May 10, 2023 | Volume 13 - Issue 1
Shainna Ali, John J. S. Harrichand, M. Ann Shillingford, Lea Herbert
Guyana has the highest rate of suicide in the Western Hemisphere. Despite this statistic, a wide gap exists in the literature regarding the exploration of mental wellness in this population. This article shares the first phase in a phenomenological study in which we explored the lived experiences of 30 Guyanese American individuals to understand how mental health is perceived. The analysis of the data revealed that participants initially perceived mental health as negative and then transitioned to a positive perception of mental health. We discuss how these perceptions affect the lived experience of the participants and present recommendations for counselors and counselor educators assisting Guyanese Americans in cultivating mental wellness.
Keywords: Guyanese American, mental health, phenomenological, mental wellness, perceptions
In 2014, the World Health Organization (WHO) reported Guyana as having the highest suicide rate in the world (44.2 suicides per 100,000 people; global average is 11.4 per 100,000 people). According to World Population Review (2023), within the Western Hemisphere, even after almost 10 years, Guyana remains the country with the highest rate of suicide—a concerning statistic. Responding to the WHO (2014) report, Arora and Persaud (2020) engaged in research to better understand the barriers Guyanese youth experience in relation to mental health help-seeking and suicide. Their research included 17 adult stakeholders (i.e., teachers, administrative staff, community workers) via focus groups, and 40 high school students who engaged in interviews. Arora and Persaud used a grounded theory approach and found the following themes as barriers to mental health help-seeking in Guyanese youth: shame and stigma about mental illness, fear of negative parental response to mental health help-seeking, and limited awareness and negative beliefs about mental health service. They recommended integrating culturally informed suicide prevention programs in schools and communities. In efforts to extend Arora and Persaud’s findings, we sought to further understand how Guyanese Americans define and experience mental health to better serve them in counseling.
Startled by the statistics presented by the WHO (2014) and Arora and Persaud (2020), we were compelled to focus our attention on this unique immigrant subgroup in the United States. It is important to note that between the WHO’s 2014 report and Aurora and Persaud’s research, no other studies related to Guyanese American suicidality are recorded in the literature. However, two studies on Guyanese American mental health emerged by Hosler and Kammer (2018) and Hosler et al. (2019). Our decision to conduct research on the Guyanese American community was further informed by Forte and colleagues’ (2018) review of immigrant literature in the United States, which stated that “immigrants and ethnic minorities may be at a higher risk for suicidal behavior as compared to the general population” (p. 1). Forte et al. found that immigrants, when compared with individuals in their homeland, were at an increased risk of experiencing mental health challenges like depression and other psychotic disorders. Currently, suicide is listed as the 10th leading cause of death overall in the United States (Heron, 2021). More specifically, within ages 10–34 and 35–44, suicide is the second and fourth leading cause of death, respectively. Heron’s (2021) report, referencing the Centers for Disease Control and Prevention (CDC), highlighted that in the United States, death by suicide (47,511) is 2.5 times higher than homicides (19,141). The prevalence of suicide among Guyanese people within and without the United States warranted further exploration of the experiences of this marginalized group.
The Guyanese American Experience
Comparing all countries with a population of at least 750,000 people, Guyana, a Caribbean nation, is said to have “the biggest share of its native-born population—36.4%—living abroad” due to remoteness and limited opportunities within the country to move from a lower to a higher socioeconomic status (Buchholz, 2022, para. 2). It is estimated that the United States is home to approximately 232,000 Guyanese Americans whose ancestry can be traced back to Guyana (United States Census Bureau, 2019), a country in the northeast of South America, bordered by Brazil, Venezuela, and Suriname. Although approximately 50% of all Guyanese immigrants in the United States reside in New York City alone (Indo-Caribbean Alliance, Inc., 2014), Guyanese people can be found across all 50 states and the District of Columbia (Statimetric, 2022). This draw to the United States, an English-speaking nation, might be linked to the fact that Guyana is the only country in South America that recognizes English as its official language (One World Nations Online, n.d.).
Like most immigrants, Guyanese immigrants travel to the United States seeking a better life and opportunities for themselves and their families. However, the process of transplanting can be bittersweet, in that Guyanese immigrants might be forced to relinquish their identity and customs and embrace American customs through assimilation (Arvelo, 2018; Cavalcanti & Schleef, 2001). For many Guyanese immigrants, being caught between leaving their homeland and beginning life in their adoptive home can lead to a cultural clash, resulting in problematic coping mechanisms (e.g., minimizing/hiding mental health challenges, cultural shedding [adopting American identity and losing cultural heritage]; Arvelo, 2018).
As discussed above, suicide in the Guyanese community is unquestionably a serious concern, but the community faces other challenges in the United States as well. For example, Hosler et al. (2019) found a statistically significant association between discrimination experience and major depressive symptoms in a sample of Guyanese Americans. However, Hosler et al. (2019) also found mean scores on the Everyday Discrimination Scale (EDS; Williams et al., 1997) were lower (i.e., less discriminatory experiences in everyday life) for Guyanese Americans when compared to other groups (Black, White, and Hispanic) because Guyanese Americans have a more cohesive interpersonal network. It would appear that Guyanese Americans experience lower everyday discrimination because they operate within interpersonal spaces that are more cohesive, yet their discriminatory experiences are positively associated with depression symptoms, which is a source of concern.
Another area of concern among Guyanese Americans is intimate partner violence (IPV), yet research remains lacking (Baboolal, 2016), leading us to draw directly from Guyanese literature. In Guyana, IPV is one of the most prevalent forms of violence (Parekh et al., 2012). As a country, although Guyana endorses the commitment to gender equality, women are the majority only in the tertiary sector (e.g., education, human services, clerical services, and tourism). Nicolas et al. (2021) stated that “domestic duties, marriage, and child-bearing, particularly for women between the ages of 25–29, have hindered their labor force participation” (p. 147). They documented that 1 in 6 Guyanese women, mostly from rural parts of the country, hold the belief that beating one’s wife is necessary (i.e., husbands are justified in beating their wives, resulting in domestic violence being a relevant mental health issue). In fact, suicide is identified as a public health issue for Guyanese women, who use it as a means of coping “with economic despair, poverty, and hopelessness . . . [and] to escape family turmoil, relationship issues, and domestic violence” (Nicolas et al., 2021, p. 148). However, even with access to mental health services increasing in Guyana, seeking out mental health care is uncommon due to stigma, lack of communication, inadequate financial resources, limited providers, and other barriers related to access (Nicolas et al., 2021). Within the U.S. literature, there remains a dearth of information on the experiences of this group as it relates to suicide and IPV. Most likely, this is a result of racial categorization within the United States, where, based on phenotype and racial composite, individuals are often lumped into one category, such as Black. As important as Guyanese literature on IPV is to inform the work of counselors, we believe it is equally important for us to engage in research regarding IPV and other mental health challenges on Guyanese Americans specifically. Learning about Guyanese Americans’ perceptions of mental health may facilitate closing the gap in the utilization of mental health services, warranting the current investigation.
Recognizing the noticeable research gap related to the mental health experiences of Guyanese Americans, we conducted a thorough review of the literature related to mental health and well-being. Through databases such as PsycINFO, ProQuest Central, Web of Science, MEDLINE, and SocINDEX, using the search terms “Guyanese Americans, Health and Wellbeing, Mental Health of Guyanese Americans, Access to Mental Health,” 54 search results were found. However, only two applicable studies were found to address Guyanese Americans’ mental health specifically (Hosler & Kammer, 2018; Hosler et al., 2019). The other search results were either not research manuscripts (i.e., reflections and newspaper articles) or addressed other constructs specific to the Guyanese people (e.g., family, education). The first study by Hosler and Kammer (2018) focused specifically on the health profiles of Guyanese immigrants in Schenectady, New York. This study was conducted with 1,861 residents between the ages of 18–64 years. Guyanese Americans from Schenectady were mostly from a low socioeconomic status, which resulted in them being less likely to have health insurance coverage, an identified place to receive care, and access to cancer screenings. They were also identified as being more likely to engage in alcohol binge drinking—all conditions of significant concern to us, resulting in the present study. In fact, Hosler and Kammer reported that Guyanese Americans are among the lowest group of those insured in the United States when compared with other minority groups such as Black and Latinx groups. Some researchers believe ethnocentric stereotyping, cultural incompetence by professionals, a lack of steady employment, and poor previous interactions with the health care system are barriers Guyanese immigrants experience when accessing medical and mental health services (Arvelo, 2018; Cheng & Robinson, 2013; Jackson et al., 2007).
The second study of Guyanese immigrants was conducted by Hosler et al. (2019) and explored everyday discrimination experiences and depressive symptoms in relation to urban Black, Hispanic, and White adults. This study included 180 Guyanese Americans (i.e., both citizens by birth and naturalized citizens/immigrants), all 18 years and older, from Schenectady, New York. The researchers found a significant independent association between the EDS score and major depressive symptoms for Guyanese Americans, suggesting that discrimination experiences might be an important social cause for depression within this community. Based on the reported challenges faced by Guyanese Americans, as well as our desire to contribute meaningfully to the extant body of literature on the Guyanese American community, we conducted a phenomenological inquiry. More specifically, we sought to better understand the lived experiences of Guyanese Americans pertaining to mental health (i.e., definitions, beliefs, practices), and how they access and incorporate mental health resources to mitigate the known mental health risks of this population in the United States, in the hopes of creating tailored methods for culturally responsive care.
Method
Because limited mental health research exists on this unique community, the present study, which is part of a larger research endeavor, sought to explore Guyanese Americans’ lived experiences with mental health. To lay the foundation of understanding, the present study focused on Guyanese Americans’ perceptions of mental health. Phenomenology, a constructivist approach, recognizes the existence of multiple realities and provides an understanding of participants’ lived experiences using their own voices (Haskins et al., 2022). We selected transcendental phenomenology (Moustakas, 1994) as the appropriate methodology for answering our research questions, as it is congruent with the counseling profession’s similar objective of understanding the human being. Akin to the practice of counseling, transcendental phenomenology emphasizes methods of the researcher to best set aside the potential clouds caused by bias in an effort to allow the explored phenomenon to surface. Transcendental phenomenology aligns with one of the core professional values in the American Counseling Association’s Code of Ethics (ACA, 2014), that of supporting “the worth, dignity, potential, and uniqueness of people within their social and cultural contexts” (p. 3). It also aligns with Ratts et al.’s (2015) Multicultural and Social Justice Counseling Competencies (MSJCC), specifically understanding the client’s worldview domain. Our focus on Guyanese Americans, an understudied minority group in the United States (Hosler & Kammer, 2018) originating from a country that has been identified as having the world’s highest suicide rate (WHO, 2014), led us to select this method so that we could maintain cognizance of our surroundings, hold respect for the population, and examine participants’ experiences (Haskins et al., 2022; Hays & Singh, 2012; Hays & Wood, 2011).
Participants
Before participants were recruited for the study, IRB approval was obtained from the university with whom Shainna Ali, M. Ann Shillingford, and Lea Herbert are affiliated. Purposive criterion sampling was used to recruit participants, leading to a sample of adults who self-identified as Guyanese American (i.e., either immigrated to the United States themselves or had at least one parent who was born in Guyana). Recruitment materials were shared with Guyanese Americans using counseling listservs (i.e., ACA–AMCD Connect and CESNET) and social media platforms (i.e., LinkedIn, Facebook, and Instagram). Members of the research team contacted all participants using email to share details regarding the study and the informed consent document, collect demographic data, and schedule individual interviews. According to qualitative research, sample size recommendations range from six to 12 participants (Creswell, 2013; Guest et al., 2006; Onwuegbuzie & Leech, 2007). Hence, we sought to recruit 15–20 participants to account for the possibility of attrition.
Our recruitment efforts yielded 73 individuals who expressed interest in the study, 60 of whom met all inclusion criteria and were initially contacted. Forty-three individuals were unable to complete an individual interview due to scheduling conflicts; hence, we secured a total of 30 participants who completed the study. Of this number, 17 participated in individual interviews and a total of 23 individuals participated in a one-time focus group to further clarify data from the individual interviews. It should be noted that 10 of the 23 focus group participants also participated in the individual interview. Further recruitment was deemed unnecessary, as the data analysis reached saturation with data from the individual interviews and focus group. We present demographic data on all participants who engaged in the study, both individual interviews and the focus group (N = 30), in Table 1.
Table 1
Participant Demographic Data
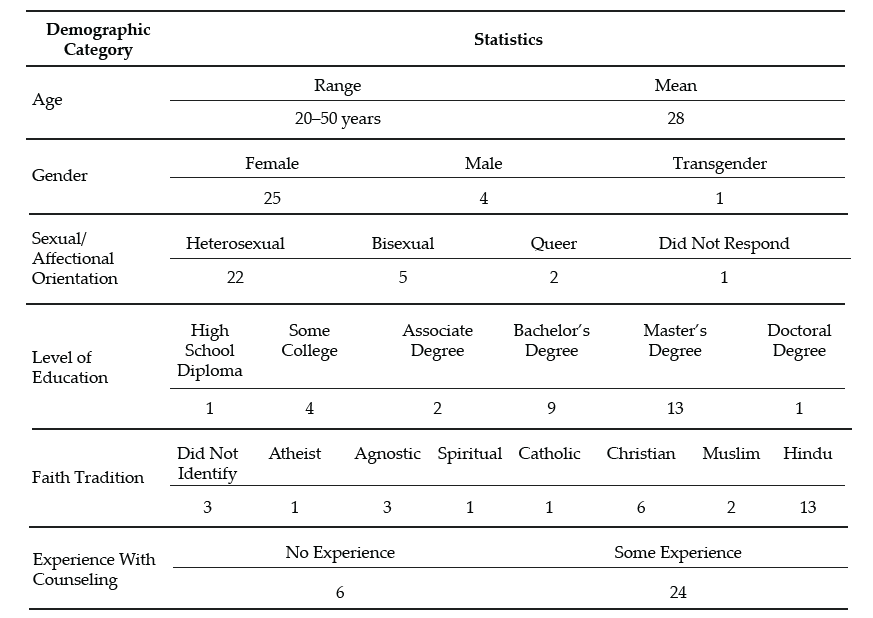
Note. This table provides a breakdown of the demographic characteristics of Guyanese American participants (N = 30).
Data Collection and Analysis
Participants engaged in a semi-structured interview lasting 30–60 minutes, conducted by Ali and Shillingford. Interviews were conducted via Zoom, audio-recorded, and transcribed verbatim. The interview protocol consisted of three primary questions, and sub-questions were used to clarify responses: 1) How do you define mental health?; 2) Who in your life has had experiences with mental health?; and 3) What experiences have you had with mental health? Prior to conducting our study, we included in our IRB documentation that data collection of individual interviews would follow saturation guidelines and that a focus group could be used for further data illumination. Following initial data analysis, we found it necessary to conduct a 1-hour follow-up focus group via Zoom to probe deeper into the data and to allow participants to clarify concepts related to emerging themes. Upon the first round of analysis, it was noted that several participants experienced a shift in perceptions regarding mental health. Focus group probes explored whether participants noticed this shift, what may have contributed to this shift, and when the shift occurred.
After all focus group and individual interviews were transcribed, we used guidelines outlined by Moustakas (1994) to analyze the data. First, we immersed ourselves in the data, reviewing each transcript individually. The transcripts were then divided equally among the four researchers, who read through each to become familiar with the data. With each transcript, we identified relevant statements reflecting participants’ lived experiences (horizontalization) as Guyanese Americans within the contexts of mental health beliefs and experiences.
Following this process, we met multiple times to review all transcripts and confer about the textural descriptions. We identified relevant codes, then synthesized the textural descriptions into themes based on commonalities, distilling the meaning expressed by participants. Then we engaged in reduction and elimination via consensus coding. This process included reading and rereading transcripts together, which followed an iterative process of reviewing the text and code, coding, rereading, and recoding, before determining which thematic content was a new horizon or new dimension of the phenomenon.
After all transcripts were analyzed following this reduction process, clustering and thematizing occurred (i.e., thematic content was clustered into core themes based on participant experiences; Hays & Singh, 2012; Moustakas, 1994). We extracted verbatim examples from the transcripts to generate a thematic and visual description of the phenomenon being examined. After completing the initial data analysis, we conducted member checking by sending each participant their individual transcript as well as the written results section. Participants were requested to provide feedback on the accuracy of their transcripts. Additionally, following the focus group and elucidation of themes all participants were offered an opportunity to member check and clarify the degree to which the results aligned with their lived experiences. The participants did not report any errors; however, clarification was offered by one participant.
Trustworthiness and Positionality
Trustworthiness is a key element of qualitative research in which the research findings accurately reflect the data (Lincoln & Guba, 1985). A critical element of maintaining research credibility is through reflexivity, wherein researchers critically examine procedures employed in relation to power, privilege, and oppression (Hunting, 2014). To safeguard against researcher bias, we worked collaboratively to establish and maintain credibility throughout data collection and analysis processes. Our research team consisted of one Indo-Guyanese American female faculty member, one Afro-Guyanese American female doctoral student, one Black female faculty member, and one Indo-Chinese-Guyanese Canadian male faculty member. All three faculty members belong to CACREP-accredited counselor education programs, and all four researchers have clinical experience working with diverse populations.
To address researcher bias, we engaged in bracketing to minimize the ways in which our experiences influence our approach to research and expectations of the outcomes of the study. Prior to data collection, we discussed our experiences in relation to Guyana, mental health in the Guyanese American community, and our roles as mental health leaders and advocates. We identified our personal experiences, acknowledged our biases, and attempted to bracket while conducting the interviews and focus group. Throughout the data collection and analysis processes, we participated in personal reflection and kept analytic memos documenting our reactions and initial thoughts about the data collected.
Before analyzing the data, we met to confirm analysis procedures, ensuring consistency. We initially analyzed data individually, then determined codes and themes as a team to reduce bias. Throughout the data analysis process, we consulted with each other, addressing questions or concerns related to the data. We also consulted with an outside researcher experienced in qualitative research to obtain critical feedback on the data analysis process and the research findings (Marshall & Rossman, 2006). Our consultant served as an external check of the research methodology and theoretical interpretation of the data.
Findings
The results of the analysis increase understanding of the lived mental health experiences of Guyanese Americans by elucidating perceptions of mental health (Creswell, 2013). All participants shared their beliefs about mental health and the direct and indirect experiences that informed their conceptualization. Three themes surfaced. The first two showed a clear divide in the data: 1) mental health being perceived as negative, stigmatized, elusive, and intimidating; and 2) mental health being perceived as positive, important, helpful, and empowering. It is important to note that these primary themes were not representative of two subsets of participants, and this extracted another theme, which centered on the tendency of participants’ beliefs to transition from negative to positive views of mental health.
The Perception of Mental Health as Negative
When exploring obstacles, subthemes emerged in which hindrances to mental health were acknowledged to exist across three levels: individual, familial, and sociocultural. In parallel, these three subthemes were echoed in the exploration of factors that participants acknowledged have contributed to their mental wellness. The following section explores the primary themes in detail by highlighting the participants’ voices in describing their lived experiences.
Mental Health Concerns Are a Sign of Weakness
All participants in the individual interviews shared that they originally believed that mental health developed out of weakness. This belief was often attributed to minimizing remarks from family members. Oftentimes these comments were paired with other suggestions of how to ameliorate symptoms such as praying more, working harder, or contributing to physical health (e.g., drinking tea). Sharon shared:
It was just like, oh no, you just need to read a book or you just need to go and do something and take your mind off of however it is you’re feeling, like there’s no reason for you to be sad, you have a roof over your head and you’re going to school and you’re doing all of these things, it doesn’t matter. There’s no reason for you to be sad or feel any type of way about anything because we provide everything for you.
Several participants noted that investment in physical wellness was preferable to mental wellness, although physical health was not genuinely prioritized. Participants shared personal and observed maladaptive coping with poor eating habits (i.e., quality and quantity) and excessive substance abuse, namely alcohol. Some participants shared that these tactics were used to manage mental health symptoms or avoidance. Christine shared, “When you’re struggling with things . . . you have nowhere to go to with them except alcohol and the bottom of a rum bottle.” Many participants recognized that coping with alcohol is normalized within the culture. Further, the commonality of these methods normalized consumption and have caused additional issues (e.g., diabetes, heart disease, alcoholism). Arjun noted:
We all have relatives that are kind of stuck on the whole drinking issue. We know a lot of them. They get together with their friends and they “lime,” as we like to call it. They drink in groups and they “gyaff,” they have fun. But it’s a completely different story when they’re by themselves and they’re drinking.
Mental Health Is Taboo
A general consensus was that all participants in the study once believed that mental health was not important and that mental health problems were shameful and not to be discussed. This consistent trend was one of the reasons that we opted to further understand responses through a focus group. Therefore, a direct probe was offered to the focus group participants to explore if they believed discussing mental health was taboo. When delving deeper into these perceptions, participants noted that these thoughts were informed by the beliefs of others and upheld in the wider cultural paradigm. All participants reported that, generally, mental health should not be talked about in order to save face and be respectful. Because mental health issues were seen to be synonymous with weakness, sharing about mental health was equated with the risk of bringing shame to oneself or to one’s family. For example, Chandra shared that “Guyanese people don’t want a kid that’s broken or a little off.” Hence, if someone opts to discuss their mental illness, it is to be done carefully, or secretly.
Most participants shared that typically, when divulging their symptoms, they went to an elder, often a parent, grandparent, or elder sibling, in an effort to keep concerns within the family system. However, many participants noted being minimized or dismissed when sharing their concerns with family members. Ramona explained her feeling that her family
is really strong about, like, don’t be selfish. And I wonder if they would categorize it under that. Like if you’re taking up too much space or time or whatever, you’re trying to center the attention on you or whatever, so that’s a self-serving thing.
A generational rule of discourse emerged from the data. Though the tendency was to keep mental health discussions within the family system, it was also atypical for a younger member to address observed issues with an elder. Several participants noted that this hidden guideline kept informed younger generations from being able to utilize their recognition of warning signs to help the given person and the family system. Arjun shared that as he’s gotten older and has learned more about mental health, he has acquired the courage to address the problems he sees with elders, including his uncle:
I said, “Uncle, what’s wrong?” And he said, “No, nothing is wrong.” But he was crying, you could see tears were streaked on his face, but he wouldn’t talk about it—he wouldn’t say anything. It’s not only one time I saw him, it’s multiple times that I’ve seen him when he has been drinking by himself, that he kind of has the same face all the time. Prior to the times that I asked him, I kind of looked at him and I kind of walked away the first couple of times. Because I was kind of like, this is not something that looked like I should butt in, as a child especially. When you’re younger, your parents tell you, “Mind your business.” Or they say, “You’re not an adult, go with the kids.” So . . . the first couple of times I saw him, I kind of avoided it.
Others Are Not To Be Trusted
Some participants noted that beyond the purpose of family protection, caution to mental health discourse was also due to lack of trust of others. Christine explained: “We had a counseling center on campus, but I was like, ‘Oh, I can’t go talk to anybody,’ because that’s what I was raised with. You don’t talk to strangers about your problems. I had to keep everything inside.” Nevertheless, some families encouraged talking to a religious leader to assist the individual in enhancing devotion and reducing mental health symptoms. Still, regarding professional mental health services, many participants believed, at least at one time, that such services are not helpful, providers are not to be trusted, assistance of that nature is for other (e.g., White) people, and succumbing to that level of desperation is a sign of weakness. When sharing about mistrust in professional mental health assistance, misconceptions and stereotypes surfaced. Ramesh shared:
Oh boy. I have to be honest with you, I feel counseling is, I’ll speak to a shrink and they’ll prescribe drugs to me, like Ritalin or . . . I was like, you know what, I’m better than that. I’m probably totally wrong about it, but that’s just the perception that I have. I’ll be laying on the couch and I’m going to speak into someone and then they’re going to prescribe drugs to me. I don’t want that. I can try to figure this out on myself by talking and trying to do things—positive behavior.
Mental Health Perceived as Positive
All participants in the individual interviews acknowledged a shift in their perceptions of mental health. Their newfound conceptualization included a holistic view of wellness in which mental wellness was seen as an important component to overall well-being and quality of life. In this newer perception, participants acknowledged the ability to consider more variables influencing mental health than they recognized in the past. For example, many participants noted a link between mind and body, versus the previously held notion that physical health is more important than mental health. A few participants noted that mental health can be influenced by genetics, while some noted that it could be influenced by personality, and others noted that it can be influenced by people and the surrounding environment.
All participants, from both the individual interviews and focus group, concurred that everyone feels mental health effects; furthermore, showing signs of a problem is not attributed to weakness. Moreover, because mental health affects everyone, a widespread belief emerged that we all have the responsibility to foster our mental wellness. Additionally, participants shared several examples of what naturally ensued without investing in strategies for mental health such as challenges with emotional regulation, coping, relationships, and worsening mental health problems.
The Transition Between Negative and Positive Perceptions
The transition between old and new conceptualizations of mental health was informed by direct and indirect experiences. All participants shared a transition in beliefs in the individual interviews, and this was explored in the focus group for further clarification. Most participants shared that their personal mental health history informed a change in their beliefs. Many of these participants noted the influence of their healing process, most notably seeking professional help. All participants, from both the individual interviews and the focus group, shared at least one example of learning about mental health by observing another person’s experience. For example, Jessie shared, “Unfortunately, I came from a home of domestic violence . . . I was around maybe six, my dad was bipolar . . . [and] he was just a wife beater. That is probably when I can recall [learning] of mental health.” Another example of learning about mental health from others is captured in Reginald’s comment:
[As] an only child . . . my parents took it upon themselves to [teach me]. . . . It wasn’t like, “Okay, sit down. Let me tell you why these things are.” It was just we’ll be talking about somebody else or going over something that happened and then they’ll explain why, but never directly for me. It was always about other people’s kids.
Many of these individuals emphasized the belief that by paying attention to others, you can learn what is helpful and unhelpful for mental health. Oftentimes this was in their own family; however, extended family and community members were also highlighted. Moreover, a few participants shared their recognition that living with someone who is struggling with their mental health may negatively impact personal wellness (e.g., be triggering). Beyond the family system, some participants noted that exposure to other cultures and perceptions of mental health informed a conceptualization of mental wellness. Seeta shared:
I had friends of other religions or like no religions. And then we would talk about a lot of different things. Like I would ask them questions like, “Oh, so how do things work in your house? Do your parents talk about your God or whatever?” And they’re like, “No.” And I’m like, “So where do your emotions come from?” And they’re like, “Well, you know, we just feel them. Some days I feel angry and some days I feel sad, some days I feel happy.” And I’m just like, “Okay, this is interesting.”
From the quote, it might appear that one’s emotions are in some way connected with God or another higher power; however, this is not something that was observed with other participants of our study. It was more common for participants to share stories of their families using religion as the solution to mental health concerns. For example, Yolanda shared:
My grandmother came when I turned 16 and she kept trying to tell my mom I was showing signs of depression. And my mom was like, “No, she’s like that all the time, like, that’s just how she is.” And my grandma was like, “That’s not normal. You should get her checked out.” And my mom kept saying, “No” and kept denying it. And then my grandma said, “You have to do something.” And then my mom replied, “Oh, I’m going to pray for her.”
In addition to personal experiences and observations of others, participants noted that improved mental health awareness and education prompted them to think critically about their mental health schemas. Ramesh shared:
My education, I always feel like this is what saved me in the end, because I was able to be around other people to know better and to come back home and be like, “Excuse me, this is not how we do things. This is not how we say things. I don’t know what it was like in Guyana.”
Some participants associated this with growing older, and others noted their personal initiative to improve mental health knowledge by following mental health pages on social media, taking a related class, and for some, becoming a part of the mental health field themselves. From this vantage point, many participants were able to equate their previously held notions with beliefs embedded in the culture such as generational rules of respect, gender differences, and the impact of colonialism. Participants, despite their gender differences, noted that within the cultural framework, the rule that mental health should not be discussed is disproportionately applicable to males. Participants shared that this is often due to the perception that it is important for men to be strong, and again, mental illness is a symptom of weakness. This was also linked to the breadwinner role and the pressure to provide for the family. However, this was only noted to have detrimental effects, as anger issues, IPV, and alcoholism were noted to arise out of this rule. Some participants noted that the survival aspect of colonialism may have contributed to the lack of privilege to focus on mental health. In addition, the history of colonialism in Guyana (i.e. slavery, indentured labor) could have informed the lack of trust in professional services.
The change in mental health conceptualization was noted to have benefits beyond the participants themselves. Some participants remarked that the shift in perception was recognized in the wider generation. Ramona reflected:
I will say that a lot of folks from my generation have been a lot more like, “Go to therapy. We should be taking care of our thoughts and our feelings or emotions.” That’s important to you in the same way that if you tore a ligament that you would need to get surgery or do whatever.
Within the newfound conceptualization of mental wellness emerged a vow of social responsibility. All participants, from both the individual interviews and the focus group, shared their intention to help others, and some even noted it as their duty. Ways to help others included advocating for mental health awareness, access, and education; helping to challenge unhelpful cultural beliefs; breaking generational cycles; and protecting others from experiencing similar struggles (e.g., child, sibling).
Discussion
The findings from this study are enlightening, and some are the first to be documented through research, even if they were observed in practice. Initial perceptions of all participants, from both the individual interviews and the focus group, were that mental health is a taboo topic and seeking mental health services is bad. These perceptions stemmed from fear, mistrust, and limited awareness of the benefits of mental health services. This is consistent with findings from Arora and Persaud (2020), who surmised that Guyanese individuals hold negative views of mental health that significantly impact their help-seeking. Furthermore, the findings point to strong familial and sociocultural influences, such as beliefs about mental health, that swayed individual perceptions of mental health, which is in keeping with recent literature on affirming cultural strengths and incorporating familial identity in working with clients of Guyanese descent (Groh et al., 2018; Nicolas et al., 2021).
