Apr 1, 2026 | Volume 16 - Issue 1
Brian J. Clarke, Michael T. Hartley, Austin M. Guida
Impostor phenomenon (IP), characterized by persistent self-doubt despite objective success, is prevalent during the early stages of counselor development, often emerging as individuals transition from training into professional practice. This study examined whether self-compassion mediates relationships between IP, resilience, and mental health among 281 counselors-in-training enrolled in departments accredited by the Council for the Accreditation of Counseling and Related Educational Programs. Mediation analyses showed that self-compassion fully mediated the effects of IP on resilience and depression and partially mediated the effect on anxiety. MANOVA results indicated that higher self-compassion corresponded with lower IP, anxiety, and depression, and greater resilience, with robust effects. Findings identify self-compassion as a developmental competency that supports balanced self-evaluation, emotional regulation, and sustainable counselor well-being. Integrating self-compassion training into counselor education and supervision may help developing counselors manage impostor-related distress, strengthen resilience, and promote ethical, sustainable professional practice.
Keywords: impostor phenomenon, counselor development, self-compassion, resilience, mental health
Building resilience and prioritizing mental health are vital during the formative stages of counselor development. During the early stages of training and supervised practice, developing counselors experience the inherent emotional demands and elevated anxiety common while learning to integrate theoretical knowledge into clinical practice (Skovholt & Trotter-Mathison, 2024; Stoltenberg & McNeill, 2010). Although these feelings may diminish with increased experience, enduring self-doubt and inadequacy may signal impostor phenomenon (Clance & Lawry, 2024). Imposter phenomenon (IP), characterized by persistent feelings of fraudulence and incompetence despite evidence of success, impacts nearly all developing counselors (Clarke et al., 2025; Tigranyan et al., 2021). Those experiencing IP may struggle to internalize mastery experiences and fail to consolidate moments of success into genuine confidence (Gadsby & Hohwy, 2024; Roskowski, 2010). Individual differences in coping with IP may be partially explained by self-compassion, which may buffer IP’s negative effects on counseling self-efficacy and well-being (Clarke et al., 2025).
The persistent fear of being exposed as a fraud becomes a harmful cycle whereby individuals ruminate on perceived shortcomings, discount positive feedback, and misattribute positive outcomes to external factors (Clance & Lawry, 2024). Behaviors associated with IP include extreme perfectionism, procrastination, and/or exhausting overpreparation, which can inhibit counselor development (Clarke et al., 2025; Nguyen, 2023). Because IP is rooted in shame and feelings of inadequacy, it contributes to isolation, burnout, and compassion fatigue (Garba et al., 2024; Ojeda, 2024).
IP undermines the reflective, relational, and self-evaluative capacities that are central to counselor development. Counselors who experience chronic self-doubt may hesitate to disclose errors in supervision, question their competence, and struggle to sustain resilience, patterns that can jeopardize client care and professional longevity (Delaney, 2018; Housenecht & Swank, 2022). Given the demands of counselor training and practice, protective factors such as resilience and self-compassion may be critical for developing counselor well-being and persistence.
Resilience is a protective factor to cope with mental distress and burnout (Gerber & Anaki, 2021; Webb & Rosenbaum, 2019). Emerging from the positive psychology movement, resilience explains why some individuals behave adaptively under great stress while others do not. Beyond recovery from adversity, resilience is a process of successful adaptation and coping during challenging or threatening circumstances (Webb & Rosenbaum, 2019). Cultivating new coping mechanisms and fostering personal growth, resilience can sustain well-being and performance during difficult experiences. The limited research on resilience among developing counselors has identified self-awareness and self-compassion as critical protective factors to cope with the emotional demands of becoming a counselor (Hou & Skovholt, 2020).
As a protective factor, self-compassion can play an important role in the resilience and mental health of developing counselors, especially in the presence of IP (Clarke et al., 2025; Neff et al., 2005). Self-compassion is comprised of three interrelated dimensions: mindfulness, common humanity, and self-kindness (Neff, 2023). Mindfulness, the core of self-compassion, involves maintaining awareness of present experiences with reduced reactivity and self-judgment. The common humanity dimension refers to the acceptance that suffering is inherent to our shared human experience. By normalizing challenging experiences, this perspective helps prevent the isolation that may arise from perceiving failures as uniquely personal. Finally, self-kindness encompasses behaviors and ways of relating intrapersonally that offer support and comfort during times of suffering or setbacks. Rather than defaulting to self-criticism, overidentification with failures, or isolation, self-compassion enables understanding and resilience, reducing the impact of IP and the fear of failure during counselor development (Clarke et al., 2025; Warren et al., 2016).
The theoretical alignment between self-compassion and resilience is rooted in their shared emphasis on adaptive emotional regulation, growth through adversity, and the development of a stable and supportive inner identity (Warren et al., 2016). Self-compassion supports sustainable resilience by reducing self-criticism and perfectionism and fostering a growth mindset (Neff, 2023; Warren et al., 2016). Indeed, a recent meta-analysis indicated that self-compassion is consistently linked to positive outcomes among mental health professionals, including enhanced competence, improved therapeutic presence, and a greater willingness to seek guidance and supervision (Crego et al., 2022).
Because of its regulating effects, self-compassion may help developing counselors to tolerate the stress of IP through improved emotional self-regulation (Crego et al., 2022; Neff, 2023). In this way, self-compassion can function as an emotion-focused coping mechanism that reduces the mental distress associated with IP (Clarke, 2024; Crego et al., 2022; Gerber & Anaki, 2021). Ultimately, when individuals experience IP-related distress, self-compassionate responses (mindfulness, common humanity, self-kindness) may interrupt the IP cycle, preserving resilience and mental health (Neff et al., 2005).
The purpose of this study is to examine how self-compassion functions as a protective factor in the relationship between IP, resilience, and mental health during counselor development. Research has found self-compassion to support resilience among health care providers (Delaney, 2018), yet much less is known about the relationship between self-compassion and resilience among developing counselors who experience IP. Addressing the negative impact of IP on counselor development, this article explores how self-compassion might mitigate IP’s negative relationships with resilience and mental health (Clarke et al, 2025; Roskowski, 2010; Tigranyan et al., 2021). The guiding research questions were:
- To what extent does self-compassion mediate the relationships between IP and the outcomes of resilience and mental health?
- How do levels of self-compassion relate to variations in IP, resilience, and mental health among the sample?
We hypothesized that IP would have a significant negative relationship with resilience and mental health, and that self-compassion will significantly mediate these negative associations. Specifically, higher levels of self-compassion will relate to lower IP and improved mental health and resilience. Our findings offer valuable insights into how self-compassion can enhance resilience and promote mental health during counselor development.
Methods
Procedure
The study received IRB approval prior to the recruitment of master’s-level counseling students from across the United States. Data were collected between April and October 2023, using an online survey disseminated via email to Council for the Accreditation of Counseling and Related Educational Programs (CACREP)–accredited program liaisons. These emails described the study and outlined informed consent procedures and inclusion criteria. Eligible participants were individuals enrolled in CACREP-accredited counseling programs aged 18 or older. After consenting, participants were presented with the measures and a demographic questionnaire developed by the authors. Engagement with the study concluded once participants either completed or exited the survey.
Participants
The sample consisted of 281 counseling students attending CACREP-accredited counseling programs from 37 U.S. states and the District of Columbia. Although the present sample consisted of counselors-in-training (CITs), the term developing counselors is used throughout this paper to reflect the broader developmental continuum that spans counselor training and early professional practice (Stoltenberg & McNeill, 2010).
Consistent with the population of CITs, most participants identified as White (n = 190, 67.29%) with lower percentages identifying as Hispanic or Latinx (n = 43, 15.2 %), Asian (n = 17, 6.0%), African American or Black (n = 13, 4.6%), multiracial (n = 13, 4.6%), American Indian or Alaskan Native (n = 3, 1.1%) and Middle Eastern (n = 2, 0.7%). The majority (n = 237, 83.7%) identified as female, with 32 (11.3%) identifying as male, 6 (2.1%) as non-binary, 4 (1.4%) as genderqueer, and 2 (0.7%) choosing not to disclose their gender identity. Participants were from clinical mental health (n = 170, 60.1%), school counseling (n = 49, 17.3%), rehabilitation counseling (n = 49, 17.3%), and marriage and family counseling (n = 13, 4.6%) programs. The average participant age was 32 years (SD = 10.35), with an age range from 21 to 67 years.
Measures
Self-Compassion Scale-Short Form (SCS-SF)
The SCS-SF is a short form of the Self-Compassion Scale (Neff, 2003), consisting of 12 self-report items selected from the original scale (Raes et al., 2011). Items are rated on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Examples include “I try to see my failings as part of the human condition” and “I’m disapproving and judgmental about my own flaws and inadequacies” (Neff, 2003, p. 2). SCS-SF scores have shown good internal consistency (α = .86), with its total scores strongly correlating with those of the full version (r = .98; Raes et al., 2011). Factor analysis has confirmed that the SCS-SF shares the same factor structure as the original scale (Neff et al., 2019; Raes et al., 2011). Scores are interpreted as levels of self-compassion: low (1–2.4), moderate (2.5–3.5), and high (3.51–5). In the present study, SCS-SF scores demonstrated good internal consistency reflected in an alpha of .85, and omega of .85.
Academic Resilience Scale-6 (ARS-6)
The ARS-6 is a concise self-report scale designed to measure academic resilience, defined as the ability to manage challenges, stress, and setbacks within a learning environment (Martin & Marsh, 2006). Items include statements such as “I’m good at bouncing back from a poor grade or difficult feedback” and “I don’t let a bad grade or feedback affect my confidence.” Responses are rated on a 7-point Likert-type response scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater academic resilience. Item and factor level construct validity was supported through factor score estimates, correlation, path analysis, and cluster analysis, showing the ARS scores were closely aligned with related constructs including self-efficacy, control, planning, low anxiety, and persistence (Martin & Marsh, 2006). ARS-6 scores have demonstrated good internal consistency, with an alpha coefficient of .89 (Martin & Marsh, 2006). In the current study, the ARS-6 scores showed acceptable reliability supported by alpha and omega scores of .83.
Clance Impostor Phenomenon Scale (CIPS-10)
The CIPS-10 (Wang et al., 2022) is a condensed, 10-item version of the original 20-item Clance Impostor Phenomenon Scale (CIPS) designed to assess impostor feelings (Clance, 1985). A systematic review by Mak et al. (2019) supported the CIPS-20 as a valid (construct, criterion, and content) measure of IP. The CIPS-10 utilizes a Likert-type response scale ranging from 1 (not at all true) to 5 (very true) and includes items from the CIPS-20, such as “I’m afraid people important to me may find out that I’m not as capable as they think I am” and “I feel my success was due to some kind of luck rather than competence.” Wang et al. (2022) reported strong internal reliability for the CIPS-10 (α = .93), with total scores closely aligning with those of the CIPS-20. Construct validity was supported through factor score estimates, revealing a single-factor structure similar to the 20-item version. In this study, CIPS-10 scores were interpreted using adjusted categories from Clance (1985): few IP (less than 20), moderate IP (20–29), frequent IP (30–39), and intense IP (40–50). Within the current sample, CIPS-10 scores demonstrated good internal consistency with an alpha of .88 and omega of .90.
Patient Health Questionnaire-4 (PHQ-4)
The PHQ-4 is a 4-item, self-report assessment screening tool for depression and anxiety (Kroenke et al., 2009). The Likert-type responses are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). A total score of 3 or more, across both items, indicates the presence of moderate-to-severe symptoms (Kroenke et al., 2009). In meta-analyses, PHQ-4 scores have shown good internal consistency (α = .89) and have yielded valid and diagnostically accurate depression and anxiety scores (Khubchandani et al., 2016; Kroenke et al, 2009). Construct validity was supported using a varimax-rotated principal components analysis conducted on the four screening items (PHQ-2 and GAD-2), yielding two components that together explained 83% of the overall variance. Likewise, criterion validity was indicated by individuals diagnosed with depression or anxiety by a health care professional scoring significantly higher on the PHQ-2, GAD-2, and PHQ-4 compared to participants without a clinical diagnosis (Khubchandani et al., 2016). In the present sample, the PHQ-4 scores showed good internal consistency with an alpha score of .87 and omega of .84.
Data Analysis
Portions of this data set informed a previously published manuscript that focused on how self-compassion can mitigate IP’s negative relationship with counselor self-efficacy (Clarke et al., 2025). Although the two manuscripts share IP and self-compassion data, the current manuscript is distinct and extends this line of inquiry by its unique focus on the benefits of self-compassion for counselor resilience and mental health, despite the presence of IP.
All analyses were performed using SPSS (v29) with a p ≤ .01 benchmark to reduce the likelihood of Type I error and ensure that the most reliable effects are interpreted as statistically meaningful. Preliminary analyses were conducted to examine statistical assumptions for the mediation and MANOVA models. Normality was confirmed for all variables via Shapiro-Wilk (all p > .05). Box’s M test supported homogeneity of variance–covariance matrices (p = .021), and observations were independent. In addition to all VIF scores being < 2, no bivariate correlations exceeded r = .80, suggesting that multicollinearity was not a concern. Collectively, these results suggest that the data met all assumptions necessary for the planned analyses (Tabachnick & Fidell, 2019).
We selected a regression-based mediation analysis because of the study’s focus on specific indirect effects of self-compassion and the moderate sample size, both of which made alternative analyses less ideal (Hayes, 2022). Because the variables tested were represented by composite scores rather than latent constructs, a mediation was statistically appropriate and provided a parsimonious method to examine self-compassion as a buffer for IP. Although cross-sectional mediation cannot establish temporal precedence or causation, it can identify statistical pathways that warrant future longitudinal investigation (Fairchild & McDaniel, 2017; Hayes, 2022). The 99% confidence intervals (CI) of the effects were derived from 10,000 bootstrap samples. If the upper and lower bounds of the CI did not include zero, they were considered statistically significant.
Finally, MANOVA was used to determine how the severity of IP affected its relationships with resilience, anxiety, depression, and self-compassion. The four levels of IP used in this analysis were defined as few, moderate, frequent, and intense IP according to the CIPS author (Clance, 1985). MANOVA effect size was described using partial eta squared values of 0.01 (small), 0.059 (medium), and 0.14 (large; Richardson, 2011). Cohen’s d was used to interpret effect sizes for follow up Tukey analyses, small effect (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8; Gignac & Szodorai, 2016).
A priori power analysis for mediation effects (Fritz & MacKinnon, 2007) indicated a minimum sample of 148 participants would provide .80 power to detect medium-sized indirect effects using bias-corrected bootstrapping. For MANOVA with three groups and four dependent variables, G*Power indicated 158 participants would yield .80 power for detecting medium effects (f² = .25). Our sample of 281 exceeded both requirements.
Results
Descriptives
Pearson correlations indicated significant (< .01) bivariate relationships among self-compassion, impostor phenomenon, depression, anxiety, and academic resilience (Table 1). There were no significant differences in self-compassion, IP, resilience, anxiety, or depression across demographics or counseling program emphasis.
Table 1
Descriptive Statistics and Bivariate Correlations
|
Mean |
SD |
1 |
2 |
3 |
4 |
|
| 1. Self-Compassion |
3.06 |
0.74 |
– |
|
|
|
| 2. Impostor Phenomenon |
32.81 |
8.22 |
−.54* |
– |
|
|
| 3. Depression |
1.27 |
1.60 |
−.42* |
.35* |
– |
|
| 4. Anxiety |
2.54 |
1.78 |
−.55* |
.46* |
.59* |
– |
| 5. Academic Resilience |
27.66 |
6.51 |
.53* |
−.36* |
−.23* |
−.40* |
*p ≤ .01.
The sample included high levels of impostor phenomenon (M = 32.81, SD = 8.22), with over 65% falling in the frequent-to-intense range. IP showed strong negative correlations with self-compassion (r = −.54) and resilience (r = −.36), and strong positive correlations with anxiety (r = .46) and depression (r = .35).
Mediation Analysis
Mediation analyses were used to explore the statistical associations among IP, self-compassion, and the outcome variables of resilience, anxiety, and depression. Results indicated that self-compassion functioned as a statistical mediator in the relationships between IP and each outcome.
Figure 1
Mediation Analysis: Impostor and Resilience
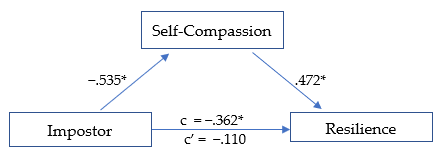
*p ≤ .01
The first model (Figure 1) was significant, R² = .290, F(1, 278) = 59.78, p < .01. The total effect (c) of IP on academic resilience was negative and significant, β = −.362, SE = .126, t = −2.868, p < .01, suggesting that higher IP scores were associated with lower resilience. When self-compassion was included in the model, the direct effect (c′) of IP on resilience was no longer significant, β = −.110, SE = .060, t = −1.838, p = .07, consistent with full statistical mediation (Hayes, 2022). The indirect pathway through self-compassion represented 69.6% of the total standardized association. IP was negatively associated with self-compassion (β = −.535, p < .01; large effect), and self-compassion was positively associated with resilience (β = .472, p < .01; large effect). The overall indirect effect was significant (β = −.252, p < .01).
Figure 2
Mediation Analysis: Impostor and Anxiety
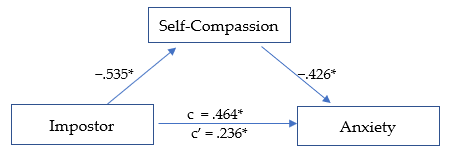
*p ≤ .01.
The second model (Figure 2) was significant, R² = .345, F(1, 278) = 73.159, p < .01. The total effect (c) of IP on anxiety was positive and significant, β = .464, SE = .053, t = 8.747, p < .01, indicating that higher IP scores were related to higher anxiety levels. After including self-compassion, the direct effect (c′) was reduced but remained significant, β = .236, SE = .057, t = 4.110, p < .01, suggesting partial statistical mediation. The indirect pathway through self-compassion accounted for 49.2% of the total standardized association. IP was negatively associated with self-compassion (β = −.535,p < .01; large effect), and self-compassion was negatively associated with anxiety (β = −.426, p < .01; medium effect). The overall indirect effect was significant, β = −.228, p < .01.
Figure 3
Mediation Analysis: Impostor and Depression
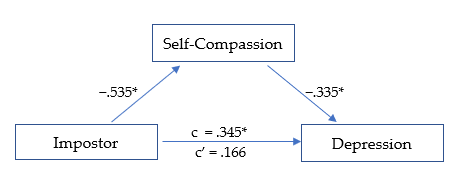
*p ≤ .01.
The third model (Figure 3) was significant, R² = .199, F(1, 278) = 34.484, p < .01. The total effect (c) of IP on depression was positive and significant, β = .345, SE = .056, t = 6.135, p < .01, indicating that higher IP scores were associated with higher depression levels. After accounting for self-compassion, the direct effect (c′) was reduced and no longer significant, β = .166, SE = .064, t = 2.611, p = .02, suggesting full statistical mediation. The indirect pathway through self-compassion represented 51.9% of the total standardized association. IP was negatively related to self-compassion (β = −.535, p < .01; large effect), and self-compassion was negatively related to depression (β = −.335, p < .01; medium effect). The overall indirect effect was significant, β = −.179, p < .01.
MANOVA
Self-compassion scores were divided into three levels (low, moderate, and high) as suggested by Neff (2003) to determine if the effect of self-compassion was consistent across each level. MANOVA analyses revealed that IP, resilience, depression, and anxiety each varied significantly based on level of self-compassion, F(8, 550) = 20.790, p < .01, Wilk’s Λ = 0.590, ηp2 = .232, indicating a large effect size.
The MANOVA results revealed that IP scores varied according to level of self-compassion, F(2, 281) = 48.807, p < .01, ηp2 = .260, with a large effect size. IP decreased significantly at each rising level of self-compassion, from low to moderate (d = 0.666, p < .01) and moderate to high (d = 0.987, p < .01), with medium and large effect sizes, respectively. The greatest decrease in IP was seen as self-compassion rose from moderate to high.
Resilience was significantly higher at each increasing level of self-compassion F(2, 281) = 39.323, p < .01, ηp2 = .221, with a large overall effect size. Resilience rose linearly across each level of self-compassion, from low to moderate (d = −0.756, p < .01), and from moderate to high (d = −0.790, p < .01), each with a medium-high effect size.
Depression scores lowered significantly as self-compassion level increased, F(2, 281) = 20.232, p < .01, ηp2 = .127, with an overall medium effect size. The decrease in depression was noted across levels of self-compassion, from low to moderate (d = 0.446, p < .01), and from moderate to high (d = 0.625, p < .01), each with a medium effect size. The largest decrease in depression was observed as self-compassion rose from moderate to high.
Anxiety scores decreased significantly as the level of self-compassion increased, F(2, 281) = 45.898, p < .01, ηp2 = .248, with a large overall effect size. Anxiety scores were lower as self-compassion rose from low to moderate (d = 0.895, p < .01), and from moderate to high (d = 0.711, p < .01), with large and medium effect sizes, respectively. The largest decrease in anxiety was noted as self-compassion increased from low to moderate.
Discussion
Our findings indicate that self-compassion is a strong protective factor and may enhance resilience and promote mental health among developing counselors, despite impostor feelings. Specifically, self-compassion fully mediated the negative relationship between IP, resilience, and depression, while partially mediating the relationship between IP and anxiety. This suggests that even when experiencing IP, higher self-compassion may help to maintain greater resilience and significantly reduced anxiety and depression. The results are promising and suggest that cultivating self-compassion may facilitate professional growth by interrupting the IP cycle. Our results offer further insights into how self-compassion can support resilience and mental health (Housenecht & Swank, 2022).
Descriptive Statistics
Descriptive analyses revealed a notably high prevalence of IP in the sample, with 96.1% (n = 270) reporting moderate to intense symptoms. Scores were skewed toward the higher end of the scale, with 65.1% of participants in the frequent-to-intense range and 21% in the highest category. Compared with earlier samples, these findings suggest that the severity of IP has increased substantially over the past 15 years (Roskowski, 2010; Tigranyan et al., 2021). For example, only 27.6% of a 2010 sample fell into the frequent-to-intense categories, compared with nearly two-thirds in the present study. Likewise, the proportion of students in the highest IP range has risen fivefold, from 4.1% in 2010 to 21% here. Although this increase may be influenced by broader cultural or educational factors, the trend underscores the importance of implementing effective coping strategies to support counselor well-being and persistence.
Consistently elevated IP scores across studies suggest that impostor feelings may be a common element of counselor development. Such feelings are often fueled by both internal and environmental pressures, particularly graduate students’ unreasonably high expectations of their performance and rapid development (Clance & Lawry, 2024). These unrealistic standards can generate unnecessary self-doubt, distorted self-assessments, and persistent self-criticism (Gadsby & Hohwy, 2024). Importantly, the current results indicate that self-compassion is a powerful counterbalance to IP. Higher self-compassion was associated with lower IP, anxiety, and depression, and with greater resilience, findings that align with previous research (Liu et al., 2023).
Mediation Models
Self-Compassion, IP, and Resilience
The first mediation analysis revealed that self-compassion fully mediated the negative relationship between IP and resilience. When accounting for self-compassion, the negative relationship between IP and resilience was rendered statistically non-significant. This outcome suggests that developing counselors with higher self-compassion may more easily adapt and recover when experiencing impostor-related distress. Self-compassion may assist key aspects of resilience, including stress management, coping with adversity, and maintaining a stable and supportive inner identity (Webb & Rosenbaum, 2019).
Although IP encourages harsh self-criticism and rumination on perceived failures, it is possible that through increased self-acceptance and soothing kindness, counselors can embody greater resilience when confronting areas of growth with less fear of failure. Additionally, a common humanity perspective can encourage acceptance of struggles as a normal part of counselor development and one shared by their peers. These soothing and normalizing aspects of self-compassion can encourage community rather than isolation when struggling, helping counselors to maintain resilience amidst adversity (Hou & Skovholt, 2020; Neff, 2023). Without effective coping practices, the challenges of counselor development can wear down resilience, creating vulnerability to mental distress, burnout, and counselor impairment (Cook et al., 2021; Gerber & Anaki, 2021).
Self-Compassion, IP, and Mental Health
Our results indicate that self-compassion is associated with less anxiety among those experiencing IP. Because anxiety is prevalent in this population and a primary emotional response to IP, efforts to increase self-compassion can have widely beneficial outcomes (Crego et al., 2022; Garba et al., 2024). The common humanity and mindfulness components of self-compassion may be critical to this outcome, as they can help limit emotional reactivity, normalize the IP experience, and reduce the isolation and fear of being exposed as an impostor (Clarke & Guida, 2025). This process involves mindfully recognizing that others share similar experiences and feelings, empowering developing counselors to seek support and reduce fear of failure (Neff, 2023). Likewise, practicing self-kindness may counter the harsh self-criticism associated with IP and encourage them to embrace the developmental process, including their imperfections (Patzak et al., 2017; Warren et al., 2016).
Anxiety and depression are closely linked and often co-occur (Beck & Alford, 2009). Though depression may not correlate as strongly with IP as anxiety does, it remains a common outcome (Garba et al., 2024). IP is persistent and sustained by cognitive distortions and misattributions, which also contribute to depressive thought patterns (Beck & Alford, 2009). However, our analysis revealed that self-compassion fully mediated the relationship between IP and depression. This suggests that a combination of mindful awareness and active self-kindness may facilitate more balanced self-assessment, countering perfectionism and harsh self-criticism commonly associated with IP (Clarke & Hartley, 2025; Pákozdy et al., 2023).
Although IP significantly predicted anxiety and depression, the buffering effect of self-compassion suggests that those with more compassionate self-perceptions may better tolerate the uncertainty and challenges common to counselor training. For example, those with a self-compassionate mindset may reinterpret failures as growth opportunities, a shift that may protect against anxious and depressive symptoms (Crego et al., 2022; Warren et al., 2016). These findings highlight the regulatory potential of self-compassion in reducing emotional reactivity to impostor-related distress.
Level of Self-Compassion in Relation to IP, Resilience, and Mental Health
MANOVA was utilized to determine whether the level of self-compassion (categorized as low, moderate, or high) was related to the level of IP, resilience, anxiety, and depression (Neff, 2003). Self-compassion had a significant positive relationship with mental health and resilience; however, the relationships varied significantly based on level of self-compassion (Figure 4). The results demonstrate that even lower levels of self-compassion were related to significantly lower IP, anxiety, and depression, as well as increased resilience. This pattern suggests that even modest improvements in self-compassion can correspond to improved well-being among developing counselors (Luo et al., 2023). For example, IP severity decreased significantly as self-compassion levels increased, revealing a linear reduction in IP from low to high self-compassion levels, with the most pronounced decrease occurring between the moderate and high categories.
Similarly, resilience scores also increased consistently across each level of self-compassion. The increase was linear, with the most substantial increase occurring when self-compassion rose from low to moderate. The steady increase in resilience across all self-compassion levels points to a possible dose-response relationship. Initial gains in self-compassion may bolster developing counselors’ ability to persevere through challenges (Neff et al., 2005), and interventions resulting in modest enhancements in self-compassion could yield significant improvements in resilience.
Figure 4
IP, Resilience, Depression, and Anxiety Across Levels of Self-Compassion
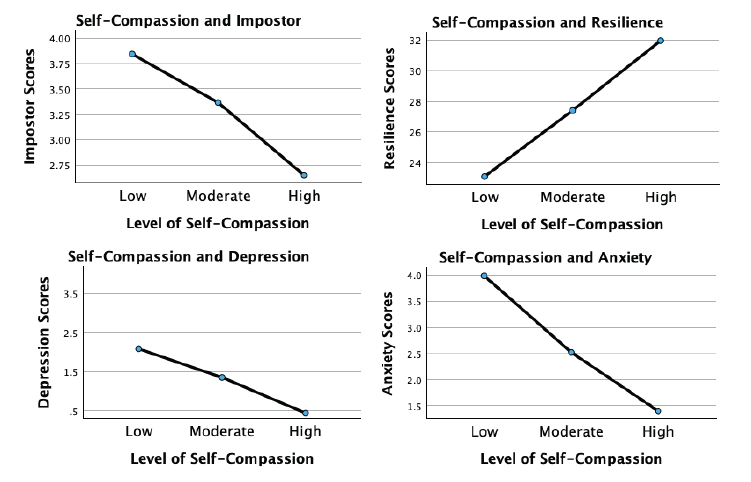
Although more variable, the association of self-compassion with anxiety and depression was similarly beneficial. Anxiety levels decreased significantly with each incremental increase in self-compassion, with the largest reduction occurring from low to moderate levels. This underscores the potential that even lower levels of self-compassion may still meaningfully alleviate anxiety. For depression, a significant decrease occurred across self-compassion levels, with the most substantial reduction noted as self-compassion increased from moderate to high. This suggests that self-compassion may interrupt the internal feedback loop of shame, self-criticism, and hopelessness that sustains depressive thinking in the context of IP.
