulin, S. E. (2018). Perfectionism and school counselors: Differences in stress, coping, and burnout. Journal of Counseling & Development, 96(4), 349–360. https://doi.org/10.1002/jcad.12218
Gnilka, P. B., Karpinski, A. C., & Smith, H. J. (2015). Factor structure of the Counselor Burnout Inventory in a sample of professional school counselors. Measurement and Evaluation in Counseling and Development, 48(3), 177–191. https://doi.org/10.1177%2F0748175615578758
Holman, L. F., Nelson, J., & Watts, R. (2019). Organizational variables contributing to school counselor burnout: An opportunity for leadership, advocacy, collaboration, and systemic change. The Professional Counselor, 9(2), 126–141. https://doi.org/10.15241/lfh.9.2.126
Kim, N., & Lambie, G. W. (2018). Burnout and implications for professional school counselors. The Professional Counselor, 8(3), 277–294. http://doi.org/10.15241/nk.8.3.277
Kolodinsky, P., Draves, P., Schroder, V., Lindsey, C., & Zlatev, M. (2009). Reported levels of satisfaction and frustration by Arizona school counselors: A desire for greater connections with students in a data-driven era. Professional School Counseling, 12(3), 193–199. https://doi.org/10.1177%2F2156759X0901200307
Lazarus, R. S. (1993). Coping theory and research: Past, present, and future. Psychosomatic Medicine, 55(3), 234–247. https://doi.org/10.1097/00006842-199305000-00002
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. Springer.
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., Ogle, N. T., Powell, M. L., Quinn, J. J., Wallace, S. L., & Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40(3), 142–154. https://doi.org/10.1080/07481756.2007.11909811
Maslach, C., & Leiter, M. P. (2017). Understanding burnout: New models. In C. L. Cooper & J. C. Quick (Eds.), The handbook of stress and health: A guide to research and practice (1st ed., pp. 36–56). Wiley-Blackwell.
McCarthy, C., Van Horn Kerne, V., Calfa, N. A., Lambert, R. G., & Guzmán, M. (2010). An exploration of school counselors’ demands and resources: Relationship to stress, biographic, and caseload characteristics. Professional School Counseling, 13(3), 146–158. https://doi.org/10.1177%2F2156759X1001300302
Moyer, M. (2011). Effects of non-guidance activities, supervision, and student-to-counselor ratios on school counselor burnout. Journal of School Counseling, 9(5), 1–30. http://www.jsc.montana.edu/articles/v9n5.pdf
Mullen, P. R., Blount, A. J., Lambie, G. W., & Chae, N. (2018). School counselors’ perceived stress, burnout, and job satisfaction. Professional School Counseling, 21(1), 1–10. https://doi.org/10.1177/2156759X18782468
Mullen, P. R., & Gutierrez, D. (2016). Burnout, stress and direct student services among school counselors. The Professional Counselor, 6(4), 344–359. http://doi.org/10.15241/pm.6.4.344
Paisley, P. O., & McMahon, H. G. (2001). School counseling for the 21st century: Challenges and opportunities. Professional School Counseling, 5(2), 106–115.
Puig, A., Baggs, A., Mixon, K., Park, Y. M., Kim, B. Y., & Lee, S. M. (2012). Relationship between job burnout and personal wellness in mental health professionals. Journal of Employment Counseling, 49(3), 98–109. https://doi.org/10.1002/j.2161-1920.2012.00010.x
Rizzo, J. R., House, R. J., & Lirtzman, S. I. (1970). Role conflict and ambiguity in complex organizations. Administrative Science Quarterly, 15(2), 150–163. https://doi.org/10.2307/2391486
Scarborough, J. L, & Culbreth, J. R. (2008). Examining discrepancies between actual and preferred practice of school counselors. Journal of Counseling & Development, 86(4), 446–459. https://doi.org/10.1002/j.1556-6678.2008.tb00533.x
Smith, P. C., Kendall, L. M., & Hulin, C. L. (1969). Measurement of satisfaction in work and retirement: A strategy for the study of attitudes. Rand McNally.
Spector, P. E. (1985). Measurement of human service staff satisfaction: Development of the Job Satisfaction Survey. American Journal of Community Psychology, 13(6), 693–713. https://doi.org/10.1007/bf00929796
Spector, P. E. (2011). Job Satisfaction Survey norms. https://shell.cas.usf.edu/~pspector/scales/jssnorms.html
Tabachnick, B. G., & Fidell, L. S. (2013). Using multivariate statistics (6th ed.). Pearson.
Trusty, J., & Brown, D. (2005). Advocacy competencies for professional school counselors. Professional School Counseling, 8(3), 259–265.
Wilkerson, K. (2009). An examination of burnout among school counselors guided by stress-strain-coping theory. Journal of Counseling & Development, 87(4), 428–437. https://doi.org/10.1002/j.1556-6678.2009.tb00127.x
Wilkerson, K., & Bellini, J. (2006). Intrapersonal and organizational factors associated with burnout among school counselors. Journal of Counseling & Development, 84(4), 440–450. https://doi.org/10.1002/j.1556-6678.2006.tb00428.x
Heather J. Fye, PhD, NCC, LPC, is an assistant professor at the University of Alabama and a certified PK–12 school counselor. Ryan M. Cook, ACS, LPC, is an assistant professor at the University of Alabama. Eric R. Baltrinic, LPCC-S, is an assistant professor at the University of Alabama. Andrea Baylin, NCC, PEL, is a doctoral student at the University of Alabama. Correspondence may be addressed to Heather Fye, Box 870231, Graves Hall 315B, Tuscaloosa, AL 35487, hjfye@ua.edu.
Sep 1, 2018 | Volume 8 - Issue 3
Nayoung Kim, Glenn W. Lambie
To prevent school counselors from experiencing feelings of burnout, identifying relevant factors is important. The purpose of this article is to review studies investigating the constructs of burnout and occupational stress in school counseling samples. Eighteen published research articles fit the inclusion criteria for this review. The researchers identified external and internal variables relating to school counselor burnout, as well as protective and risk factors. The review identified that school counselors’ higher level of burnout correlated with having non-counseling duties, being assigned large caseloads, working in schools that did not meet adequate yearly progress (AYP) status, experiencing a lack of supervision, possessing greater emotion-oriented stress coping scores, providing fewer direct student services, and having greater perceived stress. In contrast, feelings of burnout among school counselors were mitigated when counselors received supervision, possessed higher task-oriented stress coping strategies, scored at higher levels of ego maturity, reported greater occupational support at their schools, had greater grit scores, and worked in schools that met AYP.
Keywords: burnout, occupational stress, school counselors, non-counseling duties, coping strategies
There are multiple definitions of burnout (e.g., Burke & Richardson, 2000; Stalker & Harvey, 2002); however, the primary consistent aspect of burnout is that it is a psychological phenomenon associated with job-related stress (Maslach, 2017). Burnout occurs when professionals are unable to meet their own needs, as well as their clients’ needs, in a high-pressure environment (Maslach, 2017). Freudenberger (1990) identified common symptoms of burnout, including negative changes in individuals’ (a) attitudes and decision making; (b) physiological states; (c) mental, emotional, and behavioral health; and (d) occupational motivation. Burnout has significant consequences, including compromised physical health, increased risk of mental health disorders (e.g., depression, substance abuse), poor job performance, absenteeism, occupational attrition, and low self-esteem (Maslach & Leiter, 2016). Burnout can also cause symptoms such as fatigue, exhaustion, and insomnia (Armon, Shirom, Shapira, & Melamed, 2008).
Burnout in School Counseling
Morse, Salyers, Rollins, Monroe-DeVita, and Pfahler (2012) identified that 21% to 67% of mental health professionals reported experiencing high levels of burnout, possibly because of dealing with high client caseloads (Ducharme, Knudsen, & Roman, 2007) or overall job effectiveness (Stalker & Harvey, 2002). In addition, Oddie and Ousley (2007) found that 21% to 48% of mental health workers reported experiencing high levels of emotional exhaustion. School counselors specifically are at risk for experiencing feelings of burnout because of their multiple job demands, including paperwork, parent conferences, school-wide testing, large caseloads, and requests from administrators (McCarthy & Lambert, 2008), and other factors such as role ambiguity and limited occupational support (Young & Lambie, 2007). The school counseling job environment, where “the demands of the work are high, but the resources to meet those demands are low” (Maslach & Goldberg, 1998, pp. 63–64), increases susceptibility to experiencing feelings of burnout (e.g., average student-to-counselor ratio being 491-to-1; National Center for Education Statistics, 2016). Stephan (2005) found that within a national sample of school counselors, 66% of middle school counselors scored at moderate to high levels of emotional exhaustion. Further, Wachter (2006) found that 20% of the school counselors in her investigation (N = 132) experienced feelings of burnout; 16% scored at moderate levels of burnout, and 4% scored at severe levels of burnout. Thus, many school counselors experience feelings of burnout that may influence their ability to provide ethical and effective counseling services to the students they serve.
