Apr 1, 2026 | Volume 16 - Issue 1
Brian J. Clarke, Michael T. Hartley, Austin M. Guida
Impostor phenomenon (IP), characterized by persistent self-doubt despite objective success, is prevalent during the early stages of counselor development, often emerging as individuals transition from training into professional practice. This study examined whether self-compassion mediates relationships between IP, resilience, and mental health among 281 counselors-in-training enrolled in departments accredited by the Council for the Accreditation of Counseling and Related Educational Programs. Mediation analyses showed that self-compassion fully mediated the effects of IP on resilience and depression and partially mediated the effect on anxiety. MANOVA results indicated that higher self-compassion corresponded with lower IP, anxiety, and depression, and greater resilience, with robust effects. Findings identify self-compassion as a developmental competency that supports balanced self-evaluation, emotional regulation, and sustainable counselor well-being. Integrating self-compassion training into counselor education and supervision may help developing counselors manage impostor-related distress, strengthen resilience, and promote ethical, sustainable professional practice.
Keywords: impostor phenomenon, counselor development, self-compassion, resilience, mental health
Building resilience and prioritizing mental health are vital during the formative stages of counselor development. During the early stages of training and supervised practice, developing counselors experience the inherent emotional demands and elevated anxiety common while learning to integrate theoretical knowledge into clinical practice (Skovholt & Trotter-Mathison, 2024; Stoltenberg & McNeill, 2010). Although these feelings may diminish with increased experience, enduring self-doubt and inadequacy may signal impostor phenomenon (Clance & Lawry, 2024). Imposter phenomenon (IP), characterized by persistent feelings of fraudulence and incompetence despite evidence of success, impacts nearly all developing counselors (Clarke et al., 2025; Tigranyan et al., 2021). Those experiencing IP may struggle to internalize mastery experiences and fail to consolidate moments of success into genuine confidence (Gadsby & Hohwy, 2024; Roskowski, 2010). Individual differences in coping with IP may be partially explained by self-compassion, which may buffer IP’s negative effects on counseling self-efficacy and well-being (Clarke et al., 2025).
The persistent fear of being exposed as a fraud becomes a harmful cycle whereby individuals ruminate on perceived shortcomings, discount positive feedback, and misattribute positive outcomes to external factors (Clance & Lawry, 2024). Behaviors associated with IP include extreme perfectionism, procrastination, and/or exhausting overpreparation, which can inhibit counselor development (Clarke et al., 2025; Nguyen, 2023). Because IP is rooted in shame and feelings of inadequacy, it contributes to isolation, burnout, and compassion fatigue (Garba et al., 2024; Ojeda, 2024).
IP undermines the reflective, relational, and self-evaluative capacities that are central to counselor development. Counselors who experience chronic self-doubt may hesitate to disclose errors in supervision, question their competence, and struggle to sustain resilience, patterns that can jeopardize client care and professional longevity (Delaney, 2018; Housenecht & Swank, 2022). Given the demands of counselor training and practice, protective factors such as resilience and self-compassion may be critical for developing counselor well-being and persistence.
Resilience is a protective factor to cope with mental distress and burnout (Gerber & Anaki, 2021; Webb & Rosenbaum, 2019). Emerging from the positive psychology movement, resilience explains why some individuals behave adaptively under great stress while others do not. Beyond recovery from adversity, resilience is a process of successful adaptation and coping during challenging or threatening circumstances (Webb & Rosenbaum, 2019). Cultivating new coping mechanisms and fostering personal growth, resilience can sustain well-being and performance during difficult experiences. The limited research on resilience among developing counselors has identified self-awareness and self-compassion as critical protective factors to cope with the emotional demands of becoming a counselor (Hou & Skovholt, 2020).
As a protective factor, self-compassion can play an important role in the resilience and mental health of developing counselors, especially in the presence of IP (Clarke et al., 2025; Neff et al., 2005). Self-compassion is comprised of three interrelated dimensions: mindfulness, common humanity, and self-kindness (Neff, 2023). Mindfulness, the core of self-compassion, involves maintaining awareness of present experiences with reduced reactivity and self-judgment. The common humanity dimension refers to the acceptance that suffering is inherent to our shared human experience. By normalizing challenging experiences, this perspective helps prevent the isolation that may arise from perceiving failures as uniquely personal. Finally, self-kindness encompasses behaviors and ways of relating intrapersonally that offer support and comfort during times of suffering or setbacks. Rather than defaulting to self-criticism, overidentification with failures, or isolation, self-compassion enables understanding and resilience, reducing the impact of IP and the fear of failure during counselor development (Clarke et al., 2025; Warren et al., 2016).
The theoretical alignment between self-compassion and resilience is rooted in their shared emphasis on adaptive emotional regulation, growth through adversity, and the development of a stable and supportive inner identity (Warren et al., 2016). Self-compassion supports sustainable resilience by reducing self-criticism and perfectionism and fostering a growth mindset (Neff, 2023; Warren et al., 2016). Indeed, a recent meta-analysis indicated that self-compassion is consistently linked to positive outcomes among mental health professionals, including enhanced competence, improved therapeutic presence, and a greater willingness to seek guidance and supervision (Crego et al., 2022).
Because of its regulating effects, self-compassion may help developing counselors to tolerate the stress of IP through improved emotional self-regulation (Crego et al., 2022; Neff, 2023). In this way, self-compassion can function as an emotion-focused coping mechanism that reduces the mental distress associated with IP (Clarke, 2024; Crego et al., 2022; Gerber & Anaki, 2021). Ultimately, when individuals experience IP-related distress, self-compassionate responses (mindfulness, common humanity, self-kindness) may interrupt the IP cycle, preserving resilience and mental health (Neff et al., 2005).
The purpose of this study is to examine how self-compassion functions as a protective factor in the relationship between IP, resilience, and mental health during counselor development. Research has found self-compassion to support resilience among health care providers (Delaney, 2018), yet much less is known about the relationship between self-compassion and resilience among developing counselors who experience IP. Addressing the negative impact of IP on counselor development, this article explores how self-compassion might mitigate IP’s negative relationships with resilience and mental health (Clarke et al, 2025; Roskowski, 2010; Tigranyan et al., 2021). The guiding research questions were:
- To what extent does self-compassion mediate the relationships between IP and the outcomes of resilience and mental health?
- How do levels of self-compassion relate to variations in IP, resilience, and mental health among the sample?
We hypothesized that IP would have a significant negative relationship with resilience and mental health, and that self-compassion will significantly mediate these negative associations. Specifically, higher levels of self-compassion will relate to lower IP and improved mental health and resilience. Our findings offer valuable insights into how self-compassion can enhance resilience and promote mental health during counselor development.
Methods
Procedure
The study received IRB approval prior to the recruitment of master’s-level counseling students from across the United States. Data were collected between April and October 2023, using an online survey disseminated via email to Council for the Accreditation of Counseling and Related Educational Programs (CACREP)–accredited program liaisons. These emails described the study and outlined informed consent procedures and inclusion criteria. Eligible participants were individuals enrolled in CACREP-accredited counseling programs aged 18 or older. After consenting, participants were presented with the measures and a demographic questionnaire developed by the authors. Engagement with the study concluded once participants either completed or exited the survey.
Participants
The sample consisted of 281 counseling students attending CACREP-accredited counseling programs from 37 U.S. states and the District of Columbia. Although the present sample consisted of counselors-in-training (CITs), the term developing counselors is used throughout this paper to reflect the broader developmental continuum that spans counselor training and early professional practice (Stoltenberg & McNeill, 2010).
Consistent with the population of CITs, most participants identified as White (n = 190, 67.29%) with lower percentages identifying as Hispanic or Latinx (n = 43, 15.2 %), Asian (n = 17, 6.0%), African American or Black (n = 13, 4.6%), multiracial (n = 13, 4.6%), American Indian or Alaskan Native (n = 3, 1.1%) and Middle Eastern (n = 2, 0.7%). The majority (n = 237, 83.7%) identified as female, with 32 (11.3%) identifying as male, 6 (2.1%) as non-binary, 4 (1.4%) as genderqueer, and 2 (0.7%) choosing not to disclose their gender identity. Participants were from clinical mental health (n = 170, 60.1%), school counseling (n = 49, 17.3%), rehabilitation counseling (n = 49, 17.3%), and marriage and family counseling (n = 13, 4.6%) programs. The average participant age was 32 years (SD = 10.35), with an age range from 21 to 67 years.
Measures
Self-Compassion Scale-Short Form (SCS-SF)
The SCS-SF is a short form of the Self-Compassion Scale (Neff, 2003), consisting of 12 self-report items selected from the original scale (Raes et al., 2011). Items are rated on a 5-point Likert-type scale ranging from 1 (almost never) to 5 (almost always). Examples include “I try to see my failings as part of the human condition” and “I’m disapproving and judgmental about my own flaws and inadequacies” (Neff, 2003, p. 2). SCS-SF scores have shown good internal consistency (α = .86), with its total scores strongly correlating with those of the full version (r = .98; Raes et al., 2011). Factor analysis has confirmed that the SCS-SF shares the same factor structure as the original scale (Neff et al., 2019; Raes et al., 2011). Scores are interpreted as levels of self-compassion: low (1–2.4), moderate (2.5–3.5), and high (3.51–5). In the present study, SCS-SF scores demonstrated good internal consistency reflected in an alpha of .85, and omega of .85.
Academic Resilience Scale-6 (ARS-6)
The ARS-6 is a concise self-report scale designed to measure academic resilience, defined as the ability to manage challenges, stress, and setbacks within a learning environment (Martin & Marsh, 2006). Items include statements such as “I’m good at bouncing back from a poor grade or difficult feedback” and “I don’t let a bad grade or feedback affect my confidence.” Responses are rated on a 7-point Likert-type response scale ranging from 1 (strongly disagree) to 7 (strongly agree), with higher scores reflecting greater academic resilience. Item and factor level construct validity was supported through factor score estimates, correlation, path analysis, and cluster analysis, showing the ARS scores were closely aligned with related constructs including self-efficacy, control, planning, low anxiety, and persistence (Martin & Marsh, 2006). ARS-6 scores have demonstrated good internal consistency, with an alpha coefficient of .89 (Martin & Marsh, 2006). In the current study, the ARS-6 scores showed acceptable reliability supported by alpha and omega scores of .83.
Clance Impostor Phenomenon Scale (CIPS-10)
The CIPS-10 (Wang et al., 2022) is a condensed, 10-item version of the original 20-item Clance Impostor Phenomenon Scale (CIPS) designed to assess impostor feelings (Clance, 1985). A systematic review by Mak et al. (2019) supported the CIPS-20 as a valid (construct, criterion, and content) measure of IP. The CIPS-10 utilizes a Likert-type response scale ranging from 1 (not at all true) to 5 (very true) and includes items from the CIPS-20, such as “I’m afraid people important to me may find out that I’m not as capable as they think I am” and “I feel my success was due to some kind of luck rather than competence.” Wang et al. (2022) reported strong internal reliability for the CIPS-10 (α = .93), with total scores closely aligning with those of the CIPS-20. Construct validity was supported through factor score estimates, revealing a single-factor structure similar to the 20-item version. In this study, CIPS-10 scores were interpreted using adjusted categories from Clance (1985): few IP (less than 20), moderate IP (20–29), frequent IP (30–39), and intense IP (40–50). Within the current sample, CIPS-10 scores demonstrated good internal consistency with an alpha of .88 and omega of .90.
Patient Health Questionnaire-4 (PHQ-4)
The PHQ-4 is a 4-item, self-report assessment screening tool for depression and anxiety (Kroenke et al., 2009). The Likert-type responses are 0 (not at all), 1 (several days), 2 (more than half the days), and 3 (nearly every day). A total score of 3 or more, across both items, indicates the presence of moderate-to-severe symptoms (Kroenke et al., 2009). In meta-analyses, PHQ-4 scores have shown good internal consistency (α = .89) and have yielded valid and diagnostically accurate depression and anxiety scores (Khubchandani et al., 2016; Kroenke et al, 2009). Construct validity was supported using a varimax-rotated principal components analysis conducted on the four screening items (PHQ-2 and GAD-2), yielding two components that together explained 83% of the overall variance. Likewise, criterion validity was indicated by individuals diagnosed with depression or anxiety by a health care professional scoring significantly higher on the PHQ-2, GAD-2, and PHQ-4 compared to participants without a clinical diagnosis (Khubchandani et al., 2016). In the present sample, the PHQ-4 scores showed good internal consistency with an alpha score of .87 and omega of .84.
Data Analysis
Portions of this data set informed a previously published manuscript that focused on how self-compassion can mitigate IP’s negative relationship with counselor self-efficacy (Clarke et al., 2025). Although the two manuscripts share IP and self-compassion data, the current manuscript is distinct and extends this line of inquiry by its unique focus on the benefits of self-compassion for counselor resilience and mental health, despite the presence of IP.
All analyses were performed using SPSS (v29) with a p ≤ .01 benchmark to reduce the likelihood of Type I error and ensure that the most reliable effects are interpreted as statistically meaningful. Preliminary analyses were conducted to examine statistical assumptions for the mediation and MANOVA models. Normality was confirmed for all variables via Shapiro-Wilk (all p > .05). Box’s M test supported homogeneity of variance–covariance matrices (p = .021), and observations were independent. In addition to all VIF scores being < 2, no bivariate correlations exceeded r = .80, suggesting that multicollinearity was not a concern. Collectively, these results suggest that the data met all assumptions necessary for the planned analyses (Tabachnick & Fidell, 2019).
We selected a regression-based mediation analysis because of the study’s focus on specific indirect effects of self-compassion and the moderate sample size, both of which made alternative analyses less ideal (Hayes, 2022). Because the variables tested were represented by composite scores rather than latent constructs, a mediation was statistically appropriate and provided a parsimonious method to examine self-compassion as a buffer for IP. Although cross-sectional mediation cannot establish temporal precedence or causation, it can identify statistical pathways that warrant future longitudinal investigation (Fairchild & McDaniel, 2017; Hayes, 2022). The 99% confidence intervals (CI) of the effects were derived from 10,000 bootstrap samples. If the upper and lower bounds of the CI did not include zero, they were considered statistically significant.
Finally, MANOVA was used to determine how the severity of IP affected its relationships with resilience, anxiety, depression, and self-compassion. The four levels of IP used in this analysis were defined as few, moderate, frequent, and intense IP according to the CIPS author (Clance, 1985). MANOVA effect size was described using partial eta squared values of 0.01 (small), 0.059 (medium), and 0.14 (large; Richardson, 2011). Cohen’s d was used to interpret effect sizes for follow up Tukey analyses, small effect (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8; Gignac & Szodorai, 2016).
A priori power analysis for mediation effects (Fritz & MacKinnon, 2007) indicated a minimum sample of 148 participants would provide .80 power to detect medium-sized indirect effects using bias-corrected bootstrapping. For MANOVA with three groups and four dependent variables, G*Power indicated 158 participants would yield .80 power for detecting medium effects (f² = .25). Our sample of 281 exceeded both requirements.
Results
Descriptives
Pearson correlations indicated significant (< .01) bivariate relationships among self-compassion, impostor phenomenon, depression, anxiety, and academic resilience (Table 1). There were no significant differences in self-compassion, IP, resilience, anxiety, or depression across demographics or counseling program emphasis.
Table 1
Descriptive Statistics and Bivariate Correlations
|
Mean |
SD |
1 |
2 |
3 |
4 |
|
| 1. Self-Compassion |
3.06 |
0.74 |
– |
|
|
|
| 2. Impostor Phenomenon |
32.81 |
8.22 |
−.54* |
– |
|
|
| 3. Depression |
1.27 |
1.60 |
−.42* |
.35* |
– |
|
| 4. Anxiety |
2.54 |
1.78 |
−.55* |
.46* |
.59* |
– |
| 5. Academic Resilience |
27.66 |
6.51 |
.53* |
−.36* |
−.23* |
−.40* |
*p ≤ .01.
The sample included high levels of impostor phenomenon (M = 32.81, SD = 8.22), with over 65% falling in the frequent-to-intense range. IP showed strong negative correlations with self-compassion (r = −.54) and resilience (r = −.36), and strong positive correlations with anxiety (r = .46) and depression (r = .35).
Mediation Analysis
Mediation analyses were used to explore the statistical associations among IP, self-compassion, and the outcome variables of resilience, anxiety, and depression. Results indicated that self-compassion functioned as a statistical mediator in the relationships between IP and each outcome.
Figure 1
Mediation Analysis: Impostor and Resilience
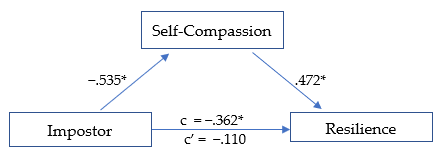
*p ≤ .01
The first model (Figure 1) was significant, R² = .290, F(1, 278) = 59.78, p < .01. The total effect (c) of IP on academic resilience was negative and significant, β = −.362, SE = .126, t = −2.868, p < .01, suggesting that higher IP scores were associated with lower resilience. When self-compassion was included in the model, the direct effect (c′) of IP on resilience was no longer significant, β = −.110, SE = .060, t = −1.838, p = .07, consistent with full statistical mediation (Hayes, 2022). The indirect pathway through self-compassion represented 69.6% of the total standardized association. IP was negatively associated with self-compassion (β = −.535, p < .01; large effect), and self-compassion was positively associated with resilience (β = .472, p < .01; large effect). The overall indirect effect was significant (β = −.252, p < .01).
Figure 2
Mediation Analysis: Impostor and Anxiety
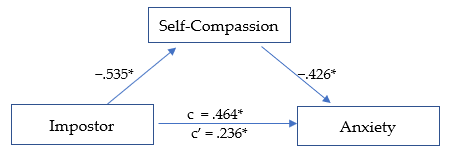
*p ≤ .01.
The second model (Figure 2) was significant, R² = .345, F(1, 278) = 73.159, p < .01. The total effect (c) of IP on anxiety was positive and significant, β = .464, SE = .053, t = 8.747, p < .01, indicating that higher IP scores were related to higher anxiety levels. After including self-compassion, the direct effect (c′) was reduced but remained significant, β = .236, SE = .057, t = 4.110, p < .01, suggesting partial statistical mediation. The indirect pathway through self-compassion accounted for 49.2% of the total standardized association. IP was negatively associated with self-compassion (β = −.535,p < .01; large effect), and self-compassion was negatively associated with anxiety (β = −.426, p < .01; medium effect). The overall indirect effect was significant, β = −.228, p < .01.
Figure 3
Mediation Analysis: Impostor and Depression
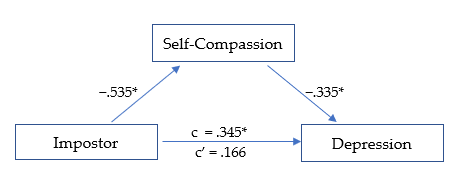
*p ≤ .01.
The third model (Figure 3) was significant, R² = .199, F(1, 278) = 34.484, p < .01. The total effect (c) of IP on depression was positive and significant, β = .345, SE = .056, t = 6.135, p < .01, indicating that higher IP scores were associated with higher depression levels. After accounting for self-compassion, the direct effect (c′) was reduced and no longer significant, β = .166, SE = .064, t = 2.611, p = .02, suggesting full statistical mediation. The indirect pathway through self-compassion represented 51.9% of the total standardized association. IP was negatively related to self-compassion (β = −.535, p < .01; large effect), and self-compassion was negatively related to depression (β = −.335, p < .01; medium effect). The overall indirect effect was significant, β = −.179, p < .01.
MANOVA
Self-compassion scores were divided into three levels (low, moderate, and high) as suggested by Neff (2003) to determine if the effect of self-compassion was consistent across each level. MANOVA analyses revealed that IP, resilience, depression, and anxiety each varied significantly based on level of self-compassion, F(8, 550) = 20.790, p < .01, Wilk’s Λ = 0.590, ηp2 = .232, indicating a large effect size.
The MANOVA results revealed that IP scores varied according to level of self-compassion, F(2, 281) = 48.807, p < .01, ηp2 = .260, with a large effect size. IP decreased significantly at each rising level of self-compassion, from low to moderate (d = 0.666, p < .01) and moderate to high (d = 0.987, p < .01), with medium and large effect sizes, respectively. The greatest decrease in IP was seen as self-compassion rose from moderate to high.
Resilience was significantly higher at each increasing level of self-compassion F(2, 281) = 39.323, p < .01, ηp2 = .221, with a large overall effect size. Resilience rose linearly across each level of self-compassion, from low to moderate (d = −0.756, p < .01), and from moderate to high (d = −0.790, p < .01), each with a medium-high effect size.
Depression scores lowered significantly as self-compassion level increased, F(2, 281) = 20.232, p < .01, ηp2 = .127, with an overall medium effect size. The decrease in depression was noted across levels of self-compassion, from low to moderate (d = 0.446, p < .01), and from moderate to high (d = 0.625, p < .01), each with a medium effect size. The largest decrease in depression was observed as self-compassion rose from moderate to high.
Anxiety scores decreased significantly as the level of self-compassion increased, F(2, 281) = 45.898, p < .01, ηp2 = .248, with a large overall effect size. Anxiety scores were lower as self-compassion rose from low to moderate (d = 0.895, p < .01), and from moderate to high (d = 0.711, p < .01), with large and medium effect sizes, respectively. The largest decrease in anxiety was noted as self-compassion increased from low to moderate.
Discussion
Our findings indicate that self-compassion is a strong protective factor and may enhance resilience and promote mental health among developing counselors, despite impostor feelings. Specifically, self-compassion fully mediated the negative relationship between IP, resilience, and depression, while partially mediating the relationship between IP and anxiety. This suggests that even when experiencing IP, higher self-compassion may help to maintain greater resilience and significantly reduced anxiety and depression. The results are promising and suggest that cultivating self-compassion may facilitate professional growth by interrupting the IP cycle. Our results offer further insights into how self-compassion can support resilience and mental health (Housenecht & Swank, 2022).
Descriptive Statistics
Descriptive analyses revealed a notably high prevalence of IP in the sample, with 96.1% (n = 270) reporting moderate to intense symptoms. Scores were skewed toward the higher end of the scale, with 65.1% of participants in the frequent-to-intense range and 21% in the highest category. Compared with earlier samples, these findings suggest that the severity of IP has increased substantially over the past 15 years (Roskowski, 2010; Tigranyan et al., 2021). For example, only 27.6% of a 2010 sample fell into the frequent-to-intense categories, compared with nearly two-thirds in the present study. Likewise, the proportion of students in the highest IP range has risen fivefold, from 4.1% in 2010 to 21% here. Although this increase may be influenced by broader cultural or educational factors, the trend underscores the importance of implementing effective coping strategies to support counselor well-being and persistence.
Consistently elevated IP scores across studies suggest that impostor feelings may be a common element of counselor development. Such feelings are often fueled by both internal and environmental pressures, particularly graduate students’ unreasonably high expectations of their performance and rapid development (Clance & Lawry, 2024). These unrealistic standards can generate unnecessary self-doubt, distorted self-assessments, and persistent self-criticism (Gadsby & Hohwy, 2024). Importantly, the current results indicate that self-compassion is a powerful counterbalance to IP. Higher self-compassion was associated with lower IP, anxiety, and depression, and with greater resilience, findings that align with previous research (Liu et al., 2023).
Mediation Models
Self-Compassion, IP, and Resilience
The first mediation analysis revealed that self-compassion fully mediated the negative relationship between IP and resilience. When accounting for self-compassion, the negative relationship between IP and resilience was rendered statistically non-significant. This outcome suggests that developing counselors with higher self-compassion may more easily adapt and recover when experiencing impostor-related distress. Self-compassion may assist key aspects of resilience, including stress management, coping with adversity, and maintaining a stable and supportive inner identity (Webb & Rosenbaum, 2019).
Although IP encourages harsh self-criticism and rumination on perceived failures, it is possible that through increased self-acceptance and soothing kindness, counselors can embody greater resilience when confronting areas of growth with less fear of failure. Additionally, a common humanity perspective can encourage acceptance of struggles as a normal part of counselor development and one shared by their peers. These soothing and normalizing aspects of self-compassion can encourage community rather than isolation when struggling, helping counselors to maintain resilience amidst adversity (Hou & Skovholt, 2020; Neff, 2023). Without effective coping practices, the challenges of counselor development can wear down resilience, creating vulnerability to mental distress, burnout, and counselor impairment (Cook et al., 2021; Gerber & Anaki, 2021).
Self-Compassion, IP, and Mental Health
Our results indicate that self-compassion is associated with less anxiety among those experiencing IP. Because anxiety is prevalent in this population and a primary emotional response to IP, efforts to increase self-compassion can have widely beneficial outcomes (Crego et al., 2022; Garba et al., 2024). The common humanity and mindfulness components of self-compassion may be critical to this outcome, as they can help limit emotional reactivity, normalize the IP experience, and reduce the isolation and fear of being exposed as an impostor (Clarke & Guida, 2025). This process involves mindfully recognizing that others share similar experiences and feelings, empowering developing counselors to seek support and reduce fear of failure (Neff, 2023). Likewise, practicing self-kindness may counter the harsh self-criticism associated with IP and encourage them to embrace the developmental process, including their imperfections (Patzak et al., 2017; Warren et al., 2016).
Anxiety and depression are closely linked and often co-occur (Beck & Alford, 2009). Though depression may not correlate as strongly with IP as anxiety does, it remains a common outcome (Garba et al., 2024). IP is persistent and sustained by cognitive distortions and misattributions, which also contribute to depressive thought patterns (Beck & Alford, 2009). However, our analysis revealed that self-compassion fully mediated the relationship between IP and depression. This suggests that a combination of mindful awareness and active self-kindness may facilitate more balanced self-assessment, countering perfectionism and harsh self-criticism commonly associated with IP (Clarke & Hartley, 2025; Pákozdy et al., 2023).
Although IP significantly predicted anxiety and depression, the buffering effect of self-compassion suggests that those with more compassionate self-perceptions may better tolerate the uncertainty and challenges common to counselor training. For example, those with a self-compassionate mindset may reinterpret failures as growth opportunities, a shift that may protect against anxious and depressive symptoms (Crego et al., 2022; Warren et al., 2016). These findings highlight the regulatory potential of self-compassion in reducing emotional reactivity to impostor-related distress.
Level of Self-Compassion in Relation to IP, Resilience, and Mental Health
MANOVA was utilized to determine whether the level of self-compassion (categorized as low, moderate, or high) was related to the level of IP, resilience, anxiety, and depression (Neff, 2003). Self-compassion had a significant positive relationship with mental health and resilience; however, the relationships varied significantly based on level of self-compassion (Figure 4). The results demonstrate that even lower levels of self-compassion were related to significantly lower IP, anxiety, and depression, as well as increased resilience. This pattern suggests that even modest improvements in self-compassion can correspond to improved well-being among developing counselors (Luo et al., 2023). For example, IP severity decreased significantly as self-compassion levels increased, revealing a linear reduction in IP from low to high self-compassion levels, with the most pronounced decrease occurring between the moderate and high categories.
Similarly, resilience scores also increased consistently across each level of self-compassion. The increase was linear, with the most substantial increase occurring when self-compassion rose from low to moderate. The steady increase in resilience across all self-compassion levels points to a possible dose-response relationship. Initial gains in self-compassion may bolster developing counselors’ ability to persevere through challenges (Neff et al., 2005), and interventions resulting in modest enhancements in self-compassion could yield significant improvements in resilience.