Discussing issues related to mental health was viewed as a sign of weakness, which translated to help-seeking being a taboo. It would appear that the stigma associated with mental health remains a common experience for Guyanese Americans, and when coupled with limited communication, insufficient funding, and lack of providers, we can see how Nicolas et al. (2021) found this to be concerning. Cultural clash, ethnocentric stereotyping, and cultural incompetency may also be responsible for Guyanese Americans being distrustful of the health care system, leading them to engage in maladaptive behaviors (i.e., avoidance, use of substances, IPV) and not receive the mental health attention and care they need (Arvelo, 2018; Cheng & Robinson, 2013; Jackson et al., 2007).
It appears that even in the face of discrimination and experiences of mental health challenges like alcoholism, depression (Hosler & Kammer, 2018), and IPV (Parekh et al., 2012), leaning on the support of the community serves to buffer against mental health challenges for Guyanese Americans. It also seems that changing mental health perceptions from negative to positive was significantly related to mental health literacy and exposure to other systems such as school, work, and community (i.e., cross-cultural exchange).
Findings that were not previously documented in the literature suggest that an integrated view of wellness enabled participants to augment their negative abstractions of mental health care. These findings serve as an indication that among Guyanese Americans, although mental health has been perceived as negative, weak, and a taboo, the narrative is beginning to shift to make space for mental health awareness, education, access, and functioning, thereby creating unique implications for counselors seeking to meet the needs of this immigrant subgroup.
Implications
In combination with prior literature, the results of this study provide a rationale for mental health counselors, marriage and family counselors, school counselors, and counselor educators to inspire dialogue to foster mental wellness. Based on the findings from this study, when working with Guyanese Americans, counselors should focus on three key strategies to support Guyanese American clients: (a) mental health awareness, (b) mental health education, and (c) mental health experience.
Mental Health Awareness
Participants in this study initially held limited views and awareness of the signs and symptoms of mental health. When awareness was heightened through various means, they were more open to exploring the benefits of services. Counselors can be instrumental in creating awareness by first raising their own awareness pertaining to cultural stigma and its influence on Guyanese Americans’ mental health. For example, unwillingness to attend counseling sessions may be linked to the culturally held perception that discussing mental health, especially beyond the core family system, is taboo. In acknowledging this, counselors can raise awareness of confidentiality, which can be seen as an alignment with the cultural notion that talking about mental health is taboo when it means talking to anyone, and the role of the counselor can be highlighted as a professional collaboration versus communal gossip. Counselors need to be mindful of the collectivistic nature of Guyanese American culture, which causes personal and familial illnesses alike to be perceived as personal problems. Rather than dismiss a client’s concerns about mental health, a counselor can benefit from exploring how the family members’ symptoms, perceptions about mental health, and willingness to adhere to treatment influence the client’s symptoms, perceptions, and commitment to counseling. Further, collectivism spans beyond the protective family system. On one hand, this community orientation can be used to explore a broad range of support, yet on the other hand, depending on the client’s experience, this may also be a widened range of societal pressure (e.g., judgment, criticism, shame).
Mental Health Education
Increased understanding of mental health appeared to have led participants to seek services and resources to increase their mental health literacy, with the hope of improving their well-being. Counselors and counselor educators can be instrumental in offering Guyanese Americans mental health education. To begin, all mental health professionals should demonstrate a posture of cultural humility when engaged in psychoeducation on mental health and wellness for this population. In order to raise awareness through education, mental health professionals are encouraged to model trust, respect, sensitivity, compassion, and a nonjudgmental stance. Within session, counselors should be prepared to offer information regarding early signs of mental illness, compounding factors (e.g., alcohol, suicidal ideation, domestic violence), obstacles (e.g., stigma), and resources. Additionally, counselors may need to offer psychoeducation on the family system, roles, dynamics, beliefs, experiences, and generational patterns that can influence individual mental health. In the event that a family member with mental health problems is unwilling to seek assistance, helping the client to better understand the diagnosis and cope personally can be empowering. Finally, to employ the collectivistic nature of Guyanese American culture, stigma can be confronted, and mental health education can be effectively offered by providing group counseling within this population. Group counseling can offer a variety of therapeutic factors that can benefit Guyanese Americans such as universality, hope, and corrective recapitulation of the primary family group (Yalom & Leszcz, 2005).
Beyond the counseling office, counselors and counselor educators should consider collaborating with culturally supportive organizations. Workshops and information sessions can be tailored to explore and address cultural, religious, ethnic, and generational differences in addition to offering mental health resources (e.g., signs, symptoms, treatment). Several of the participants in our study shared that access to psychology courses in school helped to improve their knowledge about mental health. In addition to these classes continuing to be offered, accessibility to such courses should be expanded. Schools and universities may benefit from offering workshops and other informational sessions to support mental health. Beyond information being offered, a follow-up may be beneficial by linking school or campus counselors in order to connect an improvement in awareness and education to action, change, and health.
Several participants shared that because of a lack of access to mental health education, their knowledge was attained through social media platforms such as Instagram and TikTok. Although the quality of mental health education was not assessed in the present study, the lack of regulation on social platforms could perpetuate misleading, confusing, and stigmatizing misinformation surrounding mental health. Counselor educators should consider their roles beyond the classroom. In addition to empowering counselor trainees to utilize the suggestions above to foster awareness and education, counselor educators can offer responsive and succinct information via social media. Whereas social media is not an appropriate platform for tailored education or services, brief information can be offered to bridge the gap between awareness, education, and access.
Mental Health Experience
Growth in awareness and knowledge around mental health resulted in participants intentionally engaging in positive experiences as a way of resisting past harmful and hurtful practices and generational patterns, reauthoring a new narrative of hope and healing. Being wellness-focused, counselors are uniquely positioned to support this community by facilitating positive experiences impacting overall mental health and well-being.
Counselors can honor clients from this community by creating safe spaces for them to share their narratives without judgment. Counselors can foster healing communities through group counseling, where clients collaboratively share each other’s mental burdens and celebrate successes (Yalom & Leszcz, 2005). Counselors can honor collectivism by encouraging clients to participate in support groups in addition to personal counseling. Counselors and counselor educators can enhance the approachability of counselors by improving their visibility in the community. Examples include a community counselor being involved in outreach with a local cultural center, a school counselor offering mentorship with student clubs, a college counselor guest-speaking at a Guyanese American student organization meeting, or a counselor educator offering tailored workshops for the community.
In addition to the aforementioned implications, we believe that in order for counselors to bridge generational gaps in counselor distrust, counselors must acknowledge the lack of representation of diversity within the profession of counseling, the predominance of Western and European cultural and psychologist-centered curriculum, and lapses in poor bioethics and power dynamics among counselors and marginalized communities (Singh et al., 2020). Next, the specific intersectional impacts suggest counselors must adapt a multicultural orientation and illuminate cultural sensitivity. When a clinician enacts cultural sensitivity in session, clients can examine their perceptions of illness and center their multiple identities (Davis et al., 2018).
Limitations and Future Research
Several limitations that arose from the research process are important to mention. All interviews were conducted virtually. Although secured virtual platforms such as Zoom are considered acceptable for research, lack of face-to-face interviewing may have excluded subtle visual cues and induced video-conferencing fatigue (Spataro, 2020). Though researchers made great attempts to increase participant comfort and review the informed consent before the interview process, it is also plausible that respondents may have censored their responses out of concern for potential breach in confidentiality. A majority of respondents are college-educated, female, first generation, and of Indo-Guyanese descent; hence, the results may not be representative of all Guyanese Americans. Additionally, aligned with phenomenological methods of exploring lived experiences, research prompts were general. Recognizing the concerning statistics surrounding suicide (WHO, 2014), a future study exploring suicidality could be beneficial. Future research might seek to explore a more diverse pool of participants, including diversity in gender, age, ethnicity, and number of years in the United States. To build on the findings from the present study, future studies should explore what factors contribute to Guyanese American mental health as well as what variables may hinder mental wellness. It may also be beneficial to include research from the perspective of children and parents to further understand the influence of family systems and cross-generational norms.
Conclusion
This study highlighted the crucial need to address the mental health literacy of Guyanese Americans. The findings illuminate Guyanese Americans’ perceptions of mental health, including the transition from negative to positive perceptions and its potential influences. Efforts should be made to promote awareness, education, and experience related to mental health awareness for Guyanese Americans. Supporting mental health may help to reduce alarming rates of mental illness in Guyanese Americans and may also have the potential to influence related groups such as Guyanese, American, and Caribbean individuals. Counselors and counselor educators have the potential to play a significant role in supporting these clients by being cognizant and informed about cultural considerations.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Arora, P. G., & Persaud, S. (2020). Suicide among Guyanese youth: Barriers to mental health help-seeking and recommendations for suicide prevention. International Journal of School & Educational Psychology, 8(1), 133–145. https://doi.org/10.1080/21683603.2019.1578313
Arvelo, S. D. (2018). Biculturalism: The lived experience of first- and second-generation Guyanese immigrants in the United States (Order No. 10749930) [Doctoral dissertation, Chicago School of Professional Psychology]. ProQuest One Academic. (2027471070).
Baboolal, A. A. (2016). Indo-Caribbean immigrant perspectives on intimate partner violence. International Journal of Criminal Justice Sciences, 11(2), 159–176. https://www.researchgate.net/publication/336926774_Indo-Caribbean_Immigrant_Perspectives_on_Intimate_Partner_Violence
Buchholz, K. (2022, November 11). The world’s biggest diasporas [Infographic]. Forbes. https://www.forbes.com/sites/katharinabuchholz/2022/11/11/the-worlds-biggest-diasporas-infographic/?sh=4185fd634bde
Cavalcanti, H. B., & Schleef, D. (2001). Cultural loss and the American dream: The immigrant experience in Barry Levinson’s Avalon. Journal of American and Comparative Cultures, 24(3–4), 11–22.
https://doi.org/10.1111/j.1537-4726.2001.2403_11.x
Cheng, T. C., & Robinson, M. A. (2013). Factors leading African Americans and Black Caribbeans to use social work services for treating mental and substance use disorders. Health & Social Work, 38(2), 99–109. https://doi.org/10.1093/hsw/hlt005
Creswell, J. W. (2013). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Davis, D. E., DeBlaere, C., Owen, J., Hook, J. N., Rivera, D. P., Choe, E., Van Tongeren, D. R., Worthington, E. L., Jr., & Placeres, V. (2018). The multicultural orientation framework: A narrative review. Psychotherapy, 55(1), 89–100. https://doi.org/10.1037/pst0000160
Forte, A., Trobia, F., Gualtieri, F., Lamis, D. A., Cardamone, G., Giallonardo, V., Fiorillo, A., Girardi, P., & Pompili, M. (2018). Suicide risk among immigrants and ethnic minorities: A literature overview. International Journal of Environmental Research and Public Health, 15(7), 1–21. https://doi.org/10.3390/ijerph15071438
Groh, C. J., Anthony, M., & Gash, J. (2018). The aftermath of suicide: A qualitative study with Guyanese families. Archives of Psychiatric Nursing, 32(3), 469–474. https://doi.org/10.1016/j.apnu.2018.01.007
Guest, G., Bunce, A., & Johnson, L. (2006). How many interviews are enough? An experiment with data saturation and variability. Field Methods, 18(1), 59–82. https://doi.org/10.1177/1525822X05279903
Haskins, N. H., Parker, J., Hughes, K. L., & Walker, U. (2022). Phenomenological research. In S. V. Flynn (Ed.), Research design for the behavioral sciences: An applied approach (pp. 299–325). Springer.
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hays, D. G., & Wood, C. (2011). Infusing qualitative traditions in counseling research designs. Journal of Counseling & Development, 89(3), 288–295. https://doi.org/10.1002/j.1556-6678.2011.tb00091.x
Heron, M. (2021). Deaths: Leading causes for 2019. National Vital Statistics Reports, 70(9), 1–113. https://doi.org/10.15620/cdc:107021
Hosler, A. S., & Kammer, J. R. (2018). A comprehensive health profile of Guyanese immigrants aged 18–64 in Schenectady, New York. Journal of Immigrant and Minority Health, 20(4), 972–980.
https://doi.org/10.1007/s10903-017-0613-5
Hosler, A. S., Kammer, J. R., & Cong, X. (2019). Everyday discrimination experience and depressive symptoms in urban Black, Guyanese, Hispanic, and White adults. Journal of the American Psychiatric Nurses Association, 25(6), 445–452. https://doi.org/10.1177/1078390318814620
Hunting, G. (2014). Intersectionality-informed qualitative research: A primer. The Institute for Intersectionality Research and Policy. https://nanopdf.com/download/intersectionality-informed-qualitative-research-a-primer-gemma-hunting_pdf
Indo-Caribbean Alliance, Inc. (2014, February 3). Population analysis of Guyanese and Trinidadians in NYC.
https://www.indocaribbean.org/blog/population-analysis-of-guyanese-and-trinidadians-in-nyc
Jackson, J. S., Neighbors, H. W., Torres, M., Martin, L. A., Williams, D., & Baser, R. (2007). Use of mental health services and subjective satisfaction with treatment among Black Caribbean immigrants: Results from the National Survey of American Life. American Journal of Public Health, 97(1), 60–67. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1716231/
Lincoln, Y. S., & Guba, E. G. (1985). Naturalistic inquiry. SAGE.
Marshall, C., & Rossman, G. B. (2006). Designing qualitative research (4th ed.). SAGE.
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Nicolas, G., Dudley-Grant, G. R., Maxie-Moreman, A., Liddell-Quintyn, E., Baussan, J., Janac, N., & McKenny, M. (2021). Psychotherapy with Caribbean women: Examples from USVI, Haiti, and Guyana. Women & Therapy, 44(1–2), 136–155. https://doi.org/10.1080/02703149.2020.1775993
One World Nations Online. (n.d.). Guyana. https://www.nationsonline.org/oneworld/guyana.htm
Onwuegbuzie, A. J., & Leech, N. L. (2007). A call for qualitative power analyses. Quality & Quantity, 41, 105–121. https://doi.org/10.1007/s11135-005-1098-1
Parekh, K. P., Russ, S., Amsalem, D. A., Rambaran, N., Langston, S., & Wright, S. W. (2012). Prevalence of intimate partner violence in patients presenting with traumatic injuries to a Guyanese emergency department. International Journal of Emergency Medicine, 5(1), 1–5. https://doi.org/10.1186/1865-1380-5-23
Ratts, M. J., Singh, A. A., Nassar-McMillan, S., Butler, S. K., & McCullough, J. R. (2015). Multicultural and social justice counseling competencies. American Counseling Association. https://www.counseling.org/docs/default-source/competencies/multicultural-and-social-justice-counseling-competencies.pdf
Singh, A. A., Appling, B., & Trepal, H. (2020). Using the Multicultural and Social Justice Counseling Competencies to decolonize counseling practice: The important roles of theory, power, and action. Journal of Counseling & Development, 98(3), 261–271. https://doi.org/10.1002/jcad.12321
Spataro, J. (2020). The future of work—the good, the challenging & the unknown. https://www.microsoft.com/en-us/microsoft-365/blog/2020/07/08/future-work-good-challenging-unknown/
Statimetric. (2022). Distribution of Guyanese people in the US. https://www.statimetric.com/us-ethnicity/Guyanese
United States Census Bureau. (2019). People reporting ancestry: American community survey. http://bit.ly/42RazKC
Williams, D. R., Yu, Y., Jackson, J. S., & Anderson, N. B. (1997). Racial differences in physical and mental health: Socio-economic status, stress and discrimination. Journal of Health Psychology, 2(3), 335–351.
https://doi.org/10.1177/135910539700200305
World Health Organization. (2014). First WHO report on suicide prevention. https://www.who.int/news/item/04-09-2014-first-who-report-on-suicide-prevention
World Population Review. (2023). Suicide rate by country 2023. https://worldpopulationreview.com/country-rankings/suicide-rate-by-country
Yalom, I. D., & Leszcz, M. (2005). The theory and practice of group psychotherapy (5th ed.). Basic Books.
Shainna Ali, PhD, NCC, ACS, LMHC, is the owner of Integrated Counseling Solutions. John J. S. Harrichand, PhD, NCC, ACS, CCMHC, CCTP, LMHC, LPC-S, is an assistant professor at The University of Texas at San Antonio. M. Ann Shillingford, PhD, is an associate professor at the University of Central Florida. Lea Herbert is a doctoral student at the University of Central Florida. Correspondence may be addressed to Shainna Ali, 3222 Corrine Drive, Orlando, FL 32803, hello@drshainna.com.
Nov 9, 2021 | Volume 11 - Issue 4
J. Claire Gregory, Claudia G. Interiano-Shiverdecker
Using Moustakas’s modification of Van Kaam’s systematic procedures for conducting transcendental phenomenological research, we explored ballet culture and identity and their impact on ballet dancers’ mental health. Participants included four current professional ballet dancers and four previous professionals. Four main themes emerged: (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) counseling and advocacy—“the dance population is unique.” Suggestions for counselors when working with professional ballet dancers and professional athletes, such as fostering awareness about ballet culture and its impact on ballet dancers’ identity and mental health, are provided. We also discuss recommendations to develop future research focusing on mental health treatment for this population.
Keywords: ballet dancers, culture, identity, phenomenological, mental health
“Dancers are the athletes of God.”—Albert Einstein
Professional ballet dancers’ mental health experiences are sparse within research literature (Clark et al., 2014; van Staden et al., 2009) and absent from the counseling literature. Most research including ballet dancers focuses primarily on eating disorders, performance enhancement (Clark et al., 2014), and injuries (Moola & Krahn, 2018). Although these topics are crucial to dancers’ wellness, explorations of ballet dancers’ mental health that do not primarily focus on eating disorders are also important. Increasing professional ballet dancer and athlete mental health research could provide counselors with deeper awareness of the populations’ needs. Further, counselors have access to the American Counseling Association’s (ACA; 2014) Code of Ethics, which is relevant for all clients, including athletic populations. However, the counseling profession lacks specific sports/athletic counseling ethical codes, competencies, and teaching guidelines (Hebard & Lamberson, 2017). The only mention of “athletic counseling guidelines” appears in a 1985 article from the Association for Counselor Education and Supervision (Hebard & Lamberson, 2017). In their initiative to increase counselor response to the need for athletic counseling, Hebard and Lamberson (2017) implored counselors to advocate for athletes’ mental health. Further, the researchers stated that it is common to view athletes as privileged and idolize them for their physical endurance; however, this perception may leave athletes vulnerable to mental health concerns. Recent examples of mental health difficulties experienced by formidable professional athletes include tennis player Naomi Osaka choosing to decline after-match news conferences to safeguard her mental health and gymnast Simone Biles removing herself from some events at the Tokyo 2020 Olympics in order to protect her mental health.
Moreover, scholars have been increasingly devoted to understanding the cultures within which performing artists are trained and developed and recognizing their role in supporting the health and well-being of the artist (Lewton-Brain, 2012; Wulff, 2008). For counselors, the ACA Code of Ethics (2014) promotes gaining knowledge, personal awareness, sensitivity, and skills pertinent to working with a diverse client population (C.2.a). However, this is difficult with limited current data or research seeking to advance knowledge of the culture of performing institutions and how they relate to artists’ mental health experiences. Therefore, an exploration of ballet culture and identity and their impact on ballet dancers’ mental health experiences could help inform counselors and counselor educators about the counseling needs of this population.
Mental Health Among Elite Athletes and Performing Artists
Because of the scant literature focusing directly on professional ballet dancers’ mental health, we included research findings from articles examining mental health among athletes and performing artists. Although differences exist between professional ballet dancers, elite athletes, and performing artists, a professional ballet dancer straddles multiple environments. For example, an elite athlete trains to win a national title or medal, possesses more than two years of experience, and trains daily to develop talent (Swann et al., 2015). Rouse and Rouse (2004) suggested that performing artists’ goals or outcomes are to create art and achieve a high performance level with audience satisfaction. Similar to these groups, a professional ballet dancer trains almost every day, which requires extreme dedication. They must comply with high physical and mental demands to develop their ballet technique for performing and entertaining audiences.
Scholars have discovered that elite athletes experience a high prevalence of anxiety, eating disorders, and depression compared to the general population (Åkesdotter et al., 2020; Gorczynski et al., 2017). At the same time, eating disorders are overrepresented in elite athlete studies because of the requirement that elite athletes maintain a specific stature for their profession (Åkesdotter et al., 2020). Interestingly, few elite athletes reported anxiety disorders even though they scored in the moderate range on the General Anxiety Disorder-7 (GAD-7; Åkesdotter et al., 2020). This could indicate that elite athletes normalize their anxiety and eating concerns, even at a clinical level. Likewise, performing artists display disproportionately high reporting rates for mental health disorders, such as depression, anxiety, and stress, when compared to the general population (Van den Eynde et al., 2016; van Rens & Heritage, 2021). Given professional ballet dancers’ emotionally demanding performance levels as performing artists and their physicality as athletes, they may share similar mental health experiences with elite athletes and performing artists, yet these experiences remain unknown.
Ballet Culture and Professional Dancers’ Mental Health
Literature exploring ballet dancers has focused on culture (Wulff, 2008), development (Pickard, 2012), emotional harm (Moola & Krahn, 2018), injury prevention (Biernacki et al., 2021), and disordered eating (Arcelus et al., 2014). Ballet, with origins in the Italian and French courts, is an age-old culture that fuses beauty and athleticism (Kirstein, 1970; Wulff, 2008). Influenced by social and cultural forces in the Western world (Kirstein, 1970), ballet culture is synonymous with tradition and hierarchy (Wulff, 2008). Ballet culture holds steadfast to idealistic tenets in which dispositions (e.g., tenacity), perceptions of an ideal body, and actions (e.g., constant rehearsals) provide dancers the ability to illustrate a story through movements (Wulff, 2008). Exquisite sets, costumes, and movements create a unique experience and can produce a visceral reaction in the audience (Moola & Krahn, 2018).
Yet a strong commitment to the art form requires ballet dancers to work with their bodies for hours, sustain injuries, and work through chronic pain (Pickard, 2012), often leading to emotional distress (Moola & Krahn, 2018). Physical requirements also make dancers three times more vulnerable, compared to non-dancers, to suffer from eating disorders, particularly anorexia nervosa and those labeled by the Diagnostic and Statistical Manual of Mental Disorders as eating disorders not otherwise specified (Arcelus et al., 2014). van Staden et al. (2009) focused directly on ballet dancers’ mental health, finding that professional ballet dancers also experience mental health concerns due to negative body image and stress. The vast majority of these studies originated from countries outside the United States, including South Africa (van Staden et al., 2009), the United Kingdom (Pickard, 2012), and Canada (Moola & Krahn, 2018). The scarcity of scholarly attention on professional ballet dancers’ mental health within the United States is concerning given the evidence of emotional distress in similar populations. Counselors may be less than effective without a clear understanding of this population’s mental health needs. Understanding the cultural context and its impact on ballet dancers’ mental health in the United States, therefore, requires further exploration.
Purpose of the Present Study
The purpose of this study was to explore ballet culture and identity and their impact on ballet dancers’ mental health experiences. The guiding research questions were (a) How do professional ballet dancers define ballet culture and identity? (b) What are the mental health experiences of professional ballet dancers? and (c) What are professional ballet dancers’ suggestions for counseling and advocating with this population?
Method
Given the purpose of this study, we chose a transcendental phenomenological approach as an appropriate method to discover and describe the essence of participants’ lived experiences. Both van Staden et al. (2009) and Moola and Krahn (2018) utilized phenomenological approaches to explore ballet dancers’ mental health and experiences of emotional harm. Originally introduced by Husserl (1970), this approach positions researchers to focus on the individual experience while also identifying commonalities across participants (Hays & Singh, 2012). Further, in transcendental phenomenology, researchers set aside preconceived ideas, seeking to add depth and breadth to people’s conscious experiences of their lives and the wider world. In Moustakas’s (1994) modification of Van Kaam’s method of transcendental phenomenology, researchers aim to collect the experiences of participants while consistently assessing and addressing their biases to produce a purer and transcended description of the researched phenomena. Because our lead author, J. Claire Gregory, possesses a background as a professional ballet dancer, the framework of transcendental phenomenology provided the needed structure for identification of biases and preconceived notions, allowing us to evaluate our positionality to the data.
Research Team Positionality
Our research team consisted of Gregory, a doctoral candidate and licensed professional counselor, and Claudia Interiano-Shiverdecker, an assistant professor in counselor education and supervision in a CACREP-accredited counselor education program. Gregory is a Caucasian female and was a professional ballet dancer for 7 years. Interiano-Shiverdecker is a Honduran female with extensive experience conducting qualitative research and clinical experience primarily focused on trauma, crisis, and grief. We have a combined 13 years in clinical practice. Moustakas implored researchers to uphold epoché, “a Greek word meaning to refrain from judgment, to abstain from or stay away from everyday, ordinary ways of perceiving things” (1994, p. 85), by bracketing their own opinions, theories, and expectations. Bracketing is a defining characteristic of transcendental phenomenology in which researchers set aside their own assumptions, to the extent possible, to allow individual experiences to emerge and inform a new perspective on the phenomenon (Moustakas, 1994). Given the composition of the research team and the methodology employed, it was vital to engage in ongoing conversations about our collaboration, data collection and analysis, participants, and the data. Therefore, we addressed specific biases by engaging in virtual weekly bracketing meetings for over a year. Before meetings, Gregory would log memos about thoughts during data collection and analysis. Interiano-Shiverdecker would serve as a consultant to address biases. The biases discussed included a desire to not focus on mental health disorders typically discussed in the literature (e.g., eating disorders) and a desire to highlight professional ballet dancers’ strengths to balance out negative stereotypes. Throughout data analysis, we noted that participants discussed other presenting mental health issues and the connection of ballet culture to the development of those issues, including eating disorders. We operated from a social constructivist research paradigm in which multiple realities of a phenomenon exist (ontology), researchers and participants co-construct knowledge (epistemology), and context is valuable (axiology; Hays & Singh, 2012). This approach primarily focused on reflecting the participants’ voices while recognizing our roles as researchers, so we intentionally did not incorporate a theoretical framework to analyze our data.
Sampling Procedures and Participants
The transcendental phenomenological research procedures we followed included (a) determining the phenomenon of interest, (b) bracketing researcher assumptions, and (c) collecting data from individuals who have directly experienced the phenomenon. Therefore, after receiving approval from our university’s IRB, we used purposive and snowball sampling to recruit professional ballet dancers in the spring and summer of 2020.
Purposive sampling allowed us to select participants for the amount of detail they could provide about the phenomenon (Hays & Singh, 2012). We intentionally recruited individuals who identified as a professional ballet dancer currently or in the past and were 18 years or older, aiming for a sample of at least five participants (Creswell, 2012). The parameters for “professional ballet dancer” were being a dancer with a professional ballet company and receiving financial payment. Gregory emailed potential participants, contacted professional ballet organizations to request distribution of the recruitment flyer among their members, and posted on Facebook groups used by professional ballet dancers. This email and post included an invitation to participate, a link to a demographic form, and an informed consent form. A total of seven eligible volunteers responded to recruitment emails and posts on Facebook groups. Through snowball sampling, we recruited one more participant. Seven of the dancers had worked with the same professional ballet company as Gregory, but only two had danced concurrently with her, which occurred 10 years prior to data collection.
All participants who contacted us about the study stayed enrolled and completed the interview session. Table 1 outlines the demographic information of each participant, with the use of pseudonyms. Five of the eight participants lived in a southern region of the United States, while three participants lived in northwest and eastern regions. All participants identified as Caucasian. Two participants currently worked as professional ballet dancers attached to a company; the other six were ballet teachers, office employees, freelance dancers, students, or nurses.
Data Collection Procedures
Moustakas (1994) recommended lengthy and in-depth interactions with participants in transcendental phenomenology in order to understand participants’ experiences of the phenomenon and the contexts that influence those experiences. Participation required professional ballet dancers to complete a demographic questionnaire, take a picture that represented their perspective on mental health while dancing professionally, and complete an individual semi-structured interview. We chose to include the picture to include creative expression, a vital element in ballet culture. The use of pictures during the interview process facilitated a representative and safe discussion around mental health. Although we did not directly analyze the pictures, they served as catalysts for interview questions. In qualitative research, photography can supplement primary data collection methods when participants struggle to utilize words alone to capture an experience (Hays & Singh, 2012).
Table 1
Participant Demographic Information
| Pseudonym |
Gender |
Age |
Race |
Professional Status |
| Abby |
F |
31 |
Caucasian |
Former Professional |
| Cleo |
F |
28 |
Caucasian |
Current Professional |
| Luna |
F |
35 |
Caucasian |
Former Professional |
| Mica |
F |
30 |
Caucasian |
Former Professional |
| Monica |
F |
37 |
Caucasian |
Former Professional |
| Paul |
M |
25 |
Caucasian |
Current Professional (Freelance) |
| Sophie |
F |
33 |
Caucasian |
Current Professional |
| Zelda |
F |
25 |
Caucasian |
Current Professional (Freelance) |
We developed a 9-item open-ended interview protocol (see Appendix) intended to explore participants’ experiences with mental health, counseling, and advocacy. Gregory conducted all interviews, which lasted from 30 to 60 minutes with an average of 40 minutes, and transcribed each interview verbatim afterward. Three interviews were in person, while six interviews occurred over the phone because of the COVID-19 pandemic. During development, we decided to begin with a simple question to help the dancer feel more at ease. In the next five questions, we utilized their picture to discuss mental health. Because the term “mental health” may or may not be known to the dancers, or it may hold stigma, we felt the picture could produce more insight and depth of the concept. Question 6 asked the dancers to consider their social context and its relation to their mental health. We also chose to include a question asking about ballet dancers’ strengths, as this seems to be rare within performing artist and athlete literature. Next, we directly asked the dancers how counselors could help and then asked a final question that created space for any other relevant thoughts. Through these interviews with eight (seven female, one male) professional ballet dancers, we reached data saturation, meaning that no new information emerged in the data creating redundancy.