School counselors may experience chronic fatigue, depersonalization, or feelings of hopelessness and leave their jobs because of the rigidity of school systems and limited support (Young & Lambie, 2007). In fact, counselors experiencing significant feelings of burnout provide reduced quality of service to their clientele because burnout relates to lower productivity, turnover intention, and a lowered level of job commitment (Maslach, Schaufeli, & Leiter, 2001). Because of the importance of preventing the burnout phenomenon, the American School Counselor Association’s (ASCA; 2016) ethical standards note that school counselors are responsible for maintaining their health, both physically and emotionally, and caring for their wellness to ensure their effective practice. The American Counseling Association’s (2014) ethical standards also state that school counselors have an ethical responsibility to monitor their feelings of burnout and remediate when their feelings potentially influence their ability to provide quality services to their stakeholders. To monitor burnout, counselors need to understand the symptoms of burnout and prevent it from happening, while maintaining their psychological well-being.
School counselors face challenges with their significant job demands (McCarthy, Van Horn Kerne, Calfa, Lambert, & Guzmán, 2010), such as large caseloads (Lambie, 2007) and extreme amounts of non-counseling duties (Moyer, 2011). In fact, school counselors report job stress and dissatisfaction when they are required to complete non-counseling duties, hindering their ability to work with their students (McCarthy et al., 2010). Examples of non-counseling duties include clerical tasks, such as scheduling students for classes; fair share, such as coordinating the standardized testing program; and administrative duties, such as substitute teaching (Scarborough, 2005). School counselors with large caseloads and high student-to-counselor ratios are more likely to experience increased feelings of burnout (Bardhoshi, Schweinle, & Duncan, 2014). Although ASCA (2015) recommends a student-to-counselor ratio of 250-to-1, the U.S. average student-to-counselor ratio is almost double the recommended proportion (491-to-1; National Center for Education Statistics, 2016).
Insufficient resources for school counselors and negative job perception increase their likelihood of experiencing feelings of burnout. Lower levels of principal support and lack of clinical supervision raise school counselors’ occupational stress (Bardhoshi et al., 2014; Moyer, 2011). For instance, school counselors with higher levels of role ambiguity are likely to experience burnout (Wilkerson & Bellini, 2006). School counselors experience role ambiguity when their responsibilities or the expected level of performance is not clearly identified (Coll & Freeman, 1997). As a result, school counselors report increased levels of stress (Culbreth, Scarborough, Banks-Johnson, & Solomon, 2005), leading to burnout and attrition from the profession (Wilkerson & Bellini, 2006). ASCA (2016) dictated that school counselors’ responsibilities include providing counseling services to students to support their development, which distinguishes them from other school personnel. With the importance of preventing burnout in school counseling, the purpose of this review is twofold: (a) to present identified factors influencing school counselors’ levels of burnout and (b) to offer strategies to assist school counselors in mitigating the feelings of burnout.
Research Examining Burnout in School Counseling
We began by conducting a formal search of electronic databases—PsycINFO, ERIC (EBSCOhost), and Academic Search Premiere—relating to school counselor burnout. The search term burnout was first used to analyze the research trend in the field. Both the search terms burnout and school counselors OR school counseling were used to collect any articles on the topic of school counselor burnout published between 2000 and 2018. An additional search was conducted with the terms occupational stress and school counselors OR school counseling to identify potential studies related to the topic in the same type of literature.
The following inclusion criteria were applied for our review: (a) investigations of school counselor burnout and occupational stress, (b) sample participants were school counselors in the United States, (c) the primary topic of the investigation was burnout and/or occupational stress, (d) articles were written in English, (e) articles were published in refereed journals, and (f) articles were published between 2000 and 2018. In addition, our review excluded literature reviews, editorials, and rejoinders. The abstracts of the articles meeting the criteria were examined and confirmed in order to be included in our review.
Our literature search based on the inclusion criteria produced 51 articles. As not all articles from the search satisfied the criteria, the articles were reviewed manually to evaluate whether they met the criteria, resulting in 35 articles not meeting criteria (e.g., conceptual articles, studies related to teachers) and 16 articles meeting all criteria. An additional literature search yielded two more studies meeting the inclusion criteria, identifying 18 studies in total. None of the identified research articles examined prevention or treatment interventions for burnout in school counselors. The 18 investigations had school counselor burnout or occupational stress as the constructs of interest. The research findings identified the positive relationships between school counselors’ burnout or occupational stress scores and the following factors: (a) non-counseling duties, (b) large caseloads, (c) not meeting adequate yearly progress (AYP) status (i.e., the expected amount of students’ academic growth per year based on the No Child Left Behind mandate [Minnesota House of Representatives, 2003]), (d) lack of supervision, (e) emotion-oriented stress coping scores, (f) grit, and (g) perceived stress.
Fourteen out of 18 articles provided information related to school counselor burnout (see Table 1 for quantitative studies and Table 2 for qualitative studies), and the other four studies investigated school counselors’ occupational stress (see Table 3). Occupational stress refers to the strain a person experiences when the perceived stress in a workplace outweighs their ability to cope (Decker & Borgen, 1993). Quantitative research methods were employed in 15 of the investigations, two used mixed-methods, and one study utilized a qualitative approach. For all 18 articles, the participants were current school counselors, and the number of participants ranged from 3 to 926. Effect sizes were categorized depending on the analysis into three groups (i.e., small, medium, and large) based on the effect size matrix from Sink and Stroh (2006), offering a better understanding of the results. Specifically, the effect size from independent samples t-test (2 groups; Cohen’s d) is interpreted as small for 0.2, medium for 0.5, and large for 0.8. For the effect size of other analyses listed in this review, including paired-samples t-tests (η2), multiple regression (R2), and analysis of variance (ANOVA; η2), 0.01 is considered as small, 0.06 as medium, and 0.14 as large.
Table 1
Summary of Quantitative/Mixed Studies Related to Professional School Counselor (PSC) Burnout
| Study |
Sample |
Variables |
Findings |
| Bain, Rueda, Mata-Villarreal, & Mundy (2011) |
PSCs in rural districts of South Texas
(N = 27)
Convenient Sampling |
Mental health awareness, the amount of time spent on academic advising
|
Feelings of burnout were reported by the majority of the PSCs (89%) in the study and many of them spent the greatest amount of time on administrative duties and the least on counseling. |
| Bardhoshi, Schweinle, & Duncan (2014) |
PSCs
(N = 212)
Random Sampling |
Non-counselor duties, school factors, five subscales of the CBI |
Non-counseling duties and school factors were associated with PSC burnout. Non-counseling duties explained the variance of the three burnout subscales: Exhaustion (11%; medium effect size), NWE (6%; medium effect size), and DPL (8%; medium effect size). Non-counseling duties and other factors (e.g., caseload, principal support) explained the variance of the four burnout subscales: Exhaustion (21%; large effect size), Incompetence (9%; medium effect size), NWE (49%; large effect size), and DPL (17%; large effect size). |
| Butler & Constantine (2005) |
PSCs
(N = 533)
Random Sampling |
Collective self-esteem, burnout, demographics |
Collective self-esteem explained 3% of the variance of PSC burnout (small effect size). In particular, PRCS (2%) and PUCS (1%) accounted for PA (both small effect sizes), and IICS explained 1% of feelings of DP and PA (both small effect sizes). Higher collective self-esteem was associated with lower PSC burnout. PSCs working in urban settings tended to have higher levels of burnout than the counterparts in other environmental settings. PSCs with experience of 20–29 years reported higher levels of burnout than the counterparts with 0–9 years of experience. PSCs with experience of 30 or more years reported higher levels of burnout than those with less experience. |
| Gnilka, Karpinski, & Smith (2015) |
PSCs
(N = 269)
Convenient Sampling |
Five subscales on the CBI |
Effect size differences were found between PSCs and other professionals in the counseling fields (Exhaustion, d = .26, small effect size; DC, d = -.50, medium effect size). Effect size differences were noted between PSCs and sexual offender and sexual abuse therapists (Exhaustion, d = .27, small effect size; DPL, d = -.23, small effect size; DC, d = -.82, large effect size). |
| Lambie (2007) |
PSCs
(N = 218)
Random Sampling
|
Ego maturity, three subscales on the MBI-HSS
|
PSCs with greater levels of ego maturity tended to have a higher level of PA than those with lower ego maturity. Ego maturity predicted PA (3.3%; small effect size). Occupational support and the subscales of burnout were correlated. Reported occupational support predicted EE (16%; large effect size), DP (12%; medium effect size), and PA (7.2%; medium effect size). |
| Limberg, Lambie, & Robinson (2016-2017) |
PSCs
(N = 437)
Random Sampling/
Purposive Sampling |
Altruistic motivation, altruistic behavior, burnout |
PSCs with greater levels of altruism had lower levels of EE and higher feelings of PA. PSC altruism explained 31.36% of the variance in EE (large effect size), and 29.16% of the variance in PA (large effect size). Self-Efficacy accounted for 14.4% of the variance in EE (large effect size) and 9% of the variance in PA (medium effect size). |
| Moyer (2011) |
PSCs
(N = 382)
Convenient Sampling |
Non-guidance activities, supervision, student-to-counselor ratios, five subscales of the CBI |
Non-guidance–related duties and clinical supervision were significant predictors of PSC burnout. Non-guidance duties (7.3%; medium effect size) and supervision (9%; medium effect size) predicted burnout.