Figure 4
IP, Resilience, Depression, and Anxiety Across Levels of Self-Compassion
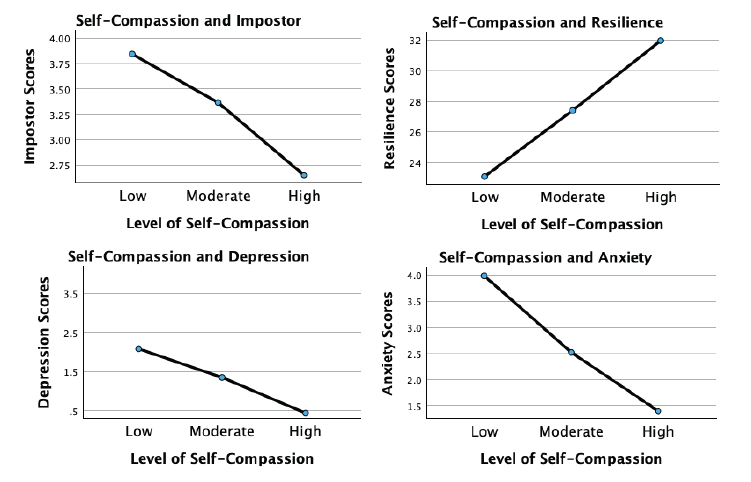
Although more variable, the association of self-compassion with anxiety and depression was similarly beneficial. Anxiety levels decreased significantly with each incremental increase in self-compassion, with the largest reduction occurring from low to moderate levels. This underscores the potential that even lower levels of self-compassion may still meaningfully alleviate anxiety. For depression, a significant decrease occurred across self-compassion levels, with the most substantial reduction noted as self-compassion increased from moderate to high. This suggests that self-compassion may interrupt the internal feedback loop of shame, self-criticism, and hopelessness that sustains depressive thinking in the context of IP.
These findings indicate that self-compassion is an important protective factor for developing counselor mental health. Contrary to expectations, even lower levels of self-compassion significantly relate to reduced IP, anxiety, and depression while increasing resilience (Luo et al., 2023). Integrating strategies to enhance self-compassion into counselor training programs could incrementally increase self-compassion, build emotional tolerance, and create a more stable internal environment from which resilience and well-being can emerge.
Implications and Future Directions for Counselor Development
Despite IP’s prevalence and association with diminished resilience and psychological distress, it remains underexamined in the counseling literature. Beyond a self-care strategy, self-compassion may build resilience and maintain mental health during and after counselor training. Integrating self-compassion into counselor education and early career development may cultivate a more supportive environment and provide counselors with evidence-based ways to manage IP and enhance resilience. Whereas, if left unaddressed, IP can lead to unnecessary distress, burnout, and professional attrition (Coaston & Lawrence, 2019; Ojeda, 2024).
Growing evidence suggests that self-compassion is vital for counselor development and ethical practice (Clarke et al., 2025; Coaston & Lawrence, 2019). The American Counseling Association (ACA) Code of Ethics (2014) emphasizes that professional counselors must engage in ongoing self-assessment and maintain their effectiveness through self-care practices. Similarly, CACREP (2023) standards require counselor education programs to integrate “self-care, self-awareness, and self-evaluation strategies for ethical and effective practice” (3.A.11.). Without meaningful coping strategies, IP can directly undermine these ethical mandates by diminishing well-being and distorting self-evaluation necessary for competent practice (Gadsby & Hohwy, 2024).
Regular engagement in reflective activities promoting balanced self-evaluation is essential to counselor development. If such exercises lack a compassionate focus, they may inadvertently reinforce impostor-related distortions by encouraging rumination and inaccurate self-critique. Matching reflective self-assessment with self-compassion practice may allow developing counselors to internalize feedback and move attention away from self-criticism and toward a growth mindset, transforming internal narratives dominated by IP (Warren et al., 2016).
Counselor educators and professional agencies can integrate self-compassion training through multiple pathways. Brief interventions, such as abbreviated versions of the Mindful Self-Compassion program (Germer & Neff, 2019), offer evidence-based approaches for enhancing counselor resilience. If limited by time and resources, supervisors and mentors can model self-compassionate practices by normalizing struggles, demonstrating constructive self-talk, and providing balanced growth-oriented feedback. The disclosure of faculty or supervisor IP experiences may be particularly powerful, reframing vulnerability and self-care as professional strengths rather than weaknesses.
Because IP is a contextual and environmentally fueled experience, counseling agencies and community mental health settings can foster organizational climates that prioritize compassion and collaboration and normalize challenges during the growth process (Coaston, 2019). When institutions reward openness, reflection, and learning from error, rather than perfection and productivity, developing counselors are more likely to engage in authentic self-assessment and seek help when struggling.
Early career peer support groups and compassion-focused initiatives can also counter the competitive, perfectionistic culture that sustains IP in professional practice (Clark et al., 2022). These approaches challenge the isolating belief that self-doubt is uniquely shameful, and foster community and belonging (Clarke & Guida, 2025; Hou & Skovholt, 2020). Future research should employ longitudinal and experimental designs to test targeted self-compassion interventions, clarifying causal relationships between self-compassion, resilience, and mental health outcomes in counselor education and professional contexts.
Clinical Supervision
Developmentally, the transition from classroom learning to applying theory and skills in clinical practice naturally provokes stress and anxiety (Skovholt & Trotter-Mathison, 2024). Although clinical supervision provides an ideal context for fostering openness and resilience (Coaston, 2019), experiencing IP may be a barrier to disclosing challenges because of emotional distress and fear of exposing perceived inadequacies (DeCandia Vitoria, 2021). Maintaining a façade of competence can compromise development and hinder the supervisory relationship (Thériault et al., 2009). These perfectionistic tendencies and IP are often motivated by context, suggesting that supervisors’ approaches may significantly alleviate these patterns.
Coaston (2019) provides a practical framework for applying self-compassion principles and philosophy in clinical supervision. Rooted in humanistic and developmental theory, this approach emphasizes that supervisors can accompany supervisees through the inevitable discomfort and vulnerability of professional growth by responding with compassion rather than judgment. By adopting a compassionate approach, the supervisory relationship can deepen, normalizing challenges and facilitating an authentic dialogue about IP-related uncertainties. In this way, clinical supervisors can address common cognitive and affective challenges.
A compassionate supervisory environment promotes balanced self-reflection and can reduce the shame-based fear of exposure that drives impostor defenses. This may allow supervisees to explore their conceptual skills openly, reframe unrealistic expectations, and persist despite challenges (Hou & Skovholt, 2020; Stoltenberg & McNeill, 2010). Future research can investigate how self-compassion contributes to the supervisory relationship, comfort with disclosure, and the integration of constructive feedback during supervised practice.
Clinical supervisors can also create a culture of shared vulnerability by modeling self-compassion and transparency about their own developmental struggles and self-doubt. This enables supervisees to internalize feedback and approach self-evaluation with less emotional reactivity. Enhancing collaboration within the alliance empowers supervisees to feel more competent in navigating their development independently (Skovholt & Trotter-Mathison, 2024). Given the potential benefits of this approach, we recommend that future research examine how embodiment and facilitation of self-compassion affect counselor development and well-being.
Limitations
Although the results of this study are encouraging, there are limitations. The cross-sectional design limits the data to a single point in time rather than showing fluctuations in self-compassion, IP, resilience, and mental health over time. Likewise, the present results do not establish causality. Replicating this study using a longitudinal approach can provide greater insight into these fluctuations. Furthermore, self-report measures introduce limitations such as social desirability bias and reliance on participant self-awareness. Likewise, individuals with a personal connection to IP may have been more likely to participate, potentially skewing results.
Participants were not asked about their matriculation status as counseling students, leaving their stage of development unknown. Future research should include clinical experience (i.e., none, practicum, internship) and matriculation status. This information would provide greater insight into how experience and counselor development interact with IP. The current study used a general IP assessment, while future research should use the Counselor Impostor Scale (CIS; Nguyen, 2023), which was published after data collection for this study was complete. The CIS is designed specifically for the counseling domain and could provide more nuanced insights. Additionally, because maladaptive coping strategies such as procrastination and perfectionism sustain IP, subsequent studies should explore these constructs, which could inform more targeted interventions.
Conclusion
The growth process during counselor training is inherently challenging and often gives rise to IP, which increases anxiety and depression while diminishing resilience. Self-compassion is a promising method for enhancing resilience and well-being, despite the presence of IP. Once learned, self-compassion is an accessible practice and relies on applying skills with which counselors are familiar, such as kindness and compassion toward themselves. The results of this study are encouraging and robust, suggesting that self-compassion can enhance resilience by supporting adaptive emotional regulation and fostering a growth-oriented mindset. Self-compassionate counselors can maintain their well-being despite experiencing IP. Importantly, the positive impact of self-compassion was consistent and significant even at lower levels, which is especially important given the prevalence and severity of IP among CITs. The findings support integrating self-compassion into counselor training and clinical supervision through modeling, training, and practice. This approach can provide effective coping for IP and improve resilience, mental health, and persistence.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/docs/default-source/default- document-library/ethics/2014-aca-code-of-ethics.pdf
Beck, A. T., & Alford, B. A. (2009). Depression: Causes and treatment (2nd ed.). University of Pennsylvania Press.
Council for the Accreditation of Counseling and Related Educational Programs (2023). 2024 standards. https://www.cacrep.org/wp-content/uploads/2023/06/2024-Standards-Combined-Version-6.27.23.pdf
Clance, P. R. (1985). Clance Impostor Phenomenon Scale (CIPS). [Database record]. APA PsycTests. https://doi.org/10.1037/t11274-000
Clance, P., & Lawry, S. (2024). Impostor phenomenon: Origins and treatment. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 17–43). American Psychological Association.
Clark, P., Holden, C., Russell, M., & Downs, H. (2022). The impostor phenomenon in mental health professionals: Relationships among compassion fatigue, burnout, and compassion satisfaction. Contemporary Family Therapy, 44(2), 185–197. https://doi.org/10.1007/s10591-021-09580-y
Clarke, B. J. (2024). Emerging adult life satisfaction and mental health: The mediating role of self-compassion and social support. Emerging Adulthood, 12(6), 1137–1147. https://doi.org/10.1177/21676968241279490
Clarke, B. J., & Guida, A. M. (2025). Self-compassion to community: The mediating effect of belonging on college student mental health and life satisfaction. Journal of College Student Mental Health. Advance online publication. https://doi.org/10.1080/28367138.2025.2552484
Clarke, B. J., & Hartley, M. T. (2025). Contemplative dispositions and mental health: The supportive role of self-compassion and mindfulness on college students’ resilience. Journal of College Student Mental Health, 39(1), 142–164. https://doi.org/10.1080/28367138.2024.2331931
Clarke, B. J., Hartley, M. T., & Button, C. (2025). Impostor phenomenon and counselor development: The critical role of self-compassion. Journal of Counseling & Development, 103(2), 149–160. https://doi.org/10.1002/jcad.12544
Coaston, S. C. (2019). Cultivating self-compassion within the supervision relationship. The Clinical Supervisor, 38(1), 79–96. https://doi.org/10.1080/07325223.2018.1525596
Coaston, S. C., & Lawrence, C. (2019). Integrating self-compassion across the counselor education curriculum. Journal of Creativity in Mental Health, 14(3), 292–305. https://doi.org/10.1080/15401383.2019.1610536
Cook, R. M., Fye, H. J., Jones, J. L., & Baltrinic, E. R. (2021). Self-reported symptoms of burnout in developing professional counselors: A content analysis. The Professional Counselor, 11(1), 31–45. https://doi.org/10.15241/rmc.11.1.31
Crego, A., Yela, J. R., Riesco-Matías, P., Gómez-Martínez, M. Á., & Vicente-Arruebarrena, A. (2022). The benefits of self-compassion in mental health professionals: A systematic review of empirical research. Psychology Research and Behavior Management, 15, 2599–2620. https://doi.org/10.2147/PRBM.S359382
DeCandia Vitoria, A. (2021). Experiential supervision: Healing impostor phenomenon from the inside out. The Clinical Supervisor, 40(2), 200–217. https://doi.org/10.1080/07325223.2020.1830215
Delaney, M. C. (2018). Caring for the caregivers: Evaluation of the effect of an eight-week pilot Mindful Self-Compassion (MSC) training program on nurses’ compassion fatigue and resilience. PLoS ONE, 13(11), e0207261. https://doi.org/10.1371/journal.pone.0207261
Fairchild, A. J., & McDaniel, H. L. (2017). Best (but oft-forgotten) practices: Mediation analysis. The American Journal of Clinical Nutrition, 105(6), 1259–1271. https://doi.org/10.3945/ajcn.117.152546
Fritz, M. S., & MacKinnon, D. P. (2007). Required sample size to detect the mediated effect. Psychological Science, 18(3), 233–239. https://doi.org/10.1111/j.1467-9280.2007.01882.x
Gadsby, S., & Hohwy, J. (2024). Negative performance evaluation in the impostor phenomenon. Current Psychology, 43, 9300–9308. https://doi.org/10.1007/s12144-023-05030-0
Garba, R., Coleman, C., & Kelley, T. (2024). The impostor phenomenon and mental health. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 61–79). American Psychological Association.
Gerber, Z., & Anaki, D. (2021). The role of self-compassion, concern for others, and basic psychological needs in the reduction of caregiving burnout. Mindfulness, 12, 741–750. https://doi.org/10.1007/s12671-020-01540-1
Germer, C., & Neff, K. (2019). Teaching the Mindful Self-Compassion program: A guide for professionals. Guilford.
Gignac, G. E., & Szodorai, E. T. (2016). Effect size guidelines for individual differences researchers. Personality and Individual Differences, 102, 74–78. https://doi.org/10.1016/j.paid.2016.06.069
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford.
Hou, J.-M., & Skovholt, T. M. (2020). Characteristics of highly resilient therapists. Journal of Counseling Psychology, 67(3), 386–400. https://doi.org/10.1037/cou0000401
Housenecht, A., & Swank, J. (2022). Motivation, belonging, and support: Examining persistence in counseling programs. Teaching and Supervision in Counseling, 4(2), Article 3. https://doi.org/10.7290/tsc04g4iv
Khubchandani, J., Brey, R., Kotecki, J., Kleinfelder, J., & Anderson, J. (2016). The psychometric properties of PHQ-4 depression and anxiety screening scale among college students. Archives of Psychiatric Nursing, 30(4), 457–462. https://doi.org/10.1016/j.apnu.2016.01.014
Kroenke, K., Spitzer, R. L., Williams, J. B. W., & Löwe, B. (2009). An ultra-brief screening scale for anxiety and depression: The PHQ–4. Psychosomatics, 50(6), 613–621.
Liu, S., Wei, M., & Russell, D. (2023). Effects of a brief self-compassion intervention for college students with impostor phenomenon. Journal of Counseling Psychology, 70(6), 711–724. https://doi.org/10.1037/cou0000703
Luo, X., Che, X., & Lei, Y. (2023). Characterizing the effects of self-compassion interventions on anxiety: Meta-analytic evidence from randomized controlled studies. Journal of Contextual Behavioral Science, 30, 132–141. https://doi.org/10.1016/j.jcbs.2023.10.004
Mak, K. K. L., Kleitman, S., & Abbott, M. J. (2019). Impostor phenomenon measurement scales: A systematic review. Frontiers in Psychology, 10, 671. https://doi.org/10.3389/fpsyg.2019.00671
Martin, A. J., & Marsh, H. W. (2006). Academic resilience and its psychological and educational correlates: A construct validity approach. Psychology in the Schools, 43(3), 267–281. https://doi.org/10.1002/pits.20149
Neff, K. (2003). Self-compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity, 2(2), 85–101. https://doi.org/10.1080/15298860309032
Neff, K. D. (2023). Self-compassion: Theory, method, research, and intervention. Annual Review of Psychology, 74, 193–218. https://doi.org/10.1146/annurev-psych-032420-031047
Neff, K. D., Hsieh, Y. P., & Dejitterat, K. (2005). Self-compassion, achievement goals, and coping with academic failure. Self and Identity, 4(3), 263–287. https://doi.org/10.1080/13576500444000317
Neff, K. D., Tóth-Király, I., Yarnell, L. M., Arimitsu, K., Castilho, P., Ghorbani, N., Guo, H. X., Hirsch, J. K., Hupfeld, J., Hutz, C. S., Kotsou, I., Lee, W. K., Montero-Marin, J., Sirois, F. M., de Souza, L. K., Svendsen, J. L., Wilkinson, R. B., & Mantzios, M. (2019). Examining the factor structure of the Self-Compassion Scale in 20 diverse samples: Support for use of a total score and six subscale scores. Psychological Assessment, 31(1), 27–45. https://doi.org/10.1037/pas0000629
Nguyen, L. T. (2023). Development and validation of the Counseling Impostor Scale (Doctoral dissertation). Texas A&M University–Corpus Christi.
Ojeda, L. (2024). Impostor phenomenon and burnout. In K. Cokley (Ed.), The impostor phenomenon: Psychological research, theory, and interventions (pp. 81–110). American Psychological Association.
Pákozdy, C., Askew, J., Dyer, J., Gately, P., Martin, L., Mavor, K. I., & Brown, G. R. (2023). The impostor phenomenon and its relationship with self-efficacy, perfectionism, and happiness in university students. Current Psychology, 43, 1–10. https://doi.org/10.1007/s12144-023-04672-4
Patzak, A., Kollmayer, M., & Schober, B. (2017). Buffering impostor feelings with kindness: The mediating role of self-compassion between gender-role orientation and the impostor phenomenon. Frontiers in Psychology, 8, Article 1289. https://doi.org/10.3389/fpsyg.2017.01289
Raes, F., Pommier, E., Neff, K. D., & Van Gucht, D. (2011). Construction and factorial validation of a short form of the Self-Compassion Scale. Clinical Psychology & Psychotherapy, 18(3), 250–255. https://doi.org/10.1002/cpp.702
Richardson, J. T. E. (2011). Eta squared and partial eta squared as measures of effect size in educational research. Educational Research Review, 6(2), 135–147. https://doi.org/10.1016/j.edurev.2010.12.001
Roskowski, J. C. R. (2010). Impostor phenomenon and counseling self-efficacy: The impact of impostor feelings (Doctoral dissertation). Ball State University.
Skovholt, T. M., & Trotter-Mathison, M. (2024). The elevated stressors of the novice practitioner. In T. M. Skovholt & M. Trotter-Mathison (Eds.), The resilient practitioner: Burnout and compassion fatigue prevention and self-care strategies for the helping professions (4th ed., pp. 42–68). Taylor & Francis.
Stoltenberg, C. D., & McNeill, B. W. (2010). IDM supervision: An integrative developmental model for supervising counselors and therapists (3rd ed.). Routledge.
Tabachnick, B. G., & Fidell, L. S. (2019). Using multivariate statistics (7th ed.). Pearson.
Thériault, A., Gazzola, N., & Richardson, B. (2009). Feelings of incompetence in developing therapists: Consequences, coping, and correctives. Canadian Journal of Counselling, 43(2), 105–119.
Tigranyan, S., Byington, D. R., Liupakorn, D., Hicks, A., Mathis, M., & Rodolfa, E. (2021). Factors related to the impostor phenomenon in psychology doctoral students. Training and Education in Professional Psychology, 15(4), 298–305. https://doi.org/10.1037/tep0000321
Wang, B., Andrews, W., Bechtoldt, M. N., Rohrmann, S., & de Vries, R. E. (2022). Validation of the short Clance Impostor Phenomenon Scale (CIPS-10). European Journal of Psychological Assessment, 40(2), 158–168. https://doi.org/10.1027/1015-5759/a000747
Warren, R., Smeets, E., & Neff, K. (2016). Self-criticism and self-compassion: Risk and resilience. Current Psychiatry, 15(12), 18–33. https://self-compassion.org/wp-content/uploads/2016/12/Self-Criticism.pdf
Webb, R. E., & Rosenbaum, P. (2019). Resilience and thinking perpendicularly: A meditation or morning jog. Journal of College Student Psychotherapy, 33(1), 75–88. https://doi.org/10.1080/87568225.2018.1449687
Brian J. Clarke, PhD, NCC, LAC, is an assistant professor at the University of Arizona. Michael T. Hartley, PhD, CRC, is a professor at the University of Arizona. Austin M. Guida, PhD, NCC, LAC, is an assistant professor at Northern Arizona University. Correspondence may be addressed to Brian J. Clarke, Department of Disability and Psychoeducational Studies, College of Education, 1430 E. 2nd Street, Room 422, Tucson, AZ, 85721-0069, bclarke14@arizona.edu.
Aug 26, 2025 | Volume 15 - Issue 3
Brandi M. Sawyer, Edith Gonzalez
The global health and economic disaster caused by the coronavirus (COVID-19) pandemic has intensified mental health needs and subsequent demands on helping professionals. Counselors, in general, are at risk of experiencing both shared traumatic realities with clients and exacerbation of occupational stressors. For rural mental health counselors, who already face enhanced stressors related to rural service provision, the impact of COVID-19 is generally unknown. Through transcendental phenomenology, this study explores the experiences of 11 rural mental health counselors practicing in Texas during the COVID-19 pandemic. Two themes emerged, revealing experiences of systemic limitations as well as counselor growth and resilience. Findings provide implications for mental health counselor training, clinical practice, and advocacy.
Keywords: COVID-19 pandemic, rural, mental health counselors, transcendental phenomenology, resilience
With over a million deaths in the United States alone (Centers for Disease Control and Prevention [CDC], n.d.) the novel coronavirus (COVID-19) pandemic created a mental health crisis that includes long-term fear, trauma, grief, isolation, and negative social patterns (Czeisler et al., 2020; Eisma et al., 2021; Elbogen et al., 2021; Prati & Mancini, 2021). The influx of mental health needs meant that practitioners had to meet the demand of providing quality counseling services for those struggling with COVID-19 pandemic–related symptoms. Mental health counselors and related professionals experienced significant increases in caseloads and the clinical severity of presenting symptoms (Czeisler et al., 2020) that added increased pressure to workload, risk of burnout, and compassion fatigue, all of which are natural occupational hazards even under typical circumstances (Litam et al., 2021; Posluns & Gall, 2020; Sprang et al., 2007).
Increases in service demand were especially problematic when considering the vast preexisting shortage of mental health service availability worldwide (Wainberg et al., 2017). For rural mental health counselors, who ordinarily experience increased mental health service shortages (Breen & Drew, 2012; Slama, 2004), these demands and lack of resources were likely more intensely highlighted as lockdowns and shelter-in-place orders further reduced service access while simultaneously increasing the need for it (Panchal et al., 2023; Prati & Mancini, 2021). Mental health professionals were suddenly forced to transition to teletherapy services, a modality not frequently used prior to the COVID-19 pandemic (Burgoyne & Cohn, 2020; Pierce et al., 2021).
Teletherapy completely reshaped the provision of counseling services and required practitioners to consider and navigate various concerns, including accessibility and advocacy issues for vulnerable populations, quality of therapeutic engagement, ethical and legal matters, financial issues, treatment effectiveness, experience limitations, and training limitations (Maurya et al., 2020). This was likely a greater adjustment for rural practitioners, as they were less likely to use this modality than their urban counterparts prior to the COVID-19 pandemic (Pierce et al., 2020). Teletherapy has its disadvantages and advantages. The disadvantages include increased complexity of ethical issues such as privacy, information security, and maintaining a professional environment and professional relationships (Burgoyne & Cohn; Pierce et al., 2021). However, teletherapy provides client accessibility to services, overcoming the most notable barrier of local practitioner shortages experienced more often by rural residents (Tarlow et al., 2020). Through teletherapy, rural residents can connect to counselors in larger populated areas, but internet connectivity to do so has been a challenge historically (Handley et al., 2014).
Rural Mental Health
Practice and clinical topics related to rural populations are relatively sparse in empirical counseling literature, and this is especially true regarding rural mental health counselors during the COVID-19 pandemic. Existing research has established the enhanced hardships faced by rural populations, including more significant mental health presentations caused by mental health stigma (Slama, 2004) and a significant lack of mental health, medical, and transportation resources (Breen & Drew, 2012; Pullen & Oser, 2014; Slama, 2004). For rural counselors, this often means bulging caseloads, professional isolation, and more complicated cases than their urban counterparts.
Although not specific to COVID-19, Fruetel et al. (2022) documented the experiences of school and clinical mental health counselors responding to crises in rural areas. Findings indicated significant hardships such as isolation and lack of crisis stabilization resources. This highlights the fact that rural counselors continue to face significant mental health challenges in the community with limited institutional and professional support, placing further demands on existing providers and thereby increasing the risk of burnout and attrition (Litam et al., 2021; Sprang et al., 2007). To further complicate matters, the COVID-19 pandemic has exacerbated practitioner experiences of vicarious trauma, fatigue, and emotional disconnection as well as feelings of incompetence (Aafjes-van Doorn et al., 2020), which likely has a compounded effect for rural mental health counselors, who face additional geographic and cultural stressors (Breen & Drew, 2012; Pullen & Oser, 2014; Slama, 2004).
Trauma and Resilience
For many counselors involved in trauma and crisis work, occupational hazards such as burnout, compassion fatigue, and vicarious trauma have been documented (Posluns & Gall, 2020; Sprang et al., 2007), but less is known about the complexities of sharing trauma and crisis simultaneously with clients. Bell and Robinson (2013) posited that such experiences evolve into a compounded experience for counselors, in which the interplay between both vicarious and direct trauma—known as shared traumatic reality—enhances the post-traumatic exposure counselors experience. The shared traumatic reality of the COVID-19 pandemic has likely intensified existing occupational hazards of stress, burnout, and compassion fatigue (Litam et al., 2021; Posluns & Gall, 2020; Sprang et al., 2007).
Examining only the negative experiences associated with long-term trauma and crisis work would be unidimensional, inaccurate, and ignoring the potential value in such meaningful work. Additionally, this one-sided position ignores the presence and value of resilience among practicing counselors. Resilience has been represented as the ability to adapt and maintain well-being during unfavorable conditions (Clauss-Ehlers, 2008) and more specifically, taking deliberate actions to sustain health during hardship (Litam et al., 2021). Fostering resilience is imperative for mental health counselors who often face vicarious trauma. Without self-care and the ability to cope positively, these professionals risk burnout and impairment (Posluns & Gall, 2020), the latter of which has strong ethical implications because it poses an emotional risk to clients (Bell & Robinson, 2013).
Lambert and Lawson (2013), who studied counselors providing services during Hurricanes Katrina and Rita, found that counselors treating survivors of those disasters experienced compassion fatigue and burnout at no greater rates than counselors in general. Interestingly, those counselors who were both survivors and treatment providers experienced compassion satisfaction and post-traumatic growth, positive counterparts to compassion fatigue and post-traumatic stress, respectively. Similarly, Litam et al. (2021) found comparable results for counselors during the COVID-19 pandemic. Although occupational hazards such as compassion fatigue, vicarious trauma, and burnout were apparent for counselors in the sample, resiliency was a positive mitigating factor. It is important to note, however, that neither study examined multicultural issues as variables, and Litam et al. noted the absence of rural counselors as a significant limitation of their study.
Although not a study conducted with counselors, Wang et al. (2021) compared coping and adjustment in rural and urban individuals in North America. Despite adverse experiences among both groups, Wang et al. found several strengths in rural populations that were undetected in their urban counterparts, including enhanced coping and adjustment. These findings imply a cultural element to trauma and disaster response. In studies specific to counselors, Crumb et al. (2021) found strengths among rural school counselors providing disaster mental health services that included deepened empathy because of co-experience; Imig (2014) also found that despite difficulties, rural counselors found meaning in difficult work.
At the time of this study, we did not find additional research examining stress, resilience, or other quantitative or qualitative inquiries of rural mental health counselors’ experiences during the COVID-19 pandemic. This paucity of literature necessitates our study, which aims to fill a gap in understanding the interplay of rural mental health constraints and COVID-19 response. Learning how rural mental health counselors manage the complexities of limited mental health and medical resources, increased service demand, and vicarious trauma is imperative to better prepare for future mass disasters while maintaining the health and well-being of practitioners. Additionally, this study provides a much-needed voice for rural counselors and can further advocacy efforts for rural communities.