These findings indicate that self-compassion is an important protective factor for developing counselor mental health. Contrary to expectations, even lower levels of self-compassion significantly relate to reduced IP, anxiety, and depression while increasing resilience (Luo et al., 2023). Integrating strategies to enhance self-compassion into counselor training programs could incrementally increase self-compassion, build emotional tolerance, and create a more stable internal environment from which resilience and well-being can emerge.
Implications and Future Directions for Counselor Development
Despite IP’s prevalence and association with diminished resilience and psychological distress, it remains underexamined in the counseling literature. Beyond a self-care strategy, self-compassion may build resilience and maintain mental health during and after counselor training. Integrating self-compassion into counselor education and early career development may cultivate a more supportive environment and provide counselors with evidence-based ways to manage IP and enhance resilience. Whereas, if left unaddressed, IP can lead to unnecessary distress, burnout, and professional attrition (Coaston & Lawrence, 2019; Ojeda, 2024).
Growing evidence suggests that self-compassion is vital for counselor development and ethical practice (Clarke et al., 2025; Coaston & Lawrence, 2019). The American Counseling Association (ACA) Code of Ethics (2014) emphasizes that professional counselors must engage in ongoing self-assessment and maintain their effectiveness through self-care practices. Similarly, CACREP (2023) standards require counselor education programs to integrate “self-care, self-awareness, and self-evaluation strategies for ethical and effective practice” (3.A.11.). Without meaningful coping strategies, IP can directly undermine these ethical mandates by diminishing well-being and distorting self-evaluation necessary for competent practice (Gadsby & Hohwy, 2024).
Regular engagement in reflective activities promoting balanced self-evaluation is essential to counselor development. If such exercises lack a compassionate focus, they may inadvertently reinforce impostor-related distortions by encouraging rumination and inaccurate self-critique. Matching reflective self-assessment with self-compassion practice may allow developing counselors to internalize feedback and move attention away from self-criticism and toward a growth mindset, transforming internal narratives dominated by IP (Warren et al., 2016).
Counselor educators and professional agencies can integrate self-compassion training through multiple pathways. Brief interventions, such as abbreviated versions of the Mindful Self-Compassion program (Germer & Neff, 2019), offer evidence-based approaches for enhancing counselor resilience. If limited by time and resources, supervisors and mentors can model self-compassionate practices by normalizing struggles, demonstrating constructive self-talk, and providing balanced growth-oriented feedback. The disclosure of faculty or supervisor IP experiences may be particularly powerful, reframing vulnerability and self-care as professional strengths rather than weaknesses.
Because IP is a contextual and environmentally fueled experience, counseling agencies and community mental health settings can foster organizational climates that prioritize compassion and collaboration and normalize challenges during the growth process (Coaston, 2019). When institutions reward openness, reflection, and learning from error, rather than perfection and productivity, developing counselors are more likely to engage in authentic self-assessment and seek help when struggling.
Early career peer support groups and compassion-focused initiatives can also counter the competitive, perfectionistic culture that sustains IP in professional practice (Clark et al., 2022). These approaches challenge the isolating belief that self-doubt is uniquely shameful, and foster community and belonging (Clarke & Guida, 2025; Hou & Skovholt, 2020). Future research should employ longitudinal and experimental designs to test targeted self-compassion interventions, clarifying causal relationships between self-compassion, resilience, and mental health outcomes in counselor education and professional contexts.
Clinical Supervision
Developmentally, the transition from classroom learning to applying theory and skills in clinical practice naturally provokes stress and anxiety (Skovholt & Trotter-Mathison, 2024). Although clinical supervision provides an ideal context for fostering openness and resilience (Coaston, 2019), experiencing IP may be a barrier to disclosing challenges because of emotional distress and fear of exposing perceived inadequacies (DeCandia Vitoria, 2021). Maintaining a façade of competence can compromise development and hinder the supervisory relationship (Thériault et al., 2009). These perfectionistic tendencies and IP are often motivated by context, suggesting that supervisors’ approaches may significantly alleviate these patterns.
Coaston (2019) provides a practical framework for applying self-compassion principles and philosophy in clinical supervision. Rooted in humanistic and developmental theory, this approach emphasizes that supervisors can accompany supervisees through the inevitable discomfort and vulnerability of professional growth by responding with compassion rather than judgment. By adopting a compassionate approach, the supervisory relationship can deepen, normalizing challenges and facilitating an authentic dialogue about IP-related uncertainties. In this way, clinical supervisors can address common cognitive and affective challenges.
A compassionate supervisory environment promotes balanced self-reflection and can reduce the shame-based fear of exposure that drives impostor defenses. This may allow supervisees to explore their conceptual skills openly, reframe unrealistic expectations, and persist despite challenges (Hou & Skovholt, 2020; Stoltenberg & McNeill, 2010). Future research can investigate how self-compassion contributes to the supervisory relationship, comfort with disclosure, and the integration of constructive feedback during supervised practice.
Clinical supervisors can also create a culture of shared vulnerability by modeling self-compassion and transparency about their own developmental struggles and self-doubt. This enables supervisees to internalize feedback and approach self-evaluation with less emotional reactivity. Enhancing collaboration within the alliance empowers supervisees to feel more competent in navigating their development independently (Skovholt & Trotter-Mathison, 2024). Given the potential benefits of this approach, we recommend that future research examine how embodiment and facilitation of self-compassion affect counselor development and well-being.
Limitations
Although the results of this study are encouraging, there are limitations. The cross-sectional design limits the data to a single point in time rather than showing fluctuations in self-compassion, IP, resilience, and mental health over time. Likewise, the present results do not establish causality. Replicating this study using a longitudinal approach can provide greater insight into these fluctuations. Furthermore, self-report measures introduce limitations such as social desirability bias and reliance on participant self-awareness. Likewise, individuals with a personal connection to IP may have been more likely to participate, potentially skewing results.
Participants were not asked about their matriculation status as counseling students, leaving their stage of development unknown. Future research should include clinical experience (i.e., none, practicum, internship) and matriculation status. This information would provide greater insight into how experience and counselor development interact with IP. The current study used a general IP assessment, while future research should use the Counselor Impostor Scale (CIS; Nguyen, 2023), which was published after data collection for this study was complete. The CIS is designed specifically for the counseling domain and could provide more nuanced insights. Additionally, because maladaptive coping strategies such as procrastination and perfectionism sustain IP, subsequent studies should explore these constructs, which could inform more targeted interventions.
Conclusion
The growth process during counselor training is inherently challenging and often gives rise to IP, which increases anxiety and depression while diminishing resilience. Self-compassion is a promising method for enhancing resilience and well-being, despite the presence of IP. Once learned, self-compassion is an accessible practice and relies on applying skills with which counselors are familiar, such as kindness and compassion toward themselves. The results of this study are encouraging and robust, suggesting that self-compassion can enhance resilience by supporting adaptive emotional regulation and fostering a growth-oriented mindset. Self-compassionate counselors can maintain their well-being despite experiencing IP. Importantly, the positive impact of self-compassion was consistent and significant even at lower levels, which is especially important given the prevalence and severity of IP among CITs. The findings support integrating self-compassion into counselor training and clinical supervision through modeling, training, and practice. This approach can provide effective coping for IP and improve resilience, mental health, and persistence.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default- document-library/ethics/2014-aca-code-of-ethics.pdf
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). University of Pennsylvania Press.
Council for the Accreditation of Counseling and Related Educational Programs (2023). 2024 standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Clance, P. R. (1985). Clance Impostor Phenomenon Scale (CIPS). [Database record]. APA PsycTests. https://doi.org/10.1037/t11274-000
Clance, P., & Lawry, S. (2024). Impostor phenomenon: Origins and treatment. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 17–43). American Psychological Association.
Clark, P., Holden, C., Russell, M., & Downs, H. (2022). The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy, 44(2), 185–197. https://doi.org/10.1007/s10591-021-09580-y
Clarke, B. J. (2024). Emerging adult life satisfaction and mental health: The mediating role of self-compassion and social support. Emerging Adulthood, 12(6), 1137–1147. https://doi.org/10.1177/21676968241279490
Clarke, B. J., & Guida, A. M. (2025). Self-compassion to community: The mediating effect of belonging on college student mental health and life satisfaction. Journal of College Student Mental Health. Advance online publication. https://doi.org/10.1080/28367138.2025.2552484
Clarke, B. J., & Hartley, M. T. (2025). Contemplative dispositions and mental health: The supportive role of self-compassion and mindfulness on college students’ resilience. Journal of College Student Mental Health, 39(1), 142–164. https://doi.org/10.1080/28367138.2024.2331931
Clarke, B. J., Hartley, M. T., & Button, C. (2025). Impostor phenomenon and counselor development: The critical role of self-compassion. Journal of Counseling & Development, 103(2), 149–160. https://doi.org/10.1002/jcad.12544
Coaston, S. C. (2019). Cultivating self-compassion within the supervision relationship. The Clinical Supervisor, 38(1), 79–96. https://doi.org/10.1080/07325223.2018.1525596
Coaston, S. C., & Lawrence, C. (2019). Integrating self-compassion across the counselor education curriculum. Journal of Creativity in Mental Health, 14(3), 292–305. https://doi.org/10.1080/15401383.2019.1610536
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in developing professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Crego, A., Yela, J. R., Riesco-Matías, P., Gómez-Martínez, M. Á., & Vicente-Arruebarrena, A. (2022). The benefits of self-compassion in mental health professionals: A systematic review of empirical research. Psychology Research and Behavior Management, 15, 2599–2620. https://doi.org/10.2147/PRBM.S359382
DeCandia Vitoria, A. (2021). Experiential supervision: Healing impostor phenomenon from the inside out. The Clinical Supervisor, 40(2), 200–217. https://doi.org/10.1080/07325223.2020.1830215
Delaney, M. C. (2018). Caring for the caregivers: Evaluation of the effect of an eight-week pilot Mindful Self-Compassion (MSC) training program on nurses’ compassion fatigue and resilience. PLoS ONE, 13(11), e0207261. https://doi.org/10.1371/journal.pone.0207261
Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gadsby, S., & Hohwy, J. (2024). Negative performance evaluation in the impostor phenomenon. Current Psychology, 43, 9300–9308. https://doi.org/10.1007/s12144-023-05030-0
Garba, R., Coleman, C., & Kelley, T. (2024). The impostor phenomenon and mental health. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 61–79). American Psychological Association.
Gerber, Z., & Anaki, D. (2021). The role of self-compassion, concern for others, and basic psychological needs in the reduction of caregiving burnout. Mindfulness, 12, 741–750. https://doi.org/10.1007/s12671-020-01540-1
Germer, C., & Neff, K. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. Guilford.
Gignac, G. E., & Szodorai, E. T. (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. https://doi.org/10.1016/j.paid.2016.06.069
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford.
Hou, J.-M., & Skovholt, T. M. (2020). Characteristics of highly resilient therapists. Journal of Counseling Psychology, 67(3), 386–400. https://doi.org/10.1037/cou0000401
Housenecht, A., & Swank, J. (2022). Motivation, belonging, and support: Examining persistence in counseling programs. Teaching and Supervision in Counseling, 4(2), Article 3. https://doi.org/10.7290/tsc04g4iv
Khubchandani, J., Brey, R., Kotecki, J., Kleinfelder, J., & Anderson, J. (2016). The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Archives of Psychiatric Nursing, 30(4), 457–462. https://doi.org/10.1016/j.apnu.2016.01.014
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Liu, S., Wei, M., & Russell, D. (2023). Effects of a brief self-compassion intervention for college students with impostor phenomenon. Journal of Counseling Psychology, 70(6), 711–724. https://doi.org/10.1037/cou0000703
Luo, X., Che, X., & Lei, Y. (2023). Characterizing the effects of self-compassion interventions on anxiety: Meta-analytic evidence from randomized controlled studies. Journal of Contextual Behavioral Science, 30, 132–141. https://doi.org/10.1016/j.jcbs.2023.10.004
Mak, K. K. L., Kleitman, S., & Abbott, M. J. (2019). Impostor phenomenon measurement scales: A systematic review. Frontiers in Psychology, 10, 671. https://doi.org/10.3389/fpsyg.2019.00671
Martin, A. J., & Marsh, H. W. (2006). Academic resilience and its psychological and educational correlates: A construct validity approach. Psychology in the Schools, 43(3), 267–281. https://doi.org/10.1002/pits.20149
Neff, K. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2023). Self-compassion: Theory, method, research, and intervention. Annual Review of Psychology, 74, 193–218. https://doi.org/10.1146/annurev-psych-032420-031047
Neff, K. D., Hsieh, Y. P., & Dejitterat, K. (2005). Self-compassion, achievement goals, and coping with academic failure. Self and Identity, 4(3), 263–287. https://doi.org/10.1080/13576500444000317
Neff, K. D., Tóth-Király, I., Yarnell, L. M., Arimitsu, K., Castilho, P., Ghorbani, N., Guo, H. X., Hirsch, J. K., Hupfeld, J., Hutz, C. S., Kotsou, I., Lee, W. K., Montero-Marin, J., Sirois, F. M., de Souza, L. K., Svendsen, J. L., Wilkinson, R. B., & Mantzios, M. (2019). Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: Support for use of a total score and six subscale scores. Psychological Assessment, 31(1), 27–45. https://doi.org/10.1037/pas0000629
Nguyen, L. T. (2023). Development and validation of the Counseling Impostor Scale (Doctoral dissertation). Texas A&M University–Corpus Christi.
Ojeda, L. (2024). Impostor phenomenon and burnout. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 81–110). American Psychological Association.
Pákozdy, C., Askew, J., Dyer, J., Gately, P., Martin, L., Mavor, K. I., & Brown, G. R. (2023). The impostor phenomenon and its relationship with self-efficacy, perfectionism, and happiness in university students. Current Psychology, 43, 1–10. https://doi.org/10.1007/s12144-023-04672-4
Patzak, A., Kollmayer, M., & Schober, B. (2017). Buffering impostor feelings with kindness: The mediating role of self-compassion between gender-role orientation and the impostor phenomenon. Frontiers in Psychology, 8, Article 1289. https://doi.org/10.3389/fpsyg.2017.01289
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Roskowski, J. C. R. (2010). Impostor phenomenon and counseling self-efficacy: The impact of impostor feelings (Doctoral dissertation). Ball State University.
Skovholt, T. M., & Trotter-Mathison, M. (2024). The elevated stressors of the novice practitioner. In T. M. Skovholt & M. Trotter-Mathison (Eds.), The resilient practitioner: Burnout and compassion fatigue prevention and self-care strategies for the helping professions (4th ed., pp. 42–68). Taylor & Francis.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Thériault, A., Gazzola, N., & Richardson, B. (2009). Feelings of incompetence in developing therapists: Consequences, coping, and correctives. Canadian Journal of Counselling, 43(2), 105–119.
Tigranyan, S., Byington, D. R., Liupakorn, D., Hicks, A., Mathis, M., & Rodolfa, E. (2021). Factors related to the impostor phenomenon in psychology doctoral students. Training and Education in Professional Psychology, 15(4), 298–305. https://doi.org/10.1037/tep0000321
Wang, B., Andrews, W., Bechtoldt, M. N., Rohrmann, S., & de Vries, R. E. (2022). Validation of the short Clance Impostor Phenomenon Scale (CIPS-10). European Journal of Psychological Assessment, 40(2), 158–168. https://doi.org/10.1027/1015-5759/a000747
Warren, R., Smeets, E., & Neff, K. (2016). Self-criticism and self-compassion: Risk and resilience. Current Psychiatry, 15(12), 18–33. https://self-compassion.org/wp-content/uploads/2016/12/Self-Criticism.pdf
Webb, R. E., & Rosenbaum, P. (2019). Resilience and thinking perpendicularly: A meditation or morning jog. Journal of College Student Psychotherapy, 33(1), 75–88. https://doi.org/10.1080/87568225.2018.1449687
Brian J. Clarke, PhD, NCC, LAC, is an assistant professor at the University of Arizona. Michael T. Hartley, PhD, CRC, is a professor at the University of Arizona. Austin M. Guida, PhD, NCC, LAC, is an assistant professor at Northern Arizona University. Correspondence may be addressed to Brian J. Clarke, Department of Disability and Psychoeducational Studies, College of Education, 1430 E. 2nd Street, Room 422, Tucson, AZ, 85721-0069, bclarke14@arizona.edu.
Mar 18, 2025 | Volume 15 - Issue 1
Zori A. Paul, Kyesha M. Isadore, Nishi Ravi, Kayla D. Lewis, Dewi Qisti, Alex Hietpas, Bergen Hermanson, Yuji Su
Queer and transgender people of color (QTPOC) face unique mental health challenges because of intersecting forms of discrimination that place them at higher risk for adverse mental health outcomes. Emerging research has begun to explore the concept of microaffirmations—small verbal or nonverbal forms of communication that signal support, encouragement, or validation—as a protective factor for marginalized populations. This study highlights how QTPOC experience and perceive microaffirmations and explores the role microaffirmations play in their mental health and well-being. Utilizing an interpretive phenomenological analysis, qualitative data were obtained from 14 QTPOC participants through semi-structured interviews. Analyses identified five superordinate themes: influence of identity development, safety with others, envisioning policy changes, representation, and internalization of perceived worth. This study demonstrates the role microaffirmations play in mitigating the negative impacts of discrimination and enhancing the well-being of QTPOC. Implications for counselors include suggestions for providing QTPOC clients with more affirming care on the micro and macro levels.
Keywords: microaffirmations, queer, transgender, people of color, mental health
The number of queer and transgender people of color (QTPOC) in the United States is increasing (Jones, 2024), leading to a greater focus on their unique experiences and mental health needs. In recent years, the visibility of QTPOC has grown, and with it, awareness of the specific challenges they face. These challenges are compounded by intersecting forms of discrimination related to both their racial/ethnic identities and their sexual and gender identities (Cyrus, 2017). Despite this increased visibility, QTPOC continue to experience significant mental health disparities, which are often overlooked in broader discussions about mental health and well-being. These mental health concerns include higher rates of depression, anxiety, and trauma, as well as increased risk of suicidal ideation compared to their White cisgender or heterosexual counterparts (Bostwick et al., 2014; Horne et al., 2022; Meyer, 2003; White Hughto et al., 2015).
Based on the existing mental health disparities among QTPOC, the need exists for enhanced awareness and education about how to promote safe and affirming therapeutic environments for QTPOC clients. Recent research indicates that QTPOC’s mental health outcomes, sense of belonging, and overall well-being are dependent on interactions with others both on the micro and macro levels. For example, how QTPOC are referred to by counselors or administrative staff and how welcomed they feel as members of their community significantly impact their overall mental health and well-being (Pflum et al., 2015). At the same time, QTPOC often experience stressors related to state and federal anti-LGBTQIA+ legislation and lack of competency from non-QTPOC counselors and other health care professionals, possibly leading to feelings of exclusion (Dispenza & O’Hara, 2016; Horne et al., 2022). Counselors and researchers have emphasized the need for addressing issues of racism, homophobia, and transphobia in clinical practices, counselor education programs, and broader societal contexts (Dispenza & O’Hara, 2016; Miller et al., 2018; Mizock & Lundquist, 2016).
Mental Health Concerns for Queer and Transgender People of Color
In recent decades, there has been an increase in research examining the social experiences of minoritized groups, including queer adults, transgender individuals, and people of color (Brooks, 1981; Flanders et al., 2019; Meyer, 2003; Testa et al., 2015). These studies have highlighted substantial disparities in mental health and well-being among these populations, often linked to experiences of discrimination and marginalization. Research indicates that QTPOC are particularly vulnerable to mental health issues because of the intersecting impacts of racism, heterosexism, and transphobia. For instance, a study examining factors related to depression and anxiety for lesbian, gay, and bisexual people of color found that both distal and proximal minority stressors accounted for 33% of the variance in participants’ mental health outcomes (Ramirez & Galupo, 2019). This dual marginalization often leads to cumulative forms of discrimination, including social exclusion from both larger society and within their own communities. QTPOC may face racism within the LGBTQIA+ community and heterosexism or transphobia within their racial and ethnic groups (Cyrus, 2017). Despite these challenges, social support and community connectedness have been identified as critical resources that can buffer the effects of stigma and promote resilience among QTPOC. For example, social support from individuals who are empathetic toward discriminatory experiences can shield young African American LGBTQIA+ youth from the distress associated with intersectional discrimination, fostering a sense of affirmation for their identities and enhancing their autonomy in help-seeking behaviors (Hailey et al., 2020).
Community connectedness has also been linked to positive outcomes among QTPOC (Roberts & Christens, 2020). Roberts and Christens (2020) found that being open about one’s sexual or gender identity (i.e., outness) is beneficial to the well-being of White participants, but not directly for Black and Latinx participants. Instead, the positive effects of outness on well-being for these groups are mediated by their connectedness to the LGBTQIA+ community (Roberts & Christens, 2020). However, the effectiveness of community connectedness can vary. For example, McConnell and colleagues (2018) reported that community connectedness had a weaker mediating effect on the relationship between stigma and stress in sexually minoritized men of color compared to their White counterparts, suggesting that racial stigma may diminish the protective effects of community connectedness. Establishing community connectedness with other QTPOC may foster positive within-community relationships that extend beyond discrete identity groups, enabling members to feel acknowledged and accepted, and leading to positive reappraisals about their identities (Ghabrial & Andersen, 2021; G. Smith et al., 2022). Despite the potential utility gained by understanding factors that promote coping and resilience, there is still a lack of research examining their impact on the mental health and well-being of QTPOC. Emerging research has begun to explore potential sources of everyday coping and resilience, such as the study of microaffirmations.
Microaffirmations
Microaffirmations are defined as small verbal or nonverbal communications that signal support, encouragement, or validation (Ellis et al., 2019; Rowe, 2008). Despite their subtle nature, microaffirmations can be intentional or unintentional, with some occurring as deliberate acts of affirmation while others emerge naturally in everyday interactions (Rowe, 2008). Rowe (2008), who first introduced the concept, posited that for underrepresented groups, daily occurrences of marginalization may go overlooked or be diminished within hierarchical power structures. As members of these groups often struggle with feeling appreciated and accepted within disempowering environments, microaffirmations may effectively counter these negative experiences by disrupting processes that promote social exclusion and oppression (Ellis et al., 2019). Microaffirmations normalize and acknowledge the contributions of marginalized individuals, offer individuals support during times of distress, and empower disenfranchised group members to leverage their strengths to maximize their potential (Rowe, 2008). In general, microaffirmations function as a tool of social reinforcement to bolster productivity by engendering a sense of belonging, fostering inclusion, and enhancing well-being (Topor et al., 2018).
Over the past decade, microaffirmations have emerged as a potential protective factor against the detrimental impact of prejudice and discrimination (Pérez Huber et al., 2021; Rolón-Dow & Davison, 2021). In particular, the underlying behavioral mechanisms of microaffirmations are implicated in reducing intergroup conflict stemming from social stratification and stigma (Jones & Rolón-Dow, 2018; Rolón-Dow & Davison, 2021). Although microaffirmations were initially developed within the workplace literature to address the experiences of cisgender women, recent work has extended the concept’s application to further marginalized groups, including people of color and the LGBTQIA+ community. Microaffirmations can play an important role in the lives of LGBTQIA+ individuals by communicating acceptance, extending social support, and affirming their identity (Flanders et al., 2019). For example, in a cross-sectional study with LGBTQIA+ adolescents, Sterzing and Gartner (2020) found that receiving microaffirmations from family members was associated with a reduction in symptoms of depression, distress, emotional dysregulation, and suicidality. Similarly, interpersonal microaffirmations have also been associated with fewer symptoms of anxiety and stress (Flanders, 2015) and are frequently referred to as impactful experiences of affirmation among bisexual people (Flanders et al., 2019). However, some studies suggest that the effects of microaffirmations may be limited or context-dependent. For example, DeLucia and Smith (2021) found that microaffirmations from mental health providers had no impact on bisexual people’s intentions to seek mental health treatment, whereas experiences of biphobia negatively influenced these intentions. Similarly, Salim et al. (2019) found no association between microaffirmations and happiness among bisexual women. These findings suggest that the effects of microaffirmations may be context-dependent, influencing some aspects of well-being while having little impact on others. Although microaffirmations may foster a sense of validation and support, they may not necessarily translate into behavioral changes, such as help-seeking. These varying results highlight the need for further research on microaffirmations to understand their impact on well-being within different social contexts and systems of power and privilege.
In contrast, research with transgender adults has shown relatively consistent and positive outcomes associated with microaffirmations. Using thematic analysis, Anzani and colleagues (2019) found that microaffirmations may strengthen the therapeutic alliance and enhance perceived treatment satisfaction and efficacy for transgender clients. Scholars have also investigated racial-specific microaffirmations, conceptualized as acts, cues, or verbal utterances that validate racial identities, acknowledge lived experiences, and promote racial justice norms (Rolón-Dow & Davison, 2021). While microaffirmations may have a lesser psychological impact, incidence rate, and intensity than microaggressions (Jones & Rolón-Dow, 2018), they may function to counteract and partially repair the cumulative effects of insidious everyday acts of racism (Pérez Huber et al., 2021). Racial microaffirmations can promote healing through shared cultural intimacy, enabling supportive community members to engage in a cumulative and responsive process of acknowledgment and support that can be both protective and restorative in the context of structural racism (Pérez Huber et al., 2021).
The Current Study
The theoretical framework for this study is grounded in Minority Stress Theory (MST; Brooks, 1981; Meyer, 2003) and Rolón-Dow and Davison’s (2021) typology of microaffirmations. MST posits that the stress experienced by individuals with stigmatized identities is not due to the identity itself but arises from external prejudice and discrimination, as well as internalized stigma (Brooks, 1981; Meyer, 2003). For QTPOC, these stressors are compounded by intersecting forms of racism, heterosexism, and transphobia. This framework highlights the unique stressors faced by QTPOC and underscores the need to understand the multifaceted nature of their experiences. In addition to MST, this study draws on the typology of racial microaffirmations from a critical race/LatCrit approach developed by Rolón-Dow and Davison (2021), which includes four forms: microrecognitions, microprotections, microtransformations, and microvalidations. Each type can be understood as different feelings arising from behaviors, verbal statements, or environmental cues. Microrecognitions involve feeling acknowledged and included (e.g., Pride flags, signage), microprotections offer a sense of being shielded from disparagement (e.g., support and advocacy from others), microtransformations foster a deep sense of belonging and capability (e.g., individuals or institutions advocating for federal and state policies that protect LGBTQ+ rights), and microvalidations affirm that one’s thoughts, feelings, and behaviors are accepted and valued (e.g., QTPOC-specific spaces). While MST has provided a valuable framework for understanding QTPOC mental health disparities, there remains a need to explore how protective factors, such as microaffirmations, can mitigate the negative impact of discrimination on QTPOC. Microaffirmations, though subtle, normalize marginalized communities’ existence and place in society and may counterbalance the pervasive negative experiences of marginalization. Despite the promising research on microaffirmations for individual marginalized groups, research specifically focusing on the impact of microaffirmations on QTPOC is still limited. Given the significant mental health disparities faced by QTPOC and the potential of microaffirmations as a protective factor, this study aimed to deepen the understanding of these dynamics and identify effective strategies for fostering resilience and improving mental health outcomes among QTPOC. The purpose of this study was to 1) explore how QTPOC describe and understand microaffirmations and 2) investigate the specific types of microaffirmations in relation to the mental health and well-being of QTPOC.
Method
The current study employed an interpretive phenomenological design. Interpretive phenomenology is a rigorous qualitative methodology that seeks to uncover participants’ meaning-making processes—comprising their understandings, perceptions, and experiences—related to their lived experiences with a particular phenomenon (J. A. Smith et al., 2009). Interpretive phenomenological analysis (IPA) focuses analytically on the personal meaning-making of participants within specific contexts (J. A. Smith et al., 2009). Through this method, themes are systematically identified and leveraged to construct interpretive descriptions of participants’ narratives, providing insight into the meanings and essences of their lived experiences with the phenomenon.