Data Analysis
We followed Moustakas’s (1994) modification of Van Kaam’s steps for data analysis, which included (a) developing clusters of meaning, (b) using significant statements and themes to write a description of what participants experienced (textural description) and how they experienced it (structural description), and (c) describing the essence of participant experience from the textural and structural descriptions. First, Gregory engaged in member checking by emailing each participant their interview transcript to ensure accuracy and provide an opportunity to redact any statements. No participant changed their transcript.
Gregory then reviewed each transcript independently, highlighting significant statements or quotes that conveyed participants’ experience. This process is known as horizontalization (Moustakas, 1994). Then, we discussed each identified statement and assigned meaning to similar statements (i.e., clusters of meaning). We used NVivo software for data analysis to ensure consistency, transparency, and accuracy. NVivo, a qualitative data analysis software, aids researchers with consistency in assigning codes to similar topics and allows the research team to cross-check codes for accuracy.
We then determined the invariant constituents, or the final code list, from redundant and ancillary information through a process of reduction and elimination. For example, we eliminated codes that did not illustrate participants’ lived experiences in relation to the purpose of this study. Through the process of reduction, we merged codes if their meaning was similar. These processes allowed us to have a final list of codes that were not repetitive and aligned with the purpose of the study. Using the final codebook, we began the recursive coding process to recode every interview and reach final consensus. Recursive coding, a qualitative data analysis technique, is very useful when analyzing interview data, allowing researchers to compact the data into different categories and illuminating patterns within the data not otherwise apparent (Hays & Singh, 2012). For example, we noticed several codes that illustrated traditions or customs, both positive and negative, that ballet dancers embraced, so we decided to categorize codes about traditions and customs, in both negative and positive categories, to illustrate ballet culture.
Following this initial coding, we explored the latent meanings and clustered invariant constituents into themes, ensuring that all themes were representative of the participants’ experiences. We then synthesized themes into textural descriptions of participants’ experiences, including verbatim quotes and emotional, social, and cultural connections to create a textural-structural description of meanings and essences of experience (Moustakas, 1994). Using the individual textural-structural descriptions, we proceeded to create composite textural and structural descriptions of reoccurring and prominent themes. Finally, Gregory engaged in the member-checking process for a second time by sending the final themes to all participants via email. Four participants responded, all supporting the final themes.
Strategies for Trustworthiness
To ensure quality, we engaged in multiple strategies to meet trustworthiness criteria, such as transferability, confirmability, dependability, and credibility. Specific strategies included using researcher triangulation, member checking, in-depth description of the analyses, and thick description of the data (Hays & Singh, 2012). Weekly meetings for a year helped reduce researcher bias through openly challenging each other with any conclusions. We also engaged in two rounds of member checking for dependability and confirmability. In addition, we utilized an external auditor with previous experience in qualitative research who was unfamiliar with ballet traditions and culture to aid in establishing confirmability of the results and credibility of our data analysis process (Hays & Singh, 2012). The auditor reviewed our NVivo file for data analysis and notes, and the final presentation of the results in a Microsoft Word document. Although the external auditor provided us with APA suggestions, she had no critical feedback regarding our analysis. Instead, she supported our findings on ballet culture that provided a new insight for counselors. Finally, we used thick description when reporting the study findings to increase trustworthiness. Utilizing thick description allowed us to depict deeper meaning and context of the data instead of only reporting the basic facts (Hays & Singh, 2012).
Results
We identified four prevalent themes about professional ballet dancers’ mental health experiences: (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) recommendations for counseling and advocacy—“the dance population is unique.”
Ballet Culture—“It’s Not All Tutus and Tiaras”
All eight participants described ballet as a unique culture with its own set of customs and ingrained traditions. One of the participants, Monica, further elucidated this point: “The traditions of ballet are very old-fashioned, but it’s beautiful when something endures and exists after hundreds of years.” Throughout their narratives, dancers mentioned patterns of “good” and “bad” sides to ballet culture. “It’s not all tutus and tiaras or the perfect life. There is so much beneath the surface,” explained Cleo. To clarify this theme, we divided it into two subthemes: negative aspects of ballet culture and positive aspects of ballet culture. Although we present this theme in two opposing subthemes for simplicity, dancers’ experiences existed along a continuum.
Negative Aspects of Ballet Culture
All of the participants shared that customs of ballet culture focused primarily on requirements indispensable to successfully performing a job that was emotionally and physically demanding. The dancers’ comments centered around physical body requirements and arduous training, highlighting the need for extreme physical athleticism to perform at a professional level. Monica explained, “They [ballet dancers] have obvious physical strength, stamina, endurance, and mind over matter for what they need to do.” “We’re a very underrated athlete,” echoed Abby. Zelda added, “I would compare us to what the world knows a little bit better as gymnastics for the Olympics.”
Although no interview questions specifically asked about the negative side to ballet, participants shared feeling constant stress, pushing their bodies and minds to their limits, worrying about body image and injuries, and feeling pressure to find and keep employment. It was commonplace for participants to experience a sense of pressure and stress from internal and external forces. For example, Paul stated, “I think about my ballet career, and I think how I was tired all the time, because I would wake up and do so much.” Echoing this feeling, Zelda shared, “I was half thriving, half dying inside.” Other participant statements emphasized feeling mentally broken with the lack of time for any outside hobby and having no power as a dancer. Abby stated, “In ballet, everything was just so competitive and mind twisting. I was raised with the idea that every day is an audition.” She added, “This could be your day, or if you don’t work hard today then 3 months from now it is going to creep up on you. So, it’s this weird, like, permanence that is doomed upon us.” According to Abby, there was a daily pressure to achieve greatness, which at times caused injury. For Cleo, a current professional ballet dancer, employment pressure and injury were prevalent: “I actually had an injury where I was not able to dance for a year. . . . I managed to sprain my ankle in three places. I had spent the entire summer rehabbing and keeping it in a boot.” Yet she explained that because she was “scared [of not being asked to return to the dance school], I danced on it for weeks after the initial injury.” Cleo also saw her peers struggling with the same issue:
My friend had food poisoning yesterday. She is still sick today and they told her she has to come in because they were setting the Adagio scene . . . she literally left class to throw up and then came back to class and the whole time was trying not to throw up.
Other professional dancers echoed these fears of financial stress and employment stability, which justified their reasons to push their minds and bodies to the limit, despite physical or mental injuries. Despite perceptions of glamour, Paul highlighted the financial strain that most ballet dancers experience by detailing how he made only “$100 a week and lived in a place that charged me $250 a month.” Even with their efforts, three participants had lost their dancing jobs. Luna believed it was her weight that got her fired, while Paul shared, “I would work super hard all day, back to the gym at night, eat super healthy, and I was still fired for not being good enough, according to my old boss.”
Positive Aspects of Ballet Culture
Despite these intense demands, all participants also discussed positive qualities of ballet culture. These included connection to others, learned adaptability, and creating a story for the audience. Paul highlighted, “Even with the bad parts, there’s a lot more good than there was bad. . . . It’s one of those things, you’re like, I love it so I’ll do it for whatever money.” Monica reflected on her career, saying, “I see fond memories and really good times.” Several participants shared how long training hours and a common goal created a unique connection to others that was difficult to experience elsewhere. Monica passionately stated that “dancers thrive in the sense of community. When you are in a company you are exactly that—part of the greater company and you work together.” Mica shared, “You aren’t really your own person when you are dancing in a professional setting.” “It helps create friends and that was the beauty behind it, you had a support system,” added Luna. Three of the dancers shared their enjoyment of creating an onstage story for the audience. Mica enjoyed how ballet “uses the body to give meaning to stories, more so than other forms of dance.” Luna shared, “We were giving back to the community and being a part of the arts. That was great. I loved that.”
Professional Ballet Dancers’ Identity—“It Is a Part of Me”
All dancers either directly or indirectly attested to a ballet identity and how it influenced their development. To display the range of experiences, we described this theme in two subthemes: ballet dancer traits and connections to their ballet dancer identities. The first subtheme illustrates aspects that ballet dancers might share, while the second theme discusses how participants connected these traits to their personal identity.
Ballet Dancer Traits
All participants shared traits they felt were central to life as a professional dancer, such as tenacity and grit, that influenced their identity during and after dancing. Luna, Mica, Sophie, and Zelda mentioned the discipline a dancer must possess for a successful ballet career. “The level of discipline, I think, is unmatched,” Mica fervently stated. Sophie, Mica, Zelda, and Paul mentioned that their determination for continuous improvement represented their role on stage and ability to maintain their jobs. Sophie expressed, “Your determination, your artistic expression, all of those things include the whole person.” The dancers expressed an ability to push through any odds knowing that, eventually, their hard work would pay off. Sophie shared:
Delayed gratification I feel is a big one [strength], especially in a society with everything now being instant and we are always on our phones, but to work on something slowly over time and be patient. Just trust that hard work pays off.
Dancers indicated a connection between their transformation as dancers and their development as adults. Cleo shared, “If you make it to a professional, you are one of the few that had a hard road, and it makes you have a very thick skin that can help in all matters of life.”
Connection to Their Ballet Dancer Identities
All dancers expressed both positive and negative emotions about their ballet identity, ranging from gratitude to contempt. Four participants expressed that dancing was not just something they did, it was who they were. For them, ballet, and the culture of ballet, were integral parts of their identity. During her interview, Zelda paused after a question about why she continues to dance and simply stated, “It is a part of me.” Sophie shared, “Over the years, I think I stuck with it because it became wrapped up in my identity a bit. This is who I am, this is what I do, this is what makes me special.” Additionally, Cleo and Sophie identified the power and connection they felt while dancing on stage. This connection gave meaning to their dance career. Sophie shared, “Somehow dance felt like it gave me the most ability to participate in music in a way I really wanted to and a kind of level of expression I never really had.”
Yet four participants also felt that their identity had evolved past ballet. “It’s a picture that represented me at a point in time, but I don’t feel it represents me anymore,” shared Mica. Paul, a freelance professional, shared, “I feel like it definitely was how I viewed myself. But I’m not 100% sure if I do or don’t feel that way now.” Monica, a former professional, explained:
Our identity is who we were and what we had, but that is not my core identity. I know who I am in my identity, and it is in Christ who made me, and also just me as a person is more than what I did and what I do on my days at a job.
Mental Health Experiences—“You Have to Compartmentalize”
Utilizing pictures to discuss mental health attended to participants’ preferred form of expression. As Zelda stated early in her interview, “I don’t know how to put it into words. It’s hard.” Despite their dedication and passion, all dancers spoke of the demanding nature of professional dancing and its impact on their mental health. Their conversation around mental health focused on two areas: perfectionism and the perfect body and compartmentalization.
Perfectionism and the Perfect Body
All dancers felt they needed an additional picture to represent the darker side of ballet or related this darker side to imperfections within the picture. Figure 1 displays Paul’s picture of artwork, which the dancer felt represented the outward appearance of perfection but included lumps of paint (i.e., imperfections), a representation of his mental health.
Figure 1
Paul’s Picture of His Mental Health Experience as a Professional Ballet Dancer

Despite there being no interview questions about their body image, seven of the eight dancers shared thoughts about body image concerns or pressure to develop a certain physique. Throughout their dancing career came numerous hours of practice in front of mirrors. Abby’s chosen picture displayed part of a bathroom mirror: “When I look into the mirror, a lot of judgments come back in, and ballet is all based off of opinions and judgments that really mess with your head.” She added, “Everything revolved around the mirror, and if the mirror said it was ok, then my brain said it was ok . . . with ballet and mental health, I feel like a lot of my mental health was based off the reflection.” Paul also shared, “I was going to the gym every single day and was in really good shape but was still told I was not in ballet shape.” Monica shared another company dancer’s experience: “Even though she was a gorgeous dancer and had the most incredible feet and legs, she was told she was overweight, and she did not know, in those days, how to deal with it.” Luna spoke openly about feelings of depression when she gained weight: “When I got fired, I would go into periods where I gained 20 pounds because of my depression. The whole reason I was fired was because I got too big.” She later added, “I started losing it when I got hired back but was not allowed to be in productions because I was too big. . . . The depression made me eat and go into a dark place.” However, Luna also spoke about current cultural changes regarding the “ideal” body shape for ballet dancers in the United States: “Nowadays I feel that they [ballet companies] have embraced differences in dancers.”
Although participants recognized the benefits of an unbreakable determination, discipline, and rigor toward their professional career, they also noted the emotional consequences of their dedicated work. Cleo best illustrated this point: “It just felt like it didn’t matter how hard I worked, it just took a toll. . . . I thought it [ballet] was beautiful, and 13 years ago I believed this, but then things started to turn darker mentally for me.” Mica shared, “I would say a lot of us, we have anxiety and depression, but we are also crazily mentally strong . . . like me, for example, I was told I was too fat from the age of 12.” With this constant stress, the dancers felt their mental health fluctuated with external forces (i.e., thoughts about not being good enough). Zelda stated, “I had constant anxiety of not being good enough.”
Compartmentalization
Another prominent subtheme for all of the dancers was compartmentalization. The dancers described compartmentalization of thoughts and feelings as a healthy coping mechanism for some and a hindrance for others. Abby and Sophie spoke about their need to separate from their feelings and thoughts to perform well. Abby told herself, “Do not think that way. You work really hard and you can put all those thoughts into a little box and hopefully, eventually, get rid of it.” She added that “when the thoughts creep up, I try to put them into my little mental box and try not to open it.” Sophie also spoke in depth about how she maintained her mental health and navigated her negative feelings:
I have to separate myself from my feelings sometimes. I have to remember that my feelings aren’t me. . . . You have to believe you can make it happen and it’s going to work out and be resilient enough to take rejection and injuries, and the uncertainty of finances. You have to hold on and believe it will happen for you. . . . Over time I have become more resilient or grounded. My mental health is very dependent on how I take care of the situations I am in.
However, several dancers also explained how this compartmentalization fostered a negative approach toward mental health, silenced their voice, and led them to bottle up their feelings. Abby described, “If you are sad and can’t handle it, then the director is going to see that, and consequences will happen . . . then it’s the worst . . . we are conditioned to accept whatever is given to us.” Cleo added, “You have to compartmentalize, to hold it in and aren’t allowed to talk about it . . . you’re not allowed to feel the validation of ‘I’m bothered by this.’ It’s almost wrong to feel bothered by this.” When analyzing the data, we noticed that the four participants who were former professional dancers noted an improvement in their mental health after their life in ballet. Sophie also illustrated changes in dancers’ mental health: “It is able to grow and change and be cultivated. So, I do not think mental health as a dancer is fixed.”
Recommendations for Counseling and Advocacy—“The Dance Population Is Unique”
As the conversation turned toward mental health experiences, all participants expressed recommendations in two areas: counseling and society’s view of ballet dancers and advocacy.
Counseling
All participants discussed recommendations for counseling when working with professional ballet dancers. Regarding counseling, Mica shared, “The dance population is unique in itself. A counselor being able to counsel to this is very important.” She further explained, “It’s not the same as advising someone who’s on a basketball team, nor is it the same as advising someone who’s on a theatre crew. It’s just different. It’s an athlete and it’s an artist.”
Abby also urged counselors to recognize trauma among this population: “I think counselors should be aware of emotional abuse and treat dancers as such.” Monica described how ballet dancers joined voices with the MeToo movement: “It just seemed like the movement of women being able to finally express what had happened to them and the abuse they had been enduring was very empowering.” At the same time, she indicated that a lot of people responded with “well that’s just what ballet is.”
Participants highlighted dancers’ absence of mental health services in their work contracts. “Just having someone to talk to would be nice. I know it’s not covered on a lot of health insurances or dancers’ insurance,” said Cleo. “It would be really cool if it were in the context of the studio and dancers could have one session a month at least . . . individual session, group sessions . . . I think a lot of people would jump at the opportunity,” stated Abby. Monica further explained how a counselor could “do a lot to sustain dancers and maybe help their careers because they might be less prone to injury if they aren’t sad and depressed or feeling alone or pushing themselves beyond their breaking point.” She added how counselors may support company staff: “I think there is a lot on the shoulders of the artistic director or one of the ballet mistresses or ballet masters to be an emotional shoulder or a listening ear.”
Another prevalent tenet woven throughout the dancers’ interviews was counselors’ awareness of ballet culture. Three dancers specifically mentioned that if counselors increased their awareness of dance careers, it might help dancers open up to counselors. Paul stated, “I think about when I was dancing, if someone had just been like ‘oh well, you don’t have to be super skinny to dance.’ I’d be like, you don’t know anything, ya know?” Another dancer shared:
Counselors may not need dance experience, but it would be helpful for the dancers if counselors at least have an idea of what a rehearsal day is . . . how many hours we are dancing, how many dancers have second jobs, how often we perform, it adds context . . . having an understanding of the rigors and demands from within the profession.
Society’s View of Ballet Dancers and Advocacy
At some point in their interviews, all participants described ballet dancers’ mental health as hidden or unknown to society, and therefore believed that the first step for advocacy required awareness. Participants explained that when people go to the theatre to watch The Nutcracker around the holiday season or attend Romeo and Juliet, they see a story, a real-time depiction of magic and narrative. Yet participants felt that this led society to view dancers as having “glamourous lifestyles” or, because of Hollywood, believe that dancers “are frail individuals that do not have a real job, throw their friends down the stairs, and steal husbands.” Cleo openly spoke about the hidden side of the ballet world when sharing her picture:
The idea is that it’s so glamorous and they have this perfect life, it’s like the same way they [society] perceive celebrities and they have these glamourous lives and everything is perfect when you see the surface and the smile you are forced to put on, but they do not see everything that goes on underneath. That’s why I love this photo: you don’t know what the person is actually feeling. . . . On the outside I am a very bubbly person, and people don’t know anything going on behind, I guess behind the curtain.
Along these same lines, participants advocated for gender equality within the profession. Although no interview questions asked about gender differences, three dancers pointed out this discrepancy by sharing that women are under extreme pressure to maintain their dance careers. Cleo and Abby also identified how most directors were male. Abby expressed this always “trying to appease the person in charge, who is almost always a man.” For five of the participants, the company director played a vital role in how they viewed themselves. Although some dancers noted overall societal changes and awareness that dancers did not have to fit “this anorexic ballerina” stereotype, some felt that overcoming long-lasting traditions in ballet culture of “skinny equals better” required significant change.
Discussion
The purpose of this qualitative study was to provide a better understanding of ballet culture and its impact on dancers’ identity and mental health. More specifically, we sought to explore different facets of professional ballet dancers’ mental health, while also providing cultural context to professional ballet dancers’ lived experiences. Our attention to cultural context is parallel to trends over the past decade reflecting scholars’ increased focus on performing artists’ training environments to understand their experiences (Lewton-Brain, 2012). Using this perspective allowed us to offer recommendations for counseling and advocacy directly inspired by the ballet dancers’ viewpoints.
The findings from this study resemble descriptions of belief systems and practices entrenched in ballet culture previously discussed in the literature (Wulff, 1998, 2008). One overarching premise presented by the dancers was their need to acquire physical strength, stamina, and a “mind over matter” attitude to have successful ballet careers. The positive and negative qualities of ballet culture created a constant push and pull; however, the participants kept dancing. They recognized their hardships and yet believed enduring them was necessary to live their dreams. The ethos of ballet culture made going through hardships—restricting eating, dancing with injuries, and other stressors—worthwhile. Without providing a justification for these physical and emotional injuries, these new findings provide context to understand ballet dancers’ ideas on body, mind, and health. As some dancers shared, ballet was more than a career to them; it was a part of them, and life without it was hard to imagine.
Participant narratives revealed the ballet dancers’ numerous strengths, such as tenacity, grit, learned adaptability, and unbreakable discipline and rigor. At the same time, participants discussed several mental health hardships. To live up to their ballet dancing goals, dancers focused on their most highly used attribute—their bodies. Because of this, body concerns were prevalent in the findings. The dancers also relayed mental struggles and with them a will to succeed and compartmentalize, to carry on for the performance and the art despite physical and/or emotional pain and at times unsupportive or even abusive environments. Their experiences seemed to align with similar concerns shared by tennis player Naomi Osaka and gymnast Simone Biles. To illustrate, Biles withdrew from part of the 2021 Olympics because of a mind and body disconnect. Her decision earned criticism from the public. She later shared her struggles with mental health concerns (i.e., depression) and how stepping down from competition allowed her to prioritize her mental health and protect her body from potential serious injury.
Our findings also aligned with similar results found with elite athletes and performing artists (Åkesdotter et al., 2020; Gorczynski et al., 2017) and ballet literature in other countries that underscore concerns with disordered eating and body image issues that run deep within ballet culture (Clark et al., 2014; van Staden et al., 2009). Participants discussed anxiety, depression, trauma, abuse, and perfectionism. Their discussions indicated a connection, with anxiety and depression feeding into restrictive eating or other types of eating disorders, and an emotional turmoil following when they were unable to have control. Comorbidity between these mental health disorders and eating disorders is prevalent in the literature, and the present findings elucidate a similar connection among professional ballet dancers.
The findings from this study add to our understanding of professional ballet dancers’ mental health across the world by presenting, to the best of our knowledge, the only study within the United States to fully focus on a qualitative exploration of professional ballet dancer mental health experiences. Our findings expand on and reinforce Hebard and Lamberson (2017), whose work implored counselors to advocate for athletes’ mental health awareness. They stressed that athletes are idolized for their physical endurance, and this perception may leave them specifically vulnerable to mental health issues. Our participants expressed a similar concern and desired counseling services integrated into their schedule and provided by a counselor possessing an understanding of the ballet culture and its specific stressors. They believed that mental health services could not only address their mental health struggles and provide trained support, but also reduce physical injuries often caused by repressed feelings of sadness, loneliness, or insecurity. Participants expressed that advocating for this population should focus on increased access to mental health service providers with an awareness of ballet culture.
Lastly, these findings elucidate a need to evaluate aspects of ballet culture ingrained in tradition that can lead to physical and emotional injuries. Conversations about ballet culture and the emphasis on “petite ballerina dancers” are slowly becoming a part of current efforts to dismantle established perceptions of beauty, athleticism, and inclusion. As Pickard (2012) stated about herself as a dancer, “My body is ballet” (p. 25), and participants expressed that for counselors to advocate for and counsel this population, building awareness about this ongoing conversation while acknowledging the impact of ballet culture on professional ballet dancers’ mindset should be a requirement.
Implications for Counseling
Because of ballet culture and traditions, ballet dancers experience intense physical and mental demands. Counselors must attempt to understand ballet culture as well as its impact on dancer identity and mental health. Counselors need to remain aware of ballet culture when broaching the topic of weight and body identity influences, requirements for a successful ballet dancer, and the relationship between ballet standards and mental health disorders. From the dancers’ perspective, their physical form is directly related to their mental state or how they view themselves. Dancers’ identities intertwine with their bodies from a young age. Although this creates many positive experiences for the dancers, they also expressed how this can lead to depression, anxiety, and other mental health disorders. Considering these experiences, we encourage counselors to support dancers with a client-centered approach and to create an atmosphere of understanding about the dancers’ physical form as integral to their identity and their profession. Utilizing a client-centered approach would allow counselors to inquire about the dancers’ professional experience and help them build an understanding of the professional demands of ballet. Additionally, we encourage counselors to help professional ballet dancers explore their internal self-talk around comparing themselves to others and their relationship with their body.
Although not as prevalent in the data, the dancer statements about abuse are just as vital for counselor awareness. As Monica stated, ballet is a culture with centuries-old traditions and, according to five of the dancers, artist leadership tends to be authoritative in nature. Ballet requires certain physical attributes and training to achieve professional status, which can manifest as abusive relationships and power struggles. We suggest that counselors help professional dancers learn when certain demands may be perceived as abuse by the world outside of the studio. Providing psychoeducation of abuse (e.g., different forms of abuse, power and control wheel) can help ballet dancers differentiate these behaviors and seek help, when needed.
Although many dancers in this study expressed wanting counseling, it seems as though they feared counselors would not understand them or why they committed to such an intense lifestyle. The central need, according to the dancers, is for counselors to be aware of the unique ballet culture. For many dancers, ballet was a part of them, their identity, and something they felt drawn to always be improving. It is not a sport or a hobby, though there seem to be some commonalities between professional ballet dancers and elite athletes. According to the literature (Åkesdotter et al., 2020; Gorczynski et al., 2017), elite athletes experience intense physical demands and elevated anxiety. Our current findings from the dancers are comparable to these features. Therefore, counselors working with dancers may find some similarities with sports counseling. However, counselors should remain aware that sports are for competition and winning, whereas ballet is an art that seeks to provide the audience enjoyment and entertainment.
Limitations and Suggestions for Future Research
As with all research, limitations exist because of many factors. For example, this study engaged a small, homogenous sample of ballet dancers with limited opportunity to dive deeply into within-group differences. All participants identified as Caucasian and many of the dancers had resided in the same geographical location at one point. We recognize that racial and geographical differences, among others, can significantly impact participants’ mental health experiences.
In addition, seven of the eight participants had experienced a prior dance connection with Gregory. Although this may have contributed to trust and more candid interviews, it is also possible that this resulted in biases despite our measures to ensure trustworthiness (e.g., weekly research meetings in order to bracket).
Another limitation is the ballet dancers’ subjective representation of their own mental health. Their illustrations of their experiences provide an inner look at their mental health yet do not guarantee an accurate or clinical representation of their experiences.
Because of the limited research examining professional ballet dancer mental health experiences, many opportunities remain open for future research. One recommendation is for future researchers to consider within-group differences (e.g., race, gender) through recruitment of a heterogenous sample. Also, considering the study’s participants all identified as Caucasian, we recommend future researchers explore the mental health experiences of minority ballet dancers, as they tend to be underrepresented in professional ballet companies in the United States. Additionally, this study included both former and current professional ballet dancers. Researchers may discover insightful data using a longitudinal study, as this could display information about the career transition period from professional dancer to former professional dancer. Other recommendations for future research include quantitative studies focusing on counseling interventions or prevention. Finally, some participants discussed instances of trauma, depression, and anxiety. Future researchers could examine specific mental health disorders and their comorbidity among ballet dancers by using the GAD-7 (Spitzer et al., 2006) for assessing anxiety and the BDI-II (Beck et al., 1996) for depression.
Conclusion
This qualitative study explored ballet culture and identity and their impact on professional ballet dancers’ mental health experiences, which resulted in the four themes of (a) ballet culture—“it’s not all tutus and tiaras”; (b) professional ballet dancers’ identity—“it is a part of me”; (c) mental health experiences—“you have to compartmentalize”; and (d) counseling and advocacy—“the dance population is unique.” A distinct culture exists for professional ballet dancers that includes traditions passed down since the 14th century. Hence, tradition, dedication, and commitment to their profession shape professional ballet dancers’ identities. Further, their identities straddle the environments of performing artists and elite athletes, creating contextually distinctive experiences. For counselors to adequately support professional ballet dancers, they must first build their awareness of ballet culture and the unique mental health needs and resiliencies of dancers.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Åkesdotter, C., Kenttä, G., Eloranta, S., & Franck, J. (2020). The prevalence of mental health problems in elite athletes. Journal of Science and Medicine in Sport, 23(4), 329–335. https://doi.org/10.1016/j.jsams.2019.10.022
American Counseling Association. (2014). ACA code of ethics. https://www.counseling.org/resources/aca-code-of-ethics.pdf
Arcelus, J., Witcomb, G. L., & Mitchell, A. (2014). Prevalence of eating disorders amongst dancers: A systemic review and meta-analysis. European Eating Disorders Review, 22(2), 92–101. https://doi.org/10.1002/erv.2271
Beck, A. T., Steer, R. A., & Brown, G. (1996). Beck Depression Inventory–II [Database record]. APA PsycTests. https://doi.org/10.1037/t00742-000
Biernacki, J. L., Stracciolini, A. S., Fraser, J., Micheli, L. J., & Sugimoto, D. (2021). Risk factors for lower-extremity injuries in female ballet dancers: A systematic review. Clinical Journal of Sports Medicine, 31(2), e64–e79.
Clark, T., Gupta, A., & Ho, C. H. (2014). Developing a dancer wellness program employing developmental evaluation. Frontiers in Psychology, 5(731), 1–9.
https://doi.org/10.3389/fpsyg.2014.00731
Creswell, J. (2012). Qualitative inquiry and research design: Choosing among five approaches (3rd ed.). SAGE.
Gorczynski, P. F., Coyle, M., & Gibson, K. (2017). Depressive symptoms in high-performance athletes and non-athletes: A comparative meta-analysis. British Journal of Sports Medicine, 51(18), 1348–1354. https://doi.org/10.1136/bjsports-2016-096455
Hays, D. G., & Singh, A. A. (2012). Qualitative inquiry in clinical and educational settings. Guilford.
Hebard, S. P., & Lamberson, K. A. (2017). Enhancing the sport counseling specialty: A call for a unified identity. The Professional Counselor, 7(4), 375–384. https://doi.org/10.15241/sph.7.4.375
Husserl, E. (1970). The crisis of European sciences and transcendental phenomenology: An introduction to phenomenological philosophy. Northwestern University Press.
Kirstein, L. (1970). Dance: A short history of classic theatrical dancing. Praeger.
Lewton-Brain, P. (2012). Conversation with a clinician: William G. Hamilton, MD – Is more always more for young dancers? International Association of Dance Medicine and Science Newsletter, 19(4).
Moola, F., & Krahn, A. (2018). A dance with many secrets: The experience of emotional harm from the perspective of past professional female ballet dancers in Canada. Journal of Aggression, Maltreatment & Trauma, 27(3), 256–274. https://doi.org/10.1080/10926771.2017.1410747
Moustakas, C. (1994). Phenomenological research methods. SAGE.