Method
The purpose of this study was to explore the experiences of rural mental health counselors during the COVID-19 pandemic and to develop a distinct picture of this population during long-term stress and disaster. We utilized a postpositivism paradigm, which allows for the acknowledgement of multiple perspectives while also striving for empirical rigor, to explore the universal experience of rural counselors during the COVID-19 pandemic (Guba & Lincoln, 1994; Hoshmand, 1996). To facilitate this exploration, we utilized a transcendental phenomenological methodology to capture the essence or true meaning of the phenomena of interest, the overall experiences, and the responses of the sample who share elements of an identity under similar conditions (Moustakas, 1994). Although postpositivism and transcendental phenomenology originate from different epistemological assumptions, one that emphasizes a reality that can be approximated through empirical observation and the other focusing on the essence of lived experience through subjective exploration, this study intentionally combined both to balance rigor and depth. Transcendental phenomenology and postpositivism have been found to complement each other through acknowledging multiple perspectives and having a top-down approach to research (Henderson, 2011; Hoshmand, 1996; Moustakas, 1994), and additional studies have utilized this paradigm and methodology (Eryaman et al., 2013; Hall et al., 2016). Nevertheless, to address potential incongruences, we utilized bracketing techniques to mitigate researcher bias and to ensure that the participants’ experiences remained central to the study. In alignment with transcendental phenomenology, we aimed to explore the lived experiences of rural mental health counselors during the COVID-19 pandemic, focusing on the perceived impacts and responses. The research questions guiding this exploration were:
- RQ1: What were the experiences of rural mental health counselors during the COVID-19 pandemic?
- RQ2: What impacts, if any, did COVID-19 have on the lives of rural mental health counselors?
- RQ3: How did rural mental health counselors respond, if at all, to the COVID-19 pandemic?
Site and Sample Selection
The sample criteria included Licensed Professional Counselors of all rankings—Licensed Professional Counselor-Associates (LPC-As), Licensed Professional Counselors (LPCs), and Licensed Professional Counselor-Supervisors (LPC-Ss)—who provided mental health counseling services in rural regions of Texas between March and December 2020. Texas was selected as a matter of convenience sampling (both Brandi M. Sawyer and Edith Gonzalez reside in Texas and are familiar with public license information) and because 76% of the state is considered fully rural. Additionally, Texas, like most other states, experienced government-mandated lockdowns, restricted social gatherings, and shuttered schools for most of 2020 (Friend, 2021; Limón, 2020), indicating that Texans experienced significant adversity from the pandemic. The criteria for rural regions were determined by the fiscal year 2022 definitions set forth by the Federal Office of Rural Health Policy (Health Resources and Services Administration, Federal Office of Rural Health Policy [FORHP], 2025).
Following approval for this study by the IRB, we obtained a list from the FORHP (2025) of counties in Texas with a completely rural status for fiscal year 2022 as an initial guide for sampling. Once the counties were identified, we used the Texas Behavioral Health Executive Council’s online search tool to obtain the names of eligible participants. This information was then used in a Google search to find addresses and emails for potential participants. In sum, we compiled a list of LPCs from 198 of 200 counties. Two counties were eliminated, as Sawyer had worked extensively in these rural counties and the likelihood that she knew potential participants was significantly increased. Email addresses, when available, were the first method of contact for recruiting participants. When not available, paper flyers were mailed to available addresses. Participants who completed the study and the final member-checking procedure received a $50 Amazon gift card. All participant recruitment and data collection took place in August and September of 2022.
Participants
Following recruitment procedures, 12 individuals volunteered to participate in this study, 11 of whom completed individual interviews. Saturation of data, when no new themes emerged during interviews and analysis (Ando et al., 2014), was reached within the 11 participants; no additional participants were needed. Eight participants identified as female, two participants identified as male, and one participant identified as transgender male. Eight participants identified as White and three identified as Hispanic or Latino. Nine of the 11 participants had master’s degrees and two held doctoral-level degrees. Years in counseling practice ranged from 1.5–30. Years in rural counseling practice also ranged from 1.5–30. Working environments varied across the 11 participants and included seven in group and private practice, three in agency and nonprofit settings, and one in an educational setting fulfilling a mental health counseling role. The sample consisted of the following current license categories: nine LPCs, one LPC-A, and one LPC-S.
Data Collection
Exploratory questions were designed to holistically capture the perceived impact of the COVID-19 pandemic, including the related thoughts, emotions, and behavioral responses as they align with the research questions exploring general experience, impact, and response. Participants chose personalized pseudonyms for anonymity and engaged in a 45–60-minute semi-structured, open-ended interview exploring their experiences working during the COVID-19 pandemic. The interview protocol included the following questions:
- What was it like to provide rural mental health counseling during the COVID-19 pandemic?
- How did you respond to the COVID-19 pandemic?
- What feelings do you experience about providing rural counseling during the COVID-19 pandemic?
- How did the COVID-19 pandemic impact your personal life?
- How did the COVID-19 pandemic impact your professional life?
- What was it like providing teletherapy during the COVID-19 pandemic?
- What is it currently like providing teletherapy?
- What is your perception of rural mental health counseling during the COVID-19 pandemic?
- How do you see your rural mental health work in the future following the COVID-19 pandemic?
Interviews were conducted and recorded via Zoom. Transcripts were first generated through a transcription application, Otter, and then verified for accuracy.
Data Analysis Procedures
Following the procedures set forth by Moustakas (1994), we used thematic analysis to evaluate data using two cycles of inductive coding. Engaging in multiple levels of inductive coding allowed us to explore themes within participant experiences while minimizing preconceived biases, a process known as epoche. The steps of coding and analysis first included preliminary horizontalization, which involved reducing narrative data into smaller units but not yet grouping data based on shared meanings. Using a spreadsheet, we achieved this by taking participant transcripts line by line, summarizing them, and placing them into columns. The next step in analysis, phenomenological reduction, involved clustering data relevant to the research questions into categories of corresponding themes and considering these from a variety of perspectives. Clustering data was done first to efficiently manage the data in order to better recognize recurring themes. We evaluated the horizontal data in the spreadsheet and clustered data from textural descriptions in various statements until no new groupings emerged. Ancillary information irrelevant to the research questions was eliminated from further coding. The final coding procedure generated the broadest themes, which were grouped based on shared meaning derived from phenomenological reduction using imaginative variation. We evaluated and interpreted the context of all codes achieved in reduction until the final themes emerged.
Strategies for Establishing Trustworthiness
We took steps to ensure trustworthiness of the findings according to Lincoln and Guba’s (1985) five tenets of trustworthiness: credibility, authenticity, transferability, dependability, and confirmability. Credibility and authenticity were achieved through in vivo and post-interview member checking to ensure accurate understanding or credibility of participant reports and by using two methods, providing ample opportunities for clarification. Another credibility validation tool, prolonged engagement, was achieved by having Sawyer interview, transcribe, check for accuracy, and conduct analysis, resulting in heightened awareness and understanding of the data. Triangulation with Gonzalez, who has different professional and personal identities, aided in furthering the inductive and methodological nature consistent with transcendental phenomenology (Moustakas, 1994).
Transferability was achieved through inductive procedures and obtaining rich details about study findings. Dependability was achieved through a rigorous methodology as outlined in Moustakas’s (1994) framework, which lends itself to examining multiple realities from an objective position. Multiple coding cycles additionally aided in dependability because they reduce abstract and biased findings. These same procedures also helped to achieve confirmability, enhancing objectivity in this qualitative research. We reduced researcher bias in interviewing and analysis through multiple coding cycles with rigorous methodology and triangulation (Lincoln & Guba, 1985).
Reflexivity
Bracketing was used to achieve reflexivity as a means to isolate and understand participant experiences apart from existing presuppositions. Sawyer has a professional identification aligning with that of rural mental health counselors. For 14 years, she has practiced mental health counseling in rural Texas, and since the onset of the COVID-19 pandemic, has provided teletherapy. She is an LPC-S and National Certified Counselor (NCC) who lives in Texas and has roots in rural Texas. Sawyer led all aspects of the research study. Gonzalez served as an external auditor for data analysis and assisted with manuscript writing. She is a counselor educator, researcher, and LPC with extensive experience in qualitative research and previous teaching experience in a rural setting. Based on Sawyer’s positionality, there were some apparent internal assumptions existing prior to the study. We assumed, based on personal and professional experiences, that participants would likely identify some hardships with rural service provision. Based on Sawyer’s work with often resilient rural clients during the last 14 years, we assumed some strengths related to rural populations would likely be identified.
In addition to bracketing, Sawyer reviewed interview questions and reflected on their cognitive reactions to the questions prior to conducting the interviews in an attempt to be aware of and set aside suppositions about the topic. Following each interview, Sawyer again reflected on personal cognitive responses to the topics, making notes as needed, and regularly reflecting on potential biases and enhancing trustworthiness with Gonzalez to counter them. As a result of such reflection, during thematic analysis, we did line-by-line coding to minimize interpretive assumptions, yielding the most objective view of sample experiences possible.
Findings
Thematic analysis rendered two themes as distinctly capturing the rural mental health counselor experience: systemic limitations and counselor growth and resilience. The codes within these themes had a 100% endorsement from the sample.
Systemic Limitations
The theme of systemic limitations was defined by participants as resource limitations within their rural communities, including significant shortages of mental health and medical services as well as services for basic needs such as food, housing, and financial assistance. Furthermore, a large majority of these clients characterized resource limitations as being both preexisting as well as exacerbated by the pandemic. For many participants, COVID-19 conditions greatly impacted their ability to provide face-to-face counseling in already resource-limited communities. Internet connectivity deficits in rural communities, which are already dealing with limited resources, were also included in this theme.
Mental health care prioritization and a lack of mental health care availability for rural clients were among the most prominent topics in participant reports. Participants shared the idea that because basic health care and other needs remained unmet in their communities, mental health care was a lower-ranking priority during the COVID-19 pandemic. One noted that “mental health had to take a second seat because their basic needs were not being met.” Another described that although mental health “maybe needed more,” other responsibilities took priority because the “importance of [mental health] was not there.” Additionally, one participant further addressed not just the need for mental health counseling services but the impact of the loss of services during the COVID-19 pandemic. She emphasized that these impacts were “more keenly” felt in rural areas due to baseline counseling resource limitations. Furthermore, one participant shared this perspective by noting the need for financial support for ongoing focus on parity in rural mental health care. Although this participant acknowledged the attention garnered by the COVID-19 pandemic for rural communities, she worried that the focus was waning too quickly.
In addition to mental health shortages, medical shortages were also prominent with rural clients. One participant, whose caseload was heavily comprised of transgender individuals, compared his experiences between metropolitan and rural areas, emphasizing the rural-specific difficulties for his clients. He went on to describe how the COVID-19 pandemic shutdowns led to a temporary loss of gender-affirming care in his community. He identified this experience as “particularly rough” for his clients who were “dealing with worrying about whether they would ever be able to access their gender-affirming health care or [have] it delayed a long time.” Limitations in resources for basic survival were also impacted during the COVID-19 pandemic, as one participant described the deepened scarcity of financial and housing assistance as well as food bank supplies. He went on to describe his community as “one of the poorest in Texas, where poverty is pronounced,” to emphasize the impact these resource shortages made in rural communities during this time.
In addition to health and other wellness services, internet connectivity deficits greatly impacted the ability for rural counselors to reach and provide services to rural clients. Nearly all participants identified geographical and/or financial barriers in rural communities obtaining internet connectivity necessary for everyday life during the COVID-19 pandemic. For those who could afford internet service, rural geography made consistent connectivity difficult. Some participants had to resort to primarily phone usage early in the COVID-19 pandemic. It was also noted that difficulties in connectivity impacted “already thin” mental health resources in rural communities and that “Wi-Fi is not as fast as it is in metro areas.” Even when some counselors attempted to have face-to-face services, they were met with difficulties in sustainability. In describing the changes to her private counseling practice, one participant described having to shutter her face-to-face business, which never rebounded after the period of shutdown between March and June 2020, and begin providing teletherapy only. This meant that there was one less in-person practice operating in a rural area where mental health resources were already limited.
Counselor Growth and Resilience
The theme of counselor growth and resilience was defined as rural counselors’ abilities to overcome significant adversities related to COVID-19 pandemic conditions in the context of their rural identification. Specifically, growth was defined as the ability to not only manage difficult circumstances but also to experience a change in themselves as an outcome of that experience. Resilience was defined as an ability to rebound or cope quickly in the face of adversity and, in the case of the COVID-19 pandemic, traumatic circumstances. Among the 11 participants, over half detailed a clear alignment between rural-specific deficits, as noted in the theme of systemic limitations, and the need to respond in resilient ways. Two participants, for example, adjusted quickly to phone counseling without face-to-face contact when rural internet connectivity and Wi-Fi availability fell short. Relatedly, another provided face-to-face services throughout the COVID-19 pandemic as the only practitioner in her area who could meet this need.
All participants described significant adverse experiences, up to and including vicarious trauma, but also an ability to cope with or make meaning of the circumstance. Collectively, participants leaned into their challenges, and many described a sense of empowerment in meeting them. For example, one participant, like most other counselors in this study, struggled significantly with the idea of teletherapy service delivery. She had difficulty adjusting treatment for her caseload, which included children coping with trauma and their families. Despite the stress described, she grew to enjoy meeting these new demands. She not only described that she “likes a challenge” but also discussed a process of using cognitive flexibility in providing herself “grace” and coping with the sudden need to learn a new skill set.
Although the ability to pivot typical practice styles during desperate times was a notable element of rural counselor growth and resiliency during the COVID-19 pandemic, so was the ability to alter beliefs and personal philosophies in order to adapt to changing times. Participants described a shift in viewpoints and flexibility to teletherapy as a modality. Although initially and fundamentally opposed to the practice, one participant reflected on the ability of professionals to shift their views. In speaking on the revolution of teletherapy in counseling, she stated that an in-person counseling modality is “not the only practice . . . we have to be flexible . . . we can’t be as old school anymore.” Similarly, another participant, also speaking on behalf of himself and rural mental health counselors, described a positive component of the pandemic: trying new things and learning that they are beneficial. He illustrated this by describing his “work–life balance” since his employers retained remote working allowances initially issued during lockdown and stay-at-home orders.
Participants illustrated cognitive flexibility in response to changes within their working world, but cognitive flexibility only represented part of the growth and resiliency among this sample. As depicted in the theme of systemic limitations, most participants provided services to clients with intensely limited resources, which naturally impacted how they typically provide counseling. In efforts to be therapeutic for his often crisis-affected clients, a participant noted that most of his work in the early months of the COVID-19 pandemic was “just letting people know that however they’re feeling is okay,” and further described, “I am good at remaining calm when the person in front of me is not . . . and appear to have at least a reasonably soothing presence.” Another participant closely mirrored these concepts in her statement that “it was, for me, a lot of just providing this space for people to have whatever feelings they had about it. And for that to be okay.” Additionally, two more participants reflected the change in focusing on immediate needs versus long-term or abstract concepts in counseling. Both described staying abreast of current events to help clients process their concerns.
As mentioned earlier, a majority of the participants noted a direct connection between rural-specific resource deprivation and the need to respond with resilience. Consequently, many participants found themselves becoming an integral part of resource seeking and attainment, which was described as a notable deviation from their typical counseling role. One participant described responding by actively providing help to clients who needed food when there were shortages due to already limited resource closures. She described this process as case management and assumed an active role in ensuring resources were obtained, including “trying to find people that could go pick up groceries and drop off at their porches.” Another similarly reflected that she did “a lot more social work . . . more connecting people with resources and that sort of thing.” She went on to note that as she adjusted her typical role from mental health counseling, the clients felt “cared for” and subsequently experienced a renewed encouragement to keep moving forward with counseling. Another participant additionally noted that gender-affirming care was already “quite difficult to find” in his rural community but became even more difficult to access due to the COVID-19 pandemic. In response, he sought out “updates through newsletters and Facebook connections with professionals” to ensure clients that the medical community was working to resolve the deficit. Collectively, these participant reports indicated that this sample of rural mental health counselors possessed the ability to shift their work and adapt to rapidly changing circumstances during the COVID-19 pandemic.
Discussion
The study explored the experiences of rural mental health counselors during the COVID-19 pandemic, revealing that participants experienced both preexisting and exacerbated systematic limitations in addition to growth and resilience during the early and more impactful phases. Systemic limitations identified by participants spanned the spectrum of human needs from food, financial, medical, transportation, and housing resources to a near absence of mental health services in their respective rural communities. Unique to rural counseling, the mass implementation of teletherapy was met with limitations involving lack of connectivity and financial means to remain online. For many participants, connectivity concerns have persisted. Unfortunately, the dearth of services for basic needs also meant an increase in the need for mental health services to cope with those hardships.
The descriptions of rural resource and funding deprivation extend and support the findings of the rural counselor hardships from other qualitative studies (Breen & Drew, 2012; Imig, 2014). The findings from this study show that despite nearly a decade, systemic changes that would otherwise bolster the quality of life or resource availability in rural communities have not been actualized. Naturally, this has created enhanced stressors for this sample of rural mental health counselors who perceived these otherwise typical limitations in their work as being grossly exacerbated during the COVID-19 pandemic.
The findings related to growth and resiliency in this study align with previous findings on counselors’ work in mass disasters (Lambert & Lawson, 2013). Most recently, Litam et al. (2021) found that counselor resiliency was associated with post-traumatic growth and compassion satisfaction, states that are in contrast with post-traumatic stress and compassion fatigue, which cause burnout. We suggest that finding one’s purpose is critical for growth, which aligns with the descriptions provided by this sample of participants. Much like the rural counselors in this study, Posluns and Gall (2020) found that maintaining awareness, finding balance, and having a flexible coping style were key to overcoming hardship. Additionally, Pow and Cashwell (2017) found that emotion-focused coping skills such as mindfulness and emotional regulation techniques were effective at mitigating the traumagenic effects of disaster work among a sample of disaster mental health counselors. The findings, combined with those on resilience practices in the current study, strongly support counselors and clients emphasizing a greater role in resilience and positive coping during disasters.
Participants also described resilience in the form of strong personal and professional support from family, friends, and colleagues, which validated findings that both personal and professional support were important for coping with adverse conditions and experiences during the COVID-19 pandemic (Aafjes-van Doorn et al., 2020). This finding is interesting in light of prior research showing that rural counselors experience isolation (Breen & Drew, 2012; Imig, 2014). They are, however, consistent with the findings of Wang et al. (2021), which showed that social connections helped rural individuals cope better than their urban counterparts during COVID-19, and Crumb et al. (2021), which indicated that social connection and rural community collaboration are helpful in coping after disaster.
Though not a theme that is uniquely tied to the rurality of the mental health counselor sample, it was evident that participants experienced intense levels of negative affect vicariously with their clients, especially during the earlier and more impactful parts of the COVID-19 pandemic. Such experiences included anxiety, uncertainty, depression, trauma, and helplessness. Findings from this study included echoes of prior research related to broader populations (Czeisler et al., 2020; Eisma et al., 2021; Elbogen et al., 2021; Prati & Mancini, 2021). In our study, these vicarious experiences intensified the natural occupational hazards (Lambert & Lawson, 2013; Litam et al., 2021) associated with professional health counseling practice and created a shared traumatic reality caused by mass disaster (Bell & Robinson, 2013). Additionally, uniquely rural hardships such as immense systemic limitations no doubt exacerbated these pandemic-related stressors as described by nearly all participants. This in turn necessitated the growth and resilience demonstrated by most of this sample in their descriptions of responding in creative and resilient ways.
Implications
Exploring the experiences of rural counselors during the COVID-19 pandemic reveals important training, clinical, and advocacy implications to consider. The findings emphasize the need for rural mental health counselors to adopt a more comprehensive approach that extends beyond traditional counseling roles. To effectively respond to sudden mass disasters or crises, like the COVID-19 pandemic, counselors must develop enhanced skills in case management, crisis intervention, referral coordination, and social service networking. Given the compounded challenges in rural settings, cultural competency training is vital for addressing the unique needs of these populations.
Mental health counselors should proactively familiarize themselves with available community resources and remain adaptable to extending services beyond conventional counseling modalities during crises. Counselors may consider expanding their training by attending workshops on advocacy and referral strategies and being more involved in networking with non-counseling resources within their clients’ communities. For those providing teletherapy services across their state or in several states, there are a few issues to consider. In addition to consulting and abiding by state laws related to interstate practice, mental health counselors should consider the location of their remote clients and at least generally link them to resources in their own communities.
Although teletherapy has proven beneficial, relying solely on virtual services is not a comprehensive solution for rural communities that lack consistent broadband access. Federal funding for increasing rural internet connectivity has been explored, as the National Telecommunication and Information Administration (n.d.) has allocated over a quarter of a million dollars to aid in increasing broadband accessibility in rural areas. However, until broadband for all is an established reality, continued advocacy is necessary to ensure rural connectivity remains a national priority.
Rural mental health counselors can further support rural clients by promoting culturally relevant resilience practices that emphasize mindfulness and emotional regulation (Pow & Cashwell, 2017) as well as self-awareness, balance, and cognitive flexibility (Posluns & Gall, 2020). For rural clients, aiding in establishing social support may better foster resilience development. Counselors can help rural clients explore, develop, and strengthen their involvement across multiple systems, including family, church, school, and the broader community to increase their capacity to cope with adversity. Further, counselors can help rural clients identify and leverage existing community strengths to mitigate the impact of resource limitations.
Advocacy and leadership are needed for promoting systemic change to drive policy and clinical practice shifts in the counseling profession (Lee & Rodgers, 2009). Advocacy efforts should prioritize systemic changes at local, state, and national levels that target funding allocations, service accessibility, and infrastructure development in rural areas. Addressing chronic resource limitations in rural areas involves advocating for increased mental health and medical funding, expanding access to basic needs, and sustaining broadband infrastructure initiatives. Prioritizing mental health care includes boosting resources, reducing stigma, and ensuring that mental health services are affordable and accessible. In these efforts, counselors can collaborate with community leaders, social service agencies, and advocacy organizations to elevate rural mental health priorities within broader policy discussions.
Finally, rural mental health counselors should recognize and enhance personal cultural strengths to overcome natural occupational hazards associated with counseling work as well as the enhanced challenges that coincide with rural practice. To maintain their own well-being amid ongoing crises, rural counselors should also engage in professional development that fosters their resilience. Implementing peer support programs, attending networking events, and participating in supervision groups can provide essential emotional support and guidance. Additionally, involvement in local, regional, and state counseling associations can further reinforce counselors’ sense of connection and reduce the isolation often associated with rural practice. This comprehensive approach will empower rural mental health counselors to better navigate the challenges they face and enhance their ability to support their clients.
Limitations and Future Research
Despite providing rich phenomenological data to understand the experiences of this sample during the COVID-19 pandemic and contributing to a relative paucity of research on this population, this study was not without limitations. Defining rurality is complex with no single definition capturing the multifaceted nature of such a culturally intricate group (Imig, 2014), and our study is no exception. For the purpose of generating accurate findings, a categorical and geographically based definition was selected. While the FORHP’s (2025) fiscal year 2022 classifications were used and represented an enhanced and more accurate definition of rural areas compared to previous definitions, it neglected to consider the descriptive or cultural aspects of rurality. Defining COVID-19 and its parameters was also a limitation. Participants, much like society, have navigated the uncertain, mutating, and episodic nature of viral outbreaks; therefore, it is difficult to define as either a historical or current event 4 years later. At the time of the study, however, participants largely viewed the most impactful degree of the COVID-19 pandemic as having occurred in earlier phases, which is helpful in ameliorating this limitation. Conversely, the length of time between the identified impactful phases in 2020 and interview time in 2022 is an additional limitation. With the passing of nearly 2 years, retrospective reflections may impact the accuracy of participants’ accounts of their experiences.
This study brings about several recommendations for future research. Future studies should continue to explore counselor experiences during mass and prolonged disasters. Despite being several years removed from the devastation of the COVID-19 pandemic, lessons of preparation and adaptability linger. In the last year, the United States has experienced Hurricane Helene in North Carolina and the Los Angeles wildfires, among hundreds of other disaster declarations (Federal Emergency Management Agency, n.d.). It is important to understand how counselors can care for their clients and themselves while navigating shared traumatic realities. Learning ways to foster resilience and post-traumatic growth is necessary to prevent counselor burnout and, ultimately, improve client care. For rural research specifically, replications of this study and related inquiries should continue to seek the most robust definition of culture; developing mixed methods approaches to capturing rurality would most likely overcome some limitations present herein. Rural cultural resilience should be a continued exploration, as much research has highlighted primarily barriers and challenges with less emphasis on resilience (Fruetel et al., 2022; Imig, 2014; Pullen & Oser, 2014; Slama, 2004; Sprang et al., 2007). Lastly, comparative analyses should be done in the future to further determine the uniqueness of rural counselor growth and resilience, as identified as a theme in this study.
Conclusion
The COVID-19 pandemic intensified mental health challenges in the United States, further straining an already overburdened health care system. Rural communities, which already experience fundamental disparities in resources and mental health care, were no exception. This study revealed both the struggles and resilience of rural mental health counselors in navigating the impacts of the COVID-19 pandemic in their communities. Identifying both exacerbated resource limitations and the need to cope and adapt with creativity and strength provides lessons for all counselors in the face of inevitable mass disasters. The findings underscore the importance of self-care, resilience-building, and leveraging community support during crises. Counselors should be well-versed in local resources and adopt broader roles. Given persistent disparities in rural health care access, ongoing advocacy remains essential.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Aafjes-van Doorn, K., Békés, V., Prout, T. A., & Hoffman, L. (2020). Psychotherapists’ vicarious traumatization during the COVID-19 pandemic. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S148–S150. https://doi.org/10.1037/tra0000868
Ando, H., Cousins, R., & Young, C. (2014). Achieving saturation in thematic analysis: Development and refinement of a codebook. Comprehensive Psychology, 3(4), 1–7. https://doi.org/10.2466/03.CP.3.4
Bell, C. H., & Robinson, E. H. (2013). Shared trauma in counseling: Information and implications for counselors. Journal of Mental Health Counseling, 35(4), 310–323. https://doi.org/10.17744/mehc.35.4.7v33258020948502
Breen, D. J., & Drew, D. L. (2012). Voices of rural counselors: Implications for counselor education and supervision. VISTAS Online, 1, 1–12. https://manifold.counseling.org/projects/vistas-online-2012/resource/voices-of-rural-counselors-implications-for-counselor-education-and-supervision
Burgoyne, N., & Cohn, A. S. (2020). Lessons from the transition to relational teletherapy during COVID-19. Family Process, 59(3), 974–988. https://doi.org/10.1111/famp.12589
Centers for Disease Control and Prevention. (n.d.). COVID-19 data tracker: Trends in United States COVID-19 deaths, emergency department (ED) visits, and test positivity by geographic area. https://covid.cdc.gov/covid-data-tracker/#trends_weeklydeaths_select_00
Clauss-Ehlers, C. S. (2008). Sociocultural factors, resilience, and coping: Support for a culturally sensitive measure of resilience. Journal of Applied Developmental Psychology, 29(3), 197–212. https://doi.org/10.1016/j.appdev.2008.02.004
Crumb, L., Appling, B., & Jones, S. (2021). Don’t wait, communicate: Rural school counselors and disaster mental health. Professional School Counseling, 25(1), 1–14. https://doi.org/10.1177/2156759X211023119
Czeisler, M. É., Lane, R. I., Petrosky, E., Wiley, J. F., Christensen, A., Njai, R., Weaver, M. D., Robbins, R., Facer-Childs, E. R., Barger, L. K., Czeisler, C. A., Howard, M. E., & Rajaratnam, S. M. W. (2020). Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24–30, 2020. Centers for Disease Control Morbidity and Mortality Weekly Report, 69(32), 1049–1057.
https://doi.org/10.15585/mmwr.mm6932a1
Eisma, M. C., Tamminga, A., Smid, G. E., & Boelen, P. A. (2021). Acute grief after deaths due to COVID-19, natural causes and unnatural causes: An empirical comparison. Journal of Affective Disorders, 278, 54–56. https://doi.org/10.1016/j.jad.2020.09.049
Elbogen, E. B., Lanier, M., Blakey, S. M., Wagner, H. R., & Tsai, J. (2021). Suicidal ideation and thoughts of self-harm during the COVID-19 pandemic: The role of COVID-19-related stress, social isolation, and financial strain. Depression and Anxiety, 38(7), 739–748. https://doi.org/10.1002/da.23162
Eryaman, M. Y., Koçer, Ö., Kana, F., & Şahin, E. Y. (2013). A transcendental phenomenological study of teachers’ self-efficacy experiences. Cadmo: Giornale Italiano di Pedagogia Sperimentale, 2, 9–33. https://doi.org/10.3280/cad2013-002002
Federal Emergency Management Agency. (n.d.). Disasters and other declarations. https://www.fema.gov/disaster/declarations
Friend, D. (2021, March 31). A timeline of Texas’ COVID-19 policies one year after “15 days to slow the Spread.” The Texan. https://thetexan.news/a-timeline-of-texas-covid-19-policies-one-year-after-15-days-to-slow-the-spread
Fruetel, K. M., Duckworth, R. C., Scott, S. L., & Fenderson, E. N. (2022). Exploring the experiences of counselors responding to crisis in rural communities. Journal of Rural Mental Health, 46(1), 40–49. https://doi.org/10.1037/rmh0000148
Guba, E. G., & Lincoln, Y. S. (1994). Competing paradigms in qualitative research. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research (1st ed.; pp. 105–117). SAGE.