Participants and Procedures
Institutional review board approval was secured prior to participant recruitment or data collection, and all participants gave consent via the online survey. Data was collected during the summer of 2023 and participants were recruited through recruitment flyers and emails via social media, LGBTQIA+ listservs, snowball sampling, and national listservs and interest networks. Eligible participants were asked to respond to an online survey to complete a brief demographic survey and were then contacted by the researchers to schedule a virtual interview. Eligibility criteria included: 18 years of age or older and capable of providing informed consent, identifying as a person of color with a marginalized sexual and/or gender identity, and currently living in the United States or U.S. territories. Interviews took place privately on a video-conferencing platform and were recorded and transcribed for data collection purposes. Participants who completed the interview were provided with a $25 e-gift card as an incentive for participation in the study. Participant demographics are presented in Table 1. All participants (N = 14) identified as a person of color; ages 22–46; sexual identities included queer, bisexual, asexual, demisexual, and gay/lesbian; gender identities included cisgender man, cisgender woman, and non-binary/gender-expansive. Racially and ethnically, participants identified as Filipino, Black/African American, Afro-Caribbean, Chinese American, Latino/a/x, Vietnamese, and Chinese. All participants held a postsecondary degree including bachelor’s, master’s, or doctorate degrees.
All participants engaged in one 60-minute semi-structured interview, which consisted of 19 open-ended questions and prompts aimed at exploring participants’ lived experiences with microaffirmations and the utility of microaffirmations in their daily lives. Drawing from Rolón-Dow & Davison’s (2021) typology of microaffirmations, the interview protocol (see Appendix) was designed to explore participants’ experiences with the four forms of microaffirmations: microrecognitions, microprotections, microtransformations, and microvalidations. For example, the question “Could you describe everyday experiences that made you feel that your thoughts, feelings, sensations, and/or behaviors associated with your lived experience as [insert identity] are accepted, legitimized, or given value?” was formulated to invite participants to reflect on whether they experienced microvalidations. This open-ended question was followed up with questions such as “If you haven’t experienced that, what do you think positive acknowledgment and understanding of your identity and lived experience would look like?” and “In what ways do you think more positive acknowledgment and understanding would impact you directly?” Audio files were recorded using a secure device and stored in a restricted access folder on the researcher’s university department server. Files were used for transcription purposes only and destroyed after the transcription process was complete.
Data Analysis
The data analysis process adhered to the established analytic procedures of IPA outlined by J. A. Smith and colleagues (2009). IPA is characterized by its interactive and inductive approach, focusing on how individuals make sense of their specific lived experiences. The interpretive nature of IPA allows for interpretations that may diverge from the participant’s original text, provided these interpretations are rooted in a close examination of the participant’s words (J. A. Smith et al., 2009).
Initially, the interviews were transcribed verbatim and meticulously reviewed by the research team to understand their context. During this preliminary phase, bracketing and initial coding were performed to describe the interview content. Each interview was individually analyzed to identify central concepts before finding commonalities across interviews (J. A. Smith et al., 2009). The researchers then utilized these initial codes and the original transcripts to identify emergent themes and patterns, employing techniques like abstraction and subsumption to develop superordinate themes. These steps were repeated for each of the participants individually to allow for new themes to emerge by case before superordinate themes were compared across participant cases corresponding to the central research questions.
Table 1
Participant Demographic Information
| Participant
(pronouns) |
Age |
Gender Identity |
Sexual Identity |
Race/Ethnicity |
Highest Degree |
| April
(she/her) |
29 |
Cisgender woman |
Asexual, Demisexual |
Chinese American |
Master’s degree |
| Baohua
(not disclosed) |
36 |
Cisgender man |
Gay |
Asian or Asian American |
Master’s degree |
| D
(she/her) |
28 |
Cisgender woman |
Lesbian, Demisexual |
Black or African American |
Master’s degree |
| Didi
(not disclosed) |
27 |
Cisgender woman |
Bisexual |
Latino/a/x or Hispanic |
Bachelor’s degree |
| Dwayne
(he/him) |
46 |
Cisgender man |
Gay |
Black or African American |
Master’s degree |
| Faith
(she/her) |
23 |
Cisgender woman |
Lesbian, Bisexual, Questioning |
Filipino |
Bachelor’s degree |
| J
(he/him) |
31 |
Cisgender man |
Bisexual |
Filipino |
Doctorate degree |
| Jane
(she/her) |
36 |
Cisgender woman |
Queer |
Black or African American |
Doctorate degree |
| Kay
(she/her) |
27 |
Cisgender woman |
Bisexual, Queer |
Black/Afro-Caribbean |
Master’s degree |
| Lucia
(they/them) |
26 |
Gender-expansive |
Queer |
Filipino |
Master’s degree |
| Nick
(he/him) |
27 |
Cisgender man |
Gay |
Black or African American |
Bachelor’s degree |
| Oliver
(he/him/any) |
22 |
Cisgender man |
Gay, Queer |
Vietnamese |
Bachelor’s degree |
| QL
(not disclosed) |
29 |
Gender-expansive |
Queer |
Chinese |
Master’s degree |
| Stacey
(she/her) |
29 |
Cisgender woman |
Bisexual |
African American & Caribbean American |
Doctorate degree |
Trustworthiness and Researcher Positionality
Our research team consisted of one Black bisexual/queer cisgender female faculty member, one Black queer genderfluid faculty member, four doctoral counseling students, and two master’s counseling students. The students on the research team identify as members of various races/ethnicities, genders, and sexual orientations. All members of the research team either work in or are enrolled in CACREP-accredited counselor education or APA-accredited counseling psychology programs, and all researchers have clinical experience working with diverse populations. To increase opportunities for candid conversations about the role of race/ethnicity, gender, sexuality, and intersectionality with participants throughout the interview process, interviews were conducted by members of the research team who identify as racially/ethnically minoritized, gender-expansive, and/or queer.
Several well-established methodological strategies were employed throughout data collection and analysis to enhance the credibility and trustworthiness of the findings. Multiple coders and peer audits of codes and themes were used to further explore themes, patterns, and interpretations; challenge assumptions; and provide additional insights. This approach is a recognized strategy for enhancing credibility in qualitative research (Yardley, 2008). The involvement of multiple coders and peer audits also served as a check against normative assumptions, prompting researchers to consider how systemic biases might influence their interpretations. Additionally, the research team conducted member checks with participants to verify the accuracy of themes and interpretations. Following the example of Lincoln and Guba (1985), the research team conducted member checks to allow participants to react to the data and the research team’s interpretations before their feedback was incorporated into the presentation of the findings. Participants who engaged in the member check process were provided with a $10 e-gift card as a token of appreciation. The participants’ feedback was not merely a validation step but also a critical engagement with their lived experiences, contributing to a more comprehensive representation of their narratives. The research team met weekly to engage in reflexive discussions about our assumptions, biases, personal worldviews, questions, and concerns related to our research processes, analyses, interpretations, and conclusions.
Results
An in-depth phenomenological analysis of the 14 participant interviews resulted in identification of five superordinate themes related to understanding the role of microaffirmations among QTPOC. Superordinate themes include influence of identity development, safety with others, envisioning policy changes, representation, and internalization of perceived worth.
Influence of Identity Development
The theme influence of identity development reflected how participants understood the utility of microaffirmations in relation to their racial, gender, and sexual identity development. Participants at earlier stages of identity development emphasized the importance of microvalidations and microrecognitions, which provided support and validation as they navigated internal conflict, such as questioning their identity or experiencing self-doubt. For example, April, a 29-year-old asexual/demisexual Chinese American woman, shared that she was still discovering her identity and sometimes felt “a little bit ambiguous about where I’m located on the map.” She highlighted how microvalidations—subtle signs of being recognized and valued—helped her feel seen and supported during this uncertain time:
The other person listening to me or asking me questions that make me feel seen . . . I would say people noticing the pieces that are authentic to who I am and people being willing to spend time listening to me and asking follow-up questions. That is affirming.
Similarly, Faith, a 23-year-old lesbian/bisexual Filipino woman, described herself as “either bisexual or gay, not sure which one yet,” and reflected on how microrecognitions, such as being acknowledged in conversations or within social settings, validated her evolving identity. These early-stage participants frequently described microvalidations and microrecognitions as pivotal in affirming their personal experiences and alleviating internal struggles with identity. In contrast, participants who were more secure and confident in their identities—representing a later stage in their identity development—emphasized a need for microprotections and microtransformations—types of microaffirmations that extend beyond individual validation to encompass broader social change. These participants valued microprotections, which offer safeguarding measures for the QTPOC community against discrimination and prejudice, and microtransformations, which focus on creating systemic changes to improve the quality of life for all QTPOC. For example, Jane, a 36-year-old queer Black woman, discussed how educators can implement microtransformations by using their influence to normalize queer identities within the classroom:
I feel like if we were to learn about [QTPOC] as historical figures and learn about them, like in health class for example, it would help us in other interpersonal contexts and making relationships. It would also normalize treating [QTPOC] as people and with kindness.
Jane’s reflection illustrates the potential for microtransformations to contribute to systemic shifts in how QTPOC are viewed and treated in society. Participants at this later stage of identity development sought microaffirmations that not only validated their personal identities but also fostered more inclusive environments through microprotections and broader societal shifts. These microprotections, such as inclusive policies in schools or workplaces, safeguard QTPOC from harmful discrimination, while microtransformations create opportunities for long-term structural changes that challenge structural inequities and create more affirming environments for QTPOC.
Safety with Others
The theme safety with others represented participants’ experiences of how microaffirmations, particularly microvalidations and microrecognitions, signaled safety in their external environments, indicating that they could express their identities without fear or discrimination. Many participants spoke about the importance of microaffirmations being a way to subtly indicate that an area or person in their external environment is less likely to discriminate, alienate, or be violent toward them. Lucia, a 26-year-old gender-expansive queer Filipino, highlighted the role of microrecognitions in fostering a sense of security: “Microaffirmations communicate safety to me, like, say, from my external environment, that I can then disclose, fully disclose, who I actually am to people . . . So [microaffirmations] are definitely an aspect of safety and being out or not.” For Lucia, small but significant acts of recognition, such as visual cues or verbal affirmations from others, provided reassurance that their identity would be accepted and protected in that space. Similarly, D, a 28-year-old lesbian/demisexual Black woman, shared that microvalidations, such as seeing the Pride flag displayed in public spaces, gave her a sense of immediate comfort and safety: “I can breathe and relax and like, oh, I can exist in this space.” These microvalidations, subtle yet powerful, signaled that the space was affirming and protective of her identity.
Beyond personal safety, participants also reflected on the protective role of microprotections. Some participants, like Jane, described how microprotections in her environment gave her confidence that she would not be alone if a negative situation occurred: “[Microaffirmations] were a sign that there was some kind of protection and backup, that if something goes wrong, that I’m not in it by myself . . . I’m not going to be piled on . . . or outwardly rejected.” This sentiment highlights how microprotections create a sense of communal support, with which participants know that others will ally with them in moments of potential conflict or discrimination. Stacey, a 29-year-old bisexual African American and Caribbean American woman, elaborated on how the cumulative effect of microaffirmations contributed to her overall sense of safety: “When you have more microaffirmations than aggressions . . . you, I, tend to feel safer.” In this instance, Stacey underscored the idea that frequent experiences of affirmation—whether through microvalidations or microrecognitions—help mitigate the impact of microaggressions, allowing her to feel more secure in her identity. Oliver, a gay/queer Vietnamese man, further reflected on how the absence of microaffirmations could leave him feeling vulnerable: “If I didn’t have the experiences of microaffirmations that I did today, I would just feel . . . less mentally secure generally.” Oliver’s observation emphasizes the protective nature of microaffirmations, in that their presence contributed not only to a sense of physical safety but also to psychological security.
Envisioning Policy Changes
The theme envisioning policy changes captured participants’ reflections on the broader implications of microaffirmations, specifically their potential to influence policy and create systemic change. Participants shared their views on both the immediate benefits of microaffirmations and their limitations in addressing larger structural issues. The role of microaffirmations was seen as a necessary component of personal healing from the often-daily trauma of microaggressions but was not sufficient to address systemic inequities. Instead, participants stated that microaffirmations should serve as stepping stones toward inclusive laws and policies. Microprotections, such as individuals expressing their support for policies that provide legal safeguards and affirming spaces, were seen as critical for improving the well-being of QTPOC. Lucia advocated for increased health and gender-affirming care protections: “We need increased protections for health and gender-affirming care, and not just in certain states but nationally.” Lucia’s desire for more inclusive policies highlights the role of microprotections in safeguarding the rights and well-being of QTPOC at a systemic level. Similarly, Stacey emphasized the need for broader legal changes to contend with book bans and the censorship of LGBTQIA+ content in public schools:
I find book bans and the banning of specific conversations in public schools to be very harmful. I primarily work with adolescents and their families, and I believe a lot of stuff starts in childhood, and if we are sending the message to children that queer people shouldn’t exist or that we can’t talk about it, it creates generations of harm.
Stacey’s reflection illustrates how microprotections can counteract systemic exclusion and ensure that QTPOC youth are represented and affirmed in public education.
Microtransformations, on the other hand, were described as the support for far-reaching changes in policies and societal norms that would fundamentally improve the daily lives of QTPOC. Kay, a bisexual/queer Black/Afro-Caribbean woman, noted that while microaffirmations were helpful in buffering the effects of daily microaggressions, they were not enough to dismantle deeply embedded systemic oppression:
So, I think microaffirmations are a buffer to all the aggressions, violence, harm, and trauma that’s happening consistently, but it doesn’t necessarily erase the harm and the violence. But it does provide, at least for me, a buffer mentally. Because I feel if I experience a microaggression, and if I internalize it, that can add to deeper trauma. And microaffirmations can help me externalize that and know that even though it hurts, that it’s not me. I’m not gonna sit in that with that person. And so, I think it’s a great buffer.
Kay’s awareness of the limitations of microaffirmations underscores the importance of advocating for systemic reforms that extend beyond individual or community-level affirmations. There was a marked urgency in advocating for national-level policy changes, such as the expansion of health care access and “full adoption rights for same-sex parents” (Baohua, a 36-year-old gay Asian man). Baohua’s comments reflect the urgent need for uniform protections and policies that support QTPOC regardless of geographic location. Dwayne, a 46-year-old Black gay man, similarly advocated for accessible and inclusive mental health care services as a form of microtransformation, stating that “Making mental health care more accessible and acceptable for all of us should be a priority.” Dwayne’s insight connects microtransformations to health equity, pointing out that long-term systemic improvements are needed to ensure that QTPOC have equal access to health services. Ultimately, dissatisfaction with current policies was prevalent, with participants advocating for equitable reforms that go beyond affirming language and instead target holistic care. Some found it challenging to specify exact policies but envisioned that supportive policies would enhance their well-being and enable easier connections, more energy, and fuller participation in daily life.
Representation
The theme of representation reflected participants’ experiences of engaging with microaffirmations that represent their lived experiences as QTPOC from external sources through visual or vocal cues, as well as participants’ creation of their own microaffirming external sources for others to feel represented through.
External Representation
Representation that was received or seen via microvalidations and microrecognitions was critical in helping participants feel affirmed in their racial/ethnic and gender/sexual identities. J, a 31-year-old bisexual Filipino man, emphasized how social media representations during Pride Month and Asian American Pacific Islander (AAPI) Heritage Month made him feel both his queer and racial identities were not only seen but celebrated:
What comes to mind right away is just Instagram stories and just seeing most of my timeline having some sort of Pride tag or Pride sticker on their stories . . . And also last month during AAPI Heritage Month, those Instagram stories and having the little sticker—it’s really nice to see a bunch of signs of like, “hey, we’re celebrating you!” and “hey, I’m a part of this group too!”
For J, these microrecognitions on social media provided him with a sense of visibility and belonging, reinforcing that the community valued his intersectional identity. Participants throughout shared that visible external representation like affirming signage, Pride flags, racially and LGBTQIA+ diverse TV shows such as Heartstopper, LGBTQIA+ bumper stickers, hashtags, social media posts, and even seeing LGBTQIA+ folks being successful in a variety of different careers were viewed as affirming of their queer identities. Having external representation through a variety of sources not only made participants feel like their identities were being celebrated, but some participants, like Kay, also believed that external representations are microprotections that are “counteracting or disrupting” people from being “harmful” and deterring discrimination.
Created Representation
Though experiencing representation was important, many found that actively creating microaffirmations and making their own representation for themselves and others was also imperative to their well-being. Many saw themselves as change agents, contributing to microtransformations by normalizing conversations about their sexual and gender identities, establishing safe spaces, and engaging in activism that benefited other QTPOC. Dwayne spoke about how his life journey recently involved stepping into a leadership role, in which he felt responsible for creating representation for others:
I guess . . . when it comes to people who are capable of trying to help others, [they realize] that there is sometimes a shortage of people who can be that spokesperson, or be that leader, to be that example, or that exemplary person. They can be in the forefront. . . . And so, I think where I’m at now, just in my life journey, is that . . . I’m coming into that space.
By creating visibility for himself, Dwayne was actively contributing to the creation of microtransformations. Stacey shared the importance of fostering inclusivity for future generations, particularly her children. She explained how creating affirming spaces at home, such as by exposing her children to diverse representations of queer families, was a way to contribute to future microprotections: “[I want to] have them reading books and you know, expose them to other queer families and let them know that this is normal.” By normalizing having conversations about the LGBTQIA+ community, not only is knowledge being shared, but the likelihood increases that youth who may resonate with identities within the community may experience less queer- and race-related microaggressions than their predecessors (Houshmand et al., 2019).
Internalization of Perceived Worth
The theme internalization of perceived worth not only highlighted participants’ internalization of microaffirmations regarding their individual and collective sense of worth but also how the source of these microaffirmations influenced their impact. Microvalidations were often described as contributing to their mental and emotional well-being. For example, Didi, a 27-year-old bisexual Latina woman, shared how microaffirmations helped her feel less overwhelmed and more validated in her identity: “[Microaffirmations] really help me feel validated and, in terms of mental health, I feel like it makes me feel less overwhelmed.” For Didi, these microvalidations provided emotional support that helped her manage the daily stressors associated with navigating stigma and other social barriers. Microrecognitions were also described as crucial in helping participants internalize a sense of worth. For some, like Nick, a 27-year-old gay Black man, internalized validation from microaffirmations not only makes participants feel like their identities as QTPOC are valid but may also provide QTPOC with “better mental health.” QL, a 29-year-old queer gender-expansive Chinese person, also spoke about how microaffirmations helped with their mental well-being and made them feel “affirmed” and “really good,” and that “in some ways it helps with the anxiety. It helps with the depression.”
Another aspect of the theme internalization of perceived worth involves the source of microaffirmations, which influenced how deeply these affirmations impacted their sense of self-worth. Microaffirmations from people with shared or similar identities were particularly meaningful, as these individuals could better understand and relate to the participants’ experiences. April explained that she primarily found validation for her identity within her relationship: “I feel that affirmation of my identifying as demisexual primarily only comes from my own relationship [with my partner].” For April, the microaffirmations she received from her partner were more impactful than those from others because they were rooted in a shared understanding of her identity and experiences. Similarly, Kay shared that the most meaningful microaffirmations often come from her queer friends who share similar marginalized identities: “The microaffirmations carry more weight when they come from my friends who are queer and/or genderfluid or trans . . . because I feel like we all know what we’re going through and we can all support each other.”
This idea that internalized perceived worth or validation comes from those with similar queer and/or trans and racial/ethnic identities was also expressed by Baohua when he described the microaffirmations he received from his friends who also identify as QTPOC, despite cultural differences:
Or maybe they experience some challenges, and I feel like that’s relatable. It’s like . . . we’re speaking in the same language. We’re experiencing similar things. . . . That kind of gives me . . . like different validation to say, hey, we are here, right? Even though that’s very old—we’re here, we’re queer, whatever. But it’s like we are here, and we are living life despite different social or political challenges that we’re facing.
Baohua’s statement highlights how microrecognitions from peers with similar identities can bolster one’s sense of worth and community, reinforcing the idea that they are not alone in their experiences.
Discussion
All 14 participants expressed various experiences of microaffirmations as queer and/or transgender people of color. Themes found in this study’s results (i.e., influence of identity development, safety with others, envisioning policy changes, representation, and internalization of perceived worth) align with and expand on the growing body of literature on microaffirmations’ role in the LGBTQIA+ community (Anzani et al., 2019; Flanders et al., 2019; Pulice-Farrow et al., 2019; Sterzing & Gartner, 2020) and marginalized racial/ethnic communities (Pérez Huber et al., 2021; Rolón-Dow & Davison, 2021). Despite the topic of microaffirmations becoming more prevalent in scholarly literature, there is still a dearth of research that looks at defining and understanding the impacts of microaffirmations for those with both marginalized gender and/or sexual identities and marginalized racial/ethnic identities. Elements of Rolón-Dow and Davison’s subcategories of microaffirmations were used as a foundation for this study’s current superordinate themes.
For the theme of influence of identity development, participants discussed their experiences with microaffirmations that supported and validated their individual identity and other microaffirmations that applied to the broader queer community. For those in the earlier stages of their identity development, the presence of microaffirmations seemed to mitigate any internalized conflict or discrimination related to their queer identities, compared to those in later stages of identity development. These findings aligned with various LGBTQIA+ identity development models, such as D’Augelli’s (1994) Model of Lesbian, Gay, and Bisexual Identity Development and the Model of Multiple Dimensions of Identity (Abes et al., 2007). It seemed that participants who were in the earlier stages of their queer and/or transgender identity development found microaffirmations to be more impactful when they were directed toward them as individuals versus those who were in later stages and had a more community/systemic viewpoint. The differences in identity developmental stages may also be explained by Roberts and Christens (2020), who reported that Black and Latinx participants, when “out,” experienced positive outcomes when they experienced a sense of connectedness to the LGBTQIA+ community. The results of this study (Roberts & Christens, 2020) suggest that those in later stages of development based on how “out” they are may have more ties to other QTPOC. Similar findings from Ghabrial and Andersen (2021) and G. Smith and colleagues (2022) further support the positive impact of community connectedness on participants’ experiences. Perhaps participants in later stages of their identity development are more likely to be out and intentional about finding QTPOC spaces, therefore feeling more validated by microaffirmations directed at the broader queer community instead of those targeting them individually.
For the theme safety with others, participants emphasized their experiences with microaffirmations that signaled safe spaces, individuals, and organizations. This theme aligns with Rolón-Dow and Davison’s (2021) subcategories of microaffirmations, specifically microvalidations and microprotections. Hudson and Romanelli’s (2020) findings, which highlight the fostering of safety and acceptance by the LGBTQ community as a strength and health-promoting factor for LGBTQ adults of color, align with this theme. Participants mentioned that being around other QTPOC allowed them to fully disclose their sexual and gender identities and authentically be themselves. Though participants primarily focused on feelings of safety regarding their marginalized sexual and/or gender identities, many, like Baohua, also mentioned examples of microaffirmations that validated and instilled feelings of safety for both these identities and their racial/ethnic identities. The microaffirmations could potentially reduce the negative mental health–related issues experienced by the participants in this study (Topor et al., 2018).
Regarding the theme envisioning policy changes, participants reflected on the broader implications of microaffirmations and their potential to influence policy and create systemic change. They shared that these microaffirmations also provided immediate benefits, supporting previous literature which reported that gender-affirming policies are associated with positive mental health outcomes among transgender individuals (Horne et al., 2022). However, many of our participants discussed the impact of current anti-LGBTQIA+ legislation and the potential effects of future legislation at both the federal and local levels on the LGBTQIA+ community. Similar to the theme influence on identity development, the centrality of community connectedness and protection was evident when participants talked about both current and future policy changes. This is supported by Hudson and Romanelli (2020), who proposed that QTPOC have a future orientation focused on investing in and improving opportunities for health and well-being for current and future community members. The fourth theme, microaffirmations as representation, was shared by participants as external representations from outside sources, as well as how participants themselves created microaffirmations for others. While previous literature (McInroy & Craig, 2017) also identified external representations of QTPOC, many participants also underlined the importance of being the provider of various forms of microaffirmations. Participants emphasized the importance of actively generating microaffirmations that provided representation for other QTPOC folks. These examples included conducting affirmative research on QTPOC, compiling resources with positive QTPOC representation, and stepping into leadership roles in the LGBTQIA+ community. Hudson and Romanelli (2020) noted that QTPOC involved in activism and advocacy were more likely to be aware of structural and social injustices that can negatively impact the well-being of individuals in the LGBTQIA+ community.
The final theme, internalization of perceived worth focuses on how microaffirmations are internalized and shape participants’ sense of self and collective worth, as well as the impact of microaffirmations based on participants’ relationship with the giver of the microaffirmations. Ghabrial (2019) suggests that for marginalized individuals, feeling that one’s marginalized identity can be viewed as a positive aspect can foster resilience and resolve when experiencing discrimination. This may explain why participants such as Didi felt less overwhelmed and participants like Stacey felt hope when receiving microaffirmations. For these two participants, their positive viewpoints on their sexual identities encouraged them not only in their identities but also in advocating for themselves and other QTPOC. Microaffirmations may therefore be one reason why QTPOC feel motivated to participate in advocacy efforts. Another element of this theme that participants discussed is the impact of internalizing perceived worth depending on the source of the microaffirmation. While microaffirmations from anyone were appreciated, some participants emphasized the positive impact of microaffirmations received from those within the LGBTQIA+ community or from close relationships, whether platonic, familial, or romantic. In a study focusing on transgender individuals and their romantic relationships, Pulice-Farrow and colleagues (2019) reported that participants found microaffirmations more meaningful when they came from romantic partners rather than strangers, as it affirmed the importance of the relationship. This idea also expands on the work by Delston (2021), who suggested that individuals from vulnerable groups seek environments where they feel valued, appreciated, and included. Delston also warns that microaffirmation recipients should be aware of where and from whom they receive microaffirmations, as they may be influenced to make life decisions based on biased external influences, such as a QTPOC only having their identity affirmed by limiting White LGBTQIA+ sources. This study’s findings indicate that microaffirmations from those in close relationships with QTPOC may have a greater impact than those from strangers or large organizations, highlighting the necessity for QTPOC to be cautious of the giver of microaffirmations and the importance of QTPOC to create intentional and affirming support systems.
Implications for Counselors
Given the nuanced understanding of microaffirmations and their profound impact on QTPOC, counselors working with this population can draw several practice implications to foster resilience and improve mental health outcomes. First, it is essential for counselors to recognize the various stages of identity development their QTPOC clients may be undergoing. Clients in the early stages of identity development may benefit significantly from microvalidations and microrecognitions that affirm their identities and experiences, helping them navigate internalized discrimination. Engaging in active listening, providing reflections and follow-up questions, and validating clients’ feelings and identities are vital strategies for those still exploring their sexual and gender identities.
Counselors must also establish environments where QTPOC clients feel safe and affirmed. This can be achieved by incorporating visible signs of support, such as Pride flags or inclusive posters, and using affirming language that communicates safety. Counselors must also check their biases, assumptions, and competencies around QTPOC identities and how they intersect (e.g., continuing education, LGBTQ+/QTPOC affirming supervision/consultation). As Delston (2021) proposed, microaffirmations may influence a person’s decisions based on who and where they came from. Well-intentioned counselors may further perpetuate harmful stereotypes or affirm QTPOC clients from a narrow White, Western perspective that limits influence from these clients’ racial/ethnic background, thereby creating an unsafe environment.
Furthermore, counselors should understand the importance of advocating for inclusive policies. Outside of sessions, counselors can educate themselves and advocate for pro-LGBTQIA+ legislation that would benefit QTPOC. By engaging in advocacy and policy work, counselors can help create a safe and supportive environment that extends beyond the counseling office. Counselors can also seek out positive representations of QTPOC in media, which may allow them to be better able to connect with clients in session by demonstrating their understanding of social and cultural references. However, non-QTPOC counselors should engage with those materials in good faith and avoid performative advocacy with clients, such as having Pride flags hanging in their office but not having resources specific to the needs of QTPOC clients. Moreover, in session, counselors can help clients outline close relationships and safe spaces affirming QTPOC clients’ identities and refer clients with limited support to QTPOC resources locally and virtually. Counselors can also incorporate expressive art therapy techniques into sessions that provide QTPOC clients creative outlets that allow them to not only express themselves but also to be productive by sharing their creations with others as a form of authentic queer representation (Buttram, 2015).
Finally, counselors can support QTPOC clients in fostering internalized worth by consistently using affirming language, adopting a strengths-based approach, and facilitating connections with other QTPOC via group counseling services or within the community. Providing psychoeducation about the impact of discrimination along with employing narrative counseling techniques can help clients reframe their personal stories. By recognizing the unique experiences and needs of QTPOC clients, counselors can play a pivotal role in fostering environments that promote mental health, resilience, and a strong sense of worth, both on an interpersonal, therapeutic level and within the broader societal context.