|
| Mullen, Blount, Lambie, & Chae (2017) |
PSCs
(N = 750)
Random Sampling |
Perceived stress, burnout, job satisfaction |
Perceived stress predicted burnout positively (large effect size) and job satisfaction negatively (large effect size). Perceived stress and burnout predicted job satisfaction (large effect size). Burnout mediated the relationship between perceived stress and job satisfaction. |
| Mullen & Crowe (2018) |
PSCs
(N = 330)
Convenient Sampling |
Grit, stress, burnout |
Grit was negatively related to burnout (small effect size) and stress (small to medium effect size). |
| Mullen & Gutierrez (2016)
|
PSCs
(N = 926)
Random Sampling
|
Burnout, perceived stress, direct student services
|
Burnout attributed to direct counseling activities (12%; medium effect size), direct curriculum activities (5%; small to medium effect size), and percentage of time at work providing direct services to students (6%; medium effect size). |
| Wachter, Clemens, & Lewis (2008) |
PSCs
(N = 249)
Random Sampling |
Demographics, stakeholder involvement, lifestyle themes, burnout |
Burnout and lifestyle themes were associated. Perfectionism subscale was negatively related to burnout, and the Self-Esteem subscale was positively related to PSC burnout. About 15.1% of the variance in burnout was accounted for by the lifestyle themes of Self-Esteem and Perfectionism (large effect size). |
| Wilkerson & Bellini (2006)
|
PSCs in northeastern U.S.
(N = 78)
Systematic Random Sampling
|
Demographics, intrapersonal, and organizational factors; three subscales on the MBI-ES |
Demographic (age, counseling experience, supervision, and student/counselor ratio), intrapersonal, and organizational factors significantly accounted for the amount of the variance in each subscale of burnout, including EE (45%; large effect size), DP (30%; large effect size), and PA (42%; large effect size). |
| Wilkerson (2009)
|
PSCs
(N = 198)
Random Sampling |
Demographic and organizational stressors and individual coping strategies; three subscales on the MBI-ES |
Demographic factors (years of experience and student/counselor ratio), organizational stress, and coping styles explained the variance of each subscale of burnout including EE (49%; large effect size), DP (27%; large effect size), and PA (36%; large effect size).
|
Table 2
Summary of Qualitative/Mixed Studies Related to Professional School Counselor Burnout
| Study |
Sample |
Topic |
Identified Themes |
| Bain, Rueda, Mata-Villarreal, & Mundy (2011) |
PSCs in rural districts of South Texas (N = 27)
Convenient Sampling |
Helpful ways to better provide mental health services at school |
Having access to additional staff and additional education and awareness in terms of helpful ways to provide mental health services at their school. |
| Bardhoshi, Schweinle, & Duncan (2014) |
PSCs
(N = 252)
Random Sampling |
a) Their experience of burnout
b) The meaning of performing non-counseling duties |
a) Lack of time, budgetary constraints, lack of resources, lack of organizational support, etc.
b) Adverse personal/professional effects, a reality of the job, reframing the duties within the context of the job. |
| Sheffield & Baker (2005) |
Female PSCs
(N = 3)
Purposive Sampling |
Burnout experience |
Important beliefs, burnout feelings, burnout attitude, (lack of) collegial support. |
Table 3
Summary of Quantitative Studies Related to Professional School Counselor Occupational Stress
| Study |
Sample |
Variables |
Findings |
| Bryant & Constantine (2006) |
Female PSCs
(N = 133)
Random Sampling |
Role balance, job satisfaction, satisfaction with life, demographics |
Multiple role balance ability and job satisfaction positively predicted overall life satisfaction. Role balance and job satisfaction explained the variance of life satisfaction (41%; large effect size). |
| Culbreth, Scarborough, Banks-Johnson, & Solomon (2005) |
PSCs
(N = 512)Stratified Random Sampling |
Role conflict, role ambiguity, role incongruence, demographics |
Perceived match between the job expectations and actual experiences predicted role-related job stress, including role conflict (7.6%; medium effect size); role incongruence (19.7%; large effect size); and role ambiguity (8.3%; medium effect size). |
| McCarthy, Van Horn Kerne, Calfa, Lambert, & Guzmán (2010) |
PSCs in Texas
(N = 227) Convenient Sampling |
Demographics, job stress, resources and demands |
Job stress was different between the resourced, balanced, and demand groups. The effect sizes were large in the differences between the demand group and the resourced group (1.62; large effect size) and the balanced group (0.70; large effect size).
|
| Rayle (2006) |
PSCs
(N = 388)Convenient Sampling |
Demographics, mattering, job-related stress |
Thirty-five percent of the variance in overall job satisfaction was explained by mattering to others at work and job-related stress (large effect size). Mattering to others (19.36%; large effect size) and job-related stress (16.81%; large effect size) explained the variance in overall job satisfaction. |
Three instruments were used to measure levels of school counselor burnout, including: (a) the Maslach Burnout Inventory (MBI; Maslach, Jackson, & Leiter, 1996), (b) the Counselor Burnout Inventory (CBI; S. M. Lee et al., 2007), and (c) the Burnout Measure Short Version (BMS; Malach-Pines, 2005). Maslach and Jackson (1981) defined burnout with three dimensions: Emotional Exhaustion (EE), Depersonalization (DP), and reduced Personal Accomplishment (PA). Emotional exhaustion is to exhaust one’s capacity to continuously involve with clients (R. T. Lee & Ashforth, 1996). Not being able to respond to clients’ needs may cause counselors to distance themselves from their job emotionally and cognitively, which is defined as depersonalization. Lastly, having a lower sense of effectiveness may reduce feelings of personal accomplishment (Maslach et al., 2001). Four studies used the MBI-Education Survey (MBI-ES), which was designed for the education population, and another study utilized the MBI-Human Services Survey (MBI-HSS), in which the word students from the MBI-ES is substituted with recipients in a third of the items (Sandoval, 1989).
Four studies used the CBI, which is a 20-item instrument with five subscales, including:
(a) Exhaustion, (b) Incompetence, (c) Negative Work Environment (NWE), (d) Devaluing Client (DC), and (e) Deterioration in Personal Life (DPL). Exhaustion is the condition of being physically and emotionally exhausted by the duties of a counselor, and incompetence focuses on counselors’ feelings of being incompetent. While negative work environment refers to the stress caused by the working environment, devaluing client is related to being unable to establish emotional connectedness with clients. Finally, deterioration in personal life assesses the level of deterioration in a counselor’s personal life. Sample items include “I feel exhausted due to my work as a counselor,” and “I feel I have poor boundaries between work and my personal life.” The internal consistency of the CBI ranged from .73 to .85 (S. M. Lee et al., 2007). In addition, three studies used the BMS (Malach-Pines, 2005), a 10-item scale in which participants rate their answers to the question “When you think about your work overall, how often do you feel the following?” in seven prompts, including: “Trapped,” “Hopeless,” and “Helpless.” The BMS is adapted from the original version of the Burnout Measure (Pines & Aronson, 1988). The internal consistency of the BMS ranged from .85 to .87 (Malach-Pines, 2005).