Hall, E., Chai, W., & Albrecht, J. A. (2016). A qualitative phenomenological exploration of teachers’ experience with nutrition education. American Journal of Health Education, 47(3), 136–148. https://doi.org/10.1080/19325037.2016.1157532
Handley, T. E., Kay-Lambkin, F. J., Inder, K. J., Attia, J. R., Lewin, T. J., & Kelly, B. J. (2014). Feasibility of internet-delivered mental health treatments for rural populations. Social Psychiatry and Psychiatric Epidemiology, 49, 275–282. https://doi.org/10.1007/s00127-013-0708-9
Health Resources and Services Administration, Federal Office of Rural Health Policy. (2025). How we define rural. https://www.hrsa.gov/rural-health/about-us/definition/index.html
Henderson, K. A. (2011). Post-positivism and the pragmatics of leisure research. Leisure Sciences, 33(4), 341–346. https://doi.org/10.1080/01490400.2011.583166
Hoshmand, L. T. (1996). Cultural psychology as metatheory. Journal of Theoretical and Philosophical Psychology, 16(1), 30–48. https://doi.org/10.1037/h0091151
Imig, A. (2014). Small but mighty: Perspectives of rural mental health counselors. The Professional Counselor, 4(4), 404–412. https://doi.org/10.15241/aii.4.4.404
Lambert, S. F., & Lawson, G. (2013). Resilience of professional counselors following Hurricanes Katrina and Rita. Journal of Counseling & Development, 91(3), 261–268. https://doi.org/10.1002/j.1556-6676.2013.00094.x
Lee, C. C., & Rodgers, R. A. (2009). Counselor advocacy: Affecting systemic change in the public arena. Journal of Counseling & Development, 87(3), 284–287. https://doi.org/10.1002/j.1556-6678.2009.tb00108.x
Limón, E. (2020, December 18). Here’s how the COVID-19 pandemic has unfolded in Texas since March. The Texas Tribune. https://www.texastribune.org/2020/07/31/coronavirus-timeline-texas
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Litam, S. D. A., Ausloos, C. D., & Harrichand, J. J. S. (2021). Stress and resilience among professional counselors during the COVID-19 pandemic. Journal of Counseling & Development, 99(4), 384–395. https://doi.org/10.1002/jcad.12391
Maurya, R. K., Bruce, M. A., & Therthani, S. (2020). Counselors’ perceptions of distance counseling: A national survey. Journal of Asia Pacific Counseling, 10(2), 1–22. https://doi.org/10.18401/2020.10.2.3
Moustakas, C. E. (1994). Phenomenological research methods. SAGE.
National Telecommunication and Information Administration. (n.d.). Broadband infrastructure program.
https://www.ntia.gov/funding-programs/internet-all/broadband-infrastructure-program
Panchal, U., Salazar de Pablo, G., Franco, M., Moreno, C., Parellada, M., Arango, C., & Fusar-Pol, P. (2023). The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. European Child & Adolescent Psychiatry, 32, 1151–1177. https://doi.org/10.1007/s00787-021-01856-w
Pierce, B. S., Perrin, P. B., & McDonald, S. D. (2020). Demographic, organizational, and clinical practice predictors of U.S. psychologists’ use of telepsychology. Professional Psychology: Research and Practice, 51(2), 184–193. https://doi.org/10.1037/pro0000267
Pierce, B. S., Perrin, P. B., Tyler, C. M., McKee, G. B., & Watson, J. D. (2021). The COVID-19 telepsychology revolution: A national study of pandemic-based changes in U.S. mental health care delivery. American Psychologist, 76(1), 14–25. https://doi.org/10.1037/amp0000722
Posluns, K., & Gall, T. L. (2020). Dear mental health practitioners, take care of yourselves: A literature review on self-care. International Journal for the Advancement of Counselling, 42, 1–20. https://doi.org/10.1007/s10447-019-09382-w
Pow, A. M., & Cashwell, C. S. (2017). Posttraumatic stress disorder and emotion-focused coping among disaster mental health counselors. Journal of Counseling & Development, 95(3), 322–331. https://doi.org/10.1002/jcad.12146
Prati, G., & Mancini, A. D. (2021). The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychological Medicine, 51(2), 201–211. https://doi.org/10.1017/S0033291721000015
Pullen, E., & Oser, C. (2014). Barriers to substance abuse treatment in rural and urban communities: Counselor perspectives. Substance Use & Misuse, 49(7), 891–901. https://doi.org/10.3109/10826084.2014.891615
Slama, K. (2004). Rural culture is a diversity issue. Minnesota Psychologist, 9–13. https://www.apa.org/practice/programs/rural/rural-culture.pdf
Sprang, G., Clark, J. J., & Whitt-Woosley, A. (2007). Compassion fatigue, compassion satisfaction, and burnout: Factors impacting a professional’s quality of life. Journal of Loss and Trauma, 12(3), 259–280. https://doi.org/10.1080/15325020701238093
Tarlow, K. R., McCord, C. E., Yuxian, D., Hammett, J., & Wills, T. (2020). Rural mental health service utilization in a Texas telepsychology clinic. Journal of Clinical Psychology, 76(6), 1004–1014.
Wainberg, M. L., Scorza, P., Shultz, J. M., Helpman, L., Mootz, J. J., Johnson, K. A., Neria, Y., Bradford, J.-M. E., Oquendo, M. A., & Arbuckle, M. R. (2017). Challenges and opportunities in global mental health: A research-to-practice perspective. Current Psychiatry Reports, 19(28), 1–10.
https://doi.org/10.1007/s11920-017-0780-z
Wang, D., Chonody, J. M., Krase, K., & Luzuriaga, L. (2021). Coping with and adapting to COVID-19 in rural United States and Canada. Families in Society: The Journal of Contemporary Social Services, 102(1), 78–90. https://doi.org/10.1177/1044389420960985
Brandi M. Sawyer, PhD, NCC, LPC-S, is an assistant professor at Bellevue University. Edith Gonzalez, PhD, NCC, LPC, is an associate professor at the Hazelden Betty Ford Graduate School. Correspondence may be addressed to Brandi M. Sawyer, 1000 Galvin Rd. S., Bellevue, NE 68005, bsawyer@bellevue.edu.
Aug 26, 2025 | Volume 15 - Issue 3
Kathleen L. Grant, Alyson Pompeo-Fargnoli, Melissa A. Alvaré
The climate crisis is having a significant impact on development and wellness. Young adults face challenges that no earlier generation has experienced, impacting their path toward wellness and thriving. This hermeneutic phenomenological study endeavored to illuminate the experiences of a group of environmentally aware young adults through semi-structured interviews. Thematic analysis, analyzed through Arnett’s theory of emerging adulthood, illustrated participants’ experiences of fear for the future, anxiety, and loss; limited coping strategies for dealing with climate-related emotions; and a perceived tension between their desire to make life choices aligned with their environmental values and a financially stable career. Recommendations for counselors to best serve this population included increasing counselors’ mental health literacy, developing specific strategies to support resilience, and exploring counselors’ ethical responsibilities as advocates.
Keywords: climate crisis, young adults, phenomenological, environmental values, resilience
The climate crisis is expected to have a profound impact on human life in the 21st century (Wuebbles et al., 2017). Evidence of the changing environment is evident everywhere, including historic storms, catastrophic wildfires, record-breaking heatwaves, and severe droughts (Intergovernmental Panel on Climate Change [IPCC], 2023). Americans increasingly believe that the climate crisis is impacting their mental health, with 57.9% of 16–25-year-olds very or extremely worried about climate change, and 38.3% indicating that feelings about climate change negatively impact their daily life (Lewandowski et al., 2024). The consequences of the climate crisis are predicted to continue profoundly impacting mental health (Clayton et al., 2021; Hickman et al., 2021; Sturm et al., 2020).
Definition of the Climate Crisis
The climate crisis poses a significant threat to the future of human civilization. Each day, millions of tons of man-made greenhouse gases, including carbon dioxide (CO2) and methane, are released into the atmosphere (Wuebbles et al., 2017). Burning fossil fuels, such as oil and natural gas, to fuel modern lifestyles is one of the most significant sources of pollution that contributes to global warming (IPCC, 2023). As greenhouse gas emissions rise, global temperatures exhibit a corresponding increase, leading to sea level rise, heat waves, floods, droughts, and severe storms (IPCC, 2023). In 2014, the United States Department of Defense reported that climate change “will likely lead to food and water shortages, pandemic disease, disputes over refugees and resources, and destruction by natural disasters in regions across the globe” (Banusiewicz, 2014, para. 3). By 2050, anywhere from 200 million to 1 billion people will be displaced from their homes, communities, and possibly countries because of climate-related events such as extreme heat, flooding, and famine (IPCC, 2023). For over three decades, the scientific community has warned of the grave danger of global warming and climate change (Borenstein, 2022). Despite the dire warnings, global greenhouse gas emissions continue to increase (World Meteorological Organization, 2020). Young adults are inheriting a world full of unprecedented and complex challenges (Hickman et al., 2021).
Impact of the Climate Crisis on Young Adults
A growing body of literature is documenting the impact of the climate crisis on mental health and wellness, particularly among young people and young adults (Clayton et al., 2021; Hart et al., 2014; Hickman et al., 2021; Sturm et al., 2020). Youth, as defined by the United Nations, encompasses individuals aged 15–24, although this definition may vary (United Nations, 2025). This age range also consists of those emerging adults in the unique developmental period of transitioning from adolescence to adulthood (Arnett, 2000). According to a large study (N = 10,000) published in The Lancet, 77% of young people (aged 16–25) surveyed reported that they think the future is frightening, and 45% indicated that their feelings about climate change had a negative impact on their daily lives (Hickman et al., 2021). Research illuminates how experiencing the direct impact of climate change, such as exposure to wildfires, floods, and displacement, can lead to acute anxiety-related responses and chronic and severe mental health disorders (Clayton et al., 2021; Watts et al., 2015).
Climate change and related disasters can cause direct anxiety-related responses and chronic and severe mental health disorders (Pihkala, 2020). A 2018 meta-analysis found an increased incidence of psychiatric disorders and psychological distress in populations exposed to environmental disaster (Beaglehole et al., 2018). Flooding and prolonged droughts have been associated with elevated anxiety levels, depression, and post-traumatic stress disorders (Hickman et al., 2021). Even among members of the population who have not been directly exposed to the impacts of climate change, such as environmental-related disasters, a simple awareness of the problem may evoke feelings of anger, powerlessness, fear, and exhaustion (Moser, 2007).
Emerging research has highlighted the mental health impact of the indirect effects of the climate crisis, such as climate anxiety (Clayton et al., 2021; Hickman et al., 2021; IPCC 2023). Climate anxiety is a response to the current and future threats of a warming planet (Clayton et al., 2021; Hickman et al., 2021). The associated feelings can include grief, fear, anger, worry, guilt, shame, and despair (Clayton et al., 2021; Doherty & Clayton, 2011). It is essential to acknowledge that scholars recognize anxiety as a natural condition of living and acknowledge its potential benefits, as it can motivate individuals to take action and effect change (Hickman et al., 2021). Climate anxiety, although it can be a complex and intense experience, can also be viewed as a congruent response to the dangers and challenges that global citizens will face now and in the future (Hickman et al., 2021).
Young people with marginalized identities will face the most devastating impacts of climate change (Watts et al., 2015). Low-income and Black, Indigenous, and other communities of color are often the most vulnerable to the worst impacts of climate change, such as flooding, drought, fire, and extreme heat (IPCC, 2023). Furthermore, because of intersectional marginalization, some individuals will be at even greater risk for severe impacts and negative mental health consequences (Hayes et al., 2018). Marginalized communities may lack access to mental health resources after traumatic weather-related events or to process the ongoing challenges associated with climate change (Hilert, 2021). The cultural stigma that reduces help-seeking behavior and lack of access to mental health services may also lead marginalized groups to suffer more from poor mental health outcomes (Priebe et al., 2012).
Research indicates that young people are particularly vulnerable to the adverse effects of climate change, largely because of their ongoing physical and mental development, their dependency on adults, and their likelihood of repeated exposure to climate-related events over time (Hart et al., 2014). However, there is a need for more research on the impact of climate change on mental health, especially as it impacts young people (Hickman et al., 2021). The counseling literature has a paucity of studies in this area (Hilert, 2021; Mongonia, 2022). As the impacts of the climate crisis continue to grow more severe, the profession must deepen its understanding of the climate crisis’s effects on young adults and explore paths toward resilience and wellness (Hickman et al., 2021).
Climate-Aware Counselors
There is a growing need for counselors who are aware of and trained in the mental health impacts of the climate crisis, including climate anxiety (Hilert, 2021). This form of counselor competency includes identifying clients who are experiencing climate-based distress and anxiety (Mongonia, 2022). Although climate anxiety has yet to receive a formal classification in the Diagnostic and Statistical Manual of Mental Disorders (DSM), it is well accepted by counselors as a fear of impending environmental collapse that elicits strong and sometimes debilitating anxiety (Thomas & Benoit, 2022). Counselors must be able to assess and understand how to treat those who present with clinically significant levels of climate anxiety that interfere with functioning and developmental tasks (Pihkala, 2020). Treatment modalities often include teaching resilience and coping skills and increasing support systems (Baudon & Jachens, 2021). Counselors are called upon to support not only their clients through their environmental action but also to take action themselves (Thomas & Benoit, 2022).
Environmental Action
One intervention that can promote positive mental health outcomes for young adults concerned about the climate crisis is climate activism or sustained efforts to effect positive change (Gislason et al., 2021). Young people have been at the forefront of creating new U.S. climate policy (see Sunrise Movement; Bauck, 2022) and driving action (Rashid, 2023). Climate action can positively bring about necessary social change and provide mental health benefits (Hart et al., 2014). Research suggests that young people engaged in climate action experience several benefits, including increased resilience, agency, a sense of purpose, and community, all of which support positive mental health outcomes (Gislason et al., 2021). However, focusing on the climate crisis can also expose individuals to difficult feelings, such as fear, sadness, loss, and hopelessness (Hickman et al., 2021). It is common for people to employ defense mechanisms, such as denial and minimization, to maintain more positive feelings and a more optimistic view of the future in response to the realities of a changing world (Doherty & Clayton, 2011).
Environmentally Aware Young People
Environmental awareness can be broadly characterized as a level of consciousness concerning the importance of the natural environment and the impact of humans’ behavior on it (Ham et al., 2016). Environmental awareness often leads to a deeper understanding of the severity of climate change and the urgency to address it (Orunbode et al., 2019). Youth awareness of the climate crisis is associated with a range of emotional and mental health impacts, such as climate anxiety and feelings of grief, loss, anger, guilt, and existential dread (Hickman et al., 2021). However, environmental awareness can also lead to increased action, a sense of purpose, and resilience building (Clayton et al., 2021).
In the 2024 American Climate Perspectives Survey, Americans aged 18–24 reported the highest levels of environmental concern among all age groups (over 80%; Speiser & Ishaq, 2024). Concern over the environment drives some young adults to action, but not all. Scholars suggest that to prevent the most severe consequences of climate change, humans must take action and alter their ways of life (IPCC, 2023; Wuebbles et al., 2017). Environmental awareness and action will be increasingly important as the impact of the climate crisis grows more pervasive and severe (IPCC, 2023). Young adults, in particular, may need to take steps to adapt to the rapidly changing planet. This study involves young people who are aware of the climate crisis, are motivated to act, and have taken a step toward creating change.
Aims of Study
This study focuses on the experiences of U.S.-based environmentally aware young adults who are moved to take action, aiming to understand their lived experiences as they transition from adolescence into adulthood. This is a significant period in life, as many young people are culminating their educational experiences and choosing who they want to be as adults, both personally and professionally (Arnett, 2014). The research questions guiding this study are: What are the lived experiences of environmentally aware young people as they transition to adulthood? How have their experiences impacted their mental health and understanding of themselves and their roles? How are their environmental experiences influencing their actions and aspirations for their futures (e.g., familial and career goals)?
Method
Hermeneutic phenomenology is a constructivist approach that scrutinizes individuals’ subjective experiences and their interpretations of those experiences, asking “what is the nature of this experience from the individual’s perspective?” (Moustakas, 1994; Ramsook, 2018). The study focused on interpreting the meaning of the lived experiences of the participants, which is crucial given that the experience of entering adulthood during the climate crisis is novel and new structures to understand the nature of this experience may be necessary. Climate engagement for emerging adults involves layered emotions, developmental stage influences, and societal pressures (Arnett, 2010; Clayton et al., 2021; Ogunbode et al., 2019). Hermeneutic phenomenology is well suited to context-rich experiences that cannot be separated from the social, political, and developmental realities in which they occur (Ramsook, 2018; van Manen, 1997). This method enabled us to explore not only what the participants said, but also how they understood themselves in this particular life stage.
Theoretical Framework
Arnett’s developmental theory of emerging adulthood provided the framework for this study. According to this theory, between the ages of 18 and 29, young people consolidate their identity and explore career paths (Arnett, 2000, 2014). This is a time of possibility, in which multiple futures are open, and instability, as individuals transition from the structure provided by their family of origin and formal education and endeavor to make career and personal choices aligned with their values and aspirations (Arnett, 2000). Social and cultural factors also influence young people as they crystallize their identities and career paths (Arnett, 2010). This theory was selected because we were interested in the dynamic interactions among experiences, emotions, and actions within a critical developmental period and how these factors shape participants. Arnett’s theory and hermeneutic phenomenology both emphasize process, interpretation, and the evolving nature of identity within a specific context.
Participants
Twelve interviewees, aged 20 to 25, participated in this research. All participants viewed climate change as an important issue and engaged in environmental action, although their methods for addressing it varied. There were seven female and five male interviewees. The majority identified as non-Hispanic White Americans, but two individuals described multiracial identities: one as South Asian and White, and the other as Asian Pacific Islander and White. All but one of the 12 participants were from a middle-class background; one described growing up in a working-class family. Eight participants were residents of New Jersey or Pennsylvania at the time of data collection, while the other four were residents of New Mexico, Colorado, Texas, and Washington, D.C.
Data Collection
To be included in this study, participants had to be aged 18–25, view climate change as an important issue, have actively engaged in some form of environmental action for at least 6 months, reside in the United States, be able to communicate in English, and consent to participate in an audio-recorded interview lasting 60–90 minutes. Following IRB approval, we contacted key informants—academics in the climate movement who are recognized as leaders because of the reach of their speaking engagements and publications, and with whom we (Kathleen L. Grant and Melissa A. Alvaré) had a prior relationship—to recommend individuals who met the selection criteria. We also utilized social media platforms, including Facebook and Instagram, and posted an IRB-approved recruitment flyer on our personal and publicly accessible sites. Snowball sampling was used, as several respondents recommended their peers for interviews. Recruitment emails described the research study, detailed the interview procedures, and invited people to contact us if they were interested in participating. Once individuals responded to these emails, they were screened to see if they met the inclusion criteria. If so, they were asked to read and sign an informed consent document and complete a demographic questionnaire before scheduling the interview.
Interview questions were designed to elicit rich descriptions of participants’ lived experiences and perspectives. We utilized Arnett’s theory of emerging adulthood, specifically the five features of identity exploration, instability, self-focus, feeling in between, and possibilities/optimism, and considered how these factors would appear in climate awareness and action (Arnett, 2010, 2014). We drew from the existing literature to develop our initial interview guide, first drafting broad, open-ended domains. Then, we met to revise them with a critical eye, working to ensure that we were not asking leading questions or probes that were overly influenced by our own biases and expectations. Taking a phenomenological approach, we also ensured that our questions were crafted to go beyond eliciting descriptions to allow us to explore the meanings participants attached to phenomena of interest (e.g., climate change and career trajectories). We then sent a draft of our interview instrument to a renowned scholar in the field of climate justice, who made recommendations for further revisions.
All interviews were conducted and recorded over Zoom by one of the three authors. In line with the phenomenological tradition and our intentions to explore topics introduced by participants, we used semi-structured interviews. The semi-structured format promoted fluidity, allowing the informal dialogue to emerge and take unexpected directions, as respondents could discuss the topics most meaningful to them (Hesse-Biber & Leavy, 2010). The interview guide included questions such as: “How has learning about the environment impacted you personally, if at all?” “Has your environmental awareness had any impact on your life goals and/or career plans?” “When you think about the future, what feelings come up for you?” and “How, if at all, do you think you have changed as a result of your involvement in environmental action?”
We asked follow-up questions based on participants’ responses and probed—when appropriate—to gain clarity and delve deeper into their experiences and viewpoints. Interviews ranged from 55 to 75 minutes in length, and participants received $15 gift cards as compensation for their time and participation. The audio files from the recorded Zoom videos were sent to a professional transcription service.
Analysis
Given our hermeneutic phenomenological design, the analysis followed van Manen’s (1997) approach, which involves a cyclical process of reading, reflecting, and writing to uncover thematic structures. Researchers (a) turn to the nature of lived experience, (b) investigate experiences as lived, (c) engage in hermeneutic phenomenological reflection, (d) engage in hermeneutic phenomenological writing, (e) maintain a robust and oriented relation, and (f) balance the research while exploring the parts and whole (van Manen, 1997, pp. 30–31). As Starks and Trinidad (2007) wrote, in coding data from phenomenological inquiries, “specific statements are analyzed and categorized into clusters of meaning” with close attention to “descriptions of what was experienced as well as how it was experienced” (pp. 1375–1376). Transcripts were divided among us for an initial pre-coding of each interview. We each engaged in preliminary note-taking, marking repeated phrases and themes, and memo writing on potential codes and sub-codes during this stage. We then met to discuss initial interpretations of interviews, emergent themes, and perceptions of the powerful and insightful stories shared by participants. At that time, we also devised an initial inductive code and created a codebook and color scheme for the next coding round. We then re-divided the transcripts and each coded four transcripts in shared Microsoft Word documents. Once all 12 interviews were coded, we met again to discuss our analyses and refine and collapse codes. We repeated this process with each reading, using four new transcripts to examine our coding processes and contribute to our analyses with the new code list and interpretations of the data.
Trustworthiness
Our research team consisted of two counselor educators and one sociologist. We identify as White, middle and upper–middle-class women, aged 35–45, with shared concerns about the climate crisis. We engaged in ongoing discussions about how our social positions, interests, and privileges influenced all phases of the research process.
Trustworthiness was established primarily through prolonged engagement, critical reflexivity, and peer debriefing. We reviewed the audio recordings and transcripts for months. Both listening to the participants’ voices in the audio recordings of interviews and prolonged engagement with the transcripts is crucial for establishing trustworthiness, as it enables the researcher to see the world from each participant’s perspective and pick up on the richness and nuance of the narratives and ensures a thorough understanding of the participants’ statements, all of which are essential for phenomenological analyses (Moustakas, 1994). We were committed to maintaining an open stance and curiosity toward participants’ experiences. Each member of the team engaged in memo writing to document our emerging interpretations and consider how personal preconceptions and backgrounds might be influencing our interpretations. These memos were shared among the team and served as starting points for critical dialogue. We responded to each other’s memos, posing alternative perspectives and challenging probes to push one another to examine how personal biases might be shaping interpretations of the data. We also met regularly to engage in reflexive practice, unpacking the data collectively, scrutinizing our codes and emerging themes, seeking data that did not support the themes that were emerging, and interrogating how personal expectations and life experiences could be influencing our analyses. Whenever we found inconsistencies in our interpretations and/or data categorization schemes, we conducted thorough discussions to reach a consensus and ensure a uniform coding process.
Findings
This study aimed to gain a deeper understanding of the experiences of young adults engaged in environmental action during the transition from late adolescence to early adulthood. In particular, this study focused on the impact of environmental awareness and action on the participants’ development, personally and professionally, as they transition into adulthood. Through a hermeneutic phenomenological analysis of the 12 in-depth interviews, three key themes emerged from the participants’ narratives: 1) Fear for the Future, Anxiety, and Loss; 2) Limited Coping Strategies;
and 3) Tension Between Making a Difference and Making a Living.
Fear for the Future, Anxiety, and Loss
The environmentally aware participants expressed fear for the future, anxiety, and loss throughout their narratives. Most discussed pervasive anxiety and fear for the future related to the climate crisis. In contrast, other participants were triggered by specific situations, such as a severe weather-related event (locally or globally) or a climate change–related news item (i.e., the release of a UN report on the climate crisis). One participant, Theodora, also reflected on the present-day harm that communities are experiencing: “And it’s here right now, and increased natural disasters are not a future thing; they’re happening. . . . It’s definitely impacted my mental health.” Mary discussed how the climate crisis is causing a “collective trauma” in her generation. She said, “I think it’s really impacting everybody because individual action feels so futile. I think we’re just feeling really lost.” Many of the participants discussed a fear for their future as adults.
The participants specifically shared their fears about the future in light of the climate crisis. They raised questions about where they will live, whether they should have children, and the state of the planet. Brianna stated that it is a “daunting and terrifying idea, if we don’t start to get it [global warming] worked out, just how much of an impact it can have on our future.” Amy stated, “I could say that the climate crisis has negatively impacted mental health . . . [I experience] anxiety and worry about the state of the planet, now and in the future.” Briana described:
It’s pretty hard to feel hopeful, especially since all of us live here in Colorado now, where fires are a big problem and stuff like that. We often have conversations where we’re like, “So the West is going to be on fire, and the Southwest won’t have water, and the coastlines are going to be flooded. Where can we live?”
Three participants (25%) discussed, without specific prompting, whether or not to have a child, as the climate crisis would profoundly impact their child’s life. Nancy stated, “I feel like my generation . . . is not the biggest about having kids. . . . There’s not going to be a good place for us to live.”
Several participants used the terms eco-anxiety and climate grief to discuss their emotional experiences related to climate change. Nancy indicated that reports of natural disasters trigger her eco-anxiety, and Carol stated that she started psychiatric medication partly because of her eco-anxiety. Evan discussed his feelings of climate grief, helplessness, and powerlessness.
Limited Coping Strategies
The participants discussed various coping strategies for dealing with their intense climate-related emotions. The main strategies were adopting a positive mindset and ignoring or withdrawing from climate information/action. These two strategies are discussed below, after which the remaining strategies are briefly discussed.