Limitations and Future Directions
This study, while providing valuable insights into the role of microaffirmations for QTPOC, has several limitations that should be noted. During the time of interviews, most participants identified as cisgender, their gender identity aligning with their sex assigned at birth, providing limiting perspectives of those with gender-expansive identities. Most participants were also Millennials (born 1981 to 1996) and older Gen Zs (born 1997 to 2010; Dimock, 2019), which limits perspectives of what may be considered microaffirmations from older generations of QTPOC who historically experienced less and/or different affirmations in their lives. Future research should aim to include a larger and more diverse sample to enhance the generalizability of the findings.
Another limitation of this study was that it did not ask participants for their regional location. Though some participants shared where they lived in their interviews, knowing regional locations may have helped to understand if participants from similar regions experienced similar types and frequency of microaffirmations. Future research should explore the experiences of QTPOC in specific geographical regions and cultural settings to capture and compare regional differences.
An additional crucial limitation is that, though the study did require participants to be currently living in the United States, there were a few participants who were either immigrants who had lived part of their developmental years in another country or were international students who came to the United States later in life. Though these participants shared their experiences, interview questions did not consider the added marginalized identities of being an immigrant/non–U.S. citizen. Future research is warranted to investigate the utility of microaffirmations for undocumented or non–U.S. citizen QTPOC. Lastly, there is a need for more intervention-based research to develop and test specific counseling strategies that effectively utilize microaffirmations to support QTPOC clients.
Conclusion
This study expanded understanding of the different subcategories of microaffirmations within the context of multiple marginalized identities, specifically being a person of color and being LGBTQIA+. The findings illustrate QTPOC perceptions of microaffirmations and their significant impact on their mental well-being. Efforts should be made to further understand the lasting impact of microaffirmations for individuals with multiple marginalized identities and how microaffirmations can encourage QTPOC and others to make macro-level changes. Counselors and researchers have a vital role in identifying and fostering microaffirmations for QTPOC across various aspects of their work.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Abes, E. S., Jones, S. R., & McEwen, M. K. (2007). Reconceptualizing the model of multiple dimensions of identity: The role of meaning-making capacity in the construction of multiple identities. Journal of College Student Development, 48(1), 1–22. https://doi.org/10.1353/csd.2007.0000
Anzani, A., Morris, E. R., & Galupo, M. P. (2019). From absence of microaggressions to seeing authentic gender: Transgender clients’ experiences with microaffirmations in therapy. Journal of LGBT Issues in Counseling, 13(4), 258–275. https://doi.org/10.1080/15538605.2019.1662359
Bostwick, W. B., Boyd, C. J., Hughes, T. L., West, B. T., & McCabe, S. E. (2014). Discrimination and mental health among lesbian, gay, and bisexual adults in the United States. American Journal of Orthopsychiatry, 84(1), 35–45. https://doi.org/10.1037/h0098851
Brooks, V. R. (1981). Minority stress and lesbian women. Lexington Books.
Buttram, M. E. (2015). The social environmental elements of resilience among vulnerable African American/Black men who have sex with men. Journal of Human Behavior in the Social Environment, 25(8), 923–933. https://doi.org/10.1080/10911359.2015.1040908
Cyrus, K. (2017). Multiple minorities as multiply marginalized: Applying the minority stress theory to LGBTQ people of color. Journal of Gay & Lesbian Mental Health, 21(3), 194–202. https://doi.org/10.1080/19359705.2017.1320739
D’Augelli, A. R. (1994). Identity development and sexual orientation: Toward a model of lesbian, gay, and bisexual development. In E. J. Trickett, R. J. Watts, & D. Birman (Eds.), Human diversity: Perspectives on people in context (pp. 312–333). Jossey-Bass.
Delston, J. B. (2021). The ethics and politics of microaffirmations. Philosophy of Management, 20(4), 411–429. https://doi.org/10.1007/s40926-021-00169-x
DeLucia, R., & Smith, N. G. (2021). The impact of provider biphobia and microaffirmations on bisexual individuals’ treatment-seeking intentions. Journal of Bisexuality, 21(2), 145–166. https://doi.org/10.1080/15299716.2021.1900020
Dimock, M. (2019, January 17). Defining generations: Where Millennials end and Generation Z begins. Pew Research Center. www.pewresearch.org/short-reads/2019/01/17/where-millennials-end-and-generation-z-begins
Dispenza, F., & O’Hara, C. (2016). Correlates of transgender and gender nonconforming counseling competencies among psychologists and mental health practitioners. Psychology of Sexual Orientation and Gender Diversity, 3(2), 156–164. https://doi.org/10.1037/sgd0000151
Ellis, J. M., Powell, C. S., Demetriou, C. P., Huerta-Bapat, C., & Panter, A. T. (2019). Examining first-generation college student lived experiences with microaggressions and microaffirmations at a predominately White public research university. Cultural Diversity & Ethnic Minority Psychology, 25(2), 266–279. https://doi.org/10.1037/cdp0000198
Flanders, C. E. (2015). Bisexual health: A daily diary analysis of stress and anxiety. Basic and Applied Social Psychology, 37(6), 319–335. https://doi.org/10.1080/01973533.2015.1079202
Flanders, C. E., Shuler, S. A., Desnoyers, S. A., & VanKim, N. A. (2019). Relationships between social support, identity, anxiety, and depression among young bisexual people of color. Journal of Bisexuality, 19(2), 253–275. https://doi.org/10.1080/15299716.2019.1617543
Ghabrial, M. A. (2019). “We can shapeshift and build bridges”: Bisexual women and gender diverse people of color on invisibility and embracing the borderlands. Journal of Bisexuality, 19(2), 169–197. https://doi.org/10.1080/15299716.2019.1617526
Ghabrial, M. A., & Andersen, J. P. (2021). Development and initial validation of the Queer People of Color Identity Affirmation Scale. Journal of Counseling Psychology, 68(1), 38–53. https://doi.org/10.1037/cou0000443
Hailey, J., Burton, W., & Arscott, J. (2020). We are family: Chosen and created families as a protective factor against racialized trauma and anti-LGBTQ oppression among African American sexual and gender minority youth. Journal of GLBT Family Studies, 16(2), 176–191.
https://doi.org/10.1080/1550428x.2020.1724133
Horne, S. G., McGinley, M., Yel, N., & Maroney, M. R. (2022). The stench of bathroom bills and anti-transgender legislation: Anxiety and depression among transgender, nonbinary, and cisgender LGBQ people during a state referendum. Journal of Counseling Psychology, 69(1), 1–13.
https://doi.org/10.1037/cou0000558
Houshmand, S., Spanierman, L. B., & De Stefano, J. (2019). “I have strong medicine, you see”: Strategic responses to racial microaggressions. Journal of Counseling Psychology, 66(6), 651–664. https://doi.org/10.1037/cou0000372
Hudson, K. D., & Romanelli, M. (2020). “We are powerful people”: Health-promoting strengths of LGBTQ communities of color. Qualitative Health Research, 30(8), 1156–1170. https://doi.org/10.1177/1049732319837572
Jones, J. M. (2024, March 13). LGBTQ+ identification in U.S. now at 7.6%. GALLUP. https://news.gallup.com/poll/611864/lgbtq-identification.aspx
Jones, J. M. & Rolón-Dow, R. (2018). Multidimensional models of microaggressions and microaffirmations. In G. C. Torino, D. P. Rivera, C. M. Capodilupo, K. L. Nadal, & D. W. Sue (Eds.), Microaggression theory: Influence and implications (pp. 32–47). Wiley. https://doi.org/10.1002/9781119466642.ch3
Lincoln, Y. S. & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
McConnell, E. A., Janulis, P., Phillips, G., II, Truong, R., & Birkett, M. (2018). Multiple minority stress and LGBT community resilience among sexual minority men. Psychology of Sexual Orientation and Gender Diversity, 5(1), 1–12. https://doi.org/10.1037/sgd0000265
McInroy, L. B., & Craig, S. L. (2017). Perspectives of LGBTQ emerging adults on the depiction and impact of LGBTQ media representation. Journal of Youth Studies, 20(1), 32–46. https://doi.org/10.1080/13676261.2016.1184243
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. https://doi.org/10.1037/0033-2909.129.5.674
Miller, M. J., Keum, B. T., Thai, C. J., Lu, Y., Truong, N. N., Huh, G. A., Li, X., Yeung, J. G., & Ahn, L. H. (2018). Practice recommendations for addressing racism: A content analysis of the counseling psychology literature. Journal of Counseling Psychology, 65(6), 669–680. https://doi.org/10.1037/cou0000306
Mizock, L., & Lundquist, C. (2016). Missteps in psychotherapy with transgender clients: Promoting gender sensitivity in counseling and psychological practice. Psychology of Sexual Orientation and Gender Diversity, 3(2), 148–155. https://doi.org/10.1037/sgd0000177
Pérez Huber, L., Gonzalez, T., Robles, G., & Solórzano, D. G. (2021). Racial microaffirmations as a response to racial microaggressions: Exploring risk and protective factors. New Ideas in Psychology, 63, 100880. https://doi.org/10.1016/j.newideapsych.2021.100880
Pflum, S. R., Testa, R. J., Balsam, K. F., Goldblum, P. B., & Bongar, B. (2015). Social support, trans community connectedness, and mental health symptoms among transgender and gender nonconforming adults. Psychology of Sexual Orientation and Gender Diversity, 2(3), 281–286. https://doi.org/10.1037/sgd0000122
Pulice-Farrow, L., Bravo, A., & Galupo, M. P. (2019). “Your gender is valid”: Microaffirmations in the romantic relationships of transgender individuals. Journal of LGBT Issues in Counseling, 13(1), 45–66. https://doi.org/10.1080/15538605.2019.1565799
Roberts, L. M., & Christens, B. D. (2020). Pathways to well-being among LGBT adults: Sociopolitical involvement, family support, outness, and community connectedness with race/ethnicity as a moderator. American Journal of Community Psychology, 67(3–4), 405–418. https://doi.org/10.1002/ajcp.12482
Rolón-Dow, R., & Davison, A. (2021). Theorizing racial microaffirmations: A Critical Race/LatCrit approach. Race Ethnicity and Education, 24(2), 245–261. https://doi.org/10.1080/13613324.2020.1798381
Rowe, M. (2008). Micro-affirmations and micro-inequities. Journal of the International Ombudsman Association, 1(1), 45–48. https://mitsloan.mit.edu/shared/ods/documents?PublicationDocumentID=5404
Salim, S., Robinson, M., & Flanders, C. E. (2019). Bisexual women’s experiences of microaggressions and microaffirmations and their relation to mental health. Psychology of Sexual Orientation and Gender Diversity, 6(3), 336–346. https://doi.org/10.1037/sgd0000329
Smith, G., Robertson, N., & Cotton, S. (2022). Transgender and gender non-conforming people’s adaptive coping responses to minority stress: A framework synthesis. Nordic Psychology, 74(3), 222–242. https://doi.org/10.1080/19012276.2021.1989708
Smith, J. A., Flowers, P., & Larkin, M. (2009). Interpretative phenomenological analysis: Theory, method and research. SAGE.
Sterzing, P. R., & Gartner, R. E. (2020). LGBTQ microaggressions and microaffirmations in families: Scale development and validation study. Journal of Homosexuality, 67(5), 600–619. https://doi.org/10.1080/00918369.2018.1553350
Testa, R. J., Habarth, J., Peta, J., Balsam, K., & Bockting, W. (2015). Development of the Gender Minority Stress and Resilience Measure. Psychology of Sexual Orientation and Gender Diversity, 2(1), 65–77. https://doi.org/10.1037/sgd0000081
Topor, A., Bøe, T. D., & Larsen, I. B. (2018). Small things, micro-affirmations and helpful professionals everyday recovery-orientated practices according to persons with mental health problems. Community Mental Health Journal, 54, 1212–1220. https://doi.org/10.1007/s10597-018-0245-9
White Hughto, J. M., Reisner, S. L., & Pachankis, J. E. (2015). Transgender stigma and health: A critical review of stigma determinants, mechanisms, and interventions. Social Science & Medicine, 147, 222–231. https://doi.org/10.1016/j.socscimed.2015.11.010
Yardley, A. (2008). Piecing together—A methodological bricolage. Forum: Qualitative Social Research, 9(2), Article 31. https://www.qualitative-research.net/index.php/fqs/article/view/416/902
Zori A. Paul, PhD, NCC, LPC (MO), is a clinical assistant professor at Marquette University. Kyesha M. Isadore, PhD, NCC, CRC, is an assistant professor at the University of Wisconsin–Madison. Nishi Ravi, MCouns, is a doctoral student at Marquette University. Kayla D. Lewis, MS, is a doctoral student at Marquette University. Dewi Qisti, MS, is a doctoral student at the University of Wisconsin–Madison. Alex Hietpas, MS, is a doctoral student at Marquette University. Bergen Hermanson, BA, is a master’s student at Marquette University. Yuji Su, BA, is a master’s student at Marquette University. Correspondence may be addressed to Zori A. Paul, Department of Counselor Education and Counseling Psychology, Schroeder Complex, 113M, Marquette University, P.O. Box 1881, Milwaukee, WI 53201-1881, zori.paul@marquette.edu.
Appendix
Interview Protocol
The interview will focus on details of participants’ experiences with microaffirmations. Participants will be asked how to describe everyday experiences and small actions that affirm their identities or impact their experiences; how different types of microaffirmations (microrecognitions, microvalidations, microtransformations, and microprotections) show up in their lives; and the impact of microaffirmations on their overall mental health and well-being. The goal of this interview is to elicit rich descriptions of participants’ experiences. The following questions and prompts will be used as a guide for the interview:
- Background Questions
a. Could you briefly explain how you refer to yourself in terms of your sexual and/or gender identity and what those labels, if you use any labels, mean to you?
b. Could you briefly explain how you refer to yourself in terms of your racial and/or ethnic identity and what those labels, if you use any labels, mean to you?
c. Can you describe a time when you felt like someone affirmed your sexual and/or gender identity?
i. If not already answered: What was your relationship to this person?
2. Microaffirmations
a. (Microrecognitions) Could you describe everyday experiences, such as actions, words, or environmental cues (like artwork, signage, symbols) that made you feel like your [insert identity] was given positive visibility and appreciation?
i. If you haven’t experienced that, what do you think positive visibility and appreciation for your identity would look like?
ii. In what ways do you think more positive visibility and appreciation for your identity would impact you directly?
b. (Microvalidations) Could you describe everyday experiences that made you feel that your thoughts, feelings, sensations, and/or behaviors associated with your lived experience as [identity] are accepted, legitimized, or given value?
i. If you haven’t experienced that, what do you think positive acknowledgment and understanding of your identity and lived experience would look like?
ii. In what ways do you think more positive acknowledgment and understanding would impact you directly?
c. (Microtransformations) Could you describe everyday experiences that made you feel that your identity as a member of [insert identity group] has been enabled, enhanced, or increased in society?
i. What do you think potential policies/initiatives that would enable, enhance, or increase your life look like?
ii. How would your life be impacted directly?
d. (Microprotections) Could you describe everyday experiences that make you feel shielded or protected from harmful or derogatory behaviors, practices, and policies tied to your identity as [insert identity]?
i. If you haven’t experienced that, what do you think potential protections or shields would look like?
ii. How would your life be impacted if you had more protection and shields?
3. Other
a. So far, we’ve been talking about positive everyday experiences that affirm your [identity]. The term we use for these everyday experiences and small actions is called microaffirmations. Can you tell us a little about the relationship of these microaffirmations with your overall mental health and well-being and how microaffirmations may impact it?
i. What do you think is the role of microaffirmations in terms of how you navigate spaces that have historically been exclusive to queer and trans people of color?
b. Is there anything we missed regarding any actions, words, or environmental cues you’ve experienced as [identity] throughout the course of your everyday life that affirms your identity and acknowledges your realized identity, and promotes social justice?
Dec 5, 2024 | Volume 14 - Issue 3
Russ Curtis, Lisen C. Roberts, Paul Stonehouse, Melodie H. Frick
Tattoo art is one of the earliest forms of self-expression, but the advent of colonialism, and its accompanying religious convictions, halted the practice in many Indigenous lands and led to widespread bias against tattooed people—a bias maintained to the present. How might the counseling profession respond to this residual bias and intentionally invoke a cultural shift destigmatizing tattoos? Through an extensive literature review, this article provides a more comprehensive understanding of tattoo-related mental health correlates, biases, and theories that enhance the effectiveness of counseling and parallel trends in the counseling profession that emphasize sociocultural influences on wellness. As a result of this survey, the authors propose a new theory of tattoo motivation, the unencumbered self theory of tattoos, which advances existing tattoo theory and aligns with current counseling trends by postulating that tattoos symbolize the uniquely human desire to transcend norms and laws imposed by external influences.
Keywords: tattoo, bias, mental health, theory, counseling
Imagine you are the parent of a 13-year-old girl. While at a parent–teacher conference, you learn your daughter is struggling with disruptive behavior and angry outbursts during class. The teacher asks if you would support your daughter seeing the school counselor and adds that the counselor is in the school building and available to speak with parents. You approach the counselor’s office, gently knock, and are welcomed by a warm, feminine-presenting adult. As the counselor offers their hand to shake, you notice an entirely tattooed forearm, and as you greet their eyes, more ink is evident on their neck.
What feelings, assumptions, or concerns emerge as you put yourself in the place of the parent in the above vignette? Despite the recent popularization of tattoos, a bias remains. Current research indicates that nearly half of adults in the United States between the ages of 18–34 have at least one tattoo (Roggenkamp et al., 2017), and the tattoo business is one of the fastest-growing enterprises, producing over a billion dollars in annual revenue (Zuckerman, 2020). This trend in tattoo art transcends the United States and is evident throughout the world (Ernst et al., 2022; Khair, 2022; Roberts, 2016). Nevertheless, bias against tattooed people remains, and women and people of color receive the brunt of this discrimination (Baumann et al., 2016; Guéguen, 2013; Kaufmann & Armstrong, 2022; Khair, 2022; Roberts, 2016). Given this meteoric resurgence in tattoo art and the discrimination that clings to it, implications for counseling practice inevitably exist.
Professional questions relevant to the counseling practice include: Is there a relationship between a desire for a tattoo and mental health? What motivates a person to seek a tattoo? In what ways may a tattoo bias subconsciously shape a counselor’s interactions with a client? How might the counseling community communicate a spirit of inclusion to the tattooed? To address these questions, this article employs the following structure. First, we provide a context for this bias by briefly examining the history and cultural perspectives of tattoos. Second, to establish the importance of this issue, we empirically demonstrate the reality of tattoo bias. Third, with this history of bias in mind, we comb the literature for research that explores the relationship between mental health and tattoos. Fourth, these relationships offer a frame of reference for our survey of established tattoo motivation theories, to which we propose an additional theory, the unencumbered self theory of tattoos, and reveal its significance within a clinical setting via a case study. Fifth, before concluding the article, we demonstrate how our inquiry’s content might be applied by enumerating our argument’s implications for the counseling profession.
Historical and Cultural Perspectives of Tattoos
The word tattoo originates from the Samoan term tatau, meaning “to tap lines on the body.” The practice of tattooing is known to have existed as early as 7000 BC, as seen on Egyptian mummies (Rohith et al., 2020). Otzi the Ice Man, dating back to 3000 BC, was discovered in 1991 with tattoos on his arms and wrist that are thought to have been applied for therapeutic purposes, a potential precursor to acupuncture (Schmid, 2013). Prior to the colonization of Indigenous lands by European countries, many tribes practiced the art of tattoo to symbolize adulthood, tribal membership, and status (Dance, 2019; Thomas et al., 2005). However, with the emergence of European imperialism, colonizers taught Indigenous people that tattoos were an abomination, scripturally prohibited, and therefore immoral. For instance, in The Holy Bible (New International Version, 1978, Leviticus 19:28) and The Qur’an (2004, Surah 7:46), specific passages forbid marking the skin.
Despite these condemnations, the practice of tattooing was not eradicated. Many cultures continued their tattoo traditions, and modern culture has adopted new traditions, which are even now expanding throughout the world (Ernst et al., 2022; Khair, 2022; Roberts, 2016). Although there is much intergroup variability, cultural identity can influence the motivation for and type of preferred tattoo. In India, for instance, tattoos often depict unique patterns specific to different tribal regions in the country. Specifically, in urbanized Indian geographic areas, there is increasing integration of tribal pattern tattoos with Western-influenced designs (Rohith et al., 2020). In Samoan culture, men receive an intricate tattoo called a pe’a while women receive a malu, both to indicate maturity (Dance, 2019). Lest the cultural importance of Indigenous tattoos be doubted, their misappropriation has resulted in litigation, thereby challenging attorneys to consider the property rights of tattoo designs (Tan, 2013).
Profoundly relevant to counseling, tattoos are often representational and symbolize something of importance. In a recent qualitative study of tattooed Middle Eastern women, Khair (2022) discovered themes related to taking ownership of their bodies in a patriarchal society and symbolism of their strength and desire to break free of patriarchal rules and religious mandates. In the United States, a study of mixed-race Americans’ tattoos revealed the most common tattoo themes include animal images and text of personally meaningful messages (Sims, 2018). In yet another group, White supremacists often get swastikas, crossed hammers, Confederate flags, and embellished Celtic crosses (Southern Poverty Law Center, 2006). Similarly, in Czech Republic prisons, the skull tattoo is a symbol representing neo-Nazi extremism, which then informs prison officials of inmates potentially becoming radicalized (Vegrichtová, 2018).
Exploring the intersection of religion and tattoos, Morello’s (2021) qualitative analysis of 21 people in three South American cities revealed that tattoos were more accepted among Catholics than evangelicals. Explained below, Morello classified the types of Christian tattoos as reversal, devotional, foundational, and then a nonreligious fourth category termed relational. According to participants, reversal tattoos symbolized regaining control of disempowering events, such as when Christians historically tattooed themselves to show Roman enslavers their devotion to Christ. Devotional tattoos were comprised of images and symbols representing religious themes (e.g., a cross), often used as a source of strength and identity. Foundational tattoos represent significant moments in life, such as major life transitions (e.g., the date of one’s conversion) or mystical experiences. Morello’s last category is akin to devotional tattoos, but the relational category was created to represent devotion to loved ones, such as images or symbols of one’s children.
In a related study examining the beliefs of religious women with and without tattoos, Morello et al. (2021) identified several common themes. This mixed methods study of 48 women in a conservative Christian college indicated that tattoos were not considered taboo by their religious friends and family and that tattooed participants spent considerable time determining which tattoo to receive. Predominant reasons for obtaining tattoos included social justice, friendship, and spiritual values. Summarizing previous research, individuals primarily choose tattoos to express their identity and uniqueness or to take ownership of their bodies. However, as discussed in the following section, there exists a bias against tattooed individuals.
Tattoo Bias
Unfortunately, with any practice that diverges from dominant cultural values, there is bias (Broussard & Harton, 2018). Although evidence indicates less discrimination against tattoos in the 21st century, negative judgments still exist explicitly and implicitly (Broussard & Harton, 2018; Williams et al., 2014; Zestcott et al., 2018). For example, Kaufmann and Armstrong (2022) found that law enforcement and the medical community hold negative sentiments toward tattooed people. They found that medical professionals who expressed negative judgments about their tattooed patients were likely to have patients not return. In fact, patients reported better rapport and increased trust with medical professionals who asked about the meaning of their tattoos. In other words, negative judgment toward, and lack of acknowledgment of, tattoos were detrimental to building the trust needed to provide optimal and consistent care (Kaufmann & Armstrong, 2022).
Unjustly, women and people of color with tattoos experience more significant discrimination than men or White people (Baumann et al., 2016; Camacho & Brown, 2018; Guégen, 2013; Solanke, 2017). For example, women encounter prejudice when failing to gain employment due to having visible tattoos regardless of having excellent job qualifications (Al-Twal & Abuhassan, 2024; Henle et al., 2022). Moreover, women of color have experienced job discrimination by being questioned if they have visible or nonvisible tattoos (i.e., inkism), being forbidden from having or being required to cover tattoos regardless of cultural relevance (e.g., covering a traditional Māori tattoo), or being required to prove that they do not have tattoos—as alleged in a legal complaint against a Singaporean airline that required female attendants to wear a swimsuit and demonstrate to their employers that they did not have tattoos (Solanke, 2017, Chapter 8). Women with tattoos also experience ambivalent sexism due to rejecting the feminine apologetic (i.e., not acting or dressing in stereotypical feminine ways); they are also perceived as wanting attention and sexually promiscuous (Heckerl, 2021). For instance, Guéguen (2013) found that women on the beach displaying a lower-back butterfly tattoo were significantly more likely to be approached by men compared to women without the tattoo, and the men interviewed indicated that they thought they had a better chance of getting a date and having sex with the tattooed women than the nontattooed women (Guéguen, 2013). In other words, men in this study had the biased perception that women with tattoos were more sexually promiscuous than nontattooed women.
This bias appears within incarceration rates as well. In a study conducted by Camacho and Brown (2018), they found that arrestees with neck tattoos were more likely to receive felony charges specifically for larceny offenses. Among these groups, Black individuals with neck tattoos were more likely than others to face felony charges (Camacho & Brown, 2018). It is also noteworthy that law enforcement catalog the tattoos of arrestees in the Registry of Distinct Marks (Miranda, 2020), which is kept in their permanent record and could potentially bias future incarceration and convictions due to the criminogenic stigmatization of individuals with tattoos (Martone, 2023; Rima et al., 2023).
Neck tattoos specifically appear to elicit bias (Baumann et al., 2016). Given two sets of photos of male and female faces, with a neck tattoo and without a visible tattoo, participants were asked to choose among the photos that they would most like to have as their surgeon. In a separate condition, participants were asked to choose who they would most like to have as their car mechanic. In both experiments, participants preferred to have a nontattooed person as their surgeon or mechanic. However, the preference was more substantial for a nontattooed surgeon than a nontattooed mechanic. Female participants assessed the tattooed faces more positively than male participants, but still preferred the nontattooed faces (Baumann et al., 2016).
Roberts (2016) suggested that although tattoos are becoming more prevalent worldwide, they are not yet entirely accepted. As such, employment discrimination occurs for people with visible tattoos. Roberts (2016) suggested employers discriminate primarily because of the fear of customer complaints and the concomitant loss of business. They further suggested that small businesses in rural areas, which tend to be more conservative, may be even more likely to refuse employment to tattooed workers.
Clients’ Perception of Tattooed Counselors
To date, very few published studies examine the perceptions of tattoos within the mental health professional arena. One exception, however, is a recent publication examining the perception of potential mental health clients of psychologists with or without tattoos. Zidenberg et al. (2022) recruited 534 participants to determine if there were negative perceptions of psychologists who had tattoos. First, participants were presented with a mock profile of a fictional clinical psychologist. Each participant was randomly assigned to view one of three images of the psychologist: with no tattoo, a neutral tattoo (a flower), or a provocative tattoo (a skull with flames). Participants then rated the counselor on perceived competence and their personal feelings toward her.
Contrary to the researchers’ initial expectations, the psychologist’s photo with the provocative tattoo was rated more likable, interesting, and confident and less lazy than the psychologist with a neutral or no tattoo. Interestingly, the psychologist’s photo without a tattoo was rated as more professional, but this did not equate to participants’ believing that the psychologist would thus provide better care. The researchers speculated that while nontattooed people are viewed as more professional, they are not necessarily who clients believe will give the best mental health care. They further hypothesized that professionalism may convey a bias of being “better than” the clients and thereby might be perceived as less authentic. Moreover, participants in this study believed they would get better help from a more “authentic” psychologist, and that the provocative tattoo communicated a sense of authenticity (Zidenberg et al., 2022).
Mental Health and Tattoos
Although early studies (e.g., Grumet, 1983) concluded that tattoos were a sign of maladjustment, contemporary research indicates that tattooed people are as healthy as nontattooed people (Mortensen et al., 2019; Pajor et al., 2015). In general, today the mere presence of a tattoo is not correlated with mental or behavioral issues (Roggenkamp et al., 2017). In fact, most people in many cultures conscientiously obtain tattoos to express themselves and honor people and causes they deeply care about (Khair, 2022; Naudé et al., 2019; Shuaib, 2020). Nevertheless, in one study of a German community (N = 1,060), which sampled people aged 14–44, 40.6% who reported childhood abuse or neglect had at least one tattoo, compared to 29.4% tattooed participants who reported no significant abuse (Ernst et al., 2022). However, Ernst et al. (2022) cautioned that the mere presence of a tattoo is not perfectly correlated with childhood abuse. Aesthetic embellishment of the body is the most common reason for getting tattoos, and it should not be considered an automatic indication of childhood abuse (Ernst et al., 2022).