Researchers investigated different factors relating to school counselor burnout within the 18 published articles. One of the studies provided descriptive statistics of school counselor burnout, comparing school counselors to other mental health professionals and showing how burnout symptoms may emerge (N = 269; Gnilka, Karpinski, & Smith, 2015). School counselors had greater levels of Exhaustion (d = .26; small effect size) and lower levels of DC (d = -.50; medium effect size) than mental health professional participants. Furthermore, school counselors had greater levels of Exhaustion (d = .27; small effect size) and lower levels of DC (d = -.82; large effect size) compared to the mental health professional participants working with sex offenders and clients that have been sexually abused. Therefore, school counselors score higher in exhaustion as compared to other mental health professionals and score lower on devaluing their clients.
Individual Factors Related to Burnout
The two categories of individual factors relating to school counselor burnout were (a) psychological constructs and (b) demographic factors. The psychological constructs included ego maturity (Lambie, 2007), collective self-esteem (Butler & Constantine, 2005), altruism (Limberg, Lambie, & Robinson, 20162017), lifestyle themes (Wachter, Clemens, & Lewis, 2008), coping styles (Wilkerson, 2009), perceived stress (Mullen, Blount, Lambie, & Chae, 2017), and grit (Mullen & Crowe, 2018). The definitions of these psychological constructs related to school counselor burnout follow.
Ego maturity refers to the fundamental element of an individual’s personality, encompassing components of self, social, cognitive, character, and moral development (Loevinger, 1976). When individuals’ egos develop, they become more individualistic, autonomous, and highly aware of themselves (Loevinger, 1976). Collective self-esteem is individuals’ perception of their identification with the social group they belong to (Bettencourt & Dorr, 1997). Altruism is the behavior driven by values or goals individuals possess or their concerns for others, aside from external rewards (Eisenberg et al., 1999). A lifestyle is an individual’s way of perceiving self, others, and the world (Mosak & Maniacci, 2000), and lifestyle themes refer to common patterns people possess in relation to their lifestyles (Mosak, 1971). Coping is defined as cognitive and behavioral efforts to deal with specific demands that take up or exceed individuals’ resources (Lazarus & Folkman, 1984), and coping styles refer to individuals’ relatively stable patterns in handling stress (Heszen-Niejodek, 1997). Perceived stress represents the extent to which individuals evaluate their situations as stressful (Cohen, 1986). Grit is “perseverance and passion for long-term goals” (Duckworth, Peterson, Matthews, & Kelly, 2007, p. 1087). Specifically, grit refers to efforts to achieve a goal despite challenges. In addition to psychological constructs, the demographic factors category included years of experience in school counseling (Butler & Constantine, 2005; Wilkerson, 2009; Wilkerson & Bellini, 2006) and age (Wilkerson & Bellini, 2006).
Psychological constructs. Seven studies identified that psychological constructs relate to school counselors’ feelings of burnout. Five of seven factors had large effect sizes, including ego maturity, altruism, lifestyle themes, coping styles, and grit, and three of the factors with large effect sizes were associated with Emotional Exhaustion (EE) among the MBI (Maslach et al., 1996) subscale scores (i.e., ego maturity, altruism, and coping styles).
Specifically, Lambie (2007) examined the directional relationship between school counselors’
(N = 218) burnout and ego maturity, identifying that those counselors with higher levels of ego maturity were likely to have greater feelings of Personal Accomplishment (PA; R2 = .033). The researcher also investigated the relationship between the school counselors’ reported occupational support and their MBI burnout subscales scores (Maslach & Jackson, 1996), identifying that each MBI subscale relates to the participants’ levels of reported occupational support; EE (large effect size; R2 = .167); DP (medium effect size; R2 = .120); and PA (medium effect size; R2 = .072). The results indicated that school counselors scoring at higher ego maturity levels had lower feelings of burnout, and counselors experiencing high levels of occupational support had significantly lower burnout scores.
The relationship between burnout and collective self-esteem was investigated within a sample of school counselors (N = 533; Butler & Constantine, 2005). The Collective Self-Esteem Scale has four subscales (Luhtanen & Crocker, 1992), including (a) Private Collective Self-Esteem (PRCS), (b) Public Collective Self-Esteem (PUCS), (c) Membership Collective Self-Esteem (MCS), and (d) Importance to Identity Collective Self-Esteem (IICS). These subscales measure individuals’ perception of social groups they belong to, including how they feel about the group (PRCS), how they perceive others feel about the group (PUCS), how they perceive themselves being a good member of the group (MCS), and how important their social group is to their self-concept (IICS). These four Collective Self-Esteem Scale subscales explained 3% of the variance in the burnout subscales (Pillai’s trace = .08, F [12, 1584] = 3.48, p < .001, η2M = .03; Maslach & Jackson, 1986).
In general, higher collective self-esteem relates to lower levels of burnout, and different dimensions of collective self-esteem relate to different components of burnout. Higher PRCS was associated with higher feelings of PA (η2 = .02), and higher PUCS was related to lower levels of EE (η2 = .01). The school counselors’ IICS subscale scores were related to their lower feelings of DP (η2 = .01) and greater feelings of PA (η2 = .01). Although a small amount of variance in burnout scores (.01–.02) was explained by the components of collective self-esteem, the positive relationship between higher PRCS and higher feelings of PA identified that positive perceptions of the group school counselors belong to might reduce their feelings of burnout. For instance, having a sense of pride as a school counselor by observing other school counselors’ hard work and good relationships with students may promote their sense of PRCS, which may lead to higher feelings of PA. Taken together, promoting school counselors’ collective self-esteem may decrease their feelings of burnout.
Limberg and colleagues (2016–2017) investigated the directional relationship between school counselors’ (N = 437) levels of altruism and burnout. The school counselors with greater levels of altruism had lower levels of EE and higher feelings of PA. Specifically, the altruism subscales of Positive Future Expectation (PFE) and Self-Efficacy from the Self-Report Altruism Scale (Rushton, Chrisjohn, & Fekken, 1981) and two subscales of burnout (MBI) correlated (χ2 = 403.611, df = 216, χ2 ratio = 1.869, p < .001). PFE and Self-Efficacy accounted for 31.36% of the variance in the EE subscale (large effect size), and 29.16% of the variance in the PA subscale (large effect size). The Self-Efficacy subscale, which involves individuals’ perceived competence in a certain skill, explained 14.4% of the variance in EE subscale scores (large effect size), and 9% of the variance in PA subscale scores (medium effect size). Therefore, the results identified that school counselors’ levels of altruism negatively contribute to their burnout scores.
Burnout was related to lifestyle themes among school counselors (N = 249; Wachter et al., 2008). Two subscales of lifestyle themes from the Kern Lifestyle Scale (Kern, 1996), Self-Esteem and Perfectionism, accounted for 15.1% of the variance in burnout (large effect size; R2 = .151). Specifically, the Perfectionism subscale was negatively related to school counselor burnout scores (Burnout Measure: Short Version; BMS; Malach-Pines, 2005), and the Self-Esteem subscale was positively related to school counselor burnout. As a result, these findings identified school counselors’ personality factors relating to their risk of burnout, supporting that higher levels of perfectionism and lower levels of self-esteem may increase the likelihood of experiencing burnout.
Two studies employed hierarchical regression analyses to examine what factors may predict burnout subscale scores of the MBI, and one of the predicting variables was coping styles (Wilkerson, 2009; Wilkerson & Bellini, 2006). Wilkerson (2009) used four-step hierarchical regression models that included demographics, organizational stressors, and coping strategies, such as task-oriented, emotion-oriented, and avoidance-oriented coping (N = 198). The models with large effect sizes explained all three MBI burnout subscales. Specifically, 49% of the variance in the EE subscale was explained (large effect size; R2 = .49); 27% of the variance in the DP subscale was accounted for (large effect size; R2 = .27); and 36% of the variance of the PA subscale was explained (large effect size; R2 = .36). The results identified school counselors’ stressor scores both at the individual and organizational levels; intrapersonal coping strategies contributed to feelings of burnout with large effect sizes in the final model. In other words, demographic factors (e.g., more school counseling experience), coping styles (e.g., more emotion-oriented and less task-oriented coping strategies), and organizational variables (e.g., lack of decision-making authority, role ambiguity, role incongruity, and role conflict) positively predicted the level of burnout among school counselors.