The majority of the participants discussed choosing to stay optimistic about the future as a coping strategy. They discussed thinking about all the people, including themselves, who are engaged in climate action to make a difference. Alex discussed guarding against negative feelings by avoiding getting “too down on myself” or adopting “too negative of an outlook” and engaging in individual action as a coping strategy. Participants elaborated on the challenges they faced in maintaining a positive perspective, especially as they age and see an increasing number of negative climate-related events. Jackson stated that it is “more and more of a struggle” to maintain a positive attitude and be motivated to take climate action.
Participants also shared examples of ignoring or withdrawing from climate-related information or action as a means of coping with negative feelings or protecting themselves. Daniel stated, “I have taken an approach of doing the most that I can in my community while choosing to stay a little ignorant on what’s happening globally.” Sarina shared, “I felt pretty stressed and sort of want . . . to give up on trying to help environmental problems because a lot of them are so far gone that it can be pretty discouraging to read about.” Mary elaborated on her emotional experience:
And it almost teaches you, I’ve found, not to feel your feelings. So in a sense, I find myself becoming more apathetic because you’re desensitized to it. You’re seeing it all the time, but you can’t feel it all the time because no one wants to stare into the impending doom of environmental decay or whatever.
Three of the participants discussed connecting with their community as a means to address their fears and concerns about the climate crisis. All three of these participants reported connecting with others who are environmentally minded or engaged in climate action. One participant discussed therapy as a strategy: “I do see a therapist occasionally. . . . She’s not trained on the eco-side of things. So she tries to understand and gets tools and whatnot, but definitely, it’s not her main area of concern. But she’s been helpful anyways.”
Two participants discussed being in nature, specifically hiking, as a coping mechanism. Mary stated, “Life outside and living a life that is environmentally based actually brings me a lot of joy, and that component of it doesn’t stress me out and give me anxiety.” Sarina shared that she does not have a clear coping strategy:
So even though me and my friends . . . are people who are trying to work towards improving things, I would say we all can feel pretty hopeless about the situation, especially [when] the current government-level response is not very strong. . . . I want to be hopeful, but I would say from a scientific perspective, it can also be pretty hard to feel hopeful for the future. Yeah, I don’t really have an answer. . . . it can be pretty overwhelming, and you just kind of have to try to think about something else. Because I guess I can remind myself I’m already working to try to increase knowledge, and that’s useful. So, I guess I’m playing some positive part, and so I can try to relieve myself with that information. But yeah, I guess I don’t really have a good way to feel better about it.
Tension Between Making a Difference and Making a Living
The participants in this study were all in a transition period between adolescence and adulthood. In their narratives, many of the participants (n = 7) expressed the tensions between their environmentally based values and the need for a job that would provide economic security. These tensions emerged as the participants struggled to make choices congruent with their stated values and career choices that might have long-term impacts, both individually and for their communities.
The role of money and financial stability was not directly probed for in the interview protocol; however, participants often brought it up when asked what prevents them from engaging in environmental action. Jackson stated, “You can either pursue this as a passion and as an ideal and as a thing to do, or you can . . . make money and have a stable life.” He went on to state:
And so I grew up with a lot of that type of thinking, of like, eventually, you’re going to have to kind of settle your own goals and ideals in order to survive in the world on your own and provide safety nets to your family later on. And so I always kind of grew with that . . . in the back of my mind, and that became more present in college. . . . I think those have been the biggest kind of like detractors . . . like “You have to choose one or the other.” Like, they [parents] weren’t necessarily discouraging my passion or any of that, they were just kind of like, “It’s one or the other.” Most people fall for the latter, and that’s kind of why we have the issues in the first place.
Evan discussed grappling with either getting paid with a traditional job or engaging in more meaningful environmental activism on a volunteer basis. He shared:
I guess, unfortunately, money is a factor. I found more ways to get paid for teaching than for volunteering my time. You have to think about, “What’s the balance of that going to be?” I need to be able to support myself, and so when I can, I will dedicate time to being active in my community and engaging with environmental issues. So, finding a balance.
Brianna, who was in law school studying environmental law, discussed the tension as she sees it:
Society . . . pins people against environmental work because it’s not lucrative, or they paint it not to be lucrative because I think people can make a decent living and know that they’re doing something beneficial. But I would say that there’s still a stigma in society just surrounding environmental work, and that if you want to make money and you want to live decently, that’s not the field to go into. I fully don’t believe in that anymore, but I think that that played a role in my choices.
Although most participants indicated that financially providing for themselves was a significant detractor from an environmentally focused career, several participants had alternative narratives. Amy, an environmental educator at a nonprofit land trust, discussed the importance of taking time in college to discover her identity and selecting a career aligned with her values, even if it was not financially lucrative. However, her financial realities were still infused into her thinking, reflected by her parents’ repeated refrain: “My parents, from day one, always said, ‘Pursue your passion, do what you love, and the money will come.’” Other participants were exploring careers in academia and research as methods to bring about change and did not mention finances as an impediment to an environmentally oriented career.
Discussion
This study aimed to gain insight into the lived experiences of environmentally aware individuals as they transition from adolescence into adulthood. Specifically, Arnett’s developmental theory of emerging adulthood was utilized to frame these experiences, as it considers the dynamic interactions among experiences, emotions, and actions within this critical developmental period between adolescence and adulthood (Arnett, 2000). In particular, Arnett’s theory provides insight into the tension and instability that young adults experience during this transition, particularly in terms of identity, career, and emotional development.
Three main themes emerged from the participants’ narratives, including feelings of fear for the future, anxiety, and loss; limited coping strategies; and tension between making a living and making a difference. Each participant described fear for the future, anxiety, and loss. These findings align with past research exploring mental health concerning the climate crisis (Gislason et al., 2021; Hickman et al., 2021; Ojala et al., 2021; Sanson et al., 2019). The depth and breadth of the participants’ descriptions of fear and anxiety suggest that thoughts, feelings, and experiences around the climate crisis impact their daily lives. Some participants reported powerful emotional responses to negative news about the climate. They were pondering significant life choices because of the climate crisis (e.g., questions about where to live and whether to have children). As previous researchers have suggested, these responses appear appropriate given the realities of the climate crisis and the expected impact it will have on their lives and those of future generations (Hickman et al., 2021). However, although participants expressed and communicated these fears and anxieties, few seemed to have comprehensive structures (psychological, behavioral, or relational) to act on their pervasive and legitimate concerns. Participants often managed complex feelings and plans independently in the absence of communities informed about their fears and realities for the future, which could help them navigate the challenges and possibilities of a life and a future heavily impacted by the climate crisis.
Although all participants experienced a range of emotional reactions to the climate crisis, they also employed various strategies to manage their feelings. The participants generally appeared to have limited strategies for dealing with challenging climate-related feelings. Most of the strategies were individualistic, and young people had to figure out how to manage their deep and complex emotions independently. Several participants discussed being optimistic as a coping strategy but also voiced that this strategy is ineffective and exhausting. Although keeping a positive attitude in the face of adversity can be beneficial, doing so without acknowledging or feeling the vast array of emotions associated with the climate crisis and their fear for their futures may be ineffective. This finding aligns with the conclusions of Hickman et al. (2021), which demonstrate that young people are facing unique stressors arising from the climate crisis that can impact their development.
Several participants discussed ignoring aspects of the climate crisis or the climate crisis itself to protect themselves. Denial is a common psychological defense to reduce climate-related distress (Doherty & Clayton, 2011). Participants noted that they disengaged from environmental action to avoid challenging feelings related to climate change. These individuals may benefit from positive strategies to manage their emotions, allowing them to take care of themselves and continue to be active citizens working toward change. Finally, participants shared coping strategies, including spending time in nature and engaging in therapy, as strategies to support their mental health. Participants also engaged with environmental communities as a coping strategy, which can be a significant influence during such a developmental period. Social and cultural factors have been shown to influence young people during the development of emerging adulthood as they crystallize their identities and career paths (Arnett, 2010). As the future will include increasingly complex and challenging climate crisis–related issues, individuals in this study may benefit from additional coping strategies, which will be further discussed in the Implications for Counseling section.
The final theme illuminated by the participants is the tension between making a difference and making a living. Participants discussed the challenges inherent in creating environmental change, often in low-paying or volunteer capacities, and the desire to support themselves financially. Although the participants were interested in environmental action, both professionally and personally, they often struggled to create a life in adulthood where they could enact their values. Participants described examples of their engagement in environmental causes in high school and college but had a more challenging time maintaining action as they transitioned to adulthood. Although part of the challenge seemed to be the lack of clear, viable paths for the participants to engage in environmental action and careers as adults, financial realities also shaped their choices. Participants viewed jobs in the environmental sector as less lucrative than others, and they would not be able to support themselves or their future families on this salary, especially if they wished to maintain the same socioeconomic level as they were offered. Additionally, the participants saw this tension as a dichotomy; they could either have a well-paying career or engage in environmental action.
Implications for Counseling
Young adults are increasingly experiencing mental health impacts of the climate crisis (Hickman et al., 2021). This study offers insight into the developmental and emotional experiences of young adult participants as they navigate the transition to adulthood, exploring how to make sense of their environmental concerns and act to create change. Counselors, including school counselors, college counselors, career counselors, and clinical mental health counselors, can play a crucial role in supporting mental health and wellness in the context of the climate crisis. Both the National Board for Certified Counselors (NBCC; 2025) and the American Counseling Association (ACA; Sturm et al., 2020) have issued statements emphasizing the need for counselors to advocate for climate action and educate themselves and others on the mental health implications of climate change.
The findings of the current study support the need for counseling services because of climate change impacts on mental health. Findings reveal that participants were experiencing challenging emotions related to the climate crisis and had limited strategies to cope with the changing world. Three implications for counseling are discussed below: increasing counselors’ climate change mental health literacy, supporting resilience, and the ethical responsibility of counselors as advocates.
Recommendation 1: Increase Counselors’ Climate Change Mental Health Literacy
Counselors must practice “within the boundaries of their competence, based on their education, training, supervised experience, state and national professional credentials, and appropriate professional experience” (ACA, 2014, Section C.2.a.). Many counselor education training programs do not cover the unique experiences and challenges individuals face because of the climate crisis, resulting in a void in counselor education training (Heiman, 2024; Hilert, 2021). Therefore, to ethically assist clients with this need, counselors must continue their education and, where necessary, seek additional supervision to treat this population. As a first step, counselors can consider learning more about the nature of the climate crisis, including the impacts on future generations (Doherty & Clayton, 2011). Publications such as the American Psychological Association’s 2021 report, Mental Health and Our Changing Climate: Impacts, Inequities, and Responses (Clayton et al., 2021), provide a comprehensive overview of the nature of the climate crisis and strategies for mental health practitioners. Counselors can also seek support, training, and consultation through membership in the Climate Psychology Alliance of North America, a community of mental health professionals who educate climate-aware practitioners (https://www.climatepsychology.us).
Participants in this study noted that their mental health practitioners were not adept at addressing their climate anxiety and trauma in sessions. Individuals may not directly broach the topics of climate anxiety, eco-grief, and weather-related PTSD; therefore, counselors must address these topics directly with clients. Climate-aware counselors must facilitate the expression of clients’ emotions about the climate crisis and help them further explore and articulate their experiences (Doherty & Clayton, 2011). Counselors can consider using interventions that facilitate emotional expression and create opportunities for adaptive behaviors (Doherty & Clayton, 2011). Interventions can also include existential therapy, particularly exploring how to find meaning, peace, joy, and hope in the face of ecological collapse and climate-related disasters (Barry, 2022; Frankl, 2006). Finally, eco-therapy is a promising modality for clients that centers healing through nurturing a stronger relationship with nature and the physical environment (Delaney, 2019). As such, it is recommended that counselors expand their knowledge of the climate crisis and its impact on mental health to serve their clients better as well as any supervisees.
Recommendation 2: Supporting Young Adult and Client Resilience
This study found that participants lacked comprehensive structures to address their climate anxiety and fears about the future. Many participants felt overwhelmed by the climate crisis, which impacted their ability to take action in the climate movement. As a coping strategy to protect themselves from difficult feelings associated with climate change, some participants withdrew from climate information or action. As challenging weather-related events and the impact of the climate crisis are expected to increase in the coming years, young adults must develop both internal and external resources to survive and thrive in a changing world (Gislason et al., 2021).
Fostering resilience is an effective strategy for supporting the mental health and well-being of young adults, including those affected by the climate crisis (Clayton et al., 2021). Resilience can be fostered through the development of both internal and external resources, and counselors can play a crucial role in this process. Internal resources can include increasing self-efficacy or young adults’ belief in their ability to overcome the stress and trauma associated with climate change. Research suggests that those who believe in their ability to withstand the challenges associated with climate change have more positive psychological outcomes than those with lower self-efficacy (Clayton et al., 2021). Belief in one’s resilience is also correlated with fewer symptoms of depression and PTSD after natural disasters (Ogunbode et al., 2019).
Counselors can support young adults in developing external resources that enhance resilience, such as fostering social connections. Social connections to peers and those of different generations can be a vital source of emotional, informational, logistical, and spiritual support (Center for the Study of Social Policy, 2019). Individuals’ ability to withstand trauma and adversity increases when they are connected to strong social networks (Clayton et al., 2021).
Finally, this study found that participants did not have clear paths to enact their environmental values in their adult lives. They faced financial and cultural pressures to choose careers that would allow them to make a living. Although this study highlights that some participants may not have had the internal and external resources to cope with the emotional stressors of engaging in climate-related work, a viable career or civic path was elusive. All counselors who work with young adults, especially school and career counselors, have the opportunity to provide resources about the wide array of jobs available in the green economy, as well as methods to include civic involvement (i.e., participation on local environmental commissions, participation in activist groups, leadership in local government advocating for green policies) when planning one’s adult life. Models of adults who engage in environmental action, both personally and professionally, must be provided to young people as examples of possible paths in adulthood. As taking action is seen to have numerous mental health benefits, specifically as it builds agency, counselors must support clients in developing the attitudes, skills, and behaviors necessary to engage in activism and advocacy (Gislason et al., 2021; Sanson et al., 2019).
Recommendation 3: Ethical Responsibility of Counselors as Climate Advocates
Counselors are ethically responsible for advocating for the well-being of their clients, as stated in the ACA Code of Ethics (2014): “When appropriate, counselors advocate at individual, group, institutional, and societal levels to address potential barriers and obstacles that inhibit access and/or the growth and development of clients” (Section A.7.a.). The climate crisis is and will continue to significantly negatively impact the growth and development of clients, with young clients and clients from historically marginalized populations such as people of color and people with low incomes among the most vulnerable (IPCC, 2023; Watts et al., 2015). Counselors’ ethical responsibility is to advocate for local, state, and national policies and practices to prevent the most dire climate outcomes and support a livable future for all. This includes the counseling profession’s call for counselors to be active in policy initiatives and advocacy related to climate change (NBCC, 2025). Such policies may consist of those that support a just transition away from fossil fuels and to renewable sources of energy; agricultural strategies that reduce emissions, shift toward more sustainable diets, and reduce food waste (United Nations Environment Programme, 2020); and nature-based solutions such as stopping deforestation and ecological degradation and moving toward ecosystem regeneration (United Nations Environment Programme, 2020). As the impacts of the climate crisis are felt most significantly in communities of color (who are more likely to be situated in floodplains, heat islands, downwind from fossil fuel-burning plants, etc.), there is an added ethical responsibility to advocate for the well-being of the most vulnerable.
Limitations and Future Research
This study had several limitations. First, the majority of participants identified as White and middle class. The study would have benefited from a greater diversity of participants to gain a broader perspective on cultural differences as they relate to the experiences of climate change, development, and mental health. Additional research is necessary to gain insight into the experiences of young adults across the intersections of identity, specifically focusing on those who will suffer the greatest impacts of the climate crisis, such as individuals from the global majority and low-income households. Secondly, all participants in this study were currently or had been previously engaged in some level of environmental action. The results of this study may not be applicable to those who are concerned about climate change but not actively engaged in taking action. Finally, although a sample size of 12 was suitable for the goals of this research and the standards of hermeneutic phenomenology (van Manen, 1997), the nature of qualitative research limits the ability to generalize these findings.
The participants in this study struggled with diverging from the status quo to make choices aligned with their values. In particular, values associated with individualism and capitalism frequently appeared as roadblocks, such as pressure to make a certain financial living and engaging with problems and solutions from an individualistic perspective. More research is needed to understand how young people challenge and resist dominant cultural values that prevent them from taking action to bring about environmental change and may contribute to poor mental health outcomes.
Conclusion
This study sheds light on the lived experiences of environmentally aware young people. Commensurate with previous findings, participants expressed fear for the future, anxiety, and loss (Hickman et al., 2021). This study highlighted the limited comprehensive strategies available to young people for addressing their climate-related emotions, which affected their ability to remain engaged in climate action. Additionally, participants felt significant cultural and financial pressure to make a living, which stood in contrast to their ability to engage in personal or professional environmental action. Counselors can support young adults by enhancing their climate-related mental health literacy, offering climate-specific interventions to increase their resilience, and engaging in social change through advocacy.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://bit.ly/acacodeofethics
Arnett, J. J. (2000). Emerging adulthood: A theory of development from the late teens through the twenties. American Psychologist, 55(5), 469–480. https://doi.org/10.1037/0003-066X.55.5.469
Arnett, J. J. (2010). Emerging adulthood(s): The cultural psychology of a new life stage. In L. A. Jensen (Ed.), Bridging cultural and developmental approaches to psychology: New syntheses in theory, research, and policy
(pp. 255–275). Oxford University Press. https://doi.org/10.1093/acprof:oso/9780195383430.003.0012
Arnett, J. J. (2014). Emerging adulthood: The winding road from the late teens through the twenties (2nd ed.). Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199929382.001.0001
Banusiewicz, J. D. (2014). Hagel to address ‘threat multiplier of climate change.’ U.S. Department of Defense. https://www.defense.gov/News/News-Stories/Article/Article/603440/hagel-to-address-threat-multiplier-of-climate-change
Barry, E. (2022, February 6). Climate change enters the therapy room. The New York Times. https://www.nytimes.com/2022/02/06/health/climate-anxiety-therapy.html
Bauck, W. (2022, November 28). Where the Sunrise Movement goes from here. Slate. https://slate.com/news-and-politics/2022/11/sunrise-movement-biden-ira-2024.html
Baudon, P., & Jachens, L. (2021). A scoping review of interventions for the treatment of eco-anxiety. International Journal of Environmental Research and Public Health, 18(18), 9636. https://doi.org/10.3390/ijerph18189636
Beaglehole, B., Mulder, R. T., Frampton, C. M., Boden, J. M., Newton-Howes, G., & Bell, C. J. (2018). Psychological distress and psychiatric disorder after natural disasters: Systematic review and meta-analysis. The British Journal of Psychiatry, 213(6), 716–722. https://doi.org/10.1192/bjp.2018.210
Borenstein, S. (2022, February 28). UN climate report: ‘Atlas of human suffering’ worse, bigger. Associated Press. https://apnews.com/article/climate-science-europe-united-nations -weather-8d5e277660f7125ffdab7a833d9856a3
Center for the Study of Social Policy. (2019). Youth thrive: Protective & promotive factors for healthy development and well-being. https://cssp.org/wp-content/uploads/2025/04/core-meanings-youth-thrive-protective-promotive-factors.pdf
Clayton, S., Manning, C., Speiser, M., & Hill, A. N. (2021). Mental health and our changing climate: Impacts, inequities, responses. American Psychological Association. https://www.apa.org/news/press/releases/mental-health-climate-change.pdf
Delaney, M. E. (2019). Nature is nurture: Counseling and the natural world. Oxford University Press.
Doherty, T. J., & Clayton, S. (2011). The psychological impacts of global climate change. American Psychologist, 66(4), 265–276. https://doi.org/10.1037/a0023141
Frankl, V. E. (2006). Man’s search for meaning: An introduction to logotherapy (4th ed.). Beacon.
Gislason, M. K., Kennedy, A. M., & Witham, S. M. (2021). The interplay between social and ecological determinants of mental health for children and youth in the climate crisis. International Journal of Environmental Research and Public Health, 18(9), 4573. https://doi.org/10.3390/ijerph18094573
Ham, M., Mrčela, D., & Horvat, M. (2016). Insights for measuring environmental awareness. Ekonomski vjesnik: Review of Contemporary Entrepreneurship, Business, and Economic Issues, 29(1), 159–176.
Hart, R., Fisher, S., & Kimiagar, B. (2014). Beyond projects: Involving children in community governance as a fundamental strategy for facing climate change. In UNICEF Office of Research (Ed.), The challenges of climate change: Children on the front line (pp. 92–97).
Hayes, K., Blashki, G., Wiseman, J., Burke, S., & Reifels, L. (2018). Climate change and mental health: Risks, impacts and priority actions. International Journal of Mental Health Systems, 12(28). https://doi.org/10.1186/s13033-018-0210-6
Heiman, N. (2024). Climate change in and out of the therapy room. Nature Climate Change, 14, 412–413.
https://doi.org/10.1038/s41558-024-01979-3
Hesse-Biber, S. N., & Leavy, P. (2010). The practice of qualitative research (2nd ed.). SAGE.
Hickman, C., Marks, E., Pihkala, P., Clayton, S., Lewandowski, R. E., Mayall, E. E., Wray, B., Mellor, C., & van Susteren, L. (2021). Climate anxiety in children and young people and their beliefs about governmental responses to climate change: A global survey. The Lancet Planetary Health, 5(12), E863–E873. https://doi.org/10.1016/S2542-5196(21)00278-3
Hilert, A. J. (2021). Counseling in the Anthropocene: Addressing social justice amid climate change. Journal of Multicultural Counseling and Development, 49(3), 175–191. https://doi.org/10.1002/jmcd.12223
Intergovernmental Panel on Climate Change. (2023). Climate change 2022: Impacts, adaptation and vulnerability: Working group II contributions to the sixth assessment report of the intergovernmental panel on climate change. Cambridge University Press. https://doi.org/10.1017/9781009325844
Lewandowski, R. E., Clayton, S. D., Olbrich, L., Sakshaug, J. W., Wray, B., & Schwartz, S. E. O., Augustinavicius, J., Howe, P. D., Parnes, M., Wright, S., Carpenter, C., Wiśniowski, A., Ruiz, D. P., & van Susteren, L. (2024). Climate emotions, thoughts, and plans among US adolescents and young adults: A cross-sectional descriptive survey and analysis by political party identification and self-reported exposure to severe weather events. The Lancet Planetary Health, 8(11), E879–E893. https://doi.org/10.1016/S2542-5196(24)00229-8
Mongonia, L. (2022). Climate change and mental health: The counseling professional’s role. Journal of Counselor Leadership and Advocacy, 9(1), 57–70. https://doi.org/10.1080/2326716X.2022.2041505
Moser, S. C. (2007). More bad news: The risk of neglecting emotional responses to climate change information. In S. C. Moser & L. Dilling (Eds.), Creating a climate for change: Communicating climate change and facilitating social change (pp. 64–80). Cambridge University Press. https://doi.org/10.1017/CBO9780511535871.006
Moustakas, C. (1994). Phenomenological research methods. SAGE.
National Board for Certified Counselors. (2025). Policy recommendations to support professional counseling in the era of climate change. https://www.nbcc.org/resources/nccs/newsletter/climate-change-policy-recommendations
Ogunbode, C. A., Böhm, G., Capstick, S. B., Demski, C., Spence, A., & Tausch, N. (2019). The resilience paradox: Flooding experience, coping and climate change mitigation intentions. Climate Policy, 19(6), 703–715. https://doi.org/10.1080/14693062.2018.1560242
Ojala, M., Cunsolo, A., Ogunbode, C. A., & Middleton, J. (2021). Anxiety, worry, and grief in a time of environmental crisis: A narrative review. Annual Review of Environment and Resources, 46, 35–58.
https://doi.org/10.1146/annurev-environ-012220-022716
Pihkala, P. (2020). Anxiety and the ecological crisis: An analysis of eco-anxiety and climate anxiety. Sustainability, 12(19), 7836. https://doi.org/10.3390/su12197836
Priebe, S., Matanov, A., Schor, R., Straßmayr, C., Barros, H., Barry, M. M., Díaz-Olalla, J. M., Gabor, E., Greacen, T., Holcnerová, P., Kluge, U., Lorant, V., Moskalewicz, J., Schene, A. H., Macassa., G., & Gaddini, A. (2012). Good practice in mental health care for socially marginalized groups in Europe: A qualitative study of expert views in 14 countries. BMC Public Health, 12, 248–260. https://doi.org/10.1186/1471-2458-12-248
Ramsook, L. (2018). A methodological approach to hermeneutic phenomenology. International Journal of Humanities and Social Sciences, 10(1), 14–24. https://ijhss.net/index.php/ijhss/article/viewFile/408/124
Rashid, S. (2023, December 7). Rising up: How youth are leading the charge for climate justice. United Nations Development Programme. https://www.undp.org/blog/rising-how-youth-are-leading-charge-climate-justice
Sanson, A. V., Van Hoorn, J., & Burke, S. E. L. (2019). Responding to the impacts of the climate crisis on children and youth. Child Development Perspectives, 13(4), 201–207. https://doi.org/10.1111/cdep.12342
Speiser, M., & Ishaq, M. (2024). Americans expect U.S. EPA to ensure a safe and healthy environment and will support climate solutions that protect health and children. https://ecoamerica.org/wp-content/uploads/2023/01/ACPS-2024-Vol-I.pdf
Starks, H., & Trinidad, S. (2007). Choose your method: A comparison of phenomenology, discourse analysis, and grounded theory. Qualitative Health Research, 17(10), 1372–1380. https://doi.org/10.1177/1049732307307031
Sturm, D. C., Daniels, J., Metz, A. L., Stauffer, M., & Reese, R. (2020). Fact sheet. American Counseling Association. https://www.counseling.org/docs/default-source/center-resources/climate-change-fact-sheet.pdf?sfvrsn=83c7222c%5C_2
Thomas, I., & Benoit, L. (2022). A guide to eco-anxiety: How to protect the planet and your mental health; What we think about when we try not to think about global warming: Toward a new psychology of climate action. Journal of the American Academy of Child & Adolescent Psychiatry, 61(2), 342–345.
https://doi.org/10.1016/j.jaac.2021.11.025
United Nations. (2025). Youth. https://www.un.org/en/global-issues/youth
United Nations Environment Programme. (2020). Emissions gap report 2020. https://www.unep.org/emissions-gap-report-2020
van Manen, M. (1997). Researching lived experience: Human science for an action sensitive pedagogy (2nd ed.). Routledge. https://doi.org/10.4324/9781315421056
Watts, N., Adger, W. N., Agnolucci, P., Blackstock, J., Byass, P., Cai, W., Chaytor, S., Colbourn, T., Collins, M., Cooper, A., Cox, P. M., Depledge, J., Drummond, P., Ekins, P., Galaz, V., Grace, D., Graham, H., Grubb, M., Haines, A., . . . Costello, A. (2015). Health and climate change: Policy responses to protect public health. The Lancet, 386(10006), 1861–1914. https://doi.org/10.1016/S0140-6736(15)60854-6
World Meteorological Organization. (2020, March 9). State of global climate 2019. https://wmo.int/publication-series/state-of-global-climate-2019
Wuebbles, D., Easterling, D. R., Hayhoe, K., Knutson, T., Kopp, R. E., Kossin, J. P., Kunkel, K. E., LeGrande, A. N., Mears, C., Sweet, W. V., Taylor, P. C., Vose, R. S., & Wehner, M. F. (2017). Our globally changing climate. In D. J. Wuebbles, D. W. Fahey, K. A. Hibbard, D. J. Dokken, B. C. Stewart, and T. K. Maycock (Eds.), Climate science special report: Fourth national climate assessment, Volume 1 (pp. 35–72). U.S. Global Change Research Program. https://www.nrc.gov/docs/ML1900/ML19008A410.pdf
Kathleen L. Grant, PhD, NCC, is an associate professor at The College of New Jersey. Alyson Pompeo-Fargnoli, PhD, NCC, LPC, is an associate professor at Monmouth University. Melissa A. Alvaré, PhD, is a lecturer at Monmouth University. Correspondence may be addressed to Kathleen L. Grant, 2000 Pennington Rd, Ewing Township, NJ 08618, grant24@tcnj.edu.