Nejedlo, R. J., Arredondo, P., & Benjamin, L. (1985). Imagine: A visionary model for counselors of tomorrow. George’s Printing.
Pickard, A. (2012). Schooling the dancer: The evolution of an identity as a ballet dancer. Research in Dance Education, 13(1), 25–46. https://doi.org/10.1080/14647893.2011.651119
Rouse, W. B., & Rouse, R. K. (2004). Teamwork in the performing arts. Proceedings of the IEEE, 92(4), 606–615. https://doi.org/10.1109/JPROC.2004.825880
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://doi.org/10.1001/archinte.166.10.1092
Swann, C., Moran, A., & Piggott, D. (2015). Defining elite athletes: Issues in the study of expert performance in sport psychology. Psychology of Sport and Exercise, 16(1), 3–14.
https://doi.org/10.1016/j.psychsport.2014.07.004
Van den Eynde, J., Fisher, A., & Sonn, C. (2016). Working in the Australian entertainment industry: Final report. Entertainment Assist, 1–181. https://crewcare.org.au/images/downloads/WorkingintheAustralianEntertainmentIndustry_FinalReport_Oct16.pdf
van Rens, F. E. C. A., & Heritage, B. (2021). Mental health of circus artists: Psychological resilience, circus factors, and demographics predict depression, anxiety, stress, and flourishing. Psychology of Sport and Exercise, 53, 101850. https://doi.org/10.1016/j.psychsport.2020.101850
van Staden, A., Myburgh, C. P. H., & Poggenpoel, M. (2009). A psycho-educational model to enhance the self-development and mental health of classical dancers. Journal of Dance Medicine & Science, 13(1), 20–28.
Wulff, H. (1998). Ballet across borders: Career and culture in the world of dancers. Berg Publishers.
Wulff, H. (2008). Ethereal expression: Paradoxes of ballet as a global physical culture. Ethnography, 9(4), 518–535. https://journals.sagepub.com/doi/10.1177/1466138108096990
J. Claire Gregory, MA, NCC, LPC, LCDC, is a doctoral candidate at the University of Texas at San Antonio. Claudia G. Interiano-Shiverdecker, PhD, is an assistant professor at the University of Texas at San Antonio. Correspondence may be addressed to J. Claire Gregory, Department of Counseling, 501 W. César E. Chávez Boulevard, San Antonio, TX 78207-4415, jessica.gregory@utsa.edu.
Appendix
Interview Protocol
- Tell me a little bit about yourself.
- Tell me about the picture you took and how this represents your understanding of mental health as a professional ballet dancer.
- Is this picture representative of your mental health? If so, how?
- What do you see here when you look at your picture?
- What are you trying to convey to someone who is looking at your picture?
- Describe how this image relates to society and what prevailing ideas about your mental health are present in this picture.
- What are some strengths about being a professional ballet dancer?
- What can we as counselors do about ballet dancers’ mental health?
- Is there anything else you would like to add?
Aug 20, 2021 | Author Videos, Volume 11 - Issue 3
Warren N. Ponder, Elizabeth A. Prosek, Tempa Sherrill
First responders are continually exposed to trauma-related events. Resilience is evidenced as a protective factor for mental health among first responders. However, there is a lack of assessments that measure the construct of resilience from a strength-based perspective. The present study used archival data from a treatment-seeking sample of 238 first responders to validate the 22-item Response to Stressful Experiences Scale (RSES-22) and its abbreviated version, the RSES-4, with two confirmatory factor analyses. Using a subsample of 190 first responders, correlational analyses were conducted of the RSES-22 and RSES-4 with measures of depressive symptoms, post-traumatic stress, anxiety, and suicidality confirming convergent and criterion validity. The two confirmatory analyses revealed a poor model fit for the RSES-22; however, the RSES-4 demonstrated an acceptable model fit. Overall, the RSES-4 may be a reliable and valid measure of resilience for treatment-seeking first responder populations.
Keywords: first responders, resilience, assessment, mental health, confirmatory factor analysis
First responder populations (i.e., law enforcement, emergency medical technicians, and fire rescue) are often repeatedly exposed to traumatic and life-threatening conditions (Greinacher et al., 2019). Researchers have concluded that such critical incidents could have a deleterious impact on first responders’ mental health, including the development of symptoms associated with post-traumatic stress, anxiety, depression, or other diagnosable mental health disorders (Donnelly & Bennett, 2014; Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). In a systematic review, Wild et al. (2020) suggested the promise of resilience-based interventions to relieve trauma-related psychological disorders among first responders. However, they noted the operationalization and measure of resilience as limitations to their intervention research. Indeed, researchers have conflicting viewpoints on how to define and assess resilience. For example, White et al. (2010) purported popular measures of resilience rely on a deficit-based approach. Counselors operate from a strength-based lens (American Counseling Association [ACA], 2014) and may prefer measures with a similar perspective. Additionally, counselors are mandated to administer assessments with acceptable psychometric properties that are normed on populations representative of the client (ACA, 2014, E.6.a., E.7.d.). For counselors working with first responder populations, resilience may be a factor of importance; however, appropriately measuring the construct warrants exploration. Therefore, the focus of this study was to validate a measure of resilience with strength-based principles among a sample of first responders.
Risk and Resilience Among First Responders
In a systematic review of the literature, Greinacher et al. (2019) described the incidents that first responders may experience as traumatic, including first-hand life-threatening events; secondary exposure and interaction with survivors of trauma; and frequent exposure to death, dead bodies, and injury. Law enforcement officers (LEOs) reported that the most severe critical incidents they encounter are making a mistake that injures or kills a colleague; having a colleague intentionally killed; and making a mistake that injures or kills a bystander (Weiss et al., 2010). Among emergency medical technicians (EMTs), critical incidents that evoked the most self-reported stress included responding to a scene involving family, friends, or others to the crew and seeing someone dying (Donnelly & Bennett, 2014). Exposure to these critical incidents may have consequences for first responders. For example, researchers concluded first responders may experience mental health symptoms as a result of the stress-related, repeated exposure (Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Moreover, considering the cumulative nature of exposure (Donnelly & Bennett, 2014), researchers concluded first responders are at increased risk for post-traumatic stress disorder (PTSD), depression, and generalized anxiety symptoms (Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Symptoms commonly experienced among first responders include those associated with post-traumatic stress, anxiety, and depression.
In a collective review of first responders, Kleim and Westphal (2011) determined a prevalence rate for PTSD of 8%–32%, which is higher than the general population lifetime rate of 6.8–7.8 % (American Psychiatric Association [APA], 2013; National Institute of Mental Health [NIMH], 2017). Some researchers have explored rates of PTSD by specific first responder population. For example, Klimley et al. (2018) concluded that 7%–19% of LEOs and 17%–22% of firefighters experience PTSD. Similarly, in a sample of LEOs, Jetelina and colleagues (2020) reported 20% of their participants met criteria for PTSD.
Generalized anxiety and depression are also prevalent mental health symptoms for first responders. Among a sample of firefighters and EMTs, 28% disclosed anxiety at moderate–severe and several levels (Jones et al., 2018). Furthermore, 17% of patrol LEOs reported an overall prevalence of generalized anxiety disorder (Jetelina et al., 2020). Additionally, first responders may be at higher risk for depression (Klimley et al., 2018), with estimated prevalence rates of 16%–26% (Kleim & Westphal, 2011). Comparatively, the past 12-month rate of major depressive disorder among the general population is 7% (APA, 2013). In a recent study, 16% of LEOs met criteria for major depressive disorder (Jetelina et al., 2020). Moreover, in a sample of firefighters and EMTs, 14% reported moderate–severe and severe depressive symptoms (Jones et al., 2018). Given these higher rates of distressful mental health symptoms, including post-traumatic stress, generalized anxiety, and depression, protective factors to reduce negative impacts are warranted.
Resilience
Broadly defined, resilience is “the ability to adopt to and rebound from change (whether it is from stress or adversity) in a healthy, positive and growth-oriented manner” (Burnett, 2017, p. 2). White and colleagues (2010) promoted a positive psychology approach to researching resilience, relying on strength-based characteristics of individuals who adapt after a stressor event. Similarly, other researchers explored how individuals’ cognitive flexibility, meaning-making, and restoration offer protection that may be collectively defined as resilience (Johnson et al., 2011).
A key element among definitions of resilience is one’s exposure to stress. Given their exposure to trauma-related incidents, first responders require the ability to cope or adapt in stressful situations (Greinacher et al., 2019). Some researchers have defined resilience as a strength-based response to stressful events (Burnett, 2017), in which healthy coping behaviors and cognitions allow individuals to overcome adverse experiences (Johnson et al., 2011; White et al., 2010). When surveyed about positive coping strategies, first responders most frequently reported resilience as important to their well-being (Crowe et al., 2017).
Researchers corroborated the potential impact of resilience for the population. For example, in samples of LEOs, researchers confirmed resilience served as a protective factor for PTSD (Klimley et al., 2018) and as a mediator between social support and PTSD symptoms (McCanlies et al., 2017). In a sample of firefighters, individual resilience mediated the indirect path between traumatic events and global perceived stress of PTSD, along with the direct path between traumatic events and PTSD symptoms (Lee et al., 2014). Their model demonstrated that those with higher levels of resilience were more protected from traumatic stress. Similarly, among emergency dispatchers, resilience was positively correlated with positive affect and post-traumatic growth, and negatively correlated with job stress (Steinkopf et al., 2018). The replete associations of resilience as a protective factor led researchers to develop resilience-based interventions. For example, researchers surmised promising results from mindfulness-based resilience interventions for firefighters (Joyce et al., 2019) and LEOs (Christopher et al., 2018). Moreover, Antony and colleagues (2020) concluded that resilience training programs demonstrated potential to reduce occupational stress among first responders.
Assessment of Resilience
Recognizing the significance of resilience as a mediating factor in PTSD among first responders and as a promising basis for interventions when working with LEOs, a reliable means to measure it among first responder clients is warranted. In a methodological review of resilience assessments, Windle and colleagues (2011) identified 19 different measures of resilience. They found 15 assessments were from original development and validation studies with four subsequent validation manuscripts from their original assessment, of which none were developed with military or first responder samples.
Subsequently, Johnson et al. (2011) developed the Response to Stressful Experiences Scale (RSES-22) to assess resilience among military populations. Unlike deficit-based assessments of resilience, they proposed a multidimensional construct representing how individuals respond to stressful experiences in adaptive or healthy ways. Cognitive flexibility, meaning-making, and restoration were identified as key elements when assessing for individuals’ characteristics connected to resilience when overcoming hardships. Initially they validated a five-factor structure for the RSES-22 with military active-duty and reserve components. Later, De La Rosa et al. (2016) re-examined the RSES-22. De La Rosa and colleagues discovered a unidimensional factor structure of the RSES-22 and validated a shorter 4-item subset of the instrument, the RSES-4, again among military populations.
It is currently unknown if the performance of the RSES-4 can be generalized to first responder populations. While there are some overlapping experiences between military populations and first responders in terms of exposure to trauma and high-risk occupations, the Substance Abuse and Mental Health Services Administration (SAMHSA; 2018) suggested differences in training and types of risk. In the counseling profession, these populations are categorized together, as evidenced by the Military and Government Counseling Association ACA division. Additionally, there may also be dual identities within the populations. For example, Lewis and Pathak (2014) found that 22% of LEOs and 15% of firefighters identified as veterans. Although the similarities of the populations may be enough to theorize the use of the same resilience measure, validation of the RSES-22 and RSES-4 among first responders remains unexamined.
Purpose of the Study
First responders are repeatedly exposed to traumatic and stressful events (Greinacher et al., 2019) and this exposure may impact their mental health, including symptoms of post-traumatic stress, anxiety, depression, and suicidality (Jetelina et al., 2020; Klimley et al., 2018). Though most measures of resilience are grounded in a deficit-based approach, researchers using a strength-based approach proposed resilience may be a protective factor for this population (Crowe et al., 2017; Wild et al., 2020). Consequently, counselors need a means to assess resilience in their clinical practice from a strength-based conceptualization of clients.
Johnson et al. (2011) offered a non-deficit approach to measuring resilience in response to stressful events associated with military service. Thus far, researchers have conducted analyses of the RSES-22 and RSES-4 with military populations (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021), but not yet with first responders. While there are some overlapping characteristics between the populations, there are also unique differences that warrant research with discrete sampling (SAMHSA, 2018). In light of the importance of resilience as a protective factor for mental health among first responders, the purpose of the current study was to confirm the reliability and validity of the RSES-22 and RSES-4 when utilized with this population. In the current study, we hypothesized the measures would perform similarly among first responders and if so, the RSES-4 would offer counselors a brief assessment option in clinical practice that is both reliable and valid.
Method
Participants
Participants in the current non-probability, purposive sample study were first responders (N = 238) seeking clinical treatment at an outpatient, mental health nonprofit organization in the Southwestern United States. Participants’ mean age was 37.53 years (SD = 10.66). The majority of participants identified as men (75.2%; n = 179), with women representing 24.8% (n = 59) of the sample. In terms of race and ethnicity, participants identified as White (78.6%; n = 187), Latino/a (11.8%; n = 28), African American or Black (5.5%; n = 13), Native American (1.7%; n = 4), Asian American (1.3%; n = 3), and multiple ethnicities (1.3%; n = 3). The participants identified as first responders in three main categories: LEO (34.9%; n = 83), EMT (28.2%; n = 67), and fire rescue (25.2%; n = 60). Among the first responders, 26.9% reported previous military affiliation. As part of the secondary analysis, we utilized a subsample (n = 190) that was reflective of the larger sample (see Table 1).
Procedure
The data for this study were collected between 2015–2020 as part of the routine clinical assessment procedures at a nonprofit organization serving military service members, first responders, frontline health care workers, and their families. The agency representatives conduct clinical assessments with clients at intake, Session 6, Session 12, and Session 18 or when clinical services are concluded. We consulted with the second author’s Institutional Review Board, which determined the research as exempt, given the de-identified, archival nature of the data. For inclusion in this analysis, data needed to represent first responders, ages 18 or older, with a completed RSES-22 at intake. The RSES-4 are four questions within the RSES-22 measure; therefore, the participants did not have to complete an additional measure. For the secondary analysis, data from participants who also completed other mental health measures at intake were also included (see Measures).
Table 1
Demographics of Sample
| Characteristic |
Sample 1
(N = 238) |
Sample 2
(n = 190) |
| Age (Years) |
|
|
| Mean |
37.53 |
37.12 |
| Median |
35.50 |
35.00 |
| SD |
10.66 |
10.30 |
| Range |
46 |
45 |
| Time in Service (Years) |
|
|
| Mean |
11.62 |
11.65 |
| Median |
10.00 |
10.00 |
| SD |
9.33 |
9.37 |
| Range |
41 |
39 |
|
n (%) |
| First Responder Type |
|
|
Emergency Medical
Technicians |
67 (28.2%) |
54 (28.4%) |
| Fire Rescue |
60 (25.2%) |
45 (23.7%) |
| Law Enforcement |
83 (34.9%) |
72 (37.9%) |
| Other |
9 (3.8%) |
5 (2.6%) |
| Two or more |
10 (4.2%) |
6 (3.2%) |
| Not reported |
9 (3.8%) |
8 (4.2%) |
| Gender |
|
|
| Women |
59 (24.8%) |
47 (24.7%) |
| Men |
179 (75.2%) |
143 (75.3%) |
| Ethnicity |
|
|
| African American/Black |
13 (5.5%) |
8 (4.2%) |
| Asian American |
3 (1.3%) |
3 (1.6%) |
| Latino(a)/Hispanic |
28 (11.8%) |
24 (12.6%) |
| Multiple Ethnicities |
3 (1.3%) |
3 (1.6%) |
| Native American |
4 (1.7%) |
3 (1.6%) |
| White |
187 (78.6%) |
149 (78.4%) |
Note. Sample 2 is a subset of Sample 1. Time in service for Sample 1, n = 225;
time in service for Sample 2, n = 190.
Measures
Response to Stressful Experiences Scale
The Response to Stressful Experiences Scale (RSES-22) is a 22-item measure to assess dimensions of resilience, including meaning-making, active coping, cognitive flexibility, spirituality, and self-efficacy (Johnson et al., 2011). Participants respond to the prompt “During and after life’s most stressful events, I tend to” on a 5-point Likert scale from 0 (not at all like me) to 4 (exactly like me). Total scores range from 0 to 88 in which higher scores represent greater resilience. Example items include see it as a challenge that will make me better, pray or meditate, and find strength in the meaning, purpose, or mission of my life. Johnson et al. (2011) reported the RSES-22 demonstrates good internal consistency (α = .92) and test-retest reliability (α = .87) among samples from military populations. Further, the developers confirmed convergent, discriminant, concurrent, and incremental criterion validity (see Johnson et al., 2011). In the current study, Cronbach’s alpha of the total score was .93.
Adapted Response to Stressful Experiences Scale
The adapted Response to Stressful Experiences Scale (RSES-4) is a 4-item measure to assess resilience as a unidimensional construct (De La Rosa et al., 2016). The prompt and Likert scale are consistent with the original RSES-22; however, it only includes four items: find a way to do what’s necessary to carry on, know I will bounce back, learn important and useful life lessons, and practice ways to handle it better next time. Total scores range from 0 to 16, with higher scores indicating greater resilience. De La Rosa et al. (2016) reported acceptable internal consistency (α = .76–.78), test-retest reliability, and demonstrated criterion validity among multiple military samples. In the current study, the Cronbach’s alpha of the total score was .74.
Patient Health Questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) is a 9-item measure to assess depressive symptoms in the past 2 weeks (Kroenke et al., 2001). Respondents rate the frequency of their symptoms on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 27, in which higher scores indicate increased severity of depressive symptoms. Example items include little interest or pleasure in doing things and feeling tired or having little energy. Kroenke et al. (2001) reported good internal consistency (α = .89) and established criterion and construct validity. In this sample, Cronbach’s alpha of the total score was .88.
PTSD Checklist-5
The PTSD Checklist-5 (PCL-5) is a 20-item measure for the presence of PTSD symptoms in the past month (Blevins et al., 2015). Participants respond on a 5-point Likert scale indicating frequency of PTSD-related symptoms from 0 (not at all) to 4 (extremely). Total scores range from 0 to 80, in which higher scores indicate more severity of PTSD-related symptoms. Example items include repeated, disturbing dreams of the stressful experience and trouble remembering important parts of the stressful experience. Blevins et al. (2015) reported good internal consistency (α = .94) and determined convergent and discriminant validity. In this sample, Cronbach’s alpha of the total score was .93.
Generalized Anxiety Disorder-7
The Generalized Anxiety Disorder-7 (GAD-7) is a 7-item measure to assess for anxiety symptoms over the past 2 weeks (Spitzer et al., 2006). Participants rate the frequency of the symptoms on a 4-point Likert scale ranging from 0 (not at all) to 3 (nearly every day). Total scores range from 0 to 21 with higher scores indicating greater severity of anxiety symptoms. Example items include not being able to stop or control worrying and becoming easily annoyed or irritable. Among patients from primary care settings, Spitzer et al. (2006) determined good internal consistency (α = .92) and established criterion, construct, and factorial validity. In this sample, Cronbach’s alpha of the total score was .91.
Suicidal Behaviors Questionnaire-Revised
The Suicidal Behaviors Questionnaire-Revised (SBQ-R) is a 4-item measure to assess suicidality (Osman et al., 2001). Each item assesses a different dimension of suicidality: lifetime ideation and attempts, frequency of ideation in the past 12 months, threat of suicidal behaviors, and likelihood of suicidal behaviors (Gutierrez et al., 2001). Total scores range from 3 to 18, with higher scores indicating more risk of suicide. Example items include How often have you thought about killing yourself in the past year? and How likely is it that you will attempt suicide someday? In a clinical sample, Osman et al. (2001) reported good internal consistency (α = .87) and established criterion validity. In this sample, Cronbach’s alpha of the total score was .85.
Data Analysis
Statistical analyses were conducted using SPSS version 26.0 and SPSS Analysis of Moment Structures (AMOS) version 26.0. We examined the dataset for missing values, replacing 0.25% (32 of 12,836 values) of data with series means. We reviewed descriptive statistics of the RSES-22 and RSES-4 scales. We determined multivariate normality as evidenced by skewness less than 2.0 and kurtosis less than 7.0 (Dimitrov, 2012). We assessed reliability for the scales by interpreting Cronbach’s alphas and inter-item correlations to confirm internal consistency.
We conducted two separate confirmatory factor analyses to determine the model fit and factorial validity of the 22-item measure and adapted 4-item measure. We used several indices to conclude model fit: minimum discrepancy per degree of freedom (CMIN/DF) and p-values, root mean residual (RMR), goodness-of-fit index (GFI), comparative fit index (CFI), Tucker-Lewis index (TLI), and the root mean square error of approximation (RMSEA). According to Dimitrov (2012), values for the CMIN/DF < 2.0,p > .05, RMR < .08, GFI > .90, CFI > .90, TLI > .90, and RMSEA < .10 provide evidence of a strong model fit. To determine criterion validity, we assessed a subsample of participants (n = 190) who had completed the RSES-22, RSES-4, and four other psychological measures (i.e., PHQ-9, PCL-5, GAD-7, and SBQ-R). We determined convergent validity by conducting bivariate correlations between the RSES-22 and RSES-4.
Results
Descriptive Analyses
We computed means, standard deviations, 95% confidence interval (CI), and score ranges for the RSES-22 and RSES-4 (Table 2). Scores on the RSES-22 ranged from 19–88. Scores on the RSES-4 ranged from 3–16. Previous researchers using the RSES-22 on military samples reported mean scores of 57.64–70.74 with standard deviations between 8.15–15.42 (Johnson et al., 2011; Prosek & Ponder, 2021). In previous research of the RSES-4 with military samples, mean scores were 9.95–11.20 with standard deviations between 3.02–3.53(De La Rosa et al., 2016; Prosek & Ponder, 2021).
Table 2
Descriptive Statistics for RSES-22 and RSES-4
| Variable |
M |
SD |
95% CI |
Score Range |
| RSES-22 scores |
60.12 |
13.76 |
58.52, 61.86 |
19–88 |
| RSES-4 scores |
11.66 |
2.62 |
11.33, 11.99 |
3–16 |
Note. N = 238. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response
to Stressful Experiences Scale 4-item adaptation.
Reliability Analyses
To determine the internal consistency of the resiliency measures, we computed Cronbach’s alphas. For the RSES-22, we found strong evidence of inter-item reliability (α = .93), which was consistent with the developers’ estimates (α = .93; Johnson et al., 2011). For the RSES-4, we assessed acceptable inter-item reliability (α = .74), which was slightly lower than previous estimates (α = .76–.78; De La Rosa et al., 2016). We calculated the correlation between items and computed the average of all the coefficients. The average inter-item correlation for the RSES-22 was .38, which falls within the acceptable range (.15–.50). The average inter-item correlation for the RSES-4 was .51, slightly above the acceptable range. Overall, evidence of internal consistency was confirmed for each scale.
Factorial Validity Analyses
We conducted two confirmatory factor analyses to assess the factor structure of the RSES-22 and RSES-4 for our sample of first responders receiving mental health services at a community clinic (Table 3). For the RSES-22, a proper solution converged in 10 iterations. Item loadings ranged between .31–.79, with 15 of 22 items loading significantly ( > .6) on the latent variable. It did not meet statistical criteria for good model fit: χ2 (209) = 825.17, p = .000, 90% CI [0.104, 0.120]. For the RSES-4, a proper solution converged in eight iterations. Item loadings ranged between .47–.80, with three of four items loading significantly ( > .6) on the latent variable. It met statistical criteria for good model fit: χ2 (2) = 5.89, p = .053, 90% CI [0.000, 0.179]. The CMIN/DF was above the suggested < 2.0 benchmark; however, the other fit indices indicated a model fit.
Table 3
Confirmatory Factor Analysis Fit Indices for RSES-22 and RSES-4
| Variable |
df |
χ2 |
CMIN/DF |
RMR |
GFI |
CFI |
TLI |
RMSEA |
90% CI |
| RSES-22 |
209 |
825.17/.000 |
3.95 |
.093 |
.749 |
.771 |
0.747 |
.112 |
0.104, 0.120 |
| RSES-4 |
2 |
5.89/.053 |
2.94 |
.020 |
.988 |
.981 |
0.944 |
.091 |
0.000, 0.179 |
Note. N = 238. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response to Stressful Experiences Scale 4-item adaptation; CMIN/DF = Minimum Discrepancy per Degree of Freedom; RMR = Root Mean Square Residual;
GFI = Goodness-of-Fit Index; CFI = Comparative Fit Index; TLI = Tucker-Lewis Index; RMSEA = Root Mean Squared Error of Approximation.
Criterion and Convergent Validity Analyses
To assess for criterion validity of the RSES-22 and RSES-4, we conducted correlational analyses with four established psychological measures (Table 4). We utilized a subsample of participants (n = 190) who completed the PHQ-9, PCL-5, GAD-7, and SBQ-R at intake. Normality of the data was not a concern because analyses established appropriate ranges for skewness and kurtosis (± 1.0). The internal consistency of the RSES-22 (α = .93) and RSES-4 (α = .77) of the subsample was comparable to the larger sample and previous studies. The RSES-22 and RSES-4 related to the psychological measures of distress in the expected direction, meaning measures were significantly and negatively related, indicating that higher resiliency scores were associated with lower scores of symptoms associated with diagnosable mental health disorders (i.e., post-traumatic stress, anxiety, depression, and suicidal behavior). We verified convergent validity with a correlational analysis of the RSES-22 and RSES-4, which demonstrated a significant and positive relationship.
Table 4
Criterion and Convergent Validity of RSES-22 and RSES-4
|
M (SD) |
Cronbach’s α |
RSES-22 |
PHQ-9 |
PCL-5 |
GAD-7 |
SBQ-R |
| RSES-22 |
60.16 (14.17) |
.93 |
— |
−.287* |
−.331* |
−.215* |
−.346* |
| RSES-4 |
11.65 (2.68) |
.77 |
.918 |
−.290* |
−.345* |
−.220* |
−.327* |
Note. n = 190. RSES-22 = Response to Stressful Experiences Scale 22-item; RSES-4 = Response to Stressful Experiences Scale 4-item adaptation; PHQ-9 = Patient Health Questionnaire-9;
PCL-5 = PTSD Checklist-5; GAD-7 = Generalized Anxiety Disorder-7; SBQ-R = Suicidal Behaviors Questionnaire-Revised.
*p < .01.
Discussion
The purpose of this study was to validate the factor structure of the RSES-22 and the abbreviated RSES-4 with a first responder sample. Aggregated means were similar to those in the articles that validated and normed the measures in military samples (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021). Additionally, the internal consistency was similar to previous studies. In the original article, Johnson et al. (2011) proposed a five-factor structure for the RSES-22, which was later established as a unidimensional assessment after further exploratory factor analysis (De La Rosa et al., 2016). Subsequently, confirmatory factor analyses with a treatment-seeking veteran population revealed that the RSES-22 demonstrated unacceptable model fit, whereas the RSES-4 demonstrated a good model fit (Prosek & Ponder, 2021). In both samples, the RSES-4 GFI, CFI, and TLI were all .944 or higher, whereas the RSES-22 GFI, CFI, and TLI were all .771 or lower. Additionally, criterion and convergent validity as measured by the PHQ-9, PCL-5, and GAD-7 in both samples were extremely close. Similarly, in this sample of treatment-seeking first responders, confirmatory factor analyses indicated an inadequate model fit for the RSES-22 and a good model fit for the RSES-4. Lastly, convergent and criterion validity were established with correlation analyses of the RSES-22 and RSES-4 with four other standardized assessment instruments (i.e., PHQ-9, PCL-5, GAD-7, SBQ-R). We concluded that among the first responder sample, the RSES-4 demonstrated acceptable psychometric properties, as well as criterion and convergent validity with other mental health variables (i.e., post-traumatic stress, anxiety, depression, and suicidal behavior).
Implications for Clinical Practice
First responders are a unique population and are regularly exposed to trauma (Donnelly & Bennett, 2014; Jetelina et al., 2020; Klimley et al., 2018; Weiss et al., 2010). Although first responders could potentially benefit from espousing resilience, they are often hesitant to seek mental health services (Crowe et al., 2017; Jones, 2017). The RSES-22 and RSES-4 were originally normed with military populations. The results of the current study indicated initial validity and reliability among a first responder population, revealing that the RSES-4 could be useful for counselors in assessing resilience.
It is important to recognize that first responders have perceived coping with traumatic stress as an individual process (Crowe et al., 2017) and may believe that seeking mental health services is counter to the emotional and physical training expectations of the profession (Crowe et al., 2015). Therefore, when first responders seek mental health care, counselors need to be prepared to provide culturally responsive services, including population-specific assessment practices and resilience-oriented care.
Jones (2017) encouraged a comprehensive intake interview and battery of appropriate assessments be conducted with first responder clients. Counselors need to balance the number of intake questions while responsibly assessing for mental health comorbidities such as post-traumatic stress, anxiety, depression, and suicidality. The RSES-4 provides counselors a brief, yet targeted assessment of resilience.
Part of what cultural competency entails is assessing constructs (e.g., resilience) that have been shown to be a protective factor against PTSD among first responders (Klimley et al., 2018). Since the items forming the RSES-4 were developed to highlight the positive characteristics of coping (Johnson et al., 2011), rather than a deficit approach, this aligns with the grounding of the counseling profession. It is also congruent with first responders’ perceptions of resilience. Indeed, in a content analysis of focus group interviews with first responders, participants defined resilience as a positive coping strategy that involves emotional regulation, perseverance, personal competence, and physical fitness (Crowe et al., 2017).