Evidence suggests that the number of tattoos as well as their placement and content better indicate potential maladjustment than the mere presence of an easily concealed tattoo. Specifically, Mortensen et al. (2019) found that participants (N = 2008 adults) who had four or more tattoos were 15.4% more likely to report having been diagnosed with a mental health problem compared to 5.8% of participants with only one tattoo. Further, 13.4% of the participants with visible tattoos reported having a mental health diagnosis, and 28.2% of the participants who self-reported having an offensive tattoo also reported having a mental health diagnosis. In other words, multiple and visible tattoos may be more closely correlated with mental and behavioral issues than the mere presence of tattoos. However, contrary to Mortensen et al. (2019), in their study of life satisfaction with a sample of 449 participants (16–58 years old), Pajor et al. (2015) used the Multidimensional Self-Esteem Inventory (MSEI; O’Brien & Epstein, 1988), a psychological assessment tool with 116 items graded on a 5-point scale and designed to measure various aspects of self-esteem. Results indicated that tattooed people reported significantly higher competence than nontattooed: 37.2 versus 33.6 (p < .001). Tattooed participants also scored significantly higher on a measure of personal power, 35.6 versus 33.5 (p < .01), and significantly lower scores on a measure of anxiety and insomnia, 1.50 versus 1.75 (p < .05). Thus, although numerous visible tattoos could potentially indicate mental or behavioral issues, the research is not conclusive, suggesting the need for counselors to open-mindedly assess each client’s motivations for obtaining tattoos.
Contrary to previous hypotheses, tattoos are rarely a form of self-harm (i.e., cutting, self-mutilation). For example, Aizenman and Jensen (2007) analyzed a sample of college students (N = 1,330; ages 17–39) to determine mental health differences between students who self-injure and those with tattoos. The majority of tattooed students reported receiving tattoos as a way to express their individuality, while students who self-injured were motivated by feelings of insecurity and loss of control. Participants also completed assessments measuring depression and self-esteem. In terms of general wellness, the self-injury group (no tattoos) reported higher mean depression scores compared to both the tattoo group’s score and the nontattooed (no self-injury) score. The self-injury group also reported lower mean self-esteem scores compared to both the tattooed and the nontattooed groups. Noteworthy is the fact that there was no significant difference between the tattooed and nontattooed groups in terms of depression and self-esteem, which further suggests that tattooed college students are no more likely to experience mental health issues than nontattooed college students.
In a more recent study to determine whether tattooing was a form of self-injury, Solís-Bravo et al. (2019) found that from a sample of 438 adolescent males, 11.5% reported engaging in nonsuicidal self-injury (NSSI), but only 1.8% indicated receiving a tattoo with the explicit intention of feeling pain. However, they also found that 62.5% of the students with tattoos self-injured compared to 10.6% of students without tattoos. Thus, with this small subsample of tattooed NSSI students, it was suggested that tattooed adolescents should be screened for potential mental health issues. Yet, considering that only eight students in this sample reported getting a tattoo to feel pain, further replication of this work is needed before confirming a conclusive relationship between tattoos and NSSI (Solís-Bravo et al., 2019).
Exploring the correlation between tattoos and premature mortality (e.g., violent death, drug overdose), Stephenson and Byard (2019) found that there was a trend for people with tattoos to die at a younger age and to experience an unnatural death compared to nontattooed people. However, these results were not statistically significant, indicating that there was no meaningful difference between age and cause of death between tattooed and nontattooed people.
More contemporary research examined the relationship between body image and tattoo acquisition (Jabłońska & Mirucka, 2023). Using a sample of 327 Polish tattooed women to examine a relationship between body image and tattoos, 45.26% reported acceptance of their appearance and a deep connection to their bodies. Researchers speculated that they received tattoos as a way to adorn their bodies and express their individuality. Another 36% reported an unstable body image, meaning they perceived both positive and negative aspects of their bodies. It was speculated that this group used tattoos to conceal perceived flaws. The remaining 18.65% held a negative body image. Although the majority of their sample held either positive or mixed body image estimations, the researchers’ speculation as to why subjects received tattoos makes it difficult to infer correlation between tattoos and well-being. Nevertheless, nearly half the sample reported appreciation for their bodies and a desire to accentuate their positive self-image with body art.
Relatedly, some trauma survivors get tattoos to symbolize what they experienced and how they have grown (Crompton et al., 2021). The semicolon is one example of this, indicating that while one life chapter may have been traumatic, that is not the end of the story. Using tattoos to navigate trauma is further supported by Kidron (2012), who noted that some descendants of Holocaust survivors replicated the number tattoo on their arms to illustrate the connection to their grandparent, redefining the tattoos from markers of trauma to markers of survival and expanding their interfamilial bond and cultural identity.
In summary, studies indicate that the mere presence of a tattoo is not significantly correlated with mental or behavioral issues. Counselors should avoid assuming that tattooed clients have mental health issues, even if multiple visible tattoos are sometimes linked with adverse health outcomes or behaviors. Because tattoos are so often attached to identity, body image, and important life events, counselors should thoroughly explore with clients why they obtained such tattoos and what they symbolize. In order to assist with such exploration, the next section identifies a number of recognized tattoo motivation theories.
Tattoo Motivation Theories
To determine effective strategies to reduce tattoo bias and counsel tattooed clients, it is important to understand the motivations and theoretical premises of why people get tattoos. This section describes recognized tattoo motivation theories. Recent findings in tattoo research cited within this article highlight the limitations of these theories and prompted us to propose our own, the unencumbered self theory of tattoos, which focuses on sociocultural influences. From this new perspective, we hope counselors will have a clearer understanding of the motivations behind getting a tattoo, which will in turn increase understanding of tattoo culture and what this implies about clients and counseling practice. To illustrate how these theoretical models might be of use in a clinical setting, in the subsequent section we provide a case study in which we discuss, compare, and contrast theories and exemplify the need for a new understanding of tattoo motivation.
Psychodynamic Theory of Tattoo
The first hypothesis for tattooing is rooted in psychodynamic theory. This theory posits that tattoos are an outward manifestation of intrapersonal conflict or unresolved psychological concerns (Grumet, 1983; Karacaoglan, 2012; Lane, 2014). The belief is that permanent skin marking serves as a visible mnemonic that prompts a defense mechanism that helps alleviate the anxiety caused by conflict within the id, ego, and superego. In other words, the symbolism embodied within the marking of the skin iteratively releases blocked psychic energy, causing temporary relief from various difficult symptoms.
Psychodynamic theory is problematic because it fails to address the alternative motivations for getting tattoos, namely, the aforementioned social–cultural perspective. Moreover, Freud’s psychoanalytic approach is rooted in Western civilization’s understanding of internal processes and is therefore heavily influenced by a European, White, male perspective of psychic processes, thus ignoring the effects of oppression and inequality on personal identity, mental health, and behavior. As was indicated in the previous research review, and as we will see in subsequent sections, current tattoo research does not support the notion that tattoos are merely the result of unconscious conflict.
Human Canvas and Upping the Ante Theories of Tattoo
Moving beyond the arguably deficit ideology of the psychodynamic theory of tattoos, Carmen et al. (2012) proposed two evolutionary theories of tattoo motivation that transcend obvious reasons like self-expression and group membership. The first theory, human canvas, argues that it is our innate longing to express the most authentic desires of our psyche through symbolic thought, originally on cave walls and later on our bodies. Their second theory, upping the ante, postulated that with increasing longevity and improved health care, the opportunities for attracting mates are more competitive, and people must devise new ways to stand out to attract mates, much like a peacock spreading its feathers.
The human canvas and upping the ante theories of tattoos are at least to some degree supported by current research (e.g., Wohlrab et al., 2007), and both theories advance our understanding of the motivation behind tattoos beyond psychodynamic theory. Indeed, people spend considerable time and thought choosing their tattoos for personal self-expression (Kaufmann & Armstrong, 2022) and to symbolize cultural traditions, sexual expression, and the love of art (Wohlrab et al., 2007). Although these theories advance tattoo theory, they fail to consider the even deeper meaning which suggests that tattoos are a way to regain bodily control and express displeasure with mandated values imposed by external influences. In essence, it is clear that tattoos are a form of self-expression, potentially to increase personal uniqueness and attractiveness, but this fails to explain what people are hoping to express. Thus, informed by contemporary tattoo research, we propose a new and expanded theory that attempts to explain the rationale behind tattoo acquisition through a wider societal lens.
The Unencumbered Self Theory of Tattoo
The unencumbered self theory of tattoos advances existing tattoo theory and aligns with current counseling trends by postulating that tattoos symbolize the uniquely human desire to transcend norms and laws imposed by external influences such as imperialism. After an exhaustive review of the tattoo literature, it is evident that the motivation to reclaim personal power from oppressive systems is one reason some people get tattoos, and this motivation is not explicitly stated within existing theories. While most closely aligned with the human canvas theory, the unencumbered self theory of tattoos differs in one subtle but essential way. The human canvas theory postulates that tattoos are a general form of self-expression (e.g., hobbies, memorials, identity, individuality). At the same time, the unencumbered self theory of tattoos suggests that specific individuals acquire tattoos as a deliberate assertion of autonomy and a repudiation of arbitrary societal norms. Take, for example, a client of Cherokee heritage who gets a tattoo depicting Cherokee syllabary. The human canvas theory would hold that this tattoo is motivated by the client’s desire to identify with her cultural heritage. The unencumbered self theory of tattoos acknowledges her desire to identify with her cultural heritage, but this desire is motivated by the need to disengage from the oppressive systems that successfully squelched her people’s values for so long.
Evidence supporting the unencumbered self theory of tattoos includes cross-cultural studies examining motivations behind obtaining tattoos (Atkinson, 2002; Khair, 2022; Kloẞ, 2022). Atkinson (2002) reported that Canadian women wore tattoos to challenge societal definitions of femininity, and Khair (2022) found that Middle Eastern women obtained tattoos primarily to express their uniqueness and to indicate ownership of their bodies. Khair (2022) stated, “In fact, women of the Middle East have been struggling to obtain the freedom of their identity due to various restrictive reasons that relate to religion” (p. 3). This sentiment is further supported by Stein (2011) who stated, “My data suggest that—rather than seeing themselves as capitulating to market forces—people think of their decision to get tattoos as an exceptionally deep expression of personal identity, as well as a dramatic declaration of autonomy” (p. 128).
Additionally supporting the cultural motivations behind obtaining tattoos, Kloẞ (2022) identified Hindu women having tattoos that symbolize both oppression from and resistance to patriarchy, colonialism, and orthodox religious beliefs. Relatedly, Stein (2011) stated that the motivation behind tattoos is, at least in part, “a defiance of patriarchal authority” (p. 113). This desire to live unencumbered is also evidenced in research indicating that tattooed people are less likely to be members of religious groups (Laumann & Derick, 2006); are less likely to conform to societal norms, as evidenced by lower scores on personality assessments measuring agreeableness and conscientiousness (Tate & Shelton, 2008); and are considered more authentic and relatable (Zidenberg et al., 2022).
The unencumbered self theory of tattoos also coincides with current research and theoretical advancements in the counseling profession. Integrative approaches, such as narrative, relational, and art therapies, illustrate how tattoos can be used to externalize issues and emotions onto the body and promote self-expression by re-authoring life stories that are freeing and healing (Alter-Muri, 2020; Covington, 2015). Further, there is an increasing interest in Indigenous healing practices and the counseling profession’s embrace of a more collaborative and collective approach to health and wellness. To illustrate how the unencumbered self theory of tattoos advances tattoo theory and serves the counseling profession, we compare and contrast the existing theories in the following case study.
Case Study and Discussion
In this fictional case study, Sage is a 28-year-old, cisgender, queer, able-bodied female whose mother is Eastern Band Cherokee and whose father identifies as Mexican American. Sage upholds many traditional Cherokee customs and regularly attends tribal council meetings as well as powwows where she dances in traditional native attire. Sage has several visible tattoos on her arms and one on the back of her neck, all of which symbolize her Cherokee heritage. She presented to counseling with increasing depression after quitting drugs and alcohol for the past year and reports being unhappy in her job with no meaningful relationships. Sage’s counselor does not have tattoos and identifies as White, female, and a social justice advocate who knows very little about people with tattoos or Cherokee customs.
From the psychodynamic theory of tattoo (Grumet, 1983), Sage’s tattoos would be considered an expression of inner conflict and unmet needs, and the counselor would ask questions hoping to uncover unconscious beliefs that are causing her depression. In this case, the counselor may not even mention her tattoos, but instead view them from a deficit lens indicating a personal problem to resolve.
In both the human canvas and upping the ante evolutionary theories of tattoos (Carmen et al., 2012), Sage’s tattoos could indicate her desire to express her individuality and enhance her attractiveness. With this in mind, the counselor is likely to acknowledge her tattoos and ask about their meaning. However, both theories fail to recognize that Sage’s tattoos may signify deeper underlying issues related to potential oppression and inequality she feels because of her race, ethnicity, and gender.
From the unencumbered self theory of tattoos, Sage’s tattoos could reflect her motivational factors, feelings of alienation, and desire to align her authentic self and heritage. From this perspective, the counselor might explore whether she has experienced discrimination and how the impact of societal marginalization shaped her current sense of self. For example, the counselor may ask, “Have you ever experienced feelings of alienation or disconnect from others, and if so, how do you think your tattoos relate to those experiences?” Another counselor probe could be, “What emotions or thoughts come up when you think about the stories or meanings behind your tattoos?” In addition, the counselor may inquire into cultural healing traditions that help Sage reclaim her authenticity and realign her with her Indigenous heritage. In this instance, the counselor may ask, “Are specific cultural or familial traditions associated with your tattoos, and how do they contribute to your sense of authenticity?” or “Have your tattoos played a role in helping you reconnect with or reclaim aspects of your cultural identity?” Ultimately, through understanding the unencumbered self theory of tattoos, the counselor can better assist Sage by gaining deeper insight into her experiences, her motivations, and the significance of her tattoos within the context of her identity and mental health journey.
In summary, clients’ motivations for tattoos are complex and include explicit explanations, such as self-expression and identity, and potentially implicit motivations, such as increased attractiveness and autonomy. Based upon the tattoo motivation research, we believe the unencumbered self theory of tattoos provides a more comprehensive understanding of the reasons people get tattoos, which appears to be motivated by boldly proclaiming their desire for autonomy and not merely to enhance personal attractiveness. With these findings in mind, the subsequent section describes how counselors, and the counseling profession more broadly, can enhance counseling practice with tattooed clients.
Implications for Counseling
Tattooed clients and counselors will become increasingly common, if not the norm. Consequently, there are clinical, professional, ethical, and societal considerations associated with the increasing popularity of tattoo art. This section addresses what counselors can do to adeptly navigate the increasing prevalence of tattoo culture and better serve their clients.
Counselors must reexamine their potential bias about tattooed clients and recognize that current research suggests they are not more likely to have mental and behavioral problems (e.g., Pajor et al., 2015). In fact, tattoos on a client might indicate their readiness for counseling by showing their strength and desire to break free of parental and societal expectations (e.g., Crompton et al., 2021). However, the number and placement of tattoos may better indicate potential mental health issues (Mortensen et al., 2019). With this in mind, asking clients about their tattoos early in the counseling relationship may help build rapport and provide potentially rich information about the client’s life story. Specifically, if the client’s tattoo is visible, it would be appropriate and possibly helpful to ask about it during intake (Kaufmann & Armstrong, 2022).
To foster genuine rapport and mitigate power imbalances in the therapeutic relationship, it is crucial for counselors to engage in self-reflection, cultivate cultural awareness and humility, and understand the potential cultural significance of tattoos (Day-Vines et al., 2018). Initiating conversations about clients’ tattoos early in counseling can be an effective strategy. Counselors might ask: “Tattoos often have special meanings or stories attached to them. What inspired you to get yours?” This approach demonstrates respect for the client’s personal and cultural narratives, promoting a more equitable and empathetic counseling environment. For instance, inquiring about a client’s neo-Nazi tattoos demonstrates the counselor’s desire to understand all aspects of the client. Despite the offensive nature of the tattoos, questioning could prompt the client to disclose personal experiences such as family addiction, abuse, poverty, insecurity, and fear of losing one’s identity in an increasingly multicultural society. These disclosures might not have emerged otherwise.
Counselors do not necessarily need to cover their tattoos, because they may help increase clients’ perception of the counselor’s relevance (Zidenberg et al., 2022). In fact, the counselor disclosing their tattoos may propel some clients to share more personally relevant information during sessions (Stein, 2011). Depending upon the client, a counselor with tattoos could broach the topic of how their tattoos symbolize their pursuit of authenticity in a society where the values of marginalized populations (e.g., women, non-White, LGBTQ) are too often not recognized, understood, or honored.
This example shows how a counselor could broach the topic of tattoos:
During our sessions, we have been exploring various aspects of identity and self-expression, which has led me to reflect on something personal I would like to share with you. As you may have noticed, I have some tattoos that hold particular significance. I have found that my tattoos remind me of essential experiences and values in my life. I share this with you because I believe it is vital for us to foster an environment of openness and authenticity in our therapeutic relationship. However, I want to emphasize that our sessions are about you and your journey. So, if you have any questions or concerns about my tattoos or anything else, please feel free to share them with me. I am here to create a safe and open space to discuss anything that comes up for you.
Thus, the counselor’s tattoo narrative may offer the client freedom to explore repressed aspects of themselves, which, once discovered, may allow for more self-awareness and appreciation, ultimately resulting in better mental health. Counselors can also simply discuss their tattoos with clients who express curiosity or concern. This approach allows the counselor to provide context and meaning behind their tattoos, potentially fostering a deeper connection and understanding between counselor and client.
However, some clients might be disinclined to continue services with an obviously tattooed counselor. As such, counselors may choose to cover their tattoos during sessions, especially if they anticipate that it may distract or discomfort certain clients. This approach can help maintain a professional appearance and minimize potential barriers to therapy. These kinds of tensions may lead to the strategic use of profile photographs on one’s counseling practice’s website. Depending on their client base and target demographics, counselors may opt for photographs that either prominently display or discreetly conceal their tattoos. Prioritizing the client’s comfort and preferences is essential. Counselors should gauge the client’s reactions and adjust their approach accordingly. In sum, the best advice for counselors with tattoos is to rely on their clinical intuition and discretion when deciding how to approach discussions about personal tattoos with clients. As with any counselor disclosure, discussing personal tattoos should be used intentionally with the client’s best interest in mind.
If a client inquires about the advisability of getting tattoos, it is essential to assist them in thoroughly processing this decision, as with any significant life choice. Be open with clients that biases against tattoos persist, with people of color and women being the most stigmatized. Regrettably, many individuals harbor negative perceptions of tattooed people, particularly regarding visible body art and content that might be deemed offensive. Counselors can ask probing questions about the client’s reasoning for obtaining tattoos, such as, “What does getting this tattoo mean to you, and how do you think it will impact your sense of identity or self-expression?” and “Have you considered any potential long-term implications of getting this tattoo, including how you might feel about it in the future or how it might affect your personal or professional life?”
The intersection of tattoos, mental health, and social justice represents a rich and largely unexplored area of research for counselor educators. As the prevalence of tattoos increases among both clients and counselors, we believe this presents a rich opportunity for personal exploration and the discovery of values and strengths, an area currently underexplored in the counseling profession. Future research on tattoos could examine their presence on counselors and clients, their effect on the therapeutic alliance, personality differences among tattooed individuals, and tattooed people’s likelihood of engaging in advocacy work. To advance dialogue and research in this domain, the Western Carolina University counseling program’s faculty, students, and graduates created the Intersection: Art, Mental Health, and Social Justice magazine (Mock et al., 2021). This publication aimed to enhance dialogue and understanding regarding tattoos. Readers are encouraged to peruse the online magazine to explore personal stories of tattooed counselors.
Conclusion
With the increasing popularity and prevalence of tattoos combined with continued cultural bias, body art is an area that warrants further research and discussion in the counseling profession. In summary, there does not appear to be significant relationship between tattooed people experiencing more mental health problems than nontattooed people. However, there is continued bias against tattooed people, and the reasons for obtaining tattoos are rooted more deeply than merely increasing personal attractiveness. As described in the unencumbered self theory of tattoos, the reemergence of tattoo art may be emblematic of the trends seen throughout the counseling profession to advance the discipline from its focus on intra- and interpersonal theories of health and wellness to include broader sociological perspectives on healing. The reemergence of tattoo art, then, could be an allegory for moving beyond the White, male, heteronormative standards that have traditionally dominated the profession, ushering forth an age of inclusivity where the rich and complex tapestry of all people’s values, traditions, and customs can be known and honored.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aizenman, M., & Jensen, M. A. C. (2007). Speaking through the body: The incidence of self-injury, piercing, and tattooing among college students. Journal of College Counseling, 10(1), 27–43. https://doi.org/10.1002/j.2161-1882.2007.tb00004.x
Alter-Muri, S. (2020). The body as canvas: Motivations, meanings, and therapeutic implications of tattoos. Art Therapy, 37(3), 139–146. https://doi.org/10.1080/07421656.2019.1679545
Al-Twal, A., & Abuhassan, R. (2024). Tattoos and career discrimination in a conservative culture: The case of Jordan. Current Psychology, 43, 11914–11923. https://doi.org/10.1007/s12144-023-05304-7
Atkinson, M. (2002). Pretty in ink: Conformity, resistance, and negotiation in women’s tattooing. Sex Roles, 47, 219–235. https://doi.org/10.1023/A:1021330609522
Baumann, C., Timming, A. R., & Gollan, P. J. (2016). Taboo tattoos? A study of the gendered effects of body art on consumers’ attitudes toward visibly tattooed front line staff. Journal of Retailing and Consumer Services, 29, 31–39. https://doi.org/10.1016/j.jretconser.2015.11.005
Broussard, K. A., & Harton, H. C. (2018). Tattoo or taboo? Tattoo stigma and negative attitudes toward tattooed individuals. The Journal of Social Psychology, 158(5), 521–540. https://doi.org/10.1080/00224545.2017.1373622
Camacho, J., & Brown, W. (2018). The evolution of the tattoo in defiance of the immutable definition of deviance: Current perceptions by law enforcement of tattooed arrestees. Deviant Behavior, 39(8), 1023–1041. https://doi.org/10.1080/01639625.2017.1395669
Carmen, R. A., Guitar, A. E., & Dillon, H. M. (2012). Ultimate answers to proximate questions: The evolutionary motivations behind tattoos and body piercings in popular culture. Review of General Psychology, 16(2), 134–143. https://doi.org/10.1037/a0027908
Covington, B. E. (2015). The sentence continues: Breaking silences and becoming authors through The Semicolon Project [Master’s thesis, James Madison University]. JMU Scholarly Commons. https://commons.lib.jmu.edu/master201019/47
Crompton, L., Amrami, G. P., Tsur, N., & Solomon, Z. (2021). Tattoos in the wake of trauma: Transforming personal stories of suffering into public stories of coping. Deviant Behavior, 42(10), 1242–1255. https://doi.org/10.1080/01639625.2020.1738641
Dance, A. (2019, April 6). How the Samoan tattoo survived colonialism. Scientific American. https://www.scientificamerican.com/article/how-the-samoan-tattoo-survived-colonialism
Day-Vines, N. L., Ammah, B. B., Steen, S., & Arnold, K. M. (2018). Getting comfortable with discomfort: Preparing counselor trainees to broach racial, ethic, and cultural factors with clients during counseling. International Journal for the Advancement of Counselling, 40(2), 89–104. https://doi.org/10.1007/s10447-017-9308-9
Ernst, M., Borkenhagen, A., Fegert, J. M., Brähler, E., & Plener, P. L. (2022). The association of childhood abuse and neglect with tattoos and piercings in the population: Evidence from a representative community survey. BMC Psychology, 10(105), 1–10. https://doi.org/10.1186/s40359-022-00811-x
Grumet, G. W. (1983). Psychodynamic implications of tattoos. American Journal of Orthopsychiatry, 53(3), 482–492. https://doi.org/10.1111/j.1939-0025.1983.tb03392.x
Guéguen, N. (2013). Effects of a tattoo on men’s behavior and attitudes towards women: An experimental field study. Archives of Sexual Behavior, 42(1), 1517–1524. https://doi.org/10.1007/s10508-013-0104-2
Heckerl, A. (2021). I can’t even wear my skin: The experiences visibly tattooed women have for rejecting hegemonic femininity (Publication No. 1099) [Master’s thesis, California State University, Monterey Bay]. Capstone Projects and Master’s Theses. https://digitalcommons.csumb.edu/caps_thes_all/1099
Henle, C. A., Shore, T. H., Murphy, K. R., & Marshall, A. D. (2022). Visible tattoos as a source of employment discrimination among female applicants for a supervisory position. Journal of Business and Psychology, 37, 107–125. https://doi.org/10.1007/s10869-021-09731-w
Jabłońska, K., & Mirucka, B. (2023). Mental body representations of women with tattoos in emerging adulthood—A cluster analysis. Archives of Women’s Mental Health, 26(4), 473–483. https://doi.org/10.1007/s00737-023-01326-z
Karacaoglan, U. (2012). Tattoo and taboo: On the meaning of tattoos in the analytic process. The International Journal of Psychoanalysis, 93(1), 5–28. https://doi.org/10.1111/j.1745-8315.2011.00497.x
Kaufmann, L., & Armstrong, M. L. (2022). The influences of tattoos on health care experiences. The Journal of Continuing Education in Nursing, 53(4), 178–184. http://doi.org/10.3928/00220124-20220311-08
Khair, N. (2022). Marketing of self: Using tattoos to symbolize ownership and control of one’s body. Narratives from Middle Eastern women. Sociology Compass, 16(7), 1–11. https://doi.org/10.1111/soc4.13002
Kidron, C. A. (2012). Breaching the wall of traumatic silence: Holocaust survivor and descendant person–object relations and the material transmission of the genocidal past. Journal of Material Culture, 17(1), 3–21. https://doi.org/10.1177/1359183511432989
Kloẞ, S. T. (2022). Embodying dependency: Caribbean godna (tattoos) as female subordination and resistance. The Journal of Latin American and Caribbean Anthropology, 27(4), 601–612. https://doi.org/10.1111/jlca.12644
Lane, D. C. (2014). Tat’s all folks: An analysis of tattoo literature. Sociology Compass, 8(4), 398–410. https://doi.org/10.1111/soc4.12142
Laumann, A. E., & Derick, A. J. (2006). Tattoos and body piercings in the United States: A national data set. Journal of the American Academy of Dermatology, 55(3), 413–421. https://doi.org/10.1016/j.jaad.2006.03.026
Martone, A. J. (2023). Scars, marks, and tattoos: How appearance influences rearrest and reconviction (Publication No. 31076097) [Master’s thesis, Sam Houston State University]. ProQuest Dissertations and Theses Global.