May 22, 2024 | Volume 14 - Issue 1
Rebekah Cole, Christine Ward, Taqueena Quintana, Elizabeth Burgin
Military spouses face many challenges as a result of the military lifestyle. Much focus has been placed on enhancing the resilience of military spouses by both the military and civilian communities. However, no research currently exists regarding spouses’ perceptions of their resilience or how they define resilience for themselves and their community. This qualitative study explored the perceptions of eight military spouses regarding their resilience through individual semi-structured interviews. The following themes emerged: 1) shaped by service member and mission priority; 2) challenges within the military lifestyle; 3) outside expectations of spouse resilience; 4) sense of responsibility for family’s resilience; 5) individual resilience; and 6) collective resilience. We discuss ways military leadership and the counseling profession can best understand and enhance the resilience of military spouses.
Keywords: military spouses, resilience, military lifestyle, perceptions, counseling
Because of the unique stressors associated with the military lifestyle, military spouses are at an increased risk for poor mental health (Donoho et al., 2018; Mailey et al., 2018; Numbers & Bruneau, 2017). They may experience mental health concerns, such as anxiety and depression, due to a number of reasons, including separation from their deployed service member, loss of support networks after a relocation, or issues with adjusting to the uncertain and frequent changes of the military (Cole et al., 2021). Additional concerns that arise, such as employment, marital, and financial issues, can also negatively affect the military spouse’s mental health (Cole et al., 2021; Mailey et al., 2018). Dorvil (2017) reported that 51% of active-duty spouses experience more stress than normal. Furthermore, 25% of military spouses meet the criteria for generalized anxiety disorder (Blue Star Families [BSF], 2021). Depression in military spouses is also higher than the rate found within the general population (Verdeli et al., 2011). As a military spouse casts aside their own personal needs to support their service member, stressors may continue to increase, which can contribute to the rise of mental health needs of military spouses (Moustafa et al., 2020).
Resilience and Military Spouses
Nature of Resilience
Given the challenges inherent in the military lifestyle and the associated mental health risks, military spouse resilience is essential. Resilience is a complex and multifaceted construct, significant to researchers, practitioners, and policymakers across numerous disciplines, including mental health and military science. The American Psychological Association (2020) defined resilience as “the process of adapting well in the face of adversity, trauma, tragedy, threats, or even significant sources of stress” (para. 4). Within the military community, resilience has been defined as the ability to withstand, recover, and grow in the face of stressors and changing demands (Meadows et al., 2015). Importantly, determinants of resilience include the interaction of biological, psychological, social, and cultural factors in response to stressors (Southwick et al., 2014). In addition to these salient variables embedded in resilience science, resilience may be operationalized as a trait (e.g., optimism), process (e.g., adaptability in changing conditions), or outcome (e.g., mental health diagnosis, post-traumatic growth; Southwick et al., 2014).
Resilience may also vary on a continuum across domains of functioning (Pietrzak & Southwick, 2011) and change as a function of development and the interaction of systems (Masten, 2014). Accordingly, a definition and operationalization of resilience may vary by population and context (Panter-Brick, 2014). During the post-9/11 era, the resilience of service members and their families received significant attention from stakeholders, including the Department of Defense (DoD) and National Academies of Sciences, Engineering, and Medicine (NASEM), both of which expressed a commitment to conducting research and establishing programming to enhance service member and military family resilience, resulting in increased awareness of the importance of service member and family resilience throughout the military community (NASEM, 2019).
Military Family Resilience
Though military families share the characteristics and challenges of their civilian counterparts, they additionally experience the demanding, high-risk nature of military duties; frequent separation and relocation; and caregiving for injured, ill, and wounded service members and veterans (Joining Forces Interagency Policy Committee, 2021). In recognition of the constellation of military-connected experiences military families face, the Defense Centers of Excellence for Psychological Health and Traumatic Brain Injury (DCoE) commissioned a review of family resilience research and relevant DoD policies to inform a definition of resilience for appropriate application to military spouses and children (Meadows et al., 2015). Meadows and colleagues (2015) proposed family resilience may be best defined as “the ability of a family to respond positively to an adverse situation and emerge from that situation feeling strengthened, more resourceful, and more confident than its prior state” (see Simon et al., 2005, for a further exploration of family resilience). Further, Meadows and colleagues identified two groups of policies delineated at the Joint Chiefs of Staff or DoD levels, or within individual branches of the military: 1) existing programs modified to augment resilience or family readiness, and 2) new programs developed to target family resilience. Programs established by these policies support access to mental health services (e.g., DoD Instruction [DoDI] 6490.06); parenting education (e.g., New Parent Support Program, DoDI 6400.05); child welfare (e.g., Family Advocacy Program, DoD Directive 6400.1); and myriad physical, psychological, social, and spiritual resources. The well-being of military families represents a critical mission for the DoD, extending beyond provision and access for families to meet their basic needs to individual service member and unit readiness, and the performance, recruitment, and retention of military personnel (NASEM, 2019).
Military Spouse Resilience
Though service member and family resilience are critical for accomplishing the DoD’s mission, focusing on the unique nature of military spouse resilience is key for understanding and supporting this population’s resilience. Counseling, psychology, sociology, and military medical professional research related to military spouse resilience has focused primarily on characteristics associated with resilience. In a study by Sinclair et al. (2019), 333 spouse participants completed a survey regarding their resilience, mental health, and well-being. The results revealed that spouses who had children, were a non-minority, had social support, had less work–family conflict, and had a partner with better mental health were more resilient. Another survey study examined the characteristics associated with resilience in Special Operations Forces military spouses, determining that community support and support from the service member was essential for spouse resilience (Richer et al., 2022). A study conducted within the communication field also explored spouses’ communicative construction of resilience during deployments. Qualitative data analysis of interviews with 24 spouses indicated how spouses use communication to reconcile their contradictory realities, which increases their resilience (Villagran et al., 2013). This resilience has also been found to be a protective factor against depression and substance abuse during military deployments (Erbes et al., 2017). Finally, a survey study of Army spouses (N = 3,036) determined that spouses who were less resilient were at higher risk for mental health diagnoses (Sullivan et al., 2021). While these studies explored the nature of resilience demonstrated by military spouses, our searches in JSTOR, PubMed, ERIC, PsycINFO, and Google Scholar did not reveal any studies regarding spouses’ perceptions of their own resilience or how they define this resilience for themselves and their community. Our study fills that research gap by exploring active-duty spouses’ perceptions and definitions of resilience.
Methods
The purpose of this qualitative study was to explore the perceptions of active-duty spouses regarding their resilience. This study was guided by the following research questions: 1) What are military spouses’ perceptions of their own resilience? and 2) How do military spouses define “resilience?” Phenomenology seeks to present a certain phenomenon in its most authentic form (Moustakas, 1994). In order to most authentically and openly describe our participants’ experiences, we chose a qualitative transcendental phenomenological approach to frame our study. This tradition of qualitative research focuses on portraying a genuine representation of the participants’ perceptions and experiences. However, the distinct feature of transcendental phenomenology is its first step, which involves the researchers recognizing and bracketing their biases so they can analyze the data without any interference (Moerer-Urdahl & Creswell, 2004). We selected this design because each of our research team members were military spouses. We therefore recognized the need to mitigate our biases in order to give a true representation of the participants’ perceptions, free from our own preconceived notions.
Participants
The participants in this study were selected based on their status as active-duty military spouses and their willingness to participate in the study. There were no other inclusion or exclusion criteria for the participants in this study. After gaining IRB approval, we used convenience sampling to recruit eight participants. In qualitative research, convenience sampling is used to recruit participants who are closely accessible to the researchers (Andrade, 2021). Our research team emailed participants that we knew through living, working, and volunteering on military bases throughout the United States and at overseas duty stations who fit the active-duty military spouse criteria for this study and asked them if they were willing to participate in the study. Once the participants expressed interest, they were provided with an information sheet regarding the study’s purpose and the nature of their involvement in the study. Participant demographics are included in Table 1. All of the participants were female and all were between the ages of 30–40. Four branches of the U.S. military, including Army, Navy, Air Force, and Marine Corps, were represented in the sample. No reservist, Coast Guard, or Space Force military spouses participated in our study. Five of our participants were White and three were Black. Their tenure as military spouses ranged from 4 years to 17 years. Five of the spouses were married to a military officer, while three of the participants were married to an enlisted service member. After interviewing these eight participants, our research team met and determined that because of the distinct common patterns we found across each of the participants’ transcripts, we had reached saturation and did not need to recruit any additional participants for our study (Saunders et al., 2018).
Table 1
Participant Demographics
| Participant |
Age |
Ethnicity |
Gender |
Branch |
Spouse’s Rank |
Years as a Spouse |
| 1 |
33 |
Black |
Female |
Air Force |
Enlisted |
4 |
| 2 |
36 |
Black |
Female |
Navy |
Enlisted |
17 |
| 3 |
31 |
White |
Female |
Army |
Officer |
7 |
| 4 |
34 |
Black |
Female |
Navy |
Enlisted |
14 |
| 5 |
36 |
White |
Female |
Marine Corps |
Officer |
12 |
| 6 |
35 |
White |
Female |
Marine Corps |
Officer |
14 |
| 7 |
40 |
White |
Female |
Navy |
Officer |
16 |
| 8 |
34 |
White |
Female |
Navy |
Officer |
10 |
Data Collection
Our research team first developed the interview protocol for the study based on a thorough review of the literature regarding resiliency within military culture as well as the challenges of the military lifestyle for military spouses. Our research team members interviewed each of the participants for 1–2 hours. These semi-structured interviews were audio recorded and transcribed verbatim by an automated transcription service. The interview questions were open-ended and focused on the spouses’ definitions of resilience and their perceptions of their resilience within the military lifestyle and culture (see Appendix for interview protocol). In addition, probing questions such as “Can you explain that a bit more?” or “Can you give any examples of what you mean by that?” were used to gather more in-depth data throughout the interviews.
Data Analysis
We followed the steps of the transcendental phenomenological data analysis process to analyze our study’s results (Moerer-Urdahl, 2004). First, each member of our research team engaged in epoche, in which we bracketed our biases as military spouses so that our own thoughts, feelings, perceptions, and experiences did not influence our interpretation of our participants’ experiences. The next step in the process was horizontalization. During this step, each member of our research team read through the interview transcripts and noted significant statements throughout so we could better understand how the participants perceived, understood, and experienced resilience. Next, we met as a research team to discuss these significant statements and organize them into themes (Moustakas, 1994). Our research team then developed textual and structural descriptions of the themes, describing not only a list of the participants’ perceptions, but also an in-depth analysis of what their perceptions of resilience entailed and how they have experienced it throughout their tenure as military spouses (Moerer-Urdal, 2004; Moustakas, 1994). We then constructed a comprehensive description of the participants’ perceptions of resilience, encapsulating the “essence of the experience” (Moerer-Urdal, 2004, p. 31).
Research Team and Strategies to Increase Trustworthiness
Our research team consisted of four university faculty members, all of whom possessed extensive experience in conducting qualitative research. Three of our research team members possess PhDs in counseling and one research team member possesses an EdD in counseling. All team members had extensive experience conducting research with military-connected communities. In addition, all of our research team members were active-duty military spouses, with years of experience as a military spouse ranging from 1–23 years.
We used several strategies to increase the credibility of our results. First, the use of an experienced research team to collectively analyze the data resulted in diverse perspectives on the emerging themes of the study. However, because each member of our research team was a military spouse, we recognized the need to bracket our own experiences and biases so that they did not interfere with our interpretation of the data. Each team member took notes on their individual biases, and our research team discussed these biases when interpreting themes. Biases held by research team members included a predisposition to believe that spouses of special warfare service members endured greater stressors and were better supported by their military communities; a belief that spouses of higher-ranking service members possessed greater knowledge of and access to resources to support social, behavioral, and mental health needs; and personal experience within the military spouse community. These biases were challenged throughout the research process by each member of the team. As each theme was identified, the team referenced individual transcripts to ensure that the interpretation was justified. We found that our biases were rightfully challenged.
Additionally, to avoid leading questions, our research team made the conscious decision not to define resilience as part of the interview and follow-up process. The team wanted to derive an organic definition of spouse resilience that was not clouded by a formal definition. In addition, we used member checking, in which we emailed the interview transcripts to the participants and asked them to verify the data. The participants responded to our request with minimal change requests related to grammatical errors in the transcriptions and validated our data. Several offered additional insight related to their definition of resilience, which was included in our data analysis.
Results
The following themes emerged from our data: 1) shaped by service member and mission priority; 2) challenges within the military lifestyle; 3) outside expectations of spouse resilience; 4) sense of responsibility for family’s resilience; 5) individual resilience; and 6) collective resilience.
Theme 1: Shaped by Service Member and Mission Priority
Military/Service Member Definition
When discussing their definition of resiliency, the spouses first considered what resiliency meant for their active-duty spouse. The participants varied in their perceptions of what resilience meant for their active-duty service member, though all defined resilience as an active process of adapting or persevering when faced with adversity, rather than a personal trait or characteristic the service member possesses. Participant 3 noted that, for their spouse, resilience was “the ability to adapt to changes that are beyond your control . . . adapting to situations in an optimistic and positive way.” Participant 6 stated that resilience for their spouse meant an “ability to bounce back from a hardship.” One participant asked their spouse to comment specifically about their definition and provided the following definition in a follow-up with the interviewer: “Resilience is how you persevere in difficult circumstances. It’s not about how hard you fall, but how quick you can get back up from being knocked down” (Participant 2 [P2]).
Some participants cited specific notions of resilience that are embedded in the service members’ military community. One Navy spouse remarked that resilience, to their spouse, meant “Don’t give up the ship” (P8). Another Navy spouse mentioned that for their spouse, resilience was “knowing how to weather the storm” (P7). Yet another spouse noted that resilience “the Marine Corps way” meant their service member must “do their job” (P4). Other participants noted that the root of resilience for the military service member stems from a place of selfless service. Participant 8 commented that the resiliency of their spouse was “more about the man standing next to me, the family I’m fighting for at home, the country I’m fighting for at home, than about their own personal needs.”
Adapting, Overcoming, and Persevering
Like their active-duty members, spouses indicated that resilience was about adapting, overcoming, and persevering in the face of obstacles. Resilience to one spouse was “being able to rebound or to overcome an obstacle” (P1); to another, resilience meant they must “be flexible, adapt with whatever, overcome whatever it is that you’re going through” (P2). Spouses noted that resilience was not a one-time event. Instead, spouses suggested that their own resilience stemmed from continually persevering. Participant 6 stated that for them, resilience meant not just “going through something difficult and making it out on the other side,” but that they then had to “keep pushing forward.” One participant indicated that their personal definition of resilience and the notion to persevere stemmed directly from their spouse: “I’ve almost kind of adopted a bit of my husband’s thought process, I guess. You just keep going to get things done” (P8).
Mindset
Our participants indicated that resilience was a mindset that one must choose and that when faced with difficulties, they chose to focus on gratitude, positivity, and growth. For example, Participant 8 stated that, although they had faced and would continue to face challenging and stressful experiences as a result of being a military spouse, they believed that “whatever may come, we’ve been very blessed in our life and we should always be thankful for the life that we have.” Another participant noted that for them, overcoming and persevering meant adopting an optimistic attitude. Specifically, the spouse stated, “sometimes you just have to kinda look at the bright side of things, and you have to find the things that work for you at each place” (P5). One participant drew resilience from a growth mindset:
I think it [resilience] is really a mindset switch. I think it’s changing from “oh this is happening to me, how horrid” to like “how can I take this horrid situation and turn it into something good?” And I think that is a big mindset switch. (P7)
Resilience Variations
Walsh (2012) described risk and resilience as a process of balancing risk and protective factors over the life span. Participants in our study expanded on that idea by suggesting that they reacted to situational challenges along a continuum:
I think what I’m saying is there’s different levels of resilience, like sometimes you have to tap into that different part of yourself. Sometimes you have to let it go and just accept the things that come, and sometimes you just gotta pick yourself up and keep on trucking. (P8)
Likewise, Participant 3 suggested that resilience takes different forms depending on the situation:
Sometimes resiliency just means like surviving day to day and other times, it means figuring out how to continue with your passions to the best of your ability while also supporting your family and your [service member spouse]. I think it’s just super unique to every situation. (P3)
Our participants also recognized that their understanding of resilience was often focused on the here and now of their situation but that their reactions to stressors had long-term effects. One participant indicated that resilience is a learning process and recognized that the stressors they overcome now prepare them to address stressors they will face in the future: “I think being able to come out of extremely, extremely stressful situations, be able to come out on the other side and [know] I’m okay and I survived this, and now I’m kind of better prepared for next time” (P6). Participant 3 wondered about the long-term ramifications of resilience in the face of prolonged adversity, stating “I may be resilient right now in the moment, but in the long term, like, how will this affect me?”
Individualized
Finally, participants defined resilience as an individualized process, stating things such as “everybody has their own unique ways of being resilient, and I think that they do what works best for their families” (P7) and “my resiliency may look different than someone else’s resiliency” (P2). One participant elaborated on this individualized approach to resilience by recognizing that each person has different risk factors that affect their response to stressors, thus affecting the way each person demonstrates resilience. This participant stated that, when viewing resilience among military spouses as a whole, it is important to
take into consideration somebody’s upbringing and the baggage that they bring into this life. We don’t know what people have gone through as kids, and that I think would have a big impact on whether or not someone can be resilient, so I don’t think it’s a one-size-fits-all. (P6)
Theme 2: Challenges Within the Military Lifestyle
Lack of Control
The spouses described the common challenges of the military lifestyle to their resilience. First, they discussed the stress of the feeling of a lack of control in their lives. One participant described how she
just found out yesterday that my husband was getting deployed and he’s leaving Sunday. And I keep hearing people say, “You have to be resilient. You’re gonna be okay!” You’re resilient, but right now, what it feels like is how much can you endure for the sake of the mission? (P1)
Another echoed this sentiment: “I have no control if the Navy says they’re going to deploy my husband. There’s nothing I can do to change that” (P8).
Constant Changes
Another common challenge mentioned among all of the participants was the constant changes they experience in their lives, including moving, career changes, and changes within their family dynamics. Because they move every few years, the spouses described how they are constantly separated from their support systems: “Even though you meet these great people, you don’t get to stay with them . . . and you’re generally not near your family, which is very hard” (P5). Another described how “Once I have started on something and I’m like, ‘This is it, we gon’ be here for a while,’ then my husband is like ‘nope. Military said we got to shift and move again’”(P2).
These constant changes resulted in career struggles for the spouses. One asked, “How can I get this [job] if I’m never at one place for long? . . . How do I uproot everything that I know or everything that I am doing to follow my service member?” (P2). Another described how “moving, changing jobs, not being able to have a secure profession, you do it because you have to . . . but that doesn’t mean that there’s not a whole lot of emotional and mental load that goes with it” (P3).
Another challenge for military spouses was constantly changing family dynamics. One described the difficulty in constantly changing work schedules: “We have to kind of get into this routine without him and then when he comes back, because it’s different while he’s away. We gotta kind of try to fit him back into our routine when he gets back” (P4). Another discussed the challenge of transitioning to being the sole caregiver during a deployment: “If I go down with COVID, what am I going to do? Because, like, I was literally IT. No one is going to want to take my kids. . . . That was the first time I ever felt, like, fearful” (P7).
Mission Priority
In addition to constant change, the spouses also mentioned the challenges of the military’s clear prioritization of the mission above military members and their families: “If something is going on at home, we’re going to take care of our active person first and worry about your family later” (P2). The participants described how this focus on the mission is so intense that it affects service members physically, which increases the burden on military spouses to care for them: “My husband’s health suffers because the mission is most important to him” (P1).
Theme 3: Outside Expectations of Spouse Resilience
Expectation to “Suck It Up”
The spouses described others’ expectations for their resilience. First, they described the military’s expectation that they “suck it up.” One described how “you have a lot of the ‘suck-it-up’ mentality, and I would say when you have the leaders who kind of fall under that, whether it’s seeking the mental health treatment or having stigmas with that” (P6). Another explained that “there’s so much focus and emphasis on just being resilient and sucking it up” so there is often a mindset of “‘Oh well, military spouses are resilient so they signed up for this, they know what it takes and they just have to get over it’” (P3). Another spouse described how “they put so much pressure on you to be like, just make it work, that you’ve gotta figure out the way to make yourself happy, and that’s hard to do” (P5). Participant 7 summed up the military spouse mentality as a whole: “You toughen up and you make it work. You know?”
The participants felt their overall resilience would be enhanced if individuals outside the military community better understood the challenges faced by military families. One participant felt the “suck it up” mentality stemmed less from the military community itself and more from outside communities who might not understand the struggles of military family life: “So when . . . you’re going through another stress of a PCS [permanent change of station], you can’t find a house, they say, well, at least you get a house allowance, at least you get free health care” (P6). Participant 3 expanded on this idea by stating, “I just honestly think that a greater understanding of what sacrifices that military spouses make . . . would increase resiliency, because there’s just so much lack of understanding what it actually entails.” Lastly, one participant mentioned a sentiment they frequently hear from others in a civilian community, expressing that it was frustrating when friends outside the military told her, “I don’t know how you do it,” to which the participant responded, “I don’t know, you just do it!”
Pressure to Be Resilient
The spouses also expressed frustration at others’ misperceptions of the expectation that they and their families demonstrate resilience: “When we call military spouses or children resilient, it just seems like a cop out and relinquishes any type of burden . . . or feeling of guilt about a situation that may cause emotional or mental damage” (P3). Another participant echoed this frustration: “Sometimes I don’t feel like I’m being resilient. Sometimes I feel like I’m just doing what needs to be done because that’s what needs to be done” (P8). Another participant described how her friends
call me Superwoman because I have all these different things going on and I always seem like I got it together. . . . It’s like saying to me that I have to keep going, no matter what, and I think people should be able to just feel defeated sometimes. Or be able to say “that was just too much for me” or “I don’t really feel like being resilient today, I kind of want to lay in bed and just be upset or sad.” (P4)
Given these expectations, one spouse pointed out the danger of expecting military children to consistently demonstrate resilience:
It’s so easy for everyone to say that military kids are always so resilient and sometimes they’re not. Sometimes they are stressed out. They are feeling the crushing weight. They feel sad but everyone keeps telling them that they’re resilient. So it almost makes it seem like . . . they aren’t allowed to feel those hard things or talk about those things or act on those feelings and emotions. (P8)
One spouse proposed a solution to these misperceptions, emphasizing that resilience is unique for military spouses and should be defined to accurately reflect the way they uniquely overcome challenges:
I think it’s important for military spouses to reappropriate that term [resilience] so that it is not weaponized, and I would like to see some sort of guidance as to how we can be resilient but in a way that positively impacts our mental health and physical health and not having to endure all of the things and all of the frustration and uncertainty that comes with the onset of having to be resilient. (P1)
Theme 4: Sense of Responsibility for Family’s Resilience
With their partners focused on the mission, the spouses described their sense of responsibility to maintain their resilience so they can care for their children in the absence of their active-duty spouse: “We have our husband or our spouses gone so much, we need to be a solid parent at home for our kiddos or our family” (P7). Participant 4 likewise described how “I kind of see myself as holding down the fort, you know, because when my husband is not home it is just me and the kids.” Another explained how “I have three little ones that’s looking up to me and I can’t slip away, depressed, because daddy’s not home” (P2). In the end, the spouses defined resilience as an obligation to their families. Participant 3 described that “I have to be that way for my children.” Participant 4 added that “I think that’s what resilience is like, knowing that you kind of have to carry the load, you know, for your whole family to try to keep us afloat.”
The participants described how this resilience is especially obligatory when the active-duty spouse is unable to be resilient:
I’m kind of taking the lead with our kids . . . but I’ve also kind of had to pour into my husband, you know, because he has those times you know where things are really, really hard for him. I’ve also been like his counselor and his doctor sometimes. (P4)
Theme 5: Individual Resilience
In response to being unable to control many aspects of the military lifestyle, most of the spouses described how they have become independent in order to withstand the constantly changing variables within the military lifestyle. One described being “pretty independent, and I think that helps a lot because I don’t rely on my spouse to do all these things I do” (P5). Another described how being independent resulted in self-confidence and resilience:
You gotta figure out how to do all of it just because you can’t ever rely on the spouse being able to help. But I think being able to come out of extremely, extremely stressful situations, be able to come out on the other side and say “I’m okay, and I survived this, and now I’m kind of better prepared for next time.” (P6)
Another spouse described how maintaining an independent identity was key to separating herself from the stressors of the military lifestyle: “That’s a really important part of being a military spouse. It doesn’t have to be a job specifically, but just something that you can be your own person separate from your husband or your spouse’s job” (P8).
The spouses also described the importance of taking care of themselves physically and mentally in order to maintain their resilience. Many described exercise as key to their mental health and wellness: “My biggest coping mechanism is exercise. I’ve found that no matter where I go, I can exercise” (P5). Another spouse described how she “tried to find a kickball team every place we’ve been to since Okinawa because I figured out it’s a stress relief” (P6). Participant 7 echoed that “working out . . . just helps me. It lowers my stress.” One spouse explained how she defaults to exercise when facing the challenges of the military lifestyle because she knows her “ability to recover quickly is directly tied to the way in which I care for myself” (P1).
Theme 6: Collective Resilience
The participants described their reliance on the collective military spouse community for their survival. One spouse, for example, described a connection with other military spouses as the difference between “doing well and barely surviving” (P6). Another spouse described her reliance on the military spouse community: “Community is what it’s all about. I can’t get through anything without community” (P7). Another spouse echoed this survival mechanism: “This is a beautiful community. It’s an amazing place . . . we all get each other. So I think there are times where it’s really hard . . . but we survive, we get through it. We’re resilient. We got the grit” (P7). Participant 1 explained exactly how the military spouse community offers this support to help spouses survive the challenges of the military lifestyle: “When time calls for it, I think, collectively, we bring our resources together to help pull other military spouses up and try to just forewarn them about what the obstacles are and what may have worked for our family” (P1).
The military spouses also described the comfort they found in other military spouses’ understanding of the challenges they face: “I think the most important part and coping is finding your community, so making sure you’re surrounding yourself with women who are going through similar experiences, or who have gone through similar experiences and similar life stages” (P3).
In the midst of this supportive community, the spouses discussed how they actively seek to comfort each other: “You’re not the only one who’s in it who’s having this issue, I understand that you’ll get through this, that we know we’ve been there, we understand how it goes” (P5). This outreach seemed to be especially helpful from spouses who were more experienced with the military lifestyle: “Having that senior spouse example has been so good. . . . She’s always been somebody who said, ‘Hey, I’ve been through a lot. If you ever have any questions, I’m always here for you’” (P8).
In addition to relying on other spouses for their own wellness and resilience, the spouses expressed pride in their ability to contribute to the military spouse community. One described how “I feel like I am a better team player. I feel like I’m more committed to helping others than I have in the past because I know that others will do the same for me” (P7). The participants also described increased self-growth as a result of being a part of a community: “I really don’t think I would have allowed myself to receive help if I hadn’t been part of this phenomenal community that is constantly supporting each other” (P7). Participant 5 echoed this sentiment: “Learning to get that help from other people is something that I feel like you have to kind of get when you are a military spouse because, otherwise, you’re going to have to do everything and you don’t have to.”
Finally, our participants frequently indicated that they felt a “sense of pride” (P7), “connection” (P4), or “camaraderie” (P8) from belonging to a group of military spouses who understood their unique situation. When asked how the military could enhance resilience for military spouses, participants commonly indicated that peer support and fostering connections with senior spouses should be a priority for military commands. One participant noted that their ability to be resilient in difficult times was related to the “opportunities” they had “to connect with other people who are going through similar stuff and who are a part of the same small community” and recommended that the military facilitate more opportunities to connect (P7). Another participant suggested that military commands should “have someone that [the spouse] can talk to” that would “help them to understand the military life whether you are a new spouse or a seasoned spouse” (P2).