Wilkerson and Bellini (2006) used three-step hierarchical regression models including demographic, intrapersonal, and organizational factors to examine the relationship between the variables and burnout among school counselors (N = 78). The school counselors’ demographic data (e.g., age, counseling experience, supervision, and student/counselor ratio), and intrapersonal (i.e., coping strategies) and organizational factors (e.g., role conflict, role ambiguity, and counselor occupational stress) significantly accounted for the variance in their burnout subscale scores on the MBI. Specifically, 45% of the variance in the EE subscale was explained (large effect size; R2 = .45), 30% of the variance in the DP subscale was accounted for (large effect size; R2 = .30), and 42% of the variance in the PA subscale was explained (large effect size; R2 = .42) by the final three-step model with the variables (i.e., counselor demographics, intrapersonal factors, and organizational factors). The findings indicated that school counselors’ emotion-oriented coping style predicted their three MBI subscale scores, supporting the importance of utilizing helpful strategies (i.e., task-oriented coping) to mitigate counselors’ feelings of burnout.
Another study examined how school counselors’ perceived stress and job satisfaction relate to burnout (Mullen et al., 2017). Specifically, perceived stress measured by the Perceived Stress Scale (Cohen, Kamarck, & Mermelstein, 1983) explained 52% of the variance in burnout (F (1, 749) = 808.55, p < .001; R2 = .52) and 25% of the variance in job satisfaction (F (1, 749) = 243.36, p < .001; R2 = .25). When both perceived stress and burnout were examined in order to test the relationship with job satisfaction, they explained 40% of the variance in job satisfaction (F (2, 747) = 246.48, p < .001; R2 = .40). In addition, the results indicated that burnout mediated the relationship between perceived stress and job satisfaction (z = -21.47, p < .001), and burnout (rs = .99) predicted job satisfaction better than perceived stress (rs = .79). Overall, perceived stress predicted burnout positively (large effect size) and job satisfaction negatively (large effect size). Both perceived stress and burnout predicted job satisfaction (large effect size).
Finally, Mullen and Crowe (2018) investigated the relationship between grit, burnout, and stress among school counselors (N = 330). The researchers found that grit was negatively correlated with burnout (r = -.22, p < .001) and stress (r = -.28, p < .001). Specifically, perseverance of effort, one of the subscales from the Grit-S (Duckworth & Quinn, 2009), was negatively related with burnout (r = -.12,
p < .05) and stress (r = -.19, p < .001). Therefore, school counselors’ level of grit may be a protective factor for burnout and stress.
Demographic factors. School counselors’ individual factors, such as age (Wilkerson & Bellini, 2006) and years of experience (Butler & Constantine, 2005; Wilkerson, 2009), correlate with feelings of burnout. Age was negatively correlated to the DP subscale (r = -.19, p < .05); therefore, older school counselors were less likely to experience burnout as compared to younger counselors (Wilkerson & Bellini, 2006). Nevertheless, the correlation between school counselors’ years of experience and burnout was inconsistent. Wilkerson and Bellini (2006) indicated that years of experience negatively correlated with the EE (r = -.26, p < .01), and DP (r = -.24, p < .05) subscales, while Butler and Constantine (2005) identified that school counselors with more years of experience scored at higher levels of burnout (MBI scores). Specifically, school counselors with 20–29 years of experience had greater DP subscale scores than those with 0–9 years of experience (F (3, 529) = 3.38, p < .05); and counselors with 30 years or more of experience had lower PA subscale scores than those with less than 20 years of experience (F (3, 529) = 3.39, p < .05). Furthermore, Wilkerson (2009) also reported that the years of experience positively correlated with the EE (ß = .21, p < .01) and DP (ß = .26, p < .01) MBI subscales in the hierarchical regression models whose variables included counselor demographics and organizational and intrapersonal variables to explain the variance of the burnout scores. Possible reasons behind the incongruent results may relate to school counselors’ role ambiguity, as counselors with less experience may experience or perceive large workloads compared to more experienced counselors. The conflicting results also may be related to other school counselor factors, such as the level of social support counselors experience at their schools. The findings identified the need for more inquiry to increase our understanding of the relationship between school counselors’ years of experience and their feelings of burnout.
Organizational Factors Relating to School Counselors Levels of Burnout
Eight organizational factors appear to correlate with school counselors’ levels of burnout, including (a) workplace (Butler & Constantine, 2005), (b) non-counseling duties such as administrative and clerical tasks (Bardhoshi et al., 2014; Moyer, 2011), (c) caseloads (Bardhoshi et al., 2014), (d) AYP (Bardhoshi et al., 2014), (e) level of principal support (Bardhoshi et al., 2014), (f) clinical supervision (Moyer, 2011), (g) student-to-counselor ratio (Wilkerson, 2009; Wilkerson & Bellini, 2006), (h) perceived work environment (Wilkerson & Bellini, 2006), and (i) direct student services (Mullen & Gutierrez, 2016). We categorize these organizational factors into two domains: (a) job responsibilities and
(b) work environment factors.
Job responsibilities. Two studies examined the relationship between school counselors’ non-counseling duties and their burnout scores. First, Bardhoshi and colleagues (2014) examined school counselors’ (N = 212) non-counseling duties and identified a significant relationship between three of the CBI subscales: (a) 11% of the variance in Exhaustion was explained (medium effect size; R2 = 0.11); (b) 6% of the variance in NWE was explained (medium effect size; R2 = 0.06); and (c) 8% of the variance in DPL was explained (medium effect size; R2 = 0.08). Taken together, the results identified that school counselors’ non-counseling duties positively predict their burnout scores.
Moyer (2011) examined how school counselors’ (N = 382) non-counseling duties (non-guidance duties) were correlated to their levels of burnout as measured by the CBI. School counselors’ non-counseling duties accounted for 7.3% of the variance in the burnout score (medium effect size; R2 = .073, ß = .27, p < .01). Receiving supervision accounted for additional variance in school counselors’ burnout scores after controlling the variance explained by non-counseling activities (medium effect size; R2 = .09, ß = -.14, p < .01). As a result, school counselors with more non-counseling duties and less clinical supervision had higher burnout scores. The findings identify the importance of clinical supervision to reduce burnout among school counselors, helping them improve their quality of counseling, which in turn may increase their sense of competence in the workplace.
Bain and colleagues (2011) investigated the mental health of school counselors in a rural setting and their percentage of workweek spent on counseling and administrative duties in South Texas (N = 27). Within this sample of school counselors, 89% had experienced feelings of burnout at least sometimes when trying to provide mental health services; specifically, 41% reported feelings of burnout, and 48% sometimes experienced burnout when providing mental health services to their students. School counselors also reported that they spent the greatest amount of time completing administrative duties and the least amount of time providing counseling services. About 48% of the counselors used more than 50% of their time completing administrative duties, such as organizing facts to report to administrators and preparing for assessments of knowledge and skills, and more than 70% of the participants spent less than 50% of their time providing counseling services. The sample size for this study was small; nevertheless, the results identified that approximately 90% of the school counselors experienced some levels of burnout and spent less time providing counseling services to their students and other stakeholders than completing administrative duties.
Finally, Mullen and Gutierrez (2016) investigated the relationship between burnout and direct student services of school counselors (N = 926). The results indicated that burnout negatively contributed to the frequency of direct counseling activities (ß = -.35, p < .001), direct curriculum activities (ß = -.22, p < .001), and percentage of time at work providing direct services to students (ß = -.24, p < .001). The findings suggest that school counselors experiencing feelings of burnout are likely to have lower numbers of direct counseling activities and curriculum activities, and spend less time offering direct services to students.
Work environment factors. School counselors’ levels of burnout may be different depending on the location of their workplace (Butler & Constantine, 2005). Specifically, school counselors working in urban settings scored higher on the EE subscale as compared to counselors in suburban, rural, and other settings (F (3, 529) = 24.66, p < .001). In addition, counselors in urban settings had higher DP subscale scores than those in other environmental settings (F (3, 529) = 13.67, p < .001). The results may relate to unique stressors school counselors in the urban settings face, including their expected proficiency in working with diverse students (Constantine et al., 2001). Overall, school counselors in urban settings were likely to experience greater feelings of burnout than those counselors in other settings, suggesting that more research is warranted to better understand possible contributors to these educators having higher MBI scores.
Factors relating to school counselors’ work correlating with their feelings of burnout include counselors’ caseloads, AYP status, principal support, and non-counseling duties. Specifically, school-related factors for counselors explained the variance of four burnout subscales of the CBI (Bardhoshi et al., 2014): (a) 21% of the variance in Exhaustion scores was explained (large effect size; R2 = 0.21, p < .001); (b) 9% of the variance in Incompetence scores was explained (medium effect size; R2 = 0.09, p < .01); (c) 49% of the variance in NWE scores was explained (large effect size; R2 = 0.49, p < .001); and (d) 17% of the variance in DPL scores was explained (large effect size; R2 = 0.17, p < .001). As a result, both school counselors’ work-related factors, such as caseloads and non-counseling duties, and their school environment (support from school staff and AYP status) correlate to their feelings of burnout. Therefore, providing sufficient support for school counselors, meeting the AYP, and reducing caseloads and non-counseling duties might mitigate feelings of burnout among school counselors.