Miranda, M. D. (2020). Tattoos and tattoo inks: Forensic considerations. WIREs Forensic Science, 2(1), 1–16. https://doi.org/10.1002/wfs2.1360
Mock, C., Jones, B., Gillespie, L., & Curtis, R. (Eds.). (2021). Intersection: Art, mental health, and social justice (Issue No. 1). Western Carolina University. https://online.fliphtml5.com/pdhbe/uinm
Morello, G. (2021). I’ve got you under my skin: Tattoos and religion in three Latin American cities. Social Compass, 68(1), 61–80. https://doi.org/10.1177/0037768620962367
Morello, G., Sanchez, M., Moreno, D., Engelmann, J., & Evangel, A. (2021). Women, tattoos, and religion an exploration into women’s inner life. Religions, 12(7), 517. https://doi.org/10.3390/rel12070517
Mortensen, K., French, M. T., & Timming, A. R. (2019). Are tattoos associated with negative health-related outcomes and risky behaviors? International Journal of Dermatology, 58(7), 816–824. https://doi.org/10.1111/ijd.14372
Naudé, L., Jordaan, J., & Bergh, L. (2019). “My body is my journal, and my tattoos are my story”: South African psychology students’ reflections on tattoo practices. Current Psychology, 38, 177–186. http://doi.org/10.1007/s12144-017-9603-y
O’Brien, E. J., & Epstein, S. (1988). The Multidimensional Self-Esteem Inventory (MSEI): Professional manual. Psychological Assessment Resources, Inc. https://www.parinc.com/products/MSEI#details
Pajor, A. J., Broniarczyk-Dyła, G., & Świtalska, J. (2015). Satisfaction with life, self-esteem and evaluation of mental health in people with tattoos or piercings. Psychiatria Polska, 49(3), 559–573. https://doi.org/10.12740/PP/27266
Rima, D., Aldabergenova, N., Sharipova, A., Atakhanova, G., & Beaver, K. M. (2023). Tattoos as a stigmatizing label implicated in being processed through the criminal justice system. Deviant Behavior, 44(11), 1701–1712. https://doi.org/10.1080/01639625.2023.2230513
Roberts, D. (2016). Using dramaturgy to better understand contemporary Western tattoos. Sociology Compass, 10(9), 795–804. https://doi.org/10.1111/soc4.12400
Roggenkamp, H., Nicholls, A., & Pierre, J. M. (2017). Tattoos as a window to the psyche: How talking about skin art can inform psychiatric practice. World Journal of Psychiatry, 7(3), 148–158. https://doi.org/10.5498/wjp.v7.i3.148
Rohith, M. M., Belcher, W. R., Roy, J., Abraham, S. O., Chakraborty, P., Nandaniya, N. J., & Johnson, A. (2020). Tattoo in forensic science: An Indian perspective. Journal of Forensic and Legal Medicine, 74, 1–10. https://doi.org/10.1016/j.jflm.2020.102022
Schmid, S. (2013). Tattoos – An historical essay. Travel Medicine and Infectious Disease, 11(6), 444–447. https://doi.org/10.1016/j.tmaid.2013.10.013
Shuaib, S. O. (2020). African traditional body art and contemporary realities. International Journal of Humanitatis Theoreticus, 3(1), 127–140. https://bit.ly/Shuaib_bodyart
Sims, J. P. (2018). “It represents me”: Tattooing mixed-race identity. Sociological Spectrum, 38(4), 243–255. https://doi.org/10.1080/02732173.2018.1478351
Solanke, I. (2017). Discrimination as stigma: A theory of anti-discrimination law. Bloomsbury.
Solís-Bravo, M. A., Flores-Rodríguez, Y., Tapia-Guillen, L. G., Gatica-Hernández, A., Guzmán-Reséndiz, M., Salinas-Torres, L. A., Vargas-Rizo, T. L., & Albores-Gallo, L. (2019). Are tattoos an indicator of severity of non-suicidal self-injury behavior in adolescents? Psychiatry Investigation, 16(7), 504–512.
https://doi.org/10.30773/pi.2019.03.06
Southern Poverty Law Center. (2006, October 19). A look at racist skinhead symbols and tattoos. The Intelligence Report. https://www.splcenter.org/fighting-hate/intelligence-report/2006/look-racist-skinhead-symbols-and-tattoos
Stein, A. (2011). The tattooed therapist: Exposure, disclosure, transference. Psychoanalysis, Culture & Society, 16, 113–131. https://doi.org/10.1057/pcs.2010.17
Stephenson, L., & Byard, R. W. (2019). Cause, manner and age of death in a series of decedents with tattoos presenting for medicolegal autopsy. Journal of Forensic and Legal Medicine, 64(1), 49–51. https://doi.org/10.1016/j.jflm.2019.04.003
Tan, L. (2013). Intellectual property law and the globalization of indigenous cultural expressions: Māori tattoo and the Whitmill versus Warner Bros. case. Theory, Culture & Society, 30(3), 61–81. https://doi.org/10.1177/0263276412474328
Tate, J. C., & Shelton, B. L. (2008). Personality correlates of tattooing and body piercing in a college sample: The kids are alright. Personality and Individual Differences, 45(4), 281–285. https://doi.org/10.1016/j.paid.2008.04.011
The Holy Bible: New International Version. (1978). The Zondervan Corporation.
The Qur’an (M. A. S. Abdel Haleem, Trans.). (2004). Oxford University Press.
Thomas, N., Cole, A., & Douglas, B. (Eds.). (2005). Tattoo: Bodies, art and exchange in the Pacific and the West. Reaktion Books.
Vegrichtová, B. (2018). Nonverbal communication of prison subculture through criminal tattoo symbols. Academic and Applied Research in Military and Public Management Science, 17(3), 179–186. https://doi.org/10.32565/aarms.2018.3.13
Williams, D. J., Thomas, J., & Christensen, C. (2014). “You need to cover your tattoos!”: Reconsidering standards of professional appearance in social work. Social Work, 59(4), 373–375. https://doi.org/10.1093/sw/swu025
Wohlrab, S., Stahl, J., & Kappeler, P. M. (2007). Modifying the body: Motivations for getting tattooed and pierced. Body Image, 4(1), 87–95. https://doi.org/10.1016/j.bodyim.2006.12.001
Zestcott, C. A., Tompkins, T. L., Kozak Williams, M., Livesay, K., & Chan, K. L. (2018). What do you think about ink? An examination of implicit and explicit attitudes toward tattooed individuals. The Journal of Social Psychology, 158(1), 7–22. https://doi.org/10.1080/00224545.2017.1297286
Zidenberg, A. M., Dutrisac, S., & Olver, M. (2022). “No ragrets”: Public perception of tattooed mental health professionals. Professional Psychology: Research and Practice, 53(3), 304–312. https://doi.org/10.1037/pro0000441
Zuckerman, A. (2020, May 13). 38 tattoo statistics: 2020/2021 industry, trends & demographics. Compare Camp. https://comparecamp.com/tattoo-statistics/
Russ Curtis, PhD, LCMHC, is a professor at Western Carolina University. Lisen C. Roberts, PhD, is an associate professor at Western Carolina University. Paul Stonehouse, PhD, is an assistant professor at Western Carolina University. Melodie H. Frick, PhD, NCC, ACS, LPC-S, is a professor at Western Carolina University. Correspondence may be addressed to Russ Curtis, Western Carolina University, 28 Schenck Parkway, Office 214, Asheville, NC 28803, curtis@wcu.edu.
Jan 17, 2024 | Volume 13 - Issue 4
Sunanda M. Sharma, Jennifer E. Bianchini, Zeynep L. Cakmak, MaryRose Kaplan, Muninder K. Ahluwalia
According to the American Counseling Association and the Council for Accreditation of Counseling and Related Educational Programs, social justice advocacy is an ethical imperative for counselors and a training standard for counseling students. As a group of socially conscious mental health counseling students and faculty, we developed and facilitated a social justice advocacy group to learn about tangible ways to engage in social justice action. Using the S-Quad model developed by Toporek and Ahluwalia, we formed and facilitated a social justice advocacy group for our peers. This paper will serve as a reflection of our experiences engaging in the process.
Keywords: social justice, advocacy, counseling students, S-Quad model, mental health
When describing the motivation for her political aspirations, Georgia gubernatorial hopeful Stacey Abrams (2019) stated, “We have to have people who understand that social justice belongs to us all.” This quote speaks to this group of authors who feel strongly about the importance of social justice in mental health counseling. This ethos served as the motivation to create a peer-led group to foster the development of our social justice advocacy skills. We used the S-Quad model (Toporek & Ahluwalia, 2020) to form and facilitate a social justice advocacy group for master’s and doctoral counseling students at our institution.
Historically, the counseling profession has been rooted in social justice advocacy (SJA) with Frank Parsons’s efforts to support White European immigrants in the United States to develop their vocational goals (Gummere, 1988; Toporek & Daniels, 2018). However, SJA has not been consistently operationalized across counselor training programs (Counselors for Social Justice [CSJ], 2020). Although ethical standards established by the American Counseling Association’s ACA Code of Ethics (ACA; 2014) encourage counselors to advocate for clients and communities when appropriate (A.7.a, A.7.b.), and training standards established by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015) state that SJA should be a part of counseling curriculum (2.F.2.b.), counselors have reported receiving little guidance about how to implement advocacy in practice (Field et al., 2019; Ratts & Greenleaf, 2018). As counseling students, we experienced the same concern. To address this gap in our educational experience, we created and facilitated a group based on the S-Quad model (strengths, solidarity, strategies, and sustainability) of SJA (Toporek & Ahluwalia, 2020). As a group of socially conscious mental health counseling students, our aim was to grow in our roles as professionals by learning about, teaching, and engaging in SJA. In the process, we learned about ourselves as budding counselors and educators.
Literature Review
In their foundational article, Vera and Speight (2003) called on the counseling profession to expand its understanding of multicultural competence; they asserted that without SJA, counselors are perpetuating the systems of oppression from which their clients are attempting to heal. Utilizing intrapsychic approaches which neglect to account for contextual factors not only perpetuates oppressive counseling practices, but it also does a disservice to those with marginalized identities (Ratts, 2009; Vera & Speight, 2003). In order to properly serve clients, counselors must step beyond the classroom, expand the original conceptualization of our roles, and explore beyond the counseling office (Ratts, 2009; Ratts & Greenleaf, 2018; Vera & Speight, 2003). Despite the increase in available resources such as the ACA Advocacy Competencies (Toporek et al., 2009) and the Multicultural and Social Justice Counseling Competencies (MSJCC; Ratts et al., 2016), the number of sociocultural forces such as racial demographics of counseling programs and reliance on theories and interventions developed for White European clients prevents social justice from being a central force in the profession (CSJ, 2020).
As mental health professionals, we are positioned to understand the impact that oppression has on health (Nadal et al., 2021), which speaks to the need for operationalizing social justice counseling and SJA so counselors may support client wellness. Counseling students require more knowledge and practice to obtain appropriate resources and tools in order to intervene and resist systemic oppression (Vera & Speight, 2003). Ratts (2009) named social justice as the “fifth force” in counseling in an attempt to concretize the relevance and importance of challenging the status quo in counseling. However, the perceived attitude of the counseling profession toward social justice is reflected in the definition of counseling. The 20/20 initiative was a movement to unify the profession and solidify professional identity by arriving at the definition of counseling. Delegates from 31 counseling-related organizations (e.g., CACREP, Chi Sigma Iota) participated in a Delphi-method study to achieve consensus on a definition; however, only 29 organizations ultimately endorsed the definition (Kaplan et al., 2014). Although the definition for counseling includes the word “empower”; it does not include the words “social justice” or “advocacy.” Thus, CSJ was one organization that did not support the new definition (Kaplan et al., 2014). Despite these challenges, Ratts and Greenleaf (2018) assert that counselors must develop the advocate part of their identity, yet they note that there is more of a focus on traditional counseling skills rather than acknowledging the shifting sociopolitical climate and equipping counselors with the skills to address these concerns. The leadership and advocacy course (or the content in another course; CACREP, 2023) in CACREP-accredited counseling doctoral programs often only focuses on leadership and advocacy within and for the profession. Although CACREP (2023) standards do not dictate the courses a counseling program must offer, there continues to be limited discussion of SJA and social justice, nor are there solid instructional methods for counselor educators to use in the classroom (Chapman-Hilliard & Parker, 2022). This situation hinders students’ understanding of the role systemic issues have on minoritized communities, further deterring people in those communities from seeking help.
As counselors and counseling students, we understand our responsibility to advocate for clients, but we feel unprepared to fulfill our ethical (and for many of us, moral) duty. We did not learn enough about the concrete, tangible skills that a professional counselor can utilize to challenge oppression and inequity. We were unable to locate any studies regarding peer-led SJA groups for counseling students, thus we hope to contribute something novel to the counseling literature and encourage counseling students to better understand and grow into their roles as social justice advocates. Counselors-in-training (CITs) and practicing counselors within the profession sometimes question the relevance of SJA and report feeling confused about how to implement SJA in counseling (Field et al., 2019; Ratts & Greenleaf, 2018). hooks (1994) notes it is imperative that a student accepts responsibility for their education and becomes “an active participant, not a passive consumer” (p. 14). Thus, we engaged in this process to support our colleagues in the counseling student body and take accountability for our education.
Taking Action: Social Justice Advocacy Group
Leading organizations in the profession claim a two-pronged approach to advocacy: one prong advocating for the legitimacy of the counseling profession, and the other advocating on behalf of the clients and students whom counselors serve (Chang et al., 2012). In our educational experience, SJA on behalf of and in partnership with clients was emphasized, but tangible interventions were not discussed. Further, systemic issues and inequities were often left unaddressed. Thus, we developed this group to more concretely address the second “prong” of advocacy in counseling. First and fourth authors Sunanda M. Sharma and MaryRose Kaplan were part of the executive board of Chi Sigma Mu (Chi Sigma Iota chapter at Montclair State University) and co-founded the social justice committee. Second and third authors Jennifer E. Bianchini and Zeynep L. Cakmak were the first members of the committee who proposed ideas and facilitated events and activities related to social justice that they felt passionately about. Bianchini proposed a social justice book club ahead of a presentation that the CSI chapter organized (hosting the authors of the book Taking Action). The book club met three times with up to three students, from whom we received feedback to help us form the SJA group.
The following semester, fifth author Muninder K. Ahluwalia proposed restructuring the book club into an advocacy group by utilizing the Taking Action text as a framework to teach students about systemic SJA. CACREP (2015) standards state that multiculturalism and social justice must be discussed throughout counseling courses (2.F.2.b.); however, in our experiences, we found that social justice is addressed as an ethical and moral imperative, but curricula do not address concrete SJA skills and strategies to combat systemic oppression. The counseling program in which the first four authors are enrolled and the fifth author is a faculty member offers a social justice counseling class as an elective. However, the class is not consistently offered every semester and has only been taught by that one faculty member. Thus, our aim with this group was to provide a space for our colleagues in which we could collaboratively learn about how to enact social justice. This section will describe the S-Quad model, explain the group structure, outline the proposed learning objectives, and provide a table that outlines the curriculum of the group.
The S-Quad Framework
As a profession, mental health counseling is positioned to “buffer” against challenges with oppression and changes to the status quo (Kivel, 2020). There is an emphasis on intrapsychic interventions to combat systemic issues, rather than attempt to uproot the oppression itself (Kivel, 2020; Ratts, 2009; Toporek, 2018). Toporek (2018) noted that upon reflection of the way the profession is positioned and her privileged identities, she developed a framework through which to take social justice action despite the challenges she continues to encounter. The S-Quad model includes four Ss for social justice advocates to formulate a way to address systemic injustices: strengths, solidarity, strategy, and sustainability (Toporek & Ahluwalia, 2020).
Strengths are described as a combination of one’s existing “skills, knowledge, and expertise” (Toporek & Ahluwalia, 2020, p. 27). Although strengths can be qualities one already has, both personal and professional, the authors also encourage budding advocates to reflect upon strengths that they would like to develop. Solidarity has multiple facets to its definition, as advocates are asked to support, honor, and respect communities they intend to engage with and to also seek support from their personal networks to remain grounded (Toporek & Ahluwalia, 2020). Solidarity is enacted through collaborative efforts and through the lens of cultural humility (Toporek & Ahluwalia, 2020). Strategy is the implementation of strengths and solidarity to construct a plan of action (Toporek & Ahluwalia, 2020). It is important to evaluate the efficacy, efficiency, and impact of different strategic plans to ensure they work toward the stated goal and—most importantly—benefit the community that the action is intended for (Toporek & Ahluwalia, 2020). Finally, a unique facet of the S-Quad model is the fourth “S,” sustainability. Sustainability addresses the wellness of advocates; without it, there is a higher likelihood they may abandon their efforts. SJA can be an enriching and healing practice, but it can also be an emotionally draining pursuit, and one can feel helpless when attempting to combat the gravity and breadth of oppression (Toporek & Ahluwalia, 2020). Thus, the authors encourage budding advocates to take an inventory of the practices that replenish and nourish them in order to remain engaged in their work.
Group Structure
Sharma proposed structuring this SJA group as a biweekly, one-hour, peer-led, open (students were free to join at any point) psychoeducation group, whose grounding framework would be the S-Quad model (Toporek & Ahluwalia, 2020). Due to COVID-19 restrictions, we facilitated the group through Zoom. The objectives of the group were: to describe all components of the S-Quad model, to describe the ethical responsibility of being a social justice advocate, to create a solidarity network of fellow advocates, to increase awareness of how one’s positionality impacts their advocacy work, and to apply the S-Quad model (Toporek, 2018) through the creation of a social justice action plan (Sheely-Moore & Kooyman, 2011). Initially, the intention was to divide each group session into two parts. The first part of the session would be didactic, in which we would discuss the “S” of that week and ground it in a case study. The second half of the session would offer members the chance to process the content so they can apply what they are learning to their social justice plan. Upon reflection and discussion as co-facilitators, we recognized the challenges associated with attempting to address so much content in a 60-minute session and collectively agreed to shift the group and make it akin to a flipped classroom by including pre-recorded didactic videos. This afforded members the chance to view the videos at their own pace and come to the session prepared to engage in dialogue.
In our experiences, instructors who taught our counseling theories courses recommended for us to select one theory to learn about before declaring our theoretical orientation. Similarly, we asked members to narrow down their focus for the purposes of this group to a cause within a community that they feel passionately about. The other structural component we addressed with group members was that this curriculum is cumulative but not necessarily linear; so, an application of the previous “S” is necessary to study the following “S.” For example, once a group member identifies their strengths, we apply those strengths to inform what strategies they will use, but it does not necessarily mean that strengths are not revisited.
Given that this was a psychoeducation group rather than a traditional course, we did not want to use typical didactic methods to engage with this material. We intentionally paired each part of the S-Quad model with a story about an advocate from a minoritized community of whom others likely may not be aware. This demonstrated that SJA is not always done on a public stage. This narrative form of teaching (Hannam et al., 2015) allowed us to contextualize stories of advocates who are quietly resisting oppression in their respective communities. We spotlighted those stories so members could feel less intimidated by the prospect of SJA. In the interest of social justice and accessibility, the Chi Sigma Iota Counseling Honor Society’s Chi Sigma Mu chapter at Montclair State University funded books for interested members so they could follow along with the activities and didactic content. After the second session, we also introduced the idea of the social justice action plan. Table 1 shows the structure/syllabus of the group that we utilized for the semester and describes the ways in which we adapted to agreed-upon changes.
Table 1
Taking Action Group Structure
| Week |
Topic & Activity Assigned |
Content/Activities |
| Week 1 |
Introducing
Taking Action
S-Quad Model |
• Purpose, rationale, and structure of group
• Group agreements/norms
• Overview of S-Quad model (Toporek & Ahluwalia, 2020)
• ADDRESSING model (Hays, 2022), a framework that explores individual identity in context
• Difference between justice, charity, philanthropy |
| Week 2 |
1st S: Strengths
Activity 4.2, p. 29**
|
• Reviewing agreed-upon group norms
• Defining strengths
• Case study: Arunachalam Muruganantham (“The Pad Man”)
Processing case study as a group
• Introducing the social action plan |
| Week 3 |
Co-facilitators reflection meeting |
• This session was initially planned to address the 2nd S in the S-Quad, but no members attended the group this day. Instead, as co-facilitators, we met to discuss the progress of the group.
|
| Week 4* |
2nd S: Solidarity
Activity 5.1, p. 55 |
• Defining solidarity
• Case study: 4 young Black women, Black Lives Matter protests
Combining strengths and solidarity
Processing case study as a group |
| Week 5 |
3rd S:
Strategy
Activity 6.1, p. 66 |
• Defining strategy
• Case study: Cakmak
Strength, solidarity, and strategy
Processing case study as a group
Cakmak’s social action plan |
| Week 6 |
4th S:
Sustainability
Activity 7.6, p. 176
|
• Defining sustainability
• Case study: Alexandria Ocasio Cortez
Strength, solidarity, strategy, and sustainability
Processing the importance and guilt of self-care
Processing burnout |
| Week 7 |
Final Group
|
• Case study
Apply ADDRESSING, S-Quad model
• Feedback from members |
*Marks shift to videos for the didactic portion
**All activities listed are from Ahluwalia & Toporek (2020).
Reflections
In this section, we offer our reflections on the group and extract salient collective themes that have come about through our processing. In our first session, we informed the group members that we intended to write a reflection paper, and they gave implicit consent to this writing; we did not collect data from group members for the purposes of this article. We begin by grounding the discussion of the group by acknowledging our positionality and social location and how that influenced how we approached our facilitation and planning of the group. Sharma, Bianchini, and Cakmak will provide their most salient takeaways from the forming and facilitation of the Taking Action group.
Positionality
Sharma identifies as a cisgender, South Asian (Indian), middle-class, able-bodied woman who is a doctoral candidate in a CACREP-accredited counseling program and a full-time lecturer in a CACREP-accredited counseling program. I bring a bicultural perspective to my counseling practice and education, and I have attended primarily White institutions (PWIs) for most of my life. As a master’s and doctoral National Board for Certified Counselors Minority Fellowship Program fellow, I learned about the importance and practice of SJA. I am a practicing clinician in private practice (working mostly with White clients), and I engage in advocacy work with South Asian intimate partner violence survivors.
Bianchini identifies as a White, cisgender woman who grew up in a predominantly White community in the United States. My family has lived in the United States for several generations and the majority of my extended family identifies as part of the middle class. I do not have any disabilities and am a practicing Christian. I am a master’s-level graduate student and joined Chi Sigma Iota’s social justice committee in my first semester of coursework.
Cakmak identifies as a Muslim American, cisgender woman of Turkish origin. I do not have any physical disabilities, but I have been diagnosed with general anxiety disorder (GAD) and major depressive disorder (MDD). I identified as part of the upper middle class in Turkey as a child, and I am middle class as an immigrant in the United States. I have two graduate degrees, one in literature and one in counseling. I have done volunteer work with underrepresented religious and cultural communities since I was in high school.
Themes
As cocreators and coauthors, we reflected on our collective and individual experiences of facilitating our Taking Action group. We each completed individual reflection sheets within 48 hours of each group session to capture our takeaways, and we processed our experiences together after each group session. We reviewed our reflection sheets individually and noted themes that arose for each of us. We then collectively reviewed the sheets to determine what themes arose across our reflection sheets. We reengaged in the reflection process as we wrote this manuscript. In this section, we highlight the major themes among our experiences.
Fear
The most significant theme of our collective experience was fear. Throughout each session, fear came up under several different guises, which served as an umbrella for additional themes: judgment, self-efficacy, and humility. Fear was the main antagonist preventing us from doing social justice work before this program. Fear of not knowing the necessary information, fear of saying or doing the wrong thing, and fear of not helping enough or adequately were examples of how this feeling manifested. However, engaging in this group helped us alleviate that fear through resources, support, and a plan of action. In the first session, we felt tentative and timid, and optimistic yet stagnant. After providing members with more information and concrete steps to create real social justice action, our fear dissipated, our passion for working as a group was ignited, and the motivation to take action began.
Judgment
In our first session, when we engaged members in a dialogue about group agreements, we noticed that there was more focus on the importance of the group serving as a judgment-free space than as a confidential one. We felt that members wanted to feel safe in the group because they feared being judged due to their self-perceived incompetence. We recognized they did not want to feel judged by others if their ideas were deemed unacceptable or incorrect. Establishing a nonjudgmental space permitted members to try, even if the outcomes were not as they hoped. We believe it allowed members to have a safe space to begin processing what they understand about SJA.
Judgment was a recurrent theme and shifted from self-judgment to judging others. Members reported feeling frustrated and upset when their peers in the program were not at the same level of advocacy awareness and action as they were. They reported feeling angry about others’ ignorance. Through a shared reflection on these feelings, the group acknowledged that the judgment of others reinforces the barriers to change that we are trying to knock down. Members recognized the importance of being humble regarding other people (another theme discussed below) and empathetic to help manage feelings of judgment.
When discussing sustainability and self-care, members and facilitators shared our hesitations to implement sustainability practices, despite it being an ethical responsibility. This hesitancy revealed itself to be motivated by self-judgment of our productivity levels. It appeared that the group members would not allow themselves the breaks they needed to provide self-care because of the importance they gave to SJA. We then discussed the need to be unapologetic in our self-care as advocates and counselors.
Self-Efficacy
Related to judgment of self and others, we found self-efficacy was another significant and recurrent theme. Almost every group member expressed that they were struggling to feel like they could contribute enough to society to perform real social justice action rather than charity. Having members share similar insecurities resulted in an insightful and vulnerable conversation that helped us to feel connected and inspired. In the second session, members reported experiencing imposter syndrome, likely resulting from their low self-efficacy in social justice work. Our self-efficacy grew throughout the sessions as members received the information and tools they needed to take concrete steps in SJA. Once we clarified a reasonable idea of what was expected of them and had some direction, they felt more prepared to take action.
Humility
Lastly, the theme of humility appeared in several different iterations. The humility through humor with which we, as facilitators, approached this process helped break the ice and create a comfortable atmosphere in our initial meeting. Humility emerged in our second session when discussing the first “S” of the S-Quad model, strengths. In our reflection process, we noted that both facilitators and members appeared to be uncomfortable when sharing what they are “good” at. We, as female-identifying co-facilitators, noted the societal pressure and shame that have historically come with feelings of discomfort for behavior commonly regarded as boastful.
In the fourth session, the group discussed the importance of humility within their community. Members discussed how it was easy to humble oneself when trying to assist a community from the outside, but that it was an important lesson that we must be humble within our own communities. Members seemed to realize that their experience of their community and identity would not be the same as the next person’s, highlighting the importance of intersectionality within the human experience.
Humility was next discussed in the fifth session in terms of failure. Members acknowledged the importance of possessing humility and patience regarding our work because we will generally fail more than we will succeed in our efforts to create change. If we never failed, we would never learn from our mistakes and there would be no more SJA to do. However, knowing this instills the hope to persevere, for you never know what your planted seeds of action will grow into.
Combining Themes
As facilitators, we noticed a parallel between what we were experiencing and our members’ experiences. From the start of our group, we felt we needed to be more qualified to be teachers of SJA. This was our campus’s first peer-led advocacy group, which meant we did not have any models to reference, and we had to rely on our own ideas, skills, and judgment. With faculty support, we went outside the confines of our curriculum because we wanted to share and engage with this content in a meaningful way. This was a large undertaking, with little training and even less confidence. Similar to what we observed in our members, we were afraid of making mistakes in the content, direction, and discussion of this group because of the weight of the topic of social justice—especially as the first group any of us attempted to create or lead. We had to adapt to constantly developing circumstances, and this felt inappropriate for us as leaders. Something we recognized much later was that we could teach and learn simultaneously; we did not need to reach a point of expertise before developing this group. Although we do not consider ourselves experts in SJA, the work we did to prepare for each session, combined with the humility with which we presented ourselves and our work, effectively allowed us to lead the group to the best of our ability.
Another source of our fear was that there was an ulterior motivation for creating this group, which was not purely social justice–oriented. We sought a sense of community, particularly given the isolating COVID-19 pandemic we were living through, and running this group gave us that community, support, and friendship. This longing for connection played into our feelings of being unqualified to do social justice work because a few of us became involved in this project out of a desire to work with friends, and not solely because we wanted to devote ourselves to social justice. However, this search for connection and participation in this SJA group gave us a passion for this work if it was not present beforehand. That feeling of connection and belonging provided us with the inner power to attempt something bigger than ourselves. The bond we authors created while facilitating this group instilled the importance of collaboration, especially when doing something new, significant, and daunting. The “S” for solidarity was also particularly salient in this case; we recognize that we could not have created or run this group alone. We needed each other to not only complete all the work required but also to hold each other accountable, support each other in times of need, and encourage each other to keep going even when our hopes dimmed. In a sense, this group and the connection to each other provided the “S” for sustainability and wellness for ourselves and our work.
While reflecting on these two sources of our fear as facilitators, we discovered our desire to make this call to the counseling profession: to strengthen the bridge between academia and counseling in practice. Applying the knowledge gained from our courses to daily practice could be less intimidating and feel more like the natural progression of our nascent counseling careers. However, once the opportunity arose to test our skills, we felt hesitant and unprepared. Creating an advocacy group is not the only venue in which this fear of practice appears. As students, we authors felt a similar fear when stepping into our practicum and internship sites. It is natural to feel afraid when seeing clients for the first time as CITs, but this fear could be lessened by academic leaders guiding students into the field before their final year of studies. If more opportunities to work with real issues affecting communities were available to students and supported by faculty, the transition between the classroom and fieldwork would feel less daunting.
Discussion
Although this project was not an empirical study, our reflective process taught us about how it feels to learn about SJA and the labor required to teach about SJA. With this knowledge, we have identified potential implications for the counseling profession and counselor education training programs. We also acknowledge the limitations of the group we formed and facilitated.