Discussion
The purpose of this study was to explore military spouses’ perceptions of their resilience and the ways in which they define resilience for their community. Our study’s results indicate that spouses’ definitions of resilience are currently shaped by service member and mission priority. Our participants also described how they often felt burdened by outside expectations of their resilience as well as by a sense of responsibility for their family’s resilience. Overall, the spouses relied on themselves and the military spouse community to overcome the challenges they faced. Participants expressed a desire for resources aimed specifically at enhancing spouse resilience and more awareness about resilience resources already in place throughout the military.
While past research has examined resilience factors in spouses such as communication skills, social support, and spousal support (Erbes et al., 2017; Richer et al., 2022; Sinclair et al., 2019; Villagran et al., 2013), our study provided new insight into military spouses’ perspectives of their resiliency. This revelation of the spouses’ worldview aids our understanding of ways to best support spouses and areas to focus on to support their resilience. Our participants’ definitions of their resilience were shaped by their relationship with their service member and the influence of the military’s mission. In addition, while past research has indicated that the military lifestyle and culture is challenging for spouses to navigate (Cole et al., 2021; DaLomba et al., 2021; Donoho et al., 2018; Mailey et al. 2018), our participants’ description of their feelings of responsibility for their family’s well-being reveals the added burden that military spouses face as they help their families navigate the military lifestyle. Finally, our participants confirmed that resiliency should be viewed as a variation and is unique to each individual (Pietrzak & Southwick, 2011). As outlined in the professional literature (Masten, 2014; Southwick et al., 2014), the participants confirmed the dynamic nature of resiliency, recognizing that sometimes they felt more resilient than at other times.
In the midst of these challenges, our participants emphasized that the military spouse community serves as a protective factor and a source of their resilience against mental health challenges. This perception of the military spouse community aligns with previous research highlighting the supportive role that spouses play for each other, so much so that it is a protective factor against suicide (Cole et al., 2021). Therefore, military leadership and the counseling community might focus on enhancing this community and connecting spouses with one another—especially more seasoned spouses with newer spouses. In addition, because military-sponsored resilience programs are often targeted to better support service member outcomes, community providers might find ways to focus on supporting the spouses and helping them to overcome the challenges they face in their daily lives.
Finally, the participants discussed how they overcame the challenges of the military lifestyle, including constant moving, deployments, and overall uncertainty, through their own individual and collective resilience. These lifestyle challenges that the participants described correspond to career struggles and shifting family dynamics that cause ongoing stress to the military spouse, both of which have been previously documented in the professional literature (Borah & Fina, 2017; Cole et al., 2021; DaLomba et al., 2021; Donoho et al., 2018; Mailey et al., 2018; Numbers & Bruneau, 2017). Currently, since the withdrawal of troops from Afghanistan, the United States is experiencing peacetime, whereas the nature of future conflicts is uncertain (Marsh & Hampton, 2022). Enhancing the resiliency of military spouses and finding solutions to ongoing stressors is key during this time of peace so that spouses are ready and able to face the stressors of future, potentially large-scale wars (Sefidan et al., 2021).
Implications for Counselors
Professional counselors are called to be trained and ready to meet the unique needs of military spouses, especially in understanding the nature of military culture and its impact on spouse mental health and well-being and enhancing spouse resilience in times of adversity (Cole, 2014). Our study echoes the continued struggles of military spouses described in the professional literature (Cole et al., 2021; Lewy et al., 2014; Runge et al., 2014), suggesting that new and innovative ways of understanding and approaching military spouse resilience is needed within the counseling community. For example, counselors might encourage spouses to explore how their resilience is shaped by the military community in order to increase self-awareness and understanding. They might also help spouses develop their independence and sense of self-efficacy while simultaneously seeking collective support within the military community. Counselors can help spouses examine their social support and help them develop their social skills so they can connect with others around them. Counselors should also help military spouses unpack their perceptions of outsiders’ expectations of their resiliency. Encouraging spouses to reflect on others’ expectations, and the ways in which these expectations impact their sense of well-being, may help define resilience for themselves and capitalize on their unique resiliencies during challenging times. Ultimately, because the military culture is so unique, counselors should seek out professional development so they can better understand how to help military spouses navigate this culture and enhance their resilience. When working with military spouses, professional counselors might explore spouses’ feelings of responsibility for their family members’ health and well-being that were described in our results. In addition, counselors can equip spouses with supportive mental health resources for their family members so they do not feel as if they need to care for them on their own. School counselors, in particular, can provide support for military-connected students at school and can connect military families with resources within both the civilian and military communities to support their mental health and resilience (Cole, 2017; Quintana & Cole, 2021).
Our participants revealed that often the expectation of resilience is burdensome for spouses, which serves as a contradiction to its purposes. Counselors are called to acknowledge the challenges of the military lifestyle and provide support for navigating these challenges, rather than expecting spouses to face these hurdles alone. In addition, counselors might focus on more holistic manifestations of resilience, recognizing that some spouses can be resilient, yet still struggle. Approaching spouses from a strengths-based perspective, rather than from a deficit perspective, can be empowering within the counseling relationship (Smith, 2006).
Limitations
Our recruitment strategy limited our sample size as we only sought participants that we knew through our military spouse networks. In addition, our sample lacked gender diversity, with all of the participants being female. Approximately 91% of active-duty service member spouses are female (DoD, 2022). However, the lack of male participants in the present study is a limitation, and the experience of male spouses is undoubtedly unique and worth exploring in greater depth. Research suggests that stressors and characteristics of resilience transcend gender categories (NASEM, 2019).
Finally, in qualitative research, the researcher’s biases may impact their interpretation of the data. As military spouses, our own experiences may have impacted the way in which we described our participants’ experiences. We took several steps to mitigate these biases, including intentionally bracketing them and engaging in peer debriefing throughout the research process.
Implications for Future Research
The participants in our study described a need for resources and programs geared specifically toward military spouses. Future research might determine how to best develop and implement these programs that will help to enhance spouse resilience. Key areas of focus may be ways to leverage the military spouse community and enhance spouse sense of self, which were two protective factors that emerged from our data. In addition, existing resilience programs within the military that are currently aimed at the active-duty population should undergo a program evaluation to determine their effectiveness with military spouses.
As a follow-up to our qualitative research, future quantitative research studies should address limitations noted previously. Specifically, future research should target a larger sample size and broader demographic of military spouses to further explore their understanding and definition of resilience. This larger and more diverse sample size would allow for greater generalizability and would assist with advocacy within the military. Finally, future qualitative research might explore the perceptions of male spouses, in particular, in order to determine their perception of resiliency and any unique areas of needed support.
Conclusion
Military spouses face a wide range of challenges as a result of the military lifestyle. They are expected to be resilient so as to overcome these challenges. However, our study reveals the often burdensome impact of these expectations on military spouses. Our results also illuminate how spouses uniquely conceptualize their own resilience, recognizing the resilience continuum and focusing on the positive impact of their protective community. Overall, the spouses took pride in themselves and their communities for their ability to overcome obstacles. These revelations are key for both the military and the counseling profession in their work to support military spouses wherever they are on this continuum and enhance their community, which is key to their well-being.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript. The opinions and assertions
expressed herein are those of the authors and
do not reflect the official policy or position of
the Uniformed Services University of the Health
Sciences or the Department of Defense.
References
American Psychological Association. (2020). Building your resilience. https://www.apa.org/topics/resilience/building-your-resilience
Andrade, C. (2021). The inconvenient truth about convenience and purposive samples. Indian Journal of Psychological Medicine, 43(1), 86–88. https://doi.org/10.1177/0253717620977000
Blue Star Families. (2021). Military Family Lifestyle Survey: 2020 comprehensive report. https://bluestarfam.org/wp-content/uploads/2021/03/BSF_MFLS_CompReport_FULL.pdf
Blue Star Families. (2023). Military Family Lifestyle Survey: 2022 comprehensive report. https://bluestarfam.org/wp-content/uploads/2023/03/BSF_MFLS_Spring23_Full_Report_Digital.pdf
Borah, E., & Fina, B. (2017). Military spouses speak up: A qualitative study of military and veteran spouses’ perspectives. Journal of Family Social Work, 20(2), 144–161. https://doi.org/10.1080/10522158.2017.1284702
Cole, R. F. (2014). Understanding military culture: A guide for professional school counselors. The Professional Counselor, 4(5), 497–504. https://doi.org/10.15241/rfc.4.5.497
Cole, R. F. (2017). Supporting students in military families during times of transition: A call for awareness and action. Professional School Counseling, 20(1), 36–43. https://doi.org/10.5330/1096-2409-20.1.36
Cole, R. F., Cowan, R. G., Dunn, H., & Lincoln, T. (2021). Military spouses’ perceptions of suicide in the military spouse community. The Professional Counselor, 11(2), 203–217.
https://doi.org/10.15241/rfc.11.2.203
DaLomba, E., Greer, M. J., Cruz, E., Harris, A., King, C., Laurel, L., McCuaig, T., & Wilder, R. (2021). The experiences of active duty military spouses with advanced degrees in maintaining and advancing their careers. Work, 68(2), 387–398. https://doi.org/10.3233/WOR-203380
Donoho, C. J., LeardMann, C., O’Malley, C. A., Walter, K. H., Riviere, L. A., Curry, J. F., & Adler, A. B. (2018). Depression among military spouses: Demographic, military, and service member psychological health risk factors. Depression and Anxiety, 35(12), 1137–1144. https://doi.org/10.1002/da.22820
Dorvil, M. (2017). 2017 survey of active-duty spouses. Office of People Analytics, U.S. Department of Defense. https://download.militaryones ource.mil/12038/MOS/Surveys/2017-Survey-of-Active-Duty-Spouses-Overview-Briefing.pdf
Erbes, C. R., Kramer, M., Arbisi, P. A., DeGarmo, D., & Polusny, M. A. (2017). Characterizing spouse/partner depression and alcohol problems over the course of military deployment. Journal of Consulting and Clinical Psychology, 85(4), 297–308. https://doi.org/10.1037/ccp0000190
Joining Forces Interagency Policy Committee. (2021). Strengthening America’s military families: Matching their devotion: Deepening our commitment to the families, caregivers, and survivors of service members and veterans. https://www.whitehouse.gov/wp-content/uploads/2021/09/Strengthening_Americas_Military_Families.pdf
Lewy, C. S., Oliver, C. M., & McFarland, B. H. (2014). Barriers to mental health treatment for military wives. Psychiatric Services, 65(9), 1170–1173. https://doi.org/10.1176/appi.ps.201300325
Mailey, E. L., Mershon, C., Joyce, J., & Irwin, B. C. (2018). “Everything else comes first”: A mixed-methods analysis of barriers to health behaviors among military spouses. BMC Public Health, 18(1013), 1–11. https://doi.org/10.1186/s12889-018-5938-z
Marsh, M. K., & Hampton, R. L. (2022). Army medicine’s critical role in large-scale combat operations: Enable the force. Military Review, 102(4), 106–113.
Masten, A. S. (2014). Global perspectives on resilience in children and youth. Child Development, 85(1), 6–20. https://doi.org/10.1111/cdev.12205
Meadows, S. O., Beckett, M. K., Bowling, K., Golinelli, D., Fisher, M. P., Martin, L. T., Meredith, L. S., & Osilla, K. C. (2015). Family resilience in the military: Definitions, models, and policies. RAND Health Quarterly, 5(3).
Moerer-Urdahl, T. & Creswell, J. W. (2004). Using transcendental phenomenology to explore the “ripple effect” in a leadership mentoring program. International Journal of Qualitative Methods, 3(2), 19–35. https://doi.org/10.1177/160940690400300202
Moustafa, A. A., Crouse, J. J., Herzallah, M. M., Salama, M., Mohamed, W., Misiak, B., Frydecka, D., Al-Dosari, N. F., Megreya, A. M., & Mattock, K. (2020). Depression following major life transitions in women: A review and theory. Psychological Reports, 123(5), 1501–1517. https://doi.org/10.1177/0033294119872209
Moustakas, C. (1994). Phenomenological research methods. SAGE.
National Academies of Sciences, Engineering, and Medicine. (2019). Strengthening the military family readiness system for a changing American society. The National Academies Press. https://doi.org/10.17226/25380
Numbers, M., & Bruneau, L. (2017). Creating connections and fostering self-growth: Gestalt group counseling for military spouses. In Ideas and Research You Can Use: VISTAS 2017.
Panter-Brick, C. (2014). Health, risk, and resilience: Interdisciplinary concepts and applications. Annual Review of Anthropology, 43, 431–448. https://doi.org/10.1146/annurev-anthro-102313-025944
Pietrzak, R. H., & Southwick, S. M. (2011). Psychological resilience in OEF-OIF veterans: Application of a novel classification approach and examination of demographic and psychosocial correlates. Journal of Affective Disorders, 133(3), 560–568.
Quintana, T. S., & Cole, R. F. (2021). Forward march: Implementing the ASCA National Model to support military-connected students. Journal of School Counseling, 19(7). http://www.jsc.montana.edu/articles/v19n7.pdf
Richer, I., Frank, C., & Guérin, E. (2022). Understanding Special Operations Forces spouses challenges and resilience: A mixed-method study. Military Behavioral Health, 10(2), 100–111.
https://doi.org/10.1080/21635781.2022.2067921
Runge, C. E., Waller, M., MacKenzie, A., & McGuire, A. C. L. (2014). Spouses of military members’ experiences and insights: Qualitative analysis of responses to an open-ended question in a survey of health and wellbeing. PloS ONE, 9(12), e114755. https://doi.org/10.1371/journal.pone.0114755
Saunders, B., Sim, J., Kingstone, T., Baker, S., Waterfield, J., Bartlam, B., Burroughs, H., & Jinks, C. (2018). Saturation in qualitative research: Exploring its conceptualization and operationalization. Quality & Quantity, 52(4), 1893–1907. https://doi.org/10.1007/s11135-017-0574-8
Sefidan, S., Pramstaller, M., La Marca, R., Wyss, T., Sadeghi-Bahmani, D., Annen, H., & Brand, S. (2021). Resilience as a protective factor in basic military training, a longitudinal study of the Swiss Armed Forces. International Journal of Environmental Research and Public Health, 18(11), 6077. https://doi.org/10.3390/ijerph18116077
Simon, J. B., Murphy, J. J., & Smith, S. M. (2005). Understanding and fostering family resilience. The Family Journal, 13(4), 427–436. https://doi.org/10.1177/1066480705278724
Sinclair, R. R., Paulson, A. L., & Riviere, L. A. (2019). The resilient spouse: Understanding factors associated with dispositional resilience among military spouses. Military Behavioral Health, 7(4), 376–390. https://doi.org/10.1080/21635781.2019.1608876
Smith, E. J. (2006). The strength-based counseling model. The Counseling Psychologist, 34(1), 13–79.
https://doi.org/10.1177/0011000005277018
Southwick, S. M., Bonanno, G. A., Masten, A. S., Panter-Brick, C., & Yehuda, R. (2014). Resilience definitions, theory, and challenges: Interdisciplinary perspectives. European Journal of Psychotraumatology, 5(1), 25338. https://doi.org/10.3402/ejpt.v5.25338
Sullivan, K. S., Hawkins, S. A., Gilreath, T. D., & Castro, C. A. (2021). Mental health outcomes associated with profiles of risk and resilience among U.S. Army spouses. Journal of Family Psychology, 35(1), 33–43. https://doi.org/10.1037/fam0000702
U.S. Department of Defense, Office of the Deputy Assistant Secretary of Defense for Military Community and Family Policy. (2022). 2021 demographics profile: Profile of the military community. https://download.militaryonesource.mil/12038/MOS/Reports/2021-demographics-report.pdf
Verdeli, H., Baily, C., Vousoura, E., Belser, A., Singla, D., & Manos, G. (2011). The case for treating depression in military spouses. Journal of Family Psychology, 25(4), 488–496. https://doi.org/10.1037/a0024525
Villagran, M., Canzona, M. R., & Ledford, C. J. W. (2013). The milspouse battle rhythm: Communicating resilience throughout the deployment cycle. Health Communication, 28(8), 778–788. https://doi.org/10.1080/10410236.2013.800441
Walsh, F. (2012). Family resilience: Strengths forged through adversity. In F. Walsh (Ed.), Normal family processes: Growing diversity and complexity (4th ed.; pp. 399–423). Guilford.
Rebekah Cole, PhD, MEd, NCC, LPC, is a research associate professor at the Uniformed Services University. Christine Ward, PhD, is an associate professor at Walsh University. Taqueena Quintana, EdD, NCC, ACS, BC-TMH, LPC, is an associate professor at Antioch University. Elizabeth Burgin, PhD, NCC, LPC, RPT, CCCPTS, is an assistant professor and program coordinator of the Military and Veterans Counseling program at William & Mary. Correspondence may be addressed to Rebekah Cole, rebekah.cole@usuhs.edu.
Appendix
Interview Protocol
- Tell me a little about your identity as a military spouse?
- What have been some of your rewarding experiences as a military spouse?
- What have been some of your stressful experiences as a military spouse?
- How have you coped with the more stressful experiences as a military spouse?
- How would you describe the military’s definition of “resilience?”
- What does the term “resilience” mean to you?
- What does the term “resilience” mean for your military partner/family?
- How would you describe the resilience of military spouses?
- In what ways have you, personally, been resilient as a military spouse?
- What would enhance the resilience of military spouses and their families, from your perspective?
- How, if at all, has your military experience enhanced your resilience?
- How, if at all, has the military’s focus on resilience presented you with challenges during your military spouse experiences?
- How, if at all, can resilience be a negative way to describe military spouses/families?
- Is there anything else about military resilience that is important to you that I did not ask about?
Aug 20, 2021 | Author Videos, Volume 11 - Issue 3
Warren N. Ponder, Elizabeth A. Prosek, Tempa Sherrill
First responders are continually exposed to trauma-related events. Resilience is evidenced as a protective factor for mental health among first responders. However, there is a lack of assessments that measure the construct of resilience from a strength-based perspective. The present study used archival data from a treatment-seeking sample of 238 first responders to validate the 22-item Response to Stressful Experiences Scale (RSES-22) and its abbreviated version, the RSES-4, with two confirmatory factor analyses. Using a subsample of 190 first responders, correlational analyses were conducted of the RSES-22 and RSES-4 with measures of depressive symptoms, post-traumatic stress, anxiety, and suicidality confirming convergent and criterion validity. The two confirmatory analyses revealed a poor model fit for the RSES-22; however, the RSES-4 demonstrated an acceptable model fit. Overall, the RSES-4 may be a reliable and valid measure of resilience for treatment-seeking first responder populations.
Keywords: first responders, resilience, assessment, mental health, confirmatory factor analysis
First responder populations (i.e., law enforcement, emergency medical technicians, and fire rescue) are often repeatedly exposed to traumatic and life-threatening conditions (Greinacher et al., 2019). Researchers have concluded that such critical incidents could have a deleterious impact on first responders’ mental health, including the development of symptoms associated with post-traumatic stress, anxiety, depression, or other diagnosable mental health disorders (Donnelly & Bennett, 2014; Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). In a systematic review, Wild et al. (2020) suggested the promise of resilience-based interventions to relieve trauma-related psychological disorders among first responders. However, they noted the operationalization and measure of resilience as limitations to their intervention research. Indeed, researchers have conflicting viewpoints on how to define and assess resilience. For example, White et al. (2010) purported popular measures of resilience rely on a deficit-based approach. Counselors operate from a strength-based lens (American Counseling Association [ACA], 2014) and may prefer measures with a similar perspective. Additionally, counselors are mandated to administer assessments with acceptable psychometric properties that are normed on populations representative of the client (ACA, 2014, E.6.a., E.7.d.). For counselors working with first responder populations, resilience may be a factor of importance; however, appropriately measuring the construct warrants exploration. Therefore, the focus of this study was to validate a measure of resilience with strength-based principles among a sample of first responders.
Risk and Resilience Among First Responders
In a systematic review of the literature, Greinacher et al. (2019) described the incidents that first responders may experience as traumatic, including first-hand life-threatening events; secondary exposure and interaction with survivors of trauma; and frequent exposure to death, dead bodies, and injury. Law enforcement officers (LEOs) reported that the most severe critical incidents they encounter are making a mistake that injures or kills a colleague; having a colleague intentionally killed; and making a mistake that injures or kills a bystander (Weiss et al., 2010). Among emergency medical technicians (EMTs), critical incidents that evoked the most self-reported stress included responding to a scene involving family, friends, or others to the crew and seeing someone dying (Donnelly & Bennett, 2014). Exposure to these critical incidents may have consequences for first responders. For example, researchers concluded first responders may experience mental health symptoms as a result of the stress-related, repeated exposure (Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Moreover, considering the cumulative nature of exposure (Donnelly & Bennett, 2014), researchers concluded first responders are at increased risk for post-traumatic stress disorder (PTSD), depression, and generalized anxiety symptoms (Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Symptoms commonly experienced among first responders include those associated with post-traumatic stress, anxiety, and depression.
In a collective review of first responders, Kleim and Westphal (2011) determined a prevalence rate for PTSD of 8%–32%, which is higher than the general population lifetime rate of 6.8–7.8 % (American Psychiatric Association [APA], 2013; National Institute of Mental Health [NIMH], 2017). Some researchers have explored rates of PTSD by specific first responder population. For example, Klimley et al. (2018) concluded that 7%–19% of LEOs and 17%–22% of firefighters experience PTSD. Similarly, in a sample of LEOs, Jetelina and colleagues (2020) reported 20% of their participants met criteria for PTSD.
Generalized anxiety and depression are also prevalent mental health symptoms for first responders. Among a sample of firefighters and EMTs, 28% disclosed anxiety at moderate–severe and several levels (Jones et al., 2018). Furthermore, 17% of patrol LEOs reported an overall prevalence of generalized anxiety disorder (Jetelina et al., 2020). Additionally, first responders may be at higher risk for depression (Klimley et al., 2018), with estimated prevalence rates of 16%–26% (Kleim & Westphal, 2011). Comparatively, the past 12-month rate of major depressive disorder among the general population is 7% (APA, 2013). In a recent study, 16% of LEOs met criteria for major depressive disorder (Jetelina et al., 2020). Moreover, in a sample of firefighters and EMTs, 14% reported moderate–severe and severe depressive symptoms (Jones et al., 2018). Given these higher rates of distressful mental health symptoms, including post-traumatic stress, generalized anxiety, and depression, protective factors to reduce negative impacts are warranted.
Resilience
Broadly defined, resilience is “the ability to adopt to and rebound from change (whether it is from stress or adversity) in a healthy, positive and growth-oriented manner” (Burnett, 2017, p. 2). White and colleagues (2010) promoted a positive psychology approach to researching resilience, relying on strength-based characteristics of individuals who adapt after a stressor event. Similarly, other researchers explored how individuals’ cognitive flexibility, meaning-making, and restoration offer protection that may be collectively defined as resilience (Johnson et al., 2011).
A key element among definitions of resilience is one’s exposure to stress. Given their exposure to trauma-related incidents, first responders require the ability to cope or adapt in stressful situations (Greinacher et al., 2019). Some researchers have defined resilience as a strength-based response to stressful events (Burnett, 2017), in which healthy coping behaviors and cognitions allow individuals to overcome adverse experiences (Johnson et al., 2011; White et al., 2010). When surveyed about positive coping strategies, first responders most frequently reported resilience as important to their well-being (Crowe et al., 2017).
Researchers corroborated the potential impact of resilience for the population. For example, in samples of LEOs, researchers confirmed resilience served as a protective factor for PTSD (Klimley et al., 2018) and as a mediator between social support and PTSD symptoms (McCanlies et al., 2017). In a sample of firefighters, individual resilience mediated the indirect path between traumatic events and global perceived stress of PTSD, along with the direct path between traumatic events and PTSD symptoms (Lee et al., 2014). Their model demonstrated that those with higher levels of resilience were more protected from traumatic stress. Similarly, among emergency dispatchers, resilience was positively correlated with positive affect and post-traumatic growth, and negatively correlated with job stress (Steinkopf et al., 2018). The replete associations of resilience as a protective factor led researchers to develop resilience-based interventions. For example, researchers surmised promising results from mindfulness-based resilience interventions for firefighters (Joyce et al., 2019) and LEOs (Christopher et al., 2018). Moreover, Antony and colleagues (2020) concluded that resilience training programs demonstrated potential to reduce occupational stress among first responders.
Assessment of Resilience
Recognizing the significance of resilience as a mediating factor in PTSD among first responders and as a promising basis for interventions when working with LEOs, a reliable means to measure it among first responder clients is warranted. In a methodological review of resilience assessments, Windle and colleagues (2011) identified 19 different measures of resilience. They found 15 assessments were from original development and validation studies with four subsequent validation manuscripts from their original assessment, of which none were developed with military or first responder samples.
Subsequently, Johnson et al. (2011) developed the Response to Stressful Experiences Scale (RSES-22) to assess resilience among military populations. Unlike deficit-based assessments of resilience, they proposed a multidimensional construct representing how individuals respond to stressful experiences in adaptive or healthy ways. Cognitive flexibility, meaning-making, and restoration were identified as key elements when assessing for individuals’ characteristics connected to resilience when overcoming hardships. Initially they validated a five-factor structure for the RSES-22 with military active-duty and reserve components. Later, De La Rosa et al. (2016) re-examined the RSES-22. De La Rosa and colleagues discovered a unidimensional factor structure of the RSES-22 and validated a shorter 4-item subset of the instrument, the RSES-4, again among military populations.
It is currently unknown if the performance of the RSES-4 can be generalized to first responder populations. While there are some overlapping experiences between military populations and first responders in terms of exposure to trauma and high-risk occupations, the Substance Abuse and Mental Health Services Administration (SAMHSA; 2018) suggested differences in training and types of risk. In the counseling profession, these populations are categorized together, as evidenced by the Military and Government Counseling Association ACA division. Additionally, there may also be dual identities within the populations. For example, Lewis and Pathak (2014) found that 22% of LEOs and 15% of firefighters identified as veterans. Although the similarities of the populations may be enough to theorize the use of the same resilience measure, validation of the RSES-22 and RSES-4 among first responders remains unexamined.
Purpose of the Study
First responders are repeatedly exposed to traumatic and stressful events (Greinacher et al., 2019) and this exposure may impact their mental health, including symptoms of post-traumatic stress, anxiety, depression, and suicidality (Jetelina et al., 2020; Klimley et al., 2018). Though most measures of resilience are grounded in a deficit-based approach, researchers using a strength-based approach proposed resilience may be a protective factor for this population (Crowe et al., 2017; Wild et al., 2020). Consequently, counselors need a means to assess resilience in their clinical practice from a strength-based conceptualization of clients.
Johnson et al. (2011) offered a non-deficit approach to measuring resilience in response to stressful events associated with military service. Thus far, researchers have conducted analyses of the RSES-22 and RSES-4 with military populations (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021), but not yet with first responders. While there are some overlapping characteristics between the populations, there are also unique differences that warrant research with discrete sampling (SAMHSA, 2018). In light of the importance of resilience as a protective factor for mental health among first responders, the purpose of the current study was to confirm the reliability and validity of the RSES-22 and RSES-4 when utilized with this population. In the current study, we hypothesized the measures would perform similarly among first responders and if so, the RSES-4 would offer counselors a brief assessment option in clinical practice that is both reliable and valid.