The RSES-4 is a brief, reliable, and valid measure of resilience with initial empirical support among a treatment-seeking first responder sample. In accordance with the ACA (2014) Code of Ethics, counselors are to administer assessments normed with the client population (E.8.). Thus, the results of the current study support counselors’ use of the measure in practice. First responder communities are facing unprecedented work tasks in response to COVID-19. Subsequently, their mental health might suffer (Centers for Disease Control and Prevention, 2020) and experts have recommended promoting resilience as a protective factor for combating the negative mental health consequences of COVID-19 (Chen & Bonanno, 2020). Therefore, the relevance of assessing resilience among first responder clients in the current context is evident.
Limitations and Future Research
This study is not without limitations. The sample of first responders was homogeneous in terms of race, ethnicity, and gender. Subsamples of first responders (i.e., LEO, EMT, fire rescue) were too small to conduct within-group analyses to determine if the factor structure of the RSES-22 and RSES-4 would perform similarly. Also, our sample of first responders included two emergency dispatchers. Researchers reported that emergency dispatchers should not be overlooked, given an estimated 13% to 15% of emergency dispatchers experience post-traumatic symptomatology (Steinkopf et al., 2018). Future researchers may develop studies that further explore how, if at all, emergency dispatchers are represented in first responder research.
Furthermore, future researchers could account for first responders who have prior military service. In a study of LEOs, Jetelina et al. (2020) found that participants with military experience were 3.76 times more likely to report mental health concerns compared to LEOs without prior military affiliation. Although we reported the prevalence rate of prior military experience in our sample, the within-group sample size was not sufficient for additional analyses. Finally, our sample represented treatment-seeking first responders. Future researchers may replicate this study with non–treatment-seeking first responder populations.
Conclusion
First responders are at risk for sustaining injuries, experiencing life-threatening events, and witnessing harm to others (Lanza et al., 2018). The nature of their exposure can be repeated and cumulative over time (Donnelly & Bennett, 2014), indicating an increased risk for post-traumatic stress, anxiety, and depressive symptoms, as well as suicidal behavior (Jones et al., 2018). Resilience is a promising protective factor that promotes wellness and healthy coping among first responders (Wild et al., 2020), and counselors may choose to routinely measure for resilience among first responder clients. The current investigation concluded that among a sample of treatment-seeking first responders, the original factor structure of the RSES-22 was unstable, although it demonstrated good reliability and validity. The adapted version, RSES-4, demonstrated good factor structure while also maintaining acceptable reliability and validity, consistent with studies of military populations (De La Rosa et al., 2016; Johnson et al., 2011; Prosek & Ponder, 2021). The RSES-4 provides counselors with a brief and strength-oriented option for measuring resilience with first responder clients.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
American Counseling Association. (2014). ACA code of ethics.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
Antony, J., Brar, R., Khan, P. A., Ghassemi, M., Nincic, V., Sharpe, J. P., Straus, S. E., & Tricco, A. C. (2020). Interventions for the prevention and management of occupational stress injury in first responders: A rapid overview of reviews. Systematic Reviews, 9(121), 1–20. https://doi.org/10.1186/s13643-020-01367-w
Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., & Domino, J. L. (2015). The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and initial psychometric evaluation. Journal of Traumatic Stress, 28(6), 489–498. https://doi.org/10.1002/jts.22059
Burnett, H. J., Jr. (2017). Revisiting the compassion fatigue, burnout, compassion satisfaction, and resilience connection among CISM responders. Journal of Police Emergency Response, 7(3), 1–10. https://doi.org/10.1177/2158244017730857
Centers for Disease Control and Prevention. (2020, June 30). Coping with stress. https://www.cdc.gov/coronavirus/2019-ncov/daily-life-coping/managing-stress-anxiety.html
Chen, S., & Bonanno, G. A. (2020). Psychological adjustment during the global outbreak of COVID-19: A resilience perspective. Psychological Trauma: Theory, Research, Practice, and Policy, 12(S1), S51–S54. https://doi.org/10.1037/tra0000685
Christopher, M. S., Hunsinger, M., Goerling, R. J., Bowen, S., Rogers, B. S., Gross, C. R., Dapolonia, E., & Pruessner, J. C. (2018). Mindfulness-based resilience training to reduce health risk, stress reactivity, and aggression among law enforcement officers: A feasibility and preliminary efficacy trial. Psychiatry Research, 264, 104–115. https://doi.org/10.1016/j.psychres.2018.03.059
Crowe, A., Glass, J. S., Lancaster, M. F., Raines, J. M., & Waggy, M. R. (2015). Mental illness stigma among first responders and the general population. Journal of Military and Government Counseling, 3(3), 132–149. http://mgcaonline.org/wp-content/uploads/2013/02/JMGC-Vol-3-Is-3.pdf
Crowe, A., Glass, J. S., Lancaster, M. F., Raines, J. M., & Waggy, M. R. (2017). A content analysis of psychological resilience among first responders. SAGE Open, 7(1), 1–9. https://doi.org/10.1177/2158244017698530
De La Rosa, G. M., Webb-Murphy, J. A., & Johnston, S. L. (2016). Development and validation of a brief measure of psychological resilience: An adaptation of the Response to Stressful Experiences Scale. Military Medicine, 181(3), 202–208. https://doi.org/10.7205/MILMED-D-15-00037
Dimitrov, D. M. (2012). Statistical methods for validation of assessment scale data in counseling and related fields. American Counseling Association.
Donnelly, E. A., & Bennett, M. (2014). Development of a critical incident stress inventory for the emergency medical services. Traumatology, 20(1), 1–8. https://doi.org/10.1177/1534765613496646
Greinacher, A., Derezza-Greeven, C., Herzog, W., & Nikendei, C. (2019). Secondary traumatization in first responders: A systematic review. European Journal of Psychotraumatology, 10(1), 1562840. https://doi.org/10.1080/20008198.2018.1562840
Gutierrez, P. M., Osman, A., Barrios, F. X., & Kopper, B. A. (2001). Development and initial validation of the Self-Harm Behavior Questionnaire. Journal of Personality Assessment, 77(3), 475–490. https://doi.org/10.1207/S15327752JPA7703_08
Jetelina, K. K., Mosberry, R. J., Gonzalez, J. R., Beauchamp, A. M., & Hall, T. (2020). Prevalence of mental illnesses and mental health care use among police officers. JAMA Network Open, 3(10), 1–12. https://doi.org/10.1001/jamanetworkopen.2020.19658
Johnson, D. C., Polusny, M. A., Erbes, C. R., King, D., King, L., Litz, B. T., Schnurr, P. P., Friedman, M., Pietrzak, R. H., & Southwick, S. M. (2011). Development and initial validation of the Response to Stressful Experiences Scale. Military Medicine, 176(2), 161–169. https://doi.org/10.7205/milmed-d-10-00258
Jones, S. (2017). Describing the mental health profile of first responders: A systematic review. Journal of the American Psychiatric Nurses Association, 23(3), 200–214. https://doi.org/10.1177/1078390317695266
Jones, S., Nagel, C., McSweeney, J., & Curran, G. (2018). Prevalence and correlates of psychiatric symptoms among first responders in a Southern state. Archives of Psychiatric Nursing, 32(6), 828–835. https://doi.org/10.1016/j.apnu.2018.06.007
Joyce, S., Tan, L., Shand, F., Bryant, R. A., & Harvey, S. B. (2019). Can resilience be measured and used to predict mental health symptomology among first responders exposed to repeated trauma? Journal of Occupational and Environmental Medicine, 61(4), 285–292. https://doi.org/10.1097/JOM.0000000000001526
Kleim, B., & Westphal, M. (2011). Mental health in first responders: A review and recommendation for prevention and intervention strategies. Traumatology, 17(4), 17–24. https://doi.org/10.1177/1534765611429079
Klimley, K. E., Van Hasselt, V. B., & Stripling, A. M. (2018). Posttraumatic stress disorder in police, firefighters, and emergency dispatchers. Aggression and Violent Behavior, 43, 33–44.
https://doi.org/10.1016/j.avb.2018.08.005
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16, 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Lanza, A., Roysircar, G., & Rodgers, S. (2018). First responder mental healthcare: Evidence-based prevention, postvention, and treatment. Professional Psychology: Research and Practice, 49(3), 193–204. https://doi.org/10.1037/pro0000192
Lee, J.-S., Ahn, Y.-S., Jeong, K.-S. Chae, J.-H., & Choi, K.-S. (2014). Resilience buffers the impact of traumatic events on the development of PTSD symptoms in firefighters. Journal of Affective Disorders, 162, 128–133. https://doi.org/10.1016/j.jad.2014.02.031
Lewis, G. B., & Pathak, R. (2014). The employment of veterans in state and local government service. State and Local Government Review, 46(2), 91–105. https://doi.org/10.1177/0160323X14537835
McCanlies, E. C., Gu, J. K., Andrew, M. E., Burchfiel, C. M., & Violanti, J. M. (2017). Resilience mediates the relationship between social support and post-traumatic stress symptoms in police officers. Journal of Emergency Management, 15(2), 107–116. https://doi.org/10.5055/jem.2017.0319
National Institute of Mental Health. (2017). Post-traumatic stress disorder. https://www.nimh.nih.gov/health/statistics/post-traumatic-stress-disorder-ptsd.shtml
Osman, A., Bagge, C. L., Gutierrez, P. M., Konick, L. C., Kopper, B. A., & Barrios, F. X. (2001). The Suicidal Behaviors Questionnaire–revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment, 8(4), 443–454. https://doi.org/10.1177/107319110100800409
Prosek, E. A., & Ponder, W. N. (2021). Validation of the Adapted Response to Stressful Experiences Scale (RSES-4) among veterans [Manuscript submitted for publication].
Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder (The GAD-7). Archives of Internal Medicine, 166(10), 1092–1097.
https://doi.org/10.1001/archinte.166.10.1092
Steinkopf, B., Reddin, R. A., Black, R. A., Van Hasselt, V. B., & Couwels, J. (2018). Assessment of stress and resiliency in emergency dispatchers. Journal of Police and Criminal Psychology, 33(4), 398–411.
https://doi.org /10.1007/s11896-018-9255-3
Substance Abuse and Mental Health Services Administration. (2018, May). First responders: Behavioral health concerns, emergency response, and trauma. Disaster Technical Assistance Center Supplemental Research Bulletin. https://www.samhsa.gov/sites/default/files/dtac/supplementalresearchbulletin-firstresponders-may2018.pdf
Weiss, D. S., Brunet, A., Best, S. R., Metzler, T. J., Liberman, A., Pole, N., Fagan, J. A., & Marmar, C. R. (2010). Frequency and severity approaches to indexing exposure to trauma: The Critical Incident History Questionnaire for police officers. Journal of Traumatic Stress, 23(6), 734–743.
https://doi.org/10.1002/jts.20576
White, B., Driver, S., & Warren, A. M. (2010). Resilience and indicators of adjustment during rehabilitation from a spinal cord injury. Rehabilitation Psychology, 55(1), 23–32. https://doi.org/10.1037/a0018451
Wild, J., El-Salahi, S., Degli Esposti, M., & Thew, G. R. (2020). Evaluating the effectiveness of a group-based resilience intervention versus psychoeducation for emergency responders in England: A randomised controlled trial. PLoS ONE, 15(11), e0241704. https://doi.org/10.1371/journal.pone.0241704
Windle, G., Bennett, K. M., & Noyes, J. (2011). A methodological review of resilience measurement scales. Health and Quality of Life Outcomes, 9, Article 8, 1–18. https://doi.org/10.1186/1477-7525-9-8
Warren N. Ponder, PhD, is Director of Outcomes and Evaluation at One Tribe Foundation. Elizabeth A. Prosek, PhD, NCC, LPC, is an associate professor at Penn State University. Tempa Sherrill, MS, LPC-S, is the founder of Stay the Course and a volunteer at One Tribe Foundation. Correspondence may be addressed to Warren N. Ponder, 855 Texas St., Suite 105, Fort Worth, TX 76102, warren@1tribefoundation.org.
Feb 26, 2021 | Volume 11 - Issue 1
David E. Jones, Jennifer S. Park, Katie Gamby, Taylor M. Bigelow, Tesfaye B. Mersha, Alonzo T. Folger
Epigenetics is the study of modifications to gene expression without an alteration to the DNA sequence. Currently there is limited translation of epigenetics to the counseling profession. The purpose of this article is to inform counseling practitioners and counselor educators about the potential role epigenetics plays in mental health. Current mental health epigenetic research supports that adverse psychosocial experiences are associated with mental health disorders such as schizophrenia, anxiety, depression, and addiction. There are also positive epigenetic associations with counseling interventions, including cognitive behavioral therapy, mindfulness, diet, and exercise. These mental health epigenetic findings have implications for the counseling profession such as engaging in early life span health prevention and wellness, attending to micro and macro environmental influences during assessment and treatment, collaborating with other health professionals in epigenetic research, and incorporating epigenetic findings into counselor education curricula that meet the standards of the Council for Accreditation of Counseling and Related Educational Programs (CACREP).
Keywords: epigenetics, mental health, counseling, prevention and wellness, counselor education
Epigenetics, defined as the study of chemical changes at the cellular level that alter gene expression but do not alter the genetic code (T.-Y. Zhang & Meaney, 2010), has emerging significance for the profession of counseling. Historically, people who studied abnormal behavior focused on determining whether the cause of poor mental health outcomes was either “nature or nurture” (i.e., either genetics or environmental factors). What we now understand is that both nature and nurture, or the interaction between the individual and their environment (e.g., neglect, trauma, substance abuse, diet, social support, exercise), can modify gene expression positively or negatively (Cohen et al., 2017; Suderman et al., 2014).
In the concept of nature and nurture, there is evidence that psychosocial experiences can change the landscape of epigenetic chemical tags across the genome. This change in landscape influences mental health concerns, such as addiction, anxiety, and depression, that are addressed by counseling practitioners (Lester et al., 2016; Provençal & Binder, 2015; Szyf et al., 2016). Because the field of epigenetics is evolving and there is limited attention to epigenetics in the counseling profession, our purpose is to inform counseling practitioners and educators about the role epigenetics may play in clinical mental health counseling.
Though many counselors and counselor educators may have taken a biology class that covered genetics sometime during their professional education, we provide pedagogical scaffolding from genetics to epigenetics. Care was taken to ensure accessibility of information for readers across this continuum of genetics knowledge. Much of what we offer below on genetics is putative knowledge, as we desire to establish a foundation for the reader in genetics so they may be able to have a greater understanding of epigenetics and a clearer comprehension of the implications we offer leading to application in counseling. We suggest readers review Brooker (2017) for more detailed information on genetics. We will present an overview of genetics and epigenetics, an examination of mental health epigenetics, and implications for the counseling profession.
Genetics
Genetics is the study of heredity (Brooker, 2017) and the cellular process by which parents pass on biological information via genes. The child inherits genetic coding from both parents. One can think of these parental genes as a recipe book for molecular operations such as the development of proteins, structure of neurons, and other functions across the human body. This total collection of the combination of genes in the human body is called the genome or genotype. The presentation of observable human traits (e.g., eye color, height, blood type) is called the phenotype. Phenotypes can be seen in our clinical work through behavior (e.g., self-injury, aggression, depression, anxiety, inattentiveness).
Before going further, it is important to establish a fundamental understanding of genetics by examining the varied molecular components and their relationships (Figure 1). Deoxyribonucleic acid (DNA) is a long-strand molecule that takes the famous double helix or ladder configuration. DNA is made up of four chemical bases called adenine (A), guanine (G), cytosine (C), and thymine (T). These form base pairs—A with T and C with G—creating a nucleic acid. The DNA is also wrapped around a specialized protein called a histone. The collection of DNA wrapped around multiple histones is called the chromatin. This wrapping process is essential for the DNA to fit within the cell nucleus. Finally, as this chromatin continues to grow, it develops a structure called a chromosome. Within every human cell nucleus, there are 23 chromosomes from each parent, totaling 46 chromosomes.
Figure 1
Gene Structure and Epigenetics
From “Epigenomics Fact Sheet,” by National Human Genome Research Institute, 2020
(https://www.genome.gov/about-genomics/fact-sheets/Epigenomics-Fact-Sheet). In the public domain.
Beyond the chromosomes, chromatin, histones, DNA, and genes, there is another key component in genetics: ribonucleic acid (RNA). RNA can be a cellular messenger that carries instructions from a DNA sequence (specific genes) to other parts of the cell (i.e., messenger RNA [mRNA]). RNA can come in several other forms as well, including transfer RNA (tRNA), microRNA (miRNA), and non-coding RNA (ncRNA). In the sections below, we elaborate on mRNA and tRNA and their impact on the genetic processes. Later in the epigenetics section, we provide fuller details on miRNA and ncRNA.
Besides the aforementioned biological aspects, it is important to understand that a child inherits genes from both parents, but they are not exactly the same genes, (i.e., alternative forms of the same gene may have differing expression). Different versions of the same gene are called alleles. Variation in an allele is one reason why we see phenotypic variation between our clients—height, weight, eye color—and this variation can contribute to mental disease susceptibility. Although there are many potential causes of poor mental health, family history is often one of the strongest risk factors because family members most closely represent the unique genetic and environmental interactions that an individual may experience. We also see this as a function of intergenerational epigenetic effects, which are covered later in this paper.
Transcription and Translation
Now that we have provided a foundation of the genetic components, we move toward the primary two-stage processes of genetics: transcription and translation (Brooker, 2017). The first step in the process of gene expression is called transcription. Transcription occurs when a sequence of DNA is copied using RNA polymerase (“ase” notes that it is an enzyme) to make mRNA for protein synthesis. We can liken transcription to the process of someone taking down information from a client’s voicemail message. In this visualization, DNA is the caller, the person writing down the message is the RNA polymerase, and the actual written message is the RNA.
A particular section of a gene, called a promotor region, is bound by the RNA polymerase (Brooker, 2017). The RNA polymerase acts like scissors to separate the double-stranded DNA helix into two strands. One of the strands, called the template, is where the RNA polymerase will read the DNA code A to T, and G to C to build mRNA. There are other modifications that must occur in eukaryotic cells such as splicing introns and exons. In short, sections of unwanted DNA, called introns, are removed by the process of splicing, and the remaining DNA codes are connected back together (exons).
Now that the mRNA has been created by the process of transcription, the next step is for the mRNA to build a protein necessary for the main functions of the body, in a process known as translation (Brooker, 2017). Here, translation is the process in which tRNA decodes or translates the mRNA into a protein in a mobile cellular factory called the ribosome. It is translating the language of a DNA sequence (gene) into the language of a protein. To do this, the tRNA uses a translation device called an anticodon. This anticodon links to the mRNA-based pairs called a codon. A codon is a trinucleotide sequence of DNA or RNA that corresponds to a specific amino acid, or building block of a protein. This process then continues to translate and connect many amino acids together until a polypeptide (a long chain of amino acids) is created. Later, these polypeptides join to form proteins. Depending on the type of cell, the protein may function in a variety of ways. For example, the neuron has several proteins for its function, and different proteins are used for memory, learning, and neuroplasticity.
Epigenetics
There is a wealth of research conducted on genetics, yet the understanding of epigenetics is more limited when focusing on mental health (Huang et al., 2017). Though the term epigenetics has been around since the 1940s, the “science” of epigenetics is in its youth. Epigenetic research in humans has grown in the last 10 years and continues to expand rapidly (Januar et al., 2015). The key concept for counselors to remember about epigenetics is that epigenetics supports the idea of coaction. Factors present in the client’s external environment (e.g., stress from caregiver neglect, foods consumed, drug intake like cigarettes) influence the expression of their genes (transcription and translation) and thus cell activity and related behavioral phenotypes. In the sections below, we will dive deeper into the understanding of epigenetic mechanisms and define key terms including epigenome, chromatin, and chemical modifications.
To start, the more formal definition of epigenetics is the differentiation of gene expression via chemical modifications upon the epigenome that do not alter the genetic code (i.e., the DNA sequence; Szyf et al., 2007). The epigenome, which is composed of chromatin (the combination of DNA and protein forming the chromosomes) and modification of DNA by chemical mechanisms (e.g., DNA methylation, histone modification), programs the process of gene expression (Szyf et al., 2007). The epigenome differs from the genome in that the chemical actions or modifications are on the outside of the genome (i.e., the DNA) or “upon” the genome. Specifically, epigenetic processes act “upon” the genome, which may open or close the chromatin to various degrees to govern access for reading DNA sequences (Figure 1). When the chromatin is opened, transcription and translation can take place; however, when the chromatin is closed, gene expression is silenced (Syzf et al., 2007).
It is important for counselors to conceptualize their client’s psychosocial environment in conjunction with the observed behavioral phenotypes, in that the client’s psychosocial environment may have partially mediated epigenetic expression (Januar et al., 2015). For example, with schizophrenia, a client’s adverse environment (e.g., early childhood trauma) influences the epigenome, or gene expression, which may contribute up to 60% of this disorder’s development (Gejman et al., 2011). Other adverse environmental influences have been associated with the development of schizophrenia, including complications during client’s prenatal development and birth, place and season of client’s birth, abuse, and parental loss (Benros et al., 2011). As we highlight below, epigenetic mechanisms (e.g., DNA methylation) may mediate between these environmental influences and genes with outcomes like schizophrenia (Cariaga-Martinez & Alelú-Paz, 2018; Tsankova et al., 2007).
Epigenetic Mechanisms
There are a variety of chemical mechanisms or tags that change the chromatin structure (either opening for expression or closing to inhibit expression). Some of the most investigated mechanisms for changes in chromatin structure are DNA methylation, histone modification, and microRNA (Benoit & Turecki, 2010; Maze & Nestler, 2011).
DNA Methylation. Methylation is the most studied epigenetic modification (Nestler et al., 2016). It occurs when a methyl group binds to a cytosine base (C) of DNA to form 5-methylcytosine. A methyl group is three hydrogens bonded to a carbon, identified as CH3. Most often, the methyl group is attached to a C followed by a G, called a CpG. These methylation changes are carried out by specific enzymes called DNA methyltransferase. These enzymes add the methyl group to the C base at the CpG site.
Methylation was initially considered irreversible, but recent research has shown that DNA methylation is more stable compared to other chemical modifications like histone modification and is therefore reversible (Nestler et al., 2016). This DNA methylation adaptability evidence is important, conceivably supporting counseling efficacy across the life span. If methylation is indeed reversible beyond 0 to 5 years of age, counseling efforts hold promise to influence mental health outcomes across the life span.
Beyond noted stability, DNA methylation is also important in that it is tissue-specific, meaning it assists in cell differentiation; it may regulate gene expression up or down and is influenced by different environmental exposures (Monk et al., 2012). For example, DNA methylation represses specific areas of a neuron’s genes, thus “turning off” their function. This stabilizes the cell by preventing any tissue-specific cell differentiation and inhibits the neuron from changing into another cell type (Szyf et al., 2016), such as becoming a lung cell later in development.
When looking at up- or downregulation, Oberlander et al. (2008) provided an example from a study using mice. When examining attachment style in mice, they found that decreased quality of mothering to offspring increased risk of anxiety, in part, because of the methylation at the glucocorticoid receptor (GR) gene and fewer GR proteins produced by the hippocampus. This change may lead to lifelong silencing or downregulation with an increased risk of anxiety to the mouse over its life span. Stevens et al. (2018) also established a link between diet, epigenetics, and DNA methylation. They found an epigenetic connection between poor dietary intake with increased risk of behavioral problems and poor mental health outcomes such as autism. The authors also remarked that further investigation is required for a clearer picture of this link and potential effects.
Histone Modification. Another process that has been extensively researched is post-translational histone modification, or changes in the histone after the translation process. The most understood histone modifications are acetylation, methylation, and phosphorylation (Nestler et al., 2016). Acetylation, the most common post-translational modification, occurs by adding an acetyl group to the histone tail, such as the amino acid lysine. The enzymes responsible for histone acetylation are histone acetyltransferases or HATs (Haggarty & Tsai, 2011). Conversely, histone deacetylases (HDACs) are enzymes that remove acetyl groups (Saavedra et al., 2016). The acetylation process promotes gene expression (Nestler et al., 2016).
Through histone methyltransferases (HMTs), histone methylation increases methylation, thereby reducing gene expression. Histone demethylases (HDMs) remove methyl groups to increase gene activity. Phosphorylation can increase or decrease gene expression. Overall, there are more than 50 known histone modifications (Nestler et al., 2016).
From a counseling perspective, it is important to note that histone modification is flexible. Unlike DNA methylation, which is more stable over a lifetime, histone modifications are more transient. To illustrate, if an acetyl group is added to a histone, it may loosen the binding between the DNA and histone, increasing transcription and thereby allowing gene expression across the life span (Nestler et al., 2016). Such acetylation processes have been found in maternal neglect to offspring (early in the life span) and mindfulness practices in adult clients (Chaix et al., 2020; Devlin et al., 2010). Yet, although histone modification can be changed across the life span (Nestler et al., 2016), it is still important for counselors to recognize the importance of early counseling interventions because of how highly active epigenetics mechanisms (e.g., DNA methylation) are in children 0 to 5 years of age.
MicroRNA. Beyond histone modification, another known mechanism is microRNA (miRNA), which is the least understood and most recently investigated epigenetic mechanism when compared to DNA methylation and histone modification (Saavedra et al., 2016). miRNA is one type of non-coding RNA (ncRNA), or RNA that is changed into proteins. Around 98% of the genome does not code for proteins, leading to a supporting hypothesis that ncRNAs play a significant role in gene expression. For example, humans and chimpanzees share 98.8% of the same DNA code. However, epigenetics and specifically ncRNA contribute to the wide phenotypic variation between the species (Zheng & Xiao, 2016). Further, Zheng and Xiao (2016) estimated that miRNA regulates up to 60% of gene expression.
miRNA has also been found to suppress and activate gene expression at the levels of transcription and translation (Saavedra et al., 2016). miRNAs affect gene expression by directly influencing mRNA. Specifically, the miRNA may attach to mRNA and “block” the mRNA from creating proteins or it may directly degrade mRNA. This then decreases the surplus of mRNA in the cell. If the miRNA binds partially with the mRNA, then it inhibits protein production; but if it binds completely, it is marked for destruction. Once the mRNA is identified for destruction, other proteins and enzymes are attracted to the mRNA, and they degrade the mRNA and eliminate it (Zheng & Xiao, 2016). Moreover, when compared to DNA methylation, which may be isolated to a single gene sequence, miRNA can target hundreds of genes (Lewis et al., 2005). Researchers have discovered that miRNA may mediate anxiety-like symptoms (Cohen et al., 2017).
Human Development and Epigenetics
Over the life of an individual, there are critical or sensitive periods in which epigenetic modifications are more heavily influenced by environmental factors (Mulligan, 2016). Early life (ages 0 to 5 years) appears to be one of the most critical time periods when epigenetics is more active. An example of this is the Dutch Famine of 1944–45, also known as the Dutch Hunger Winter (Champagne, 2010; Szyf, 2009). The Nazis occupied the Netherlands and restricted food to the country, bringing about a famine. The individual daily caloric intake estimate varied between 400 and 1800 calories at the climax of the famine. Most notably, women who gave birth during this time experienced the impact of low maternal caloric intake, which impacted their child and the child’s health outcomes into adulthood. One discovery was that male children had a higher risk of adulthood obesity if their famine exposure occurred early in gestation versus a male fetus who experienced famine in late gestation. Findings suggested that fetuses who experienced restricted caloric intake during the development of their autonomic nervous system may have an increased risk of heart disease in adulthood. The findings of epigenetic mechanisms at work between mother and child during a famine are flagrant enough, yet epigenetic researchers have also discovered that epigenetic tags carry across generations, called genomic imprinting (Arnaud, 2010; Yehuda et al., 2016; T.-Y. Zhang & Meaney, 2010).
Genomic imprinting can be defined as the passing on of certain epigenetic modifications to the fetus by parents (Arnaud, 2010). It is allele-specific, and approximately half of the imprinting an offspring receives is from the mother. The imprinting mechanism marks certain areas, or loci, of offspring’s genes as active or repressed. For instance, the loci may exhibit increased or decreased methylation.
An imprinting example is evident in the IGF-2 (insulin-like growth factor II) gene and those fetuses exposed to the Dutch Hunger Winter (Heijmans et al., 2008). Sixty years after the famine, a decrease in DNA methylation on IGF-2 was found in adults with fetal exposure during the famine compared to their older siblings. Researchers also found these intergenerational imprinting effects associated with the grandchildren of women who were pregnant during the Dutch Hunger Winter. Similar imprinting is also apparent in Holocaust survivors (Yehuda et al., 2016) and children born to mothers who experienced PTSD from the World Trade Center collapse of 9/11 (Yehuda et al., 2005). These imprinting mechanisms are important for counselors to understand in that we see the interplay between the client and the environment across generations. The client becomes the embodiment of their environment at the cellular level. This is no longer the dichotomous “nature vs. nurture” debate but the passing on of biological effects from one generation to another through the interplay of nature and nurture.
Epigenetics and Mental Health Disorders
Now we turn our focus to the influence of epigenetics on the profession of counseling. What we do know is that epigenetic mechanisms, (e.g., DNA methylation, histone modifications, miRNA) are associated with various mental health disorders. It is hypothesized that epigenetics contributes to the development of mental disorders after exposure to environmental stressors, such as traumatic life events, but it may also have positive effects based on salutary environments (Syzf, 2009; Yehuda et al., 2005). We will review only those mental health epigenetic findings that have significant implications relative to clinical disorders such as stress, anxiety, childhood maltreatment, depression, schizophrenia, and addiction. We will also offer epigenetic outcomes associated with treatment, including cognitive behavioral therapy (CBT; Roberts et al., 2015), meditation (Chaix et al., 2020), and antidepressants (Lüscher & Möhler, 2019).