Implications
Per our experience, we believe social justice counseling—and advocacy skills more specifically—must have a more prominent place in counseling curricula. Potential solutions may include consistently operationalizing social justice counseling and SJA in counselor training programs (CSJ, 2020). Furthermore, it is imperative to have more guidance from our institutional standards such as CACREP (2023) and to have more ethical standards regarding SJA in the next iteration of the ACA Code of Ethics. CACREP (2023) requirements establish content that should be covered throughout all coursework, rather than specific classes; however, each program might have a different approach to operationalize these standards because they are vaguely defined (Austin & Austin, 2020). For example, in the current CACREP (2023) standards, there is more frequent mention of social justice compared to the 2016 CACREP standards; however, there is still ambiguity about how this may present in a counseling course. Standard 3.B.1 (CACREP, 2023) says that counseling curricula must state how “theories and models of multicultural counseling, social justice, and advocacy” are addressed, but there is no mention of techniques, interventions, or skills for SJA. As a point of comparison, there are specific guidelines with respect to content like group counseling which delineate time that students must spend engaged in direct experience. However, it appears that social justice and SJA are still referred to in broader terms with fewer contingencies about how they must be addressed. We recognize that out-of-class work like advocacy might be left out of the curriculum because there are many required courses and training standards filling up students’ time in graduate school (Vera & Speight, 2003). However, we urge counseling leaders to consider the importance of SJA and the core role it plays in our healing work and our counseling identity.
Limitations and Future Directions
This group was developed and facilitated to encourage counseling students to develop their social justice advocate identity, but it was not an empirical study, and our collective reflections can only offer so much insight to facilitating such groups in the future. As this was an extracurricular group for which attendees took time out of their personal schedules, we do not know what motivated our peers to attend sessions that we offered. This would be important knowledge to address in future offerings of this group and to understand students’ attitudes toward social justice in counseling. Another limitation of our group was our inability to reach students who are unsure of what social justice is and might not recognize it as an inherent and imperative part of mental health counseling. Practicum and other service-learning opportunities for SJA within the profession have been explored in the literature (Farrell et al., 2020; Field et al., 2019; Langellier et al., 2020), but perhaps peer encouragement can help CITs to feel more confident as advocates. Although we intentionally kept the group open for accessibility, new introductions and catching up took time away from the group plan and content. We do not have data to explicate a group like this, but we hope our master’s and doctoral peers feel encouraged to start similar groups within their own programs. Finally, we wrote this article more than a year after our group ended; although we relied on our reflection sheets and notes from our experience, we are aware that there may be gaps in our recollections.
For future groups, we would be interested to complete an empirical study through an IRB in order to collect data regarding peer-led SJA groups. Screening or surveys before and after the group could not only provide valuable data, but also offer guidance for attendees even before the group starts and an opportunity for reflection after the group ends. Our decision to keep our group open led to attrition of members; thus, empirical studies might also investigate factors that contribute to student engagement. Collecting quantitative and qualitative data may provide further insight into effective strategies for describing and encouraging students to engage in concrete SJA skill development.
Conclusion
The experience of facilitating an SJA group was new, challenging, transformative, and important to our growth as CITs and budding counselor educators. As counselors, we understand our ethical duty to engage in SJA; however, we have not had adequate training in tangible strategies to utilize when advocating on behalf of our clients. The S-Quad model is an important guide that helped facilitate our understanding of how to implement SJA as mental health professionals. As co-facilitators and coauthors, we learned a great deal about ourselves as developing social justice advocates, CEs, and CITs and confronted fears parallel to those of the group members. Although SJA is a growing focus in the counseling literature, there is a great deal of research and training that must continue to occur so current and future counselors can develop their social justice advocate identities.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Abrams, S. (2019, January). 3 questions to ask yourself about everything you do [Video]. TED Talks. https://www.youtube.com/watch?v=3zJHwOwirjA
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default-document-library/2014-code-of-ethics-finaladdress.pdf?sfvrsn=96b532c_8
Austin, J. T., II, & Austin, J. A. (2020). The counselor educator’s guide: Practical in-class strategies and activities. Springer.
Chang, C. Y., Barrio Minton, C. A., Dixon, A. L., Myers, J. E., & Sweeney, T. J. (Eds.). (2012). Professional counseling excellence through leadership and advocacy (1st ed.). Routledge.
Chapman-Hilliard, C., & Parker, B. (2022). Embodied social justice learning: Considerations for curriculum development and training in counseling programs. Journal for Social Action in Counseling and Psychology, 14(1), 77–93. https://doi.org/10.33043/JSACP.14.1.77-93
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. https://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Council for Accreditation of Counseling and Related Educational Programs. (2023). 2024 CACREP standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Counselors for Social Justice. (2020). A call for social justice in the American Counseling Association (ACA). Journal for Social Action in Counseling and Psychology, 12(1), 2–12. https://doi.org/10.33043/JSACP.12.1.2-12
Farrell, I. C., DeDiego, A. C., & Marshall, R. C. (2020). Service learning to foster advocacy training in CACREP accredited programs. Journal of Creativity in Mental Health, 15(4), 522–534. https://doi.org/10.1080/15401383.2020.1733724
Field, T. A., Ghoston, M. R., Grimes, T. O., Sturm, D. C., Kaur, M., Aninditya, A., & Toomey, M. (2019). Trainee counselor development of social justice counseling competencies. Journal for Social Action in Counseling and Psychology, 11(1), 33–50. https://doi.org/10.33043/JSACP.11.1.33-50
Gummere, R. M., Jr. (1988). The counselor as prophet: Frank Parsons, 1854–1908. Journal of Counseling & Development, 66(9), 402–405. https://doi.org/10.1002/j.1556-6676.1988.tb00899.x
Hannam, F. D. (2015). Teaching through narrative. Forum on Public Policy Online, 2015(2).
Hays, P. A. (2022). Addressing cultural complexities in counseling and clinical practice: An intersectional approach (4th ed.). American Psychological Association.
hooks, b. (1994). Teaching to transgress: Education as the practice of freedom. Routledge.
Kaplan, D. M., Tarvydas, V. M., & Gladding, S. T. (2014). 20/20: A vision for the future of counseling: The new consensus definition of counseling. Journal of Counseling & Development, 92(3), 366–372. https://doi.org/10.1002/j.1556-6676.2014.00164.x
Kivel, P. (2020). Social service or social change? Who benefits from your work. https://paulkivel.com/wp-content/uploads/2011/07/Social-Service-or-Social-Change-2020-Update.pdf
Langellier, K. A., Astramovich, R. L., & Horn, E. A. D. (2020). Infusing service learning into the counselor education curriculum. The Professional Counselor, 10(2), 194–203. https://doi.org/10.15241/kal.10.2.194
Nadal, K. L., King, R., Sissoko, D. R. G., Floyd, N., & Hines, D. (2021). The legacies of systemic and internalized oppression: Experiences of microaggressions, imposter phenomenon, and stereotype threat on historically marginalized groups. New Ideas in Psychology, 63, 1–9. https://doi.org/10.1016/j.newideapsych.2021.100895
Ratts, M. J. (2009). Social justice counseling: Toward the development of a fifth force among counseling paradigms. The Journal of Humanistic Counseling, Education and Development, 48(2), 160–172.
https://doi.org/10.1002/j.2161-1939.2009.tb00076.x
Ratts, M. J., & Greenleaf, A. T. (2018). Counselor–advocate–scholar model: Changing the dominant discourse in counseling. Journal of Multicultural Counseling and Development, 46(2), 78–96. https://doi.org/10.1002/jmcd.12094
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K, & McCullough, J. R. (2016). Multicultural and social justice counseling competencies: Guidelines for the counseling profession. Journal of Multicultural Counseling and Development, 44(1), 28–48. https://doi.org/10.1002/jmcd.12035
Sheely-Moore, A. I., & Kooyman, L. (2011). Infusing multicultural and social justice competencies within counseling practice: A guide for trainers. Adultspan Journal, 10(2), 102–109. https://doi.org/10.1002/j.2161-0029.2011.tb00129.x
Toporek, R. L. (2018). Strength, solidarity, strategy and sustainability: A counseling psychologist’s guide to social action. The European Journal of Counselling Psychology, 7(1), 90–110. https://doi.org/10.5964/ejcop.v7i1.153
Toporek, R. L., & Ahluwalia, M. K. (2020). Taking action: Creating social change through strength, solidarity, strategy and sustainability. Cognella.
Toporek, R. L., & Daniels, J. (2018). American Counseling Association advocacy competencies (updated 2018). American Counseling Association. https://www.counseling.org/docs/default-source/competencies/aca-advocacy-competencies-updated-may-2020.pdf
Toporek, R. L., Lewis, J. A., & Crethar, H. C. (2009). Promoting systemic change through the ACA advocacy competencies. Journal of Counseling & Development, 87(3), 260–268. https://doi.org/10.1002/j.1556-6678.2009.tb00105.x
Vera, E. M., & Speight, S. L. (2003). Multicultural competence, social justice, and counseling psychology: Expanding our roles. The Counseling Psychologist, 31(3), 253–272. https://doi.org/10.1177/0011000003031003001
Sunanda M. Sharma, MS, NCC, LPC (NJ), LPCC (OH), is a lecturer at Wright State University. Jennifer E. Bianchini, BFA, is a master’s student at Montclair State University. Zeynep L. Cakmak, MA, LAC (NJ), is a mental health counselor at Montclair State University. MaryRose Kaplan, PhD, NCC, LPC, is a school counselor and adjunct professor at Montclair State University. Muninder K. Ahluwalia, PhD, is a professor at Montclair State University. Correspondence may be addressed to Sunanda M. Sharma, 3640 Colonel Glenn Hwy., Millett Hall 370, Dayton, OH 45435, sharmas1@montclair.edu.
Oct 31, 2023 | Volume 13 - Issue 3
Wesley B. Webber, W. Leigh Atherton, Kelli S. Russell, Hilary J. Flint, Stephen J. Leierer
The COVID-19 pandemic and efforts to manage it have affected mental health around the world. Although early research on the COVID-19 pandemic showed a general decline in mental health after the pandemic began, mental health in later stages of the pandemic might be improving alongside other changes (e.g., availability of vaccines, return to in-person activities). The present study utilized data from a mental health service intervention for individuals at a southeastern university who were exposed to COVID-19 following the university’s return to in-person operations. This study tested whether time period (August–September 2021 vs. January–February 2022) predicted individuals’ likelihood of being mild or above in depression and anxiety ratings. Results showed that individuals were more likely to be mild or above in both depression and anxiety ratings during August–September of 2021 than January–February of 2022. Suggestions for future research and implications for professional counselors are discussed.
Keywords: COVID-19, mental health, depression, anxiety, university
The novel coronavirus (COVID-19), first detected in 2019, spread globally at a rapid pace, with the first confirmed case in the United States occurring on January 20, 2020, in the state of Washington (Centers for Disease Control and Prevention [CDC], 2023). By April 2020, the United States had the most reported deaths in the world due to COVID-19. It was not until December of 2020 that the first round of vaccines, authorized under emergency use authorization, was made available (Food and Drug Administration [FDA], 2021). As of October 2022 in the United States, a total of 97,063,357 cases of COVID-19 had been reported, from which there were 1,065,152 COVID-19–related deaths (CDC, 2023). A reported 111,367,843 individuals aged 5 and above in the United States had received their first booster dose of a COVID-19 vaccine as of October 2022 (CDC, 2023). Previous research has shown that the COVID-19 pandemic and efforts to manage it (e.g., lockdowns, quarantine, isolation) had negative effects on mental health in the United States and internationally (Huckins et al., 2020; Pierce et al., 2020; Son et al., 2020). Based on the extended duration of the pandemic and changes that have occurred during it (e.g., vaccine availability, lessening of initial social restrictions), more recent research has investigated possible changes in mental health in later stages of the COVID-19 pandemic (Fioravanti et al., 2022; McLeish et al., 2022; Tang et al., 2022). The present study adds to this literature by exploring whether psychosocial symptomatology (i.e., depression and anxiety) at a university in the Southeastern United States differed in individuals exposed to COVID-19 during August–September 2021 as compared to individuals exposed to COVID-19 during January–February 2022 (following the university’s return to on-campus operations in August 2021).
Challenges to Mental Health During the COVID-19 Pandemic
Since the beginning of the COVID-19 pandemic, conceptual and empirical research has focused on ways in which the pandemic and associated stressors might impact mental health (Bzdok & Dunbar, 2020; Marroquín et al., 2020; Şimşir et al., 2022). Implementation of lockdowns to deter spread of the virus led to concerns that social isolation might have severe impacts on mental health (Bzdok & Dunbar, 2020). This hypothesis was empirically supported, as stay-at-home orders and individuals’ reported levels of social distancing were positively associated with depression and anxiety (Marroquín et al., 2020). Individuals’ views on the COVID-19 pandemic evolved quickly at the outset of the pandemic, and perceptions of risk were shown to increase during the pandemic’s first week in the United States (Wise et al., 2020). Growing awareness of the dangers of the virus likely had deleterious effects on mental health; Şimşir et al. (2022) found through a meta-analysis that fear of COVID-19 was associated with a variety of mental health problems. Mental health was also negatively affected by stigmatization associated with the COVID-19 pandemic, as was the case for those exposed to COVID-19 while at their place of work (Schubert et al., 2021). Such stigmatization associated with COVID-19 exposure was found to increase risk for depression and anxiety (Schubert et al., 2021).
The lockdowns and social distancing measures that accompanied early stages of the COVID-19 pandemic also resulted in changes to routines that likely impacted mental health. For some individuals facing lockdowns or other disruptions to typical routines, reductions in physical activity occurred. Individuals who reported greater impact of COVID-19 on their level of physical activity showed greater symptoms of depression and anxiety (Silva et al., 2022). Early in the COVID-19 pandemic, based on people’s increased time spent at home and their concerns about COVID-19 developments, some people increased their media usage (e.g., news outlets, social media). Such increases in media usage were associated with decreases in mental health (Meyer et al., 2020; Riehm et al., 2020). The COVID-19 pandemic had less significant impact on mental health for those with greater tolerance of uncertainty (Rettie & Daniels, 2021) and psychological flexibility (Dawson & Golijani-Moghaddam, 2020). Thus, some individuals were uniquely suited to face the many changes and stressors brought about by the COVID-19 pandemic.
One population that previous research has identified as being especially at risk for negative mental health outcomes during the COVID-19 pandemic is college students (Xiong et al., 2020). For college students, the COVID-19 pandemic occurred alongside other stressors known to be typical for this population such as adjusting to leaving home, navigating new peer groups, and making career decisions (Beiter et al., 2015; Liu et al., 2019). Thus, for many college students, the COVID-19 pandemic disrupted a period of life already filled with many transitions. For example, shortly after the COVID-19 pandemic began, many college students were forced to leave their dormitories and peers as universities transitioned to online delivery of classes (Copeland et al., 2021). Xiong et al. (2020) found through a systematic review that college students were especially vulnerable to negative mental health outcomes at the outset of the COVID-19 pandemic as compared to others in the general population. In the United States, college students’ reported degree of life disruption due to the COVID-19 pandemic was positively associated with depression at the conclusion of the spring 2020 semester (Stamatis et al., 2022). During fall 2020, COVID-19 concerns and previous COVID-19 infection were each found to be associated with higher levels of depression and anxiety among U.S. college students (Oh et al., 2021). Overall, previous research has supported the notion that changes associated with the COVID-19 pandemic had general negative effects on mental health in the general population and in college students specifically.
Changes in Psychosocial Symptomatology Across the COVID-19 Pandemic
Although research has shown that the COVID-19 pandemic introduced unprecedented challenges and stressors that were associated with mental health problems, another important direction for research has been to characterize overall changes in psychosocial symptomatology as the COVID-19 pandemic progressed. Such research is important given that individuals might psychologically adapt to constant COVID-19 stressors or might benefit from changes that have occurred as the COVID-19 pandemic has progressed (e.g., vaccine availability, lessening of societal restrictions). Initial longitudinal studies comparing individuals’ symptomatology before the COVID-19 pandemic and after its beginning showed that mental health deteriorated after the COVID-19 pandemic began (Elmer et al., 2020; Huckins et al., 2020; Pierce et al., 2020). Prati and Mancini (2021) conducted a meta-analysis of 28 studies that used longitudinal or natural experimental designs and found that depression and anxiety showed small but statistically significant increases after implementation of the initial lockdowns in response to COVID-19. The various changes to ways of life associated with the COVID-19 pandemic appeared to result in a general deterioration in mental health.
Previous research has also explored possible changes in mental health beyond those that were observed in the initial phase of the COVID-19 pandemic. In support of the notion that individuals adapted to changes associated with the COVID-19 pandemic, Fancourt et al. (2021) found that anxiety and depression decreased across the initial lockdown period in the United Kingdom. In contrast, Ozamiz-Etxebarria et al. (2020) found that levels of depression and anxiety were higher 3 weeks into the initial lockdown period in Spain as compared to the beginning of the lockdown. Fioravanti et al. (2022) assessed psychological symptoms longitudinally in an Italian sample at three time points—the beginning of the COVID-19 pandemic and first lockdown (March 2020), the end of the first lockdown phase (May 2020), and during a second wave of COVID-19 with increased societal restrictions (November 2020). Their findings pointed to possible influences of COVID-19 waves and societal restrictions on specific psychosocial symptoms. Specifically, depression, anxiety, obsessive-compulsive disorder, and post-traumatic stress disorder all decreased at the end of the first lockdown phase (Fioravanti et al., 2022). However, all symptoms besides obsessive-compulsive disorder significantly increased from the end of the first lockdown phase to the second wave of COVID-19 (Fioravanti et al., 2022).
Recent research on mental health among college students in later stages of the COVID-19 pandemic has also focused on possible mental health changes over time (McLeish et al., 2022; Tang et al., 2022). Tang et al. (2022) reported reductions in anxiety and depression in a longitudinal study of university students in the United Kingdom between a first time point (July–September 2020, after the end of lockdown) and a second time point (January–March 2021, when vaccinations were becoming available). In contrast, McLeish et al. (2022) found through a repeated cross-sectional study that depression and anxiety among students at a specific university increased from spring 2020 to fall 2020, with the increases being maintained in spring 2021. The authors noted that vaccines were not widely available at the university until the end of spring 2021 (McLeish et al., 2022). Thus, recent studies have found mixed results as to whether psychosocial symptomatology improved over time during the COVID-19 pandemic. These discrepancies may be due to contextual differences between studies (e.g., differences in data collection time periods, availability of vaccines, or levels of COVID-19 restrictions being implemented during data collection).
The Present Study
The present study was conducted based on the need for continued research on mental health across the evolving COVID-19 pandemic and based on previous conflicting findings on possible mental health changes in later stages of the COVID-19 pandemic. Given previous research showing detrimental effects of the COVID-19 pandemic on mental health in the general population and in college students, the present study utilized data from a university population. Specifically, an archival dataset was used in the present study to examine data collected during 2021–2022 at a university in the Southeastern United States and to test whether time period would predict severity of depression and anxiety symptoms. Individuals in the study had been exposed to COVID-19 between August–September 2021 or between January–February 2022 and had requested a mental health contact during university-conducted contact tracing. These two time periods corresponded to surges in COVID-19 cases at the university due to the delta and omicron COVID-19 variants, respectively. August–September 2021 also coincided with a return to on-campus operations at the university and therefore captured psychosocial symptomatology at the beginning of a significant transition in the COVID-19 pandemic (i.e., a return to organized in-person activities on a college campus during the evolving pandemic). This study was designed to answer the following research questions:
- Among those requesting mental health contact after COVID-19 exposure, was the likelihood of having at least mild depression symptoms different for those whose contact occurred between August–September 2021 as compared to those whose contact occurred between January–February 2022?
- Among those requesting mental health contact after COVID-19 exposure, was the likelihood of having at least mild anxiety symptoms different for those whose contact occurred between August–September 2021 as compared to those whose contact occurred between January–February 2022?
Method
Design
A retrospective research design was used to analyze the possible effect of time period on severity of depression and anxiety symptoms among members of a university population who had been exposed to COVID-19 and requested a mental health check-in. The study used a de-identified dataset obtained from the service providers who completed the mental health check-in. We confirmed through consultation with the IRB that the use of archival, de-identified data does not necessitate IRB review.
COVID-19 Mental Health Check-In Dataset
The archival, de-identified dataset used in the present study was compiled as part of a mental health service occurring between February 2021 and February 2022. Participants in the dataset had tested positive for COVID-19 or been exposed to COVID-19 without a positive test. During university-conducted contact tracing, they were offered and elected to receive a subsequent mental health check-in. Individuals who were contact traced and thereby offered a mental health check-in had become known to contact tracers through one of two routes: (a) they reported their own COVID-19 diagnosis or exposure through a self-reporting mechanism as instructed by the university, or (b) they were reported by another individual as having been diagnosed with or exposed to COVID-19. The dataset used in this study included data collected during the mental health check-ins for those who elected to receive them. This data was collected over the phone and documented in RedCap (a secure web browser–based survey protocol designed for clinical research) at the time of the phone call or within 24 hours. The dataset consisted of data for 211 individuals’ check-ins. For each check-in, the dataset included participants’ demographic information, screening data (for depression, anxiety, and trauma), identified needs of the participant, resources shared with the participant, and the date of data entry.
The present study focused on check-in data for all individuals from the COVID-19 Mental Health Check-in Dataset whose check-in had occurred during one of the two time periods of focus—August–September 2021 or January–February 2022. These two time periods corresponded to surges in COVID-19 cases at the university associated with the delta and omicron COVID-19 variants, respectively. The 149 individuals who checked in during these 4 months represented 70.62% of the total number of check-ins over the 12-month dataset (N = 211), reflecting the surges in COVID-19 cases during these two periods. Of the 149 individuals in the present study, 96 (64.43%) received their check-in during August–September 2021, and 53 (35.57%) received their check-in during January–February 2022. The selection of these two time periods from the larger dataset allowed for comparison of psychosocial symptomatology during comparable levels of COVID-19 infection (i.e., surges associated with two subsequent COVID-19 variants) at comparable points in subsequent academic semesters (i.e., the first 2 months of the fall 2021 and spring 2022 semesters). The present study used only the screening data for depression and anxiety, as the scales for each of these constructs showed good internal consistency (Cronbach’s alpha > .80).
Participants
The sample in the present study consisted of 149 individuals. The selected individuals’ ages ranged from 17 to 52 (M = 22.21, SD = 7.43). With regard to gender, 67.11% identified as female, 32.21% as male, and 0.67% as non-binary. The reported races of individuals in the study were as follows: 60.4% White, 20.13% African American, 6.71% Hispanic, 3.36% Other, 2.68% Two or more races, 1.34% Middle Eastern, 1.34% Native American, and 0.67% Asian. Some participants preferred not to indicate their race (3.36%). In responding to a question about their ethnicity, 87.25% of individuals identified as not Latinx, 9.40% identified as Latinx, and 3.36% preferred not to answer. With regard to academic level/job title, 32.89% were freshmen, 20.13% were sophomores, 14.09% were juniors, 15.44% were seniors, 7.38% were graduate students, 8.05% were faculty/staff, and 2.01% preferred not to answer. Regarding employment, 53.69% were not employed (including students), 30.20% were employed part-time, 12.75% were employed full-time, and 3.36% preferred not to answer. The relationship statuses of individuals were reported as the following: 87.92% single (never married), 4.7% married, 2.01% single but cohabitating with a significant other, 1.34% in a domestic partnership or civil union, 1.34% separated, 0.67% divorced, and 2.01% preferred not to answer. Table 1 summarizes demographic responses within each of the two time periods and for the full sample.
Measures
Demographic Questionnaire
Participants responded to seven demographic questions (age, gender, race, ethnicity, academic year/job title, current employment status, and relationship status). They were informed that this information was optional and that they could choose not to answer particular questions.
Table 1
Demographic Characteristics of the Sample
|
Demographic
Characteristic |
|
| August–September 2021 |
January–February 2022 |
Full Sample |
|
n |
% |
n |
% |
n |
% |
| Gender |
|
|
|
|
|
|
| Female |
69 |
71.88 |
31 |
58.49 |
100 |
67.11 |
| Male |
27 |
28.13 |
21 |
39.62 |
48 |
32.21 |
| Non-binary |
0 |
0 |
1 |
1.89 |
1 |
0.67 |
| Race |
|
|
|
|
|
|
| White |
56 |
58.33 |
34 |
64.15 |
90 |
60.40 |
| African American |
23 |
23.96 |
7 |
13.21 |
30 |
20.13 |
| Hispanic |
8 |
8.33 |
2 |
3.77 |
10 |
6.71 |
| Other race |
1 |
1.04 |
4 |
7.55 |
5 |
3.36 |
| Two or more races |
4 |
4.17 |
0 |
0 |
4 |
2.68 |
| Middle Eastern |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Native American |
1 |
1.04 |
1 |
1.89 |
2 |
1.34 |
| Asian |
1 |
1.04 |
0 |
0 |
1 |
0.67 |
| Prefer not to answer |
0 |
0 |
5 |
9.43 |
5 |
3.36 |
| Ethnicity |
|
|
|
|
|
|
| Not Latinx |
82 |
85.42 |
48 |
90.57 |
130 |
87.25 |
| Latinx |
12 |
12.50 |
2 |
3.77 |
14 |
9.40 |
| Prefer not to answer |
2 |
2.08 |
3 |
5.66 |
5 |
3.36 |
| Academic Year / Job Title |
|
|
|
|
|
|
| Freshman |
38 |
39.58 |
11 |
20.75 |
49 |
32.89 |
| Sophomore |
18 |
18.75 |
12 |
22.64 |
30 |
20.13 |
| Junior |
15 |
15.63 |
6 |
11.32 |
21 |
14.09 |
| Senior |
15 |
15.63 |
8 |
15.09 |
23 |
15.44 |
| Graduate Student |
6 |
6.25 |
5 |
9.43 |
11 |
7.38 |
| Faculty/Staff |
4 |
4.17 |
8 |
15.09 |
12 |
8.05 |
| Prefer not to answer |
0 |
0 |
3 |
5.66 |
3 |
2.01 |
| Employment |
|
|
|
|
|
|
| Not Employed (including student) |
62 |
64.58 |
18 |
33.96 |
80 |
53.69 |
| Employed Part-Time |
26 |
27.08 |
19 |
35.85 |
45 |
30.20 |
| Employed Full-Time |
8 |
8.33 |
11 |
20.75 |
19 |
12.75 |
| Prefer not to answer |
0 |
0 |
5 |
9.43 |
5 |
3.36 |
| Relationship Status |
|
|
|
|
|
|
| Single, never married |
87 |
90.63 |
44 |
83.02 |
131 |
87.92 |
| Married |
3 |
3.13 |
4 |
7.55 |
7 |
4.70 |
| Single, but cohabitating with a
significant other |
2 |
2.08 |
1 |
1.89 |
3 |
2.01 |
| In a domestic partnership or civil union |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Separated |
2 |
2.08 |
0 |
0 |
2 |
1.34 |
| Divorced |
0 |
0 |
1 |
1.89 |
1 |
0.67 |
| Prefer not to answer |
0 |
0 |
3 |
5.66 |
3 |
2.01 |
| Note. Average age was 21.51 (SD = 6.98) in August–September 2021 group, 23.49 (SD = 8.11) in January–February 2022 group, and 22.21 (SD = 7.43) in the full sample. |
Patient Health Questionnaire-9 (PHQ-9)
The Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., 2001) is a 9-item self-report questionnaire that measures the frequency and severity of depression symptoms over the past 2 weeks. The PHQ-9 has been validated for screening for depression in the general population (Kroenke et al., 2001; Martin et al., 2006). The questionnaire measures frequency of symptoms such as “feeling down, depressed, or hopeless,” and “little interest or pleasure in doing things.” The PHQ-9 uses a 4-point Likert scale to measure frequency of symptoms over the past 2 weeks with the response options of not at all, several days, more than half the days, and nearly every day. Scores of 0, 1, 2, and 3 are assigned to each of the four response categories, and a PHQ-9 total score is derived by adding the scores for each of the nine PHQ-9 items. Minimal depression is indicated by PHQ-9 total scores of 0–4, mild depression by scores of 5–9, moderate depression by scores of 10–14, moderately severe depression by scores of 15–19, and severe depression by scores of 20–27. Question 9 on the PHQ-9 is a single screening question assessing suicide risk. Interviewers were trained in appropriate protocol in the event of a positive screen for this question. Cronbach’s alpha for the PHQ-9 in the present study was .86.