Student-to-counselor ratio (Wilkerson, 2009) and perceived work environment (e.g., role conflict; Wilkerson & Bellini, 2006) were identified as predictive factors for school counselor burnout. Wilkerson (2009) found that the hierarchical regression models with variables of demographic data (e.g., years of experience), organizational stressors (e.g., counselor–teacher professional relationships), and coping strategies (e.g., task-oriented coping) explained all three subscale scores of the MBI in a sample of school counselors (N = 198): EE (R2 = .49; large effect size), DP (R2 = .27; large effect size), and PA (R2 = 36; large effect size). Similarly, Wilkerson and Bellini (2006) identified that school counselors’ demographic, intrapersonal, and organizational factors accounted for variance in all three MBI subscale scores, including the EE, DP, and PA subscales (45%, 30%, and 42%, respectively; all large effect sizes). The findings from these studies support that environmental factors relate to school counselor burnout.
Identified Themes From Qualitative Studies
One qualitative study and two mixed-methods studies explored themes relating to school counselor burnout and ways to improve their service, which may offer ways to prevent burnout. Bardhoshi and colleagues (2014) examined how school counselors experienced burnout. Specifically, the emergent themes identified for school counselors’ feelings of burnout organized around four areas including (a) lack of time, (b) budgetary constraints, (c) lack of resources, and (d) lack of organizational support. When school counselors were asked about the meaning of performing non-counseling duties, they stated adverse personal and professional effects, the realities of practice, and reframing the duties within the context of the job. One participant described burnout stating, “It means that I am no longer helpful to my students. I feel like I’m extremely tired and overworked and consequently my effectiveness as a school counselor is negatively impacted” (p. 437).
These themes aligned with existing qualitative research examining school counselors’ feelings of burnout (N = 3; Sheffield & Baker, 2005), including (a) important beliefs, (b) burnout feelings, (c) burnout attitude, and (d) lack of collegial support. One of the participants stated, “I didn’t think I was doing any good for anybody . . . I just can’t go on this way” (p. 181). Another participant stated, “You get to the point where it is no longer fun coming to work or when you are just tired [and] don’t want to deal with anyone” (p. 182). Finally, Bain and colleagues (2011) explored helpful ways to better provide mental health services at school with 27 school counselors in rural districts of South Texas. The results identified that having access to more staff and additional education and awareness of mental health services at their school was needed. Overall, these studies identified common themes of school counselors’ need for collegial support and resources, such as a school climate encouraging collaboration, and identifying gaps in the needs and realities of school counselors (Bardhoshi et al., 2014), as well as reducing the amount of stressful, non-counseling–related work they perform.
Occupational Stress
Researchers examined which factors may influence school counselors’ job stress or job satisfaction, including (a) counselors’ perceived match between job expectations and their actual experiences (Culbreth et al., 2005), (b) the amount of resources in their work environment (McCarthy et al., 2010), (c) mattering to others (Rayle, 2006), and (d) role balance ability (Bryant & Constantine, 2006). Perceived match between initial expectations of the job and actual experiences as a school counselor was the most significant predictor of lower role stress demonstrated by each subscale score of the Role Questionnaire (N = 512; Culbreth et al., 2005): role conflict (medium effect size; R2 = .076); role incongruence (large effect size; R2 = .197); and role ambiguity (medium effect size; R2 = .083). School counseling students reported not feeling trained enough because of the significant amount of non-counseling–related duties, which increased their sense of role conflict.
Graduating from a program accredited by the Council for Accreditation of Counseling and Related Educational Programs accounted for 1.2% of the variance in school counselors’ perceived readiness for the job (small effect size; r = .111, p < .05; Culbreth et al., 2005). School counselors’ balance between job demand and resources was another important factor for their job stress. Moreover, McCarthy and colleagues (2010) identified that perceived job stress and work environment in terms of demands and resources were correlated (N = 227; F (2, 206) = 44.77, p < .001). School counselors with resources, such as other counselors in general or as mentors, and support from administrators scored lower on levels of job stress. The effect size for the difference between the demand and the resourced groups was 1.62 (large effect size), and between the demand and balanced groups was 0.70 (large effect size). In other words, school counselors with more work-related resources were likely to experience lower levels of job stress.
Several factors are related to job satisfaction for school counselors. Rayle (2006) investigated the relationship between school counselors’ (N = 388) mattering to others at work scores and job-related stress scores, and their overall job satisfaction scores. The School Counselor Mattering Survey developed for this study included seven items asking participants to rate their perceived mattering to others, including their students, administrators, and the parents and teachers they worked with. School counselors’ mattering to others at work scores and job-related stress scores explained 35% of the variance in their overall job satisfaction (large effect size; ηp² = .62). Specifically, school counselors’ job satisfaction correlated with mattering to others at work scores (large effect size; r = .44, p < .001) and their job-related stress scores (large effect size; r = -.41, p < .001). In addition, school counselors’ mattering to others scores were negatively associated with their job-related stress scores (r = -.54, p < .001; large effect size). The findings suggest that school counselors’ perceived mattering to others at work and job-related stress predict their overall job satisfaction, and mattering to others at work relates to their job-related stress.
In addition, Bryant and Constantine (2006) investigated the relationship between female school counselors’ (N = 133) role balance, job satisfaction, and life satisfaction. After controlling for demographic information (age, years of school counseling experience, and location of school), role balance and job satisfaction scores correlated with their satisfaction with life scores (large effect size; R2 = .41). As a result, school counselors’ multiple role balance ability and job satisfaction scores positively predicted their overall life satisfaction scores. In sum, these findings identified factors related to school counselors’ job satisfaction, including mattering to others at work, job-related stress, and life satisfaction.
Discussion
Because of the dearth of literature examining school counselor burnout or occupational stress, we reviewed 18 investigations based on the inclusion criteria and included articles focusing on the topic that were published between 2000 and 2018 in refereed journals and identified internal and external factors relating to the phenomena. Specific factors were identified relating to school counselor burnout or stress and their environment, including responsibilities not related to counseling, large caseloads, AYP status, and role confusion. The findings suggest the importance of school counselors asserting themselves to focus on mandated tasks (i.e., counseling) in order to experience less burnout. In addition, it is imperative to train school counseling students to understand the reality of practice, such as other job responsibilities and school climates, and inform them on the necessity of counselors advocating for themselves in order to overcome role confusion and avoid large caseloads. Furthermore, several resources were identified to mitigate burnout among school counselors. Clinical supervision from a competent supervisor is essential for school counselors to get support and learn how to intervene with their clients effectively. In addition, peer supervision or consultation from colleagues may benefit school counselors in sharing their difficulties and gaining other professionals’ perspectives (Butler & Constantine, 2005). Task-oriented coping skills which can be learned in the school counseling programs were also related to a reduced level of burnout among school counselors.
Limitations
Our review needs to be interpreted with some caution, as it is limited to the 18 published studies meeting the inclusion criteria. Therefore, additional research investigating school counselor burnout is needed to further our understanding of this significant construct that may influence the services school counselors provide to their stakeholders. In addition, the reviewed studies include methodological limitations (e.g., sample size, self-report data), further supporting the need for increased research examining the construct of burnout in school counseling. Moreover, no research was identified examining interventions to possibly reduce counselor feelings of burnout.
Implications for School Counseling
Although no studies were identified that investigated treatments for school counselor burnout, research from other similar professions may provide insight for developing coping strategies for school counselors addressing their feelings of burnout. Awa, Plaumann, and Walter (2010) reviewed 25 intervention studies for burnout prevention whose participants included employees from diverse occupations. Seventeen out of 25 studies employed person-directed interventions and indicated the positive effects of the interventions, including cognitive behavioral training (Gorter, Eijkman, & Hoogstraten, 2001), psychosocial skill training (Ewers, Bradshaw, McGovern, & Ewers, 2002), and recreational music making (Bittman, Bruhn, Stevens, Westengard, & Umbach, 2003). Two studies used organization-directed interventions, and one of the studies reduced burnout by using cognitive behavioral techniques, management skill training, and social support (Halbesleben, Osburn, & Mumford, 2006). The other six investigations explored the effects of combined (person- and organization-directed) interventions in reducing burnout. The examples of combined interventions to mitigate counselors’ feeling of burnout include professional supervision (Melchior et al., 1996); work schedule reorganization and lectures (Innstrand, Espnes, & Mykletun, 2004); and participatory action research, communication, social support, and coping skills (Le Blanc, Hox, Schaufeli, Taris, & Peeters, 2007). Overall, Awa and colleagues (2010) identified positive impacts of burnout intervention programs, suggesting potential benefits of these treatment programs for school counselors.