Stress and Anxiety
Stress, especially during early life stages, causes long-term effects for neuronal pathways and gene expression (Lester et al., 2016; Palmisano & Pandey, 2017; Perroud et al., 2011; Roberts et al., 2015; Szyf, 2009; T.-Y. Zhang & Meaney, 2010). Currently, research supports the mediating effects of stress on epigenetics through DNA methylation, especially within the gestational environment (Lester & Marsit, 2018). DNA methylation has been associated with upregulation of the hypothalamic-pituitary-adrenal (HPA) axis, increasing anxiety symptoms (McGowan et al., 2009; Oberlander et al., 2008; Romens et al., 2015; Shimada-Sugimoto et al., 2015; Tsankova et al., 2007). DNA methylation has also been linked with increased levels of cortisol for newborns of depressed mothers. This points to an increased HPA stress response in the newborn (Oberlander et al., 2008). Ouellet-Morin et al. (2013) also looked at DNA methylation and stress. They conducted a longitudinal twin study on the effect of bullying on the serotonin transporter gene (SERT) for monozygotic twins and found increased levels of SERT DNA methylation in victims compared to their non-bullied monozygotic co-twin. Finally, Roberts et al. (2015) examined the effect of CBT on DNA methylation for children with severe anxiety, specifically testing changes in the FKBP5 gene. Although the results were not statistically significant, they may be clinically significant. Research participants with a higher DNA methylation on the FKBP5 gene had poorer response to CBT treatment.
Beyond DNA methylation, other researchers have investigated miRNA and its association with stress and anxiety. A study by Harris and Seckl (2011) found that fetal rodents with increased exposure to maternal cortisol suffered from lower birth weights and heightened anxiety. Similarly, Cohen et al. (2017) investigated anxiety in rats for a specific miRNA called miR-101a-3p. The researchers selectively bred rats, one group with low anxiety and the other with high anxiety traits. They then overexpressed miR-101a-3p in low-anxiety rats to see if that would induce greater expressions of anxiety symptomatology. The investigators observed increased anxiety behaviors when increasing the expression of miR-101a-3p in low-anxiety rats. The researchers postulated that miRNA may be a mediator of anxiety-like behaviors. Finally, paternal chronic stress in rats has been associated with intergenerational impact on offspring’s HPA axis with sperm cells having increased miRNAs, potentially indicating susceptibility of epigenetic preprogramming in male germ cells post-fertilization (Rodgers et al., 2013). The evidence suggests that paternal stress reprograms the HPA stress response during conception. This reprogramming may begin a cascading effect on the offspring’s HPA, creating dysregulation that is associated with disorders like schizophrenia, autism, and depression later in adulthood.
Though some researchers have indicated a negative association between anxiety and epigenetics, others have found positive effects between epigenetics and anxiety. A seminal study by Weaver et al. (2005) illustrated the flexibility of an offspring’s biological system to negative and positive environmental cues. Weaver et al. looked at HPA response of rodent pups who received low licking and grooming from their mother (a negative environmental effect) who exhibited higher HPA response to environmental cues in adulthood. Epigenetically, they found lower DNA methylation in a specific promotor region in these adult rodents. They hypothesized that they could reverse this hypomethylation by giving an infusion of methionine, an essential amino acid that is a methyl group donor. They discovered the ability to reverse low methylation, which improved the minimally licked and groomed adult rodents’ response to stress. This connects with counseling in that epigenetic information is not set for life but reversible through interventions such as diet.
Others have investigated mindfulness and its epigenetic effects on stress. Chaix et al. (2020) looked at DNA methylation at the genome level for differences between skilled meditators who meditated for an 8-hour interval compared to members of a control group who engaged in leisure activities for 8 hours. The control group did not have any changes in genome DNA methylation, but the skilled meditators showed 61 differentially methylated sites post-intervention. This evidence can potentially support the use of mindfulness with our clients as an intervention for treatment of stress.
Childhood Maltreatment
Childhood maltreatment includes sexual abuse, physical abuse and/or neglect, and emotional abuse and/or neglect. Through this lens, Suderman et al. (2014) examined differences in 45-year-old males’ blood samples between those who experienced abuse in childhood and those who did not, with the aim of determining whether gene promoter DNA methylation is linked with child abuse. After 30 years, the researchers found different DNA methylation patterns between abused versus non-abused individuals and that a specific hypermethylation of a gene was linked with the adults who experienced child abuse. Suderman et al. (2014) believed that adversity, such as child abuse, reorganizes biological pathways that last into adulthood. These DNA methylation differences have been associated with biological pathways leading to cancer, obesity, diabetes, and other inflammatory paths.
Other researchers have also found epigenetic interactions at CpG sites predicting depression and anxiety in participants who experienced abuse. Though these interactions were not statistically significant (Smearman et al., 2016), increased methylation at specific promoter regions was discovered (Perroud et al., 2011; Romens et al., 2015). Furthermore, in a hallmark study, McGowan et al. (2009) discovered that people with child abuse histories who completed suicide possessed hypermethylation of a particular promotor region when compared to controls. Perroud et al. (2011) noted that frequency, age of onset, and severity of maltreatment correlated positively with increased methylation in adult participants suffering from borderline personality disorder, depression, and PTSD. Yehuda et al. (2016) reported that in a smaller subset of an overall sample of Holocaust survivors, the impact of trauma was intergenerationally associated with increased DNA methylation. Continued study of these particular regions may provide evidence of DNA methylation as a predictor of risk in developing anxiety or depressive disorders.
Major Depressive Disorder
Most studies of mental illness, genetics, and depression have used stress animal models. Through these models, histone modification, chromatin remodeling, miRNA, and DNA methylation mechanisms have been found in rats and mice (Albert et al., 2019; Nestler et al., 2016). When an animal or human experiences early life stress, epigenetic biomarkers may serve to detect the development or progression of major depressive disorder (Saavedra et al., 2016). Additionally, histone modification markers may also indicate an increase in depression (Tsankova et al., 2007; Turecki, 2014). Beyond animal models, Januar et al. (2015) found that buccal tissue in older patients with major depressive disorder provided evidence that the BDNF gene modulates depression through hypermethylation of specific CpGs in promoter regions.
Lastly, certain miRNAs may serve as potential biomarkers for major depressive disorder. miRNA may be used in the pharmacologic treatment of depressive disorders (Saavedra et al., 2016). Tsankova et al. (2007) and Saavedra et al. (2016) noted that certain epigenetic mechanisms that influence gene expression may be useful as antidepressant treatments. Medication may induce neurogenesis and greater plasticity in synapses through upregulation and downregulation of miRNAs (Bocchio-Chiavetto et al., 2013; Lüscher & Möhler, 2019). This points to the potential use of epigenetic “engineering” for reducing depression progression and symptomology where a counselor could refer a client for epigenetic antidepressant treatments.
Maternal Depression
Maternal prenatal depression may program the postnatal HPA axis in infants’ responses to the caretaking environment. Such programming may result in decreased expression of certain genes associated with lesser DNA methylation in infants, depending on which trimester maternal depression was most severe, and increased HPA reactivity (Devlin et al., 2010). Further, Devlin et al. discovered that maternal depression in the second trimester affected newborns’ DNA methylation patterns. However, the authors offered key limitations in their study, namely the sample was predominantly male and depressive characteristics differed based on age. Conradt et al. (2016) reported that prenatal depression in mothers may be associated with higher DNA methylation in infants. However, maternal sensitivity (i.e., ability of mother to respond to infants’ needs positively, such as positive touch, attending to distress, and basic social-emotional needs) toward infants buffered the extent of methylation, which points to environmental influences. This finding highlights the risk of infant exposure to maternal depression in conjunction with maternal sensitivity. Yet, overall, the evidence suggests that epigenetic mechanisms are at play across critical periods—prenatal, postnatal, and beyond—that have implications for offspring. When a fetus or offspring experiences adverse conditions, such as maternal depression, there is an increased likelihood of “impaired cognitive, behavioral, and social functioning . . . [including] psychiatric disorders throughout the adult life” (Vaiserman & Koliada, 2017, p. 1). For the practicing counselor, we suggest that clinical work with expecting mothers has the potential to reduce such risk based on these epigenetic findings.
Schizophrenia
Accumulated evidence suggests that schizophrenia arises from the interaction between genetics and the client’s environment (Smigielski et al., 2020). Epigenetics is considered a mediator between a client’s genetics and environment with research showing moderate support for this position. DNA methylation, histone modifications, mRNA, and miRNA epigenetic mechanisms have been linked with schizophrenia (Boks et al., 2018; Cheah et al., 2017; Okazaki et al., 2019).
DNA methylation is a main focus in schizophrenia epigenetic research (Cariaga-Martinez & Alelú-Paz , 2018). For example, Fisher et al. (2015) conducted a longitudinal study investigating epigenetic differences between monozygotic twins who demonstrated differences in psychotic symptoms; at age 12, one twin was symptomatic and the other was asymptomatic. Fisher et al. found DNA methylation differences between these twins. The longitudinal twin study design allowed for the control of genetic contributions to the outcome as well as other internal and external threats. Further, it pointed to a stronger association between epigenetics and schizophrenia.
From a clinical perspective, Ma et al. (2018) identified a potential epigenetic biomarker for detecting schizophrenia. The authors were able to identify three specific miRNAs that may work in combination as a biomarker for the condition. According to the authors, this finding may be helpful in the future for diagnosis and monitoring treatment outcomes. We speculate that future counselors may have biomarker tests conducted as part of the diagnostic process and in monitoring treatment effectiveness with alternation in miRNA levels.
Addiction
In addictions, a diversity of epigenetic mechanisms have been identified (e.g., DNA methylation, histone acetylation, mRNA, miRNA) across various substance use disorders: cocaine, amphetamine, methamphetamine, and alcohol (Hamilton & Nestler, 2019). Moreover, these epigenetic processes have been hypothesized to contribute to the addiction process by mediating seeking behaviors via dopamine in the neurological system. Also, Hamilton and Nestler (2019) found that epigenetic mechanisms have the potential to combat addiction processes, but further research is needed.
Cadet et al. (2016) conducted a review of cocaine, methamphetamine, and epigenetics in animal models (mice and rats). Chronic cocaine use was linked with histone acetylation in the dopamine system and DNA methylation for both chronic and acute administrations. They concluded that epigenetics may be a facilitating factor for cocaine abuse. Others have supported this conclusion for cocaine specifically, in that cocaine alters the chromatin structure by increasing histone acetylation, thereby temporarily inducing addictive behaviors (Maze & Nestler, 2011; Tsankova et al., 2007). From a treatment perspective, Wright et al. (2015) reported, in a sample of rats, that an injected methyl supplementation appeared to attenuate cocaine-seeking behavior when compared to the control group associated with cocaine-induced DNA methylation.
Regarding methamphetamines, during their review, Cadet et al. (2016) discovered that there were only a few extant studies on epigenetics and methamphetamines. Numachi et al. (2004) linked extended use of methamphetamines to changes in DNA methylation patterns, which seemed to increase vulnerability to neurochemical effects. More recently, Jayanthi et al. (2014) discovered that chronic methamphetamine use in rats induced histone hypoacetylation, making it more difficult for transcription to occur and potentially supporting the addiction process. To counter this histone hypoacetylation, the authors treated the mice with valproic acid, which inhibited the histone hypoacetylation. This study may evidence potential psychopharmacological treatments in the future at the epigenetic level for methamphetamine addiction.
H. Zhang and Gelernter (2017) reviewed the literature on DNA methylation and alcohol use disorder (AUD) and found mixed results. The authors discovered that individuals with an AUD exhibited DNA hypermethylation and hypomethylation in a variety of promoter regions. They also noted generalization limitations due to small tissue samples from the same regions of postmortem brains. They suggested that DNA methylation may account for “missing heritability” (p. 510) among individuals with AUDs.
Histone deacetylation has also been connected to chromatin closing or silencing for chronic users of alcohol, which may be involved in the maintenance of an AUD. Palmisano and Pandey (2017) suggested that there are epigenetic mediating factors between comorbidity of AUDs and anxiety disorders. On a positive note, exercise has been found to have opposite epigenetic modifications when comparing a healthy exercise group to a group who experience AUDs in terms of DNA methylation at CpG sites (Chen et al., 2018). Thus, counselors may incorporate such aspects in psychoeducation when recommending exercise in goal setting and other treatment interventions.
To summarize, epigenetics has been linked to several disorders such as anxiety, stress, depression, schizophrenia, and addiction (Albert et al., 2019; Cadet et al., 2016; Lester et al., 2016; Palmisano & Pandey, 2017; Smigielski et al., 2020). DNA methylation and miRNA may have mediating effects for mental health concerns such as anxiety (Harris & Seckl, 2011; Romens et al., 2015). Additionally, epigenetic mediating effects have also been discovered in major depressive disorder, maternal depression, and addiction (Albert et al., 2019; Conradt et al., 2016; Hamilton & Nestler, 2019). Moreover, epigenetic imprinting has been associated with trauma and stress, as found in Holocaust survivors and their children (Yehuda et al., 2016). Overall, “evidence accumulates that exposure to social stressors in [childhood], puberty, adolescence, and adulthood can influence behavioral, cellular, and molecular phenotypes and . . . are mediated by epigenetic mechanisms” (Pishva et al., 2014, p. 342).
Implications
A key aim in providing a primer on epigenetics, specifically the coaction between a client’s biology and environment on gene expression, is to illuminate opportunities for counselors to prevent and intervene upon mental health concerns. This is most relevant based on the evidence that epigenetic processes change over a client’s lifetime because of environmental influences, meaning that the client is not in a fixed state per traditional gene theory (Nestler et al., 2016). Epigenetics provides an alternate view of nature and nurture, demonstrating that epigenetic tags may not only be influenced by unfavorable environmental influences (e.g., maternal depression, trauma, bullying, child abuse and neglect) but also by favorable environments and activities (e.g., mindfulness, CBT, exercise, diet, nurturing; Chaix et al., 2020; Chen et al., 2018; Conradt et al., 2016; Roberts et al., 2015; Stevens et al., 2018). Understanding the flexibility of epigenetics has the potential to engender hope for our clients and to guide our work as counselors and counselor educators, because our genetic destinies are not fixed as we once theorized in gene theory.
Bioecological Conceptualization: Proximal and Distal Impact and Interventions
The impact of epigenetics on the counseling profession can be understood using Bronfenbrenner’s (1979) bioecological model. The bioecological model conceptualizes a client’s function over time based on the coaction between the client and their environment (Broderick & Blewitt, 2015; Jones & Tang, 2015). The client’s environment can have both beneficial and deleterious proximal and distal effects. These effects are like concentric rings around the client, which Bronfenbrenner called “subsystems.” The most proximate subsystem is the microsystem, the environment that has a direct influence on the client, such as parents, teachers, classmates, coworkers, relatives, etc. The next level is the mesosystem, in which the micro entities interact with one another or intersect with influence on the client (e.g., school and home intersect to influence client’s thinking and behavior). The next system, called the exosystem, begins the level of indirect influence. This may include neighborhood factors such as the availability of fresh produce, safe neighborhoods, social safety net programs, and employment opportunities. The last subsystem is the macrosystem. This system consists of the cultural norms, values, and biases that influence all other systems. The final aspect of this model, called the chronosystem, takes into account development over time. The chronosystem directs the counselor’s attention to developmental periods that have differing risks and opportunities, or what can be called “critical” developmental periods.
Below we conceptualize epigenetic counseling implications using Bronfenbrenner’s model but simplify it by grouping systems: proximal effects (micro/meso level) labeled as micro effects and distal effects (exo/macro level) labeled as macro effects. We will also apply the chronosystem by focusing on critical developmental periods that are salient when applying epigenetics to counseling. Ultimately, our central focus is the client and the concentric influences of micro and macro effects. To begin, we will first focus on the important contribution of epigenetics during the critical developmental period of 0 to 5 years of age with implications at the micro and macro levels.
Epigenetics Supports Early Life Span Interventions
Though the evidence does support epigenetic flexibility across a client’s life span, we know that early adverse life events may alter a child’s epigenome with mediating effects on development and behavior (Lester & Marsit, 2018). We also know that epigenetic processes are most active in the first 5 years of life (Mulligan, 2016; Syzf et al., 2016). These early insults to the genome may elicit poor mental health into adulthood such as anxiety, depression, schizophrenia, and addiction. For example, a client who grew up in an urban environment with a traditionally marginalized group status and parents who experienced drug dependence has an increased risk for schizophrenia above and beyond the genetic, inherited risk. These adverse childhood experiences have the potential to modify the epigenome, increasing the likelihood of developing mental health concerns, including schizophrenia (Cariaga-Martinez & Alelú-Paz, 2018).
At the micro level, the caregiver can be a salutary effect against adverse environmental conditions (Oberlander et al. 2008; Weaver et al., 2005). Prenatally, counseling can work with parents before birth to generate healthy coping strategies (e.g., reduce substance abuse), flexible and adaptive caregiver functioning, and effective parenting strategies. An example of this is to use parent–child interactive therapy (PCIT) pre-clinically, or before the child evidences a disorder (Lieneman et al., 2017). Preventive services using PCIT have been documented as effective with externalizing behaviors, child maltreatment, and developmental delays. Additional micro-level interventions can be found in the use of home-visiting programs to improve child outcomes prenatally to 5 years of age where positive parenting and other combined interventions are utilized to improve the health of mother, father, and child (Every Child Succeeds, 2019; Healthy Families New York, 2021).
Clinically, epigenetics points to earlier care and treatment to prevent the emergence of mental disorders (e.g., major depressive disorder, schizophrenia). Also, epigenetic research has provided evidence that environmental change can be equally important as client change. Regarding treatment planning, examining the client’s individual level factors or microsystem (e.g., physical health, mental status, education, race, gender) as well as their macrosystem (e.g., social stigma, poverty, housing quality, green space, pollution) may be crucial before considering what kind of modifications and/or interventions are most appropriate. For example, if a 9-year-old White female presents to a counselor for behavioral concerns in school, it is important for the counselor to gather a holistic life history to build an informed picture of the many variables collectively impacting the child’s behavior at each level. At the micro level, a counselor will evaluate for childhood maltreatment, but from an epigenetic lens, other proximal environmental factors could be important to screen for such as poverty, maternal depression, nutrition, classroom dynamics, and exercise (McEwen & McEwen, 2017; Mulligan, 2016). If the 9-year-old child is experiencing parental neglect and food insecurity, the clinician can treat the client’s individual needs at the micro level (i.e., working with the family system to overcome any neglect by using treatments such as PCIT, and direct referral to social workers and other agencies to provide food and shelter to meet basic needs).
The science of epigenetics may also inform action taken during assessment and case conceptualization based on the coaction of environment with a client over time. Although intervention at 0–5 years of age is most preventative, it is not practical in all cases. Using assessments that collect information on an adult client’s early life may help inform case conceptualization and allow the integration of epigenetics into counseling theories to better understand the etiology of a client’s presenting problem(s). For example, using an adverse childhood experiences assessment may help identify individuals at higher risk of epigenetic concerns. Epigenetics highlights the impact of client–environment interaction and its influence (positive or negative) on overall health. Additionally, early life adversity increases the likelihood of poor health outcomes such as heart disease, anxiety, and depression. However, these poor consequences could be mediated by talking with clients about the importance of exercise and its benefit on epigenetics and, by extension, mental health.
At the macro level, examples could include the reduction of hostile environments (e.g., institutional racism, neighborhood violence, limited employment opportunities, low wages, air pollutants, water pollutants), advocacy for statutes, regulations to decrease instability such as unfair housing in low-income neighborhoods, establishing partnerships in the development of community-based and school-based prevention programs, and applying early interventions such as mindfulness to reduce the effects of stress (Chaix et al., 2020). To illustrate, postnatal depression symptom severity has been associated with residential stability (Jones et al., 2018). By developing policies that would increase housing security, a reduction in maternal depression symptom severity could potentially reduce the DNA methylation that is associated with upregulation of the HPA and child reactivity, but this would need to be investigated further for confirmation. According to Rutten et al. (2013), this change may also increase the resiliency of children by reducing their experience of chronic stress, as sustained maternal depression severity often impacts caregiving because of unstable housing.
Although members of the counseling profession have known the significance of early intervention for years, this epigenetic understanding confirms why human growth and development is a core component of our counseling professional identity (Remley & Herlihy, 2020) and provides a supporting rationale for our efforts. Additionally, epigenetic tags have the potential to cross generations via the process of imprinting (Yehuda et al., 2016). This has potential implications across the life span.
In summary, critical developmental periods must be a focal point for counseling interventions, necessitating upstream action rather than our current dominant approach of downstream activities and a shift toward primary prevention over predominantly tertiary prevention. Such primary prevention would reduce stress and trauma for children before signs and symptoms become apparent and attend to the development and sustainability of healthy environments that would increase both client and community wellness.
Epigenetics Supports Counseling Advocacy and Social Justice Efforts
When reflecting on the implications of epigenetics, it is apparent that place, context, and the client’s environment are critical factors for best positioning them for healthy outcomes, engendering a push for advocacy and social justice for clients. Because environments have no boundaries, it is important to think of advocacy across many systems: towns, counties, states, countries, and the world. This reinforces the call for counselors and counselor educators to move beyond the walls of their workplaces in order to collaborate within the larger mental health field (e.g., clinical mental health, school, marriage and family, addiction, rehabilitation). Additionally, said knowledge compels connection with other professions—such as social workers, physicians, psychologists, engineers, housing developers, public health administrators, and members of nonprofit and faith-based organizations, etc.—to enact change on a wider scale and to improve the conditions for clients at a systemic level.
This collaboration also calls for engaging at local and international levels. Global human rights issues such as sex trafficking cross countries, regions, and local communities and necessitate collaboration to ameliorate these practices and the associated trauma. For starters, the American Counseling Association and the International Association for Counseling could partner with other organizations such as the Child Defense Fund to assist in meeting their mission to level the playing field for all children in the United States. At the local level, counselors and counselor educators could collaborate with local children’s hospitals and configure a plan to meet common goals to improve children’s health and wellness.
Counseling Research and Epigenetics
Research primarily affects clients on a macro level but can trickle down to directly engage clients within our clinical work and practice. Counselors and counselor educators can partner with members of other disciplines to further the work with epigenetic biomarkers (e.g., depression and DNA methylation). Counseling researchers can also investigate how talk therapy and other adjuncts, such as diet and exercise, may improve our clients’ treatment outcomes. As counseling researchers, we can develop research agendas around intervention and prevention for those 0–5 years of age and create and evaluate programs for this age group while also creating community partnerships as noted above. An example of this partnership is The John Hopkins Center for Prevention and Early Intervention. The creators of this program developed sustainable partnerships with public schools, mental health systems, state-level educational programs, universities, and federal programs to focus on early interventions that are school-based and beyond. They collaborated to develop, evaluate, and deliver a variety of programs and research activities to improve outcomes for children and adolescents. They have created dozens of publications based on these efforts that help move the discipline forward. In one such publication, Guintivano et al. (2014) looked at epigenetic and genetic biomarkers for predicting suicide.
Counselor Education, CACREP, and Epigenetics
The counselor educational system affects clients distally but also holds implications for the work counselors conduct at the client level. Counselor educators can provide a more robust understanding of epigenetics to counseling students across the counselor education curriculum. These efforts can include introducing epigenetics in theories, diagnosis, treatment, human and family development, practicum and internship, assessment, professional orientation, and social and cultural foundations courses. By assisting counseling students to comprehend the relationship between client and environment, as well as the importance of prevention, educators will increase their students’ ability to carry out a holistic approach with clients and attend to the foundational emphases of the counseling profession on wellness and prevention. Moreover, by learning to include epigenetics in case conceptualization, students can gain a more robust understanding of the determinants of symptomology, potential etiology at the cellular level, and epigenetically supported treatments such as CBT and mindfulness.
It is fairly simple to integrate epigenetics education into programs accredited by the Council for Accreditation of Counseling and Related Educational Programs (CACREP; 2015). To begin, counselor educators can integrate epigenetics education into professional counseling orientation and ethical practice courses. As counselor educators discuss the history and philosophy of the counseling profession, particularly from a wellness and prevention lens (CACREP, 2015, 2.F.1.a), counselor educators can discuss the connection between epigenetics and wellness. Wellness is a foundational value for the counseling profession and is a part of the definition of counseling (Kaplan et al., 2014). Many wellness models (both theoretical and evidence-based) are rooted in the promotion of a holistic balance of the client in a variety of facets and contexts (Myers & Sweeney, 2011). We can continue to support these findings by integrating epigenetics within our conversations about wellness, as we have epigenetic evidence that the positive or negative coaction between the individual and their environment can impact a person toward increased or decreased wellness.
Counselor educators can also integrate epigenetics education into Social and Cultural Diversity and Human Growth and Development courses. Within Social and Cultural Diversity courses, counselor educators can address how negative environmental conditions have negative influences on offspring. This is evidenced by the discrimination against Jews and its imprinting that crosses generations (Yehuda et al., 2016). Counselor educators can discuss how discrimination and barriers to positive environmental conditions can impact someone at the epigenetic level (CACREP, 2015, 2.F.2.h). Within Human Growth and Development, counselor educators can discuss how the study of epigenetics provides us a biological theory to understand how development is influenced by environment across the life span (CACREP, 2015, 2.F.3.a, c, d, f). In particular, it can provide an etiology of how negative factors change epigenetic tags, which are correlated with negative mental health that may become full-blown mental health disorders later in adulthood (CACREP, 2015, 2.F.3.c, d, e, g).
Additionally, counselor educators can integrate epigenetic education within specialty counseling areas. Several studies (Maze & Nestler, 2011; Palmisano & Pandey, 2017; Tsankova et al., 2007; Wong et al., 2011; H. Zhang & Gelernter, 2017) have noted how epigenetic mechanisms may support the addiction process and counselor educators can interweave this information when discussing theories and models of addiction and mental health problems (CACREP, 2015, 5.A.1.b; 5.C.1.d; 5.C.2.g). Counselor educators can also discuss epigenetics as it applies to counseling practice. Because epigenetics research supports treatments like CBT, mindfulness, nutrition, and exercise (Chaix et al., 2020; Chen et al., 2018; Roberts et al., 2015; Stevens et al., 2018), counselor educators can address these topics in courses when discussing techniques and interventions that work toward prevention and treatment of mental health issues (CACREP, 2015, 5.C.3.b).
Generally, CACREP (2015) standards support programs that infuse counseling-related research into the curriculum (2.E). We support the integration of articles, books, websites, and videos that will engender an understanding of epigenetics across the curriculum, so long as the integration supports student learning and practice.
Conclusion and Future Directions
In summary, there are numerous epigenetic processes at work in the symptoms we attend to as counselors. We have provided information that illustrates how epigenetics may mediate outcomes such as depression, anxiety, schizophrenia, and addiction. We have also illustrated how CBT, exercise, diet, and meditation may have positive epigenetic influences supporting our craft. We have discovered that epigenetic processes are most malleable in early life. This information offers incremental evidence for our actions as professional counselors, educators, and researchers, leading to a potential examination of our efforts in areas of prevention, social justice, clinical practice, and counseling program development. However, we must note that epigenetics as a science is relatively new and much of the research is correlational.
Based on the current limits of epigenetic science and a lack of investigation of mental health epigenetics in professional counseling, one of our first recommendations for future research efforts is to collaborate across professions with other researchers such as geneticists, as we did for this manuscript. From this partnership, our profession’s connection to epigenetics is elucidated. Interdisciplinary collaboration allows the professional counselor to offer their expertise in mental health and the geneticist their deep understanding of epigenetics and the tools to examine the nature and nurture relationships in mental health outcomes. We can also make efforts to look at our wellness-based preventions and interventions to document changes at the epigenetic level in our clients and communities. Ideally, as the science of epigenetics advances, we will have epigenetic research in our profession of counseling that is beyond correlation and evidences the effectiveness of our work down to the cellular level.
Conflict of Interest and Funding Disclosure
The development of this manuscript was supported
in part by a Cincinnati Children’s Hospital Medical
Center Trustee Award and by a grant from the
National Heart, Lung, and Blood Institute (HL132344).
The authors reported no conflict of interest.
References
Albert, P. R., Le François, B., & Vahid-Ansari, F. (2019). Genetic, epigenetic and posttranscriptional mechanisms for treatment of major depression: The 5-HT1A receptor gene as a paradigm. Journal of Psychiatry & Neuroscience, 44(3), 164–176. https://doi.org/10.1503/jpn.180209
Arnaud, P. (2010). Genomic imprinting in germ cells: Imprints are under control. Reproduction, 140(3), 411–423. https://doi.org/10.1530/REP-10-0173
Benoit, L., & Turecki, G. (2010). The epigenetics of suicide: Explaining the biological effects of early life environmental adversity. Archives of Suicide Research, 14(4), 291–310.
https://doi.org/10.1080/13811118.2010.524025
Benros, M. E., Nielsen, P. R., Nordentoft, M., Eaton, W. W., Dalton, S. O., & Mortensen, P. B. (2011). Autoimmune diseases and severe infections as risk factors for schizophrenia: A 30-year population-based register study. The American Journal of Psychiatry, 168(12), 1303–1310. https://doi.org/10.1176/appi.ajp.2011.11030516
Bocchio-Chiavetto, L., Maffioletti, E., Bettinsoli, P., Giovannini, C., Bignotti, S., Tardito, D., Corrada, D., Milanesi, L., & Gennarelli, M. (2013). Blood microRNA changes in depressed patients during antidepressant treatment. European Neuropsychopharmacology, 23(7), 602–611. https://doi.org/10.1016/j.euroneuro.2012.06.013
Boks, M. P., Houtepen, L. C., Xu, Z., He, Y., Ursini, G., Maihofer, A. X., Rajarajan, P., Yu, Q., Xu, H., Wu, Y., Wang, S., Shi, J. P., Hulshoff Pol, H. E., Strengman, E., Rutten, B. P. F., Jaffe, A. E., Kleinman, J. E., Baker, D. G., Hol, E. M., . . . Kahn, R. S. (2018). Genetic vulnerability to DUSP22 promoter hypermethylation is involved in the relation between in utero famine exposure and schizophrenia. Nature Partner Journals Schizophrenia, 4(1), 1–8. https://doi.org/10.1038/s41537-018-0058-4
Broderick, P. C., & Blewitt, P. (2015). The life span: Human development for helping professionals (4th ed.). Pearson.