Generalized Anxiety Disorder 7-Item Scale (GAD-7)
The Generalized Anxiety Disorder 7-Item Scale (GAD-7; Spitzer et al., 2006) is a 7-item self-report anxiety questionnaire that measures the frequency and severity of anxiety symptoms over the past 2 weeks. The GAD-7 has demonstrated reliability and validity as a measure of anxiety in the general population (Löwe et al., 2008). The questionnaire measures symptoms such as “feeling nervous, anxious, or on edge,” and “not being able to stop or control worrying.” The format of the GAD-7 is similar to the PHQ-9, using a 4-point Likert scale to measure frequency of symptoms over the past 2 weeks with response options of not at all, several days, more than half the days, and nearly every day. GAD-7 scores are calculated by assigning scores of 0, 1, 2, and 3 for response categories and then adding the scores from the 7 items to derive a total score ranging from 0 to 21. Minimal anxiety is indicated by total scores of 0–4, mild anxiety by scores of 5–9, moderate anxiety by scores of 10–14, and severe anxiety by scores of 15– 21. Cronbach’s alpha for the GAD-7 in the present study was .86.
Analytic Strategy
Total scores for the PHQ-9 and GAD-7 were found to be positively skewed for both groups of participants. Binary logistic regression was therefore an appropriate method of analysis for this dataset, as binary logistic regression does not require normality of dependent variables (Tabachnick & Fidell, 2019). For two separate binary logistic regression models, individuals were classified as being either minimal or mild or above in depression (PHQ-9) and anxiety (GAD-7) to create binary outcome variables. This choice of cutoff allowed each model (with time period as predictor) to satisfy the recommendation of Peduzzi et al. (1996) that there be at least 10 cases per outcome per predictor in binary logistic regression.
Prior to performing these intended primary analyses to answer the research questions, preliminary analyses were conducted to determine whether adding control variables to the logistic regression models was warranted. Chi-square tests of independence, Fisher-Freeman-Halton Exact tests, Fisher’s Exact tests, and an independent samples t-test were used to test for possible differences between the two time periods in individuals’ responses to demographic questions. In cases in which responses to demographic questions were shown to be significantly different across the two groups, appropriate tests were used to determine whether the demographic responses in question were associated with either of the two intended dependent variables.
Following the preliminary analyses, the intended two binary logistic regressions were conducted to answer the research questions. In the first binary logistic regression, time period was the predictor
(1 = August–September 2021, 0 = January–February 2022) and PHQ-9 depression category was the outcome (1 = mild or above, 0 = minimal). In the second logistic regression, time period was the predictor (1 = August–September 2021, 0 = January–February 2022) and GAD-7 anxiety category was the outcome (1 = mild or above, 0 = minimal). All analyses were conducted using SPSS Version 28.
Results
Preliminary Demographic Analyses
Prior to the primary analyses, preliminary analyses were conducted to determine whether the two groups differed in their responses to demographic questions. Fisher-Freeman-Halton Exact tests and an independent samples t-test were used to test for differences between groups in their responses to the seven demographic questions. Two of the seven tests were statistically significant at Bonferroni-corrected alpha level. Specifically, Fisher-Freeman-Halton Exact tests found significant differences between time periods on the race (p = .004) and employment (p < .001) demographic variables.
Based on the above significant results for the race and employment variables across the time periods, 2 x 2 tests were conducted to test for differences between specific race responses and specific employment responses across the two time periods. For these 2 x 2 tests, a chi-square test of independence was used when all expected cell counts were 5 or greater and Fisher’s Exact test was used when any expected cell counts were less than 5. To follow up the significant result for race, 2 x 2 tests were conducted for all pairs of race responses in which 2 x 2 tests were possible (i.e., in which there was at least one observation for each of the two race responses at both time periods). These follow-up 2 x 2 tests of responses to the race question across time periods found no statistically significant differences between pairs of race responses across time periods using Bonferroni-corrected alpha level. Follow-up 2 x 2 tests comparing all pairs of responses to the employment question across time periods found two statistically significant differences using Bonferroni-corrected alpha level. A chi-square test of independence showed that individuals were more likely to be employed full-time during January–February 2022 than August–September 2021 as compared to those not employed (including students), X2 (1, N = 99) = 9.29, p = .002. Fisher’s Exact test showed that individuals were more likely to indicate “prefer not to answer” during January–February 2022 than during August–September 2021 as compared to those indicating “not employed (including students),” p = .001.
The statistically significant tests for race and employment across time periods were followed up with additional tests to determine if depression or anxiety category (minimal vs. mild or above for each) was associated with individuals’ responses to the relevant race and employment questions. A Fisher-Freeman-Halton Exact test showed that depression category was not associated with individuals’ responses to the race question, p = .099. A Fisher-Freeman-Halton Exact test also showed that individuals’ anxiety category was not associated with individuals’ responses to the race question,
p = .386. With regard to employment, tests of association were conducted between the intended dependent variables and the specific employment responses that were found to differ between the two groups. A chi-square test of independence showed that individuals’ status as “not employed” vs. “employed full-time” was not associated with depression category, X2 (1, N = 99) = .63, p = .429. A chi-square test of independence also showed that these employment statuses were not associated with anxiety category, X2 (1, N = 99) = .27, p = .601. Similarly, Fisher’s Exact tests showed that individuals’ employment responses of “prefer not to answer” vs. “not employed (including students)” were not associated with depression category (p = .156) or anxiety category (p = .317). These results were interpreted as indicating that the ways in which individuals in the two time periods differed demographically did not have significant impact on the study’s dependent variables of interest. Therefore, binary logistic regressions were conducted with only time period as a predictor of each dependent variable.
Relationship Between Time Period and Severity of Depression Symptoms
Most individuals in the study were in the minimal depression range on the PHQ-9 as compared to the other four categories. Figure 1 shows the percentage of individuals falling into each of the five PHQ-9 categories during each of the two time periods.
Figure 1
Percentages of Individuals Falling Into Each of the PHQ-9 Categories for Each of the Two Time Periods
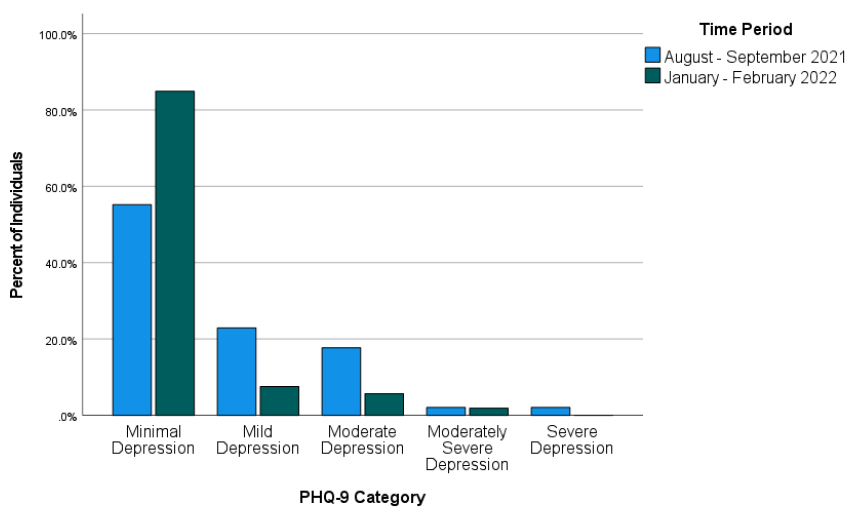
Across both time periods combined (August–September 2021 and January–February 2022), 51 individuals (34.23%) were mild or above in depression while 98 (65.77%) were in the minimal range. Binary logistic regression was used to test whether time period predicted severity of depression symptoms. Time period was entered as a predictor (1 = August–September 2021, 0 = January–February 2022) of depression (1 = mild or above, 0 = minimal depression). The overall binary logistic regression model was found to be statistically significant, χ2(1) = 14.46, p < .001, Cox & Snell R2 = .092, Nagelkerke R2 = .128. In the model, time period was found to be a significant predictor of depression, Wald χ2(1) = 12.17, B = 1.52, SE = .44, p < .001. The model estimated that the odds of being mild or above in depression were 4.56 times higher during August–September 2021 than during January–February 2022 for individuals requesting a mental health check-in following COVID-19 exposure. Specifically, the predicted odds of being mild or above in depression were .81 during August–September 2021 and .18 during January–February 2022.
Relationship Between Time Period and Severity of Anxiety Symptoms
Most individuals in the study were in the minimal anxiety range on the GAD-7 as compared to the other three categories. Figure 2 shows the percentage of individuals falling into each of the four GAD-7 categories during each of the two time periods.
Figure 2
Percentages of Individuals Falling Into Each of the GAD-7 Categories for Each of the Two Time Periods
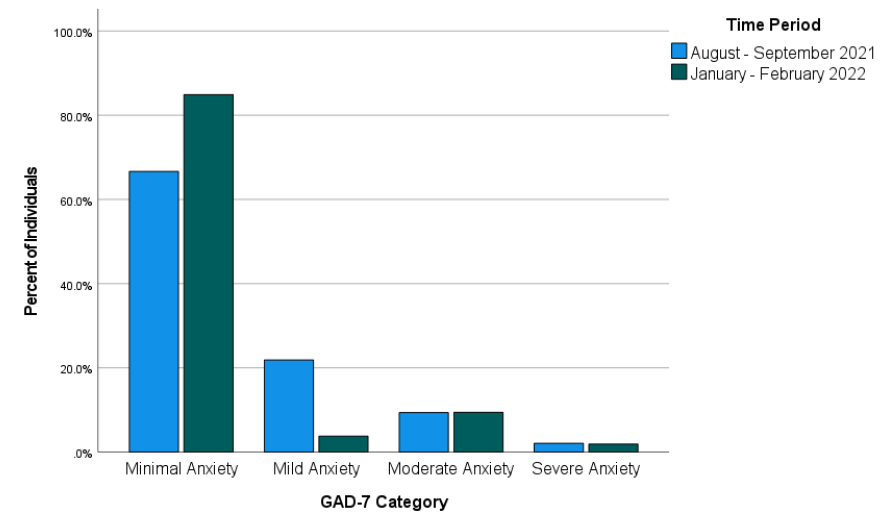
Across both time periods combined, 40 individuals (26.85%) reported anxiety at levels of mild or above and 109 individuals (73.15%) reported minimal anxiety. Binary logistic regression was used to test whether time period predicted severity of anxiety symptoms. Time period was entered as a predictor (1 = August–September 2021, 0 = January–February 2022) of anxiety (1 = mild or above, 0 = minimal anxiety). The overall binary logistic regression model was statistically significant, χ2(1) = 6.16, p = .013, Cox & Snell R2 = .041, Nagelkerke R2 = .059. In the model, time period was a significant predictor of anxiety, Wald χ2(1) = 5.51, B = 1.03, SE = .44, p = .019. Odds of being mild or above in anxiety were estimated by the model to be 2.81 times higher during August–September 2021 than during January–February 2022 for individuals requesting a mental health check-in after exposure to COVID-19. Specifically, the predicted odds of being mild or above in anxiety were .50 during August–September 2021 and .18 during January–February 2022.
Discussion
This study examined whether time period would predict severity of depression and anxiety symptoms in a sample of individuals exposed to COVID-19 at a university in the Southeastern United States. More specifically, the study addressed the possibility that the likelihood of being mild or above in depression and anxiety would differ between two time periods following the university’s return to in-person operations in August 2021. The results of the study showed that the likelihood of being mild or above in depression and the likelihood of being mild or above in anxiety after exposure to COVID-19 were both higher during August–September 2021 than during January–February 2022. This finding is in line with previous research that found improvements in psychosocial symptomatology in later stages of the COVID-19 pandemic (Tang et al., 2022) and in contrast to research that did not find such improvements (McLeish et al., 2022). Based on the results of the present study, it appears likely that factors that differed between the two assessed time periods (first two months of fall 2021 vs. first two months of spring 2022) contributed to the observed difference in likelihood of depression and anxiety symptoms. McLeish et al. (2022) noted that vaccines were not widely available in their study that did not find such differences, while Tang et al. (2022), who did find significant differences, noted that vaccines were available at their second data collection point (January–March 2021). For individuals in the present study, COVID-19 vaccinations were available. Vaccination was strongly encouraged by university administrators following the return to campus, and more individuals on campus were vaccinated in spring 2022 than in fall 2021. Vaccinations might have lessened individuals’ COVID-19 concerns and contributed to more positive psychosocial outcomes during spring 2022 than fall 2021.
Besides vaccinations possibly lessening depression and anxiety symptoms, other environmental circumstances might also have played a role. The two time periods on which this study focused also differed in their proximity to a significant environmental event—a return to in-person operations on the campus where the individuals studied and/or worked. Early research on the mental health impact of COVID-19 highlighted the negative mental health effects of factors such as reduced physical activity (Silva et al., 2022), life disruptions due to the COVID-19 pandemic (Stamatis et al., 2022), and social distancing (Marroquín et al., 2020). Therefore, it is possible that symptoms of depression and anxiety in spring 2022 were affected by changes in specific circumstances known to have negatively impacted mental health earlier in the COVID-19 pandemic. For example, individuals’ physical activity likely increased because of a return to campus, and they might have perceived less disruption to their lives through being able to resume in-person activities. Although individuals in the present study who were exposed to COVID-19 during the first 2 months after the return to campus might have reaped some benefits from the return to more normal environmental circumstances, they might also have faced a period of adjustment. In contrast, individuals exposed to COVID-19 between January and February 2022 might have been more readjusted and reaped greater benefits from the return to campus, thereby reducing depression and anxiety symptoms.
Implications
This study’s findings on psychosocial symptomatology across time during the COVID-19 pandemic have important implications for the work of counselors. Based on the results of the present study, counselors planning outreach efforts to individuals exposed to COVID-19 should consider that as time passes, these individuals might be more stable with regard to symptoms of depression and anxiety. However, some individuals directly affected by COVID-19 might still be interested in receiving mental health information despite low levels of depression and anxiety. Many individuals in the present study scored as minimal in depression and anxiety but were still interested in receiving a mental health check-in. Thus, counselors should advocate for mental health information and resources to be made available to individuals who are known to be facing stressors related to COVID-19. Counselors should be prepared to have conversations to determine the contextual needs of individuals exposed to COVID-19 rather than relying only on standardized measures of psychosocial symptomatology. For example, counselors working with employees (such as university employees in the present study) should be attentive to the possibility that employees exposed to COVID-19 may be concerned about facing stigma in their workplace due to their exposure (Schubert et al., 2021).
Given that the present study focused on individuals from a university population, the study’s results also have specific implications for college counselors. College counselors should develop approaches to reach students during circumstances that might make traditional outreach challenging. For example, the present study used data from a mental health intervention in which service providers collaborated with university contact tracers to safely provide mental health resources by telephone to individuals exposed to COVID-19. College counselors should be prepared to connect clients with services at a distance. Previous research during the COVID-19 pandemic found that college students were interested in using teletherapy and online self-help resources, particularly if such services were made available for free (Ahuvia et al., 2022).
Besides preparing for flexible modes of service delivery, college counselors should be prepared to deliver interventions most likely to be useful to college students during the COVID-19 pandemic or similar pandemics. Those recently exposed to COVID-19 might benefit from discussing possible fears associated with COVID-19, experiences of stigmatization they might have experienced due to their exposure, and ways to maintain mental health during any period of quarantine or isolation that might be required. Those not recently exposed to COVID-19 might instead benefit from interventions that address other issues that might have resulted from the COVID-19 pandemic or societal responses to it. For example, if circumstances associated with the COVID-19 pandemic led to reductions in a client’s amount of exercise, a counselor can help the client identify ways they might increase their physical activity. Interventions promoting physical activity were found to reduce anxiety and depression in college students during the COVID-19 pandemic (Luo et al., 2022).
Limitations
This study had limitations that should be considered. First, with the study being retrospective and using secondary data from a clinical intervention, it was not possible to include measures that might have better clarified mechanisms of the changes that were observed in psychosocial symptoms. Thus, the possible explanations above of what might have driven these changes are tentative and future research should test them more directly. Second, individuals in the present study were likely to have been in greater distress than the general university population based on their exposure to COVID-19, which might limit the generalizability of the study’s findings. Third, individuals in the present study were from a single university in the Southeastern United States. Thus, our findings might not generalize to other regions where university-related COVID-19 policies might have differed. Fourth, the decision to create a binary independent variable to reflect time periods (August–September 2021 and January–February 2022) in the present study also entails a limitation. This decision was justifiable on the basis that it allowed for comparisons of individuals at similar points in academic semesters and during comparable periods of COVID-19 infection. However, this analysis decision means that inferences from the study’s results are limited to the two specific time periods that were analyzed. Fifth, individuals in the present study responded to items on the GAD-7 and PHQ-9 through a phone conversation with interviewers. Interviewer-administered surveys have been previously associated with greater tendencies toward socially desirable responses than self-administered surveys (Bowling, 2005). This might limit the present study’s generalizability in contexts where self-administrations of the GAD-7 and PHQ-9 are used.
Future Research
The results of this study provide important directions for future research. Future researchers who can conduct prospective studies or who have access to larger retrospective datasets should aim to determine specific factors that might lead to improvement in mental health outcomes over time during the COVID-19 pandemic. Knowledge produced by such studies could contribute to clinical applications in the future regarding COVID-19 or other pandemics that might occur. Relatedly, future research with larger samples of demographically diverse participants should explore possible demographic differences in specific mental health trajectories in later stages of the COVID-19 pandemic.
Future research should continue to focus specifically on those who are interested in mental health information and interventions during the COVID-19 pandemic. To follow up this study’s findings, future quantitative and qualitative studies should aim to identify which individuals are interested in receiving mental health services and determine the best ways to deliver services to them. As a globally experienced stressor, the COVID-19 pandemic might have changed some individuals’ views of mental health and/or their receptiveness to mental health outreach. More specifically, some might be more receptive to available mental health information even at lower thresholds of anxiety, depression, or other psychosocial symptoms. Such clients might be interested in preventive services or their interest in mental health information might be driven by other factors. Future studies should address these possibilities more directly than was possible in the present retrospective study.
Conclusion
Overall, the present study provided a positive picture regarding psychosocial symptomatology in later stages of the COVID-19 pandemic. Results from this study of students and employees at a university in the Southeastern Unites States following their return to campus found that many individuals requesting mental health information after exposure to COVID-19 showed minimal levels of depression and anxiety. Individuals in the study were more likely to be in these minimal ranges during January–February 2022 than August–September 2021. COVID-19 will continue to have effects in individuals’ lives through future infections and potentially through lasting effects of previous stages of the COVID-19 pandemic. As organized in-person activities resume and COVID-19 infections continue, counseling researchers and practitioners should continue efforts to best characterize and address individuals’ mental health needs associated with the COVID-19 pandemic.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Ahuvia, I. L., Sung, J. Y., Dobias, M. L., Nelson, B. D., Richmond, L. L., London, B., & Schleider, J. L. (2022). College student interest in teletherapy and self-guided mental health supports during the COVID-19 pandemic. Journal of American College Health. Advance online publication.
https://doi.org/10.1080/07448481.2022.2062245
Beiter, R., Nash, R., McCrady, M., Rhoades, D., Linscomb, M., Clarahan, M., & Sammut, S. (2015). The prevalence and correlates of depression, anxiety, and stress in a sample of college students. Journal of Affective Disorders, 173, 90–96. https://doi.org/10.1016/j.jad.2014.10.054
Bowling, A. (2005). Mode of questionnaire administration can have serious effects on data quality. Journal of Public Health, 27(3), 281–291. https://doi.org/10.1093/pubmed/fdi031
Bzdok, D., & Dunbar, R. I. M. (2020). The neurobiology of social distance. Trends in Cognitive Sciences, 24(9), 717–733. https://doi.org/10.1016/j.tics.2020.05.016
Centers for Disease Control and Prevention. (2023, March 15). COVID-19 timeline. https://www.cdc.gov/museum/timeline/covid19.html
Copeland, W. E., McGinnis, E., Bai, Y., Adams, Z., Nardone, H., Devadanam, V., Rettew, J., & Hudziak, J. J. (2021). Impact of COVID-19 pandemic on college student mental health and wellness. Journal of the American Academy of Child & Adolescent Psychiatry, 60(1), 134–141.e2. https://doi.org/10.1016/j.jaac.2020.08.466
Dawson, D. L., & Golijani-Moghaddam, N. (2020). COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. Journal of Contextual Behavioral Science, 17, 126–134.
https://doi.org/10.1016/j.jcbs.2020.07.010
Elmer, T., Mepham, K., & Stadtfeld, C. (2020). Students under lockdown: Comparisons of students’ social networks and mental health before and during the COVID-19 crisis in Switzerland. PLoS ONE, 15(7), Article e0236337. https://doi.org/10.1371/journal.pone.0236337
Fancourt, D., Steptoe, A., & Bu, F. (2021). Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: A longitudinal observational study. The Lancet Psychiatry, 8(2), 141–149. https://doi.org/10.1016/S2215-0366(20)30482-X
Fioravanti, G., Benucci, S. B., Prostamo, A., Banchi, V., & Casale, S. (2022). Effects of the COVID-19 pandemic on psychological health in a sample of Italian adults: A three-wave longitudinal study. Psychiatry Research, 315, Article 114705. https://doi.org/10.1016/j.psychres.2022.114705
Food and Drug Administration. (2021, August 23). FDA approves first COVID-19 vaccine. https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine
Huckins, J. F., daSilva, A. W., Wang, W., Hedlund, E., Rogers, C., Nepal, S. K., Wu, J., Obuchi, M., Murphy, E. I., Meyer, M. L., Wagner, D. D., Holtzheimer, P. E., & Campbell, A. T. (2020). Mental health and behavior of college students during the early phases of the COVID-19 pandemic: Longitudinal smartphone and ecological momentary assessment study. Journal of Medical Internet Research, 22(6), Article e20185.
https://doi.org/10.2196/20185
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Liu, C. H., Stevens, C., Wong, S. H. M., Yasui, M., & Chen, J. A. (2019). The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: Implications for addressing disparities in service use. Depression and Anxiety, 36(1), 8–17. https://doi.org/10.1002/da.22830
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., & Herzberg, P. Y. (2008). Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Medical Care, 46(3), 266–274. https://doi.org/10.1097/MLR.0b013e318160d093
Luo, Q., Zhang, P., Liu, Y., Ma, X., & Jennings, G. (2022). Intervention of physical activity for university students with anxiety and depression during the COVID-19 pandemic prevention and control period: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 19(22), 15338. https://doi.org/10.3390/ijerph192215338
Marroquín, B., Vine, V., & Morgan, R. (2020). Mental health during the COVID-19 pandemic: Effects of stay-at-home policies, social distancing behavior, and social resources. Psychiatry Research, 293, Article 113419. https://doi.org/10.1016/j.psychres.2020.113419
Martin, A., Rief, W., Klaiberg, A., & Braehler, E. (2006). Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. General Hospital Psychiatry, 28(1), 71–77.
https://doi.org/10.1016/j.genhosppsych.2005.07.003
McLeish, A. C., Walker, K. L., & Hart, J. L. (2022). Changes in internalizing symptoms and anxiety sensitivity among college students during the COVID-19 pandemic. Journal of Psychopathology and Behavioral Assessment, 44, 1021–1028. https://doi.org/10.1007/s10862-022-09990-8
Meyer, J., McDowell, C., Lansing, J., Brower, C., Smith, L., Tully, M., & Herring, M. (2020). Changes in physical activity and sedentary behavior in response to COVID-19 and their associations with mental health in 3052 US adults. International Journal of Environmental Research and Public Health, 17(18), Article 6469.
https://doi.org/10.3390/ijerph17186469
Oh, H., Marinovich, C., Rajkumar, R., Besecker, M., Zhou, S., Jacob, L., Koyanagi, A., & Smith, L. (2021). COVID-19 dimensions are related to depression and anxiety among US college students: Findings from the Healthy Minds Survey 2020. Journal of Affective Disorders, 292, 270–275. https://doi.org/10.1016/j.jad.2021.05.121
Ozamiz-Etxebarria, N., Idoiaga Mondragon, N., Dosil Santamaría, M., & Picaza Gorrotxategi, M. (2020). Psychological symptoms during the two stages of lockdown in response to the COVID-19 outbreak: An investigation in a sample of citizens in Northern Spain. Frontiers in Psychology, 11, Article 1491.
https://doi.org/10.3389/fpsyg.2020.01491
Peduzzi, P., Concato, J., Kemper, E., Holford, T. R., & Feinstein, A. R. (1996). A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology, 49(12), 1373–1379. https://doi.org/10.1016/S0895-4356(96)00236-3
Pierce, M., Hope, H., Ford, T., Hatch, S., Hotopf, M., John, A., Kontopantelis, E., Webb, R., Wessely, S., McManus, S., & Abel, K. M. (2020). Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. The Lancet Psychiatry, 7(10), 883–892.
https://doi.org/10.1016/S2215-0366(20)30308-4
Prati, G., & Mancini, A. D. (2021). The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychological Medicine, 51(2), 201–211. https://doi.org/10.1017/S0033291721000015
Rettie, H., & Daniels, J. (2021). Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. American Psychologist, 76(3), 427–437. https://doi.org/10.1037/amp0000710
Riehm, K. E., Holingue, C., Kalb, L. G., Bennett, D., Kapteyn, A., Jiang, Q., Veldhuis, C. B., Johnson, R. M., Fallin, M. D., Kreuter, F., Stuart, E. A., & Thrul, J. (2020). Associations between media exposure and mental distress among U.S. adults at the beginning of the COVID-19 pandemic. American Journal of Preventive Medicine, 59(5), 630–638. https://doi.org/10.1016/j.amepre.2020.06.008
Schubert, M., Ludwig, J., Freiberg, A., Hahne, T. M., Romero Starke, K., Girbig, M., Faller, G., Apfelbacher, C., von dem Knesebeck, O., & Seidler, A. (2021). Stigmatization from work-related COVID-19 exposure: A systematic review with meta-analysis. International Journal of Environmental Research and Public Health, 18(12), 6183. https://doi.org/10.3390/ijerph18126183
Silva, D. T. C., Prado, W. L., Cucato, G. G., Correia, M. A., Ritti-Dias, R. M., Lofrano-Prado, M. C., Tebar, W. R., & Christofaro, D. G. D. (2022). Impact of COVID-19 pandemic on physical activity level and screen time is associated with decreased mental health in Brazillian adults: A cross-sectional epidemiological study. Psychiatry Research, 314, Article 114657. https://doi.org/10.1016/j.psychres.2022.114657
Şimşir, Z., Koç, H., Seki, T., & Griffiths, M. D. (2022). The relationship between fear of COVID-19 and mental health problems: A meta-analysis. Death Studies, 46(3), 515–523. https://doi.org/10.1080/07481187.2021.1889097
Son, C., Hegde, S., Smith, A., Wang, X., & Sasangohar, F. (2020). Effects of COVID-19 on college students’ mental health in the United States: Interview survey study. Journal of Medical Internet Research, 22(9), Article e21279. https://doi.org/10.2196/21279
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097.
https://doi.org/10.1001/archinte.166.10.1092
Stamatis, C. A., Broos, H. C., Hudiburgh, S. E., Dale, S. K., & Timpano, K. R. (2022). A longitudinal investigation of COVID-19 pandemic experiences and mental health among university students. British Journal of Clinical Psychology, 61(2), 385–404. https://doi.org/10.1111/bjc.12351
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Tang, N. K. Y., McEnery, K. A. M., Chandler, L., Toro, C., Walasek, L., Friend, H., Gu, S., Singh, S. P., & Meyer, C. (2022). Pandemic and student mental health: Mental health symptoms amongst university students and young adults after the first cycle of lockdown in the UK. BJPsych Open, 8(4), Article e138.
https://doi.org/10.1192/bjo.2022.523
Wise, T., Zbozinek, T. D., Michelini, G., Hagan, C. C., & Mobbs, D. (2020). Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States.
Royal Society Open Science, 7(9), Article 200742. https://doi.org/10.1098/rsos.200742
Xiong, J., Lipsitz, O., Nasri, F., Lui, L. M. W., Gill, H., Phan, L., Chen-Li, D., Iacobucci, M., Ho, R., Majeed, A., & McIntyre, R. S. (2020). Impact of COVID-19 pandemic on mental health in the general population: A systematic review. Journal of Affective Disorders, 277, 55–64. https://doi.org/10.1016/j.jad.2020.08.001
Wesley B. Webber, PhD, NCC, is a postdoctoral scholar at East Carolina University. W. Leigh Atherton, PhD, LCMHCS, LCAS, CCS, CRC, is an associate professor and program director at East Carolina University. Kelli S. Russell, MPH, RHEd, is a teaching assistant professor at East Carolina University. Hilary J. Flint, NCC, LCMHCA, is a clinical counselor at C&C Betterworks. Stephen J. Leierer, PhD, is a research associate at the Florida State University Career Center. Correspondence may be addressed to Wesley B. Webber, Department of Addictions and Rehabilitation Studies, Mail Stop 677, East Carolina University, 1000 East 5th Street, Greenville, NC 27858-4353, webberw21@ecu.edu.