In addition, Krasner and colleagues (2009) reported the effectiveness of their continuing medical education program for physicians to reduce burnout, which involves mindfulness, self-awareness, and communication skills. Educating for mindfulness strategies, self-awareness, and communication skills also may be helpful for school counselors. Providing a supportive environment and acknowledging school counselors’ work may help them increase their sense of matter in their workplace. Lacking empirical studies identifying treatment outcomes for burnout in school counselors, research on decreasing the level of school counselor burnout should be examined both deeply and extensively. Furthermore, intervention programs to prevent and intervene with school counselors’ burnout and occupational stress at the individual and organizational levels are warranted. The efforts to prevent burnout may lead to school counselors providing better quality of services, benefitting the counselors and the students they serve.
Our review indicated that school counselors’ responsibilities, such as non-counseling duties and dealing with large caseloads, hindered counselors from maintaining their wellness. Additionally, experiencing role conflict and employing emotion-oriented coping skills increased their feelings of burnout. Therefore, school counselor preparation programs need to incorporate into their curriculum the characteristics of their future work environment that may involve potential risk factors for burnout. Furthermore, developing school counselors’ own strategies and practicing beneficial skills such as task-oriented coping skills may be helpful for them in decreasing their likelihood of experiencing burnout.
Conclusion
Preventing and reducing school counselors’ feelings of burnout is important to ensure counselors’ ability to provide ethical and effective services to their stakeholders. Failure to address work-related stress in school counselors may cause reduced quality of their service and increased counselor attrition from the profession. Although more investigations examining burnout in school counselors are warranted, this manuscript is the first systematic review of burnout in school counseling, offering increased insight into this significant job-related psychological phenomenon.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). 2014 ACA code of ethics. Alexandria, VA: Author.
American School Counselor Association. (2015). Student-to-school-counselor ratio 2015–2016. Retrieved from https://www.schoolcounselor.org/asca/media/asca/home/Ratios15-16.pdf
American School Counselor Association. (2016). ASCA ethical standards for school counselors. Alexandria, VA: Author.
Armon, G., Shirom, A., Shapira, I., & Melamed, S. (2008). On the nature of burnout–insomnia relationships: A prospective study of employed adults. Journal of Psychosomatic Research, 65, 5–12.
doi:10.1016/j.jpsychores.2008.01.012
Awa, W. L., Plaumann, M., & Walter, U. (2010). Burnout prevention: A review of intervention programs. Patient Education and Counseling, 78, 184–190. doi:10.1016/j.pec.2009.04.008
Bain, S. F., Rueda, B., Mata-Villarreal, J., & Mundy, M.-A. (2011). Assessing mental health needs of rural schools in South Texas: Counselors’ perspectives. Research in Higher Education Journal, 14, 1–11.
Bardhoshi, G., Schweinle, A., & Duncan, K. (2014). Understanding the impact of school factors on school counselor burnout: A mixed-methods study. The Professional Counselor, 4, 426–443. doi:10.15241/gb.4.5.426
Bettencourt, B. A., & Dorr, N. (1997). Collective self-esteem as a mediator of the relationship between allocentrism and subjective well-being. Personality and Social Psychology Bulletin, 23, 955–964.
Bittman, B., Bruhn, K. T., Stevens, C., Westengard, J., & Umbach, P. O. (2003). Recreational music-making: A cost-effective group interdisciplinary strategy for reducing burnout and improving mood states in long-term care workers. Advances in Mind Body Medicine, 19(3/4), 4–15.
Bryant, R. M., & Constantine, M. G. (2006). Multiple role balance, job satisfaction, and life satisfaction in women school counselors. Professional School Counseling, 9, 265–271.
Burke, R. J., & Richardson, A. M. (2000). Psychological burnout in organizations. In R. T. Golembiewski (Ed.), Handbook of Organizational Behavior (pp. 327–368). New York, NY: Marcel Dekker, Inc.
Butler, S. K., & Constantine, M. G. (2005). Collective self-esteem and burnout in professional school counselors. Professional School Counseling, 9, 55–62.
Cohen, S. (1986). Contrasting the Hassles Scale and the Perceived Stress Scale: Who’s really measuring appraised stress? American Psychologist, 41, 716–718. doi:10.1037/0003-066X.41.6.716
Cohen, S., Kamarck, T., &Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24, 385–396. doi:10.2307/2136404
Coll, K. M., & Freeman, B. (1997). Role conflict among elementary school counselors: A national comparison with middle and secondary school counselors. Elementary School Guidance & Counseling, 31, 251–261.
Constantine, M. G., Arorash, T. J., Barakett, M. D., Blackmon, S. M., Donnelly, P. C., & Edles, P. A. (2001). School counselor’s universal-diverse orientation and aspects of their multicultural counseling competence. Professional School Counseling, 5, 13–18.
Culbreth, J. R., Scarborough, J. L., Banks-Johnson, A., & Solomon, S. (2005). Role stress among practicing school counselors. Counselor Education and Supervision, 45, 58–71.
doi:10.1002/j.1556-6978.2005.tb00130.x
Decker, P. J., & Borgen, F. H. (1993). Dimensions of work appraisal: Stress, strain, coping, job satisfaction, and negative affectivity. Journal of Counseling Psychology, 40, 470–478.
Ducharme, L. J., Knudsen, H. K., & Roman, P. M. (2007). Emotional exhaustion and turnover intention in human service occupations: The protective role of coworker support. Sociological Spectrum, 28, 81–104.
Duckworth, A. L., Peterson, C., Matthews, M. D., & Kelly, D. R. (2007). Grit: perseverance and passion for long-term goals. Journal of Personality and Social Psychology, 92, 1087–1101.
Duckworth, A. L., & Quinn, P. D. (2009). Development and validation of the Short Grit Scale (Grit-S). Journal of Personality Assessment, 91, 166–174. doi:10.1080/00223890802634290
Eisenberg, N., Guthrie, I. K., Murphy, B. C., Shepard, S. A., Cumberland, A., & Carlo, G. (1999). Consistency and development of prosocial dispositions: A longitudinal study. Child Development, 70, 1360–1372.
Ewers, P., Bradshaw, T., McGovern, J., & Ewers, B. (2002). Does training in psychosocial interventions reduce burnout rates in forensic nurses? Journal of Advanced Nursing, 37, 470–476.
doi:10.1046/j.1365-2648.2002.02115.x
Freudenberger, H. J. (1990). Caring for the caregiver: Recognizing and dealing with burnout. In J. Nottingham & H. Nottingham (Eds.), The professional and family caregiver—Dilemmas, rewards, and new directions (pp. 20–27). Americus, GA: Georgia Southwestern State University.
Gnilka, P. B., Karpinski, A. C., & Smith, H. J. (2015). Factor structure of the counselor burnout inventory in a sample of professional school counselors. Measurement and Evaluation in Counseling and Development, 48, 177–191. doi:10.1177/0748175615578758
Gorter, R. C., Eijkman, M. A., & Hoogstraten, J. (2001). A career counseling program for dentists: Effects on burnout. Patient Education and Counseling, 43, 23–30.
Halbesleben, J. R., Osburn, H. K., & Mumford, M. D. (2006). Action research as a burnout intervention: Reducing burnout in the Federal Fire Service. The Journal of Applied Behavioral Science, 42, 244–266. doi:10.1177/0021886305285031
Innstrand, S. T., Espnes, G. A., & Mykletun, R. (2004). Job stress, burnout and job satisfaction: An intervention study for staff working with people with intellectual disabilities. Journal of Applied Research in Intellectual Disabilities, 17, 119–126. doi:10.1111/j.1360-2322.2004.00189.x
Kern, R. M. (1996). Lifestyle questionnaire inventory. In D. Eckstein & L. Baruth (Eds.), The theory and practice of lifestyle assessment (pp. 243–256). Dubuque, IA: Kendall/Hunt.
Krasner, M. S., Epstein, R. M., Beckman, H., Suchman, A. L., Chapman, B., Mooney, C. J., & Quill, T. E. (2009). Association of an educational program in mindful communication with burnout, empathy, and attitudes among primary care physicians. JAMA, 302, 1284–1293.