Bronfenbrenner, U. (1979). The ecology of human development: Experiments by nature and design. Harvard University Press.
Brooker, R. J. (2017). Genetics: Analysis and principles (6th ed.). McGraw-Hill.
Cadet, J. L., McCoy, M. T., & Jayanthi, S. (2016). Epigenetics and addiction. Clinical Pharmacology & Therapeutics, 99(5), 502–511. https://doi.org/10.1002/cpt.345
Cariaga-Martinez, A., & Alelú-Paz, R. (2018). Epigenetic and schizophrenia. In F. Durbano (Ed.), Psychotic disorders – An update (pp. 147–162). IntechOpen. https://doi.org/10.5772/intechopen.73242
Chaix, R., Fagny, M., Cosin-Tomás, M., Alvarez-López, M., Lemee, L., Regnault, B., Davidson, R. J., Lutz, A., & Kaliman, P. (2020). Differential DNA methylation in experienced meditators after an intensive day of mindfulness-based practice: Implications for immune-related pathways. Brain, Behavior, and Immunity, 84, 36–44. https://doi.org/10.1016/j.bbi.2019.11.003
Champagne, F. A. (2010). Early adversity and developmental outcomes: Interaction between genetics, epigenetics, and social experiences across the life span. Perspectives on Psychological Science, 5(5), 564–574.
https://doi.org/10.1177/1745691610383494
Cheah, S.-Y., Lawford, B. R., Young, R. M., Morris, C. P., & Voisey, J. (2017). mRNA expression and DNA methylation analysis of serotonin receptor 2A (HTR2A) in the human schizophrenic brain. Genes, 8(1), 1–11. https://doi.org/10.3390/genes8010014
Chen, J., Hutchinson, K. E., Bryan, A. D., Filbey, F. M., Calhoun, V. D., Claus, E. D., Lin, D., Sui, J., Du, Y., & Liu, J. (2018). Opposite epigenetic associations with alcohol use and exercise intervention. Frontiers in Psychiatry, 9(594), 1–12. https://doi.org/10.3389/fpsyt.2018.00594
Cohen, J. L., Jackson, N. L., Ballestas, M. E., Webb, W. M., Lubin, F. D., & Clinton, S. M. (2017). miR-101a-3p and Ezh2 modulate anxiety-like behavior in high-responder rats. European Journal of Neuroscience, 46(7), 2241–2252.
Conradt, E., Hawes, K., Guerin, D., Armstrong, D. A., Marsit, C. J., Tronick, E., & Lester, B. M. (2016). The contributions of maternal sensitivity and maternal depressive symptoms to epigenetic processes and neuroendocrine functioning. Child Development, 87(1), 73–85. https://doi.org/10.1111/cdev.12483
Council for Accreditation of Counseling and Related Educational Programs. (2015). 2016 CACREP standards. http://www.cacrep.org/wp-content/uploads/2017/08/2016-Standards-with-citations.pdf
Devlin, A. M., Brain, U., Austin, J., & Oberlander, T. F. (2010). Prenatal exposure to maternal depressed mood and the MTHFR C677T variant affect SLC6A4 methylation in infants at birth. PloS ONE, 5(8), e12201.
https://doi.org/10.1371/journal.pone.0012201
Every Child Succeeds. (2019). 2019 report to the community. https://static1.squarespace.com/static/5df9251a492
ba56bc96bc96f/t/5e73b2a333e8127c09daabf2/1584640684722/Final2019Report.pdf
Fisher, H. L., Murphy, T. M., Arseneault, L., Caspi, A., Moffitt, T. E., Viana, J., Hannon, E., Pidsley, R., Burrage, J., Dempster, E. L., Wong, C. C. Y., Pariante, C. M., & Mill, J. (2015). Methylomic analysis of monozygotic twins discordant for childhood psychotic symptoms. Epigenetics, 10(11), 1014–1023.
https://doi.org/10.1080/15592294.2015.1099797
Gejman, P. V., Sanders, A. R., & Kendler, K. S. (2011). Genetics of schizophrenia: New findings and challenges. Annual Review of Genomics and Human Genetics, 12, 121–144.
https://doi.org/10.1146/annurev-genom-082410-101459
Guintivano, J., Brown, T., Newcomer, A., Jones, M., Cox, O., Maher, B. S., Eaton, W. W., Payne, J. L., Wilcox, H. C., & Kaminsky, Z. A. (2014). Identification and replication of a combined epigenetic and genetic biomarker predicting suicide and suicidal behaviors. The American Journal of Psychiatry, 171(12), 1287–1296.
https://doi.org/10.1176/appi.ajp.2014.14010008
Haggarty, S. J., & Tsai, L.-H. (2011). Probing the role of HDACs and mechanisms of chromatin-mediated neuroplasticity. Neurobiology of Learning and Memory, 96(1), 41–52. https://doi.org/10.1016/j.nlm.2011.04.009
Hamilton, P. J., & Nestler, E. J. (2019). Epigenetics and addiction. Current Opinion in Neurobiology, 59, 128–136. https://doi.org/10.1016/j.conb.2019.05.005
Harris, A., & Seckl, J. (2011). Glucocorticoids, prenatal stress and the programming of disease. Hormones and Behavior, 59(3), 279–289. https://doi.org/10.1016/j.yhbeh.2010.06.007
Healthy Families New York. (2021, January 4). [Website.] https://www.healthyfamiliesnewyork.org
Heijmans, B. T., Tobi, E. W., Stein, A. D., Putter, H., Blauw, G. J., Susser, E. S., Slagboom, P. E., & Lumey, L. H. (2008). Persistent epigenetic differences associated with prenatal exposure to famine in humans. Proceedings of the National Academy of Sciences, 105(44), 17046–17049. https://doi.org/10.1073/pnas.0806560105
Huang, W.-C., Ferris, E., Cheng, T., Hörndli, C. S., Gleason, K., Tamminga, C., Wagner, J. D., Boucher, K. M., Christian, J. L., & Gregg, C. (2017). Diverse non-genetic, allele-specific expression effects shape genetic architecture at the cellular level in the mammalian brain. Neuron, 93(5), 1094–1109.e7.
https://doi.org/10.1016/j.neuron.2017.01.033
Januar, V., Ancelin, M.-L., Ritchie, K., Saffery, R., & Ryan, J. (2015). BDNF promoter methylation and genetic variation in late-life depression. Translational Psychiatry, 5, e619. https://doi.org/10.1038/tp.2015.114
Jayanthi, S., McCoy, M. T., Chen, B., Britt, J. P., Kourrich, S., Yau, H.-J., Ladenheim, B., Krasnova, I. N., Bonci, A., & Cadet, J. L. (2014). Methamphetamine downregulates striatal glutamate receptors via diverse epigenetic mechanisms. Biological Psychiatry, 76(1), 47–56. https://doi.org/10.1016/j.biopsych.2013.09.034
Jones, D. E., & Tang, M. (2015). Health inequality: What counselors need to know to act. In Ideas and research you can use: VISTAS 2015. https://www.counseling.org/docs/default-source/vistas/article_60785a22f16116603abcacff0000bee5e7.pdf?sfvrsn=4
Jones, D. E., Tang, M., Folger, A., Ammerman, R. T., Hossain, M. M., Short, J. A., & Van Ginkel, J. B. (2018). Neighborhood effects on PND symptom severity for women enrolled in a home visiting program. Community Mental Health Journal, 54(4), 420–428. https://doi.org/10.1007/s10597-017-0175-y
Kaplan, D. M., Tarvydas, V. M., & Gladding, S. T. (2014). 20/20: A vision for the future of counseling: The new consensus definition of counseling. Journaling of Counseling & Development, 92, 366–372. https://www.counseling.org/docs/default-source/20-20/2020-jcd-article-consensus-definition.pdf?sfvrsn=76017f2c_2
Lester, B. M., Conradt, E., & Marsit, C. (2016). Introduction to the special section on epigenetics. Child Development, 87(1), 29–37. https://doi.org/10.1111/cdev.12489
Lester, B. M., & Marsit, C. J. (2018). Epigenetic mechanisms in the placenta related to infant neurodevelopment. Epigenomics, 10(3), 321–333. https://doi.org/10.2217/epi-2016-0171
Lewis, B. P., Burge, C. B., & Bartel, D. P. (2005). Conserved seed pairing, often flanked by adenosines, indicates that thousands of human genes are microRNA targets. Cell, 120(1), 15–20.
https://doi.org/10.1016/j.cell.2004.12.035
Lieneman, C. C., Brabson, L. A., Highlander, A., Wallace, N. M., & McNeil, C. B. (2017). Parent–child interaction therapy: Current perspectives. Psychology Research and Behavior Management, 10, 239–256.
https://doi.org/10.2147/PRBM.S91200
Lüscher, B., & Möhler, H. (2019). Brexanolone, a neurosteroid antidepressant, vindicates the GABAergic deficit hypothesis of depression and may foster resilience. F1000Research, 8(May), 1–14.
https://doi.org/10.12688/f1000research.18758.1
Ma, J., Shang, S., Wang, J., Zhang, T., Nie, F., Song, X., Zhao, H., Zhu, C., Zhang, R., & Hao, D. (2018). Identification of miR-22-3p, miR-92a-3p, and miR-137 in peripheral blood as biomarker for schizophrenia. Psychiatry Research, 265, 70–76. https://doi.org/10.1016/j.psychres.2018.03.080
Maze, I., & Nestler, E. J. (2011). The epigenetic landscape of addiction. Annals of the New York Academy of Sciences, 1216(1), 99–113. https://doi.org/10.1111/j.1749-6632.2010.05893.x
McEwen, C. A., & McEwen, B. S. (2017). Social structure, adversity, toxic stress, and intergenerational poverty: An early childhood model. Annual Review of Sociology, 43, 445–472.
https://doi.org/10.1146/annurev-soc-060116-053252
McGowan, P. O., Sasaki, A., D’Alessio, A. C., Dymov, S., Labonté, B., Szyf, M., Turecki, G., & Meaney, M. J. (2009). Epigenetic regulation of the glucocorticoid receptor in human brain associates with childhood abuse. Nature Neuroscience, 12(3), 342–348. https://doi.org/10.1038/nn.2270
Monk, C., Spicer, J., & Champagne, F. A. (2012). Linking prenatal maternal adversity to developmental outcomes in infants: The role of epigenetic pathways. Development and Psychopathology, 24(4), 1361–1376.
https://doi.org/10.1017/S0954579412000764
Mulligan, C. J. (2016). Early environments, stress, and the epigenetics of human health. Annual Review of Anthropology, 45(1), 233–249. https://doi.org/10.1146/annurev-anthro-102215-095954
Myers, J. E., & Sweeney, T. J. (2011). Wellness counseling: The evidence base for practice. Journal of Counseling & Development, 86(4), 482–493. https://doi.org/10.1002/j.1556-6678.2008.tb00536.x
National Human Genome Research Institute. (2020). Epigenomics fact sheet. https://www.genome.gov/about-genomics/fact-sheets/Epigenomics-Fact-Sheet
Nestler, E. J., Peña, C. J., Kundakovic, M., Mitchell, A., & Akbarian, S. (2016). Epigenetic basis of mental illness. The Neuroscientist, 22(5), 447–463. https://doi.org/10.1177/1073858415608147
Numachi, Y., Yoshida, S., Yamashita, M., Fujiyama, K., Naka, M., Matsuoka, H., Sato, M., & Sora, I. (2004). Psychostimulant alters expression of DNA methlytransferase mRNA in the rat brain. Annals of the New York Academy of Sciences, 1025(1), 102–109. https://doi.org/10.1196/annals.1316.013
Oberlander, T. F., Weinberg, J., Papsdorf, M., Grunau, R., Misri, S., & Devlin, A. M. (2008). Prenatal exposure to maternal depression, neonatal methylation of human glucocorticoid receptor gene (NR3C1) and infant cortisol stress responses. Epigenetics, 3(2), 97–106. https://doi.org/10.4161/epi.3.2.6034
Okazaki, S., Otsuka, I., Numata, S., Horai, T., Mouri, K., Boku, S., Ohmori, T., Sora, I., & Hishimoto, A. (2019). Epigenetic clock analysis of blood samples from Japanese schizophrenia patients. npj Schizophrenia, 5(9), 1–7. https://doi.org/10.1038/s41537-019-0072-1
Ouellet-Morin, I., Wong, C. C. Y., Danese, A., Pariante, C. M., Papadopoulos, A. S., Mill, J., & Arseneault, L. (2013). Increased serotonin transporter gene (SERT) DNA methylation is associated with bullying victimization and blunted cortisol response to stress in childhood: A longitudinal study of discordant monozygotic twins. Psychology of Medicine, 43(9), 1813–1823. https://doi.org/10.107/S0033291712002784
Palmisano, M., & Pandey, S. C. (2017). Epigenetic mechanisms of alcoholism and stress-related disorders. Alcohol, 60, 7–18. https://doi.org/10.1016/j.alcohol.2017.01.001
Perroud, N., Paoloni-Giacobino, A., Prada, P., Olié, E., Salzmann, A., Nicastro, R., Guillaume, S., Mouthon, D.,
Stouder, C., Dieben, K., Huguelet, P., Courtet, P., & Malafosse, A. (2011). Increased methylation of glucocorticoid receptor gene (NR3C1) in adults with a history of childhood maltreatment: A link with the severity and type of trauma. Translational Psychiatry, 1, e59. https://doi.org/10.1038/tp.2011.60
Pishva, E., Kenis, G., van den Hove, D., Lesch, K.-P., Boks, M. P. M., van Os, J., & Rutten, B. P. F. (2014). The epigenome and postnatal environmental influences in psychotic disorders. Social Psychiatry and Psychiatric Epidemiology, 49, 337–348. https://doi.org/10.1007/s00127-014-0831-2
Provençal, N., & Binder, E. B. (2015). The effects of early life stress on the epigenome: From the womb to adulthood and even before. Experimental Neurology, 268, 10–20. https://doi.org/10.1016/j.expneurol.2014.09.001
Remley, T. P., Jr., & Herlihy, B. (2020). Ethical, legal, and professional issues in counseling (6th ed.). Pearson.
Roberts, S., Keers, R., Lester, K. J., Coleman, J. R. I., Breen, G., Arendt, K., Blatter-Meunier, J., Cooper, P., Creswell, C., Fjermestad, K., Havik, O. E., Herren, C., Hogendoorn, S. M., Hudson, J. L., Krause, K., Lyneham, H. J., Morris, T., Nauta, M., Rapee, R. M., . . . Wong, C. C. Y. (2015). HPA axis related genes and response to psychological therapies: Genetics and epigenetics. Depression and Anxiety, 32(12), 861–870.
https://doi.org/10.1002/da.22430
Rodgers, A. B., Morgan, C. P., Bronson, S. L., Revello, S., & Bale, T. L. (2013). Paternal stress exposure alters sperm microRNA content and reprograms offspring HPA stress axis regulation. Journal of Neuroscience, 33(21), 9003–9012. https://doi.org/10.1523/JNEUROSCI.0914-13.2013
Romens, S. E., McDonald, J., Svaren, J., & Pollak, S. D. (2015). Associations between early life stress and gene methylation in children. Child Development, 86(1), 303–309. https://doi.org/10.1111/cdev.12270
Rutten, B. P. F., Hammels, C., Geschwind, N., Menne-Lothmann, C., Pishva, E., Schruers, K., van den Hove, D.,
Kenis, G., van Os, J., & Wichers, M. (2013). Resilence in mental health: Linking psychological and neurobiological perspectives. Acta Psychiatrica Scandinavica, 128(1), 3–20. https://doi.org/10.1111/acps.12095
Saavedra, K., Molina-Márquez, A. M., Saavedra, N., Zambrano, T., & Salazar, L. A. (2016). Epigenetic modifications of major depressive disorder. International Journal of Molecular Sciences, 17(8), 1279.
https://doi.org/10.3390/ijms17081279
Shimada-Sugimoto, M., Otowa, T., & Hettema, J. M. (2015). Genetics of anxiety disorders: Genetic epidemiological and molecular studies in humans. Psychiatry and Clinical Neurosciences, 69(7), 388–401.
https://doi.org/10.1111/pcn.12291
Smearman, E. L., Almli, L. M., Conneely, K. N., Brody, G. H., Sales, J. M., Bradley, B., Ressler, K. J., & Smith, A. K.
(2016). Oxytocin receptor genetic and epigenetic variations: Association with child abuse and adult psychiatric symptoms. Child Development, 87(1), 122–134. https://doi.org/10.1111/cdev.12493
Smigielski, L., Jagannath, V., Rössler, W., Walitza, S., & Grünblatt, E. (2020). Epigenetic mechanisms in schizophrenia and other psychotic disorders: A systematic review of empirical human findings. Molecular Psychiatry, 25, 1718–1748. https://doi.org/10.1038/s41380-019-0601-3
Stevens, A. J., Rucklidge, J. J., & Kennedy, M. A. (2018). Epigenetics, nutrition and mental health: Is there a relationship? Nutritional Neuroscience, 21(9), 602–613. https://doi.org/10.1080/1028415X.2017.1331524
Suderman, M., Borghol, N., Pappas, J. J., Pinto Pereira, S. M., Pembrey, M., Hertzman, C., Power, C., & Szyf, M. (2014). Childhood abuse is associated with methylation of multiple loci in adult DNA. BMC Medical Genomics, 7, 1–12. https://doi.org/10.1186/1755-8794-7-13
Szyf, M. (2009). The early life environment and the epigenome. Biochimica et Biophysica Acta, 1790(9), 878–885. https://doi.org/10.1016/j.bbagen.2009.01.009
Szyf, M., Tang, Y.-Y., Hill, K. G., & Musci, R. (2016). The dynamic epigenome and its implications for behavioral interventions: A role for epigenetics to inform disorder prevention and health promotion. Translational Behavioral Medicine, 6(1), 55–62. https://doi.org/10.1007/s13142-016-0387-7
Szyf, M., Weaver, I., & Meaney, M. (2007). Maternal care, the epigenome and phenotypic differences in behavior. Reproductive Toxicology, 24(1), 9–19. https://doi.org/10.1016/j.reprotox.2007.05.001
Tsankova, N., Renthal, W., Kumar, A., & Nestler, E. J. (2007). Epigenetic regulation in psychiatric disorders. Nature Reviews Neuroscience, 8, 355–367. https://doi.org/10.1038/nrn2132
Turecki, G. (2014). Epigenetics and suicidal behavior research pathways. American Journal of Preventive Medicine, 47(3), S144–S151. https://doi.org/10.1016/j.amepre.2014.06.011
Vaiserman, A. M., & Koliada, A. K. (2017). Early-life adversity and long-term neurobehavioral outcomes: Epigenome as a bridge? Human Genomics, 11(34), 1–15. https://doi.org/10.1186/s40246-017-0129-z
Weaver, I. C. G., Champagne, F. A., Brown, S. E., Dymov, S., Sharma, S., Meaney, M. J., & Szyf, M. (2005). Reversal of maternal programming of stress responses in adult offspring through methyl supplementation: Altering epigenetic marking later in life. Journal of Neuroscience, 25(47), 11045–11054.
https://doi.org/10.1523/JNEUROSCI.3652-05.2005
Wong, C. C. Y., Mill, J., & Fernandes, C. (2011). Drugs and addiction: An introduction to epigenetics. Addiction, 106(3), 480–489. https://doi.org/10.1111/j.1360-0443.2010.03321.x
Wright, K. N., Hollis, F., Duclot, F., Dossat, A. M., Strong, C. E., Francis, T. C., Mercer, R., Feng, J., Dietz, D. M., Lobo, M. K., Nestler, E. J., & Kabbaj, M. (2015). Methyl supplementation attenuates cocaine-seeking behaviors and cocaine-induced c-Fos activation in a DNA methylation-dependent manner. The Journal of Neuroscience, 35(23), 8948–8958. https://doi.org/10.1523/JNEUROSCI.5227-14.2015
Yehuda, R., Daskalakis, N. P., Bierer, L. M., Bader, H. N., Klengel, T., Holsboer, F., & Binder, E. B. (2016). Holocaust exposure induced intergenerational effects on FKBP5 methylation. Biological Psychiatry, 80, 372–380. https://doi.org/10.1016/j.biopsych.2015.08.005
Yehuda, R., Engel, S. M., Brand, S. R., Seckl, J., Marcus, S. M., & Berkowitz, G. S. (2005). Transgenerational effects of posttraumatic stress disorder in babies of mothers exposed to the World Trade Center attacks during pregnancy. The Journal of Clinical Endocrinology & Metabolism, 90(7), 4115–4118.
https://doi.org/10.1210/jc.2005-0550
Zhang, H., & Gelernter, J. (2017). Review: DNA methylation and alcohol use disorders: Progress and challenges. The American Journal on Addictions, 26(5), 502–515. https://doi.org/10.1111/ajad.12465
Zhang, T.-Y., & Meaney, M. J. (2010). Epigenetics and the environmental regulation of the genome and its function. Annual Review of Psychology, 61, 439–466. https://doi.org/10.1146/annurev.psych.60.110707.163625
Zheng, J., & Xiao, X. (2016). Epigenetic modifications and developmental origin of health and diseases (DOHaD). In Y. Dincer (Ed.), Epigenetics: Mechanisms and clinical perspectives (pp. 1–14). Nova Biomedical.
David E. Jones, EdD, NCC, LPC, is an assistant professor at Liberty University. Jennifer S. Park, PhD, NCC, ACS, LPC, is an assistant professor at Colorado Christian University. Katie Gamby, PhD, LPC, CWC, is an assistant professor at Malone University. Taylor M. Bigelow, PhD, is an assistant professor at the University of New Haven. Tesfaye B. Mersha, PhD, is an associate professor at the Cincinnati Children’s Hospital Medical Center (CCMHC), University of Cincinnati College of Medicine. Alonzo T. Folger, PhD, MS, is an assistant professor at the CCMHC, University of Cincinnati College of Medicine. Correspondence may be addressed to David E. Jones, 1971 University Blvd., Lynchburg, VA 24515, dejones14@liberty.edu.
Mar 9, 2020 | Volume 10 - Issue 1
Michael T. Kalkbrenner
College counselors work collaboratively with professionals in a variety of disciplines in higher education to coordinate gatekeeper training to prepare university community members to recognize and refer students in mental distress to support services. This article describes the cross-validation of scores on the Mental Distress Response Scale (MDRS), a questionnaire for appraising university community members’ responses to encountering a student in mental distress, with a sample of faculty members. A confirmatory factor analysis revealed the dimensions of the MDRS were estimated adequately. Results also revealed demographic differences in faculty members’ responses to encountering a student in mental distress. The MDRS has implications for augmenting the outreach efforts of college counselors. For example, the MDRS has potential utility for enhancing campus-wide mental health screening efforts. The MDRS also has implications for supporting psychoeducation efforts, including gatekeeper training workshops, for professional counselors practicing in college settings.
Keywords: Mental Distress Response Scale, mental health, college counselors, gatekeeper, outreach
College counselors play crucial roles in supporting students’ personal, social, and academic growth, as well as students’ success (Golightly et al., 2017). Outreach and prevention programming, including campus violence prevention and supporting college student mental health, are two key elements in the practice of college counselors (Brunner et al., 2014; Golightly et al., 2017). Addressing these two key areas has become increasingly challenging in recent years because of the prevalence of campus violence incidents, including mass shootings in the most severe cases, and the frequency of mental health distress among college students, which has increased substantially since the new millennium (Auerbach et al., 2016; Barrett, 2014; Vieselmeyer et al., 2017). In fact, supporting college student mental health has become one of the greatest challenges that institutions of higher education are facing (Reynolds, 2013).
Most college students suffering from mental health issues do not seek treatment (Downs & Eisenberg, 2012). In response, college counselors, student affairs professionals, and higher education administrators are working collaboratively to develop and implement mental health awareness initiatives and gatekeeper training workshops, which include training university community members (e.g., students, faculty, and staff) as referral agents to recognize and refer students who are showing warning signs for suicide or other mental health issues to support services (Albright & Schwartz, 2017; Hodges et al., 2017). Faculty members are particularly valuable referral agents, as they tend to interact with large groups of students on frequent occasions, and they generally report positive attitudes about supporting college student mental health (Albright & Schwartz, 2017; Kalkbrenner, 2016).
Despite the utility of faculty members as gatekeepers for recognizing and referring students to the university counseling center and to other resources, the results of a recent national survey indicated that a significant proportion of faculty members (63%) do not refer a student in mental distress to support services (Albright & Schwartz, 2017). The literature is lacking research on how faculty members are likely to respond to encountering a student in mental distress, including but not limited to making a faculty-to-student referral to mental health support services. The primary aim of this investigation was to confirm the psychometric properties of the Mental Distress Response Scale (MDRS), a screening tool for measuring university community members’ responses to encountering a student in mental distress. Past investigators validated the MDRS for use with 4-year university students (Kalkbrenner & Flinn, 2020) and community college students (Kalkbrenner, 2019). If found valid for use with faculty members, college counselors could find the MDRS useful for screening and promoting faculty-to-student mental health support. A review of the extant literature is provided in the following section.
Mental Health and the State of Higher Education
Active shooter incidents on college campuses are some of the most tragic events in American history (Kalkbrenner, 2016). The 2015 massacre that occurred on a college campus in Oregon received attention at the highest level of government; former President Barack Obama urged the nation to decide when voting “whether this cause of continuing death for innocent people should be a relevant factor.” (Vanderhart et al., 2015, section A, p. 1). Seung-Hui Cho was a perpetrator of another one of these tragedies at Virginia Polytechnic Institute in 2007. According to Cho’s mother, he had a history of social isolation and unresolved mental health issues (Klienfield, 2007). Without treatment, the effects of mental health disorders can be debilitating and widespread for students, including impairments in academic functioning, attrition, self-harm, social isolation, and suicide or homicide in the most serious cases (Kalkbrenner, 2016; Shuchman, 2007). The early detection and treatment of students who are at risk for mental health disorders is a harm-prevention strategy for reducing campus violence incidents and promoting college student mental health (Futo, 2011; Kalkbrenner, 2016). Consequently, the practice of college counselors involves deploying outreach and systems-level mental health support interventions (Albright & Schwartz, 2017; Brunner et al., 2014; Golightly et al., 2017).
The Role of College Counselors in Providing Systems-Level Interventions
Providing individual counseling is a key role of college counselors (Golightly et al., 2017). In recent years, however, the practice of college counselors has been extended to providing systems-level and preventative mental health interventions to meet the growing mental health needs of college student populations (Brunner et al., 2014; Golightly et al., 2017). In particular, college counselors and their constituents engage in both campus-wide and targeted prevention and outreach programs (Golightly et al., 2017; Lynch & Glass, 2019), including gatekeeper training workshops to prepare university community members as referral agents or train them to recognize and refer students at risk for suicide and other mental health issues to the university counseling center (Albright & Schwartz, 2017; Brunner et al., 2014). These collaborative, educative, and preventative efforts are particularly crucial given the increase in both the severity and complexity of mental health disorders among college students (Gallagher, 2015; Reetz et al., 2016). The findings of past investigators suggest that faculty members are particularly viable referral agents for recognizing and referring students in mental distress to the counseling center (Kalkbrenner, 2016; Margrove et al., 2014).
Faculty Members as Referral Agents
Faculty members have a propensity to serve as referral agents (i.e., recognize and refer students in mental distress to resources) because of their frequent contact with students and their generally positive attitudes and willingness to support their students’ mental and physical wellness (Albright & Schwartz, 2017). Albright and Schwartz (2017) found that approximately 95% of faculty members and staff considered connecting students in mental distress to resources as one of their roles and responsibilities. Similarly, Margrove et al. (2014) found that 64% of untrained university staff members expressed a desire to receive training to recognize warning signs of mental health disorders in students.
Past investigators extended the line of research on the utility of faculty members as gatekeepers by identifying demographic differences by gender and help-seeking history (previous attendance in counseling) in faculty members’ tendency to support college student mental health (Kalkbrenner & Carlisle, 2019; Kalkbrenner & Sink, 2018). In particular, Kalkbrenner and Sink (2018) identified gender as a significant predictor of faculty-to-student counseling referrals, with faculty who identified as female more likely to make faculty-to-student referrals to the counseling center compared to their male counterparts. Similarly, Kalkbrenner and Carlisle (2019) found that faculty members’ awareness of warning signs for mental distress in students was a significant positive predictor of faculty-to-student referrals to the counseling center. In addition, faculty members with a help-seeking history (previous attendance in counseling) were significantly more aware of warning signs for mental distress in their students compared to faculty without a help-seeking history (Kalkbrenner & Carlisle, 2019).
Faculty Members’ Responses to Encountering a Student in Mental Distress
Despite the growing body of literature on institutional agents’ participation in gatekeeper training (i.e., recognize and refer), research on the measurement and appraisal of how faculty members are likely to respond when encountering a student in mental distress is in its infancy. The results of a recent national survey of college students (N = 51,294) and faculty members (N = 14,548) were troubling, as 63% of faculty members did not refer a student in psychological distress to mental health support services (Albright & Schwartz, 2017). Making a referral to the university counseling center is one possible response of students and faculty members to encountering a peer or student in mental distress (Kalkbrenner & Sink, 2018). However, the findings of Albright and Schwartz (2017) highlight a gap in the literature regarding how university community members are likely to respond when encountering a student in mental distress, including but not limited to making a faculty-to-student referral to the college counseling center.