Method
Participants
Participants in the current non-probability, purposive sample study were first responders (N = 238) seeking clinical treatment at an outpatient, mental health nonprofit organization in the Southwestern United States. Participants’ mean age was 37.53 years (SD = 10.66). The majority of participants identified as men (75.2%; n = 179), with women representing 24.8% (n = 59) of the sample. In terms of race and ethnicity, participants identified as White (78.6%; n = 187), Latino/a (11.8%; n = 28), African American or Black (5.5%; n = 13), Native American (1.7%; n = 4), Asian American (1.3%; n = 3), and multiple ethnicities (1.3%; n = 3). The participants identified as first responders in three main categories: LEO (34.9%; n = 83), EMT (28.2%; n = 67), and fire rescue (25.2%; n = 60). Among the first responders, 26.9% reported previous military affiliation. As part of the secondary analysis, we utilized a subsample (n = 190) that was reflective of the larger sample (see Table 1).
Procedure
The data for this study were collected between 2015–2020 as part of the routine clinical assessment procedures at a nonprofit organization serving military service members, first responders, frontline health care workers, and their families. The agency representatives conduct clinical assessments with clients at intake, Session 6, Session 12, and Session 18 or when clinical services are concluded. We consulted with the second author’s Institutional Review Board, which determined the research as exempt, given the de-identified, archival nature of the data. For inclusion in this analysis, data needed to represent first responders, ages 18 or older, with a completed RSES-22 at intake. The RSES-4 are four questions within the RSES-22 measure; therefore, the participants did not have to complete an additional measure. For the secondary analysis, data from participants who also completed other mental health measures at intake were also included (see Measures).
Table 1
Demographics of Sample
| Characteristic |
Sample 1
(N = 238) |
Sample 2
(n = 190) |
| Age (Years) |
|
|
| Mean |
37.53 |
37.12 |
| Median |
35.50 |
35.00 |
| SD |
10.66 |
10.30 |
| Range |
46 |
45 |
| Time in Service (Years) |
|
|
| Mean |
11.62 |
11.65 |
| Median |
10.00 |
10.00 |
| SD |
9.33 |
9.37 |
| Range |
41 |
39 |
|
n (%) |
| First Responder Type |
|
|
Emergency Medical
Technicians |
67 (28.2%) |
54 (28.4%) |
| Fire Rescue |
60 (25.2%) |
45 (23.7%) |
| Law Enforcement |
83 (34.9%) |
72 (37.9%) |
| Other |
9 (3.8%) |
5 (2.6%) |
| Two or more |
10 (4.2%) |
6 (3.2%) |
| Not reported |
9 (3.8%) |
8 (4.2%) |
| Gender |
|
|
| Women |
59 (24.8%) |
47 (24.7%) |
| Men |
179 (75.2%) |
143 (75.3%) |
| Ethnicity |
|
|
| African American/Black |
13 (5.5%) |
8 (4.2%) |
| Asian American |
3 (1.3%) |
3 (1.6%) |
| Latino(a)/Hispanic |
28 (11.8%) |
24 (12.6%) |
| Multiple Ethnicities |
3 (1.3%) |
3 (1.6%) |
| Native American |
4 (1.7%) |
3 (1.6%) |
| White |
187 (78.6%) |
149 (78.4%) |
Note. Sample 2 is a subset of Sample 1. Time in service for Sample 1, n = 225;
time in service for Sample 2, n = 190.
Measures
Response to Stressful Experiences Scale
The Response to Stressful Experiences Scale (RSES-22) is a 22-item measure to assess dimensions of resilience, including meaning-making, active coping, cognitive flexibility, spirituality, and self-efficacy (Johnson et al., 2011). Participants respond to the prompt “During and after life’s most stressful events, I tend to” on a 5-point Likert scale from 0 (not at all like me) to 4 (exactly like me). Total scores range from 0 to 88 in which higher scores represent greater resilience. Example items include see it as a challenge that will make me better, pray or meditate, and find strength in the meaning, purpose, or mission of my life. Johnson et al. (2011) reported the RSES-22 demonstrates good internal consistency (α = .92) and test-retest reliability (α = .87) among samples from military populations. Further, the developers confirmed convergent, discriminant, concurrent, and incremental criterion validity (see Johnson et al., 2011). In the current study, Cronbach’s alpha of the total score was .93.
Adapted Response to Stressful Experiences Scale
The adapted Response to Stressful Experiences Scale (RSES-4) is a 4-item measure to assess resilience as a unidimensional construct (De La Rosa et al., 2016). The prompt and Likert scale are consistent with the original RSES-22; however, it only includes four items: find a way to do what’s necessary to carry on, know I will bounce back, learn important and useful life lessons, and practice ways to handle it better next time. Total scores range from 0 to 16, with higher scores indicating greater resilience. De La Rosa et al. (2016) reported acceptable internal consistency (α = .76–.78), test-retest reliability, and demonstrated criterion validity among multiple military samples. In the current study, the Cronbach’s alpha of the total score was .74.
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) is a 9-item measure to assess depressive symptoms in the past 2 weeks (Kroenke et al., 2001). Respondents rate the frequency of their symptoms on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 27, in which higher scores indicate increased severity of depressive symptoms. Example items include little interest or pleasure in doing things and feeling tired or having little energy. Kroenke et al. (2001) reported good internal consistency (α = .89) and established criterion and construct validity. In this sample, Cronbach’s alpha of the total score was .88.
PTSD Checklist-5
The PTSD Checklist-5 (PCL-5) is a 20-item measure for the presence of PTSD symptoms in the past month (Blevins et al., 2015). Participants respond on a 5-point Likert scale indicating frequency of PTSD-related symptoms from 0 (not at all) to 4 (extremely). Total scores range from 0 to 80, in which higher scores indicate more severity of PTSD-related symptoms. Example items include repeated, disturbing dreams of the stressful experience and trouble remembering important parts of the stressful experience. Blevins et al. (2015) reported good internal consistency (α = .94) and determined convergent and discriminant validity. In this sample, Cronbach’s alpha of the total score was .93.
Generalized Anxiety Disorder-7
The Generalized Anxiety Disorder-7 (GAD-7) is a 7-item measure to assess for anxiety symptoms over the past 2 weeks (Spitzer et al., 2006). Participants rate the frequency of the symptoms on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 21 with higher scores indicating greater severity of anxiety symptoms. Example items include not being able to stop or control worrying and becoming easily annoyed or irritable. Among patients from primary care settings, Spitzer et al. (2006) determined good internal consistency (α = .92) and established criterion, construct, and factorial validity. In this sample, Cronbach’s alpha of the total score was .91.
Suicidal Behaviors Questionnaire-Revised
The Suicidal Behaviors Questionnaire-Revised (SBQ-R) is a 4-item measure to assess suicidality (Osman et al., 2001). Each item assesses a different dimension of suicidality: lifetime ideation and attempts, frequency of ideation in the past 12 months, threat of suicidal behaviors, and likelihood of suicidal behaviors (Gutierrez et al., 2001). Total scores range from 3 to 18, with higher scores indicating more risk of suicide. Example items include How often have you thought about killing yourself in the past year? and How likely is it that you will attempt suicide someday? In a clinical sample, Osman et al. (2001) reported good internal consistency (α = .87) and established criterion validity. In this sample, Cronbach’s alpha of the total score was .85.
Data Analysis
Statistical analyses were conducted using SPSS version 26.0 and SPSS Analysis of Moment Structures (AMOS) version 26.0. We examined the dataset for missing values, replacing 0.25% (32 of 12,836 values) of data with series means. We reviewed descriptive statistics of the RSES-22 and RSES-4 scales. We determined multivariate normality as evidenced by skewness less than 2.0 and kurtosis less than 7.0 (Dimitrov, 2012). We assessed reliability for the scales by interpreting Cronbach’s alphas and inter-item correlations to confirm internal consistency.
We conducted two separate confirmatory factor analyses to determine the model fit and factorial validity of the 22-item measure and adapted 4-item measure. We used several indices to conclude model fit: minimum discrepancy per degree of freedom (CMIN/DF) and p-values, root mean residual (RMR), goodness-of-fit index (GFI), comparative fit index (CFI), Tucker-Lewis index (TLI), and the root mean square error of approximation (RMSEA). According to Dimitrov (2012), values for the CMIN/DF < 2.0,p > .05, RMR < .08, GFI > .90, CFI > .90, TLI > .90, and RMSEA < .10 provide evidence of a strong model fit. To determine criterion validity, we assessed a subsample of participants (n = 190) who had completed the RSES-22, RSES-4, and four other psychological measures (i.e., PHQ-9, PCL-5, GAD-7, and SBQ-R). We determined convergent validity by conducting bivariate correlations between the RSES-22 and RSES-4.
Results
Descriptive Analyses
We computed means, standard deviations, 95% confidence interval (CI), and score ranges for the RSES-22 and RSES-4 (Table 2). Scores on the RSES-22 ranged from 19–88. Scores on the RSES-4 ranged from 3–16. Previous researchers using the RSES-22 on military samples reported mean scores of 57.64–70.74 with standard deviations between 8.15–15.42 (Johnson et al., 2011; Prosek & Ponder, 2021). In previous research of the RSES-4 with military samples, mean scores were 9.95–11.20 with standard deviations between 3.02–3.53(De La Rosa et al., 2016; Prosek & Ponder, 2021).
Table 2
Descriptive Statistics for RSES-22 and RSES-4
| Variable |
M |
SD |
95% CI |
Score Range |
| RSES-22 scores |
60.12 |
13.76 |
58.52, 61.86 |
19–88 |
| RSES-4 scores |
11.66 |
2.62 |
11.33, 11.99 |
3–16 |
Note. N = 238. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response
to Stressful Experiences Scale 4-item adaptation.
Reliability Analyses
To determine the internal consistency of the resiliency measures, we computed Cronbach’s alphas. For the RSES-22, we found strong evidence of inter-item reliability (α = .93), which was consistent with the developers’ estimates (α = .93; Johnson et al., 2011). For the RSES-4, we assessed acceptable inter-item reliability (α = .74), which was slightly lower than previous estimates (α = .76–.78; De La Rosa et al., 2016). We calculated the correlation between items and computed the average of all the coefficients. The average inter-item correlation for the RSES-22 was .38, which falls within the acceptable range (.15–.50). The average inter-item correlation for the RSES-4 was .51, slightly above the acceptable range. Overall, evidence of internal consistency was confirmed for each scale.
Factorial Validity Analyses
We conducted two confirmatory factor analyses to assess the factor structure of the RSES-22 and RSES-4 for our sample of first responders receiving mental health services at a community clinic (Table 3). For the RSES-22, a proper solution converged in 10 iterations. Item loadings ranged between .31–.79, with 15 of 22 items loading significantly ( > .6) on the latent variable. It did not meet statistical criteria for good model fit: χ2 (209) = 825.17, p = .000, 90% CI [0.104, 0.120]. For the RSES-4, a proper solution converged in eight iterations. Item loadings ranged between .47–.80, with three of four items loading significantly ( > .6) on the latent variable. It met statistical criteria for good model fit: χ2 (2) = 5.89, p = .053, 90% CI [0.000, 0.179]. The CMIN/DF was above the suggested < 2.0 benchmark; however, the other fit indices indicated a model fit.
Table 3
Confirmatory Factor Analysis Fit Indices for RSES-22 and RSES-4
| Variable |
df |
χ2 |
CMIN/DF |
RMR |
GFI |
CFI |
TLI |
RMSEA |
90% CI |
| RSES-22 |
209 |
825.17/.000 |
3.95 |
.093 |
.749 |
.771 |
0.747 |
.112 |
0.104, 0.120 |
| RSES-4 |
2 |
5.89/.053 |
2.94 |
.020 |
.988 |
.981 |
0.944 |
.091 |
0.000, 0.179 |
Note. N = 238. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response to Stressful Experiences Scale 4-item adaptation; CMIN/DF = Minimum Discrepancy per Degree of Freedom; RMR = Root Mean Square Residual;
GFI = Goodness-of-Fit Index; CFI = Comparative Fit Index; TLI = Tucker-Lewis Index; RMSEA = Root Mean Squared Error of Approximation.
Criterion and Convergent Validity Analyses
To assess for criterion validity of the RSES-22 and RSES-4, we conducted correlational analyses with four established psychological measures (Table 4). We utilized a subsample of participants (n = 190) who completed the PHQ-9, PCL-5, GAD-7, and SBQ-R at intake. Normality of the data was not a concern because analyses established appropriate ranges for skewness and kurtosis (± 1.0). The internal consistency of the RSES-22 (α = .93) and RSES-4 (α = .77) of the subsample was comparable to the larger sample and previous studies. The RSES-22 and RSES-4 related to the psychological measures of distress in the expected direction, meaning measures were significantly and negatively related, indicating that higher resiliency scores were associated with lower scores of symptoms associated with diagnosable mental health disorders (i.e., post-traumatic stress, anxiety, depression, and suicidal behavior). We verified convergent validity with a correlational analysis of the RSES-22 and RSES-4, which demonstrated a significant and positive relationship.
Table 4
Criterion and Convergent Validity of RSES-22 and RSES-4
|
M (SD) |
Cronbach’s α |
RSES-22 |
PHQ-9 |
PCL-5 |
GAD-7 |
SBQ-R |
| RSES-22 |
60.16 (14.17) |
.93 |
— |
−.287* |
−.331* |
−.215* |
−.346* |
| RSES-4 |
11.65 (2.68) |
.77 |
.918 |
−.290* |
−.345* |
−.220* |
−.327* |
Note. n = 190. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response to Stressful Experiences Scale 4-item adaptation; PHQ-9 = Patient Health Questionnaire-9;
PCL-5 = PTSD Checklist-5; GAD-7 = Generalized Anxiety Disorder-7; SBQ-R = Suicidal Behaviors Questionnaire-Revised.
*p < .01.
Discussion
The purpose of this study was to validate the factor structure of the RSES-22 and the abbreviated RSES-4 with a first responder sample. Aggregated means were similar to those in the articles that validated and normed the measures in military samples (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021). Additionally, the internal consistency was similar to previous studies. In the original article, Johnson et al. (2011) proposed a five-factor structure for the RSES-22, which was later established as a unidimensional assessment after further exploratory factor analysis (De La Rosa et al., 2016). Subsequently, confirmatory factor analyses with a treatment-seeking veteran population revealed that the RSES-22 demonstrated unacceptable model fit, whereas the RSES-4 demonstrated a good model fit (Prosek & Ponder, 2021). In both samples, the RSES-4 GFI, CFI, and TLI were all .944 or higher, whereas the RSES-22 GFI, CFI, and TLI were all .771 or lower. Additionally, criterion and convergent validity as measured by the PHQ-9, PCL-5, and GAD-7 in both samples were extremely close. Similarly, in this sample of treatment-seeking first responders, confirmatory factor analyses indicated an inadequate model fit for the RSES-22 and a good model fit for the RSES-4. Lastly, convergent and criterion validity were established with correlation analyses of the RSES-22 and RSES-4 with four other standardized assessment instruments (i.e., PHQ-9, PCL-5, GAD-7, SBQ-R). We concluded that among the first responder sample, the RSES-4 demonstrated acceptable psychometric properties, as well as criterion and convergent validity with other mental health variables (i.e., post-traumatic stress, anxiety, depression, and suicidal behavior).
Implications for Clinical Practice
First responders are a unique population and are regularly exposed to trauma (Donnelly & Bennett, 2014; Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Although first responders could potentially benefit from espousing resilience, they are often hesitant to seek mental health services (Crowe et al., 2017; Jones, 2017). The RSES-22 and RSES-4 were originally normed with military populations. The results of the current study indicated initial validity and reliability among a first responder population, revealing that the RSES-4 could be useful for counselors in assessing resilience.
It is important to recognize that first responders have perceived coping with traumatic stress as an individual process (Crowe et al., 2017) and may believe that seeking mental health services is counter to the emotional and physical training expectations of the profession (Crowe et al., 2015). Therefore, when first responders seek mental health care, counselors need to be prepared to provide culturally responsive services, including population-specific assessment practices and resilience-oriented care.
Jones (2017) encouraged a comprehensive intake interview and battery of appropriate assessments be conducted with first responder clients. Counselors need to balance the number of intake questions while responsibly assessing for mental health comorbidities such as post-traumatic stress, anxiety, depression, and suicidality. The RSES-4 provides counselors a brief, yet targeted assessment of resilience.
Part of what cultural competency entails is assessing constructs (e.g., resilience) that have been shown to be a protective factor against PTSD among first responders (Klimley et al., 2018). Since the items forming the RSES-4 were developed to highlight the positive characteristics of coping (Johnson et al., 2011), rather than a deficit approach, this aligns with the grounding of the counseling profession. It is also congruent with first responders’ perceptions of resilience. Indeed, in a content analysis of focus group interviews with first responders, participants defined resilience as a positive coping strategy that involves emotional regulation, perseverance, personal competence, and physical fitness (Crowe et al., 2017).
The RSES-4 is a brief, reliable, and valid measure of resilience with initial empirical support among a treatment-seeking first responder sample. In accordance with the ACA (2014) Code of Ethics, counselors are to administer assessments normed with the client population (E.8.). Thus, the results of the current study support counselors’ use of the measure in practice. First responder communities are facing unprecedented work tasks in response to COVID-19. Subsequently, their mental health might suffer (Centers for Disease Control and Prevention, 2020) and experts have recommended promoting resilience as a protective factor for combating the negative mental health consequences of COVID-19 (Chen & Bonanno, 2020). Therefore, the relevance of assessing resilience among first responder clients in the current context is evident.
Limitations and Future Research
This study is not without limitations. The sample of first responders was homogeneous in terms of race, ethnicity, and gender. Subsamples of first responders (i.e., LEO, EMT, fire rescue) were too small to conduct within-group analyses to determine if the factor structure of the RSES-22 and RSES-4 would perform similarly. Also, our sample of first responders included two emergency dispatchers. Researchers reported that emergency dispatchers should not be overlooked, given an estimated 13% to 15% of emergency dispatchers experience post-traumatic symptomatology (Steinkopf et al., 2018). Future researchers may develop studies that further explore how, if at all, emergency dispatchers are represented in first responder research.
Furthermore, future researchers could account for first responders who have prior military service. In a study of LEOs, Jetelina et al. (2020) found that participants with military experience were 3.76 times more likely to report mental health concerns compared to LEOs without prior military affiliation. Although we reported the prevalence rate of prior military experience in our sample, the within-group sample size was not sufficient for additional analyses. Finally, our sample represented treatment-seeking first responders. Future researchers may replicate this study with non–treatment-seeking first responder populations.
Conclusion
First responders are at risk for sustaining injuries, experiencing life-threatening events, and witnessing harm to others (Lanza et al., 2018). The nature of their exposure can be repeated and cumulative over time (Donnelly & Bennett, 2014), indicating an increased risk for post-traumatic stress, anxiety, and depressive symptoms, as well as suicidal behavior (Jones et al., 2018). Resilience is a promising protective factor that promotes wellness and healthy coping among first responders (Wild et al., 2020), and counselors may choose to routinely measure for resilience among first responder clients. The current investigation concluded that among a sample of treatment-seeking first responders, the original factor structure of the RSES-22 was unstable, although it demonstrated good reliability and validity. The adapted version, RSES-4, demonstrated good factor structure while also maintaining acceptable reliability and validity, consistent with studies of military populations (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021). The RSES-4 provides counselors with a brief and strength-oriented option for measuring resilience with first responder clients.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Antony, J., Brar, R., Khan, P. A., Ghassemi, M., Nincic, V., Sharpe, J. P., Straus, S. E., & Tricco, A. C. (2020). Interventions for the prevention and management of occupational stress injury in first responders: A rapid overview of reviews. Systematic Reviews, 9(121), 1–20. https://doi.org/10.1186/s13643-020-01367-w
Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., & Domino, J. L. (2015). The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress, 28(6), 489–498. https://doi.org/10.1002/jts.22059
Burnett, H. J., Jr. (2017). Revisiting the compassion fatigue, burnout, compassion satisfaction, and resilience connection among CISM responders. Journal of Police Emergency Response, 7(3), 1–10. https://doi.org/10.1177/2158244017730857
Centers for Disease Control and Prevention. (2020, June 30). Coping with stress. https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html
Chen, S., & Bonanno, G. A. (2020). Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S51–S54. https://doi.org/10.1037/tra0000685
Christopher, M. S., Hunsinger, M., Goerling, R. J., Bowen, S., Rogers, B. S., Gross, C. R., Dapolonia, E., & Pruessner, J. C. (2018). Mindfulness-based resilience training to reduce health risk, stress reactivity, and aggression among law enforcement officers: A feasibility and preliminary efficacy trial. Psychiatry Research, 264, 104–115. https://doi.org/10.1016/j.psychres.2018.03.059
Crowe, A., Glass, J. S., Lancaster, M. F., Raines, J. M., & Waggy, M. R. (2015). Mental illness stigma among first responders and the general population. Journal of Military and Government Counseling, 3(3), 132–149. http://mgcaonline.org/wp-content/uploads/2013/02/JMGC-Vol-3-Is-3.pdf
Crowe, A., Glass, J. S., Lancaster, M. F., Raines, J. M., & Waggy, M. R. (2017). A content analysis of psychological resilience among first responders. SAGE Open, 7(1), 1–9. https://doi.org/10.1177/2158244017698530
De La Rosa, G. M., Webb-Murphy, J. A., & Johnston, S. L. (2016). Development and validation of a brief measure of psychological resilience: An adaptation of the Response to Stressful Experiences Scale. Military Medicine, 181(3), 202–208. https://doi.org/10.7205/MILMED-D-15-00037
Dimitrov, D. M. (2012). Statistical methods for validation of assessment scale data in counseling and related fields. American Counseling Association.
Donnelly, E. A., & Bennett, M. (2014). Development of a critical incident stress inventory for the emergency medical services. Traumatology, 20(1), 1–8. https://doi.org/10.1177/1534765613496646
Greinacher, A., Derezza-Greeven, C., Herzog, W., & Nikendei, C. (2019). Secondary traumatization in first responders: A systematic review. European Journal of Psychotraumatology, 10(1), 1562840. https://doi.org/10.1080/20008198.2018.1562840
Gutierrez, P. M., Osman, A., Barrios, F. X., & Kopper, B. A. (2001). Development and initial validation of the Self-Harm Behavior Questionnaire. Journal of Personality Assessment, 77(3), 475–490. https://doi.org/10.1207/S15327752JPA7703_08
Jetelina, K. K., Mosberry, R. J., Gonzalez, J. R., Beauchamp, A. M., & Hall, T. (2020). Prevalence of mental illnesses and mental health care use among police officers. JAMA Network Open, 3(10), 1–12. https://doi.org/10.1001/jamanetworkopen.2020.19658
Johnson, D. C., Polusny, M. A., Erbes, C. R., King, D., King, L., Litz, B. T., Schnurr, P. P., Friedman, M., Pietrzak, R. H., & Southwick, S. M. (2011). Development and initial validation of the Response to Stressful Experiences Scale. Military Medicine, 176(2), 161–169. https://doi.org/10.7205/milmed-d-10-00258
Jones, S. (2017). Describing the mental health profile of first responders: A systematic review. Journal of the American Psychiatric Nurses Association, 23(3), 200–214. https://doi.org/10.1177/1078390317695266
Jones, S., Nagel, C., McSweeney, J., & Curran, G. (2018). Prevalence and correlates of psychiatric symptoms among first responders in a Southern state. Archives of Psychiatric Nursing, 32(6), 828–835. https://doi.org/10.1016/j.apnu.2018.06.007
Joyce, S., Tan, L., Shand, F., Bryant, R. A., & Harvey, S. B. (2019). Can resilience be measured and used to predict mental health symptomology among first responders exposed to repeated trauma? Journal of Occupational and Environmental Medicine, 61(4), 285–292. https://doi.org/10.1097/JOM.0000000000001526
Kleim, B., & Westphal, M. (2011). Mental health in first responders: A review and recommendation for prevention and intervention strategies. Traumatology, 17(4), 17–24. https://doi.org/10.1177/1534765611429079
Klimley, K. E., Van Hasselt, V. B., & Stripling, A. M. (2018). Posttraumatic stress disorder in police, firefighters, and emergency dispatchers. Aggression and Violent Behavior, 43, 33–44.
https://doi.org/10.1016/j.avb.2018.08.005
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Lanza, A., Roysircar, G., & Rodgers, S. (2018). First responder mental healthcare: Evidence-based prevention, postvention, and treatment. Professional Psychology: Research and Practice, 49(3), 193–204. https://doi.org/10.1037/pro0000192
Lee, J.-S., Ahn, Y.-S., Jeong, K.-S. Chae, J.-H., & Choi, K.-S. (2014). Resilience buffers the impact of traumatic events on the development of PTSD symptoms in firefighters. Journal of Affective Disorders, 162, 128–133. https://doi.org/10.1016/j.jad.2014.02.031
Lewis, G. B., & Pathak, R. (2014). The employment of veterans in state and local government service. State and Local Government Review, 46(2), 91–105. https://doi.org/10.1177/0160323X14537835
McCanlies, E. C., Gu, J. K., Andrew, M. E., Burchfiel, C. M., & Violanti, J. M. (2017). Resilience mediates the relationship between social support and post-traumatic stress symptoms in police officers. Journal of Emergency Management, 15(2), 107–116. https://doi.org/10.5055/jem.2017.0319
National Institute of Mental Health. (2017). Post-traumatic stress disorder. https://www.nimh.nih.gov/health/statistics/post-traumatic-stress-disorder-ptsd.shtml
Osman, A., Bagge, C. L., Gutierrez, P. M., Konick, L. C., Kopper, B. A., & Barrios, F. X. (2001). The Suicidal Behaviors Questionnaire–revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment, 8(4), 443–454. https://doi.org/10.1177/107319110100800409
Prosek, E. A., & Ponder, W. N. (2021). Validation of the Adapted Response to Stressful Experiences Scale (RSES-4) among veterans [Manuscript submitted for publication].
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder (The GAD-7). Archives of Internal Medicine, 166(10), 1092–1097.
https://doi.org/10.1001/archinte.166.10.1092
Steinkopf, B., Reddin, R. A., Black, R. A., Van Hasselt, V. B., & Couwels, J. (2018). Assessment of stress and resiliency in emergency dispatchers. Journal of Police and Criminal Psychology, 33(4), 398–411.
https://doi.org /10.1007/s11896-018-9255-3
Substance Abuse and Mental Health Services Administration. (2018, May). First responders: Behavioral health concerns, emergency response, and trauma. Disaster Technical Assistance Center Supplemental Research Bulletin. https://www.samhsa.gov/sites/default/files/dtac/supplementalresearchbulletin-firstresponders-may2018.pdf
Weiss, D. S., Brunet, A., Best, S. R., Metzler, T. J., Liberman, A., Pole, N., Fagan, J. A., & Marmar, C. R. (2010). Frequency and severity approaches to indexing exposure to trauma: The Critical Incident History Questionnaire for police officers. Journal of Traumatic Stress, 23(6), 734–743.
https://doi.org/10.1002/jts.20576
White, B., Driver, S., & Warren, A. M. (2010). Resilience and indicators of adjustment during rehabilitation from a spinal cord injury. Rehabilitation Psychology, 55(1), 23–32. https://doi.org/10.1037/a0018451
Wild, J., El-Salahi, S., Degli Esposti, M., & Thew, G. R. (2020). Evaluating the effectiveness of a group-based resilience intervention versus psychoeducation for emergency responders in England: A randomised controlled trial. PLoS ONE, 15(11), e0241704. https://doi.org/10.1371/journal.pone.0241704
Windle, G., Bennett, K. M., & Noyes, J. (2011). A methodological review of resilience measurement scales. Health and Quality of Life Outcomes, 9, Article 8, 1–18. https://doi.org/10.1186/1477-7525-9-8
Warren N. Ponder, PhD, is Director of Outcomes and Evaluation at One Tribe Foundation. Elizabeth A. Prosek, PhD, NCC, LPC, is an associate professor at Penn State University. Tempa Sherrill, MS, LPC-S, is the founder of Stay the Course and a volunteer at One Tribe Foundation. Correspondence may be addressed to Warren N. Ponder, 855 Texas St., Suite 105, Fort Worth, TX 76102, warren@1tribefoundation.org.