Lambie, G. W. (2007). The contribution of ego development level to burnout in school counselors: Implications for professional school counseling. Journal of Counseling & Development, 85, 82–88. doi:10.1002/j.1556-6678.2007.tb00447.x
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York, NY: Springer.
Le Blanc, P. M., Hox, J. J., Schaufeli, W. B., Taris, T. W., & Peeters, M. C. (2007). Take care! The evaluation of a team-based burnout intervention program for oncology care providers. Journal of Applied Psychology, 92, 213–227.
Lee, R. T., & Ashforth, B. E. (1996). A meta-analytic examination of the correlates of the three dimensions of job burnout. Journal of Applied Psychology, 81, 123–133.
Lee, S. M., Baker, C. R., Cho, S. H., Heckathorn, D. E., Holland, M. W., Newgent, R. A., . . . Yu, K. (2007). Development and initial psychometrics of the Counselor Burnout Inventory. Measurement and Evaluation in Counseling and Development, 40, 142–154. doi:10.1080/07481756.2007.11909811
Limberg, D., Lambie, G., & Robinson, E. H. (2016–2017). The contribution of school counselors’ altruism to their degree of burnout. Professional School Counseling, 20, 127–138. doi:10.5330/1096-2409-20.1.127
Loevinger, J. (1976). Ego development. San Francisco, CA: Jossey-Bass.
Luhtanen, R., & Crocker, J. (1992). A collective self-esteem scale: Self-evaluation of one’s social identity. Personality and Social Psychology Bulletin, 18, 302–318. doi:10.1177/0146167292183006
Malach-Pines, A. (2005). The burnout measure, short version. International Journal of Stress Management, 12, 78–88. doi:10.1037/1072-5245.12.1.78
Maslach, C. (2017). Finding solutions to the problem of burnout. Consulting Psychology Journal: Practice and Research, 69, 143–152. doi:10.1037/cpb0000090
Maslach, C., & Goldberg, J. (1998). Prevention of burnout: New perspectives. Applied and Preventive Psychology, 7, 63–74. doi:10.1016/S0962-1849(98)80022-X
Maslach, C., & Jackson, S. E. (1986). The Maslach Burnout Inventory (2nd ed.). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., & Jackson, S. E. (1996). Maslach Burnout Inventory–Human Service Survey (MBI-HSS). In C. Maslach, S. E. Jackson, & M. P. Leiter (Eds.), Maslach Burnout Inventory Manual (3rd ed., pp. 3–17). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., Jackson, S. E., & Leiter, M. P. (1996). The Maslach Burnout Inventory manual (3rd ed.). Palo Alto, CA: Consulting Psychologists Press.
Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15, 103–111. doi:10.1002/wps.20311
Maslach, C., Schaufeli, W. B., & Leiter, M. P. (2001). Job burnout. Annual Review of Psychology, 52, 397–422. doi:10.1146/annurev.psych.52.1.397
McCarthy, C. J., & Lambert, R. G. (2008). Counselor appraisal of resources and demands. Charlotte, NC: Center for Educational Measurement and Evaluation.
McCarthy, C., Van Horn Kerne, V., Calfa, N. A., Lambert, R. G., & Guzmán, M. (2010). An exploration of school counselors’ demands and resources: Relationship to stress, biographic, and caseload characteristics. Professional School Counseling, 13, 146–158.
Melchior, M. E., Phihpsen, H., Abu-Saad, H. H., Halfens, R. J., van de Berg, A. A., & Gassman, P. (1996). The effectiveness of primary nursing on burnout among psychiatric nurses in long-stay settings. Journal of Advanced Nursing, 24, 694–702.
Minnesota House of Representatives. (2003). Adequate yearly progress under the No Child Left Behind Act. House Research. Retrieved from http://www.house.leg.state.mn.us/hrd/pubs/ss/ssayp.pdf
Morse, G., Salyers, M. P., Rollins, A. L., Monroe-DeVita, M., & Pfahler, C. (2012). Burnout in mental health services: A review of the problem and its remediation. Administration and Policy in Mental Health and Mental Health Services Research, 39, 341–352. doi:10.1007/s10488-011-0352-1
Mosak, H. H. (1971). Lifestyle. In A. G. Nikelly (Ed.), Applications of Adlerian theory: Techniques for behavior change. Springfield, IL: Charles C. Thomas.
Mosak, H., & Maniacci, M. (2000). A primer of Adlerian psychology: The analytic–behavioral–cognitive psychology of Alfred Adler. Philadelphia, PA: Brunner/Mazel.
Moyer, M. (2011). Effects of non-guidance activities, supervision, and student-to-counselor ratios on school counselor burnout. Journal of School Counseling, 9(5), n5.
Mullen, P. R., Blount, A. J., Lambie, G. W., & Chae, N. (2017). School counselors’ perceived stress, burnout, and job satisfaction. Professional School Counseling, 21, 1–10. doi:10.1177/2156759X18782468
Mullen, P. R., & Crowe, A. (2018). A psychometric investigation of the short grit scale with a sample of school counselors. Measurement and Evaluation in Counseling and Development, 51, 151–162.
doi:10.1080/07481756.2018.1435194
Mullen, P. R., & Gutierrez, D. (2016). Burnout, stress and direct student services among school counselors. The Professional Counselor, 6, 344–359. doi:10.15241/pm.6.4.344
National Center for Education Statistics. (2016). Documentation to the 2014-15 Common Core of Data. Retrieved from https://nces.ed.gov/ccd/pdf/2016077_Documentation_062916.pdf
Oddie, S., & Ousley, L. (2007). Assessing burn-out and occupational stressors in a medium secure service. The British Journal of Forensic Practice, 9(2), 32–48.
Pines, A., & Aronson, E. (1988). Career burnout: Causes and cures. New York, NY: Free Press.
Rayle, A. D. (2006). Do school counselors matter? Mattering as a moderator between job stress and job satisfaction. Professional School Counseling, 9, 206–215. doi:10.1177/2156759X0500900310
Rushton, J. P., Chrisjohn, R. D., & Fekken, G. C. (1981). The altruistic personality and the self-report altruism scale. Personality and Individual Differences, 2, 293–302.
Sandoval, J. (1989). Review of the Maslach Burnout Inventory, second edition. In J. C. Conoley & J. J. Kramer (Eds.), The Tenth Mental Measurements Yearbook (pp. 475–476). Lincoln, NE: The University of Nebraska Press.
Scarborough, J. L. (2005). The school counselor activity rating scale: An instrument for gathering process data. Professional School Counseling, 8, 274–283.
Sheffield, D. S., & Baker, S. B. (2005). Themes from retrospective interviews of school counselors who experienced burnout. Hacettepe Üniversitesi Eğitim Fakültesi Dergisi, 29, 177–186.
Sink, C. A., & Stroh, H. R. (2006). Practical significance: The use of effect sizes in school counseling
research. Professional School Counseling, 9, 401–411. doi:10.5330/prsc.9.4.283746k664204023
Stalker, C., & Harvey, C. (2002). Professional burnout: A review of theory, research, and prevention. Brantford, ON, Canada: Wilfrid Laurier University.
Stephan, J. B. (2005). School environment and counselor resources: A predictive model of school counselor burnout (Doctoral dissertation). Retrieved from https://libres.uncg.edu/ir/uncg/f/umi-uncg-1060.pdf
Wachter, C. A. (2006). Crisis in the schools: Crisis, crisis intervention training, and school counselor burnout (Doctoral dissertation). Retrieved from https://libres.uncg.edu/ir/uncg/f/umi-uncg-1190.pdf
Wachter, C. A., Clemens, E. V., & Lewis, T. F. (2008). Exploring school counselor burnout and school counselor involvement of parents and administrators through an Adlerian theoretical framework. Journal of Individual Psychology, 64, 432–449.
Wilkerson, K. (2009). An examination of burnout among school counselors guided by stress-strain-coping theory. Journal of Counseling & Development, 87, 428–437. doi:10.1002/j.1556-6678.2009.tb00127.x
Wilkerson, K., & Bellini, J. (2006). Intrapersonal and organizational factors associated with burnout among school counselors. Journal of Counseling & Development, 84, 440–450.
doi:10.1002/j.1556-6678.2006.tb00428.x
Young, M. E., & Lambie, G. W. (2007). Wellness in school and mental health systems: Organizational influences. The Journal of Humanistic Counseling, Education and Development, 46, 98–113. doi:10.1002/j.2161-1939.2007.tb00028.x