To begin filling this gap in the literature, Kalkbrenner and Flinn (2020) developed, validated, and cross-validated scores on the MDRS to assess 4-year university students’ responses to encountering a student in mental distress, including but not limited to making a referral to mental health support services. In a series of two major phases of psychometric analyses, Kalkbrenner and Flinn identified and confirmed two dimensions or subscales of the MDRS, including Diminish/Avoid and Approach/Encourage, with two large samples of undergraduate students. The Diminish/Avoid subscale measures adverse or inactive responses of university community members to encountering a student in mental distress (e.g., stay away from the person or warn the person that mental issues are perceived as a weakness). The Approach/Encourage subscale appraises facilitative or helpful responses of university community members when encountering a student in mental distress that are likely to help connect the person to resources (e.g., talking to a college counselor or suggesting that the person go to the campus counseling or health center). However, the psychometric properties of the MDRS have not been tested with faculty members. If found valid for such purposes, the MDRS could be a useful tool that college counselors and their constituents can use to screen and promote faculty-to-student referrals to mental health support services. In particular, the following research questions were posed: (1) Does the two-dimensional hypothesized MDRS model fit with a sample of faculty members? and (2) To what extent are there demographic differences in faculty members’ responses to encountering a student in mental distress?
Method
Participants and Procedures
Data were collected electronically from faculty members using Qualtrics, a secure e-survey platform. A nonprobability sampling procedure was used by sending a recruitment email message with an electronic link to the survey to 1,000 faculty members who were teaching at least one course at a research-intensive, mid-Atlantic public university at the time of data collection. A total of 221 faculty members clicked on the electronic link to the survey and 11 responses were omitted from the data set because of 100% missing data, resulting in a useable sample size of 210, yielding a response rate of 21%. This response rate is consistent with the response rates of other investigators (e.g., Brockelman & Scheyett, 2015; Kalkbrenner & Carlisle, 2019) who conducted survey research with faculty members. For gender, 58% (n = 122) identified as female, 41% (n = 86) as male, and 0.5% (n = 1) as non-binary or third gender, and 0.5% (n = 1) did not specify their gender. For ethnicity, 79.0% (n = 166) identified as Caucasian, 6.2% (n = 11) as African American, 3.8% (n = 8) as Hispanic or Latinx, 2.9% (n = 6) as Asian, 2.9% (n = 6) as multiethnic, 0.5% (n = 1) as Hindu, and 0.5% (n = 1) as Irish, and 5.2% (n = 11) did not specify their ethnic identity. Participants ranged in age from 31 to 78 (M = 50; SD = 11). Participants represented all of the academic colleges in the university, including 28.6% (n = 60) Arts and Letters, 22.9% (n = 48) Education, 18.1% (n = 38) Sciences, 12.9% (n = 27) Health Sciences, 9% (n = 19) Engineering and Technology, and 7.6% (n = 16) Business, while 1% (n = 2) of participants did not specify their college.
Instrumentation
Demographic questionnaire
Following informed consent, participants were asked to indicate that they met the inclusion criteria for participation, including (1) employment as a faculty member, and (2) teaching at least one course at the time of data collection. Participants then responded to a succession of demographic items about their gender, ethnicity, age, academic college, and highest level of education completed. Lastly, respondents indicated their rank and help-seeking history (previous attendance in counseling or no previous attendance in counseling) and if they had referred at least one student to mental health support services.
Mental Distress Response Scale (MDRS)
The MDRS is a screening tool comprised of two subscales (Approach/Encourage and Diminish/Avoid) for measuring university community members’ responses to encountering a student in mental distress (Kalkbrenner & Flinn, 2020). The items that mark the Approach/Encourage subscale appraise responses to mental distress that are consistent with providing support and encouragement to a student in mental distress (e.g., “suggest that they go to the health center on campus”). The Diminish/Avoid subscale measures adverse or inactive responses to encountering a student in mental distress (e.g., “try to ignore your concern”). Kalkbrenner and Flinn (2020) found adequate reliability evidence for an attitudinal measure (α > 0.70) and initial validity evidence for the MDRS in two major phases of analyses (exploratory and confirmatory factor analysis [CFA]) with two samples of college students. Kalkbrenner (2019) extended the line of research on the utility of the MDRS for use with community college students and found adequate reliability (α > 0.80) and validity evidence (single and multiple-group confirmatory analysis).
Data Analysis
A CFA based on structural equation modeling was computed using IBM SPSS Amos version 25 to cross-validate scores on the MDRS with a sample of faculty members (research question #1). Using a maximum likelihood estimation method, the following goodness-of-fit indices and thresholds for defining model fit were investigated based on the recommendations of Byrne (2016) and Hooper et al. (2008): Chi square absolute fit index (CMIN, non-significant p-value with an x2/df ratio < 3), comparative fit index (CFI > 0.95), incremental fit index (IFI > 0.95), Tucker-Lewis index (TLI > 0.95), goodness-of-fit index (GFI > 0.95), root mean square error of approximation (RMSEA < 0.07), and standardized root mean square residual (SRMR < 0.08). Based on the findings of past investigators (e.g., Kalkbrenner & Sink, 2018) regarding demographic differences in faculty members’ propensity to support college student mental health, a 2 X 2 (gender X help-seeking history) MANOVA was computed to investigate demographic differences in faculty members’ responses to encountering a student in mental distress (research question #2). The independent variables included gender (male or female) and help-seeking history (previous attendance in counseling or no previous attendance in counseling). Discriminant analysis was used as the post hoc procedure for significant findings in the MANOVA (Warne, 2014). The researcher examined both main effects and interaction effects and applied Bonferroni adjustments to control for the familywise error rate.
Results
CFA
The researcher ensured that the data set met the necessary assumptions for CFA (Byrne, 2016; Field, 2018). A missing values analysis revealed that less than 5% of data was missing for all MDRS items. Little’s Missing Completely at Random (MCAR) test revealed that the data was missing at random: χ2 (387) = 407.98, p = 0.22. Expectation maximization was used to impute missing values. Outliers were winsorized (Field, 2018) and skewness and kurtosis values for the MDRS items (see Table 1) were largely consistent with a normal distribution (+ 1; Mvududu & Sink, 2013). Inter-item correlations between the 10 items were favorable for CFA, and Mahalanobis d2 indices revealed no extreme multivariate outliers. The researcher ensured that the sample size was sufficient for CFA by following the guidelines provided by Mvududu and Sink (2013), including at least 10 participants per estimated parameter with a sample > 200.
Table 1
Descriptive Statistics for MDRS Items
| Item Content |
M |
SD |
Skew |
Kurtosis |
| 1. I would stay away from this person |
49.83 |
9.46 |
1.11 |
0.22 |
| 2. Suggest that they go to the health center on campus |
50.15 |
9.48 |
-0.60 |
-0.08 |
| 3. Try to ignore your concern |
49.74 |
9.08 |
1.07 |
1.08 |
| 4. Take them to a party |
49.21 |
3.11 |
0.70 |
0.81 |
| 5. Tell them to “tough it out” because they will feel better over time |
49.73 |
8.94 |
1.32 |
1.26 |
| 6. Suggest that they see a medical doctor on campus |
50.00 |
9.98 |
-0.24 |
-0.06 |
| 7. Avoid this person |
49.70 |
9.02 |
1.80 |
1.33 |
| 8. Suggest that they see a medical doctor in the community |
50.00 |
9.98 |
-0.49 |
-0.10 |
| 9. Warn the person that others are likely to see their mental health issues as a weakness |
49.31 |
7.14 |
1.90 |
1.59 |
| 10. Talk to a counselor about your concern |
50.00 |
9.97 |
-0.83 |
0.15 |
SEKurtosis = 0.15, SESkewness = 0.17.
Note. Values were winsorized and reported as standardized t-scores (M = 50; SD = 10).
The 10 MDRS items (see Table 1) were entered in the CFA. A strong model fit emerged based on the GFI recommended by Byrne (2016) and Hooper et al. (2008). The CMIN absolute fit index demonstrated no significant differences between the hypothesized model and the data: χ2 (34) = 42.41, p = 0.15, CMIN/df = 1.25. In addition, the CFI = 0.98, GFI = 0.96, IFI = 0.98, TLI = 0.98, RMSEA = 0.03, 90% confidence interval [<.00, .06], and SRMR = 0.05 also demonstrated a strong model fit. Internal consistency reliability analyses (Cronbach’s coefficient alpha) revealed satisfactory reliability coefficients for an attitudinal measure, Diminish/Avoid (α = 0.73) and Approach/Encourage (α = 0.70). In addition, the path model coefficient (-0.04) between factors supported the structural validity of the scales (see Figure 1).
Figure 1
Confirmatory Factor Analysis Path Diagram for the Mental Distress Response Scale
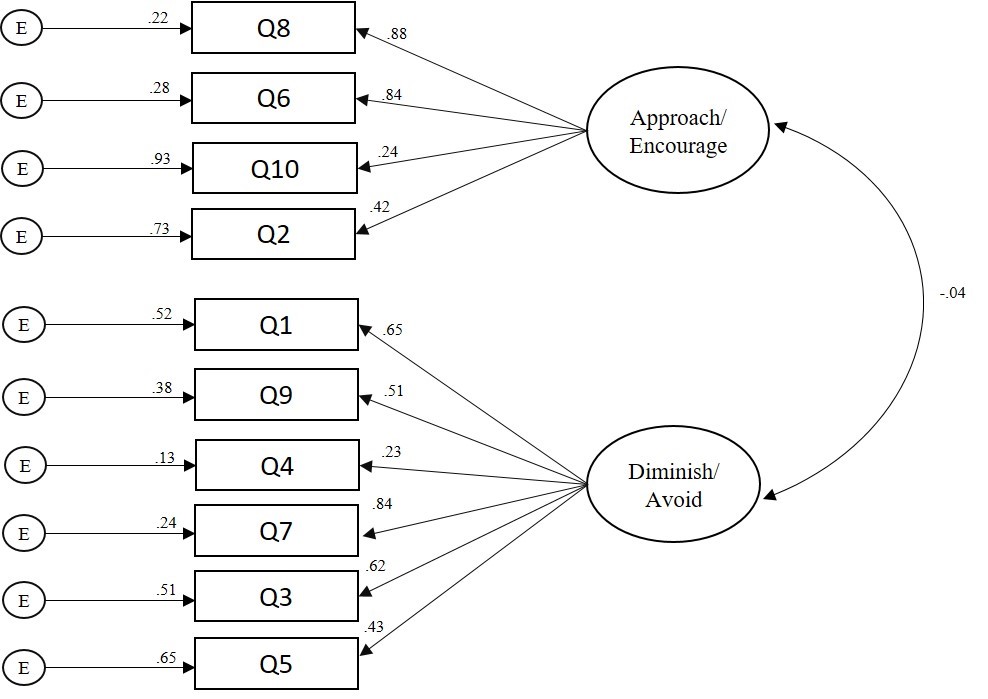
Note. CFA = confirmatory factor analysis, MDRS = Mental Distress Response Scale.
Multivariate Analysis
A 2 X 2 (gender X help-seeking history) MANOVA was computed to investigate demographic differences in faculty members’ responses to encountering a student in mental distress (research question #2). G*Power was used to conduct an a priori power analysis (Faul et al., 2007) and revealed that a minimum sample size of 151 would provide a 95% power estimate, α = .05, with a moderate effect size, F2(v) = 0.063. A significant main effect emerged for gender: F(3, 196) = 8.27, p < 0.001, Wilks’ λ = 0.92, = 0.08. The MANOVA was followed up with a post hoc discriminant analysis based on the recommendations of Warne (2014). The discriminant function significantly discriminated between groups: Wilks’ λ = 0.91, X2 = 18.85, df = 2, p < 0.001. The correlations between the latent factors and discriminant function showed that Diminish/Avoid loaded more strongly on the function (r = 0.98) than Approach/Encourage (r = 0.29), suggesting that Diminish/Avoid contributed the most to group separation in gender. The mean discriminant score on the function was -0.27 for participants who identified as female and 0.37 for participants who identified as male.
Discussion
The results of tests of internal consistency reliability (Cronbach’s coefficient alpha), CFA, and correlations between factors supported the psychometric properties of the MDRS with a sample of faculty members. The results of the CFA were promising as GFI demonstrated a strong model fit between the two-dimensional hypothesized MDRS model and a sample of faculty members (research question #1). In particular, based on one of the most conservative and rigorous absolute fit indices, the CMIN (Byrne, 2016; Credé & Harms, 2015), the researchers retained the null hypothesis—there were no significant differences between the hypothesized factor structure of the MDRS and a sample of faculty members. The strong model fit suggests that Approach/Encourage and Diminish/Avoid are two latent variables that comprise faculty members’ responses to encountering a student in mental distress. The findings of the CFA add to the extant literature about the utility of the MDRS for use with 4-year university students (Kalkbrenner & Flinn, 2020), community college students (Kalkbrenner, 2019), and now with faculty members.
An investigation of the path model coefficient between subscales (see Figure 1) revealed a small and negative association between factors, which supports the structural validity of the MDRS. In particular, the low and negative relationship between the Approach/Encourage and Diminish/Avoid subscales indicates that the dimensions of the MDRS are measuring discrete dimensions of a related construct. As expected, faculty members who scored higher on the Approach/Encourage subscale tended to score lower on the Diminish/Avoid subscale. However, the low strength of the association between factors suggests that faculty members’ responses to encountering a student in mental distress might not always be linear (e.g., a strong positive approach/encourage response might not always be associated with a strong negative diminish/avoid response). Haines et al. (2017) demonstrated that factors in the environment and temperament of a person showing signs of mental distress were significant predictors of mental health support staff’s perceptions of work safety. It is possible that under one set of circumstances faculty members might have an approach/encourage response to mental distress. However, under a difference set of circumstances, a faculty member might have a diminish/avoid response. For example, the extent to which a faculty member feels threatened or unsafe might mediate their propensity of having diminish/avoid or approach/encourage responses. Future research is needed to evaluate this possibility.
Consistent with the findings of previous researchers (Kalkbrenner & Carlisle, 2019; Kalkbrenner & Sink, 2018), the present investigators found that faculty members who identified as male were more likely to report a diminish/avoid response to encountering a student in mental distress compared to female faculty members. Similarly, Kalkbrenner and Sink (2018) found that male faculty members were less likely to make faculty-to-student referrals to the counseling center, and Kalkbrenner and Carlisle (2019) found that male faculty members were less likely to recognize warning signs of mental distress in college students. Similarly, the multivariate results of the present investigation revealed that male faculty members were more likely to report a diminish/avoid response to encountering a student in mental distress when compared to female faculty members. The synthesized findings of Kalkbrenner and Carlisle (2019), Kalkbrenner and Sink (2018), and the present investigation suggest that faculty members who identify as male might be less likely to recognize and refer a student in mental distress to mental health support services. The MDRS has valuable implications for enhancing the practice of professional counselors in college settings.
Implications for Counseling Practice
Outreach, consultation, and psychoeducation are essential components in the practice of college counselors (Brunner et al., 2014; Golightly et al., 2017). The findings of the present investigation have a number of practical implications for enhancing college counselors’ outreach and psychoeducation work—for example, gatekeeper workshops geared toward promoting faculty-to-student referrals to mental health support resources. The complex and multidimensional nature of college student mental health issues calls for interdisciplinary collaboration between college counselors and professionals in a variety of disciplinary orientations in higher education (Eells & Rockland-Miller, 2011; Hodges et al., 2017). College counselors can take leadership roles in coordinating these collaborative efforts to support college student mental health. In particular, college counselors can work with student affairs officials, higher education administrators, and their constituents, and attend new faculty orientations as well as department meetings to administer the MDRS, establish relationships with faculty, and discuss the benefits of gatekeeper training as well as supporting college student mental health. The results of the MDRS can be used to gain insight into the types of responses that faculty members are likely to have when encountering a student in mental distress. This information can be used to structure the content of gatekeeper training workshops aimed at promoting faculty-to-student referrals to mental health support services. Specifically, college counselors might consider the utility of integrating brief interventions and skills training components into gatekeeper training workshops. Motivational interviewing, for example, is an evidence-based, brief approach to counseling that includes both person-centered and directive underpinnings with utility for increasing clients’ intrinsic motivation to make positive changes in their lives (Iarussi, 2013; Resnicow & McMaster, 2012). Professional counselors who practice in higher education are already using motivational interviewing to promote college student development and mental health (Iarussi, 2013). Although future research is needed, integrating motivational interviewing principles (e.g., expressing empathy, rolling with resistance, developing discrepancies, and supporting self-efficacy; Iarussi, 2013) into gatekeeper training workshops might increase faculty members’ commitment to supporting college student mental health.
The MDRS has the potential to enhance college counselors’ outreach and mental health screening efforts (Golightly et al., 2017). College counselors can incorporate the MDRS into batteries of pretest/posttest measures (e.g., the MDRS with a referral self-efficacy measure) for evaluating the effectiveness of mental health awareness initiatives and gatekeeper training programs for faculty and other members of the campus community. If administered widely, the MDRS might have utility for assessing faculty members’ responses to students in mental distress across time and among various campus ecological systems, providing data to drive the prioritization and allocation of outreach efforts aimed at facilitating and maintaining referral networks for connecting students in mental distress to support services.
The results of the present study have policy implications related to campus violence prevention programming. The sharp increase in campus violence incidents has resulted in several universities implementing threat assessment teams as a harm-prevention measure (Eells & Rockland-Miller, 2011). Threat assessment teams involve an interdisciplinary collaboration of university faculty and staff for the purposes of recognizing and responding to students who are at risk of posing a threat to themselves or to others. College counselors can take leadership roles in establishing and supporting threat assessment teams at their universities. College counselors can administer the MDRS to faculty and staff and use the results as one way to identify potential threat assessment team members. University community members who score higher on the Approach/Encourage scale might be inclined to serve on threat assessment teams because of their propensity to support college student mental health. The brevity (10 questions) and versatility of administration (paper copy or electronically via laptop, smartphone, or tablet) of the MDRS adds to the practicality of the measure. Specifically, it might be practical for college counselors and their constituents to administer the MDRS during new faculty orientations, annual opening programs, or department meetings, or via email to faculty and staff. Results can potentially be used to recruit threat assessment team members.
Our findings indicate that when compared to their female counterparts, male faculty members might be more likely to have a diminish/avoid response when encountering a student in mental distress. College counselors might consider working collaboratively with student affairs professionals to implement gatekeeper training and mental health awareness workshops in academic departments that are comprised of high proportions of male faculty members. It is possible that male faculty members are unaware of how to identify warning signs of mental distress in their students (Kalkbrenner & Carlisle, 2019). College counselors might consider the utility of distributing psychoeducation resources for recognizing students in mental distress to faculty and staff. As just one example, the REDFLAGS model is an acronym of eight red flags or warning signs for identifying students who might be struggling with mental health issues (Kalkbrenner, 2016). Kalkbrenner and Carlisle (2019) demonstrated that the REDFLAGS model is a promising psychoeducational tool, as faculty members’ awareness of the red flags was a significant positive predictor of faculty-to-student referrals to the counseling center. The REDFLAGS model appears to be a practical resource for college counselors that can be distributed to faculty electronically or by paper copy, or posted as a flyer (Kalkbrenner, 2016; Kalkbrenner & Carlisle, 2019).
Limitations and Future Research
The findings of the present study should be considered within the context of the limitations. A number of methodological limitations (e.g., self-report bias and social desirability) can influence the validity of psychometric designs. In addition, the dichotomous nature of the faculty-to-student counseling referral variable (referred or not referred) did not provide data on the frequency of referrals. Future researchers should use a continuous variable (e.g., the number of student referrals to the counseling center in the past 2 years) to appraise faculty-to-student referrals. Future researchers can further test the psychometric properties of the MDRS through cross-validating scores on the measure with additional, unique populations of faculty members from a variety of different geographic and social locations. Invariance testing can be computed to examine the degree to which the MDRS and its dimensions maintain psychometric equivalence across different populations of faculty members. In addition, the criterion validity of the MDRS can be examined by testing the extent to which respondents’ MDRS scores are predictors of their frequency of student referrals to the counseling center and to other resources. Furthermore, future qualitative research is needed to investigate faculty members’ unique experiences around supporting college student mental health.
The low and negative association between the Approach/Encourage and Diminish/Avoid subscales suggests that faculty members might have an approach/encourage response to encountering a student in mental distress under one set of circumstances; however, they might have a diminish/avoid response under a difference set of circumstances. Future investigators might test the extent to which attitudinal variables mediate respondents’ MDRS scores—for example, the extent to which faculty members’ sense of safety predicts their MDRS scores. In addition, given the widespread public perception of individuals living with mental illness as violent and dangerous (Varshney et al., 2016), future researchers might identify demographic and background differences (particularly mental health stigma) among participants’ MDRS scores.
Summary and Conclusion
Mental health outreach and screening are essential components in the practice of college counselors, including training referral agents to recognize and refer students who might be struggling with mental health distress to support services (Golightly et al., 2017). Taken together, the results of the present study indicate that the MDRS and its dimensions were estimated sufficiently with a sample of faculty members. Our findings confirmed the two-dimensional hypothesized model for the types of responses that faculty might have when encountering a student showing signs of mental distress. In particular, the results of a CFA provided support for the MDRS and its dimensions, confirming a two-dimensional construct for the types of responses (approach/encourage and diminish/avoid) that faculty members might have when encountering a student in mental distress. Considering the utility of faculty members as gatekeepers and referral agents (Hodges et al., 2017; Kalkbrenner, 2016), researchers, practitioners, and policymakers may find the MDRS a useful screening tool for identifying the ways in which faculty members are likely to respond when encountering a student in mental distress. Results can be used to inform the content of mental health awareness initiatives and gatekeeper training programs aimed at promoting approach/encourage responses to connect students who need mental health support to the appropriate resources.
Conflict of Interest and Funding Disclosure
The authors reported no conflict of interest
or funding contributions for the development
of this manuscript.
References
Albright, G. & Schwartz, V. (2017). Are campuses ready to support students in distress?: A survey of 65,177 faculty, staff, and students in 100+ colleges and universities. https://www.jedfoundation.org/wp-content/uploads/2017/10/Kognito-JED-Are-Campuses-Ready-to-Support-Students-in-Distress.pdf
Auerbach, R. P., Alonso, J., Axinn, W. G., Cuijpers, P., Ebert, D. D., Green, J. G., Hwang, I., Kessler, R. C., Liu, H., Mortier, P., Nock, M. K., Pinder-Amaker, S., Sampson, N. A., Aguilar-Gaxiola, S., Al-Hamzawi, A., Andrade, L. H., Benjet, C., Caldas-de-Almeida, J. M., Demyttenaere, K., . . . Bruffaerts, R. (2016). Mental disorders among college students in the World Health Organization World Mental Health Surveys. Psychological Medicine, 46, 2955–2970. https://doi.org/10.1017/S0033291716001665
Barrett, D. (2014, September 24). Mass shootings on the rise, FBI says. The Wall Street Journal. http://online.wsj.com/articles/mass-shootings-on-the-rise-fbi-says-1411574475
Brockelman, K. F., & Scheyett, A. M. (2015). Faculty perceptions of accommodations, strategies, and psychiatric advance directives for university students with mental illnesses. Psychiatric Rehabilitation Journal, 38, 342–348. https://doi.org/10.1037/prj0000143
Brunner, J. L., Wallace, D. L., Reymann, L. S., Sellers, J.-J., & McCabe, A. G. (2014). College counseling today: Contemporary students and how counseling centers meet their needs. Journal of College Student Psychotherapy, 28, 257–324. https://doi.org/10.1080/87568225.2014.948770
Byrne, B. M. (2016). Structural equation modeling with AMOS: Basic concepts, applications, and programming (3rd ed.). Routledge.
Credé, M., & Harms, P. D. (2015). 25 years of higher-order confirmatory factor analysis in the organizational sciences: A critical review and development of reporting recommendations. Journal of Organizational Behavior, 36, 845–872. https://doi.org/10.1002/job.2008
Downs, M. F., & Eisenberg, D. (2012). Help seeking and treatment use among suicidal college students. Journal of American College Health, 60, 104–114. https://doi.org/10.1080/07448481.2011.619611
Eells, G. T., & Rockland-Miller, H. S. (2011). Assessing and responding to disturbed and disturbing students: Understanding the role of administrative teams in institutions of higher education. Journal of College Student Psychotherapy, 25, 8–23. https://doi.org/10.1080/87568225.2011.532470
Faul, F., Erdfelder, E., Lang, A.-G., & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191. https://doi.org/10.3758/BF03193146
Field, A. (2018). Discovering statistics using IBM SPSS Statistics (5th ed.). SAGE.
Futo, J. (2011). Dealing with mental health issues on campus starts with early recognition and intervention. Campus Law Enforcement Journal, 41, 22–23.
Gallagher, R. P. (2015). National survey of college counseling centers 2014. http://d-scholarship.pitt.edu/id/eprint/28178
Golightly, T., Thorne, K., Iglesias, A., Huebner, E., Michaelson-Chmelir, T., Yang, J., & Greco, K. (2017). Outreach as intervention: The evolution of outreach and preventive programming on college campuses. Psychological Services, 14, 451–460. https://doi.org/10.1037/ser0000198
Haines, A., Brown, A., McCabe, R., Rogerson, M., & Whittington, R. (2017). Factors impacting perceived safety among staff working on mental health wards. BJPsych Open, 3, 204–211.
https://doi.org/10.1192/bjpo.bp.117.005280
Hodges, S. J., Shelton, K., & King Lyn, M. M. (2017). The college and university counseling manual: Integrating essential services across the campus. Springer.
Hooper, D., Coughlan, J., & Mullen, M. R. (2008). Structural equation modelling: Guidelines for determining model fit. The Electronic Journal of Business Research Methods, 6, 53–60.
Iarussi, M. M. (2013). Examining how motivational interviewing may foster college student development. Journal of College Counseling, 16(2), 158–175. https://doi.org/10.1002/j.2161-1882.2013.00034.x
Kalkbrenner, M. T. (2016). Recognizing and supporting students with mental health disorders: The REDFLAGS Model. Journal of Education and Training, 3, 1–13. https://doi.org/10.5296/jet.v3i1.8141
Kalkbrenner, M. T. (2019). Peer-to-peer mental health support on community college campuses: Examining the factorial invariance of the Mental Distress Response Scale. Community College Journal of Research and Practice. https://doi.org/10.1080/10668926.2019.1645056
Kalkbrenner, M. T., & Carlisle, K. L. (2019). Faculty members and college counseling: Utility of The REDFLAGS Model. Journal of College Student Psychotherapy. https://doi.org/10.1080/87568225.2019.1621230
Kalkbrenner, M. T., & Flinn, R. F. (2020). Development, validation, and cross-validation of the Mental Distress Reaction Scale (MDRS). Journal of College Student Development.
Kalkbrenner, M. T., & Sink, C. A. (2018). Development and validation of the College Mental Health Perceived Competency Scale. The Professional Counselor, 8, 175–189. https://doi.org/10.15241/mtk.8.2.175
Kleinfield, N. R. (2007, April 22). Before deadly rage, a life consumed by a troubling silence. The New York Times. http://www.nytimes.com/2007/04/22/us/22vatech.html?pagewanted=all
Lynch, R. J., & Glass, C. R. (2019). The development of the Secondary Trauma in Student Affairs Professionals Scale (STSAP). Journal of Student Affairs Research and Practice, 56, 1–18.
https://doi.org/10.1080/19496591.2018.1474757
Margrove, K. L., Gustowska, M., & Grove, L. S. (2014). Provision of support for psychological distress by university staff, and receptiveness to mental health training. Journal of Further and Higher Education, 38, 90–106. https://doi.org/10.1080/0309877X.2012.699518
Mvududu, N. H., & Sink, C. A. (2013). Factor analysis in counseling research and practice. Counseling Outcome Research and Evaluation, 4, 75–98. https://doi.org/10.1177/2150137813494766
Reetz, D. R., Bershad, C., LeViness, P., & Whitlock, M. (2016). The Association for University and College Counseling Center Directors annual survey. https://www.aucccd.org/assets/documents/aucccd%202016%
20monograph%20-%20public.pdf
Resnicow, K., & McMaster, F. (2012). Motivational interviewing: Moving from why to how with autonomy support. International Journal of Behavioral Nutrition and Physical Activity, 9, 19.
https://doi.org/10.1186/1479-5868-9-19
Reynolds, A. L. (2013). College student concerns: Perceptions of student affairs practitioners. Journal of College Student Development, 54, 98–104. https://doi.org/ 10.1353/csd.2013.0001
Shuchman, M. (2007). Falling through the cracks—Virginia Tech and the restructuring of college mental health services. The New England Journal of Medicine, 357, 105–110. https://doi.org/10.1056/NEJMp078096
Vanderhart, D., Johnson, K., & Turkewitz, J. (2015, October 2). Oregon shooting at Umpqua College kills 10, sheriff says. The New York Times. https://www.nytimes.com/2015/10/02/us/oregon-shooting-umpqua-community-college.html?smid=pl-share
Varshney, M., Mahapatra, A., Krishnan, V., Gupta, R., & Deb, K. S. (2016). Violence and mental illness: What is the true story? Journal of Epidemiology & Community Health, 70, 223–225.
https://doi.org/10.1136/jech-2015-205546
Vieselmeyer, J., Holguin, J., & Mezulis, A. (2017). The role of resilience and gratitude in posttraumatic stress and growth following a campus shooting. Psychological Trauma: Theory, Research, Practice, and Policy, 9, 62–69. https://doi.org/10.1037/tra0000149
Warne, R. T. (2014). A primer on multivariate analysis of variance (MANOVA) for behavioral scientists. Practical Assessment, Research & Evaluation, 19(17), 1–10.
Michael T. Kalkbrenner, PhD, NCC, is an assistant professor at New Mexico State University. Correspondence can be addressed to Michael Kalkbrenner, 1220 Stewart St., OH202B, NMSU, Las Cruces, NM 88001, mkalk001@nmsu.edu.
